User login
Future of Lupus Treatments Looks Brighter With Multiple Promising Therapeutic Approaches
VIENNA — It may have been a while since there have been any major breakthroughs in the treatment of systemic lupus erythematosus (SLE), but there are high hopes that this is a situation that may be about to change, experts agreed at the annual European Congress of Rheumatology.
“It’s an incredibly vivid area of development,” Laurent Arnaud, MD, PhD, professor of rheumatology at the University of Strasbourg in Strasbourg, France, said during one of the first sessions of the meeting. He reported that there were at least 17 phase 2 and 14 phase 3 trials that were expected to start within the next few years, all with investigational agents that target different immune cells or pathways that have been implicated in the pathogenesis of SLE.

In a systematic review published last year, Dr. Arnaud and coauthors found that there were 92 investigational biologic or novel targeted agents in various phases of clinical testing. This included B-cell–targeting agents such as ianalumab, plasma cell-targeting agents such as daratumumab, and drugs with novel mechanisms of action such as KPG-818, which targets the CRL4-Cereblon (CRBN) E3 ubiquitin ligase complex. Phase 2 data on all three of these investigational agents were presented during various sessions at EULAR 2024, all with positive results, suggesting that their further development in SLE is worth pursuing.
There are of course “many more candidates in the pipeline,” Dr. Arnaud said. “I’m very happy that I think we are going to see great days for lupus right in front of our eyes.”
Targeting B Cells
Drugs that target B cells have been at the forefront of lupus treatment for several years, as David Isenberg, MD, professor of rheumatology at University College London, pointed out during an interview for EULAR TV.
“It’s clearly important to target the cells which are likely to be causing the problem in lupus, and in the main, that tends to be B cells,” he said.
Dr. Isenberg, who is renowned for his work with the B-cell–targeting agent rituximab, added: “But we know that obviously T cells integrate with B cells, so anything which interrupts the link between the T cell and the B cell is likely to be important.”
Chimeric Antigen Receptor (CAR) T-Cell Therapy ‘Revolution’
One new way of targeting B cells is with CAR T-cell therapy, which David D’Cruz , MD, PhD, a consultant rheumatologist for Guy’s and St. Thomas’ Hospital NHS Foundation Trust in London, picked as one of the “most striking” topics highlighted at EULAR 2024.
This is “truly personalized medicine,” Dr. D’Cruz said. This is an autologous therapy because a patient’s T cells are removed by leukapheresis, transfected with a CAR T vector directed against a component of the B cell, and then returned to them.
“I do feel that we’re on the cusp of a major revolution,” Dr. D’Cruz told this news organization. Not only in lupus but also in other rheumatic conditions that have proved really difficult to treat, such as systemic sclerosis and myositis, he said.
“Basically, it’s a very powerful B-cell–depleting tool, but it’s much more profound B-cell–depleting tool than, for example, rituximab or belimumab,” explained Dr. D’Cruz. “What you’re doing is reprogramming T cells to attack the B cells.”
Although rituximab and belimumab clear all the B cells in the circulation, there are still some cells left behind in the bone marrow, “and it’s very difficult to get rid of those,” Dr. D’Cruz said. “What CAR T-cell therapy appears to do is wipe out all the CD19-positive B cells everywhere, in the blood and the tissue. So you get a really profound B-cell depletion.”
Eric Morand, MBBS, PhD, head of rheumatology at Monash Health in Melbourne, Australia, told this news organization that there was obviously “a lot of buzz” about CAR T-cell therapy.

“We’re waiting to see if the exciting data from Erlangen can be reproduced in other centers with other CAR T products to show that it is a universal effect. We haven’t seen that yet, but I think we will by next year.”
Cost and expertise are two major considerations and potential limiting factors, however, as Dr. D’Cruz and Dr. Isenberg both pointed out in separate interviews with this news organization.
Dr. D’Cruz said: “It’s very expensive, it takes a while, and it doesn’t always work is what I’m hearing. It’s usually successful, but again, a little bit depends on the technique and the people doing the process.”
Dr. Isenberg said: “CAR T-cell therapy is, I think, very exciting because it does look to be quite promising. But as it costs 350,000 euros per patient, I don’t think that it is going to be widely adopted.”
Even if it could be afforded by certain centers in the West, he added, this just would not be feasible in poorer nations. “So, we’ve got to find other effective, cheaper ways to go,” Dr. Isenberg said.
“I think there are some very interesting ideas with monoclonal antibodies which target at least two different targets — one on the B cell, one on the T cell — and that could well be the way to take this forward,” he suggested.
Ianalumab ‘Double Blocking’ B Cells
Another way could be to develop more potent B-cell–depleting drugs, as Nancy Agmon-Levin , MD, head of the Clinical Immunology, Angioedema and Allergy Unit, Lupus and Autoimmune Diseases Clinic, at Sheba Medical Center, Tel Aviv University in Tel Aviv, Israel, reported during one of the clinical abstract sessions at EULAR 2024.
Dr. Agmon-Levin presented data on 67 individuals with SLE who had participated in a multicenter phase 2 study of ianalumab, a fully human immunoglobulin (Ig) G1 monoclonal antibody that results in a “double blocking of the B-cell lineage.”
Ianalumab targets the B-cell–activating factor receptor (BAFFR), but what makes it distinct from other BAFF-targeting drugs is that it has had a fructose molecule removed from its Fc portion, which renders it more likely to trigger antibody-dependent cellular cytotoxicity.
“This is a B-cell depletion therapy,” Agmon-Levin said, but it also blocks BAFFR-mediated survival of B cells, so the subsequent recuperation process of BAFFR-expressing B cells is affected, leading to continued B-cell depletion.
The phase 2 study she presented consisted of an initial 28-week, double-blind period, during which time participants had been randomly allocated to receive either subcutaneous injections of ianalumab 300 mg or a matching placebo every 4 weeks. This was followed by a 24-week, open-label period where all participants were treated with ianalumab, and then an off-treatment, minimal follow-up period that lasted up to 68 weeks, with continued data collection for safety.
The primary outcome measure was a composite of meeting criteria for the SLE Responder Index 4 and a sustained reduction in corticosteroid use at 28 weeks. This was achieved in 15 of the 34 (44.1%) people treated with ianalumab vs only 3 (9.1%) of the 33 people who had been given a placebo.
Dr. Agmon-Levin reported that the effect on this outcome was sustained to the end of the open-label period, at 1 year, in 15 (45.5%) of 33 participants who had continued treatment with ianalumab and achieved in 13 (40.6%) of 32 participants who had switched from placebo to ianalumab treatment.
Moreover, longer durations of treatment were associated with a host of improved outcomes, Dr. Agmon-Levin said: “Treatment was improved along the 52 weeks, and we can see from the LLDAS [Lupus Low Disease Activity State], DORIS [Definition Of Remission In SLE], and SRI-6 and -8 that as you continue the therapy, you improve the outcomes.”
The potential benefits of ianalumab in the treatment of SLE and lupus nephritis will now be further examined in the phase 3 SIRIUS-SLE1 , SIRIUS-SLE2, and SIRIUS-LN trials, which are estimated to provide initial results in 2027 and complete in early 2029 or 2030.
Targeting Plasma Cells With Daratumumab
Another drug showing signs that it might be useful as a treatment for SLE is daratumumab, as Tobias Alexander, MD, of Charité — Universitätsmedizin Berlin, reported during one of the late-breaking abstract sessions at EULAR 2024.
“Daratumumab is a human, first-in-class anti-CD38 antibody that efficiently depletes plasma cells,” Dr. Alexander said. CD38 is both a receptor and an enzyme, and while it is found on the surface of most immune cells, it’s particularly expressed by plasma cells, he added.
Daratumumab is not a total newcomer, however, as it’s already approved for the treatment of multiple myeloma under the trade name Darzalex. The rationale for using it in SLE comes from two case reports, Dr. Alexander explained. The first, published in 2020 in The New England Journal of Medicine, involved two patients with severe and life-threatening lupus who were given off-label treatment for a period of 4 weeks and experienced good clinical and serologic responses. The second, published last year in Nature Medicine, involved six patients with refractory lupus nephritis, five of whom had a clinical response at 6 months.
“On this background, we conducted an investigator-initiated trial, which was an open-label, single-center, proof-of-concept study,” Dr. Alexander said. A total of 10 female patients whose ages ranged from 24 to 43 years were included in the phase 2 trial that was dubbed DARALUP. For inclusion, all had to have a Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) of four or more for clinical manifestations, have been treated with at least two prior disease-modifying drugs to no avail, and be anti–double-stranded DNA (anti-dsDNA) antibody positive. Dr. Alexander reported that the median baseline SLEDAI-2K score was 12 and ranged from 8 to 20, with the number of prior therapies ranging from two to nine.
Daratumumab was given at a dose of 1800 mg via subcutaneous injection every week for 8 weeks. This is the same dose that is used to treat multiple myeloma, Dr. Alexander explained, although the dosing is not stopped. The reason for stopping after 8 weeks in the current trial was to be able to see what happened once the treatment was stopped. The follow-up was for 36 weeks.
Dr. Alexander reported that there was a “very dramatic and significant” effect on the primary endpoint of a reduction in anti-dsDNA antibody levels, decreasing from a median of 166.3 U/mL at baseline to 61.1 U/mL at week 12 (P = .002). Alongside, there was a reduction in the SLEDAI-2K score from 12 to 4 within 12 weeks, which was sustained at the 36-week follow-up assessment. Improvements in skin, joint, kidney, and level of proteinuria were also seen.
Although all patients experienced adverse events, none were serious. Infections and infestations (mostly nasopharyngitis, COVID-19, and gastroenteritis) were the most common, experienced by 80% of the participants; 70% had injection site reactions or fatigue, 60% had gastrointestinal symptoms, 50% had a fall of IgG < 5 g/L, 40% had headache, and 20% had back pain.
“This is a positive trial. I think we could demonstrate that [daratumumab] produced very strong, rapid, and durable clinical improvements,” Dr. Alexander said. “We think that targeting CD38 is relevant; plasma cells had been depleted based on the reduction of anti-dsDNA antibodies,” he added.
From the audience, however, Peter Nash, MBBS, of Griffith University in Brisbane, Australia, questioned whether the results could be attributed to “a steroid effect” because patients had been treated with oral dexamethasone throughout the study.
Dr. Alexander noted that steroid use had been part of the treatment schedule but acknowledged it was a possible confounder.
“I think we can be confident that [daratumumab] had a major effect on plasma cells decreasing…because we see that also the vaccine titers decreased,” Dr. Alexander said. “Time will tell, but even more important is the durability of the responses over time, which you don’t achieve under steroids.”
KPG-818’s Novel Mechanism of Action
Elsewhere at EULAR 2024, positive results of another phase 2 study involving a drug with an entirely different mechanism of action, KPG-818, were reported in a poster presentation. KPG-818 modulates CRBN, which results in the degradation of two transcription factors (Aiolos and Ikaros) that are involved in the development, maturation, and proliferation of innate and adaptive immune cells and have been linked to genetic risk in SLE, according to the poster’s authors. It is currently in development for the treatment of SLE, Behçet disease, inflammatory bowel disease, multiple myeloma, and non-Hodgkin lymphoma.
Yao Wang, MD, chief medical officer of KPG-818’s developer Kangpu Biopharmaceuticals, Hefei, China, and associates found that oral doses of 0.15 or 0.6 mg KPG-818 were “generally well-tolerated” and produced immunomodulatory changes that could be beneficial in people with SLE over a 12-week treatment period.
“Only two new agents have been approved for the treatment of SLE in the past five decades in USA and Europe,” Dr. Wang and team wrote, which highlights “a significant unmet need for more effective and safe treatment options.”
They believe that KPG-818 might well fit the bill based on the results of their study, in which 35 of 37 recruited patients completed the treatment. Compared with placebo, they observed reduced numbers of total B cells, Aiolos+ T and B cells, and increased Treg cells.
SLEDAI-2K and Cutaneous Lupus Erythematosus Disease Area and Severity Index activity scores in the 0.15-mg group were improved relative to baseline and placebo.
“The proof-of-concept findings suggest a favorable benefit/risk ratio in SLE for KPG-818,” Dr. Wang and coauthors said, supporting its further development in SLE.
Need for Treatments
Dr. Isenberg told this news organization that both daratumumab and KPG-818 would be welcome additions as treatment options if further trials proved their worth.
“The great frustration about lupus is that, compared to patients with rheumatoid arthritis, the choice has been so limited,” Dr. Isenberg said. Aside from rituximab (Rituxan) and belimumab (Benlysta), which are used with certain restrictions, there are no other biologic targeted treatments available in the United Kingdom. Anifrolumab (Saphnelo) has a license in the United States and some European countries but is not yet available for him to use in his practice.
Daratumumab and KPG-818 are “different types of molecules, and if they work that will be great. It would be nice to have the choice,” Dr. Isenberg said. “Whether they will be as effective as I think rituximab is, I don’t know, but these are some very encouraging results.”
Of course, these are all phase 2 trials, and the “big problem” is that such positive results do not always translate when it comes to phase 3, as Dr. D’Cruz told this news organization.
“Until a few years ago, there had been about 25 or 30 industry-led trails, and they’d all failed, except for belimumab and anifrolumab,” Dr. D’Cruz said. These drugs were found to work and be generally safe in phase 1 and 2 trials, but “when they come to phase 3, they all seem to fail, and we don’t know why.”
These are large global studies, D’Cruz added, observing that problems with patient selection, steroid use, and choice of outcome measures were possible factors for why the EXPLORER and LUNAR studies had shown no benefit for rituximab despite the drug being widely used to treat SLE.
Dr. Isenberg, who has coauthored an article on the topic of why drugs seem to fail at the final hurdle, noted: “I think it has a lot to do with the nature of the disease. It’s a complicated disease.” From having “savvy physicians doing the trials for you” to the placebo response, there are “a whole bunch or reasons why these things haven’t worked in lupus.”
Dr. Morand commented: “We’ve got many programs in phase 2 and 3, and because there’s so many, they’re all facing recruitment challenges, and as a consequence of so much activity, every program is going a little slower than hoped for.”
As for other drugs on the horizon, Dr. Morand noted: “We’re very optimistic about things like litifilimab and deucravacitinib; that’s two examples that are in phase 3. Earlier in the program of development, [there are] a huge range of targets being addressed. The future looks bright. But we might have to wait a while.”
Dr. Arnaud has consulted for AstraZeneca, AbbVie, Alpine Immune Sciences, Biogen, Bristol Myers Squibb, Boehringer Ingelheim, Chugai Pharmaceutical, GlaxoSmithKline, Grifols, Janssen, Kezar Life Sciences, LFB, Lilly, Medac, Merck, Novartis, Pfizer, Roche, and UCB. Dr. Isenberg has served as an adviser to Merck Serono, AstraZeneca, Eli Lilly, Servier, and ImmuPharma. Any honoraria received is passed on to a local arthritis charity connected to his hospital. Dr. D’Cruz has served as a consultant and advisory board member for GlaxoSmithKline and CSL Vifor. Dr. Morand has received research support, consultancy fees, or both from multiple pharmaceutical companies paid to his institution including AbbVie, Amgen, AstraZeneca, Biogen, Bristol Myers Squibb, Eli Lilly, EMD Serono, Dragonfly, Genentech, GlaxoSmithKline, Janssen, Novartis, RemeGen, Takeda, UCB, and Zenas. The ianalumab trial presented by Dr. Agmon-Levin was sponsored by Novartis Pharma; however, she reported having no conflicts of interest. The DARALUP study was an investigator-initiated trial supported by Janssen. Dr. Alexander has received consulting fees, study support, honoraria, and travel grants from various pharmaceutical companies including AbbVie, Amgen, AstraZeneca, Bayer, GlaxoSmithKline, Janssen, and Lilly. Dr. Nash has consulted for The Rheumatology Education Group Consultants. The KPG-818 study reported by Dr. Wang was sponsored by Kangpu Biopharmaceuticals.
A version of this article first appeared on Medscape.com.
VIENNA — It may have been a while since there have been any major breakthroughs in the treatment of systemic lupus erythematosus (SLE), but there are high hopes that this is a situation that may be about to change, experts agreed at the annual European Congress of Rheumatology.
“It’s an incredibly vivid area of development,” Laurent Arnaud, MD, PhD, professor of rheumatology at the University of Strasbourg in Strasbourg, France, said during one of the first sessions of the meeting. He reported that there were at least 17 phase 2 and 14 phase 3 trials that were expected to start within the next few years, all with investigational agents that target different immune cells or pathways that have been implicated in the pathogenesis of SLE.
In a systematic review published last year, Dr. Arnaud and coauthors found that there were 92 investigational biologic or novel targeted agents in various phases of clinical testing. This included B-cell–targeting agents such as ianalumab, plasma cell-targeting agents such as daratumumab, and drugs with novel mechanisms of action such as KPG-818, which targets the CRL4-Cereblon (CRBN) E3 ubiquitin ligase complex. Phase 2 data on all three of these investigational agents were presented during various sessions at EULAR 2024, all with positive results, suggesting that their further development in SLE is worth pursuing.
There are of course “many more candidates in the pipeline,” Dr. Arnaud said. “I’m very happy that I think we are going to see great days for lupus right in front of our eyes.”
Targeting B Cells
Drugs that target B cells have been at the forefront of lupus treatment for several years, as David Isenberg, MD, professor of rheumatology at University College London, pointed out during an interview for EULAR TV.
“It’s clearly important to target the cells which are likely to be causing the problem in lupus, and in the main, that tends to be B cells,” he said.
Dr. Isenberg, who is renowned for his work with the B-cell–targeting agent rituximab, added: “But we know that obviously T cells integrate with B cells, so anything which interrupts the link between the T cell and the B cell is likely to be important.”
Chimeric Antigen Receptor (CAR) T-Cell Therapy ‘Revolution’
One new way of targeting B cells is with CAR T-cell therapy, which David D’Cruz , MD, PhD, a consultant rheumatologist for Guy’s and St. Thomas’ Hospital NHS Foundation Trust in London, picked as one of the “most striking” topics highlighted at EULAR 2024.
This is “truly personalized medicine,” Dr. D’Cruz said. This is an autologous therapy because a patient’s T cells are removed by leukapheresis, transfected with a CAR T vector directed against a component of the B cell, and then returned to them.
“I do feel that we’re on the cusp of a major revolution,” Dr. D’Cruz told this news organization. Not only in lupus but also in other rheumatic conditions that have proved really difficult to treat, such as systemic sclerosis and myositis, he said.
“Basically, it’s a very powerful B-cell–depleting tool, but it’s much more profound B-cell–depleting tool than, for example, rituximab or belimumab,” explained Dr. D’Cruz. “What you’re doing is reprogramming T cells to attack the B cells.”
Although rituximab and belimumab clear all the B cells in the circulation, there are still some cells left behind in the bone marrow, “and it’s very difficult to get rid of those,” Dr. D’Cruz said. “What CAR T-cell therapy appears to do is wipe out all the CD19-positive B cells everywhere, in the blood and the tissue. So you get a really profound B-cell depletion.”
Eric Morand, MBBS, PhD, head of rheumatology at Monash Health in Melbourne, Australia, told this news organization that there was obviously “a lot of buzz” about CAR T-cell therapy.
“We’re waiting to see if the exciting data from Erlangen can be reproduced in other centers with other CAR T products to show that it is a universal effect. We haven’t seen that yet, but I think we will by next year.”
Cost and expertise are two major considerations and potential limiting factors, however, as Dr. D’Cruz and Dr. Isenberg both pointed out in separate interviews with this news organization.
Dr. D’Cruz said: “It’s very expensive, it takes a while, and it doesn’t always work is what I’m hearing. It’s usually successful, but again, a little bit depends on the technique and the people doing the process.”
Dr. Isenberg said: “CAR T-cell therapy is, I think, very exciting because it does look to be quite promising. But as it costs 350,000 euros per patient, I don’t think that it is going to be widely adopted.”
Even if it could be afforded by certain centers in the West, he added, this just would not be feasible in poorer nations. “So, we’ve got to find other effective, cheaper ways to go,” Dr. Isenberg said.
“I think there are some very interesting ideas with monoclonal antibodies which target at least two different targets — one on the B cell, one on the T cell — and that could well be the way to take this forward,” he suggested.
Ianalumab ‘Double Blocking’ B Cells
Another way could be to develop more potent B-cell–depleting drugs, as Nancy Agmon-Levin , MD, head of the Clinical Immunology, Angioedema and Allergy Unit, Lupus and Autoimmune Diseases Clinic, at Sheba Medical Center, Tel Aviv University in Tel Aviv, Israel, reported during one of the clinical abstract sessions at EULAR 2024.
Dr. Agmon-Levin presented data on 67 individuals with SLE who had participated in a multicenter phase 2 study of ianalumab, a fully human immunoglobulin (Ig) G1 monoclonal antibody that results in a “double blocking of the B-cell lineage.”
Ianalumab targets the B-cell–activating factor receptor (BAFFR), but what makes it distinct from other BAFF-targeting drugs is that it has had a fructose molecule removed from its Fc portion, which renders it more likely to trigger antibody-dependent cellular cytotoxicity.
“This is a B-cell depletion therapy,” Agmon-Levin said, but it also blocks BAFFR-mediated survival of B cells, so the subsequent recuperation process of BAFFR-expressing B cells is affected, leading to continued B-cell depletion.
The phase 2 study she presented consisted of an initial 28-week, double-blind period, during which time participants had been randomly allocated to receive either subcutaneous injections of ianalumab 300 mg or a matching placebo every 4 weeks. This was followed by a 24-week, open-label period where all participants were treated with ianalumab, and then an off-treatment, minimal follow-up period that lasted up to 68 weeks, with continued data collection for safety.
The primary outcome measure was a composite of meeting criteria for the SLE Responder Index 4 and a sustained reduction in corticosteroid use at 28 weeks. This was achieved in 15 of the 34 (44.1%) people treated with ianalumab vs only 3 (9.1%) of the 33 people who had been given a placebo.
Dr. Agmon-Levin reported that the effect on this outcome was sustained to the end of the open-label period, at 1 year, in 15 (45.5%) of 33 participants who had continued treatment with ianalumab and achieved in 13 (40.6%) of 32 participants who had switched from placebo to ianalumab treatment.
Moreover, longer durations of treatment were associated with a host of improved outcomes, Dr. Agmon-Levin said: “Treatment was improved along the 52 weeks, and we can see from the LLDAS [Lupus Low Disease Activity State], DORIS [Definition Of Remission In SLE], and SRI-6 and -8 that as you continue the therapy, you improve the outcomes.”
The potential benefits of ianalumab in the treatment of SLE and lupus nephritis will now be further examined in the phase 3 SIRIUS-SLE1 , SIRIUS-SLE2, and SIRIUS-LN trials, which are estimated to provide initial results in 2027 and complete in early 2029 or 2030.
Targeting Plasma Cells With Daratumumab
Another drug showing signs that it might be useful as a treatment for SLE is daratumumab, as Tobias Alexander, MD, of Charité — Universitätsmedizin Berlin, reported during one of the late-breaking abstract sessions at EULAR 2024.
“Daratumumab is a human, first-in-class anti-CD38 antibody that efficiently depletes plasma cells,” Dr. Alexander said. CD38 is both a receptor and an enzyme, and while it is found on the surface of most immune cells, it’s particularly expressed by plasma cells, he added.
Daratumumab is not a total newcomer, however, as it’s already approved for the treatment of multiple myeloma under the trade name Darzalex. The rationale for using it in SLE comes from two case reports, Dr. Alexander explained. The first, published in 2020 in The New England Journal of Medicine, involved two patients with severe and life-threatening lupus who were given off-label treatment for a period of 4 weeks and experienced good clinical and serologic responses. The second, published last year in Nature Medicine, involved six patients with refractory lupus nephritis, five of whom had a clinical response at 6 months.
“On this background, we conducted an investigator-initiated trial, which was an open-label, single-center, proof-of-concept study,” Dr. Alexander said. A total of 10 female patients whose ages ranged from 24 to 43 years were included in the phase 2 trial that was dubbed DARALUP. For inclusion, all had to have a Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) of four or more for clinical manifestations, have been treated with at least two prior disease-modifying drugs to no avail, and be anti–double-stranded DNA (anti-dsDNA) antibody positive. Dr. Alexander reported that the median baseline SLEDAI-2K score was 12 and ranged from 8 to 20, with the number of prior therapies ranging from two to nine.
Daratumumab was given at a dose of 1800 mg via subcutaneous injection every week for 8 weeks. This is the same dose that is used to treat multiple myeloma, Dr. Alexander explained, although the dosing is not stopped. The reason for stopping after 8 weeks in the current trial was to be able to see what happened once the treatment was stopped. The follow-up was for 36 weeks.
Dr. Alexander reported that there was a “very dramatic and significant” effect on the primary endpoint of a reduction in anti-dsDNA antibody levels, decreasing from a median of 166.3 U/mL at baseline to 61.1 U/mL at week 12 (P = .002). Alongside, there was a reduction in the SLEDAI-2K score from 12 to 4 within 12 weeks, which was sustained at the 36-week follow-up assessment. Improvements in skin, joint, kidney, and level of proteinuria were also seen.
Although all patients experienced adverse events, none were serious. Infections and infestations (mostly nasopharyngitis, COVID-19, and gastroenteritis) were the most common, experienced by 80% of the participants; 70% had injection site reactions or fatigue, 60% had gastrointestinal symptoms, 50% had a fall of IgG < 5 g/L, 40% had headache, and 20% had back pain.
“This is a positive trial. I think we could demonstrate that [daratumumab] produced very strong, rapid, and durable clinical improvements,” Dr. Alexander said. “We think that targeting CD38 is relevant; plasma cells had been depleted based on the reduction of anti-dsDNA antibodies,” he added.
From the audience, however, Peter Nash, MBBS, of Griffith University in Brisbane, Australia, questioned whether the results could be attributed to “a steroid effect” because patients had been treated with oral dexamethasone throughout the study.
Dr. Alexander noted that steroid use had been part of the treatment schedule but acknowledged it was a possible confounder.
“I think we can be confident that [daratumumab] had a major effect on plasma cells decreasing…because we see that also the vaccine titers decreased,” Dr. Alexander said. “Time will tell, but even more important is the durability of the responses over time, which you don’t achieve under steroids.”
KPG-818’s Novel Mechanism of Action
Elsewhere at EULAR 2024, positive results of another phase 2 study involving a drug with an entirely different mechanism of action, KPG-818, were reported in a poster presentation. KPG-818 modulates CRBN, which results in the degradation of two transcription factors (Aiolos and Ikaros) that are involved in the development, maturation, and proliferation of innate and adaptive immune cells and have been linked to genetic risk in SLE, according to the poster’s authors. It is currently in development for the treatment of SLE, Behçet disease, inflammatory bowel disease, multiple myeloma, and non-Hodgkin lymphoma.
Yao Wang, MD, chief medical officer of KPG-818’s developer Kangpu Biopharmaceuticals, Hefei, China, and associates found that oral doses of 0.15 or 0.6 mg KPG-818 were “generally well-tolerated” and produced immunomodulatory changes that could be beneficial in people with SLE over a 12-week treatment period.
“Only two new agents have been approved for the treatment of SLE in the past five decades in USA and Europe,” Dr. Wang and team wrote, which highlights “a significant unmet need for more effective and safe treatment options.”
They believe that KPG-818 might well fit the bill based on the results of their study, in which 35 of 37 recruited patients completed the treatment. Compared with placebo, they observed reduced numbers of total B cells, Aiolos+ T and B cells, and increased Treg cells.
SLEDAI-2K and Cutaneous Lupus Erythematosus Disease Area and Severity Index activity scores in the 0.15-mg group were improved relative to baseline and placebo.
“The proof-of-concept findings suggest a favorable benefit/risk ratio in SLE for KPG-818,” Dr. Wang and coauthors said, supporting its further development in SLE.
Need for Treatments
Dr. Isenberg told this news organization that both daratumumab and KPG-818 would be welcome additions as treatment options if further trials proved their worth.
“The great frustration about lupus is that, compared to patients with rheumatoid arthritis, the choice has been so limited,” Dr. Isenberg said. Aside from rituximab (Rituxan) and belimumab (Benlysta), which are used with certain restrictions, there are no other biologic targeted treatments available in the United Kingdom. Anifrolumab (Saphnelo) has a license in the United States and some European countries but is not yet available for him to use in his practice.
Daratumumab and KPG-818 are “different types of molecules, and if they work that will be great. It would be nice to have the choice,” Dr. Isenberg said. “Whether they will be as effective as I think rituximab is, I don’t know, but these are some very encouraging results.”
Of course, these are all phase 2 trials, and the “big problem” is that such positive results do not always translate when it comes to phase 3, as Dr. D’Cruz told this news organization.
“Until a few years ago, there had been about 25 or 30 industry-led trails, and they’d all failed, except for belimumab and anifrolumab,” Dr. D’Cruz said. These drugs were found to work and be generally safe in phase 1 and 2 trials, but “when they come to phase 3, they all seem to fail, and we don’t know why.”
These are large global studies, D’Cruz added, observing that problems with patient selection, steroid use, and choice of outcome measures were possible factors for why the EXPLORER and LUNAR studies had shown no benefit for rituximab despite the drug being widely used to treat SLE.
Dr. Isenberg, who has coauthored an article on the topic of why drugs seem to fail at the final hurdle, noted: “I think it has a lot to do with the nature of the disease. It’s a complicated disease.” From having “savvy physicians doing the trials for you” to the placebo response, there are “a whole bunch or reasons why these things haven’t worked in lupus.”
Dr. Morand commented: “We’ve got many programs in phase 2 and 3, and because there’s so many, they’re all facing recruitment challenges, and as a consequence of so much activity, every program is going a little slower than hoped for.”
As for other drugs on the horizon, Dr. Morand noted: “We’re very optimistic about things like litifilimab and deucravacitinib; that’s two examples that are in phase 3. Earlier in the program of development, [there are] a huge range of targets being addressed. The future looks bright. But we might have to wait a while.”
Dr. Arnaud has consulted for AstraZeneca, AbbVie, Alpine Immune Sciences, Biogen, Bristol Myers Squibb, Boehringer Ingelheim, Chugai Pharmaceutical, GlaxoSmithKline, Grifols, Janssen, Kezar Life Sciences, LFB, Lilly, Medac, Merck, Novartis, Pfizer, Roche, and UCB. Dr. Isenberg has served as an adviser to Merck Serono, AstraZeneca, Eli Lilly, Servier, and ImmuPharma. Any honoraria received is passed on to a local arthritis charity connected to his hospital. Dr. D’Cruz has served as a consultant and advisory board member for GlaxoSmithKline and CSL Vifor. Dr. Morand has received research support, consultancy fees, or both from multiple pharmaceutical companies paid to his institution including AbbVie, Amgen, AstraZeneca, Biogen, Bristol Myers Squibb, Eli Lilly, EMD Serono, Dragonfly, Genentech, GlaxoSmithKline, Janssen, Novartis, RemeGen, Takeda, UCB, and Zenas. The ianalumab trial presented by Dr. Agmon-Levin was sponsored by Novartis Pharma; however, she reported having no conflicts of interest. The DARALUP study was an investigator-initiated trial supported by Janssen. Dr. Alexander has received consulting fees, study support, honoraria, and travel grants from various pharmaceutical companies including AbbVie, Amgen, AstraZeneca, Bayer, GlaxoSmithKline, Janssen, and Lilly. Dr. Nash has consulted for The Rheumatology Education Group Consultants. The KPG-818 study reported by Dr. Wang was sponsored by Kangpu Biopharmaceuticals.
A version of this article first appeared on Medscape.com.
VIENNA — It may have been a while since there have been any major breakthroughs in the treatment of systemic lupus erythematosus (SLE), but there are high hopes that this is a situation that may be about to change, experts agreed at the annual European Congress of Rheumatology.
“It’s an incredibly vivid area of development,” Laurent Arnaud, MD, PhD, professor of rheumatology at the University of Strasbourg in Strasbourg, France, said during one of the first sessions of the meeting. He reported that there were at least 17 phase 2 and 14 phase 3 trials that were expected to start within the next few years, all with investigational agents that target different immune cells or pathways that have been implicated in the pathogenesis of SLE.
In a systematic review published last year, Dr. Arnaud and coauthors found that there were 92 investigational biologic or novel targeted agents in various phases of clinical testing. This included B-cell–targeting agents such as ianalumab, plasma cell-targeting agents such as daratumumab, and drugs with novel mechanisms of action such as KPG-818, which targets the CRL4-Cereblon (CRBN) E3 ubiquitin ligase complex. Phase 2 data on all three of these investigational agents were presented during various sessions at EULAR 2024, all with positive results, suggesting that their further development in SLE is worth pursuing.
There are of course “many more candidates in the pipeline,” Dr. Arnaud said. “I’m very happy that I think we are going to see great days for lupus right in front of our eyes.”
Targeting B Cells
Drugs that target B cells have been at the forefront of lupus treatment for several years, as David Isenberg, MD, professor of rheumatology at University College London, pointed out during an interview for EULAR TV.
“It’s clearly important to target the cells which are likely to be causing the problem in lupus, and in the main, that tends to be B cells,” he said.
Dr. Isenberg, who is renowned for his work with the B-cell–targeting agent rituximab, added: “But we know that obviously T cells integrate with B cells, so anything which interrupts the link between the T cell and the B cell is likely to be important.”
Chimeric Antigen Receptor (CAR) T-Cell Therapy ‘Revolution’
One new way of targeting B cells is with CAR T-cell therapy, which David D’Cruz , MD, PhD, a consultant rheumatologist for Guy’s and St. Thomas’ Hospital NHS Foundation Trust in London, picked as one of the “most striking” topics highlighted at EULAR 2024.
This is “truly personalized medicine,” Dr. D’Cruz said. This is an autologous therapy because a patient’s T cells are removed by leukapheresis, transfected with a CAR T vector directed against a component of the B cell, and then returned to them.
“I do feel that we’re on the cusp of a major revolution,” Dr. D’Cruz told this news organization. Not only in lupus but also in other rheumatic conditions that have proved really difficult to treat, such as systemic sclerosis and myositis, he said.
“Basically, it’s a very powerful B-cell–depleting tool, but it’s much more profound B-cell–depleting tool than, for example, rituximab or belimumab,” explained Dr. D’Cruz. “What you’re doing is reprogramming T cells to attack the B cells.”
Although rituximab and belimumab clear all the B cells in the circulation, there are still some cells left behind in the bone marrow, “and it’s very difficult to get rid of those,” Dr. D’Cruz said. “What CAR T-cell therapy appears to do is wipe out all the CD19-positive B cells everywhere, in the blood and the tissue. So you get a really profound B-cell depletion.”
Eric Morand, MBBS, PhD, head of rheumatology at Monash Health in Melbourne, Australia, told this news organization that there was obviously “a lot of buzz” about CAR T-cell therapy.
“We’re waiting to see if the exciting data from Erlangen can be reproduced in other centers with other CAR T products to show that it is a universal effect. We haven’t seen that yet, but I think we will by next year.”
Cost and expertise are two major considerations and potential limiting factors, however, as Dr. D’Cruz and Dr. Isenberg both pointed out in separate interviews with this news organization.
Dr. D’Cruz said: “It’s very expensive, it takes a while, and it doesn’t always work is what I’m hearing. It’s usually successful, but again, a little bit depends on the technique and the people doing the process.”
Dr. Isenberg said: “CAR T-cell therapy is, I think, very exciting because it does look to be quite promising. But as it costs 350,000 euros per patient, I don’t think that it is going to be widely adopted.”
Even if it could be afforded by certain centers in the West, he added, this just would not be feasible in poorer nations. “So, we’ve got to find other effective, cheaper ways to go,” Dr. Isenberg said.
“I think there are some very interesting ideas with monoclonal antibodies which target at least two different targets — one on the B cell, one on the T cell — and that could well be the way to take this forward,” he suggested.
Ianalumab ‘Double Blocking’ B Cells
Another way could be to develop more potent B-cell–depleting drugs, as Nancy Agmon-Levin , MD, head of the Clinical Immunology, Angioedema and Allergy Unit, Lupus and Autoimmune Diseases Clinic, at Sheba Medical Center, Tel Aviv University in Tel Aviv, Israel, reported during one of the clinical abstract sessions at EULAR 2024.
Dr. Agmon-Levin presented data on 67 individuals with SLE who had participated in a multicenter phase 2 study of ianalumab, a fully human immunoglobulin (Ig) G1 monoclonal antibody that results in a “double blocking of the B-cell lineage.”
Ianalumab targets the B-cell–activating factor receptor (BAFFR), but what makes it distinct from other BAFF-targeting drugs is that it has had a fructose molecule removed from its Fc portion, which renders it more likely to trigger antibody-dependent cellular cytotoxicity.
“This is a B-cell depletion therapy,” Agmon-Levin said, but it also blocks BAFFR-mediated survival of B cells, so the subsequent recuperation process of BAFFR-expressing B cells is affected, leading to continued B-cell depletion.
The phase 2 study she presented consisted of an initial 28-week, double-blind period, during which time participants had been randomly allocated to receive either subcutaneous injections of ianalumab 300 mg or a matching placebo every 4 weeks. This was followed by a 24-week, open-label period where all participants were treated with ianalumab, and then an off-treatment, minimal follow-up period that lasted up to 68 weeks, with continued data collection for safety.
The primary outcome measure was a composite of meeting criteria for the SLE Responder Index 4 and a sustained reduction in corticosteroid use at 28 weeks. This was achieved in 15 of the 34 (44.1%) people treated with ianalumab vs only 3 (9.1%) of the 33 people who had been given a placebo.
Dr. Agmon-Levin reported that the effect on this outcome was sustained to the end of the open-label period, at 1 year, in 15 (45.5%) of 33 participants who had continued treatment with ianalumab and achieved in 13 (40.6%) of 32 participants who had switched from placebo to ianalumab treatment.
Moreover, longer durations of treatment were associated with a host of improved outcomes, Dr. Agmon-Levin said: “Treatment was improved along the 52 weeks, and we can see from the LLDAS [Lupus Low Disease Activity State], DORIS [Definition Of Remission In SLE], and SRI-6 and -8 that as you continue the therapy, you improve the outcomes.”
The potential benefits of ianalumab in the treatment of SLE and lupus nephritis will now be further examined in the phase 3 SIRIUS-SLE1 , SIRIUS-SLE2, and SIRIUS-LN trials, which are estimated to provide initial results in 2027 and complete in early 2029 or 2030.
Targeting Plasma Cells With Daratumumab
Another drug showing signs that it might be useful as a treatment for SLE is daratumumab, as Tobias Alexander, MD, of Charité — Universitätsmedizin Berlin, reported during one of the late-breaking abstract sessions at EULAR 2024.
“Daratumumab is a human, first-in-class anti-CD38 antibody that efficiently depletes plasma cells,” Dr. Alexander said. CD38 is both a receptor and an enzyme, and while it is found on the surface of most immune cells, it’s particularly expressed by plasma cells, he added.
Daratumumab is not a total newcomer, however, as it’s already approved for the treatment of multiple myeloma under the trade name Darzalex. The rationale for using it in SLE comes from two case reports, Dr. Alexander explained. The first, published in 2020 in The New England Journal of Medicine, involved two patients with severe and life-threatening lupus who were given off-label treatment for a period of 4 weeks and experienced good clinical and serologic responses. The second, published last year in Nature Medicine, involved six patients with refractory lupus nephritis, five of whom had a clinical response at 6 months.
“On this background, we conducted an investigator-initiated trial, which was an open-label, single-center, proof-of-concept study,” Dr. Alexander said. A total of 10 female patients whose ages ranged from 24 to 43 years were included in the phase 2 trial that was dubbed DARALUP. For inclusion, all had to have a Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) of four or more for clinical manifestations, have been treated with at least two prior disease-modifying drugs to no avail, and be anti–double-stranded DNA (anti-dsDNA) antibody positive. Dr. Alexander reported that the median baseline SLEDAI-2K score was 12 and ranged from 8 to 20, with the number of prior therapies ranging from two to nine.
Daratumumab was given at a dose of 1800 mg via subcutaneous injection every week for 8 weeks. This is the same dose that is used to treat multiple myeloma, Dr. Alexander explained, although the dosing is not stopped. The reason for stopping after 8 weeks in the current trial was to be able to see what happened once the treatment was stopped. The follow-up was for 36 weeks.
Dr. Alexander reported that there was a “very dramatic and significant” effect on the primary endpoint of a reduction in anti-dsDNA antibody levels, decreasing from a median of 166.3 U/mL at baseline to 61.1 U/mL at week 12 (P = .002). Alongside, there was a reduction in the SLEDAI-2K score from 12 to 4 within 12 weeks, which was sustained at the 36-week follow-up assessment. Improvements in skin, joint, kidney, and level of proteinuria were also seen.
Although all patients experienced adverse events, none were serious. Infections and infestations (mostly nasopharyngitis, COVID-19, and gastroenteritis) were the most common, experienced by 80% of the participants; 70% had injection site reactions or fatigue, 60% had gastrointestinal symptoms, 50% had a fall of IgG < 5 g/L, 40% had headache, and 20% had back pain.
“This is a positive trial. I think we could demonstrate that [daratumumab] produced very strong, rapid, and durable clinical improvements,” Dr. Alexander said. “We think that targeting CD38 is relevant; plasma cells had been depleted based on the reduction of anti-dsDNA antibodies,” he added.
From the audience, however, Peter Nash, MBBS, of Griffith University in Brisbane, Australia, questioned whether the results could be attributed to “a steroid effect” because patients had been treated with oral dexamethasone throughout the study.
Dr. Alexander noted that steroid use had been part of the treatment schedule but acknowledged it was a possible confounder.
“I think we can be confident that [daratumumab] had a major effect on plasma cells decreasing…because we see that also the vaccine titers decreased,” Dr. Alexander said. “Time will tell, but even more important is the durability of the responses over time, which you don’t achieve under steroids.”
KPG-818’s Novel Mechanism of Action
Elsewhere at EULAR 2024, positive results of another phase 2 study involving a drug with an entirely different mechanism of action, KPG-818, were reported in a poster presentation. KPG-818 modulates CRBN, which results in the degradation of two transcription factors (Aiolos and Ikaros) that are involved in the development, maturation, and proliferation of innate and adaptive immune cells and have been linked to genetic risk in SLE, according to the poster’s authors. It is currently in development for the treatment of SLE, Behçet disease, inflammatory bowel disease, multiple myeloma, and non-Hodgkin lymphoma.
Yao Wang, MD, chief medical officer of KPG-818’s developer Kangpu Biopharmaceuticals, Hefei, China, and associates found that oral doses of 0.15 or 0.6 mg KPG-818 were “generally well-tolerated” and produced immunomodulatory changes that could be beneficial in people with SLE over a 12-week treatment period.
“Only two new agents have been approved for the treatment of SLE in the past five decades in USA and Europe,” Dr. Wang and team wrote, which highlights “a significant unmet need for more effective and safe treatment options.”
They believe that KPG-818 might well fit the bill based on the results of their study, in which 35 of 37 recruited patients completed the treatment. Compared with placebo, they observed reduced numbers of total B cells, Aiolos+ T and B cells, and increased Treg cells.
SLEDAI-2K and Cutaneous Lupus Erythematosus Disease Area and Severity Index activity scores in the 0.15-mg group were improved relative to baseline and placebo.
“The proof-of-concept findings suggest a favorable benefit/risk ratio in SLE for KPG-818,” Dr. Wang and coauthors said, supporting its further development in SLE.
Need for Treatments
Dr. Isenberg told this news organization that both daratumumab and KPG-818 would be welcome additions as treatment options if further trials proved their worth.
“The great frustration about lupus is that, compared to patients with rheumatoid arthritis, the choice has been so limited,” Dr. Isenberg said. Aside from rituximab (Rituxan) and belimumab (Benlysta), which are used with certain restrictions, there are no other biologic targeted treatments available in the United Kingdom. Anifrolumab (Saphnelo) has a license in the United States and some European countries but is not yet available for him to use in his practice.
Daratumumab and KPG-818 are “different types of molecules, and if they work that will be great. It would be nice to have the choice,” Dr. Isenberg said. “Whether they will be as effective as I think rituximab is, I don’t know, but these are some very encouraging results.”
Of course, these are all phase 2 trials, and the “big problem” is that such positive results do not always translate when it comes to phase 3, as Dr. D’Cruz told this news organization.
“Until a few years ago, there had been about 25 or 30 industry-led trails, and they’d all failed, except for belimumab and anifrolumab,” Dr. D’Cruz said. These drugs were found to work and be generally safe in phase 1 and 2 trials, but “when they come to phase 3, they all seem to fail, and we don’t know why.”
These are large global studies, D’Cruz added, observing that problems with patient selection, steroid use, and choice of outcome measures were possible factors for why the EXPLORER and LUNAR studies had shown no benefit for rituximab despite the drug being widely used to treat SLE.
Dr. Isenberg, who has coauthored an article on the topic of why drugs seem to fail at the final hurdle, noted: “I think it has a lot to do with the nature of the disease. It’s a complicated disease.” From having “savvy physicians doing the trials for you” to the placebo response, there are “a whole bunch or reasons why these things haven’t worked in lupus.”
Dr. Morand commented: “We’ve got many programs in phase 2 and 3, and because there’s so many, they’re all facing recruitment challenges, and as a consequence of so much activity, every program is going a little slower than hoped for.”
As for other drugs on the horizon, Dr. Morand noted: “We’re very optimistic about things like litifilimab and deucravacitinib; that’s two examples that are in phase 3. Earlier in the program of development, [there are] a huge range of targets being addressed. The future looks bright. But we might have to wait a while.”
Dr. Arnaud has consulted for AstraZeneca, AbbVie, Alpine Immune Sciences, Biogen, Bristol Myers Squibb, Boehringer Ingelheim, Chugai Pharmaceutical, GlaxoSmithKline, Grifols, Janssen, Kezar Life Sciences, LFB, Lilly, Medac, Merck, Novartis, Pfizer, Roche, and UCB. Dr. Isenberg has served as an adviser to Merck Serono, AstraZeneca, Eli Lilly, Servier, and ImmuPharma. Any honoraria received is passed on to a local arthritis charity connected to his hospital. Dr. D’Cruz has served as a consultant and advisory board member for GlaxoSmithKline and CSL Vifor. Dr. Morand has received research support, consultancy fees, or both from multiple pharmaceutical companies paid to his institution including AbbVie, Amgen, AstraZeneca, Biogen, Bristol Myers Squibb, Eli Lilly, EMD Serono, Dragonfly, Genentech, GlaxoSmithKline, Janssen, Novartis, RemeGen, Takeda, UCB, and Zenas. The ianalumab trial presented by Dr. Agmon-Levin was sponsored by Novartis Pharma; however, she reported having no conflicts of interest. The DARALUP study was an investigator-initiated trial supported by Janssen. Dr. Alexander has received consulting fees, study support, honoraria, and travel grants from various pharmaceutical companies including AbbVie, Amgen, AstraZeneca, Bayer, GlaxoSmithKline, Janssen, and Lilly. Dr. Nash has consulted for The Rheumatology Education Group Consultants. The KPG-818 study reported by Dr. Wang was sponsored by Kangpu Biopharmaceuticals.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
Trends in Rheumatic Disease Pain Management Show Decline in Opioid Use
TOPLINE:
Since 2014, opioid use for autoimmune rheumatic diseases decreased by 15% annually while other management modalities increased or stabilized.
METHODOLOGY:
- Researchers analyzed de-identified US claims data from the MarketScan Database from 2007-2021.
- The study included nearly 142,000 patients with autoimmune rheumatic diseases: 10,927 with ankylosing spondylitis (AS); 21,438 with psoriatic arthritis (PsA); 71,393 with rheumatoid arthritis (RA); 16,718 with Sjögren disease; 18,018 with systemic lupus erythematosus; and 3468 with systemic sclerosis.
- Primary outcome was opioid use annual trends, with secondary outcomes including trends in the use of anticonvulsants, antidepressants, skeletal muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), topical pain medications, and physical or occupational therapy.
TAKEAWAY:
- The incidence of opioid use increased annually by 4% until 2014 and decreased annually by 15% after 2014.
- NSAID use increased 2% annually until 2014, then declined by 5% afterward.
- The proportion of patients utilizing physical therapy or anticonvulsants doubled from 2008 to 2020.
- NSAID prescriptions were highest in AS, PsA, and RA, while they were lowest in Sjögren disease and systemic sclerosis.
IN PRACTICE:
“Our work, along with the published literature, highlights the need for future studies to evaluate the effectiveness of pain management modality changes over time and to understand the possible effects that changes have had on outcomes such as quality of life, disability, health status, and function,” wrote the authors of the study.
SOURCE:
The study was led by Titilola Falasinnu, PhD, Stanford University School of Medicine, Stanford, California. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study relied on administrative claims data, which did not contain information on use of over-the-counter medications like NSAIDs and topical analgesics. The study did not include the duration of pain treatment modalities, making it difficult to differentiate between acute and chronic use. The analysis did not include race or ethnicity, which is important for understanding pain outcomes across different sociodemographic groups.
DISCLOSURES:
The study was supported by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Since 2014, opioid use for autoimmune rheumatic diseases decreased by 15% annually while other management modalities increased or stabilized.
METHODOLOGY:
- Researchers analyzed de-identified US claims data from the MarketScan Database from 2007-2021.
- The study included nearly 142,000 patients with autoimmune rheumatic diseases: 10,927 with ankylosing spondylitis (AS); 21,438 with psoriatic arthritis (PsA); 71,393 with rheumatoid arthritis (RA); 16,718 with Sjögren disease; 18,018 with systemic lupus erythematosus; and 3468 with systemic sclerosis.
- Primary outcome was opioid use annual trends, with secondary outcomes including trends in the use of anticonvulsants, antidepressants, skeletal muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), topical pain medications, and physical or occupational therapy.
TAKEAWAY:
- The incidence of opioid use increased annually by 4% until 2014 and decreased annually by 15% after 2014.
- NSAID use increased 2% annually until 2014, then declined by 5% afterward.
- The proportion of patients utilizing physical therapy or anticonvulsants doubled from 2008 to 2020.
- NSAID prescriptions were highest in AS, PsA, and RA, while they were lowest in Sjögren disease and systemic sclerosis.
IN PRACTICE:
“Our work, along with the published literature, highlights the need for future studies to evaluate the effectiveness of pain management modality changes over time and to understand the possible effects that changes have had on outcomes such as quality of life, disability, health status, and function,” wrote the authors of the study.
SOURCE:
The study was led by Titilola Falasinnu, PhD, Stanford University School of Medicine, Stanford, California. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study relied on administrative claims data, which did not contain information on use of over-the-counter medications like NSAIDs and topical analgesics. The study did not include the duration of pain treatment modalities, making it difficult to differentiate between acute and chronic use. The analysis did not include race or ethnicity, which is important for understanding pain outcomes across different sociodemographic groups.
DISCLOSURES:
The study was supported by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Since 2014, opioid use for autoimmune rheumatic diseases decreased by 15% annually while other management modalities increased or stabilized.
METHODOLOGY:
- Researchers analyzed de-identified US claims data from the MarketScan Database from 2007-2021.
- The study included nearly 142,000 patients with autoimmune rheumatic diseases: 10,927 with ankylosing spondylitis (AS); 21,438 with psoriatic arthritis (PsA); 71,393 with rheumatoid arthritis (RA); 16,718 with Sjögren disease; 18,018 with systemic lupus erythematosus; and 3468 with systemic sclerosis.
- Primary outcome was opioid use annual trends, with secondary outcomes including trends in the use of anticonvulsants, antidepressants, skeletal muscle relaxants, nonsteroidal anti-inflammatory drugs (NSAIDs), topical pain medications, and physical or occupational therapy.
TAKEAWAY:
- The incidence of opioid use increased annually by 4% until 2014 and decreased annually by 15% after 2014.
- NSAID use increased 2% annually until 2014, then declined by 5% afterward.
- The proportion of patients utilizing physical therapy or anticonvulsants doubled from 2008 to 2020.
- NSAID prescriptions were highest in AS, PsA, and RA, while they were lowest in Sjögren disease and systemic sclerosis.
IN PRACTICE:
“Our work, along with the published literature, highlights the need for future studies to evaluate the effectiveness of pain management modality changes over time and to understand the possible effects that changes have had on outcomes such as quality of life, disability, health status, and function,” wrote the authors of the study.
SOURCE:
The study was led by Titilola Falasinnu, PhD, Stanford University School of Medicine, Stanford, California. It was published online in The Lancet Rheumatology.
LIMITATIONS:
The study relied on administrative claims data, which did not contain information on use of over-the-counter medications like NSAIDs and topical analgesics. The study did not include the duration of pain treatment modalities, making it difficult to differentiate between acute and chronic use. The analysis did not include race or ethnicity, which is important for understanding pain outcomes across different sociodemographic groups.
DISCLOSURES:
The study was supported by grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
FDA Expands Dostarlimab-gxly Approval for Endometrial Cancer
Prior FDA approval of the combination was granted for adults with primary advanced or recurrent endometrial cancer that was mismatch repair deficient (dMMR) or microsatellite instability–high (MSI-H).
The expanded approval, granted following a priority review, was based on efficacy and safety demonstrated in the randomized, controlled, multicenter RUBY trial, which included 494 patients who were randomized to receive the dostarlimab-gxly regimen or placebo plus carboplatin and paclitaxel, followed by placebo.
Researchers observed a significant improvement in median overall survival with treatment vs placebo in the overall population — 44.6 vs 28.2 months, respectively (hazard ratio [HR], 0.69). Median progression-free survival was also significantly better in the treatment vs placebo group — 11.8 vs 7.9 months, respectively (HR, 0.64).
“Today’s expanded approval will offer even more patients the opportunity for improved outcomes,” Matthew Powell, MD, of Washington University School of Medicine, and principal investigator on the RUBY trial, said in a press release. “This is the only immuno-oncology treatment regimen that has shown a statistically significant overall survival benefit for the full patient population, which is a meaningful step forward in treating this challenging cancer.”
Adverse reactions occurring in at least 20% of patients receiving dostarlimab-gxly include anemia, increased creatinine levels, peripheral neuropathy, decreased white blood cell counts, fatigue, nausea, alopecia, low platelet counts, increased glucose levels, lymphopenia, neutropenia, liver function test abnormalities, arthralgia, rash, constipation, diarrhea, decreased albumin levels, abdominal pain, dyspnea, decreased appetite, increased amylase levels, urinary tract infection, and vomiting. Immune-mediated adverse reactions with dostarlimab-gxly were similar to those previously reported.
The recommended dostarlimab-gxly dose, according to the full prescribing information, is 500 mg every 3 weeks for six cycles administered before carboplatin and paclitaxel if given on the same day, followed by 1000 mg monotherapy every 6 weeks until disease progression or unacceptable toxicity, or up to 3 years.
A version of this article first appeared on Medscape.com.
Prior FDA approval of the combination was granted for adults with primary advanced or recurrent endometrial cancer that was mismatch repair deficient (dMMR) or microsatellite instability–high (MSI-H).
The expanded approval, granted following a priority review, was based on efficacy and safety demonstrated in the randomized, controlled, multicenter RUBY trial, which included 494 patients who were randomized to receive the dostarlimab-gxly regimen or placebo plus carboplatin and paclitaxel, followed by placebo.
Researchers observed a significant improvement in median overall survival with treatment vs placebo in the overall population — 44.6 vs 28.2 months, respectively (hazard ratio [HR], 0.69). Median progression-free survival was also significantly better in the treatment vs placebo group — 11.8 vs 7.9 months, respectively (HR, 0.64).
“Today’s expanded approval will offer even more patients the opportunity for improved outcomes,” Matthew Powell, MD, of Washington University School of Medicine, and principal investigator on the RUBY trial, said in a press release. “This is the only immuno-oncology treatment regimen that has shown a statistically significant overall survival benefit for the full patient population, which is a meaningful step forward in treating this challenging cancer.”
Adverse reactions occurring in at least 20% of patients receiving dostarlimab-gxly include anemia, increased creatinine levels, peripheral neuropathy, decreased white blood cell counts, fatigue, nausea, alopecia, low platelet counts, increased glucose levels, lymphopenia, neutropenia, liver function test abnormalities, arthralgia, rash, constipation, diarrhea, decreased albumin levels, abdominal pain, dyspnea, decreased appetite, increased amylase levels, urinary tract infection, and vomiting. Immune-mediated adverse reactions with dostarlimab-gxly were similar to those previously reported.
The recommended dostarlimab-gxly dose, according to the full prescribing information, is 500 mg every 3 weeks for six cycles administered before carboplatin and paclitaxel if given on the same day, followed by 1000 mg monotherapy every 6 weeks until disease progression or unacceptable toxicity, or up to 3 years.
A version of this article first appeared on Medscape.com.
Prior FDA approval of the combination was granted for adults with primary advanced or recurrent endometrial cancer that was mismatch repair deficient (dMMR) or microsatellite instability–high (MSI-H).
The expanded approval, granted following a priority review, was based on efficacy and safety demonstrated in the randomized, controlled, multicenter RUBY trial, which included 494 patients who were randomized to receive the dostarlimab-gxly regimen or placebo plus carboplatin and paclitaxel, followed by placebo.
Researchers observed a significant improvement in median overall survival with treatment vs placebo in the overall population — 44.6 vs 28.2 months, respectively (hazard ratio [HR], 0.69). Median progression-free survival was also significantly better in the treatment vs placebo group — 11.8 vs 7.9 months, respectively (HR, 0.64).
“Today’s expanded approval will offer even more patients the opportunity for improved outcomes,” Matthew Powell, MD, of Washington University School of Medicine, and principal investigator on the RUBY trial, said in a press release. “This is the only immuno-oncology treatment regimen that has shown a statistically significant overall survival benefit for the full patient population, which is a meaningful step forward in treating this challenging cancer.”
Adverse reactions occurring in at least 20% of patients receiving dostarlimab-gxly include anemia, increased creatinine levels, peripheral neuropathy, decreased white blood cell counts, fatigue, nausea, alopecia, low platelet counts, increased glucose levels, lymphopenia, neutropenia, liver function test abnormalities, arthralgia, rash, constipation, diarrhea, decreased albumin levels, abdominal pain, dyspnea, decreased appetite, increased amylase levels, urinary tract infection, and vomiting. Immune-mediated adverse reactions with dostarlimab-gxly were similar to those previously reported.
The recommended dostarlimab-gxly dose, according to the full prescribing information, is 500 mg every 3 weeks for six cycles administered before carboplatin and paclitaxel if given on the same day, followed by 1000 mg monotherapy every 6 weeks until disease progression or unacceptable toxicity, or up to 3 years.
A version of this article first appeared on Medscape.com.
High Prevalence of Anxiety, Depression, Fibromyalgia With RA and OA Signals Need for Screening
TOPLINE:
About 40% of patients with osteoarthritis (OA) and 36% with rheumatoid arthritis (RA) screened positive for anxiety, depression, and/or fibromyalgia as part of routine visits to an academic medical center, and these comorbidities were linked to poorer patient status measures, highlighting the need for routine screening in clinical practice.
METHODOLOGY:
- This retrospective cross-sectional study analyzed the prevalence of anxiety, depression, and fibromyalgia in 366 patients with OA (mean age, 66.6 years) and 488 patients with RA (mean age, 56.9 years) who were in routine care at an academic center from 2011 to 2022.
- All participants were required to have complete Multidimensional Health Assessment Questionnaire (MDHAQ) data available for the analysis.
- The MDHAQ included indices to assess the overall patient status and screen for anxiety, depression, and fibromyalgia.
- The overall patient status was measured using the Routine Assessment of Patient Index Data 3 (RAPID3), which comprised the physical function, pain, and patient global scores.
- The prevalence of each comorbidity and its association with patient status was analyzed using unadjusted and age-adjusted odds ratios (ORs) and 95% CIs.
TAKEAWAY:
- Among the patients with OA, 40.4% were screened positive for at least one of the three indices indicating patient distress (anxiety, depression, and fibromyalgia). Among patients with RA, the proportion was 36.3%.
- Among the patients who screened positive for at least one index, about 20% screened positive for all three indices related to anxiety, depression, and fibromyalgia.
- In patients with OA, a poorer patient status (RAPID3, ≥ 12 vs < 12) increased the likelihood of anxiety (OR, 3.93; 95% CI, 2.24-7.23), depression (OR, 3.79; 95% CI, 2.01-7.73), and fibromyalgia (OR, 6.70; 95% CI, 3.36-14.99).
- Similarly, the odds of all three comorbidities increased in the patients with RA who had worsened patient status.
IN PRACTICE:
“Screening for [anxiety, depression, and/or fibromyalgia] can be incorporated feasibly into routine clinical care using a single MDHAQ to better inform health professionals concerning patient status, prognosis, and response to treatments,” the authors wrote.
SOURCE:
The study was led by Juan Schmukler, MD, Rush University Medical Center, Chicago, and was published online on July 16, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The analyses were cross-sectional, and whether anxiety, depression, and fibromyalgia had preceded or followed the onset of OA or RA was not known. Information on the clinical variables associated with anxiety, depression, and fibromyalgia, such as body mass index, medication history, and other comorbid conditions, was not available. All the patients were seen at a single rheumatology site, which may have limited the generalizability of the observations.
DISCLOSURES:
This study did not disclose any sources of funding. One author disclosed receiving grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. One author reported numerous financial relationships with companies in the medical industry, and another reported holding a copyright and trademark on MDHAQ and RAPID3.
This article was created using several editorial tools, including AI, as a part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
About 40% of patients with osteoarthritis (OA) and 36% with rheumatoid arthritis (RA) screened positive for anxiety, depression, and/or fibromyalgia as part of routine visits to an academic medical center, and these comorbidities were linked to poorer patient status measures, highlighting the need for routine screening in clinical practice.
METHODOLOGY:
- This retrospective cross-sectional study analyzed the prevalence of anxiety, depression, and fibromyalgia in 366 patients with OA (mean age, 66.6 years) and 488 patients with RA (mean age, 56.9 years) who were in routine care at an academic center from 2011 to 2022.
- All participants were required to have complete Multidimensional Health Assessment Questionnaire (MDHAQ) data available for the analysis.
- The MDHAQ included indices to assess the overall patient status and screen for anxiety, depression, and fibromyalgia.
- The overall patient status was measured using the Routine Assessment of Patient Index Data 3 (RAPID3), which comprised the physical function, pain, and patient global scores.
- The prevalence of each comorbidity and its association with patient status was analyzed using unadjusted and age-adjusted odds ratios (ORs) and 95% CIs.
TAKEAWAY:
- Among the patients with OA, 40.4% were screened positive for at least one of the three indices indicating patient distress (anxiety, depression, and fibromyalgia). Among patients with RA, the proportion was 36.3%.
- Among the patients who screened positive for at least one index, about 20% screened positive for all three indices related to anxiety, depression, and fibromyalgia.
- In patients with OA, a poorer patient status (RAPID3, ≥ 12 vs < 12) increased the likelihood of anxiety (OR, 3.93; 95% CI, 2.24-7.23), depression (OR, 3.79; 95% CI, 2.01-7.73), and fibromyalgia (OR, 6.70; 95% CI, 3.36-14.99).
- Similarly, the odds of all three comorbidities increased in the patients with RA who had worsened patient status.
IN PRACTICE:
“Screening for [anxiety, depression, and/or fibromyalgia] can be incorporated feasibly into routine clinical care using a single MDHAQ to better inform health professionals concerning patient status, prognosis, and response to treatments,” the authors wrote.
SOURCE:
The study was led by Juan Schmukler, MD, Rush University Medical Center, Chicago, and was published online on July 16, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The analyses were cross-sectional, and whether anxiety, depression, and fibromyalgia had preceded or followed the onset of OA or RA was not known. Information on the clinical variables associated with anxiety, depression, and fibromyalgia, such as body mass index, medication history, and other comorbid conditions, was not available. All the patients were seen at a single rheumatology site, which may have limited the generalizability of the observations.
DISCLOSURES:
This study did not disclose any sources of funding. One author disclosed receiving grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. One author reported numerous financial relationships with companies in the medical industry, and another reported holding a copyright and trademark on MDHAQ and RAPID3.
This article was created using several editorial tools, including AI, as a part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
About 40% of patients with osteoarthritis (OA) and 36% with rheumatoid arthritis (RA) screened positive for anxiety, depression, and/or fibromyalgia as part of routine visits to an academic medical center, and these comorbidities were linked to poorer patient status measures, highlighting the need for routine screening in clinical practice.
METHODOLOGY:
- This retrospective cross-sectional study analyzed the prevalence of anxiety, depression, and fibromyalgia in 366 patients with OA (mean age, 66.6 years) and 488 patients with RA (mean age, 56.9 years) who were in routine care at an academic center from 2011 to 2022.
- All participants were required to have complete Multidimensional Health Assessment Questionnaire (MDHAQ) data available for the analysis.
- The MDHAQ included indices to assess the overall patient status and screen for anxiety, depression, and fibromyalgia.
- The overall patient status was measured using the Routine Assessment of Patient Index Data 3 (RAPID3), which comprised the physical function, pain, and patient global scores.
- The prevalence of each comorbidity and its association with patient status was analyzed using unadjusted and age-adjusted odds ratios (ORs) and 95% CIs.
TAKEAWAY:
- Among the patients with OA, 40.4% were screened positive for at least one of the three indices indicating patient distress (anxiety, depression, and fibromyalgia). Among patients with RA, the proportion was 36.3%.
- Among the patients who screened positive for at least one index, about 20% screened positive for all three indices related to anxiety, depression, and fibromyalgia.
- In patients with OA, a poorer patient status (RAPID3, ≥ 12 vs < 12) increased the likelihood of anxiety (OR, 3.93; 95% CI, 2.24-7.23), depression (OR, 3.79; 95% CI, 2.01-7.73), and fibromyalgia (OR, 6.70; 95% CI, 3.36-14.99).
- Similarly, the odds of all three comorbidities increased in the patients with RA who had worsened patient status.
IN PRACTICE:
“Screening for [anxiety, depression, and/or fibromyalgia] can be incorporated feasibly into routine clinical care using a single MDHAQ to better inform health professionals concerning patient status, prognosis, and response to treatments,” the authors wrote.
SOURCE:
The study was led by Juan Schmukler, MD, Rush University Medical Center, Chicago, and was published online on July 16, 2024, in ACR Open Rheumatology.
LIMITATIONS:
The analyses were cross-sectional, and whether anxiety, depression, and fibromyalgia had preceded or followed the onset of OA or RA was not known. Information on the clinical variables associated with anxiety, depression, and fibromyalgia, such as body mass index, medication history, and other comorbid conditions, was not available. All the patients were seen at a single rheumatology site, which may have limited the generalizability of the observations.
DISCLOSURES:
This study did not disclose any sources of funding. One author disclosed receiving grants from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. One author reported numerous financial relationships with companies in the medical industry, and another reported holding a copyright and trademark on MDHAQ and RAPID3.
This article was created using several editorial tools, including AI, as a part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Self-Rated Health Predicts Hospitalization and Death
Adults who self-rated their health as poor in middle age were at least three times more likely to die or be hospitalized when older than those who self-rated their health as excellent, based on data from nearly 15,000 individuals.
Previous research has shown that self-rated health is an independent predictor of hospitalization or death, but the effects of individual subject-specific risks on these outcomes has not been examined, wrote Scott Z. Mu, MD, of the Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, and colleagues.
In a study published in the Journal of General Internal Medicine, the researchers reviewed data from 14,937 members of the Atherosclerosis Risk in Communities (ARIC) cohort, a community-based prospective study of middle-aged men and women that began with their enrollment from 1987 to 1989. The primary outcome was the association between baseline self-rated health and subsequent recurrent hospitalizations and deaths over a median follow-up period of 27.7 years.
At baseline, 34% of the participants rated their health as excellent, 47% good, 16% fair, and 3% poor. After the median follow-up, 39%, 51%, 67%, and 83% of individuals who rated their health as excellent, good, fair, and poor, respectively, had died.
The researchers used a recurrent events survival model that adjusted for clinical and demographic factors and also allowed for dependency between the rates of hospitalization and hazards of death.
After controlling for demographics and medical history, a lower self-rating of health was associated with increased rates of hospitalization and death. Compared with individuals with baseline reports of excellent health, hospitalization rates were 1.22, 2.01, and 3.13 times higher for those with baseline reports of good, fair, or poor health, respectively. Similarly, compared with individuals with baseline reports of excellent health, hazards of death were 1.30, 2.15, and 3.40 for those with baseline reports of good, fair, or poor health, respectively.
Overall, individuals who reported poor health at baseline were significantly more likely than those who reported excellent health to be older (57.0 years vs 53.0 years), obese (44% vs 18%), and current smokers (39% vs 21%). Those who reported poor health at baseline also were significantly more likely than those who reported excellent health to have a history of cancer (9.5% vs 4.4%), emphysema/COPD (18% vs 2.3%), coronary heart disease (21% vs 1.6%), myocardial infarction (19% vs 1.3%), heart failure (25% vs. 1.2%), hypertension (67% vs 19%), or diabetes (39% vs 4.6%).
Potential explanations for the independent association between poor self-rated health and poor outcomes include the ability of self-rated health to capture health information not accounted for by traditional risk factors, the researchers wrote in their discussion. “Another explanation is that self-rated health reflects subconscious bodily sensations that provide a direct sense of health unavailable to external observation,” they said. Alternatively, self-rated health may reinforce beneficial behaviors in those with higher self-rated health and harmful behaviors in those with lower self-rated health, they said.
The findings were limited by several factors including the measurement of self-rated health and the validity of hospitalization as a proxy for morbidity, the researchers noted. Other limitations include the use of models instead of repeated self-rated health measures, and a lack of data on interventions to directly or indirectly improve self-rated health, the researchers noted.
However, the study shows the potential value of self-rated health in routine clinical care to predict future hospitalizations, they said. “Clinicians can use this simple and convenient measure for individual patients to provide more accurate and personalized risk assessments,” they said.
Looking ahead, the current study findings also support the need for more research into the routine assessment not only of self-rated health but also targeted interventions to improve self-rated health and its determinants, the researchers concluded. The ARIC study has been supported by the National Heart, Lung, and Blood Institute, National Institutes of Health. Dr. Mu disclosed support from the National Heart, Lung, and Blood Institute.
Adults who self-rated their health as poor in middle age were at least three times more likely to die or be hospitalized when older than those who self-rated their health as excellent, based on data from nearly 15,000 individuals.
Previous research has shown that self-rated health is an independent predictor of hospitalization or death, but the effects of individual subject-specific risks on these outcomes has not been examined, wrote Scott Z. Mu, MD, of the Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, and colleagues.
In a study published in the Journal of General Internal Medicine, the researchers reviewed data from 14,937 members of the Atherosclerosis Risk in Communities (ARIC) cohort, a community-based prospective study of middle-aged men and women that began with their enrollment from 1987 to 1989. The primary outcome was the association between baseline self-rated health and subsequent recurrent hospitalizations and deaths over a median follow-up period of 27.7 years.
At baseline, 34% of the participants rated their health as excellent, 47% good, 16% fair, and 3% poor. After the median follow-up, 39%, 51%, 67%, and 83% of individuals who rated their health as excellent, good, fair, and poor, respectively, had died.
The researchers used a recurrent events survival model that adjusted for clinical and demographic factors and also allowed for dependency between the rates of hospitalization and hazards of death.
After controlling for demographics and medical history, a lower self-rating of health was associated with increased rates of hospitalization and death. Compared with individuals with baseline reports of excellent health, hospitalization rates were 1.22, 2.01, and 3.13 times higher for those with baseline reports of good, fair, or poor health, respectively. Similarly, compared with individuals with baseline reports of excellent health, hazards of death were 1.30, 2.15, and 3.40 for those with baseline reports of good, fair, or poor health, respectively.
Overall, individuals who reported poor health at baseline were significantly more likely than those who reported excellent health to be older (57.0 years vs 53.0 years), obese (44% vs 18%), and current smokers (39% vs 21%). Those who reported poor health at baseline also were significantly more likely than those who reported excellent health to have a history of cancer (9.5% vs 4.4%), emphysema/COPD (18% vs 2.3%), coronary heart disease (21% vs 1.6%), myocardial infarction (19% vs 1.3%), heart failure (25% vs. 1.2%), hypertension (67% vs 19%), or diabetes (39% vs 4.6%).
Potential explanations for the independent association between poor self-rated health and poor outcomes include the ability of self-rated health to capture health information not accounted for by traditional risk factors, the researchers wrote in their discussion. “Another explanation is that self-rated health reflects subconscious bodily sensations that provide a direct sense of health unavailable to external observation,” they said. Alternatively, self-rated health may reinforce beneficial behaviors in those with higher self-rated health and harmful behaviors in those with lower self-rated health, they said.
The findings were limited by several factors including the measurement of self-rated health and the validity of hospitalization as a proxy for morbidity, the researchers noted. Other limitations include the use of models instead of repeated self-rated health measures, and a lack of data on interventions to directly or indirectly improve self-rated health, the researchers noted.
However, the study shows the potential value of self-rated health in routine clinical care to predict future hospitalizations, they said. “Clinicians can use this simple and convenient measure for individual patients to provide more accurate and personalized risk assessments,” they said.
Looking ahead, the current study findings also support the need for more research into the routine assessment not only of self-rated health but also targeted interventions to improve self-rated health and its determinants, the researchers concluded. The ARIC study has been supported by the National Heart, Lung, and Blood Institute, National Institutes of Health. Dr. Mu disclosed support from the National Heart, Lung, and Blood Institute.
Adults who self-rated their health as poor in middle age were at least three times more likely to die or be hospitalized when older than those who self-rated their health as excellent, based on data from nearly 15,000 individuals.
Previous research has shown that self-rated health is an independent predictor of hospitalization or death, but the effects of individual subject-specific risks on these outcomes has not been examined, wrote Scott Z. Mu, MD, of the Johns Hopkins Bloomberg School of Public Health, Baltimore, Maryland, and colleagues.
In a study published in the Journal of General Internal Medicine, the researchers reviewed data from 14,937 members of the Atherosclerosis Risk in Communities (ARIC) cohort, a community-based prospective study of middle-aged men and women that began with their enrollment from 1987 to 1989. The primary outcome was the association between baseline self-rated health and subsequent recurrent hospitalizations and deaths over a median follow-up period of 27.7 years.
At baseline, 34% of the participants rated their health as excellent, 47% good, 16% fair, and 3% poor. After the median follow-up, 39%, 51%, 67%, and 83% of individuals who rated their health as excellent, good, fair, and poor, respectively, had died.
The researchers used a recurrent events survival model that adjusted for clinical and demographic factors and also allowed for dependency between the rates of hospitalization and hazards of death.
After controlling for demographics and medical history, a lower self-rating of health was associated with increased rates of hospitalization and death. Compared with individuals with baseline reports of excellent health, hospitalization rates were 1.22, 2.01, and 3.13 times higher for those with baseline reports of good, fair, or poor health, respectively. Similarly, compared with individuals with baseline reports of excellent health, hazards of death were 1.30, 2.15, and 3.40 for those with baseline reports of good, fair, or poor health, respectively.
Overall, individuals who reported poor health at baseline were significantly more likely than those who reported excellent health to be older (57.0 years vs 53.0 years), obese (44% vs 18%), and current smokers (39% vs 21%). Those who reported poor health at baseline also were significantly more likely than those who reported excellent health to have a history of cancer (9.5% vs 4.4%), emphysema/COPD (18% vs 2.3%), coronary heart disease (21% vs 1.6%), myocardial infarction (19% vs 1.3%), heart failure (25% vs. 1.2%), hypertension (67% vs 19%), or diabetes (39% vs 4.6%).
Potential explanations for the independent association between poor self-rated health and poor outcomes include the ability of self-rated health to capture health information not accounted for by traditional risk factors, the researchers wrote in their discussion. “Another explanation is that self-rated health reflects subconscious bodily sensations that provide a direct sense of health unavailable to external observation,” they said. Alternatively, self-rated health may reinforce beneficial behaviors in those with higher self-rated health and harmful behaviors in those with lower self-rated health, they said.
The findings were limited by several factors including the measurement of self-rated health and the validity of hospitalization as a proxy for morbidity, the researchers noted. Other limitations include the use of models instead of repeated self-rated health measures, and a lack of data on interventions to directly or indirectly improve self-rated health, the researchers noted.
However, the study shows the potential value of self-rated health in routine clinical care to predict future hospitalizations, they said. “Clinicians can use this simple and convenient measure for individual patients to provide more accurate and personalized risk assessments,” they said.
Looking ahead, the current study findings also support the need for more research into the routine assessment not only of self-rated health but also targeted interventions to improve self-rated health and its determinants, the researchers concluded. The ARIC study has been supported by the National Heart, Lung, and Blood Institute, National Institutes of Health. Dr. Mu disclosed support from the National Heart, Lung, and Blood Institute.
Wearables May Confirm Sleep Disruption Impact on Chronic Disease
Rapid eye movement (REM) sleep, deep sleep, and sleep irregularity were significantly associated with increased risk for a range of chronic diseases, based on a new study of > 6000 individuals.
“Most of what we think we know about sleep patterns in adults comes from either self-report surveys, which are widely used but have all sorts of problems with over- and under-estimating sleep duration and quality, or single-night sleep studies,” corresponding author Evan L. Brittain, MD, of Vanderbilt University, Nashville, Tennessee, said in an interview.
The single-night study yields the highest quality data but is limited by extrapolating a single night’s sleep to represent habitual sleep patterns, which is often not the case, he said. In the current study, published in Nature Medicine, “we had a unique opportunity to understand sleep using a large cohort of individuals using wearable devices that measure sleep duration, quality, and variability. The All of Us Research Program is the first to link wearables data to the electronic health record at scale and allowed us to study long-term, real-world sleep behavior,” Dr. Brittain said.
The timing of the study is important because the American Heart Association now recognizes sleep as a key component of heart health, and public awareness of the value of sleep is increasing, he added.
The researchers reviewed objectively measured, longitudinal sleep data from 6785 adults who used commercial wearable devices (Fitbit) linked to electronic health record data in the All of Us Research Program. The median age of the participants was 50.2 years, 71% were women, and 84% self-identified as White individuals. The median period of sleep monitoring was 4.5 years.
REM sleep and deep sleep were inversely associated with the odds of incident heart rhythm and heart rate abnormalities. A higher percentage of deep sleep was associated with reduced odds of atrial fibrillation (OR, 0.87), major depressive disorder (OR, 0.93), and anxiety disorder (OR, 0.94).
Increased irregular sleep was significantly associated with increased odds of incident obesity (OR, 1.49), hyperlipidemia (OR, 1.39), and hypertension (OR, 1.56), as well as major depressive disorder (OR, 1.75), anxiety disorder (OR, 1.55), and bipolar disorder (OR, 2.27).
The researchers also identified J-shaped associations between average daily sleep duration and hypertension (P for nonlinearity = .003), as well as major depressive disorder and generalized anxiety disorder (both P < .001).
The study was limited by several factors including the relatively young, White, and female study population. However, the results illustrate how sleep stages, duration, and regularity are associated with chronic disease development, and may inform evidence-based recommendations on healthy sleeping habits, the researchers wrote.
Findings Support Need for Sleep Consistency
“The biggest surprise for me was the impact of sleep variability of health,” Dr. Brittain told this news organization. “The more your sleep duration varies, the higher your risk of numerous chronic diseases across the entire spectrum of organ systems. Sleep duration and quality were also important but that was less surprising,” he said.
The clinical implications of the findings are that sleep duration, quality, and variability are all important, said Dr. Brittain. “To me, the easiest finding to translate into the clinic is the importance of reducing the variability of sleep duration as much as possible,” he said. For patients, that means explaining that they need to go to sleep and wake up at roughly the same time night to night, he said.
“Commercial wearable devices are not perfect compared with research grade devices, but our study showed that they nonetheless collect clinically relevant information,” Dr. Brittain added. “For patients who own a device, I have adopted the practice of reviewing my patients’ sleep and activity data which gives objective insight into behavior that is not always accurate through routine questioning,” he said.
As for other limitations, “Our cohort was limited to individuals who already owned a Fitbit; not surprisingly, these individuals differ from a random sample of the community in important ways, both demographic and behavioral, and our findings need to be validated in a more diverse population,” said Dr. Brittain.
Looking ahead, “we are interested in using commercial devices as a tool for sleep interventions to test the impact of improving sleep hygiene on chronic disease incidence, severity, and progression,” he said.
Device Data Will Evolve to Inform Patient Care
“With the increasing use of commercial wearable devices, it is crucial to identify and understand the data they can collect,” said Arianne K. Baldomero, MD, a pulmonologist and assistant professor of medicine at the University of Minnesota, Minneapolis, in an interview. “This study specifically analyzed sleep data from Fitbit devices among participants in the All of Us Research Program to assess sleep patterns and their association with chronic disease risk,” said Dr. Baldomero, who was not involved in the study.
The significant relationships between sleep patterns and risk for chronic diseases were not surprising, said Dr. Baldomero. The findings of an association between shorter sleep duration and greater sleep irregularity with obesity and sleep apnea validated previous studies in large-scale population surveys, she said. Findings from the current study also reflect data from the literature on sleep duration associated with hypertension, major depressive disorder, and generalized anxiety findings, she added.
“This study reinforces the importance of adequate sleep, typically around 7 hours per night, and suggests that insufficient or poor-quality sleep may be associated with chronic diseases,” Dr. Baldomero told this news organization. “Pulmonologists should remain vigilant about sleep-related issues, and consider further investigation and referrals to sleep specialty clinics for patients suspected of having sleep disturbances,” she said.
“What remains unclear is whether abnormal sleep patterns are a cause or an effect of chronic diseases,” Dr. Baldomero noted. “Additionally, it is essential to ensure that these devices accurately capture sleep patterns and continue to validate their data against gold standard measures of sleep disturbances,” she said.
The study was based on work that was partially funded by an unrestricted gift from Google, and the study itself was supported by National Institutes of Health. Dr. Brittain disclosed received research funds unrelated to this work from United Therapeutics. Dr. Baldomero had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Rapid eye movement (REM) sleep, deep sleep, and sleep irregularity were significantly associated with increased risk for a range of chronic diseases, based on a new study of > 6000 individuals.
“Most of what we think we know about sleep patterns in adults comes from either self-report surveys, which are widely used but have all sorts of problems with over- and under-estimating sleep duration and quality, or single-night sleep studies,” corresponding author Evan L. Brittain, MD, of Vanderbilt University, Nashville, Tennessee, said in an interview.
The single-night study yields the highest quality data but is limited by extrapolating a single night’s sleep to represent habitual sleep patterns, which is often not the case, he said. In the current study, published in Nature Medicine, “we had a unique opportunity to understand sleep using a large cohort of individuals using wearable devices that measure sleep duration, quality, and variability. The All of Us Research Program is the first to link wearables data to the electronic health record at scale and allowed us to study long-term, real-world sleep behavior,” Dr. Brittain said.
The timing of the study is important because the American Heart Association now recognizes sleep as a key component of heart health, and public awareness of the value of sleep is increasing, he added.
The researchers reviewed objectively measured, longitudinal sleep data from 6785 adults who used commercial wearable devices (Fitbit) linked to electronic health record data in the All of Us Research Program. The median age of the participants was 50.2 years, 71% were women, and 84% self-identified as White individuals. The median period of sleep monitoring was 4.5 years.
REM sleep and deep sleep were inversely associated with the odds of incident heart rhythm and heart rate abnormalities. A higher percentage of deep sleep was associated with reduced odds of atrial fibrillation (OR, 0.87), major depressive disorder (OR, 0.93), and anxiety disorder (OR, 0.94).
Increased irregular sleep was significantly associated with increased odds of incident obesity (OR, 1.49), hyperlipidemia (OR, 1.39), and hypertension (OR, 1.56), as well as major depressive disorder (OR, 1.75), anxiety disorder (OR, 1.55), and bipolar disorder (OR, 2.27).
The researchers also identified J-shaped associations between average daily sleep duration and hypertension (P for nonlinearity = .003), as well as major depressive disorder and generalized anxiety disorder (both P < .001).
The study was limited by several factors including the relatively young, White, and female study population. However, the results illustrate how sleep stages, duration, and regularity are associated with chronic disease development, and may inform evidence-based recommendations on healthy sleeping habits, the researchers wrote.
Findings Support Need for Sleep Consistency
“The biggest surprise for me was the impact of sleep variability of health,” Dr. Brittain told this news organization. “The more your sleep duration varies, the higher your risk of numerous chronic diseases across the entire spectrum of organ systems. Sleep duration and quality were also important but that was less surprising,” he said.
The clinical implications of the findings are that sleep duration, quality, and variability are all important, said Dr. Brittain. “To me, the easiest finding to translate into the clinic is the importance of reducing the variability of sleep duration as much as possible,” he said. For patients, that means explaining that they need to go to sleep and wake up at roughly the same time night to night, he said.
“Commercial wearable devices are not perfect compared with research grade devices, but our study showed that they nonetheless collect clinically relevant information,” Dr. Brittain added. “For patients who own a device, I have adopted the practice of reviewing my patients’ sleep and activity data which gives objective insight into behavior that is not always accurate through routine questioning,” he said.
As for other limitations, “Our cohort was limited to individuals who already owned a Fitbit; not surprisingly, these individuals differ from a random sample of the community in important ways, both demographic and behavioral, and our findings need to be validated in a more diverse population,” said Dr. Brittain.
Looking ahead, “we are interested in using commercial devices as a tool for sleep interventions to test the impact of improving sleep hygiene on chronic disease incidence, severity, and progression,” he said.
Device Data Will Evolve to Inform Patient Care
“With the increasing use of commercial wearable devices, it is crucial to identify and understand the data they can collect,” said Arianne K. Baldomero, MD, a pulmonologist and assistant professor of medicine at the University of Minnesota, Minneapolis, in an interview. “This study specifically analyzed sleep data from Fitbit devices among participants in the All of Us Research Program to assess sleep patterns and their association with chronic disease risk,” said Dr. Baldomero, who was not involved in the study.
The significant relationships between sleep patterns and risk for chronic diseases were not surprising, said Dr. Baldomero. The findings of an association between shorter sleep duration and greater sleep irregularity with obesity and sleep apnea validated previous studies in large-scale population surveys, she said. Findings from the current study also reflect data from the literature on sleep duration associated with hypertension, major depressive disorder, and generalized anxiety findings, she added.
“This study reinforces the importance of adequate sleep, typically around 7 hours per night, and suggests that insufficient or poor-quality sleep may be associated with chronic diseases,” Dr. Baldomero told this news organization. “Pulmonologists should remain vigilant about sleep-related issues, and consider further investigation and referrals to sleep specialty clinics for patients suspected of having sleep disturbances,” she said.
“What remains unclear is whether abnormal sleep patterns are a cause or an effect of chronic diseases,” Dr. Baldomero noted. “Additionally, it is essential to ensure that these devices accurately capture sleep patterns and continue to validate their data against gold standard measures of sleep disturbances,” she said.
The study was based on work that was partially funded by an unrestricted gift from Google, and the study itself was supported by National Institutes of Health. Dr. Brittain disclosed received research funds unrelated to this work from United Therapeutics. Dr. Baldomero had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Rapid eye movement (REM) sleep, deep sleep, and sleep irregularity were significantly associated with increased risk for a range of chronic diseases, based on a new study of > 6000 individuals.
“Most of what we think we know about sleep patterns in adults comes from either self-report surveys, which are widely used but have all sorts of problems with over- and under-estimating sleep duration and quality, or single-night sleep studies,” corresponding author Evan L. Brittain, MD, of Vanderbilt University, Nashville, Tennessee, said in an interview.
The single-night study yields the highest quality data but is limited by extrapolating a single night’s sleep to represent habitual sleep patterns, which is often not the case, he said. In the current study, published in Nature Medicine, “we had a unique opportunity to understand sleep using a large cohort of individuals using wearable devices that measure sleep duration, quality, and variability. The All of Us Research Program is the first to link wearables data to the electronic health record at scale and allowed us to study long-term, real-world sleep behavior,” Dr. Brittain said.
The timing of the study is important because the American Heart Association now recognizes sleep as a key component of heart health, and public awareness of the value of sleep is increasing, he added.
The researchers reviewed objectively measured, longitudinal sleep data from 6785 adults who used commercial wearable devices (Fitbit) linked to electronic health record data in the All of Us Research Program. The median age of the participants was 50.2 years, 71% were women, and 84% self-identified as White individuals. The median period of sleep monitoring was 4.5 years.
REM sleep and deep sleep were inversely associated with the odds of incident heart rhythm and heart rate abnormalities. A higher percentage of deep sleep was associated with reduced odds of atrial fibrillation (OR, 0.87), major depressive disorder (OR, 0.93), and anxiety disorder (OR, 0.94).
Increased irregular sleep was significantly associated with increased odds of incident obesity (OR, 1.49), hyperlipidemia (OR, 1.39), and hypertension (OR, 1.56), as well as major depressive disorder (OR, 1.75), anxiety disorder (OR, 1.55), and bipolar disorder (OR, 2.27).
The researchers also identified J-shaped associations between average daily sleep duration and hypertension (P for nonlinearity = .003), as well as major depressive disorder and generalized anxiety disorder (both P < .001).
The study was limited by several factors including the relatively young, White, and female study population. However, the results illustrate how sleep stages, duration, and regularity are associated with chronic disease development, and may inform evidence-based recommendations on healthy sleeping habits, the researchers wrote.
Findings Support Need for Sleep Consistency
“The biggest surprise for me was the impact of sleep variability of health,” Dr. Brittain told this news organization. “The more your sleep duration varies, the higher your risk of numerous chronic diseases across the entire spectrum of organ systems. Sleep duration and quality were also important but that was less surprising,” he said.
The clinical implications of the findings are that sleep duration, quality, and variability are all important, said Dr. Brittain. “To me, the easiest finding to translate into the clinic is the importance of reducing the variability of sleep duration as much as possible,” he said. For patients, that means explaining that they need to go to sleep and wake up at roughly the same time night to night, he said.
“Commercial wearable devices are not perfect compared with research grade devices, but our study showed that they nonetheless collect clinically relevant information,” Dr. Brittain added. “For patients who own a device, I have adopted the practice of reviewing my patients’ sleep and activity data which gives objective insight into behavior that is not always accurate through routine questioning,” he said.
As for other limitations, “Our cohort was limited to individuals who already owned a Fitbit; not surprisingly, these individuals differ from a random sample of the community in important ways, both demographic and behavioral, and our findings need to be validated in a more diverse population,” said Dr. Brittain.
Looking ahead, “we are interested in using commercial devices as a tool for sleep interventions to test the impact of improving sleep hygiene on chronic disease incidence, severity, and progression,” he said.
Device Data Will Evolve to Inform Patient Care
“With the increasing use of commercial wearable devices, it is crucial to identify and understand the data they can collect,” said Arianne K. Baldomero, MD, a pulmonologist and assistant professor of medicine at the University of Minnesota, Minneapolis, in an interview. “This study specifically analyzed sleep data from Fitbit devices among participants in the All of Us Research Program to assess sleep patterns and their association with chronic disease risk,” said Dr. Baldomero, who was not involved in the study.
The significant relationships between sleep patterns and risk for chronic diseases were not surprising, said Dr. Baldomero. The findings of an association between shorter sleep duration and greater sleep irregularity with obesity and sleep apnea validated previous studies in large-scale population surveys, she said. Findings from the current study also reflect data from the literature on sleep duration associated with hypertension, major depressive disorder, and generalized anxiety findings, she added.
“This study reinforces the importance of adequate sleep, typically around 7 hours per night, and suggests that insufficient or poor-quality sleep may be associated with chronic diseases,” Dr. Baldomero told this news organization. “Pulmonologists should remain vigilant about sleep-related issues, and consider further investigation and referrals to sleep specialty clinics for patients suspected of having sleep disturbances,” she said.
“What remains unclear is whether abnormal sleep patterns are a cause or an effect of chronic diseases,” Dr. Baldomero noted. “Additionally, it is essential to ensure that these devices accurately capture sleep patterns and continue to validate their data against gold standard measures of sleep disturbances,” she said.
The study was based on work that was partially funded by an unrestricted gift from Google, and the study itself was supported by National Institutes of Health. Dr. Brittain disclosed received research funds unrelated to this work from United Therapeutics. Dr. Baldomero had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
When Is Sexual Behavior Out of Control?
A 25-year-old man comes in with a pulled muscle. You ask if he has anything else to discuss. Sheepishly, he says he is concerned about his use of pornography.
A 45-year-old woman struggling with depression finds herself persistently seeking sex outside the bounds of her long-term relationship. Her partner is threatening to leave. She is devastated and tells you she doesn’t understand her own behavior.
Do these patients have some form of sex addiction? How should a primary care clinician intervene? Is a referral to a 12-step program for sex addiction the right choice? What other options exist? Is a diagnosis — let alone treatment — possible or appropriate?
‘Who Are You Calling “Abnormal” ’?
Normal is not a meaningful concept in human sexual behavior. To quote the sex therapist Marty Klein, PhD: “Normal is just a setting on the dryer.”
The same goes among partners: What is “normal” for one person in a sexual relationship may discomfit another. In partnerships, we have differences around all sorts of issues, from finances to parenting to how to load the dishwasher. Why should sex, sexual desire, and sexual frequency be different?
Remember: Shame, fear, and secrecy often play a role in perpetuating behaviors that cause distress. Helping our patients accept and embrace their whole selves can provide important healing, relief from anxiety, and may even help them regulate their actions. Feeling less shame, fear, and secrecy may facilitate safer choices about sex, as well as testing and treatment for sexually transmitted infections.
The International Classification of Diseases-11 includes compulsive sexual behavior disorder (CSBD)as an attempt to create consensus around a complicated, and hotly debated, problem to facilitate diagnosis and research. Syndromes similar to CSBD have had many names: “hypersexual disorder,” “sexual addiction,” “sexual compulsivity,” and “out-of-control sexual behavior.” A sizable cohort of the sexuality research community casts doubt on whether CSBD is even a discrete diagnosis.
According to the ICD-11, CSBD is characterized by “intense, repetitive sexual impulses or urges that are experienced as irresistible or uncontrollable” and result in significant distress or functional impairment.
This diagnosis has several important rule-outs. First, paraphilias, defined as a set of nonconsensual sexual behaviors and interests, are excluded. Another is that distress exclusively related to moral judgment or social disapproval is not sufficient for a diagnosis of CSBD. Finally, the diagnosis hinges on distress and does not rely on frequency of any type of sexual behavior. Some people experience significant distress over behaviors in which they engage infrequently, whereas others may have no distress from activities in which they engage quite frequently.
In one study from Germany, 5% of men and 3% of women met criteria for CSBD. A small US study found the number to be 10% and 7%, respectively. The diagnosis is not simple. Compulsive sexual behavior can be secondary to other mental health or medical conditions. Behaviors sometimes confused with CSBD can result from neurologic diseases, such as frontal brain lesions or frontotemporal dementia, as well as the use of substances and medications that enhance dopaminergic activity.
Impaired control over sexual impulses occurs in manic and hypomanic episodes. Compulsive sexual behavior frequently co-occurs with mood disorders, obsessive-compulsive disorder, attention-deficit/hyperactivity disorder, and substance use disorders. Those meeting criteria for CSBD may engage in sexual behaviors as a way of coping with depression, anxiety, boredom, loneliness, or other negative affective states.
The diagnosis of CSBD may be useful for clinicians. However, many, perhaps most, patients who present with concerns about their sexual behavior will fail to meet most criteria for CSBD. Their problem is of shorter duration, related to morality, external disapproval, lack of sexual health information, and anxiety about diverse erotic interests. It may be helpful for them to understand that they are not in the grip of a lifelong disorder but are experiencing common life challenges.
Societal concerns about sexually explicit media, often called pornography, are complex, conflicting, and catastrophizing. Some studies indicate that sexually explicit media are positive for both individual and relational sexual satisfaction; other studies have found negative effects on sexual function. Concerns about pornography often are conflated with taboos about solo sexual activity. Ironically, use of pornography is associated with fear of addiction to pornography, creating a spiral of negative self-perception.
Consequences of sexual behavior may induce distress, even if a person doesn’t meet criteria for CSBD, such as potential dissolution of a marriage, loss of a job, excessive spending, sexually transmitted infections, other health concerns, and even legal problems. Sexual behavior might not be the central issue but rather an offshoot of relational distress, a mental health disorder, or a dysfunctional coping style.
Guilt and shame can act as potent contributors to maintaining the behaviors as well as promoting secrecy around them. Sexual medicine experts recommend avoiding interventions that increase the experience of discrimination and stigma and avoiding the pathologization of the behaviors of sexually diverse individuals. As in so many aspects of medical care, we must walk in our patients’ shoes and avoid imposing on them our own moral or religious values.
What Can a Primary Care Provider Do?
When a patient is concerned about sexual behavior that feels out of control, primary care providers have an important role in evaluating for neurologic disease or side effects related to the use of medication or other substances, and facilitating psychiatric assessment to evaluate for mental health comorbidities, past trauma, and associated attachment disorders.
Our patients need resources to tease out the individual and relational problems that may arise. Seek out well-trained sex therapy colleagues in your community. The American Association of Sexuality Educators, Counselors, and Therapists (AASECT) is one certifying body in the United States for sex therapy.
Because of the heterogeneity of those who present with out-of-control sexual behavior, no one treatment fits all. Twelve-step programs, especially those with a focus on sexual “abstinence,” may not be the best choice. Many psychotherapeutic modalities are effective and often focus on addressing underlying or unrecognized mental health concerns, provide training on self-regulation and urge management, and relationship skills. Most important, the therapist needs to be sexologically informed and aware of their own biases around sexuality. Medical treatments are not recommended without concurrent psychological intervention.
Relational sex therapy can help couples create clear relational agreements that work for both parties (or, in polyamorous relationships, everyone involved). Relational distress also may be a stimulus for individual psychotherapy.
Back to these two patients.
The 25-year-old could be counseled that use of sexually explicit media and solo sex are not inherently bad or damaging. When used for pleasure and enjoyment, they do not lead to problems with partnered sex or cause sexual dysfunction. Counseling him to move toward social engagement and life goals, rather than away from pornography, may be all that is necessary.
Our second patient probably will need more intensive treatment, including medication management for her mood and referral to a certified sex therapist who has expertise in working with out-of-control sexual behavior. When she returns to see you in follow-up, she ideally expresses reduced shame, more autonomy, and renewed connection to her values, and she is keeping her relational agreements without sacrificing her sexual needs.
Dr. Kranz is medical director, Rochester Center for Sexual Wellness; assistant professor of Clinical Family Medicine and Obstetrics and Gynecology, University of Rochester Medical Center, Rochester, New York. Dr. Kranz has disclosed no relevant financial relationships. Dr. Rosen is director of Behavioral Health, Rochester Center for Sexual Wellness, Rochester, New York. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
A 25-year-old man comes in with a pulled muscle. You ask if he has anything else to discuss. Sheepishly, he says he is concerned about his use of pornography.
A 45-year-old woman struggling with depression finds herself persistently seeking sex outside the bounds of her long-term relationship. Her partner is threatening to leave. She is devastated and tells you she doesn’t understand her own behavior.
Do these patients have some form of sex addiction? How should a primary care clinician intervene? Is a referral to a 12-step program for sex addiction the right choice? What other options exist? Is a diagnosis — let alone treatment — possible or appropriate?
‘Who Are You Calling “Abnormal” ’?
Normal is not a meaningful concept in human sexual behavior. To quote the sex therapist Marty Klein, PhD: “Normal is just a setting on the dryer.”
The same goes among partners: What is “normal” for one person in a sexual relationship may discomfit another. In partnerships, we have differences around all sorts of issues, from finances to parenting to how to load the dishwasher. Why should sex, sexual desire, and sexual frequency be different?
Remember: Shame, fear, and secrecy often play a role in perpetuating behaviors that cause distress. Helping our patients accept and embrace their whole selves can provide important healing, relief from anxiety, and may even help them regulate their actions. Feeling less shame, fear, and secrecy may facilitate safer choices about sex, as well as testing and treatment for sexually transmitted infections.
The International Classification of Diseases-11 includes compulsive sexual behavior disorder (CSBD)as an attempt to create consensus around a complicated, and hotly debated, problem to facilitate diagnosis and research. Syndromes similar to CSBD have had many names: “hypersexual disorder,” “sexual addiction,” “sexual compulsivity,” and “out-of-control sexual behavior.” A sizable cohort of the sexuality research community casts doubt on whether CSBD is even a discrete diagnosis.
According to the ICD-11, CSBD is characterized by “intense, repetitive sexual impulses or urges that are experienced as irresistible or uncontrollable” and result in significant distress or functional impairment.
This diagnosis has several important rule-outs. First, paraphilias, defined as a set of nonconsensual sexual behaviors and interests, are excluded. Another is that distress exclusively related to moral judgment or social disapproval is not sufficient for a diagnosis of CSBD. Finally, the diagnosis hinges on distress and does not rely on frequency of any type of sexual behavior. Some people experience significant distress over behaviors in which they engage infrequently, whereas others may have no distress from activities in which they engage quite frequently.
In one study from Germany, 5% of men and 3% of women met criteria for CSBD. A small US study found the number to be 10% and 7%, respectively. The diagnosis is not simple. Compulsive sexual behavior can be secondary to other mental health or medical conditions. Behaviors sometimes confused with CSBD can result from neurologic diseases, such as frontal brain lesions or frontotemporal dementia, as well as the use of substances and medications that enhance dopaminergic activity.
Impaired control over sexual impulses occurs in manic and hypomanic episodes. Compulsive sexual behavior frequently co-occurs with mood disorders, obsessive-compulsive disorder, attention-deficit/hyperactivity disorder, and substance use disorders. Those meeting criteria for CSBD may engage in sexual behaviors as a way of coping with depression, anxiety, boredom, loneliness, or other negative affective states.
The diagnosis of CSBD may be useful for clinicians. However, many, perhaps most, patients who present with concerns about their sexual behavior will fail to meet most criteria for CSBD. Their problem is of shorter duration, related to morality, external disapproval, lack of sexual health information, and anxiety about diverse erotic interests. It may be helpful for them to understand that they are not in the grip of a lifelong disorder but are experiencing common life challenges.
Societal concerns about sexually explicit media, often called pornography, are complex, conflicting, and catastrophizing. Some studies indicate that sexually explicit media are positive for both individual and relational sexual satisfaction; other studies have found negative effects on sexual function. Concerns about pornography often are conflated with taboos about solo sexual activity. Ironically, use of pornography is associated with fear of addiction to pornography, creating a spiral of negative self-perception.
Consequences of sexual behavior may induce distress, even if a person doesn’t meet criteria for CSBD, such as potential dissolution of a marriage, loss of a job, excessive spending, sexually transmitted infections, other health concerns, and even legal problems. Sexual behavior might not be the central issue but rather an offshoot of relational distress, a mental health disorder, or a dysfunctional coping style.
Guilt and shame can act as potent contributors to maintaining the behaviors as well as promoting secrecy around them. Sexual medicine experts recommend avoiding interventions that increase the experience of discrimination and stigma and avoiding the pathologization of the behaviors of sexually diverse individuals. As in so many aspects of medical care, we must walk in our patients’ shoes and avoid imposing on them our own moral or religious values.
What Can a Primary Care Provider Do?
When a patient is concerned about sexual behavior that feels out of control, primary care providers have an important role in evaluating for neurologic disease or side effects related to the use of medication or other substances, and facilitating psychiatric assessment to evaluate for mental health comorbidities, past trauma, and associated attachment disorders.
Our patients need resources to tease out the individual and relational problems that may arise. Seek out well-trained sex therapy colleagues in your community. The American Association of Sexuality Educators, Counselors, and Therapists (AASECT) is one certifying body in the United States for sex therapy.
Because of the heterogeneity of those who present with out-of-control sexual behavior, no one treatment fits all. Twelve-step programs, especially those with a focus on sexual “abstinence,” may not be the best choice. Many psychotherapeutic modalities are effective and often focus on addressing underlying or unrecognized mental health concerns, provide training on self-regulation and urge management, and relationship skills. Most important, the therapist needs to be sexologically informed and aware of their own biases around sexuality. Medical treatments are not recommended without concurrent psychological intervention.
Relational sex therapy can help couples create clear relational agreements that work for both parties (or, in polyamorous relationships, everyone involved). Relational distress also may be a stimulus for individual psychotherapy.
Back to these two patients.
The 25-year-old could be counseled that use of sexually explicit media and solo sex are not inherently bad or damaging. When used for pleasure and enjoyment, they do not lead to problems with partnered sex or cause sexual dysfunction. Counseling him to move toward social engagement and life goals, rather than away from pornography, may be all that is necessary.
Our second patient probably will need more intensive treatment, including medication management for her mood and referral to a certified sex therapist who has expertise in working with out-of-control sexual behavior. When she returns to see you in follow-up, she ideally expresses reduced shame, more autonomy, and renewed connection to her values, and she is keeping her relational agreements without sacrificing her sexual needs.
Dr. Kranz is medical director, Rochester Center for Sexual Wellness; assistant professor of Clinical Family Medicine and Obstetrics and Gynecology, University of Rochester Medical Center, Rochester, New York. Dr. Kranz has disclosed no relevant financial relationships. Dr. Rosen is director of Behavioral Health, Rochester Center for Sexual Wellness, Rochester, New York. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
A 25-year-old man comes in with a pulled muscle. You ask if he has anything else to discuss. Sheepishly, he says he is concerned about his use of pornography.
A 45-year-old woman struggling with depression finds herself persistently seeking sex outside the bounds of her long-term relationship. Her partner is threatening to leave. She is devastated and tells you she doesn’t understand her own behavior.
Do these patients have some form of sex addiction? How should a primary care clinician intervene? Is a referral to a 12-step program for sex addiction the right choice? What other options exist? Is a diagnosis — let alone treatment — possible or appropriate?
‘Who Are You Calling “Abnormal” ’?
Normal is not a meaningful concept in human sexual behavior. To quote the sex therapist Marty Klein, PhD: “Normal is just a setting on the dryer.”
The same goes among partners: What is “normal” for one person in a sexual relationship may discomfit another. In partnerships, we have differences around all sorts of issues, from finances to parenting to how to load the dishwasher. Why should sex, sexual desire, and sexual frequency be different?
Remember: Shame, fear, and secrecy often play a role in perpetuating behaviors that cause distress. Helping our patients accept and embrace their whole selves can provide important healing, relief from anxiety, and may even help them regulate their actions. Feeling less shame, fear, and secrecy may facilitate safer choices about sex, as well as testing and treatment for sexually transmitted infections.
The International Classification of Diseases-11 includes compulsive sexual behavior disorder (CSBD)as an attempt to create consensus around a complicated, and hotly debated, problem to facilitate diagnosis and research. Syndromes similar to CSBD have had many names: “hypersexual disorder,” “sexual addiction,” “sexual compulsivity,” and “out-of-control sexual behavior.” A sizable cohort of the sexuality research community casts doubt on whether CSBD is even a discrete diagnosis.
According to the ICD-11, CSBD is characterized by “intense, repetitive sexual impulses or urges that are experienced as irresistible or uncontrollable” and result in significant distress or functional impairment.
This diagnosis has several important rule-outs. First, paraphilias, defined as a set of nonconsensual sexual behaviors and interests, are excluded. Another is that distress exclusively related to moral judgment or social disapproval is not sufficient for a diagnosis of CSBD. Finally, the diagnosis hinges on distress and does not rely on frequency of any type of sexual behavior. Some people experience significant distress over behaviors in which they engage infrequently, whereas others may have no distress from activities in which they engage quite frequently.
In one study from Germany, 5% of men and 3% of women met criteria for CSBD. A small US study found the number to be 10% and 7%, respectively. The diagnosis is not simple. Compulsive sexual behavior can be secondary to other mental health or medical conditions. Behaviors sometimes confused with CSBD can result from neurologic diseases, such as frontal brain lesions or frontotemporal dementia, as well as the use of substances and medications that enhance dopaminergic activity.
Impaired control over sexual impulses occurs in manic and hypomanic episodes. Compulsive sexual behavior frequently co-occurs with mood disorders, obsessive-compulsive disorder, attention-deficit/hyperactivity disorder, and substance use disorders. Those meeting criteria for CSBD may engage in sexual behaviors as a way of coping with depression, anxiety, boredom, loneliness, or other negative affective states.
The diagnosis of CSBD may be useful for clinicians. However, many, perhaps most, patients who present with concerns about their sexual behavior will fail to meet most criteria for CSBD. Their problem is of shorter duration, related to morality, external disapproval, lack of sexual health information, and anxiety about diverse erotic interests. It may be helpful for them to understand that they are not in the grip of a lifelong disorder but are experiencing common life challenges.
Societal concerns about sexually explicit media, often called pornography, are complex, conflicting, and catastrophizing. Some studies indicate that sexually explicit media are positive for both individual and relational sexual satisfaction; other studies have found negative effects on sexual function. Concerns about pornography often are conflated with taboos about solo sexual activity. Ironically, use of pornography is associated with fear of addiction to pornography, creating a spiral of negative self-perception.
Consequences of sexual behavior may induce distress, even if a person doesn’t meet criteria for CSBD, such as potential dissolution of a marriage, loss of a job, excessive spending, sexually transmitted infections, other health concerns, and even legal problems. Sexual behavior might not be the central issue but rather an offshoot of relational distress, a mental health disorder, or a dysfunctional coping style.
Guilt and shame can act as potent contributors to maintaining the behaviors as well as promoting secrecy around them. Sexual medicine experts recommend avoiding interventions that increase the experience of discrimination and stigma and avoiding the pathologization of the behaviors of sexually diverse individuals. As in so many aspects of medical care, we must walk in our patients’ shoes and avoid imposing on them our own moral or religious values.
What Can a Primary Care Provider Do?
When a patient is concerned about sexual behavior that feels out of control, primary care providers have an important role in evaluating for neurologic disease or side effects related to the use of medication or other substances, and facilitating psychiatric assessment to evaluate for mental health comorbidities, past trauma, and associated attachment disorders.
Our patients need resources to tease out the individual and relational problems that may arise. Seek out well-trained sex therapy colleagues in your community. The American Association of Sexuality Educators, Counselors, and Therapists (AASECT) is one certifying body in the United States for sex therapy.
Because of the heterogeneity of those who present with out-of-control sexual behavior, no one treatment fits all. Twelve-step programs, especially those with a focus on sexual “abstinence,” may not be the best choice. Many psychotherapeutic modalities are effective and often focus on addressing underlying or unrecognized mental health concerns, provide training on self-regulation and urge management, and relationship skills. Most important, the therapist needs to be sexologically informed and aware of their own biases around sexuality. Medical treatments are not recommended without concurrent psychological intervention.
Relational sex therapy can help couples create clear relational agreements that work for both parties (or, in polyamorous relationships, everyone involved). Relational distress also may be a stimulus for individual psychotherapy.
Back to these two patients.
The 25-year-old could be counseled that use of sexually explicit media and solo sex are not inherently bad or damaging. When used for pleasure and enjoyment, they do not lead to problems with partnered sex or cause sexual dysfunction. Counseling him to move toward social engagement and life goals, rather than away from pornography, may be all that is necessary.
Our second patient probably will need more intensive treatment, including medication management for her mood and referral to a certified sex therapist who has expertise in working with out-of-control sexual behavior. When she returns to see you in follow-up, she ideally expresses reduced shame, more autonomy, and renewed connection to her values, and she is keeping her relational agreements without sacrificing her sexual needs.
Dr. Kranz is medical director, Rochester Center for Sexual Wellness; assistant professor of Clinical Family Medicine and Obstetrics and Gynecology, University of Rochester Medical Center, Rochester, New York. Dr. Kranz has disclosed no relevant financial relationships. Dr. Rosen is director of Behavioral Health, Rochester Center for Sexual Wellness, Rochester, New York. He has disclosed no relevant financial relationships.
A version of this article appeared on Medscape.com.
Ozempic Curbs Hunger – And Not Just for Food
This transcript has been edited for clarity.
If you’ve been paying attention only to the headlines, when you think of “Ozempic” you’ll think of a few things: a blockbuster weight loss drug or the tip of the spear of a completely new industry — why not? A drug so popular that the people it was invented for (those with diabetes) can’t even get it.
Ozempic and other GLP-1 receptor agonists are undeniable game changers. Insofar as obesity is the number-one public health risk in the United States, antiobesity drugs hold immense promise even if all they do is reduce obesity.
In 2023, an article in Scientific Reports presented data suggesting that people on Ozempic might be reducing their alcohol intake, not just their total calories.
A 2024 article in Molecular Psychiatry found that the drug might positively impact cannabis use disorder. An article from Brain Sciences suggests that the drug reduces compulsive shopping.
A picture is starting to form, a picture that suggests these drugs curb hunger both literally and figuratively. That GLP-1 receptor agonists like Ozempic and Mounjaro are fundamentally anticonsumption drugs. In a society that — some would argue — is plagued by overconsumption, these drugs might be just what the doctor ordered.
If only they could stop people from smoking.
Oh, wait — they can.
At least it seems they can, based on a new study appearing in Annals of Internal Medicine.
Before we get too excited, this is not a randomized trial. There actually was a small randomized trial of exenatide (Byetta), which is in the same class as Ozempic but probably a bit less potent, with promising results for smoking cessation. 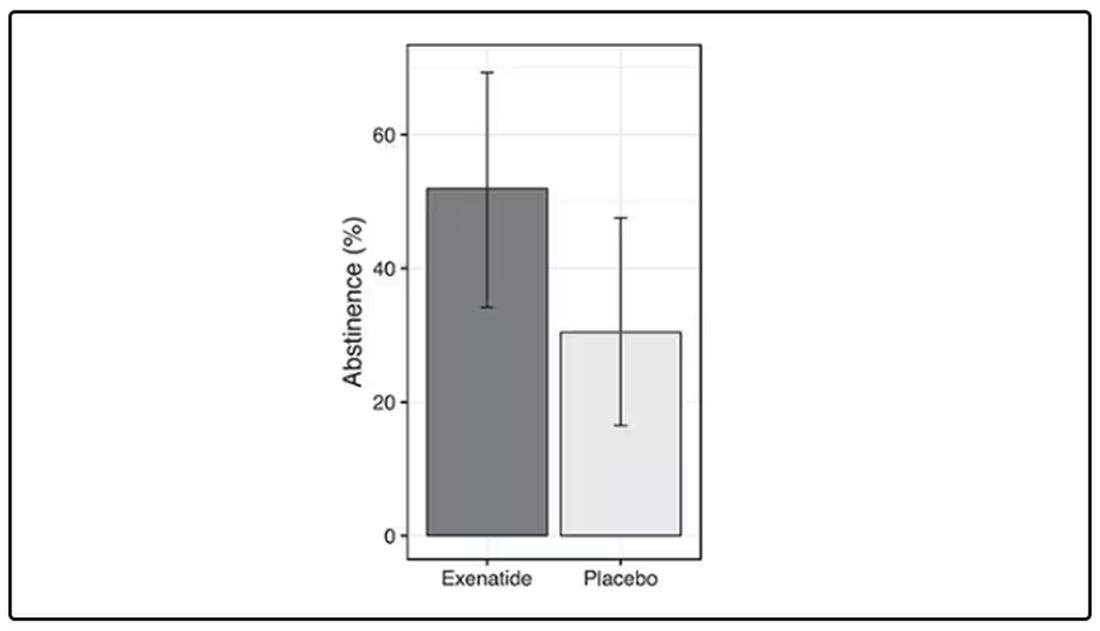
But Byetta is the weaker drug in this class; the market leader is Ozempic. So how can you figure out whether Ozempic can reduce smoking without doing a huge and expensive randomized trial? You can do what Nora Volkow and colleagues from the National Institute on Drug Abuse did: a target trial emulation study.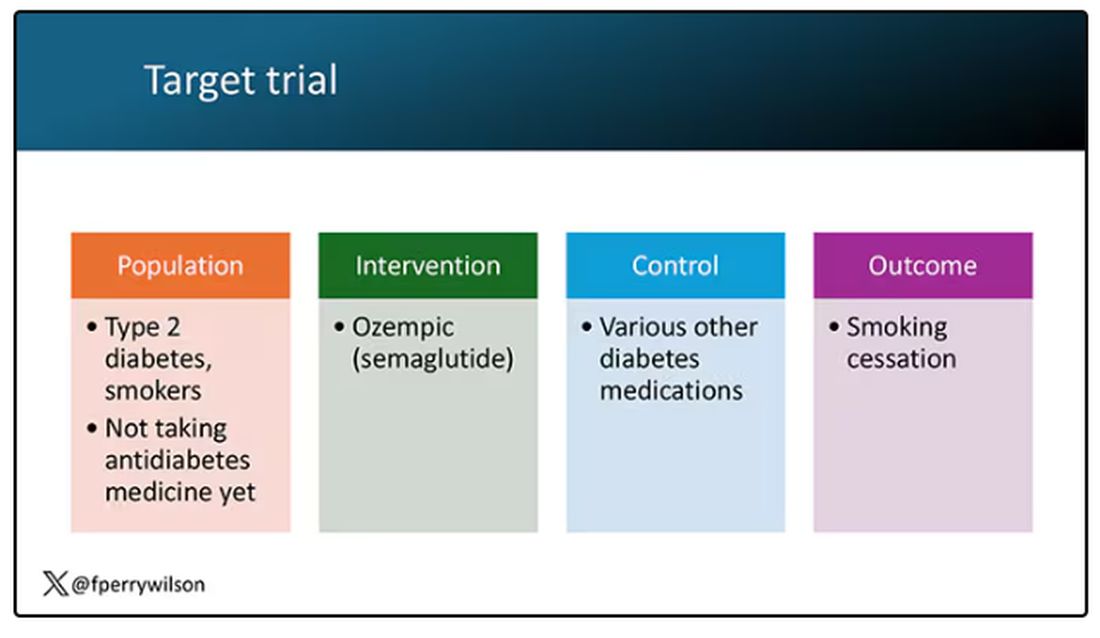
A target trial emulation study is more or less what it sounds like. First, you decide what your dream randomized controlled trial would be and you plan it all out in great detail. You define the population you would recruit, with all the relevant inclusion and exclusion criteria. You define the intervention and the control, and you define the outcome.
But you don’t actually do the trial. You could if someone would lend you $10-$50 million, but assuming you don’t have that lying around, you do the next best thing, which is to dig into a medical record database to find all the people who would be eligible for your imaginary trial. And you analyze them.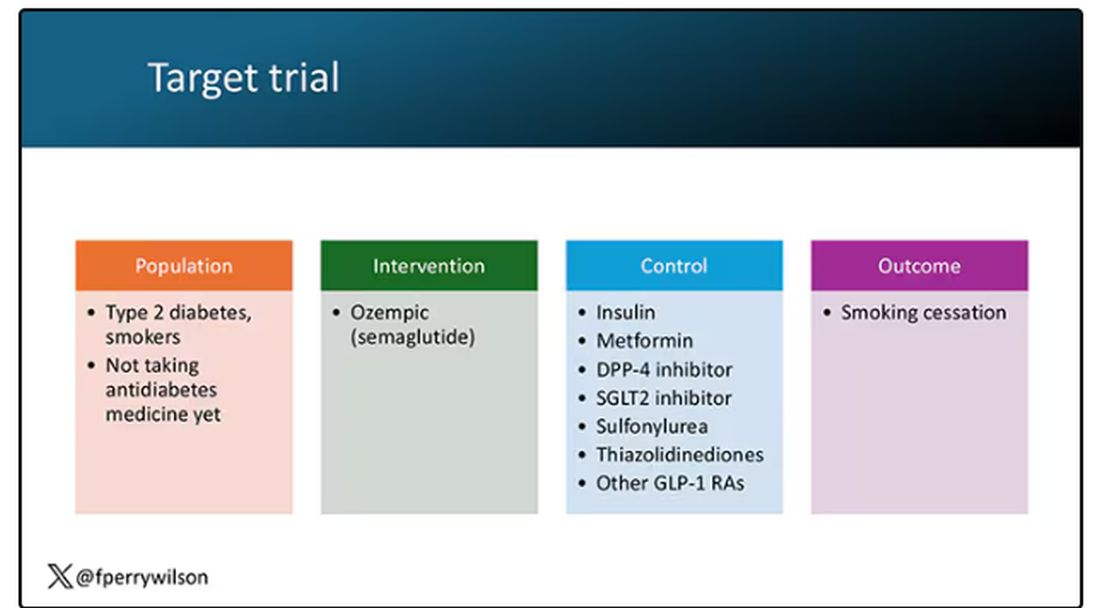
The authors wanted to study the effect of Ozempic on smoking among people with diabetes; that’s why all the comparator agents are antidiabetes drugs. They figured out whether these folks were smoking on the basis of a medical record diagnosis of tobacco use disorder before they started one of the drugs of interest. This code is fairly specific: If a patient has it, you can be pretty sure they are smoking. But it’s not very sensitive; not every smoker has this diagnostic code. This is an age-old limitation of using EHR data instead of asking patients, but it’s part of the tradeoff for not having to spend $50 million.
After applying all those inclusion and exclusion criteria, they have a defined population who could be in their dream trial. And, as luck would have it, some of those people really were treated with Ozempic and some really were treated with those other agents. Although decisions about what to prescribe were not randomized, the authors account for this confounding-by-indication using propensity-score matching. You can find a little explainer on propensity-score matching in an earlier column here. 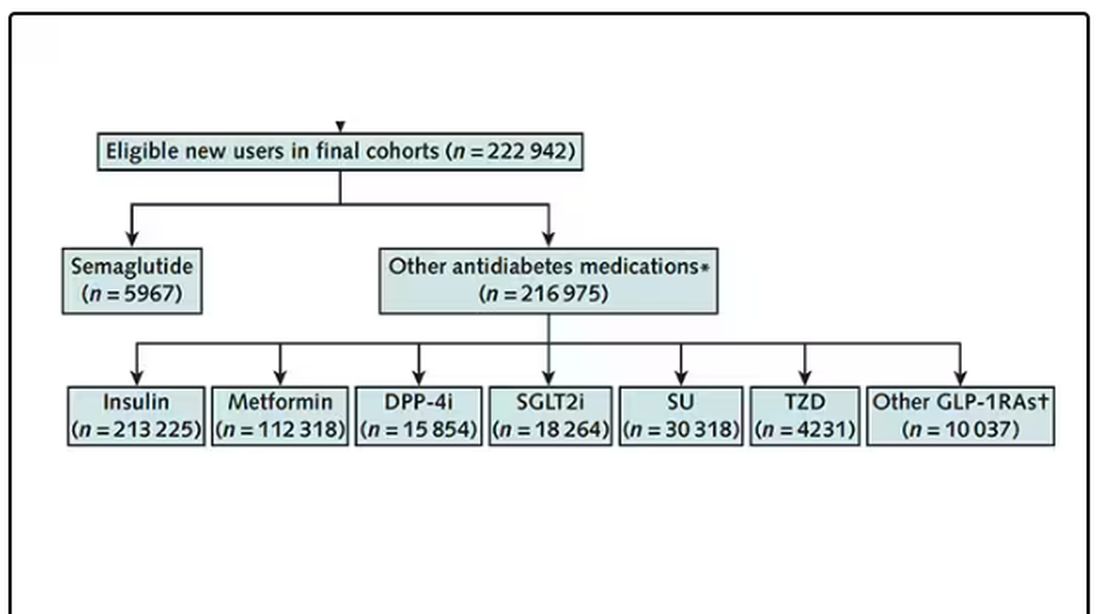
It’s easy enough, using the EHR, to figure out who has diabetes and who got which drug. But how do you know who quit smoking? Remember, everyone had a diagnosis code for tobacco use disorder prior to starting Ozempic or a comparator drug. The authors decided that if the patient had a medical visit where someone again coded tobacco-use disorder, they were still smoking. If someone prescribed smoking cessation meds like a nicotine patch or varenicline, they were obviously still smoking. If someone billed for tobacco-cessation counseling, the patient is still smoking. We’ll get back to the implications of this outcome definition in a minute.
Let’s talk about the results, which are pretty intriguing. 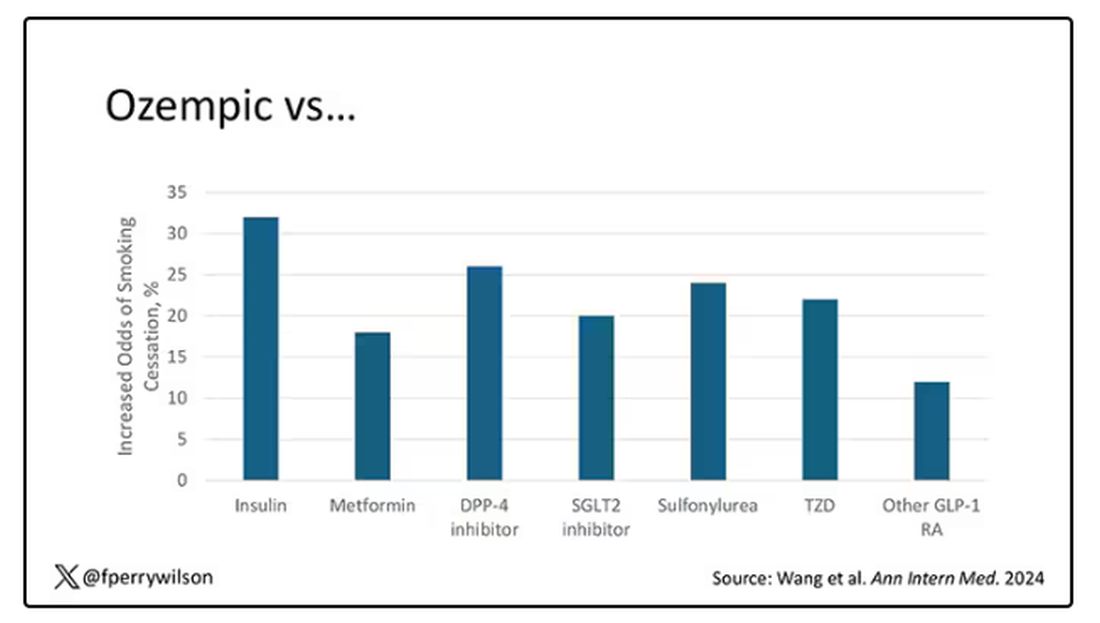
When Ozempic is compared with insulin among smokers with diabetes, those on Ozempic were about 30% more likely to quit smoking. They were about 18% more likely to quit smoking than those who took metformin. They were even slightly more likely to quit smoking than those on other GLP-1 receptor antagonists, though I should note that Mounjaro, which is probably the more potent GLP-1 drug in terms of weight loss, was not among the comparators.
This is pretty impressive for a drug that was not designed to be a smoking cessation drug. It speaks to this emerging idea that these drugs do more than curb appetite by slowing down gastric emptying or something. They work in the brain, modulating some of the reward circuitry that keeps us locked into our bad habits.
There are, of course, some caveats. As I pointed out, this study captured the idea of “still smoking” through the use of administrative codes in the EHR and prescription of smoking cessation aids. You could see similar results if taking Ozempic makes people less likely to address their smoking at all; maybe they shut down the doctor before they even talk about it, or there is too much to discuss during these visits to even get to the subject of smoking. You could also see results like this if people taking Ozempic had fewer visits overall, but the authors showed that that, at least, was not the case.
I’m inclined to believe that this effect is real, simply because we keep seeing signals from multiple sources. If that turns out to be the case, these new “weight loss” drugs may prove to be much more than that; they may turn out to be the drugs that can finally save us from ourselves.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If you’ve been paying attention only to the headlines, when you think of “Ozempic” you’ll think of a few things: a blockbuster weight loss drug or the tip of the spear of a completely new industry — why not? A drug so popular that the people it was invented for (those with diabetes) can’t even get it.
Ozempic and other GLP-1 receptor agonists are undeniable game changers. Insofar as obesity is the number-one public health risk in the United States, antiobesity drugs hold immense promise even if all they do is reduce obesity.
In 2023, an article in Scientific Reports presented data suggesting that people on Ozempic might be reducing their alcohol intake, not just their total calories.
A 2024 article in Molecular Psychiatry found that the drug might positively impact cannabis use disorder. An article from Brain Sciences suggests that the drug reduces compulsive shopping.
A picture is starting to form, a picture that suggests these drugs curb hunger both literally and figuratively. That GLP-1 receptor agonists like Ozempic and Mounjaro are fundamentally anticonsumption drugs. In a society that — some would argue — is plagued by overconsumption, these drugs might be just what the doctor ordered.
If only they could stop people from smoking.
Oh, wait — they can.
At least it seems they can, based on a new study appearing in Annals of Internal Medicine.
Before we get too excited, this is not a randomized trial. There actually was a small randomized trial of exenatide (Byetta), which is in the same class as Ozempic but probably a bit less potent, with promising results for smoking cessation.
But Byetta is the weaker drug in this class; the market leader is Ozempic. So how can you figure out whether Ozempic can reduce smoking without doing a huge and expensive randomized trial? You can do what Nora Volkow and colleagues from the National Institute on Drug Abuse did: a target trial emulation study.
A target trial emulation study is more or less what it sounds like. First, you decide what your dream randomized controlled trial would be and you plan it all out in great detail. You define the population you would recruit, with all the relevant inclusion and exclusion criteria. You define the intervention and the control, and you define the outcome.
But you don’t actually do the trial. You could if someone would lend you $10-$50 million, but assuming you don’t have that lying around, you do the next best thing, which is to dig into a medical record database to find all the people who would be eligible for your imaginary trial. And you analyze them.
The authors wanted to study the effect of Ozempic on smoking among people with diabetes; that’s why all the comparator agents are antidiabetes drugs. They figured out whether these folks were smoking on the basis of a medical record diagnosis of tobacco use disorder before they started one of the drugs of interest. This code is fairly specific: If a patient has it, you can be pretty sure they are smoking. But it’s not very sensitive; not every smoker has this diagnostic code. This is an age-old limitation of using EHR data instead of asking patients, but it’s part of the tradeoff for not having to spend $50 million.
After applying all those inclusion and exclusion criteria, they have a defined population who could be in their dream trial. And, as luck would have it, some of those people really were treated with Ozempic and some really were treated with those other agents. Although decisions about what to prescribe were not randomized, the authors account for this confounding-by-indication using propensity-score matching. You can find a little explainer on propensity-score matching in an earlier column here.
It’s easy enough, using the EHR, to figure out who has diabetes and who got which drug. But how do you know who quit smoking? Remember, everyone had a diagnosis code for tobacco use disorder prior to starting Ozempic or a comparator drug. The authors decided that if the patient had a medical visit where someone again coded tobacco-use disorder, they were still smoking. If someone prescribed smoking cessation meds like a nicotine patch or varenicline, they were obviously still smoking. If someone billed for tobacco-cessation counseling, the patient is still smoking. We’ll get back to the implications of this outcome definition in a minute.
Let’s talk about the results, which are pretty intriguing.
When Ozempic is compared with insulin among smokers with diabetes, those on Ozempic were about 30% more likely to quit smoking. They were about 18% more likely to quit smoking than those who took metformin. They were even slightly more likely to quit smoking than those on other GLP-1 receptor antagonists, though I should note that Mounjaro, which is probably the more potent GLP-1 drug in terms of weight loss, was not among the comparators.
This is pretty impressive for a drug that was not designed to be a smoking cessation drug. It speaks to this emerging idea that these drugs do more than curb appetite by slowing down gastric emptying or something. They work in the brain, modulating some of the reward circuitry that keeps us locked into our bad habits.
There are, of course, some caveats. As I pointed out, this study captured the idea of “still smoking” through the use of administrative codes in the EHR and prescription of smoking cessation aids. You could see similar results if taking Ozempic makes people less likely to address their smoking at all; maybe they shut down the doctor before they even talk about it, or there is too much to discuss during these visits to even get to the subject of smoking. You could also see results like this if people taking Ozempic had fewer visits overall, but the authors showed that that, at least, was not the case.
I’m inclined to believe that this effect is real, simply because we keep seeing signals from multiple sources. If that turns out to be the case, these new “weight loss” drugs may prove to be much more than that; they may turn out to be the drugs that can finally save us from ourselves.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
If you’ve been paying attention only to the headlines, when you think of “Ozempic” you’ll think of a few things: a blockbuster weight loss drug or the tip of the spear of a completely new industry — why not? A drug so popular that the people it was invented for (those with diabetes) can’t even get it.
Ozempic and other GLP-1 receptor agonists are undeniable game changers. Insofar as obesity is the number-one public health risk in the United States, antiobesity drugs hold immense promise even if all they do is reduce obesity.
In 2023, an article in Scientific Reports presented data suggesting that people on Ozempic might be reducing their alcohol intake, not just their total calories.
A 2024 article in Molecular Psychiatry found that the drug might positively impact cannabis use disorder. An article from Brain Sciences suggests that the drug reduces compulsive shopping.
A picture is starting to form, a picture that suggests these drugs curb hunger both literally and figuratively. That GLP-1 receptor agonists like Ozempic and Mounjaro are fundamentally anticonsumption drugs. In a society that — some would argue — is plagued by overconsumption, these drugs might be just what the doctor ordered.
If only they could stop people from smoking.
Oh, wait — they can.
At least it seems they can, based on a new study appearing in Annals of Internal Medicine.
Before we get too excited, this is not a randomized trial. There actually was a small randomized trial of exenatide (Byetta), which is in the same class as Ozempic but probably a bit less potent, with promising results for smoking cessation.
But Byetta is the weaker drug in this class; the market leader is Ozempic. So how can you figure out whether Ozempic can reduce smoking without doing a huge and expensive randomized trial? You can do what Nora Volkow and colleagues from the National Institute on Drug Abuse did: a target trial emulation study.
A target trial emulation study is more or less what it sounds like. First, you decide what your dream randomized controlled trial would be and you plan it all out in great detail. You define the population you would recruit, with all the relevant inclusion and exclusion criteria. You define the intervention and the control, and you define the outcome.
But you don’t actually do the trial. You could if someone would lend you $10-$50 million, but assuming you don’t have that lying around, you do the next best thing, which is to dig into a medical record database to find all the people who would be eligible for your imaginary trial. And you analyze them.
The authors wanted to study the effect of Ozempic on smoking among people with diabetes; that’s why all the comparator agents are antidiabetes drugs. They figured out whether these folks were smoking on the basis of a medical record diagnosis of tobacco use disorder before they started one of the drugs of interest. This code is fairly specific: If a patient has it, you can be pretty sure they are smoking. But it’s not very sensitive; not every smoker has this diagnostic code. This is an age-old limitation of using EHR data instead of asking patients, but it’s part of the tradeoff for not having to spend $50 million.
After applying all those inclusion and exclusion criteria, they have a defined population who could be in their dream trial. And, as luck would have it, some of those people really were treated with Ozempic and some really were treated with those other agents. Although decisions about what to prescribe were not randomized, the authors account for this confounding-by-indication using propensity-score matching. You can find a little explainer on propensity-score matching in an earlier column here.
It’s easy enough, using the EHR, to figure out who has diabetes and who got which drug. But how do you know who quit smoking? Remember, everyone had a diagnosis code for tobacco use disorder prior to starting Ozempic or a comparator drug. The authors decided that if the patient had a medical visit where someone again coded tobacco-use disorder, they were still smoking. If someone prescribed smoking cessation meds like a nicotine patch or varenicline, they were obviously still smoking. If someone billed for tobacco-cessation counseling, the patient is still smoking. We’ll get back to the implications of this outcome definition in a minute.
Let’s talk about the results, which are pretty intriguing.
When Ozempic is compared with insulin among smokers with diabetes, those on Ozempic were about 30% more likely to quit smoking. They were about 18% more likely to quit smoking than those who took metformin. They were even slightly more likely to quit smoking than those on other GLP-1 receptor antagonists, though I should note that Mounjaro, which is probably the more potent GLP-1 drug in terms of weight loss, was not among the comparators.
This is pretty impressive for a drug that was not designed to be a smoking cessation drug. It speaks to this emerging idea that these drugs do more than curb appetite by slowing down gastric emptying or something. They work in the brain, modulating some of the reward circuitry that keeps us locked into our bad habits.
There are, of course, some caveats. As I pointed out, this study captured the idea of “still smoking” through the use of administrative codes in the EHR and prescription of smoking cessation aids. You could see similar results if taking Ozempic makes people less likely to address their smoking at all; maybe they shut down the doctor before they even talk about it, or there is too much to discuss during these visits to even get to the subject of smoking. You could also see results like this if people taking Ozempic had fewer visits overall, but the authors showed that that, at least, was not the case.
I’m inclined to believe that this effect is real, simply because we keep seeing signals from multiple sources. If that turns out to be the case, these new “weight loss” drugs may prove to be much more than that; they may turn out to be the drugs that can finally save us from ourselves.
Dr. Wilson is associate professor of medicine and public health and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Connecticut. He has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Vasculopathy Can Vary in Patients With Idiopathic Pulmonary Arterial Hypertension
Approximately half of adults with idiopathic pulmonary arterial hypertension (IPAH) had nonplexiform vasculopathy characterized in part by severe pulmonary microvascular remodeling, based on data from 50 individuals.
The clinical phenotype of IPAH was historically described as a rapidly progressive rare disease in young women and characterized by plexiform lesions, wrote Esther J. Nossent, MD, of Amsterdam University Medical Centers, Amsterdam, the Netherlands, and colleagues. However, the patient population with IPAH has become older and predominantly men, and the nature of vascular phenotypes and histologic patterns in patients with contemporary IPAH has not been well studied, the researchers said.
In a cross-sectional study published in CHEST, the researchers reviewed lung histology data from 50 adults with IPAH that had been assessed by two experienced pathologists. The mean age of the patients was 52 years and 58% were women. Based on a histopathologic evaluation, 24 patients had nonplexiform vasculopathy (48%) and 26 had plexiform vasculopathy (52%). Notably, microvascular remodeling involving arterioles and venules was substantial in patients with nonplexiform vasculopathy but mild or absent in those with plexiform vasculopathy, the researchers wrote.
The researchers also compared the clinical characteristics of patients with plexiform vs nonplexiform vasculopathy. Hemodynamic parameters were similar in both patient groups. However, those with nonplexiform vasculopathy were significantly older than those with plexiform vasculopathy (60 years vs 44 years), were more likely to be men (67% vs 20%), and had a lower diffusing capacity of the lungs for carbon monoxide (DLCO) at diagnosis (all P < .001). Patients with nonplexiform vasculopathy also were significantly more likely than those with plexiform vasculopathy to have a history of smoking (P = .03). Genetic testing revealed no mutations in established PAH genes in the nonplexiform group.
Low DLCO has been associated with worse outcomes regardless of hemodynamic response, the researchers noted. In the current study, “a DLCO of < 45% almost perfectly identified patients with nonplexiform vasculopathy with prominent pulmonary microvascular disease,” they said.
The findings were limited by several factors, including the small study population and the higher frequency of surgical lung biopsies in the nonplexiform group vs the plexiform group, which is not part of the general workup of patients with IPAH, the researchers noted.
, they said. However, the results suggest that differences between patients with IPAH with plexiform vasculopathy and those with nonplexiform vasculopathy could ultimately inform targeted treatment strategies.
“Recognizing these clinical phenotypes allows revisiting current datasets to understand better the potential future clinical consequences of the vascular phenotypes for treatment response and clinical outcome,” the researchers concluded.
Findings May Inform More Targeted Therapy
“Any investigation that adds substantive insight into a complex disease that can translate into a better understanding of clinical patient phenotypes and eventually into improved treatments and patient outcomes has relevance at any time,” Paul Forfia, MD, professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, said in an interview.
“There is focus on the antiproliferative forms of pulmonary arterial hypertension–specific therapy, and the results of the current study may have implications to these therapies,” said Dr. Forfia, who was not involved in the current study.
“In the current study, the investigators show that 48% of patients that were traditionally categorized as IPAH had a vascular phenotype that is not considered ‘typical’ or classic for IPAH,” Dr. Forfia told this news organization. “These findings highlight a significant heterogeneity of the pulmonary vascular phenotype within IPAH, which raises the question of whether the nonplexiform patient would be less responsive to the novel, antiproliferative forms of therapy,” he said.
The new findings are quite interesting but not surprising, Dr. Forfia said. “The World Symposia diagnostic groupings for pulmonary hypertension are a very important and necessary form of categorization and differentiation amongst forms of PH [pulmonary hypertension], and these groupings make a best attempt based on available evidence to separate patients of varying PH pathophysiology, both in terms of diagnosis and in how PH patients are treated,” he explained.
“However, clinical experts in PH have known that subphenotypes of PH pathophysiology exist within group I PAH, as well as in PH related to left heart disease (group 2), chronic respiratory disease (group 3), and chronic thromboembolic disease (group 4),” he said.
Findings from the current study reinforce the importance of clinical and physiological phenotyping of each patient, which can help in terms of therapy selection and in managing expectations in response to therapy, Dr. Forfia added.
“Perhaps the most evident and important clinical implication from the current study is to remind clinicians treating patients with PH that heterogeneity exists within the vascular phenotype and clinical makeup of patients even within the same type of PAH,” Dr. Forfia said. “With this insight, clinicians are more informed and thus more apt to consider nuances in the diagnosis, treatment, and expectations for treatment response within PAH,” he said.
Dr. Forfia also highlighted the potential implications of the association between cigarette smoking and the nonplexiform vascular phenotype. “This association was present in the absence of radiographic evidence of emphysema and raises the provocative notion that cigarette smoking may lead to pulmonary vascular abnormalities, perhaps even PAH, in patients without a diagnosis of emphysema,” he said.
“An important limitation from the current study is that the vascular phenotypes observed within their cohort of IPAH patients were obtained from histopathology specimens at the time of autopsy, explant at the time of lung transplantation, and surgical lung biopsy spanning over a 22-year period,” Dr. Forfia noted. Additional research is needed to explore how vascular phenotypic differences can be appreciated in the absence of histopathology and how these differences could impact therapy selection and patient outcomes, he said.
The study received no outside funding. Dr. Nossent disclosed receiving speaker fees from Janssen, MSD, and United Therapeutics/Ferrer and consulting fees from Janssen and United Therapeutics/Ferrer. Dr. Forfia had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately half of adults with idiopathic pulmonary arterial hypertension (IPAH) had nonplexiform vasculopathy characterized in part by severe pulmonary microvascular remodeling, based on data from 50 individuals.
The clinical phenotype of IPAH was historically described as a rapidly progressive rare disease in young women and characterized by plexiform lesions, wrote Esther J. Nossent, MD, of Amsterdam University Medical Centers, Amsterdam, the Netherlands, and colleagues. However, the patient population with IPAH has become older and predominantly men, and the nature of vascular phenotypes and histologic patterns in patients with contemporary IPAH has not been well studied, the researchers said.
In a cross-sectional study published in CHEST, the researchers reviewed lung histology data from 50 adults with IPAH that had been assessed by two experienced pathologists. The mean age of the patients was 52 years and 58% were women. Based on a histopathologic evaluation, 24 patients had nonplexiform vasculopathy (48%) and 26 had plexiform vasculopathy (52%). Notably, microvascular remodeling involving arterioles and venules was substantial in patients with nonplexiform vasculopathy but mild or absent in those with plexiform vasculopathy, the researchers wrote.
The researchers also compared the clinical characteristics of patients with plexiform vs nonplexiform vasculopathy. Hemodynamic parameters were similar in both patient groups. However, those with nonplexiform vasculopathy were significantly older than those with plexiform vasculopathy (60 years vs 44 years), were more likely to be men (67% vs 20%), and had a lower diffusing capacity of the lungs for carbon monoxide (DLCO) at diagnosis (all P < .001). Patients with nonplexiform vasculopathy also were significantly more likely than those with plexiform vasculopathy to have a history of smoking (P = .03). Genetic testing revealed no mutations in established PAH genes in the nonplexiform group.
Low DLCO has been associated with worse outcomes regardless of hemodynamic response, the researchers noted. In the current study, “a DLCO of < 45% almost perfectly identified patients with nonplexiform vasculopathy with prominent pulmonary microvascular disease,” they said.
The findings were limited by several factors, including the small study population and the higher frequency of surgical lung biopsies in the nonplexiform group vs the plexiform group, which is not part of the general workup of patients with IPAH, the researchers noted.
, they said. However, the results suggest that differences between patients with IPAH with plexiform vasculopathy and those with nonplexiform vasculopathy could ultimately inform targeted treatment strategies.
“Recognizing these clinical phenotypes allows revisiting current datasets to understand better the potential future clinical consequences of the vascular phenotypes for treatment response and clinical outcome,” the researchers concluded.
Findings May Inform More Targeted Therapy
“Any investigation that adds substantive insight into a complex disease that can translate into a better understanding of clinical patient phenotypes and eventually into improved treatments and patient outcomes has relevance at any time,” Paul Forfia, MD, professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, said in an interview.
“There is focus on the antiproliferative forms of pulmonary arterial hypertension–specific therapy, and the results of the current study may have implications to these therapies,” said Dr. Forfia, who was not involved in the current study.
“In the current study, the investigators show that 48% of patients that were traditionally categorized as IPAH had a vascular phenotype that is not considered ‘typical’ or classic for IPAH,” Dr. Forfia told this news organization. “These findings highlight a significant heterogeneity of the pulmonary vascular phenotype within IPAH, which raises the question of whether the nonplexiform patient would be less responsive to the novel, antiproliferative forms of therapy,” he said.
The new findings are quite interesting but not surprising, Dr. Forfia said. “The World Symposia diagnostic groupings for pulmonary hypertension are a very important and necessary form of categorization and differentiation amongst forms of PH [pulmonary hypertension], and these groupings make a best attempt based on available evidence to separate patients of varying PH pathophysiology, both in terms of diagnosis and in how PH patients are treated,” he explained.
“However, clinical experts in PH have known that subphenotypes of PH pathophysiology exist within group I PAH, as well as in PH related to left heart disease (group 2), chronic respiratory disease (group 3), and chronic thromboembolic disease (group 4),” he said.
Findings from the current study reinforce the importance of clinical and physiological phenotyping of each patient, which can help in terms of therapy selection and in managing expectations in response to therapy, Dr. Forfia added.
“Perhaps the most evident and important clinical implication from the current study is to remind clinicians treating patients with PH that heterogeneity exists within the vascular phenotype and clinical makeup of patients even within the same type of PAH,” Dr. Forfia said. “With this insight, clinicians are more informed and thus more apt to consider nuances in the diagnosis, treatment, and expectations for treatment response within PAH,” he said.
Dr. Forfia also highlighted the potential implications of the association between cigarette smoking and the nonplexiform vascular phenotype. “This association was present in the absence of radiographic evidence of emphysema and raises the provocative notion that cigarette smoking may lead to pulmonary vascular abnormalities, perhaps even PAH, in patients without a diagnosis of emphysema,” he said.
“An important limitation from the current study is that the vascular phenotypes observed within their cohort of IPAH patients were obtained from histopathology specimens at the time of autopsy, explant at the time of lung transplantation, and surgical lung biopsy spanning over a 22-year period,” Dr. Forfia noted. Additional research is needed to explore how vascular phenotypic differences can be appreciated in the absence of histopathology and how these differences could impact therapy selection and patient outcomes, he said.
The study received no outside funding. Dr. Nossent disclosed receiving speaker fees from Janssen, MSD, and United Therapeutics/Ferrer and consulting fees from Janssen and United Therapeutics/Ferrer. Dr. Forfia had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
Approximately half of adults with idiopathic pulmonary arterial hypertension (IPAH) had nonplexiform vasculopathy characterized in part by severe pulmonary microvascular remodeling, based on data from 50 individuals.
The clinical phenotype of IPAH was historically described as a rapidly progressive rare disease in young women and characterized by plexiform lesions, wrote Esther J. Nossent, MD, of Amsterdam University Medical Centers, Amsterdam, the Netherlands, and colleagues. However, the patient population with IPAH has become older and predominantly men, and the nature of vascular phenotypes and histologic patterns in patients with contemporary IPAH has not been well studied, the researchers said.
In a cross-sectional study published in CHEST, the researchers reviewed lung histology data from 50 adults with IPAH that had been assessed by two experienced pathologists. The mean age of the patients was 52 years and 58% were women. Based on a histopathologic evaluation, 24 patients had nonplexiform vasculopathy (48%) and 26 had plexiform vasculopathy (52%). Notably, microvascular remodeling involving arterioles and venules was substantial in patients with nonplexiform vasculopathy but mild or absent in those with plexiform vasculopathy, the researchers wrote.
The researchers also compared the clinical characteristics of patients with plexiform vs nonplexiform vasculopathy. Hemodynamic parameters were similar in both patient groups. However, those with nonplexiform vasculopathy were significantly older than those with plexiform vasculopathy (60 years vs 44 years), were more likely to be men (67% vs 20%), and had a lower diffusing capacity of the lungs for carbon monoxide (DLCO) at diagnosis (all P < .001). Patients with nonplexiform vasculopathy also were significantly more likely than those with plexiform vasculopathy to have a history of smoking (P = .03). Genetic testing revealed no mutations in established PAH genes in the nonplexiform group.
Low DLCO has been associated with worse outcomes regardless of hemodynamic response, the researchers noted. In the current study, “a DLCO of < 45% almost perfectly identified patients with nonplexiform vasculopathy with prominent pulmonary microvascular disease,” they said.
The findings were limited by several factors, including the small study population and the higher frequency of surgical lung biopsies in the nonplexiform group vs the plexiform group, which is not part of the general workup of patients with IPAH, the researchers noted.
, they said. However, the results suggest that differences between patients with IPAH with plexiform vasculopathy and those with nonplexiform vasculopathy could ultimately inform targeted treatment strategies.
“Recognizing these clinical phenotypes allows revisiting current datasets to understand better the potential future clinical consequences of the vascular phenotypes for treatment response and clinical outcome,” the researchers concluded.
Findings May Inform More Targeted Therapy
“Any investigation that adds substantive insight into a complex disease that can translate into a better understanding of clinical patient phenotypes and eventually into improved treatments and patient outcomes has relevance at any time,” Paul Forfia, MD, professor of medicine at the Lewis Katz School of Medicine at Temple University, Philadelphia, said in an interview.
“There is focus on the antiproliferative forms of pulmonary arterial hypertension–specific therapy, and the results of the current study may have implications to these therapies,” said Dr. Forfia, who was not involved in the current study.
“In the current study, the investigators show that 48% of patients that were traditionally categorized as IPAH had a vascular phenotype that is not considered ‘typical’ or classic for IPAH,” Dr. Forfia told this news organization. “These findings highlight a significant heterogeneity of the pulmonary vascular phenotype within IPAH, which raises the question of whether the nonplexiform patient would be less responsive to the novel, antiproliferative forms of therapy,” he said.
The new findings are quite interesting but not surprising, Dr. Forfia said. “The World Symposia diagnostic groupings for pulmonary hypertension are a very important and necessary form of categorization and differentiation amongst forms of PH [pulmonary hypertension], and these groupings make a best attempt based on available evidence to separate patients of varying PH pathophysiology, both in terms of diagnosis and in how PH patients are treated,” he explained.
“However, clinical experts in PH have known that subphenotypes of PH pathophysiology exist within group I PAH, as well as in PH related to left heart disease (group 2), chronic respiratory disease (group 3), and chronic thromboembolic disease (group 4),” he said.
Findings from the current study reinforce the importance of clinical and physiological phenotyping of each patient, which can help in terms of therapy selection and in managing expectations in response to therapy, Dr. Forfia added.
“Perhaps the most evident and important clinical implication from the current study is to remind clinicians treating patients with PH that heterogeneity exists within the vascular phenotype and clinical makeup of patients even within the same type of PAH,” Dr. Forfia said. “With this insight, clinicians are more informed and thus more apt to consider nuances in the diagnosis, treatment, and expectations for treatment response within PAH,” he said.
Dr. Forfia also highlighted the potential implications of the association between cigarette smoking and the nonplexiform vascular phenotype. “This association was present in the absence of radiographic evidence of emphysema and raises the provocative notion that cigarette smoking may lead to pulmonary vascular abnormalities, perhaps even PAH, in patients without a diagnosis of emphysema,” he said.
“An important limitation from the current study is that the vascular phenotypes observed within their cohort of IPAH patients were obtained from histopathology specimens at the time of autopsy, explant at the time of lung transplantation, and surgical lung biopsy spanning over a 22-year period,” Dr. Forfia noted. Additional research is needed to explore how vascular phenotypic differences can be appreciated in the absence of histopathology and how these differences could impact therapy selection and patient outcomes, he said.
The study received no outside funding. Dr. Nossent disclosed receiving speaker fees from Janssen, MSD, and United Therapeutics/Ferrer and consulting fees from Janssen and United Therapeutics/Ferrer. Dr. Forfia had no financial conflicts to disclose.
A version of this article first appeared on Medscape.com.
FDA Expands Darzalex Faspro Indication in Myeloma
Approval followed priority review and was based on efficacy and safety findings from the open-label PERSEUS trial involving 709 patients under age 70 years who were randomized to receive bortezomib, lenalidomide, and dexamethasone alone or in combination with daratumumab and hyaluronidase-fihj, according to the FDA.
Compared with bortezomib, lenalidomide, and dexamethasone alone, the addition of daratumumab and hyaluronidase-fihj resulted in a 60% reduction in the risk for disease progression or death (hazard ratio, 0.40). Median progression-free survival was not reached in either group.
Adverse reactions occurring in ≥ 20% of patients were peripheral neuropathy, fatigue, edema, pyrexia, upper respiratory infection, constipation, diarrhea, musculoskeletal pain, insomnia, and rash.
The recommended dosage for this indication is 1800 mg daratumumab and 30,000 units hyaluronidase, according to the full prescribing information.
Daratumumab and hyaluronidase-fihj, which was first approved in 2020, has a range of other indications in multiple myeloma.
A version of this article first appeared on Medscape.com.
Approval followed priority review and was based on efficacy and safety findings from the open-label PERSEUS trial involving 709 patients under age 70 years who were randomized to receive bortezomib, lenalidomide, and dexamethasone alone or in combination with daratumumab and hyaluronidase-fihj, according to the FDA.
Compared with bortezomib, lenalidomide, and dexamethasone alone, the addition of daratumumab and hyaluronidase-fihj resulted in a 60% reduction in the risk for disease progression or death (hazard ratio, 0.40). Median progression-free survival was not reached in either group.
Adverse reactions occurring in ≥ 20% of patients were peripheral neuropathy, fatigue, edema, pyrexia, upper respiratory infection, constipation, diarrhea, musculoskeletal pain, insomnia, and rash.
The recommended dosage for this indication is 1800 mg daratumumab and 30,000 units hyaluronidase, according to the full prescribing information.
Daratumumab and hyaluronidase-fihj, which was first approved in 2020, has a range of other indications in multiple myeloma.
A version of this article first appeared on Medscape.com.
Approval followed priority review and was based on efficacy and safety findings from the open-label PERSEUS trial involving 709 patients under age 70 years who were randomized to receive bortezomib, lenalidomide, and dexamethasone alone or in combination with daratumumab and hyaluronidase-fihj, according to the FDA.
Compared with bortezomib, lenalidomide, and dexamethasone alone, the addition of daratumumab and hyaluronidase-fihj resulted in a 60% reduction in the risk for disease progression or death (hazard ratio, 0.40). Median progression-free survival was not reached in either group.
Adverse reactions occurring in ≥ 20% of patients were peripheral neuropathy, fatigue, edema, pyrexia, upper respiratory infection, constipation, diarrhea, musculoskeletal pain, insomnia, and rash.
The recommended dosage for this indication is 1800 mg daratumumab and 30,000 units hyaluronidase, according to the full prescribing information.
Daratumumab and hyaluronidase-fihj, which was first approved in 2020, has a range of other indications in multiple myeloma.
A version of this article first appeared on Medscape.com.