User login
Migraine and menopause: Longitudinal study shows what to expect
SAN FRANCISCO – What can women with migraine expect during the menopausal transition?
About 60% will experience a change in their headache pattern. And for 60% of that group, it’s a change for the worse, Yu-Chen Cheng, MD, reported at the annual meeting of the American Headache Society.
She presented a retrospective longitudinal study of 60 women with a preexisting history of migraine who were followed through the menopausal transition. All had long-term medical records available, including brain imaging results and hormonal laboratory data.
The impetus for the study was the fact that even though three-quarters of America’s estimated 38 million migraineurs are women, all of whom will eventually undergo menopause, the question of what happens to them headache-wise as they go through this process of permanent cessation of ovarian function has received little research attention.

“This longitudinal study addresses the pattern of change of migraine during menopausal transition, an important but underestimated and undermanaged issue. We need more awareness of this. We hope in the future that physicians can pay more attention to this and provide better treatment for our patients with impaired quality of life,” said Dr. Cheng, a neurologist and postdoctoral fellow at Massachusetts General Hospital and Harvard Medical School, Boston.
Of the 35 women who experienced a change in their migraine attacks in association with menopause, the change occurred perimenopausally or postmenopausally – that is, after the final menstrual period – in 84% of cases. Premenopausal change in migraine in women who hadn’t yet missed a menstrual period in the past 12 months was a less frequent event.
No significant demographic differences existed between the 35 women with migraine change during the menopausal transition and the 25 women whose headache pattern remained stable. However, there were significant differences between the two groups in terms of the change over time in serum estradiol and follicle-stimulating hormone (FSH) levels. The median estradiol level in women whose migraine pattern remained stable went from 29 pg/mL premenopausally to 16.5 pg/mL post menopause, a statistically nonsignificant difference. In contrast, the median estradiol in women who experienced a change in migraine pattern dropped from 52.6 pg/mL premenopausally to 22.5 pg/mL post menopause, which was a significant difference.
Similarly, the pre- to postmenopause change in median FSH from 38.6 to 62.8 IU/L in the stable migraine group didn’t attain statistical significance, while the bigger shift in the migraine change group – from 13.5 IU/L premenopausally to 62.2 IU/L post menopause, was statistically significant.
“So we can say there’s a greater hormonal change in the migraine change group for women in the menopausal transition,” the neurologist said. “This suggests the possibility that a significant steep decline in estradiol level may stimulate migraine change.”
Brain imaging findings in the two groups were similar: Nearly two-thirds of women in both groups had normal brain MRI results, while the rest had nonspecific findings.
Several female headache specialists in the audience rose to thank Dr. Cheng for shining new light on a major understudied issue with far-reaching quality-of-life implications. Could hormone replacement therapy possibly prevent worsening of migraine attacks in association with menopause? she was asked.
Dr. Cheng noted that hormone replacement therapy was used by about two-thirds of women whose migraines remained stable and a similar proportion of those whose headaches changed. But the study wasn’t designed or sized to examine any possible migraine-preventive effect of hormone therapy. That would properly be addressed in a large prospective study. Anecdotally, however, it has been her clinical impression as well as that of some of her fellow neurologists at Massachusetts General that hormone replacement therapy does seem to protect against worsening migraine attacks in menopause, she added.
Dr. Cheng reported having no financial conflicts regarding her National Institutes of Health–funded study.
SOURCE: Cheng Y-C and Maleki N. Headache. 2018;58:71. Abstract OR16.
SAN FRANCISCO – What can women with migraine expect during the menopausal transition?
About 60% will experience a change in their headache pattern. And for 60% of that group, it’s a change for the worse, Yu-Chen Cheng, MD, reported at the annual meeting of the American Headache Society.
She presented a retrospective longitudinal study of 60 women with a preexisting history of migraine who were followed through the menopausal transition. All had long-term medical records available, including brain imaging results and hormonal laboratory data.
The impetus for the study was the fact that even though three-quarters of America’s estimated 38 million migraineurs are women, all of whom will eventually undergo menopause, the question of what happens to them headache-wise as they go through this process of permanent cessation of ovarian function has received little research attention.
“This longitudinal study addresses the pattern of change of migraine during menopausal transition, an important but underestimated and undermanaged issue. We need more awareness of this. We hope in the future that physicians can pay more attention to this and provide better treatment for our patients with impaired quality of life,” said Dr. Cheng, a neurologist and postdoctoral fellow at Massachusetts General Hospital and Harvard Medical School, Boston.
Of the 35 women who experienced a change in their migraine attacks in association with menopause, the change occurred perimenopausally or postmenopausally – that is, after the final menstrual period – in 84% of cases. Premenopausal change in migraine in women who hadn’t yet missed a menstrual period in the past 12 months was a less frequent event.
No significant demographic differences existed between the 35 women with migraine change during the menopausal transition and the 25 women whose headache pattern remained stable. However, there were significant differences between the two groups in terms of the change over time in serum estradiol and follicle-stimulating hormone (FSH) levels. The median estradiol level in women whose migraine pattern remained stable went from 29 pg/mL premenopausally to 16.5 pg/mL post menopause, a statistically nonsignificant difference. In contrast, the median estradiol in women who experienced a change in migraine pattern dropped from 52.6 pg/mL premenopausally to 22.5 pg/mL post menopause, which was a significant difference.
Similarly, the pre- to postmenopause change in median FSH from 38.6 to 62.8 IU/L in the stable migraine group didn’t attain statistical significance, while the bigger shift in the migraine change group – from 13.5 IU/L premenopausally to 62.2 IU/L post menopause, was statistically significant.
“So we can say there’s a greater hormonal change in the migraine change group for women in the menopausal transition,” the neurologist said. “This suggests the possibility that a significant steep decline in estradiol level may stimulate migraine change.”
Brain imaging findings in the two groups were similar: Nearly two-thirds of women in both groups had normal brain MRI results, while the rest had nonspecific findings.
Several female headache specialists in the audience rose to thank Dr. Cheng for shining new light on a major understudied issue with far-reaching quality-of-life implications. Could hormone replacement therapy possibly prevent worsening of migraine attacks in association with menopause? she was asked.
Dr. Cheng noted that hormone replacement therapy was used by about two-thirds of women whose migraines remained stable and a similar proportion of those whose headaches changed. But the study wasn’t designed or sized to examine any possible migraine-preventive effect of hormone therapy. That would properly be addressed in a large prospective study. Anecdotally, however, it has been her clinical impression as well as that of some of her fellow neurologists at Massachusetts General that hormone replacement therapy does seem to protect against worsening migraine attacks in menopause, she added.
Dr. Cheng reported having no financial conflicts regarding her National Institutes of Health–funded study.
SOURCE: Cheng Y-C and Maleki N. Headache. 2018;58:71. Abstract OR16.
SAN FRANCISCO – What can women with migraine expect during the menopausal transition?
About 60% will experience a change in their headache pattern. And for 60% of that group, it’s a change for the worse, Yu-Chen Cheng, MD, reported at the annual meeting of the American Headache Society.
She presented a retrospective longitudinal study of 60 women with a preexisting history of migraine who were followed through the menopausal transition. All had long-term medical records available, including brain imaging results and hormonal laboratory data.
The impetus for the study was the fact that even though three-quarters of America’s estimated 38 million migraineurs are women, all of whom will eventually undergo menopause, the question of what happens to them headache-wise as they go through this process of permanent cessation of ovarian function has received little research attention.
“This longitudinal study addresses the pattern of change of migraine during menopausal transition, an important but underestimated and undermanaged issue. We need more awareness of this. We hope in the future that physicians can pay more attention to this and provide better treatment for our patients with impaired quality of life,” said Dr. Cheng, a neurologist and postdoctoral fellow at Massachusetts General Hospital and Harvard Medical School, Boston.
Of the 35 women who experienced a change in their migraine attacks in association with menopause, the change occurred perimenopausally or postmenopausally – that is, after the final menstrual period – in 84% of cases. Premenopausal change in migraine in women who hadn’t yet missed a menstrual period in the past 12 months was a less frequent event.
No significant demographic differences existed between the 35 women with migraine change during the menopausal transition and the 25 women whose headache pattern remained stable. However, there were significant differences between the two groups in terms of the change over time in serum estradiol and follicle-stimulating hormone (FSH) levels. The median estradiol level in women whose migraine pattern remained stable went from 29 pg/mL premenopausally to 16.5 pg/mL post menopause, a statistically nonsignificant difference. In contrast, the median estradiol in women who experienced a change in migraine pattern dropped from 52.6 pg/mL premenopausally to 22.5 pg/mL post menopause, which was a significant difference.
Similarly, the pre- to postmenopause change in median FSH from 38.6 to 62.8 IU/L in the stable migraine group didn’t attain statistical significance, while the bigger shift in the migraine change group – from 13.5 IU/L premenopausally to 62.2 IU/L post menopause, was statistically significant.
“So we can say there’s a greater hormonal change in the migraine change group for women in the menopausal transition,” the neurologist said. “This suggests the possibility that a significant steep decline in estradiol level may stimulate migraine change.”
Brain imaging findings in the two groups were similar: Nearly two-thirds of women in both groups had normal brain MRI results, while the rest had nonspecific findings.
Several female headache specialists in the audience rose to thank Dr. Cheng for shining new light on a major understudied issue with far-reaching quality-of-life implications. Could hormone replacement therapy possibly prevent worsening of migraine attacks in association with menopause? she was asked.
Dr. Cheng noted that hormone replacement therapy was used by about two-thirds of women whose migraines remained stable and a similar proportion of those whose headaches changed. But the study wasn’t designed or sized to examine any possible migraine-preventive effect of hormone therapy. That would properly be addressed in a large prospective study. Anecdotally, however, it has been her clinical impression as well as that of some of her fellow neurologists at Massachusetts General that hormone replacement therapy does seem to protect against worsening migraine attacks in menopause, she added.
Dr. Cheng reported having no financial conflicts regarding her National Institutes of Health–funded study.
SOURCE: Cheng Y-C and Maleki N. Headache. 2018;58:71. Abstract OR16.
REPORTING FROM THE AHS ANNUAL MEETING
Key clinical point: For migraineurs, the menopausal transition is a time of change in headache pattern, often for the worse.
Major finding: Sixty percent of migraineurs experienced a change in headache pattern during the menopausal transition, and for 60% of them it involved worsening migraine intensity and/or frequency.
Study details: This retrospective longitudinal study followed 60 women with migraine before and through the menopausal transition.
Disclosures: The presenter reported having no financial conflicts regarding her National Institutes of Health–funded study.
Source: Cheng Y-C and Maleki N. Headache. 2018;58:71. Abstract OR16.
Economic Stewardship in Acne Management
We are fortunate to have plentiful acne treatment options available that cater to each patient’s clinical examination, predispositions, and triggers, but the choices are daunting amidst the vast prescription and over-the-counter (OTC) topicals available along with disparate insurance and cost nuances. In addition, when prescribing generic oral therapies, it is complicated to parse out regional differences in price, supply, and insurance coverage to advocate best for each patient and land upon the delicate balance between efficacy, safety, and financial stewardship, both at an individual and community level. I will outline some challenges and solutions to the management of acne amidst these complicated factors.
Oral Therapies
For isotretinoin, generic choices, cost, and tiering within insurance plans are perpetual moving targets despite the drug being the only member of its class.1 Prescriber resources include tandem searches of electronic medical record price estimates within each insurance formulary, individual pharmacy search engines, and compilation mobile applications such as GoodRx to select the most affordable version for each patient. As an example of a regional trend, isotretinoin generic coverage by one provider in Pennsylvania shifted earlier this year so that every patient, whether new to isotretinoin or midcourse, required a new prior authorization with more stringent coverage requirements including failure of 2 oral antibiotics. Swiftly thereafter, efforts across the state driven by the Pennsylvania Academy of Dermatology and Dermatologic Surgery and its members and fueled by poignant patient vignettes about fragmented and substandard patient care helped to reverse this policy and remove the prior authorization mandate.2
Tetracyclines have experienced broad cost swings, mostly based on disruption of manufacturing at the limited number of distribution sites in the United States. In 2011, a tetracycline shortage arose due to a major manufacturer’s recall3 and persisted with subsequent material shortages, as doxycycline became the preferred and cheaper member of the class. Doxycycline price tag hikes then occurred following Hurricane Sandy when an East Coast manufacturing site was damaged.3 Spironolactone backorder also has been frequent due to recent raw material shortages and delays in production,3 forcing pharmacies to refill small amounts of medication in various dosage forms despite patients owing the same copayment per prescription.
Topical Therapies
Topical retinoid prescription affordability has always been fraught with difficulty owing to age cutoffs because it is often restricted to patients younger than 25 or 40 years, depending on the plan,4,5 but the availability of adapalene gel 0.1% as an OTC preparation in 2016 has broadened retinoid access and use.6 Prescription benzoyl peroxide (BPO) products alone or in combination with retinoids or topical antibiotics (or other combination topical therapies) comprise a large number of branded prescriptions often not covered by insurance or are only affordable using proprietary and intermittently available coupon cards (eg, BPO-clindamycin, clindamycin-tretinoin, BPO-adapalene); therefore, prescribers tend to dispense the individual ingredients and instruct the patient to compound them at home. Furthermore, BPO products can be purchased in effective concentrations as OTC products, and patients looking to procure more affordable, albeit less effective, topical retinoids that also have less irritation potential reach for OTC nightly retinol creams nestled in the antiaging section of the pharmacy.7
Opportunities to be involved in the larger scaffold of patient advocacy also are plentiful at the state and national levels. For example, with the support of dermatology state societies and the American Academy of Dermatology Association, Pennsylvania House Bill 22118 and similar bills in other states call for reversal of the gag clause that prevents pharmacists from disclosing the best medication price to patients. Also guided by the American Academy of Dermatology Association, prior authorization model legislation to promote transparency across insurers in this haphazard process is emerging across the country.9,10
Final Thoughts
These examples of acne medication access and cost quandaries serve to embody the daily problem-solving that dermatologists execute as part of their growing administrative and economic duties. They also represent worthy efforts to consider on behalf of patients, their pocketbooks, and the prudent use of their dermatologists’ time.
- Borgonjen RJ, de Lange JA, van de Kerkhof PCM. Guideline-based clinical decision support in acne patients receiving isotretinoin: improving adherence and cost-effectiveness. J Eur Acad Dermatol Venereol. 2017;31:e440-e442.
- Oral isotretinoin therapy update. Highmark website. https://content.highmarkprc.com/Files/NewsletterNotices/HotTopics/ht-all-isotretinoin-therapy-update-051718.pdf. Published May 17, 2018. Accessed June 29, 2018.
- Drug shortages. US Food & Drug Administration website. https://www.fda.gov/drugs/drugsafety/drugshortages/default.htm. Updated June 19, 2018. Accessed June 19, 2018.
- Retinoids prior authorization criteria. Blue Cross and Blue Shield of Illinois website. https://www.bcbsil.com/provider/pdf/retinoids.pdf. Published March 2008. Accessed June 18, 2018.
- Davis SA, Huang KE, Feldman SR, et al. Trends in ambulatory health care usage for adult acne. J Cutan Med Surg. 2015;19:377-379.
- FDA approves Differin gel 0.1% for over-the-counter use to treat acne [press release]. Silver Spring, MD: US Food & Drug Administration; July 8, 2016.
- Rosamilia LL. Over-the-counter treatments for acne and rosacea. Semin Cutan Med Surg. 2016;35:87-95.
- An Act Providing for Consumer Prescription Drug Pricing Disclosure, HB 2211, Regular Sess (Pa 2018).
- An Act Providing for Preauthorizations Conducted by Utilization Review Entities Relating to Health Care Services, HB 1293, Regular Sess (Pa 2017).
- Step therapy legislation. American Academy of Dermatology website. https://www.aad.org/advocacy/state-policy/step-therapy-legislation. Accessed June 19, 2018.
We are fortunate to have plentiful acne treatment options available that cater to each patient’s clinical examination, predispositions, and triggers, but the choices are daunting amidst the vast prescription and over-the-counter (OTC) topicals available along with disparate insurance and cost nuances. In addition, when prescribing generic oral therapies, it is complicated to parse out regional differences in price, supply, and insurance coverage to advocate best for each patient and land upon the delicate balance between efficacy, safety, and financial stewardship, both at an individual and community level. I will outline some challenges and solutions to the management of acne amidst these complicated factors.
Oral Therapies
For isotretinoin, generic choices, cost, and tiering within insurance plans are perpetual moving targets despite the drug being the only member of its class.1 Prescriber resources include tandem searches of electronic medical record price estimates within each insurance formulary, individual pharmacy search engines, and compilation mobile applications such as GoodRx to select the most affordable version for each patient. As an example of a regional trend, isotretinoin generic coverage by one provider in Pennsylvania shifted earlier this year so that every patient, whether new to isotretinoin or midcourse, required a new prior authorization with more stringent coverage requirements including failure of 2 oral antibiotics. Swiftly thereafter, efforts across the state driven by the Pennsylvania Academy of Dermatology and Dermatologic Surgery and its members and fueled by poignant patient vignettes about fragmented and substandard patient care helped to reverse this policy and remove the prior authorization mandate.2
Tetracyclines have experienced broad cost swings, mostly based on disruption of manufacturing at the limited number of distribution sites in the United States. In 2011, a tetracycline shortage arose due to a major manufacturer’s recall3 and persisted with subsequent material shortages, as doxycycline became the preferred and cheaper member of the class. Doxycycline price tag hikes then occurred following Hurricane Sandy when an East Coast manufacturing site was damaged.3 Spironolactone backorder also has been frequent due to recent raw material shortages and delays in production,3 forcing pharmacies to refill small amounts of medication in various dosage forms despite patients owing the same copayment per prescription.
Topical Therapies
Topical retinoid prescription affordability has always been fraught with difficulty owing to age cutoffs because it is often restricted to patients younger than 25 or 40 years, depending on the plan,4,5 but the availability of adapalene gel 0.1% as an OTC preparation in 2016 has broadened retinoid access and use.6 Prescription benzoyl peroxide (BPO) products alone or in combination with retinoids or topical antibiotics (or other combination topical therapies) comprise a large number of branded prescriptions often not covered by insurance or are only affordable using proprietary and intermittently available coupon cards (eg, BPO-clindamycin, clindamycin-tretinoin, BPO-adapalene); therefore, prescribers tend to dispense the individual ingredients and instruct the patient to compound them at home. Furthermore, BPO products can be purchased in effective concentrations as OTC products, and patients looking to procure more affordable, albeit less effective, topical retinoids that also have less irritation potential reach for OTC nightly retinol creams nestled in the antiaging section of the pharmacy.7
Opportunities to be involved in the larger scaffold of patient advocacy also are plentiful at the state and national levels. For example, with the support of dermatology state societies and the American Academy of Dermatology Association, Pennsylvania House Bill 22118 and similar bills in other states call for reversal of the gag clause that prevents pharmacists from disclosing the best medication price to patients. Also guided by the American Academy of Dermatology Association, prior authorization model legislation to promote transparency across insurers in this haphazard process is emerging across the country.9,10
Final Thoughts
These examples of acne medication access and cost quandaries serve to embody the daily problem-solving that dermatologists execute as part of their growing administrative and economic duties. They also represent worthy efforts to consider on behalf of patients, their pocketbooks, and the prudent use of their dermatologists’ time.
We are fortunate to have plentiful acne treatment options available that cater to each patient’s clinical examination, predispositions, and triggers, but the choices are daunting amidst the vast prescription and over-the-counter (OTC) topicals available along with disparate insurance and cost nuances. In addition, when prescribing generic oral therapies, it is complicated to parse out regional differences in price, supply, and insurance coverage to advocate best for each patient and land upon the delicate balance between efficacy, safety, and financial stewardship, both at an individual and community level. I will outline some challenges and solutions to the management of acne amidst these complicated factors.
Oral Therapies
For isotretinoin, generic choices, cost, and tiering within insurance plans are perpetual moving targets despite the drug being the only member of its class.1 Prescriber resources include tandem searches of electronic medical record price estimates within each insurance formulary, individual pharmacy search engines, and compilation mobile applications such as GoodRx to select the most affordable version for each patient. As an example of a regional trend, isotretinoin generic coverage by one provider in Pennsylvania shifted earlier this year so that every patient, whether new to isotretinoin or midcourse, required a new prior authorization with more stringent coverage requirements including failure of 2 oral antibiotics. Swiftly thereafter, efforts across the state driven by the Pennsylvania Academy of Dermatology and Dermatologic Surgery and its members and fueled by poignant patient vignettes about fragmented and substandard patient care helped to reverse this policy and remove the prior authorization mandate.2
Tetracyclines have experienced broad cost swings, mostly based on disruption of manufacturing at the limited number of distribution sites in the United States. In 2011, a tetracycline shortage arose due to a major manufacturer’s recall3 and persisted with subsequent material shortages, as doxycycline became the preferred and cheaper member of the class. Doxycycline price tag hikes then occurred following Hurricane Sandy when an East Coast manufacturing site was damaged.3 Spironolactone backorder also has been frequent due to recent raw material shortages and delays in production,3 forcing pharmacies to refill small amounts of medication in various dosage forms despite patients owing the same copayment per prescription.
Topical Therapies
Topical retinoid prescription affordability has always been fraught with difficulty owing to age cutoffs because it is often restricted to patients younger than 25 or 40 years, depending on the plan,4,5 but the availability of adapalene gel 0.1% as an OTC preparation in 2016 has broadened retinoid access and use.6 Prescription benzoyl peroxide (BPO) products alone or in combination with retinoids or topical antibiotics (or other combination topical therapies) comprise a large number of branded prescriptions often not covered by insurance or are only affordable using proprietary and intermittently available coupon cards (eg, BPO-clindamycin, clindamycin-tretinoin, BPO-adapalene); therefore, prescribers tend to dispense the individual ingredients and instruct the patient to compound them at home. Furthermore, BPO products can be purchased in effective concentrations as OTC products, and patients looking to procure more affordable, albeit less effective, topical retinoids that also have less irritation potential reach for OTC nightly retinol creams nestled in the antiaging section of the pharmacy.7
Opportunities to be involved in the larger scaffold of patient advocacy also are plentiful at the state and national levels. For example, with the support of dermatology state societies and the American Academy of Dermatology Association, Pennsylvania House Bill 22118 and similar bills in other states call for reversal of the gag clause that prevents pharmacists from disclosing the best medication price to patients. Also guided by the American Academy of Dermatology Association, prior authorization model legislation to promote transparency across insurers in this haphazard process is emerging across the country.9,10
Final Thoughts
These examples of acne medication access and cost quandaries serve to embody the daily problem-solving that dermatologists execute as part of their growing administrative and economic duties. They also represent worthy efforts to consider on behalf of patients, their pocketbooks, and the prudent use of their dermatologists’ time.
- Borgonjen RJ, de Lange JA, van de Kerkhof PCM. Guideline-based clinical decision support in acne patients receiving isotretinoin: improving adherence and cost-effectiveness. J Eur Acad Dermatol Venereol. 2017;31:e440-e442.
- Oral isotretinoin therapy update. Highmark website. https://content.highmarkprc.com/Files/NewsletterNotices/HotTopics/ht-all-isotretinoin-therapy-update-051718.pdf. Published May 17, 2018. Accessed June 29, 2018.
- Drug shortages. US Food & Drug Administration website. https://www.fda.gov/drugs/drugsafety/drugshortages/default.htm. Updated June 19, 2018. Accessed June 19, 2018.
- Retinoids prior authorization criteria. Blue Cross and Blue Shield of Illinois website. https://www.bcbsil.com/provider/pdf/retinoids.pdf. Published March 2008. Accessed June 18, 2018.
- Davis SA, Huang KE, Feldman SR, et al. Trends in ambulatory health care usage for adult acne. J Cutan Med Surg. 2015;19:377-379.
- FDA approves Differin gel 0.1% for over-the-counter use to treat acne [press release]. Silver Spring, MD: US Food & Drug Administration; July 8, 2016.
- Rosamilia LL. Over-the-counter treatments for acne and rosacea. Semin Cutan Med Surg. 2016;35:87-95.
- An Act Providing for Consumer Prescription Drug Pricing Disclosure, HB 2211, Regular Sess (Pa 2018).
- An Act Providing for Preauthorizations Conducted by Utilization Review Entities Relating to Health Care Services, HB 1293, Regular Sess (Pa 2017).
- Step therapy legislation. American Academy of Dermatology website. https://www.aad.org/advocacy/state-policy/step-therapy-legislation. Accessed June 19, 2018.
- Borgonjen RJ, de Lange JA, van de Kerkhof PCM. Guideline-based clinical decision support in acne patients receiving isotretinoin: improving adherence and cost-effectiveness. J Eur Acad Dermatol Venereol. 2017;31:e440-e442.
- Oral isotretinoin therapy update. Highmark website. https://content.highmarkprc.com/Files/NewsletterNotices/HotTopics/ht-all-isotretinoin-therapy-update-051718.pdf. Published May 17, 2018. Accessed June 29, 2018.
- Drug shortages. US Food & Drug Administration website. https://www.fda.gov/drugs/drugsafety/drugshortages/default.htm. Updated June 19, 2018. Accessed June 19, 2018.
- Retinoids prior authorization criteria. Blue Cross and Blue Shield of Illinois website. https://www.bcbsil.com/provider/pdf/retinoids.pdf. Published March 2008. Accessed June 18, 2018.
- Davis SA, Huang KE, Feldman SR, et al. Trends in ambulatory health care usage for adult acne. J Cutan Med Surg. 2015;19:377-379.
- FDA approves Differin gel 0.1% for over-the-counter use to treat acne [press release]. Silver Spring, MD: US Food & Drug Administration; July 8, 2016.
- Rosamilia LL. Over-the-counter treatments for acne and rosacea. Semin Cutan Med Surg. 2016;35:87-95.
- An Act Providing for Consumer Prescription Drug Pricing Disclosure, HB 2211, Regular Sess (Pa 2018).
- An Act Providing for Preauthorizations Conducted by Utilization Review Entities Relating to Health Care Services, HB 1293, Regular Sess (Pa 2017).
- Step therapy legislation. American Academy of Dermatology website. https://www.aad.org/advocacy/state-policy/step-therapy-legislation. Accessed June 19, 2018.

ICD use curbed in hospitals named in federal lawsuit
A 2005 update in Medicare reimbursement policy had a modest effect on the use of implantable cardioverter defibrillators for primary prevention, but it took a whistle-blower and a federal lawsuit to bring the numbers down substantially.
Usage dropped just slightly from 2007 to 2009, after Medicare updated its appropriate use criteria, Nihar R. Desai, MD, MPH, and his colleagues reported in JAMA. From 2010 to 2011, after the Department of Justice suit became public knowledge, the declines were significantly greater: 7.4% in hospitals that eventually settled for a total of $280 million, and 4.7% in hospitals that weren’t named in the suit.
The government launched the suit in 2010, after a whistle-blower used Medicare data to allege that many hospitals weren’t waiting the appropriate amount of time to implant an implantable cardioverter defibrillator (ICD) after a heart attack or coronary revascularization, wrote Dr. Desai of Yale University, New Haven, Conn., and his team. These procedures would have been against the 2005 Centers for Medicare & Medicaid Services National Coverage Determination (NCD), which required delaying implantation for 40 days after a heart attack and 90 days after a revascularization.
Just a year after the suit was filed, an independent investigator concluded that 22.5% of the ICDs implanted from 2006 to 2009 for primary prevention were not evidence based.
Dr. Desai and his coauthors used CMS data to examine changes in the proportion of primary-prevention ICD implantations at hospitals that eventually settled the suit, and those that did not. The study spanned 2007-2015 and comprised 1,809 U.S. hospitals in the National Cardiovascular Data Registry ICD Registry; of these, 452 hospitals that had done 99,591 procedures reached settlements.
After the steeper drops in 2010 and 2011, the number of procedures leveled off. From July 2011 to 2015, the proportions of ICDs not meeting the NCD criteria were similar and stable in both hospital settlement groups, with an annual change of −0.5% for settlement hospitals and −0.4% for nonsettlement hospitals, the team wrote.
Despite the changes, there was “persistent variation” among hospitals, with more than 14% of the primary-prevention ICDs not meeting NCD criteria at some of the worst-performing hospitals.
The decreases weren’t just in Medicare beneficiaries, though. Hospitals were rethinking this indication for ICD use in everyone, although the investigators found no evidence that the changing clinical landscape endangered the health of patients.
“The analyses of secondary prevention ICDs do not suggest that access to necessary procedures was negatively affected by the investigation. … These analyses offer some reassurance, but further research into hospital responses to the investigation could offer additional insights about possible unintended consequences,” the investigators wrote.
The study was sponsored by the Agency for Healthcare Research and Quality. Dr. Desai had no financial disclosures.
SOURCE: Desai NR et al. JAMA. 2018; 320: 63-71.
The federal investigation into inappropriate use of implanted cardioverter defibrillators (ICDs) appeared to be highly effective, both in recovering costs and changing behavior at hospitals.
Even though individuals were not the focus of the investigation, many physicians sensed a new exposure to civil liability, if not criminal penalties, and felt accused of providing substandard care. Did this investigation have the intended effect of improving care?
The numbers suggest it did.
The observed decrease in use raises the question of whether appropriate ICDs were also avoided, a potential unintended consequence of the investigation. The study by Desai et al noted that ICD implantations for secondary prevention remained relatively stable during this period, suggesting that appropriate ICD use likely did not decline substantially.
The investigation also clearly showed the power of a large, financially intimidating legal action.
The mere announcement of the investigation appeared to have a large and immediate influence on prompting hospitals to limit inappropriate ICD implantation for primary prevention. As a form of audit and feedback, the Department of Justice investigation appeared to be highly effective in changing practice. Past studies of audit and feedback show relatively modest effects on changing physician behavior, although these studies did not involve allegations of fraud with financial penalties. Clearly, the reward or penalty attached to the feedback influences clinician behavior with penalties likely more effective in promoting change.
Paul A. Heidenreich, MD, professor of cardiovascular medicine at Stanford (Calif.) University, made these comments in an accompanying editorial (JAMA. 2018; 320:40-2).
The federal investigation into inappropriate use of implanted cardioverter defibrillators (ICDs) appeared to be highly effective, both in recovering costs and changing behavior at hospitals.
Even though individuals were not the focus of the investigation, many physicians sensed a new exposure to civil liability, if not criminal penalties, and felt accused of providing substandard care. Did this investigation have the intended effect of improving care?
The numbers suggest it did.
The observed decrease in use raises the question of whether appropriate ICDs were also avoided, a potential unintended consequence of the investigation. The study by Desai et al noted that ICD implantations for secondary prevention remained relatively stable during this period, suggesting that appropriate ICD use likely did not decline substantially.
The investigation also clearly showed the power of a large, financially intimidating legal action.
The mere announcement of the investigation appeared to have a large and immediate influence on prompting hospitals to limit inappropriate ICD implantation for primary prevention. As a form of audit and feedback, the Department of Justice investigation appeared to be highly effective in changing practice. Past studies of audit and feedback show relatively modest effects on changing physician behavior, although these studies did not involve allegations of fraud with financial penalties. Clearly, the reward or penalty attached to the feedback influences clinician behavior with penalties likely more effective in promoting change.
Paul A. Heidenreich, MD, professor of cardiovascular medicine at Stanford (Calif.) University, made these comments in an accompanying editorial (JAMA. 2018; 320:40-2).
The federal investigation into inappropriate use of implanted cardioverter defibrillators (ICDs) appeared to be highly effective, both in recovering costs and changing behavior at hospitals.
Even though individuals were not the focus of the investigation, many physicians sensed a new exposure to civil liability, if not criminal penalties, and felt accused of providing substandard care. Did this investigation have the intended effect of improving care?
The numbers suggest it did.
The observed decrease in use raises the question of whether appropriate ICDs were also avoided, a potential unintended consequence of the investigation. The study by Desai et al noted that ICD implantations for secondary prevention remained relatively stable during this period, suggesting that appropriate ICD use likely did not decline substantially.
The investigation also clearly showed the power of a large, financially intimidating legal action.
The mere announcement of the investigation appeared to have a large and immediate influence on prompting hospitals to limit inappropriate ICD implantation for primary prevention. As a form of audit and feedback, the Department of Justice investigation appeared to be highly effective in changing practice. Past studies of audit and feedback show relatively modest effects on changing physician behavior, although these studies did not involve allegations of fraud with financial penalties. Clearly, the reward or penalty attached to the feedback influences clinician behavior with penalties likely more effective in promoting change.
Paul A. Heidenreich, MD, professor of cardiovascular medicine at Stanford (Calif.) University, made these comments in an accompanying editorial (JAMA. 2018; 320:40-2).
A 2005 update in Medicare reimbursement policy had a modest effect on the use of implantable cardioverter defibrillators for primary prevention, but it took a whistle-blower and a federal lawsuit to bring the numbers down substantially.
Usage dropped just slightly from 2007 to 2009, after Medicare updated its appropriate use criteria, Nihar R. Desai, MD, MPH, and his colleagues reported in JAMA. From 2010 to 2011, after the Department of Justice suit became public knowledge, the declines were significantly greater: 7.4% in hospitals that eventually settled for a total of $280 million, and 4.7% in hospitals that weren’t named in the suit.
The government launched the suit in 2010, after a whistle-blower used Medicare data to allege that many hospitals weren’t waiting the appropriate amount of time to implant an implantable cardioverter defibrillator (ICD) after a heart attack or coronary revascularization, wrote Dr. Desai of Yale University, New Haven, Conn., and his team. These procedures would have been against the 2005 Centers for Medicare & Medicaid Services National Coverage Determination (NCD), which required delaying implantation for 40 days after a heart attack and 90 days after a revascularization.
Just a year after the suit was filed, an independent investigator concluded that 22.5% of the ICDs implanted from 2006 to 2009 for primary prevention were not evidence based.
Dr. Desai and his coauthors used CMS data to examine changes in the proportion of primary-prevention ICD implantations at hospitals that eventually settled the suit, and those that did not. The study spanned 2007-2015 and comprised 1,809 U.S. hospitals in the National Cardiovascular Data Registry ICD Registry; of these, 452 hospitals that had done 99,591 procedures reached settlements.
After the steeper drops in 2010 and 2011, the number of procedures leveled off. From July 2011 to 2015, the proportions of ICDs not meeting the NCD criteria were similar and stable in both hospital settlement groups, with an annual change of −0.5% for settlement hospitals and −0.4% for nonsettlement hospitals, the team wrote.
Despite the changes, there was “persistent variation” among hospitals, with more than 14% of the primary-prevention ICDs not meeting NCD criteria at some of the worst-performing hospitals.
The decreases weren’t just in Medicare beneficiaries, though. Hospitals were rethinking this indication for ICD use in everyone, although the investigators found no evidence that the changing clinical landscape endangered the health of patients.
“The analyses of secondary prevention ICDs do not suggest that access to necessary procedures was negatively affected by the investigation. … These analyses offer some reassurance, but further research into hospital responses to the investigation could offer additional insights about possible unintended consequences,” the investigators wrote.
The study was sponsored by the Agency for Healthcare Research and Quality. Dr. Desai had no financial disclosures.
SOURCE: Desai NR et al. JAMA. 2018; 320: 63-71.
A 2005 update in Medicare reimbursement policy had a modest effect on the use of implantable cardioverter defibrillators for primary prevention, but it took a whistle-blower and a federal lawsuit to bring the numbers down substantially.
Usage dropped just slightly from 2007 to 2009, after Medicare updated its appropriate use criteria, Nihar R. Desai, MD, MPH, and his colleagues reported in JAMA. From 2010 to 2011, after the Department of Justice suit became public knowledge, the declines were significantly greater: 7.4% in hospitals that eventually settled for a total of $280 million, and 4.7% in hospitals that weren’t named in the suit.
The government launched the suit in 2010, after a whistle-blower used Medicare data to allege that many hospitals weren’t waiting the appropriate amount of time to implant an implantable cardioverter defibrillator (ICD) after a heart attack or coronary revascularization, wrote Dr. Desai of Yale University, New Haven, Conn., and his team. These procedures would have been against the 2005 Centers for Medicare & Medicaid Services National Coverage Determination (NCD), which required delaying implantation for 40 days after a heart attack and 90 days after a revascularization.
Just a year after the suit was filed, an independent investigator concluded that 22.5% of the ICDs implanted from 2006 to 2009 for primary prevention were not evidence based.
Dr. Desai and his coauthors used CMS data to examine changes in the proportion of primary-prevention ICD implantations at hospitals that eventually settled the suit, and those that did not. The study spanned 2007-2015 and comprised 1,809 U.S. hospitals in the National Cardiovascular Data Registry ICD Registry; of these, 452 hospitals that had done 99,591 procedures reached settlements.
After the steeper drops in 2010 and 2011, the number of procedures leveled off. From July 2011 to 2015, the proportions of ICDs not meeting the NCD criteria were similar and stable in both hospital settlement groups, with an annual change of −0.5% for settlement hospitals and −0.4% for nonsettlement hospitals, the team wrote.
Despite the changes, there was “persistent variation” among hospitals, with more than 14% of the primary-prevention ICDs not meeting NCD criteria at some of the worst-performing hospitals.
The decreases weren’t just in Medicare beneficiaries, though. Hospitals were rethinking this indication for ICD use in everyone, although the investigators found no evidence that the changing clinical landscape endangered the health of patients.
“The analyses of secondary prevention ICDs do not suggest that access to necessary procedures was negatively affected by the investigation. … These analyses offer some reassurance, but further research into hospital responses to the investigation could offer additional insights about possible unintended consequences,” the investigators wrote.
The study was sponsored by the Agency for Healthcare Research and Quality. Dr. Desai had no financial disclosures.
SOURCE: Desai NR et al. JAMA. 2018; 320: 63-71.
FROM JAMA
Key clinical point: A federal lawsuit against hospitals changed the practice of using implantable cardioverter defibrillators for primary prevention.
Major finding: In the year after the Department of Justice lawsuit was announced, ICD for primary prevention use dropped 7.4% in hospitals that settled and dropped 4.7% in hospitals that were nonsettlers.
Study details: An analysis of data from the Centers for Medicare & Medicaid Services.
Disclosures: The Agency for Healthcare Research and Quality sponsored the study. Dr. Desai had no financial disclosures.
Source: Desai NR et al. JAMA. 2018; 320:63-71.
Rapid venetoclax dose escalation aids relapsed CLL
STOCKHOLM – Patients with chronic lymphocytic leukemia (CLL) who experience relapse after therapy with a B-cell receptor signaling inhibitor tend to have a swiftly progressive disease course that requires immediate intervention. For these patients, a rapid venetoclax dose-escalation protocol may be a safe way to quickly regain disease control, and possibly bridge to salvage therapies, investigators reported.
Of 15 patients with CLL who relapsed after treatment with a B-cell receptor inhibitor (BCRi), all were able to get to their target dose of venetoclax under close inpatient monitoring at a median of 12 days, compared with the 35 days usually required for venetoclax dose escalation, reported Farrukh T. Awan, MD, of Ohio State University Comprehensive Cancer Center in Columbus, and his colleagues.
Only two patients developed clinical tumor lysis syndrome (TLS), a common occurrence with venetoclax therapy, and this adverse event was manageable, Dr. Awan said at the annual congress of the European Hematology Association.
“The reason why we have been doing a slow ramp up on venetoclax is the original toxicity issues that we saw early on,” he said in an interview. “But unfortunately, a lot of patients are progressing on these new agents and have very rapid disease progression, and what we have seen is that if you stop the ibrutinib, the disease progresses very quickly, and by the time they can get up to the effective dose of venetoclax, they’re too sick to continue, or they might even die from disease progression.”
To combat this problem, Dr. Awan and his colleagues developed a rapid dose escalation protocol that would ramp up from 20 mg to 400 mg, with increases every 1 or 2 days depending on tolerability and incident TLS. Lab tests for TLS were evaluated every 4-8 hours.
All patients were closely monitored in the hospital, and all were started on allopurinol or other uric acid–lowering agents before starting on venetoclax.
The investigators reported safety and efficacy outcomes for the patients in a retrospective analysis.
The median age of the patients, 12 men and 3 women, was 65 years (range, 58-86 years). Seven patients had Eastern Cooperative Oncology Group Performance Status of 0, seven had an ECOG score of 1, and one had a score of 2-4.
Ten patients had most recently been treated with a BCRi, either a Bruton’s tyrosine kinase inhibitor (ibrutinib or acalabrutinib), idelalisib, or entospletinib. Three patients received ibrutinib plus chemotherapy, and two received rituximab and dexamethasone followed by rituximab maintenance.
The median time to full venetoclax dose was 12 days (range, 5-21 days) and all 15 patients reached the target dose. The mean length of stay during the ramp-up period was 9.5 days (range, 6-22 days).
The incidence of clinical TLS was 13.2%, occurring in two patients, one at the initial 20-mg dose, and one at the 200-mg dose level. Another five patients had asymptomatic TLS. Other treatment-related adverse events were anemia in seven patients, neutropenia in six patients, thrombocytopenia in five patients, and lung infection in one patient.
Twelve patients had a partial response, one had stable disease, and two had progressive disease. The mean time to best response was 71 days.
One-year progression-free survival was 49%, and 1-year overall survival was 68%.
The investigators found that for patients who still have some disease control with a BCRi, it may be possible to keep them on that drug while transitioning to venetoclax. The rapid dose escalation protocol should only be attempted in highly experience comprehensive cancer centers, Dr. Awan said.
“Under very close monitoring in an experienced inpatient setting, where the nurses are very used to doing this on a weekly basis in a very high volume center, I think that our data show that we could do this without affecting toxicity significantly or mortality,” he said.
Venetoclax therapy could buy enough time for patients to bridge to other options, such as chimeric antigen receptor (CAR) T-cell therapy or allogeneic stem cell transplant, he noted.
“But if we had waited 4 weeks, most of these patients would not have made it,” he said.
The study was internally funded. Dr. Awan reported research funding from Gilead, Pharmacyclics, AbbVie, and Janssen.
SOURCE: Koenig K et al. EHA Congress, Abstract PF357.
STOCKHOLM – Patients with chronic lymphocytic leukemia (CLL) who experience relapse after therapy with a B-cell receptor signaling inhibitor tend to have a swiftly progressive disease course that requires immediate intervention. For these patients, a rapid venetoclax dose-escalation protocol may be a safe way to quickly regain disease control, and possibly bridge to salvage therapies, investigators reported.
Of 15 patients with CLL who relapsed after treatment with a B-cell receptor inhibitor (BCRi), all were able to get to their target dose of venetoclax under close inpatient monitoring at a median of 12 days, compared with the 35 days usually required for venetoclax dose escalation, reported Farrukh T. Awan, MD, of Ohio State University Comprehensive Cancer Center in Columbus, and his colleagues.
Only two patients developed clinical tumor lysis syndrome (TLS), a common occurrence with venetoclax therapy, and this adverse event was manageable, Dr. Awan said at the annual congress of the European Hematology Association.
“The reason why we have been doing a slow ramp up on venetoclax is the original toxicity issues that we saw early on,” he said in an interview. “But unfortunately, a lot of patients are progressing on these new agents and have very rapid disease progression, and what we have seen is that if you stop the ibrutinib, the disease progresses very quickly, and by the time they can get up to the effective dose of venetoclax, they’re too sick to continue, or they might even die from disease progression.”
To combat this problem, Dr. Awan and his colleagues developed a rapid dose escalation protocol that would ramp up from 20 mg to 400 mg, with increases every 1 or 2 days depending on tolerability and incident TLS. Lab tests for TLS were evaluated every 4-8 hours.
All patients were closely monitored in the hospital, and all were started on allopurinol or other uric acid–lowering agents before starting on venetoclax.
The investigators reported safety and efficacy outcomes for the patients in a retrospective analysis.
The median age of the patients, 12 men and 3 women, was 65 years (range, 58-86 years). Seven patients had Eastern Cooperative Oncology Group Performance Status of 0, seven had an ECOG score of 1, and one had a score of 2-4.
Ten patients had most recently been treated with a BCRi, either a Bruton’s tyrosine kinase inhibitor (ibrutinib or acalabrutinib), idelalisib, or entospletinib. Three patients received ibrutinib plus chemotherapy, and two received rituximab and dexamethasone followed by rituximab maintenance.
The median time to full venetoclax dose was 12 days (range, 5-21 days) and all 15 patients reached the target dose. The mean length of stay during the ramp-up period was 9.5 days (range, 6-22 days).
The incidence of clinical TLS was 13.2%, occurring in two patients, one at the initial 20-mg dose, and one at the 200-mg dose level. Another five patients had asymptomatic TLS. Other treatment-related adverse events were anemia in seven patients, neutropenia in six patients, thrombocytopenia in five patients, and lung infection in one patient.
Twelve patients had a partial response, one had stable disease, and two had progressive disease. The mean time to best response was 71 days.
One-year progression-free survival was 49%, and 1-year overall survival was 68%.
The investigators found that for patients who still have some disease control with a BCRi, it may be possible to keep them on that drug while transitioning to venetoclax. The rapid dose escalation protocol should only be attempted in highly experience comprehensive cancer centers, Dr. Awan said.
“Under very close monitoring in an experienced inpatient setting, where the nurses are very used to doing this on a weekly basis in a very high volume center, I think that our data show that we could do this without affecting toxicity significantly or mortality,” he said.
Venetoclax therapy could buy enough time for patients to bridge to other options, such as chimeric antigen receptor (CAR) T-cell therapy or allogeneic stem cell transplant, he noted.
“But if we had waited 4 weeks, most of these patients would not have made it,” he said.
The study was internally funded. Dr. Awan reported research funding from Gilead, Pharmacyclics, AbbVie, and Janssen.
SOURCE: Koenig K et al. EHA Congress, Abstract PF357.
STOCKHOLM – Patients with chronic lymphocytic leukemia (CLL) who experience relapse after therapy with a B-cell receptor signaling inhibitor tend to have a swiftly progressive disease course that requires immediate intervention. For these patients, a rapid venetoclax dose-escalation protocol may be a safe way to quickly regain disease control, and possibly bridge to salvage therapies, investigators reported.
Of 15 patients with CLL who relapsed after treatment with a B-cell receptor inhibitor (BCRi), all were able to get to their target dose of venetoclax under close inpatient monitoring at a median of 12 days, compared with the 35 days usually required for venetoclax dose escalation, reported Farrukh T. Awan, MD, of Ohio State University Comprehensive Cancer Center in Columbus, and his colleagues.
Only two patients developed clinical tumor lysis syndrome (TLS), a common occurrence with venetoclax therapy, and this adverse event was manageable, Dr. Awan said at the annual congress of the European Hematology Association.
“The reason why we have been doing a slow ramp up on venetoclax is the original toxicity issues that we saw early on,” he said in an interview. “But unfortunately, a lot of patients are progressing on these new agents and have very rapid disease progression, and what we have seen is that if you stop the ibrutinib, the disease progresses very quickly, and by the time they can get up to the effective dose of venetoclax, they’re too sick to continue, or they might even die from disease progression.”
To combat this problem, Dr. Awan and his colleagues developed a rapid dose escalation protocol that would ramp up from 20 mg to 400 mg, with increases every 1 or 2 days depending on tolerability and incident TLS. Lab tests for TLS were evaluated every 4-8 hours.
All patients were closely monitored in the hospital, and all were started on allopurinol or other uric acid–lowering agents before starting on venetoclax.
The investigators reported safety and efficacy outcomes for the patients in a retrospective analysis.
The median age of the patients, 12 men and 3 women, was 65 years (range, 58-86 years). Seven patients had Eastern Cooperative Oncology Group Performance Status of 0, seven had an ECOG score of 1, and one had a score of 2-4.
Ten patients had most recently been treated with a BCRi, either a Bruton’s tyrosine kinase inhibitor (ibrutinib or acalabrutinib), idelalisib, or entospletinib. Three patients received ibrutinib plus chemotherapy, and two received rituximab and dexamethasone followed by rituximab maintenance.
The median time to full venetoclax dose was 12 days (range, 5-21 days) and all 15 patients reached the target dose. The mean length of stay during the ramp-up period was 9.5 days (range, 6-22 days).
The incidence of clinical TLS was 13.2%, occurring in two patients, one at the initial 20-mg dose, and one at the 200-mg dose level. Another five patients had asymptomatic TLS. Other treatment-related adverse events were anemia in seven patients, neutropenia in six patients, thrombocytopenia in five patients, and lung infection in one patient.
Twelve patients had a partial response, one had stable disease, and two had progressive disease. The mean time to best response was 71 days.
One-year progression-free survival was 49%, and 1-year overall survival was 68%.
The investigators found that for patients who still have some disease control with a BCRi, it may be possible to keep them on that drug while transitioning to venetoclax. The rapid dose escalation protocol should only be attempted in highly experience comprehensive cancer centers, Dr. Awan said.
“Under very close monitoring in an experienced inpatient setting, where the nurses are very used to doing this on a weekly basis in a very high volume center, I think that our data show that we could do this without affecting toxicity significantly or mortality,” he said.
Venetoclax therapy could buy enough time for patients to bridge to other options, such as chimeric antigen receptor (CAR) T-cell therapy or allogeneic stem cell transplant, he noted.
“But if we had waited 4 weeks, most of these patients would not have made it,” he said.
The study was internally funded. Dr. Awan reported research funding from Gilead, Pharmacyclics, AbbVie, and Janssen.
SOURCE: Koenig K et al. EHA Congress, Abstract PF357.
REPORTING FROM THE EHA CONGRESS
Key clinical point:
Major finding: All patients reached the target dose of venetoclax, with only two cases of manageable clinical tumor lysis syndrome.
Study details: Retrospective analysis of outcomes for 15 patients with CLL who relapsed after treatment with a B-cell receptor signaling inhibitor.
Disclosures: The study was internally funded. Dr. Awan reported research funding from Gilead, Pharmacyclics, AbbVie, and Janssen.
Source: Koenig K et al. EHA Congress, Abstract PF357.
Under the Cover of Darkness
When he was about 12, a now 41-year-old man noticed that the skin on his left chest was darkening. For several years afterward, the darkness spread and deepened, and the area became hairy. In young adulthood, he experienced occasional outbreaks of what looked like acne on the lesion; this eventually cleared.
He now finds the hairiness increasingly bothersome, so he shaves the worst parts of it. Upon consulting his primary care provider, he was assured that the lesion is “a birthmark.” Unsatisfied with this answer, the patient took the advice of a friend and decided to consult dermatology.
EXAMINATION
A polygonal, hyperpigmented, hypertrichotic patch covers most of the patient’s left pectoral area. The lateral margin is irregular but well-defined. There is obvious partial regrowth of the shaved hair on the lateral margin, but it stops abruptly at that point.

The breast and surrounding tissue appear normal. No areas of hyperpigmentation or hypertrichosis are seen elsewhere.
What is the diagnosis?
DISCUSSION
First described by William Becker in 1948 (and subsequently named for him), the Becker nevus (BN) received little research attention until a French study of 20,000 young men showed a prevalence of 0.5%. Nearly half of the subjects had first noticed the lesion before the age of 10—a somewhat surprising finding, since abundant evidence implicates androgens in its genesis. (This is supported by the condition’s predominance in males, the increased numbers of androgen receptors and melanocytes in the affected skin, and the prevalence of hypertrichosis.)
The researchers were also surprised to find that only 30% of the reported lesions occurred above the nipple, because the first descriptions of BN gave the impression that the shoulder and chest were most commonly affected. We now know that BN can also be found on arms and legs.
Usually a benign condition, BN can be associated with skeletal or soft-tissue deformities in the affected area (eg, ipsilateral breast hypoplasia). Malignancies—most notably melanoma—have also been reported with BN but are especially uncommon.
The differential includes the café-au-lait macules of neurofibromatosis, Albright disease, and congenital melanocytic nevus. The history of BN (ie, presentation, hypertrichosis, gender of patient, and distribution) usually allow a clinical diagnosis.
Treatment is limited to laser hair removal or laser removal or reduction of pigment.
TAKE-HOME LEARNING POINTS
- Becker nevus (BN) is far more common in males than females.
- BN typically manifests during puberty, which aligns with the suspected androgenic etiology.
- Though the shoulders and chest are the most commonly affected areas, BNs can also appear on the flank, arms, or legs.
- The lesions are rarely associated with serious pathology; hypoplasia of the ipsilateral breast is the most common of these complications.
When he was about 12, a now 41-year-old man noticed that the skin on his left chest was darkening. For several years afterward, the darkness spread and deepened, and the area became hairy. In young adulthood, he experienced occasional outbreaks of what looked like acne on the lesion; this eventually cleared.
He now finds the hairiness increasingly bothersome, so he shaves the worst parts of it. Upon consulting his primary care provider, he was assured that the lesion is “a birthmark.” Unsatisfied with this answer, the patient took the advice of a friend and decided to consult dermatology.
EXAMINATION
A polygonal, hyperpigmented, hypertrichotic patch covers most of the patient’s left pectoral area. The lateral margin is irregular but well-defined. There is obvious partial regrowth of the shaved hair on the lateral margin, but it stops abruptly at that point.
The breast and surrounding tissue appear normal. No areas of hyperpigmentation or hypertrichosis are seen elsewhere.
What is the diagnosis?
DISCUSSION
First described by William Becker in 1948 (and subsequently named for him), the Becker nevus (BN) received little research attention until a French study of 20,000 young men showed a prevalence of 0.5%. Nearly half of the subjects had first noticed the lesion before the age of 10—a somewhat surprising finding, since abundant evidence implicates androgens in its genesis. (This is supported by the condition’s predominance in males, the increased numbers of androgen receptors and melanocytes in the affected skin, and the prevalence of hypertrichosis.)
The researchers were also surprised to find that only 30% of the reported lesions occurred above the nipple, because the first descriptions of BN gave the impression that the shoulder and chest were most commonly affected. We now know that BN can also be found on arms and legs.
Usually a benign condition, BN can be associated with skeletal or soft-tissue deformities in the affected area (eg, ipsilateral breast hypoplasia). Malignancies—most notably melanoma—have also been reported with BN but are especially uncommon.
The differential includes the café-au-lait macules of neurofibromatosis, Albright disease, and congenital melanocytic nevus. The history of BN (ie, presentation, hypertrichosis, gender of patient, and distribution) usually allow a clinical diagnosis.
Treatment is limited to laser hair removal or laser removal or reduction of pigment.
TAKE-HOME LEARNING POINTS
- Becker nevus (BN) is far more common in males than females.
- BN typically manifests during puberty, which aligns with the suspected androgenic etiology.
- Though the shoulders and chest are the most commonly affected areas, BNs can also appear on the flank, arms, or legs.
- The lesions are rarely associated with serious pathology; hypoplasia of the ipsilateral breast is the most common of these complications.
When he was about 12, a now 41-year-old man noticed that the skin on his left chest was darkening. For several years afterward, the darkness spread and deepened, and the area became hairy. In young adulthood, he experienced occasional outbreaks of what looked like acne on the lesion; this eventually cleared.
He now finds the hairiness increasingly bothersome, so he shaves the worst parts of it. Upon consulting his primary care provider, he was assured that the lesion is “a birthmark.” Unsatisfied with this answer, the patient took the advice of a friend and decided to consult dermatology.
EXAMINATION
A polygonal, hyperpigmented, hypertrichotic patch covers most of the patient’s left pectoral area. The lateral margin is irregular but well-defined. There is obvious partial regrowth of the shaved hair on the lateral margin, but it stops abruptly at that point.
The breast and surrounding tissue appear normal. No areas of hyperpigmentation or hypertrichosis are seen elsewhere.
What is the diagnosis?
DISCUSSION
First described by William Becker in 1948 (and subsequently named for him), the Becker nevus (BN) received little research attention until a French study of 20,000 young men showed a prevalence of 0.5%. Nearly half of the subjects had first noticed the lesion before the age of 10—a somewhat surprising finding, since abundant evidence implicates androgens in its genesis. (This is supported by the condition’s predominance in males, the increased numbers of androgen receptors and melanocytes in the affected skin, and the prevalence of hypertrichosis.)
The researchers were also surprised to find that only 30% of the reported lesions occurred above the nipple, because the first descriptions of BN gave the impression that the shoulder and chest were most commonly affected. We now know that BN can also be found on arms and legs.
Usually a benign condition, BN can be associated with skeletal or soft-tissue deformities in the affected area (eg, ipsilateral breast hypoplasia). Malignancies—most notably melanoma—have also been reported with BN but are especially uncommon.
The differential includes the café-au-lait macules of neurofibromatosis, Albright disease, and congenital melanocytic nevus. The history of BN (ie, presentation, hypertrichosis, gender of patient, and distribution) usually allow a clinical diagnosis.
Treatment is limited to laser hair removal or laser removal or reduction of pigment.
TAKE-HOME LEARNING POINTS
- Becker nevus (BN) is far more common in males than females.
- BN typically manifests during puberty, which aligns with the suspected androgenic etiology.
- Though the shoulders and chest are the most commonly affected areas, BNs can also appear on the flank, arms, or legs.
- The lesions are rarely associated with serious pathology; hypoplasia of the ipsilateral breast is the most common of these complications.

New pediatric hypertension guidelines increased hypertension prevalence
New clinical among at-risk youth, according to findings published in Pediatrics.
In a clinical practice guideline (CPG) published in 2017, the American Academy of Pediatrics updated its 2004 guideline to include new reference tables for BP values in addition to new definitions of elevated BP and hypertension, including absolute BP cutoff values for adolescents aged 13 years and older (Pediatrics. 2017 Sep;140[6]:e20173035). This was intended to “emulate the recently updated adult hypertension guidelines and to simplify the process of identifying and classifying hypertension in adolescents,” wrote Michael Khoury, MD, of the Heart Institute at Cincinnati Children’s Hospital Medical Center, and his coauthors.
To evaluate the impact of the new guidelines on the prevalence of hypertension and associations with target organ damage, the investigators used data from a study on obesity and type 2 diabetes in 364 patients aged 10-17 years; 59% were obese, and 30% had type 2 diabetes. Three groups were identified: patients with obesity and type 2 diabetes, patients with obesity but no type 2 diabetes, and healthy (“lean”) controls.
Patients fasted overnight for a minimum of 10 hours, after which body mass index was calculated, blood pressure was taken, and anthropometric, laboratory, echocardiography, and carotid assessments were performed. Average BP measurements were categorized according to the 2004 guideline and to the new CPG.
In carotid ultrasonography assessments, a composite of carotid intima-media thickness was formed from the average of three sites, and a composite carotid intima-media thickness greater than or equal to the 90th percentile of that measured in the lean patients, who were the controls, was considered abnormal. In echocardiography assessments, left ventricular mass (LVM) and LVM index were calculated. Elevated LVM was defined by the pediatric cutoff of LVM index greater than or equal to 38.6 g/m.
For diastolic function, tissue Doppler velocities under the 10th percentile and an average early left ventricular filling/peak early myocardial velocity ratio greater than or equal to the 90th percentile in controls were considered abnormal. Lastly, pulse wave velocity (PWV) was measured to determine arterial stiffness, and a PWV greater than or equal to the 90th percentile for the controls was considered abnormal.
BP classification under the new guideline resulted in an increased prevalence of hypertension at 13% (10% stage 1, 3% stage 2), compared with the 2004 guideline at 8% (6% stage 1, 2% stage 2), with a P value of .007.
Of the 75 patients classified as having elevated BP in the 2004 guideline, 19 (25%) were reclassified as having stage 1 hypertension under the CPG. These 19 patients were older, compared with patients who remained in the elevated blood pressure category (16.5 ± 0.9 vs. 15.5 ± 1.7 years; P = .02). The patients who were reclassified also had higher body mass indexes (38.8 ± 8.2 vs. 33.6 ± 7.4; P = .01) and diastolic blood pressures (76.5 mm Hg ± 8.7 vs. 62.1 ± 12.2 mm Hg; P less than .001), Dr. Khoury and his colleagues reported.
Reclassification to a higher BP category was associated with increased odds of an abnormal target organ damage (TOD) values, and both guidelines produced similar odds, “suggesting that the two guidelines produce similar associations with TOD,” the authors wrote. Reclassification based on the CPG definition accounted for 31% of patients with increased LVM, compared with 20% as defined in the 2004 guideline (P less than .001), and for 33% of patients with abnormal PWV, compared with 23% in the 2004 guideline, suggesting improved sensitivity of hypertension categorization in detecting LVM. A similar effect was seen in other measures of TOD, the authors noted.
The findings suggest that, combined with the increased prevalence of hypertension under the new guidelines, “the CPG may contribute to an increased detection of abnormal LVM and other measures of TOD,” the authors wrote. “This, in turn, may contribute to risk stratification in clinical decision making for youth presenting with BP concerns,” they concluded.
The study was supported by a National Institutes of Health grant. The authors had no relevant disclosures.
SOURCE: Khoury M et al. Pediatrics. 2018 Jul 5. doi: 10.1542/peds.2018-0245.
New clinical among at-risk youth, according to findings published in Pediatrics.
In a clinical practice guideline (CPG) published in 2017, the American Academy of Pediatrics updated its 2004 guideline to include new reference tables for BP values in addition to new definitions of elevated BP and hypertension, including absolute BP cutoff values for adolescents aged 13 years and older (Pediatrics. 2017 Sep;140[6]:e20173035). This was intended to “emulate the recently updated adult hypertension guidelines and to simplify the process of identifying and classifying hypertension in adolescents,” wrote Michael Khoury, MD, of the Heart Institute at Cincinnati Children’s Hospital Medical Center, and his coauthors.
To evaluate the impact of the new guidelines on the prevalence of hypertension and associations with target organ damage, the investigators used data from a study on obesity and type 2 diabetes in 364 patients aged 10-17 years; 59% were obese, and 30% had type 2 diabetes. Three groups were identified: patients with obesity and type 2 diabetes, patients with obesity but no type 2 diabetes, and healthy (“lean”) controls.
Patients fasted overnight for a minimum of 10 hours, after which body mass index was calculated, blood pressure was taken, and anthropometric, laboratory, echocardiography, and carotid assessments were performed. Average BP measurements were categorized according to the 2004 guideline and to the new CPG.
In carotid ultrasonography assessments, a composite of carotid intima-media thickness was formed from the average of three sites, and a composite carotid intima-media thickness greater than or equal to the 90th percentile of that measured in the lean patients, who were the controls, was considered abnormal. In echocardiography assessments, left ventricular mass (LVM) and LVM index were calculated. Elevated LVM was defined by the pediatric cutoff of LVM index greater than or equal to 38.6 g/m.
For diastolic function, tissue Doppler velocities under the 10th percentile and an average early left ventricular filling/peak early myocardial velocity ratio greater than or equal to the 90th percentile in controls were considered abnormal. Lastly, pulse wave velocity (PWV) was measured to determine arterial stiffness, and a PWV greater than or equal to the 90th percentile for the controls was considered abnormal.
BP classification under the new guideline resulted in an increased prevalence of hypertension at 13% (10% stage 1, 3% stage 2), compared with the 2004 guideline at 8% (6% stage 1, 2% stage 2), with a P value of .007.
Of the 75 patients classified as having elevated BP in the 2004 guideline, 19 (25%) were reclassified as having stage 1 hypertension under the CPG. These 19 patients were older, compared with patients who remained in the elevated blood pressure category (16.5 ± 0.9 vs. 15.5 ± 1.7 years; P = .02). The patients who were reclassified also had higher body mass indexes (38.8 ± 8.2 vs. 33.6 ± 7.4; P = .01) and diastolic blood pressures (76.5 mm Hg ± 8.7 vs. 62.1 ± 12.2 mm Hg; P less than .001), Dr. Khoury and his colleagues reported.
Reclassification to a higher BP category was associated with increased odds of an abnormal target organ damage (TOD) values, and both guidelines produced similar odds, “suggesting that the two guidelines produce similar associations with TOD,” the authors wrote. Reclassification based on the CPG definition accounted for 31% of patients with increased LVM, compared with 20% as defined in the 2004 guideline (P less than .001), and for 33% of patients with abnormal PWV, compared with 23% in the 2004 guideline, suggesting improved sensitivity of hypertension categorization in detecting LVM. A similar effect was seen in other measures of TOD, the authors noted.
The findings suggest that, combined with the increased prevalence of hypertension under the new guidelines, “the CPG may contribute to an increased detection of abnormal LVM and other measures of TOD,” the authors wrote. “This, in turn, may contribute to risk stratification in clinical decision making for youth presenting with BP concerns,” they concluded.
The study was supported by a National Institutes of Health grant. The authors had no relevant disclosures.
SOURCE: Khoury M et al. Pediatrics. 2018 Jul 5. doi: 10.1542/peds.2018-0245.
New clinical among at-risk youth, according to findings published in Pediatrics.
In a clinical practice guideline (CPG) published in 2017, the American Academy of Pediatrics updated its 2004 guideline to include new reference tables for BP values in addition to new definitions of elevated BP and hypertension, including absolute BP cutoff values for adolescents aged 13 years and older (Pediatrics. 2017 Sep;140[6]:e20173035). This was intended to “emulate the recently updated adult hypertension guidelines and to simplify the process of identifying and classifying hypertension in adolescents,” wrote Michael Khoury, MD, of the Heart Institute at Cincinnati Children’s Hospital Medical Center, and his coauthors.
To evaluate the impact of the new guidelines on the prevalence of hypertension and associations with target organ damage, the investigators used data from a study on obesity and type 2 diabetes in 364 patients aged 10-17 years; 59% were obese, and 30% had type 2 diabetes. Three groups were identified: patients with obesity and type 2 diabetes, patients with obesity but no type 2 diabetes, and healthy (“lean”) controls.
Patients fasted overnight for a minimum of 10 hours, after which body mass index was calculated, blood pressure was taken, and anthropometric, laboratory, echocardiography, and carotid assessments were performed. Average BP measurements were categorized according to the 2004 guideline and to the new CPG.
In carotid ultrasonography assessments, a composite of carotid intima-media thickness was formed from the average of three sites, and a composite carotid intima-media thickness greater than or equal to the 90th percentile of that measured in the lean patients, who were the controls, was considered abnormal. In echocardiography assessments, left ventricular mass (LVM) and LVM index were calculated. Elevated LVM was defined by the pediatric cutoff of LVM index greater than or equal to 38.6 g/m.
For diastolic function, tissue Doppler velocities under the 10th percentile and an average early left ventricular filling/peak early myocardial velocity ratio greater than or equal to the 90th percentile in controls were considered abnormal. Lastly, pulse wave velocity (PWV) was measured to determine arterial stiffness, and a PWV greater than or equal to the 90th percentile for the controls was considered abnormal.
BP classification under the new guideline resulted in an increased prevalence of hypertension at 13% (10% stage 1, 3% stage 2), compared with the 2004 guideline at 8% (6% stage 1, 2% stage 2), with a P value of .007.
Of the 75 patients classified as having elevated BP in the 2004 guideline, 19 (25%) were reclassified as having stage 1 hypertension under the CPG. These 19 patients were older, compared with patients who remained in the elevated blood pressure category (16.5 ± 0.9 vs. 15.5 ± 1.7 years; P = .02). The patients who were reclassified also had higher body mass indexes (38.8 ± 8.2 vs. 33.6 ± 7.4; P = .01) and diastolic blood pressures (76.5 mm Hg ± 8.7 vs. 62.1 ± 12.2 mm Hg; P less than .001), Dr. Khoury and his colleagues reported.
Reclassification to a higher BP category was associated with increased odds of an abnormal target organ damage (TOD) values, and both guidelines produced similar odds, “suggesting that the two guidelines produce similar associations with TOD,” the authors wrote. Reclassification based on the CPG definition accounted for 31% of patients with increased LVM, compared with 20% as defined in the 2004 guideline (P less than .001), and for 33% of patients with abnormal PWV, compared with 23% in the 2004 guideline, suggesting improved sensitivity of hypertension categorization in detecting LVM. A similar effect was seen in other measures of TOD, the authors noted.
The findings suggest that, combined with the increased prevalence of hypertension under the new guidelines, “the CPG may contribute to an increased detection of abnormal LVM and other measures of TOD,” the authors wrote. “This, in turn, may contribute to risk stratification in clinical decision making for youth presenting with BP concerns,” they concluded.
The study was supported by a National Institutes of Health grant. The authors had no relevant disclosures.
SOURCE: Khoury M et al. Pediatrics. 2018 Jul 5. doi: 10.1542/peds.2018-0245.
FROM PEDIATRICS
Key clinical point: New clinical guidelines for pediatric hypertension resulted in increased prevalence of the condition and improved sensitivity in detecting target organ damage.
Major finding: BP classification under the new guideline resulted in an increased hypertension prevalence of 13% versus 8% with the 2004 guideline (P = .007).
Study details: The impact of the new guidelines was evaluated using data on 364 patients aged 10-18 years in an obesity and type 2 diabetes mellitus trial.
Disclosures: The study was supported by a National Institutes of Health grant. The authors had no relevant disclosures to report.
Source: Khoury M et al. Pediatrics. 2018 Jul 5. doi: 10.1542/peds.2018-0245.
AGA CPU: Extraesophageal symptoms attributed to GERD
When patients lack typical symptoms of gastroesophageal reflux disease (GERD) and have extraesophageal symptoms, ENT, allergy, and pulmonary work-ups are “essential and often should be performed initially,” experts note in an American Gastroenterological Association clinical practice update.
Extraesophageal symptoms often are unrelated to GERD or are multifactorial, wrote Michael F. Vaezi, MD, PhD, of Vanderbilt University Medical Center in Nashville, Tenn., and his associates in Clinical Gastroenterology and Hepatology. Gastroenterologists often are asked to look for reflux as the cause of extraesophageal symptoms before other etiologies have been ruled out.
Proposed extraesophageal manifestations of GERD range from chronic throat clearing and dysphonia to otitis, pulmonary fibrosis, laryngeal cancer, and even lung transplant rejection. Stronger evidence links GERD with symptoms of asthma, cough, and hoarseness, the experts note. “When less stringent criteria are used, the attributions are broader and could include sore throat, sinusitis, ear pain, and pulmonary fibrosis.”
When asked to assess whether GERD is causing extraesophageal symptoms, consider the “constellation” of patient presentation, test results, and treatment response, according to the clinical practice update. No diagnostic tests “unequivocally link any suspected extraesophageal symptom to GERD.” For patients who have both extraesophageal symptoms and typical symptoms of GERD, the authors suggest an evaluator regimen of 6-8 weeks of empiric, aggressive (twice-daily) proton pump inhibitor (PPI) therapy. If aggressive acid suppression therapy appears to improve extraesophageal symptoms, patients should be titrated to the lowest effective treatment dose.If symptoms persist despite an aggressive trial of a PPI, and patients have a body mass index under 25, and a seemingly low probability of GERD, then the experts recommend pH testing “off” therapy and seeking other etiologies for extraesophageal symptoms. If symptoms persist and a patients’ BMI exceeds 25 with a high suspicion of GERD, they recommend evaluations for concomitant asthma or lung disease. If these work-ups are positive, they recommend multichannel intraluminal impedance testing or pH monitoring on treatment.
The clinical practice update strongly discourages surgical treatment of extraesophageal GERD symptoms except in specific populations, such as when patients have objective signs of treatment-refractory GERD and have not responded to comprehensive therapy for other possible causes of extraesophageal symptoms. Recent data suggest that surgery can benefit patients with confirmed structural defects, such as hiatal hernia, which are causing symptomatic, volume-based regurgitation, the experts note. Ideally, these patients should first undergo pH and impedance monitoring to objectively measure the effects of reflux. Additionally, surgical fundoplication “might be beneficial” for patients whose extraesophageal symptoms clearly have responded to PPI therapy but who refuse long-term PPI therapy or who develop unacceptable side effects.
The practice update also extensively discusses the role of testing to evaluate the role of GERD in extraesophageal symptoms. Barium esophagography is insensitive for GERD and is useful only for evaluating dysphagia and the size and type of a hiatal hernia, the experts note. Abnormal laryngoscopy or pharyngoscopic findings are more useful but should not be the “initial driving force” behind a GERD diagnosis and do not necessarily link GERD to extraesophageal symptoms. Likewise, esophagogastroduodenoscopy can identify esophagitis, which signifies GERD but does not establish it as etiologic.
Positive ambulatory pH or impedance monitoring or pharyngeal pH tests also do not definitively link reflux to suspected extraesophageal symptoms, the experts note. They suggest considering “on” therapy monitoring to evaluate treatment efficacy and to time reflux events relative to symptoms in patients with esophagitis, Barrett’s esophagus, or a large hiatal hernia. Conversely, they recommend considering “off” treatment testing to rule out GERD in patients who have no history of confirmed or suspected reflux and who have not responded to PPI therapy.
Novel tests, such as salivary pepsin and mucosal impedance, have “no clear role in establishing GERD as the cause of extraesophageal symptoms,” the experts emphasize. Clinician scientists also debate the exact pathophysiology of extraesophageal GERD sequelae. While chronic exposure to gastric refluxate clearly can harm proximal structures such as the pharynx, larynx, and bronchial tree, it remains unclear how much acid is necessary to cause injury and whether bile, pepsin, or neurogenic stimulation play a role.
Dr. Vaezi reported having no conflicts of interest. Senior author Frank Zerbib, MD, PhD, reported receiving devices for research purposes from Medtronic and Sandhill Scientific.
SOURCE: Vaezi MF et al. Clin Gastroenterol Hepatol. 2018 Feb 7. doi: 10.1016/j.cgh.2018.02.001.
When patients lack typical symptoms of gastroesophageal reflux disease (GERD) and have extraesophageal symptoms, ENT, allergy, and pulmonary work-ups are “essential and often should be performed initially,” experts note in an American Gastroenterological Association clinical practice update.
Extraesophageal symptoms often are unrelated to GERD or are multifactorial, wrote Michael F. Vaezi, MD, PhD, of Vanderbilt University Medical Center in Nashville, Tenn., and his associates in Clinical Gastroenterology and Hepatology. Gastroenterologists often are asked to look for reflux as the cause of extraesophageal symptoms before other etiologies have been ruled out.
Proposed extraesophageal manifestations of GERD range from chronic throat clearing and dysphonia to otitis, pulmonary fibrosis, laryngeal cancer, and even lung transplant rejection. Stronger evidence links GERD with symptoms of asthma, cough, and hoarseness, the experts note. “When less stringent criteria are used, the attributions are broader and could include sore throat, sinusitis, ear pain, and pulmonary fibrosis.”
When asked to assess whether GERD is causing extraesophageal symptoms, consider the “constellation” of patient presentation, test results, and treatment response, according to the clinical practice update. No diagnostic tests “unequivocally link any suspected extraesophageal symptom to GERD.” For patients who have both extraesophageal symptoms and typical symptoms of GERD, the authors suggest an evaluator regimen of 6-8 weeks of empiric, aggressive (twice-daily) proton pump inhibitor (PPI) therapy. If aggressive acid suppression therapy appears to improve extraesophageal symptoms, patients should be titrated to the lowest effective treatment dose.If symptoms persist despite an aggressive trial of a PPI, and patients have a body mass index under 25, and a seemingly low probability of GERD, then the experts recommend pH testing “off” therapy and seeking other etiologies for extraesophageal symptoms. If symptoms persist and a patients’ BMI exceeds 25 with a high suspicion of GERD, they recommend evaluations for concomitant asthma or lung disease. If these work-ups are positive, they recommend multichannel intraluminal impedance testing or pH monitoring on treatment.
The clinical practice update strongly discourages surgical treatment of extraesophageal GERD symptoms except in specific populations, such as when patients have objective signs of treatment-refractory GERD and have not responded to comprehensive therapy for other possible causes of extraesophageal symptoms. Recent data suggest that surgery can benefit patients with confirmed structural defects, such as hiatal hernia, which are causing symptomatic, volume-based regurgitation, the experts note. Ideally, these patients should first undergo pH and impedance monitoring to objectively measure the effects of reflux. Additionally, surgical fundoplication “might be beneficial” for patients whose extraesophageal symptoms clearly have responded to PPI therapy but who refuse long-term PPI therapy or who develop unacceptable side effects.
The practice update also extensively discusses the role of testing to evaluate the role of GERD in extraesophageal symptoms. Barium esophagography is insensitive for GERD and is useful only for evaluating dysphagia and the size and type of a hiatal hernia, the experts note. Abnormal laryngoscopy or pharyngoscopic findings are more useful but should not be the “initial driving force” behind a GERD diagnosis and do not necessarily link GERD to extraesophageal symptoms. Likewise, esophagogastroduodenoscopy can identify esophagitis, which signifies GERD but does not establish it as etiologic.
Positive ambulatory pH or impedance monitoring or pharyngeal pH tests also do not definitively link reflux to suspected extraesophageal symptoms, the experts note. They suggest considering “on” therapy monitoring to evaluate treatment efficacy and to time reflux events relative to symptoms in patients with esophagitis, Barrett’s esophagus, or a large hiatal hernia. Conversely, they recommend considering “off” treatment testing to rule out GERD in patients who have no history of confirmed or suspected reflux and who have not responded to PPI therapy.
Novel tests, such as salivary pepsin and mucosal impedance, have “no clear role in establishing GERD as the cause of extraesophageal symptoms,” the experts emphasize. Clinician scientists also debate the exact pathophysiology of extraesophageal GERD sequelae. While chronic exposure to gastric refluxate clearly can harm proximal structures such as the pharynx, larynx, and bronchial tree, it remains unclear how much acid is necessary to cause injury and whether bile, pepsin, or neurogenic stimulation play a role.
Dr. Vaezi reported having no conflicts of interest. Senior author Frank Zerbib, MD, PhD, reported receiving devices for research purposes from Medtronic and Sandhill Scientific.
SOURCE: Vaezi MF et al. Clin Gastroenterol Hepatol. 2018 Feb 7. doi: 10.1016/j.cgh.2018.02.001.
When patients lack typical symptoms of gastroesophageal reflux disease (GERD) and have extraesophageal symptoms, ENT, allergy, and pulmonary work-ups are “essential and often should be performed initially,” experts note in an American Gastroenterological Association clinical practice update.
Extraesophageal symptoms often are unrelated to GERD or are multifactorial, wrote Michael F. Vaezi, MD, PhD, of Vanderbilt University Medical Center in Nashville, Tenn., and his associates in Clinical Gastroenterology and Hepatology. Gastroenterologists often are asked to look for reflux as the cause of extraesophageal symptoms before other etiologies have been ruled out.
Proposed extraesophageal manifestations of GERD range from chronic throat clearing and dysphonia to otitis, pulmonary fibrosis, laryngeal cancer, and even lung transplant rejection. Stronger evidence links GERD with symptoms of asthma, cough, and hoarseness, the experts note. “When less stringent criteria are used, the attributions are broader and could include sore throat, sinusitis, ear pain, and pulmonary fibrosis.”
When asked to assess whether GERD is causing extraesophageal symptoms, consider the “constellation” of patient presentation, test results, and treatment response, according to the clinical practice update. No diagnostic tests “unequivocally link any suspected extraesophageal symptom to GERD.” For patients who have both extraesophageal symptoms and typical symptoms of GERD, the authors suggest an evaluator regimen of 6-8 weeks of empiric, aggressive (twice-daily) proton pump inhibitor (PPI) therapy. If aggressive acid suppression therapy appears to improve extraesophageal symptoms, patients should be titrated to the lowest effective treatment dose.If symptoms persist despite an aggressive trial of a PPI, and patients have a body mass index under 25, and a seemingly low probability of GERD, then the experts recommend pH testing “off” therapy and seeking other etiologies for extraesophageal symptoms. If symptoms persist and a patients’ BMI exceeds 25 with a high suspicion of GERD, they recommend evaluations for concomitant asthma or lung disease. If these work-ups are positive, they recommend multichannel intraluminal impedance testing or pH monitoring on treatment.
The clinical practice update strongly discourages surgical treatment of extraesophageal GERD symptoms except in specific populations, such as when patients have objective signs of treatment-refractory GERD and have not responded to comprehensive therapy for other possible causes of extraesophageal symptoms. Recent data suggest that surgery can benefit patients with confirmed structural defects, such as hiatal hernia, which are causing symptomatic, volume-based regurgitation, the experts note. Ideally, these patients should first undergo pH and impedance monitoring to objectively measure the effects of reflux. Additionally, surgical fundoplication “might be beneficial” for patients whose extraesophageal symptoms clearly have responded to PPI therapy but who refuse long-term PPI therapy or who develop unacceptable side effects.
The practice update also extensively discusses the role of testing to evaluate the role of GERD in extraesophageal symptoms. Barium esophagography is insensitive for GERD and is useful only for evaluating dysphagia and the size and type of a hiatal hernia, the experts note. Abnormal laryngoscopy or pharyngoscopic findings are more useful but should not be the “initial driving force” behind a GERD diagnosis and do not necessarily link GERD to extraesophageal symptoms. Likewise, esophagogastroduodenoscopy can identify esophagitis, which signifies GERD but does not establish it as etiologic.
Positive ambulatory pH or impedance monitoring or pharyngeal pH tests also do not definitively link reflux to suspected extraesophageal symptoms, the experts note. They suggest considering “on” therapy monitoring to evaluate treatment efficacy and to time reflux events relative to symptoms in patients with esophagitis, Barrett’s esophagus, or a large hiatal hernia. Conversely, they recommend considering “off” treatment testing to rule out GERD in patients who have no history of confirmed or suspected reflux and who have not responded to PPI therapy.
Novel tests, such as salivary pepsin and mucosal impedance, have “no clear role in establishing GERD as the cause of extraesophageal symptoms,” the experts emphasize. Clinician scientists also debate the exact pathophysiology of extraesophageal GERD sequelae. While chronic exposure to gastric refluxate clearly can harm proximal structures such as the pharynx, larynx, and bronchial tree, it remains unclear how much acid is necessary to cause injury and whether bile, pepsin, or neurogenic stimulation play a role.
Dr. Vaezi reported having no conflicts of interest. Senior author Frank Zerbib, MD, PhD, reported receiving devices for research purposes from Medtronic and Sandhill Scientific.
SOURCE: Vaezi MF et al. Clin Gastroenterol Hepatol. 2018 Feb 7. doi: 10.1016/j.cgh.2018.02.001.
Caring Under a Microscope
I write this editorial at the end of June as summer officially begins. Much of the country—my New Mexico home included—is suffering under an unbearable heat wave in which even those without belief pray for rain. Summer for many is associated with vacations, family trips, and happy hours in the swimming pool among other enjoyable activities that provide a welcome and much deserved break from routine and relief from the grind of work and school. In the words of the George Gershwin tune, “Summertime, and the livin’ is easy.”
In stark contrast to this season, where there is more lightness in being, is the heaviness of the news reports about the Department of Veteran Affairs (VA) that have been featured in the media and the federal press. I suspect I am not alone in having a hard time opening those e-mails; feeling once more the weight of failure on the VA and the employees who have dedicated a good part of their careers to its mission. Even for the VA, June has seen an exceptional string of bad press. I ask as you read this column to think about what the adjective bad means in this context. In the conclusion to this column, I will suggest that the meaning is multivalent.
Among the most distressing stories was the USA Today and Boston Globe headline, “Secret VA nursing home ratings hide poor quality of care from the public.”2 In an all too predictable sequence, this led justifiably to a cascade of demands from the fifth estate, congressional representatives, the administration, veterans and their families, and watchdog organizations for release of the data, investigation of the allegedly deplorable conditions, and rapid fixes to the problems along with the punishment of the guilty.
As an ethicist I am committed to the principles of transparency and accountability that these entities rightly adjure in the wake of any disclosure of a breach of duty to treat each veteran with the best we have—especially the disabled, elderly, and vulnerable. But I have come to believe that the way in which this cycle of scandal and reaction plays out over and over again in VA facilities across the country, what I call “caring under the microscope,” is actually undermining the righteous goals it seeks to achieve.
I encourage you to try this online. Search for the phrase, “VA under microscope” and see what you get. Briefly read the summary, or the entire story if you have the inclination, and then take a few minutes to reflect on the emotional impact of what you read. Under a microscope is an idiom coined to capture the experience of being the object of close inspection and intense scrutiny. As most everyone knows from their own science education, microscopes magnify images that cannot normally be seen with the human eye, allowing us to observe a more detailed and focused image. The microscope surely helped revolutionize medicine and science. But what effect does such amplified and constant observation have on VA employees?3
For the thousands of staff members who do their job every day with all the empathy and skill, integrity, and dedication they can muster, there is demoralization. Researchers in the health professions describe it as “a feeling state of dejection, hopelessness, and a sense of personal ‘incompetence’ that may be tied to a loss of or threat to one’s own goals or values. It has an existential dimension when beliefs and values about oneself are disconfirmed.”4 If you are a nurse assigned to one of VA’s nursing homes, daily striving to ensure patients are clean and comfortable, or a therapist in a continuing living center using all your training to maximize an elder’s mobility and participation in activities, you might well begin to doubt your ability as a professional and question the worth of your work. This is exactly the opposite outcome that the microscopic oversight is intended to attain.
The impact of demoralization on health professionals directly contributes to unprecedented burnout and turnover. Were this not damaging enough, it also has an insidious rippling effect—like contaminated groundwater that poisons where it should be reviving. The humanistic, even spiritual, heart of all the health professions is the relationship between the practitioner and the patient, ideally a relationship of mutual respect and trust. Waves of negative news triggering harsh and unyielding criticism distort even the strongest, purest therapeutic alliances with fear and distrust, just as a microscope not properly focused changes a beautiful image into a blurred muddle.
Worried families of veterans staring at this picture invariably are drawn into the hyper media focus, feeling alarmed and betrayed, even when their loved one may be receiving excellent VA care. In 20 years as a physician and ethicist in VA hospitals, clinics, and community living centers, I know well that bad things happen to good people (both patients and staff). Yet VA patients, families, and staff are seldom offered the wider corrective vision that would note that bad things also happen in other health care institutions and good care is delivered in the VA. Acting Secretary of Veterans Affairs Peter O’Rourke crisply summarized in his response to the nursing home story.5
No veteran or any other human being in a VA or any other nursing home should ever be medicated into a zombie state or left alone in pain like those patients reported in the news story. And if the USA Today story improves the care of a single VA patient, then good has been done at least in the short run. Yet we must also take the long view and consider the moral and psychological outcome of prolonged demoralization on the very staff who must carry out the congressional mandates.
In the same time frame as the nursing home scandal, the VA Office of Inspector General also issued a report on the continued understaffing in the VA.6 This may be the most concerning aftermath of demoralization. One of my best residents had thought about the VA but in the end made a different choice when he completed his training. When I asked him why he told me, “I am afraid to end up in the newspaper.”
Summer will go by far too quickly. Enjoy it while you can so that with renewed strength we may all search for a better way that the light of truth and heat of power can do what they must while also not withering the spirit of caring that animates the people of the VA.
1. Camus A. O’Brien J, trans. The Myth of Sisyphus and Other Essays. New York, New York: Vintage Books, 1955.
2. Slack D, Estes A. Secret VA nursing home ratings hide poor quality of care from the public. USA Today. June 17, 2018. https://www.usatoday.com/story/news/politics/2018/06/17/secret-va-nursing-home-ratings-hide-poor-quality-care/674829002. Accessed June 25, 2018.
3. Gabel S. Demoralization in health professional practice: development, amelioration, and, implications for continuing education.” J Contin Educ Health Prof. 2013;33(2):118-126.
4. Hanlon A. How the microscope redefined the fact. T he Atlantic. February 11, 2016. https://www.theatlantic.com/technology/archive/2016/02/microscope-history-data/462234. Accessed June 27, 2018.
5. O’Rourke P. VA: USA Today’s article is misleading. USA Today. June 20, 2018. https://www.usatoday.com/story/opinion/2018/06/20/va-usa-today-article-misleading-editorials-debates/36223067. Updated June 21, 2018. Accessed June 27, 2018.
6. US Department of Veterans Affairs, Office of the Inspector General. OIG determination of Veterans Health Administration’s occupational staffing shortages. https://www.va.gov/oig/pubs/VAOIG-18-01693-196.pdf. Published June 14, 2018. Accessed June 25, 2018.
I write this editorial at the end of June as summer officially begins. Much of the country—my New Mexico home included—is suffering under an unbearable heat wave in which even those without belief pray for rain. Summer for many is associated with vacations, family trips, and happy hours in the swimming pool among other enjoyable activities that provide a welcome and much deserved break from routine and relief from the grind of work and school. In the words of the George Gershwin tune, “Summertime, and the livin’ is easy.”
In stark contrast to this season, where there is more lightness in being, is the heaviness of the news reports about the Department of Veteran Affairs (VA) that have been featured in the media and the federal press. I suspect I am not alone in having a hard time opening those e-mails; feeling once more the weight of failure on the VA and the employees who have dedicated a good part of their careers to its mission. Even for the VA, June has seen an exceptional string of bad press. I ask as you read this column to think about what the adjective bad means in this context. In the conclusion to this column, I will suggest that the meaning is multivalent.
Among the most distressing stories was the USA Today and Boston Globe headline, “Secret VA nursing home ratings hide poor quality of care from the public.”2 In an all too predictable sequence, this led justifiably to a cascade of demands from the fifth estate, congressional representatives, the administration, veterans and their families, and watchdog organizations for release of the data, investigation of the allegedly deplorable conditions, and rapid fixes to the problems along with the punishment of the guilty.
As an ethicist I am committed to the principles of transparency and accountability that these entities rightly adjure in the wake of any disclosure of a breach of duty to treat each veteran with the best we have—especially the disabled, elderly, and vulnerable. But I have come to believe that the way in which this cycle of scandal and reaction plays out over and over again in VA facilities across the country, what I call “caring under the microscope,” is actually undermining the righteous goals it seeks to achieve.
I encourage you to try this online. Search for the phrase, “VA under microscope” and see what you get. Briefly read the summary, or the entire story if you have the inclination, and then take a few minutes to reflect on the emotional impact of what you read. Under a microscope is an idiom coined to capture the experience of being the object of close inspection and intense scrutiny. As most everyone knows from their own science education, microscopes magnify images that cannot normally be seen with the human eye, allowing us to observe a more detailed and focused image. The microscope surely helped revolutionize medicine and science. But what effect does such amplified and constant observation have on VA employees?3
For the thousands of staff members who do their job every day with all the empathy and skill, integrity, and dedication they can muster, there is demoralization. Researchers in the health professions describe it as “a feeling state of dejection, hopelessness, and a sense of personal ‘incompetence’ that may be tied to a loss of or threat to one’s own goals or values. It has an existential dimension when beliefs and values about oneself are disconfirmed.”4 If you are a nurse assigned to one of VA’s nursing homes, daily striving to ensure patients are clean and comfortable, or a therapist in a continuing living center using all your training to maximize an elder’s mobility and participation in activities, you might well begin to doubt your ability as a professional and question the worth of your work. This is exactly the opposite outcome that the microscopic oversight is intended to attain.
The impact of demoralization on health professionals directly contributes to unprecedented burnout and turnover. Were this not damaging enough, it also has an insidious rippling effect—like contaminated groundwater that poisons where it should be reviving. The humanistic, even spiritual, heart of all the health professions is the relationship between the practitioner and the patient, ideally a relationship of mutual respect and trust. Waves of negative news triggering harsh and unyielding criticism distort even the strongest, purest therapeutic alliances with fear and distrust, just as a microscope not properly focused changes a beautiful image into a blurred muddle.
Worried families of veterans staring at this picture invariably are drawn into the hyper media focus, feeling alarmed and betrayed, even when their loved one may be receiving excellent VA care. In 20 years as a physician and ethicist in VA hospitals, clinics, and community living centers, I know well that bad things happen to good people (both patients and staff). Yet VA patients, families, and staff are seldom offered the wider corrective vision that would note that bad things also happen in other health care institutions and good care is delivered in the VA. Acting Secretary of Veterans Affairs Peter O’Rourke crisply summarized in his response to the nursing home story.5
No veteran or any other human being in a VA or any other nursing home should ever be medicated into a zombie state or left alone in pain like those patients reported in the news story. And if the USA Today story improves the care of a single VA patient, then good has been done at least in the short run. Yet we must also take the long view and consider the moral and psychological outcome of prolonged demoralization on the very staff who must carry out the congressional mandates.
In the same time frame as the nursing home scandal, the VA Office of Inspector General also issued a report on the continued understaffing in the VA.6 This may be the most concerning aftermath of demoralization. One of my best residents had thought about the VA but in the end made a different choice when he completed his training. When I asked him why he told me, “I am afraid to end up in the newspaper.”
Summer will go by far too quickly. Enjoy it while you can so that with renewed strength we may all search for a better way that the light of truth and heat of power can do what they must while also not withering the spirit of caring that animates the people of the VA.
I write this editorial at the end of June as summer officially begins. Much of the country—my New Mexico home included—is suffering under an unbearable heat wave in which even those without belief pray for rain. Summer for many is associated with vacations, family trips, and happy hours in the swimming pool among other enjoyable activities that provide a welcome and much deserved break from routine and relief from the grind of work and school. In the words of the George Gershwin tune, “Summertime, and the livin’ is easy.”
In stark contrast to this season, where there is more lightness in being, is the heaviness of the news reports about the Department of Veteran Affairs (VA) that have been featured in the media and the federal press. I suspect I am not alone in having a hard time opening those e-mails; feeling once more the weight of failure on the VA and the employees who have dedicated a good part of their careers to its mission. Even for the VA, June has seen an exceptional string of bad press. I ask as you read this column to think about what the adjective bad means in this context. In the conclusion to this column, I will suggest that the meaning is multivalent.
Among the most distressing stories was the USA Today and Boston Globe headline, “Secret VA nursing home ratings hide poor quality of care from the public.”2 In an all too predictable sequence, this led justifiably to a cascade of demands from the fifth estate, congressional representatives, the administration, veterans and their families, and watchdog organizations for release of the data, investigation of the allegedly deplorable conditions, and rapid fixes to the problems along with the punishment of the guilty.
As an ethicist I am committed to the principles of transparency and accountability that these entities rightly adjure in the wake of any disclosure of a breach of duty to treat each veteran with the best we have—especially the disabled, elderly, and vulnerable. But I have come to believe that the way in which this cycle of scandal and reaction plays out over and over again in VA facilities across the country, what I call “caring under the microscope,” is actually undermining the righteous goals it seeks to achieve.
I encourage you to try this online. Search for the phrase, “VA under microscope” and see what you get. Briefly read the summary, or the entire story if you have the inclination, and then take a few minutes to reflect on the emotional impact of what you read. Under a microscope is an idiom coined to capture the experience of being the object of close inspection and intense scrutiny. As most everyone knows from their own science education, microscopes magnify images that cannot normally be seen with the human eye, allowing us to observe a more detailed and focused image. The microscope surely helped revolutionize medicine and science. But what effect does such amplified and constant observation have on VA employees?3
For the thousands of staff members who do their job every day with all the empathy and skill, integrity, and dedication they can muster, there is demoralization. Researchers in the health professions describe it as “a feeling state of dejection, hopelessness, and a sense of personal ‘incompetence’ that may be tied to a loss of or threat to one’s own goals or values. It has an existential dimension when beliefs and values about oneself are disconfirmed.”4 If you are a nurse assigned to one of VA’s nursing homes, daily striving to ensure patients are clean and comfortable, or a therapist in a continuing living center using all your training to maximize an elder’s mobility and participation in activities, you might well begin to doubt your ability as a professional and question the worth of your work. This is exactly the opposite outcome that the microscopic oversight is intended to attain.
The impact of demoralization on health professionals directly contributes to unprecedented burnout and turnover. Were this not damaging enough, it also has an insidious rippling effect—like contaminated groundwater that poisons where it should be reviving. The humanistic, even spiritual, heart of all the health professions is the relationship between the practitioner and the patient, ideally a relationship of mutual respect and trust. Waves of negative news triggering harsh and unyielding criticism distort even the strongest, purest therapeutic alliances with fear and distrust, just as a microscope not properly focused changes a beautiful image into a blurred muddle.
Worried families of veterans staring at this picture invariably are drawn into the hyper media focus, feeling alarmed and betrayed, even when their loved one may be receiving excellent VA care. In 20 years as a physician and ethicist in VA hospitals, clinics, and community living centers, I know well that bad things happen to good people (both patients and staff). Yet VA patients, families, and staff are seldom offered the wider corrective vision that would note that bad things also happen in other health care institutions and good care is delivered in the VA. Acting Secretary of Veterans Affairs Peter O’Rourke crisply summarized in his response to the nursing home story.5
No veteran or any other human being in a VA or any other nursing home should ever be medicated into a zombie state or left alone in pain like those patients reported in the news story. And if the USA Today story improves the care of a single VA patient, then good has been done at least in the short run. Yet we must also take the long view and consider the moral and psychological outcome of prolonged demoralization on the very staff who must carry out the congressional mandates.
In the same time frame as the nursing home scandal, the VA Office of Inspector General also issued a report on the continued understaffing in the VA.6 This may be the most concerning aftermath of demoralization. One of my best residents had thought about the VA but in the end made a different choice when he completed his training. When I asked him why he told me, “I am afraid to end up in the newspaper.”
Summer will go by far too quickly. Enjoy it while you can so that with renewed strength we may all search for a better way that the light of truth and heat of power can do what they must while also not withering the spirit of caring that animates the people of the VA.
1. Camus A. O’Brien J, trans. The Myth of Sisyphus and Other Essays. New York, New York: Vintage Books, 1955.
2. Slack D, Estes A. Secret VA nursing home ratings hide poor quality of care from the public. USA Today. June 17, 2018. https://www.usatoday.com/story/news/politics/2018/06/17/secret-va-nursing-home-ratings-hide-poor-quality-care/674829002. Accessed June 25, 2018.
3. Gabel S. Demoralization in health professional practice: development, amelioration, and, implications for continuing education.” J Contin Educ Health Prof. 2013;33(2):118-126.
4. Hanlon A. How the microscope redefined the fact. T he Atlantic. February 11, 2016. https://www.theatlantic.com/technology/archive/2016/02/microscope-history-data/462234. Accessed June 27, 2018.
5. O’Rourke P. VA: USA Today’s article is misleading. USA Today. June 20, 2018. https://www.usatoday.com/story/opinion/2018/06/20/va-usa-today-article-misleading-editorials-debates/36223067. Updated June 21, 2018. Accessed June 27, 2018.
6. US Department of Veterans Affairs, Office of the Inspector General. OIG determination of Veterans Health Administration’s occupational staffing shortages. https://www.va.gov/oig/pubs/VAOIG-18-01693-196.pdf. Published June 14, 2018. Accessed June 25, 2018.
1. Camus A. O’Brien J, trans. The Myth of Sisyphus and Other Essays. New York, New York: Vintage Books, 1955.
2. Slack D, Estes A. Secret VA nursing home ratings hide poor quality of care from the public. USA Today. June 17, 2018. https://www.usatoday.com/story/news/politics/2018/06/17/secret-va-nursing-home-ratings-hide-poor-quality-care/674829002. Accessed June 25, 2018.
3. Gabel S. Demoralization in health professional practice: development, amelioration, and, implications for continuing education.” J Contin Educ Health Prof. 2013;33(2):118-126.
4. Hanlon A. How the microscope redefined the fact. T he Atlantic. February 11, 2016. https://www.theatlantic.com/technology/archive/2016/02/microscope-history-data/462234. Accessed June 27, 2018.
5. O’Rourke P. VA: USA Today’s article is misleading. USA Today. June 20, 2018. https://www.usatoday.com/story/opinion/2018/06/20/va-usa-today-article-misleading-editorials-debates/36223067. Updated June 21, 2018. Accessed June 27, 2018.
6. US Department of Veterans Affairs, Office of the Inspector General. OIG determination of Veterans Health Administration’s occupational staffing shortages. https://www.va.gov/oig/pubs/VAOIG-18-01693-196.pdf. Published June 14, 2018. Accessed June 25, 2018.

Do carbs drive obesity? With evidence inconclusive, debate continues
While the debate continues, David S. Ludwig, MD, PhD, and Cara B. Ebbeling, PhD, argued in a recent clinical review that diet does indeed affect metabolism and body composition.
While evidence from human studies remains limited, animal research findings are consistent with a carbohydrate-insulin model of obesity, according to Dr. Ludwig and Dr. Ebbeling, who are with the New Balance Foundation Obesity Prevention Center at Boston Children’s Hospital and Harvard Medical School.
The carbohydrate-insulin model holds that eating processed, high–glycemic load carbohydrates causes hormonal changes that promote calorie deposition in fat tissue, aggravate hunger, and reduce energy expenditure, they said in JAMA Internal Medicine.
“The conventional way of thinking assumes that the individual has primary control over their calorie balance, and thus, bases conventional treatment on a target of establishing a negative energy balance – so that is 1,000 variations of the ‘eat less, move more’ recommendation,” Dr. Ludwig said in an interview.
The alternative to that established view has proven controversial. The Endocrine Society, in a recent scientific statement, said diet’s effect on obesity risk is largely explainable by calorie intake, rather than some special adverse effect on internal metabolism or energy expenditure.
“Stated differently, ‘a calorie is a calorie,’ ” the authors of the scientific statement said. “Thus, habitual consumption of highly palatable and energy-dense diets predispose to excess weight gain irrespective of macronutrient content.”
Others have sought to refute the carbohydrate-insulin hypothesis in recent reviews, such as an invited commentary in JAMA Internal Medicine by Kevin D. Hall, PhD, of the National Institute of Diabetes and Digestive and Kidney Diseases, and his coauthors.
“Although it is plausible that variables related to insulin signaling could be involved in obesity pathogenesis, the hypothesis that carbohydrate-stimulated insulin secretion is the primary cause of common obesity via direct effects on adipocytes is difficult to reconcile with current evidence,” Dr. Hall and his coauthors wrote in the commentary (JAMA Intern Med. 2018 Jul 2. doi: 10.1001/jamainternmed.2018.2920).
The conventional calorie balance model is a “straw man” that omits neuroendocrine mechanisms known to regulate homeostasis, added Dr. Hall and his coauthors, stating that accurate models of obesity should include physiological processes resisting weight loss and promoting weight gain.
“They might claim that this is a straw man argument, but I would claim that there is a case of the emperor’s new clothing,” Dr. Ludwig countered in the interview. “They argue that body weight is controlled by biology, and that that’s recognized in the conventional view, but how does that view inform treatment in any way? In the absence of any specific testable hypotheses for why the obesity epidemic has emerged so suddenly, conventional recommendations inevitably resort to advice to ‘eat less and move more.’ ”
Dr. Ludwig and Dr. Ebbeling have both conducted research studies examining the carbohydrate-insulin model, or the view that a high-carbohydrate diet results in postprandial hyperinsulinemia and promotes deposition of calories in adipocytes, leading to weight gain through slowing metabolism, increased hunger, or both.
In a study published in the Lancet, Dr. Ludwig and his coinvestigators found that rats fed a high–glycemic index (GI) diet for 18 weeks had more body fat (97.8 grams vs. 57.3 grams; P = .0152) and less lean body mass versus rats fed a low-GI diet. Rats on the high-GI diet also had greater increases over time in blood glucose and plasma insulin after oral glucose. Similarly, mice on a high-GI diet had nearly twice the body fat of mice on low-GI diet, after 9 weeks of feeding (Lancet. 2004 Aug 28. doi: 10.1016/S0140-6736(04)16937-7).
“There’s no way to explain that finding in view of the conventional view that all calories are alike to the body,” Dr. Ludwig said.
“Contrary to prediction of the conventional model, the inherently lower energy density of low-fat diets does not spontaneously produce sustained weight loss. In fact, several recent meta-analyses found that low-fat diets are inferior to all higher-fat [and thus low-glycemic] comparisons. However, these studies characteristically rely on dietary counseling, a method with limitations for testing mechanistic hypotheses owing to varying levels of noncompliance over the long-term,” Dr. Ludwig and Dr. Ebbeling wrote.
Criticisms that claim to refute the carbohydrate-insulin hypothesis are based in part on misinterpretation of recent feeding studies, according to Dr. Ludwig and Dr. Ebbeling. Multiple studies testing whether or not high–glycemic load meals lead to increased fat storage have reported no meaningful differences between low-fat and low-carbohydrate diets. However, these short-term studies, mostly 2 weeks in duration, preclude definitive findings, according to the review.
That’s because the process of adapting to a high-fat diet after having consumed a high-carbohydrate diet takes weeks, which is a well-recognized phenomenon, Dr. Ludwig said.
“If you put sedentary people into military boot camp and tested their biological state after 6 days, you’d probably find that they were fatigued, weak, and had higher inflammation in their muscles, but clearly, you wouldn’t conclude that fitness training is bad for your health,” he said in the interview. “But yet, these are the sort of data that are being used to ‘falsify’ the carbohydrate-insulin model.
“We acknowledge that there aren’t definitive human data,” he continued, “but the conventional model has failed to both explain the obesity epidemic and control it, and the latest public health data suggests that rates are higher today than ever before, despite 50 years of focusing on calorie balance.”
SOURCE: Ludwig DS et al. JAMA Intern Med. 2018 Jul 2. doi:10.1001/jamainternmed.2018.2933.
While the debate continues, David S. Ludwig, MD, PhD, and Cara B. Ebbeling, PhD, argued in a recent clinical review that diet does indeed affect metabolism and body composition.
While evidence from human studies remains limited, animal research findings are consistent with a carbohydrate-insulin model of obesity, according to Dr. Ludwig and Dr. Ebbeling, who are with the New Balance Foundation Obesity Prevention Center at Boston Children’s Hospital and Harvard Medical School.
The carbohydrate-insulin model holds that eating processed, high–glycemic load carbohydrates causes hormonal changes that promote calorie deposition in fat tissue, aggravate hunger, and reduce energy expenditure, they said in JAMA Internal Medicine.
“The conventional way of thinking assumes that the individual has primary control over their calorie balance, and thus, bases conventional treatment on a target of establishing a negative energy balance – so that is 1,000 variations of the ‘eat less, move more’ recommendation,” Dr. Ludwig said in an interview.
The alternative to that established view has proven controversial. The Endocrine Society, in a recent scientific statement, said diet’s effect on obesity risk is largely explainable by calorie intake, rather than some special adverse effect on internal metabolism or energy expenditure.
“Stated differently, ‘a calorie is a calorie,’ ” the authors of the scientific statement said. “Thus, habitual consumption of highly palatable and energy-dense diets predispose to excess weight gain irrespective of macronutrient content.”
Others have sought to refute the carbohydrate-insulin hypothesis in recent reviews, such as an invited commentary in JAMA Internal Medicine by Kevin D. Hall, PhD, of the National Institute of Diabetes and Digestive and Kidney Diseases, and his coauthors.
“Although it is plausible that variables related to insulin signaling could be involved in obesity pathogenesis, the hypothesis that carbohydrate-stimulated insulin secretion is the primary cause of common obesity via direct effects on adipocytes is difficult to reconcile with current evidence,” Dr. Hall and his coauthors wrote in the commentary (JAMA Intern Med. 2018 Jul 2. doi: 10.1001/jamainternmed.2018.2920).
The conventional calorie balance model is a “straw man” that omits neuroendocrine mechanisms known to regulate homeostasis, added Dr. Hall and his coauthors, stating that accurate models of obesity should include physiological processes resisting weight loss and promoting weight gain.
“They might claim that this is a straw man argument, but I would claim that there is a case of the emperor’s new clothing,” Dr. Ludwig countered in the interview. “They argue that body weight is controlled by biology, and that that’s recognized in the conventional view, but how does that view inform treatment in any way? In the absence of any specific testable hypotheses for why the obesity epidemic has emerged so suddenly, conventional recommendations inevitably resort to advice to ‘eat less and move more.’ ”
Dr. Ludwig and Dr. Ebbeling have both conducted research studies examining the carbohydrate-insulin model, or the view that a high-carbohydrate diet results in postprandial hyperinsulinemia and promotes deposition of calories in adipocytes, leading to weight gain through slowing metabolism, increased hunger, or both.
In a study published in the Lancet, Dr. Ludwig and his coinvestigators found that rats fed a high–glycemic index (GI) diet for 18 weeks had more body fat (97.8 grams vs. 57.3 grams; P = .0152) and less lean body mass versus rats fed a low-GI diet. Rats on the high-GI diet also had greater increases over time in blood glucose and plasma insulin after oral glucose. Similarly, mice on a high-GI diet had nearly twice the body fat of mice on low-GI diet, after 9 weeks of feeding (Lancet. 2004 Aug 28. doi: 10.1016/S0140-6736(04)16937-7).
“There’s no way to explain that finding in view of the conventional view that all calories are alike to the body,” Dr. Ludwig said.
“Contrary to prediction of the conventional model, the inherently lower energy density of low-fat diets does not spontaneously produce sustained weight loss. In fact, several recent meta-analyses found that low-fat diets are inferior to all higher-fat [and thus low-glycemic] comparisons. However, these studies characteristically rely on dietary counseling, a method with limitations for testing mechanistic hypotheses owing to varying levels of noncompliance over the long-term,” Dr. Ludwig and Dr. Ebbeling wrote.
Criticisms that claim to refute the carbohydrate-insulin hypothesis are based in part on misinterpretation of recent feeding studies, according to Dr. Ludwig and Dr. Ebbeling. Multiple studies testing whether or not high–glycemic load meals lead to increased fat storage have reported no meaningful differences between low-fat and low-carbohydrate diets. However, these short-term studies, mostly 2 weeks in duration, preclude definitive findings, according to the review.
That’s because the process of adapting to a high-fat diet after having consumed a high-carbohydrate diet takes weeks, which is a well-recognized phenomenon, Dr. Ludwig said.
“If you put sedentary people into military boot camp and tested their biological state after 6 days, you’d probably find that they were fatigued, weak, and had higher inflammation in their muscles, but clearly, you wouldn’t conclude that fitness training is bad for your health,” he said in the interview. “But yet, these are the sort of data that are being used to ‘falsify’ the carbohydrate-insulin model.
“We acknowledge that there aren’t definitive human data,” he continued, “but the conventional model has failed to both explain the obesity epidemic and control it, and the latest public health data suggests that rates are higher today than ever before, despite 50 years of focusing on calorie balance.”
SOURCE: Ludwig DS et al. JAMA Intern Med. 2018 Jul 2. doi:10.1001/jamainternmed.2018.2933.
While the debate continues, David S. Ludwig, MD, PhD, and Cara B. Ebbeling, PhD, argued in a recent clinical review that diet does indeed affect metabolism and body composition.
While evidence from human studies remains limited, animal research findings are consistent with a carbohydrate-insulin model of obesity, according to Dr. Ludwig and Dr. Ebbeling, who are with the New Balance Foundation Obesity Prevention Center at Boston Children’s Hospital and Harvard Medical School.
The carbohydrate-insulin model holds that eating processed, high–glycemic load carbohydrates causes hormonal changes that promote calorie deposition in fat tissue, aggravate hunger, and reduce energy expenditure, they said in JAMA Internal Medicine.
“The conventional way of thinking assumes that the individual has primary control over their calorie balance, and thus, bases conventional treatment on a target of establishing a negative energy balance – so that is 1,000 variations of the ‘eat less, move more’ recommendation,” Dr. Ludwig said in an interview.
The alternative to that established view has proven controversial. The Endocrine Society, in a recent scientific statement, said diet’s effect on obesity risk is largely explainable by calorie intake, rather than some special adverse effect on internal metabolism or energy expenditure.
“Stated differently, ‘a calorie is a calorie,’ ” the authors of the scientific statement said. “Thus, habitual consumption of highly palatable and energy-dense diets predispose to excess weight gain irrespective of macronutrient content.”
Others have sought to refute the carbohydrate-insulin hypothesis in recent reviews, such as an invited commentary in JAMA Internal Medicine by Kevin D. Hall, PhD, of the National Institute of Diabetes and Digestive and Kidney Diseases, and his coauthors.
“Although it is plausible that variables related to insulin signaling could be involved in obesity pathogenesis, the hypothesis that carbohydrate-stimulated insulin secretion is the primary cause of common obesity via direct effects on adipocytes is difficult to reconcile with current evidence,” Dr. Hall and his coauthors wrote in the commentary (JAMA Intern Med. 2018 Jul 2. doi: 10.1001/jamainternmed.2018.2920).
The conventional calorie balance model is a “straw man” that omits neuroendocrine mechanisms known to regulate homeostasis, added Dr. Hall and his coauthors, stating that accurate models of obesity should include physiological processes resisting weight loss and promoting weight gain.
“They might claim that this is a straw man argument, but I would claim that there is a case of the emperor’s new clothing,” Dr. Ludwig countered in the interview. “They argue that body weight is controlled by biology, and that that’s recognized in the conventional view, but how does that view inform treatment in any way? In the absence of any specific testable hypotheses for why the obesity epidemic has emerged so suddenly, conventional recommendations inevitably resort to advice to ‘eat less and move more.’ ”
Dr. Ludwig and Dr. Ebbeling have both conducted research studies examining the carbohydrate-insulin model, or the view that a high-carbohydrate diet results in postprandial hyperinsulinemia and promotes deposition of calories in adipocytes, leading to weight gain through slowing metabolism, increased hunger, or both.
In a study published in the Lancet, Dr. Ludwig and his coinvestigators found that rats fed a high–glycemic index (GI) diet for 18 weeks had more body fat (97.8 grams vs. 57.3 grams; P = .0152) and less lean body mass versus rats fed a low-GI diet. Rats on the high-GI diet also had greater increases over time in blood glucose and plasma insulin after oral glucose. Similarly, mice on a high-GI diet had nearly twice the body fat of mice on low-GI diet, after 9 weeks of feeding (Lancet. 2004 Aug 28. doi: 10.1016/S0140-6736(04)16937-7).
“There’s no way to explain that finding in view of the conventional view that all calories are alike to the body,” Dr. Ludwig said.
“Contrary to prediction of the conventional model, the inherently lower energy density of low-fat diets does not spontaneously produce sustained weight loss. In fact, several recent meta-analyses found that low-fat diets are inferior to all higher-fat [and thus low-glycemic] comparisons. However, these studies characteristically rely on dietary counseling, a method with limitations for testing mechanistic hypotheses owing to varying levels of noncompliance over the long-term,” Dr. Ludwig and Dr. Ebbeling wrote.
Criticisms that claim to refute the carbohydrate-insulin hypothesis are based in part on misinterpretation of recent feeding studies, according to Dr. Ludwig and Dr. Ebbeling. Multiple studies testing whether or not high–glycemic load meals lead to increased fat storage have reported no meaningful differences between low-fat and low-carbohydrate diets. However, these short-term studies, mostly 2 weeks in duration, preclude definitive findings, according to the review.
That’s because the process of adapting to a high-fat diet after having consumed a high-carbohydrate diet takes weeks, which is a well-recognized phenomenon, Dr. Ludwig said.
“If you put sedentary people into military boot camp and tested their biological state after 6 days, you’d probably find that they were fatigued, weak, and had higher inflammation in their muscles, but clearly, you wouldn’t conclude that fitness training is bad for your health,” he said in the interview. “But yet, these are the sort of data that are being used to ‘falsify’ the carbohydrate-insulin model.
“We acknowledge that there aren’t definitive human data,” he continued, “but the conventional model has failed to both explain the obesity epidemic and control it, and the latest public health data suggests that rates are higher today than ever before, despite 50 years of focusing on calorie balance.”
SOURCE: Ludwig DS et al. JAMA Intern Med. 2018 Jul 2. doi:10.1001/jamainternmed.2018.2933.
FROM JAMA INTERNAL MEDICINE
Diet and Dermatology: Google Search Results for Acne, Psoriasis, and Eczema
Researching medical information currently is the third most common use of the Internet in the United States,1 with the majority of adults using the Web as their first source for health information before seeing a physician.2 When assessing health-related information online, resources can be grouped into 4 categories: (1) those attributed to self-proclaimed experts, (2) promotional, (3) social media, and (4) educational.3 Access to such a wide range of sources may give readers the opportunity to share personal anecdotes and opinions, thereby serving as a forum for information that essentially cannot be validated. Although such websites may include useful information and cite current literature, in other instances health-related information may be misleading or fabricated.3
In a study evaluating 291 skin conditions and related Google trends, acne, psoriasis, and eczema were among the most burdensome diseases, with acne yielding the highest number of search results.4 Results of the study indicated a positive correlation between disease burden and online search interest.4 The impact of these online searches and the validity of Google search results are topics worth considering, as more dermatology patients are relying on holistic and nonpharmaceutical approaches to treatment and disease management.5 The purpose of this study was to evaluate content on diet and dermatology available on the Internet for acne, psoriasis, and eczema.
Methods
Google searches were performed in December 2017 using the terms diet and acne, diet and psoriasis, and diet and eczema. The first 10 results for each respective search were reviewed for recommendations about which foods to incorporate in the diet and which to avoid. They also were classified according to the following 4 website categories: (1) those attributed to self-proclaimed experts, (2) promotional, (3) social media, and (4) educational. The recommendations gathered from the 30 websites were then compared to the current literature assessing the impact of diet on these respective conditions by conducting PubMed searches of articles indexed for MEDLINE using the same terms.
Results
The results of this study are outlined in the eTable.

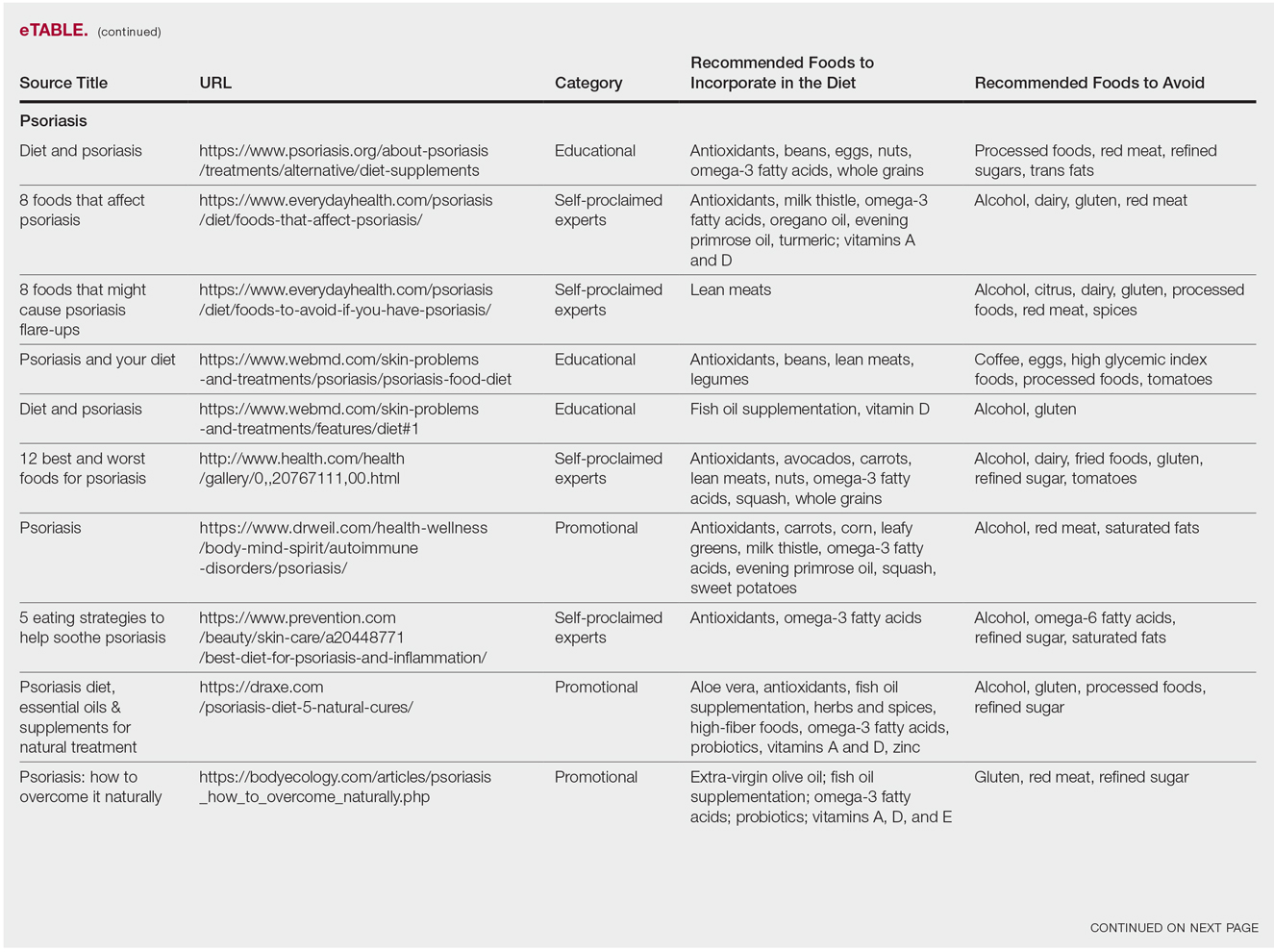
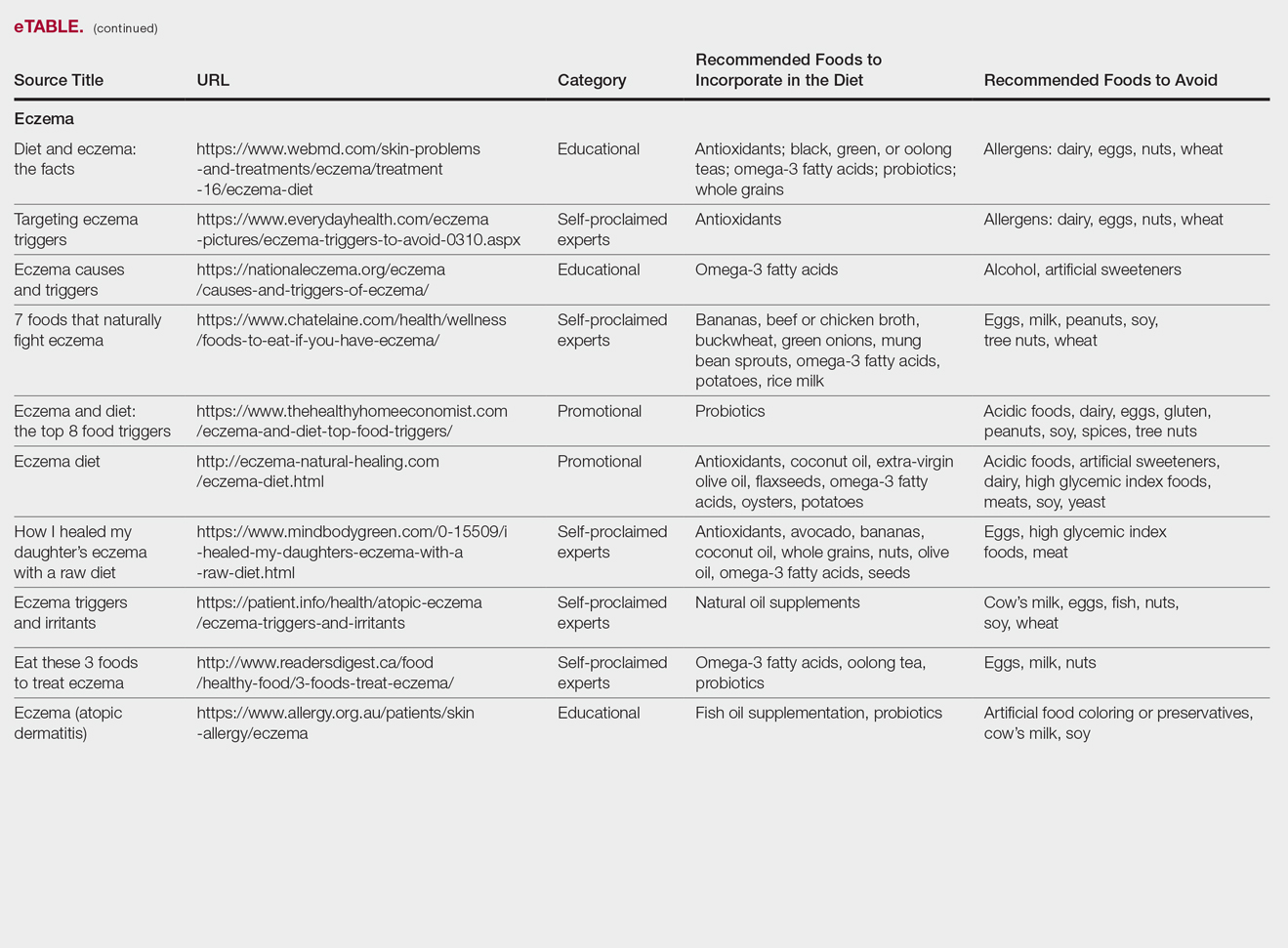
Acne
Our Google search using the term diet and acne produced 17,500,000 results. Of the first 10 search results, 40% (4/10) were websites attributed to self-proclaimed experts, 40% (4/10) were educational resources, and 20% (2/10) were promotional websites. Most of the websites advised acne patients to avoid high glycemic index foods (90% [9/10]) and dairy products (90% [9/10]). When discussing which foods to include in the diet, 70% (7/10) of websites recommended that patients incorporate omega-3 fatty acids and antioxidants in the diet.
Research has shown that a low glycemic index diet can lead to a decrease in patients’ acne lesion counts in some instances.6,7 In a case-controlled study of 2258 patients on a popular weight loss diet that emphasized low glycemic index foods, 87% of participants reported a reduction in acne and 91% reported a decrease in their dosage or number of acne medications.7 Still, the exact correlation between acne development and consumption of glycemic index foods has not been confirmed. However, high glycemic index diets have been linked to hyperinsulinemia, indicating that insulin levels may play a role in acne formation.8 The majority of other currently available studies evaluated the potential link between dairy consumption and acne. A retrospective analysis of 47,355 women spanning 12 weeks showed a positive link between increased dairy consumption, specifically skim milk, and acne formation. Despite the positive trend, limitations such as recall bias made it difficult to draw a conclusion based on these findings.9 However, results of a longitudinal questionnaire-based population study evaluating the impact of dairy consumption on acne in 2489 adolescent patients confirmed a positive correlation.10 Studies conducted in 2009 and 2011 concluded that milk consumption results in elevated insulinlike growth factor 1 levels, which were linked to comedogenesis.8,11
Currently, there are well-described mechanisms to explain the association of dairy consumption and glycemic index with acne. Confirming a correlation between acne development and dairy consumption suggests that a dairy-free diet may benefit acne patients.5 Other trials indicate that low glycemic index diets are beneficial in treating acne.6,7 Therefore, some of the recommendations made in our search results may be of merit; however, there is minimal evidence proving the benefits of the other dietary recommendations made in the websites we evaluated.
Psoriasis
Our Google search using the term diet and psoriasis yielded a total of 9,420,000 results. Of the first 10 search results, 40% (4/10) were websites attributed to self-proclaimed experts, 30% (3/10) were promotional, and 30% (3/10) were educational. Seventy percent (7/10) of websites recommended avoiding alcohol and 60% (6/10) recommended avoiding gluten, with others discouraging consumption of red meat. Most of the websites encouraged patients to consume omega-3 fatty acids and antioxidants, while a few also recommended vitamins A, D, and E, as well as evening primrose oil supplements.
Although current research indicates a positive correlation between excessive alcohol use and psoriasis severity, it is still unclear whether alcohol consumption can be directly linked to the disease.12-14 Likewise, despite belief that increased oxidative stress likely contributes to inflammation in psoriasis, there is little evidence linking antioxidants to improvement in psoriasis symptoms.12 However, the current literature is inconsistent regarding the effects of fish oil supplementation on psoriasis.12 In a randomized double-blind study of 145 patients, there was no significant difference in psoriasis area and severity index scores between a control group and a treatment group receiving fish oil supplementation.15 In another RCT of 45 participants, those given daily very long-chain omega-3 fatty acid supplements saw no difference in psoriasis symptoms.15 Despite debate, literature assessing the impact of gluten-free diets has described improvement in psoriasis lesions in patients with celiac-specific antibodies.16 Although some observational studies described vitamin D supplementation to be beneficial in the treatment of psoriatic lesions, a more recent RCT found no significant difference between control and treatment groups.17-19
Studies also have revealed that certain eating patterns, such as those associated with the Mediterranean diet that is rich in fruits, vegetables, whole grains, and omega-3 fatty acids may be linked to improved endothelial function scores and reduced C-reactive protein and IL-18levels.20,21 In a double-blind RCT of 75 patients with plaque psoriasis, mean (SD) psoriasis area and severity index scores decreased by 11.2 (9.8) in a group treated with omega-3 fatty acids compared to 7.5 (8.8) with omega-6 fatty acids (P=.048).22
Although excessive alcohol use may be linked to psoriasis, there is no conclusive evidence indicating causation, thereby discrediting online claims.12-14 Research has revealed that gluten-free diets in psoriasis patients with celiac disease may improve psoriasis treatment16; however, sufficient evidence is lacking for diets low in gluten and high in polyunsaturated fatty acids or antioxidant supplementation. Of the dietary supplements recommended in the search results we reviewed, fish oil appears to be the most promising, but no recommendations can be made based on the current research.
Eczema
Our Google search using the term diet and eczema yielded 1,160,000 results, with 50% (5/10) of websites attributed to self-proclaimed experts, 30% (3/10) to educational websites, and 20% (2/10) to promotional sites. Of the first 10 results, 80% (8/10) recommended that patients with eczema avoid milk/dairy and 50% (5/10) advised to avoid soy and wheat/gluten. Other websites indicated to avoid eggs, nuts, and artificial sweeteners. Patients were encouraged to incorporate omega-3 fatty acids in their diets, and a few sites recommended bananas, coconut oil, olive oil, and various teas.
In a review of 11 studies with a total of 596 participants, supplementation with vitamins D and E, fish oil, olive oil, and linoleic acid was evaluated for the treatment of eczema.23 Although results indicated modest improvement of eczema severity with supplementation of fish oil, evidence favoring this treatment is limited and unconvincing. Furthermore, some evidence indicates that elimination diets are only appropriate for patients with food allergies.24 In a study evaluating an egg-free and dairy-free diet for eczema patients, only participants with positive egg-specific serum IgE levels saw improvement in disease severity.23 Even though IgE-mediated food allergies have been reported in 40% of children with moderate eczema, the contribution of these allergies to eczema is questionable.25
There is little evidence in the literature to indicate a definitive correlation between the foods mentioned in the search results we evaluated and the development of eczema; however, for patients with food allergies and eczema, elimination diets may decrease disease severity.25,26 There is insufficient evidence to suggest a benefit from evening primrose oil or fish oil supplementation, thereby debunking claims found online.
Comment
Although our Google search results included a wide range of sources and information regarding diet and dermatologic conditions such as acne, psoriasis, and eczema, most of the information we found was either unfounded or misleading. Study limitations in the current literature include small sample size, potential recall bias, lack of appropriate controls, incomplete reported results, and the failure to clearly define skin changes.
When considering the accuracy and type of information regarding skin conditions that is available on the Internet, it is important to note that most of the results we reviewed were webpages attributed to self-proclaimed experts. Although educational websites also were included in the search results, whether or not patients prefer or understand the content of such websites is still unknown; therefore, health organizations should consider revising online patient education materials to allow universal comprehension.27
Furthermore, it is important to consider the impact that widespread Internet access may have on the physician-patient relationship. Having access to health-related information online and being able to potentially self-diagnose could delay or deter patients from seeking professional advice or care.3 A study evaluating the impact of online searches on the physician-patient relationship among 175 patients determined that 36.5% of patients gathered information online prior to their consultation with a physician, while 67.3% chose to complement the information given to them by their physician with online resources.28 Based on these statistics, it is important that physicians be up-to-date with Internet discourse to discredit unfounded recommendations. Ultimately, when it comes to diet and dermatology, patients ought to be skeptical of the information currently available on the Internet, given that most of it is unsubstantiated by medical research.
- Fox S. Online health search 2006. Pew Research Center website. http://www.pewinternet.org/2006/10/29/online-health-search-2006/. Published October 29, 2006. Accessed May 3, 2018.
- Prestin A, Vieux SN, Chou WY. Is online health activity alive and well or flatlining? findings from 10 years of the health information national trends survey. J Health Commun. 2015;20:790-798.
- Zeichner JA, Del Rosso JQ. Acne and the internet. Dermatol Clin. 2016;34:129-132.
- Whitsitt J, Karimkhani C, Boyers LN, et al. Comparing burden of dermatologic disease to search interest on Google trends. Dermatol Online J. 2015;21. pii:13030/qt5xg811qp.
- Shokeen D. Influence of diet in acne vulgaris and atopic dermatitis. Cutis. 2016;98:E28-E29.
- Veith WB, Silverberg NB. The association of acne vulgaris with diet. Cutis. 2011;88:84-91.
- Rouhani P. Acne improves with a popular, low glycemic diet from South Beach. J Am Acad Dermatol. 2009;60(3, suppl 1):P706.
- Melnick BC. Evidence for acne-promoting effect of milk and other insulinotropic dairy products. Nestle Nutr Worksop Ser Pediatr Program. 2011;67:131-145.
- Adebamowo CA, Spiegelman D, Berkey CS, et al. High school dietary diary intake and teenage acne. J Am Acad Dermatol. 2005;52:207-214.
- Ulvestad M, Bjertness E, Dalgard F, et al. Acne and dairy products in adolescence: results from a Norwegian longitudinal study [published online July 16, 2016]. J Eur Acad Dermatol Venereol. 2017;31:530-535.
- Melnick BC, Schmitz G. Role of insulin, insulin like growth factor 1, hyperglycemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009;18:833-841.
- Murzaku EC, Bronsnick T, Rao BK. Diet in dermatology: part II. melanoma, chronic urticaria, and psoriasis. J Am Acad Dermatol. 2014;71:1053.E1-1053.E16.
- Tobin AM, Higgins EM, Norris S, et al. Prevalence of psoriasis in patients with alcoholic liver disease. Clin Exp Dermatol. 2009;34:698-701.
- Kirby B, Richards HL, Mason DL, et al. Alcohol consumption and psychological distress in patients with psoriasis. Br J Dermatol. 2008;158:138-140.
- Søyland E, Funk J, Rajika G, et al. Effect of dietary supplementation with very long-chain n-3 fatty acids in patients with psoriasis. N Engl J Med. 1993;328:1812-1816.
- Michaëlsson G, Gerdén B, Hagforsen E, et al. Psoriasis patients with antibodies to gliadin can be improved by a gluten-free diet. Br J Dermatol. 2000;142:44-51.
- Morimoto S, Yoshikawa K. Psoriasis and vitamin D3. a review of our experience. Arch Dermatol. 1989;125:231-234.
- Smith EL, Pincus SH, Donovan L, et al. A novel approach for the evaluation and treatment of psoriasis. oral or topical use of 1,25-dihydroxyvitamin D3 can be a safe and effective therapy for psoriasis. J Am Acad Dermatol. 1988;19:516-528.
- Siddiqui MA, Al-Khawajah MM. Vitamin D3 and psoriasis: a randomized double-blind placebo-controlled study. J Dermatol Treat. 1990;1:243-245.
- Wang Y, Gao H, Loyd CM, et al. Chronic skin-specific inflammation promotes vascular inflammation and thrombosis. J Invest Dermatol. 2012;132:2067-2075.
- Barrea L, Nappi F, Di Somma C, et al. Environmental risk factors in psoriasis: the point of view of the nutritionist. Int J Environ Res Public Health. 2016;13. pii:E743. doi:10.3390/ijerph13070743.
- Mayser P, Mrowietz U, Arenberger P, et al. Omega-3 fatty acid-based lipid infusion in patients with chronic plaque psoriasis: results of a double-blind, randomized, placebo-controlled, multicenter trial. J Am Acad Dermatol. 1998;38:539-547.
- Bath-Hextall FJ, Jenkinson C, Humphreys R, et al. Dietary supplements for established atopic eczema. Cochrane Database Syst Rev. 2012;2:CD005205.
- Bronsnick T, Murzaku EC, Rao BK. Diet in dermatology: part I. atopic dermatitis, acne, and nonmelanoma skin cancer [published online November 15, 2014]. J Am Acad Dermatol. 2014;71:1039.E1-1039.E12.
- Campbell DE. The role of food allergy in childhood atopic dermatitis. J Paediatr Child Health. 2012;48:1058-1064.
- Werfel T, Erdmann S, Fuchs T, et al. Approach to suspected food allergy in atopic dermatitis. guideline of the Task Force on Food Allergy of the German Society of Allergology and Clinical Immunology (DGAKI) and the Medical Association of German Allergologists (ADA) and the German Society of Pediatric Allergology (GPA). J Dtsch Dermatol Ges. 2009;3:265-271.
- John AM, John ES, Hansberry DR, et al. Assessment of online patient education materials from major dermatologic associations. J Clin Aesthet Dermatol. 2016;9:23-28.
- Orgaz-Molina J, Cotugno M, Girón-Prieto MS, et al. A study of internet searches for medical information in dermatology patients: the patient-physician relationship. Actas Dermosifiliogr. 2015;106:493-499.
Researching medical information currently is the third most common use of the Internet in the United States,1 with the majority of adults using the Web as their first source for health information before seeing a physician.2 When assessing health-related information online, resources can be grouped into 4 categories: (1) those attributed to self-proclaimed experts, (2) promotional, (3) social media, and (4) educational.3 Access to such a wide range of sources may give readers the opportunity to share personal anecdotes and opinions, thereby serving as a forum for information that essentially cannot be validated. Although such websites may include useful information and cite current literature, in other instances health-related information may be misleading or fabricated.3
In a study evaluating 291 skin conditions and related Google trends, acne, psoriasis, and eczema were among the most burdensome diseases, with acne yielding the highest number of search results.4 Results of the study indicated a positive correlation between disease burden and online search interest.4 The impact of these online searches and the validity of Google search results are topics worth considering, as more dermatology patients are relying on holistic and nonpharmaceutical approaches to treatment and disease management.5 The purpose of this study was to evaluate content on diet and dermatology available on the Internet for acne, psoriasis, and eczema.
Methods
Google searches were performed in December 2017 using the terms diet and acne, diet and psoriasis, and diet and eczema. The first 10 results for each respective search were reviewed for recommendations about which foods to incorporate in the diet and which to avoid. They also were classified according to the following 4 website categories: (1) those attributed to self-proclaimed experts, (2) promotional, (3) social media, and (4) educational. The recommendations gathered from the 30 websites were then compared to the current literature assessing the impact of diet on these respective conditions by conducting PubMed searches of articles indexed for MEDLINE using the same terms.
Results
The results of this study are outlined in the eTable.
Acne
Our Google search using the term diet and acne produced 17,500,000 results. Of the first 10 search results, 40% (4/10) were websites attributed to self-proclaimed experts, 40% (4/10) were educational resources, and 20% (2/10) were promotional websites. Most of the websites advised acne patients to avoid high glycemic index foods (90% [9/10]) and dairy products (90% [9/10]). When discussing which foods to include in the diet, 70% (7/10) of websites recommended that patients incorporate omega-3 fatty acids and antioxidants in the diet.
Research has shown that a low glycemic index diet can lead to a decrease in patients’ acne lesion counts in some instances.6,7 In a case-controlled study of 2258 patients on a popular weight loss diet that emphasized low glycemic index foods, 87% of participants reported a reduction in acne and 91% reported a decrease in their dosage or number of acne medications.7 Still, the exact correlation between acne development and consumption of glycemic index foods has not been confirmed. However, high glycemic index diets have been linked to hyperinsulinemia, indicating that insulin levels may play a role in acne formation.8 The majority of other currently available studies evaluated the potential link between dairy consumption and acne. A retrospective analysis of 47,355 women spanning 12 weeks showed a positive link between increased dairy consumption, specifically skim milk, and acne formation. Despite the positive trend, limitations such as recall bias made it difficult to draw a conclusion based on these findings.9 However, results of a longitudinal questionnaire-based population study evaluating the impact of dairy consumption on acne in 2489 adolescent patients confirmed a positive correlation.10 Studies conducted in 2009 and 2011 concluded that milk consumption results in elevated insulinlike growth factor 1 levels, which were linked to comedogenesis.8,11
Currently, there are well-described mechanisms to explain the association of dairy consumption and glycemic index with acne. Confirming a correlation between acne development and dairy consumption suggests that a dairy-free diet may benefit acne patients.5 Other trials indicate that low glycemic index diets are beneficial in treating acne.6,7 Therefore, some of the recommendations made in our search results may be of merit; however, there is minimal evidence proving the benefits of the other dietary recommendations made in the websites we evaluated.
Psoriasis
Our Google search using the term diet and psoriasis yielded a total of 9,420,000 results. Of the first 10 search results, 40% (4/10) were websites attributed to self-proclaimed experts, 30% (3/10) were promotional, and 30% (3/10) were educational. Seventy percent (7/10) of websites recommended avoiding alcohol and 60% (6/10) recommended avoiding gluten, with others discouraging consumption of red meat. Most of the websites encouraged patients to consume omega-3 fatty acids and antioxidants, while a few also recommended vitamins A, D, and E, as well as evening primrose oil supplements.
Although current research indicates a positive correlation between excessive alcohol use and psoriasis severity, it is still unclear whether alcohol consumption can be directly linked to the disease.12-14 Likewise, despite belief that increased oxidative stress likely contributes to inflammation in psoriasis, there is little evidence linking antioxidants to improvement in psoriasis symptoms.12 However, the current literature is inconsistent regarding the effects of fish oil supplementation on psoriasis.12 In a randomized double-blind study of 145 patients, there was no significant difference in psoriasis area and severity index scores between a control group and a treatment group receiving fish oil supplementation.15 In another RCT of 45 participants, those given daily very long-chain omega-3 fatty acid supplements saw no difference in psoriasis symptoms.15 Despite debate, literature assessing the impact of gluten-free diets has described improvement in psoriasis lesions in patients with celiac-specific antibodies.16 Although some observational studies described vitamin D supplementation to be beneficial in the treatment of psoriatic lesions, a more recent RCT found no significant difference between control and treatment groups.17-19
Studies also have revealed that certain eating patterns, such as those associated with the Mediterranean diet that is rich in fruits, vegetables, whole grains, and omega-3 fatty acids may be linked to improved endothelial function scores and reduced C-reactive protein and IL-18levels.20,21 In a double-blind RCT of 75 patients with plaque psoriasis, mean (SD) psoriasis area and severity index scores decreased by 11.2 (9.8) in a group treated with omega-3 fatty acids compared to 7.5 (8.8) with omega-6 fatty acids (P=.048).22
Although excessive alcohol use may be linked to psoriasis, there is no conclusive evidence indicating causation, thereby discrediting online claims.12-14 Research has revealed that gluten-free diets in psoriasis patients with celiac disease may improve psoriasis treatment16; however, sufficient evidence is lacking for diets low in gluten and high in polyunsaturated fatty acids or antioxidant supplementation. Of the dietary supplements recommended in the search results we reviewed, fish oil appears to be the most promising, but no recommendations can be made based on the current research.
Eczema
Our Google search using the term diet and eczema yielded 1,160,000 results, with 50% (5/10) of websites attributed to self-proclaimed experts, 30% (3/10) to educational websites, and 20% (2/10) to promotional sites. Of the first 10 results, 80% (8/10) recommended that patients with eczema avoid milk/dairy and 50% (5/10) advised to avoid soy and wheat/gluten. Other websites indicated to avoid eggs, nuts, and artificial sweeteners. Patients were encouraged to incorporate omega-3 fatty acids in their diets, and a few sites recommended bananas, coconut oil, olive oil, and various teas.
In a review of 11 studies with a total of 596 participants, supplementation with vitamins D and E, fish oil, olive oil, and linoleic acid was evaluated for the treatment of eczema.23 Although results indicated modest improvement of eczema severity with supplementation of fish oil, evidence favoring this treatment is limited and unconvincing. Furthermore, some evidence indicates that elimination diets are only appropriate for patients with food allergies.24 In a study evaluating an egg-free and dairy-free diet for eczema patients, only participants with positive egg-specific serum IgE levels saw improvement in disease severity.23 Even though IgE-mediated food allergies have been reported in 40% of children with moderate eczema, the contribution of these allergies to eczema is questionable.25
There is little evidence in the literature to indicate a definitive correlation between the foods mentioned in the search results we evaluated and the development of eczema; however, for patients with food allergies and eczema, elimination diets may decrease disease severity.25,26 There is insufficient evidence to suggest a benefit from evening primrose oil or fish oil supplementation, thereby debunking claims found online.
Comment
Although our Google search results included a wide range of sources and information regarding diet and dermatologic conditions such as acne, psoriasis, and eczema, most of the information we found was either unfounded or misleading. Study limitations in the current literature include small sample size, potential recall bias, lack of appropriate controls, incomplete reported results, and the failure to clearly define skin changes.
When considering the accuracy and type of information regarding skin conditions that is available on the Internet, it is important to note that most of the results we reviewed were webpages attributed to self-proclaimed experts. Although educational websites also were included in the search results, whether or not patients prefer or understand the content of such websites is still unknown; therefore, health organizations should consider revising online patient education materials to allow universal comprehension.27
Furthermore, it is important to consider the impact that widespread Internet access may have on the physician-patient relationship. Having access to health-related information online and being able to potentially self-diagnose could delay or deter patients from seeking professional advice or care.3 A study evaluating the impact of online searches on the physician-patient relationship among 175 patients determined that 36.5% of patients gathered information online prior to their consultation with a physician, while 67.3% chose to complement the information given to them by their physician with online resources.28 Based on these statistics, it is important that physicians be up-to-date with Internet discourse to discredit unfounded recommendations. Ultimately, when it comes to diet and dermatology, patients ought to be skeptical of the information currently available on the Internet, given that most of it is unsubstantiated by medical research.
Researching medical information currently is the third most common use of the Internet in the United States,1 with the majority of adults using the Web as their first source for health information before seeing a physician.2 When assessing health-related information online, resources can be grouped into 4 categories: (1) those attributed to self-proclaimed experts, (2) promotional, (3) social media, and (4) educational.3 Access to such a wide range of sources may give readers the opportunity to share personal anecdotes and opinions, thereby serving as a forum for information that essentially cannot be validated. Although such websites may include useful information and cite current literature, in other instances health-related information may be misleading or fabricated.3
In a study evaluating 291 skin conditions and related Google trends, acne, psoriasis, and eczema were among the most burdensome diseases, with acne yielding the highest number of search results.4 Results of the study indicated a positive correlation between disease burden and online search interest.4 The impact of these online searches and the validity of Google search results are topics worth considering, as more dermatology patients are relying on holistic and nonpharmaceutical approaches to treatment and disease management.5 The purpose of this study was to evaluate content on diet and dermatology available on the Internet for acne, psoriasis, and eczema.
Methods
Google searches were performed in December 2017 using the terms diet and acne, diet and psoriasis, and diet and eczema. The first 10 results for each respective search were reviewed for recommendations about which foods to incorporate in the diet and which to avoid. They also were classified according to the following 4 website categories: (1) those attributed to self-proclaimed experts, (2) promotional, (3) social media, and (4) educational. The recommendations gathered from the 30 websites were then compared to the current literature assessing the impact of diet on these respective conditions by conducting PubMed searches of articles indexed for MEDLINE using the same terms.
Results
The results of this study are outlined in the eTable.
Acne
Our Google search using the term diet and acne produced 17,500,000 results. Of the first 10 search results, 40% (4/10) were websites attributed to self-proclaimed experts, 40% (4/10) were educational resources, and 20% (2/10) were promotional websites. Most of the websites advised acne patients to avoid high glycemic index foods (90% [9/10]) and dairy products (90% [9/10]). When discussing which foods to include in the diet, 70% (7/10) of websites recommended that patients incorporate omega-3 fatty acids and antioxidants in the diet.
Research has shown that a low glycemic index diet can lead to a decrease in patients’ acne lesion counts in some instances.6,7 In a case-controlled study of 2258 patients on a popular weight loss diet that emphasized low glycemic index foods, 87% of participants reported a reduction in acne and 91% reported a decrease in their dosage or number of acne medications.7 Still, the exact correlation between acne development and consumption of glycemic index foods has not been confirmed. However, high glycemic index diets have been linked to hyperinsulinemia, indicating that insulin levels may play a role in acne formation.8 The majority of other currently available studies evaluated the potential link between dairy consumption and acne. A retrospective analysis of 47,355 women spanning 12 weeks showed a positive link between increased dairy consumption, specifically skim milk, and acne formation. Despite the positive trend, limitations such as recall bias made it difficult to draw a conclusion based on these findings.9 However, results of a longitudinal questionnaire-based population study evaluating the impact of dairy consumption on acne in 2489 adolescent patients confirmed a positive correlation.10 Studies conducted in 2009 and 2011 concluded that milk consumption results in elevated insulinlike growth factor 1 levels, which were linked to comedogenesis.8,11
Currently, there are well-described mechanisms to explain the association of dairy consumption and glycemic index with acne. Confirming a correlation between acne development and dairy consumption suggests that a dairy-free diet may benefit acne patients.5 Other trials indicate that low glycemic index diets are beneficial in treating acne.6,7 Therefore, some of the recommendations made in our search results may be of merit; however, there is minimal evidence proving the benefits of the other dietary recommendations made in the websites we evaluated.
Psoriasis
Our Google search using the term diet and psoriasis yielded a total of 9,420,000 results. Of the first 10 search results, 40% (4/10) were websites attributed to self-proclaimed experts, 30% (3/10) were promotional, and 30% (3/10) were educational. Seventy percent (7/10) of websites recommended avoiding alcohol and 60% (6/10) recommended avoiding gluten, with others discouraging consumption of red meat. Most of the websites encouraged patients to consume omega-3 fatty acids and antioxidants, while a few also recommended vitamins A, D, and E, as well as evening primrose oil supplements.
Although current research indicates a positive correlation between excessive alcohol use and psoriasis severity, it is still unclear whether alcohol consumption can be directly linked to the disease.12-14 Likewise, despite belief that increased oxidative stress likely contributes to inflammation in psoriasis, there is little evidence linking antioxidants to improvement in psoriasis symptoms.12 However, the current literature is inconsistent regarding the effects of fish oil supplementation on psoriasis.12 In a randomized double-blind study of 145 patients, there was no significant difference in psoriasis area and severity index scores between a control group and a treatment group receiving fish oil supplementation.15 In another RCT of 45 participants, those given daily very long-chain omega-3 fatty acid supplements saw no difference in psoriasis symptoms.15 Despite debate, literature assessing the impact of gluten-free diets has described improvement in psoriasis lesions in patients with celiac-specific antibodies.16 Although some observational studies described vitamin D supplementation to be beneficial in the treatment of psoriatic lesions, a more recent RCT found no significant difference between control and treatment groups.17-19
Studies also have revealed that certain eating patterns, such as those associated with the Mediterranean diet that is rich in fruits, vegetables, whole grains, and omega-3 fatty acids may be linked to improved endothelial function scores and reduced C-reactive protein and IL-18levels.20,21 In a double-blind RCT of 75 patients with plaque psoriasis, mean (SD) psoriasis area and severity index scores decreased by 11.2 (9.8) in a group treated with omega-3 fatty acids compared to 7.5 (8.8) with omega-6 fatty acids (P=.048).22
Although excessive alcohol use may be linked to psoriasis, there is no conclusive evidence indicating causation, thereby discrediting online claims.12-14 Research has revealed that gluten-free diets in psoriasis patients with celiac disease may improve psoriasis treatment16; however, sufficient evidence is lacking for diets low in gluten and high in polyunsaturated fatty acids or antioxidant supplementation. Of the dietary supplements recommended in the search results we reviewed, fish oil appears to be the most promising, but no recommendations can be made based on the current research.
Eczema
Our Google search using the term diet and eczema yielded 1,160,000 results, with 50% (5/10) of websites attributed to self-proclaimed experts, 30% (3/10) to educational websites, and 20% (2/10) to promotional sites. Of the first 10 results, 80% (8/10) recommended that patients with eczema avoid milk/dairy and 50% (5/10) advised to avoid soy and wheat/gluten. Other websites indicated to avoid eggs, nuts, and artificial sweeteners. Patients were encouraged to incorporate omega-3 fatty acids in their diets, and a few sites recommended bananas, coconut oil, olive oil, and various teas.
In a review of 11 studies with a total of 596 participants, supplementation with vitamins D and E, fish oil, olive oil, and linoleic acid was evaluated for the treatment of eczema.23 Although results indicated modest improvement of eczema severity with supplementation of fish oil, evidence favoring this treatment is limited and unconvincing. Furthermore, some evidence indicates that elimination diets are only appropriate for patients with food allergies.24 In a study evaluating an egg-free and dairy-free diet for eczema patients, only participants with positive egg-specific serum IgE levels saw improvement in disease severity.23 Even though IgE-mediated food allergies have been reported in 40% of children with moderate eczema, the contribution of these allergies to eczema is questionable.25
There is little evidence in the literature to indicate a definitive correlation between the foods mentioned in the search results we evaluated and the development of eczema; however, for patients with food allergies and eczema, elimination diets may decrease disease severity.25,26 There is insufficient evidence to suggest a benefit from evening primrose oil or fish oil supplementation, thereby debunking claims found online.
Comment
Although our Google search results included a wide range of sources and information regarding diet and dermatologic conditions such as acne, psoriasis, and eczema, most of the information we found was either unfounded or misleading. Study limitations in the current literature include small sample size, potential recall bias, lack of appropriate controls, incomplete reported results, and the failure to clearly define skin changes.
When considering the accuracy and type of information regarding skin conditions that is available on the Internet, it is important to note that most of the results we reviewed were webpages attributed to self-proclaimed experts. Although educational websites also were included in the search results, whether or not patients prefer or understand the content of such websites is still unknown; therefore, health organizations should consider revising online patient education materials to allow universal comprehension.27
Furthermore, it is important to consider the impact that widespread Internet access may have on the physician-patient relationship. Having access to health-related information online and being able to potentially self-diagnose could delay or deter patients from seeking professional advice or care.3 A study evaluating the impact of online searches on the physician-patient relationship among 175 patients determined that 36.5% of patients gathered information online prior to their consultation with a physician, while 67.3% chose to complement the information given to them by their physician with online resources.28 Based on these statistics, it is important that physicians be up-to-date with Internet discourse to discredit unfounded recommendations. Ultimately, when it comes to diet and dermatology, patients ought to be skeptical of the information currently available on the Internet, given that most of it is unsubstantiated by medical research.
- Fox S. Online health search 2006. Pew Research Center website. http://www.pewinternet.org/2006/10/29/online-health-search-2006/. Published October 29, 2006. Accessed May 3, 2018.
- Prestin A, Vieux SN, Chou WY. Is online health activity alive and well or flatlining? findings from 10 years of the health information national trends survey. J Health Commun. 2015;20:790-798.
- Zeichner JA, Del Rosso JQ. Acne and the internet. Dermatol Clin. 2016;34:129-132.
- Whitsitt J, Karimkhani C, Boyers LN, et al. Comparing burden of dermatologic disease to search interest on Google trends. Dermatol Online J. 2015;21. pii:13030/qt5xg811qp.
- Shokeen D. Influence of diet in acne vulgaris and atopic dermatitis. Cutis. 2016;98:E28-E29.
- Veith WB, Silverberg NB. The association of acne vulgaris with diet. Cutis. 2011;88:84-91.
- Rouhani P. Acne improves with a popular, low glycemic diet from South Beach. J Am Acad Dermatol. 2009;60(3, suppl 1):P706.
- Melnick BC. Evidence for acne-promoting effect of milk and other insulinotropic dairy products. Nestle Nutr Worksop Ser Pediatr Program. 2011;67:131-145.
- Adebamowo CA, Spiegelman D, Berkey CS, et al. High school dietary diary intake and teenage acne. J Am Acad Dermatol. 2005;52:207-214.
- Ulvestad M, Bjertness E, Dalgard F, et al. Acne and dairy products in adolescence: results from a Norwegian longitudinal study [published online July 16, 2016]. J Eur Acad Dermatol Venereol. 2017;31:530-535.
- Melnick BC, Schmitz G. Role of insulin, insulin like growth factor 1, hyperglycemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009;18:833-841.
- Murzaku EC, Bronsnick T, Rao BK. Diet in dermatology: part II. melanoma, chronic urticaria, and psoriasis. J Am Acad Dermatol. 2014;71:1053.E1-1053.E16.
- Tobin AM, Higgins EM, Norris S, et al. Prevalence of psoriasis in patients with alcoholic liver disease. Clin Exp Dermatol. 2009;34:698-701.
- Kirby B, Richards HL, Mason DL, et al. Alcohol consumption and psychological distress in patients with psoriasis. Br J Dermatol. 2008;158:138-140.
- Søyland E, Funk J, Rajika G, et al. Effect of dietary supplementation with very long-chain n-3 fatty acids in patients with psoriasis. N Engl J Med. 1993;328:1812-1816.
- Michaëlsson G, Gerdén B, Hagforsen E, et al. Psoriasis patients with antibodies to gliadin can be improved by a gluten-free diet. Br J Dermatol. 2000;142:44-51.
- Morimoto S, Yoshikawa K. Psoriasis and vitamin D3. a review of our experience. Arch Dermatol. 1989;125:231-234.
- Smith EL, Pincus SH, Donovan L, et al. A novel approach for the evaluation and treatment of psoriasis. oral or topical use of 1,25-dihydroxyvitamin D3 can be a safe and effective therapy for psoriasis. J Am Acad Dermatol. 1988;19:516-528.
- Siddiqui MA, Al-Khawajah MM. Vitamin D3 and psoriasis: a randomized double-blind placebo-controlled study. J Dermatol Treat. 1990;1:243-245.
- Wang Y, Gao H, Loyd CM, et al. Chronic skin-specific inflammation promotes vascular inflammation and thrombosis. J Invest Dermatol. 2012;132:2067-2075.
- Barrea L, Nappi F, Di Somma C, et al. Environmental risk factors in psoriasis: the point of view of the nutritionist. Int J Environ Res Public Health. 2016;13. pii:E743. doi:10.3390/ijerph13070743.
- Mayser P, Mrowietz U, Arenberger P, et al. Omega-3 fatty acid-based lipid infusion in patients with chronic plaque psoriasis: results of a double-blind, randomized, placebo-controlled, multicenter trial. J Am Acad Dermatol. 1998;38:539-547.
- Bath-Hextall FJ, Jenkinson C, Humphreys R, et al. Dietary supplements for established atopic eczema. Cochrane Database Syst Rev. 2012;2:CD005205.
- Bronsnick T, Murzaku EC, Rao BK. Diet in dermatology: part I. atopic dermatitis, acne, and nonmelanoma skin cancer [published online November 15, 2014]. J Am Acad Dermatol. 2014;71:1039.E1-1039.E12.
- Campbell DE. The role of food allergy in childhood atopic dermatitis. J Paediatr Child Health. 2012;48:1058-1064.
- Werfel T, Erdmann S, Fuchs T, et al. Approach to suspected food allergy in atopic dermatitis. guideline of the Task Force on Food Allergy of the German Society of Allergology and Clinical Immunology (DGAKI) and the Medical Association of German Allergologists (ADA) and the German Society of Pediatric Allergology (GPA). J Dtsch Dermatol Ges. 2009;3:265-271.
- John AM, John ES, Hansberry DR, et al. Assessment of online patient education materials from major dermatologic associations. J Clin Aesthet Dermatol. 2016;9:23-28.
- Orgaz-Molina J, Cotugno M, Girón-Prieto MS, et al. A study of internet searches for medical information in dermatology patients: the patient-physician relationship. Actas Dermosifiliogr. 2015;106:493-499.
- Fox S. Online health search 2006. Pew Research Center website. http://www.pewinternet.org/2006/10/29/online-health-search-2006/. Published October 29, 2006. Accessed May 3, 2018.
- Prestin A, Vieux SN, Chou WY. Is online health activity alive and well or flatlining? findings from 10 years of the health information national trends survey. J Health Commun. 2015;20:790-798.
- Zeichner JA, Del Rosso JQ. Acne and the internet. Dermatol Clin. 2016;34:129-132.
- Whitsitt J, Karimkhani C, Boyers LN, et al. Comparing burden of dermatologic disease to search interest on Google trends. Dermatol Online J. 2015;21. pii:13030/qt5xg811qp.
- Shokeen D. Influence of diet in acne vulgaris and atopic dermatitis. Cutis. 2016;98:E28-E29.
- Veith WB, Silverberg NB. The association of acne vulgaris with diet. Cutis. 2011;88:84-91.
- Rouhani P. Acne improves with a popular, low glycemic diet from South Beach. J Am Acad Dermatol. 2009;60(3, suppl 1):P706.
- Melnick BC. Evidence for acne-promoting effect of milk and other insulinotropic dairy products. Nestle Nutr Worksop Ser Pediatr Program. 2011;67:131-145.
- Adebamowo CA, Spiegelman D, Berkey CS, et al. High school dietary diary intake and teenage acne. J Am Acad Dermatol. 2005;52:207-214.
- Ulvestad M, Bjertness E, Dalgard F, et al. Acne and dairy products in adolescence: results from a Norwegian longitudinal study [published online July 16, 2016]. J Eur Acad Dermatol Venereol. 2017;31:530-535.
- Melnick BC, Schmitz G. Role of insulin, insulin like growth factor 1, hyperglycemic food and milk consumption in the pathogenesis of acne vulgaris. Exp Dermatol. 2009;18:833-841.
- Murzaku EC, Bronsnick T, Rao BK. Diet in dermatology: part II. melanoma, chronic urticaria, and psoriasis. J Am Acad Dermatol. 2014;71:1053.E1-1053.E16.
- Tobin AM, Higgins EM, Norris S, et al. Prevalence of psoriasis in patients with alcoholic liver disease. Clin Exp Dermatol. 2009;34:698-701.
- Kirby B, Richards HL, Mason DL, et al. Alcohol consumption and psychological distress in patients with psoriasis. Br J Dermatol. 2008;158:138-140.
- Søyland E, Funk J, Rajika G, et al. Effect of dietary supplementation with very long-chain n-3 fatty acids in patients with psoriasis. N Engl J Med. 1993;328:1812-1816.
- Michaëlsson G, Gerdén B, Hagforsen E, et al. Psoriasis patients with antibodies to gliadin can be improved by a gluten-free diet. Br J Dermatol. 2000;142:44-51.
- Morimoto S, Yoshikawa K. Psoriasis and vitamin D3. a review of our experience. Arch Dermatol. 1989;125:231-234.
- Smith EL, Pincus SH, Donovan L, et al. A novel approach for the evaluation and treatment of psoriasis. oral or topical use of 1,25-dihydroxyvitamin D3 can be a safe and effective therapy for psoriasis. J Am Acad Dermatol. 1988;19:516-528.
- Siddiqui MA, Al-Khawajah MM. Vitamin D3 and psoriasis: a randomized double-blind placebo-controlled study. J Dermatol Treat. 1990;1:243-245.
- Wang Y, Gao H, Loyd CM, et al. Chronic skin-specific inflammation promotes vascular inflammation and thrombosis. J Invest Dermatol. 2012;132:2067-2075.
- Barrea L, Nappi F, Di Somma C, et al. Environmental risk factors in psoriasis: the point of view of the nutritionist. Int J Environ Res Public Health. 2016;13. pii:E743. doi:10.3390/ijerph13070743.
- Mayser P, Mrowietz U, Arenberger P, et al. Omega-3 fatty acid-based lipid infusion in patients with chronic plaque psoriasis: results of a double-blind, randomized, placebo-controlled, multicenter trial. J Am Acad Dermatol. 1998;38:539-547.
- Bath-Hextall FJ, Jenkinson C, Humphreys R, et al. Dietary supplements for established atopic eczema. Cochrane Database Syst Rev. 2012;2:CD005205.
- Bronsnick T, Murzaku EC, Rao BK. Diet in dermatology: part I. atopic dermatitis, acne, and nonmelanoma skin cancer [published online November 15, 2014]. J Am Acad Dermatol. 2014;71:1039.E1-1039.E12.
- Campbell DE. The role of food allergy in childhood atopic dermatitis. J Paediatr Child Health. 2012;48:1058-1064.
- Werfel T, Erdmann S, Fuchs T, et al. Approach to suspected food allergy in atopic dermatitis. guideline of the Task Force on Food Allergy of the German Society of Allergology and Clinical Immunology (DGAKI) and the Medical Association of German Allergologists (ADA) and the German Society of Pediatric Allergology (GPA). J Dtsch Dermatol Ges. 2009;3:265-271.
- John AM, John ES, Hansberry DR, et al. Assessment of online patient education materials from major dermatologic associations. J Clin Aesthet Dermatol. 2016;9:23-28.
- Orgaz-Molina J, Cotugno M, Girón-Prieto MS, et al. A study of internet searches for medical information in dermatology patients: the patient-physician relationship. Actas Dermosifiliogr. 2015;106:493-499.
Practice Points
- It is important physicians be well-informed regarding Internet discourse to discredit unfounded recommendations.
- It is likely that patients seeking medical advice regarding their dermatologic condition and treatment will have done prior research on the Internet.
- Oftentimes, the information on educational health websites can be confusing to patients.
- Because of widespread Internet access to health-related information, patients may opt to self-diagnose and therefore delay seeking professional care.
