User login
Alzheimer’s Transmissible Via Stem Cell Transplantation?
Studies in preclinical models hint that familial Alzheimer’s disease (AD) may be transmissible via bone marrow transplant, but the researchers and outside experts caution against making the immediate leap to humans.
These pathologic features included compromised blood-brain barrier integrity, heightened cerebral vascular neoangiogenesis, elevated brain-associated beta-amyloid levels, and cognitive impairment.
In addition, symptoms of cognitive decline presented rapidly — 6 months after transplant in the APP-knockout mice and 9 months in the wild-type mice vs 12 months shown previously in AD transgenic mice.
“Contrary to prevailing beliefs regarding AD occurring solely in familial or sporadic forms, our study reveals an unexpected transplantable form of AD in a preclinical model, suggesting potential iatrogenic transmission in AD patients,” the investigators, led by Wilfred Jefferies, DPhil, write.
Although this is probably an “infrequent” occurrence, it’s still “concerning,” Dr. Jefferies told this news organization, and it suggests that “human donors of blood, tissue, organ, and stem cells should be screened to prevent its inadvertent transfer of disease during blood product transfusions and cellular therapies.”
The study was published March 28 in Stem Cell Reports.
Intriguing, but Limited Human Relevance
The researchers note the study also demonstrates that beta-amyloid accumulation originating outside of the central nervous system contributes to AD pathology, providing an opportunity for the development of new biomarkers for AD.
Several experts weighed in on this research in a statement from the UK-based nonprofit and independent Science Media Centre (SMC).
David Curtis, MBBS, MD, PhD, with University College London’s Genetics Institute, United Kingdom, noted that the study suggests that “theoretically there could be a risk of acquiring Alzheimer’s disease if one received a stem cell transplant from somebody carrying the severe, familial form of the disease. However, this form is extremely rare so in practice the risk seems low and there are many safeguards around stem cell transplantation. I do not see that the risks extend to other areas such as organ transplantation or blood transfusion because these procedures do not involve large numbers of stem cells which can go on to form glial cells.”
Paul Morgan, PhD, with UK Dementia Research Institute Cardiff, Cardiff University, said the study is “scientifically intriguing” in demonstrating in this “very specific experimental situation, that bone marrow cells are sufficient to transfer the gene and the disease. Relevance to human organ and cell transplant is limited.”
Morgan cautioned against making the “gargantuan leap to propose that tissue, organ and cell transplantation, and even blood transfusion, carry a risk of transferring Alzheimer’s disease and other neuropathologies in man.”
Bart De Strooper, MD, PhD, with University College London, agreed. “There is not sufficient evidence here to suggest that anyone receiving a bone marrow transplant is at risk of developing Alzheimer’s disease as a result of the procedure, and nobody should forgo a transplant for this reason,” he said in the SMC release.
The study had no specific funding. The authors hold equity in the start-up company, Cava Healthcare, which possesses intellectual property related to these findings. This had no role in the study design, data collection, analysis, or interpretation of data, or in the writing of the paper. Morgan, De Strooper, and Curtis have no relevant disclosures.
A version of this article appeared on Medscape.com.
Studies in preclinical models hint that familial Alzheimer’s disease (AD) may be transmissible via bone marrow transplant, but the researchers and outside experts caution against making the immediate leap to humans.
These pathologic features included compromised blood-brain barrier integrity, heightened cerebral vascular neoangiogenesis, elevated brain-associated beta-amyloid levels, and cognitive impairment.
In addition, symptoms of cognitive decline presented rapidly — 6 months after transplant in the APP-knockout mice and 9 months in the wild-type mice vs 12 months shown previously in AD transgenic mice.
“Contrary to prevailing beliefs regarding AD occurring solely in familial or sporadic forms, our study reveals an unexpected transplantable form of AD in a preclinical model, suggesting potential iatrogenic transmission in AD patients,” the investigators, led by Wilfred Jefferies, DPhil, write.
Although this is probably an “infrequent” occurrence, it’s still “concerning,” Dr. Jefferies told this news organization, and it suggests that “human donors of blood, tissue, organ, and stem cells should be screened to prevent its inadvertent transfer of disease during blood product transfusions and cellular therapies.”
The study was published March 28 in Stem Cell Reports.
Intriguing, but Limited Human Relevance
The researchers note the study also demonstrates that beta-amyloid accumulation originating outside of the central nervous system contributes to AD pathology, providing an opportunity for the development of new biomarkers for AD.
Several experts weighed in on this research in a statement from the UK-based nonprofit and independent Science Media Centre (SMC).
David Curtis, MBBS, MD, PhD, with University College London’s Genetics Institute, United Kingdom, noted that the study suggests that “theoretically there could be a risk of acquiring Alzheimer’s disease if one received a stem cell transplant from somebody carrying the severe, familial form of the disease. However, this form is extremely rare so in practice the risk seems low and there are many safeguards around stem cell transplantation. I do not see that the risks extend to other areas such as organ transplantation or blood transfusion because these procedures do not involve large numbers of stem cells which can go on to form glial cells.”
Paul Morgan, PhD, with UK Dementia Research Institute Cardiff, Cardiff University, said the study is “scientifically intriguing” in demonstrating in this “very specific experimental situation, that bone marrow cells are sufficient to transfer the gene and the disease. Relevance to human organ and cell transplant is limited.”
Morgan cautioned against making the “gargantuan leap to propose that tissue, organ and cell transplantation, and even blood transfusion, carry a risk of transferring Alzheimer’s disease and other neuropathologies in man.”
Bart De Strooper, MD, PhD, with University College London, agreed. “There is not sufficient evidence here to suggest that anyone receiving a bone marrow transplant is at risk of developing Alzheimer’s disease as a result of the procedure, and nobody should forgo a transplant for this reason,” he said in the SMC release.
The study had no specific funding. The authors hold equity in the start-up company, Cava Healthcare, which possesses intellectual property related to these findings. This had no role in the study design, data collection, analysis, or interpretation of data, or in the writing of the paper. Morgan, De Strooper, and Curtis have no relevant disclosures.
A version of this article appeared on Medscape.com.
Studies in preclinical models hint that familial Alzheimer’s disease (AD) may be transmissible via bone marrow transplant, but the researchers and outside experts caution against making the immediate leap to humans.
These pathologic features included compromised blood-brain barrier integrity, heightened cerebral vascular neoangiogenesis, elevated brain-associated beta-amyloid levels, and cognitive impairment.
In addition, symptoms of cognitive decline presented rapidly — 6 months after transplant in the APP-knockout mice and 9 months in the wild-type mice vs 12 months shown previously in AD transgenic mice.
“Contrary to prevailing beliefs regarding AD occurring solely in familial or sporadic forms, our study reveals an unexpected transplantable form of AD in a preclinical model, suggesting potential iatrogenic transmission in AD patients,” the investigators, led by Wilfred Jefferies, DPhil, write.
Although this is probably an “infrequent” occurrence, it’s still “concerning,” Dr. Jefferies told this news organization, and it suggests that “human donors of blood, tissue, organ, and stem cells should be screened to prevent its inadvertent transfer of disease during blood product transfusions and cellular therapies.”
The study was published March 28 in Stem Cell Reports.
Intriguing, but Limited Human Relevance
The researchers note the study also demonstrates that beta-amyloid accumulation originating outside of the central nervous system contributes to AD pathology, providing an opportunity for the development of new biomarkers for AD.
Several experts weighed in on this research in a statement from the UK-based nonprofit and independent Science Media Centre (SMC).
David Curtis, MBBS, MD, PhD, with University College London’s Genetics Institute, United Kingdom, noted that the study suggests that “theoretically there could be a risk of acquiring Alzheimer’s disease if one received a stem cell transplant from somebody carrying the severe, familial form of the disease. However, this form is extremely rare so in practice the risk seems low and there are many safeguards around stem cell transplantation. I do not see that the risks extend to other areas such as organ transplantation or blood transfusion because these procedures do not involve large numbers of stem cells which can go on to form glial cells.”
Paul Morgan, PhD, with UK Dementia Research Institute Cardiff, Cardiff University, said the study is “scientifically intriguing” in demonstrating in this “very specific experimental situation, that bone marrow cells are sufficient to transfer the gene and the disease. Relevance to human organ and cell transplant is limited.”
Morgan cautioned against making the “gargantuan leap to propose that tissue, organ and cell transplantation, and even blood transfusion, carry a risk of transferring Alzheimer’s disease and other neuropathologies in man.”
Bart De Strooper, MD, PhD, with University College London, agreed. “There is not sufficient evidence here to suggest that anyone receiving a bone marrow transplant is at risk of developing Alzheimer’s disease as a result of the procedure, and nobody should forgo a transplant for this reason,” he said in the SMC release.
The study had no specific funding. The authors hold equity in the start-up company, Cava Healthcare, which possesses intellectual property related to these findings. This had no role in the study design, data collection, analysis, or interpretation of data, or in the writing of the paper. Morgan, De Strooper, and Curtis have no relevant disclosures.
A version of this article appeared on Medscape.com.
FROM STEM CELL REPORTS
Magnesium Spray for Better Sleep? Experts Weigh In
As your patient’s scheduled bedtime is approaching, they begin to worry another restless night is looming. Could magnesium oil spray actually help them sleep? Some — even doctors — are sharing testimonials about how this simple tactic transformed their sleep quality. Experts suggest some sleep improvement is possible, though it does not negate the need for treatment, and should not be used in patients with cardiovascular disease.
Take Daniel Barrett, MD, a board-certified plastic surgeon and owner of Barrett Plastic Surgery in Beverly Hills, as an example. He decided to test whether magnesium oil could indeed give him a sleepy sensation and shared his experience. Dr. Barrett sprayed magnesium oil on his feet — until they felt “slippery and wet,” he said — and put his socks back on. (He said magnesium is absorbed more easily through the skin. Putting it on the skin helps this mineral get into the lymphatics and circulatory system, offering a way to get a higher concentration of magnesium in the bloodstream. The pores on the feet are also said to be the largest on the body, making them an ideal place for absorption.)
“My central nervous system had calmed down a bit — it’s similar to what I feel when I take oral magnesium as well. It took about 15 minutes to feel the effect,” Dr. Barrett said.
Research shows that magnesium blocks N-methyl-D-aspartate (a receptor that can hinder sleep) and stimulates gamma-aminobutyric acid (a receptor that can promote good sleep), said Dennis Auckley, MD, director of MetroHealth’s Center for Sleep Medicine. And studies looking at the effects of oral magnesium have shown that taking it may be linked to better self-reported sleep quality and less daytime sleepiness, he said. But traditional magnesium supplements taken orally can sometimes come with side effects in your gut, so putting magnesium on the skin could help to avoid this.
Magnesium oil on the feet could also help with certain sleep disturbances, such as nocturnal leg cramps and restless legs syndrome, said Sam Kashani, MD, a sleep medicine specialist and assistant clinical professor at UCLA Medical School. (Nocturnal leg cramps – one of the most common secondary factors of insomnia and sleep disturbances in older adults – includes sudden, painful contractions in the lower leg muscles while sleeping. Restless legs syndrome, on the other hand, is like nocturnal leg cramps, but minus the painful contractions, said Dr. Kashani.)
“Magnesium is a mineral that does have some benefit with regard to reducing the muscle tightness and promoting a little bit more of relaxation of the muscles,” Dr. Kashani said. “This [magnesium oil on your soles] could be beneficial for these types of sleep problems.”
Still, sleep medicine experts stressed that putting magnesium oil on your feet should not be viewed a cure-all for sleep troubles.
“High-quality scientific evidence supporting magnesium as a sleep remedy is severely limited,” said Emerson Wickwire, PhD, an American Academy of Sleep Medicine spokesperson and section head of sleep medicine at the University of Maryland Medical School. “Certainly, magnesium is not supported as a treatment for sleep disorders.”
If your patients plan to use magnesium oil on their feet to help them sleep, make sure they carefully follow the directions to make sure they are taking the proper dosage. Most importantly, patients with a history of cardiovascular complications, or issues with the heart and blood vessels should consult their doctor.
“Magnesium is an electrolyte that has multiple roles and functions in the body, including within our cardiovascular system,” Dr. Kashani said. “So, if you are somebody who has heart troubles, you definitely want to talk to your primary doctor about any kind of supplements that you are taking, including magnesium.”
A version of this article appeared on WebMD.com.
As your patient’s scheduled bedtime is approaching, they begin to worry another restless night is looming. Could magnesium oil spray actually help them sleep? Some — even doctors — are sharing testimonials about how this simple tactic transformed their sleep quality. Experts suggest some sleep improvement is possible, though it does not negate the need for treatment, and should not be used in patients with cardiovascular disease.
Take Daniel Barrett, MD, a board-certified plastic surgeon and owner of Barrett Plastic Surgery in Beverly Hills, as an example. He decided to test whether magnesium oil could indeed give him a sleepy sensation and shared his experience. Dr. Barrett sprayed magnesium oil on his feet — until they felt “slippery and wet,” he said — and put his socks back on. (He said magnesium is absorbed more easily through the skin. Putting it on the skin helps this mineral get into the lymphatics and circulatory system, offering a way to get a higher concentration of magnesium in the bloodstream. The pores on the feet are also said to be the largest on the body, making them an ideal place for absorption.)
“My central nervous system had calmed down a bit — it’s similar to what I feel when I take oral magnesium as well. It took about 15 minutes to feel the effect,” Dr. Barrett said.
Research shows that magnesium blocks N-methyl-D-aspartate (a receptor that can hinder sleep) and stimulates gamma-aminobutyric acid (a receptor that can promote good sleep), said Dennis Auckley, MD, director of MetroHealth’s Center for Sleep Medicine. And studies looking at the effects of oral magnesium have shown that taking it may be linked to better self-reported sleep quality and less daytime sleepiness, he said. But traditional magnesium supplements taken orally can sometimes come with side effects in your gut, so putting magnesium on the skin could help to avoid this.
Magnesium oil on the feet could also help with certain sleep disturbances, such as nocturnal leg cramps and restless legs syndrome, said Sam Kashani, MD, a sleep medicine specialist and assistant clinical professor at UCLA Medical School. (Nocturnal leg cramps – one of the most common secondary factors of insomnia and sleep disturbances in older adults – includes sudden, painful contractions in the lower leg muscles while sleeping. Restless legs syndrome, on the other hand, is like nocturnal leg cramps, but minus the painful contractions, said Dr. Kashani.)
“Magnesium is a mineral that does have some benefit with regard to reducing the muscle tightness and promoting a little bit more of relaxation of the muscles,” Dr. Kashani said. “This [magnesium oil on your soles] could be beneficial for these types of sleep problems.”
Still, sleep medicine experts stressed that putting magnesium oil on your feet should not be viewed a cure-all for sleep troubles.
“High-quality scientific evidence supporting magnesium as a sleep remedy is severely limited,” said Emerson Wickwire, PhD, an American Academy of Sleep Medicine spokesperson and section head of sleep medicine at the University of Maryland Medical School. “Certainly, magnesium is not supported as a treatment for sleep disorders.”
If your patients plan to use magnesium oil on their feet to help them sleep, make sure they carefully follow the directions to make sure they are taking the proper dosage. Most importantly, patients with a history of cardiovascular complications, or issues with the heart and blood vessels should consult their doctor.
“Magnesium is an electrolyte that has multiple roles and functions in the body, including within our cardiovascular system,” Dr. Kashani said. “So, if you are somebody who has heart troubles, you definitely want to talk to your primary doctor about any kind of supplements that you are taking, including magnesium.”
A version of this article appeared on WebMD.com.
As your patient’s scheduled bedtime is approaching, they begin to worry another restless night is looming. Could magnesium oil spray actually help them sleep? Some — even doctors — are sharing testimonials about how this simple tactic transformed their sleep quality. Experts suggest some sleep improvement is possible, though it does not negate the need for treatment, and should not be used in patients with cardiovascular disease.
Take Daniel Barrett, MD, a board-certified plastic surgeon and owner of Barrett Plastic Surgery in Beverly Hills, as an example. He decided to test whether magnesium oil could indeed give him a sleepy sensation and shared his experience. Dr. Barrett sprayed magnesium oil on his feet — until they felt “slippery and wet,” he said — and put his socks back on. (He said magnesium is absorbed more easily through the skin. Putting it on the skin helps this mineral get into the lymphatics and circulatory system, offering a way to get a higher concentration of magnesium in the bloodstream. The pores on the feet are also said to be the largest on the body, making them an ideal place for absorption.)
“My central nervous system had calmed down a bit — it’s similar to what I feel when I take oral magnesium as well. It took about 15 minutes to feel the effect,” Dr. Barrett said.
Research shows that magnesium blocks N-methyl-D-aspartate (a receptor that can hinder sleep) and stimulates gamma-aminobutyric acid (a receptor that can promote good sleep), said Dennis Auckley, MD, director of MetroHealth’s Center for Sleep Medicine. And studies looking at the effects of oral magnesium have shown that taking it may be linked to better self-reported sleep quality and less daytime sleepiness, he said. But traditional magnesium supplements taken orally can sometimes come with side effects in your gut, so putting magnesium on the skin could help to avoid this.
Magnesium oil on the feet could also help with certain sleep disturbances, such as nocturnal leg cramps and restless legs syndrome, said Sam Kashani, MD, a sleep medicine specialist and assistant clinical professor at UCLA Medical School. (Nocturnal leg cramps – one of the most common secondary factors of insomnia and sleep disturbances in older adults – includes sudden, painful contractions in the lower leg muscles while sleeping. Restless legs syndrome, on the other hand, is like nocturnal leg cramps, but minus the painful contractions, said Dr. Kashani.)
“Magnesium is a mineral that does have some benefit with regard to reducing the muscle tightness and promoting a little bit more of relaxation of the muscles,” Dr. Kashani said. “This [magnesium oil on your soles] could be beneficial for these types of sleep problems.”
Still, sleep medicine experts stressed that putting magnesium oil on your feet should not be viewed a cure-all for sleep troubles.
“High-quality scientific evidence supporting magnesium as a sleep remedy is severely limited,” said Emerson Wickwire, PhD, an American Academy of Sleep Medicine spokesperson and section head of sleep medicine at the University of Maryland Medical School. “Certainly, magnesium is not supported as a treatment for sleep disorders.”
If your patients plan to use magnesium oil on their feet to help them sleep, make sure they carefully follow the directions to make sure they are taking the proper dosage. Most importantly, patients with a history of cardiovascular complications, or issues with the heart and blood vessels should consult their doctor.
“Magnesium is an electrolyte that has multiple roles and functions in the body, including within our cardiovascular system,” Dr. Kashani said. “So, if you are somebody who has heart troubles, you definitely want to talk to your primary doctor about any kind of supplements that you are taking, including magnesium.”
A version of this article appeared on WebMD.com.
Women’s Cancers: Clinicians Research, Advise on Sexual Dysfunction
Decreased sexual function is a side effect of many types of cancer, notably uterine, cervical, ovarian, and breast cancer, that often goes unaddressed, according to the authors of several studies presented at the Society of Gynecologic Oncology (SGO)’s Annual Meeting on Women’s Cancer.
Patients want to talk about sex, but not necessarily at the start of their diagnosis or treatment, suggest the findings of a study presented at the meeting. Jesse T. Brewer of Weill Cornell Medicine in New York City and colleagues enrolled 63 patients who underwent surgery with documented hereditary breast cancer, ovarian cancer, or Lynch syndrome in a cross-sectional survey.
Overall, 86% said that sexuality and intimacy were very or somewhat important, and 78% said that the healthcare team addressing the issue was very or somewhat important, the researchers found. However, only 40% of the respondents said that they wanted to discuss sexuality at the time of diagnosis because the idea was too overwhelming.

Oncologists are more aware of sexual side effects and the potential for sexual issues that persist long after treatment, but many patients may not have opportunities to talk about sexual concerns, said Don S. Dizon, MD, an oncologist specializing in women’s cancers at Brown University, Providence, Rhode Island, in an interview.
“It is important that we [oncologists] be the ones to open the door to these conversations; people with cancer will not bring it up spontaneously, for fear of making their provider uncomfortable, especially if they’ve never been asked about it before,” Dr. Dizon said in an interview.
He advised clinicians to find a network within their health systems so they can refer patients to specialized services, such as sex therapy, couples counseling, pelvic rehabilitation, or menopausal experts as needed.
In another study presented at the meeting, Naaman Mehta, MD, of NYU Langone Health, and colleagues reviewed data from 166 healthcare providers who completed a 23-item survey about evaluating and managing sexual health concerns of their patients. Most of the respondents were gynecologic oncologists (93.4%), but one radiation oncologist and 10 other healthcare providers also completed the survey.
Overall, approximately 60% of the respondents routinely asked about the sexual health concerns of their patients, and 98% of these said they believed that sexual health discussions should be held with a gynecologic oncologist. Just over half (54%) also said that the patient should be the one to initiate a discussion of sexual health concerns.
Female providers were significantly more likely to discuss sexual health with patients, compared with male providers, after controlling for the hospital setting and training level, the researchers noted (odds ratio, 1.4;P < .01).
The results suggest a need for more ways to integrate sexual health screening into gynecologic oncologic clinics, the researchers concluded.
The provider survey findings are similar to the results of a survey conducted by Dr. Dizon and colleagues in 2007. In that study, less than half of respondents took a sexual history, but 80% felt there was insufficient time to explore sexual issues.
“It is critical to understand that people with cancer do not expect their oncologists to be sexual health experts, but as with all other side effects caused by treatment and the diagnosis, we can be the ones who recognize it,” Dr. Dizon noted, in an interview.
Common Complaints and Causes
In Dr. Dizon’s experience, local symptoms including vaginal dryness, pain with penetration, and vaginal thinning, are common sexual complaints in women with cancer, as are systemic issues such as lack of interest and menopause-type symptoms.
“For those undergoing radiation, the vaginal tunnel can actually develop adhesions, and if not treated proactively this can lead to vaginal stenosis,” said Dr. Dizon, who was not involved in the studies presented at the meeting.

Comorbidities such as diabetes, cardiovascular disease, and musculoskeletal conditions can contribute to sexual issues in women with cancer, according to Nora Lersch, DNP, FNP-BC, AOCNP, and Nicole Dreibelbis, CRNP, the authors of other research presented at the meeting.
Culture, religion, fitness level, history of sexual violence, and gender spectrum health also play a role, as do anxiety and depression, dementia, and substance abuse disorders, the authors wrote in their presentation, “Prioritizing Sexual Health in Gynecological Oncology Care.”
Low libido is a frequent complaint across all cancer types, Ms. Dreibelbis, a nurse practitioner specializing in gynecologic oncology at the UPMC Hillman Cancer Center, Pittsburgh, Pennsylvania, said in an interview.

“Breast cancer patients, especially those on [aromatase inhibitor] therapy, often experience vaginal dryness and therefore dyspareunia,” she added.
The pelvic floor muscles, with their important role in sexual response, can be weakened by cancer treatment or surgery, and the pudendal nerves, which are the primary nerves responsible for sexual response in women, can be affected as well, Dr. Lersch and Ms. Dreibelbis wrote.
Taking Sex Seriously
Researchers are exploring the impact of different cancer prevention treatments for women to mitigate sexual side effects, as illustrated by another study presented at the meeting.

Dr. Barbara Norquist, MD, a gynecologic oncologist at the University of Washington, Seattle, and colleagues compared the sexual function and menopausal symptoms of patients at high risk of ovarian carcinoma who underwent either interval salpingectomy/delayed oophorectomy (ISDO) or risk-reducing salpingo-oophorectomy (RRSO).
“For patients at high risk for ovarian cancer, surgical removal of the tubes and ovaries is the mainstay of prevention, as screening is not effective at reducing death from ovarian cancer. As a result of surgery, many patients become suddenly postmenopausal from losing their ovaries,” Dr. Norquist said in an interview.
Some patients delay surgery out of concern for health and quality of life, including sexual function, she said.
In the study (known as the WISP trial) the researchers compared data from 166 patients who underwent immediate removal of the fallopian tubes and ovaries and 171 who underwent fallopian tube removal and delayed oophorectomy. All patients completed questionnaires about sexual function. The primary outcome was change in sexual function based on the sexual function index (FSFI) from baseline to 6 months after surgery.
Overall, changes in sexual function were significantly greater in the immediate oophorectomy group, compared with the delayed oophorectomy group at 6 months (33% vs 17%) and also at 12 months (43% vs 20%).
A further review of patients using hormone therapy showed that those in the immediate oophorectomy group still had greater decreases in sexual function, compared with the delayed group, though the difference between groups of patients using hormone therapy was less dramatic.
“I was surprised that, even with hormone replacement therapy, patients undergoing removal of the ovaries still had significant detrimental changes to sexual function when compared to those having the tubes removed, although this was even worse in those who could not take HRT,” Dr. Norquist said, in an interview. “I was reassured that menopausal symptoms in general were well managed with HRT, as these patients did not score differently on menopause symptoms, compared with those having their tubes removed,” she said.
Patients deserve accurate information about predicted changes in menopausal symptoms and sexual function as a result of ovary removal, and HRT should be provided when there is no contraindication, Dr. Norquist told this news organization.
Dr. Norquist and colleagues are awaiting the results of clinical trials investigating the safety of salpingectomy with delayed oophorectomy in terms of ovarian cancer prevention, but more research is needed to identify optimal management of the menopausal and sexual side effects associated with surgical menopause, she noted.
“Findings from the WISP study show the importance of hormones in women undergoing prophylactic surgery,” Dr. Dizon said. The findings indicate that salpingectomy has less of a negative influence on sexual function compared to removal of the ovaries, and the impact of hormone therapy and the relatively young age of the patients who took hormones reinforces current knowledge about hormones and sex, he added.
Barriers and Solutions
Barriers to asking women with cancer about sexual issues reported by providers include limited time, lack of training in sexual health, a desire to avoid offending the patient or making them uncomfortable, and uncertainty about how to answer the questions, Dr. Lersch and Ms. Dreibelbis wrote in their presentation.
Barriers to asking healthcare providers about their sexual issues reported by patients include the beliefs that the clinician should initiate the discussion, that sexual function will not be taken seriously, and that they might make the provider uncomfortable.
“Fortunately, more information and research has been done on sexual health and gynecological cancer in recent years, so oncologists are becoming more aware of the issues women may have,” said Dr. Lersch who is an oncology nurse practitioner at Providence Franz Cancer Institute in Portland, Oregon, in an interview.
Telling patients early in their cancer treatment about potential sexual side effects and opportunities for help is essential, she added.
Although oncologists have become more aware of the importance of sexual health and well-being for their patients, “I think there has historically been a disconnect in including sexual health education in medical training,” Ms. Dreibelbis said in an interview.
Dr. Lersch and Ms. Dreibelbis advised a multidimensional approach to managing sexual problems in cancer patients that includes consideration of biological and psychological symptoms, but also social, cultural, and interpersonal factors, in their presentation.
Their suggestions include discussing dyspareunia with their patients, asking for details such as whether the pain is internal or external, whether it occurs with activities outside of sex including masturbation, and whether bleeding is present.
Oncology therapies and surgeries can decrease or eliminate an individual’s ability to produce their own lubricant; for example, removal of the cervix eliminates cervical mucous, which helps with internal lubrication, they wrote in their presentation.
For patients with dyspareunia, Dr. Lersch and Ms. Dreibelbis recommend a vaginal moisturizer especially formulated for vaginal tissue that can be absorbed by the mucosal tissue of the vagina. Use of this type of product can increase the effectiveness of lubricants and help restore integrity of the vaginal tissue. Such moisturizers are available as gels, creams, or suppositories over the counter, and do not contain hormones.
Vaginal estrogen can be helpful for burning, itching, irritation, tissue fragility, and pain with sex, according to Dr. Lersch and Ms. Dreibelbis. Adequate estrogen therapy can promote normalization of vaginal pH and microflora, as well increase vaginal secretion and reduce pain and dryness with intercourse, the presenters stated in their presentation. In addition, dilator therapy can be used to help prevent vaginal stenosis, and penetration bumpers can help relieve discomfort during intercourse, they wrote.
Looking ahead, more research is needed to serve a wider patient population, Ms. Dreibelbis said, in an interview.
“LGBTQIA [individuals] have not been included in sexual health research and there are more people than ever who identify within this group of people. I know there has also been some very early work on shielding the clitoris from the impacts of radiation, and I believe this is extremely important up-and-coming research,” she said.
Dr. Lersch, Ms. Dreibelbi, Dr. Dizon, Dr. Norquist, Ms. Brewer, and Dr. Mehta had no financial conflicts to disclose.
Decreased sexual function is a side effect of many types of cancer, notably uterine, cervical, ovarian, and breast cancer, that often goes unaddressed, according to the authors of several studies presented at the Society of Gynecologic Oncology (SGO)’s Annual Meeting on Women’s Cancer.
Patients want to talk about sex, but not necessarily at the start of their diagnosis or treatment, suggest the findings of a study presented at the meeting. Jesse T. Brewer of Weill Cornell Medicine in New York City and colleagues enrolled 63 patients who underwent surgery with documented hereditary breast cancer, ovarian cancer, or Lynch syndrome in a cross-sectional survey.
Overall, 86% said that sexuality and intimacy were very or somewhat important, and 78% said that the healthcare team addressing the issue was very or somewhat important, the researchers found. However, only 40% of the respondents said that they wanted to discuss sexuality at the time of diagnosis because the idea was too overwhelming.
Oncologists are more aware of sexual side effects and the potential for sexual issues that persist long after treatment, but many patients may not have opportunities to talk about sexual concerns, said Don S. Dizon, MD, an oncologist specializing in women’s cancers at Brown University, Providence, Rhode Island, in an interview.
“It is important that we [oncologists] be the ones to open the door to these conversations; people with cancer will not bring it up spontaneously, for fear of making their provider uncomfortable, especially if they’ve never been asked about it before,” Dr. Dizon said in an interview.
He advised clinicians to find a network within their health systems so they can refer patients to specialized services, such as sex therapy, couples counseling, pelvic rehabilitation, or menopausal experts as needed.
In another study presented at the meeting, Naaman Mehta, MD, of NYU Langone Health, and colleagues reviewed data from 166 healthcare providers who completed a 23-item survey about evaluating and managing sexual health concerns of their patients. Most of the respondents were gynecologic oncologists (93.4%), but one radiation oncologist and 10 other healthcare providers also completed the survey.
Overall, approximately 60% of the respondents routinely asked about the sexual health concerns of their patients, and 98% of these said they believed that sexual health discussions should be held with a gynecologic oncologist. Just over half (54%) also said that the patient should be the one to initiate a discussion of sexual health concerns.
Female providers were significantly more likely to discuss sexual health with patients, compared with male providers, after controlling for the hospital setting and training level, the researchers noted (odds ratio, 1.4;P < .01).
The results suggest a need for more ways to integrate sexual health screening into gynecologic oncologic clinics, the researchers concluded.
The provider survey findings are similar to the results of a survey conducted by Dr. Dizon and colleagues in 2007. In that study, less than half of respondents took a sexual history, but 80% felt there was insufficient time to explore sexual issues.
“It is critical to understand that people with cancer do not expect their oncologists to be sexual health experts, but as with all other side effects caused by treatment and the diagnosis, we can be the ones who recognize it,” Dr. Dizon noted, in an interview.
Common Complaints and Causes
In Dr. Dizon’s experience, local symptoms including vaginal dryness, pain with penetration, and vaginal thinning, are common sexual complaints in women with cancer, as are systemic issues such as lack of interest and menopause-type symptoms.
“For those undergoing radiation, the vaginal tunnel can actually develop adhesions, and if not treated proactively this can lead to vaginal stenosis,” said Dr. Dizon, who was not involved in the studies presented at the meeting.
Comorbidities such as diabetes, cardiovascular disease, and musculoskeletal conditions can contribute to sexual issues in women with cancer, according to Nora Lersch, DNP, FNP-BC, AOCNP, and Nicole Dreibelbis, CRNP, the authors of other research presented at the meeting.
Culture, religion, fitness level, history of sexual violence, and gender spectrum health also play a role, as do anxiety and depression, dementia, and substance abuse disorders, the authors wrote in their presentation, “Prioritizing Sexual Health in Gynecological Oncology Care.”
Low libido is a frequent complaint across all cancer types, Ms. Dreibelbis, a nurse practitioner specializing in gynecologic oncology at the UPMC Hillman Cancer Center, Pittsburgh, Pennsylvania, said in an interview.
“Breast cancer patients, especially those on [aromatase inhibitor] therapy, often experience vaginal dryness and therefore dyspareunia,” she added.
The pelvic floor muscles, with their important role in sexual response, can be weakened by cancer treatment or surgery, and the pudendal nerves, which are the primary nerves responsible for sexual response in women, can be affected as well, Dr. Lersch and Ms. Dreibelbis wrote.
Taking Sex Seriously
Researchers are exploring the impact of different cancer prevention treatments for women to mitigate sexual side effects, as illustrated by another study presented at the meeting.
Dr. Barbara Norquist, MD, a gynecologic oncologist at the University of Washington, Seattle, and colleagues compared the sexual function and menopausal symptoms of patients at high risk of ovarian carcinoma who underwent either interval salpingectomy/delayed oophorectomy (ISDO) or risk-reducing salpingo-oophorectomy (RRSO).
“For patients at high risk for ovarian cancer, surgical removal of the tubes and ovaries is the mainstay of prevention, as screening is not effective at reducing death from ovarian cancer. As a result of surgery, many patients become suddenly postmenopausal from losing their ovaries,” Dr. Norquist said in an interview.
Some patients delay surgery out of concern for health and quality of life, including sexual function, she said.
In the study (known as the WISP trial) the researchers compared data from 166 patients who underwent immediate removal of the fallopian tubes and ovaries and 171 who underwent fallopian tube removal and delayed oophorectomy. All patients completed questionnaires about sexual function. The primary outcome was change in sexual function based on the sexual function index (FSFI) from baseline to 6 months after surgery.
Overall, changes in sexual function were significantly greater in the immediate oophorectomy group, compared with the delayed oophorectomy group at 6 months (33% vs 17%) and also at 12 months (43% vs 20%).
A further review of patients using hormone therapy showed that those in the immediate oophorectomy group still had greater decreases in sexual function, compared with the delayed group, though the difference between groups of patients using hormone therapy was less dramatic.
“I was surprised that, even with hormone replacement therapy, patients undergoing removal of the ovaries still had significant detrimental changes to sexual function when compared to those having the tubes removed, although this was even worse in those who could not take HRT,” Dr. Norquist said, in an interview. “I was reassured that menopausal symptoms in general were well managed with HRT, as these patients did not score differently on menopause symptoms, compared with those having their tubes removed,” she said.
Patients deserve accurate information about predicted changes in menopausal symptoms and sexual function as a result of ovary removal, and HRT should be provided when there is no contraindication, Dr. Norquist told this news organization.
Dr. Norquist and colleagues are awaiting the results of clinical trials investigating the safety of salpingectomy with delayed oophorectomy in terms of ovarian cancer prevention, but more research is needed to identify optimal management of the menopausal and sexual side effects associated with surgical menopause, she noted.
“Findings from the WISP study show the importance of hormones in women undergoing prophylactic surgery,” Dr. Dizon said. The findings indicate that salpingectomy has less of a negative influence on sexual function compared to removal of the ovaries, and the impact of hormone therapy and the relatively young age of the patients who took hormones reinforces current knowledge about hormones and sex, he added.
Barriers and Solutions
Barriers to asking women with cancer about sexual issues reported by providers include limited time, lack of training in sexual health, a desire to avoid offending the patient or making them uncomfortable, and uncertainty about how to answer the questions, Dr. Lersch and Ms. Dreibelbis wrote in their presentation.
Barriers to asking healthcare providers about their sexual issues reported by patients include the beliefs that the clinician should initiate the discussion, that sexual function will not be taken seriously, and that they might make the provider uncomfortable.
“Fortunately, more information and research has been done on sexual health and gynecological cancer in recent years, so oncologists are becoming more aware of the issues women may have,” said Dr. Lersch who is an oncology nurse practitioner at Providence Franz Cancer Institute in Portland, Oregon, in an interview.
Telling patients early in their cancer treatment about potential sexual side effects and opportunities for help is essential, she added.
Although oncologists have become more aware of the importance of sexual health and well-being for their patients, “I think there has historically been a disconnect in including sexual health education in medical training,” Ms. Dreibelbis said in an interview.
Dr. Lersch and Ms. Dreibelbis advised a multidimensional approach to managing sexual problems in cancer patients that includes consideration of biological and psychological symptoms, but also social, cultural, and interpersonal factors, in their presentation.
Their suggestions include discussing dyspareunia with their patients, asking for details such as whether the pain is internal or external, whether it occurs with activities outside of sex including masturbation, and whether bleeding is present.
Oncology therapies and surgeries can decrease or eliminate an individual’s ability to produce their own lubricant; for example, removal of the cervix eliminates cervical mucous, which helps with internal lubrication, they wrote in their presentation.
For patients with dyspareunia, Dr. Lersch and Ms. Dreibelbis recommend a vaginal moisturizer especially formulated for vaginal tissue that can be absorbed by the mucosal tissue of the vagina. Use of this type of product can increase the effectiveness of lubricants and help restore integrity of the vaginal tissue. Such moisturizers are available as gels, creams, or suppositories over the counter, and do not contain hormones.
Vaginal estrogen can be helpful for burning, itching, irritation, tissue fragility, and pain with sex, according to Dr. Lersch and Ms. Dreibelbis. Adequate estrogen therapy can promote normalization of vaginal pH and microflora, as well increase vaginal secretion and reduce pain and dryness with intercourse, the presenters stated in their presentation. In addition, dilator therapy can be used to help prevent vaginal stenosis, and penetration bumpers can help relieve discomfort during intercourse, they wrote.
Looking ahead, more research is needed to serve a wider patient population, Ms. Dreibelbis said, in an interview.
“LGBTQIA [individuals] have not been included in sexual health research and there are more people than ever who identify within this group of people. I know there has also been some very early work on shielding the clitoris from the impacts of radiation, and I believe this is extremely important up-and-coming research,” she said.
Dr. Lersch, Ms. Dreibelbi, Dr. Dizon, Dr. Norquist, Ms. Brewer, and Dr. Mehta had no financial conflicts to disclose.
Decreased sexual function is a side effect of many types of cancer, notably uterine, cervical, ovarian, and breast cancer, that often goes unaddressed, according to the authors of several studies presented at the Society of Gynecologic Oncology (SGO)’s Annual Meeting on Women’s Cancer.
Patients want to talk about sex, but not necessarily at the start of their diagnosis or treatment, suggest the findings of a study presented at the meeting. Jesse T. Brewer of Weill Cornell Medicine in New York City and colleagues enrolled 63 patients who underwent surgery with documented hereditary breast cancer, ovarian cancer, or Lynch syndrome in a cross-sectional survey.
Overall, 86% said that sexuality and intimacy were very or somewhat important, and 78% said that the healthcare team addressing the issue was very or somewhat important, the researchers found. However, only 40% of the respondents said that they wanted to discuss sexuality at the time of diagnosis because the idea was too overwhelming.
Oncologists are more aware of sexual side effects and the potential for sexual issues that persist long after treatment, but many patients may not have opportunities to talk about sexual concerns, said Don S. Dizon, MD, an oncologist specializing in women’s cancers at Brown University, Providence, Rhode Island, in an interview.
“It is important that we [oncologists] be the ones to open the door to these conversations; people with cancer will not bring it up spontaneously, for fear of making their provider uncomfortable, especially if they’ve never been asked about it before,” Dr. Dizon said in an interview.
He advised clinicians to find a network within their health systems so they can refer patients to specialized services, such as sex therapy, couples counseling, pelvic rehabilitation, or menopausal experts as needed.
In another study presented at the meeting, Naaman Mehta, MD, of NYU Langone Health, and colleagues reviewed data from 166 healthcare providers who completed a 23-item survey about evaluating and managing sexual health concerns of their patients. Most of the respondents were gynecologic oncologists (93.4%), but one radiation oncologist and 10 other healthcare providers also completed the survey.
Overall, approximately 60% of the respondents routinely asked about the sexual health concerns of their patients, and 98% of these said they believed that sexual health discussions should be held with a gynecologic oncologist. Just over half (54%) also said that the patient should be the one to initiate a discussion of sexual health concerns.
Female providers were significantly more likely to discuss sexual health with patients, compared with male providers, after controlling for the hospital setting and training level, the researchers noted (odds ratio, 1.4;P < .01).
The results suggest a need for more ways to integrate sexual health screening into gynecologic oncologic clinics, the researchers concluded.
The provider survey findings are similar to the results of a survey conducted by Dr. Dizon and colleagues in 2007. In that study, less than half of respondents took a sexual history, but 80% felt there was insufficient time to explore sexual issues.
“It is critical to understand that people with cancer do not expect their oncologists to be sexual health experts, but as with all other side effects caused by treatment and the diagnosis, we can be the ones who recognize it,” Dr. Dizon noted, in an interview.
Common Complaints and Causes
In Dr. Dizon’s experience, local symptoms including vaginal dryness, pain with penetration, and vaginal thinning, are common sexual complaints in women with cancer, as are systemic issues such as lack of interest and menopause-type symptoms.
“For those undergoing radiation, the vaginal tunnel can actually develop adhesions, and if not treated proactively this can lead to vaginal stenosis,” said Dr. Dizon, who was not involved in the studies presented at the meeting.
Comorbidities such as diabetes, cardiovascular disease, and musculoskeletal conditions can contribute to sexual issues in women with cancer, according to Nora Lersch, DNP, FNP-BC, AOCNP, and Nicole Dreibelbis, CRNP, the authors of other research presented at the meeting.
Culture, religion, fitness level, history of sexual violence, and gender spectrum health also play a role, as do anxiety and depression, dementia, and substance abuse disorders, the authors wrote in their presentation, “Prioritizing Sexual Health in Gynecological Oncology Care.”
Low libido is a frequent complaint across all cancer types, Ms. Dreibelbis, a nurse practitioner specializing in gynecologic oncology at the UPMC Hillman Cancer Center, Pittsburgh, Pennsylvania, said in an interview.
“Breast cancer patients, especially those on [aromatase inhibitor] therapy, often experience vaginal dryness and therefore dyspareunia,” she added.
The pelvic floor muscles, with their important role in sexual response, can be weakened by cancer treatment or surgery, and the pudendal nerves, which are the primary nerves responsible for sexual response in women, can be affected as well, Dr. Lersch and Ms. Dreibelbis wrote.
Taking Sex Seriously
Researchers are exploring the impact of different cancer prevention treatments for women to mitigate sexual side effects, as illustrated by another study presented at the meeting.
Dr. Barbara Norquist, MD, a gynecologic oncologist at the University of Washington, Seattle, and colleagues compared the sexual function and menopausal symptoms of patients at high risk of ovarian carcinoma who underwent either interval salpingectomy/delayed oophorectomy (ISDO) or risk-reducing salpingo-oophorectomy (RRSO).
“For patients at high risk for ovarian cancer, surgical removal of the tubes and ovaries is the mainstay of prevention, as screening is not effective at reducing death from ovarian cancer. As a result of surgery, many patients become suddenly postmenopausal from losing their ovaries,” Dr. Norquist said in an interview.
Some patients delay surgery out of concern for health and quality of life, including sexual function, she said.
In the study (known as the WISP trial) the researchers compared data from 166 patients who underwent immediate removal of the fallopian tubes and ovaries and 171 who underwent fallopian tube removal and delayed oophorectomy. All patients completed questionnaires about sexual function. The primary outcome was change in sexual function based on the sexual function index (FSFI) from baseline to 6 months after surgery.
Overall, changes in sexual function were significantly greater in the immediate oophorectomy group, compared with the delayed oophorectomy group at 6 months (33% vs 17%) and also at 12 months (43% vs 20%).
A further review of patients using hormone therapy showed that those in the immediate oophorectomy group still had greater decreases in sexual function, compared with the delayed group, though the difference between groups of patients using hormone therapy was less dramatic.
“I was surprised that, even with hormone replacement therapy, patients undergoing removal of the ovaries still had significant detrimental changes to sexual function when compared to those having the tubes removed, although this was even worse in those who could not take HRT,” Dr. Norquist said, in an interview. “I was reassured that menopausal symptoms in general were well managed with HRT, as these patients did not score differently on menopause symptoms, compared with those having their tubes removed,” she said.
Patients deserve accurate information about predicted changes in menopausal symptoms and sexual function as a result of ovary removal, and HRT should be provided when there is no contraindication, Dr. Norquist told this news organization.
Dr. Norquist and colleagues are awaiting the results of clinical trials investigating the safety of salpingectomy with delayed oophorectomy in terms of ovarian cancer prevention, but more research is needed to identify optimal management of the menopausal and sexual side effects associated with surgical menopause, she noted.
“Findings from the WISP study show the importance of hormones in women undergoing prophylactic surgery,” Dr. Dizon said. The findings indicate that salpingectomy has less of a negative influence on sexual function compared to removal of the ovaries, and the impact of hormone therapy and the relatively young age of the patients who took hormones reinforces current knowledge about hormones and sex, he added.
Barriers and Solutions
Barriers to asking women with cancer about sexual issues reported by providers include limited time, lack of training in sexual health, a desire to avoid offending the patient or making them uncomfortable, and uncertainty about how to answer the questions, Dr. Lersch and Ms. Dreibelbis wrote in their presentation.
Barriers to asking healthcare providers about their sexual issues reported by patients include the beliefs that the clinician should initiate the discussion, that sexual function will not be taken seriously, and that they might make the provider uncomfortable.
“Fortunately, more information and research has been done on sexual health and gynecological cancer in recent years, so oncologists are becoming more aware of the issues women may have,” said Dr. Lersch who is an oncology nurse practitioner at Providence Franz Cancer Institute in Portland, Oregon, in an interview.
Telling patients early in their cancer treatment about potential sexual side effects and opportunities for help is essential, she added.
Although oncologists have become more aware of the importance of sexual health and well-being for their patients, “I think there has historically been a disconnect in including sexual health education in medical training,” Ms. Dreibelbis said in an interview.
Dr. Lersch and Ms. Dreibelbis advised a multidimensional approach to managing sexual problems in cancer patients that includes consideration of biological and psychological symptoms, but also social, cultural, and interpersonal factors, in their presentation.
Their suggestions include discussing dyspareunia with their patients, asking for details such as whether the pain is internal or external, whether it occurs with activities outside of sex including masturbation, and whether bleeding is present.
Oncology therapies and surgeries can decrease or eliminate an individual’s ability to produce their own lubricant; for example, removal of the cervix eliminates cervical mucous, which helps with internal lubrication, they wrote in their presentation.
For patients with dyspareunia, Dr. Lersch and Ms. Dreibelbis recommend a vaginal moisturizer especially formulated for vaginal tissue that can be absorbed by the mucosal tissue of the vagina. Use of this type of product can increase the effectiveness of lubricants and help restore integrity of the vaginal tissue. Such moisturizers are available as gels, creams, or suppositories over the counter, and do not contain hormones.
Vaginal estrogen can be helpful for burning, itching, irritation, tissue fragility, and pain with sex, according to Dr. Lersch and Ms. Dreibelbis. Adequate estrogen therapy can promote normalization of vaginal pH and microflora, as well increase vaginal secretion and reduce pain and dryness with intercourse, the presenters stated in their presentation. In addition, dilator therapy can be used to help prevent vaginal stenosis, and penetration bumpers can help relieve discomfort during intercourse, they wrote.
Looking ahead, more research is needed to serve a wider patient population, Ms. Dreibelbis said, in an interview.
“LGBTQIA [individuals] have not been included in sexual health research and there are more people than ever who identify within this group of people. I know there has also been some very early work on shielding the clitoris from the impacts of radiation, and I believe this is extremely important up-and-coming research,” she said.
Dr. Lersch, Ms. Dreibelbi, Dr. Dizon, Dr. Norquist, Ms. Brewer, and Dr. Mehta had no financial conflicts to disclose.
FROM SGO 2024
Sarcopenia With Obesity Increases Risk for Death
TOPLINE:
Patients with sarcopenic obesity (SO) are at a greater risk for earlier death, but screening for muscle function could offer an opportunity for intervention.
METHODOLOGY:
- The proportion of older adults living with high body fat and/or low muscle function and mass has risen in recent years, but sarcopenia and SO are undiagnosed conditions.
- Researchers evaluated 5888 individuals who participated in a population-based cohort study in the Netherlands: Participants were largely of European descent (98%); the mean age of participants was 69.5 years, and 56.8% were female.
- Participants were included if they had available measurements of handgrip strength and had received a dual-energy x-ray absorptiometry scan.
- Sarcopenia was defined by researchers in JAMA Network Open as having low handgrip strength and was confirmed with a low appendicular skeletal muscle mass index; SO was defined as a body mass index (BMI) over 27, having low handgrip strength, a high fat percentage, and/or a low appendicular skeletal muscle index, which were defined as altered body composition (BC).
TAKEAWAY:
- Participants with SO and one BC component were at a higher risk for all-cause mortality (hazard ratio [HR], 1.94; 95% CI, 1.60-2.33).
- Participants with SO and both components of BC had almost three times the risk for mortality as those without (HR, 2.84; 95% CI, 1.97-4.11).
IN PRACTICE:
“These results suggest that screening for SO might be implemented in primary care. In addition, early nonpharmacologic interventions, such as nutrition and exercise training, should be included to delay the onset of and to treat sarcopenia, especially SO,” the researchers wrote.
SOURCE:
Yves Boirie, MD, PhD, of the Human Nutrition Unit at Université Clermont Auvergne in Clermont-Ferrand, France, is the corresponding author for this study. The study was funded by the Netherlands Organisation for Health Research and Development, the French National Research Agency, and the European Union’s Horizon 2020 research and innovation program, among others.
LIMITATIONS:
The researchers also did not consider specific causes of death. Because the most participants had European ancestry, the results cannot be generalized.
DISCLOSURES:
Various authors report receiving grants from the Agence Nationale de la Recherche and Agencia Estatal de Investigación. Other authors report being members of advisory board panels for Pfizer, Eli Lilly, Novo Nordisk, and Nutricia Research.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with sarcopenic obesity (SO) are at a greater risk for earlier death, but screening for muscle function could offer an opportunity for intervention.
METHODOLOGY:
- The proportion of older adults living with high body fat and/or low muscle function and mass has risen in recent years, but sarcopenia and SO are undiagnosed conditions.
- Researchers evaluated 5888 individuals who participated in a population-based cohort study in the Netherlands: Participants were largely of European descent (98%); the mean age of participants was 69.5 years, and 56.8% were female.
- Participants were included if they had available measurements of handgrip strength and had received a dual-energy x-ray absorptiometry scan.
- Sarcopenia was defined by researchers in JAMA Network Open as having low handgrip strength and was confirmed with a low appendicular skeletal muscle mass index; SO was defined as a body mass index (BMI) over 27, having low handgrip strength, a high fat percentage, and/or a low appendicular skeletal muscle index, which were defined as altered body composition (BC).
TAKEAWAY:
- Participants with SO and one BC component were at a higher risk for all-cause mortality (hazard ratio [HR], 1.94; 95% CI, 1.60-2.33).
- Participants with SO and both components of BC had almost three times the risk for mortality as those without (HR, 2.84; 95% CI, 1.97-4.11).
IN PRACTICE:
“These results suggest that screening for SO might be implemented in primary care. In addition, early nonpharmacologic interventions, such as nutrition and exercise training, should be included to delay the onset of and to treat sarcopenia, especially SO,” the researchers wrote.
SOURCE:
Yves Boirie, MD, PhD, of the Human Nutrition Unit at Université Clermont Auvergne in Clermont-Ferrand, France, is the corresponding author for this study. The study was funded by the Netherlands Organisation for Health Research and Development, the French National Research Agency, and the European Union’s Horizon 2020 research and innovation program, among others.
LIMITATIONS:
The researchers also did not consider specific causes of death. Because the most participants had European ancestry, the results cannot be generalized.
DISCLOSURES:
Various authors report receiving grants from the Agence Nationale de la Recherche and Agencia Estatal de Investigación. Other authors report being members of advisory board panels for Pfizer, Eli Lilly, Novo Nordisk, and Nutricia Research.
A version of this article appeared on Medscape.com.
TOPLINE:
Patients with sarcopenic obesity (SO) are at a greater risk for earlier death, but screening for muscle function could offer an opportunity for intervention.
METHODOLOGY:
- The proportion of older adults living with high body fat and/or low muscle function and mass has risen in recent years, but sarcopenia and SO are undiagnosed conditions.
- Researchers evaluated 5888 individuals who participated in a population-based cohort study in the Netherlands: Participants were largely of European descent (98%); the mean age of participants was 69.5 years, and 56.8% were female.
- Participants were included if they had available measurements of handgrip strength and had received a dual-energy x-ray absorptiometry scan.
- Sarcopenia was defined by researchers in JAMA Network Open as having low handgrip strength and was confirmed with a low appendicular skeletal muscle mass index; SO was defined as a body mass index (BMI) over 27, having low handgrip strength, a high fat percentage, and/or a low appendicular skeletal muscle index, which were defined as altered body composition (BC).
TAKEAWAY:
- Participants with SO and one BC component were at a higher risk for all-cause mortality (hazard ratio [HR], 1.94; 95% CI, 1.60-2.33).
- Participants with SO and both components of BC had almost three times the risk for mortality as those without (HR, 2.84; 95% CI, 1.97-4.11).
IN PRACTICE:
“These results suggest that screening for SO might be implemented in primary care. In addition, early nonpharmacologic interventions, such as nutrition and exercise training, should be included to delay the onset of and to treat sarcopenia, especially SO,” the researchers wrote.
SOURCE:
Yves Boirie, MD, PhD, of the Human Nutrition Unit at Université Clermont Auvergne in Clermont-Ferrand, France, is the corresponding author for this study. The study was funded by the Netherlands Organisation for Health Research and Development, the French National Research Agency, and the European Union’s Horizon 2020 research and innovation program, among others.
LIMITATIONS:
The researchers also did not consider specific causes of death. Because the most participants had European ancestry, the results cannot be generalized.
DISCLOSURES:
Various authors report receiving grants from the Agence Nationale de la Recherche and Agencia Estatal de Investigación. Other authors report being members of advisory board panels for Pfizer, Eli Lilly, Novo Nordisk, and Nutricia Research.
A version of this article appeared on Medscape.com.
Linaclotide Succeeds for Functional Constipation in Children
, according to data from 330 individuals.
“Functional constipation is prevalent in pediatrics and is associated with chronic burdensome symptoms and impaired quality of life with an unmet need for treatment options for this age group,” corresponding study author Julie Khlevner, MD, AGAF, a pediatric gastroenterologist at Columbia University Vagelos College of Physicians and Surgeons, New York, said in an interview.

“Linaclotide has been approved for adults with chronic idiopathic constipation and irritable bowel syndrome with constipation, but its efficacy and safety in pediatric patients were unknown. Therefore, evaluating its use in this population was crucial to provide evidence-based treatment option,” she said.
In a study published in The Lancet Gastroenterology & Hepatology, the researchers randomized 166 pediatric patients with functional constipation to 72 micrograms of linaclotide once daily for 12 weeks and 164 to a placebo. The study was conducted at 64 clinic or hospital sites across 7 countries between October 1, 2019, and March 21, 2022. Approximately half (55%) of the patients were female.
The primary outcome was a change from baseline to 12 weeks in the frequency of spontaneous bowel movements (SBMs) per week, with no rescue medication on the day of or before the bowel movement. The secondary endpoint was change in stool consistency from baseline to 12 weeks. The mean frequency for SBMs at baseline was 1.16 per week in patients randomized to linaclotide and 1.28 for those randomized to placebo; these rates increased to 3.41 and 2.29, respectively, over the study period. The linaclotide patients showed a significantly greater improvement over placebo patients based on least-squares mean change from baseline (2.22 vs. 1.05, P = .0001).
In a subgroup analysis by age, the response was stronger in younger patients aged 6-11 years than in those aged 12-17 years, the researchers noted. This difference might stem from different pathophysiological mechanisms between older and younger ages, such as withholding behavior, they added.
Linaclotide was well tolerated overall; the most frequently reported treatment-emergent events were diarrhea (seven linaclotide patients and three placebo patients). In addition, five linaclotide patients and four placebo patients developed COVID-19 during treatment. No deaths occurred during the study, but one serious adverse event involving severe diarrhea, dehydration, and hospitalization, occurred in a 17-year-old female patient, but resolved after administration of intravenous fluids, the researchers noted.
Clinical Implications and Next Steps
The study findings reflect previous research on linaclotide in adults, Dr. Khlevner said. “The significant improvement in spontaneous bowel movements frequency and stool consistency with linaclotide compared to placebo is consistent with its mechanism of action as a guanylate cyclase C agonist,” she noted.
In clinical practice, barriers to the use of linaclotide may include lack of awareness of linaclotide’s safety and efficacy profile, and of its Food and Drug Administration approval for use in children aged 6-17 years with functional constipation, said Dr. Khlevner. “Additionally, access to the medication and insurance coverage may be potential barriers for some patients.” However, “some of these barriers can be overcome through education and training of healthcare providers regarding the appropriate use of linaclotide in pediatric patients with functional constipation,” she added.
The findings were limited by several factors including potential measurement bias and selection bias, lack of assessment of lifestyle modifications as confounding factors, and lack of quality-of-life assessment, the researchers noted. Other limitations included the relatively short 12-week treatment duration, which may not fully capture long-term safety and efficacy, and the focus on patients aged 6-17 years, Dr. Khlevner told this news organization.
“Future research could address these limitations through longer-term studies with broader age ranges and incorporating patient-reported outcomes in real world situations to assess the overall impact of linaclotide treatment on pediatric patients with functional constipation,” she said.
Study Supports Noninvasive Treatment Option
An alternative medication for children with functional constipation who do not respond to current therapies could prevent the use of more invasive interventions such as frequent enemas or antegrade enemas, Stephen M. Borowitz, MD, professor of pediatrics at the University of Virginia, Charlottesville, said in an interview.
Dr. Borowitz said he was not surprised by study findings. “Given the mechanism of action of the drug, I would expect the majority of children with functional constipation to respond in the sense of having more frequent and softer stools,” he said. “The bigger question, which wasn’t answered, is whether children who fail more conservative therapies respond to linaclotide,” said Dr. Borowitz, who was not involved in the study. “This was a phase 3 trial of otherwise healthy children with functional constipation and we know the majority of these children will respond to aggressive management with osmotic stool softeners, plus or minus a stimulant like senna coupled with lifestyle modifications (such as drinking more fluid, regular toileting, and appropriate toileting behaviors),” he said.
The greatest short-term barrier to the expanded use of linaclotide in clinical practice will likely be cost, and whether insurance will cover the drug, Dr. Borowitz told this news organization. Insurance coverage may not be an option until the child has failed more conservative, less expensive therapies, he said.
Also, the current study was a placebo-controlled trial, and not a comparison between linaclotide and polyethylene glycol, plus or minus senna, with other routine interventions, he said.
Looking ahead, “now that we know linaclotide is better than placebo, we need to know if it is as good, better, or worse than other proven interventions, and perhaps even more importantly, is it effective among children who have failed more conservative management,” Dr. Borowitz said. “We also need to know long-term risks, and given that the majority of childhood constipation develops before age 6 years, whether the drug can be used in younger children,” he emphasized. If so, studies need to examine whether linaclotide alters the natural history of the problem, he added. Previous studies suggest that the longer the symptom goes on, the harder it is to undo the secondary behaviors that result, such as withholding, pelvic floor dysfunction, and toileting refusal, he noted.
The study was supported by AbbVie and Ironwood Pharmaceuticals. The lead author, Carlo Di Lorenzo, MD, disclosed consulting fees from AbbVie, Ironwood Pharmaceuticals, Mallinckrodt, NeurAxis, QOL Medical, and Takeda. Dr. Khlevner disclosed honoraria from Abbott Pediatric Nutrition and participation on a data safety monitoring board and advisory board for AbbVie. Dr. Borowitz had no financial conflicts to disclose.
, according to data from 330 individuals.
“Functional constipation is prevalent in pediatrics and is associated with chronic burdensome symptoms and impaired quality of life with an unmet need for treatment options for this age group,” corresponding study author Julie Khlevner, MD, AGAF, a pediatric gastroenterologist at Columbia University Vagelos College of Physicians and Surgeons, New York, said in an interview.
“Linaclotide has been approved for adults with chronic idiopathic constipation and irritable bowel syndrome with constipation, but its efficacy and safety in pediatric patients were unknown. Therefore, evaluating its use in this population was crucial to provide evidence-based treatment option,” she said.
In a study published in The Lancet Gastroenterology & Hepatology, the researchers randomized 166 pediatric patients with functional constipation to 72 micrograms of linaclotide once daily for 12 weeks and 164 to a placebo. The study was conducted at 64 clinic or hospital sites across 7 countries between October 1, 2019, and March 21, 2022. Approximately half (55%) of the patients were female.
The primary outcome was a change from baseline to 12 weeks in the frequency of spontaneous bowel movements (SBMs) per week, with no rescue medication on the day of or before the bowel movement. The secondary endpoint was change in stool consistency from baseline to 12 weeks. The mean frequency for SBMs at baseline was 1.16 per week in patients randomized to linaclotide and 1.28 for those randomized to placebo; these rates increased to 3.41 and 2.29, respectively, over the study period. The linaclotide patients showed a significantly greater improvement over placebo patients based on least-squares mean change from baseline (2.22 vs. 1.05, P = .0001).
In a subgroup analysis by age, the response was stronger in younger patients aged 6-11 years than in those aged 12-17 years, the researchers noted. This difference might stem from different pathophysiological mechanisms between older and younger ages, such as withholding behavior, they added.
Linaclotide was well tolerated overall; the most frequently reported treatment-emergent events were diarrhea (seven linaclotide patients and three placebo patients). In addition, five linaclotide patients and four placebo patients developed COVID-19 during treatment. No deaths occurred during the study, but one serious adverse event involving severe diarrhea, dehydration, and hospitalization, occurred in a 17-year-old female patient, but resolved after administration of intravenous fluids, the researchers noted.
Clinical Implications and Next Steps
The study findings reflect previous research on linaclotide in adults, Dr. Khlevner said. “The significant improvement in spontaneous bowel movements frequency and stool consistency with linaclotide compared to placebo is consistent with its mechanism of action as a guanylate cyclase C agonist,” she noted.
In clinical practice, barriers to the use of linaclotide may include lack of awareness of linaclotide’s safety and efficacy profile, and of its Food and Drug Administration approval for use in children aged 6-17 years with functional constipation, said Dr. Khlevner. “Additionally, access to the medication and insurance coverage may be potential barriers for some patients.” However, “some of these barriers can be overcome through education and training of healthcare providers regarding the appropriate use of linaclotide in pediatric patients with functional constipation,” she added.
The findings were limited by several factors including potential measurement bias and selection bias, lack of assessment of lifestyle modifications as confounding factors, and lack of quality-of-life assessment, the researchers noted. Other limitations included the relatively short 12-week treatment duration, which may not fully capture long-term safety and efficacy, and the focus on patients aged 6-17 years, Dr. Khlevner told this news organization.
“Future research could address these limitations through longer-term studies with broader age ranges and incorporating patient-reported outcomes in real world situations to assess the overall impact of linaclotide treatment on pediatric patients with functional constipation,” she said.
Study Supports Noninvasive Treatment Option
An alternative medication for children with functional constipation who do not respond to current therapies could prevent the use of more invasive interventions such as frequent enemas or antegrade enemas, Stephen M. Borowitz, MD, professor of pediatrics at the University of Virginia, Charlottesville, said in an interview.
Dr. Borowitz said he was not surprised by study findings. “Given the mechanism of action of the drug, I would expect the majority of children with functional constipation to respond in the sense of having more frequent and softer stools,” he said. “The bigger question, which wasn’t answered, is whether children who fail more conservative therapies respond to linaclotide,” said Dr. Borowitz, who was not involved in the study. “This was a phase 3 trial of otherwise healthy children with functional constipation and we know the majority of these children will respond to aggressive management with osmotic stool softeners, plus or minus a stimulant like senna coupled with lifestyle modifications (such as drinking more fluid, regular toileting, and appropriate toileting behaviors),” he said.
The greatest short-term barrier to the expanded use of linaclotide in clinical practice will likely be cost, and whether insurance will cover the drug, Dr. Borowitz told this news organization. Insurance coverage may not be an option until the child has failed more conservative, less expensive therapies, he said.
Also, the current study was a placebo-controlled trial, and not a comparison between linaclotide and polyethylene glycol, plus or minus senna, with other routine interventions, he said.
Looking ahead, “now that we know linaclotide is better than placebo, we need to know if it is as good, better, or worse than other proven interventions, and perhaps even more importantly, is it effective among children who have failed more conservative management,” Dr. Borowitz said. “We also need to know long-term risks, and given that the majority of childhood constipation develops before age 6 years, whether the drug can be used in younger children,” he emphasized. If so, studies need to examine whether linaclotide alters the natural history of the problem, he added. Previous studies suggest that the longer the symptom goes on, the harder it is to undo the secondary behaviors that result, such as withholding, pelvic floor dysfunction, and toileting refusal, he noted.
The study was supported by AbbVie and Ironwood Pharmaceuticals. The lead author, Carlo Di Lorenzo, MD, disclosed consulting fees from AbbVie, Ironwood Pharmaceuticals, Mallinckrodt, NeurAxis, QOL Medical, and Takeda. Dr. Khlevner disclosed honoraria from Abbott Pediatric Nutrition and participation on a data safety monitoring board and advisory board for AbbVie. Dr. Borowitz had no financial conflicts to disclose.
, according to data from 330 individuals.
“Functional constipation is prevalent in pediatrics and is associated with chronic burdensome symptoms and impaired quality of life with an unmet need for treatment options for this age group,” corresponding study author Julie Khlevner, MD, AGAF, a pediatric gastroenterologist at Columbia University Vagelos College of Physicians and Surgeons, New York, said in an interview.
“Linaclotide has been approved for adults with chronic idiopathic constipation and irritable bowel syndrome with constipation, but its efficacy and safety in pediatric patients were unknown. Therefore, evaluating its use in this population was crucial to provide evidence-based treatment option,” she said.
In a study published in The Lancet Gastroenterology & Hepatology, the researchers randomized 166 pediatric patients with functional constipation to 72 micrograms of linaclotide once daily for 12 weeks and 164 to a placebo. The study was conducted at 64 clinic or hospital sites across 7 countries between October 1, 2019, and March 21, 2022. Approximately half (55%) of the patients were female.
The primary outcome was a change from baseline to 12 weeks in the frequency of spontaneous bowel movements (SBMs) per week, with no rescue medication on the day of or before the bowel movement. The secondary endpoint was change in stool consistency from baseline to 12 weeks. The mean frequency for SBMs at baseline was 1.16 per week in patients randomized to linaclotide and 1.28 for those randomized to placebo; these rates increased to 3.41 and 2.29, respectively, over the study period. The linaclotide patients showed a significantly greater improvement over placebo patients based on least-squares mean change from baseline (2.22 vs. 1.05, P = .0001).
In a subgroup analysis by age, the response was stronger in younger patients aged 6-11 years than in those aged 12-17 years, the researchers noted. This difference might stem from different pathophysiological mechanisms between older and younger ages, such as withholding behavior, they added.
Linaclotide was well tolerated overall; the most frequently reported treatment-emergent events were diarrhea (seven linaclotide patients and three placebo patients). In addition, five linaclotide patients and four placebo patients developed COVID-19 during treatment. No deaths occurred during the study, but one serious adverse event involving severe diarrhea, dehydration, and hospitalization, occurred in a 17-year-old female patient, but resolved after administration of intravenous fluids, the researchers noted.
Clinical Implications and Next Steps
The study findings reflect previous research on linaclotide in adults, Dr. Khlevner said. “The significant improvement in spontaneous bowel movements frequency and stool consistency with linaclotide compared to placebo is consistent with its mechanism of action as a guanylate cyclase C agonist,” she noted.
In clinical practice, barriers to the use of linaclotide may include lack of awareness of linaclotide’s safety and efficacy profile, and of its Food and Drug Administration approval for use in children aged 6-17 years with functional constipation, said Dr. Khlevner. “Additionally, access to the medication and insurance coverage may be potential barriers for some patients.” However, “some of these barriers can be overcome through education and training of healthcare providers regarding the appropriate use of linaclotide in pediatric patients with functional constipation,” she added.
The findings were limited by several factors including potential measurement bias and selection bias, lack of assessment of lifestyle modifications as confounding factors, and lack of quality-of-life assessment, the researchers noted. Other limitations included the relatively short 12-week treatment duration, which may not fully capture long-term safety and efficacy, and the focus on patients aged 6-17 years, Dr. Khlevner told this news organization.
“Future research could address these limitations through longer-term studies with broader age ranges and incorporating patient-reported outcomes in real world situations to assess the overall impact of linaclotide treatment on pediatric patients with functional constipation,” she said.
Study Supports Noninvasive Treatment Option
An alternative medication for children with functional constipation who do not respond to current therapies could prevent the use of more invasive interventions such as frequent enemas or antegrade enemas, Stephen M. Borowitz, MD, professor of pediatrics at the University of Virginia, Charlottesville, said in an interview.
Dr. Borowitz said he was not surprised by study findings. “Given the mechanism of action of the drug, I would expect the majority of children with functional constipation to respond in the sense of having more frequent and softer stools,” he said. “The bigger question, which wasn’t answered, is whether children who fail more conservative therapies respond to linaclotide,” said Dr. Borowitz, who was not involved in the study. “This was a phase 3 trial of otherwise healthy children with functional constipation and we know the majority of these children will respond to aggressive management with osmotic stool softeners, plus or minus a stimulant like senna coupled with lifestyle modifications (such as drinking more fluid, regular toileting, and appropriate toileting behaviors),” he said.
The greatest short-term barrier to the expanded use of linaclotide in clinical practice will likely be cost, and whether insurance will cover the drug, Dr. Borowitz told this news organization. Insurance coverage may not be an option until the child has failed more conservative, less expensive therapies, he said.
Also, the current study was a placebo-controlled trial, and not a comparison between linaclotide and polyethylene glycol, plus or minus senna, with other routine interventions, he said.
Looking ahead, “now that we know linaclotide is better than placebo, we need to know if it is as good, better, or worse than other proven interventions, and perhaps even more importantly, is it effective among children who have failed more conservative management,” Dr. Borowitz said. “We also need to know long-term risks, and given that the majority of childhood constipation develops before age 6 years, whether the drug can be used in younger children,” he emphasized. If so, studies need to examine whether linaclotide alters the natural history of the problem, he added. Previous studies suggest that the longer the symptom goes on, the harder it is to undo the secondary behaviors that result, such as withholding, pelvic floor dysfunction, and toileting refusal, he noted.
The study was supported by AbbVie and Ironwood Pharmaceuticals. The lead author, Carlo Di Lorenzo, MD, disclosed consulting fees from AbbVie, Ironwood Pharmaceuticals, Mallinckrodt, NeurAxis, QOL Medical, and Takeda. Dr. Khlevner disclosed honoraria from Abbott Pediatric Nutrition and participation on a data safety monitoring board and advisory board for AbbVie. Dr. Borowitz had no financial conflicts to disclose.
FROM THE LANCET GASTROENTEROLOGY & HEPATOLOGY
Lab Tests Are Key for Diagnosing Chickenpox
, according to a report featured in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
Only about half of clinically diagnosed varicella cases — cases diagnosed by examining rashes without laboratory testing — were positive for the varicella-zoster virus (VZV), suggesting lab testing is important to avoid consequences such as children being kept out of school longer than necessary.
Clinical diagnosis continues to be the primary method for diagnosing varicella, said authors of the report, led by Alison Ruprecht, MPH, a state epidemiologist with the MDH. But the signs and symptoms of those who have received the varicella vaccine (including fewer skin lesions, mostly maculopapular) make it difficult to diagnose.
Minnesota Offers Free Tests
In December 2016, the MDH expanded polymerase chain reaction (PCR) laboratory testing for varicella in the state. The program reached out to clinicians through newsletters, webinars, advisories, and conferences describing the importance of lab testing when clinicians suspect a patient’s rash is varicella. The department also offered free testing at MDH Public Health Laboratory (PHL) through an agreement with the CDC and follow-up, if needed, with clinicians on testing practices.
MDH also provided specimen collection kits (containing a collection swab for vesicular fluid and slides for collection of scabs or scraping of maculopapular lesions) to clinics. Free testing was available for people with suspected varicella, including those who had been clinically diagnosed, or people who self-reported suspected varicella or whose school or child care reported the suspected cases. In addition to testing for varicella, MDH-PHL performed PCR testing for herpes simplex virus 1 (HSV-1), herpes simplex virus 2 (HSV-2), and enterovirus on all samples.
The state then saw lab-confirmed varicella cases double from 17% (235 of 1,426) during January 2013–November 2016 to 36% (619 of 1,717) during December 2016–March 2023 (P < .001).
During December 2016–March 2023, MDH-PHL tested specimens for 420 patients with suspected varicella; the median patient age was 5 years (range = 0-68 years). Of those, 23% provided specimens collected at home.
Clinical Diagnosis Versus Lab Test Confirmation
The researchers found that among 208 patients receiving a clinical diagnosis of varicella after only examination at a medical facility, fewer than half (45%) had positive varicella-zoster virus (VZV) lab test results. VZV detection was 66% lower in those who received varicella vaccine compared with those who did not.
The researchers acknowledged that outreach, at-home specimen collection, and free testing likely increased lab testing numbers.
They added that, “This increase in varicella testing likely also contributed to an increase in appropriate clinical management and school exclusion recommendations for suspect varicella cases.
“Clinicians should incorporate routine laboratory testing whenever varicella is suspected,” the researchers wrote. “Public health and school health professionals should emphasize the importance of laboratory confirmation in their recommendations to clinicians and parents.”
Presentation May Also Be Different in Immunocompromised
Sam Dominguez, MD, infectious disease specialist at Children’s Colorado in Aurora, who was not part of the research, said in addition to presentation being harder to recognize in those who are vaccinated, varicella is harder to diagnose in the immunocompromised population, where the rash may not be as prominent or more localized or appear in any number of atypical presentations.
In addition, he said, clinicians don’t see many cases these days. “Providers aren’t as familiar with what varicella looks like, especially younger providers who weren’t trained in the prevaccination era,” he said.
Cost is often an issue with lab testing as well as turn-around time and access, he said, and those factors can be barriers.
Dr. Dominguez said some classic presentations are easily diagnosed as varicella. “If you have a normal, healthy kid, who you’re seeing in the outpatient world who presents with a very classic rash for chickenpox, I don’t think laboratory testing is necessarily warranted in that scenario.”
But when clinicians aren’t confident in their diagnosis, “I think in those scenarios, testing can be very helpful in terms of management from a treatment standpoint as well as a potential infection control standpoint,” he said.
The authors reported no relevant financial relationships. Dr. Dominguez is a consultant for diagnostic companies Karius and BioFire. He has grant support from Pfizer and BioFire.
, according to a report featured in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
Only about half of clinically diagnosed varicella cases — cases diagnosed by examining rashes without laboratory testing — were positive for the varicella-zoster virus (VZV), suggesting lab testing is important to avoid consequences such as children being kept out of school longer than necessary.
Clinical diagnosis continues to be the primary method for diagnosing varicella, said authors of the report, led by Alison Ruprecht, MPH, a state epidemiologist with the MDH. But the signs and symptoms of those who have received the varicella vaccine (including fewer skin lesions, mostly maculopapular) make it difficult to diagnose.
Minnesota Offers Free Tests
In December 2016, the MDH expanded polymerase chain reaction (PCR) laboratory testing for varicella in the state. The program reached out to clinicians through newsletters, webinars, advisories, and conferences describing the importance of lab testing when clinicians suspect a patient’s rash is varicella. The department also offered free testing at MDH Public Health Laboratory (PHL) through an agreement with the CDC and follow-up, if needed, with clinicians on testing practices.
MDH also provided specimen collection kits (containing a collection swab for vesicular fluid and slides for collection of scabs or scraping of maculopapular lesions) to clinics. Free testing was available for people with suspected varicella, including those who had been clinically diagnosed, or people who self-reported suspected varicella or whose school or child care reported the suspected cases. In addition to testing for varicella, MDH-PHL performed PCR testing for herpes simplex virus 1 (HSV-1), herpes simplex virus 2 (HSV-2), and enterovirus on all samples.
The state then saw lab-confirmed varicella cases double from 17% (235 of 1,426) during January 2013–November 2016 to 36% (619 of 1,717) during December 2016–March 2023 (P < .001).
During December 2016–March 2023, MDH-PHL tested specimens for 420 patients with suspected varicella; the median patient age was 5 years (range = 0-68 years). Of those, 23% provided specimens collected at home.
Clinical Diagnosis Versus Lab Test Confirmation
The researchers found that among 208 patients receiving a clinical diagnosis of varicella after only examination at a medical facility, fewer than half (45%) had positive varicella-zoster virus (VZV) lab test results. VZV detection was 66% lower in those who received varicella vaccine compared with those who did not.
The researchers acknowledged that outreach, at-home specimen collection, and free testing likely increased lab testing numbers.
They added that, “This increase in varicella testing likely also contributed to an increase in appropriate clinical management and school exclusion recommendations for suspect varicella cases.
“Clinicians should incorporate routine laboratory testing whenever varicella is suspected,” the researchers wrote. “Public health and school health professionals should emphasize the importance of laboratory confirmation in their recommendations to clinicians and parents.”
Presentation May Also Be Different in Immunocompromised
Sam Dominguez, MD, infectious disease specialist at Children’s Colorado in Aurora, who was not part of the research, said in addition to presentation being harder to recognize in those who are vaccinated, varicella is harder to diagnose in the immunocompromised population, where the rash may not be as prominent or more localized or appear in any number of atypical presentations.
In addition, he said, clinicians don’t see many cases these days. “Providers aren’t as familiar with what varicella looks like, especially younger providers who weren’t trained in the prevaccination era,” he said.
Cost is often an issue with lab testing as well as turn-around time and access, he said, and those factors can be barriers.
Dr. Dominguez said some classic presentations are easily diagnosed as varicella. “If you have a normal, healthy kid, who you’re seeing in the outpatient world who presents with a very classic rash for chickenpox, I don’t think laboratory testing is necessarily warranted in that scenario.”
But when clinicians aren’t confident in their diagnosis, “I think in those scenarios, testing can be very helpful in terms of management from a treatment standpoint as well as a potential infection control standpoint,” he said.
The authors reported no relevant financial relationships. Dr. Dominguez is a consultant for diagnostic companies Karius and BioFire. He has grant support from Pfizer and BioFire.
, according to a report featured in the Centers for Disease Control and Prevention’s Morbidity and Mortality Weekly Report.
Only about half of clinically diagnosed varicella cases — cases diagnosed by examining rashes without laboratory testing — were positive for the varicella-zoster virus (VZV), suggesting lab testing is important to avoid consequences such as children being kept out of school longer than necessary.
Clinical diagnosis continues to be the primary method for diagnosing varicella, said authors of the report, led by Alison Ruprecht, MPH, a state epidemiologist with the MDH. But the signs and symptoms of those who have received the varicella vaccine (including fewer skin lesions, mostly maculopapular) make it difficult to diagnose.
Minnesota Offers Free Tests
In December 2016, the MDH expanded polymerase chain reaction (PCR) laboratory testing for varicella in the state. The program reached out to clinicians through newsletters, webinars, advisories, and conferences describing the importance of lab testing when clinicians suspect a patient’s rash is varicella. The department also offered free testing at MDH Public Health Laboratory (PHL) through an agreement with the CDC and follow-up, if needed, with clinicians on testing practices.
MDH also provided specimen collection kits (containing a collection swab for vesicular fluid and slides for collection of scabs or scraping of maculopapular lesions) to clinics. Free testing was available for people with suspected varicella, including those who had been clinically diagnosed, or people who self-reported suspected varicella or whose school or child care reported the suspected cases. In addition to testing for varicella, MDH-PHL performed PCR testing for herpes simplex virus 1 (HSV-1), herpes simplex virus 2 (HSV-2), and enterovirus on all samples.
The state then saw lab-confirmed varicella cases double from 17% (235 of 1,426) during January 2013–November 2016 to 36% (619 of 1,717) during December 2016–March 2023 (P < .001).
During December 2016–March 2023, MDH-PHL tested specimens for 420 patients with suspected varicella; the median patient age was 5 years (range = 0-68 years). Of those, 23% provided specimens collected at home.
Clinical Diagnosis Versus Lab Test Confirmation
The researchers found that among 208 patients receiving a clinical diagnosis of varicella after only examination at a medical facility, fewer than half (45%) had positive varicella-zoster virus (VZV) lab test results. VZV detection was 66% lower in those who received varicella vaccine compared with those who did not.
The researchers acknowledged that outreach, at-home specimen collection, and free testing likely increased lab testing numbers.
They added that, “This increase in varicella testing likely also contributed to an increase in appropriate clinical management and school exclusion recommendations for suspect varicella cases.
“Clinicians should incorporate routine laboratory testing whenever varicella is suspected,” the researchers wrote. “Public health and school health professionals should emphasize the importance of laboratory confirmation in their recommendations to clinicians and parents.”
Presentation May Also Be Different in Immunocompromised
Sam Dominguez, MD, infectious disease specialist at Children’s Colorado in Aurora, who was not part of the research, said in addition to presentation being harder to recognize in those who are vaccinated, varicella is harder to diagnose in the immunocompromised population, where the rash may not be as prominent or more localized or appear in any number of atypical presentations.
In addition, he said, clinicians don’t see many cases these days. “Providers aren’t as familiar with what varicella looks like, especially younger providers who weren’t trained in the prevaccination era,” he said.
Cost is often an issue with lab testing as well as turn-around time and access, he said, and those factors can be barriers.
Dr. Dominguez said some classic presentations are easily diagnosed as varicella. “If you have a normal, healthy kid, who you’re seeing in the outpatient world who presents with a very classic rash for chickenpox, I don’t think laboratory testing is necessarily warranted in that scenario.”
But when clinicians aren’t confident in their diagnosis, “I think in those scenarios, testing can be very helpful in terms of management from a treatment standpoint as well as a potential infection control standpoint,” he said.
The authors reported no relevant financial relationships. Dr. Dominguez is a consultant for diagnostic companies Karius and BioFire. He has grant support from Pfizer and BioFire.
FROM MMWR
ASCO Releases Vaccination Guidelines for Adults With Cancer
TOPLINE:
“Optimizing vaccination status should be considered a key element in the care of patients with cancer,” according to the authors of newly released American of Clinical Oncology (ASCO) guidelines.
METHODOLOGY:
- “Infections are the second most common cause of noncancer-related mortality within the first year after a cancer diagnosis,” highlighting the need for oncologists to help ensure patients are up to date on key vaccines, an ASCO panel of experts wrote.
- The expert panel reviewed the existing evidence and made recommendations to guide vaccination of adults with solid tumors or hematologic malignancies, including those who received hematopoietic stem-cell transplantation (HSCT), chimeric antigen T-cell (CAR T-cell) therapy and B-cell-depleting therapy, as well as guide vaccination of their household contacts.
- The panel reviewed 102 publications, including 24 systematic reviews, 14 randomized controlled trials, and 64 nonrandomized studies.
- Vaccines evaluated included those for COVID-19, influenza, hepatitis A and B, respiratory syncytial virus, Tdap, human papillomavirus, inactivated polio, and rabies.
- The authors noted that patients’ underlying immune status and their cancer therapy could affect vaccination and revaccination strategies compared with recommendations for a general adult population without cancer.
TAKEAWAY:
- The first step is to determine patients’ vaccination status and ensure adults newly diagnosed with cancer (as well as their household contacts) are up to date on seasonal and age or risk-based vaccines before starting their cancer treatment. If there are gaps, patients would ideally receive their vaccinations 2-4 weeks before their cancer treatment begins; however, non-live vaccines can be given during or after treatment.
- The authors recommended complete revaccination of patients 6-12 months following HSCT to restore vaccine-induced immunity. The caveats: COVID-19, influenza, and pneumococcal vaccines can be given as early as 3 months after transplant, and patients should receive live and live attenuated vaccines only in the absence of active GVHD or immunosuppression and only ≥ 2 years following HSCT.
- After CAR T-cell therapy directed against B-cell antigens (CD19/BCMA), patients should not receive influenza and COVID-19 vaccines sooner than 3 months after completing therapy and nonlive vaccines should not be given before 6 months.
- After B-cell depleting therapy, revaccinate patients for COVID-19 only and no sooner than 6 months after completing treatment. Long-term survivors of hematologic cancer with or without active disease or those with long-standing B-cell dysfunction or hypogammaglobulinemia from therapy or B-cell lineage malignancies should receive the recommended nonlive vaccines.
- Adults with solid and hematologic cancers traveling to an area of risk should follow the CDC standard recommendations for the destination. Hepatitis A, intramuscular typhoid vaccine, inactivated polio, hepatitis B, rabies, meningococcal, and nonlive Japanese encephalitis vaccines are safe.
IN PRACTICE:
“Enhancing vaccine uptake against preventable illnesses will help the community and improve the quality of care for patients with cancer,” the authors said. “Clinicians play a critical role in helping the patient and caregiver to understand the potential benefits and risks of recommended vaccination[s]. In addition, clinicians should provide authoritative resources, such as fact-based vaccine informational handouts and Internet sites, to help patients and caregivers learn more about the topic.”
SOURCE:
Mini Kamboj, MD, with Memorial Sloan Kettering Cancer Center, New York City, and Elise Kohn, MD, with the National Cancer Institute, Rockville, Maryland, served as cochairs for the expert panel. The guideline was published March 18 in the Journal of Clinical Oncology.
LIMITATIONS:
The evidence for some vaccines in cancer patients continues to evolve, particularly for new vaccines like COVID-19 vaccines.
DISCLOSURES:
This research had no commercial funding. Disclosures for the guideline panel are available with the original article.
A version of this article appeared on Medscape.com.
TOPLINE:
“Optimizing vaccination status should be considered a key element in the care of patients with cancer,” according to the authors of newly released American of Clinical Oncology (ASCO) guidelines.
METHODOLOGY:
- “Infections are the second most common cause of noncancer-related mortality within the first year after a cancer diagnosis,” highlighting the need for oncologists to help ensure patients are up to date on key vaccines, an ASCO panel of experts wrote.
- The expert panel reviewed the existing evidence and made recommendations to guide vaccination of adults with solid tumors or hematologic malignancies, including those who received hematopoietic stem-cell transplantation (HSCT), chimeric antigen T-cell (CAR T-cell) therapy and B-cell-depleting therapy, as well as guide vaccination of their household contacts.
- The panel reviewed 102 publications, including 24 systematic reviews, 14 randomized controlled trials, and 64 nonrandomized studies.
- Vaccines evaluated included those for COVID-19, influenza, hepatitis A and B, respiratory syncytial virus, Tdap, human papillomavirus, inactivated polio, and rabies.
- The authors noted that patients’ underlying immune status and their cancer therapy could affect vaccination and revaccination strategies compared with recommendations for a general adult population without cancer.
TAKEAWAY:
- The first step is to determine patients’ vaccination status and ensure adults newly diagnosed with cancer (as well as their household contacts) are up to date on seasonal and age or risk-based vaccines before starting their cancer treatment. If there are gaps, patients would ideally receive their vaccinations 2-4 weeks before their cancer treatment begins; however, non-live vaccines can be given during or after treatment.
- The authors recommended complete revaccination of patients 6-12 months following HSCT to restore vaccine-induced immunity. The caveats: COVID-19, influenza, and pneumococcal vaccines can be given as early as 3 months after transplant, and patients should receive live and live attenuated vaccines only in the absence of active GVHD or immunosuppression and only ≥ 2 years following HSCT.
- After CAR T-cell therapy directed against B-cell antigens (CD19/BCMA), patients should not receive influenza and COVID-19 vaccines sooner than 3 months after completing therapy and nonlive vaccines should not be given before 6 months.
- After B-cell depleting therapy, revaccinate patients for COVID-19 only and no sooner than 6 months after completing treatment. Long-term survivors of hematologic cancer with or without active disease or those with long-standing B-cell dysfunction or hypogammaglobulinemia from therapy or B-cell lineage malignancies should receive the recommended nonlive vaccines.
- Adults with solid and hematologic cancers traveling to an area of risk should follow the CDC standard recommendations for the destination. Hepatitis A, intramuscular typhoid vaccine, inactivated polio, hepatitis B, rabies, meningococcal, and nonlive Japanese encephalitis vaccines are safe.
IN PRACTICE:
“Enhancing vaccine uptake against preventable illnesses will help the community and improve the quality of care for patients with cancer,” the authors said. “Clinicians play a critical role in helping the patient and caregiver to understand the potential benefits and risks of recommended vaccination[s]. In addition, clinicians should provide authoritative resources, such as fact-based vaccine informational handouts and Internet sites, to help patients and caregivers learn more about the topic.”
SOURCE:
Mini Kamboj, MD, with Memorial Sloan Kettering Cancer Center, New York City, and Elise Kohn, MD, with the National Cancer Institute, Rockville, Maryland, served as cochairs for the expert panel. The guideline was published March 18 in the Journal of Clinical Oncology.
LIMITATIONS:
The evidence for some vaccines in cancer patients continues to evolve, particularly for new vaccines like COVID-19 vaccines.
DISCLOSURES:
This research had no commercial funding. Disclosures for the guideline panel are available with the original article.
A version of this article appeared on Medscape.com.
TOPLINE:
“Optimizing vaccination status should be considered a key element in the care of patients with cancer,” according to the authors of newly released American of Clinical Oncology (ASCO) guidelines.
METHODOLOGY:
- “Infections are the second most common cause of noncancer-related mortality within the first year after a cancer diagnosis,” highlighting the need for oncologists to help ensure patients are up to date on key vaccines, an ASCO panel of experts wrote.
- The expert panel reviewed the existing evidence and made recommendations to guide vaccination of adults with solid tumors or hematologic malignancies, including those who received hematopoietic stem-cell transplantation (HSCT), chimeric antigen T-cell (CAR T-cell) therapy and B-cell-depleting therapy, as well as guide vaccination of their household contacts.
- The panel reviewed 102 publications, including 24 systematic reviews, 14 randomized controlled trials, and 64 nonrandomized studies.
- Vaccines evaluated included those for COVID-19, influenza, hepatitis A and B, respiratory syncytial virus, Tdap, human papillomavirus, inactivated polio, and rabies.
- The authors noted that patients’ underlying immune status and their cancer therapy could affect vaccination and revaccination strategies compared with recommendations for a general adult population without cancer.
TAKEAWAY:
- The first step is to determine patients’ vaccination status and ensure adults newly diagnosed with cancer (as well as their household contacts) are up to date on seasonal and age or risk-based vaccines before starting their cancer treatment. If there are gaps, patients would ideally receive their vaccinations 2-4 weeks before their cancer treatment begins; however, non-live vaccines can be given during or after treatment.
- The authors recommended complete revaccination of patients 6-12 months following HSCT to restore vaccine-induced immunity. The caveats: COVID-19, influenza, and pneumococcal vaccines can be given as early as 3 months after transplant, and patients should receive live and live attenuated vaccines only in the absence of active GVHD or immunosuppression and only ≥ 2 years following HSCT.
- After CAR T-cell therapy directed against B-cell antigens (CD19/BCMA), patients should not receive influenza and COVID-19 vaccines sooner than 3 months after completing therapy and nonlive vaccines should not be given before 6 months.
- After B-cell depleting therapy, revaccinate patients for COVID-19 only and no sooner than 6 months after completing treatment. Long-term survivors of hematologic cancer with or without active disease or those with long-standing B-cell dysfunction or hypogammaglobulinemia from therapy or B-cell lineage malignancies should receive the recommended nonlive vaccines.
- Adults with solid and hematologic cancers traveling to an area of risk should follow the CDC standard recommendations for the destination. Hepatitis A, intramuscular typhoid vaccine, inactivated polio, hepatitis B, rabies, meningococcal, and nonlive Japanese encephalitis vaccines are safe.
IN PRACTICE:
“Enhancing vaccine uptake against preventable illnesses will help the community and improve the quality of care for patients with cancer,” the authors said. “Clinicians play a critical role in helping the patient and caregiver to understand the potential benefits and risks of recommended vaccination[s]. In addition, clinicians should provide authoritative resources, such as fact-based vaccine informational handouts and Internet sites, to help patients and caregivers learn more about the topic.”
SOURCE:
Mini Kamboj, MD, with Memorial Sloan Kettering Cancer Center, New York City, and Elise Kohn, MD, with the National Cancer Institute, Rockville, Maryland, served as cochairs for the expert panel. The guideline was published March 18 in the Journal of Clinical Oncology.
LIMITATIONS:
The evidence for some vaccines in cancer patients continues to evolve, particularly for new vaccines like COVID-19 vaccines.
DISCLOSURES:
This research had no commercial funding. Disclosures for the guideline panel are available with the original article.
A version of this article appeared on Medscape.com.
No Increased Stroke Risk After COVID-19 Bivalent Vaccine
TOPLINE:
, a new study of Medicare beneficiaries showed.
METHODOLOGY:
- The analysis included 5.4 million people age ≥ 65 years who received either the Pfizer-BioNTech COVID-19 bivalent vaccine or the Moderna bivalent vaccine, or the Pfizer vaccine and a high-dose or adjuvanted concomitant influenza vaccine (ie, administered on the same day).
- A total of 11,001 of the cohort experienced a stroke in the first 90 days after vaccination.
- The main outcome was stroke risk (nonhemorrhagic stroke, transient ischemic attack [TIA], or hemorrhagic stroke) during the 1- to 21-day or 22- to 42-day window after vaccination vs the 43- to 90-day control window.
- The mean age of participants was 74 years, and 56% were female.
TAKEAWAY:
- There was no statistically significant association with either brand of the COVID-19 bivalent vaccine or any of the stroke outcomes during the 1- to 21-day or 22- to 42-day risk window compared with the 43- to 90-day control window (incidence rate ratio [IRR] range, 0.72-1.12).
- Vaccination with COVID-19 bivalent vaccine plus a high-dose or adjuvanted influenza vaccine (n = 4596) was associated with a significantly greater risk for nonhemorrhagic stroke 22-42 days after vaccination with Pfizer-BioNTech (IRR, 1.20; risk difference/100,000 doses, 3.13) and an increase in TIA risk 1-21 days after vaccination with Moderna (IRR, 1.35; risk difference/100,000 doses, 3.33).
- There was a significant association between vaccination with a high-dose or adjuvanted influenza vaccine (n = 21,345) and nonhemorrhagic stroke 22-42 days after vaccination (IRR, 1.09; risk difference/100,000 doses, 1.65).
IN PRACTICE:
“The clinical significance of the risk of stroke after vaccination must be carefully considered together with the significant benefits of receiving an influenza vaccination,” the authors wrote. “Because the framework of the current self-controlled case series study does not compare the populations who were vaccinated vs those who were unvaccinated, it does not account for the reduced rate of severe influenza after vaccination. More studies are needed to better understand the association between high-dose or adjuvanted influenza vaccination and stroke.”
SOURCE:
Yun Lu, PhD, of the Center for Biologics Evaluation and Research, US Food and Drug Administration, Silver Spring, Maryland, was the lead and corresponding author of the study. It was published online on March 19 in JAMA.
LIMITATIONS:
Some stroke cases may have been missed or misclassified. The study included only vaccinated individuals — a population considered to have health-seeking behaviors — which may limit the generalizability of the findings. The study was conducted using COVID-19 bivalent vaccines, which are no longer available.
DISCLOSURES:
This work was funded by the US Food and Drug Administration through an interagency agreement with the Centers for Medicare & Medicaid Services. Dr. Lu reported no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article appeared on Medscape.com.
TOPLINE:
, a new study of Medicare beneficiaries showed.
METHODOLOGY:
- The analysis included 5.4 million people age ≥ 65 years who received either the Pfizer-BioNTech COVID-19 bivalent vaccine or the Moderna bivalent vaccine, or the Pfizer vaccine and a high-dose or adjuvanted concomitant influenza vaccine (ie, administered on the same day).
- A total of 11,001 of the cohort experienced a stroke in the first 90 days after vaccination.
- The main outcome was stroke risk (nonhemorrhagic stroke, transient ischemic attack [TIA], or hemorrhagic stroke) during the 1- to 21-day or 22- to 42-day window after vaccination vs the 43- to 90-day control window.
- The mean age of participants was 74 years, and 56% were female.
TAKEAWAY:
- There was no statistically significant association with either brand of the COVID-19 bivalent vaccine or any of the stroke outcomes during the 1- to 21-day or 22- to 42-day risk window compared with the 43- to 90-day control window (incidence rate ratio [IRR] range, 0.72-1.12).
- Vaccination with COVID-19 bivalent vaccine plus a high-dose or adjuvanted influenza vaccine (n = 4596) was associated with a significantly greater risk for nonhemorrhagic stroke 22-42 days after vaccination with Pfizer-BioNTech (IRR, 1.20; risk difference/100,000 doses, 3.13) and an increase in TIA risk 1-21 days after vaccination with Moderna (IRR, 1.35; risk difference/100,000 doses, 3.33).
- There was a significant association between vaccination with a high-dose or adjuvanted influenza vaccine (n = 21,345) and nonhemorrhagic stroke 22-42 days after vaccination (IRR, 1.09; risk difference/100,000 doses, 1.65).
IN PRACTICE:
“The clinical significance of the risk of stroke after vaccination must be carefully considered together with the significant benefits of receiving an influenza vaccination,” the authors wrote. “Because the framework of the current self-controlled case series study does not compare the populations who were vaccinated vs those who were unvaccinated, it does not account for the reduced rate of severe influenza after vaccination. More studies are needed to better understand the association between high-dose or adjuvanted influenza vaccination and stroke.”
SOURCE:
Yun Lu, PhD, of the Center for Biologics Evaluation and Research, US Food and Drug Administration, Silver Spring, Maryland, was the lead and corresponding author of the study. It was published online on March 19 in JAMA.
LIMITATIONS:
Some stroke cases may have been missed or misclassified. The study included only vaccinated individuals — a population considered to have health-seeking behaviors — which may limit the generalizability of the findings. The study was conducted using COVID-19 bivalent vaccines, which are no longer available.
DISCLOSURES:
This work was funded by the US Food and Drug Administration through an interagency agreement with the Centers for Medicare & Medicaid Services. Dr. Lu reported no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article appeared on Medscape.com.
TOPLINE:
, a new study of Medicare beneficiaries showed.
METHODOLOGY:
- The analysis included 5.4 million people age ≥ 65 years who received either the Pfizer-BioNTech COVID-19 bivalent vaccine or the Moderna bivalent vaccine, or the Pfizer vaccine and a high-dose or adjuvanted concomitant influenza vaccine (ie, administered on the same day).
- A total of 11,001 of the cohort experienced a stroke in the first 90 days after vaccination.
- The main outcome was stroke risk (nonhemorrhagic stroke, transient ischemic attack [TIA], or hemorrhagic stroke) during the 1- to 21-day or 22- to 42-day window after vaccination vs the 43- to 90-day control window.
- The mean age of participants was 74 years, and 56% were female.
TAKEAWAY:
- There was no statistically significant association with either brand of the COVID-19 bivalent vaccine or any of the stroke outcomes during the 1- to 21-day or 22- to 42-day risk window compared with the 43- to 90-day control window (incidence rate ratio [IRR] range, 0.72-1.12).
- Vaccination with COVID-19 bivalent vaccine plus a high-dose or adjuvanted influenza vaccine (n = 4596) was associated with a significantly greater risk for nonhemorrhagic stroke 22-42 days after vaccination with Pfizer-BioNTech (IRR, 1.20; risk difference/100,000 doses, 3.13) and an increase in TIA risk 1-21 days after vaccination with Moderna (IRR, 1.35; risk difference/100,000 doses, 3.33).
- There was a significant association between vaccination with a high-dose or adjuvanted influenza vaccine (n = 21,345) and nonhemorrhagic stroke 22-42 days after vaccination (IRR, 1.09; risk difference/100,000 doses, 1.65).
IN PRACTICE:
“The clinical significance of the risk of stroke after vaccination must be carefully considered together with the significant benefits of receiving an influenza vaccination,” the authors wrote. “Because the framework of the current self-controlled case series study does not compare the populations who were vaccinated vs those who were unvaccinated, it does not account for the reduced rate of severe influenza after vaccination. More studies are needed to better understand the association between high-dose or adjuvanted influenza vaccination and stroke.”
SOURCE:
Yun Lu, PhD, of the Center for Biologics Evaluation and Research, US Food and Drug Administration, Silver Spring, Maryland, was the lead and corresponding author of the study. It was published online on March 19 in JAMA.
LIMITATIONS:
Some stroke cases may have been missed or misclassified. The study included only vaccinated individuals — a population considered to have health-seeking behaviors — which may limit the generalizability of the findings. The study was conducted using COVID-19 bivalent vaccines, which are no longer available.
DISCLOSURES:
This work was funded by the US Food and Drug Administration through an interagency agreement with the Centers for Medicare & Medicaid Services. Dr. Lu reported no relevant financial relationships. The other authors’ disclosures are listed in the original paper.
A version of this article appeared on Medscape.com.
Could Regular, Daytime Naps Increase Glucose Levels?
TOPLINE:
Long naps of an hour or more, naps in the morning, or regular siestas may increase blood glucose levels in older people with type 2 diabetes (T2D).
METHODOLOGY:
- Napping is common in China and other cultures and may play a role in cardiometabolic health, but previous studies on the relationship between napping and glycemic control in T2D have reported conflicting results.
- In a cross-sectional study, the researchers assessed 226 individuals with T2D (median age, 67 years; about half women; mostly retired) from two community healthcare centers in China between May 2023 and July 2023.
- Using questionnaires, the participants were evaluated for A1c levels, as well as frequency, duration (shorter or longer than 1 hour), timing, and type of napping behavior (restorative for lack of sleep vs appetitive by habit or for enjoyment).
- Multivariate analysis controlled for age, sex, body mass index, T2D treatment regimen, diabetes duration, cognitive impairment, depression, night sleep duration, and insomnia symptoms.
TAKEAWAY:
- Among 180 participants who reported napping, 61 (33.9%) took long naps of 60 minutes and more, 162 (90%) reported afternoon napping, and 131 (72.8%) displayed appetitive napping.
- Restorative napping was linked to lower A1c levels than appetitive napping (β, −0.176; P = 0.028).
- Napping frequency was not associated with A1c levels.
IN PRACTICE:
“In clinical practice, healthcare professionals may offer tips about napping, eg, taking a nap less than an hour, taking a nap in the afternoon instead of in the morning, avoiding appetitive napping,” the authors concluded.
SOURCE:
The study, from corresponding author Bingqian Zhu, PhD, of the Shanghai Jiao Tong University School of Nursing, Shanghai, was published in Frontiers in Endocrinology.
LIMITATIONS:
The participants were older individuals, mostly retired, who may have had less need for restorative napping and more time for appetitive napping, limiting generalizability. The sample size may have been too small to find a link to napping frequency. Self-reported data could introduce recall bias. Only A1c levels were used as a measure of glycemic control.
DISCLOSURES:
The study was supported by the National Natural Science Foundation of China and other sources. The authors declared no potential conflict of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Long naps of an hour or more, naps in the morning, or regular siestas may increase blood glucose levels in older people with type 2 diabetes (T2D).
METHODOLOGY:
- Napping is common in China and other cultures and may play a role in cardiometabolic health, but previous studies on the relationship between napping and glycemic control in T2D have reported conflicting results.
- In a cross-sectional study, the researchers assessed 226 individuals with T2D (median age, 67 years; about half women; mostly retired) from two community healthcare centers in China between May 2023 and July 2023.
- Using questionnaires, the participants were evaluated for A1c levels, as well as frequency, duration (shorter or longer than 1 hour), timing, and type of napping behavior (restorative for lack of sleep vs appetitive by habit or for enjoyment).
- Multivariate analysis controlled for age, sex, body mass index, T2D treatment regimen, diabetes duration, cognitive impairment, depression, night sleep duration, and insomnia symptoms.
TAKEAWAY:
- Among 180 participants who reported napping, 61 (33.9%) took long naps of 60 minutes and more, 162 (90%) reported afternoon napping, and 131 (72.8%) displayed appetitive napping.
- Restorative napping was linked to lower A1c levels than appetitive napping (β, −0.176; P = 0.028).
- Napping frequency was not associated with A1c levels.
IN PRACTICE:
“In clinical practice, healthcare professionals may offer tips about napping, eg, taking a nap less than an hour, taking a nap in the afternoon instead of in the morning, avoiding appetitive napping,” the authors concluded.
SOURCE:
The study, from corresponding author Bingqian Zhu, PhD, of the Shanghai Jiao Tong University School of Nursing, Shanghai, was published in Frontiers in Endocrinology.
LIMITATIONS:
The participants were older individuals, mostly retired, who may have had less need for restorative napping and more time for appetitive napping, limiting generalizability. The sample size may have been too small to find a link to napping frequency. Self-reported data could introduce recall bias. Only A1c levels were used as a measure of glycemic control.
DISCLOSURES:
The study was supported by the National Natural Science Foundation of China and other sources. The authors declared no potential conflict of interest.
A version of this article appeared on Medscape.com.
TOPLINE:
Long naps of an hour or more, naps in the morning, or regular siestas may increase blood glucose levels in older people with type 2 diabetes (T2D).
METHODOLOGY:
- Napping is common in China and other cultures and may play a role in cardiometabolic health, but previous studies on the relationship between napping and glycemic control in T2D have reported conflicting results.
- In a cross-sectional study, the researchers assessed 226 individuals with T2D (median age, 67 years; about half women; mostly retired) from two community healthcare centers in China between May 2023 and July 2023.
- Using questionnaires, the participants were evaluated for A1c levels, as well as frequency, duration (shorter or longer than 1 hour), timing, and type of napping behavior (restorative for lack of sleep vs appetitive by habit or for enjoyment).
- Multivariate analysis controlled for age, sex, body mass index, T2D treatment regimen, diabetes duration, cognitive impairment, depression, night sleep duration, and insomnia symptoms.
TAKEAWAY:
- Among 180 participants who reported napping, 61 (33.9%) took long naps of 60 minutes and more, 162 (90%) reported afternoon napping, and 131 (72.8%) displayed appetitive napping.
- Restorative napping was linked to lower A1c levels than appetitive napping (β, −0.176; P = 0.028).
- Napping frequency was not associated with A1c levels.
IN PRACTICE:
“In clinical practice, healthcare professionals may offer tips about napping, eg, taking a nap less than an hour, taking a nap in the afternoon instead of in the morning, avoiding appetitive napping,” the authors concluded.
SOURCE:
The study, from corresponding author Bingqian Zhu, PhD, of the Shanghai Jiao Tong University School of Nursing, Shanghai, was published in Frontiers in Endocrinology.
LIMITATIONS:
The participants were older individuals, mostly retired, who may have had less need for restorative napping and more time for appetitive napping, limiting generalizability. The sample size may have been too small to find a link to napping frequency. Self-reported data could introduce recall bias. Only A1c levels were used as a measure of glycemic control.
DISCLOSURES:
The study was supported by the National Natural Science Foundation of China and other sources. The authors declared no potential conflict of interest.
A version of this article appeared on Medscape.com.
Ultrasound and Its Role In Diagnosing and Managing Endometriosis
Introduction: Imaging for Endometriosis — A Necessary Prerequisite
While the gold standard in the diagnosis of endometriosis remains laparoscopy, it is now recognized that thorough evaluation via ultrasound offers an acceptable, less expensive, and less invasive alternative. It is especially useful for the diagnosis of deep infiltrative disease, which penetrates more than 5 mm into the peritoneum, ovarian endometrioma, and when anatomic distortion occurs, such as to the path of the ureter.
Besides establishing the diagnosis, ultrasound imaging has become, along with MRI, the most important aid for proper preoperative planning. Not only does imaging provide the surgeon and patient with knowledge regarding the extent of the upcoming procedure, but it also allows the minimally invasive gynecologic (MIG) surgeon to involve colleagues, such as colorectal surgeons or urologists. For example, deep infiltrative endometriosis penetrating into the bowel mucosa will require a discoid or segmental bowel resection.

While many endometriosis experts rely on MRI, many MIG surgeons are dependent on ultrasound. I would not consider taking a patient with signs and symptoms suggestive of endometriosis to surgery without 2D/3D transvaginal ultrasound. If the patient possesses a uterus, a saline-infused sonogram is performed to potentially diagnose adenomyosis.
It is a pleasure and honor to welcome Professor Caterina Exacoustos MD, PhD, associate professor of ob.gyn. at the University of Rome “Tor Vergata,” to this edition of the Master Class in Gynecologic Surgery to discuss “Ultrasound and Its Role in the Diagnosis of and Management of Endometriosis, Including DIE.”
Prof. Exacoustos’ main areas of interest are endometriosis and benign diseases including uterine pathology and infertility. Her extensive body of work comprises over 120 scientific publications and numerous book chapters both in English and in Italian.
Prof. Exacoustos continues to be one of the most well respected lecturers speaking about ultrasound throughout the world.
Dr. Miller is professor of obstetrics and gynecology, department of clinical sciences, Rosalind Franklin University of Medicine and Science, North Chicago. Dr. Miller has no conflicts of interest to report.
Ultrasound and Its Role In Diagnosing and Managing Endometriosis
Endometriosis affects approximately 10%-20% of premenopausal women worldwide. It is the leading cause of chronic pelvic pain, is often associated with infertility, and has a significant impact on quality of life. Although the natural history of endometriosis remains unknown, emerging evidence suggests that the pathophysiological steps of initiation and development of endometriosis must occur earlier in the lifespan. Most notably, the onset of endometriosis-associated pain symptoms is often reported during adolescence and young adulthood.1
While many patients with endometriosis are referred with dysmenorrhea at a young age, at age ≤ 25 years,2 symptoms are often highly underestimated and considered to be normal and transient.3,4 Clinical and pelvic exams are often negative in young women, and delays in endometriosis diagnosis are well known.
The presentation of primary dysmenorrhea with no anatomical cause embodies the paradigm that dysmenorrhea in adolescents is most often an insignificant disorder. This perspective is probably a root cause of delayed endometriosis diagnosis in young patients. However, another issue behind delayed diagnosis is the reluctance of the physician to perform a diagnostic laparoscopy — historically the gold standard for diagnosing endometriosis — for seemingly common symptoms such as dysmenorrhea in young patients.
Today we know that there are typical aspects of ultrasound imaging that identify endometriosis in the pelvis, and notably, the 2022 European Society for Human Reproduction and Embryology (ESHRE) endometriosis guideline5 recognizes imaging (ultrasound or MRI) as the standard for endometriosis diagnosis without requiring laparoscopic or histological confirmation.
An early and noninvasive method of diagnosis aids in timely diagnosis and provides for the timely initiation of medical management to improve quality of life and prevent progression of disease (Figure 1).
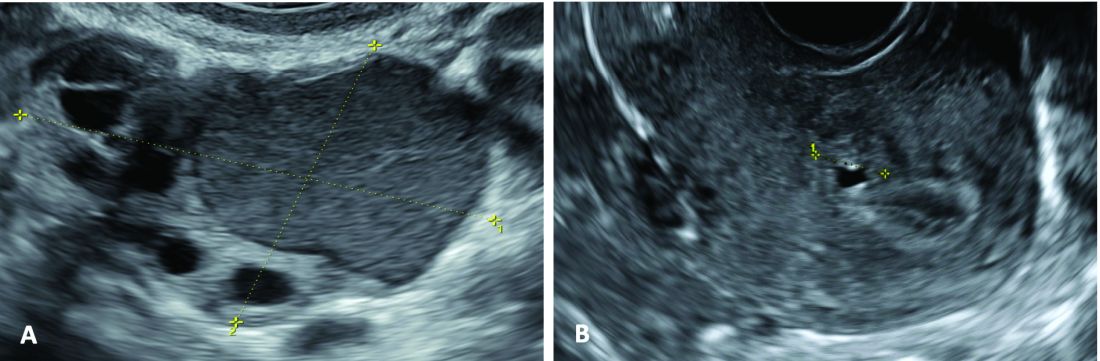
(A. Transvaginal ultrasound appearance of a small ovarian endometrioma in a 16-year-old girl. Note the unilocular cyst with ground glass echogenicity surrounded by multifollicular ovarian tissue. B. Ultrasound image of a retroverted uterus of an 18-year-old girl with focal adenomyosis of the posterior wall. Note the round cystic anechoic areas in the inner myometrium or junctional zone. The small intra-myometrial cyst is surrounded by a hyperechoic ring).
Indeed, the typical appearance of endometriotic pelvic lesions on transvaginal sonography, such as endometriomas and rectal deep infiltrating endometriosis (DIE) — as well as adenomyosis – can be medically treated without histologic confirmation .
When surgery is advisable, ultrasound findings also play a valuable role in presurgical staging, planning, and counseling for patients of all ages. Determining the extent and location of DIE preoperatively, for instance, facilitates the engagement of the appropriate surgical specialists so that multiple surgeries can be avoided. It also enables patients to be optimally informed before surgery of possible outcomes and complications.
Moreover, in the context of infertility, ultrasound can be a valuable tool for understanding uterine pathology and assessing for adenomyosis so that affected patients may be treated surgically or medically before turning to assisted reproductive technology.
Uniformity, Standardization in the Sonographic Assessment
In Europe, as in the United States, transvaginal sonography (TVS) is the first-line imaging tool for the diagnosis and management of endometriosis. In Europe, many ob.gyns. perform ultrasound themselves, as do treating surgeons. When diagnostic findings are negative but clinical suspicion is high, MRI is often utilized. Laparoscopy may then be considered in patients with negative imaging results.
Efforts to standardize terms, definitions, measurements, and sonographic features of different types of endometriosis have been made to make it easier for physicians to share data and communicate with each other. A lack of uniformity has contributed to variability in the reported diagnostic accuracy of TVS.
About 10 years ago, in one such effort, we assessed the accuracy of TVS for DIE by comparing TVS results with laparoscopic/histologic findings, and developed an ultrasound mapping system to accurately record the location, size and depth of lesions visualized by TVS. The accuracy of TVS ranged from 76% for the diagnosis of vaginal endometriosis to 97% for the diagnosis of bladder lesions and posterior cul-de-sac obliteration. Accuracy was 93% and 91% for detecting ureteral involvement (right and left); 87% for uterosacral ligament endometriotic lesions; and 87% for parametrial involvement.6
Shortly after, with a focus on DIE, expert sonographers and physician-sonographers from across Europe — as well as some experts from Australia, Japan, Brazil, Chile, and the United States (Y. Osuga from Brigham and Women’s Hospital and Harvard Medical School) — came together to agree on a uniform approach to the sonographic evaluation for suspected endometriosis and a standardization of terminology.
The consensus opinion from the International Deep Endometriosis Analysis (IDEA) group details four steps for examining women with suspected DIE: 1) Evaluation of the uterus and adnexa, 2) evaluation of transvaginal sonographic “soft markers” (ie. site-specific tenderness and ovarian mobility), 3) assessment of the status of the posterior cul-de-sac using real-time ultrasound-based “sliding sign,” and 4) assessment for DIE nodules in the anterior and posterior compartments.7
Our paper describing a mapping system and the IDEA paper describe how to detect deep endometriosis in the pelvis by utilizing an ultrasound view of normal anatomy and pelvic organ structure to provide landmarks for accurately defining the site of DIE lesions (Figure 2).
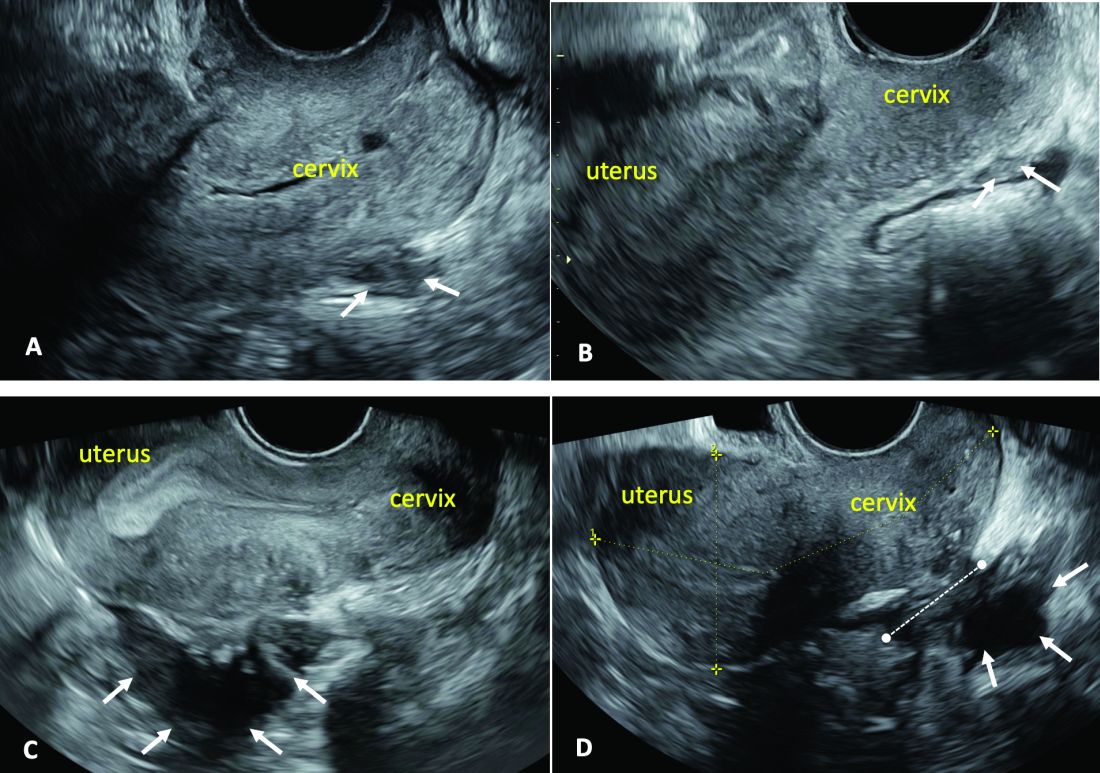
(A. Ultrasound appearance of a small DIE lesion of the retrocervical area [white arrows], which involved the torus uterinum and the right uterosacral ligament [USL]. The lesion appears as hypoechoic tissue with irregular margins caused by the fibrosis induced by the DIE. B. TVS appearance of small nodules of DIE of the left USL. Note the small retrocervical DIE lesion [white arrows], which appears hypoechoic due to the infiltration of the hyperechoic USL. C) Ultrasound appearance of a DIE nodule of the recto-sigmoid wall. Note the hypoechoic thickening of the muscular layers of the bowel wall attached to the corpus of the uterus and the adenomyosis of the posterior wall. The retrocervical area is free. D. TVS appearance of nodules of DIE of the lower rectal wall. Note the hypoechoic lesion [white arrows] of the rectum is attached to a retrocervical DIE fibrosis of the torus and USL [white dotted line]).
So-called rectovaginal endometriosis can be well assessed, for instance, since the involvement of the rectum, sigmoid colon, vaginal wall, rectovaginal septum, and posterior cul-de-sac uterosacral ligament can be seen by ultrasound as a single structure, making the location, size, and depth of any lesions discernible.
Again, this evaluation of the extent of disease is important for presurgical assessment so the surgeon can organize the right team and time of surgery and so the patient can be counseled on the advantages and possible complications of the treatment.
Notably, an accurate ultrasound description of pelvic endometriosis is helpful for accurate classification of disease. Endometriosis classification systems such as that of the American Association of Gynecologic Laparoscopists (AAGL)8 and the American Society of Reproductive Medicine (ASRM),9 as well as the #Enzian surgical description system,10 have been adapted to cover findings from ultrasound as well as MRI imaging.
A Systematic Evaluation
In keeping with the IDEA consensus opinion and based on our years of experience at the University of Rome, I advise that patients with typical pain symptoms of endometriosis or infertility undergo an accurate sonographic assessment of the pelvis with particular evaluation not only of the uterus and ovaries but of all pelvic retroperitoneal spaces.
The TVS examination should start with a slightly filled bladder, which permits a better evaluation of the bladder walls and the presence of endometriotic nodules. These nodules appear as hyperechoic linear or spherical lesions bulging toward the lumen and involving the serosa, muscularis, or (sub)mucosa of the bladder.
Then, an accurate evaluation of the uterus in 2D and 3D permits the diagnosis of adenomyosis. 3D sonographic evaluation of the myometrium and of the junctional zone are important; alteration and infiltration of the junctional zone and the presence of small adenomyotic cysts in the inner or outer myometrium are direct, specific signs of adenomyosis and should be ruled out in patients with dysmenorrhea, heavy menstrual bleeding, infertility, and pregnancy complications.
Endometriomas of the ovaries can be easily detected as having the typical appearance of a cyst with ground glass content. Adhesions of the ovaries and the uterus also should be evaluated with a dynamic ultrasound approach that utilizes the sliding sign and mobilization by palpation of the organs during the TVS scan.
Finally, the posterior and lateral retroperitoneal compartments should be carefully evaluated, with symptoms guiding the TVS examination whenever possible. Deep endometriotic nodules of the rectum appear as hypoechoic lesions or linear or nodular retroperitoneal thickening with irregular borders, penetrating into the intestinal wall and distorting its normal structure. In young patients, it seems very important to assess for small lesions below the peritoneum between the vagina and rectum, and in the parametria and around the ureter and nerves — lesions that, notably, would not be seen by diagnostic laparoscopy.
The Evaluation of Young Patients
In adolescent and young patients, endometriosis and adenomyosis are often present with small lesions and shallow tissue invasion, making a very careful and experienced approach to ultrasound essential for detection. Endometriomas are often of small diameter, and DIE is not always easily diagnosed because retroperitoneal lesions are similarly very small.
In a series of 270 adolescents (ages 12-20) who were referred to our outpatient gynecologic ultrasound unit over a 5-year period for various indications, at least one ultrasound feature of endometriosis was observed in 13.3%. In those with dysmenorrhea, the detection of endometriosis increased to 21%. Endometrioma was the most common type of endometriosis we found in the study, but DIE and adenomyosis were found in 4%-11%.
Although endometriotic lesions typically are small in young patients, they are often associated with severe pain symptoms, including chronic pelvic pain, dysmenorrhea, dyspareunia, dysuria, and dyschezia, all of which can have a serious effect on the quality of life of these young women. These symptoms keep them away from school during menstruation, away from sports, and cause painful intercourse and infertility. In young patients, an accurate TVS can provide a lot of information, and the ability to detect retroperitoneal endometriotic lesions and adenomyosis is probably better than with purely diagnostic laparoscopy, which would evaluate only superficial lesions.
TVS or, when needed, transrectal ultrasound, can enable adequate treatment and follow-up of the disease and its symptoms. There are no guidelines recommending adequate follow-up times to evaluate the effectiveness of medical therapy in patients with ultrasound signs of endometriosis. (Likewise, there are no indications for follow-up in patients with severe dysmenorrhea without ultrasound signs of endometriosis.) Certainly, our studies suggest careful evaluation over time of young patients with severe dysmenorrhea by serial ultrasound scans. With such follow-up, disease progress can be monitored and the medical or surgical treatment approach modified if needed.
The diagnosis of endometriosis at a young age has significant benefits not only in avoiding or reducing progression of the disease, but also in improving quality of life and aiding women in their desire for pregnancy.
Dr. Exacoustos is associate professor of ob.gyn. at the University of Rome “Tor Vergata.” She has no conflicts of interest to report.
References
1. Zondervan KT et al. N Engl J Med. 2020;382:1244-56.
2. Greene R et al. Fertil Steril. 2009;91:32-9.
3. Chapron C et al. J Pediatr Adolesc Gynecol. 2011;24:S7-12.
4. Randhawa AE et al. J Pediatr Adolesc Gynecol. 2021;34:643-8.
5. Becker CM et al. Hum Reprod Open. 2022(2):hoac009.
6. Exacoustos C et al. Fertil Steril. 2014;102:143-9. 7. Guerriero S et al. Ultrasound Obstet Gynecol. 2016;48(3):318-32.
8. Abrao MS et al. J Minim Invasive Gynecol. 2021;28:1941-50.9. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997;67:817-21. 10. Keckstein J et al. Acta Obstet Gynecol Scand. 2021;100:1165-75.
11. Martire FG et al. Fertil Steril. 2020;114(5):1049-57.
Introduction: Imaging for Endometriosis — A Necessary Prerequisite
While the gold standard in the diagnosis of endometriosis remains laparoscopy, it is now recognized that thorough evaluation via ultrasound offers an acceptable, less expensive, and less invasive alternative. It is especially useful for the diagnosis of deep infiltrative disease, which penetrates more than 5 mm into the peritoneum, ovarian endometrioma, and when anatomic distortion occurs, such as to the path of the ureter.
Besides establishing the diagnosis, ultrasound imaging has become, along with MRI, the most important aid for proper preoperative planning. Not only does imaging provide the surgeon and patient with knowledge regarding the extent of the upcoming procedure, but it also allows the minimally invasive gynecologic (MIG) surgeon to involve colleagues, such as colorectal surgeons or urologists. For example, deep infiltrative endometriosis penetrating into the bowel mucosa will require a discoid or segmental bowel resection.
While many endometriosis experts rely on MRI, many MIG surgeons are dependent on ultrasound. I would not consider taking a patient with signs and symptoms suggestive of endometriosis to surgery without 2D/3D transvaginal ultrasound. If the patient possesses a uterus, a saline-infused sonogram is performed to potentially diagnose adenomyosis.
It is a pleasure and honor to welcome Professor Caterina Exacoustos MD, PhD, associate professor of ob.gyn. at the University of Rome “Tor Vergata,” to this edition of the Master Class in Gynecologic Surgery to discuss “Ultrasound and Its Role in the Diagnosis of and Management of Endometriosis, Including DIE.”
Prof. Exacoustos’ main areas of interest are endometriosis and benign diseases including uterine pathology and infertility. Her extensive body of work comprises over 120 scientific publications and numerous book chapters both in English and in Italian.
Prof. Exacoustos continues to be one of the most well respected lecturers speaking about ultrasound throughout the world.
Dr. Miller is professor of obstetrics and gynecology, department of clinical sciences, Rosalind Franklin University of Medicine and Science, North Chicago. Dr. Miller has no conflicts of interest to report.
Ultrasound and Its Role In Diagnosing and Managing Endometriosis
Endometriosis affects approximately 10%-20% of premenopausal women worldwide. It is the leading cause of chronic pelvic pain, is often associated with infertility, and has a significant impact on quality of life. Although the natural history of endometriosis remains unknown, emerging evidence suggests that the pathophysiological steps of initiation and development of endometriosis must occur earlier in the lifespan. Most notably, the onset of endometriosis-associated pain symptoms is often reported during adolescence and young adulthood.1
While many patients with endometriosis are referred with dysmenorrhea at a young age, at age ≤ 25 years,2 symptoms are often highly underestimated and considered to be normal and transient.3,4 Clinical and pelvic exams are often negative in young women, and delays in endometriosis diagnosis are well known.
The presentation of primary dysmenorrhea with no anatomical cause embodies the paradigm that dysmenorrhea in adolescents is most often an insignificant disorder. This perspective is probably a root cause of delayed endometriosis diagnosis in young patients. However, another issue behind delayed diagnosis is the reluctance of the physician to perform a diagnostic laparoscopy — historically the gold standard for diagnosing endometriosis — for seemingly common symptoms such as dysmenorrhea in young patients.
Today we know that there are typical aspects of ultrasound imaging that identify endometriosis in the pelvis, and notably, the 2022 European Society for Human Reproduction and Embryology (ESHRE) endometriosis guideline5 recognizes imaging (ultrasound or MRI) as the standard for endometriosis diagnosis without requiring laparoscopic or histological confirmation.
An early and noninvasive method of diagnosis aids in timely diagnosis and provides for the timely initiation of medical management to improve quality of life and prevent progression of disease (Figure 1).
(A. Transvaginal ultrasound appearance of a small ovarian endometrioma in a 16-year-old girl. Note the unilocular cyst with ground glass echogenicity surrounded by multifollicular ovarian tissue. B. Ultrasound image of a retroverted uterus of an 18-year-old girl with focal adenomyosis of the posterior wall. Note the round cystic anechoic areas in the inner myometrium or junctional zone. The small intra-myometrial cyst is surrounded by a hyperechoic ring).
Indeed, the typical appearance of endometriotic pelvic lesions on transvaginal sonography, such as endometriomas and rectal deep infiltrating endometriosis (DIE) — as well as adenomyosis – can be medically treated without histologic confirmation .
When surgery is advisable, ultrasound findings also play a valuable role in presurgical staging, planning, and counseling for patients of all ages. Determining the extent and location of DIE preoperatively, for instance, facilitates the engagement of the appropriate surgical specialists so that multiple surgeries can be avoided. It also enables patients to be optimally informed before surgery of possible outcomes and complications.
Moreover, in the context of infertility, ultrasound can be a valuable tool for understanding uterine pathology and assessing for adenomyosis so that affected patients may be treated surgically or medically before turning to assisted reproductive technology.
Uniformity, Standardization in the Sonographic Assessment
In Europe, as in the United States, transvaginal sonography (TVS) is the first-line imaging tool for the diagnosis and management of endometriosis. In Europe, many ob.gyns. perform ultrasound themselves, as do treating surgeons. When diagnostic findings are negative but clinical suspicion is high, MRI is often utilized. Laparoscopy may then be considered in patients with negative imaging results.
Efforts to standardize terms, definitions, measurements, and sonographic features of different types of endometriosis have been made to make it easier for physicians to share data and communicate with each other. A lack of uniformity has contributed to variability in the reported diagnostic accuracy of TVS.
About 10 years ago, in one such effort, we assessed the accuracy of TVS for DIE by comparing TVS results with laparoscopic/histologic findings, and developed an ultrasound mapping system to accurately record the location, size and depth of lesions visualized by TVS. The accuracy of TVS ranged from 76% for the diagnosis of vaginal endometriosis to 97% for the diagnosis of bladder lesions and posterior cul-de-sac obliteration. Accuracy was 93% and 91% for detecting ureteral involvement (right and left); 87% for uterosacral ligament endometriotic lesions; and 87% for parametrial involvement.6
Shortly after, with a focus on DIE, expert sonographers and physician-sonographers from across Europe — as well as some experts from Australia, Japan, Brazil, Chile, and the United States (Y. Osuga from Brigham and Women’s Hospital and Harvard Medical School) — came together to agree on a uniform approach to the sonographic evaluation for suspected endometriosis and a standardization of terminology.
The consensus opinion from the International Deep Endometriosis Analysis (IDEA) group details four steps for examining women with suspected DIE: 1) Evaluation of the uterus and adnexa, 2) evaluation of transvaginal sonographic “soft markers” (ie. site-specific tenderness and ovarian mobility), 3) assessment of the status of the posterior cul-de-sac using real-time ultrasound-based “sliding sign,” and 4) assessment for DIE nodules in the anterior and posterior compartments.7
Our paper describing a mapping system and the IDEA paper describe how to detect deep endometriosis in the pelvis by utilizing an ultrasound view of normal anatomy and pelvic organ structure to provide landmarks for accurately defining the site of DIE lesions (Figure 2).
(A. Ultrasound appearance of a small DIE lesion of the retrocervical area [white arrows], which involved the torus uterinum and the right uterosacral ligament [USL]. The lesion appears as hypoechoic tissue with irregular margins caused by the fibrosis induced by the DIE. B. TVS appearance of small nodules of DIE of the left USL. Note the small retrocervical DIE lesion [white arrows], which appears hypoechoic due to the infiltration of the hyperechoic USL. C) Ultrasound appearance of a DIE nodule of the recto-sigmoid wall. Note the hypoechoic thickening of the muscular layers of the bowel wall attached to the corpus of the uterus and the adenomyosis of the posterior wall. The retrocervical area is free. D. TVS appearance of nodules of DIE of the lower rectal wall. Note the hypoechoic lesion [white arrows] of the rectum is attached to a retrocervical DIE fibrosis of the torus and USL [white dotted line]).
So-called rectovaginal endometriosis can be well assessed, for instance, since the involvement of the rectum, sigmoid colon, vaginal wall, rectovaginal septum, and posterior cul-de-sac uterosacral ligament can be seen by ultrasound as a single structure, making the location, size, and depth of any lesions discernible.
Again, this evaluation of the extent of disease is important for presurgical assessment so the surgeon can organize the right team and time of surgery and so the patient can be counseled on the advantages and possible complications of the treatment.
Notably, an accurate ultrasound description of pelvic endometriosis is helpful for accurate classification of disease. Endometriosis classification systems such as that of the American Association of Gynecologic Laparoscopists (AAGL)8 and the American Society of Reproductive Medicine (ASRM),9 as well as the #Enzian surgical description system,10 have been adapted to cover findings from ultrasound as well as MRI imaging.
A Systematic Evaluation
In keeping with the IDEA consensus opinion and based on our years of experience at the University of Rome, I advise that patients with typical pain symptoms of endometriosis or infertility undergo an accurate sonographic assessment of the pelvis with particular evaluation not only of the uterus and ovaries but of all pelvic retroperitoneal spaces.
The TVS examination should start with a slightly filled bladder, which permits a better evaluation of the bladder walls and the presence of endometriotic nodules. These nodules appear as hyperechoic linear or spherical lesions bulging toward the lumen and involving the serosa, muscularis, or (sub)mucosa of the bladder.
Then, an accurate evaluation of the uterus in 2D and 3D permits the diagnosis of adenomyosis. 3D sonographic evaluation of the myometrium and of the junctional zone are important; alteration and infiltration of the junctional zone and the presence of small adenomyotic cysts in the inner or outer myometrium are direct, specific signs of adenomyosis and should be ruled out in patients with dysmenorrhea, heavy menstrual bleeding, infertility, and pregnancy complications.
Endometriomas of the ovaries can be easily detected as having the typical appearance of a cyst with ground glass content. Adhesions of the ovaries and the uterus also should be evaluated with a dynamic ultrasound approach that utilizes the sliding sign and mobilization by palpation of the organs during the TVS scan.
Finally, the posterior and lateral retroperitoneal compartments should be carefully evaluated, with symptoms guiding the TVS examination whenever possible. Deep endometriotic nodules of the rectum appear as hypoechoic lesions or linear or nodular retroperitoneal thickening with irregular borders, penetrating into the intestinal wall and distorting its normal structure. In young patients, it seems very important to assess for small lesions below the peritoneum between the vagina and rectum, and in the parametria and around the ureter and nerves — lesions that, notably, would not be seen by diagnostic laparoscopy.
The Evaluation of Young Patients
In adolescent and young patients, endometriosis and adenomyosis are often present with small lesions and shallow tissue invasion, making a very careful and experienced approach to ultrasound essential for detection. Endometriomas are often of small diameter, and DIE is not always easily diagnosed because retroperitoneal lesions are similarly very small.
In a series of 270 adolescents (ages 12-20) who were referred to our outpatient gynecologic ultrasound unit over a 5-year period for various indications, at least one ultrasound feature of endometriosis was observed in 13.3%. In those with dysmenorrhea, the detection of endometriosis increased to 21%. Endometrioma was the most common type of endometriosis we found in the study, but DIE and adenomyosis were found in 4%-11%.
Although endometriotic lesions typically are small in young patients, they are often associated with severe pain symptoms, including chronic pelvic pain, dysmenorrhea, dyspareunia, dysuria, and dyschezia, all of which can have a serious effect on the quality of life of these young women. These symptoms keep them away from school during menstruation, away from sports, and cause painful intercourse and infertility. In young patients, an accurate TVS can provide a lot of information, and the ability to detect retroperitoneal endometriotic lesions and adenomyosis is probably better than with purely diagnostic laparoscopy, which would evaluate only superficial lesions.
TVS or, when needed, transrectal ultrasound, can enable adequate treatment and follow-up of the disease and its symptoms. There are no guidelines recommending adequate follow-up times to evaluate the effectiveness of medical therapy in patients with ultrasound signs of endometriosis. (Likewise, there are no indications for follow-up in patients with severe dysmenorrhea without ultrasound signs of endometriosis.) Certainly, our studies suggest careful evaluation over time of young patients with severe dysmenorrhea by serial ultrasound scans. With such follow-up, disease progress can be monitored and the medical or surgical treatment approach modified if needed.
The diagnosis of endometriosis at a young age has significant benefits not only in avoiding or reducing progression of the disease, but also in improving quality of life and aiding women in their desire for pregnancy.
Dr. Exacoustos is associate professor of ob.gyn. at the University of Rome “Tor Vergata.” She has no conflicts of interest to report.
References
1. Zondervan KT et al. N Engl J Med. 2020;382:1244-56.
2. Greene R et al. Fertil Steril. 2009;91:32-9.
3. Chapron C et al. J Pediatr Adolesc Gynecol. 2011;24:S7-12.
4. Randhawa AE et al. J Pediatr Adolesc Gynecol. 2021;34:643-8.
5. Becker CM et al. Hum Reprod Open. 2022(2):hoac009.
6. Exacoustos C et al. Fertil Steril. 2014;102:143-9. 7. Guerriero S et al. Ultrasound Obstet Gynecol. 2016;48(3):318-32.
8. Abrao MS et al. J Minim Invasive Gynecol. 2021;28:1941-50.9. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997;67:817-21. 10. Keckstein J et al. Acta Obstet Gynecol Scand. 2021;100:1165-75.
11. Martire FG et al. Fertil Steril. 2020;114(5):1049-57.
Introduction: Imaging for Endometriosis — A Necessary Prerequisite
While the gold standard in the diagnosis of endometriosis remains laparoscopy, it is now recognized that thorough evaluation via ultrasound offers an acceptable, less expensive, and less invasive alternative. It is especially useful for the diagnosis of deep infiltrative disease, which penetrates more than 5 mm into the peritoneum, ovarian endometrioma, and when anatomic distortion occurs, such as to the path of the ureter.
Besides establishing the diagnosis, ultrasound imaging has become, along with MRI, the most important aid for proper preoperative planning. Not only does imaging provide the surgeon and patient with knowledge regarding the extent of the upcoming procedure, but it also allows the minimally invasive gynecologic (MIG) surgeon to involve colleagues, such as colorectal surgeons or urologists. For example, deep infiltrative endometriosis penetrating into the bowel mucosa will require a discoid or segmental bowel resection.
While many endometriosis experts rely on MRI, many MIG surgeons are dependent on ultrasound. I would not consider taking a patient with signs and symptoms suggestive of endometriosis to surgery without 2D/3D transvaginal ultrasound. If the patient possesses a uterus, a saline-infused sonogram is performed to potentially diagnose adenomyosis.
It is a pleasure and honor to welcome Professor Caterina Exacoustos MD, PhD, associate professor of ob.gyn. at the University of Rome “Tor Vergata,” to this edition of the Master Class in Gynecologic Surgery to discuss “Ultrasound and Its Role in the Diagnosis of and Management of Endometriosis, Including DIE.”
Prof. Exacoustos’ main areas of interest are endometriosis and benign diseases including uterine pathology and infertility. Her extensive body of work comprises over 120 scientific publications and numerous book chapters both in English and in Italian.
Prof. Exacoustos continues to be one of the most well respected lecturers speaking about ultrasound throughout the world.
Dr. Miller is professor of obstetrics and gynecology, department of clinical sciences, Rosalind Franklin University of Medicine and Science, North Chicago. Dr. Miller has no conflicts of interest to report.
Ultrasound and Its Role In Diagnosing and Managing Endometriosis
Endometriosis affects approximately 10%-20% of premenopausal women worldwide. It is the leading cause of chronic pelvic pain, is often associated with infertility, and has a significant impact on quality of life. Although the natural history of endometriosis remains unknown, emerging evidence suggests that the pathophysiological steps of initiation and development of endometriosis must occur earlier in the lifespan. Most notably, the onset of endometriosis-associated pain symptoms is often reported during adolescence and young adulthood.1
While many patients with endometriosis are referred with dysmenorrhea at a young age, at age ≤ 25 years,2 symptoms are often highly underestimated and considered to be normal and transient.3,4 Clinical and pelvic exams are often negative in young women, and delays in endometriosis diagnosis are well known.
The presentation of primary dysmenorrhea with no anatomical cause embodies the paradigm that dysmenorrhea in adolescents is most often an insignificant disorder. This perspective is probably a root cause of delayed endometriosis diagnosis in young patients. However, another issue behind delayed diagnosis is the reluctance of the physician to perform a diagnostic laparoscopy — historically the gold standard for diagnosing endometriosis — for seemingly common symptoms such as dysmenorrhea in young patients.
Today we know that there are typical aspects of ultrasound imaging that identify endometriosis in the pelvis, and notably, the 2022 European Society for Human Reproduction and Embryology (ESHRE) endometriosis guideline5 recognizes imaging (ultrasound or MRI) as the standard for endometriosis diagnosis without requiring laparoscopic or histological confirmation.
An early and noninvasive method of diagnosis aids in timely diagnosis and provides for the timely initiation of medical management to improve quality of life and prevent progression of disease (Figure 1).
(A. Transvaginal ultrasound appearance of a small ovarian endometrioma in a 16-year-old girl. Note the unilocular cyst with ground glass echogenicity surrounded by multifollicular ovarian tissue. B. Ultrasound image of a retroverted uterus of an 18-year-old girl with focal adenomyosis of the posterior wall. Note the round cystic anechoic areas in the inner myometrium or junctional zone. The small intra-myometrial cyst is surrounded by a hyperechoic ring).
Indeed, the typical appearance of endometriotic pelvic lesions on transvaginal sonography, such as endometriomas and rectal deep infiltrating endometriosis (DIE) — as well as adenomyosis – can be medically treated without histologic confirmation .
When surgery is advisable, ultrasound findings also play a valuable role in presurgical staging, planning, and counseling for patients of all ages. Determining the extent and location of DIE preoperatively, for instance, facilitates the engagement of the appropriate surgical specialists so that multiple surgeries can be avoided. It also enables patients to be optimally informed before surgery of possible outcomes and complications.
Moreover, in the context of infertility, ultrasound can be a valuable tool for understanding uterine pathology and assessing for adenomyosis so that affected patients may be treated surgically or medically before turning to assisted reproductive technology.
Uniformity, Standardization in the Sonographic Assessment
In Europe, as in the United States, transvaginal sonography (TVS) is the first-line imaging tool for the diagnosis and management of endometriosis. In Europe, many ob.gyns. perform ultrasound themselves, as do treating surgeons. When diagnostic findings are negative but clinical suspicion is high, MRI is often utilized. Laparoscopy may then be considered in patients with negative imaging results.
Efforts to standardize terms, definitions, measurements, and sonographic features of different types of endometriosis have been made to make it easier for physicians to share data and communicate with each other. A lack of uniformity has contributed to variability in the reported diagnostic accuracy of TVS.
About 10 years ago, in one such effort, we assessed the accuracy of TVS for DIE by comparing TVS results with laparoscopic/histologic findings, and developed an ultrasound mapping system to accurately record the location, size and depth of lesions visualized by TVS. The accuracy of TVS ranged from 76% for the diagnosis of vaginal endometriosis to 97% for the diagnosis of bladder lesions and posterior cul-de-sac obliteration. Accuracy was 93% and 91% for detecting ureteral involvement (right and left); 87% for uterosacral ligament endometriotic lesions; and 87% for parametrial involvement.6
Shortly after, with a focus on DIE, expert sonographers and physician-sonographers from across Europe — as well as some experts from Australia, Japan, Brazil, Chile, and the United States (Y. Osuga from Brigham and Women’s Hospital and Harvard Medical School) — came together to agree on a uniform approach to the sonographic evaluation for suspected endometriosis and a standardization of terminology.
The consensus opinion from the International Deep Endometriosis Analysis (IDEA) group details four steps for examining women with suspected DIE: 1) Evaluation of the uterus and adnexa, 2) evaluation of transvaginal sonographic “soft markers” (ie. site-specific tenderness and ovarian mobility), 3) assessment of the status of the posterior cul-de-sac using real-time ultrasound-based “sliding sign,” and 4) assessment for DIE nodules in the anterior and posterior compartments.7
Our paper describing a mapping system and the IDEA paper describe how to detect deep endometriosis in the pelvis by utilizing an ultrasound view of normal anatomy and pelvic organ structure to provide landmarks for accurately defining the site of DIE lesions (Figure 2).
(A. Ultrasound appearance of a small DIE lesion of the retrocervical area [white arrows], which involved the torus uterinum and the right uterosacral ligament [USL]. The lesion appears as hypoechoic tissue with irregular margins caused by the fibrosis induced by the DIE. B. TVS appearance of small nodules of DIE of the left USL. Note the small retrocervical DIE lesion [white arrows], which appears hypoechoic due to the infiltration of the hyperechoic USL. C) Ultrasound appearance of a DIE nodule of the recto-sigmoid wall. Note the hypoechoic thickening of the muscular layers of the bowel wall attached to the corpus of the uterus and the adenomyosis of the posterior wall. The retrocervical area is free. D. TVS appearance of nodules of DIE of the lower rectal wall. Note the hypoechoic lesion [white arrows] of the rectum is attached to a retrocervical DIE fibrosis of the torus and USL [white dotted line]).
So-called rectovaginal endometriosis can be well assessed, for instance, since the involvement of the rectum, sigmoid colon, vaginal wall, rectovaginal septum, and posterior cul-de-sac uterosacral ligament can be seen by ultrasound as a single structure, making the location, size, and depth of any lesions discernible.
Again, this evaluation of the extent of disease is important for presurgical assessment so the surgeon can organize the right team and time of surgery and so the patient can be counseled on the advantages and possible complications of the treatment.
Notably, an accurate ultrasound description of pelvic endometriosis is helpful for accurate classification of disease. Endometriosis classification systems such as that of the American Association of Gynecologic Laparoscopists (AAGL)8 and the American Society of Reproductive Medicine (ASRM),9 as well as the #Enzian surgical description system,10 have been adapted to cover findings from ultrasound as well as MRI imaging.
A Systematic Evaluation
In keeping with the IDEA consensus opinion and based on our years of experience at the University of Rome, I advise that patients with typical pain symptoms of endometriosis or infertility undergo an accurate sonographic assessment of the pelvis with particular evaluation not only of the uterus and ovaries but of all pelvic retroperitoneal spaces.
The TVS examination should start with a slightly filled bladder, which permits a better evaluation of the bladder walls and the presence of endometriotic nodules. These nodules appear as hyperechoic linear or spherical lesions bulging toward the lumen and involving the serosa, muscularis, or (sub)mucosa of the bladder.
Then, an accurate evaluation of the uterus in 2D and 3D permits the diagnosis of adenomyosis. 3D sonographic evaluation of the myometrium and of the junctional zone are important; alteration and infiltration of the junctional zone and the presence of small adenomyotic cysts in the inner or outer myometrium are direct, specific signs of adenomyosis and should be ruled out in patients with dysmenorrhea, heavy menstrual bleeding, infertility, and pregnancy complications.
Endometriomas of the ovaries can be easily detected as having the typical appearance of a cyst with ground glass content. Adhesions of the ovaries and the uterus also should be evaluated with a dynamic ultrasound approach that utilizes the sliding sign and mobilization by palpation of the organs during the TVS scan.
Finally, the posterior and lateral retroperitoneal compartments should be carefully evaluated, with symptoms guiding the TVS examination whenever possible. Deep endometriotic nodules of the rectum appear as hypoechoic lesions or linear or nodular retroperitoneal thickening with irregular borders, penetrating into the intestinal wall and distorting its normal structure. In young patients, it seems very important to assess for small lesions below the peritoneum between the vagina and rectum, and in the parametria and around the ureter and nerves — lesions that, notably, would not be seen by diagnostic laparoscopy.
The Evaluation of Young Patients
In adolescent and young patients, endometriosis and adenomyosis are often present with small lesions and shallow tissue invasion, making a very careful and experienced approach to ultrasound essential for detection. Endometriomas are often of small diameter, and DIE is not always easily diagnosed because retroperitoneal lesions are similarly very small.
In a series of 270 adolescents (ages 12-20) who were referred to our outpatient gynecologic ultrasound unit over a 5-year period for various indications, at least one ultrasound feature of endometriosis was observed in 13.3%. In those with dysmenorrhea, the detection of endometriosis increased to 21%. Endometrioma was the most common type of endometriosis we found in the study, but DIE and adenomyosis were found in 4%-11%.
Although endometriotic lesions typically are small in young patients, they are often associated with severe pain symptoms, including chronic pelvic pain, dysmenorrhea, dyspareunia, dysuria, and dyschezia, all of which can have a serious effect on the quality of life of these young women. These symptoms keep them away from school during menstruation, away from sports, and cause painful intercourse and infertility. In young patients, an accurate TVS can provide a lot of information, and the ability to detect retroperitoneal endometriotic lesions and adenomyosis is probably better than with purely diagnostic laparoscopy, which would evaluate only superficial lesions.
TVS or, when needed, transrectal ultrasound, can enable adequate treatment and follow-up of the disease and its symptoms. There are no guidelines recommending adequate follow-up times to evaluate the effectiveness of medical therapy in patients with ultrasound signs of endometriosis. (Likewise, there are no indications for follow-up in patients with severe dysmenorrhea without ultrasound signs of endometriosis.) Certainly, our studies suggest careful evaluation over time of young patients with severe dysmenorrhea by serial ultrasound scans. With such follow-up, disease progress can be monitored and the medical or surgical treatment approach modified if needed.
The diagnosis of endometriosis at a young age has significant benefits not only in avoiding or reducing progression of the disease, but also in improving quality of life and aiding women in their desire for pregnancy.
Dr. Exacoustos is associate professor of ob.gyn. at the University of Rome “Tor Vergata.” She has no conflicts of interest to report.
References
1. Zondervan KT et al. N Engl J Med. 2020;382:1244-56.
2. Greene R et al. Fertil Steril. 2009;91:32-9.
3. Chapron C et al. J Pediatr Adolesc Gynecol. 2011;24:S7-12.
4. Randhawa AE et al. J Pediatr Adolesc Gynecol. 2021;34:643-8.
5. Becker CM et al. Hum Reprod Open. 2022(2):hoac009.
6. Exacoustos C et al. Fertil Steril. 2014;102:143-9. 7. Guerriero S et al. Ultrasound Obstet Gynecol. 2016;48(3):318-32.
8. Abrao MS et al. J Minim Invasive Gynecol. 2021;28:1941-50.9. Revised American Society for Reproductive Medicine classification of endometriosis: 1996. Fertil Steril. 1997;67:817-21. 10. Keckstein J et al. Acta Obstet Gynecol Scand. 2021;100:1165-75.
11. Martire FG et al. Fertil Steril. 2020;114(5):1049-57.
