User login
AVAHO 2022: The Necessity of Self-care in Cancer Care
Bernadette Heron, PharmD, summarizes the offerings at the AVAHO 2022 meeting, from the standard sharing of updates across disciplines and specialties to the more specific focus on the role of self-care in cancer care.
Importantly, Dr Heron underscores the connection between the concept of self-care and the implements required for its realization in the clinical setting, resulting in an assortment of tools that practitioners can draw on as they continue the conversation that drives the evolution of cancer care.
Bernadette Heron, PharmD, summarizes the offerings at the AVAHO 2022 meeting, from the standard sharing of updates across disciplines and specialties to the more specific focus on the role of self-care in cancer care.
Importantly, Dr Heron underscores the connection between the concept of self-care and the implements required for its realization in the clinical setting, resulting in an assortment of tools that practitioners can draw on as they continue the conversation that drives the evolution of cancer care.
Bernadette Heron, PharmD, summarizes the offerings at the AVAHO 2022 meeting, from the standard sharing of updates across disciplines and specialties to the more specific focus on the role of self-care in cancer care.
Importantly, Dr Heron underscores the connection between the concept of self-care and the implements required for its realization in the clinical setting, resulting in an assortment of tools that practitioners can draw on as they continue the conversation that drives the evolution of cancer care.






AVAHO 2022: An Opportunity to Recharge
Lauren Cliffel, MSW, describes how the AVAHO 2022 meeting and the main theme of "Self-care in Cancer Care" reestablished the feelings of joy and compassion that led her to choose a career as a cancer care provider in the first place.
The inclusive character of even the larger sessions this year is noted, in which all interdisciplinary contributors to cancer care were addressed as central to the delivery of an informed and effective care of patients and, importantly, how this care is enhanced by a restored sense of purpose among all those engaged in the specialty of oncology.
Lauren Cliffel, MSW, describes how the AVAHO 2022 meeting and the main theme of "Self-care in Cancer Care" reestablished the feelings of joy and compassion that led her to choose a career as a cancer care provider in the first place.
The inclusive character of even the larger sessions this year is noted, in which all interdisciplinary contributors to cancer care were addressed as central to the delivery of an informed and effective care of patients and, importantly, how this care is enhanced by a restored sense of purpose among all those engaged in the specialty of oncology.
Lauren Cliffel, MSW, describes how the AVAHO 2022 meeting and the main theme of "Self-care in Cancer Care" reestablished the feelings of joy and compassion that led her to choose a career as a cancer care provider in the first place.
The inclusive character of even the larger sessions this year is noted, in which all interdisciplinary contributors to cancer care were addressed as central to the delivery of an informed and effective care of patients and, importantly, how this care is enhanced by a restored sense of purpose among all those engaged in the specialty of oncology.



Airways Disorders Network
Bronchiectasis Section
Antibiotics in non–cystic fibrosis bronchiectasis: new perspectives
There is a paucity of high-quality evidence for prophylactic antibiotics, though guidelines support this practice, particularly for adults with three or more exacerbations a year. A recent Cochrane database review (Spencer, et al. Cochrane Database Syst Rev. 2022;1[1]:CD013254) examined eight RCTs, with interventions ranging from 16 to 48 weeks, involving 2,180 adults and found little net benefit for prophylactic cycled antibiotics (fluoroquinolones, beta-lactams, and aminoglycosides) in terms of outcomes viz time-to-first-exacerbation and duration of exacerbations, but more than doubled the risk of emerging resistance.
Clinical equipoise exists regarding the duration of antibiotics during exacerbations. Guidelines favor 14 days. A recent RCT (Pallavi, et al. Eur Respir J. 2021;58:2004388) examined the feasibility of bacterial load-guided therapy in 47 participants with bronchiectasis requiring IV antibiotics.
Patients were randomized to either 14 days of antibiotics or treatment guided by bacterial load (BLGG). The 88% of participants in the BLGG group were able to stop antibiotics by day 8, and potentially 81% of participants in the 14-day group could have stopped antibiotics at day 8. Median time to next exacerbation was much longer – 60 days (18-110 days) in the in BLGG group vs 27.5 days (12.5-60 days) in the 14-day group vs (P = .0034). A larger multicenter RCT may clarify the benefits of this approach to shortening duration of antibiotic therapy in patients with bronchiectasis exacerbations.
O’Neil Green, MBBS, FCCP
Member-at-Large
Bronchiectasis Section
Antibiotics in non–cystic fibrosis bronchiectasis: new perspectives
There is a paucity of high-quality evidence for prophylactic antibiotics, though guidelines support this practice, particularly for adults with three or more exacerbations a year. A recent Cochrane database review (Spencer, et al. Cochrane Database Syst Rev. 2022;1[1]:CD013254) examined eight RCTs, with interventions ranging from 16 to 48 weeks, involving 2,180 adults and found little net benefit for prophylactic cycled antibiotics (fluoroquinolones, beta-lactams, and aminoglycosides) in terms of outcomes viz time-to-first-exacerbation and duration of exacerbations, but more than doubled the risk of emerging resistance.
Clinical equipoise exists regarding the duration of antibiotics during exacerbations. Guidelines favor 14 days. A recent RCT (Pallavi, et al. Eur Respir J. 2021;58:2004388) examined the feasibility of bacterial load-guided therapy in 47 participants with bronchiectasis requiring IV antibiotics.
Patients were randomized to either 14 days of antibiotics or treatment guided by bacterial load (BLGG). The 88% of participants in the BLGG group were able to stop antibiotics by day 8, and potentially 81% of participants in the 14-day group could have stopped antibiotics at day 8. Median time to next exacerbation was much longer – 60 days (18-110 days) in the in BLGG group vs 27.5 days (12.5-60 days) in the 14-day group vs (P = .0034). A larger multicenter RCT may clarify the benefits of this approach to shortening duration of antibiotic therapy in patients with bronchiectasis exacerbations.
O’Neil Green, MBBS, FCCP
Member-at-Large
Bronchiectasis Section
Antibiotics in non–cystic fibrosis bronchiectasis: new perspectives
There is a paucity of high-quality evidence for prophylactic antibiotics, though guidelines support this practice, particularly for adults with three or more exacerbations a year. A recent Cochrane database review (Spencer, et al. Cochrane Database Syst Rev. 2022;1[1]:CD013254) examined eight RCTs, with interventions ranging from 16 to 48 weeks, involving 2,180 adults and found little net benefit for prophylactic cycled antibiotics (fluoroquinolones, beta-lactams, and aminoglycosides) in terms of outcomes viz time-to-first-exacerbation and duration of exacerbations, but more than doubled the risk of emerging resistance.
Clinical equipoise exists regarding the duration of antibiotics during exacerbations. Guidelines favor 14 days. A recent RCT (Pallavi, et al. Eur Respir J. 2021;58:2004388) examined the feasibility of bacterial load-guided therapy in 47 participants with bronchiectasis requiring IV antibiotics.
Patients were randomized to either 14 days of antibiotics or treatment guided by bacterial load (BLGG). The 88% of participants in the BLGG group were able to stop antibiotics by day 8, and potentially 81% of participants in the 14-day group could have stopped antibiotics at day 8. Median time to next exacerbation was much longer – 60 days (18-110 days) in the in BLGG group vs 27.5 days (12.5-60 days) in the 14-day group vs (P = .0034). A larger multicenter RCT may clarify the benefits of this approach to shortening duration of antibiotic therapy in patients with bronchiectasis exacerbations.
O’Neil Green, MBBS, FCCP
Member-at-Large
ICU telemedicine turns 40
connected with intensivists at the University Hospitals of Cleveland (Grundy, et al. Crit Care Med. 1982;10[7]:471). After this proof-of-concept report, however, ICU telemedicine gained little traction for nearly 20 years, until Johns Hopkins Hospital established a continuously monitored ICU telemedicine service in a nonintensivist staffed surgical ICU. Their pre/post analysis suggested a 64% decrease in severity-adjusted ICU mortality and greater than 30% decrease in ICU length of stay, ICU complications, and costs (Rosenfeld, et al. Crit Care Med. 2000;28[12]:3925).
Along with better and less costly telemedicine technology, rapid adoption of electronic medical records, and a nationwide intensivist shortage, this and other evidence for the service’s clinical and cost effectiveness has spurred explosive growth in ICU telemedicine in the succeeding 2 decades, with at least 18% of hospitals and 28% of ICU beds supported by ICU telemedicine by 2018 (Ofoma, et al. Crit Care Explor. 2021;4[3]:e0468).
Importantly, what “ICU telemedicine” represents varies substantially across hospitals and even across ICUs within systems. Two-way audiovisual technology is the defining feature, and at a minimum, programs provide intensivists and/or nurses who respond to consultation requests. Commonly, telemedicine clinicians directly connect with patients; monitor labs, hemodynamics, and alarms; and proactively contact on-site clinicians with recommendations or place orders directly into the electronic health record depending on whether the clinician acts as the patients’ primary, co-managing, or consultant provider. A centralized hub and spoke model with telemedicine personnel located at a single, remote center is the most common and best studied ICU telemedicine design. Additional staffing may include respiratory therapists, pharmacists, and advanced practice clinicians in coverage models that range from 24/7 to nocturnal and can also differ in whether patients are monitored continuously or on an as needed basis, triggered by alarms or clinician/nursing concerns.
On-demand services may extend to support for teams responding to medical emergencies inside and sometimes outside the ICU. Another equally important role that ICU telemedicine can provide is helping ensure facilities adhere to ICU quality metrics, such as ventilator bundles, DVT prophylaxis, and daily SAT/SBT.
Unsurprisingly, integrating ICU telemedicine into an existing system is very costly and complex, requiring substantial and thoughtful process redesign to maximize fiscal and clinical return on investment. One vendor of proprietary telemedicine technology, Philips eICU, estimates an implementation cost of $50,000 to $100,000 per bed with annual overhead, software maintenance, and IT staffing of ~20% of implementation costs in addition to clinician staffing of $1-2 million per 100 beds. However, some (but not all) evidence suggests that ICU telemedicine programs pay for themselves over time. An influential report from Sentara Healthcare, an early adopter of ICU telemedicine, described equipment costs of more than $1 million for a total of 103 critical care beds but attributed savings of $460,000 per month to decreased length of stay (Coustasse, et al. The Permanente Journal. 2014;18[4]:76).
Cost savings are great, of course, but ICU telemedicine’s potential to improve clinical outcomes is the real priority. While Sentara’s early report included a 27% decrease in ICU mortality after telemedicine adoption, a 2011 meta-analysis of 13 studies, including 35 ICUs and over 40,000 patients, suggested decreased ICU mortality and LOS with a statistically significant effect on overall hospital mortality and LOS (Young, et al. Arch Intern Med. 2011;171[6]:498). This highlights the Achilles heel of ICU telemedicine evidence: the pretest/posttest studies that dominate this field and likely contribute substantially to the inconsistencies in the evidence base.
In the absence of risk adjustment and control groups, many studies observed postimplementation changes that may reflect trends in patient mix or the effects of unrelated practice changes rather than the causal influence of ICU telemedicine. In fact, in studies using more robust methods, ICU telemedicine’s effect size has been smaller or nonexistent. For example, in 2016, Kahn and colleagues used CMS data to evaluate 132 ICU telemedicine programs using 389 matched controlled hospitals. There was a slight reduction in 90-day mortality (OR=0.96, CI 0.94-0.98) with only 12% showing a statistically significant reduction in mortality. Interestingly, hospitals in urban areas demonstrated greater benefit than rural facilities (Kahn, et al. Medical Care. 2016;54[3]:319).
The heterogeneity of the studied programs (e.g., primary vs consultative role, on-demand vs proactive involvement) and recipient ICUs (e.g., rural vs tertiary care facility, presence of bedside intensivists) further hinders a clear answer to the key question: Would ICU telemedicine benefit my hospital? Fortunately, some recent, well-designed studies have attempted to understand which attributes of ICU telemedicine programs provide results and which ICUs will see the most benefit. In a cohort of 118,990 patients across 56 ICUs, four interventions were associated with lower mortality and reduced LOS: (1) evaluation of patients within 1 hour of ICU admission, (2) frequent leadership review of performance data, (3) ICU best practice compliance, and (4) prompt response to alerts (Lilly, et al. Chest. 2014;145[3]:500). Kahn and colleagues have also investigated this issue, conducting an in-depth ethnographic evaluation of 10 hospitals identified in their 2016 study to have positive, neutral, or negative outcomes after ICU telemedicine implementation (Kahn, et al. Am J Respir Crit Care Med. 2019;199[8]:970). They found that successful programs:
(1) provided consistent services matched to recipient needs;
(2) provided services both proactively and reactively without being obtrusive;
(3) embedded routine engagements unobtrusively into usual routines;
(4) had engaged leadership who set clear expectations and mediated conflicts; and
(5) had bedside clinicians who valued and sought out telemedicine participation in care.
The authors concluded that, “the true value of ICU telemedicine lies not in whether the technology exists but in how it is applied.” However, another recent analysis also suggested that, rather than telemedicine or recipient ICU design, targeting underperforming recipient ICU performance may be the key determinant of whether ICU telemedicine implementation improves outcomes (Fusaro, et al. Crit Care Med. 2019; 47[4]:501). While the finding may reflect regression to the mean, the idea that ICUs with above-expected mortality derive greater benefit from ICU telemedicine support than already well-performing ICUs is certainly logical.
As COVID-19 strained health care systems across the country, we and others found ways to use ICU telemedicine to preserve optimal care delivery for critically ill patients. Our program at Intermountain Healthcare – already supporting 17 ICUs within our 24-hospital health system, as well as 10 external ICUs with experienced critical care physicians, nurses, respiratory therapists, and pharmacists – took on increased responsibility for ICU load balancing and interhospital transfers.
Leveraging telemedicine services also helped community ICUs care for sicker, more complex patients than usual and aided nonintensivist physicians called upon to manage critically ill patients in ad hoc ICUs at referral hospitals. While the pandemic certainly stressed ICU staff, we suspect that telemedicine’s ability to balance caseloads and distribute clinical tasks helped mitigate these stresses. At age 40, ICU telemedicine is both mature and still growing, with continued expansion of bed coverage and the range of services available. Looking ahead, as we confront a national shortage of intensivists, ICU telemedicine likely represents a cost effective and efficient strategy to maintain critical care capacity with the potential to ensure low-cost, high-quality care for all, regardless of location.
Dr. Graham and Dr. Peltan are with the Division of Pulmonary & Critical Care Medicine, Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City, Utah; and Dr. Peltan is also with the Division of Pulmonary & Critical Care Medicine, Department of Medicine, Intermountain Medical Center, Murray, Utah.
connected with intensivists at the University Hospitals of Cleveland (Grundy, et al. Crit Care Med. 1982;10[7]:471). After this proof-of-concept report, however, ICU telemedicine gained little traction for nearly 20 years, until Johns Hopkins Hospital established a continuously monitored ICU telemedicine service in a nonintensivist staffed surgical ICU. Their pre/post analysis suggested a 64% decrease in severity-adjusted ICU mortality and greater than 30% decrease in ICU length of stay, ICU complications, and costs (Rosenfeld, et al. Crit Care Med. 2000;28[12]:3925).
Along with better and less costly telemedicine technology, rapid adoption of electronic medical records, and a nationwide intensivist shortage, this and other evidence for the service’s clinical and cost effectiveness has spurred explosive growth in ICU telemedicine in the succeeding 2 decades, with at least 18% of hospitals and 28% of ICU beds supported by ICU telemedicine by 2018 (Ofoma, et al. Crit Care Explor. 2021;4[3]:e0468).
Importantly, what “ICU telemedicine” represents varies substantially across hospitals and even across ICUs within systems. Two-way audiovisual technology is the defining feature, and at a minimum, programs provide intensivists and/or nurses who respond to consultation requests. Commonly, telemedicine clinicians directly connect with patients; monitor labs, hemodynamics, and alarms; and proactively contact on-site clinicians with recommendations or place orders directly into the electronic health record depending on whether the clinician acts as the patients’ primary, co-managing, or consultant provider. A centralized hub and spoke model with telemedicine personnel located at a single, remote center is the most common and best studied ICU telemedicine design. Additional staffing may include respiratory therapists, pharmacists, and advanced practice clinicians in coverage models that range from 24/7 to nocturnal and can also differ in whether patients are monitored continuously or on an as needed basis, triggered by alarms or clinician/nursing concerns.
On-demand services may extend to support for teams responding to medical emergencies inside and sometimes outside the ICU. Another equally important role that ICU telemedicine can provide is helping ensure facilities adhere to ICU quality metrics, such as ventilator bundles, DVT prophylaxis, and daily SAT/SBT.
Unsurprisingly, integrating ICU telemedicine into an existing system is very costly and complex, requiring substantial and thoughtful process redesign to maximize fiscal and clinical return on investment. One vendor of proprietary telemedicine technology, Philips eICU, estimates an implementation cost of $50,000 to $100,000 per bed with annual overhead, software maintenance, and IT staffing of ~20% of implementation costs in addition to clinician staffing of $1-2 million per 100 beds. However, some (but not all) evidence suggests that ICU telemedicine programs pay for themselves over time. An influential report from Sentara Healthcare, an early adopter of ICU telemedicine, described equipment costs of more than $1 million for a total of 103 critical care beds but attributed savings of $460,000 per month to decreased length of stay (Coustasse, et al. The Permanente Journal. 2014;18[4]:76).
Cost savings are great, of course, but ICU telemedicine’s potential to improve clinical outcomes is the real priority. While Sentara’s early report included a 27% decrease in ICU mortality after telemedicine adoption, a 2011 meta-analysis of 13 studies, including 35 ICUs and over 40,000 patients, suggested decreased ICU mortality and LOS with a statistically significant effect on overall hospital mortality and LOS (Young, et al. Arch Intern Med. 2011;171[6]:498). This highlights the Achilles heel of ICU telemedicine evidence: the pretest/posttest studies that dominate this field and likely contribute substantially to the inconsistencies in the evidence base.
In the absence of risk adjustment and control groups, many studies observed postimplementation changes that may reflect trends in patient mix or the effects of unrelated practice changes rather than the causal influence of ICU telemedicine. In fact, in studies using more robust methods, ICU telemedicine’s effect size has been smaller or nonexistent. For example, in 2016, Kahn and colleagues used CMS data to evaluate 132 ICU telemedicine programs using 389 matched controlled hospitals. There was a slight reduction in 90-day mortality (OR=0.96, CI 0.94-0.98) with only 12% showing a statistically significant reduction in mortality. Interestingly, hospitals in urban areas demonstrated greater benefit than rural facilities (Kahn, et al. Medical Care. 2016;54[3]:319).
The heterogeneity of the studied programs (e.g., primary vs consultative role, on-demand vs proactive involvement) and recipient ICUs (e.g., rural vs tertiary care facility, presence of bedside intensivists) further hinders a clear answer to the key question: Would ICU telemedicine benefit my hospital? Fortunately, some recent, well-designed studies have attempted to understand which attributes of ICU telemedicine programs provide results and which ICUs will see the most benefit. In a cohort of 118,990 patients across 56 ICUs, four interventions were associated with lower mortality and reduced LOS: (1) evaluation of patients within 1 hour of ICU admission, (2) frequent leadership review of performance data, (3) ICU best practice compliance, and (4) prompt response to alerts (Lilly, et al. Chest. 2014;145[3]:500). Kahn and colleagues have also investigated this issue, conducting an in-depth ethnographic evaluation of 10 hospitals identified in their 2016 study to have positive, neutral, or negative outcomes after ICU telemedicine implementation (Kahn, et al. Am J Respir Crit Care Med. 2019;199[8]:970). They found that successful programs:
(1) provided consistent services matched to recipient needs;
(2) provided services both proactively and reactively without being obtrusive;
(3) embedded routine engagements unobtrusively into usual routines;
(4) had engaged leadership who set clear expectations and mediated conflicts; and
(5) had bedside clinicians who valued and sought out telemedicine participation in care.
The authors concluded that, “the true value of ICU telemedicine lies not in whether the technology exists but in how it is applied.” However, another recent analysis also suggested that, rather than telemedicine or recipient ICU design, targeting underperforming recipient ICU performance may be the key determinant of whether ICU telemedicine implementation improves outcomes (Fusaro, et al. Crit Care Med. 2019; 47[4]:501). While the finding may reflect regression to the mean, the idea that ICUs with above-expected mortality derive greater benefit from ICU telemedicine support than already well-performing ICUs is certainly logical.
As COVID-19 strained health care systems across the country, we and others found ways to use ICU telemedicine to preserve optimal care delivery for critically ill patients. Our program at Intermountain Healthcare – already supporting 17 ICUs within our 24-hospital health system, as well as 10 external ICUs with experienced critical care physicians, nurses, respiratory therapists, and pharmacists – took on increased responsibility for ICU load balancing and interhospital transfers.
Leveraging telemedicine services also helped community ICUs care for sicker, more complex patients than usual and aided nonintensivist physicians called upon to manage critically ill patients in ad hoc ICUs at referral hospitals. While the pandemic certainly stressed ICU staff, we suspect that telemedicine’s ability to balance caseloads and distribute clinical tasks helped mitigate these stresses. At age 40, ICU telemedicine is both mature and still growing, with continued expansion of bed coverage and the range of services available. Looking ahead, as we confront a national shortage of intensivists, ICU telemedicine likely represents a cost effective and efficient strategy to maintain critical care capacity with the potential to ensure low-cost, high-quality care for all, regardless of location.
Dr. Graham and Dr. Peltan are with the Division of Pulmonary & Critical Care Medicine, Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City, Utah; and Dr. Peltan is also with the Division of Pulmonary & Critical Care Medicine, Department of Medicine, Intermountain Medical Center, Murray, Utah.
connected with intensivists at the University Hospitals of Cleveland (Grundy, et al. Crit Care Med. 1982;10[7]:471). After this proof-of-concept report, however, ICU telemedicine gained little traction for nearly 20 years, until Johns Hopkins Hospital established a continuously monitored ICU telemedicine service in a nonintensivist staffed surgical ICU. Their pre/post analysis suggested a 64% decrease in severity-adjusted ICU mortality and greater than 30% decrease in ICU length of stay, ICU complications, and costs (Rosenfeld, et al. Crit Care Med. 2000;28[12]:3925).
Along with better and less costly telemedicine technology, rapid adoption of electronic medical records, and a nationwide intensivist shortage, this and other evidence for the service’s clinical and cost effectiveness has spurred explosive growth in ICU telemedicine in the succeeding 2 decades, with at least 18% of hospitals and 28% of ICU beds supported by ICU telemedicine by 2018 (Ofoma, et al. Crit Care Explor. 2021;4[3]:e0468).
Importantly, what “ICU telemedicine” represents varies substantially across hospitals and even across ICUs within systems. Two-way audiovisual technology is the defining feature, and at a minimum, programs provide intensivists and/or nurses who respond to consultation requests. Commonly, telemedicine clinicians directly connect with patients; monitor labs, hemodynamics, and alarms; and proactively contact on-site clinicians with recommendations or place orders directly into the electronic health record depending on whether the clinician acts as the patients’ primary, co-managing, or consultant provider. A centralized hub and spoke model with telemedicine personnel located at a single, remote center is the most common and best studied ICU telemedicine design. Additional staffing may include respiratory therapists, pharmacists, and advanced practice clinicians in coverage models that range from 24/7 to nocturnal and can also differ in whether patients are monitored continuously or on an as needed basis, triggered by alarms or clinician/nursing concerns.
On-demand services may extend to support for teams responding to medical emergencies inside and sometimes outside the ICU. Another equally important role that ICU telemedicine can provide is helping ensure facilities adhere to ICU quality metrics, such as ventilator bundles, DVT prophylaxis, and daily SAT/SBT.
Unsurprisingly, integrating ICU telemedicine into an existing system is very costly and complex, requiring substantial and thoughtful process redesign to maximize fiscal and clinical return on investment. One vendor of proprietary telemedicine technology, Philips eICU, estimates an implementation cost of $50,000 to $100,000 per bed with annual overhead, software maintenance, and IT staffing of ~20% of implementation costs in addition to clinician staffing of $1-2 million per 100 beds. However, some (but not all) evidence suggests that ICU telemedicine programs pay for themselves over time. An influential report from Sentara Healthcare, an early adopter of ICU telemedicine, described equipment costs of more than $1 million for a total of 103 critical care beds but attributed savings of $460,000 per month to decreased length of stay (Coustasse, et al. The Permanente Journal. 2014;18[4]:76).
Cost savings are great, of course, but ICU telemedicine’s potential to improve clinical outcomes is the real priority. While Sentara’s early report included a 27% decrease in ICU mortality after telemedicine adoption, a 2011 meta-analysis of 13 studies, including 35 ICUs and over 40,000 patients, suggested decreased ICU mortality and LOS with a statistically significant effect on overall hospital mortality and LOS (Young, et al. Arch Intern Med. 2011;171[6]:498). This highlights the Achilles heel of ICU telemedicine evidence: the pretest/posttest studies that dominate this field and likely contribute substantially to the inconsistencies in the evidence base.
In the absence of risk adjustment and control groups, many studies observed postimplementation changes that may reflect trends in patient mix or the effects of unrelated practice changes rather than the causal influence of ICU telemedicine. In fact, in studies using more robust methods, ICU telemedicine’s effect size has been smaller or nonexistent. For example, in 2016, Kahn and colleagues used CMS data to evaluate 132 ICU telemedicine programs using 389 matched controlled hospitals. There was a slight reduction in 90-day mortality (OR=0.96, CI 0.94-0.98) with only 12% showing a statistically significant reduction in mortality. Interestingly, hospitals in urban areas demonstrated greater benefit than rural facilities (Kahn, et al. Medical Care. 2016;54[3]:319).
The heterogeneity of the studied programs (e.g., primary vs consultative role, on-demand vs proactive involvement) and recipient ICUs (e.g., rural vs tertiary care facility, presence of bedside intensivists) further hinders a clear answer to the key question: Would ICU telemedicine benefit my hospital? Fortunately, some recent, well-designed studies have attempted to understand which attributes of ICU telemedicine programs provide results and which ICUs will see the most benefit. In a cohort of 118,990 patients across 56 ICUs, four interventions were associated with lower mortality and reduced LOS: (1) evaluation of patients within 1 hour of ICU admission, (2) frequent leadership review of performance data, (3) ICU best practice compliance, and (4) prompt response to alerts (Lilly, et al. Chest. 2014;145[3]:500). Kahn and colleagues have also investigated this issue, conducting an in-depth ethnographic evaluation of 10 hospitals identified in their 2016 study to have positive, neutral, or negative outcomes after ICU telemedicine implementation (Kahn, et al. Am J Respir Crit Care Med. 2019;199[8]:970). They found that successful programs:
(1) provided consistent services matched to recipient needs;
(2) provided services both proactively and reactively without being obtrusive;
(3) embedded routine engagements unobtrusively into usual routines;
(4) had engaged leadership who set clear expectations and mediated conflicts; and
(5) had bedside clinicians who valued and sought out telemedicine participation in care.
The authors concluded that, “the true value of ICU telemedicine lies not in whether the technology exists but in how it is applied.” However, another recent analysis also suggested that, rather than telemedicine or recipient ICU design, targeting underperforming recipient ICU performance may be the key determinant of whether ICU telemedicine implementation improves outcomes (Fusaro, et al. Crit Care Med. 2019; 47[4]:501). While the finding may reflect regression to the mean, the idea that ICUs with above-expected mortality derive greater benefit from ICU telemedicine support than already well-performing ICUs is certainly logical.
As COVID-19 strained health care systems across the country, we and others found ways to use ICU telemedicine to preserve optimal care delivery for critically ill patients. Our program at Intermountain Healthcare – already supporting 17 ICUs within our 24-hospital health system, as well as 10 external ICUs with experienced critical care physicians, nurses, respiratory therapists, and pharmacists – took on increased responsibility for ICU load balancing and interhospital transfers.
Leveraging telemedicine services also helped community ICUs care for sicker, more complex patients than usual and aided nonintensivist physicians called upon to manage critically ill patients in ad hoc ICUs at referral hospitals. While the pandemic certainly stressed ICU staff, we suspect that telemedicine’s ability to balance caseloads and distribute clinical tasks helped mitigate these stresses. At age 40, ICU telemedicine is both mature and still growing, with continued expansion of bed coverage and the range of services available. Looking ahead, as we confront a national shortage of intensivists, ICU telemedicine likely represents a cost effective and efficient strategy to maintain critical care capacity with the potential to ensure low-cost, high-quality care for all, regardless of location.
Dr. Graham and Dr. Peltan are with the Division of Pulmonary & Critical Care Medicine, Department of Internal Medicine, University of Utah School of Medicine, Salt Lake City, Utah; and Dr. Peltan is also with the Division of Pulmonary & Critical Care Medicine, Department of Medicine, Intermountain Medical Center, Murray, Utah.
Board of Regents meeting, August 16, 2022
The CHEST Board of Regents (BOR) convened a hybrid meeting in Atlanta prior to the pulmonary board review course. Hopefully, many of you had the opportunity to participate in that excellent learning experience. The function of the BOR is to provide direction and oversight for the organization’s strategy and goals, including the development of the many programs that are so expertly crafted by our talented staff, with contributions from our volunteers. Our EVP/CEO, Dr. Robert Musacchio, opened the meeting with a review of the organization’s mid-year progress toward achieving these annual goals. Despite the current economic turmoil and need for flexibility in our COVID landscape, CHEST is on track to meet or exceed the majority of the stated goals. The team continues efforts to achieve our key metrics related to increasing learners, members, and growth in revenue – we anticipate the upcoming annual meeting will only bolster our progress.
Every BOR meeting includes a report from the Finance Committee, which is thoroughly reviewed by the BOR. CHEST investments have fared no better than the rest of the country, but our investment advisors assure us that things will improve.
Similar updates were given by the President of the CHEST Foundation, Dr. Ian Nathanson, who noted that the Foundation will be celebrating its 25th anniversary during CHEST 2022. I would like to personally encourage you to donate and make this year the best year of fundraising. We are eager to bolster our community and patients after the long journey through COVID. Every donation enables more investment in creating access to the profession and in piloting programs across our communities that improve access to care. Thank you to those who have already contributed.
The morning session was completed with excellent presentations by the Chief Learning Officer/Education SVP, Richard Schuch and Publisher/Communications SVP, Nicki Augustyn. Rich provided an update on the education strategy and how it will change to keep up with the ever-changing needs of learners. He also made the observation that CHEST cannot do this alone, and partnering with companies to assist in new methods of content delivery will be important for the future of the organization. Nicki presented data regarding the current membership structure, as well as the effect of the pandemic on membership over the last 2 years.
In the afternoon session, the BOR and staff spent over 2 hours on the topic of advocacy. CHEST has become more active in the area of advocacy for both patients and the medical profession, specifically in the areas of pulmonary, critical care, and sleep medicine. The Health Policy and Advocacy Committee (HPAC) currently has workgroups working in five different areas, including: oxygen, pulmonary rehabilitation, coding and billing, noninvasive ventilation, and tobacco and vaping. However, CHEST is often asked to sign on to or support the advocacy efforts of other organizations, including other medical societies, patient groups, and industry groups. At times, the decision to support or not support is easy. While there is a process to make that decision, this session helped better define the process and started to create some norms around when CHEST itself should lead its own statement on a particular issue.
The BOR will meet a total of six times this year, either remotely or in person, to make certain that CHEST continues to fulfill its mission “to champion the prevention, diagnosis, and treatment of chest diseases through education, communication, and research.”
The CHEST Board of Regents (BOR) convened a hybrid meeting in Atlanta prior to the pulmonary board review course. Hopefully, many of you had the opportunity to participate in that excellent learning experience. The function of the BOR is to provide direction and oversight for the organization’s strategy and goals, including the development of the many programs that are so expertly crafted by our talented staff, with contributions from our volunteers. Our EVP/CEO, Dr. Robert Musacchio, opened the meeting with a review of the organization’s mid-year progress toward achieving these annual goals. Despite the current economic turmoil and need for flexibility in our COVID landscape, CHEST is on track to meet or exceed the majority of the stated goals. The team continues efforts to achieve our key metrics related to increasing learners, members, and growth in revenue – we anticipate the upcoming annual meeting will only bolster our progress.
Every BOR meeting includes a report from the Finance Committee, which is thoroughly reviewed by the BOR. CHEST investments have fared no better than the rest of the country, but our investment advisors assure us that things will improve.
Similar updates were given by the President of the CHEST Foundation, Dr. Ian Nathanson, who noted that the Foundation will be celebrating its 25th anniversary during CHEST 2022. I would like to personally encourage you to donate and make this year the best year of fundraising. We are eager to bolster our community and patients after the long journey through COVID. Every donation enables more investment in creating access to the profession and in piloting programs across our communities that improve access to care. Thank you to those who have already contributed.
The morning session was completed with excellent presentations by the Chief Learning Officer/Education SVP, Richard Schuch and Publisher/Communications SVP, Nicki Augustyn. Rich provided an update on the education strategy and how it will change to keep up with the ever-changing needs of learners. He also made the observation that CHEST cannot do this alone, and partnering with companies to assist in new methods of content delivery will be important for the future of the organization. Nicki presented data regarding the current membership structure, as well as the effect of the pandemic on membership over the last 2 years.
In the afternoon session, the BOR and staff spent over 2 hours on the topic of advocacy. CHEST has become more active in the area of advocacy for both patients and the medical profession, specifically in the areas of pulmonary, critical care, and sleep medicine. The Health Policy and Advocacy Committee (HPAC) currently has workgroups working in five different areas, including: oxygen, pulmonary rehabilitation, coding and billing, noninvasive ventilation, and tobacco and vaping. However, CHEST is often asked to sign on to or support the advocacy efforts of other organizations, including other medical societies, patient groups, and industry groups. At times, the decision to support or not support is easy. While there is a process to make that decision, this session helped better define the process and started to create some norms around when CHEST itself should lead its own statement on a particular issue.
The BOR will meet a total of six times this year, either remotely or in person, to make certain that CHEST continues to fulfill its mission “to champion the prevention, diagnosis, and treatment of chest diseases through education, communication, and research.”
The CHEST Board of Regents (BOR) convened a hybrid meeting in Atlanta prior to the pulmonary board review course. Hopefully, many of you had the opportunity to participate in that excellent learning experience. The function of the BOR is to provide direction and oversight for the organization’s strategy and goals, including the development of the many programs that are so expertly crafted by our talented staff, with contributions from our volunteers. Our EVP/CEO, Dr. Robert Musacchio, opened the meeting with a review of the organization’s mid-year progress toward achieving these annual goals. Despite the current economic turmoil and need for flexibility in our COVID landscape, CHEST is on track to meet or exceed the majority of the stated goals. The team continues efforts to achieve our key metrics related to increasing learners, members, and growth in revenue – we anticipate the upcoming annual meeting will only bolster our progress.
Every BOR meeting includes a report from the Finance Committee, which is thoroughly reviewed by the BOR. CHEST investments have fared no better than the rest of the country, but our investment advisors assure us that things will improve.
Similar updates were given by the President of the CHEST Foundation, Dr. Ian Nathanson, who noted that the Foundation will be celebrating its 25th anniversary during CHEST 2022. I would like to personally encourage you to donate and make this year the best year of fundraising. We are eager to bolster our community and patients after the long journey through COVID. Every donation enables more investment in creating access to the profession and in piloting programs across our communities that improve access to care. Thank you to those who have already contributed.
The morning session was completed with excellent presentations by the Chief Learning Officer/Education SVP, Richard Schuch and Publisher/Communications SVP, Nicki Augustyn. Rich provided an update on the education strategy and how it will change to keep up with the ever-changing needs of learners. He also made the observation that CHEST cannot do this alone, and partnering with companies to assist in new methods of content delivery will be important for the future of the organization. Nicki presented data regarding the current membership structure, as well as the effect of the pandemic on membership over the last 2 years.
In the afternoon session, the BOR and staff spent over 2 hours on the topic of advocacy. CHEST has become more active in the area of advocacy for both patients and the medical profession, specifically in the areas of pulmonary, critical care, and sleep medicine. The Health Policy and Advocacy Committee (HPAC) currently has workgroups working in five different areas, including: oxygen, pulmonary rehabilitation, coding and billing, noninvasive ventilation, and tobacco and vaping. However, CHEST is often asked to sign on to or support the advocacy efforts of other organizations, including other medical societies, patient groups, and industry groups. At times, the decision to support or not support is easy. While there is a process to make that decision, this session helped better define the process and started to create some norms around when CHEST itself should lead its own statement on a particular issue.
The BOR will meet a total of six times this year, either remotely or in person, to make certain that CHEST continues to fulfill its mission “to champion the prevention, diagnosis, and treatment of chest diseases through education, communication, and research.”
Noninvasive combination procedure effective for upper arm fat reduction, muscle toning
DENVER – , according to results from a study that analyzed results with MRI and other measures at two dermatology practices.
Simultaneous use of HIFEM and RF has been shown to be safe and effective “for fat reduction and muscle toning in various body parts,” lead study author Carolyn Jacob, MD, founder and director of Chicago Cosmetic Surgery and Dermatology, wrote in an abstract presented at the annual meeting of the American Society for Dermatologic Surgery. This study investigated the effect of the HIFEM and RF procedure on muscle toning and adipose tissue in the upper arms.

In what Dr. Jacob described as the first study of its kind because magnetic resonance imaging (MRI) was used to evaluate results, she and her coauthors enrolled 34 patients aged 23-72 years at two centers who had a BMI in the range of 18.5-33.9 kg/m2. The patients underwent four 30-minute bilateral procedures over the upper arms spaced 1 week apart with the Emsculpt NEO (BTL Aesthetics), which simultaneously delivers HIFEM and RF therapy.
NEO small sized applicators were used, which at the time of the study were under investigation but have since been cleared for use with the device. According to the manufacturer’s website, Emsculpt NEO is indicated for noninvasive lipolysis of the abdomen and thighs and reduction in the circumference of the abdomen and thighs in patients with skin types I-VI; and for noninvasive lipolysis of the upper arms “limited to skin types II and III and BMI 30 or under.”
The investigators measured changes in fat and triceps muscle tissue via MRI at baseline, 1-month, and 3-month follow-up visits. They also obtained digital photographs, administered patient questionnaires regarding comfort and satisfaction, and monitored safety of the treatments.
Of the 28 patients who completed their 1-month follow-up visit, analysis of MRI images showed a 22.3% average decrease in fat tissue from baseline MRIs (a decrease of 4.0 ± 1.2 mm; P < .01) and a 21.5% average increase in muscle mass (an increase of 8.2 ± 2.3 mm; P < .001). For the 25 patients who completed their 3-month follow-up visit, analysis of MRI images showed a 25.5% average decrease in fat tissue (a decrease of 4.9 ± 1.5 mm; P < .01) and a 23.9% average increase in muscle mass (an increase of 8.9 ± 2.0 mm; P < .001).
The analysis of questionnaires revealed high patient satisfaction with the results (87.1%), high comfort during the treatment (91.2%), and a low Visual Analogue Scale (VAS) score (1.6 ± 2.0) used to evaluate pain.
“This study shows that HIFEM and RF consistently increases muscle and decreases fat,” Dr. Jacob said in an interview. “It’s the only study on the triceps showing MRI evidence of fat loss with a nonsurgical body shaping device.”
She characterized the learning curve for the Emsculpt NEO as “small, as the previous Emsculpt small applicators have a similar fit.”
Pooja Sodha, MD, director of the center for laser and cosmetic dermatology at George Washington University, Washington, who was asked to comment on the study, said that the combination of radiofrequency energy and high-intensity focused electromagnetic technology triggers heat-induced damage of adipose tissue and muscle strengthening, respectively, to improve overall appearance and tone.
“Simultaneous delivery is the key here, and the real technological superhero, allowing us to take advantage of the synergistic effects of the muscle contractions and the tissue heating,” Dr. Sodha told this news organization. “Earlier this year, we saw published data on success with abdominal contouring with similar fat reduction and muscle enhancement as reported in this study, and these results persisted at 6 months,” with some declines noted at that time, she said.
“It is very encouraging and exciting to have similar effectiveness and safety for the arms, with such high satisfaction and comfort,” she added.
Dr. Jacob disclosed that she has conducted research studies for BTL Aesthetics since 2017 and is a member of the company’s advisory board. Dr. Sodha reported having no financial disclosures.
DENVER – , according to results from a study that analyzed results with MRI and other measures at two dermatology practices.
Simultaneous use of HIFEM and RF has been shown to be safe and effective “for fat reduction and muscle toning in various body parts,” lead study author Carolyn Jacob, MD, founder and director of Chicago Cosmetic Surgery and Dermatology, wrote in an abstract presented at the annual meeting of the American Society for Dermatologic Surgery. This study investigated the effect of the HIFEM and RF procedure on muscle toning and adipose tissue in the upper arms.
In what Dr. Jacob described as the first study of its kind because magnetic resonance imaging (MRI) was used to evaluate results, she and her coauthors enrolled 34 patients aged 23-72 years at two centers who had a BMI in the range of 18.5-33.9 kg/m2. The patients underwent four 30-minute bilateral procedures over the upper arms spaced 1 week apart with the Emsculpt NEO (BTL Aesthetics), which simultaneously delivers HIFEM and RF therapy.
NEO small sized applicators were used, which at the time of the study were under investigation but have since been cleared for use with the device. According to the manufacturer’s website, Emsculpt NEO is indicated for noninvasive lipolysis of the abdomen and thighs and reduction in the circumference of the abdomen and thighs in patients with skin types I-VI; and for noninvasive lipolysis of the upper arms “limited to skin types II and III and BMI 30 or under.”
The investigators measured changes in fat and triceps muscle tissue via MRI at baseline, 1-month, and 3-month follow-up visits. They also obtained digital photographs, administered patient questionnaires regarding comfort and satisfaction, and monitored safety of the treatments.
Of the 28 patients who completed their 1-month follow-up visit, analysis of MRI images showed a 22.3% average decrease in fat tissue from baseline MRIs (a decrease of 4.0 ± 1.2 mm; P < .01) and a 21.5% average increase in muscle mass (an increase of 8.2 ± 2.3 mm; P < .001). For the 25 patients who completed their 3-month follow-up visit, analysis of MRI images showed a 25.5% average decrease in fat tissue (a decrease of 4.9 ± 1.5 mm; P < .01) and a 23.9% average increase in muscle mass (an increase of 8.9 ± 2.0 mm; P < .001).
The analysis of questionnaires revealed high patient satisfaction with the results (87.1%), high comfort during the treatment (91.2%), and a low Visual Analogue Scale (VAS) score (1.6 ± 2.0) used to evaluate pain.
“This study shows that HIFEM and RF consistently increases muscle and decreases fat,” Dr. Jacob said in an interview. “It’s the only study on the triceps showing MRI evidence of fat loss with a nonsurgical body shaping device.”
She characterized the learning curve for the Emsculpt NEO as “small, as the previous Emsculpt small applicators have a similar fit.”
Pooja Sodha, MD, director of the center for laser and cosmetic dermatology at George Washington University, Washington, who was asked to comment on the study, said that the combination of radiofrequency energy and high-intensity focused electromagnetic technology triggers heat-induced damage of adipose tissue and muscle strengthening, respectively, to improve overall appearance and tone.
“Simultaneous delivery is the key here, and the real technological superhero, allowing us to take advantage of the synergistic effects of the muscle contractions and the tissue heating,” Dr. Sodha told this news organization. “Earlier this year, we saw published data on success with abdominal contouring with similar fat reduction and muscle enhancement as reported in this study, and these results persisted at 6 months,” with some declines noted at that time, she said.
“It is very encouraging and exciting to have similar effectiveness and safety for the arms, with such high satisfaction and comfort,” she added.
Dr. Jacob disclosed that she has conducted research studies for BTL Aesthetics since 2017 and is a member of the company’s advisory board. Dr. Sodha reported having no financial disclosures.
DENVER – , according to results from a study that analyzed results with MRI and other measures at two dermatology practices.
Simultaneous use of HIFEM and RF has been shown to be safe and effective “for fat reduction and muscle toning in various body parts,” lead study author Carolyn Jacob, MD, founder and director of Chicago Cosmetic Surgery and Dermatology, wrote in an abstract presented at the annual meeting of the American Society for Dermatologic Surgery. This study investigated the effect of the HIFEM and RF procedure on muscle toning and adipose tissue in the upper arms.
In what Dr. Jacob described as the first study of its kind because magnetic resonance imaging (MRI) was used to evaluate results, she and her coauthors enrolled 34 patients aged 23-72 years at two centers who had a BMI in the range of 18.5-33.9 kg/m2. The patients underwent four 30-minute bilateral procedures over the upper arms spaced 1 week apart with the Emsculpt NEO (BTL Aesthetics), which simultaneously delivers HIFEM and RF therapy.
NEO small sized applicators were used, which at the time of the study were under investigation but have since been cleared for use with the device. According to the manufacturer’s website, Emsculpt NEO is indicated for noninvasive lipolysis of the abdomen and thighs and reduction in the circumference of the abdomen and thighs in patients with skin types I-VI; and for noninvasive lipolysis of the upper arms “limited to skin types II and III and BMI 30 or under.”
The investigators measured changes in fat and triceps muscle tissue via MRI at baseline, 1-month, and 3-month follow-up visits. They also obtained digital photographs, administered patient questionnaires regarding comfort and satisfaction, and monitored safety of the treatments.
Of the 28 patients who completed their 1-month follow-up visit, analysis of MRI images showed a 22.3% average decrease in fat tissue from baseline MRIs (a decrease of 4.0 ± 1.2 mm; P < .01) and a 21.5% average increase in muscle mass (an increase of 8.2 ± 2.3 mm; P < .001). For the 25 patients who completed their 3-month follow-up visit, analysis of MRI images showed a 25.5% average decrease in fat tissue (a decrease of 4.9 ± 1.5 mm; P < .01) and a 23.9% average increase in muscle mass (an increase of 8.9 ± 2.0 mm; P < .001).
The analysis of questionnaires revealed high patient satisfaction with the results (87.1%), high comfort during the treatment (91.2%), and a low Visual Analogue Scale (VAS) score (1.6 ± 2.0) used to evaluate pain.
“This study shows that HIFEM and RF consistently increases muscle and decreases fat,” Dr. Jacob said in an interview. “It’s the only study on the triceps showing MRI evidence of fat loss with a nonsurgical body shaping device.”
She characterized the learning curve for the Emsculpt NEO as “small, as the previous Emsculpt small applicators have a similar fit.”
Pooja Sodha, MD, director of the center for laser and cosmetic dermatology at George Washington University, Washington, who was asked to comment on the study, said that the combination of radiofrequency energy and high-intensity focused electromagnetic technology triggers heat-induced damage of adipose tissue and muscle strengthening, respectively, to improve overall appearance and tone.
“Simultaneous delivery is the key here, and the real technological superhero, allowing us to take advantage of the synergistic effects of the muscle contractions and the tissue heating,” Dr. Sodha told this news organization. “Earlier this year, we saw published data on success with abdominal contouring with similar fat reduction and muscle enhancement as reported in this study, and these results persisted at 6 months,” with some declines noted at that time, she said.
“It is very encouraging and exciting to have similar effectiveness and safety for the arms, with such high satisfaction and comfort,” she added.
Dr. Jacob disclosed that she has conducted research studies for BTL Aesthetics since 2017 and is a member of the company’s advisory board. Dr. Sodha reported having no financial disclosures.
AT ASDS 2022
‘Low and Slow’ hyperthermic treatment being evaluated for superficial and nodular BCCs
DENVER –
At the annual meeting of the American Society for Dermatologic Surgery, Christopher Zachary, MD, and colleagues described a novel, noninvasive standardized controlled hyperthermia and mapping protocol (CHAMP) designed to help clinicians with margin assessment and treatment of superficial and nodular basal cell cancers (BCCs). “There’s considerable interest on the part of the public in having CHAMP treatment for their BCCs,” Dr. Zachary, professor and chair emeritus, University of California, Irvine, told this news organization in advance of the meeting.
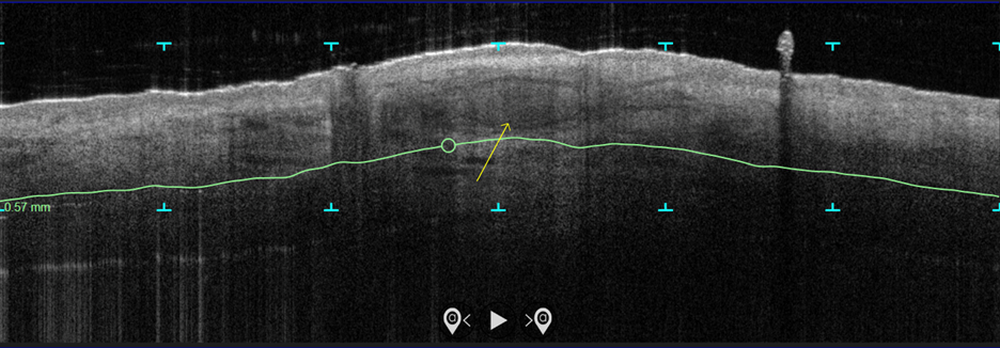
In the study, which is being conducted at three centers and plans to enroll 100 patients, more than 70 patients with biopsy-proven superficial and nodular BCCs have been scanned with the VivoSight Dx optical coherence tomography (OCT) device to map BCC tumor margins. Next, they were treated with the Sciton 1,064-nm Er:YAG laser equipped with a 4-mm beam diameter scan pattern with no overlap and an 8-millisecond pulse duration, randomized to either 120 J/cm2 pulses, until tissue graying and contraction was observed, or a novel controlled hyperthermia technique known as “Low and Slow” using repeated 25 J/cm2 pulses under thermal camera imaging to maintain a consistent temperature of 55º C for 60 seconds.
The researchers reassessed the tissue response both clinically and by OCT at 3 months and the patients were retreated with the same method if residual BCC was demonstrated. At 3-12 months post treatment, the lesion sites were saucerized and examined histologically by step sections to confirm clearance.
“In contrast to the more commonly performed ‘standard’ long-pulse 1,064-nm laser tumor coagulation, where the end point is graying and contraction of tissue, the new controlled ‘Low and Slow’ technique heats the tissue to 55º C for 60 seconds, avoids ulceration, and induces apoptotic tumor disappearance by a caspase-3 and -7 mechanism,” Dr. Zachary explained in an interview. “It’s a gentler process that allows patients an alternative to second intention wounds that occur after electrodessication and curettage or Mohs,” he added, noting that CHAMP is not intended for the treatment of more complex, large, recurrent, or infiltrative BCCs.
In both study arms, the majority of patients enrolled to date have been found to be free of tumor at 3 months by clinical and OCT examination. “The study is ongoing, but the current numbers indicate that 9 out of 10 superficial and nodular BCCs are free of tumor at 3-12 months after the last treatment,” Dr. Zachary said. The standard-treatment arm, where tissue was treated to a gray color with tissue contraction, generally resulted in more blistering and tissue necrosis with prolonged healing, compared with the Low and Slow–controlled hyperthermia arm. BCC lesions treated in the controlled hyperthermia arm had a lilac gray color with “a surprising increase” in the Doppler blood flow rate, compared with those in the standard-treatment arm, he noted.
“Blood flow following the standard technique is dramatically reduced immediately post treatment, which accounts in part for the frequent ulceration and slow healing in that group,” Dr. Zachary said.
He acknowledged certain limitations of the study, including its relatively small sample size and the fact that the optimal treatment parameters of the Low and Slow technique have yet to be realized. “It could be that we will achieve better results at 50º C for 70 seconds or similar,” he said. “While this technique will not in any way reduce the great benefits of Mohs surgery for complex BCCs, it will benefit those with simpler superficial and nodular BCCs, particularly in those who are not good surgical candidates.”
As an aside, Dr. Zachary supports the increased use of OCT scanners to improve the ability to diagnose and assess the lateral and deep margins of skin cancers. “I think that all dermatology residents should understand how to use these devices,” he said. “I’m convinced they are going to be useful in their clinical practice in the future.”
Keith L. Duffy, MD, who was asked to comment on the work, said that the study demonstrates novel ways to use existing and developing technologies in dermatology and highlights the intersection of aesthetic, surgical, and medical dermatology. “CHAMP is promising as shown by the data in the abstract and I am eager to see the final results of the study with an eye toward final cure rate and cosmesis,” said Dr. Duffy, associate professor of dermatology at the University of Utah, Salt Lake City.
“In my estimation, this technology will need to prove to be superior in one or both of these parameters in order to be considered a first- or second-line therapy,” he added. “My practice for these types of basal cell carcinomas is a simple one pass of curettage with aluminum chloride or pressure for hemostasis. The healing is fast, the cosmesis is excellent, and the cure rate is more than 90% for this simple in-office destruction. However, for those with access to this technology and proficiency with its use, CHAMP may become a viable alternative to our existing destructive methods. I look forward to seeing the published results of this multicenter trial.”
This study is being funded by Michelson Diagnostics. Sciton provided the long-pulsed 1,064-nm lasers devices being used in the trial. Neither Dr. Zachary nor Dr. Duffy reported having relevant disclosures.
DENVER –
At the annual meeting of the American Society for Dermatologic Surgery, Christopher Zachary, MD, and colleagues described a novel, noninvasive standardized controlled hyperthermia and mapping protocol (CHAMP) designed to help clinicians with margin assessment and treatment of superficial and nodular basal cell cancers (BCCs). “There’s considerable interest on the part of the public in having CHAMP treatment for their BCCs,” Dr. Zachary, professor and chair emeritus, University of California, Irvine, told this news organization in advance of the meeting.
In the study, which is being conducted at three centers and plans to enroll 100 patients, more than 70 patients with biopsy-proven superficial and nodular BCCs have been scanned with the VivoSight Dx optical coherence tomography (OCT) device to map BCC tumor margins. Next, they were treated with the Sciton 1,064-nm Er:YAG laser equipped with a 4-mm beam diameter scan pattern with no overlap and an 8-millisecond pulse duration, randomized to either 120 J/cm2 pulses, until tissue graying and contraction was observed, or a novel controlled hyperthermia technique known as “Low and Slow” using repeated 25 J/cm2 pulses under thermal camera imaging to maintain a consistent temperature of 55º C for 60 seconds.
The researchers reassessed the tissue response both clinically and by OCT at 3 months and the patients were retreated with the same method if residual BCC was demonstrated. At 3-12 months post treatment, the lesion sites were saucerized and examined histologically by step sections to confirm clearance.
“In contrast to the more commonly performed ‘standard’ long-pulse 1,064-nm laser tumor coagulation, where the end point is graying and contraction of tissue, the new controlled ‘Low and Slow’ technique heats the tissue to 55º C for 60 seconds, avoids ulceration, and induces apoptotic tumor disappearance by a caspase-3 and -7 mechanism,” Dr. Zachary explained in an interview. “It’s a gentler process that allows patients an alternative to second intention wounds that occur after electrodessication and curettage or Mohs,” he added, noting that CHAMP is not intended for the treatment of more complex, large, recurrent, or infiltrative BCCs.
In both study arms, the majority of patients enrolled to date have been found to be free of tumor at 3 months by clinical and OCT examination. “The study is ongoing, but the current numbers indicate that 9 out of 10 superficial and nodular BCCs are free of tumor at 3-12 months after the last treatment,” Dr. Zachary said. The standard-treatment arm, where tissue was treated to a gray color with tissue contraction, generally resulted in more blistering and tissue necrosis with prolonged healing, compared with the Low and Slow–controlled hyperthermia arm. BCC lesions treated in the controlled hyperthermia arm had a lilac gray color with “a surprising increase” in the Doppler blood flow rate, compared with those in the standard-treatment arm, he noted.
“Blood flow following the standard technique is dramatically reduced immediately post treatment, which accounts in part for the frequent ulceration and slow healing in that group,” Dr. Zachary said.
He acknowledged certain limitations of the study, including its relatively small sample size and the fact that the optimal treatment parameters of the Low and Slow technique have yet to be realized. “It could be that we will achieve better results at 50º C for 70 seconds or similar,” he said. “While this technique will not in any way reduce the great benefits of Mohs surgery for complex BCCs, it will benefit those with simpler superficial and nodular BCCs, particularly in those who are not good surgical candidates.”
As an aside, Dr. Zachary supports the increased use of OCT scanners to improve the ability to diagnose and assess the lateral and deep margins of skin cancers. “I think that all dermatology residents should understand how to use these devices,” he said. “I’m convinced they are going to be useful in their clinical practice in the future.”
Keith L. Duffy, MD, who was asked to comment on the work, said that the study demonstrates novel ways to use existing and developing technologies in dermatology and highlights the intersection of aesthetic, surgical, and medical dermatology. “CHAMP is promising as shown by the data in the abstract and I am eager to see the final results of the study with an eye toward final cure rate and cosmesis,” said Dr. Duffy, associate professor of dermatology at the University of Utah, Salt Lake City.
“In my estimation, this technology will need to prove to be superior in one or both of these parameters in order to be considered a first- or second-line therapy,” he added. “My practice for these types of basal cell carcinomas is a simple one pass of curettage with aluminum chloride or pressure for hemostasis. The healing is fast, the cosmesis is excellent, and the cure rate is more than 90% for this simple in-office destruction. However, for those with access to this technology and proficiency with its use, CHAMP may become a viable alternative to our existing destructive methods. I look forward to seeing the published results of this multicenter trial.”
This study is being funded by Michelson Diagnostics. Sciton provided the long-pulsed 1,064-nm lasers devices being used in the trial. Neither Dr. Zachary nor Dr. Duffy reported having relevant disclosures.
DENVER –
At the annual meeting of the American Society for Dermatologic Surgery, Christopher Zachary, MD, and colleagues described a novel, noninvasive standardized controlled hyperthermia and mapping protocol (CHAMP) designed to help clinicians with margin assessment and treatment of superficial and nodular basal cell cancers (BCCs). “There’s considerable interest on the part of the public in having CHAMP treatment for their BCCs,” Dr. Zachary, professor and chair emeritus, University of California, Irvine, told this news organization in advance of the meeting.
In the study, which is being conducted at three centers and plans to enroll 100 patients, more than 70 patients with biopsy-proven superficial and nodular BCCs have been scanned with the VivoSight Dx optical coherence tomography (OCT) device to map BCC tumor margins. Next, they were treated with the Sciton 1,064-nm Er:YAG laser equipped with a 4-mm beam diameter scan pattern with no overlap and an 8-millisecond pulse duration, randomized to either 120 J/cm2 pulses, until tissue graying and contraction was observed, or a novel controlled hyperthermia technique known as “Low and Slow” using repeated 25 J/cm2 pulses under thermal camera imaging to maintain a consistent temperature of 55º C for 60 seconds.
The researchers reassessed the tissue response both clinically and by OCT at 3 months and the patients were retreated with the same method if residual BCC was demonstrated. At 3-12 months post treatment, the lesion sites were saucerized and examined histologically by step sections to confirm clearance.
“In contrast to the more commonly performed ‘standard’ long-pulse 1,064-nm laser tumor coagulation, where the end point is graying and contraction of tissue, the new controlled ‘Low and Slow’ technique heats the tissue to 55º C for 60 seconds, avoids ulceration, and induces apoptotic tumor disappearance by a caspase-3 and -7 mechanism,” Dr. Zachary explained in an interview. “It’s a gentler process that allows patients an alternative to second intention wounds that occur after electrodessication and curettage or Mohs,” he added, noting that CHAMP is not intended for the treatment of more complex, large, recurrent, or infiltrative BCCs.
In both study arms, the majority of patients enrolled to date have been found to be free of tumor at 3 months by clinical and OCT examination. “The study is ongoing, but the current numbers indicate that 9 out of 10 superficial and nodular BCCs are free of tumor at 3-12 months after the last treatment,” Dr. Zachary said. The standard-treatment arm, where tissue was treated to a gray color with tissue contraction, generally resulted in more blistering and tissue necrosis with prolonged healing, compared with the Low and Slow–controlled hyperthermia arm. BCC lesions treated in the controlled hyperthermia arm had a lilac gray color with “a surprising increase” in the Doppler blood flow rate, compared with those in the standard-treatment arm, he noted.
“Blood flow following the standard technique is dramatically reduced immediately post treatment, which accounts in part for the frequent ulceration and slow healing in that group,” Dr. Zachary said.
He acknowledged certain limitations of the study, including its relatively small sample size and the fact that the optimal treatment parameters of the Low and Slow technique have yet to be realized. “It could be that we will achieve better results at 50º C for 70 seconds or similar,” he said. “While this technique will not in any way reduce the great benefits of Mohs surgery for complex BCCs, it will benefit those with simpler superficial and nodular BCCs, particularly in those who are not good surgical candidates.”
As an aside, Dr. Zachary supports the increased use of OCT scanners to improve the ability to diagnose and assess the lateral and deep margins of skin cancers. “I think that all dermatology residents should understand how to use these devices,” he said. “I’m convinced they are going to be useful in their clinical practice in the future.”
Keith L. Duffy, MD, who was asked to comment on the work, said that the study demonstrates novel ways to use existing and developing technologies in dermatology and highlights the intersection of aesthetic, surgical, and medical dermatology. “CHAMP is promising as shown by the data in the abstract and I am eager to see the final results of the study with an eye toward final cure rate and cosmesis,” said Dr. Duffy, associate professor of dermatology at the University of Utah, Salt Lake City.
“In my estimation, this technology will need to prove to be superior in one or both of these parameters in order to be considered a first- or second-line therapy,” he added. “My practice for these types of basal cell carcinomas is a simple one pass of curettage with aluminum chloride or pressure for hemostasis. The healing is fast, the cosmesis is excellent, and the cure rate is more than 90% for this simple in-office destruction. However, for those with access to this technology and proficiency with its use, CHAMP may become a viable alternative to our existing destructive methods. I look forward to seeing the published results of this multicenter trial.”
This study is being funded by Michelson Diagnostics. Sciton provided the long-pulsed 1,064-nm lasers devices being used in the trial. Neither Dr. Zachary nor Dr. Duffy reported having relevant disclosures.
AT ASDS 2022
Liquid injectable silicone safe for acne scarring in dark-skinned patients, study finds
DENVER – Highly , results from a recent study showed.
“Acne is pervasive, and acne scarring disproportionately affects darker skin types,” lead study author Nicole Salame, MD, told this news organization in advance of the annual meeting of the American Society for Dermatologic Surgery, where she presented the results of the study. “Treatment of acne scarring in darker skin is also particularly challenging since resurfacing can be problematic. Numerous treatment options exist but vary in effectiveness, sustainability, and side-effect profile, especially for patients with darker skin.”

Highly purified liquid injectable silicone (also known as LIS) is approved by the Food and Drug Administration for treating intraocular tamponade of retinal detachment, and has been used off label for skin augmentation. A 2005 study of LIS for five patients with acne scarring, with up to 30 years of follow-up, showed efficacy and preservation of product without complications for depressed, broad-based acne scars .
“Use of LIS as a permanent treatment for acne scarring in darker skin types has yet to be evaluated,” said Dr. Salame, a 4th-year dermatology resident at Emory University, Atlanta. “Our study is the first to retrospectively evaluate the safety and efficacy of highly purified LIS for the treatment of acne scars in all skin types.”
Dr. Salame and coauthor Harold J. Brody, MD, evaluated the charts of 96 patients with a mean age of 51 years who received highly purified LIS for the treatment of acne scars at Dr. Brody’s Atlanta-based private dermatology practice between July 2010 and March 2021. Of the 96 patients, 31 had darker skin types (20 were Fitzpatrick skin type IV and 11 were Fitzpatrick skin type V). Dr. Brody performed all treatments: a total of 206 in the 96 patients.
The average time of follow-up was 6.31 years; 19 patients had a follow-up of 1-3 years, 25 had a follow-up of 3-5 years, and 52 had a follow-up of greater than 5 years. The researchers did not observe any complications along the course of the patients’ treatments, and no patients reported complications or dissatisfaction with treatment.
“Among the most impressive findings of our study was the permanence of effectiveness of LIS for acne scarring in patients who had treatment over a decade before,” Dr. Salame said. “Our longest follow up was 12 years. These patients continued to show improvement in their acne scarring years after treatment with LIS, even as they lost collagen and volume in their face with advancing age.”
In addition, she said, none of the patients experienced complications of granulomatous reactions, migration, or extrusion of product, which were previously documented with the use of macrodroplet injectable silicone techniques. “This is likely due to the consistent use of the microdroplet injection technique in our study – less than 0.01 cc per injection at minimum 6- to 8-week intervals or more,” Dr. Salame said.
Lawrence J. Green, MD, of the department of dermatology at George Washington University, Washington, who was asked to comment on the study, said that the findings “show safety and durability of highly purified microdroplet liquid silicone to treat acne scars. The numbers of patients reviewed are small and selective (one highly skilled dermatologist), but with the right material (highly purified liquid silicone) and in a qualified and experienced physician’s hand, this treatment seems like a great option.”
Dr. Salame acknowledged certain limitations of the study, including its single-center, retrospective design. “Future prospective studies with larger patient populations of all skin types recruited from multiple centers may be needed,” she said.
The researchers reported having no relevant conflicts of interest or funding sources to disclose. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
DENVER – Highly , results from a recent study showed.
“Acne is pervasive, and acne scarring disproportionately affects darker skin types,” lead study author Nicole Salame, MD, told this news organization in advance of the annual meeting of the American Society for Dermatologic Surgery, where she presented the results of the study. “Treatment of acne scarring in darker skin is also particularly challenging since resurfacing can be problematic. Numerous treatment options exist but vary in effectiveness, sustainability, and side-effect profile, especially for patients with darker skin.”
Highly purified liquid injectable silicone (also known as LIS) is approved by the Food and Drug Administration for treating intraocular tamponade of retinal detachment, and has been used off label for skin augmentation. A 2005 study of LIS for five patients with acne scarring, with up to 30 years of follow-up, showed efficacy and preservation of product without complications for depressed, broad-based acne scars .
“Use of LIS as a permanent treatment for acne scarring in darker skin types has yet to be evaluated,” said Dr. Salame, a 4th-year dermatology resident at Emory University, Atlanta. “Our study is the first to retrospectively evaluate the safety and efficacy of highly purified LIS for the treatment of acne scars in all skin types.”
Dr. Salame and coauthor Harold J. Brody, MD, evaluated the charts of 96 patients with a mean age of 51 years who received highly purified LIS for the treatment of acne scars at Dr. Brody’s Atlanta-based private dermatology practice between July 2010 and March 2021. Of the 96 patients, 31 had darker skin types (20 were Fitzpatrick skin type IV and 11 were Fitzpatrick skin type V). Dr. Brody performed all treatments: a total of 206 in the 96 patients.
The average time of follow-up was 6.31 years; 19 patients had a follow-up of 1-3 years, 25 had a follow-up of 3-5 years, and 52 had a follow-up of greater than 5 years. The researchers did not observe any complications along the course of the patients’ treatments, and no patients reported complications or dissatisfaction with treatment.
“Among the most impressive findings of our study was the permanence of effectiveness of LIS for acne scarring in patients who had treatment over a decade before,” Dr. Salame said. “Our longest follow up was 12 years. These patients continued to show improvement in their acne scarring years after treatment with LIS, even as they lost collagen and volume in their face with advancing age.”
In addition, she said, none of the patients experienced complications of granulomatous reactions, migration, or extrusion of product, which were previously documented with the use of macrodroplet injectable silicone techniques. “This is likely due to the consistent use of the microdroplet injection technique in our study – less than 0.01 cc per injection at minimum 6- to 8-week intervals or more,” Dr. Salame said.
Lawrence J. Green, MD, of the department of dermatology at George Washington University, Washington, who was asked to comment on the study, said that the findings “show safety and durability of highly purified microdroplet liquid silicone to treat acne scars. The numbers of patients reviewed are small and selective (one highly skilled dermatologist), but with the right material (highly purified liquid silicone) and in a qualified and experienced physician’s hand, this treatment seems like a great option.”
Dr. Salame acknowledged certain limitations of the study, including its single-center, retrospective design. “Future prospective studies with larger patient populations of all skin types recruited from multiple centers may be needed,” she said.
The researchers reported having no relevant conflicts of interest or funding sources to disclose. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
DENVER – Highly , results from a recent study showed.
“Acne is pervasive, and acne scarring disproportionately affects darker skin types,” lead study author Nicole Salame, MD, told this news organization in advance of the annual meeting of the American Society for Dermatologic Surgery, where she presented the results of the study. “Treatment of acne scarring in darker skin is also particularly challenging since resurfacing can be problematic. Numerous treatment options exist but vary in effectiveness, sustainability, and side-effect profile, especially for patients with darker skin.”
Highly purified liquid injectable silicone (also known as LIS) is approved by the Food and Drug Administration for treating intraocular tamponade of retinal detachment, and has been used off label for skin augmentation. A 2005 study of LIS for five patients with acne scarring, with up to 30 years of follow-up, showed efficacy and preservation of product without complications for depressed, broad-based acne scars .
“Use of LIS as a permanent treatment for acne scarring in darker skin types has yet to be evaluated,” said Dr. Salame, a 4th-year dermatology resident at Emory University, Atlanta. “Our study is the first to retrospectively evaluate the safety and efficacy of highly purified LIS for the treatment of acne scars in all skin types.”
Dr. Salame and coauthor Harold J. Brody, MD, evaluated the charts of 96 patients with a mean age of 51 years who received highly purified LIS for the treatment of acne scars at Dr. Brody’s Atlanta-based private dermatology practice between July 2010 and March 2021. Of the 96 patients, 31 had darker skin types (20 were Fitzpatrick skin type IV and 11 were Fitzpatrick skin type V). Dr. Brody performed all treatments: a total of 206 in the 96 patients.
The average time of follow-up was 6.31 years; 19 patients had a follow-up of 1-3 years, 25 had a follow-up of 3-5 years, and 52 had a follow-up of greater than 5 years. The researchers did not observe any complications along the course of the patients’ treatments, and no patients reported complications or dissatisfaction with treatment.
“Among the most impressive findings of our study was the permanence of effectiveness of LIS for acne scarring in patients who had treatment over a decade before,” Dr. Salame said. “Our longest follow up was 12 years. These patients continued to show improvement in their acne scarring years after treatment with LIS, even as they lost collagen and volume in their face with advancing age.”
In addition, she said, none of the patients experienced complications of granulomatous reactions, migration, or extrusion of product, which were previously documented with the use of macrodroplet injectable silicone techniques. “This is likely due to the consistent use of the microdroplet injection technique in our study – less than 0.01 cc per injection at minimum 6- to 8-week intervals or more,” Dr. Salame said.
Lawrence J. Green, MD, of the department of dermatology at George Washington University, Washington, who was asked to comment on the study, said that the findings “show safety and durability of highly purified microdroplet liquid silicone to treat acne scars. The numbers of patients reviewed are small and selective (one highly skilled dermatologist), but with the right material (highly purified liquid silicone) and in a qualified and experienced physician’s hand, this treatment seems like a great option.”
Dr. Salame acknowledged certain limitations of the study, including its single-center, retrospective design. “Future prospective studies with larger patient populations of all skin types recruited from multiple centers may be needed,” she said.
The researchers reported having no relevant conflicts of interest or funding sources to disclose. Dr. Green disclosed that he is a speaker, consultant, or investigator for numerous pharmaceutical companies.
AT ASDS 2022
Blindness from PRP injections a rare but potentially devastating side effect
DENVER – None of the cases involved scalp injections.
“Both soft tissue fillers and [PRP] are common injection-type treatments that dermatologists perform on the head and neck area,” lead study author Sean Wu, MD, said in an interview in advance of the annual meeting of the American Society for Dermatologic Surgery, where he presented the results during an oral abstract session. “Fillers are usually used to replace volume and fill in lines while PRP is usually used for skin rejuvenation and certain forms of hair loss. We know that fillers may rarely cause blindness if accidentally injected into a facial artery.”
Certain facial areas such as the glabella, nose, and forehead are considered high risk for blindness with filler injections. But whether PRP injections in those areas may also result in blindness is not yet known, so Dr. Wu and his colleagues, Xu He, MD, and Robert Weiss, MD, at the Maryland Laser, Skin, and Vein Institute in Hunt Valley, Md., performed what is believed to be the first systematic review of the topic. In January 2022 they searched the PubMed database, which yielded 224 articles from which they selected four for full review. The results were recently published in Dermatologic Surgery.
Collectively, the four articles reported a total of seven patients with unilateral vision loss or impairment following PRP injection. They ranged in age from 41 to 63 years. Skin rejuvenation was the indication for PRP injection in six patients and temporomandibular joint (TMJ) disorder in one. Three of the cases occurred in Venezuela while one each occurred in the United States, the United Kingdom, and Malaysia. All patients had signs of arterial occlusion or ischemia on retinal examination or imaging.

Dr. Wu and colleagues found that the glabella was the most common site of injection associated with vision loss (five cases), followed by the forehead (two cases), and one case each in the lateral canthus, nasolabial fold, and the TMJ. In all but two cases, vision loss occurred immediately after injection. (The number of injections exceeded seven because two patients received PRP in more than one site.)
Associated symptoms included ocular pain, fullness, eyelid ptosis, headache, nausea, vomiting, dizziness, tinnitus, and urinary urgency. At their initial ophthalmology evaluation, six patients had no light perception in the affected eye. Only one patient reported recovery of visual acuity at 3 months but with residual deficits on eye exam. This person had been evaluated and treated by an ophthalmologist within 3 hours of symptom onset.
“The other cases reported complete blindness in one eye,” Dr. Wu said. “There is no reversing agent for PRP, unlike for many fillers, so there is no clear-cut solution for this issue.”
Based on the results of the systematic review, Dr. Wu concluded that blindness is a rare complication of PRP. “We should take the same precautions when injecting PRP on the face as we do when injecting fillers,” he advised. “This may include not injecting in high-risk areas and aspirating prior to injection to make sure we are not accidentally injecting into an artery.”
It was “notable,” he added, that no cases of blindness occurred following scalp injections of PRP for hair loss, indicating “that this use of PRP is likely very safe from a vision loss standpoint.”
Dr. Wu acknowledged certain imitations of the analysis, including the low quality of some case reports/series. “There is a notable lack of detail on the PRP injection technique, as the authors of the case reports were generally not the PRP injectors themselves,” he said. “There was also no attempt at treatment in a series of four cases.”
Asked to comment on the review, Terrence Keaney, MD, founder and director of SkinDC, in Arlington, Va., said that the analysis underscores the importance of considering blindness as a possible side effect when injecting PRP into the face. “Using techniques that can minimize intravascular injections including the use of cannulas, aspiration, and larger needle size may help reduce this rare side effect,” said Dr. Keaney, a clinical associate professor of dermatology at George Washington University, Washington.

“It is important to recognize the lack of cases of blindness when injecting the scalp, one of the most popular PRP injection locations. This reduced risk may be due to the reduced communication between the scalp vasculature and the ophthalmic vasculature,” he added.
The study authors reported having no financial disclosures. Dr. Keaney disclosed that he is a member of the advisory board for Crown Aesthetics.
DENVER – None of the cases involved scalp injections.
“Both soft tissue fillers and [PRP] are common injection-type treatments that dermatologists perform on the head and neck area,” lead study author Sean Wu, MD, said in an interview in advance of the annual meeting of the American Society for Dermatologic Surgery, where he presented the results during an oral abstract session. “Fillers are usually used to replace volume and fill in lines while PRP is usually used for skin rejuvenation and certain forms of hair loss. We know that fillers may rarely cause blindness if accidentally injected into a facial artery.”
Certain facial areas such as the glabella, nose, and forehead are considered high risk for blindness with filler injections. But whether PRP injections in those areas may also result in blindness is not yet known, so Dr. Wu and his colleagues, Xu He, MD, and Robert Weiss, MD, at the Maryland Laser, Skin, and Vein Institute in Hunt Valley, Md., performed what is believed to be the first systematic review of the topic. In January 2022 they searched the PubMed database, which yielded 224 articles from which they selected four for full review. The results were recently published in Dermatologic Surgery.
Collectively, the four articles reported a total of seven patients with unilateral vision loss or impairment following PRP injection. They ranged in age from 41 to 63 years. Skin rejuvenation was the indication for PRP injection in six patients and temporomandibular joint (TMJ) disorder in one. Three of the cases occurred in Venezuela while one each occurred in the United States, the United Kingdom, and Malaysia. All patients had signs of arterial occlusion or ischemia on retinal examination or imaging.
Dr. Wu and colleagues found that the glabella was the most common site of injection associated with vision loss (five cases), followed by the forehead (two cases), and one case each in the lateral canthus, nasolabial fold, and the TMJ. In all but two cases, vision loss occurred immediately after injection. (The number of injections exceeded seven because two patients received PRP in more than one site.)
Associated symptoms included ocular pain, fullness, eyelid ptosis, headache, nausea, vomiting, dizziness, tinnitus, and urinary urgency. At their initial ophthalmology evaluation, six patients had no light perception in the affected eye. Only one patient reported recovery of visual acuity at 3 months but with residual deficits on eye exam. This person had been evaluated and treated by an ophthalmologist within 3 hours of symptom onset.
“The other cases reported complete blindness in one eye,” Dr. Wu said. “There is no reversing agent for PRP, unlike for many fillers, so there is no clear-cut solution for this issue.”
Based on the results of the systematic review, Dr. Wu concluded that blindness is a rare complication of PRP. “We should take the same precautions when injecting PRP on the face as we do when injecting fillers,” he advised. “This may include not injecting in high-risk areas and aspirating prior to injection to make sure we are not accidentally injecting into an artery.”
It was “notable,” he added, that no cases of blindness occurred following scalp injections of PRP for hair loss, indicating “that this use of PRP is likely very safe from a vision loss standpoint.”
Dr. Wu acknowledged certain imitations of the analysis, including the low quality of some case reports/series. “There is a notable lack of detail on the PRP injection technique, as the authors of the case reports were generally not the PRP injectors themselves,” he said. “There was also no attempt at treatment in a series of four cases.”
Asked to comment on the review, Terrence Keaney, MD, founder and director of SkinDC, in Arlington, Va., said that the analysis underscores the importance of considering blindness as a possible side effect when injecting PRP into the face. “Using techniques that can minimize intravascular injections including the use of cannulas, aspiration, and larger needle size may help reduce this rare side effect,” said Dr. Keaney, a clinical associate professor of dermatology at George Washington University, Washington.
“It is important to recognize the lack of cases of blindness when injecting the scalp, one of the most popular PRP injection locations. This reduced risk may be due to the reduced communication between the scalp vasculature and the ophthalmic vasculature,” he added.
The study authors reported having no financial disclosures. Dr. Keaney disclosed that he is a member of the advisory board for Crown Aesthetics.
DENVER – None of the cases involved scalp injections.
“Both soft tissue fillers and [PRP] are common injection-type treatments that dermatologists perform on the head and neck area,” lead study author Sean Wu, MD, said in an interview in advance of the annual meeting of the American Society for Dermatologic Surgery, where he presented the results during an oral abstract session. “Fillers are usually used to replace volume and fill in lines while PRP is usually used for skin rejuvenation and certain forms of hair loss. We know that fillers may rarely cause blindness if accidentally injected into a facial artery.”
Certain facial areas such as the glabella, nose, and forehead are considered high risk for blindness with filler injections. But whether PRP injections in those areas may also result in blindness is not yet known, so Dr. Wu and his colleagues, Xu He, MD, and Robert Weiss, MD, at the Maryland Laser, Skin, and Vein Institute in Hunt Valley, Md., performed what is believed to be the first systematic review of the topic. In January 2022 they searched the PubMed database, which yielded 224 articles from which they selected four for full review. The results were recently published in Dermatologic Surgery.
Collectively, the four articles reported a total of seven patients with unilateral vision loss or impairment following PRP injection. They ranged in age from 41 to 63 years. Skin rejuvenation was the indication for PRP injection in six patients and temporomandibular joint (TMJ) disorder in one. Three of the cases occurred in Venezuela while one each occurred in the United States, the United Kingdom, and Malaysia. All patients had signs of arterial occlusion or ischemia on retinal examination or imaging.
Dr. Wu and colleagues found that the glabella was the most common site of injection associated with vision loss (five cases), followed by the forehead (two cases), and one case each in the lateral canthus, nasolabial fold, and the TMJ. In all but two cases, vision loss occurred immediately after injection. (The number of injections exceeded seven because two patients received PRP in more than one site.)
Associated symptoms included ocular pain, fullness, eyelid ptosis, headache, nausea, vomiting, dizziness, tinnitus, and urinary urgency. At their initial ophthalmology evaluation, six patients had no light perception in the affected eye. Only one patient reported recovery of visual acuity at 3 months but with residual deficits on eye exam. This person had been evaluated and treated by an ophthalmologist within 3 hours of symptom onset.
“The other cases reported complete blindness in one eye,” Dr. Wu said. “There is no reversing agent for PRP, unlike for many fillers, so there is no clear-cut solution for this issue.”
Based on the results of the systematic review, Dr. Wu concluded that blindness is a rare complication of PRP. “We should take the same precautions when injecting PRP on the face as we do when injecting fillers,” he advised. “This may include not injecting in high-risk areas and aspirating prior to injection to make sure we are not accidentally injecting into an artery.”
It was “notable,” he added, that no cases of blindness occurred following scalp injections of PRP for hair loss, indicating “that this use of PRP is likely very safe from a vision loss standpoint.”
Dr. Wu acknowledged certain imitations of the analysis, including the low quality of some case reports/series. “There is a notable lack of detail on the PRP injection technique, as the authors of the case reports were generally not the PRP injectors themselves,” he said. “There was also no attempt at treatment in a series of four cases.”
Asked to comment on the review, Terrence Keaney, MD, founder and director of SkinDC, in Arlington, Va., said that the analysis underscores the importance of considering blindness as a possible side effect when injecting PRP into the face. “Using techniques that can minimize intravascular injections including the use of cannulas, aspiration, and larger needle size may help reduce this rare side effect,” said Dr. Keaney, a clinical associate professor of dermatology at George Washington University, Washington.
“It is important to recognize the lack of cases of blindness when injecting the scalp, one of the most popular PRP injection locations. This reduced risk may be due to the reduced communication between the scalp vasculature and the ophthalmic vasculature,” he added.
The study authors reported having no financial disclosures. Dr. Keaney disclosed that he is a member of the advisory board for Crown Aesthetics.
AT ASDS 2022
Pulmonary Vascular Disease & Cardiovascular Disease Network
Cardiovascular Medicine & Surgery Section
Emerging role of cardiopulmonary obstetric critical care
, with 23.8 women dying per 100,000 live births (Hoyert DL, Miniño AM. Maternal mortality in the United States. National Vital Statistics Reports; vol 69 no 2. Hyattsville, MD: National Center for Health Statistics. 2020). The care of this vulnerable population testifies to the quality of care provided across the country. Some of these poor outcomes are directly attributed to in-hospital deaths due to preexisting or newly discovered heart or lung diseases, such as valvular heart diseases, cardiomyopathies, pulmonary arterial hypertension, eclampsia, or other etiologies. With the development of advanced heart and lung programs across the nation capable of providing mechanical circulatory support and extracorporeal life support, we believe that incorporating a heart-lung-OB team approach to high-risk cases can identify knowledge gaps early and predict and prevent maternal complications.
In this proposed model, patients funnel to the hub facility to be cared for by a team of intensive care physicians, advanced heart failure physicians, cardiovascular and obstetric anesthesiologists, and maternal/fetal medicine physicians, with the potential addition of an adult ECMO team member.
A team huddle, using a virtual platform, would be organized by a designated OB coordinator at the patient’s admission with follow-up huddles every 2 to 3 days, to ensure the team stays engaged through delivery into the postpartum period. Value could be added with subsequent cardiac or pulmonary rehabilitation. With an emphasis on shared decision making, we can make it a national priority to save every woman during the birthing process.
Bindu Akkanti, MD, FCCP, Member-at-Large
Mark Warner, MD, FCCP, Member-at-Large
Cardiovascular Medicine & Surgery Section
Emerging role of cardiopulmonary obstetric critical care
, with 23.8 women dying per 100,000 live births (Hoyert DL, Miniño AM. Maternal mortality in the United States. National Vital Statistics Reports; vol 69 no 2. Hyattsville, MD: National Center for Health Statistics. 2020). The care of this vulnerable population testifies to the quality of care provided across the country. Some of these poor outcomes are directly attributed to in-hospital deaths due to preexisting or newly discovered heart or lung diseases, such as valvular heart diseases, cardiomyopathies, pulmonary arterial hypertension, eclampsia, or other etiologies. With the development of advanced heart and lung programs across the nation capable of providing mechanical circulatory support and extracorporeal life support, we believe that incorporating a heart-lung-OB team approach to high-risk cases can identify knowledge gaps early and predict and prevent maternal complications.
In this proposed model, patients funnel to the hub facility to be cared for by a team of intensive care physicians, advanced heart failure physicians, cardiovascular and obstetric anesthesiologists, and maternal/fetal medicine physicians, with the potential addition of an adult ECMO team member.
A team huddle, using a virtual platform, would be organized by a designated OB coordinator at the patient’s admission with follow-up huddles every 2 to 3 days, to ensure the team stays engaged through delivery into the postpartum period. Value could be added with subsequent cardiac or pulmonary rehabilitation. With an emphasis on shared decision making, we can make it a national priority to save every woman during the birthing process.
Bindu Akkanti, MD, FCCP, Member-at-Large
Mark Warner, MD, FCCP, Member-at-Large
Cardiovascular Medicine & Surgery Section
Emerging role of cardiopulmonary obstetric critical care
, with 23.8 women dying per 100,000 live births (Hoyert DL, Miniño AM. Maternal mortality in the United States. National Vital Statistics Reports; vol 69 no 2. Hyattsville, MD: National Center for Health Statistics. 2020). The care of this vulnerable population testifies to the quality of care provided across the country. Some of these poor outcomes are directly attributed to in-hospital deaths due to preexisting or newly discovered heart or lung diseases, such as valvular heart diseases, cardiomyopathies, pulmonary arterial hypertension, eclampsia, or other etiologies. With the development of advanced heart and lung programs across the nation capable of providing mechanical circulatory support and extracorporeal life support, we believe that incorporating a heart-lung-OB team approach to high-risk cases can identify knowledge gaps early and predict and prevent maternal complications.
In this proposed model, patients funnel to the hub facility to be cared for by a team of intensive care physicians, advanced heart failure physicians, cardiovascular and obstetric anesthesiologists, and maternal/fetal medicine physicians, with the potential addition of an adult ECMO team member.
A team huddle, using a virtual platform, would be organized by a designated OB coordinator at the patient’s admission with follow-up huddles every 2 to 3 days, to ensure the team stays engaged through delivery into the postpartum period. Value could be added with subsequent cardiac or pulmonary rehabilitation. With an emphasis on shared decision making, we can make it a national priority to save every woman during the birthing process.
Bindu Akkanti, MD, FCCP, Member-at-Large
Mark Warner, MD, FCCP, Member-at-Large