User login
Postextubation laryngeal injury has lasting effects
(ALgI), and the injury is associated with worse breathing and speaking at 10 weeks, according to a study published in Critical Care Medicine (2019 Dec;47[12]:1669-1706). The researchers, led by Alexander Gelbard, MD, of Vanderbilt Medical Center, Nashville, Tenn., found that higher body mass index, diabetes, and larger endotracheal tube (ETT) size were all associated with heightened risk.
The investigators assert that comparatively scarce data are available about how patients fare after receiving mechanical ventilation, and how adverse effects might interfere with recovery and return to daily activity. The larynx is rarely examined after extubation, and laryngeal injury may initially appear to be minor. Restricted glottic mobility therefore tends to be diagnosed after discharge, leaving critical care specialists unaware of the long-term impact.
The findings of the study should be a wake-up call for the development of guidelines for recognition and management of laryngeal injuries, according to John Robert Gowardman, MD, of Royal Brisbane (Australia) and Women’s Hospital, who wrote an accompanying editorial (Crit Care Med, 2019 Dec;47[12]:1802-04).
In addition, findings that ETT size, diabetes, and BMI represent risk factors for injury should help identify patients at risk, and the “practice of ‘putting in the biggest ETT just in case’ needs to be balanced against the dangers of an undersized ETT ... we should ask, ‘can my patient be safely managed with a smaller ETT?’ ” wrote Dr. Gowardman.
The researchers followed 100 consecutive adult patients who were examined with nasolaryngoscopy following an intubation of greater than 12 hours at Vanderbilt University Medical Center. They recorded baseline comorbidities and other factors. Fifty seven patients had an ALgI, defined as having glottic mucosal ulceration/granulation or subglottic granulation tissue/stenosis at the time of endoscopy. Nineteen patients had granulation tissue, 48 had posterior glottic ulceration, and 8 had subglottic mucosal ulceration.
Ten weeks after extubation, all patients were contacted by phone and asked to answer the Voice Handicap Index (VHI)-10 and the Clinical Chronic Obstructive Pulmonary Disease Questionnaire (CCQ). The questioner did not know the results of the patient’s endoscopy. Patients with ALgI were heavier on average (mean difference, 14 kg; BMI difference, 3.8 kg/m2), were more likely to have type 2 diabetes (46% versus 21%), and had more severe illness (median Charlson Comorbidity Index, 3.00 versus 2.00).
Sixty-seven patients completed the 10-week questionnaires, including 40 patients with ALgI and 27 without ALgI. Injury was associated with reports of worse breathing (median CCQ, 1.05 versus 0.20; P less than .001), as well as worse patient-reported voice outcomes (median VHI, 2 versus 0; P = .005).
ETT size appeared to be an important factor, according to multivariate analyses. Use of a 7.0 ETT was associated with lower frequency of injury than 7.5 (adjusted odds ratio, 0.04; P = .004) and 8.0 (OR, 0.03; P = .004). There was no significant difference between the 7.5 and 8.0 sizes.
The presence of type 2 diabetes altered the risk associated with BMI (P = .003 for interaction). Among patients who did not have type 2 diabetes, ALgI went up as a function of increasing BMI. Still, injury risk was higher in the presence of type 2 diabetes across all BMI ranges.
The Vanderbilt Institute for Clinical and Translational Research funded the study. Dr. Gowardman has no relevant disclosures.
SOURCE: Shinn JR et al. Crit Care Med;2019 Dec;47(12):1669-1706 .
(ALgI), and the injury is associated with worse breathing and speaking at 10 weeks, according to a study published in Critical Care Medicine (2019 Dec;47[12]:1669-1706). The researchers, led by Alexander Gelbard, MD, of Vanderbilt Medical Center, Nashville, Tenn., found that higher body mass index, diabetes, and larger endotracheal tube (ETT) size were all associated with heightened risk.
The investigators assert that comparatively scarce data are available about how patients fare after receiving mechanical ventilation, and how adverse effects might interfere with recovery and return to daily activity. The larynx is rarely examined after extubation, and laryngeal injury may initially appear to be minor. Restricted glottic mobility therefore tends to be diagnosed after discharge, leaving critical care specialists unaware of the long-term impact.
The findings of the study should be a wake-up call for the development of guidelines for recognition and management of laryngeal injuries, according to John Robert Gowardman, MD, of Royal Brisbane (Australia) and Women’s Hospital, who wrote an accompanying editorial (Crit Care Med, 2019 Dec;47[12]:1802-04).
In addition, findings that ETT size, diabetes, and BMI represent risk factors for injury should help identify patients at risk, and the “practice of ‘putting in the biggest ETT just in case’ needs to be balanced against the dangers of an undersized ETT ... we should ask, ‘can my patient be safely managed with a smaller ETT?’ ” wrote Dr. Gowardman.
The researchers followed 100 consecutive adult patients who were examined with nasolaryngoscopy following an intubation of greater than 12 hours at Vanderbilt University Medical Center. They recorded baseline comorbidities and other factors. Fifty seven patients had an ALgI, defined as having glottic mucosal ulceration/granulation or subglottic granulation tissue/stenosis at the time of endoscopy. Nineteen patients had granulation tissue, 48 had posterior glottic ulceration, and 8 had subglottic mucosal ulceration.
Ten weeks after extubation, all patients were contacted by phone and asked to answer the Voice Handicap Index (VHI)-10 and the Clinical Chronic Obstructive Pulmonary Disease Questionnaire (CCQ). The questioner did not know the results of the patient’s endoscopy. Patients with ALgI were heavier on average (mean difference, 14 kg; BMI difference, 3.8 kg/m2), were more likely to have type 2 diabetes (46% versus 21%), and had more severe illness (median Charlson Comorbidity Index, 3.00 versus 2.00).
Sixty-seven patients completed the 10-week questionnaires, including 40 patients with ALgI and 27 without ALgI. Injury was associated with reports of worse breathing (median CCQ, 1.05 versus 0.20; P less than .001), as well as worse patient-reported voice outcomes (median VHI, 2 versus 0; P = .005).
ETT size appeared to be an important factor, according to multivariate analyses. Use of a 7.0 ETT was associated with lower frequency of injury than 7.5 (adjusted odds ratio, 0.04; P = .004) and 8.0 (OR, 0.03; P = .004). There was no significant difference between the 7.5 and 8.0 sizes.
The presence of type 2 diabetes altered the risk associated with BMI (P = .003 for interaction). Among patients who did not have type 2 diabetes, ALgI went up as a function of increasing BMI. Still, injury risk was higher in the presence of type 2 diabetes across all BMI ranges.
The Vanderbilt Institute for Clinical and Translational Research funded the study. Dr. Gowardman has no relevant disclosures.
SOURCE: Shinn JR et al. Crit Care Med;2019 Dec;47(12):1669-1706 .
(ALgI), and the injury is associated with worse breathing and speaking at 10 weeks, according to a study published in Critical Care Medicine (2019 Dec;47[12]:1669-1706). The researchers, led by Alexander Gelbard, MD, of Vanderbilt Medical Center, Nashville, Tenn., found that higher body mass index, diabetes, and larger endotracheal tube (ETT) size were all associated with heightened risk.
The investigators assert that comparatively scarce data are available about how patients fare after receiving mechanical ventilation, and how adverse effects might interfere with recovery and return to daily activity. The larynx is rarely examined after extubation, and laryngeal injury may initially appear to be minor. Restricted glottic mobility therefore tends to be diagnosed after discharge, leaving critical care specialists unaware of the long-term impact.
The findings of the study should be a wake-up call for the development of guidelines for recognition and management of laryngeal injuries, according to John Robert Gowardman, MD, of Royal Brisbane (Australia) and Women’s Hospital, who wrote an accompanying editorial (Crit Care Med, 2019 Dec;47[12]:1802-04).
In addition, findings that ETT size, diabetes, and BMI represent risk factors for injury should help identify patients at risk, and the “practice of ‘putting in the biggest ETT just in case’ needs to be balanced against the dangers of an undersized ETT ... we should ask, ‘can my patient be safely managed with a smaller ETT?’ ” wrote Dr. Gowardman.
The researchers followed 100 consecutive adult patients who were examined with nasolaryngoscopy following an intubation of greater than 12 hours at Vanderbilt University Medical Center. They recorded baseline comorbidities and other factors. Fifty seven patients had an ALgI, defined as having glottic mucosal ulceration/granulation or subglottic granulation tissue/stenosis at the time of endoscopy. Nineteen patients had granulation tissue, 48 had posterior glottic ulceration, and 8 had subglottic mucosal ulceration.
Ten weeks after extubation, all patients were contacted by phone and asked to answer the Voice Handicap Index (VHI)-10 and the Clinical Chronic Obstructive Pulmonary Disease Questionnaire (CCQ). The questioner did not know the results of the patient’s endoscopy. Patients with ALgI were heavier on average (mean difference, 14 kg; BMI difference, 3.8 kg/m2), were more likely to have type 2 diabetes (46% versus 21%), and had more severe illness (median Charlson Comorbidity Index, 3.00 versus 2.00).
Sixty-seven patients completed the 10-week questionnaires, including 40 patients with ALgI and 27 without ALgI. Injury was associated with reports of worse breathing (median CCQ, 1.05 versus 0.20; P less than .001), as well as worse patient-reported voice outcomes (median VHI, 2 versus 0; P = .005).
ETT size appeared to be an important factor, according to multivariate analyses. Use of a 7.0 ETT was associated with lower frequency of injury than 7.5 (adjusted odds ratio, 0.04; P = .004) and 8.0 (OR, 0.03; P = .004). There was no significant difference between the 7.5 and 8.0 sizes.
The presence of type 2 diabetes altered the risk associated with BMI (P = .003 for interaction). Among patients who did not have type 2 diabetes, ALgI went up as a function of increasing BMI. Still, injury risk was higher in the presence of type 2 diabetes across all BMI ranges.
The Vanderbilt Institute for Clinical and Translational Research funded the study. Dr. Gowardman has no relevant disclosures.
SOURCE: Shinn JR et al. Crit Care Med;2019 Dec;47(12):1669-1706 .
FROM CRITICAL CARE MEDICINE
Overcoming barriers to clinical trial enrollment in patients with bone and soft tissue sarcoma: a paradigm for an increasingly heterogeneous cancer population
Introduction
The development of new cancer therapies relies on the successful development and completion of clinical trials. While clinical trials have led to significant improvements in cancer treatment, the success is dependent upon patient enrollment and participation. Unfortunately, fewer than 5% of adult patients enroll in trials.1-3 This represents a significant barrier to the development and approval of new cancer treatments. Reasons for low accrual into trials are multifactorial, but include structural barriers (eg, clinic access), clinical barriers (eg, eligibility criteria), and physician and patient attitudes towards trial enrollment.4,5 One study at the University of California Davis Cancer Center reported 49% of patients declined participation despite meeting eligibility criteria,3,6 suggesting that psychosocial barriers such as knowledge of trials and attitudes towards clinical research are a major impediment to accrual.7-9
Bone and soft tissue sarcoma represent a heterogeneous group of tumors of mesenchymal origin that are an important cause of morbidity and mortality. Local disease is often treated with a multidisciplinary approach including surgery, radiation, and systemic therapy. Metastatic disease is predominantly treated palliatively with systemic therapy.10 Given its rarity and heterogeneity, trial accrual is of particular importance in sarcoma and often requires multiple sites to enroll adequate numbers of patients. While sarcoma represents <1% of adult malignancies overall, it constitutes ~15% of malignancies in the adolescent and young adult (AYA) population (15- 39 years old).11,12 Sarcoma represents a patient population in which low trial accrual has been correlated with lack of progress in cancer-related outcomes in both the adult and AYA populations.13 The reasons for low accrual rates among patients with sarcoma are poorly understood.
Sarcomas represent a molecularly and biologically heterogeneous group of malignancies with over 100 different subtypes.12 As a result, there has been significant interest in performing molecular profiling, or genetic sequencing, to identify “targetable” mutations. Targetable mutations refer to a specific genetic change identified within the tumor molecular profile for which there is a specific drug that may demonstrate activity against a particular tumor. Given the widespread utilization of this technology in sarcoma, identifying and understanding patient perceptions with regard to molecular profiling is critically important in this disease.14
In this study, we use a cross-sectional design to describe patient perceptions of trial enrollment among patients with bone and soft tissue sarcoma through validated measures, including attitudes towards clinical trials, knowledge of clinical trials, and perceived ability (ie, self-efficacy) to carry out actions involved in making an informed decision about clinical trial participation, receptivity to learning more about clinical trials, and willingness to participate in clinical trials.6 In addition, we describe this patient cohort’s perceptions of molecular profiling, as current and future trials are increasingly driven by molecular or other biomarkers.
Methods
This was a cross-sectional electronic survey study of patients with bone and soft tissue sarcoma treated at Northwestern Medicine (NM) over a 5-year period. NM Enterprise Data Warehouse (NMEDW) is a single, comprehensive, and integrated repository of all clinical and research data sources within NM. The study was approved by the Northwestern University Institutional Review Board.
Survey
The investigators designed a self-administered, online survey, which was built using Research Electronic Data Capture (REDCap). The survey consisted of three sections that were answered using skip logic—a custom path through the survey that varied based on patients’ answers: (1) Patient demographic information and trial perceptions (answered by all patients); (2) Thoughts about molecular profiling (answered by patients who answered “yes” to the question, “Have you heard about molecular profiling of tumors?”); and (3) Considerations to undergo molecular profiling (answered by patients who answered “yes” to the question, “Have you undergone profiling of your cancer?”).
Clinical trial perceptions included questions assessing (1) patient knowledge about trials; (2) patient attitudes toward trials; (3) perceived ability (ie, self-efficacy) to carry out actions involved in making an informed decision about trial participation; (4) receptivity to learning more about trials; and (5) willingness to participate in trials. These outcome measures had been previously developed and pilot tested for reliability and validity (TABLE 1).6
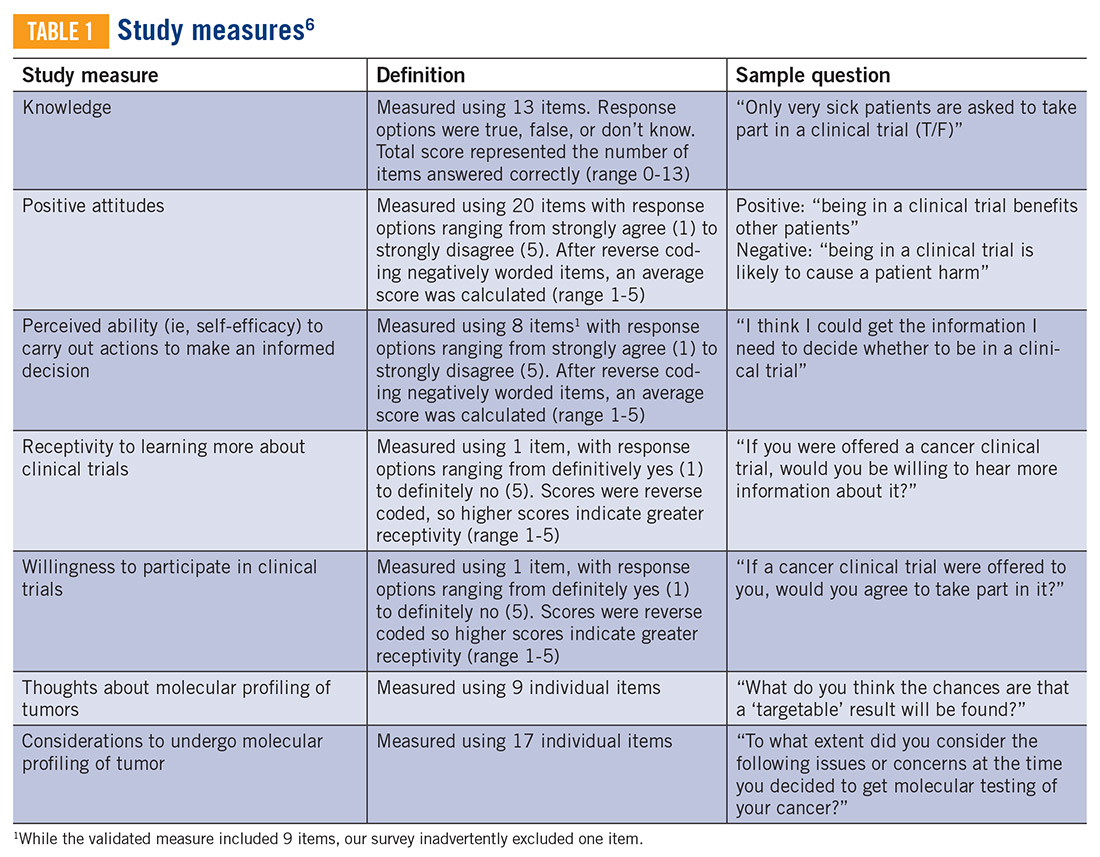
Thoughts about molecular profiling of tumors were assessed using nine items (TABLE 1). Of these, items assessing potential benefit or harm of molecular profiling were assessed using a 7-step Likert scale. Items assessing maximal benefit or harm of therapy, importance of quality vs length of life, and concern about the cost of molecular testing were assessed using a 5-step Likert scale. The study team developed and piloted these questions because there is no validated survey assessing these domains.
Considerations to undergo molecular profiling were assessed using 17 items. Items were in response to the question, “To what extent did you consider the following issues or concerns at the time you decided to get molecular testing of your cancer?” Responses were assessed using a 5-point Likert scale.
Data Collection
Patients 18 years and older evaluated at NM between November 20, 2012, and November 20, 2017, with a diagnosis of sarcoma were identified by query of the NMEDW by ICD-10 codes (C40, C41.9, C44.99, C45-49, C55, C71.9, D48, D49.9, and M12.20) or equivalent ICD-9 codes. Patients were subsequently excluded if they did not have a diagnosis of bone or soft tissue sarcoma, no e-mail address listed, had died, or had not been evaluated at an NM clinic in the previous 5 years. Patients with a diagnosis of gastrointestinal stromal tumor and Kaposi’s sarcoma were also excluded.
A personalized contact e-mail was sent to patients containing an explanation of the survey and an internet link to the electronic survey through REDCap from January 2018 to March 2018. If patients did not respond to the survey, two follow-up reminder e-mails were sent 2 and 4 days following the initial survey. The link was protected so that each patient could complete the survey only once. Responses were collected through the REDCap platform. Patients read and signed an electronic consent form prior to completing the survey.
Upon completion of the survey, patients were offered a $50 VISA gift card as compensation, with an option to donate their compensation to the Robert H. Lurie Comprehensive Cancer Center Sarcoma Research Fund.
Over the described survey period, open clinical trials for patients with bone and soft tissue sarcoma available at NM were evaluated. The number of patients screened and accrued to each trial were recorded.
Statistical analysis
Responses were separated from the personal data for complete anonymization. Descriptive statistical analysis was performed for demographics and disease variables and were summarized using frequencies and percentages. Median and range were used for age. Correlations between continuous variables were analyzed using Spearman correlations. Scores were compared between subgroups using the Mann-Whitney test. Descriptive statistics for knowledge, attitude, and ability scores include means and 95% confidence intervals. Correlations were interpreted as small (r=0.10), medium (r=0.30), or large (r=0.50).15 Statistical significance was indicated when P<0.05.
Results
Patients
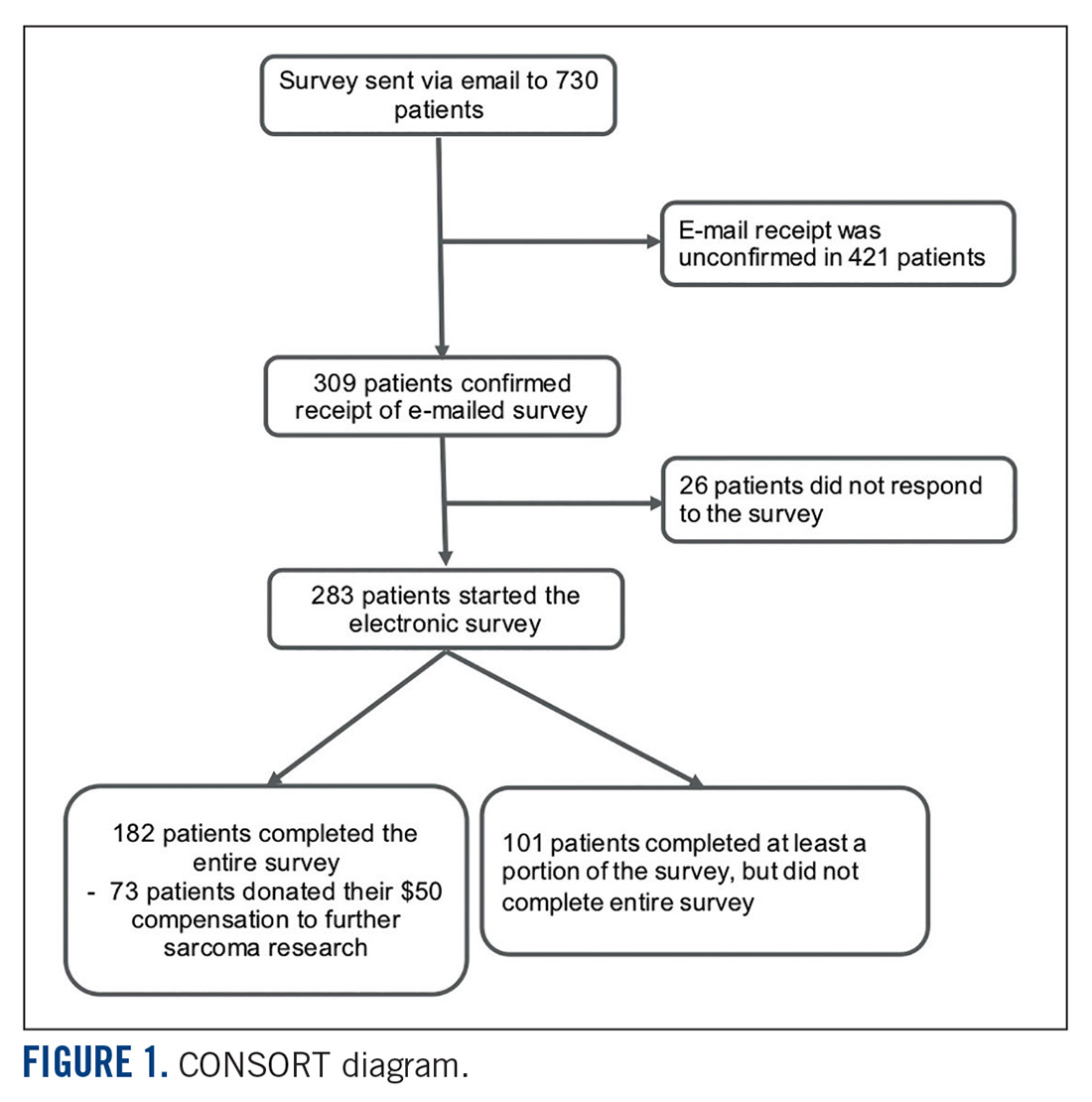
Seven hundred fifty patients were eligible to participate in the survey and received the initial and two follow-up e-mails. Twenty e-mailed surveys bounced back. Three hundred nine patients opened the initial e-mail and 283 patients (37.7% of total and 91.6% of opened) completed at least a portion of the survey, with 182 patients completing the entire survey (FIGURE 1). Data for analysis were used from patients who completed at least a portion of the survey.
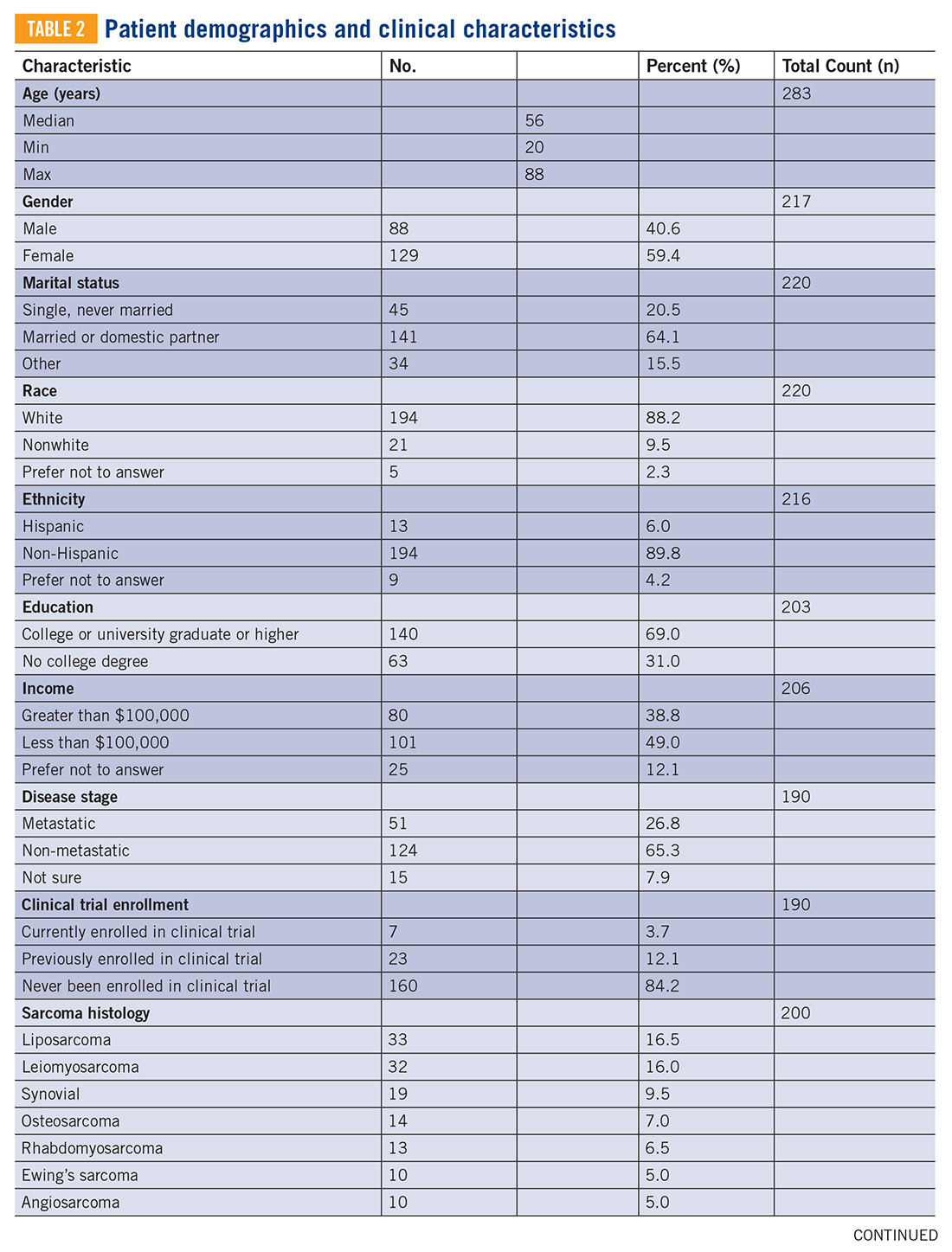
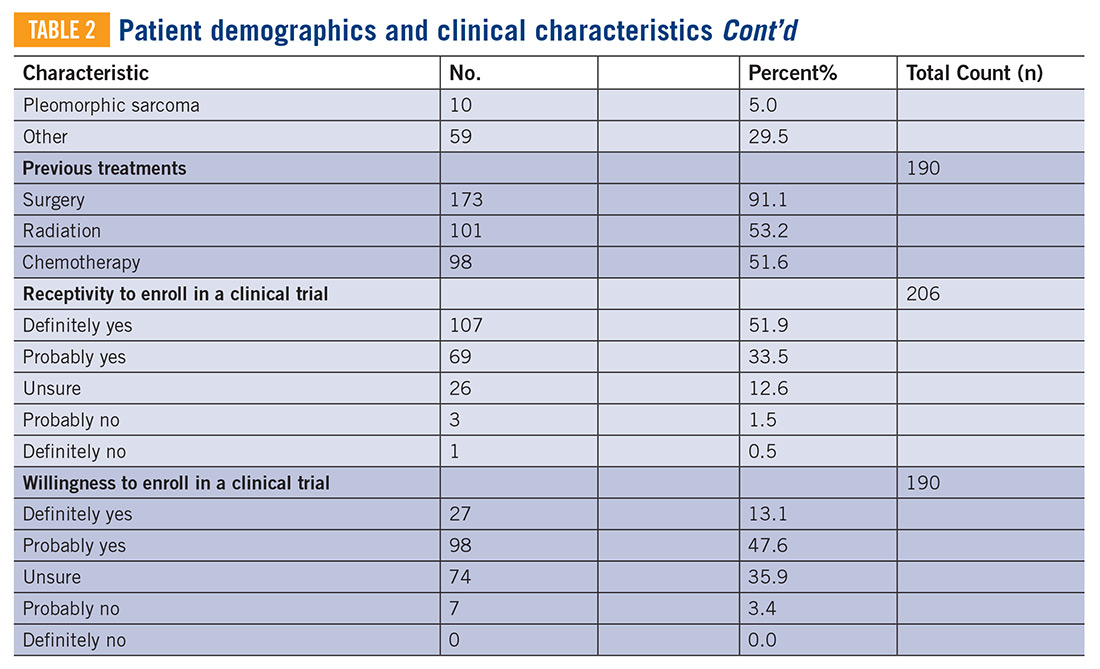
Baseline characteristics of patients who responded can be seen in TABLE 2. Patients had a median age of 56, the majority were female (59.4%), white (88.2%), and most had college or university graduate degrees or higher educational level (69.0%). Patients had various different histological subtypes, with the most common being liposarcoma (16.5%) and leiomyosarcoma (16.0%). Slightly more than a quarter (26.8%) of patients had metastatic disease, and 84.2% had never been enrolled in a clinical trial. Previous treatments included surgery (91.1%), radiation (53.2%), and chemotherapy (51.6%). Prior to completing the survey, 85.4% reported being receptive to a cancer clinical trial, while 60.7% of patients reported willingness to participate in a clinical trial.
Knowledge, attitudes, and perceived ability
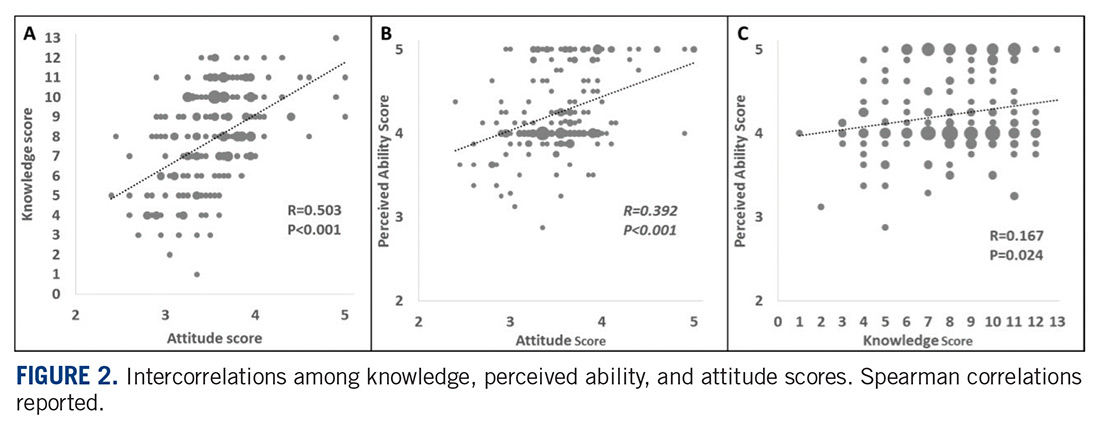
A statistically significant correlation was observed between greater knowledge of trials and more positive attitudes towards trials (P<0.001; r=0.5, FIGURE 2A). In relating patient attitudes with perceived ability, again a significant correlation was seen (P<0.001; r=0.4, FIGURE 2B). In contrast, knowledge had a weak correlation with perceived ability (P=0.024; r=0.2, FIGURE 2C). There was no difference regarding patient knowledge, attitudes, or perceived ability by age, gender, race, or income.
Knowledge, attitudes, perceived ability, and clinical trial enrollment
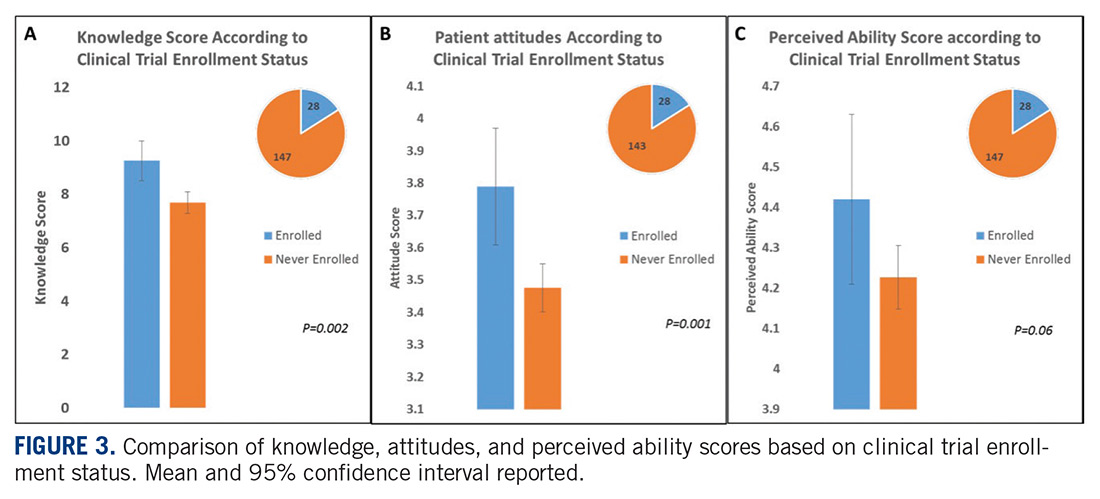
Thirty patients reported clinical trial experience (either previously or currently enrolled in trials) and 160 patients were never enrolled. Of the 30 patients with trial experience, 7 reported being currently enrolled, while 23 reported previous enrollment. Of these patients, 16 had metastatic disease, while 12 had non-metastatic disease, and 2 were unsure whether or not they had metastatic disease.
Patients with previous clinical trial exposure (currently or previously enrolled in clinical trials) demonstrated significantly greater trial knowledge, with a mean knowledge score of 9.3 (CI 8.5-10.0) compared with 7.7 (CI 7.3-8.1) among patients without trial exposure (P=0.002; FIGURE 3A). Similarly, patients with trial experience also had statistically significant more positive attitudes towards trials as compared with patients with no trial experience, with a mean attitude score of 3.8 (CI 3.6-4.0) and 3.5 (CI 3.4-3.6), respectively (P=0.001; FIGURE 3B). While numerically patients with trial experience have greater perceived ability compared with patients with no trial experience, with a mean score of 4.4 (CI 4.2-4.6) and 4.2 (CI 4.1-4.3), respectively, this difference did not reach statistical significance (FIGURE 3C).
Knowledge, attitudes, perceived ability, and disease stage
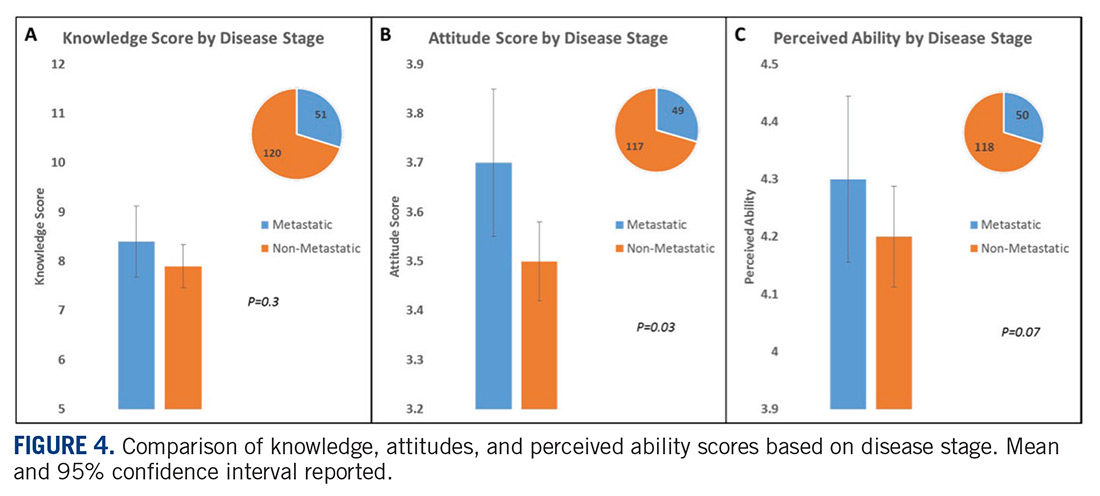
An analysis was performed comparing patients with metastatic vs non-metastatic disease. It was observed that patients with metastatic disease had similar knowledge of trials compared with non-metastatic patients, with a mean knowledge score of 8.4 (CI 7.7- 9.1) and 7.9 (CI 7.5-8.4), respectively, (P=0.3; FIGURE 4A). In contrast, patients with metastatic disease had more positive attitudes compared with non-metastatic patients, with a mean score of 3.7 (CI 3.5-3.8) and 3.5 (CI 3.4-3.6), respectively, which was statistically significant (P=0.03; FIGURE 4B). There was no difference in perceived ability in metastatic vs non-metastatic patients (FIGURE 4C).
Thoughts about molecular profiling
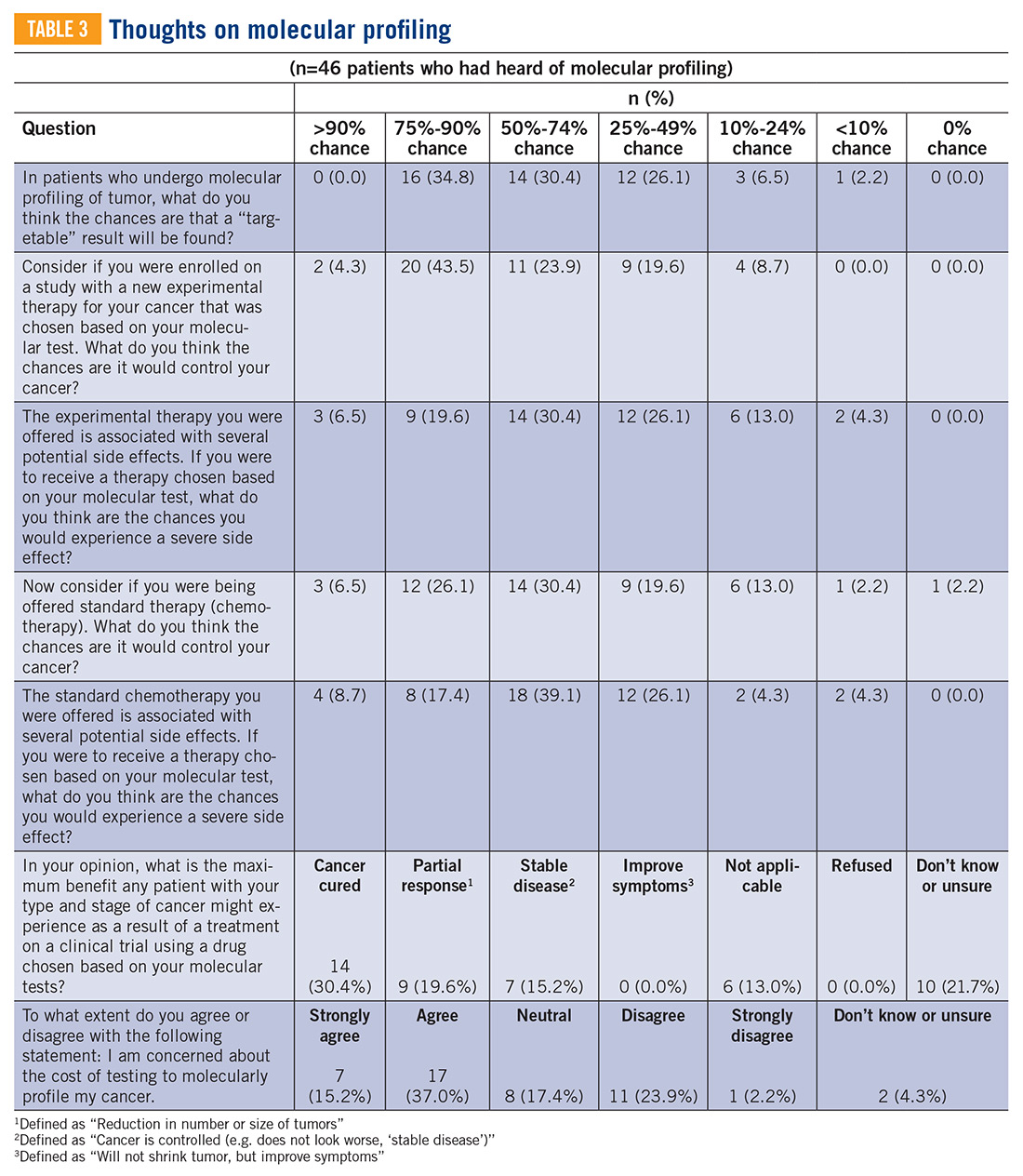
Of the total number of patients, 46 patients had heard of molecular profiling and were presented with questions regarding their thoughts (TABLE 3). Approximately two-thirds (65.2%) thought there would be a 50% or greater likelihood of finding a targetable result in their tumor molecular profile. A majority (71.7%) of patients thought that a new experimental therapy chosen based on a patient’s tumor molecular profile would have at least a 50% chance of controlling the cancer. Somewhat less than a third (30.4%) of patients thought that total cure is the maximal benefit a patient could experience as a result of a treatment on a clinical trial using a drug chosen based on molecular tests. About half (52.2%) of patients agreed with the statement, “I am concerned about the cost of the test to molecularly profile my cancer.”
Considerations to undergo molecular profiling
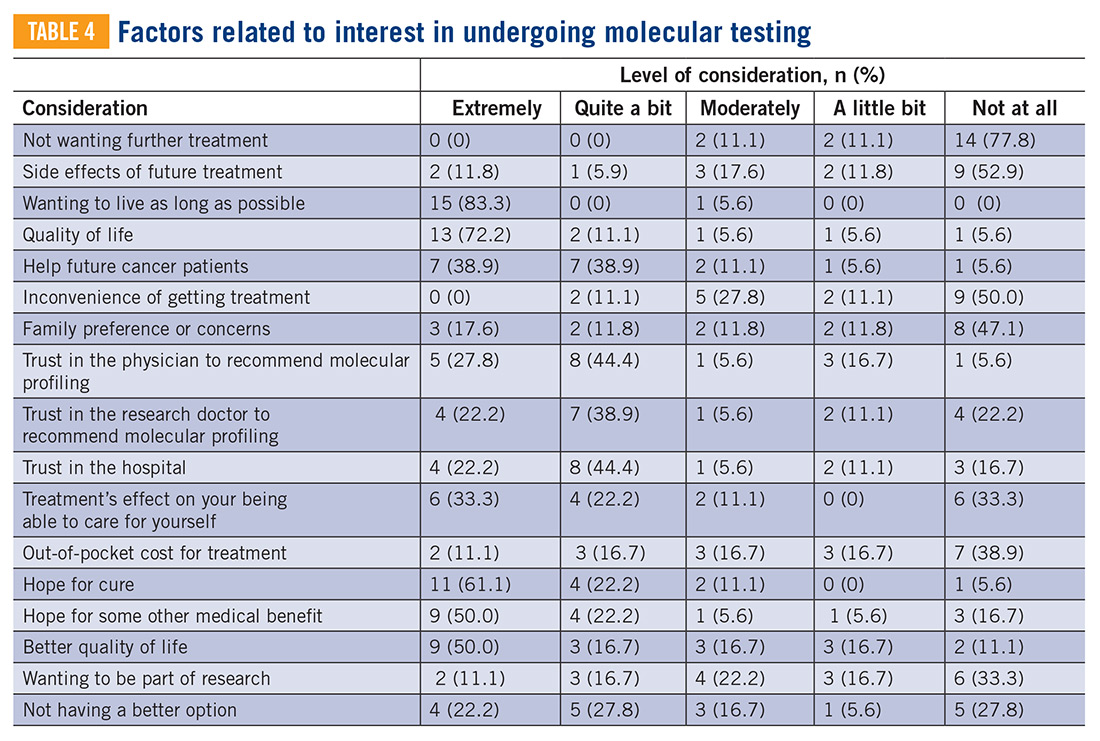
Eighteen patients had undergone molecular profiling of their tumor. These patients were posed the question, “To what extent did you consider the following issues or concerns at the time you decided to get molecular testing of your cancer?” (TABLE 4). A majority (83.3%) of patients stated that wanting to live as long as possible was important, and 72.2% of patients stated that quality of life was important. A majority (83.3%) of patients stated that hope for a cure was an extremely or quite a bit important consideration. Helping future cancer patients was extremely or quite a bit important for 77.8% of patients, while wanting to be a part of research was not at all or of little importance in 50.0% of patients.
Clinical trials at NM
Twenty-four clinical trials were available at NM between the years 2012 and 2017 for patients with bone and soft tissue sarcoma. Of these trials, 3 of 24 were for non-metastatic patients, while the remaining 21 were open only to metastatic patients. The median number of patients screened per trial was 11 (range 0-66) and the median number of patients accrued per trial was 9 (range 0-58). Of the 24 trials, 17 were not subtype specific (13 included soft tissue sarcoma alone while 4 included both bone and soft tissue sarcoma). The remaining 7 trials were sarcoma subtype specific (eg, angiosarcoma, liposarcoma, etc). Trials available at NM during this period are included in TABLE 5. There were 318 patients screened and 262 patients accrued to sarcoma trials over this time period, with a screen failure rate of 17.6% overall.

Discussion
Our study sought to describe perceptions of clinical trial enrollment among patients with bone and soft tissue sarcoma in order to elucidate and overcome barriers to enrollment, which to the best of our knowledge had not been previously described. Using previously validated patient- reported outcomes in the literature,6 our data reveal a correlation between knowledge of trials and more positive attitudes towards trials. This underscores the importance of awareness and educational strategies in this cancer population as a whole. Interventions should focus on patient perceptions that contribute to lack of participation, such as fear of side effects, loss of control (eg, idea of placebo or randomization), logistical challenges (eg, additional time or convenient location), and cost.3,5,7,16,17 For example, patients concerned about randomization should be educated on equipoise and other ethical considerations in trial design.5 Previous research has suggested that a multimedia psychoeducational intervention was effective in improving attitudes toward trials.6 Educating patients on the essential role of trials in oncology care, as demonstrated by the vast number of new drug approvals in recent years, is an essential strategy to improve attitudes, and subsequently leads to higher patient accrual rates.
In our study, both knowledge and at titudes were increased in patients with previous trial exposure. This suggests that either patients with greater knowledge and more positive attitudes are more likely to enroll in trials, or that patients with direct trial exposure are more knowledgeable and develop more positive attitudes. Our patient population was overall receptive to learning more about clinical trials (85.4%) and willing to participate (65.8%). At the same time, our study demonstrated low to medium correlations between attitudes and perceived ability to take steps towards making an informed decision to enroll in a trial (r=0.4), which may partially be explained by the absence of a tangible trial opportunity. While we did not assess specifically whether patients in our study were offered a trial, there was a substantial trial menu at NM with limited screen failures and decent trial accrual over the time frame of our study. This underscores the importance not only of patient-focused strategies to increase educational and attitudinal resources, but also a need to focus on research-site optimization that includes opening of multiple trials in various settings, systematic pre-screening of patients, and eligibility criteria that are inclusive and rational.5
The patient population with metastatic disease demonstrated more positive attitudes towards enrolling in clinical trials. This cohort accrued well to clinical trials, with 21 of 24 trials enrolling specifically patients with metastatic disease. Of the patients who responded to our survey, patients with previous trial exposure were enriched for patients with metastatic disease (53.3% metastatic among previous trial exposure versus 26.8% metastatic overall). These observations are likely reflective of the need for novel therapies in this disease setting. At the same time, approximately 25% of patients with localized soft tissue sarcoma will develop distant metastatic disease after successful treatment of their primary tumor, which increases to 40% to 50% in larger and higher-grade tumors.18 Three of 24 trials were open for patients with non-metastatic disease, of which one managed to accrue patients. Patients with non-metastatic disease had more negative attitudes towards trial enrollment. These disproportionate findings suggest a need for interventions to increase patient awareness and attitudes towards trial enrollment among this patient population and the importance of research-site optimization for trial opportunities across disease states.
Molecular profiling of tumors and biomarker identification has become a critical component of further characterizing cancer subtypes. In our study, a majority (65.2%) thought there would be a 50% or greater likelihood of finding a targetable result in their molecular profile. Molecular data on 5,749 bone and soft tissue sarcomas suggested that 9.5% of tumors demonstrate a “targetable result,” defined as a new molecular finding for which there is an FDA-approved drug for malignancies other than sarcoma (eg, BRAF V600E, Her2, etc.),19 suggesting an overestimation in our patient cohort of the likelihood of benefit of molecular profiling. These results highlight that the growing use of molecular profiling has increased the need for educational and supportive resources to help patients understand the utility of molecular profiling and aid in shared decision-making surrounding the results.
At the same time, the importance of identifying a targetable mutation in patients with sarcoma cannot be understated. As a recent example of this paradigm, tumors that harbor fusions with the neurotrophic receptor tyrosine kinase 1, 2, or 3 (NTRK1, 2, and 3) have a high response rate (~75%) to drugs that target these fusions, such as larotrectinib and entrectinib.13 Molecular profiling and identification of predictive biomarkers in small patient subsets has led to great challenges in trial design and research-site optimization. Novel designs that incorporate molecular profiling,20 such as the Lung- MAP trial21 and NCI’s Molecular Analysis for Therapy Choice (MATCH) trial,22 are emerging to identify new therapies for small patient subsets. As a rare and increasingly heterogeneous cancer, sarcoma represents a paradigm to provide insight into optimizing patient perceptions and research enterprises to maximize clinical trial enrollment.
Some limitations of our study include a homogeneous and selected patient population that was predominantly Caucasian and highly educated. Therefore, these findings should not be extrapolated to other populations with barriers to trial accrual, such as lower socioeconomic or minority populations. The low response rate and failure of some to complete the survey may have introduced some bias. Additionally, our data include self-reported outcomes, which could have affected our results. Finally, the limited number of patients who had undergone or heard of molecular profiling limited our ability to draw definitive conclusions, and should be assessed in larger patient cohorts.
While our paper addresses a unique population—the sarcoma patient—similar themes and issues pertain to all oncology patients. A recent review was published in the American Society of Clinical Oncology Educational Book23 looking at methods to overcome barriers to clinical trial enrollment. Their paper clearly illustrates mechanisms to assist with overcoming financial burdens associated with cancer clinical trials, overcoming barriers as they relate to patient and clinician difficulty in coping with the uncertainty inherent in clinical trial participation, and highlight the role of a patient navigator in clinical trial participation.
Conclusions
Interventions aimed at increasing awareness, knowledge, and attitudes towards clinical trials among sarcoma patients may lead to increased trial enrollment and greater progress in cancer treatment in this population. In addition to patient- focused interventions, thoughtful and strategic clinical trial designs that allow for the development of biomarker- driven therapeutics, while at the same time optimizing patient accrual rates, should be developed. Evaluation of barriers to clinical trial enrollment and molecular profiling of tumors among bone and soft tissue sarcoma patients at an academic center can serve as a paradigm to overcome barriers to enrollment in the era of an increasingly heterogeneous cancer population. TSJ
1. Go RS, Frisby KA, Lee JA, et al. Clinical trial accrual among new cancer patients at a community-based cancer center. Cancer. 2006;106(2):426-433.
2. Murthy VH, Krumholz HM, Gross CP. Participation in cancer clinical trials: Race-, sex-, and age-based disparities. JAMA. 2004; 291(22):2720-2726.
3. Lara PN Jr, Higdon R, Lim N, et al. Prospective evaluation of cancer clinical trial accrual patterns: identifying potential barriers to enrollment. J Clin Oncol. 2001;19(6):1728-1733.
4. Unger JM, Cook E, Tai E, Bleyer A. The role of clinical trial participation in cancer research: barriers, evidence, and strategies. Am Soc Clin Oncol Educ Book. 2016;35:185-198.
5. Cancer Action Network American Cancer Society. Barriers to patient enrollment in therapeutic clinical trials for cancer. 2018: https:// www.fightcancer.org/policy-resources/clinical- trial-barriers#figures. Accessed March 14, 2019.
6. Jacobsen PB, Wells KJ, Meade CD, et al. Effects of a brief multimedia psychoeducational intervention on the attitudes and interest of patients with cancer regarding clinical trial participation: a multicenter randomized controlled trial. J Clin Oncol. 2012;30(20):2516-2521.
7. Meropol NJ, Buzaglo JS, Millard J, et al. Barriers to clinical trial participation as perceived by oncologists and patients. J Natl Compr Canc Netw. 2007;5(8):655-664.
8. Cox K, McGarry J. Why patients don’t take part in cancer clinical trials: an overview of the literature. Eur J Cancer Care (Engl). 2003;12(2): 114-122.
9. Mills EJ, Seely D, Rachlis B, et al. Barriers to participation in clinical trials of cancer: a meta- analysis and systematic review of patient-reported factors. Lancet Oncol. 2006;7(2):141-148.
10. National Comprehensive Cancer Network. Soft Tissue Sarcoma (Version 4.2019). https:// www.nccn.org/professionals/physician_gls/ pdf/sarcoma.pdf. Accessed October 30, 2019.
11. Nass SJ, Beaupin LK, Demark-Wahnefried W, et al. Identifying and addressing the needs of adolescents and young adults with cancer: summary of an Institute of Medicine workshop. Oncologist. 2015;20(2):186-195.
12. Wilky BA, Villalobos VM. Emerging role for precision therapy through next-generation sequencing for sarcomas. JCO Precision Oncol. 2018(2):1-4.
13. Bleyer A, Montello M, Budd T, Saxman S. National survival trends of young adults with sarcoma: lack of progress is associated with lack of clinical trial participation. Cancer. 2005;103(9):1891-1897.
14. Gornick MC, Cobain E, Le LQ, et al. Oncologists’ use of genomic sequencing data to inform clinical management. JCO Precision Oncol. 2018(2):1-13.
15. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: L. Erlbaum Associates; 1988.
16. Unger JM, Hershman DL, Albain KS, et al. Patient income level and cancer clinical trial participation. J Clin Oncol. 2013;31(5):536- 542.
17. Javid SH, Unger JM, Gralow JR, et al. A prospective analysis of the influence of older age on physician and patient decision-making when considering enrollment in breast cancer clinical trials (SWOG S0316). Oncologist. 2012;17(9):1180-1190.
18. Singhi EK, Moore DC, Muslimani A. Metastatic soft tissue sarcomas: a review of treatment and new pharmacotherapies. P T. 2018;43(7): 410-429.
19. Gounder MM, Ali SM, Robinson V, et al. Impact of next-generation sequencing (NGS) on diagnostic and therapeutic options in soft-tissue and bone sarcoma. J Clin Oncol. 2017;35(15_suppl):abstr 11001.
20. Woodcock J, LaVange LM. Master protocols to study multiple therapies, multiple diseases, or both. N Engl J Med. 2017;377(1):62-70.
21. Steuer CE, Papadimitrakopoulou V, Herbst RS, et al. Innovative clinical trials: the LUNGMAP study. Clin Pharmacol Ther. 2015;97(5): 488-491.
22. McNeil C. NCI-MATCH launch highlights new trial design in precision-medicine era. J Natl Cancer Inst. 2015;107(7).
23. Nipp RD, Hong K, Paskett ED. Overcoming barriers to clinical trial enrollment. Am Soc Clin Oncol Educ Book. 2019;39:105-114.
Introduction
The development of new cancer therapies relies on the successful development and completion of clinical trials. While clinical trials have led to significant improvements in cancer treatment, the success is dependent upon patient enrollment and participation. Unfortunately, fewer than 5% of adult patients enroll in trials.1-3 This represents a significant barrier to the development and approval of new cancer treatments. Reasons for low accrual into trials are multifactorial, but include structural barriers (eg, clinic access), clinical barriers (eg, eligibility criteria), and physician and patient attitudes towards trial enrollment.4,5 One study at the University of California Davis Cancer Center reported 49% of patients declined participation despite meeting eligibility criteria,3,6 suggesting that psychosocial barriers such as knowledge of trials and attitudes towards clinical research are a major impediment to accrual.7-9
Bone and soft tissue sarcoma represent a heterogeneous group of tumors of mesenchymal origin that are an important cause of morbidity and mortality. Local disease is often treated with a multidisciplinary approach including surgery, radiation, and systemic therapy. Metastatic disease is predominantly treated palliatively with systemic therapy.10 Given its rarity and heterogeneity, trial accrual is of particular importance in sarcoma and often requires multiple sites to enroll adequate numbers of patients. While sarcoma represents <1% of adult malignancies overall, it constitutes ~15% of malignancies in the adolescent and young adult (AYA) population (15- 39 years old).11,12 Sarcoma represents a patient population in which low trial accrual has been correlated with lack of progress in cancer-related outcomes in both the adult and AYA populations.13 The reasons for low accrual rates among patients with sarcoma are poorly understood.
Sarcomas represent a molecularly and biologically heterogeneous group of malignancies with over 100 different subtypes.12 As a result, there has been significant interest in performing molecular profiling, or genetic sequencing, to identify “targetable” mutations. Targetable mutations refer to a specific genetic change identified within the tumor molecular profile for which there is a specific drug that may demonstrate activity against a particular tumor. Given the widespread utilization of this technology in sarcoma, identifying and understanding patient perceptions with regard to molecular profiling is critically important in this disease.14
In this study, we use a cross-sectional design to describe patient perceptions of trial enrollment among patients with bone and soft tissue sarcoma through validated measures, including attitudes towards clinical trials, knowledge of clinical trials, and perceived ability (ie, self-efficacy) to carry out actions involved in making an informed decision about clinical trial participation, receptivity to learning more about clinical trials, and willingness to participate in clinical trials.6 In addition, we describe this patient cohort’s perceptions of molecular profiling, as current and future trials are increasingly driven by molecular or other biomarkers.
Methods
This was a cross-sectional electronic survey study of patients with bone and soft tissue sarcoma treated at Northwestern Medicine (NM) over a 5-year period. NM Enterprise Data Warehouse (NMEDW) is a single, comprehensive, and integrated repository of all clinical and research data sources within NM. The study was approved by the Northwestern University Institutional Review Board.
Survey
The investigators designed a self-administered, online survey, which was built using Research Electronic Data Capture (REDCap). The survey consisted of three sections that were answered using skip logic—a custom path through the survey that varied based on patients’ answers: (1) Patient demographic information and trial perceptions (answered by all patients); (2) Thoughts about molecular profiling (answered by patients who answered “yes” to the question, “Have you heard about molecular profiling of tumors?”); and (3) Considerations to undergo molecular profiling (answered by patients who answered “yes” to the question, “Have you undergone profiling of your cancer?”).
Clinical trial perceptions included questions assessing (1) patient knowledge about trials; (2) patient attitudes toward trials; (3) perceived ability (ie, self-efficacy) to carry out actions involved in making an informed decision about trial participation; (4) receptivity to learning more about trials; and (5) willingness to participate in trials. These outcome measures had been previously developed and pilot tested for reliability and validity (TABLE 1).6
Thoughts about molecular profiling of tumors were assessed using nine items (TABLE 1). Of these, items assessing potential benefit or harm of molecular profiling were assessed using a 7-step Likert scale. Items assessing maximal benefit or harm of therapy, importance of quality vs length of life, and concern about the cost of molecular testing were assessed using a 5-step Likert scale. The study team developed and piloted these questions because there is no validated survey assessing these domains.
Considerations to undergo molecular profiling were assessed using 17 items. Items were in response to the question, “To what extent did you consider the following issues or concerns at the time you decided to get molecular testing of your cancer?” Responses were assessed using a 5-point Likert scale.
Data Collection
Patients 18 years and older evaluated at NM between November 20, 2012, and November 20, 2017, with a diagnosis of sarcoma were identified by query of the NMEDW by ICD-10 codes (C40, C41.9, C44.99, C45-49, C55, C71.9, D48, D49.9, and M12.20) or equivalent ICD-9 codes. Patients were subsequently excluded if they did not have a diagnosis of bone or soft tissue sarcoma, no e-mail address listed, had died, or had not been evaluated at an NM clinic in the previous 5 years. Patients with a diagnosis of gastrointestinal stromal tumor and Kaposi’s sarcoma were also excluded.
A personalized contact e-mail was sent to patients containing an explanation of the survey and an internet link to the electronic survey through REDCap from January 2018 to March 2018. If patients did not respond to the survey, two follow-up reminder e-mails were sent 2 and 4 days following the initial survey. The link was protected so that each patient could complete the survey only once. Responses were collected through the REDCap platform. Patients read and signed an electronic consent form prior to completing the survey.
Upon completion of the survey, patients were offered a $50 VISA gift card as compensation, with an option to donate their compensation to the Robert H. Lurie Comprehensive Cancer Center Sarcoma Research Fund.
Over the described survey period, open clinical trials for patients with bone and soft tissue sarcoma available at NM were evaluated. The number of patients screened and accrued to each trial were recorded.
Statistical analysis
Responses were separated from the personal data for complete anonymization. Descriptive statistical analysis was performed for demographics and disease variables and were summarized using frequencies and percentages. Median and range were used for age. Correlations between continuous variables were analyzed using Spearman correlations. Scores were compared between subgroups using the Mann-Whitney test. Descriptive statistics for knowledge, attitude, and ability scores include means and 95% confidence intervals. Correlations were interpreted as small (r=0.10), medium (r=0.30), or large (r=0.50).15 Statistical significance was indicated when P<0.05.
Results
Patients
Seven hundred fifty patients were eligible to participate in the survey and received the initial and two follow-up e-mails. Twenty e-mailed surveys bounced back. Three hundred nine patients opened the initial e-mail and 283 patients (37.7% of total and 91.6% of opened) completed at least a portion of the survey, with 182 patients completing the entire survey (FIGURE 1). Data for analysis were used from patients who completed at least a portion of the survey.
Baseline characteristics of patients who responded can be seen in TABLE 2. Patients had a median age of 56, the majority were female (59.4%), white (88.2%), and most had college or university graduate degrees or higher educational level (69.0%). Patients had various different histological subtypes, with the most common being liposarcoma (16.5%) and leiomyosarcoma (16.0%). Slightly more than a quarter (26.8%) of patients had metastatic disease, and 84.2% had never been enrolled in a clinical trial. Previous treatments included surgery (91.1%), radiation (53.2%), and chemotherapy (51.6%). Prior to completing the survey, 85.4% reported being receptive to a cancer clinical trial, while 60.7% of patients reported willingness to participate in a clinical trial.
Knowledge, attitudes, and perceived ability
A statistically significant correlation was observed between greater knowledge of trials and more positive attitudes towards trials (P<0.001; r=0.5, FIGURE 2A). In relating patient attitudes with perceived ability, again a significant correlation was seen (P<0.001; r=0.4, FIGURE 2B). In contrast, knowledge had a weak correlation with perceived ability (P=0.024; r=0.2, FIGURE 2C). There was no difference regarding patient knowledge, attitudes, or perceived ability by age, gender, race, or income.
Knowledge, attitudes, perceived ability, and clinical trial enrollment
Thirty patients reported clinical trial experience (either previously or currently enrolled in trials) and 160 patients were never enrolled. Of the 30 patients with trial experience, 7 reported being currently enrolled, while 23 reported previous enrollment. Of these patients, 16 had metastatic disease, while 12 had non-metastatic disease, and 2 were unsure whether or not they had metastatic disease.
Patients with previous clinical trial exposure (currently or previously enrolled in clinical trials) demonstrated significantly greater trial knowledge, with a mean knowledge score of 9.3 (CI 8.5-10.0) compared with 7.7 (CI 7.3-8.1) among patients without trial exposure (P=0.002; FIGURE 3A). Similarly, patients with trial experience also had statistically significant more positive attitudes towards trials as compared with patients with no trial experience, with a mean attitude score of 3.8 (CI 3.6-4.0) and 3.5 (CI 3.4-3.6), respectively (P=0.001; FIGURE 3B). While numerically patients with trial experience have greater perceived ability compared with patients with no trial experience, with a mean score of 4.4 (CI 4.2-4.6) and 4.2 (CI 4.1-4.3), respectively, this difference did not reach statistical significance (FIGURE 3C).
Knowledge, attitudes, perceived ability, and disease stage
An analysis was performed comparing patients with metastatic vs non-metastatic disease. It was observed that patients with metastatic disease had similar knowledge of trials compared with non-metastatic patients, with a mean knowledge score of 8.4 (CI 7.7- 9.1) and 7.9 (CI 7.5-8.4), respectively, (P=0.3; FIGURE 4A). In contrast, patients with metastatic disease had more positive attitudes compared with non-metastatic patients, with a mean score of 3.7 (CI 3.5-3.8) and 3.5 (CI 3.4-3.6), respectively, which was statistically significant (P=0.03; FIGURE 4B). There was no difference in perceived ability in metastatic vs non-metastatic patients (FIGURE 4C).
Thoughts about molecular profiling
Of the total number of patients, 46 patients had heard of molecular profiling and were presented with questions regarding their thoughts (TABLE 3). Approximately two-thirds (65.2%) thought there would be a 50% or greater likelihood of finding a targetable result in their tumor molecular profile. A majority (71.7%) of patients thought that a new experimental therapy chosen based on a patient’s tumor molecular profile would have at least a 50% chance of controlling the cancer. Somewhat less than a third (30.4%) of patients thought that total cure is the maximal benefit a patient could experience as a result of a treatment on a clinical trial using a drug chosen based on molecular tests. About half (52.2%) of patients agreed with the statement, “I am concerned about the cost of the test to molecularly profile my cancer.”
Considerations to undergo molecular profiling
Eighteen patients had undergone molecular profiling of their tumor. These patients were posed the question, “To what extent did you consider the following issues or concerns at the time you decided to get molecular testing of your cancer?” (TABLE 4). A majority (83.3%) of patients stated that wanting to live as long as possible was important, and 72.2% of patients stated that quality of life was important. A majority (83.3%) of patients stated that hope for a cure was an extremely or quite a bit important consideration. Helping future cancer patients was extremely or quite a bit important for 77.8% of patients, while wanting to be a part of research was not at all or of little importance in 50.0% of patients.
Clinical trials at NM
Twenty-four clinical trials were available at NM between the years 2012 and 2017 for patients with bone and soft tissue sarcoma. Of these trials, 3 of 24 were for non-metastatic patients, while the remaining 21 were open only to metastatic patients. The median number of patients screened per trial was 11 (range 0-66) and the median number of patients accrued per trial was 9 (range 0-58). Of the 24 trials, 17 were not subtype specific (13 included soft tissue sarcoma alone while 4 included both bone and soft tissue sarcoma). The remaining 7 trials were sarcoma subtype specific (eg, angiosarcoma, liposarcoma, etc). Trials available at NM during this period are included in TABLE 5. There were 318 patients screened and 262 patients accrued to sarcoma trials over this time period, with a screen failure rate of 17.6% overall.
Discussion
Our study sought to describe perceptions of clinical trial enrollment among patients with bone and soft tissue sarcoma in order to elucidate and overcome barriers to enrollment, which to the best of our knowledge had not been previously described. Using previously validated patient- reported outcomes in the literature,6 our data reveal a correlation between knowledge of trials and more positive attitudes towards trials. This underscores the importance of awareness and educational strategies in this cancer population as a whole. Interventions should focus on patient perceptions that contribute to lack of participation, such as fear of side effects, loss of control (eg, idea of placebo or randomization), logistical challenges (eg, additional time or convenient location), and cost.3,5,7,16,17 For example, patients concerned about randomization should be educated on equipoise and other ethical considerations in trial design.5 Previous research has suggested that a multimedia psychoeducational intervention was effective in improving attitudes toward trials.6 Educating patients on the essential role of trials in oncology care, as demonstrated by the vast number of new drug approvals in recent years, is an essential strategy to improve attitudes, and subsequently leads to higher patient accrual rates.
In our study, both knowledge and at titudes were increased in patients with previous trial exposure. This suggests that either patients with greater knowledge and more positive attitudes are more likely to enroll in trials, or that patients with direct trial exposure are more knowledgeable and develop more positive attitudes. Our patient population was overall receptive to learning more about clinical trials (85.4%) and willing to participate (65.8%). At the same time, our study demonstrated low to medium correlations between attitudes and perceived ability to take steps towards making an informed decision to enroll in a trial (r=0.4), which may partially be explained by the absence of a tangible trial opportunity. While we did not assess specifically whether patients in our study were offered a trial, there was a substantial trial menu at NM with limited screen failures and decent trial accrual over the time frame of our study. This underscores the importance not only of patient-focused strategies to increase educational and attitudinal resources, but also a need to focus on research-site optimization that includes opening of multiple trials in various settings, systematic pre-screening of patients, and eligibility criteria that are inclusive and rational.5
The patient population with metastatic disease demonstrated more positive attitudes towards enrolling in clinical trials. This cohort accrued well to clinical trials, with 21 of 24 trials enrolling specifically patients with metastatic disease. Of the patients who responded to our survey, patients with previous trial exposure were enriched for patients with metastatic disease (53.3% metastatic among previous trial exposure versus 26.8% metastatic overall). These observations are likely reflective of the need for novel therapies in this disease setting. At the same time, approximately 25% of patients with localized soft tissue sarcoma will develop distant metastatic disease after successful treatment of their primary tumor, which increases to 40% to 50% in larger and higher-grade tumors.18 Three of 24 trials were open for patients with non-metastatic disease, of which one managed to accrue patients. Patients with non-metastatic disease had more negative attitudes towards trial enrollment. These disproportionate findings suggest a need for interventions to increase patient awareness and attitudes towards trial enrollment among this patient population and the importance of research-site optimization for trial opportunities across disease states.
Molecular profiling of tumors and biomarker identification has become a critical component of further characterizing cancer subtypes. In our study, a majority (65.2%) thought there would be a 50% or greater likelihood of finding a targetable result in their molecular profile. Molecular data on 5,749 bone and soft tissue sarcomas suggested that 9.5% of tumors demonstrate a “targetable result,” defined as a new molecular finding for which there is an FDA-approved drug for malignancies other than sarcoma (eg, BRAF V600E, Her2, etc.),19 suggesting an overestimation in our patient cohort of the likelihood of benefit of molecular profiling. These results highlight that the growing use of molecular profiling has increased the need for educational and supportive resources to help patients understand the utility of molecular profiling and aid in shared decision-making surrounding the results.
At the same time, the importance of identifying a targetable mutation in patients with sarcoma cannot be understated. As a recent example of this paradigm, tumors that harbor fusions with the neurotrophic receptor tyrosine kinase 1, 2, or 3 (NTRK1, 2, and 3) have a high response rate (~75%) to drugs that target these fusions, such as larotrectinib and entrectinib.13 Molecular profiling and identification of predictive biomarkers in small patient subsets has led to great challenges in trial design and research-site optimization. Novel designs that incorporate molecular profiling,20 such as the Lung- MAP trial21 and NCI’s Molecular Analysis for Therapy Choice (MATCH) trial,22 are emerging to identify new therapies for small patient subsets. As a rare and increasingly heterogeneous cancer, sarcoma represents a paradigm to provide insight into optimizing patient perceptions and research enterprises to maximize clinical trial enrollment.
Some limitations of our study include a homogeneous and selected patient population that was predominantly Caucasian and highly educated. Therefore, these findings should not be extrapolated to other populations with barriers to trial accrual, such as lower socioeconomic or minority populations. The low response rate and failure of some to complete the survey may have introduced some bias. Additionally, our data include self-reported outcomes, which could have affected our results. Finally, the limited number of patients who had undergone or heard of molecular profiling limited our ability to draw definitive conclusions, and should be assessed in larger patient cohorts.
While our paper addresses a unique population—the sarcoma patient—similar themes and issues pertain to all oncology patients. A recent review was published in the American Society of Clinical Oncology Educational Book23 looking at methods to overcome barriers to clinical trial enrollment. Their paper clearly illustrates mechanisms to assist with overcoming financial burdens associated with cancer clinical trials, overcoming barriers as they relate to patient and clinician difficulty in coping with the uncertainty inherent in clinical trial participation, and highlight the role of a patient navigator in clinical trial participation.
Conclusions
Interventions aimed at increasing awareness, knowledge, and attitudes towards clinical trials among sarcoma patients may lead to increased trial enrollment and greater progress in cancer treatment in this population. In addition to patient- focused interventions, thoughtful and strategic clinical trial designs that allow for the development of biomarker- driven therapeutics, while at the same time optimizing patient accrual rates, should be developed. Evaluation of barriers to clinical trial enrollment and molecular profiling of tumors among bone and soft tissue sarcoma patients at an academic center can serve as a paradigm to overcome barriers to enrollment in the era of an increasingly heterogeneous cancer population. TSJ
Introduction
The development of new cancer therapies relies on the successful development and completion of clinical trials. While clinical trials have led to significant improvements in cancer treatment, the success is dependent upon patient enrollment and participation. Unfortunately, fewer than 5% of adult patients enroll in trials.1-3 This represents a significant barrier to the development and approval of new cancer treatments. Reasons for low accrual into trials are multifactorial, but include structural barriers (eg, clinic access), clinical barriers (eg, eligibility criteria), and physician and patient attitudes towards trial enrollment.4,5 One study at the University of California Davis Cancer Center reported 49% of patients declined participation despite meeting eligibility criteria,3,6 suggesting that psychosocial barriers such as knowledge of trials and attitudes towards clinical research are a major impediment to accrual.7-9
Bone and soft tissue sarcoma represent a heterogeneous group of tumors of mesenchymal origin that are an important cause of morbidity and mortality. Local disease is often treated with a multidisciplinary approach including surgery, radiation, and systemic therapy. Metastatic disease is predominantly treated palliatively with systemic therapy.10 Given its rarity and heterogeneity, trial accrual is of particular importance in sarcoma and often requires multiple sites to enroll adequate numbers of patients. While sarcoma represents <1% of adult malignancies overall, it constitutes ~15% of malignancies in the adolescent and young adult (AYA) population (15- 39 years old).11,12 Sarcoma represents a patient population in which low trial accrual has been correlated with lack of progress in cancer-related outcomes in both the adult and AYA populations.13 The reasons for low accrual rates among patients with sarcoma are poorly understood.
Sarcomas represent a molecularly and biologically heterogeneous group of malignancies with over 100 different subtypes.12 As a result, there has been significant interest in performing molecular profiling, or genetic sequencing, to identify “targetable” mutations. Targetable mutations refer to a specific genetic change identified within the tumor molecular profile for which there is a specific drug that may demonstrate activity against a particular tumor. Given the widespread utilization of this technology in sarcoma, identifying and understanding patient perceptions with regard to molecular profiling is critically important in this disease.14
In this study, we use a cross-sectional design to describe patient perceptions of trial enrollment among patients with bone and soft tissue sarcoma through validated measures, including attitudes towards clinical trials, knowledge of clinical trials, and perceived ability (ie, self-efficacy) to carry out actions involved in making an informed decision about clinical trial participation, receptivity to learning more about clinical trials, and willingness to participate in clinical trials.6 In addition, we describe this patient cohort’s perceptions of molecular profiling, as current and future trials are increasingly driven by molecular or other biomarkers.
Methods
This was a cross-sectional electronic survey study of patients with bone and soft tissue sarcoma treated at Northwestern Medicine (NM) over a 5-year period. NM Enterprise Data Warehouse (NMEDW) is a single, comprehensive, and integrated repository of all clinical and research data sources within NM. The study was approved by the Northwestern University Institutional Review Board.
Survey
The investigators designed a self-administered, online survey, which was built using Research Electronic Data Capture (REDCap). The survey consisted of three sections that were answered using skip logic—a custom path through the survey that varied based on patients’ answers: (1) Patient demographic information and trial perceptions (answered by all patients); (2) Thoughts about molecular profiling (answered by patients who answered “yes” to the question, “Have you heard about molecular profiling of tumors?”); and (3) Considerations to undergo molecular profiling (answered by patients who answered “yes” to the question, “Have you undergone profiling of your cancer?”).
Clinical trial perceptions included questions assessing (1) patient knowledge about trials; (2) patient attitudes toward trials; (3) perceived ability (ie, self-efficacy) to carry out actions involved in making an informed decision about trial participation; (4) receptivity to learning more about trials; and (5) willingness to participate in trials. These outcome measures had been previously developed and pilot tested for reliability and validity (TABLE 1).6
Thoughts about molecular profiling of tumors were assessed using nine items (TABLE 1). Of these, items assessing potential benefit or harm of molecular profiling were assessed using a 7-step Likert scale. Items assessing maximal benefit or harm of therapy, importance of quality vs length of life, and concern about the cost of molecular testing were assessed using a 5-step Likert scale. The study team developed and piloted these questions because there is no validated survey assessing these domains.
Considerations to undergo molecular profiling were assessed using 17 items. Items were in response to the question, “To what extent did you consider the following issues or concerns at the time you decided to get molecular testing of your cancer?” Responses were assessed using a 5-point Likert scale.
Data Collection
Patients 18 years and older evaluated at NM between November 20, 2012, and November 20, 2017, with a diagnosis of sarcoma were identified by query of the NMEDW by ICD-10 codes (C40, C41.9, C44.99, C45-49, C55, C71.9, D48, D49.9, and M12.20) or equivalent ICD-9 codes. Patients were subsequently excluded if they did not have a diagnosis of bone or soft tissue sarcoma, no e-mail address listed, had died, or had not been evaluated at an NM clinic in the previous 5 years. Patients with a diagnosis of gastrointestinal stromal tumor and Kaposi’s sarcoma were also excluded.
A personalized contact e-mail was sent to patients containing an explanation of the survey and an internet link to the electronic survey through REDCap from January 2018 to March 2018. If patients did not respond to the survey, two follow-up reminder e-mails were sent 2 and 4 days following the initial survey. The link was protected so that each patient could complete the survey only once. Responses were collected through the REDCap platform. Patients read and signed an electronic consent form prior to completing the survey.
Upon completion of the survey, patients were offered a $50 VISA gift card as compensation, with an option to donate their compensation to the Robert H. Lurie Comprehensive Cancer Center Sarcoma Research Fund.
Over the described survey period, open clinical trials for patients with bone and soft tissue sarcoma available at NM were evaluated. The number of patients screened and accrued to each trial were recorded.
Statistical analysis
Responses were separated from the personal data for complete anonymization. Descriptive statistical analysis was performed for demographics and disease variables and were summarized using frequencies and percentages. Median and range were used for age. Correlations between continuous variables were analyzed using Spearman correlations. Scores were compared between subgroups using the Mann-Whitney test. Descriptive statistics for knowledge, attitude, and ability scores include means and 95% confidence intervals. Correlations were interpreted as small (r=0.10), medium (r=0.30), or large (r=0.50).15 Statistical significance was indicated when P<0.05.
Results
Patients
Seven hundred fifty patients were eligible to participate in the survey and received the initial and two follow-up e-mails. Twenty e-mailed surveys bounced back. Three hundred nine patients opened the initial e-mail and 283 patients (37.7% of total and 91.6% of opened) completed at least a portion of the survey, with 182 patients completing the entire survey (FIGURE 1). Data for analysis were used from patients who completed at least a portion of the survey.
Baseline characteristics of patients who responded can be seen in TABLE 2. Patients had a median age of 56, the majority were female (59.4%), white (88.2%), and most had college or university graduate degrees or higher educational level (69.0%). Patients had various different histological subtypes, with the most common being liposarcoma (16.5%) and leiomyosarcoma (16.0%). Slightly more than a quarter (26.8%) of patients had metastatic disease, and 84.2% had never been enrolled in a clinical trial. Previous treatments included surgery (91.1%), radiation (53.2%), and chemotherapy (51.6%). Prior to completing the survey, 85.4% reported being receptive to a cancer clinical trial, while 60.7% of patients reported willingness to participate in a clinical trial.
Knowledge, attitudes, and perceived ability
A statistically significant correlation was observed between greater knowledge of trials and more positive attitudes towards trials (P<0.001; r=0.5, FIGURE 2A). In relating patient attitudes with perceived ability, again a significant correlation was seen (P<0.001; r=0.4, FIGURE 2B). In contrast, knowledge had a weak correlation with perceived ability (P=0.024; r=0.2, FIGURE 2C). There was no difference regarding patient knowledge, attitudes, or perceived ability by age, gender, race, or income.
Knowledge, attitudes, perceived ability, and clinical trial enrollment
Thirty patients reported clinical trial experience (either previously or currently enrolled in trials) and 160 patients were never enrolled. Of the 30 patients with trial experience, 7 reported being currently enrolled, while 23 reported previous enrollment. Of these patients, 16 had metastatic disease, while 12 had non-metastatic disease, and 2 were unsure whether or not they had metastatic disease.
Patients with previous clinical trial exposure (currently or previously enrolled in clinical trials) demonstrated significantly greater trial knowledge, with a mean knowledge score of 9.3 (CI 8.5-10.0) compared with 7.7 (CI 7.3-8.1) among patients without trial exposure (P=0.002; FIGURE 3A). Similarly, patients with trial experience also had statistically significant more positive attitudes towards trials as compared with patients with no trial experience, with a mean attitude score of 3.8 (CI 3.6-4.0) and 3.5 (CI 3.4-3.6), respectively (P=0.001; FIGURE 3B). While numerically patients with trial experience have greater perceived ability compared with patients with no trial experience, with a mean score of 4.4 (CI 4.2-4.6) and 4.2 (CI 4.1-4.3), respectively, this difference did not reach statistical significance (FIGURE 3C).
Knowledge, attitudes, perceived ability, and disease stage
An analysis was performed comparing patients with metastatic vs non-metastatic disease. It was observed that patients with metastatic disease had similar knowledge of trials compared with non-metastatic patients, with a mean knowledge score of 8.4 (CI 7.7- 9.1) and 7.9 (CI 7.5-8.4), respectively, (P=0.3; FIGURE 4A). In contrast, patients with metastatic disease had more positive attitudes compared with non-metastatic patients, with a mean score of 3.7 (CI 3.5-3.8) and 3.5 (CI 3.4-3.6), respectively, which was statistically significant (P=0.03; FIGURE 4B). There was no difference in perceived ability in metastatic vs non-metastatic patients (FIGURE 4C).
Thoughts about molecular profiling
Of the total number of patients, 46 patients had heard of molecular profiling and were presented with questions regarding their thoughts (TABLE 3). Approximately two-thirds (65.2%) thought there would be a 50% or greater likelihood of finding a targetable result in their tumor molecular profile. A majority (71.7%) of patients thought that a new experimental therapy chosen based on a patient’s tumor molecular profile would have at least a 50% chance of controlling the cancer. Somewhat less than a third (30.4%) of patients thought that total cure is the maximal benefit a patient could experience as a result of a treatment on a clinical trial using a drug chosen based on molecular tests. About half (52.2%) of patients agreed with the statement, “I am concerned about the cost of the test to molecularly profile my cancer.”
Considerations to undergo molecular profiling
Eighteen patients had undergone molecular profiling of their tumor. These patients were posed the question, “To what extent did you consider the following issues or concerns at the time you decided to get molecular testing of your cancer?” (TABLE 4). A majority (83.3%) of patients stated that wanting to live as long as possible was important, and 72.2% of patients stated that quality of life was important. A majority (83.3%) of patients stated that hope for a cure was an extremely or quite a bit important consideration. Helping future cancer patients was extremely or quite a bit important for 77.8% of patients, while wanting to be a part of research was not at all or of little importance in 50.0% of patients.
Clinical trials at NM
Twenty-four clinical trials were available at NM between the years 2012 and 2017 for patients with bone and soft tissue sarcoma. Of these trials, 3 of 24 were for non-metastatic patients, while the remaining 21 were open only to metastatic patients. The median number of patients screened per trial was 11 (range 0-66) and the median number of patients accrued per trial was 9 (range 0-58). Of the 24 trials, 17 were not subtype specific (13 included soft tissue sarcoma alone while 4 included both bone and soft tissue sarcoma). The remaining 7 trials were sarcoma subtype specific (eg, angiosarcoma, liposarcoma, etc). Trials available at NM during this period are included in TABLE 5. There were 318 patients screened and 262 patients accrued to sarcoma trials over this time period, with a screen failure rate of 17.6% overall.
Discussion
Our study sought to describe perceptions of clinical trial enrollment among patients with bone and soft tissue sarcoma in order to elucidate and overcome barriers to enrollment, which to the best of our knowledge had not been previously described. Using previously validated patient- reported outcomes in the literature,6 our data reveal a correlation between knowledge of trials and more positive attitudes towards trials. This underscores the importance of awareness and educational strategies in this cancer population as a whole. Interventions should focus on patient perceptions that contribute to lack of participation, such as fear of side effects, loss of control (eg, idea of placebo or randomization), logistical challenges (eg, additional time or convenient location), and cost.3,5,7,16,17 For example, patients concerned about randomization should be educated on equipoise and other ethical considerations in trial design.5 Previous research has suggested that a multimedia psychoeducational intervention was effective in improving attitudes toward trials.6 Educating patients on the essential role of trials in oncology care, as demonstrated by the vast number of new drug approvals in recent years, is an essential strategy to improve attitudes, and subsequently leads to higher patient accrual rates.
In our study, both knowledge and at titudes were increased in patients with previous trial exposure. This suggests that either patients with greater knowledge and more positive attitudes are more likely to enroll in trials, or that patients with direct trial exposure are more knowledgeable and develop more positive attitudes. Our patient population was overall receptive to learning more about clinical trials (85.4%) and willing to participate (65.8%). At the same time, our study demonstrated low to medium correlations between attitudes and perceived ability to take steps towards making an informed decision to enroll in a trial (r=0.4), which may partially be explained by the absence of a tangible trial opportunity. While we did not assess specifically whether patients in our study were offered a trial, there was a substantial trial menu at NM with limited screen failures and decent trial accrual over the time frame of our study. This underscores the importance not only of patient-focused strategies to increase educational and attitudinal resources, but also a need to focus on research-site optimization that includes opening of multiple trials in various settings, systematic pre-screening of patients, and eligibility criteria that are inclusive and rational.5
The patient population with metastatic disease demonstrated more positive attitudes towards enrolling in clinical trials. This cohort accrued well to clinical trials, with 21 of 24 trials enrolling specifically patients with metastatic disease. Of the patients who responded to our survey, patients with previous trial exposure were enriched for patients with metastatic disease (53.3% metastatic among previous trial exposure versus 26.8% metastatic overall). These observations are likely reflective of the need for novel therapies in this disease setting. At the same time, approximately 25% of patients with localized soft tissue sarcoma will develop distant metastatic disease after successful treatment of their primary tumor, which increases to 40% to 50% in larger and higher-grade tumors.18 Three of 24 trials were open for patients with non-metastatic disease, of which one managed to accrue patients. Patients with non-metastatic disease had more negative attitudes towards trial enrollment. These disproportionate findings suggest a need for interventions to increase patient awareness and attitudes towards trial enrollment among this patient population and the importance of research-site optimization for trial opportunities across disease states.
Molecular profiling of tumors and biomarker identification has become a critical component of further characterizing cancer subtypes. In our study, a majority (65.2%) thought there would be a 50% or greater likelihood of finding a targetable result in their molecular profile. Molecular data on 5,749 bone and soft tissue sarcomas suggested that 9.5% of tumors demonstrate a “targetable result,” defined as a new molecular finding for which there is an FDA-approved drug for malignancies other than sarcoma (eg, BRAF V600E, Her2, etc.),19 suggesting an overestimation in our patient cohort of the likelihood of benefit of molecular profiling. These results highlight that the growing use of molecular profiling has increased the need for educational and supportive resources to help patients understand the utility of molecular profiling and aid in shared decision-making surrounding the results.
At the same time, the importance of identifying a targetable mutation in patients with sarcoma cannot be understated. As a recent example of this paradigm, tumors that harbor fusions with the neurotrophic receptor tyrosine kinase 1, 2, or 3 (NTRK1, 2, and 3) have a high response rate (~75%) to drugs that target these fusions, such as larotrectinib and entrectinib.13 Molecular profiling and identification of predictive biomarkers in small patient subsets has led to great challenges in trial design and research-site optimization. Novel designs that incorporate molecular profiling,20 such as the Lung- MAP trial21 and NCI’s Molecular Analysis for Therapy Choice (MATCH) trial,22 are emerging to identify new therapies for small patient subsets. As a rare and increasingly heterogeneous cancer, sarcoma represents a paradigm to provide insight into optimizing patient perceptions and research enterprises to maximize clinical trial enrollment.
Some limitations of our study include a homogeneous and selected patient population that was predominantly Caucasian and highly educated. Therefore, these findings should not be extrapolated to other populations with barriers to trial accrual, such as lower socioeconomic or minority populations. The low response rate and failure of some to complete the survey may have introduced some bias. Additionally, our data include self-reported outcomes, which could have affected our results. Finally, the limited number of patients who had undergone or heard of molecular profiling limited our ability to draw definitive conclusions, and should be assessed in larger patient cohorts.
While our paper addresses a unique population—the sarcoma patient—similar themes and issues pertain to all oncology patients. A recent review was published in the American Society of Clinical Oncology Educational Book23 looking at methods to overcome barriers to clinical trial enrollment. Their paper clearly illustrates mechanisms to assist with overcoming financial burdens associated with cancer clinical trials, overcoming barriers as they relate to patient and clinician difficulty in coping with the uncertainty inherent in clinical trial participation, and highlight the role of a patient navigator in clinical trial participation.
Conclusions
Interventions aimed at increasing awareness, knowledge, and attitudes towards clinical trials among sarcoma patients may lead to increased trial enrollment and greater progress in cancer treatment in this population. In addition to patient- focused interventions, thoughtful and strategic clinical trial designs that allow for the development of biomarker- driven therapeutics, while at the same time optimizing patient accrual rates, should be developed. Evaluation of barriers to clinical trial enrollment and molecular profiling of tumors among bone and soft tissue sarcoma patients at an academic center can serve as a paradigm to overcome barriers to enrollment in the era of an increasingly heterogeneous cancer population. TSJ
1. Go RS, Frisby KA, Lee JA, et al. Clinical trial accrual among new cancer patients at a community-based cancer center. Cancer. 2006;106(2):426-433.
2. Murthy VH, Krumholz HM, Gross CP. Participation in cancer clinical trials: Race-, sex-, and age-based disparities. JAMA. 2004; 291(22):2720-2726.
3. Lara PN Jr, Higdon R, Lim N, et al. Prospective evaluation of cancer clinical trial accrual patterns: identifying potential barriers to enrollment. J Clin Oncol. 2001;19(6):1728-1733.
4. Unger JM, Cook E, Tai E, Bleyer A. The role of clinical trial participation in cancer research: barriers, evidence, and strategies. Am Soc Clin Oncol Educ Book. 2016;35:185-198.
5. Cancer Action Network American Cancer Society. Barriers to patient enrollment in therapeutic clinical trials for cancer. 2018: https:// www.fightcancer.org/policy-resources/clinical- trial-barriers#figures. Accessed March 14, 2019.
6. Jacobsen PB, Wells KJ, Meade CD, et al. Effects of a brief multimedia psychoeducational intervention on the attitudes and interest of patients with cancer regarding clinical trial participation: a multicenter randomized controlled trial. J Clin Oncol. 2012;30(20):2516-2521.
7. Meropol NJ, Buzaglo JS, Millard J, et al. Barriers to clinical trial participation as perceived by oncologists and patients. J Natl Compr Canc Netw. 2007;5(8):655-664.
8. Cox K, McGarry J. Why patients don’t take part in cancer clinical trials: an overview of the literature. Eur J Cancer Care (Engl). 2003;12(2): 114-122.
9. Mills EJ, Seely D, Rachlis B, et al. Barriers to participation in clinical trials of cancer: a meta- analysis and systematic review of patient-reported factors. Lancet Oncol. 2006;7(2):141-148.
10. National Comprehensive Cancer Network. Soft Tissue Sarcoma (Version 4.2019). https:// www.nccn.org/professionals/physician_gls/ pdf/sarcoma.pdf. Accessed October 30, 2019.
11. Nass SJ, Beaupin LK, Demark-Wahnefried W, et al. Identifying and addressing the needs of adolescents and young adults with cancer: summary of an Institute of Medicine workshop. Oncologist. 2015;20(2):186-195.
12. Wilky BA, Villalobos VM. Emerging role for precision therapy through next-generation sequencing for sarcomas. JCO Precision Oncol. 2018(2):1-4.
13. Bleyer A, Montello M, Budd T, Saxman S. National survival trends of young adults with sarcoma: lack of progress is associated with lack of clinical trial participation. Cancer. 2005;103(9):1891-1897.
14. Gornick MC, Cobain E, Le LQ, et al. Oncologists’ use of genomic sequencing data to inform clinical management. JCO Precision Oncol. 2018(2):1-13.
15. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: L. Erlbaum Associates; 1988.
16. Unger JM, Hershman DL, Albain KS, et al. Patient income level and cancer clinical trial participation. J Clin Oncol. 2013;31(5):536- 542.
17. Javid SH, Unger JM, Gralow JR, et al. A prospective analysis of the influence of older age on physician and patient decision-making when considering enrollment in breast cancer clinical trials (SWOG S0316). Oncologist. 2012;17(9):1180-1190.
18. Singhi EK, Moore DC, Muslimani A. Metastatic soft tissue sarcomas: a review of treatment and new pharmacotherapies. P T. 2018;43(7): 410-429.
19. Gounder MM, Ali SM, Robinson V, et al. Impact of next-generation sequencing (NGS) on diagnostic and therapeutic options in soft-tissue and bone sarcoma. J Clin Oncol. 2017;35(15_suppl):abstr 11001.
20. Woodcock J, LaVange LM. Master protocols to study multiple therapies, multiple diseases, or both. N Engl J Med. 2017;377(1):62-70.
21. Steuer CE, Papadimitrakopoulou V, Herbst RS, et al. Innovative clinical trials: the LUNGMAP study. Clin Pharmacol Ther. 2015;97(5): 488-491.
22. McNeil C. NCI-MATCH launch highlights new trial design in precision-medicine era. J Natl Cancer Inst. 2015;107(7).
23. Nipp RD, Hong K, Paskett ED. Overcoming barriers to clinical trial enrollment. Am Soc Clin Oncol Educ Book. 2019;39:105-114.
1. Go RS, Frisby KA, Lee JA, et al. Clinical trial accrual among new cancer patients at a community-based cancer center. Cancer. 2006;106(2):426-433.
2. Murthy VH, Krumholz HM, Gross CP. Participation in cancer clinical trials: Race-, sex-, and age-based disparities. JAMA. 2004; 291(22):2720-2726.
3. Lara PN Jr, Higdon R, Lim N, et al. Prospective evaluation of cancer clinical trial accrual patterns: identifying potential barriers to enrollment. J Clin Oncol. 2001;19(6):1728-1733.
4. Unger JM, Cook E, Tai E, Bleyer A. The role of clinical trial participation in cancer research: barriers, evidence, and strategies. Am Soc Clin Oncol Educ Book. 2016;35:185-198.
5. Cancer Action Network American Cancer Society. Barriers to patient enrollment in therapeutic clinical trials for cancer. 2018: https:// www.fightcancer.org/policy-resources/clinical- trial-barriers#figures. Accessed March 14, 2019.
6. Jacobsen PB, Wells KJ, Meade CD, et al. Effects of a brief multimedia psychoeducational intervention on the attitudes and interest of patients with cancer regarding clinical trial participation: a multicenter randomized controlled trial. J Clin Oncol. 2012;30(20):2516-2521.
7. Meropol NJ, Buzaglo JS, Millard J, et al. Barriers to clinical trial participation as perceived by oncologists and patients. J Natl Compr Canc Netw. 2007;5(8):655-664.
8. Cox K, McGarry J. Why patients don’t take part in cancer clinical trials: an overview of the literature. Eur J Cancer Care (Engl). 2003;12(2): 114-122.
9. Mills EJ, Seely D, Rachlis B, et al. Barriers to participation in clinical trials of cancer: a meta- analysis and systematic review of patient-reported factors. Lancet Oncol. 2006;7(2):141-148.
10. National Comprehensive Cancer Network. Soft Tissue Sarcoma (Version 4.2019). https:// www.nccn.org/professionals/physician_gls/ pdf/sarcoma.pdf. Accessed October 30, 2019.
11. Nass SJ, Beaupin LK, Demark-Wahnefried W, et al. Identifying and addressing the needs of adolescents and young adults with cancer: summary of an Institute of Medicine workshop. Oncologist. 2015;20(2):186-195.
12. Wilky BA, Villalobos VM. Emerging role for precision therapy through next-generation sequencing for sarcomas. JCO Precision Oncol. 2018(2):1-4.
13. Bleyer A, Montello M, Budd T, Saxman S. National survival trends of young adults with sarcoma: lack of progress is associated with lack of clinical trial participation. Cancer. 2005;103(9):1891-1897.
14. Gornick MC, Cobain E, Le LQ, et al. Oncologists’ use of genomic sequencing data to inform clinical management. JCO Precision Oncol. 2018(2):1-13.
15. Cohen J. Statistical Power Analysis for the Behavioral Sciences. 2nd ed. Hillsdale, NJ: L. Erlbaum Associates; 1988.
16. Unger JM, Hershman DL, Albain KS, et al. Patient income level and cancer clinical trial participation. J Clin Oncol. 2013;31(5):536- 542.
17. Javid SH, Unger JM, Gralow JR, et al. A prospective analysis of the influence of older age on physician and patient decision-making when considering enrollment in breast cancer clinical trials (SWOG S0316). Oncologist. 2012;17(9):1180-1190.
18. Singhi EK, Moore DC, Muslimani A. Metastatic soft tissue sarcomas: a review of treatment and new pharmacotherapies. P T. 2018;43(7): 410-429.
19. Gounder MM, Ali SM, Robinson V, et al. Impact of next-generation sequencing (NGS) on diagnostic and therapeutic options in soft-tissue and bone sarcoma. J Clin Oncol. 2017;35(15_suppl):abstr 11001.
20. Woodcock J, LaVange LM. Master protocols to study multiple therapies, multiple diseases, or both. N Engl J Med. 2017;377(1):62-70.
21. Steuer CE, Papadimitrakopoulou V, Herbst RS, et al. Innovative clinical trials: the LUNGMAP study. Clin Pharmacol Ther. 2015;97(5): 488-491.
22. McNeil C. NCI-MATCH launch highlights new trial design in precision-medicine era. J Natl Cancer Inst. 2015;107(7).
23. Nipp RD, Hong K, Paskett ED. Overcoming barriers to clinical trial enrollment. Am Soc Clin Oncol Educ Book. 2019;39:105-114.
Pimavanserin reduced dementia-related psychotic symptoms without affecting cognition
SAN DIEGO – Pimavanserin, a second-generation antipsychotic approved for hallucinations and delusions in patients with Parkinson’s disease, may also be helpful for psychotic symptoms in other dementia patients, Erin P. Foff, MD, said at the Clinical Trials on Alzheimer’s Disease conference.

In fact, the phase 3 HARMONY trial was stopped early, after an interim efficacy analysis determined that treatment with pimavanserin (Nuplazid) had achieved its primary endpoint – a statistically significant threefold reduction in the risk of relapse (P less than .0033).
Importantly, pimavanserin didn’t significantly affect cognition nor, at least in this controlled setting, did it appear to increase falls or other adverse events often seen with antipsychotic use in elderly patients, said Dr. Foff, clinical lead for the dementia-related psychosis program at Acadia Pharmaceuticals, which makes the drug and sponsored the study.
Based on the positive results, Acadia intends to submit a supplemental new drug application for this indication, according to an investor presentation posted on the company website.
“There is a critical need for an intervention [for psychosis symptoms] in this population,” Dr. Foff said. “We saw a robust response that was well tolerated and well maintained with no negative impact on cognitive scores.”
The second-generation antipsychotic was approved in 2016 for treating hallucinations and delusions in patients with Parkinson’s disease.
The drug is a selective antagonist of 5-HT2 receptors, with low affinity for dopamine receptors. This slightly differentiates it from other second-generation antipsychotics that affect dopamine receptors as well as 5-HT2 receptors.
HARMONY was not a typical placebo-controlled, randomized efficacy trial. Rather, it employed a two-phase design: an open-label treatment response period followed by a placebo-controlled randomization limited to open-label responders. Overall, HARMONY involved 392 patients with mild to severe dementia of numerous etiologies, including Alzheimer’s disease (66.8%), Parkinson’s disease dementia (14.3%), frontotemporal dementia (1.8%), vascular dementia (9.7%), and dementia with Lewy bodies (7.4%). All patients entered a 12-week, open-label period during which they received pimavanserin 34 mg daily. The primary endpoint was a combination of least a 30% reduction on the total Scale for the Assessment of Positive Symptom–Hallucinations and Delusions (SAPS-HD) scale plus a score of 1-2 on the Clinical Global Impressions–Improvement (CGI-I) scale, meaning better or very much better.
At 12 weeks, all responders were then randomized to placebo or continued therapy for 26 weeks. The primary endpoint was relapse, defined as at least a 30% worsening of the SAPS-HD relative to open-label baseline, plus a CGI-I score of 6-7 (worse or very much worse).
Patients were aged a mean of 74 years. Most (about 90%) were living at home. Visual hallucinations occurred in 80% and delusions in 83%. At baseline, the mean SAPS-HD score was 24.4, and the mean CGI-Severity score was 4.7. The mean Mini-Mental State Exam (MMSE) score was 16.7.
In the open-label period, pimavanserin reduced the SAPS-HD score at 12 weeks by a mean of 75%. Symptoms began to decline in the first week of treatment, with continuing improvement throughout the treatment period. By week 4, 30% had hit the response target. This number increased steadily, with 51% responding by week 4, 75% by week 8, and 88% by week 12.
By probable diagnosis, response rates were 59.8% in Alzheimer’s patients, 45.5% for those with Lewy body dementia, 71.2% among patients with Parkinson’s disease, 71% in patients with vascular dementia, and 50% in patients with frontotemporal dementia. In the final analysis, 80% of patients overall were considered responders.
The randomized potion began immediately thereafter with no washout period. About 62% (194) of the entire cohort – all responders – entered into the placebo-controlled phase. The remaining patients were either not responders (20%), dropped out because of an adverse event (7.7%), or left the study for unspecified reasons (10%). There was one death, which was not related to the study medication. A total of 41 patients were still being treated when the study was discontinued, and they were excluded from the final analysis.
When the randomized study ended, relapses had occurred in 28.3% of those taking placebo and in 12.6% of those taking pimavanserin – a statistically significant difference (hazard ratio, 0.353). This translated to a 180% reduction in relapse.
The rate of adverse events was similar in both active and placebo groups (41% vs. 36.6%). Serious adverse events occurred in 4.8% and 3.6%, respectively. The most commonly reported adverse events were headache (9.5% vs. 4.5%) and urinary tract infection (6.7% vs. 3.6%). Asthenia occurred in 2.9% of treated patients and 0.9% of placebo patients, but no falls were reported. Anxiety and dizziness were also reported in three patients taking the study medication.
Three patients (2.9%) experienced a prolonged QT phase on ECG, with a mean delay of 5.4 milliseconds from baseline. “Pimavanserin is known to have this effect of QT prolongation,” Dr. Foff said. “This 5.4-ms change is exactly in line with what we already know about pimavanserin and is not clinically significant. We saw no effect on motor function, consistent with the mechanism of action, and very low levels of agitation or aggression.”
Pimavanserin didn’t significantly change cognition from baseline in the open-label period, and in the randomized period, MMSE never differed significantly between groups.
The company also conducted an exploratory subgroup analysis that looked at placebo versus pimavanserin relapse by probable clinical diagnosis. Among the types of dementia, relapse rates for placebo versus pimavanserin were 23% versus 13% among Alzheimer’s patients, 67% versus 0% in Lewy body dementia patients, 50% versus 7% in patients with Parkinson’s, and 17% each among vascular dementia patients. Only one patient in the randomized period had frontotemporal dementia, and that patient relapsed on treatment.
Whether pimavanserin is effective specifically for psychosis in Alzheimer’s disease patients, however, remains in question. In 2018, Acadia published a negative phase 2 trial in a targeted group of 181 Alzheimer’s patients. The primary outcome in each study was mean change on the Neuropsychiatric Inventory–Nursing Home Version psychosis score (NPI-NH-PS). Clive Ballard, MD, of the University of Exeter (England), was the primary investigator.
After 6 weeks, those taking pimavanserin had a 3.76-point change in the NPI-NH-PS, compared with a 1.93-point change in the placebo group. The mean 1.84-point difference was not statistically significant.
This Alzheimer’s-only cohort group also experienced more adverse events than the HARMONY mixed-diagnosis cohort did, although the differences between pimavanserin and placebo groups were not significant. Adverse events included falls (23% of each group) and agitation (21% with pimavanserin vs. 14% with placebo). Cognition was unaffected.
Later that year, Acadia published a subgroup analysis of the same cohort parsing response by symptom severity, again with Dr. Ballard as the lead investigator.
The analysis focused on 57 patients with a baseline NPI-NH-PS of at least 12, indicating severe symptoms of psychosis.
Treatment effects were more pronounced in this group, significantly favoring pimavanserin. On the NPI-NH-PS, 88.9% of the pimavanserin group and 43.3% of the placebo group had at least a 30% improvement; 77.8% and 43.3% experienced at least a 50% improvement. The rate of serious adverse events was similar (18% with pimavanserin and 17% with placebo) and cognition was unaffected. Falls occurred in 14% of the treated group and 20% of the placebo group.
“These findings coupled with the results from other studies of pimavanserin suggest a potential role for pimavanserin in treating psychosis in patients across a range of neuropsychiatric conditions,” Dr. Ballard wrote.
SOURCE: Foff EP et al. CTAD 2019, Late-breaker 1
SAN DIEGO – Pimavanserin, a second-generation antipsychotic approved for hallucinations and delusions in patients with Parkinson’s disease, may also be helpful for psychotic symptoms in other dementia patients, Erin P. Foff, MD, said at the Clinical Trials on Alzheimer’s Disease conference.
In fact, the phase 3 HARMONY trial was stopped early, after an interim efficacy analysis determined that treatment with pimavanserin (Nuplazid) had achieved its primary endpoint – a statistically significant threefold reduction in the risk of relapse (P less than .0033).
Importantly, pimavanserin didn’t significantly affect cognition nor, at least in this controlled setting, did it appear to increase falls or other adverse events often seen with antipsychotic use in elderly patients, said Dr. Foff, clinical lead for the dementia-related psychosis program at Acadia Pharmaceuticals, which makes the drug and sponsored the study.
Based on the positive results, Acadia intends to submit a supplemental new drug application for this indication, according to an investor presentation posted on the company website.
“There is a critical need for an intervention [for psychosis symptoms] in this population,” Dr. Foff said. “We saw a robust response that was well tolerated and well maintained with no negative impact on cognitive scores.”
The second-generation antipsychotic was approved in 2016 for treating hallucinations and delusions in patients with Parkinson’s disease.
The drug is a selective antagonist of 5-HT2 receptors, with low affinity for dopamine receptors. This slightly differentiates it from other second-generation antipsychotics that affect dopamine receptors as well as 5-HT2 receptors.
HARMONY was not a typical placebo-controlled, randomized efficacy trial. Rather, it employed a two-phase design: an open-label treatment response period followed by a placebo-controlled randomization limited to open-label responders. Overall, HARMONY involved 392 patients with mild to severe dementia of numerous etiologies, including Alzheimer’s disease (66.8%), Parkinson’s disease dementia (14.3%), frontotemporal dementia (1.8%), vascular dementia (9.7%), and dementia with Lewy bodies (7.4%). All patients entered a 12-week, open-label period during which they received pimavanserin 34 mg daily. The primary endpoint was a combination of least a 30% reduction on the total Scale for the Assessment of Positive Symptom–Hallucinations and Delusions (SAPS-HD) scale plus a score of 1-2 on the Clinical Global Impressions–Improvement (CGI-I) scale, meaning better or very much better.
At 12 weeks, all responders were then randomized to placebo or continued therapy for 26 weeks. The primary endpoint was relapse, defined as at least a 30% worsening of the SAPS-HD relative to open-label baseline, plus a CGI-I score of 6-7 (worse or very much worse).
Patients were aged a mean of 74 years. Most (about 90%) were living at home. Visual hallucinations occurred in 80% and delusions in 83%. At baseline, the mean SAPS-HD score was 24.4, and the mean CGI-Severity score was 4.7. The mean Mini-Mental State Exam (MMSE) score was 16.7.
In the open-label period, pimavanserin reduced the SAPS-HD score at 12 weeks by a mean of 75%. Symptoms began to decline in the first week of treatment, with continuing improvement throughout the treatment period. By week 4, 30% had hit the response target. This number increased steadily, with 51% responding by week 4, 75% by week 8, and 88% by week 12.
By probable diagnosis, response rates were 59.8% in Alzheimer’s patients, 45.5% for those with Lewy body dementia, 71.2% among patients with Parkinson’s disease, 71% in patients with vascular dementia, and 50% in patients with frontotemporal dementia. In the final analysis, 80% of patients overall were considered responders.
The randomized potion began immediately thereafter with no washout period. About 62% (194) of the entire cohort – all responders – entered into the placebo-controlled phase. The remaining patients were either not responders (20%), dropped out because of an adverse event (7.7%), or left the study for unspecified reasons (10%). There was one death, which was not related to the study medication. A total of 41 patients were still being treated when the study was discontinued, and they were excluded from the final analysis.
When the randomized study ended, relapses had occurred in 28.3% of those taking placebo and in 12.6% of those taking pimavanserin – a statistically significant difference (hazard ratio, 0.353). This translated to a 180% reduction in relapse.
The rate of adverse events was similar in both active and placebo groups (41% vs. 36.6%). Serious adverse events occurred in 4.8% and 3.6%, respectively. The most commonly reported adverse events were headache (9.5% vs. 4.5%) and urinary tract infection (6.7% vs. 3.6%). Asthenia occurred in 2.9% of treated patients and 0.9% of placebo patients, but no falls were reported. Anxiety and dizziness were also reported in three patients taking the study medication.
Three patients (2.9%) experienced a prolonged QT phase on ECG, with a mean delay of 5.4 milliseconds from baseline. “Pimavanserin is known to have this effect of QT prolongation,” Dr. Foff said. “This 5.4-ms change is exactly in line with what we already know about pimavanserin and is not clinically significant. We saw no effect on motor function, consistent with the mechanism of action, and very low levels of agitation or aggression.”
Pimavanserin didn’t significantly change cognition from baseline in the open-label period, and in the randomized period, MMSE never differed significantly between groups.
The company also conducted an exploratory subgroup analysis that looked at placebo versus pimavanserin relapse by probable clinical diagnosis. Among the types of dementia, relapse rates for placebo versus pimavanserin were 23% versus 13% among Alzheimer’s patients, 67% versus 0% in Lewy body dementia patients, 50% versus 7% in patients with Parkinson’s, and 17% each among vascular dementia patients. Only one patient in the randomized period had frontotemporal dementia, and that patient relapsed on treatment.
Whether pimavanserin is effective specifically for psychosis in Alzheimer’s disease patients, however, remains in question. In 2018, Acadia published a negative phase 2 trial in a targeted group of 181 Alzheimer’s patients. The primary outcome in each study was mean change on the Neuropsychiatric Inventory–Nursing Home Version psychosis score (NPI-NH-PS). Clive Ballard, MD, of the University of Exeter (England), was the primary investigator.
After 6 weeks, those taking pimavanserin had a 3.76-point change in the NPI-NH-PS, compared with a 1.93-point change in the placebo group. The mean 1.84-point difference was not statistically significant.
This Alzheimer’s-only cohort group also experienced more adverse events than the HARMONY mixed-diagnosis cohort did, although the differences between pimavanserin and placebo groups were not significant. Adverse events included falls (23% of each group) and agitation (21% with pimavanserin vs. 14% with placebo). Cognition was unaffected.
Later that year, Acadia published a subgroup analysis of the same cohort parsing response by symptom severity, again with Dr. Ballard as the lead investigator.
The analysis focused on 57 patients with a baseline NPI-NH-PS of at least 12, indicating severe symptoms of psychosis.
Treatment effects were more pronounced in this group, significantly favoring pimavanserin. On the NPI-NH-PS, 88.9% of the pimavanserin group and 43.3% of the placebo group had at least a 30% improvement; 77.8% and 43.3% experienced at least a 50% improvement. The rate of serious adverse events was similar (18% with pimavanserin and 17% with placebo) and cognition was unaffected. Falls occurred in 14% of the treated group and 20% of the placebo group.
“These findings coupled with the results from other studies of pimavanserin suggest a potential role for pimavanserin in treating psychosis in patients across a range of neuropsychiatric conditions,” Dr. Ballard wrote.
SOURCE: Foff EP et al. CTAD 2019, Late-breaker 1
SAN DIEGO – Pimavanserin, a second-generation antipsychotic approved for hallucinations and delusions in patients with Parkinson’s disease, may also be helpful for psychotic symptoms in other dementia patients, Erin P. Foff, MD, said at the Clinical Trials on Alzheimer’s Disease conference.
In fact, the phase 3 HARMONY trial was stopped early, after an interim efficacy analysis determined that treatment with pimavanserin (Nuplazid) had achieved its primary endpoint – a statistically significant threefold reduction in the risk of relapse (P less than .0033).
Importantly, pimavanserin didn’t significantly affect cognition nor, at least in this controlled setting, did it appear to increase falls or other adverse events often seen with antipsychotic use in elderly patients, said Dr. Foff, clinical lead for the dementia-related psychosis program at Acadia Pharmaceuticals, which makes the drug and sponsored the study.
Based on the positive results, Acadia intends to submit a supplemental new drug application for this indication, according to an investor presentation posted on the company website.
“There is a critical need for an intervention [for psychosis symptoms] in this population,” Dr. Foff said. “We saw a robust response that was well tolerated and well maintained with no negative impact on cognitive scores.”
The second-generation antipsychotic was approved in 2016 for treating hallucinations and delusions in patients with Parkinson’s disease.
The drug is a selective antagonist of 5-HT2 receptors, with low affinity for dopamine receptors. This slightly differentiates it from other second-generation antipsychotics that affect dopamine receptors as well as 5-HT2 receptors.
HARMONY was not a typical placebo-controlled, randomized efficacy trial. Rather, it employed a two-phase design: an open-label treatment response period followed by a placebo-controlled randomization limited to open-label responders. Overall, HARMONY involved 392 patients with mild to severe dementia of numerous etiologies, including Alzheimer’s disease (66.8%), Parkinson’s disease dementia (14.3%), frontotemporal dementia (1.8%), vascular dementia (9.7%), and dementia with Lewy bodies (7.4%). All patients entered a 12-week, open-label period during which they received pimavanserin 34 mg daily. The primary endpoint was a combination of least a 30% reduction on the total Scale for the Assessment of Positive Symptom–Hallucinations and Delusions (SAPS-HD) scale plus a score of 1-2 on the Clinical Global Impressions–Improvement (CGI-I) scale, meaning better or very much better.
At 12 weeks, all responders were then randomized to placebo or continued therapy for 26 weeks. The primary endpoint was relapse, defined as at least a 30% worsening of the SAPS-HD relative to open-label baseline, plus a CGI-I score of 6-7 (worse or very much worse).
Patients were aged a mean of 74 years. Most (about 90%) were living at home. Visual hallucinations occurred in 80% and delusions in 83%. At baseline, the mean SAPS-HD score was 24.4, and the mean CGI-Severity score was 4.7. The mean Mini-Mental State Exam (MMSE) score was 16.7.
In the open-label period, pimavanserin reduced the SAPS-HD score at 12 weeks by a mean of 75%. Symptoms began to decline in the first week of treatment, with continuing improvement throughout the treatment period. By week 4, 30% had hit the response target. This number increased steadily, with 51% responding by week 4, 75% by week 8, and 88% by week 12.
By probable diagnosis, response rates were 59.8% in Alzheimer’s patients, 45.5% for those with Lewy body dementia, 71.2% among patients with Parkinson’s disease, 71% in patients with vascular dementia, and 50% in patients with frontotemporal dementia. In the final analysis, 80% of patients overall were considered responders.
The randomized potion began immediately thereafter with no washout period. About 62% (194) of the entire cohort – all responders – entered into the placebo-controlled phase. The remaining patients were either not responders (20%), dropped out because of an adverse event (7.7%), or left the study for unspecified reasons (10%). There was one death, which was not related to the study medication. A total of 41 patients were still being treated when the study was discontinued, and they were excluded from the final analysis.
When the randomized study ended, relapses had occurred in 28.3% of those taking placebo and in 12.6% of those taking pimavanserin – a statistically significant difference (hazard ratio, 0.353). This translated to a 180% reduction in relapse.
The rate of adverse events was similar in both active and placebo groups (41% vs. 36.6%). Serious adverse events occurred in 4.8% and 3.6%, respectively. The most commonly reported adverse events were headache (9.5% vs. 4.5%) and urinary tract infection (6.7% vs. 3.6%). Asthenia occurred in 2.9% of treated patients and 0.9% of placebo patients, but no falls were reported. Anxiety and dizziness were also reported in three patients taking the study medication.
Three patients (2.9%) experienced a prolonged QT phase on ECG, with a mean delay of 5.4 milliseconds from baseline. “Pimavanserin is known to have this effect of QT prolongation,” Dr. Foff said. “This 5.4-ms change is exactly in line with what we already know about pimavanserin and is not clinically significant. We saw no effect on motor function, consistent with the mechanism of action, and very low levels of agitation or aggression.”
Pimavanserin didn’t significantly change cognition from baseline in the open-label period, and in the randomized period, MMSE never differed significantly between groups.
The company also conducted an exploratory subgroup analysis that looked at placebo versus pimavanserin relapse by probable clinical diagnosis. Among the types of dementia, relapse rates for placebo versus pimavanserin were 23% versus 13% among Alzheimer’s patients, 67% versus 0% in Lewy body dementia patients, 50% versus 7% in patients with Parkinson’s, and 17% each among vascular dementia patients. Only one patient in the randomized period had frontotemporal dementia, and that patient relapsed on treatment.
Whether pimavanserin is effective specifically for psychosis in Alzheimer’s disease patients, however, remains in question. In 2018, Acadia published a negative phase 2 trial in a targeted group of 181 Alzheimer’s patients. The primary outcome in each study was mean change on the Neuropsychiatric Inventory–Nursing Home Version psychosis score (NPI-NH-PS). Clive Ballard, MD, of the University of Exeter (England), was the primary investigator.
After 6 weeks, those taking pimavanserin had a 3.76-point change in the NPI-NH-PS, compared with a 1.93-point change in the placebo group. The mean 1.84-point difference was not statistically significant.
This Alzheimer’s-only cohort group also experienced more adverse events than the HARMONY mixed-diagnosis cohort did, although the differences between pimavanserin and placebo groups were not significant. Adverse events included falls (23% of each group) and agitation (21% with pimavanserin vs. 14% with placebo). Cognition was unaffected.
Later that year, Acadia published a subgroup analysis of the same cohort parsing response by symptom severity, again with Dr. Ballard as the lead investigator.
The analysis focused on 57 patients with a baseline NPI-NH-PS of at least 12, indicating severe symptoms of psychosis.
Treatment effects were more pronounced in this group, significantly favoring pimavanserin. On the NPI-NH-PS, 88.9% of the pimavanserin group and 43.3% of the placebo group had at least a 30% improvement; 77.8% and 43.3% experienced at least a 50% improvement. The rate of serious adverse events was similar (18% with pimavanserin and 17% with placebo) and cognition was unaffected. Falls occurred in 14% of the treated group and 20% of the placebo group.
“These findings coupled with the results from other studies of pimavanserin suggest a potential role for pimavanserin in treating psychosis in patients across a range of neuropsychiatric conditions,” Dr. Ballard wrote.
SOURCE: Foff EP et al. CTAD 2019, Late-breaker 1
REPORTING FROM CTAD 2019
Promising new neoadjuvant strategy in luminal B breast cancer
SAN ANTONIO – The combination of ribociclib and letrozole proved to be an attractive alternative to standard multidrug neoadjuvant chemotherapy for women with high-risk luminal B breast cancer in the exploratory phase 2 SOLTI-1402/CORALLEEN trial.

Neoadjuvant therapy with ribociclib (Kisqali), an inhibitor of cyclin-dependent kinases 4 and 6 (CDK4/6), in combination with the aromatase inhibitor letrozole (Femara) proved as effective for presurgical molecular disease downstaging as standard multiagent chemotherapy, but with considerably less toxicity, Joaquín Gavilá, MD, reported at the San Antonio Breast Cancer Symposium.
“We believe that these results suggest that in clinically high-risk luminal B disease, a chemotherapy-free treatment strategy based upon CDK4/6 inhibition is worth exploring in future neoadjuvant trials,” declared Dr. Gavilá, a medical oncologist at the Valencia (Spain) Institute of Oncology.
SOLTI-1402/CORALLEEN was an open-label, multicenter trial involving 106 postmenopausal women with hormone receptor–positive and HER2-negative stage I-IIIA breast cancer, an operable tumor size of at least 2 cm measured by MRI, and high-risk luminal B subtype disease as defined via the Prosigna genomic tumor profiling test, also known as PAM50, on which they had a baseline median Risk of Recurrence (ROR) score of 74 out of a possible 100 points. The luminal B subtype accounts for 30%-40% of all hormone receptor–positive/HER2-negative breast cancer and carries a greater than 10% risk of distant recurrence at 10 years.
The women were randomized to 6 months of neoadjuvant therapy involving one of two regimens: six 28-day cycles of oral ribociclib at 600 mg once daily for 3 weeks followed by 1 week off plus daily oral letrozole at 2.5 mg/day; or four cycles of intravenous doxorubicin at 60 mg/m2 and cyclophosphamide at 600 mg/m2 every 21 days, then weekly intravenous paclitaxel at 80 mg/m2 for 12 weeks.
The primary study endpoint was achievement of a low ROR score at the time of surgery: that is, a score below 40 points if pathologically node-negative at surgery, and below 15 with one to three positive nodes, which are the cutoffs for a less than 10% risk of distant recurrence at 10 years. A low ROR score was accomplished in 47% of the ribociclib/letrozole group and 46% of patients on standard multiagent chemotherapy. The median ROR score improved from 74 points at baseline to 18 in the investigational treatment arm and 25 in the standard chemotherapy arm.
“In other words, we observed that nearly half of the patients were downstaged from high risk to low risk in both treatment arms,” Dr. Gavilá noted.
Another 31% of patients in both treatment arms were ROR-intermediate at surgery.
The reduction in ROR score at day 15 of the study was more pronounced in the ribociclib/letrozole group than in the chemotherapy arm.
Turning to secondary outcomes, Dr. Gavilá noted that a Residual Cancer Burden score of 0 or 1, correlating with a pathologic complete response or minimal residual disease at time of surgery, was documented in 6% of the ribociclib/letrozole group and 12% of the chemotherapy group. A Preoperative Endocrine Prognostic Index (PEPI) score of 0 was attained in 22% of the novel treatment group and similarly in 17% of those on chemotherapy. Median levels of the tumor cell proliferation biomarker Ki 67 improved from 32% at baseline to 3% in the ribociclib/letrozole group and 10% in the chemotherapy arm. Eighty-eight percent of the ribociclib/letrozole group converted from luminal B to the less aggressive luminal A intrinsic subtype, as did 83% of patients following neoadjuvant chemotherapy.
The rate of serious adverse events was 4% in the ribociclib/letrozole group and 15% in the chemotherapy arm. The most common grade 3 or higher adverse event was neutropenia in both study arms, followed by increased transaminase levels in the ribociclib/letrozole group and febrile neutropenia in the chemotherapy arm. Fifty-nine percent of the ribociclib/letrozole group experienced an adverse event leading to dose reduction or temporary interruption of treatment, as did 83% of the chemotherapy group.
The SOLTI-1402/CORALLEEN trial was sponsored by Novartis, the Breast Cancer Research Foundation, The American Association for Cancer Research, and the Breast Cancer Now Career Catalyst. Dr. Gavilá reported serving as a consultant to Novartis, Roche, and MSD.
Simultaneously with Dr. Gavilá’s presentation in San Antonio, the study results were published online in The Lancet Oncology.
In an accompanying editorial, Massimo Cristofanilli, MD, opined that while the novel neoadjuvant treatment strategy tested in SOLTI-1402/CORALLEEN is promising, the most important concept introduced in the study is that a molecular subtyping tool such the Prosigna test can be used to assess the success of neoadjuvant therapy.
“The increasing availability of molecular testing in both the primary and metastatic setting is contributing to a change in the ability to stratify, select, and monitor disease biology and molecular evolution. This is resulting in the introduction of new frameworks in breast cancer treatments with potentially profound effects on patient outcomes and quality of life,” according to Dr. Cristofanilli, professor of medicine at Northwestern University, Chicago.
SOURCE: Gavilá J. SABCS 2019 Abstract GS2-06.
SAN ANTONIO – The combination of ribociclib and letrozole proved to be an attractive alternative to standard multidrug neoadjuvant chemotherapy for women with high-risk luminal B breast cancer in the exploratory phase 2 SOLTI-1402/CORALLEEN trial.
Neoadjuvant therapy with ribociclib (Kisqali), an inhibitor of cyclin-dependent kinases 4 and 6 (CDK4/6), in combination with the aromatase inhibitor letrozole (Femara) proved as effective for presurgical molecular disease downstaging as standard multiagent chemotherapy, but with considerably less toxicity, Joaquín Gavilá, MD, reported at the San Antonio Breast Cancer Symposium.
“We believe that these results suggest that in clinically high-risk luminal B disease, a chemotherapy-free treatment strategy based upon CDK4/6 inhibition is worth exploring in future neoadjuvant trials,” declared Dr. Gavilá, a medical oncologist at the Valencia (Spain) Institute of Oncology.
SOLTI-1402/CORALLEEN was an open-label, multicenter trial involving 106 postmenopausal women with hormone receptor–positive and HER2-negative stage I-IIIA breast cancer, an operable tumor size of at least 2 cm measured by MRI, and high-risk luminal B subtype disease as defined via the Prosigna genomic tumor profiling test, also known as PAM50, on which they had a baseline median Risk of Recurrence (ROR) score of 74 out of a possible 100 points. The luminal B subtype accounts for 30%-40% of all hormone receptor–positive/HER2-negative breast cancer and carries a greater than 10% risk of distant recurrence at 10 years.
The women were randomized to 6 months of neoadjuvant therapy involving one of two regimens: six 28-day cycles of oral ribociclib at 600 mg once daily for 3 weeks followed by 1 week off plus daily oral letrozole at 2.5 mg/day; or four cycles of intravenous doxorubicin at 60 mg/m2 and cyclophosphamide at 600 mg/m2 every 21 days, then weekly intravenous paclitaxel at 80 mg/m2 for 12 weeks.
The primary study endpoint was achievement of a low ROR score at the time of surgery: that is, a score below 40 points if pathologically node-negative at surgery, and below 15 with one to three positive nodes, which are the cutoffs for a less than 10% risk of distant recurrence at 10 years. A low ROR score was accomplished in 47% of the ribociclib/letrozole group and 46% of patients on standard multiagent chemotherapy. The median ROR score improved from 74 points at baseline to 18 in the investigational treatment arm and 25 in the standard chemotherapy arm.
“In other words, we observed that nearly half of the patients were downstaged from high risk to low risk in both treatment arms,” Dr. Gavilá noted.
Another 31% of patients in both treatment arms were ROR-intermediate at surgery.
The reduction in ROR score at day 15 of the study was more pronounced in the ribociclib/letrozole group than in the chemotherapy arm.
Turning to secondary outcomes, Dr. Gavilá noted that a Residual Cancer Burden score of 0 or 1, correlating with a pathologic complete response or minimal residual disease at time of surgery, was documented in 6% of the ribociclib/letrozole group and 12% of the chemotherapy group. A Preoperative Endocrine Prognostic Index (PEPI) score of 0 was attained in 22% of the novel treatment group and similarly in 17% of those on chemotherapy. Median levels of the tumor cell proliferation biomarker Ki 67 improved from 32% at baseline to 3% in the ribociclib/letrozole group and 10% in the chemotherapy arm. Eighty-eight percent of the ribociclib/letrozole group converted from luminal B to the less aggressive luminal A intrinsic subtype, as did 83% of patients following neoadjuvant chemotherapy.
The rate of serious adverse events was 4% in the ribociclib/letrozole group and 15% in the chemotherapy arm. The most common grade 3 or higher adverse event was neutropenia in both study arms, followed by increased transaminase levels in the ribociclib/letrozole group and febrile neutropenia in the chemotherapy arm. Fifty-nine percent of the ribociclib/letrozole group experienced an adverse event leading to dose reduction or temporary interruption of treatment, as did 83% of the chemotherapy group.
The SOLTI-1402/CORALLEEN trial was sponsored by Novartis, the Breast Cancer Research Foundation, The American Association for Cancer Research, and the Breast Cancer Now Career Catalyst. Dr. Gavilá reported serving as a consultant to Novartis, Roche, and MSD.
Simultaneously with Dr. Gavilá’s presentation in San Antonio, the study results were published online in The Lancet Oncology.
In an accompanying editorial, Massimo Cristofanilli, MD, opined that while the novel neoadjuvant treatment strategy tested in SOLTI-1402/CORALLEEN is promising, the most important concept introduced in the study is that a molecular subtyping tool such the Prosigna test can be used to assess the success of neoadjuvant therapy.
“The increasing availability of molecular testing in both the primary and metastatic setting is contributing to a change in the ability to stratify, select, and monitor disease biology and molecular evolution. This is resulting in the introduction of new frameworks in breast cancer treatments with potentially profound effects on patient outcomes and quality of life,” according to Dr. Cristofanilli, professor of medicine at Northwestern University, Chicago.
SOURCE: Gavilá J. SABCS 2019 Abstract GS2-06.
SAN ANTONIO – The combination of ribociclib and letrozole proved to be an attractive alternative to standard multidrug neoadjuvant chemotherapy for women with high-risk luminal B breast cancer in the exploratory phase 2 SOLTI-1402/CORALLEEN trial.
Neoadjuvant therapy with ribociclib (Kisqali), an inhibitor of cyclin-dependent kinases 4 and 6 (CDK4/6), in combination with the aromatase inhibitor letrozole (Femara) proved as effective for presurgical molecular disease downstaging as standard multiagent chemotherapy, but with considerably less toxicity, Joaquín Gavilá, MD, reported at the San Antonio Breast Cancer Symposium.
“We believe that these results suggest that in clinically high-risk luminal B disease, a chemotherapy-free treatment strategy based upon CDK4/6 inhibition is worth exploring in future neoadjuvant trials,” declared Dr. Gavilá, a medical oncologist at the Valencia (Spain) Institute of Oncology.
SOLTI-1402/CORALLEEN was an open-label, multicenter trial involving 106 postmenopausal women with hormone receptor–positive and HER2-negative stage I-IIIA breast cancer, an operable tumor size of at least 2 cm measured by MRI, and high-risk luminal B subtype disease as defined via the Prosigna genomic tumor profiling test, also known as PAM50, on which they had a baseline median Risk of Recurrence (ROR) score of 74 out of a possible 100 points. The luminal B subtype accounts for 30%-40% of all hormone receptor–positive/HER2-negative breast cancer and carries a greater than 10% risk of distant recurrence at 10 years.
The women were randomized to 6 months of neoadjuvant therapy involving one of two regimens: six 28-day cycles of oral ribociclib at 600 mg once daily for 3 weeks followed by 1 week off plus daily oral letrozole at 2.5 mg/day; or four cycles of intravenous doxorubicin at 60 mg/m2 and cyclophosphamide at 600 mg/m2 every 21 days, then weekly intravenous paclitaxel at 80 mg/m2 for 12 weeks.
The primary study endpoint was achievement of a low ROR score at the time of surgery: that is, a score below 40 points if pathologically node-negative at surgery, and below 15 with one to three positive nodes, which are the cutoffs for a less than 10% risk of distant recurrence at 10 years. A low ROR score was accomplished in 47% of the ribociclib/letrozole group and 46% of patients on standard multiagent chemotherapy. The median ROR score improved from 74 points at baseline to 18 in the investigational treatment arm and 25 in the standard chemotherapy arm.
“In other words, we observed that nearly half of the patients were downstaged from high risk to low risk in both treatment arms,” Dr. Gavilá noted.
Another 31% of patients in both treatment arms were ROR-intermediate at surgery.
The reduction in ROR score at day 15 of the study was more pronounced in the ribociclib/letrozole group than in the chemotherapy arm.
Turning to secondary outcomes, Dr. Gavilá noted that a Residual Cancer Burden score of 0 or 1, correlating with a pathologic complete response or minimal residual disease at time of surgery, was documented in 6% of the ribociclib/letrozole group and 12% of the chemotherapy group. A Preoperative Endocrine Prognostic Index (PEPI) score of 0 was attained in 22% of the novel treatment group and similarly in 17% of those on chemotherapy. Median levels of the tumor cell proliferation biomarker Ki 67 improved from 32% at baseline to 3% in the ribociclib/letrozole group and 10% in the chemotherapy arm. Eighty-eight percent of the ribociclib/letrozole group converted from luminal B to the less aggressive luminal A intrinsic subtype, as did 83% of patients following neoadjuvant chemotherapy.
The rate of serious adverse events was 4% in the ribociclib/letrozole group and 15% in the chemotherapy arm. The most common grade 3 or higher adverse event was neutropenia in both study arms, followed by increased transaminase levels in the ribociclib/letrozole group and febrile neutropenia in the chemotherapy arm. Fifty-nine percent of the ribociclib/letrozole group experienced an adverse event leading to dose reduction or temporary interruption of treatment, as did 83% of the chemotherapy group.
The SOLTI-1402/CORALLEEN trial was sponsored by Novartis, the Breast Cancer Research Foundation, The American Association for Cancer Research, and the Breast Cancer Now Career Catalyst. Dr. Gavilá reported serving as a consultant to Novartis, Roche, and MSD.
Simultaneously with Dr. Gavilá’s presentation in San Antonio, the study results were published online in The Lancet Oncology.
In an accompanying editorial, Massimo Cristofanilli, MD, opined that while the novel neoadjuvant treatment strategy tested in SOLTI-1402/CORALLEEN is promising, the most important concept introduced in the study is that a molecular subtyping tool such the Prosigna test can be used to assess the success of neoadjuvant therapy.
“The increasing availability of molecular testing in both the primary and metastatic setting is contributing to a change in the ability to stratify, select, and monitor disease biology and molecular evolution. This is resulting in the introduction of new frameworks in breast cancer treatments with potentially profound effects on patient outcomes and quality of life,” according to Dr. Cristofanilli, professor of medicine at Northwestern University, Chicago.
SOURCE: Gavilá J. SABCS 2019 Abstract GS2-06.
REPORTING FROM SABCS 2019
Switch to biologic for RA more about prescribers than patients
The length of time a patient with rheumatoid arthritis takes a conventional synthetic disease-modifying antirheumatic drug (csDMARD) such as methotrexate before switching to a biologic DMARD varies widely, and the variation is largely related to differences in prescriber preference, researchers say.
They found that 65% of the variation was attributed to differences between prescribers rather than patient variables. Another 4.6% was associated with regional differences in biologic DMARD use, and 30.4% of the variation was unexplained.
“Although disparities in access to biologic DMARDs increased in this study, the overall prescription percentage decreased relative to the population of active medication users with RA. This suggests that despite rheumatologists prescribing fewer biologic DMARDs on average per patient per unit of time, variations in the prescription of biologic DMARDs continue to grow,” the researchers explain.
The clinical implications of these differences in prescriber preferences are unclear, but the findings “show that between-prescriber differences exist in health care delivery for patients with RA, despite identical health insurance coverage,” they continue.
Mark Tatangelo of the University of Toronto and colleagues published their findings online Dec. 6, 2019, in JAMA Network Open.
They examined factors associated with the length of time from first csDMARD to receipt of first biologic in a retrospective cohort study using administrative data for 17,672 patients with RA and identical single-payer health insurance coverage in Ontario.
Patients were aged 67 years or older, had incident RA, and had received at least one csDMARD. The observation window was 2002 to 2015. During the study 719 patients (4.1%) received a first biologic DMARD. The primary outcome was time from first csDMARD to receipt of first biologic DMARD.
In an invited commentary, Natalie McCormick, PhD, from the clinical epidemiology program at Massachusetts General Hospital in Boston, writes: “A distinctive feature of the report by Tatangelo et al. was the emphasis on longer time to initiation of biologic therapy as an ideal outcome.”
Factors associated with a quicker move from csDMARDs to biologic DMARDs included younger age, female sex, living in an urban area close to prescribers, and longer disease duration. The shift to biologic DMARDs was also earlier for prescribers who were more recent graduates, in urban areas, and in areas with a greater supply of rheumatologists.
Dr. McCormick suggests that the association between earlier biologic DMARD use and higher concentration of rheumatologists might indicate that “peer effects” influence prescribing decisions.
Factors associated with a more prolonged time on csDMARDs before beginning a biologic DMARD included older age, male sex, and distance to the nearest rheumatologist.
Immigrants born outside of Canada were 41% less likely to have begun biologic DMARDs. “While its mechanism and implications warrant further investigation, this finding is novel and compelling, and it could become increasingly important,” Dr. McCormick writes.
The variation in highest biologic DMARD use, compared with lowest use among the regions in Ontario rose from 1.8% in 2002 to 8.7% in 2015. In models adjusted for age, sex, calendar year, and all patient and physician covariates, regional differences accounted for 4.6% of the variation in biologic DMARD prescription.
“A 4.6% difference in time to receipt of biologic DMARDs between regions should be considered problematic in the absence of other explanatory factors,” the authors write. “For example, every 1% increase in biologic prescriptions among a population of 72,000 funded patients with RA costs approximately CaD $10.8 million (U.S. $8.25 million) per year (assuming 10% biologics penetration and CaD $15,000 annually per biologic DMARD prescription [U.S. $11,460]).”
They explain that reducing the highest spending region in Ontario to the average spend would save approximately CaD $6 million to $8 million (U.S. $4.6 million to $6.1 million) per year, whereas increasing biologic use in the underserved regions to the population average would cost about CaD $6 million to $8 million (U.S. $4.6 million to $6.1 million).
Dr. McCormick writes that both undertreatment and overtreatment need more study and adds that the age gradient identified in this study “may reflect an ongoing bias against prescribing biologic DMARDs to elderly patients, despite a lack of evidence that older patients have a higher risk of infections or other adverse events.”
Dr. McCormick and the researchers emphasize that the decision to begin biologic DMARDs should not be taken lightly. “[S]mall changes in time to first biologic DMARD have major clinical and economic impacts. From a clinical perspective, the prescription of a biologic DMARD represents a transition to a more complex care plan, with less data to support the next prescription choice after the first biologic DMARD,” the authors warn.
This study was funded by grants from the Canadian Institute of Health Research, the Arthritis Society, the Ontario Drug Policy Research and Effectiveness Network, and the Canadian Institute of Health Research Drug Safety and Effectiveness Network. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care.
Several study authors report receiving consulting fees from Amgen, Covance, Roche, Novartis, Sanofi, Merck, and Eli Lilly; grants and consulting fees from AbbVie, Janssen Pharmaceuticals, Hospira, Merck, Pfizer, Sanofi, and Novartis; and grants from Amgen, Eli Lilly, Celgene, Medexus, Medreleaf, Roche, and Union Chimique Belge.
Dr. McCormick reports a fellowship award from the Canadian Institutes of Health Research.
SOURCES: Tatangelo M et al. JAMA Netw Open. 2019;2(12):e1917053. doi: 10.1001/jamanetworkopen.2019.17053; McCormick N. JAMA Netw Open. 2019;2(12):e1917065. doi: 10.1001/jamanetworkopen.2019.17065
This story first appeared on Medscape.com.
The length of time a patient with rheumatoid arthritis takes a conventional synthetic disease-modifying antirheumatic drug (csDMARD) such as methotrexate before switching to a biologic DMARD varies widely, and the variation is largely related to differences in prescriber preference, researchers say.
They found that 65% of the variation was attributed to differences between prescribers rather than patient variables. Another 4.6% was associated with regional differences in biologic DMARD use, and 30.4% of the variation was unexplained.
“Although disparities in access to biologic DMARDs increased in this study, the overall prescription percentage decreased relative to the population of active medication users with RA. This suggests that despite rheumatologists prescribing fewer biologic DMARDs on average per patient per unit of time, variations in the prescription of biologic DMARDs continue to grow,” the researchers explain.
The clinical implications of these differences in prescriber preferences are unclear, but the findings “show that between-prescriber differences exist in health care delivery for patients with RA, despite identical health insurance coverage,” they continue.
Mark Tatangelo of the University of Toronto and colleagues published their findings online Dec. 6, 2019, in JAMA Network Open.
They examined factors associated with the length of time from first csDMARD to receipt of first biologic in a retrospective cohort study using administrative data for 17,672 patients with RA and identical single-payer health insurance coverage in Ontario.
Patients were aged 67 years or older, had incident RA, and had received at least one csDMARD. The observation window was 2002 to 2015. During the study 719 patients (4.1%) received a first biologic DMARD. The primary outcome was time from first csDMARD to receipt of first biologic DMARD.
In an invited commentary, Natalie McCormick, PhD, from the clinical epidemiology program at Massachusetts General Hospital in Boston, writes: “A distinctive feature of the report by Tatangelo et al. was the emphasis on longer time to initiation of biologic therapy as an ideal outcome.”
Factors associated with a quicker move from csDMARDs to biologic DMARDs included younger age, female sex, living in an urban area close to prescribers, and longer disease duration. The shift to biologic DMARDs was also earlier for prescribers who were more recent graduates, in urban areas, and in areas with a greater supply of rheumatologists.
Dr. McCormick suggests that the association between earlier biologic DMARD use and higher concentration of rheumatologists might indicate that “peer effects” influence prescribing decisions.
Factors associated with a more prolonged time on csDMARDs before beginning a biologic DMARD included older age, male sex, and distance to the nearest rheumatologist.
Immigrants born outside of Canada were 41% less likely to have begun biologic DMARDs. “While its mechanism and implications warrant further investigation, this finding is novel and compelling, and it could become increasingly important,” Dr. McCormick writes.
The variation in highest biologic DMARD use, compared with lowest use among the regions in Ontario rose from 1.8% in 2002 to 8.7% in 2015. In models adjusted for age, sex, calendar year, and all patient and physician covariates, regional differences accounted for 4.6% of the variation in biologic DMARD prescription.
“A 4.6% difference in time to receipt of biologic DMARDs between regions should be considered problematic in the absence of other explanatory factors,” the authors write. “For example, every 1% increase in biologic prescriptions among a population of 72,000 funded patients with RA costs approximately CaD $10.8 million (U.S. $8.25 million) per year (assuming 10% biologics penetration and CaD $15,000 annually per biologic DMARD prescription [U.S. $11,460]).”
They explain that reducing the highest spending region in Ontario to the average spend would save approximately CaD $6 million to $8 million (U.S. $4.6 million to $6.1 million) per year, whereas increasing biologic use in the underserved regions to the population average would cost about CaD $6 million to $8 million (U.S. $4.6 million to $6.1 million).
Dr. McCormick writes that both undertreatment and overtreatment need more study and adds that the age gradient identified in this study “may reflect an ongoing bias against prescribing biologic DMARDs to elderly patients, despite a lack of evidence that older patients have a higher risk of infections or other adverse events.”
Dr. McCormick and the researchers emphasize that the decision to begin biologic DMARDs should not be taken lightly. “[S]mall changes in time to first biologic DMARD have major clinical and economic impacts. From a clinical perspective, the prescription of a biologic DMARD represents a transition to a more complex care plan, with less data to support the next prescription choice after the first biologic DMARD,” the authors warn.
This study was funded by grants from the Canadian Institute of Health Research, the Arthritis Society, the Ontario Drug Policy Research and Effectiveness Network, and the Canadian Institute of Health Research Drug Safety and Effectiveness Network. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care.
Several study authors report receiving consulting fees from Amgen, Covance, Roche, Novartis, Sanofi, Merck, and Eli Lilly; grants and consulting fees from AbbVie, Janssen Pharmaceuticals, Hospira, Merck, Pfizer, Sanofi, and Novartis; and grants from Amgen, Eli Lilly, Celgene, Medexus, Medreleaf, Roche, and Union Chimique Belge.
Dr. McCormick reports a fellowship award from the Canadian Institutes of Health Research.
SOURCES: Tatangelo M et al. JAMA Netw Open. 2019;2(12):e1917053. doi: 10.1001/jamanetworkopen.2019.17053; McCormick N. JAMA Netw Open. 2019;2(12):e1917065. doi: 10.1001/jamanetworkopen.2019.17065
This story first appeared on Medscape.com.
The length of time a patient with rheumatoid arthritis takes a conventional synthetic disease-modifying antirheumatic drug (csDMARD) such as methotrexate before switching to a biologic DMARD varies widely, and the variation is largely related to differences in prescriber preference, researchers say.
They found that 65% of the variation was attributed to differences between prescribers rather than patient variables. Another 4.6% was associated with regional differences in biologic DMARD use, and 30.4% of the variation was unexplained.
“Although disparities in access to biologic DMARDs increased in this study, the overall prescription percentage decreased relative to the population of active medication users with RA. This suggests that despite rheumatologists prescribing fewer biologic DMARDs on average per patient per unit of time, variations in the prescription of biologic DMARDs continue to grow,” the researchers explain.
The clinical implications of these differences in prescriber preferences are unclear, but the findings “show that between-prescriber differences exist in health care delivery for patients with RA, despite identical health insurance coverage,” they continue.
Mark Tatangelo of the University of Toronto and colleagues published their findings online Dec. 6, 2019, in JAMA Network Open.
They examined factors associated with the length of time from first csDMARD to receipt of first biologic in a retrospective cohort study using administrative data for 17,672 patients with RA and identical single-payer health insurance coverage in Ontario.
Patients were aged 67 years or older, had incident RA, and had received at least one csDMARD. The observation window was 2002 to 2015. During the study 719 patients (4.1%) received a first biologic DMARD. The primary outcome was time from first csDMARD to receipt of first biologic DMARD.
In an invited commentary, Natalie McCormick, PhD, from the clinical epidemiology program at Massachusetts General Hospital in Boston, writes: “A distinctive feature of the report by Tatangelo et al. was the emphasis on longer time to initiation of biologic therapy as an ideal outcome.”
Factors associated with a quicker move from csDMARDs to biologic DMARDs included younger age, female sex, living in an urban area close to prescribers, and longer disease duration. The shift to biologic DMARDs was also earlier for prescribers who were more recent graduates, in urban areas, and in areas with a greater supply of rheumatologists.
Dr. McCormick suggests that the association between earlier biologic DMARD use and higher concentration of rheumatologists might indicate that “peer effects” influence prescribing decisions.
Factors associated with a more prolonged time on csDMARDs before beginning a biologic DMARD included older age, male sex, and distance to the nearest rheumatologist.
Immigrants born outside of Canada were 41% less likely to have begun biologic DMARDs. “While its mechanism and implications warrant further investigation, this finding is novel and compelling, and it could become increasingly important,” Dr. McCormick writes.
The variation in highest biologic DMARD use, compared with lowest use among the regions in Ontario rose from 1.8% in 2002 to 8.7% in 2015. In models adjusted for age, sex, calendar year, and all patient and physician covariates, regional differences accounted for 4.6% of the variation in biologic DMARD prescription.
“A 4.6% difference in time to receipt of biologic DMARDs between regions should be considered problematic in the absence of other explanatory factors,” the authors write. “For example, every 1% increase in biologic prescriptions among a population of 72,000 funded patients with RA costs approximately CaD $10.8 million (U.S. $8.25 million) per year (assuming 10% biologics penetration and CaD $15,000 annually per biologic DMARD prescription [U.S. $11,460]).”
They explain that reducing the highest spending region in Ontario to the average spend would save approximately CaD $6 million to $8 million (U.S. $4.6 million to $6.1 million) per year, whereas increasing biologic use in the underserved regions to the population average would cost about CaD $6 million to $8 million (U.S. $4.6 million to $6.1 million).
Dr. McCormick writes that both undertreatment and overtreatment need more study and adds that the age gradient identified in this study “may reflect an ongoing bias against prescribing biologic DMARDs to elderly patients, despite a lack of evidence that older patients have a higher risk of infections or other adverse events.”
Dr. McCormick and the researchers emphasize that the decision to begin biologic DMARDs should not be taken lightly. “[S]mall changes in time to first biologic DMARD have major clinical and economic impacts. From a clinical perspective, the prescription of a biologic DMARD represents a transition to a more complex care plan, with less data to support the next prescription choice after the first biologic DMARD,” the authors warn.
This study was funded by grants from the Canadian Institute of Health Research, the Arthritis Society, the Ontario Drug Policy Research and Effectiveness Network, and the Canadian Institute of Health Research Drug Safety and Effectiveness Network. This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health and Long-Term Care.
Several study authors report receiving consulting fees from Amgen, Covance, Roche, Novartis, Sanofi, Merck, and Eli Lilly; grants and consulting fees from AbbVie, Janssen Pharmaceuticals, Hospira, Merck, Pfizer, Sanofi, and Novartis; and grants from Amgen, Eli Lilly, Celgene, Medexus, Medreleaf, Roche, and Union Chimique Belge.
Dr. McCormick reports a fellowship award from the Canadian Institutes of Health Research.
SOURCES: Tatangelo M et al. JAMA Netw Open. 2019;2(12):e1917053. doi: 10.1001/jamanetworkopen.2019.17053; McCormick N. JAMA Netw Open. 2019;2(12):e1917065. doi: 10.1001/jamanetworkopen.2019.17065
This story first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
APHINITY 6-year data: Benefit ongoing in HER2+ early BC, no significant OS benefit
SAN ANTONIO – Adding pertuzumab to trastuzumab and chemotherapy after surgery for HER2-positive early breast cancer continued to show a slight, but statistically nonsignificant overall survival benefit, compared with placebo, at a preplanned 6-year interim analysis of the phase 3 APHINITY trial.

Invasive disease-free survival (IDFS) was significantly improved with pertuzumab at this second interim analysis, and node-positive patients continued to derive the greatest benefit, as was the case in the primary analysis reported in the New England Journal of Medicine in 2017, Martine Piccart, MD, PhD, reported at the San Antonio Breast Cancer Symposium.
At a median of 74.1 months of follow-up, overall survival (OS) was 94.8% in 2,400 patients in the pertuzumab arm, compared with 93.9% in 2,405 patients in the placebo arm (hazard ratio, 0.85), said Dr. Piccart of Institut Jules Bordet, Brussels.
She noted that a “very stringent” P value of.0012 was required for statistical significance in this interim OS analysis.
IDFS rates at follow-up were 90.6% vs. 87.8% in the intent-to-treat population, a difference caused mainly by a reduction in distant and loco-regional recurrence, she noted.
“[That translates] to a 2.8% absolute improvement with pertuzumab at 6 years,” she said, adding that the risk of both distant and loco-regional recurrences was reduced with pertuzumab. “The rate of [central nervous system] metastases, contralateral invasive breast cancers, and death without a prior event – not different between the two treatment groups.”
In the node-positive cohort, the 6-year IDFS rates were 87.9% vs. 83.4% with pertuzumab vs. placebo (4.5% absolute benefit; HR, 0.72), showing a clear benefit.
“In contrast, no treatment effect is detected in the node-negative population [95.0% and 94.9%, respectively; HR, 1.02],” she said.
Importantly, the clinical benefits were seen regardless of hormone receptor status (HRs, 0.73 and 0.83 for hormone receptor–positive and –negative disease, respectively), she said, noting that this finding differs from the 3-year analysis, which suggested an enhanced benefit only in the hormone receptor–negative cohort.
“These [hormone receptor–negative] patients still benefit from pertuzumab ... but interestingly, now the curves are diverging in the hormone receptor–positive population, and there is a benefit emerging,” she said.
An updated descriptive analysis of cardiac safety was also performed, and no new safety concerns emerged, Dr. Piccart said.
“What is important to remember is the rate of severe cardiac events is below 1% in both groups (0.8% and 0.3% with pertuzumab and placebo),” she said.
APHINITY is a randomized, multicenter, double-blind, placebo-controlled trial which previously demonstrated that pertuzumab added to standard chemotherapy plus 1 year of trastuzumab in operable HER2-positive breast cancer was associated with modest but statistically significant improvement in IDFS, compared with placebo and chemotherapy plus trastuzumab (HR, 0.81; P = .04).
The effect was more pronounced in node-negative patients (HR, 0.77) and hormone receptor–negative patients (HR, 0.76).
Patients with node-positive or high-risk node-negative, HER2-positive, operable early breast cancer were enrolled between November 2011 and August 2013, and the primary analysis was conducted at 45.4 months of follow-up. Based on those findings, pertuzumab in combination with trastuzumab was approved for high-risk early HER2-positive breast cancer patients.
The first interim OS analysis was conducted at that time, and no significant treatment effect was observed, Dr. Piccart said.
The 6-year findings demonstrate that the small OS benefit and the statistically significant IDFS benefit with pertuzumab in this setting is maintained, with the node-positive population deriving the greatest benefit.
“Further follow-up will be very important to determine whether there is a survival benefit associated with pertuzumab administration in early HER2-positive breast cancer,” she said, noting that a calendar-driven third interim OS analysis is planned in 2.5 years.
The APHINITY trial is funded by Roche. Dr. Piccart reported receiving consulting fees from Roche and research funding to her institution from Roche and several other companies. She also is a consultant for the advisory boards of AstraZeneca, Camel-IDS, Crescendo Biologics, Debiopharm, G1 Therapeutics, Huya Bioscience International, and Immunomedics.
SOURCE: Piccart M et al. SABCS 2019, Abstract GS1-04.
SAN ANTONIO – Adding pertuzumab to trastuzumab and chemotherapy after surgery for HER2-positive early breast cancer continued to show a slight, but statistically nonsignificant overall survival benefit, compared with placebo, at a preplanned 6-year interim analysis of the phase 3 APHINITY trial.
Invasive disease-free survival (IDFS) was significantly improved with pertuzumab at this second interim analysis, and node-positive patients continued to derive the greatest benefit, as was the case in the primary analysis reported in the New England Journal of Medicine in 2017, Martine Piccart, MD, PhD, reported at the San Antonio Breast Cancer Symposium.
At a median of 74.1 months of follow-up, overall survival (OS) was 94.8% in 2,400 patients in the pertuzumab arm, compared with 93.9% in 2,405 patients in the placebo arm (hazard ratio, 0.85), said Dr. Piccart of Institut Jules Bordet, Brussels.
She noted that a “very stringent” P value of.0012 was required for statistical significance in this interim OS analysis.
IDFS rates at follow-up were 90.6% vs. 87.8% in the intent-to-treat population, a difference caused mainly by a reduction in distant and loco-regional recurrence, she noted.
“[That translates] to a 2.8% absolute improvement with pertuzumab at 6 years,” she said, adding that the risk of both distant and loco-regional recurrences was reduced with pertuzumab. “The rate of [central nervous system] metastases, contralateral invasive breast cancers, and death without a prior event – not different between the two treatment groups.”
In the node-positive cohort, the 6-year IDFS rates were 87.9% vs. 83.4% with pertuzumab vs. placebo (4.5% absolute benefit; HR, 0.72), showing a clear benefit.
“In contrast, no treatment effect is detected in the node-negative population [95.0% and 94.9%, respectively; HR, 1.02],” she said.
Importantly, the clinical benefits were seen regardless of hormone receptor status (HRs, 0.73 and 0.83 for hormone receptor–positive and –negative disease, respectively), she said, noting that this finding differs from the 3-year analysis, which suggested an enhanced benefit only in the hormone receptor–negative cohort.
“These [hormone receptor–negative] patients still benefit from pertuzumab ... but interestingly, now the curves are diverging in the hormone receptor–positive population, and there is a benefit emerging,” she said.
An updated descriptive analysis of cardiac safety was also performed, and no new safety concerns emerged, Dr. Piccart said.
“What is important to remember is the rate of severe cardiac events is below 1% in both groups (0.8% and 0.3% with pertuzumab and placebo),” she said.
APHINITY is a randomized, multicenter, double-blind, placebo-controlled trial which previously demonstrated that pertuzumab added to standard chemotherapy plus 1 year of trastuzumab in operable HER2-positive breast cancer was associated with modest but statistically significant improvement in IDFS, compared with placebo and chemotherapy plus trastuzumab (HR, 0.81; P = .04).
The effect was more pronounced in node-negative patients (HR, 0.77) and hormone receptor–negative patients (HR, 0.76).
Patients with node-positive or high-risk node-negative, HER2-positive, operable early breast cancer were enrolled between November 2011 and August 2013, and the primary analysis was conducted at 45.4 months of follow-up. Based on those findings, pertuzumab in combination with trastuzumab was approved for high-risk early HER2-positive breast cancer patients.
The first interim OS analysis was conducted at that time, and no significant treatment effect was observed, Dr. Piccart said.
The 6-year findings demonstrate that the small OS benefit and the statistically significant IDFS benefit with pertuzumab in this setting is maintained, with the node-positive population deriving the greatest benefit.
“Further follow-up will be very important to determine whether there is a survival benefit associated with pertuzumab administration in early HER2-positive breast cancer,” she said, noting that a calendar-driven third interim OS analysis is planned in 2.5 years.
The APHINITY trial is funded by Roche. Dr. Piccart reported receiving consulting fees from Roche and research funding to her institution from Roche and several other companies. She also is a consultant for the advisory boards of AstraZeneca, Camel-IDS, Crescendo Biologics, Debiopharm, G1 Therapeutics, Huya Bioscience International, and Immunomedics.
SOURCE: Piccart M et al. SABCS 2019, Abstract GS1-04.
SAN ANTONIO – Adding pertuzumab to trastuzumab and chemotherapy after surgery for HER2-positive early breast cancer continued to show a slight, but statistically nonsignificant overall survival benefit, compared with placebo, at a preplanned 6-year interim analysis of the phase 3 APHINITY trial.
Invasive disease-free survival (IDFS) was significantly improved with pertuzumab at this second interim analysis, and node-positive patients continued to derive the greatest benefit, as was the case in the primary analysis reported in the New England Journal of Medicine in 2017, Martine Piccart, MD, PhD, reported at the San Antonio Breast Cancer Symposium.
At a median of 74.1 months of follow-up, overall survival (OS) was 94.8% in 2,400 patients in the pertuzumab arm, compared with 93.9% in 2,405 patients in the placebo arm (hazard ratio, 0.85), said Dr. Piccart of Institut Jules Bordet, Brussels.
She noted that a “very stringent” P value of.0012 was required for statistical significance in this interim OS analysis.
IDFS rates at follow-up were 90.6% vs. 87.8% in the intent-to-treat population, a difference caused mainly by a reduction in distant and loco-regional recurrence, she noted.
“[That translates] to a 2.8% absolute improvement with pertuzumab at 6 years,” she said, adding that the risk of both distant and loco-regional recurrences was reduced with pertuzumab. “The rate of [central nervous system] metastases, contralateral invasive breast cancers, and death without a prior event – not different between the two treatment groups.”
In the node-positive cohort, the 6-year IDFS rates were 87.9% vs. 83.4% with pertuzumab vs. placebo (4.5% absolute benefit; HR, 0.72), showing a clear benefit.
“In contrast, no treatment effect is detected in the node-negative population [95.0% and 94.9%, respectively; HR, 1.02],” she said.
Importantly, the clinical benefits were seen regardless of hormone receptor status (HRs, 0.73 and 0.83 for hormone receptor–positive and –negative disease, respectively), she said, noting that this finding differs from the 3-year analysis, which suggested an enhanced benefit only in the hormone receptor–negative cohort.
“These [hormone receptor–negative] patients still benefit from pertuzumab ... but interestingly, now the curves are diverging in the hormone receptor–positive population, and there is a benefit emerging,” she said.
An updated descriptive analysis of cardiac safety was also performed, and no new safety concerns emerged, Dr. Piccart said.
“What is important to remember is the rate of severe cardiac events is below 1% in both groups (0.8% and 0.3% with pertuzumab and placebo),” she said.
APHINITY is a randomized, multicenter, double-blind, placebo-controlled trial which previously demonstrated that pertuzumab added to standard chemotherapy plus 1 year of trastuzumab in operable HER2-positive breast cancer was associated with modest but statistically significant improvement in IDFS, compared with placebo and chemotherapy plus trastuzumab (HR, 0.81; P = .04).
The effect was more pronounced in node-negative patients (HR, 0.77) and hormone receptor–negative patients (HR, 0.76).
Patients with node-positive or high-risk node-negative, HER2-positive, operable early breast cancer were enrolled between November 2011 and August 2013, and the primary analysis was conducted at 45.4 months of follow-up. Based on those findings, pertuzumab in combination with trastuzumab was approved for high-risk early HER2-positive breast cancer patients.
The first interim OS analysis was conducted at that time, and no significant treatment effect was observed, Dr. Piccart said.
The 6-year findings demonstrate that the small OS benefit and the statistically significant IDFS benefit with pertuzumab in this setting is maintained, with the node-positive population deriving the greatest benefit.
“Further follow-up will be very important to determine whether there is a survival benefit associated with pertuzumab administration in early HER2-positive breast cancer,” she said, noting that a calendar-driven third interim OS analysis is planned in 2.5 years.
The APHINITY trial is funded by Roche. Dr. Piccart reported receiving consulting fees from Roche and research funding to her institution from Roche and several other companies. She also is a consultant for the advisory boards of AstraZeneca, Camel-IDS, Crescendo Biologics, Debiopharm, G1 Therapeutics, Huya Bioscience International, and Immunomedics.
SOURCE: Piccart M et al. SABCS 2019, Abstract GS1-04.
REPORTING FROM SABCS 2019
Emergency physicians not yet embracing buprenorphine for opioid users
SAN DIEGO – Emergency physicians can be persuaded to follow a recommended strategy to prescribe buprenorphine to patients with opioid addictions and to refer them to follow-up care, Kathryn F. Hawk, MD, said at the annual meeting of the American Academy of Addiction Psychiatry.
“People are willing to change their practices and evolve as long as they have the support to do so,” Dr. Hawk, assistant professor of emergency medicine at Yale University, New Haven, Conn., said at the meeting.
Dr. Hawk highlighted a landmark 2015 study led by Yale colleagues that compared three strategies to treating patients with opioid use disorder in the emergency department. Researchers randomly assigned 329 patients to 1) referral to treatment; 2) brief intervention and facilitated referral to community-based treatment services; and 3) emergency department-initiated treatment with buprenorphine/naloxone (Suboxone) plus referral to primary care for 10-week follow-up.
At 30 days, 78% of patients in the third group were in addiction treatment vs. 37% in the first group and 45% in the second group. (P less than .001). However, the percentage of patients in the groups who had negative urine screens for opioids were not statistically different (JAMA. 2015. Apr 28;313[16]:1636-44).
Both the American College of Emergency Physicians (ACEP) and the American College of Medical Toxicology have endorsed the use of buprenorphine in the ED “as a bridge to long-term addiction treatment,” said Dr. Hawk, who also is affiliated with Yale New Haven Hospital.
Emergency department physicians, however, have been reluctant to start prescribing buprenorphine and get more deeply involved in referrals to care, said E. Jennifer Edelman, MD, associate professor of general internal medicine at Yale. She described the results of a 2017-2019 survey of 268 medical professionals at urban emergency departments in Seattle, Cincinnati, New York City, and Baltimore. Only 20% of the survey respondents said they were “ready” to initiate the buprenorphine treatment protocol.
Researchers also held focus groups with 74 clinicians who offered insight into their hesitation. “That’s not something that we’re even really taught in medical school and certainly not in our training as emergency physicians,” one faculty member said. “It is this detox black box across the street, and that’s how it is in many places.”
Another faculty member expressed regret about the current system: “I feel like this is particularly vulnerable patient population [and] we’re just saying, ‘Here’s a sheet. Call some numbers. Good luck.’ That’s the way it feels when I discharge these folks.” And a resident said: “We can’t provide all of that care up front. It’s just too time-consuming, and there are other patients to see.”
But not all of the findings were grim.
Dr. Edelman said.
According to her, strategies aimed at boosting the Suboxone approach include establishing protocols, and providing leadership support and resources. Addiction psychiatrists also can be helpful, she said.
“Let’s think about partnering together to bridge that gap,” she said. One idea: Invite emergency physicians to observe a treatment initiation.
“Showing how you counsel patients to start medication at home would be really a wonderful way to facilitate practices in the emergency department,” she said.
Another idea, she said, is to “give them feedback on their patients.” If an emergency physician refers a patient and they walk in the door, “let them know how they did. That’s going to be really, really powerful.”
ACEP and the American Society of Addiction Medicine have created a tool aimed at helping facilitate the use of buprenorphine and naloxone in the emergency department.
Dr. Hawk and Dr. Edelman reported no relevant disclosures.
SAN DIEGO – Emergency physicians can be persuaded to follow a recommended strategy to prescribe buprenorphine to patients with opioid addictions and to refer them to follow-up care, Kathryn F. Hawk, MD, said at the annual meeting of the American Academy of Addiction Psychiatry.
“People are willing to change their practices and evolve as long as they have the support to do so,” Dr. Hawk, assistant professor of emergency medicine at Yale University, New Haven, Conn., said at the meeting.
Dr. Hawk highlighted a landmark 2015 study led by Yale colleagues that compared three strategies to treating patients with opioid use disorder in the emergency department. Researchers randomly assigned 329 patients to 1) referral to treatment; 2) brief intervention and facilitated referral to community-based treatment services; and 3) emergency department-initiated treatment with buprenorphine/naloxone (Suboxone) plus referral to primary care for 10-week follow-up.
At 30 days, 78% of patients in the third group were in addiction treatment vs. 37% in the first group and 45% in the second group. (P less than .001). However, the percentage of patients in the groups who had negative urine screens for opioids were not statistically different (JAMA. 2015. Apr 28;313[16]:1636-44).
Both the American College of Emergency Physicians (ACEP) and the American College of Medical Toxicology have endorsed the use of buprenorphine in the ED “as a bridge to long-term addiction treatment,” said Dr. Hawk, who also is affiliated with Yale New Haven Hospital.
Emergency department physicians, however, have been reluctant to start prescribing buprenorphine and get more deeply involved in referrals to care, said E. Jennifer Edelman, MD, associate professor of general internal medicine at Yale. She described the results of a 2017-2019 survey of 268 medical professionals at urban emergency departments in Seattle, Cincinnati, New York City, and Baltimore. Only 20% of the survey respondents said they were “ready” to initiate the buprenorphine treatment protocol.
Researchers also held focus groups with 74 clinicians who offered insight into their hesitation. “That’s not something that we’re even really taught in medical school and certainly not in our training as emergency physicians,” one faculty member said. “It is this detox black box across the street, and that’s how it is in many places.”
Another faculty member expressed regret about the current system: “I feel like this is particularly vulnerable patient population [and] we’re just saying, ‘Here’s a sheet. Call some numbers. Good luck.’ That’s the way it feels when I discharge these folks.” And a resident said: “We can’t provide all of that care up front. It’s just too time-consuming, and there are other patients to see.”
But not all of the findings were grim.
Dr. Edelman said.
According to her, strategies aimed at boosting the Suboxone approach include establishing protocols, and providing leadership support and resources. Addiction psychiatrists also can be helpful, she said.
“Let’s think about partnering together to bridge that gap,” she said. One idea: Invite emergency physicians to observe a treatment initiation.
“Showing how you counsel patients to start medication at home would be really a wonderful way to facilitate practices in the emergency department,” she said.
Another idea, she said, is to “give them feedback on their patients.” If an emergency physician refers a patient and they walk in the door, “let them know how they did. That’s going to be really, really powerful.”
ACEP and the American Society of Addiction Medicine have created a tool aimed at helping facilitate the use of buprenorphine and naloxone in the emergency department.
Dr. Hawk and Dr. Edelman reported no relevant disclosures.
SAN DIEGO – Emergency physicians can be persuaded to follow a recommended strategy to prescribe buprenorphine to patients with opioid addictions and to refer them to follow-up care, Kathryn F. Hawk, MD, said at the annual meeting of the American Academy of Addiction Psychiatry.
“People are willing to change their practices and evolve as long as they have the support to do so,” Dr. Hawk, assistant professor of emergency medicine at Yale University, New Haven, Conn., said at the meeting.
Dr. Hawk highlighted a landmark 2015 study led by Yale colleagues that compared three strategies to treating patients with opioid use disorder in the emergency department. Researchers randomly assigned 329 patients to 1) referral to treatment; 2) brief intervention and facilitated referral to community-based treatment services; and 3) emergency department-initiated treatment with buprenorphine/naloxone (Suboxone) plus referral to primary care for 10-week follow-up.
At 30 days, 78% of patients in the third group were in addiction treatment vs. 37% in the first group and 45% in the second group. (P less than .001). However, the percentage of patients in the groups who had negative urine screens for opioids were not statistically different (JAMA. 2015. Apr 28;313[16]:1636-44).
Both the American College of Emergency Physicians (ACEP) and the American College of Medical Toxicology have endorsed the use of buprenorphine in the ED “as a bridge to long-term addiction treatment,” said Dr. Hawk, who also is affiliated with Yale New Haven Hospital.
Emergency department physicians, however, have been reluctant to start prescribing buprenorphine and get more deeply involved in referrals to care, said E. Jennifer Edelman, MD, associate professor of general internal medicine at Yale. She described the results of a 2017-2019 survey of 268 medical professionals at urban emergency departments in Seattle, Cincinnati, New York City, and Baltimore. Only 20% of the survey respondents said they were “ready” to initiate the buprenorphine treatment protocol.
Researchers also held focus groups with 74 clinicians who offered insight into their hesitation. “That’s not something that we’re even really taught in medical school and certainly not in our training as emergency physicians,” one faculty member said. “It is this detox black box across the street, and that’s how it is in many places.”
Another faculty member expressed regret about the current system: “I feel like this is particularly vulnerable patient population [and] we’re just saying, ‘Here’s a sheet. Call some numbers. Good luck.’ That’s the way it feels when I discharge these folks.” And a resident said: “We can’t provide all of that care up front. It’s just too time-consuming, and there are other patients to see.”
But not all of the findings were grim.
Dr. Edelman said.
According to her, strategies aimed at boosting the Suboxone approach include establishing protocols, and providing leadership support and resources. Addiction psychiatrists also can be helpful, she said.
“Let’s think about partnering together to bridge that gap,” she said. One idea: Invite emergency physicians to observe a treatment initiation.
“Showing how you counsel patients to start medication at home would be really a wonderful way to facilitate practices in the emergency department,” she said.
Another idea, she said, is to “give them feedback on their patients.” If an emergency physician refers a patient and they walk in the door, “let them know how they did. That’s going to be really, really powerful.”
ACEP and the American Society of Addiction Medicine have created a tool aimed at helping facilitate the use of buprenorphine and naloxone in the emergency department.
Dr. Hawk and Dr. Edelman reported no relevant disclosures.
REPORTING FROM AAAP 2019
Albinism awareness goes global in dermatologists’ nonprofit work
A dermatologist-led nonprofit organization has entered into a

Representatives from the New York–based NYDG Foundation, including dermatologist David Colbert, MD, recently signed the agreement with the United Nations High Commissioner for Human Rights. At the center of the inclusivity efforts is the foundation’s ColorFull campaign, which aims to shape a collective response to the discrimination and violence that individuals with albinism face around the world.
“We really need to build more inclusive and communal health care systems for all. Partnering with the United Nations will help us to reach our goals and build stronger bonds with those health care providers working with one of the most marginalized and vulnerable groups in Africa,” Dr. Colbert said in an interview.
Stylish images of individuals with albinism, including prominent model Diandra Forrest, anchor the ColorFull campaign’s messaging; Ms. Forrest is featured in a video posted by the United Nations in November announcing the joint human rights campaign. Because the consequences of albinism can be deadly serious for affected individuals in many parts of the world, awareness is desperately needed, participants in NYDG’s work and in Standing Voice, another nonprofit that provides resources for people with albinism in East Africa, emphasized in interviews.
Striving to do good work
Stephan Bognar, a seasoned leader of international nonprofits, has teamed up with Dr. Colbert, NYDG Foundation’s founding physician, to craft the international campaign to raise awareness of albinism and increase acceptance of those with the condition. “You don’t always have to stand alone to break down the walls of exclusion. The fight for social justice and human rights for persons with albinism requires a collective responsibility,” Mr. Bognar said in an interview.

Dr. Colbert, senior partner of the New York Dermatology Group, a large Manhattan-based practice, founded the nonprofit when he became involved in wound-care efforts in Haiti following the 2010 earthquake. The foundation has since supported such philanthropic efforts as helping people with albinism, offering scholarships, and raising awareness of the importance of sun protection among youth athletes.
“One day, 3 years ago or so, I was reading the New York Times and I came across this article – it was called ‘The Hunted,’ ” Dr. Colbert recalled. “It was something I knew nothing about. In Eastern Africa, people with albinism are often hunted down for body parts and their lives are at risk” from being hunted and murdered – but also because their body parts are used for witchcraft and magic, he noted.
“I was captivated by that, and I remember I called Stephan, and I said, ‘I have a project for you.’ ” Because of extensive previous work with international nongovernmental organizations and the United Nations, Mr. Bognar, who is now the executive director of the NYDG Foundation, “had the pedigree to make things happen instead of spinning our wheels,” Dr. Colbert said.

Albinism is more common by a factor of about 10 in certain sub-Saharan African populations in Tanzania and Malawi, compared with worldwide prevalence. The condition is stigmatized, but people with albinism are also believed to possess some magical powers. People with albinism are attacked, maimed, and even killed for their body parts, which are used by traditional “witch doctors” in ceremonies designed to generate wealth and good fortune. Raping a woman with albinism is thought by some to cure HIV/AIDS and infertility.
If African individuals with albinism escapes these horrors, they are still at high risk of developing a disfiguring, or even fatal, skin cancer. Even in higher-resource countries and in places farther from the equator, though, people with albinism still need stringent sun-exposure precautions and frequent dermatologic surveillance.
Philanthropic work in dermatology
Despite his busy practice, Dr. Colbert said he has found great satisfaction in pursuing philanthropic work. For physicians considering similar efforts, he said that genuine engagement with the issue is critical and global travel isn’t necessary to make a real difference.
“I think that, first, this should be something that you’re interested in and that you have the means to make some impact,” Dr. Colbert said. “Doing something doesn’t need to be a global campaign. You don’t need to have a home run – every little thing counts. Catching one squamous cell cancer on one patient with albinism makes a difference. But if you want to go bigger, you have to look at your community and see who has the resources and who might also be interested” in a cause you’re passionate about.
He added that a busy physician shouldn’t expect to do it all. “You have to find the right partner because we as physicians are taking care of our patients and paying the rent, so taking on a partner who is trained to do that can ... help you achieve what you envision.”
Though the NYDG Foundation has funded trips to Africa and participates in teledermatology there, Dr. Colbert said that the awareness campaign the NYDG is cosponsoring with the United Nations is of fundamental importance as well. “This is a really great example of the positive impact that social media can have on our society – in a good way, instead of a negative or self-serving way,” he said.
“I think that the ColorFull campaign will normalize the idea of people who are living without melanin in their skin. It keeps it out of the realm of ‘Don’t say anything.’ People don’t know what it means, so if we bring out the science, and show successful people who have normal lives, who have children, and we explain what it is, it demystifies it – and everybody wins. ... We’re all just people, no matter how many melanin granules we have.”
Dr. Colbert reported that he has no relevant conflicts of interest.
Standing Voice also provides resources in East Africa
The work of other nongovernmental organizations is also making a difference for people in East Africa with albinism.
Standing Voice is a United Kingdom–based nonprofit that provides education and resources that include sunscreen, as well as assessment and treatment of skin conditions for people with albinism in Tanzania and Malawi.

This and other work by Standing Voice were on display in an exhibit at the World Congress of Dermatology meeting in Milan in June 2019. In an interview at the meeting, Dr. Sharp, who spent his childhood in East Africa, contrasted access to dermatology care in the United States and United Kingdom with that in Africa, where an entire country may have hardly more than a few dermatologists.

“I go about three times a year, for about a week,” explained Dr. Sharp. “I’ll do a workshop to teach basic skin surgery techniques – excisions and biopsies. Very simple stuff. I’ll teach skin grafting as well because some of these patients have large lesions that won’t close directly,” he said. “On the whole, we like to use good grafts, rather than flaps, because often a local flap is just moving sun-damaged skin.”

Many patients have to travel great distances to reach a facility where general anesthesia and a full operating room suite are available, resources that are in high demand in resource-restricted African nations, according to Dr. Sharp. Teaching African practitioners regional anesthesia techniques that can be used for skin cancer surgery also helps ensure that more patients with albinism and squamous cell carcinoma can be treated – and treated closer to home.

Dr. Sharp reported that he has no relevant conflicts of interest.
A dermatologist-led nonprofit organization has entered into a
Representatives from the New York–based NYDG Foundation, including dermatologist David Colbert, MD, recently signed the agreement with the United Nations High Commissioner for Human Rights. At the center of the inclusivity efforts is the foundation’s ColorFull campaign, which aims to shape a collective response to the discrimination and violence that individuals with albinism face around the world.
“We really need to build more inclusive and communal health care systems for all. Partnering with the United Nations will help us to reach our goals and build stronger bonds with those health care providers working with one of the most marginalized and vulnerable groups in Africa,” Dr. Colbert said in an interview.
Stylish images of individuals with albinism, including prominent model Diandra Forrest, anchor the ColorFull campaign’s messaging; Ms. Forrest is featured in a video posted by the United Nations in November announcing the joint human rights campaign. Because the consequences of albinism can be deadly serious for affected individuals in many parts of the world, awareness is desperately needed, participants in NYDG’s work and in Standing Voice, another nonprofit that provides resources for people with albinism in East Africa, emphasized in interviews.
Striving to do good work
Stephan Bognar, a seasoned leader of international nonprofits, has teamed up with Dr. Colbert, NYDG Foundation’s founding physician, to craft the international campaign to raise awareness of albinism and increase acceptance of those with the condition. “You don’t always have to stand alone to break down the walls of exclusion. The fight for social justice and human rights for persons with albinism requires a collective responsibility,” Mr. Bognar said in an interview.
Dr. Colbert, senior partner of the New York Dermatology Group, a large Manhattan-based practice, founded the nonprofit when he became involved in wound-care efforts in Haiti following the 2010 earthquake. The foundation has since supported such philanthropic efforts as helping people with albinism, offering scholarships, and raising awareness of the importance of sun protection among youth athletes.
“One day, 3 years ago or so, I was reading the New York Times and I came across this article – it was called ‘The Hunted,’ ” Dr. Colbert recalled. “It was something I knew nothing about. In Eastern Africa, people with albinism are often hunted down for body parts and their lives are at risk” from being hunted and murdered – but also because their body parts are used for witchcraft and magic, he noted.
“I was captivated by that, and I remember I called Stephan, and I said, ‘I have a project for you.’ ” Because of extensive previous work with international nongovernmental organizations and the United Nations, Mr. Bognar, who is now the executive director of the NYDG Foundation, “had the pedigree to make things happen instead of spinning our wheels,” Dr. Colbert said.
Albinism is more common by a factor of about 10 in certain sub-Saharan African populations in Tanzania and Malawi, compared with worldwide prevalence. The condition is stigmatized, but people with albinism are also believed to possess some magical powers. People with albinism are attacked, maimed, and even killed for their body parts, which are used by traditional “witch doctors” in ceremonies designed to generate wealth and good fortune. Raping a woman with albinism is thought by some to cure HIV/AIDS and infertility.
If African individuals with albinism escapes these horrors, they are still at high risk of developing a disfiguring, or even fatal, skin cancer. Even in higher-resource countries and in places farther from the equator, though, people with albinism still need stringent sun-exposure precautions and frequent dermatologic surveillance.
Philanthropic work in dermatology
Despite his busy practice, Dr. Colbert said he has found great satisfaction in pursuing philanthropic work. For physicians considering similar efforts, he said that genuine engagement with the issue is critical and global travel isn’t necessary to make a real difference.
“I think that, first, this should be something that you’re interested in and that you have the means to make some impact,” Dr. Colbert said. “Doing something doesn’t need to be a global campaign. You don’t need to have a home run – every little thing counts. Catching one squamous cell cancer on one patient with albinism makes a difference. But if you want to go bigger, you have to look at your community and see who has the resources and who might also be interested” in a cause you’re passionate about.
He added that a busy physician shouldn’t expect to do it all. “You have to find the right partner because we as physicians are taking care of our patients and paying the rent, so taking on a partner who is trained to do that can ... help you achieve what you envision.”
Though the NYDG Foundation has funded trips to Africa and participates in teledermatology there, Dr. Colbert said that the awareness campaign the NYDG is cosponsoring with the United Nations is of fundamental importance as well. “This is a really great example of the positive impact that social media can have on our society – in a good way, instead of a negative or self-serving way,” he said.
“I think that the ColorFull campaign will normalize the idea of people who are living without melanin in their skin. It keeps it out of the realm of ‘Don’t say anything.’ People don’t know what it means, so if we bring out the science, and show successful people who have normal lives, who have children, and we explain what it is, it demystifies it – and everybody wins. ... We’re all just people, no matter how many melanin granules we have.”
Dr. Colbert reported that he has no relevant conflicts of interest.
Standing Voice also provides resources in East Africa
The work of other nongovernmental organizations is also making a difference for people in East Africa with albinism.
Standing Voice is a United Kingdom–based nonprofit that provides education and resources that include sunscreen, as well as assessment and treatment of skin conditions for people with albinism in Tanzania and Malawi.
This and other work by Standing Voice were on display in an exhibit at the World Congress of Dermatology meeting in Milan in June 2019. In an interview at the meeting, Dr. Sharp, who spent his childhood in East Africa, contrasted access to dermatology care in the United States and United Kingdom with that in Africa, where an entire country may have hardly more than a few dermatologists.
“I go about three times a year, for about a week,” explained Dr. Sharp. “I’ll do a workshop to teach basic skin surgery techniques – excisions and biopsies. Very simple stuff. I’ll teach skin grafting as well because some of these patients have large lesions that won’t close directly,” he said. “On the whole, we like to use good grafts, rather than flaps, because often a local flap is just moving sun-damaged skin.”
Many patients have to travel great distances to reach a facility where general anesthesia and a full operating room suite are available, resources that are in high demand in resource-restricted African nations, according to Dr. Sharp. Teaching African practitioners regional anesthesia techniques that can be used for skin cancer surgery also helps ensure that more patients with albinism and squamous cell carcinoma can be treated – and treated closer to home.
Dr. Sharp reported that he has no relevant conflicts of interest.
A dermatologist-led nonprofit organization has entered into a
Representatives from the New York–based NYDG Foundation, including dermatologist David Colbert, MD, recently signed the agreement with the United Nations High Commissioner for Human Rights. At the center of the inclusivity efforts is the foundation’s ColorFull campaign, which aims to shape a collective response to the discrimination and violence that individuals with albinism face around the world.
“We really need to build more inclusive and communal health care systems for all. Partnering with the United Nations will help us to reach our goals and build stronger bonds with those health care providers working with one of the most marginalized and vulnerable groups in Africa,” Dr. Colbert said in an interview.
Stylish images of individuals with albinism, including prominent model Diandra Forrest, anchor the ColorFull campaign’s messaging; Ms. Forrest is featured in a video posted by the United Nations in November announcing the joint human rights campaign. Because the consequences of albinism can be deadly serious for affected individuals in many parts of the world, awareness is desperately needed, participants in NYDG’s work and in Standing Voice, another nonprofit that provides resources for people with albinism in East Africa, emphasized in interviews.
Striving to do good work
Stephan Bognar, a seasoned leader of international nonprofits, has teamed up with Dr. Colbert, NYDG Foundation’s founding physician, to craft the international campaign to raise awareness of albinism and increase acceptance of those with the condition. “You don’t always have to stand alone to break down the walls of exclusion. The fight for social justice and human rights for persons with albinism requires a collective responsibility,” Mr. Bognar said in an interview.
Dr. Colbert, senior partner of the New York Dermatology Group, a large Manhattan-based practice, founded the nonprofit when he became involved in wound-care efforts in Haiti following the 2010 earthquake. The foundation has since supported such philanthropic efforts as helping people with albinism, offering scholarships, and raising awareness of the importance of sun protection among youth athletes.
“One day, 3 years ago or so, I was reading the New York Times and I came across this article – it was called ‘The Hunted,’ ” Dr. Colbert recalled. “It was something I knew nothing about. In Eastern Africa, people with albinism are often hunted down for body parts and their lives are at risk” from being hunted and murdered – but also because their body parts are used for witchcraft and magic, he noted.
“I was captivated by that, and I remember I called Stephan, and I said, ‘I have a project for you.’ ” Because of extensive previous work with international nongovernmental organizations and the United Nations, Mr. Bognar, who is now the executive director of the NYDG Foundation, “had the pedigree to make things happen instead of spinning our wheels,” Dr. Colbert said.
Albinism is more common by a factor of about 10 in certain sub-Saharan African populations in Tanzania and Malawi, compared with worldwide prevalence. The condition is stigmatized, but people with albinism are also believed to possess some magical powers. People with albinism are attacked, maimed, and even killed for their body parts, which are used by traditional “witch doctors” in ceremonies designed to generate wealth and good fortune. Raping a woman with albinism is thought by some to cure HIV/AIDS and infertility.
If African individuals with albinism escapes these horrors, they are still at high risk of developing a disfiguring, or even fatal, skin cancer. Even in higher-resource countries and in places farther from the equator, though, people with albinism still need stringent sun-exposure precautions and frequent dermatologic surveillance.
Philanthropic work in dermatology
Despite his busy practice, Dr. Colbert said he has found great satisfaction in pursuing philanthropic work. For physicians considering similar efforts, he said that genuine engagement with the issue is critical and global travel isn’t necessary to make a real difference.
“I think that, first, this should be something that you’re interested in and that you have the means to make some impact,” Dr. Colbert said. “Doing something doesn’t need to be a global campaign. You don’t need to have a home run – every little thing counts. Catching one squamous cell cancer on one patient with albinism makes a difference. But if you want to go bigger, you have to look at your community and see who has the resources and who might also be interested” in a cause you’re passionate about.
He added that a busy physician shouldn’t expect to do it all. “You have to find the right partner because we as physicians are taking care of our patients and paying the rent, so taking on a partner who is trained to do that can ... help you achieve what you envision.”
Though the NYDG Foundation has funded trips to Africa and participates in teledermatology there, Dr. Colbert said that the awareness campaign the NYDG is cosponsoring with the United Nations is of fundamental importance as well. “This is a really great example of the positive impact that social media can have on our society – in a good way, instead of a negative or self-serving way,” he said.
“I think that the ColorFull campaign will normalize the idea of people who are living without melanin in their skin. It keeps it out of the realm of ‘Don’t say anything.’ People don’t know what it means, so if we bring out the science, and show successful people who have normal lives, who have children, and we explain what it is, it demystifies it – and everybody wins. ... We’re all just people, no matter how many melanin granules we have.”
Dr. Colbert reported that he has no relevant conflicts of interest.
Standing Voice also provides resources in East Africa
The work of other nongovernmental organizations is also making a difference for people in East Africa with albinism.
Standing Voice is a United Kingdom–based nonprofit that provides education and resources that include sunscreen, as well as assessment and treatment of skin conditions for people with albinism in Tanzania and Malawi.
This and other work by Standing Voice were on display in an exhibit at the World Congress of Dermatology meeting in Milan in June 2019. In an interview at the meeting, Dr. Sharp, who spent his childhood in East Africa, contrasted access to dermatology care in the United States and United Kingdom with that in Africa, where an entire country may have hardly more than a few dermatologists.
“I go about three times a year, for about a week,” explained Dr. Sharp. “I’ll do a workshop to teach basic skin surgery techniques – excisions and biopsies. Very simple stuff. I’ll teach skin grafting as well because some of these patients have large lesions that won’t close directly,” he said. “On the whole, we like to use good grafts, rather than flaps, because often a local flap is just moving sun-damaged skin.”
Many patients have to travel great distances to reach a facility where general anesthesia and a full operating room suite are available, resources that are in high demand in resource-restricted African nations, according to Dr. Sharp. Teaching African practitioners regional anesthesia techniques that can be used for skin cancer surgery also helps ensure that more patients with albinism and squamous cell carcinoma can be treated – and treated closer to home.
Dr. Sharp reported that he has no relevant conflicts of interest.
Asthma exacerbation in pregnancy impacts mothers, infants
Women with asthma who suffer asthma exacerbation while pregnant are at increased risk for complications during pregnancy and delivery, and their infants are at increased risk for respiratory problems, according to data from a longitudinal study of 58,524 women with asthma.

“Asthma exacerbation during pregnancy has been found to be associated with adverse perinatal and pregnancy outcomes such as low birth weight, small for gestational age, preterm delivery, congenital malformation, preeclampsia, and perinatal mortality,” but previous studies have been small and limited to comparisons of asthmatic and nonasthmatic women, wrote Kawsari Abdullah, PhD, of Children’s Hospital of Eastern Ontario, Ottawa, and colleagues.
To determine the impact of asthma exacerbation on maternal and fetal outcomes, the researchers analyzed data from the Ontario Asthma Surveillance Information System to identify women with asthma who had at least one pregnancy resulting in a live or still birth between 2006 and 2012.
Overall, significantly more women with exacerbated asthma had preeclampsia or pregnancy-induced hypertension, compared with asthmatic women who had no exacerbations, at 5% vs. 4% and 7% vs. 5%, respectively (P less than .001), according to the study published in the European Respiratory Journal.
Adverse perinatal outcomes were significantly more likely among babies of mothers with exacerbated asthma, compared with those who had no exacerbations, including low birth weight (7% vs. 5%), small for gestational age (3% vs. 2%), preterm birth (8% vs. 7%), and congenital malformation (6% vs. 5%). All P values were less than .001, except for small for gestational age, which was P = .008.
In addition, significantly more babies of asthmatic women with exacerbated asthma during pregnancy had respiratory problems including asthma and pneumonia, compared with those of asthmatic women who had no exacerbations during pregnancy, at 38% vs. 31% and 24% vs. 22% (P less than .001 for both). The researchers found no significant interactions between maternal age and smoking and asthma exacerbations.
The findings were limited by several factors, including the lack of a validated algorithm for asthma exacerbation, which the researchers defined as five or more visits to a general practice clinician for asthma during pregnancy. Other limitations included the lack of categorizing asthma exacerbation by severity, and the inability to include the potential effects of asthma medication on maternal and fetal outcomes, Dr. Abdullah and colleagues noted.
However, the results were strengthened by the large sample size and ability to follow babies from birth until 5 years of age, they said.
“Targeting women with asthma during pregnancy and ensuring appropriate asthma management and postpartum follow-up may help to reduce the risk of pregnancy complications, adverse perinatal outcomes, and early childhood respiratory disorders,” they concluded.

This study is important because asthma is a common, potentially serious medical condition that complicates approximately 4%-8% of pregnancies, and one in three women with asthma experience an exacerbation during pregnancy, Iris Krishna, MD, a specialist in maternal/fetal medicine at Emory University, Atlanta, said in an interview.
“This study is unique in that it uses population-level data to assess the association between an asthma exacerbation during pregnancy and adverse perinatal outcomes,” Dr. Krishna said. “After adjusting for confounders, and consistent with previous studies, study findings suggest an increased risk for women with asthma who have an asthma exacerbation during pregnancy for preeclampsia [odds ratio, 1.3; P less than .001], pregnancy-induced hypertension [OR, 1.17; P less than .05], low-birth-weight infant [OR, 1.14; P less than .05], preterm birth [OR, 1.14; P less than .05], and congenital malformations [OR, 1.21; P less than .001].”
Dr. Krishna also noted the impact on early childhood outcomes. “In this study, children born to women who had an asthma exacerbation during pregnancy had a 23% higher risk of developing asthma before 5 years of age, which is consistent with previous studies. [The] investigators also reported a 12% higher risk of having pneumonia during the first 5 years of life for children born to women who had an asthma exacerbation during pregnancy.”
“Previous studies have suggested children born to mothers with uncontrolled asthma have an increased risk for respiratory infections, but this study is the first to report an association with pneumonia,” she said. This increased risk for childhood respiratory disorders warrants further study.
Consequently, “Women with asthma during pregnancy should have appropriate management to ensure good control to optimize pregnancy outcome,” Dr. Krishna emphasized. “Women who experience asthma exacerbations in pregnancy are at increased risk for preeclampsia, [pregnancy-induced hypertension], low birth weight, and preterm delivery and may require closer monitoring.”
The study was supported by the Institute for Clinical Evaluative Sciences. The researchers and Dr. Krishna had no financial conflicts to disclose.
SOURCE: Abdullah K et al. Eur Respir J. 2019 Nov 26. doi: 10.1183/13993003.01335-2019.
Women with asthma who suffer asthma exacerbation while pregnant are at increased risk for complications during pregnancy and delivery, and their infants are at increased risk for respiratory problems, according to data from a longitudinal study of 58,524 women with asthma.
“Asthma exacerbation during pregnancy has been found to be associated with adverse perinatal and pregnancy outcomes such as low birth weight, small for gestational age, preterm delivery, congenital malformation, preeclampsia, and perinatal mortality,” but previous studies have been small and limited to comparisons of asthmatic and nonasthmatic women, wrote Kawsari Abdullah, PhD, of Children’s Hospital of Eastern Ontario, Ottawa, and colleagues.
To determine the impact of asthma exacerbation on maternal and fetal outcomes, the researchers analyzed data from the Ontario Asthma Surveillance Information System to identify women with asthma who had at least one pregnancy resulting in a live or still birth between 2006 and 2012.
Overall, significantly more women with exacerbated asthma had preeclampsia or pregnancy-induced hypertension, compared with asthmatic women who had no exacerbations, at 5% vs. 4% and 7% vs. 5%, respectively (P less than .001), according to the study published in the European Respiratory Journal.
Adverse perinatal outcomes were significantly more likely among babies of mothers with exacerbated asthma, compared with those who had no exacerbations, including low birth weight (7% vs. 5%), small for gestational age (3% vs. 2%), preterm birth (8% vs. 7%), and congenital malformation (6% vs. 5%). All P values were less than .001, except for small for gestational age, which was P = .008.
In addition, significantly more babies of asthmatic women with exacerbated asthma during pregnancy had respiratory problems including asthma and pneumonia, compared with those of asthmatic women who had no exacerbations during pregnancy, at 38% vs. 31% and 24% vs. 22% (P less than .001 for both). The researchers found no significant interactions between maternal age and smoking and asthma exacerbations.
The findings were limited by several factors, including the lack of a validated algorithm for asthma exacerbation, which the researchers defined as five or more visits to a general practice clinician for asthma during pregnancy. Other limitations included the lack of categorizing asthma exacerbation by severity, and the inability to include the potential effects of asthma medication on maternal and fetal outcomes, Dr. Abdullah and colleagues noted.
However, the results were strengthened by the large sample size and ability to follow babies from birth until 5 years of age, they said.
“Targeting women with asthma during pregnancy and ensuring appropriate asthma management and postpartum follow-up may help to reduce the risk of pregnancy complications, adverse perinatal outcomes, and early childhood respiratory disorders,” they concluded.
This study is important because asthma is a common, potentially serious medical condition that complicates approximately 4%-8% of pregnancies, and one in three women with asthma experience an exacerbation during pregnancy, Iris Krishna, MD, a specialist in maternal/fetal medicine at Emory University, Atlanta, said in an interview.
“This study is unique in that it uses population-level data to assess the association between an asthma exacerbation during pregnancy and adverse perinatal outcomes,” Dr. Krishna said. “After adjusting for confounders, and consistent with previous studies, study findings suggest an increased risk for women with asthma who have an asthma exacerbation during pregnancy for preeclampsia [odds ratio, 1.3; P less than .001], pregnancy-induced hypertension [OR, 1.17; P less than .05], low-birth-weight infant [OR, 1.14; P less than .05], preterm birth [OR, 1.14; P less than .05], and congenital malformations [OR, 1.21; P less than .001].”
Dr. Krishna also noted the impact on early childhood outcomes. “In this study, children born to women who had an asthma exacerbation during pregnancy had a 23% higher risk of developing asthma before 5 years of age, which is consistent with previous studies. [The] investigators also reported a 12% higher risk of having pneumonia during the first 5 years of life for children born to women who had an asthma exacerbation during pregnancy.”
“Previous studies have suggested children born to mothers with uncontrolled asthma have an increased risk for respiratory infections, but this study is the first to report an association with pneumonia,” she said. This increased risk for childhood respiratory disorders warrants further study.
Consequently, “Women with asthma during pregnancy should have appropriate management to ensure good control to optimize pregnancy outcome,” Dr. Krishna emphasized. “Women who experience asthma exacerbations in pregnancy are at increased risk for preeclampsia, [pregnancy-induced hypertension], low birth weight, and preterm delivery and may require closer monitoring.”
The study was supported by the Institute for Clinical Evaluative Sciences. The researchers and Dr. Krishna had no financial conflicts to disclose.
SOURCE: Abdullah K et al. Eur Respir J. 2019 Nov 26. doi: 10.1183/13993003.01335-2019.
Women with asthma who suffer asthma exacerbation while pregnant are at increased risk for complications during pregnancy and delivery, and their infants are at increased risk for respiratory problems, according to data from a longitudinal study of 58,524 women with asthma.
“Asthma exacerbation during pregnancy has been found to be associated with adverse perinatal and pregnancy outcomes such as low birth weight, small for gestational age, preterm delivery, congenital malformation, preeclampsia, and perinatal mortality,” but previous studies have been small and limited to comparisons of asthmatic and nonasthmatic women, wrote Kawsari Abdullah, PhD, of Children’s Hospital of Eastern Ontario, Ottawa, and colleagues.
To determine the impact of asthma exacerbation on maternal and fetal outcomes, the researchers analyzed data from the Ontario Asthma Surveillance Information System to identify women with asthma who had at least one pregnancy resulting in a live or still birth between 2006 and 2012.
Overall, significantly more women with exacerbated asthma had preeclampsia or pregnancy-induced hypertension, compared with asthmatic women who had no exacerbations, at 5% vs. 4% and 7% vs. 5%, respectively (P less than .001), according to the study published in the European Respiratory Journal.
Adverse perinatal outcomes were significantly more likely among babies of mothers with exacerbated asthma, compared with those who had no exacerbations, including low birth weight (7% vs. 5%), small for gestational age (3% vs. 2%), preterm birth (8% vs. 7%), and congenital malformation (6% vs. 5%). All P values were less than .001, except for small for gestational age, which was P = .008.
In addition, significantly more babies of asthmatic women with exacerbated asthma during pregnancy had respiratory problems including asthma and pneumonia, compared with those of asthmatic women who had no exacerbations during pregnancy, at 38% vs. 31% and 24% vs. 22% (P less than .001 for both). The researchers found no significant interactions between maternal age and smoking and asthma exacerbations.
The findings were limited by several factors, including the lack of a validated algorithm for asthma exacerbation, which the researchers defined as five or more visits to a general practice clinician for asthma during pregnancy. Other limitations included the lack of categorizing asthma exacerbation by severity, and the inability to include the potential effects of asthma medication on maternal and fetal outcomes, Dr. Abdullah and colleagues noted.
However, the results were strengthened by the large sample size and ability to follow babies from birth until 5 years of age, they said.
“Targeting women with asthma during pregnancy and ensuring appropriate asthma management and postpartum follow-up may help to reduce the risk of pregnancy complications, adverse perinatal outcomes, and early childhood respiratory disorders,” they concluded.
This study is important because asthma is a common, potentially serious medical condition that complicates approximately 4%-8% of pregnancies, and one in three women with asthma experience an exacerbation during pregnancy, Iris Krishna, MD, a specialist in maternal/fetal medicine at Emory University, Atlanta, said in an interview.
“This study is unique in that it uses population-level data to assess the association between an asthma exacerbation during pregnancy and adverse perinatal outcomes,” Dr. Krishna said. “After adjusting for confounders, and consistent with previous studies, study findings suggest an increased risk for women with asthma who have an asthma exacerbation during pregnancy for preeclampsia [odds ratio, 1.3; P less than .001], pregnancy-induced hypertension [OR, 1.17; P less than .05], low-birth-weight infant [OR, 1.14; P less than .05], preterm birth [OR, 1.14; P less than .05], and congenital malformations [OR, 1.21; P less than .001].”
Dr. Krishna also noted the impact on early childhood outcomes. “In this study, children born to women who had an asthma exacerbation during pregnancy had a 23% higher risk of developing asthma before 5 years of age, which is consistent with previous studies. [The] investigators also reported a 12% higher risk of having pneumonia during the first 5 years of life for children born to women who had an asthma exacerbation during pregnancy.”
“Previous studies have suggested children born to mothers with uncontrolled asthma have an increased risk for respiratory infections, but this study is the first to report an association with pneumonia,” she said. This increased risk for childhood respiratory disorders warrants further study.
Consequently, “Women with asthma during pregnancy should have appropriate management to ensure good control to optimize pregnancy outcome,” Dr. Krishna emphasized. “Women who experience asthma exacerbations in pregnancy are at increased risk for preeclampsia, [pregnancy-induced hypertension], low birth weight, and preterm delivery and may require closer monitoring.”
The study was supported by the Institute for Clinical Evaluative Sciences. The researchers and Dr. Krishna had no financial conflicts to disclose.
SOURCE: Abdullah K et al. Eur Respir J. 2019 Nov 26. doi: 10.1183/13993003.01335-2019.
FROM THE EUROPEAN RESPIRATORY JOURNAL

Do women with diabetes need more CVD risk reduction than men?
BUSAN, SOUTH KOREA – Whether cardiovascular disease risk reduction efforts should be more aggressive in women than men with diabetes depends on how you interpret the data.
Two experts came to different conclusions on this question during a heated, but jovial, debate last week here at the International Diabetes Federation 2019 Congress.
Endocrinologist David Simmons, MB, BChir, Western Sydney University, Campbelltown, Australia, argued that diabetes erases the well-described life expectancy advantage of 4-7 years that women experience over men in the general population.
He also highlighted the fact that the heightened risk is of particular concern in both younger women and those with prior gestational diabetes.
But Timothy Davis, BMedSc, MB, BS, DPhil, an endocrinologist and general physician at Fremantle (Australia) Hospital, countered that the data only show the diabetes-attributable excess cardiovascular risk is higher in women than men, but that the absolute risk is actually greater in men.
Moreover, he argued, at least in type 1 diabetes, there is no evidence that more aggressive cardiovascular risk factor management improves outcomes.
Yes: Diabetes eliminates female CVD protection
Dr. Simmons began by pointing out that, although on average women die at an older age than men, it has been known for over 40 years that this “female protection” is lost in insulin-treated women, particularly as a result of their increased risk for cardiovascular disease.
In a 2015 meta-analysis of 26 studies, women with type 1 diabetes were found to have about a 37% greater risk of all-cause mortality, compared with men with the condition when mortality is contrasted with that of the general population, and twice the risk of both fatal and nonfatal vascular events.
The risk appeared to be greater in women who were younger at the time of diabetes diagnosis. “This is a really important point – the time we would want to intervene,” Dr. Simmons said.
In another meta-analysis of 30 studies including 2,307,694 individuals with type 2 diabetes and 252,491 deaths, the pooled women-to-men ratio of the standardized mortality ratio for all-cause mortality was 1.14.
In those with versus without type 2 diabetes, the pooled standardized mortality ratio in women was 2.30 and in men was 1.94, both significant, compared with those without diabetes.
And in a 2006 meta-analysis of 22 studies involving individuals with type 2 diabetes, the pooled data showed a 46% excess relative risk using standardized mortality ratios in women versus men for fatal coronary artery disease.
Meanwhile, in a 2018 meta-analysis of 68 studies involving nearly 1 million adults examining differences in occlusive vascular disease, after controlling for major vascular risk factors, diabetes roughly doubled the risk for occlusive vascular mortality in men (relative risk, 2.10), but tripled it in women (3.00).
Women with diabetes aged 35-59 years had the highest relative risk for death over follow-up across all age and sex groups: They had 5.5 times the excess risk, compared with those without diabetes, while the excess risk for men of that age was 2.3-fold.
“So very clearly, it’s these young women who are most at risk, “emphasized Dr. Simmons, who is an investigator for Novo Nordisk and a speaker for Medtronic, Novo Nordisk, and Sanofi.
Are disparities because of differences in cvd risk factor management?
The question has arisen whether the female/male differences might be because of differences in cardiovascular risk factor management, Simmons noted.
A 2015 American Heart Association statement laid out the evidence for lower prescribing of statins, aspirin, beta-blockers, and ACE inhibitors in women, compared with men, Dr. Simmons said.
And some studies suggest medication adherence is lower in women than men.
In terms of medications, fenofibrate appears to produce better outcomes in women than men, but there is no evidence of gender differences in the effects of statins, ACE inhibitors, or aspirin, Simmons said.
He also outlined the results of a 2008 study of 78,254 patients with acute myocardial infarction from 420 U.S. hospitals in 2001-2006.
Women were older, had more comorbidities, less often presented with ST-elevation myocardial infarction (STEMI), and had a higher rate of unadjusted in-hospital death (8.2% vs. 5.7%; P less than .0001) than men. Of the participants, 33% of women had diabetes, compared with 28% of men.
The in-hospital mortality difference disappeared after multivariable adjustment, but women with STEMI still had higher adjusted mortality rates than men.
“The underuse of evidence-based treatments and delayed reperfusion in women represent potential opportunities for reducing sex disparities in care and outcome after acute myocardial infarction,” the authors concluded.
“It’s very clear amongst our cardiology colleagues that something needs to be done and that we need more aggressive cardiological risk reduction in women,” Dr. Simmons said.
“The AHA has already decided this. It’s already a policy. So why are we having this debate?” he wondered.
He also pointed out that women with prior gestational diabetes are an exceptionally high–risk group, with a twofold excess risk for cardiovascular disease within the first 10 years post partum.
“We need to do something about this particularly high-risk group, independent of debates about gender,” Dr. Simmons emphasized. “Clearly, women with diabetes warrant more aggressive cardiovascular risk reduction than men with diabetes, especially at those younger ages,” he concluded.
No: Confusion about relative risk within each sex and absolute risk
Dr. Davis began his counterargument by stating that estimation of absolute vascular risk is an established part of strategies to prevent cardiovascular disease, including in diabetes.
And that risk, he stressed, is actually higher in men.
“Male sex is a consistent adverse risk factor in cardiovascular disease event prediction equations in type 2 diabetes. Identifying absolute risk is important,” he said, noting risk calculators include male sex, such as the risk engine derived from the United Kingdom Prospective Diabetes Trial.
And in the Australian population-based Fremantle study, of which Dr. Davis is an author, the absolute 5-year incidence rates for all outcomes – including myocardial infarction, stroke, heart failure, lower extremity amputation, cardiovascular mortality, and all-cause mortality – were consistently higher in men versus women in the first phase, which began in the 1990s and included 1,426 individuals with diabetes (91% had type 2 diabetes).
In the ongoing second phase, which began in 2008 with 1,732 participants, overall rates of those outcomes are lower and the discrepancy between men and women has narrowed, Dr. Davis noted.
Overall, the Fremantle study data “suggest that women with type 2 diabetes do not need more aggressive cardiovascular reduction than men with type 2 diabetes because they are not at increased absolute vascular risk,” he stressed.
And in a “sensitivity analysis” of two areas in Finland, the authors concluded that the stronger effect of type 2 diabetes on the risk of congenital heart disease (CHD) in women, compared with men was in part explained by a heavier risk factor burden and a greater effect of blood pressure and atherogenic dyslipidemia in women with diabetes, he explained.
The Finnish authors wrote, “In terms of absolute risk of CHD death or a major CHD event, diabetes almost completely abolished the female protection from CHD.”
But, Dr. Davis emphasized, rates were not higher in females.
So then, “why is there the view that women with type 2 diabetes need more aggressive cardiovascular risk reduction than men with diabetes?
“It probably comes back to confusion based on absolute risk versus a comparison of relative risk within each sex,” he asserted.
ADA Standards of Medical Care 2019 don’t mention gender
Lastly, in a meta-analysis published just in July this year involving more than 5 million participants, compared with men with diabetes, women with diabetes had a 58% and 13% greater risk of CHD and all-cause mortality, respectively.
“This points to an urgent need to develop sex- and gender-specific risk assessment strategies and therapeutic interventions that target diabetes management in the context of CHD prevention,” the authors concluded.
But, Dr. Davis noted, “It is not absolute vascular risk. It’s a relative risk compared across the two genders. In the paper, there is no mention of absolute vascular risk.
“Greater CVD mortality in women with and without diabetes, versus men, doesn’t mean there’s also an absolute vascular increase in women versus men with diabetes,” he said.
Moreover, Dr. Davis pointed out that in an editorial accompanying the 2015 meta-analysis in type 1 diabetes, Simmons had actually stated that absolute mortality rates are highest in men.
“I don’t know what happened to his epidemiology knowledge in the last 4 years but it seems to have gone backwards,” he joked to his debate opponent.
And, Dr. Davis asserted, even if there were a higher risk in women with type 1 diabetes, there is no evidence that cardiovascular risk reduction measures affect endpoints in that patient population. Only about 8% of people with diabetes in statin trials had type 1 diabetes.
Indeed, he noted, in the American Diabetes Association Standards of Medical Care in Diabetes – 2019, the treatment goals for individual cardiovascular risk factors do not mention gender.
What’s more, Dr. David said, there is evidence that women are significantly less likely than men to take prescribed statins and are more likely to have an eating disorder and underdose insulin, “suggesting significant issues with compliance. ... So, trying to get more intensive risk reduction in women may be a challenge.”
“Women with diabetes do not need more aggressive cardiovascular risk reduction than men with diabetes, irrespective of type,” he concluded.
A version of this story originally appeared on medscape.com.
BUSAN, SOUTH KOREA – Whether cardiovascular disease risk reduction efforts should be more aggressive in women than men with diabetes depends on how you interpret the data.
Two experts came to different conclusions on this question during a heated, but jovial, debate last week here at the International Diabetes Federation 2019 Congress.
Endocrinologist David Simmons, MB, BChir, Western Sydney University, Campbelltown, Australia, argued that diabetes erases the well-described life expectancy advantage of 4-7 years that women experience over men in the general population.
He also highlighted the fact that the heightened risk is of particular concern in both younger women and those with prior gestational diabetes.
But Timothy Davis, BMedSc, MB, BS, DPhil, an endocrinologist and general physician at Fremantle (Australia) Hospital, countered that the data only show the diabetes-attributable excess cardiovascular risk is higher in women than men, but that the absolute risk is actually greater in men.
Moreover, he argued, at least in type 1 diabetes, there is no evidence that more aggressive cardiovascular risk factor management improves outcomes.
Yes: Diabetes eliminates female CVD protection
Dr. Simmons began by pointing out that, although on average women die at an older age than men, it has been known for over 40 years that this “female protection” is lost in insulin-treated women, particularly as a result of their increased risk for cardiovascular disease.
In a 2015 meta-analysis of 26 studies, women with type 1 diabetes were found to have about a 37% greater risk of all-cause mortality, compared with men with the condition when mortality is contrasted with that of the general population, and twice the risk of both fatal and nonfatal vascular events.
The risk appeared to be greater in women who were younger at the time of diabetes diagnosis. “This is a really important point – the time we would want to intervene,” Dr. Simmons said.
In another meta-analysis of 30 studies including 2,307,694 individuals with type 2 diabetes and 252,491 deaths, the pooled women-to-men ratio of the standardized mortality ratio for all-cause mortality was 1.14.
In those with versus without type 2 diabetes, the pooled standardized mortality ratio in women was 2.30 and in men was 1.94, both significant, compared with those without diabetes.
And in a 2006 meta-analysis of 22 studies involving individuals with type 2 diabetes, the pooled data showed a 46% excess relative risk using standardized mortality ratios in women versus men for fatal coronary artery disease.
Meanwhile, in a 2018 meta-analysis of 68 studies involving nearly 1 million adults examining differences in occlusive vascular disease, after controlling for major vascular risk factors, diabetes roughly doubled the risk for occlusive vascular mortality in men (relative risk, 2.10), but tripled it in women (3.00).
Women with diabetes aged 35-59 years had the highest relative risk for death over follow-up across all age and sex groups: They had 5.5 times the excess risk, compared with those without diabetes, while the excess risk for men of that age was 2.3-fold.
“So very clearly, it’s these young women who are most at risk, “emphasized Dr. Simmons, who is an investigator for Novo Nordisk and a speaker for Medtronic, Novo Nordisk, and Sanofi.
Are disparities because of differences in cvd risk factor management?
The question has arisen whether the female/male differences might be because of differences in cardiovascular risk factor management, Simmons noted.
A 2015 American Heart Association statement laid out the evidence for lower prescribing of statins, aspirin, beta-blockers, and ACE inhibitors in women, compared with men, Dr. Simmons said.
And some studies suggest medication adherence is lower in women than men.
In terms of medications, fenofibrate appears to produce better outcomes in women than men, but there is no evidence of gender differences in the effects of statins, ACE inhibitors, or aspirin, Simmons said.
He also outlined the results of a 2008 study of 78,254 patients with acute myocardial infarction from 420 U.S. hospitals in 2001-2006.
Women were older, had more comorbidities, less often presented with ST-elevation myocardial infarction (STEMI), and had a higher rate of unadjusted in-hospital death (8.2% vs. 5.7%; P less than .0001) than men. Of the participants, 33% of women had diabetes, compared with 28% of men.
The in-hospital mortality difference disappeared after multivariable adjustment, but women with STEMI still had higher adjusted mortality rates than men.
“The underuse of evidence-based treatments and delayed reperfusion in women represent potential opportunities for reducing sex disparities in care and outcome after acute myocardial infarction,” the authors concluded.
“It’s very clear amongst our cardiology colleagues that something needs to be done and that we need more aggressive cardiological risk reduction in women,” Dr. Simmons said.
“The AHA has already decided this. It’s already a policy. So why are we having this debate?” he wondered.
He also pointed out that women with prior gestational diabetes are an exceptionally high–risk group, with a twofold excess risk for cardiovascular disease within the first 10 years post partum.
“We need to do something about this particularly high-risk group, independent of debates about gender,” Dr. Simmons emphasized. “Clearly, women with diabetes warrant more aggressive cardiovascular risk reduction than men with diabetes, especially at those younger ages,” he concluded.
No: Confusion about relative risk within each sex and absolute risk
Dr. Davis began his counterargument by stating that estimation of absolute vascular risk is an established part of strategies to prevent cardiovascular disease, including in diabetes.
And that risk, he stressed, is actually higher in men.
“Male sex is a consistent adverse risk factor in cardiovascular disease event prediction equations in type 2 diabetes. Identifying absolute risk is important,” he said, noting risk calculators include male sex, such as the risk engine derived from the United Kingdom Prospective Diabetes Trial.
And in the Australian population-based Fremantle study, of which Dr. Davis is an author, the absolute 5-year incidence rates for all outcomes – including myocardial infarction, stroke, heart failure, lower extremity amputation, cardiovascular mortality, and all-cause mortality – were consistently higher in men versus women in the first phase, which began in the 1990s and included 1,426 individuals with diabetes (91% had type 2 diabetes).
In the ongoing second phase, which began in 2008 with 1,732 participants, overall rates of those outcomes are lower and the discrepancy between men and women has narrowed, Dr. Davis noted.
Overall, the Fremantle study data “suggest that women with type 2 diabetes do not need more aggressive cardiovascular reduction than men with type 2 diabetes because they are not at increased absolute vascular risk,” he stressed.
And in a “sensitivity analysis” of two areas in Finland, the authors concluded that the stronger effect of type 2 diabetes on the risk of congenital heart disease (CHD) in women, compared with men was in part explained by a heavier risk factor burden and a greater effect of blood pressure and atherogenic dyslipidemia in women with diabetes, he explained.
The Finnish authors wrote, “In terms of absolute risk of CHD death or a major CHD event, diabetes almost completely abolished the female protection from CHD.”
But, Dr. Davis emphasized, rates were not higher in females.
So then, “why is there the view that women with type 2 diabetes need more aggressive cardiovascular risk reduction than men with diabetes?
“It probably comes back to confusion based on absolute risk versus a comparison of relative risk within each sex,” he asserted.
ADA Standards of Medical Care 2019 don’t mention gender
Lastly, in a meta-analysis published just in July this year involving more than 5 million participants, compared with men with diabetes, women with diabetes had a 58% and 13% greater risk of CHD and all-cause mortality, respectively.
“This points to an urgent need to develop sex- and gender-specific risk assessment strategies and therapeutic interventions that target diabetes management in the context of CHD prevention,” the authors concluded.
But, Dr. Davis noted, “It is not absolute vascular risk. It’s a relative risk compared across the two genders. In the paper, there is no mention of absolute vascular risk.
“Greater CVD mortality in women with and without diabetes, versus men, doesn’t mean there’s also an absolute vascular increase in women versus men with diabetes,” he said.
Moreover, Dr. Davis pointed out that in an editorial accompanying the 2015 meta-analysis in type 1 diabetes, Simmons had actually stated that absolute mortality rates are highest in men.
“I don’t know what happened to his epidemiology knowledge in the last 4 years but it seems to have gone backwards,” he joked to his debate opponent.
And, Dr. Davis asserted, even if there were a higher risk in women with type 1 diabetes, there is no evidence that cardiovascular risk reduction measures affect endpoints in that patient population. Only about 8% of people with diabetes in statin trials had type 1 diabetes.
Indeed, he noted, in the American Diabetes Association Standards of Medical Care in Diabetes – 2019, the treatment goals for individual cardiovascular risk factors do not mention gender.
What’s more, Dr. David said, there is evidence that women are significantly less likely than men to take prescribed statins and are more likely to have an eating disorder and underdose insulin, “suggesting significant issues with compliance. ... So, trying to get more intensive risk reduction in women may be a challenge.”
“Women with diabetes do not need more aggressive cardiovascular risk reduction than men with diabetes, irrespective of type,” he concluded.
A version of this story originally appeared on medscape.com.
BUSAN, SOUTH KOREA – Whether cardiovascular disease risk reduction efforts should be more aggressive in women than men with diabetes depends on how you interpret the data.
Two experts came to different conclusions on this question during a heated, but jovial, debate last week here at the International Diabetes Federation 2019 Congress.
Endocrinologist David Simmons, MB, BChir, Western Sydney University, Campbelltown, Australia, argued that diabetes erases the well-described life expectancy advantage of 4-7 years that women experience over men in the general population.
He also highlighted the fact that the heightened risk is of particular concern in both younger women and those with prior gestational diabetes.
But Timothy Davis, BMedSc, MB, BS, DPhil, an endocrinologist and general physician at Fremantle (Australia) Hospital, countered that the data only show the diabetes-attributable excess cardiovascular risk is higher in women than men, but that the absolute risk is actually greater in men.
Moreover, he argued, at least in type 1 diabetes, there is no evidence that more aggressive cardiovascular risk factor management improves outcomes.
Yes: Diabetes eliminates female CVD protection
Dr. Simmons began by pointing out that, although on average women die at an older age than men, it has been known for over 40 years that this “female protection” is lost in insulin-treated women, particularly as a result of their increased risk for cardiovascular disease.
In a 2015 meta-analysis of 26 studies, women with type 1 diabetes were found to have about a 37% greater risk of all-cause mortality, compared with men with the condition when mortality is contrasted with that of the general population, and twice the risk of both fatal and nonfatal vascular events.
The risk appeared to be greater in women who were younger at the time of diabetes diagnosis. “This is a really important point – the time we would want to intervene,” Dr. Simmons said.
In another meta-analysis of 30 studies including 2,307,694 individuals with type 2 diabetes and 252,491 deaths, the pooled women-to-men ratio of the standardized mortality ratio for all-cause mortality was 1.14.
In those with versus without type 2 diabetes, the pooled standardized mortality ratio in women was 2.30 and in men was 1.94, both significant, compared with those without diabetes.
And in a 2006 meta-analysis of 22 studies involving individuals with type 2 diabetes, the pooled data showed a 46% excess relative risk using standardized mortality ratios in women versus men for fatal coronary artery disease.
Meanwhile, in a 2018 meta-analysis of 68 studies involving nearly 1 million adults examining differences in occlusive vascular disease, after controlling for major vascular risk factors, diabetes roughly doubled the risk for occlusive vascular mortality in men (relative risk, 2.10), but tripled it in women (3.00).
Women with diabetes aged 35-59 years had the highest relative risk for death over follow-up across all age and sex groups: They had 5.5 times the excess risk, compared with those without diabetes, while the excess risk for men of that age was 2.3-fold.
“So very clearly, it’s these young women who are most at risk, “emphasized Dr. Simmons, who is an investigator for Novo Nordisk and a speaker for Medtronic, Novo Nordisk, and Sanofi.
Are disparities because of differences in cvd risk factor management?
The question has arisen whether the female/male differences might be because of differences in cardiovascular risk factor management, Simmons noted.
A 2015 American Heart Association statement laid out the evidence for lower prescribing of statins, aspirin, beta-blockers, and ACE inhibitors in women, compared with men, Dr. Simmons said.
And some studies suggest medication adherence is lower in women than men.
In terms of medications, fenofibrate appears to produce better outcomes in women than men, but there is no evidence of gender differences in the effects of statins, ACE inhibitors, or aspirin, Simmons said.
He also outlined the results of a 2008 study of 78,254 patients with acute myocardial infarction from 420 U.S. hospitals in 2001-2006.
Women were older, had more comorbidities, less often presented with ST-elevation myocardial infarction (STEMI), and had a higher rate of unadjusted in-hospital death (8.2% vs. 5.7%; P less than .0001) than men. Of the participants, 33% of women had diabetes, compared with 28% of men.
The in-hospital mortality difference disappeared after multivariable adjustment, but women with STEMI still had higher adjusted mortality rates than men.
“The underuse of evidence-based treatments and delayed reperfusion in women represent potential opportunities for reducing sex disparities in care and outcome after acute myocardial infarction,” the authors concluded.
“It’s very clear amongst our cardiology colleagues that something needs to be done and that we need more aggressive cardiological risk reduction in women,” Dr. Simmons said.
“The AHA has already decided this. It’s already a policy. So why are we having this debate?” he wondered.
He also pointed out that women with prior gestational diabetes are an exceptionally high–risk group, with a twofold excess risk for cardiovascular disease within the first 10 years post partum.
“We need to do something about this particularly high-risk group, independent of debates about gender,” Dr. Simmons emphasized. “Clearly, women with diabetes warrant more aggressive cardiovascular risk reduction than men with diabetes, especially at those younger ages,” he concluded.
No: Confusion about relative risk within each sex and absolute risk
Dr. Davis began his counterargument by stating that estimation of absolute vascular risk is an established part of strategies to prevent cardiovascular disease, including in diabetes.
And that risk, he stressed, is actually higher in men.
“Male sex is a consistent adverse risk factor in cardiovascular disease event prediction equations in type 2 diabetes. Identifying absolute risk is important,” he said, noting risk calculators include male sex, such as the risk engine derived from the United Kingdom Prospective Diabetes Trial.
And in the Australian population-based Fremantle study, of which Dr. Davis is an author, the absolute 5-year incidence rates for all outcomes – including myocardial infarction, stroke, heart failure, lower extremity amputation, cardiovascular mortality, and all-cause mortality – were consistently higher in men versus women in the first phase, which began in the 1990s and included 1,426 individuals with diabetes (91% had type 2 diabetes).
In the ongoing second phase, which began in 2008 with 1,732 participants, overall rates of those outcomes are lower and the discrepancy between men and women has narrowed, Dr. Davis noted.
Overall, the Fremantle study data “suggest that women with type 2 diabetes do not need more aggressive cardiovascular reduction than men with type 2 diabetes because they are not at increased absolute vascular risk,” he stressed.
And in a “sensitivity analysis” of two areas in Finland, the authors concluded that the stronger effect of type 2 diabetes on the risk of congenital heart disease (CHD) in women, compared with men was in part explained by a heavier risk factor burden and a greater effect of blood pressure and atherogenic dyslipidemia in women with diabetes, he explained.
The Finnish authors wrote, “In terms of absolute risk of CHD death or a major CHD event, diabetes almost completely abolished the female protection from CHD.”
But, Dr. Davis emphasized, rates were not higher in females.
So then, “why is there the view that women with type 2 diabetes need more aggressive cardiovascular risk reduction than men with diabetes?
“It probably comes back to confusion based on absolute risk versus a comparison of relative risk within each sex,” he asserted.
ADA Standards of Medical Care 2019 don’t mention gender
Lastly, in a meta-analysis published just in July this year involving more than 5 million participants, compared with men with diabetes, women with diabetes had a 58% and 13% greater risk of CHD and all-cause mortality, respectively.
“This points to an urgent need to develop sex- and gender-specific risk assessment strategies and therapeutic interventions that target diabetes management in the context of CHD prevention,” the authors concluded.
But, Dr. Davis noted, “It is not absolute vascular risk. It’s a relative risk compared across the two genders. In the paper, there is no mention of absolute vascular risk.
“Greater CVD mortality in women with and without diabetes, versus men, doesn’t mean there’s also an absolute vascular increase in women versus men with diabetes,” he said.
Moreover, Dr. Davis pointed out that in an editorial accompanying the 2015 meta-analysis in type 1 diabetes, Simmons had actually stated that absolute mortality rates are highest in men.
“I don’t know what happened to his epidemiology knowledge in the last 4 years but it seems to have gone backwards,” he joked to his debate opponent.
And, Dr. Davis asserted, even if there were a higher risk in women with type 1 diabetes, there is no evidence that cardiovascular risk reduction measures affect endpoints in that patient population. Only about 8% of people with diabetes in statin trials had type 1 diabetes.
Indeed, he noted, in the American Diabetes Association Standards of Medical Care in Diabetes – 2019, the treatment goals for individual cardiovascular risk factors do not mention gender.
What’s more, Dr. David said, there is evidence that women are significantly less likely than men to take prescribed statins and are more likely to have an eating disorder and underdose insulin, “suggesting significant issues with compliance. ... So, trying to get more intensive risk reduction in women may be a challenge.”
“Women with diabetes do not need more aggressive cardiovascular risk reduction than men with diabetes, irrespective of type,” he concluded.
A version of this story originally appeared on medscape.com.