User login
Gout too often treated only in emergency department
Only about one in three patients seen in the emergency department of an academic health system for acute gout had a follow-up visit that addressed this condition, Lesley Jackson, MD, of the University of Alabama at Birmingham, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network (G-CAN).
Dr. Jackson presented research done on patients seen within her university’s health system, looking at 72 patients seen in the ED between September 2021 and February 2022. Medications prescribed at discharge from the ED included corticosteroids (46 patients, or 64%), opioids (45 patients, 63%), NSAIDs (31 patients, 43%), and colchicine (23 patients, 32%).
Only 26 patients, or about 36%, had a subsequent outpatient visit in the UAB health system addressing gout, she said. Of 33 patients with any outpatient follow-up visit within the UAB system, 21 were within 1 month after the index ED visit, followed by 3 more prior to 3 months, and 9 more after 3 months.
The limitations of the study includes its collection of data from a single institution. But the results highlight the need for improved quality of care for gout, with too many people being treated for this condition primarily in the ED, she said.
In an email exchange arranged by the Arthritis Foundation, Herbert S. B. Baraf, MD, said he agreed that patients too often limit their treatment for gout to seeking care for acute attacks in the ED.
Because of competing demands, physicians working there are more to take a “Band-Aid” approach and not impress upon patients that gout is a lifelong condition that needs follow-up and monitoring, said Dr. Baraf, clinical professor of medicine at George Washington University, Washington, and an associate clinical professor at the University of Maryland, Baltimore. He retired from private practice in 2022.
“This problem is akin to the patient who has a hip fracture due to osteoporosis who gets a surgical repair but is never referred for osteoporotic management,” wrote Dr. Baraf, who is a former board member of the Arthritis Foundation.
He suggested viewing gout as a form of arthritis that has two components.
“The first, that which brings the patient to seek medical care, is the often exquisitely painful attack of pain and swelling in a joint or joints that comes on acutely,” he wrote. “Calming these attacks are the focus of the patient and the doctor, who does the evaluation as relief of pain and inflammation is the most pressing task at hand.”
But equally important is the second element, addressing the cause of these flare ups of arthritis, he wrote. Elevated uric acid leads to crystalline deposits of urate in the joints, particularly in the feet, ankles, knees, and hands. Over time, these deposits generate seemingly random flare ups of acute joint pain in one or more of these areas.
“Thus, when a patient presents to an emergency room with a first or second attack of gout, pain relief is the primary focus of the visit,” Dr. Baraf wrote. “But if over time that is the only focus, and the elevation of serum uric acid is not addressed, deposits will continue to mount and flare ups will occur with increasing frequency and severity.”
This study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Jackson has no relevant financial disclosures.
Only about one in three patients seen in the emergency department of an academic health system for acute gout had a follow-up visit that addressed this condition, Lesley Jackson, MD, of the University of Alabama at Birmingham, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network (G-CAN).
Dr. Jackson presented research done on patients seen within her university’s health system, looking at 72 patients seen in the ED between September 2021 and February 2022. Medications prescribed at discharge from the ED included corticosteroids (46 patients, or 64%), opioids (45 patients, 63%), NSAIDs (31 patients, 43%), and colchicine (23 patients, 32%).
Only 26 patients, or about 36%, had a subsequent outpatient visit in the UAB health system addressing gout, she said. Of 33 patients with any outpatient follow-up visit within the UAB system, 21 were within 1 month after the index ED visit, followed by 3 more prior to 3 months, and 9 more after 3 months.
The limitations of the study includes its collection of data from a single institution. But the results highlight the need for improved quality of care for gout, with too many people being treated for this condition primarily in the ED, she said.
In an email exchange arranged by the Arthritis Foundation, Herbert S. B. Baraf, MD, said he agreed that patients too often limit their treatment for gout to seeking care for acute attacks in the ED.
Because of competing demands, physicians working there are more to take a “Band-Aid” approach and not impress upon patients that gout is a lifelong condition that needs follow-up and monitoring, said Dr. Baraf, clinical professor of medicine at George Washington University, Washington, and an associate clinical professor at the University of Maryland, Baltimore. He retired from private practice in 2022.
“This problem is akin to the patient who has a hip fracture due to osteoporosis who gets a surgical repair but is never referred for osteoporotic management,” wrote Dr. Baraf, who is a former board member of the Arthritis Foundation.
He suggested viewing gout as a form of arthritis that has two components.
“The first, that which brings the patient to seek medical care, is the often exquisitely painful attack of pain and swelling in a joint or joints that comes on acutely,” he wrote. “Calming these attacks are the focus of the patient and the doctor, who does the evaluation as relief of pain and inflammation is the most pressing task at hand.”
But equally important is the second element, addressing the cause of these flare ups of arthritis, he wrote. Elevated uric acid leads to crystalline deposits of urate in the joints, particularly in the feet, ankles, knees, and hands. Over time, these deposits generate seemingly random flare ups of acute joint pain in one or more of these areas.
“Thus, when a patient presents to an emergency room with a first or second attack of gout, pain relief is the primary focus of the visit,” Dr. Baraf wrote. “But if over time that is the only focus, and the elevation of serum uric acid is not addressed, deposits will continue to mount and flare ups will occur with increasing frequency and severity.”
This study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Jackson has no relevant financial disclosures.
Only about one in three patients seen in the emergency department of an academic health system for acute gout had a follow-up visit that addressed this condition, Lesley Jackson, MD, of the University of Alabama at Birmingham, reported at the annual research symposium of the Gout, Hyperuricemia, and Crystal Associated Disease Network (G-CAN).
Dr. Jackson presented research done on patients seen within her university’s health system, looking at 72 patients seen in the ED between September 2021 and February 2022. Medications prescribed at discharge from the ED included corticosteroids (46 patients, or 64%), opioids (45 patients, 63%), NSAIDs (31 patients, 43%), and colchicine (23 patients, 32%).
Only 26 patients, or about 36%, had a subsequent outpatient visit in the UAB health system addressing gout, she said. Of 33 patients with any outpatient follow-up visit within the UAB system, 21 were within 1 month after the index ED visit, followed by 3 more prior to 3 months, and 9 more after 3 months.
The limitations of the study includes its collection of data from a single institution. But the results highlight the need for improved quality of care for gout, with too many people being treated for this condition primarily in the ED, she said.
In an email exchange arranged by the Arthritis Foundation, Herbert S. B. Baraf, MD, said he agreed that patients too often limit their treatment for gout to seeking care for acute attacks in the ED.
Because of competing demands, physicians working there are more to take a “Band-Aid” approach and not impress upon patients that gout is a lifelong condition that needs follow-up and monitoring, said Dr. Baraf, clinical professor of medicine at George Washington University, Washington, and an associate clinical professor at the University of Maryland, Baltimore. He retired from private practice in 2022.
“This problem is akin to the patient who has a hip fracture due to osteoporosis who gets a surgical repair but is never referred for osteoporotic management,” wrote Dr. Baraf, who is a former board member of the Arthritis Foundation.
He suggested viewing gout as a form of arthritis that has two components.
“The first, that which brings the patient to seek medical care, is the often exquisitely painful attack of pain and swelling in a joint or joints that comes on acutely,” he wrote. “Calming these attacks are the focus of the patient and the doctor, who does the evaluation as relief of pain and inflammation is the most pressing task at hand.”
But equally important is the second element, addressing the cause of these flare ups of arthritis, he wrote. Elevated uric acid leads to crystalline deposits of urate in the joints, particularly in the feet, ankles, knees, and hands. Over time, these deposits generate seemingly random flare ups of acute joint pain in one or more of these areas.
“Thus, when a patient presents to an emergency room with a first or second attack of gout, pain relief is the primary focus of the visit,” Dr. Baraf wrote. “But if over time that is the only focus, and the elevation of serum uric acid is not addressed, deposits will continue to mount and flare ups will occur with increasing frequency and severity.”
This study was supported by a grant from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. Dr. Jackson has no relevant financial disclosures.
FROM G-CAN 2022
Hyaluronidase for Skin Necrosis Induced by Amiodarone
To the Editor:
Amiodarone is an oral or intravenous (IV) drug commonly used to treat supraventricular and ventricular arrhythmia as well as atrial fibrillation.1 Adverse drug reactions associated with the use of amiodarone include pulmonary, gastrointestinal, thyroid, ocular, neurologic, and cutaneous reactions.1 Long-term use of amiodarone—typically more than 4 months—can lead to slate-gray skin discoloration and photosensitivity, both of which can be reversed with drug withdrawal.2,3 Phlebitis also has been described in less than 3% of patients who receive peripheral IV administration of amiodarone.4
Amiodarone-induced skin necrosis due to extravasation is a rare complication of this antiarrhythmic medication, with only 3 reported cases in the literature according to a PubMed search of articles indexed for MEDLINE using the search terms amiodarone and skin and (necrosis or ischemia or extravasation or reaction).5–7 Although hyaluronidase is a known therapy for extravasation of fluids, including parenteral nutrition and chemotherapy, its use for the treatment of extravasation from amiodarone is not well documented.6 We report a case of skin necrosis of the left dorsal forearm and the left dorsal and ventral hand following infusion of amiodarone through a peripheral IV line, which was treated with injections of hyaluronidase.
A 77-year-old man was admitted to the emergency department for sepsis secondary to cholangitis in the setting of an obstructive gallbladder stone. His medical history was notable for multivessel coronary artery disease and atrial flutter treated with ablation. One day after admission, endoscopic retrograde cholangiopancreatography was attempted and aborted due to atrial fibrillation with rapid ventricular response. A second endoscopic retrograde cholangiopancreatography attempt was made 4 days later, during which the patient underwent cardiac arrest. During this event, amiodarone was administered in a 200-mL solution (1.8 mg/mL) in 5% dextrose through a peripheral IV line in the left forearm. The patient was stabilized and transferred to the intensive care unit.
Twenty-four hours after amiodarone administration, erythema was noted on the left dorsal forearm. Within hours, the digits of the hand became a dark, dusky color, which spread to involve the forearm. Surgical debridement was not deemed necessary; the left arm was elevated, and warm compresses were applied regularly. Within the next week, the skin of the left hand and dorsal forearm had progressively worsened and took on a well-demarcated, dusky blue hue surrounded by an erythematous border involving the proximal forearm and upper arm (Figure 1A). The skin was fragile and had overlying bullae (Figure 1B).

Hyaluronidase (1000 U) was injected into the surrounding areas of erythema, which resolved from the left proximal forearm to the elbow within 2 days after injection (Figure 2). The dusky violaceous patches were persistent, and the necrotic bullae were unchanged. Hyaluronidase (1000 U) was injected into necrotic skin of the left dorsal forearm and dorsal and ventral hand. No improvement was noted on subsequent evaluations of this area. While still an inpatient, he received wound care and twice-daily Doppler ultrasounds in the areas of necrosis. The patient lost sensation in the left hand with increased soft tissue necrosis and developed an eschar on the left dorsal forearm. Due to the progressive loss of function and necrosis, a partial forearm amputation was performed that healed well, and the patient experienced improvement in range of motion of the left upper extremity.

Well-known adverse reactions of amiodarone treatment include pulmonary fibrosis, hepatic dysfunction, hypothyroidism and hyperthyroidism, peripheral neuropathy, and corneal deposits.1 Cutaneous adverse reactions include photosensitivity (phototoxic and photoallergic reactions), hyperpigmentation, pseudoporphyria, and linear IgA bullous dermatosis. Less commonly, it also can cause urticaria, pruritus, erythema nodosum, purpura, and toxic epidermal necrolysis.3 Amiodarone-induced skin necrosis is rare, first described by Russell and Saltissi5 in 2006 in a 60-year-old man who developed dark discoloration and edema of the forearm 24 hours after initiation of an amiodarone peripheral IV. The patient was treated with hot or cold packs and steroid cream per the pharmaceutical company’s recommendations; however, patient outcomes were not discussed.5 A 77-year-old man who received subcutaneous amiodarone due to misplaced vascular access developed edema and bullae of the forearm followed by tissue necrosis, resulting in notably reduced mobility.6 Fox et al7 described a 60-year-old man who developed atrial fibrillation after emergent spinal fusion and laminectomy. He received intradermal hyaluronidase administration within 24 hours of developing severe pain from extravasation induced by amiodarone with no adverse outcomes and full recovery.7
There are numerous properties of amiodarone that may have resulted in the skin necrosis seen in these cases. The acidic pH (3.5–4.5) of amiodarone can contribute to coagulative necrosis, cellular desiccation, eschar formation, and edema.8 It also can contain additives such as polysorbate and benzyl alcohol, which may contribute to the drug’s vesicant properties.9
Current recommendations for IV administration of amiodarone include delivery through a central vein with high concentrations (>2 mg/mL) because peripheral infusion is slower and may cause phlebitis.4 In-line filters also may be a potential method of preventing phlebitis with peripheral IV administration of amiodarone.10 Extravasation of amiodarone can be treated nonpharmacologically with limb elevation and warm compresses, as these methods may promote vasodilation and enhance drug removal.5-7 However, when extravasation leads to progressive erythema and skin necrosis or is refractory to these therapies, intradermal injection of hyaluronidase should be considered. Hyaluronidase mediates the degradation of hyaluronic acid in the extracellular matrix, allowing for increased permeability of injected fluids into tissues and diluting the concentration of toxins at the site of exposure.9,11 It has been used to treat extravasation of fluids such as parenteral nutrition, electrolyte infusion, antibiotics, aminophylline, mannitol, and chemotherapy.11 Although hyaluronidase has been recognized as therapeutic for extravasation, there is no established consistent dosing or proper technique. In the setting of infiltration of chemotherapy, doses of hyaluronidase ranging from 150 to 1500 U/mL can be subcutaneously or intradermally injected into the site within 1 hour of extravasation. Side effects of using hyaluronidase are rare, including local pruritus, allergic reactions, urticaria, and angioedema.12
The patient described by Fox et al7 who fully recovered from amiodarone extravasation after hyaluronidase injections likely benefited from quick intervention, as he received amiodarone within 24 hours of the care team identifying initial erythema. Although our patient did have improvement of the areas of erythema on the forearm, evidence of skin and subcutaneous tissue necrosis on the left hand and proximal forearm was already apparent and not reversible, most likely caused by late intervention of intradermal hyaluronidase almost a week after the extravasation event. It is important to identify amiodarone as the source of extravasation and administer intradermal hyaluronidase in a timely fashion for extravasation refractory to conventional measurements to prevent progression to severe tissue damage.
Our case draws attention to the risk for skin necrosis with peripheral IV administration of amiodarone. Interventions include limb elevation, warm compresses, and consideration of intradermal hyaluronidase within 24 hours of extravasation, as this may reduce the severity of subsequent tissue damage with minimal side effects.
- Epstein AE, Olshansky B, Naccarelli GV, et al. Practical management guide for clinicians who treat patients with amiodarone. Am J Med. 2016;129:468-475. doi:10.1016/j.amjmed.2015.08.039
- Harris L, McKenna WJ, Rowland E, et al. Side effects of long-term amiodarone therapy. Circulation. 1983;67:45-51. doi:10.1161/01.cir.67.1.45
- Jaworski K, Walecka I, Rudnicka L, et al. Cutaneous adverse reactions of amiodarone. Med Sci Monit. 2014;20:2369-2372. doi:10.12659/MSM.890881
- Kowey Peter R, Marinchak Roger A, Rials Seth J, et al. Intravenous amiodarone. J Am Coll Cardiol. 1997;29:1190-1198. doi:10.1016/S0735-1097(97)00069-7
- Russell SJ, Saltissi S. Amiodarone induced skin necrosis. Heart. 2006;92:1395. doi:10.1136/hrt.2005.086157
- Grove EL. Skin necrosis and consequences of accidental subcutaneous administration of amiodarone. Ugeskr Laeger. 2015;177:V66928.
- Fox AN, Villanueva R, Miller JL. Management of amiodarone extravasation with intradermal hyaluronidase. Am J Health Syst Pharm. 2017;74:1545-1548. doi:10.2146/ajhp160737
- Reynolds PM, MacLaren R, Mueller SW, et al. Management of extravasation injuries: a focused evaluation of noncytotoxic medications. Pharmacotherapy. 2014;34:617-632. doi:https://doi.org/10.1002/phar.1396
- Le A, Patel S. Extravasation of noncytotoxic drugs: a review of the literature. Ann Pharmacother. 2014;48:870-886. doi:10.1177/1060028014527820
- Slim AM, Roth JE, Duffy B, et al. The incidence of phlebitis with intravenous amiodarone at guideline dose recommendations. Mil Med. 2007;172:1279-1283.
- Girish KS, Kemparaju K. The magic glue hyaluronan and its eraser hyaluronidase: a biological overview. Life Sci. 2007;80:1921-1943. doi:10.1016/j.lfs.2007.02.037
- Jung H. Hyaluronidase: an overview of its properties, applications, and side effects. Arch Plast Surg. 2020;47:297-300. doi:10.5999/aps.2020.00752
To the Editor:
Amiodarone is an oral or intravenous (IV) drug commonly used to treat supraventricular and ventricular arrhythmia as well as atrial fibrillation.1 Adverse drug reactions associated with the use of amiodarone include pulmonary, gastrointestinal, thyroid, ocular, neurologic, and cutaneous reactions.1 Long-term use of amiodarone—typically more than 4 months—can lead to slate-gray skin discoloration and photosensitivity, both of which can be reversed with drug withdrawal.2,3 Phlebitis also has been described in less than 3% of patients who receive peripheral IV administration of amiodarone.4
Amiodarone-induced skin necrosis due to extravasation is a rare complication of this antiarrhythmic medication, with only 3 reported cases in the literature according to a PubMed search of articles indexed for MEDLINE using the search terms amiodarone and skin and (necrosis or ischemia or extravasation or reaction).5–7 Although hyaluronidase is a known therapy for extravasation of fluids, including parenteral nutrition and chemotherapy, its use for the treatment of extravasation from amiodarone is not well documented.6 We report a case of skin necrosis of the left dorsal forearm and the left dorsal and ventral hand following infusion of amiodarone through a peripheral IV line, which was treated with injections of hyaluronidase.
A 77-year-old man was admitted to the emergency department for sepsis secondary to cholangitis in the setting of an obstructive gallbladder stone. His medical history was notable for multivessel coronary artery disease and atrial flutter treated with ablation. One day after admission, endoscopic retrograde cholangiopancreatography was attempted and aborted due to atrial fibrillation with rapid ventricular response. A second endoscopic retrograde cholangiopancreatography attempt was made 4 days later, during which the patient underwent cardiac arrest. During this event, amiodarone was administered in a 200-mL solution (1.8 mg/mL) in 5% dextrose through a peripheral IV line in the left forearm. The patient was stabilized and transferred to the intensive care unit.
Twenty-four hours after amiodarone administration, erythema was noted on the left dorsal forearm. Within hours, the digits of the hand became a dark, dusky color, which spread to involve the forearm. Surgical debridement was not deemed necessary; the left arm was elevated, and warm compresses were applied regularly. Within the next week, the skin of the left hand and dorsal forearm had progressively worsened and took on a well-demarcated, dusky blue hue surrounded by an erythematous border involving the proximal forearm and upper arm (Figure 1A). The skin was fragile and had overlying bullae (Figure 1B).
Hyaluronidase (1000 U) was injected into the surrounding areas of erythema, which resolved from the left proximal forearm to the elbow within 2 days after injection (Figure 2). The dusky violaceous patches were persistent, and the necrotic bullae were unchanged. Hyaluronidase (1000 U) was injected into necrotic skin of the left dorsal forearm and dorsal and ventral hand. No improvement was noted on subsequent evaluations of this area. While still an inpatient, he received wound care and twice-daily Doppler ultrasounds in the areas of necrosis. The patient lost sensation in the left hand with increased soft tissue necrosis and developed an eschar on the left dorsal forearm. Due to the progressive loss of function and necrosis, a partial forearm amputation was performed that healed well, and the patient experienced improvement in range of motion of the left upper extremity.
Well-known adverse reactions of amiodarone treatment include pulmonary fibrosis, hepatic dysfunction, hypothyroidism and hyperthyroidism, peripheral neuropathy, and corneal deposits.1 Cutaneous adverse reactions include photosensitivity (phototoxic and photoallergic reactions), hyperpigmentation, pseudoporphyria, and linear IgA bullous dermatosis. Less commonly, it also can cause urticaria, pruritus, erythema nodosum, purpura, and toxic epidermal necrolysis.3 Amiodarone-induced skin necrosis is rare, first described by Russell and Saltissi5 in 2006 in a 60-year-old man who developed dark discoloration and edema of the forearm 24 hours after initiation of an amiodarone peripheral IV. The patient was treated with hot or cold packs and steroid cream per the pharmaceutical company’s recommendations; however, patient outcomes were not discussed.5 A 77-year-old man who received subcutaneous amiodarone due to misplaced vascular access developed edema and bullae of the forearm followed by tissue necrosis, resulting in notably reduced mobility.6 Fox et al7 described a 60-year-old man who developed atrial fibrillation after emergent spinal fusion and laminectomy. He received intradermal hyaluronidase administration within 24 hours of developing severe pain from extravasation induced by amiodarone with no adverse outcomes and full recovery.7
There are numerous properties of amiodarone that may have resulted in the skin necrosis seen in these cases. The acidic pH (3.5–4.5) of amiodarone can contribute to coagulative necrosis, cellular desiccation, eschar formation, and edema.8 It also can contain additives such as polysorbate and benzyl alcohol, which may contribute to the drug’s vesicant properties.9
Current recommendations for IV administration of amiodarone include delivery through a central vein with high concentrations (>2 mg/mL) because peripheral infusion is slower and may cause phlebitis.4 In-line filters also may be a potential method of preventing phlebitis with peripheral IV administration of amiodarone.10 Extravasation of amiodarone can be treated nonpharmacologically with limb elevation and warm compresses, as these methods may promote vasodilation and enhance drug removal.5-7 However, when extravasation leads to progressive erythema and skin necrosis or is refractory to these therapies, intradermal injection of hyaluronidase should be considered. Hyaluronidase mediates the degradation of hyaluronic acid in the extracellular matrix, allowing for increased permeability of injected fluids into tissues and diluting the concentration of toxins at the site of exposure.9,11 It has been used to treat extravasation of fluids such as parenteral nutrition, electrolyte infusion, antibiotics, aminophylline, mannitol, and chemotherapy.11 Although hyaluronidase has been recognized as therapeutic for extravasation, there is no established consistent dosing or proper technique. In the setting of infiltration of chemotherapy, doses of hyaluronidase ranging from 150 to 1500 U/mL can be subcutaneously or intradermally injected into the site within 1 hour of extravasation. Side effects of using hyaluronidase are rare, including local pruritus, allergic reactions, urticaria, and angioedema.12
The patient described by Fox et al7 who fully recovered from amiodarone extravasation after hyaluronidase injections likely benefited from quick intervention, as he received amiodarone within 24 hours of the care team identifying initial erythema. Although our patient did have improvement of the areas of erythema on the forearm, evidence of skin and subcutaneous tissue necrosis on the left hand and proximal forearm was already apparent and not reversible, most likely caused by late intervention of intradermal hyaluronidase almost a week after the extravasation event. It is important to identify amiodarone as the source of extravasation and administer intradermal hyaluronidase in a timely fashion for extravasation refractory to conventional measurements to prevent progression to severe tissue damage.
Our case draws attention to the risk for skin necrosis with peripheral IV administration of amiodarone. Interventions include limb elevation, warm compresses, and consideration of intradermal hyaluronidase within 24 hours of extravasation, as this may reduce the severity of subsequent tissue damage with minimal side effects.
To the Editor:
Amiodarone is an oral or intravenous (IV) drug commonly used to treat supraventricular and ventricular arrhythmia as well as atrial fibrillation.1 Adverse drug reactions associated with the use of amiodarone include pulmonary, gastrointestinal, thyroid, ocular, neurologic, and cutaneous reactions.1 Long-term use of amiodarone—typically more than 4 months—can lead to slate-gray skin discoloration and photosensitivity, both of which can be reversed with drug withdrawal.2,3 Phlebitis also has been described in less than 3% of patients who receive peripheral IV administration of amiodarone.4
Amiodarone-induced skin necrosis due to extravasation is a rare complication of this antiarrhythmic medication, with only 3 reported cases in the literature according to a PubMed search of articles indexed for MEDLINE using the search terms amiodarone and skin and (necrosis or ischemia or extravasation or reaction).5–7 Although hyaluronidase is a known therapy for extravasation of fluids, including parenteral nutrition and chemotherapy, its use for the treatment of extravasation from amiodarone is not well documented.6 We report a case of skin necrosis of the left dorsal forearm and the left dorsal and ventral hand following infusion of amiodarone through a peripheral IV line, which was treated with injections of hyaluronidase.
A 77-year-old man was admitted to the emergency department for sepsis secondary to cholangitis in the setting of an obstructive gallbladder stone. His medical history was notable for multivessel coronary artery disease and atrial flutter treated with ablation. One day after admission, endoscopic retrograde cholangiopancreatography was attempted and aborted due to atrial fibrillation with rapid ventricular response. A second endoscopic retrograde cholangiopancreatography attempt was made 4 days later, during which the patient underwent cardiac arrest. During this event, amiodarone was administered in a 200-mL solution (1.8 mg/mL) in 5% dextrose through a peripheral IV line in the left forearm. The patient was stabilized and transferred to the intensive care unit.
Twenty-four hours after amiodarone administration, erythema was noted on the left dorsal forearm. Within hours, the digits of the hand became a dark, dusky color, which spread to involve the forearm. Surgical debridement was not deemed necessary; the left arm was elevated, and warm compresses were applied regularly. Within the next week, the skin of the left hand and dorsal forearm had progressively worsened and took on a well-demarcated, dusky blue hue surrounded by an erythematous border involving the proximal forearm and upper arm (Figure 1A). The skin was fragile and had overlying bullae (Figure 1B).
Hyaluronidase (1000 U) was injected into the surrounding areas of erythema, which resolved from the left proximal forearm to the elbow within 2 days after injection (Figure 2). The dusky violaceous patches were persistent, and the necrotic bullae were unchanged. Hyaluronidase (1000 U) was injected into necrotic skin of the left dorsal forearm and dorsal and ventral hand. No improvement was noted on subsequent evaluations of this area. While still an inpatient, he received wound care and twice-daily Doppler ultrasounds in the areas of necrosis. The patient lost sensation in the left hand with increased soft tissue necrosis and developed an eschar on the left dorsal forearm. Due to the progressive loss of function and necrosis, a partial forearm amputation was performed that healed well, and the patient experienced improvement in range of motion of the left upper extremity.
Well-known adverse reactions of amiodarone treatment include pulmonary fibrosis, hepatic dysfunction, hypothyroidism and hyperthyroidism, peripheral neuropathy, and corneal deposits.1 Cutaneous adverse reactions include photosensitivity (phototoxic and photoallergic reactions), hyperpigmentation, pseudoporphyria, and linear IgA bullous dermatosis. Less commonly, it also can cause urticaria, pruritus, erythema nodosum, purpura, and toxic epidermal necrolysis.3 Amiodarone-induced skin necrosis is rare, first described by Russell and Saltissi5 in 2006 in a 60-year-old man who developed dark discoloration and edema of the forearm 24 hours after initiation of an amiodarone peripheral IV. The patient was treated with hot or cold packs and steroid cream per the pharmaceutical company’s recommendations; however, patient outcomes were not discussed.5 A 77-year-old man who received subcutaneous amiodarone due to misplaced vascular access developed edema and bullae of the forearm followed by tissue necrosis, resulting in notably reduced mobility.6 Fox et al7 described a 60-year-old man who developed atrial fibrillation after emergent spinal fusion and laminectomy. He received intradermal hyaluronidase administration within 24 hours of developing severe pain from extravasation induced by amiodarone with no adverse outcomes and full recovery.7
There are numerous properties of amiodarone that may have resulted in the skin necrosis seen in these cases. The acidic pH (3.5–4.5) of amiodarone can contribute to coagulative necrosis, cellular desiccation, eschar formation, and edema.8 It also can contain additives such as polysorbate and benzyl alcohol, which may contribute to the drug’s vesicant properties.9
Current recommendations for IV administration of amiodarone include delivery through a central vein with high concentrations (>2 mg/mL) because peripheral infusion is slower and may cause phlebitis.4 In-line filters also may be a potential method of preventing phlebitis with peripheral IV administration of amiodarone.10 Extravasation of amiodarone can be treated nonpharmacologically with limb elevation and warm compresses, as these methods may promote vasodilation and enhance drug removal.5-7 However, when extravasation leads to progressive erythema and skin necrosis or is refractory to these therapies, intradermal injection of hyaluronidase should be considered. Hyaluronidase mediates the degradation of hyaluronic acid in the extracellular matrix, allowing for increased permeability of injected fluids into tissues and diluting the concentration of toxins at the site of exposure.9,11 It has been used to treat extravasation of fluids such as parenteral nutrition, electrolyte infusion, antibiotics, aminophylline, mannitol, and chemotherapy.11 Although hyaluronidase has been recognized as therapeutic for extravasation, there is no established consistent dosing or proper technique. In the setting of infiltration of chemotherapy, doses of hyaluronidase ranging from 150 to 1500 U/mL can be subcutaneously or intradermally injected into the site within 1 hour of extravasation. Side effects of using hyaluronidase are rare, including local pruritus, allergic reactions, urticaria, and angioedema.12
The patient described by Fox et al7 who fully recovered from amiodarone extravasation after hyaluronidase injections likely benefited from quick intervention, as he received amiodarone within 24 hours of the care team identifying initial erythema. Although our patient did have improvement of the areas of erythema on the forearm, evidence of skin and subcutaneous tissue necrosis on the left hand and proximal forearm was already apparent and not reversible, most likely caused by late intervention of intradermal hyaluronidase almost a week after the extravasation event. It is important to identify amiodarone as the source of extravasation and administer intradermal hyaluronidase in a timely fashion for extravasation refractory to conventional measurements to prevent progression to severe tissue damage.
Our case draws attention to the risk for skin necrosis with peripheral IV administration of amiodarone. Interventions include limb elevation, warm compresses, and consideration of intradermal hyaluronidase within 24 hours of extravasation, as this may reduce the severity of subsequent tissue damage with minimal side effects.
- Epstein AE, Olshansky B, Naccarelli GV, et al. Practical management guide for clinicians who treat patients with amiodarone. Am J Med. 2016;129:468-475. doi:10.1016/j.amjmed.2015.08.039
- Harris L, McKenna WJ, Rowland E, et al. Side effects of long-term amiodarone therapy. Circulation. 1983;67:45-51. doi:10.1161/01.cir.67.1.45
- Jaworski K, Walecka I, Rudnicka L, et al. Cutaneous adverse reactions of amiodarone. Med Sci Monit. 2014;20:2369-2372. doi:10.12659/MSM.890881
- Kowey Peter R, Marinchak Roger A, Rials Seth J, et al. Intravenous amiodarone. J Am Coll Cardiol. 1997;29:1190-1198. doi:10.1016/S0735-1097(97)00069-7
- Russell SJ, Saltissi S. Amiodarone induced skin necrosis. Heart. 2006;92:1395. doi:10.1136/hrt.2005.086157
- Grove EL. Skin necrosis and consequences of accidental subcutaneous administration of amiodarone. Ugeskr Laeger. 2015;177:V66928.
- Fox AN, Villanueva R, Miller JL. Management of amiodarone extravasation with intradermal hyaluronidase. Am J Health Syst Pharm. 2017;74:1545-1548. doi:10.2146/ajhp160737
- Reynolds PM, MacLaren R, Mueller SW, et al. Management of extravasation injuries: a focused evaluation of noncytotoxic medications. Pharmacotherapy. 2014;34:617-632. doi:https://doi.org/10.1002/phar.1396
- Le A, Patel S. Extravasation of noncytotoxic drugs: a review of the literature. Ann Pharmacother. 2014;48:870-886. doi:10.1177/1060028014527820
- Slim AM, Roth JE, Duffy B, et al. The incidence of phlebitis with intravenous amiodarone at guideline dose recommendations. Mil Med. 2007;172:1279-1283.
- Girish KS, Kemparaju K. The magic glue hyaluronan and its eraser hyaluronidase: a biological overview. Life Sci. 2007;80:1921-1943. doi:10.1016/j.lfs.2007.02.037
- Jung H. Hyaluronidase: an overview of its properties, applications, and side effects. Arch Plast Surg. 2020;47:297-300. doi:10.5999/aps.2020.00752
- Epstein AE, Olshansky B, Naccarelli GV, et al. Practical management guide for clinicians who treat patients with amiodarone. Am J Med. 2016;129:468-475. doi:10.1016/j.amjmed.2015.08.039
- Harris L, McKenna WJ, Rowland E, et al. Side effects of long-term amiodarone therapy. Circulation. 1983;67:45-51. doi:10.1161/01.cir.67.1.45
- Jaworski K, Walecka I, Rudnicka L, et al. Cutaneous adverse reactions of amiodarone. Med Sci Monit. 2014;20:2369-2372. doi:10.12659/MSM.890881
- Kowey Peter R, Marinchak Roger A, Rials Seth J, et al. Intravenous amiodarone. J Am Coll Cardiol. 1997;29:1190-1198. doi:10.1016/S0735-1097(97)00069-7
- Russell SJ, Saltissi S. Amiodarone induced skin necrosis. Heart. 2006;92:1395. doi:10.1136/hrt.2005.086157
- Grove EL. Skin necrosis and consequences of accidental subcutaneous administration of amiodarone. Ugeskr Laeger. 2015;177:V66928.
- Fox AN, Villanueva R, Miller JL. Management of amiodarone extravasation with intradermal hyaluronidase. Am J Health Syst Pharm. 2017;74:1545-1548. doi:10.2146/ajhp160737
- Reynolds PM, MacLaren R, Mueller SW, et al. Management of extravasation injuries: a focused evaluation of noncytotoxic medications. Pharmacotherapy. 2014;34:617-632. doi:https://doi.org/10.1002/phar.1396
- Le A, Patel S. Extravasation of noncytotoxic drugs: a review of the literature. Ann Pharmacother. 2014;48:870-886. doi:10.1177/1060028014527820
- Slim AM, Roth JE, Duffy B, et al. The incidence of phlebitis with intravenous amiodarone at guideline dose recommendations. Mil Med. 2007;172:1279-1283.
- Girish KS, Kemparaju K. The magic glue hyaluronan and its eraser hyaluronidase: a biological overview. Life Sci. 2007;80:1921-1943. doi:10.1016/j.lfs.2007.02.037
- Jung H. Hyaluronidase: an overview of its properties, applications, and side effects. Arch Plast Surg. 2020;47:297-300. doi:10.5999/aps.2020.00752
Practice Points
- Intravenous amiodarone administered peripherally can induce skin extravasation, leading to necrosis.
- Dermatologists should be aware that early intervention with intradermal hyaluronidase may reduce the severity of tissue damage caused by amiodarone-induced skin necrosis.

Genital Lentiginosis: A Benign Pigmentary Abnormality Often Raising Concern for Melanoma
To the Editor:
Genital lentiginosis (also known as mucosal melanotic macules, vulvar melanosis, penile melanosis, and penile lentigines) occurs in men and women.1 Lesions present in adult life as multifocal, asymmetrical, pigmented patches that can have a mottled appearance or exhibit skip areas. The irregular appearance of the pigmented areas often raises concern for melanoma. Biopsy reveals increased pigmentation along the basal layer of the epidermis; the irregular distribution of single melanocytes and pagetoid spread typical of melanoma in situ is not identified.

Genital lentiginosis usually occurs as an isolated finding; however, the condition can be a manifestation of Laugier-Hunziker syndrome, Carney complex, and Bannayan-Riley-Ruvalcaba syndrome.1-3 When it occurs as an isolated finding, the patient can be reassured and treatment is unnecessary. Because genital lentiginosis may mimic the appearance of melanoma, it is important for physicians to differentiate the two and make a correct diagnosis. We present a case of genital lentiginosis that mimicked vulvar melanoma.
.")
A 64-year-old woman was referred by her gynecologist to dermatology to rule out vulvar melanoma. The patient had a history of hypothyroidism and hypercholesterolemia but was otherwise in good health. Genital examination revealed asymptomatic pigmented macules and patches of unknown duration (Figure 1). Specimens were taken from 3 areas by punch biopsy to clarify the diagnosis. All 3 specimens showed identical features including basilar pigmentation, occasional melanophages in the papillary dermis, and no evidence of nests or pagetoid spread of atypical melanocytes (Figures 2 and 3). Histologic findings were diagnostic for genital lentiginosis. The patient was reassured, and no treatment was provided. At 6-month follow-up there was no change in clinical appearance.
.")
Genital lentiginosis is characterized by brown lesions that can have a mottled appearance and often are associated with skip areas.1 Lesions can be strikingly irregular and darkly pigmented.
Although the lesions of genital lentiginosis most often are isolated findings, they can be a clue to several uncommon syndromes such as autosomal-dominant Bannayan-Riley-Ruvalcaba syndrome, which is associated with genital lentiginosis, intestinal polyposis, and macrocephaly.3 Vascular malformations, lipomatosis, verrucal keratoses, and acrochordons can occur. Bannayan-Riley-Ruvalcaba syndrome and Cowden syndrome may share genetic linkage; mutations in the tumor suppressor PTEN (phosphatase and tensin homolog deleted on chromosome ten) has been implicated in both syndromes.4 Underlying Carney complex should be excluded when genital lentiginosis is encountered.
Genital lentiginosis is idiopathic in most instances, but reports of lesions occurring after annular lichen planus suggest a possible mechanism.5 The disappearance of lentigines after imatinib therapy suggests a role for c-kit, a receptor tyrosine kinase that is involved in intracellular signaling, in some cases.6 At times, lesions can simulate trichrome vitiligo or have a reticulate pattern.7
Men and women present at different points in the course of disease. Men often present with penile lesions 14 years after onset, on average; they notice a gradual increase in the size of lesions. Because women can have greater difficulty self-examining the genital region, they tend to present much later in the course but often within a few months after initial inspection.1,8
Genital lentiginosis can mimic melanoma with nonhomogeneous pigmentation, asymmetry, and unilateral distribution, which makes dermoscopic assessment of colors helpful in narrowing the differential diagnosis. Melanoma is associated with combinations of gray, red, blue, and white, which are not found in genital lentiginosis.9
Biopsy of a genital lentigo is diagnostic, distinguishing the lesion from melanoma—failing to reveal the atypical melanocytes and pagetoid spread characteristic of melanoma in situ. Histologic findings can cause diagnostic difficulties when concurrent lichen sclerosus is associated with genital lentigines or nevi.10
Lentigines on sun-damaged skin or in the setting of xeroderma pigmentosum have been associated with melanoma,11-13 but genital lentigines are not considered a form of precancerous melanosis. In women, early diagnosis is important when there is concern for melanoma because the prognosis for vulvar melanoma is improved in thin lesions.14
Other entities in the differential include secondary syphilis, which commonly presents as macules and scaly papules and can be found on mucosal surfaces such as the oral cavity,15 as well as Kaposi sarcoma, which is characterized by purplish, brown, or black macules, plaques, and nodules, more commonly in immunosuppressed patients.16
To avoid unwarranted concern and unnecessary surgery, dermatologists should be aware of genital lentigines and their characteristic presentation in adults.
- Hwang L, Wilson H, Orengo I. Off-center fold: irregular, pigmented genital macules. Arch Dermatol. 2000;136:1559-1564. doi:10.1001/archderm.136.12.1559-b
- Rhodes AR, Silverman RA, Harrist TJ, et al. Mucocutaneous lentigines, cardiomucocutaneous myxomas, and multiple blue nevi: the “LAMB” syndrome. J Am Acad Dermatol. 1984;10:72-82. doi:10.1016/s0190-9622(84)80047-x
- Erkek E, Hizel S, Sanl C, et al. Clinical and histopathological findings in Bannayan-Riley-Ruvalcaba syndrome. J Am Acad Dermatol. 2005;53:639-643. doi:10.1016/j.jaad.2005.06.022
- Blum RR, Rahimizadeh A, Kardon N, et al. Genital lentigines in a 6-year-old boy with a family history of Cowden’s disease: clinical and genetic evidence of the linkage between Bannayan-Riley-Ruvalcaba syndrome and Cowden’s disease. J Cutan Med Surg. 2001;5:228-230. doi:10.1177/120347540100500307
- Isbary G, Dyall-Smith D, Coras-Stepanek B, et al. Penile lentigo (genital mucosal macule) following annular lichen planus: a possible association? Australas J Dermatol. 2014;55:159-161. doi:10.1111/ajd.12169
- Campbell T, Felsten L, Moore J. Disappearance of lentigines in a patient receiving imatinib treatment for familial gastrointestinal stromal tumor syndrome. Arch Dermatol. 2009;145:1313-1316. doi:10.1001/archdermatol.2009.263
- Romero- A, R, , et al. Reticulate genital pigmentation associated with localized vitiligo. Arch Dermatol. 2010; 146:574-575. doi:10.1001/archdermatol.2010.69
- Barnhill RL, Albert LS, Shama SK, et al. Genital lentiginosis: a clinical and histopathologic study. J Am Acad Dermatol. 1990;22:453-460. doi:10.1016/0190-9622(90)70064-o
- De Giorgi V, Gori A, Salvati L, et al. Clinical and dermoscopic features of vulvar melanosis over the last 20 years. JAMA Dermatol. 2020;156:1185–1191. doi:10.1001/jamadermatol.2020.2528
- El Shabrawi-Caelen L, Soyer HP, Schaeppi H, et al. Genital lentigines and melanocytic nevi with superimposed lichen sclerosus: a diagnostic challenge. J Am Acad Dermatol. 2004;50:690-694. doi:10.1016/j.jaad.2003.09.034
- Shatkin M, Helm MF, Muhlbauer A, et al. Solar lentigo evolving into fatal metastatic melanoma in a patient who initially refused surgery. N A J Med Sci. 2020;1:28-31. doi:10.7156/najms.2020.1301028
- Stern JB, Peck GL, Haupt HM, et al. Malignant melanoma in xeroderma pigmentosum: search for a precursor lesion. J Am Acad Dermatol. 1993;28:591-594. doi:10.1016/0190-9622(93)70079-9
- Byrom L, Barksdale S, Weedon D, et al. Unstable solar lentigo: a defined separate entity. Australas J Dermatol. 2016;57:229-234. doi:10.1111/ajd.12447
- Panizzon RG. Vulvar melanoma. Semin Dermatol. 1996;15:67-70. doi:10.1016/s1085-5629(96)80021-6
- Chapel TA. The signs and symptoms of secondary syphilis. Sex Transm Dis. 1980;7:161-164. doi:10.1097/00007435-198010000-00002
- Schwartz RA. Kaposi’s sarcoma: an update. J Surg Oncol. 2004;87:146-151. doi:10.1002/jso.20090
To the Editor:
Genital lentiginosis (also known as mucosal melanotic macules, vulvar melanosis, penile melanosis, and penile lentigines) occurs in men and women.1 Lesions present in adult life as multifocal, asymmetrical, pigmented patches that can have a mottled appearance or exhibit skip areas. The irregular appearance of the pigmented areas often raises concern for melanoma. Biopsy reveals increased pigmentation along the basal layer of the epidermis; the irregular distribution of single melanocytes and pagetoid spread typical of melanoma in situ is not identified.
Genital lentiginosis usually occurs as an isolated finding; however, the condition can be a manifestation of Laugier-Hunziker syndrome, Carney complex, and Bannayan-Riley-Ruvalcaba syndrome.1-3 When it occurs as an isolated finding, the patient can be reassured and treatment is unnecessary. Because genital lentiginosis may mimic the appearance of melanoma, it is important for physicians to differentiate the two and make a correct diagnosis. We present a case of genital lentiginosis that mimicked vulvar melanoma.
A 64-year-old woman was referred by her gynecologist to dermatology to rule out vulvar melanoma. The patient had a history of hypothyroidism and hypercholesterolemia but was otherwise in good health. Genital examination revealed asymptomatic pigmented macules and patches of unknown duration (Figure 1). Specimens were taken from 3 areas by punch biopsy to clarify the diagnosis. All 3 specimens showed identical features including basilar pigmentation, occasional melanophages in the papillary dermis, and no evidence of nests or pagetoid spread of atypical melanocytes (Figures 2 and 3). Histologic findings were diagnostic for genital lentiginosis. The patient was reassured, and no treatment was provided. At 6-month follow-up there was no change in clinical appearance.
Genital lentiginosis is characterized by brown lesions that can have a mottled appearance and often are associated with skip areas.1 Lesions can be strikingly irregular and darkly pigmented.
Although the lesions of genital lentiginosis most often are isolated findings, they can be a clue to several uncommon syndromes such as autosomal-dominant Bannayan-Riley-Ruvalcaba syndrome, which is associated with genital lentiginosis, intestinal polyposis, and macrocephaly.3 Vascular malformations, lipomatosis, verrucal keratoses, and acrochordons can occur. Bannayan-Riley-Ruvalcaba syndrome and Cowden syndrome may share genetic linkage; mutations in the tumor suppressor PTEN (phosphatase and tensin homolog deleted on chromosome ten) has been implicated in both syndromes.4 Underlying Carney complex should be excluded when genital lentiginosis is encountered.
Genital lentiginosis is idiopathic in most instances, but reports of lesions occurring after annular lichen planus suggest a possible mechanism.5 The disappearance of lentigines after imatinib therapy suggests a role for c-kit, a receptor tyrosine kinase that is involved in intracellular signaling, in some cases.6 At times, lesions can simulate trichrome vitiligo or have a reticulate pattern.7
Men and women present at different points in the course of disease. Men often present with penile lesions 14 years after onset, on average; they notice a gradual increase in the size of lesions. Because women can have greater difficulty self-examining the genital region, they tend to present much later in the course but often within a few months after initial inspection.1,8
Genital lentiginosis can mimic melanoma with nonhomogeneous pigmentation, asymmetry, and unilateral distribution, which makes dermoscopic assessment of colors helpful in narrowing the differential diagnosis. Melanoma is associated with combinations of gray, red, blue, and white, which are not found in genital lentiginosis.9
Biopsy of a genital lentigo is diagnostic, distinguishing the lesion from melanoma—failing to reveal the atypical melanocytes and pagetoid spread characteristic of melanoma in situ. Histologic findings can cause diagnostic difficulties when concurrent lichen sclerosus is associated with genital lentigines or nevi.10
Lentigines on sun-damaged skin or in the setting of xeroderma pigmentosum have been associated with melanoma,11-13 but genital lentigines are not considered a form of precancerous melanosis. In women, early diagnosis is important when there is concern for melanoma because the prognosis for vulvar melanoma is improved in thin lesions.14
Other entities in the differential include secondary syphilis, which commonly presents as macules and scaly papules and can be found on mucosal surfaces such as the oral cavity,15 as well as Kaposi sarcoma, which is characterized by purplish, brown, or black macules, plaques, and nodules, more commonly in immunosuppressed patients.16
To avoid unwarranted concern and unnecessary surgery, dermatologists should be aware of genital lentigines and their characteristic presentation in adults.
To the Editor:
Genital lentiginosis (also known as mucosal melanotic macules, vulvar melanosis, penile melanosis, and penile lentigines) occurs in men and women.1 Lesions present in adult life as multifocal, asymmetrical, pigmented patches that can have a mottled appearance or exhibit skip areas. The irregular appearance of the pigmented areas often raises concern for melanoma. Biopsy reveals increased pigmentation along the basal layer of the epidermis; the irregular distribution of single melanocytes and pagetoid spread typical of melanoma in situ is not identified.
Genital lentiginosis usually occurs as an isolated finding; however, the condition can be a manifestation of Laugier-Hunziker syndrome, Carney complex, and Bannayan-Riley-Ruvalcaba syndrome.1-3 When it occurs as an isolated finding, the patient can be reassured and treatment is unnecessary. Because genital lentiginosis may mimic the appearance of melanoma, it is important for physicians to differentiate the two and make a correct diagnosis. We present a case of genital lentiginosis that mimicked vulvar melanoma.
A 64-year-old woman was referred by her gynecologist to dermatology to rule out vulvar melanoma. The patient had a history of hypothyroidism and hypercholesterolemia but was otherwise in good health. Genital examination revealed asymptomatic pigmented macules and patches of unknown duration (Figure 1). Specimens were taken from 3 areas by punch biopsy to clarify the diagnosis. All 3 specimens showed identical features including basilar pigmentation, occasional melanophages in the papillary dermis, and no evidence of nests or pagetoid spread of atypical melanocytes (Figures 2 and 3). Histologic findings were diagnostic for genital lentiginosis. The patient was reassured, and no treatment was provided. At 6-month follow-up there was no change in clinical appearance.
Genital lentiginosis is characterized by brown lesions that can have a mottled appearance and often are associated with skip areas.1 Lesions can be strikingly irregular and darkly pigmented.
Although the lesions of genital lentiginosis most often are isolated findings, they can be a clue to several uncommon syndromes such as autosomal-dominant Bannayan-Riley-Ruvalcaba syndrome, which is associated with genital lentiginosis, intestinal polyposis, and macrocephaly.3 Vascular malformations, lipomatosis, verrucal keratoses, and acrochordons can occur. Bannayan-Riley-Ruvalcaba syndrome and Cowden syndrome may share genetic linkage; mutations in the tumor suppressor PTEN (phosphatase and tensin homolog deleted on chromosome ten) has been implicated in both syndromes.4 Underlying Carney complex should be excluded when genital lentiginosis is encountered.
Genital lentiginosis is idiopathic in most instances, but reports of lesions occurring after annular lichen planus suggest a possible mechanism.5 The disappearance of lentigines after imatinib therapy suggests a role for c-kit, a receptor tyrosine kinase that is involved in intracellular signaling, in some cases.6 At times, lesions can simulate trichrome vitiligo or have a reticulate pattern.7
Men and women present at different points in the course of disease. Men often present with penile lesions 14 years after onset, on average; they notice a gradual increase in the size of lesions. Because women can have greater difficulty self-examining the genital region, they tend to present much later in the course but often within a few months after initial inspection.1,8
Genital lentiginosis can mimic melanoma with nonhomogeneous pigmentation, asymmetry, and unilateral distribution, which makes dermoscopic assessment of colors helpful in narrowing the differential diagnosis. Melanoma is associated with combinations of gray, red, blue, and white, which are not found in genital lentiginosis.9
Biopsy of a genital lentigo is diagnostic, distinguishing the lesion from melanoma—failing to reveal the atypical melanocytes and pagetoid spread characteristic of melanoma in situ. Histologic findings can cause diagnostic difficulties when concurrent lichen sclerosus is associated with genital lentigines or nevi.10
Lentigines on sun-damaged skin or in the setting of xeroderma pigmentosum have been associated with melanoma,11-13 but genital lentigines are not considered a form of precancerous melanosis. In women, early diagnosis is important when there is concern for melanoma because the prognosis for vulvar melanoma is improved in thin lesions.14
Other entities in the differential include secondary syphilis, which commonly presents as macules and scaly papules and can be found on mucosal surfaces such as the oral cavity,15 as well as Kaposi sarcoma, which is characterized by purplish, brown, or black macules, plaques, and nodules, more commonly in immunosuppressed patients.16
To avoid unwarranted concern and unnecessary surgery, dermatologists should be aware of genital lentigines and their characteristic presentation in adults.
- Hwang L, Wilson H, Orengo I. Off-center fold: irregular, pigmented genital macules. Arch Dermatol. 2000;136:1559-1564. doi:10.1001/archderm.136.12.1559-b
- Rhodes AR, Silverman RA, Harrist TJ, et al. Mucocutaneous lentigines, cardiomucocutaneous myxomas, and multiple blue nevi: the “LAMB” syndrome. J Am Acad Dermatol. 1984;10:72-82. doi:10.1016/s0190-9622(84)80047-x
- Erkek E, Hizel S, Sanl C, et al. Clinical and histopathological findings in Bannayan-Riley-Ruvalcaba syndrome. J Am Acad Dermatol. 2005;53:639-643. doi:10.1016/j.jaad.2005.06.022
- Blum RR, Rahimizadeh A, Kardon N, et al. Genital lentigines in a 6-year-old boy with a family history of Cowden’s disease: clinical and genetic evidence of the linkage between Bannayan-Riley-Ruvalcaba syndrome and Cowden’s disease. J Cutan Med Surg. 2001;5:228-230. doi:10.1177/120347540100500307
- Isbary G, Dyall-Smith D, Coras-Stepanek B, et al. Penile lentigo (genital mucosal macule) following annular lichen planus: a possible association? Australas J Dermatol. 2014;55:159-161. doi:10.1111/ajd.12169
- Campbell T, Felsten L, Moore J. Disappearance of lentigines in a patient receiving imatinib treatment for familial gastrointestinal stromal tumor syndrome. Arch Dermatol. 2009;145:1313-1316. doi:10.1001/archdermatol.2009.263
- Romero- A, R, , et al. Reticulate genital pigmentation associated with localized vitiligo. Arch Dermatol. 2010; 146:574-575. doi:10.1001/archdermatol.2010.69
- Barnhill RL, Albert LS, Shama SK, et al. Genital lentiginosis: a clinical and histopathologic study. J Am Acad Dermatol. 1990;22:453-460. doi:10.1016/0190-9622(90)70064-o
- De Giorgi V, Gori A, Salvati L, et al. Clinical and dermoscopic features of vulvar melanosis over the last 20 years. JAMA Dermatol. 2020;156:1185–1191. doi:10.1001/jamadermatol.2020.2528
- El Shabrawi-Caelen L, Soyer HP, Schaeppi H, et al. Genital lentigines and melanocytic nevi with superimposed lichen sclerosus: a diagnostic challenge. J Am Acad Dermatol. 2004;50:690-694. doi:10.1016/j.jaad.2003.09.034
- Shatkin M, Helm MF, Muhlbauer A, et al. Solar lentigo evolving into fatal metastatic melanoma in a patient who initially refused surgery. N A J Med Sci. 2020;1:28-31. doi:10.7156/najms.2020.1301028
- Stern JB, Peck GL, Haupt HM, et al. Malignant melanoma in xeroderma pigmentosum: search for a precursor lesion. J Am Acad Dermatol. 1993;28:591-594. doi:10.1016/0190-9622(93)70079-9
- Byrom L, Barksdale S, Weedon D, et al. Unstable solar lentigo: a defined separate entity. Australas J Dermatol. 2016;57:229-234. doi:10.1111/ajd.12447
- Panizzon RG. Vulvar melanoma. Semin Dermatol. 1996;15:67-70. doi:10.1016/s1085-5629(96)80021-6
- Chapel TA. The signs and symptoms of secondary syphilis. Sex Transm Dis. 1980;7:161-164. doi:10.1097/00007435-198010000-00002
- Schwartz RA. Kaposi’s sarcoma: an update. J Surg Oncol. 2004;87:146-151. doi:10.1002/jso.20090
- Hwang L, Wilson H, Orengo I. Off-center fold: irregular, pigmented genital macules. Arch Dermatol. 2000;136:1559-1564. doi:10.1001/archderm.136.12.1559-b
- Rhodes AR, Silverman RA, Harrist TJ, et al. Mucocutaneous lentigines, cardiomucocutaneous myxomas, and multiple blue nevi: the “LAMB” syndrome. J Am Acad Dermatol. 1984;10:72-82. doi:10.1016/s0190-9622(84)80047-x
- Erkek E, Hizel S, Sanl C, et al. Clinical and histopathological findings in Bannayan-Riley-Ruvalcaba syndrome. J Am Acad Dermatol. 2005;53:639-643. doi:10.1016/j.jaad.2005.06.022
- Blum RR, Rahimizadeh A, Kardon N, et al. Genital lentigines in a 6-year-old boy with a family history of Cowden’s disease: clinical and genetic evidence of the linkage between Bannayan-Riley-Ruvalcaba syndrome and Cowden’s disease. J Cutan Med Surg. 2001;5:228-230. doi:10.1177/120347540100500307
- Isbary G, Dyall-Smith D, Coras-Stepanek B, et al. Penile lentigo (genital mucosal macule) following annular lichen planus: a possible association? Australas J Dermatol. 2014;55:159-161. doi:10.1111/ajd.12169
- Campbell T, Felsten L, Moore J. Disappearance of lentigines in a patient receiving imatinib treatment for familial gastrointestinal stromal tumor syndrome. Arch Dermatol. 2009;145:1313-1316. doi:10.1001/archdermatol.2009.263
- Romero- A, R, , et al. Reticulate genital pigmentation associated with localized vitiligo. Arch Dermatol. 2010; 146:574-575. doi:10.1001/archdermatol.2010.69
- Barnhill RL, Albert LS, Shama SK, et al. Genital lentiginosis: a clinical and histopathologic study. J Am Acad Dermatol. 1990;22:453-460. doi:10.1016/0190-9622(90)70064-o
- De Giorgi V, Gori A, Salvati L, et al. Clinical and dermoscopic features of vulvar melanosis over the last 20 years. JAMA Dermatol. 2020;156:1185–1191. doi:10.1001/jamadermatol.2020.2528
- El Shabrawi-Caelen L, Soyer HP, Schaeppi H, et al. Genital lentigines and melanocytic nevi with superimposed lichen sclerosus: a diagnostic challenge. J Am Acad Dermatol. 2004;50:690-694. doi:10.1016/j.jaad.2003.09.034
- Shatkin M, Helm MF, Muhlbauer A, et al. Solar lentigo evolving into fatal metastatic melanoma in a patient who initially refused surgery. N A J Med Sci. 2020;1:28-31. doi:10.7156/najms.2020.1301028
- Stern JB, Peck GL, Haupt HM, et al. Malignant melanoma in xeroderma pigmentosum: search for a precursor lesion. J Am Acad Dermatol. 1993;28:591-594. doi:10.1016/0190-9622(93)70079-9
- Byrom L, Barksdale S, Weedon D, et al. Unstable solar lentigo: a defined separate entity. Australas J Dermatol. 2016;57:229-234. doi:10.1111/ajd.12447
- Panizzon RG. Vulvar melanoma. Semin Dermatol. 1996;15:67-70. doi:10.1016/s1085-5629(96)80021-6
- Chapel TA. The signs and symptoms of secondary syphilis. Sex Transm Dis. 1980;7:161-164. doi:10.1097/00007435-198010000-00002
- Schwartz RA. Kaposi’s sarcoma: an update. J Surg Oncol. 2004;87:146-151. doi:10.1002/jso.20090
Practice Points
- The irregular appearance of genital lentiginosis—multifocal, asymmetric, irregular, and darkly pigmented patches—often raises concern for melanoma but is benign.
- Certain genetic conditions can present with genital lentiginosis.
- Dermoscopic assessment of the lesion color is highly helpful in narrowing the differential diagnosis; seeing no gray, red, blue, or white makes melanoma less likely.
- Be aware of genital lentigines and their characteristic presentation in adulthood to avoid unwarranted concern and unneeded surgery.

Commentary: Novel Migraine Treatment Side Effects, November 2022
Calcitonin gene-related peptide (CGRP) antagonist medications are becoming more and more of a mainstay of both migraine prevention and acute treatment. Four CGRP monoclonal antibody medications and three oral CGRP antagonists are now available for prevention and acute treatment of migraine. When this class of medications was developed, many patients and providers were initially concerned regarding any potentially unanticipated long-term adverse events. The first CGRP antagonist medication, erenumab, was associated with constipation, and, although this has not been formally reported with other CGRP medications, there is some anecdotal evidence of gastrointestinal (GI) discomfort with both oral and other monoclonal antibody medications in this class. In 2021, erenumab was also reported to be associated with hypertension and a formal warning was issued for this.
Before CGRP was used for migraine prevention, it had been known to be a potent vasodilator. Although the randomized controlled trials (RCT) for all CGRP medications included a longitudinal review of blood pressure (BP) measures, none of those initial trials revealed an increased risk for hypertension or other cardiovascular events or concerns. Some of the initial trials even included patients at higher cardiovascular risk. Migraine itself is associated with an increased vascular risk; it is therefore extremely important to determine whether a potential treatment may be increasing this risk further.
In the study by de Vries and colleagues, all patients were started on either erenumab or fremanezumab and were included if they had a follow-up blood pressure measurement within 6 months. All patients had at least8 migraine days per month and had used four or more preventive medications. Patients taking erenumab were first started at 70 mg monthly and were optionally increased to 140 mg after 3 months. Fremanezumab was always given at a dose of 225 mg monthly (as opposed to 675 mg every 3 months). BP data were collected at baseline and followed up at every visit, with a maximum of 12 months of review. Patients were excluded if their baseline BP was measured while they were undergoing tapering an antihypertensive medication at the same time that they were starting the CGRP antagonist. Patients already treated for hypertension were included only if there were no changes to their hypertensive regimen.
Patients were also compared with a control group with a similar distribution in sex, age, and diagnosis, and who were not taking any migraine preventive medication that would affect their BP. Control group BP was also measured at least two different time points 1-3 months from baseline.
A total of 211 patients were enrolled: 109 in the erenumab group and 87 in the fremanezumab group. The erenumab group was also associated with an increase in both systolic BP (SBP) and diastolic BP (DBP) (SBP ≤ 9 mm Hg; DBP ≤ 6.3 mm Hg). The fremanezumab group had a lower increase in SBP (1 mm Hg) and no increase in DBP. Nine patients were started on antihypertensive medications, five of them after the baseline BP recording only. There was no change over time in the control group.
As noted, CGRP has a potent vasodilatory effect. Although not proven, a theory has been posited that CGRP receptor antagonist medications are somewhat more likely to lead to systemic adverse effects than are ligand-blocking medications. This may, at least in part, explain why erenumab appears to have more associated GI discomfort and constipation as well as a vascular effect with hypertension. In light of these findings, it is absolutely necessary for the additional CGRP medications to also be studied for these potential risk factors.
With the advent of novel acute treatments for migraine, many providers ask themselves what the potential risks and benefits are for each new class of drugs developed and approved over the past few years. Johnston and colleagues reviewed five recently published RCT to compare risk-benefit profiles for lasmiditan, rimegepant, and ubrogepant. Lasmiditan is the only medication in the ditan class, a serotonin (5HT-1F) receptor agonist medication approved for the acute treatment of migraine. Rimegepant and ubrogepant are oral CGRP antagonists.
Lasmiditan does have a potential risk for impairment while driving due to excessive sedation and dizziness; it is also more likely than the CGRP medications to lead to the development of medication overuse headache. The CGRP medications, however, are associated with a smaller responder rate for headache freedom at 2 hours. The investigators reviewed the data published in five RCT to develop a statistically based decision-making process that correlates with the number needed to treat vs the number needed to harm for all three of these medications. The number needed to treat is a statistically defined parameter that characterizes the number of patients that need to be treated with an intervention to achieve a positive event. The number needed to harm refers to an additional negative event relative to the reference treatment (placebo in the case of an RCT).
The reviewed studies compared multiple dosages of these medications. Efficacy outcomes were pain relief and pain freedom at 2 hours, sustained pain relief from 2 to 24 hours, and freedom from the most bothersome symptom at 2 hours. Safety outcomes were dizziness and nausea.
The number needed to treat was the lowest for 200 mg lasmiditan (twice the highest recommended acute dose), followed by 75 mg rimegepant. The number needed to harm was highest for 25 mg ubrogepant (half of the lowest recommended acute dose). Nausea was lowest for 75 mg rimegepant.
An individualized approach is always recommended when considering both preventive and acute treatments for migraine. It is definitely worth keeping these results in mind when discussing potential acute treatment options with patients. This is especially true when considering patients who may be more likely to experience either dizziness or nausea with other acute treatments. It is also worth individualizing a potential acute treatment when a patient experiences rapid-onset migraine symptoms. Further investigations into both acute and preventive treatments would enlighten and further individualize our clinical approaches.
Erenumab currently carries a prescriber warning for constipation. Although there has been some anecdotal evidence for constipation with other CGRP antagonists, this has never fully been investigated. Currently, the other CGRP medication options have fewer side effects and not all are associated with constipation. Kudrow and colleagues sought to review the incidence of constipation, and GI motility in general, with both erenumab and galcanezumab. Their hypothesis was that a single dose of erenumab would be associated with delayed GI motility and a single dose of galcanezumab would not be.
This study was conducted as a multicenter trial with single-blinding. A total of 65 patients were enrolled and given either 140 mg erenumab or 240 mg galcanezumab (the loading dose). GI motility was measured via a wireless motility capsule at baseline before treatment and repeated at 2 weeks. This test is approved by the US Food and Drug Administration for evaluation of gastric transit time in patients with suspected gastroparesis and for evaluation of colonic transit time in patients with chronic idiopathic constipation. Patients with prior GI symptoms were excluded, as were patients taking a tricyclic antidepressant or a calcium-channel blocker, owing to known constipation with these agents.
The primary endpoint in this study was change from a baseline colonic transit time 2 weeks after injection with the CGRP monoclonal antibody. Secondary endpoints included change from baseline in whole-gut transit time, gastric emptying time, small-bowel transfer time, and combined small- and large-bowel transfer time. The Gastrointestinal Symptom Rating Scale (GSRS) was also used, evaluating abdominal pain, reflux, indigestion, constipation, and diarrhea based on a 7-point response, ranging from no discomfort to very severe discomfort.
The primary endpoint of baseline change in colonic transit time was not statistically significant between the groups: A mean change of 5.8 hours was noted for erenumab and 5.4 hours for galcanezumab. Most secondary endpoints were also not statistically significantly different between the two groups. Small-bowel transit time was decreased in the galcanezumab group. When the patient-reported scales were reviewed, spontaneous bowel movements decreased significantly in the erenumab group, a finding that was not seen in the galcanezumab group and was statistically significant. The GSRS also showed a small but statistically significant change in the erenumab group.
This study does appear to show a significant difference in the two CGRP antagonist medications. The full side-effect profiles of the four CGRP monoclonal antibodies and three oral CGRP blocking medications available remain unknown. Further head-to-head comparisons will allow better differentiation of these options and better individualization of patient care.
Calcitonin gene-related peptide (CGRP) antagonist medications are becoming more and more of a mainstay of both migraine prevention and acute treatment. Four CGRP monoclonal antibody medications and three oral CGRP antagonists are now available for prevention and acute treatment of migraine. When this class of medications was developed, many patients and providers were initially concerned regarding any potentially unanticipated long-term adverse events. The first CGRP antagonist medication, erenumab, was associated with constipation, and, although this has not been formally reported with other CGRP medications, there is some anecdotal evidence of gastrointestinal (GI) discomfort with both oral and other monoclonal antibody medications in this class. In 2021, erenumab was also reported to be associated with hypertension and a formal warning was issued for this.
Before CGRP was used for migraine prevention, it had been known to be a potent vasodilator. Although the randomized controlled trials (RCT) for all CGRP medications included a longitudinal review of blood pressure (BP) measures, none of those initial trials revealed an increased risk for hypertension or other cardiovascular events or concerns. Some of the initial trials even included patients at higher cardiovascular risk. Migraine itself is associated with an increased vascular risk; it is therefore extremely important to determine whether a potential treatment may be increasing this risk further.
In the study by de Vries and colleagues, all patients were started on either erenumab or fremanezumab and were included if they had a follow-up blood pressure measurement within 6 months. All patients had at least8 migraine days per month and had used four or more preventive medications. Patients taking erenumab were first started at 70 mg monthly and were optionally increased to 140 mg after 3 months. Fremanezumab was always given at a dose of 225 mg monthly (as opposed to 675 mg every 3 months). BP data were collected at baseline and followed up at every visit, with a maximum of 12 months of review. Patients were excluded if their baseline BP was measured while they were undergoing tapering an antihypertensive medication at the same time that they were starting the CGRP antagonist. Patients already treated for hypertension were included only if there were no changes to their hypertensive regimen.
Patients were also compared with a control group with a similar distribution in sex, age, and diagnosis, and who were not taking any migraine preventive medication that would affect their BP. Control group BP was also measured at least two different time points 1-3 months from baseline.
A total of 211 patients were enrolled: 109 in the erenumab group and 87 in the fremanezumab group. The erenumab group was also associated with an increase in both systolic BP (SBP) and diastolic BP (DBP) (SBP ≤ 9 mm Hg; DBP ≤ 6.3 mm Hg). The fremanezumab group had a lower increase in SBP (1 mm Hg) and no increase in DBP. Nine patients were started on antihypertensive medications, five of them after the baseline BP recording only. There was no change over time in the control group.
As noted, CGRP has a potent vasodilatory effect. Although not proven, a theory has been posited that CGRP receptor antagonist medications are somewhat more likely to lead to systemic adverse effects than are ligand-blocking medications. This may, at least in part, explain why erenumab appears to have more associated GI discomfort and constipation as well as a vascular effect with hypertension. In light of these findings, it is absolutely necessary for the additional CGRP medications to also be studied for these potential risk factors.
With the advent of novel acute treatments for migraine, many providers ask themselves what the potential risks and benefits are for each new class of drugs developed and approved over the past few years. Johnston and colleagues reviewed five recently published RCT to compare risk-benefit profiles for lasmiditan, rimegepant, and ubrogepant. Lasmiditan is the only medication in the ditan class, a serotonin (5HT-1F) receptor agonist medication approved for the acute treatment of migraine. Rimegepant and ubrogepant are oral CGRP antagonists.
Lasmiditan does have a potential risk for impairment while driving due to excessive sedation and dizziness; it is also more likely than the CGRP medications to lead to the development of medication overuse headache. The CGRP medications, however, are associated with a smaller responder rate for headache freedom at 2 hours. The investigators reviewed the data published in five RCT to develop a statistically based decision-making process that correlates with the number needed to treat vs the number needed to harm for all three of these medications. The number needed to treat is a statistically defined parameter that characterizes the number of patients that need to be treated with an intervention to achieve a positive event. The number needed to harm refers to an additional negative event relative to the reference treatment (placebo in the case of an RCT).
The reviewed studies compared multiple dosages of these medications. Efficacy outcomes were pain relief and pain freedom at 2 hours, sustained pain relief from 2 to 24 hours, and freedom from the most bothersome symptom at 2 hours. Safety outcomes were dizziness and nausea.
The number needed to treat was the lowest for 200 mg lasmiditan (twice the highest recommended acute dose), followed by 75 mg rimegepant. The number needed to harm was highest for 25 mg ubrogepant (half of the lowest recommended acute dose). Nausea was lowest for 75 mg rimegepant.
An individualized approach is always recommended when considering both preventive and acute treatments for migraine. It is definitely worth keeping these results in mind when discussing potential acute treatment options with patients. This is especially true when considering patients who may be more likely to experience either dizziness or nausea with other acute treatments. It is also worth individualizing a potential acute treatment when a patient experiences rapid-onset migraine symptoms. Further investigations into both acute and preventive treatments would enlighten and further individualize our clinical approaches.
Erenumab currently carries a prescriber warning for constipation. Although there has been some anecdotal evidence for constipation with other CGRP antagonists, this has never fully been investigated. Currently, the other CGRP medication options have fewer side effects and not all are associated with constipation. Kudrow and colleagues sought to review the incidence of constipation, and GI motility in general, with both erenumab and galcanezumab. Their hypothesis was that a single dose of erenumab would be associated with delayed GI motility and a single dose of galcanezumab would not be.
This study was conducted as a multicenter trial with single-blinding. A total of 65 patients were enrolled and given either 140 mg erenumab or 240 mg galcanezumab (the loading dose). GI motility was measured via a wireless motility capsule at baseline before treatment and repeated at 2 weeks. This test is approved by the US Food and Drug Administration for evaluation of gastric transit time in patients with suspected gastroparesis and for evaluation of colonic transit time in patients with chronic idiopathic constipation. Patients with prior GI symptoms were excluded, as were patients taking a tricyclic antidepressant or a calcium-channel blocker, owing to known constipation with these agents.
The primary endpoint in this study was change from a baseline colonic transit time 2 weeks after injection with the CGRP monoclonal antibody. Secondary endpoints included change from baseline in whole-gut transit time, gastric emptying time, small-bowel transfer time, and combined small- and large-bowel transfer time. The Gastrointestinal Symptom Rating Scale (GSRS) was also used, evaluating abdominal pain, reflux, indigestion, constipation, and diarrhea based on a 7-point response, ranging from no discomfort to very severe discomfort.
The primary endpoint of baseline change in colonic transit time was not statistically significant between the groups: A mean change of 5.8 hours was noted for erenumab and 5.4 hours for galcanezumab. Most secondary endpoints were also not statistically significantly different between the two groups. Small-bowel transit time was decreased in the galcanezumab group. When the patient-reported scales were reviewed, spontaneous bowel movements decreased significantly in the erenumab group, a finding that was not seen in the galcanezumab group and was statistically significant. The GSRS also showed a small but statistically significant change in the erenumab group.
This study does appear to show a significant difference in the two CGRP antagonist medications. The full side-effect profiles of the four CGRP monoclonal antibodies and three oral CGRP blocking medications available remain unknown. Further head-to-head comparisons will allow better differentiation of these options and better individualization of patient care.
Calcitonin gene-related peptide (CGRP) antagonist medications are becoming more and more of a mainstay of both migraine prevention and acute treatment. Four CGRP monoclonal antibody medications and three oral CGRP antagonists are now available for prevention and acute treatment of migraine. When this class of medications was developed, many patients and providers were initially concerned regarding any potentially unanticipated long-term adverse events. The first CGRP antagonist medication, erenumab, was associated with constipation, and, although this has not been formally reported with other CGRP medications, there is some anecdotal evidence of gastrointestinal (GI) discomfort with both oral and other monoclonal antibody medications in this class. In 2021, erenumab was also reported to be associated with hypertension and a formal warning was issued for this.
Before CGRP was used for migraine prevention, it had been known to be a potent vasodilator. Although the randomized controlled trials (RCT) for all CGRP medications included a longitudinal review of blood pressure (BP) measures, none of those initial trials revealed an increased risk for hypertension or other cardiovascular events or concerns. Some of the initial trials even included patients at higher cardiovascular risk. Migraine itself is associated with an increased vascular risk; it is therefore extremely important to determine whether a potential treatment may be increasing this risk further.
In the study by de Vries and colleagues, all patients were started on either erenumab or fremanezumab and were included if they had a follow-up blood pressure measurement within 6 months. All patients had at least8 migraine days per month and had used four or more preventive medications. Patients taking erenumab were first started at 70 mg monthly and were optionally increased to 140 mg after 3 months. Fremanezumab was always given at a dose of 225 mg monthly (as opposed to 675 mg every 3 months). BP data were collected at baseline and followed up at every visit, with a maximum of 12 months of review. Patients were excluded if their baseline BP was measured while they were undergoing tapering an antihypertensive medication at the same time that they were starting the CGRP antagonist. Patients already treated for hypertension were included only if there were no changes to their hypertensive regimen.
Patients were also compared with a control group with a similar distribution in sex, age, and diagnosis, and who were not taking any migraine preventive medication that would affect their BP. Control group BP was also measured at least two different time points 1-3 months from baseline.
A total of 211 patients were enrolled: 109 in the erenumab group and 87 in the fremanezumab group. The erenumab group was also associated with an increase in both systolic BP (SBP) and diastolic BP (DBP) (SBP ≤ 9 mm Hg; DBP ≤ 6.3 mm Hg). The fremanezumab group had a lower increase in SBP (1 mm Hg) and no increase in DBP. Nine patients were started on antihypertensive medications, five of them after the baseline BP recording only. There was no change over time in the control group.
As noted, CGRP has a potent vasodilatory effect. Although not proven, a theory has been posited that CGRP receptor antagonist medications are somewhat more likely to lead to systemic adverse effects than are ligand-blocking medications. This may, at least in part, explain why erenumab appears to have more associated GI discomfort and constipation as well as a vascular effect with hypertension. In light of these findings, it is absolutely necessary for the additional CGRP medications to also be studied for these potential risk factors.
With the advent of novel acute treatments for migraine, many providers ask themselves what the potential risks and benefits are for each new class of drugs developed and approved over the past few years. Johnston and colleagues reviewed five recently published RCT to compare risk-benefit profiles for lasmiditan, rimegepant, and ubrogepant. Lasmiditan is the only medication in the ditan class, a serotonin (5HT-1F) receptor agonist medication approved for the acute treatment of migraine. Rimegepant and ubrogepant are oral CGRP antagonists.
Lasmiditan does have a potential risk for impairment while driving due to excessive sedation and dizziness; it is also more likely than the CGRP medications to lead to the development of medication overuse headache. The CGRP medications, however, are associated with a smaller responder rate for headache freedom at 2 hours. The investigators reviewed the data published in five RCT to develop a statistically based decision-making process that correlates with the number needed to treat vs the number needed to harm for all three of these medications. The number needed to treat is a statistically defined parameter that characterizes the number of patients that need to be treated with an intervention to achieve a positive event. The number needed to harm refers to an additional negative event relative to the reference treatment (placebo in the case of an RCT).
The reviewed studies compared multiple dosages of these medications. Efficacy outcomes were pain relief and pain freedom at 2 hours, sustained pain relief from 2 to 24 hours, and freedom from the most bothersome symptom at 2 hours. Safety outcomes were dizziness and nausea.
The number needed to treat was the lowest for 200 mg lasmiditan (twice the highest recommended acute dose), followed by 75 mg rimegepant. The number needed to harm was highest for 25 mg ubrogepant (half of the lowest recommended acute dose). Nausea was lowest for 75 mg rimegepant.
An individualized approach is always recommended when considering both preventive and acute treatments for migraine. It is definitely worth keeping these results in mind when discussing potential acute treatment options with patients. This is especially true when considering patients who may be more likely to experience either dizziness or nausea with other acute treatments. It is also worth individualizing a potential acute treatment when a patient experiences rapid-onset migraine symptoms. Further investigations into both acute and preventive treatments would enlighten and further individualize our clinical approaches.
Erenumab currently carries a prescriber warning for constipation. Although there has been some anecdotal evidence for constipation with other CGRP antagonists, this has never fully been investigated. Currently, the other CGRP medication options have fewer side effects and not all are associated with constipation. Kudrow and colleagues sought to review the incidence of constipation, and GI motility in general, with both erenumab and galcanezumab. Their hypothesis was that a single dose of erenumab would be associated with delayed GI motility and a single dose of galcanezumab would not be.
This study was conducted as a multicenter trial with single-blinding. A total of 65 patients were enrolled and given either 140 mg erenumab or 240 mg galcanezumab (the loading dose). GI motility was measured via a wireless motility capsule at baseline before treatment and repeated at 2 weeks. This test is approved by the US Food and Drug Administration for evaluation of gastric transit time in patients with suspected gastroparesis and for evaluation of colonic transit time in patients with chronic idiopathic constipation. Patients with prior GI symptoms were excluded, as were patients taking a tricyclic antidepressant or a calcium-channel blocker, owing to known constipation with these agents.
The primary endpoint in this study was change from a baseline colonic transit time 2 weeks after injection with the CGRP monoclonal antibody. Secondary endpoints included change from baseline in whole-gut transit time, gastric emptying time, small-bowel transfer time, and combined small- and large-bowel transfer time. The Gastrointestinal Symptom Rating Scale (GSRS) was also used, evaluating abdominal pain, reflux, indigestion, constipation, and diarrhea based on a 7-point response, ranging from no discomfort to very severe discomfort.
The primary endpoint of baseline change in colonic transit time was not statistically significant between the groups: A mean change of 5.8 hours was noted for erenumab and 5.4 hours for galcanezumab. Most secondary endpoints were also not statistically significantly different between the two groups. Small-bowel transit time was decreased in the galcanezumab group. When the patient-reported scales were reviewed, spontaneous bowel movements decreased significantly in the erenumab group, a finding that was not seen in the galcanezumab group and was statistically significant. The GSRS also showed a small but statistically significant change in the erenumab group.
This study does appear to show a significant difference in the two CGRP antagonist medications. The full side-effect profiles of the four CGRP monoclonal antibodies and three oral CGRP blocking medications available remain unknown. Further head-to-head comparisons will allow better differentiation of these options and better individualization of patient care.
How to prevent a feared complication after joint replacement
Knee and hip replacements can improve how well patients get around and can significantly increase their quality of life. But if a bone near the new joint breaks, the injury can be a major setback for the patient’s mobility, and the consequences can be life-threatening.
The proportion of patients who experience a periprosthetic fracture within 5 years of total hip arthroplasty is 0.9%. After total knee arthroplasty (TKA), the proportion is 0.6%, research shows.
Those rates might seem low. But given that more than a million of these joint replacement surgeries are performed each year in the United States – they are the most common inpatient surgical procedures among people aged 65 and older – thousands of revision surgeries due to periprosthetic fractures occur each year.
Primary care clinicians who make their patients’ bone health a priority early on – years before surgery, ideally – may help patients enjoy the benefits of new joints long term.

At the 2022 annual Santa Fe Bone Symposium this summer, Susan V. Bukata, MD, professor and chair of orthopedics at the University of California, San Diego, showed an image of “what we’re trying to avoid” – a patient with a broken bone and infection. Unfortunately, Dr. Bukata said, the patient’s clinicians had not adequately addressed her skeletal health before the injury.
“This is a complete disaster for this person who went in having a total hip to improve their function and now will probably never walk normally on that leg,” Dr. Bukata said at the meeting.
The patient eventually underwent total femur replacement. Five surgeries were required to clear the infection.
Medical and surgical advances have allowed more people – including older patients and those with other medical conditions – to undergo joint replacement surgery, including replacement of knees, hips, and shoulders.
The surgeries often are performed for adults whose bones are thinning. Sometimes surgeons don’t realize just how thin a patient’s bone is until they are operating.
Prioritizing bone health
In patients with osteoporosis, the bone surrounding the new joint is weaker than the metal of the prosthesis, and the metal can rip out of the bone, Dr. Bukata told this news organization. A periprosthetic fracture should be recognized as an osteoporotic fracture, too, although these fractures have not typically been categorized that way, she said.
People live with total joints in place for as long as 40 years, and fractures around the implants are “one of the fastest growing injuries that we are seeing in older patients,” Dr. Bukata said. “People don’t think of those as osteoporotic fractures. But a 90-year-old who falls and breaks next to their total knee, if they didn’t have that total knee in place, everybody would be, like, ‘Oh, that’s an osteoporotic fracture.’ ”
Periprosthetic fractures tend not to occur right after surgery but rather after the bone continues to lose density as the patient ages, Dr. Bukata said.
Missed chances
One approach to preventing periprosthetic fractures could involve prioritizing bone health earlier in life and diagnosing and treating osteoporosis well before a patient is scheduled for surgery.
A patient’s initial visit to their primary care doctor because of joint pain is an opportunity to check on and promote their bone health, given that they might be a candidate for surgery in the future, Dr. Bukata said.
Ahead of a scheduled surgery, patients can see endocrinologists or rheumatologists to receive medication to try to strengthen bones. Doctors may be limited in how much of a difference they can make in a matter of several weeks or months with these drugs, however. These patients still likely will need to be treated as if they have osteoporosis, Dr. Bukata said.
When surgeons realize that a patient has weaker bones while they are in the middle of an operation, they should emphasize the importance of bone health after the procedure, Dr. Bukata said.
Strengthening, maintaining, and protecting bone should be seen as a long-term investment in the patient’s success after a joint replacement. That said, “There is no clear evidence or protocol for us to follow,” she said. “The mantra at UCSD now is, let’s keep it simple. Get the patient on track. And then we can always refine things as we continue to treat the patient.”
Health systems should establish routines in which bone health is discussed before surgery in the way patient education programs address smoking cessation, nutrition, and weight management, Dr. Bukata said. Another step in the right direction could involve setting electronic medical records to automatically order assessments of bone health when a surgeon books a case.

Linda A. Russell, MD, rheumatologist and director of perioperative medicine at the Hospital for Special Surgery in New York, said periprosthetic fractures are a “complication we fear.”
“It’s a big deal to try to repair it,” Dr. Russell said. “Sometimes you need to revise the joint, or sometimes you need to put lots more hardware in.” Surgeons increasingly appreciate the need to pay attention to the quality of the bone before they operate, she said.
Nevertheless, Dr. Russell does not necessarily say that such cases call for alarm or particularly aggressive treatment regimens – just regular bone health evaluations before and after surgery to see whether patients have osteoporosis and are candidates for treatment.
Lifelong effort
In some ways, to address bone health at the time of surgery may be too late.
Bone health “is not something that you can have as an afterthought when you’re 75 years old,” said Elizabeth Matzkin, MD, chief of women’s sports medicine at Brigham and Women’s Hospital, in Boston.
The chance of being able to rebuild bone mass at that age is slim. If patients maximize bone density when they are young, they can afford to lose some bone mass each year as they age.
To that end, a healthy diet, exercise, not smoking, and cutting back on alcohol can help, she said.
For Dr. Matzkin, a fragility fracture is a red flag that the patient’s bone density is probably not optimal. In such cases, she prepares for various scenarios during surgery, such as a screw not holding in a low-density bone.
Recently published research reflects that prior fragility fractures are a significant risk factor for complications after surgery, including periprosthetic fractures.
Edward J. Testa, MD, of Brown University, Providence, R.I., and colleagues analyzed insurance claims to compare outcomes for 24,398 patients who had experienced a fragility fracture – that is, a break caused by low-velocity trauma such as a fall – during the 3 years before their TKA procedure and a matched group of patients who were similar in many respects but who had not had a fragility fracture in the 3 years before surgery.
Dr. Testa’s group found that a history of fragility fracture was associated with higher rates of complications in the year after surgery, including hospital readmissions (hazard ratio = 1.30; 95% CI, 1.22-1.38), periprosthetic fractures (odds ratio = 2.72; 95% CI, 1.89-3.99), and secondary fragility fractures (OR = 4.62; 95% CI, 4.19-5.12). Patients who had previously experienced fragility fractures also experienced dislocated prostheses (OR = 1.76; 95% CI, 1.22-2.56) and periprosthetic infections (OR = 1.49; 95% CI, 1.29-1.71) at higher rates.
The rates of complications were similar regardless of whether patients had filled a prescription for medications used to treat osteoporosis, including bisphosphonates, vitamin D replacement, raloxifene, and denosumab, the researchers reported.
The lack of a clear association between these treatments and patient outcomes could be related to an insufficient duration of pharmacotherapy before or after TKA, poor medication adherence, or small sample sizes, Dr. Testa said.
Given the findings, which were published online in the Journal of Arthroplasty, “patients with a history of fragility fracture should be identified and counseled appropriately for a possible increased risk of the aforementioned complications, and optimized when possible, prior to undergoing TKA,” Dr. Testa told this news organization. “Ultimately, the decision to move forward with surgery is far more complex than the identification of this sole, yet important, risk factor for certain postoperative, implant-related complications.”
Treatment gaps
Prior research has shown that women aged 70 years and older are at higher risk for periprosthetic fractures. Many women in this age group who could receive treatment for osteoporosis do not, and major treatment gaps exist worldwide, noted Neil Binkley, MD, with the University of Wisconsin–Madison, in a separate talk at the Santa Fe Bone Symposium.
Ensuring adequate protein intake and addressing the risk of falling are other measures that clinicians can take to promote healthy bones, apart from prescribing drugs, he said.
Unpublished data from one group show that nearly 90% of periprosthetic fractures may result from falls, while about 8% may be spontaneous. “We need to be thinking about falls,” Dr. Binkley said.
Dr. Bukata has consulted for Amgen, Radius, and Solarea Bio and has served on a speakers bureau for Radius. She also is a board member for the Orthopaedic Research Society and the American Academy of Orthopaedic Surgeons Board of Specialty Societies. Dr. Binkley has received research support from Radius and has consulted for Amgen.
A version of this article first appeared on Medscape.com.
Knee and hip replacements can improve how well patients get around and can significantly increase their quality of life. But if a bone near the new joint breaks, the injury can be a major setback for the patient’s mobility, and the consequences can be life-threatening.
The proportion of patients who experience a periprosthetic fracture within 5 years of total hip arthroplasty is 0.9%. After total knee arthroplasty (TKA), the proportion is 0.6%, research shows.
Those rates might seem low. But given that more than a million of these joint replacement surgeries are performed each year in the United States – they are the most common inpatient surgical procedures among people aged 65 and older – thousands of revision surgeries due to periprosthetic fractures occur each year.
Primary care clinicians who make their patients’ bone health a priority early on – years before surgery, ideally – may help patients enjoy the benefits of new joints long term.
At the 2022 annual Santa Fe Bone Symposium this summer, Susan V. Bukata, MD, professor and chair of orthopedics at the University of California, San Diego, showed an image of “what we’re trying to avoid” – a patient with a broken bone and infection. Unfortunately, Dr. Bukata said, the patient’s clinicians had not adequately addressed her skeletal health before the injury.
“This is a complete disaster for this person who went in having a total hip to improve their function and now will probably never walk normally on that leg,” Dr. Bukata said at the meeting.
The patient eventually underwent total femur replacement. Five surgeries were required to clear the infection.
Medical and surgical advances have allowed more people – including older patients and those with other medical conditions – to undergo joint replacement surgery, including replacement of knees, hips, and shoulders.
The surgeries often are performed for adults whose bones are thinning. Sometimes surgeons don’t realize just how thin a patient’s bone is until they are operating.
Prioritizing bone health
In patients with osteoporosis, the bone surrounding the new joint is weaker than the metal of the prosthesis, and the metal can rip out of the bone, Dr. Bukata told this news organization. A periprosthetic fracture should be recognized as an osteoporotic fracture, too, although these fractures have not typically been categorized that way, she said.
People live with total joints in place for as long as 40 years, and fractures around the implants are “one of the fastest growing injuries that we are seeing in older patients,” Dr. Bukata said. “People don’t think of those as osteoporotic fractures. But a 90-year-old who falls and breaks next to their total knee, if they didn’t have that total knee in place, everybody would be, like, ‘Oh, that’s an osteoporotic fracture.’ ”
Periprosthetic fractures tend not to occur right after surgery but rather after the bone continues to lose density as the patient ages, Dr. Bukata said.
Missed chances
One approach to preventing periprosthetic fractures could involve prioritizing bone health earlier in life and diagnosing and treating osteoporosis well before a patient is scheduled for surgery.
A patient’s initial visit to their primary care doctor because of joint pain is an opportunity to check on and promote their bone health, given that they might be a candidate for surgery in the future, Dr. Bukata said.
Ahead of a scheduled surgery, patients can see endocrinologists or rheumatologists to receive medication to try to strengthen bones. Doctors may be limited in how much of a difference they can make in a matter of several weeks or months with these drugs, however. These patients still likely will need to be treated as if they have osteoporosis, Dr. Bukata said.
When surgeons realize that a patient has weaker bones while they are in the middle of an operation, they should emphasize the importance of bone health after the procedure, Dr. Bukata said.
Strengthening, maintaining, and protecting bone should be seen as a long-term investment in the patient’s success after a joint replacement. That said, “There is no clear evidence or protocol for us to follow,” she said. “The mantra at UCSD now is, let’s keep it simple. Get the patient on track. And then we can always refine things as we continue to treat the patient.”
Health systems should establish routines in which bone health is discussed before surgery in the way patient education programs address smoking cessation, nutrition, and weight management, Dr. Bukata said. Another step in the right direction could involve setting electronic medical records to automatically order assessments of bone health when a surgeon books a case.
Linda A. Russell, MD, rheumatologist and director of perioperative medicine at the Hospital for Special Surgery in New York, said periprosthetic fractures are a “complication we fear.”
“It’s a big deal to try to repair it,” Dr. Russell said. “Sometimes you need to revise the joint, or sometimes you need to put lots more hardware in.” Surgeons increasingly appreciate the need to pay attention to the quality of the bone before they operate, she said.
Nevertheless, Dr. Russell does not necessarily say that such cases call for alarm or particularly aggressive treatment regimens – just regular bone health evaluations before and after surgery to see whether patients have osteoporosis and are candidates for treatment.
Lifelong effort
In some ways, to address bone health at the time of surgery may be too late.
Bone health “is not something that you can have as an afterthought when you’re 75 years old,” said Elizabeth Matzkin, MD, chief of women’s sports medicine at Brigham and Women’s Hospital, in Boston.
The chance of being able to rebuild bone mass at that age is slim. If patients maximize bone density when they are young, they can afford to lose some bone mass each year as they age.
To that end, a healthy diet, exercise, not smoking, and cutting back on alcohol can help, she said.
For Dr. Matzkin, a fragility fracture is a red flag that the patient’s bone density is probably not optimal. In such cases, she prepares for various scenarios during surgery, such as a screw not holding in a low-density bone.
Recently published research reflects that prior fragility fractures are a significant risk factor for complications after surgery, including periprosthetic fractures.
Edward J. Testa, MD, of Brown University, Providence, R.I., and colleagues analyzed insurance claims to compare outcomes for 24,398 patients who had experienced a fragility fracture – that is, a break caused by low-velocity trauma such as a fall – during the 3 years before their TKA procedure and a matched group of patients who were similar in many respects but who had not had a fragility fracture in the 3 years before surgery.
Dr. Testa’s group found that a history of fragility fracture was associated with higher rates of complications in the year after surgery, including hospital readmissions (hazard ratio = 1.30; 95% CI, 1.22-1.38), periprosthetic fractures (odds ratio = 2.72; 95% CI, 1.89-3.99), and secondary fragility fractures (OR = 4.62; 95% CI, 4.19-5.12). Patients who had previously experienced fragility fractures also experienced dislocated prostheses (OR = 1.76; 95% CI, 1.22-2.56) and periprosthetic infections (OR = 1.49; 95% CI, 1.29-1.71) at higher rates.
The rates of complications were similar regardless of whether patients had filled a prescription for medications used to treat osteoporosis, including bisphosphonates, vitamin D replacement, raloxifene, and denosumab, the researchers reported.
The lack of a clear association between these treatments and patient outcomes could be related to an insufficient duration of pharmacotherapy before or after TKA, poor medication adherence, or small sample sizes, Dr. Testa said.
Given the findings, which were published online in the Journal of Arthroplasty, “patients with a history of fragility fracture should be identified and counseled appropriately for a possible increased risk of the aforementioned complications, and optimized when possible, prior to undergoing TKA,” Dr. Testa told this news organization. “Ultimately, the decision to move forward with surgery is far more complex than the identification of this sole, yet important, risk factor for certain postoperative, implant-related complications.”
Treatment gaps
Prior research has shown that women aged 70 years and older are at higher risk for periprosthetic fractures. Many women in this age group who could receive treatment for osteoporosis do not, and major treatment gaps exist worldwide, noted Neil Binkley, MD, with the University of Wisconsin–Madison, in a separate talk at the Santa Fe Bone Symposium.
Ensuring adequate protein intake and addressing the risk of falling are other measures that clinicians can take to promote healthy bones, apart from prescribing drugs, he said.
Unpublished data from one group show that nearly 90% of periprosthetic fractures may result from falls, while about 8% may be spontaneous. “We need to be thinking about falls,” Dr. Binkley said.
Dr. Bukata has consulted for Amgen, Radius, and Solarea Bio and has served on a speakers bureau for Radius. She also is a board member for the Orthopaedic Research Society and the American Academy of Orthopaedic Surgeons Board of Specialty Societies. Dr. Binkley has received research support from Radius and has consulted for Amgen.
A version of this article first appeared on Medscape.com.
Knee and hip replacements can improve how well patients get around and can significantly increase their quality of life. But if a bone near the new joint breaks, the injury can be a major setback for the patient’s mobility, and the consequences can be life-threatening.
The proportion of patients who experience a periprosthetic fracture within 5 years of total hip arthroplasty is 0.9%. After total knee arthroplasty (TKA), the proportion is 0.6%, research shows.
Those rates might seem low. But given that more than a million of these joint replacement surgeries are performed each year in the United States – they are the most common inpatient surgical procedures among people aged 65 and older – thousands of revision surgeries due to periprosthetic fractures occur each year.
Primary care clinicians who make their patients’ bone health a priority early on – years before surgery, ideally – may help patients enjoy the benefits of new joints long term.
At the 2022 annual Santa Fe Bone Symposium this summer, Susan V. Bukata, MD, professor and chair of orthopedics at the University of California, San Diego, showed an image of “what we’re trying to avoid” – a patient with a broken bone and infection. Unfortunately, Dr. Bukata said, the patient’s clinicians had not adequately addressed her skeletal health before the injury.
“This is a complete disaster for this person who went in having a total hip to improve their function and now will probably never walk normally on that leg,” Dr. Bukata said at the meeting.
The patient eventually underwent total femur replacement. Five surgeries were required to clear the infection.
Medical and surgical advances have allowed more people – including older patients and those with other medical conditions – to undergo joint replacement surgery, including replacement of knees, hips, and shoulders.
The surgeries often are performed for adults whose bones are thinning. Sometimes surgeons don’t realize just how thin a patient’s bone is until they are operating.
Prioritizing bone health
In patients with osteoporosis, the bone surrounding the new joint is weaker than the metal of the prosthesis, and the metal can rip out of the bone, Dr. Bukata told this news organization. A periprosthetic fracture should be recognized as an osteoporotic fracture, too, although these fractures have not typically been categorized that way, she said.
People live with total joints in place for as long as 40 years, and fractures around the implants are “one of the fastest growing injuries that we are seeing in older patients,” Dr. Bukata said. “People don’t think of those as osteoporotic fractures. But a 90-year-old who falls and breaks next to their total knee, if they didn’t have that total knee in place, everybody would be, like, ‘Oh, that’s an osteoporotic fracture.’ ”
Periprosthetic fractures tend not to occur right after surgery but rather after the bone continues to lose density as the patient ages, Dr. Bukata said.
Missed chances
One approach to preventing periprosthetic fractures could involve prioritizing bone health earlier in life and diagnosing and treating osteoporosis well before a patient is scheduled for surgery.
A patient’s initial visit to their primary care doctor because of joint pain is an opportunity to check on and promote their bone health, given that they might be a candidate for surgery in the future, Dr. Bukata said.
Ahead of a scheduled surgery, patients can see endocrinologists or rheumatologists to receive medication to try to strengthen bones. Doctors may be limited in how much of a difference they can make in a matter of several weeks or months with these drugs, however. These patients still likely will need to be treated as if they have osteoporosis, Dr. Bukata said.
When surgeons realize that a patient has weaker bones while they are in the middle of an operation, they should emphasize the importance of bone health after the procedure, Dr. Bukata said.
Strengthening, maintaining, and protecting bone should be seen as a long-term investment in the patient’s success after a joint replacement. That said, “There is no clear evidence or protocol for us to follow,” she said. “The mantra at UCSD now is, let’s keep it simple. Get the patient on track. And then we can always refine things as we continue to treat the patient.”
Health systems should establish routines in which bone health is discussed before surgery in the way patient education programs address smoking cessation, nutrition, and weight management, Dr. Bukata said. Another step in the right direction could involve setting electronic medical records to automatically order assessments of bone health when a surgeon books a case.
Linda A. Russell, MD, rheumatologist and director of perioperative medicine at the Hospital for Special Surgery in New York, said periprosthetic fractures are a “complication we fear.”
“It’s a big deal to try to repair it,” Dr. Russell said. “Sometimes you need to revise the joint, or sometimes you need to put lots more hardware in.” Surgeons increasingly appreciate the need to pay attention to the quality of the bone before they operate, she said.
Nevertheless, Dr. Russell does not necessarily say that such cases call for alarm or particularly aggressive treatment regimens – just regular bone health evaluations before and after surgery to see whether patients have osteoporosis and are candidates for treatment.
Lifelong effort
In some ways, to address bone health at the time of surgery may be too late.
Bone health “is not something that you can have as an afterthought when you’re 75 years old,” said Elizabeth Matzkin, MD, chief of women’s sports medicine at Brigham and Women’s Hospital, in Boston.
The chance of being able to rebuild bone mass at that age is slim. If patients maximize bone density when they are young, they can afford to lose some bone mass each year as they age.
To that end, a healthy diet, exercise, not smoking, and cutting back on alcohol can help, she said.
For Dr. Matzkin, a fragility fracture is a red flag that the patient’s bone density is probably not optimal. In such cases, she prepares for various scenarios during surgery, such as a screw not holding in a low-density bone.
Recently published research reflects that prior fragility fractures are a significant risk factor for complications after surgery, including periprosthetic fractures.
Edward J. Testa, MD, of Brown University, Providence, R.I., and colleagues analyzed insurance claims to compare outcomes for 24,398 patients who had experienced a fragility fracture – that is, a break caused by low-velocity trauma such as a fall – during the 3 years before their TKA procedure and a matched group of patients who were similar in many respects but who had not had a fragility fracture in the 3 years before surgery.
Dr. Testa’s group found that a history of fragility fracture was associated with higher rates of complications in the year after surgery, including hospital readmissions (hazard ratio = 1.30; 95% CI, 1.22-1.38), periprosthetic fractures (odds ratio = 2.72; 95% CI, 1.89-3.99), and secondary fragility fractures (OR = 4.62; 95% CI, 4.19-5.12). Patients who had previously experienced fragility fractures also experienced dislocated prostheses (OR = 1.76; 95% CI, 1.22-2.56) and periprosthetic infections (OR = 1.49; 95% CI, 1.29-1.71) at higher rates.
The rates of complications were similar regardless of whether patients had filled a prescription for medications used to treat osteoporosis, including bisphosphonates, vitamin D replacement, raloxifene, and denosumab, the researchers reported.
The lack of a clear association between these treatments and patient outcomes could be related to an insufficient duration of pharmacotherapy before or after TKA, poor medication adherence, or small sample sizes, Dr. Testa said.
Given the findings, which were published online in the Journal of Arthroplasty, “patients with a history of fragility fracture should be identified and counseled appropriately for a possible increased risk of the aforementioned complications, and optimized when possible, prior to undergoing TKA,” Dr. Testa told this news organization. “Ultimately, the decision to move forward with surgery is far more complex than the identification of this sole, yet important, risk factor for certain postoperative, implant-related complications.”
Treatment gaps
Prior research has shown that women aged 70 years and older are at higher risk for periprosthetic fractures. Many women in this age group who could receive treatment for osteoporosis do not, and major treatment gaps exist worldwide, noted Neil Binkley, MD, with the University of Wisconsin–Madison, in a separate talk at the Santa Fe Bone Symposium.
Ensuring adequate protein intake and addressing the risk of falling are other measures that clinicians can take to promote healthy bones, apart from prescribing drugs, he said.
Unpublished data from one group show that nearly 90% of periprosthetic fractures may result from falls, while about 8% may be spontaneous. “We need to be thinking about falls,” Dr. Binkley said.
Dr. Bukata has consulted for Amgen, Radius, and Solarea Bio and has served on a speakers bureau for Radius. She also is a board member for the Orthopaedic Research Society and the American Academy of Orthopaedic Surgeons Board of Specialty Societies. Dr. Binkley has received research support from Radius and has consulted for Amgen.
A version of this article first appeared on Medscape.com.
Mid-October flulike illness cases higher than past 5 years
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”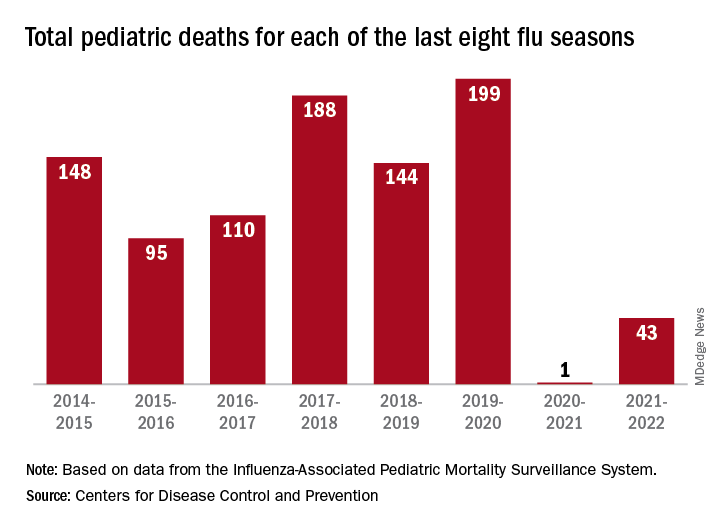
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Outpatient visits for influenzalike illness (ILI), which includes influenza, SARS-CoV-2, and RSV, were higher after 3 weeks than for any of the previous five flu seasons: 3.3% of visits reported through the CDC’s Outpatient Influenza-like Illness Surveillance Network involved ILI as of Oct. 22. The highest comparable rate in the previous 5 years was the 1.9% recorded in late October of 2021, shortly after the definition of ILI was changed to also include illnesses other than influenza.
This season’s higher flu activity is in contrast to the previous two, which were unusually mild. The change, however, is not unexpected, as William Schaffner, MD, an infectious disease expert and professor of preventive medicine at Vanderbilt University, recently told CNN.
“Here we are in the middle of October – not the middle of November – we’re already seeing scattered influenza cases, even hospitalized influenza cases, around the country,” he said. “So we know that this virus is now spreading out in the community already. It’s gathering speed already. It looks to me to be about a month early.”
One indication of the mildness of the previous two flu seasons was the number of deaths, both pediatric and overall. Influenza-associated pediatric deaths had averaged about 110 per season over the previous eight seasons, compared with just 1 for 2020-2021 and 43 in 2021-2022. Overall flu deaths never reached 1% of all weekly deaths for either season, well below baseline levels for the flu, which range from 5.5% to 6.8%, CDC data show.
Other indicators of early severity
This season’s early rise in viral activity also can be seen in hospitalizations. The cumulative rate of flu-related admissions was 1.5 per 100,000 population as of Oct. 22, higher than the rate observed in the comparable week of previous seasons going back to 2010-2011, according to the CDC’s Influenza Hospitalization Surveillance Network.
A look at state reports of ILI outpatient visit rates shows that the District of Columbia and South Carolina are already in the very high range of the CDC’s severity scale, while 11 states are in the high range. Again going back to 2010-2011, no jurisdiction has ever been in the very high range this early in the season, based on data from the Outpatient Influenza-like Illness Surveillance Network.
Patients at risk for Barrett’s esophagus rarely screened
Adults with chronic gastroesophageal reflux disease (GERD) are at increased risk for Barrett’s esophagus (BE) – the precursor to esophageal adenocarcinoma (EAC) – but most don’t undergo recommended screening, new research shows.
Jennifer Kolb, MD, with the University of California, Los Angeles, and colleagues surveyed 472 adults with chronic GERD who qualify for BE screening and had a recent visit with their primary care provider.
In this diverse population of people at risk for BE and EAC, only 13% had ever been advised to undergo endoscopy to screen for BE and only 5% actually had a prior screening, the study notes.
“These results make it clear that screening is rarely done,” Dr. Kolb told this news organization.
The results of the survey are published online in the American Journal of Gastroenterology.
Concern high, understanding low
Esophageal cancer and BE have increased among middle-aged adults over roughly the past 5 years, and this increase is not because of better or more frequent screening, as reported previously by this news organization.
In fact, the majority of patients who develop EAC do not have a prior diagnosis of BE, which highlights the failure of current BE screening practices, Dr. Kolb and colleagues point out.
Professional gastroenterology society guidelines recommend screening for BE using upper endoscopy for at-risk individuals, which includes those with chronic GERD, along with other risk factors such as age older than 50 years, male sex, white race, smoking, obesity, and family history of BE or EAC.
In the current survey, most individuals said early detection of BE/EAC is important and leads to better outcomes, but most had poor overall knowledge of risk factors and indications for screening.
Only about two-thirds of respondents correctly identified BE risk factors, and only about 20% believed BE screening was necessary with GERD, the researchers note.
Roughly two-thirds of individuals wanted to prioritize BE screening and felt that getting an upper endoscopy would ease their concern.
Yet, 40% had no prior esophagogastroduodenoscopy. These individuals were less knowledgeable about BE/EAC risk and screening recommendations and identified more barriers to completing endoscopy.
“While minorities were most concerned about developing Barrett’s esophagus and cancer, they reported more barriers to screening compared to White participants,” Dr. Kolb said.
Addressing knowledge gaps
The primary care clinician is often the first line for patients with symptomatic acid reflux and the gateway for preventive cancer screening.
Yet, research has shown that primary care clinicians often have trouble identifying who should be screened for BE, and competing clinical issues make it challenging to implement BE screening.
“As gastroenterologists, we must partner with our primary care colleagues to help increase awareness of this lethal disease and improve recognition of risk factors so that eligible patients can be identified and referred for screening,” Dr. Kolb said.
Reached for comment, Seth Gross, MD, clinical chief of the division of gastroenterology and hepatology at New York University Langone Health, said the results “shed light on the fact that patients with GERD don’t have the knowledge of when they should get medical attention and possibly endoscopy.”
“We may need to do a better job of educating our colleagues and patients to know when to seek specialists to potentially get an endoscopy,” Dr. Gross said.
About 90% of esophageal cancers are diagnosed outside of surveillance programs, noted Prasad G. Iyer, MD, a gastroenterologist at Mayo Clinic in Rochester, Minn.
“Patients didn’t even know that they had Barrett’s [esophagus], so they were never under surveillance. They only come to attention after they have trouble with food sticking, and they can’t swallow solid food,” said Dr. Iyer, who wasn’t involved in the survey.
“Unfortunately, there are just so many cancers and so many issues that primary care providers have to deal with that I think this may not be getting the attention it deserves,” he said.
Access to endoscopy is also likely a barrier, Dr. Iyer noted.
“The waiting list may be several months, and I think providers may focus on other things,” he said.
Less-invasive screening options
Fear of endoscopy may be another issue.
In their survey, Dr. Kolb and colleagues found that 20% of respondents reported fear of discomfort with endoscopy as a barrier to completing screening.
But less-invasive screening options are increasingly available or in development.
This includes Cytosponge, a swallowable capsule containing a compressed sponge attached to a string. When withdrawn, the sponge contains esophageal cytology samples that can be used to identify biomarkers for BE.
In a guideline released last spring, the American College of Gastroenterology endorsed Cytosponge as a nonendoscopic BE screening modality, as published in the American Journal of Gastroenterology.
“The strength of the recommendation is conditional, but it’s the first time where [the ACG] is saying that this may be an option for people,” Dr. Gross said.
This research was funded by the American College of Gastroenterology. Dr. Kolb, Dr. Gross, and Dr. Iyer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adults with chronic gastroesophageal reflux disease (GERD) are at increased risk for Barrett’s esophagus (BE) – the precursor to esophageal adenocarcinoma (EAC) – but most don’t undergo recommended screening, new research shows.
Jennifer Kolb, MD, with the University of California, Los Angeles, and colleagues surveyed 472 adults with chronic GERD who qualify for BE screening and had a recent visit with their primary care provider.
In this diverse population of people at risk for BE and EAC, only 13% had ever been advised to undergo endoscopy to screen for BE and only 5% actually had a prior screening, the study notes.
“These results make it clear that screening is rarely done,” Dr. Kolb told this news organization.
The results of the survey are published online in the American Journal of Gastroenterology.
Concern high, understanding low
Esophageal cancer and BE have increased among middle-aged adults over roughly the past 5 years, and this increase is not because of better or more frequent screening, as reported previously by this news organization.
In fact, the majority of patients who develop EAC do not have a prior diagnosis of BE, which highlights the failure of current BE screening practices, Dr. Kolb and colleagues point out.
Professional gastroenterology society guidelines recommend screening for BE using upper endoscopy for at-risk individuals, which includes those with chronic GERD, along with other risk factors such as age older than 50 years, male sex, white race, smoking, obesity, and family history of BE or EAC.
In the current survey, most individuals said early detection of BE/EAC is important and leads to better outcomes, but most had poor overall knowledge of risk factors and indications for screening.
Only about two-thirds of respondents correctly identified BE risk factors, and only about 20% believed BE screening was necessary with GERD, the researchers note.
Roughly two-thirds of individuals wanted to prioritize BE screening and felt that getting an upper endoscopy would ease their concern.
Yet, 40% had no prior esophagogastroduodenoscopy. These individuals were less knowledgeable about BE/EAC risk and screening recommendations and identified more barriers to completing endoscopy.
“While minorities were most concerned about developing Barrett’s esophagus and cancer, they reported more barriers to screening compared to White participants,” Dr. Kolb said.
Addressing knowledge gaps
The primary care clinician is often the first line for patients with symptomatic acid reflux and the gateway for preventive cancer screening.
Yet, research has shown that primary care clinicians often have trouble identifying who should be screened for BE, and competing clinical issues make it challenging to implement BE screening.
“As gastroenterologists, we must partner with our primary care colleagues to help increase awareness of this lethal disease and improve recognition of risk factors so that eligible patients can be identified and referred for screening,” Dr. Kolb said.
Reached for comment, Seth Gross, MD, clinical chief of the division of gastroenterology and hepatology at New York University Langone Health, said the results “shed light on the fact that patients with GERD don’t have the knowledge of when they should get medical attention and possibly endoscopy.”
“We may need to do a better job of educating our colleagues and patients to know when to seek specialists to potentially get an endoscopy,” Dr. Gross said.
About 90% of esophageal cancers are diagnosed outside of surveillance programs, noted Prasad G. Iyer, MD, a gastroenterologist at Mayo Clinic in Rochester, Minn.
“Patients didn’t even know that they had Barrett’s [esophagus], so they were never under surveillance. They only come to attention after they have trouble with food sticking, and they can’t swallow solid food,” said Dr. Iyer, who wasn’t involved in the survey.
“Unfortunately, there are just so many cancers and so many issues that primary care providers have to deal with that I think this may not be getting the attention it deserves,” he said.
Access to endoscopy is also likely a barrier, Dr. Iyer noted.
“The waiting list may be several months, and I think providers may focus on other things,” he said.
Less-invasive screening options
Fear of endoscopy may be another issue.
In their survey, Dr. Kolb and colleagues found that 20% of respondents reported fear of discomfort with endoscopy as a barrier to completing screening.
But less-invasive screening options are increasingly available or in development.
This includes Cytosponge, a swallowable capsule containing a compressed sponge attached to a string. When withdrawn, the sponge contains esophageal cytology samples that can be used to identify biomarkers for BE.
In a guideline released last spring, the American College of Gastroenterology endorsed Cytosponge as a nonendoscopic BE screening modality, as published in the American Journal of Gastroenterology.
“The strength of the recommendation is conditional, but it’s the first time where [the ACG] is saying that this may be an option for people,” Dr. Gross said.
This research was funded by the American College of Gastroenterology. Dr. Kolb, Dr. Gross, and Dr. Iyer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Adults with chronic gastroesophageal reflux disease (GERD) are at increased risk for Barrett’s esophagus (BE) – the precursor to esophageal adenocarcinoma (EAC) – but most don’t undergo recommended screening, new research shows.
Jennifer Kolb, MD, with the University of California, Los Angeles, and colleagues surveyed 472 adults with chronic GERD who qualify for BE screening and had a recent visit with their primary care provider.
In this diverse population of people at risk for BE and EAC, only 13% had ever been advised to undergo endoscopy to screen for BE and only 5% actually had a prior screening, the study notes.
“These results make it clear that screening is rarely done,” Dr. Kolb told this news organization.
The results of the survey are published online in the American Journal of Gastroenterology.
Concern high, understanding low
Esophageal cancer and BE have increased among middle-aged adults over roughly the past 5 years, and this increase is not because of better or more frequent screening, as reported previously by this news organization.
In fact, the majority of patients who develop EAC do not have a prior diagnosis of BE, which highlights the failure of current BE screening practices, Dr. Kolb and colleagues point out.
Professional gastroenterology society guidelines recommend screening for BE using upper endoscopy for at-risk individuals, which includes those with chronic GERD, along with other risk factors such as age older than 50 years, male sex, white race, smoking, obesity, and family history of BE or EAC.
In the current survey, most individuals said early detection of BE/EAC is important and leads to better outcomes, but most had poor overall knowledge of risk factors and indications for screening.
Only about two-thirds of respondents correctly identified BE risk factors, and only about 20% believed BE screening was necessary with GERD, the researchers note.
Roughly two-thirds of individuals wanted to prioritize BE screening and felt that getting an upper endoscopy would ease their concern.
Yet, 40% had no prior esophagogastroduodenoscopy. These individuals were less knowledgeable about BE/EAC risk and screening recommendations and identified more barriers to completing endoscopy.
“While minorities were most concerned about developing Barrett’s esophagus and cancer, they reported more barriers to screening compared to White participants,” Dr. Kolb said.
Addressing knowledge gaps
The primary care clinician is often the first line for patients with symptomatic acid reflux and the gateway for preventive cancer screening.
Yet, research has shown that primary care clinicians often have trouble identifying who should be screened for BE, and competing clinical issues make it challenging to implement BE screening.
“As gastroenterologists, we must partner with our primary care colleagues to help increase awareness of this lethal disease and improve recognition of risk factors so that eligible patients can be identified and referred for screening,” Dr. Kolb said.
Reached for comment, Seth Gross, MD, clinical chief of the division of gastroenterology and hepatology at New York University Langone Health, said the results “shed light on the fact that patients with GERD don’t have the knowledge of when they should get medical attention and possibly endoscopy.”
“We may need to do a better job of educating our colleagues and patients to know when to seek specialists to potentially get an endoscopy,” Dr. Gross said.
About 90% of esophageal cancers are diagnosed outside of surveillance programs, noted Prasad G. Iyer, MD, a gastroenterologist at Mayo Clinic in Rochester, Minn.
“Patients didn’t even know that they had Barrett’s [esophagus], so they were never under surveillance. They only come to attention after they have trouble with food sticking, and they can’t swallow solid food,” said Dr. Iyer, who wasn’t involved in the survey.
“Unfortunately, there are just so many cancers and so many issues that primary care providers have to deal with that I think this may not be getting the attention it deserves,” he said.
Access to endoscopy is also likely a barrier, Dr. Iyer noted.
“The waiting list may be several months, and I think providers may focus on other things,” he said.
Less-invasive screening options
Fear of endoscopy may be another issue.
In their survey, Dr. Kolb and colleagues found that 20% of respondents reported fear of discomfort with endoscopy as a barrier to completing screening.
But less-invasive screening options are increasingly available or in development.
This includes Cytosponge, a swallowable capsule containing a compressed sponge attached to a string. When withdrawn, the sponge contains esophageal cytology samples that can be used to identify biomarkers for BE.
In a guideline released last spring, the American College of Gastroenterology endorsed Cytosponge as a nonendoscopic BE screening modality, as published in the American Journal of Gastroenterology.
“The strength of the recommendation is conditional, but it’s the first time where [the ACG] is saying that this may be an option for people,” Dr. Gross said.
This research was funded by the American College of Gastroenterology. Dr. Kolb, Dr. Gross, and Dr. Iyer report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM AMERICAN JOURNAL OF GASTROENTEROLOGY
FDA rejects bulevirtide for hepatitis D
The U.S. Food and Drug Administration (FDA) has declined to approve bulevirtide, Gilead Sciences’ drug for the treatment of hepatitis delta virus (HDV) infection and compensated liver disease.
In a complete response letter, the FDA voiced concerns over the production and delivery of bulevirtide, an investigational, first-in-class HDV entry-inhibitor that received conditional approved in Europe in 2020.
The FDA did not request new studies to evaluate the safety and efficacy of bulevirtide.
As reported previously by this news organization, data from an ongoing phase 3 trial showed that after 48 weeks of treatment, almost half of those treated with bulevirtide achieved the combined primary endpoint of reduced or undetectable HDV RNA levels and normalized alanine aminotransferase levels.
Chronic HDV infection is the most severe form of viral hepatitis. It is associated with a poor prognosis and high mortality rates.
There are currently no approved treatments for HDV in the United States. Bulevirtide was granted breakthrough therapy and orphan drug designations by the FDA.
Merdad Parsey, MD, PhD, chief medical officer, Gilead Sciences, wrote in a news release that the company looks forward to “continuing our active discussions with FDA so that we may bring bulevirtide to people living with HDV in the U.S. as soon as possible.”
This is the second manufacturing-related complete response letter Gilead has received in the past 8 months. In March, the FDA rejected the long-acting HIV drug lenacapavir. The drug was sanctioned in Europe and the United Kingdom in September.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration (FDA) has declined to approve bulevirtide, Gilead Sciences’ drug for the treatment of hepatitis delta virus (HDV) infection and compensated liver disease.
In a complete response letter, the FDA voiced concerns over the production and delivery of bulevirtide, an investigational, first-in-class HDV entry-inhibitor that received conditional approved in Europe in 2020.
The FDA did not request new studies to evaluate the safety and efficacy of bulevirtide.
As reported previously by this news organization, data from an ongoing phase 3 trial showed that after 48 weeks of treatment, almost half of those treated with bulevirtide achieved the combined primary endpoint of reduced or undetectable HDV RNA levels and normalized alanine aminotransferase levels.
Chronic HDV infection is the most severe form of viral hepatitis. It is associated with a poor prognosis and high mortality rates.
There are currently no approved treatments for HDV in the United States. Bulevirtide was granted breakthrough therapy and orphan drug designations by the FDA.
Merdad Parsey, MD, PhD, chief medical officer, Gilead Sciences, wrote in a news release that the company looks forward to “continuing our active discussions with FDA so that we may bring bulevirtide to people living with HDV in the U.S. as soon as possible.”
This is the second manufacturing-related complete response letter Gilead has received in the past 8 months. In March, the FDA rejected the long-acting HIV drug lenacapavir. The drug was sanctioned in Europe and the United Kingdom in September.
A version of this article first appeared on Medscape.com.
The U.S. Food and Drug Administration (FDA) has declined to approve bulevirtide, Gilead Sciences’ drug for the treatment of hepatitis delta virus (HDV) infection and compensated liver disease.
In a complete response letter, the FDA voiced concerns over the production and delivery of bulevirtide, an investigational, first-in-class HDV entry-inhibitor that received conditional approved in Europe in 2020.
The FDA did not request new studies to evaluate the safety and efficacy of bulevirtide.
As reported previously by this news organization, data from an ongoing phase 3 trial showed that after 48 weeks of treatment, almost half of those treated with bulevirtide achieved the combined primary endpoint of reduced or undetectable HDV RNA levels and normalized alanine aminotransferase levels.
Chronic HDV infection is the most severe form of viral hepatitis. It is associated with a poor prognosis and high mortality rates.
There are currently no approved treatments for HDV in the United States. Bulevirtide was granted breakthrough therapy and orphan drug designations by the FDA.
Merdad Parsey, MD, PhD, chief medical officer, Gilead Sciences, wrote in a news release that the company looks forward to “continuing our active discussions with FDA so that we may bring bulevirtide to people living with HDV in the U.S. as soon as possible.”
This is the second manufacturing-related complete response letter Gilead has received in the past 8 months. In March, the FDA rejected the long-acting HIV drug lenacapavir. The drug was sanctioned in Europe and the United Kingdom in September.
A version of this article first appeared on Medscape.com.
Crusty ear

The physician used a curette to perform a shave biopsy; pathology results indicated this was a poorly differentiated squamous cell carcinoma (SCC). Cutaneous SCC is the second most common skin cancer in the United States (after basal cell carcinoma) and increases in frequency with age and cumulative sun damage. It is the most common skin cancer in patients who are Black.
SCC is frequently found on the head and neck, including the ear, but is less commonly found within the conchal bowl (as seen here). Often, SCC manifests as a rough plaque or dome-shaped papule in a sun damaged location, but it may occasionally manifest as an ulcer. While most patients are cured with outpatient surgery, an estimated 8000 patients will develop nodal metastasis and 3000 patients will die from the disease in the United States annually.1 Chronically immunosuppressed patients, such as organ transplant recipients, are at high risk.
This patient underwent Mohs microsurgery (MMS) and clear margins were achieved after 2 stages. The resulting defect was repaired with a full-thickness graft from the postauricular fold. MMS is an excellent technique for keratinocyte carcinomas (SCC and basal cell carcinomas) of the head and neck, recurrent skin cancers on the trunk and extremities, high-risk cancer subtypes, and tumors with indistinct clinical borders. Follow-up for patients with SCCs includes full skin exams every 6 months for 2 years.
The American Academy of Dermatology offers a complimentary Mohs Surgery Appropriate Use Criteria App that assists in determining when Mohs surgery is appropriate, based on multiple tumor characteristics.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Waldman A, Schmults C. Cutaneous squamous cell carcinoma. Hematol Oncol Clin North Am. 2019;33:1-12. doi:10.1016/j.hoc.2018.08.001
The physician used a curette to perform a shave biopsy; pathology results indicated this was a poorly differentiated squamous cell carcinoma (SCC). Cutaneous SCC is the second most common skin cancer in the United States (after basal cell carcinoma) and increases in frequency with age and cumulative sun damage. It is the most common skin cancer in patients who are Black.
SCC is frequently found on the head and neck, including the ear, but is less commonly found within the conchal bowl (as seen here). Often, SCC manifests as a rough plaque or dome-shaped papule in a sun damaged location, but it may occasionally manifest as an ulcer. While most patients are cured with outpatient surgery, an estimated 8000 patients will develop nodal metastasis and 3000 patients will die from the disease in the United States annually.1 Chronically immunosuppressed patients, such as organ transplant recipients, are at high risk.
This patient underwent Mohs microsurgery (MMS) and clear margins were achieved after 2 stages. The resulting defect was repaired with a full-thickness graft from the postauricular fold. MMS is an excellent technique for keratinocyte carcinomas (SCC and basal cell carcinomas) of the head and neck, recurrent skin cancers on the trunk and extremities, high-risk cancer subtypes, and tumors with indistinct clinical borders. Follow-up for patients with SCCs includes full skin exams every 6 months for 2 years.
The American Academy of Dermatology offers a complimentary Mohs Surgery Appropriate Use Criteria App that assists in determining when Mohs surgery is appropriate, based on multiple tumor characteristics.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
The physician used a curette to perform a shave biopsy; pathology results indicated this was a poorly differentiated squamous cell carcinoma (SCC). Cutaneous SCC is the second most common skin cancer in the United States (after basal cell carcinoma) and increases in frequency with age and cumulative sun damage. It is the most common skin cancer in patients who are Black.
SCC is frequently found on the head and neck, including the ear, but is less commonly found within the conchal bowl (as seen here). Often, SCC manifests as a rough plaque or dome-shaped papule in a sun damaged location, but it may occasionally manifest as an ulcer. While most patients are cured with outpatient surgery, an estimated 8000 patients will develop nodal metastasis and 3000 patients will die from the disease in the United States annually.1 Chronically immunosuppressed patients, such as organ transplant recipients, are at high risk.
This patient underwent Mohs microsurgery (MMS) and clear margins were achieved after 2 stages. The resulting defect was repaired with a full-thickness graft from the postauricular fold. MMS is an excellent technique for keratinocyte carcinomas (SCC and basal cell carcinomas) of the head and neck, recurrent skin cancers on the trunk and extremities, high-risk cancer subtypes, and tumors with indistinct clinical borders. Follow-up for patients with SCCs includes full skin exams every 6 months for 2 years.
The American Academy of Dermatology offers a complimentary Mohs Surgery Appropriate Use Criteria App that assists in determining when Mohs surgery is appropriate, based on multiple tumor characteristics.
Photos and text for Photo Rounds Friday courtesy of Jonathan Karnes, MD (copyright retained). Dr. Karnes is the medical director of MDFMR Dermatology Services, Augusta, ME.
1. Waldman A, Schmults C. Cutaneous squamous cell carcinoma. Hematol Oncol Clin North Am. 2019;33:1-12. doi:10.1016/j.hoc.2018.08.001
1. Waldman A, Schmults C. Cutaneous squamous cell carcinoma. Hematol Oncol Clin North Am. 2019;33:1-12. doi:10.1016/j.hoc.2018.08.001

Major depression treatments boost brain connectivity
VIENNA – , new research suggests.
In a “repeat” MRI study, adult participants with MDD had significantly lower brain connectivity compared with their healthy peers at baseline – but showed significant improvement at the 6-week follow-up. These improvements were associated with decreases in symptom severity, independent of whether they received electroconvulsive therapy (ECT) or other treatment modalities.
“This means that the brain structure of patients with serious clinical depression is not as fixed as we thought, and we can improve brain structure within a short time frame [of] around 6 weeks,” lead author Jonathan Repple, MD, now professor of predictive psychiatry at the University of Frankfurt, Germany, said in a release.
“This gives hope to patients who believe nothing can change and they have to live with a disease forever because it is ‘set in stone’ in their brain,” he added.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
‘Easily understandable picture’
Dr. Repple said in an interview that the investigators “were surprised to see how plastic” the brain could be.
“I’ve done a lot of imaging studies in the past where we looked at differences in depression vs. healthy controls, and then maybe had tiny effects. But we’ve never seen such a clear and easily understandable picture, where we see a deficit at the beginning and then a significant increase in whatever biomarker we were looking at, that even correlated with how successful the treatment was,” he said.
Dr. Repple noted that “this is the thing everyone is looking for when we’re talking about a biomarker: That we see this exact pattern” – and it is why they are so excited about the results.
However, he cautioned that the study included a “small sample” and the results need to be independently replicated.
“If this can be replicated, this might be a very good target for future intervention studies,” Dr. Repple said.
The investigators noted that altered brain structural connectivity has been implicated before in the pathophysiology of MDD.
However, it is not clear whether these changes are stable over time and indicate a biological predisposition, or are markers of current disease severity and can be altered by effective treatment.
To investigate further, the researchers used gray matter T1-weighted MRI to define nodes in the brain and diffusion-weighted imaging (DWI)-based tractography to determine connections between the nodes, to create a structural connectome or white matter network.
They performed assessments at baseline and at 6 weeks’ follow-up in 123 participants diagnosed with current MDD and receiving inpatient treatment, and 55 participants who acted as the healthy controls group.
Among the patients with MDD, 56 were treated with ECT and 67 received other antidepressant care, including psychological therapy or medications. Some patients had received all three treatment modalities.
Significant interactions
Results showed a significant interaction by group and time between the baseline and 6-week follow-up assessments (P < .05).
This was partly driven by the MDD group having a significantly lower connectivity strength at baseline than the healthy controls group (P < .05).
It was also partly driven by patients showing a significant improvement in connectivity strength between the baseline and follow-up assessments (P < .05), a pattern that was not seen in the nonpatients.
This increase in connectivity strength was associated with a significant decrease in depression symptom severity (P < .05). This was independent of the treatment modality, indicating that it was not linked to the use of ECT.
Dr. Repple acknowledged the relatively short follow-up period of the study, and added that he is not aware of longitudinal studies of the structural connectome with a longer follow-up.
He pointed out that the structural connectivity of the brain decreases with age, but there have been no studies that have assessed patients with depression and “measured the same person again after 2, 4, 6, or 8 years.”
Dr. Repple reported that the investigators will be following up with their participants, “so hopefully in a few years we’ll have more information on that.
“One thing I also need to stress is that, when we’re looking at the MRI brain scans, we see an increase in connectivity strength, but we really can’t say what the molecular mechanisms behind it are,” he said. “This is a black box for us.”
Several unanswered questions
Commenting in the release, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said this was a “very interesting and difficult study to perform.”
However, Dr. Ruhe, who was not involved in the research, told this news organization that it is “very difficult to connect the lack of brain connectivity to the patient symptomatology because there is a huge gap between them.”
The problem is that, despite “lots of evidence” that they are effective, “we currently don’t know how antidepressant therapies work” in terms of their underlying mechanisms of action, he said.
“We think that these types of therapies all modulate the plasticity of the brain,” said Dr. Ruhe. “What this study showed is there are changes that you can detect even in 6 weeks,” although they may have been observed even sooner with a shorter follow-up.
He noted that big questions are whether the change is specific to the treatment given, and “can you modulate different brain network dysfunctions with different treatments?”
Moreover, he wondered if a brain scan could indicate which type of treatment should be used. “This is, of course, very new and very challenging, and we don’t know yet, but we should be pursuing this,” Dr. Ruhe said.
Another question is whether or not the brain connectivity changes shown in the study represent a persistent change – “and whether this is a persistent change that is associated with a consistent and persistent relief of depression.
“Again, this is something that needs to be followed up,” said Dr. Ruhe.
No funding was declared. The study authors and Dr. Ruhe report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA – , new research suggests.
In a “repeat” MRI study, adult participants with MDD had significantly lower brain connectivity compared with their healthy peers at baseline – but showed significant improvement at the 6-week follow-up. These improvements were associated with decreases in symptom severity, independent of whether they received electroconvulsive therapy (ECT) or other treatment modalities.
“This means that the brain structure of patients with serious clinical depression is not as fixed as we thought, and we can improve brain structure within a short time frame [of] around 6 weeks,” lead author Jonathan Repple, MD, now professor of predictive psychiatry at the University of Frankfurt, Germany, said in a release.
“This gives hope to patients who believe nothing can change and they have to live with a disease forever because it is ‘set in stone’ in their brain,” he added.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
‘Easily understandable picture’
Dr. Repple said in an interview that the investigators “were surprised to see how plastic” the brain could be.
“I’ve done a lot of imaging studies in the past where we looked at differences in depression vs. healthy controls, and then maybe had tiny effects. But we’ve never seen such a clear and easily understandable picture, where we see a deficit at the beginning and then a significant increase in whatever biomarker we were looking at, that even correlated with how successful the treatment was,” he said.
Dr. Repple noted that “this is the thing everyone is looking for when we’re talking about a biomarker: That we see this exact pattern” – and it is why they are so excited about the results.
However, he cautioned that the study included a “small sample” and the results need to be independently replicated.
“If this can be replicated, this might be a very good target for future intervention studies,” Dr. Repple said.
The investigators noted that altered brain structural connectivity has been implicated before in the pathophysiology of MDD.
However, it is not clear whether these changes are stable over time and indicate a biological predisposition, or are markers of current disease severity and can be altered by effective treatment.
To investigate further, the researchers used gray matter T1-weighted MRI to define nodes in the brain and diffusion-weighted imaging (DWI)-based tractography to determine connections between the nodes, to create a structural connectome or white matter network.
They performed assessments at baseline and at 6 weeks’ follow-up in 123 participants diagnosed with current MDD and receiving inpatient treatment, and 55 participants who acted as the healthy controls group.
Among the patients with MDD, 56 were treated with ECT and 67 received other antidepressant care, including psychological therapy or medications. Some patients had received all three treatment modalities.
Significant interactions
Results showed a significant interaction by group and time between the baseline and 6-week follow-up assessments (P < .05).
This was partly driven by the MDD group having a significantly lower connectivity strength at baseline than the healthy controls group (P < .05).
It was also partly driven by patients showing a significant improvement in connectivity strength between the baseline and follow-up assessments (P < .05), a pattern that was not seen in the nonpatients.
This increase in connectivity strength was associated with a significant decrease in depression symptom severity (P < .05). This was independent of the treatment modality, indicating that it was not linked to the use of ECT.
Dr. Repple acknowledged the relatively short follow-up period of the study, and added that he is not aware of longitudinal studies of the structural connectome with a longer follow-up.
He pointed out that the structural connectivity of the brain decreases with age, but there have been no studies that have assessed patients with depression and “measured the same person again after 2, 4, 6, or 8 years.”
Dr. Repple reported that the investigators will be following up with their participants, “so hopefully in a few years we’ll have more information on that.
“One thing I also need to stress is that, when we’re looking at the MRI brain scans, we see an increase in connectivity strength, but we really can’t say what the molecular mechanisms behind it are,” he said. “This is a black box for us.”
Several unanswered questions
Commenting in the release, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said this was a “very interesting and difficult study to perform.”
However, Dr. Ruhe, who was not involved in the research, told this news organization that it is “very difficult to connect the lack of brain connectivity to the patient symptomatology because there is a huge gap between them.”
The problem is that, despite “lots of evidence” that they are effective, “we currently don’t know how antidepressant therapies work” in terms of their underlying mechanisms of action, he said.
“We think that these types of therapies all modulate the plasticity of the brain,” said Dr. Ruhe. “What this study showed is there are changes that you can detect even in 6 weeks,” although they may have been observed even sooner with a shorter follow-up.
He noted that big questions are whether the change is specific to the treatment given, and “can you modulate different brain network dysfunctions with different treatments?”
Moreover, he wondered if a brain scan could indicate which type of treatment should be used. “This is, of course, very new and very challenging, and we don’t know yet, but we should be pursuing this,” Dr. Ruhe said.
Another question is whether or not the brain connectivity changes shown in the study represent a persistent change – “and whether this is a persistent change that is associated with a consistent and persistent relief of depression.
“Again, this is something that needs to be followed up,” said Dr. Ruhe.
No funding was declared. The study authors and Dr. Ruhe report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
VIENNA – , new research suggests.
In a “repeat” MRI study, adult participants with MDD had significantly lower brain connectivity compared with their healthy peers at baseline – but showed significant improvement at the 6-week follow-up. These improvements were associated with decreases in symptom severity, independent of whether they received electroconvulsive therapy (ECT) or other treatment modalities.
“This means that the brain structure of patients with serious clinical depression is not as fixed as we thought, and we can improve brain structure within a short time frame [of] around 6 weeks,” lead author Jonathan Repple, MD, now professor of predictive psychiatry at the University of Frankfurt, Germany, said in a release.
“This gives hope to patients who believe nothing can change and they have to live with a disease forever because it is ‘set in stone’ in their brain,” he added.
The findings were presented at the 35th European College of Neuropsychopharmacology (ECNP) Congress.
‘Easily understandable picture’
Dr. Repple said in an interview that the investigators “were surprised to see how plastic” the brain could be.
“I’ve done a lot of imaging studies in the past where we looked at differences in depression vs. healthy controls, and then maybe had tiny effects. But we’ve never seen such a clear and easily understandable picture, where we see a deficit at the beginning and then a significant increase in whatever biomarker we were looking at, that even correlated with how successful the treatment was,” he said.
Dr. Repple noted that “this is the thing everyone is looking for when we’re talking about a biomarker: That we see this exact pattern” – and it is why they are so excited about the results.
However, he cautioned that the study included a “small sample” and the results need to be independently replicated.
“If this can be replicated, this might be a very good target for future intervention studies,” Dr. Repple said.
The investigators noted that altered brain structural connectivity has been implicated before in the pathophysiology of MDD.
However, it is not clear whether these changes are stable over time and indicate a biological predisposition, or are markers of current disease severity and can be altered by effective treatment.
To investigate further, the researchers used gray matter T1-weighted MRI to define nodes in the brain and diffusion-weighted imaging (DWI)-based tractography to determine connections between the nodes, to create a structural connectome or white matter network.
They performed assessments at baseline and at 6 weeks’ follow-up in 123 participants diagnosed with current MDD and receiving inpatient treatment, and 55 participants who acted as the healthy controls group.
Among the patients with MDD, 56 were treated with ECT and 67 received other antidepressant care, including psychological therapy or medications. Some patients had received all three treatment modalities.
Significant interactions
Results showed a significant interaction by group and time between the baseline and 6-week follow-up assessments (P < .05).
This was partly driven by the MDD group having a significantly lower connectivity strength at baseline than the healthy controls group (P < .05).
It was also partly driven by patients showing a significant improvement in connectivity strength between the baseline and follow-up assessments (P < .05), a pattern that was not seen in the nonpatients.
This increase in connectivity strength was associated with a significant decrease in depression symptom severity (P < .05). This was independent of the treatment modality, indicating that it was not linked to the use of ECT.
Dr. Repple acknowledged the relatively short follow-up period of the study, and added that he is not aware of longitudinal studies of the structural connectome with a longer follow-up.
He pointed out that the structural connectivity of the brain decreases with age, but there have been no studies that have assessed patients with depression and “measured the same person again after 2, 4, 6, or 8 years.”
Dr. Repple reported that the investigators will be following up with their participants, “so hopefully in a few years we’ll have more information on that.
“One thing I also need to stress is that, when we’re looking at the MRI brain scans, we see an increase in connectivity strength, but we really can’t say what the molecular mechanisms behind it are,” he said. “This is a black box for us.”
Several unanswered questions
Commenting in the release, Eric Ruhe, MD, PhD, Radboud University Medical Center, Nijmegen, the Netherlands, said this was a “very interesting and difficult study to perform.”
However, Dr. Ruhe, who was not involved in the research, told this news organization that it is “very difficult to connect the lack of brain connectivity to the patient symptomatology because there is a huge gap between them.”
The problem is that, despite “lots of evidence” that they are effective, “we currently don’t know how antidepressant therapies work” in terms of their underlying mechanisms of action, he said.
“We think that these types of therapies all modulate the plasticity of the brain,” said Dr. Ruhe. “What this study showed is there are changes that you can detect even in 6 weeks,” although they may have been observed even sooner with a shorter follow-up.
He noted that big questions are whether the change is specific to the treatment given, and “can you modulate different brain network dysfunctions with different treatments?”
Moreover, he wondered if a brain scan could indicate which type of treatment should be used. “This is, of course, very new and very challenging, and we don’t know yet, but we should be pursuing this,” Dr. Ruhe said.
Another question is whether or not the brain connectivity changes shown in the study represent a persistent change – “and whether this is a persistent change that is associated with a consistent and persistent relief of depression.
“Again, this is something that needs to be followed up,” said Dr. Ruhe.
No funding was declared. The study authors and Dr. Ruhe report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
AT ECNP 2022