User login
COVID-related harm to HCWs must be tracked more rigorously: NAS panel
A panel of scientific experts is urging the nation to do more to track morbidity and mortality among health care workers (HCWs), given the large and disproportionate number who have been infected with or died from SARS-CoV-2.
The National Academies of Sciences, Engineering, and Medicine’s Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats issued a 10-page “rapid expert consultation” on what is known about deaths and mental health problems among HCWs associated with the COVID-19 pandemic and how to protect workers.
“The absence of a uniform national framework and inconsistent requirements across states for collecting, recording, and reporting HCW mortality and morbidity data associated with COVID-19 impairs anyone’s ability to make comparisons, do combined analyses, or draw conclusions about the scale of the problem,” says the panel in the report.
Mental health, in particular, needs to be examined, it says. Although the data are still limited, the prevalence of burnout and suicide “points to a serious concern,” according to the report.
“As with mortality due to COVID-19, there are currently no national systems nor reporting standards for morbidity measures related to the pandemic, such as mental health status, provider well-being, and other psychological effects on HCWs,” the report says.
A more robust national system that collected data on circumstances and interventions that may raise or lower risk, as well as on where the infection occurred, “would support the adoption of effective mitigation strategies,” says the report. It would also facilitate epidemiologic studies on risk factors, such as face-to-face contact with COVID-19 patients and the availability and use of personal protective equipment (PPE). Studies could also examine the impact of institutional requirements for masking.
Studies have consistently shown that universal mask wearing and access to appropriate PPE support the physical safety and mental health of HCWs, says the report.
Track scale of crisis
The committee cited many gaps in the current system. The Occupational Safety and Health Administration, for instance, doesn’t count deaths from occupationally acquired infection. Many states don’t report COVID-19 deaths by profession. The Centers for Disease Control and Prevention (CDC) relies on case report forms from local health departments for all COVID-19 cases, which typically are lacking in specifics, such as occupation or job setting, says the committee’s report.
As of Nov. 3, the CDC had reported 786 deaths among HCWs that were attributable to COVID-19 – a far lower number than other sources have reported.
The committee notes that much could be done immediately. A National Academy of Medicine panel on clinician well-being and resilience in August recommended that the CDC establish a national epidemiologic tracking program to measure HCWs’ well-being, assess the acute and long-term effects of COVID-19 on those workers, and report on the outcomes of interventions.
Such a program “is needed to comprehensively acknowledge the scale of the COVID-19 crisis and protect the health care workforce that is already stretched to the breaking point in many locations,” the committee says in its report.
A version of this article originally appeared on Medscape.com.
A panel of scientific experts is urging the nation to do more to track morbidity and mortality among health care workers (HCWs), given the large and disproportionate number who have been infected with or died from SARS-CoV-2.
The National Academies of Sciences, Engineering, and Medicine’s Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats issued a 10-page “rapid expert consultation” on what is known about deaths and mental health problems among HCWs associated with the COVID-19 pandemic and how to protect workers.
“The absence of a uniform national framework and inconsistent requirements across states for collecting, recording, and reporting HCW mortality and morbidity data associated with COVID-19 impairs anyone’s ability to make comparisons, do combined analyses, or draw conclusions about the scale of the problem,” says the panel in the report.
Mental health, in particular, needs to be examined, it says. Although the data are still limited, the prevalence of burnout and suicide “points to a serious concern,” according to the report.
“As with mortality due to COVID-19, there are currently no national systems nor reporting standards for morbidity measures related to the pandemic, such as mental health status, provider well-being, and other psychological effects on HCWs,” the report says.
A more robust national system that collected data on circumstances and interventions that may raise or lower risk, as well as on where the infection occurred, “would support the adoption of effective mitigation strategies,” says the report. It would also facilitate epidemiologic studies on risk factors, such as face-to-face contact with COVID-19 patients and the availability and use of personal protective equipment (PPE). Studies could also examine the impact of institutional requirements for masking.
Studies have consistently shown that universal mask wearing and access to appropriate PPE support the physical safety and mental health of HCWs, says the report.
Track scale of crisis
The committee cited many gaps in the current system. The Occupational Safety and Health Administration, for instance, doesn’t count deaths from occupationally acquired infection. Many states don’t report COVID-19 deaths by profession. The Centers for Disease Control and Prevention (CDC) relies on case report forms from local health departments for all COVID-19 cases, which typically are lacking in specifics, such as occupation or job setting, says the committee’s report.
As of Nov. 3, the CDC had reported 786 deaths among HCWs that were attributable to COVID-19 – a far lower number than other sources have reported.
The committee notes that much could be done immediately. A National Academy of Medicine panel on clinician well-being and resilience in August recommended that the CDC establish a national epidemiologic tracking program to measure HCWs’ well-being, assess the acute and long-term effects of COVID-19 on those workers, and report on the outcomes of interventions.
Such a program “is needed to comprehensively acknowledge the scale of the COVID-19 crisis and protect the health care workforce that is already stretched to the breaking point in many locations,” the committee says in its report.
A version of this article originally appeared on Medscape.com.
A panel of scientific experts is urging the nation to do more to track morbidity and mortality among health care workers (HCWs), given the large and disproportionate number who have been infected with or died from SARS-CoV-2.
The National Academies of Sciences, Engineering, and Medicine’s Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats issued a 10-page “rapid expert consultation” on what is known about deaths and mental health problems among HCWs associated with the COVID-19 pandemic and how to protect workers.
“The absence of a uniform national framework and inconsistent requirements across states for collecting, recording, and reporting HCW mortality and morbidity data associated with COVID-19 impairs anyone’s ability to make comparisons, do combined analyses, or draw conclusions about the scale of the problem,” says the panel in the report.
Mental health, in particular, needs to be examined, it says. Although the data are still limited, the prevalence of burnout and suicide “points to a serious concern,” according to the report.
“As with mortality due to COVID-19, there are currently no national systems nor reporting standards for morbidity measures related to the pandemic, such as mental health status, provider well-being, and other psychological effects on HCWs,” the report says.
A more robust national system that collected data on circumstances and interventions that may raise or lower risk, as well as on where the infection occurred, “would support the adoption of effective mitigation strategies,” says the report. It would also facilitate epidemiologic studies on risk factors, such as face-to-face contact with COVID-19 patients and the availability and use of personal protective equipment (PPE). Studies could also examine the impact of institutional requirements for masking.
Studies have consistently shown that universal mask wearing and access to appropriate PPE support the physical safety and mental health of HCWs, says the report.
Track scale of crisis
The committee cited many gaps in the current system. The Occupational Safety and Health Administration, for instance, doesn’t count deaths from occupationally acquired infection. Many states don’t report COVID-19 deaths by profession. The Centers for Disease Control and Prevention (CDC) relies on case report forms from local health departments for all COVID-19 cases, which typically are lacking in specifics, such as occupation or job setting, says the committee’s report.
As of Nov. 3, the CDC had reported 786 deaths among HCWs that were attributable to COVID-19 – a far lower number than other sources have reported.
The committee notes that much could be done immediately. A National Academy of Medicine panel on clinician well-being and resilience in August recommended that the CDC establish a national epidemiologic tracking program to measure HCWs’ well-being, assess the acute and long-term effects of COVID-19 on those workers, and report on the outcomes of interventions.
Such a program “is needed to comprehensively acknowledge the scale of the COVID-19 crisis and protect the health care workforce that is already stretched to the breaking point in many locations,” the committee says in its report.
A version of this article originally appeared on Medscape.com.
Coronavirus has infected over 2% of U.S. children
After last week’s ever-so-slightly positive news, the COVID-19 numbers in children have gone back to their old ways.
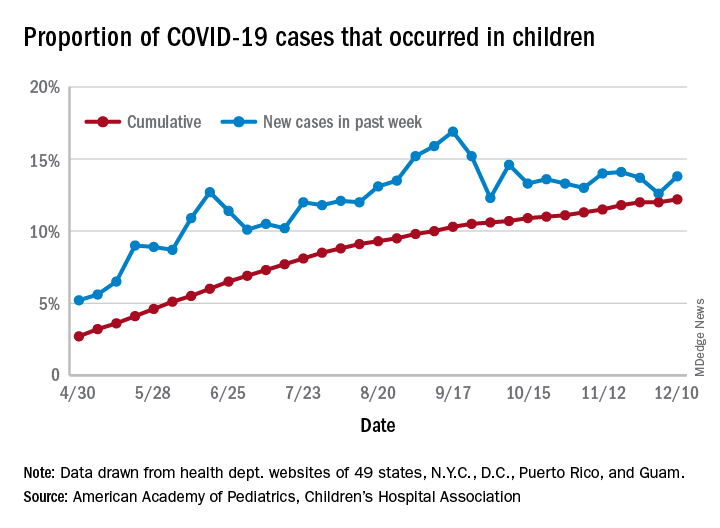
For the week ending Dec. 10, there were 178,823 new COVID-19 cases reported in U.S. children, the highest weekly total yet during the pandemic. The number of new cases had dropped the week before after setting a new high of almost 154,000 during the last full week of November, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
A new weekly high has been seen in 9 of the last 10 weeks, during which time the weekly total of child cases has gone from just over 40,000 (week ending Oct. 8) to almost 179,000, the two organizations said.
and that 2.1% of all children (2,179 per 100,000) in the United States have been infected with the coronavirus, the AAP and CHA said in their weekly report, which includes health department data from 49 states (New York does not report age distribution), the District of Columbia, New York City, Puerto Rico, and Guam.
The cumulative proportion of 12.2% has been exceeded in 27 states, as well as Puerto Rico and Guam, with the highest coming in Wyoming (21.3%), South Carolina (18.1%), and Tennessee (18.1%) and the lowest in Florida (6.7%, but the state uses an age range of 0-14 years) and New Jersey (7.6%), the AAP/CHA data show.
In a separate statement, AAP president Sally Goza, MD, welcomed the approval of the Pfizer-BioNTech COVID-19 vaccine but noted that the “virus is at unprecedented levels in nearly every community in the U.S., and in many areas, our health care system is terribly overburdened. The vaccine will not solve this overnight. I urge everyone to continue to practice social distancing, and wear masks or cloth face coverings, and get a flu shot, so we can protect the people we care about.”
Dr. Goza continued: “We applaud Pfizer-BioNTech for including children ages 12 through 17 in their clinical trials and we look forward to learning more about the data from children aged 12-15. We also want to acknowledge the discussion during the committee meeting on including 16- to 17-year-olds in the EUA [emergency-use authorization]. We believe that discussion underscores the need to keep expanding these trials to the pediatric population so we can collect robust data on this age group.”
[email protected]
After last week’s ever-so-slightly positive news, the COVID-19 numbers in children have gone back to their old ways.
For the week ending Dec. 10, there were 178,823 new COVID-19 cases reported in U.S. children, the highest weekly total yet during the pandemic. The number of new cases had dropped the week before after setting a new high of almost 154,000 during the last full week of November, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
A new weekly high has been seen in 9 of the last 10 weeks, during which time the weekly total of child cases has gone from just over 40,000 (week ending Oct. 8) to almost 179,000, the two organizations said.
and that 2.1% of all children (2,179 per 100,000) in the United States have been infected with the coronavirus, the AAP and CHA said in their weekly report, which includes health department data from 49 states (New York does not report age distribution), the District of Columbia, New York City, Puerto Rico, and Guam.
The cumulative proportion of 12.2% has been exceeded in 27 states, as well as Puerto Rico and Guam, with the highest coming in Wyoming (21.3%), South Carolina (18.1%), and Tennessee (18.1%) and the lowest in Florida (6.7%, but the state uses an age range of 0-14 years) and New Jersey (7.6%), the AAP/CHA data show.
In a separate statement, AAP president Sally Goza, MD, welcomed the approval of the Pfizer-BioNTech COVID-19 vaccine but noted that the “virus is at unprecedented levels in nearly every community in the U.S., and in many areas, our health care system is terribly overburdened. The vaccine will not solve this overnight. I urge everyone to continue to practice social distancing, and wear masks or cloth face coverings, and get a flu shot, so we can protect the people we care about.”
Dr. Goza continued: “We applaud Pfizer-BioNTech for including children ages 12 through 17 in their clinical trials and we look forward to learning more about the data from children aged 12-15. We also want to acknowledge the discussion during the committee meeting on including 16- to 17-year-olds in the EUA [emergency-use authorization]. We believe that discussion underscores the need to keep expanding these trials to the pediatric population so we can collect robust data on this age group.”
[email protected]
After last week’s ever-so-slightly positive news, the COVID-19 numbers in children have gone back to their old ways.
For the week ending Dec. 10, there were 178,823 new COVID-19 cases reported in U.S. children, the highest weekly total yet during the pandemic. The number of new cases had dropped the week before after setting a new high of almost 154,000 during the last full week of November, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association.
A new weekly high has been seen in 9 of the last 10 weeks, during which time the weekly total of child cases has gone from just over 40,000 (week ending Oct. 8) to almost 179,000, the two organizations said.
and that 2.1% of all children (2,179 per 100,000) in the United States have been infected with the coronavirus, the AAP and CHA said in their weekly report, which includes health department data from 49 states (New York does not report age distribution), the District of Columbia, New York City, Puerto Rico, and Guam.
The cumulative proportion of 12.2% has been exceeded in 27 states, as well as Puerto Rico and Guam, with the highest coming in Wyoming (21.3%), South Carolina (18.1%), and Tennessee (18.1%) and the lowest in Florida (6.7%, but the state uses an age range of 0-14 years) and New Jersey (7.6%), the AAP/CHA data show.
In a separate statement, AAP president Sally Goza, MD, welcomed the approval of the Pfizer-BioNTech COVID-19 vaccine but noted that the “virus is at unprecedented levels in nearly every community in the U.S., and in many areas, our health care system is terribly overburdened. The vaccine will not solve this overnight. I urge everyone to continue to practice social distancing, and wear masks or cloth face coverings, and get a flu shot, so we can protect the people we care about.”
Dr. Goza continued: “We applaud Pfizer-BioNTech for including children ages 12 through 17 in their clinical trials and we look forward to learning more about the data from children aged 12-15. We also want to acknowledge the discussion during the committee meeting on including 16- to 17-year-olds in the EUA [emergency-use authorization]. We believe that discussion underscores the need to keep expanding these trials to the pediatric population so we can collect robust data on this age group.”
[email protected]
PTSD, depression combo tied to high risk for early death in women
Middle-aged women with PTSD and comorbid depression have a nearly fourfold increased risk for early death from a variety of causes in comparison with their peers who do not have those conditions, new research shows.
“Women with more severe symptoms of depression and PTSD were more at risk, compared with those with fewer symptoms or women with symptoms of only PTSD or only depression,” lead investigator Andrea Roberts, PhD, Harvard School of Public Health, Boston, said in an interview.
Health care providers “should be aware that mental health is a critical component of overall health and is tightly entwined with physical health. Identifying and treating mental health issues should be a foundational part of general health practice,” said Dr. Roberts.
The study was published online Dec. 4 in JAMA Network Open.
Mental health fundamental to survival
The researchers studied more than 51,000 mostly White women from the Nurses Health Study II who were followed for 9 years (2008-2017). At baseline in 2008, the women were aged between 43 and 64 years (mean age, 53.3 years).
Women with high levels of PTSD (six or seven symptoms) and probable depression were nearly four times more likely to die during follow-up than their peers who did not have these conditions (hazard ratio, 3.8; 95% confidence interval, 2.65-5.45; P < .001).
With adjustment for health factors such as smoking and body mass index, women with a high level of PTSD and depression remained at increased risk for early death (HR, 3.11; 95% CI, 2.16-4.47; P < .001).
The risk for early death was also elevated among women with moderate PTSD (four or five symptoms) and depression (HR, 2.03; 95% CI, 1.35-3.03; P < .001) and women with subclinical PTSD and depression (HR, 2.85; 95% CI, 1.99-4.07; P < .001) compared with those who did not have PTSD or depression.
Among women with PTSD symptoms and depression, the incidence of death from nearly all major causes was increased, including death from cardiovascular disease, respiratory disease, type 2 diabetes, unintentional injury, suicide, and other causes.
“These findings provide further evidence that mental health is fundamental to physical health – and to our very survival. We ignore our emotional well-being at our peril,” senior author Karestan Koenen, PhD, said in a news release.
New knowledge
Commenting on the findings, Jennifer Sumner, PhD, said that it’s “critical to appreciate the physical health consequences of psychopathology in individuals who have experienced trauma. This study adds to a growing literature demonstrating that the impact extends far beyond emotional health.
“Furthermore, these results highlight the potential value of promoting healthy lifestyle changes in order to reduce the elevated mortality risk in trauma-exposed individuals with co-occurring PTSD and depression,” said Dr. Sumner, who is with the department of psychology, University of California, Los Angeles.
She noted that this study builds on other work that links PTSD to mortality in men.
“Most work on posttraumatic psychopathology and physical health has actually been conducted in predominantly male samples of veterans, so said Dr. Sumner.
“It’s also important to note that PTSD and depression are more prevalent in women than in men, so demonstrating these associations in women is particularly relevant,” she added.
Funding for the study was provided by the National Institutes of Heath. The authors disclosed no relevant financial relationships. Dr. Sumner has collaborated with the study investigators on prior studies.
A version of this article originally appeared on Medscape.com.
Middle-aged women with PTSD and comorbid depression have a nearly fourfold increased risk for early death from a variety of causes in comparison with their peers who do not have those conditions, new research shows.
“Women with more severe symptoms of depression and PTSD were more at risk, compared with those with fewer symptoms or women with symptoms of only PTSD or only depression,” lead investigator Andrea Roberts, PhD, Harvard School of Public Health, Boston, said in an interview.
Health care providers “should be aware that mental health is a critical component of overall health and is tightly entwined with physical health. Identifying and treating mental health issues should be a foundational part of general health practice,” said Dr. Roberts.
The study was published online Dec. 4 in JAMA Network Open.
Mental health fundamental to survival
The researchers studied more than 51,000 mostly White women from the Nurses Health Study II who were followed for 9 years (2008-2017). At baseline in 2008, the women were aged between 43 and 64 years (mean age, 53.3 years).
Women with high levels of PTSD (six or seven symptoms) and probable depression were nearly four times more likely to die during follow-up than their peers who did not have these conditions (hazard ratio, 3.8; 95% confidence interval, 2.65-5.45; P < .001).
With adjustment for health factors such as smoking and body mass index, women with a high level of PTSD and depression remained at increased risk for early death (HR, 3.11; 95% CI, 2.16-4.47; P < .001).
The risk for early death was also elevated among women with moderate PTSD (four or five symptoms) and depression (HR, 2.03; 95% CI, 1.35-3.03; P < .001) and women with subclinical PTSD and depression (HR, 2.85; 95% CI, 1.99-4.07; P < .001) compared with those who did not have PTSD or depression.
Among women with PTSD symptoms and depression, the incidence of death from nearly all major causes was increased, including death from cardiovascular disease, respiratory disease, type 2 diabetes, unintentional injury, suicide, and other causes.
“These findings provide further evidence that mental health is fundamental to physical health – and to our very survival. We ignore our emotional well-being at our peril,” senior author Karestan Koenen, PhD, said in a news release.
New knowledge
Commenting on the findings, Jennifer Sumner, PhD, said that it’s “critical to appreciate the physical health consequences of psychopathology in individuals who have experienced trauma. This study adds to a growing literature demonstrating that the impact extends far beyond emotional health.
“Furthermore, these results highlight the potential value of promoting healthy lifestyle changes in order to reduce the elevated mortality risk in trauma-exposed individuals with co-occurring PTSD and depression,” said Dr. Sumner, who is with the department of psychology, University of California, Los Angeles.
She noted that this study builds on other work that links PTSD to mortality in men.
“Most work on posttraumatic psychopathology and physical health has actually been conducted in predominantly male samples of veterans, so said Dr. Sumner.
“It’s also important to note that PTSD and depression are more prevalent in women than in men, so demonstrating these associations in women is particularly relevant,” she added.
Funding for the study was provided by the National Institutes of Heath. The authors disclosed no relevant financial relationships. Dr. Sumner has collaborated with the study investigators on prior studies.
A version of this article originally appeared on Medscape.com.
Middle-aged women with PTSD and comorbid depression have a nearly fourfold increased risk for early death from a variety of causes in comparison with their peers who do not have those conditions, new research shows.
“Women with more severe symptoms of depression and PTSD were more at risk, compared with those with fewer symptoms or women with symptoms of only PTSD or only depression,” lead investigator Andrea Roberts, PhD, Harvard School of Public Health, Boston, said in an interview.
Health care providers “should be aware that mental health is a critical component of overall health and is tightly entwined with physical health. Identifying and treating mental health issues should be a foundational part of general health practice,” said Dr. Roberts.
The study was published online Dec. 4 in JAMA Network Open.
Mental health fundamental to survival
The researchers studied more than 51,000 mostly White women from the Nurses Health Study II who were followed for 9 years (2008-2017). At baseline in 2008, the women were aged between 43 and 64 years (mean age, 53.3 years).
Women with high levels of PTSD (six or seven symptoms) and probable depression were nearly four times more likely to die during follow-up than their peers who did not have these conditions (hazard ratio, 3.8; 95% confidence interval, 2.65-5.45; P < .001).
With adjustment for health factors such as smoking and body mass index, women with a high level of PTSD and depression remained at increased risk for early death (HR, 3.11; 95% CI, 2.16-4.47; P < .001).
The risk for early death was also elevated among women with moderate PTSD (four or five symptoms) and depression (HR, 2.03; 95% CI, 1.35-3.03; P < .001) and women with subclinical PTSD and depression (HR, 2.85; 95% CI, 1.99-4.07; P < .001) compared with those who did not have PTSD or depression.
Among women with PTSD symptoms and depression, the incidence of death from nearly all major causes was increased, including death from cardiovascular disease, respiratory disease, type 2 diabetes, unintentional injury, suicide, and other causes.
“These findings provide further evidence that mental health is fundamental to physical health – and to our very survival. We ignore our emotional well-being at our peril,” senior author Karestan Koenen, PhD, said in a news release.
New knowledge
Commenting on the findings, Jennifer Sumner, PhD, said that it’s “critical to appreciate the physical health consequences of psychopathology in individuals who have experienced trauma. This study adds to a growing literature demonstrating that the impact extends far beyond emotional health.
“Furthermore, these results highlight the potential value of promoting healthy lifestyle changes in order to reduce the elevated mortality risk in trauma-exposed individuals with co-occurring PTSD and depression,” said Dr. Sumner, who is with the department of psychology, University of California, Los Angeles.
She noted that this study builds on other work that links PTSD to mortality in men.
“Most work on posttraumatic psychopathology and physical health has actually been conducted in predominantly male samples of veterans, so said Dr. Sumner.
“It’s also important to note that PTSD and depression are more prevalent in women than in men, so demonstrating these associations in women is particularly relevant,” she added.
Funding for the study was provided by the National Institutes of Heath. The authors disclosed no relevant financial relationships. Dr. Sumner has collaborated with the study investigators on prior studies.
A version of this article originally appeared on Medscape.com.
Genetic mutation burden can predict prognosis for myelodysplastic syndrome
Key clinical point: A mutation load of the gene U2AF1 (VAF > 40%) was an independent indicator of lower 1-year survival in adults with myelodysplastic syndrome.
Major finding: Myelodysplastic syndrome patients with a higher mutation load of U2AF1 (VAF > 40%) had a significantly lower 1-year survival rate compared to those with a mutation load of VAF 40 or lower (46.1% and 80.5%, respectively, P= 0.027).
Study details: The data come from genetic analyses of 234 myelodysplastic syndrome patients aged 17 to 86 years; a total of 51 patients had an U2AF1 mutation at 52 mutation sites.
Disclosures: The study was supported by the National Natural Science Foundation of China; Henan Natural Science Foundation of China and by the Henan Medical Science and Technology Research Project, Key Scientific Research Project of Henan Provincial Education Department. The researchers had no financial conflicts to disclose.
Source: Wang H et al. Sci Rep. 2020 Oct 29. doi: 10.1038/s41598-020-74744-z.
Key clinical point: A mutation load of the gene U2AF1 (VAF > 40%) was an independent indicator of lower 1-year survival in adults with myelodysplastic syndrome.
Major finding: Myelodysplastic syndrome patients with a higher mutation load of U2AF1 (VAF > 40%) had a significantly lower 1-year survival rate compared to those with a mutation load of VAF 40 or lower (46.1% and 80.5%, respectively, P= 0.027).
Study details: The data come from genetic analyses of 234 myelodysplastic syndrome patients aged 17 to 86 years; a total of 51 patients had an U2AF1 mutation at 52 mutation sites.
Disclosures: The study was supported by the National Natural Science Foundation of China; Henan Natural Science Foundation of China and by the Henan Medical Science and Technology Research Project, Key Scientific Research Project of Henan Provincial Education Department. The researchers had no financial conflicts to disclose.
Source: Wang H et al. Sci Rep. 2020 Oct 29. doi: 10.1038/s41598-020-74744-z.
Key clinical point: A mutation load of the gene U2AF1 (VAF > 40%) was an independent indicator of lower 1-year survival in adults with myelodysplastic syndrome.
Major finding: Myelodysplastic syndrome patients with a higher mutation load of U2AF1 (VAF > 40%) had a significantly lower 1-year survival rate compared to those with a mutation load of VAF 40 or lower (46.1% and 80.5%, respectively, P= 0.027).
Study details: The data come from genetic analyses of 234 myelodysplastic syndrome patients aged 17 to 86 years; a total of 51 patients had an U2AF1 mutation at 52 mutation sites.
Disclosures: The study was supported by the National Natural Science Foundation of China; Henan Natural Science Foundation of China and by the Henan Medical Science and Technology Research Project, Key Scientific Research Project of Henan Provincial Education Department. The researchers had no financial conflicts to disclose.
Source: Wang H et al. Sci Rep. 2020 Oct 29. doi: 10.1038/s41598-020-74744-z.
Novel gene fusions surface more often in acute myeloid leukemia vs. myelodysplastic syndrome
Key clinical point: Novel gene fusions may have a role in developing biomarkers for monitoring of minimal residual disease (MRD) in patients with acute myeloid leukemia and myelodysplastic syndrome.
Major finding: Overall, gene fusion events occurred in 37% of patients with acute myeloid leukemia compared to 3% of those with myelodysplastic syndrome. In addition, 67% of AML patients had TB53 mutations and 71% had complex karyotypes, compared with 26% and 21%, respectively, of MDS patients.
Study details: The data come from a review of gene transcripts from 572 adults with acute myeloid leukemia and 630 with myelodysplastic syndrome.
Disclosures: The study received no outside funding. Lead author Dr. Stengel had no financial conflicts to disclose.
Source: Stengel A et al. Blood Adv. 2020 Nov 10. doi: 10.1182/bloodadvances.2020003007.
Key clinical point: Novel gene fusions may have a role in developing biomarkers for monitoring of minimal residual disease (MRD) in patients with acute myeloid leukemia and myelodysplastic syndrome.
Major finding: Overall, gene fusion events occurred in 37% of patients with acute myeloid leukemia compared to 3% of those with myelodysplastic syndrome. In addition, 67% of AML patients had TB53 mutations and 71% had complex karyotypes, compared with 26% and 21%, respectively, of MDS patients.
Study details: The data come from a review of gene transcripts from 572 adults with acute myeloid leukemia and 630 with myelodysplastic syndrome.
Disclosures: The study received no outside funding. Lead author Dr. Stengel had no financial conflicts to disclose.
Source: Stengel A et al. Blood Adv. 2020 Nov 10. doi: 10.1182/bloodadvances.2020003007.
Key clinical point: Novel gene fusions may have a role in developing biomarkers for monitoring of minimal residual disease (MRD) in patients with acute myeloid leukemia and myelodysplastic syndrome.
Major finding: Overall, gene fusion events occurred in 37% of patients with acute myeloid leukemia compared to 3% of those with myelodysplastic syndrome. In addition, 67% of AML patients had TB53 mutations and 71% had complex karyotypes, compared with 26% and 21%, respectively, of MDS patients.
Study details: The data come from a review of gene transcripts from 572 adults with acute myeloid leukemia and 630 with myelodysplastic syndrome.
Disclosures: The study received no outside funding. Lead author Dr. Stengel had no financial conflicts to disclose.
Source: Stengel A et al. Blood Adv. 2020 Nov 10. doi: 10.1182/bloodadvances.2020003007.
Azacitidine shows safety but lacks effectiveness for relapse reduction in myelodysplastic syndrome and acute myeloid leukemia
Key clinical point: Azacitidine was safe but had no significant impact on relapse-free survival after transplant in in patients with acute myeloid leukemia/myelodysplastic syndrome
Major finding: Median relapse-free survival (RFS) was 2.07 years in the azacitidine group vs. 1.28 years in the control group (P = .19).
Study details: The data come from a phase 3 open-label randomized trial of 187 patients aged 18 to 75 years with acute myeloid leukemia/myelodysplastic syndrome (AML/MDS); patients received 32 mg/m2 of azacitidine daily for 5 days every 28 days for 12 cycles.
Disclosures: The study was supported by Celgene Pharmaceuticals. Lead author Dr. Oran disclosed serving as a consultant for Celgene and receiving research funding from AROG Pharmaceuticals and Astex Pharmaceuticals.
Source: Oran B et al. Blood Adv. 2020 Nov 10. doi: 10.1182/bloodadvances.2020002544.
Key clinical point: Azacitidine was safe but had no significant impact on relapse-free survival after transplant in in patients with acute myeloid leukemia/myelodysplastic syndrome
Major finding: Median relapse-free survival (RFS) was 2.07 years in the azacitidine group vs. 1.28 years in the control group (P = .19).
Study details: The data come from a phase 3 open-label randomized trial of 187 patients aged 18 to 75 years with acute myeloid leukemia/myelodysplastic syndrome (AML/MDS); patients received 32 mg/m2 of azacitidine daily for 5 days every 28 days for 12 cycles.
Disclosures: The study was supported by Celgene Pharmaceuticals. Lead author Dr. Oran disclosed serving as a consultant for Celgene and receiving research funding from AROG Pharmaceuticals and Astex Pharmaceuticals.
Source: Oran B et al. Blood Adv. 2020 Nov 10. doi: 10.1182/bloodadvances.2020002544.
Key clinical point: Azacitidine was safe but had no significant impact on relapse-free survival after transplant in in patients with acute myeloid leukemia/myelodysplastic syndrome
Major finding: Median relapse-free survival (RFS) was 2.07 years in the azacitidine group vs. 1.28 years in the control group (P = .19).
Study details: The data come from a phase 3 open-label randomized trial of 187 patients aged 18 to 75 years with acute myeloid leukemia/myelodysplastic syndrome (AML/MDS); patients received 32 mg/m2 of azacitidine daily for 5 days every 28 days for 12 cycles.
Disclosures: The study was supported by Celgene Pharmaceuticals. Lead author Dr. Oran disclosed serving as a consultant for Celgene and receiving research funding from AROG Pharmaceuticals and Astex Pharmaceuticals.
Source: Oran B et al. Blood Adv. 2020 Nov 10. doi: 10.1182/bloodadvances.2020002544.
Imetelstat curbs need for blood transfusions in myelodysplastic syndrome
Key clinical point: Imetelstat increased transfusion independence for patients with lower risk myelodysplastic syndromes who were resistant or refractory to treatment with erythropoiesis-stimulating agent.
Major finding: At 8 weeks, 37% of the patients were red blood cell transfusion independent, with an average duration of 65 weeks.
Study details: The data come from a phase II study of 57 adult patients with lower-risk myelodysplastic syndromes dependent on red blood cell transfusion and relapsed or refractory to erythropoiesis-stimulating agent; patients received imetelstat with a primary endpoint of red blood cell transfusion independence at 8 weeks.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Steensma DP et al. J Clin Oncol. 2020 Oct 27. doi: 10.1200/JCO.20.01895.
Key clinical point: Imetelstat increased transfusion independence for patients with lower risk myelodysplastic syndromes who were resistant or refractory to treatment with erythropoiesis-stimulating agent.
Major finding: At 8 weeks, 37% of the patients were red blood cell transfusion independent, with an average duration of 65 weeks.
Study details: The data come from a phase II study of 57 adult patients with lower-risk myelodysplastic syndromes dependent on red blood cell transfusion and relapsed or refractory to erythropoiesis-stimulating agent; patients received imetelstat with a primary endpoint of red blood cell transfusion independence at 8 weeks.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Steensma DP et al. J Clin Oncol. 2020 Oct 27. doi: 10.1200/JCO.20.01895.
Key clinical point: Imetelstat increased transfusion independence for patients with lower risk myelodysplastic syndromes who were resistant or refractory to treatment with erythropoiesis-stimulating agent.
Major finding: At 8 weeks, 37% of the patients were red blood cell transfusion independent, with an average duration of 65 weeks.
Study details: The data come from a phase II study of 57 adult patients with lower-risk myelodysplastic syndromes dependent on red blood cell transfusion and relapsed or refractory to erythropoiesis-stimulating agent; patients received imetelstat with a primary endpoint of red blood cell transfusion independence at 8 weeks.
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Steensma DP et al. J Clin Oncol. 2020 Oct 27. doi: 10.1200/JCO.20.01895.
Food supplements improve mitochondrial respiration in myelodysplastic syndrome
Key clinical point: Food supplements coenzyme Q10 and carnitine significantly improved mitochondrial respiration in patients with low-risk myelodysplastic syndrome
Major finding: A total of 6 patients (21.4%) achieved hematological improvement based on the International Working Group (IWG) response criteria for MDS after 6 months.
Study details: The data come from an open-label study of 33 adults with myelodysplastic syndrome aged 56 to 93 years who received a combination of coenzyme Q10 at 180 mg/day L-carnitine at 2000 mg/ day, and a standard vitamin-mineral complex daily.
Disclosures: The study was supported by the Rising Tide Foundation and Israel Society of Hematology and Blood Transfusion. The researchers had no financial conflicts to disclose.
Source: Filanovsky K et al. Mediterr J Hemtol Infec Dis. 2020 Nov 1. doi: 10.4084/MJHID.2020.072.
Key clinical point: Food supplements coenzyme Q10 and carnitine significantly improved mitochondrial respiration in patients with low-risk myelodysplastic syndrome
Major finding: A total of 6 patients (21.4%) achieved hematological improvement based on the International Working Group (IWG) response criteria for MDS after 6 months.
Study details: The data come from an open-label study of 33 adults with myelodysplastic syndrome aged 56 to 93 years who received a combination of coenzyme Q10 at 180 mg/day L-carnitine at 2000 mg/ day, and a standard vitamin-mineral complex daily.
Disclosures: The study was supported by the Rising Tide Foundation and Israel Society of Hematology and Blood Transfusion. The researchers had no financial conflicts to disclose.
Source: Filanovsky K et al. Mediterr J Hemtol Infec Dis. 2020 Nov 1. doi: 10.4084/MJHID.2020.072.
Key clinical point: Food supplements coenzyme Q10 and carnitine significantly improved mitochondrial respiration in patients with low-risk myelodysplastic syndrome
Major finding: A total of 6 patients (21.4%) achieved hematological improvement based on the International Working Group (IWG) response criteria for MDS after 6 months.
Study details: The data come from an open-label study of 33 adults with myelodysplastic syndrome aged 56 to 93 years who received a combination of coenzyme Q10 at 180 mg/day L-carnitine at 2000 mg/ day, and a standard vitamin-mineral complex daily.
Disclosures: The study was supported by the Rising Tide Foundation and Israel Society of Hematology and Blood Transfusion. The researchers had no financial conflicts to disclose.
Source: Filanovsky K et al. Mediterr J Hemtol Infec Dis. 2020 Nov 1. doi: 10.4084/MJHID.2020.072.
Monthly azacitidine injections reduce relapse in acute myeloid leukemia and myelodysplastic syndrome
Key clinical point: The financial burden of monthly azacitidine must be weighed against the benefits of treatment, but patients with acute myeloid leukemia and myelodysplastic syndrome have few options.
Major finding: A total of 31 patients with measurable residual disease at baseline were relapse-free and alive after 6 months of monthly injection treatment with azacitidine.
Study details: The data come from a review of the pros and cons of the RELAZA-2, a German-multicentered, open-label, single-arm, phase II study of azacitidine in 53 adult patients who developed measurable residual disease after treatment for acute myeloid leukemia or advanced myelodysplastic syndrome; 29 after chemotherapy and 24 after allogeneic hematopoietic stem cell transplantation (ASCT).
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Pan J et al. Front Oncol. 2020 Oct 22. doi: 10.3389/fonc.2020.576924.
Key clinical point: The financial burden of monthly azacitidine must be weighed against the benefits of treatment, but patients with acute myeloid leukemia and myelodysplastic syndrome have few options.
Major finding: A total of 31 patients with measurable residual disease at baseline were relapse-free and alive after 6 months of monthly injection treatment with azacitidine.
Study details: The data come from a review of the pros and cons of the RELAZA-2, a German-multicentered, open-label, single-arm, phase II study of azacitidine in 53 adult patients who developed measurable residual disease after treatment for acute myeloid leukemia or advanced myelodysplastic syndrome; 29 after chemotherapy and 24 after allogeneic hematopoietic stem cell transplantation (ASCT).
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Pan J et al. Front Oncol. 2020 Oct 22. doi: 10.3389/fonc.2020.576924.
Key clinical point: The financial burden of monthly azacitidine must be weighed against the benefits of treatment, but patients with acute myeloid leukemia and myelodysplastic syndrome have few options.
Major finding: A total of 31 patients with measurable residual disease at baseline were relapse-free and alive after 6 months of monthly injection treatment with azacitidine.
Study details: The data come from a review of the pros and cons of the RELAZA-2, a German-multicentered, open-label, single-arm, phase II study of azacitidine in 53 adult patients who developed measurable residual disease after treatment for acute myeloid leukemia or advanced myelodysplastic syndrome; 29 after chemotherapy and 24 after allogeneic hematopoietic stem cell transplantation (ASCT).
Disclosures: The study received no outside funding. The researchers had no financial conflicts to disclose.
Source: Pan J et al. Front Oncol. 2020 Oct 22. doi: 10.3389/fonc.2020.576924.
Synthetic retinoid shows potential for myeloid malignancies
Key clinical point: A novel retinoic acid receptor alpha agonist appeared safe in a phase 1 study of patients with relapsed and refractory high-grade myelodysplastic syndrome or acute myelogenous leukemia.
Major finding: A total of 4 of 11 patients (36%) had stable disease or better after two 28-day treatment cycles; the study ended early because of an inadequate supply of the drug.
Study details: The data come from a phase 1 dose-escalation study of the novel retinoic acid receptor alpha agonist IRX195183; 11 adults aged 18 to 60 years with relapsed or refractory myelodysplastic syndrome or acute myelogenous leukemia received the drug for two 28-day cycles with dosage starting at 50 mg daily or 75 mg daily.
Disclosures: The study was supported by the National Heart, Lung, and Blood Institute, the National Cancer Institute, the Leukemia and Lymphoma Society, and the Augustine Fellowship. IRX195183 was provided by Io Therapeutics, Inc. Lead author Dr. Ambinder had no financial conflicts to disclose. Several coauthors are authors on a patent for the use of IRX195183.
Source: Ambinder AJ et al. Front Oncol. 2020 Oct 23. doi: 10.3389/fonc.2020.587062.
Key clinical point: A novel retinoic acid receptor alpha agonist appeared safe in a phase 1 study of patients with relapsed and refractory high-grade myelodysplastic syndrome or acute myelogenous leukemia.
Major finding: A total of 4 of 11 patients (36%) had stable disease or better after two 28-day treatment cycles; the study ended early because of an inadequate supply of the drug.
Study details: The data come from a phase 1 dose-escalation study of the novel retinoic acid receptor alpha agonist IRX195183; 11 adults aged 18 to 60 years with relapsed or refractory myelodysplastic syndrome or acute myelogenous leukemia received the drug for two 28-day cycles with dosage starting at 50 mg daily or 75 mg daily.
Disclosures: The study was supported by the National Heart, Lung, and Blood Institute, the National Cancer Institute, the Leukemia and Lymphoma Society, and the Augustine Fellowship. IRX195183 was provided by Io Therapeutics, Inc. Lead author Dr. Ambinder had no financial conflicts to disclose. Several coauthors are authors on a patent for the use of IRX195183.
Source: Ambinder AJ et al. Front Oncol. 2020 Oct 23. doi: 10.3389/fonc.2020.587062.
Key clinical point: A novel retinoic acid receptor alpha agonist appeared safe in a phase 1 study of patients with relapsed and refractory high-grade myelodysplastic syndrome or acute myelogenous leukemia.
Major finding: A total of 4 of 11 patients (36%) had stable disease or better after two 28-day treatment cycles; the study ended early because of an inadequate supply of the drug.
Study details: The data come from a phase 1 dose-escalation study of the novel retinoic acid receptor alpha agonist IRX195183; 11 adults aged 18 to 60 years with relapsed or refractory myelodysplastic syndrome or acute myelogenous leukemia received the drug for two 28-day cycles with dosage starting at 50 mg daily or 75 mg daily.
Disclosures: The study was supported by the National Heart, Lung, and Blood Institute, the National Cancer Institute, the Leukemia and Lymphoma Society, and the Augustine Fellowship. IRX195183 was provided by Io Therapeutics, Inc. Lead author Dr. Ambinder had no financial conflicts to disclose. Several coauthors are authors on a patent for the use of IRX195183.
Source: Ambinder AJ et al. Front Oncol. 2020 Oct 23. doi: 10.3389/fonc.2020.587062.