User login
Oophorectomy for premenopausal breast cancer
One-quarter of patients with breast cancer are diagnosed at a premenopausal age and these young women may be directed to discuss oophorectomy with their ob.gyn. This may be because of the discovery of a deleterious BRCA gene mutation, which places them at increased risk for ovarian cancer, but oophorectomy may also be a therapeutic option for their breast cancer: 60% of premenopausal breast cancers are hormone receptor–positive. Ovarian ablation has been associated with improved overall survival and disease-free survival among these patients.1
Estrogen is an important promoter of breast cancer and is predominantly derived from ovarian tissue in premenopausal women. However, in postmenopausal women, the majority of estrogen is produced peripherally through the conversion of androgens to estrogen via the enzyme aromatase. Aromatase inhibitors, such as exemestane, anastrazole, and letrazole, are drugs which block this conversion in peripheral tissues. They are contraindicated in premenopausal women with intact ovarian function, because there is a reflex pituitary stimulation of ovarian estrogen release in response to suppression of peripheral conversion of androgens. For such patients, ovarian function must be ablated either with surgery or with gonadotropin-releasing hormone (GnRH) analogues such as leuprorelin and goserelin if aromatase inhibitors are desired.

In these trials, ovarian ablation was achieved either reversibly with GnRH analogues or permanently and irreversibly with oophorectomy. No studies have compared the survival benefit of these two approaches; however, surgical ovarian ablation is immediate, reliable, and has been shown to be the most cost-effective method.4 It is a good option for women who struggle with adherence to repeated appointments for injections. It also substantially reduces the risk for ovarian cancer, which is elevated among this population of patients, even among those without a deleterious BRCA gene mutation.
BRCA populations
For women with BRCA germline mutations and a history of breast cancer, oophorectomy is associated with a 70% risk of all-cause mortality, including a 60% reduction in breast cancer mortality. This effect is inclusive of patients with “triple-negative,” hormone receptor–negative tumors. The positive effect on breast cancer mortality is predominantly seen among BRCA-1 mutation carriers, and if the oophorectomy is performed within 2 years of diagnosis.5
Technique
When performing oophorectomy either for breast cancer or because of a hereditary cancer syndrome such as BRCA mutation, it is important to ensure that the ovarian vessel pedicle is transected at least 2 cm from its insertion in the ovary. This prevents leaving a residual ovarian remnant. In order to do this, it may be necessary to skeletonize the ovarian vessels free from their physiological attachments to the sigmoid colon on the left, and terminal ileum and cecum on the right. It is also important to ensure that the ureter is not invested in this more proximal segment of ovarian vessels. To prevent this, the retroperitoneal space can be opened lateral to and parallel with the ovarian vessels, and the “medial leaf” of the broad ligament swept medially to expose the ureter as it crosses the bifurcation of the external and internal iliac arteries at the pelvic brim. With the ureter in view, a window can then be made in the “medial leaf” above the ureter and below the ovary and ovarian vessels, in doing so creating a skeletonized ovarian vessel segment which can be sealed and cut 2 cm or more from its insertion in the ovary.
The fallopian tubes should be removed with the ovarian specimens, with attention made to removing the fallopian tube at its junction with the uterine cornua. It should be noted that the majority of fallopian tube cancers arise in the fimbriated end of the tube, and cornual tubal malignancies are fairly uncommon.
The decision about whether or not to perform hysterectomy at the time of salpingo-oophorectomy is complex. In patients without hereditary cancer syndromes, such as BRCA or Lynch syndrome, hysterectomy likely offers no benefit to the patient who is undergoing a procedure for the purpose of ovarian ablation. An argument has been made that hysterectomy can eliminate the increased endometrial cancer risk associated with tamoxifen. However, given the previously discussed data, after oophorectomy, aromatase inhibitors are the preferred treatment option, and tamoxifen can be avoided. If a patient has unrelated underlying uterine pathology a hysterectomy might be indicated. Women with BRCA germline mutations, particularly women with BRCA-1 mutations, may be at increased risk for uterine serous carcinoma, and in these patients, hysterectomy at the time of oophorectomy can be discussed and offered, though as yet, it is not a guideline recommendation for all patients.6 Patients who ask to “just take everything out while you are there” without a clear indication for hysterectomy should be counseled that hysterectomy is associated with increased risk, recovery, and cost, compared with bilateral salpingo-oophorectomy. Among patients with elevated surgical risk (such as morbid obesity, known adhesive disease, increased venous thromboembolism risk, diabetes, and so on) it may not always be appropriate to extend the complexity of the procedure given the limited benefit.
Consequences of ovarian ablation
It should be noted that ovarian ablation in the TEXT and SOFT trials was not associated with an increase in overall survival for women with premenopausal breast cancer. Alternatively, large, observational studies such as the Nurses’ Health Study have shown that premenopausal oophorectomy without hormone replacement therapy is associated with increased all-cause mortality. This is primarily driven by the increased cardiopulmonary risk (heart attack and stroke), deaths after osteoporotic hip fractures, and the increased risk for lung and colon cancer.7,8
It is normal for young patients to have heightened concerns regarding their risk of recurrence from their cancer, and less concerned by threats to their health in decades to come. However, it is important to discuss this data with the patient and allow for her to make an informed decision about her immediate versus future risks. If she determines that she is not interested in permanent ovarian ablation with oophorectomy because of either surgical risks, concerns regarding permanent infertility, or increased all-cause mortality, she still has an option for medical ovarian ablation with GnRH analogues in the treatment of her breast cancer.
Hormone replacement therapy postoperatively
Women who undergo oophorectomy for the treatment of breast cancer should not be offered hormone replacement therapy. This is true even for “triple-negative” or hormone receptor–negative breast cancers as there is still some observed benefit of ovarian ablation, and risk from exogenous hormone administration in these women. Alternatively, postoperative hormone replacement therapy remains safe until the age of natural menopause among premenopausal patients with BRCA germline mutations without a preceding breast cancer diagnosis.
Surgical ovarian ablation with bilateral salpingo-oophorectomy is a valuable strategy in the adjuvant therapy of premenopausal breast cancer, particularly among BRCA mutation carriers and women with hormone receptor–positive disease, or among women who find adherence to medical ablation difficult. Patients should be carefully counseled that this may introduce increased long-term cardiovascular risks for them.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Early Breast Cancer Trialists’ Collaborative Group. Lancet. 1996 Nov 2;348:1189-96.
2. Pagani O et al. N Engl J Med. 2014 Jul 10;371(12):107-18.
3. Francis PA et al. N Engl J Med. 2015 Jan 29;372(5):436-46.
4. Ferrandina G et al. Clin Drug Investig. 2017 Nov;37(11):1093-102.
5. Finch AP et al. J Clin Oncol. 2014 May 20;32(15):1547-53.
6. Shu CA et al. JAMA Oncol. 2016 Nov 1;2(11):1434-40.
7. Parker WH et al. Obstet Gynecol. 2013 Apr;121(4):709-16.
8. Rivera CM et al. Menopause. 2009 Jan-Feb;16:15-23.
One-quarter of patients with breast cancer are diagnosed at a premenopausal age and these young women may be directed to discuss oophorectomy with their ob.gyn. This may be because of the discovery of a deleterious BRCA gene mutation, which places them at increased risk for ovarian cancer, but oophorectomy may also be a therapeutic option for their breast cancer: 60% of premenopausal breast cancers are hormone receptor–positive. Ovarian ablation has been associated with improved overall survival and disease-free survival among these patients.1
Estrogen is an important promoter of breast cancer and is predominantly derived from ovarian tissue in premenopausal women. However, in postmenopausal women, the majority of estrogen is produced peripherally through the conversion of androgens to estrogen via the enzyme aromatase. Aromatase inhibitors, such as exemestane, anastrazole, and letrazole, are drugs which block this conversion in peripheral tissues. They are contraindicated in premenopausal women with intact ovarian function, because there is a reflex pituitary stimulation of ovarian estrogen release in response to suppression of peripheral conversion of androgens. For such patients, ovarian function must be ablated either with surgery or with gonadotropin-releasing hormone (GnRH) analogues such as leuprorelin and goserelin if aromatase inhibitors are desired.
In these trials, ovarian ablation was achieved either reversibly with GnRH analogues or permanently and irreversibly with oophorectomy. No studies have compared the survival benefit of these two approaches; however, surgical ovarian ablation is immediate, reliable, and has been shown to be the most cost-effective method.4 It is a good option for women who struggle with adherence to repeated appointments for injections. It also substantially reduces the risk for ovarian cancer, which is elevated among this population of patients, even among those without a deleterious BRCA gene mutation.
BRCA populations
For women with BRCA germline mutations and a history of breast cancer, oophorectomy is associated with a 70% risk of all-cause mortality, including a 60% reduction in breast cancer mortality. This effect is inclusive of patients with “triple-negative,” hormone receptor–negative tumors. The positive effect on breast cancer mortality is predominantly seen among BRCA-1 mutation carriers, and if the oophorectomy is performed within 2 years of diagnosis.5
Technique
When performing oophorectomy either for breast cancer or because of a hereditary cancer syndrome such as BRCA mutation, it is important to ensure that the ovarian vessel pedicle is transected at least 2 cm from its insertion in the ovary. This prevents leaving a residual ovarian remnant. In order to do this, it may be necessary to skeletonize the ovarian vessels free from their physiological attachments to the sigmoid colon on the left, and terminal ileum and cecum on the right. It is also important to ensure that the ureter is not invested in this more proximal segment of ovarian vessels. To prevent this, the retroperitoneal space can be opened lateral to and parallel with the ovarian vessels, and the “medial leaf” of the broad ligament swept medially to expose the ureter as it crosses the bifurcation of the external and internal iliac arteries at the pelvic brim. With the ureter in view, a window can then be made in the “medial leaf” above the ureter and below the ovary and ovarian vessels, in doing so creating a skeletonized ovarian vessel segment which can be sealed and cut 2 cm or more from its insertion in the ovary.
The fallopian tubes should be removed with the ovarian specimens, with attention made to removing the fallopian tube at its junction with the uterine cornua. It should be noted that the majority of fallopian tube cancers arise in the fimbriated end of the tube, and cornual tubal malignancies are fairly uncommon.
The decision about whether or not to perform hysterectomy at the time of salpingo-oophorectomy is complex. In patients without hereditary cancer syndromes, such as BRCA or Lynch syndrome, hysterectomy likely offers no benefit to the patient who is undergoing a procedure for the purpose of ovarian ablation. An argument has been made that hysterectomy can eliminate the increased endometrial cancer risk associated with tamoxifen. However, given the previously discussed data, after oophorectomy, aromatase inhibitors are the preferred treatment option, and tamoxifen can be avoided. If a patient has unrelated underlying uterine pathology a hysterectomy might be indicated. Women with BRCA germline mutations, particularly women with BRCA-1 mutations, may be at increased risk for uterine serous carcinoma, and in these patients, hysterectomy at the time of oophorectomy can be discussed and offered, though as yet, it is not a guideline recommendation for all patients.6 Patients who ask to “just take everything out while you are there” without a clear indication for hysterectomy should be counseled that hysterectomy is associated with increased risk, recovery, and cost, compared with bilateral salpingo-oophorectomy. Among patients with elevated surgical risk (such as morbid obesity, known adhesive disease, increased venous thromboembolism risk, diabetes, and so on) it may not always be appropriate to extend the complexity of the procedure given the limited benefit.
Consequences of ovarian ablation
It should be noted that ovarian ablation in the TEXT and SOFT trials was not associated with an increase in overall survival for women with premenopausal breast cancer. Alternatively, large, observational studies such as the Nurses’ Health Study have shown that premenopausal oophorectomy without hormone replacement therapy is associated with increased all-cause mortality. This is primarily driven by the increased cardiopulmonary risk (heart attack and stroke), deaths after osteoporotic hip fractures, and the increased risk for lung and colon cancer.7,8
It is normal for young patients to have heightened concerns regarding their risk of recurrence from their cancer, and less concerned by threats to their health in decades to come. However, it is important to discuss this data with the patient and allow for her to make an informed decision about her immediate versus future risks. If she determines that she is not interested in permanent ovarian ablation with oophorectomy because of either surgical risks, concerns regarding permanent infertility, or increased all-cause mortality, she still has an option for medical ovarian ablation with GnRH analogues in the treatment of her breast cancer.
Hormone replacement therapy postoperatively
Women who undergo oophorectomy for the treatment of breast cancer should not be offered hormone replacement therapy. This is true even for “triple-negative” or hormone receptor–negative breast cancers as there is still some observed benefit of ovarian ablation, and risk from exogenous hormone administration in these women. Alternatively, postoperative hormone replacement therapy remains safe until the age of natural menopause among premenopausal patients with BRCA germline mutations without a preceding breast cancer diagnosis.
Surgical ovarian ablation with bilateral salpingo-oophorectomy is a valuable strategy in the adjuvant therapy of premenopausal breast cancer, particularly among BRCA mutation carriers and women with hormone receptor–positive disease, or among women who find adherence to medical ablation difficult. Patients should be carefully counseled that this may introduce increased long-term cardiovascular risks for them.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Early Breast Cancer Trialists’ Collaborative Group. Lancet. 1996 Nov 2;348:1189-96.
2. Pagani O et al. N Engl J Med. 2014 Jul 10;371(12):107-18.
3. Francis PA et al. N Engl J Med. 2015 Jan 29;372(5):436-46.
4. Ferrandina G et al. Clin Drug Investig. 2017 Nov;37(11):1093-102.
5. Finch AP et al. J Clin Oncol. 2014 May 20;32(15):1547-53.
6. Shu CA et al. JAMA Oncol. 2016 Nov 1;2(11):1434-40.
7. Parker WH et al. Obstet Gynecol. 2013 Apr;121(4):709-16.
8. Rivera CM et al. Menopause. 2009 Jan-Feb;16:15-23.
One-quarter of patients with breast cancer are diagnosed at a premenopausal age and these young women may be directed to discuss oophorectomy with their ob.gyn. This may be because of the discovery of a deleterious BRCA gene mutation, which places them at increased risk for ovarian cancer, but oophorectomy may also be a therapeutic option for their breast cancer: 60% of premenopausal breast cancers are hormone receptor–positive. Ovarian ablation has been associated with improved overall survival and disease-free survival among these patients.1
Estrogen is an important promoter of breast cancer and is predominantly derived from ovarian tissue in premenopausal women. However, in postmenopausal women, the majority of estrogen is produced peripherally through the conversion of androgens to estrogen via the enzyme aromatase. Aromatase inhibitors, such as exemestane, anastrazole, and letrazole, are drugs which block this conversion in peripheral tissues. They are contraindicated in premenopausal women with intact ovarian function, because there is a reflex pituitary stimulation of ovarian estrogen release in response to suppression of peripheral conversion of androgens. For such patients, ovarian function must be ablated either with surgery or with gonadotropin-releasing hormone (GnRH) analogues such as leuprorelin and goserelin if aromatase inhibitors are desired.
In these trials, ovarian ablation was achieved either reversibly with GnRH analogues or permanently and irreversibly with oophorectomy. No studies have compared the survival benefit of these two approaches; however, surgical ovarian ablation is immediate, reliable, and has been shown to be the most cost-effective method.4 It is a good option for women who struggle with adherence to repeated appointments for injections. It also substantially reduces the risk for ovarian cancer, which is elevated among this population of patients, even among those without a deleterious BRCA gene mutation.
BRCA populations
For women with BRCA germline mutations and a history of breast cancer, oophorectomy is associated with a 70% risk of all-cause mortality, including a 60% reduction in breast cancer mortality. This effect is inclusive of patients with “triple-negative,” hormone receptor–negative tumors. The positive effect on breast cancer mortality is predominantly seen among BRCA-1 mutation carriers, and if the oophorectomy is performed within 2 years of diagnosis.5
Technique
When performing oophorectomy either for breast cancer or because of a hereditary cancer syndrome such as BRCA mutation, it is important to ensure that the ovarian vessel pedicle is transected at least 2 cm from its insertion in the ovary. This prevents leaving a residual ovarian remnant. In order to do this, it may be necessary to skeletonize the ovarian vessels free from their physiological attachments to the sigmoid colon on the left, and terminal ileum and cecum on the right. It is also important to ensure that the ureter is not invested in this more proximal segment of ovarian vessels. To prevent this, the retroperitoneal space can be opened lateral to and parallel with the ovarian vessels, and the “medial leaf” of the broad ligament swept medially to expose the ureter as it crosses the bifurcation of the external and internal iliac arteries at the pelvic brim. With the ureter in view, a window can then be made in the “medial leaf” above the ureter and below the ovary and ovarian vessels, in doing so creating a skeletonized ovarian vessel segment which can be sealed and cut 2 cm or more from its insertion in the ovary.
The fallopian tubes should be removed with the ovarian specimens, with attention made to removing the fallopian tube at its junction with the uterine cornua. It should be noted that the majority of fallopian tube cancers arise in the fimbriated end of the tube, and cornual tubal malignancies are fairly uncommon.
The decision about whether or not to perform hysterectomy at the time of salpingo-oophorectomy is complex. In patients without hereditary cancer syndromes, such as BRCA or Lynch syndrome, hysterectomy likely offers no benefit to the patient who is undergoing a procedure for the purpose of ovarian ablation. An argument has been made that hysterectomy can eliminate the increased endometrial cancer risk associated with tamoxifen. However, given the previously discussed data, after oophorectomy, aromatase inhibitors are the preferred treatment option, and tamoxifen can be avoided. If a patient has unrelated underlying uterine pathology a hysterectomy might be indicated. Women with BRCA germline mutations, particularly women with BRCA-1 mutations, may be at increased risk for uterine serous carcinoma, and in these patients, hysterectomy at the time of oophorectomy can be discussed and offered, though as yet, it is not a guideline recommendation for all patients.6 Patients who ask to “just take everything out while you are there” without a clear indication for hysterectomy should be counseled that hysterectomy is associated with increased risk, recovery, and cost, compared with bilateral salpingo-oophorectomy. Among patients with elevated surgical risk (such as morbid obesity, known adhesive disease, increased venous thromboembolism risk, diabetes, and so on) it may not always be appropriate to extend the complexity of the procedure given the limited benefit.
Consequences of ovarian ablation
It should be noted that ovarian ablation in the TEXT and SOFT trials was not associated with an increase in overall survival for women with premenopausal breast cancer. Alternatively, large, observational studies such as the Nurses’ Health Study have shown that premenopausal oophorectomy without hormone replacement therapy is associated with increased all-cause mortality. This is primarily driven by the increased cardiopulmonary risk (heart attack and stroke), deaths after osteoporotic hip fractures, and the increased risk for lung and colon cancer.7,8
It is normal for young patients to have heightened concerns regarding their risk of recurrence from their cancer, and less concerned by threats to their health in decades to come. However, it is important to discuss this data with the patient and allow for her to make an informed decision about her immediate versus future risks. If she determines that she is not interested in permanent ovarian ablation with oophorectomy because of either surgical risks, concerns regarding permanent infertility, or increased all-cause mortality, she still has an option for medical ovarian ablation with GnRH analogues in the treatment of her breast cancer.
Hormone replacement therapy postoperatively
Women who undergo oophorectomy for the treatment of breast cancer should not be offered hormone replacement therapy. This is true even for “triple-negative” or hormone receptor–negative breast cancers as there is still some observed benefit of ovarian ablation, and risk from exogenous hormone administration in these women. Alternatively, postoperative hormone replacement therapy remains safe until the age of natural menopause among premenopausal patients with BRCA germline mutations without a preceding breast cancer diagnosis.
Surgical ovarian ablation with bilateral salpingo-oophorectomy is a valuable strategy in the adjuvant therapy of premenopausal breast cancer, particularly among BRCA mutation carriers and women with hormone receptor–positive disease, or among women who find adherence to medical ablation difficult. Patients should be carefully counseled that this may introduce increased long-term cardiovascular risks for them.
Dr. Rossi is an assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill.
References
1. Early Breast Cancer Trialists’ Collaborative Group. Lancet. 1996 Nov 2;348:1189-96.
2. Pagani O et al. N Engl J Med. 2014 Jul 10;371(12):107-18.
3. Francis PA et al. N Engl J Med. 2015 Jan 29;372(5):436-46.
4. Ferrandina G et al. Clin Drug Investig. 2017 Nov;37(11):1093-102.
5. Finch AP et al. J Clin Oncol. 2014 May 20;32(15):1547-53.
6. Shu CA et al. JAMA Oncol. 2016 Nov 1;2(11):1434-40.
7. Parker WH et al. Obstet Gynecol. 2013 Apr;121(4):709-16.
8. Rivera CM et al. Menopause. 2009 Jan-Feb;16:15-23.
New remote monitoring system lessens symptoms in head and neck cancer
A new system for remotely assessing and transmitting selected vitals and self-reported measures reduces symptom severity among patients with head and neck cancer receiving radiation therapy, in a randomized trial reported at a press briefing held before the annual meeting of the American Society of Clinical Oncology.
“Head and neck cancer patients who receive radiation treatment have a high symptom burden and also are at increased risk for dehydration during treatment,” said lead study author Susan K. Peterson, PhD, a professor in the department of behavioral science at the University of Texas MD Anderson Cancer Center, Houston. “Previously, we have shown that it was feasible to use mobile and sensor technology to identify treatment-related symptoms and early dehydration risk in patients receiving radiation treatment as part of their outpatient care.”
In the new trial, the investigators tested the CYCORE system (Cyberinfrastructure for Comparative Effectiveness Research), which consists of a Bluetooth-enabled weight scale and blood pressure cuff, and a mobile tablet with a symptom-tracking app that sends information directly to the physician each weekday. A network hub/router was set up in patients’ homes to transmit their sensor readouts, and the mobile app transmitted their symptom data to secure firewall-protected computers. “CYCORE also included a software infrastructure that enabled the analysis and viewing of data in near-real time and was compliant with safety and security and confidentiality standards,” Dr. Peterson noted.
Main trial results showed that compared with peers receiving only usual care (weekly visits with the radiation oncologist), patients receiving usual care augmented with the CYCORE system had lower mean scores on a 10-point scale for general symptoms (0.5-point difference) and for symptoms specific to head and neck cancer (0.6-point difference). In addition, daily remote tracking of patient well-being allowed clinicians to more rapidly detect and respond to symptoms.
“This is important because symptoms can affects patients’ ability to tolerate treatment and can also impact their quality of life during treatment,” Dr. Peterson said.
The mean age of the patients was 60 years; the oldest was 86 years old. “This supports the notion that the use of technology-based interventions can be feasible in older patients,” she maintained. In addition, patients in the CYCORE group showed at least 80% adherence to the daily monitoring tasks.
“We believe that good patient adherence plus the fact that this imposed minimal burden on clinicians for the monitoring supports the use of systems like CYCORE during intensive treatment periods in cancer care, and that using sensor and mobile technology to monitor patients during critical periods of outpatient care can provide a timely source of information for clinical decision making and may ultimately improve quality of life and health outcomes,” Dr. Peterson concluded. “Our next steps would be to explore ways to implement this as part of clinical care, including in community cancer centers, where most patients receive their care.”
“This is yet another application of technology-enabled sharing of information generated at home,” said ASCO President Bruce E. Johnson, MD, FASCO, noting that a similar study last year showed better patient-reported experience and overall survival.
Such technology will likely be increasingly used to obtain timely information that ultimately leads to a reduction in complications, he speculated.
“This information in head and neck cancer is particularly important because patients commonly get a lot of side effects when attempting to swallow enough fluids, such that some centers end up putting a feeding tube into the stomach because it’s so difficult to swallow,” added Dr. Johnson, who is also a professor of medicine at the Dana-Farber Cancer Institute and a leader of the Dana-Farber/Harvard Cancer Center Lung Cancer Program, Boston. “So this is a particularly important clinical application in cancer.”
Study details
The trial population consisted of 357 patients undergoing radiation therapy for head and neck cancer. “We believe that this is the first and largest study of its kind in head and neck cancer,” Dr. Peterson said.
The severity of symptoms and their interference with daily activities were assessed at serial time points with the MD Anderson Symptom Inventory.
In the CYCORE group, 87% of patients measured their blood pressure daily, 86% measured their weight daily, and 80% used the symptom-tracking app daily.
At the end of radiation therapy, the CYCORE patients had lower (i.e., better) mean scores for general symptoms (e.g., pain, nausea, fatigue) relative to usual care counterparts (2.9 vs. 3.4), with a difference still evident 6-8 weeks later (1.6 vs. 1.9) (P = .007).
In addition, the CYCORE patients had lower mean scores for symptoms specific to head and neck cancer (e.g., dysphagia, pain, rash) at the end of radiation therapy (4.2 vs. 4.8), with a difference still evident 6-8 weeks later (1.7 vs. 2.1) (P = .009).
The groups fared essentially the same with respect to scores assessing interference of symptoms with activities of daily living.
Dr. Peterson disclosed that she had no relevant conflicts of interest. The study received funding from the National Institutes of Health.
SOURCE: Peterson et al. ASCO 2018, Abstract 6063.
A new system for remotely assessing and transmitting selected vitals and self-reported measures reduces symptom severity among patients with head and neck cancer receiving radiation therapy, in a randomized trial reported at a press briefing held before the annual meeting of the American Society of Clinical Oncology.
“Head and neck cancer patients who receive radiation treatment have a high symptom burden and also are at increased risk for dehydration during treatment,” said lead study author Susan K. Peterson, PhD, a professor in the department of behavioral science at the University of Texas MD Anderson Cancer Center, Houston. “Previously, we have shown that it was feasible to use mobile and sensor technology to identify treatment-related symptoms and early dehydration risk in patients receiving radiation treatment as part of their outpatient care.”
In the new trial, the investigators tested the CYCORE system (Cyberinfrastructure for Comparative Effectiveness Research), which consists of a Bluetooth-enabled weight scale and blood pressure cuff, and a mobile tablet with a symptom-tracking app that sends information directly to the physician each weekday. A network hub/router was set up in patients’ homes to transmit their sensor readouts, and the mobile app transmitted their symptom data to secure firewall-protected computers. “CYCORE also included a software infrastructure that enabled the analysis and viewing of data in near-real time and was compliant with safety and security and confidentiality standards,” Dr. Peterson noted.
Main trial results showed that compared with peers receiving only usual care (weekly visits with the radiation oncologist), patients receiving usual care augmented with the CYCORE system had lower mean scores on a 10-point scale for general symptoms (0.5-point difference) and for symptoms specific to head and neck cancer (0.6-point difference). In addition, daily remote tracking of patient well-being allowed clinicians to more rapidly detect and respond to symptoms.
“This is important because symptoms can affects patients’ ability to tolerate treatment and can also impact their quality of life during treatment,” Dr. Peterson said.
The mean age of the patients was 60 years; the oldest was 86 years old. “This supports the notion that the use of technology-based interventions can be feasible in older patients,” she maintained. In addition, patients in the CYCORE group showed at least 80% adherence to the daily monitoring tasks.
“We believe that good patient adherence plus the fact that this imposed minimal burden on clinicians for the monitoring supports the use of systems like CYCORE during intensive treatment periods in cancer care, and that using sensor and mobile technology to monitor patients during critical periods of outpatient care can provide a timely source of information for clinical decision making and may ultimately improve quality of life and health outcomes,” Dr. Peterson concluded. “Our next steps would be to explore ways to implement this as part of clinical care, including in community cancer centers, where most patients receive their care.”
“This is yet another application of technology-enabled sharing of information generated at home,” said ASCO President Bruce E. Johnson, MD, FASCO, noting that a similar study last year showed better patient-reported experience and overall survival.
Such technology will likely be increasingly used to obtain timely information that ultimately leads to a reduction in complications, he speculated.
“This information in head and neck cancer is particularly important because patients commonly get a lot of side effects when attempting to swallow enough fluids, such that some centers end up putting a feeding tube into the stomach because it’s so difficult to swallow,” added Dr. Johnson, who is also a professor of medicine at the Dana-Farber Cancer Institute and a leader of the Dana-Farber/Harvard Cancer Center Lung Cancer Program, Boston. “So this is a particularly important clinical application in cancer.”
Study details
The trial population consisted of 357 patients undergoing radiation therapy for head and neck cancer. “We believe that this is the first and largest study of its kind in head and neck cancer,” Dr. Peterson said.
The severity of symptoms and their interference with daily activities were assessed at serial time points with the MD Anderson Symptom Inventory.
In the CYCORE group, 87% of patients measured their blood pressure daily, 86% measured their weight daily, and 80% used the symptom-tracking app daily.
At the end of radiation therapy, the CYCORE patients had lower (i.e., better) mean scores for general symptoms (e.g., pain, nausea, fatigue) relative to usual care counterparts (2.9 vs. 3.4), with a difference still evident 6-8 weeks later (1.6 vs. 1.9) (P = .007).
In addition, the CYCORE patients had lower mean scores for symptoms specific to head and neck cancer (e.g., dysphagia, pain, rash) at the end of radiation therapy (4.2 vs. 4.8), with a difference still evident 6-8 weeks later (1.7 vs. 2.1) (P = .009).
The groups fared essentially the same with respect to scores assessing interference of symptoms with activities of daily living.
Dr. Peterson disclosed that she had no relevant conflicts of interest. The study received funding from the National Institutes of Health.
SOURCE: Peterson et al. ASCO 2018, Abstract 6063.
A new system for remotely assessing and transmitting selected vitals and self-reported measures reduces symptom severity among patients with head and neck cancer receiving radiation therapy, in a randomized trial reported at a press briefing held before the annual meeting of the American Society of Clinical Oncology.
“Head and neck cancer patients who receive radiation treatment have a high symptom burden and also are at increased risk for dehydration during treatment,” said lead study author Susan K. Peterson, PhD, a professor in the department of behavioral science at the University of Texas MD Anderson Cancer Center, Houston. “Previously, we have shown that it was feasible to use mobile and sensor technology to identify treatment-related symptoms and early dehydration risk in patients receiving radiation treatment as part of their outpatient care.”
In the new trial, the investigators tested the CYCORE system (Cyberinfrastructure for Comparative Effectiveness Research), which consists of a Bluetooth-enabled weight scale and blood pressure cuff, and a mobile tablet with a symptom-tracking app that sends information directly to the physician each weekday. A network hub/router was set up in patients’ homes to transmit their sensor readouts, and the mobile app transmitted their symptom data to secure firewall-protected computers. “CYCORE also included a software infrastructure that enabled the analysis and viewing of data in near-real time and was compliant with safety and security and confidentiality standards,” Dr. Peterson noted.
Main trial results showed that compared with peers receiving only usual care (weekly visits with the radiation oncologist), patients receiving usual care augmented with the CYCORE system had lower mean scores on a 10-point scale for general symptoms (0.5-point difference) and for symptoms specific to head and neck cancer (0.6-point difference). In addition, daily remote tracking of patient well-being allowed clinicians to more rapidly detect and respond to symptoms.
“This is important because symptoms can affects patients’ ability to tolerate treatment and can also impact their quality of life during treatment,” Dr. Peterson said.
The mean age of the patients was 60 years; the oldest was 86 years old. “This supports the notion that the use of technology-based interventions can be feasible in older patients,” she maintained. In addition, patients in the CYCORE group showed at least 80% adherence to the daily monitoring tasks.
“We believe that good patient adherence plus the fact that this imposed minimal burden on clinicians for the monitoring supports the use of systems like CYCORE during intensive treatment periods in cancer care, and that using sensor and mobile technology to monitor patients during critical periods of outpatient care can provide a timely source of information for clinical decision making and may ultimately improve quality of life and health outcomes,” Dr. Peterson concluded. “Our next steps would be to explore ways to implement this as part of clinical care, including in community cancer centers, where most patients receive their care.”
“This is yet another application of technology-enabled sharing of information generated at home,” said ASCO President Bruce E. Johnson, MD, FASCO, noting that a similar study last year showed better patient-reported experience and overall survival.
Such technology will likely be increasingly used to obtain timely information that ultimately leads to a reduction in complications, he speculated.
“This information in head and neck cancer is particularly important because patients commonly get a lot of side effects when attempting to swallow enough fluids, such that some centers end up putting a feeding tube into the stomach because it’s so difficult to swallow,” added Dr. Johnson, who is also a professor of medicine at the Dana-Farber Cancer Institute and a leader of the Dana-Farber/Harvard Cancer Center Lung Cancer Program, Boston. “So this is a particularly important clinical application in cancer.”
Study details
The trial population consisted of 357 patients undergoing radiation therapy for head and neck cancer. “We believe that this is the first and largest study of its kind in head and neck cancer,” Dr. Peterson said.
The severity of symptoms and their interference with daily activities were assessed at serial time points with the MD Anderson Symptom Inventory.
In the CYCORE group, 87% of patients measured their blood pressure daily, 86% measured their weight daily, and 80% used the symptom-tracking app daily.
At the end of radiation therapy, the CYCORE patients had lower (i.e., better) mean scores for general symptoms (e.g., pain, nausea, fatigue) relative to usual care counterparts (2.9 vs. 3.4), with a difference still evident 6-8 weeks later (1.6 vs. 1.9) (P = .007).
In addition, the CYCORE patients had lower mean scores for symptoms specific to head and neck cancer (e.g., dysphagia, pain, rash) at the end of radiation therapy (4.2 vs. 4.8), with a difference still evident 6-8 weeks later (1.7 vs. 2.1) (P = .009).
The groups fared essentially the same with respect to scores assessing interference of symptoms with activities of daily living.
Dr. Peterson disclosed that she had no relevant conflicts of interest. The study received funding from the National Institutes of Health.
SOURCE: Peterson et al. ASCO 2018, Abstract 6063.
REPORTING FROM ASCO 2018
Key clinical point: .
Major finding: Compared with usual care, the system for tracking and transmitting vitals and self-reported measures through sensor and mobile devices was associated with milder general symptoms (0.5-point difference) and head and neck cancer symptoms (0.6-point difference).
Study details: A randomized controlled trial among 357 patients with head and neck cancer undergoing radiation therapy.
Disclosures: Dr. Peterson disclosed that she had no conflicts of interest. The study received funding from the National Institutes of Health.
Source: Peterson et al. ASCO 2018, Abstract 6063.
2018 AAN Post Meeting Highlights

Solitary Angiokeratoma of the Vulva Mimicking Malignant Melanoma
To the Editor:
Angiokeratoma is a benign vascular tumor characterized by several dilated vessels in the superficial dermis accompanied by epidermal hyperplasia and hyperkeratosis.1 Angiokeratoma of the vulva is a rare clinical finding, usually involving multiple lesions as part of the Fordyce type.2 Solitary angiokeratoma occurs predominantly on the lower legs,3 and although other locations have been described, the presence of a solitary angiokeratoma on the vulva is rare.4 We report 2 cases of solitary angiokeratoma on the vulva that was misdiagnosed as malignant melanoma. Both patients were referred to our center for evaluation and excision.
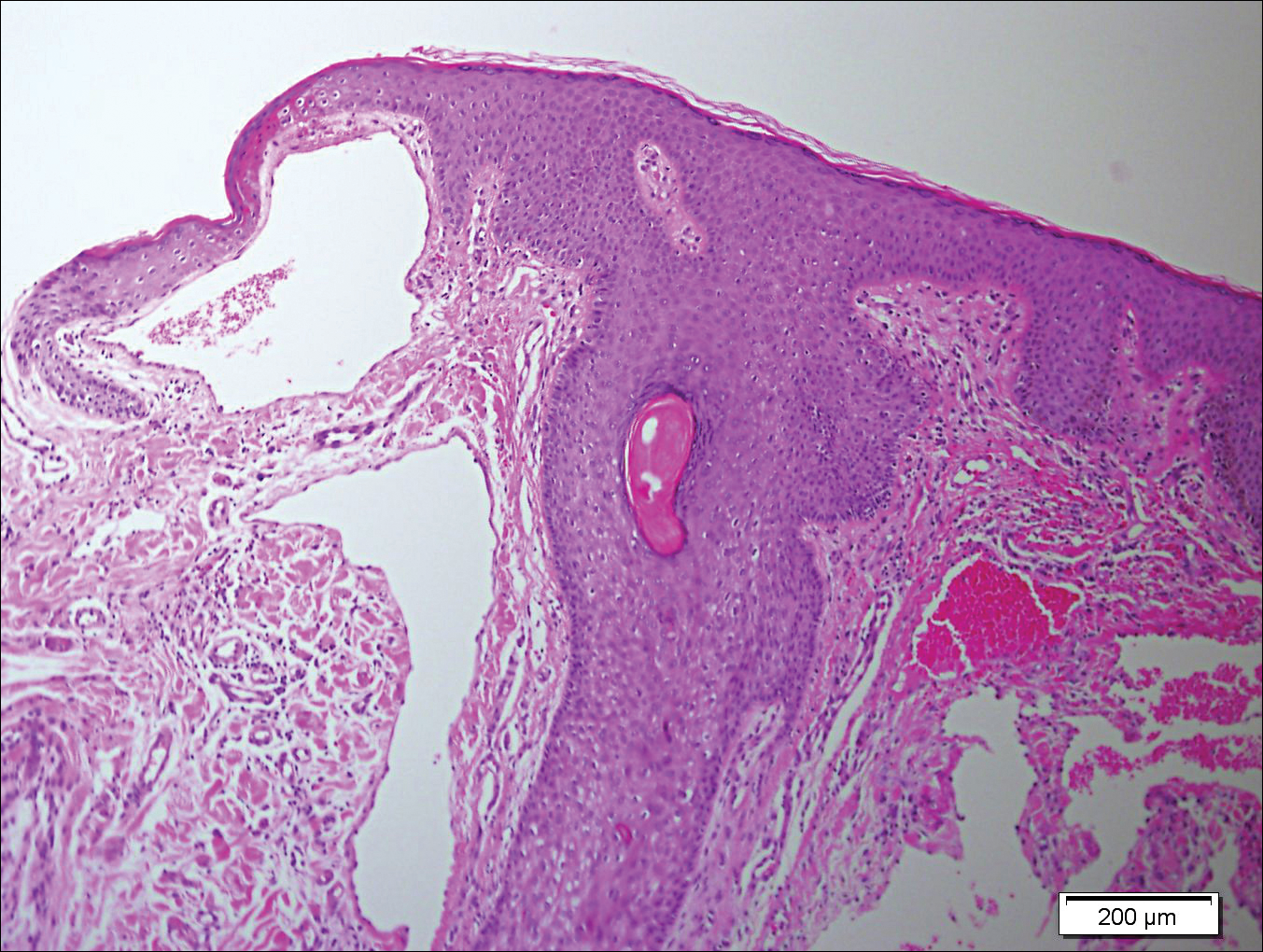
A 65-year-old woman (patient 1) and a 67-year-old woman (patient 2) presented with a bluish black, growing, asymptomatic lesion on the right (Figure 1) and left labia majora, respectively. Both patients were referred by outside physicians for excision because of suspected malignant melanoma. Physical examinations revealed bluish black globular nodules that measured 0.5 and 0.3 cm in diameter, respectively. Dermoscopy (patient 1) revealed dark lacunae. Histopathologic examination of the vulvar lesion (patient 2) showed dilated, blood-filled, vascular spaces in the papillary dermis, accompanied by overlying acanthosis, hyperkeratosis, and papillomatosis that was consistent with angiokeratoma (Figure 2).

Angiokeratoma, particularly the solitary type, often is misdiagnosed. Clinical differential diagnoses may include a wide range of pathologic conditions, including condyloma acuminata, basal cell carcinoma, pyogenic granuloma, lymphangioma, nevi, condyloma lata, nodular prurigo, seborrheic keratosis, granuloma inguinale, and deep fungal infection.2,5 However, due to its quickly growing nature and its dark complexion, malignant melanoma often is initially diagnosed. Because patients affected by angiokeratoma of the vulva usually are aged 20 to 40 years,5 and vulvar melanoma is typical for middle-aged women (median age, 68 years),6 this misdiagnosis is more likely in older patients. It should be noted that a high index of suspicion for melanoma often is present when examining the vulva, considering that this area is difficult to monitor, and there is an especially poor prognosis of vulvar melanoma due to its late detection.6,7
In the past, biopsy was considered mandatory for confirming the diagnosis of vulvar angiokeratoma.5,8,9 However, dermoscopy has emerged as a valuable tool for diagnosis of angiokeratoma10 and also was helpful as a diagnostic aid in one of our patients (patient 1). Therefore, we believe that dermoscopy should be performed prior to a biopsy of angiokeratomas of the vulva.
- Requena L, Sangueza OP. Cutaneous vascular anomalies. part I. hamartomas, malformations, and dilation of preexisting vessels. J Am Acad Dermatol. 1997;37:523-549.
- Schiller PI, Itin PH. Angiokeratomas: an update. Dermatology. 1996;193:275-282.
- Gomi H, Eriyama Y, Horikawa E, et al. Solitary angiokeratoma. J Dermatol. 1988;15:349-350.
- Yamazaki M, Hiruma M, Irie H, et al. Angiokeratoma of the clitoris: a subtype of angiokeratoma vulvae. J Dermatol. 1992;19:553-555.
- Cohen PR, Young AW Jr, Tovell HM. Angiokeratoma of the vulva: diagnosis and review of the literature. Obstet Gynecol Surv. 1989;44:339-346.
- Sugiyama VE, Chan JK, Shin JY, et al. Vulvar melanoma: a multivariable analysis of 644 patients. Obstet Gynecol. 2007;110:296-301.
- De Simone P, Silipo V, Buccini P, et al. Vulvar melanoma: a report of 10 cases and review of the literature. Melanoma Res. 2008;18:127-133.
- Novick NL. Angiokeratoma vulvae. J Am Acad Dermatol. 1985;12:561-563.
- Yigiter M, Arda IS, Tosun E, et al. Angiokeratoma of clitoris: a rare lesion in an adolescent girl. Urology. 2008;71:604-606.
- Zaballos P, Daufi C, Puig S, et al. Dermoscopy of solitary angiokeratomas: a morphological study. Arch Dermatol. 2007;143:318-325.
To the Editor:
Angiokeratoma is a benign vascular tumor characterized by several dilated vessels in the superficial dermis accompanied by epidermal hyperplasia and hyperkeratosis.1 Angiokeratoma of the vulva is a rare clinical finding, usually involving multiple lesions as part of the Fordyce type.2 Solitary angiokeratoma occurs predominantly on the lower legs,3 and although other locations have been described, the presence of a solitary angiokeratoma on the vulva is rare.4 We report 2 cases of solitary angiokeratoma on the vulva that was misdiagnosed as malignant melanoma. Both patients were referred to our center for evaluation and excision.
A 65-year-old woman (patient 1) and a 67-year-old woman (patient 2) presented with a bluish black, growing, asymptomatic lesion on the right (Figure 1) and left labia majora, respectively. Both patients were referred by outside physicians for excision because of suspected malignant melanoma. Physical examinations revealed bluish black globular nodules that measured 0.5 and 0.3 cm in diameter, respectively. Dermoscopy (patient 1) revealed dark lacunae. Histopathologic examination of the vulvar lesion (patient 2) showed dilated, blood-filled, vascular spaces in the papillary dermis, accompanied by overlying acanthosis, hyperkeratosis, and papillomatosis that was consistent with angiokeratoma (Figure 2).
Angiokeratoma, particularly the solitary type, often is misdiagnosed. Clinical differential diagnoses may include a wide range of pathologic conditions, including condyloma acuminata, basal cell carcinoma, pyogenic granuloma, lymphangioma, nevi, condyloma lata, nodular prurigo, seborrheic keratosis, granuloma inguinale, and deep fungal infection.2,5 However, due to its quickly growing nature and its dark complexion, malignant melanoma often is initially diagnosed. Because patients affected by angiokeratoma of the vulva usually are aged 20 to 40 years,5 and vulvar melanoma is typical for middle-aged women (median age, 68 years),6 this misdiagnosis is more likely in older patients. It should be noted that a high index of suspicion for melanoma often is present when examining the vulva, considering that this area is difficult to monitor, and there is an especially poor prognosis of vulvar melanoma due to its late detection.6,7
In the past, biopsy was considered mandatory for confirming the diagnosis of vulvar angiokeratoma.5,8,9 However, dermoscopy has emerged as a valuable tool for diagnosis of angiokeratoma10 and also was helpful as a diagnostic aid in one of our patients (patient 1). Therefore, we believe that dermoscopy should be performed prior to a biopsy of angiokeratomas of the vulva.
To the Editor:
Angiokeratoma is a benign vascular tumor characterized by several dilated vessels in the superficial dermis accompanied by epidermal hyperplasia and hyperkeratosis.1 Angiokeratoma of the vulva is a rare clinical finding, usually involving multiple lesions as part of the Fordyce type.2 Solitary angiokeratoma occurs predominantly on the lower legs,3 and although other locations have been described, the presence of a solitary angiokeratoma on the vulva is rare.4 We report 2 cases of solitary angiokeratoma on the vulva that was misdiagnosed as malignant melanoma. Both patients were referred to our center for evaluation and excision.
A 65-year-old woman (patient 1) and a 67-year-old woman (patient 2) presented with a bluish black, growing, asymptomatic lesion on the right (Figure 1) and left labia majora, respectively. Both patients were referred by outside physicians for excision because of suspected malignant melanoma. Physical examinations revealed bluish black globular nodules that measured 0.5 and 0.3 cm in diameter, respectively. Dermoscopy (patient 1) revealed dark lacunae. Histopathologic examination of the vulvar lesion (patient 2) showed dilated, blood-filled, vascular spaces in the papillary dermis, accompanied by overlying acanthosis, hyperkeratosis, and papillomatosis that was consistent with angiokeratoma (Figure 2).
Angiokeratoma, particularly the solitary type, often is misdiagnosed. Clinical differential diagnoses may include a wide range of pathologic conditions, including condyloma acuminata, basal cell carcinoma, pyogenic granuloma, lymphangioma, nevi, condyloma lata, nodular prurigo, seborrheic keratosis, granuloma inguinale, and deep fungal infection.2,5 However, due to its quickly growing nature and its dark complexion, malignant melanoma often is initially diagnosed. Because patients affected by angiokeratoma of the vulva usually are aged 20 to 40 years,5 and vulvar melanoma is typical for middle-aged women (median age, 68 years),6 this misdiagnosis is more likely in older patients. It should be noted that a high index of suspicion for melanoma often is present when examining the vulva, considering that this area is difficult to monitor, and there is an especially poor prognosis of vulvar melanoma due to its late detection.6,7
In the past, biopsy was considered mandatory for confirming the diagnosis of vulvar angiokeratoma.5,8,9 However, dermoscopy has emerged as a valuable tool for diagnosis of angiokeratoma10 and also was helpful as a diagnostic aid in one of our patients (patient 1). Therefore, we believe that dermoscopy should be performed prior to a biopsy of angiokeratomas of the vulva.
- Requena L, Sangueza OP. Cutaneous vascular anomalies. part I. hamartomas, malformations, and dilation of preexisting vessels. J Am Acad Dermatol. 1997;37:523-549.
- Schiller PI, Itin PH. Angiokeratomas: an update. Dermatology. 1996;193:275-282.
- Gomi H, Eriyama Y, Horikawa E, et al. Solitary angiokeratoma. J Dermatol. 1988;15:349-350.
- Yamazaki M, Hiruma M, Irie H, et al. Angiokeratoma of the clitoris: a subtype of angiokeratoma vulvae. J Dermatol. 1992;19:553-555.
- Cohen PR, Young AW Jr, Tovell HM. Angiokeratoma of the vulva: diagnosis and review of the literature. Obstet Gynecol Surv. 1989;44:339-346.
- Sugiyama VE, Chan JK, Shin JY, et al. Vulvar melanoma: a multivariable analysis of 644 patients. Obstet Gynecol. 2007;110:296-301.
- De Simone P, Silipo V, Buccini P, et al. Vulvar melanoma: a report of 10 cases and review of the literature. Melanoma Res. 2008;18:127-133.
- Novick NL. Angiokeratoma vulvae. J Am Acad Dermatol. 1985;12:561-563.
- Yigiter M, Arda IS, Tosun E, et al. Angiokeratoma of clitoris: a rare lesion in an adolescent girl. Urology. 2008;71:604-606.
- Zaballos P, Daufi C, Puig S, et al. Dermoscopy of solitary angiokeratomas: a morphological study. Arch Dermatol. 2007;143:318-325.
- Requena L, Sangueza OP. Cutaneous vascular anomalies. part I. hamartomas, malformations, and dilation of preexisting vessels. J Am Acad Dermatol. 1997;37:523-549.
- Schiller PI, Itin PH. Angiokeratomas: an update. Dermatology. 1996;193:275-282.
- Gomi H, Eriyama Y, Horikawa E, et al. Solitary angiokeratoma. J Dermatol. 1988;15:349-350.
- Yamazaki M, Hiruma M, Irie H, et al. Angiokeratoma of the clitoris: a subtype of angiokeratoma vulvae. J Dermatol. 1992;19:553-555.
- Cohen PR, Young AW Jr, Tovell HM. Angiokeratoma of the vulva: diagnosis and review of the literature. Obstet Gynecol Surv. 1989;44:339-346.
- Sugiyama VE, Chan JK, Shin JY, et al. Vulvar melanoma: a multivariable analysis of 644 patients. Obstet Gynecol. 2007;110:296-301.
- De Simone P, Silipo V, Buccini P, et al. Vulvar melanoma: a report of 10 cases and review of the literature. Melanoma Res. 2008;18:127-133.
- Novick NL. Angiokeratoma vulvae. J Am Acad Dermatol. 1985;12:561-563.
- Yigiter M, Arda IS, Tosun E, et al. Angiokeratoma of clitoris: a rare lesion in an adolescent girl. Urology. 2008;71:604-606.
- Zaballos P, Daufi C, Puig S, et al. Dermoscopy of solitary angiokeratomas: a morphological study. Arch Dermatol. 2007;143:318-325.
Practice Points
- Solitary angiokeratoma of the vulva often is misdiagnosed as malignant melanoma due to its rapid growth and dark color.
- Dermoscopy is a valuable tool for diagnosing vulvar angiokeratoma to avoid unnecessary excisions.

CRC recurrence surveillance studies: No benefit to high-intensity strategy
More frequent follow-up with computed tomography of the thorax and abdomen and serum carcinoembyronic antigen (CEA) testing does not significantly improve mortality rates or improve time to detection of recurrence, results of two studies published in JAMA have suggested.*
In COLOFOL, a randomized clinical trial including more than 2,500 patients with stage II or III colorectal cancer, more frequent follow-up with CT of the thorax and abdomen and serum CEA did not significantly improve 5-year overall mortality or colorectal cancer–specific mortality rates.
In the second study, a retrospective cohort analysis of the National Cancer Database (NCDB) including more than 8,500 patients with stage I-III colorectal cancer, investigators found no significant association between the surveillance testing frequency and time to detection of disease recurrence.
Taken together, these findings suggest a need to revisit clinical practice guidelines, Hanna K. Sanoff, MD, of the University of North Carolina at Chapel Hill said in a related editorial (for details, see “Views on the News”).
The COLOFOL randomized trial, reported by Henrik T. Sørensen, DMSc, head of the department of clinical epidemiology at Aarhus (Denmark) University Hospital, and his colleagues, included 2,509 patients with stage II or III colorectal cancer.
“The question of appropriate follow-up intervals has been controversial, and varying intensity of follow-up has been used within and among countries,” Dr. Sørensen and his coauthors said.
Patients were randomized either to a high-frequency group, in which CT and CEA testing were conducted at 6, 12, 18, 24, and 36 months after surgery, or to a low-frequency group that received testing only at 12 and 36 months after surgery.
Results of COLOFOL showed that the 5-year colorectal cancer–specific mortality rate was similar: 10.6% for the high-frequency follow-up group versus 11.4% for the low frequency group (risk difference, 0.8%; 95%confidence interval, –1.7% to 3.3%; P = .52).
Likewise, 5-year overall mortality was 13.0% for the high-frequency group and 14.1% for the low-frequency follow-up groups (risk difference, 1.1%; 95% CI, –1.6% to 3.8%; P = .43
High-intensity testing did result in recurrences being detected earlier; nevertheless, this did not translate into a reduced mortality rate, investigators said.
The retrospective NCDB analysis, reported by George J. Chang, MD, of University of Texas MD Anderson Cancer Center, Houston, and his coauthors, included 8,529 patients with stage I-III colorectal cancer treated at 1,175 facilities.
Facilities designated as high intensity for imaging performed a mean of 2.87 imaging tests over 3 years, compared with 1.63 for facilities designated as low intensity. Median time to detection of recurrence was similar between arms, at 15.1 months for patients treated at centers with high-intensity surveillance versus 16.0 months for those treated at low-intensity surveillance centers (hazard ratio, 0.99; 95% CI, 0.90-1.09).
High-intensity CEA testing facilities performed a mean of 4.31 tests within 3 years versus 1.63 for low-intensity facilities. Again, investigators found similar median time to detection of recurrence for high- and low-intensity facilities (15.9 months versus 15.3 months, respectively; hazard ratio, 1.00; 95% CI, 0.90-1.11)
Previously, the Follow-up After Colorectal Surgery (FACS) study, a randomized controlled trial, showed no survival benefit to more frequent testing, Dr. Chang and his colleagues noted.
“Based on these data and the recent FACS trial, current National Comprehensive Cancer Network (NCCN) guideline recommendations could be considered overtesting given the absence of improvement in recurrence detection or survival,” they wrote, noting that the NCCN guidelines have suggested CT testing every 6 months for 3 years.
Disclosures for the COLOFOL trial included one investigator who reported potential conflicts of interest with Janssen-Cilag and Merck Serono. For the NCDB study, one coauthor reported a potential conflict of interest related to Johnson & Johnson. No other disclosures were reported.
SOURCES: Sørensen HT et al. JAMA Oncol. 2018 May 22. doi: 10.1001/jama.2018.5623; Chang GJ et al. JAMA Oncol. 2018 May 22. doi; 10.1001/jama.2018.5816.
Correction, 6/8/18: An earlier version of this article misstated the name of the journal in which this study was published.
Clinical practice guidelines should be reevaluated in light of the findings of these two studies, according to Hanna K. Sanoff, MD.
While the studies both have methodological limitations, the need to revisit recommendations is important given the potential harms associated with more frequent testing, Dr. Sanoff said in an accompanying editorial.
“Because of their designs, results of the COLOFOL trial and the NCDB study should not be considered precise estimates of the effect of surveillance on survival,” she wrote. “However, as gold standard randomized controlled trial evidence is unlikely to become available, decisions must be made on the basis of these imperfect, although methodologically sound, reports.”
Both studies found that a high-intensity surveillance strategy offered no significant differences in key outcomes versus a low-intensity strategy. However, the NCDB study was a retrospective cohort analysis, so the results should be viewed in light of the inherent limitations of that study approach.
Similarly, although the COLOFOL study is randomized, it should be viewed as a pragmatic study, according to Dr. Sanoff, since investigators made several practical design decisions to ensure that patients would be enrolled and the study completed. For example, the eligibility criteria were not stringent with regard to confirming metastatic disease at entry.
Even so, the results of the trial are corroborated by another pragmatic randomized controlled trial, the Follow-up After Colorectal Surgery (FACS) study, which also showed no benefit to more frequent testing.
“There is now a considerable body of evidence that imaging and CEA testing more often than every year does little to improve survival in a meaningful way,” Dr. Sanoff said in her editorial.
Hanna K. Sanoff, MD, is with the division of hematology/oncology at the University of North Carolina at Chapel Hill. These comments are derived from her editorial in JAMA Oncology. Dr. Sanoff reported no conflicts of interest relevant to her work on the editorial.
Clinical practice guidelines should be reevaluated in light of the findings of these two studies, according to Hanna K. Sanoff, MD.
While the studies both have methodological limitations, the need to revisit recommendations is important given the potential harms associated with more frequent testing, Dr. Sanoff said in an accompanying editorial.
“Because of their designs, results of the COLOFOL trial and the NCDB study should not be considered precise estimates of the effect of surveillance on survival,” she wrote. “However, as gold standard randomized controlled trial evidence is unlikely to become available, decisions must be made on the basis of these imperfect, although methodologically sound, reports.”
Both studies found that a high-intensity surveillance strategy offered no significant differences in key outcomes versus a low-intensity strategy. However, the NCDB study was a retrospective cohort analysis, so the results should be viewed in light of the inherent limitations of that study approach.
Similarly, although the COLOFOL study is randomized, it should be viewed as a pragmatic study, according to Dr. Sanoff, since investigators made several practical design decisions to ensure that patients would be enrolled and the study completed. For example, the eligibility criteria were not stringent with regard to confirming metastatic disease at entry.
Even so, the results of the trial are corroborated by another pragmatic randomized controlled trial, the Follow-up After Colorectal Surgery (FACS) study, which also showed no benefit to more frequent testing.
“There is now a considerable body of evidence that imaging and CEA testing more often than every year does little to improve survival in a meaningful way,” Dr. Sanoff said in her editorial.
Hanna K. Sanoff, MD, is with the division of hematology/oncology at the University of North Carolina at Chapel Hill. These comments are derived from her editorial in JAMA Oncology. Dr. Sanoff reported no conflicts of interest relevant to her work on the editorial.
Clinical practice guidelines should be reevaluated in light of the findings of these two studies, according to Hanna K. Sanoff, MD.
While the studies both have methodological limitations, the need to revisit recommendations is important given the potential harms associated with more frequent testing, Dr. Sanoff said in an accompanying editorial.
“Because of their designs, results of the COLOFOL trial and the NCDB study should not be considered precise estimates of the effect of surveillance on survival,” she wrote. “However, as gold standard randomized controlled trial evidence is unlikely to become available, decisions must be made on the basis of these imperfect, although methodologically sound, reports.”
Both studies found that a high-intensity surveillance strategy offered no significant differences in key outcomes versus a low-intensity strategy. However, the NCDB study was a retrospective cohort analysis, so the results should be viewed in light of the inherent limitations of that study approach.
Similarly, although the COLOFOL study is randomized, it should be viewed as a pragmatic study, according to Dr. Sanoff, since investigators made several practical design decisions to ensure that patients would be enrolled and the study completed. For example, the eligibility criteria were not stringent with regard to confirming metastatic disease at entry.
Even so, the results of the trial are corroborated by another pragmatic randomized controlled trial, the Follow-up After Colorectal Surgery (FACS) study, which also showed no benefit to more frequent testing.
“There is now a considerable body of evidence that imaging and CEA testing more often than every year does little to improve survival in a meaningful way,” Dr. Sanoff said in her editorial.
Hanna K. Sanoff, MD, is with the division of hematology/oncology at the University of North Carolina at Chapel Hill. These comments are derived from her editorial in JAMA Oncology. Dr. Sanoff reported no conflicts of interest relevant to her work on the editorial.
More frequent follow-up with computed tomography of the thorax and abdomen and serum carcinoembyronic antigen (CEA) testing does not significantly improve mortality rates or improve time to detection of recurrence, results of two studies published in JAMA have suggested.*
In COLOFOL, a randomized clinical trial including more than 2,500 patients with stage II or III colorectal cancer, more frequent follow-up with CT of the thorax and abdomen and serum CEA did not significantly improve 5-year overall mortality or colorectal cancer–specific mortality rates.
In the second study, a retrospective cohort analysis of the National Cancer Database (NCDB) including more than 8,500 patients with stage I-III colorectal cancer, investigators found no significant association between the surveillance testing frequency and time to detection of disease recurrence.
Taken together, these findings suggest a need to revisit clinical practice guidelines, Hanna K. Sanoff, MD, of the University of North Carolina at Chapel Hill said in a related editorial (for details, see “Views on the News”).
The COLOFOL randomized trial, reported by Henrik T. Sørensen, DMSc, head of the department of clinical epidemiology at Aarhus (Denmark) University Hospital, and his colleagues, included 2,509 patients with stage II or III colorectal cancer.
“The question of appropriate follow-up intervals has been controversial, and varying intensity of follow-up has been used within and among countries,” Dr. Sørensen and his coauthors said.
Patients were randomized either to a high-frequency group, in which CT and CEA testing were conducted at 6, 12, 18, 24, and 36 months after surgery, or to a low-frequency group that received testing only at 12 and 36 months after surgery.
Results of COLOFOL showed that the 5-year colorectal cancer–specific mortality rate was similar: 10.6% for the high-frequency follow-up group versus 11.4% for the low frequency group (risk difference, 0.8%; 95%confidence interval, –1.7% to 3.3%; P = .52).
Likewise, 5-year overall mortality was 13.0% for the high-frequency group and 14.1% for the low-frequency follow-up groups (risk difference, 1.1%; 95% CI, –1.6% to 3.8%; P = .43
High-intensity testing did result in recurrences being detected earlier; nevertheless, this did not translate into a reduced mortality rate, investigators said.
The retrospective NCDB analysis, reported by George J. Chang, MD, of University of Texas MD Anderson Cancer Center, Houston, and his coauthors, included 8,529 patients with stage I-III colorectal cancer treated at 1,175 facilities.
Facilities designated as high intensity for imaging performed a mean of 2.87 imaging tests over 3 years, compared with 1.63 for facilities designated as low intensity. Median time to detection of recurrence was similar between arms, at 15.1 months for patients treated at centers with high-intensity surveillance versus 16.0 months for those treated at low-intensity surveillance centers (hazard ratio, 0.99; 95% CI, 0.90-1.09).
High-intensity CEA testing facilities performed a mean of 4.31 tests within 3 years versus 1.63 for low-intensity facilities. Again, investigators found similar median time to detection of recurrence for high- and low-intensity facilities (15.9 months versus 15.3 months, respectively; hazard ratio, 1.00; 95% CI, 0.90-1.11)
Previously, the Follow-up After Colorectal Surgery (FACS) study, a randomized controlled trial, showed no survival benefit to more frequent testing, Dr. Chang and his colleagues noted.
“Based on these data and the recent FACS trial, current National Comprehensive Cancer Network (NCCN) guideline recommendations could be considered overtesting given the absence of improvement in recurrence detection or survival,” they wrote, noting that the NCCN guidelines have suggested CT testing every 6 months for 3 years.
Disclosures for the COLOFOL trial included one investigator who reported potential conflicts of interest with Janssen-Cilag and Merck Serono. For the NCDB study, one coauthor reported a potential conflict of interest related to Johnson & Johnson. No other disclosures were reported.
SOURCES: Sørensen HT et al. JAMA Oncol. 2018 May 22. doi: 10.1001/jama.2018.5623; Chang GJ et al. JAMA Oncol. 2018 May 22. doi; 10.1001/jama.2018.5816.
Correction, 6/8/18: An earlier version of this article misstated the name of the journal in which this study was published.
More frequent follow-up with computed tomography of the thorax and abdomen and serum carcinoembyronic antigen (CEA) testing does not significantly improve mortality rates or improve time to detection of recurrence, results of two studies published in JAMA have suggested.*
In COLOFOL, a randomized clinical trial including more than 2,500 patients with stage II or III colorectal cancer, more frequent follow-up with CT of the thorax and abdomen and serum CEA did not significantly improve 5-year overall mortality or colorectal cancer–specific mortality rates.
In the second study, a retrospective cohort analysis of the National Cancer Database (NCDB) including more than 8,500 patients with stage I-III colorectal cancer, investigators found no significant association between the surveillance testing frequency and time to detection of disease recurrence.
Taken together, these findings suggest a need to revisit clinical practice guidelines, Hanna K. Sanoff, MD, of the University of North Carolina at Chapel Hill said in a related editorial (for details, see “Views on the News”).
The COLOFOL randomized trial, reported by Henrik T. Sørensen, DMSc, head of the department of clinical epidemiology at Aarhus (Denmark) University Hospital, and his colleagues, included 2,509 patients with stage II or III colorectal cancer.
“The question of appropriate follow-up intervals has been controversial, and varying intensity of follow-up has been used within and among countries,” Dr. Sørensen and his coauthors said.
Patients were randomized either to a high-frequency group, in which CT and CEA testing were conducted at 6, 12, 18, 24, and 36 months after surgery, or to a low-frequency group that received testing only at 12 and 36 months after surgery.
Results of COLOFOL showed that the 5-year colorectal cancer–specific mortality rate was similar: 10.6% for the high-frequency follow-up group versus 11.4% for the low frequency group (risk difference, 0.8%; 95%confidence interval, –1.7% to 3.3%; P = .52).
Likewise, 5-year overall mortality was 13.0% for the high-frequency group and 14.1% for the low-frequency follow-up groups (risk difference, 1.1%; 95% CI, –1.6% to 3.8%; P = .43
High-intensity testing did result in recurrences being detected earlier; nevertheless, this did not translate into a reduced mortality rate, investigators said.
The retrospective NCDB analysis, reported by George J. Chang, MD, of University of Texas MD Anderson Cancer Center, Houston, and his coauthors, included 8,529 patients with stage I-III colorectal cancer treated at 1,175 facilities.
Facilities designated as high intensity for imaging performed a mean of 2.87 imaging tests over 3 years, compared with 1.63 for facilities designated as low intensity. Median time to detection of recurrence was similar between arms, at 15.1 months for patients treated at centers with high-intensity surveillance versus 16.0 months for those treated at low-intensity surveillance centers (hazard ratio, 0.99; 95% CI, 0.90-1.09).
High-intensity CEA testing facilities performed a mean of 4.31 tests within 3 years versus 1.63 for low-intensity facilities. Again, investigators found similar median time to detection of recurrence for high- and low-intensity facilities (15.9 months versus 15.3 months, respectively; hazard ratio, 1.00; 95% CI, 0.90-1.11)
Previously, the Follow-up After Colorectal Surgery (FACS) study, a randomized controlled trial, showed no survival benefit to more frequent testing, Dr. Chang and his colleagues noted.
“Based on these data and the recent FACS trial, current National Comprehensive Cancer Network (NCCN) guideline recommendations could be considered overtesting given the absence of improvement in recurrence detection or survival,” they wrote, noting that the NCCN guidelines have suggested CT testing every 6 months for 3 years.
Disclosures for the COLOFOL trial included one investigator who reported potential conflicts of interest with Janssen-Cilag and Merck Serono. For the NCDB study, one coauthor reported a potential conflict of interest related to Johnson & Johnson. No other disclosures were reported.
SOURCES: Sørensen HT et al. JAMA Oncol. 2018 May 22. doi: 10.1001/jama.2018.5623; Chang GJ et al. JAMA Oncol. 2018 May 22. doi; 10.1001/jama.2018.5816.
Correction, 6/8/18: An earlier version of this article misstated the name of the journal in which this study was published.
FROM JAMA
Key clinical point: In a randomized study, more frequent follow-up with CT of the thorax and abdomen and serum carcinoembryonic antigen (CEA) did not significantly improve mortality rates. In a retrospective study, there was no association found between frequency of testing and time to detection of recurrence.
Major finding: In the randomized trial, the 5-year colorectal cancer–specific mortality rate was 10.6% for high-frequency follow-up versus 11.4% for low frequency (risk difference, 0.8%; 95% confidence interval, –1.7% to 3.3%; P = .52). In the retrospective study, the median time to detection of recurrence was 15.1 months versus 16.0 months, respectively, for patients treated at centers with high- or low-intensity imaging surveillance (difference, –0.95 months; 95% CI, –2.59 to 0.68; hazard ratio, 0.99), with similar results for high- versus low-intensity CEA testing.
Study details: The COLOFOL randomized clinical trial, which included 2,509 patients with stage II or III colorectal cancer, and a retrospective cohort study of the National Cancer Database (NCDB), which included 8,529 patients with stage I-III colorectal cancer.
Disclosures: For the COLOFOL trial, one investigator reported disclosures with Janssen-Cilag and Merck Serono. For the NCDB study, one coauthor reported a disclosure related to Johnson & Johnson. No other disclosures were reported.
Source: Sørensen HT et al. JAMA Oncol. 2018 May 22. doi: 10.1001/jama.2018.5623; Chang GJ et al. JAMA Oncol. 2018 May 22. doi: 10.1001/jama.2018.5816.
New criteria slightly improved melanoma staging
Use of the recently updated AJCC Cancer Staging Manual, 8th edition, produced about 10% better accuracy when interpreting T1a invasive melanomas in a national study.
For stage T1b or greater cases, using the AJCC 8 instead of the AJCC 7 yielded about 6% higher concordance between interpretations and consensus reference diagnoses, said Joann G. Elmore, MD, MPH, of the David Geffen School of Medicine at the University of California, Los Angeles, and her associates. “Intraobserver reproducibility of diagnoses also improved,” but “concordance and reproducibility remain low,” the researchers wrote. The report was published in JAMA Open Network.
For the study, 187 pathologists each interpreted one of five glass slide sets of melanocytic skin biopsies. At least 8 months later, they interpreted the same set again, both times recording their interpretations on the online Pathology Assessment Tool and Hierarchy for Diagnosis (MPATH-Dx). Researchers then used AJCC 7 and AJCC 8 criteria to group these interpretations into one of five MPATH-Dx classes. The final analysis included only the 116 cases of invasive melanoma, because changes in the AJCC 8 criteria affected only MPATH-Dx classes IV (T1a) and V (T1b and higher), the investigators explained.
For T1a invasive melanomas, overall concordance between interpretations and consensus diagnoses rose from 44% (95% confidence interval, 41%-48%) under the AJCC 7 criteria to 54% (95% CI, 51%-57%) under the AJCC 8 criteria. For stage T1b or higher lesions, concordance rose from 72% to 78%. Intrapathologist reproducibility improved from 59% to 64% for T1a cases and from 74% to 77% for T1b or higher cases. Thus, the AJCC 8 produced “modest” improvements in concordance and reproducibility over the AJCC 7, the researchers said.
One of the most likely explanations is that the AJCC 8 eliminated dermal mitotic activity as a criterion for T1b melanomas, which is “potentially unreliable” in thin lesions, they added. Persistently low concordance and reproducibility “suggest that conventional histopathology has been parsed to a degree that falls below the limits of reliability,” they concluded.
The National Cancer Institute provided funding. Dr. Elmore disclosed ties to Myriad Genetics, SciBase, and the National Institutes of Health.
SOURCE: Elmore JG et al. JAMA Network Open. 2018 May 18. doi: 10.1001/jamanetworkopen.2018.0083.
Compared with the seventh edition, use of the eighth AJCC Cancer Staging Manual (AJCC 8) produced “modest but significant improvements” in reproducibility and concordance when microstaging cutaneous melanoma, Peter M. Ferguson, MBChB, PhD, FRCPA, Jeffrey E. Gershenwald, MD, and Richard A. Scolyer, MD, FRCPA, wrote in an editorial accompanying the study.
But the study revealed “significant” shortcomings in reproducibility, they added. Future studies should explore the reproducibility of individual AJCC parameters and how experience and access to relevant case data affects reproducibility, they wrote.
The study used the Melanocytic Pathology Assessment Tool and Hierarchy for Diagnosis system instead of classifying cases by AJCC tumor categories. Consequently, pathologists collapsed several AJCC tumor subcategories into the Melanoma Pathology Study class V, which limited interpretability of results for T1b melanomas, an important threshold for recommending sentinel node biopsy. “[We] have published higher rates of concordance using AJCC 7 criteria, albeit with access to clinical information and reporting by a small number of pathologists with expertise reporting melanomas at a high-volume referral center,” the editorialists emphasized.
Dr. Ferguson and Dr. Scolyer are with the University of Sydney. Dr. Gershenwald is with the University of Texas MD Anderson Cancer Center, Houston. The editorialists disclosed support from the Robert and Lynne Grossman Family Foundation, the Michael and Patricia Booker Melanoma Research Endowment, Melanoma Institute Australia, the Deborah and John McMurtrie Melanoma Institute Australia Pathology Fellowship, and the Australian National Health and Medical Research Council Fellowship. Dr. Gershenwald disclosed ties to Merck, Syndax, Castle Biosciences, and the AJCC (JAMA Network Open. 2018 May 18. doi: 10.1001/jamanetworkopen.2018.0086 ).
Compared with the seventh edition, use of the eighth AJCC Cancer Staging Manual (AJCC 8) produced “modest but significant improvements” in reproducibility and concordance when microstaging cutaneous melanoma, Peter M. Ferguson, MBChB, PhD, FRCPA, Jeffrey E. Gershenwald, MD, and Richard A. Scolyer, MD, FRCPA, wrote in an editorial accompanying the study.
But the study revealed “significant” shortcomings in reproducibility, they added. Future studies should explore the reproducibility of individual AJCC parameters and how experience and access to relevant case data affects reproducibility, they wrote.
The study used the Melanocytic Pathology Assessment Tool and Hierarchy for Diagnosis system instead of classifying cases by AJCC tumor categories. Consequently, pathologists collapsed several AJCC tumor subcategories into the Melanoma Pathology Study class V, which limited interpretability of results for T1b melanomas, an important threshold for recommending sentinel node biopsy. “[We] have published higher rates of concordance using AJCC 7 criteria, albeit with access to clinical information and reporting by a small number of pathologists with expertise reporting melanomas at a high-volume referral center,” the editorialists emphasized.
Dr. Ferguson and Dr. Scolyer are with the University of Sydney. Dr. Gershenwald is with the University of Texas MD Anderson Cancer Center, Houston. The editorialists disclosed support from the Robert and Lynne Grossman Family Foundation, the Michael and Patricia Booker Melanoma Research Endowment, Melanoma Institute Australia, the Deborah and John McMurtrie Melanoma Institute Australia Pathology Fellowship, and the Australian National Health and Medical Research Council Fellowship. Dr. Gershenwald disclosed ties to Merck, Syndax, Castle Biosciences, and the AJCC (JAMA Network Open. 2018 May 18. doi: 10.1001/jamanetworkopen.2018.0086 ).
Compared with the seventh edition, use of the eighth AJCC Cancer Staging Manual (AJCC 8) produced “modest but significant improvements” in reproducibility and concordance when microstaging cutaneous melanoma, Peter M. Ferguson, MBChB, PhD, FRCPA, Jeffrey E. Gershenwald, MD, and Richard A. Scolyer, MD, FRCPA, wrote in an editorial accompanying the study.
But the study revealed “significant” shortcomings in reproducibility, they added. Future studies should explore the reproducibility of individual AJCC parameters and how experience and access to relevant case data affects reproducibility, they wrote.
The study used the Melanocytic Pathology Assessment Tool and Hierarchy for Diagnosis system instead of classifying cases by AJCC tumor categories. Consequently, pathologists collapsed several AJCC tumor subcategories into the Melanoma Pathology Study class V, which limited interpretability of results for T1b melanomas, an important threshold for recommending sentinel node biopsy. “[We] have published higher rates of concordance using AJCC 7 criteria, albeit with access to clinical information and reporting by a small number of pathologists with expertise reporting melanomas at a high-volume referral center,” the editorialists emphasized.
Dr. Ferguson and Dr. Scolyer are with the University of Sydney. Dr. Gershenwald is with the University of Texas MD Anderson Cancer Center, Houston. The editorialists disclosed support from the Robert and Lynne Grossman Family Foundation, the Michael and Patricia Booker Melanoma Research Endowment, Melanoma Institute Australia, the Deborah and John McMurtrie Melanoma Institute Australia Pathology Fellowship, and the Australian National Health and Medical Research Council Fellowship. Dr. Gershenwald disclosed ties to Merck, Syndax, Castle Biosciences, and the AJCC (JAMA Network Open. 2018 May 18. doi: 10.1001/jamanetworkopen.2018.0086 ).
Use of the recently updated AJCC Cancer Staging Manual, 8th edition, produced about 10% better accuracy when interpreting T1a invasive melanomas in a national study.
For stage T1b or greater cases, using the AJCC 8 instead of the AJCC 7 yielded about 6% higher concordance between interpretations and consensus reference diagnoses, said Joann G. Elmore, MD, MPH, of the David Geffen School of Medicine at the University of California, Los Angeles, and her associates. “Intraobserver reproducibility of diagnoses also improved,” but “concordance and reproducibility remain low,” the researchers wrote. The report was published in JAMA Open Network.
For the study, 187 pathologists each interpreted one of five glass slide sets of melanocytic skin biopsies. At least 8 months later, they interpreted the same set again, both times recording their interpretations on the online Pathology Assessment Tool and Hierarchy for Diagnosis (MPATH-Dx). Researchers then used AJCC 7 and AJCC 8 criteria to group these interpretations into one of five MPATH-Dx classes. The final analysis included only the 116 cases of invasive melanoma, because changes in the AJCC 8 criteria affected only MPATH-Dx classes IV (T1a) and V (T1b and higher), the investigators explained.
For T1a invasive melanomas, overall concordance between interpretations and consensus diagnoses rose from 44% (95% confidence interval, 41%-48%) under the AJCC 7 criteria to 54% (95% CI, 51%-57%) under the AJCC 8 criteria. For stage T1b or higher lesions, concordance rose from 72% to 78%. Intrapathologist reproducibility improved from 59% to 64% for T1a cases and from 74% to 77% for T1b or higher cases. Thus, the AJCC 8 produced “modest” improvements in concordance and reproducibility over the AJCC 7, the researchers said.
One of the most likely explanations is that the AJCC 8 eliminated dermal mitotic activity as a criterion for T1b melanomas, which is “potentially unreliable” in thin lesions, they added. Persistently low concordance and reproducibility “suggest that conventional histopathology has been parsed to a degree that falls below the limits of reliability,” they concluded.
The National Cancer Institute provided funding. Dr. Elmore disclosed ties to Myriad Genetics, SciBase, and the National Institutes of Health.
SOURCE: Elmore JG et al. JAMA Network Open. 2018 May 18. doi: 10.1001/jamanetworkopen.2018.0083.
Use of the recently updated AJCC Cancer Staging Manual, 8th edition, produced about 10% better accuracy when interpreting T1a invasive melanomas in a national study.
For stage T1b or greater cases, using the AJCC 8 instead of the AJCC 7 yielded about 6% higher concordance between interpretations and consensus reference diagnoses, said Joann G. Elmore, MD, MPH, of the David Geffen School of Medicine at the University of California, Los Angeles, and her associates. “Intraobserver reproducibility of diagnoses also improved,” but “concordance and reproducibility remain low,” the researchers wrote. The report was published in JAMA Open Network.
For the study, 187 pathologists each interpreted one of five glass slide sets of melanocytic skin biopsies. At least 8 months later, they interpreted the same set again, both times recording their interpretations on the online Pathology Assessment Tool and Hierarchy for Diagnosis (MPATH-Dx). Researchers then used AJCC 7 and AJCC 8 criteria to group these interpretations into one of five MPATH-Dx classes. The final analysis included only the 116 cases of invasive melanoma, because changes in the AJCC 8 criteria affected only MPATH-Dx classes IV (T1a) and V (T1b and higher), the investigators explained.
For T1a invasive melanomas, overall concordance between interpretations and consensus diagnoses rose from 44% (95% confidence interval, 41%-48%) under the AJCC 7 criteria to 54% (95% CI, 51%-57%) under the AJCC 8 criteria. For stage T1b or higher lesions, concordance rose from 72% to 78%. Intrapathologist reproducibility improved from 59% to 64% for T1a cases and from 74% to 77% for T1b or higher cases. Thus, the AJCC 8 produced “modest” improvements in concordance and reproducibility over the AJCC 7, the researchers said.
One of the most likely explanations is that the AJCC 8 eliminated dermal mitotic activity as a criterion for T1b melanomas, which is “potentially unreliable” in thin lesions, they added. Persistently low concordance and reproducibility “suggest that conventional histopathology has been parsed to a degree that falls below the limits of reliability,” they concluded.
The National Cancer Institute provided funding. Dr. Elmore disclosed ties to Myriad Genetics, SciBase, and the National Institutes of Health.
SOURCE: Elmore JG et al. JAMA Network Open. 2018 May 18. doi: 10.1001/jamanetworkopen.2018.0083.
FROM JAMA NETWORK OPEN
Key clinical point: Use of the recently updated AJCC Cancer Staging Manual, 8th edition, somewhat improved concordance and reproducibility for invasive melanoma, compared with the previous edition.
Major finding: For diagnoses of T1a invasive melanoma, concordance with consensus diagnoses rose from 44% with the AJCC 7 to 54% with the AJCC 8. For T1b, concordance rose from 72% to 78%.
Study details: Interpretations of 116 invasive melanomas by 187 pathologists.
Disclosures: The National Cancer Institute provided funding. Dr. Elmore disclosed ties to Myriad Genetics, SciBase, and the National Institutes of Health.
Source: Elmore JG et al. JAMA Network Open. 2018 May 18. doi: 10.1001/jamanetworkopen.2018.0083.
IBD upped Parkinson’s risk in large study
Patients with inflammatory bowel disease were about 22% more likely to develop Parkinson’s disease than were unaffected peers in a population-based cohort study spanning more than 3 decades.
The finding “strengthens the theory of a ‘gut-brain axis,’ in which the intestinal environment influences the functioning of the central nervous system and intestinal imbalance may precede Parkinson’s disease,” wrote Marie Villumsen, PhD, of Bispebjerg and Frederiksberg Hospital in Copenhagen, with her associates.
Thus, clinicians should be vigilant for parkinsonism in patients with inflammatory bowel disease (IBD), the researchers wrote on May 21 in Gut. “Although the absolute risk of Parkinson’s disease [among patients with IBD] remains low, our study points to overlapping pathogenic mechanisms which merit further investigation, as they may represent targets for future therapeutic interventions.”
Gastrointestinal dysfunction can be one of the earliest manifestations of Parkinson’s disease, the researchers noted. Both neurodegenerative disorders and IBD involve chronic inflammation, and both Crohn’s disease and Parkinson’s disease have been linked to aberrations of the LRRK2 gene, which helps regulate inflammation and clearance of alpha-sinuclein, a key component of neuronal Lewy bodies in Parkinson’s disease.
To assess whether IBD directly increases the risk of Parkinson’s disease, the investigators studied individuals from the Danish National Patient Register, which covers all hospitalizations and outpatient visits in Denmark. They matched 76,477 patients with IBD with 7.5 million unaffected individuals of the same sex and age during 1977-2014. Patients with IBD had significantly more comorbidities (P less than .001) than individuals without IBD, so the researchers also controlled for Charlson Comorbidity Index.
In the adjusted analyses, IBD significantly increased the risk of developing Parkinson’s disease among both men (hazard ratio, 1.2) and women (HR, 1.23), irrespective of follow-up time and regardless of whether patients were less than 40 years old (HR, 1.22), 40-65 years old (HR, 1.25), or older than 65 years (HR, 1.30). The association between IBD and Parkinson’s disease also held up after accounting for the possibility that early gut symptoms of Parkinson’s disease were sometimes misdiagnosed as IBD, the researchers wrote.
Interestingly, stratifying by IBD subtype showed that the statistically significant risk factor was ulcerative colitis (HR, 1.35; 95% confidence interval, 1.20-1.52), not Crohn’s disease (HR, 1.12; 95% CI, 0.89-1.40). Prior studies have found that cigarette smoking reduces the risk of both Parkinson’s disease and ulcerative colitis, the investigators noted. They called for additional studies of intestinal inflammation in Parkinson’s disease and the role of the brain-gut axis in the etiology of parkinsonism.
Parkinsonforeningen, Landsforeningen Multipel System Atrofi, and Aage og Johanne Louis-Hansens Fond provided support. The investigators declared no competing interests.
SOURCE: Villumsen M et al. Gut. 2018 May 21. doi: 10.1136/gutjnl-2017-315666.
Patients with inflammatory bowel disease were about 22% more likely to develop Parkinson’s disease than were unaffected peers in a population-based cohort study spanning more than 3 decades.
The finding “strengthens the theory of a ‘gut-brain axis,’ in which the intestinal environment influences the functioning of the central nervous system and intestinal imbalance may precede Parkinson’s disease,” wrote Marie Villumsen, PhD, of Bispebjerg and Frederiksberg Hospital in Copenhagen, with her associates.
Thus, clinicians should be vigilant for parkinsonism in patients with inflammatory bowel disease (IBD), the researchers wrote on May 21 in Gut. “Although the absolute risk of Parkinson’s disease [among patients with IBD] remains low, our study points to overlapping pathogenic mechanisms which merit further investigation, as they may represent targets for future therapeutic interventions.”
Gastrointestinal dysfunction can be one of the earliest manifestations of Parkinson’s disease, the researchers noted. Both neurodegenerative disorders and IBD involve chronic inflammation, and both Crohn’s disease and Parkinson’s disease have been linked to aberrations of the LRRK2 gene, which helps regulate inflammation and clearance of alpha-sinuclein, a key component of neuronal Lewy bodies in Parkinson’s disease.
To assess whether IBD directly increases the risk of Parkinson’s disease, the investigators studied individuals from the Danish National Patient Register, which covers all hospitalizations and outpatient visits in Denmark. They matched 76,477 patients with IBD with 7.5 million unaffected individuals of the same sex and age during 1977-2014. Patients with IBD had significantly more comorbidities (P less than .001) than individuals without IBD, so the researchers also controlled for Charlson Comorbidity Index.
In the adjusted analyses, IBD significantly increased the risk of developing Parkinson’s disease among both men (hazard ratio, 1.2) and women (HR, 1.23), irrespective of follow-up time and regardless of whether patients were less than 40 years old (HR, 1.22), 40-65 years old (HR, 1.25), or older than 65 years (HR, 1.30). The association between IBD and Parkinson’s disease also held up after accounting for the possibility that early gut symptoms of Parkinson’s disease were sometimes misdiagnosed as IBD, the researchers wrote.
Interestingly, stratifying by IBD subtype showed that the statistically significant risk factor was ulcerative colitis (HR, 1.35; 95% confidence interval, 1.20-1.52), not Crohn’s disease (HR, 1.12; 95% CI, 0.89-1.40). Prior studies have found that cigarette smoking reduces the risk of both Parkinson’s disease and ulcerative colitis, the investigators noted. They called for additional studies of intestinal inflammation in Parkinson’s disease and the role of the brain-gut axis in the etiology of parkinsonism.
Parkinsonforeningen, Landsforeningen Multipel System Atrofi, and Aage og Johanne Louis-Hansens Fond provided support. The investigators declared no competing interests.
SOURCE: Villumsen M et al. Gut. 2018 May 21. doi: 10.1136/gutjnl-2017-315666.
Patients with inflammatory bowel disease were about 22% more likely to develop Parkinson’s disease than were unaffected peers in a population-based cohort study spanning more than 3 decades.
The finding “strengthens the theory of a ‘gut-brain axis,’ in which the intestinal environment influences the functioning of the central nervous system and intestinal imbalance may precede Parkinson’s disease,” wrote Marie Villumsen, PhD, of Bispebjerg and Frederiksberg Hospital in Copenhagen, with her associates.
Thus, clinicians should be vigilant for parkinsonism in patients with inflammatory bowel disease (IBD), the researchers wrote on May 21 in Gut. “Although the absolute risk of Parkinson’s disease [among patients with IBD] remains low, our study points to overlapping pathogenic mechanisms which merit further investigation, as they may represent targets for future therapeutic interventions.”
Gastrointestinal dysfunction can be one of the earliest manifestations of Parkinson’s disease, the researchers noted. Both neurodegenerative disorders and IBD involve chronic inflammation, and both Crohn’s disease and Parkinson’s disease have been linked to aberrations of the LRRK2 gene, which helps regulate inflammation and clearance of alpha-sinuclein, a key component of neuronal Lewy bodies in Parkinson’s disease.
To assess whether IBD directly increases the risk of Parkinson’s disease, the investigators studied individuals from the Danish National Patient Register, which covers all hospitalizations and outpatient visits in Denmark. They matched 76,477 patients with IBD with 7.5 million unaffected individuals of the same sex and age during 1977-2014. Patients with IBD had significantly more comorbidities (P less than .001) than individuals without IBD, so the researchers also controlled for Charlson Comorbidity Index.
In the adjusted analyses, IBD significantly increased the risk of developing Parkinson’s disease among both men (hazard ratio, 1.2) and women (HR, 1.23), irrespective of follow-up time and regardless of whether patients were less than 40 years old (HR, 1.22), 40-65 years old (HR, 1.25), or older than 65 years (HR, 1.30). The association between IBD and Parkinson’s disease also held up after accounting for the possibility that early gut symptoms of Parkinson’s disease were sometimes misdiagnosed as IBD, the researchers wrote.
Interestingly, stratifying by IBD subtype showed that the statistically significant risk factor was ulcerative colitis (HR, 1.35; 95% confidence interval, 1.20-1.52), not Crohn’s disease (HR, 1.12; 95% CI, 0.89-1.40). Prior studies have found that cigarette smoking reduces the risk of both Parkinson’s disease and ulcerative colitis, the investigators noted. They called for additional studies of intestinal inflammation in Parkinson’s disease and the role of the brain-gut axis in the etiology of parkinsonism.
Parkinsonforeningen, Landsforeningen Multipel System Atrofi, and Aage og Johanne Louis-Hansens Fond provided support. The investigators declared no competing interests.
SOURCE: Villumsen M et al. Gut. 2018 May 21. doi: 10.1136/gutjnl-2017-315666.
FROM GUT
Key clinical point:
Major finding: After accounting for comorbidities, individuals with IBD were about 22% more likely to develop Parkinson’s disease compared with individuals without IBD (hazard ratio, 1.22; 95% confidence interval, 1.09-1.35).
Study details: A population-based cohort study of 76,477 individuals with IBD and 7.5 million unaffected persons.
Disclosures: Parkinsonforeningen, Landsforeningen Multipel System Atrofi, and Aage og Johanne Louis-Hansens Fond provided support. The investigators declared no competing interests.
Source: Villumsen M et al. Gut. 2018 May 21. doi: 10.1136/gutjnl-2017-315666.
Physical therapy, exercise still relevant for ankylosing spondylitis
CAMBRIDGE, MASS. – , according to Angelo Papachristos, an advanced physiotherapist at St. Michaels Hospital in Toronto.
Speaking in an education session at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN), Mr. Papachristos said that therapy should be introduced at diagnosis, individualized, and constantly reevaluated.
“There is no one recommendation,” he said. “Therapy should be monitored and adjusted over time depending on how the patient responds.”
Mr. Papachristos drew attention to two portions of recommendations from the American College of Sports Medicine (ACSM).
First, that scientific evidence demonstrates that the beneficial effects of exercise are indisputable and that the benefits far outweigh the risks.
Second, that a program of regular exercise that includes cardiorespiratory, resistance, flexibility, and neuromotor aspects to improve and maintain fitness and health is essential for most adults.
How much exercise to prescribe and when to introduce exercise remains a question.
The ACSM recommends moderate-intensity cardiovascular exercise for 30 minutes or more each day or 150 minutes per week, resistance training, neuromotor exercise, and flexibility training at least twice each week.
In a 2011 literature review published in Arthritis Care & Research, researchers analyzed 12 studies (826 total patients) to find out if exercise had actual potential for patients with ankylosing spondylitis. They used three criteria: whether the programs were designed using ACSM recommendations, if/how physiological responses were measured, and whether adherence to programs was monitored.
Of the 12 trials, 5 included cardiovascular exercise, 5 included strength training, 11 included flexibility, and 4 reported program adherence.
Only one trial met ACSM recommendations for intensity, duration, frequency, and length of exercise period. That trial showed the greatest improvement in aerobic capacity (Arthritis Car Res. 2011 Apr;63[4]:597-603).
“The literature isn’t impressive,” said Mr. Papachristos. “But, that’s because it isn’t uniform. No specific protocol is being followed.”
He compared what he believes is happening with what he believes to be a better alternative.
What he calls the hit-them-with-everything approach includes diagnosis, NSAIDs, biologics, smoking cessation at the same time as exercise that includes posture, swimming, strength, and aerobic conditioning. According to Mr. Papachristos, this approach can lead to patient burnout.
Indeed, research from 2010 published in the Journal of Rheumatology showed that 40% of patients with ankylosing spondylitis said that exercise takes too much time, 60% said that exercise is hard work, 60% reported being fatigued by exercise, and 20% said that their family members did not encourage exercise (J Rheumatol. 2010 Mar 1. doi: 10.3899/jrheum.090655).
To combat burnout and improve patient outcomes, Mr. Papachristos suggested an alternative approach whereby patients would begin with diagnosis and medication, but disease education and a baseline fitness assessment would also be a priority. The first 6-9 months following diagnosis would then be used to evaluate a patient’s home and work/school ergonomic situation to assess needs. During this time, the patient would be introduced to basic exercises for range of motion and flexibility. Throughout this approach, the patient would be consistently reevaluated and, if appropriate, would slowly ramp up exercise efforts. At 12 months, the patients could graduate to core cervical and lumbar strength before reaching cardiovascular and sports recreation at 12-18 months following diagnosis.
Mr. Papachristos concluded that the coordination between physical therapist, primary care provider, and rheumatologist is of the utmost importance.
“It’s just like anything else – if we’re all on the same page, it’s better for the patient,” he said. “Patients should be encouraged on lifestyle and wellness management with the goal of lifelong regular exercise.”
Mr. Papachristos reported having no disclosures.
CAMBRIDGE, MASS. – , according to Angelo Papachristos, an advanced physiotherapist at St. Michaels Hospital in Toronto.
Speaking in an education session at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN), Mr. Papachristos said that therapy should be introduced at diagnosis, individualized, and constantly reevaluated.
“There is no one recommendation,” he said. “Therapy should be monitored and adjusted over time depending on how the patient responds.”
Mr. Papachristos drew attention to two portions of recommendations from the American College of Sports Medicine (ACSM).
First, that scientific evidence demonstrates that the beneficial effects of exercise are indisputable and that the benefits far outweigh the risks.
Second, that a program of regular exercise that includes cardiorespiratory, resistance, flexibility, and neuromotor aspects to improve and maintain fitness and health is essential for most adults.
How much exercise to prescribe and when to introduce exercise remains a question.
The ACSM recommends moderate-intensity cardiovascular exercise for 30 minutes or more each day or 150 minutes per week, resistance training, neuromotor exercise, and flexibility training at least twice each week.
In a 2011 literature review published in Arthritis Care & Research, researchers analyzed 12 studies (826 total patients) to find out if exercise had actual potential for patients with ankylosing spondylitis. They used three criteria: whether the programs were designed using ACSM recommendations, if/how physiological responses were measured, and whether adherence to programs was monitored.
Of the 12 trials, 5 included cardiovascular exercise, 5 included strength training, 11 included flexibility, and 4 reported program adherence.
Only one trial met ACSM recommendations for intensity, duration, frequency, and length of exercise period. That trial showed the greatest improvement in aerobic capacity (Arthritis Car Res. 2011 Apr;63[4]:597-603).
“The literature isn’t impressive,” said Mr. Papachristos. “But, that’s because it isn’t uniform. No specific protocol is being followed.”
He compared what he believes is happening with what he believes to be a better alternative.
What he calls the hit-them-with-everything approach includes diagnosis, NSAIDs, biologics, smoking cessation at the same time as exercise that includes posture, swimming, strength, and aerobic conditioning. According to Mr. Papachristos, this approach can lead to patient burnout.
Indeed, research from 2010 published in the Journal of Rheumatology showed that 40% of patients with ankylosing spondylitis said that exercise takes too much time, 60% said that exercise is hard work, 60% reported being fatigued by exercise, and 20% said that their family members did not encourage exercise (J Rheumatol. 2010 Mar 1. doi: 10.3899/jrheum.090655).
To combat burnout and improve patient outcomes, Mr. Papachristos suggested an alternative approach whereby patients would begin with diagnosis and medication, but disease education and a baseline fitness assessment would also be a priority. The first 6-9 months following diagnosis would then be used to evaluate a patient’s home and work/school ergonomic situation to assess needs. During this time, the patient would be introduced to basic exercises for range of motion and flexibility. Throughout this approach, the patient would be consistently reevaluated and, if appropriate, would slowly ramp up exercise efforts. At 12 months, the patients could graduate to core cervical and lumbar strength before reaching cardiovascular and sports recreation at 12-18 months following diagnosis.
Mr. Papachristos concluded that the coordination between physical therapist, primary care provider, and rheumatologist is of the utmost importance.
“It’s just like anything else – if we’re all on the same page, it’s better for the patient,” he said. “Patients should be encouraged on lifestyle and wellness management with the goal of lifelong regular exercise.”
Mr. Papachristos reported having no disclosures.
CAMBRIDGE, MASS. – , according to Angelo Papachristos, an advanced physiotherapist at St. Michaels Hospital in Toronto.
Speaking in an education session at the annual meeting of the Spondyloarthritis Research and Treatment Network (SPARTAN), Mr. Papachristos said that therapy should be introduced at diagnosis, individualized, and constantly reevaluated.
“There is no one recommendation,” he said. “Therapy should be monitored and adjusted over time depending on how the patient responds.”
Mr. Papachristos drew attention to two portions of recommendations from the American College of Sports Medicine (ACSM).
First, that scientific evidence demonstrates that the beneficial effects of exercise are indisputable and that the benefits far outweigh the risks.
Second, that a program of regular exercise that includes cardiorespiratory, resistance, flexibility, and neuromotor aspects to improve and maintain fitness and health is essential for most adults.
How much exercise to prescribe and when to introduce exercise remains a question.
The ACSM recommends moderate-intensity cardiovascular exercise for 30 minutes or more each day or 150 minutes per week, resistance training, neuromotor exercise, and flexibility training at least twice each week.
In a 2011 literature review published in Arthritis Care & Research, researchers analyzed 12 studies (826 total patients) to find out if exercise had actual potential for patients with ankylosing spondylitis. They used three criteria: whether the programs were designed using ACSM recommendations, if/how physiological responses were measured, and whether adherence to programs was monitored.
Of the 12 trials, 5 included cardiovascular exercise, 5 included strength training, 11 included flexibility, and 4 reported program adherence.
Only one trial met ACSM recommendations for intensity, duration, frequency, and length of exercise period. That trial showed the greatest improvement in aerobic capacity (Arthritis Car Res. 2011 Apr;63[4]:597-603).
“The literature isn’t impressive,” said Mr. Papachristos. “But, that’s because it isn’t uniform. No specific protocol is being followed.”
He compared what he believes is happening with what he believes to be a better alternative.
What he calls the hit-them-with-everything approach includes diagnosis, NSAIDs, biologics, smoking cessation at the same time as exercise that includes posture, swimming, strength, and aerobic conditioning. According to Mr. Papachristos, this approach can lead to patient burnout.
Indeed, research from 2010 published in the Journal of Rheumatology showed that 40% of patients with ankylosing spondylitis said that exercise takes too much time, 60% said that exercise is hard work, 60% reported being fatigued by exercise, and 20% said that their family members did not encourage exercise (J Rheumatol. 2010 Mar 1. doi: 10.3899/jrheum.090655).
To combat burnout and improve patient outcomes, Mr. Papachristos suggested an alternative approach whereby patients would begin with diagnosis and medication, but disease education and a baseline fitness assessment would also be a priority. The first 6-9 months following diagnosis would then be used to evaluate a patient’s home and work/school ergonomic situation to assess needs. During this time, the patient would be introduced to basic exercises for range of motion and flexibility. Throughout this approach, the patient would be consistently reevaluated and, if appropriate, would slowly ramp up exercise efforts. At 12 months, the patients could graduate to core cervical and lumbar strength before reaching cardiovascular and sports recreation at 12-18 months following diagnosis.
Mr. Papachristos concluded that the coordination between physical therapist, primary care provider, and rheumatologist is of the utmost importance.
“It’s just like anything else – if we’re all on the same page, it’s better for the patient,” he said. “Patients should be encouraged on lifestyle and wellness management with the goal of lifelong regular exercise.”
Mr. Papachristos reported having no disclosures.
REPORTING FROM SPARTAN
Four-meter gait speed predicts mortality in IPF
SAN DIEGO – Among patients with idiopathic pulmonary fibrosis (IPF), an improvement in 4-meter gait speed with pulmonary rehabilitation is an independent predictor of all-cause mortality at 1 year, suggest results from a multicenter study presented at an international conference of the American Thoracic Society.
In all, 11% of patients died within 1 year of completing pulmonary rehabilitation.

“Mortality is an attractive endpoint in IPF clinical research but requires large sample sizes and long follow-up duration, making clinical trials expensive and challenging to undertake,” lead study author Claire M. Nolan, MSc, said at the conference.
“Consequently, there is much interest in surrogate endpoints of mortality. In the elderly population, a lot of work has been done on performance measures, in particular the 4-meter gait test. It’s a simple test to do from the assessor’s perspective, because you just need a 4-meter corridor and a stopwatch. From the patient’s perspective, they only have to walk at their usual speed, making it feasible in most settings.”
The study by Ms. Nolan, a National Institute for Health Research fellow, and her associates, involved recruiting 90 IPF patients referred to three outpatient pulmonary rehabilitation programs in London. All patients underwent the following assessments before and after 8 weeks of pulmonary rehabilitation: spirometry; Medical Research Council dyspnea score; anthropometry; 4-meter gait speed; incremental shuttle walk test, and King’s Brief Interstitial Lung Disease questionnaire. Ms. Nolan, a respiratory physiotherapist with the Harefield Pulmonary Rehabilitation and Muscle Research Group, Royal Brompton and Harefield NHS Foundation Trust, Harefield, London, and her associates drew from national databases to obtain data on all-cause mortality 1 year following pulmonary rehabilitation.
“We also identified a cutpoint, so if patients improved their walking speed by 0.009 meters per second or above, that was associated with a longer survival time at 1 year (area under the curve of 0.76, for sensitivity of 69.6% and a specificity of 70%; P less than 0.01),” she said.* “Among patients who achieved that cutpoint or exceeded it, only 5% of them died in the 1-year follow-up period, compared with 23% in the group that didn’t achieve that cutpoint. That’s quite a big difference, but this requires external validation in another population.”
To determine the 4-meter gait speed change cut-off that best discriminated between patients who died and survived, the investigators plotted receiver operating characteristic curves. For validation, they conducted a Kaplan-Meier analysis to assess time to death, with significance assessed via the log-rank test. Finally, they used a multivariate Cox proportional hazards model to characterize the relationship between 4-meter gait speed change and all-cause mortality, adjusting for independent predictors of mortality (age, previous respiratory hospitalizations in the past year, forced vital capacity percent predicted) and baseline 4-meter gait speed.
At baseline, 70% of the 90 patients were male, mean age was 74 years, mean forced vital capacity was 72.8% predicted, and mean Medical Research Council dyspnea score was 3. In addition, mean body mass index was 27.2 kg/m2, mean 4-meter gait speed was 0.92 meters per second, mean incremental shuttle walk test measurement was 271 meters, and mean King’s Brief Interstitial Lung Disease total score was 56.4. Following 8 weeks of pulmonary rehabilitation, the patients’ 4-meter gait speed improved significantly by a mean of 0.15 meters per second (P less than .001). All other variables also improved significantly, with the exception of forced vital capacity.
In an interview, Ms. Nolan characterized the results as “one piece of the puzzle in answering whether 4-meter gait speed is a useful test for clinicians and researchers. It needs to be taken in the context of 4-meter gait speed in other populations as well as with what we’re finding in patients with IPF. We know that this test is reliable, valid, and responsive to treatment. Now we know that it has predictive capacity as well.”
During her presentation, she cited potential reasons why change in gait speed is associated with survival. “Firstly, gait speed has been described as a clinical indicator of multisystem well-being and the ‘sixth vital sign,’ ”she said. “Walking ability and speed rely on multiple factors and the integration of many systems, cardiovascular and otherwise. We know that pulmonary rehab has multiple benefits and improves these systems, and it’s plausible that change in gait speed may be a surrogate marker for, say, improvement in exercise capacity or health status. But the precise mechanism requires verification.”
Ms. Nolan acknowledged certain limitations of the study, including the fact that contemporaneous measurement of full lung function testing and pulmonary hypertension diagnosis were not available at the time of the study. “Therefore, we were unable to account for [diffusing capacity of the lung for carbon monoxide] and pulmonary hypertension diagnosis,” she said. “Secondly, we were unable to identify the precise cause of death from the national database of harm and care records, but this corroborates previous data which suggest that it’s difficult to reliably discern if a death is IPF- or non-IPF related. Lastly, we know that the benefits of pulmonary rehab experienced by IPF patients tend to wane after 6 months. It would be interesting to compare the short-term improvements in gait speed that we observed to more sustained improvements, to identify whether this impacts prognostability.”
National Institute for Health Research funded the study. Ms. Nolan reported having no financial disclosures.
*Correction, 5/23/18: An earlier version of this article misstated the 4-meter gait speed cutoff point.
SOURCE: Nolan CM et al. ATS 2018, Abstract A2456.
SAN DIEGO – Among patients with idiopathic pulmonary fibrosis (IPF), an improvement in 4-meter gait speed with pulmonary rehabilitation is an independent predictor of all-cause mortality at 1 year, suggest results from a multicenter study presented at an international conference of the American Thoracic Society.
In all, 11% of patients died within 1 year of completing pulmonary rehabilitation.
“Mortality is an attractive endpoint in IPF clinical research but requires large sample sizes and long follow-up duration, making clinical trials expensive and challenging to undertake,” lead study author Claire M. Nolan, MSc, said at the conference.
“Consequently, there is much interest in surrogate endpoints of mortality. In the elderly population, a lot of work has been done on performance measures, in particular the 4-meter gait test. It’s a simple test to do from the assessor’s perspective, because you just need a 4-meter corridor and a stopwatch. From the patient’s perspective, they only have to walk at their usual speed, making it feasible in most settings.”
The study by Ms. Nolan, a National Institute for Health Research fellow, and her associates, involved recruiting 90 IPF patients referred to three outpatient pulmonary rehabilitation programs in London. All patients underwent the following assessments before and after 8 weeks of pulmonary rehabilitation: spirometry; Medical Research Council dyspnea score; anthropometry; 4-meter gait speed; incremental shuttle walk test, and King’s Brief Interstitial Lung Disease questionnaire. Ms. Nolan, a respiratory physiotherapist with the Harefield Pulmonary Rehabilitation and Muscle Research Group, Royal Brompton and Harefield NHS Foundation Trust, Harefield, London, and her associates drew from national databases to obtain data on all-cause mortality 1 year following pulmonary rehabilitation.
“We also identified a cutpoint, so if patients improved their walking speed by 0.009 meters per second or above, that was associated with a longer survival time at 1 year (area under the curve of 0.76, for sensitivity of 69.6% and a specificity of 70%; P less than 0.01),” she said.* “Among patients who achieved that cutpoint or exceeded it, only 5% of them died in the 1-year follow-up period, compared with 23% in the group that didn’t achieve that cutpoint. That’s quite a big difference, but this requires external validation in another population.”
To determine the 4-meter gait speed change cut-off that best discriminated between patients who died and survived, the investigators plotted receiver operating characteristic curves. For validation, they conducted a Kaplan-Meier analysis to assess time to death, with significance assessed via the log-rank test. Finally, they used a multivariate Cox proportional hazards model to characterize the relationship between 4-meter gait speed change and all-cause mortality, adjusting for independent predictors of mortality (age, previous respiratory hospitalizations in the past year, forced vital capacity percent predicted) and baseline 4-meter gait speed.
At baseline, 70% of the 90 patients were male, mean age was 74 years, mean forced vital capacity was 72.8% predicted, and mean Medical Research Council dyspnea score was 3. In addition, mean body mass index was 27.2 kg/m2, mean 4-meter gait speed was 0.92 meters per second, mean incremental shuttle walk test measurement was 271 meters, and mean King’s Brief Interstitial Lung Disease total score was 56.4. Following 8 weeks of pulmonary rehabilitation, the patients’ 4-meter gait speed improved significantly by a mean of 0.15 meters per second (P less than .001). All other variables also improved significantly, with the exception of forced vital capacity.
In an interview, Ms. Nolan characterized the results as “one piece of the puzzle in answering whether 4-meter gait speed is a useful test for clinicians and researchers. It needs to be taken in the context of 4-meter gait speed in other populations as well as with what we’re finding in patients with IPF. We know that this test is reliable, valid, and responsive to treatment. Now we know that it has predictive capacity as well.”
During her presentation, she cited potential reasons why change in gait speed is associated with survival. “Firstly, gait speed has been described as a clinical indicator of multisystem well-being and the ‘sixth vital sign,’ ”she said. “Walking ability and speed rely on multiple factors and the integration of many systems, cardiovascular and otherwise. We know that pulmonary rehab has multiple benefits and improves these systems, and it’s plausible that change in gait speed may be a surrogate marker for, say, improvement in exercise capacity or health status. But the precise mechanism requires verification.”
Ms. Nolan acknowledged certain limitations of the study, including the fact that contemporaneous measurement of full lung function testing and pulmonary hypertension diagnosis were not available at the time of the study. “Therefore, we were unable to account for [diffusing capacity of the lung for carbon monoxide] and pulmonary hypertension diagnosis,” she said. “Secondly, we were unable to identify the precise cause of death from the national database of harm and care records, but this corroborates previous data which suggest that it’s difficult to reliably discern if a death is IPF- or non-IPF related. Lastly, we know that the benefits of pulmonary rehab experienced by IPF patients tend to wane after 6 months. It would be interesting to compare the short-term improvements in gait speed that we observed to more sustained improvements, to identify whether this impacts prognostability.”
National Institute for Health Research funded the study. Ms. Nolan reported having no financial disclosures.
*Correction, 5/23/18: An earlier version of this article misstated the 4-meter gait speed cutoff point.
SOURCE: Nolan CM et al. ATS 2018, Abstract A2456.
SAN DIEGO – Among patients with idiopathic pulmonary fibrosis (IPF), an improvement in 4-meter gait speed with pulmonary rehabilitation is an independent predictor of all-cause mortality at 1 year, suggest results from a multicenter study presented at an international conference of the American Thoracic Society.
In all, 11% of patients died within 1 year of completing pulmonary rehabilitation.
“Mortality is an attractive endpoint in IPF clinical research but requires large sample sizes and long follow-up duration, making clinical trials expensive and challenging to undertake,” lead study author Claire M. Nolan, MSc, said at the conference.
“Consequently, there is much interest in surrogate endpoints of mortality. In the elderly population, a lot of work has been done on performance measures, in particular the 4-meter gait test. It’s a simple test to do from the assessor’s perspective, because you just need a 4-meter corridor and a stopwatch. From the patient’s perspective, they only have to walk at their usual speed, making it feasible in most settings.”
The study by Ms. Nolan, a National Institute for Health Research fellow, and her associates, involved recruiting 90 IPF patients referred to three outpatient pulmonary rehabilitation programs in London. All patients underwent the following assessments before and after 8 weeks of pulmonary rehabilitation: spirometry; Medical Research Council dyspnea score; anthropometry; 4-meter gait speed; incremental shuttle walk test, and King’s Brief Interstitial Lung Disease questionnaire. Ms. Nolan, a respiratory physiotherapist with the Harefield Pulmonary Rehabilitation and Muscle Research Group, Royal Brompton and Harefield NHS Foundation Trust, Harefield, London, and her associates drew from national databases to obtain data on all-cause mortality 1 year following pulmonary rehabilitation.
“We also identified a cutpoint, so if patients improved their walking speed by 0.009 meters per second or above, that was associated with a longer survival time at 1 year (area under the curve of 0.76, for sensitivity of 69.6% and a specificity of 70%; P less than 0.01),” she said.* “Among patients who achieved that cutpoint or exceeded it, only 5% of them died in the 1-year follow-up period, compared with 23% in the group that didn’t achieve that cutpoint. That’s quite a big difference, but this requires external validation in another population.”
To determine the 4-meter gait speed change cut-off that best discriminated between patients who died and survived, the investigators plotted receiver operating characteristic curves. For validation, they conducted a Kaplan-Meier analysis to assess time to death, with significance assessed via the log-rank test. Finally, they used a multivariate Cox proportional hazards model to characterize the relationship between 4-meter gait speed change and all-cause mortality, adjusting for independent predictors of mortality (age, previous respiratory hospitalizations in the past year, forced vital capacity percent predicted) and baseline 4-meter gait speed.
At baseline, 70% of the 90 patients were male, mean age was 74 years, mean forced vital capacity was 72.8% predicted, and mean Medical Research Council dyspnea score was 3. In addition, mean body mass index was 27.2 kg/m2, mean 4-meter gait speed was 0.92 meters per second, mean incremental shuttle walk test measurement was 271 meters, and mean King’s Brief Interstitial Lung Disease total score was 56.4. Following 8 weeks of pulmonary rehabilitation, the patients’ 4-meter gait speed improved significantly by a mean of 0.15 meters per second (P less than .001). All other variables also improved significantly, with the exception of forced vital capacity.
In an interview, Ms. Nolan characterized the results as “one piece of the puzzle in answering whether 4-meter gait speed is a useful test for clinicians and researchers. It needs to be taken in the context of 4-meter gait speed in other populations as well as with what we’re finding in patients with IPF. We know that this test is reliable, valid, and responsive to treatment. Now we know that it has predictive capacity as well.”
During her presentation, she cited potential reasons why change in gait speed is associated with survival. “Firstly, gait speed has been described as a clinical indicator of multisystem well-being and the ‘sixth vital sign,’ ”she said. “Walking ability and speed rely on multiple factors and the integration of many systems, cardiovascular and otherwise. We know that pulmonary rehab has multiple benefits and improves these systems, and it’s plausible that change in gait speed may be a surrogate marker for, say, improvement in exercise capacity or health status. But the precise mechanism requires verification.”
Ms. Nolan acknowledged certain limitations of the study, including the fact that contemporaneous measurement of full lung function testing and pulmonary hypertension diagnosis were not available at the time of the study. “Therefore, we were unable to account for [diffusing capacity of the lung for carbon monoxide] and pulmonary hypertension diagnosis,” she said. “Secondly, we were unable to identify the precise cause of death from the national database of harm and care records, but this corroborates previous data which suggest that it’s difficult to reliably discern if a death is IPF- or non-IPF related. Lastly, we know that the benefits of pulmonary rehab experienced by IPF patients tend to wane after 6 months. It would be interesting to compare the short-term improvements in gait speed that we observed to more sustained improvements, to identify whether this impacts prognostability.”
National Institute for Health Research funded the study. Ms. Nolan reported having no financial disclosures.
*Correction, 5/23/18: An earlier version of this article misstated the 4-meter gait speed cutoff point.
SOURCE: Nolan CM et al. ATS 2018, Abstract A2456.
AT ATS 2018
Key clinical point: Change in 4-meter gait speed following pulmonary rehabilitation is an independent predictor of all-cause mortality at 1 year in patients with IPF.
Major finding: IPF patients who improved their 4-meter walking speed by 0.009 meters per second or more were more likely to be alive 1 year following pulmonary rehabilitation, compared with those who did not reach that cut point (P less than .01).
Study details: A multicenter study of 90 IPF patients who underwent 8 weeks of pulmonary rehabilitation.
Disclosures: The National Institute for Health Research funded the study. Ms. Nolan reported having no financial disclosures.
Source: Nolan, CM et al. ATS 2018, Abstract A2456.
Dear VESS Members and Attendees: Welcome to Spring Meeting
On the advent of this year’s Society for Vascular Surgery’s (SVS) Vascular Annual Meeting (VAM), I would like to welcome you to the 2018 annual spring meeting for VESS, which convenes in conjunction with VAM on June 20 at the Hynes Convention Center in Boston. Our Wednesday program looks very diverse and outstanding, covering key topics in aortic and branch aortic, cerebrovascular, lower extremity, venous disease, hemodialysis, physician wellness/burnout, academic issues, and the medical management of vascular disease. Thank you to Matthew Smeds and the rest of the program committee for putting together such an engaging lineup for this year’s spring meeting! I would also encourage you to visit our industry sponsors for this event; exhibits will be available for perusal June 21-22 within the convention center. Finally, we will be cosponsoring an event Thursday, June 21, at 7 p.m. in the Independence West Room of the Sheraton Hotel as a Networking Reception for Women, Diversity, and Young Surgeons. All residents and students are invited to attend this networking reception hosted by SVS and VESS. Thanks also to the SVS for hosting this meeting and for the ongoing collaboration we have enjoyed between our societies!

VESS members and leadership have continued to elevate the practice of vascular surgery and the research that has defined it. The more than 40-year history of this society is well outlined by Dr. Vik Kashyap in J Vasc Surg 2014;60(4):1123-4. VESS remains focused on engaging vascular trainees and vascular surgeons within a framework of collegial academic excellence. We continue to support research through grant funding at both the trainee and young investigator levels, and our presenters at both the spring VESS/VAM and Winter Annual Meetings enjoy a very high acceptance rate for publication of their findings. For more information about VESS, just visit vesurgery.org. The leadership for this society is proud of what it stands for. We are committed to exploring relevant and educational topics in vascular surgery. We hope this year’s spring meeting enhances your understanding and practice of vascular surgery. See you June 20th!
Jon Eliason, MD
VESS President
On the advent of this year’s Society for Vascular Surgery’s (SVS) Vascular Annual Meeting (VAM), I would like to welcome you to the 2018 annual spring meeting for VESS, which convenes in conjunction with VAM on June 20 at the Hynes Convention Center in Boston. Our Wednesday program looks very diverse and outstanding, covering key topics in aortic and branch aortic, cerebrovascular, lower extremity, venous disease, hemodialysis, physician wellness/burnout, academic issues, and the medical management of vascular disease. Thank you to Matthew Smeds and the rest of the program committee for putting together such an engaging lineup for this year’s spring meeting! I would also encourage you to visit our industry sponsors for this event; exhibits will be available for perusal June 21-22 within the convention center. Finally, we will be cosponsoring an event Thursday, June 21, at 7 p.m. in the Independence West Room of the Sheraton Hotel as a Networking Reception for Women, Diversity, and Young Surgeons. All residents and students are invited to attend this networking reception hosted by SVS and VESS. Thanks also to the SVS for hosting this meeting and for the ongoing collaboration we have enjoyed between our societies!
VESS members and leadership have continued to elevate the practice of vascular surgery and the research that has defined it. The more than 40-year history of this society is well outlined by Dr. Vik Kashyap in J Vasc Surg 2014;60(4):1123-4. VESS remains focused on engaging vascular trainees and vascular surgeons within a framework of collegial academic excellence. We continue to support research through grant funding at both the trainee and young investigator levels, and our presenters at both the spring VESS/VAM and Winter Annual Meetings enjoy a very high acceptance rate for publication of their findings. For more information about VESS, just visit vesurgery.org. The leadership for this society is proud of what it stands for. We are committed to exploring relevant and educational topics in vascular surgery. We hope this year’s spring meeting enhances your understanding and practice of vascular surgery. See you June 20th!
Jon Eliason, MD
VESS President
On the advent of this year’s Society for Vascular Surgery’s (SVS) Vascular Annual Meeting (VAM), I would like to welcome you to the 2018 annual spring meeting for VESS, which convenes in conjunction with VAM on June 20 at the Hynes Convention Center in Boston. Our Wednesday program looks very diverse and outstanding, covering key topics in aortic and branch aortic, cerebrovascular, lower extremity, venous disease, hemodialysis, physician wellness/burnout, academic issues, and the medical management of vascular disease. Thank you to Matthew Smeds and the rest of the program committee for putting together such an engaging lineup for this year’s spring meeting! I would also encourage you to visit our industry sponsors for this event; exhibits will be available for perusal June 21-22 within the convention center. Finally, we will be cosponsoring an event Thursday, June 21, at 7 p.m. in the Independence West Room of the Sheraton Hotel as a Networking Reception for Women, Diversity, and Young Surgeons. All residents and students are invited to attend this networking reception hosted by SVS and VESS. Thanks also to the SVS for hosting this meeting and for the ongoing collaboration we have enjoyed between our societies!
VESS members and leadership have continued to elevate the practice of vascular surgery and the research that has defined it. The more than 40-year history of this society is well outlined by Dr. Vik Kashyap in J Vasc Surg 2014;60(4):1123-4. VESS remains focused on engaging vascular trainees and vascular surgeons within a framework of collegial academic excellence. We continue to support research through grant funding at both the trainee and young investigator levels, and our presenters at both the spring VESS/VAM and Winter Annual Meetings enjoy a very high acceptance rate for publication of their findings. For more information about VESS, just visit vesurgery.org. The leadership for this society is proud of what it stands for. We are committed to exploring relevant and educational topics in vascular surgery. We hope this year’s spring meeting enhances your understanding and practice of vascular surgery. See you June 20th!
Jon Eliason, MD
VESS President