User login
‘Why did I choose this?’ Tackling burnout in oncology
MADRID – “Why did I choose this?”
That is the core question a Portuguese oncologist posed from the audience during a session at the annual meeting of the European Society for Medical Oncology (ESMO) that was dedicated to building a sustainable oncology workforce.
“Ten, twenty years ago, being a doctor was a dream,” she said, but right now doctors are underpaid, under strain, and have very few resources.
This oncologist is hardly alone.
A survey from ESMO conducted almost a decade ago found that more than 50% of oncologists across Europe, many of whom were early in their careers, reported being burned out.
This, Dr. Lim said, “was the starting point,” well before the COVID pandemic struck.
More recently, the pandemic has taken its own toll on the well-being of oncologists. A survey presented at ESMO 2020 revealed that 38% of participants, spanning 101 countries, reported experiencing burnout, and 66% said they were not able to perform their job.
Medscape’s 2023 Physician Burnout and Depression Report highlighted similar burnout rates, with 53% of U.S. physicians and 52% of oncologists saying they felt burned out, compared with about 42% in 2018, before the pandemic.
The oncology workforce is in crisis in every country, said Dr. Lim, from the Cancer Dynamics Lab, the Francis Crick Institute, London.
Burnout, characterized by emotional exhaustion, depersonalization or feelings of cynicism, and a low sense of personal accomplishment, can result in a poor work-life balance as well as poor mental and physical health. Factors linked to burnout include social isolation, increased workload, reduced quality of work, lack of control over work, and stressful professional experiences.
Together, these factors can affect patient care and further exacerbate staffing issues, Dr. Lim said.
Staffing shortages are common. Oncologists often work long hours or on weekends to cover gaps caused by staffing shortages. Recent data revealed that in high-income countries, there are on average 0.65 medical oncologists and 0.25 radiation oncologists per 100 patients — a situation made worse by professionals taking early retirement or leaving medicine during the pandemic.
“We have seen that the shortage of human resources in many countries as well as the increasing workload related to the increasing number of cancers,” as well as patients surviving longer, have increased pressures on the healthcare system, Andrés Cervantes, MD, PhD, president of ESMO, explained in a press conference.
While tackling these oncology workforce problems requires smaller, local changes to a physician’s daily routine, “the real change,” Dr. Lim said, lies at an infrastructure level.
In response to this chronic and growing problem, ESMO launched its Resilience Task Force in 2020 to evaluate burnout and well-being. The task force plans to publish a position paper in which it will propose a set of recommendations regarding the psychosocial risks of burnout as well as flexible work patterns, well-being resources, and targeted support.
A panel of experts at the meeting touched on some of these solutions.
Dealing with staff shortages is a must, said Jean-Yves Blay, MD, PhD, during the session. “It’s a simple mathematical equation,” Dr. Blay said. “We must increase the number of doctors in medical schools and the number of nurses and healthcare professionals in all schools.” Improving staffing would also help reduce chronic workload issues.
Resilience training should also be incorporated into physician training starting in medical school. Teaching oncologists how to deal with bad news and to cope when patients dies is particularly important.
“I was not taught that,” said the oncologist from Portugal. “I had to learn that at my own cost.”
The good news is that it’s possible to develop resiliency skills over time, said Claire Hardy, PhD, from Lancaster University, United Kingdom, who agreed that training programs could be one approach to improve oncologists’ work life.
However, a person’s needs are determined by their institution and personal responsibilities. “No one knows your job better than you,” Dr. Hardy said. “No one knows better than you where the inefficiencies are, where the bureaucracy is that could be taken away, or it could be done by somebody whose role it is to sort all that out.”
But having this understanding is not enough. Physician also need to feel “psychological safety to be able to speak out and say that something isn’t working right now or is too much,” or, “I’m spending too much time doing this.”
In other words, oncologists need to be able to set boundaries and say no.
Dr. Hardy said this concept “has been around a while, but it’s really gaining momentum,” and being able to discuss these issues in a forum such as the ESMO Congress is a promising start.
Dr. Lim has relationships with Janseen and SEOM. No other relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
MADRID – “Why did I choose this?”
That is the core question a Portuguese oncologist posed from the audience during a session at the annual meeting of the European Society for Medical Oncology (ESMO) that was dedicated to building a sustainable oncology workforce.
“Ten, twenty years ago, being a doctor was a dream,” she said, but right now doctors are underpaid, under strain, and have very few resources.
This oncologist is hardly alone.
A survey from ESMO conducted almost a decade ago found that more than 50% of oncologists across Europe, many of whom were early in their careers, reported being burned out.
This, Dr. Lim said, “was the starting point,” well before the COVID pandemic struck.
More recently, the pandemic has taken its own toll on the well-being of oncologists. A survey presented at ESMO 2020 revealed that 38% of participants, spanning 101 countries, reported experiencing burnout, and 66% said they were not able to perform their job.
Medscape’s 2023 Physician Burnout and Depression Report highlighted similar burnout rates, with 53% of U.S. physicians and 52% of oncologists saying they felt burned out, compared with about 42% in 2018, before the pandemic.
The oncology workforce is in crisis in every country, said Dr. Lim, from the Cancer Dynamics Lab, the Francis Crick Institute, London.
Burnout, characterized by emotional exhaustion, depersonalization or feelings of cynicism, and a low sense of personal accomplishment, can result in a poor work-life balance as well as poor mental and physical health. Factors linked to burnout include social isolation, increased workload, reduced quality of work, lack of control over work, and stressful professional experiences.
Together, these factors can affect patient care and further exacerbate staffing issues, Dr. Lim said.
Staffing shortages are common. Oncologists often work long hours or on weekends to cover gaps caused by staffing shortages. Recent data revealed that in high-income countries, there are on average 0.65 medical oncologists and 0.25 radiation oncologists per 100 patients — a situation made worse by professionals taking early retirement or leaving medicine during the pandemic.
“We have seen that the shortage of human resources in many countries as well as the increasing workload related to the increasing number of cancers,” as well as patients surviving longer, have increased pressures on the healthcare system, Andrés Cervantes, MD, PhD, president of ESMO, explained in a press conference.
While tackling these oncology workforce problems requires smaller, local changes to a physician’s daily routine, “the real change,” Dr. Lim said, lies at an infrastructure level.
In response to this chronic and growing problem, ESMO launched its Resilience Task Force in 2020 to evaluate burnout and well-being. The task force plans to publish a position paper in which it will propose a set of recommendations regarding the psychosocial risks of burnout as well as flexible work patterns, well-being resources, and targeted support.
A panel of experts at the meeting touched on some of these solutions.
Dealing with staff shortages is a must, said Jean-Yves Blay, MD, PhD, during the session. “It’s a simple mathematical equation,” Dr. Blay said. “We must increase the number of doctors in medical schools and the number of nurses and healthcare professionals in all schools.” Improving staffing would also help reduce chronic workload issues.
Resilience training should also be incorporated into physician training starting in medical school. Teaching oncologists how to deal with bad news and to cope when patients dies is particularly important.
“I was not taught that,” said the oncologist from Portugal. “I had to learn that at my own cost.”
The good news is that it’s possible to develop resiliency skills over time, said Claire Hardy, PhD, from Lancaster University, United Kingdom, who agreed that training programs could be one approach to improve oncologists’ work life.
However, a person’s needs are determined by their institution and personal responsibilities. “No one knows your job better than you,” Dr. Hardy said. “No one knows better than you where the inefficiencies are, where the bureaucracy is that could be taken away, or it could be done by somebody whose role it is to sort all that out.”
But having this understanding is not enough. Physician also need to feel “psychological safety to be able to speak out and say that something isn’t working right now or is too much,” or, “I’m spending too much time doing this.”
In other words, oncologists need to be able to set boundaries and say no.
Dr. Hardy said this concept “has been around a while, but it’s really gaining momentum,” and being able to discuss these issues in a forum such as the ESMO Congress is a promising start.
Dr. Lim has relationships with Janseen and SEOM. No other relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
MADRID – “Why did I choose this?”
That is the core question a Portuguese oncologist posed from the audience during a session at the annual meeting of the European Society for Medical Oncology (ESMO) that was dedicated to building a sustainable oncology workforce.
“Ten, twenty years ago, being a doctor was a dream,” she said, but right now doctors are underpaid, under strain, and have very few resources.
This oncologist is hardly alone.
A survey from ESMO conducted almost a decade ago found that more than 50% of oncologists across Europe, many of whom were early in their careers, reported being burned out.
This, Dr. Lim said, “was the starting point,” well before the COVID pandemic struck.
More recently, the pandemic has taken its own toll on the well-being of oncologists. A survey presented at ESMO 2020 revealed that 38% of participants, spanning 101 countries, reported experiencing burnout, and 66% said they were not able to perform their job.
Medscape’s 2023 Physician Burnout and Depression Report highlighted similar burnout rates, with 53% of U.S. physicians and 52% of oncologists saying they felt burned out, compared with about 42% in 2018, before the pandemic.
The oncology workforce is in crisis in every country, said Dr. Lim, from the Cancer Dynamics Lab, the Francis Crick Institute, London.
Burnout, characterized by emotional exhaustion, depersonalization or feelings of cynicism, and a low sense of personal accomplishment, can result in a poor work-life balance as well as poor mental and physical health. Factors linked to burnout include social isolation, increased workload, reduced quality of work, lack of control over work, and stressful professional experiences.
Together, these factors can affect patient care and further exacerbate staffing issues, Dr. Lim said.
Staffing shortages are common. Oncologists often work long hours or on weekends to cover gaps caused by staffing shortages. Recent data revealed that in high-income countries, there are on average 0.65 medical oncologists and 0.25 radiation oncologists per 100 patients — a situation made worse by professionals taking early retirement or leaving medicine during the pandemic.
“We have seen that the shortage of human resources in many countries as well as the increasing workload related to the increasing number of cancers,” as well as patients surviving longer, have increased pressures on the healthcare system, Andrés Cervantes, MD, PhD, president of ESMO, explained in a press conference.
While tackling these oncology workforce problems requires smaller, local changes to a physician’s daily routine, “the real change,” Dr. Lim said, lies at an infrastructure level.
In response to this chronic and growing problem, ESMO launched its Resilience Task Force in 2020 to evaluate burnout and well-being. The task force plans to publish a position paper in which it will propose a set of recommendations regarding the psychosocial risks of burnout as well as flexible work patterns, well-being resources, and targeted support.
A panel of experts at the meeting touched on some of these solutions.
Dealing with staff shortages is a must, said Jean-Yves Blay, MD, PhD, during the session. “It’s a simple mathematical equation,” Dr. Blay said. “We must increase the number of doctors in medical schools and the number of nurses and healthcare professionals in all schools.” Improving staffing would also help reduce chronic workload issues.
Resilience training should also be incorporated into physician training starting in medical school. Teaching oncologists how to deal with bad news and to cope when patients dies is particularly important.
“I was not taught that,” said the oncologist from Portugal. “I had to learn that at my own cost.”
The good news is that it’s possible to develop resiliency skills over time, said Claire Hardy, PhD, from Lancaster University, United Kingdom, who agreed that training programs could be one approach to improve oncologists’ work life.
However, a person’s needs are determined by their institution and personal responsibilities. “No one knows your job better than you,” Dr. Hardy said. “No one knows better than you where the inefficiencies are, where the bureaucracy is that could be taken away, or it could be done by somebody whose role it is to sort all that out.”
But having this understanding is not enough. Physician also need to feel “psychological safety to be able to speak out and say that something isn’t working right now or is too much,” or, “I’m spending too much time doing this.”
In other words, oncologists need to be able to set boundaries and say no.
Dr. Hardy said this concept “has been around a while, but it’s really gaining momentum,” and being able to discuss these issues in a forum such as the ESMO Congress is a promising start.
Dr. Lim has relationships with Janseen and SEOM. No other relevant financial relationships were disclosed.
A version of this article first appeared on Medscape.com.
FROM ESMO 2023
FDA OKs ivosidenib for IDH1-mutated myelodysplastic syndromes
The agency also approved the Abbott RealTime IDH1 Assay to test for the mutation.

Almost 4% of the 16,000 people diagnosed with MDS in the United States each year carry an isocitrate dehydrogenase-1 (IDH1) mutation, which increases their risk for poor outcomes, such as transformation to acute myeloid leukemia, Servier explained in a press announcement.
Ivosidenib is an IDH1 inhibitor that has previously been approved for IDH1-mutated AML and locally advanced or metastatic cholangiocarcinoma. The new approval makes it the only targeted therapy approved for relapsed or refractory MDS with the mutation, Servier said.
The FDA approval was based on a phase 1 study in 18 adults aged 61-82 years with IDH1-mutated relapsed or refractory MDS. Patients started at a dose of 500 mg daily in 28-day cycles until disease progression, unacceptable toxicity, or hematopoietic stem cell transplantation. Median treatment duration was 9.3 months, and one patient went on to receive a transplant.
Overall survival was a median of 35.7 months. Fifteen patients (83.3%) had an objective response and 7 (38.9%) went into complete remission after a median of 1.9 months of treatment. The median duration of remission had not been reached at data cutoff.
Among the 9 patients dependent on RBC or platelet transfusions at baseline, 6 (66.7%) no longer needed them during any 56-day post-baseline period.
Grade 3/4 adverse events in 5% or more of patients included arthralgia, hypertension, fatigue, mucositis, and leukocytosis.
Labeling carries a boxed warning of potentially fatal differentiation syndrome. Ivosidenib can also cause QTc prolongation.
A version of this article first appeared on Medscape.com.
The agency also approved the Abbott RealTime IDH1 Assay to test for the mutation.
Almost 4% of the 16,000 people diagnosed with MDS in the United States each year carry an isocitrate dehydrogenase-1 (IDH1) mutation, which increases their risk for poor outcomes, such as transformation to acute myeloid leukemia, Servier explained in a press announcement.
Ivosidenib is an IDH1 inhibitor that has previously been approved for IDH1-mutated AML and locally advanced or metastatic cholangiocarcinoma. The new approval makes it the only targeted therapy approved for relapsed or refractory MDS with the mutation, Servier said.
The FDA approval was based on a phase 1 study in 18 adults aged 61-82 years with IDH1-mutated relapsed or refractory MDS. Patients started at a dose of 500 mg daily in 28-day cycles until disease progression, unacceptable toxicity, or hematopoietic stem cell transplantation. Median treatment duration was 9.3 months, and one patient went on to receive a transplant.
Overall survival was a median of 35.7 months. Fifteen patients (83.3%) had an objective response and 7 (38.9%) went into complete remission after a median of 1.9 months of treatment. The median duration of remission had not been reached at data cutoff.
Among the 9 patients dependent on RBC or platelet transfusions at baseline, 6 (66.7%) no longer needed them during any 56-day post-baseline period.
Grade 3/4 adverse events in 5% or more of patients included arthralgia, hypertension, fatigue, mucositis, and leukocytosis.
Labeling carries a boxed warning of potentially fatal differentiation syndrome. Ivosidenib can also cause QTc prolongation.
A version of this article first appeared on Medscape.com.
The agency also approved the Abbott RealTime IDH1 Assay to test for the mutation.
Almost 4% of the 16,000 people diagnosed with MDS in the United States each year carry an isocitrate dehydrogenase-1 (IDH1) mutation, which increases their risk for poor outcomes, such as transformation to acute myeloid leukemia, Servier explained in a press announcement.
Ivosidenib is an IDH1 inhibitor that has previously been approved for IDH1-mutated AML and locally advanced or metastatic cholangiocarcinoma. The new approval makes it the only targeted therapy approved for relapsed or refractory MDS with the mutation, Servier said.
The FDA approval was based on a phase 1 study in 18 adults aged 61-82 years with IDH1-mutated relapsed or refractory MDS. Patients started at a dose of 500 mg daily in 28-day cycles until disease progression, unacceptable toxicity, or hematopoietic stem cell transplantation. Median treatment duration was 9.3 months, and one patient went on to receive a transplant.
Overall survival was a median of 35.7 months. Fifteen patients (83.3%) had an objective response and 7 (38.9%) went into complete remission after a median of 1.9 months of treatment. The median duration of remission had not been reached at data cutoff.
Among the 9 patients dependent on RBC or platelet transfusions at baseline, 6 (66.7%) no longer needed them during any 56-day post-baseline period.
Grade 3/4 adverse events in 5% or more of patients included arthralgia, hypertension, fatigue, mucositis, and leukocytosis.
Labeling carries a boxed warning of potentially fatal differentiation syndrome. Ivosidenib can also cause QTc prolongation.
A version of this article first appeared on Medscape.com.
Enfortumab vedotin/pembrolizumab hailed as new standard for upfront mUC
following a phase 3 trial presented at the 2023 European Society for Medical Oncology annual meeting.
The combination soundly beat the current standard of care – platinum-based chemotherapy – with a median overall survival of 31.5 months among 442 subjects versus 16.1 months among 444 randomized to gemcitabine with cisplatin or carboplatin, an unprecedented 53% drop in the risk of mortality (P < .00001).
The elimination of chemotherapy also meant that there were substantially fewer grade 3 or higher adverse events with the new combination.
“This is the first time we’ve managed to beat chemotherapy in the first-line setting for overall survival despite multiple previous attempts.” The 30% remission rate with enfortumab vedotin plus pembrolizumab “is not something we’ve seen before,” said lead investigator Thomas Powles, MBBS, MD, a urologic oncologist and researcher at the University of London, who presented the findings.
“We welcome a new standard of care in the management of advanced, metastatic urothelial carcinoma, enfortumab vedotin plus pembrolizumab,” said Andrea Apolo, MD, a urologic oncology researcher at the National Cancer Institute in Bethesda, Md., and discussant on the trial, dubbed EV-302/KEYNOTE-A39.
The news overshadowed a second trial presented immediately after Dr. Powles’ that also showed improvement in overall survival versus standard platinum-based chemotherapy, CheckMate 901.
Instead of replacing chemotherapy, CheckMate 901 added nivolumab. With 304 patients randomized to each arm, nivolumab add-on led to a median overall survival of 21.7 months versus 18.9 months with stand-alone gemcitabine/cisplatin, a 22% drop in the risk of mortality (P = .0171).
It’s the first time that adding immunotherapy to first-line chemotherapy improved survival in metastatic urothelial carcinoma, said lead investigator Michiel van der Heijden, MD, PhD, a urologic oncologist and researcher at the Netherlands Cancer Institute, Amsterdam.
After decades of stagnation, Dr. Apolo said, it’s “monumental for our field” to have two trials that beat chemotherapy in the first-line setting.
However, she said that the much better survival with enfortumab vedotin/pembrolizumab means that the combination now “takes first place as the best first-line regimen in urothelial carcinoma.”
Major disruptions in the treatment paradigm
The crowning of a new first-line standard for locally advanced/metastatic urothelial carcinoma means that everything else in the treatment paradigm has to shift, Dr. Apolo said, and there are many new questions that need to be answered.
Among the most pressing, should the previous first-line standard – platinum-based chemotherapy – now move to the second line and be considered the treatment of choice after progression? Also, is there still a role for the previous second-line standards, pembrolizumab and other immunotherapies, if pembrolizumab fails in the first line?
Dr. Apolo said investigators also need to figure out if there is a role for enfortumab vedotin/pembrolizumab in earlier-stage disease, such as muscle-invasive bladder cancer, and if the dose and duration of enfortumab vedotin can be reduced to limit its peculiar ocular and other toxicities.
Finally, “we must discuss cost,” she said. Enfortumab vedotin plus pembrolizumab (EV+P) is expensive. “Will payers be able to afford” it?
Dr. Powles, the lead investigator on EV-302/KEYNOTE-A39, said he doesn’t know how negotiations are going with payers, but that he hopes they move quickly. “We’ve seen transformative results” with the combination for even aggressive cancers in very sick people. “I think it’s going to be a challenge with patients not to talk about these data.”
EV-302/KEYNOTE-059 details
Merck, the maker of pembrolizumab, and the makers/marketers of enfortumab vedotin, Astellas and Seagen, said they will use EV-302/KEYNOTE-059 to seek a first-line indication for locally advanced/metastatic urothelial carcinoma from the U.S. Food and Drug Administration and other regulators.
They also said the results serve as the confirmation FDA required when it gave accelerated approval to the combination in April 2023 for cisplatin-ineligible patients based on tumor response rates and response durability, according to press releases from the companies.
Pembrolizumab (P) in the trial was dosed at 200 mg on the first day of 3-week treatment cycles to a maximum of 35 cycles; enfortumab vedotin (EV) was given on the first and eighth day of the cycle with no limit in the number of cycles until progression or unacceptable toxicity.
Cisplatin or carboplatin (C) in the control arm was delivered on the first day and gemcitabine (G) on the first and eighth days for up to six 3-week cycles.
Patients in both arms were split about equally between performance statuses of 0 or 1; less than 4% in each group had statuses of 2.
Echoing the overall survival (OS) results, progression-free survival (PFS) was a median of 12.5 months with EV-P versus 6.3 months with GC, a 55% drop in the risk of progression or death (P < .00001).
The results held regardless of PD-L1 expression, cisplatin eligibility, and the presence or absence of visceral metastases.
Follow-up treatments in the trial begin to address Dr. Apolo’s questions: Almost 60% of GC patients went on to a PD-1/L1 for subsequent maintenance or progression, and almost a quarter of EV+P patients went on to subsequent platinum-based chemotherapy.
Grade 3 or higher adverse events occurred in 55.9% of subjects in the EV+P group versus 69.5% in the GC arm.
The most common in the chemotherapy arm were anemia, neutropenia, thrombocytopenia, fatigue, and nausea. The most common with EV+P were skin reactions, hyperglycemia, neutropenia, peripheral neuropathy, diarrhea, and anemia,
CheckMate 901 details
In CheckMate 901, gemcitabine and cisplatin were administered on the first day of 3-week treatment cycles for up to 6 cycles; subjects randomized to nivolumab add-on received 360 mg on day 1 of each cycle, followed by 480 mg every 4 weeks until disease progression or unacceptable toxicity for up to 2 years.
PFS results again mirrored OS, with a median PFS of 7.9 months in the nivolumab arm versus 7.6 months with stand-alone chemotherapy, a 28% drop in the risk of progression or death (P = .0012).
Although OS and PFS benefits were statistically significant overall, they were not significant in subgroup analyses of patients 65 years and older, women, or in patients with liver metastases.
Trends in OS and PFS actually favored chemotherapy in the 40 U.S. subjects (HR OS, 1.92; 95% confidence interval, 0.95-3.88).
The rate of grade 3 or higher adverse events was 61.8% with nivolumab add-on versus 51.7% with chemotherapy alone. Anemia and neutropenia were the most common in both arms, and higher in the nivolumab group.
EV-302/KEYNOTE-A39 was funded by Seagen, Astellas, and Merck. CheckMate 901 was funded by Bristol-Myers Squibb, the maker of nivolumab.
Dr. Powles reported extensive financial ties to pharmaceutical companies, including being an advisor to and receiving research funding from Bristol-Myers Squibb, Merck, SeaGen, and Astellas, as well as travel expenses from Merck. Among other disclosures, Dr. Heijden is an advisor to Seagen and an advisor and researcher for Bristol-Myers Squibb. Dr. Apolo is an unpaid consultant to Merck, Astellas, Seagen, Bristol-Myers Squibb, and other companies.
following a phase 3 trial presented at the 2023 European Society for Medical Oncology annual meeting.
The combination soundly beat the current standard of care – platinum-based chemotherapy – with a median overall survival of 31.5 months among 442 subjects versus 16.1 months among 444 randomized to gemcitabine with cisplatin or carboplatin, an unprecedented 53% drop in the risk of mortality (P < .00001).
The elimination of chemotherapy also meant that there were substantially fewer grade 3 or higher adverse events with the new combination.
“This is the first time we’ve managed to beat chemotherapy in the first-line setting for overall survival despite multiple previous attempts.” The 30% remission rate with enfortumab vedotin plus pembrolizumab “is not something we’ve seen before,” said lead investigator Thomas Powles, MBBS, MD, a urologic oncologist and researcher at the University of London, who presented the findings.
“We welcome a new standard of care in the management of advanced, metastatic urothelial carcinoma, enfortumab vedotin plus pembrolizumab,” said Andrea Apolo, MD, a urologic oncology researcher at the National Cancer Institute in Bethesda, Md., and discussant on the trial, dubbed EV-302/KEYNOTE-A39.
The news overshadowed a second trial presented immediately after Dr. Powles’ that also showed improvement in overall survival versus standard platinum-based chemotherapy, CheckMate 901.
Instead of replacing chemotherapy, CheckMate 901 added nivolumab. With 304 patients randomized to each arm, nivolumab add-on led to a median overall survival of 21.7 months versus 18.9 months with stand-alone gemcitabine/cisplatin, a 22% drop in the risk of mortality (P = .0171).
It’s the first time that adding immunotherapy to first-line chemotherapy improved survival in metastatic urothelial carcinoma, said lead investigator Michiel van der Heijden, MD, PhD, a urologic oncologist and researcher at the Netherlands Cancer Institute, Amsterdam.
After decades of stagnation, Dr. Apolo said, it’s “monumental for our field” to have two trials that beat chemotherapy in the first-line setting.
However, she said that the much better survival with enfortumab vedotin/pembrolizumab means that the combination now “takes first place as the best first-line regimen in urothelial carcinoma.”
Major disruptions in the treatment paradigm
The crowning of a new first-line standard for locally advanced/metastatic urothelial carcinoma means that everything else in the treatment paradigm has to shift, Dr. Apolo said, and there are many new questions that need to be answered.
Among the most pressing, should the previous first-line standard – platinum-based chemotherapy – now move to the second line and be considered the treatment of choice after progression? Also, is there still a role for the previous second-line standards, pembrolizumab and other immunotherapies, if pembrolizumab fails in the first line?
Dr. Apolo said investigators also need to figure out if there is a role for enfortumab vedotin/pembrolizumab in earlier-stage disease, such as muscle-invasive bladder cancer, and if the dose and duration of enfortumab vedotin can be reduced to limit its peculiar ocular and other toxicities.
Finally, “we must discuss cost,” she said. Enfortumab vedotin plus pembrolizumab (EV+P) is expensive. “Will payers be able to afford” it?
Dr. Powles, the lead investigator on EV-302/KEYNOTE-A39, said he doesn’t know how negotiations are going with payers, but that he hopes they move quickly. “We’ve seen transformative results” with the combination for even aggressive cancers in very sick people. “I think it’s going to be a challenge with patients not to talk about these data.”
EV-302/KEYNOTE-059 details
Merck, the maker of pembrolizumab, and the makers/marketers of enfortumab vedotin, Astellas and Seagen, said they will use EV-302/KEYNOTE-059 to seek a first-line indication for locally advanced/metastatic urothelial carcinoma from the U.S. Food and Drug Administration and other regulators.
They also said the results serve as the confirmation FDA required when it gave accelerated approval to the combination in April 2023 for cisplatin-ineligible patients based on tumor response rates and response durability, according to press releases from the companies.
Pembrolizumab (P) in the trial was dosed at 200 mg on the first day of 3-week treatment cycles to a maximum of 35 cycles; enfortumab vedotin (EV) was given on the first and eighth day of the cycle with no limit in the number of cycles until progression or unacceptable toxicity.
Cisplatin or carboplatin (C) in the control arm was delivered on the first day and gemcitabine (G) on the first and eighth days for up to six 3-week cycles.
Patients in both arms were split about equally between performance statuses of 0 or 1; less than 4% in each group had statuses of 2.
Echoing the overall survival (OS) results, progression-free survival (PFS) was a median of 12.5 months with EV-P versus 6.3 months with GC, a 55% drop in the risk of progression or death (P < .00001).
The results held regardless of PD-L1 expression, cisplatin eligibility, and the presence or absence of visceral metastases.
Follow-up treatments in the trial begin to address Dr. Apolo’s questions: Almost 60% of GC patients went on to a PD-1/L1 for subsequent maintenance or progression, and almost a quarter of EV+P patients went on to subsequent platinum-based chemotherapy.
Grade 3 or higher adverse events occurred in 55.9% of subjects in the EV+P group versus 69.5% in the GC arm.
The most common in the chemotherapy arm were anemia, neutropenia, thrombocytopenia, fatigue, and nausea. The most common with EV+P were skin reactions, hyperglycemia, neutropenia, peripheral neuropathy, diarrhea, and anemia,
CheckMate 901 details
In CheckMate 901, gemcitabine and cisplatin were administered on the first day of 3-week treatment cycles for up to 6 cycles; subjects randomized to nivolumab add-on received 360 mg on day 1 of each cycle, followed by 480 mg every 4 weeks until disease progression or unacceptable toxicity for up to 2 years.
PFS results again mirrored OS, with a median PFS of 7.9 months in the nivolumab arm versus 7.6 months with stand-alone chemotherapy, a 28% drop in the risk of progression or death (P = .0012).
Although OS and PFS benefits were statistically significant overall, they were not significant in subgroup analyses of patients 65 years and older, women, or in patients with liver metastases.
Trends in OS and PFS actually favored chemotherapy in the 40 U.S. subjects (HR OS, 1.92; 95% confidence interval, 0.95-3.88).
The rate of grade 3 or higher adverse events was 61.8% with nivolumab add-on versus 51.7% with chemotherapy alone. Anemia and neutropenia were the most common in both arms, and higher in the nivolumab group.
EV-302/KEYNOTE-A39 was funded by Seagen, Astellas, and Merck. CheckMate 901 was funded by Bristol-Myers Squibb, the maker of nivolumab.
Dr. Powles reported extensive financial ties to pharmaceutical companies, including being an advisor to and receiving research funding from Bristol-Myers Squibb, Merck, SeaGen, and Astellas, as well as travel expenses from Merck. Among other disclosures, Dr. Heijden is an advisor to Seagen and an advisor and researcher for Bristol-Myers Squibb. Dr. Apolo is an unpaid consultant to Merck, Astellas, Seagen, Bristol-Myers Squibb, and other companies.
following a phase 3 trial presented at the 2023 European Society for Medical Oncology annual meeting.
The combination soundly beat the current standard of care – platinum-based chemotherapy – with a median overall survival of 31.5 months among 442 subjects versus 16.1 months among 444 randomized to gemcitabine with cisplatin or carboplatin, an unprecedented 53% drop in the risk of mortality (P < .00001).
The elimination of chemotherapy also meant that there were substantially fewer grade 3 or higher adverse events with the new combination.
“This is the first time we’ve managed to beat chemotherapy in the first-line setting for overall survival despite multiple previous attempts.” The 30% remission rate with enfortumab vedotin plus pembrolizumab “is not something we’ve seen before,” said lead investigator Thomas Powles, MBBS, MD, a urologic oncologist and researcher at the University of London, who presented the findings.
“We welcome a new standard of care in the management of advanced, metastatic urothelial carcinoma, enfortumab vedotin plus pembrolizumab,” said Andrea Apolo, MD, a urologic oncology researcher at the National Cancer Institute in Bethesda, Md., and discussant on the trial, dubbed EV-302/KEYNOTE-A39.
The news overshadowed a second trial presented immediately after Dr. Powles’ that also showed improvement in overall survival versus standard platinum-based chemotherapy, CheckMate 901.
Instead of replacing chemotherapy, CheckMate 901 added nivolumab. With 304 patients randomized to each arm, nivolumab add-on led to a median overall survival of 21.7 months versus 18.9 months with stand-alone gemcitabine/cisplatin, a 22% drop in the risk of mortality (P = .0171).
It’s the first time that adding immunotherapy to first-line chemotherapy improved survival in metastatic urothelial carcinoma, said lead investigator Michiel van der Heijden, MD, PhD, a urologic oncologist and researcher at the Netherlands Cancer Institute, Amsterdam.
After decades of stagnation, Dr. Apolo said, it’s “monumental for our field” to have two trials that beat chemotherapy in the first-line setting.
However, she said that the much better survival with enfortumab vedotin/pembrolizumab means that the combination now “takes first place as the best first-line regimen in urothelial carcinoma.”
Major disruptions in the treatment paradigm
The crowning of a new first-line standard for locally advanced/metastatic urothelial carcinoma means that everything else in the treatment paradigm has to shift, Dr. Apolo said, and there are many new questions that need to be answered.
Among the most pressing, should the previous first-line standard – platinum-based chemotherapy – now move to the second line and be considered the treatment of choice after progression? Also, is there still a role for the previous second-line standards, pembrolizumab and other immunotherapies, if pembrolizumab fails in the first line?
Dr. Apolo said investigators also need to figure out if there is a role for enfortumab vedotin/pembrolizumab in earlier-stage disease, such as muscle-invasive bladder cancer, and if the dose and duration of enfortumab vedotin can be reduced to limit its peculiar ocular and other toxicities.
Finally, “we must discuss cost,” she said. Enfortumab vedotin plus pembrolizumab (EV+P) is expensive. “Will payers be able to afford” it?
Dr. Powles, the lead investigator on EV-302/KEYNOTE-A39, said he doesn’t know how negotiations are going with payers, but that he hopes they move quickly. “We’ve seen transformative results” with the combination for even aggressive cancers in very sick people. “I think it’s going to be a challenge with patients not to talk about these data.”
EV-302/KEYNOTE-059 details
Merck, the maker of pembrolizumab, and the makers/marketers of enfortumab vedotin, Astellas and Seagen, said they will use EV-302/KEYNOTE-059 to seek a first-line indication for locally advanced/metastatic urothelial carcinoma from the U.S. Food and Drug Administration and other regulators.
They also said the results serve as the confirmation FDA required when it gave accelerated approval to the combination in April 2023 for cisplatin-ineligible patients based on tumor response rates and response durability, according to press releases from the companies.
Pembrolizumab (P) in the trial was dosed at 200 mg on the first day of 3-week treatment cycles to a maximum of 35 cycles; enfortumab vedotin (EV) was given on the first and eighth day of the cycle with no limit in the number of cycles until progression or unacceptable toxicity.
Cisplatin or carboplatin (C) in the control arm was delivered on the first day and gemcitabine (G) on the first and eighth days for up to six 3-week cycles.
Patients in both arms were split about equally between performance statuses of 0 or 1; less than 4% in each group had statuses of 2.
Echoing the overall survival (OS) results, progression-free survival (PFS) was a median of 12.5 months with EV-P versus 6.3 months with GC, a 55% drop in the risk of progression or death (P < .00001).
The results held regardless of PD-L1 expression, cisplatin eligibility, and the presence or absence of visceral metastases.
Follow-up treatments in the trial begin to address Dr. Apolo’s questions: Almost 60% of GC patients went on to a PD-1/L1 for subsequent maintenance or progression, and almost a quarter of EV+P patients went on to subsequent platinum-based chemotherapy.
Grade 3 or higher adverse events occurred in 55.9% of subjects in the EV+P group versus 69.5% in the GC arm.
The most common in the chemotherapy arm were anemia, neutropenia, thrombocytopenia, fatigue, and nausea. The most common with EV+P were skin reactions, hyperglycemia, neutropenia, peripheral neuropathy, diarrhea, and anemia,
CheckMate 901 details
In CheckMate 901, gemcitabine and cisplatin were administered on the first day of 3-week treatment cycles for up to 6 cycles; subjects randomized to nivolumab add-on received 360 mg on day 1 of each cycle, followed by 480 mg every 4 weeks until disease progression or unacceptable toxicity for up to 2 years.
PFS results again mirrored OS, with a median PFS of 7.9 months in the nivolumab arm versus 7.6 months with stand-alone chemotherapy, a 28% drop in the risk of progression or death (P = .0012).
Although OS and PFS benefits were statistically significant overall, they were not significant in subgroup analyses of patients 65 years and older, women, or in patients with liver metastases.
Trends in OS and PFS actually favored chemotherapy in the 40 U.S. subjects (HR OS, 1.92; 95% confidence interval, 0.95-3.88).
The rate of grade 3 or higher adverse events was 61.8% with nivolumab add-on versus 51.7% with chemotherapy alone. Anemia and neutropenia were the most common in both arms, and higher in the nivolumab group.
EV-302/KEYNOTE-A39 was funded by Seagen, Astellas, and Merck. CheckMate 901 was funded by Bristol-Myers Squibb, the maker of nivolumab.
Dr. Powles reported extensive financial ties to pharmaceutical companies, including being an advisor to and receiving research funding from Bristol-Myers Squibb, Merck, SeaGen, and Astellas, as well as travel expenses from Merck. Among other disclosures, Dr. Heijden is an advisor to Seagen and an advisor and researcher for Bristol-Myers Squibb. Dr. Apolo is an unpaid consultant to Merck, Astellas, Seagen, Bristol-Myers Squibb, and other companies.
FROM ESMO 2023
The sobering facts about alcohol and cancer
There is an urgent need to raise global awareness about the direct link between alcohol consumption and cancer risk.
That message was delivered by Isabelle Soerjomataram, PhD, with the International Agency for Research on Cancer (IARC), Lyon, France, at a session devoted to alcohol and cancer at the annual meeting of the European Society for Medical Oncology.
Dr. Soerjomataram told the audience. “Health professionals – oncologists, nurses, medical doctors, GPs – have an important role in increasing awareness and bringing this knowledge to people, which may lead to reduced consumption.”
Session chair Gilberto Morgan, MD, medical oncologist, Skåne University Hospital, Lund, Sweden, agreed.
Dr. Morgan noted that healthcare professionals tend to downplay their influence over patients’ drinking habits and often don’t address these behaviors.
But that needs to change.
“We have absolutely no problem asking patients if they take supplements or vitamins or if they’re eating [healthy],” Dr. Morgan said. “So, what is the difference? Why not recommend that they cut down their alcohol intake and leave it up to everybody’s personal choice to do it or not?”
In the session, Dr. Soerjomataram highlighted the global statistics on alcohol use. IARC data show, for instance, that nearly half (46%) of the world’s population consumes alcohol, with rates higher in men (54%) than women (38%).
How much are people drinking?
Globally, on average, the amount comes to about six liters of pure ethanol per year per drinker, or about one wine bottle per week. However, consumption patterns vary widely by country. In France, people consume about 12 liters per year or about two wine bottles per week.
Dr. Soerjomataram stressed the link between alcohol consumption and cancer.
According to IARC data, heavy drinking – defined as more than 60 g/day or about six daily drinks – accounts for 47% of the alcohol-attributable cancers. Risky drinking – between 20 and 60 g/day – accounts for 29%, she explained, while moderate drinking – less than 20 g/day or about two daily drinks – accounts for roughly 14% of cases of alcohol-attributable cancers.
Globally, alcohol intake accounted for 4% of all cancers diagnosed in 2020, according to a 2021 analysis by IARC.
In the United Kingdom alone, “alcohol drinking caused nearly 17,000 cases of cancer in 2020,” Dr. Soerjomataram said, and breast cancer made up almost one in four of those new cases.
In addition to breast cancer, six other cancer types – oral cavity, pharyngeal, laryngeal, esophageal, colorectal, and liver cancer – can be attributed to alcohol consumption, and emerging evidence suggests stomach and pancreatic cancer may be as well.
The good news, said Dr. Soerjomataram, is that long-term trends show declines in alcohol drinking in many countries, including the high wine-producing countries of France and Italy, where large reductions in consumption have been noted since the peak of intake in the 1920s.
“If it’s possible in these countries, I can imagine it’s possible elsewhere,” said Dr. Soerjomataram.
Dr. Soerjomataram and Dr. Morgan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There is an urgent need to raise global awareness about the direct link between alcohol consumption and cancer risk.
That message was delivered by Isabelle Soerjomataram, PhD, with the International Agency for Research on Cancer (IARC), Lyon, France, at a session devoted to alcohol and cancer at the annual meeting of the European Society for Medical Oncology.
Dr. Soerjomataram told the audience. “Health professionals – oncologists, nurses, medical doctors, GPs – have an important role in increasing awareness and bringing this knowledge to people, which may lead to reduced consumption.”
Session chair Gilberto Morgan, MD, medical oncologist, Skåne University Hospital, Lund, Sweden, agreed.
Dr. Morgan noted that healthcare professionals tend to downplay their influence over patients’ drinking habits and often don’t address these behaviors.
But that needs to change.
“We have absolutely no problem asking patients if they take supplements or vitamins or if they’re eating [healthy],” Dr. Morgan said. “So, what is the difference? Why not recommend that they cut down their alcohol intake and leave it up to everybody’s personal choice to do it or not?”
In the session, Dr. Soerjomataram highlighted the global statistics on alcohol use. IARC data show, for instance, that nearly half (46%) of the world’s population consumes alcohol, with rates higher in men (54%) than women (38%).
How much are people drinking?
Globally, on average, the amount comes to about six liters of pure ethanol per year per drinker, or about one wine bottle per week. However, consumption patterns vary widely by country. In France, people consume about 12 liters per year or about two wine bottles per week.
Dr. Soerjomataram stressed the link between alcohol consumption and cancer.
According to IARC data, heavy drinking – defined as more than 60 g/day or about six daily drinks – accounts for 47% of the alcohol-attributable cancers. Risky drinking – between 20 and 60 g/day – accounts for 29%, she explained, while moderate drinking – less than 20 g/day or about two daily drinks – accounts for roughly 14% of cases of alcohol-attributable cancers.
Globally, alcohol intake accounted for 4% of all cancers diagnosed in 2020, according to a 2021 analysis by IARC.
In the United Kingdom alone, “alcohol drinking caused nearly 17,000 cases of cancer in 2020,” Dr. Soerjomataram said, and breast cancer made up almost one in four of those new cases.
In addition to breast cancer, six other cancer types – oral cavity, pharyngeal, laryngeal, esophageal, colorectal, and liver cancer – can be attributed to alcohol consumption, and emerging evidence suggests stomach and pancreatic cancer may be as well.
The good news, said Dr. Soerjomataram, is that long-term trends show declines in alcohol drinking in many countries, including the high wine-producing countries of France and Italy, where large reductions in consumption have been noted since the peak of intake in the 1920s.
“If it’s possible in these countries, I can imagine it’s possible elsewhere,” said Dr. Soerjomataram.
Dr. Soerjomataram and Dr. Morgan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
There is an urgent need to raise global awareness about the direct link between alcohol consumption and cancer risk.
That message was delivered by Isabelle Soerjomataram, PhD, with the International Agency for Research on Cancer (IARC), Lyon, France, at a session devoted to alcohol and cancer at the annual meeting of the European Society for Medical Oncology.
Dr. Soerjomataram told the audience. “Health professionals – oncologists, nurses, medical doctors, GPs – have an important role in increasing awareness and bringing this knowledge to people, which may lead to reduced consumption.”
Session chair Gilberto Morgan, MD, medical oncologist, Skåne University Hospital, Lund, Sweden, agreed.
Dr. Morgan noted that healthcare professionals tend to downplay their influence over patients’ drinking habits and often don’t address these behaviors.
But that needs to change.
“We have absolutely no problem asking patients if they take supplements or vitamins or if they’re eating [healthy],” Dr. Morgan said. “So, what is the difference? Why not recommend that they cut down their alcohol intake and leave it up to everybody’s personal choice to do it or not?”
In the session, Dr. Soerjomataram highlighted the global statistics on alcohol use. IARC data show, for instance, that nearly half (46%) of the world’s population consumes alcohol, with rates higher in men (54%) than women (38%).
How much are people drinking?
Globally, on average, the amount comes to about six liters of pure ethanol per year per drinker, or about one wine bottle per week. However, consumption patterns vary widely by country. In France, people consume about 12 liters per year or about two wine bottles per week.
Dr. Soerjomataram stressed the link between alcohol consumption and cancer.
According to IARC data, heavy drinking – defined as more than 60 g/day or about six daily drinks – accounts for 47% of the alcohol-attributable cancers. Risky drinking – between 20 and 60 g/day – accounts for 29%, she explained, while moderate drinking – less than 20 g/day or about two daily drinks – accounts for roughly 14% of cases of alcohol-attributable cancers.
Globally, alcohol intake accounted for 4% of all cancers diagnosed in 2020, according to a 2021 analysis by IARC.
In the United Kingdom alone, “alcohol drinking caused nearly 17,000 cases of cancer in 2020,” Dr. Soerjomataram said, and breast cancer made up almost one in four of those new cases.
In addition to breast cancer, six other cancer types – oral cavity, pharyngeal, laryngeal, esophageal, colorectal, and liver cancer – can be attributed to alcohol consumption, and emerging evidence suggests stomach and pancreatic cancer may be as well.
The good news, said Dr. Soerjomataram, is that long-term trends show declines in alcohol drinking in many countries, including the high wine-producing countries of France and Italy, where large reductions in consumption have been noted since the peak of intake in the 1920s.
“If it’s possible in these countries, I can imagine it’s possible elsewhere,” said Dr. Soerjomataram.
Dr. Soerjomataram and Dr. Morgan report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ESMO 2023
This drug works, but wait till you hear what’s in it
This transcript has been edited for clarity.
As some of you may know, I do a fair amount of clinical research developing and evaluating artificial intelligence (AI) models, particularly machine learning algorithms that predict certain outcomes.
A thorny issue that comes up as algorithms have gotten more complicated is “explainability.” The problem is that AI can be a black box. Even if you have a model that is very accurate at predicting death, clinicians don’t trust it unless you can explain how it makes its predictions – how it works. “It just works” is not good enough to build trust.
It’s easier to build trust when you’re talking about a medication rather than a computer program. When a new blood pressure drug comes out that lowers blood pressure, importantly, we know why it lowers blood pressure. Every drug has a mechanism of action and, for most of the drugs in our arsenal, we know what that mechanism is.
But what if there were a drug – or better yet, a treatment – that worked? And I can honestly say we have no idea how it works. That’s what came across my desk today in what I believe is the largest, most rigorous trial of a traditional Chinese medication in history.
“Traditional Chinese medicine” is an omnibus term that refers to a class of therapies and health practices that are fundamentally different from how we practice medicine in the West.
It’s a highly personalized practice, with practitioners using often esoteric means to choose what substance to give what patient. That personalization makes traditional Chinese medicine nearly impossible to study in the typical randomized trial framework because treatments are not chosen solely on the basis of disease states.
The lack of scientific rigor in traditional Chinese medicine means that it is rife with practices and beliefs that can legitimately be called pseudoscience. As a nephrologist who has treated someone for “Chinese herb nephropathy,” I can tell you that some of the practices may be actively harmful.
But that doesn’t mean there is nothing there. I do not subscribe to the “argument from antiquity” – the idea that because something has been done for a long time it must be correct. But at the same time, traditional and non–science-based medicine practices could still identify therapies that work.
And with that, let me introduce you to Tongxinluo. Tongxinluo literally means “to open the network of the heart,” and it is a substance that has been used for centuries by traditional Chinese medicine practitioners to treat angina but was approved by the Chinese state medicine agency for use in 1996.
Like many traditional Chinese medicine preparations, Tongxinluo is not a single chemical – far from it. It is a powder made from a variety of plant and insect parts, as you can see here.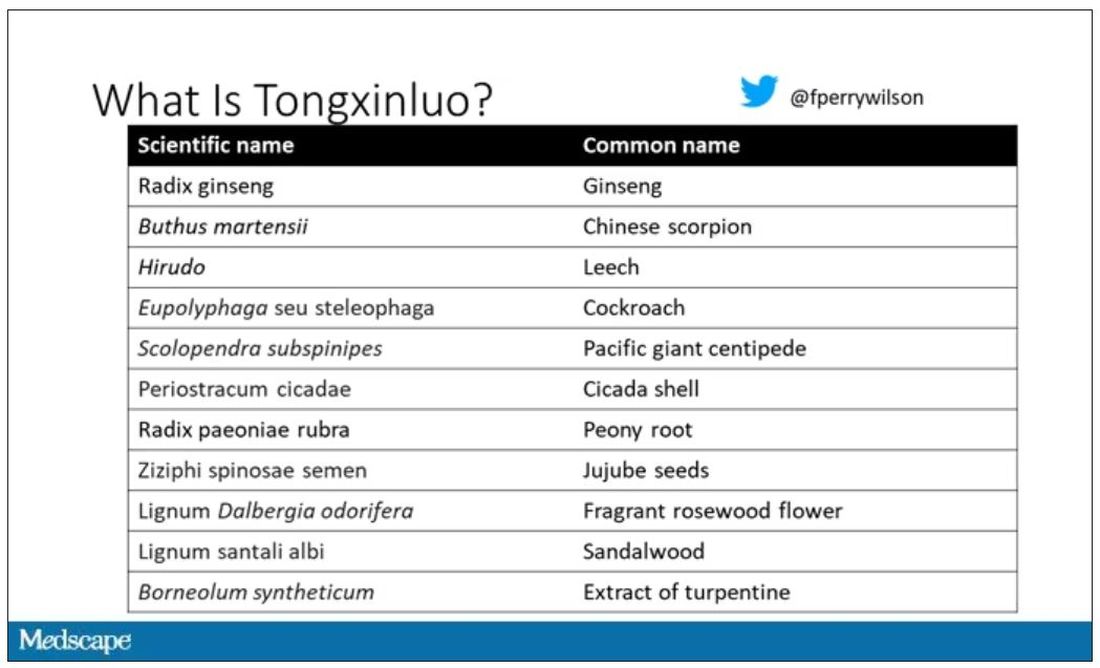
I can’t imagine running a trial of this concoction in the United States; I just don’t see an institutional review board signing off, given the ingredient list.
But let’s set that aside and talk about the study itself.
While I don’t have access to any primary data, the write-up of the study suggests that it was highly rigorous. Chinese researchers randomized 3,797 patients with ST-elevation MI to take Tongxinluo – four capsules, three times a day for 12 months – or matching placebo. The placebo was designed to look just like the Tongxinluo capsules and, if the capsules were opened, to smell like them as well.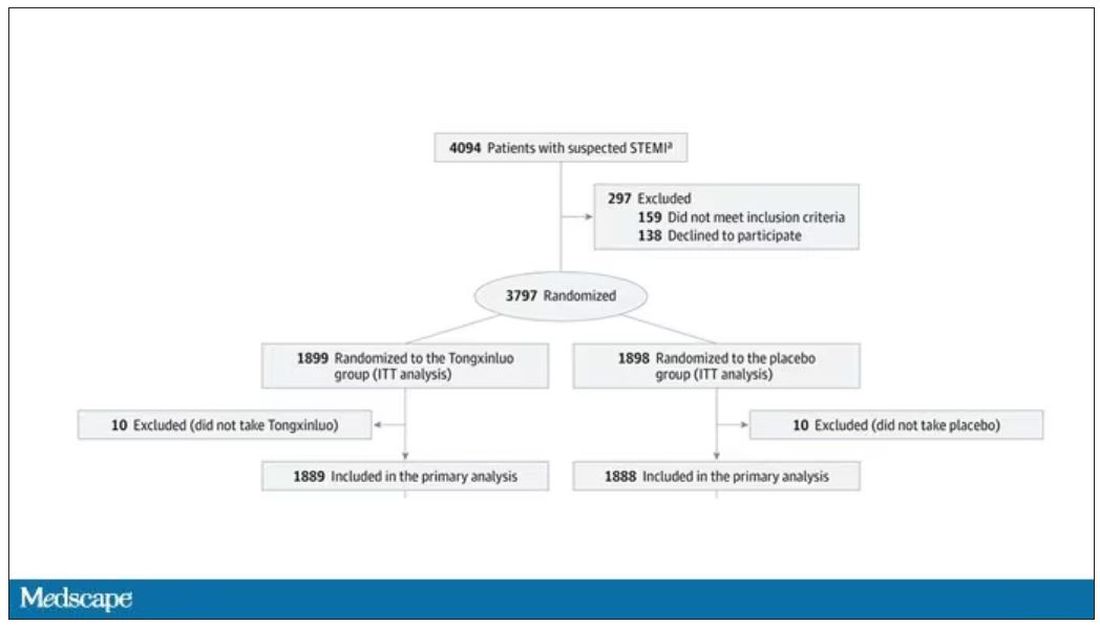
Researchers and participants were blinded, and the statistical analysis was done both by the primary team and an independent research agency, also in China.
And the results were pretty good. The primary outcome, 30-day major cardiovascular and cerebral events, were significantly lower in the intervention group than in the placebo group.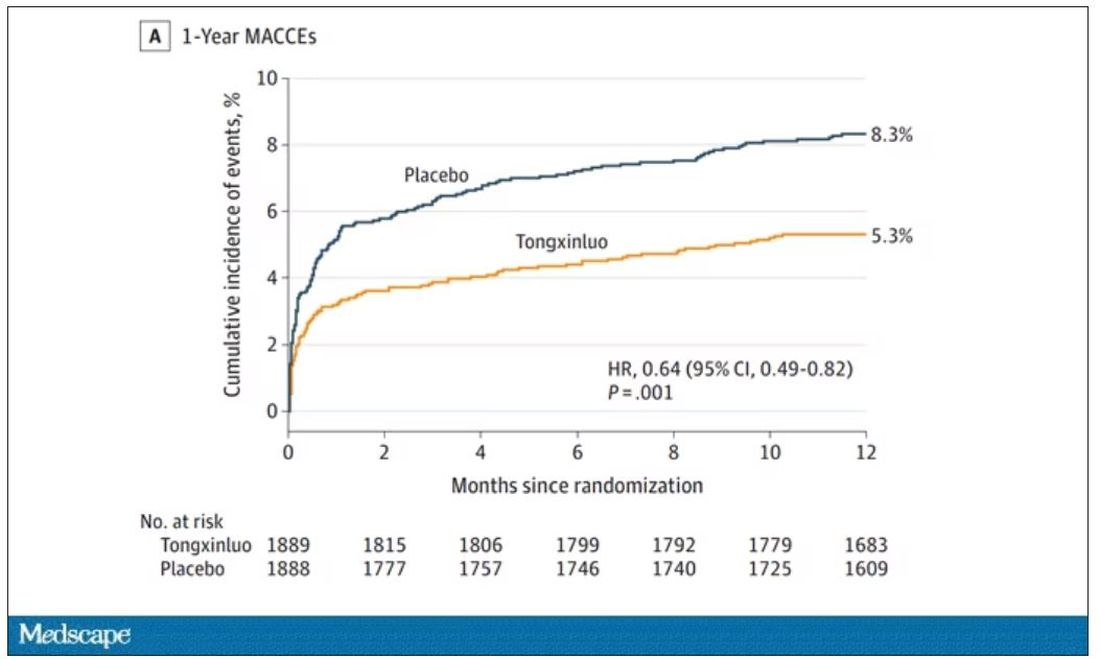
One-year outcomes were similarly good; 8.3% of the placebo group suffered a major cardiovascular or cerebral event in that time frame, compared with 5.3% of the Tongxinluo group. In short, if this were a pure chemical compound from a major pharmaceutical company, well, you might be seeing a new treatment for heart attack – and a boost in stock price.
But there are some issues here, generalizability being a big one. This study was done entirely in China, so its applicability to a more diverse population is unclear. Moreover, the quality of post-MI care in this study is quite a bit worse than what we’d see here in the United States, with just over 50% of patients being discharged on a beta-blocker, for example.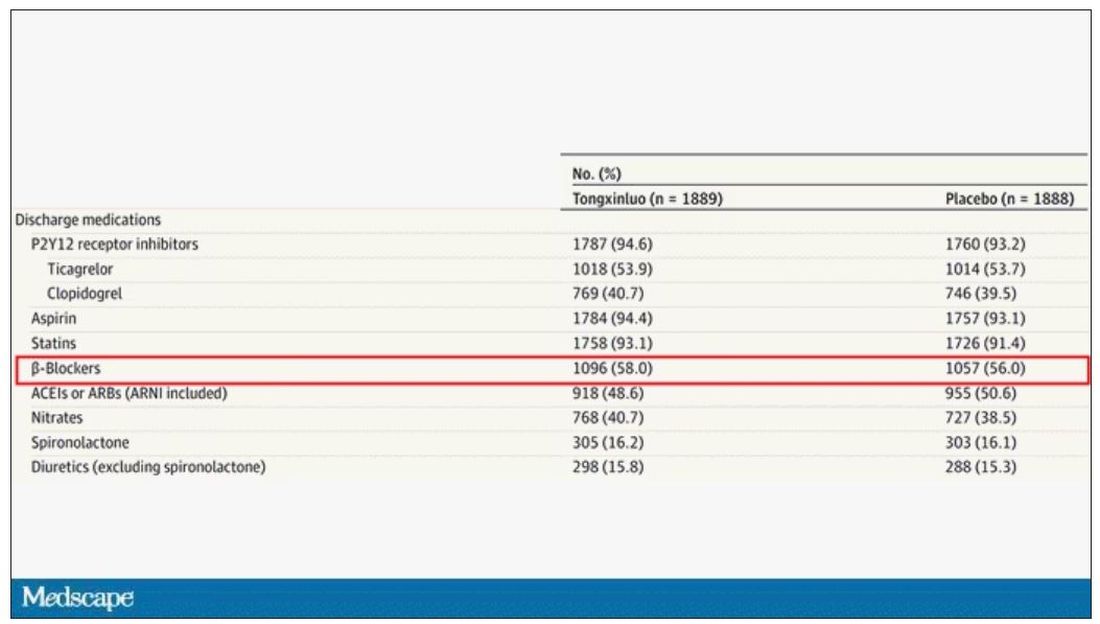
But issues of generalizability and potentially substandard supplementary treatments are the usual reasons we worry about new medication trials. And those concerns seem to pale before the big one I have here which is, you know – we don’t know why this works.
Is it the extract of leech in the preparation perhaps thinning the blood a bit? Or is it the antioxidants in the ginseng, or something from the Pacific centipede or the sandalwood?
This trial doesn’t read to me as a vindication of traditional Chinese medicine but rather as an example of missed opportunity. More rigorous scientific study over the centuries that Tongxinluo has been used could have identified one, or perhaps more, compounds with strong therapeutic potential.
Purity of medical substances is incredibly important. Pure substances have predictable effects and side effects. Pure substances interact with other treatments we give patients in predictable ways. Pure substances can be quantified for purity by third parties, they can be manufactured according to accepted standards, and they can be assessed for adulteration. In short, pure substances pose less risk.
Now, I know that may come off as particularly sterile. Some people will feel that a “natural” substance has some inherent benefit over pure compounds. And, of course, there is something soothing about imagining a traditional preparation handed down over centuries, being prepared with care by a single practitioner, in contrast to the sterile industrial processes of a for-profit pharmaceutical company. I get it. But natural is not the same as safe. I am glad I have access to purified aspirin and don’t have to chew willow bark. I like my pure penicillin and am glad I don’t have to make a mold slurry to treat a bacterial infection.
I applaud the researchers for subjecting Tongxinluo to the rigor of a well-designed trial. They have generated data that are incredibly exciting, but not because we have a new treatment for ST-elevation MI on our hands; it’s because we have a map to a new treatment. The next big thing in heart attack care is not the mixture that is Tongxinluo, but it might be in the mixture.
A version of this article first appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available now.
This transcript has been edited for clarity.
As some of you may know, I do a fair amount of clinical research developing and evaluating artificial intelligence (AI) models, particularly machine learning algorithms that predict certain outcomes.
A thorny issue that comes up as algorithms have gotten more complicated is “explainability.” The problem is that AI can be a black box. Even if you have a model that is very accurate at predicting death, clinicians don’t trust it unless you can explain how it makes its predictions – how it works. “It just works” is not good enough to build trust.
It’s easier to build trust when you’re talking about a medication rather than a computer program. When a new blood pressure drug comes out that lowers blood pressure, importantly, we know why it lowers blood pressure. Every drug has a mechanism of action and, for most of the drugs in our arsenal, we know what that mechanism is.
But what if there were a drug – or better yet, a treatment – that worked? And I can honestly say we have no idea how it works. That’s what came across my desk today in what I believe is the largest, most rigorous trial of a traditional Chinese medication in history.
“Traditional Chinese medicine” is an omnibus term that refers to a class of therapies and health practices that are fundamentally different from how we practice medicine in the West.
It’s a highly personalized practice, with practitioners using often esoteric means to choose what substance to give what patient. That personalization makes traditional Chinese medicine nearly impossible to study in the typical randomized trial framework because treatments are not chosen solely on the basis of disease states.
The lack of scientific rigor in traditional Chinese medicine means that it is rife with practices and beliefs that can legitimately be called pseudoscience. As a nephrologist who has treated someone for “Chinese herb nephropathy,” I can tell you that some of the practices may be actively harmful.
But that doesn’t mean there is nothing there. I do not subscribe to the “argument from antiquity” – the idea that because something has been done for a long time it must be correct. But at the same time, traditional and non–science-based medicine practices could still identify therapies that work.
And with that, let me introduce you to Tongxinluo. Tongxinluo literally means “to open the network of the heart,” and it is a substance that has been used for centuries by traditional Chinese medicine practitioners to treat angina but was approved by the Chinese state medicine agency for use in 1996.
Like many traditional Chinese medicine preparations, Tongxinluo is not a single chemical – far from it. It is a powder made from a variety of plant and insect parts, as you can see here.
I can’t imagine running a trial of this concoction in the United States; I just don’t see an institutional review board signing off, given the ingredient list.
But let’s set that aside and talk about the study itself.
While I don’t have access to any primary data, the write-up of the study suggests that it was highly rigorous. Chinese researchers randomized 3,797 patients with ST-elevation MI to take Tongxinluo – four capsules, three times a day for 12 months – or matching placebo. The placebo was designed to look just like the Tongxinluo capsules and, if the capsules were opened, to smell like them as well.
Researchers and participants were blinded, and the statistical analysis was done both by the primary team and an independent research agency, also in China.
And the results were pretty good. The primary outcome, 30-day major cardiovascular and cerebral events, were significantly lower in the intervention group than in the placebo group.
One-year outcomes were similarly good; 8.3% of the placebo group suffered a major cardiovascular or cerebral event in that time frame, compared with 5.3% of the Tongxinluo group. In short, if this were a pure chemical compound from a major pharmaceutical company, well, you might be seeing a new treatment for heart attack – and a boost in stock price.
But there are some issues here, generalizability being a big one. This study was done entirely in China, so its applicability to a more diverse population is unclear. Moreover, the quality of post-MI care in this study is quite a bit worse than what we’d see here in the United States, with just over 50% of patients being discharged on a beta-blocker, for example.
But issues of generalizability and potentially substandard supplementary treatments are the usual reasons we worry about new medication trials. And those concerns seem to pale before the big one I have here which is, you know – we don’t know why this works.
Is it the extract of leech in the preparation perhaps thinning the blood a bit? Or is it the antioxidants in the ginseng, or something from the Pacific centipede or the sandalwood?
This trial doesn’t read to me as a vindication of traditional Chinese medicine but rather as an example of missed opportunity. More rigorous scientific study over the centuries that Tongxinluo has been used could have identified one, or perhaps more, compounds with strong therapeutic potential.
Purity of medical substances is incredibly important. Pure substances have predictable effects and side effects. Pure substances interact with other treatments we give patients in predictable ways. Pure substances can be quantified for purity by third parties, they can be manufactured according to accepted standards, and they can be assessed for adulteration. In short, pure substances pose less risk.
Now, I know that may come off as particularly sterile. Some people will feel that a “natural” substance has some inherent benefit over pure compounds. And, of course, there is something soothing about imagining a traditional preparation handed down over centuries, being prepared with care by a single practitioner, in contrast to the sterile industrial processes of a for-profit pharmaceutical company. I get it. But natural is not the same as safe. I am glad I have access to purified aspirin and don’t have to chew willow bark. I like my pure penicillin and am glad I don’t have to make a mold slurry to treat a bacterial infection.
I applaud the researchers for subjecting Tongxinluo to the rigor of a well-designed trial. They have generated data that are incredibly exciting, but not because we have a new treatment for ST-elevation MI on our hands; it’s because we have a map to a new treatment. The next big thing in heart attack care is not the mixture that is Tongxinluo, but it might be in the mixture.
A version of this article first appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available now.
This transcript has been edited for clarity.
As some of you may know, I do a fair amount of clinical research developing and evaluating artificial intelligence (AI) models, particularly machine learning algorithms that predict certain outcomes.
A thorny issue that comes up as algorithms have gotten more complicated is “explainability.” The problem is that AI can be a black box. Even if you have a model that is very accurate at predicting death, clinicians don’t trust it unless you can explain how it makes its predictions – how it works. “It just works” is not good enough to build trust.
It’s easier to build trust when you’re talking about a medication rather than a computer program. When a new blood pressure drug comes out that lowers blood pressure, importantly, we know why it lowers blood pressure. Every drug has a mechanism of action and, for most of the drugs in our arsenal, we know what that mechanism is.
But what if there were a drug – or better yet, a treatment – that worked? And I can honestly say we have no idea how it works. That’s what came across my desk today in what I believe is the largest, most rigorous trial of a traditional Chinese medication in history.
“Traditional Chinese medicine” is an omnibus term that refers to a class of therapies and health practices that are fundamentally different from how we practice medicine in the West.
It’s a highly personalized practice, with practitioners using often esoteric means to choose what substance to give what patient. That personalization makes traditional Chinese medicine nearly impossible to study in the typical randomized trial framework because treatments are not chosen solely on the basis of disease states.
The lack of scientific rigor in traditional Chinese medicine means that it is rife with practices and beliefs that can legitimately be called pseudoscience. As a nephrologist who has treated someone for “Chinese herb nephropathy,” I can tell you that some of the practices may be actively harmful.
But that doesn’t mean there is nothing there. I do not subscribe to the “argument from antiquity” – the idea that because something has been done for a long time it must be correct. But at the same time, traditional and non–science-based medicine practices could still identify therapies that work.
And with that, let me introduce you to Tongxinluo. Tongxinluo literally means “to open the network of the heart,” and it is a substance that has been used for centuries by traditional Chinese medicine practitioners to treat angina but was approved by the Chinese state medicine agency for use in 1996.
Like many traditional Chinese medicine preparations, Tongxinluo is not a single chemical – far from it. It is a powder made from a variety of plant and insect parts, as you can see here.
I can’t imagine running a trial of this concoction in the United States; I just don’t see an institutional review board signing off, given the ingredient list.
But let’s set that aside and talk about the study itself.
While I don’t have access to any primary data, the write-up of the study suggests that it was highly rigorous. Chinese researchers randomized 3,797 patients with ST-elevation MI to take Tongxinluo – four capsules, three times a day for 12 months – or matching placebo. The placebo was designed to look just like the Tongxinluo capsules and, if the capsules were opened, to smell like them as well.
Researchers and participants were blinded, and the statistical analysis was done both by the primary team and an independent research agency, also in China.
And the results were pretty good. The primary outcome, 30-day major cardiovascular and cerebral events, were significantly lower in the intervention group than in the placebo group.
One-year outcomes were similarly good; 8.3% of the placebo group suffered a major cardiovascular or cerebral event in that time frame, compared with 5.3% of the Tongxinluo group. In short, if this were a pure chemical compound from a major pharmaceutical company, well, you might be seeing a new treatment for heart attack – and a boost in stock price.
But there are some issues here, generalizability being a big one. This study was done entirely in China, so its applicability to a more diverse population is unclear. Moreover, the quality of post-MI care in this study is quite a bit worse than what we’d see here in the United States, with just over 50% of patients being discharged on a beta-blocker, for example.
But issues of generalizability and potentially substandard supplementary treatments are the usual reasons we worry about new medication trials. And those concerns seem to pale before the big one I have here which is, you know – we don’t know why this works.
Is it the extract of leech in the preparation perhaps thinning the blood a bit? Or is it the antioxidants in the ginseng, or something from the Pacific centipede or the sandalwood?
This trial doesn’t read to me as a vindication of traditional Chinese medicine but rather as an example of missed opportunity. More rigorous scientific study over the centuries that Tongxinluo has been used could have identified one, or perhaps more, compounds with strong therapeutic potential.
Purity of medical substances is incredibly important. Pure substances have predictable effects and side effects. Pure substances interact with other treatments we give patients in predictable ways. Pure substances can be quantified for purity by third parties, they can be manufactured according to accepted standards, and they can be assessed for adulteration. In short, pure substances pose less risk.
Now, I know that may come off as particularly sterile. Some people will feel that a “natural” substance has some inherent benefit over pure compounds. And, of course, there is something soothing about imagining a traditional preparation handed down over centuries, being prepared with care by a single practitioner, in contrast to the sterile industrial processes of a for-profit pharmaceutical company. I get it. But natural is not the same as safe. I am glad I have access to purified aspirin and don’t have to chew willow bark. I like my pure penicillin and am glad I don’t have to make a mold slurry to treat a bacterial infection.
I applaud the researchers for subjecting Tongxinluo to the rigor of a well-designed trial. They have generated data that are incredibly exciting, but not because we have a new treatment for ST-elevation MI on our hands; it’s because we have a map to a new treatment. The next big thing in heart attack care is not the mixture that is Tongxinluo, but it might be in the mixture.
A version of this article first appeared on Medscape.com.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and on Medscape. He tweets @fperrywilson and his new book, “How Medicine Works and When It Doesn’t,” is available now.
‘Frame running’ may help boost physical activity in MS
MILAN – , a pilot study suggests.
“Frame running” uses a three-wheeled frame with a saddle and body supports but no pedals to allow individuals with disabilities and balance impairments to walk and run under their own power.
Eight individuals with multiple sclerosis and moderate to severe walking impairments took part in a 12-week frame running intervention, which improved both objective physical performance and patient-reported outcomes measures.
“Frame running presents a feasible and enjoyable exercise option for people with multiple sclerosis,” lead author Gary McEwan, PhD, research fellow at the Centre for Health, Activity and Rehabilitation Research at Queen Margaret University, Edinburgh, and colleagues conclude.
It may, they add, “have potential to improve measures of physical function and the ability to perform mobility-related daily activities.”
The findings were presented at the 9th Joint ECTRIMS-ACTRIMS Meeting.
Dearth of exercise opportunities
The authors note regular physical activity and exercise are “amongst the most important adjunct therapies for managing the symptoms of multiple sclerosis,” and yet people with the disease are significantly less physically active than the general population.
This is particularly the case for individuals at the upper end of the disability spectrum, they continue, and may reflect the “relative dearth of exercise opportunities that are suitable for those with more severe mobility impairments.”
In recent years, frame running has emerged as a form of exercise that allows individuals with walking difficulties to engage in moderate to vigorous physical activity in a safe manner, but its feasibility in multiple sclerosis has not been investigated.
The researchers recruited people with multiple sclerosis who had moderate to severe walking impairments to take part in a 12-week frame running intervention, comprising a 1-hour session every week.
The 6-minute frame running test (6MFRT) and an adapted shuttle frame running test (SFRT) were used to assess physical function at baseline and after the intervention. Recruitment, retention, and attendance rates were recorded.
The participants also completed a series of patient-reported outcome measures, alongside the Canadian Occupational Performance Measure, to calculate self-perceived abilities in activities of daily living, and semistructured interviews to capture their experiences of the intervention.
The camaraderie of physical activity
With six females and two males enrolled in the study, the team reported that the recruitment rate was 47.1%, the retention rate was 75%, and attendance was 86.7%. No adverse events were reported, they note.
The results indicate there were improvements in performance on the physical measures, with small effect sizes on both the 6MFRT (d = 0.37) and the SFRT (d = 0.30).
There were also improvements on the Multiple Sclerosis Walking Scale (d = 0.27), the Fatigue Scale for Motor and Cognitive Functions (d = 0.20), and the Exercise Self-Efficacy Scale (d = 0.46), again with small effect sizes.
A medium effect size was seen for improvements on the Godin Leisure Time Exercise Questionnaire (d = 0.73), and 80% of the participants reported “changes in performance and in satisfaction with their activities of daily living,” the team says.
The qualitative data also suggested the patients found frame running to be “safe and enjoyable,” with key highlights being the “social aspect and camaraderie developed amongst participants.”
Mix of physical interventions
Approached for comment, Robert Motl, MD, professor of kinesiology and nutrition, College of Applied Health Sciences, University of Illinois at Chicago, said it “makes a lot of sense” that frame running can improve walking-related outcomes.
He told this news organization that, “for people who have balance-related problems, using their legs in that rhythmical way could really have some great benefits for walking.”
However, Dr. Motl said he is a “little more skeptical about the benefits for balance, because to improve balance you have to be doing something that challenges upright posture.”
With the frame, “I don’t think you’re having to regulate upright posture while you’re doing that intervention, because you have stability with three points and the ground,” he said. “So, I wonder a little bit about that as an outcome.”
Dr. Motl nevertheless underlined that walking can certainly improve physical activity, “and all the other things like vascular function, cardiovascular fitness,” and so on.
Consequently, frame running “could be part of the mix of things for people who are having a disability, particularly individuals who have some balance dysfunction and [for whom] ambulating might put them at risk of falling.”
The study was supported by a research grant from the Multiple Sclerosis Society UK. The study authors and Dr. Modl report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MILAN – , a pilot study suggests.
“Frame running” uses a three-wheeled frame with a saddle and body supports but no pedals to allow individuals with disabilities and balance impairments to walk and run under their own power.
Eight individuals with multiple sclerosis and moderate to severe walking impairments took part in a 12-week frame running intervention, which improved both objective physical performance and patient-reported outcomes measures.
“Frame running presents a feasible and enjoyable exercise option for people with multiple sclerosis,” lead author Gary McEwan, PhD, research fellow at the Centre for Health, Activity and Rehabilitation Research at Queen Margaret University, Edinburgh, and colleagues conclude.
It may, they add, “have potential to improve measures of physical function and the ability to perform mobility-related daily activities.”
The findings were presented at the 9th Joint ECTRIMS-ACTRIMS Meeting.
Dearth of exercise opportunities
The authors note regular physical activity and exercise are “amongst the most important adjunct therapies for managing the symptoms of multiple sclerosis,” and yet people with the disease are significantly less physically active than the general population.
This is particularly the case for individuals at the upper end of the disability spectrum, they continue, and may reflect the “relative dearth of exercise opportunities that are suitable for those with more severe mobility impairments.”
In recent years, frame running has emerged as a form of exercise that allows individuals with walking difficulties to engage in moderate to vigorous physical activity in a safe manner, but its feasibility in multiple sclerosis has not been investigated.
The researchers recruited people with multiple sclerosis who had moderate to severe walking impairments to take part in a 12-week frame running intervention, comprising a 1-hour session every week.
The 6-minute frame running test (6MFRT) and an adapted shuttle frame running test (SFRT) were used to assess physical function at baseline and after the intervention. Recruitment, retention, and attendance rates were recorded.
The participants also completed a series of patient-reported outcome measures, alongside the Canadian Occupational Performance Measure, to calculate self-perceived abilities in activities of daily living, and semistructured interviews to capture their experiences of the intervention.
The camaraderie of physical activity
With six females and two males enrolled in the study, the team reported that the recruitment rate was 47.1%, the retention rate was 75%, and attendance was 86.7%. No adverse events were reported, they note.
The results indicate there were improvements in performance on the physical measures, with small effect sizes on both the 6MFRT (d = 0.37) and the SFRT (d = 0.30).
There were also improvements on the Multiple Sclerosis Walking Scale (d = 0.27), the Fatigue Scale for Motor and Cognitive Functions (d = 0.20), and the Exercise Self-Efficacy Scale (d = 0.46), again with small effect sizes.
A medium effect size was seen for improvements on the Godin Leisure Time Exercise Questionnaire (d = 0.73), and 80% of the participants reported “changes in performance and in satisfaction with their activities of daily living,” the team says.
The qualitative data also suggested the patients found frame running to be “safe and enjoyable,” with key highlights being the “social aspect and camaraderie developed amongst participants.”
Mix of physical interventions
Approached for comment, Robert Motl, MD, professor of kinesiology and nutrition, College of Applied Health Sciences, University of Illinois at Chicago, said it “makes a lot of sense” that frame running can improve walking-related outcomes.
He told this news organization that, “for people who have balance-related problems, using their legs in that rhythmical way could really have some great benefits for walking.”
However, Dr. Motl said he is a “little more skeptical about the benefits for balance, because to improve balance you have to be doing something that challenges upright posture.”
With the frame, “I don’t think you’re having to regulate upright posture while you’re doing that intervention, because you have stability with three points and the ground,” he said. “So, I wonder a little bit about that as an outcome.”
Dr. Motl nevertheless underlined that walking can certainly improve physical activity, “and all the other things like vascular function, cardiovascular fitness,” and so on.
Consequently, frame running “could be part of the mix of things for people who are having a disability, particularly individuals who have some balance dysfunction and [for whom] ambulating might put them at risk of falling.”
The study was supported by a research grant from the Multiple Sclerosis Society UK. The study authors and Dr. Modl report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
MILAN – , a pilot study suggests.
“Frame running” uses a three-wheeled frame with a saddle and body supports but no pedals to allow individuals with disabilities and balance impairments to walk and run under their own power.
Eight individuals with multiple sclerosis and moderate to severe walking impairments took part in a 12-week frame running intervention, which improved both objective physical performance and patient-reported outcomes measures.
“Frame running presents a feasible and enjoyable exercise option for people with multiple sclerosis,” lead author Gary McEwan, PhD, research fellow at the Centre for Health, Activity and Rehabilitation Research at Queen Margaret University, Edinburgh, and colleagues conclude.
It may, they add, “have potential to improve measures of physical function and the ability to perform mobility-related daily activities.”
The findings were presented at the 9th Joint ECTRIMS-ACTRIMS Meeting.
Dearth of exercise opportunities
The authors note regular physical activity and exercise are “amongst the most important adjunct therapies for managing the symptoms of multiple sclerosis,” and yet people with the disease are significantly less physically active than the general population.
This is particularly the case for individuals at the upper end of the disability spectrum, they continue, and may reflect the “relative dearth of exercise opportunities that are suitable for those with more severe mobility impairments.”
In recent years, frame running has emerged as a form of exercise that allows individuals with walking difficulties to engage in moderate to vigorous physical activity in a safe manner, but its feasibility in multiple sclerosis has not been investigated.
The researchers recruited people with multiple sclerosis who had moderate to severe walking impairments to take part in a 12-week frame running intervention, comprising a 1-hour session every week.
The 6-minute frame running test (6MFRT) and an adapted shuttle frame running test (SFRT) were used to assess physical function at baseline and after the intervention. Recruitment, retention, and attendance rates were recorded.
The participants also completed a series of patient-reported outcome measures, alongside the Canadian Occupational Performance Measure, to calculate self-perceived abilities in activities of daily living, and semistructured interviews to capture their experiences of the intervention.
The camaraderie of physical activity
With six females and two males enrolled in the study, the team reported that the recruitment rate was 47.1%, the retention rate was 75%, and attendance was 86.7%. No adverse events were reported, they note.
The results indicate there were improvements in performance on the physical measures, with small effect sizes on both the 6MFRT (d = 0.37) and the SFRT (d = 0.30).
There were also improvements on the Multiple Sclerosis Walking Scale (d = 0.27), the Fatigue Scale for Motor and Cognitive Functions (d = 0.20), and the Exercise Self-Efficacy Scale (d = 0.46), again with small effect sizes.
A medium effect size was seen for improvements on the Godin Leisure Time Exercise Questionnaire (d = 0.73), and 80% of the participants reported “changes in performance and in satisfaction with their activities of daily living,” the team says.
The qualitative data also suggested the patients found frame running to be “safe and enjoyable,” with key highlights being the “social aspect and camaraderie developed amongst participants.”
Mix of physical interventions
Approached for comment, Robert Motl, MD, professor of kinesiology and nutrition, College of Applied Health Sciences, University of Illinois at Chicago, said it “makes a lot of sense” that frame running can improve walking-related outcomes.
He told this news organization that, “for people who have balance-related problems, using their legs in that rhythmical way could really have some great benefits for walking.”
However, Dr. Motl said he is a “little more skeptical about the benefits for balance, because to improve balance you have to be doing something that challenges upright posture.”
With the frame, “I don’t think you’re having to regulate upright posture while you’re doing that intervention, because you have stability with three points and the ground,” he said. “So, I wonder a little bit about that as an outcome.”
Dr. Motl nevertheless underlined that walking can certainly improve physical activity, “and all the other things like vascular function, cardiovascular fitness,” and so on.
Consequently, frame running “could be part of the mix of things for people who are having a disability, particularly individuals who have some balance dysfunction and [for whom] ambulating might put them at risk of falling.”
The study was supported by a research grant from the Multiple Sclerosis Society UK. The study authors and Dr. Modl report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ECTRIMS 2023
Hitting the snooze button may provide cognitive benefit
TOPLINE:
Challenging conventional wisdom,
METHODOLOGY:
- Researchers did two studies to determine why intermittent morning alarms are used and how they affect sleep, cognition, cortisol, and mood.
- Study 1 was a survey of 1,732 healthy adults (mean age 34 years; 66% women) designed to elucidate the characteristics of people who snooze and why they choose to delay their waking in this way.
- Study 2 was a within-subject polysomnography study of 31 healthy habitual snoozers (mean age 27 years; 18 women) designed to explore the acute effects of snoozing on sleep architecture, sleepiness, cognitive ability, mood, and cortisol awakening response.
TAKEAWAY:
- Overall, 69% reported using the snooze button or setting multiple alarms at least sometimes, most often on workdays (71%), with an average snooze time per morning of 22 minutes.
- Sleep quality did not differ between snoozers and nonsnoozers, but snoozers were more likely to feel mentally drowsy on waking (odds ratio, 3.0; P < .001) and had slightly shorter sleep time on workdays (13 minutes).
- In the polysomnography study, compared with waking up abruptly, 30 minutes of snoozing in the morning improved or did not affect performance on standard cognitive tests completed directly on final awakening.
- Snoozing resulted in about 6 minutes of lost sleep, but it prevented awakening from slow-wave sleep and had no clear effects on the cortisol awakening response, morning sleepiness, mood, or overnight sleep architecture.
IN PRACTICE:
“The findings indicate that there is no reason to stop snoozing in the morning if you enjoy it, at least not for snooze times around 30 minutes. In fact, it may even help those with morning drowsiness to be slightly more awake once they get up,” corresponding author Tina Sundelin, PhD, of Stockholm University, said in a statement.
SOURCE:
The study was published online in the Journal of Sleep Research.
LIMITATIONS:
Study 1 focused on waking preferences in a convenience sample of adults. Study 2 included only habitual snoozers making it difficult to generalize the findings to people who don’t usually snooze. The study investigated only the effect of 30 minutes of snoozing on the studied parameters. It’s possible that shorter or longer snooze times have different cognitive effects.
DISCLOSURES:
Support for the study was provided by the Stress Research Institute, Stockholm University, and a grant from Vetenskapsrådet. The authors disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Challenging conventional wisdom,
METHODOLOGY:
- Researchers did two studies to determine why intermittent morning alarms are used and how they affect sleep, cognition, cortisol, and mood.
- Study 1 was a survey of 1,732 healthy adults (mean age 34 years; 66% women) designed to elucidate the characteristics of people who snooze and why they choose to delay their waking in this way.
- Study 2 was a within-subject polysomnography study of 31 healthy habitual snoozers (mean age 27 years; 18 women) designed to explore the acute effects of snoozing on sleep architecture, sleepiness, cognitive ability, mood, and cortisol awakening response.
TAKEAWAY:
- Overall, 69% reported using the snooze button or setting multiple alarms at least sometimes, most often on workdays (71%), with an average snooze time per morning of 22 minutes.
- Sleep quality did not differ between snoozers and nonsnoozers, but snoozers were more likely to feel mentally drowsy on waking (odds ratio, 3.0; P < .001) and had slightly shorter sleep time on workdays (13 minutes).
- In the polysomnography study, compared with waking up abruptly, 30 minutes of snoozing in the morning improved or did not affect performance on standard cognitive tests completed directly on final awakening.
- Snoozing resulted in about 6 minutes of lost sleep, but it prevented awakening from slow-wave sleep and had no clear effects on the cortisol awakening response, morning sleepiness, mood, or overnight sleep architecture.
IN PRACTICE:
“The findings indicate that there is no reason to stop snoozing in the morning if you enjoy it, at least not for snooze times around 30 minutes. In fact, it may even help those with morning drowsiness to be slightly more awake once they get up,” corresponding author Tina Sundelin, PhD, of Stockholm University, said in a statement.
SOURCE:
The study was published online in the Journal of Sleep Research.
LIMITATIONS:
Study 1 focused on waking preferences in a convenience sample of adults. Study 2 included only habitual snoozers making it difficult to generalize the findings to people who don’t usually snooze. The study investigated only the effect of 30 minutes of snoozing on the studied parameters. It’s possible that shorter or longer snooze times have different cognitive effects.
DISCLOSURES:
Support for the study was provided by the Stress Research Institute, Stockholm University, and a grant from Vetenskapsrådet. The authors disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
TOPLINE:
Challenging conventional wisdom,
METHODOLOGY:
- Researchers did two studies to determine why intermittent morning alarms are used and how they affect sleep, cognition, cortisol, and mood.
- Study 1 was a survey of 1,732 healthy adults (mean age 34 years; 66% women) designed to elucidate the characteristics of people who snooze and why they choose to delay their waking in this way.
- Study 2 was a within-subject polysomnography study of 31 healthy habitual snoozers (mean age 27 years; 18 women) designed to explore the acute effects of snoozing on sleep architecture, sleepiness, cognitive ability, mood, and cortisol awakening response.
TAKEAWAY:
- Overall, 69% reported using the snooze button or setting multiple alarms at least sometimes, most often on workdays (71%), with an average snooze time per morning of 22 minutes.
- Sleep quality did not differ between snoozers and nonsnoozers, but snoozers were more likely to feel mentally drowsy on waking (odds ratio, 3.0; P < .001) and had slightly shorter sleep time on workdays (13 minutes).
- In the polysomnography study, compared with waking up abruptly, 30 minutes of snoozing in the morning improved or did not affect performance on standard cognitive tests completed directly on final awakening.
- Snoozing resulted in about 6 minutes of lost sleep, but it prevented awakening from slow-wave sleep and had no clear effects on the cortisol awakening response, morning sleepiness, mood, or overnight sleep architecture.
IN PRACTICE:
“The findings indicate that there is no reason to stop snoozing in the morning if you enjoy it, at least not for snooze times around 30 minutes. In fact, it may even help those with morning drowsiness to be slightly more awake once they get up,” corresponding author Tina Sundelin, PhD, of Stockholm University, said in a statement.
SOURCE:
The study was published online in the Journal of Sleep Research.
LIMITATIONS:
Study 1 focused on waking preferences in a convenience sample of adults. Study 2 included only habitual snoozers making it difficult to generalize the findings to people who don’t usually snooze. The study investigated only the effect of 30 minutes of snoozing on the studied parameters. It’s possible that shorter or longer snooze times have different cognitive effects.
DISCLOSURES:
Support for the study was provided by the Stress Research Institute, Stockholm University, and a grant from Vetenskapsrådet. The authors disclosed no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
Physical activity in children tied to increased brain volume
TOPLINE:
METHODOLOGY:
- Investigators used data on 1,088 children (52% girls) in the Generation R Study, a 4-year longitudinal population-based cohort study in Rotterdam, the Netherlands.
- At age 10 years, children and their caregivers reported on children’s level of physical activity and sports involvement.
- Investigators measured changes in participants’ brain volume via MRI at ages 10 and 14 years.
TAKEAWAY:
- Every 1 additional hour per week in sports participation was associated with a 64.0-mm3 larger volume change in subcortical gray matter (P = .04).
- Every 1 additional hour per week in total physical activity was associated with a 154.0-mm3 larger volume change in total white matter (P = .02).
- Total physical activity reported by any source (P = .03) and child reports of outdoor play (P = .01) were associated with increased amygdala volume over time.
- Total physical activity reported by the children was associated with hippocampal volume increases (P = .02).
IN PRACTICE:
“Physical activity is one of the most promising environmental exposures favorably influencing health across the lifespan,” the authors write. “This study adds to prior literature by highlighting the neurodevelopmental benefits physical activity may have on the architecture of the amygdala and hippocampus.”
SOURCE:
The study was led by Fernando Estévez-López, PhD, of the Harvard T.H. Chan School of Public Health, Boston, the SPORT Research Group and CERNEP Research Center at the University of Almería (Spain), and Erasmus MC University Medical Centre, Rotterdam, the Netherlands. It was published online on in JAMA Network Open.
LIMITATIONS:
The study only accounted for confounders at baseline, does not establish causation, and utilized unvalidated questionnaires to gather information on physical activity.
DISCLOSURES:
Individual authors report receiving financial support, but there was no specific funding for this study. Dr. Estévez-López reports no relevant financial conflicts. Full disclosures are available in the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Investigators used data on 1,088 children (52% girls) in the Generation R Study, a 4-year longitudinal population-based cohort study in Rotterdam, the Netherlands.
- At age 10 years, children and their caregivers reported on children’s level of physical activity and sports involvement.
- Investigators measured changes in participants’ brain volume via MRI at ages 10 and 14 years.
TAKEAWAY:
- Every 1 additional hour per week in sports participation was associated with a 64.0-mm3 larger volume change in subcortical gray matter (P = .04).
- Every 1 additional hour per week in total physical activity was associated with a 154.0-mm3 larger volume change in total white matter (P = .02).
- Total physical activity reported by any source (P = .03) and child reports of outdoor play (P = .01) were associated with increased amygdala volume over time.
- Total physical activity reported by the children was associated with hippocampal volume increases (P = .02).
IN PRACTICE:
“Physical activity is one of the most promising environmental exposures favorably influencing health across the lifespan,” the authors write. “This study adds to prior literature by highlighting the neurodevelopmental benefits physical activity may have on the architecture of the amygdala and hippocampus.”
SOURCE:
The study was led by Fernando Estévez-López, PhD, of the Harvard T.H. Chan School of Public Health, Boston, the SPORT Research Group and CERNEP Research Center at the University of Almería (Spain), and Erasmus MC University Medical Centre, Rotterdam, the Netherlands. It was published online on in JAMA Network Open.
LIMITATIONS:
The study only accounted for confounders at baseline, does not establish causation, and utilized unvalidated questionnaires to gather information on physical activity.
DISCLOSURES:
Individual authors report receiving financial support, but there was no specific funding for this study. Dr. Estévez-López reports no relevant financial conflicts. Full disclosures are available in the original article.
A version of this article first appeared on Medscape.com.
TOPLINE:
METHODOLOGY:
- Investigators used data on 1,088 children (52% girls) in the Generation R Study, a 4-year longitudinal population-based cohort study in Rotterdam, the Netherlands.
- At age 10 years, children and their caregivers reported on children’s level of physical activity and sports involvement.
- Investigators measured changes in participants’ brain volume via MRI at ages 10 and 14 years.
TAKEAWAY:
- Every 1 additional hour per week in sports participation was associated with a 64.0-mm3 larger volume change in subcortical gray matter (P = .04).
- Every 1 additional hour per week in total physical activity was associated with a 154.0-mm3 larger volume change in total white matter (P = .02).
- Total physical activity reported by any source (P = .03) and child reports of outdoor play (P = .01) were associated with increased amygdala volume over time.
- Total physical activity reported by the children was associated with hippocampal volume increases (P = .02).
IN PRACTICE:
“Physical activity is one of the most promising environmental exposures favorably influencing health across the lifespan,” the authors write. “This study adds to prior literature by highlighting the neurodevelopmental benefits physical activity may have on the architecture of the amygdala and hippocampus.”
SOURCE:
The study was led by Fernando Estévez-López, PhD, of the Harvard T.H. Chan School of Public Health, Boston, the SPORT Research Group and CERNEP Research Center at the University of Almería (Spain), and Erasmus MC University Medical Centre, Rotterdam, the Netherlands. It was published online on in JAMA Network Open.
LIMITATIONS:
The study only accounted for confounders at baseline, does not establish causation, and utilized unvalidated questionnaires to gather information on physical activity.
DISCLOSURES:
Individual authors report receiving financial support, but there was no specific funding for this study. Dr. Estévez-López reports no relevant financial conflicts. Full disclosures are available in the original article.
A version of this article first appeared on Medscape.com.
Postmenopausal stress linked to mood, cognitive symptoms
PHILADELPHIA – , according to research presented at the annual meeting of the Menopause Society (formerly the North American Menopause Society).
“This work suggests that markers of hypothalamic-pituitary-axis activation that capture total cortisol secretion over multiple months, [such as] hair cortisol, strongly correlate with cognitive performance on attention and working memory tasks, whereas measures of more acute cortisol, [such as] salivary cortisol, may be more strongly associated with depression symptom severity and verbal learning,” Christina Metcalf, PhD, an assistant professor of psychiatry in the Colorado Center for Women’s Behavioral Health and Wellness at the University of Colorado at Denver, Aurora, told attendees. “Given the associations with chronic stress, there’s a lot of potential here to increase our knowledge about how women are doing and managing stress and life stressors during this life transition,” she said.

The study involved collecting hair and saliva samples from 43 healthy women in late perimenopause or early postmenopause with an average age of 51. The participants were predominantly white and college educated. The hair sample was taken within 2 cm of the scalp, and the saliva samples were collected the day after the hair sample collection, at the start and end of a 30-minute rest period that took place between 2:00 and 3:00 p.m. local time.
All the participants had an intact uterus and at least one ovary. None of the participants were current smokers or had recent alcohol or drug dependence, and none had used hormones within the previous 6 months. The study also excluded women who were pregnant or breastfeeding, who had bleached hair or no hair, who were taking steroids, beta blockers or opioid medication, and who had recently taken NSAIDS.
Measuring hair cortisol more feasible
The study was conducted remotely, with participants using video conferencing to communicate with the study personnel and then completing study procedures at home, including 2 days of cognitive testing with the California Verbal Learning Test – Third Edition and the n-back and continuous performance tasks. The participants also completed the Center for Epidemiologic Studies Depression Scale (CES-D).
Participants with higher levels of hair cortisol and salivary cortisol also had more severe depression symptoms (P < .001). Hair cortisol was also significantly associated with attention and working memory: Women with higher levels had fewer correct answers on the 0-back and 1-back trials (P < .01) and made more mistakes on the 2-back trial (P < .001). They also scored with less specificity on the continuous performance tasks (P = .022).
Although no association existed between hair cortisol levels and verbal learning or verbal memory (P > .05), participants with higher hair cortisol did score worse on the immediate recall trials (P = .034). Salivary cortisol levels, on the other hand, showed no association with memory recall trials, attention or working memory (P > .05).
Measuring cortisol from hair samples is more feasible than using saliva samples and may offer valuable insights regarding hypothalamic-pituitary-axis activity “to consider alongside the cognitive and mental health of late peri-/early postmenopausal women,” Dr. Metcalf told attendees. The next step is to find out whether the hypothalamic-pituitary-axis axis is a modifiable biomarker that can be used to improve executive function.
The study was limited by its small population, its cross-sectional design, and the lack of covariates in the current analyses.
Monitor symptoms in midlife
Hadine Joffe, MD, MSc, a professor of psychiatry and executive director of the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said the study findings were not surprising given how common the complaints of stress and depressive symptoms are.

“Mood changes are linked with acute, immediate cortisol levels at the same point in time, and cognitive symptoms were linked to more chronically elevated cortisol levels,” Dr. Joffe said in an interview. “Women and their providers should monitor for these challenging brain symptoms in midlife as they affect performance and quality of life and are linked with changes in the HPA axis as stress biomarkers.”
Because the study is small and has a cross-sectional design, it’s not possible to determine the direction of the associations or to make any inferences about causation, Dr. Joffe said.
“We cannot make the conclusion that stress is adversely affecting mood and cognitive performance given the design limitations. It is possible that mood and cognitive issues contributed to these stress markers,” Dr. Joffe said.“However, it is known that the experience of stress is linked with vulnerability to mood and cognitive symptoms, and also that mood and cognitive symptoms induce significant stress.”
The research was funded by the Menopause Society, Colorado University, the Ludeman Family Center for Women’s Health Research, the National Institute of Mental Health, and the National Institute of Aging. Dr. Metcalf had no disclosures. Dr. Joffe has received grant support from Merck, Pfizer and Sage, and has been a consultant or advisor for Bayer, Merck and Hello Therapeutics.
PHILADELPHIA – , according to research presented at the annual meeting of the Menopause Society (formerly the North American Menopause Society).
“This work suggests that markers of hypothalamic-pituitary-axis activation that capture total cortisol secretion over multiple months, [such as] hair cortisol, strongly correlate with cognitive performance on attention and working memory tasks, whereas measures of more acute cortisol, [such as] salivary cortisol, may be more strongly associated with depression symptom severity and verbal learning,” Christina Metcalf, PhD, an assistant professor of psychiatry in the Colorado Center for Women’s Behavioral Health and Wellness at the University of Colorado at Denver, Aurora, told attendees. “Given the associations with chronic stress, there’s a lot of potential here to increase our knowledge about how women are doing and managing stress and life stressors during this life transition,” she said.
The study involved collecting hair and saliva samples from 43 healthy women in late perimenopause or early postmenopause with an average age of 51. The participants were predominantly white and college educated. The hair sample was taken within 2 cm of the scalp, and the saliva samples were collected the day after the hair sample collection, at the start and end of a 30-minute rest period that took place between 2:00 and 3:00 p.m. local time.
All the participants had an intact uterus and at least one ovary. None of the participants were current smokers or had recent alcohol or drug dependence, and none had used hormones within the previous 6 months. The study also excluded women who were pregnant or breastfeeding, who had bleached hair or no hair, who were taking steroids, beta blockers or opioid medication, and who had recently taken NSAIDS.
Measuring hair cortisol more feasible
The study was conducted remotely, with participants using video conferencing to communicate with the study personnel and then completing study procedures at home, including 2 days of cognitive testing with the California Verbal Learning Test – Third Edition and the n-back and continuous performance tasks. The participants also completed the Center for Epidemiologic Studies Depression Scale (CES-D).
Participants with higher levels of hair cortisol and salivary cortisol also had more severe depression symptoms (P < .001). Hair cortisol was also significantly associated with attention and working memory: Women with higher levels had fewer correct answers on the 0-back and 1-back trials (P < .01) and made more mistakes on the 2-back trial (P < .001). They also scored with less specificity on the continuous performance tasks (P = .022).
Although no association existed between hair cortisol levels and verbal learning or verbal memory (P > .05), participants with higher hair cortisol did score worse on the immediate recall trials (P = .034). Salivary cortisol levels, on the other hand, showed no association with memory recall trials, attention or working memory (P > .05).
Measuring cortisol from hair samples is more feasible than using saliva samples and may offer valuable insights regarding hypothalamic-pituitary-axis activity “to consider alongside the cognitive and mental health of late peri-/early postmenopausal women,” Dr. Metcalf told attendees. The next step is to find out whether the hypothalamic-pituitary-axis axis is a modifiable biomarker that can be used to improve executive function.
The study was limited by its small population, its cross-sectional design, and the lack of covariates in the current analyses.
Monitor symptoms in midlife
Hadine Joffe, MD, MSc, a professor of psychiatry and executive director of the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said the study findings were not surprising given how common the complaints of stress and depressive symptoms are.
“Mood changes are linked with acute, immediate cortisol levels at the same point in time, and cognitive symptoms were linked to more chronically elevated cortisol levels,” Dr. Joffe said in an interview. “Women and their providers should monitor for these challenging brain symptoms in midlife as they affect performance and quality of life and are linked with changes in the HPA axis as stress biomarkers.”
Because the study is small and has a cross-sectional design, it’s not possible to determine the direction of the associations or to make any inferences about causation, Dr. Joffe said.
“We cannot make the conclusion that stress is adversely affecting mood and cognitive performance given the design limitations. It is possible that mood and cognitive issues contributed to these stress markers,” Dr. Joffe said.“However, it is known that the experience of stress is linked with vulnerability to mood and cognitive symptoms, and also that mood and cognitive symptoms induce significant stress.”
The research was funded by the Menopause Society, Colorado University, the Ludeman Family Center for Women’s Health Research, the National Institute of Mental Health, and the National Institute of Aging. Dr. Metcalf had no disclosures. Dr. Joffe has received grant support from Merck, Pfizer and Sage, and has been a consultant or advisor for Bayer, Merck and Hello Therapeutics.
PHILADELPHIA – , according to research presented at the annual meeting of the Menopause Society (formerly the North American Menopause Society).
“This work suggests that markers of hypothalamic-pituitary-axis activation that capture total cortisol secretion over multiple months, [such as] hair cortisol, strongly correlate with cognitive performance on attention and working memory tasks, whereas measures of more acute cortisol, [such as] salivary cortisol, may be more strongly associated with depression symptom severity and verbal learning,” Christina Metcalf, PhD, an assistant professor of psychiatry in the Colorado Center for Women’s Behavioral Health and Wellness at the University of Colorado at Denver, Aurora, told attendees. “Given the associations with chronic stress, there’s a lot of potential here to increase our knowledge about how women are doing and managing stress and life stressors during this life transition,” she said.
The study involved collecting hair and saliva samples from 43 healthy women in late perimenopause or early postmenopause with an average age of 51. The participants were predominantly white and college educated. The hair sample was taken within 2 cm of the scalp, and the saliva samples were collected the day after the hair sample collection, at the start and end of a 30-minute rest period that took place between 2:00 and 3:00 p.m. local time.
All the participants had an intact uterus and at least one ovary. None of the participants were current smokers or had recent alcohol or drug dependence, and none had used hormones within the previous 6 months. The study also excluded women who were pregnant or breastfeeding, who had bleached hair or no hair, who were taking steroids, beta blockers or opioid medication, and who had recently taken NSAIDS.
Measuring hair cortisol more feasible
The study was conducted remotely, with participants using video conferencing to communicate with the study personnel and then completing study procedures at home, including 2 days of cognitive testing with the California Verbal Learning Test – Third Edition and the n-back and continuous performance tasks. The participants also completed the Center for Epidemiologic Studies Depression Scale (CES-D).
Participants with higher levels of hair cortisol and salivary cortisol also had more severe depression symptoms (P < .001). Hair cortisol was also significantly associated with attention and working memory: Women with higher levels had fewer correct answers on the 0-back and 1-back trials (P < .01) and made more mistakes on the 2-back trial (P < .001). They also scored with less specificity on the continuous performance tasks (P = .022).
Although no association existed between hair cortisol levels and verbal learning or verbal memory (P > .05), participants with higher hair cortisol did score worse on the immediate recall trials (P = .034). Salivary cortisol levels, on the other hand, showed no association with memory recall trials, attention or working memory (P > .05).
Measuring cortisol from hair samples is more feasible than using saliva samples and may offer valuable insights regarding hypothalamic-pituitary-axis activity “to consider alongside the cognitive and mental health of late peri-/early postmenopausal women,” Dr. Metcalf told attendees. The next step is to find out whether the hypothalamic-pituitary-axis axis is a modifiable biomarker that can be used to improve executive function.
The study was limited by its small population, its cross-sectional design, and the lack of covariates in the current analyses.
Monitor symptoms in midlife
Hadine Joffe, MD, MSc, a professor of psychiatry and executive director of the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and Harvard Medical School, both in Boston, said the study findings were not surprising given how common the complaints of stress and depressive symptoms are.
“Mood changes are linked with acute, immediate cortisol levels at the same point in time, and cognitive symptoms were linked to more chronically elevated cortisol levels,” Dr. Joffe said in an interview. “Women and their providers should monitor for these challenging brain symptoms in midlife as they affect performance and quality of life and are linked with changes in the HPA axis as stress biomarkers.”
Because the study is small and has a cross-sectional design, it’s not possible to determine the direction of the associations or to make any inferences about causation, Dr. Joffe said.
“We cannot make the conclusion that stress is adversely affecting mood and cognitive performance given the design limitations. It is possible that mood and cognitive issues contributed to these stress markers,” Dr. Joffe said.“However, it is known that the experience of stress is linked with vulnerability to mood and cognitive symptoms, and also that mood and cognitive symptoms induce significant stress.”
The research was funded by the Menopause Society, Colorado University, the Ludeman Family Center for Women’s Health Research, the National Institute of Mental Health, and the National Institute of Aging. Dr. Metcalf had no disclosures. Dr. Joffe has received grant support from Merck, Pfizer and Sage, and has been a consultant or advisor for Bayer, Merck and Hello Therapeutics.
AT NAMS 2023
Specialized care may curb suicide risk in veterans with disabilities
TOPLINE:
Investigators speculate that veteran status may mitigate suicide risk given increased provision of disability-related care through the Department of Veterans Affairs, but they acknowledge that more research is needed to confirm this theory.
METHODOLOGY:
- The study includes analysis of self-reported data collected from 2015 to 2020 from 231,000 NSDUH respondents, 9% of whom were veterans; 20% reported at least one disability.
- Respondents were asked questions about suicide, veteran status, and the number and type of disability they had, if applicable.
- Disabilities included those related to hearing, sight, and concentration, memory, decision-making, ambulation, or functional status (at home or outside the home).
TAKEAWAY:
- Overall, 4.4% of the sample reported suicide ideation, planning, or attempt.
- Among participants with one disability, being a veteran was associated with a 43% lower risk of suicide planning (adjusted odds ratio, 0.57; P = .03).
- Among those with two disabilities, veterans had a 54% lower likelihood of having a history of suicide attempt, compared with nonveterans (aOR, 0.46; P = .02).
- Compared with U.S. veterans reporting 1, 2, and ≥ 3 disabilities, U.S. veterans with no disabilities were 50%, 160%, and 127% more likely, respectively, to report suicidal ideation.
IN PRACTICE:
“The observed buffering effect of veteran status among people with a disability may be reflective of characteristics of disability-related care offered through the Department of Veterans Affairs,” the authors write. “It is possible that VA services could act as a protective factor for suicide-related outcomes for veterans with disabilities by improving access, quality of care, and understanding of their disability context.”
SOURCE:
Rebecca K. Blais, PhD, of Arizona State University, Tempe, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
Assessments were based on self-reported information and there was no information about disability severity, which may have influenced suicide risk among veterans and nonveterans.
DISCLOSURES:
Coauthor Anne Kirby, PhD, received grants from the National Institute of Mental Health during the conduct of the study as well as grants from the U.S. Centers for Disease Control and Prevention and personal fees from University of Pittsburgh outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
Investigators speculate that veteran status may mitigate suicide risk given increased provision of disability-related care through the Department of Veterans Affairs, but they acknowledge that more research is needed to confirm this theory.
METHODOLOGY:
- The study includes analysis of self-reported data collected from 2015 to 2020 from 231,000 NSDUH respondents, 9% of whom were veterans; 20% reported at least one disability.
- Respondents were asked questions about suicide, veteran status, and the number and type of disability they had, if applicable.
- Disabilities included those related to hearing, sight, and concentration, memory, decision-making, ambulation, or functional status (at home or outside the home).
TAKEAWAY:
- Overall, 4.4% of the sample reported suicide ideation, planning, or attempt.
- Among participants with one disability, being a veteran was associated with a 43% lower risk of suicide planning (adjusted odds ratio, 0.57; P = .03).
- Among those with two disabilities, veterans had a 54% lower likelihood of having a history of suicide attempt, compared with nonveterans (aOR, 0.46; P = .02).
- Compared with U.S. veterans reporting 1, 2, and ≥ 3 disabilities, U.S. veterans with no disabilities were 50%, 160%, and 127% more likely, respectively, to report suicidal ideation.
IN PRACTICE:
“The observed buffering effect of veteran status among people with a disability may be reflective of characteristics of disability-related care offered through the Department of Veterans Affairs,” the authors write. “It is possible that VA services could act as a protective factor for suicide-related outcomes for veterans with disabilities by improving access, quality of care, and understanding of their disability context.”
SOURCE:
Rebecca K. Blais, PhD, of Arizona State University, Tempe, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
Assessments were based on self-reported information and there was no information about disability severity, which may have influenced suicide risk among veterans and nonveterans.
DISCLOSURES:
Coauthor Anne Kirby, PhD, received grants from the National Institute of Mental Health during the conduct of the study as well as grants from the U.S. Centers for Disease Control and Prevention and personal fees from University of Pittsburgh outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.
TOPLINE:
Investigators speculate that veteran status may mitigate suicide risk given increased provision of disability-related care through the Department of Veterans Affairs, but they acknowledge that more research is needed to confirm this theory.
METHODOLOGY:
- The study includes analysis of self-reported data collected from 2015 to 2020 from 231,000 NSDUH respondents, 9% of whom were veterans; 20% reported at least one disability.
- Respondents were asked questions about suicide, veteran status, and the number and type of disability they had, if applicable.
- Disabilities included those related to hearing, sight, and concentration, memory, decision-making, ambulation, or functional status (at home or outside the home).
TAKEAWAY:
- Overall, 4.4% of the sample reported suicide ideation, planning, or attempt.
- Among participants with one disability, being a veteran was associated with a 43% lower risk of suicide planning (adjusted odds ratio, 0.57; P = .03).
- Among those with two disabilities, veterans had a 54% lower likelihood of having a history of suicide attempt, compared with nonveterans (aOR, 0.46; P = .02).
- Compared with U.S. veterans reporting 1, 2, and ≥ 3 disabilities, U.S. veterans with no disabilities were 50%, 160%, and 127% more likely, respectively, to report suicidal ideation.
IN PRACTICE:
“The observed buffering effect of veteran status among people with a disability may be reflective of characteristics of disability-related care offered through the Department of Veterans Affairs,” the authors write. “It is possible that VA services could act as a protective factor for suicide-related outcomes for veterans with disabilities by improving access, quality of care, and understanding of their disability context.”
SOURCE:
Rebecca K. Blais, PhD, of Arizona State University, Tempe, led the study, which was published online in JAMA Network Open.
LIMITATIONS:
Assessments were based on self-reported information and there was no information about disability severity, which may have influenced suicide risk among veterans and nonveterans.
DISCLOSURES:
Coauthor Anne Kirby, PhD, received grants from the National Institute of Mental Health during the conduct of the study as well as grants from the U.S. Centers for Disease Control and Prevention and personal fees from University of Pittsburgh outside the submitted work. No other disclosures were reported.
A version of this article first appeared on Medscape.com.