User login
Gout flares linked to transient jump in MI, stroke risk
There is evidence that gout and heart disease are mechanistically linked by inflammation and patients with gout are at elevated risk for cardiovascular disease (CVD). But do gout flares, on their own, affect short-term risk for CV events? A new analysis based on records from British medical practices suggests that might be the case.
Risk for myocardial infarction or stroke climbed in the weeks after individual gout flare-ups in the study’s more than 60,000 patients with a recent gout diagnosis. The jump in risk, significant but small in absolute terms, held for about 4 months in the case-control study before going away.
A sensitivity analysis that excluded patients who already had CVD when their gout was diagnosed yielded similar results.
The observational study isn’t able to show that gout flares themselves transiently raise the risk for MI or stroke, but it’s enough to send a cautionary message to physicians who care for patients with gout, rheumatologist Abhishek Abhishek, PhD, Nottingham (England) City Hospital, said in an interview.
In such patients who also have conditions like hypertension, diabetes, or dyslipidemia, or a history of heart disease, he said, it’s important “to manage risk factors really aggressively, knowing that when these patients have a gout flare, there’s a temporary increase in risk of a cardiovascular event.”
Managing their absolute CV risk – whether with drug therapy, lifestyle changes, or other interventions – should help limit the transient jump in risk for MI or stroke following a gout flare, proposed Dr. Abhishek, who is senior author on the study published in JAMA, with lead author Edoardo Cipolletta, MD, also from Nottingham City Hospital.
First robust evidence
The case-control study, which involved more than 60,000 patients with a recent gout diagnosis, some who went on to have MI or stroke, looked at rates of such events at different time intervals after gout flares. Those who experienced such events showed a more than 90% increased likelihood of a gout flare-up in the preceding 60 days, a greater than 50% chance of a flare between 60 and 120 days before the event, but no increased likelihood prior to 120 days before the event.
Such a link between gout flares and CV events “has been suspected but never proven,” observed rheumatologist Hyon K. Choi, MD, Harvard Medical School, Boston, who was not associated with the analysis. “This is the first time it has actually been shown in a robust way,” he said in an interview.
The study suggests a “likely causative relationship” between gout flares and CV events, but – as the published report noted – has limitations like any observational study, said Dr. Choi, who also directs the Gout & Crystal Arthropathy Center at Massachusetts General Hospital, Boston. “Hopefully, this can be replicated in other cohorts.”
The analysis controlled for a number of relevant potential confounders, he noted, but couldn’t account for all issues that could argue against gout flares as a direct cause of the MIs and strokes.
Gout attacks are a complex experience with a range of potential indirect effects on CV risk, Dr. Choi observed. They can immobilize patients, possibly raising their risk for thrombotic events, for example. They can be exceptionally painful, which causes stress and can lead to frequent or chronic use of glucocorticoids or NSAIDs, all of which can exacerbate high blood pressure and possibly worsen CV risk.
A unique insight
The timing of gout flares relative to acute vascular events hasn’t been fully explored, observed an accompanying editorial. The current study’s “unique insight,” it stated, “is that disease activity from gout was associated with an incremental increase in risk for acute vascular events during the time period immediately following the gout flare.”
Although the study is observational, a “large body of evidence from animal and human research, mechanistic insights, and clinical interventions” support an association between flares and vascular events and “make a causal link eminently reasonable,” stated the editorialists, Jeffrey L. Anderson, MD, and Kirk U. Knowlton, MD, both with Intermountain Medical Center, Salt Lake City, Utah.
The findings, they wrote, “should alert clinicians and patients to the increased cardiovascular risk in the weeks beginning after a gout flare and should focus attention on optimizing preventive measures.” Those can include “lifestyle measures and standard risk-factor control including adherence to diet, statins, anti-inflammatory drugs (e.g., aspirin, colchicine), smoking cessation, diabetic and blood pressure control, and antithrombotic medications as indicated.”
Dr. Choi said the current results argue for more liberal use of colchicine, and for preferring colchicine over other anti-inflammatories, in patients with gout and traditional CV risk factors, given multiple randomized trials supporting the drug’s use in such cases. “If you use colchicine, you are covering their heart disease risk as well as their gout. It’s two birds with one stone.”
Nested case-control study
The investigators accessed electronic health records from 96,153 patients with recently diagnosed gout in England from 1997 to 2020; the cohort’s mean age was about 76 years, and 69% of participants were men. They matched 10,475 patients with at least one CV event to 52,099 others who didn’t have such an event by age, sex, and time from gout diagnosis. In each matched set of patients, those not experiencing a CV event were assigned a flare-to-event interval based on their matching with patients who did experience such an event.
Those with CV events, compared with patients without an event, had a greater than 90% increased likelihood of experiencing a gout flare-up in the 60 days preceding the event, a more than 50% greater chance of a flare-up 60-120 days before the CV event, but no increased likelihood more than 120 days before the event.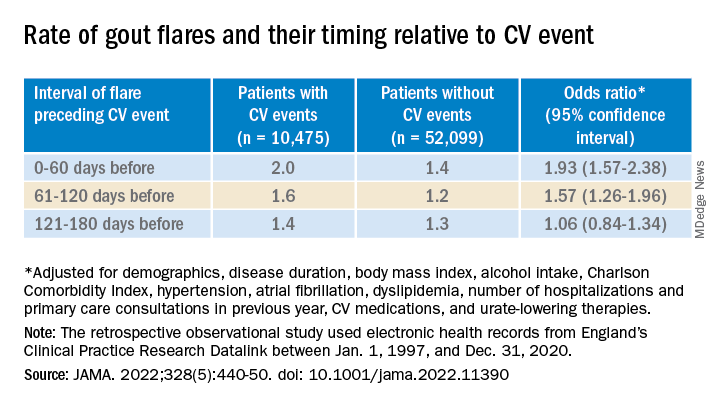
A self-controlled case series based on the same overall cohort with gout yielded similar results while sidestepping any potential for residual confounding, an inherent concern with any case–control analysis, the report notes. It involved 1,421 patients with one or more gout flare and at least one MI or stroke after the diagnosis of gout.
Among that cohort, the CV-event incidence rate ratio, adjusted for age and season of the year, by time interval after a gout flare, was 1.89 (95% confidence interval, 1.54-2.30) at 0-60 days, 1.64 (95% CI, 1.45-1.86) at 61-120 days, and1.29 (95% CI, 1.02-1.64) at 121-180 days.
Also similar, the report noted, were results of several sensitivity analyses, including one that excluded patients with confirmed CVD before their gout diagnosis; another that left out patients at low to moderate CV risk; and one that considered only gout flares treated with colchicine, corticosteroids, or NSAIDs.
The incremental CV event risks observed after flares in the study were small, which “has implications for both cost effectiveness and clinical relevance,” observed Dr. Anderson and Dr. Knowlton.
“An alternative to universal augmentation of cardiovascular risk prevention with therapies among patients with gout flares,” they wrote, would be “to further stratify risk by defining a group at highest near-term risk.” Such interventions could potentially be guided by markers of CV risk such as, for example, levels of high-sensitivity C-reactive protein or lipoprotein(a), or plaque burden on coronary-artery calcium scans.
Dr. Abhishek, Dr. Cipolletta, and the other authors reported no competing interests. Dr. Choi disclosed research support from Ironwood and Horizon; and consulting fees from Ironwood, Selecta, Horizon, Takeda, Kowa, and Vaxart. Dr. Anderson disclosed receiving grants to his institution from Novartis and Milestone.
A version of this article first appeared on Medscape.com.
There is evidence that gout and heart disease are mechanistically linked by inflammation and patients with gout are at elevated risk for cardiovascular disease (CVD). But do gout flares, on their own, affect short-term risk for CV events? A new analysis based on records from British medical practices suggests that might be the case.
Risk for myocardial infarction or stroke climbed in the weeks after individual gout flare-ups in the study’s more than 60,000 patients with a recent gout diagnosis. The jump in risk, significant but small in absolute terms, held for about 4 months in the case-control study before going away.
A sensitivity analysis that excluded patients who already had CVD when their gout was diagnosed yielded similar results.
The observational study isn’t able to show that gout flares themselves transiently raise the risk for MI or stroke, but it’s enough to send a cautionary message to physicians who care for patients with gout, rheumatologist Abhishek Abhishek, PhD, Nottingham (England) City Hospital, said in an interview.
In such patients who also have conditions like hypertension, diabetes, or dyslipidemia, or a history of heart disease, he said, it’s important “to manage risk factors really aggressively, knowing that when these patients have a gout flare, there’s a temporary increase in risk of a cardiovascular event.”
Managing their absolute CV risk – whether with drug therapy, lifestyle changes, or other interventions – should help limit the transient jump in risk for MI or stroke following a gout flare, proposed Dr. Abhishek, who is senior author on the study published in JAMA, with lead author Edoardo Cipolletta, MD, also from Nottingham City Hospital.
First robust evidence
The case-control study, which involved more than 60,000 patients with a recent gout diagnosis, some who went on to have MI or stroke, looked at rates of such events at different time intervals after gout flares. Those who experienced such events showed a more than 90% increased likelihood of a gout flare-up in the preceding 60 days, a greater than 50% chance of a flare between 60 and 120 days before the event, but no increased likelihood prior to 120 days before the event.
Such a link between gout flares and CV events “has been suspected but never proven,” observed rheumatologist Hyon K. Choi, MD, Harvard Medical School, Boston, who was not associated with the analysis. “This is the first time it has actually been shown in a robust way,” he said in an interview.
The study suggests a “likely causative relationship” between gout flares and CV events, but – as the published report noted – has limitations like any observational study, said Dr. Choi, who also directs the Gout & Crystal Arthropathy Center at Massachusetts General Hospital, Boston. “Hopefully, this can be replicated in other cohorts.”
The analysis controlled for a number of relevant potential confounders, he noted, but couldn’t account for all issues that could argue against gout flares as a direct cause of the MIs and strokes.
Gout attacks are a complex experience with a range of potential indirect effects on CV risk, Dr. Choi observed. They can immobilize patients, possibly raising their risk for thrombotic events, for example. They can be exceptionally painful, which causes stress and can lead to frequent or chronic use of glucocorticoids or NSAIDs, all of which can exacerbate high blood pressure and possibly worsen CV risk.
A unique insight
The timing of gout flares relative to acute vascular events hasn’t been fully explored, observed an accompanying editorial. The current study’s “unique insight,” it stated, “is that disease activity from gout was associated with an incremental increase in risk for acute vascular events during the time period immediately following the gout flare.”
Although the study is observational, a “large body of evidence from animal and human research, mechanistic insights, and clinical interventions” support an association between flares and vascular events and “make a causal link eminently reasonable,” stated the editorialists, Jeffrey L. Anderson, MD, and Kirk U. Knowlton, MD, both with Intermountain Medical Center, Salt Lake City, Utah.
The findings, they wrote, “should alert clinicians and patients to the increased cardiovascular risk in the weeks beginning after a gout flare and should focus attention on optimizing preventive measures.” Those can include “lifestyle measures and standard risk-factor control including adherence to diet, statins, anti-inflammatory drugs (e.g., aspirin, colchicine), smoking cessation, diabetic and blood pressure control, and antithrombotic medications as indicated.”
Dr. Choi said the current results argue for more liberal use of colchicine, and for preferring colchicine over other anti-inflammatories, in patients with gout and traditional CV risk factors, given multiple randomized trials supporting the drug’s use in such cases. “If you use colchicine, you are covering their heart disease risk as well as their gout. It’s two birds with one stone.”
Nested case-control study
The investigators accessed electronic health records from 96,153 patients with recently diagnosed gout in England from 1997 to 2020; the cohort’s mean age was about 76 years, and 69% of participants were men. They matched 10,475 patients with at least one CV event to 52,099 others who didn’t have such an event by age, sex, and time from gout diagnosis. In each matched set of patients, those not experiencing a CV event were assigned a flare-to-event interval based on their matching with patients who did experience such an event.
Those with CV events, compared with patients without an event, had a greater than 90% increased likelihood of experiencing a gout flare-up in the 60 days preceding the event, a more than 50% greater chance of a flare-up 60-120 days before the CV event, but no increased likelihood more than 120 days before the event.
A self-controlled case series based on the same overall cohort with gout yielded similar results while sidestepping any potential for residual confounding, an inherent concern with any case–control analysis, the report notes. It involved 1,421 patients with one or more gout flare and at least one MI or stroke after the diagnosis of gout.
Among that cohort, the CV-event incidence rate ratio, adjusted for age and season of the year, by time interval after a gout flare, was 1.89 (95% confidence interval, 1.54-2.30) at 0-60 days, 1.64 (95% CI, 1.45-1.86) at 61-120 days, and1.29 (95% CI, 1.02-1.64) at 121-180 days.
Also similar, the report noted, were results of several sensitivity analyses, including one that excluded patients with confirmed CVD before their gout diagnosis; another that left out patients at low to moderate CV risk; and one that considered only gout flares treated with colchicine, corticosteroids, or NSAIDs.
The incremental CV event risks observed after flares in the study were small, which “has implications for both cost effectiveness and clinical relevance,” observed Dr. Anderson and Dr. Knowlton.
“An alternative to universal augmentation of cardiovascular risk prevention with therapies among patients with gout flares,” they wrote, would be “to further stratify risk by defining a group at highest near-term risk.” Such interventions could potentially be guided by markers of CV risk such as, for example, levels of high-sensitivity C-reactive protein or lipoprotein(a), or plaque burden on coronary-artery calcium scans.
Dr. Abhishek, Dr. Cipolletta, and the other authors reported no competing interests. Dr. Choi disclosed research support from Ironwood and Horizon; and consulting fees from Ironwood, Selecta, Horizon, Takeda, Kowa, and Vaxart. Dr. Anderson disclosed receiving grants to his institution from Novartis and Milestone.
A version of this article first appeared on Medscape.com.
There is evidence that gout and heart disease are mechanistically linked by inflammation and patients with gout are at elevated risk for cardiovascular disease (CVD). But do gout flares, on their own, affect short-term risk for CV events? A new analysis based on records from British medical practices suggests that might be the case.
Risk for myocardial infarction or stroke climbed in the weeks after individual gout flare-ups in the study’s more than 60,000 patients with a recent gout diagnosis. The jump in risk, significant but small in absolute terms, held for about 4 months in the case-control study before going away.
A sensitivity analysis that excluded patients who already had CVD when their gout was diagnosed yielded similar results.
The observational study isn’t able to show that gout flares themselves transiently raise the risk for MI or stroke, but it’s enough to send a cautionary message to physicians who care for patients with gout, rheumatologist Abhishek Abhishek, PhD, Nottingham (England) City Hospital, said in an interview.
In such patients who also have conditions like hypertension, diabetes, or dyslipidemia, or a history of heart disease, he said, it’s important “to manage risk factors really aggressively, knowing that when these patients have a gout flare, there’s a temporary increase in risk of a cardiovascular event.”
Managing their absolute CV risk – whether with drug therapy, lifestyle changes, or other interventions – should help limit the transient jump in risk for MI or stroke following a gout flare, proposed Dr. Abhishek, who is senior author on the study published in JAMA, with lead author Edoardo Cipolletta, MD, also from Nottingham City Hospital.
First robust evidence
The case-control study, which involved more than 60,000 patients with a recent gout diagnosis, some who went on to have MI or stroke, looked at rates of such events at different time intervals after gout flares. Those who experienced such events showed a more than 90% increased likelihood of a gout flare-up in the preceding 60 days, a greater than 50% chance of a flare between 60 and 120 days before the event, but no increased likelihood prior to 120 days before the event.
Such a link between gout flares and CV events “has been suspected but never proven,” observed rheumatologist Hyon K. Choi, MD, Harvard Medical School, Boston, who was not associated with the analysis. “This is the first time it has actually been shown in a robust way,” he said in an interview.
The study suggests a “likely causative relationship” between gout flares and CV events, but – as the published report noted – has limitations like any observational study, said Dr. Choi, who also directs the Gout & Crystal Arthropathy Center at Massachusetts General Hospital, Boston. “Hopefully, this can be replicated in other cohorts.”
The analysis controlled for a number of relevant potential confounders, he noted, but couldn’t account for all issues that could argue against gout flares as a direct cause of the MIs and strokes.
Gout attacks are a complex experience with a range of potential indirect effects on CV risk, Dr. Choi observed. They can immobilize patients, possibly raising their risk for thrombotic events, for example. They can be exceptionally painful, which causes stress and can lead to frequent or chronic use of glucocorticoids or NSAIDs, all of which can exacerbate high blood pressure and possibly worsen CV risk.
A unique insight
The timing of gout flares relative to acute vascular events hasn’t been fully explored, observed an accompanying editorial. The current study’s “unique insight,” it stated, “is that disease activity from gout was associated with an incremental increase in risk for acute vascular events during the time period immediately following the gout flare.”
Although the study is observational, a “large body of evidence from animal and human research, mechanistic insights, and clinical interventions” support an association between flares and vascular events and “make a causal link eminently reasonable,” stated the editorialists, Jeffrey L. Anderson, MD, and Kirk U. Knowlton, MD, both with Intermountain Medical Center, Salt Lake City, Utah.
The findings, they wrote, “should alert clinicians and patients to the increased cardiovascular risk in the weeks beginning after a gout flare and should focus attention on optimizing preventive measures.” Those can include “lifestyle measures and standard risk-factor control including adherence to diet, statins, anti-inflammatory drugs (e.g., aspirin, colchicine), smoking cessation, diabetic and blood pressure control, and antithrombotic medications as indicated.”
Dr. Choi said the current results argue for more liberal use of colchicine, and for preferring colchicine over other anti-inflammatories, in patients with gout and traditional CV risk factors, given multiple randomized trials supporting the drug’s use in such cases. “If you use colchicine, you are covering their heart disease risk as well as their gout. It’s two birds with one stone.”
Nested case-control study
The investigators accessed electronic health records from 96,153 patients with recently diagnosed gout in England from 1997 to 2020; the cohort’s mean age was about 76 years, and 69% of participants were men. They matched 10,475 patients with at least one CV event to 52,099 others who didn’t have such an event by age, sex, and time from gout diagnosis. In each matched set of patients, those not experiencing a CV event were assigned a flare-to-event interval based on their matching with patients who did experience such an event.
Those with CV events, compared with patients without an event, had a greater than 90% increased likelihood of experiencing a gout flare-up in the 60 days preceding the event, a more than 50% greater chance of a flare-up 60-120 days before the CV event, but no increased likelihood more than 120 days before the event.
A self-controlled case series based on the same overall cohort with gout yielded similar results while sidestepping any potential for residual confounding, an inherent concern with any case–control analysis, the report notes. It involved 1,421 patients with one or more gout flare and at least one MI or stroke after the diagnosis of gout.
Among that cohort, the CV-event incidence rate ratio, adjusted for age and season of the year, by time interval after a gout flare, was 1.89 (95% confidence interval, 1.54-2.30) at 0-60 days, 1.64 (95% CI, 1.45-1.86) at 61-120 days, and1.29 (95% CI, 1.02-1.64) at 121-180 days.
Also similar, the report noted, were results of several sensitivity analyses, including one that excluded patients with confirmed CVD before their gout diagnosis; another that left out patients at low to moderate CV risk; and one that considered only gout flares treated with colchicine, corticosteroids, or NSAIDs.
The incremental CV event risks observed after flares in the study were small, which “has implications for both cost effectiveness and clinical relevance,” observed Dr. Anderson and Dr. Knowlton.
“An alternative to universal augmentation of cardiovascular risk prevention with therapies among patients with gout flares,” they wrote, would be “to further stratify risk by defining a group at highest near-term risk.” Such interventions could potentially be guided by markers of CV risk such as, for example, levels of high-sensitivity C-reactive protein or lipoprotein(a), or plaque burden on coronary-artery calcium scans.
Dr. Abhishek, Dr. Cipolletta, and the other authors reported no competing interests. Dr. Choi disclosed research support from Ironwood and Horizon; and consulting fees from Ironwood, Selecta, Horizon, Takeda, Kowa, and Vaxart. Dr. Anderson disclosed receiving grants to his institution from Novartis and Milestone.
A version of this article first appeared on Medscape.com.
FROM JAMA
Taste dysfunction in head and neck cancer due to radiation dose
finds a new study from JAMA Otolaryngology–Head & Neck Surgery.
Taste dysfunction can affect up to 90% of patients undergoing radiotherapy for head and neck cancer. While the ability to taste usually returns after the treatment concludes, some patients can still feel the lingering effects of radiotherapy on taste function long after the treatment concludes. It can lead to weight loss and dry mouth which can, in turn, negatively affect quality of life.
“Taste dysfunction has profound effects on quality of life in patients with head and neck cancer, and the oral cavity dose could be significantly lower with modern radiotherapy techniques,” wrote the researchers, who were led by Miao-Fen Chen, MD, PhD, of Chang Gung University, Taoyuan City, Taiwan. “This study provides useful dose constraints of the oral cavity that may be associated with reduced taste dysfunction.”
Degradation of taste is an important quality of life factor for head and neck cancer patients. A 2021 systematic review published in the journal Radiotherapy and Oncology found that acute taste dysfunction affected 96% of patients as measured objectively, and 79% as measured subjectively. While most patients recover an estimated 23-53% of patients experience long-term dysfunction.
In 2019, a study published in the journal Chemical Senses found that 31% of head and neck cancer patients had long-term changes to taste at 27 months after intensity-modulated radiotherapy (IMRT), with dysfunction associated with glossectomy and oral cavity radiation doses greater than 50 Gy, but the study only used one quality of life subjective measure to evaluate taste function.
In the new JAMA study, researchers reported the results of a longitudinal using the whole-mouth solution method for basic tastes, including salt, sweet, sour, and bitter.
Study methodology
The study included 87 patients (mean age, 58 years; 90% men) who were enrolled between 2017 and 2020 from a single hospital. 45 patients received primary intensity-modulated radiotherapy and 42 received postoperative radiotherapy. 78 patients received volumetric arc therapy, and 9 received intensity-modulated radiotherapy. The radiotherapy was directed to minimize the effect on the parotid glands and oral cavity.
Researchers measured taste dysfunction according to detection thresholds based on solutions with different concentrations. After moving the solution around the mouth and spitting it out, patients were asked to identify taste components. Following a water rinse, they tested a solution with another concentration of taste components. A number was assigned based on the concentration level they were able to detect, with nigher numbers indicating greater sensitivity.
Two to four weeks after initiation of radiotherapy, there were drops in taste scores for salt (4.7 to 1.4), sweet (4.2 to 1.8), sour (4.5 to 2.3), and bitter (4.7 to 1.2). 1 week after radiotherapy, those mean scores increased to 2.6, 2.6, 2.9, and 2.3 respectively. Over the following 3 months, mean scores reflected general recovery to near preradiotherapy levels (4.2, 3.9, 4.1, and 4.0, respectively). At 6 months and 1 year, the scores were equivalent to preradiotherapy levels.
Objective taste tests were performed on 81 participants. 33.3% had taste dysfunction 6 months after radiotherapy. 6 months after, 8.9% had taste dysfunction. At 3 months following radiotherapy, taste dysfunction was associated with an oral cavity mean dose of 4,000 cGy or higher (relative risk, 2.87; 95% confidence interval, 1.21-6.81) or 5,000 cGy or higher (RR, 2.04; 95% CI, 1.12-3.72). At 6 months, taste dysfunction was predicted by glossectomy (RR, 5.63; 95% CI, 1.12-28.15) and oral cavity mean dose 5,000 cGy or greater (RR, 7.79; 95% CI, 0.93-64.92).
The researchers quantified the relationship between mean oral cavity dose and probability of developing taste dysfunction at 3 and 6 months. 3 months after radiotherapy, 25 Gy predicted a 15% chance, 38 Gy predicted a 25% chance, and 60 Gy predicted a 50% chance. At 6 months, the numbers were 57, 60, and 64 Gy.
The study was limited by being conducted at a single center and its small sample size, and it recruited patients varied significantly in treatment modality and disease subtype.
finds a new study from JAMA Otolaryngology–Head & Neck Surgery.
Taste dysfunction can affect up to 90% of patients undergoing radiotherapy for head and neck cancer. While the ability to taste usually returns after the treatment concludes, some patients can still feel the lingering effects of radiotherapy on taste function long after the treatment concludes. It can lead to weight loss and dry mouth which can, in turn, negatively affect quality of life.
“Taste dysfunction has profound effects on quality of life in patients with head and neck cancer, and the oral cavity dose could be significantly lower with modern radiotherapy techniques,” wrote the researchers, who were led by Miao-Fen Chen, MD, PhD, of Chang Gung University, Taoyuan City, Taiwan. “This study provides useful dose constraints of the oral cavity that may be associated with reduced taste dysfunction.”
Degradation of taste is an important quality of life factor for head and neck cancer patients. A 2021 systematic review published in the journal Radiotherapy and Oncology found that acute taste dysfunction affected 96% of patients as measured objectively, and 79% as measured subjectively. While most patients recover an estimated 23-53% of patients experience long-term dysfunction.
In 2019, a study published in the journal Chemical Senses found that 31% of head and neck cancer patients had long-term changes to taste at 27 months after intensity-modulated radiotherapy (IMRT), with dysfunction associated with glossectomy and oral cavity radiation doses greater than 50 Gy, but the study only used one quality of life subjective measure to evaluate taste function.
In the new JAMA study, researchers reported the results of a longitudinal using the whole-mouth solution method for basic tastes, including salt, sweet, sour, and bitter.
Study methodology
The study included 87 patients (mean age, 58 years; 90% men) who were enrolled between 2017 and 2020 from a single hospital. 45 patients received primary intensity-modulated radiotherapy and 42 received postoperative radiotherapy. 78 patients received volumetric arc therapy, and 9 received intensity-modulated radiotherapy. The radiotherapy was directed to minimize the effect on the parotid glands and oral cavity.
Researchers measured taste dysfunction according to detection thresholds based on solutions with different concentrations. After moving the solution around the mouth and spitting it out, patients were asked to identify taste components. Following a water rinse, they tested a solution with another concentration of taste components. A number was assigned based on the concentration level they were able to detect, with nigher numbers indicating greater sensitivity.
Two to four weeks after initiation of radiotherapy, there were drops in taste scores for salt (4.7 to 1.4), sweet (4.2 to 1.8), sour (4.5 to 2.3), and bitter (4.7 to 1.2). 1 week after radiotherapy, those mean scores increased to 2.6, 2.6, 2.9, and 2.3 respectively. Over the following 3 months, mean scores reflected general recovery to near preradiotherapy levels (4.2, 3.9, 4.1, and 4.0, respectively). At 6 months and 1 year, the scores were equivalent to preradiotherapy levels.
Objective taste tests were performed on 81 participants. 33.3% had taste dysfunction 6 months after radiotherapy. 6 months after, 8.9% had taste dysfunction. At 3 months following radiotherapy, taste dysfunction was associated with an oral cavity mean dose of 4,000 cGy or higher (relative risk, 2.87; 95% confidence interval, 1.21-6.81) or 5,000 cGy or higher (RR, 2.04; 95% CI, 1.12-3.72). At 6 months, taste dysfunction was predicted by glossectomy (RR, 5.63; 95% CI, 1.12-28.15) and oral cavity mean dose 5,000 cGy or greater (RR, 7.79; 95% CI, 0.93-64.92).
The researchers quantified the relationship between mean oral cavity dose and probability of developing taste dysfunction at 3 and 6 months. 3 months after radiotherapy, 25 Gy predicted a 15% chance, 38 Gy predicted a 25% chance, and 60 Gy predicted a 50% chance. At 6 months, the numbers were 57, 60, and 64 Gy.
The study was limited by being conducted at a single center and its small sample size, and it recruited patients varied significantly in treatment modality and disease subtype.
finds a new study from JAMA Otolaryngology–Head & Neck Surgery.
Taste dysfunction can affect up to 90% of patients undergoing radiotherapy for head and neck cancer. While the ability to taste usually returns after the treatment concludes, some patients can still feel the lingering effects of radiotherapy on taste function long after the treatment concludes. It can lead to weight loss and dry mouth which can, in turn, negatively affect quality of life.
“Taste dysfunction has profound effects on quality of life in patients with head and neck cancer, and the oral cavity dose could be significantly lower with modern radiotherapy techniques,” wrote the researchers, who were led by Miao-Fen Chen, MD, PhD, of Chang Gung University, Taoyuan City, Taiwan. “This study provides useful dose constraints of the oral cavity that may be associated with reduced taste dysfunction.”
Degradation of taste is an important quality of life factor for head and neck cancer patients. A 2021 systematic review published in the journal Radiotherapy and Oncology found that acute taste dysfunction affected 96% of patients as measured objectively, and 79% as measured subjectively. While most patients recover an estimated 23-53% of patients experience long-term dysfunction.
In 2019, a study published in the journal Chemical Senses found that 31% of head and neck cancer patients had long-term changes to taste at 27 months after intensity-modulated radiotherapy (IMRT), with dysfunction associated with glossectomy and oral cavity radiation doses greater than 50 Gy, but the study only used one quality of life subjective measure to evaluate taste function.
In the new JAMA study, researchers reported the results of a longitudinal using the whole-mouth solution method for basic tastes, including salt, sweet, sour, and bitter.
Study methodology
The study included 87 patients (mean age, 58 years; 90% men) who were enrolled between 2017 and 2020 from a single hospital. 45 patients received primary intensity-modulated radiotherapy and 42 received postoperative radiotherapy. 78 patients received volumetric arc therapy, and 9 received intensity-modulated radiotherapy. The radiotherapy was directed to minimize the effect on the parotid glands and oral cavity.
Researchers measured taste dysfunction according to detection thresholds based on solutions with different concentrations. After moving the solution around the mouth and spitting it out, patients were asked to identify taste components. Following a water rinse, they tested a solution with another concentration of taste components. A number was assigned based on the concentration level they were able to detect, with nigher numbers indicating greater sensitivity.
Two to four weeks after initiation of radiotherapy, there were drops in taste scores for salt (4.7 to 1.4), sweet (4.2 to 1.8), sour (4.5 to 2.3), and bitter (4.7 to 1.2). 1 week after radiotherapy, those mean scores increased to 2.6, 2.6, 2.9, and 2.3 respectively. Over the following 3 months, mean scores reflected general recovery to near preradiotherapy levels (4.2, 3.9, 4.1, and 4.0, respectively). At 6 months and 1 year, the scores were equivalent to preradiotherapy levels.
Objective taste tests were performed on 81 participants. 33.3% had taste dysfunction 6 months after radiotherapy. 6 months after, 8.9% had taste dysfunction. At 3 months following radiotherapy, taste dysfunction was associated with an oral cavity mean dose of 4,000 cGy or higher (relative risk, 2.87; 95% confidence interval, 1.21-6.81) or 5,000 cGy or higher (RR, 2.04; 95% CI, 1.12-3.72). At 6 months, taste dysfunction was predicted by glossectomy (RR, 5.63; 95% CI, 1.12-28.15) and oral cavity mean dose 5,000 cGy or greater (RR, 7.79; 95% CI, 0.93-64.92).
The researchers quantified the relationship between mean oral cavity dose and probability of developing taste dysfunction at 3 and 6 months. 3 months after radiotherapy, 25 Gy predicted a 15% chance, 38 Gy predicted a 25% chance, and 60 Gy predicted a 50% chance. At 6 months, the numbers were 57, 60, and 64 Gy.
The study was limited by being conducted at a single center and its small sample size, and it recruited patients varied significantly in treatment modality and disease subtype.
FROM JAMA OTOLARYNGOLOGY–HEAD AND NECK SURGERY
Ustekinumab becomes second biologic approved for PsA in kids
The Food and Drug Administration has approved the dual interleukin-12 and IL-23 inhibitor ustekinumab (Stelara) for the treatment of juvenile psoriatic arthritis (jPsA) in patients aged 6 years and older, according to an Aug. 1 announcement from its manufacturer, Janssen.
The approval makes jPsA the sixth approved indication for ustekinumab, which include active psoriatic arthritis in adults, moderate to severe plaque psoriasis in both adults and children aged 6 years or older who are candidates for phototherapy or systemic therapy, moderately to severely active Crohn’s disease in adults, and moderately to severely active ulcerative colitis in adults.
In addition, ustekinumab is now the second biologic to be approved for jPsA, following the agency’s December 2021 approval of secukinumab (Cosentyx) to treat jPsA in children and adolescents aged 2 years and older as well as enthesitis-related arthritis in children and adolescents aged 4 years and older.
In pediatric patients, ustekinumab is administered as a subcutaneous injection dosed four times per year after two starter doses.
Ustekinumab’s approval is based on “an extrapolation of the established data and existing safety profile” of ustekinumab in multiple phase 3 studies in adult and pediatric patients with moderate to severe plaque psoriasis and adult patients with active PsA, according to Janssen.
“With the limited availability of pediatric patients for clinical trial inclusion, researchers can extrapolate data from trials with adults to determine the potential efficacy and tolerability of a treatment for a pediatric population,” according to the October 2021 announcement from the company that the Biologics License Application had been submitted to the FDA.
Juvenile arthritis occurs in an estimated 20-45 children per 100,000 in the United States, with about 5% of those children having jPsA, according to the National Psoriasis Foundation.
The prescribing information for ustekinumab includes specific warnings and areas of concern. The drug should not be administered to individuals with known hypersensitivity to ustekinumab. The drug may lower the ability of the immune system to fight infections and may increase risk of infections, sometimes serious, and a test for tuberculosis infection should be given before administration.
Patients taking ustekinumab should not be given a live vaccine, and their doctors should be informed if anyone in their household needs a live vaccine. They also should not receive the BCG vaccine during the 1 year before receiving the drug or 1 year after they stop taking it, according to Johnson & Johnson.
The most common adverse effects include nasal congestion, sore throat, runny nose, upper respiratory infections, fever, headache, tiredness, itching, nausea and vomiting, redness at the injection site, vaginal yeast infections, urinary tract infections, sinus infection, bronchitis, diarrhea, stomach pain, and joint pain.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the dual interleukin-12 and IL-23 inhibitor ustekinumab (Stelara) for the treatment of juvenile psoriatic arthritis (jPsA) in patients aged 6 years and older, according to an Aug. 1 announcement from its manufacturer, Janssen.
The approval makes jPsA the sixth approved indication for ustekinumab, which include active psoriatic arthritis in adults, moderate to severe plaque psoriasis in both adults and children aged 6 years or older who are candidates for phototherapy or systemic therapy, moderately to severely active Crohn’s disease in adults, and moderately to severely active ulcerative colitis in adults.
In addition, ustekinumab is now the second biologic to be approved for jPsA, following the agency’s December 2021 approval of secukinumab (Cosentyx) to treat jPsA in children and adolescents aged 2 years and older as well as enthesitis-related arthritis in children and adolescents aged 4 years and older.
In pediatric patients, ustekinumab is administered as a subcutaneous injection dosed four times per year after two starter doses.
Ustekinumab’s approval is based on “an extrapolation of the established data and existing safety profile” of ustekinumab in multiple phase 3 studies in adult and pediatric patients with moderate to severe plaque psoriasis and adult patients with active PsA, according to Janssen.
“With the limited availability of pediatric patients for clinical trial inclusion, researchers can extrapolate data from trials with adults to determine the potential efficacy and tolerability of a treatment for a pediatric population,” according to the October 2021 announcement from the company that the Biologics License Application had been submitted to the FDA.
Juvenile arthritis occurs in an estimated 20-45 children per 100,000 in the United States, with about 5% of those children having jPsA, according to the National Psoriasis Foundation.
The prescribing information for ustekinumab includes specific warnings and areas of concern. The drug should not be administered to individuals with known hypersensitivity to ustekinumab. The drug may lower the ability of the immune system to fight infections and may increase risk of infections, sometimes serious, and a test for tuberculosis infection should be given before administration.
Patients taking ustekinumab should not be given a live vaccine, and their doctors should be informed if anyone in their household needs a live vaccine. They also should not receive the BCG vaccine during the 1 year before receiving the drug or 1 year after they stop taking it, according to Johnson & Johnson.
The most common adverse effects include nasal congestion, sore throat, runny nose, upper respiratory infections, fever, headache, tiredness, itching, nausea and vomiting, redness at the injection site, vaginal yeast infections, urinary tract infections, sinus infection, bronchitis, diarrhea, stomach pain, and joint pain.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has approved the dual interleukin-12 and IL-23 inhibitor ustekinumab (Stelara) for the treatment of juvenile psoriatic arthritis (jPsA) in patients aged 6 years and older, according to an Aug. 1 announcement from its manufacturer, Janssen.
The approval makes jPsA the sixth approved indication for ustekinumab, which include active psoriatic arthritis in adults, moderate to severe plaque psoriasis in both adults and children aged 6 years or older who are candidates for phototherapy or systemic therapy, moderately to severely active Crohn’s disease in adults, and moderately to severely active ulcerative colitis in adults.
In addition, ustekinumab is now the second biologic to be approved for jPsA, following the agency’s December 2021 approval of secukinumab (Cosentyx) to treat jPsA in children and adolescents aged 2 years and older as well as enthesitis-related arthritis in children and adolescents aged 4 years and older.
In pediatric patients, ustekinumab is administered as a subcutaneous injection dosed four times per year after two starter doses.
Ustekinumab’s approval is based on “an extrapolation of the established data and existing safety profile” of ustekinumab in multiple phase 3 studies in adult and pediatric patients with moderate to severe plaque psoriasis and adult patients with active PsA, according to Janssen.
“With the limited availability of pediatric patients for clinical trial inclusion, researchers can extrapolate data from trials with adults to determine the potential efficacy and tolerability of a treatment for a pediatric population,” according to the October 2021 announcement from the company that the Biologics License Application had been submitted to the FDA.
Juvenile arthritis occurs in an estimated 20-45 children per 100,000 in the United States, with about 5% of those children having jPsA, according to the National Psoriasis Foundation.
The prescribing information for ustekinumab includes specific warnings and areas of concern. The drug should not be administered to individuals with known hypersensitivity to ustekinumab. The drug may lower the ability of the immune system to fight infections and may increase risk of infections, sometimes serious, and a test for tuberculosis infection should be given before administration.
Patients taking ustekinumab should not be given a live vaccine, and their doctors should be informed if anyone in their household needs a live vaccine. They also should not receive the BCG vaccine during the 1 year before receiving the drug or 1 year after they stop taking it, according to Johnson & Johnson.
The most common adverse effects include nasal congestion, sore throat, runny nose, upper respiratory infections, fever, headache, tiredness, itching, nausea and vomiting, redness at the injection site, vaginal yeast infections, urinary tract infections, sinus infection, bronchitis, diarrhea, stomach pain, and joint pain.
A version of this article first appeared on Medscape.com.
Commentary: Treating Gastric Cancer Subtypes, August 2022
Patients with stage II or III gastric cancer are treated with surgical resection and perioperative chemotherapy. Platinum agents have established activity in this disease. Combination chemotherapy FLOT (5-fluorouracil, oxaliplatin, and docetaxel) is now standard perioperative treatment for resectable gastric cancer.1 The study by Slagter and colleagues evaluated whether cisplatin was noninferior to oxaliplatin when used in the treatment of early-stage gastric cancer. Prior to the incorporation of FLOT into standard treatment practice, patients were treated with ECX (epirubicin, cisplatin, and docetaxel), as per the MAGIC trial.2 In the metastatic setting, chemotherapy regimens with either cisplatin or oxaliplatin as a choice of platinum agent have comparable activity against these tumors. Oxaliplatin activity has been shown to be noninferior to cisplatin in the randomized REAL2 trial in metastatic setting.3
The study by Slagter and colleagues is a post hoc analysis of 781 patients with resectable gastric cancer who were enrolled in the CRITICS trial. This analysis demonstrated that chemotherapy regimens containing oxaliplatin and cisplatin had comparable 5-year overall survival rates. Not surprisingly, oxaliplatin was associated with higher neurotoxicity. Based on this analysis, it is likely safe to conclude that, just as in the advanced setting, cisplatin and oxaliplatin have similar activity in early-stage disease.
Mismatch repair protein deficient or microsatellite unstable gastric cancer (MSI-H) represent unique subtypes of gastric cancer, with distinct biologic behaviors and treatment responses. The efficacy of chemotherapy in patients with early-stage MSI-H tumors has been questioned previously. Similar to MSI-H colorectal cancers, the benefit of chemotherapy in resectable MSI-H gastric and esophagogastric junction tumors appears to be less robust than in microsatellite stable (MSS) tumors. In the exploratory analysis of patients with MSI-H tumors enrolled in the perioperative MAGIC trial, patients with MSI-H tumors had better prognosis when treated with surgery alone and potentially experienced detrimental effects from chemotherapy.4 The retrospective analysis by Vos and colleagues adds to the body of knowledge about early-stage MSI-H gastric cancers. They evaluated 535 patients with early-stage disease who were treated with surgery alone or surgery plus perioperative therapy between 2000 and 2018. The overall survival in 82 patients with MSI-H tumors was 20% better than in those with MSS disease. This favorable outcome was seen irrespective of whether chemotherapy was given. Though these results suggest that chemotherapy may not be necessary in the treatment of these tumors and there are emerging data regarding the activity of immune checkpoint inhibitors in this setting, these results should definitely be investigated further in prospective studies.5 However, in the absence of prospective randomized data, it is difficult to recommend deviating from the established standard of care with FLOT, especially for patients undergoing curative intent treatment.
A study by Yukami and colleagues evaluated whether the presence of liver metastasis, which have been shown to be enriched in immunosuppressive cells in the preclinical setting, had any bearing on the activity of immune checkpoint inhibitors alone or in combination with multi-tyrosine kinase inhibitors. The analysis included 54 patients enrolled in a phase 1b trial of REGONIVO (regorafenib and nivolumab) and a phase 2 trial of LENPEM (lenvatinib and pembrolizumab). With a median follow up of 14 months, there was no significant difference in the efficacy of the above regimens (overall survival, progression-free survival, and objective response rate) between patients with and without liver metastasis. The promising activity of these combinations is continuing with longer follow-up. The above regimens should be investigated further in larger prospective studies irrespective of metastatic sites.
Additional References
1. Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393:1948-1957. Doi: 10.1016/S0140-6736(18)32557-1
2. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11-20. Doi: 10.1056/NEJMoa055531
3. Cunningham D, Starling N, Rao S, et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med. 2008;358:36-46. Doi: 10.1056/NEJMoa073149
4. Smyth EC, Wotherspoon A, Peckitt C, et al. Mismatch repair deficiency, microsatellite instability, and survival: an exploratory analysis of the Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial. JAMA Oncol. 2017;3:1197-1203. Doi: 10.1001/jamaoncol.2016.6762
5. Andre T, Tougeron D, Piessen G, et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in patients (pts) with localized microsatellite instability-high (MSI)/mismatch repair deficient (dMMR) oeso-gastric adenocarcinoma (OGA): the GERCOR NEONIPIGA phase II study. J Clin Oncol. 2022;40:244-244. Doi: 10.1200/JCO.2022.40.4_suppl.244
Patients with stage II or III gastric cancer are treated with surgical resection and perioperative chemotherapy. Platinum agents have established activity in this disease. Combination chemotherapy FLOT (5-fluorouracil, oxaliplatin, and docetaxel) is now standard perioperative treatment for resectable gastric cancer.1 The study by Slagter and colleagues evaluated whether cisplatin was noninferior to oxaliplatin when used in the treatment of early-stage gastric cancer. Prior to the incorporation of FLOT into standard treatment practice, patients were treated with ECX (epirubicin, cisplatin, and docetaxel), as per the MAGIC trial.2 In the metastatic setting, chemotherapy regimens with either cisplatin or oxaliplatin as a choice of platinum agent have comparable activity against these tumors. Oxaliplatin activity has been shown to be noninferior to cisplatin in the randomized REAL2 trial in metastatic setting.3
The study by Slagter and colleagues is a post hoc analysis of 781 patients with resectable gastric cancer who were enrolled in the CRITICS trial. This analysis demonstrated that chemotherapy regimens containing oxaliplatin and cisplatin had comparable 5-year overall survival rates. Not surprisingly, oxaliplatin was associated with higher neurotoxicity. Based on this analysis, it is likely safe to conclude that, just as in the advanced setting, cisplatin and oxaliplatin have similar activity in early-stage disease.
Mismatch repair protein deficient or microsatellite unstable gastric cancer (MSI-H) represent unique subtypes of gastric cancer, with distinct biologic behaviors and treatment responses. The efficacy of chemotherapy in patients with early-stage MSI-H tumors has been questioned previously. Similar to MSI-H colorectal cancers, the benefit of chemotherapy in resectable MSI-H gastric and esophagogastric junction tumors appears to be less robust than in microsatellite stable (MSS) tumors. In the exploratory analysis of patients with MSI-H tumors enrolled in the perioperative MAGIC trial, patients with MSI-H tumors had better prognosis when treated with surgery alone and potentially experienced detrimental effects from chemotherapy.4 The retrospective analysis by Vos and colleagues adds to the body of knowledge about early-stage MSI-H gastric cancers. They evaluated 535 patients with early-stage disease who were treated with surgery alone or surgery plus perioperative therapy between 2000 and 2018. The overall survival in 82 patients with MSI-H tumors was 20% better than in those with MSS disease. This favorable outcome was seen irrespective of whether chemotherapy was given. Though these results suggest that chemotherapy may not be necessary in the treatment of these tumors and there are emerging data regarding the activity of immune checkpoint inhibitors in this setting, these results should definitely be investigated further in prospective studies.5 However, in the absence of prospective randomized data, it is difficult to recommend deviating from the established standard of care with FLOT, especially for patients undergoing curative intent treatment.
A study by Yukami and colleagues evaluated whether the presence of liver metastasis, which have been shown to be enriched in immunosuppressive cells in the preclinical setting, had any bearing on the activity of immune checkpoint inhibitors alone or in combination with multi-tyrosine kinase inhibitors. The analysis included 54 patients enrolled in a phase 1b trial of REGONIVO (regorafenib and nivolumab) and a phase 2 trial of LENPEM (lenvatinib and pembrolizumab). With a median follow up of 14 months, there was no significant difference in the efficacy of the above regimens (overall survival, progression-free survival, and objective response rate) between patients with and without liver metastasis. The promising activity of these combinations is continuing with longer follow-up. The above regimens should be investigated further in larger prospective studies irrespective of metastatic sites.
Additional References
1. Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393:1948-1957. Doi: 10.1016/S0140-6736(18)32557-1
2. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11-20. Doi: 10.1056/NEJMoa055531
3. Cunningham D, Starling N, Rao S, et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med. 2008;358:36-46. Doi: 10.1056/NEJMoa073149
4. Smyth EC, Wotherspoon A, Peckitt C, et al. Mismatch repair deficiency, microsatellite instability, and survival: an exploratory analysis of the Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial. JAMA Oncol. 2017;3:1197-1203. Doi: 10.1001/jamaoncol.2016.6762
5. Andre T, Tougeron D, Piessen G, et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in patients (pts) with localized microsatellite instability-high (MSI)/mismatch repair deficient (dMMR) oeso-gastric adenocarcinoma (OGA): the GERCOR NEONIPIGA phase II study. J Clin Oncol. 2022;40:244-244. Doi: 10.1200/JCO.2022.40.4_suppl.244
Patients with stage II or III gastric cancer are treated with surgical resection and perioperative chemotherapy. Platinum agents have established activity in this disease. Combination chemotherapy FLOT (5-fluorouracil, oxaliplatin, and docetaxel) is now standard perioperative treatment for resectable gastric cancer.1 The study by Slagter and colleagues evaluated whether cisplatin was noninferior to oxaliplatin when used in the treatment of early-stage gastric cancer. Prior to the incorporation of FLOT into standard treatment practice, patients were treated with ECX (epirubicin, cisplatin, and docetaxel), as per the MAGIC trial.2 In the metastatic setting, chemotherapy regimens with either cisplatin or oxaliplatin as a choice of platinum agent have comparable activity against these tumors. Oxaliplatin activity has been shown to be noninferior to cisplatin in the randomized REAL2 trial in metastatic setting.3
The study by Slagter and colleagues is a post hoc analysis of 781 patients with resectable gastric cancer who were enrolled in the CRITICS trial. This analysis demonstrated that chemotherapy regimens containing oxaliplatin and cisplatin had comparable 5-year overall survival rates. Not surprisingly, oxaliplatin was associated with higher neurotoxicity. Based on this analysis, it is likely safe to conclude that, just as in the advanced setting, cisplatin and oxaliplatin have similar activity in early-stage disease.
Mismatch repair protein deficient or microsatellite unstable gastric cancer (MSI-H) represent unique subtypes of gastric cancer, with distinct biologic behaviors and treatment responses. The efficacy of chemotherapy in patients with early-stage MSI-H tumors has been questioned previously. Similar to MSI-H colorectal cancers, the benefit of chemotherapy in resectable MSI-H gastric and esophagogastric junction tumors appears to be less robust than in microsatellite stable (MSS) tumors. In the exploratory analysis of patients with MSI-H tumors enrolled in the perioperative MAGIC trial, patients with MSI-H tumors had better prognosis when treated with surgery alone and potentially experienced detrimental effects from chemotherapy.4 The retrospective analysis by Vos and colleagues adds to the body of knowledge about early-stage MSI-H gastric cancers. They evaluated 535 patients with early-stage disease who were treated with surgery alone or surgery plus perioperative therapy between 2000 and 2018. The overall survival in 82 patients with MSI-H tumors was 20% better than in those with MSS disease. This favorable outcome was seen irrespective of whether chemotherapy was given. Though these results suggest that chemotherapy may not be necessary in the treatment of these tumors and there are emerging data regarding the activity of immune checkpoint inhibitors in this setting, these results should definitely be investigated further in prospective studies.5 However, in the absence of prospective randomized data, it is difficult to recommend deviating from the established standard of care with FLOT, especially for patients undergoing curative intent treatment.
A study by Yukami and colleagues evaluated whether the presence of liver metastasis, which have been shown to be enriched in immunosuppressive cells in the preclinical setting, had any bearing on the activity of immune checkpoint inhibitors alone or in combination with multi-tyrosine kinase inhibitors. The analysis included 54 patients enrolled in a phase 1b trial of REGONIVO (regorafenib and nivolumab) and a phase 2 trial of LENPEM (lenvatinib and pembrolizumab). With a median follow up of 14 months, there was no significant difference in the efficacy of the above regimens (overall survival, progression-free survival, and objective response rate) between patients with and without liver metastasis. The promising activity of these combinations is continuing with longer follow-up. The above regimens should be investigated further in larger prospective studies irrespective of metastatic sites.
Additional References
1. Al-Batran SE, Homann N, Pauligk C, et al. Perioperative chemotherapy with fluorouracil plus leucovorin, oxaliplatin, and docetaxel versus fluorouracil or capecitabine plus cisplatin and epirubicin for locally advanced, resectable gastric or gastro-oesophageal junction adenocarcinoma (FLOT4): a randomised, phase 2/3 trial. Lancet. 2019;393:1948-1957. Doi: 10.1016/S0140-6736(18)32557-1
2. Cunningham D, Allum WH, Stenning SP, et al. Perioperative chemotherapy versus surgery alone for resectable gastroesophageal cancer. N Engl J Med. 2006;355:11-20. Doi: 10.1056/NEJMoa055531
3. Cunningham D, Starling N, Rao S, et al. Capecitabine and oxaliplatin for advanced esophagogastric cancer. N Engl J Med. 2008;358:36-46. Doi: 10.1056/NEJMoa073149
4. Smyth EC, Wotherspoon A, Peckitt C, et al. Mismatch repair deficiency, microsatellite instability, and survival: an exploratory analysis of the Medical Research Council Adjuvant Gastric Infusional Chemotherapy (MAGIC) trial. JAMA Oncol. 2017;3:1197-1203. Doi: 10.1001/jamaoncol.2016.6762
5. Andre T, Tougeron D, Piessen G, et al. Neoadjuvant nivolumab plus ipilimumab and adjuvant nivolumab in patients (pts) with localized microsatellite instability-high (MSI)/mismatch repair deficient (dMMR) oeso-gastric adenocarcinoma (OGA): the GERCOR NEONIPIGA phase II study. J Clin Oncol. 2022;40:244-244. Doi: 10.1200/JCO.2022.40.4_suppl.244
Commentary: Diabetes Drug Comparisons, August 2022

Meta-analyses of sodium-glucose cotransporter 2 inhibitor (SGLT2i) outcome trials have shown reductions in all-cause and cardiovascular mortality, but dipeptidyl peptidase 4 inhibitors (DPP4i) have been neutral for these outcomes. In a Taiwanese retrospective cohort study, Chung and colleagues compared 53,264 pairs of propensity-matched patients with type 2 diabetes who were treated with either an SGLT2i or DPP4i. They not only reported relative risk reductions of 34% and 32% for all-cause death and cardiovascular death, respectively, but also a reduction in cancer death of 27% and a reduction in noncancer, noncardiovascular death of 38%. Although limited by its retrospective, observational design, the finding of a benefit of SGLT2i treatment on both cancer death and noncancer, noncardiovascular death would benefit from further research.
In another large Taiwanese retrospective cohort study with propensity matching, Chan and colleagues compared patients treated with SGLT2i, DPP4i, and glucagon-like peptide 1 receptor agonists (GLP-1RA), with a main study outcome of new-onset atrial fibrillation (AF). They noted that SGLT2i treatment was associated with a 10% and 36% lower risk for AF compared with DPP4i and GLP-1RA treatment, respectively. These results are consistent with meta-analyses of SGLT2i outcome trials that have demonstrated reductions in AF with SGLT2i vs placebo. Perhaps it is time to recognize that another clinical benefit of the SGLT2i class is the reduction in risk for AF.
Although GLP-1RA have been linked to an increased risk for gallbladder-related events in many studies, there has been little data suggesting an increased risk with DPP4i. He and colleagues have published a pairwise meta-analysis of 82 randomized clinical trials and found that DPP4i compared with placebo or nonincretin drugs increased the risk for gallbladder or biliary diseases by 1.22-fold, with 11 more events per 10,000 person years. In a network meta-analysis of 184 randomized trials, they also found that DPP4i treatment increased the risk for gallbladder or biliary diseases compared with SGLT2i but not compared with GLP-1RA. This was the first meta-analysis to systematically study the association between DPP4i and gallbladder-related diseases. Although the absolute risk is small, clinicians need to be aware of this link and consider this adverse effect when deciding about the risks vs benefits of DPP4i treatment.
Individuals with obesity and prediabetes are at greater risk for type 2 diabetes. Trials of lifestyle modification and antiobesity agents have shown that restoration to normoglycemia can occur with weight loss. Phase 3A studies of the antiobesity agent semaglutide (2.4 mg/week) included 3375 individuals with prediabetes across three trials. In a post hoc analysis of these patients with prediabetes, Perreault and colleagues found that after 68 weeks of treatment, there was a much higher likelihood of normoglycemia with 2.4 mg/week of semaglutide compared with placebo. Though definite conclusions are limited owing to the post hoc nature of this analysis, these results make it very likely that the ongoing STEP 10 trial of 2.4 mg semaglutide vs placebo (201 participants with obesity and prediabetes) will probably show a significant benefit on the primary outcome of change to normoglycemia.
Meta-analyses of sodium-glucose cotransporter 2 inhibitor (SGLT2i) outcome trials have shown reductions in all-cause and cardiovascular mortality, but dipeptidyl peptidase 4 inhibitors (DPP4i) have been neutral for these outcomes. In a Taiwanese retrospective cohort study, Chung and colleagues compared 53,264 pairs of propensity-matched patients with type 2 diabetes who were treated with either an SGLT2i or DPP4i. They not only reported relative risk reductions of 34% and 32% for all-cause death and cardiovascular death, respectively, but also a reduction in cancer death of 27% and a reduction in noncancer, noncardiovascular death of 38%. Although limited by its retrospective, observational design, the finding of a benefit of SGLT2i treatment on both cancer death and noncancer, noncardiovascular death would benefit from further research.
In another large Taiwanese retrospective cohort study with propensity matching, Chan and colleagues compared patients treated with SGLT2i, DPP4i, and glucagon-like peptide 1 receptor agonists (GLP-1RA), with a main study outcome of new-onset atrial fibrillation (AF). They noted that SGLT2i treatment was associated with a 10% and 36% lower risk for AF compared with DPP4i and GLP-1RA treatment, respectively. These results are consistent with meta-analyses of SGLT2i outcome trials that have demonstrated reductions in AF with SGLT2i vs placebo. Perhaps it is time to recognize that another clinical benefit of the SGLT2i class is the reduction in risk for AF.
Although GLP-1RA have been linked to an increased risk for gallbladder-related events in many studies, there has been little data suggesting an increased risk with DPP4i. He and colleagues have published a pairwise meta-analysis of 82 randomized clinical trials and found that DPP4i compared with placebo or nonincretin drugs increased the risk for gallbladder or biliary diseases by 1.22-fold, with 11 more events per 10,000 person years. In a network meta-analysis of 184 randomized trials, they also found that DPP4i treatment increased the risk for gallbladder or biliary diseases compared with SGLT2i but not compared with GLP-1RA. This was the first meta-analysis to systematically study the association between DPP4i and gallbladder-related diseases. Although the absolute risk is small, clinicians need to be aware of this link and consider this adverse effect when deciding about the risks vs benefits of DPP4i treatment.
Individuals with obesity and prediabetes are at greater risk for type 2 diabetes. Trials of lifestyle modification and antiobesity agents have shown that restoration to normoglycemia can occur with weight loss. Phase 3A studies of the antiobesity agent semaglutide (2.4 mg/week) included 3375 individuals with prediabetes across three trials. In a post hoc analysis of these patients with prediabetes, Perreault and colleagues found that after 68 weeks of treatment, there was a much higher likelihood of normoglycemia with 2.4 mg/week of semaglutide compared with placebo. Though definite conclusions are limited owing to the post hoc nature of this analysis, these results make it very likely that the ongoing STEP 10 trial of 2.4 mg semaglutide vs placebo (201 participants with obesity and prediabetes) will probably show a significant benefit on the primary outcome of change to normoglycemia.
Meta-analyses of sodium-glucose cotransporter 2 inhibitor (SGLT2i) outcome trials have shown reductions in all-cause and cardiovascular mortality, but dipeptidyl peptidase 4 inhibitors (DPP4i) have been neutral for these outcomes. In a Taiwanese retrospective cohort study, Chung and colleagues compared 53,264 pairs of propensity-matched patients with type 2 diabetes who were treated with either an SGLT2i or DPP4i. They not only reported relative risk reductions of 34% and 32% for all-cause death and cardiovascular death, respectively, but also a reduction in cancer death of 27% and a reduction in noncancer, noncardiovascular death of 38%. Although limited by its retrospective, observational design, the finding of a benefit of SGLT2i treatment on both cancer death and noncancer, noncardiovascular death would benefit from further research.
In another large Taiwanese retrospective cohort study with propensity matching, Chan and colleagues compared patients treated with SGLT2i, DPP4i, and glucagon-like peptide 1 receptor agonists (GLP-1RA), with a main study outcome of new-onset atrial fibrillation (AF). They noted that SGLT2i treatment was associated with a 10% and 36% lower risk for AF compared with DPP4i and GLP-1RA treatment, respectively. These results are consistent with meta-analyses of SGLT2i outcome trials that have demonstrated reductions in AF with SGLT2i vs placebo. Perhaps it is time to recognize that another clinical benefit of the SGLT2i class is the reduction in risk for AF.
Although GLP-1RA have been linked to an increased risk for gallbladder-related events in many studies, there has been little data suggesting an increased risk with DPP4i. He and colleagues have published a pairwise meta-analysis of 82 randomized clinical trials and found that DPP4i compared with placebo or nonincretin drugs increased the risk for gallbladder or biliary diseases by 1.22-fold, with 11 more events per 10,000 person years. In a network meta-analysis of 184 randomized trials, they also found that DPP4i treatment increased the risk for gallbladder or biliary diseases compared with SGLT2i but not compared with GLP-1RA. This was the first meta-analysis to systematically study the association between DPP4i and gallbladder-related diseases. Although the absolute risk is small, clinicians need to be aware of this link and consider this adverse effect when deciding about the risks vs benefits of DPP4i treatment.
Individuals with obesity and prediabetes are at greater risk for type 2 diabetes. Trials of lifestyle modification and antiobesity agents have shown that restoration to normoglycemia can occur with weight loss. Phase 3A studies of the antiobesity agent semaglutide (2.4 mg/week) included 3375 individuals with prediabetes across three trials. In a post hoc analysis of these patients with prediabetes, Perreault and colleagues found that after 68 weeks of treatment, there was a much higher likelihood of normoglycemia with 2.4 mg/week of semaglutide compared with placebo. Though definite conclusions are limited owing to the post hoc nature of this analysis, these results make it very likely that the ongoing STEP 10 trial of 2.4 mg semaglutide vs placebo (201 participants with obesity and prediabetes) will probably show a significant benefit on the primary outcome of change to normoglycemia.
Commentary: Concomitant Lung Disease, Drug Efficacy, and Potential Misdiagnosis in RA, August 2022

Interstitial lung disease (ILD) is a serious and not infrequent complication of rheumatoid arthritis (RA). Despite the use of several immunosuppressive medications for ILD as well as others for RA, the most effective treatment for both is yet unclear. Prior cross-sectional, retrospective, and open-label registry studies have suggested that abatacept can be used in patients with RA-ILD, with stability or improvement in pulmonary parameters in a majority of patients. Mena-Vazquez and colleagues present the results of a prospective, observational cohort study with 57 patients from multiple centers in Spain. Similar to previously published results, this study found stability or improvement in pulmonary function tests in 70% of patients as well as improvement in RA disease activity. A relatively high proportion of patients (25 in 57) experienced infections. The study lends further weight to the proposal that abatacept is a reasonable choice in patients with RA-ILD for treatment of both joint and pulmonary inflammation, given the lack of randomized controlled trials.
Lauper and colleagues published the results of a large cohort study of more than 30,000 treatment courses in patients with RA, looking at the efficacy of different biologics and a Janus kinase (JAK) inhibitor. Discontinuation of therapy was used as the primary efficacy outcome, and one secondary outcome was low disease activity based on Clinical Disease Activity Index (CDAI) at 12 months. Over 17,000 courses were anti–tumor necrosis factor (TNF) therapy, with about 7000 JAK-inhibitor therapy courses and the remainder an interleukin 6 (IL-6) inhibitor or abatacept therapy; individual data was only available from 13 to 17 registries (depending on the parameter of interest). Overall, IL-6 inhibitors and JAK inhibitors were less frequently stopped for ineffectiveness compared with anti-TNF agents, but were more frequently stopped owing to adverse events. Drug retention rates also varied between different countries, suggesting that prescription pattern differences may affect the primary outcome. In terms of CDAI, response rates at 1 year were similar between anti-TNF agents, JAK inhibitors, and IL-6 inhibitors and was slightly lower for abatacept. This real-world study does support similar efficacy between these classes of medications, though further conclusions are somewhat hampered by the lack of individual data.
A study in Japan by Mori and colleagues looked at biologic disease-modifying antirheumatic drugs (bDMARD) (TNF inhibitors and an IL-6 inhibitor) and tofacitinib discontinuation in a cohort of 97 patients with RA . Patients were required to initially be in a high or moderate disease activity state prior to treatment, then in remission or a low disease activity state with treatment for more than 48 weeks. Mean follow-up was 2.1 years and disease flare occurred in about 75% of patients at about 1.6 years after medication discontinuation. Though bDMARD- or targeted synthetic DMARD (tsDMARD)–free remission was not "durable" for most patients, the majority of those patients who experienced flares improved with resumption of their previous medication. Though it is reassuring that most study patients were able to discontinue their bDMARD or tsDMARD medication for a period of time, the fact that most experienced flares within 2 years suggests that discontinuation of these medications in patients with high disease activity is not a viable long-term approach.
Krekeler and colleagues performed a retrospective analysis of about 500 patients seen in a single rheumatology clinic to evaluate possible misdiagnosis of RA. The diagnosis of calcium pyrophosphate deposition disease (CPPD), as well as the presence of radiographic chondrocalcinosis, were more frequently found among patients diagnosed with seronegative RA vs those diagnosed with seropositive RA, particularly RA in the wrists. The CPPD diagnosis was made by rheumatologists on the basis of the presence of radiographic chondrocalcinosis along with typical joint swelling and signs of inflammation. Because chondrocalcinosis was part of the CPPD diagnosis, it is unsurprising that both followed similar patterns. Whether patients with CPPD were actually misdiagnosed as having seronegative RA is unclear from this retrospective study; as the authors note, chondrocalcinosis itself has been found to be associated with older age and osteoarthritis in prior studies, particularly in the knee. However, the study confirms that alternative diagnoses in seronegative RA should be considered.
Interstitial lung disease (ILD) is a serious and not infrequent complication of rheumatoid arthritis (RA). Despite the use of several immunosuppressive medications for ILD as well as others for RA, the most effective treatment for both is yet unclear. Prior cross-sectional, retrospective, and open-label registry studies have suggested that abatacept can be used in patients with RA-ILD, with stability or improvement in pulmonary parameters in a majority of patients. Mena-Vazquez and colleagues present the results of a prospective, observational cohort study with 57 patients from multiple centers in Spain. Similar to previously published results, this study found stability or improvement in pulmonary function tests in 70% of patients as well as improvement in RA disease activity. A relatively high proportion of patients (25 in 57) experienced infections. The study lends further weight to the proposal that abatacept is a reasonable choice in patients with RA-ILD for treatment of both joint and pulmonary inflammation, given the lack of randomized controlled trials.
Lauper and colleagues published the results of a large cohort study of more than 30,000 treatment courses in patients with RA, looking at the efficacy of different biologics and a Janus kinase (JAK) inhibitor. Discontinuation of therapy was used as the primary efficacy outcome, and one secondary outcome was low disease activity based on Clinical Disease Activity Index (CDAI) at 12 months. Over 17,000 courses were anti–tumor necrosis factor (TNF) therapy, with about 7000 JAK-inhibitor therapy courses and the remainder an interleukin 6 (IL-6) inhibitor or abatacept therapy; individual data was only available from 13 to 17 registries (depending on the parameter of interest). Overall, IL-6 inhibitors and JAK inhibitors were less frequently stopped for ineffectiveness compared with anti-TNF agents, but were more frequently stopped owing to adverse events. Drug retention rates also varied between different countries, suggesting that prescription pattern differences may affect the primary outcome. In terms of CDAI, response rates at 1 year were similar between anti-TNF agents, JAK inhibitors, and IL-6 inhibitors and was slightly lower for abatacept. This real-world study does support similar efficacy between these classes of medications, though further conclusions are somewhat hampered by the lack of individual data.
A study in Japan by Mori and colleagues looked at biologic disease-modifying antirheumatic drugs (bDMARD) (TNF inhibitors and an IL-6 inhibitor) and tofacitinib discontinuation in a cohort of 97 patients with RA . Patients were required to initially be in a high or moderate disease activity state prior to treatment, then in remission or a low disease activity state with treatment for more than 48 weeks. Mean follow-up was 2.1 years and disease flare occurred in about 75% of patients at about 1.6 years after medication discontinuation. Though bDMARD- or targeted synthetic DMARD (tsDMARD)–free remission was not "durable" for most patients, the majority of those patients who experienced flares improved with resumption of their previous medication. Though it is reassuring that most study patients were able to discontinue their bDMARD or tsDMARD medication for a period of time, the fact that most experienced flares within 2 years suggests that discontinuation of these medications in patients with high disease activity is not a viable long-term approach.
Krekeler and colleagues performed a retrospective analysis of about 500 patients seen in a single rheumatology clinic to evaluate possible misdiagnosis of RA. The diagnosis of calcium pyrophosphate deposition disease (CPPD), as well as the presence of radiographic chondrocalcinosis, were more frequently found among patients diagnosed with seronegative RA vs those diagnosed with seropositive RA, particularly RA in the wrists. The CPPD diagnosis was made by rheumatologists on the basis of the presence of radiographic chondrocalcinosis along with typical joint swelling and signs of inflammation. Because chondrocalcinosis was part of the CPPD diagnosis, it is unsurprising that both followed similar patterns. Whether patients with CPPD were actually misdiagnosed as having seronegative RA is unclear from this retrospective study; as the authors note, chondrocalcinosis itself has been found to be associated with older age and osteoarthritis in prior studies, particularly in the knee. However, the study confirms that alternative diagnoses in seronegative RA should be considered.
Interstitial lung disease (ILD) is a serious and not infrequent complication of rheumatoid arthritis (RA). Despite the use of several immunosuppressive medications for ILD as well as others for RA, the most effective treatment for both is yet unclear. Prior cross-sectional, retrospective, and open-label registry studies have suggested that abatacept can be used in patients with RA-ILD, with stability or improvement in pulmonary parameters in a majority of patients. Mena-Vazquez and colleagues present the results of a prospective, observational cohort study with 57 patients from multiple centers in Spain. Similar to previously published results, this study found stability or improvement in pulmonary function tests in 70% of patients as well as improvement in RA disease activity. A relatively high proportion of patients (25 in 57) experienced infections. The study lends further weight to the proposal that abatacept is a reasonable choice in patients with RA-ILD for treatment of both joint and pulmonary inflammation, given the lack of randomized controlled trials.
Lauper and colleagues published the results of a large cohort study of more than 30,000 treatment courses in patients with RA, looking at the efficacy of different biologics and a Janus kinase (JAK) inhibitor. Discontinuation of therapy was used as the primary efficacy outcome, and one secondary outcome was low disease activity based on Clinical Disease Activity Index (CDAI) at 12 months. Over 17,000 courses were anti–tumor necrosis factor (TNF) therapy, with about 7000 JAK-inhibitor therapy courses and the remainder an interleukin 6 (IL-6) inhibitor or abatacept therapy; individual data was only available from 13 to 17 registries (depending on the parameter of interest). Overall, IL-6 inhibitors and JAK inhibitors were less frequently stopped for ineffectiveness compared with anti-TNF agents, but were more frequently stopped owing to adverse events. Drug retention rates also varied between different countries, suggesting that prescription pattern differences may affect the primary outcome. In terms of CDAI, response rates at 1 year were similar between anti-TNF agents, JAK inhibitors, and IL-6 inhibitors and was slightly lower for abatacept. This real-world study does support similar efficacy between these classes of medications, though further conclusions are somewhat hampered by the lack of individual data.
A study in Japan by Mori and colleagues looked at biologic disease-modifying antirheumatic drugs (bDMARD) (TNF inhibitors and an IL-6 inhibitor) and tofacitinib discontinuation in a cohort of 97 patients with RA . Patients were required to initially be in a high or moderate disease activity state prior to treatment, then in remission or a low disease activity state with treatment for more than 48 weeks. Mean follow-up was 2.1 years and disease flare occurred in about 75% of patients at about 1.6 years after medication discontinuation. Though bDMARD- or targeted synthetic DMARD (tsDMARD)–free remission was not "durable" for most patients, the majority of those patients who experienced flares improved with resumption of their previous medication. Though it is reassuring that most study patients were able to discontinue their bDMARD or tsDMARD medication for a period of time, the fact that most experienced flares within 2 years suggests that discontinuation of these medications in patients with high disease activity is not a viable long-term approach.
Krekeler and colleagues performed a retrospective analysis of about 500 patients seen in a single rheumatology clinic to evaluate possible misdiagnosis of RA. The diagnosis of calcium pyrophosphate deposition disease (CPPD), as well as the presence of radiographic chondrocalcinosis, were more frequently found among patients diagnosed with seronegative RA vs those diagnosed with seropositive RA, particularly RA in the wrists. The CPPD diagnosis was made by rheumatologists on the basis of the presence of radiographic chondrocalcinosis along with typical joint swelling and signs of inflammation. Because chondrocalcinosis was part of the CPPD diagnosis, it is unsurprising that both followed similar patterns. Whether patients with CPPD were actually misdiagnosed as having seronegative RA is unclear from this retrospective study; as the authors note, chondrocalcinosis itself has been found to be associated with older age and osteoarthritis in prior studies, particularly in the knee. However, the study confirms that alternative diagnoses in seronegative RA should be considered.
Commentary: Adjuvant Chemotherapy in Stage II Colon Cancer, August 2022

This month brought us findings from DYNAMIC, a randomized trial of circulating tumor DNA (ctDNA), which aimed to provide guidance on the use of adjuvant chemotherapy in stage II colon cancer. This study has already been touted on oncology Twitter as a massive breakthrough for identifying patients with stage II colon cancer who would benefit from adjuvant chemotherapy. Does the reality live up to the hype? Let's break it down.
Patients with resected stage II colon cancer were eligible for enrollment. Two thirds of patients were randomly assigned to the ctDNA guidance arm, whereas the remaining third had chemotherapy guidance based on clinicopathologic high-risk features (T4, poor differentiation, < 12 lymph nodes in surgical sample, lymphovascular invasion, tumor perforation, or bowel obstruction). Chemotherapy choice was left up to the clinician and could be an oxaliplatin-based doublet or a single-agent fluoropyrimidine. The primary endpoint was recurrence-free survival at 2 years. A key secondary endpoint was chemotherapy treatment frequency by arm. A total of 459 patients were enrolled from 23 Australian centers over 4 years. Approximately 40% of patients were considered to be at high risk for recurrence on the basis of their tumors' clinicopathologic features. Approximately 20% of patients had tumors that were mismatch repair deficient.
There was no difference in 2-year recurrence-free survival between the two arms (93.5% vs 92.4%; 95% CI -4.1 to 6.2). This met criteria for noninferiority. However, chemotherapy administration in the two arms was markedly different. A significantly greater proportion of patients randomly assigned to the standard management arm received chemotherapy (28% vs 15%; relative risk [RR] 1.82; 95% CI 1.25-2.65). However, a significantly greater proportion of patients guided by ctDNA received an oxaliplatin-based doublet (62% vs 10%; RR 2.39; 95% CI 1.62-3.52). Clearly, when clinicians were presented with a positive ctDNA test, they overwhelmingly opted to give an oxaliplatin-based doublet rather than a single-agent fluoropyrimidine. Oxaliplatin's use in stage II colon cancer remains very controversial; it is oxaliplatin that causes most of the long-term toxicity associated with adjuvant chemotherapy for colorectal cancer. Although ctDNA testing might lower the total proportion of patients who received adjuvant treatment, it significantly raised the proportion who received oxaliplatin. I doubt this is a worthy trade-off.
Furthermore, clinicopathologic factors were still highly relevant in patients with ctDNA-negative results. Among ctDNA-negative patients, 3-year recurrence-free survival was higher in patients with clinicopathologic low-risk cancers than in those with high-risk cancers (96.7% vs 85.1%; hazard ratio 3.04; 95% CI 1.26-7.34). This strongly suggests that ctDNA testing is unlikely to replace clinicopathologic high-risk features in the real-world practice of clinical oncology. Rather, ctDNA testing will probably be added to the list of high-risk features, prompting use of more chemotherapy, not less, for stage II colon cancer.
A more useful study, in my opinion, should be performed in stage III colon cancer. Patients with stage III colon cancer receive chemotherapy without exception, although we know from MOSAIC that the absolute benefit of chemotherapy in stage III colon cancer is modest. What proportion of these patients who have a negative ctDNA test might be able to either forgo treatment completely or have treatment with a fluoropyrimidine only? That's something I would be very interested to find out.
This month brought us findings from DYNAMIC, a randomized trial of circulating tumor DNA (ctDNA), which aimed to provide guidance on the use of adjuvant chemotherapy in stage II colon cancer. This study has already been touted on oncology Twitter as a massive breakthrough for identifying patients with stage II colon cancer who would benefit from adjuvant chemotherapy. Does the reality live up to the hype? Let's break it down.
Patients with resected stage II colon cancer were eligible for enrollment. Two thirds of patients were randomly assigned to the ctDNA guidance arm, whereas the remaining third had chemotherapy guidance based on clinicopathologic high-risk features (T4, poor differentiation, < 12 lymph nodes in surgical sample, lymphovascular invasion, tumor perforation, or bowel obstruction). Chemotherapy choice was left up to the clinician and could be an oxaliplatin-based doublet or a single-agent fluoropyrimidine. The primary endpoint was recurrence-free survival at 2 years. A key secondary endpoint was chemotherapy treatment frequency by arm. A total of 459 patients were enrolled from 23 Australian centers over 4 years. Approximately 40% of patients were considered to be at high risk for recurrence on the basis of their tumors' clinicopathologic features. Approximately 20% of patients had tumors that were mismatch repair deficient.
There was no difference in 2-year recurrence-free survival between the two arms (93.5% vs 92.4%; 95% CI -4.1 to 6.2). This met criteria for noninferiority. However, chemotherapy administration in the two arms was markedly different. A significantly greater proportion of patients randomly assigned to the standard management arm received chemotherapy (28% vs 15%; relative risk [RR] 1.82; 95% CI 1.25-2.65). However, a significantly greater proportion of patients guided by ctDNA received an oxaliplatin-based doublet (62% vs 10%; RR 2.39; 95% CI 1.62-3.52). Clearly, when clinicians were presented with a positive ctDNA test, they overwhelmingly opted to give an oxaliplatin-based doublet rather than a single-agent fluoropyrimidine. Oxaliplatin's use in stage II colon cancer remains very controversial; it is oxaliplatin that causes most of the long-term toxicity associated with adjuvant chemotherapy for colorectal cancer. Although ctDNA testing might lower the total proportion of patients who received adjuvant treatment, it significantly raised the proportion who received oxaliplatin. I doubt this is a worthy trade-off.
Furthermore, clinicopathologic factors were still highly relevant in patients with ctDNA-negative results. Among ctDNA-negative patients, 3-year recurrence-free survival was higher in patients with clinicopathologic low-risk cancers than in those with high-risk cancers (96.7% vs 85.1%; hazard ratio 3.04; 95% CI 1.26-7.34). This strongly suggests that ctDNA testing is unlikely to replace clinicopathologic high-risk features in the real-world practice of clinical oncology. Rather, ctDNA testing will probably be added to the list of high-risk features, prompting use of more chemotherapy, not less, for stage II colon cancer.
A more useful study, in my opinion, should be performed in stage III colon cancer. Patients with stage III colon cancer receive chemotherapy without exception, although we know from MOSAIC that the absolute benefit of chemotherapy in stage III colon cancer is modest. What proportion of these patients who have a negative ctDNA test might be able to either forgo treatment completely or have treatment with a fluoropyrimidine only? That's something I would be very interested to find out.
This month brought us findings from DYNAMIC, a randomized trial of circulating tumor DNA (ctDNA), which aimed to provide guidance on the use of adjuvant chemotherapy in stage II colon cancer. This study has already been touted on oncology Twitter as a massive breakthrough for identifying patients with stage II colon cancer who would benefit from adjuvant chemotherapy. Does the reality live up to the hype? Let's break it down.
Patients with resected stage II colon cancer were eligible for enrollment. Two thirds of patients were randomly assigned to the ctDNA guidance arm, whereas the remaining third had chemotherapy guidance based on clinicopathologic high-risk features (T4, poor differentiation, < 12 lymph nodes in surgical sample, lymphovascular invasion, tumor perforation, or bowel obstruction). Chemotherapy choice was left up to the clinician and could be an oxaliplatin-based doublet or a single-agent fluoropyrimidine. The primary endpoint was recurrence-free survival at 2 years. A key secondary endpoint was chemotherapy treatment frequency by arm. A total of 459 patients were enrolled from 23 Australian centers over 4 years. Approximately 40% of patients were considered to be at high risk for recurrence on the basis of their tumors' clinicopathologic features. Approximately 20% of patients had tumors that were mismatch repair deficient.
There was no difference in 2-year recurrence-free survival between the two arms (93.5% vs 92.4%; 95% CI -4.1 to 6.2). This met criteria for noninferiority. However, chemotherapy administration in the two arms was markedly different. A significantly greater proportion of patients randomly assigned to the standard management arm received chemotherapy (28% vs 15%; relative risk [RR] 1.82; 95% CI 1.25-2.65). However, a significantly greater proportion of patients guided by ctDNA received an oxaliplatin-based doublet (62% vs 10%; RR 2.39; 95% CI 1.62-3.52). Clearly, when clinicians were presented with a positive ctDNA test, they overwhelmingly opted to give an oxaliplatin-based doublet rather than a single-agent fluoropyrimidine. Oxaliplatin's use in stage II colon cancer remains very controversial; it is oxaliplatin that causes most of the long-term toxicity associated with adjuvant chemotherapy for colorectal cancer. Although ctDNA testing might lower the total proportion of patients who received adjuvant treatment, it significantly raised the proportion who received oxaliplatin. I doubt this is a worthy trade-off.
Furthermore, clinicopathologic factors were still highly relevant in patients with ctDNA-negative results. Among ctDNA-negative patients, 3-year recurrence-free survival was higher in patients with clinicopathologic low-risk cancers than in those with high-risk cancers (96.7% vs 85.1%; hazard ratio 3.04; 95% CI 1.26-7.34). This strongly suggests that ctDNA testing is unlikely to replace clinicopathologic high-risk features in the real-world practice of clinical oncology. Rather, ctDNA testing will probably be added to the list of high-risk features, prompting use of more chemotherapy, not less, for stage II colon cancer.
A more useful study, in my opinion, should be performed in stage III colon cancer. Patients with stage III colon cancer receive chemotherapy without exception, although we know from MOSAIC that the absolute benefit of chemotherapy in stage III colon cancer is modest. What proportion of these patients who have a negative ctDNA test might be able to either forgo treatment completely or have treatment with a fluoropyrimidine only? That's something I would be very interested to find out.
Commentary: Exercise, Mental Health, and Checkpoint Inhibitors in PsA, August 2022

Biomechanical stress and trauma are important factors driving the development and progression of psoriatic arthritis (PsA). On the other hand, physical exercise is beneficial for patients with arthritis. However, there is concern that high-intensity interval training (HIIT) may worsen PsA. Hypothesizing that bone marrow edema changes could occur in patients with PsA after HIIT despite no reported changes in disease activity by clinical examination, Chronaiou and colleagues aimed to assess whether HIIT in PsA patients led to MRI-detectable changes in the axial skeleton. Comparing 19 PsA patients who went through 11 weeks of HIIT with 20 patients who had no change in physical exercise habits, they found no significant changes in bone marrow edema on MRI images of the spine after HIIT. Thus, the 11-week HIIT regimen may be safe in PsA.
Mental health problems are often underestimated in psoriatic disease. Lada and colleagues aimed to estimate the prevalence of depression in patients with psoriatic disease and determine whether PsA is associated with higher depression and anxiety in patients with psoriasis. Analyzing data from British Association of Dermatologists Biologic and Immunomodulators Register (BADBIR) participants (540 with psoriasis and 167 with both psoriasis and PsA) who had completed the Hospital Anxiety and Depression Scale (HADS), they found that the prevalence of depression was higher in patients with PsA (32%) than in patients without PsA (22.7%) using a HADS cutoff of 8 (odds ratio 1.66; 95% CI 1.13--2.43). Pain mediated the effect of PsA on depression and anxiety.
Inhibitors of interleukin (IL)-23 are safe and efficacious in the treatment of psoriasis and PsA. However, changes in composite PsA indices have not been investigated in detail. Using pooled data from the phase 3 DISCOVER-1 (n = 381) and DISCOVER-2 (n = 739) studies, Coates and colleagues demonstrated that a significantly higher proportion of patients receiving guselkumab every 4 or 8 weeks vs placebo achieved low disease activity according to the Disease Activity Index for PsA (DAPSA) at week 8 (19.8%/17.3% vs 8.1%), DAPSA remission at week 12 (4.3%/4.3% vs 0.5%), minimal disease activity at week 16 (14.7%/16.5% vs 4.6%; all P < .001), and very low disease activity at week 24 (6.4%/4.3% vs 1.3%; P < .05), with improvements maintained until week 52. Thus, compared with placebo, treatment with guselkumab leads to early and sustained benefits for patients with PsA.
Similarly, Ostor and colleagues demonstrated in the phase 3 KEEPsAKE2 trial, which included 443 patients with PsA, that, at week 24, patients receiving risankizumab report a significantly greater improvement in the mean pain index score (-14.7 vs -6.5; P < .001), fatigue score (4.9 vs 2.6; P < .01), patient's global assessment of disease activity (-16.5 vs -7.7; P < .001), general health status (0.09 vs 0.01; P < .001), and physical functioning (5.1 vs 2.0; P < .001) compared with placebo.
In another study, treatment with bimekizumab, an inhibitor of IL-17A and IL-17F, was associated with sustained improvement in patient-reported outcomes. Mease and colleagues report that, at week 48, there was a substantial improvement in mean arthritis pain (29.9 points), fatigue (2.4 points), Health Assessment Questionnaire-Disability Index (0.43 points), and Physical Component Summary score (9.1 points), with improvements sustained till week 152. High proportions of patients achieved the Patient Acceptable Symptom State at weeks 48 (75.2%) and 152 (65.0%). Thus, inhibitors of IL-23 and IL-17 have established efficacy in the treatment of PsA.
Biomechanical stress and trauma are important factors driving the development and progression of psoriatic arthritis (PsA). On the other hand, physical exercise is beneficial for patients with arthritis. However, there is concern that high-intensity interval training (HIIT) may worsen PsA. Hypothesizing that bone marrow edema changes could occur in patients with PsA after HIIT despite no reported changes in disease activity by clinical examination, Chronaiou and colleagues aimed to assess whether HIIT in PsA patients led to MRI-detectable changes in the axial skeleton. Comparing 19 PsA patients who went through 11 weeks of HIIT with 20 patients who had no change in physical exercise habits, they found no significant changes in bone marrow edema on MRI images of the spine after HIIT. Thus, the 11-week HIIT regimen may be safe in PsA.
Mental health problems are often underestimated in psoriatic disease. Lada and colleagues aimed to estimate the prevalence of depression in patients with psoriatic disease and determine whether PsA is associated with higher depression and anxiety in patients with psoriasis. Analyzing data from British Association of Dermatologists Biologic and Immunomodulators Register (BADBIR) participants (540 with psoriasis and 167 with both psoriasis and PsA) who had completed the Hospital Anxiety and Depression Scale (HADS), they found that the prevalence of depression was higher in patients with PsA (32%) than in patients without PsA (22.7%) using a HADS cutoff of 8 (odds ratio 1.66; 95% CI 1.13--2.43). Pain mediated the effect of PsA on depression and anxiety.
Inhibitors of interleukin (IL)-23 are safe and efficacious in the treatment of psoriasis and PsA. However, changes in composite PsA indices have not been investigated in detail. Using pooled data from the phase 3 DISCOVER-1 (n = 381) and DISCOVER-2 (n = 739) studies, Coates and colleagues demonstrated that a significantly higher proportion of patients receiving guselkumab every 4 or 8 weeks vs placebo achieved low disease activity according to the Disease Activity Index for PsA (DAPSA) at week 8 (19.8%/17.3% vs 8.1%), DAPSA remission at week 12 (4.3%/4.3% vs 0.5%), minimal disease activity at week 16 (14.7%/16.5% vs 4.6%; all P < .001), and very low disease activity at week 24 (6.4%/4.3% vs 1.3%; P < .05), with improvements maintained until week 52. Thus, compared with placebo, treatment with guselkumab leads to early and sustained benefits for patients with PsA.
Similarly, Ostor and colleagues demonstrated in the phase 3 KEEPsAKE2 trial, which included 443 patients with PsA, that, at week 24, patients receiving risankizumab report a significantly greater improvement in the mean pain index score (-14.7 vs -6.5; P < .001), fatigue score (4.9 vs 2.6; P < .01), patient's global assessment of disease activity (-16.5 vs -7.7; P < .001), general health status (0.09 vs 0.01; P < .001), and physical functioning (5.1 vs 2.0; P < .001) compared with placebo.
In another study, treatment with bimekizumab, an inhibitor of IL-17A and IL-17F, was associated with sustained improvement in patient-reported outcomes. Mease and colleagues report that, at week 48, there was a substantial improvement in mean arthritis pain (29.9 points), fatigue (2.4 points), Health Assessment Questionnaire-Disability Index (0.43 points), and Physical Component Summary score (9.1 points), with improvements sustained till week 152. High proportions of patients achieved the Patient Acceptable Symptom State at weeks 48 (75.2%) and 152 (65.0%). Thus, inhibitors of IL-23 and IL-17 have established efficacy in the treatment of PsA.
Biomechanical stress and trauma are important factors driving the development and progression of psoriatic arthritis (PsA). On the other hand, physical exercise is beneficial for patients with arthritis. However, there is concern that high-intensity interval training (HIIT) may worsen PsA. Hypothesizing that bone marrow edema changes could occur in patients with PsA after HIIT despite no reported changes in disease activity by clinical examination, Chronaiou and colleagues aimed to assess whether HIIT in PsA patients led to MRI-detectable changes in the axial skeleton. Comparing 19 PsA patients who went through 11 weeks of HIIT with 20 patients who had no change in physical exercise habits, they found no significant changes in bone marrow edema on MRI images of the spine after HIIT. Thus, the 11-week HIIT regimen may be safe in PsA.
Mental health problems are often underestimated in psoriatic disease. Lada and colleagues aimed to estimate the prevalence of depression in patients with psoriatic disease and determine whether PsA is associated with higher depression and anxiety in patients with psoriasis. Analyzing data from British Association of Dermatologists Biologic and Immunomodulators Register (BADBIR) participants (540 with psoriasis and 167 with both psoriasis and PsA) who had completed the Hospital Anxiety and Depression Scale (HADS), they found that the prevalence of depression was higher in patients with PsA (32%) than in patients without PsA (22.7%) using a HADS cutoff of 8 (odds ratio 1.66; 95% CI 1.13--2.43). Pain mediated the effect of PsA on depression and anxiety.
Inhibitors of interleukin (IL)-23 are safe and efficacious in the treatment of psoriasis and PsA. However, changes in composite PsA indices have not been investigated in detail. Using pooled data from the phase 3 DISCOVER-1 (n = 381) and DISCOVER-2 (n = 739) studies, Coates and colleagues demonstrated that a significantly higher proportion of patients receiving guselkumab every 4 or 8 weeks vs placebo achieved low disease activity according to the Disease Activity Index for PsA (DAPSA) at week 8 (19.8%/17.3% vs 8.1%), DAPSA remission at week 12 (4.3%/4.3% vs 0.5%), minimal disease activity at week 16 (14.7%/16.5% vs 4.6%; all P < .001), and very low disease activity at week 24 (6.4%/4.3% vs 1.3%; P < .05), with improvements maintained until week 52. Thus, compared with placebo, treatment with guselkumab leads to early and sustained benefits for patients with PsA.
Similarly, Ostor and colleagues demonstrated in the phase 3 KEEPsAKE2 trial, which included 443 patients with PsA, that, at week 24, patients receiving risankizumab report a significantly greater improvement in the mean pain index score (-14.7 vs -6.5; P < .001), fatigue score (4.9 vs 2.6; P < .01), patient's global assessment of disease activity (-16.5 vs -7.7; P < .001), general health status (0.09 vs 0.01; P < .001), and physical functioning (5.1 vs 2.0; P < .001) compared with placebo.
In another study, treatment with bimekizumab, an inhibitor of IL-17A and IL-17F, was associated with sustained improvement in patient-reported outcomes. Mease and colleagues report that, at week 48, there was a substantial improvement in mean arthritis pain (29.9 points), fatigue (2.4 points), Health Assessment Questionnaire-Disability Index (0.43 points), and Physical Component Summary score (9.1 points), with improvements sustained till week 152. High proportions of patients achieved the Patient Acceptable Symptom State at weeks 48 (75.2%) and 152 (65.0%). Thus, inhibitors of IL-23 and IL-17 have established efficacy in the treatment of PsA.
Mixed results for intensive home care for psychiatric crises
Intensive home treatment may offer an alternative to inpatient care for patients in acute psychiatric crisis – but the intervention is no outright substitute, new research suggests.
However, there was no difference between treatment groups in improvement in quality of life or patient satisfaction; and a reduction in symptom severity noted after 6 weeks of home treatment faded within 6 months.

“We found no differences in admission rates either, which suggests that intensive home treatment is not a substitute for inpatient care but a different treatment opportunity for psychiatric patients in crisis,” Jurgen Cornelis, MD, Arkin Institute for Mental Health, Amsterdam, and colleagues write.
The findings were published online in The Lancet Psychiatry.
Increasingly popular
“Intensive home treatment is increasingly popular as an alternative to hospitalization. It was developed to prevent or reduce levels of inpatient care and facilitate the transition between inpatient care and low-intensity outpatient care,” the investigators write.
However, there have previously been only two randomized controlled trials published that assessed this type of care, resulting in “somewhat conflicting findings,” they add.
For the current study, participants presented to psychiatric emergency wards at two medical centers in the Netherlands. They were included only if they were able to offer informed consent within 14 days.
The intensive home treatment group (n = 183) worked with a multidisciplinary team that designed a care plan tailored to their specific crisis. Treatment components included pharmacotherapy, up to three home visits each day, psychoeducation, brief supportive and cognitive behavioral therapy, social care, and support and empowerment of the patient’s informal care system.
The usual care group (n = 63) commonly received a combination of highly intensive inpatient treatment in the first phase and outpatient treatment up to two times a week in the second phase. Treatment included similar components as those in intensive home treatment.
The most common primary clinical diagnosis in both groups was mood disorder, followed by psychotic disorders, personality disorders, or anxiety disorders.
The home treatment group had a significantly higher total mean item score on the Brief Psychiatric Rating Scale (BPRS) at baseline (2.23 vs. 2.04, P = .04).
Mixed results
Results at 6 weeks showed the number of hospital days was 25.3% lower in the home treatment group, compared with those who received usual care.
That trend continued at 1 year, with the intensive home treatment group recording 36.6% fewer hospital days than the usual care group (mean, 42.5 days vs. 67 days, respectively; P = .03).
However, the number of patients who were admitted in the first 6 weeks and at 1 year stayed the same, as did the mean number of admissions per patient over 12 months.
The home treatment group reported significantly fewer symptoms on the BPRS depression and anxiety scale at 6 weeks, compared with the usual treatment group (P = .025), but that difference was not maintained after 6 months.
The number of adverse events, including suicide attempts, was similar between the groups. Three patients in the home treatment group and two in the usual care group died by suicide.
“Future research should focus on which components of intensive home treatment or hospitalization can be used when, for whom, and meet which goals, so that both hospital care and intensive home treatment can be used proportionally and efficiently for patients in psychiatric crisis,” the investigators write.
Not generalizable?
In an accompanying editorial, Claire Henderson, PhD, Institute of Psychiatry, Psychology, and Neuroscience at King’s College London, noted that generalizing the study’s results to other countries could be problematic, especially to regions such as North America, which have shorter lengths of stay for psychiatric hospitalization.

“Future trials looking at intensive home treatment would be most informative if done in countries with relatively short lengths of stay, and without separate crisis services for people receiving assertive community treatment,” Dr. Henderson writes.
The study was funded by De Stichting tot Steun Vereniging voor Christelijke Verzorging van Geestes-en Zenuwzieken. The investigators and Dr. Henderson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Intensive home treatment may offer an alternative to inpatient care for patients in acute psychiatric crisis – but the intervention is no outright substitute, new research suggests.
However, there was no difference between treatment groups in improvement in quality of life or patient satisfaction; and a reduction in symptom severity noted after 6 weeks of home treatment faded within 6 months.
“We found no differences in admission rates either, which suggests that intensive home treatment is not a substitute for inpatient care but a different treatment opportunity for psychiatric patients in crisis,” Jurgen Cornelis, MD, Arkin Institute for Mental Health, Amsterdam, and colleagues write.
The findings were published online in The Lancet Psychiatry.
Increasingly popular
“Intensive home treatment is increasingly popular as an alternative to hospitalization. It was developed to prevent or reduce levels of inpatient care and facilitate the transition between inpatient care and low-intensity outpatient care,” the investigators write.
However, there have previously been only two randomized controlled trials published that assessed this type of care, resulting in “somewhat conflicting findings,” they add.
For the current study, participants presented to psychiatric emergency wards at two medical centers in the Netherlands. They were included only if they were able to offer informed consent within 14 days.
The intensive home treatment group (n = 183) worked with a multidisciplinary team that designed a care plan tailored to their specific crisis. Treatment components included pharmacotherapy, up to three home visits each day, psychoeducation, brief supportive and cognitive behavioral therapy, social care, and support and empowerment of the patient’s informal care system.
The usual care group (n = 63) commonly received a combination of highly intensive inpatient treatment in the first phase and outpatient treatment up to two times a week in the second phase. Treatment included similar components as those in intensive home treatment.
The most common primary clinical diagnosis in both groups was mood disorder, followed by psychotic disorders, personality disorders, or anxiety disorders.
The home treatment group had a significantly higher total mean item score on the Brief Psychiatric Rating Scale (BPRS) at baseline (2.23 vs. 2.04, P = .04).
Mixed results
Results at 6 weeks showed the number of hospital days was 25.3% lower in the home treatment group, compared with those who received usual care.
That trend continued at 1 year, with the intensive home treatment group recording 36.6% fewer hospital days than the usual care group (mean, 42.5 days vs. 67 days, respectively; P = .03).
However, the number of patients who were admitted in the first 6 weeks and at 1 year stayed the same, as did the mean number of admissions per patient over 12 months.
The home treatment group reported significantly fewer symptoms on the BPRS depression and anxiety scale at 6 weeks, compared with the usual treatment group (P = .025), but that difference was not maintained after 6 months.
The number of adverse events, including suicide attempts, was similar between the groups. Three patients in the home treatment group and two in the usual care group died by suicide.
“Future research should focus on which components of intensive home treatment or hospitalization can be used when, for whom, and meet which goals, so that both hospital care and intensive home treatment can be used proportionally and efficiently for patients in psychiatric crisis,” the investigators write.
Not generalizable?
In an accompanying editorial, Claire Henderson, PhD, Institute of Psychiatry, Psychology, and Neuroscience at King’s College London, noted that generalizing the study’s results to other countries could be problematic, especially to regions such as North America, which have shorter lengths of stay for psychiatric hospitalization.
“Future trials looking at intensive home treatment would be most informative if done in countries with relatively short lengths of stay, and without separate crisis services for people receiving assertive community treatment,” Dr. Henderson writes.
The study was funded by De Stichting tot Steun Vereniging voor Christelijke Verzorging van Geestes-en Zenuwzieken. The investigators and Dr. Henderson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Intensive home treatment may offer an alternative to inpatient care for patients in acute psychiatric crisis – but the intervention is no outright substitute, new research suggests.
However, there was no difference between treatment groups in improvement in quality of life or patient satisfaction; and a reduction in symptom severity noted after 6 weeks of home treatment faded within 6 months.
“We found no differences in admission rates either, which suggests that intensive home treatment is not a substitute for inpatient care but a different treatment opportunity for psychiatric patients in crisis,” Jurgen Cornelis, MD, Arkin Institute for Mental Health, Amsterdam, and colleagues write.
The findings were published online in The Lancet Psychiatry.
Increasingly popular
“Intensive home treatment is increasingly popular as an alternative to hospitalization. It was developed to prevent or reduce levels of inpatient care and facilitate the transition between inpatient care and low-intensity outpatient care,” the investigators write.
However, there have previously been only two randomized controlled trials published that assessed this type of care, resulting in “somewhat conflicting findings,” they add.
For the current study, participants presented to psychiatric emergency wards at two medical centers in the Netherlands. They were included only if they were able to offer informed consent within 14 days.
The intensive home treatment group (n = 183) worked with a multidisciplinary team that designed a care plan tailored to their specific crisis. Treatment components included pharmacotherapy, up to three home visits each day, psychoeducation, brief supportive and cognitive behavioral therapy, social care, and support and empowerment of the patient’s informal care system.
The usual care group (n = 63) commonly received a combination of highly intensive inpatient treatment in the first phase and outpatient treatment up to two times a week in the second phase. Treatment included similar components as those in intensive home treatment.
The most common primary clinical diagnosis in both groups was mood disorder, followed by psychotic disorders, personality disorders, or anxiety disorders.
The home treatment group had a significantly higher total mean item score on the Brief Psychiatric Rating Scale (BPRS) at baseline (2.23 vs. 2.04, P = .04).
Mixed results
Results at 6 weeks showed the number of hospital days was 25.3% lower in the home treatment group, compared with those who received usual care.
That trend continued at 1 year, with the intensive home treatment group recording 36.6% fewer hospital days than the usual care group (mean, 42.5 days vs. 67 days, respectively; P = .03).
However, the number of patients who were admitted in the first 6 weeks and at 1 year stayed the same, as did the mean number of admissions per patient over 12 months.
The home treatment group reported significantly fewer symptoms on the BPRS depression and anxiety scale at 6 weeks, compared with the usual treatment group (P = .025), but that difference was not maintained after 6 months.
The number of adverse events, including suicide attempts, was similar between the groups. Three patients in the home treatment group and two in the usual care group died by suicide.
“Future research should focus on which components of intensive home treatment or hospitalization can be used when, for whom, and meet which goals, so that both hospital care and intensive home treatment can be used proportionally and efficiently for patients in psychiatric crisis,” the investigators write.
Not generalizable?
In an accompanying editorial, Claire Henderson, PhD, Institute of Psychiatry, Psychology, and Neuroscience at King’s College London, noted that generalizing the study’s results to other countries could be problematic, especially to regions such as North America, which have shorter lengths of stay for psychiatric hospitalization.
“Future trials looking at intensive home treatment would be most informative if done in countries with relatively short lengths of stay, and without separate crisis services for people receiving assertive community treatment,” Dr. Henderson writes.
The study was funded by De Stichting tot Steun Vereniging voor Christelijke Verzorging van Geestes-en Zenuwzieken. The investigators and Dr. Henderson have reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE LANCET PSYCHIATRY
Is Lp(a) a marker for aortic calcium onset?
Lipoprotein(a) has long been thought to be a potential marker of aortic valve disease, and the population-based Rotterdam Study in the Netherlands has reported that Lp(a) has a strong association with new-onset aortic valve calcium (AVC), but not necessarily with progression of aortic valve disease.
Reporting in the European Heart Journal, the study authors analyzed data on 922 participants in the Rotterdam Study whose Lp(a) was measured along with a computed tomography scan upon enrollment, followed by CT scan 14 years later. At baseline, 702 participants didn’t have AVC, but the follow-up scan identified new-onset AVC in 415 (59.1%).

The investigators found an association between Lp(a) concentration and baseline AVC, with an odds ratio of 1.43 for each 50 mg/dL higher Lp(a) (95% confidence interval, 1.15-1.79), as well as new-onset AVC, with an OR of 1.30 for each 50 mg/dL increase in Lp(a) (95% CI, 1.02-1.65). However, the study found no association between rising Lp(a) levels and AVC progression; it found only an association between baseline AVC score and progression (P < .001).
‘Trigger’ for calcification but not progression
“This suggests that Lp(a) is an important trigger in the initiation of aortic valve calcification, but once the valve is calcified, disease progression may be primarily driven by other factors such as the baseline calcium burden of the valve and likely other unknown factors,” senior study author Daniel Bos, MD, PhD, said in e-mailed comments.
Dr. Bos and coauthors claim this is the first study to show that even minor AVC progresses independently of Lp(a).
“There are previous studies that showed a possible relationship between Lp(a) [and] progression of aortic valve calcium,” he said. “Our study suggests that the most meaningful benefit of Lp(a) lowering may actually be prior to the onset of aortic valve calcification.”
While no treatments have been approved for lowering Lp(a), the study findings could be meaningful if trials, including the ongoing phase 3 Lp(a) HORIZON trial of the investigational antisense agent pelacarsen (NCT04023552), show promising results, Dr. Bos said. Citing Lp(a) HORIZON, he said, “If the study shows Lp(a) lowering leads to a reduction in incident cardiovascular disease, similar strategies may be applied to prevent, rather than slow down, progression of aortic valve calcification.”
Dr. Bos called the Rotterdam Study results “an important first pointer into that direction.” He added, “We will need randomized trials to provide a definitive answer to the question whether Lp(a) lowering may prevent aortic valve calcium.”
Focus on AVC is study ‘weakness’
The study findings raise a key question for clinical trials of investigative Lp(a)-lowering therapies as well as how to use those therapies to treat aortic valve disease, said Christie Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston.

The findings could be “problematic” for these clinical trials, he said. “This study is just looking at calcium progression,” Dr. Ballantyne noted. “What we want to know about clinically is the progression to aortic stenosis, and then in particular to progression from mild disease to moderate or severe disease, because once you get into more severe disease, one has to do an intervention with either surgery or TAVR [transcatheter aortic valve replacement].”
He considered the study’s focus on AVC rather than aortic valve function a weakness and noted that only 14 study participants had TAVR. “We’re going to need much bigger numbers to look into this question of progression, including progression to severe diseases,” he said.
However, the Rotterdam Study showed the importance of CT in evaluating AVC, which can easily be done in other trials to further explore the association between Lp(a) and AVC, Dr. Ballantyne said.
Dr. Bos has no relevant disclosures. Study coauthors disclosed relationships with Amgen, Sanofi, Reservlogix, Athera, Experio, Novartis and Ionis Pharmaceuticals. Dr. Ballantyne disclosed relationships with Amgen and Novartis.
Lipoprotein(a) has long been thought to be a potential marker of aortic valve disease, and the population-based Rotterdam Study in the Netherlands has reported that Lp(a) has a strong association with new-onset aortic valve calcium (AVC), but not necessarily with progression of aortic valve disease.
Reporting in the European Heart Journal, the study authors analyzed data on 922 participants in the Rotterdam Study whose Lp(a) was measured along with a computed tomography scan upon enrollment, followed by CT scan 14 years later. At baseline, 702 participants didn’t have AVC, but the follow-up scan identified new-onset AVC in 415 (59.1%).
The investigators found an association between Lp(a) concentration and baseline AVC, with an odds ratio of 1.43 for each 50 mg/dL higher Lp(a) (95% confidence interval, 1.15-1.79), as well as new-onset AVC, with an OR of 1.30 for each 50 mg/dL increase in Lp(a) (95% CI, 1.02-1.65). However, the study found no association between rising Lp(a) levels and AVC progression; it found only an association between baseline AVC score and progression (P < .001).
‘Trigger’ for calcification but not progression
“This suggests that Lp(a) is an important trigger in the initiation of aortic valve calcification, but once the valve is calcified, disease progression may be primarily driven by other factors such as the baseline calcium burden of the valve and likely other unknown factors,” senior study author Daniel Bos, MD, PhD, said in e-mailed comments.
Dr. Bos and coauthors claim this is the first study to show that even minor AVC progresses independently of Lp(a).
“There are previous studies that showed a possible relationship between Lp(a) [and] progression of aortic valve calcium,” he said. “Our study suggests that the most meaningful benefit of Lp(a) lowering may actually be prior to the onset of aortic valve calcification.”
While no treatments have been approved for lowering Lp(a), the study findings could be meaningful if trials, including the ongoing phase 3 Lp(a) HORIZON trial of the investigational antisense agent pelacarsen (NCT04023552), show promising results, Dr. Bos said. Citing Lp(a) HORIZON, he said, “If the study shows Lp(a) lowering leads to a reduction in incident cardiovascular disease, similar strategies may be applied to prevent, rather than slow down, progression of aortic valve calcification.”
Dr. Bos called the Rotterdam Study results “an important first pointer into that direction.” He added, “We will need randomized trials to provide a definitive answer to the question whether Lp(a) lowering may prevent aortic valve calcium.”
Focus on AVC is study ‘weakness’
The study findings raise a key question for clinical trials of investigative Lp(a)-lowering therapies as well as how to use those therapies to treat aortic valve disease, said Christie Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston.
The findings could be “problematic” for these clinical trials, he said. “This study is just looking at calcium progression,” Dr. Ballantyne noted. “What we want to know about clinically is the progression to aortic stenosis, and then in particular to progression from mild disease to moderate or severe disease, because once you get into more severe disease, one has to do an intervention with either surgery or TAVR [transcatheter aortic valve replacement].”
He considered the study’s focus on AVC rather than aortic valve function a weakness and noted that only 14 study participants had TAVR. “We’re going to need much bigger numbers to look into this question of progression, including progression to severe diseases,” he said.
However, the Rotterdam Study showed the importance of CT in evaluating AVC, which can easily be done in other trials to further explore the association between Lp(a) and AVC, Dr. Ballantyne said.
Dr. Bos has no relevant disclosures. Study coauthors disclosed relationships with Amgen, Sanofi, Reservlogix, Athera, Experio, Novartis and Ionis Pharmaceuticals. Dr. Ballantyne disclosed relationships with Amgen and Novartis.
Lipoprotein(a) has long been thought to be a potential marker of aortic valve disease, and the population-based Rotterdam Study in the Netherlands has reported that Lp(a) has a strong association with new-onset aortic valve calcium (AVC), but not necessarily with progression of aortic valve disease.
Reporting in the European Heart Journal, the study authors analyzed data on 922 participants in the Rotterdam Study whose Lp(a) was measured along with a computed tomography scan upon enrollment, followed by CT scan 14 years later. At baseline, 702 participants didn’t have AVC, but the follow-up scan identified new-onset AVC in 415 (59.1%).
The investigators found an association between Lp(a) concentration and baseline AVC, with an odds ratio of 1.43 for each 50 mg/dL higher Lp(a) (95% confidence interval, 1.15-1.79), as well as new-onset AVC, with an OR of 1.30 for each 50 mg/dL increase in Lp(a) (95% CI, 1.02-1.65). However, the study found no association between rising Lp(a) levels and AVC progression; it found only an association between baseline AVC score and progression (P < .001).
‘Trigger’ for calcification but not progression
“This suggests that Lp(a) is an important trigger in the initiation of aortic valve calcification, but once the valve is calcified, disease progression may be primarily driven by other factors such as the baseline calcium burden of the valve and likely other unknown factors,” senior study author Daniel Bos, MD, PhD, said in e-mailed comments.
Dr. Bos and coauthors claim this is the first study to show that even minor AVC progresses independently of Lp(a).
“There are previous studies that showed a possible relationship between Lp(a) [and] progression of aortic valve calcium,” he said. “Our study suggests that the most meaningful benefit of Lp(a) lowering may actually be prior to the onset of aortic valve calcification.”
While no treatments have been approved for lowering Lp(a), the study findings could be meaningful if trials, including the ongoing phase 3 Lp(a) HORIZON trial of the investigational antisense agent pelacarsen (NCT04023552), show promising results, Dr. Bos said. Citing Lp(a) HORIZON, he said, “If the study shows Lp(a) lowering leads to a reduction in incident cardiovascular disease, similar strategies may be applied to prevent, rather than slow down, progression of aortic valve calcification.”
Dr. Bos called the Rotterdam Study results “an important first pointer into that direction.” He added, “We will need randomized trials to provide a definitive answer to the question whether Lp(a) lowering may prevent aortic valve calcium.”
Focus on AVC is study ‘weakness’
The study findings raise a key question for clinical trials of investigative Lp(a)-lowering therapies as well as how to use those therapies to treat aortic valve disease, said Christie Ballantyne, MD, chief of cardiology at Baylor College of Medicine in Houston.
The findings could be “problematic” for these clinical trials, he said. “This study is just looking at calcium progression,” Dr. Ballantyne noted. “What we want to know about clinically is the progression to aortic stenosis, and then in particular to progression from mild disease to moderate or severe disease, because once you get into more severe disease, one has to do an intervention with either surgery or TAVR [transcatheter aortic valve replacement].”
He considered the study’s focus on AVC rather than aortic valve function a weakness and noted that only 14 study participants had TAVR. “We’re going to need much bigger numbers to look into this question of progression, including progression to severe diseases,” he said.
However, the Rotterdam Study showed the importance of CT in evaluating AVC, which can easily be done in other trials to further explore the association between Lp(a) and AVC, Dr. Ballantyne said.
Dr. Bos has no relevant disclosures. Study coauthors disclosed relationships with Amgen, Sanofi, Reservlogix, Athera, Experio, Novartis and Ionis Pharmaceuticals. Dr. Ballantyne disclosed relationships with Amgen and Novartis.
FROM THE EUROPEAN HEART JOURNAL