User login
Mantle Cell Lymphoma: Drug Combo Improves PFS
Still, “in the countries where ibrutinib is indicated, this combination should be a new standard therapy for relapsed/refractory mantle cell lymphoma,” Michael Wang, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in a media briefing at the annual meeting of the American Society of Hematology.
Its use would be off label, according to the authors of the industry-funded trial, because no nation has approved the combination therapy for MCL, a rare, aggressive form of non-Hodgkin lymphoma.
As Dr. Wang noted, ibrutinib (a Bruton tyrosine kinase inhibitor) is approved by the Food and Drug Administration to treat MCL, while venetoclax (a BCL-2 inhibitor) is approved for chronic lymphocytic leukemia and previously untreated acute myeloid leukemia. “The combination of these two agents leverages complementary modes of action and has demonstrated synergistic anti-tumor activity in preclinical models of mantle cell lymphoma,” he said. And “in patients with relapsed/refractory mantle cell lymphoma, promising clinical activity has also been observed in early-phase studies.”
For the multinational, randomized, phase 3, double-blind SYMPATICO study, researchers assigned 267 adults with relapsed/refractory MCL after 1-5 prior therapies 1:1 to receive oral ibrutinib 560 mg daily with oral venetoclax (standard 5-wk ramp-up to a target dose of 400 mg once daily) or placebo for 2 years. Then they continued with ibrutinib alone until progressive disease or unacceptable toxicity.
The study began in 2017. The median age of patients was 68, and the numbers of patients in each group were 134 (both drugs) and 133 (ibrutinib plus placebo).
At a median of 51.2 months, median PFS — the primary endpoint — was higher in the combination group vs. ibrutinib alone (31.9 vs. 22.1 months, hazard ratio [HR]=0.65, 95% CI, 0.47–0.88, P = .0052). While overall survival was higher in the combination group vs. ibrutinib alone, an interim analysis found that the difference was not statistically significant (44.9 months vs. 38.6 months, 95% CI, HR = 0.85, 0.62-1.19, P = .3465).
When questioned about this finding at the ASH news briefing, Dr. Wang said that 170 events are needed for a full overall survival analysis, and there are just 144 now. The study may reach that point in early 2025, he said.
Over a median treatment duration of 22.0 months for the combination treatment and 17.7 months for ibrutinib alone, grade ≥ 3 adverse events occurred in 84% and 76% of patients, respectively. At 60%, the level of serious adverse events was the same in both groups.
In an interview, Brian T. Hill, MD, PhD, of Cleveland Clinic, noted that in general, MCL “has a pretty relentless pattern of relapses and disease progression without an easy cure in the vast majority of patients.”
Ibrutinib has revolutionized treatment over the past decade with generally manageable side effects, and clinicians are now turning to other Bruton tyrosine kinase inhibitors, he said. Still, “there is a need for improving the durability and the response rates second-line treatment or beyond,” Dr. Hill said.
The new study is important since it’s the first randomized trial “that demonstrates that additional venetoclax significantly improves not only response rates, but also progression-free survival with a trend toward overall survival,” he said. “The toxicity profile doesn’t really seem to be significantly more worse than what we might expect with each agent given individually.”
However, Dr. Hill noted that “it’s a relatively small study and relatively short follow-up.”
It may be difficult to get an ibrutinib-venetoclax combination approved today since ibrutinib is no longer the preferred Bruton tyrosine kinase inhibitor for clinicians, he said.
Pharmacyclics, maker of ibrutinib, is the study sponsor and Janssen is a collaborator.
Dr. Wang reports research funding Acerta Pharma, AstraZeneca, BeiGene, BioInvent, Celgene, Genentech, Innocare, Janssen, Juno Therapeutics, Kite Pharma, Lilly, Loxo Oncology, Molecular Templates, Oncternal, Pharmacyclics, and VelosBio. Other authors report multiple and various relationships with industry. Dr. Hill discloses research funding and consulting relationships with Pharmacyclics, AbbVie, BeiGene, and AstraZeneca.
Still, “in the countries where ibrutinib is indicated, this combination should be a new standard therapy for relapsed/refractory mantle cell lymphoma,” Michael Wang, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in a media briefing at the annual meeting of the American Society of Hematology.
Its use would be off label, according to the authors of the industry-funded trial, because no nation has approved the combination therapy for MCL, a rare, aggressive form of non-Hodgkin lymphoma.
As Dr. Wang noted, ibrutinib (a Bruton tyrosine kinase inhibitor) is approved by the Food and Drug Administration to treat MCL, while venetoclax (a BCL-2 inhibitor) is approved for chronic lymphocytic leukemia and previously untreated acute myeloid leukemia. “The combination of these two agents leverages complementary modes of action and has demonstrated synergistic anti-tumor activity in preclinical models of mantle cell lymphoma,” he said. And “in patients with relapsed/refractory mantle cell lymphoma, promising clinical activity has also been observed in early-phase studies.”
For the multinational, randomized, phase 3, double-blind SYMPATICO study, researchers assigned 267 adults with relapsed/refractory MCL after 1-5 prior therapies 1:1 to receive oral ibrutinib 560 mg daily with oral venetoclax (standard 5-wk ramp-up to a target dose of 400 mg once daily) or placebo for 2 years. Then they continued with ibrutinib alone until progressive disease or unacceptable toxicity.
The study began in 2017. The median age of patients was 68, and the numbers of patients in each group were 134 (both drugs) and 133 (ibrutinib plus placebo).
At a median of 51.2 months, median PFS — the primary endpoint — was higher in the combination group vs. ibrutinib alone (31.9 vs. 22.1 months, hazard ratio [HR]=0.65, 95% CI, 0.47–0.88, P = .0052). While overall survival was higher in the combination group vs. ibrutinib alone, an interim analysis found that the difference was not statistically significant (44.9 months vs. 38.6 months, 95% CI, HR = 0.85, 0.62-1.19, P = .3465).
When questioned about this finding at the ASH news briefing, Dr. Wang said that 170 events are needed for a full overall survival analysis, and there are just 144 now. The study may reach that point in early 2025, he said.
Over a median treatment duration of 22.0 months for the combination treatment and 17.7 months for ibrutinib alone, grade ≥ 3 adverse events occurred in 84% and 76% of patients, respectively. At 60%, the level of serious adverse events was the same in both groups.
In an interview, Brian T. Hill, MD, PhD, of Cleveland Clinic, noted that in general, MCL “has a pretty relentless pattern of relapses and disease progression without an easy cure in the vast majority of patients.”
Ibrutinib has revolutionized treatment over the past decade with generally manageable side effects, and clinicians are now turning to other Bruton tyrosine kinase inhibitors, he said. Still, “there is a need for improving the durability and the response rates second-line treatment or beyond,” Dr. Hill said.
The new study is important since it’s the first randomized trial “that demonstrates that additional venetoclax significantly improves not only response rates, but also progression-free survival with a trend toward overall survival,” he said. “The toxicity profile doesn’t really seem to be significantly more worse than what we might expect with each agent given individually.”
However, Dr. Hill noted that “it’s a relatively small study and relatively short follow-up.”
It may be difficult to get an ibrutinib-venetoclax combination approved today since ibrutinib is no longer the preferred Bruton tyrosine kinase inhibitor for clinicians, he said.
Pharmacyclics, maker of ibrutinib, is the study sponsor and Janssen is a collaborator.
Dr. Wang reports research funding Acerta Pharma, AstraZeneca, BeiGene, BioInvent, Celgene, Genentech, Innocare, Janssen, Juno Therapeutics, Kite Pharma, Lilly, Loxo Oncology, Molecular Templates, Oncternal, Pharmacyclics, and VelosBio. Other authors report multiple and various relationships with industry. Dr. Hill discloses research funding and consulting relationships with Pharmacyclics, AbbVie, BeiGene, and AstraZeneca.
Still, “in the countries where ibrutinib is indicated, this combination should be a new standard therapy for relapsed/refractory mantle cell lymphoma,” Michael Wang, MD, of the University of Texas MD Anderson Cancer Center, Houston, said in a media briefing at the annual meeting of the American Society of Hematology.
Its use would be off label, according to the authors of the industry-funded trial, because no nation has approved the combination therapy for MCL, a rare, aggressive form of non-Hodgkin lymphoma.
As Dr. Wang noted, ibrutinib (a Bruton tyrosine kinase inhibitor) is approved by the Food and Drug Administration to treat MCL, while venetoclax (a BCL-2 inhibitor) is approved for chronic lymphocytic leukemia and previously untreated acute myeloid leukemia. “The combination of these two agents leverages complementary modes of action and has demonstrated synergistic anti-tumor activity in preclinical models of mantle cell lymphoma,” he said. And “in patients with relapsed/refractory mantle cell lymphoma, promising clinical activity has also been observed in early-phase studies.”
For the multinational, randomized, phase 3, double-blind SYMPATICO study, researchers assigned 267 adults with relapsed/refractory MCL after 1-5 prior therapies 1:1 to receive oral ibrutinib 560 mg daily with oral venetoclax (standard 5-wk ramp-up to a target dose of 400 mg once daily) or placebo for 2 years. Then they continued with ibrutinib alone until progressive disease or unacceptable toxicity.
The study began in 2017. The median age of patients was 68, and the numbers of patients in each group were 134 (both drugs) and 133 (ibrutinib plus placebo).
At a median of 51.2 months, median PFS — the primary endpoint — was higher in the combination group vs. ibrutinib alone (31.9 vs. 22.1 months, hazard ratio [HR]=0.65, 95% CI, 0.47–0.88, P = .0052). While overall survival was higher in the combination group vs. ibrutinib alone, an interim analysis found that the difference was not statistically significant (44.9 months vs. 38.6 months, 95% CI, HR = 0.85, 0.62-1.19, P = .3465).
When questioned about this finding at the ASH news briefing, Dr. Wang said that 170 events are needed for a full overall survival analysis, and there are just 144 now. The study may reach that point in early 2025, he said.
Over a median treatment duration of 22.0 months for the combination treatment and 17.7 months for ibrutinib alone, grade ≥ 3 adverse events occurred in 84% and 76% of patients, respectively. At 60%, the level of serious adverse events was the same in both groups.
In an interview, Brian T. Hill, MD, PhD, of Cleveland Clinic, noted that in general, MCL “has a pretty relentless pattern of relapses and disease progression without an easy cure in the vast majority of patients.”
Ibrutinib has revolutionized treatment over the past decade with generally manageable side effects, and clinicians are now turning to other Bruton tyrosine kinase inhibitors, he said. Still, “there is a need for improving the durability and the response rates second-line treatment or beyond,” Dr. Hill said.
The new study is important since it’s the first randomized trial “that demonstrates that additional venetoclax significantly improves not only response rates, but also progression-free survival with a trend toward overall survival,” he said. “The toxicity profile doesn’t really seem to be significantly more worse than what we might expect with each agent given individually.”
However, Dr. Hill noted that “it’s a relatively small study and relatively short follow-up.”
It may be difficult to get an ibrutinib-venetoclax combination approved today since ibrutinib is no longer the preferred Bruton tyrosine kinase inhibitor for clinicians, he said.
Pharmacyclics, maker of ibrutinib, is the study sponsor and Janssen is a collaborator.
Dr. Wang reports research funding Acerta Pharma, AstraZeneca, BeiGene, BioInvent, Celgene, Genentech, Innocare, Janssen, Juno Therapeutics, Kite Pharma, Lilly, Loxo Oncology, Molecular Templates, Oncternal, Pharmacyclics, and VelosBio. Other authors report multiple and various relationships with industry. Dr. Hill discloses research funding and consulting relationships with Pharmacyclics, AbbVie, BeiGene, and AstraZeneca.
FROM ASH 2023
‘Baby TAM’ effective, tolerable for breast cancer prevention
SAN ANTONIO — The drug can reduce incidence of breast cancer in high-risk individuals, but side effects that mimic menopause have led to low rates of uptake. Lower-dose tamoxifen aims to reduce those side effects, but there remains some uncertainty about the minimum dose required to maintain efficacy.
The TAM-01 study, first published in 2019, demonstrated that a 5-mg dose of tamoxifen led to a reduction in recurrence of invasive breast cancer or ductal carcinoma in situ (DCIS). At the San Antonio Breast Cancer Symposium, two studies were presented that provided insight into dose efficacy and likelihood of medication adherence in women taking baby TAM.
“We all know that women who are at increased risk for breast cancer may benefit from the use of tamoxifen to help lower their risk, although historical uptake to tamoxifen in the prevention setting has been quite low,” said Lauren Cornell, MD, during a presentation. Her team investigated the impact of patient counseling on how well they understood their risk, as well as their likelihood of adherence to the medication.
The study included 41 women, and 31 completed follow-up at 1 year. “We saw that 90% of our patients reported good or complete understanding of their breast cancer risk after the consultation, emphasizing the benefit of that consult, and 73% reported that the availability of baby tamoxifen helped in their decision to consider a preventative medication,” said Dr. Cornell during her presentation. After 1 year of follow-up, 74% said that they had initiated baby tamoxifen, and 78% of those who started taking the drug were still taking it at 1 year.
Participants who continued to take baby TAM at 1 year had a higher estimated breast cancer risk (IBIS 10-year risk, 12.7% vs 7.6%; P = .027) than those who discontinued. “We saw that uptake to baby TAM after informed discussion in patients who qualify is high, especially in those patients with high risk and intraepithelial lesions or DCIS, and adherence and tolerability at 1 year follow up is improved, compared to what we would expect with traditional dosing of tamoxifen. It’s important to note that the NCCN guidelines and the ASCO clinical practice update now include low-dose tamoxifen as an option for select women, and future randomized control trials on de-escalation of tamoxifen and high-risk patients based on their risk model assessment still need to be done. Future study should also focus on markers to identify candidates best suited for low versus standard dose of tamoxifen,” said Dr. Cornell, who is an assistant professor of medicine at Mayo Clinic Florida in Jacksonville.
At another SABCS session, Per Hall, MD, PhD, discussed findings from the previously published KARISMA-2 study, which examined efficacy of various doses of tamoxifen. A total of 1440 participants, 240 in each arm, received tamoxifen doses of 20 mg, 10 mg, 5 mg, 2.5 mg, 1 mg, or placebo. During his talk, Dr. Hall pointed out that measuring outcomes would take a very large number of participants to identify small differences in breast cancer rates. Therefore, the researchers examined breast density changes as a proxy. As a noninferiority outcome, the researchers used the proportion of women in each arm who achieved the median decrease in breast density seen at 20 mg of tamoxifen, which is 10.1%.
The women underwent mammograms at baseline and again at 6 months to determine change in breast density. Among all women in the study, the proportion of patients who had a similar breast density reduction as the 20-mg dose were very similar in the 10 mg (50.0%; P = .002), 5 mg (49.3%; P < .001), and 2.5 mg (52.5%; P < .001) groups. The 1 mg group had a proportion of 39.5% (P = .138), while the placebo group had 38.9% (P = .161). However, the results were driven by premenopausal women, where the values were 63.3%, 70.7%, 74.4%, and 69.7% in the 20-mg, 10-mg, 5-mg, and 2.5-mg groups, respectively, and 32.9% at 1 mg and 29.7% on placebo. In postmenopausal women, the values were 41.9%, 36.7%, 33.3%, and 41.9% in the 20-mg, 10-mg, 5-mg, and 2.5-mg groups, with values of 44.2% in the 1-mg group and 43.8% in the placebo group.
The median density change was 18.5% in premenopausal women and 4.0% in postmenopausal women.
“We didn’t see anything in the postmenopausal women. The decrease for those on 20 milligrams and those on placebo were exactly the same. Why this is, we still don’t know because we do know that tamoxifen in the adjuvant setting could be used for postmenopausal women. It could be that 6 months is too short of a time [to see a benefit]. We don’t know,” said Dr. Hall, who is a medical epidemiologist and biostatistician at Karolinska Institutet, Stockholm, Sweden.
Severe vasomotor side effects like hot flashes, cold flashes, and night sweats were reduced by about 50% in the lower tamoxifen doses, compared with 20 mg.
Dr. Hall also pointed out that tamoxifen is a prodrug. The CYP2D6 enzyme produces a range of metabolites, with endoxifen having the strongest affinity to the estrogen receptor and being present at the highest plasma concentration. He showed a table of endoxifen plasma levels at various tamoxifen doses in women of various metabolizer status, ranging from poor to ultrafast. Among intermediate, normal, and ultrarapid metabolizers, 5- and 10-mg doses produced plasma endoxifen levels ranging from 2.4 to 6.2 ng/mL, which represents a good therapeutic window. “For intermediate and normal metabolizers, it could be that 5 mg [of tamoxifen] is enough, but I want to underline that we didn’t use breast cancer incidence or recurrence in this study, we used density change, so we should be careful when we use these results,” said Dr. Hall. His group is now conducting the KARISMA Endoxifen trial, which will test endoxifen directly at doses of 1 and 2 mg.
Dr. Cornell has no relevant financial disclosures. Dr. Hall is a member of the scientific advisory board for Atossa Therapeutics.
SAN ANTONIO — The drug can reduce incidence of breast cancer in high-risk individuals, but side effects that mimic menopause have led to low rates of uptake. Lower-dose tamoxifen aims to reduce those side effects, but there remains some uncertainty about the minimum dose required to maintain efficacy.
The TAM-01 study, first published in 2019, demonstrated that a 5-mg dose of tamoxifen led to a reduction in recurrence of invasive breast cancer or ductal carcinoma in situ (DCIS). At the San Antonio Breast Cancer Symposium, two studies were presented that provided insight into dose efficacy and likelihood of medication adherence in women taking baby TAM.
“We all know that women who are at increased risk for breast cancer may benefit from the use of tamoxifen to help lower their risk, although historical uptake to tamoxifen in the prevention setting has been quite low,” said Lauren Cornell, MD, during a presentation. Her team investigated the impact of patient counseling on how well they understood their risk, as well as their likelihood of adherence to the medication.
The study included 41 women, and 31 completed follow-up at 1 year. “We saw that 90% of our patients reported good or complete understanding of their breast cancer risk after the consultation, emphasizing the benefit of that consult, and 73% reported that the availability of baby tamoxifen helped in their decision to consider a preventative medication,” said Dr. Cornell during her presentation. After 1 year of follow-up, 74% said that they had initiated baby tamoxifen, and 78% of those who started taking the drug were still taking it at 1 year.
Participants who continued to take baby TAM at 1 year had a higher estimated breast cancer risk (IBIS 10-year risk, 12.7% vs 7.6%; P = .027) than those who discontinued. “We saw that uptake to baby TAM after informed discussion in patients who qualify is high, especially in those patients with high risk and intraepithelial lesions or DCIS, and adherence and tolerability at 1 year follow up is improved, compared to what we would expect with traditional dosing of tamoxifen. It’s important to note that the NCCN guidelines and the ASCO clinical practice update now include low-dose tamoxifen as an option for select women, and future randomized control trials on de-escalation of tamoxifen and high-risk patients based on their risk model assessment still need to be done. Future study should also focus on markers to identify candidates best suited for low versus standard dose of tamoxifen,” said Dr. Cornell, who is an assistant professor of medicine at Mayo Clinic Florida in Jacksonville.
At another SABCS session, Per Hall, MD, PhD, discussed findings from the previously published KARISMA-2 study, which examined efficacy of various doses of tamoxifen. A total of 1440 participants, 240 in each arm, received tamoxifen doses of 20 mg, 10 mg, 5 mg, 2.5 mg, 1 mg, or placebo. During his talk, Dr. Hall pointed out that measuring outcomes would take a very large number of participants to identify small differences in breast cancer rates. Therefore, the researchers examined breast density changes as a proxy. As a noninferiority outcome, the researchers used the proportion of women in each arm who achieved the median decrease in breast density seen at 20 mg of tamoxifen, which is 10.1%.
The women underwent mammograms at baseline and again at 6 months to determine change in breast density. Among all women in the study, the proportion of patients who had a similar breast density reduction as the 20-mg dose were very similar in the 10 mg (50.0%; P = .002), 5 mg (49.3%; P < .001), and 2.5 mg (52.5%; P < .001) groups. The 1 mg group had a proportion of 39.5% (P = .138), while the placebo group had 38.9% (P = .161). However, the results were driven by premenopausal women, where the values were 63.3%, 70.7%, 74.4%, and 69.7% in the 20-mg, 10-mg, 5-mg, and 2.5-mg groups, respectively, and 32.9% at 1 mg and 29.7% on placebo. In postmenopausal women, the values were 41.9%, 36.7%, 33.3%, and 41.9% in the 20-mg, 10-mg, 5-mg, and 2.5-mg groups, with values of 44.2% in the 1-mg group and 43.8% in the placebo group.
The median density change was 18.5% in premenopausal women and 4.0% in postmenopausal women.
“We didn’t see anything in the postmenopausal women. The decrease for those on 20 milligrams and those on placebo were exactly the same. Why this is, we still don’t know because we do know that tamoxifen in the adjuvant setting could be used for postmenopausal women. It could be that 6 months is too short of a time [to see a benefit]. We don’t know,” said Dr. Hall, who is a medical epidemiologist and biostatistician at Karolinska Institutet, Stockholm, Sweden.
Severe vasomotor side effects like hot flashes, cold flashes, and night sweats were reduced by about 50% in the lower tamoxifen doses, compared with 20 mg.
Dr. Hall also pointed out that tamoxifen is a prodrug. The CYP2D6 enzyme produces a range of metabolites, with endoxifen having the strongest affinity to the estrogen receptor and being present at the highest plasma concentration. He showed a table of endoxifen plasma levels at various tamoxifen doses in women of various metabolizer status, ranging from poor to ultrafast. Among intermediate, normal, and ultrarapid metabolizers, 5- and 10-mg doses produced plasma endoxifen levels ranging from 2.4 to 6.2 ng/mL, which represents a good therapeutic window. “For intermediate and normal metabolizers, it could be that 5 mg [of tamoxifen] is enough, but I want to underline that we didn’t use breast cancer incidence or recurrence in this study, we used density change, so we should be careful when we use these results,” said Dr. Hall. His group is now conducting the KARISMA Endoxifen trial, which will test endoxifen directly at doses of 1 and 2 mg.
Dr. Cornell has no relevant financial disclosures. Dr. Hall is a member of the scientific advisory board for Atossa Therapeutics.
SAN ANTONIO — The drug can reduce incidence of breast cancer in high-risk individuals, but side effects that mimic menopause have led to low rates of uptake. Lower-dose tamoxifen aims to reduce those side effects, but there remains some uncertainty about the minimum dose required to maintain efficacy.
The TAM-01 study, first published in 2019, demonstrated that a 5-mg dose of tamoxifen led to a reduction in recurrence of invasive breast cancer or ductal carcinoma in situ (DCIS). At the San Antonio Breast Cancer Symposium, two studies were presented that provided insight into dose efficacy and likelihood of medication adherence in women taking baby TAM.
“We all know that women who are at increased risk for breast cancer may benefit from the use of tamoxifen to help lower their risk, although historical uptake to tamoxifen in the prevention setting has been quite low,” said Lauren Cornell, MD, during a presentation. Her team investigated the impact of patient counseling on how well they understood their risk, as well as their likelihood of adherence to the medication.
The study included 41 women, and 31 completed follow-up at 1 year. “We saw that 90% of our patients reported good or complete understanding of their breast cancer risk after the consultation, emphasizing the benefit of that consult, and 73% reported that the availability of baby tamoxifen helped in their decision to consider a preventative medication,” said Dr. Cornell during her presentation. After 1 year of follow-up, 74% said that they had initiated baby tamoxifen, and 78% of those who started taking the drug were still taking it at 1 year.
Participants who continued to take baby TAM at 1 year had a higher estimated breast cancer risk (IBIS 10-year risk, 12.7% vs 7.6%; P = .027) than those who discontinued. “We saw that uptake to baby TAM after informed discussion in patients who qualify is high, especially in those patients with high risk and intraepithelial lesions or DCIS, and adherence and tolerability at 1 year follow up is improved, compared to what we would expect with traditional dosing of tamoxifen. It’s important to note that the NCCN guidelines and the ASCO clinical practice update now include low-dose tamoxifen as an option for select women, and future randomized control trials on de-escalation of tamoxifen and high-risk patients based on their risk model assessment still need to be done. Future study should also focus on markers to identify candidates best suited for low versus standard dose of tamoxifen,” said Dr. Cornell, who is an assistant professor of medicine at Mayo Clinic Florida in Jacksonville.
At another SABCS session, Per Hall, MD, PhD, discussed findings from the previously published KARISMA-2 study, which examined efficacy of various doses of tamoxifen. A total of 1440 participants, 240 in each arm, received tamoxifen doses of 20 mg, 10 mg, 5 mg, 2.5 mg, 1 mg, or placebo. During his talk, Dr. Hall pointed out that measuring outcomes would take a very large number of participants to identify small differences in breast cancer rates. Therefore, the researchers examined breast density changes as a proxy. As a noninferiority outcome, the researchers used the proportion of women in each arm who achieved the median decrease in breast density seen at 20 mg of tamoxifen, which is 10.1%.
The women underwent mammograms at baseline and again at 6 months to determine change in breast density. Among all women in the study, the proportion of patients who had a similar breast density reduction as the 20-mg dose were very similar in the 10 mg (50.0%; P = .002), 5 mg (49.3%; P < .001), and 2.5 mg (52.5%; P < .001) groups. The 1 mg group had a proportion of 39.5% (P = .138), while the placebo group had 38.9% (P = .161). However, the results were driven by premenopausal women, where the values were 63.3%, 70.7%, 74.4%, and 69.7% in the 20-mg, 10-mg, 5-mg, and 2.5-mg groups, respectively, and 32.9% at 1 mg and 29.7% on placebo. In postmenopausal women, the values were 41.9%, 36.7%, 33.3%, and 41.9% in the 20-mg, 10-mg, 5-mg, and 2.5-mg groups, with values of 44.2% in the 1-mg group and 43.8% in the placebo group.
The median density change was 18.5% in premenopausal women and 4.0% in postmenopausal women.
“We didn’t see anything in the postmenopausal women. The decrease for those on 20 milligrams and those on placebo were exactly the same. Why this is, we still don’t know because we do know that tamoxifen in the adjuvant setting could be used for postmenopausal women. It could be that 6 months is too short of a time [to see a benefit]. We don’t know,” said Dr. Hall, who is a medical epidemiologist and biostatistician at Karolinska Institutet, Stockholm, Sweden.
Severe vasomotor side effects like hot flashes, cold flashes, and night sweats were reduced by about 50% in the lower tamoxifen doses, compared with 20 mg.
Dr. Hall also pointed out that tamoxifen is a prodrug. The CYP2D6 enzyme produces a range of metabolites, with endoxifen having the strongest affinity to the estrogen receptor and being present at the highest plasma concentration. He showed a table of endoxifen plasma levels at various tamoxifen doses in women of various metabolizer status, ranging from poor to ultrafast. Among intermediate, normal, and ultrarapid metabolizers, 5- and 10-mg doses produced plasma endoxifen levels ranging from 2.4 to 6.2 ng/mL, which represents a good therapeutic window. “For intermediate and normal metabolizers, it could be that 5 mg [of tamoxifen] is enough, but I want to underline that we didn’t use breast cancer incidence or recurrence in this study, we used density change, so we should be careful when we use these results,” said Dr. Hall. His group is now conducting the KARISMA Endoxifen trial, which will test endoxifen directly at doses of 1 and 2 mg.
Dr. Cornell has no relevant financial disclosures. Dr. Hall is a member of the scientific advisory board for Atossa Therapeutics.
FROM SABCS 2023
Anti-Rheumatic Drugs Linked to Reduced Thyroid Disease Incidence
TOPLINE:
Patients with rheumatoid arthritis (RA) in a large Swedish population cohort show a reduced incidence of autoimmune thyroid diseases, such as hypothyroidism or hyperthyroidism, after being diagnosed with RA, with the effect being more pronounced among those treated with disease-modifying anti-rheumatic drugs (DMARDs), particularly TNF-inhibitors.
Although DMARDs are commonly used in the treatment of RA, the drugs are rarely used to treat autoimmune thyroid diseases. The new results support theories raised in previous smaller studies that DMARDs could have a protective effect against thyroid disease.
METHODOLOGY:
- The study involved 13,731 patients with new-onset RA who were listed in the Swedish Rheumatology Quality Register between 2006 and 2018.
- The patients were matched for sex, age, and residential area with up to five reference individuals in the general population of 63,201 comparators.
- Overall, patients with RA were 64.7% female, with a mean age of 59. They were followed up with their matched comparators until the development of autoimmune thyroid disease, death, emigration, or the end of the study period, December 2019.
- The relative risks of autoimmune thyroid disease following a diagnosis of RA and with treatment with DMARDs were compared with those risks in the general population.
- Participants with a non-autoimmune cause for thyroxine prescription were excluded, as were those with an autoimmune thyroid disease at the time of RA diagnosis.
TAKEAWAY:
- Following their RA diagnosis, 321 (2.3%) of patients developed an autoimmune thyroid disease, compared with 1838 (2.9%) in the general population comparators, representing an incidence of 3.7 vs 4.6 per 1000 person-years (hazard ratio [HR], 0.81).
- The lower incidence of autoimmune thyroid disease was more pronounced with longer RA duration. For instance, at 10-14 years after an RA diagnosis, the incidence was 2.9 vs. 4.5 autoimmune thyroid disease events per 1000 person-years, respectively (HR, 0.64).
- The decreased risk of incident autoimmune thyroid disease among RA patients compared with the general population was strongest among patients treated with biologic DMARDs (bDMARD), with an HR of 0.54.
- The reduced incidence of autoimmune thyroid disease with bDMARD use was most pronounced among users of TNF-inhibitors (HR, 0.67).
- The lower incidence of autoimmune thyroid disease following a diagnosis of RA contrasts with previous studies showing an increased risk for thyroid disease associated with RA.
- However, the decreased risk of thyroid disease following bDMARD treatment supports the theory that immunomodulatory treatment could also have an effect of blunting the inflammatory processes that can lead to overt clinical autoimmune thyroid disease.
IN PRACTICE:
“To our knowledge, no previous study has investigated whether the risk of new-onset autoimmune thyroid disease is affected by RA treatment in early RA,” the authors report.
“Our results demonstrate that compared to the general population, patients with RA treated with bDMARDs, TNF-inhibitors in particular, are at decreased risk of developing autoimmune thyroid disease, a finding that calls for replication and may open for drug-repurposing studies,” they note.
SOURCE:
The study was conducted by first author Kristin Waldenlind, PhD, of the Department of Medicine, Solna, Division of Clinical Epidemiology, Karolinska Institutet, Stockholm, Sweden, and colleagues. It was published online November 27 in the Journal of Internal Medicine.
LIMITATIONS:
The study lacked details on participants’ thyroid autoantibody and hormone levels.
The presence of autoimmune thyroid disease was determined based on prescriptions for thyroxine, hence the authors cannot exclude the possibility of a lower threshold for thyroxine prescription among patients treated with DMARDs.
Information was not available on potential risk factors for RA and autoimmune thyroid disease that might have introduced confounding, such as smoking or obesity.
DISCLOSURES:
The study received funding from the Swedish Research Council, the Swedish Heart Lung Foundation, Vinnova, and Region Stockholm/Karolinska Institutet (ALF). The authors’ disclosures are detailed in the published study.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with rheumatoid arthritis (RA) in a large Swedish population cohort show a reduced incidence of autoimmune thyroid diseases, such as hypothyroidism or hyperthyroidism, after being diagnosed with RA, with the effect being more pronounced among those treated with disease-modifying anti-rheumatic drugs (DMARDs), particularly TNF-inhibitors.
Although DMARDs are commonly used in the treatment of RA, the drugs are rarely used to treat autoimmune thyroid diseases. The new results support theories raised in previous smaller studies that DMARDs could have a protective effect against thyroid disease.
METHODOLOGY:
- The study involved 13,731 patients with new-onset RA who were listed in the Swedish Rheumatology Quality Register between 2006 and 2018.
- The patients were matched for sex, age, and residential area with up to five reference individuals in the general population of 63,201 comparators.
- Overall, patients with RA were 64.7% female, with a mean age of 59. They were followed up with their matched comparators until the development of autoimmune thyroid disease, death, emigration, or the end of the study period, December 2019.
- The relative risks of autoimmune thyroid disease following a diagnosis of RA and with treatment with DMARDs were compared with those risks in the general population.
- Participants with a non-autoimmune cause for thyroxine prescription were excluded, as were those with an autoimmune thyroid disease at the time of RA diagnosis.
TAKEAWAY:
- Following their RA diagnosis, 321 (2.3%) of patients developed an autoimmune thyroid disease, compared with 1838 (2.9%) in the general population comparators, representing an incidence of 3.7 vs 4.6 per 1000 person-years (hazard ratio [HR], 0.81).
- The lower incidence of autoimmune thyroid disease was more pronounced with longer RA duration. For instance, at 10-14 years after an RA diagnosis, the incidence was 2.9 vs. 4.5 autoimmune thyroid disease events per 1000 person-years, respectively (HR, 0.64).
- The decreased risk of incident autoimmune thyroid disease among RA patients compared with the general population was strongest among patients treated with biologic DMARDs (bDMARD), with an HR of 0.54.
- The reduced incidence of autoimmune thyroid disease with bDMARD use was most pronounced among users of TNF-inhibitors (HR, 0.67).
- The lower incidence of autoimmune thyroid disease following a diagnosis of RA contrasts with previous studies showing an increased risk for thyroid disease associated with RA.
- However, the decreased risk of thyroid disease following bDMARD treatment supports the theory that immunomodulatory treatment could also have an effect of blunting the inflammatory processes that can lead to overt clinical autoimmune thyroid disease.
IN PRACTICE:
“To our knowledge, no previous study has investigated whether the risk of new-onset autoimmune thyroid disease is affected by RA treatment in early RA,” the authors report.
“Our results demonstrate that compared to the general population, patients with RA treated with bDMARDs, TNF-inhibitors in particular, are at decreased risk of developing autoimmune thyroid disease, a finding that calls for replication and may open for drug-repurposing studies,” they note.
SOURCE:
The study was conducted by first author Kristin Waldenlind, PhD, of the Department of Medicine, Solna, Division of Clinical Epidemiology, Karolinska Institutet, Stockholm, Sweden, and colleagues. It was published online November 27 in the Journal of Internal Medicine.
LIMITATIONS:
The study lacked details on participants’ thyroid autoantibody and hormone levels.
The presence of autoimmune thyroid disease was determined based on prescriptions for thyroxine, hence the authors cannot exclude the possibility of a lower threshold for thyroxine prescription among patients treated with DMARDs.
Information was not available on potential risk factors for RA and autoimmune thyroid disease that might have introduced confounding, such as smoking or obesity.
DISCLOSURES:
The study received funding from the Swedish Research Council, the Swedish Heart Lung Foundation, Vinnova, and Region Stockholm/Karolinska Institutet (ALF). The authors’ disclosures are detailed in the published study.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with rheumatoid arthritis (RA) in a large Swedish population cohort show a reduced incidence of autoimmune thyroid diseases, such as hypothyroidism or hyperthyroidism, after being diagnosed with RA, with the effect being more pronounced among those treated with disease-modifying anti-rheumatic drugs (DMARDs), particularly TNF-inhibitors.
Although DMARDs are commonly used in the treatment of RA, the drugs are rarely used to treat autoimmune thyroid diseases. The new results support theories raised in previous smaller studies that DMARDs could have a protective effect against thyroid disease.
METHODOLOGY:
- The study involved 13,731 patients with new-onset RA who were listed in the Swedish Rheumatology Quality Register between 2006 and 2018.
- The patients were matched for sex, age, and residential area with up to five reference individuals in the general population of 63,201 comparators.
- Overall, patients with RA were 64.7% female, with a mean age of 59. They were followed up with their matched comparators until the development of autoimmune thyroid disease, death, emigration, or the end of the study period, December 2019.
- The relative risks of autoimmune thyroid disease following a diagnosis of RA and with treatment with DMARDs were compared with those risks in the general population.
- Participants with a non-autoimmune cause for thyroxine prescription were excluded, as were those with an autoimmune thyroid disease at the time of RA diagnosis.
TAKEAWAY:
- Following their RA diagnosis, 321 (2.3%) of patients developed an autoimmune thyroid disease, compared with 1838 (2.9%) in the general population comparators, representing an incidence of 3.7 vs 4.6 per 1000 person-years (hazard ratio [HR], 0.81).
- The lower incidence of autoimmune thyroid disease was more pronounced with longer RA duration. For instance, at 10-14 years after an RA diagnosis, the incidence was 2.9 vs. 4.5 autoimmune thyroid disease events per 1000 person-years, respectively (HR, 0.64).
- The decreased risk of incident autoimmune thyroid disease among RA patients compared with the general population was strongest among patients treated with biologic DMARDs (bDMARD), with an HR of 0.54.
- The reduced incidence of autoimmune thyroid disease with bDMARD use was most pronounced among users of TNF-inhibitors (HR, 0.67).
- The lower incidence of autoimmune thyroid disease following a diagnosis of RA contrasts with previous studies showing an increased risk for thyroid disease associated with RA.
- However, the decreased risk of thyroid disease following bDMARD treatment supports the theory that immunomodulatory treatment could also have an effect of blunting the inflammatory processes that can lead to overt clinical autoimmune thyroid disease.
IN PRACTICE:
“To our knowledge, no previous study has investigated whether the risk of new-onset autoimmune thyroid disease is affected by RA treatment in early RA,” the authors report.
“Our results demonstrate that compared to the general population, patients with RA treated with bDMARDs, TNF-inhibitors in particular, are at decreased risk of developing autoimmune thyroid disease, a finding that calls for replication and may open for drug-repurposing studies,” they note.
SOURCE:
The study was conducted by first author Kristin Waldenlind, PhD, of the Department of Medicine, Solna, Division of Clinical Epidemiology, Karolinska Institutet, Stockholm, Sweden, and colleagues. It was published online November 27 in the Journal of Internal Medicine.
LIMITATIONS:
The study lacked details on participants’ thyroid autoantibody and hormone levels.
The presence of autoimmune thyroid disease was determined based on prescriptions for thyroxine, hence the authors cannot exclude the possibility of a lower threshold for thyroxine prescription among patients treated with DMARDs.
Information was not available on potential risk factors for RA and autoimmune thyroid disease that might have introduced confounding, such as smoking or obesity.
DISCLOSURES:
The study received funding from the Swedish Research Council, the Swedish Heart Lung Foundation, Vinnova, and Region Stockholm/Karolinska Institutet (ALF). The authors’ disclosures are detailed in the published study.
A version of this article appeared on Medscape.com.
Sotatercept Endorsed for PAH by ICER
In a new report, the Midwest Institute for Clinical and Economic Review’s (ICER) Comparative Effectiveness Public Advisory Council concluded that the Merck drug sotatercept, currently under review by the US Food and Drug Administration (FDA), has a high certainty of at least a small net health benefit to patients with pulmonary arterial hypertension (PAH) when added to background therapy. The limited availability of evidence means that the benefit could range from minimal to substantial, according to the authors.
Sotatercept, administered by injection every 3 weeks, is a first-in-class activin signaling inhibitor. It counters cell proliferation and decreases inflammation in vessel walls, which may lead to improved pulmonary blood flow. The US FDA is considering it for approval through a biologics license application, with a decision expected by March 26, 2024.
There remains a great deal of uncertainty surrounding the long-term benefits of sotatercept. It’s possible that the drug is disease-modifying, but there isn’t yet any proof, according to Greg Curfman, MD, who attended a virtual ICER public meeting on December 1 that summarized the report and accepted public comments. “I’m still wondering the extent to which disease-modifying issue here is more aspirational at this point than really documented,” said Dr. Curfman, who is an associated professor of medicine at Harvard Medical School and executive editor of the Journal of the American Medical Association.
Current PAH treatment consists of vasodilators, including phosphodiesterase-5 inhibitors (PDE5i), guanylate cyclase stimulators, endothelin receptor antagonists (ERA), prostacyclin analogues (prostanoids), and a prostacyclin receptor agonist. The 2022 European Society of Cardiology and the European Respiratory Society clinical practice guideline recommends that low- and intermediate-risk patients should be started on ERA/PDE5i combination therapy, while high-risk patients should also be given an intravenous or subcutaneous prostacyclin analogue, referred to as triple therapy.
Sotatercept’s regulatory approval hinges on the phase 3 STELLAR trial, which included 323 patients with World Health Organization functional class (WHO-FC) II and III PAH who were randomized to 0.75 mg/kg sotatercept in addition to background double or triple therapy, or background therapy alone. The mean age was 48 years, and the mean time since diagnosis was 8.8 years. About 40% received infused prostacyclin therapy at baseline. At 24 weeks, the median change in 6-min walking distance (6mWD) was 40.8 m longer in the sotatercept group. More patients in the sotatercept group experienced WHO-FC improvement (29.4% vs 13.8%). Those in the sotatercept group also experienced an 84% reduction in risk for clinical worsening or death. PAH-specific quality of life scales did not show a difference between the two groups. Open-label extension trials have shown that benefits are maintained for up to 2 years. Adverse events likely related to sotatercept included telangiectasias, increased hemoglobin levels, and bleeding events.
Along with its benefits, the report authors suggest that the subcutaneous delivery of sotatercept may be less burdensome to patients than some other PAH treatments, especially inhaled and intravenous prostanoids. “However, uncertainty remains about sotatercept’s efficacy in sicker populations and in those with connective tissue disease, and about the durability of effect,” the authors wrote.
A lack of long-term data leaves open the question of its effect on mortality and unknown adverse effects.
Using a de novo decision analytic model, the authors estimated that sotatercept treatment would lead to a longer time without symptoms at rest and more quality-adjusted life years, life years, and equal value life years. They determined the health benefit price benchmark for sotatercept to be between $18,700 and $36,200 per year. “The long-term conventional cost-effectiveness of sotatercept is largely dependent on the long-term effect of sotatercept on improving functional class and slowing the worsening in functional class; however, controlled trial evidence for sotatercept is limited to 24 weeks. Long-term data are necessary to reduce the uncertainty in sotatercept’s long-term effect on improving functional class and slowing the worsening in functional class,” the authors wrote.
During the online meeting, Dr. Curfman took note of the fact that the STELLAR trial reported a median value of increase in 6mWD, rather than a mean, and the 40-m improvement is close to the value accepted as clinically meaningful. “So that tells us that half the patients had less than a clinically important improvement in the six-minute walk distance. We should be putting that in perspective,” said Dr. Curfman.
Another attendee pointed out that the open-label PULSAR extension trial showed that the proportion of patients in the sotatercept arm who were functional class I rose from 7.5% at the end of the trial to 20.6% at the end of the open-label period and wondered if that could be a sign of disease-modifying activity. “I think that’s a remarkable piece of data. I don’t recall seeing that in any other open label [trial of a PAH therapy] — that much of an improvement in getting to our best functional status,” said Marc Simon, MD, professor of medicine and director of the Pulmonary Hypertension Center at the University of California, San Francisco, who was a coauthor of the report.
Dr. Curfman has no relevant financial disclosures. Dr. Simon has consulted for Merck.
A version of this article appeared on Medscape.com.
In a new report, the Midwest Institute for Clinical and Economic Review’s (ICER) Comparative Effectiveness Public Advisory Council concluded that the Merck drug sotatercept, currently under review by the US Food and Drug Administration (FDA), has a high certainty of at least a small net health benefit to patients with pulmonary arterial hypertension (PAH) when added to background therapy. The limited availability of evidence means that the benefit could range from minimal to substantial, according to the authors.
Sotatercept, administered by injection every 3 weeks, is a first-in-class activin signaling inhibitor. It counters cell proliferation and decreases inflammation in vessel walls, which may lead to improved pulmonary blood flow. The US FDA is considering it for approval through a biologics license application, with a decision expected by March 26, 2024.
There remains a great deal of uncertainty surrounding the long-term benefits of sotatercept. It’s possible that the drug is disease-modifying, but there isn’t yet any proof, according to Greg Curfman, MD, who attended a virtual ICER public meeting on December 1 that summarized the report and accepted public comments. “I’m still wondering the extent to which disease-modifying issue here is more aspirational at this point than really documented,” said Dr. Curfman, who is an associated professor of medicine at Harvard Medical School and executive editor of the Journal of the American Medical Association.
Current PAH treatment consists of vasodilators, including phosphodiesterase-5 inhibitors (PDE5i), guanylate cyclase stimulators, endothelin receptor antagonists (ERA), prostacyclin analogues (prostanoids), and a prostacyclin receptor agonist. The 2022 European Society of Cardiology and the European Respiratory Society clinical practice guideline recommends that low- and intermediate-risk patients should be started on ERA/PDE5i combination therapy, while high-risk patients should also be given an intravenous or subcutaneous prostacyclin analogue, referred to as triple therapy.
Sotatercept’s regulatory approval hinges on the phase 3 STELLAR trial, which included 323 patients with World Health Organization functional class (WHO-FC) II and III PAH who were randomized to 0.75 mg/kg sotatercept in addition to background double or triple therapy, or background therapy alone. The mean age was 48 years, and the mean time since diagnosis was 8.8 years. About 40% received infused prostacyclin therapy at baseline. At 24 weeks, the median change in 6-min walking distance (6mWD) was 40.8 m longer in the sotatercept group. More patients in the sotatercept group experienced WHO-FC improvement (29.4% vs 13.8%). Those in the sotatercept group also experienced an 84% reduction in risk for clinical worsening or death. PAH-specific quality of life scales did not show a difference between the two groups. Open-label extension trials have shown that benefits are maintained for up to 2 years. Adverse events likely related to sotatercept included telangiectasias, increased hemoglobin levels, and bleeding events.
Along with its benefits, the report authors suggest that the subcutaneous delivery of sotatercept may be less burdensome to patients than some other PAH treatments, especially inhaled and intravenous prostanoids. “However, uncertainty remains about sotatercept’s efficacy in sicker populations and in those with connective tissue disease, and about the durability of effect,” the authors wrote.
A lack of long-term data leaves open the question of its effect on mortality and unknown adverse effects.
Using a de novo decision analytic model, the authors estimated that sotatercept treatment would lead to a longer time without symptoms at rest and more quality-adjusted life years, life years, and equal value life years. They determined the health benefit price benchmark for sotatercept to be between $18,700 and $36,200 per year. “The long-term conventional cost-effectiveness of sotatercept is largely dependent on the long-term effect of sotatercept on improving functional class and slowing the worsening in functional class; however, controlled trial evidence for sotatercept is limited to 24 weeks. Long-term data are necessary to reduce the uncertainty in sotatercept’s long-term effect on improving functional class and slowing the worsening in functional class,” the authors wrote.
During the online meeting, Dr. Curfman took note of the fact that the STELLAR trial reported a median value of increase in 6mWD, rather than a mean, and the 40-m improvement is close to the value accepted as clinically meaningful. “So that tells us that half the patients had less than a clinically important improvement in the six-minute walk distance. We should be putting that in perspective,” said Dr. Curfman.
Another attendee pointed out that the open-label PULSAR extension trial showed that the proportion of patients in the sotatercept arm who were functional class I rose from 7.5% at the end of the trial to 20.6% at the end of the open-label period and wondered if that could be a sign of disease-modifying activity. “I think that’s a remarkable piece of data. I don’t recall seeing that in any other open label [trial of a PAH therapy] — that much of an improvement in getting to our best functional status,” said Marc Simon, MD, professor of medicine and director of the Pulmonary Hypertension Center at the University of California, San Francisco, who was a coauthor of the report.
Dr. Curfman has no relevant financial disclosures. Dr. Simon has consulted for Merck.
A version of this article appeared on Medscape.com.
In a new report, the Midwest Institute for Clinical and Economic Review’s (ICER) Comparative Effectiveness Public Advisory Council concluded that the Merck drug sotatercept, currently under review by the US Food and Drug Administration (FDA), has a high certainty of at least a small net health benefit to patients with pulmonary arterial hypertension (PAH) when added to background therapy. The limited availability of evidence means that the benefit could range from minimal to substantial, according to the authors.
Sotatercept, administered by injection every 3 weeks, is a first-in-class activin signaling inhibitor. It counters cell proliferation and decreases inflammation in vessel walls, which may lead to improved pulmonary blood flow. The US FDA is considering it for approval through a biologics license application, with a decision expected by March 26, 2024.
There remains a great deal of uncertainty surrounding the long-term benefits of sotatercept. It’s possible that the drug is disease-modifying, but there isn’t yet any proof, according to Greg Curfman, MD, who attended a virtual ICER public meeting on December 1 that summarized the report and accepted public comments. “I’m still wondering the extent to which disease-modifying issue here is more aspirational at this point than really documented,” said Dr. Curfman, who is an associated professor of medicine at Harvard Medical School and executive editor of the Journal of the American Medical Association.
Current PAH treatment consists of vasodilators, including phosphodiesterase-5 inhibitors (PDE5i), guanylate cyclase stimulators, endothelin receptor antagonists (ERA), prostacyclin analogues (prostanoids), and a prostacyclin receptor agonist. The 2022 European Society of Cardiology and the European Respiratory Society clinical practice guideline recommends that low- and intermediate-risk patients should be started on ERA/PDE5i combination therapy, while high-risk patients should also be given an intravenous or subcutaneous prostacyclin analogue, referred to as triple therapy.
Sotatercept’s regulatory approval hinges on the phase 3 STELLAR trial, which included 323 patients with World Health Organization functional class (WHO-FC) II and III PAH who were randomized to 0.75 mg/kg sotatercept in addition to background double or triple therapy, or background therapy alone. The mean age was 48 years, and the mean time since diagnosis was 8.8 years. About 40% received infused prostacyclin therapy at baseline. At 24 weeks, the median change in 6-min walking distance (6mWD) was 40.8 m longer in the sotatercept group. More patients in the sotatercept group experienced WHO-FC improvement (29.4% vs 13.8%). Those in the sotatercept group also experienced an 84% reduction in risk for clinical worsening or death. PAH-specific quality of life scales did not show a difference between the two groups. Open-label extension trials have shown that benefits are maintained for up to 2 years. Adverse events likely related to sotatercept included telangiectasias, increased hemoglobin levels, and bleeding events.
Along with its benefits, the report authors suggest that the subcutaneous delivery of sotatercept may be less burdensome to patients than some other PAH treatments, especially inhaled and intravenous prostanoids. “However, uncertainty remains about sotatercept’s efficacy in sicker populations and in those with connective tissue disease, and about the durability of effect,” the authors wrote.
A lack of long-term data leaves open the question of its effect on mortality and unknown adverse effects.
Using a de novo decision analytic model, the authors estimated that sotatercept treatment would lead to a longer time without symptoms at rest and more quality-adjusted life years, life years, and equal value life years. They determined the health benefit price benchmark for sotatercept to be between $18,700 and $36,200 per year. “The long-term conventional cost-effectiveness of sotatercept is largely dependent on the long-term effect of sotatercept on improving functional class and slowing the worsening in functional class; however, controlled trial evidence for sotatercept is limited to 24 weeks. Long-term data are necessary to reduce the uncertainty in sotatercept’s long-term effect on improving functional class and slowing the worsening in functional class,” the authors wrote.
During the online meeting, Dr. Curfman took note of the fact that the STELLAR trial reported a median value of increase in 6mWD, rather than a mean, and the 40-m improvement is close to the value accepted as clinically meaningful. “So that tells us that half the patients had less than a clinically important improvement in the six-minute walk distance. We should be putting that in perspective,” said Dr. Curfman.
Another attendee pointed out that the open-label PULSAR extension trial showed that the proportion of patients in the sotatercept arm who were functional class I rose from 7.5% at the end of the trial to 20.6% at the end of the open-label period and wondered if that could be a sign of disease-modifying activity. “I think that’s a remarkable piece of data. I don’t recall seeing that in any other open label [trial of a PAH therapy] — that much of an improvement in getting to our best functional status,” said Marc Simon, MD, professor of medicine and director of the Pulmonary Hypertension Center at the University of California, San Francisco, who was a coauthor of the report.
Dr. Curfman has no relevant financial disclosures. Dr. Simon has consulted for Merck.
A version of this article appeared on Medscape.com.
Living in a Food Swamp Tied to High Breast Cancer Mortality
SAN ANTONIO — a novel ecological study has found.
“Food deserts and food swamps are both bad, but it’s worse in food swamps,” Malcolm Bevel, PhD, MSPH, with Augusta University in Georgia, said in an interview.
He presented his research at the San Antonio Breast Cancer Symposium.
Breast cancer is the fourth leading cause of cancer death in the United States and is one of 13 obesity-related cancers. Healthy food consumption is a protective factor shown to decrease obesity risk and postmenopausal breast cancer mortality.
However, residing in food deserts or food swamps reduces access to healthy foods and has been severely understudied regarding postmenopausal breast cancer mortality, Dr. Bevel explained.
To investigate, Dr. Bevel and colleagues did a cross-sectional, ecological analysis where they merged 2010 to 2020 postmenopausal breast cancer mortality data from the Centers for Disease Control and Prevention (CDC) with aggregated 2012 to 2020 data from the US Department of Agriculture Food Environment Atlas.
A food swamp score was calculated as the ratio of fast-food and convenience stores to grocery stores and farmer’s markets.
A food desert score was calculated as the proportion of residents living more than 1 mile (urban) or 10 miles (rural) from a grocery store and household income ≤ 200% of the federal poverty threshold.
The researchers categorized food deserts and food swamps as low, moderate, or high, with higher scores denoting counties with fewer resources for healthy food.
Counties with high postmenopausal breast cancer mortality rates had a higher percentage of non-Hispanic Black population (5.8% vs. 2.1%), poverty rates (17.2% vs 14.2%), and adult obesity (32.5% vs 32%) and diabetes rates (11.8% vs 10.5%), compared with counties with low postmenopausal breast cancer mortality rates, Dr. Bevel reported.
The age-adjusted odds of counties having high postmenopausal breast cancer mortality was 53% higher in counties with high food desert scores (adjusted odds ratio [aOR] 1.53; 95% CI, 1.26 - 1.88), and over twofold higher in those with high food swamp scores (aOR, 2.09; 95% CI: 1.69 - 2.58).
In fully adjusted models, the likelihood of counties having moderate postmenopausal breast cancer mortality rates was 32% higher in those with moderate food swamp scores (aOR, 1.32; 95% CI, 1.03 - 1.70).
Growing Epidemic Requires System Change
These findings are in line with another study by Dr. Bevel and his colleagues published earlier this year in JAMA Oncology.
In that study, communities with easy access to fast food were 77% more likely to have high levels of obesity-related cancer mortality, as reported by this news organization.
There is a “growing epidemic” of food deserts and food swamps in the US, which could be due to systemic issues such as gentrification/redlining and lack of investment with chain grocery stores that provide healthy food options, said Dr. Bevel.
Local policymakers and community stakeholders could implement culturally tailored, sustainable interventions for obesity and obesity-related cancer prevention, including postmenopausal breast cancer. These could include creating more walkable neighborhoods and community vegetable gardens, he suggested.
“This is an important study demonstrating how the environment impacts outcomes in postmenopausal women diagnosed with breast cancer,” said Lia Scott, PhD, MPH, discussant for the study.
“Most of the literature is primarily focused on food deserts to characterize the food environment. However, these authors looked at both food deserts and food swamps. And even after adjusting for various factors and age, counties with high food swamp scores at greater odds of having higher postmenopausal breast cancer mortality rates,” said Dr. Scott, who is from Georgia State University School of Public Health in Atlanta.
“There is a clear need for systems change. With ecological studies like this one, we could potentially drive policy by providing actionable data,” she added.
The study had no specific funding. Dr. Bevel and Dr. Scott report no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN ANTONIO — a novel ecological study has found.
“Food deserts and food swamps are both bad, but it’s worse in food swamps,” Malcolm Bevel, PhD, MSPH, with Augusta University in Georgia, said in an interview.
He presented his research at the San Antonio Breast Cancer Symposium.
Breast cancer is the fourth leading cause of cancer death in the United States and is one of 13 obesity-related cancers. Healthy food consumption is a protective factor shown to decrease obesity risk and postmenopausal breast cancer mortality.
However, residing in food deserts or food swamps reduces access to healthy foods and has been severely understudied regarding postmenopausal breast cancer mortality, Dr. Bevel explained.
To investigate, Dr. Bevel and colleagues did a cross-sectional, ecological analysis where they merged 2010 to 2020 postmenopausal breast cancer mortality data from the Centers for Disease Control and Prevention (CDC) with aggregated 2012 to 2020 data from the US Department of Agriculture Food Environment Atlas.
A food swamp score was calculated as the ratio of fast-food and convenience stores to grocery stores and farmer’s markets.
A food desert score was calculated as the proportion of residents living more than 1 mile (urban) or 10 miles (rural) from a grocery store and household income ≤ 200% of the federal poverty threshold.
The researchers categorized food deserts and food swamps as low, moderate, or high, with higher scores denoting counties with fewer resources for healthy food.
Counties with high postmenopausal breast cancer mortality rates had a higher percentage of non-Hispanic Black population (5.8% vs. 2.1%), poverty rates (17.2% vs 14.2%), and adult obesity (32.5% vs 32%) and diabetes rates (11.8% vs 10.5%), compared with counties with low postmenopausal breast cancer mortality rates, Dr. Bevel reported.
The age-adjusted odds of counties having high postmenopausal breast cancer mortality was 53% higher in counties with high food desert scores (adjusted odds ratio [aOR] 1.53; 95% CI, 1.26 - 1.88), and over twofold higher in those with high food swamp scores (aOR, 2.09; 95% CI: 1.69 - 2.58).
In fully adjusted models, the likelihood of counties having moderate postmenopausal breast cancer mortality rates was 32% higher in those with moderate food swamp scores (aOR, 1.32; 95% CI, 1.03 - 1.70).
Growing Epidemic Requires System Change
These findings are in line with another study by Dr. Bevel and his colleagues published earlier this year in JAMA Oncology.
In that study, communities with easy access to fast food were 77% more likely to have high levels of obesity-related cancer mortality, as reported by this news organization.
There is a “growing epidemic” of food deserts and food swamps in the US, which could be due to systemic issues such as gentrification/redlining and lack of investment with chain grocery stores that provide healthy food options, said Dr. Bevel.
Local policymakers and community stakeholders could implement culturally tailored, sustainable interventions for obesity and obesity-related cancer prevention, including postmenopausal breast cancer. These could include creating more walkable neighborhoods and community vegetable gardens, he suggested.
“This is an important study demonstrating how the environment impacts outcomes in postmenopausal women diagnosed with breast cancer,” said Lia Scott, PhD, MPH, discussant for the study.
“Most of the literature is primarily focused on food deserts to characterize the food environment. However, these authors looked at both food deserts and food swamps. And even after adjusting for various factors and age, counties with high food swamp scores at greater odds of having higher postmenopausal breast cancer mortality rates,” said Dr. Scott, who is from Georgia State University School of Public Health in Atlanta.
“There is a clear need for systems change. With ecological studies like this one, we could potentially drive policy by providing actionable data,” she added.
The study had no specific funding. Dr. Bevel and Dr. Scott report no relevant financial relationships.
A version of this article appeared on Medscape.com.
SAN ANTONIO — a novel ecological study has found.
“Food deserts and food swamps are both bad, but it’s worse in food swamps,” Malcolm Bevel, PhD, MSPH, with Augusta University in Georgia, said in an interview.
He presented his research at the San Antonio Breast Cancer Symposium.
Breast cancer is the fourth leading cause of cancer death in the United States and is one of 13 obesity-related cancers. Healthy food consumption is a protective factor shown to decrease obesity risk and postmenopausal breast cancer mortality.
However, residing in food deserts or food swamps reduces access to healthy foods and has been severely understudied regarding postmenopausal breast cancer mortality, Dr. Bevel explained.
To investigate, Dr. Bevel and colleagues did a cross-sectional, ecological analysis where they merged 2010 to 2020 postmenopausal breast cancer mortality data from the Centers for Disease Control and Prevention (CDC) with aggregated 2012 to 2020 data from the US Department of Agriculture Food Environment Atlas.
A food swamp score was calculated as the ratio of fast-food and convenience stores to grocery stores and farmer’s markets.
A food desert score was calculated as the proportion of residents living more than 1 mile (urban) or 10 miles (rural) from a grocery store and household income ≤ 200% of the federal poverty threshold.
The researchers categorized food deserts and food swamps as low, moderate, or high, with higher scores denoting counties with fewer resources for healthy food.
Counties with high postmenopausal breast cancer mortality rates had a higher percentage of non-Hispanic Black population (5.8% vs. 2.1%), poverty rates (17.2% vs 14.2%), and adult obesity (32.5% vs 32%) and diabetes rates (11.8% vs 10.5%), compared with counties with low postmenopausal breast cancer mortality rates, Dr. Bevel reported.
The age-adjusted odds of counties having high postmenopausal breast cancer mortality was 53% higher in counties with high food desert scores (adjusted odds ratio [aOR] 1.53; 95% CI, 1.26 - 1.88), and over twofold higher in those with high food swamp scores (aOR, 2.09; 95% CI: 1.69 - 2.58).
In fully adjusted models, the likelihood of counties having moderate postmenopausal breast cancer mortality rates was 32% higher in those with moderate food swamp scores (aOR, 1.32; 95% CI, 1.03 - 1.70).
Growing Epidemic Requires System Change
These findings are in line with another study by Dr. Bevel and his colleagues published earlier this year in JAMA Oncology.
In that study, communities with easy access to fast food were 77% more likely to have high levels of obesity-related cancer mortality, as reported by this news organization.
There is a “growing epidemic” of food deserts and food swamps in the US, which could be due to systemic issues such as gentrification/redlining and lack of investment with chain grocery stores that provide healthy food options, said Dr. Bevel.
Local policymakers and community stakeholders could implement culturally tailored, sustainable interventions for obesity and obesity-related cancer prevention, including postmenopausal breast cancer. These could include creating more walkable neighborhoods and community vegetable gardens, he suggested.
“This is an important study demonstrating how the environment impacts outcomes in postmenopausal women diagnosed with breast cancer,” said Lia Scott, PhD, MPH, discussant for the study.
“Most of the literature is primarily focused on food deserts to characterize the food environment. However, these authors looked at both food deserts and food swamps. And even after adjusting for various factors and age, counties with high food swamp scores at greater odds of having higher postmenopausal breast cancer mortality rates,” said Dr. Scott, who is from Georgia State University School of Public Health in Atlanta.
“There is a clear need for systems change. With ecological studies like this one, we could potentially drive policy by providing actionable data,” she added.
The study had no specific funding. Dr. Bevel and Dr. Scott report no relevant financial relationships.
A version of this article appeared on Medscape.com.
FROM SABCS 2023
Oncotype Score Helps Avoid Unnecessary Radiation in DCIS
SAN ANTONIO — There’s a long-standing concern among oncologists that many women with ductal carcinoma in situ (DCIS), a potential precursor to invasive breast cancer, receive more treatment than they need. The potential for overtreatment largely revolves around the extent of surgery and the use of radiation.
Using the Oncotype DX Breast DCIS Score test, a laboratory test that estimates DCIS recurrence risk, may help identify patients with low-risk DCIS who can safely avoid adjuvant radiation after surgery, according to new research (abstract GS03-01) presented at the San Antonio Breast Cancer Symposium.
Low-risk patients who skipped adjuvant radiotherapy after breast-conserving surgery demonstrated similar 5-year recurrence rates compared with high-risk patients who received adjuvant radiotherapy.
This is the first prospective study to evaluate radiation decisions among patients with DCIS.
Lead author Seema A. Khan, MD, who presented the research, called the findings “reassuring.”
However, “we need larger and better trials” as well as longer follow-up to confirm this less-is-more approach, said Dr. Khan, a breast cancer surgeon and researcher at Northwestern University, Chicago.
Virginia Kaklamani, MD, who moderated the presentation, noted that it is good to finally have prospective data on this topic. And although they are not definitive, “I personally think these results should be used” for counseling, said Dr. Kaklamani, leader of the breast cancer program at UT Health San Antonio.
To reduce the risk for DCIS recurrence or progression to invasive breast cancer, most patients with DCIS undergo breast-conserving surgery followed by adjuvant radiotherapy, Dr. Khan explained. Instead of breast-conserving surgery, about one in four patients opt for mastectomy.
Earlier results from this trial revealed that MRI helped identify patients who can safely receive breast-conserving surgery instead of mastectomy.
The current results assessed whether the Oncotype DX score can guide radiation treatment decisions.
The study included 171 patients with DCIS who had wide local excisions after MRI confirmed that they could forgo more extensive surgery.
Surgical specimens were then sent for testing to determine the DCIS score using the 12-gene Oncotype DX test.
Women who scored < 39 points on the 100-point Oncotype DX scale were considered to be at low risk for recurrence and were advised to skip radiation. Women who scored > 39 were advised to undergo radiation. Overall, 93% of the patients followed the radiation recommendations: 75 of 82 patients (91.4%) deemed as low risk skipped adjuvant radiotherapy and 84 of 89 patients (94.4%) deemed as high risk had radiotherapy.
At a median follow-up of 5 years, 5.1% (4 of 82) of low-risk patients experienced a recurrence vs. 4.5% (4 of 89) of higher-risk patients.
Recurrence rates among patients who followed the radiation recommendations mirrored these overall findings: 5.5% of 75 patients with low-risk DCIS who skipped radiotherapy experienced disease recurrence vs. 4.8% of 84 patients with high-risk DCIS who received radiotherapy.
Age did not appear to affect the outcomes. Among the 33 women younger than 50 years, two experienced a recurrence (4%), both invasive. One occurred in the low-risk group and the other in the higher-risk group. Among the 138 older women, six had recurrences, three in each group, and one recurrence in each was invasive.
In short, “women who skipped radiation based on this score did not experience an excess risk of” ipsilateral recurrence over 5 years, said Dr. Khan.
Overall, the study offers “strong evidence” that the DCIS score might help “prevent excessive treatment for some patients,” she concluded, adding that 10-year outcomes will be reported.
The work was funded by the National Cancer Institute. Dr. Khan has no conflicts of interest. Dr. Kaklamani has extensive industry ties, including being a speaker for Pfizer, Genentech, Novartis, and AstraZeneca.
A version in the article appeared on Medscape.com.
SAN ANTONIO — There’s a long-standing concern among oncologists that many women with ductal carcinoma in situ (DCIS), a potential precursor to invasive breast cancer, receive more treatment than they need. The potential for overtreatment largely revolves around the extent of surgery and the use of radiation.
Using the Oncotype DX Breast DCIS Score test, a laboratory test that estimates DCIS recurrence risk, may help identify patients with low-risk DCIS who can safely avoid adjuvant radiation after surgery, according to new research (abstract GS03-01) presented at the San Antonio Breast Cancer Symposium.
Low-risk patients who skipped adjuvant radiotherapy after breast-conserving surgery demonstrated similar 5-year recurrence rates compared with high-risk patients who received adjuvant radiotherapy.
This is the first prospective study to evaluate radiation decisions among patients with DCIS.
Lead author Seema A. Khan, MD, who presented the research, called the findings “reassuring.”
However, “we need larger and better trials” as well as longer follow-up to confirm this less-is-more approach, said Dr. Khan, a breast cancer surgeon and researcher at Northwestern University, Chicago.
Virginia Kaklamani, MD, who moderated the presentation, noted that it is good to finally have prospective data on this topic. And although they are not definitive, “I personally think these results should be used” for counseling, said Dr. Kaklamani, leader of the breast cancer program at UT Health San Antonio.
To reduce the risk for DCIS recurrence or progression to invasive breast cancer, most patients with DCIS undergo breast-conserving surgery followed by adjuvant radiotherapy, Dr. Khan explained. Instead of breast-conserving surgery, about one in four patients opt for mastectomy.
Earlier results from this trial revealed that MRI helped identify patients who can safely receive breast-conserving surgery instead of mastectomy.
The current results assessed whether the Oncotype DX score can guide radiation treatment decisions.
The study included 171 patients with DCIS who had wide local excisions after MRI confirmed that they could forgo more extensive surgery.
Surgical specimens were then sent for testing to determine the DCIS score using the 12-gene Oncotype DX test.
Women who scored < 39 points on the 100-point Oncotype DX scale were considered to be at low risk for recurrence and were advised to skip radiation. Women who scored > 39 were advised to undergo radiation. Overall, 93% of the patients followed the radiation recommendations: 75 of 82 patients (91.4%) deemed as low risk skipped adjuvant radiotherapy and 84 of 89 patients (94.4%) deemed as high risk had radiotherapy.
At a median follow-up of 5 years, 5.1% (4 of 82) of low-risk patients experienced a recurrence vs. 4.5% (4 of 89) of higher-risk patients.
Recurrence rates among patients who followed the radiation recommendations mirrored these overall findings: 5.5% of 75 patients with low-risk DCIS who skipped radiotherapy experienced disease recurrence vs. 4.8% of 84 patients with high-risk DCIS who received radiotherapy.
Age did not appear to affect the outcomes. Among the 33 women younger than 50 years, two experienced a recurrence (4%), both invasive. One occurred in the low-risk group and the other in the higher-risk group. Among the 138 older women, six had recurrences, three in each group, and one recurrence in each was invasive.
In short, “women who skipped radiation based on this score did not experience an excess risk of” ipsilateral recurrence over 5 years, said Dr. Khan.
Overall, the study offers “strong evidence” that the DCIS score might help “prevent excessive treatment for some patients,” she concluded, adding that 10-year outcomes will be reported.
The work was funded by the National Cancer Institute. Dr. Khan has no conflicts of interest. Dr. Kaklamani has extensive industry ties, including being a speaker for Pfizer, Genentech, Novartis, and AstraZeneca.
A version in the article appeared on Medscape.com.
SAN ANTONIO — There’s a long-standing concern among oncologists that many women with ductal carcinoma in situ (DCIS), a potential precursor to invasive breast cancer, receive more treatment than they need. The potential for overtreatment largely revolves around the extent of surgery and the use of radiation.
Using the Oncotype DX Breast DCIS Score test, a laboratory test that estimates DCIS recurrence risk, may help identify patients with low-risk DCIS who can safely avoid adjuvant radiation after surgery, according to new research (abstract GS03-01) presented at the San Antonio Breast Cancer Symposium.
Low-risk patients who skipped adjuvant radiotherapy after breast-conserving surgery demonstrated similar 5-year recurrence rates compared with high-risk patients who received adjuvant radiotherapy.
This is the first prospective study to evaluate radiation decisions among patients with DCIS.
Lead author Seema A. Khan, MD, who presented the research, called the findings “reassuring.”
However, “we need larger and better trials” as well as longer follow-up to confirm this less-is-more approach, said Dr. Khan, a breast cancer surgeon and researcher at Northwestern University, Chicago.
Virginia Kaklamani, MD, who moderated the presentation, noted that it is good to finally have prospective data on this topic. And although they are not definitive, “I personally think these results should be used” for counseling, said Dr. Kaklamani, leader of the breast cancer program at UT Health San Antonio.
To reduce the risk for DCIS recurrence or progression to invasive breast cancer, most patients with DCIS undergo breast-conserving surgery followed by adjuvant radiotherapy, Dr. Khan explained. Instead of breast-conserving surgery, about one in four patients opt for mastectomy.
Earlier results from this trial revealed that MRI helped identify patients who can safely receive breast-conserving surgery instead of mastectomy.
The current results assessed whether the Oncotype DX score can guide radiation treatment decisions.
The study included 171 patients with DCIS who had wide local excisions after MRI confirmed that they could forgo more extensive surgery.
Surgical specimens were then sent for testing to determine the DCIS score using the 12-gene Oncotype DX test.
Women who scored < 39 points on the 100-point Oncotype DX scale were considered to be at low risk for recurrence and were advised to skip radiation. Women who scored > 39 were advised to undergo radiation. Overall, 93% of the patients followed the radiation recommendations: 75 of 82 patients (91.4%) deemed as low risk skipped adjuvant radiotherapy and 84 of 89 patients (94.4%) deemed as high risk had radiotherapy.
At a median follow-up of 5 years, 5.1% (4 of 82) of low-risk patients experienced a recurrence vs. 4.5% (4 of 89) of higher-risk patients.
Recurrence rates among patients who followed the radiation recommendations mirrored these overall findings: 5.5% of 75 patients with low-risk DCIS who skipped radiotherapy experienced disease recurrence vs. 4.8% of 84 patients with high-risk DCIS who received radiotherapy.
Age did not appear to affect the outcomes. Among the 33 women younger than 50 years, two experienced a recurrence (4%), both invasive. One occurred in the low-risk group and the other in the higher-risk group. Among the 138 older women, six had recurrences, three in each group, and one recurrence in each was invasive.
In short, “women who skipped radiation based on this score did not experience an excess risk of” ipsilateral recurrence over 5 years, said Dr. Khan.
Overall, the study offers “strong evidence” that the DCIS score might help “prevent excessive treatment for some patients,” she concluded, adding that 10-year outcomes will be reported.
The work was funded by the National Cancer Institute. Dr. Khan has no conflicts of interest. Dr. Kaklamani has extensive industry ties, including being a speaker for Pfizer, Genentech, Novartis, and AstraZeneca.
A version in the article appeared on Medscape.com.
FROM SABCS 2023
2023 Update on minimally invasive gynecologic surgery
It has been an incredible year for complex gynecology and minimally invasive gynecologic surgery (MIGS), with several outstanding new findings and reviews in 2023. The surgical community continues to push the envelope and emphasize the value of this specialty for women’s health.
Endometriosis and adenomyosis were at the center of several large cohort studies and systematic reviews that reassessed what we know about how to evaluate and treat these challenging diseases, including both surgical and nonsurgical approaches, with an emphasis on fertility-sparing modalities.1-8 In addition, a focus on quality of life, patient-centered care, and racial biases allowed us to reflect on our own practice patterns and keep the patient at the center of care models.9-13 Finally, there was a clear expansion in the use of technologies such as artificial intelligence (AI) and machine learning for care and novel minimally invasive tools.14
In this Update, we highlight and expand on how several particularly important developments are likely to make a difference in our clinical management.
New classification system for cesarean scar ectopic pregnancy with defined surgical guidance has 97% treatment success rate
Ban Y, Shen J, Wang X, et al. Cesarean scar ectopic pregnancy clinical classification system with recommended surgical strategy. Obstet Gynecol. 2023;141:927-936. doi:10.1097/AOG.0000000000005113
A large multiarmed study by Ban and colleagues used multivariable modeling to formulate and test a classification system and recommended surgical treatment strategies for patients with a cesarean scar ectopic pregnancy (CSP).15 In the study, 273 patients were included in the predictive modeling group, 118 in the internal validation group, and 564 within the model testing cohort. Classifications were based on 2 independent risk factors for intraoperative hemorrhage: anterior myometrial thickness and mean diameter of gestational sac (MSD).
Classification types
The 3 main CSP types were defined based on the anterior myometrial thickness at the cesarean section scar (type I, > 3 mm; type II, 1–3 mm; type III, ≤ 1 mm) and subtyped based on the MSD (type IIa, MSD ≤ 30 mm; type IIb, MSD > 30 mm; type IIIa, MSD ≤ 50 mm; type IIIb, MSD > 50 mm).
The subgroups were matched with recommended surgical strategy using expert opinion: Type I CSP was treated with suction dilation and aspiration (D&A) under ultrasound guidance, with or without hysteroscopy. Type IIa CSP was treated with suction D&A with hysteroscopy under ultrasound guidance. Type IIb CSP was treated with hysteroscopy with laparoscopic monitoring or excision, or transvaginal excision. Type IIIa CSP was treated with laparoscopic excision or transvaginal excision. Type IIIb CSP was treated with laparoscopic excision after uterine artery embolization or laparotomy (TABLE).15
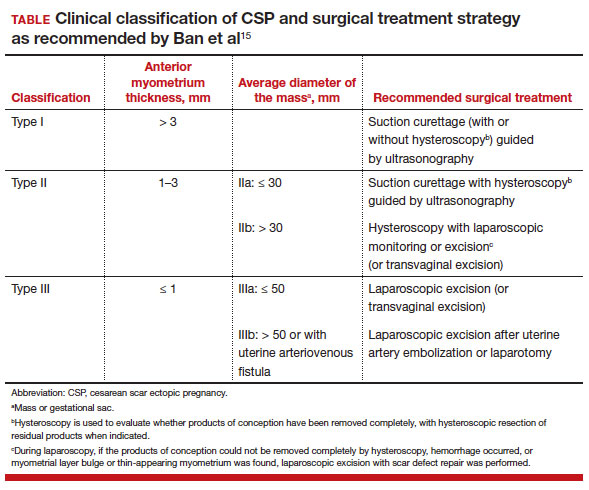
Treatment outcomes
These guidelines were tested on a cohort of 564 patients between 2014 and 2022. Using these treatment guidelines, the overall treatment success rate was 97.5%; 85% of patients had a negative serum ß-human chorionic gonadotropin (ß-hCG) level within 3 weeks, and 95.2% of patients resumed menstrual cycles within 8 weeks. Successful treatment was defined as:
- complete resection of the products of conception
- no need to shift to a second-line surgical strategy
- no major complications
- no readmission for additional treatment
- serum ß-hCG levels that returned to normal within 4 weeks.
Although the incidence of CSP is reported to be around 1:2,000 pregnancies, these rare findings frequently cause a clinical conundrum.16 This thoughtful study by Ban and colleagues provides guidance with the creation of a classification system aimed at decreasing the severe morbidity that can come from mismanagement of these problematic pregnancies using predictive quantitative measures. In our own practice, we have used classification (type 1 endogenic or type 2 exogenic), mean gestational sac diameter, and overlying myometrial thickness when weighing options for treatment. However, decisions have been made on a case-by-case basis and expert opinion without specific cutoffs. Having defined parameters to more accurately classify the type of ectopic pregnancy is essential for communicating risk factors with all team members and for research purposes. The treatment algorithm proposed and tested in this study is logical with good outcomes in the test group. We applaud the authors of this study on a rare but potentially morbid pregnancy outcome. Of note, this study does not discuss nonsurgical alternatives for treatment, such as intra-sac methotrexate injection, which is another option used in select patients at our institution.
Continue to: Pre-op hormonal treatment of endometriosis found to be protective against post-op complications...
Pre-op hormonal treatment of endometriosis found to be protective against post-op complications
Casarin J, Ghezzi F, Mueller M, et al. Surgical outcomes and complications of laparoscopic hysterectomy for endometriosis: a multicentric cohort study. J Minim Invasive Gynecol. 2023;30:587-592. doi:1016/j.jmig.2023.03.018
In a large European multicenter retrospective cohort study, Casarin and colleagues evaluated perioperative complications during laparoscopic hysterectomy for endometriosis or adenomyosis in 995 patients treated from 2010 to 2020.2
Reported intraoperative data included the frequency of ureterolysis (26.8%), deep nodule resection (30%) and posterior adhesiolysis (38.9%), unilateral salpingo-oophorectomy (15.1%), bilateral salpingo-oophorectomy (26.8%), estimated blood loss (mean, 100 mL), and adverse events. Intraoperative complications occurred in 3% of cases (including bladder/bowel injury or need for transfusion).
Postoperative complications occurred in 13.8% of cases, and 9.3% had a major event, including vaginal cuff dehiscence, fever, abscess, and fistula.
Factors associated with postoperative complications
In a multivariate analysis, the authors found that increased operative time, younger age at surgery, previous surgery for endometriosis, and occurrence of intraoperative complications were associated with Clavien-Dindo score grade 2 or greater postoperative complications.
Medical treatment for endometriosis with estro-progestin or progestin medications, however, was found to be protective, with an odds ratio of 0.50 (95% confidence interval, 0.31–0.81).
It is well known that endometriosis is a risk factor for surgical complications. The reported complication rates in this cohort were relatively high, with nearly 10% of patients sustaining a major event postoperatively. While surgical risk is multifactorial and includes factors that are difficult to capture, including surgeon experience and patient population baseline risk, the relatively high incidence reported should be cause for pause and be incorporated in patient counseling. Of note, this cohort did undergo a large number of higher order dissections and a high number of bilateral salpingo-oophorectomies (26.8%), which suggests a high-risk population.
What we found most interesting, however, was the positive finding that medication administration was protective against complications. The authors suggested that the antiinflammatory effects of hormone suppressive medications may be the key. Although this was a retrospective cohort study, the significant risk reduction seen is extremely compelling. A randomized clinical trial corroborating these findings would be instrumental. Endometriosis acts similarly to cancer in its progressive spread and destruction of surrounding tissues. As is increasingly supported in the oncologic literature, perhaps neoadjuvant therapy should be the standard for our “benign” high-risk endometriosis surgeries, with hormonal suppression serving as our chemotherapy. In our own practices, we may be more likely to encourage preoperative medication management, citing this added benefit to patients.
Diaphragmatic endometriosis prevalence higher than previously reported
Pagano F, Schwander A, Vaineau C, et al. True prevalence of diaphragmatic endometriosis and its association with severe endometriosis: a call for awareness and investigation. J Minim Invasive Gynecol. 2023;30:329-334. doi:10.1016/j.jmig.2023.01.006
Pagano and colleagues conducted an impressive large prospective cohort study that included more than 1,300 patients with histologically proven endometriosis.1 Each patient underwent a systematic evaluation and reporting of intraoperative findings, including bilateral evaluation for diaphragmatic endometriosis (DE).
Patients with DE had high rates of infertility and high-stage disease
In this cohort, 4.7% of patients were found to have diaphragmatic disease; 92.3% of these cases had DE involving the right diaphragm. Patients with DE had a higher rate of infertility than those without DE (nearly 50%), but otherwise they had no difference in typical endometriosis symptoms (dysmenorrhea, dyspareunia, dyschezia, dysuria). In this cohort, 27.4% had diaphragmatic symptoms (right shoulder pain, cough, cyclic dyspnea).
Patients found to have DE had higher rates of stage III/IV disease (78.4%), and the left pelvis was affected in more patients (73.8%).
The prevalence of DE in this large cohort evaluated by endometriosis surgeons was far higher than previously reported rates of DE (0.19%–1.5% for abdominal endometriosis cases).17,18 Although admittedly this center cares for a larger portion of women with high-stage disease than many nonspecialty centers do, it still begs the question: Are we as a specialty underdiagnosing diaphragmatic endometriosis, especially in our patients with more severe endometriosis? Because nearly 5% of endometriosis patients could have DE, a thoughtful and systematic approach to the abdominal survey and diaphragm should be performed for each case. Adding questions about diaphragmatic symptoms to our preoperative evaluation may help to identify about one-quarter of these complicated patients preoperatively to aid in counseling and surgical planning. Patients to be specifically mindful about include those with high-stage disease, especially left-sided disease, and those with infertility (although this could be a secondary association given the larger proportion of patients with stage III/IV disease with infertility, and no multivariate analysis was performed). This study serves as a thoughtful reminder of this important subject.
A word on fertility-sparing treatments for adenomyosis
Several interesting and thoughtful studies were published on the fertility-sparing management of adenomyosis.6-8 These included a comparison of fertility outcomes following excisional and nonexcisional therapies,6 a systematic review of the literature that compared recurrence rates following procedural and surgical treatments,8 and outcomes after use of a novel therapy (percutaneous microwave ablation) for the treatment of adenomyosis.7
Although our critical evaluation of these studies found that they are not robust enough to yet change our practice, we want to applaud the authors on their discerning questions and on taking the initial steps to answer critical questions, including:
- What is the best uterine-sparing method for treatment of diffuse adenomyosis?
- Are radiofrequency or microwave ablation procedures the future of adenomyosis care?
- How do we counsel patients about fertility potential following procedural treatments?
- Pagano F, Schwander A, Vaineau C, et al. True prevalence of diaphragmatic endometriosis and its association with severe endometriosis: a call for awareness and investigation. J Minim Invasive Gynecol. 2023;30:329-334. doi:10.1016 /j.jmig.2023.01.006
- Casarin J, Ghezzi F, Mueller M, et al. Surgical outcomes and complications of laparoscopic hysterectomy for endometriosis: a multicentric cohort study. J Minim Invasive Gynecol. 2023;30:587-592. doi:1016/j.jmig.2023.03.018
- Abrao MS, Andres MP, Gingold JA, et al. Preoperative ultrasound scoring of endometriosis by AAGL 2021 endometriosis classification is concordant with laparoscopic surgical findings and distinguishes early from advanced stages. J Minim Invasive Gynecol. 2023;30:363-373. doi:10.1016 /j.jmig.2022.11.003
- Meyer R, Siedhoff M, Truong M, et al. Risk factors for major complications following minimally invasive surgeries for endometriosis in the United States. J Minim Invasive Gynecol. 2023;30:820-826. doi:10.1016/j.jmig.2023.06.002
- Davenport S, Smith D, Green DJ. Barriers to a timely diagnosis of endometriosis. Obstet Gynecol. 2023;142:571-583. doi:10.1097/AOG.0000000000005255
- Jiang L, Han Y, Song Z, et al. Pregnancy outcomes after uterus-sparing operative treatment for adenomyosis: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2023:30:543-554. doi:10.1016/j.jmig.2023.03.015
- Li S, Li Z, Lin M, et al. Efficacy of transabdominal ultrasoundguided percutaneous microwave ablation in the treatment of symptomatic adenomyosis: a retrospective cohort study. J Minim Invasive Gynecol. 2023;30:137-146. doi:10.1016/j.jmig.2022.11.004
- Liu L, Tian H, Lin D, et al. Risk of recurrence and reintervention after uterine-sparing interventions for symptomatic adenomyosis: a systematic review and metaanalysis. Obstet Gynecol. 2023;141:711-723. doi:10.1097 /AOG.0000000000005080
- Chang OH, Tewari S, Yao M, et al. Who places high value on the uterus? A cross-sectional survey study evaluating predictors for uterine preservation. J Minim Invasive Gynecol. 2023;30:131-136. doi:10.1016/j.jmig.2022.10.012
- Carey ET, Moore KJ, McClurg AB, et al. Racial disparities in hysterectomy route for benign disease: examining trends and perioperative complications from 2007 to 2018 using the NSQIP database. J Minim Invasive Gynecol. 2023;30:627-634. doi:10.1016/j.jmig.2023.03.024
- Frisch EH, Mitchell J, Yao M, et al. The impact of fertility goals on long-term quality of life in reproductive-aged women who underwent myomectomy versus hysterectomy for uterine fibroids. J Minim Invasive Gynecol. 2023;30:642-651. doi:10.1016/j.jmig.2023.04.003 1
- Robinson WR, Mathias JG, Wood ME, et al. Ethnoracial differences in premenopausal hysterectomy: the role of symptom severity. Obstet Gynecol. 2023;142:350-359. doi:10.1097 /AOG.0000000000005225
- Harris HR, Peres LC, Johnson CE, et al. Racial differences in the association of endometriosis and uterine leiomyomas with the risk of ovarian cancer. Obstet Gynecol. 2023;141:11241138. doi:10.1097/AOG.0000000000005191
- Atia O, Hazan E, Rotem R, et al. A scoring system developed by a machine learning algorithm to better predict adnexal torsion. J Minim Invasive Gynecol. 2023;30:486-493. doi:10.1016/j.jmig.2023.02.008
- Ban Y, Shen J, Wang X, et al. Cesarean scar ectopic pregnancy clinical classification system with recommended surgical strategy. Obstet Gynecol. 2023;141:927-936. doi:10.1097 /AOG.0000000000005113
- Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies. Obstet Gynecol. 2006;107:1373-1381. doi:10.1097/01.AOG.0000218690.24494.ce
- Scioscia M, Bruni F, Ceccaroni M, et al. Distribution of endometriotic lesions in endometriosis stage IV supports the menstrual reflux theory and requires specific preoperative assessment and therapy. Acta Obstet Gynecol Scand. 2011;90:136-139. doi:10.1111/j.1600-0412.2010.01008.x
- Wetzel A, Philip C-A, Golfier F, et al. Surgical management of diaphragmatic and thoracic endometriosis: a French multicentric descriptive study. J Gynecol Obstet Hum Reprod. 2021;50:102147. doi:10.1016/j.jogoh.2021.102147
It has been an incredible year for complex gynecology and minimally invasive gynecologic surgery (MIGS), with several outstanding new findings and reviews in 2023. The surgical community continues to push the envelope and emphasize the value of this specialty for women’s health.
Endometriosis and adenomyosis were at the center of several large cohort studies and systematic reviews that reassessed what we know about how to evaluate and treat these challenging diseases, including both surgical and nonsurgical approaches, with an emphasis on fertility-sparing modalities.1-8 In addition, a focus on quality of life, patient-centered care, and racial biases allowed us to reflect on our own practice patterns and keep the patient at the center of care models.9-13 Finally, there was a clear expansion in the use of technologies such as artificial intelligence (AI) and machine learning for care and novel minimally invasive tools.14
In this Update, we highlight and expand on how several particularly important developments are likely to make a difference in our clinical management.
New classification system for cesarean scar ectopic pregnancy with defined surgical guidance has 97% treatment success rate
Ban Y, Shen J, Wang X, et al. Cesarean scar ectopic pregnancy clinical classification system with recommended surgical strategy. Obstet Gynecol. 2023;141:927-936. doi:10.1097/AOG.0000000000005113
A large multiarmed study by Ban and colleagues used multivariable modeling to formulate and test a classification system and recommended surgical treatment strategies for patients with a cesarean scar ectopic pregnancy (CSP).15 In the study, 273 patients were included in the predictive modeling group, 118 in the internal validation group, and 564 within the model testing cohort. Classifications were based on 2 independent risk factors for intraoperative hemorrhage: anterior myometrial thickness and mean diameter of gestational sac (MSD).
Classification types
The 3 main CSP types were defined based on the anterior myometrial thickness at the cesarean section scar (type I, > 3 mm; type II, 1–3 mm; type III, ≤ 1 mm) and subtyped based on the MSD (type IIa, MSD ≤ 30 mm; type IIb, MSD > 30 mm; type IIIa, MSD ≤ 50 mm; type IIIb, MSD > 50 mm).
The subgroups were matched with recommended surgical strategy using expert opinion: Type I CSP was treated with suction dilation and aspiration (D&A) under ultrasound guidance, with or without hysteroscopy. Type IIa CSP was treated with suction D&A with hysteroscopy under ultrasound guidance. Type IIb CSP was treated with hysteroscopy with laparoscopic monitoring or excision, or transvaginal excision. Type IIIa CSP was treated with laparoscopic excision or transvaginal excision. Type IIIb CSP was treated with laparoscopic excision after uterine artery embolization or laparotomy (TABLE).15
Treatment outcomes
These guidelines were tested on a cohort of 564 patients between 2014 and 2022. Using these treatment guidelines, the overall treatment success rate was 97.5%; 85% of patients had a negative serum ß-human chorionic gonadotropin (ß-hCG) level within 3 weeks, and 95.2% of patients resumed menstrual cycles within 8 weeks. Successful treatment was defined as:
- complete resection of the products of conception
- no need to shift to a second-line surgical strategy
- no major complications
- no readmission for additional treatment
- serum ß-hCG levels that returned to normal within 4 weeks.
Although the incidence of CSP is reported to be around 1:2,000 pregnancies, these rare findings frequently cause a clinical conundrum.16 This thoughtful study by Ban and colleagues provides guidance with the creation of a classification system aimed at decreasing the severe morbidity that can come from mismanagement of these problematic pregnancies using predictive quantitative measures. In our own practice, we have used classification (type 1 endogenic or type 2 exogenic), mean gestational sac diameter, and overlying myometrial thickness when weighing options for treatment. However, decisions have been made on a case-by-case basis and expert opinion without specific cutoffs. Having defined parameters to more accurately classify the type of ectopic pregnancy is essential for communicating risk factors with all team members and for research purposes. The treatment algorithm proposed and tested in this study is logical with good outcomes in the test group. We applaud the authors of this study on a rare but potentially morbid pregnancy outcome. Of note, this study does not discuss nonsurgical alternatives for treatment, such as intra-sac methotrexate injection, which is another option used in select patients at our institution.
Continue to: Pre-op hormonal treatment of endometriosis found to be protective against post-op complications...
Pre-op hormonal treatment of endometriosis found to be protective against post-op complications
Casarin J, Ghezzi F, Mueller M, et al. Surgical outcomes and complications of laparoscopic hysterectomy for endometriosis: a multicentric cohort study. J Minim Invasive Gynecol. 2023;30:587-592. doi:1016/j.jmig.2023.03.018
In a large European multicenter retrospective cohort study, Casarin and colleagues evaluated perioperative complications during laparoscopic hysterectomy for endometriosis or adenomyosis in 995 patients treated from 2010 to 2020.2
Reported intraoperative data included the frequency of ureterolysis (26.8%), deep nodule resection (30%) and posterior adhesiolysis (38.9%), unilateral salpingo-oophorectomy (15.1%), bilateral salpingo-oophorectomy (26.8%), estimated blood loss (mean, 100 mL), and adverse events. Intraoperative complications occurred in 3% of cases (including bladder/bowel injury or need for transfusion).
Postoperative complications occurred in 13.8% of cases, and 9.3% had a major event, including vaginal cuff dehiscence, fever, abscess, and fistula.
Factors associated with postoperative complications
In a multivariate analysis, the authors found that increased operative time, younger age at surgery, previous surgery for endometriosis, and occurrence of intraoperative complications were associated with Clavien-Dindo score grade 2 or greater postoperative complications.
Medical treatment for endometriosis with estro-progestin or progestin medications, however, was found to be protective, with an odds ratio of 0.50 (95% confidence interval, 0.31–0.81).
It is well known that endometriosis is a risk factor for surgical complications. The reported complication rates in this cohort were relatively high, with nearly 10% of patients sustaining a major event postoperatively. While surgical risk is multifactorial and includes factors that are difficult to capture, including surgeon experience and patient population baseline risk, the relatively high incidence reported should be cause for pause and be incorporated in patient counseling. Of note, this cohort did undergo a large number of higher order dissections and a high number of bilateral salpingo-oophorectomies (26.8%), which suggests a high-risk population.
What we found most interesting, however, was the positive finding that medication administration was protective against complications. The authors suggested that the antiinflammatory effects of hormone suppressive medications may be the key. Although this was a retrospective cohort study, the significant risk reduction seen is extremely compelling. A randomized clinical trial corroborating these findings would be instrumental. Endometriosis acts similarly to cancer in its progressive spread and destruction of surrounding tissues. As is increasingly supported in the oncologic literature, perhaps neoadjuvant therapy should be the standard for our “benign” high-risk endometriosis surgeries, with hormonal suppression serving as our chemotherapy. In our own practices, we may be more likely to encourage preoperative medication management, citing this added benefit to patients.
Diaphragmatic endometriosis prevalence higher than previously reported
Pagano F, Schwander A, Vaineau C, et al. True prevalence of diaphragmatic endometriosis and its association with severe endometriosis: a call for awareness and investigation. J Minim Invasive Gynecol. 2023;30:329-334. doi:10.1016/j.jmig.2023.01.006
Pagano and colleagues conducted an impressive large prospective cohort study that included more than 1,300 patients with histologically proven endometriosis.1 Each patient underwent a systematic evaluation and reporting of intraoperative findings, including bilateral evaluation for diaphragmatic endometriosis (DE).
Patients with DE had high rates of infertility and high-stage disease
In this cohort, 4.7% of patients were found to have diaphragmatic disease; 92.3% of these cases had DE involving the right diaphragm. Patients with DE had a higher rate of infertility than those without DE (nearly 50%), but otherwise they had no difference in typical endometriosis symptoms (dysmenorrhea, dyspareunia, dyschezia, dysuria). In this cohort, 27.4% had diaphragmatic symptoms (right shoulder pain, cough, cyclic dyspnea).
Patients found to have DE had higher rates of stage III/IV disease (78.4%), and the left pelvis was affected in more patients (73.8%).
The prevalence of DE in this large cohort evaluated by endometriosis surgeons was far higher than previously reported rates of DE (0.19%–1.5% for abdominal endometriosis cases).17,18 Although admittedly this center cares for a larger portion of women with high-stage disease than many nonspecialty centers do, it still begs the question: Are we as a specialty underdiagnosing diaphragmatic endometriosis, especially in our patients with more severe endometriosis? Because nearly 5% of endometriosis patients could have DE, a thoughtful and systematic approach to the abdominal survey and diaphragm should be performed for each case. Adding questions about diaphragmatic symptoms to our preoperative evaluation may help to identify about one-quarter of these complicated patients preoperatively to aid in counseling and surgical planning. Patients to be specifically mindful about include those with high-stage disease, especially left-sided disease, and those with infertility (although this could be a secondary association given the larger proportion of patients with stage III/IV disease with infertility, and no multivariate analysis was performed). This study serves as a thoughtful reminder of this important subject.
A word on fertility-sparing treatments for adenomyosis
Several interesting and thoughtful studies were published on the fertility-sparing management of adenomyosis.6-8 These included a comparison of fertility outcomes following excisional and nonexcisional therapies,6 a systematic review of the literature that compared recurrence rates following procedural and surgical treatments,8 and outcomes after use of a novel therapy (percutaneous microwave ablation) for the treatment of adenomyosis.7
Although our critical evaluation of these studies found that they are not robust enough to yet change our practice, we want to applaud the authors on their discerning questions and on taking the initial steps to answer critical questions, including:
- What is the best uterine-sparing method for treatment of diffuse adenomyosis?
- Are radiofrequency or microwave ablation procedures the future of adenomyosis care?
- How do we counsel patients about fertility potential following procedural treatments?
It has been an incredible year for complex gynecology and minimally invasive gynecologic surgery (MIGS), with several outstanding new findings and reviews in 2023. The surgical community continues to push the envelope and emphasize the value of this specialty for women’s health.
Endometriosis and adenomyosis were at the center of several large cohort studies and systematic reviews that reassessed what we know about how to evaluate and treat these challenging diseases, including both surgical and nonsurgical approaches, with an emphasis on fertility-sparing modalities.1-8 In addition, a focus on quality of life, patient-centered care, and racial biases allowed us to reflect on our own practice patterns and keep the patient at the center of care models.9-13 Finally, there was a clear expansion in the use of technologies such as artificial intelligence (AI) and machine learning for care and novel minimally invasive tools.14
In this Update, we highlight and expand on how several particularly important developments are likely to make a difference in our clinical management.
New classification system for cesarean scar ectopic pregnancy with defined surgical guidance has 97% treatment success rate
Ban Y, Shen J, Wang X, et al. Cesarean scar ectopic pregnancy clinical classification system with recommended surgical strategy. Obstet Gynecol. 2023;141:927-936. doi:10.1097/AOG.0000000000005113
A large multiarmed study by Ban and colleagues used multivariable modeling to formulate and test a classification system and recommended surgical treatment strategies for patients with a cesarean scar ectopic pregnancy (CSP).15 In the study, 273 patients were included in the predictive modeling group, 118 in the internal validation group, and 564 within the model testing cohort. Classifications were based on 2 independent risk factors for intraoperative hemorrhage: anterior myometrial thickness and mean diameter of gestational sac (MSD).
Classification types
The 3 main CSP types were defined based on the anterior myometrial thickness at the cesarean section scar (type I, > 3 mm; type II, 1–3 mm; type III, ≤ 1 mm) and subtyped based on the MSD (type IIa, MSD ≤ 30 mm; type IIb, MSD > 30 mm; type IIIa, MSD ≤ 50 mm; type IIIb, MSD > 50 mm).
The subgroups were matched with recommended surgical strategy using expert opinion: Type I CSP was treated with suction dilation and aspiration (D&A) under ultrasound guidance, with or without hysteroscopy. Type IIa CSP was treated with suction D&A with hysteroscopy under ultrasound guidance. Type IIb CSP was treated with hysteroscopy with laparoscopic monitoring or excision, or transvaginal excision. Type IIIa CSP was treated with laparoscopic excision or transvaginal excision. Type IIIb CSP was treated with laparoscopic excision after uterine artery embolization or laparotomy (TABLE).15
Treatment outcomes
These guidelines were tested on a cohort of 564 patients between 2014 and 2022. Using these treatment guidelines, the overall treatment success rate was 97.5%; 85% of patients had a negative serum ß-human chorionic gonadotropin (ß-hCG) level within 3 weeks, and 95.2% of patients resumed menstrual cycles within 8 weeks. Successful treatment was defined as:
- complete resection of the products of conception
- no need to shift to a second-line surgical strategy
- no major complications
- no readmission for additional treatment
- serum ß-hCG levels that returned to normal within 4 weeks.
Although the incidence of CSP is reported to be around 1:2,000 pregnancies, these rare findings frequently cause a clinical conundrum.16 This thoughtful study by Ban and colleagues provides guidance with the creation of a classification system aimed at decreasing the severe morbidity that can come from mismanagement of these problematic pregnancies using predictive quantitative measures. In our own practice, we have used classification (type 1 endogenic or type 2 exogenic), mean gestational sac diameter, and overlying myometrial thickness when weighing options for treatment. However, decisions have been made on a case-by-case basis and expert opinion without specific cutoffs. Having defined parameters to more accurately classify the type of ectopic pregnancy is essential for communicating risk factors with all team members and for research purposes. The treatment algorithm proposed and tested in this study is logical with good outcomes in the test group. We applaud the authors of this study on a rare but potentially morbid pregnancy outcome. Of note, this study does not discuss nonsurgical alternatives for treatment, such as intra-sac methotrexate injection, which is another option used in select patients at our institution.
Continue to: Pre-op hormonal treatment of endometriosis found to be protective against post-op complications...
Pre-op hormonal treatment of endometriosis found to be protective against post-op complications
Casarin J, Ghezzi F, Mueller M, et al. Surgical outcomes and complications of laparoscopic hysterectomy for endometriosis: a multicentric cohort study. J Minim Invasive Gynecol. 2023;30:587-592. doi:1016/j.jmig.2023.03.018
In a large European multicenter retrospective cohort study, Casarin and colleagues evaluated perioperative complications during laparoscopic hysterectomy for endometriosis or adenomyosis in 995 patients treated from 2010 to 2020.2
Reported intraoperative data included the frequency of ureterolysis (26.8%), deep nodule resection (30%) and posterior adhesiolysis (38.9%), unilateral salpingo-oophorectomy (15.1%), bilateral salpingo-oophorectomy (26.8%), estimated blood loss (mean, 100 mL), and adverse events. Intraoperative complications occurred in 3% of cases (including bladder/bowel injury or need for transfusion).
Postoperative complications occurred in 13.8% of cases, and 9.3% had a major event, including vaginal cuff dehiscence, fever, abscess, and fistula.
Factors associated with postoperative complications
In a multivariate analysis, the authors found that increased operative time, younger age at surgery, previous surgery for endometriosis, and occurrence of intraoperative complications were associated with Clavien-Dindo score grade 2 or greater postoperative complications.
Medical treatment for endometriosis with estro-progestin or progestin medications, however, was found to be protective, with an odds ratio of 0.50 (95% confidence interval, 0.31–0.81).
It is well known that endometriosis is a risk factor for surgical complications. The reported complication rates in this cohort were relatively high, with nearly 10% of patients sustaining a major event postoperatively. While surgical risk is multifactorial and includes factors that are difficult to capture, including surgeon experience and patient population baseline risk, the relatively high incidence reported should be cause for pause and be incorporated in patient counseling. Of note, this cohort did undergo a large number of higher order dissections and a high number of bilateral salpingo-oophorectomies (26.8%), which suggests a high-risk population.
What we found most interesting, however, was the positive finding that medication administration was protective against complications. The authors suggested that the antiinflammatory effects of hormone suppressive medications may be the key. Although this was a retrospective cohort study, the significant risk reduction seen is extremely compelling. A randomized clinical trial corroborating these findings would be instrumental. Endometriosis acts similarly to cancer in its progressive spread and destruction of surrounding tissues. As is increasingly supported in the oncologic literature, perhaps neoadjuvant therapy should be the standard for our “benign” high-risk endometriosis surgeries, with hormonal suppression serving as our chemotherapy. In our own practices, we may be more likely to encourage preoperative medication management, citing this added benefit to patients.
Diaphragmatic endometriosis prevalence higher than previously reported
Pagano F, Schwander A, Vaineau C, et al. True prevalence of diaphragmatic endometriosis and its association with severe endometriosis: a call for awareness and investigation. J Minim Invasive Gynecol. 2023;30:329-334. doi:10.1016/j.jmig.2023.01.006
Pagano and colleagues conducted an impressive large prospective cohort study that included more than 1,300 patients with histologically proven endometriosis.1 Each patient underwent a systematic evaluation and reporting of intraoperative findings, including bilateral evaluation for diaphragmatic endometriosis (DE).
Patients with DE had high rates of infertility and high-stage disease
In this cohort, 4.7% of patients were found to have diaphragmatic disease; 92.3% of these cases had DE involving the right diaphragm. Patients with DE had a higher rate of infertility than those without DE (nearly 50%), but otherwise they had no difference in typical endometriosis symptoms (dysmenorrhea, dyspareunia, dyschezia, dysuria). In this cohort, 27.4% had diaphragmatic symptoms (right shoulder pain, cough, cyclic dyspnea).
Patients found to have DE had higher rates of stage III/IV disease (78.4%), and the left pelvis was affected in more patients (73.8%).
The prevalence of DE in this large cohort evaluated by endometriosis surgeons was far higher than previously reported rates of DE (0.19%–1.5% for abdominal endometriosis cases).17,18 Although admittedly this center cares for a larger portion of women with high-stage disease than many nonspecialty centers do, it still begs the question: Are we as a specialty underdiagnosing diaphragmatic endometriosis, especially in our patients with more severe endometriosis? Because nearly 5% of endometriosis patients could have DE, a thoughtful and systematic approach to the abdominal survey and diaphragm should be performed for each case. Adding questions about diaphragmatic symptoms to our preoperative evaluation may help to identify about one-quarter of these complicated patients preoperatively to aid in counseling and surgical planning. Patients to be specifically mindful about include those with high-stage disease, especially left-sided disease, and those with infertility (although this could be a secondary association given the larger proportion of patients with stage III/IV disease with infertility, and no multivariate analysis was performed). This study serves as a thoughtful reminder of this important subject.
A word on fertility-sparing treatments for adenomyosis
Several interesting and thoughtful studies were published on the fertility-sparing management of adenomyosis.6-8 These included a comparison of fertility outcomes following excisional and nonexcisional therapies,6 a systematic review of the literature that compared recurrence rates following procedural and surgical treatments,8 and outcomes after use of a novel therapy (percutaneous microwave ablation) for the treatment of adenomyosis.7
Although our critical evaluation of these studies found that they are not robust enough to yet change our practice, we want to applaud the authors on their discerning questions and on taking the initial steps to answer critical questions, including:
- What is the best uterine-sparing method for treatment of diffuse adenomyosis?
- Are radiofrequency or microwave ablation procedures the future of adenomyosis care?
- How do we counsel patients about fertility potential following procedural treatments?
- Pagano F, Schwander A, Vaineau C, et al. True prevalence of diaphragmatic endometriosis and its association with severe endometriosis: a call for awareness and investigation. J Minim Invasive Gynecol. 2023;30:329-334. doi:10.1016 /j.jmig.2023.01.006
- Casarin J, Ghezzi F, Mueller M, et al. Surgical outcomes and complications of laparoscopic hysterectomy for endometriosis: a multicentric cohort study. J Minim Invasive Gynecol. 2023;30:587-592. doi:1016/j.jmig.2023.03.018
- Abrao MS, Andres MP, Gingold JA, et al. Preoperative ultrasound scoring of endometriosis by AAGL 2021 endometriosis classification is concordant with laparoscopic surgical findings and distinguishes early from advanced stages. J Minim Invasive Gynecol. 2023;30:363-373. doi:10.1016 /j.jmig.2022.11.003
- Meyer R, Siedhoff M, Truong M, et al. Risk factors for major complications following minimally invasive surgeries for endometriosis in the United States. J Minim Invasive Gynecol. 2023;30:820-826. doi:10.1016/j.jmig.2023.06.002
- Davenport S, Smith D, Green DJ. Barriers to a timely diagnosis of endometriosis. Obstet Gynecol. 2023;142:571-583. doi:10.1097/AOG.0000000000005255
- Jiang L, Han Y, Song Z, et al. Pregnancy outcomes after uterus-sparing operative treatment for adenomyosis: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2023:30:543-554. doi:10.1016/j.jmig.2023.03.015
- Li S, Li Z, Lin M, et al. Efficacy of transabdominal ultrasoundguided percutaneous microwave ablation in the treatment of symptomatic adenomyosis: a retrospective cohort study. J Minim Invasive Gynecol. 2023;30:137-146. doi:10.1016/j.jmig.2022.11.004
- Liu L, Tian H, Lin D, et al. Risk of recurrence and reintervention after uterine-sparing interventions for symptomatic adenomyosis: a systematic review and metaanalysis. Obstet Gynecol. 2023;141:711-723. doi:10.1097 /AOG.0000000000005080
- Chang OH, Tewari S, Yao M, et al. Who places high value on the uterus? A cross-sectional survey study evaluating predictors for uterine preservation. J Minim Invasive Gynecol. 2023;30:131-136. doi:10.1016/j.jmig.2022.10.012
- Carey ET, Moore KJ, McClurg AB, et al. Racial disparities in hysterectomy route for benign disease: examining trends and perioperative complications from 2007 to 2018 using the NSQIP database. J Minim Invasive Gynecol. 2023;30:627-634. doi:10.1016/j.jmig.2023.03.024
- Frisch EH, Mitchell J, Yao M, et al. The impact of fertility goals on long-term quality of life in reproductive-aged women who underwent myomectomy versus hysterectomy for uterine fibroids. J Minim Invasive Gynecol. 2023;30:642-651. doi:10.1016/j.jmig.2023.04.003 1
- Robinson WR, Mathias JG, Wood ME, et al. Ethnoracial differences in premenopausal hysterectomy: the role of symptom severity. Obstet Gynecol. 2023;142:350-359. doi:10.1097 /AOG.0000000000005225
- Harris HR, Peres LC, Johnson CE, et al. Racial differences in the association of endometriosis and uterine leiomyomas with the risk of ovarian cancer. Obstet Gynecol. 2023;141:11241138. doi:10.1097/AOG.0000000000005191
- Atia O, Hazan E, Rotem R, et al. A scoring system developed by a machine learning algorithm to better predict adnexal torsion. J Minim Invasive Gynecol. 2023;30:486-493. doi:10.1016/j.jmig.2023.02.008
- Ban Y, Shen J, Wang X, et al. Cesarean scar ectopic pregnancy clinical classification system with recommended surgical strategy. Obstet Gynecol. 2023;141:927-936. doi:10.1097 /AOG.0000000000005113
- Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies. Obstet Gynecol. 2006;107:1373-1381. doi:10.1097/01.AOG.0000218690.24494.ce
- Scioscia M, Bruni F, Ceccaroni M, et al. Distribution of endometriotic lesions in endometriosis stage IV supports the menstrual reflux theory and requires specific preoperative assessment and therapy. Acta Obstet Gynecol Scand. 2011;90:136-139. doi:10.1111/j.1600-0412.2010.01008.x
- Wetzel A, Philip C-A, Golfier F, et al. Surgical management of diaphragmatic and thoracic endometriosis: a French multicentric descriptive study. J Gynecol Obstet Hum Reprod. 2021;50:102147. doi:10.1016/j.jogoh.2021.102147
- Pagano F, Schwander A, Vaineau C, et al. True prevalence of diaphragmatic endometriosis and its association with severe endometriosis: a call for awareness and investigation. J Minim Invasive Gynecol. 2023;30:329-334. doi:10.1016 /j.jmig.2023.01.006
- Casarin J, Ghezzi F, Mueller M, et al. Surgical outcomes and complications of laparoscopic hysterectomy for endometriosis: a multicentric cohort study. J Minim Invasive Gynecol. 2023;30:587-592. doi:1016/j.jmig.2023.03.018
- Abrao MS, Andres MP, Gingold JA, et al. Preoperative ultrasound scoring of endometriosis by AAGL 2021 endometriosis classification is concordant with laparoscopic surgical findings and distinguishes early from advanced stages. J Minim Invasive Gynecol. 2023;30:363-373. doi:10.1016 /j.jmig.2022.11.003
- Meyer R, Siedhoff M, Truong M, et al. Risk factors for major complications following minimally invasive surgeries for endometriosis in the United States. J Minim Invasive Gynecol. 2023;30:820-826. doi:10.1016/j.jmig.2023.06.002
- Davenport S, Smith D, Green DJ. Barriers to a timely diagnosis of endometriosis. Obstet Gynecol. 2023;142:571-583. doi:10.1097/AOG.0000000000005255
- Jiang L, Han Y, Song Z, et al. Pregnancy outcomes after uterus-sparing operative treatment for adenomyosis: a systematic review and meta-analysis. J Minim Invasive Gynecol. 2023:30:543-554. doi:10.1016/j.jmig.2023.03.015
- Li S, Li Z, Lin M, et al. Efficacy of transabdominal ultrasoundguided percutaneous microwave ablation in the treatment of symptomatic adenomyosis: a retrospective cohort study. J Minim Invasive Gynecol. 2023;30:137-146. doi:10.1016/j.jmig.2022.11.004
- Liu L, Tian H, Lin D, et al. Risk of recurrence and reintervention after uterine-sparing interventions for symptomatic adenomyosis: a systematic review and metaanalysis. Obstet Gynecol. 2023;141:711-723. doi:10.1097 /AOG.0000000000005080
- Chang OH, Tewari S, Yao M, et al. Who places high value on the uterus? A cross-sectional survey study evaluating predictors for uterine preservation. J Minim Invasive Gynecol. 2023;30:131-136. doi:10.1016/j.jmig.2022.10.012
- Carey ET, Moore KJ, McClurg AB, et al. Racial disparities in hysterectomy route for benign disease: examining trends and perioperative complications from 2007 to 2018 using the NSQIP database. J Minim Invasive Gynecol. 2023;30:627-634. doi:10.1016/j.jmig.2023.03.024
- Frisch EH, Mitchell J, Yao M, et al. The impact of fertility goals on long-term quality of life in reproductive-aged women who underwent myomectomy versus hysterectomy for uterine fibroids. J Minim Invasive Gynecol. 2023;30:642-651. doi:10.1016/j.jmig.2023.04.003 1
- Robinson WR, Mathias JG, Wood ME, et al. Ethnoracial differences in premenopausal hysterectomy: the role of symptom severity. Obstet Gynecol. 2023;142:350-359. doi:10.1097 /AOG.0000000000005225
- Harris HR, Peres LC, Johnson CE, et al. Racial differences in the association of endometriosis and uterine leiomyomas with the risk of ovarian cancer. Obstet Gynecol. 2023;141:11241138. doi:10.1097/AOG.0000000000005191
- Atia O, Hazan E, Rotem R, et al. A scoring system developed by a machine learning algorithm to better predict adnexal torsion. J Minim Invasive Gynecol. 2023;30:486-493. doi:10.1016/j.jmig.2023.02.008
- Ban Y, Shen J, Wang X, et al. Cesarean scar ectopic pregnancy clinical classification system with recommended surgical strategy. Obstet Gynecol. 2023;141:927-936. doi:10.1097 /AOG.0000000000005113
- Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies. Obstet Gynecol. 2006;107:1373-1381. doi:10.1097/01.AOG.0000218690.24494.ce
- Scioscia M, Bruni F, Ceccaroni M, et al. Distribution of endometriotic lesions in endometriosis stage IV supports the menstrual reflux theory and requires specific preoperative assessment and therapy. Acta Obstet Gynecol Scand. 2011;90:136-139. doi:10.1111/j.1600-0412.2010.01008.x
- Wetzel A, Philip C-A, Golfier F, et al. Surgical management of diaphragmatic and thoracic endometriosis: a French multicentric descriptive study. J Gynecol Obstet Hum Reprod. 2021;50:102147. doi:10.1016/j.jogoh.2021.102147
CGRP in migraine prodrome can stop headache, reduce severity
BARCELONA, SPAIN — In the randomized, placebo-controlled crossover PRODROME trial, treatment with ubrogepant (Ubrelvy) 100 mg, one of the new CGRP receptor antagonists, during the prodrome prevented the development of moderate/severe headache at both 24 hours and 48 hours post-dose. The medication also reduced headache of any intensity within 24 hours and functional disability compared with placebo.
“This represents a totally different way of treating a migraine attack – to treat it before the headache starts. This is a paradigm shift in the way we approach the acute treatment of migraine,” study investigator Peter Goadsby, MBBS, MD, PhD, professor of neurology at Kings College London, UK, said in an interview.
The findings were presented at 17th European Headache Congress (EHC) and were also recently published online in The Lancet.
A New Way to Manage Migraine?
The prodrome is usually the earliest phase of a migraine attack and is believed to be experienced by the vast majority of patients with migraine. It consists of various symptoms, including sensitivity to light, fatigue, mood changes, cognitive dysfunction, craving certain foods, and neck pain, which can occur several hours or days before onset.
Dr. Goadsby notes that, at present, there isn’t very much a patient can do about the prodrome.
“We advise patients if they feel an attack is coming not to do anything that might make it worse and make sure they have their acute treatment available for when the headache phase starts. So, we just advise people to prepare for the attack rather than doing anything specific to stop it. But with new data from this study, we now have something that can be done. Patients have an option,” he said.
Dr. Goadsby explained that currently patients are not encouraged to use acute migraine medications such as triptans in the prodrome phase.
“There is actually no evidence that taking a triptan during the prodromal phase works. The advice is to take a triptan as soon as the headache starts, but not before the headache starts.”
He noted that there is also the problem of medication overuse that is seen with triptans, and most other medications used to treat acute migraine, which leads to medication overuse headache, “so we don’t like to encourage patients to increase the frequency of taking triptans for this reason.”
But ubrogepant and other members of the “gepant” class do not seem to have the propensity for medication overuse problems. “Rather, the more a patient takes the less likely they are to get a headache as these drugs also have a preventative effect,” Dr. Goadsby said.
Major Reduction in Severity
The PRODROME trial was conducted at 75 sites in the United States in 518 patients who had at least a 1-year history of migraine with or without aura and a history of two to eight migraine attacks per month with moderate to severe headache in each of the 3 months before study entry.
Participants underwent a rigorous screening period during which they were required to show that they could identify prodromal symptoms that were reliably followed by migraine headache within 1-6 hours.
They were randomly assigned to receive either placebo to treat the first qualifying prodrome event and ubrogepant 100 mg to treat the second qualifying prodrome event or vice versa, with instructions to take the study drug at the onset of the prodrome event.
Efficacy assessments during the double-blind treatment period were recorded by the participant in an electronic diary. On identifying a qualifying prodrome, the patient recorded prodromal symptoms, and was then required to report the absence or presence of a headache at regular intervals up to 48 hours after the study drug dose. If a headache was reported, participants rated the intensity as mild, moderate, or severe and reported whether rescue medication was taken to treat it.
The primary endpoint was absence of moderate or severe intensity headache within 24 hours after study-drug dose. This occurred after 46% of 418 qualifying prodrome events that had been treated with ubrogepant and after 29% of 423 qualifying prodrome events that had been treated with placebo (odds ratio, 2.09; 95% CI, 1.63 - 2.69; P < .0001).
“The incidence of moderate to severe headache was almost halved when ubrogepant was taken in the prodrome,” Dr. Goadsby reported.
Ubrogepant also showed similar impressive results for the secondary endpoints in the absence of moderate to severe headache within 48 hours post-dose and the absence of any headache of any intensity at 24 hours.
Little to No Disability
The researchers also evaluated functional ability, and more participants reported “no disability or able to function normally” during the 24 hours after treatment with ubrogepant than after placebo (OR, 1.66; P < .0001).
Other findings showed that the prodromal symptoms themselves, such as light sensitivity and cognitive dysfunction, were also reduced with ubrogepant.
Dr. Goadsby said he was pleased but not surprised by the results, as the “gepant” class of drugs are used in both the acute treatment of migraine and as preventive agents, although different agents have been approved for different indications in this regard.
“The ‘gepants’ are a class of medication that can be used in almost any way in migraine — to treat an acute migraine headache, to prevent migraine if taken chronically, and now we see that they can also stop a migraine from developing if taken during the initial prodromal phase. That’s unique for a migraine medication,” he said.
While the current study was conducted with ubrogepant, Dr. Goadsby suspects that any of the “gepants” would probably have a similar effect.
He noted that the prodromal phase of migraine has only just started to be explored, with functional imaging studies showing that structural brain changes occur during this phase.
Dr. Goadsby said the current study opens up a whole new area of interest, emphasizing the clinical value of identifying the prodrome in individuals with migraine, better characterizing the symptomology of the prodrome and understanding more about how to treat it.
“It’s the ultimate way of treating migraine early, and by taking this type of medication in the prodromal phase, patients may be able to stop having pain. That’s quite an implication,” he concluded.
The PRODROME study was funded by AbbVie. Dr. Goadsby reports personal fees from AbbVie.
A version of this article appeared on Medscape.com.
BARCELONA, SPAIN — In the randomized, placebo-controlled crossover PRODROME trial, treatment with ubrogepant (Ubrelvy) 100 mg, one of the new CGRP receptor antagonists, during the prodrome prevented the development of moderate/severe headache at both 24 hours and 48 hours post-dose. The medication also reduced headache of any intensity within 24 hours and functional disability compared with placebo.
“This represents a totally different way of treating a migraine attack – to treat it before the headache starts. This is a paradigm shift in the way we approach the acute treatment of migraine,” study investigator Peter Goadsby, MBBS, MD, PhD, professor of neurology at Kings College London, UK, said in an interview.
The findings were presented at 17th European Headache Congress (EHC) and were also recently published online in The Lancet.
A New Way to Manage Migraine?
The prodrome is usually the earliest phase of a migraine attack and is believed to be experienced by the vast majority of patients with migraine. It consists of various symptoms, including sensitivity to light, fatigue, mood changes, cognitive dysfunction, craving certain foods, and neck pain, which can occur several hours or days before onset.
Dr. Goadsby notes that, at present, there isn’t very much a patient can do about the prodrome.
“We advise patients if they feel an attack is coming not to do anything that might make it worse and make sure they have their acute treatment available for when the headache phase starts. So, we just advise people to prepare for the attack rather than doing anything specific to stop it. But with new data from this study, we now have something that can be done. Patients have an option,” he said.
Dr. Goadsby explained that currently patients are not encouraged to use acute migraine medications such as triptans in the prodrome phase.
“There is actually no evidence that taking a triptan during the prodromal phase works. The advice is to take a triptan as soon as the headache starts, but not before the headache starts.”
He noted that there is also the problem of medication overuse that is seen with triptans, and most other medications used to treat acute migraine, which leads to medication overuse headache, “so we don’t like to encourage patients to increase the frequency of taking triptans for this reason.”
But ubrogepant and other members of the “gepant” class do not seem to have the propensity for medication overuse problems. “Rather, the more a patient takes the less likely they are to get a headache as these drugs also have a preventative effect,” Dr. Goadsby said.
Major Reduction in Severity
The PRODROME trial was conducted at 75 sites in the United States in 518 patients who had at least a 1-year history of migraine with or without aura and a history of two to eight migraine attacks per month with moderate to severe headache in each of the 3 months before study entry.
Participants underwent a rigorous screening period during which they were required to show that they could identify prodromal symptoms that were reliably followed by migraine headache within 1-6 hours.
They were randomly assigned to receive either placebo to treat the first qualifying prodrome event and ubrogepant 100 mg to treat the second qualifying prodrome event or vice versa, with instructions to take the study drug at the onset of the prodrome event.
Efficacy assessments during the double-blind treatment period were recorded by the participant in an electronic diary. On identifying a qualifying prodrome, the patient recorded prodromal symptoms, and was then required to report the absence or presence of a headache at regular intervals up to 48 hours after the study drug dose. If a headache was reported, participants rated the intensity as mild, moderate, or severe and reported whether rescue medication was taken to treat it.
The primary endpoint was absence of moderate or severe intensity headache within 24 hours after study-drug dose. This occurred after 46% of 418 qualifying prodrome events that had been treated with ubrogepant and after 29% of 423 qualifying prodrome events that had been treated with placebo (odds ratio, 2.09; 95% CI, 1.63 - 2.69; P < .0001).
“The incidence of moderate to severe headache was almost halved when ubrogepant was taken in the prodrome,” Dr. Goadsby reported.
Ubrogepant also showed similar impressive results for the secondary endpoints in the absence of moderate to severe headache within 48 hours post-dose and the absence of any headache of any intensity at 24 hours.
Little to No Disability
The researchers also evaluated functional ability, and more participants reported “no disability or able to function normally” during the 24 hours after treatment with ubrogepant than after placebo (OR, 1.66; P < .0001).
Other findings showed that the prodromal symptoms themselves, such as light sensitivity and cognitive dysfunction, were also reduced with ubrogepant.
Dr. Goadsby said he was pleased but not surprised by the results, as the “gepant” class of drugs are used in both the acute treatment of migraine and as preventive agents, although different agents have been approved for different indications in this regard.
“The ‘gepants’ are a class of medication that can be used in almost any way in migraine — to treat an acute migraine headache, to prevent migraine if taken chronically, and now we see that they can also stop a migraine from developing if taken during the initial prodromal phase. That’s unique for a migraine medication,” he said.
While the current study was conducted with ubrogepant, Dr. Goadsby suspects that any of the “gepants” would probably have a similar effect.
He noted that the prodromal phase of migraine has only just started to be explored, with functional imaging studies showing that structural brain changes occur during this phase.
Dr. Goadsby said the current study opens up a whole new area of interest, emphasizing the clinical value of identifying the prodrome in individuals with migraine, better characterizing the symptomology of the prodrome and understanding more about how to treat it.
“It’s the ultimate way of treating migraine early, and by taking this type of medication in the prodromal phase, patients may be able to stop having pain. That’s quite an implication,” he concluded.
The PRODROME study was funded by AbbVie. Dr. Goadsby reports personal fees from AbbVie.
A version of this article appeared on Medscape.com.
BARCELONA, SPAIN — In the randomized, placebo-controlled crossover PRODROME trial, treatment with ubrogepant (Ubrelvy) 100 mg, one of the new CGRP receptor antagonists, during the prodrome prevented the development of moderate/severe headache at both 24 hours and 48 hours post-dose. The medication also reduced headache of any intensity within 24 hours and functional disability compared with placebo.
“This represents a totally different way of treating a migraine attack – to treat it before the headache starts. This is a paradigm shift in the way we approach the acute treatment of migraine,” study investigator Peter Goadsby, MBBS, MD, PhD, professor of neurology at Kings College London, UK, said in an interview.
The findings were presented at 17th European Headache Congress (EHC) and were also recently published online in The Lancet.
A New Way to Manage Migraine?
The prodrome is usually the earliest phase of a migraine attack and is believed to be experienced by the vast majority of patients with migraine. It consists of various symptoms, including sensitivity to light, fatigue, mood changes, cognitive dysfunction, craving certain foods, and neck pain, which can occur several hours or days before onset.
Dr. Goadsby notes that, at present, there isn’t very much a patient can do about the prodrome.
“We advise patients if they feel an attack is coming not to do anything that might make it worse and make sure they have their acute treatment available for when the headache phase starts. So, we just advise people to prepare for the attack rather than doing anything specific to stop it. But with new data from this study, we now have something that can be done. Patients have an option,” he said.
Dr. Goadsby explained that currently patients are not encouraged to use acute migraine medications such as triptans in the prodrome phase.
“There is actually no evidence that taking a triptan during the prodromal phase works. The advice is to take a triptan as soon as the headache starts, but not before the headache starts.”
He noted that there is also the problem of medication overuse that is seen with triptans, and most other medications used to treat acute migraine, which leads to medication overuse headache, “so we don’t like to encourage patients to increase the frequency of taking triptans for this reason.”
But ubrogepant and other members of the “gepant” class do not seem to have the propensity for medication overuse problems. “Rather, the more a patient takes the less likely they are to get a headache as these drugs also have a preventative effect,” Dr. Goadsby said.
Major Reduction in Severity
The PRODROME trial was conducted at 75 sites in the United States in 518 patients who had at least a 1-year history of migraine with or without aura and a history of two to eight migraine attacks per month with moderate to severe headache in each of the 3 months before study entry.
Participants underwent a rigorous screening period during which they were required to show that they could identify prodromal symptoms that were reliably followed by migraine headache within 1-6 hours.
They were randomly assigned to receive either placebo to treat the first qualifying prodrome event and ubrogepant 100 mg to treat the second qualifying prodrome event or vice versa, with instructions to take the study drug at the onset of the prodrome event.
Efficacy assessments during the double-blind treatment period were recorded by the participant in an electronic diary. On identifying a qualifying prodrome, the patient recorded prodromal symptoms, and was then required to report the absence or presence of a headache at regular intervals up to 48 hours after the study drug dose. If a headache was reported, participants rated the intensity as mild, moderate, or severe and reported whether rescue medication was taken to treat it.
The primary endpoint was absence of moderate or severe intensity headache within 24 hours after study-drug dose. This occurred after 46% of 418 qualifying prodrome events that had been treated with ubrogepant and after 29% of 423 qualifying prodrome events that had been treated with placebo (odds ratio, 2.09; 95% CI, 1.63 - 2.69; P < .0001).
“The incidence of moderate to severe headache was almost halved when ubrogepant was taken in the prodrome,” Dr. Goadsby reported.
Ubrogepant also showed similar impressive results for the secondary endpoints in the absence of moderate to severe headache within 48 hours post-dose and the absence of any headache of any intensity at 24 hours.
Little to No Disability
The researchers also evaluated functional ability, and more participants reported “no disability or able to function normally” during the 24 hours after treatment with ubrogepant than after placebo (OR, 1.66; P < .0001).
Other findings showed that the prodromal symptoms themselves, such as light sensitivity and cognitive dysfunction, were also reduced with ubrogepant.
Dr. Goadsby said he was pleased but not surprised by the results, as the “gepant” class of drugs are used in both the acute treatment of migraine and as preventive agents, although different agents have been approved for different indications in this regard.
“The ‘gepants’ are a class of medication that can be used in almost any way in migraine — to treat an acute migraine headache, to prevent migraine if taken chronically, and now we see that they can also stop a migraine from developing if taken during the initial prodromal phase. That’s unique for a migraine medication,” he said.
While the current study was conducted with ubrogepant, Dr. Goadsby suspects that any of the “gepants” would probably have a similar effect.
He noted that the prodromal phase of migraine has only just started to be explored, with functional imaging studies showing that structural brain changes occur during this phase.
Dr. Goadsby said the current study opens up a whole new area of interest, emphasizing the clinical value of identifying the prodrome in individuals with migraine, better characterizing the symptomology of the prodrome and understanding more about how to treat it.
“It’s the ultimate way of treating migraine early, and by taking this type of medication in the prodromal phase, patients may be able to stop having pain. That’s quite an implication,” he concluded.
The PRODROME study was funded by AbbVie. Dr. Goadsby reports personal fees from AbbVie.
A version of this article appeared on Medscape.com.
FROM EHC 2023
Why Are Prion Diseases on the Rise?
This transcript has been edited for clarity.
In 1986, in Britain, cattle started dying.
The condition, quickly nicknamed “mad cow disease,” was clearly infectious, but the particular pathogen was difficult to identify. By 1993, 120,000 cattle in Britain were identified as being infected. As yet, no human cases had occurred and the UK government insisted that cattle were a dead-end host for the pathogen. By the mid-1990s, however, multiple human cases, attributable to ingestion of meat and organs from infected cattle, were discovered. In humans, variant Creutzfeldt-Jakob disease (CJD) was a media sensation — a nearly uniformly fatal, untreatable condition with a rapid onset of dementia, mobility issues characterized by jerky movements, and autopsy reports finding that the brain itself had turned into a spongy mess.
The United States banned UK beef imports in 1996 and only lifted the ban in 2020.
The disease was made all the more mysterious because the pathogen involved was not a bacterium, parasite, or virus, but a protein — or a proteinaceous infectious particle, shortened to “prion.”
Prions are misfolded proteins that aggregate in cells — in this case, in nerve cells. But what makes prions different from other misfolded proteins is that the misfolded protein catalyzes the conversion of its non-misfolded counterpart into the misfolded configuration. It creates a chain reaction, leading to rapid accumulation of misfolded proteins and cell death.
And, like a time bomb, we all have prion protein inside us. In its normally folded state, the function of prion protein remains unclear — knockout mice do okay without it — but it is also highly conserved across mammalian species, so it probably does something worthwhile, perhaps protecting nerve fibers.
Far more common than humans contracting mad cow disease is the condition known as sporadic CJD, responsible for 85% of all cases of prion-induced brain disease. The cause of sporadic CJD is unknown.
But one thing is known: Cases are increasing.
I don’t want you to freak out; we are not in the midst of a CJD epidemic. But it’s been a while since I’ve seen people discussing the condition — which remains as horrible as it was in the 1990s — and a new research letter appearing in JAMA Neurology brought it back to the top of my mind.
Researchers, led by Matthew Crane at Hopkins, used the CDC’s WONDER cause-of-death database, which pulls diagnoses from death certificates. Normally, I’m not a fan of using death certificates for cause-of-death analyses, but in this case I’ll give it a pass. Assuming that the diagnosis of CJD is made, it would be really unlikely for it not to appear on a death certificate.
The main findings are seen here. 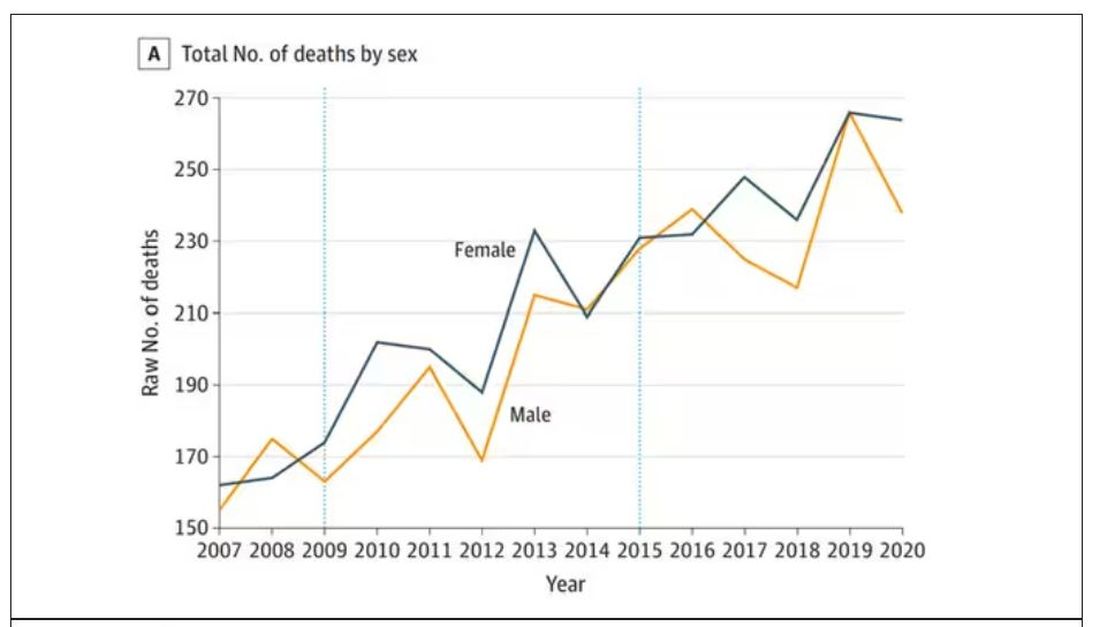
Note that we can’t tell whether these are sporadic CJD cases or variant CJD cases or even familial CJD cases; however, unless there has been a dramatic change in epidemiology, the vast majority of these will be sporadic.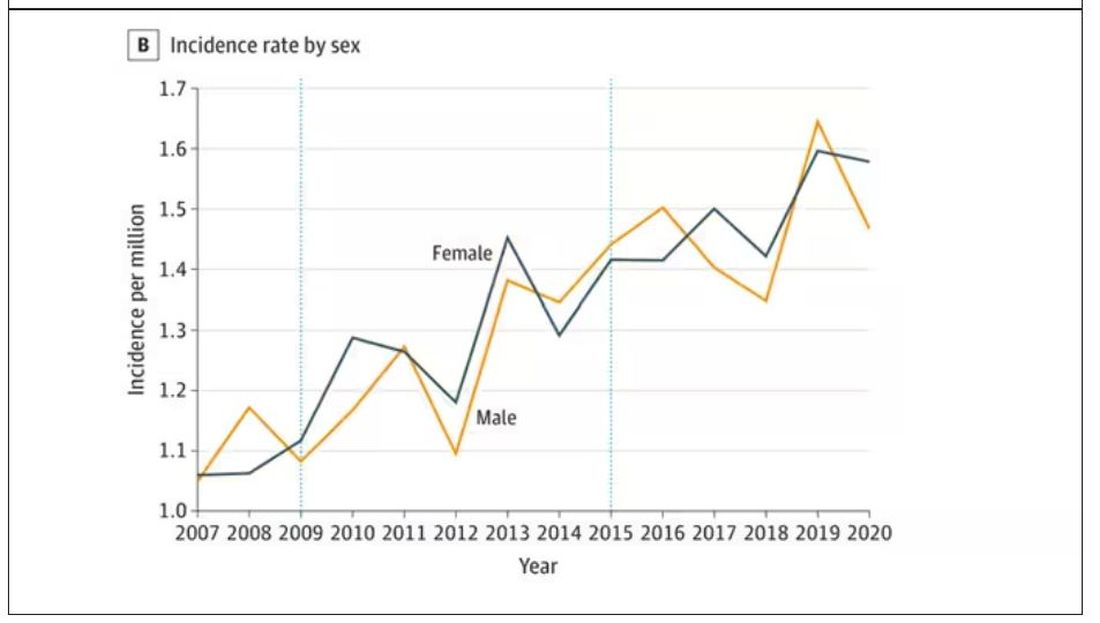
The question is, why are there more cases?
Whenever this type of question comes up with any disease, there are basically three possibilities:
First, there may be an increase in the susceptible, or at-risk, population. In this case, we know that older people are at higher risk of developing sporadic CJD, and over time, the population has aged. To be fair, the authors adjusted for this and still saw an increase, though it was attenuated.
Second, we might be better at diagnosing the condition. A lot has happened since the mid-1990s, when the diagnosis was based more or less on symptoms. The advent of more sophisticated MRI protocols as well as a new diagnostic test called “real-time quaking-induced conversion testing” may mean we are just better at detecting people with this disease.
Third (and most concerning), a new exposure has occurred. What that exposure might be, where it might come from, is anyone’s guess. It’s hard to do broad-scale epidemiology on very rare diseases.
But given these findings, it seems that a bit more surveillance for this rare but devastating condition is well merited.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now.
F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
In 1986, in Britain, cattle started dying.
The condition, quickly nicknamed “mad cow disease,” was clearly infectious, but the particular pathogen was difficult to identify. By 1993, 120,000 cattle in Britain were identified as being infected. As yet, no human cases had occurred and the UK government insisted that cattle were a dead-end host for the pathogen. By the mid-1990s, however, multiple human cases, attributable to ingestion of meat and organs from infected cattle, were discovered. In humans, variant Creutzfeldt-Jakob disease (CJD) was a media sensation — a nearly uniformly fatal, untreatable condition with a rapid onset of dementia, mobility issues characterized by jerky movements, and autopsy reports finding that the brain itself had turned into a spongy mess.
The United States banned UK beef imports in 1996 and only lifted the ban in 2020.
The disease was made all the more mysterious because the pathogen involved was not a bacterium, parasite, or virus, but a protein — or a proteinaceous infectious particle, shortened to “prion.”
Prions are misfolded proteins that aggregate in cells — in this case, in nerve cells. But what makes prions different from other misfolded proteins is that the misfolded protein catalyzes the conversion of its non-misfolded counterpart into the misfolded configuration. It creates a chain reaction, leading to rapid accumulation of misfolded proteins and cell death.
And, like a time bomb, we all have prion protein inside us. In its normally folded state, the function of prion protein remains unclear — knockout mice do okay without it — but it is also highly conserved across mammalian species, so it probably does something worthwhile, perhaps protecting nerve fibers.
Far more common than humans contracting mad cow disease is the condition known as sporadic CJD, responsible for 85% of all cases of prion-induced brain disease. The cause of sporadic CJD is unknown.
But one thing is known: Cases are increasing.
I don’t want you to freak out; we are not in the midst of a CJD epidemic. But it’s been a while since I’ve seen people discussing the condition — which remains as horrible as it was in the 1990s — and a new research letter appearing in JAMA Neurology brought it back to the top of my mind.
Researchers, led by Matthew Crane at Hopkins, used the CDC’s WONDER cause-of-death database, which pulls diagnoses from death certificates. Normally, I’m not a fan of using death certificates for cause-of-death analyses, but in this case I’ll give it a pass. Assuming that the diagnosis of CJD is made, it would be really unlikely for it not to appear on a death certificate.
The main findings are seen here.
Note that we can’t tell whether these are sporadic CJD cases or variant CJD cases or even familial CJD cases; however, unless there has been a dramatic change in epidemiology, the vast majority of these will be sporadic.
The question is, why are there more cases?
Whenever this type of question comes up with any disease, there are basically three possibilities:
First, there may be an increase in the susceptible, or at-risk, population. In this case, we know that older people are at higher risk of developing sporadic CJD, and over time, the population has aged. To be fair, the authors adjusted for this and still saw an increase, though it was attenuated.
Second, we might be better at diagnosing the condition. A lot has happened since the mid-1990s, when the diagnosis was based more or less on symptoms. The advent of more sophisticated MRI protocols as well as a new diagnostic test called “real-time quaking-induced conversion testing” may mean we are just better at detecting people with this disease.
Third (and most concerning), a new exposure has occurred. What that exposure might be, where it might come from, is anyone’s guess. It’s hard to do broad-scale epidemiology on very rare diseases.
But given these findings, it seems that a bit more surveillance for this rare but devastating condition is well merited.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now.
F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
In 1986, in Britain, cattle started dying.
The condition, quickly nicknamed “mad cow disease,” was clearly infectious, but the particular pathogen was difficult to identify. By 1993, 120,000 cattle in Britain were identified as being infected. As yet, no human cases had occurred and the UK government insisted that cattle were a dead-end host for the pathogen. By the mid-1990s, however, multiple human cases, attributable to ingestion of meat and organs from infected cattle, were discovered. In humans, variant Creutzfeldt-Jakob disease (CJD) was a media sensation — a nearly uniformly fatal, untreatable condition with a rapid onset of dementia, mobility issues characterized by jerky movements, and autopsy reports finding that the brain itself had turned into a spongy mess.
The United States banned UK beef imports in 1996 and only lifted the ban in 2020.
The disease was made all the more mysterious because the pathogen involved was not a bacterium, parasite, or virus, but a protein — or a proteinaceous infectious particle, shortened to “prion.”
Prions are misfolded proteins that aggregate in cells — in this case, in nerve cells. But what makes prions different from other misfolded proteins is that the misfolded protein catalyzes the conversion of its non-misfolded counterpart into the misfolded configuration. It creates a chain reaction, leading to rapid accumulation of misfolded proteins and cell death.
And, like a time bomb, we all have prion protein inside us. In its normally folded state, the function of prion protein remains unclear — knockout mice do okay without it — but it is also highly conserved across mammalian species, so it probably does something worthwhile, perhaps protecting nerve fibers.
Far more common than humans contracting mad cow disease is the condition known as sporadic CJD, responsible for 85% of all cases of prion-induced brain disease. The cause of sporadic CJD is unknown.
But one thing is known: Cases are increasing.
I don’t want you to freak out; we are not in the midst of a CJD epidemic. But it’s been a while since I’ve seen people discussing the condition — which remains as horrible as it was in the 1990s — and a new research letter appearing in JAMA Neurology brought it back to the top of my mind.
Researchers, led by Matthew Crane at Hopkins, used the CDC’s WONDER cause-of-death database, which pulls diagnoses from death certificates. Normally, I’m not a fan of using death certificates for cause-of-death analyses, but in this case I’ll give it a pass. Assuming that the diagnosis of CJD is made, it would be really unlikely for it not to appear on a death certificate.
The main findings are seen here.
Note that we can’t tell whether these are sporadic CJD cases or variant CJD cases or even familial CJD cases; however, unless there has been a dramatic change in epidemiology, the vast majority of these will be sporadic.
The question is, why are there more cases?
Whenever this type of question comes up with any disease, there are basically three possibilities:
First, there may be an increase in the susceptible, or at-risk, population. In this case, we know that older people are at higher risk of developing sporadic CJD, and over time, the population has aged. To be fair, the authors adjusted for this and still saw an increase, though it was attenuated.
Second, we might be better at diagnosing the condition. A lot has happened since the mid-1990s, when the diagnosis was based more or less on symptoms. The advent of more sophisticated MRI protocols as well as a new diagnostic test called “real-time quaking-induced conversion testing” may mean we are just better at detecting people with this disease.
Third (and most concerning), a new exposure has occurred. What that exposure might be, where it might come from, is anyone’s guess. It’s hard to do broad-scale epidemiology on very rare diseases.
But given these findings, it seems that a bit more surveillance for this rare but devastating condition is well merited.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and public health and director of Yale’s Clinical and Translational Research Accelerator. His science communication work can be found in the Huffington Post, on NPR, and here on Medscape. He tweets @fperrywilson and his new book, How Medicine Works and When It Doesn’t, is available now.
F. Perry Wilson, MD, MSCE, has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Is migraine really a female disorder?
BARCELONA, SPAIN — Migraine is widely considered a predominantly female disorder. Its frequency, duration, and severity tend to be higher in women, and women are also more likely than men to receive a migraine diagnosis. However, gender expectations, differences in the likelihood of self-reporting, and problems with how migraine is classified make it difficult to estimate its true prevalence in men and women.
Different Symptoms
Headache disorders are estimated to affect 50% of the general population ; tension-type headache and migraine are the two most common. According to epidemiologic studies, migraine is more prevalent in women, with a female-to-male ratio of 3:1. There are numerous studies of why this might be, most of which focus largely on female-related factors, such as hormones and the menstrual cycle.
“Despite many years of research, there isn’t one clear factor explaining this substantial difference between women and men,” said Tobias Kurth of Charité – Universitätsmedizin Berlin, Germany. “So the question is: Are we missing something else?”
One factor in these perceived sex differences in migraine is that women seem to report their migraines differently from men, and they also have different symptoms. For example, women are more likely than men to report severe pain, and their migraine attacks are more often accompanied by photophobia, phonophobia, and nausea, whereas men’s migraines are more often accompanied by aura.
“By favoring female symptoms, the classification system may not be picking up male symptoms because they’re not being classified in the right way,” Dr. Kurth said, with one consequence being that migraine is underdiagnosed in men. “Before trying to understand the biological and behavioral reasons for these sex differences, we first need to consider these methodological challenges that we all apply knowingly or unknowingly.”
Christian Lampl, professor of neurology at Konventhospital der Barmherzigen Brüder Linz, Austria, and president of the European Headache Federation, said in an interview, “I’m convinced that this 3:1 ratio which has been stated for decades is wrong, but we still don’t have the data. The criteria we have [for classifying migraine] are useful for clinical trials, but they are useless for determining the male-to-female ratio.
“We need a new definition of migraine,” he added. “Migraine is an episode, not an attack. Attacks have a sudden onset, and migraine onset is not sudden — it is an episode with a headache attack.”
Inadequate Menopause Services
Professor Anne MacGregor of St. Bartholomew’s Hospital in London, United Kingdom, specializes in migraine and women’s health. She presented data showing that migraine is underdiagnosed in women; one reason being that the disorder receives inadequate attention from healthcare professionals at specialist menopause services.
Menopause is associated with an increased prevalence of migraine, but women do not discuss headache symptoms at specialist menopause services, Dr. MacGregor said.
She then described unpublished results from a survey of 117 women attending the specialist menopause service at St. Bartholomew’s Hospital. Among the respondents, 34% reported experiencing episodic migraine and an additional 8% reported having chronic migraine.
“Within this population of women who were not reporting headache as a symptom [to the menopause service until asked in the survey], 42% of them were positive for a diagnosis of migraine,” said Dr. MacGregor. “They were mostly relying on prescribed paracetamol and codeine, or buying it over the counter, and only 22% of them were receiving triptans.
“They are clearly being undertreated,” she added. “Part of this issue is that they didn’t spontaneously report headache as a menopause symptom, so they weren’t consulting for headache to their primary care physicians.”
Correct diagnosis by a consultant is a prerequisite for receiving appropriate migraine treatment. Yet, according to a US study published in 2012, only 45.5% of women with episodic migraine consulted a prescribing healthcare professional. Of those who consulted, 89% were diagnosed correctly, and only 68% of those received the appropriate treatment.
A larger, more recent study confirmed that there is a massive unmet need for improving care in this patient population. The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study, which analyzed data from nearly 90,000 participants, showed that just 4.8% of people with chronic migraine received consultation, correct diagnosis, and treatment, with 89% of women with chronic migraine left undiagnosed.
The OVERCOME Study further revealed that although many people with migraine were repeat consulters, they were consulting their physicians for other health problems.
“This makes it very clear that people in other specialties need to be more aware about picking up and diagnosing headache,” said MacGregor. “That’s where the real need is in managing headache. We have the treatments, but if the patients can’t access them, they’re not much good to them.”
A version of this article appeared on Medscape.com.
BARCELONA, SPAIN — Migraine is widely considered a predominantly female disorder. Its frequency, duration, and severity tend to be higher in women, and women are also more likely than men to receive a migraine diagnosis. However, gender expectations, differences in the likelihood of self-reporting, and problems with how migraine is classified make it difficult to estimate its true prevalence in men and women.
Different Symptoms
Headache disorders are estimated to affect 50% of the general population ; tension-type headache and migraine are the two most common. According to epidemiologic studies, migraine is more prevalent in women, with a female-to-male ratio of 3:1. There are numerous studies of why this might be, most of which focus largely on female-related factors, such as hormones and the menstrual cycle.
“Despite many years of research, there isn’t one clear factor explaining this substantial difference between women and men,” said Tobias Kurth of Charité – Universitätsmedizin Berlin, Germany. “So the question is: Are we missing something else?”
One factor in these perceived sex differences in migraine is that women seem to report their migraines differently from men, and they also have different symptoms. For example, women are more likely than men to report severe pain, and their migraine attacks are more often accompanied by photophobia, phonophobia, and nausea, whereas men’s migraines are more often accompanied by aura.
“By favoring female symptoms, the classification system may not be picking up male symptoms because they’re not being classified in the right way,” Dr. Kurth said, with one consequence being that migraine is underdiagnosed in men. “Before trying to understand the biological and behavioral reasons for these sex differences, we first need to consider these methodological challenges that we all apply knowingly or unknowingly.”
Christian Lampl, professor of neurology at Konventhospital der Barmherzigen Brüder Linz, Austria, and president of the European Headache Federation, said in an interview, “I’m convinced that this 3:1 ratio which has been stated for decades is wrong, but we still don’t have the data. The criteria we have [for classifying migraine] are useful for clinical trials, but they are useless for determining the male-to-female ratio.
“We need a new definition of migraine,” he added. “Migraine is an episode, not an attack. Attacks have a sudden onset, and migraine onset is not sudden — it is an episode with a headache attack.”
Inadequate Menopause Services
Professor Anne MacGregor of St. Bartholomew’s Hospital in London, United Kingdom, specializes in migraine and women’s health. She presented data showing that migraine is underdiagnosed in women; one reason being that the disorder receives inadequate attention from healthcare professionals at specialist menopause services.
Menopause is associated with an increased prevalence of migraine, but women do not discuss headache symptoms at specialist menopause services, Dr. MacGregor said.
She then described unpublished results from a survey of 117 women attending the specialist menopause service at St. Bartholomew’s Hospital. Among the respondents, 34% reported experiencing episodic migraine and an additional 8% reported having chronic migraine.
“Within this population of women who were not reporting headache as a symptom [to the menopause service until asked in the survey], 42% of them were positive for a diagnosis of migraine,” said Dr. MacGregor. “They were mostly relying on prescribed paracetamol and codeine, or buying it over the counter, and only 22% of them were receiving triptans.
“They are clearly being undertreated,” she added. “Part of this issue is that they didn’t spontaneously report headache as a menopause symptom, so they weren’t consulting for headache to their primary care physicians.”
Correct diagnosis by a consultant is a prerequisite for receiving appropriate migraine treatment. Yet, according to a US study published in 2012, only 45.5% of women with episodic migraine consulted a prescribing healthcare professional. Of those who consulted, 89% were diagnosed correctly, and only 68% of those received the appropriate treatment.
A larger, more recent study confirmed that there is a massive unmet need for improving care in this patient population. The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study, which analyzed data from nearly 90,000 participants, showed that just 4.8% of people with chronic migraine received consultation, correct diagnosis, and treatment, with 89% of women with chronic migraine left undiagnosed.
The OVERCOME Study further revealed that although many people with migraine were repeat consulters, they were consulting their physicians for other health problems.
“This makes it very clear that people in other specialties need to be more aware about picking up and diagnosing headache,” said MacGregor. “That’s where the real need is in managing headache. We have the treatments, but if the patients can’t access them, they’re not much good to them.”
A version of this article appeared on Medscape.com.
BARCELONA, SPAIN — Migraine is widely considered a predominantly female disorder. Its frequency, duration, and severity tend to be higher in women, and women are also more likely than men to receive a migraine diagnosis. However, gender expectations, differences in the likelihood of self-reporting, and problems with how migraine is classified make it difficult to estimate its true prevalence in men and women.
Different Symptoms
Headache disorders are estimated to affect 50% of the general population ; tension-type headache and migraine are the two most common. According to epidemiologic studies, migraine is more prevalent in women, with a female-to-male ratio of 3:1. There are numerous studies of why this might be, most of which focus largely on female-related factors, such as hormones and the menstrual cycle.
“Despite many years of research, there isn’t one clear factor explaining this substantial difference between women and men,” said Tobias Kurth of Charité – Universitätsmedizin Berlin, Germany. “So the question is: Are we missing something else?”
One factor in these perceived sex differences in migraine is that women seem to report their migraines differently from men, and they also have different symptoms. For example, women are more likely than men to report severe pain, and their migraine attacks are more often accompanied by photophobia, phonophobia, and nausea, whereas men’s migraines are more often accompanied by aura.
“By favoring female symptoms, the classification system may not be picking up male symptoms because they’re not being classified in the right way,” Dr. Kurth said, with one consequence being that migraine is underdiagnosed in men. “Before trying to understand the biological and behavioral reasons for these sex differences, we first need to consider these methodological challenges that we all apply knowingly or unknowingly.”
Christian Lampl, professor of neurology at Konventhospital der Barmherzigen Brüder Linz, Austria, and president of the European Headache Federation, said in an interview, “I’m convinced that this 3:1 ratio which has been stated for decades is wrong, but we still don’t have the data. The criteria we have [for classifying migraine] are useful for clinical trials, but they are useless for determining the male-to-female ratio.
“We need a new definition of migraine,” he added. “Migraine is an episode, not an attack. Attacks have a sudden onset, and migraine onset is not sudden — it is an episode with a headache attack.”
Inadequate Menopause Services
Professor Anne MacGregor of St. Bartholomew’s Hospital in London, United Kingdom, specializes in migraine and women’s health. She presented data showing that migraine is underdiagnosed in women; one reason being that the disorder receives inadequate attention from healthcare professionals at specialist menopause services.
Menopause is associated with an increased prevalence of migraine, but women do not discuss headache symptoms at specialist menopause services, Dr. MacGregor said.
She then described unpublished results from a survey of 117 women attending the specialist menopause service at St. Bartholomew’s Hospital. Among the respondents, 34% reported experiencing episodic migraine and an additional 8% reported having chronic migraine.
“Within this population of women who were not reporting headache as a symptom [to the menopause service until asked in the survey], 42% of them were positive for a diagnosis of migraine,” said Dr. MacGregor. “They were mostly relying on prescribed paracetamol and codeine, or buying it over the counter, and only 22% of them were receiving triptans.
“They are clearly being undertreated,” she added. “Part of this issue is that they didn’t spontaneously report headache as a menopause symptom, so they weren’t consulting for headache to their primary care physicians.”
Correct diagnosis by a consultant is a prerequisite for receiving appropriate migraine treatment. Yet, according to a US study published in 2012, only 45.5% of women with episodic migraine consulted a prescribing healthcare professional. Of those who consulted, 89% were diagnosed correctly, and only 68% of those received the appropriate treatment.
A larger, more recent study confirmed that there is a massive unmet need for improving care in this patient population. The Chronic Migraine Epidemiology and Outcomes (CaMEO) Study, which analyzed data from nearly 90,000 participants, showed that just 4.8% of people with chronic migraine received consultation, correct diagnosis, and treatment, with 89% of women with chronic migraine left undiagnosed.
The OVERCOME Study further revealed that although many people with migraine were repeat consulters, they were consulting their physicians for other health problems.
“This makes it very clear that people in other specialties need to be more aware about picking up and diagnosing headache,” said MacGregor. “That’s where the real need is in managing headache. We have the treatments, but if the patients can’t access them, they’re not much good to them.”
A version of this article appeared on Medscape.com.
FROM EHC 2023