User login
Eruptive Syringoma Manifesting as a Widespread Rash in 3 Patients
To the Editor:
Syringoma is a relatively common benign adnexal neoplasm originating in the ducts of eccrine sweat glands. It can be
A 28-year-old man presented with multiple asymptomatic papules on the trunk and upper arms of 20 years’ duration (patient 1). He had been diagnosed with Darier disease 3 years prior to the current presentation and was treated with oral and topical retinoic acid without a response. After 3 months of oral treatment, the retinoic acid was stopped due to elevated liver enzymes. Physical examination at the current presentation revealed multiple smooth, firm, nonfused, 1- to 4-mm
A 27-year-old woman presented with widespread asymptomatic papules

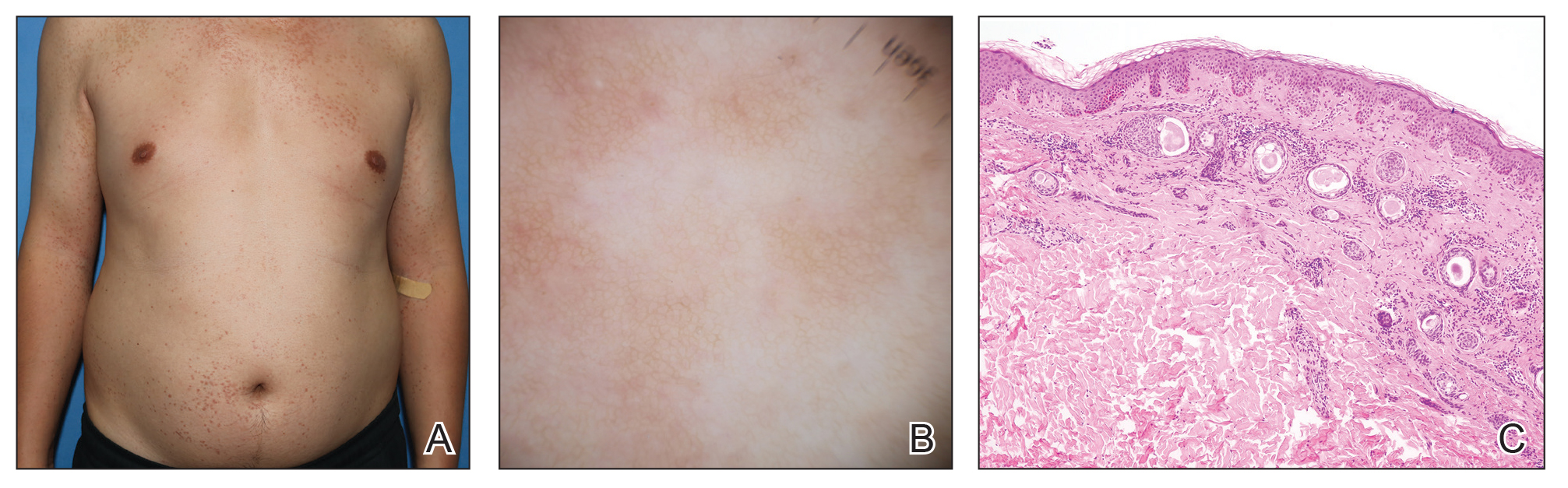
A 43-year-old man who was otherwise healthy presented with brownish flat-topped papules on the chest and abdomen of 19 years’ duration (Figure 3A)(patient 3). The lesions had remained stable and did not progress. He denied any treatment.
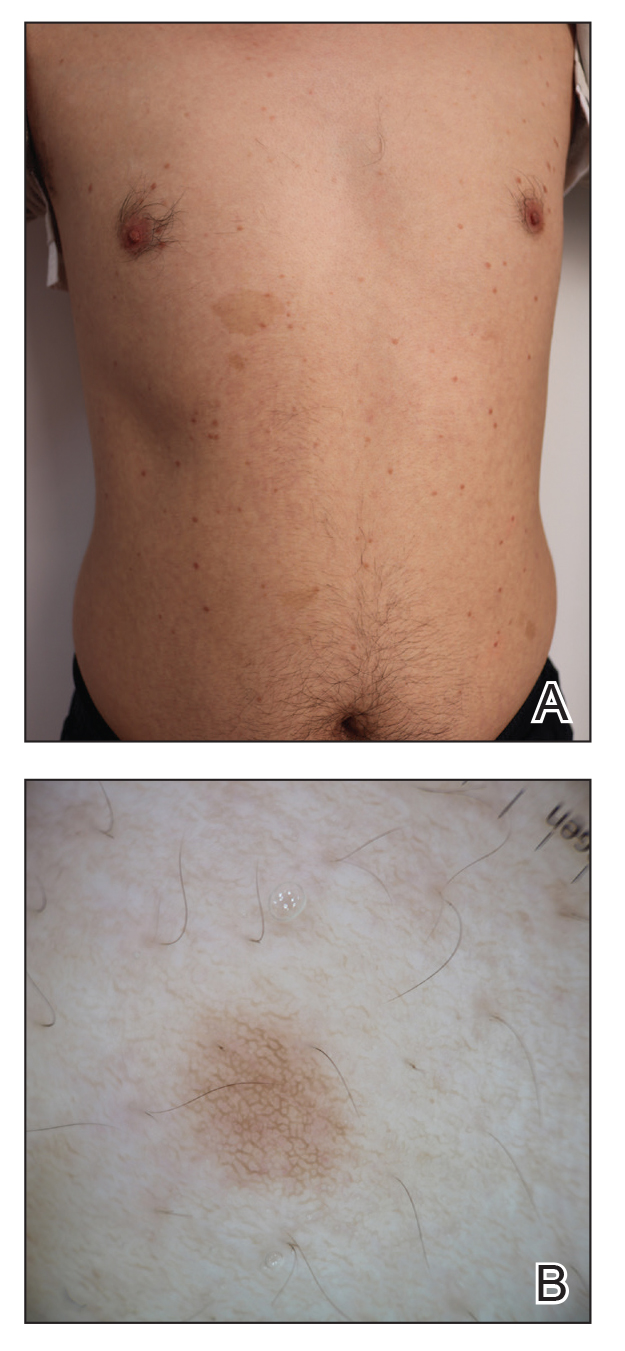
All 3 patients demonstrated classic histopathologic features of syringoma, and none had a family history of similar skin lesions. The clinical and dermoscopic findings along with the histopathology in all 3 patients were consistent with ES.
The pathogenesis of ES is
- Williams K, Shinkai K. Evaluation and management of the patient with multiple syringomas: a systematic review of the literature. J Am Acad Dermatol. 2016;74:1234-1240.e1239. doi:10.1016/j.jaad.2015.12.006
- Jacquet L, Darier J.
Hidradénomes éruptifs, I.épithéliomes adenoids des glandes sudoripares ou adénomes sudoripares. Ann Dermatol Venerol. 1887;8:317-323. - Huang A, Taylor G, Liebman TN. Generalized eruptive syringomas. Dermatol Online J. 2017;23:13030/qt0hb8q22g..
- Maeda T, Natsuga K, Nishie W, et al. Extensive eruptive syringoma after liver transplantation. Acta Derm Venereol. 2018;98:119-120. doi:10.2340/00015555-2814
- Lerner TH, Barr RJ, Dolezal JF, et al. Syringomatous hyperplasia and eccrine squamous syringometaplasia associated with benoxaprofen therapy. Arch Dermatol. 1987;123:1202-1204. doi:10.1001/archderm.1987.01660330113022
- Ozturk F, Ermertcan AT, Bilac C, et al.
A case report of postpubertal eruptive syringoma triggered with antiepileptic drugs. J Drugs Dermatol. 2010;9:707-710. - Guitart J, Rosenbaum MM, Requena L. ‘Eruptive syringoma’: a misnomer for a reactive eccrine gland ductal proliferation? J Cutan Pathol. 2003;30:202-205. doi:10.1034/j.1600-0560.2003.00023.x
- Dupre A, Carrere S, Bonafe JL, et al. Eruptive generalized syringomas, milium and atrophoderma vermiculata. Nicolau and Balus’ syndrome (author’s transl). Dermatologica. 1981;162:281-286.
- Schepis C, Torre V, Siragusa M, et al. Eruptive syringomas with calcium deposits in a young woman with Down’s syndrome. Dermatology. 2001;203:345-347. doi:10.1159/000051788
- Samia AM, Donthi D, Nenow J, et al. A case study and review of literature of eruptive syringoma in a six-year-old. Cureus. 2021;13:E14634. doi:10.7759/cureus.14634
- Soler-Carrillo J, Estrach T, Mascaró JM. Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15:242-246. doi:10.1046/j.1468-3083.2001.00235.x
- Aleissa M, Aljarbou O, AlJasser MI. Dermoscopy of eruptive syringoma. Skin Appendage Disord. 2021;7:401-403. doi:10.1159/000515443
- Botsali A, Caliskan E, Coskun A, et al. Eruptive syringoma: two cases with dermoscopic features. Skin Appendage Disord. 2020;6:319-322. doi:10.1159/000508656
- Dutra Rezende H, Madia ACT, Elias BM, et al. Comment on: eruptive syringoma—two cases with dermoscopic features. Skin Appendage Disord. 2022;8:81-82. doi:10.1159/000518158
- Silva-Hirschberg C, Cabrera R, Rollán MP, et al. Darier disease: the use of dermoscopy in monitoring acitretin treatment. An Bras Dermatol. 2022;97:644-647. doi:10.1016/j.abd.2021.05.021
- Singal A, Kaur I, Jakhar D. Fox-Fordyce disease: dermoscopic perspective. Skin Appendage Disord. 2020;6:247-249. doi:10.1159/000508201
- Brau Javier CN, Morales A, Sanchez JL. Histopathology attributes of Fox-Fordyce disease. Int J Dermatol. 2012;51:1313-1318. doi:10.1159/000508201
- Horie K, Shinkuma S, Fujita Y, et al. Efficacy of N-(3,4-dimethoxycinnamoyl)-anthranilic acid (tranilast) against eruptive syringoma: report of two cases and review of published work. J Dermatol. 2012;39:1044-1046. doi:10.1111/j.1346-8138.2012.01612.x
- Sanchez TS, Dauden E, Casas AP, et al. Eruptive pruritic syringomas: treatment with topical atropine. J Am Acad Dermatol. 2001;44:148-149. doi:10.1067/mjd.2001.109854
To the Editor:
Syringoma is a relatively common benign adnexal neoplasm originating in the ducts of eccrine sweat glands. It can be
A 28-year-old man presented with multiple asymptomatic papules on the trunk and upper arms of 20 years’ duration (patient 1). He had been diagnosed with Darier disease 3 years prior to the current presentation and was treated with oral and topical retinoic acid without a response. After 3 months of oral treatment, the retinoic acid was stopped due to elevated liver enzymes. Physical examination at the current presentation revealed multiple smooth, firm, nonfused, 1- to 4-mm
A 27-year-old woman presented with widespread asymptomatic papules
A 43-year-old man who was otherwise healthy presented with brownish flat-topped papules on the chest and abdomen of 19 years’ duration (Figure 3A)(patient 3). The lesions had remained stable and did not progress. He denied any treatment.
All 3 patients demonstrated classic histopathologic features of syringoma, and none had a family history of similar skin lesions. The clinical and dermoscopic findings along with the histopathology in all 3 patients were consistent with ES.
The pathogenesis of ES is
To the Editor:
Syringoma is a relatively common benign adnexal neoplasm originating in the ducts of eccrine sweat glands. It can be
A 28-year-old man presented with multiple asymptomatic papules on the trunk and upper arms of 20 years’ duration (patient 1). He had been diagnosed with Darier disease 3 years prior to the current presentation and was treated with oral and topical retinoic acid without a response. After 3 months of oral treatment, the retinoic acid was stopped due to elevated liver enzymes. Physical examination at the current presentation revealed multiple smooth, firm, nonfused, 1- to 4-mm
A 27-year-old woman presented with widespread asymptomatic papules
A 43-year-old man who was otherwise healthy presented with brownish flat-topped papules on the chest and abdomen of 19 years’ duration (Figure 3A)(patient 3). The lesions had remained stable and did not progress. He denied any treatment.
All 3 patients demonstrated classic histopathologic features of syringoma, and none had a family history of similar skin lesions. The clinical and dermoscopic findings along with the histopathology in all 3 patients were consistent with ES.
The pathogenesis of ES is
- Williams K, Shinkai K. Evaluation and management of the patient with multiple syringomas: a systematic review of the literature. J Am Acad Dermatol. 2016;74:1234-1240.e1239. doi:10.1016/j.jaad.2015.12.006
- Jacquet L, Darier J.
Hidradénomes éruptifs, I.épithéliomes adenoids des glandes sudoripares ou adénomes sudoripares. Ann Dermatol Venerol. 1887;8:317-323. - Huang A, Taylor G, Liebman TN. Generalized eruptive syringomas. Dermatol Online J. 2017;23:13030/qt0hb8q22g..
- Maeda T, Natsuga K, Nishie W, et al. Extensive eruptive syringoma after liver transplantation. Acta Derm Venereol. 2018;98:119-120. doi:10.2340/00015555-2814
- Lerner TH, Barr RJ, Dolezal JF, et al. Syringomatous hyperplasia and eccrine squamous syringometaplasia associated with benoxaprofen therapy. Arch Dermatol. 1987;123:1202-1204. doi:10.1001/archderm.1987.01660330113022
- Ozturk F, Ermertcan AT, Bilac C, et al.
A case report of postpubertal eruptive syringoma triggered with antiepileptic drugs. J Drugs Dermatol. 2010;9:707-710. - Guitart J, Rosenbaum MM, Requena L. ‘Eruptive syringoma’: a misnomer for a reactive eccrine gland ductal proliferation? J Cutan Pathol. 2003;30:202-205. doi:10.1034/j.1600-0560.2003.00023.x
- Dupre A, Carrere S, Bonafe JL, et al. Eruptive generalized syringomas, milium and atrophoderma vermiculata. Nicolau and Balus’ syndrome (author’s transl). Dermatologica. 1981;162:281-286.
- Schepis C, Torre V, Siragusa M, et al. Eruptive syringomas with calcium deposits in a young woman with Down’s syndrome. Dermatology. 2001;203:345-347. doi:10.1159/000051788
- Samia AM, Donthi D, Nenow J, et al. A case study and review of literature of eruptive syringoma in a six-year-old. Cureus. 2021;13:E14634. doi:10.7759/cureus.14634
- Soler-Carrillo J, Estrach T, Mascaró JM. Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15:242-246. doi:10.1046/j.1468-3083.2001.00235.x
- Aleissa M, Aljarbou O, AlJasser MI. Dermoscopy of eruptive syringoma. Skin Appendage Disord. 2021;7:401-403. doi:10.1159/000515443
- Botsali A, Caliskan E, Coskun A, et al. Eruptive syringoma: two cases with dermoscopic features. Skin Appendage Disord. 2020;6:319-322. doi:10.1159/000508656
- Dutra Rezende H, Madia ACT, Elias BM, et al. Comment on: eruptive syringoma—two cases with dermoscopic features. Skin Appendage Disord. 2022;8:81-82. doi:10.1159/000518158
- Silva-Hirschberg C, Cabrera R, Rollán MP, et al. Darier disease: the use of dermoscopy in monitoring acitretin treatment. An Bras Dermatol. 2022;97:644-647. doi:10.1016/j.abd.2021.05.021
- Singal A, Kaur I, Jakhar D. Fox-Fordyce disease: dermoscopic perspective. Skin Appendage Disord. 2020;6:247-249. doi:10.1159/000508201
- Brau Javier CN, Morales A, Sanchez JL. Histopathology attributes of Fox-Fordyce disease. Int J Dermatol. 2012;51:1313-1318. doi:10.1159/000508201
- Horie K, Shinkuma S, Fujita Y, et al. Efficacy of N-(3,4-dimethoxycinnamoyl)-anthranilic acid (tranilast) against eruptive syringoma: report of two cases and review of published work. J Dermatol. 2012;39:1044-1046. doi:10.1111/j.1346-8138.2012.01612.x
- Sanchez TS, Dauden E, Casas AP, et al. Eruptive pruritic syringomas: treatment with topical atropine. J Am Acad Dermatol. 2001;44:148-149. doi:10.1067/mjd.2001.109854
- Williams K, Shinkai K. Evaluation and management of the patient with multiple syringomas: a systematic review of the literature. J Am Acad Dermatol. 2016;74:1234-1240.e1239. doi:10.1016/j.jaad.2015.12.006
- Jacquet L, Darier J.
Hidradénomes éruptifs, I.épithéliomes adenoids des glandes sudoripares ou adénomes sudoripares. Ann Dermatol Venerol. 1887;8:317-323. - Huang A, Taylor G, Liebman TN. Generalized eruptive syringomas. Dermatol Online J. 2017;23:13030/qt0hb8q22g..
- Maeda T, Natsuga K, Nishie W, et al. Extensive eruptive syringoma after liver transplantation. Acta Derm Venereol. 2018;98:119-120. doi:10.2340/00015555-2814
- Lerner TH, Barr RJ, Dolezal JF, et al. Syringomatous hyperplasia and eccrine squamous syringometaplasia associated with benoxaprofen therapy. Arch Dermatol. 1987;123:1202-1204. doi:10.1001/archderm.1987.01660330113022
- Ozturk F, Ermertcan AT, Bilac C, et al.
A case report of postpubertal eruptive syringoma triggered with antiepileptic drugs. J Drugs Dermatol. 2010;9:707-710. - Guitart J, Rosenbaum MM, Requena L. ‘Eruptive syringoma’: a misnomer for a reactive eccrine gland ductal proliferation? J Cutan Pathol. 2003;30:202-205. doi:10.1034/j.1600-0560.2003.00023.x
- Dupre A, Carrere S, Bonafe JL, et al. Eruptive generalized syringomas, milium and atrophoderma vermiculata. Nicolau and Balus’ syndrome (author’s transl). Dermatologica. 1981;162:281-286.
- Schepis C, Torre V, Siragusa M, et al. Eruptive syringomas with calcium deposits in a young woman with Down’s syndrome. Dermatology. 2001;203:345-347. doi:10.1159/000051788
- Samia AM, Donthi D, Nenow J, et al. A case study and review of literature of eruptive syringoma in a six-year-old. Cureus. 2021;13:E14634. doi:10.7759/cureus.14634
- Soler-Carrillo J, Estrach T, Mascaró JM. Eruptive syringoma: 27 new cases and review of the literature. J Eur Acad Dermatol Venereol. 2001;15:242-246. doi:10.1046/j.1468-3083.2001.00235.x
- Aleissa M, Aljarbou O, AlJasser MI. Dermoscopy of eruptive syringoma. Skin Appendage Disord. 2021;7:401-403. doi:10.1159/000515443
- Botsali A, Caliskan E, Coskun A, et al. Eruptive syringoma: two cases with dermoscopic features. Skin Appendage Disord. 2020;6:319-322. doi:10.1159/000508656
- Dutra Rezende H, Madia ACT, Elias BM, et al. Comment on: eruptive syringoma—two cases with dermoscopic features. Skin Appendage Disord. 2022;8:81-82. doi:10.1159/000518158
- Silva-Hirschberg C, Cabrera R, Rollán MP, et al. Darier disease: the use of dermoscopy in monitoring acitretin treatment. An Bras Dermatol. 2022;97:644-647. doi:10.1016/j.abd.2021.05.021
- Singal A, Kaur I, Jakhar D. Fox-Fordyce disease: dermoscopic perspective. Skin Appendage Disord. 2020;6:247-249. doi:10.1159/000508201
- Brau Javier CN, Morales A, Sanchez JL. Histopathology attributes of Fox-Fordyce disease. Int J Dermatol. 2012;51:1313-1318. doi:10.1159/000508201
- Horie K, Shinkuma S, Fujita Y, et al. Efficacy of N-(3,4-dimethoxycinnamoyl)-anthranilic acid (tranilast) against eruptive syringoma: report of two cases and review of published work. J Dermatol. 2012;39:1044-1046. doi:10.1111/j.1346-8138.2012.01612.x
- Sanchez TS, Dauden E, Casas AP, et al. Eruptive pruritic syringomas: treatment with topical atropine. J Am Acad Dermatol. 2001;44:148-149. doi:10.1067/mjd.2001.109854
Practice Points
- Eruptive syringoma (ES) is a benign cutaneous adnexal neoplasm that typically does not require treatment.
- Dermoscopy and biopsy are helpful for the diagnosis of ES, which often is missed or misdiagnosed clinically.
Sjögren Disease Treatments in Early Trials Have Mostly Positive Results
VIENNA — Nipocalimab, iscalimab, and tibulizumab, but not lusvertikimab, appear to be promising new agents for Sjögren disease that warrant further investigation, suggest the results of four separate early clinical trials reported at the recent annual European Congress of Rheumatology (EULAR).
This is potentially good news for patients, as discovering new treatments that work for managing the various symptoms of Sjögren disease is a high priority, Jacques-Eric Gottenberg, MD, PhD, said when he presented the results of the phase 2 DAHLIAS study of nipocalimab during a late-breaking abstract session.
“All patients suffer from high burden of symptoms — pain, fatigue, and dryness; nearly 50% of patients have systemic complications; mortality is increased, so there is a high unmet need since no specific drug has been accepted so far,” said Dr. Gottenberg, who works at Strasbourg University Hospital in Strasbourg, France.
“The pathogenesis of the disease involves high B-cell activation, resulting in high IgG levels, and secretion of autoantibodies,” such as anti-Ro, anti-La, anti-Sjögren’s syndrome type A (anti-SSA), and anti-Sjögren’s syndrome type B antibodies, Dr. Gottenberg said.
Thus, one approach to reducing the disease burden is to try to lower circulating immunoglobulin G (IgG) levels and IgG-associated autoantibodies, which is how the monoclonal antibody nipocalimab works. Nipocalimab essentially blocks the interaction of IgG with the neonatal fragment crystallizable receptor and has already been shown to have efficacy in other autoimmune conditions such as myasthenia gravis and fetal and neonatal hemolytic disease, although not as hoped in rheumatoid arthritis.
The DAHLIAS Phase 2 Study
Now, results from the DAHLIAS study show that nipocalimab may also work in Sjögren disease, with significant improvement vs placebo seen in the primary endpoint of the total EULAR Sjögren’s Syndrome Disease Activity Index (clinESSDAI) at 24 weeks for one of the two doses of the drug that were tested.
The multicenter, placebo-controlled, double-blind study was conducted in 163 patients with moderate to severely active primary Sjögren disease. The latter was determined by having a clinESSDAI of 6 or higher and seropositivity for anti-Ro60, anti-Ro52, or both autoantibodies.
Dr. Gottenberg reported that the mean age of patients was 48 years; the majority (92.6%) were women and of White ethnicity (90.8%). The baseline clinESSDAI was a mean of 9.9; 98.1% had anti-Ro60, 80.6% had anti-Ro52, and 71.9% had anti-La antibodies.
In addition to standard of care, patients were randomly allocated to receive intravenous treatment every 2 weeks with nipocalimab 5 mg/kg or 15 mg/kg, or placebo.
At 24 weeks, the least squares mean (LSM) change in clinESSDAI from baseline was −3.74 for placebo, −4.08 for nipocalimab 5 mg/kg (P = not significant vs placebo), and −6.40 for nipocalimab 15 mg/kg (P = .02 vs placebo).
Nipocalimab 15 mg/kg also “demonstrated similar and consistent trends in other key efficacy endpoints,” Dr. Gottenberg said. This included improvements in the ESSDAI and EULAR Sjögren’s Syndrome Patient Reported Index (ESSPRI) and composite measures such as the Sjögren’s Tool for Assessing Response (STAR), Composite of Relevant Endpoints for Sjögren’s Syndrome (CRESS), and the Disease Activity Level. There were also improvements in the unstimulated salivary flow rate.
Safety findings showed no new concerns, with adverse events reported in 62.5% of placebo-treated patients and by 79.2% and 79.6% of patients receiving nipocalimab 5 mg/kg and 15 mg/kg, respectively. Serious adverse events were reported in a respective 5.4%, 7.5%, and 7.4%, including severe infections or infections requiring intravenous anti-infectives in 1.8%, 3.8%, and 1.9% of participants, although none was thought to be related to the study treatment. No opportunistic infections or any deaths were reported.
Thomas Schindler, PhD, senior clinical scientist at F. Hoffmann-La Roche Ltd., in Basel, Switzerland, commented from the audience: “This was a very impressive set of results, and I’m very surprised that its safety profile is so benign.”
Dr. Schindler wanted to know if there were any changes in the serum albumin level and if this manifested as any laboratory abnormalities, but there were no reported cases of severe hypoalbuminemia in the study.
The TWINSS Phase 2 Study
Similarly hopeful results were reported for iscalimab, a fully human IgG1 anti-CD40 monoclonal antibody that is given by subcutaneous injection, during a clinical abstracts session. Xavier Mariette, MD, PhD, head of the Rheumatology Department at Bicêtre Hospital, Paris-Saclay University in Paris, France, reported updated results of the phase 2b dose-ranging TWINSS study, showing sustained benefits at 48 weeks. The primary endpoint results at 24 weeks were recently published in The Lancet.
TWINSS was set up to assess the safety and efficacy of iscalimab given every 2 weeks vs placebo in two distinct cohorts of patients with Sjögren disease — one with moderate to severe disease with both systemic and symptomatic involvement and the other with low systemic involvement but high symptom burden.
Whereas patients in the first cohort who had moderate to severe disease (n = 173) were randomly allocated to one of three doses (150, 300, and 600 mg) of iscalimab or placebo for the initial 24 weeks, those in the second cohort (n = 100) were randomly allocated to a 600-mg dose or placebo. After the double-blind period ended, patients taking iscalimab continued on the dose they were taking for another 24 weeks, with those in the placebo arms switching to the 600-mg dose in cohort 1 and the 300-mg dose in cohort 2.
Topline results for those in cohort 1 with moderate to severe Sjögren disease were that the significant improvements in ESSDAI that had been seen at week 24 were maintained in those who continued iscalimab and improved in those who had switched from placebo.
LSM change from baseline in ESSDAI vs placebo at week 24 had been −3.0, −1.4, and −2.9 for the 150-, 300-, and 600-mg doses of iscalimab, respectively. Results at week 48 were a respective −7.6, −5.7, and −7.9. The LSM change for the placebo-treated patients who had switched to the 600-mg dose was −6.7.
Dr. Mariette reported “consistent improvement” in patient-reported outcomes, including ESSPRI, the Sjögren’s Syndrome Symptom Diary, Functional Assessment of Chronic Illness Therapy-Fatigue measure, and the Impact of Dry Eye on Everyday Life instrument. There was also a significant improvement in stimulated salivary flow rates.
Similar benefits were seen in the second cohort of patients who did not have systemic involvement but had a high burden of symptoms, with improved ESSPRI scores of a LSM change from baseline vs placebo of −2.29 for patients continuing iscalimab 600 mg treatment and −1.14 for those taking the 300-mg dose after being treated with placebo. Improvements were also seen in the other patient-reported outcomes used.
Regarding safety, Dr. Mariette reported that there were “no specific issues” seen in the patients who switched from placebo to iscalimab, either at the 300-mg or 600-mg dose. Any adverse event occurred in around 80% of placebo-treated patients and roughly 90% of those given iscalimab, and serious adverse events occurred in 11.4%, 14.3%, and 11.4% pf patients treated with iscalimab 150, 300, and 600 mg, and 4.9% of those given placebo and then 600 mg iscalimab.
“The safety seems equivalent to patients having received iscalimab from the beginning of the trial,” Dr. Mariette said, adding “the risk-benefit [analysis] seems positive in patients up to week 48.”
Phase 1 Trial of Tibulizumab
Further positive early trial results were reported by Michael Howell, PhD, chief scientific officer for Zura Bio, a biotech company based in Henderson, Nevada. During a poster tour at EULAR 2024, Dr. Howell presented some preliminary findings from a phase 1 trial of tibulizumab, a dual antagonist of interleukin (IL)-17A and the B-cell–activating factor (BAFF) engineered by fusing elements of ixekizumab (Taltz) and tabalumab together.
“The headline result for me is that the molecule does what it’s supposed to,” Dr. Howell told this news organization. “We have potent engagement of the IL-17 and BAFF pathways, and this sets the tone for additional exploration in rheumatologic diseases where there’s known activation of those two pathways,” he said.
Dr. Howell reported that total B-cell counts and lower levels of type 1 T helper cells were seen during the trial.
Over the years, Dr. Howell, an immunologist, has been involved in the development of many therapeutics, such as risankizumab (Skyrizi) and spesolimab (Spevigo).
“When I look at the molecules and the opportunity we have to do broader antagonism of pathways in a safe aspect, this is probably one of the most exciting,” he said.
The trial he presented included 25 people with a confirmed diagnosis of Sjögren disease and anti-SSA or anti-SSB antibodies. Patients received tibulizumab or a placebo for a total of 12 weeks via a subcutaneous injection. Various doses were tested: 30 mg, 100 mg, or 300 mg every 4 weeks, or 300 mg every 2 weeks.
Serum levels of both BAFF and IL-17A increased as expected in the tibulizumab-treated patients, and Dr. Howell reported that “it’s well tolerated. There’s no adverse event profile that caused any concern.”
As a phase 1 study, it was not powered to look at efficacy, but there were positive signals, Dr. Howell said, meaning that the drug is likely to be tested further in a phase 2 trial.
Lusvertikimab Phase 2 Trial
During the same poster tour, the null findings of a phase 2 trial of the anti-IL-7 monoclonal antibody lusvertikimab were presented by Benjamin Fisher, MD, professor of rheumatology at Birmingham University in Birmingham, England.
Dr. Fisher told this news organization: “It’s a negative study, at least over the 3-month period that we’ve studied it.” Whether longer durations of treatment may be needed is a question that currently cannot be answered, he added.
A total of 48 patients with Sjögren disease had been included in the trial from 19 different centers in Europe, the United States, and Australia. The mean age of the participants was 53.7 years, 87% were women, and the mean duration of disease was 5.0 years. Baseline ESSDAI and ESSPRI were 12.1 and 7.0, respectively. Half were receiving other background treatment, and 72.9% were anti-Ro or anti-SSA positive.
Lusvertikimab 750 mg or a matching placebo was given via intravenous infusion at weeks 0, 2, 4, 7, and 10.
The primary endpoint was the mean change in ESSDAI from baseline to week 13, which was the same, at −3.9, in both groups. There was also no significant difference between the groups in any of the other secondary endpoints that were used, including ESSPRI, Schirmer’s test, the ocular staining score, salivary flow rate, physician and patient global assessment, assessment of fatigue, quality of life, or the composite measures STAR and CRESS.
“This isn’t going anywhere,” said Dr. Fisher, asking what was going to happen next and if this meant the end of IL-7-focused therapy.
“For years, there’s been quite a lot of interest in this,” Dr. Fisher said. Sjögren disease is characterized by a sort of focal inflammation of the saliva glands, which is composed of both T and B cells in the early stages, probably a T-cell component and a B-cell component, he explained.
“IL-7 is thought to be an important cytokine for homeostasis of the T-cell compartment, so for maintenance of T central memory and effector memory cells,” he said. “So, the idea is that, if you block IL-7, you switch off T cells, and you may rebalance the immune system towards a more regulatory phenotype. Just that it didn’t work,” Dr. Fisher said.
“There’s large unmet need,” he said. “Sjögren’s is associated with poor health-related quality of life, [and] a large part that is symptom-driven — dryness and fatigue — which we have no real interventions yet for patients; there’s no licensed therapeutics for it.”
Dr. Fisher cited ianalumab as one of the front-runners for becoming the first licensed treatment for Sjögren disease. The novel BAFF-targeting antibody is already in phase 3 trials and is also showing promise for the treatment of systemic lupus erythematosus.
“Then there are CD40-targeting drugs; the ones most advanced are dazodalibep and iscalimab.” Commenting on the potential of iscalimab, Dr. Fisher said that it “seems to work — it improves systemic disease activity; it also leads to some symptomatic improvement, which has been difficult to demonstrate in Sjögren’s.”
Dr. Fisher added that “the nipocalimab data looks interesting, as do data on TYK2 inhibition.”
The DAHLIAS study was funded by Janssen Research & Development. Dr. Gottenberg has consulted for AbbVie, Bristol Myers Squibb (BMS), Galapagos, Gilead, Janssen, Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Sanofi, and UCB. The TWINSS study was funded by Novartis. Dr. Mariette has consulted for BMS, Galapagos, GlaxoSmithKline, Novartis, Pfizer, and Servier. The tibulizumab phase 1 study was funded by Eli Lilly & Company. Dr. Howell is an employee of the developer, Zura Bio. The Institut de Recherches Internationales Servier sponsored the lusvertikimab trial. Dr. Fisher has consulted for Novartis, Roche, BMS, Galapagos, Janssen, Servier, UCB, and Sanofi and received funding to his institution for collaborative research from Janssen, Celgene, Galapagos, and Servier.
A version of this article first appeared on Medscape.com.
VIENNA — Nipocalimab, iscalimab, and tibulizumab, but not lusvertikimab, appear to be promising new agents for Sjögren disease that warrant further investigation, suggest the results of four separate early clinical trials reported at the recent annual European Congress of Rheumatology (EULAR).
This is potentially good news for patients, as discovering new treatments that work for managing the various symptoms of Sjögren disease is a high priority, Jacques-Eric Gottenberg, MD, PhD, said when he presented the results of the phase 2 DAHLIAS study of nipocalimab during a late-breaking abstract session.
“All patients suffer from high burden of symptoms — pain, fatigue, and dryness; nearly 50% of patients have systemic complications; mortality is increased, so there is a high unmet need since no specific drug has been accepted so far,” said Dr. Gottenberg, who works at Strasbourg University Hospital in Strasbourg, France.
“The pathogenesis of the disease involves high B-cell activation, resulting in high IgG levels, and secretion of autoantibodies,” such as anti-Ro, anti-La, anti-Sjögren’s syndrome type A (anti-SSA), and anti-Sjögren’s syndrome type B antibodies, Dr. Gottenberg said.
Thus, one approach to reducing the disease burden is to try to lower circulating immunoglobulin G (IgG) levels and IgG-associated autoantibodies, which is how the monoclonal antibody nipocalimab works. Nipocalimab essentially blocks the interaction of IgG with the neonatal fragment crystallizable receptor and has already been shown to have efficacy in other autoimmune conditions such as myasthenia gravis and fetal and neonatal hemolytic disease, although not as hoped in rheumatoid arthritis.
The DAHLIAS Phase 2 Study
Now, results from the DAHLIAS study show that nipocalimab may also work in Sjögren disease, with significant improvement vs placebo seen in the primary endpoint of the total EULAR Sjögren’s Syndrome Disease Activity Index (clinESSDAI) at 24 weeks for one of the two doses of the drug that were tested.
The multicenter, placebo-controlled, double-blind study was conducted in 163 patients with moderate to severely active primary Sjögren disease. The latter was determined by having a clinESSDAI of 6 or higher and seropositivity for anti-Ro60, anti-Ro52, or both autoantibodies.
Dr. Gottenberg reported that the mean age of patients was 48 years; the majority (92.6%) were women and of White ethnicity (90.8%). The baseline clinESSDAI was a mean of 9.9; 98.1% had anti-Ro60, 80.6% had anti-Ro52, and 71.9% had anti-La antibodies.
In addition to standard of care, patients were randomly allocated to receive intravenous treatment every 2 weeks with nipocalimab 5 mg/kg or 15 mg/kg, or placebo.
At 24 weeks, the least squares mean (LSM) change in clinESSDAI from baseline was −3.74 for placebo, −4.08 for nipocalimab 5 mg/kg (P = not significant vs placebo), and −6.40 for nipocalimab 15 mg/kg (P = .02 vs placebo).
Nipocalimab 15 mg/kg also “demonstrated similar and consistent trends in other key efficacy endpoints,” Dr. Gottenberg said. This included improvements in the ESSDAI and EULAR Sjögren’s Syndrome Patient Reported Index (ESSPRI) and composite measures such as the Sjögren’s Tool for Assessing Response (STAR), Composite of Relevant Endpoints for Sjögren’s Syndrome (CRESS), and the Disease Activity Level. There were also improvements in the unstimulated salivary flow rate.
Safety findings showed no new concerns, with adverse events reported in 62.5% of placebo-treated patients and by 79.2% and 79.6% of patients receiving nipocalimab 5 mg/kg and 15 mg/kg, respectively. Serious adverse events were reported in a respective 5.4%, 7.5%, and 7.4%, including severe infections or infections requiring intravenous anti-infectives in 1.8%, 3.8%, and 1.9% of participants, although none was thought to be related to the study treatment. No opportunistic infections or any deaths were reported.
Thomas Schindler, PhD, senior clinical scientist at F. Hoffmann-La Roche Ltd., in Basel, Switzerland, commented from the audience: “This was a very impressive set of results, and I’m very surprised that its safety profile is so benign.”
Dr. Schindler wanted to know if there were any changes in the serum albumin level and if this manifested as any laboratory abnormalities, but there were no reported cases of severe hypoalbuminemia in the study.
The TWINSS Phase 2 Study
Similarly hopeful results were reported for iscalimab, a fully human IgG1 anti-CD40 monoclonal antibody that is given by subcutaneous injection, during a clinical abstracts session. Xavier Mariette, MD, PhD, head of the Rheumatology Department at Bicêtre Hospital, Paris-Saclay University in Paris, France, reported updated results of the phase 2b dose-ranging TWINSS study, showing sustained benefits at 48 weeks. The primary endpoint results at 24 weeks were recently published in The Lancet.
TWINSS was set up to assess the safety and efficacy of iscalimab given every 2 weeks vs placebo in two distinct cohorts of patients with Sjögren disease — one with moderate to severe disease with both systemic and symptomatic involvement and the other with low systemic involvement but high symptom burden.
Whereas patients in the first cohort who had moderate to severe disease (n = 173) were randomly allocated to one of three doses (150, 300, and 600 mg) of iscalimab or placebo for the initial 24 weeks, those in the second cohort (n = 100) were randomly allocated to a 600-mg dose or placebo. After the double-blind period ended, patients taking iscalimab continued on the dose they were taking for another 24 weeks, with those in the placebo arms switching to the 600-mg dose in cohort 1 and the 300-mg dose in cohort 2.
Topline results for those in cohort 1 with moderate to severe Sjögren disease were that the significant improvements in ESSDAI that had been seen at week 24 were maintained in those who continued iscalimab and improved in those who had switched from placebo.
LSM change from baseline in ESSDAI vs placebo at week 24 had been −3.0, −1.4, and −2.9 for the 150-, 300-, and 600-mg doses of iscalimab, respectively. Results at week 48 were a respective −7.6, −5.7, and −7.9. The LSM change for the placebo-treated patients who had switched to the 600-mg dose was −6.7.
Dr. Mariette reported “consistent improvement” in patient-reported outcomes, including ESSPRI, the Sjögren’s Syndrome Symptom Diary, Functional Assessment of Chronic Illness Therapy-Fatigue measure, and the Impact of Dry Eye on Everyday Life instrument. There was also a significant improvement in stimulated salivary flow rates.
Similar benefits were seen in the second cohort of patients who did not have systemic involvement but had a high burden of symptoms, with improved ESSPRI scores of a LSM change from baseline vs placebo of −2.29 for patients continuing iscalimab 600 mg treatment and −1.14 for those taking the 300-mg dose after being treated with placebo. Improvements were also seen in the other patient-reported outcomes used.
Regarding safety, Dr. Mariette reported that there were “no specific issues” seen in the patients who switched from placebo to iscalimab, either at the 300-mg or 600-mg dose. Any adverse event occurred in around 80% of placebo-treated patients and roughly 90% of those given iscalimab, and serious adverse events occurred in 11.4%, 14.3%, and 11.4% pf patients treated with iscalimab 150, 300, and 600 mg, and 4.9% of those given placebo and then 600 mg iscalimab.
“The safety seems equivalent to patients having received iscalimab from the beginning of the trial,” Dr. Mariette said, adding “the risk-benefit [analysis] seems positive in patients up to week 48.”
Phase 1 Trial of Tibulizumab
Further positive early trial results were reported by Michael Howell, PhD, chief scientific officer for Zura Bio, a biotech company based in Henderson, Nevada. During a poster tour at EULAR 2024, Dr. Howell presented some preliminary findings from a phase 1 trial of tibulizumab, a dual antagonist of interleukin (IL)-17A and the B-cell–activating factor (BAFF) engineered by fusing elements of ixekizumab (Taltz) and tabalumab together.
“The headline result for me is that the molecule does what it’s supposed to,” Dr. Howell told this news organization. “We have potent engagement of the IL-17 and BAFF pathways, and this sets the tone for additional exploration in rheumatologic diseases where there’s known activation of those two pathways,” he said.
Dr. Howell reported that total B-cell counts and lower levels of type 1 T helper cells were seen during the trial.
Over the years, Dr. Howell, an immunologist, has been involved in the development of many therapeutics, such as risankizumab (Skyrizi) and spesolimab (Spevigo).
“When I look at the molecules and the opportunity we have to do broader antagonism of pathways in a safe aspect, this is probably one of the most exciting,” he said.
The trial he presented included 25 people with a confirmed diagnosis of Sjögren disease and anti-SSA or anti-SSB antibodies. Patients received tibulizumab or a placebo for a total of 12 weeks via a subcutaneous injection. Various doses were tested: 30 mg, 100 mg, or 300 mg every 4 weeks, or 300 mg every 2 weeks.
Serum levels of both BAFF and IL-17A increased as expected in the tibulizumab-treated patients, and Dr. Howell reported that “it’s well tolerated. There’s no adverse event profile that caused any concern.”
As a phase 1 study, it was not powered to look at efficacy, but there were positive signals, Dr. Howell said, meaning that the drug is likely to be tested further in a phase 2 trial.
Lusvertikimab Phase 2 Trial
During the same poster tour, the null findings of a phase 2 trial of the anti-IL-7 monoclonal antibody lusvertikimab were presented by Benjamin Fisher, MD, professor of rheumatology at Birmingham University in Birmingham, England.
Dr. Fisher told this news organization: “It’s a negative study, at least over the 3-month period that we’ve studied it.” Whether longer durations of treatment may be needed is a question that currently cannot be answered, he added.
A total of 48 patients with Sjögren disease had been included in the trial from 19 different centers in Europe, the United States, and Australia. The mean age of the participants was 53.7 years, 87% were women, and the mean duration of disease was 5.0 years. Baseline ESSDAI and ESSPRI were 12.1 and 7.0, respectively. Half were receiving other background treatment, and 72.9% were anti-Ro or anti-SSA positive.
Lusvertikimab 750 mg or a matching placebo was given via intravenous infusion at weeks 0, 2, 4, 7, and 10.
The primary endpoint was the mean change in ESSDAI from baseline to week 13, which was the same, at −3.9, in both groups. There was also no significant difference between the groups in any of the other secondary endpoints that were used, including ESSPRI, Schirmer’s test, the ocular staining score, salivary flow rate, physician and patient global assessment, assessment of fatigue, quality of life, or the composite measures STAR and CRESS.
“This isn’t going anywhere,” said Dr. Fisher, asking what was going to happen next and if this meant the end of IL-7-focused therapy.
“For years, there’s been quite a lot of interest in this,” Dr. Fisher said. Sjögren disease is characterized by a sort of focal inflammation of the saliva glands, which is composed of both T and B cells in the early stages, probably a T-cell component and a B-cell component, he explained.
“IL-7 is thought to be an important cytokine for homeostasis of the T-cell compartment, so for maintenance of T central memory and effector memory cells,” he said. “So, the idea is that, if you block IL-7, you switch off T cells, and you may rebalance the immune system towards a more regulatory phenotype. Just that it didn’t work,” Dr. Fisher said.
“There’s large unmet need,” he said. “Sjögren’s is associated with poor health-related quality of life, [and] a large part that is symptom-driven — dryness and fatigue — which we have no real interventions yet for patients; there’s no licensed therapeutics for it.”
Dr. Fisher cited ianalumab as one of the front-runners for becoming the first licensed treatment for Sjögren disease. The novel BAFF-targeting antibody is already in phase 3 trials and is also showing promise for the treatment of systemic lupus erythematosus.
“Then there are CD40-targeting drugs; the ones most advanced are dazodalibep and iscalimab.” Commenting on the potential of iscalimab, Dr. Fisher said that it “seems to work — it improves systemic disease activity; it also leads to some symptomatic improvement, which has been difficult to demonstrate in Sjögren’s.”
Dr. Fisher added that “the nipocalimab data looks interesting, as do data on TYK2 inhibition.”
The DAHLIAS study was funded by Janssen Research & Development. Dr. Gottenberg has consulted for AbbVie, Bristol Myers Squibb (BMS), Galapagos, Gilead, Janssen, Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Sanofi, and UCB. The TWINSS study was funded by Novartis. Dr. Mariette has consulted for BMS, Galapagos, GlaxoSmithKline, Novartis, Pfizer, and Servier. The tibulizumab phase 1 study was funded by Eli Lilly & Company. Dr. Howell is an employee of the developer, Zura Bio. The Institut de Recherches Internationales Servier sponsored the lusvertikimab trial. Dr. Fisher has consulted for Novartis, Roche, BMS, Galapagos, Janssen, Servier, UCB, and Sanofi and received funding to his institution for collaborative research from Janssen, Celgene, Galapagos, and Servier.
A version of this article first appeared on Medscape.com.
VIENNA — Nipocalimab, iscalimab, and tibulizumab, but not lusvertikimab, appear to be promising new agents for Sjögren disease that warrant further investigation, suggest the results of four separate early clinical trials reported at the recent annual European Congress of Rheumatology (EULAR).
This is potentially good news for patients, as discovering new treatments that work for managing the various symptoms of Sjögren disease is a high priority, Jacques-Eric Gottenberg, MD, PhD, said when he presented the results of the phase 2 DAHLIAS study of nipocalimab during a late-breaking abstract session.
“All patients suffer from high burden of symptoms — pain, fatigue, and dryness; nearly 50% of patients have systemic complications; mortality is increased, so there is a high unmet need since no specific drug has been accepted so far,” said Dr. Gottenberg, who works at Strasbourg University Hospital in Strasbourg, France.
“The pathogenesis of the disease involves high B-cell activation, resulting in high IgG levels, and secretion of autoantibodies,” such as anti-Ro, anti-La, anti-Sjögren’s syndrome type A (anti-SSA), and anti-Sjögren’s syndrome type B antibodies, Dr. Gottenberg said.
Thus, one approach to reducing the disease burden is to try to lower circulating immunoglobulin G (IgG) levels and IgG-associated autoantibodies, which is how the monoclonal antibody nipocalimab works. Nipocalimab essentially blocks the interaction of IgG with the neonatal fragment crystallizable receptor and has already been shown to have efficacy in other autoimmune conditions such as myasthenia gravis and fetal and neonatal hemolytic disease, although not as hoped in rheumatoid arthritis.
The DAHLIAS Phase 2 Study
Now, results from the DAHLIAS study show that nipocalimab may also work in Sjögren disease, with significant improvement vs placebo seen in the primary endpoint of the total EULAR Sjögren’s Syndrome Disease Activity Index (clinESSDAI) at 24 weeks for one of the two doses of the drug that were tested.
The multicenter, placebo-controlled, double-blind study was conducted in 163 patients with moderate to severely active primary Sjögren disease. The latter was determined by having a clinESSDAI of 6 or higher and seropositivity for anti-Ro60, anti-Ro52, or both autoantibodies.
Dr. Gottenberg reported that the mean age of patients was 48 years; the majority (92.6%) were women and of White ethnicity (90.8%). The baseline clinESSDAI was a mean of 9.9; 98.1% had anti-Ro60, 80.6% had anti-Ro52, and 71.9% had anti-La antibodies.
In addition to standard of care, patients were randomly allocated to receive intravenous treatment every 2 weeks with nipocalimab 5 mg/kg or 15 mg/kg, or placebo.
At 24 weeks, the least squares mean (LSM) change in clinESSDAI from baseline was −3.74 for placebo, −4.08 for nipocalimab 5 mg/kg (P = not significant vs placebo), and −6.40 for nipocalimab 15 mg/kg (P = .02 vs placebo).
Nipocalimab 15 mg/kg also “demonstrated similar and consistent trends in other key efficacy endpoints,” Dr. Gottenberg said. This included improvements in the ESSDAI and EULAR Sjögren’s Syndrome Patient Reported Index (ESSPRI) and composite measures such as the Sjögren’s Tool for Assessing Response (STAR), Composite of Relevant Endpoints for Sjögren’s Syndrome (CRESS), and the Disease Activity Level. There were also improvements in the unstimulated salivary flow rate.
Safety findings showed no new concerns, with adverse events reported in 62.5% of placebo-treated patients and by 79.2% and 79.6% of patients receiving nipocalimab 5 mg/kg and 15 mg/kg, respectively. Serious adverse events were reported in a respective 5.4%, 7.5%, and 7.4%, including severe infections or infections requiring intravenous anti-infectives in 1.8%, 3.8%, and 1.9% of participants, although none was thought to be related to the study treatment. No opportunistic infections or any deaths were reported.
Thomas Schindler, PhD, senior clinical scientist at F. Hoffmann-La Roche Ltd., in Basel, Switzerland, commented from the audience: “This was a very impressive set of results, and I’m very surprised that its safety profile is so benign.”
Dr. Schindler wanted to know if there were any changes in the serum albumin level and if this manifested as any laboratory abnormalities, but there were no reported cases of severe hypoalbuminemia in the study.
The TWINSS Phase 2 Study
Similarly hopeful results were reported for iscalimab, a fully human IgG1 anti-CD40 monoclonal antibody that is given by subcutaneous injection, during a clinical abstracts session. Xavier Mariette, MD, PhD, head of the Rheumatology Department at Bicêtre Hospital, Paris-Saclay University in Paris, France, reported updated results of the phase 2b dose-ranging TWINSS study, showing sustained benefits at 48 weeks. The primary endpoint results at 24 weeks were recently published in The Lancet.
TWINSS was set up to assess the safety and efficacy of iscalimab given every 2 weeks vs placebo in two distinct cohorts of patients with Sjögren disease — one with moderate to severe disease with both systemic and symptomatic involvement and the other with low systemic involvement but high symptom burden.
Whereas patients in the first cohort who had moderate to severe disease (n = 173) were randomly allocated to one of three doses (150, 300, and 600 mg) of iscalimab or placebo for the initial 24 weeks, those in the second cohort (n = 100) were randomly allocated to a 600-mg dose or placebo. After the double-blind period ended, patients taking iscalimab continued on the dose they were taking for another 24 weeks, with those in the placebo arms switching to the 600-mg dose in cohort 1 and the 300-mg dose in cohort 2.
Topline results for those in cohort 1 with moderate to severe Sjögren disease were that the significant improvements in ESSDAI that had been seen at week 24 were maintained in those who continued iscalimab and improved in those who had switched from placebo.
LSM change from baseline in ESSDAI vs placebo at week 24 had been −3.0, −1.4, and −2.9 for the 150-, 300-, and 600-mg doses of iscalimab, respectively. Results at week 48 were a respective −7.6, −5.7, and −7.9. The LSM change for the placebo-treated patients who had switched to the 600-mg dose was −6.7.
Dr. Mariette reported “consistent improvement” in patient-reported outcomes, including ESSPRI, the Sjögren’s Syndrome Symptom Diary, Functional Assessment of Chronic Illness Therapy-Fatigue measure, and the Impact of Dry Eye on Everyday Life instrument. There was also a significant improvement in stimulated salivary flow rates.
Similar benefits were seen in the second cohort of patients who did not have systemic involvement but had a high burden of symptoms, with improved ESSPRI scores of a LSM change from baseline vs placebo of −2.29 for patients continuing iscalimab 600 mg treatment and −1.14 for those taking the 300-mg dose after being treated with placebo. Improvements were also seen in the other patient-reported outcomes used.
Regarding safety, Dr. Mariette reported that there were “no specific issues” seen in the patients who switched from placebo to iscalimab, either at the 300-mg or 600-mg dose. Any adverse event occurred in around 80% of placebo-treated patients and roughly 90% of those given iscalimab, and serious adverse events occurred in 11.4%, 14.3%, and 11.4% pf patients treated with iscalimab 150, 300, and 600 mg, and 4.9% of those given placebo and then 600 mg iscalimab.
“The safety seems equivalent to patients having received iscalimab from the beginning of the trial,” Dr. Mariette said, adding “the risk-benefit [analysis] seems positive in patients up to week 48.”
Phase 1 Trial of Tibulizumab
Further positive early trial results were reported by Michael Howell, PhD, chief scientific officer for Zura Bio, a biotech company based in Henderson, Nevada. During a poster tour at EULAR 2024, Dr. Howell presented some preliminary findings from a phase 1 trial of tibulizumab, a dual antagonist of interleukin (IL)-17A and the B-cell–activating factor (BAFF) engineered by fusing elements of ixekizumab (Taltz) and tabalumab together.
“The headline result for me is that the molecule does what it’s supposed to,” Dr. Howell told this news organization. “We have potent engagement of the IL-17 and BAFF pathways, and this sets the tone for additional exploration in rheumatologic diseases where there’s known activation of those two pathways,” he said.
Dr. Howell reported that total B-cell counts and lower levels of type 1 T helper cells were seen during the trial.
Over the years, Dr. Howell, an immunologist, has been involved in the development of many therapeutics, such as risankizumab (Skyrizi) and spesolimab (Spevigo).
“When I look at the molecules and the opportunity we have to do broader antagonism of pathways in a safe aspect, this is probably one of the most exciting,” he said.
The trial he presented included 25 people with a confirmed diagnosis of Sjögren disease and anti-SSA or anti-SSB antibodies. Patients received tibulizumab or a placebo for a total of 12 weeks via a subcutaneous injection. Various doses were tested: 30 mg, 100 mg, or 300 mg every 4 weeks, or 300 mg every 2 weeks.
Serum levels of both BAFF and IL-17A increased as expected in the tibulizumab-treated patients, and Dr. Howell reported that “it’s well tolerated. There’s no adverse event profile that caused any concern.”
As a phase 1 study, it was not powered to look at efficacy, but there were positive signals, Dr. Howell said, meaning that the drug is likely to be tested further in a phase 2 trial.
Lusvertikimab Phase 2 Trial
During the same poster tour, the null findings of a phase 2 trial of the anti-IL-7 monoclonal antibody lusvertikimab were presented by Benjamin Fisher, MD, professor of rheumatology at Birmingham University in Birmingham, England.
Dr. Fisher told this news organization: “It’s a negative study, at least over the 3-month period that we’ve studied it.” Whether longer durations of treatment may be needed is a question that currently cannot be answered, he added.
A total of 48 patients with Sjögren disease had been included in the trial from 19 different centers in Europe, the United States, and Australia. The mean age of the participants was 53.7 years, 87% were women, and the mean duration of disease was 5.0 years. Baseline ESSDAI and ESSPRI were 12.1 and 7.0, respectively. Half were receiving other background treatment, and 72.9% were anti-Ro or anti-SSA positive.
Lusvertikimab 750 mg or a matching placebo was given via intravenous infusion at weeks 0, 2, 4, 7, and 10.
The primary endpoint was the mean change in ESSDAI from baseline to week 13, which was the same, at −3.9, in both groups. There was also no significant difference between the groups in any of the other secondary endpoints that were used, including ESSPRI, Schirmer’s test, the ocular staining score, salivary flow rate, physician and patient global assessment, assessment of fatigue, quality of life, or the composite measures STAR and CRESS.
“This isn’t going anywhere,” said Dr. Fisher, asking what was going to happen next and if this meant the end of IL-7-focused therapy.
“For years, there’s been quite a lot of interest in this,” Dr. Fisher said. Sjögren disease is characterized by a sort of focal inflammation of the saliva glands, which is composed of both T and B cells in the early stages, probably a T-cell component and a B-cell component, he explained.
“IL-7 is thought to be an important cytokine for homeostasis of the T-cell compartment, so for maintenance of T central memory and effector memory cells,” he said. “So, the idea is that, if you block IL-7, you switch off T cells, and you may rebalance the immune system towards a more regulatory phenotype. Just that it didn’t work,” Dr. Fisher said.
“There’s large unmet need,” he said. “Sjögren’s is associated with poor health-related quality of life, [and] a large part that is symptom-driven — dryness and fatigue — which we have no real interventions yet for patients; there’s no licensed therapeutics for it.”
Dr. Fisher cited ianalumab as one of the front-runners for becoming the first licensed treatment for Sjögren disease. The novel BAFF-targeting antibody is already in phase 3 trials and is also showing promise for the treatment of systemic lupus erythematosus.
“Then there are CD40-targeting drugs; the ones most advanced are dazodalibep and iscalimab.” Commenting on the potential of iscalimab, Dr. Fisher said that it “seems to work — it improves systemic disease activity; it also leads to some symptomatic improvement, which has been difficult to demonstrate in Sjögren’s.”
Dr. Fisher added that “the nipocalimab data looks interesting, as do data on TYK2 inhibition.”
The DAHLIAS study was funded by Janssen Research & Development. Dr. Gottenberg has consulted for AbbVie, Bristol Myers Squibb (BMS), Galapagos, Gilead, Janssen, Lilly, Merck Sharp & Dohme, Novartis, Pfizer, Sanofi, and UCB. The TWINSS study was funded by Novartis. Dr. Mariette has consulted for BMS, Galapagos, GlaxoSmithKline, Novartis, Pfizer, and Servier. The tibulizumab phase 1 study was funded by Eli Lilly & Company. Dr. Howell is an employee of the developer, Zura Bio. The Institut de Recherches Internationales Servier sponsored the lusvertikimab trial. Dr. Fisher has consulted for Novartis, Roche, BMS, Galapagos, Janssen, Servier, UCB, and Sanofi and received funding to his institution for collaborative research from Janssen, Celgene, Galapagos, and Servier.
A version of this article first appeared on Medscape.com.
FROM EULAR 2024
Saxophone Penis: A Forgotten Manifestation of Hidradenitis Suppurativa
To the Editor:
Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease affecting 1% to 4% of Europeans. It is characterized by recurrent inflamed nodules, abscesses, and sinus tracts in intertriginous regions.1 The genital area is affected in 11% of cases2 and usually is connected to severe forms of HS in both men and women.3 The prevalence of HS-associated genital lymphedema remains unknown.
Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation of the major penile lymphatic vessels that cause fibrosis of the surrounding connective tissue. Poor blood flow further causes contracture and distortion of the penile axis.4 Saxophone penis also has been associated with primary lymphedema, lymphogranuloma venereum, filariasis,5 and administration of paraffin injections.6 We describe 3 men with HS who presented with saxophone penis.
A 33-year-old man with Hurley stage III HS presented with a medical history of groin lesions and progressive penoscrotal edema of 13 years’ duration. He had a body mass index (BMI) of 37, no family history of HS or comorbidities, and a 15-year history of smoking 20 cigarettes per day. After repeated surgical drainage of the HS lesions as well as antibiotic treatment with clindamycin 600 mg/d and rifampicin 600 mg/d, the patient was kept on a maintenance therapy with adalimumab 40 mg/wk. Due to lack of response, treatment was discontinued at week 16. Clindamycin and rifampicin 300 mg were immediately reintroduced with no benefit on the genital lesions. The patient underwent genital reconstruction, including penile degloving, scrotoplasty, infrapubic fat pad removal, and perineoplasty (Figure 1). The patient currently is not undergoing any therapies.
A 55-year-old man presented with Hurley stage II HS of 33 years’ duration. He had a BMI of 52; a history of hypertension, hyperuricemia, severe hip and knee osteoarthritis, and orchiopexy in childhood; a smoking history of 40 cigarettes per day; and an alcohol consumption history of 200 mL per day since 18 years of age. He had radical excision of axillary lesions 8 years prior. One year later, he was treated with concomitant clindamycin and rifampicin 300 mg twice daily for 3 months with no desirable effects. Adalimumab 40 mg/wk was initiated. After 12 weeks of treatment, he experienced 80% improvement in all areas except the genital region. He continued adalimumab for 3 years with good clinical response in all HS-affected sites except the genital region.
A 66-year-old man presented with Hurley stage III HS of 37 years’ duration. He had a smoking history of 10 cigarettes per day for 30 years, a BMI of 24.6, and a medical history of long-standing hypertension and hypothyroidism. A 3-month course of clindamycin and rifampicin 600 mg/d was ineffective; adalimumab 40 mg/wk was initiated. All affected areas improved, except for the saxophone penis. He continues his fifth year of therapy with adalimumab (Figure 2).

Hidradenitis suppurativa is associated with chronic pain, purulent malodor, and scarring with structural deformity. Repetitive inflammation causes fibrosis, scar formation, and soft-tissue destruction of lymphatic vessels, leading to lymphedema; primary lymphedema of the genitals in men has been reported to result in a saxophone penis.4
The only approved biologic treatments for moderate to severe HS are the tumor necrosis factor α inhibitor adalimumab and anti-IL-17 secukinumab.1 All 3 of our patients with HS were treated with adalimumab with reasonable success; however, the penile condition remained refractory, which we speculate may be due to adalimumab’s ability to control only active inflammatory lesions but not scars or fibrotic tissue.7 Higher adalimumab dosages were unlikely to be beneficial for their penile condition; some improvements have been reported following fluoroquinolone therapy. To our knowledge, there is no effective medical treatment for saxophone penis. However, surgery showed good results in one of our patients. Among our 3 adalimumab-treated patients, only 1 patient had corrective surgery that resulted in improvement in the penile deformity, further confirming adalimumab’s limited role in genital lymphedema.7 Extensive resection of the lymphedematous tissue, scrotoplasty, and Charles procedure are treatment options.8
Genital lymphedema has been associated with lymphangiectasia, lymphangioma circumscriptum, infections, and neoplasms such as lymphangiosarcoma and squamous cell carcinoma.9 Our patients reported discomfort, hygiene issues, and swelling. One patient reported micturition, and 2 patients reported sexual dysfunction.
Saxophone penis remains a disabling sequela of HS. Early diagnosis and treatment of HS may help prevent development of this condition.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Fertitta L, Hotz C, Wolkenstein P, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34:839-845.
- Micieli R, Alavi A. Lymphedema in patients with hidradenitis suppurativa: a systematic review of published literature. Int J Dermatol. 2018;57:1471-1480.
- Maatouk I, Moutran R. Saxophone penis. JAMA Dermatol. 2013;149:802.
- Koley S, Mandal RK. Saxophone penis after unilateral inguinal bubo of lymphogranuloma venereum. Indian J Sex Transm Dis AIDS. 2013;34:149-151.
- D’Antuono A, Lambertini M, Gaspari V, et al. Visual dermatology: self-induced chronic saxophone penis due to paraffin injections. J Cutan Med Surg. 2019;23:330.
- Musumeci ML, Scilletta A, Sorci F, et al. Genital lymphedema associated with hidradenitis suppurativa unresponsive to adalimumab treatment. JAAD Case Rep. 2019;5:326-328.
- Jain V, Singh S, Garge S, et al. Saxophone penis due to primary lymphoedema. J Indian Assoc Pediatr Surg. 2009;14:230-231.
- Moosbrugger EA, Mutasim DF. Hidradenitis suppurativa complicated by severe lymphedema and lymphangiectasias. J Am Acad Dermatol. 2011;64:1223-1224.
To the Editor:
Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease affecting 1% to 4% of Europeans. It is characterized by recurrent inflamed nodules, abscesses, and sinus tracts in intertriginous regions.1 The genital area is affected in 11% of cases2 and usually is connected to severe forms of HS in both men and women.3 The prevalence of HS-associated genital lymphedema remains unknown.
Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation of the major penile lymphatic vessels that cause fibrosis of the surrounding connective tissue. Poor blood flow further causes contracture and distortion of the penile axis.4 Saxophone penis also has been associated with primary lymphedema, lymphogranuloma venereum, filariasis,5 and administration of paraffin injections.6 We describe 3 men with HS who presented with saxophone penis.
A 33-year-old man with Hurley stage III HS presented with a medical history of groin lesions and progressive penoscrotal edema of 13 years’ duration. He had a body mass index (BMI) of 37, no family history of HS or comorbidities, and a 15-year history of smoking 20 cigarettes per day. After repeated surgical drainage of the HS lesions as well as antibiotic treatment with clindamycin 600 mg/d and rifampicin 600 mg/d, the patient was kept on a maintenance therapy with adalimumab 40 mg/wk. Due to lack of response, treatment was discontinued at week 16. Clindamycin and rifampicin 300 mg were immediately reintroduced with no benefit on the genital lesions. The patient underwent genital reconstruction, including penile degloving, scrotoplasty, infrapubic fat pad removal, and perineoplasty (Figure 1). The patient currently is not undergoing any therapies.
A 55-year-old man presented with Hurley stage II HS of 33 years’ duration. He had a BMI of 52; a history of hypertension, hyperuricemia, severe hip and knee osteoarthritis, and orchiopexy in childhood; a smoking history of 40 cigarettes per day; and an alcohol consumption history of 200 mL per day since 18 years of age. He had radical excision of axillary lesions 8 years prior. One year later, he was treated with concomitant clindamycin and rifampicin 300 mg twice daily for 3 months with no desirable effects. Adalimumab 40 mg/wk was initiated. After 12 weeks of treatment, he experienced 80% improvement in all areas except the genital region. He continued adalimumab for 3 years with good clinical response in all HS-affected sites except the genital region.
A 66-year-old man presented with Hurley stage III HS of 37 years’ duration. He had a smoking history of 10 cigarettes per day for 30 years, a BMI of 24.6, and a medical history of long-standing hypertension and hypothyroidism. A 3-month course of clindamycin and rifampicin 600 mg/d was ineffective; adalimumab 40 mg/wk was initiated. All affected areas improved, except for the saxophone penis. He continues his fifth year of therapy with adalimumab (Figure 2).
Hidradenitis suppurativa is associated with chronic pain, purulent malodor, and scarring with structural deformity. Repetitive inflammation causes fibrosis, scar formation, and soft-tissue destruction of lymphatic vessels, leading to lymphedema; primary lymphedema of the genitals in men has been reported to result in a saxophone penis.4
The only approved biologic treatments for moderate to severe HS are the tumor necrosis factor α inhibitor adalimumab and anti-IL-17 secukinumab.1 All 3 of our patients with HS were treated with adalimumab with reasonable success; however, the penile condition remained refractory, which we speculate may be due to adalimumab’s ability to control only active inflammatory lesions but not scars or fibrotic tissue.7 Higher adalimumab dosages were unlikely to be beneficial for their penile condition; some improvements have been reported following fluoroquinolone therapy. To our knowledge, there is no effective medical treatment for saxophone penis. However, surgery showed good results in one of our patients. Among our 3 adalimumab-treated patients, only 1 patient had corrective surgery that resulted in improvement in the penile deformity, further confirming adalimumab’s limited role in genital lymphedema.7 Extensive resection of the lymphedematous tissue, scrotoplasty, and Charles procedure are treatment options.8
Genital lymphedema has been associated with lymphangiectasia, lymphangioma circumscriptum, infections, and neoplasms such as lymphangiosarcoma and squamous cell carcinoma.9 Our patients reported discomfort, hygiene issues, and swelling. One patient reported micturition, and 2 patients reported sexual dysfunction.
Saxophone penis remains a disabling sequela of HS. Early diagnosis and treatment of HS may help prevent development of this condition.
To the Editor:
Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease affecting 1% to 4% of Europeans. It is characterized by recurrent inflamed nodules, abscesses, and sinus tracts in intertriginous regions.1 The genital area is affected in 11% of cases2 and usually is connected to severe forms of HS in both men and women.3 The prevalence of HS-associated genital lymphedema remains unknown.
Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation of the major penile lymphatic vessels that cause fibrosis of the surrounding connective tissue. Poor blood flow further causes contracture and distortion of the penile axis.4 Saxophone penis also has been associated with primary lymphedema, lymphogranuloma venereum, filariasis,5 and administration of paraffin injections.6 We describe 3 men with HS who presented with saxophone penis.
A 33-year-old man with Hurley stage III HS presented with a medical history of groin lesions and progressive penoscrotal edema of 13 years’ duration. He had a body mass index (BMI) of 37, no family history of HS or comorbidities, and a 15-year history of smoking 20 cigarettes per day. After repeated surgical drainage of the HS lesions as well as antibiotic treatment with clindamycin 600 mg/d and rifampicin 600 mg/d, the patient was kept on a maintenance therapy with adalimumab 40 mg/wk. Due to lack of response, treatment was discontinued at week 16. Clindamycin and rifampicin 300 mg were immediately reintroduced with no benefit on the genital lesions. The patient underwent genital reconstruction, including penile degloving, scrotoplasty, infrapubic fat pad removal, and perineoplasty (Figure 1). The patient currently is not undergoing any therapies.
A 55-year-old man presented with Hurley stage II HS of 33 years’ duration. He had a BMI of 52; a history of hypertension, hyperuricemia, severe hip and knee osteoarthritis, and orchiopexy in childhood; a smoking history of 40 cigarettes per day; and an alcohol consumption history of 200 mL per day since 18 years of age. He had radical excision of axillary lesions 8 years prior. One year later, he was treated with concomitant clindamycin and rifampicin 300 mg twice daily for 3 months with no desirable effects. Adalimumab 40 mg/wk was initiated. After 12 weeks of treatment, he experienced 80% improvement in all areas except the genital region. He continued adalimumab for 3 years with good clinical response in all HS-affected sites except the genital region.
A 66-year-old man presented with Hurley stage III HS of 37 years’ duration. He had a smoking history of 10 cigarettes per day for 30 years, a BMI of 24.6, and a medical history of long-standing hypertension and hypothyroidism. A 3-month course of clindamycin and rifampicin 600 mg/d was ineffective; adalimumab 40 mg/wk was initiated. All affected areas improved, except for the saxophone penis. He continues his fifth year of therapy with adalimumab (Figure 2).
Hidradenitis suppurativa is associated with chronic pain, purulent malodor, and scarring with structural deformity. Repetitive inflammation causes fibrosis, scar formation, and soft-tissue destruction of lymphatic vessels, leading to lymphedema; primary lymphedema of the genitals in men has been reported to result in a saxophone penis.4
The only approved biologic treatments for moderate to severe HS are the tumor necrosis factor α inhibitor adalimumab and anti-IL-17 secukinumab.1 All 3 of our patients with HS were treated with adalimumab with reasonable success; however, the penile condition remained refractory, which we speculate may be due to adalimumab’s ability to control only active inflammatory lesions but not scars or fibrotic tissue.7 Higher adalimumab dosages were unlikely to be beneficial for their penile condition; some improvements have been reported following fluoroquinolone therapy. To our knowledge, there is no effective medical treatment for saxophone penis. However, surgery showed good results in one of our patients. Among our 3 adalimumab-treated patients, only 1 patient had corrective surgery that resulted in improvement in the penile deformity, further confirming adalimumab’s limited role in genital lymphedema.7 Extensive resection of the lymphedematous tissue, scrotoplasty, and Charles procedure are treatment options.8
Genital lymphedema has been associated with lymphangiectasia, lymphangioma circumscriptum, infections, and neoplasms such as lymphangiosarcoma and squamous cell carcinoma.9 Our patients reported discomfort, hygiene issues, and swelling. One patient reported micturition, and 2 patients reported sexual dysfunction.
Saxophone penis remains a disabling sequela of HS. Early diagnosis and treatment of HS may help prevent development of this condition.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Fertitta L, Hotz C, Wolkenstein P, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34:839-845.
- Micieli R, Alavi A. Lymphedema in patients with hidradenitis suppurativa: a systematic review of published literature. Int J Dermatol. 2018;57:1471-1480.
- Maatouk I, Moutran R. Saxophone penis. JAMA Dermatol. 2013;149:802.
- Koley S, Mandal RK. Saxophone penis after unilateral inguinal bubo of lymphogranuloma venereum. Indian J Sex Transm Dis AIDS. 2013;34:149-151.
- D’Antuono A, Lambertini M, Gaspari V, et al. Visual dermatology: self-induced chronic saxophone penis due to paraffin injections. J Cutan Med Surg. 2019;23:330.
- Musumeci ML, Scilletta A, Sorci F, et al. Genital lymphedema associated with hidradenitis suppurativa unresponsive to adalimumab treatment. JAAD Case Rep. 2019;5:326-328.
- Jain V, Singh S, Garge S, et al. Saxophone penis due to primary lymphoedema. J Indian Assoc Pediatr Surg. 2009;14:230-231.
- Moosbrugger EA, Mutasim DF. Hidradenitis suppurativa complicated by severe lymphedema and lymphangiectasias. J Am Acad Dermatol. 2011;64:1223-1224.
- Lee EY, Alhusayen R, Lansang P, et al. What is hidradenitis suppurativa? Can Fam Physician. 2017;63:114-120.
- Fertitta L, Hotz C, Wolkenstein P, et al. Efficacy and satisfaction of surgical treatment for hidradenitis suppurativa. J Eur Acad Dermatol Venereol. 2020;34:839-845.
- Micieli R, Alavi A. Lymphedema in patients with hidradenitis suppurativa: a systematic review of published literature. Int J Dermatol. 2018;57:1471-1480.
- Maatouk I, Moutran R. Saxophone penis. JAMA Dermatol. 2013;149:802.
- Koley S, Mandal RK. Saxophone penis after unilateral inguinal bubo of lymphogranuloma venereum. Indian J Sex Transm Dis AIDS. 2013;34:149-151.
- D’Antuono A, Lambertini M, Gaspari V, et al. Visual dermatology: self-induced chronic saxophone penis due to paraffin injections. J Cutan Med Surg. 2019;23:330.
- Musumeci ML, Scilletta A, Sorci F, et al. Genital lymphedema associated with hidradenitis suppurativa unresponsive to adalimumab treatment. JAAD Case Rep. 2019;5:326-328.
- Jain V, Singh S, Garge S, et al. Saxophone penis due to primary lymphoedema. J Indian Assoc Pediatr Surg. 2009;14:230-231.
- Moosbrugger EA, Mutasim DF. Hidradenitis suppurativa complicated by severe lymphedema and lymphangiectasias. J Am Acad Dermatol. 2011;64:1223-1224.
Practice Points
- Hidradenitis suppurativa (HS) is a multifactorial chronic inflammatory skin disease.
- Saxophone penis is a specific penile malformation characterized by a saxophone shape due to inflammation.
- Repetitive inflammation within the context of HS may cause structural deformity of the penis, resulting in a saxophone penis.
- Early diagnosis and treatment of HS may help prevent development of this condition.

Government Accuses Health System of Paying Docs Outrageous Salaries for Patient Referrals
Strapped for cash and searching for new profits, Tennessee-based Erlanger Health System illegally paid excessive salaries to physicians in exchange for patient referrals, the US government alleged in a federal lawsuit.
Erlanger changed its compensation model to entice revenue-generating doctors, paying some two to three times the median salary for their specialty, according to the complaint.
The physicians in turn referred numerous patients to Erlanger, and the health system submitted claims to Medicare for the referred services in violation of the Stark Law, according to the suit, filed in US District Court for the Western District of North Carolina.
The government’s complaint “serves as a warning” to healthcare providers who try to boost profits through improper financial arrangements with referring physicians, said Tamala E. Miles, Special Agent in Charge for the US Department of Health and Human Services (HHS) Office of Inspector General (OIG).
In a statement provided to this news organization, Erlanger denied the allegations and said it would “vigorously” defend the lawsuit.
“Erlanger paid physicians based on amounts that outside experts advised was fair market value,” Erlanger officials said in the statement. “Erlanger did not pay for referrals. A complete picture of the facts will demonstrate that the allegations lack merit and tell a very different story than what the government now claims.”
The Erlanger case is a reminder to physicians to consult their own knowledgeable advisors when considering financial arrangements with hospitals, said William Sarraille, JD, adjunct professor for the University of Maryland Francis King Carey School of Law in Baltimore and a regulatory consultant.
“There is a tendency by physicians when contracting ... to rely on [hospitals’] perceived compliance and legal expertise,” Mr. Sarraille told this news organization. “This case illustrates the risks in doing so. Sometimes bigger doesn’t translate into more sophisticated or more effective from a compliance perspective.”
Stark Law Prohibits Kickbacks
The Stark Law prohibits hospitals from billing the Centers for Medicare & Medicaid Services (CMS) for services referred by a physician with whom the hospital has an improper financial relationship.
CMS paid Erlanger about $27.8 million for claims stemming from the improper financial arrangements, the government contends.
“HHS-OIG will continue to investigate such deals to prevent financial arrangements that could compromise impartial medical judgment, increase healthcare costs, and erode public trust in the healthcare system,” Ms. Miles said in a statement.
Suit: Health System’s Money Woes Led to Illegal Arrangements
Erlanger’s financial troubles allegedly started after a previous run-in with the US government over false claims.
In 2005, Erlanger Health System agreed to pay the government $40 million to resolve allegations that it knowingly submitted false claims to Medicare, according to the government’s complaint. At the time, Erlanger entered into a Corporate Integrity Agreement (CIA) with the OIG that required Erlanger to put controls in place to ensure its financial relationships did not violate the Stark Law.
Erlanger’s agreement with OIG ended in 2010. Over the next 3 years, the health system lost nearly $32 million and in fiscal year 2013, had only 65 days of cash on hand, according to the government’s lawsuit.
Beginning in 2013, Erlanger allegedly implemented a strategy to increase profits by employing more physicians, particularly specialists from competing hospitals whose patients would need costly hospital stays, according to the complaint.
Once hired, Erlanger’s physicians were expected to treat patients at Erlanger’s hospitals and refer them to other providers within the health system, the suit claims. Erlanger also relaxed or eliminated the oversight and controls on physician compensation put in place under the CIA. For example, Erlanger’s CEO signed some compensation contracts before its chief compliance officer could review them and no longer allowed the compliance officer to vote on whether to approve compensation arrangements, according to the complaint.
Erlanger also changed its compensation model to include large salaries for medical director and academic positions and allegedly paid such salaries to physicians without ensuring the required work was performed. As a result, Erlanger physicians with profitable referrals were among the highest paid in the nation for their specialties, the government claims. For example, according to the complaint:
- Erlanger paid an electrophysiologist an annual clinical salary of $816,701, a medical director salary of $101,080, an academic salary of $59,322, and a productivity incentive based on work relative value units (wRVUs). The medical director and academic salaries paid were near the 90th percentile of comparable salaries in the specialty.
- The health system paid a neurosurgeon a base salary of $654,735, a productivity incentive based on wRVUs, and payments for excess call coverage ranging from $400 to $1000 per 24-hour shift. In 2016, the neurosurgeon made $500,000 in excess call payments.
- Erlanger paid a cardiothoracic surgeon a base clinical salary of $1,070,000, a sign-on bonus of $150,000, a retention bonus of $100,000 (payable in the 4th year of the contract), and a program incentive of up to $150,000 per year.
In addition, Erlanger ignored patient safety concerns about some of its high revenue-generating physicians, the government claims.
For instance, Erlanger received multiple complaints that a cardiothoracic surgeon was misusing an expensive form of life support in which pumps and oxygenators take over heart and lung function. Overuse of the equipment prolonged patients’ hospital stays and increased the hospital fees generated by the surgeon, according to the complaint. Staff also raised concerns about the cardiothoracic surgeon’s patient outcomes.
But Erlanger disregarded the concerns and in 2018, increased the cardiothoracic surgeon’s retention bonus from $100,000 to $250,000, the suit alleges. A year later, the health system increased his base salary from $1,070,000 to $1,195,000.
Health care compensation and billing consultants alerted Erlanger that it was overpaying salaries and handing out bonuses based on measures that overstated the work physicians were performing, but Erlanger ignored the warnings, according to the complaint.
Administrators allegedly resisted efforts by the chief compliance officer to hire an outside consultant to review its compensation models. Erlanger fired the compliance officer in 2019.
The former chief compliance officer and another administrator filed a whistleblower lawsuit against Erlanger in 2021. The two administrators are relators in the government’s July 2024 lawsuit.
How to Protect Yourself From Illegal Hospital Deals
The Erlanger case is the latest in a series of recent complaints by the federal government involving financial arrangements between hospitals and physicians.
In December 2023, Indianapolis-based Community Health Network Inc. agreed to pay the government $345 million to resolve claims that it paid physicians above fair market value and awarded bonuses tied to referrals in violation of the Stark Law.
Also in 2023, Saginaw, Michigan–based Covenant HealthCare and two physicians paid the government $69 million to settle allegations that administrators engaged in improper financial arrangements with referring physicians and a physician-owned investment group. In another 2023 case, Massachusetts Eye and Ear in Boston agreed to pay $5.7 million to resolve claims that some of its physician compensation plans violated the Stark Law.
Before you enter into a financial arrangement with a hospital, it’s also important to examine what percentile the aggregate compensation would reflect, law professor Mr. Sarraille said. The Erlanger case highlights federal officials’ suspicion of compensation, in aggregate, that exceeds the 90th percentile and increased attention to compensation that exceeds the 75th percentile, he said.
To research compensation levels, doctors can review the Medical Group Management Association’s annual compensation report or search its compensation data.
Before signing any contracts, Mr. Sarraille suggests, physicians should also consider whether the hospital shares the same values. Ask physicians at the hospital what they have to say about the hospital’s culture, vision, and values. Have physicians left the hospital after their practices were acquired? Consider speaking with them to learn why.
Keep in mind that a doctor’s reputation could be impacted by a compliance complaint, regardless of whether it’s directed at the hospital and not the employed physician, Mr. Sarraille said.
“The [Erlanger] complaint focuses on the compensation of specific, named physicians saying they were wildly overcompensated,” he said. “The implication is that they sold their referral power in exchange for a pay day. It’s a bad look, no matter how the case evolves from here.”
Physicians could also face their own liability risk under the Stark Law and False Claims Act, depending on the circumstances. In the event of related quality-of-care issues, medical liability could come into play, Mr. Sarraille noted. In such cases, plaintiffs’ attorneys may see an opportunity to boost their claims with allegations that the patient harm was a function of “chasing compensation dollars,” Mr. Sarraille said.
“Where that happens, plaintiff lawyers see the potential for crippling punitive damages, which might not be covered by an insurer,” he said.
A version of this article appeared on Medscape.com.
Strapped for cash and searching for new profits, Tennessee-based Erlanger Health System illegally paid excessive salaries to physicians in exchange for patient referrals, the US government alleged in a federal lawsuit.
Erlanger changed its compensation model to entice revenue-generating doctors, paying some two to three times the median salary for their specialty, according to the complaint.
The physicians in turn referred numerous patients to Erlanger, and the health system submitted claims to Medicare for the referred services in violation of the Stark Law, according to the suit, filed in US District Court for the Western District of North Carolina.
The government’s complaint “serves as a warning” to healthcare providers who try to boost profits through improper financial arrangements with referring physicians, said Tamala E. Miles, Special Agent in Charge for the US Department of Health and Human Services (HHS) Office of Inspector General (OIG).
In a statement provided to this news organization, Erlanger denied the allegations and said it would “vigorously” defend the lawsuit.
“Erlanger paid physicians based on amounts that outside experts advised was fair market value,” Erlanger officials said in the statement. “Erlanger did not pay for referrals. A complete picture of the facts will demonstrate that the allegations lack merit and tell a very different story than what the government now claims.”
The Erlanger case is a reminder to physicians to consult their own knowledgeable advisors when considering financial arrangements with hospitals, said William Sarraille, JD, adjunct professor for the University of Maryland Francis King Carey School of Law in Baltimore and a regulatory consultant.
“There is a tendency by physicians when contracting ... to rely on [hospitals’] perceived compliance and legal expertise,” Mr. Sarraille told this news organization. “This case illustrates the risks in doing so. Sometimes bigger doesn’t translate into more sophisticated or more effective from a compliance perspective.”
Stark Law Prohibits Kickbacks
The Stark Law prohibits hospitals from billing the Centers for Medicare & Medicaid Services (CMS) for services referred by a physician with whom the hospital has an improper financial relationship.
CMS paid Erlanger about $27.8 million for claims stemming from the improper financial arrangements, the government contends.
“HHS-OIG will continue to investigate such deals to prevent financial arrangements that could compromise impartial medical judgment, increase healthcare costs, and erode public trust in the healthcare system,” Ms. Miles said in a statement.
Suit: Health System’s Money Woes Led to Illegal Arrangements
Erlanger’s financial troubles allegedly started after a previous run-in with the US government over false claims.
In 2005, Erlanger Health System agreed to pay the government $40 million to resolve allegations that it knowingly submitted false claims to Medicare, according to the government’s complaint. At the time, Erlanger entered into a Corporate Integrity Agreement (CIA) with the OIG that required Erlanger to put controls in place to ensure its financial relationships did not violate the Stark Law.
Erlanger’s agreement with OIG ended in 2010. Over the next 3 years, the health system lost nearly $32 million and in fiscal year 2013, had only 65 days of cash on hand, according to the government’s lawsuit.
Beginning in 2013, Erlanger allegedly implemented a strategy to increase profits by employing more physicians, particularly specialists from competing hospitals whose patients would need costly hospital stays, according to the complaint.
Once hired, Erlanger’s physicians were expected to treat patients at Erlanger’s hospitals and refer them to other providers within the health system, the suit claims. Erlanger also relaxed or eliminated the oversight and controls on physician compensation put in place under the CIA. For example, Erlanger’s CEO signed some compensation contracts before its chief compliance officer could review them and no longer allowed the compliance officer to vote on whether to approve compensation arrangements, according to the complaint.
Erlanger also changed its compensation model to include large salaries for medical director and academic positions and allegedly paid such salaries to physicians without ensuring the required work was performed. As a result, Erlanger physicians with profitable referrals were among the highest paid in the nation for their specialties, the government claims. For example, according to the complaint:
- Erlanger paid an electrophysiologist an annual clinical salary of $816,701, a medical director salary of $101,080, an academic salary of $59,322, and a productivity incentive based on work relative value units (wRVUs). The medical director and academic salaries paid were near the 90th percentile of comparable salaries in the specialty.
- The health system paid a neurosurgeon a base salary of $654,735, a productivity incentive based on wRVUs, and payments for excess call coverage ranging from $400 to $1000 per 24-hour shift. In 2016, the neurosurgeon made $500,000 in excess call payments.
- Erlanger paid a cardiothoracic surgeon a base clinical salary of $1,070,000, a sign-on bonus of $150,000, a retention bonus of $100,000 (payable in the 4th year of the contract), and a program incentive of up to $150,000 per year.
In addition, Erlanger ignored patient safety concerns about some of its high revenue-generating physicians, the government claims.
For instance, Erlanger received multiple complaints that a cardiothoracic surgeon was misusing an expensive form of life support in which pumps and oxygenators take over heart and lung function. Overuse of the equipment prolonged patients’ hospital stays and increased the hospital fees generated by the surgeon, according to the complaint. Staff also raised concerns about the cardiothoracic surgeon’s patient outcomes.
But Erlanger disregarded the concerns and in 2018, increased the cardiothoracic surgeon’s retention bonus from $100,000 to $250,000, the suit alleges. A year later, the health system increased his base salary from $1,070,000 to $1,195,000.
Health care compensation and billing consultants alerted Erlanger that it was overpaying salaries and handing out bonuses based on measures that overstated the work physicians were performing, but Erlanger ignored the warnings, according to the complaint.
Administrators allegedly resisted efforts by the chief compliance officer to hire an outside consultant to review its compensation models. Erlanger fired the compliance officer in 2019.
The former chief compliance officer and another administrator filed a whistleblower lawsuit against Erlanger in 2021. The two administrators are relators in the government’s July 2024 lawsuit.
How to Protect Yourself From Illegal Hospital Deals
The Erlanger case is the latest in a series of recent complaints by the federal government involving financial arrangements between hospitals and physicians.
In December 2023, Indianapolis-based Community Health Network Inc. agreed to pay the government $345 million to resolve claims that it paid physicians above fair market value and awarded bonuses tied to referrals in violation of the Stark Law.
Also in 2023, Saginaw, Michigan–based Covenant HealthCare and two physicians paid the government $69 million to settle allegations that administrators engaged in improper financial arrangements with referring physicians and a physician-owned investment group. In another 2023 case, Massachusetts Eye and Ear in Boston agreed to pay $5.7 million to resolve claims that some of its physician compensation plans violated the Stark Law.
Before you enter into a financial arrangement with a hospital, it’s also important to examine what percentile the aggregate compensation would reflect, law professor Mr. Sarraille said. The Erlanger case highlights federal officials’ suspicion of compensation, in aggregate, that exceeds the 90th percentile and increased attention to compensation that exceeds the 75th percentile, he said.
To research compensation levels, doctors can review the Medical Group Management Association’s annual compensation report or search its compensation data.
Before signing any contracts, Mr. Sarraille suggests, physicians should also consider whether the hospital shares the same values. Ask physicians at the hospital what they have to say about the hospital’s culture, vision, and values. Have physicians left the hospital after their practices were acquired? Consider speaking with them to learn why.
Keep in mind that a doctor’s reputation could be impacted by a compliance complaint, regardless of whether it’s directed at the hospital and not the employed physician, Mr. Sarraille said.
“The [Erlanger] complaint focuses on the compensation of specific, named physicians saying they were wildly overcompensated,” he said. “The implication is that they sold their referral power in exchange for a pay day. It’s a bad look, no matter how the case evolves from here.”
Physicians could also face their own liability risk under the Stark Law and False Claims Act, depending on the circumstances. In the event of related quality-of-care issues, medical liability could come into play, Mr. Sarraille noted. In such cases, plaintiffs’ attorneys may see an opportunity to boost their claims with allegations that the patient harm was a function of “chasing compensation dollars,” Mr. Sarraille said.
“Where that happens, plaintiff lawyers see the potential for crippling punitive damages, which might not be covered by an insurer,” he said.
A version of this article appeared on Medscape.com.
Strapped for cash and searching for new profits, Tennessee-based Erlanger Health System illegally paid excessive salaries to physicians in exchange for patient referrals, the US government alleged in a federal lawsuit.
Erlanger changed its compensation model to entice revenue-generating doctors, paying some two to three times the median salary for their specialty, according to the complaint.
The physicians in turn referred numerous patients to Erlanger, and the health system submitted claims to Medicare for the referred services in violation of the Stark Law, according to the suit, filed in US District Court for the Western District of North Carolina.
The government’s complaint “serves as a warning” to healthcare providers who try to boost profits through improper financial arrangements with referring physicians, said Tamala E. Miles, Special Agent in Charge for the US Department of Health and Human Services (HHS) Office of Inspector General (OIG).
In a statement provided to this news organization, Erlanger denied the allegations and said it would “vigorously” defend the lawsuit.
“Erlanger paid physicians based on amounts that outside experts advised was fair market value,” Erlanger officials said in the statement. “Erlanger did not pay for referrals. A complete picture of the facts will demonstrate that the allegations lack merit and tell a very different story than what the government now claims.”
The Erlanger case is a reminder to physicians to consult their own knowledgeable advisors when considering financial arrangements with hospitals, said William Sarraille, JD, adjunct professor for the University of Maryland Francis King Carey School of Law in Baltimore and a regulatory consultant.
“There is a tendency by physicians when contracting ... to rely on [hospitals’] perceived compliance and legal expertise,” Mr. Sarraille told this news organization. “This case illustrates the risks in doing so. Sometimes bigger doesn’t translate into more sophisticated or more effective from a compliance perspective.”
Stark Law Prohibits Kickbacks
The Stark Law prohibits hospitals from billing the Centers for Medicare & Medicaid Services (CMS) for services referred by a physician with whom the hospital has an improper financial relationship.
CMS paid Erlanger about $27.8 million for claims stemming from the improper financial arrangements, the government contends.
“HHS-OIG will continue to investigate such deals to prevent financial arrangements that could compromise impartial medical judgment, increase healthcare costs, and erode public trust in the healthcare system,” Ms. Miles said in a statement.
Suit: Health System’s Money Woes Led to Illegal Arrangements
Erlanger’s financial troubles allegedly started after a previous run-in with the US government over false claims.
In 2005, Erlanger Health System agreed to pay the government $40 million to resolve allegations that it knowingly submitted false claims to Medicare, according to the government’s complaint. At the time, Erlanger entered into a Corporate Integrity Agreement (CIA) with the OIG that required Erlanger to put controls in place to ensure its financial relationships did not violate the Stark Law.
Erlanger’s agreement with OIG ended in 2010. Over the next 3 years, the health system lost nearly $32 million and in fiscal year 2013, had only 65 days of cash on hand, according to the government’s lawsuit.
Beginning in 2013, Erlanger allegedly implemented a strategy to increase profits by employing more physicians, particularly specialists from competing hospitals whose patients would need costly hospital stays, according to the complaint.
Once hired, Erlanger’s physicians were expected to treat patients at Erlanger’s hospitals and refer them to other providers within the health system, the suit claims. Erlanger also relaxed or eliminated the oversight and controls on physician compensation put in place under the CIA. For example, Erlanger’s CEO signed some compensation contracts before its chief compliance officer could review them and no longer allowed the compliance officer to vote on whether to approve compensation arrangements, according to the complaint.
Erlanger also changed its compensation model to include large salaries for medical director and academic positions and allegedly paid such salaries to physicians without ensuring the required work was performed. As a result, Erlanger physicians with profitable referrals were among the highest paid in the nation for their specialties, the government claims. For example, according to the complaint:
- Erlanger paid an electrophysiologist an annual clinical salary of $816,701, a medical director salary of $101,080, an academic salary of $59,322, and a productivity incentive based on work relative value units (wRVUs). The medical director and academic salaries paid were near the 90th percentile of comparable salaries in the specialty.
- The health system paid a neurosurgeon a base salary of $654,735, a productivity incentive based on wRVUs, and payments for excess call coverage ranging from $400 to $1000 per 24-hour shift. In 2016, the neurosurgeon made $500,000 in excess call payments.
- Erlanger paid a cardiothoracic surgeon a base clinical salary of $1,070,000, a sign-on bonus of $150,000, a retention bonus of $100,000 (payable in the 4th year of the contract), and a program incentive of up to $150,000 per year.
In addition, Erlanger ignored patient safety concerns about some of its high revenue-generating physicians, the government claims.
For instance, Erlanger received multiple complaints that a cardiothoracic surgeon was misusing an expensive form of life support in which pumps and oxygenators take over heart and lung function. Overuse of the equipment prolonged patients’ hospital stays and increased the hospital fees generated by the surgeon, according to the complaint. Staff also raised concerns about the cardiothoracic surgeon’s patient outcomes.
But Erlanger disregarded the concerns and in 2018, increased the cardiothoracic surgeon’s retention bonus from $100,000 to $250,000, the suit alleges. A year later, the health system increased his base salary from $1,070,000 to $1,195,000.
Health care compensation and billing consultants alerted Erlanger that it was overpaying salaries and handing out bonuses based on measures that overstated the work physicians were performing, but Erlanger ignored the warnings, according to the complaint.
Administrators allegedly resisted efforts by the chief compliance officer to hire an outside consultant to review its compensation models. Erlanger fired the compliance officer in 2019.
The former chief compliance officer and another administrator filed a whistleblower lawsuit against Erlanger in 2021. The two administrators are relators in the government’s July 2024 lawsuit.
How to Protect Yourself From Illegal Hospital Deals
The Erlanger case is the latest in a series of recent complaints by the federal government involving financial arrangements between hospitals and physicians.
In December 2023, Indianapolis-based Community Health Network Inc. agreed to pay the government $345 million to resolve claims that it paid physicians above fair market value and awarded bonuses tied to referrals in violation of the Stark Law.
Also in 2023, Saginaw, Michigan–based Covenant HealthCare and two physicians paid the government $69 million to settle allegations that administrators engaged in improper financial arrangements with referring physicians and a physician-owned investment group. In another 2023 case, Massachusetts Eye and Ear in Boston agreed to pay $5.7 million to resolve claims that some of its physician compensation plans violated the Stark Law.
Before you enter into a financial arrangement with a hospital, it’s also important to examine what percentile the aggregate compensation would reflect, law professor Mr. Sarraille said. The Erlanger case highlights federal officials’ suspicion of compensation, in aggregate, that exceeds the 90th percentile and increased attention to compensation that exceeds the 75th percentile, he said.
To research compensation levels, doctors can review the Medical Group Management Association’s annual compensation report or search its compensation data.
Before signing any contracts, Mr. Sarraille suggests, physicians should also consider whether the hospital shares the same values. Ask physicians at the hospital what they have to say about the hospital’s culture, vision, and values. Have physicians left the hospital after their practices were acquired? Consider speaking with them to learn why.
Keep in mind that a doctor’s reputation could be impacted by a compliance complaint, regardless of whether it’s directed at the hospital and not the employed physician, Mr. Sarraille said.
“The [Erlanger] complaint focuses on the compensation of specific, named physicians saying they were wildly overcompensated,” he said. “The implication is that they sold their referral power in exchange for a pay day. It’s a bad look, no matter how the case evolves from here.”
Physicians could also face their own liability risk under the Stark Law and False Claims Act, depending on the circumstances. In the event of related quality-of-care issues, medical liability could come into play, Mr. Sarraille noted. In such cases, plaintiffs’ attorneys may see an opportunity to boost their claims with allegations that the patient harm was a function of “chasing compensation dollars,” Mr. Sarraille said.
“Where that happens, plaintiff lawyers see the potential for crippling punitive damages, which might not be covered by an insurer,” he said.
A version of this article appeared on Medscape.com.
Air Pollution and Genetics May Raise Risk for Lupus
TOPLINE:
Chronic exposure to air pollutants such as fine particulate matter ≤ 2.5 μm in diameter (PM2.5), particulate matter ≤ 10 μm in diameter (PM10), nitrogen dioxide (NO2), and nitrogen oxides (NOX) increased the risk for systemic lupus erythematosus (SLE) onset. The risk was highest among those with high genetic risk and high air-pollution exposure.
METHODOLOGY:
- Researchers prospectively investigated the association between long-term exposure to air pollutants and incident SLE in 459,815 participants from the UK Biobank.
- A land-use regression model was used to quantify the annual average air pollution concentrations, including PM2.5, PM10, NO2, and NOX.
- The genetic susceptibility to lupus was assessed using polygenic risk scores (PRS), and the participants were classified into low–, intermediate–, or high–genetic-risk groups based on the tertiles of PRS.
- The joint effect of air pollutants and genetic susceptibility to lupus on the risk for incident SLE was evaluated, with the reference group consisting of participants with a low genetic risk and low exposure to air pollution.
TAKEAWAY:
- Over a median follow-up period of 11.77 years, 399 new cases of SLE were identified.
- The odds of developing SLE were higher among participants with high genetic risk than among those with low genetic risk (hazard ratio [HR], 3.45; P < .001 for trend).
- The risk for developing SLE was even higher among participants with a high genetic risk and high exposure to PM2.5 (adjusted HR [aHR], 4.16; 95% CI, 2.67-6.49), PM10 (aHR, 5.31; 95% CI, 3.30-8.55), NO2 (aHR, 5.61; 95% CI, 3.45-9.13), and NOX (aHR, 4.80; 95% CI, 3.00-7.66) than among with those with a low genetic risk and low exposure to air pollutants.
IN PRACTICE:
“Findings can inform the development of stricter air quality regulations to mitigate exposure to harmful pollutants, thereby reducing the risk of SLE,” the authors wrote.
SOURCE:
The study was led by Meiqi Xing, MASc, Huazhong University of Science and Technology, Wuhan, China. It was published online in Arthritis & Rheumatology.
LIMITATIONS:
The study participants were enrolled voluntarily, which may have led to selection bias because they might have been healthier or more health conscious. The study did not consider the specific components of air pollutants, particularly particulate matter, which may have varying effects on the incidence of SLE. Other air pollutants such as ozone, sulfur dioxide, and carbon monoxide were not included in the analysis.
DISCLOSURES:
This study did not disclose any funding source. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Chronic exposure to air pollutants such as fine particulate matter ≤ 2.5 μm in diameter (PM2.5), particulate matter ≤ 10 μm in diameter (PM10), nitrogen dioxide (NO2), and nitrogen oxides (NOX) increased the risk for systemic lupus erythematosus (SLE) onset. The risk was highest among those with high genetic risk and high air-pollution exposure.
METHODOLOGY:
- Researchers prospectively investigated the association between long-term exposure to air pollutants and incident SLE in 459,815 participants from the UK Biobank.
- A land-use regression model was used to quantify the annual average air pollution concentrations, including PM2.5, PM10, NO2, and NOX.
- The genetic susceptibility to lupus was assessed using polygenic risk scores (PRS), and the participants were classified into low–, intermediate–, or high–genetic-risk groups based on the tertiles of PRS.
- The joint effect of air pollutants and genetic susceptibility to lupus on the risk for incident SLE was evaluated, with the reference group consisting of participants with a low genetic risk and low exposure to air pollution.
TAKEAWAY:
- Over a median follow-up period of 11.77 years, 399 new cases of SLE were identified.
- The odds of developing SLE were higher among participants with high genetic risk than among those with low genetic risk (hazard ratio [HR], 3.45; P < .001 for trend).
- The risk for developing SLE was even higher among participants with a high genetic risk and high exposure to PM2.5 (adjusted HR [aHR], 4.16; 95% CI, 2.67-6.49), PM10 (aHR, 5.31; 95% CI, 3.30-8.55), NO2 (aHR, 5.61; 95% CI, 3.45-9.13), and NOX (aHR, 4.80; 95% CI, 3.00-7.66) than among with those with a low genetic risk and low exposure to air pollutants.
IN PRACTICE:
“Findings can inform the development of stricter air quality regulations to mitigate exposure to harmful pollutants, thereby reducing the risk of SLE,” the authors wrote.
SOURCE:
The study was led by Meiqi Xing, MASc, Huazhong University of Science and Technology, Wuhan, China. It was published online in Arthritis & Rheumatology.
LIMITATIONS:
The study participants were enrolled voluntarily, which may have led to selection bias because they might have been healthier or more health conscious. The study did not consider the specific components of air pollutants, particularly particulate matter, which may have varying effects on the incidence of SLE. Other air pollutants such as ozone, sulfur dioxide, and carbon monoxide were not included in the analysis.
DISCLOSURES:
This study did not disclose any funding source. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Chronic exposure to air pollutants such as fine particulate matter ≤ 2.5 μm in diameter (PM2.5), particulate matter ≤ 10 μm in diameter (PM10), nitrogen dioxide (NO2), and nitrogen oxides (NOX) increased the risk for systemic lupus erythematosus (SLE) onset. The risk was highest among those with high genetic risk and high air-pollution exposure.
METHODOLOGY:
- Researchers prospectively investigated the association between long-term exposure to air pollutants and incident SLE in 459,815 participants from the UK Biobank.
- A land-use regression model was used to quantify the annual average air pollution concentrations, including PM2.5, PM10, NO2, and NOX.
- The genetic susceptibility to lupus was assessed using polygenic risk scores (PRS), and the participants were classified into low–, intermediate–, or high–genetic-risk groups based on the tertiles of PRS.
- The joint effect of air pollutants and genetic susceptibility to lupus on the risk for incident SLE was evaluated, with the reference group consisting of participants with a low genetic risk and low exposure to air pollution.
TAKEAWAY:
- Over a median follow-up period of 11.77 years, 399 new cases of SLE were identified.
- The odds of developing SLE were higher among participants with high genetic risk than among those with low genetic risk (hazard ratio [HR], 3.45; P < .001 for trend).
- The risk for developing SLE was even higher among participants with a high genetic risk and high exposure to PM2.5 (adjusted HR [aHR], 4.16; 95% CI, 2.67-6.49), PM10 (aHR, 5.31; 95% CI, 3.30-8.55), NO2 (aHR, 5.61; 95% CI, 3.45-9.13), and NOX (aHR, 4.80; 95% CI, 3.00-7.66) than among with those with a low genetic risk and low exposure to air pollutants.
IN PRACTICE:
“Findings can inform the development of stricter air quality regulations to mitigate exposure to harmful pollutants, thereby reducing the risk of SLE,” the authors wrote.
SOURCE:
The study was led by Meiqi Xing, MASc, Huazhong University of Science and Technology, Wuhan, China. It was published online in Arthritis & Rheumatology.
LIMITATIONS:
The study participants were enrolled voluntarily, which may have led to selection bias because they might have been healthier or more health conscious. The study did not consider the specific components of air pollutants, particularly particulate matter, which may have varying effects on the incidence of SLE. Other air pollutants such as ozone, sulfur dioxide, and carbon monoxide were not included in the analysis.
DISCLOSURES:
This study did not disclose any funding source. The authors declared no conflicts of interest.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Non-Prescription Semaglutide Purchased Online Poses Risks
Semaglutide products sold online without a prescription may pose multiple risks to consumers, new research found.
Of six test purchases of semaglutide products offered online without a prescription, only three were actually received. The other three vendors demanded additional payment. Of the three delivered, one was potentially contaminated, and all three contained higher concentrations of semaglutide than indicated on the label, potentially resulting in an overdose.
“Semaglutide products are actively being sold without prescription by illegal online pharmacies, with vendors shipping unregistered and falsified products,” wrote Amir Reza Ashraf, PharmD, of the University of Pécs, Hungary, and colleagues in their paper, published online on August 2, 2024, in JAMA Network Open.
The study was conducted in July 2023, but its publication comes a week after the US Food and Drug Administration (FDA) issued an alert about dosing errors in compounded semaglutide, which typically does require a prescription.
Study coauthor Tim K. Mackey, PhD, told this news organization, “Compounding pharmacies are another element of this risk that has become more prominent now but arguably have more controls if prescribed appropriately, while the traditional ‘no-prescription’ online market still exists and will continue to evolve.”
Overall, said Dr. Mackey, professor of global health at the University of California San Diego and director of the Global Health Policy and Data Institute,
He advises clinicians to actively discuss with their patients the risks associated with semaglutide and, specifically, the dangers of buying it online. “Clinicians can act as a primary information source for patient safety information by letting their patients know about these risks ... and also asking where patients get their medications in case they are concerned about reports of adverse events or other patient safety issues.”
Buyer Beware: Online Semaglutide Purchases Not as They Seem
The investigators began by searching online for websites advertising semaglutide without a prescription. They ordered products from six online vendors that showed up prominently in the searches. Of those, three offered prefilled 0.25 mg/dose semaglutide injection pens, while the other three sold vials of lyophilized semaglutide powder to be reconstituted to solution for injection. Prices for the smallest dose and quantity ranged from $113 to $360.
Only three of the ordered products — all vials — actually showed up. The advertised prefilled pens were all nondelivery scams, with requests for an extra payment of $650-$1200 purportedly to clear customs. This was confirmed as fraudulent by customs agencies, the authors noted.
The three vial products were received and assessed physically, of both the packaging and the actual product, by liquid chromatography-mass spectrometry to determine purity and peptide concentration, and microbiologically, to examine sterility.
Using a checklist from the International Pharmaceutical Federation, Dr. Ashraf and colleagues found “clear discrepancies in regulatory registration information, accurate labeling, and evidence products were likely unregistered or unlicensed.”
Quality testing showed that one sample had an elevated presence of endotoxin suggesting possible contamination. While all three actually did contain semaglutide, the measured content exceeded the labeled amount by 29%-39%, posing a risk that users could receive up to 39% more than intended per injection, “particularly concerning if a consumer has to reconstitute and self-inject,” Dr. Mackey noted.
At least one of these sites in this study, “semaspace.com,” was subsequently sent a warning letter by the FDA for unauthorized semaglutide sale, Mackey noted.
Unfortunately, he told this news organization, these dangers are likely to persist. “There is a strong market opportunity to introduce counterfeit and unauthorized versions of semaglutide. Counterfeiters will continue to innovate with where they sell products, what products they offer, and how they mislead consumers about the safety and legality of what they are offering online. We are likely just at the beginning of counterfeiting of semaglutide, and it is likely that these false products will become endemic in our supply chain.”
The research was supported by the Hungarian Scientific Research Fund. The authors had no further disclosures.
A version of this article appeared on Medscape.com.
Semaglutide products sold online without a prescription may pose multiple risks to consumers, new research found.
Of six test purchases of semaglutide products offered online without a prescription, only three were actually received. The other three vendors demanded additional payment. Of the three delivered, one was potentially contaminated, and all three contained higher concentrations of semaglutide than indicated on the label, potentially resulting in an overdose.
“Semaglutide products are actively being sold without prescription by illegal online pharmacies, with vendors shipping unregistered and falsified products,” wrote Amir Reza Ashraf, PharmD, of the University of Pécs, Hungary, and colleagues in their paper, published online on August 2, 2024, in JAMA Network Open.
The study was conducted in July 2023, but its publication comes a week after the US Food and Drug Administration (FDA) issued an alert about dosing errors in compounded semaglutide, which typically does require a prescription.
Study coauthor Tim K. Mackey, PhD, told this news organization, “Compounding pharmacies are another element of this risk that has become more prominent now but arguably have more controls if prescribed appropriately, while the traditional ‘no-prescription’ online market still exists and will continue to evolve.”
Overall, said Dr. Mackey, professor of global health at the University of California San Diego and director of the Global Health Policy and Data Institute,
He advises clinicians to actively discuss with their patients the risks associated with semaglutide and, specifically, the dangers of buying it online. “Clinicians can act as a primary information source for patient safety information by letting their patients know about these risks ... and also asking where patients get their medications in case they are concerned about reports of adverse events or other patient safety issues.”
Buyer Beware: Online Semaglutide Purchases Not as They Seem
The investigators began by searching online for websites advertising semaglutide without a prescription. They ordered products from six online vendors that showed up prominently in the searches. Of those, three offered prefilled 0.25 mg/dose semaglutide injection pens, while the other three sold vials of lyophilized semaglutide powder to be reconstituted to solution for injection. Prices for the smallest dose and quantity ranged from $113 to $360.
Only three of the ordered products — all vials — actually showed up. The advertised prefilled pens were all nondelivery scams, with requests for an extra payment of $650-$1200 purportedly to clear customs. This was confirmed as fraudulent by customs agencies, the authors noted.
The three vial products were received and assessed physically, of both the packaging and the actual product, by liquid chromatography-mass spectrometry to determine purity and peptide concentration, and microbiologically, to examine sterility.
Using a checklist from the International Pharmaceutical Federation, Dr. Ashraf and colleagues found “clear discrepancies in regulatory registration information, accurate labeling, and evidence products were likely unregistered or unlicensed.”
Quality testing showed that one sample had an elevated presence of endotoxin suggesting possible contamination. While all three actually did contain semaglutide, the measured content exceeded the labeled amount by 29%-39%, posing a risk that users could receive up to 39% more than intended per injection, “particularly concerning if a consumer has to reconstitute and self-inject,” Dr. Mackey noted.
At least one of these sites in this study, “semaspace.com,” was subsequently sent a warning letter by the FDA for unauthorized semaglutide sale, Mackey noted.
Unfortunately, he told this news organization, these dangers are likely to persist. “There is a strong market opportunity to introduce counterfeit and unauthorized versions of semaglutide. Counterfeiters will continue to innovate with where they sell products, what products they offer, and how they mislead consumers about the safety and legality of what they are offering online. We are likely just at the beginning of counterfeiting of semaglutide, and it is likely that these false products will become endemic in our supply chain.”
The research was supported by the Hungarian Scientific Research Fund. The authors had no further disclosures.
A version of this article appeared on Medscape.com.
Semaglutide products sold online without a prescription may pose multiple risks to consumers, new research found.
Of six test purchases of semaglutide products offered online without a prescription, only three were actually received. The other three vendors demanded additional payment. Of the three delivered, one was potentially contaminated, and all three contained higher concentrations of semaglutide than indicated on the label, potentially resulting in an overdose.
“Semaglutide products are actively being sold without prescription by illegal online pharmacies, with vendors shipping unregistered and falsified products,” wrote Amir Reza Ashraf, PharmD, of the University of Pécs, Hungary, and colleagues in their paper, published online on August 2, 2024, in JAMA Network Open.
The study was conducted in July 2023, but its publication comes a week after the US Food and Drug Administration (FDA) issued an alert about dosing errors in compounded semaglutide, which typically does require a prescription.
Study coauthor Tim K. Mackey, PhD, told this news organization, “Compounding pharmacies are another element of this risk that has become more prominent now but arguably have more controls if prescribed appropriately, while the traditional ‘no-prescription’ online market still exists and will continue to evolve.”
Overall, said Dr. Mackey, professor of global health at the University of California San Diego and director of the Global Health Policy and Data Institute,
He advises clinicians to actively discuss with their patients the risks associated with semaglutide and, specifically, the dangers of buying it online. “Clinicians can act as a primary information source for patient safety information by letting their patients know about these risks ... and also asking where patients get their medications in case they are concerned about reports of adverse events or other patient safety issues.”
Buyer Beware: Online Semaglutide Purchases Not as They Seem
The investigators began by searching online for websites advertising semaglutide without a prescription. They ordered products from six online vendors that showed up prominently in the searches. Of those, three offered prefilled 0.25 mg/dose semaglutide injection pens, while the other three sold vials of lyophilized semaglutide powder to be reconstituted to solution for injection. Prices for the smallest dose and quantity ranged from $113 to $360.
Only three of the ordered products — all vials — actually showed up. The advertised prefilled pens were all nondelivery scams, with requests for an extra payment of $650-$1200 purportedly to clear customs. This was confirmed as fraudulent by customs agencies, the authors noted.
The three vial products were received and assessed physically, of both the packaging and the actual product, by liquid chromatography-mass spectrometry to determine purity and peptide concentration, and microbiologically, to examine sterility.
Using a checklist from the International Pharmaceutical Federation, Dr. Ashraf and colleagues found “clear discrepancies in regulatory registration information, accurate labeling, and evidence products were likely unregistered or unlicensed.”
Quality testing showed that one sample had an elevated presence of endotoxin suggesting possible contamination. While all three actually did contain semaglutide, the measured content exceeded the labeled amount by 29%-39%, posing a risk that users could receive up to 39% more than intended per injection, “particularly concerning if a consumer has to reconstitute and self-inject,” Dr. Mackey noted.
At least one of these sites in this study, “semaspace.com,” was subsequently sent a warning letter by the FDA for unauthorized semaglutide sale, Mackey noted.
Unfortunately, he told this news organization, these dangers are likely to persist. “There is a strong market opportunity to introduce counterfeit and unauthorized versions of semaglutide. Counterfeiters will continue to innovate with where they sell products, what products they offer, and how they mislead consumers about the safety and legality of what they are offering online. We are likely just at the beginning of counterfeiting of semaglutide, and it is likely that these false products will become endemic in our supply chain.”
The research was supported by the Hungarian Scientific Research Fund. The authors had no further disclosures.
A version of this article appeared on Medscape.com.
SUNY Downstate Emergency Medicine Doc Charged With $1.5M Fraud
In a case that spotlights the importance of comprehensive financial controls in medical offices,
Michael Lucchesi, MD, who had served as chairman of Emergency Medicine at SUNY Downstate Medical Center in New York City, was arraigned on July 9 and pleaded not guilty. Dr. Lucchesi’s attorney, Earl Ward, did not respond to messages from this news organization, but he told the New York Post that “the funds he used were not stolen funds.”
Dr. Lucchesi, who’s in his late 60s, faces nine counts of first- and second-degree grand larceny, first-degree falsifying business records, and third-degree criminal tax fraud. According to a press statement from the district attorney of Kings County, which encompasses the borough of Brooklyn, Dr. Lucchesi is accused of using his clinical practice’s business card for cash advances (about $115,000), high-end pet care ($176,000), personal travel ($348,000), gym membership and personal training ($109,000), catering ($52,000), tuition payments for his children ($46,000), and other expenses such as online shopping, flowers, liquor, and electronics.
Most of the alleged pet care spending — $120,000 — went to the Green Leaf Pet Resort, which has two locations in New Jersey, including one with “56 acres of nature and lots of tail wagging.” Some of the alleged spending on gym membership was at the New York Sports Clubs chain, where monthly membership tops out at $139.99.
The alleged spending occurred between 2016 and 2023 and was discovered by SUNY Downstate during an audit. Dr. Lucchesi reportedly left his position at the hospital, where he made $399,712 in 2022 as a professor, according to public records.
“As a high-ranking doctor at this vital healthcare institution, this defendant was entrusted with access to significant funds, which he allegedly exploited, stealing more than 1 million dollars to pay for a lavish lifestyle,” District Attorney Eric Gonzalez said in a statement.
SUNY Downstate is in a fight for its life amid efforts by New York Governor Kathy Hochul to shut it down. According to The New York Times, it is the only state-run hospital in New York City.
Dr. Lucchesi, who had previously served as the hospital’s chief medical officer and acting head, was released without bail. His next court date is September 25, 2024.
Size of Alleged Theft Is ‘Very Unusual’
David P. Weber, JD, DBA, a professor and fraud specialist at Salisbury University, Salisbury, Maryland, told this news organization that the fraudulent use of a business or purchase credit card is a form of embezzlement and “one of the most frequently seen types of frauds against organizations.”
William J. Kresse, JD, MSA, CPA/CFF, who studies fraud at Governors State University in University Park, Illinois, noted in an interview with this news organization that the high amount of alleged fraud in this case is “very unusual,” as is the period it is said to have occurred (over 6 years).
Mr. Kresse highlighted a 2024 report by the Association of Certified Fraud Examiners, which found that the median fraud loss in healthcare, on the basis of 117 cases, is $100,000. The most common form of fraud in the industry is corruption (47%), followed by billing (38%), noncash theft such as inventory (22%), and expense reimbursement (21%).
The details of the current case suggest that “SUNY Downstate had weak or insufficient internal controls to prevent this type of fraud,” Salisbury University’s Mr. Weber said. “However, research also makes clear that the tenure and position of the perpetrator play a significant role in the size of the fraud. Internal controls are supposed to apply to all employees, but the higher in the organization the perpetrator is, the easier it can be to engage in fraud.”
Even Small Medical Offices Can Act to Prevent Fraud
What can be done to prevent this kind of fraud? “Each employee should be required to submit actual receipts or scanned copies, and the reimbursement requests should be reviewed and inputted by a separate department or office of the organization to ensure that the expenses are legitimate,” Mr. Weber said. “In addition, all credit card statements should be available for review by the organization either simultaneously with the bill going to the employee or available for audit or review at any time without notification to the employee. Expenses that are in certain categories should be prohibited automatically and coded to the card so such a charge is rejected by the credit card bank.”
Smaller businesses — like many medical practices — may not have the manpower to handle these roles. In that case, Mr. Weber said, “The key is segregation or separation of duties. The bookkeeper cannot be the person receiving the bank statements, the payments from patients, and the invoices from vendors. There needs to be at least one other person in the loop to have some level of control.”
One strategy, he said, “is that the practice should institute a policy that only the doctor or owner of the practice can receive the mail, not the bookkeeper. Even if the practice leader does not actually review the bank statements, simply opening them before handing them off to the bookkeeper can provide a level of deterrence [since] the employee may get caught if someone else is reviewing the bank statements.”
A version of this article first appeared on Medscape.com.
In a case that spotlights the importance of comprehensive financial controls in medical offices,
Michael Lucchesi, MD, who had served as chairman of Emergency Medicine at SUNY Downstate Medical Center in New York City, was arraigned on July 9 and pleaded not guilty. Dr. Lucchesi’s attorney, Earl Ward, did not respond to messages from this news organization, but he told the New York Post that “the funds he used were not stolen funds.”
Dr. Lucchesi, who’s in his late 60s, faces nine counts of first- and second-degree grand larceny, first-degree falsifying business records, and third-degree criminal tax fraud. According to a press statement from the district attorney of Kings County, which encompasses the borough of Brooklyn, Dr. Lucchesi is accused of using his clinical practice’s business card for cash advances (about $115,000), high-end pet care ($176,000), personal travel ($348,000), gym membership and personal training ($109,000), catering ($52,000), tuition payments for his children ($46,000), and other expenses such as online shopping, flowers, liquor, and electronics.
Most of the alleged pet care spending — $120,000 — went to the Green Leaf Pet Resort, which has two locations in New Jersey, including one with “56 acres of nature and lots of tail wagging.” Some of the alleged spending on gym membership was at the New York Sports Clubs chain, where monthly membership tops out at $139.99.
The alleged spending occurred between 2016 and 2023 and was discovered by SUNY Downstate during an audit. Dr. Lucchesi reportedly left his position at the hospital, where he made $399,712 in 2022 as a professor, according to public records.
“As a high-ranking doctor at this vital healthcare institution, this defendant was entrusted with access to significant funds, which he allegedly exploited, stealing more than 1 million dollars to pay for a lavish lifestyle,” District Attorney Eric Gonzalez said in a statement.
SUNY Downstate is in a fight for its life amid efforts by New York Governor Kathy Hochul to shut it down. According to The New York Times, it is the only state-run hospital in New York City.
Dr. Lucchesi, who had previously served as the hospital’s chief medical officer and acting head, was released without bail. His next court date is September 25, 2024.
Size of Alleged Theft Is ‘Very Unusual’
David P. Weber, JD, DBA, a professor and fraud specialist at Salisbury University, Salisbury, Maryland, told this news organization that the fraudulent use of a business or purchase credit card is a form of embezzlement and “one of the most frequently seen types of frauds against organizations.”
William J. Kresse, JD, MSA, CPA/CFF, who studies fraud at Governors State University in University Park, Illinois, noted in an interview with this news organization that the high amount of alleged fraud in this case is “very unusual,” as is the period it is said to have occurred (over 6 years).
Mr. Kresse highlighted a 2024 report by the Association of Certified Fraud Examiners, which found that the median fraud loss in healthcare, on the basis of 117 cases, is $100,000. The most common form of fraud in the industry is corruption (47%), followed by billing (38%), noncash theft such as inventory (22%), and expense reimbursement (21%).
The details of the current case suggest that “SUNY Downstate had weak or insufficient internal controls to prevent this type of fraud,” Salisbury University’s Mr. Weber said. “However, research also makes clear that the tenure and position of the perpetrator play a significant role in the size of the fraud. Internal controls are supposed to apply to all employees, but the higher in the organization the perpetrator is, the easier it can be to engage in fraud.”
Even Small Medical Offices Can Act to Prevent Fraud
What can be done to prevent this kind of fraud? “Each employee should be required to submit actual receipts or scanned copies, and the reimbursement requests should be reviewed and inputted by a separate department or office of the organization to ensure that the expenses are legitimate,” Mr. Weber said. “In addition, all credit card statements should be available for review by the organization either simultaneously with the bill going to the employee or available for audit or review at any time without notification to the employee. Expenses that are in certain categories should be prohibited automatically and coded to the card so such a charge is rejected by the credit card bank.”
Smaller businesses — like many medical practices — may not have the manpower to handle these roles. In that case, Mr. Weber said, “The key is segregation or separation of duties. The bookkeeper cannot be the person receiving the bank statements, the payments from patients, and the invoices from vendors. There needs to be at least one other person in the loop to have some level of control.”
One strategy, he said, “is that the practice should institute a policy that only the doctor or owner of the practice can receive the mail, not the bookkeeper. Even if the practice leader does not actually review the bank statements, simply opening them before handing them off to the bookkeeper can provide a level of deterrence [since] the employee may get caught if someone else is reviewing the bank statements.”
A version of this article first appeared on Medscape.com.
In a case that spotlights the importance of comprehensive financial controls in medical offices,
Michael Lucchesi, MD, who had served as chairman of Emergency Medicine at SUNY Downstate Medical Center in New York City, was arraigned on July 9 and pleaded not guilty. Dr. Lucchesi’s attorney, Earl Ward, did not respond to messages from this news organization, but he told the New York Post that “the funds he used were not stolen funds.”
Dr. Lucchesi, who’s in his late 60s, faces nine counts of first- and second-degree grand larceny, first-degree falsifying business records, and third-degree criminal tax fraud. According to a press statement from the district attorney of Kings County, which encompasses the borough of Brooklyn, Dr. Lucchesi is accused of using his clinical practice’s business card for cash advances (about $115,000), high-end pet care ($176,000), personal travel ($348,000), gym membership and personal training ($109,000), catering ($52,000), tuition payments for his children ($46,000), and other expenses such as online shopping, flowers, liquor, and electronics.
Most of the alleged pet care spending — $120,000 — went to the Green Leaf Pet Resort, which has two locations in New Jersey, including one with “56 acres of nature and lots of tail wagging.” Some of the alleged spending on gym membership was at the New York Sports Clubs chain, where monthly membership tops out at $139.99.
The alleged spending occurred between 2016 and 2023 and was discovered by SUNY Downstate during an audit. Dr. Lucchesi reportedly left his position at the hospital, where he made $399,712 in 2022 as a professor, according to public records.
“As a high-ranking doctor at this vital healthcare institution, this defendant was entrusted with access to significant funds, which he allegedly exploited, stealing more than 1 million dollars to pay for a lavish lifestyle,” District Attorney Eric Gonzalez said in a statement.
SUNY Downstate is in a fight for its life amid efforts by New York Governor Kathy Hochul to shut it down. According to The New York Times, it is the only state-run hospital in New York City.
Dr. Lucchesi, who had previously served as the hospital’s chief medical officer and acting head, was released without bail. His next court date is September 25, 2024.
Size of Alleged Theft Is ‘Very Unusual’
David P. Weber, JD, DBA, a professor and fraud specialist at Salisbury University, Salisbury, Maryland, told this news organization that the fraudulent use of a business or purchase credit card is a form of embezzlement and “one of the most frequently seen types of frauds against organizations.”
William J. Kresse, JD, MSA, CPA/CFF, who studies fraud at Governors State University in University Park, Illinois, noted in an interview with this news organization that the high amount of alleged fraud in this case is “very unusual,” as is the period it is said to have occurred (over 6 years).
Mr. Kresse highlighted a 2024 report by the Association of Certified Fraud Examiners, which found that the median fraud loss in healthcare, on the basis of 117 cases, is $100,000. The most common form of fraud in the industry is corruption (47%), followed by billing (38%), noncash theft such as inventory (22%), and expense reimbursement (21%).
The details of the current case suggest that “SUNY Downstate had weak or insufficient internal controls to prevent this type of fraud,” Salisbury University’s Mr. Weber said. “However, research also makes clear that the tenure and position of the perpetrator play a significant role in the size of the fraud. Internal controls are supposed to apply to all employees, but the higher in the organization the perpetrator is, the easier it can be to engage in fraud.”
Even Small Medical Offices Can Act to Prevent Fraud
What can be done to prevent this kind of fraud? “Each employee should be required to submit actual receipts or scanned copies, and the reimbursement requests should be reviewed and inputted by a separate department or office of the organization to ensure that the expenses are legitimate,” Mr. Weber said. “In addition, all credit card statements should be available for review by the organization either simultaneously with the bill going to the employee or available for audit or review at any time without notification to the employee. Expenses that are in certain categories should be prohibited automatically and coded to the card so such a charge is rejected by the credit card bank.”
Smaller businesses — like many medical practices — may not have the manpower to handle these roles. In that case, Mr. Weber said, “The key is segregation or separation of duties. The bookkeeper cannot be the person receiving the bank statements, the payments from patients, and the invoices from vendors. There needs to be at least one other person in the loop to have some level of control.”
One strategy, he said, “is that the practice should institute a policy that only the doctor or owner of the practice can receive the mail, not the bookkeeper. Even if the practice leader does not actually review the bank statements, simply opening them before handing them off to the bookkeeper can provide a level of deterrence [since] the employee may get caught if someone else is reviewing the bank statements.”
A version of this article first appeared on Medscape.com.
Fruits and Vegetables May Promote Kidney and Cardiovascular Health in Hypertensive Patients
Progression of chronic kidney disease (CKD) and cardiovascular disease risk in hypertensive adults was significantly slower among those who consumed more fruits and vegetables or oral sodium bicarbonate, compared with controls who received usual care.
A primary focus on pharmacologic strategies has failed to reduced hypertension-related CKD and cardiovascular disease mortality, Nimrit Goraya, MD, of Texas A&M Health Sciences Center College of Medicine, Temple, and colleagues wrote. High-acid diets (those with greater amounts of animal-sourced foods) have been associated with increased incidence and progression of CKD and with increased risk of cardiovascular disease.
Diets high in fruits and vegetables are associated with reduced CKD and cardiovascular disease but are not routinely used as part of hypertension treatment. The researchers hypothesized that dietary acid reduction could slow kidney disease progression and reduce cardiovascular disease risk.
In a study published in The American Journal of Medicine, the researchers randomized 153 adults aged 18-70 years with hypertension and CKD to fruits and vegetables, oral sodium bicarbonate (NaHCO3), or usual care; 51 to each group. The fruit and vegetable group received 2-4 cups daily of base-producing food items including apples, apricots, oranges, peaches, pears, raisins, strawberries, carrots, cauliflower, eggplant, lettuce, potatoes, spinach, tomatoes, and zucchini. Participants were not instructed how to incorporate these foods into their diets. The sodium bicarbonate group received an average of four to five NaHCO3 tablets daily (650 mg), divided into two doses.
The mean age of the participants was 48.8 years, 51% were female, and 47% were African American. The primary outcome was CKD progression and cardiovascular disease risk over 5 years. All participants met criteria at baseline for macroalbuminuria (a urine albumin to creatinine ratio of at least 200 mg/g) and were considered at increased risk for CKD progression.
Over the 5-year follow-up, CKD progression was significantly slower in the groups receiving fruits and vegetables and oral sodium bicarbonate, compared with usual care, based on trajectories showing a lower decline of estimated glomerular filtration rates (mean declines of 1.08 and 1.17 for fruits/vegetables and NaHCO3, respectively, vs 19.4 for usual care, P < .001 for both).
However, systolic blood pressure and subsequent cardiovascular disease risk indicators were lower only in the fruit and vegetable group, compared with both the NaHCO3 or usual-care groups over the long term. “Specifically, with fruits and vegetables, systolic blood pressure, plasma LDL and Lp(a) cholesterol, and body mass index decreased from baseline, consistent with better cardiovascular disease protection,” the researchers wrote. The protection against cardiovascular disease in the fruits and vegetables group occurred with lower doses of antihypertensive and statin medications and was not affected by baseline differences in medication doses.
The findings were limited by several factors, including the lack of data on compliance with the NaHCO3 supplements, although urine net acid excretion in this group suggested increased alkali intake similar to that provided by fruits and vegetables, the researchers noted. Other limitations included the focus only on individuals with very high albuminuria.
More basic science studies are needed to explore how the potential vascular injury suggested by albuminuria affects CKD progression and cardiovascular disease, and clinical studies are needed to assess the impact of dietary acid reduction on patients with lower levels of albuminuria that the current study, the researchers said.
However, the results suggest that consuming fruits and vegetables, rather than NaHCO3, is the preferred strategy for dietary acid reduction for patients with primary hypertension and CKD, they concluded. The findings also support routine measurement of urine albumin-to-creatinine ratios in hypertensive patients to identify CKD and assess risk for progression and subsequent cardiovascular disease.
The study was supported by the Larry and Jane Woirhaye Memorial Endowment in Renal Research at the Texas Tech University Health Sciences Center, the University Medical Center (both in Lubbock, Texas), the Endowment, Academic Operations Division of Baylor Scott & White Health, and the Episcopal Health Foundation. The researchers had no financial conflicts to disclose.
Progression of chronic kidney disease (CKD) and cardiovascular disease risk in hypertensive adults was significantly slower among those who consumed more fruits and vegetables or oral sodium bicarbonate, compared with controls who received usual care.
A primary focus on pharmacologic strategies has failed to reduced hypertension-related CKD and cardiovascular disease mortality, Nimrit Goraya, MD, of Texas A&M Health Sciences Center College of Medicine, Temple, and colleagues wrote. High-acid diets (those with greater amounts of animal-sourced foods) have been associated with increased incidence and progression of CKD and with increased risk of cardiovascular disease.
Diets high in fruits and vegetables are associated with reduced CKD and cardiovascular disease but are not routinely used as part of hypertension treatment. The researchers hypothesized that dietary acid reduction could slow kidney disease progression and reduce cardiovascular disease risk.
In a study published in The American Journal of Medicine, the researchers randomized 153 adults aged 18-70 years with hypertension and CKD to fruits and vegetables, oral sodium bicarbonate (NaHCO3), or usual care; 51 to each group. The fruit and vegetable group received 2-4 cups daily of base-producing food items including apples, apricots, oranges, peaches, pears, raisins, strawberries, carrots, cauliflower, eggplant, lettuce, potatoes, spinach, tomatoes, and zucchini. Participants were not instructed how to incorporate these foods into their diets. The sodium bicarbonate group received an average of four to five NaHCO3 tablets daily (650 mg), divided into two doses.
The mean age of the participants was 48.8 years, 51% were female, and 47% were African American. The primary outcome was CKD progression and cardiovascular disease risk over 5 years. All participants met criteria at baseline for macroalbuminuria (a urine albumin to creatinine ratio of at least 200 mg/g) and were considered at increased risk for CKD progression.
Over the 5-year follow-up, CKD progression was significantly slower in the groups receiving fruits and vegetables and oral sodium bicarbonate, compared with usual care, based on trajectories showing a lower decline of estimated glomerular filtration rates (mean declines of 1.08 and 1.17 for fruits/vegetables and NaHCO3, respectively, vs 19.4 for usual care, P < .001 for both).
However, systolic blood pressure and subsequent cardiovascular disease risk indicators were lower only in the fruit and vegetable group, compared with both the NaHCO3 or usual-care groups over the long term. “Specifically, with fruits and vegetables, systolic blood pressure, plasma LDL and Lp(a) cholesterol, and body mass index decreased from baseline, consistent with better cardiovascular disease protection,” the researchers wrote. The protection against cardiovascular disease in the fruits and vegetables group occurred with lower doses of antihypertensive and statin medications and was not affected by baseline differences in medication doses.
The findings were limited by several factors, including the lack of data on compliance with the NaHCO3 supplements, although urine net acid excretion in this group suggested increased alkali intake similar to that provided by fruits and vegetables, the researchers noted. Other limitations included the focus only on individuals with very high albuminuria.
More basic science studies are needed to explore how the potential vascular injury suggested by albuminuria affects CKD progression and cardiovascular disease, and clinical studies are needed to assess the impact of dietary acid reduction on patients with lower levels of albuminuria that the current study, the researchers said.
However, the results suggest that consuming fruits and vegetables, rather than NaHCO3, is the preferred strategy for dietary acid reduction for patients with primary hypertension and CKD, they concluded. The findings also support routine measurement of urine albumin-to-creatinine ratios in hypertensive patients to identify CKD and assess risk for progression and subsequent cardiovascular disease.
The study was supported by the Larry and Jane Woirhaye Memorial Endowment in Renal Research at the Texas Tech University Health Sciences Center, the University Medical Center (both in Lubbock, Texas), the Endowment, Academic Operations Division of Baylor Scott & White Health, and the Episcopal Health Foundation. The researchers had no financial conflicts to disclose.
Progression of chronic kidney disease (CKD) and cardiovascular disease risk in hypertensive adults was significantly slower among those who consumed more fruits and vegetables or oral sodium bicarbonate, compared with controls who received usual care.
A primary focus on pharmacologic strategies has failed to reduced hypertension-related CKD and cardiovascular disease mortality, Nimrit Goraya, MD, of Texas A&M Health Sciences Center College of Medicine, Temple, and colleagues wrote. High-acid diets (those with greater amounts of animal-sourced foods) have been associated with increased incidence and progression of CKD and with increased risk of cardiovascular disease.
Diets high in fruits and vegetables are associated with reduced CKD and cardiovascular disease but are not routinely used as part of hypertension treatment. The researchers hypothesized that dietary acid reduction could slow kidney disease progression and reduce cardiovascular disease risk.
In a study published in The American Journal of Medicine, the researchers randomized 153 adults aged 18-70 years with hypertension and CKD to fruits and vegetables, oral sodium bicarbonate (NaHCO3), or usual care; 51 to each group. The fruit and vegetable group received 2-4 cups daily of base-producing food items including apples, apricots, oranges, peaches, pears, raisins, strawberries, carrots, cauliflower, eggplant, lettuce, potatoes, spinach, tomatoes, and zucchini. Participants were not instructed how to incorporate these foods into their diets. The sodium bicarbonate group received an average of four to five NaHCO3 tablets daily (650 mg), divided into two doses.
The mean age of the participants was 48.8 years, 51% were female, and 47% were African American. The primary outcome was CKD progression and cardiovascular disease risk over 5 years. All participants met criteria at baseline for macroalbuminuria (a urine albumin to creatinine ratio of at least 200 mg/g) and were considered at increased risk for CKD progression.
Over the 5-year follow-up, CKD progression was significantly slower in the groups receiving fruits and vegetables and oral sodium bicarbonate, compared with usual care, based on trajectories showing a lower decline of estimated glomerular filtration rates (mean declines of 1.08 and 1.17 for fruits/vegetables and NaHCO3, respectively, vs 19.4 for usual care, P < .001 for both).
However, systolic blood pressure and subsequent cardiovascular disease risk indicators were lower only in the fruit and vegetable group, compared with both the NaHCO3 or usual-care groups over the long term. “Specifically, with fruits and vegetables, systolic blood pressure, plasma LDL and Lp(a) cholesterol, and body mass index decreased from baseline, consistent with better cardiovascular disease protection,” the researchers wrote. The protection against cardiovascular disease in the fruits and vegetables group occurred with lower doses of antihypertensive and statin medications and was not affected by baseline differences in medication doses.
The findings were limited by several factors, including the lack of data on compliance with the NaHCO3 supplements, although urine net acid excretion in this group suggested increased alkali intake similar to that provided by fruits and vegetables, the researchers noted. Other limitations included the focus only on individuals with very high albuminuria.
More basic science studies are needed to explore how the potential vascular injury suggested by albuminuria affects CKD progression and cardiovascular disease, and clinical studies are needed to assess the impact of dietary acid reduction on patients with lower levels of albuminuria that the current study, the researchers said.
However, the results suggest that consuming fruits and vegetables, rather than NaHCO3, is the preferred strategy for dietary acid reduction for patients with primary hypertension and CKD, they concluded. The findings also support routine measurement of urine albumin-to-creatinine ratios in hypertensive patients to identify CKD and assess risk for progression and subsequent cardiovascular disease.
The study was supported by the Larry and Jane Woirhaye Memorial Endowment in Renal Research at the Texas Tech University Health Sciences Center, the University Medical Center (both in Lubbock, Texas), the Endowment, Academic Operations Division of Baylor Scott & White Health, and the Episcopal Health Foundation. The researchers had no financial conflicts to disclose.
FROM THE AMERICAN JOURNAL OF MEDICINE
FDA Approves First Engineered Cell Therapy for a Solid Tumor
Afami-cel — the first engineered cell therapy for a solid tumor — is indicated specifically for adults with unresectable or metastatic synovial sarcoma who have received prior chemotherapy, are positive for several human leukocyte antigens (HLAs), and whose tumors express melanoma-associated antigen A4, as determined by FDA-authorized companion diagnostic devices.
The single-dose treatment targets solid tumors expressing melanoma-associated antigen A4, a protein highly expressed in synovial sarcoma.
Synovial sarcoma is a rare form of cancer, which affects about 1000 people in the US each year. Malignant cells develop and form a tumor in soft tissues, often in the extremities.
“Adults with metastatic synovial sarcoma, a life-threatening form of cancer, often face limited treatment options in addition to the risk of cancer spread or recurrence,” Nicole Verdun, MD, director of the Office of Therapeutic Products in the FDA’s Center for Biologics Evaluation and Research, said in the agency press release announcing the approval. “Today’s approval represents a significant milestone in the development of an innovative, safe and effective therapy for patients with this rare but potentially fatal disease.”
T-cell receptor therapy, like chimeric antigen receptor (CAR) T-cell (CAR-T) therapy, involves altering patient T cells to fight cancer. While CAR-T therapy inserts an artificial receptor to target a specific surface protein on cancer cells, the T-cell receptor therapy modifies existing receptors to recognize an array of antigens on the surface of cancer cells — a promising strategy for targeting solid tumors.
The accelerated approval of afami-cel was based on the phase 2 SPEARHEAD-1 trial in 44 patients with synovial sarcoma who received a single infusion of the therapy. The trial had enrolled 52 patients, but 8 did not receive afami-cel, including 3 who died and 1 who withdrew.
According to the FDA announcement, the overall response rate was 43.2%, with a median time to response of 4.9 weeks. The median duration of response was 6 months (95% CI, 4.6 months to not reached). Among patients who responded, 39% had a duration of response of 12 months or longer.
“These results suggest that a one-time treatment with afami-cel has the potential to extend life while allowing responders to go off chemotherapy,” said lead investigator Sandra D’Angelo, MD, a sarcoma specialist at Memorial Sloan Kettering Cancer Center in New York City, in a company press release.
The prescribing information includes a boxed warning for serious or fatal cytokine release syndrome.
The most common nonlaboratory adverse reactions, occurring in at least 20% of patients, included cytokine release syndrome, nausea, vomiting, fatigue, infections, pyrexia, constipation, dyspnea, tachycardia, hypotension, diarrhea, and edema. The most common grade 3 or 4 laboratory abnormalities, occurring in at least 20% of patients, included decreased lymphocyte count, neutrophil count, white cell blood count, red blood cell, and platelet count.
The recommended dose is between 2.68x109 to 10x109 MAGE-A4 T-cell receptor–positive T-cells. The FDA notice specifies not using a leukodepleting filter or prophylactic systemic corticosteroids.
The list price for the one-time therapy is $727,000, according to Fierce Pharma.
A version of this article first appeared on Medscape.com.
Afami-cel — the first engineered cell therapy for a solid tumor — is indicated specifically for adults with unresectable or metastatic synovial sarcoma who have received prior chemotherapy, are positive for several human leukocyte antigens (HLAs), and whose tumors express melanoma-associated antigen A4, as determined by FDA-authorized companion diagnostic devices.
The single-dose treatment targets solid tumors expressing melanoma-associated antigen A4, a protein highly expressed in synovial sarcoma.
Synovial sarcoma is a rare form of cancer, which affects about 1000 people in the US each year. Malignant cells develop and form a tumor in soft tissues, often in the extremities.
“Adults with metastatic synovial sarcoma, a life-threatening form of cancer, often face limited treatment options in addition to the risk of cancer spread or recurrence,” Nicole Verdun, MD, director of the Office of Therapeutic Products in the FDA’s Center for Biologics Evaluation and Research, said in the agency press release announcing the approval. “Today’s approval represents a significant milestone in the development of an innovative, safe and effective therapy for patients with this rare but potentially fatal disease.”
T-cell receptor therapy, like chimeric antigen receptor (CAR) T-cell (CAR-T) therapy, involves altering patient T cells to fight cancer. While CAR-T therapy inserts an artificial receptor to target a specific surface protein on cancer cells, the T-cell receptor therapy modifies existing receptors to recognize an array of antigens on the surface of cancer cells — a promising strategy for targeting solid tumors.
The accelerated approval of afami-cel was based on the phase 2 SPEARHEAD-1 trial in 44 patients with synovial sarcoma who received a single infusion of the therapy. The trial had enrolled 52 patients, but 8 did not receive afami-cel, including 3 who died and 1 who withdrew.
According to the FDA announcement, the overall response rate was 43.2%, with a median time to response of 4.9 weeks. The median duration of response was 6 months (95% CI, 4.6 months to not reached). Among patients who responded, 39% had a duration of response of 12 months or longer.
“These results suggest that a one-time treatment with afami-cel has the potential to extend life while allowing responders to go off chemotherapy,” said lead investigator Sandra D’Angelo, MD, a sarcoma specialist at Memorial Sloan Kettering Cancer Center in New York City, in a company press release.
The prescribing information includes a boxed warning for serious or fatal cytokine release syndrome.
The most common nonlaboratory adverse reactions, occurring in at least 20% of patients, included cytokine release syndrome, nausea, vomiting, fatigue, infections, pyrexia, constipation, dyspnea, tachycardia, hypotension, diarrhea, and edema. The most common grade 3 or 4 laboratory abnormalities, occurring in at least 20% of patients, included decreased lymphocyte count, neutrophil count, white cell blood count, red blood cell, and platelet count.
The recommended dose is between 2.68x109 to 10x109 MAGE-A4 T-cell receptor–positive T-cells. The FDA notice specifies not using a leukodepleting filter or prophylactic systemic corticosteroids.
The list price for the one-time therapy is $727,000, according to Fierce Pharma.
A version of this article first appeared on Medscape.com.
Afami-cel — the first engineered cell therapy for a solid tumor — is indicated specifically for adults with unresectable or metastatic synovial sarcoma who have received prior chemotherapy, are positive for several human leukocyte antigens (HLAs), and whose tumors express melanoma-associated antigen A4, as determined by FDA-authorized companion diagnostic devices.
The single-dose treatment targets solid tumors expressing melanoma-associated antigen A4, a protein highly expressed in synovial sarcoma.
Synovial sarcoma is a rare form of cancer, which affects about 1000 people in the US each year. Malignant cells develop and form a tumor in soft tissues, often in the extremities.
“Adults with metastatic synovial sarcoma, a life-threatening form of cancer, often face limited treatment options in addition to the risk of cancer spread or recurrence,” Nicole Verdun, MD, director of the Office of Therapeutic Products in the FDA’s Center for Biologics Evaluation and Research, said in the agency press release announcing the approval. “Today’s approval represents a significant milestone in the development of an innovative, safe and effective therapy for patients with this rare but potentially fatal disease.”
T-cell receptor therapy, like chimeric antigen receptor (CAR) T-cell (CAR-T) therapy, involves altering patient T cells to fight cancer. While CAR-T therapy inserts an artificial receptor to target a specific surface protein on cancer cells, the T-cell receptor therapy modifies existing receptors to recognize an array of antigens on the surface of cancer cells — a promising strategy for targeting solid tumors.
The accelerated approval of afami-cel was based on the phase 2 SPEARHEAD-1 trial in 44 patients with synovial sarcoma who received a single infusion of the therapy. The trial had enrolled 52 patients, but 8 did not receive afami-cel, including 3 who died and 1 who withdrew.
According to the FDA announcement, the overall response rate was 43.2%, with a median time to response of 4.9 weeks. The median duration of response was 6 months (95% CI, 4.6 months to not reached). Among patients who responded, 39% had a duration of response of 12 months or longer.
“These results suggest that a one-time treatment with afami-cel has the potential to extend life while allowing responders to go off chemotherapy,” said lead investigator Sandra D’Angelo, MD, a sarcoma specialist at Memorial Sloan Kettering Cancer Center in New York City, in a company press release.
The prescribing information includes a boxed warning for serious or fatal cytokine release syndrome.
The most common nonlaboratory adverse reactions, occurring in at least 20% of patients, included cytokine release syndrome, nausea, vomiting, fatigue, infections, pyrexia, constipation, dyspnea, tachycardia, hypotension, diarrhea, and edema. The most common grade 3 or 4 laboratory abnormalities, occurring in at least 20% of patients, included decreased lymphocyte count, neutrophil count, white cell blood count, red blood cell, and platelet count.
The recommended dose is between 2.68x109 to 10x109 MAGE-A4 T-cell receptor–positive T-cells. The FDA notice specifies not using a leukodepleting filter or prophylactic systemic corticosteroids.
The list price for the one-time therapy is $727,000, according to Fierce Pharma.
A version of this article first appeared on Medscape.com.