User login
Coronavirus can spread to heart, brain days after infection
The coronavirus that causes COVID-19 can spread to the heart and brain within days of infection and can survive for months in organs, according to a new study by the National Institutes of Health.
The virus can spread to almost every organ system in the body, which could contribute to the ongoing symptoms seen in “long COVID” patients, the study authors wrote. The study is considered one of the most comprehensive reviews of how the virus replicates in human cells and persists in the human body. It is under review for publication in the journal Nature.
“This is remarkably important work,” Ziyad Al-Aly, MD, director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System, told Bloomberg News. Dr. Al-Aly wasn’t involved with the NIH study but has researched the long-term effects of COVID-19.
“For a long time now, we have been scratching our heads and asking why long COVID seems to affect so many organ systems,” he said. “This paper sheds some light and may help explain why long COVID can occur even in people who had mild or asymptomatic acute disease.”
The NIH researchers sampled and analyzed tissues from autopsies on 44 patients who died after contracting the coronavirus during the first year of the pandemic. They found persistent virus particles in multiple parts of the body, including the heart and brain, for as long as 230 days after symptoms began. This could represent infection with defective virus particles, they said, which has also been seen in persistent infections among measles patients.
“We don’t yet know what burden of chronic illness will result in years to come,” Raina MacIntyre, PhD, a professor of global biosecurity at the University of New South Wales, Sydney, told Bloomberg News.
“Will we see young-onset cardiac failure in survivors or early-onset dementia?” she asked. “These are unanswered questions which call for a precautionary public health approach to mitigation of the spread of this virus.”
Unlike other COVID-19 autopsy research, the NIH team had a more comprehensive postmortem tissue collection process, which typically occurred within a day of the patient’s death, Bloomberg News reported. The researchers also used a variety of ways to preserve tissue to figure out viral levels. They were able to grow the virus collected from several tissues, including the heart, lungs, small intestine, and adrenal glands.
“Our results collectively show that, while the highest burden of SARS-CoV-2 is in the airways and lung, the virus can disseminate early during infection and infect cells throughout the entire body, including widely throughout the brain,” the study authors wrote.
A version of this article first appeared on WebMD.com.
The coronavirus that causes COVID-19 can spread to the heart and brain within days of infection and can survive for months in organs, according to a new study by the National Institutes of Health.
The virus can spread to almost every organ system in the body, which could contribute to the ongoing symptoms seen in “long COVID” patients, the study authors wrote. The study is considered one of the most comprehensive reviews of how the virus replicates in human cells and persists in the human body. It is under review for publication in the journal Nature.
“This is remarkably important work,” Ziyad Al-Aly, MD, director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System, told Bloomberg News. Dr. Al-Aly wasn’t involved with the NIH study but has researched the long-term effects of COVID-19.
“For a long time now, we have been scratching our heads and asking why long COVID seems to affect so many organ systems,” he said. “This paper sheds some light and may help explain why long COVID can occur even in people who had mild or asymptomatic acute disease.”
The NIH researchers sampled and analyzed tissues from autopsies on 44 patients who died after contracting the coronavirus during the first year of the pandemic. They found persistent virus particles in multiple parts of the body, including the heart and brain, for as long as 230 days after symptoms began. This could represent infection with defective virus particles, they said, which has also been seen in persistent infections among measles patients.
“We don’t yet know what burden of chronic illness will result in years to come,” Raina MacIntyre, PhD, a professor of global biosecurity at the University of New South Wales, Sydney, told Bloomberg News.
“Will we see young-onset cardiac failure in survivors or early-onset dementia?” she asked. “These are unanswered questions which call for a precautionary public health approach to mitigation of the spread of this virus.”
Unlike other COVID-19 autopsy research, the NIH team had a more comprehensive postmortem tissue collection process, which typically occurred within a day of the patient’s death, Bloomberg News reported. The researchers also used a variety of ways to preserve tissue to figure out viral levels. They were able to grow the virus collected from several tissues, including the heart, lungs, small intestine, and adrenal glands.
“Our results collectively show that, while the highest burden of SARS-CoV-2 is in the airways and lung, the virus can disseminate early during infection and infect cells throughout the entire body, including widely throughout the brain,” the study authors wrote.
A version of this article first appeared on WebMD.com.
The coronavirus that causes COVID-19 can spread to the heart and brain within days of infection and can survive for months in organs, according to a new study by the National Institutes of Health.
The virus can spread to almost every organ system in the body, which could contribute to the ongoing symptoms seen in “long COVID” patients, the study authors wrote. The study is considered one of the most comprehensive reviews of how the virus replicates in human cells and persists in the human body. It is under review for publication in the journal Nature.
“This is remarkably important work,” Ziyad Al-Aly, MD, director of the Clinical Epidemiology Center at the Veterans Affairs St. Louis Health Care System, told Bloomberg News. Dr. Al-Aly wasn’t involved with the NIH study but has researched the long-term effects of COVID-19.
“For a long time now, we have been scratching our heads and asking why long COVID seems to affect so many organ systems,” he said. “This paper sheds some light and may help explain why long COVID can occur even in people who had mild or asymptomatic acute disease.”
The NIH researchers sampled and analyzed tissues from autopsies on 44 patients who died after contracting the coronavirus during the first year of the pandemic. They found persistent virus particles in multiple parts of the body, including the heart and brain, for as long as 230 days after symptoms began. This could represent infection with defective virus particles, they said, which has also been seen in persistent infections among measles patients.
“We don’t yet know what burden of chronic illness will result in years to come,” Raina MacIntyre, PhD, a professor of global biosecurity at the University of New South Wales, Sydney, told Bloomberg News.
“Will we see young-onset cardiac failure in survivors or early-onset dementia?” she asked. “These are unanswered questions which call for a precautionary public health approach to mitigation of the spread of this virus.”
Unlike other COVID-19 autopsy research, the NIH team had a more comprehensive postmortem tissue collection process, which typically occurred within a day of the patient’s death, Bloomberg News reported. The researchers also used a variety of ways to preserve tissue to figure out viral levels. They were able to grow the virus collected from several tissues, including the heart, lungs, small intestine, and adrenal glands.
“Our results collectively show that, while the highest burden of SARS-CoV-2 is in the airways and lung, the virus can disseminate early during infection and infect cells throughout the entire body, including widely throughout the brain,” the study authors wrote.
A version of this article first appeared on WebMD.com.
Omega-3 supplementation improves sleep, mood in breast cancer patients on hormone therapy
After 4 weeks of treatment, patients who received omega-3 reported better sleep, depression, and mood outcomes than those who received placebo.
Estrogen-receptor inhibitors are used to treat breast cancer with positive hormone receptors in combination with other therapies. However, the drugs can lead to long-term side effects, including hot flashes, night sweats, and changes to mood and sleep.
These side effects are often treated with selective serotonin reuptake inhibitors and some anticonvulsant drugs. Omega-3 supplements contain various polyunsaturated fatty acids, which influence cell signaling and contribute to the production of bioactive fat mediators that counter inflammation. They are widely used in cardiovascular disease, breast cancer, rheumatoid arthritis, depression, and other cognitive disorders. They also appear to amplify the antitumor efficacy of tamoxifen through the inhibition of proliferative and antiapoptotic pathways that that are influenced by estrogen-receptor signaling.
“This study showed that omega-3 supplementation can improve mood and sleep disorder in women suffering from breast cancer while they (are) managing with antihormone drugs. … this supplement can be proposed for the treatment of these patients,” wrote researchers led by Azadeh Moghaddas, MD, PhD, who is an associate professor of clinical pharmacy and pharmacy practice at Isfahan (Iran) University of Medical Sciences.
The study was made available as a preprint on ResearchSquare and has not yet been peer reviewed. It included 60 patients who were screened for baseline mood disorders using the hospital anxiety and depression scale (HADS), then randomized to 2 mg omega-3 per day for 4 weeks, or placebo.
Studies have shown that omega-3 supplementation improves menopause and mood symptoms in postmenopausal women without cancer.
Omega-3 supplementation has neuroprotective effects and improved brain function and mood in rats, and a 2019 review suggested that the evidence is strong enough to warrant clinical studies.
To determine if the supplement was also safe and effective in women with breast cancer undergoing hormone therapy, the researchers analyzed data from 32 patients in the intervention group and 28 patients in the placebo group.
At 4 weeks of follow-up, patients in the intervention group had significantly lower values on the Center for Epidemiological Studies-Depression scale (mean, 22.8 vs. 30.8; P < .001), Profile of Mood State (mean, 30.8 versus 39.5; P<.001), and Pittsburgh Sleep Quality Index (mean, 4.6 vs. 5.9; P = .04). There were no statistically significant changes in these values in the placebo group.
At 4 weeks, paired samples t-test comparisons between the intervention and the placebo groups revealed lower scores in the intervention group for mean scores in the PSQI subscales subjective sleep quality (0.8 vs. 1.4; P = .002), delay in falling asleep (1.1 vs. 1.6; P = .02), and sleep disturbances (0.8 vs. 1.1; P = .005).
There were no significant adverse reactions in either group.
The study is limited by its small sample size and the short follow-up period.
The study was funded by Isfahan University of Medical Sciences. The authors declare no other conflicts of interest.
After 4 weeks of treatment, patients who received omega-3 reported better sleep, depression, and mood outcomes than those who received placebo.
Estrogen-receptor inhibitors are used to treat breast cancer with positive hormone receptors in combination with other therapies. However, the drugs can lead to long-term side effects, including hot flashes, night sweats, and changes to mood and sleep.
These side effects are often treated with selective serotonin reuptake inhibitors and some anticonvulsant drugs. Omega-3 supplements contain various polyunsaturated fatty acids, which influence cell signaling and contribute to the production of bioactive fat mediators that counter inflammation. They are widely used in cardiovascular disease, breast cancer, rheumatoid arthritis, depression, and other cognitive disorders. They also appear to amplify the antitumor efficacy of tamoxifen through the inhibition of proliferative and antiapoptotic pathways that that are influenced by estrogen-receptor signaling.
“This study showed that omega-3 supplementation can improve mood and sleep disorder in women suffering from breast cancer while they (are) managing with antihormone drugs. … this supplement can be proposed for the treatment of these patients,” wrote researchers led by Azadeh Moghaddas, MD, PhD, who is an associate professor of clinical pharmacy and pharmacy practice at Isfahan (Iran) University of Medical Sciences.
The study was made available as a preprint on ResearchSquare and has not yet been peer reviewed. It included 60 patients who were screened for baseline mood disorders using the hospital anxiety and depression scale (HADS), then randomized to 2 mg omega-3 per day for 4 weeks, or placebo.
Studies have shown that omega-3 supplementation improves menopause and mood symptoms in postmenopausal women without cancer.
Omega-3 supplementation has neuroprotective effects and improved brain function and mood in rats, and a 2019 review suggested that the evidence is strong enough to warrant clinical studies.
To determine if the supplement was also safe and effective in women with breast cancer undergoing hormone therapy, the researchers analyzed data from 32 patients in the intervention group and 28 patients in the placebo group.
At 4 weeks of follow-up, patients in the intervention group had significantly lower values on the Center for Epidemiological Studies-Depression scale (mean, 22.8 vs. 30.8; P < .001), Profile of Mood State (mean, 30.8 versus 39.5; P<.001), and Pittsburgh Sleep Quality Index (mean, 4.6 vs. 5.9; P = .04). There were no statistically significant changes in these values in the placebo group.
At 4 weeks, paired samples t-test comparisons between the intervention and the placebo groups revealed lower scores in the intervention group for mean scores in the PSQI subscales subjective sleep quality (0.8 vs. 1.4; P = .002), delay in falling asleep (1.1 vs. 1.6; P = .02), and sleep disturbances (0.8 vs. 1.1; P = .005).
There were no significant adverse reactions in either group.
The study is limited by its small sample size and the short follow-up period.
The study was funded by Isfahan University of Medical Sciences. The authors declare no other conflicts of interest.
After 4 weeks of treatment, patients who received omega-3 reported better sleep, depression, and mood outcomes than those who received placebo.
Estrogen-receptor inhibitors are used to treat breast cancer with positive hormone receptors in combination with other therapies. However, the drugs can lead to long-term side effects, including hot flashes, night sweats, and changes to mood and sleep.
These side effects are often treated with selective serotonin reuptake inhibitors and some anticonvulsant drugs. Omega-3 supplements contain various polyunsaturated fatty acids, which influence cell signaling and contribute to the production of bioactive fat mediators that counter inflammation. They are widely used in cardiovascular disease, breast cancer, rheumatoid arthritis, depression, and other cognitive disorders. They also appear to amplify the antitumor efficacy of tamoxifen through the inhibition of proliferative and antiapoptotic pathways that that are influenced by estrogen-receptor signaling.
“This study showed that omega-3 supplementation can improve mood and sleep disorder in women suffering from breast cancer while they (are) managing with antihormone drugs. … this supplement can be proposed for the treatment of these patients,” wrote researchers led by Azadeh Moghaddas, MD, PhD, who is an associate professor of clinical pharmacy and pharmacy practice at Isfahan (Iran) University of Medical Sciences.
The study was made available as a preprint on ResearchSquare and has not yet been peer reviewed. It included 60 patients who were screened for baseline mood disorders using the hospital anxiety and depression scale (HADS), then randomized to 2 mg omega-3 per day for 4 weeks, or placebo.
Studies have shown that omega-3 supplementation improves menopause and mood symptoms in postmenopausal women without cancer.
Omega-3 supplementation has neuroprotective effects and improved brain function and mood in rats, and a 2019 review suggested that the evidence is strong enough to warrant clinical studies.
To determine if the supplement was also safe and effective in women with breast cancer undergoing hormone therapy, the researchers analyzed data from 32 patients in the intervention group and 28 patients in the placebo group.
At 4 weeks of follow-up, patients in the intervention group had significantly lower values on the Center for Epidemiological Studies-Depression scale (mean, 22.8 vs. 30.8; P < .001), Profile of Mood State (mean, 30.8 versus 39.5; P<.001), and Pittsburgh Sleep Quality Index (mean, 4.6 vs. 5.9; P = .04). There were no statistically significant changes in these values in the placebo group.
At 4 weeks, paired samples t-test comparisons between the intervention and the placebo groups revealed lower scores in the intervention group for mean scores in the PSQI subscales subjective sleep quality (0.8 vs. 1.4; P = .002), delay in falling asleep (1.1 vs. 1.6; P = .02), and sleep disturbances (0.8 vs. 1.1; P = .005).
There were no significant adverse reactions in either group.
The study is limited by its small sample size and the short follow-up period.
The study was funded by Isfahan University of Medical Sciences. The authors declare no other conflicts of interest.
FROM RESEARCHSQUARE
NSCLC Diagnosis
Children and COVID: Nearly 200,000 new cases reported in 1 week
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Available state data show that 198,551 child COVID cases were added during the week of Dec. 17-23 – up by 16.8% from the nearly 170,000 new cases reported the previous week and the highest 7-day figure since Sept. 17-23, when 207,000 cases were reported, the AAP and the CHA said in their weekly COVID report. Since Oct. 22-28, when the weekly count dropped to a seasonal low, the weekly count has nearly doubled.
The largest shares of the nearly 199,000 new cases were divided pretty equally between the Northeast and the South, while the West had just a small bump in cases and the Midwest was in the middle. The largest statewide percent increases came in the New England states, along with New Jersey, the District of Columbia, and Puerto Rico. New York State does not report age ranges for COVID cases, the AAP/CHA report noted.
Emergency department visits and hospital admissions are following a similar trend, as both have risen considerably over the last 2 months, data from the Centers for Disease Control and Prevention show.
COVID-related ED visits for children aged 0-11 years – measured as a proportion of all ED visits – are nearing the pandemic high of 4.1% set in late August, while visits in 12- to 15-year-olds have risen from 1.4% in early November to 5.6% on Dec. 24 and 16- to 17-year-olds have gone from 1.5% to 6% over the same period of time, the CDC reported on its COVID Data Tracker.
As for hospital admissions in children aged 0-17 years, the rate was down to 0.19 per 100,000 population on Nov. 11 but had risen to 0.38 per 100,000 as of Dec. 24. The highest point reached in children during the pandemic was 0.46 per 100,000 in early September, the CDC said.
On Dec. 23, 367 children were admitted to hospitals in the United States, the highest number since Sept. 7, when 374 were hospitalized. The highest 1-day total over the course of the pandemic, 394, came just a week before that, Aug. 31, according to the Department of Health & Human Services.
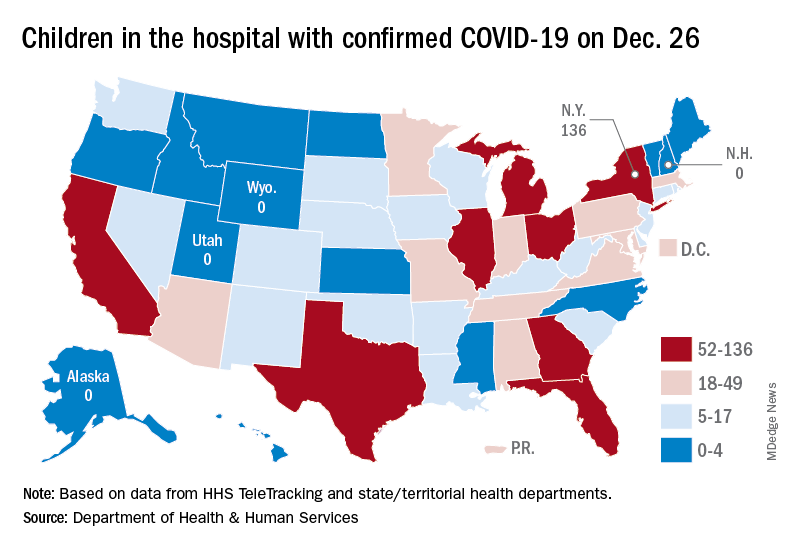
A look at the most recent HHS data shows that 1,161 children were being hospitalized in pediatric inpatient beds with confirmed COVID-19 on Dec. 26. The highest number by state was in New York (136), followed by Texas (90) and Illinois and Ohio, both with 83. There were four states – Alaska, New Hampshire, Utah, and Wyoming – with no hospitalized children, the HHS said. Puerto Rico, meanwhile, had 28 children in the hospital with COVID, more than 38 states.
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Available state data show that 198,551 child COVID cases were added during the week of Dec. 17-23 – up by 16.8% from the nearly 170,000 new cases reported the previous week and the highest 7-day figure since Sept. 17-23, when 207,000 cases were reported, the AAP and the CHA said in their weekly COVID report. Since Oct. 22-28, when the weekly count dropped to a seasonal low, the weekly count has nearly doubled.
The largest shares of the nearly 199,000 new cases were divided pretty equally between the Northeast and the South, while the West had just a small bump in cases and the Midwest was in the middle. The largest statewide percent increases came in the New England states, along with New Jersey, the District of Columbia, and Puerto Rico. New York State does not report age ranges for COVID cases, the AAP/CHA report noted.
Emergency department visits and hospital admissions are following a similar trend, as both have risen considerably over the last 2 months, data from the Centers for Disease Control and Prevention show.
COVID-related ED visits for children aged 0-11 years – measured as a proportion of all ED visits – are nearing the pandemic high of 4.1% set in late August, while visits in 12- to 15-year-olds have risen from 1.4% in early November to 5.6% on Dec. 24 and 16- to 17-year-olds have gone from 1.5% to 6% over the same period of time, the CDC reported on its COVID Data Tracker.
As for hospital admissions in children aged 0-17 years, the rate was down to 0.19 per 100,000 population on Nov. 11 but had risen to 0.38 per 100,000 as of Dec. 24. The highest point reached in children during the pandemic was 0.46 per 100,000 in early September, the CDC said.
On Dec. 23, 367 children were admitted to hospitals in the United States, the highest number since Sept. 7, when 374 were hospitalized. The highest 1-day total over the course of the pandemic, 394, came just a week before that, Aug. 31, according to the Department of Health & Human Services.
A look at the most recent HHS data shows that 1,161 children were being hospitalized in pediatric inpatient beds with confirmed COVID-19 on Dec. 26. The highest number by state was in New York (136), followed by Texas (90) and Illinois and Ohio, both with 83. There were four states – Alaska, New Hampshire, Utah, and Wyoming – with no hospitalized children, the HHS said. Puerto Rico, meanwhile, had 28 children in the hospital with COVID, more than 38 states.
, according to the American Academy of Pediatrics and the Children’s Hospital Association.
Available state data show that 198,551 child COVID cases were added during the week of Dec. 17-23 – up by 16.8% from the nearly 170,000 new cases reported the previous week and the highest 7-day figure since Sept. 17-23, when 207,000 cases were reported, the AAP and the CHA said in their weekly COVID report. Since Oct. 22-28, when the weekly count dropped to a seasonal low, the weekly count has nearly doubled.
The largest shares of the nearly 199,000 new cases were divided pretty equally between the Northeast and the South, while the West had just a small bump in cases and the Midwest was in the middle. The largest statewide percent increases came in the New England states, along with New Jersey, the District of Columbia, and Puerto Rico. New York State does not report age ranges for COVID cases, the AAP/CHA report noted.
Emergency department visits and hospital admissions are following a similar trend, as both have risen considerably over the last 2 months, data from the Centers for Disease Control and Prevention show.
COVID-related ED visits for children aged 0-11 years – measured as a proportion of all ED visits – are nearing the pandemic high of 4.1% set in late August, while visits in 12- to 15-year-olds have risen from 1.4% in early November to 5.6% on Dec. 24 and 16- to 17-year-olds have gone from 1.5% to 6% over the same period of time, the CDC reported on its COVID Data Tracker.
As for hospital admissions in children aged 0-17 years, the rate was down to 0.19 per 100,000 population on Nov. 11 but had risen to 0.38 per 100,000 as of Dec. 24. The highest point reached in children during the pandemic was 0.46 per 100,000 in early September, the CDC said.
On Dec. 23, 367 children were admitted to hospitals in the United States, the highest number since Sept. 7, when 374 were hospitalized. The highest 1-day total over the course of the pandemic, 394, came just a week before that, Aug. 31, according to the Department of Health & Human Services.
A look at the most recent HHS data shows that 1,161 children were being hospitalized in pediatric inpatient beds with confirmed COVID-19 on Dec. 26. The highest number by state was in New York (136), followed by Texas (90) and Illinois and Ohio, both with 83. There were four states – Alaska, New Hampshire, Utah, and Wyoming – with no hospitalized children, the HHS said. Puerto Rico, meanwhile, had 28 children in the hospital with COVID, more than 38 states.
Most cancer patients with breakthrough COVID-19 infection experience severe outcomes
Of 54 fully vaccinated patients with cancer and COVID-19, 35 (65%) were hospitalized, 10 (19%) were admitted to the intensive care unit or required mechanical ventilation, and 7 (13%) died within 30 days.
Although the study did not assess the rate of breakthrough infection among fully vaccinated patients with cancer, the findings do underscore the need for continued vigilance in protecting this vulnerable patient population by vaccinating close contacts, administering boosters, social distancing, and mask-wearing.
“Overall, vaccination remains an invaluable strategy in protecting vulnerable populations, including patients with cancer, against COVID-19. However, patients with cancer who develop breakthrough infection despite full vaccination remain at risk of severe outcomes,” Andrew L. Schmidt, MB, of Dana-Farber Cancer Institute, Boston, and associates wrote.
The analysis, which appeared online in Annals of Oncology Dec. 24 as a pre-proof but has not yet been peer reviewed, analyzed registry data from 1,787 adults with current or prior invasive cancer and laboratory-confirmed COVID-19 between Nov. 1, 2020, and May 31, 2021, before COVID vaccination was widespread. Of those, 1,656 (93%) were unvaccinated, 77 (4%) were partially vaccinated, and 54 (3%) were considered fully vaccinated at the time of COVID-19 infection.
Of the fully vaccinated patients with breakthrough infection, 52 (96%) experienced a severe outcome: two-thirds had to be hospitalized, nearly 1 in 5 went to the ICU or needed mechanical ventilation, and 13% died within 30 days.
“Comparable rates were observed in the unvaccinated group,” the investigators write, adding that there was no statistical difference in 30-day mortality between the fully vaccinated patients and the unvaccinated cohort (adjusted odds ratio, 1.08).
Factors associated with increased 30-day mortality among unvaccinated patients included lymphopenia (aOR, 1.68), comorbidities (aORs, 1.66-2.10), worse performance status (aORs, 2.26-4.34), and baseline cancer status (active/progressing vs. not active/ progressing, aOR, 6.07).
No significant differences were observed in ICU, mechanical ventilation, or hospitalization rates between the vaccinated and unvaccinated cohort after adjustment for confounders (aORs,1.13 and 1.25, respectively).
Notably, patients with an underlying hematologic malignancy were overrepresented among those with breakthrough COVID-19 (35% vs. 20%). Compared with those with solid cancers, patients with hematologic malignancies also had significantly higher rates of ICU admission, mechanical ventilation, and hospitalization.
This finding is “consistent with evidence that these patients may have a blunted serologic response to vaccination secondary to disease or therapy,” the authors note.
Although the investigators did not evaluate the risk of breakthrough infection post vaccination, recent research indicates that receiving a COVID-19 booster increases antibody levels among patients with cancer under active treatment and thus may provide additional protection against the virus.
Given the risk of breakthrough infection and severe outcomes in patients with cancer, the authors propose that “a mitigation approach that includes vaccination of close contacts, boosters, social distancing, and mask-wearing in public should be continued for the foreseeable future.” However, “additional research is needed to further categorize the patients that remain at risk of symptomatic COVID-19 following vaccination and test strategies that may reduce this risk.”
The findings are from a pre-proof that has not yet been peer reviewed or published. First author Dr. Schmidt reported nonfinancial support from Astellas, nonfinancial support from Pfizer, outside the submitted work. Other coauthors reported a range of disclosures as well. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
Of 54 fully vaccinated patients with cancer and COVID-19, 35 (65%) were hospitalized, 10 (19%) were admitted to the intensive care unit or required mechanical ventilation, and 7 (13%) died within 30 days.
Although the study did not assess the rate of breakthrough infection among fully vaccinated patients with cancer, the findings do underscore the need for continued vigilance in protecting this vulnerable patient population by vaccinating close contacts, administering boosters, social distancing, and mask-wearing.
“Overall, vaccination remains an invaluable strategy in protecting vulnerable populations, including patients with cancer, against COVID-19. However, patients with cancer who develop breakthrough infection despite full vaccination remain at risk of severe outcomes,” Andrew L. Schmidt, MB, of Dana-Farber Cancer Institute, Boston, and associates wrote.
The analysis, which appeared online in Annals of Oncology Dec. 24 as a pre-proof but has not yet been peer reviewed, analyzed registry data from 1,787 adults with current or prior invasive cancer and laboratory-confirmed COVID-19 between Nov. 1, 2020, and May 31, 2021, before COVID vaccination was widespread. Of those, 1,656 (93%) were unvaccinated, 77 (4%) were partially vaccinated, and 54 (3%) were considered fully vaccinated at the time of COVID-19 infection.
Of the fully vaccinated patients with breakthrough infection, 52 (96%) experienced a severe outcome: two-thirds had to be hospitalized, nearly 1 in 5 went to the ICU or needed mechanical ventilation, and 13% died within 30 days.
“Comparable rates were observed in the unvaccinated group,” the investigators write, adding that there was no statistical difference in 30-day mortality between the fully vaccinated patients and the unvaccinated cohort (adjusted odds ratio, 1.08).
Factors associated with increased 30-day mortality among unvaccinated patients included lymphopenia (aOR, 1.68), comorbidities (aORs, 1.66-2.10), worse performance status (aORs, 2.26-4.34), and baseline cancer status (active/progressing vs. not active/ progressing, aOR, 6.07).
No significant differences were observed in ICU, mechanical ventilation, or hospitalization rates between the vaccinated and unvaccinated cohort after adjustment for confounders (aORs,1.13 and 1.25, respectively).
Notably, patients with an underlying hematologic malignancy were overrepresented among those with breakthrough COVID-19 (35% vs. 20%). Compared with those with solid cancers, patients with hematologic malignancies also had significantly higher rates of ICU admission, mechanical ventilation, and hospitalization.
This finding is “consistent with evidence that these patients may have a blunted serologic response to vaccination secondary to disease or therapy,” the authors note.
Although the investigators did not evaluate the risk of breakthrough infection post vaccination, recent research indicates that receiving a COVID-19 booster increases antibody levels among patients with cancer under active treatment and thus may provide additional protection against the virus.
Given the risk of breakthrough infection and severe outcomes in patients with cancer, the authors propose that “a mitigation approach that includes vaccination of close contacts, boosters, social distancing, and mask-wearing in public should be continued for the foreseeable future.” However, “additional research is needed to further categorize the patients that remain at risk of symptomatic COVID-19 following vaccination and test strategies that may reduce this risk.”
The findings are from a pre-proof that has not yet been peer reviewed or published. First author Dr. Schmidt reported nonfinancial support from Astellas, nonfinancial support from Pfizer, outside the submitted work. Other coauthors reported a range of disclosures as well. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
Of 54 fully vaccinated patients with cancer and COVID-19, 35 (65%) were hospitalized, 10 (19%) were admitted to the intensive care unit or required mechanical ventilation, and 7 (13%) died within 30 days.
Although the study did not assess the rate of breakthrough infection among fully vaccinated patients with cancer, the findings do underscore the need for continued vigilance in protecting this vulnerable patient population by vaccinating close contacts, administering boosters, social distancing, and mask-wearing.
“Overall, vaccination remains an invaluable strategy in protecting vulnerable populations, including patients with cancer, against COVID-19. However, patients with cancer who develop breakthrough infection despite full vaccination remain at risk of severe outcomes,” Andrew L. Schmidt, MB, of Dana-Farber Cancer Institute, Boston, and associates wrote.
The analysis, which appeared online in Annals of Oncology Dec. 24 as a pre-proof but has not yet been peer reviewed, analyzed registry data from 1,787 adults with current or prior invasive cancer and laboratory-confirmed COVID-19 between Nov. 1, 2020, and May 31, 2021, before COVID vaccination was widespread. Of those, 1,656 (93%) were unvaccinated, 77 (4%) were partially vaccinated, and 54 (3%) were considered fully vaccinated at the time of COVID-19 infection.
Of the fully vaccinated patients with breakthrough infection, 52 (96%) experienced a severe outcome: two-thirds had to be hospitalized, nearly 1 in 5 went to the ICU or needed mechanical ventilation, and 13% died within 30 days.
“Comparable rates were observed in the unvaccinated group,” the investigators write, adding that there was no statistical difference in 30-day mortality between the fully vaccinated patients and the unvaccinated cohort (adjusted odds ratio, 1.08).
Factors associated with increased 30-day mortality among unvaccinated patients included lymphopenia (aOR, 1.68), comorbidities (aORs, 1.66-2.10), worse performance status (aORs, 2.26-4.34), and baseline cancer status (active/progressing vs. not active/ progressing, aOR, 6.07).
No significant differences were observed in ICU, mechanical ventilation, or hospitalization rates between the vaccinated and unvaccinated cohort after adjustment for confounders (aORs,1.13 and 1.25, respectively).
Notably, patients with an underlying hematologic malignancy were overrepresented among those with breakthrough COVID-19 (35% vs. 20%). Compared with those with solid cancers, patients with hematologic malignancies also had significantly higher rates of ICU admission, mechanical ventilation, and hospitalization.
This finding is “consistent with evidence that these patients may have a blunted serologic response to vaccination secondary to disease or therapy,” the authors note.
Although the investigators did not evaluate the risk of breakthrough infection post vaccination, recent research indicates that receiving a COVID-19 booster increases antibody levels among patients with cancer under active treatment and thus may provide additional protection against the virus.
Given the risk of breakthrough infection and severe outcomes in patients with cancer, the authors propose that “a mitigation approach that includes vaccination of close contacts, boosters, social distancing, and mask-wearing in public should be continued for the foreseeable future.” However, “additional research is needed to further categorize the patients that remain at risk of symptomatic COVID-19 following vaccination and test strategies that may reduce this risk.”
The findings are from a pre-proof that has not yet been peer reviewed or published. First author Dr. Schmidt reported nonfinancial support from Astellas, nonfinancial support from Pfizer, outside the submitted work. Other coauthors reported a range of disclosures as well. The full list can be found with the original article.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF ONCOLOGY
FDA gives nod to tralokinumab for adults with moderate to severe AD
whose disease is not well controlled with topical prescription therapies or when those therapies are not advisable.

Administered subcutaneously, tralokinumab is a fully human IgG4 monoclonal antibody that specifically binds to interleukin-13, a key driver of underlying inflammation in AD. The drug, which has been developed by LEO Pharma, comes as a single-dose (150 mg) prefilled syringe with needle guard.
In two pivotal phase 3 trials, ECZTRA 1 and ECZTRA 2, tralokinumab monotherapy was superior to placebo at week 16 for all primary and secondary endpoints. For example, at week 16, for the ECZTRA 1 and 2 monotherapy trials, respectively, 16% and 21% of patients treated with tralokinumab 300 mg every other week achieved clear or almost clear skin (IGA 0/1) versus 7% and 9% with placebo.
In addition, 25% and 33% of patients treated with tralokinumab 300 mg every other week achieved an improvement of 75% or more in the Eczema Area and Severity Index score (EASI-75) versus 13% and 10% with placebo. At 52 weeks, 51% and 60% of patients who responded at week 16 maintained IGA 0/1 response with tralokinumab 300 mg every other week in ECZTRA 1 and 2, respectively.
Finally, 60% and 57% of patients who responded at week 16 maintained EASI-75 response with tralokinumab 300 mg every other week.
In the drug’s third pivotal trial, ECZTRA 3, researchers evaluated the efficacy and safety of tralokinumab 300 mg in combination with topical corticosteroids (TCS) as needed in adults with moderate to severe atopic dermatitis who are candidates for systemic therapy. At week 16, 38% of patients treated with tralokinumab 300 mg every other week plus TCS achieved clear or almost clear skin (IGA 0/1) versus 27% with placebo plus TCS. In addition, 56% of patients treated with tralokinumab 300 mg every other week plus TCS achieved an improvement of 75% or more in the EASI-75 versus 37% with placebo plus TCS. At 32 weeks, 89% and 92% of patients who responded at week 16 maintained response (IGA 0/1 and EASI-75, respectively) with tralokinumab 300 mg every other week.
A link to prescribing information can be found here. Tralokinumab is expected to be available by February 2022.
whose disease is not well controlled with topical prescription therapies or when those therapies are not advisable.
Administered subcutaneously, tralokinumab is a fully human IgG4 monoclonal antibody that specifically binds to interleukin-13, a key driver of underlying inflammation in AD. The drug, which has been developed by LEO Pharma, comes as a single-dose (150 mg) prefilled syringe with needle guard.
In two pivotal phase 3 trials, ECZTRA 1 and ECZTRA 2, tralokinumab monotherapy was superior to placebo at week 16 for all primary and secondary endpoints. For example, at week 16, for the ECZTRA 1 and 2 monotherapy trials, respectively, 16% and 21% of patients treated with tralokinumab 300 mg every other week achieved clear or almost clear skin (IGA 0/1) versus 7% and 9% with placebo.
In addition, 25% and 33% of patients treated with tralokinumab 300 mg every other week achieved an improvement of 75% or more in the Eczema Area and Severity Index score (EASI-75) versus 13% and 10% with placebo. At 52 weeks, 51% and 60% of patients who responded at week 16 maintained IGA 0/1 response with tralokinumab 300 mg every other week in ECZTRA 1 and 2, respectively.
Finally, 60% and 57% of patients who responded at week 16 maintained EASI-75 response with tralokinumab 300 mg every other week.
In the drug’s third pivotal trial, ECZTRA 3, researchers evaluated the efficacy and safety of tralokinumab 300 mg in combination with topical corticosteroids (TCS) as needed in adults with moderate to severe atopic dermatitis who are candidates for systemic therapy. At week 16, 38% of patients treated with tralokinumab 300 mg every other week plus TCS achieved clear or almost clear skin (IGA 0/1) versus 27% with placebo plus TCS. In addition, 56% of patients treated with tralokinumab 300 mg every other week plus TCS achieved an improvement of 75% or more in the EASI-75 versus 37% with placebo plus TCS. At 32 weeks, 89% and 92% of patients who responded at week 16 maintained response (IGA 0/1 and EASI-75, respectively) with tralokinumab 300 mg every other week.
A link to prescribing information can be found here. Tralokinumab is expected to be available by February 2022.
whose disease is not well controlled with topical prescription therapies or when those therapies are not advisable.
Administered subcutaneously, tralokinumab is a fully human IgG4 monoclonal antibody that specifically binds to interleukin-13, a key driver of underlying inflammation in AD. The drug, which has been developed by LEO Pharma, comes as a single-dose (150 mg) prefilled syringe with needle guard.
In two pivotal phase 3 trials, ECZTRA 1 and ECZTRA 2, tralokinumab monotherapy was superior to placebo at week 16 for all primary and secondary endpoints. For example, at week 16, for the ECZTRA 1 and 2 monotherapy trials, respectively, 16% and 21% of patients treated with tralokinumab 300 mg every other week achieved clear or almost clear skin (IGA 0/1) versus 7% and 9% with placebo.
In addition, 25% and 33% of patients treated with tralokinumab 300 mg every other week achieved an improvement of 75% or more in the Eczema Area and Severity Index score (EASI-75) versus 13% and 10% with placebo. At 52 weeks, 51% and 60% of patients who responded at week 16 maintained IGA 0/1 response with tralokinumab 300 mg every other week in ECZTRA 1 and 2, respectively.
Finally, 60% and 57% of patients who responded at week 16 maintained EASI-75 response with tralokinumab 300 mg every other week.
In the drug’s third pivotal trial, ECZTRA 3, researchers evaluated the efficacy and safety of tralokinumab 300 mg in combination with topical corticosteroids (TCS) as needed in adults with moderate to severe atopic dermatitis who are candidates for systemic therapy. At week 16, 38% of patients treated with tralokinumab 300 mg every other week plus TCS achieved clear or almost clear skin (IGA 0/1) versus 27% with placebo plus TCS. In addition, 56% of patients treated with tralokinumab 300 mg every other week plus TCS achieved an improvement of 75% or more in the EASI-75 versus 37% with placebo plus TCS. At 32 weeks, 89% and 92% of patients who responded at week 16 maintained response (IGA 0/1 and EASI-75, respectively) with tralokinumab 300 mg every other week.
A link to prescribing information can be found here. Tralokinumab is expected to be available by February 2022.
Gender-based pay inequity in gastroenterology
In 2017, the number of women students entering medical school surpassed that of men.1 However, the future generation of women doctors is unlikely to be paid the same as their male colleagues for equal work unless something changes in health care. About 34% of gastroenterology fellows are women,2 and there are increasing proportions of women in all academic and community practices, as well as in leadership positions.

Despite this progress, equity in pay between male and female physicians has been unequal in many areas of the country, despite the same level of training.3 Doximity, a social network for physicians, surveyed 65,000 doctors in the United States and found a difference in pay between male and female physicians who worked full time.4 This is an issue that the medical field has been aware of for many years, and articles have been published on this topic in several medical journals.5-11 Doximity found that women physicians are paid less than men, although the extent of the difference varies among regions.

In 2017, per the Doximity report, the field of gastroenterology was one of the top five specialties with the biggest pay gap: Women gastroenterologists earn 19% less (or $86,447) than men gastroenterologists. This study did not differentiate among practice types (academic, private practice, hospital, or multispecialty), but it did break down the data for all physicians into general groups of owner/partner, independent contractor, and employee – it found a gender-based gap in pay among all three of these groups. For owner/partners, the gap was a $114,590 (27.2%) difference.4 According to Doximity survey data from 2018, gastroenterology is no longer in the top five specialties with the largest gender pay gap, indicating the gap is shrinking but still exists.12
A questionnaire sent to gastroenterologists 3, 5, or 10 years after they completed their fellowships (in 1993 or 1995) revealed that after 3 years women earned 23% less per hour than men, and at 5 years, the gap had decreased to 19% less per hour.6-7 The statistical data showed that the mean annual gross income of males was significantly higher at 3 years and 5 years.7 Unfortunately, at 10 years the income gap increased up to 22%.6 The researchers found that female gastroenterologists at academic centers earned 39% less than male gastroenterologists at academic centers, whereas women at nonacademic centers earned 24% less than men, despite similar work hours and call schedules.6-7
Desai and colleauges analyzed health care provider reimbursement data for various medical specialties using the 2014 Medicare Fee-for-Service Provider Utilization and Payment Data Physician and Other Supplier Public Use File, and they found a disparity in reimbursements of female versus male physicians.11 Female physicians received significantly lower Medicare reimbursements in 11 of 13 medical specialties,4 despite adjustments for productivity, work hours, and years of experience. Factors that might affect Medicare reimbursement include variations in payment among different locations, types of service provided, location of procedures performed (hospital vs. clinic), and missing data because of privacy concerns.
Among medical specialties, the gender-based payment gap is highest among vascular surgeons, followed by occupational medicine physicians, gastroenterologists, pediatric endocrinologists, and rheumatologists. In these specialties, men earn approximately 20% more than women (approximately $89,000 more for a male vascular surgeon or about $45,000 more for a male pediatric rheumatologist).4
Gender-based gaps in pay, leadership opportunities, and other opportunities exist in the health care field regardless of whether physicians are employed at academic institutions, community-based private practices, or large health care systems. Women physicians occupy fewer leadership positions, and female physician leaders have greater disparities in pay, compared with men than women who are not in leadership positions.6,10 A 2016 survey of the 50 medical schools with the largest amounts of funding from the National Institutes of Health revealed that only 13% of the department leaders were women.
The Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aimed to close the salary gap between men and women.13 So why are women paid less than men for the same work? Some researchers have proposed “gender differences in negotiation skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.”8,10
The fee for service model based on relative value units can result in lower pay for female physicians, who spend more time with patients, compared with male physicians, because of fewer billable RVUs per hour and per day.15
What should be done?
The American Medical Women’s Association leadership stated that the key to pay equity is transparency, which has been a struggle. Some states, such as New York, require state contractors, including providers that work with the state health department, to disclose salary information. Because of the persistent gender gap in pay in all medical specialties (even after adjustments for age, experience, faculty rank, and measures of research productivity and clinical revenue), the American Medical Association House of Delegates announced a plan to balance salaries within the AMA, and in medicine overall, by promoting research, action, and advocacy.14 In the American College of Physicians, 37% of the members are women. This organization published a position paper in 2018 on gender disparity in pay, and proposed solutions included reviewing and addressing recruitment and advancement of women and other underrepresented groups.15
The executive director of Indiana University’s National Center of Excellence in Women’s Health in Indianapolis, Theresa Rohr-Kirchgraber, MD, who is a professor of clinical care and pediatrics, said that women physicians should bill and code in ways that better reflect the services they provide. Women should also demand more transparency in salaries and push to remove patient satisfaction scores from being a factor in salary determination.16
It is also important to note that there are medical groups and hospitals at which disparities in gender pay might not be an issue, because of physician compensation models. These include but are not limited to Kaiser Permanente and large private practice groups (such as MNGI Digestive Health). For example, with MNGI Digestive Health, shareholder track, ambulatory surgical center distributions are based on full-time equivalent status and not on production. Shareholder compensation is transparent and communicated to all. For Kaiser Permanente, salary is based on specialty and years of service. We will have the opportunity to evaluate the effects of different compensation models as health care delivery moves toward value-based care.
There is a limitation in data presented, as we were unable to obtain specialty salary data from the Association of American Medical Colleges or Medical Group Management Association to confirm findings from the Doximity survey, etc.
Conclusions
It is important to acknowledge that we have made great strides in ensuring gender diversity in the field of gastroenterology. All professional medical and gastroenterological societies are working to address gender disparities in compensation and leadership opportunities. Medical schools and fellowship programs have incorporated training on negotiation skills into their curriculums. The medical profession and overall society will benefit from providing thriving workplaces to female physicians, allowing them to achieve their full potential by ensuring gender equity in compensation and opportunities.
Dr. Perera is a gastroenterologist at Advocate Aurora Health, Grafton, Wisc. Dr. Toriz is a gastroenterologist, treasurer, and board member, MNGI Digestive Health, Bloomington, Minn. They disclosed having no relevant conflicts of interest.
References
1. The American Association of Medical Colleges. “More Women Than Men Enrolled in U.S. Medical schools in 2017.” 2017 Dec 17. http://news.aamc.org/press-releases/article/applicants-enrollment
2. The American Association of Medical Colleges data. https://aamc.org/downlaod/280338/data/tablel3.pdf
3. CBS Business. “The gender pay gap for women doctors is big – and getting worse.” 2018 Mar 14. https://money.CNN.com/2018/03/14/news/economy/gender-pay-gap-doctors/index.html4. Doximity. “Doxmity 2018 Physician Compensation Report.” 2018 Mar 27. https://blog.doximity.com/articles/doximity-2018-physician-compensation-report
5. Tomer G et al. Gastroenterology. 2015;60: 481-5.
6. Singh A et al. Am J Gastroenterol. 2008 Jul;103(7):1589-95.
7. Burke CA et al. Am J Gastroenterol. 2005 Feb;100(2):259-64.
8. Achkar E. Am J Gastroenterol. 2008 Jul;103(7):1587-8.
9. Hoff TJ. Inquiry. 2004;41(3):301-15.
10. Weaver AC et al. J Hosp Med. 2015 Aug;10(8):486-90.
11. Desai T et al. Postgrad Med J. 2016 Oct;92(1092):571-5.
12. Doximity. “Women in Medicine: The Gender Pay Gap” 2018 Oct 2. https://blog.finder.doximity.info/women-in-medicine-the-gender-pay-gap
13. H.R.438. Fair Pay Act of 2013. 113th Congress (2013-2014)
14. O’Reilly KB. American Medical Association. “Physicians adopt plan to combat pay gap in medicine.” 2018 Jun 13. https://www.ama-assn.org/delivering-care/health-equity/physicians-adopt-plan-combat-pay-gap-medicine
15. Butkus R et al. Ann Intern Med. 2018 May 15;168(10):721-3.
16. Commins J. “5 Reasons Women Doctors Earn Less Than Men.” Health Leaders. 2018 Aug 6. https://www.healthleadersmedia.com/clinical-care /5-reasons-women-doctors-earn-less-men
In 2017, the number of women students entering medical school surpassed that of men.1 However, the future generation of women doctors is unlikely to be paid the same as their male colleagues for equal work unless something changes in health care. About 34% of gastroenterology fellows are women,2 and there are increasing proportions of women in all academic and community practices, as well as in leadership positions.
Despite this progress, equity in pay between male and female physicians has been unequal in many areas of the country, despite the same level of training.3 Doximity, a social network for physicians, surveyed 65,000 doctors in the United States and found a difference in pay between male and female physicians who worked full time.4 This is an issue that the medical field has been aware of for many years, and articles have been published on this topic in several medical journals.5-11 Doximity found that women physicians are paid less than men, although the extent of the difference varies among regions.
In 2017, per the Doximity report, the field of gastroenterology was one of the top five specialties with the biggest pay gap: Women gastroenterologists earn 19% less (or $86,447) than men gastroenterologists. This study did not differentiate among practice types (academic, private practice, hospital, or multispecialty), but it did break down the data for all physicians into general groups of owner/partner, independent contractor, and employee – it found a gender-based gap in pay among all three of these groups. For owner/partners, the gap was a $114,590 (27.2%) difference.4 According to Doximity survey data from 2018, gastroenterology is no longer in the top five specialties with the largest gender pay gap, indicating the gap is shrinking but still exists.12
A questionnaire sent to gastroenterologists 3, 5, or 10 years after they completed their fellowships (in 1993 or 1995) revealed that after 3 years women earned 23% less per hour than men, and at 5 years, the gap had decreased to 19% less per hour.6-7 The statistical data showed that the mean annual gross income of males was significantly higher at 3 years and 5 years.7 Unfortunately, at 10 years the income gap increased up to 22%.6 The researchers found that female gastroenterologists at academic centers earned 39% less than male gastroenterologists at academic centers, whereas women at nonacademic centers earned 24% less than men, despite similar work hours and call schedules.6-7
Desai and colleauges analyzed health care provider reimbursement data for various medical specialties using the 2014 Medicare Fee-for-Service Provider Utilization and Payment Data Physician and Other Supplier Public Use File, and they found a disparity in reimbursements of female versus male physicians.11 Female physicians received significantly lower Medicare reimbursements in 11 of 13 medical specialties,4 despite adjustments for productivity, work hours, and years of experience. Factors that might affect Medicare reimbursement include variations in payment among different locations, types of service provided, location of procedures performed (hospital vs. clinic), and missing data because of privacy concerns.
Among medical specialties, the gender-based payment gap is highest among vascular surgeons, followed by occupational medicine physicians, gastroenterologists, pediatric endocrinologists, and rheumatologists. In these specialties, men earn approximately 20% more than women (approximately $89,000 more for a male vascular surgeon or about $45,000 more for a male pediatric rheumatologist).4
Gender-based gaps in pay, leadership opportunities, and other opportunities exist in the health care field regardless of whether physicians are employed at academic institutions, community-based private practices, or large health care systems. Women physicians occupy fewer leadership positions, and female physician leaders have greater disparities in pay, compared with men than women who are not in leadership positions.6,10 A 2016 survey of the 50 medical schools with the largest amounts of funding from the National Institutes of Health revealed that only 13% of the department leaders were women.
The Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aimed to close the salary gap between men and women.13 So why are women paid less than men for the same work? Some researchers have proposed “gender differences in negotiation skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.”8,10
The fee for service model based on relative value units can result in lower pay for female physicians, who spend more time with patients, compared with male physicians, because of fewer billable RVUs per hour and per day.15
What should be done?
The American Medical Women’s Association leadership stated that the key to pay equity is transparency, which has been a struggle. Some states, such as New York, require state contractors, including providers that work with the state health department, to disclose salary information. Because of the persistent gender gap in pay in all medical specialties (even after adjustments for age, experience, faculty rank, and measures of research productivity and clinical revenue), the American Medical Association House of Delegates announced a plan to balance salaries within the AMA, and in medicine overall, by promoting research, action, and advocacy.14 In the American College of Physicians, 37% of the members are women. This organization published a position paper in 2018 on gender disparity in pay, and proposed solutions included reviewing and addressing recruitment and advancement of women and other underrepresented groups.15
The executive director of Indiana University’s National Center of Excellence in Women’s Health in Indianapolis, Theresa Rohr-Kirchgraber, MD, who is a professor of clinical care and pediatrics, said that women physicians should bill and code in ways that better reflect the services they provide. Women should also demand more transparency in salaries and push to remove patient satisfaction scores from being a factor in salary determination.16
It is also important to note that there are medical groups and hospitals at which disparities in gender pay might not be an issue, because of physician compensation models. These include but are not limited to Kaiser Permanente and large private practice groups (such as MNGI Digestive Health). For example, with MNGI Digestive Health, shareholder track, ambulatory surgical center distributions are based on full-time equivalent status and not on production. Shareholder compensation is transparent and communicated to all. For Kaiser Permanente, salary is based on specialty and years of service. We will have the opportunity to evaluate the effects of different compensation models as health care delivery moves toward value-based care.
There is a limitation in data presented, as we were unable to obtain specialty salary data from the Association of American Medical Colleges or Medical Group Management Association to confirm findings from the Doximity survey, etc.
Conclusions
It is important to acknowledge that we have made great strides in ensuring gender diversity in the field of gastroenterology. All professional medical and gastroenterological societies are working to address gender disparities in compensation and leadership opportunities. Medical schools and fellowship programs have incorporated training on negotiation skills into their curriculums. The medical profession and overall society will benefit from providing thriving workplaces to female physicians, allowing them to achieve their full potential by ensuring gender equity in compensation and opportunities.
Dr. Perera is a gastroenterologist at Advocate Aurora Health, Grafton, Wisc. Dr. Toriz is a gastroenterologist, treasurer, and board member, MNGI Digestive Health, Bloomington, Minn. They disclosed having no relevant conflicts of interest.
References
1. The American Association of Medical Colleges. “More Women Than Men Enrolled in U.S. Medical schools in 2017.” 2017 Dec 17. http://news.aamc.org/press-releases/article/applicants-enrollment
2. The American Association of Medical Colleges data. https://aamc.org/downlaod/280338/data/tablel3.pdf
3. CBS Business. “The gender pay gap for women doctors is big – and getting worse.” 2018 Mar 14. https://money.CNN.com/2018/03/14/news/economy/gender-pay-gap-doctors/index.html4. Doximity. “Doxmity 2018 Physician Compensation Report.” 2018 Mar 27. https://blog.doximity.com/articles/doximity-2018-physician-compensation-report
5. Tomer G et al. Gastroenterology. 2015;60: 481-5.
6. Singh A et al. Am J Gastroenterol. 2008 Jul;103(7):1589-95.
7. Burke CA et al. Am J Gastroenterol. 2005 Feb;100(2):259-64.
8. Achkar E. Am J Gastroenterol. 2008 Jul;103(7):1587-8.
9. Hoff TJ. Inquiry. 2004;41(3):301-15.
10. Weaver AC et al. J Hosp Med. 2015 Aug;10(8):486-90.
11. Desai T et al. Postgrad Med J. 2016 Oct;92(1092):571-5.
12. Doximity. “Women in Medicine: The Gender Pay Gap” 2018 Oct 2. https://blog.finder.doximity.info/women-in-medicine-the-gender-pay-gap
13. H.R.438. Fair Pay Act of 2013. 113th Congress (2013-2014)
14. O’Reilly KB. American Medical Association. “Physicians adopt plan to combat pay gap in medicine.” 2018 Jun 13. https://www.ama-assn.org/delivering-care/health-equity/physicians-adopt-plan-combat-pay-gap-medicine
15. Butkus R et al. Ann Intern Med. 2018 May 15;168(10):721-3.
16. Commins J. “5 Reasons Women Doctors Earn Less Than Men.” Health Leaders. 2018 Aug 6. https://www.healthleadersmedia.com/clinical-care /5-reasons-women-doctors-earn-less-men
In 2017, the number of women students entering medical school surpassed that of men.1 However, the future generation of women doctors is unlikely to be paid the same as their male colleagues for equal work unless something changes in health care. About 34% of gastroenterology fellows are women,2 and there are increasing proportions of women in all academic and community practices, as well as in leadership positions.
Despite this progress, equity in pay between male and female physicians has been unequal in many areas of the country, despite the same level of training.3 Doximity, a social network for physicians, surveyed 65,000 doctors in the United States and found a difference in pay between male and female physicians who worked full time.4 This is an issue that the medical field has been aware of for many years, and articles have been published on this topic in several medical journals.5-11 Doximity found that women physicians are paid less than men, although the extent of the difference varies among regions.
In 2017, per the Doximity report, the field of gastroenterology was one of the top five specialties with the biggest pay gap: Women gastroenterologists earn 19% less (or $86,447) than men gastroenterologists. This study did not differentiate among practice types (academic, private practice, hospital, or multispecialty), but it did break down the data for all physicians into general groups of owner/partner, independent contractor, and employee – it found a gender-based gap in pay among all three of these groups. For owner/partners, the gap was a $114,590 (27.2%) difference.4 According to Doximity survey data from 2018, gastroenterology is no longer in the top five specialties with the largest gender pay gap, indicating the gap is shrinking but still exists.12
A questionnaire sent to gastroenterologists 3, 5, or 10 years after they completed their fellowships (in 1993 or 1995) revealed that after 3 years women earned 23% less per hour than men, and at 5 years, the gap had decreased to 19% less per hour.6-7 The statistical data showed that the mean annual gross income of males was significantly higher at 3 years and 5 years.7 Unfortunately, at 10 years the income gap increased up to 22%.6 The researchers found that female gastroenterologists at academic centers earned 39% less than male gastroenterologists at academic centers, whereas women at nonacademic centers earned 24% less than men, despite similar work hours and call schedules.6-7
Desai and colleauges analyzed health care provider reimbursement data for various medical specialties using the 2014 Medicare Fee-for-Service Provider Utilization and Payment Data Physician and Other Supplier Public Use File, and they found a disparity in reimbursements of female versus male physicians.11 Female physicians received significantly lower Medicare reimbursements in 11 of 13 medical specialties,4 despite adjustments for productivity, work hours, and years of experience. Factors that might affect Medicare reimbursement include variations in payment among different locations, types of service provided, location of procedures performed (hospital vs. clinic), and missing data because of privacy concerns.
Among medical specialties, the gender-based payment gap is highest among vascular surgeons, followed by occupational medicine physicians, gastroenterologists, pediatric endocrinologists, and rheumatologists. In these specialties, men earn approximately 20% more than women (approximately $89,000 more for a male vascular surgeon or about $45,000 more for a male pediatric rheumatologist).4
Gender-based gaps in pay, leadership opportunities, and other opportunities exist in the health care field regardless of whether physicians are employed at academic institutions, community-based private practices, or large health care systems. Women physicians occupy fewer leadership positions, and female physician leaders have greater disparities in pay, compared with men than women who are not in leadership positions.6,10 A 2016 survey of the 50 medical schools with the largest amounts of funding from the National Institutes of Health revealed that only 13% of the department leaders were women.
The Fair Pay Act of 2013 and the Paycheck Fairness Act of 2014 aimed to close the salary gap between men and women.13 So why are women paid less than men for the same work? Some researchers have proposed “gender differences in negotiation skills, lack of opportunities to join networks of influence within organizations, and implicit or explicit bias and discrimination.”8,10
The fee for service model based on relative value units can result in lower pay for female physicians, who spend more time with patients, compared with male physicians, because of fewer billable RVUs per hour and per day.15
What should be done?
The American Medical Women’s Association leadership stated that the key to pay equity is transparency, which has been a struggle. Some states, such as New York, require state contractors, including providers that work with the state health department, to disclose salary information. Because of the persistent gender gap in pay in all medical specialties (even after adjustments for age, experience, faculty rank, and measures of research productivity and clinical revenue), the American Medical Association House of Delegates announced a plan to balance salaries within the AMA, and in medicine overall, by promoting research, action, and advocacy.14 In the American College of Physicians, 37% of the members are women. This organization published a position paper in 2018 on gender disparity in pay, and proposed solutions included reviewing and addressing recruitment and advancement of women and other underrepresented groups.15
The executive director of Indiana University’s National Center of Excellence in Women’s Health in Indianapolis, Theresa Rohr-Kirchgraber, MD, who is a professor of clinical care and pediatrics, said that women physicians should bill and code in ways that better reflect the services they provide. Women should also demand more transparency in salaries and push to remove patient satisfaction scores from being a factor in salary determination.16
It is also important to note that there are medical groups and hospitals at which disparities in gender pay might not be an issue, because of physician compensation models. These include but are not limited to Kaiser Permanente and large private practice groups (such as MNGI Digestive Health). For example, with MNGI Digestive Health, shareholder track, ambulatory surgical center distributions are based on full-time equivalent status and not on production. Shareholder compensation is transparent and communicated to all. For Kaiser Permanente, salary is based on specialty and years of service. We will have the opportunity to evaluate the effects of different compensation models as health care delivery moves toward value-based care.
There is a limitation in data presented, as we were unable to obtain specialty salary data from the Association of American Medical Colleges or Medical Group Management Association to confirm findings from the Doximity survey, etc.
Conclusions
It is important to acknowledge that we have made great strides in ensuring gender diversity in the field of gastroenterology. All professional medical and gastroenterological societies are working to address gender disparities in compensation and leadership opportunities. Medical schools and fellowship programs have incorporated training on negotiation skills into their curriculums. The medical profession and overall society will benefit from providing thriving workplaces to female physicians, allowing them to achieve their full potential by ensuring gender equity in compensation and opportunities.
Dr. Perera is a gastroenterologist at Advocate Aurora Health, Grafton, Wisc. Dr. Toriz is a gastroenterologist, treasurer, and board member, MNGI Digestive Health, Bloomington, Minn. They disclosed having no relevant conflicts of interest.
References
1. The American Association of Medical Colleges. “More Women Than Men Enrolled in U.S. Medical schools in 2017.” 2017 Dec 17. http://news.aamc.org/press-releases/article/applicants-enrollment
2. The American Association of Medical Colleges data. https://aamc.org/downlaod/280338/data/tablel3.pdf
3. CBS Business. “The gender pay gap for women doctors is big – and getting worse.” 2018 Mar 14. https://money.CNN.com/2018/03/14/news/economy/gender-pay-gap-doctors/index.html4. Doximity. “Doxmity 2018 Physician Compensation Report.” 2018 Mar 27. https://blog.doximity.com/articles/doximity-2018-physician-compensation-report
5. Tomer G et al. Gastroenterology. 2015;60: 481-5.
6. Singh A et al. Am J Gastroenterol. 2008 Jul;103(7):1589-95.
7. Burke CA et al. Am J Gastroenterol. 2005 Feb;100(2):259-64.
8. Achkar E. Am J Gastroenterol. 2008 Jul;103(7):1587-8.
9. Hoff TJ. Inquiry. 2004;41(3):301-15.
10. Weaver AC et al. J Hosp Med. 2015 Aug;10(8):486-90.
11. Desai T et al. Postgrad Med J. 2016 Oct;92(1092):571-5.
12. Doximity. “Women in Medicine: The Gender Pay Gap” 2018 Oct 2. https://blog.finder.doximity.info/women-in-medicine-the-gender-pay-gap
13. H.R.438. Fair Pay Act of 2013. 113th Congress (2013-2014)
14. O’Reilly KB. American Medical Association. “Physicians adopt plan to combat pay gap in medicine.” 2018 Jun 13. https://www.ama-assn.org/delivering-care/health-equity/physicians-adopt-plan-combat-pay-gap-medicine
15. Butkus R et al. Ann Intern Med. 2018 May 15;168(10):721-3.
16. Commins J. “5 Reasons Women Doctors Earn Less Than Men.” Health Leaders. 2018 Aug 6. https://www.healthleadersmedia.com/clinical-care /5-reasons-women-doctors-earn-less-men