User login
Novel ddPCR assay precisely measures CAR T-cells after infusion
A novel quantitative assay used with flow cytometry helps to precisely measure chimeric antigen receptor (CAR) T-cell engraftment and in vivo expansion to predict patient outcomes after CAR T-cell infusion, according to researchers at the Fondazione IRCCS Istituto Nazionale Tumorion in Milan.
Higher frequencies of CAR-positive T cells at day 9 after infusion, as measured using the polymerase chain reaction (PCR)-based assay, accurately distinguished responders from nonresponders, Paolo Corradini, MD, said at the 3rd European CAR T-cell Meeting.
The findings, first presented in December at the American Society of Hematology annual conference, suggest the assay could improve treatment decision-making, Dr. Corradini of the University of Milan said at the meeting, which is jointly sponsored by the European Society for Blood and Marrow Transplantation and the European Hematology Association
He and his colleagues prospectively collected samples from 16 patients with diffuse large B-cell lymphoma, 5 with transformed follicular lymphoma, and 7 with primary mediastinal B-cell lymphoma who were treated with either axicabtagene ciloleucel (axi-cel; Yescarta) or tisagenlecleucel (tisa-cal; Kymriah) between November 2019 and July 2020. CAR T cells were monitored using flow cytometry.
Pivotal trial data and subsequent findings with respect to tisa-cel and axi-cel have demonstrated that CAR T-cell engraftment and in vivo expansion have a crucial impact on disease response and toxicity: a cut-off value of CAR+ cells at day 9 greater than 24.5/microliters distinguished responders from nonresponders with a sensitivity of 87.5% and specificity of 81%, Dr. Corradini noted.
“But we have also devised a methodology by digital droplet PCR (ddPCR) recently that correlates perfectly with the flow cytometry data,” he said, adding that the assay is “easy and allowed precise enumeration of the CAR T cells in the blood of the patient.”
The R square (coefficient of determination) for ddPCR and flow cytometry was 0.9995 and 0.9997 for tisa-cel and axi-cel, respectively (P < .0001 for each). This is particularly useful for assessing whether low CAR T-cell levels on flow cytometry are background signals resulting from nonspecific binding of the antibodies or true low levels, and the findings therefore have implications for improving clinical decision-making and outcomes in CAR T-cell therapy recipients, he said.
A novel quantitative assay used with flow cytometry helps to precisely measure chimeric antigen receptor (CAR) T-cell engraftment and in vivo expansion to predict patient outcomes after CAR T-cell infusion, according to researchers at the Fondazione IRCCS Istituto Nazionale Tumorion in Milan.
Higher frequencies of CAR-positive T cells at day 9 after infusion, as measured using the polymerase chain reaction (PCR)-based assay, accurately distinguished responders from nonresponders, Paolo Corradini, MD, said at the 3rd European CAR T-cell Meeting.
The findings, first presented in December at the American Society of Hematology annual conference, suggest the assay could improve treatment decision-making, Dr. Corradini of the University of Milan said at the meeting, which is jointly sponsored by the European Society for Blood and Marrow Transplantation and the European Hematology Association
He and his colleagues prospectively collected samples from 16 patients with diffuse large B-cell lymphoma, 5 with transformed follicular lymphoma, and 7 with primary mediastinal B-cell lymphoma who were treated with either axicabtagene ciloleucel (axi-cel; Yescarta) or tisagenlecleucel (tisa-cal; Kymriah) between November 2019 and July 2020. CAR T cells were monitored using flow cytometry.
Pivotal trial data and subsequent findings with respect to tisa-cel and axi-cel have demonstrated that CAR T-cell engraftment and in vivo expansion have a crucial impact on disease response and toxicity: a cut-off value of CAR+ cells at day 9 greater than 24.5/microliters distinguished responders from nonresponders with a sensitivity of 87.5% and specificity of 81%, Dr. Corradini noted.
“But we have also devised a methodology by digital droplet PCR (ddPCR) recently that correlates perfectly with the flow cytometry data,” he said, adding that the assay is “easy and allowed precise enumeration of the CAR T cells in the blood of the patient.”
The R square (coefficient of determination) for ddPCR and flow cytometry was 0.9995 and 0.9997 for tisa-cel and axi-cel, respectively (P < .0001 for each). This is particularly useful for assessing whether low CAR T-cell levels on flow cytometry are background signals resulting from nonspecific binding of the antibodies or true low levels, and the findings therefore have implications for improving clinical decision-making and outcomes in CAR T-cell therapy recipients, he said.
A novel quantitative assay used with flow cytometry helps to precisely measure chimeric antigen receptor (CAR) T-cell engraftment and in vivo expansion to predict patient outcomes after CAR T-cell infusion, according to researchers at the Fondazione IRCCS Istituto Nazionale Tumorion in Milan.
Higher frequencies of CAR-positive T cells at day 9 after infusion, as measured using the polymerase chain reaction (PCR)-based assay, accurately distinguished responders from nonresponders, Paolo Corradini, MD, said at the 3rd European CAR T-cell Meeting.
The findings, first presented in December at the American Society of Hematology annual conference, suggest the assay could improve treatment decision-making, Dr. Corradini of the University of Milan said at the meeting, which is jointly sponsored by the European Society for Blood and Marrow Transplantation and the European Hematology Association
He and his colleagues prospectively collected samples from 16 patients with diffuse large B-cell lymphoma, 5 with transformed follicular lymphoma, and 7 with primary mediastinal B-cell lymphoma who were treated with either axicabtagene ciloleucel (axi-cel; Yescarta) or tisagenlecleucel (tisa-cal; Kymriah) between November 2019 and July 2020. CAR T cells were monitored using flow cytometry.
Pivotal trial data and subsequent findings with respect to tisa-cel and axi-cel have demonstrated that CAR T-cell engraftment and in vivo expansion have a crucial impact on disease response and toxicity: a cut-off value of CAR+ cells at day 9 greater than 24.5/microliters distinguished responders from nonresponders with a sensitivity of 87.5% and specificity of 81%, Dr. Corradini noted.
“But we have also devised a methodology by digital droplet PCR (ddPCR) recently that correlates perfectly with the flow cytometry data,” he said, adding that the assay is “easy and allowed precise enumeration of the CAR T cells in the blood of the patient.”
The R square (coefficient of determination) for ddPCR and flow cytometry was 0.9995 and 0.9997 for tisa-cel and axi-cel, respectively (P < .0001 for each). This is particularly useful for assessing whether low CAR T-cell levels on flow cytometry are background signals resulting from nonspecific binding of the antibodies or true low levels, and the findings therefore have implications for improving clinical decision-making and outcomes in CAR T-cell therapy recipients, he said.
REPORTING FROM CART21
Hospitalizations for food anaphylaxis triple, but deaths down in United Kingdom
The rate of hospital admissions in the United Kingdom for food-induced anaphylaxis more than tripled over the 20 years from 1998 to 2018, but the case fatality rate fell by more than half, researchers report in BMJ.
“Cow’s milk is increasingly identified as the culprit allergen for fatal food reactions and is now the commonest cause of fatal anaphylaxis in children,” write Alessia Baseggio Conrado, PhD, a biochemist with the National Heart and Lung Institute at Imperial College London, and colleagues. “More education is needed to highlight the specific risks posed by cow’s milk to people who are allergic to increase awareness among food businesses.”
Whereas recognition of the risks posed by nut allergies has increased, people think milk allergy is mild, says senior author Paul. J. Turner, BMBCh, PhD, an allergist/immunologist at Imperial College. “This is often true in very young children, but school-aged children who still have milk allergy tend to have a more allergic profile, often with other allergies, including asthma,” Dr. Turner told this news organization. “Also, milk is very common in our diet, and you don’t need much milk to achieve a decent dose of allergen.”
During the study period, 101,891 people were hospitalized for anaphylaxis; 30,700 cases (30%) were coded as having been triggered by food.
These food-related admissions represent an increase from 1.23 to 4.04 per 100,000 population per year, for an annual increase of 5.7% (95% confidence interval, 5.5-5.9; P < .001), the authors write.
The largest jump occurred among children younger than 15 years, for whom admissions rose from 2.1 to 9.2 per 100,000 population per year, an annual increase of 6.6% (95% CI, 6.3-7.0). The annual increases were 5.9% (95% CI, 5.6-6.2) among persons aged 15 to 59 years and 2.1% (95% CI, 1.8-3.1) among those aged 60 years and older.
The investigators used data from England, Scotland, Wales, and Northern Ireland to track temporal trends and age and sex distributions for hospital admissions for which the primary diagnosis was anaphylaxis attributable to both food and nonfood triggers. These data were compared with nationally reported fatalities.
Over the 20-year period, 152 deaths were attributed to likely food-induced anaphylaxis. During that time, the case fatality rate for confirmed fatal food anaphylaxis fell from 0.7% to 0.19% (rate ratio, 0.931; 95% CI, 0.904-0.959; P < .001) and declined to 0.30% for suspected fatal food anaphylaxis (rate ratio, 0.970; 95% CI, 0.945-0.996; P = .024).
Between 1992 and 2018, at least 46% of all anaphylactic fatalities were deemed to be triggered by peanut or tree nut. Among school-aged children, 26% of anaphylactic fatalities were attributed to cow’s milk.
Not surprisingly, during the study period, there was an increase of 336% in prescriptions for adrenaline autoinjectors. Such prescriptions increased 11% per year.
Global trend
The data extend findings Dr. Turner and colleagues reported for England and Wales in 2014 regarding the entire United Kingdom population and align with epidemiologic trends in hospital admissions for anaphylaxis in the United States and Australia.
The researchers say better recognition and management of anaphylaxis could partly explain the decrease in fatalities, but the rise in hospitalizations remains puzzling. “Whether a true increase in the prevalence of anaphylaxis has occurred (rather than a reduction in the threshold to admit patients presenting with anaphylaxis) is unclear because evidence is lacking for an increase in prevalence of food allergy in the [United Kingdom] (and elsewhere) over the same time period,” they write.
Ronna L. Campbell, MD, PhD, an emergency physician at the Mayo Clinic in Rochester, Minn., has noted similar trends in the United States. “It may be that anaphylaxis recognition and diagnosis have improved, resulting in earlier administration of epinephrine,” Dr. Campbell said in an interview. “So while cases are increasing, earlier recognition and treatment result in decreased fatalities.” She is unaware of any new guidelines recommending increased hospitalization that would explain the puzzling rise in admissions.
According to the study authors, the clinical criteria used to diagnose anaphylaxis in the United Kingdom did not change during the study period. Although national guidance recommending the hospitalization of children younger than 16 who are suspected of having anaphylaxis was introduced in 2011 and may have boosted admissions, the year-on-year rate of increase has persisted since 2014. “Therefore the increase over the past 5 years cannot be attributed to the impact of the guidance,” they write.
The study was funded by grants from the U.K. Medical Research Council and U.K. Food Standards Agency. Two coauthors have disclosed financial relationships with industry outside of the submitted work. Dr. Conrado has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com
The rate of hospital admissions in the United Kingdom for food-induced anaphylaxis more than tripled over the 20 years from 1998 to 2018, but the case fatality rate fell by more than half, researchers report in BMJ.
“Cow’s milk is increasingly identified as the culprit allergen for fatal food reactions and is now the commonest cause of fatal anaphylaxis in children,” write Alessia Baseggio Conrado, PhD, a biochemist with the National Heart and Lung Institute at Imperial College London, and colleagues. “More education is needed to highlight the specific risks posed by cow’s milk to people who are allergic to increase awareness among food businesses.”
Whereas recognition of the risks posed by nut allergies has increased, people think milk allergy is mild, says senior author Paul. J. Turner, BMBCh, PhD, an allergist/immunologist at Imperial College. “This is often true in very young children, but school-aged children who still have milk allergy tend to have a more allergic profile, often with other allergies, including asthma,” Dr. Turner told this news organization. “Also, milk is very common in our diet, and you don’t need much milk to achieve a decent dose of allergen.”
During the study period, 101,891 people were hospitalized for anaphylaxis; 30,700 cases (30%) were coded as having been triggered by food.
These food-related admissions represent an increase from 1.23 to 4.04 per 100,000 population per year, for an annual increase of 5.7% (95% confidence interval, 5.5-5.9; P < .001), the authors write.
The largest jump occurred among children younger than 15 years, for whom admissions rose from 2.1 to 9.2 per 100,000 population per year, an annual increase of 6.6% (95% CI, 6.3-7.0). The annual increases were 5.9% (95% CI, 5.6-6.2) among persons aged 15 to 59 years and 2.1% (95% CI, 1.8-3.1) among those aged 60 years and older.
The investigators used data from England, Scotland, Wales, and Northern Ireland to track temporal trends and age and sex distributions for hospital admissions for which the primary diagnosis was anaphylaxis attributable to both food and nonfood triggers. These data were compared with nationally reported fatalities.
Over the 20-year period, 152 deaths were attributed to likely food-induced anaphylaxis. During that time, the case fatality rate for confirmed fatal food anaphylaxis fell from 0.7% to 0.19% (rate ratio, 0.931; 95% CI, 0.904-0.959; P < .001) and declined to 0.30% for suspected fatal food anaphylaxis (rate ratio, 0.970; 95% CI, 0.945-0.996; P = .024).
Between 1992 and 2018, at least 46% of all anaphylactic fatalities were deemed to be triggered by peanut or tree nut. Among school-aged children, 26% of anaphylactic fatalities were attributed to cow’s milk.
Not surprisingly, during the study period, there was an increase of 336% in prescriptions for adrenaline autoinjectors. Such prescriptions increased 11% per year.
Global trend
The data extend findings Dr. Turner and colleagues reported for England and Wales in 2014 regarding the entire United Kingdom population and align with epidemiologic trends in hospital admissions for anaphylaxis in the United States and Australia.
The researchers say better recognition and management of anaphylaxis could partly explain the decrease in fatalities, but the rise in hospitalizations remains puzzling. “Whether a true increase in the prevalence of anaphylaxis has occurred (rather than a reduction in the threshold to admit patients presenting with anaphylaxis) is unclear because evidence is lacking for an increase in prevalence of food allergy in the [United Kingdom] (and elsewhere) over the same time period,” they write.
Ronna L. Campbell, MD, PhD, an emergency physician at the Mayo Clinic in Rochester, Minn., has noted similar trends in the United States. “It may be that anaphylaxis recognition and diagnosis have improved, resulting in earlier administration of epinephrine,” Dr. Campbell said in an interview. “So while cases are increasing, earlier recognition and treatment result in decreased fatalities.” She is unaware of any new guidelines recommending increased hospitalization that would explain the puzzling rise in admissions.
According to the study authors, the clinical criteria used to diagnose anaphylaxis in the United Kingdom did not change during the study period. Although national guidance recommending the hospitalization of children younger than 16 who are suspected of having anaphylaxis was introduced in 2011 and may have boosted admissions, the year-on-year rate of increase has persisted since 2014. “Therefore the increase over the past 5 years cannot be attributed to the impact of the guidance,” they write.
The study was funded by grants from the U.K. Medical Research Council and U.K. Food Standards Agency. Two coauthors have disclosed financial relationships with industry outside of the submitted work. Dr. Conrado has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com
The rate of hospital admissions in the United Kingdom for food-induced anaphylaxis more than tripled over the 20 years from 1998 to 2018, but the case fatality rate fell by more than half, researchers report in BMJ.
“Cow’s milk is increasingly identified as the culprit allergen for fatal food reactions and is now the commonest cause of fatal anaphylaxis in children,” write Alessia Baseggio Conrado, PhD, a biochemist with the National Heart and Lung Institute at Imperial College London, and colleagues. “More education is needed to highlight the specific risks posed by cow’s milk to people who are allergic to increase awareness among food businesses.”
Whereas recognition of the risks posed by nut allergies has increased, people think milk allergy is mild, says senior author Paul. J. Turner, BMBCh, PhD, an allergist/immunologist at Imperial College. “This is often true in very young children, but school-aged children who still have milk allergy tend to have a more allergic profile, often with other allergies, including asthma,” Dr. Turner told this news organization. “Also, milk is very common in our diet, and you don’t need much milk to achieve a decent dose of allergen.”
During the study period, 101,891 people were hospitalized for anaphylaxis; 30,700 cases (30%) were coded as having been triggered by food.
These food-related admissions represent an increase from 1.23 to 4.04 per 100,000 population per year, for an annual increase of 5.7% (95% confidence interval, 5.5-5.9; P < .001), the authors write.
The largest jump occurred among children younger than 15 years, for whom admissions rose from 2.1 to 9.2 per 100,000 population per year, an annual increase of 6.6% (95% CI, 6.3-7.0). The annual increases were 5.9% (95% CI, 5.6-6.2) among persons aged 15 to 59 years and 2.1% (95% CI, 1.8-3.1) among those aged 60 years and older.
The investigators used data from England, Scotland, Wales, and Northern Ireland to track temporal trends and age and sex distributions for hospital admissions for which the primary diagnosis was anaphylaxis attributable to both food and nonfood triggers. These data were compared with nationally reported fatalities.
Over the 20-year period, 152 deaths were attributed to likely food-induced anaphylaxis. During that time, the case fatality rate for confirmed fatal food anaphylaxis fell from 0.7% to 0.19% (rate ratio, 0.931; 95% CI, 0.904-0.959; P < .001) and declined to 0.30% for suspected fatal food anaphylaxis (rate ratio, 0.970; 95% CI, 0.945-0.996; P = .024).
Between 1992 and 2018, at least 46% of all anaphylactic fatalities were deemed to be triggered by peanut or tree nut. Among school-aged children, 26% of anaphylactic fatalities were attributed to cow’s milk.
Not surprisingly, during the study period, there was an increase of 336% in prescriptions for adrenaline autoinjectors. Such prescriptions increased 11% per year.
Global trend
The data extend findings Dr. Turner and colleagues reported for England and Wales in 2014 regarding the entire United Kingdom population and align with epidemiologic trends in hospital admissions for anaphylaxis in the United States and Australia.
The researchers say better recognition and management of anaphylaxis could partly explain the decrease in fatalities, but the rise in hospitalizations remains puzzling. “Whether a true increase in the prevalence of anaphylaxis has occurred (rather than a reduction in the threshold to admit patients presenting with anaphylaxis) is unclear because evidence is lacking for an increase in prevalence of food allergy in the [United Kingdom] (and elsewhere) over the same time period,” they write.
Ronna L. Campbell, MD, PhD, an emergency physician at the Mayo Clinic in Rochester, Minn., has noted similar trends in the United States. “It may be that anaphylaxis recognition and diagnosis have improved, resulting in earlier administration of epinephrine,” Dr. Campbell said in an interview. “So while cases are increasing, earlier recognition and treatment result in decreased fatalities.” She is unaware of any new guidelines recommending increased hospitalization that would explain the puzzling rise in admissions.
According to the study authors, the clinical criteria used to diagnose anaphylaxis in the United Kingdom did not change during the study period. Although national guidance recommending the hospitalization of children younger than 16 who are suspected of having anaphylaxis was introduced in 2011 and may have boosted admissions, the year-on-year rate of increase has persisted since 2014. “Therefore the increase over the past 5 years cannot be attributed to the impact of the guidance,” they write.
The study was funded by grants from the U.K. Medical Research Council and U.K. Food Standards Agency. Two coauthors have disclosed financial relationships with industry outside of the submitted work. Dr. Conrado has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com
Important lessons about telehealth
Telehealth exploded into the public consciousness this year as a way for clinicians and patients to safely connect during the COVID-19 crisis. While telehealth has been part of care delivery at Providence St. Joseph Health (PSJH) for more than a decade, it transitioned almost overnight from an offering most often focused on serving patients in rural areas to a way for any patient to get the care they need virtually whether in a hospital, outpatient facility, or from the comfort and safety of their own home.
Telehealth growth was fueled by changes in regulation and reimbursement during the public health emergency enabling providers to see new and established patients at home across all payer types. To put this growth into perspective, the large PSJH system averaged a few thousand video visits per month in January and February 2020. As COVID transmission spread and lockdowns began, that number climbed to over 15,000 video visits in March to a height of more than 150,000 video visits in May. As of the end of October 2020, PSJH has conducted more than 1.2 million video visits since the beginning of January, steadily accounting for 20%-25% of total visit volume.
Going virtual with gastroenterology
PSJH gastroenterology providers have been a part of this wave, conducting more than 12,000 video visits so far this year (as documented in our Epic EMR), which has been an entirely new method of care delivery for most of these clinicians. We also have many affiliated, private practice gastroenterology providers who practice in our facilities and transitioned quickly to video for outpatient care. Pre- and postprocedure follow-up visits were some of the most common visit types that went virtual, along with new patient visits to establish care and existing patient visits to check in on the status of a health condition, medication, or other concern. Complementary services for gastroenterology patients were transitioned to video over the past 8 months as well. Care management, nutrition services, online support groups, bariatric care information sessions, behavioral health, and more are now available for patients to access virtually.
Remembering it’s not about the tech
New technologies can be challenging to adopt – especially at a pace as rapid as it was this year. Fortunately for PSJH, we had inpatient and outpatient video platforms already in place and an experienced internal telehealth team to scale them quickly to providers and caregivers across system. But even with those advantages, it was still a huge challenge to transition so many providers and caregivers to video visits in such a short time without change management hurdles and bumps along the way.
Too often, there is an overemphasis placed on the technology. It’s a tool, and some technologies are better than others, and they continue to evolve over time. True success or failure lies in the clinical and operational work flows and how well the providers and care teams engage with and adapt them. We found that the providers and staff members willing to venture outside their comfort zone of “how we’ve always done it” and collaborate on the transition to virtual care had the best results. Openness and flexibility to trying new things and using temporary workarounds if existing functionality didn’t meet the need was key to transitioning quickly. Then, by listening to ideas from and sharing feedback among providers, clinics, and geographies, we were able to identify fixes and optimizations that needed to be made to improve the experience for all.
Selecting a video visit platform
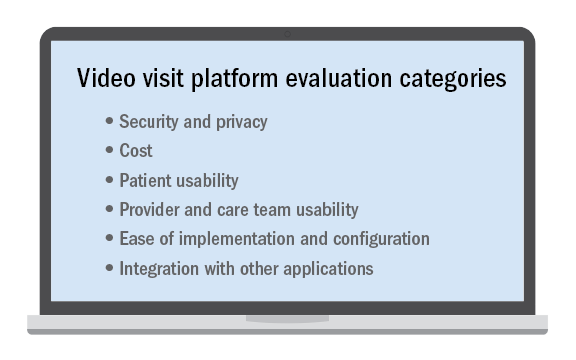
No telehealth platform is perfect and meets every patient, provider, and staff need or request despite what a technology vendor may claim. This is especially true in a large and/or diverse system with many different types of clinical use cases. Determining the “must-have” requirements from among those that may be important or simply nice to have is critical when selecting the video visit platform to use.
It’s not an easy decision and nearly impossible to please everyone. Ensuring that there are clinician, operator, and technical stakeholders all contributing to the requirements and decision-making is essential. While some may prefer a “best-of-breed” solution that does one thing very well, it may have to be paired with a set of other complimentary applications to meet all of the organization’s needs. Alternatively, there may be a platform with an expansive feature set but not all of the features are as strong as desired. Then there are solutions that integrate with your existing applications, which is a compelling option to consider.
Regardless of the tool chosen, best-practice work flows, easy-to-follow documentation, a mix of different training options, and internal technical help that responds quickly is key to implementing it successfully. And once implemented, optimization is an ongoing process to make it easier, faster, and better.
Looking ahead
As we came to the end of 2020, all providers and health systems were paying close attention to the Centers for Medicaid & Medicare Services and state-level regulations and reimbursement changes for 2021 to evaluate the impact on telehealth after the public health emergency and COVID-19 waivers are ended. Advocacy efforts are urging lawmakers to not lose the gains that were made during this time and have enabled millions of patients to access care more easily – changes which we believe they will now expect as an option going forward.
We at Providence believe telehealth’s future is a bright one, especially where value-based/managed care arrangements with payers are in place. In addition to integrating video visits and consults into normal clinical practice, we see further growth in serving patients at home with remote patient monitoring and other home-based programs that leverage connected devices and virtual tools. We also anticipate more providers will acquire licenses in other states to virtually care for patients who lack access to specialty services in their own community, which increases access where it is most needed. After 2020, we hope that telehealth will no longer be a specialized service only some patients can receive but a normal way of delivering care to all.
Ms. Winkelman is the system director of telehealth product development and delivery at Providence St. Joseph Health. Providence is the third-largest nonprofit health system in the United States with 51 hospitals, more than 800 clinics, and a comprehensive range of health and social services across Alaska, California, Montana, New Mexico, Oregon, Texas, and Washington.
Telehealth exploded into the public consciousness this year as a way for clinicians and patients to safely connect during the COVID-19 crisis. While telehealth has been part of care delivery at Providence St. Joseph Health (PSJH) for more than a decade, it transitioned almost overnight from an offering most often focused on serving patients in rural areas to a way for any patient to get the care they need virtually whether in a hospital, outpatient facility, or from the comfort and safety of their own home.
Telehealth growth was fueled by changes in regulation and reimbursement during the public health emergency enabling providers to see new and established patients at home across all payer types. To put this growth into perspective, the large PSJH system averaged a few thousand video visits per month in January and February 2020. As COVID transmission spread and lockdowns began, that number climbed to over 15,000 video visits in March to a height of more than 150,000 video visits in May. As of the end of October 2020, PSJH has conducted more than 1.2 million video visits since the beginning of January, steadily accounting for 20%-25% of total visit volume.
Going virtual with gastroenterology
PSJH gastroenterology providers have been a part of this wave, conducting more than 12,000 video visits so far this year (as documented in our Epic EMR), which has been an entirely new method of care delivery for most of these clinicians. We also have many affiliated, private practice gastroenterology providers who practice in our facilities and transitioned quickly to video for outpatient care. Pre- and postprocedure follow-up visits were some of the most common visit types that went virtual, along with new patient visits to establish care and existing patient visits to check in on the status of a health condition, medication, or other concern. Complementary services for gastroenterology patients were transitioned to video over the past 8 months as well. Care management, nutrition services, online support groups, bariatric care information sessions, behavioral health, and more are now available for patients to access virtually.
Remembering it’s not about the tech
New technologies can be challenging to adopt – especially at a pace as rapid as it was this year. Fortunately for PSJH, we had inpatient and outpatient video platforms already in place and an experienced internal telehealth team to scale them quickly to providers and caregivers across system. But even with those advantages, it was still a huge challenge to transition so many providers and caregivers to video visits in such a short time without change management hurdles and bumps along the way.
Too often, there is an overemphasis placed on the technology. It’s a tool, and some technologies are better than others, and they continue to evolve over time. True success or failure lies in the clinical and operational work flows and how well the providers and care teams engage with and adapt them. We found that the providers and staff members willing to venture outside their comfort zone of “how we’ve always done it” and collaborate on the transition to virtual care had the best results. Openness and flexibility to trying new things and using temporary workarounds if existing functionality didn’t meet the need was key to transitioning quickly. Then, by listening to ideas from and sharing feedback among providers, clinics, and geographies, we were able to identify fixes and optimizations that needed to be made to improve the experience for all.
Selecting a video visit platform
No telehealth platform is perfect and meets every patient, provider, and staff need or request despite what a technology vendor may claim. This is especially true in a large and/or diverse system with many different types of clinical use cases. Determining the “must-have” requirements from among those that may be important or simply nice to have is critical when selecting the video visit platform to use.
It’s not an easy decision and nearly impossible to please everyone. Ensuring that there are clinician, operator, and technical stakeholders all contributing to the requirements and decision-making is essential. While some may prefer a “best-of-breed” solution that does one thing very well, it may have to be paired with a set of other complimentary applications to meet all of the organization’s needs. Alternatively, there may be a platform with an expansive feature set but not all of the features are as strong as desired. Then there are solutions that integrate with your existing applications, which is a compelling option to consider.
Regardless of the tool chosen, best-practice work flows, easy-to-follow documentation, a mix of different training options, and internal technical help that responds quickly is key to implementing it successfully. And once implemented, optimization is an ongoing process to make it easier, faster, and better.
Looking ahead
As we came to the end of 2020, all providers and health systems were paying close attention to the Centers for Medicaid & Medicare Services and state-level regulations and reimbursement changes for 2021 to evaluate the impact on telehealth after the public health emergency and COVID-19 waivers are ended. Advocacy efforts are urging lawmakers to not lose the gains that were made during this time and have enabled millions of patients to access care more easily – changes which we believe they will now expect as an option going forward.
We at Providence believe telehealth’s future is a bright one, especially where value-based/managed care arrangements with payers are in place. In addition to integrating video visits and consults into normal clinical practice, we see further growth in serving patients at home with remote patient monitoring and other home-based programs that leverage connected devices and virtual tools. We also anticipate more providers will acquire licenses in other states to virtually care for patients who lack access to specialty services in their own community, which increases access where it is most needed. After 2020, we hope that telehealth will no longer be a specialized service only some patients can receive but a normal way of delivering care to all.
Ms. Winkelman is the system director of telehealth product development and delivery at Providence St. Joseph Health. Providence is the third-largest nonprofit health system in the United States with 51 hospitals, more than 800 clinics, and a comprehensive range of health and social services across Alaska, California, Montana, New Mexico, Oregon, Texas, and Washington.
Telehealth exploded into the public consciousness this year as a way for clinicians and patients to safely connect during the COVID-19 crisis. While telehealth has been part of care delivery at Providence St. Joseph Health (PSJH) for more than a decade, it transitioned almost overnight from an offering most often focused on serving patients in rural areas to a way for any patient to get the care they need virtually whether in a hospital, outpatient facility, or from the comfort and safety of their own home.
Telehealth growth was fueled by changes in regulation and reimbursement during the public health emergency enabling providers to see new and established patients at home across all payer types. To put this growth into perspective, the large PSJH system averaged a few thousand video visits per month in January and February 2020. As COVID transmission spread and lockdowns began, that number climbed to over 15,000 video visits in March to a height of more than 150,000 video visits in May. As of the end of October 2020, PSJH has conducted more than 1.2 million video visits since the beginning of January, steadily accounting for 20%-25% of total visit volume.
Going virtual with gastroenterology
PSJH gastroenterology providers have been a part of this wave, conducting more than 12,000 video visits so far this year (as documented in our Epic EMR), which has been an entirely new method of care delivery for most of these clinicians. We also have many affiliated, private practice gastroenterology providers who practice in our facilities and transitioned quickly to video for outpatient care. Pre- and postprocedure follow-up visits were some of the most common visit types that went virtual, along with new patient visits to establish care and existing patient visits to check in on the status of a health condition, medication, or other concern. Complementary services for gastroenterology patients were transitioned to video over the past 8 months as well. Care management, nutrition services, online support groups, bariatric care information sessions, behavioral health, and more are now available for patients to access virtually.
Remembering it’s not about the tech
New technologies can be challenging to adopt – especially at a pace as rapid as it was this year. Fortunately for PSJH, we had inpatient and outpatient video platforms already in place and an experienced internal telehealth team to scale them quickly to providers and caregivers across system. But even with those advantages, it was still a huge challenge to transition so many providers and caregivers to video visits in such a short time without change management hurdles and bumps along the way.
Too often, there is an overemphasis placed on the technology. It’s a tool, and some technologies are better than others, and they continue to evolve over time. True success or failure lies in the clinical and operational work flows and how well the providers and care teams engage with and adapt them. We found that the providers and staff members willing to venture outside their comfort zone of “how we’ve always done it” and collaborate on the transition to virtual care had the best results. Openness and flexibility to trying new things and using temporary workarounds if existing functionality didn’t meet the need was key to transitioning quickly. Then, by listening to ideas from and sharing feedback among providers, clinics, and geographies, we were able to identify fixes and optimizations that needed to be made to improve the experience for all.
Selecting a video visit platform
No telehealth platform is perfect and meets every patient, provider, and staff need or request despite what a technology vendor may claim. This is especially true in a large and/or diverse system with many different types of clinical use cases. Determining the “must-have” requirements from among those that may be important or simply nice to have is critical when selecting the video visit platform to use.
It’s not an easy decision and nearly impossible to please everyone. Ensuring that there are clinician, operator, and technical stakeholders all contributing to the requirements and decision-making is essential. While some may prefer a “best-of-breed” solution that does one thing very well, it may have to be paired with a set of other complimentary applications to meet all of the organization’s needs. Alternatively, there may be a platform with an expansive feature set but not all of the features are as strong as desired. Then there are solutions that integrate with your existing applications, which is a compelling option to consider.
Regardless of the tool chosen, best-practice work flows, easy-to-follow documentation, a mix of different training options, and internal technical help that responds quickly is key to implementing it successfully. And once implemented, optimization is an ongoing process to make it easier, faster, and better.
Looking ahead
As we came to the end of 2020, all providers and health systems were paying close attention to the Centers for Medicaid & Medicare Services and state-level regulations and reimbursement changes for 2021 to evaluate the impact on telehealth after the public health emergency and COVID-19 waivers are ended. Advocacy efforts are urging lawmakers to not lose the gains that were made during this time and have enabled millions of patients to access care more easily – changes which we believe they will now expect as an option going forward.
We at Providence believe telehealth’s future is a bright one, especially where value-based/managed care arrangements with payers are in place. In addition to integrating video visits and consults into normal clinical practice, we see further growth in serving patients at home with remote patient monitoring and other home-based programs that leverage connected devices and virtual tools. We also anticipate more providers will acquire licenses in other states to virtually care for patients who lack access to specialty services in their own community, which increases access where it is most needed. After 2020, we hope that telehealth will no longer be a specialized service only some patients can receive but a normal way of delivering care to all.
Ms. Winkelman is the system director of telehealth product development and delivery at Providence St. Joseph Health. Providence is the third-largest nonprofit health system in the United States with 51 hospitals, more than 800 clinics, and a comprehensive range of health and social services across Alaska, California, Montana, New Mexico, Oregon, Texas, and Washington.
How a gift of stock to the AGA Research Foundation can be a win-win
If you own stock that’s increased in value since you purchased it (and you’ve owned it for at least 1 year), you have a unique opportunity for philanthropy. When you donate securities to the AGA Research Foundation, you receive the same income tax savings (if you itemize) that you would if you wrote the AGA Research Foundation a check, but with the added benefit of eliminating capital gains taxes on the transfer, which can be as high as 20%.
Making a gift of securities to support the AGA Research Foundation’s mission to raise funds to support young researchers in gastroenterology and hepatology is as easy as instructing your broker to transfer the shares. Using assets other than cash also allows you more flexibility when planning your gift.
Benefits:
- Receive an income tax deduction for gifts of securities if you itemize.
- Provide relief from capital gains tax with gifts of securities.
- Help fulfill our mission with your contribution.
Take the next step:
The AGA Research Foundation can help clarify and document the steps to donate stock to us. Contact us at [email protected] to make your donation.
If you own stock that’s increased in value since you purchased it (and you’ve owned it for at least 1 year), you have a unique opportunity for philanthropy. When you donate securities to the AGA Research Foundation, you receive the same income tax savings (if you itemize) that you would if you wrote the AGA Research Foundation a check, but with the added benefit of eliminating capital gains taxes on the transfer, which can be as high as 20%.
Making a gift of securities to support the AGA Research Foundation’s mission to raise funds to support young researchers in gastroenterology and hepatology is as easy as instructing your broker to transfer the shares. Using assets other than cash also allows you more flexibility when planning your gift.
Benefits:
- Receive an income tax deduction for gifts of securities if you itemize.
- Provide relief from capital gains tax with gifts of securities.
- Help fulfill our mission with your contribution.
Take the next step:
The AGA Research Foundation can help clarify and document the steps to donate stock to us. Contact us at [email protected] to make your donation.
If you own stock that’s increased in value since you purchased it (and you’ve owned it for at least 1 year), you have a unique opportunity for philanthropy. When you donate securities to the AGA Research Foundation, you receive the same income tax savings (if you itemize) that you would if you wrote the AGA Research Foundation a check, but with the added benefit of eliminating capital gains taxes on the transfer, which can be as high as 20%.
Making a gift of securities to support the AGA Research Foundation’s mission to raise funds to support young researchers in gastroenterology and hepatology is as easy as instructing your broker to transfer the shares. Using assets other than cash also allows you more flexibility when planning your gift.
Benefits:
- Receive an income tax deduction for gifts of securities if you itemize.
- Provide relief from capital gains tax with gifts of securities.
- Help fulfill our mission with your contribution.
Take the next step:
The AGA Research Foundation can help clarify and document the steps to donate stock to us. Contact us at [email protected] to make your donation.
Registration for DDW® 2021 is now open
Join your colleagues in the digestive disease community at the most prestigious meeting for GI professionals. Registration for Digestive Disease Week® (DDW) 2021 is now open. Register on or before March 31 to receive a discounted rate. AGA member trainees, postdoctoral fellows, medical residents and students also receive complimentary registration during this early bird period.
In 2021, DDW moves online as a fully virtual meeting, taking place May 21–23, 2021. While DDW Virtual™ will look a little different, we’re excited by opportunities the new format provides to learn, share, and connect, such as the following:
- Explore today’s most pressing topics and new developments, shared in oral abstract and ePoster presentations.
- Gain the kind of insight that you can’t get out of a textbook, presented in sessions led by top GI and hepatology experts.
- Network and build connections with your colleagues in an engaging, interactive setting.
Learn more and register at ddw.org.
Join your colleagues in the digestive disease community at the most prestigious meeting for GI professionals. Registration for Digestive Disease Week® (DDW) 2021 is now open. Register on or before March 31 to receive a discounted rate. AGA member trainees, postdoctoral fellows, medical residents and students also receive complimentary registration during this early bird period.
In 2021, DDW moves online as a fully virtual meeting, taking place May 21–23, 2021. While DDW Virtual™ will look a little different, we’re excited by opportunities the new format provides to learn, share, and connect, such as the following:
- Explore today’s most pressing topics and new developments, shared in oral abstract and ePoster presentations.
- Gain the kind of insight that you can’t get out of a textbook, presented in sessions led by top GI and hepatology experts.
- Network and build connections with your colleagues in an engaging, interactive setting.
Learn more and register at ddw.org.
Join your colleagues in the digestive disease community at the most prestigious meeting for GI professionals. Registration for Digestive Disease Week® (DDW) 2021 is now open. Register on or before March 31 to receive a discounted rate. AGA member trainees, postdoctoral fellows, medical residents and students also receive complimentary registration during this early bird period.
In 2021, DDW moves online as a fully virtual meeting, taking place May 21–23, 2021. While DDW Virtual™ will look a little different, we’re excited by opportunities the new format provides to learn, share, and connect, such as the following:
- Explore today’s most pressing topics and new developments, shared in oral abstract and ePoster presentations.
- Gain the kind of insight that you can’t get out of a textbook, presented in sessions led by top GI and hepatology experts.
- Network and build connections with your colleagues in an engaging, interactive setting.
Learn more and register at ddw.org.
Meet the 2021 AGA Fellowship inductees
Join the GI community in a round of applause for the 120 members adding the designation “AGAF” in their professional activities. Along with a recognition pin and certificate of acceptance, American Gastroenterological Association President Bishr Omary commends the group in the AGA Community for their superior professional achievements and contributions to the field of gastroenterology. See the full list and join the discussion at https://community.gastro.org.
Join the GI community in a round of applause for the 120 members adding the designation “AGAF” in their professional activities. Along with a recognition pin and certificate of acceptance, American Gastroenterological Association President Bishr Omary commends the group in the AGA Community for their superior professional achievements and contributions to the field of gastroenterology. See the full list and join the discussion at https://community.gastro.org.
Join the GI community in a round of applause for the 120 members adding the designation “AGAF” in their professional activities. Along with a recognition pin and certificate of acceptance, American Gastroenterological Association President Bishr Omary commends the group in the AGA Community for their superior professional achievements and contributions to the field of gastroenterology. See the full list and join the discussion at https://community.gastro.org.
Advocacy in gastroenterology: Advancing health policies for our patients and our profession
Physician advocacy is an important tool for health care professionals to protect patients and the vitality of the profession. Medical associations across the spectrum participate in advocacy because of its value in preserving the beneficial role of physicians in health care policy decision making. This is especially true for specialty physician associations, like the American Gastroenterological Association, which represents more than 9,000 U.S. GI physicians and researchers. Advocacy allows for the voice of GIs and their patients to be heard on Capitol Hill, in the White House, and among various regulatory agencies. When we advocate as a profession, we help ensure good policies gain momentum and halt harmful legislative or regulatory efforts from enactment.
What is physician advocacy?
Physicians are advocating every day for their patients by helping patients make the right decisions about their care. This naturally translates into advocacy at the health policy level. Advocacy is lobbying. While that word may take on a negative meaning for some, it also means being a persuasive communicator, passionate educator, and a leader. National associations, like AGA, often call on members to do just that: educate lawmakers on policies affecting GI, communicate how policies could affect lawmakers’ constituencies back in their respective districts, and lead others to support GI policy agendas.
Physician advocacy works. AGA had its busiest year for policy work, but this was coupled with a large uptick in GI advocacy engagement. The public health emergency placed many burdens on the health care community and our profession. However, through our advocacy work, we also saw many changes, including increased federal research funding for digestive diseases and GI cancers, passage of legislation to remove patients’ barriers to colorectal cancer screening, increased regulatory and reimbursement flexibilities incorporated to ensure physicians could continue to deliver timely care, and creation of federal financial and small business relief programs to support gastroenterology practices.
Physician advocacy in GI is especially critical because specialty care is often viewed as having a smaller voice when compared with those of the larger bodies, such as primary care, surgery, or emergency physicians. As a health care specialty with a known shortage across the United States, we need all the help we can get to inform policy makers of our position on controversial policies. In many cases, non–health care professionals are informing policy makers on how to address issues that impact our profession. Additionally, there is a lack of knowledge about health care complexities and needs among decision makers who are ultimately determining how health care is delivered. As health care experts, we are best suited to educate lawmakers on the true impact of health policies. If we do not engage and educate policy makers, our profession and patients will suffer the consequences.
GI policy priorities for 2021
AGA will continue its advocacy work in 2021 on the following issues and encourage you and your colleagues to get involved:
Administrative burden relief
Utilization management protocols, like prior authorizations and step therapy, continue to increase and force physicians and their staff to spend hours of extra work time each week to process the paperwork. Prior authorizations are especially troublesome because they have increased for upper GI procedures and other common procedures. Step therapy protocols have also increased for IBD patients on biologics or other high-cost therapies, resulting in patients not receiving effective therapies as determined by their physician in a timely manner.
Patient access and protections
Coverage
Coverage for patients includes the following two areas:
COVID-19 relief: The public health emergency has weakened the health care workforce with physician practices and researchers facing financial instability and threatened patient access to specialty care. To support the health care community and to combat the pandemic, the following is necessary: Increased access to personal protective equipment and medical supplies for testing and vaccination distribution and increased rapid tests, testing sites, and health care workers. The public health emergency response also requires a stronger emphasis on health equity given the disproportionate impact it has had on communities of color.
- Preserving Affordable Care Act patient protections: The Supreme Court will rule on the Affordable Care Act, a decision which threatens to dismantle the law, including provisions that require insurers to cover preexisting conditions and preventive services. With patients delaying screenings because of the COVID-19 pandemic and the increased incidence among minority and younger populations, it is imperative that preventative screening services – like colorectal cancer screenings – remain fully covered by payers. Moreover, because of the nature of GI diseases, patients often develop multiple conditions throughout their lifetime. The preexisting conditions protections in the ACA ensure that GI patients can gain the insurance coverage they need to obtain quality treatment.
Choice
Health plans and pharmacy benefit managers are using burdensome practices, such as step therapy, to limit patient access to drugs and biologics. These practices disrupt treatment and restrict individuals with digestive diseases from the medicines that work best for them.
Affordability
High out-of-pocket drug and biologics costs limit access to necessary therapies for people with digestive diseases, such as Crohn’s disease and ulcerative colitis. High out-of-pocket costs contribute to noncompliance, which in turn results in disease progression and complications and increases in overall health care costs.
Research funding
Sustainable long-term funding for federal research is critical to ensure the United States remains a leading contributor to innovative research breakthroughs. Under the current appropriations process in Congress, federal research funding can vary dramatically from year to year. Often enough, research funding for the next fiscal year is delayed by politics in Congress that result in continuing resolutions to fund the government and U.S. research institutions. Unstable funding causes a turbulent environment for investigators and is a deterrent for new investigators entering the field.
Member engagement
GIs need to engage in the policymaking process as there are too many threats and opportunities in today’s policy arena. The effectiveness of AGA’s advocacy work in the federal government is contingent upon members’ engagement in public policy. To increase physician advocacy and AGA member engagement, AGA offers the following avenues for members:
AGA political action committee
Political engagement is a powerful tool physician advocates can use to increase the visibility of GI on Capitol Hill. Political action committees (PACs) help provide access to lawmakers and their staff so that our advocates can educate them on the rationale for supporting our clinical and research priorities. Although PACs do not guarantee successes in Congress, it is important to note that contributions to legislators’ campaigns help them to be run more smoothly and effectively and allow the legislators to continue to serve their constituents. AGA PAC is a bipartisan political arm of AGA and is the only PAC dedicated to gastroenterology. Learn more at gastro.org/AGA-PAC.
Grassroots engagement
Build a relationship with your elected officials and their health policy staff by communicating with them often and offering to serve as a resource to the office on issues related to specialty medicine. AGA makes this easy with its online advocacy action center: gastro.quorum.us. Find out who your lawmakers are and research their background, engage them by email or Twitter on priority policy issues, and share stories with AGA staff about your interactions with congressional offices.
Congressional Advocates Program
This program creates a national grassroots network of engaged gastroenterologists interested in advocating for our profession and patients. Congressional Advocates are mentored and receive year-round advocacy training by AGA leadership and staff. Learn more at gastro.org/advocacy-and-policy/congressional-advocates-program.
Start advocating for gastroenterology
A new session of Congress has just begun, a new administration with a heavy health care agenda was elected into office, and gastroenterology needs your voice more than ever as we advocate for what really matters to us and our patients.
Join your colleagues at AGA’s spring virtual Advocacy Day on April 22, 2021. The event allows AGA members to meet with lawmakers and health policy staff virtually to educate them on the priority issues affecting our profession.
AGA staff makes it easy for you to participate. Webinar trainings, meeting schedules, and talking points will be provided to you ahead of time. For this event, we will speak to lawmakers about increasing federal research funding, addressing regulatory burdens like prior authorizations and step therapy protocols, and ensuring gastroenterologists and investigators have continued support during the COVID-19 pandemic.
For more information, visit gastro.org/aga-advocacy-day or contact AGA’s senior public policy coordinator, Jonathan Sollish, at [email protected].
Physician advocacy is an important tool for health care professionals to protect patients and the vitality of the profession. Medical associations across the spectrum participate in advocacy because of its value in preserving the beneficial role of physicians in health care policy decision making. This is especially true for specialty physician associations, like the American Gastroenterological Association, which represents more than 9,000 U.S. GI physicians and researchers. Advocacy allows for the voice of GIs and their patients to be heard on Capitol Hill, in the White House, and among various regulatory agencies. When we advocate as a profession, we help ensure good policies gain momentum and halt harmful legislative or regulatory efforts from enactment.
What is physician advocacy?
Physicians are advocating every day for their patients by helping patients make the right decisions about their care. This naturally translates into advocacy at the health policy level. Advocacy is lobbying. While that word may take on a negative meaning for some, it also means being a persuasive communicator, passionate educator, and a leader. National associations, like AGA, often call on members to do just that: educate lawmakers on policies affecting GI, communicate how policies could affect lawmakers’ constituencies back in their respective districts, and lead others to support GI policy agendas.
Physician advocacy works. AGA had its busiest year for policy work, but this was coupled with a large uptick in GI advocacy engagement. The public health emergency placed many burdens on the health care community and our profession. However, through our advocacy work, we also saw many changes, including increased federal research funding for digestive diseases and GI cancers, passage of legislation to remove patients’ barriers to colorectal cancer screening, increased regulatory and reimbursement flexibilities incorporated to ensure physicians could continue to deliver timely care, and creation of federal financial and small business relief programs to support gastroenterology practices.
Physician advocacy in GI is especially critical because specialty care is often viewed as having a smaller voice when compared with those of the larger bodies, such as primary care, surgery, or emergency physicians. As a health care specialty with a known shortage across the United States, we need all the help we can get to inform policy makers of our position on controversial policies. In many cases, non–health care professionals are informing policy makers on how to address issues that impact our profession. Additionally, there is a lack of knowledge about health care complexities and needs among decision makers who are ultimately determining how health care is delivered. As health care experts, we are best suited to educate lawmakers on the true impact of health policies. If we do not engage and educate policy makers, our profession and patients will suffer the consequences.
GI policy priorities for 2021
AGA will continue its advocacy work in 2021 on the following issues and encourage you and your colleagues to get involved:
Administrative burden relief
Utilization management protocols, like prior authorizations and step therapy, continue to increase and force physicians and their staff to spend hours of extra work time each week to process the paperwork. Prior authorizations are especially troublesome because they have increased for upper GI procedures and other common procedures. Step therapy protocols have also increased for IBD patients on biologics or other high-cost therapies, resulting in patients not receiving effective therapies as determined by their physician in a timely manner.
Patient access and protections
Coverage
Coverage for patients includes the following two areas:
COVID-19 relief: The public health emergency has weakened the health care workforce with physician practices and researchers facing financial instability and threatened patient access to specialty care. To support the health care community and to combat the pandemic, the following is necessary: Increased access to personal protective equipment and medical supplies for testing and vaccination distribution and increased rapid tests, testing sites, and health care workers. The public health emergency response also requires a stronger emphasis on health equity given the disproportionate impact it has had on communities of color.
- Preserving Affordable Care Act patient protections: The Supreme Court will rule on the Affordable Care Act, a decision which threatens to dismantle the law, including provisions that require insurers to cover preexisting conditions and preventive services. With patients delaying screenings because of the COVID-19 pandemic and the increased incidence among minority and younger populations, it is imperative that preventative screening services – like colorectal cancer screenings – remain fully covered by payers. Moreover, because of the nature of GI diseases, patients often develop multiple conditions throughout their lifetime. The preexisting conditions protections in the ACA ensure that GI patients can gain the insurance coverage they need to obtain quality treatment.
Choice
Health plans and pharmacy benefit managers are using burdensome practices, such as step therapy, to limit patient access to drugs and biologics. These practices disrupt treatment and restrict individuals with digestive diseases from the medicines that work best for them.
Affordability
High out-of-pocket drug and biologics costs limit access to necessary therapies for people with digestive diseases, such as Crohn’s disease and ulcerative colitis. High out-of-pocket costs contribute to noncompliance, which in turn results in disease progression and complications and increases in overall health care costs.
Research funding
Sustainable long-term funding for federal research is critical to ensure the United States remains a leading contributor to innovative research breakthroughs. Under the current appropriations process in Congress, federal research funding can vary dramatically from year to year. Often enough, research funding for the next fiscal year is delayed by politics in Congress that result in continuing resolutions to fund the government and U.S. research institutions. Unstable funding causes a turbulent environment for investigators and is a deterrent for new investigators entering the field.
Member engagement
GIs need to engage in the policymaking process as there are too many threats and opportunities in today’s policy arena. The effectiveness of AGA’s advocacy work in the federal government is contingent upon members’ engagement in public policy. To increase physician advocacy and AGA member engagement, AGA offers the following avenues for members:
AGA political action committee
Political engagement is a powerful tool physician advocates can use to increase the visibility of GI on Capitol Hill. Political action committees (PACs) help provide access to lawmakers and their staff so that our advocates can educate them on the rationale for supporting our clinical and research priorities. Although PACs do not guarantee successes in Congress, it is important to note that contributions to legislators’ campaigns help them to be run more smoothly and effectively and allow the legislators to continue to serve their constituents. AGA PAC is a bipartisan political arm of AGA and is the only PAC dedicated to gastroenterology. Learn more at gastro.org/AGA-PAC.
Grassroots engagement
Build a relationship with your elected officials and their health policy staff by communicating with them often and offering to serve as a resource to the office on issues related to specialty medicine. AGA makes this easy with its online advocacy action center: gastro.quorum.us. Find out who your lawmakers are and research their background, engage them by email or Twitter on priority policy issues, and share stories with AGA staff about your interactions with congressional offices.
Congressional Advocates Program
This program creates a national grassroots network of engaged gastroenterologists interested in advocating for our profession and patients. Congressional Advocates are mentored and receive year-round advocacy training by AGA leadership and staff. Learn more at gastro.org/advocacy-and-policy/congressional-advocates-program.
Start advocating for gastroenterology
A new session of Congress has just begun, a new administration with a heavy health care agenda was elected into office, and gastroenterology needs your voice more than ever as we advocate for what really matters to us and our patients.
Join your colleagues at AGA’s spring virtual Advocacy Day on April 22, 2021. The event allows AGA members to meet with lawmakers and health policy staff virtually to educate them on the priority issues affecting our profession.
AGA staff makes it easy for you to participate. Webinar trainings, meeting schedules, and talking points will be provided to you ahead of time. For this event, we will speak to lawmakers about increasing federal research funding, addressing regulatory burdens like prior authorizations and step therapy protocols, and ensuring gastroenterologists and investigators have continued support during the COVID-19 pandemic.
For more information, visit gastro.org/aga-advocacy-day or contact AGA’s senior public policy coordinator, Jonathan Sollish, at [email protected].
Physician advocacy is an important tool for health care professionals to protect patients and the vitality of the profession. Medical associations across the spectrum participate in advocacy because of its value in preserving the beneficial role of physicians in health care policy decision making. This is especially true for specialty physician associations, like the American Gastroenterological Association, which represents more than 9,000 U.S. GI physicians and researchers. Advocacy allows for the voice of GIs and their patients to be heard on Capitol Hill, in the White House, and among various regulatory agencies. When we advocate as a profession, we help ensure good policies gain momentum and halt harmful legislative or regulatory efforts from enactment.
What is physician advocacy?
Physicians are advocating every day for their patients by helping patients make the right decisions about their care. This naturally translates into advocacy at the health policy level. Advocacy is lobbying. While that word may take on a negative meaning for some, it also means being a persuasive communicator, passionate educator, and a leader. National associations, like AGA, often call on members to do just that: educate lawmakers on policies affecting GI, communicate how policies could affect lawmakers’ constituencies back in their respective districts, and lead others to support GI policy agendas.
Physician advocacy works. AGA had its busiest year for policy work, but this was coupled with a large uptick in GI advocacy engagement. The public health emergency placed many burdens on the health care community and our profession. However, through our advocacy work, we also saw many changes, including increased federal research funding for digestive diseases and GI cancers, passage of legislation to remove patients’ barriers to colorectal cancer screening, increased regulatory and reimbursement flexibilities incorporated to ensure physicians could continue to deliver timely care, and creation of federal financial and small business relief programs to support gastroenterology practices.
Physician advocacy in GI is especially critical because specialty care is often viewed as having a smaller voice when compared with those of the larger bodies, such as primary care, surgery, or emergency physicians. As a health care specialty with a known shortage across the United States, we need all the help we can get to inform policy makers of our position on controversial policies. In many cases, non–health care professionals are informing policy makers on how to address issues that impact our profession. Additionally, there is a lack of knowledge about health care complexities and needs among decision makers who are ultimately determining how health care is delivered. As health care experts, we are best suited to educate lawmakers on the true impact of health policies. If we do not engage and educate policy makers, our profession and patients will suffer the consequences.
GI policy priorities for 2021
AGA will continue its advocacy work in 2021 on the following issues and encourage you and your colleagues to get involved:
Administrative burden relief
Utilization management protocols, like prior authorizations and step therapy, continue to increase and force physicians and their staff to spend hours of extra work time each week to process the paperwork. Prior authorizations are especially troublesome because they have increased for upper GI procedures and other common procedures. Step therapy protocols have also increased for IBD patients on biologics or other high-cost therapies, resulting in patients not receiving effective therapies as determined by their physician in a timely manner.
Patient access and protections
Coverage
Coverage for patients includes the following two areas:
COVID-19 relief: The public health emergency has weakened the health care workforce with physician practices and researchers facing financial instability and threatened patient access to specialty care. To support the health care community and to combat the pandemic, the following is necessary: Increased access to personal protective equipment and medical supplies for testing and vaccination distribution and increased rapid tests, testing sites, and health care workers. The public health emergency response also requires a stronger emphasis on health equity given the disproportionate impact it has had on communities of color.
- Preserving Affordable Care Act patient protections: The Supreme Court will rule on the Affordable Care Act, a decision which threatens to dismantle the law, including provisions that require insurers to cover preexisting conditions and preventive services. With patients delaying screenings because of the COVID-19 pandemic and the increased incidence among minority and younger populations, it is imperative that preventative screening services – like colorectal cancer screenings – remain fully covered by payers. Moreover, because of the nature of GI diseases, patients often develop multiple conditions throughout their lifetime. The preexisting conditions protections in the ACA ensure that GI patients can gain the insurance coverage they need to obtain quality treatment.
Choice
Health plans and pharmacy benefit managers are using burdensome practices, such as step therapy, to limit patient access to drugs and biologics. These practices disrupt treatment and restrict individuals with digestive diseases from the medicines that work best for them.
Affordability
High out-of-pocket drug and biologics costs limit access to necessary therapies for people with digestive diseases, such as Crohn’s disease and ulcerative colitis. High out-of-pocket costs contribute to noncompliance, which in turn results in disease progression and complications and increases in overall health care costs.
Research funding
Sustainable long-term funding for federal research is critical to ensure the United States remains a leading contributor to innovative research breakthroughs. Under the current appropriations process in Congress, federal research funding can vary dramatically from year to year. Often enough, research funding for the next fiscal year is delayed by politics in Congress that result in continuing resolutions to fund the government and U.S. research institutions. Unstable funding causes a turbulent environment for investigators and is a deterrent for new investigators entering the field.
Member engagement
GIs need to engage in the policymaking process as there are too many threats and opportunities in today’s policy arena. The effectiveness of AGA’s advocacy work in the federal government is contingent upon members’ engagement in public policy. To increase physician advocacy and AGA member engagement, AGA offers the following avenues for members:
AGA political action committee
Political engagement is a powerful tool physician advocates can use to increase the visibility of GI on Capitol Hill. Political action committees (PACs) help provide access to lawmakers and their staff so that our advocates can educate them on the rationale for supporting our clinical and research priorities. Although PACs do not guarantee successes in Congress, it is important to note that contributions to legislators’ campaigns help them to be run more smoothly and effectively and allow the legislators to continue to serve their constituents. AGA PAC is a bipartisan political arm of AGA and is the only PAC dedicated to gastroenterology. Learn more at gastro.org/AGA-PAC.
Grassroots engagement
Build a relationship with your elected officials and their health policy staff by communicating with them often and offering to serve as a resource to the office on issues related to specialty medicine. AGA makes this easy with its online advocacy action center: gastro.quorum.us. Find out who your lawmakers are and research their background, engage them by email or Twitter on priority policy issues, and share stories with AGA staff about your interactions with congressional offices.
Congressional Advocates Program
This program creates a national grassroots network of engaged gastroenterologists interested in advocating for our profession and patients. Congressional Advocates are mentored and receive year-round advocacy training by AGA leadership and staff. Learn more at gastro.org/advocacy-and-policy/congressional-advocates-program.
Start advocating for gastroenterology
A new session of Congress has just begun, a new administration with a heavy health care agenda was elected into office, and gastroenterology needs your voice more than ever as we advocate for what really matters to us and our patients.
Join your colleagues at AGA’s spring virtual Advocacy Day on April 22, 2021. The event allows AGA members to meet with lawmakers and health policy staff virtually to educate them on the priority issues affecting our profession.
AGA staff makes it easy for you to participate. Webinar trainings, meeting schedules, and talking points will be provided to you ahead of time. For this event, we will speak to lawmakers about increasing federal research funding, addressing regulatory burdens like prior authorizations and step therapy protocols, and ensuring gastroenterologists and investigators have continued support during the COVID-19 pandemic.
For more information, visit gastro.org/aga-advocacy-day or contact AGA’s senior public policy coordinator, Jonathan Sollish, at [email protected].
PET predicts response to endocrine therapy in ER+ breast cancer
Endocrine therapy is the standard of care for estrogen receptor–positive (ER+) breast cancer, but only about half of women respond. At present, there is no method for identifying the women who are likely – and also unlikely – to respond.
But a new approach looks to be useful. It involves a trial of estrogen followed by imaging that measures the function of estrogen receptors in the cancer cells.
This functional testing of estrogen receptors on breast cancer cells was perfectly accurate in predicting endocrine therapy response in 43 postmenopausal women with advanced ER+ disease, say researchers from Washington University, St. Louis, led by Farrokh Dehdashti, MD.
“There is an unmet clinical need to develop more precise predictive biomarkers. The results of this study are extremely promising,” they conclude.
The study was published online in Nature Communications.
For the study, the women were first infused with a radioactive progestin analog – 21-[18F]fluorofuranylnorprogesterone (FFNP) – that binds progesterone receptors. About 40 minutes later, they had a PET scan to assess its uptake, an indication of progesterone-receptor abundance.
The women were then given three 200-mg doses of estradiol over 24 hours.
The FFNP infusion and PET scan were repeated the next day.
Estradiol will cause cancer cells with functional estrogen receptors to produce more progesterone receptors, so increased uptake of the radioactive analog indicates functional estrogen receptors that will respond to endocrine therapy. If estrogen receptors are not functional, and therefore not amenable to endocrine therapy (ET), estradiol will not upregulate progesterone receptors.
The results proved the theory. FFNP uptake increased more than 6.7% in 28 subjects and a median of 25.4%. All 28 women responded to subsequent ET, including 15 partial responses and 13 women with stable disease at 6 months.
Median survival was not reached after a median follow up of 27.1 months.
Uptake increased no more than 6.7% in 15 subjects and, in fact, fell a median of 0.7% from baseline. None of these women responded to ET. The median survival was 22.6 months.
“We observed 100% agreement between the response to estrogen challenge and the response to hormone therapy. … This method should work for any therapy that depends on a functional estrogen receptor, and it could provide valuable information to oncologists deciding how best to treat their patients,” Dr. Dehdashti said in a press release.
A larger multicenter confirmation trial is in the works.
Oncology needs “to get away from empiric therapies and make therapy more individualized” to save patients from the morbidity and expense of ineffective treatment and wasting time when other options are available, Dr. Dehdashti told this news organization.
“It would be a good thing if we could identify endocrine-resistant patients,” said Charles Shapiro, MD, a professor and director of translational breast cancer research at Mount Sinai Hospital, New York.
However, he wondered “about the exportability to less resource-intensive community settings where most oncology care occurs. This technology, assuming the results are confirmed in a larger study, [needs] a cost-effectiveness analysis” vs. the empiric approach, Dr. Shapiro said in an interview.
The women taking part in this study were a median of 60 years old, and most had metastatic disease. PET imaging extended from the base of the skull to the upper thighs, with data derived from bone, lung, breast, and other tumor sites. ET options included aromatase inhibitors, fulvestrant, and tamoxifen in combination with other agents.
Almost three-quarters of the women had prior systemic treatment, most often a hormone therapy–based regimen. Prior treatment had no effect on FFNP uptake.
There were no adverse events with the radiotracer, but the estradiol made a few women nauseous, among other transient discomforts, the team reported.
The work was funded by the National Cancer Institute and Washington University, St. Louis. Dr. Shapiro and Dr. Dehdashti have disclosed no relevant financial relationships. Several investigators reported consulting fees and/or other ties to a number of companies, including Pfizer, Merck, Avid Radiopharmaceutical, and Radius Health.
A version of this article first appeared on Medscape.com.
Endocrine therapy is the standard of care for estrogen receptor–positive (ER+) breast cancer, but only about half of women respond. At present, there is no method for identifying the women who are likely – and also unlikely – to respond.
But a new approach looks to be useful. It involves a trial of estrogen followed by imaging that measures the function of estrogen receptors in the cancer cells.
This functional testing of estrogen receptors on breast cancer cells was perfectly accurate in predicting endocrine therapy response in 43 postmenopausal women with advanced ER+ disease, say researchers from Washington University, St. Louis, led by Farrokh Dehdashti, MD.
“There is an unmet clinical need to develop more precise predictive biomarkers. The results of this study are extremely promising,” they conclude.
The study was published online in Nature Communications.
For the study, the women were first infused with a radioactive progestin analog – 21-[18F]fluorofuranylnorprogesterone (FFNP) – that binds progesterone receptors. About 40 minutes later, they had a PET scan to assess its uptake, an indication of progesterone-receptor abundance.
The women were then given three 200-mg doses of estradiol over 24 hours.
The FFNP infusion and PET scan were repeated the next day.
Estradiol will cause cancer cells with functional estrogen receptors to produce more progesterone receptors, so increased uptake of the radioactive analog indicates functional estrogen receptors that will respond to endocrine therapy. If estrogen receptors are not functional, and therefore not amenable to endocrine therapy (ET), estradiol will not upregulate progesterone receptors.
The results proved the theory. FFNP uptake increased more than 6.7% in 28 subjects and a median of 25.4%. All 28 women responded to subsequent ET, including 15 partial responses and 13 women with stable disease at 6 months.
Median survival was not reached after a median follow up of 27.1 months.
Uptake increased no more than 6.7% in 15 subjects and, in fact, fell a median of 0.7% from baseline. None of these women responded to ET. The median survival was 22.6 months.
“We observed 100% agreement between the response to estrogen challenge and the response to hormone therapy. … This method should work for any therapy that depends on a functional estrogen receptor, and it could provide valuable information to oncologists deciding how best to treat their patients,” Dr. Dehdashti said in a press release.
A larger multicenter confirmation trial is in the works.
Oncology needs “to get away from empiric therapies and make therapy more individualized” to save patients from the morbidity and expense of ineffective treatment and wasting time when other options are available, Dr. Dehdashti told this news organization.
“It would be a good thing if we could identify endocrine-resistant patients,” said Charles Shapiro, MD, a professor and director of translational breast cancer research at Mount Sinai Hospital, New York.
However, he wondered “about the exportability to less resource-intensive community settings where most oncology care occurs. This technology, assuming the results are confirmed in a larger study, [needs] a cost-effectiveness analysis” vs. the empiric approach, Dr. Shapiro said in an interview.
The women taking part in this study were a median of 60 years old, and most had metastatic disease. PET imaging extended from the base of the skull to the upper thighs, with data derived from bone, lung, breast, and other tumor sites. ET options included aromatase inhibitors, fulvestrant, and tamoxifen in combination with other agents.
Almost three-quarters of the women had prior systemic treatment, most often a hormone therapy–based regimen. Prior treatment had no effect on FFNP uptake.
There were no adverse events with the radiotracer, but the estradiol made a few women nauseous, among other transient discomforts, the team reported.
The work was funded by the National Cancer Institute and Washington University, St. Louis. Dr. Shapiro and Dr. Dehdashti have disclosed no relevant financial relationships. Several investigators reported consulting fees and/or other ties to a number of companies, including Pfizer, Merck, Avid Radiopharmaceutical, and Radius Health.
A version of this article first appeared on Medscape.com.
Endocrine therapy is the standard of care for estrogen receptor–positive (ER+) breast cancer, but only about half of women respond. At present, there is no method for identifying the women who are likely – and also unlikely – to respond.
But a new approach looks to be useful. It involves a trial of estrogen followed by imaging that measures the function of estrogen receptors in the cancer cells.
This functional testing of estrogen receptors on breast cancer cells was perfectly accurate in predicting endocrine therapy response in 43 postmenopausal women with advanced ER+ disease, say researchers from Washington University, St. Louis, led by Farrokh Dehdashti, MD.
“There is an unmet clinical need to develop more precise predictive biomarkers. The results of this study are extremely promising,” they conclude.
The study was published online in Nature Communications.
For the study, the women were first infused with a radioactive progestin analog – 21-[18F]fluorofuranylnorprogesterone (FFNP) – that binds progesterone receptors. About 40 minutes later, they had a PET scan to assess its uptake, an indication of progesterone-receptor abundance.
The women were then given three 200-mg doses of estradiol over 24 hours.
The FFNP infusion and PET scan were repeated the next day.
Estradiol will cause cancer cells with functional estrogen receptors to produce more progesterone receptors, so increased uptake of the radioactive analog indicates functional estrogen receptors that will respond to endocrine therapy. If estrogen receptors are not functional, and therefore not amenable to endocrine therapy (ET), estradiol will not upregulate progesterone receptors.
The results proved the theory. FFNP uptake increased more than 6.7% in 28 subjects and a median of 25.4%. All 28 women responded to subsequent ET, including 15 partial responses and 13 women with stable disease at 6 months.
Median survival was not reached after a median follow up of 27.1 months.
Uptake increased no more than 6.7% in 15 subjects and, in fact, fell a median of 0.7% from baseline. None of these women responded to ET. The median survival was 22.6 months.
“We observed 100% agreement between the response to estrogen challenge and the response to hormone therapy. … This method should work for any therapy that depends on a functional estrogen receptor, and it could provide valuable information to oncologists deciding how best to treat their patients,” Dr. Dehdashti said in a press release.
A larger multicenter confirmation trial is in the works.
Oncology needs “to get away from empiric therapies and make therapy more individualized” to save patients from the morbidity and expense of ineffective treatment and wasting time when other options are available, Dr. Dehdashti told this news organization.
“It would be a good thing if we could identify endocrine-resistant patients,” said Charles Shapiro, MD, a professor and director of translational breast cancer research at Mount Sinai Hospital, New York.
However, he wondered “about the exportability to less resource-intensive community settings where most oncology care occurs. This technology, assuming the results are confirmed in a larger study, [needs] a cost-effectiveness analysis” vs. the empiric approach, Dr. Shapiro said in an interview.
The women taking part in this study were a median of 60 years old, and most had metastatic disease. PET imaging extended from the base of the skull to the upper thighs, with data derived from bone, lung, breast, and other tumor sites. ET options included aromatase inhibitors, fulvestrant, and tamoxifen in combination with other agents.
Almost three-quarters of the women had prior systemic treatment, most often a hormone therapy–based regimen. Prior treatment had no effect on FFNP uptake.
There were no adverse events with the radiotracer, but the estradiol made a few women nauseous, among other transient discomforts, the team reported.
The work was funded by the National Cancer Institute and Washington University, St. Louis. Dr. Shapiro and Dr. Dehdashti have disclosed no relevant financial relationships. Several investigators reported consulting fees and/or other ties to a number of companies, including Pfizer, Merck, Avid Radiopharmaceutical, and Radius Health.
A version of this article first appeared on Medscape.com.
Eruptive Annular Papules on the Trunk of an Organ Transplant Recipient
The Diagnosis: Epidermodysplasia Verruciformis
Histopathologic examination of our patient's biopsy specimen revealed mild acanthosis with prominent hypergranulosis and enlarged keratinocytes with blue-gray cytoplasm (Figure). A diagnosis of acquired epidermodysplasia verruciformis (EV) was rendered. The patient was treated with photodynamic therapy utilizing 5-aminolevulinic acid.
Epidermodysplasia verruciformis is characterized by susceptibility to human papillomavirus (HPV) infections via a defect in cellular immunity. Epidermodysplasia verruciformis was first described as an autosomal-recessive genodermatosis, but it can be acquired in immunosuppressed states with an atypical clinical appearance.1 There are few case reports in skin of color. Acquired EV appears in patients with acquired immunodeficiencies that are susceptible to EV-causing HPVs via a similar mechanism found in inherited EV.2 The most common HPV serotypes involved in EV are HPV-5 and HPV-8. The duration of immunosuppression has been found to be positively correlated with the risk for EV development, with the majority of patients developing lesions after 5 years of immunosuppression.3 There is an approximately 60% risk of malignant transformation of EV lesions into nonmelanoma skin cancer.2 This risk is believed to be lower in patients with darker skin.4
Preventative measures including sun protection and annual surveillance are crucial in EV patients given the high rate of malignant transformation in sun-exposed lesions.5 Treatment options for EV are anecdotal and have variable results, ranging from topicals including 5-fluorouracil and imiquimod to systemic medications including acitretin and interferon.3 Photodynamic therapy can be used for extensive EV. Surgical modalities and other destructive methods also have been tried.6
Epidermodysplasia verruciformis often can be confused with similar dermatoses. Porokeratosis appears as annular pink papules with waferlike peripheral scales. Tinea versicolor is a dermatophyte infection caused by Malassezia furfur and presents as multiple dyspigmented, finely scaling, thin papules and plaques. Subacute cutaneous lupus erythematosus presents as pink, scaly, annular or psoriasiform papules and plaques most commonly on the trunk. Discoid lupus erythematosus presents as pink, hypopigmented or depigmented, atrophic plaques with a peripheral rim of erythema that indicates activity. Secondary syphilis, commonly denoted as the "great mimicker," presents as psoriasiform papules and plaques among other variable morphologies.
- Sa NB, Guerini MB, Barbato MT, et al. Epidermodysplasia verruciformis: clinical presentation with varied forms of lesions. An Bras Dermatol. 2011;86(4 suppl 1):S57-S60.
- Rogers HD, Macgregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:315-320.
- Henley JK, Hossler EW. Acquired epidermodysplasia verruciformis occurring in a renal transplant recipient. Cutis. 2017;99:E9-E12.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Fox SH, Elston DM. Epidermodysplasia verruciformis and the risk for malignancy. Cutis. 2016;98:E10-E12.
- Shruti S, Siraj F, Singh A, et al. Epidermodysplasia verruciformis: three case reports and a brief review. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26:59-61.
The Diagnosis: Epidermodysplasia Verruciformis
Histopathologic examination of our patient's biopsy specimen revealed mild acanthosis with prominent hypergranulosis and enlarged keratinocytes with blue-gray cytoplasm (Figure). A diagnosis of acquired epidermodysplasia verruciformis (EV) was rendered. The patient was treated with photodynamic therapy utilizing 5-aminolevulinic acid.
Epidermodysplasia verruciformis is characterized by susceptibility to human papillomavirus (HPV) infections via a defect in cellular immunity. Epidermodysplasia verruciformis was first described as an autosomal-recessive genodermatosis, but it can be acquired in immunosuppressed states with an atypical clinical appearance.1 There are few case reports in skin of color. Acquired EV appears in patients with acquired immunodeficiencies that are susceptible to EV-causing HPVs via a similar mechanism found in inherited EV.2 The most common HPV serotypes involved in EV are HPV-5 and HPV-8. The duration of immunosuppression has been found to be positively correlated with the risk for EV development, with the majority of patients developing lesions after 5 years of immunosuppression.3 There is an approximately 60% risk of malignant transformation of EV lesions into nonmelanoma skin cancer.2 This risk is believed to be lower in patients with darker skin.4
Preventative measures including sun protection and annual surveillance are crucial in EV patients given the high rate of malignant transformation in sun-exposed lesions.5 Treatment options for EV are anecdotal and have variable results, ranging from topicals including 5-fluorouracil and imiquimod to systemic medications including acitretin and interferon.3 Photodynamic therapy can be used for extensive EV. Surgical modalities and other destructive methods also have been tried.6
Epidermodysplasia verruciformis often can be confused with similar dermatoses. Porokeratosis appears as annular pink papules with waferlike peripheral scales. Tinea versicolor is a dermatophyte infection caused by Malassezia furfur and presents as multiple dyspigmented, finely scaling, thin papules and plaques. Subacute cutaneous lupus erythematosus presents as pink, scaly, annular or psoriasiform papules and plaques most commonly on the trunk. Discoid lupus erythematosus presents as pink, hypopigmented or depigmented, atrophic plaques with a peripheral rim of erythema that indicates activity. Secondary syphilis, commonly denoted as the "great mimicker," presents as psoriasiform papules and plaques among other variable morphologies.
The Diagnosis: Epidermodysplasia Verruciformis
Histopathologic examination of our patient's biopsy specimen revealed mild acanthosis with prominent hypergranulosis and enlarged keratinocytes with blue-gray cytoplasm (Figure). A diagnosis of acquired epidermodysplasia verruciformis (EV) was rendered. The patient was treated with photodynamic therapy utilizing 5-aminolevulinic acid.
Epidermodysplasia verruciformis is characterized by susceptibility to human papillomavirus (HPV) infections via a defect in cellular immunity. Epidermodysplasia verruciformis was first described as an autosomal-recessive genodermatosis, but it can be acquired in immunosuppressed states with an atypical clinical appearance.1 There are few case reports in skin of color. Acquired EV appears in patients with acquired immunodeficiencies that are susceptible to EV-causing HPVs via a similar mechanism found in inherited EV.2 The most common HPV serotypes involved in EV are HPV-5 and HPV-8. The duration of immunosuppression has been found to be positively correlated with the risk for EV development, with the majority of patients developing lesions after 5 years of immunosuppression.3 There is an approximately 60% risk of malignant transformation of EV lesions into nonmelanoma skin cancer.2 This risk is believed to be lower in patients with darker skin.4
Preventative measures including sun protection and annual surveillance are crucial in EV patients given the high rate of malignant transformation in sun-exposed lesions.5 Treatment options for EV are anecdotal and have variable results, ranging from topicals including 5-fluorouracil and imiquimod to systemic medications including acitretin and interferon.3 Photodynamic therapy can be used for extensive EV. Surgical modalities and other destructive methods also have been tried.6
Epidermodysplasia verruciformis often can be confused with similar dermatoses. Porokeratosis appears as annular pink papules with waferlike peripheral scales. Tinea versicolor is a dermatophyte infection caused by Malassezia furfur and presents as multiple dyspigmented, finely scaling, thin papules and plaques. Subacute cutaneous lupus erythematosus presents as pink, scaly, annular or psoriasiform papules and plaques most commonly on the trunk. Discoid lupus erythematosus presents as pink, hypopigmented or depigmented, atrophic plaques with a peripheral rim of erythema that indicates activity. Secondary syphilis, commonly denoted as the "great mimicker," presents as psoriasiform papules and plaques among other variable morphologies.
- Sa NB, Guerini MB, Barbato MT, et al. Epidermodysplasia verruciformis: clinical presentation with varied forms of lesions. An Bras Dermatol. 2011;86(4 suppl 1):S57-S60.
- Rogers HD, Macgregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:315-320.
- Henley JK, Hossler EW. Acquired epidermodysplasia verruciformis occurring in a renal transplant recipient. Cutis. 2017;99:E9-E12.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Fox SH, Elston DM. Epidermodysplasia verruciformis and the risk for malignancy. Cutis. 2016;98:E10-E12.
- Shruti S, Siraj F, Singh A, et al. Epidermodysplasia verruciformis: three case reports and a brief review. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26:59-61.
- Sa NB, Guerini MB, Barbato MT, et al. Epidermodysplasia verruciformis: clinical presentation with varied forms of lesions. An Bras Dermatol. 2011;86(4 suppl 1):S57-S60.
- Rogers HD, Macgregor JL, Nord KM, et al. Acquired epidermodysplasia verruciformis. J Am Acad Dermatol. 2009;60:315-320.
- Henley JK, Hossler EW. Acquired epidermodysplasia verruciformis occurring in a renal transplant recipient. Cutis. 2017;99:E9-E12.
- Jacyk WK, De Villiers EM. Epidermodysplasia verruciformis in Africans. Int J Dermatol. 1993;32:806-810.
- Fox SH, Elston DM. Epidermodysplasia verruciformis and the risk for malignancy. Cutis. 2016;98:E10-E12.
- Shruti S, Siraj F, Singh A, et al. Epidermodysplasia verruciformis: three case reports and a brief review. Acta Dermatovenerol Alp Pannonica Adriat. 2017;26:59-61.
A 50-year-old Black woman with systemic lupus erythematosus and a renal transplant 15 years prior due to lupus nephritis presented with a nonpruritic rash on the abdomen of 1 year’s duration. Her immunosuppressive regimen consisted of tacrolimus, azathioprine, and prednisone. Physical examination revealed numerous monomorphic, annular, hyperpigmented, and thin papules with central clearing present on the abdomen extending to the flanks and groin. The patient denied any family history of similar lesions. A 4-mm punch biopsy of an abdominal lesion was performed.
ASDSA warns of rogue insulin pen use for DIY fillers
.
In the safety warning, issued on Feb. 18, the ASDSA reported that ASDSA members, all board-certified dermatologists, have seen evidence online of young people using so-called “hyaluron pens” to inject hyaluronic acid filler in the epidermal and upper dermal skin.
The pens being used and promoted in social media for do-it-yourself filler injections are medical devices originally developed for insulin injections. “The use of air pressure technology causes these pens to deliver the hyaluronic acid to insert nanoscale molecules of the filler through the skin,” according to the ASDSA statement. Marketing materials state that the pens can be used to create volume and shape in the lips, and to improve the appearance of nasolabial lines, marionette lines, brow lines known as “elevens,” and forehead wrinkles. Claims that the hyaluronic acid only reaches the papillary layer of the dermis, and is therefore safe, do not alleviate the risk of injury in inexperienced hands, the ASDSA statement points out.
“We are concerned about California children falling prey to products that are not appropriate and safe for them to use,” Elan Newland, MD, member of the ASDSA and the California Society for Dermatology and Dermatological Surgery (CalDerm), said in the statement. “The power of social media is very strong, especially for impressionable teenagers. CalDerm supports alerting consumers and regulators of the dangers of these pens,” he said.

“TikTok is proving to be an extremely powerful platform to communicate, entertain, and even educate, which is why many physicians are getting involved and finding success there. Unfortunately, just like the World Wide Web, there is misinformation there and even dangerous lies,” Sandra Lee, MD, who practices in Upland, Calif. (and is also known as “Dr. Pimple Popper”), said in the statement.
“It’s very concerning to see young people posting a How To on injecting their own lips with hyaluronic acid serum using an ‘airgun’ pen, which acts much like a BB gun to push with force the product under the skin,” she added. “So many things can go wrong.”
The ASDSA has contacted the Food and Drug Administration to report these safety concerns. “In addition, the ASDSA is alerting state medical and estheticians’ boards regarding these patient safety concerns and alerting consumers directly about the risks through social media and other education materials,” according to the statement.
.
In the safety warning, issued on Feb. 18, the ASDSA reported that ASDSA members, all board-certified dermatologists, have seen evidence online of young people using so-called “hyaluron pens” to inject hyaluronic acid filler in the epidermal and upper dermal skin.
The pens being used and promoted in social media for do-it-yourself filler injections are medical devices originally developed for insulin injections. “The use of air pressure technology causes these pens to deliver the hyaluronic acid to insert nanoscale molecules of the filler through the skin,” according to the ASDSA statement. Marketing materials state that the pens can be used to create volume and shape in the lips, and to improve the appearance of nasolabial lines, marionette lines, brow lines known as “elevens,” and forehead wrinkles. Claims that the hyaluronic acid only reaches the papillary layer of the dermis, and is therefore safe, do not alleviate the risk of injury in inexperienced hands, the ASDSA statement points out.
“We are concerned about California children falling prey to products that are not appropriate and safe for them to use,” Elan Newland, MD, member of the ASDSA and the California Society for Dermatology and Dermatological Surgery (CalDerm), said in the statement. “The power of social media is very strong, especially for impressionable teenagers. CalDerm supports alerting consumers and regulators of the dangers of these pens,” he said.
“TikTok is proving to be an extremely powerful platform to communicate, entertain, and even educate, which is why many physicians are getting involved and finding success there. Unfortunately, just like the World Wide Web, there is misinformation there and even dangerous lies,” Sandra Lee, MD, who practices in Upland, Calif. (and is also known as “Dr. Pimple Popper”), said in the statement.
“It’s very concerning to see young people posting a How To on injecting their own lips with hyaluronic acid serum using an ‘airgun’ pen, which acts much like a BB gun to push with force the product under the skin,” she added. “So many things can go wrong.”
The ASDSA has contacted the Food and Drug Administration to report these safety concerns. “In addition, the ASDSA is alerting state medical and estheticians’ boards regarding these patient safety concerns and alerting consumers directly about the risks through social media and other education materials,” according to the statement.
.
In the safety warning, issued on Feb. 18, the ASDSA reported that ASDSA members, all board-certified dermatologists, have seen evidence online of young people using so-called “hyaluron pens” to inject hyaluronic acid filler in the epidermal and upper dermal skin.
The pens being used and promoted in social media for do-it-yourself filler injections are medical devices originally developed for insulin injections. “The use of air pressure technology causes these pens to deliver the hyaluronic acid to insert nanoscale molecules of the filler through the skin,” according to the ASDSA statement. Marketing materials state that the pens can be used to create volume and shape in the lips, and to improve the appearance of nasolabial lines, marionette lines, brow lines known as “elevens,” and forehead wrinkles. Claims that the hyaluronic acid only reaches the papillary layer of the dermis, and is therefore safe, do not alleviate the risk of injury in inexperienced hands, the ASDSA statement points out.
“We are concerned about California children falling prey to products that are not appropriate and safe for them to use,” Elan Newland, MD, member of the ASDSA and the California Society for Dermatology and Dermatological Surgery (CalDerm), said in the statement. “The power of social media is very strong, especially for impressionable teenagers. CalDerm supports alerting consumers and regulators of the dangers of these pens,” he said.
“TikTok is proving to be an extremely powerful platform to communicate, entertain, and even educate, which is why many physicians are getting involved and finding success there. Unfortunately, just like the World Wide Web, there is misinformation there and even dangerous lies,” Sandra Lee, MD, who practices in Upland, Calif. (and is also known as “Dr. Pimple Popper”), said in the statement.
“It’s very concerning to see young people posting a How To on injecting their own lips with hyaluronic acid serum using an ‘airgun’ pen, which acts much like a BB gun to push with force the product under the skin,” she added. “So many things can go wrong.”
The ASDSA has contacted the Food and Drug Administration to report these safety concerns. “In addition, the ASDSA is alerting state medical and estheticians’ boards regarding these patient safety concerns and alerting consumers directly about the risks through social media and other education materials,” according to the statement.