User login
Oral Therapy for Aerococcus urinae Bacteremia and Thoracic Spondylodiscitis of Presumed Urinary Origin
Aerococcus urinae (A urinae), a gram-positive coccus readily mistaken for a Staphylococcus species, was first identified in 1992.1-3 It now reportedly accounts for 0.2% to 0.8% of clinical urine isolates.4-6 A urinae bacteriuria is typically asymptomatic and mainly occurs in women.7-9 Symptomatic A urinae urinary tract infection (UTI) occurs predominantly in older men with underlying urologic abnormalities.4-10
Serious A urinae infections are rare. The first 2 reported cases involved men with A urinae endocarditis, one of whom died.11,12 To date, only 8 cases of spondylodiscitis due to A urinae have been reported.13-20 Optimal treatment for invasive A urinae infection is undefined; however, the reported cases were treated successfully with diverse antibiotic regimen combinations; all including a β-lactam and beginning with at least 2 weeks of IV antibiotics.13-20 We describe a man with A urinae bacteremia and spondylodiscitis, presumably arising from a urinary source in the setting of bladder outlet obstruction, who was treated successfully.
Case Presentation
A 74-year-old man with morbid obesity, type 2 diabetes mellitus, stage 2 chronic kidney disease, and tobacco use presented to the emergency department after 2 weeks of progressive, nonradiating, midthoracic back pain, lower extremity weakness, gait imbalance, fatigue, anorexia, rigors, and subjective fevers. On presentation, he was afebrile and hemodynamically stable. A physical examination revealed point tenderness of the midthoracic vertebrae, nontender costovertebral angles, diffusely decreased strength, nonsustained clonus in both lower extremities, inguinal intertrigo, and a buried penis with purulent meatal discharge.
Laboratory results indicated a white blood cell (WBC) count of 13.5 K/μL (reference range, 4.0-11.0), absolute neutrophil count of 11.48 K/μL (reference range, 2.0-7.7), C-reactive protein (CRP) level of 225.3 mg/L (reference range, ≤ 5.0), erythrocyte sedimentation rate of 85 mm/h (reference range, 5-15), serum blood urea nitrogen of 76 mg/dL (reference range, 8-26), and serum creatinine (SCr) of 1.9 mg/dL (reference range, 1.1-1.4). A urinalysis showed positive leukocyte esterase, WBC clumps, and little bacteria. Abdominal/pelvic computed tomography showed spondylodiscitis-like changes at T7-T8, bilateral perinephric fat stranding, bladder distension, and bladder wall thickening.
The patient was presumed to have discitis secondary to a UTI, with possible pyelonephritis, and was given empiric vancomycin and ceftriaxone. Spinal magnetic resonance imaging with contrast supported spondylodiscitis at T7-T8, extending to T8-T9. Preliminary results from the admission blood and urine cultures showed gram-positive cocci in clusters, which were presumed initially to be Staphylococcus aureus (S aureus).
The final urine culture report listed multiple organisms, predominantly A urinae (Table 1); 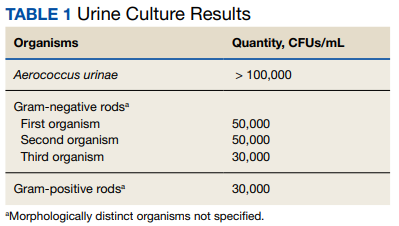
On hospital day 6, the patient’s back pain had resolved, micturition was normal, appetite had normalized, and SCr was minimally above baseline (1.4 mg/dL). He insisted on completing antibiotic treatment at home and had no other medical indication for continued hospitalization. Thus, antibiotic therapy was changed to an all-oral regimen of amoxicillin 1 g 3 times daily for 10 days and levofloxacin 750 mg daily for 6 weeks, and the patient was discharged to home.
The patient returned 5 days postdischarge due to anuria. Investigation showed severe acute kidney injury (SCr, 6.8 mg/dL) and bladder outlet obstruction due to phimosis and urethral meatal stenosis. Urinalysis was unremarkable. His CRP had declined from 225 mg/L (initial admission) to 154 mg/L. A urinae culture and 2 sets of blood cultures were finalized as no growth. He was diagnosed with postrenal acute kidney injury and underwent meatal dilation and Foley catheterization but declined surgical correction. When seen in the clinic 2 months postantimicrobial therapy, the patient had normal micturition, no symptoms or signs of infection, and steadily down-trending inflammatory markers.
Discussion
A urinae, historically considered a rare pathogen, has been identified with increasing frequency in urine cultures due to improved microbiologic diagnostic techniques. However, there are only 8 reported cases of A urinae spondylodiscitis. Urinary pathology is an accepted risk factor for A urinae infections; consequently, we suspect that our patient’s urinary outflow obstruction and poor genitourinary hygiene were related to his invasive A urinae infection.10,21,22 We surmise that he had a chronic urinary outflow obstruction contributing to his infection, as evidenced by imaging findings, while the phimosis and urethral meatal stenosis were most likely infectious sequelae considering his anuria and acute kidney injury 5 days postdischarge. Indeed, the correlation between A urinae and urinary tract pathology may justify an evaluation for urinary pathology in any man with A urinae infection, regardless of the presence of symptoms.
By contrast, the implications of A urinae bacteriuria remain unclear. From a public health perspective, A urinae bacteriuria is rare, but the infectious mechanism remains undetermined with a case report suggesting the possibility of sexual transmission.4-6,23 In our case, the patient was not sexually active and had no clear origin of infection. Considering the potential severity of infection, more studies are needed to determine the infectious mechanism of A urinae.
In terms of infectious morbidity, the results seem to vary by sex. In a retrospective study of about 30,000 clinical urine samples, 62 (58 from women, 4 from men) yielded A urinae. The 62 corresponding patients lacked systemic infectious complications, leading the authors to conclude that A urinae is a relatively avirulent organism.24 Although possibly true in women, we are wary of drawing conclusions, especially regarding men, from a study that included only 62 urine samples were A urinae–positive, with only 4 from men. More evidence is needed to define the prognostic implications of A urinae bacteriuria in men.
As illustrated by the present case and previous reports, severe A urinae infections can occur, and the contributory factors deserve consideration. In our patient, the actual mechanism for bacteremia remains unclear. The initial concern for acute pyelonephritis was prompted by a computed tomography finding of bilateral perinephric fat stranding. This finding was questioned because it is common in older patients without infection, hence, is highly nonspecific. A correlation with urinary outflow obstruction may be an important clue in cases like this one.25,26
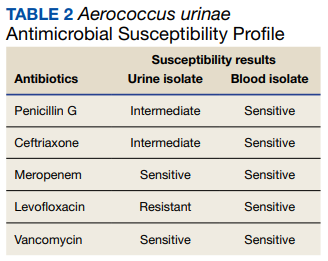
Furthermore, whether the urinary tract truly was the source of the patient’s bacteremia is clouded by the differing antimicrobial susceptibility patterns of the A urinae blood and urine isolates. The simplest explanation for this discordance may be that all the isolates shared a common initial origin but adapted to different environments in the host (perhaps over time) or laboratory, producing phenotypic variation. Alternatively, the infection could have been polyclonal from the onset, with sampling error leading to the differing detected susceptibility patterns, or the blood and urine isolates may have represented independent acquisition events, involving distinct A urinae strains. Unfortunately (from an academic perspective), given patient preferences and recommendations from the infectious disease consultant, no bone biopsy was done for histology and culture to confirm infection and to allow comparative strain identification if A urinae was isolated.
Optimal treatment for A urinae spondylodiscitis has yet to be established. β-lactams have shown good clinical efficacy despite being bacteriostatic in vitro.27 Early in vitro studies showed synergistic bactericidal synergistic activity with penicillin plus aminoglycoside combination therapies.27-30 Cases of endocarditis have been successfully treated mainly with the combination of a β-lactam plus aminoglycoside combination therapy.30,31 Previous cases of spondylodiscitis have been treated successfully with diverse antimicrobial agents, including clindamycin, β-lactams, cephalosporins, fluoroquinolones, and aminoglycosides.14
Our patient improved rapidly while receiving empiric therapy with vancomycin and ceftriaxone and tolerated a rapid transition to oral amoxicillin and levofloxacin. This is the shortest IV treatment course for A urinae spondylodiscitis reported to date. We suspect that such rapid IV-to-oral transitions will suffice in most stable patients with A urinae spondylodiscitis or other invasive A urinae infections in line with the results of the OVIVA and POET trials.32,33
Conclusions
We believe A urinae UTI in the absence of obvious predisposing factors should prompt evaluation for urinary outflow obstruction. Despite improved laboratory diagnostic techniques, spondylodiscitis related to A urinae remains a rare entity and thus definitive treatment recommendations are difficult to make. However, we suspect that in many cases it is reasonable to extrapolate from the results of the POET and OVIVA trials and rapidly transition therapy of A urinae spondylodiscitis from IV to oral antibiotics. We suspect a review of the US Department of Veterans Affairs population might uncover a higher incidence of A urinae infection than previously estimated due to the population demographics and the epidemiology of A urinae.
1. Christensen JJ, Korner B, Kjaergaard H. Aerococcus-like organism—an unnoticed urinary tract pathogen. APMIS. 1989;97(6):539-546. doi:10.1111/j.1699-0463.1989.tb00828.x
2. Aguirre M, Collins MD. Phylogenetic analysis of some Aerococcus-like organisms from urinary tract infections: description of Aerococcus urinae sp. nov. J Gen Microbiol. 1992;138(2):401-405. doi:10.1099/00221287-138-2-401
3. Williams RE, Hirch A, Cowan ST. Aerococcus, a new bacterial genus. J Gen Microbiol. 1953;8(3):475-480. doi:10.1099/00221287-8-3-475
4. Kline KA, Lewis AL. Gram-positive uropathogens, polymicrobial urinary tract infection, and the emerging microbiota of the urinary tract. Microbiol Spectr. 2016;4(2). doi:10.1128/microbiolspec.UTI-0012-2012
5. Schuur PM, Kasteren ME, Sabbe L, Vos MC, Janssens MM, Buiting AG. Urinary tract infections with Aerococcus urinae in the south of The Netherlands. Eur J Clin Microbiol Infect Dis. 1997;16(12):871-875. doi:10.1007/BF01700552
6. Grude N, Tveten Y. Aerococcus urinae og urinveisinfeksjon [Aerococcus urinae and urinary tract infection]. Tidsskr Nor Laegeforen. 2002;122(2):174-175.
7. Narayanasamy S, King K, Dennison A, Spelman DW, Aung AK. Clinical characteristics and laboratory identification of Aerococcus infections: an Australian tertiary centre perspective. Int J Microbiol. 2017;2017. doi:10.1155/2017/5684614
8. Hilt EE, McKinley K, Pearce MM, et al. Urine is not sterile: use of enhanced urine culture techniques to detect resident bacterial flora in the adult female bladder. J Clin Microbiol. 2014;52(3):871-876. doi:10.1128/JCM.02876-13
9. Pearce MM, Hilt EE, Rosenfeld AB, et al. The female urinary microbiome: a comparison of women with and without urgency urinary incontinence. mBio. 2014;5(4):e01283-14. doi:10.1128/mBio.01283-14
10. Sahu KK, Lal A, Mishra AK, Abraham GM. Aerococcus-related infections and their significance: a 9-year retrospective study. J Microsc Ultrastruct. 2021;9(1):18-25. doi:10.4103/JMAU.JMAU_61_19
11. Skov RL, Klarlund M, Thorsen S. Fatal endocarditis due to Aerococcus urinae. Diagn Microbiol Infect Dis. 1995;21(4):219-221. doi:10.1016/0732-8893(95)00037-b
12. Kristensen B, Nielsen G. Endocarditis caused by Aerococcus urinae, a newly recognized pathogen. Eur J Clin Microbiol Infect Dis. 1995;14(1):49-51. doi:10.1007/BF02112619
13. Astudillo L, Sailler L, Porte L, Lefevre JC, Massip P, Arlet-Suau E. Spondylodiscitis due to Aerococcus urinae: a first report. Scand J Infect Dis. 2003;35(11-12):890-891. doi:10.1080/00365540310016664
14. Lyagoubi A, Souffi C, Baroiller V, Vallee E. Spondylodiscitis: an increasingly described localization. EJIFCC. 2020;31(2):169-173.
15. Jerome M, Slim J, Sison R, Marton R. A case of Aerococcus urinae vertebral osteomyelitis. J Glob Infect Dis. 2015;7(2):85-86. doi:10.4103/0974-777X.157246
16. Tekin A, Tekin G, Turunç T, Demiroğlu Z, Kizilkiliç O. Infective endocarditis and spondylodiscitis in a patient due to Aerococcus urinae: first report. Int J Cardiol. 2007;115(3):402-403. doi:10.1016/j.ijcard.2006.01.046
17. Rougier E, Braud A, Argemi X, et al. Spondylodiscitis due to Aerococcus urinae and literature review. Infection. 2018;46(3):419-421. doi:10.1007/s15010-017-1106-0
18. Degroote E, Yildiz H, Lecouvet F, Verroken A, Belkhir L. Aerococcus urinae: an underestimated cause of spine infection? Case report and review of the literature. Acta Clin Belg. 2018;73(6):444-447. doi:10.1080/17843286.2018.1443003
19. Torres-Martos E, Pérez-Cortés S, Sánchez-Calvo JM, López-Prieto MD. Spondylodiscitis due to Aerococcus urinae infection in an elderly immunocompetent patient. Enferm Infecc Microbiol Clin. 2017;35(10):682-684. doi:10.1016/j.eimc.2017.02.005
20. Senneby E, Petersson AC, Rasmussen M. Clinical and microbiological features of bacteraemia with Aerococcus urinae. Clin Microbiol Infect. 2012;18(6):546-550. doi:10.1111/j.1469-0691.2011.03609.x
21. Sunnerhagen T, Nilson B, Olaison L, Rasmussen M. Clinical and microbiological features of infective endocarditis caused by aerococci. Infection. 2016;44(2):167-173. doi:10.1007/s15010-015-0812-8
22. de Jong MF, Soetekouw R, ten Kate RW, Veenendaal D. Aerococcus urinae: severe and fatal bloodstream infections and endocarditis. J Clin Microbiol. 2010;48(9):3445-3447. doi:10.1128/JCM.00835-10
23. Babaeer AA, Nader C, Iacoviello V, Tomera K. Necrotizing urethritis due to Aerococcus urinae. Case Rep Urol. 2015;2015:136147. doi:10.1155/2015/136147
24. Sierra-Hoffman M, Watkins K, Jinadatha C, Fader R, Carpenter JL. Clinical significance of Aerococcus urinae: a retrospective review. Diagn Microbiol Infect Dis. 2005;53(4):289-292. doi:10.1016/j.diagmicrobio.2005.06.021
25. Fukami H, Takeuchi Y, Kagaya S, et al. Perirenal fat stranding is not a powerful diagnostic tool for acute pyelonephritis. Int J Gen Med. 2017;10:137-144. doi:10.2147/IJGM.S133685
26. Han NY, Sung DJ, Kim MJ, Park BJ, Sim KC, Cho SB. Perirenal fat stranding on CT: is there an association with bladder outlet obstruction? Br J Radiol. 2016;89(1063):20160195. doi:10.1259/bjr.20160195
27. Hirzel C, Hirzberger L, Furrer H, Endimiani A. Bactericidal activity of penicillin, ceftriaxone, gentamicin and daptomycin alone and in combination against Aerococcus urinae. Int J Antimicrob Agents. 2016;48(3):271-276. doi:10.1016/j.ijantimicag.2016.05.007
28. Zbinden R, Santanam P, Hunziker L, Leuzinger B, von Graevenitz A. Endocarditis due to Aerococcus urinae: diagnostic tests, fatty acid composition and killing kinetics. Infection. 1999;27(2):122-124. doi:10.1007/BF02560511
29. Skov R, Christensen JJ, Korner B, Frimodt-Møller N, Espersen F. In vitro antimicrobial susceptibility of Aerococcus urinae to 14 antibiotics, and time-kill curves for penicillin, gentamicin and vancomycin. J Antimicrob Chemother. 2001;48(5):653-658. doi:10.1093/jac/48.5.653
30. Ebnöther C, Altwegg M, Gottschalk J, Seebach JD, Kronenberg A. Aerococcus urinae endocarditis: case report and review of the literature. Infection. 2002;30(5):310-313. doi:10.1007/s15010-002-3106-x
31. Tai DBG, Go JR, Fida M, Saleh OA. Management and treatment of Aerococcus bacteremia and endocarditis. Int J Infect Dis. 2021;102:584-589. doi:10.1016/j.ijid.2020.10.096
32. Li H-K, Rombach I, Zambellas R, et al; OVIVA Trial Collaborators. Oral versus intravenous antibiotics for bone and joint infection. N Engl J Med. 2019;380(5):425-436. doi:10.1056/NEJMoa1710926
33. Iversen K, Ihlemann N, Gill SU, et al. Partial oral versus intravenous antibiotic treatment of endocarditis. N Engl J Med. 2019;380(5):415-424. doi:10.1056/NEJMoa1808312
Aerococcus urinae (A urinae), a gram-positive coccus readily mistaken for a Staphylococcus species, was first identified in 1992.1-3 It now reportedly accounts for 0.2% to 0.8% of clinical urine isolates.4-6 A urinae bacteriuria is typically asymptomatic and mainly occurs in women.7-9 Symptomatic A urinae urinary tract infection (UTI) occurs predominantly in older men with underlying urologic abnormalities.4-10
Serious A urinae infections are rare. The first 2 reported cases involved men with A urinae endocarditis, one of whom died.11,12 To date, only 8 cases of spondylodiscitis due to A urinae have been reported.13-20 Optimal treatment for invasive A urinae infection is undefined; however, the reported cases were treated successfully with diverse antibiotic regimen combinations; all including a β-lactam and beginning with at least 2 weeks of IV antibiotics.13-20 We describe a man with A urinae bacteremia and spondylodiscitis, presumably arising from a urinary source in the setting of bladder outlet obstruction, who was treated successfully.
Case Presentation
A 74-year-old man with morbid obesity, type 2 diabetes mellitus, stage 2 chronic kidney disease, and tobacco use presented to the emergency department after 2 weeks of progressive, nonradiating, midthoracic back pain, lower extremity weakness, gait imbalance, fatigue, anorexia, rigors, and subjective fevers. On presentation, he was afebrile and hemodynamically stable. A physical examination revealed point tenderness of the midthoracic vertebrae, nontender costovertebral angles, diffusely decreased strength, nonsustained clonus in both lower extremities, inguinal intertrigo, and a buried penis with purulent meatal discharge.
Laboratory results indicated a white blood cell (WBC) count of 13.5 K/μL (reference range, 4.0-11.0), absolute neutrophil count of 11.48 K/μL (reference range, 2.0-7.7), C-reactive protein (CRP) level of 225.3 mg/L (reference range, ≤ 5.0), erythrocyte sedimentation rate of 85 mm/h (reference range, 5-15), serum blood urea nitrogen of 76 mg/dL (reference range, 8-26), and serum creatinine (SCr) of 1.9 mg/dL (reference range, 1.1-1.4). A urinalysis showed positive leukocyte esterase, WBC clumps, and little bacteria. Abdominal/pelvic computed tomography showed spondylodiscitis-like changes at T7-T8, bilateral perinephric fat stranding, bladder distension, and bladder wall thickening.
The patient was presumed to have discitis secondary to a UTI, with possible pyelonephritis, and was given empiric vancomycin and ceftriaxone. Spinal magnetic resonance imaging with contrast supported spondylodiscitis at T7-T8, extending to T8-T9. Preliminary results from the admission blood and urine cultures showed gram-positive cocci in clusters, which were presumed initially to be Staphylococcus aureus (S aureus).
The final urine culture report listed multiple organisms, predominantly A urinae (Table 1);
On hospital day 6, the patient’s back pain had resolved, micturition was normal, appetite had normalized, and SCr was minimally above baseline (1.4 mg/dL). He insisted on completing antibiotic treatment at home and had no other medical indication for continued hospitalization. Thus, antibiotic therapy was changed to an all-oral regimen of amoxicillin 1 g 3 times daily for 10 days and levofloxacin 750 mg daily for 6 weeks, and the patient was discharged to home.
The patient returned 5 days postdischarge due to anuria. Investigation showed severe acute kidney injury (SCr, 6.8 mg/dL) and bladder outlet obstruction due to phimosis and urethral meatal stenosis. Urinalysis was unremarkable. His CRP had declined from 225 mg/L (initial admission) to 154 mg/L. A urinae culture and 2 sets of blood cultures were finalized as no growth. He was diagnosed with postrenal acute kidney injury and underwent meatal dilation and Foley catheterization but declined surgical correction. When seen in the clinic 2 months postantimicrobial therapy, the patient had normal micturition, no symptoms or signs of infection, and steadily down-trending inflammatory markers.
Discussion
A urinae, historically considered a rare pathogen, has been identified with increasing frequency in urine cultures due to improved microbiologic diagnostic techniques. However, there are only 8 reported cases of A urinae spondylodiscitis. Urinary pathology is an accepted risk factor for A urinae infections; consequently, we suspect that our patient’s urinary outflow obstruction and poor genitourinary hygiene were related to his invasive A urinae infection.10,21,22 We surmise that he had a chronic urinary outflow obstruction contributing to his infection, as evidenced by imaging findings, while the phimosis and urethral meatal stenosis were most likely infectious sequelae considering his anuria and acute kidney injury 5 days postdischarge. Indeed, the correlation between A urinae and urinary tract pathology may justify an evaluation for urinary pathology in any man with A urinae infection, regardless of the presence of symptoms.
By contrast, the implications of A urinae bacteriuria remain unclear. From a public health perspective, A urinae bacteriuria is rare, but the infectious mechanism remains undetermined with a case report suggesting the possibility of sexual transmission.4-6,23 In our case, the patient was not sexually active and had no clear origin of infection. Considering the potential severity of infection, more studies are needed to determine the infectious mechanism of A urinae.
In terms of infectious morbidity, the results seem to vary by sex. In a retrospective study of about 30,000 clinical urine samples, 62 (58 from women, 4 from men) yielded A urinae. The 62 corresponding patients lacked systemic infectious complications, leading the authors to conclude that A urinae is a relatively avirulent organism.24 Although possibly true in women, we are wary of drawing conclusions, especially regarding men, from a study that included only 62 urine samples were A urinae–positive, with only 4 from men. More evidence is needed to define the prognostic implications of A urinae bacteriuria in men.
As illustrated by the present case and previous reports, severe A urinae infections can occur, and the contributory factors deserve consideration. In our patient, the actual mechanism for bacteremia remains unclear. The initial concern for acute pyelonephritis was prompted by a computed tomography finding of bilateral perinephric fat stranding. This finding was questioned because it is common in older patients without infection, hence, is highly nonspecific. A correlation with urinary outflow obstruction may be an important clue in cases like this one.25,26
Furthermore, whether the urinary tract truly was the source of the patient’s bacteremia is clouded by the differing antimicrobial susceptibility patterns of the A urinae blood and urine isolates. The simplest explanation for this discordance may be that all the isolates shared a common initial origin but adapted to different environments in the host (perhaps over time) or laboratory, producing phenotypic variation. Alternatively, the infection could have been polyclonal from the onset, with sampling error leading to the differing detected susceptibility patterns, or the blood and urine isolates may have represented independent acquisition events, involving distinct A urinae strains. Unfortunately (from an academic perspective), given patient preferences and recommendations from the infectious disease consultant, no bone biopsy was done for histology and culture to confirm infection and to allow comparative strain identification if A urinae was isolated.
Optimal treatment for A urinae spondylodiscitis has yet to be established. β-lactams have shown good clinical efficacy despite being bacteriostatic in vitro.27 Early in vitro studies showed synergistic bactericidal synergistic activity with penicillin plus aminoglycoside combination therapies.27-30 Cases of endocarditis have been successfully treated mainly with the combination of a β-lactam plus aminoglycoside combination therapy.30,31 Previous cases of spondylodiscitis have been treated successfully with diverse antimicrobial agents, including clindamycin, β-lactams, cephalosporins, fluoroquinolones, and aminoglycosides.14
Our patient improved rapidly while receiving empiric therapy with vancomycin and ceftriaxone and tolerated a rapid transition to oral amoxicillin and levofloxacin. This is the shortest IV treatment course for A urinae spondylodiscitis reported to date. We suspect that such rapid IV-to-oral transitions will suffice in most stable patients with A urinae spondylodiscitis or other invasive A urinae infections in line with the results of the OVIVA and POET trials.32,33
Conclusions
We believe A urinae UTI in the absence of obvious predisposing factors should prompt evaluation for urinary outflow obstruction. Despite improved laboratory diagnostic techniques, spondylodiscitis related to A urinae remains a rare entity and thus definitive treatment recommendations are difficult to make. However, we suspect that in many cases it is reasonable to extrapolate from the results of the POET and OVIVA trials and rapidly transition therapy of A urinae spondylodiscitis from IV to oral antibiotics. We suspect a review of the US Department of Veterans Affairs population might uncover a higher incidence of A urinae infection than previously estimated due to the population demographics and the epidemiology of A urinae.
Aerococcus urinae (A urinae), a gram-positive coccus readily mistaken for a Staphylococcus species, was first identified in 1992.1-3 It now reportedly accounts for 0.2% to 0.8% of clinical urine isolates.4-6 A urinae bacteriuria is typically asymptomatic and mainly occurs in women.7-9 Symptomatic A urinae urinary tract infection (UTI) occurs predominantly in older men with underlying urologic abnormalities.4-10
Serious A urinae infections are rare. The first 2 reported cases involved men with A urinae endocarditis, one of whom died.11,12 To date, only 8 cases of spondylodiscitis due to A urinae have been reported.13-20 Optimal treatment for invasive A urinae infection is undefined; however, the reported cases were treated successfully with diverse antibiotic regimen combinations; all including a β-lactam and beginning with at least 2 weeks of IV antibiotics.13-20 We describe a man with A urinae bacteremia and spondylodiscitis, presumably arising from a urinary source in the setting of bladder outlet obstruction, who was treated successfully.
Case Presentation
A 74-year-old man with morbid obesity, type 2 diabetes mellitus, stage 2 chronic kidney disease, and tobacco use presented to the emergency department after 2 weeks of progressive, nonradiating, midthoracic back pain, lower extremity weakness, gait imbalance, fatigue, anorexia, rigors, and subjective fevers. On presentation, he was afebrile and hemodynamically stable. A physical examination revealed point tenderness of the midthoracic vertebrae, nontender costovertebral angles, diffusely decreased strength, nonsustained clonus in both lower extremities, inguinal intertrigo, and a buried penis with purulent meatal discharge.
Laboratory results indicated a white blood cell (WBC) count of 13.5 K/μL (reference range, 4.0-11.0), absolute neutrophil count of 11.48 K/μL (reference range, 2.0-7.7), C-reactive protein (CRP) level of 225.3 mg/L (reference range, ≤ 5.0), erythrocyte sedimentation rate of 85 mm/h (reference range, 5-15), serum blood urea nitrogen of 76 mg/dL (reference range, 8-26), and serum creatinine (SCr) of 1.9 mg/dL (reference range, 1.1-1.4). A urinalysis showed positive leukocyte esterase, WBC clumps, and little bacteria. Abdominal/pelvic computed tomography showed spondylodiscitis-like changes at T7-T8, bilateral perinephric fat stranding, bladder distension, and bladder wall thickening.
The patient was presumed to have discitis secondary to a UTI, with possible pyelonephritis, and was given empiric vancomycin and ceftriaxone. Spinal magnetic resonance imaging with contrast supported spondylodiscitis at T7-T8, extending to T8-T9. Preliminary results from the admission blood and urine cultures showed gram-positive cocci in clusters, which were presumed initially to be Staphylococcus aureus (S aureus).
The final urine culture report listed multiple organisms, predominantly A urinae (Table 1);
On hospital day 6, the patient’s back pain had resolved, micturition was normal, appetite had normalized, and SCr was minimally above baseline (1.4 mg/dL). He insisted on completing antibiotic treatment at home and had no other medical indication for continued hospitalization. Thus, antibiotic therapy was changed to an all-oral regimen of amoxicillin 1 g 3 times daily for 10 days and levofloxacin 750 mg daily for 6 weeks, and the patient was discharged to home.
The patient returned 5 days postdischarge due to anuria. Investigation showed severe acute kidney injury (SCr, 6.8 mg/dL) and bladder outlet obstruction due to phimosis and urethral meatal stenosis. Urinalysis was unremarkable. His CRP had declined from 225 mg/L (initial admission) to 154 mg/L. A urinae culture and 2 sets of blood cultures were finalized as no growth. He was diagnosed with postrenal acute kidney injury and underwent meatal dilation and Foley catheterization but declined surgical correction. When seen in the clinic 2 months postantimicrobial therapy, the patient had normal micturition, no symptoms or signs of infection, and steadily down-trending inflammatory markers.
Discussion
A urinae, historically considered a rare pathogen, has been identified with increasing frequency in urine cultures due to improved microbiologic diagnostic techniques. However, there are only 8 reported cases of A urinae spondylodiscitis. Urinary pathology is an accepted risk factor for A urinae infections; consequently, we suspect that our patient’s urinary outflow obstruction and poor genitourinary hygiene were related to his invasive A urinae infection.10,21,22 We surmise that he had a chronic urinary outflow obstruction contributing to his infection, as evidenced by imaging findings, while the phimosis and urethral meatal stenosis were most likely infectious sequelae considering his anuria and acute kidney injury 5 days postdischarge. Indeed, the correlation between A urinae and urinary tract pathology may justify an evaluation for urinary pathology in any man with A urinae infection, regardless of the presence of symptoms.
By contrast, the implications of A urinae bacteriuria remain unclear. From a public health perspective, A urinae bacteriuria is rare, but the infectious mechanism remains undetermined with a case report suggesting the possibility of sexual transmission.4-6,23 In our case, the patient was not sexually active and had no clear origin of infection. Considering the potential severity of infection, more studies are needed to determine the infectious mechanism of A urinae.
In terms of infectious morbidity, the results seem to vary by sex. In a retrospective study of about 30,000 clinical urine samples, 62 (58 from women, 4 from men) yielded A urinae. The 62 corresponding patients lacked systemic infectious complications, leading the authors to conclude that A urinae is a relatively avirulent organism.24 Although possibly true in women, we are wary of drawing conclusions, especially regarding men, from a study that included only 62 urine samples were A urinae–positive, with only 4 from men. More evidence is needed to define the prognostic implications of A urinae bacteriuria in men.
As illustrated by the present case and previous reports, severe A urinae infections can occur, and the contributory factors deserve consideration. In our patient, the actual mechanism for bacteremia remains unclear. The initial concern for acute pyelonephritis was prompted by a computed tomography finding of bilateral perinephric fat stranding. This finding was questioned because it is common in older patients without infection, hence, is highly nonspecific. A correlation with urinary outflow obstruction may be an important clue in cases like this one.25,26
Furthermore, whether the urinary tract truly was the source of the patient’s bacteremia is clouded by the differing antimicrobial susceptibility patterns of the A urinae blood and urine isolates. The simplest explanation for this discordance may be that all the isolates shared a common initial origin but adapted to different environments in the host (perhaps over time) or laboratory, producing phenotypic variation. Alternatively, the infection could have been polyclonal from the onset, with sampling error leading to the differing detected susceptibility patterns, or the blood and urine isolates may have represented independent acquisition events, involving distinct A urinae strains. Unfortunately (from an academic perspective), given patient preferences and recommendations from the infectious disease consultant, no bone biopsy was done for histology and culture to confirm infection and to allow comparative strain identification if A urinae was isolated.
Optimal treatment for A urinae spondylodiscitis has yet to be established. β-lactams have shown good clinical efficacy despite being bacteriostatic in vitro.27 Early in vitro studies showed synergistic bactericidal synergistic activity with penicillin plus aminoglycoside combination therapies.27-30 Cases of endocarditis have been successfully treated mainly with the combination of a β-lactam plus aminoglycoside combination therapy.30,31 Previous cases of spondylodiscitis have been treated successfully with diverse antimicrobial agents, including clindamycin, β-lactams, cephalosporins, fluoroquinolones, and aminoglycosides.14
Our patient improved rapidly while receiving empiric therapy with vancomycin and ceftriaxone and tolerated a rapid transition to oral amoxicillin and levofloxacin. This is the shortest IV treatment course for A urinae spondylodiscitis reported to date. We suspect that such rapid IV-to-oral transitions will suffice in most stable patients with A urinae spondylodiscitis or other invasive A urinae infections in line with the results of the OVIVA and POET trials.32,33
Conclusions
We believe A urinae UTI in the absence of obvious predisposing factors should prompt evaluation for urinary outflow obstruction. Despite improved laboratory diagnostic techniques, spondylodiscitis related to A urinae remains a rare entity and thus definitive treatment recommendations are difficult to make. However, we suspect that in many cases it is reasonable to extrapolate from the results of the POET and OVIVA trials and rapidly transition therapy of A urinae spondylodiscitis from IV to oral antibiotics. We suspect a review of the US Department of Veterans Affairs population might uncover a higher incidence of A urinae infection than previously estimated due to the population demographics and the epidemiology of A urinae.
1. Christensen JJ, Korner B, Kjaergaard H. Aerococcus-like organism—an unnoticed urinary tract pathogen. APMIS. 1989;97(6):539-546. doi:10.1111/j.1699-0463.1989.tb00828.x
2. Aguirre M, Collins MD. Phylogenetic analysis of some Aerococcus-like organisms from urinary tract infections: description of Aerococcus urinae sp. nov. J Gen Microbiol. 1992;138(2):401-405. doi:10.1099/00221287-138-2-401
3. Williams RE, Hirch A, Cowan ST. Aerococcus, a new bacterial genus. J Gen Microbiol. 1953;8(3):475-480. doi:10.1099/00221287-8-3-475
4. Kline KA, Lewis AL. Gram-positive uropathogens, polymicrobial urinary tract infection, and the emerging microbiota of the urinary tract. Microbiol Spectr. 2016;4(2). doi:10.1128/microbiolspec.UTI-0012-2012
5. Schuur PM, Kasteren ME, Sabbe L, Vos MC, Janssens MM, Buiting AG. Urinary tract infections with Aerococcus urinae in the south of The Netherlands. Eur J Clin Microbiol Infect Dis. 1997;16(12):871-875. doi:10.1007/BF01700552
6. Grude N, Tveten Y. Aerococcus urinae og urinveisinfeksjon [Aerococcus urinae and urinary tract infection]. Tidsskr Nor Laegeforen. 2002;122(2):174-175.
7. Narayanasamy S, King K, Dennison A, Spelman DW, Aung AK. Clinical characteristics and laboratory identification of Aerococcus infections: an Australian tertiary centre perspective. Int J Microbiol. 2017;2017. doi:10.1155/2017/5684614
8. Hilt EE, McKinley K, Pearce MM, et al. Urine is not sterile: use of enhanced urine culture techniques to detect resident bacterial flora in the adult female bladder. J Clin Microbiol. 2014;52(3):871-876. doi:10.1128/JCM.02876-13
9. Pearce MM, Hilt EE, Rosenfeld AB, et al. The female urinary microbiome: a comparison of women with and without urgency urinary incontinence. mBio. 2014;5(4):e01283-14. doi:10.1128/mBio.01283-14
10. Sahu KK, Lal A, Mishra AK, Abraham GM. Aerococcus-related infections and their significance: a 9-year retrospective study. J Microsc Ultrastruct. 2021;9(1):18-25. doi:10.4103/JMAU.JMAU_61_19
11. Skov RL, Klarlund M, Thorsen S. Fatal endocarditis due to Aerococcus urinae. Diagn Microbiol Infect Dis. 1995;21(4):219-221. doi:10.1016/0732-8893(95)00037-b
12. Kristensen B, Nielsen G. Endocarditis caused by Aerococcus urinae, a newly recognized pathogen. Eur J Clin Microbiol Infect Dis. 1995;14(1):49-51. doi:10.1007/BF02112619
13. Astudillo L, Sailler L, Porte L, Lefevre JC, Massip P, Arlet-Suau E. Spondylodiscitis due to Aerococcus urinae: a first report. Scand J Infect Dis. 2003;35(11-12):890-891. doi:10.1080/00365540310016664
14. Lyagoubi A, Souffi C, Baroiller V, Vallee E. Spondylodiscitis: an increasingly described localization. EJIFCC. 2020;31(2):169-173.
15. Jerome M, Slim J, Sison R, Marton R. A case of Aerococcus urinae vertebral osteomyelitis. J Glob Infect Dis. 2015;7(2):85-86. doi:10.4103/0974-777X.157246
16. Tekin A, Tekin G, Turunç T, Demiroğlu Z, Kizilkiliç O. Infective endocarditis and spondylodiscitis in a patient due to Aerococcus urinae: first report. Int J Cardiol. 2007;115(3):402-403. doi:10.1016/j.ijcard.2006.01.046
17. Rougier E, Braud A, Argemi X, et al. Spondylodiscitis due to Aerococcus urinae and literature review. Infection. 2018;46(3):419-421. doi:10.1007/s15010-017-1106-0
18. Degroote E, Yildiz H, Lecouvet F, Verroken A, Belkhir L. Aerococcus urinae: an underestimated cause of spine infection? Case report and review of the literature. Acta Clin Belg. 2018;73(6):444-447. doi:10.1080/17843286.2018.1443003
19. Torres-Martos E, Pérez-Cortés S, Sánchez-Calvo JM, López-Prieto MD. Spondylodiscitis due to Aerococcus urinae infection in an elderly immunocompetent patient. Enferm Infecc Microbiol Clin. 2017;35(10):682-684. doi:10.1016/j.eimc.2017.02.005
20. Senneby E, Petersson AC, Rasmussen M. Clinical and microbiological features of bacteraemia with Aerococcus urinae. Clin Microbiol Infect. 2012;18(6):546-550. doi:10.1111/j.1469-0691.2011.03609.x
21. Sunnerhagen T, Nilson B, Olaison L, Rasmussen M. Clinical and microbiological features of infective endocarditis caused by aerococci. Infection. 2016;44(2):167-173. doi:10.1007/s15010-015-0812-8
22. de Jong MF, Soetekouw R, ten Kate RW, Veenendaal D. Aerococcus urinae: severe and fatal bloodstream infections and endocarditis. J Clin Microbiol. 2010;48(9):3445-3447. doi:10.1128/JCM.00835-10
23. Babaeer AA, Nader C, Iacoviello V, Tomera K. Necrotizing urethritis due to Aerococcus urinae. Case Rep Urol. 2015;2015:136147. doi:10.1155/2015/136147
24. Sierra-Hoffman M, Watkins K, Jinadatha C, Fader R, Carpenter JL. Clinical significance of Aerococcus urinae: a retrospective review. Diagn Microbiol Infect Dis. 2005;53(4):289-292. doi:10.1016/j.diagmicrobio.2005.06.021
25. Fukami H, Takeuchi Y, Kagaya S, et al. Perirenal fat stranding is not a powerful diagnostic tool for acute pyelonephritis. Int J Gen Med. 2017;10:137-144. doi:10.2147/IJGM.S133685
26. Han NY, Sung DJ, Kim MJ, Park BJ, Sim KC, Cho SB. Perirenal fat stranding on CT: is there an association with bladder outlet obstruction? Br J Radiol. 2016;89(1063):20160195. doi:10.1259/bjr.20160195
27. Hirzel C, Hirzberger L, Furrer H, Endimiani A. Bactericidal activity of penicillin, ceftriaxone, gentamicin and daptomycin alone and in combination against Aerococcus urinae. Int J Antimicrob Agents. 2016;48(3):271-276. doi:10.1016/j.ijantimicag.2016.05.007
28. Zbinden R, Santanam P, Hunziker L, Leuzinger B, von Graevenitz A. Endocarditis due to Aerococcus urinae: diagnostic tests, fatty acid composition and killing kinetics. Infection. 1999;27(2):122-124. doi:10.1007/BF02560511
29. Skov R, Christensen JJ, Korner B, Frimodt-Møller N, Espersen F. In vitro antimicrobial susceptibility of Aerococcus urinae to 14 antibiotics, and time-kill curves for penicillin, gentamicin and vancomycin. J Antimicrob Chemother. 2001;48(5):653-658. doi:10.1093/jac/48.5.653
30. Ebnöther C, Altwegg M, Gottschalk J, Seebach JD, Kronenberg A. Aerococcus urinae endocarditis: case report and review of the literature. Infection. 2002;30(5):310-313. doi:10.1007/s15010-002-3106-x
31. Tai DBG, Go JR, Fida M, Saleh OA. Management and treatment of Aerococcus bacteremia and endocarditis. Int J Infect Dis. 2021;102:584-589. doi:10.1016/j.ijid.2020.10.096
32. Li H-K, Rombach I, Zambellas R, et al; OVIVA Trial Collaborators. Oral versus intravenous antibiotics for bone and joint infection. N Engl J Med. 2019;380(5):425-436. doi:10.1056/NEJMoa1710926
33. Iversen K, Ihlemann N, Gill SU, et al. Partial oral versus intravenous antibiotic treatment of endocarditis. N Engl J Med. 2019;380(5):415-424. doi:10.1056/NEJMoa1808312
1. Christensen JJ, Korner B, Kjaergaard H. Aerococcus-like organism—an unnoticed urinary tract pathogen. APMIS. 1989;97(6):539-546. doi:10.1111/j.1699-0463.1989.tb00828.x
2. Aguirre M, Collins MD. Phylogenetic analysis of some Aerococcus-like organisms from urinary tract infections: description of Aerococcus urinae sp. nov. J Gen Microbiol. 1992;138(2):401-405. doi:10.1099/00221287-138-2-401
3. Williams RE, Hirch A, Cowan ST. Aerococcus, a new bacterial genus. J Gen Microbiol. 1953;8(3):475-480. doi:10.1099/00221287-8-3-475
4. Kline KA, Lewis AL. Gram-positive uropathogens, polymicrobial urinary tract infection, and the emerging microbiota of the urinary tract. Microbiol Spectr. 2016;4(2). doi:10.1128/microbiolspec.UTI-0012-2012
5. Schuur PM, Kasteren ME, Sabbe L, Vos MC, Janssens MM, Buiting AG. Urinary tract infections with Aerococcus urinae in the south of The Netherlands. Eur J Clin Microbiol Infect Dis. 1997;16(12):871-875. doi:10.1007/BF01700552
6. Grude N, Tveten Y. Aerococcus urinae og urinveisinfeksjon [Aerococcus urinae and urinary tract infection]. Tidsskr Nor Laegeforen. 2002;122(2):174-175.
7. Narayanasamy S, King K, Dennison A, Spelman DW, Aung AK. Clinical characteristics and laboratory identification of Aerococcus infections: an Australian tertiary centre perspective. Int J Microbiol. 2017;2017. doi:10.1155/2017/5684614
8. Hilt EE, McKinley K, Pearce MM, et al. Urine is not sterile: use of enhanced urine culture techniques to detect resident bacterial flora in the adult female bladder. J Clin Microbiol. 2014;52(3):871-876. doi:10.1128/JCM.02876-13
9. Pearce MM, Hilt EE, Rosenfeld AB, et al. The female urinary microbiome: a comparison of women with and without urgency urinary incontinence. mBio. 2014;5(4):e01283-14. doi:10.1128/mBio.01283-14
10. Sahu KK, Lal A, Mishra AK, Abraham GM. Aerococcus-related infections and their significance: a 9-year retrospective study. J Microsc Ultrastruct. 2021;9(1):18-25. doi:10.4103/JMAU.JMAU_61_19
11. Skov RL, Klarlund M, Thorsen S. Fatal endocarditis due to Aerococcus urinae. Diagn Microbiol Infect Dis. 1995;21(4):219-221. doi:10.1016/0732-8893(95)00037-b
12. Kristensen B, Nielsen G. Endocarditis caused by Aerococcus urinae, a newly recognized pathogen. Eur J Clin Microbiol Infect Dis. 1995;14(1):49-51. doi:10.1007/BF02112619
13. Astudillo L, Sailler L, Porte L, Lefevre JC, Massip P, Arlet-Suau E. Spondylodiscitis due to Aerococcus urinae: a first report. Scand J Infect Dis. 2003;35(11-12):890-891. doi:10.1080/00365540310016664
14. Lyagoubi A, Souffi C, Baroiller V, Vallee E. Spondylodiscitis: an increasingly described localization. EJIFCC. 2020;31(2):169-173.
15. Jerome M, Slim J, Sison R, Marton R. A case of Aerococcus urinae vertebral osteomyelitis. J Glob Infect Dis. 2015;7(2):85-86. doi:10.4103/0974-777X.157246
16. Tekin A, Tekin G, Turunç T, Demiroğlu Z, Kizilkiliç O. Infective endocarditis and spondylodiscitis in a patient due to Aerococcus urinae: first report. Int J Cardiol. 2007;115(3):402-403. doi:10.1016/j.ijcard.2006.01.046
17. Rougier E, Braud A, Argemi X, et al. Spondylodiscitis due to Aerococcus urinae and literature review. Infection. 2018;46(3):419-421. doi:10.1007/s15010-017-1106-0
18. Degroote E, Yildiz H, Lecouvet F, Verroken A, Belkhir L. Aerococcus urinae: an underestimated cause of spine infection? Case report and review of the literature. Acta Clin Belg. 2018;73(6):444-447. doi:10.1080/17843286.2018.1443003
19. Torres-Martos E, Pérez-Cortés S, Sánchez-Calvo JM, López-Prieto MD. Spondylodiscitis due to Aerococcus urinae infection in an elderly immunocompetent patient. Enferm Infecc Microbiol Clin. 2017;35(10):682-684. doi:10.1016/j.eimc.2017.02.005
20. Senneby E, Petersson AC, Rasmussen M. Clinical and microbiological features of bacteraemia with Aerococcus urinae. Clin Microbiol Infect. 2012;18(6):546-550. doi:10.1111/j.1469-0691.2011.03609.x
21. Sunnerhagen T, Nilson B, Olaison L, Rasmussen M. Clinical and microbiological features of infective endocarditis caused by aerococci. Infection. 2016;44(2):167-173. doi:10.1007/s15010-015-0812-8
22. de Jong MF, Soetekouw R, ten Kate RW, Veenendaal D. Aerococcus urinae: severe and fatal bloodstream infections and endocarditis. J Clin Microbiol. 2010;48(9):3445-3447. doi:10.1128/JCM.00835-10
23. Babaeer AA, Nader C, Iacoviello V, Tomera K. Necrotizing urethritis due to Aerococcus urinae. Case Rep Urol. 2015;2015:136147. doi:10.1155/2015/136147
24. Sierra-Hoffman M, Watkins K, Jinadatha C, Fader R, Carpenter JL. Clinical significance of Aerococcus urinae: a retrospective review. Diagn Microbiol Infect Dis. 2005;53(4):289-292. doi:10.1016/j.diagmicrobio.2005.06.021
25. Fukami H, Takeuchi Y, Kagaya S, et al. Perirenal fat stranding is not a powerful diagnostic tool for acute pyelonephritis. Int J Gen Med. 2017;10:137-144. doi:10.2147/IJGM.S133685
26. Han NY, Sung DJ, Kim MJ, Park BJ, Sim KC, Cho SB. Perirenal fat stranding on CT: is there an association with bladder outlet obstruction? Br J Radiol. 2016;89(1063):20160195. doi:10.1259/bjr.20160195
27. Hirzel C, Hirzberger L, Furrer H, Endimiani A. Bactericidal activity of penicillin, ceftriaxone, gentamicin and daptomycin alone and in combination against Aerococcus urinae. Int J Antimicrob Agents. 2016;48(3):271-276. doi:10.1016/j.ijantimicag.2016.05.007
28. Zbinden R, Santanam P, Hunziker L, Leuzinger B, von Graevenitz A. Endocarditis due to Aerococcus urinae: diagnostic tests, fatty acid composition and killing kinetics. Infection. 1999;27(2):122-124. doi:10.1007/BF02560511
29. Skov R, Christensen JJ, Korner B, Frimodt-Møller N, Espersen F. In vitro antimicrobial susceptibility of Aerococcus urinae to 14 antibiotics, and time-kill curves for penicillin, gentamicin and vancomycin. J Antimicrob Chemother. 2001;48(5):653-658. doi:10.1093/jac/48.5.653
30. Ebnöther C, Altwegg M, Gottschalk J, Seebach JD, Kronenberg A. Aerococcus urinae endocarditis: case report and review of the literature. Infection. 2002;30(5):310-313. doi:10.1007/s15010-002-3106-x
31. Tai DBG, Go JR, Fida M, Saleh OA. Management and treatment of Aerococcus bacteremia and endocarditis. Int J Infect Dis. 2021;102:584-589. doi:10.1016/j.ijid.2020.10.096
32. Li H-K, Rombach I, Zambellas R, et al; OVIVA Trial Collaborators. Oral versus intravenous antibiotics for bone and joint infection. N Engl J Med. 2019;380(5):425-436. doi:10.1056/NEJMoa1710926
33. Iversen K, Ihlemann N, Gill SU, et al. Partial oral versus intravenous antibiotic treatment of endocarditis. N Engl J Med. 2019;380(5):415-424. doi:10.1056/NEJMoa1808312
Liver cancer exacts high financial toll on older adults
In the first year after a diagnosis of HCC, median Medicare payments exceed $65,000 and out-of-pocket costs top $10,000.
Even after adjustment for the presence of cirrhosis and its related costs, patients with HCC still have Medicare payments exceeding $50,000 and out-of-pocket costs topping $7000.
Amit Singal, MD, of UT Southwestern Medical Center in Dallas, and colleagues reported their findings in Clinical Gastroenterology and Hepatology.
Common and costly
HCC, the most common type of primary liver cancer, is a leading cause of death in patients with cirrhosis and is projected to become the third leading cause of cancer-related death in the United States by 2040, the researchers wrote.
The treatment landscape for HCC has changed over the past decade, with expanded surgical options, introduction of radiation-based therapies, and approval of immunotherapies – all of which are costly.
Yet the magnitude of financial burden of HCC therapy has been understudied, the researchers noted.
To investigate, Dr. Singal and colleagues evaluated Surveillance, Epidemiology, and End Results (SEER)–Medicare data for 4,525 adults with traditional Medicare coverage who were diagnosed with HCC between 2011 and 2015 and a propensity-matched cohort of 4,525 adults with cirrhosis but no HCC as a comparator group to tease out HCC-specific costs beyond those related to cirrhosis. Patients in Medicare managed care were excluded because their cost information is not available in the database.
In the first year after a diagnosis of HCC, the median total Medicare payments were $66,338 (interquartile range [IQR], $30,931-$158,740) and patient liabilities (a proxy for out-of-pocket costs) were $10,008 (IQR, $5,427-$19,669).
First-year costs were higher for patients with HCC than matched patients without HCC; the former group incurred median incremental Medicare payments of $50,110 (IQR, $14,242-$136,239) and patient liabilities of $7,166 (IQR, $2,401-$16,099), the investigators found.
Patients with early-stage HCC had lower incremental patient liabilities (median, $4,195 vs. $8,238) and Medicare payments (median, $28,207 vs. $59,509) than did their peers with larger tumor burden.
NAFLD notably tied to higher costs
Factors associated with higher HCC-related costs were nonalcoholic fatty liver disease (NAFLD) etiology, higher comorbidities, presence of ascites and hepatic encephalopathy, and larger tumor burden.
The researchers said that the link between NAFLD and higher costs is notable, given that NAFLD is an increasingly common underlying cause of HCC.
The link between larger tumor burden and higher costs underscores “another benefit of HCC surveillance and early detection,” they added.
“By separating the financial liabilities borne by patients and Medicare, we provide a clearer outlook of how cancer-related costs are distributed between patients and public payers,” Dr. Singal and colleagues said.
“Our findings will inform policy interventions and will help formulate better financial supports targeting the most vulnerable HCC patients,” they concluded.
The study had no commercial funding. Dr. Singal has been on advisory boards and served as a consultant for Wako Diagnostics, Glycotest, Exact Sciences, Roche, Genentech, Bayer, Eisai, BMS, Exelixis, AstraZeneca, and TARGET RWE.
A version of this article first appeared on Medscape.com.
In the first year after a diagnosis of HCC, median Medicare payments exceed $65,000 and out-of-pocket costs top $10,000.
Even after adjustment for the presence of cirrhosis and its related costs, patients with HCC still have Medicare payments exceeding $50,000 and out-of-pocket costs topping $7000.
Amit Singal, MD, of UT Southwestern Medical Center in Dallas, and colleagues reported their findings in Clinical Gastroenterology and Hepatology.
Common and costly
HCC, the most common type of primary liver cancer, is a leading cause of death in patients with cirrhosis and is projected to become the third leading cause of cancer-related death in the United States by 2040, the researchers wrote.
The treatment landscape for HCC has changed over the past decade, with expanded surgical options, introduction of radiation-based therapies, and approval of immunotherapies – all of which are costly.
Yet the magnitude of financial burden of HCC therapy has been understudied, the researchers noted.
To investigate, Dr. Singal and colleagues evaluated Surveillance, Epidemiology, and End Results (SEER)–Medicare data for 4,525 adults with traditional Medicare coverage who were diagnosed with HCC between 2011 and 2015 and a propensity-matched cohort of 4,525 adults with cirrhosis but no HCC as a comparator group to tease out HCC-specific costs beyond those related to cirrhosis. Patients in Medicare managed care were excluded because their cost information is not available in the database.
In the first year after a diagnosis of HCC, the median total Medicare payments were $66,338 (interquartile range [IQR], $30,931-$158,740) and patient liabilities (a proxy for out-of-pocket costs) were $10,008 (IQR, $5,427-$19,669).
First-year costs were higher for patients with HCC than matched patients without HCC; the former group incurred median incremental Medicare payments of $50,110 (IQR, $14,242-$136,239) and patient liabilities of $7,166 (IQR, $2,401-$16,099), the investigators found.
Patients with early-stage HCC had lower incremental patient liabilities (median, $4,195 vs. $8,238) and Medicare payments (median, $28,207 vs. $59,509) than did their peers with larger tumor burden.
NAFLD notably tied to higher costs
Factors associated with higher HCC-related costs were nonalcoholic fatty liver disease (NAFLD) etiology, higher comorbidities, presence of ascites and hepatic encephalopathy, and larger tumor burden.
The researchers said that the link between NAFLD and higher costs is notable, given that NAFLD is an increasingly common underlying cause of HCC.
The link between larger tumor burden and higher costs underscores “another benefit of HCC surveillance and early detection,” they added.
“By separating the financial liabilities borne by patients and Medicare, we provide a clearer outlook of how cancer-related costs are distributed between patients and public payers,” Dr. Singal and colleagues said.
“Our findings will inform policy interventions and will help formulate better financial supports targeting the most vulnerable HCC patients,” they concluded.
The study had no commercial funding. Dr. Singal has been on advisory boards and served as a consultant for Wako Diagnostics, Glycotest, Exact Sciences, Roche, Genentech, Bayer, Eisai, BMS, Exelixis, AstraZeneca, and TARGET RWE.
A version of this article first appeared on Medscape.com.
In the first year after a diagnosis of HCC, median Medicare payments exceed $65,000 and out-of-pocket costs top $10,000.
Even after adjustment for the presence of cirrhosis and its related costs, patients with HCC still have Medicare payments exceeding $50,000 and out-of-pocket costs topping $7000.
Amit Singal, MD, of UT Southwestern Medical Center in Dallas, and colleagues reported their findings in Clinical Gastroenterology and Hepatology.
Common and costly
HCC, the most common type of primary liver cancer, is a leading cause of death in patients with cirrhosis and is projected to become the third leading cause of cancer-related death in the United States by 2040, the researchers wrote.
The treatment landscape for HCC has changed over the past decade, with expanded surgical options, introduction of radiation-based therapies, and approval of immunotherapies – all of which are costly.
Yet the magnitude of financial burden of HCC therapy has been understudied, the researchers noted.
To investigate, Dr. Singal and colleagues evaluated Surveillance, Epidemiology, and End Results (SEER)–Medicare data for 4,525 adults with traditional Medicare coverage who were diagnosed with HCC between 2011 and 2015 and a propensity-matched cohort of 4,525 adults with cirrhosis but no HCC as a comparator group to tease out HCC-specific costs beyond those related to cirrhosis. Patients in Medicare managed care were excluded because their cost information is not available in the database.
In the first year after a diagnosis of HCC, the median total Medicare payments were $66,338 (interquartile range [IQR], $30,931-$158,740) and patient liabilities (a proxy for out-of-pocket costs) were $10,008 (IQR, $5,427-$19,669).
First-year costs were higher for patients with HCC than matched patients without HCC; the former group incurred median incremental Medicare payments of $50,110 (IQR, $14,242-$136,239) and patient liabilities of $7,166 (IQR, $2,401-$16,099), the investigators found.
Patients with early-stage HCC had lower incremental patient liabilities (median, $4,195 vs. $8,238) and Medicare payments (median, $28,207 vs. $59,509) than did their peers with larger tumor burden.
NAFLD notably tied to higher costs
Factors associated with higher HCC-related costs were nonalcoholic fatty liver disease (NAFLD) etiology, higher comorbidities, presence of ascites and hepatic encephalopathy, and larger tumor burden.
The researchers said that the link between NAFLD and higher costs is notable, given that NAFLD is an increasingly common underlying cause of HCC.
The link between larger tumor burden and higher costs underscores “another benefit of HCC surveillance and early detection,” they added.
“By separating the financial liabilities borne by patients and Medicare, we provide a clearer outlook of how cancer-related costs are distributed between patients and public payers,” Dr. Singal and colleagues said.
“Our findings will inform policy interventions and will help formulate better financial supports targeting the most vulnerable HCC patients,” they concluded.
The study had no commercial funding. Dr. Singal has been on advisory boards and served as a consultant for Wako Diagnostics, Glycotest, Exact Sciences, Roche, Genentech, Bayer, Eisai, BMS, Exelixis, AstraZeneca, and TARGET RWE.
A version of this article first appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Therapeutic Approaches in Advanced Breast Cancer
More than 280,000 women in the United States will be diagnosed with invasive breast cancer this year. For those with metastatic breast cancer with distant spread, the 5-year survival rate is approximately 28%. Whether advanced disease is discovered at initial diagnosis or in relapsed disease, it is imperative to understand the molecular characteristics of the metastatic tumor.
Dr Susan Domchek, from the University of Pennsylvania, discusses the importance of retesting for estrogen receptor, progesterone receptor, and HER2/neu on a metastatic tumor focus in order to identify potential discordance between the primary cancer and metastatic disease.
Additionally, Dr Domchek discusses the importance of molecular testing for targetable mutations, including P13K and germline BRCA1/2, for which approved therapies have shown survival benefit.
The list of targetable mutations in breast cancer continues to expand. In the tumor-agnostic studies, pembrolizumab has shown survival benefit in tumors that have mismatch repair deficiency and microsatellite instability, and TRK inhibitors have shown efficacy in tumors positive for NTRK fusions. Numerous clinical trials are available looking at additional molecular-based therapies.
--
Susan M. Domchek, MD, Basser Professor, Department of Oncology; Executive Director, Basser Center for BRCA, Abramson Cancer Center, University of Pennsylvania, Philadelphia
Susan M. Domchek, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: AstraZeneca; Clovis; Bristol Myers Squibb
More than 280,000 women in the United States will be diagnosed with invasive breast cancer this year. For those with metastatic breast cancer with distant spread, the 5-year survival rate is approximately 28%. Whether advanced disease is discovered at initial diagnosis or in relapsed disease, it is imperative to understand the molecular characteristics of the metastatic tumor.
Dr Susan Domchek, from the University of Pennsylvania, discusses the importance of retesting for estrogen receptor, progesterone receptor, and HER2/neu on a metastatic tumor focus in order to identify potential discordance between the primary cancer and metastatic disease.
Additionally, Dr Domchek discusses the importance of molecular testing for targetable mutations, including P13K and germline BRCA1/2, for which approved therapies have shown survival benefit.
The list of targetable mutations in breast cancer continues to expand. In the tumor-agnostic studies, pembrolizumab has shown survival benefit in tumors that have mismatch repair deficiency and microsatellite instability, and TRK inhibitors have shown efficacy in tumors positive for NTRK fusions. Numerous clinical trials are available looking at additional molecular-based therapies.
--
Susan M. Domchek, MD, Basser Professor, Department of Oncology; Executive Director, Basser Center for BRCA, Abramson Cancer Center, University of Pennsylvania, Philadelphia
Susan M. Domchek, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: AstraZeneca; Clovis; Bristol Myers Squibb
More than 280,000 women in the United States will be diagnosed with invasive breast cancer this year. For those with metastatic breast cancer with distant spread, the 5-year survival rate is approximately 28%. Whether advanced disease is discovered at initial diagnosis or in relapsed disease, it is imperative to understand the molecular characteristics of the metastatic tumor.
Dr Susan Domchek, from the University of Pennsylvania, discusses the importance of retesting for estrogen receptor, progesterone receptor, and HER2/neu on a metastatic tumor focus in order to identify potential discordance between the primary cancer and metastatic disease.
Additionally, Dr Domchek discusses the importance of molecular testing for targetable mutations, including P13K and germline BRCA1/2, for which approved therapies have shown survival benefit.
The list of targetable mutations in breast cancer continues to expand. In the tumor-agnostic studies, pembrolizumab has shown survival benefit in tumors that have mismatch repair deficiency and microsatellite instability, and TRK inhibitors have shown efficacy in tumors positive for NTRK fusions. Numerous clinical trials are available looking at additional molecular-based therapies.
--
Susan M. Domchek, MD, Basser Professor, Department of Oncology; Executive Director, Basser Center for BRCA, Abramson Cancer Center, University of Pennsylvania, Philadelphia
Susan M. Domchek, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: AstraZeneca; Clovis; Bristol Myers Squibb

CTC-guided therapy beats physician choice in metastatic breast cancer
SAN ANTONIO – When choosing between chemotherapy and endocrine therapy for patients with hormone receptor (HR)+/HER2- metastatic breast cancer, allowing the results from a blood test that measures circulating tumor cell (CTC) count to overrule physician’s choice of therapy can significantly improve overall survival.
But One expert reacting to the findings says probably not, and another pointed out that the CTC count test used in the trial (CellSearch), although approved by the Food and Drug Administration, is not widely used in clinical practice.
The findings comes from updated results from the STIC CTC study.
“When the trial was designed, the question related to the choice between single-agent endocrine therapy and chemotherapy [in] first-line therapy,” explained study presenter François-Clément Bidard, MD, PhD, professor of medical oncology at Institut Curie and Versailles Saint-Quentin University, Paris.
Since then, the first-line treatment has changed and can now can also include cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors, but Dr. Bidard said the results are still clinically relevant.
Nowadays, endocrine therapy plus CDK4/6 inhibitors is the “preferred option for treatment-naive patients, but the dilemma between endocrine therapy and chemotherapy remains after disease progression on adjuvant or first-line therapy with CDK4/6 inhibitors, where current guidelines advocate in favor of endocrine therapy, despite its short-lived efficacy.”
“In that scenario, based on the STIC CTC trial results, the CTC count in combination with predictive biomarkers, whenever available, may help customize the early use of chemotherapy or antibody-drug conjugates, which are becoming more and more attractive,” Dr. Bidard said.
The research was presented here at the San Antonio Breast Cancer Symposium (SABCS).
The study involved more than 750 patients with HR+/HER2- metastatic breast cancer randomly assigned to physician choice or CTC-guided therapy, although the physician decision and the recommendation based on the CTC count was recorded in both groups.
Using the CellSearch (Menarini Silicon Biosystems) to perform the CTC count at baseline only, the team defined patients as low or high risk, with low-risk patients deemed to need only endocrine therapy and high-risk patients recommended chemotherapy.
Physicians based their decisions on current guidelines and their clinical experience.
In the 25% of cases where CTC count would recommend chemotherapy while the physician would recommend endocrine therapy, following the CTC count–based choice resulted in a 35% improvement in progression-free survival (PFS) and a 47% increase in overall survival.
In all other situations, including those when the CTC count recommended endocrine therapy in contrast to the physicians, or the approximately 60% of cases in which the two were in agreement, there was no difference in survival outcomes between the approaches.
Reacting to the findings, Nancy Chan, MD, medical oncologist and the director of breast cancer clinical research at NYU Langone’s Perlmutter Cancer Center, said that the “goal is really to understand how we can personalize treatment options for patients.”
Another aim is to avoid performing a tumor biopsy, if possible, “as that has increased morbidity for patients.”
She noted also that choosing between endocrine therapy and chemotherapy is a “big decision.” These researchers “really wanted to help some patients get less chemotherapy,” as they felt that “some patients are getting too much” as they are not really that high risk and should get endocrine therapy instead.
However, Dr. Chan said that the CTC count is a “complicated concept” and is “not something we’re all using in our clinical practice yet.”
With regard to the approximately 40% discordance between the CTC- and physician-guided choices, Dr. Chan said that clinicians are perhaps not as accurate as they believed in predicting risk when relying on the clinical or pathological features of the tumor.
On Twitter, Guilherme Nader-Marta, MD, Jules Bordet Institute, Université Libre de Bruxelles, Belgium, commented that the question behind the study was whether CTC measurement is a “clinically useful strategy for first-line treatment decision-making.”
“Amazingly,” he continued, the trial went “straight to the point” to answer the question and showed that CTC-based decisions can offer a survival benefit.
Daniel F. Hayes, MD, co-director of the Breast Oncology Program at the University of Michigan Comprehensive Cancer Center, Ann Arbor, echoed these thoughts, saying that the goals of therapy are to make patients live longer and “better.”
He said that the point of any clinical biomarker is not only to show that testing for it offers “analytical validity” but that it also provides “clinical utility” in that it can guide treatment decisions to improve outcomes.
Dr. Hayes, who was not involved in the study but has worked for many years on the development of CellSearch, said that the results do not make it clear whether measuring CTC counts meets the definition of clinical utility, but it’s “very close.”
On the other hand, the analytical validity of the test is “excellent,” and, in that context, was well-chosen, he said, adding that the endpoint of the trial “is the one most important to us: improvement in overall survival.”
Dr. Hayes noted that the magnitude of benefit from CTC-guided therapy was “moderate,” although that is a “matter of perception,” and the “level of evidence is probably 2 or 3.” Although the trial was prospective, he said, the key results were in a “relatively small” subgroup.
The question is, Dr. Hayes continued: “Is this enough to change practice? My conclusions are: probably not.”
Although patients rated as low risk based on their low CTC count avoided chemotherapy, “it’s not clear to me that this whole thing is sufficient for clinical utility in context of what we know today.” The key issue, however, is who decides whether CTC counts are measured and whether they will be used to guide therapy decisions – will it be the patient, the caregiver, an expert guidelines panel, or third party payers/society?
Study details
In his presentation, Dr. Bidard explained that CTC count is an FDA-approved standardized liquid biopsy biomarker, with a count of greater than or equal to 5 cells per 7.5 mL of blood deemed an adverse prognostic marker, regardless of the line of therapy, with a grade 1 level of evidence.
Previous studies have indicated that a high CTC count is strongly associated with overall survival, at a hazard ratio of 2.78.
Crucially, the CTC count “complements” and does not duplicate standard clinicopathological prognostic factors, Dr. Bidard said.
To determine the potential of the CTC count as an aid to treatment decisions, Dr. Bidard and colleagues conducted a trial in pre- and postmenopausal women with untreated HR+/HER2- metastatic breast cancer who were able to receive either endocrine therapy or chemotherapy.
They were randomly assigned to either a standard group, in which the treatment decision followed the physician’s choice, regardless of their CTC count, or to a CTC group, in which the physicians made a treatment recommendation but the choice was driven by the CTC count.
Dr. Bidard reminded the audience that the primary endpoint of PFS to demonstrate the non-inferiority of CTC versus physician treatment decisions has already been met, with the results published in 2020. Those results came from an analysis of 788 patients enrolled between February 2012 and July 2016 at 17 sites in France and showed after 42 months of follow-up that the median PFS in the CTC arm was 15.6 months versus 14 months in the physician choice arm, at a hazard ratio of 0.92.
The current pre-planned analysis involved 755 patients who were followed up for a median of 57 months by the time the trial was stopped in 2021.
In the standard treatment arm, endocrine therapy was favored by physicians in 72.7% of cases (Clin-low), while 27.3% were given chemotherapy (Clin-high).
In the CTC group, 73.5% of patients were recommended to have endocrine therapy by their physician based on their clinical characteristics (Clin-low), whereas 26.5% were suggested to have chemotherapy (Clin-high).
In contrast, 60.1% of patients in the standard arm would have received endocrine therapy based on their CTC count (CTC-low), and 39.9% chemotherapy (CTC-high), while 63.4% of those in the CTC arm were given endocrine therapy based on their CTC count (CTC-low), and 36.6% were assigned to chemotherapy (CTC-high).
Once the allocated treatment was known in both treatment groups, the physicians were free to choose between endocrine therapy (mostly a single-agent aromatase inhibitor or fulvestrant) and chemotherapy (mostly paclitaxel or capecitabine).
Although CDK4/6 inhibitors were not approved at the time of enrollment, 42.2% of patients across both treatment groups received one of these drugs as a second-line or later therapy.
Guiding treatment decisions
Dr. Bidard said that, overall, more patients in the CTC arm were assigned to chemotherapy, at a difference of 9.7%. There was approximately 60% concordance between physician- and CTC-guided treatment choices; in other words, patients were recommended the same treatment by the two approaches in both treatment groups.
In these patients, there was no significant difference in overall survival between the physician choice and CTC groups, at a median of 45.5 months versus 51.3 months (hazard ratio, 0.85; P = .11).
The updated PFS data revealed a median PFS of 15.7 months in the CTC group versus 13.8 months, again at a nonsignificant HR of 0.94.
These results, Dr. Bidard said, indicate that CTC-based treatment choices are “safe.”
However, there was discordance between physician and CTC-based treatment choices in around 40% of cases, meaning that the two approaches recommended different therapies.
The physician recommended endocrine therapy, in contrast to the CTC count indicating chemotherapy, in 25% of patients (Clin-low/CTC-high), whereas 13.6% of cases were recommended chemotherapy while their CTC count indicated otherwise (Clin-high/CTC-low).
In Clin-low/CTC-high patients, this resulted in 26.1% of patients in the standard group receiving endocrine therapy when their CTC count indicated chemotherapy, while 23.9% of patients in the CTC group received chemotherapy even though their physician did not recommended it.
Comparing these two groups, the researchers found that patients in the CTC group had a significantly longer PFS, at 15.7 months versus 10 months (HR, 0.65; P = .005). They also had a significantly longer median overall survival, at a median of 51.8 months versus 35.4 months with physician choice (HR, 0.53; P = .001).
Among Clin-high/CTC-low, there was no benefit from physician’s choice of chemotherapy over the CTC-guided recommendation of endocrine therapy, at an HR for PFS of 1.14 for CTC- versus physician-guided therapy (P = .54), and an HR for overall survival of 0.88 (P = .64).
Dr. Bidard highlighted that the treatment effects were seen across prespecified subgroups.
The study was funded by the Institut National du Cancer, the Institut Curie SIRIC2 program, and Menarini Silicon Biosystems. Dr. Chan reports no relevant financial relationships. Dr. Hayes and Dr. Bidard reported relationships with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
SAN ANTONIO – When choosing between chemotherapy and endocrine therapy for patients with hormone receptor (HR)+/HER2- metastatic breast cancer, allowing the results from a blood test that measures circulating tumor cell (CTC) count to overrule physician’s choice of therapy can significantly improve overall survival.
But One expert reacting to the findings says probably not, and another pointed out that the CTC count test used in the trial (CellSearch), although approved by the Food and Drug Administration, is not widely used in clinical practice.
The findings comes from updated results from the STIC CTC study.
“When the trial was designed, the question related to the choice between single-agent endocrine therapy and chemotherapy [in] first-line therapy,” explained study presenter François-Clément Bidard, MD, PhD, professor of medical oncology at Institut Curie and Versailles Saint-Quentin University, Paris.
Since then, the first-line treatment has changed and can now can also include cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors, but Dr. Bidard said the results are still clinically relevant.
Nowadays, endocrine therapy plus CDK4/6 inhibitors is the “preferred option for treatment-naive patients, but the dilemma between endocrine therapy and chemotherapy remains after disease progression on adjuvant or first-line therapy with CDK4/6 inhibitors, where current guidelines advocate in favor of endocrine therapy, despite its short-lived efficacy.”
“In that scenario, based on the STIC CTC trial results, the CTC count in combination with predictive biomarkers, whenever available, may help customize the early use of chemotherapy or antibody-drug conjugates, which are becoming more and more attractive,” Dr. Bidard said.
The research was presented here at the San Antonio Breast Cancer Symposium (SABCS).
The study involved more than 750 patients with HR+/HER2- metastatic breast cancer randomly assigned to physician choice or CTC-guided therapy, although the physician decision and the recommendation based on the CTC count was recorded in both groups.
Using the CellSearch (Menarini Silicon Biosystems) to perform the CTC count at baseline only, the team defined patients as low or high risk, with low-risk patients deemed to need only endocrine therapy and high-risk patients recommended chemotherapy.
Physicians based their decisions on current guidelines and their clinical experience.
In the 25% of cases where CTC count would recommend chemotherapy while the physician would recommend endocrine therapy, following the CTC count–based choice resulted in a 35% improvement in progression-free survival (PFS) and a 47% increase in overall survival.
In all other situations, including those when the CTC count recommended endocrine therapy in contrast to the physicians, or the approximately 60% of cases in which the two were in agreement, there was no difference in survival outcomes between the approaches.
Reacting to the findings, Nancy Chan, MD, medical oncologist and the director of breast cancer clinical research at NYU Langone’s Perlmutter Cancer Center, said that the “goal is really to understand how we can personalize treatment options for patients.”
Another aim is to avoid performing a tumor biopsy, if possible, “as that has increased morbidity for patients.”
She noted also that choosing between endocrine therapy and chemotherapy is a “big decision.” These researchers “really wanted to help some patients get less chemotherapy,” as they felt that “some patients are getting too much” as they are not really that high risk and should get endocrine therapy instead.
However, Dr. Chan said that the CTC count is a “complicated concept” and is “not something we’re all using in our clinical practice yet.”
With regard to the approximately 40% discordance between the CTC- and physician-guided choices, Dr. Chan said that clinicians are perhaps not as accurate as they believed in predicting risk when relying on the clinical or pathological features of the tumor.
On Twitter, Guilherme Nader-Marta, MD, Jules Bordet Institute, Université Libre de Bruxelles, Belgium, commented that the question behind the study was whether CTC measurement is a “clinically useful strategy for first-line treatment decision-making.”
“Amazingly,” he continued, the trial went “straight to the point” to answer the question and showed that CTC-based decisions can offer a survival benefit.
Daniel F. Hayes, MD, co-director of the Breast Oncology Program at the University of Michigan Comprehensive Cancer Center, Ann Arbor, echoed these thoughts, saying that the goals of therapy are to make patients live longer and “better.”
He said that the point of any clinical biomarker is not only to show that testing for it offers “analytical validity” but that it also provides “clinical utility” in that it can guide treatment decisions to improve outcomes.
Dr. Hayes, who was not involved in the study but has worked for many years on the development of CellSearch, said that the results do not make it clear whether measuring CTC counts meets the definition of clinical utility, but it’s “very close.”
On the other hand, the analytical validity of the test is “excellent,” and, in that context, was well-chosen, he said, adding that the endpoint of the trial “is the one most important to us: improvement in overall survival.”
Dr. Hayes noted that the magnitude of benefit from CTC-guided therapy was “moderate,” although that is a “matter of perception,” and the “level of evidence is probably 2 or 3.” Although the trial was prospective, he said, the key results were in a “relatively small” subgroup.
The question is, Dr. Hayes continued: “Is this enough to change practice? My conclusions are: probably not.”
Although patients rated as low risk based on their low CTC count avoided chemotherapy, “it’s not clear to me that this whole thing is sufficient for clinical utility in context of what we know today.” The key issue, however, is who decides whether CTC counts are measured and whether they will be used to guide therapy decisions – will it be the patient, the caregiver, an expert guidelines panel, or third party payers/society?
Study details
In his presentation, Dr. Bidard explained that CTC count is an FDA-approved standardized liquid biopsy biomarker, with a count of greater than or equal to 5 cells per 7.5 mL of blood deemed an adverse prognostic marker, regardless of the line of therapy, with a grade 1 level of evidence.
Previous studies have indicated that a high CTC count is strongly associated with overall survival, at a hazard ratio of 2.78.
Crucially, the CTC count “complements” and does not duplicate standard clinicopathological prognostic factors, Dr. Bidard said.
To determine the potential of the CTC count as an aid to treatment decisions, Dr. Bidard and colleagues conducted a trial in pre- and postmenopausal women with untreated HR+/HER2- metastatic breast cancer who were able to receive either endocrine therapy or chemotherapy.
They were randomly assigned to either a standard group, in which the treatment decision followed the physician’s choice, regardless of their CTC count, or to a CTC group, in which the physicians made a treatment recommendation but the choice was driven by the CTC count.
Dr. Bidard reminded the audience that the primary endpoint of PFS to demonstrate the non-inferiority of CTC versus physician treatment decisions has already been met, with the results published in 2020. Those results came from an analysis of 788 patients enrolled between February 2012 and July 2016 at 17 sites in France and showed after 42 months of follow-up that the median PFS in the CTC arm was 15.6 months versus 14 months in the physician choice arm, at a hazard ratio of 0.92.
The current pre-planned analysis involved 755 patients who were followed up for a median of 57 months by the time the trial was stopped in 2021.
In the standard treatment arm, endocrine therapy was favored by physicians in 72.7% of cases (Clin-low), while 27.3% were given chemotherapy (Clin-high).
In the CTC group, 73.5% of patients were recommended to have endocrine therapy by their physician based on their clinical characteristics (Clin-low), whereas 26.5% were suggested to have chemotherapy (Clin-high).
In contrast, 60.1% of patients in the standard arm would have received endocrine therapy based on their CTC count (CTC-low), and 39.9% chemotherapy (CTC-high), while 63.4% of those in the CTC arm were given endocrine therapy based on their CTC count (CTC-low), and 36.6% were assigned to chemotherapy (CTC-high).
Once the allocated treatment was known in both treatment groups, the physicians were free to choose between endocrine therapy (mostly a single-agent aromatase inhibitor or fulvestrant) and chemotherapy (mostly paclitaxel or capecitabine).
Although CDK4/6 inhibitors were not approved at the time of enrollment, 42.2% of patients across both treatment groups received one of these drugs as a second-line or later therapy.
Guiding treatment decisions
Dr. Bidard said that, overall, more patients in the CTC arm were assigned to chemotherapy, at a difference of 9.7%. There was approximately 60% concordance between physician- and CTC-guided treatment choices; in other words, patients were recommended the same treatment by the two approaches in both treatment groups.
In these patients, there was no significant difference in overall survival between the physician choice and CTC groups, at a median of 45.5 months versus 51.3 months (hazard ratio, 0.85; P = .11).
The updated PFS data revealed a median PFS of 15.7 months in the CTC group versus 13.8 months, again at a nonsignificant HR of 0.94.
These results, Dr. Bidard said, indicate that CTC-based treatment choices are “safe.”
However, there was discordance between physician and CTC-based treatment choices in around 40% of cases, meaning that the two approaches recommended different therapies.
The physician recommended endocrine therapy, in contrast to the CTC count indicating chemotherapy, in 25% of patients (Clin-low/CTC-high), whereas 13.6% of cases were recommended chemotherapy while their CTC count indicated otherwise (Clin-high/CTC-low).
In Clin-low/CTC-high patients, this resulted in 26.1% of patients in the standard group receiving endocrine therapy when their CTC count indicated chemotherapy, while 23.9% of patients in the CTC group received chemotherapy even though their physician did not recommended it.
Comparing these two groups, the researchers found that patients in the CTC group had a significantly longer PFS, at 15.7 months versus 10 months (HR, 0.65; P = .005). They also had a significantly longer median overall survival, at a median of 51.8 months versus 35.4 months with physician choice (HR, 0.53; P = .001).
Among Clin-high/CTC-low, there was no benefit from physician’s choice of chemotherapy over the CTC-guided recommendation of endocrine therapy, at an HR for PFS of 1.14 for CTC- versus physician-guided therapy (P = .54), and an HR for overall survival of 0.88 (P = .64).
Dr. Bidard highlighted that the treatment effects were seen across prespecified subgroups.
The study was funded by the Institut National du Cancer, the Institut Curie SIRIC2 program, and Menarini Silicon Biosystems. Dr. Chan reports no relevant financial relationships. Dr. Hayes and Dr. Bidard reported relationships with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
SAN ANTONIO – When choosing between chemotherapy and endocrine therapy for patients with hormone receptor (HR)+/HER2- metastatic breast cancer, allowing the results from a blood test that measures circulating tumor cell (CTC) count to overrule physician’s choice of therapy can significantly improve overall survival.
But One expert reacting to the findings says probably not, and another pointed out that the CTC count test used in the trial (CellSearch), although approved by the Food and Drug Administration, is not widely used in clinical practice.
The findings comes from updated results from the STIC CTC study.
“When the trial was designed, the question related to the choice between single-agent endocrine therapy and chemotherapy [in] first-line therapy,” explained study presenter François-Clément Bidard, MD, PhD, professor of medical oncology at Institut Curie and Versailles Saint-Quentin University, Paris.
Since then, the first-line treatment has changed and can now can also include cyclin-dependent kinase 4 and 6 (CDK4/6) inhibitors, but Dr. Bidard said the results are still clinically relevant.
Nowadays, endocrine therapy plus CDK4/6 inhibitors is the “preferred option for treatment-naive patients, but the dilemma between endocrine therapy and chemotherapy remains after disease progression on adjuvant or first-line therapy with CDK4/6 inhibitors, where current guidelines advocate in favor of endocrine therapy, despite its short-lived efficacy.”
“In that scenario, based on the STIC CTC trial results, the CTC count in combination with predictive biomarkers, whenever available, may help customize the early use of chemotherapy or antibody-drug conjugates, which are becoming more and more attractive,” Dr. Bidard said.
The research was presented here at the San Antonio Breast Cancer Symposium (SABCS).
The study involved more than 750 patients with HR+/HER2- metastatic breast cancer randomly assigned to physician choice or CTC-guided therapy, although the physician decision and the recommendation based on the CTC count was recorded in both groups.
Using the CellSearch (Menarini Silicon Biosystems) to perform the CTC count at baseline only, the team defined patients as low or high risk, with low-risk patients deemed to need only endocrine therapy and high-risk patients recommended chemotherapy.
Physicians based their decisions on current guidelines and their clinical experience.
In the 25% of cases where CTC count would recommend chemotherapy while the physician would recommend endocrine therapy, following the CTC count–based choice resulted in a 35% improvement in progression-free survival (PFS) and a 47% increase in overall survival.
In all other situations, including those when the CTC count recommended endocrine therapy in contrast to the physicians, or the approximately 60% of cases in which the two were in agreement, there was no difference in survival outcomes between the approaches.
Reacting to the findings, Nancy Chan, MD, medical oncologist and the director of breast cancer clinical research at NYU Langone’s Perlmutter Cancer Center, said that the “goal is really to understand how we can personalize treatment options for patients.”
Another aim is to avoid performing a tumor biopsy, if possible, “as that has increased morbidity for patients.”
She noted also that choosing between endocrine therapy and chemotherapy is a “big decision.” These researchers “really wanted to help some patients get less chemotherapy,” as they felt that “some patients are getting too much” as they are not really that high risk and should get endocrine therapy instead.
However, Dr. Chan said that the CTC count is a “complicated concept” and is “not something we’re all using in our clinical practice yet.”
With regard to the approximately 40% discordance between the CTC- and physician-guided choices, Dr. Chan said that clinicians are perhaps not as accurate as they believed in predicting risk when relying on the clinical or pathological features of the tumor.
On Twitter, Guilherme Nader-Marta, MD, Jules Bordet Institute, Université Libre de Bruxelles, Belgium, commented that the question behind the study was whether CTC measurement is a “clinically useful strategy for first-line treatment decision-making.”
“Amazingly,” he continued, the trial went “straight to the point” to answer the question and showed that CTC-based decisions can offer a survival benefit.
Daniel F. Hayes, MD, co-director of the Breast Oncology Program at the University of Michigan Comprehensive Cancer Center, Ann Arbor, echoed these thoughts, saying that the goals of therapy are to make patients live longer and “better.”
He said that the point of any clinical biomarker is not only to show that testing for it offers “analytical validity” but that it also provides “clinical utility” in that it can guide treatment decisions to improve outcomes.
Dr. Hayes, who was not involved in the study but has worked for many years on the development of CellSearch, said that the results do not make it clear whether measuring CTC counts meets the definition of clinical utility, but it’s “very close.”
On the other hand, the analytical validity of the test is “excellent,” and, in that context, was well-chosen, he said, adding that the endpoint of the trial “is the one most important to us: improvement in overall survival.”
Dr. Hayes noted that the magnitude of benefit from CTC-guided therapy was “moderate,” although that is a “matter of perception,” and the “level of evidence is probably 2 or 3.” Although the trial was prospective, he said, the key results were in a “relatively small” subgroup.
The question is, Dr. Hayes continued: “Is this enough to change practice? My conclusions are: probably not.”
Although patients rated as low risk based on their low CTC count avoided chemotherapy, “it’s not clear to me that this whole thing is sufficient for clinical utility in context of what we know today.” The key issue, however, is who decides whether CTC counts are measured and whether they will be used to guide therapy decisions – will it be the patient, the caregiver, an expert guidelines panel, or third party payers/society?
Study details
In his presentation, Dr. Bidard explained that CTC count is an FDA-approved standardized liquid biopsy biomarker, with a count of greater than or equal to 5 cells per 7.5 mL of blood deemed an adverse prognostic marker, regardless of the line of therapy, with a grade 1 level of evidence.
Previous studies have indicated that a high CTC count is strongly associated with overall survival, at a hazard ratio of 2.78.
Crucially, the CTC count “complements” and does not duplicate standard clinicopathological prognostic factors, Dr. Bidard said.
To determine the potential of the CTC count as an aid to treatment decisions, Dr. Bidard and colleagues conducted a trial in pre- and postmenopausal women with untreated HR+/HER2- metastatic breast cancer who were able to receive either endocrine therapy or chemotherapy.
They were randomly assigned to either a standard group, in which the treatment decision followed the physician’s choice, regardless of their CTC count, or to a CTC group, in which the physicians made a treatment recommendation but the choice was driven by the CTC count.
Dr. Bidard reminded the audience that the primary endpoint of PFS to demonstrate the non-inferiority of CTC versus physician treatment decisions has already been met, with the results published in 2020. Those results came from an analysis of 788 patients enrolled between February 2012 and July 2016 at 17 sites in France and showed after 42 months of follow-up that the median PFS in the CTC arm was 15.6 months versus 14 months in the physician choice arm, at a hazard ratio of 0.92.
The current pre-planned analysis involved 755 patients who were followed up for a median of 57 months by the time the trial was stopped in 2021.
In the standard treatment arm, endocrine therapy was favored by physicians in 72.7% of cases (Clin-low), while 27.3% were given chemotherapy (Clin-high).
In the CTC group, 73.5% of patients were recommended to have endocrine therapy by their physician based on their clinical characteristics (Clin-low), whereas 26.5% were suggested to have chemotherapy (Clin-high).
In contrast, 60.1% of patients in the standard arm would have received endocrine therapy based on their CTC count (CTC-low), and 39.9% chemotherapy (CTC-high), while 63.4% of those in the CTC arm were given endocrine therapy based on their CTC count (CTC-low), and 36.6% were assigned to chemotherapy (CTC-high).
Once the allocated treatment was known in both treatment groups, the physicians were free to choose between endocrine therapy (mostly a single-agent aromatase inhibitor or fulvestrant) and chemotherapy (mostly paclitaxel or capecitabine).
Although CDK4/6 inhibitors were not approved at the time of enrollment, 42.2% of patients across both treatment groups received one of these drugs as a second-line or later therapy.
Guiding treatment decisions
Dr. Bidard said that, overall, more patients in the CTC arm were assigned to chemotherapy, at a difference of 9.7%. There was approximately 60% concordance between physician- and CTC-guided treatment choices; in other words, patients were recommended the same treatment by the two approaches in both treatment groups.
In these patients, there was no significant difference in overall survival between the physician choice and CTC groups, at a median of 45.5 months versus 51.3 months (hazard ratio, 0.85; P = .11).
The updated PFS data revealed a median PFS of 15.7 months in the CTC group versus 13.8 months, again at a nonsignificant HR of 0.94.
These results, Dr. Bidard said, indicate that CTC-based treatment choices are “safe.”
However, there was discordance between physician and CTC-based treatment choices in around 40% of cases, meaning that the two approaches recommended different therapies.
The physician recommended endocrine therapy, in contrast to the CTC count indicating chemotherapy, in 25% of patients (Clin-low/CTC-high), whereas 13.6% of cases were recommended chemotherapy while their CTC count indicated otherwise (Clin-high/CTC-low).
In Clin-low/CTC-high patients, this resulted in 26.1% of patients in the standard group receiving endocrine therapy when their CTC count indicated chemotherapy, while 23.9% of patients in the CTC group received chemotherapy even though their physician did not recommended it.
Comparing these two groups, the researchers found that patients in the CTC group had a significantly longer PFS, at 15.7 months versus 10 months (HR, 0.65; P = .005). They also had a significantly longer median overall survival, at a median of 51.8 months versus 35.4 months with physician choice (HR, 0.53; P = .001).
Among Clin-high/CTC-low, there was no benefit from physician’s choice of chemotherapy over the CTC-guided recommendation of endocrine therapy, at an HR for PFS of 1.14 for CTC- versus physician-guided therapy (P = .54), and an HR for overall survival of 0.88 (P = .64).
Dr. Bidard highlighted that the treatment effects were seen across prespecified subgroups.
The study was funded by the Institut National du Cancer, the Institut Curie SIRIC2 program, and Menarini Silicon Biosystems. Dr. Chan reports no relevant financial relationships. Dr. Hayes and Dr. Bidard reported relationships with numerous pharmaceutical companies.
A version of this article first appeared on Medscape.com.
AT SABCS 2022
Cancer researcher banned from federal funding for faking data in nearly 400 images in 16 grant applications
according to a U.S. government research watchdog.
Alice C. Chang, PhD, whose publications and grants listed her name as Chun-Ju Chang, received nearly $700,000 in funding from the National Institutes of Health through grant applications that the U.S. Office of Research Integrity said contained fake data. She will be banned from receiving federal grants for a decade – a more severe sanction than ORI has typically imposed in recent years.
In its findings, ORI said Dr. Chang, who was an associate professor of basic medical sciences at Purdue’s College of Veterinary Medicine, West Lafayette, Ind., “knowingly, intentionally, or recklessly falsified and/or fabricated data from the same mouse models or cell lines by reusing the data, with or without manipulation, to represent unrelated experiments from different mouse models or cell lines with different treatments in three hundred eighty-four (384) figure panels in sixteen (16) grant applications.”
Two of the grant applications were funded. Dr. Chang received $688,196 from the National Cancer Institute, a division of NIH, from 2018 to 2019 for “Targeting metformin-directed stem cell fate in triple negative breast cancer.” The other grant ORI says was submitted in 2014 and funded, “Targeting cell polarity machinery to exhaust breast cancer stem cell pool,” does not show up in NIH RePorter. The rest of the grants were not approved.
We found a Chun-Ju Chang who is dean of the College of Life Sciences at China Medical University in Taiwan and has published papers with a group that Chun-Ju Chang at Purdue also published with. She did not immediately respond to our request for comment.
ORI’s finding also stated Dr. Chang faked data in two papers supported by government funding by reusing figures reporting gene expression in mice and cells after drug treatments, relabeling them to say they showed the results of different experiments. According to the agency, she has agreed to request corrections for the papers:
“Leptin–STAT3–G9a Signaling Promotes Obesity-Mediated Breast Cancer Progression,” published in May 2015 in Cancer Research and cited 83 times, according to Clarivate’s Web of Science.
“Retinoic acid directs breast cancer cell state changes through regulation of TET2-PKC-zeta pathway,” published in February 2017 in Oncogene and cited 26 times.
Between the two papers and 15 of the grant applications, ORI said that Dr. Chang reused gene expression data, sometimes with manipulation, in 119 figure panels. She reused other types of data and images in hundreds of figures across multiple grant applications, ORI found.
As well as correcting the two papers, Dr. Chang agreed to a 10-year ban from all federal contracting, including grant funding. She also agreed not to serve in any advisory or consulting role with the U.S. Public Health Service, which includes the NIH, for that time period.
A version of this article first appeared on Retraction Watch.
according to a U.S. government research watchdog.
Alice C. Chang, PhD, whose publications and grants listed her name as Chun-Ju Chang, received nearly $700,000 in funding from the National Institutes of Health through grant applications that the U.S. Office of Research Integrity said contained fake data. She will be banned from receiving federal grants for a decade – a more severe sanction than ORI has typically imposed in recent years.
In its findings, ORI said Dr. Chang, who was an associate professor of basic medical sciences at Purdue’s College of Veterinary Medicine, West Lafayette, Ind., “knowingly, intentionally, or recklessly falsified and/or fabricated data from the same mouse models or cell lines by reusing the data, with or without manipulation, to represent unrelated experiments from different mouse models or cell lines with different treatments in three hundred eighty-four (384) figure panels in sixteen (16) grant applications.”
Two of the grant applications were funded. Dr. Chang received $688,196 from the National Cancer Institute, a division of NIH, from 2018 to 2019 for “Targeting metformin-directed stem cell fate in triple negative breast cancer.” The other grant ORI says was submitted in 2014 and funded, “Targeting cell polarity machinery to exhaust breast cancer stem cell pool,” does not show up in NIH RePorter. The rest of the grants were not approved.
We found a Chun-Ju Chang who is dean of the College of Life Sciences at China Medical University in Taiwan and has published papers with a group that Chun-Ju Chang at Purdue also published with. She did not immediately respond to our request for comment.
ORI’s finding also stated Dr. Chang faked data in two papers supported by government funding by reusing figures reporting gene expression in mice and cells after drug treatments, relabeling them to say they showed the results of different experiments. According to the agency, she has agreed to request corrections for the papers:
“Leptin–STAT3–G9a Signaling Promotes Obesity-Mediated Breast Cancer Progression,” published in May 2015 in Cancer Research and cited 83 times, according to Clarivate’s Web of Science.
“Retinoic acid directs breast cancer cell state changes through regulation of TET2-PKC-zeta pathway,” published in February 2017 in Oncogene and cited 26 times.
Between the two papers and 15 of the grant applications, ORI said that Dr. Chang reused gene expression data, sometimes with manipulation, in 119 figure panels. She reused other types of data and images in hundreds of figures across multiple grant applications, ORI found.
As well as correcting the two papers, Dr. Chang agreed to a 10-year ban from all federal contracting, including grant funding. She also agreed not to serve in any advisory or consulting role with the U.S. Public Health Service, which includes the NIH, for that time period.
A version of this article first appeared on Retraction Watch.
according to a U.S. government research watchdog.
Alice C. Chang, PhD, whose publications and grants listed her name as Chun-Ju Chang, received nearly $700,000 in funding from the National Institutes of Health through grant applications that the U.S. Office of Research Integrity said contained fake data. She will be banned from receiving federal grants for a decade – a more severe sanction than ORI has typically imposed in recent years.
In its findings, ORI said Dr. Chang, who was an associate professor of basic medical sciences at Purdue’s College of Veterinary Medicine, West Lafayette, Ind., “knowingly, intentionally, or recklessly falsified and/or fabricated data from the same mouse models or cell lines by reusing the data, with or without manipulation, to represent unrelated experiments from different mouse models or cell lines with different treatments in three hundred eighty-four (384) figure panels in sixteen (16) grant applications.”
Two of the grant applications were funded. Dr. Chang received $688,196 from the National Cancer Institute, a division of NIH, from 2018 to 2019 for “Targeting metformin-directed stem cell fate in triple negative breast cancer.” The other grant ORI says was submitted in 2014 and funded, “Targeting cell polarity machinery to exhaust breast cancer stem cell pool,” does not show up in NIH RePorter. The rest of the grants were not approved.
We found a Chun-Ju Chang who is dean of the College of Life Sciences at China Medical University in Taiwan and has published papers with a group that Chun-Ju Chang at Purdue also published with. She did not immediately respond to our request for comment.
ORI’s finding also stated Dr. Chang faked data in two papers supported by government funding by reusing figures reporting gene expression in mice and cells after drug treatments, relabeling them to say they showed the results of different experiments. According to the agency, she has agreed to request corrections for the papers:
“Leptin–STAT3–G9a Signaling Promotes Obesity-Mediated Breast Cancer Progression,” published in May 2015 in Cancer Research and cited 83 times, according to Clarivate’s Web of Science.
“Retinoic acid directs breast cancer cell state changes through regulation of TET2-PKC-zeta pathway,” published in February 2017 in Oncogene and cited 26 times.
Between the two papers and 15 of the grant applications, ORI said that Dr. Chang reused gene expression data, sometimes with manipulation, in 119 figure panels. She reused other types of data and images in hundreds of figures across multiple grant applications, ORI found.
As well as correcting the two papers, Dr. Chang agreed to a 10-year ban from all federal contracting, including grant funding. She also agreed not to serve in any advisory or consulting role with the U.S. Public Health Service, which includes the NIH, for that time period.
A version of this article first appeared on Retraction Watch.
Nitroglycerin’s safety and value examined
He has stable angina, having chest pain with exercise. He uses sublingual nitroglycerin (SL NTG prn) about three times a month. His blood pressure is 140/70 mm Hg. His pulse is 60 beats per minute. His current medications are lisinopril, atorvastatin, aspirin, and SL NTG tablets as needed.
What would you recommend?
A. No sildenafil; refer to urologist for other ED options.
B. Okay to use sildenafil if greater than 6 hours from NTG use.
C. Recommend tadalafil.
Is coprescribing nitrates and phosphodiesterase inhibitors safe?
The FDA warns against the use of phosphodiesterase inhibitors in patients taking nitrates. Combining nitrates with phosphodiesterase type 5 (PDE5) inhibitors is contraindicated because of a synergistic blood pressure lowering effect.1 This warning/contraindication was based on theoretical concerns, as well as concern that of the first 130 deaths reported in patients who took sildenafil, 16 of the patients also were taking nitrates.2
Parker and colleagues studied the safety of giving IV nitroglycerin to patients with coronary artery disease (CAD) who have taken sildenafil.3 The study was a randomized, placebo-controlled, crossover trial. Participants received sildenafil 100 mg or placebo, then received intravenous NTG. Patients who received sildenafil had a 4-6 mm Hg systolic BP drop compared with those who took the placebo. There was no difference in severe events between the sildenafil and placebo groups. The blood levels of nitroglycerin in this study were very likely much higher than the levels that occur with SL NTG.
A recent study by Holt et al. looked at overall cardiovascular outcomes with coprescribing nitrates and phosphodiesterase inhibitors.4 The study was a case crossover design, using a nationwide Danish health registry over the period of 2000-2018. In 2000, the rate of coprescribing of phosphodiesterase inhibitors in ischemic heart disease patients on nitrates was .9 per 100 persons/year and rose to 19.5 prescriptions per 100 persons/year in 2018. During this same time, no statistically significant association was found between the coprescription of nitrates with PDE5 inhibitors and the risk for MI, cardiac arrest, syncope, stroke, or an adverse drug event.
Does nitroglycerin response help determine cause of chest pain?
Nitroglycerin response has long been used as a clinical indicator on whether a patient’s chest pain is cardiac or not. Eric A. Shry, MD, and his colleagues looked at the usefulness of nitroglycerin response in the treatment of chest pain as a predictor of ischemic chest pain in an emergency department setting.5
The study was a retrospective review of 223 patients who presented to the emergency department over a 5-month period with ongoing chest pain. They looked at patients who had ongoing chest pain in the emergency department, received nitroglycerin, and did not receive any therapy other than aspirin within 10 minutes of receiving nitroglycerin. Response to the drug was compared with the final diagnosis of cardiac versus noncardiac chest pain.
Of the patients with a final determination of cardiac chest pain, 88% had a nitroglycerin response, whereas 92% of the patients with noncardiac chest pain had a nitroglycerin response (P = .50).
Deborah B. Diercks, MD, and her colleagues looked at improvement in chest pain scores in the emergency department in patients treated with nitroglycerin and whether it correlated with a cardiac etiology of chest pain.6 The study was a prospective, observational study of 664 patients in an urban tertiary care emergency department over a 16-month period. An 11-point numeric chest pain scale was assessed and recorded by research assistants before and 5 minutes after receiving nitroglycerin. The scale ranged from 0 (no pain) to 10 (worst pain imaginable).
A final diagnosis of a cardiac etiology for chest pain was found in 18% of the patients in the study. Of the patients who had cardiac-related chest pain, 20% had no reduction in pain with nitroglycerin, compared with 19% of the patients without cardiac-related chest pain.
A complete or significant reduction in chest pain occurred with nitroglycerin in 31% of patients with cardiac chest pain and 27% of the patients without cardiac chest pain (P = .76).
Nitroglycerin response does not appear to be helpful in distinguishing cardiac from noncardiac chest pain, but a study by His and colleagues offers an interesting twist.7
The authors of this research studied 118 patients looking to see if the side effect of headache with nitroglycerin was more common in patients who did not have CAD than in those who did. All the patients had a varying degree of relief of chest pain with NTG administration within 10 minutes. In patients with normal coronary arteries or minimal CAD, 73% had headache caused by NTG, whereas in patients with obstructive CAD, only 23% had headache after NTG use.
Take-home messages
- Short acting nitroglycerin may not be a contraindication for phosphodiesterase inhibitor use.
- More data are still needed.
- Nitroglycerin response does not help distinguish chest pain from CAD from noncardiac causes.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Schwartz BG, Kloner RA. Drug interactions with phosphodiesterase-5 inhibitors used for the treatment of erectile dysfunction or pulmonary hypertension. Circulation. 2010;122:88-95.
2. Kloner RA, Zusman RM. Cardiovascular effects of sildenafil citrate and recommendations for its use. Am J Cardiol. 1999 Sep 9;84(5B):11N-17N.
3. Parker JD et al. Safety of intravenous nitroglycerin after administration of sildenafil citrate to men with coronary artery disease: A double-blind, placebo-controlled, randomized, crossover trial. Crit Care Med. 2007;35:1863-8.
4. Holt A et al. Adverse events associated with coprescription of phosphodiesterase type inhibitors and oral organic nitrates in male patients with ischemic heart disease. Ann Intern Med. 2022 Jun;175(6):774-82.
5. Shry EA et al. Usefulness of the response to sublingual nitroglycerin as a predictor of ischemic chest pain in the emergency department. Am J Cardiol. 2002 Dec 1;90(11):1264-6.
6. Diercks DB et al. Changes in the numeric descriptive scale for pain after sublingual nitroglycerin do not predict cardiac etiology of chest pain. Ann Emerg Med. 2005 Jun;45(6):581-5.
7. His DH et al. Headache response to glyceryl trinitrate in patients with and without obstructive coronary artery disease. Heart 2005;91:1164-6.
He has stable angina, having chest pain with exercise. He uses sublingual nitroglycerin (SL NTG prn) about three times a month. His blood pressure is 140/70 mm Hg. His pulse is 60 beats per minute. His current medications are lisinopril, atorvastatin, aspirin, and SL NTG tablets as needed.
What would you recommend?
A. No sildenafil; refer to urologist for other ED options.
B. Okay to use sildenafil if greater than 6 hours from NTG use.
C. Recommend tadalafil.
Is coprescribing nitrates and phosphodiesterase inhibitors safe?
The FDA warns against the use of phosphodiesterase inhibitors in patients taking nitrates. Combining nitrates with phosphodiesterase type 5 (PDE5) inhibitors is contraindicated because of a synergistic blood pressure lowering effect.1 This warning/contraindication was based on theoretical concerns, as well as concern that of the first 130 deaths reported in patients who took sildenafil, 16 of the patients also were taking nitrates.2
Parker and colleagues studied the safety of giving IV nitroglycerin to patients with coronary artery disease (CAD) who have taken sildenafil.3 The study was a randomized, placebo-controlled, crossover trial. Participants received sildenafil 100 mg or placebo, then received intravenous NTG. Patients who received sildenafil had a 4-6 mm Hg systolic BP drop compared with those who took the placebo. There was no difference in severe events between the sildenafil and placebo groups. The blood levels of nitroglycerin in this study were very likely much higher than the levels that occur with SL NTG.
A recent study by Holt et al. looked at overall cardiovascular outcomes with coprescribing nitrates and phosphodiesterase inhibitors.4 The study was a case crossover design, using a nationwide Danish health registry over the period of 2000-2018. In 2000, the rate of coprescribing of phosphodiesterase inhibitors in ischemic heart disease patients on nitrates was .9 per 100 persons/year and rose to 19.5 prescriptions per 100 persons/year in 2018. During this same time, no statistically significant association was found between the coprescription of nitrates with PDE5 inhibitors and the risk for MI, cardiac arrest, syncope, stroke, or an adverse drug event.
Does nitroglycerin response help determine cause of chest pain?
Nitroglycerin response has long been used as a clinical indicator on whether a patient’s chest pain is cardiac or not. Eric A. Shry, MD, and his colleagues looked at the usefulness of nitroglycerin response in the treatment of chest pain as a predictor of ischemic chest pain in an emergency department setting.5
The study was a retrospective review of 223 patients who presented to the emergency department over a 5-month period with ongoing chest pain. They looked at patients who had ongoing chest pain in the emergency department, received nitroglycerin, and did not receive any therapy other than aspirin within 10 minutes of receiving nitroglycerin. Response to the drug was compared with the final diagnosis of cardiac versus noncardiac chest pain.
Of the patients with a final determination of cardiac chest pain, 88% had a nitroglycerin response, whereas 92% of the patients with noncardiac chest pain had a nitroglycerin response (P = .50).
Deborah B. Diercks, MD, and her colleagues looked at improvement in chest pain scores in the emergency department in patients treated with nitroglycerin and whether it correlated with a cardiac etiology of chest pain.6 The study was a prospective, observational study of 664 patients in an urban tertiary care emergency department over a 16-month period. An 11-point numeric chest pain scale was assessed and recorded by research assistants before and 5 minutes after receiving nitroglycerin. The scale ranged from 0 (no pain) to 10 (worst pain imaginable).
A final diagnosis of a cardiac etiology for chest pain was found in 18% of the patients in the study. Of the patients who had cardiac-related chest pain, 20% had no reduction in pain with nitroglycerin, compared with 19% of the patients without cardiac-related chest pain.
A complete or significant reduction in chest pain occurred with nitroglycerin in 31% of patients with cardiac chest pain and 27% of the patients without cardiac chest pain (P = .76).
Nitroglycerin response does not appear to be helpful in distinguishing cardiac from noncardiac chest pain, but a study by His and colleagues offers an interesting twist.7
The authors of this research studied 118 patients looking to see if the side effect of headache with nitroglycerin was more common in patients who did not have CAD than in those who did. All the patients had a varying degree of relief of chest pain with NTG administration within 10 minutes. In patients with normal coronary arteries or minimal CAD, 73% had headache caused by NTG, whereas in patients with obstructive CAD, only 23% had headache after NTG use.
Take-home messages
- Short acting nitroglycerin may not be a contraindication for phosphodiesterase inhibitor use.
- More data are still needed.
- Nitroglycerin response does not help distinguish chest pain from CAD from noncardiac causes.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Schwartz BG, Kloner RA. Drug interactions with phosphodiesterase-5 inhibitors used for the treatment of erectile dysfunction or pulmonary hypertension. Circulation. 2010;122:88-95.
2. Kloner RA, Zusman RM. Cardiovascular effects of sildenafil citrate and recommendations for its use. Am J Cardiol. 1999 Sep 9;84(5B):11N-17N.
3. Parker JD et al. Safety of intravenous nitroglycerin after administration of sildenafil citrate to men with coronary artery disease: A double-blind, placebo-controlled, randomized, crossover trial. Crit Care Med. 2007;35:1863-8.
4. Holt A et al. Adverse events associated with coprescription of phosphodiesterase type inhibitors and oral organic nitrates in male patients with ischemic heart disease. Ann Intern Med. 2022 Jun;175(6):774-82.
5. Shry EA et al. Usefulness of the response to sublingual nitroglycerin as a predictor of ischemic chest pain in the emergency department. Am J Cardiol. 2002 Dec 1;90(11):1264-6.
6. Diercks DB et al. Changes in the numeric descriptive scale for pain after sublingual nitroglycerin do not predict cardiac etiology of chest pain. Ann Emerg Med. 2005 Jun;45(6):581-5.
7. His DH et al. Headache response to glyceryl trinitrate in patients with and without obstructive coronary artery disease. Heart 2005;91:1164-6.
He has stable angina, having chest pain with exercise. He uses sublingual nitroglycerin (SL NTG prn) about three times a month. His blood pressure is 140/70 mm Hg. His pulse is 60 beats per minute. His current medications are lisinopril, atorvastatin, aspirin, and SL NTG tablets as needed.
What would you recommend?
A. No sildenafil; refer to urologist for other ED options.
B. Okay to use sildenafil if greater than 6 hours from NTG use.
C. Recommend tadalafil.
Is coprescribing nitrates and phosphodiesterase inhibitors safe?
The FDA warns against the use of phosphodiesterase inhibitors in patients taking nitrates. Combining nitrates with phosphodiesterase type 5 (PDE5) inhibitors is contraindicated because of a synergistic blood pressure lowering effect.1 This warning/contraindication was based on theoretical concerns, as well as concern that of the first 130 deaths reported in patients who took sildenafil, 16 of the patients also were taking nitrates.2
Parker and colleagues studied the safety of giving IV nitroglycerin to patients with coronary artery disease (CAD) who have taken sildenafil.3 The study was a randomized, placebo-controlled, crossover trial. Participants received sildenafil 100 mg or placebo, then received intravenous NTG. Patients who received sildenafil had a 4-6 mm Hg systolic BP drop compared with those who took the placebo. There was no difference in severe events between the sildenafil and placebo groups. The blood levels of nitroglycerin in this study were very likely much higher than the levels that occur with SL NTG.
A recent study by Holt et al. looked at overall cardiovascular outcomes with coprescribing nitrates and phosphodiesterase inhibitors.4 The study was a case crossover design, using a nationwide Danish health registry over the period of 2000-2018. In 2000, the rate of coprescribing of phosphodiesterase inhibitors in ischemic heart disease patients on nitrates was .9 per 100 persons/year and rose to 19.5 prescriptions per 100 persons/year in 2018. During this same time, no statistically significant association was found between the coprescription of nitrates with PDE5 inhibitors and the risk for MI, cardiac arrest, syncope, stroke, or an adverse drug event.
Does nitroglycerin response help determine cause of chest pain?
Nitroglycerin response has long been used as a clinical indicator on whether a patient’s chest pain is cardiac or not. Eric A. Shry, MD, and his colleagues looked at the usefulness of nitroglycerin response in the treatment of chest pain as a predictor of ischemic chest pain in an emergency department setting.5
The study was a retrospective review of 223 patients who presented to the emergency department over a 5-month period with ongoing chest pain. They looked at patients who had ongoing chest pain in the emergency department, received nitroglycerin, and did not receive any therapy other than aspirin within 10 minutes of receiving nitroglycerin. Response to the drug was compared with the final diagnosis of cardiac versus noncardiac chest pain.
Of the patients with a final determination of cardiac chest pain, 88% had a nitroglycerin response, whereas 92% of the patients with noncardiac chest pain had a nitroglycerin response (P = .50).
Deborah B. Diercks, MD, and her colleagues looked at improvement in chest pain scores in the emergency department in patients treated with nitroglycerin and whether it correlated with a cardiac etiology of chest pain.6 The study was a prospective, observational study of 664 patients in an urban tertiary care emergency department over a 16-month period. An 11-point numeric chest pain scale was assessed and recorded by research assistants before and 5 minutes after receiving nitroglycerin. The scale ranged from 0 (no pain) to 10 (worst pain imaginable).
A final diagnosis of a cardiac etiology for chest pain was found in 18% of the patients in the study. Of the patients who had cardiac-related chest pain, 20% had no reduction in pain with nitroglycerin, compared with 19% of the patients without cardiac-related chest pain.
A complete or significant reduction in chest pain occurred with nitroglycerin in 31% of patients with cardiac chest pain and 27% of the patients without cardiac chest pain (P = .76).
Nitroglycerin response does not appear to be helpful in distinguishing cardiac from noncardiac chest pain, but a study by His and colleagues offers an interesting twist.7
The authors of this research studied 118 patients looking to see if the side effect of headache with nitroglycerin was more common in patients who did not have CAD than in those who did. All the patients had a varying degree of relief of chest pain with NTG administration within 10 minutes. In patients with normal coronary arteries or minimal CAD, 73% had headache caused by NTG, whereas in patients with obstructive CAD, only 23% had headache after NTG use.
Take-home messages
- Short acting nitroglycerin may not be a contraindication for phosphodiesterase inhibitor use.
- More data are still needed.
- Nitroglycerin response does not help distinguish chest pain from CAD from noncardiac causes.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and he serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Schwartz BG, Kloner RA. Drug interactions with phosphodiesterase-5 inhibitors used for the treatment of erectile dysfunction or pulmonary hypertension. Circulation. 2010;122:88-95.
2. Kloner RA, Zusman RM. Cardiovascular effects of sildenafil citrate and recommendations for its use. Am J Cardiol. 1999 Sep 9;84(5B):11N-17N.
3. Parker JD et al. Safety of intravenous nitroglycerin after administration of sildenafil citrate to men with coronary artery disease: A double-blind, placebo-controlled, randomized, crossover trial. Crit Care Med. 2007;35:1863-8.
4. Holt A et al. Adverse events associated with coprescription of phosphodiesterase type inhibitors and oral organic nitrates in male patients with ischemic heart disease. Ann Intern Med. 2022 Jun;175(6):774-82.
5. Shry EA et al. Usefulness of the response to sublingual nitroglycerin as a predictor of ischemic chest pain in the emergency department. Am J Cardiol. 2002 Dec 1;90(11):1264-6.
6. Diercks DB et al. Changes in the numeric descriptive scale for pain after sublingual nitroglycerin do not predict cardiac etiology of chest pain. Ann Emerg Med. 2005 Jun;45(6):581-5.
7. His DH et al. Headache response to glyceryl trinitrate in patients with and without obstructive coronary artery disease. Heart 2005;91:1164-6.
Dupilumab significantly improves markers of AD severity in pediatric patients
A registry-based study provides further evidence that treatment with dupilumab significantly reduces severity and symptoms of atopic dermatitis (AD) in clinical practice.
Dupilumab also decreased severity-associated biomarkers in pediatric patients with moderate to severe AD, researchers in the Netherlands reported.
Obtaining serum biomarkers is not the current standard in everyday practice, but studying them may improve understanding of who might respond best to dupilumab, said Jessica Hui, MD, a pediatric allergist and immunologist at National Jewish Health in Denver, in an email comment to this news organization.
“AD is heterogeneous, as each patient may have different presentations and underlying biology,” said Dr. Hui, who wasn’t involved in the research. “Studying biomarkers can eventually assist us in providing targeted therapy to each individual patient.”
Dr. Hui added, “As blood biomarkers can inform us of severity and treatment response, we can be hopeful that this will assist us in the management of AD patients in the future.”
Examining effect on disease severity
Dupilumab, a monoclonal antibody that inhibits interleukin (IL)-4 and IL-13 signaling, is approved in Europe and the United States to treat moderate to severe AD in patients 6 months of age or older, and to treat certain other inflammatory conditions.
Phase 3 studies show that dupilumab is effective for improving AD symptoms and quality of life in pediatric patients, but few clinical practice studies have researched the effect of the therapy on severity- and disease-related biomarkers in this population, the study authors write.
The study was published online in Pediatric Allergy Immunology.
In a new study, a team led by Esmé Kamphuis, MD, of the University of Groningen, the Netherlands, and colleagues evaluated the efficacy and safety of a 28-week dupilumab treatment course in 61 pediatric patients with moderate to severe AD. Additionally, the investigators examined the effect of this treatment regimen on serum biomarkers associated with disease severity.
Patients in the study were registered in the multicenter BioDay registry, which includes patients with moderate to severe AD receiving biologics or small-molecule agents. The AD cohort included children between 6 and 12 years of age (n = 16) and adolescents between 12 and less than 18 years of age (n = 45), all of whom received dupilumab on a dosing regimen indicated by age and body weight.
Over one-third (36.1%) of dupilumab-treated patients achieved an Investigator Global Assessment score of “almost clear” by 28 weeks of treatment. Approximately 75.4% of patients reached an Eczema Area and Severity Index (EASI) of 50, 49.2% reached EASI-75, and 24.6% reached EASI-90 at the 7-month follow-up.
Among patient-reported outcomes, 84.7% experienced improvements of 4 or more points on the Patient-Oriented Eczema Measure after the 28-week dupilumab treatment. In addition, improvements of 4 or more points on the Numeric Rating Scale for pruritus and pain were achieved by 45.3% and 77.4% of patients, respectively.
The most frequently reported side effects included conjunctivitis (n = 10) and headache (n = 4).
Of the 19 severity-associated serum biomarkers measured at baseline, week 4, and week 16, markers related to AD severity and treatment response significantly decreased during treatment (thymus- and activation-regulated chemokine, pulmonary and activation-regulated chemokine, periostin, soluble IL-2 receptor alpha).
A predicted EASI, calculated from selected biomarkers, demonstrated a significant association with disease severity in the cohort.
Implications for practice
When asked to comment on the study findings, Raegan Hunt, MD, the division chief of pediatric dermatology at Texas Children’s Hospital in Houston, said it is important to validate the changes in AD serum biomarkers in pediatric patients on dupilumab therapy, given that this treatment has historically been better studied in adults.
“This study adds to daily practice outcomes data, which in many cases is more relevant to the everyday care of patients than structured clinical trial data,” said Dr. Hunt, an associate professor at the Baylor College of Medicine, Houston.
Dr. Hunt, who didn’t participate in the study, noted that more research is needed on the adverse effects of dupilumab in the pediatric AD population.
Dr. Hui added that there is a lack of clear understanding of the exact underlying mechanisms for certain side effects, such as conjunctivitis, warranting further study.
The study’s BioDay registry is funded by Sanofi/Regeneron, AbbVie, Leo Pharma, Pfizer, and Eli Lilly. Several study coauthors report relationships with several pharmaceutical companies. Dr. Hunt and Dr. Hui report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A registry-based study provides further evidence that treatment with dupilumab significantly reduces severity and symptoms of atopic dermatitis (AD) in clinical practice.
Dupilumab also decreased severity-associated biomarkers in pediatric patients with moderate to severe AD, researchers in the Netherlands reported.
Obtaining serum biomarkers is not the current standard in everyday practice, but studying them may improve understanding of who might respond best to dupilumab, said Jessica Hui, MD, a pediatric allergist and immunologist at National Jewish Health in Denver, in an email comment to this news organization.
“AD is heterogeneous, as each patient may have different presentations and underlying biology,” said Dr. Hui, who wasn’t involved in the research. “Studying biomarkers can eventually assist us in providing targeted therapy to each individual patient.”
Dr. Hui added, “As blood biomarkers can inform us of severity and treatment response, we can be hopeful that this will assist us in the management of AD patients in the future.”
Examining effect on disease severity
Dupilumab, a monoclonal antibody that inhibits interleukin (IL)-4 and IL-13 signaling, is approved in Europe and the United States to treat moderate to severe AD in patients 6 months of age or older, and to treat certain other inflammatory conditions.
Phase 3 studies show that dupilumab is effective for improving AD symptoms and quality of life in pediatric patients, but few clinical practice studies have researched the effect of the therapy on severity- and disease-related biomarkers in this population, the study authors write.
The study was published online in Pediatric Allergy Immunology.
In a new study, a team led by Esmé Kamphuis, MD, of the University of Groningen, the Netherlands, and colleagues evaluated the efficacy and safety of a 28-week dupilumab treatment course in 61 pediatric patients with moderate to severe AD. Additionally, the investigators examined the effect of this treatment regimen on serum biomarkers associated with disease severity.
Patients in the study were registered in the multicenter BioDay registry, which includes patients with moderate to severe AD receiving biologics or small-molecule agents. The AD cohort included children between 6 and 12 years of age (n = 16) and adolescents between 12 and less than 18 years of age (n = 45), all of whom received dupilumab on a dosing regimen indicated by age and body weight.
Over one-third (36.1%) of dupilumab-treated patients achieved an Investigator Global Assessment score of “almost clear” by 28 weeks of treatment. Approximately 75.4% of patients reached an Eczema Area and Severity Index (EASI) of 50, 49.2% reached EASI-75, and 24.6% reached EASI-90 at the 7-month follow-up.
Among patient-reported outcomes, 84.7% experienced improvements of 4 or more points on the Patient-Oriented Eczema Measure after the 28-week dupilumab treatment. In addition, improvements of 4 or more points on the Numeric Rating Scale for pruritus and pain were achieved by 45.3% and 77.4% of patients, respectively.
The most frequently reported side effects included conjunctivitis (n = 10) and headache (n = 4).
Of the 19 severity-associated serum biomarkers measured at baseline, week 4, and week 16, markers related to AD severity and treatment response significantly decreased during treatment (thymus- and activation-regulated chemokine, pulmonary and activation-regulated chemokine, periostin, soluble IL-2 receptor alpha).
A predicted EASI, calculated from selected biomarkers, demonstrated a significant association with disease severity in the cohort.
Implications for practice
When asked to comment on the study findings, Raegan Hunt, MD, the division chief of pediatric dermatology at Texas Children’s Hospital in Houston, said it is important to validate the changes in AD serum biomarkers in pediatric patients on dupilumab therapy, given that this treatment has historically been better studied in adults.
“This study adds to daily practice outcomes data, which in many cases is more relevant to the everyday care of patients than structured clinical trial data,” said Dr. Hunt, an associate professor at the Baylor College of Medicine, Houston.
Dr. Hunt, who didn’t participate in the study, noted that more research is needed on the adverse effects of dupilumab in the pediatric AD population.
Dr. Hui added that there is a lack of clear understanding of the exact underlying mechanisms for certain side effects, such as conjunctivitis, warranting further study.
The study’s BioDay registry is funded by Sanofi/Regeneron, AbbVie, Leo Pharma, Pfizer, and Eli Lilly. Several study coauthors report relationships with several pharmaceutical companies. Dr. Hunt and Dr. Hui report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A registry-based study provides further evidence that treatment with dupilumab significantly reduces severity and symptoms of atopic dermatitis (AD) in clinical practice.
Dupilumab also decreased severity-associated biomarkers in pediatric patients with moderate to severe AD, researchers in the Netherlands reported.
Obtaining serum biomarkers is not the current standard in everyday practice, but studying them may improve understanding of who might respond best to dupilumab, said Jessica Hui, MD, a pediatric allergist and immunologist at National Jewish Health in Denver, in an email comment to this news organization.
“AD is heterogeneous, as each patient may have different presentations and underlying biology,” said Dr. Hui, who wasn’t involved in the research. “Studying biomarkers can eventually assist us in providing targeted therapy to each individual patient.”
Dr. Hui added, “As blood biomarkers can inform us of severity and treatment response, we can be hopeful that this will assist us in the management of AD patients in the future.”
Examining effect on disease severity
Dupilumab, a monoclonal antibody that inhibits interleukin (IL)-4 and IL-13 signaling, is approved in Europe and the United States to treat moderate to severe AD in patients 6 months of age or older, and to treat certain other inflammatory conditions.
Phase 3 studies show that dupilumab is effective for improving AD symptoms and quality of life in pediatric patients, but few clinical practice studies have researched the effect of the therapy on severity- and disease-related biomarkers in this population, the study authors write.
The study was published online in Pediatric Allergy Immunology.
In a new study, a team led by Esmé Kamphuis, MD, of the University of Groningen, the Netherlands, and colleagues evaluated the efficacy and safety of a 28-week dupilumab treatment course in 61 pediatric patients with moderate to severe AD. Additionally, the investigators examined the effect of this treatment regimen on serum biomarkers associated with disease severity.
Patients in the study were registered in the multicenter BioDay registry, which includes patients with moderate to severe AD receiving biologics or small-molecule agents. The AD cohort included children between 6 and 12 years of age (n = 16) and adolescents between 12 and less than 18 years of age (n = 45), all of whom received dupilumab on a dosing regimen indicated by age and body weight.
Over one-third (36.1%) of dupilumab-treated patients achieved an Investigator Global Assessment score of “almost clear” by 28 weeks of treatment. Approximately 75.4% of patients reached an Eczema Area and Severity Index (EASI) of 50, 49.2% reached EASI-75, and 24.6% reached EASI-90 at the 7-month follow-up.
Among patient-reported outcomes, 84.7% experienced improvements of 4 or more points on the Patient-Oriented Eczema Measure after the 28-week dupilumab treatment. In addition, improvements of 4 or more points on the Numeric Rating Scale for pruritus and pain were achieved by 45.3% and 77.4% of patients, respectively.
The most frequently reported side effects included conjunctivitis (n = 10) and headache (n = 4).
Of the 19 severity-associated serum biomarkers measured at baseline, week 4, and week 16, markers related to AD severity and treatment response significantly decreased during treatment (thymus- and activation-regulated chemokine, pulmonary and activation-regulated chemokine, periostin, soluble IL-2 receptor alpha).
A predicted EASI, calculated from selected biomarkers, demonstrated a significant association with disease severity in the cohort.
Implications for practice
When asked to comment on the study findings, Raegan Hunt, MD, the division chief of pediatric dermatology at Texas Children’s Hospital in Houston, said it is important to validate the changes in AD serum biomarkers in pediatric patients on dupilumab therapy, given that this treatment has historically been better studied in adults.
“This study adds to daily practice outcomes data, which in many cases is more relevant to the everyday care of patients than structured clinical trial data,” said Dr. Hunt, an associate professor at the Baylor College of Medicine, Houston.
Dr. Hunt, who didn’t participate in the study, noted that more research is needed on the adverse effects of dupilumab in the pediatric AD population.
Dr. Hui added that there is a lack of clear understanding of the exact underlying mechanisms for certain side effects, such as conjunctivitis, warranting further study.
The study’s BioDay registry is funded by Sanofi/Regeneron, AbbVie, Leo Pharma, Pfizer, and Eli Lilly. Several study coauthors report relationships with several pharmaceutical companies. Dr. Hunt and Dr. Hui report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PEDIATRIC ALLERGY IMMUNOLOGY
Women can safely interrupt endocrine therapy to pursue pregnancy
without affecting their short-term disease outcomes, suggest results from the prospective POSITIVE trial.
The study involved more than 500 premenopausal women from 20 countries who had received at least 18 months of endocrine therapy for HR+ breast cancer. After a 3-month washout, they were given 2 years to conceive, deliver, and breastfeed a baby before resuming treatment.
Crucially, taking a treatment break had no impact on recurrence rates, with the 3-year breast cancer–free interval (BCFI) failure rate of nearly 9% comparing favorably with historical controls.
Moreover, almost three-quarters of women achieved at least one pregnancy, the majority within 2 years, and the vast majority had resumed endocrine therapy by the end of the study period.
The research was presented at the San Antonio Breast Cancer Symposium.
“These data stress the need to incorporate patient-centered reproductive health care, treatments, and choices in the treatment and follow-up of our young women with breast cancer so that they can not only survive, but thrive in their survivorship,” said study presenter Ann Partridge, MD, MPH, vice chair of medical oncology at Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, both in Boston.
She noted, however, that the results so far are from a 3-year follow-up. The team now plans on following the women for “at least a decade ... to monitor for independent therapy resumption, and disease outcomes, because of course there is great concern about the late return” of HR+ breast cancer.
This point was also raised by Marleen I. Meyers, MD, a medical oncologist New York University Langone Perlmutter Cancer Center, who was not involved in the study. While she praised the study as offering the “first real evidence” that treatment can be interrupted safely, she said she would be “cautious, as the follow-up is short and we know that hormone positive breast cancer can recur within 10 years of diagnosis and beyond.”
Meyer also emphasized that “the potential loss of fertility and ability to have biologic children ... [is] one of the most devastating results for young women with breast cancer.”
“We have come a long way with fertility preservation,” Dr. Meyers continued, but waiting to complete the recommended 5-10 years of endocrine therapy “makes the possibility of carrying a child less realistic.”
“This study offers hope for some women with hormone receptor–positive breast cancer to be able to interrupt cancer treatment and still have good outcomes,” she said.
Dr. Partridge said that “women are often discouraged” from becoming pregnant, in addition to which giving adjuvant endocrine therapy for the standard 5-10 years “compromises conception” in women with HR+ disease.
POSITIVE was a single-arm trial involving premenopausal women aged up to 42 years at study entry. They were required to have undergone at least 18 months and no more than 30 months of adjuvant endocrine therapy for stage I-III HR+ breast cancer, with no clinical evidence of recurrence. The women could also have undergone prior neoadjuvant chemotherapy with or without fertility preservation.
Women halted endocrine therapy within 1 month of trial enrollment and then underwent a 3-month washout period before having up to 2 years to attempt pregnancy, and to conceive, give birth to, and breastfeed a baby. They were then “strongly recommended” to resume endocrine therapy to complete the planned 5-10 years of treatment, with follow-up planned for up to 10 years.
In all, 518 women were enrolled at 116 centers in 20 countries on four continents, of whom 516 were available for the primary efficacy analysis. The median time from breast cancer diagnosis to enrollment was 29 months.
The median age of the participants at enrollment was 37 years, and 75% had no prior births. Stage I or II disease was diagnosed in 93%. The median duration of endocrine therapy prior to enrollment was 23.4 months.
Selective estrogen receptor modulators were given alone in 42% of patients, while 36% had a SERM plus ovarian function suppression. A further 16% of women received an aromatase inhibitor alongside ovarian function suppression. The majority (62%) of women had received prior neoadjuvant chemotherapy.
The primary endpoint of 3-year BCFI was measured after a median follow-up of 41 months. There were 44 events, with a 3-year BCFI failure rate of 8.9%. The 3-year distant recurrence–free interval (DRFI) failure rate was calculated at 4.5%, with 22 events.
To provide an external control, the researchers examined data from the SOFT and TEXT trials to assemble a cohort of 1,499 women balanced for patient, disease, and treatment characteristics.
This revealed no significant differences in BCFI between the two groups (hazard ratio, 0.81; 95% confidence interval, 0.57-1.15) and a difference in BCFI rates at 3 years of 0.2% between the SOFT, TEXT, and POSITIVE trials.
There was also no significant difference in DRFI rates (HR, 0.70; 95% CI, 0.44-1.12), with a 3-year rate difference of 1.4%.
For the secondary endpoint analysis, the team included 497 women from the POSITIVE cohort, of whom 368 (74%) had at least one pregnancy, giving a total of 507 pregnancies. At least one live birth was recorded in 64% of the women, or 86% of those who became pregnant.
Dr. Partridge noted that around 43% of women used some form of assisted reproductive technology at some point during the study period.
Pregnancy complications were observed in 11% of pregnancies, the most common of which were hypertension/preeclampsia in 3%, and diabetes in 2%.
There were a total of 350 live births in 317 women, including 335 singleton births and 15 sets of twins. Only 8% of the offspring had a low birth weight, and 2% had a birth defect. Breastfeeding was reported by 62% of women.
Conducting an 18-month landmark analysis, the team found that pregnancy did not increase BCFI rates, at an HR versus nonpregnant women of 0.53 after controlling for age, body mass index, lymph node status, prior chemotherapy, and prior aromatase inhibitor therapy.
At 48 months of follow-up, 76% of women had resumed endocrine therapy. A further 8% of women had cancer recurrence or death before they could restart therapy, while 15% had not yet resumed treatment for other reasons.
Among disease-free women who had not resumed endocrine therapy, 79% reported at their most recent follow-up continuing to pursue pregnancy, having an active or recent pregnancy, or continuing to breastfeed as the reason.
Commenting on the study, Jennifer K. Litton, MD, vice president of clinical research at University of Texas MD Anderson Cancer Center, Houston, said that this was a “challenging study to design and execute.”
“It gives us really a first look into the safety of a practice that was already happening,” she commented, and emphasized that the interruption of treatment to pursue pregnancy remains “an exceptionally individual decision.”
Dr. Litton also underlined that these results apply only to endocrine therapy and not to women on other therapies such as abemaciclib, for example, for which the course should be “fully completed” before considering any treatment interruptions.
She added more generally that “we need to continue to improve discussing fertility concerns with our breast cancer patients who want future pregnancies.”
The study was sponsored and conducted by the International Breast Cancer Study Group, a division of ETOP IBCSG Partners Foundation, and by the Alliance for Clinical Trials in Oncology in North America, in collaboration with the Breast International Group. Dr. Partridge and Dr. Litton reported no relevant relationships.
A version of this article first appeared on Medscape.com.
without affecting their short-term disease outcomes, suggest results from the prospective POSITIVE trial.
The study involved more than 500 premenopausal women from 20 countries who had received at least 18 months of endocrine therapy for HR+ breast cancer. After a 3-month washout, they were given 2 years to conceive, deliver, and breastfeed a baby before resuming treatment.
Crucially, taking a treatment break had no impact on recurrence rates, with the 3-year breast cancer–free interval (BCFI) failure rate of nearly 9% comparing favorably with historical controls.
Moreover, almost three-quarters of women achieved at least one pregnancy, the majority within 2 years, and the vast majority had resumed endocrine therapy by the end of the study period.
The research was presented at the San Antonio Breast Cancer Symposium.
“These data stress the need to incorporate patient-centered reproductive health care, treatments, and choices in the treatment and follow-up of our young women with breast cancer so that they can not only survive, but thrive in their survivorship,” said study presenter Ann Partridge, MD, MPH, vice chair of medical oncology at Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, both in Boston.
She noted, however, that the results so far are from a 3-year follow-up. The team now plans on following the women for “at least a decade ... to monitor for independent therapy resumption, and disease outcomes, because of course there is great concern about the late return” of HR+ breast cancer.
This point was also raised by Marleen I. Meyers, MD, a medical oncologist New York University Langone Perlmutter Cancer Center, who was not involved in the study. While she praised the study as offering the “first real evidence” that treatment can be interrupted safely, she said she would be “cautious, as the follow-up is short and we know that hormone positive breast cancer can recur within 10 years of diagnosis and beyond.”
Meyer also emphasized that “the potential loss of fertility and ability to have biologic children ... [is] one of the most devastating results for young women with breast cancer.”
“We have come a long way with fertility preservation,” Dr. Meyers continued, but waiting to complete the recommended 5-10 years of endocrine therapy “makes the possibility of carrying a child less realistic.”
“This study offers hope for some women with hormone receptor–positive breast cancer to be able to interrupt cancer treatment and still have good outcomes,” she said.
Dr. Partridge said that “women are often discouraged” from becoming pregnant, in addition to which giving adjuvant endocrine therapy for the standard 5-10 years “compromises conception” in women with HR+ disease.
POSITIVE was a single-arm trial involving premenopausal women aged up to 42 years at study entry. They were required to have undergone at least 18 months and no more than 30 months of adjuvant endocrine therapy for stage I-III HR+ breast cancer, with no clinical evidence of recurrence. The women could also have undergone prior neoadjuvant chemotherapy with or without fertility preservation.
Women halted endocrine therapy within 1 month of trial enrollment and then underwent a 3-month washout period before having up to 2 years to attempt pregnancy, and to conceive, give birth to, and breastfeed a baby. They were then “strongly recommended” to resume endocrine therapy to complete the planned 5-10 years of treatment, with follow-up planned for up to 10 years.
In all, 518 women were enrolled at 116 centers in 20 countries on four continents, of whom 516 were available for the primary efficacy analysis. The median time from breast cancer diagnosis to enrollment was 29 months.
The median age of the participants at enrollment was 37 years, and 75% had no prior births. Stage I or II disease was diagnosed in 93%. The median duration of endocrine therapy prior to enrollment was 23.4 months.
Selective estrogen receptor modulators were given alone in 42% of patients, while 36% had a SERM plus ovarian function suppression. A further 16% of women received an aromatase inhibitor alongside ovarian function suppression. The majority (62%) of women had received prior neoadjuvant chemotherapy.
The primary endpoint of 3-year BCFI was measured after a median follow-up of 41 months. There were 44 events, with a 3-year BCFI failure rate of 8.9%. The 3-year distant recurrence–free interval (DRFI) failure rate was calculated at 4.5%, with 22 events.
To provide an external control, the researchers examined data from the SOFT and TEXT trials to assemble a cohort of 1,499 women balanced for patient, disease, and treatment characteristics.
This revealed no significant differences in BCFI between the two groups (hazard ratio, 0.81; 95% confidence interval, 0.57-1.15) and a difference in BCFI rates at 3 years of 0.2% between the SOFT, TEXT, and POSITIVE trials.
There was also no significant difference in DRFI rates (HR, 0.70; 95% CI, 0.44-1.12), with a 3-year rate difference of 1.4%.
For the secondary endpoint analysis, the team included 497 women from the POSITIVE cohort, of whom 368 (74%) had at least one pregnancy, giving a total of 507 pregnancies. At least one live birth was recorded in 64% of the women, or 86% of those who became pregnant.
Dr. Partridge noted that around 43% of women used some form of assisted reproductive technology at some point during the study period.
Pregnancy complications were observed in 11% of pregnancies, the most common of which were hypertension/preeclampsia in 3%, and diabetes in 2%.
There were a total of 350 live births in 317 women, including 335 singleton births and 15 sets of twins. Only 8% of the offspring had a low birth weight, and 2% had a birth defect. Breastfeeding was reported by 62% of women.
Conducting an 18-month landmark analysis, the team found that pregnancy did not increase BCFI rates, at an HR versus nonpregnant women of 0.53 after controlling for age, body mass index, lymph node status, prior chemotherapy, and prior aromatase inhibitor therapy.
At 48 months of follow-up, 76% of women had resumed endocrine therapy. A further 8% of women had cancer recurrence or death before they could restart therapy, while 15% had not yet resumed treatment for other reasons.
Among disease-free women who had not resumed endocrine therapy, 79% reported at their most recent follow-up continuing to pursue pregnancy, having an active or recent pregnancy, or continuing to breastfeed as the reason.
Commenting on the study, Jennifer K. Litton, MD, vice president of clinical research at University of Texas MD Anderson Cancer Center, Houston, said that this was a “challenging study to design and execute.”
“It gives us really a first look into the safety of a practice that was already happening,” she commented, and emphasized that the interruption of treatment to pursue pregnancy remains “an exceptionally individual decision.”
Dr. Litton also underlined that these results apply only to endocrine therapy and not to women on other therapies such as abemaciclib, for example, for which the course should be “fully completed” before considering any treatment interruptions.
She added more generally that “we need to continue to improve discussing fertility concerns with our breast cancer patients who want future pregnancies.”
The study was sponsored and conducted by the International Breast Cancer Study Group, a division of ETOP IBCSG Partners Foundation, and by the Alliance for Clinical Trials in Oncology in North America, in collaboration with the Breast International Group. Dr. Partridge and Dr. Litton reported no relevant relationships.
A version of this article first appeared on Medscape.com.
without affecting their short-term disease outcomes, suggest results from the prospective POSITIVE trial.
The study involved more than 500 premenopausal women from 20 countries who had received at least 18 months of endocrine therapy for HR+ breast cancer. After a 3-month washout, they were given 2 years to conceive, deliver, and breastfeed a baby before resuming treatment.
Crucially, taking a treatment break had no impact on recurrence rates, with the 3-year breast cancer–free interval (BCFI) failure rate of nearly 9% comparing favorably with historical controls.
Moreover, almost three-quarters of women achieved at least one pregnancy, the majority within 2 years, and the vast majority had resumed endocrine therapy by the end of the study period.
The research was presented at the San Antonio Breast Cancer Symposium.
“These data stress the need to incorporate patient-centered reproductive health care, treatments, and choices in the treatment and follow-up of our young women with breast cancer so that they can not only survive, but thrive in their survivorship,” said study presenter Ann Partridge, MD, MPH, vice chair of medical oncology at Dana-Farber Cancer Institute and professor of medicine at Harvard Medical School, both in Boston.
She noted, however, that the results so far are from a 3-year follow-up. The team now plans on following the women for “at least a decade ... to monitor for independent therapy resumption, and disease outcomes, because of course there is great concern about the late return” of HR+ breast cancer.
This point was also raised by Marleen I. Meyers, MD, a medical oncologist New York University Langone Perlmutter Cancer Center, who was not involved in the study. While she praised the study as offering the “first real evidence” that treatment can be interrupted safely, she said she would be “cautious, as the follow-up is short and we know that hormone positive breast cancer can recur within 10 years of diagnosis and beyond.”
Meyer also emphasized that “the potential loss of fertility and ability to have biologic children ... [is] one of the most devastating results for young women with breast cancer.”
“We have come a long way with fertility preservation,” Dr. Meyers continued, but waiting to complete the recommended 5-10 years of endocrine therapy “makes the possibility of carrying a child less realistic.”
“This study offers hope for some women with hormone receptor–positive breast cancer to be able to interrupt cancer treatment and still have good outcomes,” she said.
Dr. Partridge said that “women are often discouraged” from becoming pregnant, in addition to which giving adjuvant endocrine therapy for the standard 5-10 years “compromises conception” in women with HR+ disease.
POSITIVE was a single-arm trial involving premenopausal women aged up to 42 years at study entry. They were required to have undergone at least 18 months and no more than 30 months of adjuvant endocrine therapy for stage I-III HR+ breast cancer, with no clinical evidence of recurrence. The women could also have undergone prior neoadjuvant chemotherapy with or without fertility preservation.
Women halted endocrine therapy within 1 month of trial enrollment and then underwent a 3-month washout period before having up to 2 years to attempt pregnancy, and to conceive, give birth to, and breastfeed a baby. They were then “strongly recommended” to resume endocrine therapy to complete the planned 5-10 years of treatment, with follow-up planned for up to 10 years.
In all, 518 women were enrolled at 116 centers in 20 countries on four continents, of whom 516 were available for the primary efficacy analysis. The median time from breast cancer diagnosis to enrollment was 29 months.
The median age of the participants at enrollment was 37 years, and 75% had no prior births. Stage I or II disease was diagnosed in 93%. The median duration of endocrine therapy prior to enrollment was 23.4 months.
Selective estrogen receptor modulators were given alone in 42% of patients, while 36% had a SERM plus ovarian function suppression. A further 16% of women received an aromatase inhibitor alongside ovarian function suppression. The majority (62%) of women had received prior neoadjuvant chemotherapy.
The primary endpoint of 3-year BCFI was measured after a median follow-up of 41 months. There were 44 events, with a 3-year BCFI failure rate of 8.9%. The 3-year distant recurrence–free interval (DRFI) failure rate was calculated at 4.5%, with 22 events.
To provide an external control, the researchers examined data from the SOFT and TEXT trials to assemble a cohort of 1,499 women balanced for patient, disease, and treatment characteristics.
This revealed no significant differences in BCFI between the two groups (hazard ratio, 0.81; 95% confidence interval, 0.57-1.15) and a difference in BCFI rates at 3 years of 0.2% between the SOFT, TEXT, and POSITIVE trials.
There was also no significant difference in DRFI rates (HR, 0.70; 95% CI, 0.44-1.12), with a 3-year rate difference of 1.4%.
For the secondary endpoint analysis, the team included 497 women from the POSITIVE cohort, of whom 368 (74%) had at least one pregnancy, giving a total of 507 pregnancies. At least one live birth was recorded in 64% of the women, or 86% of those who became pregnant.
Dr. Partridge noted that around 43% of women used some form of assisted reproductive technology at some point during the study period.
Pregnancy complications were observed in 11% of pregnancies, the most common of which were hypertension/preeclampsia in 3%, and diabetes in 2%.
There were a total of 350 live births in 317 women, including 335 singleton births and 15 sets of twins. Only 8% of the offspring had a low birth weight, and 2% had a birth defect. Breastfeeding was reported by 62% of women.
Conducting an 18-month landmark analysis, the team found that pregnancy did not increase BCFI rates, at an HR versus nonpregnant women of 0.53 after controlling for age, body mass index, lymph node status, prior chemotherapy, and prior aromatase inhibitor therapy.
At 48 months of follow-up, 76% of women had resumed endocrine therapy. A further 8% of women had cancer recurrence or death before they could restart therapy, while 15% had not yet resumed treatment for other reasons.
Among disease-free women who had not resumed endocrine therapy, 79% reported at their most recent follow-up continuing to pursue pregnancy, having an active or recent pregnancy, or continuing to breastfeed as the reason.
Commenting on the study, Jennifer K. Litton, MD, vice president of clinical research at University of Texas MD Anderson Cancer Center, Houston, said that this was a “challenging study to design and execute.”
“It gives us really a first look into the safety of a practice that was already happening,” she commented, and emphasized that the interruption of treatment to pursue pregnancy remains “an exceptionally individual decision.”
Dr. Litton also underlined that these results apply only to endocrine therapy and not to women on other therapies such as abemaciclib, for example, for which the course should be “fully completed” before considering any treatment interruptions.
She added more generally that “we need to continue to improve discussing fertility concerns with our breast cancer patients who want future pregnancies.”
The study was sponsored and conducted by the International Breast Cancer Study Group, a division of ETOP IBCSG Partners Foundation, and by the Alliance for Clinical Trials in Oncology in North America, in collaboration with the Breast International Group. Dr. Partridge and Dr. Litton reported no relevant relationships.
A version of this article first appeared on Medscape.com.
FROM SABCS 2022
Key research on TNBC: Top five picks from SABCS
SAN ANTONIO – While , research highlighting new findings in triple-negative breast cancer (TNBC) stood out as well.
This news organization spoke with SABCS program director Virginia Kaklamani, MD, leader of the Breast Cancer Program at UT Health, San Antonio, and Kevin Kalinsky, MD, a medical oncologist and director of the Glenn Family Breast Center at the Winship Cancer Institute of Emory University in Atlanta, about the TNBC data that caught their eye and what the findings could mean for clinical practice.
1. Carboplatin for TNBC
Dr. Kalinsky’s first pick was a study on the impact of platinum therapy on long-term TNBC outcomes.
The phase 3 randomized controlled trial, presented in general session (GS) 5-01, explored whether adding carboplatin to sequential taxane-anthracycline neoadjuvant chemotherapy for patients with TNBC improved disease-free survival, pathologic complete response, or overall survival.
Overall, 365 patients received carboplatin, and 355 did not. At a median follow-up of 67.6 months, the 5-year disease-free survival rate was 70.6% in the carboplatin group vs. 64.5% in the control arm (hazard ratio, 0.79); the 5-year overall survival was also higher in the carboplatin group (74.0% vs. 66.7%; HR, 0.75). Pathologic complete response occurred in 55.2% of carboplatin patients, vs. 41.5% of control patients.
“These results are important,” Dr. Kalinsky said. “The results of this study suggest that there is a benefit to the TNBC population from being treated with carboplatin.”
Dr. Kalinsky cautioned, however, that despite the encouraging results, it remains unclear whether there is a specific biomarker for selecting patients who may derive the most benefit from treatment with carboplatin. “This remains an outstanding question,” he said.
2. Risk of contralateral breast cancer
Women with breast cancer who have germline pathogenic variants in BRCA1, BRCA2, CHEK2, or PALB2 had nearly double the risk of contralateral breast cancer in comparison with patients without those variants, according to recent data presented at the meeting (GS4-04).
Researchers estimated the risk of contralateral breast cancer in women with pathogenic variants in comparison with control patients. They found that having ATM does not increase this risk.
“The reason this study is important is that many women with these mutations want to have a bilateral mastectomy, but thus far, the data have been unclear, and the question is, are they going to benefit from having a bilateral mastectomy?” said Dr. Kaklamani. “The results of this study help shine a light on what mutations might warrant a bilateral mastectomy. Most of these patients are going to be triple negative.”
Hal Burstein, MD, also weighed in, saying the “data should allow many to avoid prophylactic mastectomy.”
3. Cemiplimab plus LAG-3 inhibitor in TNBC
Another session that caught Dr. Kalinsky’s attention explored results from the I-SPY2 trial (GS5-03), which evaluated the use of the checkpoint inhibitior cemiplimab in combination with LAG-3 inhibitor REGN3767 for patients with early-stage, high-risk, HER2-negative breast cancer.
Among the 73 patients with HER2-negative disease who received cemiplimab plus REGN3767, 33 had TNBC. The control group included 357 patients with HER2-negative tumors, of whom 156 had TNBC. Overall, the combination of a LAG-3 and anti-PD1 inhibitor resulted in a pathologic complete response rate of 60% for patients with TNBC and 37% for patients with HR-positive disease.
“We know that checkpoint inhibitors benefit patients with TNBC, and there has been a lot of interest in looking beyond checkpoint inhibition,” said Dr. Kalinsky, who is a coinvestigator on the I-SPY trial. “LAG-3 has been a target of interest, and this is the first study looking in the neoadjuvant setting of giving a LAG-3 inhibitor along with a checkpoint inhibitor.”
4. Efficacy vs. side effect profile of cemiplimab
Taking adverse events of immune checkpoint inhibitors into account is also important. Dr. Kalinsky and colleagues presented research on the efficacy as well as the side-effect profile associated with cemiplimab (PD11-01) among patients in the I-SPY trial.
Overall, cemiplimab was associated with a higher pathologic complete response rate for patients with TNBC (55%), compared with control patients who received paclitaxel followed by doxorubicin/cyclophosphamide (29%). The rate of immune-related adverse events was higher in the cemiplimab group: hypothyroidism, 3% vs. 0%; adrenal insufficiency, 6% vs. 0%; hyperthyroid, 8% vs. 0%; and thyroiditis, 3% vs. 0%. However, only one case of grade 3 adrenal insufficiency occurred in the cemiplimab arm.
“I really think the key takeaway is not just the efficacy that is seen in the HER2-negative population but also what the side-effect profile is going to be,” Dr. Kalinsky said.
5. Olaparib or carboplatinum?
Dr. Kaklamani highlighted data from the GeparOLA study (GS5-02), which evaluated the efficacy and safety of using olaparib instead of carboplatinum along with paclitaxel as neoadjuvant chemotherapy in early-stage HER2-negative breast cancer.
The results of the study indicate that among patients in the cohort with HER2-negative homologous recombination deficiency tumors – those with a g/tBRCA mutation – the two groups had similar pathologic complete responses. Overall, patients in the olaparib group had more invasive disease-free survival events (15 vs. 3), more distant disease-free survival events (11 vs. 2), and more deaths (6 vs. 1). However, when comparing patients with a g/tBRCA mutation, outcomes were comparable in both arms.
“The majority of these patients were triple negative, and I think the importance here is that this [study] shows us whether we should be adding olaparib in some patients who have a homologous recombination deficiency,” Dr. Kaklamani said.
A version of this article first appeared on Medscape.com.
SAN ANTONIO – While , research highlighting new findings in triple-negative breast cancer (TNBC) stood out as well.
This news organization spoke with SABCS program director Virginia Kaklamani, MD, leader of the Breast Cancer Program at UT Health, San Antonio, and Kevin Kalinsky, MD, a medical oncologist and director of the Glenn Family Breast Center at the Winship Cancer Institute of Emory University in Atlanta, about the TNBC data that caught their eye and what the findings could mean for clinical practice.
1. Carboplatin for TNBC
Dr. Kalinsky’s first pick was a study on the impact of platinum therapy on long-term TNBC outcomes.
The phase 3 randomized controlled trial, presented in general session (GS) 5-01, explored whether adding carboplatin to sequential taxane-anthracycline neoadjuvant chemotherapy for patients with TNBC improved disease-free survival, pathologic complete response, or overall survival.
Overall, 365 patients received carboplatin, and 355 did not. At a median follow-up of 67.6 months, the 5-year disease-free survival rate was 70.6% in the carboplatin group vs. 64.5% in the control arm (hazard ratio, 0.79); the 5-year overall survival was also higher in the carboplatin group (74.0% vs. 66.7%; HR, 0.75). Pathologic complete response occurred in 55.2% of carboplatin patients, vs. 41.5% of control patients.
“These results are important,” Dr. Kalinsky said. “The results of this study suggest that there is a benefit to the TNBC population from being treated with carboplatin.”
Dr. Kalinsky cautioned, however, that despite the encouraging results, it remains unclear whether there is a specific biomarker for selecting patients who may derive the most benefit from treatment with carboplatin. “This remains an outstanding question,” he said.
2. Risk of contralateral breast cancer
Women with breast cancer who have germline pathogenic variants in BRCA1, BRCA2, CHEK2, or PALB2 had nearly double the risk of contralateral breast cancer in comparison with patients without those variants, according to recent data presented at the meeting (GS4-04).
Researchers estimated the risk of contralateral breast cancer in women with pathogenic variants in comparison with control patients. They found that having ATM does not increase this risk.
“The reason this study is important is that many women with these mutations want to have a bilateral mastectomy, but thus far, the data have been unclear, and the question is, are they going to benefit from having a bilateral mastectomy?” said Dr. Kaklamani. “The results of this study help shine a light on what mutations might warrant a bilateral mastectomy. Most of these patients are going to be triple negative.”
Hal Burstein, MD, also weighed in, saying the “data should allow many to avoid prophylactic mastectomy.”
3. Cemiplimab plus LAG-3 inhibitor in TNBC
Another session that caught Dr. Kalinsky’s attention explored results from the I-SPY2 trial (GS5-03), which evaluated the use of the checkpoint inhibitior cemiplimab in combination with LAG-3 inhibitor REGN3767 for patients with early-stage, high-risk, HER2-negative breast cancer.
Among the 73 patients with HER2-negative disease who received cemiplimab plus REGN3767, 33 had TNBC. The control group included 357 patients with HER2-negative tumors, of whom 156 had TNBC. Overall, the combination of a LAG-3 and anti-PD1 inhibitor resulted in a pathologic complete response rate of 60% for patients with TNBC and 37% for patients with HR-positive disease.
“We know that checkpoint inhibitors benefit patients with TNBC, and there has been a lot of interest in looking beyond checkpoint inhibition,” said Dr. Kalinsky, who is a coinvestigator on the I-SPY trial. “LAG-3 has been a target of interest, and this is the first study looking in the neoadjuvant setting of giving a LAG-3 inhibitor along with a checkpoint inhibitor.”
4. Efficacy vs. side effect profile of cemiplimab
Taking adverse events of immune checkpoint inhibitors into account is also important. Dr. Kalinsky and colleagues presented research on the efficacy as well as the side-effect profile associated with cemiplimab (PD11-01) among patients in the I-SPY trial.
Overall, cemiplimab was associated with a higher pathologic complete response rate for patients with TNBC (55%), compared with control patients who received paclitaxel followed by doxorubicin/cyclophosphamide (29%). The rate of immune-related adverse events was higher in the cemiplimab group: hypothyroidism, 3% vs. 0%; adrenal insufficiency, 6% vs. 0%; hyperthyroid, 8% vs. 0%; and thyroiditis, 3% vs. 0%. However, only one case of grade 3 adrenal insufficiency occurred in the cemiplimab arm.
“I really think the key takeaway is not just the efficacy that is seen in the HER2-negative population but also what the side-effect profile is going to be,” Dr. Kalinsky said.
5. Olaparib or carboplatinum?
Dr. Kaklamani highlighted data from the GeparOLA study (GS5-02), which evaluated the efficacy and safety of using olaparib instead of carboplatinum along with paclitaxel as neoadjuvant chemotherapy in early-stage HER2-negative breast cancer.
The results of the study indicate that among patients in the cohort with HER2-negative homologous recombination deficiency tumors – those with a g/tBRCA mutation – the two groups had similar pathologic complete responses. Overall, patients in the olaparib group had more invasive disease-free survival events (15 vs. 3), more distant disease-free survival events (11 vs. 2), and more deaths (6 vs. 1). However, when comparing patients with a g/tBRCA mutation, outcomes were comparable in both arms.
“The majority of these patients were triple negative, and I think the importance here is that this [study] shows us whether we should be adding olaparib in some patients who have a homologous recombination deficiency,” Dr. Kaklamani said.
A version of this article first appeared on Medscape.com.
SAN ANTONIO – While , research highlighting new findings in triple-negative breast cancer (TNBC) stood out as well.
This news organization spoke with SABCS program director Virginia Kaklamani, MD, leader of the Breast Cancer Program at UT Health, San Antonio, and Kevin Kalinsky, MD, a medical oncologist and director of the Glenn Family Breast Center at the Winship Cancer Institute of Emory University in Atlanta, about the TNBC data that caught their eye and what the findings could mean for clinical practice.
1. Carboplatin for TNBC
Dr. Kalinsky’s first pick was a study on the impact of platinum therapy on long-term TNBC outcomes.
The phase 3 randomized controlled trial, presented in general session (GS) 5-01, explored whether adding carboplatin to sequential taxane-anthracycline neoadjuvant chemotherapy for patients with TNBC improved disease-free survival, pathologic complete response, or overall survival.
Overall, 365 patients received carboplatin, and 355 did not. At a median follow-up of 67.6 months, the 5-year disease-free survival rate was 70.6% in the carboplatin group vs. 64.5% in the control arm (hazard ratio, 0.79); the 5-year overall survival was also higher in the carboplatin group (74.0% vs. 66.7%; HR, 0.75). Pathologic complete response occurred in 55.2% of carboplatin patients, vs. 41.5% of control patients.
“These results are important,” Dr. Kalinsky said. “The results of this study suggest that there is a benefit to the TNBC population from being treated with carboplatin.”
Dr. Kalinsky cautioned, however, that despite the encouraging results, it remains unclear whether there is a specific biomarker for selecting patients who may derive the most benefit from treatment with carboplatin. “This remains an outstanding question,” he said.
2. Risk of contralateral breast cancer
Women with breast cancer who have germline pathogenic variants in BRCA1, BRCA2, CHEK2, or PALB2 had nearly double the risk of contralateral breast cancer in comparison with patients without those variants, according to recent data presented at the meeting (GS4-04).
Researchers estimated the risk of contralateral breast cancer in women with pathogenic variants in comparison with control patients. They found that having ATM does not increase this risk.
“The reason this study is important is that many women with these mutations want to have a bilateral mastectomy, but thus far, the data have been unclear, and the question is, are they going to benefit from having a bilateral mastectomy?” said Dr. Kaklamani. “The results of this study help shine a light on what mutations might warrant a bilateral mastectomy. Most of these patients are going to be triple negative.”
Hal Burstein, MD, also weighed in, saying the “data should allow many to avoid prophylactic mastectomy.”
3. Cemiplimab plus LAG-3 inhibitor in TNBC
Another session that caught Dr. Kalinsky’s attention explored results from the I-SPY2 trial (GS5-03), which evaluated the use of the checkpoint inhibitior cemiplimab in combination with LAG-3 inhibitor REGN3767 for patients with early-stage, high-risk, HER2-negative breast cancer.
Among the 73 patients with HER2-negative disease who received cemiplimab plus REGN3767, 33 had TNBC. The control group included 357 patients with HER2-negative tumors, of whom 156 had TNBC. Overall, the combination of a LAG-3 and anti-PD1 inhibitor resulted in a pathologic complete response rate of 60% for patients with TNBC and 37% for patients with HR-positive disease.
“We know that checkpoint inhibitors benefit patients with TNBC, and there has been a lot of interest in looking beyond checkpoint inhibition,” said Dr. Kalinsky, who is a coinvestigator on the I-SPY trial. “LAG-3 has been a target of interest, and this is the first study looking in the neoadjuvant setting of giving a LAG-3 inhibitor along with a checkpoint inhibitor.”
4. Efficacy vs. side effect profile of cemiplimab
Taking adverse events of immune checkpoint inhibitors into account is also important. Dr. Kalinsky and colleagues presented research on the efficacy as well as the side-effect profile associated with cemiplimab (PD11-01) among patients in the I-SPY trial.
Overall, cemiplimab was associated with a higher pathologic complete response rate for patients with TNBC (55%), compared with control patients who received paclitaxel followed by doxorubicin/cyclophosphamide (29%). The rate of immune-related adverse events was higher in the cemiplimab group: hypothyroidism, 3% vs. 0%; adrenal insufficiency, 6% vs. 0%; hyperthyroid, 8% vs. 0%; and thyroiditis, 3% vs. 0%. However, only one case of grade 3 adrenal insufficiency occurred in the cemiplimab arm.
“I really think the key takeaway is not just the efficacy that is seen in the HER2-negative population but also what the side-effect profile is going to be,” Dr. Kalinsky said.
5. Olaparib or carboplatinum?
Dr. Kaklamani highlighted data from the GeparOLA study (GS5-02), which evaluated the efficacy and safety of using olaparib instead of carboplatinum along with paclitaxel as neoadjuvant chemotherapy in early-stage HER2-negative breast cancer.
The results of the study indicate that among patients in the cohort with HER2-negative homologous recombination deficiency tumors – those with a g/tBRCA mutation – the two groups had similar pathologic complete responses. Overall, patients in the olaparib group had more invasive disease-free survival events (15 vs. 3), more distant disease-free survival events (11 vs. 2), and more deaths (6 vs. 1). However, when comparing patients with a g/tBRCA mutation, outcomes were comparable in both arms.
“The majority of these patients were triple negative, and I think the importance here is that this [study] shows us whether we should be adding olaparib in some patients who have a homologous recombination deficiency,” Dr. Kaklamani said.
A version of this article first appeared on Medscape.com.
AT SABCS 2022