User login
Tax Questions Frequently Asked by Physicians
Physicians spend years of their lives in education and training. There are countless hours devoted to studying, researching, and clinical training, not to mention residency and possible fellowships. Then literally overnight, they transition out of a resident salary into a full-time attending pay with little to no education around what to do with this significant increase in salary.
Every job position is unique in terms of benefits, how compensation is earned, job expectations, etc. But they all share one thing in common — taxes. Increased income comes with increased taxes.

FAQ 1. What is the difference between W2 income and 1099 income?
A: If you are a W2 employee, your employer is responsible for paying half of your Social Security and Medicare taxes. You, as the employee, are then responsible only for the remaining half of your Social Security and Medicare taxes. Additionally, your employer will withhold these taxes, along with federal income taxes, from your paycheck each pay period. You are not responsible for remitting any taxes to the IRS or state agencies, as your employer will do this for you. As a W2 employee, you are not able to deduct any employee expenses against your income.

As a 1099 contractor, you are considered self-employed and are responsible for the employer and employee portion of the Social Security and Medicare taxes. You are also responsible for remitting these taxes, as well as quarterly estimated federal withholding, to the IRS and state agencies. You can deduct work-related expenses against your 1099 income.
Both types of income have pros and cons. Either of these can be more beneficial to a specific situation.
FAQ 2. How do I know if I am withholding enough taxes?
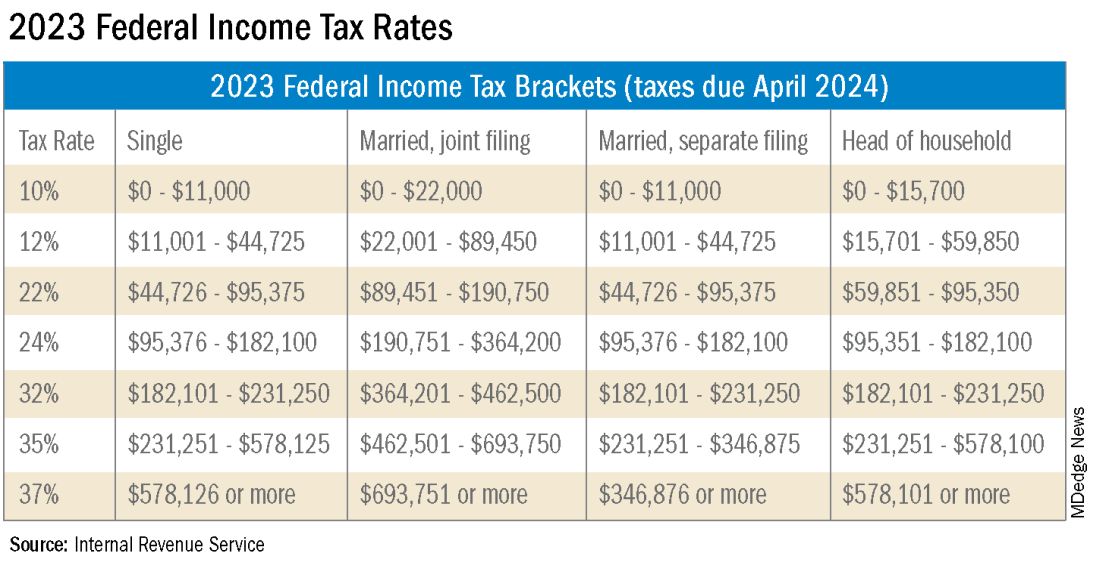
A: This is a very common issue I see, especially with physicians who are transitioning out of training into their full-time attending salary. Because this transition happens mid-year, often the first half of the year you are withholding at a rate much lower than what you will be earning as an attending and end up with a tax surprise at filing. One way to remedy this is to look at how much taxes are being withheld from your paycheck and compare this to what tax bracket you anticipate to be in, depending on filing status (Figure 1). If you do this and realize you are not withholding enough taxes, you can submit an amended form W4 to your employer to have additional withholding taken out each pay period.
FAQ 3. I am a 1099 contractor; do I need a PLLC, and should I file as an S-Corporation?
A: The term “S-Corp” gets mentioned often related to 1099 contractors and can be extremely beneficial from a tax savings perspective. Often physicians may moonlight — in addition to working in their W2 positions — and would receive this compensation as a 1099 contractor rather than an employee. This is an example of when a Professional Limited Liability Company (PLLC) might be advisable. A PLLC is created at a state level and helps shield owners from potential litigation. The owner of a PLLC pays Social Security and Medicare taxes on all income earned from the entity, and the PLLC is included in the owner’s individual income tax return.
A Small-Corporation (S-Corporation) is a tax classification that passes income through to the owners. The PLLC is now taxed as an S-Corporation, rather than a disregarded entity. The shareholders of the S-Corporation are required to pay a reasonable salary (W2 income). The remaining income passes through to the owner and is not subject to Social Security and Medicare taxes, only federal income tax. This taxation status requires an additional tax return and payroll service. Because there are additional expenses with being taxed as an S-Corporation, a cost-benefit analysis should be done before changing the tax classification to confirm that the tax savings are greater than the additional costs.
FAQ 4. What is the ‘backdoor Roth’ strategy? Should I implement it?
A: A Roth IRA is a specific type of Individual Retirement Account (IRA) that is funded with after-tax dollars. The contributions and growth in a Roth IRA can be withdrawn at retirement, tax free. As physicians who are typically high earners, you are not able to contribute directly to a Roth IRA because of income limitations. This is where the Roth conversion strategy — the backdoor Roth — comes into play. This strategy allows you to make a nondeductible traditional IRA contribution and then convert those dollars into a Roth IRA. In 2023, you can contribute up to $6,500 into this type of account. There are many additional considerations that must be made before implementing this strategy. Discussion with a financial advisor or CPA is recommended.
FAQ 5. I’ve always done my own taxes. Do I need to hire a CPA?
A: For many physicians, especially during training, your tax situation may not warrant the need for a Certified Public Accountant (CPA). However, as your income and tax complexity increase, working with a CPA not only decreases your risk for error, but also helps ensure you are not overpaying in taxes. There are many different types of services that a CPA can offer, the most basic being tax preparation. This is simply compiling your tax return based on the circumstances that occurred in the prior year. Tax planning is an additional level of service that may not be included in tax preparation cost. Tax planning is a proactive approach to taxes and helps maximize tax savings opportunities before return preparation. When interviewing a potential CPA, you can ask what level of services are included in the fees quoted.
These are just a few of the questions I regularly answer related to physicians’ taxation. The tax code is complex and ever changing. Recommendations that are made today might not be applicable or advisable in the future to any given situation. Working with a professional can ensure you have the most up-to-date and accurate information related to your taxes.
Ms. Anderson is with Physician’s Resource Services and is on Instagram @physiciansrs . Dr. Anderson is a CA-1 Resident in Anesthesia at Baylor Scott and White Health. The authors have no conflicts of interest.
Physicians spend years of their lives in education and training. There are countless hours devoted to studying, researching, and clinical training, not to mention residency and possible fellowships. Then literally overnight, they transition out of a resident salary into a full-time attending pay with little to no education around what to do with this significant increase in salary.
Every job position is unique in terms of benefits, how compensation is earned, job expectations, etc. But they all share one thing in common — taxes. Increased income comes with increased taxes.
FAQ 1. What is the difference between W2 income and 1099 income?
A: If you are a W2 employee, your employer is responsible for paying half of your Social Security and Medicare taxes. You, as the employee, are then responsible only for the remaining half of your Social Security and Medicare taxes. Additionally, your employer will withhold these taxes, along with federal income taxes, from your paycheck each pay period. You are not responsible for remitting any taxes to the IRS or state agencies, as your employer will do this for you. As a W2 employee, you are not able to deduct any employee expenses against your income.
As a 1099 contractor, you are considered self-employed and are responsible for the employer and employee portion of the Social Security and Medicare taxes. You are also responsible for remitting these taxes, as well as quarterly estimated federal withholding, to the IRS and state agencies. You can deduct work-related expenses against your 1099 income.
Both types of income have pros and cons. Either of these can be more beneficial to a specific situation.
FAQ 2. How do I know if I am withholding enough taxes?
A: This is a very common issue I see, especially with physicians who are transitioning out of training into their full-time attending salary. Because this transition happens mid-year, often the first half of the year you are withholding at a rate much lower than what you will be earning as an attending and end up with a tax surprise at filing. One way to remedy this is to look at how much taxes are being withheld from your paycheck and compare this to what tax bracket you anticipate to be in, depending on filing status (Figure 1). If you do this and realize you are not withholding enough taxes, you can submit an amended form W4 to your employer to have additional withholding taken out each pay period.
FAQ 3. I am a 1099 contractor; do I need a PLLC, and should I file as an S-Corporation?
A: The term “S-Corp” gets mentioned often related to 1099 contractors and can be extremely beneficial from a tax savings perspective. Often physicians may moonlight — in addition to working in their W2 positions — and would receive this compensation as a 1099 contractor rather than an employee. This is an example of when a Professional Limited Liability Company (PLLC) might be advisable. A PLLC is created at a state level and helps shield owners from potential litigation. The owner of a PLLC pays Social Security and Medicare taxes on all income earned from the entity, and the PLLC is included in the owner’s individual income tax return.
A Small-Corporation (S-Corporation) is a tax classification that passes income through to the owners. The PLLC is now taxed as an S-Corporation, rather than a disregarded entity. The shareholders of the S-Corporation are required to pay a reasonable salary (W2 income). The remaining income passes through to the owner and is not subject to Social Security and Medicare taxes, only federal income tax. This taxation status requires an additional tax return and payroll service. Because there are additional expenses with being taxed as an S-Corporation, a cost-benefit analysis should be done before changing the tax classification to confirm that the tax savings are greater than the additional costs.
FAQ 4. What is the ‘backdoor Roth’ strategy? Should I implement it?
A: A Roth IRA is a specific type of Individual Retirement Account (IRA) that is funded with after-tax dollars. The contributions and growth in a Roth IRA can be withdrawn at retirement, tax free. As physicians who are typically high earners, you are not able to contribute directly to a Roth IRA because of income limitations. This is where the Roth conversion strategy — the backdoor Roth — comes into play. This strategy allows you to make a nondeductible traditional IRA contribution and then convert those dollars into a Roth IRA. In 2023, you can contribute up to $6,500 into this type of account. There are many additional considerations that must be made before implementing this strategy. Discussion with a financial advisor or CPA is recommended.
FAQ 5. I’ve always done my own taxes. Do I need to hire a CPA?
A: For many physicians, especially during training, your tax situation may not warrant the need for a Certified Public Accountant (CPA). However, as your income and tax complexity increase, working with a CPA not only decreases your risk for error, but also helps ensure you are not overpaying in taxes. There are many different types of services that a CPA can offer, the most basic being tax preparation. This is simply compiling your tax return based on the circumstances that occurred in the prior year. Tax planning is an additional level of service that may not be included in tax preparation cost. Tax planning is a proactive approach to taxes and helps maximize tax savings opportunities before return preparation. When interviewing a potential CPA, you can ask what level of services are included in the fees quoted.
These are just a few of the questions I regularly answer related to physicians’ taxation. The tax code is complex and ever changing. Recommendations that are made today might not be applicable or advisable in the future to any given situation. Working with a professional can ensure you have the most up-to-date and accurate information related to your taxes.
Ms. Anderson is with Physician’s Resource Services and is on Instagram @physiciansrs . Dr. Anderson is a CA-1 Resident in Anesthesia at Baylor Scott and White Health. The authors have no conflicts of interest.
Physicians spend years of their lives in education and training. There are countless hours devoted to studying, researching, and clinical training, not to mention residency and possible fellowships. Then literally overnight, they transition out of a resident salary into a full-time attending pay with little to no education around what to do with this significant increase in salary.
Every job position is unique in terms of benefits, how compensation is earned, job expectations, etc. But they all share one thing in common — taxes. Increased income comes with increased taxes.
FAQ 1. What is the difference between W2 income and 1099 income?
A: If you are a W2 employee, your employer is responsible for paying half of your Social Security and Medicare taxes. You, as the employee, are then responsible only for the remaining half of your Social Security and Medicare taxes. Additionally, your employer will withhold these taxes, along with federal income taxes, from your paycheck each pay period. You are not responsible for remitting any taxes to the IRS or state agencies, as your employer will do this for you. As a W2 employee, you are not able to deduct any employee expenses against your income.
As a 1099 contractor, you are considered self-employed and are responsible for the employer and employee portion of the Social Security and Medicare taxes. You are also responsible for remitting these taxes, as well as quarterly estimated federal withholding, to the IRS and state agencies. You can deduct work-related expenses against your 1099 income.
Both types of income have pros and cons. Either of these can be more beneficial to a specific situation.
FAQ 2. How do I know if I am withholding enough taxes?
A: This is a very common issue I see, especially with physicians who are transitioning out of training into their full-time attending salary. Because this transition happens mid-year, often the first half of the year you are withholding at a rate much lower than what you will be earning as an attending and end up with a tax surprise at filing. One way to remedy this is to look at how much taxes are being withheld from your paycheck and compare this to what tax bracket you anticipate to be in, depending on filing status (Figure 1). If you do this and realize you are not withholding enough taxes, you can submit an amended form W4 to your employer to have additional withholding taken out each pay period.
FAQ 3. I am a 1099 contractor; do I need a PLLC, and should I file as an S-Corporation?
A: The term “S-Corp” gets mentioned often related to 1099 contractors and can be extremely beneficial from a tax savings perspective. Often physicians may moonlight — in addition to working in their W2 positions — and would receive this compensation as a 1099 contractor rather than an employee. This is an example of when a Professional Limited Liability Company (PLLC) might be advisable. A PLLC is created at a state level and helps shield owners from potential litigation. The owner of a PLLC pays Social Security and Medicare taxes on all income earned from the entity, and the PLLC is included in the owner’s individual income tax return.
A Small-Corporation (S-Corporation) is a tax classification that passes income through to the owners. The PLLC is now taxed as an S-Corporation, rather than a disregarded entity. The shareholders of the S-Corporation are required to pay a reasonable salary (W2 income). The remaining income passes through to the owner and is not subject to Social Security and Medicare taxes, only federal income tax. This taxation status requires an additional tax return and payroll service. Because there are additional expenses with being taxed as an S-Corporation, a cost-benefit analysis should be done before changing the tax classification to confirm that the tax savings are greater than the additional costs.
FAQ 4. What is the ‘backdoor Roth’ strategy? Should I implement it?
A: A Roth IRA is a specific type of Individual Retirement Account (IRA) that is funded with after-tax dollars. The contributions and growth in a Roth IRA can be withdrawn at retirement, tax free. As physicians who are typically high earners, you are not able to contribute directly to a Roth IRA because of income limitations. This is where the Roth conversion strategy — the backdoor Roth — comes into play. This strategy allows you to make a nondeductible traditional IRA contribution and then convert those dollars into a Roth IRA. In 2023, you can contribute up to $6,500 into this type of account. There are many additional considerations that must be made before implementing this strategy. Discussion with a financial advisor or CPA is recommended.
FAQ 5. I’ve always done my own taxes. Do I need to hire a CPA?
A: For many physicians, especially during training, your tax situation may not warrant the need for a Certified Public Accountant (CPA). However, as your income and tax complexity increase, working with a CPA not only decreases your risk for error, but also helps ensure you are not overpaying in taxes. There are many different types of services that a CPA can offer, the most basic being tax preparation. This is simply compiling your tax return based on the circumstances that occurred in the prior year. Tax planning is an additional level of service that may not be included in tax preparation cost. Tax planning is a proactive approach to taxes and helps maximize tax savings opportunities before return preparation. When interviewing a potential CPA, you can ask what level of services are included in the fees quoted.
These are just a few of the questions I regularly answer related to physicians’ taxation. The tax code is complex and ever changing. Recommendations that are made today might not be applicable or advisable in the future to any given situation. Working with a professional can ensure you have the most up-to-date and accurate information related to your taxes.
Ms. Anderson is with Physician’s Resource Services and is on Instagram @physiciansrs . Dr. Anderson is a CA-1 Resident in Anesthesia at Baylor Scott and White Health. The authors have no conflicts of interest.
Roflumilast foam gets nod as new option for seborrheic dermatitis
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
Survival-Toxicity Trade-off With T-DM1 in HER+ Breast Cancer
SAN ANTONIO — in older patients with advanced human epidermal growth factor receptor 2–positive (HER2+) breast cancer, although toxicity is much lower, results from the HERB TEA study show.
Overall, the standard-of-care triple regimen of monoclonal antibodies pertuzumab and trastuzumab plus docetaxel remains the “first-line treatment for HER2-positive advanced breast cancer, regardless of age,” said study author Akihiko Shimomura, MD, PhD, who presented the findings (abstract RF02-04) on December 7 at the San Antonio Breast Cancer Symposium.
However, he noted that the standard-of-care regimen appears to be “intolerable mentally and physically” in those older than 65 years, and “impairs” quality of life.
Therefore a “new standard treatment with less toxicity and noninferior efficacy for older patients is needed,” said Dr. Shimomura, Department of Breast and Medical Oncology, National Center for Global Health and Medicine, Tokyo.
Dr. Shimomura and colleagues recruited patients aged 65 years or older with advanced HER2+ breast cancer who had received no prior chemotherapy for metastatic breast cancer and had a good performance status.
Patients were randomly assigned to either pertuzumab and trastuzumab plus docetaxel or T-DM1 until disease progression. The planned sample size was 250 patients, but the study was terminated after 148 participants were recruited because an interim analysis showed that T-DM1 failed to show noninferiority.
Among 75 patients assigned to the standard-of-care regimen, the mean age was 71 years, with 64% aged 65-74 years. Sixty-five percent had stage IV disease, and 35% had relapsed. These baseline characteristics were similar among the 73 patients given T-DM1.
At the data cutoff of June 15, 2023, the median progression-free survival was comparable between the two groups, at 15.6 months with the triple therapy vs 11.3 months with T-DM1 (hazard ratio [HR], 1.358; P =.1236).
There was also no significant difference in overall survival between the two groups (HR, 1.263; P =.95322).
However, T-DM1 failed to meet its primary endpoint of noninferiority to pertuzumab and trastuzumab plus docetaxel, defined as a hazard ratio for overall survival of 1.35.
Nevertheless, T-DM1 was associated with significantly less toxicity than the standard-of care-regimen, with rates of grade 3 or worse adverse events of 36.1% vs 56.8%, Shimomura reported.
The most common hematologic adverse events with the triple therapy were leukopenia (34.2%) and neutropenia (52.0%), whereas thrombocytopenia was the most common event with T-DM1 (16.7%).
Liver toxicities were also increased with the antibody-drug conjugate, whereas fatigue, diarrhea, and appetite loss were more frequently seen with the standard-of-care regimen.
Although T-DM1 did not achieve noninferiority, given its lower toxicity profile, a “detailed analysis, including geriatric assessment, is needed to identify the patient population for whom T-DM1 may be used as first line treatment,” said Shimomura.
Virginia Kaklamani, MD, codirector of the SABCS and leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center, Texas, said in an interview that the trial shows T-DM1 could be “a good alternative to our first line therapy in HER2+ metastatic breast cancer” for some patients.
“It is, however, unlikely to change the standard of care due to several changes in the field including the results from the KATHERINE trial and the DESTINY-Breast trials,” she said.
The study was funded by the Japanese National Cancer Center. Dr. Shimomura declares relationships with Daiichi Sankyo, Pfizer, AstraZeneca K.K., Chugai Pharmaceutical Co. Ltd, Eli Lilly Japan K.K., MSD Co. Ltd, Eisai Co. Ltd, Gilead Sciences, and Taiho Pharmaceutical Co. Ltd.
A version of this article appeared on Medscape.com.
SAN ANTONIO — in older patients with advanced human epidermal growth factor receptor 2–positive (HER2+) breast cancer, although toxicity is much lower, results from the HERB TEA study show.
Overall, the standard-of-care triple regimen of monoclonal antibodies pertuzumab and trastuzumab plus docetaxel remains the “first-line treatment for HER2-positive advanced breast cancer, regardless of age,” said study author Akihiko Shimomura, MD, PhD, who presented the findings (abstract RF02-04) on December 7 at the San Antonio Breast Cancer Symposium.
However, he noted that the standard-of-care regimen appears to be “intolerable mentally and physically” in those older than 65 years, and “impairs” quality of life.
Therefore a “new standard treatment with less toxicity and noninferior efficacy for older patients is needed,” said Dr. Shimomura, Department of Breast and Medical Oncology, National Center for Global Health and Medicine, Tokyo.
Dr. Shimomura and colleagues recruited patients aged 65 years or older with advanced HER2+ breast cancer who had received no prior chemotherapy for metastatic breast cancer and had a good performance status.
Patients were randomly assigned to either pertuzumab and trastuzumab plus docetaxel or T-DM1 until disease progression. The planned sample size was 250 patients, but the study was terminated after 148 participants were recruited because an interim analysis showed that T-DM1 failed to show noninferiority.
Among 75 patients assigned to the standard-of-care regimen, the mean age was 71 years, with 64% aged 65-74 years. Sixty-five percent had stage IV disease, and 35% had relapsed. These baseline characteristics were similar among the 73 patients given T-DM1.
At the data cutoff of June 15, 2023, the median progression-free survival was comparable between the two groups, at 15.6 months with the triple therapy vs 11.3 months with T-DM1 (hazard ratio [HR], 1.358; P =.1236).
There was also no significant difference in overall survival between the two groups (HR, 1.263; P =.95322).
However, T-DM1 failed to meet its primary endpoint of noninferiority to pertuzumab and trastuzumab plus docetaxel, defined as a hazard ratio for overall survival of 1.35.
Nevertheless, T-DM1 was associated with significantly less toxicity than the standard-of care-regimen, with rates of grade 3 or worse adverse events of 36.1% vs 56.8%, Shimomura reported.
The most common hematologic adverse events with the triple therapy were leukopenia (34.2%) and neutropenia (52.0%), whereas thrombocytopenia was the most common event with T-DM1 (16.7%).
Liver toxicities were also increased with the antibody-drug conjugate, whereas fatigue, diarrhea, and appetite loss were more frequently seen with the standard-of-care regimen.
Although T-DM1 did not achieve noninferiority, given its lower toxicity profile, a “detailed analysis, including geriatric assessment, is needed to identify the patient population for whom T-DM1 may be used as first line treatment,” said Shimomura.
Virginia Kaklamani, MD, codirector of the SABCS and leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center, Texas, said in an interview that the trial shows T-DM1 could be “a good alternative to our first line therapy in HER2+ metastatic breast cancer” for some patients.
“It is, however, unlikely to change the standard of care due to several changes in the field including the results from the KATHERINE trial and the DESTINY-Breast trials,” she said.
The study was funded by the Japanese National Cancer Center. Dr. Shimomura declares relationships with Daiichi Sankyo, Pfizer, AstraZeneca K.K., Chugai Pharmaceutical Co. Ltd, Eli Lilly Japan K.K., MSD Co. Ltd, Eisai Co. Ltd, Gilead Sciences, and Taiho Pharmaceutical Co. Ltd.
A version of this article appeared on Medscape.com.
SAN ANTONIO — in older patients with advanced human epidermal growth factor receptor 2–positive (HER2+) breast cancer, although toxicity is much lower, results from the HERB TEA study show.
Overall, the standard-of-care triple regimen of monoclonal antibodies pertuzumab and trastuzumab plus docetaxel remains the “first-line treatment for HER2-positive advanced breast cancer, regardless of age,” said study author Akihiko Shimomura, MD, PhD, who presented the findings (abstract RF02-04) on December 7 at the San Antonio Breast Cancer Symposium.
However, he noted that the standard-of-care regimen appears to be “intolerable mentally and physically” in those older than 65 years, and “impairs” quality of life.
Therefore a “new standard treatment with less toxicity and noninferior efficacy for older patients is needed,” said Dr. Shimomura, Department of Breast and Medical Oncology, National Center for Global Health and Medicine, Tokyo.
Dr. Shimomura and colleagues recruited patients aged 65 years or older with advanced HER2+ breast cancer who had received no prior chemotherapy for metastatic breast cancer and had a good performance status.
Patients were randomly assigned to either pertuzumab and trastuzumab plus docetaxel or T-DM1 until disease progression. The planned sample size was 250 patients, but the study was terminated after 148 participants were recruited because an interim analysis showed that T-DM1 failed to show noninferiority.
Among 75 patients assigned to the standard-of-care regimen, the mean age was 71 years, with 64% aged 65-74 years. Sixty-five percent had stage IV disease, and 35% had relapsed. These baseline characteristics were similar among the 73 patients given T-DM1.
At the data cutoff of June 15, 2023, the median progression-free survival was comparable between the two groups, at 15.6 months with the triple therapy vs 11.3 months with T-DM1 (hazard ratio [HR], 1.358; P =.1236).
There was also no significant difference in overall survival between the two groups (HR, 1.263; P =.95322).
However, T-DM1 failed to meet its primary endpoint of noninferiority to pertuzumab and trastuzumab plus docetaxel, defined as a hazard ratio for overall survival of 1.35.
Nevertheless, T-DM1 was associated with significantly less toxicity than the standard-of care-regimen, with rates of grade 3 or worse adverse events of 36.1% vs 56.8%, Shimomura reported.
The most common hematologic adverse events with the triple therapy were leukopenia (34.2%) and neutropenia (52.0%), whereas thrombocytopenia was the most common event with T-DM1 (16.7%).
Liver toxicities were also increased with the antibody-drug conjugate, whereas fatigue, diarrhea, and appetite loss were more frequently seen with the standard-of-care regimen.
Although T-DM1 did not achieve noninferiority, given its lower toxicity profile, a “detailed analysis, including geriatric assessment, is needed to identify the patient population for whom T-DM1 may be used as first line treatment,” said Shimomura.
Virginia Kaklamani, MD, codirector of the SABCS and leader of the Breast Cancer Program at the UT Health San Antonio Cancer Center, Texas, said in an interview that the trial shows T-DM1 could be “a good alternative to our first line therapy in HER2+ metastatic breast cancer” for some patients.
“It is, however, unlikely to change the standard of care due to several changes in the field including the results from the KATHERINE trial and the DESTINY-Breast trials,” she said.
The study was funded by the Japanese National Cancer Center. Dr. Shimomura declares relationships with Daiichi Sankyo, Pfizer, AstraZeneca K.K., Chugai Pharmaceutical Co. Ltd, Eli Lilly Japan K.K., MSD Co. Ltd, Eisai Co. Ltd, Gilead Sciences, and Taiho Pharmaceutical Co. Ltd.
A version of this article appeared on Medscape.com.
AT SABCS 2023
Deciphering the usefulness of probiotics
The idea of the use of probiotics has a history going back more than a century when Russian scientist, Elie Metchnikoff, theorized that lactic acid bacteria may offer health benefits as well as promote longevity. In the early 1900s, intestinal disorders were frequently treated with nonpathogenic bacteria to replace gut microbes.
Today, the market is flooded with products from foods to prescription medications containing probiotics that extol their health benefits. It has been estimated that the global market for probiotics is more than $32 billion dollars annually and is expected to increase 8% per year.

As family doctors, patients come to us with many questions about the use of probiotics. Look online or on store shelves — there are so many types, doses, and brands of probiotics it is hard to decipher which are worth using. We older doctors never received much education about them.
Earlier this year, the World Gastroenterology Organization (WGO) developed recommendations around the use of probiotics and defined them as “live microbes that have been shown in controlled human studies to impart a health benefit.” Their recommendation is to use the strains that have been shown to be beneficial for the condition they claim to help and have been shown to do so in controlled studies. The dosage advised should be that shown to be useful in studies.
While this is an easy statement to make, it is much less so in clinical practice. The guidelines do a good job breaking down the conditions they help and the strains that have shown to be beneficial for specific conditions.
There have been claims that probiotics have been shown to be beneficial in colorectal cancer. While there have been some studies to show that they can improve markers associated with colorectal cancer, there are no data that probiotics actually do much in terms of prevention. Eating a healthy diet is more helpful here.
One area where probiotics have been shown to be beneficial is in the prevention of antibiotic-associated diarrhea. This makes sense since we know that antibiotics can kill the “good bacteria” lining the gut wall and probiotics work to replace them. Other conditions where these agents have been shown to be beneficial include radiation-induced diarrhea, acute diarrhea, irritable bowel syndrome, and colic in breast-fed infants.
The guideline contains good evidence of where and which types of probiotics are useful and it is good to look at the charts in the paper to see the specific strains recommended. It also contains an extensive reference section, and as primary care physicians, it is imperative that we educate ourselves on these agents.
While probiotics are typically sold as supplements, we should not dismiss them summarily. It is easy to do that when supplemental products are marketed and sold unethically with no clinical evidence of benefit. We need to remember that just because something is a supplement doesn’t necessarily mean that it was not studied.
Family physicians need to be able to educate their patients and answer their questions. When we don’t have the answers, we need to find them. Any time our patient doesn’t get good information from us, they will probably go to the Internet and get bad advice from someone else.
There is much ongoing research about the gut microbiome and the bacteria that can be found in the gut. Researchers are looking into the “gut-brain” axis but there is not much good evidence of this link yet. There is no evidence that probiotics can cure Alzheimer’s disease or Parkinsonism. The future may reveal different stories, but for now, we need to follow the evidence we have available.
There are many outlandish claims about what the gut microbiome is responsible for and can do for health. It is easy to have a knee-jerk reaction when anyone brings it up in conversation. We need to arm ourselves with the evidence. We are stewards of the health and safety of our patients.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. She was paid by Pfizer as a consultant on Paxlovid and is the editor in chief of Physician’s Weekly.
The idea of the use of probiotics has a history going back more than a century when Russian scientist, Elie Metchnikoff, theorized that lactic acid bacteria may offer health benefits as well as promote longevity. In the early 1900s, intestinal disorders were frequently treated with nonpathogenic bacteria to replace gut microbes.
Today, the market is flooded with products from foods to prescription medications containing probiotics that extol their health benefits. It has been estimated that the global market for probiotics is more than $32 billion dollars annually and is expected to increase 8% per year.
As family doctors, patients come to us with many questions about the use of probiotics. Look online or on store shelves — there are so many types, doses, and brands of probiotics it is hard to decipher which are worth using. We older doctors never received much education about them.
Earlier this year, the World Gastroenterology Organization (WGO) developed recommendations around the use of probiotics and defined them as “live microbes that have been shown in controlled human studies to impart a health benefit.” Their recommendation is to use the strains that have been shown to be beneficial for the condition they claim to help and have been shown to do so in controlled studies. The dosage advised should be that shown to be useful in studies.
While this is an easy statement to make, it is much less so in clinical practice. The guidelines do a good job breaking down the conditions they help and the strains that have shown to be beneficial for specific conditions.
There have been claims that probiotics have been shown to be beneficial in colorectal cancer. While there have been some studies to show that they can improve markers associated with colorectal cancer, there are no data that probiotics actually do much in terms of prevention. Eating a healthy diet is more helpful here.
One area where probiotics have been shown to be beneficial is in the prevention of antibiotic-associated diarrhea. This makes sense since we know that antibiotics can kill the “good bacteria” lining the gut wall and probiotics work to replace them. Other conditions where these agents have been shown to be beneficial include radiation-induced diarrhea, acute diarrhea, irritable bowel syndrome, and colic in breast-fed infants.
The guideline contains good evidence of where and which types of probiotics are useful and it is good to look at the charts in the paper to see the specific strains recommended. It also contains an extensive reference section, and as primary care physicians, it is imperative that we educate ourselves on these agents.
While probiotics are typically sold as supplements, we should not dismiss them summarily. It is easy to do that when supplemental products are marketed and sold unethically with no clinical evidence of benefit. We need to remember that just because something is a supplement doesn’t necessarily mean that it was not studied.
Family physicians need to be able to educate their patients and answer their questions. When we don’t have the answers, we need to find them. Any time our patient doesn’t get good information from us, they will probably go to the Internet and get bad advice from someone else.
There is much ongoing research about the gut microbiome and the bacteria that can be found in the gut. Researchers are looking into the “gut-brain” axis but there is not much good evidence of this link yet. There is no evidence that probiotics can cure Alzheimer’s disease or Parkinsonism. The future may reveal different stories, but for now, we need to follow the evidence we have available.
There are many outlandish claims about what the gut microbiome is responsible for and can do for health. It is easy to have a knee-jerk reaction when anyone brings it up in conversation. We need to arm ourselves with the evidence. We are stewards of the health and safety of our patients.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. She was paid by Pfizer as a consultant on Paxlovid and is the editor in chief of Physician’s Weekly.
The idea of the use of probiotics has a history going back more than a century when Russian scientist, Elie Metchnikoff, theorized that lactic acid bacteria may offer health benefits as well as promote longevity. In the early 1900s, intestinal disorders were frequently treated with nonpathogenic bacteria to replace gut microbes.
Today, the market is flooded with products from foods to prescription medications containing probiotics that extol their health benefits. It has been estimated that the global market for probiotics is more than $32 billion dollars annually and is expected to increase 8% per year.
As family doctors, patients come to us with many questions about the use of probiotics. Look online or on store shelves — there are so many types, doses, and brands of probiotics it is hard to decipher which are worth using. We older doctors never received much education about them.
Earlier this year, the World Gastroenterology Organization (WGO) developed recommendations around the use of probiotics and defined them as “live microbes that have been shown in controlled human studies to impart a health benefit.” Their recommendation is to use the strains that have been shown to be beneficial for the condition they claim to help and have been shown to do so in controlled studies. The dosage advised should be that shown to be useful in studies.
While this is an easy statement to make, it is much less so in clinical practice. The guidelines do a good job breaking down the conditions they help and the strains that have shown to be beneficial for specific conditions.
There have been claims that probiotics have been shown to be beneficial in colorectal cancer. While there have been some studies to show that they can improve markers associated with colorectal cancer, there are no data that probiotics actually do much in terms of prevention. Eating a healthy diet is more helpful here.
One area where probiotics have been shown to be beneficial is in the prevention of antibiotic-associated diarrhea. This makes sense since we know that antibiotics can kill the “good bacteria” lining the gut wall and probiotics work to replace them. Other conditions where these agents have been shown to be beneficial include radiation-induced diarrhea, acute diarrhea, irritable bowel syndrome, and colic in breast-fed infants.
The guideline contains good evidence of where and which types of probiotics are useful and it is good to look at the charts in the paper to see the specific strains recommended. It also contains an extensive reference section, and as primary care physicians, it is imperative that we educate ourselves on these agents.
While probiotics are typically sold as supplements, we should not dismiss them summarily. It is easy to do that when supplemental products are marketed and sold unethically with no clinical evidence of benefit. We need to remember that just because something is a supplement doesn’t necessarily mean that it was not studied.
Family physicians need to be able to educate their patients and answer their questions. When we don’t have the answers, we need to find them. Any time our patient doesn’t get good information from us, they will probably go to the Internet and get bad advice from someone else.
There is much ongoing research about the gut microbiome and the bacteria that can be found in the gut. Researchers are looking into the “gut-brain” axis but there is not much good evidence of this link yet. There is no evidence that probiotics can cure Alzheimer’s disease or Parkinsonism. The future may reveal different stories, but for now, we need to follow the evidence we have available.
There are many outlandish claims about what the gut microbiome is responsible for and can do for health. It is easy to have a knee-jerk reaction when anyone brings it up in conversation. We need to arm ourselves with the evidence. We are stewards of the health and safety of our patients.
Dr. Girgis practices family medicine in South River, N.J., and is a clinical assistant professor of family medicine at Robert Wood Johnson Medical School, New Brunswick, N.J. She was paid by Pfizer as a consultant on Paxlovid and is the editor in chief of Physician’s Weekly.
Pregnancy safe after BRCA-mutated breast cancer
SAN ANTONIO — New research provides some reassuring news for young women hoping to become pregnant after a diagnosis of BRCA-mutated breast cancer.
said Jame Abraham, MD, chair of Hematology & Medical Oncology at the Cleveland Clinic, who was not involved in the research.
The analysis, presented at the San Antonio Breast Cancer Symposium, revealed no issue with women becoming pregnant and carrying a healthy baby to term and reported no sign of worse disease outcomes among BRCA carriers following diagnosis and treatment.
“The final and most important conclusion from our study is that conceiving after proper breast cancer treatment and follow-up should not be contraindicated anymore in young BRCA carriers,” a message of particular importance for oncofertility counseling, lead investigator Matteo Lambertini, MD, a breast cancer oncologist at the University of Genova, Italy, said during his SABCS presentation.
The study was published December 7 in JAMA to coincide with his presentation.
Although pregnancy after breast cancer is generally considered safe, limited data exist for BRCA carriers in particular, Dr. Lambertini said.
The current analysis represents the largest look into the matter to date. The study included 4732 young women from across the globe who had been diagnosed with stage I-III invasive breast cancer. These women, all BRCA carriers, were 40 years or younger (median age at diagnosis, 35 years).
The team compared outcomes between 659 patients who had at least one pregnancy over a median follow-up of almost 8 years with 4073 women who did not become pregnant.
Dr. Lambertini and colleagues reported a median time of 3.5 years from breast cancer diagnosis to conception. Overall, about 1 in 5 young BRCA carriers (22%) conceived within 10 years after their breast cancer diagnosis. Of the 80% of patients with a completed pregnancy, 91% delivered at term and only 4 infants (0.9%) had documented congenital anomalies.
In short, “the rate of pregnancy, fetal, and obstetric complications was low and in line with the expectations in a population of women with similar age and no history of breast cancer,” Dr. Lambertini said. The team cautioned, however, that the data was extracted from oncology medical records, which might have underreported maternal and fetal outcomes.
Disease-free survival was similar among women who became pregnant and those who did not after breast cancer (adjusted HR, 0.99; 95% CI, 0.81-1.20).
When looking at the specific BRCA gene, differences did emerge. BRCA1 carriers had better disease-free survival after pregnancy (aHR, 0.80), while BRCA2 carriers appeared to have worse disease-free survival after pregnancy (aHR, 1.55).
For reasons that remain unclear, the researchers also found that BRCA1 carriers who got pregnant had significantly better breast cancer-specific survival (aHR, 0.59; P < .01) and overall survival (aHR, 0.58; P < .01). These women tended to have HR-negative breast cancer, which the authors also found was associated with improved survival after pregnancy (aHR, 0.76).
It’s possible, the team posited, that hormone receptor status played a role in the observed survival benefit. It’s also possible that these women were healthier overall.
The overall survival advantage, however, did not extend to BRCA2 carriers, who tended to have hormone receptor-positive disease. Hormone receptor-positive status did not appear to have a significant impact on survival (aHR, 1.30; 95% CI, 0.95-1.76).
“While the results appear reassuring for BRCA1 carriers, more caution is needed to counsel BRCA2 carriers, “ the investigators wrote.
The study was funded by the Italian Association for Cancer Research, Gilead, and others. Investigators had numerous ties to industry, including Dr. Lambertini, who is an adviser and speaker for Roche, Pfizer, Novartis, and others. The full list of disclosures can be found with the original article.
A version of this article appeared on Medscape.com.
SAN ANTONIO — New research provides some reassuring news for young women hoping to become pregnant after a diagnosis of BRCA-mutated breast cancer.
said Jame Abraham, MD, chair of Hematology & Medical Oncology at the Cleveland Clinic, who was not involved in the research.
The analysis, presented at the San Antonio Breast Cancer Symposium, revealed no issue with women becoming pregnant and carrying a healthy baby to term and reported no sign of worse disease outcomes among BRCA carriers following diagnosis and treatment.
“The final and most important conclusion from our study is that conceiving after proper breast cancer treatment and follow-up should not be contraindicated anymore in young BRCA carriers,” a message of particular importance for oncofertility counseling, lead investigator Matteo Lambertini, MD, a breast cancer oncologist at the University of Genova, Italy, said during his SABCS presentation.
The study was published December 7 in JAMA to coincide with his presentation.
Although pregnancy after breast cancer is generally considered safe, limited data exist for BRCA carriers in particular, Dr. Lambertini said.
The current analysis represents the largest look into the matter to date. The study included 4732 young women from across the globe who had been diagnosed with stage I-III invasive breast cancer. These women, all BRCA carriers, were 40 years or younger (median age at diagnosis, 35 years).
The team compared outcomes between 659 patients who had at least one pregnancy over a median follow-up of almost 8 years with 4073 women who did not become pregnant.
Dr. Lambertini and colleagues reported a median time of 3.5 years from breast cancer diagnosis to conception. Overall, about 1 in 5 young BRCA carriers (22%) conceived within 10 years after their breast cancer diagnosis. Of the 80% of patients with a completed pregnancy, 91% delivered at term and only 4 infants (0.9%) had documented congenital anomalies.
In short, “the rate of pregnancy, fetal, and obstetric complications was low and in line with the expectations in a population of women with similar age and no history of breast cancer,” Dr. Lambertini said. The team cautioned, however, that the data was extracted from oncology medical records, which might have underreported maternal and fetal outcomes.
Disease-free survival was similar among women who became pregnant and those who did not after breast cancer (adjusted HR, 0.99; 95% CI, 0.81-1.20).
When looking at the specific BRCA gene, differences did emerge. BRCA1 carriers had better disease-free survival after pregnancy (aHR, 0.80), while BRCA2 carriers appeared to have worse disease-free survival after pregnancy (aHR, 1.55).
For reasons that remain unclear, the researchers also found that BRCA1 carriers who got pregnant had significantly better breast cancer-specific survival (aHR, 0.59; P < .01) and overall survival (aHR, 0.58; P < .01). These women tended to have HR-negative breast cancer, which the authors also found was associated with improved survival after pregnancy (aHR, 0.76).
It’s possible, the team posited, that hormone receptor status played a role in the observed survival benefit. It’s also possible that these women were healthier overall.
The overall survival advantage, however, did not extend to BRCA2 carriers, who tended to have hormone receptor-positive disease. Hormone receptor-positive status did not appear to have a significant impact on survival (aHR, 1.30; 95% CI, 0.95-1.76).
“While the results appear reassuring for BRCA1 carriers, more caution is needed to counsel BRCA2 carriers, “ the investigators wrote.
The study was funded by the Italian Association for Cancer Research, Gilead, and others. Investigators had numerous ties to industry, including Dr. Lambertini, who is an adviser and speaker for Roche, Pfizer, Novartis, and others. The full list of disclosures can be found with the original article.
A version of this article appeared on Medscape.com.
SAN ANTONIO — New research provides some reassuring news for young women hoping to become pregnant after a diagnosis of BRCA-mutated breast cancer.
said Jame Abraham, MD, chair of Hematology & Medical Oncology at the Cleveland Clinic, who was not involved in the research.
The analysis, presented at the San Antonio Breast Cancer Symposium, revealed no issue with women becoming pregnant and carrying a healthy baby to term and reported no sign of worse disease outcomes among BRCA carriers following diagnosis and treatment.
“The final and most important conclusion from our study is that conceiving after proper breast cancer treatment and follow-up should not be contraindicated anymore in young BRCA carriers,” a message of particular importance for oncofertility counseling, lead investigator Matteo Lambertini, MD, a breast cancer oncologist at the University of Genova, Italy, said during his SABCS presentation.
The study was published December 7 in JAMA to coincide with his presentation.
Although pregnancy after breast cancer is generally considered safe, limited data exist for BRCA carriers in particular, Dr. Lambertini said.
The current analysis represents the largest look into the matter to date. The study included 4732 young women from across the globe who had been diagnosed with stage I-III invasive breast cancer. These women, all BRCA carriers, were 40 years or younger (median age at diagnosis, 35 years).
The team compared outcomes between 659 patients who had at least one pregnancy over a median follow-up of almost 8 years with 4073 women who did not become pregnant.
Dr. Lambertini and colleagues reported a median time of 3.5 years from breast cancer diagnosis to conception. Overall, about 1 in 5 young BRCA carriers (22%) conceived within 10 years after their breast cancer diagnosis. Of the 80% of patients with a completed pregnancy, 91% delivered at term and only 4 infants (0.9%) had documented congenital anomalies.
In short, “the rate of pregnancy, fetal, and obstetric complications was low and in line with the expectations in a population of women with similar age and no history of breast cancer,” Dr. Lambertini said. The team cautioned, however, that the data was extracted from oncology medical records, which might have underreported maternal and fetal outcomes.
Disease-free survival was similar among women who became pregnant and those who did not after breast cancer (adjusted HR, 0.99; 95% CI, 0.81-1.20).
When looking at the specific BRCA gene, differences did emerge. BRCA1 carriers had better disease-free survival after pregnancy (aHR, 0.80), while BRCA2 carriers appeared to have worse disease-free survival after pregnancy (aHR, 1.55).
For reasons that remain unclear, the researchers also found that BRCA1 carriers who got pregnant had significantly better breast cancer-specific survival (aHR, 0.59; P < .01) and overall survival (aHR, 0.58; P < .01). These women tended to have HR-negative breast cancer, which the authors also found was associated with improved survival after pregnancy (aHR, 0.76).
It’s possible, the team posited, that hormone receptor status played a role in the observed survival benefit. It’s also possible that these women were healthier overall.
The overall survival advantage, however, did not extend to BRCA2 carriers, who tended to have hormone receptor-positive disease. Hormone receptor-positive status did not appear to have a significant impact on survival (aHR, 1.30; 95% CI, 0.95-1.76).
“While the results appear reassuring for BRCA1 carriers, more caution is needed to counsel BRCA2 carriers, “ the investigators wrote.
The study was funded by the Italian Association for Cancer Research, Gilead, and others. Investigators had numerous ties to industry, including Dr. Lambertini, who is an adviser and speaker for Roche, Pfizer, Novartis, and others. The full list of disclosures can be found with the original article.
A version of this article appeared on Medscape.com.
FROM SABCS 2023
Caring for LGBTQ+ Patients with IBD
Cases
Patient 1: 55-year-old cis-male, who identifies as gay, has ulcerative colitis that has been refractory to multiple biologic therapies. His provider recommends a total proctocolectomy with ileal pouch anal anastomosis (TPC with IPAA), but the patient has questions regarding sexual function following surgery. Specifically, he is wondering when, or if, he can resume receptive anal intercourse. How would you counsel him?
Patient 2: 25-year-old, trans-female, status-post vaginoplasty with use of sigmoid colon and with well-controlled ulcerative colitis, presents with vaginal discharge, weight loss, and rectal bleeding. How do you explain what has happened to her? During your discussion, she also asks you why her chart continues to use her “dead name.” How do you respond?
Patient 3: 32-year-old, cis-female, G2P2, who identifies as a lesbian, has active ulcerative colitis. She wants to discuss medical or surgical therapy and future pregnancies. How would you counsel her?
Many gastroenterologists would likely know how to address patient 3’s concerns, but the concerns of patients 1 and 2 often go unaddressed or dismissed. Numerous studies and surveys have been conducted on patients with inflammatory bowel disease (IBD), but the focus of these studies has always been through a heteronormative cisgender lens. The focus of many studies is on fertility or sexual health and function in cisgender, heteronormative individuals.1-3 In the last few years, however, there has been increasing awareness of the health disparities, stigma, and discrimination that sexual and gender minorities (SGM) experience.4-6 For the purposes of this discussion, individuals within the lesbian, gay, bisexual, transgender, queer/questioning, intersex, and asexual (LGBTQIA+) community will be referred to as SGM. We recognize that even this exhaustive listing above does not acknowledge the full spectrum of diversity within the SGM community.
Clinical Care/Competency for SGM with IBD is Lacking
Almost 10% of the US population identifies as some form of SGM, and that number can be higher within the younger generations.4 SGM patients tend to delay or avoid seeking health care due to concern for provider mistreatment or lack of regard for their individual concerns. Additionally, there are several gaps in clinical knowledge about caring for SGM individuals. Little is known regarding the incidence or prevalence of IBD in SGM populations, but it is perceived to be similar to cisgender heterosexual individuals. Furthermore, as Newman et al. highlighted in their systematic review published in May 2023, there is a lack of guidance regarding sexual activity in the setting of IBD in SGM individuals.5 There is also a significant lack of knowledge on the impact of gender-affirming care on the natural history and treatments of IBD in transgender and gender non-conforming (TGNC) individuals. This can impact providers’ comfort and competence in caring for TGNC individuals.

Another important point to make is that the SGM community still faces discrimination due to sexual orientation or gender identity to this day, which impacts the quality and delivery of their care.7 Culturally-competent care should include care that is free from stigma, implicit and explicit biases, and discrimination. In 2011, an Institute of Medicine report documented, among other issues, provider discomfort in delivering care to SGM patients.8 While SGM individuals prefer a provider who acknowledges their sexual orientation and gender identity and treats them with the dignity and respect they deserve, many SGM individuals share valid concerns regarding their safety, which impact their desire to disclose their identity to health care providers.9 This certainly can have an impact on the quality of care they receive, including important health maintenance milestones and cancer screenings.10
An internal survey at our institution of providers (nurses, physician assistants, surgeons, and physicians) found that among 85 responders, 70% have cared for SGM who have undergone TPC with ileal pouch anal anastomosis (IPAA). Of these, 75% did not ask about sexual orientation or practices before pouch formation (though almost all of them agreed it would be important to ask). A total of 55% were comfortable in discussing SGM-related concerns; 53% did not feel comfortable discussing sexual orientation or practices; and in particular when it came to anoreceptive intercourse (ARI), 73% did not feel confident discussing recommendations.11
All of these issues highlight the importance of developing curricula that focus on reducing implicit and explicit biases towards SGM individuals and increasing the competence of providers to take care of SGM individuals in a safe space.

Additionally, it further justifies the need for ethical research that focuses on the needs of SGM individuals to guide evidence-based approaches to care. Given the implicit and explicit heterosexism and transphobia in society and many health care systems, Rainbows in Gastro was formed as an advocacy group for SGM patients, trainees, and staff in gastroenterology and hepatology.4
Research in SGM and IBD is lacking
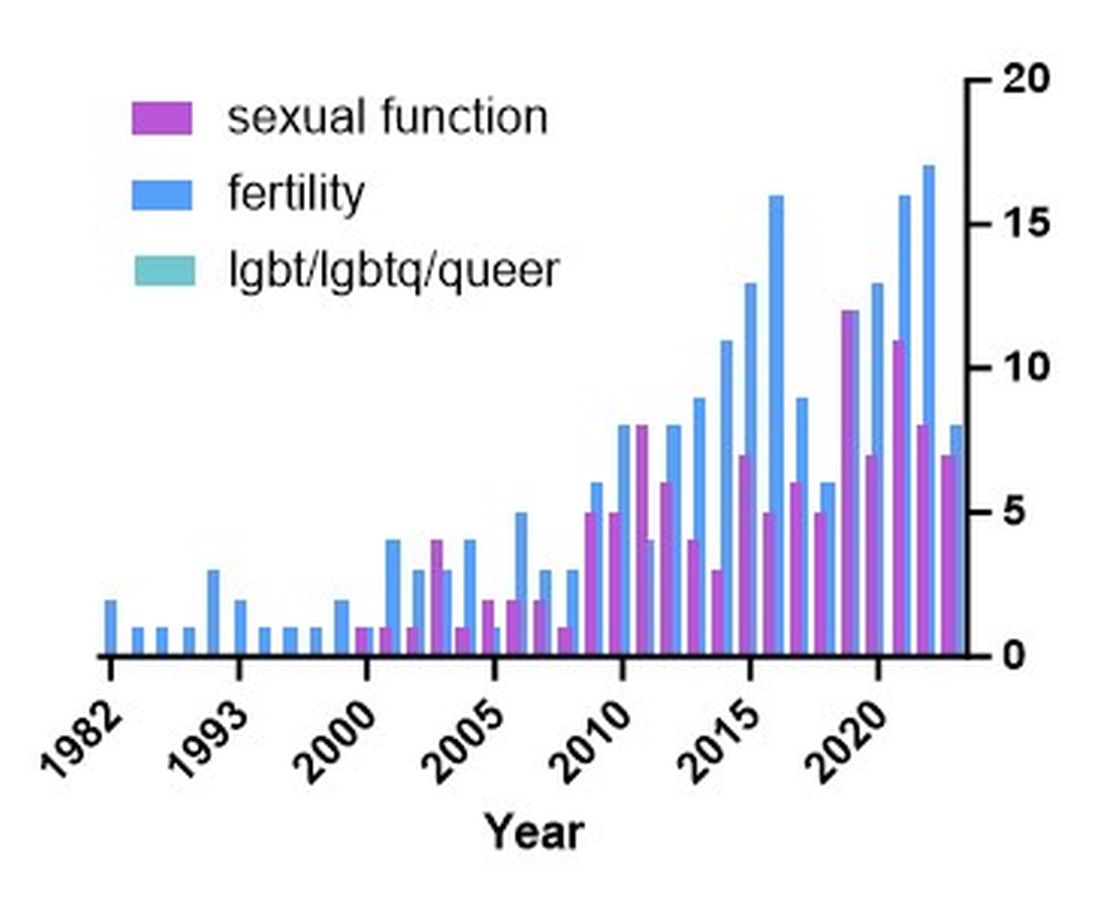
There are additional needs for research in IBD and how it pertains to the needs of SGM individuals. Figure 1 highlights the lack of PubMed results for the search terms “IBD + LGBT,” “IBD + LGBTQ,” or “IBD + queer.” In contrast, the search terms “IBD + fertility” and “IBD + sexual dysfunction” generate many results. Even a systemic review conducted by Newman et al. of multiple databases in 2022 found only seven articles that demonstrated appropriately performed studies on SGM patients with IBD.5 This highlights the significant dearth of research in the realm of SGM health in IBD.
Newman and colleagues have recently published research considerations for SGM individuals. They highlighted the need to include understanding the “unique combination of psychosocial, biomedical, and legal experiences” that results in different needs and outcomes. There were several areas identified, including minority stress, which comes from existence of being SGM, especially as transgender individuals face increasing legal challenges in a variety of settings, not just healthcare.6 In a retrospective chart review investigating social determinants of health in SGM-IBD populations,12 36% of patients reported some level of social isolation, and almost 50% reported some level of stress. A total of 40% of them self-reported some perceived level of risk with respect to employment, and 17% reported depression. Given that this was a chart review and not a strict questionnaire, this study was certainly limited, and we would hypothesize that these numbers are therefore underestimating the true proportion of SGM-IBD patients who deal with employment concerns, social isolation, or psychological distress.
What Next? Back to the Patients
Circling back to our patients from the introduction, how would you counsel each of them? In patient 1’s case, we would inform him that pelvic surgery can increase the risk for sexual dysfunction, such as erectile dysfunction. He additionally would be advised during a staged TPC with IPAA, he may experience issues with body image. However, should he desire to participate in receptive anal intercourse after completion of his surgeries, the general recommendation would be to wait at least 6 months and with proven remission. It should further be noted that these are not formalized recommendations, only highlighting the need for more research and consensus on standards of care for SGM patients. He should finally be told that because he has ulcerative colitis, removal of the colon does not remove the risk for future intestinal involvement such as possible pouchitis.
In patient 2’s case, she is likely experiencing diversion vaginitis related to use of her colon for her neo-vagina. She should undergo colonoscopy and vaginoscopy in addition to standard work-up for her known ulcerative colitis.13 Management should be done in a multidisciplinary approach between the IBD provider, gynecologist, and gender-affirming provider. The electronic medical record should be updated to reflect the patient’s preferred name, pronouns, and gender identity, and her medical records, including automated clinical reports, should be updated accordingly.
As for patient 3, she would be counseled according to well-documented guidelines on pregnancy and IBD, including risks of medications (such as Jak inhibitors or methotrexate) versus the risk of uncontrolled IBD during pregnancy.1
Regardless of a patient’s gender identity or sexual orientation, patient-centered, culturally competent, and sensitive care should be provided. At Mayo Clinic in Rochester, we started one of the first Pride in IBD Clinics, which focuses on the care of SGM individuals with IBD. Our focus is to address the needs of patients who belong to the SGM community in a wholistic approach within a safe space (https://www.youtube.com/watch?v=pYa_zYaCA6M; https://www.mayoclinic.org/departments-centers/inflammatory-bowel-disease-clinic/overview/ovc-20357763). Our process of developing the clinic included training all staff on proper communication and cultural sensitivity for the SGM community.
Furthermore, providing welcoming and affirming signs of inclusivity for SGM individuals at the provider’s office — including but not limited to rainbow progressive flags, gender-neutral bathroom signs, or pronoun pins on provider identification badges (see Figure 2) — are usually appreciated by patients. Ensuring that patient education materials do not assume gender (for example, using the term “parents” rather than “mother and father”) and using gender neutral terms on intake forms is very important. Inclusive communication includes providers introducing themselves by preferred name and pronouns, asking the patients to introduce themselves, and welcoming them to share their pronouns. These simple actions can provide an atmosphere of safety for SGM patients, which would serve to enhance the quality of care we can provide for them.
For Resources and Further Reading: CDC,14 the Fenway Institute’s National LGBTQIA+ Health Education Center,15 and US Department of Health and Human Services.16
Dr. Chiang and Dr. Chedid are both in the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota. Dr. Chedid is also with the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic. Neither of the authors have any relevant conflicts of interest. They are on X, formerly Twitter: @dr_davidchiang , @VictorChedidMD .
CITATIONS
1. Mahadevan U et al. Inflammatory bowel disease in pregnancy clinical care pathway: A report from the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology. 2019;156:1508-24.
2. Pires F et al. A survey on the impact of IBD in sexual health: Into intimacy. Medicine (Baltimore). 2022;101:e32279.
3. Mules TC et al. The impact of disease activity on sexual and erectile dysfunction in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2023;29:1244-54.
4. Duong N et al. Overcoming disparities for sexual and gender minority patients and providers in gastroenterology and hepatology: Introduction to Rainbows in Gastro. Lancet Gastroenterol Hepatol. 2023;8:299-301.
5. Newman KL et al. A systematic review of inflammatory bowel disease epidemiology and health outcomes in sexual and gender minority individuals. Gastroenterology. 2023;164:866-71.
6. Newman KL et al. Research considerations in Digestive and liver disease in transgender and gender-diverse populations. Gastroenterology. 2023;165:523-28 e1.
7. Velez C et al. Digestive health in sexual and gender minority populations. Am J Gastroenterol. 2022;117:865-75.
8. Medicine Io. Washington (DC): The National Academies Press, 2011.
9. Austin EL. Sexual orientation disclosure to health care providers among urban and non-urban southern lesbians. Women Health. 2013;53:41-55.
10. Oladeru OT et al. Breast and cervical cancer screening disparities in transgender people. Am J Clin Oncol. 2022;45:116-21.
11. Vinsard DG et al. Healthcare providers’ perspectives on anoreceptive intercourse in sexual and gender minorities with ileal pouch anal anastomosis. Digestive Disease Week (DDW). Chicago, IL, 2023.
12. Ghusn W et al. Social determinants of health in LGBTQIA+ patients with inflammatory bowel disease. American College of Gastroenterology (ACG). Charlotte, NC, 2022.
13. Grasman ME et al. Neovaginal sparing in a transgender woman with ulcerative colitis. Clin Gastroenterol Hepatol. 2016;14:e73-4.
14. Prevention CfDCa. Lesbian, Gay, Bisexual, and Transgender Health — https://www.cdc.gov/lgbthealth/index.htm.
15. Institute TF. National LGBTQIA+ Health Education Center — https://www.lgbtqiahealtheducation.org/.
16. Services UDoHaH. LGBTQI+ Resources — https://www.hhs.gov/programs/topic-sites/lgbtqi/resources/index.html.
Cases
Patient 1: 55-year-old cis-male, who identifies as gay, has ulcerative colitis that has been refractory to multiple biologic therapies. His provider recommends a total proctocolectomy with ileal pouch anal anastomosis (TPC with IPAA), but the patient has questions regarding sexual function following surgery. Specifically, he is wondering when, or if, he can resume receptive anal intercourse. How would you counsel him?
Patient 2: 25-year-old, trans-female, status-post vaginoplasty with use of sigmoid colon and with well-controlled ulcerative colitis, presents with vaginal discharge, weight loss, and rectal bleeding. How do you explain what has happened to her? During your discussion, she also asks you why her chart continues to use her “dead name.” How do you respond?
Patient 3: 32-year-old, cis-female, G2P2, who identifies as a lesbian, has active ulcerative colitis. She wants to discuss medical or surgical therapy and future pregnancies. How would you counsel her?
Many gastroenterologists would likely know how to address patient 3’s concerns, but the concerns of patients 1 and 2 often go unaddressed or dismissed. Numerous studies and surveys have been conducted on patients with inflammatory bowel disease (IBD), but the focus of these studies has always been through a heteronormative cisgender lens. The focus of many studies is on fertility or sexual health and function in cisgender, heteronormative individuals.1-3 In the last few years, however, there has been increasing awareness of the health disparities, stigma, and discrimination that sexual and gender minorities (SGM) experience.4-6 For the purposes of this discussion, individuals within the lesbian, gay, bisexual, transgender, queer/questioning, intersex, and asexual (LGBTQIA+) community will be referred to as SGM. We recognize that even this exhaustive listing above does not acknowledge the full spectrum of diversity within the SGM community.
Clinical Care/Competency for SGM with IBD is Lacking
Almost 10% of the US population identifies as some form of SGM, and that number can be higher within the younger generations.4 SGM patients tend to delay or avoid seeking health care due to concern for provider mistreatment or lack of regard for their individual concerns. Additionally, there are several gaps in clinical knowledge about caring for SGM individuals. Little is known regarding the incidence or prevalence of IBD in SGM populations, but it is perceived to be similar to cisgender heterosexual individuals. Furthermore, as Newman et al. highlighted in their systematic review published in May 2023, there is a lack of guidance regarding sexual activity in the setting of IBD in SGM individuals.5 There is also a significant lack of knowledge on the impact of gender-affirming care on the natural history and treatments of IBD in transgender and gender non-conforming (TGNC) individuals. This can impact providers’ comfort and competence in caring for TGNC individuals.
Another important point to make is that the SGM community still faces discrimination due to sexual orientation or gender identity to this day, which impacts the quality and delivery of their care.7 Culturally-competent care should include care that is free from stigma, implicit and explicit biases, and discrimination. In 2011, an Institute of Medicine report documented, among other issues, provider discomfort in delivering care to SGM patients.8 While SGM individuals prefer a provider who acknowledges their sexual orientation and gender identity and treats them with the dignity and respect they deserve, many SGM individuals share valid concerns regarding their safety, which impact their desire to disclose their identity to health care providers.9 This certainly can have an impact on the quality of care they receive, including important health maintenance milestones and cancer screenings.10
An internal survey at our institution of providers (nurses, physician assistants, surgeons, and physicians) found that among 85 responders, 70% have cared for SGM who have undergone TPC with ileal pouch anal anastomosis (IPAA). Of these, 75% did not ask about sexual orientation or practices before pouch formation (though almost all of them agreed it would be important to ask). A total of 55% were comfortable in discussing SGM-related concerns; 53% did not feel comfortable discussing sexual orientation or practices; and in particular when it came to anoreceptive intercourse (ARI), 73% did not feel confident discussing recommendations.11
All of these issues highlight the importance of developing curricula that focus on reducing implicit and explicit biases towards SGM individuals and increasing the competence of providers to take care of SGM individuals in a safe space.
Additionally, it further justifies the need for ethical research that focuses on the needs of SGM individuals to guide evidence-based approaches to care. Given the implicit and explicit heterosexism and transphobia in society and many health care systems, Rainbows in Gastro was formed as an advocacy group for SGM patients, trainees, and staff in gastroenterology and hepatology.4
Research in SGM and IBD is lacking
There are additional needs for research in IBD and how it pertains to the needs of SGM individuals. Figure 1 highlights the lack of PubMed results for the search terms “IBD + LGBT,” “IBD + LGBTQ,” or “IBD + queer.” In contrast, the search terms “IBD + fertility” and “IBD + sexual dysfunction” generate many results. Even a systemic review conducted by Newman et al. of multiple databases in 2022 found only seven articles that demonstrated appropriately performed studies on SGM patients with IBD.5 This highlights the significant dearth of research in the realm of SGM health in IBD.
Newman and colleagues have recently published research considerations for SGM individuals. They highlighted the need to include understanding the “unique combination of psychosocial, biomedical, and legal experiences” that results in different needs and outcomes. There were several areas identified, including minority stress, which comes from existence of being SGM, especially as transgender individuals face increasing legal challenges in a variety of settings, not just healthcare.6 In a retrospective chart review investigating social determinants of health in SGM-IBD populations,12 36% of patients reported some level of social isolation, and almost 50% reported some level of stress. A total of 40% of them self-reported some perceived level of risk with respect to employment, and 17% reported depression. Given that this was a chart review and not a strict questionnaire, this study was certainly limited, and we would hypothesize that these numbers are therefore underestimating the true proportion of SGM-IBD patients who deal with employment concerns, social isolation, or psychological distress.
What Next? Back to the Patients
Circling back to our patients from the introduction, how would you counsel each of them? In patient 1’s case, we would inform him that pelvic surgery can increase the risk for sexual dysfunction, such as erectile dysfunction. He additionally would be advised during a staged TPC with IPAA, he may experience issues with body image. However, should he desire to participate in receptive anal intercourse after completion of his surgeries, the general recommendation would be to wait at least 6 months and with proven remission. It should further be noted that these are not formalized recommendations, only highlighting the need for more research and consensus on standards of care for SGM patients. He should finally be told that because he has ulcerative colitis, removal of the colon does not remove the risk for future intestinal involvement such as possible pouchitis.
In patient 2’s case, she is likely experiencing diversion vaginitis related to use of her colon for her neo-vagina. She should undergo colonoscopy and vaginoscopy in addition to standard work-up for her known ulcerative colitis.13 Management should be done in a multidisciplinary approach between the IBD provider, gynecologist, and gender-affirming provider. The electronic medical record should be updated to reflect the patient’s preferred name, pronouns, and gender identity, and her medical records, including automated clinical reports, should be updated accordingly.
As for patient 3, she would be counseled according to well-documented guidelines on pregnancy and IBD, including risks of medications (such as Jak inhibitors or methotrexate) versus the risk of uncontrolled IBD during pregnancy.1
Regardless of a patient’s gender identity or sexual orientation, patient-centered, culturally competent, and sensitive care should be provided. At Mayo Clinic in Rochester, we started one of the first Pride in IBD Clinics, which focuses on the care of SGM individuals with IBD. Our focus is to address the needs of patients who belong to the SGM community in a wholistic approach within a safe space (https://www.youtube.com/watch?v=pYa_zYaCA6M; https://www.mayoclinic.org/departments-centers/inflammatory-bowel-disease-clinic/overview/ovc-20357763). Our process of developing the clinic included training all staff on proper communication and cultural sensitivity for the SGM community.
Furthermore, providing welcoming and affirming signs of inclusivity for SGM individuals at the provider’s office — including but not limited to rainbow progressive flags, gender-neutral bathroom signs, or pronoun pins on provider identification badges (see Figure 2) — are usually appreciated by patients. Ensuring that patient education materials do not assume gender (for example, using the term “parents” rather than “mother and father”) and using gender neutral terms on intake forms is very important. Inclusive communication includes providers introducing themselves by preferred name and pronouns, asking the patients to introduce themselves, and welcoming them to share their pronouns. These simple actions can provide an atmosphere of safety for SGM patients, which would serve to enhance the quality of care we can provide for them.
For Resources and Further Reading: CDC,14 the Fenway Institute’s National LGBTQIA+ Health Education Center,15 and US Department of Health and Human Services.16
Dr. Chiang and Dr. Chedid are both in the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota. Dr. Chedid is also with the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic. Neither of the authors have any relevant conflicts of interest. They are on X, formerly Twitter: @dr_davidchiang , @VictorChedidMD .
CITATIONS
1. Mahadevan U et al. Inflammatory bowel disease in pregnancy clinical care pathway: A report from the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology. 2019;156:1508-24.
2. Pires F et al. A survey on the impact of IBD in sexual health: Into intimacy. Medicine (Baltimore). 2022;101:e32279.
3. Mules TC et al. The impact of disease activity on sexual and erectile dysfunction in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2023;29:1244-54.
4. Duong N et al. Overcoming disparities for sexual and gender minority patients and providers in gastroenterology and hepatology: Introduction to Rainbows in Gastro. Lancet Gastroenterol Hepatol. 2023;8:299-301.
5. Newman KL et al. A systematic review of inflammatory bowel disease epidemiology and health outcomes in sexual and gender minority individuals. Gastroenterology. 2023;164:866-71.
6. Newman KL et al. Research considerations in Digestive and liver disease in transgender and gender-diverse populations. Gastroenterology. 2023;165:523-28 e1.
7. Velez C et al. Digestive health in sexual and gender minority populations. Am J Gastroenterol. 2022;117:865-75.
8. Medicine Io. Washington (DC): The National Academies Press, 2011.
9. Austin EL. Sexual orientation disclosure to health care providers among urban and non-urban southern lesbians. Women Health. 2013;53:41-55.
10. Oladeru OT et al. Breast and cervical cancer screening disparities in transgender people. Am J Clin Oncol. 2022;45:116-21.
11. Vinsard DG et al. Healthcare providers’ perspectives on anoreceptive intercourse in sexual and gender minorities with ileal pouch anal anastomosis. Digestive Disease Week (DDW). Chicago, IL, 2023.
12. Ghusn W et al. Social determinants of health in LGBTQIA+ patients with inflammatory bowel disease. American College of Gastroenterology (ACG). Charlotte, NC, 2022.
13. Grasman ME et al. Neovaginal sparing in a transgender woman with ulcerative colitis. Clin Gastroenterol Hepatol. 2016;14:e73-4.
14. Prevention CfDCa. Lesbian, Gay, Bisexual, and Transgender Health — https://www.cdc.gov/lgbthealth/index.htm.
15. Institute TF. National LGBTQIA+ Health Education Center — https://www.lgbtqiahealtheducation.org/.
16. Services UDoHaH. LGBTQI+ Resources — https://www.hhs.gov/programs/topic-sites/lgbtqi/resources/index.html.
Cases
Patient 1: 55-year-old cis-male, who identifies as gay, has ulcerative colitis that has been refractory to multiple biologic therapies. His provider recommends a total proctocolectomy with ileal pouch anal anastomosis (TPC with IPAA), but the patient has questions regarding sexual function following surgery. Specifically, he is wondering when, or if, he can resume receptive anal intercourse. How would you counsel him?
Patient 2: 25-year-old, trans-female, status-post vaginoplasty with use of sigmoid colon and with well-controlled ulcerative colitis, presents with vaginal discharge, weight loss, and rectal bleeding. How do you explain what has happened to her? During your discussion, she also asks you why her chart continues to use her “dead name.” How do you respond?
Patient 3: 32-year-old, cis-female, G2P2, who identifies as a lesbian, has active ulcerative colitis. She wants to discuss medical or surgical therapy and future pregnancies. How would you counsel her?
Many gastroenterologists would likely know how to address patient 3’s concerns, but the concerns of patients 1 and 2 often go unaddressed or dismissed. Numerous studies and surveys have been conducted on patients with inflammatory bowel disease (IBD), but the focus of these studies has always been through a heteronormative cisgender lens. The focus of many studies is on fertility or sexual health and function in cisgender, heteronormative individuals.1-3 In the last few years, however, there has been increasing awareness of the health disparities, stigma, and discrimination that sexual and gender minorities (SGM) experience.4-6 For the purposes of this discussion, individuals within the lesbian, gay, bisexual, transgender, queer/questioning, intersex, and asexual (LGBTQIA+) community will be referred to as SGM. We recognize that even this exhaustive listing above does not acknowledge the full spectrum of diversity within the SGM community.
Clinical Care/Competency for SGM with IBD is Lacking
Almost 10% of the US population identifies as some form of SGM, and that number can be higher within the younger generations.4 SGM patients tend to delay or avoid seeking health care due to concern for provider mistreatment or lack of regard for their individual concerns. Additionally, there are several gaps in clinical knowledge about caring for SGM individuals. Little is known regarding the incidence or prevalence of IBD in SGM populations, but it is perceived to be similar to cisgender heterosexual individuals. Furthermore, as Newman et al. highlighted in their systematic review published in May 2023, there is a lack of guidance regarding sexual activity in the setting of IBD in SGM individuals.5 There is also a significant lack of knowledge on the impact of gender-affirming care on the natural history and treatments of IBD in transgender and gender non-conforming (TGNC) individuals. This can impact providers’ comfort and competence in caring for TGNC individuals.
Another important point to make is that the SGM community still faces discrimination due to sexual orientation or gender identity to this day, which impacts the quality and delivery of their care.7 Culturally-competent care should include care that is free from stigma, implicit and explicit biases, and discrimination. In 2011, an Institute of Medicine report documented, among other issues, provider discomfort in delivering care to SGM patients.8 While SGM individuals prefer a provider who acknowledges their sexual orientation and gender identity and treats them with the dignity and respect they deserve, many SGM individuals share valid concerns regarding their safety, which impact their desire to disclose their identity to health care providers.9 This certainly can have an impact on the quality of care they receive, including important health maintenance milestones and cancer screenings.10
An internal survey at our institution of providers (nurses, physician assistants, surgeons, and physicians) found that among 85 responders, 70% have cared for SGM who have undergone TPC with ileal pouch anal anastomosis (IPAA). Of these, 75% did not ask about sexual orientation or practices before pouch formation (though almost all of them agreed it would be important to ask). A total of 55% were comfortable in discussing SGM-related concerns; 53% did not feel comfortable discussing sexual orientation or practices; and in particular when it came to anoreceptive intercourse (ARI), 73% did not feel confident discussing recommendations.11
All of these issues highlight the importance of developing curricula that focus on reducing implicit and explicit biases towards SGM individuals and increasing the competence of providers to take care of SGM individuals in a safe space.
Additionally, it further justifies the need for ethical research that focuses on the needs of SGM individuals to guide evidence-based approaches to care. Given the implicit and explicit heterosexism and transphobia in society and many health care systems, Rainbows in Gastro was formed as an advocacy group for SGM patients, trainees, and staff in gastroenterology and hepatology.4
Research in SGM and IBD is lacking
There are additional needs for research in IBD and how it pertains to the needs of SGM individuals. Figure 1 highlights the lack of PubMed results for the search terms “IBD + LGBT,” “IBD + LGBTQ,” or “IBD + queer.” In contrast, the search terms “IBD + fertility” and “IBD + sexual dysfunction” generate many results. Even a systemic review conducted by Newman et al. of multiple databases in 2022 found only seven articles that demonstrated appropriately performed studies on SGM patients with IBD.5 This highlights the significant dearth of research in the realm of SGM health in IBD.
Newman and colleagues have recently published research considerations for SGM individuals. They highlighted the need to include understanding the “unique combination of psychosocial, biomedical, and legal experiences” that results in different needs and outcomes. There were several areas identified, including minority stress, which comes from existence of being SGM, especially as transgender individuals face increasing legal challenges in a variety of settings, not just healthcare.6 In a retrospective chart review investigating social determinants of health in SGM-IBD populations,12 36% of patients reported some level of social isolation, and almost 50% reported some level of stress. A total of 40% of them self-reported some perceived level of risk with respect to employment, and 17% reported depression. Given that this was a chart review and not a strict questionnaire, this study was certainly limited, and we would hypothesize that these numbers are therefore underestimating the true proportion of SGM-IBD patients who deal with employment concerns, social isolation, or psychological distress.
What Next? Back to the Patients
Circling back to our patients from the introduction, how would you counsel each of them? In patient 1’s case, we would inform him that pelvic surgery can increase the risk for sexual dysfunction, such as erectile dysfunction. He additionally would be advised during a staged TPC with IPAA, he may experience issues with body image. However, should he desire to participate in receptive anal intercourse after completion of his surgeries, the general recommendation would be to wait at least 6 months and with proven remission. It should further be noted that these are not formalized recommendations, only highlighting the need for more research and consensus on standards of care for SGM patients. He should finally be told that because he has ulcerative colitis, removal of the colon does not remove the risk for future intestinal involvement such as possible pouchitis.
In patient 2’s case, she is likely experiencing diversion vaginitis related to use of her colon for her neo-vagina. She should undergo colonoscopy and vaginoscopy in addition to standard work-up for her known ulcerative colitis.13 Management should be done in a multidisciplinary approach between the IBD provider, gynecologist, and gender-affirming provider. The electronic medical record should be updated to reflect the patient’s preferred name, pronouns, and gender identity, and her medical records, including automated clinical reports, should be updated accordingly.
As for patient 3, she would be counseled according to well-documented guidelines on pregnancy and IBD, including risks of medications (such as Jak inhibitors or methotrexate) versus the risk of uncontrolled IBD during pregnancy.1
Regardless of a patient’s gender identity or sexual orientation, patient-centered, culturally competent, and sensitive care should be provided. At Mayo Clinic in Rochester, we started one of the first Pride in IBD Clinics, which focuses on the care of SGM individuals with IBD. Our focus is to address the needs of patients who belong to the SGM community in a wholistic approach within a safe space (https://www.youtube.com/watch?v=pYa_zYaCA6M; https://www.mayoclinic.org/departments-centers/inflammatory-bowel-disease-clinic/overview/ovc-20357763). Our process of developing the clinic included training all staff on proper communication and cultural sensitivity for the SGM community.
Furthermore, providing welcoming and affirming signs of inclusivity for SGM individuals at the provider’s office — including but not limited to rainbow progressive flags, gender-neutral bathroom signs, or pronoun pins on provider identification badges (see Figure 2) — are usually appreciated by patients. Ensuring that patient education materials do not assume gender (for example, using the term “parents” rather than “mother and father”) and using gender neutral terms on intake forms is very important. Inclusive communication includes providers introducing themselves by preferred name and pronouns, asking the patients to introduce themselves, and welcoming them to share their pronouns. These simple actions can provide an atmosphere of safety for SGM patients, which would serve to enhance the quality of care we can provide for them.
For Resources and Further Reading: CDC,14 the Fenway Institute’s National LGBTQIA+ Health Education Center,15 and US Department of Health and Human Services.16
Dr. Chiang and Dr. Chedid are both in the Division of Gastroenterology and Hepatology, Mayo Clinic, Rochester, Minnesota. Dr. Chedid is also with the Robert D. and Patricia E. Kern Center for the Science of Health Care Delivery, Mayo Clinic. Neither of the authors have any relevant conflicts of interest. They are on X, formerly Twitter: @dr_davidchiang , @VictorChedidMD .
CITATIONS
1. Mahadevan U et al. Inflammatory bowel disease in pregnancy clinical care pathway: A report from the American Gastroenterological Association IBD Parenthood Project Working Group. Gastroenterology. 2019;156:1508-24.
2. Pires F et al. A survey on the impact of IBD in sexual health: Into intimacy. Medicine (Baltimore). 2022;101:e32279.
3. Mules TC et al. The impact of disease activity on sexual and erectile dysfunction in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2023;29:1244-54.
4. Duong N et al. Overcoming disparities for sexual and gender minority patients and providers in gastroenterology and hepatology: Introduction to Rainbows in Gastro. Lancet Gastroenterol Hepatol. 2023;8:299-301.
5. Newman KL et al. A systematic review of inflammatory bowel disease epidemiology and health outcomes in sexual and gender minority individuals. Gastroenterology. 2023;164:866-71.
6. Newman KL et al. Research considerations in Digestive and liver disease in transgender and gender-diverse populations. Gastroenterology. 2023;165:523-28 e1.
7. Velez C et al. Digestive health in sexual and gender minority populations. Am J Gastroenterol. 2022;117:865-75.
8. Medicine Io. Washington (DC): The National Academies Press, 2011.
9. Austin EL. Sexual orientation disclosure to health care providers among urban and non-urban southern lesbians. Women Health. 2013;53:41-55.
10. Oladeru OT et al. Breast and cervical cancer screening disparities in transgender people. Am J Clin Oncol. 2022;45:116-21.
11. Vinsard DG et al. Healthcare providers’ perspectives on anoreceptive intercourse in sexual and gender minorities with ileal pouch anal anastomosis. Digestive Disease Week (DDW). Chicago, IL, 2023.
12. Ghusn W et al. Social determinants of health in LGBTQIA+ patients with inflammatory bowel disease. American College of Gastroenterology (ACG). Charlotte, NC, 2022.
13. Grasman ME et al. Neovaginal sparing in a transgender woman with ulcerative colitis. Clin Gastroenterol Hepatol. 2016;14:e73-4.
14. Prevention CfDCa. Lesbian, Gay, Bisexual, and Transgender Health — https://www.cdc.gov/lgbthealth/index.htm.
15. Institute TF. National LGBTQIA+ Health Education Center — https://www.lgbtqiahealtheducation.org/.
16. Services UDoHaH. LGBTQI+ Resources — https://www.hhs.gov/programs/topic-sites/lgbtqi/resources/index.html.
‘We Will Rock You’ Into Real-time Diabetes Control
, reveals a series of experiments.
The research was published in The Lancet Diabetes & Endocrinology.
After developing a cell line in which music-sensitive calcium channels triggered the release of insulin-containing vesicles, the researchers conducted a series of studies identifying the optimal frequency, pitch, and volume of sounds for triggering release.
After settling on low-bass heavy popular music, they tested their system on mice with type 1 diabetes that had the insulin-releasing cells implanted in their abdomen. Applying the music directly at 60 dB led to near wild-type levels of insulin in the blood within 15 minutes.
“With only 4 hours required for a full refill, [the system] can provide several therapeutic doses a day,” says Martin Fussenegger, PhD, professor of biotechnology and bioengineering, Department of Biosystems Science and Engineering, ETH Zurich, Basel, Switzerland, and colleagues.
“This would match the typical needs of people with type 2 diabetes consuming three meals a day, and for whom administration of prandial insulin is an established treatment option, as they do not have capability for early postprandial insulin secretion from preformed insulin.”
As the system requires nothing more than portable battery-powered commercially available loudspeakers, the multiple daily dosing of biopharmaceuticals becomes “straightforward in the absence of medical infrastructure or staff, simply by having the patient listen to the prescribed music.”
It therefore “could be an interesting option for cell-based therapies, especially where the need for frequent dosing raises compliance issues.”
It is a “very exciting piece of work, no doubt,” said Anandwardhan A. Hardikar, PhD, group leader, Diabetes and Islet Biology Group, Translational Health Research Institute, Western Sydney University, Penrith NSW, Australia.
He pointed out that the concept of using music to drive gene expression “is something we’ve known for the last 20 years,” but bringing the different strands of research together to generate cells that can be implanted into mice is “an amazing idea.”
Dr. Hardikar, who was not involved in the study, said, however, the publication of the study as a correspondence “does not allow for a lot of the detail that I would have expected as an academic,” and consequently some questions remain.
The most important is whether the music itself is required to trigger the insulin release, as opposed simply to sounds in general.
Is Music or Sound the “Trigger?”
Music is “frequency, it’s the amplitude of the waveform, and it’s the duration for which those waveforms are present,” he noted, but the same profile can be achieved by cutting up and editing the melody so it becomes a jumble of sounds.
For Dr. Hardikar, the “best control” for the study would be to have no music as well as the edited song, with “bits of pieces” played randomly so “it sounds like it’s the same frequency and amplitude.”
Then it would be clear whether the effect is owing to the “noise, or we have to appreciate the melody.”
The other outstanding question is whether the results “can directly translate to larger animals,” such as humans, Dr. Hardikar said.
The authors point out that when translated into mechanical vibrations in the middle ear, the acoustic waves of music activate mechanosensitive ion channels, a form of trigger that is seen across the animal kingdom.
They go on to highlight that while gene switches have been developed for use in next-generation cell-based therapies for a range of conditions, small-molecular trigger compounds face a number of challenges and may cause adverse effects.
With “traceless triggers” such as light, ultrasound, magnetic fields, radio waves, electricity, and heat also facing issues, there is a “need for new switching modalities.”
The researchers therefore developed a music-inducible cellular control (MUSIC) system, which leverages the known intracellular calcium surge in response to music, via calcium-permeable mechanosensitive channels, to drive the release of biopharmaceuticals from vesicles.
They then generated MUSIC-controlled insulin-releasing cell lines, finding that, using a customized box containing off-the-shelf loudspeakers, they could induce channel activation and insulin release with 60 dB at 50 Hz, which is “within the safe range for the human ear.”
Further experiments revealed that insulin release was greatest at 50-100 Hz, and higher than that seen with potassium chloride, the “gold-standard” depolarization control for calcium channels.
The researchers then showed that with optimal stimulation at 50 Hz and 60 dB, channel activation and subsequent insulin release required at least 3 seconds of continuous music, “which might protect the cellular device from inadvertent activation during everyday activities.”
Next, they examined the impact of different musical genres on insulin release, finding that low-bass heavy popular music and movie soundtracks induced maximum release, while the responses were more diverse to classical and guitar-based music.
Specifically, “We Will Rock You,” by the British rock band Queen, induced the release of 70% of available insulin within 5 minutes and 100% within 15 minutes. This, the team notes, is “similar to the dynamics of glucose-triggered insulin release by human pancreatic islets.”
Exposing the cells to a second music session at different intervals revealed that full insulin refill was achieved within 4 hours, which “would be appropriate to attenuate glycemic excursions associated with typical dietary habits.”
Finally, the researchers tested the system in vivo, constructing a box with two off-the-shelf loudspeakers that focuses acoustic waves, via deflectors, onto the abdomens of mice with type 1 diabetes.
Exposing the mice, which had been implanted with microencapsulated MUSIC cells in the peritoneum, to low-bass acoustic waves at 60 dB (50 m/s2) for 15 minutes allowed them to achieve near wild-type levels of insulin in the blood and restored normoglycemia.
Moreover, “Queen’s song ‘We Will Rock You’ generated sufficient insulin to rapidly attenuate postprandial glycemic excursions during glucose tolerance tests,” the team says.
In contrast, animals without implants, or those that had implants but did not have music immersion, remained severely hyperglycemic, they add.
They also note that the effect was seen only when the sound waves “directly impinge on the skin just above the implantation site” for at least 15 minutes, with no increase in insulin release observed with commercially available headphones or ear plugs, such as Apple AirPods, or with loud environmental noises.
Consequently, “therapeutic MUSIC sessions would still be compatible with listening to other types of music or listening to all types of music via headphones,” the researchers write, and are “compatible with standard drug administration schemes.”
The study was supported by a European Research Council advanced grant and in part by the Swiss National Science Foundation NCCR Molecular Systems Engineering. One author acknowledges the support of the Chinese Scholarship Council.
No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
, reveals a series of experiments.
The research was published in The Lancet Diabetes & Endocrinology.
After developing a cell line in which music-sensitive calcium channels triggered the release of insulin-containing vesicles, the researchers conducted a series of studies identifying the optimal frequency, pitch, and volume of sounds for triggering release.
After settling on low-bass heavy popular music, they tested their system on mice with type 1 diabetes that had the insulin-releasing cells implanted in their abdomen. Applying the music directly at 60 dB led to near wild-type levels of insulin in the blood within 15 minutes.
“With only 4 hours required for a full refill, [the system] can provide several therapeutic doses a day,” says Martin Fussenegger, PhD, professor of biotechnology and bioengineering, Department of Biosystems Science and Engineering, ETH Zurich, Basel, Switzerland, and colleagues.
“This would match the typical needs of people with type 2 diabetes consuming three meals a day, and for whom administration of prandial insulin is an established treatment option, as they do not have capability for early postprandial insulin secretion from preformed insulin.”
As the system requires nothing more than portable battery-powered commercially available loudspeakers, the multiple daily dosing of biopharmaceuticals becomes “straightforward in the absence of medical infrastructure or staff, simply by having the patient listen to the prescribed music.”
It therefore “could be an interesting option for cell-based therapies, especially where the need for frequent dosing raises compliance issues.”
It is a “very exciting piece of work, no doubt,” said Anandwardhan A. Hardikar, PhD, group leader, Diabetes and Islet Biology Group, Translational Health Research Institute, Western Sydney University, Penrith NSW, Australia.
He pointed out that the concept of using music to drive gene expression “is something we’ve known for the last 20 years,” but bringing the different strands of research together to generate cells that can be implanted into mice is “an amazing idea.”
Dr. Hardikar, who was not involved in the study, said, however, the publication of the study as a correspondence “does not allow for a lot of the detail that I would have expected as an academic,” and consequently some questions remain.
The most important is whether the music itself is required to trigger the insulin release, as opposed simply to sounds in general.
Is Music or Sound the “Trigger?”
Music is “frequency, it’s the amplitude of the waveform, and it’s the duration for which those waveforms are present,” he noted, but the same profile can be achieved by cutting up and editing the melody so it becomes a jumble of sounds.
For Dr. Hardikar, the “best control” for the study would be to have no music as well as the edited song, with “bits of pieces” played randomly so “it sounds like it’s the same frequency and amplitude.”
Then it would be clear whether the effect is owing to the “noise, or we have to appreciate the melody.”
The other outstanding question is whether the results “can directly translate to larger animals,” such as humans, Dr. Hardikar said.
The authors point out that when translated into mechanical vibrations in the middle ear, the acoustic waves of music activate mechanosensitive ion channels, a form of trigger that is seen across the animal kingdom.
They go on to highlight that while gene switches have been developed for use in next-generation cell-based therapies for a range of conditions, small-molecular trigger compounds face a number of challenges and may cause adverse effects.
With “traceless triggers” such as light, ultrasound, magnetic fields, radio waves, electricity, and heat also facing issues, there is a “need for new switching modalities.”
The researchers therefore developed a music-inducible cellular control (MUSIC) system, which leverages the known intracellular calcium surge in response to music, via calcium-permeable mechanosensitive channels, to drive the release of biopharmaceuticals from vesicles.
They then generated MUSIC-controlled insulin-releasing cell lines, finding that, using a customized box containing off-the-shelf loudspeakers, they could induce channel activation and insulin release with 60 dB at 50 Hz, which is “within the safe range for the human ear.”
Further experiments revealed that insulin release was greatest at 50-100 Hz, and higher than that seen with potassium chloride, the “gold-standard” depolarization control for calcium channels.
The researchers then showed that with optimal stimulation at 50 Hz and 60 dB, channel activation and subsequent insulin release required at least 3 seconds of continuous music, “which might protect the cellular device from inadvertent activation during everyday activities.”
Next, they examined the impact of different musical genres on insulin release, finding that low-bass heavy popular music and movie soundtracks induced maximum release, while the responses were more diverse to classical and guitar-based music.
Specifically, “We Will Rock You,” by the British rock band Queen, induced the release of 70% of available insulin within 5 minutes and 100% within 15 minutes. This, the team notes, is “similar to the dynamics of glucose-triggered insulin release by human pancreatic islets.”
Exposing the cells to a second music session at different intervals revealed that full insulin refill was achieved within 4 hours, which “would be appropriate to attenuate glycemic excursions associated with typical dietary habits.”
Finally, the researchers tested the system in vivo, constructing a box with two off-the-shelf loudspeakers that focuses acoustic waves, via deflectors, onto the abdomens of mice with type 1 diabetes.
Exposing the mice, which had been implanted with microencapsulated MUSIC cells in the peritoneum, to low-bass acoustic waves at 60 dB (50 m/s2) for 15 minutes allowed them to achieve near wild-type levels of insulin in the blood and restored normoglycemia.
Moreover, “Queen’s song ‘We Will Rock You’ generated sufficient insulin to rapidly attenuate postprandial glycemic excursions during glucose tolerance tests,” the team says.
In contrast, animals without implants, or those that had implants but did not have music immersion, remained severely hyperglycemic, they add.
They also note that the effect was seen only when the sound waves “directly impinge on the skin just above the implantation site” for at least 15 minutes, with no increase in insulin release observed with commercially available headphones or ear plugs, such as Apple AirPods, or with loud environmental noises.
Consequently, “therapeutic MUSIC sessions would still be compatible with listening to other types of music or listening to all types of music via headphones,” the researchers write, and are “compatible with standard drug administration schemes.”
The study was supported by a European Research Council advanced grant and in part by the Swiss National Science Foundation NCCR Molecular Systems Engineering. One author acknowledges the support of the Chinese Scholarship Council.
No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
, reveals a series of experiments.
The research was published in The Lancet Diabetes & Endocrinology.
After developing a cell line in which music-sensitive calcium channels triggered the release of insulin-containing vesicles, the researchers conducted a series of studies identifying the optimal frequency, pitch, and volume of sounds for triggering release.
After settling on low-bass heavy popular music, they tested their system on mice with type 1 diabetes that had the insulin-releasing cells implanted in their abdomen. Applying the music directly at 60 dB led to near wild-type levels of insulin in the blood within 15 minutes.
“With only 4 hours required for a full refill, [the system] can provide several therapeutic doses a day,” says Martin Fussenegger, PhD, professor of biotechnology and bioengineering, Department of Biosystems Science and Engineering, ETH Zurich, Basel, Switzerland, and colleagues.
“This would match the typical needs of people with type 2 diabetes consuming three meals a day, and for whom administration of prandial insulin is an established treatment option, as they do not have capability for early postprandial insulin secretion from preformed insulin.”
As the system requires nothing more than portable battery-powered commercially available loudspeakers, the multiple daily dosing of biopharmaceuticals becomes “straightforward in the absence of medical infrastructure or staff, simply by having the patient listen to the prescribed music.”
It therefore “could be an interesting option for cell-based therapies, especially where the need for frequent dosing raises compliance issues.”
It is a “very exciting piece of work, no doubt,” said Anandwardhan A. Hardikar, PhD, group leader, Diabetes and Islet Biology Group, Translational Health Research Institute, Western Sydney University, Penrith NSW, Australia.
He pointed out that the concept of using music to drive gene expression “is something we’ve known for the last 20 years,” but bringing the different strands of research together to generate cells that can be implanted into mice is “an amazing idea.”
Dr. Hardikar, who was not involved in the study, said, however, the publication of the study as a correspondence “does not allow for a lot of the detail that I would have expected as an academic,” and consequently some questions remain.
The most important is whether the music itself is required to trigger the insulin release, as opposed simply to sounds in general.
Is Music or Sound the “Trigger?”
Music is “frequency, it’s the amplitude of the waveform, and it’s the duration for which those waveforms are present,” he noted, but the same profile can be achieved by cutting up and editing the melody so it becomes a jumble of sounds.
For Dr. Hardikar, the “best control” for the study would be to have no music as well as the edited song, with “bits of pieces” played randomly so “it sounds like it’s the same frequency and amplitude.”
Then it would be clear whether the effect is owing to the “noise, or we have to appreciate the melody.”
The other outstanding question is whether the results “can directly translate to larger animals,” such as humans, Dr. Hardikar said.
The authors point out that when translated into mechanical vibrations in the middle ear, the acoustic waves of music activate mechanosensitive ion channels, a form of trigger that is seen across the animal kingdom.
They go on to highlight that while gene switches have been developed for use in next-generation cell-based therapies for a range of conditions, small-molecular trigger compounds face a number of challenges and may cause adverse effects.
With “traceless triggers” such as light, ultrasound, magnetic fields, radio waves, electricity, and heat also facing issues, there is a “need for new switching modalities.”
The researchers therefore developed a music-inducible cellular control (MUSIC) system, which leverages the known intracellular calcium surge in response to music, via calcium-permeable mechanosensitive channels, to drive the release of biopharmaceuticals from vesicles.
They then generated MUSIC-controlled insulin-releasing cell lines, finding that, using a customized box containing off-the-shelf loudspeakers, they could induce channel activation and insulin release with 60 dB at 50 Hz, which is “within the safe range for the human ear.”
Further experiments revealed that insulin release was greatest at 50-100 Hz, and higher than that seen with potassium chloride, the “gold-standard” depolarization control for calcium channels.
The researchers then showed that with optimal stimulation at 50 Hz and 60 dB, channel activation and subsequent insulin release required at least 3 seconds of continuous music, “which might protect the cellular device from inadvertent activation during everyday activities.”
Next, they examined the impact of different musical genres on insulin release, finding that low-bass heavy popular music and movie soundtracks induced maximum release, while the responses were more diverse to classical and guitar-based music.
Specifically, “We Will Rock You,” by the British rock band Queen, induced the release of 70% of available insulin within 5 minutes and 100% within 15 minutes. This, the team notes, is “similar to the dynamics of glucose-triggered insulin release by human pancreatic islets.”
Exposing the cells to a second music session at different intervals revealed that full insulin refill was achieved within 4 hours, which “would be appropriate to attenuate glycemic excursions associated with typical dietary habits.”
Finally, the researchers tested the system in vivo, constructing a box with two off-the-shelf loudspeakers that focuses acoustic waves, via deflectors, onto the abdomens of mice with type 1 diabetes.
Exposing the mice, which had been implanted with microencapsulated MUSIC cells in the peritoneum, to low-bass acoustic waves at 60 dB (50 m/s2) for 15 minutes allowed them to achieve near wild-type levels of insulin in the blood and restored normoglycemia.
Moreover, “Queen’s song ‘We Will Rock You’ generated sufficient insulin to rapidly attenuate postprandial glycemic excursions during glucose tolerance tests,” the team says.
In contrast, animals without implants, or those that had implants but did not have music immersion, remained severely hyperglycemic, they add.
They also note that the effect was seen only when the sound waves “directly impinge on the skin just above the implantation site” for at least 15 minutes, with no increase in insulin release observed with commercially available headphones or ear plugs, such as Apple AirPods, or with loud environmental noises.
Consequently, “therapeutic MUSIC sessions would still be compatible with listening to other types of music or listening to all types of music via headphones,” the researchers write, and are “compatible with standard drug administration schemes.”
The study was supported by a European Research Council advanced grant and in part by the Swiss National Science Foundation NCCR Molecular Systems Engineering. One author acknowledges the support of the Chinese Scholarship Council.
No relevant financial relationships were declared.
A version of this article appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
What causes obesity? More science points to the brain
For much of his life, 32-year-old Michael Smith had a war going on in his head.
After a big meal, he knew he should be full. But an inexplicable hunger would drive him to pick up the fork again.
Cravings for fried chicken or gummy bears overwhelmed him, fueling late-night DoorDash orders that — despite their bounty of fat and sugar — never satisfied him.
He recalls waking up on the couch, half-eaten takeout in his lap, feeling sluggish and out of control.
“It was like I was food drunk,” recalls Smith, who lives in Boston. “I had a moment I looked at myself in the mirror. I was around 380 pounds, and I said, ‘OK, something has got to give.’ “
Smith is among the 42% of U.S. adults living with obesity, a misunderstood and stubbornly hard-to-manage condition that doctors have only recently begun to call a disease. Its root causes have been debated for decades, with studies suggesting everything from genes to lifestyle to a shifting food supply loaded with carbohydrates and ultra-processed foods. Solutions have long targeted self-discipline and a simple “eat less, move more” strategy with remarkably grim results.
Those who successfully slim down tend to gain back 50% of that weight within 2 years, and 80% within 5 years. Meanwhile, the obesity epidemic marches on.
But a new frontier of brain-based therapies — from GLP-1 agonist drugs thought to act on reward and appetite centers to deep brain stimulation aimed at resetting neural circuits — has kindled hope among patients like Smith and the doctors who treat them. The treatments, and theories behind them, are not without controversy. They’re expensive, have side effects, and, critics contend, pull focus from diet and exercise.
But most agree that in the battle against obesity, one crucial organ has been overlooked.
“Obesity, in almost all circumstances, is most likely a disorder of the brain,” said Casey Halpern, MD, associate professor of neurosurgery at the University of Pennsylvania. “What these individuals need is not simply more willpower, but the therapeutic equivalent of an electrician that can make right these connections inside their brain.”
A Break in the Machine
Throughout the day, the machine that is our brain is constantly humming in the background, taking in subtle signals from our gut, hormones, and environment to determine when we’re hungry, how food makes us feel, and whether we are taking in enough energy, or expending too much, to survive.
said Kevin Hall, PhD, an obesity researcher with the National Institute of Diabetes and Digestive and Kidney Diseases. “I liken it to holding your breath. I can do that for a period of time, and I have some conscious control. But eventually, physiology wins out.”
Mounting evidence suggests that in people with obesity, something in the machine is broken.
One seminal 2001 study in The Lancet suggested that, like people addicted to cocaine or alcohol, they lack receptors to the feel-good brain chemical dopamine and overeat in pursuit of the pleasure they lack.
A recent study, not yet published, from Dr. Hall’s lab drew a slightly different conclusion, suggesting that people with obesity actually have too much dopamine, filling up those receptors so the pleasure spike from eating doesn’t feel like much.
“It’s kind of like trying to shout in a noisy room. You’re going to have to shout louder to have the same effect,” said Dr. Hall.
Gut-brain pathways that tell us we’re full may also be impaired.
In another study, Yale researchers tube-fed 500 calories of sugar or fat directly into the stomachs of 28 lean people and 30 people with obesity. Then they observed brain activity using functional magnetic resonance imaging (fMRI).
In lean people, about 30 regions of the brain quieted after the meal, including parts of the striatum (associated with cravings).
In those with obesity, the brain barely responded at all.
“In my clinic, patients will often say ‘I just finished my dinner, but it doesn’t feel like it,’” said senior author Mireille Serlie, MD, PhD, an obesity researcher at the Yale School of Medicine. “It may be that this nutrient-sensing interaction between the gut and the brain is less pronounced or comes too late for them after the meal.”
Dr. Halpern recently identified a brain circuit linking a memory center (hippocampus) to an appetite control region (hypothalamus). In people with obesity and binge eating disorder, the circuit appears jammed. This may cause them to, in a sense, forget they just ate.
“Some of their eating episodes are almost dissociative — they’re not realizing how much they are eating and can’t keep track of it,” he said.
Another brain system works to maintain longer-term homeostasis — or weight stability. Like a set thermostat, it kicks on to trigger hunger and fatigue when it senses we’re low on fat.
The hormone leptin, found in fat cells, sends signals to the hypothalamus to let it know how much energy we have on board.
“If leptin levels go up, it signals the brain that you have too much fat and you should eat less to return to the starting point,” said Rockefeller University geneticist Jeffrey Friedman, MD, PhD, who discovered the hormone in 1994. “If you have too little fat and leptin is low, that will stimulate appetite to return you to the starting point.”
In people with obesity, he said, the thermostat — or set point the body seeks to maintain — is too high.
All this raises a crucial question: How do these circuits and pathways malfunction in the first place?
What Breaks the Brain?
Genes, scientists agree, play a role.
Studies show that genetics underlie as much as 75% of people’s differences in body mass index (BMI), with certain gene combinations raising obesity risk in particular environments.
While hundreds of genes are believed to have a small effect, about a dozen single genes are thought to have a large effect. (Notably, most influence brain function.) For instance, about 6% of people with severe obesity since childhood have mutations in a gene called MC4R (melanocortin 4 receptor), which influences leptin signaling.
Still, genetics alone cannot account for the explosion in obesity in the U.S. over the last 50 years, says epidemiologist Deirdre Tobias, ScD, assistant professor of medicine at Harvard Medical School.
At the population level, “our genes don’t change that much in less than a generation,” she said.
But our food supply has.
Ultra-processed foods — those containing hydrogenated oils, high-fructose corn syrup, flavoring agents, emulsifiers, and other manufactured ingredients — now make up about 60% of the food supply.
“The evidence is fairly consistent indicating that there’s something about these foods that is possibly causing obesity,” said Tobias.
In one telling 2019 study, Dr. Hall and his colleagues brought 20 men and women into a study center to live for a month and tightly controlled their food intake and activity. One group was provided with meals with 80% of calories from ultra-processed food. The other was given meals with no processed food.
The three daily meals provided had the same calories, sugars, fats, fiber, and carbohydrates, and people were told to eat as much as they wanted.
Those on the ultra-processed diet ate about 500 calories more per day, ate faster, and gained weight. Those on the unprocessed diet lost weight.
“This is a stark example of how, when you can change the food environment, you cause really remarkable changes in food intake without people even being aware that they are overeating,” said Dr. Hall.
Just what it is about these relatively novel foods that may trigger overeating is unclear. It could be the crunch, the lack of water content, the engineered balance of sugar/salt/fat, their easy-to-devour texture, or something else.
Some research suggests that the foods may interfere with gut-brain signaling that tells the brain you’re full.
“Evidence is amassing that the nutritional content of processed foods is not accurately conveyed to the brain,” Dana M. Small, PhD, a neuroscientist at Yale, wrote in a recent perspective paper in Science.
Even more concerning: Some animal studies suggest processed foods reprogram the brain to dislike healthy foods.
And once these brain changes are made, they are hard to reverse.
“The problem is, our brain is not wired for this,” said Dr. Halpern. “We are not evolved to eat the food we are eating, so our brain adapts, but it adapts in a negative way that puts us at risk.”
That’s why changing the food environment via public policy must be part of the solution in combating obesity, Dr. Tobias said.
A New Era of Brain-Based Solutions
In the spring of 2021, after years of trying and failing to lose weight via the “move more, eat less” model, Michael Smith began to take a medication called Vyvanse. The drug was approved in 2008 for attention deficit hyperactivity disorder, but since it also influences levels of the hormones dopamine and norepinephrine to reduce cravings, it is now frequently prescribed for binge eating disorder.
“That was pretty much how I got rid of my first 60 to 70 pounds,” Smith said.
A few months later, after he hit a plateau, he had surgery to shrink the size of his stomach — a decision he now second-guesses.
While it kept him from overeating for a time, the fried chicken and gummy bear cravings returned a few months later.
His doctor, Fatima Cody Stanford, MD, put him on a second medication: semaglutide, or Wegovy, the weekly shot approved for weight loss in 2021. It works, in part, by mimicking glucagon-like peptide-1 (GLP-1), a key gut hormone that lets your brain know you are full.
The weight began to fall off again.
Smith’s success story is just one of many that Dr. Stanford, an obesity medicine doctor-scientist at Harvard, has heard in her office in recent years.
“I do not believe these drugs are a panacea,” she said. “There are nonresponders, and those are the patients I take off the medication. But for the high-responders, and there are many of them, they are telling me, ‘Oh my gosh. For the first time in my life, I am not constantly thinking about eating. My life has changed.’”
A Multi-Pronged Approach
Dr. Halpern, at Penn, has also been hearing success stories.
In recent years, he has placed permanent electrodes in the brains of three people with grade III, or severe, obesity and binge eating disorder.
All had tried exercise, dieting, support groups, medication, and weight loss surgery to no avail.
The electrodes modulate an area in the center of the brain called the nucleus accumbens, which in mice studies has been shown to reduce cravings when stimulated.
Thus far, all three are seeing promising results.
“It’s not like I don’t think about food at all,” one of them, Robyn Baldwin, told The New York Times. “But I’m no longer a craving person.”
Dr. Halpern is now extending the trial to more patients and hopes to ultimately include other areas of the brain, including those that involve memory.
He imagines a day when people with severe obesity, who have failed conventional treatments, can walk into a clinic and have their brain circuits assessed to see which ones may be misfiring.
Many might find relief with noninvasive brain stimulation, like transcranial magnetic stimulation (already in use for depression). Others might need a more extreme approach, like the deep brain stimulation, or DBS, therapy Dr. Halpern used.
“Obviously, DBS is hard to scale, so it would have to be reserved for the most severe patients,” he said.
Still, not everyone believes brain-based drugs and surgeries are the answer.
David Ludwig, MD, PhD, a professor of nutrition at the Harvard School of Public Health, played a key role in the discovery of GLP-1 and acknowledges that “of course” the brain influences body composition. But to him, explaining obesity as a disease of the brain oversimplifies it, discounting metabolic factors such as a tendency to store too much fat.
He noted that it’s hard to get drug companies, or any agencies, to fund large clinical trials on simple things like low-carbohydrate diets or exercise programs.
“We need all the tools we can get in the battle against the obesity epidemic, and new technologies are worth exploring,” he said. “However, the success of these drugs should not lead us to deprioritize diet and lifestyle interventions.”
Dr. Stanford, who has received consulting fees from Wegovy, believes the future of treatment lies in a multi-pronged approach, with surgery, medication, and lifestyle changes coalescing in a lasting, but fragile, remission.
“Unfortunately, there is no cure for obesity,” said Dr. Stanford, whose patients often have setbacks and must try new strategies. “There are treatments that work for a while, but they are constantly pushing up against this origin in the brain.”
Smith says understanding this has been a big part of his success.
He is now a leaner and healthier 5-foot-6 and 204 pounds. In addition to taking his medication, he walks to work, goes to the gym twice a week, limits his portions, and tries to reframe the way he thinks about food, viewing it as fuel rather than an indulgence.
Sometimes, when he looks in the mirror, he is reminded of his 380-pound self, and it scares him. He doesn’t want to go back there. He’s confident now that he won’t have to.
“There is this misconception out there that you just need to put the fork down, but I’m learning it’s more complicated than that,” he said. “I intend to treat this as the illness that it is and do what I need to combat it so I’m able to keep this new reality I have built for myself.”
A version of this article appeared on WebMD.com .
For much of his life, 32-year-old Michael Smith had a war going on in his head.
After a big meal, he knew he should be full. But an inexplicable hunger would drive him to pick up the fork again.
Cravings for fried chicken or gummy bears overwhelmed him, fueling late-night DoorDash orders that — despite their bounty of fat and sugar — never satisfied him.
He recalls waking up on the couch, half-eaten takeout in his lap, feeling sluggish and out of control.
“It was like I was food drunk,” recalls Smith, who lives in Boston. “I had a moment I looked at myself in the mirror. I was around 380 pounds, and I said, ‘OK, something has got to give.’ “
Smith is among the 42% of U.S. adults living with obesity, a misunderstood and stubbornly hard-to-manage condition that doctors have only recently begun to call a disease. Its root causes have been debated for decades, with studies suggesting everything from genes to lifestyle to a shifting food supply loaded with carbohydrates and ultra-processed foods. Solutions have long targeted self-discipline and a simple “eat less, move more” strategy with remarkably grim results.
Those who successfully slim down tend to gain back 50% of that weight within 2 years, and 80% within 5 years. Meanwhile, the obesity epidemic marches on.
But a new frontier of brain-based therapies — from GLP-1 agonist drugs thought to act on reward and appetite centers to deep brain stimulation aimed at resetting neural circuits — has kindled hope among patients like Smith and the doctors who treat them. The treatments, and theories behind them, are not without controversy. They’re expensive, have side effects, and, critics contend, pull focus from diet and exercise.
But most agree that in the battle against obesity, one crucial organ has been overlooked.
“Obesity, in almost all circumstances, is most likely a disorder of the brain,” said Casey Halpern, MD, associate professor of neurosurgery at the University of Pennsylvania. “What these individuals need is not simply more willpower, but the therapeutic equivalent of an electrician that can make right these connections inside their brain.”
A Break in the Machine
Throughout the day, the machine that is our brain is constantly humming in the background, taking in subtle signals from our gut, hormones, and environment to determine when we’re hungry, how food makes us feel, and whether we are taking in enough energy, or expending too much, to survive.
said Kevin Hall, PhD, an obesity researcher with the National Institute of Diabetes and Digestive and Kidney Diseases. “I liken it to holding your breath. I can do that for a period of time, and I have some conscious control. But eventually, physiology wins out.”
Mounting evidence suggests that in people with obesity, something in the machine is broken.
One seminal 2001 study in The Lancet suggested that, like people addicted to cocaine or alcohol, they lack receptors to the feel-good brain chemical dopamine and overeat in pursuit of the pleasure they lack.
A recent study, not yet published, from Dr. Hall’s lab drew a slightly different conclusion, suggesting that people with obesity actually have too much dopamine, filling up those receptors so the pleasure spike from eating doesn’t feel like much.
“It’s kind of like trying to shout in a noisy room. You’re going to have to shout louder to have the same effect,” said Dr. Hall.
Gut-brain pathways that tell us we’re full may also be impaired.
In another study, Yale researchers tube-fed 500 calories of sugar or fat directly into the stomachs of 28 lean people and 30 people with obesity. Then they observed brain activity using functional magnetic resonance imaging (fMRI).
In lean people, about 30 regions of the brain quieted after the meal, including parts of the striatum (associated with cravings).
In those with obesity, the brain barely responded at all.
“In my clinic, patients will often say ‘I just finished my dinner, but it doesn’t feel like it,’” said senior author Mireille Serlie, MD, PhD, an obesity researcher at the Yale School of Medicine. “It may be that this nutrient-sensing interaction between the gut and the brain is less pronounced or comes too late for them after the meal.”
Dr. Halpern recently identified a brain circuit linking a memory center (hippocampus) to an appetite control region (hypothalamus). In people with obesity and binge eating disorder, the circuit appears jammed. This may cause them to, in a sense, forget they just ate.
“Some of their eating episodes are almost dissociative — they’re not realizing how much they are eating and can’t keep track of it,” he said.
Another brain system works to maintain longer-term homeostasis — or weight stability. Like a set thermostat, it kicks on to trigger hunger and fatigue when it senses we’re low on fat.
The hormone leptin, found in fat cells, sends signals to the hypothalamus to let it know how much energy we have on board.
“If leptin levels go up, it signals the brain that you have too much fat and you should eat less to return to the starting point,” said Rockefeller University geneticist Jeffrey Friedman, MD, PhD, who discovered the hormone in 1994. “If you have too little fat and leptin is low, that will stimulate appetite to return you to the starting point.”
In people with obesity, he said, the thermostat — or set point the body seeks to maintain — is too high.
All this raises a crucial question: How do these circuits and pathways malfunction in the first place?
What Breaks the Brain?
Genes, scientists agree, play a role.
Studies show that genetics underlie as much as 75% of people’s differences in body mass index (BMI), with certain gene combinations raising obesity risk in particular environments.
While hundreds of genes are believed to have a small effect, about a dozen single genes are thought to have a large effect. (Notably, most influence brain function.) For instance, about 6% of people with severe obesity since childhood have mutations in a gene called MC4R (melanocortin 4 receptor), which influences leptin signaling.
Still, genetics alone cannot account for the explosion in obesity in the U.S. over the last 50 years, says epidemiologist Deirdre Tobias, ScD, assistant professor of medicine at Harvard Medical School.
At the population level, “our genes don’t change that much in less than a generation,” she said.
But our food supply has.
Ultra-processed foods — those containing hydrogenated oils, high-fructose corn syrup, flavoring agents, emulsifiers, and other manufactured ingredients — now make up about 60% of the food supply.
“The evidence is fairly consistent indicating that there’s something about these foods that is possibly causing obesity,” said Tobias.
In one telling 2019 study, Dr. Hall and his colleagues brought 20 men and women into a study center to live for a month and tightly controlled their food intake and activity. One group was provided with meals with 80% of calories from ultra-processed food. The other was given meals with no processed food.
The three daily meals provided had the same calories, sugars, fats, fiber, and carbohydrates, and people were told to eat as much as they wanted.
Those on the ultra-processed diet ate about 500 calories more per day, ate faster, and gained weight. Those on the unprocessed diet lost weight.
“This is a stark example of how, when you can change the food environment, you cause really remarkable changes in food intake without people even being aware that they are overeating,” said Dr. Hall.
Just what it is about these relatively novel foods that may trigger overeating is unclear. It could be the crunch, the lack of water content, the engineered balance of sugar/salt/fat, their easy-to-devour texture, or something else.
Some research suggests that the foods may interfere with gut-brain signaling that tells the brain you’re full.
“Evidence is amassing that the nutritional content of processed foods is not accurately conveyed to the brain,” Dana M. Small, PhD, a neuroscientist at Yale, wrote in a recent perspective paper in Science.
Even more concerning: Some animal studies suggest processed foods reprogram the brain to dislike healthy foods.
And once these brain changes are made, they are hard to reverse.
“The problem is, our brain is not wired for this,” said Dr. Halpern. “We are not evolved to eat the food we are eating, so our brain adapts, but it adapts in a negative way that puts us at risk.”
That’s why changing the food environment via public policy must be part of the solution in combating obesity, Dr. Tobias said.
A New Era of Brain-Based Solutions
In the spring of 2021, after years of trying and failing to lose weight via the “move more, eat less” model, Michael Smith began to take a medication called Vyvanse. The drug was approved in 2008 for attention deficit hyperactivity disorder, but since it also influences levels of the hormones dopamine and norepinephrine to reduce cravings, it is now frequently prescribed for binge eating disorder.
“That was pretty much how I got rid of my first 60 to 70 pounds,” Smith said.
A few months later, after he hit a plateau, he had surgery to shrink the size of his stomach — a decision he now second-guesses.
While it kept him from overeating for a time, the fried chicken and gummy bear cravings returned a few months later.
His doctor, Fatima Cody Stanford, MD, put him on a second medication: semaglutide, or Wegovy, the weekly shot approved for weight loss in 2021. It works, in part, by mimicking glucagon-like peptide-1 (GLP-1), a key gut hormone that lets your brain know you are full.
The weight began to fall off again.
Smith’s success story is just one of many that Dr. Stanford, an obesity medicine doctor-scientist at Harvard, has heard in her office in recent years.
“I do not believe these drugs are a panacea,” she said. “There are nonresponders, and those are the patients I take off the medication. But for the high-responders, and there are many of them, they are telling me, ‘Oh my gosh. For the first time in my life, I am not constantly thinking about eating. My life has changed.’”
A Multi-Pronged Approach
Dr. Halpern, at Penn, has also been hearing success stories.
In recent years, he has placed permanent electrodes in the brains of three people with grade III, or severe, obesity and binge eating disorder.
All had tried exercise, dieting, support groups, medication, and weight loss surgery to no avail.
The electrodes modulate an area in the center of the brain called the nucleus accumbens, which in mice studies has been shown to reduce cravings when stimulated.
Thus far, all three are seeing promising results.
“It’s not like I don’t think about food at all,” one of them, Robyn Baldwin, told The New York Times. “But I’m no longer a craving person.”
Dr. Halpern is now extending the trial to more patients and hopes to ultimately include other areas of the brain, including those that involve memory.
He imagines a day when people with severe obesity, who have failed conventional treatments, can walk into a clinic and have their brain circuits assessed to see which ones may be misfiring.
Many might find relief with noninvasive brain stimulation, like transcranial magnetic stimulation (already in use for depression). Others might need a more extreme approach, like the deep brain stimulation, or DBS, therapy Dr. Halpern used.
“Obviously, DBS is hard to scale, so it would have to be reserved for the most severe patients,” he said.
Still, not everyone believes brain-based drugs and surgeries are the answer.
David Ludwig, MD, PhD, a professor of nutrition at the Harvard School of Public Health, played a key role in the discovery of GLP-1 and acknowledges that “of course” the brain influences body composition. But to him, explaining obesity as a disease of the brain oversimplifies it, discounting metabolic factors such as a tendency to store too much fat.
He noted that it’s hard to get drug companies, or any agencies, to fund large clinical trials on simple things like low-carbohydrate diets or exercise programs.
“We need all the tools we can get in the battle against the obesity epidemic, and new technologies are worth exploring,” he said. “However, the success of these drugs should not lead us to deprioritize diet and lifestyle interventions.”
Dr. Stanford, who has received consulting fees from Wegovy, believes the future of treatment lies in a multi-pronged approach, with surgery, medication, and lifestyle changes coalescing in a lasting, but fragile, remission.
“Unfortunately, there is no cure for obesity,” said Dr. Stanford, whose patients often have setbacks and must try new strategies. “There are treatments that work for a while, but they are constantly pushing up against this origin in the brain.”
Smith says understanding this has been a big part of his success.
He is now a leaner and healthier 5-foot-6 and 204 pounds. In addition to taking his medication, he walks to work, goes to the gym twice a week, limits his portions, and tries to reframe the way he thinks about food, viewing it as fuel rather than an indulgence.
Sometimes, when he looks in the mirror, he is reminded of his 380-pound self, and it scares him. He doesn’t want to go back there. He’s confident now that he won’t have to.
“There is this misconception out there that you just need to put the fork down, but I’m learning it’s more complicated than that,” he said. “I intend to treat this as the illness that it is and do what I need to combat it so I’m able to keep this new reality I have built for myself.”
A version of this article appeared on WebMD.com .
For much of his life, 32-year-old Michael Smith had a war going on in his head.
After a big meal, he knew he should be full. But an inexplicable hunger would drive him to pick up the fork again.
Cravings for fried chicken or gummy bears overwhelmed him, fueling late-night DoorDash orders that — despite their bounty of fat and sugar — never satisfied him.
He recalls waking up on the couch, half-eaten takeout in his lap, feeling sluggish and out of control.
“It was like I was food drunk,” recalls Smith, who lives in Boston. “I had a moment I looked at myself in the mirror. I was around 380 pounds, and I said, ‘OK, something has got to give.’ “
Smith is among the 42% of U.S. adults living with obesity, a misunderstood and stubbornly hard-to-manage condition that doctors have only recently begun to call a disease. Its root causes have been debated for decades, with studies suggesting everything from genes to lifestyle to a shifting food supply loaded with carbohydrates and ultra-processed foods. Solutions have long targeted self-discipline and a simple “eat less, move more” strategy with remarkably grim results.
Those who successfully slim down tend to gain back 50% of that weight within 2 years, and 80% within 5 years. Meanwhile, the obesity epidemic marches on.
But a new frontier of brain-based therapies — from GLP-1 agonist drugs thought to act on reward and appetite centers to deep brain stimulation aimed at resetting neural circuits — has kindled hope among patients like Smith and the doctors who treat them. The treatments, and theories behind them, are not without controversy. They’re expensive, have side effects, and, critics contend, pull focus from diet and exercise.
But most agree that in the battle against obesity, one crucial organ has been overlooked.
“Obesity, in almost all circumstances, is most likely a disorder of the brain,” said Casey Halpern, MD, associate professor of neurosurgery at the University of Pennsylvania. “What these individuals need is not simply more willpower, but the therapeutic equivalent of an electrician that can make right these connections inside their brain.”
A Break in the Machine
Throughout the day, the machine that is our brain is constantly humming in the background, taking in subtle signals from our gut, hormones, and environment to determine when we’re hungry, how food makes us feel, and whether we are taking in enough energy, or expending too much, to survive.
said Kevin Hall, PhD, an obesity researcher with the National Institute of Diabetes and Digestive and Kidney Diseases. “I liken it to holding your breath. I can do that for a period of time, and I have some conscious control. But eventually, physiology wins out.”
Mounting evidence suggests that in people with obesity, something in the machine is broken.
One seminal 2001 study in The Lancet suggested that, like people addicted to cocaine or alcohol, they lack receptors to the feel-good brain chemical dopamine and overeat in pursuit of the pleasure they lack.
A recent study, not yet published, from Dr. Hall’s lab drew a slightly different conclusion, suggesting that people with obesity actually have too much dopamine, filling up those receptors so the pleasure spike from eating doesn’t feel like much.
“It’s kind of like trying to shout in a noisy room. You’re going to have to shout louder to have the same effect,” said Dr. Hall.
Gut-brain pathways that tell us we’re full may also be impaired.
In another study, Yale researchers tube-fed 500 calories of sugar or fat directly into the stomachs of 28 lean people and 30 people with obesity. Then they observed brain activity using functional magnetic resonance imaging (fMRI).
In lean people, about 30 regions of the brain quieted after the meal, including parts of the striatum (associated with cravings).
In those with obesity, the brain barely responded at all.
“In my clinic, patients will often say ‘I just finished my dinner, but it doesn’t feel like it,’” said senior author Mireille Serlie, MD, PhD, an obesity researcher at the Yale School of Medicine. “It may be that this nutrient-sensing interaction between the gut and the brain is less pronounced or comes too late for them after the meal.”
Dr. Halpern recently identified a brain circuit linking a memory center (hippocampus) to an appetite control region (hypothalamus). In people with obesity and binge eating disorder, the circuit appears jammed. This may cause them to, in a sense, forget they just ate.
“Some of their eating episodes are almost dissociative — they’re not realizing how much they are eating and can’t keep track of it,” he said.
Another brain system works to maintain longer-term homeostasis — or weight stability. Like a set thermostat, it kicks on to trigger hunger and fatigue when it senses we’re low on fat.
The hormone leptin, found in fat cells, sends signals to the hypothalamus to let it know how much energy we have on board.
“If leptin levels go up, it signals the brain that you have too much fat and you should eat less to return to the starting point,” said Rockefeller University geneticist Jeffrey Friedman, MD, PhD, who discovered the hormone in 1994. “If you have too little fat and leptin is low, that will stimulate appetite to return you to the starting point.”
In people with obesity, he said, the thermostat — or set point the body seeks to maintain — is too high.
All this raises a crucial question: How do these circuits and pathways malfunction in the first place?
What Breaks the Brain?
Genes, scientists agree, play a role.
Studies show that genetics underlie as much as 75% of people’s differences in body mass index (BMI), with certain gene combinations raising obesity risk in particular environments.
While hundreds of genes are believed to have a small effect, about a dozen single genes are thought to have a large effect. (Notably, most influence brain function.) For instance, about 6% of people with severe obesity since childhood have mutations in a gene called MC4R (melanocortin 4 receptor), which influences leptin signaling.
Still, genetics alone cannot account for the explosion in obesity in the U.S. over the last 50 years, says epidemiologist Deirdre Tobias, ScD, assistant professor of medicine at Harvard Medical School.
At the population level, “our genes don’t change that much in less than a generation,” she said.
But our food supply has.
Ultra-processed foods — those containing hydrogenated oils, high-fructose corn syrup, flavoring agents, emulsifiers, and other manufactured ingredients — now make up about 60% of the food supply.
“The evidence is fairly consistent indicating that there’s something about these foods that is possibly causing obesity,” said Tobias.
In one telling 2019 study, Dr. Hall and his colleagues brought 20 men and women into a study center to live for a month and tightly controlled their food intake and activity. One group was provided with meals with 80% of calories from ultra-processed food. The other was given meals with no processed food.
The three daily meals provided had the same calories, sugars, fats, fiber, and carbohydrates, and people were told to eat as much as they wanted.
Those on the ultra-processed diet ate about 500 calories more per day, ate faster, and gained weight. Those on the unprocessed diet lost weight.
“This is a stark example of how, when you can change the food environment, you cause really remarkable changes in food intake without people even being aware that they are overeating,” said Dr. Hall.
Just what it is about these relatively novel foods that may trigger overeating is unclear. It could be the crunch, the lack of water content, the engineered balance of sugar/salt/fat, their easy-to-devour texture, or something else.
Some research suggests that the foods may interfere with gut-brain signaling that tells the brain you’re full.
“Evidence is amassing that the nutritional content of processed foods is not accurately conveyed to the brain,” Dana M. Small, PhD, a neuroscientist at Yale, wrote in a recent perspective paper in Science.
Even more concerning: Some animal studies suggest processed foods reprogram the brain to dislike healthy foods.
And once these brain changes are made, they are hard to reverse.
“The problem is, our brain is not wired for this,” said Dr. Halpern. “We are not evolved to eat the food we are eating, so our brain adapts, but it adapts in a negative way that puts us at risk.”
That’s why changing the food environment via public policy must be part of the solution in combating obesity, Dr. Tobias said.
A New Era of Brain-Based Solutions
In the spring of 2021, after years of trying and failing to lose weight via the “move more, eat less” model, Michael Smith began to take a medication called Vyvanse. The drug was approved in 2008 for attention deficit hyperactivity disorder, but since it also influences levels of the hormones dopamine and norepinephrine to reduce cravings, it is now frequently prescribed for binge eating disorder.
“That was pretty much how I got rid of my first 60 to 70 pounds,” Smith said.
A few months later, after he hit a plateau, he had surgery to shrink the size of his stomach — a decision he now second-guesses.
While it kept him from overeating for a time, the fried chicken and gummy bear cravings returned a few months later.
His doctor, Fatima Cody Stanford, MD, put him on a second medication: semaglutide, or Wegovy, the weekly shot approved for weight loss in 2021. It works, in part, by mimicking glucagon-like peptide-1 (GLP-1), a key gut hormone that lets your brain know you are full.
The weight began to fall off again.
Smith’s success story is just one of many that Dr. Stanford, an obesity medicine doctor-scientist at Harvard, has heard in her office in recent years.
“I do not believe these drugs are a panacea,” she said. “There are nonresponders, and those are the patients I take off the medication. But for the high-responders, and there are many of them, they are telling me, ‘Oh my gosh. For the first time in my life, I am not constantly thinking about eating. My life has changed.’”
A Multi-Pronged Approach
Dr. Halpern, at Penn, has also been hearing success stories.
In recent years, he has placed permanent electrodes in the brains of three people with grade III, or severe, obesity and binge eating disorder.
All had tried exercise, dieting, support groups, medication, and weight loss surgery to no avail.
The electrodes modulate an area in the center of the brain called the nucleus accumbens, which in mice studies has been shown to reduce cravings when stimulated.
Thus far, all three are seeing promising results.
“It’s not like I don’t think about food at all,” one of them, Robyn Baldwin, told The New York Times. “But I’m no longer a craving person.”
Dr. Halpern is now extending the trial to more patients and hopes to ultimately include other areas of the brain, including those that involve memory.
He imagines a day when people with severe obesity, who have failed conventional treatments, can walk into a clinic and have their brain circuits assessed to see which ones may be misfiring.
Many might find relief with noninvasive brain stimulation, like transcranial magnetic stimulation (already in use for depression). Others might need a more extreme approach, like the deep brain stimulation, or DBS, therapy Dr. Halpern used.
“Obviously, DBS is hard to scale, so it would have to be reserved for the most severe patients,” he said.
Still, not everyone believes brain-based drugs and surgeries are the answer.
David Ludwig, MD, PhD, a professor of nutrition at the Harvard School of Public Health, played a key role in the discovery of GLP-1 and acknowledges that “of course” the brain influences body composition. But to him, explaining obesity as a disease of the brain oversimplifies it, discounting metabolic factors such as a tendency to store too much fat.
He noted that it’s hard to get drug companies, or any agencies, to fund large clinical trials on simple things like low-carbohydrate diets or exercise programs.
“We need all the tools we can get in the battle against the obesity epidemic, and new technologies are worth exploring,” he said. “However, the success of these drugs should not lead us to deprioritize diet and lifestyle interventions.”
Dr. Stanford, who has received consulting fees from Wegovy, believes the future of treatment lies in a multi-pronged approach, with surgery, medication, and lifestyle changes coalescing in a lasting, but fragile, remission.
“Unfortunately, there is no cure for obesity,” said Dr. Stanford, whose patients often have setbacks and must try new strategies. “There are treatments that work for a while, but they are constantly pushing up against this origin in the brain.”
Smith says understanding this has been a big part of his success.
He is now a leaner and healthier 5-foot-6 and 204 pounds. In addition to taking his medication, he walks to work, goes to the gym twice a week, limits his portions, and tries to reframe the way he thinks about food, viewing it as fuel rather than an indulgence.
Sometimes, when he looks in the mirror, he is reminded of his 380-pound self, and it scares him. He doesn’t want to go back there. He’s confident now that he won’t have to.
“There is this misconception out there that you just need to put the fork down, but I’m learning it’s more complicated than that,” he said. “I intend to treat this as the illness that it is and do what I need to combat it so I’m able to keep this new reality I have built for myself.”
A version of this article appeared on WebMD.com .
Early evidence supports psilocybin for bipolar depression
, a small, nonrandomized clinical trial shows. However, the investigators and other outside experts warn these results should not be overinterpreted.
Three weeks after receiving psilocybin and psychotherapy, all 15 participants’ depression scores dropped by an average of 24 points. Twelve met criteria for response and 11 for remission.
This benefit lasted until the 12-week mark, with 12 participants (80%) meeting criteria for both response and remission. There were no reports of mixed or manic symptoms, psychotic symptoms, or suicidal ideation.
Given the study’s small, open-label design, the findings should be interpreted cautiously, but the investigators say the results are promising.
“The results we saw from this trial are encouraging and further support the clinical study of psychedelics in patients with treatment-resistant bipolar II,” lead investigator Scott T. Aaronson, MD, chief science officer of the Institute for Advanced Diagnostics and Therapeutics at Sheppard Pratt Health System in Baltimore, Maryland, remarked in a press release. “One participant compared the transformation she experienced to taking a deep breath after breathing through a straw for years.”
The findings were published online on December 6, 2023, in JAMA Psychiatry.
Underserved Population
Previous studies show that psilocybin is effective in reducing the symptoms of treatment-resistant depression, major depressive disorder, and anorexia nervosa, most with only mild to moderate adverse effects.
Individuals with bipolar disorder (BPD) have been excluded from psilocybin studies in the last two decades. Investigators attribute this to anecdotal evidence that psychedelics may result in manic episodes in patients with BPD, even though empirical evidence of those effects is limited.
This study included 15 participants (9 female; mean age, 37.8 years) with BDII who had experienced an episode for more than 3 months and failed at least two medications within the current episode.
Participants stopped all psychotropic medications at least 2 weeks prior to the trial and received 25 mg of synthetic COMP360 psilocybin in a controlled setting. Psychotherapy included three sessions before dosing, one during the 8-hour dosing day, and three integration sessions posttreatment.
Depression was measured with the Montgomery Ǻsberg Depression Rating Scale (MADRS) at six points during the 12-week study.
By week 3, all 15 participants had lower MADRS scores, with a mean decrease of 24 points (P < .001). Twelve participants met the response criteria of ≥ 50% reduction in MADRS scores, and 11 met the criteria for remission of a MADRS score of ≤ 10 (both P < .001).
MADRS scores at each posttreatment time point were significantly lower than they were at baseline and the improvement persisted at 12 weeks.
Participants were also monitored for mania and suicidality at various time points during the study, and no significant changes were found from baseline.
“As a first open-label foray into this underserved and treatment-resistant population, care should be taken not to overinterpret the findings,” the authors note, adding that the findings may not apply to patients with BDI or BDII in a mixed or hypomanic phase of their illness.
No Definitive Conclusion
In an accompanying editorial, David B. Yaden, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland, and colleagues write that the findings are “tantalizingly suggestive,” but ultimately say nothing definitive about the efficacy of psilocybin for BDII.
“The danger is that some individuals will see the large (yet uncontrolled) effect size and believe that a new treatment of bipolar II has been discovered that is substantially better than all other treatments, while neglecting to mention the lack of control condition and substantial psychosocial support included in the study,” Dr. Yaden and colleagues wrote.
They also cautioned that due to the study’s limitations, which include its small sample size and lack of a control group, “it is imperative that the large effect size before to after the study is not overinterpreted.”
However, Dr. Yaden and colleagues also characterized the safety data as “compelling,” noting the safety profile could affect exclusion criteria in future studies involving people with BPD.
“The results of the present study provide preliminary evidence that perhaps those with bipolar II can be safely included in study samples without undue risk of triggering hypomanic episodes,” they wrote. “It also suggests re-evaluation of the need to exclude individuals with mere family history of bipolar II, which several studies do.”
The study was funded by COMPASS Pathways, who provided the study drug. Dr. Aaronson reported grants and nonfinancial support (supply of drug) from COMPASS Pathways during the conduct of the study and personal fees from LivaNova, Neuronetics, Genomind, and Sage Therapeutics outside the submitted work. Other disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
, a small, nonrandomized clinical trial shows. However, the investigators and other outside experts warn these results should not be overinterpreted.
Three weeks after receiving psilocybin and psychotherapy, all 15 participants’ depression scores dropped by an average of 24 points. Twelve met criteria for response and 11 for remission.
This benefit lasted until the 12-week mark, with 12 participants (80%) meeting criteria for both response and remission. There were no reports of mixed or manic symptoms, psychotic symptoms, or suicidal ideation.
Given the study’s small, open-label design, the findings should be interpreted cautiously, but the investigators say the results are promising.
“The results we saw from this trial are encouraging and further support the clinical study of psychedelics in patients with treatment-resistant bipolar II,” lead investigator Scott T. Aaronson, MD, chief science officer of the Institute for Advanced Diagnostics and Therapeutics at Sheppard Pratt Health System in Baltimore, Maryland, remarked in a press release. “One participant compared the transformation she experienced to taking a deep breath after breathing through a straw for years.”
The findings were published online on December 6, 2023, in JAMA Psychiatry.
Underserved Population
Previous studies show that psilocybin is effective in reducing the symptoms of treatment-resistant depression, major depressive disorder, and anorexia nervosa, most with only mild to moderate adverse effects.
Individuals with bipolar disorder (BPD) have been excluded from psilocybin studies in the last two decades. Investigators attribute this to anecdotal evidence that psychedelics may result in manic episodes in patients with BPD, even though empirical evidence of those effects is limited.
This study included 15 participants (9 female; mean age, 37.8 years) with BDII who had experienced an episode for more than 3 months and failed at least two medications within the current episode.
Participants stopped all psychotropic medications at least 2 weeks prior to the trial and received 25 mg of synthetic COMP360 psilocybin in a controlled setting. Psychotherapy included three sessions before dosing, one during the 8-hour dosing day, and three integration sessions posttreatment.
Depression was measured with the Montgomery Ǻsberg Depression Rating Scale (MADRS) at six points during the 12-week study.
By week 3, all 15 participants had lower MADRS scores, with a mean decrease of 24 points (P < .001). Twelve participants met the response criteria of ≥ 50% reduction in MADRS scores, and 11 met the criteria for remission of a MADRS score of ≤ 10 (both P < .001).
MADRS scores at each posttreatment time point were significantly lower than they were at baseline and the improvement persisted at 12 weeks.
Participants were also monitored for mania and suicidality at various time points during the study, and no significant changes were found from baseline.
“As a first open-label foray into this underserved and treatment-resistant population, care should be taken not to overinterpret the findings,” the authors note, adding that the findings may not apply to patients with BDI or BDII in a mixed or hypomanic phase of their illness.
No Definitive Conclusion
In an accompanying editorial, David B. Yaden, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland, and colleagues write that the findings are “tantalizingly suggestive,” but ultimately say nothing definitive about the efficacy of psilocybin for BDII.
“The danger is that some individuals will see the large (yet uncontrolled) effect size and believe that a new treatment of bipolar II has been discovered that is substantially better than all other treatments, while neglecting to mention the lack of control condition and substantial psychosocial support included in the study,” Dr. Yaden and colleagues wrote.
They also cautioned that due to the study’s limitations, which include its small sample size and lack of a control group, “it is imperative that the large effect size before to after the study is not overinterpreted.”
However, Dr. Yaden and colleagues also characterized the safety data as “compelling,” noting the safety profile could affect exclusion criteria in future studies involving people with BPD.
“The results of the present study provide preliminary evidence that perhaps those with bipolar II can be safely included in study samples without undue risk of triggering hypomanic episodes,” they wrote. “It also suggests re-evaluation of the need to exclude individuals with mere family history of bipolar II, which several studies do.”
The study was funded by COMPASS Pathways, who provided the study drug. Dr. Aaronson reported grants and nonfinancial support (supply of drug) from COMPASS Pathways during the conduct of the study and personal fees from LivaNova, Neuronetics, Genomind, and Sage Therapeutics outside the submitted work. Other disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
, a small, nonrandomized clinical trial shows. However, the investigators and other outside experts warn these results should not be overinterpreted.
Three weeks after receiving psilocybin and psychotherapy, all 15 participants’ depression scores dropped by an average of 24 points. Twelve met criteria for response and 11 for remission.
This benefit lasted until the 12-week mark, with 12 participants (80%) meeting criteria for both response and remission. There were no reports of mixed or manic symptoms, psychotic symptoms, or suicidal ideation.
Given the study’s small, open-label design, the findings should be interpreted cautiously, but the investigators say the results are promising.
“The results we saw from this trial are encouraging and further support the clinical study of psychedelics in patients with treatment-resistant bipolar II,” lead investigator Scott T. Aaronson, MD, chief science officer of the Institute for Advanced Diagnostics and Therapeutics at Sheppard Pratt Health System in Baltimore, Maryland, remarked in a press release. “One participant compared the transformation she experienced to taking a deep breath after breathing through a straw for years.”
The findings were published online on December 6, 2023, in JAMA Psychiatry.
Underserved Population
Previous studies show that psilocybin is effective in reducing the symptoms of treatment-resistant depression, major depressive disorder, and anorexia nervosa, most with only mild to moderate adverse effects.
Individuals with bipolar disorder (BPD) have been excluded from psilocybin studies in the last two decades. Investigators attribute this to anecdotal evidence that psychedelics may result in manic episodes in patients with BPD, even though empirical evidence of those effects is limited.
This study included 15 participants (9 female; mean age, 37.8 years) with BDII who had experienced an episode for more than 3 months and failed at least two medications within the current episode.
Participants stopped all psychotropic medications at least 2 weeks prior to the trial and received 25 mg of synthetic COMP360 psilocybin in a controlled setting. Psychotherapy included three sessions before dosing, one during the 8-hour dosing day, and three integration sessions posttreatment.
Depression was measured with the Montgomery Ǻsberg Depression Rating Scale (MADRS) at six points during the 12-week study.
By week 3, all 15 participants had lower MADRS scores, with a mean decrease of 24 points (P < .001). Twelve participants met the response criteria of ≥ 50% reduction in MADRS scores, and 11 met the criteria for remission of a MADRS score of ≤ 10 (both P < .001).
MADRS scores at each posttreatment time point were significantly lower than they were at baseline and the improvement persisted at 12 weeks.
Participants were also monitored for mania and suicidality at various time points during the study, and no significant changes were found from baseline.
“As a first open-label foray into this underserved and treatment-resistant population, care should be taken not to overinterpret the findings,” the authors note, adding that the findings may not apply to patients with BDI or BDII in a mixed or hypomanic phase of their illness.
No Definitive Conclusion
In an accompanying editorial, David B. Yaden, PhD, Johns Hopkins University School of Medicine, Baltimore, Maryland, and colleagues write that the findings are “tantalizingly suggestive,” but ultimately say nothing definitive about the efficacy of psilocybin for BDII.
“The danger is that some individuals will see the large (yet uncontrolled) effect size and believe that a new treatment of bipolar II has been discovered that is substantially better than all other treatments, while neglecting to mention the lack of control condition and substantial psychosocial support included in the study,” Dr. Yaden and colleagues wrote.
They also cautioned that due to the study’s limitations, which include its small sample size and lack of a control group, “it is imperative that the large effect size before to after the study is not overinterpreted.”
However, Dr. Yaden and colleagues also characterized the safety data as “compelling,” noting the safety profile could affect exclusion criteria in future studies involving people with BPD.
“The results of the present study provide preliminary evidence that perhaps those with bipolar II can be safely included in study samples without undue risk of triggering hypomanic episodes,” they wrote. “It also suggests re-evaluation of the need to exclude individuals with mere family history of bipolar II, which several studies do.”
The study was funded by COMPASS Pathways, who provided the study drug. Dr. Aaronson reported grants and nonfinancial support (supply of drug) from COMPASS Pathways during the conduct of the study and personal fees from LivaNova, Neuronetics, Genomind, and Sage Therapeutics outside the submitted work. Other disclosures are noted in the original article.
A version of this article appeared on Medscape.com.
FROM JAMA PSYCHIATRY
FDA approves implant for glaucoma
The iDose TR (Glaukos Corp) is inserted into a corneal incision on the temple side of the eye. Pivotal phase 3 clinical trials showed the treatment resulted in sustained reductions in IOP for 3 months ranging from 6.6 to 8.4 mm Hg, comparable to reductions with topical timolol 0.5% drops used twice daily. Normal IOP is 10-21 mm Hg, and glaucoma treatments are designed to reduce high IOP into the normal range.
Glaukos Corp said that it intends a commercial launch of the implant early in 2024, with a wholesale cost of $13,950 per implant.
Travoprost is a prostaglandin analog that has been long used as a topical formulation for lowering IOP in OAG and OHT. Timolol is a topical beta-blocker widely used for the same indications.
iDose TR comes in a preloaded handheld injector designed to deliver the implant into the sclera of the eye. The implant seats in the junction of the iris, sclera, and cornea.
In two phase 3 clinical trials, 81% of patients who received the iDose TR did not require supplemental drops to reduce IOP after 12 months compared with 95% of those who receive timolol alone.
The phase 3 trials included 1150 participants across 89 clinical sites. Both trials, GC-010 and GC-012, met the primary endpoints through 3 months and demonstrated a favorable tolerability and safety profile through 12 months, according to results that John Berdahl, MD, a researcher with Vance Thompson Vision in Sioux Falls, South Dakota, and an investigator for Glaukos, presented in May at the annual meeting of the American Society of Cataract and Refractive Surgery.
Based on these outcomes, the FDA concluded in the prescribing information that iDose TR demonstrated noninferiority to topical timolol in reduction of IOP during the first 3 months of treatment. The agency also noted that use of iDose TR did not demonstrate noninferiority over the next 9 months.
In the controlled studies, the most common ocular adverse reactions reported in 2% to 6% of patients who received iDose TR were increases in IOP , iritis, dry eye, and defects of the visual field, most of which were said to be mild and transient in nature.
A version of this article appeared on Medscape.com.
The iDose TR (Glaukos Corp) is inserted into a corneal incision on the temple side of the eye. Pivotal phase 3 clinical trials showed the treatment resulted in sustained reductions in IOP for 3 months ranging from 6.6 to 8.4 mm Hg, comparable to reductions with topical timolol 0.5% drops used twice daily. Normal IOP is 10-21 mm Hg, and glaucoma treatments are designed to reduce high IOP into the normal range.
Glaukos Corp said that it intends a commercial launch of the implant early in 2024, with a wholesale cost of $13,950 per implant.
Travoprost is a prostaglandin analog that has been long used as a topical formulation for lowering IOP in OAG and OHT. Timolol is a topical beta-blocker widely used for the same indications.
iDose TR comes in a preloaded handheld injector designed to deliver the implant into the sclera of the eye. The implant seats in the junction of the iris, sclera, and cornea.
In two phase 3 clinical trials, 81% of patients who received the iDose TR did not require supplemental drops to reduce IOP after 12 months compared with 95% of those who receive timolol alone.
The phase 3 trials included 1150 participants across 89 clinical sites. Both trials, GC-010 and GC-012, met the primary endpoints through 3 months and demonstrated a favorable tolerability and safety profile through 12 months, according to results that John Berdahl, MD, a researcher with Vance Thompson Vision in Sioux Falls, South Dakota, and an investigator for Glaukos, presented in May at the annual meeting of the American Society of Cataract and Refractive Surgery.
Based on these outcomes, the FDA concluded in the prescribing information that iDose TR demonstrated noninferiority to topical timolol in reduction of IOP during the first 3 months of treatment. The agency also noted that use of iDose TR did not demonstrate noninferiority over the next 9 months.
In the controlled studies, the most common ocular adverse reactions reported in 2% to 6% of patients who received iDose TR were increases in IOP , iritis, dry eye, and defects of the visual field, most of which were said to be mild and transient in nature.
A version of this article appeared on Medscape.com.
The iDose TR (Glaukos Corp) is inserted into a corneal incision on the temple side of the eye. Pivotal phase 3 clinical trials showed the treatment resulted in sustained reductions in IOP for 3 months ranging from 6.6 to 8.4 mm Hg, comparable to reductions with topical timolol 0.5% drops used twice daily. Normal IOP is 10-21 mm Hg, and glaucoma treatments are designed to reduce high IOP into the normal range.
Glaukos Corp said that it intends a commercial launch of the implant early in 2024, with a wholesale cost of $13,950 per implant.
Travoprost is a prostaglandin analog that has been long used as a topical formulation for lowering IOP in OAG and OHT. Timolol is a topical beta-blocker widely used for the same indications.
iDose TR comes in a preloaded handheld injector designed to deliver the implant into the sclera of the eye. The implant seats in the junction of the iris, sclera, and cornea.
In two phase 3 clinical trials, 81% of patients who received the iDose TR did not require supplemental drops to reduce IOP after 12 months compared with 95% of those who receive timolol alone.
The phase 3 trials included 1150 participants across 89 clinical sites. Both trials, GC-010 and GC-012, met the primary endpoints through 3 months and demonstrated a favorable tolerability and safety profile through 12 months, according to results that John Berdahl, MD, a researcher with Vance Thompson Vision in Sioux Falls, South Dakota, and an investigator for Glaukos, presented in May at the annual meeting of the American Society of Cataract and Refractive Surgery.
Based on these outcomes, the FDA concluded in the prescribing information that iDose TR demonstrated noninferiority to topical timolol in reduction of IOP during the first 3 months of treatment. The agency also noted that use of iDose TR did not demonstrate noninferiority over the next 9 months.
In the controlled studies, the most common ocular adverse reactions reported in 2% to 6% of patients who received iDose TR were increases in IOP , iritis, dry eye, and defects of the visual field, most of which were said to be mild and transient in nature.
A version of this article appeared on Medscape.com.