User login
Ultrasound-guided nerve blocks improve fracture pain
results from a meta-analysis published in BMC Anesthesiology show.
With the caveat that the quality of evidence in most trials in the analysis is low owing to a lack of blinding and other factors, “our review suggests that, among patients suffering from a hip fracture, a preoperative ultrasound-guided peripheral nerve block is associated with a significant pain reduction and reduced need for systemic analgesics compared to conventional analgesia,” reported the authors.
“Our results may also indicate a lower risk of delirium, serious adverse events and higher patient satisfaction in patients receiving an ultrasound-guided peripheral nerve block,” they added.
Because hip fractures commonly affect older populations and those who are frail, treatment of the substantial pain that can occur perioperatively is a challenge.
Peripheral nerve blocks have been shown to reduce pain within 30 minutes of the block placement; however, most studies have primarily included blocks that use anatomic landmarks or nerve stimulation for guidance. However, the use of ultrasound guidance with the nerve block should improve efficacy, the authors noted.
“It seems intuitive that using ultrasound-guidance should be more effective than using a blind technique, since it allows a trained physician to deposit the local anesthetic with much more precision,” they wrote.
To evaluate the data from studies that have looked at ultrasound-guided peripheral nerve blocks, Oskar Wilborg Exsteen, of the department of anesthesiology and intensive care, Copenhagen University Hospital and Nordsjællands Hospital, Hillerød, Denmark, and colleagues identified 12 randomized controlled trials, involving a combined total of 976 participants, for the meta-analysis.
The studies included 509 participants who received ultrasound-guided peripheral nerve blocks, specifically the femoral nerve block and fascia iliaca block, and 476 who were randomly assigned to control groups.
Overall, those treated with the nerve blocks showed significantly greater reductions in pain measured closest to 2 hours of block placement, compared with conventional analgesia, with a mean reduction of 2.26 points on the Visual Analogue Scale (VAS) (range, 0-10; P < .001).
Ultrasound-guided peripheral nerve block use was associated with lower preoperative usage of analgesic intravenous morphine equivalents in milligram, reported in four of the trials (random effects model mean difference, –5.34; P = .003).
Delirium was also significantly lower with the nerve blocks (risk ratio, 0.6; P = 0.03), as were serious adverse events, compared with standard analgesia (RR, 0.33; P = .006), whereas patient satisfaction was significantly higher with the nerve blocks (mean VAS difference, 25.9 [score 0-100]; P < .001).
Seven of the studies had monitored for serious adverse events or complications related to the nerve blocks, but none reported any complications directly related to the ultrasound-guided peripheral nerve blocks.
Owing to the inability to conduct blinded comparisons, clinical heterogeneity, and other caveats, the quality of evidence was ultimately judged to be “low” or “very low”; however, the observed benefits are nevertheless relevant, the authors concluded.
“Despite the low quality of evidence, ultrasound-guided blocks were associated with benefits compared to conventional systemic analgesia,” they said.
Key caveats include that the morphine reductions observed with the nerve blocks were not substantial, they noted. “The opioid-sparing effect seems small and may be of less clinical importance.” The decreases in opioid consumption, as well as pain reduction in the analysis, are in fact similar to those observed with conventional, peripheral nerve blocks that did not use ultrasound guidance, compared with standard pain management.
No trials were identified that directly compared ultrasound-guided peripheral nerve blocks with nerve block techniques that didn’t use ultrasound.
However, the other noted improvements carry more weight, the authors said.
“The potential for higher patient satisfaction and reduction in serious adverse events and delirium may be of clinical importance,” they wrote.
Ultrasound-guided peripheral nerve blocks not always accessible
Of note, the use of ultrasound-guided peripheral nerve blocks appears to be somewhat low, with one observational trend study of national data in the United States showing that, among patients receiving a peripheral nerve block for hip arthroplasty, only 3.2% of the procedures were performed using ultrasound guidance.
Stephen C. Haskins, MD, a coauthor on that study, said that the low utilization underscores that, in real-world practice, an ultrasound-guided approach isn’t always convenient.
“I think our findings demonstrate a common misconception that exists for those of us that work at academic institutions and/or within the ivory towers of regional anesthesia, which is that everyone is performing cutting edge ultrasound-guided techniques for all procedures,” Dr. Haskins, an associate attending anesthesiologist and chief medical diversity officer with the department of anesthesiology, critical care & pain management at the Hospital for Special Surgery in New York, said in an interview.
However, “there are many limitations to use of ultrasound for these blocks, including limited access to machines, limited access to training, and limited interest and support from our surgical colleagues,” he explained.
“Ultimately, the best nerve block is the one performed in a timely and successful fashion, regardless of technique,” he said. “But we will continue to see a trend towards ultrasound use in the future due to increasing access in the form of portability and affordability.”
Haskins noted that newer ultrasound-guided nerve blocks that were not reviewed in the study, such as the pericapsular nerve group block, regional block, and supra-inguinal fascia iliaca block, which provide additional benefits such as avoiding quadriceps weakness.
Jeff Gadsden, MD, chief of the orthopedics, plastic, and regional anesthesiology division at Duke University Medical Center, Durham, N.C., agreed, noting that much has changed since some of the older studies in the analysis, that date back to 2010.
“A fascia iliaca block done in 2022 looks a lot different than it did in 2012, and we would expect it to be more consistent, reliable and longer-lasting with current techniques and technology,” he said in an interview. “So, if anything, I would expect the findings of this analysis to undersell the benefits of peripheral nerve blocks in this population.”
Although the quality of evidence in the meta-analysis is described as “low,” the downsides of the procedures are few, and “the potential benefits [of ultrasound-guided peripheral nerve blocks] are just too good to ignore,” Dr. Gadsden emphasized.
“If we can avoid or reduce opioids in this population and at the same time reduce the acute pain from the injury, there is no question that the incidence of delirium will go down,” he said. “Delirium is associated with a number of poor outcomes following hip fracture, including increased mortality.
“The bottom line is that the risk/benefit ratio is so far in favor of performing the blocks that even in the face of ‘modest’ levels of evidence, we should all be doing these.”
The authors, Dr. Haskins, and Dr. Gadsden had no disclosures relating to the study to report.
A version of this article first appeared on Medscape.com.
results from a meta-analysis published in BMC Anesthesiology show.
With the caveat that the quality of evidence in most trials in the analysis is low owing to a lack of blinding and other factors, “our review suggests that, among patients suffering from a hip fracture, a preoperative ultrasound-guided peripheral nerve block is associated with a significant pain reduction and reduced need for systemic analgesics compared to conventional analgesia,” reported the authors.
“Our results may also indicate a lower risk of delirium, serious adverse events and higher patient satisfaction in patients receiving an ultrasound-guided peripheral nerve block,” they added.
Because hip fractures commonly affect older populations and those who are frail, treatment of the substantial pain that can occur perioperatively is a challenge.
Peripheral nerve blocks have been shown to reduce pain within 30 minutes of the block placement; however, most studies have primarily included blocks that use anatomic landmarks or nerve stimulation for guidance. However, the use of ultrasound guidance with the nerve block should improve efficacy, the authors noted.
“It seems intuitive that using ultrasound-guidance should be more effective than using a blind technique, since it allows a trained physician to deposit the local anesthetic with much more precision,” they wrote.
To evaluate the data from studies that have looked at ultrasound-guided peripheral nerve blocks, Oskar Wilborg Exsteen, of the department of anesthesiology and intensive care, Copenhagen University Hospital and Nordsjællands Hospital, Hillerød, Denmark, and colleagues identified 12 randomized controlled trials, involving a combined total of 976 participants, for the meta-analysis.
The studies included 509 participants who received ultrasound-guided peripheral nerve blocks, specifically the femoral nerve block and fascia iliaca block, and 476 who were randomly assigned to control groups.
Overall, those treated with the nerve blocks showed significantly greater reductions in pain measured closest to 2 hours of block placement, compared with conventional analgesia, with a mean reduction of 2.26 points on the Visual Analogue Scale (VAS) (range, 0-10; P < .001).
Ultrasound-guided peripheral nerve block use was associated with lower preoperative usage of analgesic intravenous morphine equivalents in milligram, reported in four of the trials (random effects model mean difference, –5.34; P = .003).
Delirium was also significantly lower with the nerve blocks (risk ratio, 0.6; P = 0.03), as were serious adverse events, compared with standard analgesia (RR, 0.33; P = .006), whereas patient satisfaction was significantly higher with the nerve blocks (mean VAS difference, 25.9 [score 0-100]; P < .001).
Seven of the studies had monitored for serious adverse events or complications related to the nerve blocks, but none reported any complications directly related to the ultrasound-guided peripheral nerve blocks.
Owing to the inability to conduct blinded comparisons, clinical heterogeneity, and other caveats, the quality of evidence was ultimately judged to be “low” or “very low”; however, the observed benefits are nevertheless relevant, the authors concluded.
“Despite the low quality of evidence, ultrasound-guided blocks were associated with benefits compared to conventional systemic analgesia,” they said.
Key caveats include that the morphine reductions observed with the nerve blocks were not substantial, they noted. “The opioid-sparing effect seems small and may be of less clinical importance.” The decreases in opioid consumption, as well as pain reduction in the analysis, are in fact similar to those observed with conventional, peripheral nerve blocks that did not use ultrasound guidance, compared with standard pain management.
No trials were identified that directly compared ultrasound-guided peripheral nerve blocks with nerve block techniques that didn’t use ultrasound.
However, the other noted improvements carry more weight, the authors said.
“The potential for higher patient satisfaction and reduction in serious adverse events and delirium may be of clinical importance,” they wrote.
Ultrasound-guided peripheral nerve blocks not always accessible
Of note, the use of ultrasound-guided peripheral nerve blocks appears to be somewhat low, with one observational trend study of national data in the United States showing that, among patients receiving a peripheral nerve block for hip arthroplasty, only 3.2% of the procedures were performed using ultrasound guidance.
Stephen C. Haskins, MD, a coauthor on that study, said that the low utilization underscores that, in real-world practice, an ultrasound-guided approach isn’t always convenient.
“I think our findings demonstrate a common misconception that exists for those of us that work at academic institutions and/or within the ivory towers of regional anesthesia, which is that everyone is performing cutting edge ultrasound-guided techniques for all procedures,” Dr. Haskins, an associate attending anesthesiologist and chief medical diversity officer with the department of anesthesiology, critical care & pain management at the Hospital for Special Surgery in New York, said in an interview.
However, “there are many limitations to use of ultrasound for these blocks, including limited access to machines, limited access to training, and limited interest and support from our surgical colleagues,” he explained.
“Ultimately, the best nerve block is the one performed in a timely and successful fashion, regardless of technique,” he said. “But we will continue to see a trend towards ultrasound use in the future due to increasing access in the form of portability and affordability.”
Haskins noted that newer ultrasound-guided nerve blocks that were not reviewed in the study, such as the pericapsular nerve group block, regional block, and supra-inguinal fascia iliaca block, which provide additional benefits such as avoiding quadriceps weakness.
Jeff Gadsden, MD, chief of the orthopedics, plastic, and regional anesthesiology division at Duke University Medical Center, Durham, N.C., agreed, noting that much has changed since some of the older studies in the analysis, that date back to 2010.
“A fascia iliaca block done in 2022 looks a lot different than it did in 2012, and we would expect it to be more consistent, reliable and longer-lasting with current techniques and technology,” he said in an interview. “So, if anything, I would expect the findings of this analysis to undersell the benefits of peripheral nerve blocks in this population.”
Although the quality of evidence in the meta-analysis is described as “low,” the downsides of the procedures are few, and “the potential benefits [of ultrasound-guided peripheral nerve blocks] are just too good to ignore,” Dr. Gadsden emphasized.
“If we can avoid or reduce opioids in this population and at the same time reduce the acute pain from the injury, there is no question that the incidence of delirium will go down,” he said. “Delirium is associated with a number of poor outcomes following hip fracture, including increased mortality.
“The bottom line is that the risk/benefit ratio is so far in favor of performing the blocks that even in the face of ‘modest’ levels of evidence, we should all be doing these.”
The authors, Dr. Haskins, and Dr. Gadsden had no disclosures relating to the study to report.
A version of this article first appeared on Medscape.com.
results from a meta-analysis published in BMC Anesthesiology show.
With the caveat that the quality of evidence in most trials in the analysis is low owing to a lack of blinding and other factors, “our review suggests that, among patients suffering from a hip fracture, a preoperative ultrasound-guided peripheral nerve block is associated with a significant pain reduction and reduced need for systemic analgesics compared to conventional analgesia,” reported the authors.
“Our results may also indicate a lower risk of delirium, serious adverse events and higher patient satisfaction in patients receiving an ultrasound-guided peripheral nerve block,” they added.
Because hip fractures commonly affect older populations and those who are frail, treatment of the substantial pain that can occur perioperatively is a challenge.
Peripheral nerve blocks have been shown to reduce pain within 30 minutes of the block placement; however, most studies have primarily included blocks that use anatomic landmarks or nerve stimulation for guidance. However, the use of ultrasound guidance with the nerve block should improve efficacy, the authors noted.
“It seems intuitive that using ultrasound-guidance should be more effective than using a blind technique, since it allows a trained physician to deposit the local anesthetic with much more precision,” they wrote.
To evaluate the data from studies that have looked at ultrasound-guided peripheral nerve blocks, Oskar Wilborg Exsteen, of the department of anesthesiology and intensive care, Copenhagen University Hospital and Nordsjællands Hospital, Hillerød, Denmark, and colleagues identified 12 randomized controlled trials, involving a combined total of 976 participants, for the meta-analysis.
The studies included 509 participants who received ultrasound-guided peripheral nerve blocks, specifically the femoral nerve block and fascia iliaca block, and 476 who were randomly assigned to control groups.
Overall, those treated with the nerve blocks showed significantly greater reductions in pain measured closest to 2 hours of block placement, compared with conventional analgesia, with a mean reduction of 2.26 points on the Visual Analogue Scale (VAS) (range, 0-10; P < .001).
Ultrasound-guided peripheral nerve block use was associated with lower preoperative usage of analgesic intravenous morphine equivalents in milligram, reported in four of the trials (random effects model mean difference, –5.34; P = .003).
Delirium was also significantly lower with the nerve blocks (risk ratio, 0.6; P = 0.03), as were serious adverse events, compared with standard analgesia (RR, 0.33; P = .006), whereas patient satisfaction was significantly higher with the nerve blocks (mean VAS difference, 25.9 [score 0-100]; P < .001).
Seven of the studies had monitored for serious adverse events or complications related to the nerve blocks, but none reported any complications directly related to the ultrasound-guided peripheral nerve blocks.
Owing to the inability to conduct blinded comparisons, clinical heterogeneity, and other caveats, the quality of evidence was ultimately judged to be “low” or “very low”; however, the observed benefits are nevertheless relevant, the authors concluded.
“Despite the low quality of evidence, ultrasound-guided blocks were associated with benefits compared to conventional systemic analgesia,” they said.
Key caveats include that the morphine reductions observed with the nerve blocks were not substantial, they noted. “The opioid-sparing effect seems small and may be of less clinical importance.” The decreases in opioid consumption, as well as pain reduction in the analysis, are in fact similar to those observed with conventional, peripheral nerve blocks that did not use ultrasound guidance, compared with standard pain management.
No trials were identified that directly compared ultrasound-guided peripheral nerve blocks with nerve block techniques that didn’t use ultrasound.
However, the other noted improvements carry more weight, the authors said.
“The potential for higher patient satisfaction and reduction in serious adverse events and delirium may be of clinical importance,” they wrote.
Ultrasound-guided peripheral nerve blocks not always accessible
Of note, the use of ultrasound-guided peripheral nerve blocks appears to be somewhat low, with one observational trend study of national data in the United States showing that, among patients receiving a peripheral nerve block for hip arthroplasty, only 3.2% of the procedures were performed using ultrasound guidance.
Stephen C. Haskins, MD, a coauthor on that study, said that the low utilization underscores that, in real-world practice, an ultrasound-guided approach isn’t always convenient.
“I think our findings demonstrate a common misconception that exists for those of us that work at academic institutions and/or within the ivory towers of regional anesthesia, which is that everyone is performing cutting edge ultrasound-guided techniques for all procedures,” Dr. Haskins, an associate attending anesthesiologist and chief medical diversity officer with the department of anesthesiology, critical care & pain management at the Hospital for Special Surgery in New York, said in an interview.
However, “there are many limitations to use of ultrasound for these blocks, including limited access to machines, limited access to training, and limited interest and support from our surgical colleagues,” he explained.
“Ultimately, the best nerve block is the one performed in a timely and successful fashion, regardless of technique,” he said. “But we will continue to see a trend towards ultrasound use in the future due to increasing access in the form of portability and affordability.”
Haskins noted that newer ultrasound-guided nerve blocks that were not reviewed in the study, such as the pericapsular nerve group block, regional block, and supra-inguinal fascia iliaca block, which provide additional benefits such as avoiding quadriceps weakness.
Jeff Gadsden, MD, chief of the orthopedics, plastic, and regional anesthesiology division at Duke University Medical Center, Durham, N.C., agreed, noting that much has changed since some of the older studies in the analysis, that date back to 2010.
“A fascia iliaca block done in 2022 looks a lot different than it did in 2012, and we would expect it to be more consistent, reliable and longer-lasting with current techniques and technology,” he said in an interview. “So, if anything, I would expect the findings of this analysis to undersell the benefits of peripheral nerve blocks in this population.”
Although the quality of evidence in the meta-analysis is described as “low,” the downsides of the procedures are few, and “the potential benefits [of ultrasound-guided peripheral nerve blocks] are just too good to ignore,” Dr. Gadsden emphasized.
“If we can avoid or reduce opioids in this population and at the same time reduce the acute pain from the injury, there is no question that the incidence of delirium will go down,” he said. “Delirium is associated with a number of poor outcomes following hip fracture, including increased mortality.
“The bottom line is that the risk/benefit ratio is so far in favor of performing the blocks that even in the face of ‘modest’ levels of evidence, we should all be doing these.”
The authors, Dr. Haskins, and Dr. Gadsden had no disclosures relating to the study to report.
A version of this article first appeared on Medscape.com.
FROM BMC ANESTHESIOLOGY
Doctors using fake positive reviews to boost business
Five years ago, Kay Dean relied upon Yelp! and Google reviews in her search for a doctor in her area. After finding a physician with fairly high reviews, Ms. Dean was shocked when her personal experience was significantly worse than patients on the review platforms.
Following her experience, Ms. Dean, a former federal government investigator, became skeptical and used her skills to investigate the practice on all review platforms. She uncovered that the practice had a review from an individual who was involved in a review trading group on Facebook, where organizations openly barter their services in exchange for positive reviews fraud.
“I discovered that the online review world was just saturated with fake reviews, much more so than I think most people are aware ... and law enforcement regulators aren’t doing anything to address the problem,” said Ms. Dean. “In this online space, it’s the Wild West; cheating is rewarded.”
Ms. Dean decided to take matters into her own hands. She created a YouTube channel called Fake Review Watch, where she exposes real businesses and their attempts to dupe potential consumers with fake positive reviews.
For example, one video analyzes an orthopedic surgeon in Manhattan with an abundance of five-star reviews. Through her detailed analysis, Ms. Dean created a spreadsheet of the 26 alleged patients of the orthopedic surgeon that had submitted glowing reviews. She looked into other businesses that the individuals had left reviews for and found a significant amount of overlap.
According to the video, 19 of the doctor’s reviewers had left high reviews for the same moving company in Las Vegas, and 18 of them reviewed the same locksmith in Texas. Overall, eight of the patients reviewed the same mover, locksmith, and hotel in New Zealand.
A matter of trust
Ms. Dean expressed the gravity of this phenomenon, especially in health care, as patients often head online first when searching for care options. Based on a survey by Software Advice, about 84% of patients use online reviews to assess a physician, and 77% use review sites as the first step in finding a doctor.
Patient trust has continued to diminish in recent years, particularly following the pandemic. In a 2021 global ranking of trust levels towards health care by country, the U.S. health care system ranked 19th, far below those of several developing countries.
Owing to the rise of fake patient reviews and their inscrutable nature, Ms. Dean advises staying away from online review platforms. Instead, she suggests sticking to the old-fashioned method of getting recommendations from friends and relatives, not virtual people.
Ms. Dean explained a few indicators that she looks for when trying to identify a fake review.
“The business has all five-star reviews, negative reviews are followed by five-star reviews, or the business has an abnormal number of positive reviews in a short period of time,” she noted. “Some businesses try to bury legitimate negative reviews by obtaining more recent, fake, positive ones. The recent reviews will contradict the specific criticisms in the negative review.”
She warned that consumers should not give credibility to reviews simply because the reviewer is dubbed “Elite” or a Google Local Guide, because she has seen plenty of these individuals posting fake reviews.
Unfortunately, review platforms haven’t been doing much self-policing. Google and Healthgrades have a series of policies against fake engagement, impersonation, misinformation, and misrepresentation, according to their websites. However, the only consequence of these violations is review removal.
Both Yelp! and Google say they have automated software that distinguishes real versus fake reviews. When Yelp! uncovers users engaging in compensation review activity, it removes their reviews, closes their account, and blocks those users from creating future Yelp! accounts.
Physicians’ basis
Moreover,
“I think there’s an erosion of business ethics because cheating is rewarded. You can’t compete in an environment where your competition is allowed to accumulate numerous fake reviews while you’re still trying to fill chairs in your business,” said Ms. Dean. “Your competition is then getting the business because the tech companies are allowing this fraud.”
Family physician and practice owner Mike Woo-Ming, MD, MPH, provides career coaching for physicians, including maintaining a good reputation – in-person and online. He has seen physicians bumping up their own five-star reviews personally as well as posting negative reviews for their competition.
“I’ve seen where they’re going to lose business, as many practices were affected through COVID,” he said. “Business owners can become desperate and may decide to start posting or buying reviews because they know people will choose certain services these days based upon reviews.”
Dr. Woo-Ming expressed his frustration with fellow physicians who give in to purchasing fake reviews, because the patients have no idea whether reviews are genuine or not.
To encourage genuine positive reviews, Dr. Woo-Ming’s practice uses a third-party app system that sends patients a follow-up email or text asking about their experience with a link to review sites.
“Honest reviews are a reflection of what I can do to improve my business. At the end of the day, if you’re truly providing great service and you’re helping people by providing great medical care, those are going to win out,” he said. “I would rather, as a responsible practice owner, improve the experience and outcome for the patient.”
A version of this article first appeared on Medscape.com.
Five years ago, Kay Dean relied upon Yelp! and Google reviews in her search for a doctor in her area. After finding a physician with fairly high reviews, Ms. Dean was shocked when her personal experience was significantly worse than patients on the review platforms.
Following her experience, Ms. Dean, a former federal government investigator, became skeptical and used her skills to investigate the practice on all review platforms. She uncovered that the practice had a review from an individual who was involved in a review trading group on Facebook, where organizations openly barter their services in exchange for positive reviews fraud.
“I discovered that the online review world was just saturated with fake reviews, much more so than I think most people are aware ... and law enforcement regulators aren’t doing anything to address the problem,” said Ms. Dean. “In this online space, it’s the Wild West; cheating is rewarded.”
Ms. Dean decided to take matters into her own hands. She created a YouTube channel called Fake Review Watch, where she exposes real businesses and their attempts to dupe potential consumers with fake positive reviews.
For example, one video analyzes an orthopedic surgeon in Manhattan with an abundance of five-star reviews. Through her detailed analysis, Ms. Dean created a spreadsheet of the 26 alleged patients of the orthopedic surgeon that had submitted glowing reviews. She looked into other businesses that the individuals had left reviews for and found a significant amount of overlap.
According to the video, 19 of the doctor’s reviewers had left high reviews for the same moving company in Las Vegas, and 18 of them reviewed the same locksmith in Texas. Overall, eight of the patients reviewed the same mover, locksmith, and hotel in New Zealand.
A matter of trust
Ms. Dean expressed the gravity of this phenomenon, especially in health care, as patients often head online first when searching for care options. Based on a survey by Software Advice, about 84% of patients use online reviews to assess a physician, and 77% use review sites as the first step in finding a doctor.
Patient trust has continued to diminish in recent years, particularly following the pandemic. In a 2021 global ranking of trust levels towards health care by country, the U.S. health care system ranked 19th, far below those of several developing countries.
Owing to the rise of fake patient reviews and their inscrutable nature, Ms. Dean advises staying away from online review platforms. Instead, she suggests sticking to the old-fashioned method of getting recommendations from friends and relatives, not virtual people.
Ms. Dean explained a few indicators that she looks for when trying to identify a fake review.
“The business has all five-star reviews, negative reviews are followed by five-star reviews, or the business has an abnormal number of positive reviews in a short period of time,” she noted. “Some businesses try to bury legitimate negative reviews by obtaining more recent, fake, positive ones. The recent reviews will contradict the specific criticisms in the negative review.”
She warned that consumers should not give credibility to reviews simply because the reviewer is dubbed “Elite” or a Google Local Guide, because she has seen plenty of these individuals posting fake reviews.
Unfortunately, review platforms haven’t been doing much self-policing. Google and Healthgrades have a series of policies against fake engagement, impersonation, misinformation, and misrepresentation, according to their websites. However, the only consequence of these violations is review removal.
Both Yelp! and Google say they have automated software that distinguishes real versus fake reviews. When Yelp! uncovers users engaging in compensation review activity, it removes their reviews, closes their account, and blocks those users from creating future Yelp! accounts.
Physicians’ basis
Moreover,
“I think there’s an erosion of business ethics because cheating is rewarded. You can’t compete in an environment where your competition is allowed to accumulate numerous fake reviews while you’re still trying to fill chairs in your business,” said Ms. Dean. “Your competition is then getting the business because the tech companies are allowing this fraud.”
Family physician and practice owner Mike Woo-Ming, MD, MPH, provides career coaching for physicians, including maintaining a good reputation – in-person and online. He has seen physicians bumping up their own five-star reviews personally as well as posting negative reviews for their competition.
“I’ve seen where they’re going to lose business, as many practices were affected through COVID,” he said. “Business owners can become desperate and may decide to start posting or buying reviews because they know people will choose certain services these days based upon reviews.”
Dr. Woo-Ming expressed his frustration with fellow physicians who give in to purchasing fake reviews, because the patients have no idea whether reviews are genuine or not.
To encourage genuine positive reviews, Dr. Woo-Ming’s practice uses a third-party app system that sends patients a follow-up email or text asking about their experience with a link to review sites.
“Honest reviews are a reflection of what I can do to improve my business. At the end of the day, if you’re truly providing great service and you’re helping people by providing great medical care, those are going to win out,” he said. “I would rather, as a responsible practice owner, improve the experience and outcome for the patient.”
A version of this article first appeared on Medscape.com.
Five years ago, Kay Dean relied upon Yelp! and Google reviews in her search for a doctor in her area. After finding a physician with fairly high reviews, Ms. Dean was shocked when her personal experience was significantly worse than patients on the review platforms.
Following her experience, Ms. Dean, a former federal government investigator, became skeptical and used her skills to investigate the practice on all review platforms. She uncovered that the practice had a review from an individual who was involved in a review trading group on Facebook, where organizations openly barter their services in exchange for positive reviews fraud.
“I discovered that the online review world was just saturated with fake reviews, much more so than I think most people are aware ... and law enforcement regulators aren’t doing anything to address the problem,” said Ms. Dean. “In this online space, it’s the Wild West; cheating is rewarded.”
Ms. Dean decided to take matters into her own hands. She created a YouTube channel called Fake Review Watch, where she exposes real businesses and their attempts to dupe potential consumers with fake positive reviews.
For example, one video analyzes an orthopedic surgeon in Manhattan with an abundance of five-star reviews. Through her detailed analysis, Ms. Dean created a spreadsheet of the 26 alleged patients of the orthopedic surgeon that had submitted glowing reviews. She looked into other businesses that the individuals had left reviews for and found a significant amount of overlap.
According to the video, 19 of the doctor’s reviewers had left high reviews for the same moving company in Las Vegas, and 18 of them reviewed the same locksmith in Texas. Overall, eight of the patients reviewed the same mover, locksmith, and hotel in New Zealand.
A matter of trust
Ms. Dean expressed the gravity of this phenomenon, especially in health care, as patients often head online first when searching for care options. Based on a survey by Software Advice, about 84% of patients use online reviews to assess a physician, and 77% use review sites as the first step in finding a doctor.
Patient trust has continued to diminish in recent years, particularly following the pandemic. In a 2021 global ranking of trust levels towards health care by country, the U.S. health care system ranked 19th, far below those of several developing countries.
Owing to the rise of fake patient reviews and their inscrutable nature, Ms. Dean advises staying away from online review platforms. Instead, she suggests sticking to the old-fashioned method of getting recommendations from friends and relatives, not virtual people.
Ms. Dean explained a few indicators that she looks for when trying to identify a fake review.
“The business has all five-star reviews, negative reviews are followed by five-star reviews, or the business has an abnormal number of positive reviews in a short period of time,” she noted. “Some businesses try to bury legitimate negative reviews by obtaining more recent, fake, positive ones. The recent reviews will contradict the specific criticisms in the negative review.”
She warned that consumers should not give credibility to reviews simply because the reviewer is dubbed “Elite” or a Google Local Guide, because she has seen plenty of these individuals posting fake reviews.
Unfortunately, review platforms haven’t been doing much self-policing. Google and Healthgrades have a series of policies against fake engagement, impersonation, misinformation, and misrepresentation, according to their websites. However, the only consequence of these violations is review removal.
Both Yelp! and Google say they have automated software that distinguishes real versus fake reviews. When Yelp! uncovers users engaging in compensation review activity, it removes their reviews, closes their account, and blocks those users from creating future Yelp! accounts.
Physicians’ basis
Moreover,
“I think there’s an erosion of business ethics because cheating is rewarded. You can’t compete in an environment where your competition is allowed to accumulate numerous fake reviews while you’re still trying to fill chairs in your business,” said Ms. Dean. “Your competition is then getting the business because the tech companies are allowing this fraud.”
Family physician and practice owner Mike Woo-Ming, MD, MPH, provides career coaching for physicians, including maintaining a good reputation – in-person and online. He has seen physicians bumping up their own five-star reviews personally as well as posting negative reviews for their competition.
“I’ve seen where they’re going to lose business, as many practices were affected through COVID,” he said. “Business owners can become desperate and may decide to start posting or buying reviews because they know people will choose certain services these days based upon reviews.”
Dr. Woo-Ming expressed his frustration with fellow physicians who give in to purchasing fake reviews, because the patients have no idea whether reviews are genuine or not.
To encourage genuine positive reviews, Dr. Woo-Ming’s practice uses a third-party app system that sends patients a follow-up email or text asking about their experience with a link to review sites.
“Honest reviews are a reflection of what I can do to improve my business. At the end of the day, if you’re truly providing great service and you’re helping people by providing great medical care, those are going to win out,” he said. “I would rather, as a responsible practice owner, improve the experience and outcome for the patient.”
A version of this article first appeared on Medscape.com.
Why our brains wear out at the end of the day
The transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Once again, we’re doing an informal journal club to talk about a really interesting study, “A Neuro-metabolic Account of Why Daylong Cognitive Work Alters the Control of Economic Decisions,” that just came out. It tries to answer the question of why our brains wear out. I’m going to put myself in the corner here. Let’s walk through this study, which appears in Current Biology, by lead author Antonius Wiehler from Paris.
The big question is what’s going on with cognitive fatigue. If you look at chess players who are exerting a lot of cognitive effort, it’s well documented that over hours of play, they get worse and make more mistakes. It takes them longer to make decisions. The question is, why?
Why does your brain get tired?
To date, it’s been a little bit hard to tease that out. Now, there is some suggestion of what is responsible for this. The cognitive control center of the brain is probably somewhere in the left lateral prefrontal cortex (LLPC).
The prefrontal cortex is responsible for higher-level thinking. It’s what causes you to be inhibited. It gets shut off by alcohol and leads to impulsive behaviors. The LLPC, according to functional MRI studies, has reduced activity as people become more and more cognitively fatigued. The LLPC helps you think through choices. As you become more fatigued, this area of the brain isn’t working as well. But why would it not work as well? What is going on in that particular part of the brain? It doesn’t seem to be something simple, like glucose levels; that’s been investigated and glucose levels are pretty constant throughout the brain, regardless of cognitive task. This paper seeks to tease out what is actually going on in the LLPC when you are becoming cognitively tired.
They did an experiment where they induced cognitive fatigue, and it sounds like a painful experiment. For more than 6 hours, volunteers completed sessions during which they had to perform cognitive switching tasks. Investigators showed participants a letter, in either red or green, and the participant would respond with whether it was a vowel or a consonant or whether it was a capital or lowercase letter, based on the color. If it’s red, say whether it’s a consonant or vowel. If it’s green, say whether it’s upper- or lowercase.
It’s hard, and doing it for 6 hours is likely to induce a lot of cognitive fatigue. They had a control group as well, which is really important here. The control group also did a task like this for 6 hours, but for them, investigators didn’t change the color as often – perhaps only once per session. For the study group, they were switching colors back and forth quite a lot. They also incorporated a memory challenge that worked in a similar way.
So, what are the readouts of this study? They had a group who went through the hard cognitive challenge and a group who went through the easy cognitive challenge. They looked at a variety of metrics. I’ll describe a few.
The first is performance decrement. Did they get it wrong? What percentage of the time did the participant say “consonant” when they should have said “lowercase?”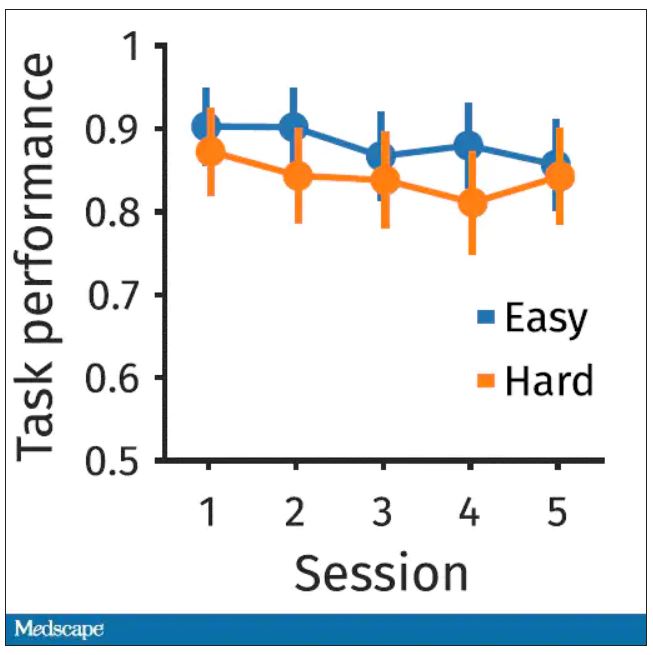
You can see here that the hard group did a little bit worse overall. It was harder, so they don’t do as well. That makes sense. But both groups kind of waned over time a little bit. It’s not as though the hard group declines much more. The slopes of those lines are pretty similar. So, not very robust findings there.
What about subjective fatigue? They asked the participants how exhausted they were from doing the tasks.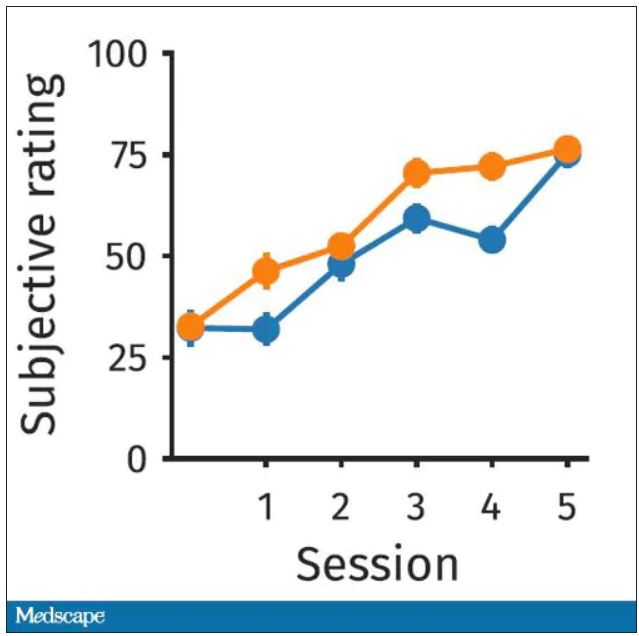
Both groups were worn out. It was a long day. There was a suggestion that the hard group became worn out a little bit sooner, but I don’t think this achieves statistical significance. Everyone was getting tired by hour 6 here.
What about response time? How quickly could the participant say “consonant,” “vowel,” “lowercase,” or “uppercase?”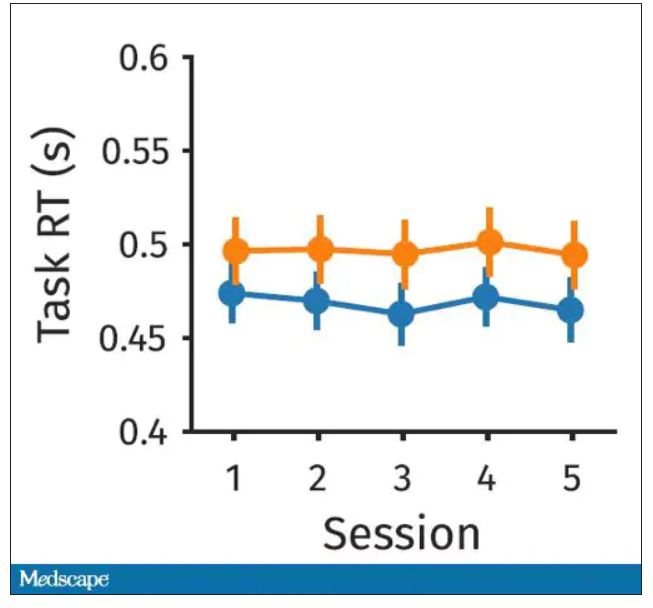
The hard group took longer to respond because it was a harder task. But over time, the response times were pretty flat.
So far there isn’t a robust readout that would make us say, oh, yeah, that is a good marker of cognitive fatigue. That’s how you measure cognitive fatigue. It’s not what people say. It’s not how quick they are. It’s not even how accurate they are.
But then the investigators got a little bit clever. Participants were asked to play a “would you rather” game, a reward game. Here are two examples.
Would you rather:
- Have a 25% chance of earning $50 OR a 95% chance of earning $17.30?
- Earn $50, but your next task session will be hard or earn $40 and your next task session will be easy?
Participants had to figure out the better odds – what should they be choosing here? They had to tease out whether they preferred lower cost lower-risk choices – when they are cognitively fatigued, which has been shown in prior studies.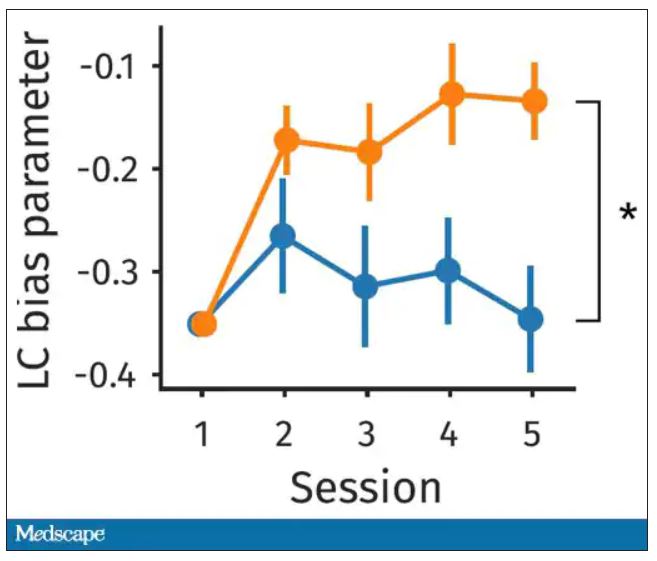
This showed a pretty dramatic difference between the groups in terms of the low-cost bias – how much more likely they were to pick the low-cost, easier choice as they became more and more cognitively fatigued. The hard group participants were more likely to pick the easy thing rather than the potentially more lucrative thing, which is really interesting when we think about how our own cognitive fatigue happens at the end of a difficult workday, how you may just be likely to go with the flow and do something easy because you just don’t have that much decision-making power left.
It would be nice to have some objective physiologic measurements for this, and they do. This is pupil dilation.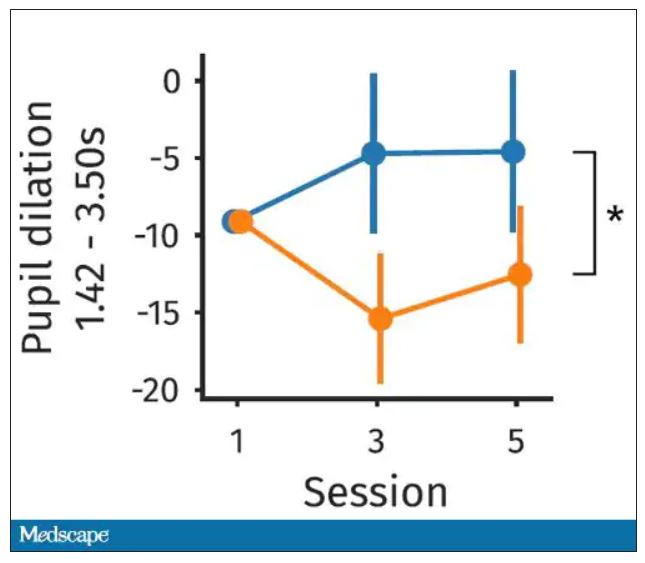
When you’re paying attention to something, your pupils dilate a little bit. They were able to show that as the hard group became more and more fatigued, pupil dilation sort of went away. In fact, if anything, their pupils constricted a little bit. But basically there was a significant difference here. The easy group’s pupils were still fine; they were still dilating. The hard group’s pupils got more sluggish. This is a physiologic correlate of what’s going on.
But again, these are all downstream of whatever is happening in the LLPC. So the real meat of this study is a functional MRI analysis, and the way they did this is pretty clever. They were looking for metabolites in the various parts of the brain using a labeled hydrogen MRI, which is even fancier than a functional MRI. It’s like MRI spectroscopy, and it can measure the levels of certain chemicals in the brain. They hypothesized that if there is a chemical that builds up when you are tired, it should build up preferentially in the LLPC.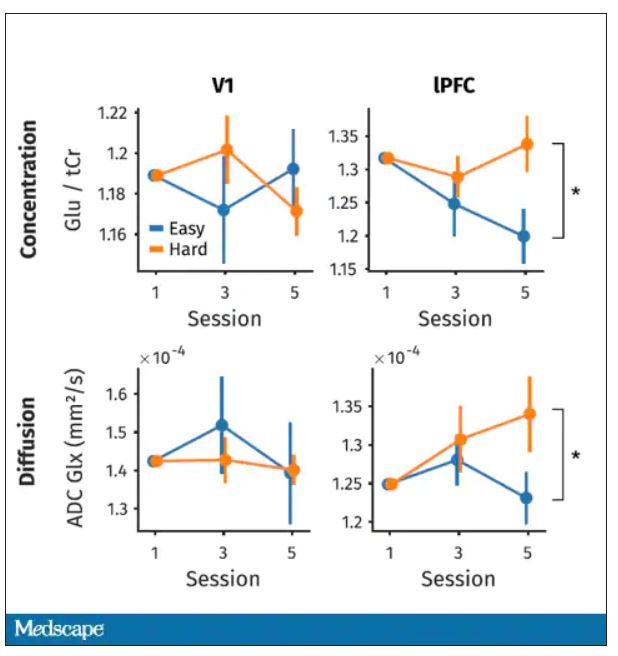
Whereas in the rest of the brain, there shouldn’t be that much difference because we know the action is happening in the LLPC. The control part of the brain is a section called V1. They looked at a variety of metabolites, but the only one that behaved the way they expected was glutamate and glutamic acid (glutamate metabolites). In the hard group, the glutamate is building up over time, so there is a higher concentration of glutamate in the LLPC but not the rest of the brain. There is also a greater diffusion of glutamate from the intracellular to the extracellular space, which suggests that it’s kind of leaking out of the cells.
So the signal here is that the thing that’s impacting that part of the brain is this buildup of glutamate. To tie this together, they showed in the scatterplot the relationship between the increase in glutamate and the low-cost bias from the decision fatigue example.
It’s not the strongest correlation, but it is statistically significant that the more glutamate in your LLPC, the more likely you are to just take the easy decision as opposed to really thinking things through. That is pretty powerful. It’s telling us that your brain making you fatigued, and making you less likely to continue to use your LLPC, may be a self-defense mechanism against a buildup of glutamate, which may be neurotoxic. And that’s a fascinating bit of homeostasis.
Of course, it makes you wonder how we might adjust glutamate levels in the brain, although maybe we should let the brain be tired if the brain wants to be tired. It reminds me of that old Far Side cartoon where the guy is raising his hand and asking: “Can I be excused? My brain is full.” That is essentially what’s happening. This part of your brain is becoming taxed and building up glutamate. There’s some kind of negative feedback loop. The authors don’t know what the receptor pathway is that down-regulates that part of the brain based on the glutamate buildup, but some kind of negative feedback loop is saying, okay, give this part of the brain a rest. Things have gone on too far here.
It’s a fascinating study, although it’s not clear what we can do with this information. It’s not clear whether we can manipulate glutamate levels in this particular part of the brain or not. But it’s nice to see some biologic correlates of a psychological phenomenon that is incredibly well described – the phenomenon of decision fatigue. I think we all feel it at the end of a hard workday. If you’ve been doing a lot of cognitively intensive tasks, you just don’t have it in you anymore. And maybe the act of a good night’s sleep is clearing out some of that glutamate in the LLPC, which lets you start over and make some good decisions again. So I hope you all make some good decisions and keep your glutamate levels low. And I’ll see you next time.
For Medscape, I’m Perry Wilson.
Dr. Wilson is an associate professor of medicine and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Once again, we’re doing an informal journal club to talk about a really interesting study, “A Neuro-metabolic Account of Why Daylong Cognitive Work Alters the Control of Economic Decisions,” that just came out. It tries to answer the question of why our brains wear out. I’m going to put myself in the corner here. Let’s walk through this study, which appears in Current Biology, by lead author Antonius Wiehler from Paris.
The big question is what’s going on with cognitive fatigue. If you look at chess players who are exerting a lot of cognitive effort, it’s well documented that over hours of play, they get worse and make more mistakes. It takes them longer to make decisions. The question is, why?
Why does your brain get tired?
To date, it’s been a little bit hard to tease that out. Now, there is some suggestion of what is responsible for this. The cognitive control center of the brain is probably somewhere in the left lateral prefrontal cortex (LLPC).
The prefrontal cortex is responsible for higher-level thinking. It’s what causes you to be inhibited. It gets shut off by alcohol and leads to impulsive behaviors. The LLPC, according to functional MRI studies, has reduced activity as people become more and more cognitively fatigued. The LLPC helps you think through choices. As you become more fatigued, this area of the brain isn’t working as well. But why would it not work as well? What is going on in that particular part of the brain? It doesn’t seem to be something simple, like glucose levels; that’s been investigated and glucose levels are pretty constant throughout the brain, regardless of cognitive task. This paper seeks to tease out what is actually going on in the LLPC when you are becoming cognitively tired.
They did an experiment where they induced cognitive fatigue, and it sounds like a painful experiment. For more than 6 hours, volunteers completed sessions during which they had to perform cognitive switching tasks. Investigators showed participants a letter, in either red or green, and the participant would respond with whether it was a vowel or a consonant or whether it was a capital or lowercase letter, based on the color. If it’s red, say whether it’s a consonant or vowel. If it’s green, say whether it’s upper- or lowercase.
It’s hard, and doing it for 6 hours is likely to induce a lot of cognitive fatigue. They had a control group as well, which is really important here. The control group also did a task like this for 6 hours, but for them, investigators didn’t change the color as often – perhaps only once per session. For the study group, they were switching colors back and forth quite a lot. They also incorporated a memory challenge that worked in a similar way.
So, what are the readouts of this study? They had a group who went through the hard cognitive challenge and a group who went through the easy cognitive challenge. They looked at a variety of metrics. I’ll describe a few.
The first is performance decrement. Did they get it wrong? What percentage of the time did the participant say “consonant” when they should have said “lowercase?”
You can see here that the hard group did a little bit worse overall. It was harder, so they don’t do as well. That makes sense. But both groups kind of waned over time a little bit. It’s not as though the hard group declines much more. The slopes of those lines are pretty similar. So, not very robust findings there.
What about subjective fatigue? They asked the participants how exhausted they were from doing the tasks.
Both groups were worn out. It was a long day. There was a suggestion that the hard group became worn out a little bit sooner, but I don’t think this achieves statistical significance. Everyone was getting tired by hour 6 here.
What about response time? How quickly could the participant say “consonant,” “vowel,” “lowercase,” or “uppercase?”
The hard group took longer to respond because it was a harder task. But over time, the response times were pretty flat.
So far there isn’t a robust readout that would make us say, oh, yeah, that is a good marker of cognitive fatigue. That’s how you measure cognitive fatigue. It’s not what people say. It’s not how quick they are. It’s not even how accurate they are.
But then the investigators got a little bit clever. Participants were asked to play a “would you rather” game, a reward game. Here are two examples.
Would you rather:
- Have a 25% chance of earning $50 OR a 95% chance of earning $17.30?
- Earn $50, but your next task session will be hard or earn $40 and your next task session will be easy?
Participants had to figure out the better odds – what should they be choosing here? They had to tease out whether they preferred lower cost lower-risk choices – when they are cognitively fatigued, which has been shown in prior studies.
This showed a pretty dramatic difference between the groups in terms of the low-cost bias – how much more likely they were to pick the low-cost, easier choice as they became more and more cognitively fatigued. The hard group participants were more likely to pick the easy thing rather than the potentially more lucrative thing, which is really interesting when we think about how our own cognitive fatigue happens at the end of a difficult workday, how you may just be likely to go with the flow and do something easy because you just don’t have that much decision-making power left.
It would be nice to have some objective physiologic measurements for this, and they do. This is pupil dilation.
When you’re paying attention to something, your pupils dilate a little bit. They were able to show that as the hard group became more and more fatigued, pupil dilation sort of went away. In fact, if anything, their pupils constricted a little bit. But basically there was a significant difference here. The easy group’s pupils were still fine; they were still dilating. The hard group’s pupils got more sluggish. This is a physiologic correlate of what’s going on.
But again, these are all downstream of whatever is happening in the LLPC. So the real meat of this study is a functional MRI analysis, and the way they did this is pretty clever. They were looking for metabolites in the various parts of the brain using a labeled hydrogen MRI, which is even fancier than a functional MRI. It’s like MRI spectroscopy, and it can measure the levels of certain chemicals in the brain. They hypothesized that if there is a chemical that builds up when you are tired, it should build up preferentially in the LLPC.
Whereas in the rest of the brain, there shouldn’t be that much difference because we know the action is happening in the LLPC. The control part of the brain is a section called V1. They looked at a variety of metabolites, but the only one that behaved the way they expected was glutamate and glutamic acid (glutamate metabolites). In the hard group, the glutamate is building up over time, so there is a higher concentration of glutamate in the LLPC but not the rest of the brain. There is also a greater diffusion of glutamate from the intracellular to the extracellular space, which suggests that it’s kind of leaking out of the cells.
So the signal here is that the thing that’s impacting that part of the brain is this buildup of glutamate. To tie this together, they showed in the scatterplot the relationship between the increase in glutamate and the low-cost bias from the decision fatigue example.
It’s not the strongest correlation, but it is statistically significant that the more glutamate in your LLPC, the more likely you are to just take the easy decision as opposed to really thinking things through. That is pretty powerful. It’s telling us that your brain making you fatigued, and making you less likely to continue to use your LLPC, may be a self-defense mechanism against a buildup of glutamate, which may be neurotoxic. And that’s a fascinating bit of homeostasis.
Of course, it makes you wonder how we might adjust glutamate levels in the brain, although maybe we should let the brain be tired if the brain wants to be tired. It reminds me of that old Far Side cartoon where the guy is raising his hand and asking: “Can I be excused? My brain is full.” That is essentially what’s happening. This part of your brain is becoming taxed and building up glutamate. There’s some kind of negative feedback loop. The authors don’t know what the receptor pathway is that down-regulates that part of the brain based on the glutamate buildup, but some kind of negative feedback loop is saying, okay, give this part of the brain a rest. Things have gone on too far here.
It’s a fascinating study, although it’s not clear what we can do with this information. It’s not clear whether we can manipulate glutamate levels in this particular part of the brain or not. But it’s nice to see some biologic correlates of a psychological phenomenon that is incredibly well described – the phenomenon of decision fatigue. I think we all feel it at the end of a hard workday. If you’ve been doing a lot of cognitively intensive tasks, you just don’t have it in you anymore. And maybe the act of a good night’s sleep is clearing out some of that glutamate in the LLPC, which lets you start over and make some good decisions again. So I hope you all make some good decisions and keep your glutamate levels low. And I’ll see you next time.
For Medscape, I’m Perry Wilson.
Dr. Wilson is an associate professor of medicine and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
Once again, we’re doing an informal journal club to talk about a really interesting study, “A Neuro-metabolic Account of Why Daylong Cognitive Work Alters the Control of Economic Decisions,” that just came out. It tries to answer the question of why our brains wear out. I’m going to put myself in the corner here. Let’s walk through this study, which appears in Current Biology, by lead author Antonius Wiehler from Paris.
The big question is what’s going on with cognitive fatigue. If you look at chess players who are exerting a lot of cognitive effort, it’s well documented that over hours of play, they get worse and make more mistakes. It takes them longer to make decisions. The question is, why?
Why does your brain get tired?
To date, it’s been a little bit hard to tease that out. Now, there is some suggestion of what is responsible for this. The cognitive control center of the brain is probably somewhere in the left lateral prefrontal cortex (LLPC).
The prefrontal cortex is responsible for higher-level thinking. It’s what causes you to be inhibited. It gets shut off by alcohol and leads to impulsive behaviors. The LLPC, according to functional MRI studies, has reduced activity as people become more and more cognitively fatigued. The LLPC helps you think through choices. As you become more fatigued, this area of the brain isn’t working as well. But why would it not work as well? What is going on in that particular part of the brain? It doesn’t seem to be something simple, like glucose levels; that’s been investigated and glucose levels are pretty constant throughout the brain, regardless of cognitive task. This paper seeks to tease out what is actually going on in the LLPC when you are becoming cognitively tired.
They did an experiment where they induced cognitive fatigue, and it sounds like a painful experiment. For more than 6 hours, volunteers completed sessions during which they had to perform cognitive switching tasks. Investigators showed participants a letter, in either red or green, and the participant would respond with whether it was a vowel or a consonant or whether it was a capital or lowercase letter, based on the color. If it’s red, say whether it’s a consonant or vowel. If it’s green, say whether it’s upper- or lowercase.
It’s hard, and doing it for 6 hours is likely to induce a lot of cognitive fatigue. They had a control group as well, which is really important here. The control group also did a task like this for 6 hours, but for them, investigators didn’t change the color as often – perhaps only once per session. For the study group, they were switching colors back and forth quite a lot. They also incorporated a memory challenge that worked in a similar way.
So, what are the readouts of this study? They had a group who went through the hard cognitive challenge and a group who went through the easy cognitive challenge. They looked at a variety of metrics. I’ll describe a few.
The first is performance decrement. Did they get it wrong? What percentage of the time did the participant say “consonant” when they should have said “lowercase?”
You can see here that the hard group did a little bit worse overall. It was harder, so they don’t do as well. That makes sense. But both groups kind of waned over time a little bit. It’s not as though the hard group declines much more. The slopes of those lines are pretty similar. So, not very robust findings there.
What about subjective fatigue? They asked the participants how exhausted they were from doing the tasks.
Both groups were worn out. It was a long day. There was a suggestion that the hard group became worn out a little bit sooner, but I don’t think this achieves statistical significance. Everyone was getting tired by hour 6 here.
What about response time? How quickly could the participant say “consonant,” “vowel,” “lowercase,” or “uppercase?”
The hard group took longer to respond because it was a harder task. But over time, the response times were pretty flat.
So far there isn’t a robust readout that would make us say, oh, yeah, that is a good marker of cognitive fatigue. That’s how you measure cognitive fatigue. It’s not what people say. It’s not how quick they are. It’s not even how accurate they are.
But then the investigators got a little bit clever. Participants were asked to play a “would you rather” game, a reward game. Here are two examples.
Would you rather:
- Have a 25% chance of earning $50 OR a 95% chance of earning $17.30?
- Earn $50, but your next task session will be hard or earn $40 and your next task session will be easy?
Participants had to figure out the better odds – what should they be choosing here? They had to tease out whether they preferred lower cost lower-risk choices – when they are cognitively fatigued, which has been shown in prior studies.
This showed a pretty dramatic difference between the groups in terms of the low-cost bias – how much more likely they were to pick the low-cost, easier choice as they became more and more cognitively fatigued. The hard group participants were more likely to pick the easy thing rather than the potentially more lucrative thing, which is really interesting when we think about how our own cognitive fatigue happens at the end of a difficult workday, how you may just be likely to go with the flow and do something easy because you just don’t have that much decision-making power left.
It would be nice to have some objective physiologic measurements for this, and they do. This is pupil dilation.
When you’re paying attention to something, your pupils dilate a little bit. They were able to show that as the hard group became more and more fatigued, pupil dilation sort of went away. In fact, if anything, their pupils constricted a little bit. But basically there was a significant difference here. The easy group’s pupils were still fine; they were still dilating. The hard group’s pupils got more sluggish. This is a physiologic correlate of what’s going on.
But again, these are all downstream of whatever is happening in the LLPC. So the real meat of this study is a functional MRI analysis, and the way they did this is pretty clever. They were looking for metabolites in the various parts of the brain using a labeled hydrogen MRI, which is even fancier than a functional MRI. It’s like MRI spectroscopy, and it can measure the levels of certain chemicals in the brain. They hypothesized that if there is a chemical that builds up when you are tired, it should build up preferentially in the LLPC.
Whereas in the rest of the brain, there shouldn’t be that much difference because we know the action is happening in the LLPC. The control part of the brain is a section called V1. They looked at a variety of metabolites, but the only one that behaved the way they expected was glutamate and glutamic acid (glutamate metabolites). In the hard group, the glutamate is building up over time, so there is a higher concentration of glutamate in the LLPC but not the rest of the brain. There is also a greater diffusion of glutamate from the intracellular to the extracellular space, which suggests that it’s kind of leaking out of the cells.
So the signal here is that the thing that’s impacting that part of the brain is this buildup of glutamate. To tie this together, they showed in the scatterplot the relationship between the increase in glutamate and the low-cost bias from the decision fatigue example.
It’s not the strongest correlation, but it is statistically significant that the more glutamate in your LLPC, the more likely you are to just take the easy decision as opposed to really thinking things through. That is pretty powerful. It’s telling us that your brain making you fatigued, and making you less likely to continue to use your LLPC, may be a self-defense mechanism against a buildup of glutamate, which may be neurotoxic. And that’s a fascinating bit of homeostasis.
Of course, it makes you wonder how we might adjust glutamate levels in the brain, although maybe we should let the brain be tired if the brain wants to be tired. It reminds me of that old Far Side cartoon where the guy is raising his hand and asking: “Can I be excused? My brain is full.” That is essentially what’s happening. This part of your brain is becoming taxed and building up glutamate. There’s some kind of negative feedback loop. The authors don’t know what the receptor pathway is that down-regulates that part of the brain based on the glutamate buildup, but some kind of negative feedback loop is saying, okay, give this part of the brain a rest. Things have gone on too far here.
It’s a fascinating study, although it’s not clear what we can do with this information. It’s not clear whether we can manipulate glutamate levels in this particular part of the brain or not. But it’s nice to see some biologic correlates of a psychological phenomenon that is incredibly well described – the phenomenon of decision fatigue. I think we all feel it at the end of a hard workday. If you’ve been doing a lot of cognitively intensive tasks, you just don’t have it in you anymore. And maybe the act of a good night’s sleep is clearing out some of that glutamate in the LLPC, which lets you start over and make some good decisions again. So I hope you all make some good decisions and keep your glutamate levels low. And I’ll see you next time.
For Medscape, I’m Perry Wilson.
Dr. Wilson is an associate professor of medicine and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
New international dermatology registry tracks monkeypox cases
The American Academy of Dermatology and the International League of Dermatological Societies (ILDS) have created a new registry that now accepts reports from health care providers worldwide about monkeypox cases and monkeypox vaccine reactions.
Patient data such as names and dates of birth will not be collected.
“As with our joint COVID-19 registry, we will be doing real-time data analysis during the outbreak,” dermatologist Esther Freeman, MD, PhD, director of MGH Global Health Dermatology at Massachusetts General Hospital, Boston, and a member of the AAD’s monkeypox task force, said in an interview. “We will to try to feed information back to our front line in terms of clinical characteristics of cases, morphology, and any unexpected findings.”
According to Dr. Freeman, the principal investigator for the COVID-19 registry, this registry has allowed the quick gathering of information about dermatologic findings of COVID-19 from over 53 countries. “We have published over 15 papers, and we share data with outside investigators wishing to do their own analysis of registry-related data,” she said. “Our most-cited paper on COVID vaccine skin reactions has been cited almost 500 times since 2021. It has been used to educate the public on vaccine side effects and to combat vaccine hesitancy.”

The monkeypox registry “doesn’t belong to any one group or person,” Dr. Freeman said. “The idea with rapid data analysis is to be able to give back to the dermatologic community what is hard for us to see with any single case: Patterns and new findings that can be helpful to share with dermatologists and other physicians worldwide, all working together to stop an outbreak.”
The American Academy of Dermatology and the International League of Dermatological Societies (ILDS) have created a new registry that now accepts reports from health care providers worldwide about monkeypox cases and monkeypox vaccine reactions.
Patient data such as names and dates of birth will not be collected.
“As with our joint COVID-19 registry, we will be doing real-time data analysis during the outbreak,” dermatologist Esther Freeman, MD, PhD, director of MGH Global Health Dermatology at Massachusetts General Hospital, Boston, and a member of the AAD’s monkeypox task force, said in an interview. “We will to try to feed information back to our front line in terms of clinical characteristics of cases, morphology, and any unexpected findings.”
According to Dr. Freeman, the principal investigator for the COVID-19 registry, this registry has allowed the quick gathering of information about dermatologic findings of COVID-19 from over 53 countries. “We have published over 15 papers, and we share data with outside investigators wishing to do their own analysis of registry-related data,” she said. “Our most-cited paper on COVID vaccine skin reactions has been cited almost 500 times since 2021. It has been used to educate the public on vaccine side effects and to combat vaccine hesitancy.”
The monkeypox registry “doesn’t belong to any one group or person,” Dr. Freeman said. “The idea with rapid data analysis is to be able to give back to the dermatologic community what is hard for us to see with any single case: Patterns and new findings that can be helpful to share with dermatologists and other physicians worldwide, all working together to stop an outbreak.”
The American Academy of Dermatology and the International League of Dermatological Societies (ILDS) have created a new registry that now accepts reports from health care providers worldwide about monkeypox cases and monkeypox vaccine reactions.
Patient data such as names and dates of birth will not be collected.
“As with our joint COVID-19 registry, we will be doing real-time data analysis during the outbreak,” dermatologist Esther Freeman, MD, PhD, director of MGH Global Health Dermatology at Massachusetts General Hospital, Boston, and a member of the AAD’s monkeypox task force, said in an interview. “We will to try to feed information back to our front line in terms of clinical characteristics of cases, morphology, and any unexpected findings.”
According to Dr. Freeman, the principal investigator for the COVID-19 registry, this registry has allowed the quick gathering of information about dermatologic findings of COVID-19 from over 53 countries. “We have published over 15 papers, and we share data with outside investigators wishing to do their own analysis of registry-related data,” she said. “Our most-cited paper on COVID vaccine skin reactions has been cited almost 500 times since 2021. It has been used to educate the public on vaccine side effects and to combat vaccine hesitancy.”
The monkeypox registry “doesn’t belong to any one group or person,” Dr. Freeman said. “The idea with rapid data analysis is to be able to give back to the dermatologic community what is hard for us to see with any single case: Patterns and new findings that can be helpful to share with dermatologists and other physicians worldwide, all working together to stop an outbreak.”
Dermatology and monkeypox: What you need to know
.

Diagnosing cases “can be hard and folks should keep a very open mind and consider monkeypox virus,” said Misha Rosenbach, MD, a University of Pennsylvania dermatologist and member of the American Academy of Dermatology’s ad hoc task force to develop monkeypox content.
Although it’s named after a primate, it turns out that monkeypox is quite the copycat. As dermatologists have learned, its lesions can look like those caused by a long list of other diseases including herpes, varicella, and syphilis. In small numbers, they can even appear to be insect bites.
To make things more complicated, a patient can have one or two lesions – or dozens. They often cluster in the anogenital area, likely reflecting transmission via sexual intercourse, unlike previous outbreaks in which lesions appeared all over the body. “We have to let go of some of our conceptions about what monkeypox might look like,” said dermatologist Esther Freeman, MD, PhD, associate professor of dermatology, Harvard University, Boston, and a member of the AAD task force.
To make things even more complicated, “the spectrum of illness that we are seeing has ranged from limited, subtle lesions to dramatic, widespread, ulcerative/necrotic lesions,” said Dr. Rosenbach, associate professor of dermatology at the University of Pennsylvania, Philadelphia.
But monkeypox has unique traits that can set it apart and pave the way toward a diagnosis, dermatologists say. And important patient data can help dermatologists gauge the likelihood of a case: Almost 99% of cases with data available have been in men, and among men with available information, 94% reported male-to-male sexual or close intimate contact during the 3 weeks before developing symptoms, according to a CDC report tracking cases from May through late July. So far, cases in women and children are extremely rare, although there have been some reported in the United States.
Are dermatologists likely to see monkeypox in the clinic? It’s unclear so far. Of four dermatologists interviewed for this article, only one has seen patients with monkeypox in person. But others say they’ve been sought for consultations. “I have been asked by infectious disease colleagues for advice remotely but have not seen it,” said dermatologist Howa Yeung, MD, MSc, assistant professor of dermatology, Emory University, Atlanta. “Most of the time, they’re catching all the symptomatic cases before any need for dermatology in-person referrals.”

Still, the rapid rate of growth of the outbreak – up from 3,487 in the United States on July 25 to 12,689 as of Aug.16 – suggests that more dermatologists will see cases, and consultations may become more common too.
Know your lesions
Lesions are the telltale signs of symptomatic monkeypox. According to a recent New England Journal of Medicine study of 528 monkeypox cases from 16 nations, diagnosed between April 27 and June 24, 2022, 95% had skin lesions (58% were vesiculopustular), most commonly in the anogenital area (73%), and on the trunk/arms/or legs (55%) and face (25%), and the palms/soles (10%).
However, “the current monkeypox outbreak often presents differently from the multiple classic vesiculopustules on the skin we see in textbooks,” Dr. Yeung said. “Sometimes people can present with throat pain or rectal pain, with isolated pharyngitis or proctitis. Sometimes there are so few lesions on the skin that it can be easily confused with a bug bite, folliculitis, herpes, dyshidrotic eczema, or other skin problems. This is where dermatologists will get consulted to clarify the diagnosis while the monkeypox PCR test is pending.”
Dr. Rosenbach, who has provided consultation services to other physicians about cases, said the lesions often appear to be vesicles or pustules, “but if you go to ‘pop’ it – e.g., for testing – it’s firm and without fluid. This is likely due to pox virus inclusion, similar to other diseases such as molluscum,” caused by another pox virus, he said. Molluscum lesions are “characteristically umbilicated, with a dimple in the center, and monkeypox lesions seem to be showing a roughly similar morphology with many bowl- or caldera-shaped lesions that are donut-like in appearance,” he added.
Over time, Dr. Rosenbach said, “lesions tend to evolve slowly from smaller flesh-colored or vaguely white firm papules to broader more umbilicated/donut-shaped lesions which may erode, ulcerate, develop a crust or scab, and then heal. The amount of scarring is not yet clear, but we anticipate it to be significant, especially in patients with more widespread or severe disease.”
Jon Peebles, MD, a dermatologist at Kaiser Permanente in Largo, Md., who has treated a few in-person monkeypox cases, said the lesions can be “exquisitely painful,” although he’s also seen patients with asymptomatic lesions. “Lesions are showing a predilection for the anogenital skin, though they can occur anywhere and not uncommonly involve the oral mucosa,” said Dr. Peebles, also a member of the AAD monkeypox task force.

Dr. Yeung said it’s important to ask patients about their sexual orientation, gender identity, and sexual behaviors. “That is the only way to know who your patients are and the only way to understand who else may be at risks and can benefit from contact tracing and additional prevention measures, such as vaccination for asymptomatic sex partners.” (The Jynneos smallpox vaccine is Food and Drug Administration–approved to prevent monkeypox, although its efficacy is not entirely clear, and there’s controversy over expanding its limited availability by administering the vaccine intradermally.)
It’s also important to keep in mind that sexually transmitted infections (STIs) are common in gay and bisexual men. “Just because the patient is diagnosed with gonorrhea or syphilis does not mean the patient cannot also have monkeypox,” Dr. Rosenbach said. Indeed, the NEJM study reported that of 377 patients screened, 29% had an STI other than HIV, mostly syphilis (9%) and gonorrhea (8%). Of all 528 patients in the study (all male or transgender/nonbinary), 41% were HIV-positive, and the median number of sex partners in the last 3 months was 5 (range, 3-15).
Testing is crucial to rule monkeypox in – or out
While monkeypox lesions can be confused for other diseases, Dr. Rosenbach said that a diagnosis can be confirmed through various tests. Varicella zoster virus (VZV) and herpes simplex virus (HSV) have distinct findings on Tzanck smears (nuclear molding, multinucleated cells), and have widely available fairly rapid tests (PCR, or in some places, DFA). “Staph and bacterial folliculitis can usually be cultured quickly,” he said. “If you have someone with no risk factors/exposure, and you test for VZV, HSV, folliculitis, and it’s negative – you should know within 24 hours in most places – then you can broaden your differential diagnosis and consider alternate explanations, including monkeypox.”
Quest Diagnostics and Labcorp, two of the largest commercial labs in the United States, are now offering monkeypox tests. Labcorp says its test has a 2- to 3-day turnaround time.
As for treatment, some physicians are prescribing off-label use of tecovirimat (also known as TPOXX or ST-246), a smallpox antiviral treatment. The CDC offers guidelines about its use. “It seems to work very fast, with patients improving in 24-72 hours,” Dr. Rosenbach said. However, “it is still very challenging to give and get. There’s a cumbersome system to prescribe it, and it needs to be shipped from the national stockpile. Dermatologists should be working with their state health department, infection control, and infectious disease doctors.”
It’s likely that dermatologists are not comfortable with the process to access the drug, he said, “but if we do not act quickly to control the current outbreak, we will all – unfortunately – need to learn to be comfortable prescribing it.”
In regard to pain control, an over-the-counter painkiller approach may be appropriate depending on comorbidities, Dr. Rosenbach said. “Some patients with very severe disease, such as perianal involvement and proctitis, have such severe pain they need to be hospitalized. This is less common.”
Recommendations pending on scarring prevention
There’s limited high-quality evidence about the prevention of scarring in diseases like monkeypox, Dr. Rosenbach noted. “Any recommendations are usually based on very small, limited, uncontrolled studies. In the case of monkeypox, truly we are off the edge of the map.”
He advises cleaning lesions with gentle soap and water – keeping in mind that contaminated towels may spread disease – and potentially using a topical ointment-based dressing such as a Vaseline/nonstick dressing or Vaseline-impregnated gauze. If there’s concern about superinfection, as can occur with staph infections, topical antibiotics such as mupirocin 2% ointment may be appropriate, he said.
“Some folks like to try silica gel sheets to prevent scarring,” Dr. Rosenbach said. “There’s not a lot of evidence to support that, but they’re unlikely to be harmful. I would personally consider them, but it really depends on the extent of disease, anatomic sites involved, and access to care.”
Emory University’s Dr. Yeung also suggested using silicone gel or sheets to optimize the scar appearance once the lesions have crusted over. “People have used lasers, microneedling, etc., to improve smallpox scar appearance,” he added, “and I’m sure dermatologists will be the ones to study what works best for treating monkeypox scars.”
As for the big picture, Dr. Yeung said that dermatologists are critical in the fight to control monkeypox: “We can help our colleagues and patients manage symptoms and wound care, advocate for vaccination and treatment, treat long-term scarring sequelae, and destigmatize LGBTQ health care.”
The dermatologists interviewed for this article report no disclosures.
.
Diagnosing cases “can be hard and folks should keep a very open mind and consider monkeypox virus,” said Misha Rosenbach, MD, a University of Pennsylvania dermatologist and member of the American Academy of Dermatology’s ad hoc task force to develop monkeypox content.
Although it’s named after a primate, it turns out that monkeypox is quite the copycat. As dermatologists have learned, its lesions can look like those caused by a long list of other diseases including herpes, varicella, and syphilis. In small numbers, they can even appear to be insect bites.
To make things more complicated, a patient can have one or two lesions – or dozens. They often cluster in the anogenital area, likely reflecting transmission via sexual intercourse, unlike previous outbreaks in which lesions appeared all over the body. “We have to let go of some of our conceptions about what monkeypox might look like,” said dermatologist Esther Freeman, MD, PhD, associate professor of dermatology, Harvard University, Boston, and a member of the AAD task force.
To make things even more complicated, “the spectrum of illness that we are seeing has ranged from limited, subtle lesions to dramatic, widespread, ulcerative/necrotic lesions,” said Dr. Rosenbach, associate professor of dermatology at the University of Pennsylvania, Philadelphia.
But monkeypox has unique traits that can set it apart and pave the way toward a diagnosis, dermatologists say. And important patient data can help dermatologists gauge the likelihood of a case: Almost 99% of cases with data available have been in men, and among men with available information, 94% reported male-to-male sexual or close intimate contact during the 3 weeks before developing symptoms, according to a CDC report tracking cases from May through late July. So far, cases in women and children are extremely rare, although there have been some reported in the United States.
Are dermatologists likely to see monkeypox in the clinic? It’s unclear so far. Of four dermatologists interviewed for this article, only one has seen patients with monkeypox in person. But others say they’ve been sought for consultations. “I have been asked by infectious disease colleagues for advice remotely but have not seen it,” said dermatologist Howa Yeung, MD, MSc, assistant professor of dermatology, Emory University, Atlanta. “Most of the time, they’re catching all the symptomatic cases before any need for dermatology in-person referrals.”
Still, the rapid rate of growth of the outbreak – up from 3,487 in the United States on July 25 to 12,689 as of Aug.16 – suggests that more dermatologists will see cases, and consultations may become more common too.
Know your lesions
Lesions are the telltale signs of symptomatic monkeypox. According to a recent New England Journal of Medicine study of 528 monkeypox cases from 16 nations, diagnosed between April 27 and June 24, 2022, 95% had skin lesions (58% were vesiculopustular), most commonly in the anogenital area (73%), and on the trunk/arms/or legs (55%) and face (25%), and the palms/soles (10%).
However, “the current monkeypox outbreak often presents differently from the multiple classic vesiculopustules on the skin we see in textbooks,” Dr. Yeung said. “Sometimes people can present with throat pain or rectal pain, with isolated pharyngitis or proctitis. Sometimes there are so few lesions on the skin that it can be easily confused with a bug bite, folliculitis, herpes, dyshidrotic eczema, or other skin problems. This is where dermatologists will get consulted to clarify the diagnosis while the monkeypox PCR test is pending.”
Dr. Rosenbach, who has provided consultation services to other physicians about cases, said the lesions often appear to be vesicles or pustules, “but if you go to ‘pop’ it – e.g., for testing – it’s firm and without fluid. This is likely due to pox virus inclusion, similar to other diseases such as molluscum,” caused by another pox virus, he said. Molluscum lesions are “characteristically umbilicated, with a dimple in the center, and monkeypox lesions seem to be showing a roughly similar morphology with many bowl- or caldera-shaped lesions that are donut-like in appearance,” he added.
Over time, Dr. Rosenbach said, “lesions tend to evolve slowly from smaller flesh-colored or vaguely white firm papules to broader more umbilicated/donut-shaped lesions which may erode, ulcerate, develop a crust or scab, and then heal. The amount of scarring is not yet clear, but we anticipate it to be significant, especially in patients with more widespread or severe disease.”
Jon Peebles, MD, a dermatologist at Kaiser Permanente in Largo, Md., who has treated a few in-person monkeypox cases, said the lesions can be “exquisitely painful,” although he’s also seen patients with asymptomatic lesions. “Lesions are showing a predilection for the anogenital skin, though they can occur anywhere and not uncommonly involve the oral mucosa,” said Dr. Peebles, also a member of the AAD monkeypox task force.
Dr. Yeung said it’s important to ask patients about their sexual orientation, gender identity, and sexual behaviors. “That is the only way to know who your patients are and the only way to understand who else may be at risks and can benefit from contact tracing and additional prevention measures, such as vaccination for asymptomatic sex partners.” (The Jynneos smallpox vaccine is Food and Drug Administration–approved to prevent monkeypox, although its efficacy is not entirely clear, and there’s controversy over expanding its limited availability by administering the vaccine intradermally.)
It’s also important to keep in mind that sexually transmitted infections (STIs) are common in gay and bisexual men. “Just because the patient is diagnosed with gonorrhea or syphilis does not mean the patient cannot also have monkeypox,” Dr. Rosenbach said. Indeed, the NEJM study reported that of 377 patients screened, 29% had an STI other than HIV, mostly syphilis (9%) and gonorrhea (8%). Of all 528 patients in the study (all male or transgender/nonbinary), 41% were HIV-positive, and the median number of sex partners in the last 3 months was 5 (range, 3-15).
Testing is crucial to rule monkeypox in – or out
While monkeypox lesions can be confused for other diseases, Dr. Rosenbach said that a diagnosis can be confirmed through various tests. Varicella zoster virus (VZV) and herpes simplex virus (HSV) have distinct findings on Tzanck smears (nuclear molding, multinucleated cells), and have widely available fairly rapid tests (PCR, or in some places, DFA). “Staph and bacterial folliculitis can usually be cultured quickly,” he said. “If you have someone with no risk factors/exposure, and you test for VZV, HSV, folliculitis, and it’s negative – you should know within 24 hours in most places – then you can broaden your differential diagnosis and consider alternate explanations, including monkeypox.”
Quest Diagnostics and Labcorp, two of the largest commercial labs in the United States, are now offering monkeypox tests. Labcorp says its test has a 2- to 3-day turnaround time.
As for treatment, some physicians are prescribing off-label use of tecovirimat (also known as TPOXX or ST-246), a smallpox antiviral treatment. The CDC offers guidelines about its use. “It seems to work very fast, with patients improving in 24-72 hours,” Dr. Rosenbach said. However, “it is still very challenging to give and get. There’s a cumbersome system to prescribe it, and it needs to be shipped from the national stockpile. Dermatologists should be working with their state health department, infection control, and infectious disease doctors.”
It’s likely that dermatologists are not comfortable with the process to access the drug, he said, “but if we do not act quickly to control the current outbreak, we will all – unfortunately – need to learn to be comfortable prescribing it.”
In regard to pain control, an over-the-counter painkiller approach may be appropriate depending on comorbidities, Dr. Rosenbach said. “Some patients with very severe disease, such as perianal involvement and proctitis, have such severe pain they need to be hospitalized. This is less common.”
Recommendations pending on scarring prevention
There’s limited high-quality evidence about the prevention of scarring in diseases like monkeypox, Dr. Rosenbach noted. “Any recommendations are usually based on very small, limited, uncontrolled studies. In the case of monkeypox, truly we are off the edge of the map.”
He advises cleaning lesions with gentle soap and water – keeping in mind that contaminated towels may spread disease – and potentially using a topical ointment-based dressing such as a Vaseline/nonstick dressing or Vaseline-impregnated gauze. If there’s concern about superinfection, as can occur with staph infections, topical antibiotics such as mupirocin 2% ointment may be appropriate, he said.
“Some folks like to try silica gel sheets to prevent scarring,” Dr. Rosenbach said. “There’s not a lot of evidence to support that, but they’re unlikely to be harmful. I would personally consider them, but it really depends on the extent of disease, anatomic sites involved, and access to care.”
Emory University’s Dr. Yeung also suggested using silicone gel or sheets to optimize the scar appearance once the lesions have crusted over. “People have used lasers, microneedling, etc., to improve smallpox scar appearance,” he added, “and I’m sure dermatologists will be the ones to study what works best for treating monkeypox scars.”
As for the big picture, Dr. Yeung said that dermatologists are critical in the fight to control monkeypox: “We can help our colleagues and patients manage symptoms and wound care, advocate for vaccination and treatment, treat long-term scarring sequelae, and destigmatize LGBTQ health care.”
The dermatologists interviewed for this article report no disclosures.
.
Diagnosing cases “can be hard and folks should keep a very open mind and consider monkeypox virus,” said Misha Rosenbach, MD, a University of Pennsylvania dermatologist and member of the American Academy of Dermatology’s ad hoc task force to develop monkeypox content.
Although it’s named after a primate, it turns out that monkeypox is quite the copycat. As dermatologists have learned, its lesions can look like those caused by a long list of other diseases including herpes, varicella, and syphilis. In small numbers, they can even appear to be insect bites.
To make things more complicated, a patient can have one or two lesions – or dozens. They often cluster in the anogenital area, likely reflecting transmission via sexual intercourse, unlike previous outbreaks in which lesions appeared all over the body. “We have to let go of some of our conceptions about what monkeypox might look like,” said dermatologist Esther Freeman, MD, PhD, associate professor of dermatology, Harvard University, Boston, and a member of the AAD task force.
To make things even more complicated, “the spectrum of illness that we are seeing has ranged from limited, subtle lesions to dramatic, widespread, ulcerative/necrotic lesions,” said Dr. Rosenbach, associate professor of dermatology at the University of Pennsylvania, Philadelphia.
But monkeypox has unique traits that can set it apart and pave the way toward a diagnosis, dermatologists say. And important patient data can help dermatologists gauge the likelihood of a case: Almost 99% of cases with data available have been in men, and among men with available information, 94% reported male-to-male sexual or close intimate contact during the 3 weeks before developing symptoms, according to a CDC report tracking cases from May through late July. So far, cases in women and children are extremely rare, although there have been some reported in the United States.
Are dermatologists likely to see monkeypox in the clinic? It’s unclear so far. Of four dermatologists interviewed for this article, only one has seen patients with monkeypox in person. But others say they’ve been sought for consultations. “I have been asked by infectious disease colleagues for advice remotely but have not seen it,” said dermatologist Howa Yeung, MD, MSc, assistant professor of dermatology, Emory University, Atlanta. “Most of the time, they’re catching all the symptomatic cases before any need for dermatology in-person referrals.”
Still, the rapid rate of growth of the outbreak – up from 3,487 in the United States on July 25 to 12,689 as of Aug.16 – suggests that more dermatologists will see cases, and consultations may become more common too.
Know your lesions
Lesions are the telltale signs of symptomatic monkeypox. According to a recent New England Journal of Medicine study of 528 monkeypox cases from 16 nations, diagnosed between April 27 and June 24, 2022, 95% had skin lesions (58% were vesiculopustular), most commonly in the anogenital area (73%), and on the trunk/arms/or legs (55%) and face (25%), and the palms/soles (10%).
However, “the current monkeypox outbreak often presents differently from the multiple classic vesiculopustules on the skin we see in textbooks,” Dr. Yeung said. “Sometimes people can present with throat pain or rectal pain, with isolated pharyngitis or proctitis. Sometimes there are so few lesions on the skin that it can be easily confused with a bug bite, folliculitis, herpes, dyshidrotic eczema, or other skin problems. This is where dermatologists will get consulted to clarify the diagnosis while the monkeypox PCR test is pending.”
Dr. Rosenbach, who has provided consultation services to other physicians about cases, said the lesions often appear to be vesicles or pustules, “but if you go to ‘pop’ it – e.g., for testing – it’s firm and without fluid. This is likely due to pox virus inclusion, similar to other diseases such as molluscum,” caused by another pox virus, he said. Molluscum lesions are “characteristically umbilicated, with a dimple in the center, and monkeypox lesions seem to be showing a roughly similar morphology with many bowl- or caldera-shaped lesions that are donut-like in appearance,” he added.
Over time, Dr. Rosenbach said, “lesions tend to evolve slowly from smaller flesh-colored or vaguely white firm papules to broader more umbilicated/donut-shaped lesions which may erode, ulcerate, develop a crust or scab, and then heal. The amount of scarring is not yet clear, but we anticipate it to be significant, especially in patients with more widespread or severe disease.”
Jon Peebles, MD, a dermatologist at Kaiser Permanente in Largo, Md., who has treated a few in-person monkeypox cases, said the lesions can be “exquisitely painful,” although he’s also seen patients with asymptomatic lesions. “Lesions are showing a predilection for the anogenital skin, though they can occur anywhere and not uncommonly involve the oral mucosa,” said Dr. Peebles, also a member of the AAD monkeypox task force.
Dr. Yeung said it’s important to ask patients about their sexual orientation, gender identity, and sexual behaviors. “That is the only way to know who your patients are and the only way to understand who else may be at risks and can benefit from contact tracing and additional prevention measures, such as vaccination for asymptomatic sex partners.” (The Jynneos smallpox vaccine is Food and Drug Administration–approved to prevent monkeypox, although its efficacy is not entirely clear, and there’s controversy over expanding its limited availability by administering the vaccine intradermally.)
It’s also important to keep in mind that sexually transmitted infections (STIs) are common in gay and bisexual men. “Just because the patient is diagnosed with gonorrhea or syphilis does not mean the patient cannot also have monkeypox,” Dr. Rosenbach said. Indeed, the NEJM study reported that of 377 patients screened, 29% had an STI other than HIV, mostly syphilis (9%) and gonorrhea (8%). Of all 528 patients in the study (all male or transgender/nonbinary), 41% were HIV-positive, and the median number of sex partners in the last 3 months was 5 (range, 3-15).
Testing is crucial to rule monkeypox in – or out
While monkeypox lesions can be confused for other diseases, Dr. Rosenbach said that a diagnosis can be confirmed through various tests. Varicella zoster virus (VZV) and herpes simplex virus (HSV) have distinct findings on Tzanck smears (nuclear molding, multinucleated cells), and have widely available fairly rapid tests (PCR, or in some places, DFA). “Staph and bacterial folliculitis can usually be cultured quickly,” he said. “If you have someone with no risk factors/exposure, and you test for VZV, HSV, folliculitis, and it’s negative – you should know within 24 hours in most places – then you can broaden your differential diagnosis and consider alternate explanations, including monkeypox.”
Quest Diagnostics and Labcorp, two of the largest commercial labs in the United States, are now offering monkeypox tests. Labcorp says its test has a 2- to 3-day turnaround time.
As for treatment, some physicians are prescribing off-label use of tecovirimat (also known as TPOXX or ST-246), a smallpox antiviral treatment. The CDC offers guidelines about its use. “It seems to work very fast, with patients improving in 24-72 hours,” Dr. Rosenbach said. However, “it is still very challenging to give and get. There’s a cumbersome system to prescribe it, and it needs to be shipped from the national stockpile. Dermatologists should be working with their state health department, infection control, and infectious disease doctors.”
It’s likely that dermatologists are not comfortable with the process to access the drug, he said, “but if we do not act quickly to control the current outbreak, we will all – unfortunately – need to learn to be comfortable prescribing it.”
In regard to pain control, an over-the-counter painkiller approach may be appropriate depending on comorbidities, Dr. Rosenbach said. “Some patients with very severe disease, such as perianal involvement and proctitis, have such severe pain they need to be hospitalized. This is less common.”
Recommendations pending on scarring prevention
There’s limited high-quality evidence about the prevention of scarring in diseases like monkeypox, Dr. Rosenbach noted. “Any recommendations are usually based on very small, limited, uncontrolled studies. In the case of monkeypox, truly we are off the edge of the map.”
He advises cleaning lesions with gentle soap and water – keeping in mind that contaminated towels may spread disease – and potentially using a topical ointment-based dressing such as a Vaseline/nonstick dressing or Vaseline-impregnated gauze. If there’s concern about superinfection, as can occur with staph infections, topical antibiotics such as mupirocin 2% ointment may be appropriate, he said.
“Some folks like to try silica gel sheets to prevent scarring,” Dr. Rosenbach said. “There’s not a lot of evidence to support that, but they’re unlikely to be harmful. I would personally consider them, but it really depends on the extent of disease, anatomic sites involved, and access to care.”
Emory University’s Dr. Yeung also suggested using silicone gel or sheets to optimize the scar appearance once the lesions have crusted over. “People have used lasers, microneedling, etc., to improve smallpox scar appearance,” he added, “and I’m sure dermatologists will be the ones to study what works best for treating monkeypox scars.”
As for the big picture, Dr. Yeung said that dermatologists are critical in the fight to control monkeypox: “We can help our colleagues and patients manage symptoms and wound care, advocate for vaccination and treatment, treat long-term scarring sequelae, and destigmatize LGBTQ health care.”
The dermatologists interviewed for this article report no disclosures.
Exaggerated Facial Lines on the Forehead and Cheeks
The Diagnosis: Pachydermoperiostosis
Histopathology of the forehead punch biopsy demonstrated sebaceous hyperplasia with an occupation rate of greater than 40%, increased mucin, elastic fiber degeneration, and fibrosis. Pachydermia is graded from 0 to 3 depending on the degree of these changes; our patient met criteria for grade 3 pachydermia (Figure 1). Radiography revealed diffuse cortical thickening of the long bones that was most marked in the left femur (Figure 2); however, no other findings were demonstrative of Paget disease.
. B, Colloidal iron stain demonstrated increased mucin (original magnification ×4). C, Verhoeff-van Gieson stain showed elastic fiber")
Pachydermoperiostosis (PDP)(also known as Touraine-Solente-Golé syndrome or primary hypertrophic osteoarthropathy) is a rare genetic condition that affects both the dermatologic and skeletal systems. Clinical features of the disease include progressive thickening and furrowing of the skin on the scalp and face (known as pachydermia), digital clubbing, and periostosis. Other potential cutaneous features include seborrhea, acne, hyperhidrosis of the palms and soles, cutis verticis gyrata, eczema, and a burning sensation of the hands and feet. Myelofibrosis and gastrointestinal abnormalities also have been reported.1

The disease typically affects males (7:1 ratio); also, men typically display a more severe phenotype of the disease.2 It most commonly begins during puberty and follows a generally progressive course of 5 to 20 years before eventually stabilizing. Both autosomal-dominant with incomplete penetrance and recessive inheritance versions of PDP can occur. Prostaglandin E2 (PGE2) has been implicated in the pathogenesis of PDP; PGE2 is important in the inflammatory response and may evolve from disrupted protein degradation pathways.3 Sasaki et al4 additionally reported that the severity of pachydermia clinically and histologically appeared to correlate with the serum PGE2 levels in affected patients. Prostaglandin E2 causes a vasodilatory effect, perhaps explaining the clubbing observed in PDP, and also modifies the activity of osteoblasts and osteoclasts, causing the bone remodeling observed in the disease.4
In our patient, the initial differential diagnosis included PDP, as well as lepromatous leprosy, acromegaly, Paget disease of the bone, amyloidosis, scleromyxedema, and cutaneous T-cell lymphoma. However, the time course of the disease, lack of numerous symmetric thickened plaques and madarosis, and pathology argued against lepromatous leprosy. Acromegaly was ruled out due to lack of macroglossia as well as laboratory analysis within reference range including IGF-1 levels and thyroid function tests. Biopsy findings ultimately ruled out amyloidosis and cutaneous T-cell lymphoma. The bone scan revealed diffuse cortical thickening consistent with PDP, and there were no other radiologic findings suggestive of Paget disease. Pachydermoperiostosis is diagnosed using the Borochowitz criteria, which entails that 2 of the following 4 fulfillment criteria must be met: familial transmission, pachydermia, digital clubbing, and/or bony involvement with evidence of radiologic alterations or pain. Our patient met all 4 criteria. The clinical manifestations of PDP are variable with respect to skin and bone changes. The various clinical expressions include the complete form (ie, pachydermia, cutis verticis gyrata, periostosis), the incomplete form (ie, absence of cutis verticis gyrata), and forme fruste (ie, pachydermia with minimal or absent periostosis).5
Management for PDP involves surgical correction for cosmesis as well as for functional concerns if present. Symptoms secondary to periostosis should be managed with symptomatic treatment such as nonsteroidal antiinflammatory drugs. Patients managed with etoricoxib, a COX-2–selective nonsteroidal anti-inflammatory drug, have had normalized inflammatory markers that resulted in the lessening of forehead skin folds. Oral aescin has been shown to relieve joint pain due to its antiedematous effect.6 Our patient received treatment with nonsteroidal anti-inflammatory drugs for symptomatic management of the associated joint pain but unfortunately was lost to follow-up.
- Castori M, Sinibaldi L, Mingarelli R, et al. Pachydermoperiostosis: an update. Clin Genet. 2005;68:477-486.
- Reginato AJ, Shipachasse V, Guerrero R. Familial idiopathic hypertrophic osteoarthropathy and cranial suture defects in children. Skel Radiol. 1982;8:105-109.
- Coggins KG, Coffman TM, Koller BH. The Hippocratic finger points the blame at PGE2. Nat Genet. 2008;40:691-692.
- Sasaki T, Niizeki H, Shimizu A, et al. Identification of mutations in the prostaglandin transporter gene SLCO2A1 and its phenotype-genotype correlation in Japanese patients with pachydermoperiostosis. J Dermatol Sci. 2012;68:36-44.
- Bhaskaranand K, Shetty RR, Bhat AK. Pachydermoperiostosis: three case reports. J Orthop Surg (Hong Kong). 2001;9:61-66.
- Zhang H, Yang B. Successful treatment of pachydermoperiostosis patients with etoricoxib, aescin, and arthroscopic synovectomy: two case reports. Medicine (Baltimore). 2017;96:E8865.
The Diagnosis: Pachydermoperiostosis
Histopathology of the forehead punch biopsy demonstrated sebaceous hyperplasia with an occupation rate of greater than 40%, increased mucin, elastic fiber degeneration, and fibrosis. Pachydermia is graded from 0 to 3 depending on the degree of these changes; our patient met criteria for grade 3 pachydermia (Figure 1). Radiography revealed diffuse cortical thickening of the long bones that was most marked in the left femur (Figure 2); however, no other findings were demonstrative of Paget disease.
Pachydermoperiostosis (PDP)(also known as Touraine-Solente-Golé syndrome or primary hypertrophic osteoarthropathy) is a rare genetic condition that affects both the dermatologic and skeletal systems. Clinical features of the disease include progressive thickening and furrowing of the skin on the scalp and face (known as pachydermia), digital clubbing, and periostosis. Other potential cutaneous features include seborrhea, acne, hyperhidrosis of the palms and soles, cutis verticis gyrata, eczema, and a burning sensation of the hands and feet. Myelofibrosis and gastrointestinal abnormalities also have been reported.1
The disease typically affects males (7:1 ratio); also, men typically display a more severe phenotype of the disease.2 It most commonly begins during puberty and follows a generally progressive course of 5 to 20 years before eventually stabilizing. Both autosomal-dominant with incomplete penetrance and recessive inheritance versions of PDP can occur. Prostaglandin E2 (PGE2) has been implicated in the pathogenesis of PDP; PGE2 is important in the inflammatory response and may evolve from disrupted protein degradation pathways.3 Sasaki et al4 additionally reported that the severity of pachydermia clinically and histologically appeared to correlate with the serum PGE2 levels in affected patients. Prostaglandin E2 causes a vasodilatory effect, perhaps explaining the clubbing observed in PDP, and also modifies the activity of osteoblasts and osteoclasts, causing the bone remodeling observed in the disease.4
In our patient, the initial differential diagnosis included PDP, as well as lepromatous leprosy, acromegaly, Paget disease of the bone, amyloidosis, scleromyxedema, and cutaneous T-cell lymphoma. However, the time course of the disease, lack of numerous symmetric thickened plaques and madarosis, and pathology argued against lepromatous leprosy. Acromegaly was ruled out due to lack of macroglossia as well as laboratory analysis within reference range including IGF-1 levels and thyroid function tests. Biopsy findings ultimately ruled out amyloidosis and cutaneous T-cell lymphoma. The bone scan revealed diffuse cortical thickening consistent with PDP, and there were no other radiologic findings suggestive of Paget disease. Pachydermoperiostosis is diagnosed using the Borochowitz criteria, which entails that 2 of the following 4 fulfillment criteria must be met: familial transmission, pachydermia, digital clubbing, and/or bony involvement with evidence of radiologic alterations or pain. Our patient met all 4 criteria. The clinical manifestations of PDP are variable with respect to skin and bone changes. The various clinical expressions include the complete form (ie, pachydermia, cutis verticis gyrata, periostosis), the incomplete form (ie, absence of cutis verticis gyrata), and forme fruste (ie, pachydermia with minimal or absent periostosis).5
Management for PDP involves surgical correction for cosmesis as well as for functional concerns if present. Symptoms secondary to periostosis should be managed with symptomatic treatment such as nonsteroidal antiinflammatory drugs. Patients managed with etoricoxib, a COX-2–selective nonsteroidal anti-inflammatory drug, have had normalized inflammatory markers that resulted in the lessening of forehead skin folds. Oral aescin has been shown to relieve joint pain due to its antiedematous effect.6 Our patient received treatment with nonsteroidal anti-inflammatory drugs for symptomatic management of the associated joint pain but unfortunately was lost to follow-up.
The Diagnosis: Pachydermoperiostosis
Histopathology of the forehead punch biopsy demonstrated sebaceous hyperplasia with an occupation rate of greater than 40%, increased mucin, elastic fiber degeneration, and fibrosis. Pachydermia is graded from 0 to 3 depending on the degree of these changes; our patient met criteria for grade 3 pachydermia (Figure 1). Radiography revealed diffuse cortical thickening of the long bones that was most marked in the left femur (Figure 2); however, no other findings were demonstrative of Paget disease.
Pachydermoperiostosis (PDP)(also known as Touraine-Solente-Golé syndrome or primary hypertrophic osteoarthropathy) is a rare genetic condition that affects both the dermatologic and skeletal systems. Clinical features of the disease include progressive thickening and furrowing of the skin on the scalp and face (known as pachydermia), digital clubbing, and periostosis. Other potential cutaneous features include seborrhea, acne, hyperhidrosis of the palms and soles, cutis verticis gyrata, eczema, and a burning sensation of the hands and feet. Myelofibrosis and gastrointestinal abnormalities also have been reported.1
The disease typically affects males (7:1 ratio); also, men typically display a more severe phenotype of the disease.2 It most commonly begins during puberty and follows a generally progressive course of 5 to 20 years before eventually stabilizing. Both autosomal-dominant with incomplete penetrance and recessive inheritance versions of PDP can occur. Prostaglandin E2 (PGE2) has been implicated in the pathogenesis of PDP; PGE2 is important in the inflammatory response and may evolve from disrupted protein degradation pathways.3 Sasaki et al4 additionally reported that the severity of pachydermia clinically and histologically appeared to correlate with the serum PGE2 levels in affected patients. Prostaglandin E2 causes a vasodilatory effect, perhaps explaining the clubbing observed in PDP, and also modifies the activity of osteoblasts and osteoclasts, causing the bone remodeling observed in the disease.4
In our patient, the initial differential diagnosis included PDP, as well as lepromatous leprosy, acromegaly, Paget disease of the bone, amyloidosis, scleromyxedema, and cutaneous T-cell lymphoma. However, the time course of the disease, lack of numerous symmetric thickened plaques and madarosis, and pathology argued against lepromatous leprosy. Acromegaly was ruled out due to lack of macroglossia as well as laboratory analysis within reference range including IGF-1 levels and thyroid function tests. Biopsy findings ultimately ruled out amyloidosis and cutaneous T-cell lymphoma. The bone scan revealed diffuse cortical thickening consistent with PDP, and there were no other radiologic findings suggestive of Paget disease. Pachydermoperiostosis is diagnosed using the Borochowitz criteria, which entails that 2 of the following 4 fulfillment criteria must be met: familial transmission, pachydermia, digital clubbing, and/or bony involvement with evidence of radiologic alterations or pain. Our patient met all 4 criteria. The clinical manifestations of PDP are variable with respect to skin and bone changes. The various clinical expressions include the complete form (ie, pachydermia, cutis verticis gyrata, periostosis), the incomplete form (ie, absence of cutis verticis gyrata), and forme fruste (ie, pachydermia with minimal or absent periostosis).5
Management for PDP involves surgical correction for cosmesis as well as for functional concerns if present. Symptoms secondary to periostosis should be managed with symptomatic treatment such as nonsteroidal antiinflammatory drugs. Patients managed with etoricoxib, a COX-2–selective nonsteroidal anti-inflammatory drug, have had normalized inflammatory markers that resulted in the lessening of forehead skin folds. Oral aescin has been shown to relieve joint pain due to its antiedematous effect.6 Our patient received treatment with nonsteroidal anti-inflammatory drugs for symptomatic management of the associated joint pain but unfortunately was lost to follow-up.
- Castori M, Sinibaldi L, Mingarelli R, et al. Pachydermoperiostosis: an update. Clin Genet. 2005;68:477-486.
- Reginato AJ, Shipachasse V, Guerrero R. Familial idiopathic hypertrophic osteoarthropathy and cranial suture defects in children. Skel Radiol. 1982;8:105-109.
- Coggins KG, Coffman TM, Koller BH. The Hippocratic finger points the blame at PGE2. Nat Genet. 2008;40:691-692.
- Sasaki T, Niizeki H, Shimizu A, et al. Identification of mutations in the prostaglandin transporter gene SLCO2A1 and its phenotype-genotype correlation in Japanese patients with pachydermoperiostosis. J Dermatol Sci. 2012;68:36-44.
- Bhaskaranand K, Shetty RR, Bhat AK. Pachydermoperiostosis: three case reports. J Orthop Surg (Hong Kong). 2001;9:61-66.
- Zhang H, Yang B. Successful treatment of pachydermoperiostosis patients with etoricoxib, aescin, and arthroscopic synovectomy: two case reports. Medicine (Baltimore). 2017;96:E8865.
- Castori M, Sinibaldi L, Mingarelli R, et al. Pachydermoperiostosis: an update. Clin Genet. 2005;68:477-486.
- Reginato AJ, Shipachasse V, Guerrero R. Familial idiopathic hypertrophic osteoarthropathy and cranial suture defects in children. Skel Radiol. 1982;8:105-109.
- Coggins KG, Coffman TM, Koller BH. The Hippocratic finger points the blame at PGE2. Nat Genet. 2008;40:691-692.
- Sasaki T, Niizeki H, Shimizu A, et al. Identification of mutations in the prostaglandin transporter gene SLCO2A1 and its phenotype-genotype correlation in Japanese patients with pachydermoperiostosis. J Dermatol Sci. 2012;68:36-44.
- Bhaskaranand K, Shetty RR, Bhat AK. Pachydermoperiostosis: three case reports. J Orthop Surg (Hong Kong). 2001;9:61-66.
- Zhang H, Yang B. Successful treatment of pachydermoperiostosis patients with etoricoxib, aescin, and arthroscopic synovectomy: two case reports. Medicine (Baltimore). 2017;96:E8865.
A 36-year-old man presented to the emergency department with an olecranon fracture after falling from a tree. The patient had a medical history of type 2 diabetes mellitus and a surgical history of facial cosmetic surgery. He underwent internal fixation with orthopedic surgery for the olecranon fracture, and dermatology subsequently was consulted due to diffuse skin changes on the face. He reported that these dermatologic changes began around 17 years of age and had progressed to the current presentation. He denied itching, burning, pain, or contact with armadillos. A family history revealed the patient’s brother also had a similar appearance. Physical examination revealed exaggerated facial lines on the forehead (top) and cheeks. Digital clubbing and skin thickening were noted on the hands (bottom) and feet; examination of the back revealed multiple hypopigmented patches. Observation of the scalp showed multiple symmetric ridges and grooves with sparse overlying hair consistent with cutis verticis gyrata. A punch biopsy of the forehead was obtained as well as bone radiography taken previously by the primary team.


Diagnostic criterion may hide borderline personality disorder
Investigators compared characteristics of almost 400 psychiatric outpatients diagnosed with BPD. About half of the participants met the suicidality/self-injury diagnostic criterion for the disorder, while the other half did not.
Results showed no differences between the two groups in degree of impairment in occupational or social functioning, comorbid psychiatric disorders, history of childhood trauma, or severity of depression, anxiety, or anger.
“Just because a person doesn’t engage in self-harm or suicidal behavior doesn’t mean that the person is free of borderline personality disorder,” lead author Mark Zimmerman, MD, professor of psychiatry and human behavior, Brown University, Providence, R.I., told this news organization.

“Clinicians need to screen for borderline personality disorder in patients with other suggestive symptoms, even if those patients don’t self-harm, just as they would for similar patients who do self-harm,” said Dr. Zimmerman, who is also the director of the Outpatient Division at the Partial Hospital Program, Rhode Island Hospital.
The findings were published online in Psychological Medicine.
A ‘polythetic diagnosis’
Dr. Zimmerman noted the impetus for conducting the study originated with a patient he saw who had all of the features of BPD except for self-harm and suicidality. However, because she didn’t have those two features, she was told by her therapist she could not have BPD.
“This sparked the idea that perhaps there are other individuals whose BPD may not be recognized because they don’t engage in self-harm or suicidal behavior,” Dr. Zimmerman said.
“Most individuals with BPD don’t present for treatment saying, ‘I’m here because I don’t have a sense of myself’ or ‘I feel empty inside’ – but they do say, ‘I’m here because I’m cutting myself’ or ‘I’m suicidal,’ ” he added.
The investigators wondered if there were other “hidden” cases of BPD that were being missed by therapists.
They had previously analyzed each diagnostic criterion for BPD to ascertain its sensitivity. “We had been interested in wanting to see whether there was a criterion so frequent in BPD that every patient with BPD has it,” Dr. Zimmerman said.
BPD is a “polythetic diagnosis,” he added. It is “based on a list of features, with a certain minimum number of those features necessary to make the diagnosis rather than one specific criterion.”
His group’s previous research showed affective instability criterion to be present in more than 90% of individuals with BPD. “It had a very high negative predictive value, meaning that if you didn’t have affective instability, you didn’t have the disorder,” he said.
“Given the clinical and public health significance of suicidal and self-harm behavior in patients with BPD, an important question is whether the absence of this criterion, which might attenuate the likelihood of recognizing and diagnosing the disorder, identifies a subgroup of patients with BPD who are ‘less borderline’ than patients with BPD who do not manifest this criterion,” the investigators write.
The researchers wanted to see if a similar finding applied to self-injury and suicidal behavior and turned to the Rhode Island Methods to Improve Diagnostic Assessment and Services (MIDAS) project to compare the demographic and clinical characteristics of patients with BPD who do and do not engage in repeated suicidal and self-harm behavior.
MIDAS project
The study population was derived from 3,800 psychiatric outpatients who had been evaluated in the MIDAS project with semi-structured diagnostic interviews.
Of these, 390 patients were diagnosed with BPD. Since the suicidality/self-harm item was not rated in one patient, the analyzed sample consisted of 389 individuals with BPD (28.3% male; mean age, 32.6 years; 86.3% White). A little more than half the participants (54%) met the BPD suicidality/ self-harm criterion.
Only one-fifth (20.5%) of patients with BPD presented with a chief complaint that was related to a feature of BPD and had received BPD as their principal diagnosis.
Patients who met the suicidality/self-injury criterion were almost twice as likely to be diagnosed with BPD as the principal diagnosis, compared with those who did not have that criterion (24.8% vs. 14.5%, respectively; P < .01).
On the other hand, there was no difference in the mean number of BPD criteria that were met, other than suicidality/self-harm, between those who did and did not present with suicidality/self-harm (5.5 ± 1.2 vs. 5.7 ± 0.8, t = 1.44). The investigators note that this finding was “not significant.”
There also was no difference between patients who did and did not meet the criterion in number of psychiatric diagnoses at time of evaluation (3.4 ± 1.9 vs. 3.5 ± 1.8, t = 0.56).
Hidden BPD
Similarly, there was no difference in any specific Axis I or personality disorder – except for generalized anxiety disorder (GAD) and histrionic personality disorder. Both were more frequent in the patients who did not meet the suicidality/self-injury criterion. However, after controlling for age, the group difference in GAD was no longer deemed significant (F = 3.45, P = .064).
By contrast, histrionic personality disorder remained significant with age as the covariate (F = 6.03, P = .015).
“The patients who met the suicidality/self-injury criterion were significantly more likely to have been hospitalized and reported more suicidal ideation at the time of the evaluation,” the researchers write. Both variables remained significant even after including age as a covariate.
There were no between-group differences on severity of depression, anxiety, or anger at initial evaluation nor were there differences in social functioning, adolescent social functioning, likelihood of persistent unemployment or receiving disability payments, childhood trauma, or neglect.
“I suspect that there are a number of individuals whose BPD is not recognized because they don’t have the more overt feature of self-injury or suicidal behavior,” said Dr. Zimmerman, noting that these patients might be considered as having “hidden” BPD.
“Repeated self-injurious and suicidal behavior is not synonymous with BPD, and clinicians should be aware that the absence of these behaviors does not rule out a diagnosis of BPD,” he added.
Stigmatizing diagnosis?
Monica Carsky, PhD, clinical assistant professor of psychology in psychiatry and senior fellow, Personality Disorders Institute, Weill Cornell Medical College, New York, said the study “will be particularly useful in the education of clinicians about the characteristics of individuals with BPD.”

Dr. Carsky, who is also an adjunct assistant professor in the NYU Postdoctoral Program in Psychoanalysis and Psychotherapy, was not involved with the study. She noted that other factors “can contribute to misdiagnosis of the borderline patients who do not have suicidality/self-harm.”
Clinicians and patients “may see BPD as a stigmatizing diagnosis so that clinicians become reluctant to make, share, and explain this personality disorder diagnosis,” she said.
Dr. Carsky suggested that increasing use of the Alternate Model for Personality Disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), which first rates the severity level of personality by assessing identity and relationship problems and then notes traits of specific personality disorders, “will help clinicians who dread telling patients they are ‘borderline.’ ”
No source of study funding has been reported. The investigators and Dr. Carsky reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators compared characteristics of almost 400 psychiatric outpatients diagnosed with BPD. About half of the participants met the suicidality/self-injury diagnostic criterion for the disorder, while the other half did not.
Results showed no differences between the two groups in degree of impairment in occupational or social functioning, comorbid psychiatric disorders, history of childhood trauma, or severity of depression, anxiety, or anger.
“Just because a person doesn’t engage in self-harm or suicidal behavior doesn’t mean that the person is free of borderline personality disorder,” lead author Mark Zimmerman, MD, professor of psychiatry and human behavior, Brown University, Providence, R.I., told this news organization.
“Clinicians need to screen for borderline personality disorder in patients with other suggestive symptoms, even if those patients don’t self-harm, just as they would for similar patients who do self-harm,” said Dr. Zimmerman, who is also the director of the Outpatient Division at the Partial Hospital Program, Rhode Island Hospital.
The findings were published online in Psychological Medicine.
A ‘polythetic diagnosis’
Dr. Zimmerman noted the impetus for conducting the study originated with a patient he saw who had all of the features of BPD except for self-harm and suicidality. However, because she didn’t have those two features, she was told by her therapist she could not have BPD.
“This sparked the idea that perhaps there are other individuals whose BPD may not be recognized because they don’t engage in self-harm or suicidal behavior,” Dr. Zimmerman said.
“Most individuals with BPD don’t present for treatment saying, ‘I’m here because I don’t have a sense of myself’ or ‘I feel empty inside’ – but they do say, ‘I’m here because I’m cutting myself’ or ‘I’m suicidal,’ ” he added.
The investigators wondered if there were other “hidden” cases of BPD that were being missed by therapists.
They had previously analyzed each diagnostic criterion for BPD to ascertain its sensitivity. “We had been interested in wanting to see whether there was a criterion so frequent in BPD that every patient with BPD has it,” Dr. Zimmerman said.
BPD is a “polythetic diagnosis,” he added. It is “based on a list of features, with a certain minimum number of those features necessary to make the diagnosis rather than one specific criterion.”
His group’s previous research showed affective instability criterion to be present in more than 90% of individuals with BPD. “It had a very high negative predictive value, meaning that if you didn’t have affective instability, you didn’t have the disorder,” he said.
“Given the clinical and public health significance of suicidal and self-harm behavior in patients with BPD, an important question is whether the absence of this criterion, which might attenuate the likelihood of recognizing and diagnosing the disorder, identifies a subgroup of patients with BPD who are ‘less borderline’ than patients with BPD who do not manifest this criterion,” the investigators write.
The researchers wanted to see if a similar finding applied to self-injury and suicidal behavior and turned to the Rhode Island Methods to Improve Diagnostic Assessment and Services (MIDAS) project to compare the demographic and clinical characteristics of patients with BPD who do and do not engage in repeated suicidal and self-harm behavior.
MIDAS project
The study population was derived from 3,800 psychiatric outpatients who had been evaluated in the MIDAS project with semi-structured diagnostic interviews.
Of these, 390 patients were diagnosed with BPD. Since the suicidality/self-harm item was not rated in one patient, the analyzed sample consisted of 389 individuals with BPD (28.3% male; mean age, 32.6 years; 86.3% White). A little more than half the participants (54%) met the BPD suicidality/ self-harm criterion.
Only one-fifth (20.5%) of patients with BPD presented with a chief complaint that was related to a feature of BPD and had received BPD as their principal diagnosis.
Patients who met the suicidality/self-injury criterion were almost twice as likely to be diagnosed with BPD as the principal diagnosis, compared with those who did not have that criterion (24.8% vs. 14.5%, respectively; P < .01).
On the other hand, there was no difference in the mean number of BPD criteria that were met, other than suicidality/self-harm, between those who did and did not present with suicidality/self-harm (5.5 ± 1.2 vs. 5.7 ± 0.8, t = 1.44). The investigators note that this finding was “not significant.”
There also was no difference between patients who did and did not meet the criterion in number of psychiatric diagnoses at time of evaluation (3.4 ± 1.9 vs. 3.5 ± 1.8, t = 0.56).
Hidden BPD
Similarly, there was no difference in any specific Axis I or personality disorder – except for generalized anxiety disorder (GAD) and histrionic personality disorder. Both were more frequent in the patients who did not meet the suicidality/self-injury criterion. However, after controlling for age, the group difference in GAD was no longer deemed significant (F = 3.45, P = .064).
By contrast, histrionic personality disorder remained significant with age as the covariate (F = 6.03, P = .015).
“The patients who met the suicidality/self-injury criterion were significantly more likely to have been hospitalized and reported more suicidal ideation at the time of the evaluation,” the researchers write. Both variables remained significant even after including age as a covariate.
There were no between-group differences on severity of depression, anxiety, or anger at initial evaluation nor were there differences in social functioning, adolescent social functioning, likelihood of persistent unemployment or receiving disability payments, childhood trauma, or neglect.
“I suspect that there are a number of individuals whose BPD is not recognized because they don’t have the more overt feature of self-injury or suicidal behavior,” said Dr. Zimmerman, noting that these patients might be considered as having “hidden” BPD.
“Repeated self-injurious and suicidal behavior is not synonymous with BPD, and clinicians should be aware that the absence of these behaviors does not rule out a diagnosis of BPD,” he added.
Stigmatizing diagnosis?
Monica Carsky, PhD, clinical assistant professor of psychology in psychiatry and senior fellow, Personality Disorders Institute, Weill Cornell Medical College, New York, said the study “will be particularly useful in the education of clinicians about the characteristics of individuals with BPD.”
Dr. Carsky, who is also an adjunct assistant professor in the NYU Postdoctoral Program in Psychoanalysis and Psychotherapy, was not involved with the study. She noted that other factors “can contribute to misdiagnosis of the borderline patients who do not have suicidality/self-harm.”
Clinicians and patients “may see BPD as a stigmatizing diagnosis so that clinicians become reluctant to make, share, and explain this personality disorder diagnosis,” she said.
Dr. Carsky suggested that increasing use of the Alternate Model for Personality Disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), which first rates the severity level of personality by assessing identity and relationship problems and then notes traits of specific personality disorders, “will help clinicians who dread telling patients they are ‘borderline.’ ”
No source of study funding has been reported. The investigators and Dr. Carsky reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Investigators compared characteristics of almost 400 psychiatric outpatients diagnosed with BPD. About half of the participants met the suicidality/self-injury diagnostic criterion for the disorder, while the other half did not.
Results showed no differences between the two groups in degree of impairment in occupational or social functioning, comorbid psychiatric disorders, history of childhood trauma, or severity of depression, anxiety, or anger.
“Just because a person doesn’t engage in self-harm or suicidal behavior doesn’t mean that the person is free of borderline personality disorder,” lead author Mark Zimmerman, MD, professor of psychiatry and human behavior, Brown University, Providence, R.I., told this news organization.
“Clinicians need to screen for borderline personality disorder in patients with other suggestive symptoms, even if those patients don’t self-harm, just as they would for similar patients who do self-harm,” said Dr. Zimmerman, who is also the director of the Outpatient Division at the Partial Hospital Program, Rhode Island Hospital.
The findings were published online in Psychological Medicine.
A ‘polythetic diagnosis’
Dr. Zimmerman noted the impetus for conducting the study originated with a patient he saw who had all of the features of BPD except for self-harm and suicidality. However, because she didn’t have those two features, she was told by her therapist she could not have BPD.
“This sparked the idea that perhaps there are other individuals whose BPD may not be recognized because they don’t engage in self-harm or suicidal behavior,” Dr. Zimmerman said.
“Most individuals with BPD don’t present for treatment saying, ‘I’m here because I don’t have a sense of myself’ or ‘I feel empty inside’ – but they do say, ‘I’m here because I’m cutting myself’ or ‘I’m suicidal,’ ” he added.
The investigators wondered if there were other “hidden” cases of BPD that were being missed by therapists.
They had previously analyzed each diagnostic criterion for BPD to ascertain its sensitivity. “We had been interested in wanting to see whether there was a criterion so frequent in BPD that every patient with BPD has it,” Dr. Zimmerman said.
BPD is a “polythetic diagnosis,” he added. It is “based on a list of features, with a certain minimum number of those features necessary to make the diagnosis rather than one specific criterion.”
His group’s previous research showed affective instability criterion to be present in more than 90% of individuals with BPD. “It had a very high negative predictive value, meaning that if you didn’t have affective instability, you didn’t have the disorder,” he said.
“Given the clinical and public health significance of suicidal and self-harm behavior in patients with BPD, an important question is whether the absence of this criterion, which might attenuate the likelihood of recognizing and diagnosing the disorder, identifies a subgroup of patients with BPD who are ‘less borderline’ than patients with BPD who do not manifest this criterion,” the investigators write.
The researchers wanted to see if a similar finding applied to self-injury and suicidal behavior and turned to the Rhode Island Methods to Improve Diagnostic Assessment and Services (MIDAS) project to compare the demographic and clinical characteristics of patients with BPD who do and do not engage in repeated suicidal and self-harm behavior.
MIDAS project
The study population was derived from 3,800 psychiatric outpatients who had been evaluated in the MIDAS project with semi-structured diagnostic interviews.
Of these, 390 patients were diagnosed with BPD. Since the suicidality/self-harm item was not rated in one patient, the analyzed sample consisted of 389 individuals with BPD (28.3% male; mean age, 32.6 years; 86.3% White). A little more than half the participants (54%) met the BPD suicidality/ self-harm criterion.
Only one-fifth (20.5%) of patients with BPD presented with a chief complaint that was related to a feature of BPD and had received BPD as their principal diagnosis.
Patients who met the suicidality/self-injury criterion were almost twice as likely to be diagnosed with BPD as the principal diagnosis, compared with those who did not have that criterion (24.8% vs. 14.5%, respectively; P < .01).
On the other hand, there was no difference in the mean number of BPD criteria that were met, other than suicidality/self-harm, between those who did and did not present with suicidality/self-harm (5.5 ± 1.2 vs. 5.7 ± 0.8, t = 1.44). The investigators note that this finding was “not significant.”
There also was no difference between patients who did and did not meet the criterion in number of psychiatric diagnoses at time of evaluation (3.4 ± 1.9 vs. 3.5 ± 1.8, t = 0.56).
Hidden BPD
Similarly, there was no difference in any specific Axis I or personality disorder – except for generalized anxiety disorder (GAD) and histrionic personality disorder. Both were more frequent in the patients who did not meet the suicidality/self-injury criterion. However, after controlling for age, the group difference in GAD was no longer deemed significant (F = 3.45, P = .064).
By contrast, histrionic personality disorder remained significant with age as the covariate (F = 6.03, P = .015).
“The patients who met the suicidality/self-injury criterion were significantly more likely to have been hospitalized and reported more suicidal ideation at the time of the evaluation,” the researchers write. Both variables remained significant even after including age as a covariate.
There were no between-group differences on severity of depression, anxiety, or anger at initial evaluation nor were there differences in social functioning, adolescent social functioning, likelihood of persistent unemployment or receiving disability payments, childhood trauma, or neglect.
“I suspect that there are a number of individuals whose BPD is not recognized because they don’t have the more overt feature of self-injury or suicidal behavior,” said Dr. Zimmerman, noting that these patients might be considered as having “hidden” BPD.
“Repeated self-injurious and suicidal behavior is not synonymous with BPD, and clinicians should be aware that the absence of these behaviors does not rule out a diagnosis of BPD,” he added.
Stigmatizing diagnosis?
Monica Carsky, PhD, clinical assistant professor of psychology in psychiatry and senior fellow, Personality Disorders Institute, Weill Cornell Medical College, New York, said the study “will be particularly useful in the education of clinicians about the characteristics of individuals with BPD.”
Dr. Carsky, who is also an adjunct assistant professor in the NYU Postdoctoral Program in Psychoanalysis and Psychotherapy, was not involved with the study. She noted that other factors “can contribute to misdiagnosis of the borderline patients who do not have suicidality/self-harm.”
Clinicians and patients “may see BPD as a stigmatizing diagnosis so that clinicians become reluctant to make, share, and explain this personality disorder diagnosis,” she said.
Dr. Carsky suggested that increasing use of the Alternate Model for Personality Disorders in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V), which first rates the severity level of personality by assessing identity and relationship problems and then notes traits of specific personality disorders, “will help clinicians who dread telling patients they are ‘borderline.’ ”
No source of study funding has been reported. The investigators and Dr. Carsky reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Children and COVID: ED visits and new admissions change course
New child cases of COVID-19 made at least a temporary transition from slow increase to decrease, and emergency department visits and new admissions seem to be following a downward trend.
, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association. For some historical perspective, the latest weekly count falls below last year’s Delta surge figure of 121,000 (Aug. 6-12) but above the summer 2020 total of 26,000 (Aug. 7-13).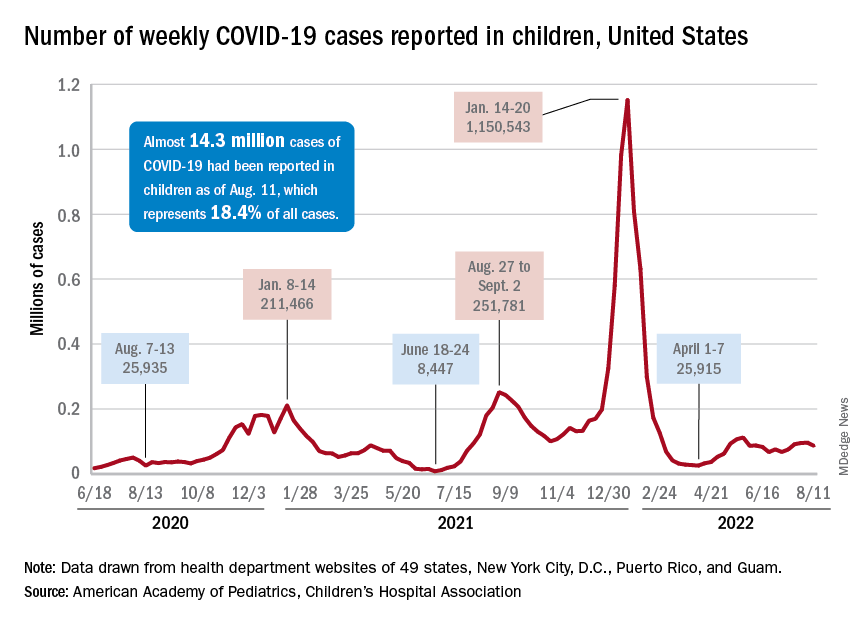
Measures of serious illness finally head downward
The prolonged rise in ED visits and new admissions over the last 5 months, which continued even through late spring when cases were declining, seems to have peaked, CDC data suggest.
That upward trend, driven largely by continued increases among younger children, peaked in late July, when 6.7% of all ED visits for children aged 0-11 years involved diagnosed COVID-19. The corresponding peaks for older children occurred around the same time but were only about half as high: 3.4% for 12- to 15-year-olds and 3.6% for those aged 16-17, the CDC reported.
The data for new admissions present a similar scenario: an increase starting in mid-April that continued unabated into late July despite the decline in new cases. By the time admissions among children aged 0-17 years peaked at 0.46 per 100,000 population in late July, they had reached the same level seen during the Delta surge. By Aug. 7, the rate of new hospitalizations was down to 0.42 per 100,000, the CDC said on its COVID Data Tracker.
The vaccine is ready for all students, but …
As children all over the country start or get ready to start a new school year, the only large-scale student vaccine mandate belongs to the District of Columbia. California has a mandate pending, but it will not go into effect until after July 1, 2023. There are, however, 20 states that have banned vaccine mandates for students, according to the National Academy for State Health Policy.
Nonmandated vaccination of the youngest children against COVID-19 continues to be slow. In the approximately 7 weeks (June 19 to Aug. 9) since the vaccine was approved for use in children younger than 5 years, just 4.4% of that age group has received at least one dose and 0.7% are fully vaccinated. Among those aged 5-11 years, who have been vaccine-eligible since early November of last year, 37.6% have received at least one dose and 30.2% are fully vaccinated, the CDC said.
New child cases of COVID-19 made at least a temporary transition from slow increase to decrease, and emergency department visits and new admissions seem to be following a downward trend.
, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association. For some historical perspective, the latest weekly count falls below last year’s Delta surge figure of 121,000 (Aug. 6-12) but above the summer 2020 total of 26,000 (Aug. 7-13).
Measures of serious illness finally head downward
The prolonged rise in ED visits and new admissions over the last 5 months, which continued even through late spring when cases were declining, seems to have peaked, CDC data suggest.
That upward trend, driven largely by continued increases among younger children, peaked in late July, when 6.7% of all ED visits for children aged 0-11 years involved diagnosed COVID-19. The corresponding peaks for older children occurred around the same time but were only about half as high: 3.4% for 12- to 15-year-olds and 3.6% for those aged 16-17, the CDC reported.
The data for new admissions present a similar scenario: an increase starting in mid-April that continued unabated into late July despite the decline in new cases. By the time admissions among children aged 0-17 years peaked at 0.46 per 100,000 population in late July, they had reached the same level seen during the Delta surge. By Aug. 7, the rate of new hospitalizations was down to 0.42 per 100,000, the CDC said on its COVID Data Tracker.
The vaccine is ready for all students, but …
As children all over the country start or get ready to start a new school year, the only large-scale student vaccine mandate belongs to the District of Columbia. California has a mandate pending, but it will not go into effect until after July 1, 2023. There are, however, 20 states that have banned vaccine mandates for students, according to the National Academy for State Health Policy.
Nonmandated vaccination of the youngest children against COVID-19 continues to be slow. In the approximately 7 weeks (June 19 to Aug. 9) since the vaccine was approved for use in children younger than 5 years, just 4.4% of that age group has received at least one dose and 0.7% are fully vaccinated. Among those aged 5-11 years, who have been vaccine-eligible since early November of last year, 37.6% have received at least one dose and 30.2% are fully vaccinated, the CDC said.
New child cases of COVID-19 made at least a temporary transition from slow increase to decrease, and emergency department visits and new admissions seem to be following a downward trend.
, according to a report from the American Academy of Pediatrics and the Children’s Hospital Association. For some historical perspective, the latest weekly count falls below last year’s Delta surge figure of 121,000 (Aug. 6-12) but above the summer 2020 total of 26,000 (Aug. 7-13).
Measures of serious illness finally head downward
The prolonged rise in ED visits and new admissions over the last 5 months, which continued even through late spring when cases were declining, seems to have peaked, CDC data suggest.
That upward trend, driven largely by continued increases among younger children, peaked in late July, when 6.7% of all ED visits for children aged 0-11 years involved diagnosed COVID-19. The corresponding peaks for older children occurred around the same time but were only about half as high: 3.4% for 12- to 15-year-olds and 3.6% for those aged 16-17, the CDC reported.
The data for new admissions present a similar scenario: an increase starting in mid-April that continued unabated into late July despite the decline in new cases. By the time admissions among children aged 0-17 years peaked at 0.46 per 100,000 population in late July, they had reached the same level seen during the Delta surge. By Aug. 7, the rate of new hospitalizations was down to 0.42 per 100,000, the CDC said on its COVID Data Tracker.
The vaccine is ready for all students, but …
As children all over the country start or get ready to start a new school year, the only large-scale student vaccine mandate belongs to the District of Columbia. California has a mandate pending, but it will not go into effect until after July 1, 2023. There are, however, 20 states that have banned vaccine mandates for students, according to the National Academy for State Health Policy.
Nonmandated vaccination of the youngest children against COVID-19 continues to be slow. In the approximately 7 weeks (June 19 to Aug. 9) since the vaccine was approved for use in children younger than 5 years, just 4.4% of that age group has received at least one dose and 0.7% are fully vaccinated. Among those aged 5-11 years, who have been vaccine-eligible since early November of last year, 37.6% have received at least one dose and 30.2% are fully vaccinated, the CDC said.
Hearing aids available in October without a prescription
The White House announced today that the Food and Drug Administration will move forward with plans to make hearing aids available over the counter in pharmacies, other retail locations, and online.
This major milestone aims to make hearing aids easier to buy and more affordable, potentially saving families thousands of dollars.
An estimated 28.8 million U.S. adults could benefit from using hearing aids, according to numbers from the National Institute on Deafness and Other Communication Disorders. But only about 16% of people aged 20-69 years who could be helped by hearing aids have ever used them.
The risk for hearing loss increases with age. Among Americans ages 70 and older, only 30% who could hear better with these devices have ever used them, the institute reports.
Once the FDA final rule takes effect, Americans with mild to moderate hearing loss will be able to buy a hearing aid without a doctor’s exam, prescription, or fitting adjustment.
President Joe Biden announced in 2021 he intended to allow hearing aids to be sold over the counter without a prescription to increase competition among manufacturers. Congress also passed bipartisan legislation in 2017 requiring the FDA to create a new category for hearing aids sold directly to consumers. Some devices intended for minors or people with severe hearing loss will remain available only with a prescription.
“This action makes good on my commitment to lower costs for American families, delivering nearly $3,000 in savings to American families for a pair of hearing aids and giving people more choices to improve their health and wellbeing,” the president said in a statement announcing the news.
The new over-the-counter hearing aids will be considered medical devices. To avoid confusion, the FDA explains the differences between hearing aids and personal sound amplification products (PSAPs). For example, PSAPs are considered electronic devices designed for people with normal hearing to use in certain situations, like birdwatching or hunting.
A version of this article first appeared on WebMD.com.
The White House announced today that the Food and Drug Administration will move forward with plans to make hearing aids available over the counter in pharmacies, other retail locations, and online.
This major milestone aims to make hearing aids easier to buy and more affordable, potentially saving families thousands of dollars.
An estimated 28.8 million U.S. adults could benefit from using hearing aids, according to numbers from the National Institute on Deafness and Other Communication Disorders. But only about 16% of people aged 20-69 years who could be helped by hearing aids have ever used them.
The risk for hearing loss increases with age. Among Americans ages 70 and older, only 30% who could hear better with these devices have ever used them, the institute reports.
Once the FDA final rule takes effect, Americans with mild to moderate hearing loss will be able to buy a hearing aid without a doctor’s exam, prescription, or fitting adjustment.
President Joe Biden announced in 2021 he intended to allow hearing aids to be sold over the counter without a prescription to increase competition among manufacturers. Congress also passed bipartisan legislation in 2017 requiring the FDA to create a new category for hearing aids sold directly to consumers. Some devices intended for minors or people with severe hearing loss will remain available only with a prescription.
“This action makes good on my commitment to lower costs for American families, delivering nearly $3,000 in savings to American families for a pair of hearing aids and giving people more choices to improve their health and wellbeing,” the president said in a statement announcing the news.
The new over-the-counter hearing aids will be considered medical devices. To avoid confusion, the FDA explains the differences between hearing aids and personal sound amplification products (PSAPs). For example, PSAPs are considered electronic devices designed for people with normal hearing to use in certain situations, like birdwatching or hunting.
A version of this article first appeared on WebMD.com.
The White House announced today that the Food and Drug Administration will move forward with plans to make hearing aids available over the counter in pharmacies, other retail locations, and online.
This major milestone aims to make hearing aids easier to buy and more affordable, potentially saving families thousands of dollars.
An estimated 28.8 million U.S. adults could benefit from using hearing aids, according to numbers from the National Institute on Deafness and Other Communication Disorders. But only about 16% of people aged 20-69 years who could be helped by hearing aids have ever used them.
The risk for hearing loss increases with age. Among Americans ages 70 and older, only 30% who could hear better with these devices have ever used them, the institute reports.
Once the FDA final rule takes effect, Americans with mild to moderate hearing loss will be able to buy a hearing aid without a doctor’s exam, prescription, or fitting adjustment.
President Joe Biden announced in 2021 he intended to allow hearing aids to be sold over the counter without a prescription to increase competition among manufacturers. Congress also passed bipartisan legislation in 2017 requiring the FDA to create a new category for hearing aids sold directly to consumers. Some devices intended for minors or people with severe hearing loss will remain available only with a prescription.
“This action makes good on my commitment to lower costs for American families, delivering nearly $3,000 in savings to American families for a pair of hearing aids and giving people more choices to improve their health and wellbeing,” the president said in a statement announcing the news.
The new over-the-counter hearing aids will be considered medical devices. To avoid confusion, the FDA explains the differences between hearing aids and personal sound amplification products (PSAPs). For example, PSAPs are considered electronic devices designed for people with normal hearing to use in certain situations, like birdwatching or hunting.
A version of this article first appeared on WebMD.com.
Psychiatrists’ income, net worth rise as COVID wanes
Last year brought welcome relief to psychiatrists, with incomes generally rising as practices reopened after COVID-19 restrictions lifted and patients ventured out of their homes.
Psychiatrists’ average annual income rose to $287,000, according to the Medscape Psychiatrist Wealth and Debt Report 2022. That is up about 4% from $275,000, which was listed in last year’s report.
However, psychiatrists still rank in the bottom third of all specialties when it comes to physicians’ income.
According to the overall Medscape Physician Wealth and Debt Report 2022, the highest-paying speciality is plastic surgery ($576,000), followed by orthopedics ($557,000) and cardiology ($490,000).
The lowest-paying areas of medicine are family medicine ($255,000), pediatrics ($244,000), and public health and preventive medicine ($243,000).
The report is based on responses from more than 13,000 physicians in 29 specialties. All were surveyed between Oct. 5, 2021 and Jan. 19, 2022.
Money-conscious?
Similar to last year’s report, three-quarters of psychiatrists have not done anything to reduce major expenses. Those who have taken cost-cutting measures cited deferring or refinancing loans, moving to a different home, or changing cars as ways to do so.
Most psychiatrists (80%) reported having avoided major financial losses, which is up slightly from last year (76%). Only 6% of psychiatrists (9% last year) reported monetary losses because of issues at their medical practice.
One-quarter reported having a stock or corporate investment go south, which is about the same as last year. In addition, 42% said that they have yet to make a particular investment mistake and 19% said that they have not made any investments.
This year, a somewhat smaller percentage of psychiatrists reported keeping their rates of saving in after-tax accounts level or at increased rates, compared with last year (47% vs. 52%).
About 28% of psychiatrists do not regularly put money into after-tax savings accounts, compared with 25% of physicians overall.
The vast majority said that they kept up with bills amid COVID, as they also did last year.
The percentage of psychiatrists who paid mortgages or other bills late during the pandemic is about the same this year as last year (3% and 5%, respectively).
That is in contrast to one 2021 industry survey, which showed that 46% of Americans missed one or more rent or mortgage payments because of COVID.
Other key findings from Medscape’s latest psychiatrist wealth and debt report include that:
- 61% live in a home of 3,000 square feet or less, which is greater that the current average size of a U.S. house (2,261 square feet)
- 22% have one or two credit cards and 42% have five or more credit cards, while the average American has four cards
- 63% differ in opinion, at least sporadically, with their significant other about spending. A Northwestern Mutual study showed that across the country, around 1 in 4 couples argue about money at least once a month.
In addition, 70% of psychiatrists said that they typically tip at least the recommended 20% for decent service, which is somewhat more generous than the average physician (64%).
A version of this article first appeared on Medscape.com.
Last year brought welcome relief to psychiatrists, with incomes generally rising as practices reopened after COVID-19 restrictions lifted and patients ventured out of their homes.
Psychiatrists’ average annual income rose to $287,000, according to the Medscape Psychiatrist Wealth and Debt Report 2022. That is up about 4% from $275,000, which was listed in last year’s report.
However, psychiatrists still rank in the bottom third of all specialties when it comes to physicians’ income.
According to the overall Medscape Physician Wealth and Debt Report 2022, the highest-paying speciality is plastic surgery ($576,000), followed by orthopedics ($557,000) and cardiology ($490,000).
The lowest-paying areas of medicine are family medicine ($255,000), pediatrics ($244,000), and public health and preventive medicine ($243,000).
The report is based on responses from more than 13,000 physicians in 29 specialties. All were surveyed between Oct. 5, 2021 and Jan. 19, 2022.
Money-conscious?
Similar to last year’s report, three-quarters of psychiatrists have not done anything to reduce major expenses. Those who have taken cost-cutting measures cited deferring or refinancing loans, moving to a different home, or changing cars as ways to do so.
Most psychiatrists (80%) reported having avoided major financial losses, which is up slightly from last year (76%). Only 6% of psychiatrists (9% last year) reported monetary losses because of issues at their medical practice.
One-quarter reported having a stock or corporate investment go south, which is about the same as last year. In addition, 42% said that they have yet to make a particular investment mistake and 19% said that they have not made any investments.
This year, a somewhat smaller percentage of psychiatrists reported keeping their rates of saving in after-tax accounts level or at increased rates, compared with last year (47% vs. 52%).
About 28% of psychiatrists do not regularly put money into after-tax savings accounts, compared with 25% of physicians overall.
The vast majority said that they kept up with bills amid COVID, as they also did last year.
The percentage of psychiatrists who paid mortgages or other bills late during the pandemic is about the same this year as last year (3% and 5%, respectively).
That is in contrast to one 2021 industry survey, which showed that 46% of Americans missed one or more rent or mortgage payments because of COVID.
Other key findings from Medscape’s latest psychiatrist wealth and debt report include that:
- 61% live in a home of 3,000 square feet or less, which is greater that the current average size of a U.S. house (2,261 square feet)
- 22% have one or two credit cards and 42% have five or more credit cards, while the average American has four cards
- 63% differ in opinion, at least sporadically, with their significant other about spending. A Northwestern Mutual study showed that across the country, around 1 in 4 couples argue about money at least once a month.
In addition, 70% of psychiatrists said that they typically tip at least the recommended 20% for decent service, which is somewhat more generous than the average physician (64%).
A version of this article first appeared on Medscape.com.
Last year brought welcome relief to psychiatrists, with incomes generally rising as practices reopened after COVID-19 restrictions lifted and patients ventured out of their homes.
Psychiatrists’ average annual income rose to $287,000, according to the Medscape Psychiatrist Wealth and Debt Report 2022. That is up about 4% from $275,000, which was listed in last year’s report.
However, psychiatrists still rank in the bottom third of all specialties when it comes to physicians’ income.
According to the overall Medscape Physician Wealth and Debt Report 2022, the highest-paying speciality is plastic surgery ($576,000), followed by orthopedics ($557,000) and cardiology ($490,000).
The lowest-paying areas of medicine are family medicine ($255,000), pediatrics ($244,000), and public health and preventive medicine ($243,000).
The report is based on responses from more than 13,000 physicians in 29 specialties. All were surveyed between Oct. 5, 2021 and Jan. 19, 2022.
Money-conscious?
Similar to last year’s report, three-quarters of psychiatrists have not done anything to reduce major expenses. Those who have taken cost-cutting measures cited deferring or refinancing loans, moving to a different home, or changing cars as ways to do so.
Most psychiatrists (80%) reported having avoided major financial losses, which is up slightly from last year (76%). Only 6% of psychiatrists (9% last year) reported monetary losses because of issues at their medical practice.
One-quarter reported having a stock or corporate investment go south, which is about the same as last year. In addition, 42% said that they have yet to make a particular investment mistake and 19% said that they have not made any investments.
This year, a somewhat smaller percentage of psychiatrists reported keeping their rates of saving in after-tax accounts level or at increased rates, compared with last year (47% vs. 52%).
About 28% of psychiatrists do not regularly put money into after-tax savings accounts, compared with 25% of physicians overall.
The vast majority said that they kept up with bills amid COVID, as they also did last year.
The percentage of psychiatrists who paid mortgages or other bills late during the pandemic is about the same this year as last year (3% and 5%, respectively).
That is in contrast to one 2021 industry survey, which showed that 46% of Americans missed one or more rent or mortgage payments because of COVID.
Other key findings from Medscape’s latest psychiatrist wealth and debt report include that:
- 61% live in a home of 3,000 square feet or less, which is greater that the current average size of a U.S. house (2,261 square feet)
- 22% have one or two credit cards and 42% have five or more credit cards, while the average American has four cards
- 63% differ in opinion, at least sporadically, with their significant other about spending. A Northwestern Mutual study showed that across the country, around 1 in 4 couples argue about money at least once a month.
In addition, 70% of psychiatrists said that they typically tip at least the recommended 20% for decent service, which is somewhat more generous than the average physician (64%).
A version of this article first appeared on Medscape.com.