User login
Barbershop BP intervention going strong at 12 months
for a black male cohort of participants, according to 12-month data from the project.
Of the 319 black, non-Hispanic male participants, 180 were randomized to participate in an intensive 6-month hypertension intervention. The study protocol allowed pharmacists, who visited participants at their barbershops, to prescribe hypertension medication under collaborative practice agreements with participants’ primary care providers (PCPs).
Compared with an active control group who received instruction about blood pressure and lifestyle modification, participants receiving the intervention saw significant reductions in systolic BP at 6 months (N Engl J Med. 2018 Apr 5;378:1291-391). From 6 months onward, participants in the intervention arm received fewer visits from pharmacists, though they still regularly visited the barbershop, where blood pressure was recorded. At the end of 12 months, systolic BP – at least 140 mm Hg at enrollment – dropped by 28.6 mm Hg from baseline in the intervention group to a mean 123.8 mm Hg. For those in the control group, the reduction in systolic BP was 7.2 mm Hg, to a mean 147.4 mm Hg. This 20.8-point difference between the two groups was highly statistically significant (P less than .0001).
“These new 12-month efficacy data are statistically indistinguishable from our previously reported 6-month data,” wrote Ciantal Blyler, PharmD, a clinical pharmacist at Cedars-Sinai Medical Center, Los Angeles, and her coauthors.
Diastolic BP, a secondary outcome measure, fell in the intervention group by 14.5 mm Hg more than in the active controls. In the intervention arm, 68% of participants reached the prespecified goal blood pressure of less than 130/80 mm Hg, while just 11% of the control group hit this target, a significant difference.
No trial participants experienced treatment-related adverse events or deaths during the 6-month extension phase.
Compared with men in the active control arm, those receiving the intervention were on a greater number of antihypertensive classes per regimen. Also, patients receiving the intervention were more likely to receive first-line drugs as add-on therapy. At the end of the 12-month period, all participants in the intensive arm were on antihypertensives, up from 57% at baseline. For the control group, antihypertensive medication use went from 53% at baseline to 65% at 6 months (P less than .001).
The intervention group saw their PCP more frequently than did the control group during the study; there was no difference in PCP visit frequency at baseline. “This suggests that the pharmacist intervention did not interfere with the patient-PCP relationship, and perhaps influenced the increase in PCP visits,” noted Dr. Blyler and her colleagues.
The investigators noted that the pharmacists’ ability to begin, titrate, and change hypertension medication under a collaborative agreement with physicians was an essential part of the program’s initial and continued success. “Perhaps the most critical first step toward widespread dissemination of our model is the expansion of collaborative practice between pharmacists and physicians, or the elimination of the requirement altogether (as in Canada and the UK),” wrote Dr. Blyler and her coauthors.
Beyond that, Dr. Blyler and her colleagues said that scalability will depend on the ability to adapt the model to create operational efficiencies while maintaining intervention potency. The time it took pharmacists to get to and from barbershops was significant, and some form of telemonitoring may work well going forward as “an appropriate means of maintaining/sustaining the intervention effect whilst also addressing this logistical inefficiency,” they said.
The study was funded by the National Institutes of Health, the California Endowment, the Lincy Foundation, the Harriet and Steven Nichols Foundation, the Smidt Heart Institute, and the Division of Community Relations and Development at Cedars-Sinai Medical Center, Los Angeles. One coauthor reported being a consultant for Recor Medical; other authors reported that they had no disclosures.
SOURCE: Blyler C et al. Circulation. 2018 Dec 17.
for a black male cohort of participants, according to 12-month data from the project.
Of the 319 black, non-Hispanic male participants, 180 were randomized to participate in an intensive 6-month hypertension intervention. The study protocol allowed pharmacists, who visited participants at their barbershops, to prescribe hypertension medication under collaborative practice agreements with participants’ primary care providers (PCPs).
Compared with an active control group who received instruction about blood pressure and lifestyle modification, participants receiving the intervention saw significant reductions in systolic BP at 6 months (N Engl J Med. 2018 Apr 5;378:1291-391). From 6 months onward, participants in the intervention arm received fewer visits from pharmacists, though they still regularly visited the barbershop, where blood pressure was recorded. At the end of 12 months, systolic BP – at least 140 mm Hg at enrollment – dropped by 28.6 mm Hg from baseline in the intervention group to a mean 123.8 mm Hg. For those in the control group, the reduction in systolic BP was 7.2 mm Hg, to a mean 147.4 mm Hg. This 20.8-point difference between the two groups was highly statistically significant (P less than .0001).
“These new 12-month efficacy data are statistically indistinguishable from our previously reported 6-month data,” wrote Ciantal Blyler, PharmD, a clinical pharmacist at Cedars-Sinai Medical Center, Los Angeles, and her coauthors.
Diastolic BP, a secondary outcome measure, fell in the intervention group by 14.5 mm Hg more than in the active controls. In the intervention arm, 68% of participants reached the prespecified goal blood pressure of less than 130/80 mm Hg, while just 11% of the control group hit this target, a significant difference.
No trial participants experienced treatment-related adverse events or deaths during the 6-month extension phase.
Compared with men in the active control arm, those receiving the intervention were on a greater number of antihypertensive classes per regimen. Also, patients receiving the intervention were more likely to receive first-line drugs as add-on therapy. At the end of the 12-month period, all participants in the intensive arm were on antihypertensives, up from 57% at baseline. For the control group, antihypertensive medication use went from 53% at baseline to 65% at 6 months (P less than .001).
The intervention group saw their PCP more frequently than did the control group during the study; there was no difference in PCP visit frequency at baseline. “This suggests that the pharmacist intervention did not interfere with the patient-PCP relationship, and perhaps influenced the increase in PCP visits,” noted Dr. Blyler and her colleagues.
The investigators noted that the pharmacists’ ability to begin, titrate, and change hypertension medication under a collaborative agreement with physicians was an essential part of the program’s initial and continued success. “Perhaps the most critical first step toward widespread dissemination of our model is the expansion of collaborative practice between pharmacists and physicians, or the elimination of the requirement altogether (as in Canada and the UK),” wrote Dr. Blyler and her coauthors.
Beyond that, Dr. Blyler and her colleagues said that scalability will depend on the ability to adapt the model to create operational efficiencies while maintaining intervention potency. The time it took pharmacists to get to and from barbershops was significant, and some form of telemonitoring may work well going forward as “an appropriate means of maintaining/sustaining the intervention effect whilst also addressing this logistical inefficiency,” they said.
The study was funded by the National Institutes of Health, the California Endowment, the Lincy Foundation, the Harriet and Steven Nichols Foundation, the Smidt Heart Institute, and the Division of Community Relations and Development at Cedars-Sinai Medical Center, Los Angeles. One coauthor reported being a consultant for Recor Medical; other authors reported that they had no disclosures.
SOURCE: Blyler C et al. Circulation. 2018 Dec 17.
for a black male cohort of participants, according to 12-month data from the project.
Of the 319 black, non-Hispanic male participants, 180 were randomized to participate in an intensive 6-month hypertension intervention. The study protocol allowed pharmacists, who visited participants at their barbershops, to prescribe hypertension medication under collaborative practice agreements with participants’ primary care providers (PCPs).
Compared with an active control group who received instruction about blood pressure and lifestyle modification, participants receiving the intervention saw significant reductions in systolic BP at 6 months (N Engl J Med. 2018 Apr 5;378:1291-391). From 6 months onward, participants in the intervention arm received fewer visits from pharmacists, though they still regularly visited the barbershop, where blood pressure was recorded. At the end of 12 months, systolic BP – at least 140 mm Hg at enrollment – dropped by 28.6 mm Hg from baseline in the intervention group to a mean 123.8 mm Hg. For those in the control group, the reduction in systolic BP was 7.2 mm Hg, to a mean 147.4 mm Hg. This 20.8-point difference between the two groups was highly statistically significant (P less than .0001).
“These new 12-month efficacy data are statistically indistinguishable from our previously reported 6-month data,” wrote Ciantal Blyler, PharmD, a clinical pharmacist at Cedars-Sinai Medical Center, Los Angeles, and her coauthors.
Diastolic BP, a secondary outcome measure, fell in the intervention group by 14.5 mm Hg more than in the active controls. In the intervention arm, 68% of participants reached the prespecified goal blood pressure of less than 130/80 mm Hg, while just 11% of the control group hit this target, a significant difference.
No trial participants experienced treatment-related adverse events or deaths during the 6-month extension phase.
Compared with men in the active control arm, those receiving the intervention were on a greater number of antihypertensive classes per regimen. Also, patients receiving the intervention were more likely to receive first-line drugs as add-on therapy. At the end of the 12-month period, all participants in the intensive arm were on antihypertensives, up from 57% at baseline. For the control group, antihypertensive medication use went from 53% at baseline to 65% at 6 months (P less than .001).
The intervention group saw their PCP more frequently than did the control group during the study; there was no difference in PCP visit frequency at baseline. “This suggests that the pharmacist intervention did not interfere with the patient-PCP relationship, and perhaps influenced the increase in PCP visits,” noted Dr. Blyler and her colleagues.
The investigators noted that the pharmacists’ ability to begin, titrate, and change hypertension medication under a collaborative agreement with physicians was an essential part of the program’s initial and continued success. “Perhaps the most critical first step toward widespread dissemination of our model is the expansion of collaborative practice between pharmacists and physicians, or the elimination of the requirement altogether (as in Canada and the UK),” wrote Dr. Blyler and her coauthors.
Beyond that, Dr. Blyler and her colleagues said that scalability will depend on the ability to adapt the model to create operational efficiencies while maintaining intervention potency. The time it took pharmacists to get to and from barbershops was significant, and some form of telemonitoring may work well going forward as “an appropriate means of maintaining/sustaining the intervention effect whilst also addressing this logistical inefficiency,” they said.
The study was funded by the National Institutes of Health, the California Endowment, the Lincy Foundation, the Harriet and Steven Nichols Foundation, the Smidt Heart Institute, and the Division of Community Relations and Development at Cedars-Sinai Medical Center, Los Angeles. One coauthor reported being a consultant for Recor Medical; other authors reported that they had no disclosures.
SOURCE: Blyler C et al. Circulation. 2018 Dec 17.
FROM CIRCULATION
Key clinical point:
Major finding: Systolic BP fell by 28.6 vs. 7.2 mm Hg for those receiving the intervention (P less than .0001).
Study details: Cluster-randomized cohort study of 319 non-Hispanic African American males with hypertension.
Disclosures: The study was funded by the National Institutes of Health, the California Endowment, the Lincy Foundation, the Harriet and Steven Nichols Foundation, the Smidt Heart Institute, and the Division of Community Relations and Development at Cedars-Sinai Medical Center, Los Angeles. One coauthor reported being a consultant for Recor Medical; other authors reported that they had no disclosures.
Source: Blyler C et al. Circulation. 2018 Dec 17.
2018 REVIEWER APPRECIATION
The JCSO Editors and editorial staff thank all those who generously contributed to the peer-review process this past year. We are mindful of the many demands on you and value the time and expertise you put in to reviewing submissions.
Click on the PDF icon at the top of this introduction for a complete list of the names of all the reviewers.
The JCSO Editors and editorial staff thank all those who generously contributed to the peer-review process this past year. We are mindful of the many demands on you and value the time and expertise you put in to reviewing submissions.
Click on the PDF icon at the top of this introduction for a complete list of the names of all the reviewers.
The JCSO Editors and editorial staff thank all those who generously contributed to the peer-review process this past year. We are mindful of the many demands on you and value the time and expertise you put in to reviewing submissions.
Click on the PDF icon at the top of this introduction for a complete list of the names of all the reviewers.
Chronic opioid use during pregnancy linked with reduced head circumference in NAS newborns
(HC), reported Craig V. Towers, MD, and his associates at the University of Tennessee Medical Center in Knoxville in Pediatrics.
In the first large prospective cohort study to compare HC in newborns being treated for NAS, a total of 858 neonates, including 429 with NAS and 429 controls, were enrolled and assessed at the University of Tennessee Medical Center, Knoxville, from April 1, 2014, to Dec. 31, 2016.
Dr. Towers and his associates found that mean HC in those neonates with NAS was significantly smaller, by 9.5 mm, than it was in controls. Of the 429 newborns with NAS, 62% had a normal HC, 30% had an HC less than the 10th percentile, and 8% had an HC less than or equal to the third percentile. Of the controls, 12% had an HC less than the 10th percentile.
The authors identified a significant 3% reduction in mean HC as well as a 2% reduction in mean birth weight. “Because newborn HC is an indirect measure of brain volume, further research is necessary to determine if this finding increases the risk for long-term neurodevelopmental delay,” they said.
Even though the newborns with NAS were found to experience greater coexposure to benzodiazepines, stimulants, marijuana, gabapentin, tobacco, and SSRIs, compared with controls, none of these coexposures was determined to be a significant risk factor for smaller head circumference at birth when individual drug exposure relationships within the newborn population alone were assessed, the researchers observed.
Dr. Towers and his associates did consider it noteworthy, however, that the majority of NAS cases included in the study were born to mothers receiving opioid agonist medication–assisted treatment (MAT), which is the recommended treatment in cases where opioid use disorder is addressed during pregnancy. Among the 429 NAS cases, the mothers of 372 (87%) were on opioid agonist MAT (320 buprenorphine and 52 methadone); the remaining 13% were born to mothers who were prescribed other opioid drugs.
There is limited data available to determine whether detoxification during pregnancy for patients with opioid use disorder (OUD) has any effect on lessening the risk of lower HC. In fact, the authors caution that detoxification during pregnancy is not recommended for managing OUD. To date, there are only a few locations in the United States and other countries offering such treatment. If the practice becomes more widespread, they cautioned, further research examining new born HC and long-term outcomes “is of paramount importance.”
Further prospective studies evaluating the effects of opioid exposure in newborns who do not develop NAS also are needed. Such data could provide clues concerning whether there is a crucial period of exposure that leads to reduced HC or whether the effects of opioid exposure are in fact cumulative. In cases where newborns are exposed as a result of maintenance MAT, through illicit use, or as a result of maternal detoxification, such studies also could assist with determining whether it is necessary to reconsider current practices for managing OUD in pregnancy.
The study was partially funded through the Blue Cross Blue Shield Research Foundation. The authors reported no relevant financial disclosures.
SOURCE: Towers CV et al. Pediatrics. 2019;143(1):e20180541.
At a time when more people in the United States are dying from opioid overdose than from automobile trauma, the number of newborns with NAS has virtually exploded, rising fivefold since 2000. In some states, more than 30 infants per 1,000 live births develop NAS “effectively transforming some NICUs into NAS wards,” Mark L. Hudak, MD, and Kartikeya Makker, MD, wrote in an accompanying editorial.
Among the strengths of the current study, they cited “universal dating of pregnancies by early ultrasound, multiple antenatal maternal urine drug tests for exposures in both cases and controls, and the use of a fairly robust statistical methodology to account for confounding exposures.”
Among the findings of the study were that, “compared with well-matched controls, newborns with NAS demonstrated a highly significant (nearly 1 cm) decrease in the mean head circumference. Another finding was that newborns with NAS showed proportionately greater decreases in head circumference than in birth weight,” the editorialists said.
Dr. Hadak and Dr. Makker noted that, while NAS can be challenging to manage, the acute effects of withdrawal are transient. The more important questions, they propose are: “What are the best methods to prevent NAS?” and “What, if any, are the long-term effects of fetal and neonatal opioid exposure on the developing child?”
Dr. Hudak and Dr. Makker question the practicality of closely following maternal opioid usage during pregnancy, but they do foresee value in the anticipated findings of a current study in which Dr. Towers and his associates are observing newborns with reduced fetal exposure to opioids who have not developed NAS.
“Additional evidence revealing that the reduction of maternal opioid use can protect normal fetal head and brain growth should energize discussion about refining the management of the opioid-maintained maternal-fetal dyad, with the goal not solely to prevent NAS but more importantly to optimize the outcome of the child,” they said.
Dr. Hudak and Dr. Makker are affiliated with the department of pediatrics at the University of Florida, Jacksonville. These comments are summarized from an editorial commenting on the study by Towers et al. (Pediatrics. 2019;143[1]:e20183376). Dr. Hudak and Dr. Makker said they had no relevant financial disclosures.
At a time when more people in the United States are dying from opioid overdose than from automobile trauma, the number of newborns with NAS has virtually exploded, rising fivefold since 2000. In some states, more than 30 infants per 1,000 live births develop NAS “effectively transforming some NICUs into NAS wards,” Mark L. Hudak, MD, and Kartikeya Makker, MD, wrote in an accompanying editorial.
Among the strengths of the current study, they cited “universal dating of pregnancies by early ultrasound, multiple antenatal maternal urine drug tests for exposures in both cases and controls, and the use of a fairly robust statistical methodology to account for confounding exposures.”
Among the findings of the study were that, “compared with well-matched controls, newborns with NAS demonstrated a highly significant (nearly 1 cm) decrease in the mean head circumference. Another finding was that newborns with NAS showed proportionately greater decreases in head circumference than in birth weight,” the editorialists said.
Dr. Hadak and Dr. Makker noted that, while NAS can be challenging to manage, the acute effects of withdrawal are transient. The more important questions, they propose are: “What are the best methods to prevent NAS?” and “What, if any, are the long-term effects of fetal and neonatal opioid exposure on the developing child?”
Dr. Hudak and Dr. Makker question the practicality of closely following maternal opioid usage during pregnancy, but they do foresee value in the anticipated findings of a current study in which Dr. Towers and his associates are observing newborns with reduced fetal exposure to opioids who have not developed NAS.
“Additional evidence revealing that the reduction of maternal opioid use can protect normal fetal head and brain growth should energize discussion about refining the management of the opioid-maintained maternal-fetal dyad, with the goal not solely to prevent NAS but more importantly to optimize the outcome of the child,” they said.
Dr. Hudak and Dr. Makker are affiliated with the department of pediatrics at the University of Florida, Jacksonville. These comments are summarized from an editorial commenting on the study by Towers et al. (Pediatrics. 2019;143[1]:e20183376). Dr. Hudak and Dr. Makker said they had no relevant financial disclosures.
At a time when more people in the United States are dying from opioid overdose than from automobile trauma, the number of newborns with NAS has virtually exploded, rising fivefold since 2000. In some states, more than 30 infants per 1,000 live births develop NAS “effectively transforming some NICUs into NAS wards,” Mark L. Hudak, MD, and Kartikeya Makker, MD, wrote in an accompanying editorial.
Among the strengths of the current study, they cited “universal dating of pregnancies by early ultrasound, multiple antenatal maternal urine drug tests for exposures in both cases and controls, and the use of a fairly robust statistical methodology to account for confounding exposures.”
Among the findings of the study were that, “compared with well-matched controls, newborns with NAS demonstrated a highly significant (nearly 1 cm) decrease in the mean head circumference. Another finding was that newborns with NAS showed proportionately greater decreases in head circumference than in birth weight,” the editorialists said.
Dr. Hadak and Dr. Makker noted that, while NAS can be challenging to manage, the acute effects of withdrawal are transient. The more important questions, they propose are: “What are the best methods to prevent NAS?” and “What, if any, are the long-term effects of fetal and neonatal opioid exposure on the developing child?”
Dr. Hudak and Dr. Makker question the practicality of closely following maternal opioid usage during pregnancy, but they do foresee value in the anticipated findings of a current study in which Dr. Towers and his associates are observing newborns with reduced fetal exposure to opioids who have not developed NAS.
“Additional evidence revealing that the reduction of maternal opioid use can protect normal fetal head and brain growth should energize discussion about refining the management of the opioid-maintained maternal-fetal dyad, with the goal not solely to prevent NAS but more importantly to optimize the outcome of the child,” they said.
Dr. Hudak and Dr. Makker are affiliated with the department of pediatrics at the University of Florida, Jacksonville. These comments are summarized from an editorial commenting on the study by Towers et al. (Pediatrics. 2019;143[1]:e20183376). Dr. Hudak and Dr. Makker said they had no relevant financial disclosures.
(HC), reported Craig V. Towers, MD, and his associates at the University of Tennessee Medical Center in Knoxville in Pediatrics.
In the first large prospective cohort study to compare HC in newborns being treated for NAS, a total of 858 neonates, including 429 with NAS and 429 controls, were enrolled and assessed at the University of Tennessee Medical Center, Knoxville, from April 1, 2014, to Dec. 31, 2016.
Dr. Towers and his associates found that mean HC in those neonates with NAS was significantly smaller, by 9.5 mm, than it was in controls. Of the 429 newborns with NAS, 62% had a normal HC, 30% had an HC less than the 10th percentile, and 8% had an HC less than or equal to the third percentile. Of the controls, 12% had an HC less than the 10th percentile.
The authors identified a significant 3% reduction in mean HC as well as a 2% reduction in mean birth weight. “Because newborn HC is an indirect measure of brain volume, further research is necessary to determine if this finding increases the risk for long-term neurodevelopmental delay,” they said.
Even though the newborns with NAS were found to experience greater coexposure to benzodiazepines, stimulants, marijuana, gabapentin, tobacco, and SSRIs, compared with controls, none of these coexposures was determined to be a significant risk factor for smaller head circumference at birth when individual drug exposure relationships within the newborn population alone were assessed, the researchers observed.
Dr. Towers and his associates did consider it noteworthy, however, that the majority of NAS cases included in the study were born to mothers receiving opioid agonist medication–assisted treatment (MAT), which is the recommended treatment in cases where opioid use disorder is addressed during pregnancy. Among the 429 NAS cases, the mothers of 372 (87%) were on opioid agonist MAT (320 buprenorphine and 52 methadone); the remaining 13% were born to mothers who were prescribed other opioid drugs.
There is limited data available to determine whether detoxification during pregnancy for patients with opioid use disorder (OUD) has any effect on lessening the risk of lower HC. In fact, the authors caution that detoxification during pregnancy is not recommended for managing OUD. To date, there are only a few locations in the United States and other countries offering such treatment. If the practice becomes more widespread, they cautioned, further research examining new born HC and long-term outcomes “is of paramount importance.”
Further prospective studies evaluating the effects of opioid exposure in newborns who do not develop NAS also are needed. Such data could provide clues concerning whether there is a crucial period of exposure that leads to reduced HC or whether the effects of opioid exposure are in fact cumulative. In cases where newborns are exposed as a result of maintenance MAT, through illicit use, or as a result of maternal detoxification, such studies also could assist with determining whether it is necessary to reconsider current practices for managing OUD in pregnancy.
The study was partially funded through the Blue Cross Blue Shield Research Foundation. The authors reported no relevant financial disclosures.
SOURCE: Towers CV et al. Pediatrics. 2019;143(1):e20180541.
(HC), reported Craig V. Towers, MD, and his associates at the University of Tennessee Medical Center in Knoxville in Pediatrics.
In the first large prospective cohort study to compare HC in newborns being treated for NAS, a total of 858 neonates, including 429 with NAS and 429 controls, were enrolled and assessed at the University of Tennessee Medical Center, Knoxville, from April 1, 2014, to Dec. 31, 2016.
Dr. Towers and his associates found that mean HC in those neonates with NAS was significantly smaller, by 9.5 mm, than it was in controls. Of the 429 newborns with NAS, 62% had a normal HC, 30% had an HC less than the 10th percentile, and 8% had an HC less than or equal to the third percentile. Of the controls, 12% had an HC less than the 10th percentile.
The authors identified a significant 3% reduction in mean HC as well as a 2% reduction in mean birth weight. “Because newborn HC is an indirect measure of brain volume, further research is necessary to determine if this finding increases the risk for long-term neurodevelopmental delay,” they said.
Even though the newborns with NAS were found to experience greater coexposure to benzodiazepines, stimulants, marijuana, gabapentin, tobacco, and SSRIs, compared with controls, none of these coexposures was determined to be a significant risk factor for smaller head circumference at birth when individual drug exposure relationships within the newborn population alone were assessed, the researchers observed.
Dr. Towers and his associates did consider it noteworthy, however, that the majority of NAS cases included in the study were born to mothers receiving opioid agonist medication–assisted treatment (MAT), which is the recommended treatment in cases where opioid use disorder is addressed during pregnancy. Among the 429 NAS cases, the mothers of 372 (87%) were on opioid agonist MAT (320 buprenorphine and 52 methadone); the remaining 13% were born to mothers who were prescribed other opioid drugs.
There is limited data available to determine whether detoxification during pregnancy for patients with opioid use disorder (OUD) has any effect on lessening the risk of lower HC. In fact, the authors caution that detoxification during pregnancy is not recommended for managing OUD. To date, there are only a few locations in the United States and other countries offering such treatment. If the practice becomes more widespread, they cautioned, further research examining new born HC and long-term outcomes “is of paramount importance.”
Further prospective studies evaluating the effects of opioid exposure in newborns who do not develop NAS also are needed. Such data could provide clues concerning whether there is a crucial period of exposure that leads to reduced HC or whether the effects of opioid exposure are in fact cumulative. In cases where newborns are exposed as a result of maintenance MAT, through illicit use, or as a result of maternal detoxification, such studies also could assist with determining whether it is necessary to reconsider current practices for managing OUD in pregnancy.
The study was partially funded through the Blue Cross Blue Shield Research Foundation. The authors reported no relevant financial disclosures.
SOURCE: Towers CV et al. Pediatrics. 2019;143(1):e20180541.
FROM PEDIATRICS
Key clinical point: Detoxification during pregnancy may be ill advised for patients with opioid use disorder.
Major finding: Head circumference was smaller by a mean 9.5 mm.
Study details: Prospective cohort study of 429 NAS neonates and 429 controls.
Disclosures: The study was partially funded through the Blue Cross Blue Shield Research Foundation. The authors reported no relevant financial disclosures.
Source: Towers CV et al. Pediatrics. 2019;143(1):e20180541.
HPV-16/-18 dramatically increases risk of high-grade CIN in young women
Young women with HPV-16/-18 are significantly more likely to develop high-grade cervical intraepithelial neoplasia (CIN), compared with young women who do not have HPV-16/-18, and therefore require close monitoring, according to a 9-year study of more than 500 women.
Specific strain of HPV had less effect on risk in women aged 30 years or older, compared with younger women, reported lead author Maria Fröberg, MD, PhD, of Karolinska University Hospital and Institute in Stockholm and her colleagues.
“With today’s introduction of HPV primary screening into several organized screening programs and with many triage algorithms available, further research is needed to ensure safe follow-up management and prevent the unnecessary treatment of transient positive HPV findings associated with regressive high-grade CIN,” the investigators wrote in Cancer.
To better understand risk associated with HPV, the investigators drew from a database of 9,464 Swedish women who were cytologically negative for cervical intraepithelial lesions or malignancy (NILM) at baseline during 2005-2007. These baseline-negative women were followed for 9 years; during this time, 96 women developed histologically confirmed, high-grade CIN (CIN2, CIN3, cervical cancer, or adenocarcinoma in situ [AIS]). For each case, five age-matched women were selected who did not develop high-grade CIN to make a control cohort of 480 women.
Approximately half of the cases had CIN2 (45.8%), and half had CIN3 or worse histopathology (CIN3+, 54.2%). HPV-16/-18 was more often associated with CIN3+, compared with CIN2 (Pearson x2, 6.12; P less than .02 [2-sided]). Women with high-grade CIN were significantly more likely to have HPV of any strain, compared with controls (odds ratio, 6.78). Women aged younger than 30 years who had HPV-16/-18 at baseline were far more likely to develop high-grade CIN (OR, 9.44) but showed less impact from other strains of HPV (OR, 2.24). In contrast, women aged 30 years or older showed similar increases in high-grade CIN risk when comparing HPV-16/-18 with other strains (OR, 8.16 vs. 9.04).
“These latter findings suggest that genotyping for HPV-16/-18 might be useful for risk stratification among younger women,” the investigators suggested, noting that “further prospective study on this topic is warranted.”
The study was funded by the Swedish Cancer Foundation, the Stockholm County Council, the Swedish Research Council, and the King Gustaf V Jubilee Fund, and the Karolinska Institute. During the study, one investigator received grants from VALGENT and the 7th Framework Programme of DG Research and Innovation (European Commission).
SOURCE: Fröberg M et al. Cancer. 2018 Dec 10. doi: 10.1002/cncr.31788.
Young women with HPV-16/-18 are significantly more likely to develop high-grade cervical intraepithelial neoplasia (CIN), compared with young women who do not have HPV-16/-18, and therefore require close monitoring, according to a 9-year study of more than 500 women.
Specific strain of HPV had less effect on risk in women aged 30 years or older, compared with younger women, reported lead author Maria Fröberg, MD, PhD, of Karolinska University Hospital and Institute in Stockholm and her colleagues.
“With today’s introduction of HPV primary screening into several organized screening programs and with many triage algorithms available, further research is needed to ensure safe follow-up management and prevent the unnecessary treatment of transient positive HPV findings associated with regressive high-grade CIN,” the investigators wrote in Cancer.
To better understand risk associated with HPV, the investigators drew from a database of 9,464 Swedish women who were cytologically negative for cervical intraepithelial lesions or malignancy (NILM) at baseline during 2005-2007. These baseline-negative women were followed for 9 years; during this time, 96 women developed histologically confirmed, high-grade CIN (CIN2, CIN3, cervical cancer, or adenocarcinoma in situ [AIS]). For each case, five age-matched women were selected who did not develop high-grade CIN to make a control cohort of 480 women.
Approximately half of the cases had CIN2 (45.8%), and half had CIN3 or worse histopathology (CIN3+, 54.2%). HPV-16/-18 was more often associated with CIN3+, compared with CIN2 (Pearson x2, 6.12; P less than .02 [2-sided]). Women with high-grade CIN were significantly more likely to have HPV of any strain, compared with controls (odds ratio, 6.78). Women aged younger than 30 years who had HPV-16/-18 at baseline were far more likely to develop high-grade CIN (OR, 9.44) but showed less impact from other strains of HPV (OR, 2.24). In contrast, women aged 30 years or older showed similar increases in high-grade CIN risk when comparing HPV-16/-18 with other strains (OR, 8.16 vs. 9.04).
“These latter findings suggest that genotyping for HPV-16/-18 might be useful for risk stratification among younger women,” the investigators suggested, noting that “further prospective study on this topic is warranted.”
The study was funded by the Swedish Cancer Foundation, the Stockholm County Council, the Swedish Research Council, and the King Gustaf V Jubilee Fund, and the Karolinska Institute. During the study, one investigator received grants from VALGENT and the 7th Framework Programme of DG Research and Innovation (European Commission).
SOURCE: Fröberg M et al. Cancer. 2018 Dec 10. doi: 10.1002/cncr.31788.
Young women with HPV-16/-18 are significantly more likely to develop high-grade cervical intraepithelial neoplasia (CIN), compared with young women who do not have HPV-16/-18, and therefore require close monitoring, according to a 9-year study of more than 500 women.
Specific strain of HPV had less effect on risk in women aged 30 years or older, compared with younger women, reported lead author Maria Fröberg, MD, PhD, of Karolinska University Hospital and Institute in Stockholm and her colleagues.
“With today’s introduction of HPV primary screening into several organized screening programs and with many triage algorithms available, further research is needed to ensure safe follow-up management and prevent the unnecessary treatment of transient positive HPV findings associated with regressive high-grade CIN,” the investigators wrote in Cancer.
To better understand risk associated with HPV, the investigators drew from a database of 9,464 Swedish women who were cytologically negative for cervical intraepithelial lesions or malignancy (NILM) at baseline during 2005-2007. These baseline-negative women were followed for 9 years; during this time, 96 women developed histologically confirmed, high-grade CIN (CIN2, CIN3, cervical cancer, or adenocarcinoma in situ [AIS]). For each case, five age-matched women were selected who did not develop high-grade CIN to make a control cohort of 480 women.
Approximately half of the cases had CIN2 (45.8%), and half had CIN3 or worse histopathology (CIN3+, 54.2%). HPV-16/-18 was more often associated with CIN3+, compared with CIN2 (Pearson x2, 6.12; P less than .02 [2-sided]). Women with high-grade CIN were significantly more likely to have HPV of any strain, compared with controls (odds ratio, 6.78). Women aged younger than 30 years who had HPV-16/-18 at baseline were far more likely to develop high-grade CIN (OR, 9.44) but showed less impact from other strains of HPV (OR, 2.24). In contrast, women aged 30 years or older showed similar increases in high-grade CIN risk when comparing HPV-16/-18 with other strains (OR, 8.16 vs. 9.04).
“These latter findings suggest that genotyping for HPV-16/-18 might be useful for risk stratification among younger women,” the investigators suggested, noting that “further prospective study on this topic is warranted.”
The study was funded by the Swedish Cancer Foundation, the Stockholm County Council, the Swedish Research Council, and the King Gustaf V Jubilee Fund, and the Karolinska Institute. During the study, one investigator received grants from VALGENT and the 7th Framework Programme of DG Research and Innovation (European Commission).
SOURCE: Fröberg M et al. Cancer. 2018 Dec 10. doi: 10.1002/cncr.31788.
FROM CANCER
Key clinical point: Women with HPV-16/-18 are at significantly higher risk of high-grade cervical intraepithelial neoplasia (CIN), compared with women without HPV-16/-18, and therefore require close monitoring.
Major finding: Women younger than 30 years who test positive for HPV-16/-18 are almost 10 times as likely to develop high-grade CIN, compared with young women negative for HPV-16/-18 (odds ratio, 9.44).
Study details: A nested case-control study involving 96 women who developed high-grade CIN over the 9-year study period, compared with 480 age-matched controls who did not develop cervical lesions.
Disclosures: The study was funded by the Swedish Cancer Foundation, the Stockholm County Council, the Swedish Research Council, and the King Gustaf V Jubilee Fund, and the Karolinska Institute. During the study, one investigator received grants from VALGENT and the 7th Framework Programme of DG Research and Innovation (European Commission).
Source: Fröberg M et al. Cancer. 2018 Dec 10. doi: 10.1002/cncr.31788.
Clinical trial: Robotic or open radical cystectomy in treating patients with bladder cancer

Patients who are recruited will undergo either open or robotic radical cystectomy. In open radical cystectomy, the surgeon cuts into the lower abdomen to expose the urinary tract in order to remove the bladder. In robotic radical cystectomy, small cuts are made in the abdomen into which a scope is inserted; with robotic help, the surgeon removes the bladder. It is currently unknown which approach results in fewer complications, better quality of life, and faster recovery time.
Patients are eligible for the study if they are indicated for radical cystectomy, have Tis-T3 urothelial cancer, and meet surgical candidate criteria. Exclusion factors include having a bulky lymphadenopathy, prior pelvic radiation, or uncontrolled coagulopathy.
The primary outcome measure is change in patient-reported quality of life, as reported using the European Organization for Research and Treatment of Cancer (EORTC)-QLQ-C30, 1 month post surgery. The secondary outcome measure is change in erectile dysfunction, as measured by the Sexual Health Inventory For Men score, over a follow-up of up to 12 months.
Recruitment ends on Oct. 12, 2019, and the estimated study completion date is Oct. 12, 2020. About 208 participants are expected to be included.
Find more information on the study page at Clinicaltrials.gov.
Patients who are recruited will undergo either open or robotic radical cystectomy. In open radical cystectomy, the surgeon cuts into the lower abdomen to expose the urinary tract in order to remove the bladder. In robotic radical cystectomy, small cuts are made in the abdomen into which a scope is inserted; with robotic help, the surgeon removes the bladder. It is currently unknown which approach results in fewer complications, better quality of life, and faster recovery time.
Patients are eligible for the study if they are indicated for radical cystectomy, have Tis-T3 urothelial cancer, and meet surgical candidate criteria. Exclusion factors include having a bulky lymphadenopathy, prior pelvic radiation, or uncontrolled coagulopathy.
The primary outcome measure is change in patient-reported quality of life, as reported using the European Organization for Research and Treatment of Cancer (EORTC)-QLQ-C30, 1 month post surgery. The secondary outcome measure is change in erectile dysfunction, as measured by the Sexual Health Inventory For Men score, over a follow-up of up to 12 months.
Recruitment ends on Oct. 12, 2019, and the estimated study completion date is Oct. 12, 2020. About 208 participants are expected to be included.
Find more information on the study page at Clinicaltrials.gov.
Patients who are recruited will undergo either open or robotic radical cystectomy. In open radical cystectomy, the surgeon cuts into the lower abdomen to expose the urinary tract in order to remove the bladder. In robotic radical cystectomy, small cuts are made in the abdomen into which a scope is inserted; with robotic help, the surgeon removes the bladder. It is currently unknown which approach results in fewer complications, better quality of life, and faster recovery time.
Patients are eligible for the study if they are indicated for radical cystectomy, have Tis-T3 urothelial cancer, and meet surgical candidate criteria. Exclusion factors include having a bulky lymphadenopathy, prior pelvic radiation, or uncontrolled coagulopathy.
The primary outcome measure is change in patient-reported quality of life, as reported using the European Organization for Research and Treatment of Cancer (EORTC)-QLQ-C30, 1 month post surgery. The secondary outcome measure is change in erectile dysfunction, as measured by the Sexual Health Inventory For Men score, over a follow-up of up to 12 months.
Recruitment ends on Oct. 12, 2019, and the estimated study completion date is Oct. 12, 2020. About 208 participants are expected to be included.
Find more information on the study page at Clinicaltrials.gov.
CPN welcomes Andrea Murru, MD, PhD, to CPN board
Clinical Psychiatry News is pleased to announce that Andrea Murru, MD, PhD, has joined the Editorial Advisory Board.
Dr. Murru is senior clinician in the bipolar disorder and sleep disorder units of the Hospital Clinic of Barcelona in Spain, and is a postdoctoral researcher of the Spanish Network of Research in Mental Health, which is led by Eduard Vieta, MD, PhD.
In addition, His research focuses on using, long-term treatments, and implementing clinical guidelines in daily practice. He also researches tolerability in patients with bipolar disorder, schizoaffective disorder, and sleep-related disorders and biomarkers.
He earned his medical degree from the University of Cagliari (Italy).
Clinical Psychiatry News is pleased to announce that Andrea Murru, MD, PhD, has joined the Editorial Advisory Board.
Dr. Murru is senior clinician in the bipolar disorder and sleep disorder units of the Hospital Clinic of Barcelona in Spain, and is a postdoctoral researcher of the Spanish Network of Research in Mental Health, which is led by Eduard Vieta, MD, PhD.
In addition, His research focuses on using, long-term treatments, and implementing clinical guidelines in daily practice. He also researches tolerability in patients with bipolar disorder, schizoaffective disorder, and sleep-related disorders and biomarkers.
He earned his medical degree from the University of Cagliari (Italy).
Clinical Psychiatry News is pleased to announce that Andrea Murru, MD, PhD, has joined the Editorial Advisory Board.
Dr. Murru is senior clinician in the bipolar disorder and sleep disorder units of the Hospital Clinic of Barcelona in Spain, and is a postdoctoral researcher of the Spanish Network of Research in Mental Health, which is led by Eduard Vieta, MD, PhD.
In addition, His research focuses on using, long-term treatments, and implementing clinical guidelines in daily practice. He also researches tolerability in patients with bipolar disorder, schizoaffective disorder, and sleep-related disorders and biomarkers.
He earned his medical degree from the University of Cagliari (Italy).
New insight gained into natural history of interstitial pneumonia with autoimmune features
CHICAGO – than are those with idiopathic interstitial lung disease who don’t meet the criteria, Michail Alevizos, MD, reported at the annual meeting of the American College of Rheumatology.

“We think this is a very novel finding. It means that patients with IPAF [interstitial pneumonia with autoimmune features] should be followed and evaluated by rheumatologists over time,” said Dr. Alevizos, who was a rheumatology fellow at Columbia University in New York at the time of the study.
Interstitial pneumonia with autoimmune features (IPAF) is a term proposed by a joint task force of the American Thoracic Society and European Respiratory Society in 2015 to describe patients diagnosed with idiopathic interstitial lung disease who possess some features of autoimmunity without meeting formal criteria for a full-blown rheumatic disease. The designation requires the presence of interstitial lung disease by imaging or biopsy, exclusion of all other etiologies, and at least one feature from within at least two of three domains: clinical, serologic, and morphologic.
The clinical domain includes Raynaud’s, palmar telangiectasias, distal digital tip ulceration, and other entities. The serologic criteria include any of a dozen possible autoantibodies. And the morphologic domain encompasses a radiographic or histopathologic pattern suggestive of organizing pneumonia, nonspecific interstitial pneumonia, or other specific abnormalities (Eur Respir J. 2015 Oct;46[4]:976-87).
The natural history of IPAF is largely unknown, which was the impetus for Dr. Alevizos’ study. He presented a single-center, retrospective study of 697 patients diagnosed with interstitial lung disease, 174 of whom had idiopathic interstitial lung disease at baseline. Fifty of the 174 met criteria for IPAF, while the other 124 did not.
During a median follow-up of 5.2 years, 8 of the 50 patients with IPAF (16%) were diagnosed with a systemic autoimmune rheumatic disease, as were 2 of the 124 non-IPAF group (1.6%). The average time to diagnosis of a formal rheumatic disease was 3.4 years in the IPAF group and 7.8 years in the comparator arm. The rheumatic diseases that arose in the IPAF group consisted of two cases of rheumatoid arthritis, two of antineutrophil cytoplasmic antibody–associated vasculitis, three of systemic sclerosis, and one of polymyositis.
In an analysis adjusted for age, sex, smoking status, and immunosuppressive therapy at baseline, patients with IPAF were 14.1 times more likely to progress to an autoimmune rheumatic disease.
In terms of distinguishing features, the IPAF patients were on average 10 years younger at baseline and more commonly female. On high-resolution CT, 82% of them displayed a pattern of nonspecific interstitial pneumonia, compared with only 15% of the non-IPAF group. Also, 96% of the IPAF patients were on immunosuppressive therapy at baseline, as were 52% of the non-IPAF group. Usual interstitial pneumonia was evident on high-resolution CT in 18% of the IPAF group, compared with 75% of patients with idiopathic interstitial pneumonia without IPAF.
Dr. Alevizos said he hopes to validate these findings in a prospective study. He reported having no financial conflicts regarding the study, which was conducted free of commercial support.
SOURCE: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.
CHICAGO – than are those with idiopathic interstitial lung disease who don’t meet the criteria, Michail Alevizos, MD, reported at the annual meeting of the American College of Rheumatology.
“We think this is a very novel finding. It means that patients with IPAF [interstitial pneumonia with autoimmune features] should be followed and evaluated by rheumatologists over time,” said Dr. Alevizos, who was a rheumatology fellow at Columbia University in New York at the time of the study.
Interstitial pneumonia with autoimmune features (IPAF) is a term proposed by a joint task force of the American Thoracic Society and European Respiratory Society in 2015 to describe patients diagnosed with idiopathic interstitial lung disease who possess some features of autoimmunity without meeting formal criteria for a full-blown rheumatic disease. The designation requires the presence of interstitial lung disease by imaging or biopsy, exclusion of all other etiologies, and at least one feature from within at least two of three domains: clinical, serologic, and morphologic.
The clinical domain includes Raynaud’s, palmar telangiectasias, distal digital tip ulceration, and other entities. The serologic criteria include any of a dozen possible autoantibodies. And the morphologic domain encompasses a radiographic or histopathologic pattern suggestive of organizing pneumonia, nonspecific interstitial pneumonia, or other specific abnormalities (Eur Respir J. 2015 Oct;46[4]:976-87).
The natural history of IPAF is largely unknown, which was the impetus for Dr. Alevizos’ study. He presented a single-center, retrospective study of 697 patients diagnosed with interstitial lung disease, 174 of whom had idiopathic interstitial lung disease at baseline. Fifty of the 174 met criteria for IPAF, while the other 124 did not.
During a median follow-up of 5.2 years, 8 of the 50 patients with IPAF (16%) were diagnosed with a systemic autoimmune rheumatic disease, as were 2 of the 124 non-IPAF group (1.6%). The average time to diagnosis of a formal rheumatic disease was 3.4 years in the IPAF group and 7.8 years in the comparator arm. The rheumatic diseases that arose in the IPAF group consisted of two cases of rheumatoid arthritis, two of antineutrophil cytoplasmic antibody–associated vasculitis, three of systemic sclerosis, and one of polymyositis.
In an analysis adjusted for age, sex, smoking status, and immunosuppressive therapy at baseline, patients with IPAF were 14.1 times more likely to progress to an autoimmune rheumatic disease.
In terms of distinguishing features, the IPAF patients were on average 10 years younger at baseline and more commonly female. On high-resolution CT, 82% of them displayed a pattern of nonspecific interstitial pneumonia, compared with only 15% of the non-IPAF group. Also, 96% of the IPAF patients were on immunosuppressive therapy at baseline, as were 52% of the non-IPAF group. Usual interstitial pneumonia was evident on high-resolution CT in 18% of the IPAF group, compared with 75% of patients with idiopathic interstitial pneumonia without IPAF.
Dr. Alevizos said he hopes to validate these findings in a prospective study. He reported having no financial conflicts regarding the study, which was conducted free of commercial support.
SOURCE: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.
CHICAGO – than are those with idiopathic interstitial lung disease who don’t meet the criteria, Michail Alevizos, MD, reported at the annual meeting of the American College of Rheumatology.
“We think this is a very novel finding. It means that patients with IPAF [interstitial pneumonia with autoimmune features] should be followed and evaluated by rheumatologists over time,” said Dr. Alevizos, who was a rheumatology fellow at Columbia University in New York at the time of the study.
Interstitial pneumonia with autoimmune features (IPAF) is a term proposed by a joint task force of the American Thoracic Society and European Respiratory Society in 2015 to describe patients diagnosed with idiopathic interstitial lung disease who possess some features of autoimmunity without meeting formal criteria for a full-blown rheumatic disease. The designation requires the presence of interstitial lung disease by imaging or biopsy, exclusion of all other etiologies, and at least one feature from within at least two of three domains: clinical, serologic, and morphologic.
The clinical domain includes Raynaud’s, palmar telangiectasias, distal digital tip ulceration, and other entities. The serologic criteria include any of a dozen possible autoantibodies. And the morphologic domain encompasses a radiographic or histopathologic pattern suggestive of organizing pneumonia, nonspecific interstitial pneumonia, or other specific abnormalities (Eur Respir J. 2015 Oct;46[4]:976-87).
The natural history of IPAF is largely unknown, which was the impetus for Dr. Alevizos’ study. He presented a single-center, retrospective study of 697 patients diagnosed with interstitial lung disease, 174 of whom had idiopathic interstitial lung disease at baseline. Fifty of the 174 met criteria for IPAF, while the other 124 did not.
During a median follow-up of 5.2 years, 8 of the 50 patients with IPAF (16%) were diagnosed with a systemic autoimmune rheumatic disease, as were 2 of the 124 non-IPAF group (1.6%). The average time to diagnosis of a formal rheumatic disease was 3.4 years in the IPAF group and 7.8 years in the comparator arm. The rheumatic diseases that arose in the IPAF group consisted of two cases of rheumatoid arthritis, two of antineutrophil cytoplasmic antibody–associated vasculitis, three of systemic sclerosis, and one of polymyositis.
In an analysis adjusted for age, sex, smoking status, and immunosuppressive therapy at baseline, patients with IPAF were 14.1 times more likely to progress to an autoimmune rheumatic disease.
In terms of distinguishing features, the IPAF patients were on average 10 years younger at baseline and more commonly female. On high-resolution CT, 82% of them displayed a pattern of nonspecific interstitial pneumonia, compared with only 15% of the non-IPAF group. Also, 96% of the IPAF patients were on immunosuppressive therapy at baseline, as were 52% of the non-IPAF group. Usual interstitial pneumonia was evident on high-resolution CT in 18% of the IPAF group, compared with 75% of patients with idiopathic interstitial pneumonia without IPAF.
Dr. Alevizos said he hopes to validate these findings in a prospective study. He reported having no financial conflicts regarding the study, which was conducted free of commercial support.
SOURCE: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.
REPORTING FROM the ACR ANNUAL MEETING
Key clinical point: The adjusted risk of progression to a systemic autoimmune rheumatic disease is 14.1 times greater in interstitial pneumonia with autoimmune features than in idiopathic interstitial lung disease without such features.
Major finding: A total of 16% of patients with interstitial pneumonia with autoimmune features progressed to a systemic autoimmune rheumatic disease during follow-up, compared with 1.6% of patients with idiopathic interstitial lung disease without such features.
Study details: This retrospective, single-center study included 174 patients with idiopathic interstitial lung disease followed for a median of 5.2 years.
Disclosures: The presenter reported having no financial conflicts regarding the study, which was conducted free of commercial support.
Source: Alevizos M et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 1305.
Drug-drug interactions in rheumatology patients on PPIs: An underappreciated problem?
CHICAGO – posing a distinct danger of unwelcome drug-drug interactions affecting the rate and extent of absorption of selected oral antirheumatic drugs, Nicholas Jones, PharmD, said at the annual meeting of the American College of Rheumatology.
Of particular interest is the fact that the oral Janus kinase inhibitors – a drug class that’s a red hot research topic now in rheumatology – are weak bases whose absorption can be greatly affected by pH-dependent solubility, according to Dr. Jones, a research scientist at Genentech in South San Francisco.
Other commonly prescribed oral antirheumatic drugs whose solubility is affected by the level of stomach acidity include azathioprine, methotrexate, mycophenolate mofetil, and sulfasalazine. On the other hand, solubility is not pH-dependent for apremilast, chloroquine, cyclophosphamide, cyclosporine, hydroxychloroquine, leflunomide, or tacrolimus.
Dr. Jones presented a retrospective analysis of proton pump inhibitor (PPI) utilization patterns during 2012-2015 in 77,034 rheumatoid arthritis and 2,224 systemic lupus erythematosus (SLE) patients included in the national Truven Health MarketScan database.
Thirty-five percent of the rheumatoid arthritis patients and 34% of SLE patients were chronic users of PPIs as defined by continuous daily use for more than a month during 2 years of follow-up. Among the SLE cohort, chronic utilization of PPIs increased stepwise with disease severity: The rate was 27% in those with mild SLE, 39% with moderate disease, and 54% among those with severe SLE.
Omeprazole was far and away the most widely used PPI. It was the one used by 53% of the RA patients who were chronic users of PPIs, followed by pantoprazole at 20% and esomeprazole at 15%. The PPI distribution pattern closely followed suit in SLE patients who were chronic users.
Esomeprazole is 60% more potent and pantoprazole 77% less potent than omeprazole, Dr. Jones noted. The pharmacokinetic clearance routes for omeprazole and esomeprazole involve CYP2C19 and CYP3A4. Clearance of pantoprazole is by those two mechanisms as well as by CYP2D6 and CYP2C9.
Dr. Jones recommended that physicians who treat rheumatoid arthritis and SLE patients be sure to ask them about concomitant use of PPIs, including OTC formulations. And clinical trialists need to be attentive to PPI usage in potential study participants.
Genentech sponsored the study.
SOURCE: Keebler D et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 228
CHICAGO – posing a distinct danger of unwelcome drug-drug interactions affecting the rate and extent of absorption of selected oral antirheumatic drugs, Nicholas Jones, PharmD, said at the annual meeting of the American College of Rheumatology.
Of particular interest is the fact that the oral Janus kinase inhibitors – a drug class that’s a red hot research topic now in rheumatology – are weak bases whose absorption can be greatly affected by pH-dependent solubility, according to Dr. Jones, a research scientist at Genentech in South San Francisco.
Other commonly prescribed oral antirheumatic drugs whose solubility is affected by the level of stomach acidity include azathioprine, methotrexate, mycophenolate mofetil, and sulfasalazine. On the other hand, solubility is not pH-dependent for apremilast, chloroquine, cyclophosphamide, cyclosporine, hydroxychloroquine, leflunomide, or tacrolimus.
Dr. Jones presented a retrospective analysis of proton pump inhibitor (PPI) utilization patterns during 2012-2015 in 77,034 rheumatoid arthritis and 2,224 systemic lupus erythematosus (SLE) patients included in the national Truven Health MarketScan database.
Thirty-five percent of the rheumatoid arthritis patients and 34% of SLE patients were chronic users of PPIs as defined by continuous daily use for more than a month during 2 years of follow-up. Among the SLE cohort, chronic utilization of PPIs increased stepwise with disease severity: The rate was 27% in those with mild SLE, 39% with moderate disease, and 54% among those with severe SLE.
Omeprazole was far and away the most widely used PPI. It was the one used by 53% of the RA patients who were chronic users of PPIs, followed by pantoprazole at 20% and esomeprazole at 15%. The PPI distribution pattern closely followed suit in SLE patients who were chronic users.
Esomeprazole is 60% more potent and pantoprazole 77% less potent than omeprazole, Dr. Jones noted. The pharmacokinetic clearance routes for omeprazole and esomeprazole involve CYP2C19 and CYP3A4. Clearance of pantoprazole is by those two mechanisms as well as by CYP2D6 and CYP2C9.
Dr. Jones recommended that physicians who treat rheumatoid arthritis and SLE patients be sure to ask them about concomitant use of PPIs, including OTC formulations. And clinical trialists need to be attentive to PPI usage in potential study participants.
Genentech sponsored the study.
SOURCE: Keebler D et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 228
CHICAGO – posing a distinct danger of unwelcome drug-drug interactions affecting the rate and extent of absorption of selected oral antirheumatic drugs, Nicholas Jones, PharmD, said at the annual meeting of the American College of Rheumatology.
Of particular interest is the fact that the oral Janus kinase inhibitors – a drug class that’s a red hot research topic now in rheumatology – are weak bases whose absorption can be greatly affected by pH-dependent solubility, according to Dr. Jones, a research scientist at Genentech in South San Francisco.
Other commonly prescribed oral antirheumatic drugs whose solubility is affected by the level of stomach acidity include azathioprine, methotrexate, mycophenolate mofetil, and sulfasalazine. On the other hand, solubility is not pH-dependent for apremilast, chloroquine, cyclophosphamide, cyclosporine, hydroxychloroquine, leflunomide, or tacrolimus.
Dr. Jones presented a retrospective analysis of proton pump inhibitor (PPI) utilization patterns during 2012-2015 in 77,034 rheumatoid arthritis and 2,224 systemic lupus erythematosus (SLE) patients included in the national Truven Health MarketScan database.
Thirty-five percent of the rheumatoid arthritis patients and 34% of SLE patients were chronic users of PPIs as defined by continuous daily use for more than a month during 2 years of follow-up. Among the SLE cohort, chronic utilization of PPIs increased stepwise with disease severity: The rate was 27% in those with mild SLE, 39% with moderate disease, and 54% among those with severe SLE.
Omeprazole was far and away the most widely used PPI. It was the one used by 53% of the RA patients who were chronic users of PPIs, followed by pantoprazole at 20% and esomeprazole at 15%. The PPI distribution pattern closely followed suit in SLE patients who were chronic users.
Esomeprazole is 60% more potent and pantoprazole 77% less potent than omeprazole, Dr. Jones noted. The pharmacokinetic clearance routes for omeprazole and esomeprazole involve CYP2C19 and CYP3A4. Clearance of pantoprazole is by those two mechanisms as well as by CYP2D6 and CYP2C9.
Dr. Jones recommended that physicians who treat rheumatoid arthritis and SLE patients be sure to ask them about concomitant use of PPIs, including OTC formulations. And clinical trialists need to be attentive to PPI usage in potential study participants.
Genentech sponsored the study.
SOURCE: Keebler D et al. Arthritis Rheumatol. 2018;70(Suppl 10): Abstract 228
REPORTING FROM the ACR ANNUAL MEETING
Key clinical point: Ask your RA and SLE patients about concomitant chronic use of PPIs to avoid drug-drug interactions.
Major finding: More than one-third of RA and SLE patients are chronic users of PPIs, which raises potential drug-drug interaction issues for many commonly prescribed oral antirheumatic drugs.
Study details: This retrospective study utilized national claims data to examine chronic use of PPIs among more than 77,000 patients with RA and 2,224 with SLE.
Disclosures: The presenter is employed at Genentech, which sponsored the study.
Source: Keebler D et al. Arthritis Rheumatol. 2018;70(Suppl 10), Abstract 228
Verrucous Coalescing Dry Papules and Plaques on the Hip and Flank
The Diagnosis: Blaschkitis
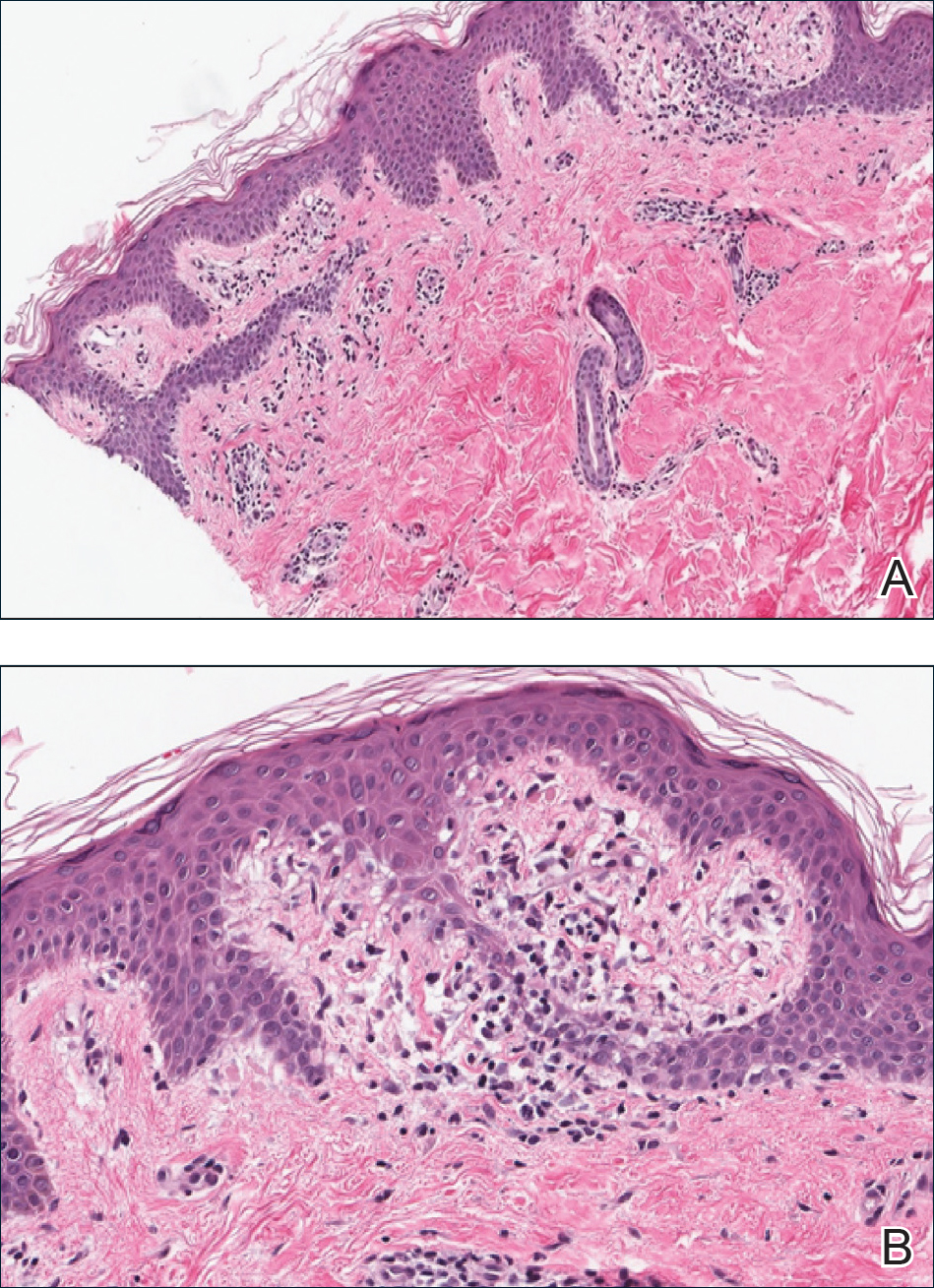
A punch biopsy from the right lateral hip was performed. Histopathologic examination revealed orthokeratosis overlying mild psoriasiform epidermal hyperplasia associated with a lichenoid infiltrate composed almost entirely of lymphocytes (Figure). The infiltrate did not entirely obscure the dermoepidermal junction and spared the adnexal structures. The clinical presentation along with histopathologic analysis confirmed a diagnosis of blaschkitis. The lesions were treated with triamcinolone ointment twice daily as needed, and the patient reported symptomatic and clinical improvement with this intervention at 4-week follow-up.
Described by Grosshans and Marot1 in 1990, blaschkitis is an acquired inflammatory dermatosis following the lines of Blaschko. It predominantly is seen on the trunk and typically presents with pruritic papules and vesicles. It frequently has a relapsing course and is more commonly found in adults. Blaschkitis is considered a form of cutaneous mosaicism representing somatic mutations affecting epidermal cell growth and migration during embryogenesis. It has been proposed that these aberrant cells are not clinically apparent at birth; however, viral infection and drug or other environmental triggers can induce antigen presentation of the clone cells activating a T cell–mediated inflammatory response.2-4
The differential diagnosis includes other acquired Blaschko-linear dermatoses such as lichen striatus, inflammatory linear verrucous epidermal nevus, unilateral lichen planus, linear lichen sclerosus, linear psoriasis, linear fixed drug reaction, lichen nitidus, and others.1,4 Given the overlap in clinical and histopathological presentations of the entities in the differential, it often is difficult to discern the etiology of the papular and vesicular eruption in question. Discrimination of one etiology from the others is further confounded by the fact that these lesions can all be pruritic and initially are treated with topical corticosteroids. A degree of clinical suspicion for blaschkitis coupled with prior understanding of lesional manifestations is helpful in this circumstance. Although classic lichen planus often affects the arms, legs, flexor surfaces, and occasionally the oral mucosa, blaschkitis generally is limited to the trunk. The lesions of lichen planus generally are violaceous, flattopped, polygonal papules that tend to coalesce. They often have a thin, transparent, and adherent scale overlying the papular lesions, and they occasionally demonstrate Wickham striae, which are faint white reticulated networks typically seen in oral mucosal lesions. In the case of lichen nitidus, lesions often follow a geometric line due to the Köbner response, whereas physical trauma from scratching or injury causes lesions to form along the line of insult. Assessing patients for any newly initiated medications can help eliminate lichenoid drug eruptions. Lichen striatus perhaps has the most overlap with blaschkitis, having been described as also following the lines of Blaschko but occurring in children rather than adults. Inflammatory linear verrucous epidermal nevi also can be distinguished from blaschkitis on this premise, as these lesions arise during the first 5 years of life and generally affect the lower extremities.4,5
Histopathology is somewhat variable but generally includes spongiotic dermatitis with concomitant interface
dermatitis characterized by T-cell infiltration. Spongiosis is a feature less commonly seen in lichen striatus. Lesions can progress over time from spongiotic dermatitis to spongiotic psoriasiform dermatitis and later to spongiotic psoriasiform lichenoid dermatitis.4 Treatment of blaschkitis should begin with reassurance of the benign nature of the dermatosis. Pruritic symptoms can be managed with a course of topical steroids.
Blaschkitis is a rare and self-limiting acquired dermatosis that should be incorporated into the differential diagnosis of Blaschko-linear dermatoses. Further investigation is needed to determine if blaschkitis and lichen striatus represent the ends of a disease spectrum or completely distinct entities.
- Grosshans E, Marot L. Blaschkitis in adults. Ann Dermatol Venereol. 1990;117:9-15.
- Müller CS, Schmaltz R, Vogt T, et al. Lichen striatus and blaschkitis: reappraisal of the concept of blaschkolinear dermatoses [published online November 29, 2010]. Br J Dermatol. 2011;164:257-262.
- Sun BK, Tsao H. X-chromosome inactivation and skin disease. J Invest Dermatol. 2008;128:2753-2759.
- Keegan BR, Kamino H, Fangman W, et al. “Pediatric blaschkitis”: expanding spectrum of childhood acquired Blaschko-linear dermatoses. Pediatr Dermatol. 2007;24:261-267.
- Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012.
The Diagnosis: Blaschkitis
A punch biopsy from the right lateral hip was performed. Histopathologic examination revealed orthokeratosis overlying mild psoriasiform epidermal hyperplasia associated with a lichenoid infiltrate composed almost entirely of lymphocytes (Figure). The infiltrate did not entirely obscure the dermoepidermal junction and spared the adnexal structures. The clinical presentation along with histopathologic analysis confirmed a diagnosis of blaschkitis. The lesions were treated with triamcinolone ointment twice daily as needed, and the patient reported symptomatic and clinical improvement with this intervention at 4-week follow-up.
Described by Grosshans and Marot1 in 1990, blaschkitis is an acquired inflammatory dermatosis following the lines of Blaschko. It predominantly is seen on the trunk and typically presents with pruritic papules and vesicles. It frequently has a relapsing course and is more commonly found in adults. Blaschkitis is considered a form of cutaneous mosaicism representing somatic mutations affecting epidermal cell growth and migration during embryogenesis. It has been proposed that these aberrant cells are not clinically apparent at birth; however, viral infection and drug or other environmental triggers can induce antigen presentation of the clone cells activating a T cell–mediated inflammatory response.2-4
The differential diagnosis includes other acquired Blaschko-linear dermatoses such as lichen striatus, inflammatory linear verrucous epidermal nevus, unilateral lichen planus, linear lichen sclerosus, linear psoriasis, linear fixed drug reaction, lichen nitidus, and others.1,4 Given the overlap in clinical and histopathological presentations of the entities in the differential, it often is difficult to discern the etiology of the papular and vesicular eruption in question. Discrimination of one etiology from the others is further confounded by the fact that these lesions can all be pruritic and initially are treated with topical corticosteroids. A degree of clinical suspicion for blaschkitis coupled with prior understanding of lesional manifestations is helpful in this circumstance. Although classic lichen planus often affects the arms, legs, flexor surfaces, and occasionally the oral mucosa, blaschkitis generally is limited to the trunk. The lesions of lichen planus generally are violaceous, flattopped, polygonal papules that tend to coalesce. They often have a thin, transparent, and adherent scale overlying the papular lesions, and they occasionally demonstrate Wickham striae, which are faint white reticulated networks typically seen in oral mucosal lesions. In the case of lichen nitidus, lesions often follow a geometric line due to the Köbner response, whereas physical trauma from scratching or injury causes lesions to form along the line of insult. Assessing patients for any newly initiated medications can help eliminate lichenoid drug eruptions. Lichen striatus perhaps has the most overlap with blaschkitis, having been described as also following the lines of Blaschko but occurring in children rather than adults. Inflammatory linear verrucous epidermal nevi also can be distinguished from blaschkitis on this premise, as these lesions arise during the first 5 years of life and generally affect the lower extremities.4,5
Histopathology is somewhat variable but generally includes spongiotic dermatitis with concomitant interface
dermatitis characterized by T-cell infiltration. Spongiosis is a feature less commonly seen in lichen striatus. Lesions can progress over time from spongiotic dermatitis to spongiotic psoriasiform dermatitis and later to spongiotic psoriasiform lichenoid dermatitis.4 Treatment of blaschkitis should begin with reassurance of the benign nature of the dermatosis. Pruritic symptoms can be managed with a course of topical steroids.
Blaschkitis is a rare and self-limiting acquired dermatosis that should be incorporated into the differential diagnosis of Blaschko-linear dermatoses. Further investigation is needed to determine if blaschkitis and lichen striatus represent the ends of a disease spectrum or completely distinct entities.
The Diagnosis: Blaschkitis
A punch biopsy from the right lateral hip was performed. Histopathologic examination revealed orthokeratosis overlying mild psoriasiform epidermal hyperplasia associated with a lichenoid infiltrate composed almost entirely of lymphocytes (Figure). The infiltrate did not entirely obscure the dermoepidermal junction and spared the adnexal structures. The clinical presentation along with histopathologic analysis confirmed a diagnosis of blaschkitis. The lesions were treated with triamcinolone ointment twice daily as needed, and the patient reported symptomatic and clinical improvement with this intervention at 4-week follow-up.
Described by Grosshans and Marot1 in 1990, blaschkitis is an acquired inflammatory dermatosis following the lines of Blaschko. It predominantly is seen on the trunk and typically presents with pruritic papules and vesicles. It frequently has a relapsing course and is more commonly found in adults. Blaschkitis is considered a form of cutaneous mosaicism representing somatic mutations affecting epidermal cell growth and migration during embryogenesis. It has been proposed that these aberrant cells are not clinically apparent at birth; however, viral infection and drug or other environmental triggers can induce antigen presentation of the clone cells activating a T cell–mediated inflammatory response.2-4
The differential diagnosis includes other acquired Blaschko-linear dermatoses such as lichen striatus, inflammatory linear verrucous epidermal nevus, unilateral lichen planus, linear lichen sclerosus, linear psoriasis, linear fixed drug reaction, lichen nitidus, and others.1,4 Given the overlap in clinical and histopathological presentations of the entities in the differential, it often is difficult to discern the etiology of the papular and vesicular eruption in question. Discrimination of one etiology from the others is further confounded by the fact that these lesions can all be pruritic and initially are treated with topical corticosteroids. A degree of clinical suspicion for blaschkitis coupled with prior understanding of lesional manifestations is helpful in this circumstance. Although classic lichen planus often affects the arms, legs, flexor surfaces, and occasionally the oral mucosa, blaschkitis generally is limited to the trunk. The lesions of lichen planus generally are violaceous, flattopped, polygonal papules that tend to coalesce. They often have a thin, transparent, and adherent scale overlying the papular lesions, and they occasionally demonstrate Wickham striae, which are faint white reticulated networks typically seen in oral mucosal lesions. In the case of lichen nitidus, lesions often follow a geometric line due to the Köbner response, whereas physical trauma from scratching or injury causes lesions to form along the line of insult. Assessing patients for any newly initiated medications can help eliminate lichenoid drug eruptions. Lichen striatus perhaps has the most overlap with blaschkitis, having been described as also following the lines of Blaschko but occurring in children rather than adults. Inflammatory linear verrucous epidermal nevi also can be distinguished from blaschkitis on this premise, as these lesions arise during the first 5 years of life and generally affect the lower extremities.4,5
Histopathology is somewhat variable but generally includes spongiotic dermatitis with concomitant interface
dermatitis characterized by T-cell infiltration. Spongiosis is a feature less commonly seen in lichen striatus. Lesions can progress over time from spongiotic dermatitis to spongiotic psoriasiform dermatitis and later to spongiotic psoriasiform lichenoid dermatitis.4 Treatment of blaschkitis should begin with reassurance of the benign nature of the dermatosis. Pruritic symptoms can be managed with a course of topical steroids.
Blaschkitis is a rare and self-limiting acquired dermatosis that should be incorporated into the differential diagnosis of Blaschko-linear dermatoses. Further investigation is needed to determine if blaschkitis and lichen striatus represent the ends of a disease spectrum or completely distinct entities.
- Grosshans E, Marot L. Blaschkitis in adults. Ann Dermatol Venereol. 1990;117:9-15.
- Müller CS, Schmaltz R, Vogt T, et al. Lichen striatus and blaschkitis: reappraisal of the concept of blaschkolinear dermatoses [published online November 29, 2010]. Br J Dermatol. 2011;164:257-262.
- Sun BK, Tsao H. X-chromosome inactivation and skin disease. J Invest Dermatol. 2008;128:2753-2759.
- Keegan BR, Kamino H, Fangman W, et al. “Pediatric blaschkitis”: expanding spectrum of childhood acquired Blaschko-linear dermatoses. Pediatr Dermatol. 2007;24:261-267.
- Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012.
- Grosshans E, Marot L. Blaschkitis in adults. Ann Dermatol Venereol. 1990;117:9-15.
- Müller CS, Schmaltz R, Vogt T, et al. Lichen striatus and blaschkitis: reappraisal of the concept of blaschkolinear dermatoses [published online November 29, 2010]. Br J Dermatol. 2011;164:257-262.
- Sun BK, Tsao H. X-chromosome inactivation and skin disease. J Invest Dermatol. 2008;128:2753-2759.
- Keegan BR, Kamino H, Fangman W, et al. “Pediatric blaschkitis”: expanding spectrum of childhood acquired Blaschko-linear dermatoses. Pediatr Dermatol. 2007;24:261-267.
- Goldsmith LA, Katz SI, Gilchrest BA, et al, eds. Fitzpatrick’s Dermatology in General Medicine. 8th ed. New York, NY: McGraw-Hill; 2012.

A 31-year-old man presented with a recurring pruritic rash on the right lateral flank and hip of 2 years’ duration. Physical examination revealed erythematous, verrucous, dry papules and plaques coalescing into larger plaques on the right flank and hip in dermatomal distributions involving the T10 and T11 dermatomes. A few papules were scattered in a linear eruption along the right flank and right upper thigh. Some postinflammatory changes were noted. No rash was noted over any other area of the body. Physical examination was otherwise unremarkable.

Data underscore the importance of lifestyle interventions in breast cancer patients
SAN ANTONIO – Data continue to underscore the benefits of lifestyle interventions in women with breast cancer, but questions remain about their effects on recurrence, according to Jennifer Ligibel, MD.
Findings from the EBBA-II trial as presented at the San Antonio Breast Cancer Symposium, for example, showed that exercise improves cardiorespiratory fitness in women with early breast cancer, and findings from the SUCCESS C study showed that breast cancer patients who completed a weight-loss intervention showed some improvements, compared with those who did not, said Dr. Ligibel of Dana-Farber Cancer Institute in Boston, who was the discussant for those and other lifestyle-intervention studies at the symposium.
SUCCESS C failed to show an overall reduction in breast cancer recurrence or survival, but weight loss among intervention-group participants was modest, and more than half of the participants dropped out of the study, so it’s hard to make any firm conclusions, she said.
Overall, the findings – in the context of what is already known about lifestyle interventions among women with breast cancer – provide “yet another reason to tell women that it’s important to exercise during treatment,” she said.

In this video interview, Dr. Ligibel discussed the studies and the implications of the findings, and also mentioned an ongoing study for which she is an investigator. In that study – the Breast Cancer Weight Loss study (BWEL) – adherence among the approximately 1,700 women enrolled has been high. “So we’re hoping that this study in a few years will give us a bit more information about the power of weight loss to potentially reduce recurrence.”
For now, the available data show that there are “lots of concrete benefits” associated with improving lifestyle in women with breast cancer, she said, noting that she tells all of her patients to live as healthy a lifestyle as possible, and especially to exercise.
SAN ANTONIO – Data continue to underscore the benefits of lifestyle interventions in women with breast cancer, but questions remain about their effects on recurrence, according to Jennifer Ligibel, MD.
Findings from the EBBA-II trial as presented at the San Antonio Breast Cancer Symposium, for example, showed that exercise improves cardiorespiratory fitness in women with early breast cancer, and findings from the SUCCESS C study showed that breast cancer patients who completed a weight-loss intervention showed some improvements, compared with those who did not, said Dr. Ligibel of Dana-Farber Cancer Institute in Boston, who was the discussant for those and other lifestyle-intervention studies at the symposium.
SUCCESS C failed to show an overall reduction in breast cancer recurrence or survival, but weight loss among intervention-group participants was modest, and more than half of the participants dropped out of the study, so it’s hard to make any firm conclusions, she said.
Overall, the findings – in the context of what is already known about lifestyle interventions among women with breast cancer – provide “yet another reason to tell women that it’s important to exercise during treatment,” she said.
In this video interview, Dr. Ligibel discussed the studies and the implications of the findings, and also mentioned an ongoing study for which she is an investigator. In that study – the Breast Cancer Weight Loss study (BWEL) – adherence among the approximately 1,700 women enrolled has been high. “So we’re hoping that this study in a few years will give us a bit more information about the power of weight loss to potentially reduce recurrence.”
For now, the available data show that there are “lots of concrete benefits” associated with improving lifestyle in women with breast cancer, she said, noting that she tells all of her patients to live as healthy a lifestyle as possible, and especially to exercise.
SAN ANTONIO – Data continue to underscore the benefits of lifestyle interventions in women with breast cancer, but questions remain about their effects on recurrence, according to Jennifer Ligibel, MD.
Findings from the EBBA-II trial as presented at the San Antonio Breast Cancer Symposium, for example, showed that exercise improves cardiorespiratory fitness in women with early breast cancer, and findings from the SUCCESS C study showed that breast cancer patients who completed a weight-loss intervention showed some improvements, compared with those who did not, said Dr. Ligibel of Dana-Farber Cancer Institute in Boston, who was the discussant for those and other lifestyle-intervention studies at the symposium.
SUCCESS C failed to show an overall reduction in breast cancer recurrence or survival, but weight loss among intervention-group participants was modest, and more than half of the participants dropped out of the study, so it’s hard to make any firm conclusions, she said.
Overall, the findings – in the context of what is already known about lifestyle interventions among women with breast cancer – provide “yet another reason to tell women that it’s important to exercise during treatment,” she said.
In this video interview, Dr. Ligibel discussed the studies and the implications of the findings, and also mentioned an ongoing study for which she is an investigator. In that study – the Breast Cancer Weight Loss study (BWEL) – adherence among the approximately 1,700 women enrolled has been high. “So we’re hoping that this study in a few years will give us a bit more information about the power of weight loss to potentially reduce recurrence.”
For now, the available data show that there are “lots of concrete benefits” associated with improving lifestyle in women with breast cancer, she said, noting that she tells all of her patients to live as healthy a lifestyle as possible, and especially to exercise.
REPORTING FROM SABCS 2018