User login
The ERAS Supplemental Application: Current Status and Recommendations for Dermatology Applicants and Programs
In the 2021-2022 residency application cycle, the Association of American Medical Colleges (AAMC) piloted a supplemental application to accompany the standard residency application submitted via the AAMC’s Electronic Residency Application Service (ERAS).1 Dermatology was 1 of 3 specialties to participate in the pilot alongside internal medicine and general surgery. The goal was to develop a tool that could align applicants with programs that best matched their career goals as well as program and geographic preferences. The Association of Professors of Dermatology Residency Program Directors Section was an early advocate for the supplemental application, and members of our leadership were involved in the design, implementation, and evaluation of the pilot supplemental application.
Participating in the supplemental application was optional for both applicants and programs. The supplemental application included a Past Experiences section, which allowed applicants to highlight their 5 most meaningful research, work, and/or volunteer experiences and to describe a challenging life event that might not otherwise be included with their application. The geographic preferences section permitted applicants to select up to 3 regions of interest as well as to indicate an urban vs rural preference. Lastly, a preference-signaling section allowed dermatology applicants to send signals to up to 3 programs of particular interest.
With the close of another application cycle, applicants and programs will begin preparing for the 2022-2023 recruitment season. In this column, we present dermatology-specific data regarding the supplemental application, highlight tentative changes for the upcoming application cycle, and offer tips for applicants and programs as we approach year 2 of the supplemental application.
Results of Supplemental Application Evaluation Surveys
During the 2021-2022 recruitment season, 93% (950/1019) of dermatology applicants submitted the supplemental application, and 87% (117/135) of dermatology residency programs participated in the pilot.2 Surveys conducted by the AAMC between October 2021 and January 2022 showed that a large majority of dermatology programs used supplemental application data during initial application review when deciding who to interview. Eighty-three percent (40/48) of program directors felt that preference signals in particular helped them identify applicants they would have otherwise overlooked. Fifty-seven percent (4288/7516) of applicants across all specialties that participated in the pilot felt that preference signals would help them be noticed by their preferred programs.2 Preference signals were not evenly distributed among dermatology programs. Programs received an average of 23 signals, with a range of 2 to 87 (AAMC, unpublished data, February 2022).
Additional questions remain to be answered: How does the number of signals received affect application review? How often do geographic and program signals convert to interview offers and matches? Regardless, enthusiasm among dermatology programs for the supplemental application remains. In a recent survey of Association of Professors of Dermatology program directors, all 43 respondents planned to participate in the supplemental application again in the upcoming year (Ilana Rosman, MD; unpublished data; February 2022). The pilot will be expanded to include at least 12 other specialties.1As many who reviewed residency applications in 2021-2022 will attest, there was difficulty accessing the supplemental application data because it was not integrated into the Program Directors’ Work Station, the ERAS platform for programs to access applications, which will be remedied for the 2022-2023 iteration. Other tentative changes include modifications to the past experiences sections and timeline of the application.2
Utilizing the Supplemental Application: Recommendations to Applicants
Format of the Application—Applicants should familiarize themselves with the format of the supplemental application in advance and give themselves sufficient time to complete the application. In general, 3 to 4 hours of focused work should be enough time. Applicants should proofread for grammar and spelling before submitting.
Past Experiences—The past experiences section is intended to provide a focused snapshot of an applicant’s most meaningful activities and unique path to residency. Applicants should answer honestly based on their interests. If a student’s focus has been on volunteerism, the bulk of their 5 experiences listed may be related to service. Similarly, a student who has focused on research may preferentially highlight those experiences. In place of the long list of research, volunteer, and work experiences in the traditional ERAS application, applicants can highlight those activities in which they have been most invested. Applicants are encouraged to reflect on all genres of activities at any stage of their careers, even those not medical in nature, including work experience, military service, college athletics, or sustained musical or artistic achievement. Applicants should explain why each experience is meaningful rather than simply describing the activity.
Applicants also have the option to share a notable challenge they have overcome. It is not expected that each applicant will complete this question; in general, applicants who have not faced notable personal or professional obstacles should avoid answering. Additionally, if these challenges have been discussed in other areas of the application—for example, in the personal statement or medical student performance evaluation—it is not necessary to restate them here, though applicants can choose to do so. Examples of topics a student might discuss include being a first-generation college or medical student, growing up in poverty, facing notable personal or family health challenges, or having limited educational opportunities. It is important to share how this experience impacted an applicant’s journey to dermatology residency.
Geographic Preferences—The geographic preferences section can be difficult for applicants to navigate, as it may involve balancing a desire to attend a residency program in a particular region vs a greater desire to simply match in dermatology. In the past, programs may have made assumptions about geographic preferences based on an applicant’s birthplace, hometown, or medical school. In the supplemental application, applicants have the opportunity to directly reveal their preferences. We encourage applicants to be candid. Selecting a geographic region will not necessarily exclude applicants from consideration at other programs. For some applicants, program qualities may be more important than geography, or there may be no regional preferences. Those applicants can choose “no geographic preference.” There is considerable variability in how programs use geographic preferences. For this reason, it is in the best interest of applicants to simply respond honestly.
Preference Signaling—Preference signaling allows applicants to signal up to 3 preferred programs. Dermatology program directors agree that applicants should not signal their home program or programs at which they did in-person away rotations, as those programs would already be aware of the applicant’s interest. Although a signal increases the chances that the application will be reviewed holistically, it does not guarantee an interview offer. Programs may differentially utilize signals depending on multiple factors, including the number of signals received. We encourage applicants to discuss preference signaling strategies with advisors and focus on signaling programs in which they have genuine interest.
Recommendations to Selection Committees and Program Directors
The intent of the supplemental application is to provide a more meaningful picture of applicants and their experiences and preferences, with the goal of optimizing applicant-program fit. Programs should explicitly define for themselves the applicant characteristics and experiences they prioritize as well as their program goals. The supplemental application offers the potential to streamline holistic application review based on these elements. The short essay answers in the past experiences section permit reviewers to quickly scan for important experiences that align with the program’s recruitment goals. Importantly, reviewers should not penalize applicants who have not completed the question regarding other impactful life experiences, as not all applicants will have relevant information to share.
Some programs may find the geographic preferences section more valuable than others. Multiple factors affect how much weight will be given to geographic preferences, including program location and other characteristics that affect the desirability of the program to applicants. The competitiveness of the field, relatively low match rate, and limited number of programs may lead to less emphasis on geographic preferences in dermatology compared to other specialties. The purpose of this section is not to exclude applicants but to give programs more information that may help with alignment.
Anecdotally, many dermatology program directors were most interested in the preference signaling section of the supplemental application. Programs should consider signals to be evidence of strong preliminary interest. Programs may utilize signals differently depending on many factors such as the overall competitiveness of the program, program location, and the total number of signals the program receives. We recommend that programs holistically review all applications accompanied by a signal. Programs that utilize a points system may choose to award a certain number of points for a signal to their program. A signal might have a higher value at a program that receives only a few signals; conversely, a program that receives a large number of signals might not place tremendous value on the signal but may use it as a tiebreaker between similarly qualified applicants. Preference signaling is solely a tool for application review; because applicants’ preferences may change after the interview process, signals should not be utilized during ranking.
Next Steps
For program directors who have excitedly awaited residency application reform, the supplemental ERAS application is an important first step. Ultimately, we hope the supplemental application supplants much of the current residency application, serving as an efficient high-yield tool for holistically evaluating applicants’ academic and service records, accomplishments, and training preferences. Arriving at a new application will undoubtedly take time and discussion among the various stakeholders. Please continue to complete surveys from the AAMC, as feedback is the best method for refining the tool to serve its intended purpose.
Optimization of the application content is only one component of the reforms needed to improve the application process. Even with a revamped application tool, holistic review is challenging when programs are inundated with an ever-increasing number of applications. As such, we encourage stakeholders to simultaneously consider other potential reforms, such as caps on the number of applications, to allow programs and applicants the best opportunity for a mutually successful match.
- Supplemental ERAS application. Association of American Medical Colleges website. Accessed May 9, 2022. https://students-residents.aamc.org/applying-residencies-eras/supplemental-eras-application-eras-2023-cycle
- Association of American Medical Colleges. Supplemental application data and reports. Accessed May 9, 2022. https://www.aamc.org/data-reports/students-residents/report/supplemental-eras-application-data-and-reports
In the 2021-2022 residency application cycle, the Association of American Medical Colleges (AAMC) piloted a supplemental application to accompany the standard residency application submitted via the AAMC’s Electronic Residency Application Service (ERAS).1 Dermatology was 1 of 3 specialties to participate in the pilot alongside internal medicine and general surgery. The goal was to develop a tool that could align applicants with programs that best matched their career goals as well as program and geographic preferences. The Association of Professors of Dermatology Residency Program Directors Section was an early advocate for the supplemental application, and members of our leadership were involved in the design, implementation, and evaluation of the pilot supplemental application.
Participating in the supplemental application was optional for both applicants and programs. The supplemental application included a Past Experiences section, which allowed applicants to highlight their 5 most meaningful research, work, and/or volunteer experiences and to describe a challenging life event that might not otherwise be included with their application. The geographic preferences section permitted applicants to select up to 3 regions of interest as well as to indicate an urban vs rural preference. Lastly, a preference-signaling section allowed dermatology applicants to send signals to up to 3 programs of particular interest.
With the close of another application cycle, applicants and programs will begin preparing for the 2022-2023 recruitment season. In this column, we present dermatology-specific data regarding the supplemental application, highlight tentative changes for the upcoming application cycle, and offer tips for applicants and programs as we approach year 2 of the supplemental application.
Results of Supplemental Application Evaluation Surveys
During the 2021-2022 recruitment season, 93% (950/1019) of dermatology applicants submitted the supplemental application, and 87% (117/135) of dermatology residency programs participated in the pilot.2 Surveys conducted by the AAMC between October 2021 and January 2022 showed that a large majority of dermatology programs used supplemental application data during initial application review when deciding who to interview. Eighty-three percent (40/48) of program directors felt that preference signals in particular helped them identify applicants they would have otherwise overlooked. Fifty-seven percent (4288/7516) of applicants across all specialties that participated in the pilot felt that preference signals would help them be noticed by their preferred programs.2 Preference signals were not evenly distributed among dermatology programs. Programs received an average of 23 signals, with a range of 2 to 87 (AAMC, unpublished data, February 2022).
Additional questions remain to be answered: How does the number of signals received affect application review? How often do geographic and program signals convert to interview offers and matches? Regardless, enthusiasm among dermatology programs for the supplemental application remains. In a recent survey of Association of Professors of Dermatology program directors, all 43 respondents planned to participate in the supplemental application again in the upcoming year (Ilana Rosman, MD; unpublished data; February 2022). The pilot will be expanded to include at least 12 other specialties.1As many who reviewed residency applications in 2021-2022 will attest, there was difficulty accessing the supplemental application data because it was not integrated into the Program Directors’ Work Station, the ERAS platform for programs to access applications, which will be remedied for the 2022-2023 iteration. Other tentative changes include modifications to the past experiences sections and timeline of the application.2
Utilizing the Supplemental Application: Recommendations to Applicants
Format of the Application—Applicants should familiarize themselves with the format of the supplemental application in advance and give themselves sufficient time to complete the application. In general, 3 to 4 hours of focused work should be enough time. Applicants should proofread for grammar and spelling before submitting.
Past Experiences—The past experiences section is intended to provide a focused snapshot of an applicant’s most meaningful activities and unique path to residency. Applicants should answer honestly based on their interests. If a student’s focus has been on volunteerism, the bulk of their 5 experiences listed may be related to service. Similarly, a student who has focused on research may preferentially highlight those experiences. In place of the long list of research, volunteer, and work experiences in the traditional ERAS application, applicants can highlight those activities in which they have been most invested. Applicants are encouraged to reflect on all genres of activities at any stage of their careers, even those not medical in nature, including work experience, military service, college athletics, or sustained musical or artistic achievement. Applicants should explain why each experience is meaningful rather than simply describing the activity.
Applicants also have the option to share a notable challenge they have overcome. It is not expected that each applicant will complete this question; in general, applicants who have not faced notable personal or professional obstacles should avoid answering. Additionally, if these challenges have been discussed in other areas of the application—for example, in the personal statement or medical student performance evaluation—it is not necessary to restate them here, though applicants can choose to do so. Examples of topics a student might discuss include being a first-generation college or medical student, growing up in poverty, facing notable personal or family health challenges, or having limited educational opportunities. It is important to share how this experience impacted an applicant’s journey to dermatology residency.
Geographic Preferences—The geographic preferences section can be difficult for applicants to navigate, as it may involve balancing a desire to attend a residency program in a particular region vs a greater desire to simply match in dermatology. In the past, programs may have made assumptions about geographic preferences based on an applicant’s birthplace, hometown, or medical school. In the supplemental application, applicants have the opportunity to directly reveal their preferences. We encourage applicants to be candid. Selecting a geographic region will not necessarily exclude applicants from consideration at other programs. For some applicants, program qualities may be more important than geography, or there may be no regional preferences. Those applicants can choose “no geographic preference.” There is considerable variability in how programs use geographic preferences. For this reason, it is in the best interest of applicants to simply respond honestly.
Preference Signaling—Preference signaling allows applicants to signal up to 3 preferred programs. Dermatology program directors agree that applicants should not signal their home program or programs at which they did in-person away rotations, as those programs would already be aware of the applicant’s interest. Although a signal increases the chances that the application will be reviewed holistically, it does not guarantee an interview offer. Programs may differentially utilize signals depending on multiple factors, including the number of signals received. We encourage applicants to discuss preference signaling strategies with advisors and focus on signaling programs in which they have genuine interest.
Recommendations to Selection Committees and Program Directors
The intent of the supplemental application is to provide a more meaningful picture of applicants and their experiences and preferences, with the goal of optimizing applicant-program fit. Programs should explicitly define for themselves the applicant characteristics and experiences they prioritize as well as their program goals. The supplemental application offers the potential to streamline holistic application review based on these elements. The short essay answers in the past experiences section permit reviewers to quickly scan for important experiences that align with the program’s recruitment goals. Importantly, reviewers should not penalize applicants who have not completed the question regarding other impactful life experiences, as not all applicants will have relevant information to share.
Some programs may find the geographic preferences section more valuable than others. Multiple factors affect how much weight will be given to geographic preferences, including program location and other characteristics that affect the desirability of the program to applicants. The competitiveness of the field, relatively low match rate, and limited number of programs may lead to less emphasis on geographic preferences in dermatology compared to other specialties. The purpose of this section is not to exclude applicants but to give programs more information that may help with alignment.
Anecdotally, many dermatology program directors were most interested in the preference signaling section of the supplemental application. Programs should consider signals to be evidence of strong preliminary interest. Programs may utilize signals differently depending on many factors such as the overall competitiveness of the program, program location, and the total number of signals the program receives. We recommend that programs holistically review all applications accompanied by a signal. Programs that utilize a points system may choose to award a certain number of points for a signal to their program. A signal might have a higher value at a program that receives only a few signals; conversely, a program that receives a large number of signals might not place tremendous value on the signal but may use it as a tiebreaker between similarly qualified applicants. Preference signaling is solely a tool for application review; because applicants’ preferences may change after the interview process, signals should not be utilized during ranking.
Next Steps
For program directors who have excitedly awaited residency application reform, the supplemental ERAS application is an important first step. Ultimately, we hope the supplemental application supplants much of the current residency application, serving as an efficient high-yield tool for holistically evaluating applicants’ academic and service records, accomplishments, and training preferences. Arriving at a new application will undoubtedly take time and discussion among the various stakeholders. Please continue to complete surveys from the AAMC, as feedback is the best method for refining the tool to serve its intended purpose.
Optimization of the application content is only one component of the reforms needed to improve the application process. Even with a revamped application tool, holistic review is challenging when programs are inundated with an ever-increasing number of applications. As such, we encourage stakeholders to simultaneously consider other potential reforms, such as caps on the number of applications, to allow programs and applicants the best opportunity for a mutually successful match.
In the 2021-2022 residency application cycle, the Association of American Medical Colleges (AAMC) piloted a supplemental application to accompany the standard residency application submitted via the AAMC’s Electronic Residency Application Service (ERAS).1 Dermatology was 1 of 3 specialties to participate in the pilot alongside internal medicine and general surgery. The goal was to develop a tool that could align applicants with programs that best matched their career goals as well as program and geographic preferences. The Association of Professors of Dermatology Residency Program Directors Section was an early advocate for the supplemental application, and members of our leadership were involved in the design, implementation, and evaluation of the pilot supplemental application.
Participating in the supplemental application was optional for both applicants and programs. The supplemental application included a Past Experiences section, which allowed applicants to highlight their 5 most meaningful research, work, and/or volunteer experiences and to describe a challenging life event that might not otherwise be included with their application. The geographic preferences section permitted applicants to select up to 3 regions of interest as well as to indicate an urban vs rural preference. Lastly, a preference-signaling section allowed dermatology applicants to send signals to up to 3 programs of particular interest.
With the close of another application cycle, applicants and programs will begin preparing for the 2022-2023 recruitment season. In this column, we present dermatology-specific data regarding the supplemental application, highlight tentative changes for the upcoming application cycle, and offer tips for applicants and programs as we approach year 2 of the supplemental application.
Results of Supplemental Application Evaluation Surveys
During the 2021-2022 recruitment season, 93% (950/1019) of dermatology applicants submitted the supplemental application, and 87% (117/135) of dermatology residency programs participated in the pilot.2 Surveys conducted by the AAMC between October 2021 and January 2022 showed that a large majority of dermatology programs used supplemental application data during initial application review when deciding who to interview. Eighty-three percent (40/48) of program directors felt that preference signals in particular helped them identify applicants they would have otherwise overlooked. Fifty-seven percent (4288/7516) of applicants across all specialties that participated in the pilot felt that preference signals would help them be noticed by their preferred programs.2 Preference signals were not evenly distributed among dermatology programs. Programs received an average of 23 signals, with a range of 2 to 87 (AAMC, unpublished data, February 2022).
Additional questions remain to be answered: How does the number of signals received affect application review? How often do geographic and program signals convert to interview offers and matches? Regardless, enthusiasm among dermatology programs for the supplemental application remains. In a recent survey of Association of Professors of Dermatology program directors, all 43 respondents planned to participate in the supplemental application again in the upcoming year (Ilana Rosman, MD; unpublished data; February 2022). The pilot will be expanded to include at least 12 other specialties.1As many who reviewed residency applications in 2021-2022 will attest, there was difficulty accessing the supplemental application data because it was not integrated into the Program Directors’ Work Station, the ERAS platform for programs to access applications, which will be remedied for the 2022-2023 iteration. Other tentative changes include modifications to the past experiences sections and timeline of the application.2
Utilizing the Supplemental Application: Recommendations to Applicants
Format of the Application—Applicants should familiarize themselves with the format of the supplemental application in advance and give themselves sufficient time to complete the application. In general, 3 to 4 hours of focused work should be enough time. Applicants should proofread for grammar and spelling before submitting.
Past Experiences—The past experiences section is intended to provide a focused snapshot of an applicant’s most meaningful activities and unique path to residency. Applicants should answer honestly based on their interests. If a student’s focus has been on volunteerism, the bulk of their 5 experiences listed may be related to service. Similarly, a student who has focused on research may preferentially highlight those experiences. In place of the long list of research, volunteer, and work experiences in the traditional ERAS application, applicants can highlight those activities in which they have been most invested. Applicants are encouraged to reflect on all genres of activities at any stage of their careers, even those not medical in nature, including work experience, military service, college athletics, or sustained musical or artistic achievement. Applicants should explain why each experience is meaningful rather than simply describing the activity.
Applicants also have the option to share a notable challenge they have overcome. It is not expected that each applicant will complete this question; in general, applicants who have not faced notable personal or professional obstacles should avoid answering. Additionally, if these challenges have been discussed in other areas of the application—for example, in the personal statement or medical student performance evaluation—it is not necessary to restate them here, though applicants can choose to do so. Examples of topics a student might discuss include being a first-generation college or medical student, growing up in poverty, facing notable personal or family health challenges, or having limited educational opportunities. It is important to share how this experience impacted an applicant’s journey to dermatology residency.
Geographic Preferences—The geographic preferences section can be difficult for applicants to navigate, as it may involve balancing a desire to attend a residency program in a particular region vs a greater desire to simply match in dermatology. In the past, programs may have made assumptions about geographic preferences based on an applicant’s birthplace, hometown, or medical school. In the supplemental application, applicants have the opportunity to directly reveal their preferences. We encourage applicants to be candid. Selecting a geographic region will not necessarily exclude applicants from consideration at other programs. For some applicants, program qualities may be more important than geography, or there may be no regional preferences. Those applicants can choose “no geographic preference.” There is considerable variability in how programs use geographic preferences. For this reason, it is in the best interest of applicants to simply respond honestly.
Preference Signaling—Preference signaling allows applicants to signal up to 3 preferred programs. Dermatology program directors agree that applicants should not signal their home program or programs at which they did in-person away rotations, as those programs would already be aware of the applicant’s interest. Although a signal increases the chances that the application will be reviewed holistically, it does not guarantee an interview offer. Programs may differentially utilize signals depending on multiple factors, including the number of signals received. We encourage applicants to discuss preference signaling strategies with advisors and focus on signaling programs in which they have genuine interest.
Recommendations to Selection Committees and Program Directors
The intent of the supplemental application is to provide a more meaningful picture of applicants and their experiences and preferences, with the goal of optimizing applicant-program fit. Programs should explicitly define for themselves the applicant characteristics and experiences they prioritize as well as their program goals. The supplemental application offers the potential to streamline holistic application review based on these elements. The short essay answers in the past experiences section permit reviewers to quickly scan for important experiences that align with the program’s recruitment goals. Importantly, reviewers should not penalize applicants who have not completed the question regarding other impactful life experiences, as not all applicants will have relevant information to share.
Some programs may find the geographic preferences section more valuable than others. Multiple factors affect how much weight will be given to geographic preferences, including program location and other characteristics that affect the desirability of the program to applicants. The competitiveness of the field, relatively low match rate, and limited number of programs may lead to less emphasis on geographic preferences in dermatology compared to other specialties. The purpose of this section is not to exclude applicants but to give programs more information that may help with alignment.
Anecdotally, many dermatology program directors were most interested in the preference signaling section of the supplemental application. Programs should consider signals to be evidence of strong preliminary interest. Programs may utilize signals differently depending on many factors such as the overall competitiveness of the program, program location, and the total number of signals the program receives. We recommend that programs holistically review all applications accompanied by a signal. Programs that utilize a points system may choose to award a certain number of points for a signal to their program. A signal might have a higher value at a program that receives only a few signals; conversely, a program that receives a large number of signals might not place tremendous value on the signal but may use it as a tiebreaker between similarly qualified applicants. Preference signaling is solely a tool for application review; because applicants’ preferences may change after the interview process, signals should not be utilized during ranking.
Next Steps
For program directors who have excitedly awaited residency application reform, the supplemental ERAS application is an important first step. Ultimately, we hope the supplemental application supplants much of the current residency application, serving as an efficient high-yield tool for holistically evaluating applicants’ academic and service records, accomplishments, and training preferences. Arriving at a new application will undoubtedly take time and discussion among the various stakeholders. Please continue to complete surveys from the AAMC, as feedback is the best method for refining the tool to serve its intended purpose.
Optimization of the application content is only one component of the reforms needed to improve the application process. Even with a revamped application tool, holistic review is challenging when programs are inundated with an ever-increasing number of applications. As such, we encourage stakeholders to simultaneously consider other potential reforms, such as caps on the number of applications, to allow programs and applicants the best opportunity for a mutually successful match.
- Supplemental ERAS application. Association of American Medical Colleges website. Accessed May 9, 2022. https://students-residents.aamc.org/applying-residencies-eras/supplemental-eras-application-eras-2023-cycle
- Association of American Medical Colleges. Supplemental application data and reports. Accessed May 9, 2022. https://www.aamc.org/data-reports/students-residents/report/supplemental-eras-application-data-and-reports
- Supplemental ERAS application. Association of American Medical Colleges website. Accessed May 9, 2022. https://students-residents.aamc.org/applying-residencies-eras/supplemental-eras-application-eras-2023-cycle
- Association of American Medical Colleges. Supplemental application data and reports. Accessed May 9, 2022. https://www.aamc.org/data-reports/students-residents/report/supplemental-eras-application-data-and-reports
Practice Points
- The Electronic Residency Application Service (ERAS) Supplemental Application was piloted in the 2021-2022 residency application cycle and was utilized by the vast majority of dermatology applicants and programs.
- Survey data suggested that both applicants and programs found the supplemental application useful, particularly the preference signaling portion.
- The supplemental application will return for the 2022-2023 application cycle and will be integrated into the MyERAS workstation platform for easier access by programs.
Going Beyond Hydroquinone: Alternative Skin Lightening Agents
Disorders of hyperpigmentation—melasma, postinflammatory hyperpigmentation, lichen planus pigmentosus, erythema dyschromicum perstans, and pigmented contact dermatitis, among others—are common and challenging to treat. Although they can affect individuals of all skin types, they most commonly are seen in skin of color; in fact, dyspigmentation is one of the most common chief concerns for which individuals of color see a dermatologist.1,2
For many years, hydroquinone (HQ) was one of the main options available for use as a lightening agent. Although effective, it has the risk of causing irritant dermatitis, potentially leading to further dyspigmentation, in addition to the risk of ochronosis with long-term use. It remains an important and useful treatment for pigmentary disorders, but there are numerous other lightening agents that also can be considered in the treatment of disorders of hyperpigmentation.
Herein, we provide recommendations for traditional and newer non-HQ lightening agents that can be considered when treating disorders of hyperpigmentation.
Traditional Non-HQ Lightening Agents
Retinoids—Retinoids are topical vitamin A derivatives that have been used safely and effectively for decades in the treatment of pigmentary disorders. Retinoids have multiple mechanisms of action in improving pigmentation. In addition to impeding tyrosinase induction, they inhibit pigment transfer to keratinocytes and lead to accelerated pigment loss due to epidermal shedding.3 Over-the-counter formulations include retinol, retinaldehyde, and adapalene. Prescription formulations include tretinoin and tazarotene in different strengths and vehicle formulations.4
Glycolic Acid—Glycolic acid is derived from sugarcane and is considered an α-hydroxy acid that leads to rapid desquamation of pigmented keratinocytes.5 Glycolic acid can not only be used in chemical peels but also in topical creams. It is the most common α-hydroxy acid peel and is sometimes paired with HQ and other topical lightening agents for increased penetration. Glycolic acid peels are available in concentrations of 20% to 70% and can be used at various depths. When used incorrectly, it can cause redness, burning, and even skin discoloration; however, when used at the proper concentrations and depth according to Fitzpatrick skin type, there typically are no notable adverse effects, and clinical results are favorable.
Kojic Acid—Kojic acid is a natural metabolite derived from fungi and is widely used in Asian countries. It works by inhibiting the catecholase activity of tyrosinase6 and typically is available in concentrations of 1% to 4%. A study suggested that a concentration of 1% or less typically is safe to use for prolonged periods without adverse effects. Although not more effective than HQ as a monotherapy, kojic acid has been shown to haveimproved efficacy when used in combination with other lightening agents.7
Azelaic Acid—Azelaic acid works by inhibiting tyrosinase, mitochondrial oxidoreductase activation, and DNA synthesis. It preferentially targets heavily pigmented melanocytes and possesses anti-inflammatory and antibacterial properties.8 A 20% concentration of azelaic acid was compared to HQ 4% for the treatment of melasma, and results revealed that the liposomal form of azelaic acid was considerably more tolerable than HQ 4% and also more effective.9
Licorice Extracts—Licorice extracts have been safely used in several cosmeceutical skin lightening products.10 The main active compounds in licorice root are glabridin and liquiritin, which work to disperse melanin. These compounds often are used topically at concentrations of 10% to 40%. A study by Amer and Metwalli11 found that topical liquiritin produced a reduction of pigmentary intensity, with 80% of patients showing an excellent response, which was described as no difference between the previously pigmented area and the normal skin surrounding it.
Aloesin—Aloesin is a low-molecular-weight glycoprotein found in aloe vera plants. Its mechanism of action includes competitive inhibition of the dihydroxyphenylalanine oxidation site, resulting in the inhibition of tyrosinase.12 It often is combined with arbutin for an enhanced lightening effect.
Niacinamide—Niacinamide is a form of vitamin B3 that works by suppressing the transfer of melanosomes to keratinocytes.13 In addition to its skin lightening effects, it also is photoprotective and antimicrobial, and its tolerability and safety have led to its inclusion in many cosmeceutical and prescription products.14
Ascorbic Acid—Ascorbic acid affects the monopherase activity of tyrosinase, thus reducing the synthesis of melanin. It also serves as an antioxidant in the skin by preventing the production of free radicals that can induce melanogenesis.15 Although it tends to be well tolerated with a low adverse effect profile, its relative instability and varying permeability can present a challenge. It is less effective as a monotherapy, so it often is combined with other lightening ingredients for greater efficacy.
Corticosteroids—Topical corticosteroids are anti-inflammatory and impact melanogenesis, though the mechanism of action of the latter has not been fully elucidated.16,17 Low- to mid-potency topical steroids often are used in conjunction with skin lightening products to diminish irritation and decrease inflammation.18 However, prolonged use of corticosteroids can lead to cutaneous adverse effects such as striae, hypopigmentation, and acne, as well as systemic side effects if there is sufficient absorption over time.
Soybean Extracts—Soybean extracts contain serine protease inhibitors that reduce the transfer of melanosomes into keratinocytes by inhibiting the PAR-2 (protease-activated receptor 2) pathway.19,20
Ellagic Acid—Ellagic acid is found in common plants such as eucalyptus and strawberry as well as green tea.21 It works as an antioxidant and decreases melanogenesis through inhibition of tyrosinase activity.
Paper Mulberry—Paper mulberry extract comes from the roots of the Broussonetia papyrifera tree and functions by inhibiting tyrosinase activity. It is widely used in South Africa and Europe.22
Resveratrol—Resveratrol is an ingredient extracted from Morus alba L and functions as an antimelanogentic agent by directly inhibiting tyrosinase as well as transcriptional and posttranscriptional processing of tyrosinase.23 It also holds antiproliferative, anti-inflammatory, and antioxidant properties and has widely been used for antiaging and skin lightening purposes.24
Newer Non-HQ Lightening Agents
Silymarin—Silymarin (also known as milk thistle [Silybum marianum]), is a polyphenolic flavonoid that possesses anticarcinogenic, antioxidant, and anti-inflammatory properties. It prevents melanin production in a dose-dependent manner by inhibiting levodopa (L-dopa) oxidation activity of tyrosinase and also reduces the expression of tyrosinase protein.25 In combination with vitamins C and E and hexylresorcinol, silymarin has been found to reduce the effects of photodamage, brighten skin, improve evenness and lines, as well as improve global facial appearance.26
Malassezin—Malassezin is an indole produced by Malessezia furfur yeast and has recently been investigated for melanogenesis suppression. Grimes et al27 assessed the efficacy of topical malassezin in 7 patients with facial hyperpigmentation applied twice daily for 14 weeks. Punch biopsies were taken at weeks 0, 8, 14, and 22. Biopsies from weeks 8 and 14 demonstrated reduced epidermal melanin compared to baseline in all participants; however, at 22 weeks, biopsies showed no difference in melanin content compared to baseline, indicating a temporary process induced by the malassezin.27 More clinical studies are needed to investigate this further.
N-acetyl-glucosamine—N-acetyl-glucosamine is an aminosaccharide that inhibits the glycosylation of tyrosinase as well as its function in melanogenesis.28 It is synthesized and included in topical products for wound healing, rhytides, moisturization, and pigmentation disorders.
Topical Tranexamic Acid—Tranexamic acid traditionally has been used orally for the treatment of menorrhagia but also has been found to be beneficial as a therapy for hyperpigmentation and erythema. Tranexamic acid interferes with plasmin activity, thus indirectly inhibiting melanogenesis while also inhibiting angiogenesis by targeting vascular endothelial growth factor (VEGF) receptors.29 It also leads to an increase in the levels of β-endorphin and μ-opioid receptors as well as the expression of estrogen receptor β on the surface of mast cells.30 Its oral benefit led to the development of topical formulations, typically in 2% to 5% concentrations. It has proven particularly beneficial in the treatment of melasma due to its effects on improving pigmentation, erythema, and skin barrier function.31 Topical tranexamic acid has a relatively high safety profile, with minor side effects such as transient skin irritation and erythema being reported.32
Cysteamine—Cysteamine inhibits tyrosinase, peroxidase, and chelating copper ions necessary for melanogenesis. It has proven to be effective in treating melasma and chronic severe postinflammatory hyperpigmentation when used in a 5% cream formulation.33,34 Lima et al35 were the first to compare the effects of topical cysteamine to HQ in the treatment of facial melasma. They found that the mean reduction in modified Melasma Area and Severity Index score was 24% for cysteamine and 41% for HQ after 60 days. There were no severe adverse effects with either treatment group.35
Final Thoughts
Hydroquinone remains the gold standard for treatment of hyperpigmentation; however, its side-effect profile and risk of ochronosis with long-term use has ushered in various other safe and effective skin lightening agents that can be used as monotherapies or in combination with other lightening agents. Many of these products also can be used effectively with procedural treatments such as chemical peels, lasers, and microneedling for enhanced absorption and efficacy. As newer agents are developed, additional well-designed studies will be needed to determine their safety and efficacy in different skin types as well as their role in the treatment of pigmentary disorders.
- Woolery-Lloyd H, Kammer JN. Treatment of hyperpigmentation. Semin Cutan Med Surg. 2011;30:171-175. doi:10.1016/j.sder.2011.06.004
- Desai SR. Hyperpigmentation therapy: a review. J Clin Aesthet Dermatol. 2014;7:13-17.
- Kligman AM, Willis I. A new formula for depigmenting human skin. Arch Dermatol. 1975;111:40-48.
- Kligman AM, Grove GL, Hirose R, et al. Topical tretinoin for photoaged skin. J Am Acad Dermatol. 1986;15(4 pt 2):836-859. doi:10.1016/s0190-9622(86)70242-9
- Sharad J. Glycolic acid peel therapy—a current review. Clin Cosmet Investig Dermatol. 2013;6:281-288. doi:10.2147/CCID.S34029
- Nautiyal A, Wairkar S. Management of hyperpigmentation: current treatments and emerging therapies. Pigment Cell Melanoma Res. 2021;34:1000-1014. doi:10.1111/pcmr.12986
- Saeedi M, Eslamifar M, Khezri K. Kojic acid applications in cosmetic and pharmaceutical preparations. Biomed Pharmacother. 2019;110:582-593. doi:10.1016/j.biopha.2018.12.006
- Schulte BC, Wu W, Rosen T. Azelaic acid: evidence-based update on mechanism of action and clinical application. J Drugs Dermatol. 2015;14:964-968.
- Akl EM. Liposomal azelaic acid 20% cream vs hydroquinone 4% cream as adjuvant to oral tranexamic acid in melasma: a comparative study [published online April 7, 2021]. J Dermatol Treat. doi:10.1080/09546634.2021.1905765
- Holloway VL. Ethnic cosmetic products. Dermatol Clin. 2003;21:743-749. doi:10.1016/s0733-8635(03)00089-5
- Amer M, Metwalli M. Topical liquiritin improves melasma. Int J Dermatol. 2000;39:299-301. doi:10.1046/j.1365-4362.2000.00943.x
- Jones K, Hughes J, Hong M, et al. Modulation of melanogenesis by aloesin: a competitive inhibitor of tyrosinase. Pigment Cell Res. 2002;15:335-340. doi:10.1034/j.1600-0749.2002.02014.x
- Hakozaki T, Minwalla L, Zhuang J, et al. The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. Br J Dermatol. 2002;147:20-31. doi:10.1046/j.1365-2133.2002.04834.x
- Wohlrab J, Kreft D. Niacinamide—mechanisms of action and its topical use in dermatology. Skin Pharmacol Physiol. 2014;27:311-315. doi:10.1159/000359974
- Fitzpatrick RE, Rostan EF. Double-blind, half-face study comparing topical vitamin C and vehicle for rejuvenation of photodamage. Dermatol Surg. 2002;28:231-236. doi:10.1046/j.1524-4725.2002.01129.x
- Mehta AB, Nadkarni NJ, Patil SP, et al. Topical corticosteroids in dermatology. Indian J Dermatol Venereol Leprol. 2016;82:371-378. doi:10.4103/0378-6323.178903
- Petit L, Piérard GE. Skin-lightening products revisited. Int J Cosmet Sci. 2003;25:169-181. doi:10.1046/j.1467-2494.2003.00182.x
- Kanwar AJ, Dhar S, Kaur S. Treatment of melasma with potent topical corticosteroids. Dermatol Basel Switz. 1994;188:170. doi:10.1159/000247129
- Paine C, Sharlow E, Liebel F, et al. An alternative approach to depigmentation by soybean extracts via inhibition of the PAR-2 pathway. J Invest Dermatol. 2001;116:587-595. doi:10.1046/j.1523-1747.2001.01291.x
- Seiberg M, Paine C, Sharlow E, et al. Inhibition of melanosome transfer results in skin lightening. J Invest Dermatol. 2000;115:162-167. doi:10.1046/j.1523-1747.2000.00035.x
- Shimogaki H, Tanaka Y, Tamai H, et al. In vitro and in vivo evaluation of ellagic acid on melanogenesis inhibition. Int J Cosmet Sci. 2000;22:291-303. doi:10.1046/j.1467-2494.2000.00023.x
- Rendon MI, Gaviria JI. Review of skin-lightening agents. Dermatol Surg. 2005;31(7 pt 2):886-889; discussion 889. doi:10.1111/j.1524-4725.2005.31736
- Na JI, Shin JW, Choi HR, et al. Resveratrol as a multifunctional topical hypopigmenting agent [published online February 22, 2019]. Int J Mol Sci. 2019;20:956. doi:10.3390/ijms20040956
- Ratz-Łyko A, Arct J. Resveratrol as an active ingredient for cosmetic and dermatological applications: a review. J Cosmet Laser Ther. 2019;21:84-90. doi:10.1080/14764172.2018.1469767
- Choo SJ, Ryoo IJ, Kim YH, et al. Silymarin inhibits melanin synthesis in melanocyte cells. J Pharm Pharmacol. 2009;61:663-667. doi:10.1211/jpp/61.05.0016
- Draelos ZD, Diaz I, Cohen A, et al. A novel skin brightening topical technology. J Cosmet Dermatol. 2020;19:3280-3285. doi:10.1111/jocd.13741
- Grimes P, Bhawan J, Howell M, et al. Histopathological changes induced by malassezin: a novel natural microbiome indole for treatment of facial hyperpigmentation. J Drugs Dermatol. 2022;21:141-145. doi:10.36849/jdd.6596
- Bissett DL. Glucosamine: an ingredient with skin and other benefits. J Cosmet Dermatol. 2006;5:309-315. doi:10.1111/j.1473-2165.2006.00277.x
- Zhu JW, Ni YJ, Tong XY, et al. Tranexamic acid inhibits angiogenesis and melanogenesis in vitro by targeting VEGF receptors. Int J Med Sci. 2020;17:903-911. doi:10.7150/ijms.44188
- Hiramoto K, Yamate Y, Sugiyama D, et al. Tranexamic acid inhibits the plasma and non-irradiated skin markers of photoaging induced by long-term UVA eye irradiation in female mice. Biomed Pharmacother. 2018;107:54-58. doi:10.1016/j.biopha.2018.07.146
- da Silva Souza ID, Lampe L, Winn D. New topical tranexamic acid derivative for the improvement of hyperpigmentation and inflammation in the sun-damaged skin. J Cosmet Dermatol. 2021;20:561-565. doi:10.1111/jocd.13545
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781. doi:10.2340/00015555-2668
- Mathe N, Balogun M, Yoo J. A case report on the use of topical cysteamine 5% cream in the management of refractory postinflammatory hyperpigmentation (PIH) resistant to triple combination cream (hydroquinone, topical corticosteroids, and retinoids). J Cosmet Dermatol. 2021;20:204-206. doi:10.1111/jocd.13755
- Mansouri P, Farshi S, Hashemi Z, et al. Evaluation of the efficacy of cysteamine 5% cream in the treatment of epidermal melasma: a randomized double-blind placebo-controlled trial. Br J Dermatol. 2015;173:209-217. doi:10.1111/bjd.13424
- Lima PB, Dias JAF, Cassiano D, et al. A comparative study of topical 5% cysteamine versus 4% hydroquinone in the treatment of facial melasma in women. Int J Dermatol. 2020;59:1531-1536. doi:10.1111/ijd.15146
Disorders of hyperpigmentation—melasma, postinflammatory hyperpigmentation, lichen planus pigmentosus, erythema dyschromicum perstans, and pigmented contact dermatitis, among others—are common and challenging to treat. Although they can affect individuals of all skin types, they most commonly are seen in skin of color; in fact, dyspigmentation is one of the most common chief concerns for which individuals of color see a dermatologist.1,2
For many years, hydroquinone (HQ) was one of the main options available for use as a lightening agent. Although effective, it has the risk of causing irritant dermatitis, potentially leading to further dyspigmentation, in addition to the risk of ochronosis with long-term use. It remains an important and useful treatment for pigmentary disorders, but there are numerous other lightening agents that also can be considered in the treatment of disorders of hyperpigmentation.
Herein, we provide recommendations for traditional and newer non-HQ lightening agents that can be considered when treating disorders of hyperpigmentation.
Traditional Non-HQ Lightening Agents
Retinoids—Retinoids are topical vitamin A derivatives that have been used safely and effectively for decades in the treatment of pigmentary disorders. Retinoids have multiple mechanisms of action in improving pigmentation. In addition to impeding tyrosinase induction, they inhibit pigment transfer to keratinocytes and lead to accelerated pigment loss due to epidermal shedding.3 Over-the-counter formulations include retinol, retinaldehyde, and adapalene. Prescription formulations include tretinoin and tazarotene in different strengths and vehicle formulations.4
Glycolic Acid—Glycolic acid is derived from sugarcane and is considered an α-hydroxy acid that leads to rapid desquamation of pigmented keratinocytes.5 Glycolic acid can not only be used in chemical peels but also in topical creams. It is the most common α-hydroxy acid peel and is sometimes paired with HQ and other topical lightening agents for increased penetration. Glycolic acid peels are available in concentrations of 20% to 70% and can be used at various depths. When used incorrectly, it can cause redness, burning, and even skin discoloration; however, when used at the proper concentrations and depth according to Fitzpatrick skin type, there typically are no notable adverse effects, and clinical results are favorable.
Kojic Acid—Kojic acid is a natural metabolite derived from fungi and is widely used in Asian countries. It works by inhibiting the catecholase activity of tyrosinase6 and typically is available in concentrations of 1% to 4%. A study suggested that a concentration of 1% or less typically is safe to use for prolonged periods without adverse effects. Although not more effective than HQ as a monotherapy, kojic acid has been shown to haveimproved efficacy when used in combination with other lightening agents.7
Azelaic Acid—Azelaic acid works by inhibiting tyrosinase, mitochondrial oxidoreductase activation, and DNA synthesis. It preferentially targets heavily pigmented melanocytes and possesses anti-inflammatory and antibacterial properties.8 A 20% concentration of azelaic acid was compared to HQ 4% for the treatment of melasma, and results revealed that the liposomal form of azelaic acid was considerably more tolerable than HQ 4% and also more effective.9
Licorice Extracts—Licorice extracts have been safely used in several cosmeceutical skin lightening products.10 The main active compounds in licorice root are glabridin and liquiritin, which work to disperse melanin. These compounds often are used topically at concentrations of 10% to 40%. A study by Amer and Metwalli11 found that topical liquiritin produced a reduction of pigmentary intensity, with 80% of patients showing an excellent response, which was described as no difference between the previously pigmented area and the normal skin surrounding it.
Aloesin—Aloesin is a low-molecular-weight glycoprotein found in aloe vera plants. Its mechanism of action includes competitive inhibition of the dihydroxyphenylalanine oxidation site, resulting in the inhibition of tyrosinase.12 It often is combined with arbutin for an enhanced lightening effect.
Niacinamide—Niacinamide is a form of vitamin B3 that works by suppressing the transfer of melanosomes to keratinocytes.13 In addition to its skin lightening effects, it also is photoprotective and antimicrobial, and its tolerability and safety have led to its inclusion in many cosmeceutical and prescription products.14
Ascorbic Acid—Ascorbic acid affects the monopherase activity of tyrosinase, thus reducing the synthesis of melanin. It also serves as an antioxidant in the skin by preventing the production of free radicals that can induce melanogenesis.15 Although it tends to be well tolerated with a low adverse effect profile, its relative instability and varying permeability can present a challenge. It is less effective as a monotherapy, so it often is combined with other lightening ingredients for greater efficacy.
Corticosteroids—Topical corticosteroids are anti-inflammatory and impact melanogenesis, though the mechanism of action of the latter has not been fully elucidated.16,17 Low- to mid-potency topical steroids often are used in conjunction with skin lightening products to diminish irritation and decrease inflammation.18 However, prolonged use of corticosteroids can lead to cutaneous adverse effects such as striae, hypopigmentation, and acne, as well as systemic side effects if there is sufficient absorption over time.
Soybean Extracts—Soybean extracts contain serine protease inhibitors that reduce the transfer of melanosomes into keratinocytes by inhibiting the PAR-2 (protease-activated receptor 2) pathway.19,20
Ellagic Acid—Ellagic acid is found in common plants such as eucalyptus and strawberry as well as green tea.21 It works as an antioxidant and decreases melanogenesis through inhibition of tyrosinase activity.
Paper Mulberry—Paper mulberry extract comes from the roots of the Broussonetia papyrifera tree and functions by inhibiting tyrosinase activity. It is widely used in South Africa and Europe.22
Resveratrol—Resveratrol is an ingredient extracted from Morus alba L and functions as an antimelanogentic agent by directly inhibiting tyrosinase as well as transcriptional and posttranscriptional processing of tyrosinase.23 It also holds antiproliferative, anti-inflammatory, and antioxidant properties and has widely been used for antiaging and skin lightening purposes.24
Newer Non-HQ Lightening Agents
Silymarin—Silymarin (also known as milk thistle [Silybum marianum]), is a polyphenolic flavonoid that possesses anticarcinogenic, antioxidant, and anti-inflammatory properties. It prevents melanin production in a dose-dependent manner by inhibiting levodopa (L-dopa) oxidation activity of tyrosinase and also reduces the expression of tyrosinase protein.25 In combination with vitamins C and E and hexylresorcinol, silymarin has been found to reduce the effects of photodamage, brighten skin, improve evenness and lines, as well as improve global facial appearance.26
Malassezin—Malassezin is an indole produced by Malessezia furfur yeast and has recently been investigated for melanogenesis suppression. Grimes et al27 assessed the efficacy of topical malassezin in 7 patients with facial hyperpigmentation applied twice daily for 14 weeks. Punch biopsies were taken at weeks 0, 8, 14, and 22. Biopsies from weeks 8 and 14 demonstrated reduced epidermal melanin compared to baseline in all participants; however, at 22 weeks, biopsies showed no difference in melanin content compared to baseline, indicating a temporary process induced by the malassezin.27 More clinical studies are needed to investigate this further.
N-acetyl-glucosamine—N-acetyl-glucosamine is an aminosaccharide that inhibits the glycosylation of tyrosinase as well as its function in melanogenesis.28 It is synthesized and included in topical products for wound healing, rhytides, moisturization, and pigmentation disorders.
Topical Tranexamic Acid—Tranexamic acid traditionally has been used orally for the treatment of menorrhagia but also has been found to be beneficial as a therapy for hyperpigmentation and erythema. Tranexamic acid interferes with plasmin activity, thus indirectly inhibiting melanogenesis while also inhibiting angiogenesis by targeting vascular endothelial growth factor (VEGF) receptors.29 It also leads to an increase in the levels of β-endorphin and μ-opioid receptors as well as the expression of estrogen receptor β on the surface of mast cells.30 Its oral benefit led to the development of topical formulations, typically in 2% to 5% concentrations. It has proven particularly beneficial in the treatment of melasma due to its effects on improving pigmentation, erythema, and skin barrier function.31 Topical tranexamic acid has a relatively high safety profile, with minor side effects such as transient skin irritation and erythema being reported.32
Cysteamine—Cysteamine inhibits tyrosinase, peroxidase, and chelating copper ions necessary for melanogenesis. It has proven to be effective in treating melasma and chronic severe postinflammatory hyperpigmentation when used in a 5% cream formulation.33,34 Lima et al35 were the first to compare the effects of topical cysteamine to HQ in the treatment of facial melasma. They found that the mean reduction in modified Melasma Area and Severity Index score was 24% for cysteamine and 41% for HQ after 60 days. There were no severe adverse effects with either treatment group.35
Final Thoughts
Hydroquinone remains the gold standard for treatment of hyperpigmentation; however, its side-effect profile and risk of ochronosis with long-term use has ushered in various other safe and effective skin lightening agents that can be used as monotherapies or in combination with other lightening agents. Many of these products also can be used effectively with procedural treatments such as chemical peels, lasers, and microneedling for enhanced absorption and efficacy. As newer agents are developed, additional well-designed studies will be needed to determine their safety and efficacy in different skin types as well as their role in the treatment of pigmentary disorders.
Disorders of hyperpigmentation—melasma, postinflammatory hyperpigmentation, lichen planus pigmentosus, erythema dyschromicum perstans, and pigmented contact dermatitis, among others—are common and challenging to treat. Although they can affect individuals of all skin types, they most commonly are seen in skin of color; in fact, dyspigmentation is one of the most common chief concerns for which individuals of color see a dermatologist.1,2
For many years, hydroquinone (HQ) was one of the main options available for use as a lightening agent. Although effective, it has the risk of causing irritant dermatitis, potentially leading to further dyspigmentation, in addition to the risk of ochronosis with long-term use. It remains an important and useful treatment for pigmentary disorders, but there are numerous other lightening agents that also can be considered in the treatment of disorders of hyperpigmentation.
Herein, we provide recommendations for traditional and newer non-HQ lightening agents that can be considered when treating disorders of hyperpigmentation.
Traditional Non-HQ Lightening Agents
Retinoids—Retinoids are topical vitamin A derivatives that have been used safely and effectively for decades in the treatment of pigmentary disorders. Retinoids have multiple mechanisms of action in improving pigmentation. In addition to impeding tyrosinase induction, they inhibit pigment transfer to keratinocytes and lead to accelerated pigment loss due to epidermal shedding.3 Over-the-counter formulations include retinol, retinaldehyde, and adapalene. Prescription formulations include tretinoin and tazarotene in different strengths and vehicle formulations.4
Glycolic Acid—Glycolic acid is derived from sugarcane and is considered an α-hydroxy acid that leads to rapid desquamation of pigmented keratinocytes.5 Glycolic acid can not only be used in chemical peels but also in topical creams. It is the most common α-hydroxy acid peel and is sometimes paired with HQ and other topical lightening agents for increased penetration. Glycolic acid peels are available in concentrations of 20% to 70% and can be used at various depths. When used incorrectly, it can cause redness, burning, and even skin discoloration; however, when used at the proper concentrations and depth according to Fitzpatrick skin type, there typically are no notable adverse effects, and clinical results are favorable.
Kojic Acid—Kojic acid is a natural metabolite derived from fungi and is widely used in Asian countries. It works by inhibiting the catecholase activity of tyrosinase6 and typically is available in concentrations of 1% to 4%. A study suggested that a concentration of 1% or less typically is safe to use for prolonged periods without adverse effects. Although not more effective than HQ as a monotherapy, kojic acid has been shown to haveimproved efficacy when used in combination with other lightening agents.7
Azelaic Acid—Azelaic acid works by inhibiting tyrosinase, mitochondrial oxidoreductase activation, and DNA synthesis. It preferentially targets heavily pigmented melanocytes and possesses anti-inflammatory and antibacterial properties.8 A 20% concentration of azelaic acid was compared to HQ 4% for the treatment of melasma, and results revealed that the liposomal form of azelaic acid was considerably more tolerable than HQ 4% and also more effective.9
Licorice Extracts—Licorice extracts have been safely used in several cosmeceutical skin lightening products.10 The main active compounds in licorice root are glabridin and liquiritin, which work to disperse melanin. These compounds often are used topically at concentrations of 10% to 40%. A study by Amer and Metwalli11 found that topical liquiritin produced a reduction of pigmentary intensity, with 80% of patients showing an excellent response, which was described as no difference between the previously pigmented area and the normal skin surrounding it.
Aloesin—Aloesin is a low-molecular-weight glycoprotein found in aloe vera plants. Its mechanism of action includes competitive inhibition of the dihydroxyphenylalanine oxidation site, resulting in the inhibition of tyrosinase.12 It often is combined with arbutin for an enhanced lightening effect.
Niacinamide—Niacinamide is a form of vitamin B3 that works by suppressing the transfer of melanosomes to keratinocytes.13 In addition to its skin lightening effects, it also is photoprotective and antimicrobial, and its tolerability and safety have led to its inclusion in many cosmeceutical and prescription products.14
Ascorbic Acid—Ascorbic acid affects the monopherase activity of tyrosinase, thus reducing the synthesis of melanin. It also serves as an antioxidant in the skin by preventing the production of free radicals that can induce melanogenesis.15 Although it tends to be well tolerated with a low adverse effect profile, its relative instability and varying permeability can present a challenge. It is less effective as a monotherapy, so it often is combined with other lightening ingredients for greater efficacy.
Corticosteroids—Topical corticosteroids are anti-inflammatory and impact melanogenesis, though the mechanism of action of the latter has not been fully elucidated.16,17 Low- to mid-potency topical steroids often are used in conjunction with skin lightening products to diminish irritation and decrease inflammation.18 However, prolonged use of corticosteroids can lead to cutaneous adverse effects such as striae, hypopigmentation, and acne, as well as systemic side effects if there is sufficient absorption over time.
Soybean Extracts—Soybean extracts contain serine protease inhibitors that reduce the transfer of melanosomes into keratinocytes by inhibiting the PAR-2 (protease-activated receptor 2) pathway.19,20
Ellagic Acid—Ellagic acid is found in common plants such as eucalyptus and strawberry as well as green tea.21 It works as an antioxidant and decreases melanogenesis through inhibition of tyrosinase activity.
Paper Mulberry—Paper mulberry extract comes from the roots of the Broussonetia papyrifera tree and functions by inhibiting tyrosinase activity. It is widely used in South Africa and Europe.22
Resveratrol—Resveratrol is an ingredient extracted from Morus alba L and functions as an antimelanogentic agent by directly inhibiting tyrosinase as well as transcriptional and posttranscriptional processing of tyrosinase.23 It also holds antiproliferative, anti-inflammatory, and antioxidant properties and has widely been used for antiaging and skin lightening purposes.24
Newer Non-HQ Lightening Agents
Silymarin—Silymarin (also known as milk thistle [Silybum marianum]), is a polyphenolic flavonoid that possesses anticarcinogenic, antioxidant, and anti-inflammatory properties. It prevents melanin production in a dose-dependent manner by inhibiting levodopa (L-dopa) oxidation activity of tyrosinase and also reduces the expression of tyrosinase protein.25 In combination with vitamins C and E and hexylresorcinol, silymarin has been found to reduce the effects of photodamage, brighten skin, improve evenness and lines, as well as improve global facial appearance.26
Malassezin—Malassezin is an indole produced by Malessezia furfur yeast and has recently been investigated for melanogenesis suppression. Grimes et al27 assessed the efficacy of topical malassezin in 7 patients with facial hyperpigmentation applied twice daily for 14 weeks. Punch biopsies were taken at weeks 0, 8, 14, and 22. Biopsies from weeks 8 and 14 demonstrated reduced epidermal melanin compared to baseline in all participants; however, at 22 weeks, biopsies showed no difference in melanin content compared to baseline, indicating a temporary process induced by the malassezin.27 More clinical studies are needed to investigate this further.
N-acetyl-glucosamine—N-acetyl-glucosamine is an aminosaccharide that inhibits the glycosylation of tyrosinase as well as its function in melanogenesis.28 It is synthesized and included in topical products for wound healing, rhytides, moisturization, and pigmentation disorders.
Topical Tranexamic Acid—Tranexamic acid traditionally has been used orally for the treatment of menorrhagia but also has been found to be beneficial as a therapy for hyperpigmentation and erythema. Tranexamic acid interferes with plasmin activity, thus indirectly inhibiting melanogenesis while also inhibiting angiogenesis by targeting vascular endothelial growth factor (VEGF) receptors.29 It also leads to an increase in the levels of β-endorphin and μ-opioid receptors as well as the expression of estrogen receptor β on the surface of mast cells.30 Its oral benefit led to the development of topical formulations, typically in 2% to 5% concentrations. It has proven particularly beneficial in the treatment of melasma due to its effects on improving pigmentation, erythema, and skin barrier function.31 Topical tranexamic acid has a relatively high safety profile, with minor side effects such as transient skin irritation and erythema being reported.32
Cysteamine—Cysteamine inhibits tyrosinase, peroxidase, and chelating copper ions necessary for melanogenesis. It has proven to be effective in treating melasma and chronic severe postinflammatory hyperpigmentation when used in a 5% cream formulation.33,34 Lima et al35 were the first to compare the effects of topical cysteamine to HQ in the treatment of facial melasma. They found that the mean reduction in modified Melasma Area and Severity Index score was 24% for cysteamine and 41% for HQ after 60 days. There were no severe adverse effects with either treatment group.35
Final Thoughts
Hydroquinone remains the gold standard for treatment of hyperpigmentation; however, its side-effect profile and risk of ochronosis with long-term use has ushered in various other safe and effective skin lightening agents that can be used as monotherapies or in combination with other lightening agents. Many of these products also can be used effectively with procedural treatments such as chemical peels, lasers, and microneedling for enhanced absorption and efficacy. As newer agents are developed, additional well-designed studies will be needed to determine their safety and efficacy in different skin types as well as their role in the treatment of pigmentary disorders.
- Woolery-Lloyd H, Kammer JN. Treatment of hyperpigmentation. Semin Cutan Med Surg. 2011;30:171-175. doi:10.1016/j.sder.2011.06.004
- Desai SR. Hyperpigmentation therapy: a review. J Clin Aesthet Dermatol. 2014;7:13-17.
- Kligman AM, Willis I. A new formula for depigmenting human skin. Arch Dermatol. 1975;111:40-48.
- Kligman AM, Grove GL, Hirose R, et al. Topical tretinoin for photoaged skin. J Am Acad Dermatol. 1986;15(4 pt 2):836-859. doi:10.1016/s0190-9622(86)70242-9
- Sharad J. Glycolic acid peel therapy—a current review. Clin Cosmet Investig Dermatol. 2013;6:281-288. doi:10.2147/CCID.S34029
- Nautiyal A, Wairkar S. Management of hyperpigmentation: current treatments and emerging therapies. Pigment Cell Melanoma Res. 2021;34:1000-1014. doi:10.1111/pcmr.12986
- Saeedi M, Eslamifar M, Khezri K. Kojic acid applications in cosmetic and pharmaceutical preparations. Biomed Pharmacother. 2019;110:582-593. doi:10.1016/j.biopha.2018.12.006
- Schulte BC, Wu W, Rosen T. Azelaic acid: evidence-based update on mechanism of action and clinical application. J Drugs Dermatol. 2015;14:964-968.
- Akl EM. Liposomal azelaic acid 20% cream vs hydroquinone 4% cream as adjuvant to oral tranexamic acid in melasma: a comparative study [published online April 7, 2021]. J Dermatol Treat. doi:10.1080/09546634.2021.1905765
- Holloway VL. Ethnic cosmetic products. Dermatol Clin. 2003;21:743-749. doi:10.1016/s0733-8635(03)00089-5
- Amer M, Metwalli M. Topical liquiritin improves melasma. Int J Dermatol. 2000;39:299-301. doi:10.1046/j.1365-4362.2000.00943.x
- Jones K, Hughes J, Hong M, et al. Modulation of melanogenesis by aloesin: a competitive inhibitor of tyrosinase. Pigment Cell Res. 2002;15:335-340. doi:10.1034/j.1600-0749.2002.02014.x
- Hakozaki T, Minwalla L, Zhuang J, et al. The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. Br J Dermatol. 2002;147:20-31. doi:10.1046/j.1365-2133.2002.04834.x
- Wohlrab J, Kreft D. Niacinamide—mechanisms of action and its topical use in dermatology. Skin Pharmacol Physiol. 2014;27:311-315. doi:10.1159/000359974
- Fitzpatrick RE, Rostan EF. Double-blind, half-face study comparing topical vitamin C and vehicle for rejuvenation of photodamage. Dermatol Surg. 2002;28:231-236. doi:10.1046/j.1524-4725.2002.01129.x
- Mehta AB, Nadkarni NJ, Patil SP, et al. Topical corticosteroids in dermatology. Indian J Dermatol Venereol Leprol. 2016;82:371-378. doi:10.4103/0378-6323.178903
- Petit L, Piérard GE. Skin-lightening products revisited. Int J Cosmet Sci. 2003;25:169-181. doi:10.1046/j.1467-2494.2003.00182.x
- Kanwar AJ, Dhar S, Kaur S. Treatment of melasma with potent topical corticosteroids. Dermatol Basel Switz. 1994;188:170. doi:10.1159/000247129
- Paine C, Sharlow E, Liebel F, et al. An alternative approach to depigmentation by soybean extracts via inhibition of the PAR-2 pathway. J Invest Dermatol. 2001;116:587-595. doi:10.1046/j.1523-1747.2001.01291.x
- Seiberg M, Paine C, Sharlow E, et al. Inhibition of melanosome transfer results in skin lightening. J Invest Dermatol. 2000;115:162-167. doi:10.1046/j.1523-1747.2000.00035.x
- Shimogaki H, Tanaka Y, Tamai H, et al. In vitro and in vivo evaluation of ellagic acid on melanogenesis inhibition. Int J Cosmet Sci. 2000;22:291-303. doi:10.1046/j.1467-2494.2000.00023.x
- Rendon MI, Gaviria JI. Review of skin-lightening agents. Dermatol Surg. 2005;31(7 pt 2):886-889; discussion 889. doi:10.1111/j.1524-4725.2005.31736
- Na JI, Shin JW, Choi HR, et al. Resveratrol as a multifunctional topical hypopigmenting agent [published online February 22, 2019]. Int J Mol Sci. 2019;20:956. doi:10.3390/ijms20040956
- Ratz-Łyko A, Arct J. Resveratrol as an active ingredient for cosmetic and dermatological applications: a review. J Cosmet Laser Ther. 2019;21:84-90. doi:10.1080/14764172.2018.1469767
- Choo SJ, Ryoo IJ, Kim YH, et al. Silymarin inhibits melanin synthesis in melanocyte cells. J Pharm Pharmacol. 2009;61:663-667. doi:10.1211/jpp/61.05.0016
- Draelos ZD, Diaz I, Cohen A, et al. A novel skin brightening topical technology. J Cosmet Dermatol. 2020;19:3280-3285. doi:10.1111/jocd.13741
- Grimes P, Bhawan J, Howell M, et al. Histopathological changes induced by malassezin: a novel natural microbiome indole for treatment of facial hyperpigmentation. J Drugs Dermatol. 2022;21:141-145. doi:10.36849/jdd.6596
- Bissett DL. Glucosamine: an ingredient with skin and other benefits. J Cosmet Dermatol. 2006;5:309-315. doi:10.1111/j.1473-2165.2006.00277.x
- Zhu JW, Ni YJ, Tong XY, et al. Tranexamic acid inhibits angiogenesis and melanogenesis in vitro by targeting VEGF receptors. Int J Med Sci. 2020;17:903-911. doi:10.7150/ijms.44188
- Hiramoto K, Yamate Y, Sugiyama D, et al. Tranexamic acid inhibits the plasma and non-irradiated skin markers of photoaging induced by long-term UVA eye irradiation in female mice. Biomed Pharmacother. 2018;107:54-58. doi:10.1016/j.biopha.2018.07.146
- da Silva Souza ID, Lampe L, Winn D. New topical tranexamic acid derivative for the improvement of hyperpigmentation and inflammation in the sun-damaged skin. J Cosmet Dermatol. 2021;20:561-565. doi:10.1111/jocd.13545
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781. doi:10.2340/00015555-2668
- Mathe N, Balogun M, Yoo J. A case report on the use of topical cysteamine 5% cream in the management of refractory postinflammatory hyperpigmentation (PIH) resistant to triple combination cream (hydroquinone, topical corticosteroids, and retinoids). J Cosmet Dermatol. 2021;20:204-206. doi:10.1111/jocd.13755
- Mansouri P, Farshi S, Hashemi Z, et al. Evaluation of the efficacy of cysteamine 5% cream in the treatment of epidermal melasma: a randomized double-blind placebo-controlled trial. Br J Dermatol. 2015;173:209-217. doi:10.1111/bjd.13424
- Lima PB, Dias JAF, Cassiano D, et al. A comparative study of topical 5% cysteamine versus 4% hydroquinone in the treatment of facial melasma in women. Int J Dermatol. 2020;59:1531-1536. doi:10.1111/ijd.15146
- Woolery-Lloyd H, Kammer JN. Treatment of hyperpigmentation. Semin Cutan Med Surg. 2011;30:171-175. doi:10.1016/j.sder.2011.06.004
- Desai SR. Hyperpigmentation therapy: a review. J Clin Aesthet Dermatol. 2014;7:13-17.
- Kligman AM, Willis I. A new formula for depigmenting human skin. Arch Dermatol. 1975;111:40-48.
- Kligman AM, Grove GL, Hirose R, et al. Topical tretinoin for photoaged skin. J Am Acad Dermatol. 1986;15(4 pt 2):836-859. doi:10.1016/s0190-9622(86)70242-9
- Sharad J. Glycolic acid peel therapy—a current review. Clin Cosmet Investig Dermatol. 2013;6:281-288. doi:10.2147/CCID.S34029
- Nautiyal A, Wairkar S. Management of hyperpigmentation: current treatments and emerging therapies. Pigment Cell Melanoma Res. 2021;34:1000-1014. doi:10.1111/pcmr.12986
- Saeedi M, Eslamifar M, Khezri K. Kojic acid applications in cosmetic and pharmaceutical preparations. Biomed Pharmacother. 2019;110:582-593. doi:10.1016/j.biopha.2018.12.006
- Schulte BC, Wu W, Rosen T. Azelaic acid: evidence-based update on mechanism of action and clinical application. J Drugs Dermatol. 2015;14:964-968.
- Akl EM. Liposomal azelaic acid 20% cream vs hydroquinone 4% cream as adjuvant to oral tranexamic acid in melasma: a comparative study [published online April 7, 2021]. J Dermatol Treat. doi:10.1080/09546634.2021.1905765
- Holloway VL. Ethnic cosmetic products. Dermatol Clin. 2003;21:743-749. doi:10.1016/s0733-8635(03)00089-5
- Amer M, Metwalli M. Topical liquiritin improves melasma. Int J Dermatol. 2000;39:299-301. doi:10.1046/j.1365-4362.2000.00943.x
- Jones K, Hughes J, Hong M, et al. Modulation of melanogenesis by aloesin: a competitive inhibitor of tyrosinase. Pigment Cell Res. 2002;15:335-340. doi:10.1034/j.1600-0749.2002.02014.x
- Hakozaki T, Minwalla L, Zhuang J, et al. The effect of niacinamide on reducing cutaneous pigmentation and suppression of melanosome transfer. Br J Dermatol. 2002;147:20-31. doi:10.1046/j.1365-2133.2002.04834.x
- Wohlrab J, Kreft D. Niacinamide—mechanisms of action and its topical use in dermatology. Skin Pharmacol Physiol. 2014;27:311-315. doi:10.1159/000359974
- Fitzpatrick RE, Rostan EF. Double-blind, half-face study comparing topical vitamin C and vehicle for rejuvenation of photodamage. Dermatol Surg. 2002;28:231-236. doi:10.1046/j.1524-4725.2002.01129.x
- Mehta AB, Nadkarni NJ, Patil SP, et al. Topical corticosteroids in dermatology. Indian J Dermatol Venereol Leprol. 2016;82:371-378. doi:10.4103/0378-6323.178903
- Petit L, Piérard GE. Skin-lightening products revisited. Int J Cosmet Sci. 2003;25:169-181. doi:10.1046/j.1467-2494.2003.00182.x
- Kanwar AJ, Dhar S, Kaur S. Treatment of melasma with potent topical corticosteroids. Dermatol Basel Switz. 1994;188:170. doi:10.1159/000247129
- Paine C, Sharlow E, Liebel F, et al. An alternative approach to depigmentation by soybean extracts via inhibition of the PAR-2 pathway. J Invest Dermatol. 2001;116:587-595. doi:10.1046/j.1523-1747.2001.01291.x
- Seiberg M, Paine C, Sharlow E, et al. Inhibition of melanosome transfer results in skin lightening. J Invest Dermatol. 2000;115:162-167. doi:10.1046/j.1523-1747.2000.00035.x
- Shimogaki H, Tanaka Y, Tamai H, et al. In vitro and in vivo evaluation of ellagic acid on melanogenesis inhibition. Int J Cosmet Sci. 2000;22:291-303. doi:10.1046/j.1467-2494.2000.00023.x
- Rendon MI, Gaviria JI. Review of skin-lightening agents. Dermatol Surg. 2005;31(7 pt 2):886-889; discussion 889. doi:10.1111/j.1524-4725.2005.31736
- Na JI, Shin JW, Choi HR, et al. Resveratrol as a multifunctional topical hypopigmenting agent [published online February 22, 2019]. Int J Mol Sci. 2019;20:956. doi:10.3390/ijms20040956
- Ratz-Łyko A, Arct J. Resveratrol as an active ingredient for cosmetic and dermatological applications: a review. J Cosmet Laser Ther. 2019;21:84-90. doi:10.1080/14764172.2018.1469767
- Choo SJ, Ryoo IJ, Kim YH, et al. Silymarin inhibits melanin synthesis in melanocyte cells. J Pharm Pharmacol. 2009;61:663-667. doi:10.1211/jpp/61.05.0016
- Draelos ZD, Diaz I, Cohen A, et al. A novel skin brightening topical technology. J Cosmet Dermatol. 2020;19:3280-3285. doi:10.1111/jocd.13741
- Grimes P, Bhawan J, Howell M, et al. Histopathological changes induced by malassezin: a novel natural microbiome indole for treatment of facial hyperpigmentation. J Drugs Dermatol. 2022;21:141-145. doi:10.36849/jdd.6596
- Bissett DL. Glucosamine: an ingredient with skin and other benefits. J Cosmet Dermatol. 2006;5:309-315. doi:10.1111/j.1473-2165.2006.00277.x
- Zhu JW, Ni YJ, Tong XY, et al. Tranexamic acid inhibits angiogenesis and melanogenesis in vitro by targeting VEGF receptors. Int J Med Sci. 2020;17:903-911. doi:10.7150/ijms.44188
- Hiramoto K, Yamate Y, Sugiyama D, et al. Tranexamic acid inhibits the plasma and non-irradiated skin markers of photoaging induced by long-term UVA eye irradiation in female mice. Biomed Pharmacother. 2018;107:54-58. doi:10.1016/j.biopha.2018.07.146
- da Silva Souza ID, Lampe L, Winn D. New topical tranexamic acid derivative for the improvement of hyperpigmentation and inflammation in the sun-damaged skin. J Cosmet Dermatol. 2021;20:561-565. doi:10.1111/jocd.13545
- Kim HJ, Moon SH, Cho SH, et al. Efficacy and safety of tranexamic acid in melasma: a meta-analysis and systematic review. Acta Derm Venereol. 2017;97:776-781. doi:10.2340/00015555-2668
- Mathe N, Balogun M, Yoo J. A case report on the use of topical cysteamine 5% cream in the management of refractory postinflammatory hyperpigmentation (PIH) resistant to triple combination cream (hydroquinone, topical corticosteroids, and retinoids). J Cosmet Dermatol. 2021;20:204-206. doi:10.1111/jocd.13755
- Mansouri P, Farshi S, Hashemi Z, et al. Evaluation of the efficacy of cysteamine 5% cream in the treatment of epidermal melasma: a randomized double-blind placebo-controlled trial. Br J Dermatol. 2015;173:209-217. doi:10.1111/bjd.13424
- Lima PB, Dias JAF, Cassiano D, et al. A comparative study of topical 5% cysteamine versus 4% hydroquinone in the treatment of facial melasma in women. Int J Dermatol. 2020;59:1531-1536. doi:10.1111/ijd.15146
Stem cell transplants for MS are a ‘reasonable option,’ but questions persist
NATIONAL HARBOR, MD. – .” But, he said, it remains unclear which patients should undergo the procedure.
An especially pressing question is “whether transplant is an alternative to our high-efficacy disease-modifying therapies” (DMTs) in some high-risk patients, Jeffrey A. Cohen, MD, director of experimental therapeutics at Cleveland Clinic’s Mellen Center, said in a presidential lecture at the annual meeting of the Consortium of Multiple Sclerosis Centers.

A handful of ongoing randomized controlled trials will bring answers, he said.
Stem cell therapy exists because there are gaps in MS treatment, Dr. Cohen said. “We have now more than 20 medications. However, none of these therapies is completely effective in all patients. In particular, there are some patients with very active disease who continue to have relapses or new MRI lesion activity despite treatment with all of the available therapies.”
And in progressive MS, the efficacy of a couple of agents is modest and mainly for people with ongoing focal lesion activity, he said. “Finally, all of these currently available therapies are intended primarily to prevent the accumulation of damage, and none of them directly promotes repair. So despite our progress in the field, there still are a number of unmet needs.”
‘Rebooting’ the immune system
Several types of stem cell therapy exist, including remyelination and anti-inflammatory therapy, Dr. Cohen said. In his lecture, he focused on immunoablative or myeloablative therapy followed by autologous hematopoietic stem cell transplantation.
This “complicated, multistep procedure” involves first eliminating the immune system to get rid of pathogenic inflammatory cells. This “big component is actually the therapy for MS. It’s also the step that has the most potential complications,” he said.
According to Dr. Cohen, the next step has been described as “rebooting” the immune system.
Does this procedure help patients with MS? In relapsing MS, reports suggest there’s “almost complete abrogation of disease activity following transplant,” he said, “a benefit that’s lasted 5-10-15 years. In addition, there’s also a benefit on the accumulation of CNS damage as measured by whole brain atrophy.”
Recent data, he said, suggests that MS patients most likely to benefit are young, developed MS relatively recently, are still ambulatory, and have highly active MS despite treatment with first- and second-line agents.
However, there have only been two randomized controlled trials of stem cell transplantation versus DMT, and Dr. Cohen said both studies have limitations. The first one, from 2015, is very small, with just 21 subjects. The second study – from 2019 – is larger (n = 103), but some patients weren’t taking higher-efficacy DMTs.
Other research is more promising: Dr. Cohen highlighted a 2017 analysis that found patients with relapsing/remitting MS who underwent stem-cell transplantation were more likely to be symptom-free at 2 years (78%-83%) than those who took DMTs in clinical trials (13%-46%).
Clinical concerns
As for side effects of stem cell transplantation, Dr. Cohen said, “most patients have some adverse effects during the procedure itself. There may be an MS relapse or pseudorelapses in association with the mobilization and the conditioning regimens.”
A wide range of other adverse effects is possible before the immune system is reconstituted, he said, including reactivation of various virus infections, such as HPV, CMV or EPV (Epstein-Barr virus), secondary autoimmune phenomenon, and secondary malignancy. EPV infection is also common after transplant, and is “probably the most troublesome posttransplant complication from a management point of view,” he said.
“Thankfully, once the patient ... recovers from the transplant procedure, late adverse effects are relatively uncommon, the most common of which would be infertility,” he said. “There have been some reports of successful pregnancies following transplant, but it’s important to advise people who are considering transplant that most men and women have infertility after the procedure. So if they desire to have children afterward, they need to be counseled on necessary preparations to do that.”
What about progressive multifocal leukoencephalopathy (PML), which seems a possible risk because of the suppression of the immune system? Dr. Cohen is aware of one case linked to a stem-cell transplant, and it may not have been caused by the procedure.
Cost is another potential obstacle, he noted. The National Multiple Sclerosis Society estimates that autologous hematopoietic stem cell transplants cost $150,000 on average in the U.S., although the expense varies widely.
Unanswered questions
Moving forward, Dr. Cohen said it remains unclear how these procedures fare against the newest generations of DMTs in MS. Five phase 3 randomized controlled trials are now trying to clarify the matter, he said, by pitting stem-cell transplantation against various MS drugs – alemtuzumab, cladribine, natalizumab, ocrelizumab, and rituximab.
There are also unanswered questions about the best conditioning regimens in the transplants, he said, and lack of clarity about where to draw the line between eligible and ineligible patients with MS. “How many DMTs does the person have to fail? What’s the upper level of disability beyond which it is unlikely to be helpful and more likely to cause harm?”
He added: “A particular profile that we’re seeing increasingly at our center is someone with very active disease and onset who gets started on a high-efficacy therapy as their first therapy and effectively stops relapses and MRI lesion activity. But within a couple of years, we can tell that they’re already starting to accumulate disability. Is this someone for whom transplant might be useful, and by extension, is transplant appropriate as the first therapy in some patients? And beyond MS, is transplant a consideration for other autoimmune CNS disorders? There are lots of unanswered questions, which future studies will hopefully begin to address.”
Dr. Cohen reports consulting for Biogen, Bristol‐Myers Squibb, Convelo, EMD Serono, GlaxoSmithKline (now GSK), Janssen, Mylan, and PSI. He serves as an editor of Multiple Sclerosis Journal.
NATIONAL HARBOR, MD. – .” But, he said, it remains unclear which patients should undergo the procedure.
An especially pressing question is “whether transplant is an alternative to our high-efficacy disease-modifying therapies” (DMTs) in some high-risk patients, Jeffrey A. Cohen, MD, director of experimental therapeutics at Cleveland Clinic’s Mellen Center, said in a presidential lecture at the annual meeting of the Consortium of Multiple Sclerosis Centers.
A handful of ongoing randomized controlled trials will bring answers, he said.
Stem cell therapy exists because there are gaps in MS treatment, Dr. Cohen said. “We have now more than 20 medications. However, none of these therapies is completely effective in all patients. In particular, there are some patients with very active disease who continue to have relapses or new MRI lesion activity despite treatment with all of the available therapies.”
And in progressive MS, the efficacy of a couple of agents is modest and mainly for people with ongoing focal lesion activity, he said. “Finally, all of these currently available therapies are intended primarily to prevent the accumulation of damage, and none of them directly promotes repair. So despite our progress in the field, there still are a number of unmet needs.”
‘Rebooting’ the immune system
Several types of stem cell therapy exist, including remyelination and anti-inflammatory therapy, Dr. Cohen said. In his lecture, he focused on immunoablative or myeloablative therapy followed by autologous hematopoietic stem cell transplantation.
This “complicated, multistep procedure” involves first eliminating the immune system to get rid of pathogenic inflammatory cells. This “big component is actually the therapy for MS. It’s also the step that has the most potential complications,” he said.
According to Dr. Cohen, the next step has been described as “rebooting” the immune system.
Does this procedure help patients with MS? In relapsing MS, reports suggest there’s “almost complete abrogation of disease activity following transplant,” he said, “a benefit that’s lasted 5-10-15 years. In addition, there’s also a benefit on the accumulation of CNS damage as measured by whole brain atrophy.”
Recent data, he said, suggests that MS patients most likely to benefit are young, developed MS relatively recently, are still ambulatory, and have highly active MS despite treatment with first- and second-line agents.
However, there have only been two randomized controlled trials of stem cell transplantation versus DMT, and Dr. Cohen said both studies have limitations. The first one, from 2015, is very small, with just 21 subjects. The second study – from 2019 – is larger (n = 103), but some patients weren’t taking higher-efficacy DMTs.
Other research is more promising: Dr. Cohen highlighted a 2017 analysis that found patients with relapsing/remitting MS who underwent stem-cell transplantation were more likely to be symptom-free at 2 years (78%-83%) than those who took DMTs in clinical trials (13%-46%).
Clinical concerns
As for side effects of stem cell transplantation, Dr. Cohen said, “most patients have some adverse effects during the procedure itself. There may be an MS relapse or pseudorelapses in association with the mobilization and the conditioning regimens.”
A wide range of other adverse effects is possible before the immune system is reconstituted, he said, including reactivation of various virus infections, such as HPV, CMV or EPV (Epstein-Barr virus), secondary autoimmune phenomenon, and secondary malignancy. EPV infection is also common after transplant, and is “probably the most troublesome posttransplant complication from a management point of view,” he said.
“Thankfully, once the patient ... recovers from the transplant procedure, late adverse effects are relatively uncommon, the most common of which would be infertility,” he said. “There have been some reports of successful pregnancies following transplant, but it’s important to advise people who are considering transplant that most men and women have infertility after the procedure. So if they desire to have children afterward, they need to be counseled on necessary preparations to do that.”
What about progressive multifocal leukoencephalopathy (PML), which seems a possible risk because of the suppression of the immune system? Dr. Cohen is aware of one case linked to a stem-cell transplant, and it may not have been caused by the procedure.
Cost is another potential obstacle, he noted. The National Multiple Sclerosis Society estimates that autologous hematopoietic stem cell transplants cost $150,000 on average in the U.S., although the expense varies widely.
Unanswered questions
Moving forward, Dr. Cohen said it remains unclear how these procedures fare against the newest generations of DMTs in MS. Five phase 3 randomized controlled trials are now trying to clarify the matter, he said, by pitting stem-cell transplantation against various MS drugs – alemtuzumab, cladribine, natalizumab, ocrelizumab, and rituximab.
There are also unanswered questions about the best conditioning regimens in the transplants, he said, and lack of clarity about where to draw the line between eligible and ineligible patients with MS. “How many DMTs does the person have to fail? What’s the upper level of disability beyond which it is unlikely to be helpful and more likely to cause harm?”
He added: “A particular profile that we’re seeing increasingly at our center is someone with very active disease and onset who gets started on a high-efficacy therapy as their first therapy and effectively stops relapses and MRI lesion activity. But within a couple of years, we can tell that they’re already starting to accumulate disability. Is this someone for whom transplant might be useful, and by extension, is transplant appropriate as the first therapy in some patients? And beyond MS, is transplant a consideration for other autoimmune CNS disorders? There are lots of unanswered questions, which future studies will hopefully begin to address.”
Dr. Cohen reports consulting for Biogen, Bristol‐Myers Squibb, Convelo, EMD Serono, GlaxoSmithKline (now GSK), Janssen, Mylan, and PSI. He serves as an editor of Multiple Sclerosis Journal.
NATIONAL HARBOR, MD. – .” But, he said, it remains unclear which patients should undergo the procedure.
An especially pressing question is “whether transplant is an alternative to our high-efficacy disease-modifying therapies” (DMTs) in some high-risk patients, Jeffrey A. Cohen, MD, director of experimental therapeutics at Cleveland Clinic’s Mellen Center, said in a presidential lecture at the annual meeting of the Consortium of Multiple Sclerosis Centers.
A handful of ongoing randomized controlled trials will bring answers, he said.
Stem cell therapy exists because there are gaps in MS treatment, Dr. Cohen said. “We have now more than 20 medications. However, none of these therapies is completely effective in all patients. In particular, there are some patients with very active disease who continue to have relapses or new MRI lesion activity despite treatment with all of the available therapies.”
And in progressive MS, the efficacy of a couple of agents is modest and mainly for people with ongoing focal lesion activity, he said. “Finally, all of these currently available therapies are intended primarily to prevent the accumulation of damage, and none of them directly promotes repair. So despite our progress in the field, there still are a number of unmet needs.”
‘Rebooting’ the immune system
Several types of stem cell therapy exist, including remyelination and anti-inflammatory therapy, Dr. Cohen said. In his lecture, he focused on immunoablative or myeloablative therapy followed by autologous hematopoietic stem cell transplantation.
This “complicated, multistep procedure” involves first eliminating the immune system to get rid of pathogenic inflammatory cells. This “big component is actually the therapy for MS. It’s also the step that has the most potential complications,” he said.
According to Dr. Cohen, the next step has been described as “rebooting” the immune system.
Does this procedure help patients with MS? In relapsing MS, reports suggest there’s “almost complete abrogation of disease activity following transplant,” he said, “a benefit that’s lasted 5-10-15 years. In addition, there’s also a benefit on the accumulation of CNS damage as measured by whole brain atrophy.”
Recent data, he said, suggests that MS patients most likely to benefit are young, developed MS relatively recently, are still ambulatory, and have highly active MS despite treatment with first- and second-line agents.
However, there have only been two randomized controlled trials of stem cell transplantation versus DMT, and Dr. Cohen said both studies have limitations. The first one, from 2015, is very small, with just 21 subjects. The second study – from 2019 – is larger (n = 103), but some patients weren’t taking higher-efficacy DMTs.
Other research is more promising: Dr. Cohen highlighted a 2017 analysis that found patients with relapsing/remitting MS who underwent stem-cell transplantation were more likely to be symptom-free at 2 years (78%-83%) than those who took DMTs in clinical trials (13%-46%).
Clinical concerns
As for side effects of stem cell transplantation, Dr. Cohen said, “most patients have some adverse effects during the procedure itself. There may be an MS relapse or pseudorelapses in association with the mobilization and the conditioning regimens.”
A wide range of other adverse effects is possible before the immune system is reconstituted, he said, including reactivation of various virus infections, such as HPV, CMV or EPV (Epstein-Barr virus), secondary autoimmune phenomenon, and secondary malignancy. EPV infection is also common after transplant, and is “probably the most troublesome posttransplant complication from a management point of view,” he said.
“Thankfully, once the patient ... recovers from the transplant procedure, late adverse effects are relatively uncommon, the most common of which would be infertility,” he said. “There have been some reports of successful pregnancies following transplant, but it’s important to advise people who are considering transplant that most men and women have infertility after the procedure. So if they desire to have children afterward, they need to be counseled on necessary preparations to do that.”
What about progressive multifocal leukoencephalopathy (PML), which seems a possible risk because of the suppression of the immune system? Dr. Cohen is aware of one case linked to a stem-cell transplant, and it may not have been caused by the procedure.
Cost is another potential obstacle, he noted. The National Multiple Sclerosis Society estimates that autologous hematopoietic stem cell transplants cost $150,000 on average in the U.S., although the expense varies widely.
Unanswered questions
Moving forward, Dr. Cohen said it remains unclear how these procedures fare against the newest generations of DMTs in MS. Five phase 3 randomized controlled trials are now trying to clarify the matter, he said, by pitting stem-cell transplantation against various MS drugs – alemtuzumab, cladribine, natalizumab, ocrelizumab, and rituximab.
There are also unanswered questions about the best conditioning regimens in the transplants, he said, and lack of clarity about where to draw the line between eligible and ineligible patients with MS. “How many DMTs does the person have to fail? What’s the upper level of disability beyond which it is unlikely to be helpful and more likely to cause harm?”
He added: “A particular profile that we’re seeing increasingly at our center is someone with very active disease and onset who gets started on a high-efficacy therapy as their first therapy and effectively stops relapses and MRI lesion activity. But within a couple of years, we can tell that they’re already starting to accumulate disability. Is this someone for whom transplant might be useful, and by extension, is transplant appropriate as the first therapy in some patients? And beyond MS, is transplant a consideration for other autoimmune CNS disorders? There are lots of unanswered questions, which future studies will hopefully begin to address.”
Dr. Cohen reports consulting for Biogen, Bristol‐Myers Squibb, Convelo, EMD Serono, GlaxoSmithKline (now GSK), Janssen, Mylan, and PSI. He serves as an editor of Multiple Sclerosis Journal.
At CMSC 2022
HIV care continuum conundrum: Challenges of out-of-care patients
Among an estimated 87% of people with HIV (PWH) whose condition has been diagnosed, roughly 66% have received medication. But only half are retained in care, leaving substantial risk for viral rebound and further HIV transmission.
A variety of factors contribute to falling out of care (OOC), a primary reason why a team from the Centers for Disease Control and Prevention reviewed over three decades of studies with the goal of identifying best practices for re-engagement.
The research, which was published in the journal AIDS, underscores the need for more customized strategies, rather than a one-size-fits-all approach, especially for historically underserved communities.
“Many study participants across the studies included in this review represented communities who have the largest challenges with remaining in care,” Darrel H. Higa, PhD, MSW, lead study author and a behavioral scientist at the CDC in Atlanta, told this news organization.
For example, “Some face barriers that may limit their access to care ... including not having health insurance or being unable to pay for doctor visits or medication, HIV-related stigma, racism, homophobia, transphobia, health literacy, and a lack of providers who specialize in HIV care,” he said.
Other challenges relate to personal barriers, such as competing priorities (for example, work or childcare), substance use, mental health disorders, transportation problems, or a lack of social support.
Even with improvements that address some of these barriers, such as expanded access to health care insurance and broader provision of medical care and HIV medications through the national Ryan White program, structural challenges and social barriers persist.
Better versus best practices
In their analysis, the CDC team expanded the scope of prior reviews by including literature published between 2000 and 2020 and further conducted meta-analyses to assess the effectiveness of five common, non mutually exclusive interventions:
- patient navigation
- appointment help/alerts
- psychosocial support
- transportation/appointment reminders
- data-to-care HIV care outcomes (using health department surveillance data and/or patient health records to identify and re-engage OOC PWH)
The majority of the 26,154 participants in 39 included studies (incorporating 42 unique interventions) were male (71%) and Black (64%); the most common time frame for OOC was between 6 and 12 months, but some studies used a time frame of 3-4 months, and others more than 12 months.
Definitions for re-engagement and retention were likewise inconsistent across studies but most commonly involved having an HIV medical visit or viral load test record between 2 and 6 months (re-engagement), and ≥ 1 medical visits in each 6-month period a minimum of 60 days apart for a period of over 2 years (retention).
This is notable, as it points to the role played – at least in part – by the care fragmentation inherent in the United States health care system. Without national indicators or thresholds for clinical outcomes, services are unlikely to reach scale.
said Mary Jane Rotheram-Borus, PhD, distinguished professor of clinical psychology and director of the Global Center for Children and Families at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles. (Dr. Rotheram-Borus authored an accompanying editorial but was not involved in the study.)
Nevertheless, review findings highlighted that overall, the five interventions appeared to improve care re-engagement (odds ratio = 1.79, 95% confidence interval, 1.36-2.36), care retention (OR = 2.01; 95% CI, 1.64-2.46), and viral suppression (OR = 2.50; 95% CI, 1.87-2.24).
Overall, the five strategies were associated with optimal re-engagement and retention in care. In addition, four of them were associated with viral suppression for PWH who were OOC during the study time frame. The one exception was data-to-care, for which the evidence supporting an association with viral suppression was unclear.
Because of the similarities between patient navigation and transportation/appointment accompaniment, the researchers also compared PWH who received combined strategies to those who did not.
“The findings suggest that patient navigation services that often include helping with transportation to appointments or accompanying PWH to appointments may be more effective compared to interventions without the combination,” explained Dr. Higa, “especially for communities with the largest challenges remaining in care.”
He added that, moving forward, many of the same strategies that help re-engage out-of-care PWH may be useful for retention. These include co-locating services, outreach, mental health services, clinical care models, telemedicine, and financial incentives.
Despite its financial investments toward ending the HIV epidemic, the United States arguably still has a long way to go to improve retention and care.
Still, Dr. Rotheram-Borus underscores the silver lining.
“The breakthroughs in medication are substantial,” she said, pointing to her own research, which has shown that at least 60% of newly infected, poor, LGBTQ+ young people up to age 24 have been linked to care and are adherent enough to be virally suppressed.
For PWH who are out of care, perhaps treatment advances – including long-acting injectables – may ultimately fill in the gaps.
Dr. Higa and Dr. Rotherum-Borus report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Among an estimated 87% of people with HIV (PWH) whose condition has been diagnosed, roughly 66% have received medication. But only half are retained in care, leaving substantial risk for viral rebound and further HIV transmission.
A variety of factors contribute to falling out of care (OOC), a primary reason why a team from the Centers for Disease Control and Prevention reviewed over three decades of studies with the goal of identifying best practices for re-engagement.
The research, which was published in the journal AIDS, underscores the need for more customized strategies, rather than a one-size-fits-all approach, especially for historically underserved communities.
“Many study participants across the studies included in this review represented communities who have the largest challenges with remaining in care,” Darrel H. Higa, PhD, MSW, lead study author and a behavioral scientist at the CDC in Atlanta, told this news organization.
For example, “Some face barriers that may limit their access to care ... including not having health insurance or being unable to pay for doctor visits or medication, HIV-related stigma, racism, homophobia, transphobia, health literacy, and a lack of providers who specialize in HIV care,” he said.
Other challenges relate to personal barriers, such as competing priorities (for example, work or childcare), substance use, mental health disorders, transportation problems, or a lack of social support.
Even with improvements that address some of these barriers, such as expanded access to health care insurance and broader provision of medical care and HIV medications through the national Ryan White program, structural challenges and social barriers persist.
Better versus best practices
In their analysis, the CDC team expanded the scope of prior reviews by including literature published between 2000 and 2020 and further conducted meta-analyses to assess the effectiveness of five common, non mutually exclusive interventions:
- patient navigation
- appointment help/alerts
- psychosocial support
- transportation/appointment reminders
- data-to-care HIV care outcomes (using health department surveillance data and/or patient health records to identify and re-engage OOC PWH)
The majority of the 26,154 participants in 39 included studies (incorporating 42 unique interventions) were male (71%) and Black (64%); the most common time frame for OOC was between 6 and 12 months, but some studies used a time frame of 3-4 months, and others more than 12 months.
Definitions for re-engagement and retention were likewise inconsistent across studies but most commonly involved having an HIV medical visit or viral load test record between 2 and 6 months (re-engagement), and ≥ 1 medical visits in each 6-month period a minimum of 60 days apart for a period of over 2 years (retention).
This is notable, as it points to the role played – at least in part – by the care fragmentation inherent in the United States health care system. Without national indicators or thresholds for clinical outcomes, services are unlikely to reach scale.
said Mary Jane Rotheram-Borus, PhD, distinguished professor of clinical psychology and director of the Global Center for Children and Families at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles. (Dr. Rotheram-Borus authored an accompanying editorial but was not involved in the study.)
Nevertheless, review findings highlighted that overall, the five interventions appeared to improve care re-engagement (odds ratio = 1.79, 95% confidence interval, 1.36-2.36), care retention (OR = 2.01; 95% CI, 1.64-2.46), and viral suppression (OR = 2.50; 95% CI, 1.87-2.24).
Overall, the five strategies were associated with optimal re-engagement and retention in care. In addition, four of them were associated with viral suppression for PWH who were OOC during the study time frame. The one exception was data-to-care, for which the evidence supporting an association with viral suppression was unclear.
Because of the similarities between patient navigation and transportation/appointment accompaniment, the researchers also compared PWH who received combined strategies to those who did not.
“The findings suggest that patient navigation services that often include helping with transportation to appointments or accompanying PWH to appointments may be more effective compared to interventions without the combination,” explained Dr. Higa, “especially for communities with the largest challenges remaining in care.”
He added that, moving forward, many of the same strategies that help re-engage out-of-care PWH may be useful for retention. These include co-locating services, outreach, mental health services, clinical care models, telemedicine, and financial incentives.
Despite its financial investments toward ending the HIV epidemic, the United States arguably still has a long way to go to improve retention and care.
Still, Dr. Rotheram-Borus underscores the silver lining.
“The breakthroughs in medication are substantial,” she said, pointing to her own research, which has shown that at least 60% of newly infected, poor, LGBTQ+ young people up to age 24 have been linked to care and are adherent enough to be virally suppressed.
For PWH who are out of care, perhaps treatment advances – including long-acting injectables – may ultimately fill in the gaps.
Dr. Higa and Dr. Rotherum-Borus report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Among an estimated 87% of people with HIV (PWH) whose condition has been diagnosed, roughly 66% have received medication. But only half are retained in care, leaving substantial risk for viral rebound and further HIV transmission.
A variety of factors contribute to falling out of care (OOC), a primary reason why a team from the Centers for Disease Control and Prevention reviewed over three decades of studies with the goal of identifying best practices for re-engagement.
The research, which was published in the journal AIDS, underscores the need for more customized strategies, rather than a one-size-fits-all approach, especially for historically underserved communities.
“Many study participants across the studies included in this review represented communities who have the largest challenges with remaining in care,” Darrel H. Higa, PhD, MSW, lead study author and a behavioral scientist at the CDC in Atlanta, told this news organization.
For example, “Some face barriers that may limit their access to care ... including not having health insurance or being unable to pay for doctor visits or medication, HIV-related stigma, racism, homophobia, transphobia, health literacy, and a lack of providers who specialize in HIV care,” he said.
Other challenges relate to personal barriers, such as competing priorities (for example, work or childcare), substance use, mental health disorders, transportation problems, or a lack of social support.
Even with improvements that address some of these barriers, such as expanded access to health care insurance and broader provision of medical care and HIV medications through the national Ryan White program, structural challenges and social barriers persist.
Better versus best practices
In their analysis, the CDC team expanded the scope of prior reviews by including literature published between 2000 and 2020 and further conducted meta-analyses to assess the effectiveness of five common, non mutually exclusive interventions:
- patient navigation
- appointment help/alerts
- psychosocial support
- transportation/appointment reminders
- data-to-care HIV care outcomes (using health department surveillance data and/or patient health records to identify and re-engage OOC PWH)
The majority of the 26,154 participants in 39 included studies (incorporating 42 unique interventions) were male (71%) and Black (64%); the most common time frame for OOC was between 6 and 12 months, but some studies used a time frame of 3-4 months, and others more than 12 months.
Definitions for re-engagement and retention were likewise inconsistent across studies but most commonly involved having an HIV medical visit or viral load test record between 2 and 6 months (re-engagement), and ≥ 1 medical visits in each 6-month period a minimum of 60 days apart for a period of over 2 years (retention).
This is notable, as it points to the role played – at least in part – by the care fragmentation inherent in the United States health care system. Without national indicators or thresholds for clinical outcomes, services are unlikely to reach scale.
said Mary Jane Rotheram-Borus, PhD, distinguished professor of clinical psychology and director of the Global Center for Children and Families at the Semel Institute for Neuroscience and Human Behavior at the University of California, Los Angeles. (Dr. Rotheram-Borus authored an accompanying editorial but was not involved in the study.)
Nevertheless, review findings highlighted that overall, the five interventions appeared to improve care re-engagement (odds ratio = 1.79, 95% confidence interval, 1.36-2.36), care retention (OR = 2.01; 95% CI, 1.64-2.46), and viral suppression (OR = 2.50; 95% CI, 1.87-2.24).
Overall, the five strategies were associated with optimal re-engagement and retention in care. In addition, four of them were associated with viral suppression for PWH who were OOC during the study time frame. The one exception was data-to-care, for which the evidence supporting an association with viral suppression was unclear.
Because of the similarities between patient navigation and transportation/appointment accompaniment, the researchers also compared PWH who received combined strategies to those who did not.
“The findings suggest that patient navigation services that often include helping with transportation to appointments or accompanying PWH to appointments may be more effective compared to interventions without the combination,” explained Dr. Higa, “especially for communities with the largest challenges remaining in care.”
He added that, moving forward, many of the same strategies that help re-engage out-of-care PWH may be useful for retention. These include co-locating services, outreach, mental health services, clinical care models, telemedicine, and financial incentives.
Despite its financial investments toward ending the HIV epidemic, the United States arguably still has a long way to go to improve retention and care.
Still, Dr. Rotheram-Borus underscores the silver lining.
“The breakthroughs in medication are substantial,” she said, pointing to her own research, which has shown that at least 60% of newly infected, poor, LGBTQ+ young people up to age 24 have been linked to care and are adherent enough to be virally suppressed.
For PWH who are out of care, perhaps treatment advances – including long-acting injectables – may ultimately fill in the gaps.
Dr. Higa and Dr. Rotherum-Borus report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Endoscopic management of duodenal and ampullary adenomas
Duodenal polyps are a relatively rare entity with a reported incidence of 0.3%-4.6%.1 There are three major types of duodenal adenomas: sporadic, nonampullary duodenal adenomas (SNDAs), adenomas in familial adenomatous polyposis syndrome, and ampullary adenomas. It is important to distinguish between the different types of duodenal polyps as the management may differ depending on the etiology.

SNDAs constitute <10% of all duodenal polyps, most commonly located in the second portion of the duodenum, and up to 85% have been shown to have malignant transformation over time.2 Most of the studies of SNDAs are small series, and there are no consensus guidelines for management. Villous features increase malignancy risk, thus resection of SNDAs is advised.3-7 It has also been shown that 72% of patients with SNDAs also have colon polyps,8 and therefore these patients should be up to date on colonoscopy screening.
Ampullary adenomas are less common, but up to half may be associated with familial adenomatous polyposis (FAP), and some may be surveyed.9 However, those that are larger than 10 mm or have villous features may raise concern for malignancy with up to half harboring small foci of adenocarcinoma.10,11 These require ERCP with ampullectomy. For the purposes of this paper, we will focus on endoscopic resection of SNDAs and ampullary adenomas.
Endoscopic mucosal resection (EMR) of duodenal polyps can be technically challenging. There are considerations specific to the duodenum: thin muscle layer, increased motility, and significant vascular supply including two major arterial supplies – the gastroduodenal artery from the celiac branch and the inferior pancreaticoduodenal artery from the superior mesenteric artery. These factors may explain higher reported rates of perforation and bleeding compared to colon EMR.

After a detailed inspection is performed to define the duodenal polyp in terms of size, location, and position relative to the ampulla, a submucosal injection is performed using a dye solution. Once adequate lift is achieved, the lesion is resected using stiff monofilament snares. If possible, resection sites are closed with hemostatic clips, although their utility in preventing delayed complications may be less than that in the colon because of increased motility causing them to become dislodged more easily. We avoid using snares larger than 2 cm given increased risk of perforation. Intraprocedural bleeding may be controlled with coagulation graspers on soft coagulation setting; using a bipolar electrocoagulation therapy or argon plasma coagulation is avoided, as these have been shown to increase rates of complications. Figure 1 provides examples of duodenal adenomas that have been resected.
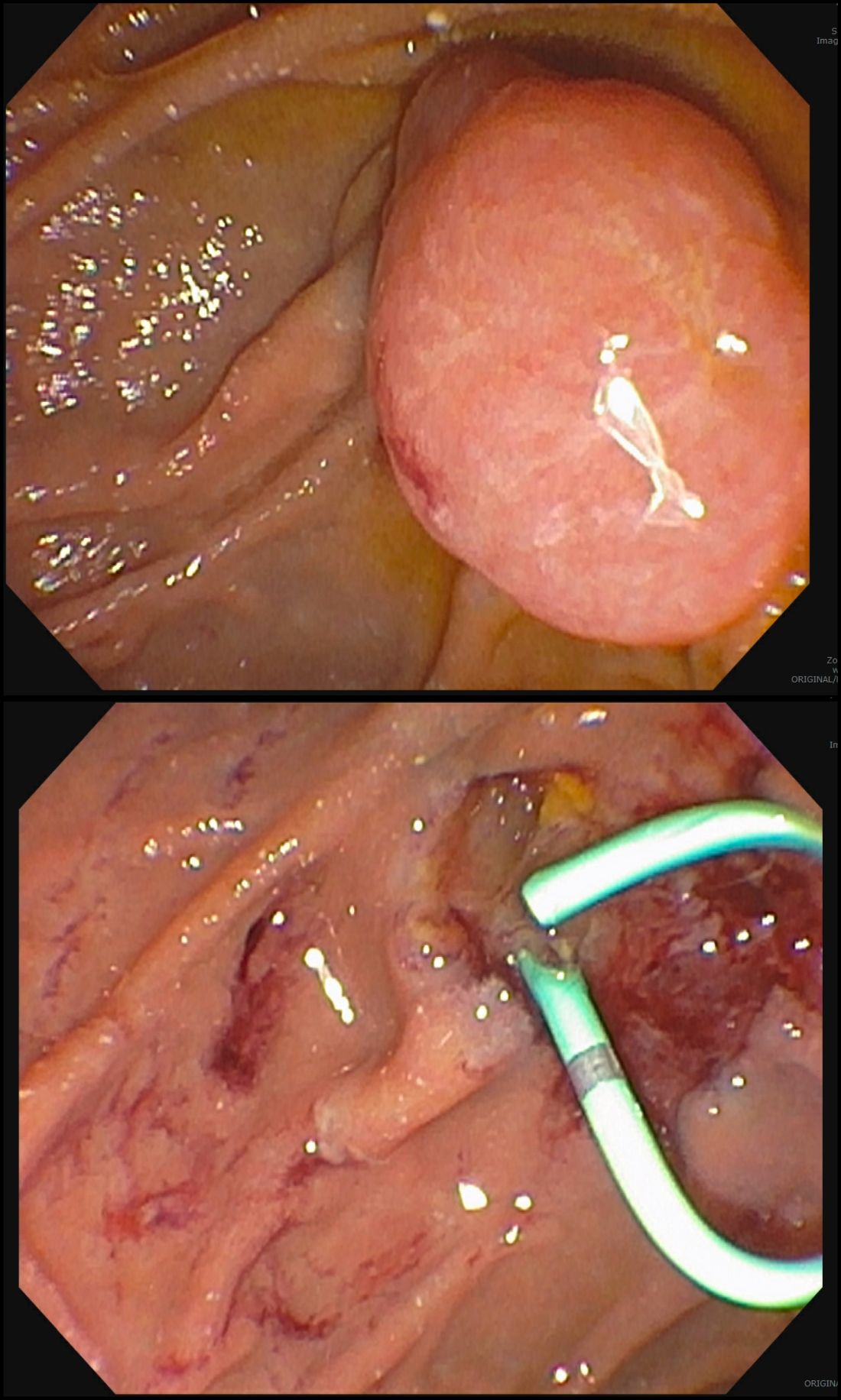
The ampullectomy technique is slightly different from duodenal EMRs and carries the additional risk of pancreatitis.12,13 In our opinion, there is low utility for submucosal injection unless there is a laterally spreading component onto the duodenal wall, as injection of the ampulla itself does not lift well and simply distorts views. Typically, both the common bile duct and the pancreatic duct are injected with contrast, and we typically perform a biliary sphincterotomy prior to ampullectomy. Based on endoscopist preference, one can also leave a guide wire in the pancreatic duct (PD) and pass the snare over it to perform resection to maintain access for a subsequent stent placement. This technique has the advantage of never losing pancreatic duct access, which can occur after resection from edema or bleeding and allows easy PD stent placement. The snare should be opened in a line corresponding to the long axis of the mound with the snare tip anchored above the apex of the papilla and snare opened and drawn down over the papilla. After resection, the PD must be stented to minimize pancreatitis risk.14 Figure 2 shows an ampullary adenoma pre and post EMR, with a PD stent.
Recurrence of duodenal adenomas, both SNDAs and ampullary, can be quite high, with reports up to 39%.15-18 Risk factors include histology and size, but interestingly were not shown to be associated with en-bloc resection.15,19 On the other hand, intraprocedural bleeding also occurs in up to 43% of patients and is associated with size, number of resections, and procedure time.20 Per 2015 ASGE Standards of Practice, duodenal lesions warrant short follow-up at 3- to 6-month intervals given high recurrence rates, then at 6- to 12-month intervals for 2-5 years thereafter.21
When a duodenal polyp is detected, it is important to determine which type of adenoma it is to guide management. There are various techniques utilized to perform duodenal EMR and ampullectomy with some highlighted in this article. It is important to understand how to recognize, prevent, and manage associated adverse events, as well as to have a surveillance plan given the risk of recurrence.
Dr. Kim has no disclosures. Dr. Siddiqui has financial relationships with Boston Scientific (research support, consulting fees, speaking honoraria); Cook, Medtronic, ConMed (consulting fees, speaking honoraria); and Pinnacle Biologic, Ovesco (speaking honoraria).
Dr. Kim is a GI fellow, section of gastroenterology, hepatology, and nutrition, department of internal medicine, University of Chicago. Dr. Siddiqui is a professor of medicine and the director of the Center for Endoscopic Research and Therapeutics (CERT), section of gastroenterology, hepatology, and nutrition, department of internal medicine, University of Chicago.
References
1. Jepsen JM et al. Scand J Gastroenterol. Jun 1994;29(6):483-7.
2. Sellner F. Cancer. 1990 Aug 15;66(4):702-15.
3. Witteman BJ et al. Neth J Med. 1993 Feb;42(1-2):5-11.
4. Reddy RR et al. J Clin Gastroenterol. 1981 Jun;3(2):139-47.
5. Sakorafas GH et al. Scand J Gastroenterol. 2000 Apr;35(4):337-44.
6. Galandiuk S et al. Ann Surg. 1988 Mar;207(3):234-9.
7. Farnell MB et al. J Gastrointest Surg. 2000 Jan-Feb;4(1):13-21, discussion 22-3.
8. Apel D et al. Gastrointest Endosc. 2004 Sep;60(3):397-9.
9. Kashiwagi H et al. Lancet. 1994 Dec 3;344(8936):1582.
10. Clary BM et al. Surgery. 2000 Jun;127(6):628-33.
11. Posner S et al. Surgery. 2000 Oct;128(4):694-701.
12. Harewood GC et al. Gastrointest Endosc. 2005 Sep;62(3):367-70.
13. Chini P et al. World J Gastrointest Endosc. 2011 Dec 16;3(12):241-7.
14. Chang WI et al. Gut Liver. May 2014;8(3):306-12.
15. Hoibian S et al. Ann Gastroenterol. 2021;34(2):169-176. doi: 10.20524/aog.2021.0581.
16. Kakushima N et al. World J Gastroenterol. 2014 Sep 21;20(35):12501-8.
17. Lienert A and Bagshaw PF. ANZ J Surg. 2007 May;77(5):371-3.
18. Singh A et al. Gastrointest Endosc. 2016 Oct;84(4):700-8.
19. Tomizawa Y and Ginsberg GG. Gastrointest Endosc. 2018 May;87(5):1270-8.
20. Klein A et al. Gastrointest Endosc. 2016 Oct;84(4):688-96.
21. Chathadi KV et al. Gastrointest Endosc. 2015 Nov;82(5):773-81.
Duodenal polyps are a relatively rare entity with a reported incidence of 0.3%-4.6%.1 There are three major types of duodenal adenomas: sporadic, nonampullary duodenal adenomas (SNDAs), adenomas in familial adenomatous polyposis syndrome, and ampullary adenomas. It is important to distinguish between the different types of duodenal polyps as the management may differ depending on the etiology.
SNDAs constitute <10% of all duodenal polyps, most commonly located in the second portion of the duodenum, and up to 85% have been shown to have malignant transformation over time.2 Most of the studies of SNDAs are small series, and there are no consensus guidelines for management. Villous features increase malignancy risk, thus resection of SNDAs is advised.3-7 It has also been shown that 72% of patients with SNDAs also have colon polyps,8 and therefore these patients should be up to date on colonoscopy screening.
Ampullary adenomas are less common, but up to half may be associated with familial adenomatous polyposis (FAP), and some may be surveyed.9 However, those that are larger than 10 mm or have villous features may raise concern for malignancy with up to half harboring small foci of adenocarcinoma.10,11 These require ERCP with ampullectomy. For the purposes of this paper, we will focus on endoscopic resection of SNDAs and ampullary adenomas.
Endoscopic mucosal resection (EMR) of duodenal polyps can be technically challenging. There are considerations specific to the duodenum: thin muscle layer, increased motility, and significant vascular supply including two major arterial supplies – the gastroduodenal artery from the celiac branch and the inferior pancreaticoduodenal artery from the superior mesenteric artery. These factors may explain higher reported rates of perforation and bleeding compared to colon EMR.
After a detailed inspection is performed to define the duodenal polyp in terms of size, location, and position relative to the ampulla, a submucosal injection is performed using a dye solution. Once adequate lift is achieved, the lesion is resected using stiff monofilament snares. If possible, resection sites are closed with hemostatic clips, although their utility in preventing delayed complications may be less than that in the colon because of increased motility causing them to become dislodged more easily. We avoid using snares larger than 2 cm given increased risk of perforation. Intraprocedural bleeding may be controlled with coagulation graspers on soft coagulation setting; using a bipolar electrocoagulation therapy or argon plasma coagulation is avoided, as these have been shown to increase rates of complications. Figure 1 provides examples of duodenal adenomas that have been resected.
The ampullectomy technique is slightly different from duodenal EMRs and carries the additional risk of pancreatitis.12,13 In our opinion, there is low utility for submucosal injection unless there is a laterally spreading component onto the duodenal wall, as injection of the ampulla itself does not lift well and simply distorts views. Typically, both the common bile duct and the pancreatic duct are injected with contrast, and we typically perform a biliary sphincterotomy prior to ampullectomy. Based on endoscopist preference, one can also leave a guide wire in the pancreatic duct (PD) and pass the snare over it to perform resection to maintain access for a subsequent stent placement. This technique has the advantage of never losing pancreatic duct access, which can occur after resection from edema or bleeding and allows easy PD stent placement. The snare should be opened in a line corresponding to the long axis of the mound with the snare tip anchored above the apex of the papilla and snare opened and drawn down over the papilla. After resection, the PD must be stented to minimize pancreatitis risk.14 Figure 2 shows an ampullary adenoma pre and post EMR, with a PD stent.
Recurrence of duodenal adenomas, both SNDAs and ampullary, can be quite high, with reports up to 39%.15-18 Risk factors include histology and size, but interestingly were not shown to be associated with en-bloc resection.15,19 On the other hand, intraprocedural bleeding also occurs in up to 43% of patients and is associated with size, number of resections, and procedure time.20 Per 2015 ASGE Standards of Practice, duodenal lesions warrant short follow-up at 3- to 6-month intervals given high recurrence rates, then at 6- to 12-month intervals for 2-5 years thereafter.21
When a duodenal polyp is detected, it is important to determine which type of adenoma it is to guide management. There are various techniques utilized to perform duodenal EMR and ampullectomy with some highlighted in this article. It is important to understand how to recognize, prevent, and manage associated adverse events, as well as to have a surveillance plan given the risk of recurrence.
Dr. Kim has no disclosures. Dr. Siddiqui has financial relationships with Boston Scientific (research support, consulting fees, speaking honoraria); Cook, Medtronic, ConMed (consulting fees, speaking honoraria); and Pinnacle Biologic, Ovesco (speaking honoraria).
Dr. Kim is a GI fellow, section of gastroenterology, hepatology, and nutrition, department of internal medicine, University of Chicago. Dr. Siddiqui is a professor of medicine and the director of the Center for Endoscopic Research and Therapeutics (CERT), section of gastroenterology, hepatology, and nutrition, department of internal medicine, University of Chicago.
References
1. Jepsen JM et al. Scand J Gastroenterol. Jun 1994;29(6):483-7.
2. Sellner F. Cancer. 1990 Aug 15;66(4):702-15.
3. Witteman BJ et al. Neth J Med. 1993 Feb;42(1-2):5-11.
4. Reddy RR et al. J Clin Gastroenterol. 1981 Jun;3(2):139-47.
5. Sakorafas GH et al. Scand J Gastroenterol. 2000 Apr;35(4):337-44.
6. Galandiuk S et al. Ann Surg. 1988 Mar;207(3):234-9.
7. Farnell MB et al. J Gastrointest Surg. 2000 Jan-Feb;4(1):13-21, discussion 22-3.
8. Apel D et al. Gastrointest Endosc. 2004 Sep;60(3):397-9.
9. Kashiwagi H et al. Lancet. 1994 Dec 3;344(8936):1582.
10. Clary BM et al. Surgery. 2000 Jun;127(6):628-33.
11. Posner S et al. Surgery. 2000 Oct;128(4):694-701.
12. Harewood GC et al. Gastrointest Endosc. 2005 Sep;62(3):367-70.
13. Chini P et al. World J Gastrointest Endosc. 2011 Dec 16;3(12):241-7.
14. Chang WI et al. Gut Liver. May 2014;8(3):306-12.
15. Hoibian S et al. Ann Gastroenterol. 2021;34(2):169-176. doi: 10.20524/aog.2021.0581.
16. Kakushima N et al. World J Gastroenterol. 2014 Sep 21;20(35):12501-8.
17. Lienert A and Bagshaw PF. ANZ J Surg. 2007 May;77(5):371-3.
18. Singh A et al. Gastrointest Endosc. 2016 Oct;84(4):700-8.
19. Tomizawa Y and Ginsberg GG. Gastrointest Endosc. 2018 May;87(5):1270-8.
20. Klein A et al. Gastrointest Endosc. 2016 Oct;84(4):688-96.
21. Chathadi KV et al. Gastrointest Endosc. 2015 Nov;82(5):773-81.
Duodenal polyps are a relatively rare entity with a reported incidence of 0.3%-4.6%.1 There are three major types of duodenal adenomas: sporadic, nonampullary duodenal adenomas (SNDAs), adenomas in familial adenomatous polyposis syndrome, and ampullary adenomas. It is important to distinguish between the different types of duodenal polyps as the management may differ depending on the etiology.
SNDAs constitute <10% of all duodenal polyps, most commonly located in the second portion of the duodenum, and up to 85% have been shown to have malignant transformation over time.2 Most of the studies of SNDAs are small series, and there are no consensus guidelines for management. Villous features increase malignancy risk, thus resection of SNDAs is advised.3-7 It has also been shown that 72% of patients with SNDAs also have colon polyps,8 and therefore these patients should be up to date on colonoscopy screening.
Ampullary adenomas are less common, but up to half may be associated with familial adenomatous polyposis (FAP), and some may be surveyed.9 However, those that are larger than 10 mm or have villous features may raise concern for malignancy with up to half harboring small foci of adenocarcinoma.10,11 These require ERCP with ampullectomy. For the purposes of this paper, we will focus on endoscopic resection of SNDAs and ampullary adenomas.
Endoscopic mucosal resection (EMR) of duodenal polyps can be technically challenging. There are considerations specific to the duodenum: thin muscle layer, increased motility, and significant vascular supply including two major arterial supplies – the gastroduodenal artery from the celiac branch and the inferior pancreaticoduodenal artery from the superior mesenteric artery. These factors may explain higher reported rates of perforation and bleeding compared to colon EMR.
After a detailed inspection is performed to define the duodenal polyp in terms of size, location, and position relative to the ampulla, a submucosal injection is performed using a dye solution. Once adequate lift is achieved, the lesion is resected using stiff monofilament snares. If possible, resection sites are closed with hemostatic clips, although their utility in preventing delayed complications may be less than that in the colon because of increased motility causing them to become dislodged more easily. We avoid using snares larger than 2 cm given increased risk of perforation. Intraprocedural bleeding may be controlled with coagulation graspers on soft coagulation setting; using a bipolar electrocoagulation therapy or argon plasma coagulation is avoided, as these have been shown to increase rates of complications. Figure 1 provides examples of duodenal adenomas that have been resected.
The ampullectomy technique is slightly different from duodenal EMRs and carries the additional risk of pancreatitis.12,13 In our opinion, there is low utility for submucosal injection unless there is a laterally spreading component onto the duodenal wall, as injection of the ampulla itself does not lift well and simply distorts views. Typically, both the common bile duct and the pancreatic duct are injected with contrast, and we typically perform a biliary sphincterotomy prior to ampullectomy. Based on endoscopist preference, one can also leave a guide wire in the pancreatic duct (PD) and pass the snare over it to perform resection to maintain access for a subsequent stent placement. This technique has the advantage of never losing pancreatic duct access, which can occur after resection from edema or bleeding and allows easy PD stent placement. The snare should be opened in a line corresponding to the long axis of the mound with the snare tip anchored above the apex of the papilla and snare opened and drawn down over the papilla. After resection, the PD must be stented to minimize pancreatitis risk.14 Figure 2 shows an ampullary adenoma pre and post EMR, with a PD stent.
Recurrence of duodenal adenomas, both SNDAs and ampullary, can be quite high, with reports up to 39%.15-18 Risk factors include histology and size, but interestingly were not shown to be associated with en-bloc resection.15,19 On the other hand, intraprocedural bleeding also occurs in up to 43% of patients and is associated with size, number of resections, and procedure time.20 Per 2015 ASGE Standards of Practice, duodenal lesions warrant short follow-up at 3- to 6-month intervals given high recurrence rates, then at 6- to 12-month intervals for 2-5 years thereafter.21
When a duodenal polyp is detected, it is important to determine which type of adenoma it is to guide management. There are various techniques utilized to perform duodenal EMR and ampullectomy with some highlighted in this article. It is important to understand how to recognize, prevent, and manage associated adverse events, as well as to have a surveillance plan given the risk of recurrence.
Dr. Kim has no disclosures. Dr. Siddiqui has financial relationships with Boston Scientific (research support, consulting fees, speaking honoraria); Cook, Medtronic, ConMed (consulting fees, speaking honoraria); and Pinnacle Biologic, Ovesco (speaking honoraria).
Dr. Kim is a GI fellow, section of gastroenterology, hepatology, and nutrition, department of internal medicine, University of Chicago. Dr. Siddiqui is a professor of medicine and the director of the Center for Endoscopic Research and Therapeutics (CERT), section of gastroenterology, hepatology, and nutrition, department of internal medicine, University of Chicago.
References
1. Jepsen JM et al. Scand J Gastroenterol. Jun 1994;29(6):483-7.
2. Sellner F. Cancer. 1990 Aug 15;66(4):702-15.
3. Witteman BJ et al. Neth J Med. 1993 Feb;42(1-2):5-11.
4. Reddy RR et al. J Clin Gastroenterol. 1981 Jun;3(2):139-47.
5. Sakorafas GH et al. Scand J Gastroenterol. 2000 Apr;35(4):337-44.
6. Galandiuk S et al. Ann Surg. 1988 Mar;207(3):234-9.
7. Farnell MB et al. J Gastrointest Surg. 2000 Jan-Feb;4(1):13-21, discussion 22-3.
8. Apel D et al. Gastrointest Endosc. 2004 Sep;60(3):397-9.
9. Kashiwagi H et al. Lancet. 1994 Dec 3;344(8936):1582.
10. Clary BM et al. Surgery. 2000 Jun;127(6):628-33.
11. Posner S et al. Surgery. 2000 Oct;128(4):694-701.
12. Harewood GC et al. Gastrointest Endosc. 2005 Sep;62(3):367-70.
13. Chini P et al. World J Gastrointest Endosc. 2011 Dec 16;3(12):241-7.
14. Chang WI et al. Gut Liver. May 2014;8(3):306-12.
15. Hoibian S et al. Ann Gastroenterol. 2021;34(2):169-176. doi: 10.20524/aog.2021.0581.
16. Kakushima N et al. World J Gastroenterol. 2014 Sep 21;20(35):12501-8.
17. Lienert A and Bagshaw PF. ANZ J Surg. 2007 May;77(5):371-3.
18. Singh A et al. Gastrointest Endosc. 2016 Oct;84(4):700-8.
19. Tomizawa Y and Ginsberg GG. Gastrointest Endosc. 2018 May;87(5):1270-8.
20. Klein A et al. Gastrointest Endosc. 2016 Oct;84(4):688-96.
21. Chathadi KV et al. Gastrointest Endosc. 2015 Nov;82(5):773-81.
Rippled Macules and Papules on the Legs
The Diagnosis: Cutaneous Amyloidosis
A punch biopsy confirmed the diagnosis of cutaneous amyloidosis, which is characterized by the deposition of amyloid proteins in the skin without systemic involvement. Subtypes of cutaneous amyloidosis include lichenoid, macular, and nodular amyloidosis. A mixed or biphasic amyloidosis can occur when both lichenoid and macular lesions are present.1 Lichenoid and macular amyloidosis generally are characterized by moderate to severe pruritus. Lichenoid amyloidosis favors the shins, calves, ankles, and extensor extremities; macular amyloidosis has a predilection for the interscapular area and less frequently the upper arms, chest, and thighs.2 Atypical variants also have been reported, including amyloidosis cutis dyschromica, poikilodermalike amyloidosis, and bullous amyloidosis, as well as incontinentia pigmenti–like, linear, and nevoid types.3 Macular amyloidosis has been reported to occur in association with progressive systemic sclerosis, primary biliary cirrhosis, systemic lupus erythematosus, paronychia, and multiple endocrine neoplasia type 2.2
Acanthosis nigricans typically presents on the neck and intertriginous areas as velvety hyperpigmented plaques. Confluent and reticulated papillomatosis also appears as slightly elevated papules; however, it occurs in the intermammary region in a reticulated pattern. Ichthyosis vulgaris also may occur on the lower extremities but presents with adherent large scales rather than papules. Keratosis pilaris may present on the proximal lower extremities with smaller, folliculocentric, fleshcolored to pink papules.
Treatment of cutaneous amyloidosis has long been challenging for dermatologists. The primary focus should be treatment of any underlying disease that is causing the pruritus and subsequent manipulation of skin lesions. Topical calcipotriol, phototherapy, oral cyclophosphamide, and Nd:YAG laser have demonstrated beneficial outcomes. IL-31 antibodies may be a potential future treatment.1
1. Weidner T, Illing T, Elsner P. Primary localized cutaneous amyloidosis: a systematic treatment review. Am J Clin Dermatol. 2017;18:629-642. doi:10.1007/s40257-017-0278-9 2. Rasi A, Khatami A, Javaheri SM. Macular amyloidosis: an assessment of prevalence, sex, and age. Int J Dermatol. 2004;43:898-899. doi:10.1111 /j.1365-4632.2004.01935.x 3. Hamie L, Haddad I, Nasser N, et al. Primary localized cutaneous amyloidosis of keratinocyte origin: an update with emphasis on atypical clinical variants [published online July 21, 2021]. 2021;22:667-680. Am J Clin Dermatol. doi:10.1007/s40257-021-00620-9
The Diagnosis: Cutaneous Amyloidosis
A punch biopsy confirmed the diagnosis of cutaneous amyloidosis, which is characterized by the deposition of amyloid proteins in the skin without systemic involvement. Subtypes of cutaneous amyloidosis include lichenoid, macular, and nodular amyloidosis. A mixed or biphasic amyloidosis can occur when both lichenoid and macular lesions are present.1 Lichenoid and macular amyloidosis generally are characterized by moderate to severe pruritus. Lichenoid amyloidosis favors the shins, calves, ankles, and extensor extremities; macular amyloidosis has a predilection for the interscapular area and less frequently the upper arms, chest, and thighs.2 Atypical variants also have been reported, including amyloidosis cutis dyschromica, poikilodermalike amyloidosis, and bullous amyloidosis, as well as incontinentia pigmenti–like, linear, and nevoid types.3 Macular amyloidosis has been reported to occur in association with progressive systemic sclerosis, primary biliary cirrhosis, systemic lupus erythematosus, paronychia, and multiple endocrine neoplasia type 2.2
Acanthosis nigricans typically presents on the neck and intertriginous areas as velvety hyperpigmented plaques. Confluent and reticulated papillomatosis also appears as slightly elevated papules; however, it occurs in the intermammary region in a reticulated pattern. Ichthyosis vulgaris also may occur on the lower extremities but presents with adherent large scales rather than papules. Keratosis pilaris may present on the proximal lower extremities with smaller, folliculocentric, fleshcolored to pink papules.
Treatment of cutaneous amyloidosis has long been challenging for dermatologists. The primary focus should be treatment of any underlying disease that is causing the pruritus and subsequent manipulation of skin lesions. Topical calcipotriol, phototherapy, oral cyclophosphamide, and Nd:YAG laser have demonstrated beneficial outcomes. IL-31 antibodies may be a potential future treatment.1
The Diagnosis: Cutaneous Amyloidosis
A punch biopsy confirmed the diagnosis of cutaneous amyloidosis, which is characterized by the deposition of amyloid proteins in the skin without systemic involvement. Subtypes of cutaneous amyloidosis include lichenoid, macular, and nodular amyloidosis. A mixed or biphasic amyloidosis can occur when both lichenoid and macular lesions are present.1 Lichenoid and macular amyloidosis generally are characterized by moderate to severe pruritus. Lichenoid amyloidosis favors the shins, calves, ankles, and extensor extremities; macular amyloidosis has a predilection for the interscapular area and less frequently the upper arms, chest, and thighs.2 Atypical variants also have been reported, including amyloidosis cutis dyschromica, poikilodermalike amyloidosis, and bullous amyloidosis, as well as incontinentia pigmenti–like, linear, and nevoid types.3 Macular amyloidosis has been reported to occur in association with progressive systemic sclerosis, primary biliary cirrhosis, systemic lupus erythematosus, paronychia, and multiple endocrine neoplasia type 2.2
Acanthosis nigricans typically presents on the neck and intertriginous areas as velvety hyperpigmented plaques. Confluent and reticulated papillomatosis also appears as slightly elevated papules; however, it occurs in the intermammary region in a reticulated pattern. Ichthyosis vulgaris also may occur on the lower extremities but presents with adherent large scales rather than papules. Keratosis pilaris may present on the proximal lower extremities with smaller, folliculocentric, fleshcolored to pink papules.
Treatment of cutaneous amyloidosis has long been challenging for dermatologists. The primary focus should be treatment of any underlying disease that is causing the pruritus and subsequent manipulation of skin lesions. Topical calcipotriol, phototherapy, oral cyclophosphamide, and Nd:YAG laser have demonstrated beneficial outcomes. IL-31 antibodies may be a potential future treatment.1
1. Weidner T, Illing T, Elsner P. Primary localized cutaneous amyloidosis: a systematic treatment review. Am J Clin Dermatol. 2017;18:629-642. doi:10.1007/s40257-017-0278-9 2. Rasi A, Khatami A, Javaheri SM. Macular amyloidosis: an assessment of prevalence, sex, and age. Int J Dermatol. 2004;43:898-899. doi:10.1111 /j.1365-4632.2004.01935.x 3. Hamie L, Haddad I, Nasser N, et al. Primary localized cutaneous amyloidosis of keratinocyte origin: an update with emphasis on atypical clinical variants [published online July 21, 2021]. 2021;22:667-680. Am J Clin Dermatol. doi:10.1007/s40257-021-00620-9
1. Weidner T, Illing T, Elsner P. Primary localized cutaneous amyloidosis: a systematic treatment review. Am J Clin Dermatol. 2017;18:629-642. doi:10.1007/s40257-017-0278-9 2. Rasi A, Khatami A, Javaheri SM. Macular amyloidosis: an assessment of prevalence, sex, and age. Int J Dermatol. 2004;43:898-899. doi:10.1111 /j.1365-4632.2004.01935.x 3. Hamie L, Haddad I, Nasser N, et al. Primary localized cutaneous amyloidosis of keratinocyte origin: an update with emphasis on atypical clinical variants [published online July 21, 2021]. 2021;22:667-680. Am J Clin Dermatol. doi:10.1007/s40257-021-00620-9
A 34-year-old woman presented to our dermatology clinic with an intensely pruritic rash on the legs of 2 years’ duration. The pruritus had waxed and waned in intensity, and the skin lesions were refractory to treatment with low-potency topical steroids. She had no other chronic medical conditions and was not taking any other medications.


‘Great optimism’ greets immunotherapy responses in dMMR rectal cancer
Thus far, the study has involved only 12 patients, but all of them have had a clinical complete response to treatment. They continue to show no signs of cancer (during follow-up ranging from 6 to 25 months) and have not undergone surgery or had radiation and chemotherapy, which are the standard treatment approaches.
The results were presented (Abstract 16) at the American Society of Clinical Oncology annual meeting and simultaneously published in the New England Journal of Medicine.
“In our study, the elimination of tumors after 6 months of therapy with PD-1 blockade enabled us to omit both chemoradiotherapy and surgery and to proceed with observation alone,” said the authors, led by Andrea Cercek, MD, Memorial Sloan Kettering Cancer Center, New York.
About 5%-10% of patients with rectal cancer have tumors with dMMR.
“The implications for quality of life are substantial, especially among patients in whom standard treatment would affect child-bearing potential [and] given that the incidence of rectal cancer is rising among young adults of childbearing age, the use of PD-1 blockade to eliminate the need for chemoradiotherapy and surgery may confer a particular benefit in that age group,” the authors wrote.
The results of the current study are cause for “great optimism, but such an approach cannot yet supplant our current curative treatment approach,” Dr. Hanna K. Sanoff, MD, University of North Carolina at Chapel Hill, wrote in an accompanying editorial.
Single-agent dostarlimab
For the study, all patients were treated with single-agent dostarlimab every 3 weeks for 6 months.
Dostarlimab is already approved by the Food and Drug Administration for use in the treatment of recurrent or advanced endometrial cancer with dMMR. Rectal cancer is an off-label use.
All patients had mismatch repair-deficient stage 2 or 3 rectal adenocarcinoma. The authors noted that these tumors respond poorly to standard chemotherapy regimens, including neoadjuvant chemotherapy. The median age of enrolled patients was 54 years and 62% were women.
For the study, investigators planned that patients who had a clinical complete response after completion of dostarlimab were to proceed to observation without undergoing either chemoradiotherapy or surgery, while those who did not have a complete response were to have received these standard treatments.
As it turned out, all 12 patients achieved a complete response and have been followed by observation alone. The median follow-up from time of enrollment to data cutoff for the 12 patients was 12 months.
“Therapeutic responses were rapid,” the authors noted, “with resolution of symptoms within 8 weeks after initiation of dostarlimab in 81% of the patients.”
To date, four patients have had 1 year of sustained clinical complete response after completion of the anti-PD-1 course.
In addition to the 12 patients documented in the study, another four patients have received at least one dose of dostarlimab and continue to receive treatment.
Adverse events occurred in most patients but none were grade 3 or higher. The most common grade 1 or 2 adverse events were rash or dermatitis, pruritus, fatigue, nausea and, in one patient, thyroid-function abnormalities.
The authors speculated that in addition to the extremely high tumor mutational burden associated with mismatch-repair deficiency, a tumor cell–extrinsic factor such as the gut microbiome may be driving the exceptionally good response to PD-1 blockade seen in this patient population.
Editorial commentary
In the editorial, Dr. Sanoff emphasized that the approach remains experimental and should not replace current curative treatment. She noted that cancer recurrences have been seen in other studies using both chemotherapy and immunotherapy.
For example, with chemotherapy and radiation, those patients who achieve a clinical complete response have a better prognosis compared with those who do not, but she cautioned that “cancer regrowth occurs in 20% to 30% of such patients when the cancer is managed nonoperatively.”
Dr. Sanoff noted that recurrences were seen when this approach of PD-1 inhibition has been used for metastatic colorectal cancer with dMMR. In the KEYNOTE-177 trial with pembrolizumab (Keytruda), only 55% of patients were reported to be alive without cancer progression at 12 months, and of the patients who initially had a strong response, only 70% had an ongoing response 3 years later.
“These recurrence dynamics may (or may not) differ between immunotherapy and chemoradiotherapy and between early and late-stage disease,” Dr. Sanoff said.
“In fact, very little is known about the duration of time needed to find out whether a clinical complete response to dostarlimab equates to cure,” she added.
In addition, Dr. Sanoff warned that the decision not to pursue further treatment and to follow patients with observation alone requires very close monitoring.
The current study was conducted at a top U.S. cancer center, Memorial Sloan Kettering Cancer Center. The authors noted that the complete responses (after a minimum of 6 months of follow-up) were measured by the combination of rectal MRI, visual endoscopic inspection, and digital rectal examination.
The completeness of these responses was further supported by the absence of residual tumor on serial endoscopic biopsies and the resolution of 18F-fluorodeoxyglucose uptake on PET scans, the authors added.
In the editorial, Dr. Sanoff said that “safe nonoperative management [also] involves access to specialty care for direct intraluminal visualization and expertise in interpretation of rectal magnetic resonance imaging ... Such expertise is not available in all communities and without it, patients could miss the opportunity for curative resection if tumor regrowth occurred.”
The study was sponsored by the Simon and Eve Colin Foundation, GlaxoSmithKline, and Stand Up to Cancer, among others.
A version of this article first appeared on Medscape.com.
Thus far, the study has involved only 12 patients, but all of them have had a clinical complete response to treatment. They continue to show no signs of cancer (during follow-up ranging from 6 to 25 months) and have not undergone surgery or had radiation and chemotherapy, which are the standard treatment approaches.
The results were presented (Abstract 16) at the American Society of Clinical Oncology annual meeting and simultaneously published in the New England Journal of Medicine.
“In our study, the elimination of tumors after 6 months of therapy with PD-1 blockade enabled us to omit both chemoradiotherapy and surgery and to proceed with observation alone,” said the authors, led by Andrea Cercek, MD, Memorial Sloan Kettering Cancer Center, New York.
About 5%-10% of patients with rectal cancer have tumors with dMMR.
“The implications for quality of life are substantial, especially among patients in whom standard treatment would affect child-bearing potential [and] given that the incidence of rectal cancer is rising among young adults of childbearing age, the use of PD-1 blockade to eliminate the need for chemoradiotherapy and surgery may confer a particular benefit in that age group,” the authors wrote.
The results of the current study are cause for “great optimism, but such an approach cannot yet supplant our current curative treatment approach,” Dr. Hanna K. Sanoff, MD, University of North Carolina at Chapel Hill, wrote in an accompanying editorial.
Single-agent dostarlimab
For the study, all patients were treated with single-agent dostarlimab every 3 weeks for 6 months.
Dostarlimab is already approved by the Food and Drug Administration for use in the treatment of recurrent or advanced endometrial cancer with dMMR. Rectal cancer is an off-label use.
All patients had mismatch repair-deficient stage 2 or 3 rectal adenocarcinoma. The authors noted that these tumors respond poorly to standard chemotherapy regimens, including neoadjuvant chemotherapy. The median age of enrolled patients was 54 years and 62% were women.
For the study, investigators planned that patients who had a clinical complete response after completion of dostarlimab were to proceed to observation without undergoing either chemoradiotherapy or surgery, while those who did not have a complete response were to have received these standard treatments.
As it turned out, all 12 patients achieved a complete response and have been followed by observation alone. The median follow-up from time of enrollment to data cutoff for the 12 patients was 12 months.
“Therapeutic responses were rapid,” the authors noted, “with resolution of symptoms within 8 weeks after initiation of dostarlimab in 81% of the patients.”
To date, four patients have had 1 year of sustained clinical complete response after completion of the anti-PD-1 course.
In addition to the 12 patients documented in the study, another four patients have received at least one dose of dostarlimab and continue to receive treatment.
Adverse events occurred in most patients but none were grade 3 or higher. The most common grade 1 or 2 adverse events were rash or dermatitis, pruritus, fatigue, nausea and, in one patient, thyroid-function abnormalities.
The authors speculated that in addition to the extremely high tumor mutational burden associated with mismatch-repair deficiency, a tumor cell–extrinsic factor such as the gut microbiome may be driving the exceptionally good response to PD-1 blockade seen in this patient population.
Editorial commentary
In the editorial, Dr. Sanoff emphasized that the approach remains experimental and should not replace current curative treatment. She noted that cancer recurrences have been seen in other studies using both chemotherapy and immunotherapy.
For example, with chemotherapy and radiation, those patients who achieve a clinical complete response have a better prognosis compared with those who do not, but she cautioned that “cancer regrowth occurs in 20% to 30% of such patients when the cancer is managed nonoperatively.”
Dr. Sanoff noted that recurrences were seen when this approach of PD-1 inhibition has been used for metastatic colorectal cancer with dMMR. In the KEYNOTE-177 trial with pembrolizumab (Keytruda), only 55% of patients were reported to be alive without cancer progression at 12 months, and of the patients who initially had a strong response, only 70% had an ongoing response 3 years later.
“These recurrence dynamics may (or may not) differ between immunotherapy and chemoradiotherapy and between early and late-stage disease,” Dr. Sanoff said.
“In fact, very little is known about the duration of time needed to find out whether a clinical complete response to dostarlimab equates to cure,” she added.
In addition, Dr. Sanoff warned that the decision not to pursue further treatment and to follow patients with observation alone requires very close monitoring.
The current study was conducted at a top U.S. cancer center, Memorial Sloan Kettering Cancer Center. The authors noted that the complete responses (after a minimum of 6 months of follow-up) were measured by the combination of rectal MRI, visual endoscopic inspection, and digital rectal examination.
The completeness of these responses was further supported by the absence of residual tumor on serial endoscopic biopsies and the resolution of 18F-fluorodeoxyglucose uptake on PET scans, the authors added.
In the editorial, Dr. Sanoff said that “safe nonoperative management [also] involves access to specialty care for direct intraluminal visualization and expertise in interpretation of rectal magnetic resonance imaging ... Such expertise is not available in all communities and without it, patients could miss the opportunity for curative resection if tumor regrowth occurred.”
The study was sponsored by the Simon and Eve Colin Foundation, GlaxoSmithKline, and Stand Up to Cancer, among others.
A version of this article first appeared on Medscape.com.
Thus far, the study has involved only 12 patients, but all of them have had a clinical complete response to treatment. They continue to show no signs of cancer (during follow-up ranging from 6 to 25 months) and have not undergone surgery or had radiation and chemotherapy, which are the standard treatment approaches.
The results were presented (Abstract 16) at the American Society of Clinical Oncology annual meeting and simultaneously published in the New England Journal of Medicine.
“In our study, the elimination of tumors after 6 months of therapy with PD-1 blockade enabled us to omit both chemoradiotherapy and surgery and to proceed with observation alone,” said the authors, led by Andrea Cercek, MD, Memorial Sloan Kettering Cancer Center, New York.
About 5%-10% of patients with rectal cancer have tumors with dMMR.
“The implications for quality of life are substantial, especially among patients in whom standard treatment would affect child-bearing potential [and] given that the incidence of rectal cancer is rising among young adults of childbearing age, the use of PD-1 blockade to eliminate the need for chemoradiotherapy and surgery may confer a particular benefit in that age group,” the authors wrote.
The results of the current study are cause for “great optimism, but such an approach cannot yet supplant our current curative treatment approach,” Dr. Hanna K. Sanoff, MD, University of North Carolina at Chapel Hill, wrote in an accompanying editorial.
Single-agent dostarlimab
For the study, all patients were treated with single-agent dostarlimab every 3 weeks for 6 months.
Dostarlimab is already approved by the Food and Drug Administration for use in the treatment of recurrent or advanced endometrial cancer with dMMR. Rectal cancer is an off-label use.
All patients had mismatch repair-deficient stage 2 or 3 rectal adenocarcinoma. The authors noted that these tumors respond poorly to standard chemotherapy regimens, including neoadjuvant chemotherapy. The median age of enrolled patients was 54 years and 62% were women.
For the study, investigators planned that patients who had a clinical complete response after completion of dostarlimab were to proceed to observation without undergoing either chemoradiotherapy or surgery, while those who did not have a complete response were to have received these standard treatments.
As it turned out, all 12 patients achieved a complete response and have been followed by observation alone. The median follow-up from time of enrollment to data cutoff for the 12 patients was 12 months.
“Therapeutic responses were rapid,” the authors noted, “with resolution of symptoms within 8 weeks after initiation of dostarlimab in 81% of the patients.”
To date, four patients have had 1 year of sustained clinical complete response after completion of the anti-PD-1 course.
In addition to the 12 patients documented in the study, another four patients have received at least one dose of dostarlimab and continue to receive treatment.
Adverse events occurred in most patients but none were grade 3 or higher. The most common grade 1 or 2 adverse events were rash or dermatitis, pruritus, fatigue, nausea and, in one patient, thyroid-function abnormalities.
The authors speculated that in addition to the extremely high tumor mutational burden associated with mismatch-repair deficiency, a tumor cell–extrinsic factor such as the gut microbiome may be driving the exceptionally good response to PD-1 blockade seen in this patient population.
Editorial commentary
In the editorial, Dr. Sanoff emphasized that the approach remains experimental and should not replace current curative treatment. She noted that cancer recurrences have been seen in other studies using both chemotherapy and immunotherapy.
For example, with chemotherapy and radiation, those patients who achieve a clinical complete response have a better prognosis compared with those who do not, but she cautioned that “cancer regrowth occurs in 20% to 30% of such patients when the cancer is managed nonoperatively.”
Dr. Sanoff noted that recurrences were seen when this approach of PD-1 inhibition has been used for metastatic colorectal cancer with dMMR. In the KEYNOTE-177 trial with pembrolizumab (Keytruda), only 55% of patients were reported to be alive without cancer progression at 12 months, and of the patients who initially had a strong response, only 70% had an ongoing response 3 years later.
“These recurrence dynamics may (or may not) differ between immunotherapy and chemoradiotherapy and between early and late-stage disease,” Dr. Sanoff said.
“In fact, very little is known about the duration of time needed to find out whether a clinical complete response to dostarlimab equates to cure,” she added.
In addition, Dr. Sanoff warned that the decision not to pursue further treatment and to follow patients with observation alone requires very close monitoring.
The current study was conducted at a top U.S. cancer center, Memorial Sloan Kettering Cancer Center. The authors noted that the complete responses (after a minimum of 6 months of follow-up) were measured by the combination of rectal MRI, visual endoscopic inspection, and digital rectal examination.
The completeness of these responses was further supported by the absence of residual tumor on serial endoscopic biopsies and the resolution of 18F-fluorodeoxyglucose uptake on PET scans, the authors added.
In the editorial, Dr. Sanoff said that “safe nonoperative management [also] involves access to specialty care for direct intraluminal visualization and expertise in interpretation of rectal magnetic resonance imaging ... Such expertise is not available in all communities and without it, patients could miss the opportunity for curative resection if tumor regrowth occurred.”
The study was sponsored by the Simon and Eve Colin Foundation, GlaxoSmithKline, and Stand Up to Cancer, among others.
A version of this article first appeared on Medscape.com.
FROM ASCO 2022
‘Remission is possible’ for patients with type 2 diabetes
A novel approach that involves sensors, artificial intelligence, and real-time individualized lifestyle guidance from an app and live coaches led to a high rate of remission of type 2 diabetes in a new study.
Specifically, among 199 patients with type 2 diabetes in India who received the app-delivered lifestyle guidance developed by Twin Health, Mountain View, Calif., mean hemoglobin A1c dropped from 9.0% to 5.7% at 6 months.

This is “huge,” Paramesh Shamanna, MD, told a press briefing at the annual scientific sessions of the American Diabetes Association. The research was presented as three posters by the group at the meeting.
Patients were a mean age of 43 and had diabetes for a mean of 3.7 years and up to 8 years.
An “unprecedented” 84% of patients had remission of diabetes at 6 months, Dr. Shamanna, medical director at Twin Health, noted.
Diabetes remission was defined according to the 2021 joint consensus statement from the ADA and other organizations as an A1c less than 6.5% without the use of diabetes medications for at least 3 months.
Importantly, patients’ time in range (percentage of time spent in target blood glucose range) increased from 53% to 81%, Dr. Shamanna pointed out. On average, patients’ waist circumference decreased by 10 cm (3.9 inches) and their weight dropped from 79 kg (approximately 174 lb) to 68 kg (150 lb).
These results are driven by “the continuous individualized and precise guidance regarding nutrition, activity, and sleep,” Dr. Shamanna said in an interview.
Remission is not reversal or cure ...
“Remission” from type 2 diabetes is not “reversal” or a “cure,” Robert A. Gabbay, MD, PhD, chief scientific and medical officer of the ADA, stressed to the press. Just like cancer, diabetes can return after remission

Therefore, it is important to follow the lifestyle guidance. Patients may still be at risk for diabetes complications after diabetes remission, so it’s also important to continue to be screened for eye disease, nerve damage, and lipid levels.
However, “remission can be made to last,” Dr. Shamanna said, by continuing to follow the lifestyle advice and getting back on track after a relapse.
“We’re in a different time right now,” Lisa Shah, MD, chief medical officer, Twin Health, noted. “This is very different from management of blood glucose to a certain number.”
This study shows that “remission [from type 2 diabetes] is possible. How you achieve it can be precise for you.”
The program is designed to consider the health and happiness of the patient, added Shashank R. Joshi, MD, chief scientist, Twin Health. “We want remission to be complication free. These findings give patients hope.”
“It’s exciting now that we can really start thinking about remission as an option for people with [type 2] diabetes, and that just provides such incredible hope for all of those living with [type 2] diabetes,” Dr. Gabbay said in an interview.
How the intervention works
The Twin Precision Treatment (TPT) intervention integrates multiple data – glucose values from a continuous glucose monitor (CGM); heart rate, activity, and sleep time from a fitness tracker; blood pressure values from a blood pressure cuff; food intake from the patient’s food log; and weight and body fat data from a smart scale – and provides the patient with precise, individualized nutrition and health guidance.
The four most critical sensors are the CGM, the fitness tracker, the smart scale, and the blood pressure cuff, Dr. Shah explained. The system gathers thousands of signals combined with patient self-reported data including mood or anxiety.
The CGM is used to build the initial nutrition guidance during the first 30 days. Once a patient is in remission, he or she can just keep the fitness tracker and smart scale.
The coaches who are part of this program include dietitians who are trained to provide compassionate patient education and help patients avoid diabetes relapse, and they are overseen by a licensed provider.
The program does not restrict calories. “It is not a diet,” Dr. Shah stressed.
The algorithm makes mini adjustments to the food a person is already eating to improve nutrition, Dr. Joshi explained. “This is personalized medicine at its best.” Patients eat food that they like and are guided to make small changes to get glucose under control and avoid glucose spikes.
The program is designed to safely deescalate diabetes medications as A1c decreases, Dr. Shamanna added.
U.S. clinical trial, health insurance coverage
The 1-year results of the current trial are expected in August, and the trial will continue for 2-=5 years, Dr. Shamanna said.
The company has started a clinical trial in the United States, with 5-year results expected in 2027.
“Currently, in the United States, we are partnering with self-insured employers and select health plans that offer [Twin Precision Treatment ] as an available benefit for their members,” Dr. Shah said. It “is suitable for most members living with type 2 diabetes, with rare exclusion situations.”
The study was funded by Twin Health. Dr. Shamanna, Dr. Shah, and Dr. Joshi are employees of Twin Health.
A version of this article first appeared on Medscape.com.
A novel approach that involves sensors, artificial intelligence, and real-time individualized lifestyle guidance from an app and live coaches led to a high rate of remission of type 2 diabetes in a new study.
Specifically, among 199 patients with type 2 diabetes in India who received the app-delivered lifestyle guidance developed by Twin Health, Mountain View, Calif., mean hemoglobin A1c dropped from 9.0% to 5.7% at 6 months.
This is “huge,” Paramesh Shamanna, MD, told a press briefing at the annual scientific sessions of the American Diabetes Association. The research was presented as three posters by the group at the meeting.
Patients were a mean age of 43 and had diabetes for a mean of 3.7 years and up to 8 years.
An “unprecedented” 84% of patients had remission of diabetes at 6 months, Dr. Shamanna, medical director at Twin Health, noted.
Diabetes remission was defined according to the 2021 joint consensus statement from the ADA and other organizations as an A1c less than 6.5% without the use of diabetes medications for at least 3 months.
Importantly, patients’ time in range (percentage of time spent in target blood glucose range) increased from 53% to 81%, Dr. Shamanna pointed out. On average, patients’ waist circumference decreased by 10 cm (3.9 inches) and their weight dropped from 79 kg (approximately 174 lb) to 68 kg (150 lb).
These results are driven by “the continuous individualized and precise guidance regarding nutrition, activity, and sleep,” Dr. Shamanna said in an interview.
Remission is not reversal or cure ...
“Remission” from type 2 diabetes is not “reversal” or a “cure,” Robert A. Gabbay, MD, PhD, chief scientific and medical officer of the ADA, stressed to the press. Just like cancer, diabetes can return after remission
Therefore, it is important to follow the lifestyle guidance. Patients may still be at risk for diabetes complications after diabetes remission, so it’s also important to continue to be screened for eye disease, nerve damage, and lipid levels.
However, “remission can be made to last,” Dr. Shamanna said, by continuing to follow the lifestyle advice and getting back on track after a relapse.
“We’re in a different time right now,” Lisa Shah, MD, chief medical officer, Twin Health, noted. “This is very different from management of blood glucose to a certain number.”
This study shows that “remission [from type 2 diabetes] is possible. How you achieve it can be precise for you.”
The program is designed to consider the health and happiness of the patient, added Shashank R. Joshi, MD, chief scientist, Twin Health. “We want remission to be complication free. These findings give patients hope.”
“It’s exciting now that we can really start thinking about remission as an option for people with [type 2] diabetes, and that just provides such incredible hope for all of those living with [type 2] diabetes,” Dr. Gabbay said in an interview.
How the intervention works
The Twin Precision Treatment (TPT) intervention integrates multiple data – glucose values from a continuous glucose monitor (CGM); heart rate, activity, and sleep time from a fitness tracker; blood pressure values from a blood pressure cuff; food intake from the patient’s food log; and weight and body fat data from a smart scale – and provides the patient with precise, individualized nutrition and health guidance.
The four most critical sensors are the CGM, the fitness tracker, the smart scale, and the blood pressure cuff, Dr. Shah explained. The system gathers thousands of signals combined with patient self-reported data including mood or anxiety.
The CGM is used to build the initial nutrition guidance during the first 30 days. Once a patient is in remission, he or she can just keep the fitness tracker and smart scale.
The coaches who are part of this program include dietitians who are trained to provide compassionate patient education and help patients avoid diabetes relapse, and they are overseen by a licensed provider.
The program does not restrict calories. “It is not a diet,” Dr. Shah stressed.
The algorithm makes mini adjustments to the food a person is already eating to improve nutrition, Dr. Joshi explained. “This is personalized medicine at its best.” Patients eat food that they like and are guided to make small changes to get glucose under control and avoid glucose spikes.
The program is designed to safely deescalate diabetes medications as A1c decreases, Dr. Shamanna added.
U.S. clinical trial, health insurance coverage
The 1-year results of the current trial are expected in August, and the trial will continue for 2-=5 years, Dr. Shamanna said.
The company has started a clinical trial in the United States, with 5-year results expected in 2027.
“Currently, in the United States, we are partnering with self-insured employers and select health plans that offer [Twin Precision Treatment ] as an available benefit for their members,” Dr. Shah said. It “is suitable for most members living with type 2 diabetes, with rare exclusion situations.”
The study was funded by Twin Health. Dr. Shamanna, Dr. Shah, and Dr. Joshi are employees of Twin Health.
A version of this article first appeared on Medscape.com.
A novel approach that involves sensors, artificial intelligence, and real-time individualized lifestyle guidance from an app and live coaches led to a high rate of remission of type 2 diabetes in a new study.
Specifically, among 199 patients with type 2 diabetes in India who received the app-delivered lifestyle guidance developed by Twin Health, Mountain View, Calif., mean hemoglobin A1c dropped from 9.0% to 5.7% at 6 months.
This is “huge,” Paramesh Shamanna, MD, told a press briefing at the annual scientific sessions of the American Diabetes Association. The research was presented as three posters by the group at the meeting.
Patients were a mean age of 43 and had diabetes for a mean of 3.7 years and up to 8 years.
An “unprecedented” 84% of patients had remission of diabetes at 6 months, Dr. Shamanna, medical director at Twin Health, noted.
Diabetes remission was defined according to the 2021 joint consensus statement from the ADA and other organizations as an A1c less than 6.5% without the use of diabetes medications for at least 3 months.
Importantly, patients’ time in range (percentage of time spent in target blood glucose range) increased from 53% to 81%, Dr. Shamanna pointed out. On average, patients’ waist circumference decreased by 10 cm (3.9 inches) and their weight dropped from 79 kg (approximately 174 lb) to 68 kg (150 lb).
These results are driven by “the continuous individualized and precise guidance regarding nutrition, activity, and sleep,” Dr. Shamanna said in an interview.
Remission is not reversal or cure ...
“Remission” from type 2 diabetes is not “reversal” or a “cure,” Robert A. Gabbay, MD, PhD, chief scientific and medical officer of the ADA, stressed to the press. Just like cancer, diabetes can return after remission
Therefore, it is important to follow the lifestyle guidance. Patients may still be at risk for diabetes complications after diabetes remission, so it’s also important to continue to be screened for eye disease, nerve damage, and lipid levels.
However, “remission can be made to last,” Dr. Shamanna said, by continuing to follow the lifestyle advice and getting back on track after a relapse.
“We’re in a different time right now,” Lisa Shah, MD, chief medical officer, Twin Health, noted. “This is very different from management of blood glucose to a certain number.”
This study shows that “remission [from type 2 diabetes] is possible. How you achieve it can be precise for you.”
The program is designed to consider the health and happiness of the patient, added Shashank R. Joshi, MD, chief scientist, Twin Health. “We want remission to be complication free. These findings give patients hope.”
“It’s exciting now that we can really start thinking about remission as an option for people with [type 2] diabetes, and that just provides such incredible hope for all of those living with [type 2] diabetes,” Dr. Gabbay said in an interview.
How the intervention works
The Twin Precision Treatment (TPT) intervention integrates multiple data – glucose values from a continuous glucose monitor (CGM); heart rate, activity, and sleep time from a fitness tracker; blood pressure values from a blood pressure cuff; food intake from the patient’s food log; and weight and body fat data from a smart scale – and provides the patient with precise, individualized nutrition and health guidance.
The four most critical sensors are the CGM, the fitness tracker, the smart scale, and the blood pressure cuff, Dr. Shah explained. The system gathers thousands of signals combined with patient self-reported data including mood or anxiety.
The CGM is used to build the initial nutrition guidance during the first 30 days. Once a patient is in remission, he or she can just keep the fitness tracker and smart scale.
The coaches who are part of this program include dietitians who are trained to provide compassionate patient education and help patients avoid diabetes relapse, and they are overseen by a licensed provider.
The program does not restrict calories. “It is not a diet,” Dr. Shah stressed.
The algorithm makes mini adjustments to the food a person is already eating to improve nutrition, Dr. Joshi explained. “This is personalized medicine at its best.” Patients eat food that they like and are guided to make small changes to get glucose under control and avoid glucose spikes.
The program is designed to safely deescalate diabetes medications as A1c decreases, Dr. Shamanna added.
U.S. clinical trial, health insurance coverage
The 1-year results of the current trial are expected in August, and the trial will continue for 2-=5 years, Dr. Shamanna said.
The company has started a clinical trial in the United States, with 5-year results expected in 2027.
“Currently, in the United States, we are partnering with self-insured employers and select health plans that offer [Twin Precision Treatment ] as an available benefit for their members,” Dr. Shah said. It “is suitable for most members living with type 2 diabetes, with rare exclusion situations.”
The study was funded by Twin Health. Dr. Shamanna, Dr. Shah, and Dr. Joshi are employees of Twin Health.
A version of this article first appeared on Medscape.com.
FROM ADA 2022
Methotrexate enhances pegloticase response in uncontrolled gout
In patients with uncontrolled gout, response rates were increased by 32% when methotrexate was used in conjunction with pegloticase versus pegloticase plus a placebo, it was reported at the annual European Congress of Rheumatology.
In the phase 4 MIRROR trial, 71% of patients who received pretreatment with methotrexate and then the combination of methotrexate and pegloticase achieved uric-acid levels lower than 6 mg/dL for more than 80% of the time during weeks 20-24 of the 52-week study. By comparison, only 39% of those treated with pegloticase plus a placebo achieved this primary endpoint (P < .0001).

“This trial confirms not only improved efficacy but improved safety in patients treated with pegloticase in combination with methotrexate 15 mg orally once weekly,” study investigator John K. Botson, MD, RPh, CCD, said in reporting the trial’s findings.
This is good news for patients, suggested two rheumatologists who were not involved in the study. The combination appears “useful for a select group of gout patients,” observed Christian Ammitzbøll, MD, PhD, from Aarhus University Hospital, Denmark.
“Very promising in refractory gout,” agreed Emre Bilgin, MD, from Ankara, Turkey.
Rationale for using methotrexate
“Oral urate lowering agents are the mainstay of treatment of gout, but there are patients that just don’t respond to oral agents,” said Dr. Botson, a rheumatologist in private practice from Anchorage, Alaska.
“These patients are very difficult to treat,” he added. “They have a lot of physical disabilities, they have high medical comorbidities, and they have a low quality of life. Their treatment options are extremely limited.”
One of the few options they have is pegloticase, a pegylated uric acid specific enzyme sold under the brand name Krystexxa for the past 12 years. It lowers serum uric acid by converting it to allantoin, which is more water soluble and thus is easier to excrete from the body.
However, one of the problems of using the drug is that anti-drug antibodies frequently develop, meaning that discontinuation rates can be as high as 50%, with around a quarter of patients at high risk of experiencing an infusion reaction.
“Methotrexate is a medication we’re very familiar with for other rheumatologic conditions that use biologic medications, and we use this to prevent anti-drug antibodies. So, the MIRROR RCT was a study we performed to examine the pegloticase therapy in combination with methotrexate co therapy,” explained Dr. Botson.
In fact, co-administration of methotrexate and pegloticase was associated with fewer infusion reactions than using pegloticase alone (3% vs. 31%).
Study design and results
A total of 152 patients were included in the trial and were treated with methotrexate at a weekly dose of 15 mg for 2 weeks before being randomized, 2:1, to either continue methotrexate and then receive intravenous pegloticase or receive the latter with a placebo. Pegloticase was given at a dose of 8 mg every 2 weeks. Treatment was for 52 weeks, with the primary endpoint of serum uric acid response tested at 6 months.
The reason for the 2-week run-in period with methotrexate was to check that patients would be able to tolerate it, Dr. Botson explained.
The mean age of patients was around 54 years, the majority (> 84%) were male and were White (69%). The average duration of gout was about 14 years, with over 74% having tophi present at screening and experiencing 10-11 flares in the previous year. Baseline serum uric acid averaged at about 9 mg/dL.
Almost three-quarters of the 100 patients (73%) who were treated with the combination completed treatment to week 24 while the corresponding percentage in the placebo arm (n = 52) was 39%. The main reason for stopping was due to lack of efficacy (27% and 61% of cases, respectively), defined as having serum uric acid levels above 6 mg/dL on two consecutive measurements.
The median time to discontinuation was 69 days for those in the placebo arm; “it was non-estimable” in the methotrexate arm, Dr. Botson reported.
The mean change in serum uric acid through to week 24 was higher in the methotrexate than placebo arm, at a respective 7.66 and 5.23 mg/dL, giving a significant mean difference of 2.43 mg/dL.
There was a “dramatic resolution of tophaceous deposits,” Dr. Botson said. Complete resolution of tophi was seen in 34.6% of methotrexate-treated patients versus 13.8% of pegloticase-placebo–treated patients (P = .043).
One of the most common adverse events associated with pegloticase treatment is gout flare, which occurred in about 70% of participants in both study arms. Overall, the addition of methotrexate did not increase the risk for adverse events in general, and of the two deaths seen in the study – both in methotrexate-treated patients – one was because of a heart attack and another due COVID-19, so they were unrelated to study treatment.
In patients with renal insufficiency
Concern was raised during the discussion, however, on how to handle methotrexate use in patients with renal insufficiency.
“That’s been a debate that we’ve had in this study and others,” said Dr. Botson, acknowledging that “methotrexate is often a concern for the nephrologist that we’re co-treating these patients with.” However, no dose adjustments were needed in the study.
“There are some other studies with other immunomodulators that do suggest that other agents could be used that may be a little less potentially renal toxic, but we didn’t see any toxicity in the patients that we had, even in those that had a reduced [glomerular filtration rate],” he added.
Dr. Botson has received research support from Horizon and Radius Health. He also acknowledged receiving speakers fees from AbbVie, Amgen, Aurinia, ChemoCentryx*, Horizon, Eli Lilly, and Novartis.
Correction, 6/7/22: The name of the company ChemoCentryx was misstated.
In patients with uncontrolled gout, response rates were increased by 32% when methotrexate was used in conjunction with pegloticase versus pegloticase plus a placebo, it was reported at the annual European Congress of Rheumatology.
In the phase 4 MIRROR trial, 71% of patients who received pretreatment with methotrexate and then the combination of methotrexate and pegloticase achieved uric-acid levels lower than 6 mg/dL for more than 80% of the time during weeks 20-24 of the 52-week study. By comparison, only 39% of those treated with pegloticase plus a placebo achieved this primary endpoint (P < .0001).
“This trial confirms not only improved efficacy but improved safety in patients treated with pegloticase in combination with methotrexate 15 mg orally once weekly,” study investigator John K. Botson, MD, RPh, CCD, said in reporting the trial’s findings.
This is good news for patients, suggested two rheumatologists who were not involved in the study. The combination appears “useful for a select group of gout patients,” observed Christian Ammitzbøll, MD, PhD, from Aarhus University Hospital, Denmark.
“Very promising in refractory gout,” agreed Emre Bilgin, MD, from Ankara, Turkey.
Rationale for using methotrexate
“Oral urate lowering agents are the mainstay of treatment of gout, but there are patients that just don’t respond to oral agents,” said Dr. Botson, a rheumatologist in private practice from Anchorage, Alaska.
“These patients are very difficult to treat,” he added. “They have a lot of physical disabilities, they have high medical comorbidities, and they have a low quality of life. Their treatment options are extremely limited.”
One of the few options they have is pegloticase, a pegylated uric acid specific enzyme sold under the brand name Krystexxa for the past 12 years. It lowers serum uric acid by converting it to allantoin, which is more water soluble and thus is easier to excrete from the body.
However, one of the problems of using the drug is that anti-drug antibodies frequently develop, meaning that discontinuation rates can be as high as 50%, with around a quarter of patients at high risk of experiencing an infusion reaction.
“Methotrexate is a medication we’re very familiar with for other rheumatologic conditions that use biologic medications, and we use this to prevent anti-drug antibodies. So, the MIRROR RCT was a study we performed to examine the pegloticase therapy in combination with methotrexate co therapy,” explained Dr. Botson.
In fact, co-administration of methotrexate and pegloticase was associated with fewer infusion reactions than using pegloticase alone (3% vs. 31%).
Study design and results
A total of 152 patients were included in the trial and were treated with methotrexate at a weekly dose of 15 mg for 2 weeks before being randomized, 2:1, to either continue methotrexate and then receive intravenous pegloticase or receive the latter with a placebo. Pegloticase was given at a dose of 8 mg every 2 weeks. Treatment was for 52 weeks, with the primary endpoint of serum uric acid response tested at 6 months.
The reason for the 2-week run-in period with methotrexate was to check that patients would be able to tolerate it, Dr. Botson explained.
The mean age of patients was around 54 years, the majority (> 84%) were male and were White (69%). The average duration of gout was about 14 years, with over 74% having tophi present at screening and experiencing 10-11 flares in the previous year. Baseline serum uric acid averaged at about 9 mg/dL.
Almost three-quarters of the 100 patients (73%) who were treated with the combination completed treatment to week 24 while the corresponding percentage in the placebo arm (n = 52) was 39%. The main reason for stopping was due to lack of efficacy (27% and 61% of cases, respectively), defined as having serum uric acid levels above 6 mg/dL on two consecutive measurements.
The median time to discontinuation was 69 days for those in the placebo arm; “it was non-estimable” in the methotrexate arm, Dr. Botson reported.
The mean change in serum uric acid through to week 24 was higher in the methotrexate than placebo arm, at a respective 7.66 and 5.23 mg/dL, giving a significant mean difference of 2.43 mg/dL.
There was a “dramatic resolution of tophaceous deposits,” Dr. Botson said. Complete resolution of tophi was seen in 34.6% of methotrexate-treated patients versus 13.8% of pegloticase-placebo–treated patients (P = .043).
One of the most common adverse events associated with pegloticase treatment is gout flare, which occurred in about 70% of participants in both study arms. Overall, the addition of methotrexate did not increase the risk for adverse events in general, and of the two deaths seen in the study – both in methotrexate-treated patients – one was because of a heart attack and another due COVID-19, so they were unrelated to study treatment.
In patients with renal insufficiency
Concern was raised during the discussion, however, on how to handle methotrexate use in patients with renal insufficiency.
“That’s been a debate that we’ve had in this study and others,” said Dr. Botson, acknowledging that “methotrexate is often a concern for the nephrologist that we’re co-treating these patients with.” However, no dose adjustments were needed in the study.
“There are some other studies with other immunomodulators that do suggest that other agents could be used that may be a little less potentially renal toxic, but we didn’t see any toxicity in the patients that we had, even in those that had a reduced [glomerular filtration rate],” he added.
Dr. Botson has received research support from Horizon and Radius Health. He also acknowledged receiving speakers fees from AbbVie, Amgen, Aurinia, ChemoCentryx*, Horizon, Eli Lilly, and Novartis.
Correction, 6/7/22: The name of the company ChemoCentryx was misstated.
In patients with uncontrolled gout, response rates were increased by 32% when methotrexate was used in conjunction with pegloticase versus pegloticase plus a placebo, it was reported at the annual European Congress of Rheumatology.
In the phase 4 MIRROR trial, 71% of patients who received pretreatment with methotrexate and then the combination of methotrexate and pegloticase achieved uric-acid levels lower than 6 mg/dL for more than 80% of the time during weeks 20-24 of the 52-week study. By comparison, only 39% of those treated with pegloticase plus a placebo achieved this primary endpoint (P < .0001).
“This trial confirms not only improved efficacy but improved safety in patients treated with pegloticase in combination with methotrexate 15 mg orally once weekly,” study investigator John K. Botson, MD, RPh, CCD, said in reporting the trial’s findings.
This is good news for patients, suggested two rheumatologists who were not involved in the study. The combination appears “useful for a select group of gout patients,” observed Christian Ammitzbøll, MD, PhD, from Aarhus University Hospital, Denmark.
“Very promising in refractory gout,” agreed Emre Bilgin, MD, from Ankara, Turkey.
Rationale for using methotrexate
“Oral urate lowering agents are the mainstay of treatment of gout, but there are patients that just don’t respond to oral agents,” said Dr. Botson, a rheumatologist in private practice from Anchorage, Alaska.
“These patients are very difficult to treat,” he added. “They have a lot of physical disabilities, they have high medical comorbidities, and they have a low quality of life. Their treatment options are extremely limited.”
One of the few options they have is pegloticase, a pegylated uric acid specific enzyme sold under the brand name Krystexxa for the past 12 years. It lowers serum uric acid by converting it to allantoin, which is more water soluble and thus is easier to excrete from the body.
However, one of the problems of using the drug is that anti-drug antibodies frequently develop, meaning that discontinuation rates can be as high as 50%, with around a quarter of patients at high risk of experiencing an infusion reaction.
“Methotrexate is a medication we’re very familiar with for other rheumatologic conditions that use biologic medications, and we use this to prevent anti-drug antibodies. So, the MIRROR RCT was a study we performed to examine the pegloticase therapy in combination with methotrexate co therapy,” explained Dr. Botson.
In fact, co-administration of methotrexate and pegloticase was associated with fewer infusion reactions than using pegloticase alone (3% vs. 31%).
Study design and results
A total of 152 patients were included in the trial and were treated with methotrexate at a weekly dose of 15 mg for 2 weeks before being randomized, 2:1, to either continue methotrexate and then receive intravenous pegloticase or receive the latter with a placebo. Pegloticase was given at a dose of 8 mg every 2 weeks. Treatment was for 52 weeks, with the primary endpoint of serum uric acid response tested at 6 months.
The reason for the 2-week run-in period with methotrexate was to check that patients would be able to tolerate it, Dr. Botson explained.
The mean age of patients was around 54 years, the majority (> 84%) were male and were White (69%). The average duration of gout was about 14 years, with over 74% having tophi present at screening and experiencing 10-11 flares in the previous year. Baseline serum uric acid averaged at about 9 mg/dL.
Almost three-quarters of the 100 patients (73%) who were treated with the combination completed treatment to week 24 while the corresponding percentage in the placebo arm (n = 52) was 39%. The main reason for stopping was due to lack of efficacy (27% and 61% of cases, respectively), defined as having serum uric acid levels above 6 mg/dL on two consecutive measurements.
The median time to discontinuation was 69 days for those in the placebo arm; “it was non-estimable” in the methotrexate arm, Dr. Botson reported.
The mean change in serum uric acid through to week 24 was higher in the methotrexate than placebo arm, at a respective 7.66 and 5.23 mg/dL, giving a significant mean difference of 2.43 mg/dL.
There was a “dramatic resolution of tophaceous deposits,” Dr. Botson said. Complete resolution of tophi was seen in 34.6% of methotrexate-treated patients versus 13.8% of pegloticase-placebo–treated patients (P = .043).
One of the most common adverse events associated with pegloticase treatment is gout flare, which occurred in about 70% of participants in both study arms. Overall, the addition of methotrexate did not increase the risk for adverse events in general, and of the two deaths seen in the study – both in methotrexate-treated patients – one was because of a heart attack and another due COVID-19, so they were unrelated to study treatment.
In patients with renal insufficiency
Concern was raised during the discussion, however, on how to handle methotrexate use in patients with renal insufficiency.
“That’s been a debate that we’ve had in this study and others,” said Dr. Botson, acknowledging that “methotrexate is often a concern for the nephrologist that we’re co-treating these patients with.” However, no dose adjustments were needed in the study.
“There are some other studies with other immunomodulators that do suggest that other agents could be used that may be a little less potentially renal toxic, but we didn’t see any toxicity in the patients that we had, even in those that had a reduced [glomerular filtration rate],” he added.
Dr. Botson has received research support from Horizon and Radius Health. He also acknowledged receiving speakers fees from AbbVie, Amgen, Aurinia, ChemoCentryx*, Horizon, Eli Lilly, and Novartis.
Correction, 6/7/22: The name of the company ChemoCentryx was misstated.
FROM THE EULAR 2022 CONGRESS
MS and COVID-19: Conflicting signs on risk but some trends are clearer
NATIONAL HARBOR, MD. – While patients with multiple sclerosis (MS) don’t seem to be more likely to be infected with COVID-19, a neurologist told colleagues, the jury is still out over whether they face a higher mortality risk, especially if they take certain disease-modifying therapies (DMTs)
In regard to MS overall, “the data is conflicting, but any increased risk of mortality appears to be slight. And it appears to be chiefly the consequences associated with comorbidities as seen in other populations,” Joseph R. Berger, MD, said at the John F. Kurtzke Memorial Lecture at the annual meeting of the Consortium of Multiple Sclerosis Centers. “If you’re old, if you’re infirm, if you have obesity and cardiovascular disease and underlying pulmonary disease, you’re at risk of dying yourself. It’s not so much the MS,” said Dr. Berger, professor of neurology at the Hospital of the University of Pennsylvania and chief of the multiple sclerosis division at the University of Pennsylvania, Philadelphia.

Dr. Berger had his own COVID-19 story to tell: He couldn’t attend the conference in person because he was quarantining in Portugal since he tested positive. At press time, he was faring well but had reported 4 days of intense back pain.
In regard to MS and COVID-19, Dr. Berger said consistent research suggests that There may be a very small increase in risk of MS relapse in patients with COVID-19, he said, but pseudorelapses are far more common. As for mortality, he highlighted a 2021 pooled analysis of 18 studies with 5,634 patients that suggested they had a crude death rate of 1.97%, standardized lethality ratio of 1.24, and a 24% increased risk of death.
Dr. Berger is skeptical of these findings, however, in light of overall death rate numbers. Early on in the pandemic, the fatality rate in China was estimated at 2.3%.
He said he’s more convinced by a retrospective 2021 German COVID-19 study that compared 551 patients with MS to 156,973 other patients and found lower rates of ICU admission (17.1% in patients with MS vs. 22.7% in those without it), ventilation (9.8% vs. 14.5%), and in‐hospital mortality (11.1% vs. 19.3%).
Meanwhile, a 2021 systematic review found no increase in mortality among 4,310 patients with MS (3% death rate, 20.7% hospitalization), but the death risk was highest among those on no DMTs and those taking anti-CD20 monoclonal antibodies. The COViMS Registry has reported similar findings regarding the anti-CD20 drugs rituximab and ocrelizumab, Dr. Berger noted, and a pooled study of Italian and French data links the monoclonal antibodies to more severe COVID. A 2021 aggregated study also linked the antibodies to increased risk of hospitalization and ICU admission.
“Anti-CD20 monoclonal antibodies appear to increase the risk of hospitalization and perhaps the acquisition of the virus, ICU admission, maybe death,” he said, with rituximab appearing to pose the most risk, followed by ocrelizumab and ofatumumab. “And it appears that the platform [older] therapies may be associated with lesser mortality.”
As for nondrug factors, Dr. Berger said, studies have linked higher risk to age, male sex, and comorbidities.
COVID-19 vaccines are another area of concern, he said. “The recommendation is to administer vaccination prior to the initiation of the anti-CD20s, alemtuzumab, and cladribine, and wait a period of time. Three months is ideal, maybe a little longer, because it appears that the antibody response seems to be best as your CD19 count starts to return.”
Finally, Dr. Berger noted that “passive vaccination” is now available via Evusheld (tixagevimab and cilgavimab) as a preexposure treatment for people with moderate to severe immune compromise who may not mount an effective immune response to COVID-19 vaccination or those who are allergic.
Dr. Berger reported multiple disclosures.
NATIONAL HARBOR, MD. – While patients with multiple sclerosis (MS) don’t seem to be more likely to be infected with COVID-19, a neurologist told colleagues, the jury is still out over whether they face a higher mortality risk, especially if they take certain disease-modifying therapies (DMTs)
In regard to MS overall, “the data is conflicting, but any increased risk of mortality appears to be slight. And it appears to be chiefly the consequences associated with comorbidities as seen in other populations,” Joseph R. Berger, MD, said at the John F. Kurtzke Memorial Lecture at the annual meeting of the Consortium of Multiple Sclerosis Centers. “If you’re old, if you’re infirm, if you have obesity and cardiovascular disease and underlying pulmonary disease, you’re at risk of dying yourself. It’s not so much the MS,” said Dr. Berger, professor of neurology at the Hospital of the University of Pennsylvania and chief of the multiple sclerosis division at the University of Pennsylvania, Philadelphia.
Dr. Berger had his own COVID-19 story to tell: He couldn’t attend the conference in person because he was quarantining in Portugal since he tested positive. At press time, he was faring well but had reported 4 days of intense back pain.
In regard to MS and COVID-19, Dr. Berger said consistent research suggests that There may be a very small increase in risk of MS relapse in patients with COVID-19, he said, but pseudorelapses are far more common. As for mortality, he highlighted a 2021 pooled analysis of 18 studies with 5,634 patients that suggested they had a crude death rate of 1.97%, standardized lethality ratio of 1.24, and a 24% increased risk of death.
Dr. Berger is skeptical of these findings, however, in light of overall death rate numbers. Early on in the pandemic, the fatality rate in China was estimated at 2.3%.
He said he’s more convinced by a retrospective 2021 German COVID-19 study that compared 551 patients with MS to 156,973 other patients and found lower rates of ICU admission (17.1% in patients with MS vs. 22.7% in those without it), ventilation (9.8% vs. 14.5%), and in‐hospital mortality (11.1% vs. 19.3%).
Meanwhile, a 2021 systematic review found no increase in mortality among 4,310 patients with MS (3% death rate, 20.7% hospitalization), but the death risk was highest among those on no DMTs and those taking anti-CD20 monoclonal antibodies. The COViMS Registry has reported similar findings regarding the anti-CD20 drugs rituximab and ocrelizumab, Dr. Berger noted, and a pooled study of Italian and French data links the monoclonal antibodies to more severe COVID. A 2021 aggregated study also linked the antibodies to increased risk of hospitalization and ICU admission.
“Anti-CD20 monoclonal antibodies appear to increase the risk of hospitalization and perhaps the acquisition of the virus, ICU admission, maybe death,” he said, with rituximab appearing to pose the most risk, followed by ocrelizumab and ofatumumab. “And it appears that the platform [older] therapies may be associated with lesser mortality.”
As for nondrug factors, Dr. Berger said, studies have linked higher risk to age, male sex, and comorbidities.
COVID-19 vaccines are another area of concern, he said. “The recommendation is to administer vaccination prior to the initiation of the anti-CD20s, alemtuzumab, and cladribine, and wait a period of time. Three months is ideal, maybe a little longer, because it appears that the antibody response seems to be best as your CD19 count starts to return.”
Finally, Dr. Berger noted that “passive vaccination” is now available via Evusheld (tixagevimab and cilgavimab) as a preexposure treatment for people with moderate to severe immune compromise who may not mount an effective immune response to COVID-19 vaccination or those who are allergic.
Dr. Berger reported multiple disclosures.
NATIONAL HARBOR, MD. – While patients with multiple sclerosis (MS) don’t seem to be more likely to be infected with COVID-19, a neurologist told colleagues, the jury is still out over whether they face a higher mortality risk, especially if they take certain disease-modifying therapies (DMTs)
In regard to MS overall, “the data is conflicting, but any increased risk of mortality appears to be slight. And it appears to be chiefly the consequences associated with comorbidities as seen in other populations,” Joseph R. Berger, MD, said at the John F. Kurtzke Memorial Lecture at the annual meeting of the Consortium of Multiple Sclerosis Centers. “If you’re old, if you’re infirm, if you have obesity and cardiovascular disease and underlying pulmonary disease, you’re at risk of dying yourself. It’s not so much the MS,” said Dr. Berger, professor of neurology at the Hospital of the University of Pennsylvania and chief of the multiple sclerosis division at the University of Pennsylvania, Philadelphia.
Dr. Berger had his own COVID-19 story to tell: He couldn’t attend the conference in person because he was quarantining in Portugal since he tested positive. At press time, he was faring well but had reported 4 days of intense back pain.
In regard to MS and COVID-19, Dr. Berger said consistent research suggests that There may be a very small increase in risk of MS relapse in patients with COVID-19, he said, but pseudorelapses are far more common. As for mortality, he highlighted a 2021 pooled analysis of 18 studies with 5,634 patients that suggested they had a crude death rate of 1.97%, standardized lethality ratio of 1.24, and a 24% increased risk of death.
Dr. Berger is skeptical of these findings, however, in light of overall death rate numbers. Early on in the pandemic, the fatality rate in China was estimated at 2.3%.
He said he’s more convinced by a retrospective 2021 German COVID-19 study that compared 551 patients with MS to 156,973 other patients and found lower rates of ICU admission (17.1% in patients with MS vs. 22.7% in those without it), ventilation (9.8% vs. 14.5%), and in‐hospital mortality (11.1% vs. 19.3%).
Meanwhile, a 2021 systematic review found no increase in mortality among 4,310 patients with MS (3% death rate, 20.7% hospitalization), but the death risk was highest among those on no DMTs and those taking anti-CD20 monoclonal antibodies. The COViMS Registry has reported similar findings regarding the anti-CD20 drugs rituximab and ocrelizumab, Dr. Berger noted, and a pooled study of Italian and French data links the monoclonal antibodies to more severe COVID. A 2021 aggregated study also linked the antibodies to increased risk of hospitalization and ICU admission.
“Anti-CD20 monoclonal antibodies appear to increase the risk of hospitalization and perhaps the acquisition of the virus, ICU admission, maybe death,” he said, with rituximab appearing to pose the most risk, followed by ocrelizumab and ofatumumab. “And it appears that the platform [older] therapies may be associated with lesser mortality.”
As for nondrug factors, Dr. Berger said, studies have linked higher risk to age, male sex, and comorbidities.
COVID-19 vaccines are another area of concern, he said. “The recommendation is to administer vaccination prior to the initiation of the anti-CD20s, alemtuzumab, and cladribine, and wait a period of time. Three months is ideal, maybe a little longer, because it appears that the antibody response seems to be best as your CD19 count starts to return.”
Finally, Dr. Berger noted that “passive vaccination” is now available via Evusheld (tixagevimab and cilgavimab) as a preexposure treatment for people with moderate to severe immune compromise who may not mount an effective immune response to COVID-19 vaccination or those who are allergic.
Dr. Berger reported multiple disclosures.
AT CMSC 2022