User login
Infectious disease fellowship matches nose-dive after pandemic bump
Just 56% of infectious disease fellowship programs filled their 2023 slots, according to new data released by the National Resident Matching Program. Infectious disease (ID) fellowships had seen a jump in applications in the previous 2 years, but these new numbers may suggest a backward slide in a specialty that for many years has struggled to recruit residents.
There are unfilled positions across the country, including in health care hot spots. In Boston, all three slots at Boston Medical Center ID fellowship program are currently empty.
“For our program, going unfilled is a pretty rare event,” said Daniel Bourque, MD, an assistant professor of infectious disease at Boston University and director of the program. “For a program in the city of Boston that’s at a large tertiary care center, that definitely was a big surprise.”
Many other ID fellowships have joined BMC in posting about their vacancies on social media, looking for residents who may not have matched in other fellowships and for physicians who initially decided not to pursue additional training but are now reconsidering.
“If you are interested in a career in this exciting field, in the amazing city of Seattle, with incredible and friendly colleagues, please contact us,” the University of Washington’s ID fellowship program tweeted. Tulane University, Creighton University, the University of Connecticut, Washington University in St. Louis, and the University of Colorado also advertised their unfilled positions.
Other ID doctors commiserated with the disappointing match year. “I made a new riddle after yesterday’s match results: In the hospital, everyone needs me. Yet, no one wants to be me. What am I? An ID doctor,” tweeted Nathan Nolan, MD, MPH, an infectious disease specialist at the Veterans Health Administration in St. Louis.
Infectious disease positions continue to grow
One contributor to this downturn could be the growing number of infectious disease programs offered, whereas the number of applicants has generally remained stable. In 2018, there were 394 slots at 151 infectious disease fellowship programs offered. For the 2023 match year, there were 441 slots at 175 programs.
At the same time, there has not been a notable rise in applicants. From match years 2018 to 2020, about 320 applicants applied for ID fellowship positions each year. There was a rise in in interest in first 2 years of the pandemic, with 404 and 387 applicants in the 2021 and 2022 match years, respectively. The most recent round suggests a return to prepandemic numbers, with 330 residents applying to ID programs.
“I think it’s fair to question whether, as a field, we should be increasing training programs and spots at this point, and if it’s better to focus on ways to increase interest and demand,” said Daniel Diekema, MD, an ID physician at Maine Medical Center in Portland. “Otherwise, we’re just going to look worse and worse every year,” he added, and the work that goes into creating these training opportunities will not have a return on investment.
More training, less pay
The fellowship recruitment issues combined with an already short supply of infectious disease specialists can be traced back to comparatively worse pay compared with other subspecialties, experts say. Infectious disease was the fifth lowest paid specialty in the 2022 Medscape Physician Compensation Report – ranking above only primary care specialties and diabetes and endocrinology.
Pursuing this subspeciality in medicine may not translate to higher pay, Dr. Diekema noted. For example, a physician who completes an internal medicine residency and then a 2- to 3-year infectious disease fellowship can make less than a physician who pursues hospital medicine directly after completing the same residency.
“You’re in a situation where you’re doing additional training to reduce your income earning potential, and that’s a very hard sales pitch to make,” he said. It’s become more difficult as student loan debts continue to increase, he added.
Because infectious disease is a cognitive specialty and does not perform procedures, it is at a disadvantage in a typical fee-for-service pay model. ID physicians also advise on hospital policies for testing and personal protective equipment, which is not always compensated, said Wendy Armstrong, MD, a professor of infectious diseases at Emory University, Atlanta.
A reflection of pandemic burnout?
Experts also wonder if the past 2 years of the pandemic and the notable burnout in ID and other in-demand specialties may have dissuaded applicants from pursuing the ID career path.
“This residency class is the class that started their training in June or July of 2020 and represent that residency class that has trained throughout the pandemic,” Dr. Bourque said. “Does [this low match rate] reflect a negative outlook on the field of ID because of COVID? Is it a reflection of trainee burnout in the setting of the pandemic?”
Dr. Diekema wonders if increased public scrutiny and politicization of the field may have discouraged residents. “The vilification of public health and [of] infectious disease experts like Dr. Fauci by significant portions of our society can be demoralizing,” he said. “People might say, ‘Why would I want to put myself through that?’ ”
But Dr. Armstrong doubts this is the case. “I’ve never had a resident tell me that was on their radar screen,” she said, noting that while there had been recent improvements in applicants, lower match numbers for ID fellowships have been a long-standing issue.
Rethinking reimbursement
Experts agree that pay issues need to be addressed to make ID a more attractive specialty. Moving away from traditional payment plans to value-based models using quality measurements specific to infectious disease could be one way to quantify the value of ID specialists in care systems.
The Infectious Diseases Society of America recently met with the panel that sets compensation rates for Medicare to discuss ways to increase compensation for ID, said IDSA president Carlos del Rio, MD. He is also a professor of medicine at Emory University.
ID specialists need to be able to put a dollar value to their policy work that’s not related to patient reimbursement, Dr. del Rio said. IDSA’s ongoing compensation initiative advocates for value-based care and provides salary negotiation tools for ID specialists, he added.
“Salaries shouldn’t simply be defined by what reimbursement is, and that’s true for other specialties,” such as hospital medicine and palliative care at many institutions, Dr. Armstrong said. “Infectious disease needs to be held at the same level of respect and value.”
But despite issues within the specialties, ID physicians remain passionate about their field.
“It is the most fascinating specialty I can ever imagine,” Dr. Armstrong said. Dr. Bourque agreed, noting the dynamic nature of specialty, with the emergence of new diseases like COVID-19 and reemergence of diseases like mpox (formerly called monkeypox), Zika, Ebola, and chikungunya in the past decade.
“There’s nothing about the field of infectious diseases that, in my mind, isn’t fascinating or rewarding enough to bring people in,” added Dr. Diekema. “The factors that are keeping people out are primarily economic factors and aspects of our health care system that need attention.”
A version of this article first appeared on Medscape.com.
Just 56% of infectious disease fellowship programs filled their 2023 slots, according to new data released by the National Resident Matching Program. Infectious disease (ID) fellowships had seen a jump in applications in the previous 2 years, but these new numbers may suggest a backward slide in a specialty that for many years has struggled to recruit residents.
There are unfilled positions across the country, including in health care hot spots. In Boston, all three slots at Boston Medical Center ID fellowship program are currently empty.
“For our program, going unfilled is a pretty rare event,” said Daniel Bourque, MD, an assistant professor of infectious disease at Boston University and director of the program. “For a program in the city of Boston that’s at a large tertiary care center, that definitely was a big surprise.”
Many other ID fellowships have joined BMC in posting about their vacancies on social media, looking for residents who may not have matched in other fellowships and for physicians who initially decided not to pursue additional training but are now reconsidering.
“If you are interested in a career in this exciting field, in the amazing city of Seattle, with incredible and friendly colleagues, please contact us,” the University of Washington’s ID fellowship program tweeted. Tulane University, Creighton University, the University of Connecticut, Washington University in St. Louis, and the University of Colorado also advertised their unfilled positions.
Other ID doctors commiserated with the disappointing match year. “I made a new riddle after yesterday’s match results: In the hospital, everyone needs me. Yet, no one wants to be me. What am I? An ID doctor,” tweeted Nathan Nolan, MD, MPH, an infectious disease specialist at the Veterans Health Administration in St. Louis.
Infectious disease positions continue to grow
One contributor to this downturn could be the growing number of infectious disease programs offered, whereas the number of applicants has generally remained stable. In 2018, there were 394 slots at 151 infectious disease fellowship programs offered. For the 2023 match year, there were 441 slots at 175 programs.
At the same time, there has not been a notable rise in applicants. From match years 2018 to 2020, about 320 applicants applied for ID fellowship positions each year. There was a rise in in interest in first 2 years of the pandemic, with 404 and 387 applicants in the 2021 and 2022 match years, respectively. The most recent round suggests a return to prepandemic numbers, with 330 residents applying to ID programs.
“I think it’s fair to question whether, as a field, we should be increasing training programs and spots at this point, and if it’s better to focus on ways to increase interest and demand,” said Daniel Diekema, MD, an ID physician at Maine Medical Center in Portland. “Otherwise, we’re just going to look worse and worse every year,” he added, and the work that goes into creating these training opportunities will not have a return on investment.
More training, less pay
The fellowship recruitment issues combined with an already short supply of infectious disease specialists can be traced back to comparatively worse pay compared with other subspecialties, experts say. Infectious disease was the fifth lowest paid specialty in the 2022 Medscape Physician Compensation Report – ranking above only primary care specialties and diabetes and endocrinology.
Pursuing this subspeciality in medicine may not translate to higher pay, Dr. Diekema noted. For example, a physician who completes an internal medicine residency and then a 2- to 3-year infectious disease fellowship can make less than a physician who pursues hospital medicine directly after completing the same residency.
“You’re in a situation where you’re doing additional training to reduce your income earning potential, and that’s a very hard sales pitch to make,” he said. It’s become more difficult as student loan debts continue to increase, he added.
Because infectious disease is a cognitive specialty and does not perform procedures, it is at a disadvantage in a typical fee-for-service pay model. ID physicians also advise on hospital policies for testing and personal protective equipment, which is not always compensated, said Wendy Armstrong, MD, a professor of infectious diseases at Emory University, Atlanta.
A reflection of pandemic burnout?
Experts also wonder if the past 2 years of the pandemic and the notable burnout in ID and other in-demand specialties may have dissuaded applicants from pursuing the ID career path.
“This residency class is the class that started their training in June or July of 2020 and represent that residency class that has trained throughout the pandemic,” Dr. Bourque said. “Does [this low match rate] reflect a negative outlook on the field of ID because of COVID? Is it a reflection of trainee burnout in the setting of the pandemic?”
Dr. Diekema wonders if increased public scrutiny and politicization of the field may have discouraged residents. “The vilification of public health and [of] infectious disease experts like Dr. Fauci by significant portions of our society can be demoralizing,” he said. “People might say, ‘Why would I want to put myself through that?’ ”
But Dr. Armstrong doubts this is the case. “I’ve never had a resident tell me that was on their radar screen,” she said, noting that while there had been recent improvements in applicants, lower match numbers for ID fellowships have been a long-standing issue.
Rethinking reimbursement
Experts agree that pay issues need to be addressed to make ID a more attractive specialty. Moving away from traditional payment plans to value-based models using quality measurements specific to infectious disease could be one way to quantify the value of ID specialists in care systems.
The Infectious Diseases Society of America recently met with the panel that sets compensation rates for Medicare to discuss ways to increase compensation for ID, said IDSA president Carlos del Rio, MD. He is also a professor of medicine at Emory University.
ID specialists need to be able to put a dollar value to their policy work that’s not related to patient reimbursement, Dr. del Rio said. IDSA’s ongoing compensation initiative advocates for value-based care and provides salary negotiation tools for ID specialists, he added.
“Salaries shouldn’t simply be defined by what reimbursement is, and that’s true for other specialties,” such as hospital medicine and palliative care at many institutions, Dr. Armstrong said. “Infectious disease needs to be held at the same level of respect and value.”
But despite issues within the specialties, ID physicians remain passionate about their field.
“It is the most fascinating specialty I can ever imagine,” Dr. Armstrong said. Dr. Bourque agreed, noting the dynamic nature of specialty, with the emergence of new diseases like COVID-19 and reemergence of diseases like mpox (formerly called monkeypox), Zika, Ebola, and chikungunya in the past decade.
“There’s nothing about the field of infectious diseases that, in my mind, isn’t fascinating or rewarding enough to bring people in,” added Dr. Diekema. “The factors that are keeping people out are primarily economic factors and aspects of our health care system that need attention.”
A version of this article first appeared on Medscape.com.
Just 56% of infectious disease fellowship programs filled their 2023 slots, according to new data released by the National Resident Matching Program. Infectious disease (ID) fellowships had seen a jump in applications in the previous 2 years, but these new numbers may suggest a backward slide in a specialty that for many years has struggled to recruit residents.
There are unfilled positions across the country, including in health care hot spots. In Boston, all three slots at Boston Medical Center ID fellowship program are currently empty.
“For our program, going unfilled is a pretty rare event,” said Daniel Bourque, MD, an assistant professor of infectious disease at Boston University and director of the program. “For a program in the city of Boston that’s at a large tertiary care center, that definitely was a big surprise.”
Many other ID fellowships have joined BMC in posting about their vacancies on social media, looking for residents who may not have matched in other fellowships and for physicians who initially decided not to pursue additional training but are now reconsidering.
“If you are interested in a career in this exciting field, in the amazing city of Seattle, with incredible and friendly colleagues, please contact us,” the University of Washington’s ID fellowship program tweeted. Tulane University, Creighton University, the University of Connecticut, Washington University in St. Louis, and the University of Colorado also advertised their unfilled positions.
Other ID doctors commiserated with the disappointing match year. “I made a new riddle after yesterday’s match results: In the hospital, everyone needs me. Yet, no one wants to be me. What am I? An ID doctor,” tweeted Nathan Nolan, MD, MPH, an infectious disease specialist at the Veterans Health Administration in St. Louis.
Infectious disease positions continue to grow
One contributor to this downturn could be the growing number of infectious disease programs offered, whereas the number of applicants has generally remained stable. In 2018, there were 394 slots at 151 infectious disease fellowship programs offered. For the 2023 match year, there were 441 slots at 175 programs.
At the same time, there has not been a notable rise in applicants. From match years 2018 to 2020, about 320 applicants applied for ID fellowship positions each year. There was a rise in in interest in first 2 years of the pandemic, with 404 and 387 applicants in the 2021 and 2022 match years, respectively. The most recent round suggests a return to prepandemic numbers, with 330 residents applying to ID programs.
“I think it’s fair to question whether, as a field, we should be increasing training programs and spots at this point, and if it’s better to focus on ways to increase interest and demand,” said Daniel Diekema, MD, an ID physician at Maine Medical Center in Portland. “Otherwise, we’re just going to look worse and worse every year,” he added, and the work that goes into creating these training opportunities will not have a return on investment.
More training, less pay
The fellowship recruitment issues combined with an already short supply of infectious disease specialists can be traced back to comparatively worse pay compared with other subspecialties, experts say. Infectious disease was the fifth lowest paid specialty in the 2022 Medscape Physician Compensation Report – ranking above only primary care specialties and diabetes and endocrinology.
Pursuing this subspeciality in medicine may not translate to higher pay, Dr. Diekema noted. For example, a physician who completes an internal medicine residency and then a 2- to 3-year infectious disease fellowship can make less than a physician who pursues hospital medicine directly after completing the same residency.
“You’re in a situation where you’re doing additional training to reduce your income earning potential, and that’s a very hard sales pitch to make,” he said. It’s become more difficult as student loan debts continue to increase, he added.
Because infectious disease is a cognitive specialty and does not perform procedures, it is at a disadvantage in a typical fee-for-service pay model. ID physicians also advise on hospital policies for testing and personal protective equipment, which is not always compensated, said Wendy Armstrong, MD, a professor of infectious diseases at Emory University, Atlanta.
A reflection of pandemic burnout?
Experts also wonder if the past 2 years of the pandemic and the notable burnout in ID and other in-demand specialties may have dissuaded applicants from pursuing the ID career path.
“This residency class is the class that started their training in June or July of 2020 and represent that residency class that has trained throughout the pandemic,” Dr. Bourque said. “Does [this low match rate] reflect a negative outlook on the field of ID because of COVID? Is it a reflection of trainee burnout in the setting of the pandemic?”
Dr. Diekema wonders if increased public scrutiny and politicization of the field may have discouraged residents. “The vilification of public health and [of] infectious disease experts like Dr. Fauci by significant portions of our society can be demoralizing,” he said. “People might say, ‘Why would I want to put myself through that?’ ”
But Dr. Armstrong doubts this is the case. “I’ve never had a resident tell me that was on their radar screen,” she said, noting that while there had been recent improvements in applicants, lower match numbers for ID fellowships have been a long-standing issue.
Rethinking reimbursement
Experts agree that pay issues need to be addressed to make ID a more attractive specialty. Moving away from traditional payment plans to value-based models using quality measurements specific to infectious disease could be one way to quantify the value of ID specialists in care systems.
The Infectious Diseases Society of America recently met with the panel that sets compensation rates for Medicare to discuss ways to increase compensation for ID, said IDSA president Carlos del Rio, MD. He is also a professor of medicine at Emory University.
ID specialists need to be able to put a dollar value to their policy work that’s not related to patient reimbursement, Dr. del Rio said. IDSA’s ongoing compensation initiative advocates for value-based care and provides salary negotiation tools for ID specialists, he added.
“Salaries shouldn’t simply be defined by what reimbursement is, and that’s true for other specialties,” such as hospital medicine and palliative care at many institutions, Dr. Armstrong said. “Infectious disease needs to be held at the same level of respect and value.”
But despite issues within the specialties, ID physicians remain passionate about their field.
“It is the most fascinating specialty I can ever imagine,” Dr. Armstrong said. Dr. Bourque agreed, noting the dynamic nature of specialty, with the emergence of new diseases like COVID-19 and reemergence of diseases like mpox (formerly called monkeypox), Zika, Ebola, and chikungunya in the past decade.
“There’s nothing about the field of infectious diseases that, in my mind, isn’t fascinating or rewarding enough to bring people in,” added Dr. Diekema. “The factors that are keeping people out are primarily economic factors and aspects of our health care system that need attention.”
A version of this article first appeared on Medscape.com.
Study: Formula-fed extreme preemies need more iron
NEW ORLEANS –
“We were surprised that, despite actually receiving more iron in total each day on average, the formula-fed infants were significantly more iron deficient than breast-fed babies. This is the opposite of what one would expect,” study lead author Grace Power, a medical student at Dalhousie University, Halifax, N.S., said in an interview. She presented the results at the annual meeting of the American Society of Hematology.

According to Ms. Power, there’s limited research into how breastfeeding and formula feeding affect iron levels in preterm infants – especially those born extremely early, between 23 and 30 weeks’ gestation.
“This kind of research is important because preterm infants are highly susceptible to iron deficiency for a number of reasons,” she said. “Iron deficiency early in life is associated with developmental and behavioral problems later on in life. That association still stands, even if the iron deficiency is corrected, so prevention is key in this population. Knowing more about how feeding type affects iron status can help us learn about ways to prevent iron deficiency in these infants in the future.”
For the study, researchers retrospectively analyzed data about all preterm infants (< 31 weeks gestation) in Nova Scotia from 2005 to 2018. Of the 392 infants in this group (55.75% male; average age, about 5 months), 285 were fed with iron-rich formula (mean intake, 1.66 mg/kg per day), and 107 were fully or partially breast fed. The two groups were similar in terms of traits such as mean birth weight and gestational age.
The formula-fed infants were more likely to develop iron deficiency (ID, 36.8%) than the breast-fed infants (20.6%; P = .002). “Mean gestational age and birth weight were both lower in the ID group. The ID group also had a higher percentage of infants born less than 1,100 g (P = .01). More babies in the ID group received at least one blood transfusion,” the researchers reported. “ID infants had a higher daily formula intake, daily iron intake from formula, and total daily iron intake combined from formula and supplements.”
Why is there such a gap between formula-fed infants and breast-fed infants? The researchers speculated that infants absorb less iron from formula versus breast milk, possibly because of the presence of lactoferrin in breast milk.
The researchers also wondered whether physicians may pull back on iron supplementation in infants who undergo blood transfusions out of fear of the risk of iron overload, which Ms. Power said can cause infection and poor growth. By doing so, they may inadvertently deprive the babies of their need for iron.
“We don’t want clinicians to assume an infant doesn’t need iron supplementation just because they’ve received a blood transfusion,” she said.
As for an overall message from the research, Ms. Power said clinicians “should be aware that formula feeding can put infants at risk for iron deficiency and consider this when making decisions about supplementation.” And she noted that guidelines from the American Academy of Pediatrics and Canadian Pediatric Society don’t highlight the importance of iron supplementation in formula-fed, very preterm infants.
In an interview, University of Michigan pediatrician Michael K. Georgieff, MD, who has studied iron supplementation, said the study’s primary findings are surprising, although it makes sense that infants with lower gestational age and birth weight would suffer from more ID. Blood transfusion can indeed raise iron levels, but it’s important to consider that these infants may already have low levels of iron.
Dr. Georgieff advised colleagues to understand the potential for various nutritional deficiencies in preterm infants well beyond the first few weeks. When the babies are handed off to other clinicians such as pediatricians, they should undergo nutritional screening at 6 months, not at a year.
Dalhousie University funded the study. The study authors and Dr. Georgieff have no disclosures.
NEW ORLEANS –
“We were surprised that, despite actually receiving more iron in total each day on average, the formula-fed infants were significantly more iron deficient than breast-fed babies. This is the opposite of what one would expect,” study lead author Grace Power, a medical student at Dalhousie University, Halifax, N.S., said in an interview. She presented the results at the annual meeting of the American Society of Hematology.
According to Ms. Power, there’s limited research into how breastfeeding and formula feeding affect iron levels in preterm infants – especially those born extremely early, between 23 and 30 weeks’ gestation.
“This kind of research is important because preterm infants are highly susceptible to iron deficiency for a number of reasons,” she said. “Iron deficiency early in life is associated with developmental and behavioral problems later on in life. That association still stands, even if the iron deficiency is corrected, so prevention is key in this population. Knowing more about how feeding type affects iron status can help us learn about ways to prevent iron deficiency in these infants in the future.”
For the study, researchers retrospectively analyzed data about all preterm infants (< 31 weeks gestation) in Nova Scotia from 2005 to 2018. Of the 392 infants in this group (55.75% male; average age, about 5 months), 285 were fed with iron-rich formula (mean intake, 1.66 mg/kg per day), and 107 were fully or partially breast fed. The two groups were similar in terms of traits such as mean birth weight and gestational age.
The formula-fed infants were more likely to develop iron deficiency (ID, 36.8%) than the breast-fed infants (20.6%; P = .002). “Mean gestational age and birth weight were both lower in the ID group. The ID group also had a higher percentage of infants born less than 1,100 g (P = .01). More babies in the ID group received at least one blood transfusion,” the researchers reported. “ID infants had a higher daily formula intake, daily iron intake from formula, and total daily iron intake combined from formula and supplements.”
Why is there such a gap between formula-fed infants and breast-fed infants? The researchers speculated that infants absorb less iron from formula versus breast milk, possibly because of the presence of lactoferrin in breast milk.
The researchers also wondered whether physicians may pull back on iron supplementation in infants who undergo blood transfusions out of fear of the risk of iron overload, which Ms. Power said can cause infection and poor growth. By doing so, they may inadvertently deprive the babies of their need for iron.
“We don’t want clinicians to assume an infant doesn’t need iron supplementation just because they’ve received a blood transfusion,” she said.
As for an overall message from the research, Ms. Power said clinicians “should be aware that formula feeding can put infants at risk for iron deficiency and consider this when making decisions about supplementation.” And she noted that guidelines from the American Academy of Pediatrics and Canadian Pediatric Society don’t highlight the importance of iron supplementation in formula-fed, very preterm infants.
In an interview, University of Michigan pediatrician Michael K. Georgieff, MD, who has studied iron supplementation, said the study’s primary findings are surprising, although it makes sense that infants with lower gestational age and birth weight would suffer from more ID. Blood transfusion can indeed raise iron levels, but it’s important to consider that these infants may already have low levels of iron.
Dr. Georgieff advised colleagues to understand the potential for various nutritional deficiencies in preterm infants well beyond the first few weeks. When the babies are handed off to other clinicians such as pediatricians, they should undergo nutritional screening at 6 months, not at a year.
Dalhousie University funded the study. The study authors and Dr. Georgieff have no disclosures.
NEW ORLEANS –
“We were surprised that, despite actually receiving more iron in total each day on average, the formula-fed infants were significantly more iron deficient than breast-fed babies. This is the opposite of what one would expect,” study lead author Grace Power, a medical student at Dalhousie University, Halifax, N.S., said in an interview. She presented the results at the annual meeting of the American Society of Hematology.
According to Ms. Power, there’s limited research into how breastfeeding and formula feeding affect iron levels in preterm infants – especially those born extremely early, between 23 and 30 weeks’ gestation.
“This kind of research is important because preterm infants are highly susceptible to iron deficiency for a number of reasons,” she said. “Iron deficiency early in life is associated with developmental and behavioral problems later on in life. That association still stands, even if the iron deficiency is corrected, so prevention is key in this population. Knowing more about how feeding type affects iron status can help us learn about ways to prevent iron deficiency in these infants in the future.”
For the study, researchers retrospectively analyzed data about all preterm infants (< 31 weeks gestation) in Nova Scotia from 2005 to 2018. Of the 392 infants in this group (55.75% male; average age, about 5 months), 285 were fed with iron-rich formula (mean intake, 1.66 mg/kg per day), and 107 were fully or partially breast fed. The two groups were similar in terms of traits such as mean birth weight and gestational age.
The formula-fed infants were more likely to develop iron deficiency (ID, 36.8%) than the breast-fed infants (20.6%; P = .002). “Mean gestational age and birth weight were both lower in the ID group. The ID group also had a higher percentage of infants born less than 1,100 g (P = .01). More babies in the ID group received at least one blood transfusion,” the researchers reported. “ID infants had a higher daily formula intake, daily iron intake from formula, and total daily iron intake combined from formula and supplements.”
Why is there such a gap between formula-fed infants and breast-fed infants? The researchers speculated that infants absorb less iron from formula versus breast milk, possibly because of the presence of lactoferrin in breast milk.
The researchers also wondered whether physicians may pull back on iron supplementation in infants who undergo blood transfusions out of fear of the risk of iron overload, which Ms. Power said can cause infection and poor growth. By doing so, they may inadvertently deprive the babies of their need for iron.
“We don’t want clinicians to assume an infant doesn’t need iron supplementation just because they’ve received a blood transfusion,” she said.
As for an overall message from the research, Ms. Power said clinicians “should be aware that formula feeding can put infants at risk for iron deficiency and consider this when making decisions about supplementation.” And she noted that guidelines from the American Academy of Pediatrics and Canadian Pediatric Society don’t highlight the importance of iron supplementation in formula-fed, very preterm infants.
In an interview, University of Michigan pediatrician Michael K. Georgieff, MD, who has studied iron supplementation, said the study’s primary findings are surprising, although it makes sense that infants with lower gestational age and birth weight would suffer from more ID. Blood transfusion can indeed raise iron levels, but it’s important to consider that these infants may already have low levels of iron.
Dr. Georgieff advised colleagues to understand the potential for various nutritional deficiencies in preterm infants well beyond the first few weeks. When the babies are handed off to other clinicians such as pediatricians, they should undergo nutritional screening at 6 months, not at a year.
Dalhousie University funded the study. The study authors and Dr. Georgieff have no disclosures.
AT ASH 2022
CLL phase 3 study: Zanubrutinib bests ibrutinib
Progression-free survival (PFS) was significantly higher for zanubrutinib versus ibrutinib, according to investigator Jennifer R. Brown, MD, PhD, director of the Center for Chronic Lymphocytic Leukemia at Dana-Farber Cancer Institute, Boston.

Cardiac safety was also better with zanubrutinib, the second-generation Bruton’s tyrosine kinase inhibitor, compared to ibrutinib, the first-in-class Bruton’s tyrosine kinase inhibitor. Dr. Brown noted that ibrutinib has “transformed CLL therapy,” despite toxicity and pharmacokinetics issues which limit its use.
Even in patients with high-risk CLL, there was a clear benefit of zanubrutinib over ibrutinib, according to Dr. Brown, who presented final results of ALPINE in a late-breaking clinical trials session at the annual meeting of the American Society of Hematology.
“I am not aware of a patient population in which I would select ibrutinib as compared to zanubrutinib,” Dr. Brown said in a press briefing on the study at the meeting.
Although not currently indicated in CLL, zanubrutinib received Food and Drug Administration approval for treatment of relapsed/refractory mantle cell lymphoma in late 2019, followed by indications in Waldenström’s macroglobulinemia and relapsed/refractory marginal zone lymphoma in 2021.
But the choice of zanubrutinib over ibrutinib in relapsed/refractory CLL is already supported in current clinical practice guidelines, Dr. Brown said.
The most recent CLL guidelines from the National Comprehensive Cancer Network (NCCN), updated Aug 30, describe zanubrutinib as a “preferred” regimen, while ibrutinib falls into the category of an “other recommended regimen.”
The zanubrutinib recommendation is category 1, meaning that it is based on high-level evidence, with uniform consensus that the intervention in appropriate, according to NCCN.
Improved safety, efficacy
Side effects have proved to be an Achilles heel for ibrutinib, which first received an FDA approval in CLL in 2014.
Across CLL studies, between 16% and 23% of CLL patients have discontinued ibrutinib treatment because of toxicities, Dr. Brown, the ALPINE investigator, said at the ASH meeting.
In addition, pharmacokinetic data suggest that at certain times between doses, the amount of ibrutinib in a patient’s system may drop below the level needed to effectively inhibit the target protein, Bruton’s tyrosine kinase.
By contrast, zanubrutinib is designed to have greater specificity for that target protein, Dr. Brown said. Furthermore, the pharmacokinetic studies have demonstrated concentrations of drug consistently above the level needed for effective inhibition – an effect that suggests potential for greater efficacy.
In the ALPINE study, 652 patients with relapsed/refractory CLL/small lymphocytic lymphoma (SLL) were randomized to zanubrutinib 160 mg twice daily or ibrutinib once daily.
With a mean follow-up of 29.6 months, zanubrutinib PFS was significantly superior to ibrutinib, according to Dr. Brown, with a hazard ratio (HR) of 0.65 and 95% confidence interval (CI) between 0.49 and 0.86.
Estimated PFS at 2 years was 79.5% in the zanubrutinib arm and 67.3% for ibrutinib, according to the ALPINE data presented.
However, the difference in PFS in favor of zanubrutinib was even more pronounced in high-risk patients, according to Dr. Brown. Among patients with chromosome 17 deletion or TP53 mutation, the PFS at 2 years was 77.6% for zanubrutinib and just 55.7% for ibrutinib, with an HR of 0.52 and 95% CI of 0.30 to 0.88.
Zanubrutinib’s safety profile was superior to ibrutinib, with serious adverse rates of 42.0% and 50.0%, respectively, and significantly lower cardiac toxicity for zanubrutinib, according to the investigators’ presentation.
Only 5.2% of patients on zanubrutinib had atrial fibrillation/flutter on study, compared to 13.3% for ibrutinib (P = .0004), while rates of serious cardiac adverse events were 1.9% and 7.7% , respectively.
Impressive benefit
The PFS benefit of zanubrutinib over ibrutinib was “quite impressive” in ALPINE, and in line with pharmacokinetic differences observed between Bruton’s tyrosine kinase inhibitors, said Stefan K. Barta, MD, associate professor of medicine at the University of Pennsylvania in Philadelphia.
“In the lab, [second-generation Bruton’s tyrosine kinase inhibitors] do hit the target better, but better doesn’t necessarily translate into good outcomes for patients – that’s a different question,” Dr. Barta said in an interview
However, the safety findings of ALPINE are particularly relevant, according to Dr. Barta, since today, many patients with CLL will receive treatment with Bruton’s tyrosine kinase inhibitors indefinitely.
In ALPINE results presented at ASH, zanubrutinib-treated patients had lower rates of atrial fibrillation and serious cardiac events, as well as zero deaths due to cardiac events, compared to six deaths in the ibrutinib group.
“Side effects make a big difference if you are on something for a long time,” Dr. Barta said. “It’s certainly a huge difference already, but then if you get the added bonus of also having an improvement in PFS, that’s a win-win.”
Dr. Brown reported disclosures related to Abbvie, Acerta/AstraZeneca, Beigene, Bristol-Myers Squibb/Juno/Celgene, Catapult, Genentech/Roche, Janssen, MEI Pharma, Morphosys AG, Novartis, Pfizer, Rigel, Gilead, Loxo/Lilly, Verastem/Secura Bio, Sun, TG Therapeutics, Invectys, Grifols Worldwide Operations, Hutchmed, iOnctura, and Pharmacyclics.
Progression-free survival (PFS) was significantly higher for zanubrutinib versus ibrutinib, according to investigator Jennifer R. Brown, MD, PhD, director of the Center for Chronic Lymphocytic Leukemia at Dana-Farber Cancer Institute, Boston.
Cardiac safety was also better with zanubrutinib, the second-generation Bruton’s tyrosine kinase inhibitor, compared to ibrutinib, the first-in-class Bruton’s tyrosine kinase inhibitor. Dr. Brown noted that ibrutinib has “transformed CLL therapy,” despite toxicity and pharmacokinetics issues which limit its use.
Even in patients with high-risk CLL, there was a clear benefit of zanubrutinib over ibrutinib, according to Dr. Brown, who presented final results of ALPINE in a late-breaking clinical trials session at the annual meeting of the American Society of Hematology.
“I am not aware of a patient population in which I would select ibrutinib as compared to zanubrutinib,” Dr. Brown said in a press briefing on the study at the meeting.
Although not currently indicated in CLL, zanubrutinib received Food and Drug Administration approval for treatment of relapsed/refractory mantle cell lymphoma in late 2019, followed by indications in Waldenström’s macroglobulinemia and relapsed/refractory marginal zone lymphoma in 2021.
But the choice of zanubrutinib over ibrutinib in relapsed/refractory CLL is already supported in current clinical practice guidelines, Dr. Brown said.
The most recent CLL guidelines from the National Comprehensive Cancer Network (NCCN), updated Aug 30, describe zanubrutinib as a “preferred” regimen, while ibrutinib falls into the category of an “other recommended regimen.”
The zanubrutinib recommendation is category 1, meaning that it is based on high-level evidence, with uniform consensus that the intervention in appropriate, according to NCCN.
Improved safety, efficacy
Side effects have proved to be an Achilles heel for ibrutinib, which first received an FDA approval in CLL in 2014.
Across CLL studies, between 16% and 23% of CLL patients have discontinued ibrutinib treatment because of toxicities, Dr. Brown, the ALPINE investigator, said at the ASH meeting.
In addition, pharmacokinetic data suggest that at certain times between doses, the amount of ibrutinib in a patient’s system may drop below the level needed to effectively inhibit the target protein, Bruton’s tyrosine kinase.
By contrast, zanubrutinib is designed to have greater specificity for that target protein, Dr. Brown said. Furthermore, the pharmacokinetic studies have demonstrated concentrations of drug consistently above the level needed for effective inhibition – an effect that suggests potential for greater efficacy.
In the ALPINE study, 652 patients with relapsed/refractory CLL/small lymphocytic lymphoma (SLL) were randomized to zanubrutinib 160 mg twice daily or ibrutinib once daily.
With a mean follow-up of 29.6 months, zanubrutinib PFS was significantly superior to ibrutinib, according to Dr. Brown, with a hazard ratio (HR) of 0.65 and 95% confidence interval (CI) between 0.49 and 0.86.
Estimated PFS at 2 years was 79.5% in the zanubrutinib arm and 67.3% for ibrutinib, according to the ALPINE data presented.
However, the difference in PFS in favor of zanubrutinib was even more pronounced in high-risk patients, according to Dr. Brown. Among patients with chromosome 17 deletion or TP53 mutation, the PFS at 2 years was 77.6% for zanubrutinib and just 55.7% for ibrutinib, with an HR of 0.52 and 95% CI of 0.30 to 0.88.
Zanubrutinib’s safety profile was superior to ibrutinib, with serious adverse rates of 42.0% and 50.0%, respectively, and significantly lower cardiac toxicity for zanubrutinib, according to the investigators’ presentation.
Only 5.2% of patients on zanubrutinib had atrial fibrillation/flutter on study, compared to 13.3% for ibrutinib (P = .0004), while rates of serious cardiac adverse events were 1.9% and 7.7% , respectively.
Impressive benefit
The PFS benefit of zanubrutinib over ibrutinib was “quite impressive” in ALPINE, and in line with pharmacokinetic differences observed between Bruton’s tyrosine kinase inhibitors, said Stefan K. Barta, MD, associate professor of medicine at the University of Pennsylvania in Philadelphia.
“In the lab, [second-generation Bruton’s tyrosine kinase inhibitors] do hit the target better, but better doesn’t necessarily translate into good outcomes for patients – that’s a different question,” Dr. Barta said in an interview
However, the safety findings of ALPINE are particularly relevant, according to Dr. Barta, since today, many patients with CLL will receive treatment with Bruton’s tyrosine kinase inhibitors indefinitely.
In ALPINE results presented at ASH, zanubrutinib-treated patients had lower rates of atrial fibrillation and serious cardiac events, as well as zero deaths due to cardiac events, compared to six deaths in the ibrutinib group.
“Side effects make a big difference if you are on something for a long time,” Dr. Barta said. “It’s certainly a huge difference already, but then if you get the added bonus of also having an improvement in PFS, that’s a win-win.”
Dr. Brown reported disclosures related to Abbvie, Acerta/AstraZeneca, Beigene, Bristol-Myers Squibb/Juno/Celgene, Catapult, Genentech/Roche, Janssen, MEI Pharma, Morphosys AG, Novartis, Pfizer, Rigel, Gilead, Loxo/Lilly, Verastem/Secura Bio, Sun, TG Therapeutics, Invectys, Grifols Worldwide Operations, Hutchmed, iOnctura, and Pharmacyclics.
Progression-free survival (PFS) was significantly higher for zanubrutinib versus ibrutinib, according to investigator Jennifer R. Brown, MD, PhD, director of the Center for Chronic Lymphocytic Leukemia at Dana-Farber Cancer Institute, Boston.
Cardiac safety was also better with zanubrutinib, the second-generation Bruton’s tyrosine kinase inhibitor, compared to ibrutinib, the first-in-class Bruton’s tyrosine kinase inhibitor. Dr. Brown noted that ibrutinib has “transformed CLL therapy,” despite toxicity and pharmacokinetics issues which limit its use.
Even in patients with high-risk CLL, there was a clear benefit of zanubrutinib over ibrutinib, according to Dr. Brown, who presented final results of ALPINE in a late-breaking clinical trials session at the annual meeting of the American Society of Hematology.
“I am not aware of a patient population in which I would select ibrutinib as compared to zanubrutinib,” Dr. Brown said in a press briefing on the study at the meeting.
Although not currently indicated in CLL, zanubrutinib received Food and Drug Administration approval for treatment of relapsed/refractory mantle cell lymphoma in late 2019, followed by indications in Waldenström’s macroglobulinemia and relapsed/refractory marginal zone lymphoma in 2021.
But the choice of zanubrutinib over ibrutinib in relapsed/refractory CLL is already supported in current clinical practice guidelines, Dr. Brown said.
The most recent CLL guidelines from the National Comprehensive Cancer Network (NCCN), updated Aug 30, describe zanubrutinib as a “preferred” regimen, while ibrutinib falls into the category of an “other recommended regimen.”
The zanubrutinib recommendation is category 1, meaning that it is based on high-level evidence, with uniform consensus that the intervention in appropriate, according to NCCN.
Improved safety, efficacy
Side effects have proved to be an Achilles heel for ibrutinib, which first received an FDA approval in CLL in 2014.
Across CLL studies, between 16% and 23% of CLL patients have discontinued ibrutinib treatment because of toxicities, Dr. Brown, the ALPINE investigator, said at the ASH meeting.
In addition, pharmacokinetic data suggest that at certain times between doses, the amount of ibrutinib in a patient’s system may drop below the level needed to effectively inhibit the target protein, Bruton’s tyrosine kinase.
By contrast, zanubrutinib is designed to have greater specificity for that target protein, Dr. Brown said. Furthermore, the pharmacokinetic studies have demonstrated concentrations of drug consistently above the level needed for effective inhibition – an effect that suggests potential for greater efficacy.
In the ALPINE study, 652 patients with relapsed/refractory CLL/small lymphocytic lymphoma (SLL) were randomized to zanubrutinib 160 mg twice daily or ibrutinib once daily.
With a mean follow-up of 29.6 months, zanubrutinib PFS was significantly superior to ibrutinib, according to Dr. Brown, with a hazard ratio (HR) of 0.65 and 95% confidence interval (CI) between 0.49 and 0.86.
Estimated PFS at 2 years was 79.5% in the zanubrutinib arm and 67.3% for ibrutinib, according to the ALPINE data presented.
However, the difference in PFS in favor of zanubrutinib was even more pronounced in high-risk patients, according to Dr. Brown. Among patients with chromosome 17 deletion or TP53 mutation, the PFS at 2 years was 77.6% for zanubrutinib and just 55.7% for ibrutinib, with an HR of 0.52 and 95% CI of 0.30 to 0.88.
Zanubrutinib’s safety profile was superior to ibrutinib, with serious adverse rates of 42.0% and 50.0%, respectively, and significantly lower cardiac toxicity for zanubrutinib, according to the investigators’ presentation.
Only 5.2% of patients on zanubrutinib had atrial fibrillation/flutter on study, compared to 13.3% for ibrutinib (P = .0004), while rates of serious cardiac adverse events were 1.9% and 7.7% , respectively.
Impressive benefit
The PFS benefit of zanubrutinib over ibrutinib was “quite impressive” in ALPINE, and in line with pharmacokinetic differences observed between Bruton’s tyrosine kinase inhibitors, said Stefan K. Barta, MD, associate professor of medicine at the University of Pennsylvania in Philadelphia.
“In the lab, [second-generation Bruton’s tyrosine kinase inhibitors] do hit the target better, but better doesn’t necessarily translate into good outcomes for patients – that’s a different question,” Dr. Barta said in an interview
However, the safety findings of ALPINE are particularly relevant, according to Dr. Barta, since today, many patients with CLL will receive treatment with Bruton’s tyrosine kinase inhibitors indefinitely.
In ALPINE results presented at ASH, zanubrutinib-treated patients had lower rates of atrial fibrillation and serious cardiac events, as well as zero deaths due to cardiac events, compared to six deaths in the ibrutinib group.
“Side effects make a big difference if you are on something for a long time,” Dr. Barta said. “It’s certainly a huge difference already, but then if you get the added bonus of also having an improvement in PFS, that’s a win-win.”
Dr. Brown reported disclosures related to Abbvie, Acerta/AstraZeneca, Beigene, Bristol-Myers Squibb/Juno/Celgene, Catapult, Genentech/Roche, Janssen, MEI Pharma, Morphosys AG, Novartis, Pfizer, Rigel, Gilead, Loxo/Lilly, Verastem/Secura Bio, Sun, TG Therapeutics, Invectys, Grifols Worldwide Operations, Hutchmed, iOnctura, and Pharmacyclics.
FROM ASH 2022
FDA approves Idacio as eighth adalimumab biosimilar in U.S.
A biosimilar drug to the tumor necrosis factor inhibitor adalimumab, marketed as Idacio (adalimumab-aacf), has been approved by the Food and Drug Administration for use in the United States, according to a press release from manufacturer Fresenius Kabi.
Idacio is a citrate-free, low-concentration formulation of adalimumab and is now approved for use for all but three of the indications that currently apply to the reference adalimumab product (Humira): rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis in adults, ankylosing spondylitis, Crohn’s disease in adults and children aged 6 years or older, ulcerative colitis in adults, and plaque psoriasis in adults. It does not apply to Humira’s indications for hidradenitis suppurativa, uveitis, or ulcerative colitis in pediatric patients aged 5 years and older.
Idacio is the eighth adalimumab biosimilar to be approved in the United States. Its approval was based on evidence of a similar profile of pharmacokinetics, safety, efficacy, and immunogenicity to Humira.
Idacio was first launched in 2019 and has been marketed in more than 37 countries worldwide, according to Fresenius Kabi. The U.S. launch is scheduled for July, and Idacio will be available as a self-administered prefilled syringe or prefilled pen.
A version of this article first appeared on Medscape.com.
A biosimilar drug to the tumor necrosis factor inhibitor adalimumab, marketed as Idacio (adalimumab-aacf), has been approved by the Food and Drug Administration for use in the United States, according to a press release from manufacturer Fresenius Kabi.
Idacio is a citrate-free, low-concentration formulation of adalimumab and is now approved for use for all but three of the indications that currently apply to the reference adalimumab product (Humira): rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis in adults, ankylosing spondylitis, Crohn’s disease in adults and children aged 6 years or older, ulcerative colitis in adults, and plaque psoriasis in adults. It does not apply to Humira’s indications for hidradenitis suppurativa, uveitis, or ulcerative colitis in pediatric patients aged 5 years and older.
Idacio is the eighth adalimumab biosimilar to be approved in the United States. Its approval was based on evidence of a similar profile of pharmacokinetics, safety, efficacy, and immunogenicity to Humira.
Idacio was first launched in 2019 and has been marketed in more than 37 countries worldwide, according to Fresenius Kabi. The U.S. launch is scheduled for July, and Idacio will be available as a self-administered prefilled syringe or prefilled pen.
A version of this article first appeared on Medscape.com.
A biosimilar drug to the tumor necrosis factor inhibitor adalimumab, marketed as Idacio (adalimumab-aacf), has been approved by the Food and Drug Administration for use in the United States, according to a press release from manufacturer Fresenius Kabi.
Idacio is a citrate-free, low-concentration formulation of adalimumab and is now approved for use for all but three of the indications that currently apply to the reference adalimumab product (Humira): rheumatoid arthritis, polyarticular juvenile idiopathic arthritis, psoriatic arthritis in adults, ankylosing spondylitis, Crohn’s disease in adults and children aged 6 years or older, ulcerative colitis in adults, and plaque psoriasis in adults. It does not apply to Humira’s indications for hidradenitis suppurativa, uveitis, or ulcerative colitis in pediatric patients aged 5 years and older.
Idacio is the eighth adalimumab biosimilar to be approved in the United States. Its approval was based on evidence of a similar profile of pharmacokinetics, safety, efficacy, and immunogenicity to Humira.
Idacio was first launched in 2019 and has been marketed in more than 37 countries worldwide, according to Fresenius Kabi. The U.S. launch is scheduled for July, and Idacio will be available as a self-administered prefilled syringe or prefilled pen.
A version of this article first appeared on Medscape.com.
Rheumatology workforce shortage demands multipronged approach
PHILADELPHIA – New rheumatology fellowships in underserved areas. Rheumatology training for nonspecialists. Telemedicine training, tools, and resources. These are a few of the remedies the American College of Rheumatology’s new Workforce Solutions Committee has concocted to address a shrinking U.S. rheumatology workforce in the face of a rising population of patients with rheumatologic diseases.
In two sessions at the ACR’s annual meeting, committee members provided insights on current workforce projections since the most recent ACR workforce study in 2015. They also outlined the 1-year-old committee’s response to bridge the looming gap in patient care. Some projects are already underway, while others have yet to be implemented and require sustained monetary and project coordination commitments to make their impacts felt across the targeted regions.

“At the current pace of physician departures from the workforce, even with fellows graduating from adult and pediatric rheumatology training programs, the subspecialty cannot be sustained,” said Daniel Battafarano, DO, chair of the Workforce Solution Committee, professor of medicine at the Uniformed Services University of the Health Sciences, Bethesda, Md., and adjunct professor at the University of Texas Health Science Center, San Antonio.
The Northwest is an example of the problem at hand. “For an adult, there’s 1.65 rheumatologists per 100,000 in 2015. In 2025, there’s going to be 0.5 [adult] rheumatologists per 100,000. That’s a problem. If you look at every region in the United States, every single region is decrementing significantly,” he said.
Even the Northeast, which boasted 3.07 adult rheumatologists per 100,000 in 2015, will drop to 1.61 in 2025. Other regions are much worse off. The Southwest will drop from 1.28 to 0.64, and North Central will drop from 1.64 to 0.69, projections show.
The situation for pediatrics “has been in a crisis since 2015,” Dr. Battafarano said. It is much worse off than the situation for adult rheumatology, with 2015 figures going from 0.17 to 0.20 in the Southwest and from 0.03 to 0.04 in the South Central region by 2025, and in the Northwest from 0.67 to 0.13 and Northeast from 0.83 to 0.16.
“The ill effects of the pandemic are immeasurable to this point, but anecdotally we know we lost colleagues to part-time employment, we saw early retirements, and that happened across the full spectrum of the United States,” he said. It’s possible that up to 10% of full-time equivalents of physicians left practice in the United States since the pandemic began.
Rheumatologists largely practice in the 392 U.S. metropolitan statistical areas (MSAs), which are defined as a “core area containing a substantial population nucleus, together with adjacent communities having a high degree of economic and social integration with that core.” The smallest MSA has nearly 59,000 people. This distribution leaves many people in the Northwest, Southwest, South Central, and North Central regions with few rheumatologists. Over 86% of locations where rheumatologists train and work are in MSAs.
“By definition, if you get into a region where there’s 60,000 people or less, you can’t support a rheumatologist,” Dr. Battafarano said. He also noted that all pediatric hospitals tend to be in dense MSAs where rheumatologists might be.
South Central region serves as an example
People in certain MSAs of the South Central region (Oklahoma, Texas, Arkansas) such as Laredo, Tex., population 281,805 – where there is no adult rheumatologist – have to drive nearly 2.5 hours to the nearest well-served MSA (San Antonio) where there is a rheumatology fellowship program and medical school.
“Texas may have rheumatologists, but it depends on where you live,” Dr. Battafarano said. “The same applies to Waco, Texas; Texarkana, Arkansas; Lawton, Oklahoma; Pine Bluff, Arkansas; and Enid, Oklahoma, and you can see the range of traveling is between 45 minutes and 2.5 hours. That’s adult rheumatology.”
People in Laredo have an even longer drive to find a pediatric rheumatologist. In pediatrics, he said, “we don’t even look at towns, we look at pediatrics by state. You can see there’s a pediatric fellowship program in Dallas, and there’s one in Houston. There’s one or two [pediatric] rheumatologists in Austin. It just depends on how quickly they burn out and how long they stay. I’m in San Antonio. We don’t have a pediatric rheumatologist in San Antonio, the seventh-largest city in the United States.”
Pediatric rheumatologists are very often found where fellowship programs are located. “Ninety-five percent or greater of pediatric rheumatologists are housed in a pediatric hospital,” Dr. Battafarano said. “There are very few adult rheumatologists who see children, for a variety of reasons.”

In a panel discussion and question-and-answer session that took place after Dr. Battafarano outlined concerns with the numbers and distribution of rheumatologists across the United States, committee member Beth Jonas, MD, professor of medicine and chief of the division of rheumatology, allergy, and immunology at the University of North Carolina at Chapel Hill, noted that the rheumatology specialty match is competitive and typically leaves close to 100 residents who had rheumatology as their first choice without a match because there are not enough fellowship positions for them to fill.
The Workforce Solutions Committee hopes to reduce this “bottleneck,” she said, by identifying institutions that are ripe for opening new fellowship programs or have existing programs that can expand their number of positions, as well as expanding musculoskeletal training among nonrheumatologists, such as primary care physicians, advanced practice providers, and sports medicine physicians.
“I think that we’re going to find ourselves needing to be more creative as we become overcome with events with shortages of physicians,” Dr. Battafarano said. He gave an example of a recent pediatric rheumatology fellow in Seattle who wanted to go back home to Montana to practice. At the same time, the pediatric program wanted her to become a faculty member, so they said they would bridge their program to her, rotating fellows and covering her while on vacation.
“That’s an example of a pediatric program spreading its wings,” he said. “I think that we need to think that way, whether we talk about urban, suburban, rural. It’s how can we stage rheumatologists in areas, how can we embrace our primary care providers, and have rheumatology health care teams so that we have rheumatology expertise located within arm’s length but also within telemedicine length.”
Interventions for 2023
As part of a report on the activities of the Workforce Solutions Committee, Dr. Jonas outlined a number of interventions that the ACR is set to launch in 2023. The committee created five intervention teams to support fellowship positions and training providers, recruitment opportunities, fostering patient-centered communities, virtual training programs, and grants for research and training. The ACR’s initial pilot interventions are focused on, but not limited to, the Northwest, Southwest, and South Central regions.
The committee identified 10 potential partner institutions to develop new fellowship programs in the Northwest, Southwest, and South Central regions: University of Nevada, Las Vegas; Texas Tech University Permian Basin Program; Baylor Scott and White Medical Center Round Rock (Tex.) Program; Texas Tech University Health Science Center El Paso Program; University of Texas at Austin Dell Medical School Program; Abrazo Health Network Program in Arizona; University of Arizona Phoenix Program; University of Arkansas (pediatric program); Oklahoma State University; and University of Texas, San Antonio (pediatric program).
Dr. Jonas explained that opening new programs in these underserved areas should help establish new rheumatologists in these areas, because studies have shown that fellows tend to stay within 100-200 miles of where they trained.
In addition to starting new programs, “if you want to grow your program, if you want to add another fellow, we can support that,” Dr. Jonas said.
To help convince institutions of the value of rheumatology care, a position paper will soon be released by the ACR that outlines the benefits of the specialty to a health care system. The paper will describe an annual preventive cost savings of $2,762 per patient who is in the care of a rheumatologist and an annual direct or downstream income of $3.5 million per rheumatologist in a community, committee members said.
To help with recruitment and retention efforts, the ACR will revise its CareerConnection website to make it more useful.
To help in developing patient-centered communities of care, there will be a discussion series with payers on topics such as access, care delivery, and financing, in which 12 payers (including Blue Cross Blue Shield, Aetna, UnitedHealthcare, and Kaiser) will discuss patient access, cost, and quality measures. An in-person payer summit is also scheduled for 2023.
Interventions to enhance rheumatology care will also keep an ongoing focus on virtual training programs for primary care physicians and advanced practice providers, including a Project ECHO (Extension for Community Healthcare Outcomes) virtual lecture and case-based training and mentoring series for nonrheumatologists, an online library of searchable topics targeted to nonrheumatologists, as well as a grand rounds podcast series on certain rheumatic diseases for residents in family medicine, internal medicine, and pediatric programs. For rheumatology educators in 2023, there also will be an online portal curated by the ACR and other sources to use as a resource for developing curriculum.

A newly revised Fundamentals of Rheumatology course started in June 2022, which can help many medical students, residents, primary care physicians, and students in rehabilitation professions to learn about rheumatologic diseases, said committee member Janet Poole, PhD, division chief, professor, and director of the occupational therapy graduate program at the University of New Mexico, Albuquerque. Grants from the Rheumatology Research Foundation are available to offset the costs of the course for attendees.
An “onboarding toolkit” for nurse practitioners and physician assistants is now available to provide advice to practices for hiring, mentoring, and conducting performance evaluations in rheumatology care teams, Dr. Poole said. And fact sheets about the roles of interprofessional team members are being revised to give nonspecialty providers a sense of what other disciplines are available to care for patients with rheumatic and musculoskeletal disorders. The Advanced Rheumatology course is also being revised and will be available in summer 2023.
Other planned interventions aim to optimize telemedicine for the rheumatology community with a telehealth curriculum for rheumatology fellows, tools to improve telehealth implementation and delivery, and educational materials for patients to optimize their participation in telehealth visits.
The committee created targeted outreach to promote all grants focused on workforce expansion. As a result, in the last year the committee noted a three- to fourfold rise in the number of grant applications, including people and programs in underserved areas that had not previously applied. The Rheumatology Research Foundation also created a baseline for measuring success of grant funding in underserved areas and earmarked funds to increase awareness of the grants and facilitate applications.

Early signs of success are evident in the Rheumatology Access Expansion initiative in the ACR’s Collaborative Initiatives (COIN) department, said committee member Rosalind Ramsey-Goldman, MD, DrPH, professor of medicine/rheumatology at Northwestern University, Chicago. A team of rheumatologists, a pharmacist, and Navajo cultural interpreters developed a 12-week rheumatoid arthritis training program for primary care physicians in the Navajo Nation American Indian reservation, where there’s a high prevalence of RA and a shortage of local rheumatology providers. Results of the pilot study were presented in a plenary session at the meeting.
COIN also worked with the ACR’s Diversity, Equity, and Inclusion task force to sponsor 2022 annual meeting attendance for 11 medical students who identify themselves as underrepresented in medicine to expose them to rheumatology early in their career, said Dr. Ramsey-Goldman. The ACR is starting a program for medical students at historically Black colleges and universities and minority-serving institutions to include mentoring, round tables, and attendance at next year’s annual meeting.
None of the rheumatologists had relevant financial disclosures.
PHILADELPHIA – New rheumatology fellowships in underserved areas. Rheumatology training for nonspecialists. Telemedicine training, tools, and resources. These are a few of the remedies the American College of Rheumatology’s new Workforce Solutions Committee has concocted to address a shrinking U.S. rheumatology workforce in the face of a rising population of patients with rheumatologic diseases.
In two sessions at the ACR’s annual meeting, committee members provided insights on current workforce projections since the most recent ACR workforce study in 2015. They also outlined the 1-year-old committee’s response to bridge the looming gap in patient care. Some projects are already underway, while others have yet to be implemented and require sustained monetary and project coordination commitments to make their impacts felt across the targeted regions.
“At the current pace of physician departures from the workforce, even with fellows graduating from adult and pediatric rheumatology training programs, the subspecialty cannot be sustained,” said Daniel Battafarano, DO, chair of the Workforce Solution Committee, professor of medicine at the Uniformed Services University of the Health Sciences, Bethesda, Md., and adjunct professor at the University of Texas Health Science Center, San Antonio.
The Northwest is an example of the problem at hand. “For an adult, there’s 1.65 rheumatologists per 100,000 in 2015. In 2025, there’s going to be 0.5 [adult] rheumatologists per 100,000. That’s a problem. If you look at every region in the United States, every single region is decrementing significantly,” he said.
Even the Northeast, which boasted 3.07 adult rheumatologists per 100,000 in 2015, will drop to 1.61 in 2025. Other regions are much worse off. The Southwest will drop from 1.28 to 0.64, and North Central will drop from 1.64 to 0.69, projections show.
The situation for pediatrics “has been in a crisis since 2015,” Dr. Battafarano said. It is much worse off than the situation for adult rheumatology, with 2015 figures going from 0.17 to 0.20 in the Southwest and from 0.03 to 0.04 in the South Central region by 2025, and in the Northwest from 0.67 to 0.13 and Northeast from 0.83 to 0.16.
“The ill effects of the pandemic are immeasurable to this point, but anecdotally we know we lost colleagues to part-time employment, we saw early retirements, and that happened across the full spectrum of the United States,” he said. It’s possible that up to 10% of full-time equivalents of physicians left practice in the United States since the pandemic began.
Rheumatologists largely practice in the 392 U.S. metropolitan statistical areas (MSAs), which are defined as a “core area containing a substantial population nucleus, together with adjacent communities having a high degree of economic and social integration with that core.” The smallest MSA has nearly 59,000 people. This distribution leaves many people in the Northwest, Southwest, South Central, and North Central regions with few rheumatologists. Over 86% of locations where rheumatologists train and work are in MSAs.
“By definition, if you get into a region where there’s 60,000 people or less, you can’t support a rheumatologist,” Dr. Battafarano said. He also noted that all pediatric hospitals tend to be in dense MSAs where rheumatologists might be.
South Central region serves as an example
People in certain MSAs of the South Central region (Oklahoma, Texas, Arkansas) such as Laredo, Tex., population 281,805 – where there is no adult rheumatologist – have to drive nearly 2.5 hours to the nearest well-served MSA (San Antonio) where there is a rheumatology fellowship program and medical school.
“Texas may have rheumatologists, but it depends on where you live,” Dr. Battafarano said. “The same applies to Waco, Texas; Texarkana, Arkansas; Lawton, Oklahoma; Pine Bluff, Arkansas; and Enid, Oklahoma, and you can see the range of traveling is between 45 minutes and 2.5 hours. That’s adult rheumatology.”
People in Laredo have an even longer drive to find a pediatric rheumatologist. In pediatrics, he said, “we don’t even look at towns, we look at pediatrics by state. You can see there’s a pediatric fellowship program in Dallas, and there’s one in Houston. There’s one or two [pediatric] rheumatologists in Austin. It just depends on how quickly they burn out and how long they stay. I’m in San Antonio. We don’t have a pediatric rheumatologist in San Antonio, the seventh-largest city in the United States.”
Pediatric rheumatologists are very often found where fellowship programs are located. “Ninety-five percent or greater of pediatric rheumatologists are housed in a pediatric hospital,” Dr. Battafarano said. “There are very few adult rheumatologists who see children, for a variety of reasons.”
In a panel discussion and question-and-answer session that took place after Dr. Battafarano outlined concerns with the numbers and distribution of rheumatologists across the United States, committee member Beth Jonas, MD, professor of medicine and chief of the division of rheumatology, allergy, and immunology at the University of North Carolina at Chapel Hill, noted that the rheumatology specialty match is competitive and typically leaves close to 100 residents who had rheumatology as their first choice without a match because there are not enough fellowship positions for them to fill.
The Workforce Solutions Committee hopes to reduce this “bottleneck,” she said, by identifying institutions that are ripe for opening new fellowship programs or have existing programs that can expand their number of positions, as well as expanding musculoskeletal training among nonrheumatologists, such as primary care physicians, advanced practice providers, and sports medicine physicians.
“I think that we’re going to find ourselves needing to be more creative as we become overcome with events with shortages of physicians,” Dr. Battafarano said. He gave an example of a recent pediatric rheumatology fellow in Seattle who wanted to go back home to Montana to practice. At the same time, the pediatric program wanted her to become a faculty member, so they said they would bridge their program to her, rotating fellows and covering her while on vacation.
“That’s an example of a pediatric program spreading its wings,” he said. “I think that we need to think that way, whether we talk about urban, suburban, rural. It’s how can we stage rheumatologists in areas, how can we embrace our primary care providers, and have rheumatology health care teams so that we have rheumatology expertise located within arm’s length but also within telemedicine length.”
Interventions for 2023
As part of a report on the activities of the Workforce Solutions Committee, Dr. Jonas outlined a number of interventions that the ACR is set to launch in 2023. The committee created five intervention teams to support fellowship positions and training providers, recruitment opportunities, fostering patient-centered communities, virtual training programs, and grants for research and training. The ACR’s initial pilot interventions are focused on, but not limited to, the Northwest, Southwest, and South Central regions.
The committee identified 10 potential partner institutions to develop new fellowship programs in the Northwest, Southwest, and South Central regions: University of Nevada, Las Vegas; Texas Tech University Permian Basin Program; Baylor Scott and White Medical Center Round Rock (Tex.) Program; Texas Tech University Health Science Center El Paso Program; University of Texas at Austin Dell Medical School Program; Abrazo Health Network Program in Arizona; University of Arizona Phoenix Program; University of Arkansas (pediatric program); Oklahoma State University; and University of Texas, San Antonio (pediatric program).
Dr. Jonas explained that opening new programs in these underserved areas should help establish new rheumatologists in these areas, because studies have shown that fellows tend to stay within 100-200 miles of where they trained.
In addition to starting new programs, “if you want to grow your program, if you want to add another fellow, we can support that,” Dr. Jonas said.
To help convince institutions of the value of rheumatology care, a position paper will soon be released by the ACR that outlines the benefits of the specialty to a health care system. The paper will describe an annual preventive cost savings of $2,762 per patient who is in the care of a rheumatologist and an annual direct or downstream income of $3.5 million per rheumatologist in a community, committee members said.
To help with recruitment and retention efforts, the ACR will revise its CareerConnection website to make it more useful.
To help in developing patient-centered communities of care, there will be a discussion series with payers on topics such as access, care delivery, and financing, in which 12 payers (including Blue Cross Blue Shield, Aetna, UnitedHealthcare, and Kaiser) will discuss patient access, cost, and quality measures. An in-person payer summit is also scheduled for 2023.
Interventions to enhance rheumatology care will also keep an ongoing focus on virtual training programs for primary care physicians and advanced practice providers, including a Project ECHO (Extension for Community Healthcare Outcomes) virtual lecture and case-based training and mentoring series for nonrheumatologists, an online library of searchable topics targeted to nonrheumatologists, as well as a grand rounds podcast series on certain rheumatic diseases for residents in family medicine, internal medicine, and pediatric programs. For rheumatology educators in 2023, there also will be an online portal curated by the ACR and other sources to use as a resource for developing curriculum.
A newly revised Fundamentals of Rheumatology course started in June 2022, which can help many medical students, residents, primary care physicians, and students in rehabilitation professions to learn about rheumatologic diseases, said committee member Janet Poole, PhD, division chief, professor, and director of the occupational therapy graduate program at the University of New Mexico, Albuquerque. Grants from the Rheumatology Research Foundation are available to offset the costs of the course for attendees.
An “onboarding toolkit” for nurse practitioners and physician assistants is now available to provide advice to practices for hiring, mentoring, and conducting performance evaluations in rheumatology care teams, Dr. Poole said. And fact sheets about the roles of interprofessional team members are being revised to give nonspecialty providers a sense of what other disciplines are available to care for patients with rheumatic and musculoskeletal disorders. The Advanced Rheumatology course is also being revised and will be available in summer 2023.
Other planned interventions aim to optimize telemedicine for the rheumatology community with a telehealth curriculum for rheumatology fellows, tools to improve telehealth implementation and delivery, and educational materials for patients to optimize their participation in telehealth visits.
The committee created targeted outreach to promote all grants focused on workforce expansion. As a result, in the last year the committee noted a three- to fourfold rise in the number of grant applications, including people and programs in underserved areas that had not previously applied. The Rheumatology Research Foundation also created a baseline for measuring success of grant funding in underserved areas and earmarked funds to increase awareness of the grants and facilitate applications.
Early signs of success are evident in the Rheumatology Access Expansion initiative in the ACR’s Collaborative Initiatives (COIN) department, said committee member Rosalind Ramsey-Goldman, MD, DrPH, professor of medicine/rheumatology at Northwestern University, Chicago. A team of rheumatologists, a pharmacist, and Navajo cultural interpreters developed a 12-week rheumatoid arthritis training program for primary care physicians in the Navajo Nation American Indian reservation, where there’s a high prevalence of RA and a shortage of local rheumatology providers. Results of the pilot study were presented in a plenary session at the meeting.
COIN also worked with the ACR’s Diversity, Equity, and Inclusion task force to sponsor 2022 annual meeting attendance for 11 medical students who identify themselves as underrepresented in medicine to expose them to rheumatology early in their career, said Dr. Ramsey-Goldman. The ACR is starting a program for medical students at historically Black colleges and universities and minority-serving institutions to include mentoring, round tables, and attendance at next year’s annual meeting.
None of the rheumatologists had relevant financial disclosures.
PHILADELPHIA – New rheumatology fellowships in underserved areas. Rheumatology training for nonspecialists. Telemedicine training, tools, and resources. These are a few of the remedies the American College of Rheumatology’s new Workforce Solutions Committee has concocted to address a shrinking U.S. rheumatology workforce in the face of a rising population of patients with rheumatologic diseases.
In two sessions at the ACR’s annual meeting, committee members provided insights on current workforce projections since the most recent ACR workforce study in 2015. They also outlined the 1-year-old committee’s response to bridge the looming gap in patient care. Some projects are already underway, while others have yet to be implemented and require sustained monetary and project coordination commitments to make their impacts felt across the targeted regions.
“At the current pace of physician departures from the workforce, even with fellows graduating from adult and pediatric rheumatology training programs, the subspecialty cannot be sustained,” said Daniel Battafarano, DO, chair of the Workforce Solution Committee, professor of medicine at the Uniformed Services University of the Health Sciences, Bethesda, Md., and adjunct professor at the University of Texas Health Science Center, San Antonio.
The Northwest is an example of the problem at hand. “For an adult, there’s 1.65 rheumatologists per 100,000 in 2015. In 2025, there’s going to be 0.5 [adult] rheumatologists per 100,000. That’s a problem. If you look at every region in the United States, every single region is decrementing significantly,” he said.
Even the Northeast, which boasted 3.07 adult rheumatologists per 100,000 in 2015, will drop to 1.61 in 2025. Other regions are much worse off. The Southwest will drop from 1.28 to 0.64, and North Central will drop from 1.64 to 0.69, projections show.
The situation for pediatrics “has been in a crisis since 2015,” Dr. Battafarano said. It is much worse off than the situation for adult rheumatology, with 2015 figures going from 0.17 to 0.20 in the Southwest and from 0.03 to 0.04 in the South Central region by 2025, and in the Northwest from 0.67 to 0.13 and Northeast from 0.83 to 0.16.
“The ill effects of the pandemic are immeasurable to this point, but anecdotally we know we lost colleagues to part-time employment, we saw early retirements, and that happened across the full spectrum of the United States,” he said. It’s possible that up to 10% of full-time equivalents of physicians left practice in the United States since the pandemic began.
Rheumatologists largely practice in the 392 U.S. metropolitan statistical areas (MSAs), which are defined as a “core area containing a substantial population nucleus, together with adjacent communities having a high degree of economic and social integration with that core.” The smallest MSA has nearly 59,000 people. This distribution leaves many people in the Northwest, Southwest, South Central, and North Central regions with few rheumatologists. Over 86% of locations where rheumatologists train and work are in MSAs.
“By definition, if you get into a region where there’s 60,000 people or less, you can’t support a rheumatologist,” Dr. Battafarano said. He also noted that all pediatric hospitals tend to be in dense MSAs where rheumatologists might be.
South Central region serves as an example
People in certain MSAs of the South Central region (Oklahoma, Texas, Arkansas) such as Laredo, Tex., population 281,805 – where there is no adult rheumatologist – have to drive nearly 2.5 hours to the nearest well-served MSA (San Antonio) where there is a rheumatology fellowship program and medical school.
“Texas may have rheumatologists, but it depends on where you live,” Dr. Battafarano said. “The same applies to Waco, Texas; Texarkana, Arkansas; Lawton, Oklahoma; Pine Bluff, Arkansas; and Enid, Oklahoma, and you can see the range of traveling is between 45 minutes and 2.5 hours. That’s adult rheumatology.”
People in Laredo have an even longer drive to find a pediatric rheumatologist. In pediatrics, he said, “we don’t even look at towns, we look at pediatrics by state. You can see there’s a pediatric fellowship program in Dallas, and there’s one in Houston. There’s one or two [pediatric] rheumatologists in Austin. It just depends on how quickly they burn out and how long they stay. I’m in San Antonio. We don’t have a pediatric rheumatologist in San Antonio, the seventh-largest city in the United States.”
Pediatric rheumatologists are very often found where fellowship programs are located. “Ninety-five percent or greater of pediatric rheumatologists are housed in a pediatric hospital,” Dr. Battafarano said. “There are very few adult rheumatologists who see children, for a variety of reasons.”
In a panel discussion and question-and-answer session that took place after Dr. Battafarano outlined concerns with the numbers and distribution of rheumatologists across the United States, committee member Beth Jonas, MD, professor of medicine and chief of the division of rheumatology, allergy, and immunology at the University of North Carolina at Chapel Hill, noted that the rheumatology specialty match is competitive and typically leaves close to 100 residents who had rheumatology as their first choice without a match because there are not enough fellowship positions for them to fill.
The Workforce Solutions Committee hopes to reduce this “bottleneck,” she said, by identifying institutions that are ripe for opening new fellowship programs or have existing programs that can expand their number of positions, as well as expanding musculoskeletal training among nonrheumatologists, such as primary care physicians, advanced practice providers, and sports medicine physicians.
“I think that we’re going to find ourselves needing to be more creative as we become overcome with events with shortages of physicians,” Dr. Battafarano said. He gave an example of a recent pediatric rheumatology fellow in Seattle who wanted to go back home to Montana to practice. At the same time, the pediatric program wanted her to become a faculty member, so they said they would bridge their program to her, rotating fellows and covering her while on vacation.
“That’s an example of a pediatric program spreading its wings,” he said. “I think that we need to think that way, whether we talk about urban, suburban, rural. It’s how can we stage rheumatologists in areas, how can we embrace our primary care providers, and have rheumatology health care teams so that we have rheumatology expertise located within arm’s length but also within telemedicine length.”
Interventions for 2023
As part of a report on the activities of the Workforce Solutions Committee, Dr. Jonas outlined a number of interventions that the ACR is set to launch in 2023. The committee created five intervention teams to support fellowship positions and training providers, recruitment opportunities, fostering patient-centered communities, virtual training programs, and grants for research and training. The ACR’s initial pilot interventions are focused on, but not limited to, the Northwest, Southwest, and South Central regions.
The committee identified 10 potential partner institutions to develop new fellowship programs in the Northwest, Southwest, and South Central regions: University of Nevada, Las Vegas; Texas Tech University Permian Basin Program; Baylor Scott and White Medical Center Round Rock (Tex.) Program; Texas Tech University Health Science Center El Paso Program; University of Texas at Austin Dell Medical School Program; Abrazo Health Network Program in Arizona; University of Arizona Phoenix Program; University of Arkansas (pediatric program); Oklahoma State University; and University of Texas, San Antonio (pediatric program).
Dr. Jonas explained that opening new programs in these underserved areas should help establish new rheumatologists in these areas, because studies have shown that fellows tend to stay within 100-200 miles of where they trained.
In addition to starting new programs, “if you want to grow your program, if you want to add another fellow, we can support that,” Dr. Jonas said.
To help convince institutions of the value of rheumatology care, a position paper will soon be released by the ACR that outlines the benefits of the specialty to a health care system. The paper will describe an annual preventive cost savings of $2,762 per patient who is in the care of a rheumatologist and an annual direct or downstream income of $3.5 million per rheumatologist in a community, committee members said.
To help with recruitment and retention efforts, the ACR will revise its CareerConnection website to make it more useful.
To help in developing patient-centered communities of care, there will be a discussion series with payers on topics such as access, care delivery, and financing, in which 12 payers (including Blue Cross Blue Shield, Aetna, UnitedHealthcare, and Kaiser) will discuss patient access, cost, and quality measures. An in-person payer summit is also scheduled for 2023.
Interventions to enhance rheumatology care will also keep an ongoing focus on virtual training programs for primary care physicians and advanced practice providers, including a Project ECHO (Extension for Community Healthcare Outcomes) virtual lecture and case-based training and mentoring series for nonrheumatologists, an online library of searchable topics targeted to nonrheumatologists, as well as a grand rounds podcast series on certain rheumatic diseases for residents in family medicine, internal medicine, and pediatric programs. For rheumatology educators in 2023, there also will be an online portal curated by the ACR and other sources to use as a resource for developing curriculum.
A newly revised Fundamentals of Rheumatology course started in June 2022, which can help many medical students, residents, primary care physicians, and students in rehabilitation professions to learn about rheumatologic diseases, said committee member Janet Poole, PhD, division chief, professor, and director of the occupational therapy graduate program at the University of New Mexico, Albuquerque. Grants from the Rheumatology Research Foundation are available to offset the costs of the course for attendees.
An “onboarding toolkit” for nurse practitioners and physician assistants is now available to provide advice to practices for hiring, mentoring, and conducting performance evaluations in rheumatology care teams, Dr. Poole said. And fact sheets about the roles of interprofessional team members are being revised to give nonspecialty providers a sense of what other disciplines are available to care for patients with rheumatic and musculoskeletal disorders. The Advanced Rheumatology course is also being revised and will be available in summer 2023.
Other planned interventions aim to optimize telemedicine for the rheumatology community with a telehealth curriculum for rheumatology fellows, tools to improve telehealth implementation and delivery, and educational materials for patients to optimize their participation in telehealth visits.
The committee created targeted outreach to promote all grants focused on workforce expansion. As a result, in the last year the committee noted a three- to fourfold rise in the number of grant applications, including people and programs in underserved areas that had not previously applied. The Rheumatology Research Foundation also created a baseline for measuring success of grant funding in underserved areas and earmarked funds to increase awareness of the grants and facilitate applications.
Early signs of success are evident in the Rheumatology Access Expansion initiative in the ACR’s Collaborative Initiatives (COIN) department, said committee member Rosalind Ramsey-Goldman, MD, DrPH, professor of medicine/rheumatology at Northwestern University, Chicago. A team of rheumatologists, a pharmacist, and Navajo cultural interpreters developed a 12-week rheumatoid arthritis training program for primary care physicians in the Navajo Nation American Indian reservation, where there’s a high prevalence of RA and a shortage of local rheumatology providers. Results of the pilot study were presented in a plenary session at the meeting.
COIN also worked with the ACR’s Diversity, Equity, and Inclusion task force to sponsor 2022 annual meeting attendance for 11 medical students who identify themselves as underrepresented in medicine to expose them to rheumatology early in their career, said Dr. Ramsey-Goldman. The ACR is starting a program for medical students at historically Black colleges and universities and minority-serving institutions to include mentoring, round tables, and attendance at next year’s annual meeting.
None of the rheumatologists had relevant financial disclosures.
AT ACR 2022
Overturning Roe: Exacerbating inequities in abortion care and ObGyn training
On a recent overnight shift, our ObGyn on-call team was urgently paged to the emergency room for a patient who was brought in hemorrhaging after having passed out mid-flight from Texas to Boston. She was 12-weeks pregnant. We rushed her to the operating room for surgical removal of the pregnancy by dilation and curettage to stop her bleeding. Landing in Massachusetts had saved her life.
The significance of this patient’s case was not lost on the multidisciplinary teams caring for her, as the—at the time—impending Roe v Wade decision weighed heavily on our minds. One of many, her story foreshadows the harrowing experiences that we anticipate in the coming months and highlights the danger that the Supreme Court has inflicted on pregnant people nationally.
The Supreme Court decision on Dobbs v Jackson condemns us as a nation in which abortion rights are no longer federally protected under Roe v Wade.1 Twenty-six states have been poised to ban abortion, and in at least 12 states, abortion is now illegal.2,3 Political decision making will soon deny pregnant people the right to bodily autonomy, and the United States will lag behind other nations in abortion access.4 As ObGyn resident physicians who practice in tertiary referral hospitals in Massachusetts, where the ROE Act protects abortion beyond 24 weeks’ gestational age, we affirm abortion as essential health care that saves lives.5
Collectively as physician residents, we have provided an abortion for the patient at 22 weeks with a desired pregnancy who would have otherwise died from high blood pressures, the patient who ended her pregnancy to expedite breast cancer treatment, and the 16-year-old who feared for her life after suffering an assault by her partner for disclosing her pregnancy. With the overturn of Roe v Wade, patients like these will suffer dramatically divergent fates as race, class, and, now more than ever, geography will impact who is able to access abortion care.
Ramifications of the overturn of Roe
History foreshadows the grim impact of repealing Roe. Ohio’s 2011 law that requires the use of the restrictive protocol approved by the US Food and Drug Administration for mifepristone administration deepened existing inequities in abortion access.6 Patients with private insurance, higher income, higher level of education, and those who were White were more likely to obtain abortion care.7 In Texas, after the implementation of SB8 and other restrictive laws, Hispanic women whose travel distance increased more than 100 miles had the greatest reduction in abortion rates.8,9 A recent study regarding banning abortion in the United States estimated a 7% increase in pregnancy-related deaths in 1 year, with a 21% increase in subsequent years.10
Inequities in abortion access subsequently will disparately increase deaths of pregnant individuals in certain populations.11,12 Communities with the highest rates of unintended pregnancy, medical comorbidities, and lack of access to abortion, as well as historically marginalized populations—including non-Hispanic Black people, LGBTQIA people, those with limited English proficiency, and undocumented persons—will experience the greatest increase in pregnancy-related deaths due to a total abortion ban.13-15
The US maternal mortality rate is already the highest among developed nations, and it will only climb if ObGyns are not appropriately trained to operate within our full scope of practice and, thus, are unable to provide the highest quality of care.16,17
Continue: Abortion is a medical treatment that requires resident training...
Abortion is a medical treatment that requires resident training
Abortion care must be protected. Uterine evacuation by medical management, suction curettage, or dilation and evacuation is indicated for undesired pregnancy, regardless of reasoning or life circumstance. Pregnancy carries inherent risks that can at times be deadly.18 Abortion serves as first-line treatment for certain life-threatening pregnancy risks, including septic miscarriage, maternal hemorrhage, early-onset severe preeclampsia, and certain health conditions.19 Surgical skills and medical management of abortion are therefore fundamental components of ObGyn care and residency training.20
In choosing to become ObGyns,and particularly in selecting our training program, the ability to provide safe abortion care was a calculated priority. A recent study on the implications of overturning Roe predicted that nearly half of ObGyn residents will likely or certainly lose access to in-state abortion training.21 As demonstrated already in states with restrictive abortion laws, we will lose an entire generation of medical professionals skilled in performing this lifesaving procedure.9,22 While privileged patients may travel across state borders to access care, ObGyn and other medical trainees who are contract bound to residency programs do not have such flexibility to seek out abortion training. Although we hope the reversal of Roe will be fleeting, the consequences of this lost generation are irreparable.23,24 For physicians like ourselves, who fortunately are trained in surgical abortions and safe management of medical terminations, the discrepancy between evidence-based guidelines and impending political restrictions is distressing. We are forced to imagine refusing patients necessary health care—or face incarceration to save their lives.
The idea of watching a patient die, whether by hemorrhage, sepsis, or suicide, while armed with the tools of safe abortion technique is horrific. As authors with roots in Texas, Michigan, and Georgia, where abortion has or will almost certainly become illegal now that Roe v Wade is overturned, this scene is personal. It affects our future patients, our families, our colleagues, and our ability to return to our home states to live and practice.
Political organizing is critical to protect and restore abortion rights and defend against conservative coercive politics.25 Nearly half of pregnancies in the United States are unintended, and more than half of these end in abortion.26,27 Threats to abortion access require action from every one of the 59% of Americans who believe abortion should remain legal.28 This is especially important from a social and racial justice perspective as abortion bans will disproportionately affect marginalized groups and further exacerbate inequities in maternal mortality.13
Call to action
Now is the time for community action for reproductive justice and human rights. We urge everyone to donate to abortion funds, vote for leaders who support reproductive justice, and petition your state legislators to codify Roe into law. Now is the time to expand legislation to protect abortion providers and our patients. To ObGyns, family medicine physicians, internists, and other reproductive health clinicians, now is the time to maximize your abortion training. Now is the time to act; otherwise, pregnant individuals will die and future generations of physicians will not have the training to save their lives. ●
- de Vogue A, Sneed T, Duster C, et al. Supreme Court overturns Roe v Wade. CNN Politics. June 24, 2022. Accessed July 19, 2022. https://www.cnn.com/2022/06/24/politics/dobbs-missis sippi-supreme-court-abortion-roe-wade/index.html
- Nash E, Cross L. 26 States are certain or likely to ban abortion without Roe: here’s which ones and why. Guttmacher Institute. October 28, 2021. Updated April 19, 2022. Accessed July 19, 2022. https://www.guttmacher.org/article/2021/10/26-states-are-certain-or-likely-ban-abortion-without-roe-heres-which-ones-and-why
- Messerly M. Abortion laws by state: where abortions are illegal after Roe v Wade overturned. Politico. June 24, 2022. Accessed July 19, 2022. https://www.politico.com/news/2022/06/24/abortion-laws-by-state-roe-v-wade-00037695
- Archie A. US would lag behind global abortion access if Roe v Wade is undone, advocates say. NPR. May 5, 2022. Accessed July 19, 2022. https://www.npr.org/2022/05/05/1096805490/abortion-access-supreme-court-roe-v-wade-united-nations
- Romo V. Massachusetts senate overrides veto, passes law expanding abortion access. NPR. December 29, 2020. Accessed July 19, 2022. https://www.npr.org/2020/12/29/951259506/massachusetts-senate-overrides-veto-passes-law-expanding-abortion-access
- Upadhyay UD, Johns NE, Combellick SL, et al. Comparison of outcomes before and after Ohio’s law mandating use of the FDA-approved protocol for medication abortion: a retrospective cohort study. PLoS Med. 2016;13:e1002110.
- Upadhyay UD, Johns NE, Cartwright AF, et al. Sociodemographic characteristics of women able to obtain medication abortion before and after Ohio’s law requiring use of the Food and Drug Administration protocol. Health Equity. 2018;2:122-130.
- Goyal V, Brooks IHM, Powers DA. Differences in abortion rates by race-ethnicity after implementation of a restrictive Texas law. Contraception. 2020;102:109-114.
- Noyes E Holder BH, Evans ML. Texas SB8 and the future of abortion care. OBG Manag. 2021;33. doi:12788/obgm.0151.
- Vilda D, Wallace ME, Daniel C, et al. State abortion policies and maternal death in the United States, 2015‒2018. Am J Public Health. 2021;111:1696-1704.
- The Lancet. Why Roe v Wade must be defended. Lancet. 2022;399:1845.
- Nambiar A, Patel S, Santiago-Munoz P, et al. Maternal morbidity and fetal outcomes among pregnant women at 22 weeks’ gestation or less with complications in two Texas hospitals after legislation on abortion. Am J Obstet Gynecol. 2022;227:648-650.e1.
- Stevenson AJ. The pregnancy-related mortality impact of a total abortion ban in the United States: a research note on increased deaths due to remaining pregnant. Demography. 2021;58:20192028.
- Medley S. Gutting abortion rights would be devastating for LGBTQ+ people. Them. September 17, 2021. Accessed July 20, 2022. https://www.them.us/story/gutting-abortion-rights-devastating-lgbtq-people
- Holter L. Detained immigrant women are facing a grueling abortion struggle. National Latina Institute for Reproductive Justice. May 10, 2017. Accessed July 20, 2022. https://www.latinainsti tute.org/es/node/4620
- Haddad LB, Nour NM. Unsafe abortion: unnecessary maternal mortality. Rev Obstet Gynecol. 2009;2:122-126.
- Tikkanen R, Gunja MZ, FitzGerald M, et al. Maternal mortality and maternity care in the United States compared to 10 other developed countries. The Commonwealth Fund. November 18, 2020. Accessed November 17, 2022. https://www .commonwealthfund.org/publications/issue -briefs/2020/nov/maternal-mortality-maternity -care-us-compared-10-countries
- Collier A-RY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews. 2019;20:e561-e574.
- ACOG practice bulletin no. 135: Second-trimester abortion. Obstet Gynecol. 2013;121:1394-1406.
- Committee on Health Care for Underserved Women. ACOG Committee opinion no. 612: Abortion training and education. Obstet Gynecol. 2014;124:1055-1059.
- Vinekar K, Karlapudi A, Nathan L, et al. Projected implications of overturning Roe v Wade on abortion training in US obstetrics and gynecology residency programs. Obstet Gynecol. 2022;140:146-149.
- Horvath S, Turk J, Steinauer J, et al. Increase in obstetrics and gynecology resident self-assessed competence in early pregnancy loss management with routine abortion care training. Obstet Gynecol. 2022;139:116-119.
- Anderson N. The fall of Roe scrambles abortion training in university hospitals. The Washington Post. June 30, 2022. Accessed July 20, 2022. https://www.washingtonpost.com/educa tion/2022/06/30/abortion-training-upheaval-dobbs/
- Weiner S. How the repeal of Roe v Wade will affect training in abortion and reproductive health. AAMC. June 24, 2022. Accessed July 20, 2022. https://www.aamc.org/news-insights/how-repeal-roe-v-wade-will-affect-training-abortion-and-reproductive-health
- Dreweke J. Coercion is at the heart of social conservatives’ reproductive health agenda. Guttmacher Institute. February 7, 2018. Accessed July 20, 2022. https://www.guttmacher.org/gpr/2018/02/coercion-heart-social-conservatives-reproduc tive-health-agenda
- Unintended pregnancy and abortion worldwide. Guttmacher Institute. March 2022. Accessed July 20, 2022. https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide
- Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374:843-852.
- Hartig H. About six-in-ten Americans say abortion should be legal in all or most cases. Pew Research Center. June 13, 2022. Accessed July 20, 2022. https://www.pewresearch.org/fact-tank/2022/06/13/about-six-in-ten-americans-say-abortion-should-be-legal-in-all-or-most-cases-2/

Samantha Truong, MD
Dr. Truong is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, Massachusetts.

Emily R. Burdette, MD, MPH
Dr. Burdette is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.

Ellen C. Murphy, MD
Dr. Murphy is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
The authors report no financial relationships relevant to this article.
Samantha Truong, MD
Dr. Truong is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, Massachusetts.
Emily R. Burdette, MD, MPH
Dr. Burdette is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
Ellen C. Murphy, MD
Dr. Murphy is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
The authors report no financial relationships relevant to this article.
Samantha Truong, MD
Dr. Truong is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston, Massachusetts.
Emily R. Burdette, MD, MPH
Dr. Burdette is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
Ellen C. Murphy, MD
Dr. Murphy is Resident, Obstetrics and Gynecology, Brigham and Women’s Hospital and Massachusetts General Hospital, Boston.
The authors report no financial relationships relevant to this article.
On a recent overnight shift, our ObGyn on-call team was urgently paged to the emergency room for a patient who was brought in hemorrhaging after having passed out mid-flight from Texas to Boston. She was 12-weeks pregnant. We rushed her to the operating room for surgical removal of the pregnancy by dilation and curettage to stop her bleeding. Landing in Massachusetts had saved her life.
The significance of this patient’s case was not lost on the multidisciplinary teams caring for her, as the—at the time—impending Roe v Wade decision weighed heavily on our minds. One of many, her story foreshadows the harrowing experiences that we anticipate in the coming months and highlights the danger that the Supreme Court has inflicted on pregnant people nationally.
The Supreme Court decision on Dobbs v Jackson condemns us as a nation in which abortion rights are no longer federally protected under Roe v Wade.1 Twenty-six states have been poised to ban abortion, and in at least 12 states, abortion is now illegal.2,3 Political decision making will soon deny pregnant people the right to bodily autonomy, and the United States will lag behind other nations in abortion access.4 As ObGyn resident physicians who practice in tertiary referral hospitals in Massachusetts, where the ROE Act protects abortion beyond 24 weeks’ gestational age, we affirm abortion as essential health care that saves lives.5
Collectively as physician residents, we have provided an abortion for the patient at 22 weeks with a desired pregnancy who would have otherwise died from high blood pressures, the patient who ended her pregnancy to expedite breast cancer treatment, and the 16-year-old who feared for her life after suffering an assault by her partner for disclosing her pregnancy. With the overturn of Roe v Wade, patients like these will suffer dramatically divergent fates as race, class, and, now more than ever, geography will impact who is able to access abortion care.
Ramifications of the overturn of Roe
History foreshadows the grim impact of repealing Roe. Ohio’s 2011 law that requires the use of the restrictive protocol approved by the US Food and Drug Administration for mifepristone administration deepened existing inequities in abortion access.6 Patients with private insurance, higher income, higher level of education, and those who were White were more likely to obtain abortion care.7 In Texas, after the implementation of SB8 and other restrictive laws, Hispanic women whose travel distance increased more than 100 miles had the greatest reduction in abortion rates.8,9 A recent study regarding banning abortion in the United States estimated a 7% increase in pregnancy-related deaths in 1 year, with a 21% increase in subsequent years.10
Inequities in abortion access subsequently will disparately increase deaths of pregnant individuals in certain populations.11,12 Communities with the highest rates of unintended pregnancy, medical comorbidities, and lack of access to abortion, as well as historically marginalized populations—including non-Hispanic Black people, LGBTQIA people, those with limited English proficiency, and undocumented persons—will experience the greatest increase in pregnancy-related deaths due to a total abortion ban.13-15
The US maternal mortality rate is already the highest among developed nations, and it will only climb if ObGyns are not appropriately trained to operate within our full scope of practice and, thus, are unable to provide the highest quality of care.16,17
Continue: Abortion is a medical treatment that requires resident training...
Abortion is a medical treatment that requires resident training
Abortion care must be protected. Uterine evacuation by medical management, suction curettage, or dilation and evacuation is indicated for undesired pregnancy, regardless of reasoning or life circumstance. Pregnancy carries inherent risks that can at times be deadly.18 Abortion serves as first-line treatment for certain life-threatening pregnancy risks, including septic miscarriage, maternal hemorrhage, early-onset severe preeclampsia, and certain health conditions.19 Surgical skills and medical management of abortion are therefore fundamental components of ObGyn care and residency training.20
In choosing to become ObGyns,and particularly in selecting our training program, the ability to provide safe abortion care was a calculated priority. A recent study on the implications of overturning Roe predicted that nearly half of ObGyn residents will likely or certainly lose access to in-state abortion training.21 As demonstrated already in states with restrictive abortion laws, we will lose an entire generation of medical professionals skilled in performing this lifesaving procedure.9,22 While privileged patients may travel across state borders to access care, ObGyn and other medical trainees who are contract bound to residency programs do not have such flexibility to seek out abortion training. Although we hope the reversal of Roe will be fleeting, the consequences of this lost generation are irreparable.23,24 For physicians like ourselves, who fortunately are trained in surgical abortions and safe management of medical terminations, the discrepancy between evidence-based guidelines and impending political restrictions is distressing. We are forced to imagine refusing patients necessary health care—or face incarceration to save their lives.
The idea of watching a patient die, whether by hemorrhage, sepsis, or suicide, while armed with the tools of safe abortion technique is horrific. As authors with roots in Texas, Michigan, and Georgia, where abortion has or will almost certainly become illegal now that Roe v Wade is overturned, this scene is personal. It affects our future patients, our families, our colleagues, and our ability to return to our home states to live and practice.
Political organizing is critical to protect and restore abortion rights and defend against conservative coercive politics.25 Nearly half of pregnancies in the United States are unintended, and more than half of these end in abortion.26,27 Threats to abortion access require action from every one of the 59% of Americans who believe abortion should remain legal.28 This is especially important from a social and racial justice perspective as abortion bans will disproportionately affect marginalized groups and further exacerbate inequities in maternal mortality.13
Call to action
Now is the time for community action for reproductive justice and human rights. We urge everyone to donate to abortion funds, vote for leaders who support reproductive justice, and petition your state legislators to codify Roe into law. Now is the time to expand legislation to protect abortion providers and our patients. To ObGyns, family medicine physicians, internists, and other reproductive health clinicians, now is the time to maximize your abortion training. Now is the time to act; otherwise, pregnant individuals will die and future generations of physicians will not have the training to save their lives. ●
On a recent overnight shift, our ObGyn on-call team was urgently paged to the emergency room for a patient who was brought in hemorrhaging after having passed out mid-flight from Texas to Boston. She was 12-weeks pregnant. We rushed her to the operating room for surgical removal of the pregnancy by dilation and curettage to stop her bleeding. Landing in Massachusetts had saved her life.
The significance of this patient’s case was not lost on the multidisciplinary teams caring for her, as the—at the time—impending Roe v Wade decision weighed heavily on our minds. One of many, her story foreshadows the harrowing experiences that we anticipate in the coming months and highlights the danger that the Supreme Court has inflicted on pregnant people nationally.
The Supreme Court decision on Dobbs v Jackson condemns us as a nation in which abortion rights are no longer federally protected under Roe v Wade.1 Twenty-six states have been poised to ban abortion, and in at least 12 states, abortion is now illegal.2,3 Political decision making will soon deny pregnant people the right to bodily autonomy, and the United States will lag behind other nations in abortion access.4 As ObGyn resident physicians who practice in tertiary referral hospitals in Massachusetts, where the ROE Act protects abortion beyond 24 weeks’ gestational age, we affirm abortion as essential health care that saves lives.5
Collectively as physician residents, we have provided an abortion for the patient at 22 weeks with a desired pregnancy who would have otherwise died from high blood pressures, the patient who ended her pregnancy to expedite breast cancer treatment, and the 16-year-old who feared for her life after suffering an assault by her partner for disclosing her pregnancy. With the overturn of Roe v Wade, patients like these will suffer dramatically divergent fates as race, class, and, now more than ever, geography will impact who is able to access abortion care.
Ramifications of the overturn of Roe
History foreshadows the grim impact of repealing Roe. Ohio’s 2011 law that requires the use of the restrictive protocol approved by the US Food and Drug Administration for mifepristone administration deepened existing inequities in abortion access.6 Patients with private insurance, higher income, higher level of education, and those who were White were more likely to obtain abortion care.7 In Texas, after the implementation of SB8 and other restrictive laws, Hispanic women whose travel distance increased more than 100 miles had the greatest reduction in abortion rates.8,9 A recent study regarding banning abortion in the United States estimated a 7% increase in pregnancy-related deaths in 1 year, with a 21% increase in subsequent years.10
Inequities in abortion access subsequently will disparately increase deaths of pregnant individuals in certain populations.11,12 Communities with the highest rates of unintended pregnancy, medical comorbidities, and lack of access to abortion, as well as historically marginalized populations—including non-Hispanic Black people, LGBTQIA people, those with limited English proficiency, and undocumented persons—will experience the greatest increase in pregnancy-related deaths due to a total abortion ban.13-15
The US maternal mortality rate is already the highest among developed nations, and it will only climb if ObGyns are not appropriately trained to operate within our full scope of practice and, thus, are unable to provide the highest quality of care.16,17
Continue: Abortion is a medical treatment that requires resident training...
Abortion is a medical treatment that requires resident training
Abortion care must be protected. Uterine evacuation by medical management, suction curettage, or dilation and evacuation is indicated for undesired pregnancy, regardless of reasoning or life circumstance. Pregnancy carries inherent risks that can at times be deadly.18 Abortion serves as first-line treatment for certain life-threatening pregnancy risks, including septic miscarriage, maternal hemorrhage, early-onset severe preeclampsia, and certain health conditions.19 Surgical skills and medical management of abortion are therefore fundamental components of ObGyn care and residency training.20
In choosing to become ObGyns,and particularly in selecting our training program, the ability to provide safe abortion care was a calculated priority. A recent study on the implications of overturning Roe predicted that nearly half of ObGyn residents will likely or certainly lose access to in-state abortion training.21 As demonstrated already in states with restrictive abortion laws, we will lose an entire generation of medical professionals skilled in performing this lifesaving procedure.9,22 While privileged patients may travel across state borders to access care, ObGyn and other medical trainees who are contract bound to residency programs do not have such flexibility to seek out abortion training. Although we hope the reversal of Roe will be fleeting, the consequences of this lost generation are irreparable.23,24 For physicians like ourselves, who fortunately are trained in surgical abortions and safe management of medical terminations, the discrepancy between evidence-based guidelines and impending political restrictions is distressing. We are forced to imagine refusing patients necessary health care—or face incarceration to save their lives.
The idea of watching a patient die, whether by hemorrhage, sepsis, or suicide, while armed with the tools of safe abortion technique is horrific. As authors with roots in Texas, Michigan, and Georgia, where abortion has or will almost certainly become illegal now that Roe v Wade is overturned, this scene is personal. It affects our future patients, our families, our colleagues, and our ability to return to our home states to live and practice.
Political organizing is critical to protect and restore abortion rights and defend against conservative coercive politics.25 Nearly half of pregnancies in the United States are unintended, and more than half of these end in abortion.26,27 Threats to abortion access require action from every one of the 59% of Americans who believe abortion should remain legal.28 This is especially important from a social and racial justice perspective as abortion bans will disproportionately affect marginalized groups and further exacerbate inequities in maternal mortality.13
Call to action
Now is the time for community action for reproductive justice and human rights. We urge everyone to donate to abortion funds, vote for leaders who support reproductive justice, and petition your state legislators to codify Roe into law. Now is the time to expand legislation to protect abortion providers and our patients. To ObGyns, family medicine physicians, internists, and other reproductive health clinicians, now is the time to maximize your abortion training. Now is the time to act; otherwise, pregnant individuals will die and future generations of physicians will not have the training to save their lives. ●
- de Vogue A, Sneed T, Duster C, et al. Supreme Court overturns Roe v Wade. CNN Politics. June 24, 2022. Accessed July 19, 2022. https://www.cnn.com/2022/06/24/politics/dobbs-missis sippi-supreme-court-abortion-roe-wade/index.html
- Nash E, Cross L. 26 States are certain or likely to ban abortion without Roe: here’s which ones and why. Guttmacher Institute. October 28, 2021. Updated April 19, 2022. Accessed July 19, 2022. https://www.guttmacher.org/article/2021/10/26-states-are-certain-or-likely-ban-abortion-without-roe-heres-which-ones-and-why
- Messerly M. Abortion laws by state: where abortions are illegal after Roe v Wade overturned. Politico. June 24, 2022. Accessed July 19, 2022. https://www.politico.com/news/2022/06/24/abortion-laws-by-state-roe-v-wade-00037695
- Archie A. US would lag behind global abortion access if Roe v Wade is undone, advocates say. NPR. May 5, 2022. Accessed July 19, 2022. https://www.npr.org/2022/05/05/1096805490/abortion-access-supreme-court-roe-v-wade-united-nations
- Romo V. Massachusetts senate overrides veto, passes law expanding abortion access. NPR. December 29, 2020. Accessed July 19, 2022. https://www.npr.org/2020/12/29/951259506/massachusetts-senate-overrides-veto-passes-law-expanding-abortion-access
- Upadhyay UD, Johns NE, Combellick SL, et al. Comparison of outcomes before and after Ohio’s law mandating use of the FDA-approved protocol for medication abortion: a retrospective cohort study. PLoS Med. 2016;13:e1002110.
- Upadhyay UD, Johns NE, Cartwright AF, et al. Sociodemographic characteristics of women able to obtain medication abortion before and after Ohio’s law requiring use of the Food and Drug Administration protocol. Health Equity. 2018;2:122-130.
- Goyal V, Brooks IHM, Powers DA. Differences in abortion rates by race-ethnicity after implementation of a restrictive Texas law. Contraception. 2020;102:109-114.
- Noyes E Holder BH, Evans ML. Texas SB8 and the future of abortion care. OBG Manag. 2021;33. doi:12788/obgm.0151.
- Vilda D, Wallace ME, Daniel C, et al. State abortion policies and maternal death in the United States, 2015‒2018. Am J Public Health. 2021;111:1696-1704.
- The Lancet. Why Roe v Wade must be defended. Lancet. 2022;399:1845.
- Nambiar A, Patel S, Santiago-Munoz P, et al. Maternal morbidity and fetal outcomes among pregnant women at 22 weeks’ gestation or less with complications in two Texas hospitals after legislation on abortion. Am J Obstet Gynecol. 2022;227:648-650.e1.
- Stevenson AJ. The pregnancy-related mortality impact of a total abortion ban in the United States: a research note on increased deaths due to remaining pregnant. Demography. 2021;58:20192028.
- Medley S. Gutting abortion rights would be devastating for LGBTQ+ people. Them. September 17, 2021. Accessed July 20, 2022. https://www.them.us/story/gutting-abortion-rights-devastating-lgbtq-people
- Holter L. Detained immigrant women are facing a grueling abortion struggle. National Latina Institute for Reproductive Justice. May 10, 2017. Accessed July 20, 2022. https://www.latinainsti tute.org/es/node/4620
- Haddad LB, Nour NM. Unsafe abortion: unnecessary maternal mortality. Rev Obstet Gynecol. 2009;2:122-126.
- Tikkanen R, Gunja MZ, FitzGerald M, et al. Maternal mortality and maternity care in the United States compared to 10 other developed countries. The Commonwealth Fund. November 18, 2020. Accessed November 17, 2022. https://www .commonwealthfund.org/publications/issue -briefs/2020/nov/maternal-mortality-maternity -care-us-compared-10-countries
- Collier A-RY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews. 2019;20:e561-e574.
- ACOG practice bulletin no. 135: Second-trimester abortion. Obstet Gynecol. 2013;121:1394-1406.
- Committee on Health Care for Underserved Women. ACOG Committee opinion no. 612: Abortion training and education. Obstet Gynecol. 2014;124:1055-1059.
- Vinekar K, Karlapudi A, Nathan L, et al. Projected implications of overturning Roe v Wade on abortion training in US obstetrics and gynecology residency programs. Obstet Gynecol. 2022;140:146-149.
- Horvath S, Turk J, Steinauer J, et al. Increase in obstetrics and gynecology resident self-assessed competence in early pregnancy loss management with routine abortion care training. Obstet Gynecol. 2022;139:116-119.
- Anderson N. The fall of Roe scrambles abortion training in university hospitals. The Washington Post. June 30, 2022. Accessed July 20, 2022. https://www.washingtonpost.com/educa tion/2022/06/30/abortion-training-upheaval-dobbs/
- Weiner S. How the repeal of Roe v Wade will affect training in abortion and reproductive health. AAMC. June 24, 2022. Accessed July 20, 2022. https://www.aamc.org/news-insights/how-repeal-roe-v-wade-will-affect-training-abortion-and-reproductive-health
- Dreweke J. Coercion is at the heart of social conservatives’ reproductive health agenda. Guttmacher Institute. February 7, 2018. Accessed July 20, 2022. https://www.guttmacher.org/gpr/2018/02/coercion-heart-social-conservatives-reproduc tive-health-agenda
- Unintended pregnancy and abortion worldwide. Guttmacher Institute. March 2022. Accessed July 20, 2022. https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide
- Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374:843-852.
- Hartig H. About six-in-ten Americans say abortion should be legal in all or most cases. Pew Research Center. June 13, 2022. Accessed July 20, 2022. https://www.pewresearch.org/fact-tank/2022/06/13/about-six-in-ten-americans-say-abortion-should-be-legal-in-all-or-most-cases-2/
- de Vogue A, Sneed T, Duster C, et al. Supreme Court overturns Roe v Wade. CNN Politics. June 24, 2022. Accessed July 19, 2022. https://www.cnn.com/2022/06/24/politics/dobbs-missis sippi-supreme-court-abortion-roe-wade/index.html
- Nash E, Cross L. 26 States are certain or likely to ban abortion without Roe: here’s which ones and why. Guttmacher Institute. October 28, 2021. Updated April 19, 2022. Accessed July 19, 2022. https://www.guttmacher.org/article/2021/10/26-states-are-certain-or-likely-ban-abortion-without-roe-heres-which-ones-and-why
- Messerly M. Abortion laws by state: where abortions are illegal after Roe v Wade overturned. Politico. June 24, 2022. Accessed July 19, 2022. https://www.politico.com/news/2022/06/24/abortion-laws-by-state-roe-v-wade-00037695
- Archie A. US would lag behind global abortion access if Roe v Wade is undone, advocates say. NPR. May 5, 2022. Accessed July 19, 2022. https://www.npr.org/2022/05/05/1096805490/abortion-access-supreme-court-roe-v-wade-united-nations
- Romo V. Massachusetts senate overrides veto, passes law expanding abortion access. NPR. December 29, 2020. Accessed July 19, 2022. https://www.npr.org/2020/12/29/951259506/massachusetts-senate-overrides-veto-passes-law-expanding-abortion-access
- Upadhyay UD, Johns NE, Combellick SL, et al. Comparison of outcomes before and after Ohio’s law mandating use of the FDA-approved protocol for medication abortion: a retrospective cohort study. PLoS Med. 2016;13:e1002110.
- Upadhyay UD, Johns NE, Cartwright AF, et al. Sociodemographic characteristics of women able to obtain medication abortion before and after Ohio’s law requiring use of the Food and Drug Administration protocol. Health Equity. 2018;2:122-130.
- Goyal V, Brooks IHM, Powers DA. Differences in abortion rates by race-ethnicity after implementation of a restrictive Texas law. Contraception. 2020;102:109-114.
- Noyes E Holder BH, Evans ML. Texas SB8 and the future of abortion care. OBG Manag. 2021;33. doi:12788/obgm.0151.
- Vilda D, Wallace ME, Daniel C, et al. State abortion policies and maternal death in the United States, 2015‒2018. Am J Public Health. 2021;111:1696-1704.
- The Lancet. Why Roe v Wade must be defended. Lancet. 2022;399:1845.
- Nambiar A, Patel S, Santiago-Munoz P, et al. Maternal morbidity and fetal outcomes among pregnant women at 22 weeks’ gestation or less with complications in two Texas hospitals after legislation on abortion. Am J Obstet Gynecol. 2022;227:648-650.e1.
- Stevenson AJ. The pregnancy-related mortality impact of a total abortion ban in the United States: a research note on increased deaths due to remaining pregnant. Demography. 2021;58:20192028.
- Medley S. Gutting abortion rights would be devastating for LGBTQ+ people. Them. September 17, 2021. Accessed July 20, 2022. https://www.them.us/story/gutting-abortion-rights-devastating-lgbtq-people
- Holter L. Detained immigrant women are facing a grueling abortion struggle. National Latina Institute for Reproductive Justice. May 10, 2017. Accessed July 20, 2022. https://www.latinainsti tute.org/es/node/4620
- Haddad LB, Nour NM. Unsafe abortion: unnecessary maternal mortality. Rev Obstet Gynecol. 2009;2:122-126.
- Tikkanen R, Gunja MZ, FitzGerald M, et al. Maternal mortality and maternity care in the United States compared to 10 other developed countries. The Commonwealth Fund. November 18, 2020. Accessed November 17, 2022. https://www .commonwealthfund.org/publications/issue -briefs/2020/nov/maternal-mortality-maternity -care-us-compared-10-countries
- Collier A-RY, Molina RL. Maternal mortality in the United States: updates on trends, causes, and solutions. Neoreviews. 2019;20:e561-e574.
- ACOG practice bulletin no. 135: Second-trimester abortion. Obstet Gynecol. 2013;121:1394-1406.
- Committee on Health Care for Underserved Women. ACOG Committee opinion no. 612: Abortion training and education. Obstet Gynecol. 2014;124:1055-1059.
- Vinekar K, Karlapudi A, Nathan L, et al. Projected implications of overturning Roe v Wade on abortion training in US obstetrics and gynecology residency programs. Obstet Gynecol. 2022;140:146-149.
- Horvath S, Turk J, Steinauer J, et al. Increase in obstetrics and gynecology resident self-assessed competence in early pregnancy loss management with routine abortion care training. Obstet Gynecol. 2022;139:116-119.
- Anderson N. The fall of Roe scrambles abortion training in university hospitals. The Washington Post. June 30, 2022. Accessed July 20, 2022. https://www.washingtonpost.com/educa tion/2022/06/30/abortion-training-upheaval-dobbs/
- Weiner S. How the repeal of Roe v Wade will affect training in abortion and reproductive health. AAMC. June 24, 2022. Accessed July 20, 2022. https://www.aamc.org/news-insights/how-repeal-roe-v-wade-will-affect-training-abortion-and-reproductive-health
- Dreweke J. Coercion is at the heart of social conservatives’ reproductive health agenda. Guttmacher Institute. February 7, 2018. Accessed July 20, 2022. https://www.guttmacher.org/gpr/2018/02/coercion-heart-social-conservatives-reproduc tive-health-agenda
- Unintended pregnancy and abortion worldwide. Guttmacher Institute. March 2022. Accessed July 20, 2022. https://www.guttmacher.org/fact-sheet/induced-abortion-worldwide
- Finer LB, Zolna MR. Declines in unintended pregnancy in the United States, 2008–2011. N Engl J Med. 2016;374:843-852.
- Hartig H. About six-in-ten Americans say abortion should be legal in all or most cases. Pew Research Center. June 13, 2022. Accessed July 20, 2022. https://www.pewresearch.org/fact-tank/2022/06/13/about-six-in-ten-americans-say-abortion-should-be-legal-in-all-or-most-cases-2/

Does fertility preservation in patients with breast cancer impact relapse rates and disease-specific mortality?
Marklund A, Lekberg T, Hedayati E, et al. Relapse rates and disease-specific mortality following procedures for fertility preservation at time of breast cancer diagnosis. JAMA Oncol. 2022;8:1438-1446. doi:10.1001/jamaoncol.2022.3677.
EXPERT COMMENTARY
Breast cancer is the most diagnosed cancer among US women after skin cancer.1 As of the end of 2020, 7.8 million women were alive who were diagnosed with breast cancer in the past 5 years, making it the world’s most prevalent cancer. Given the wide reach of breast cancer and the increase in its distant stage by more than 4% per year in women of reproductive age (20–39 years), clinicians are urged to address fertility preservation due to reproductive compromise of gonadotoxic therapies and gonadectomy.2 To predict the risk of infertility following chemotherapy, a Cyclophosphamide Equivalent Dose (CED) calculator can be used. A CED of 4,000 mg/m2 has been associated with a significant risk of infertility.3
In 2012, the American Society for Reproductive Medicine removed the experimental label of oocyte cryopreservation then recently endorsed ovarian cryopreservation, thereby providing acceptable procedures for fertility preservation.4 Gonadotropin-releasing hormone agonist use during chemotherapy, which is used to protect the ovary in premenopausal women against the effects of chemotherapy, has been shown to have inconsistent findings and should not replace the established modalities of oocyte/embryo/ovarian tissue cryopreservation.2,5
Details of the study
While studies have been reassuring that ovarian stimulation for fertility preservation in women with breast cancer does not worsen the prognosis, findings are limited by short-term follow-up.6
The recent study by Marklund and colleagues presented an analysis of breast cancer relapse and mortality following fertility preservation with and without hormonal stimulation. In their prospective cohort study of 425 Swedish women who underwent fertility preservation, the authors categorized patients into 2 groups: oocyte and embryo cryopreservation by ovarian hormonal stimulation and ovarian tissue cryopreservation without hormonal stimulation. The control group included 850 women with breast cancer who did not undergo fertility preservation. The cohort and the control groups were matched on age, calendar period of diagnosis, and region. Three Swedish registers for breast cancer were used to obtain the study cohort, and for each participant, 2 breast cancer patients who were unexposed to fertility preservation were used for comparison. The primary outcome was mortality while the secondary outcome was any event of death due to breast cancer or relapse.
Results. A total of 1,275 women were studied at the time of breast cancer diagnosis. After stratification, which included age, parity at diagnosis, tumor size, number of lymph node metastases, and estrogen receptor status, disease-specific mortality was similar in all categories of women, that is, hormonal fertility preservation, nonhormonal fertility preservation, and controls. In the subcohort of 723 women, the adjusted rate of relapse and disease-specific mortality remained the same among all groups.
Study strengths and limitations
This study prompts several areas of criticism. The follow-up of breast cancer patients was only 5 years, adding to the limitations of short-term monitoring seen in prior studies. The authors also considered a delay in pregnancy attempts following breast cancer treatment of hormonally sensitive cancers of 5 to 10 years. However, the long-term safety of pregnancy following breast cancer has shown a statistically significantly superior disease-free survival (DFS) in patients who became pregnant less than 2 years from diagnosis and no difference in those who became pregnant 2 or more years from diagnosis.7
Only 58 women in the nonhormonal fertility preservation group (ovarian tissue cryopreservation) were studied, which may limit an adequate evaluation although it is not expected to negatively impact breast cancer prognosis. Another area of potential bias was the use of only a subcohort to assess relapse-free survival as opposed to the entire cohort that was used to assess mortality.
Strengths of this study include obligatory reporting to the registry and equal access to anticancer treatment and fertility preservation in Sweden. Ovarian stimulating drugs were examined, as letrozole is often used in breast cancer patients to maintain lower estradiol levels due to aromatase inhibition. Nevertheless, this study did not demonstrate a difference in mortality with or without letrozole use. ●
Marklund and colleagues’ findings revealed no increase of breast cancer relapse and mortality following fertility preservation with or without hormonal stimulation. They also propose a “healthy user effect” whereby a woman who feels healthy may choose to undergo fertility preservation, thereby biasing the outcome by having a better survival.8
Future studies with longer follow-up are needed to address the hormonal impact of fertility preservation, if any, on breast cancer DFS and mortality, as well as to evaluate subsequent pregnancy outcomes, stratified for medication treatment type via the CED calculator. To date, evidence continues to support fertility preservation options that use hormonal ovarian stimulation in breast cancer patients as apparently safe for, at least, up to 5 years of follow-up.
MARK P. TROLICE, MD
- Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72:524-541. doi:10.3322/caac.21754.
- Oktay K, Harvey BE, Partridge AH, et al. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;1;36:1994-2001. doi:10.1200/JCO.2018.78.1914.
- Fertility Preservation in Pittsburgh. CED calculator. Accessed November 14, 2022. https://fertilitypreservationpittsburgh.org/fertility-resources/fertility-risk-calculator/
- Practice Committee of the American Society for Reproductive Medicine. Fertility preservation in patients undergoing gonadotoxic therapy or gonadectomy: a committee opinion. Fertil Steril. 2019;112:1022-1033. doi:10.1016/j.fertnstert.2019.09.013.
- Blumenfeld Z. Fertility preservation using GnRH agonists: rationale, possible mechanisms, and explanation of controversy. Clin Med Insights Reprod Health. 2019;13: 1179558119870163. doi:10.1177/1179558119870163.
- Beebeejaun Y, Athithan A, Copeland TP, et al. Risk of breast cancer in women treated with ovarian stimulation drugs for infertility: a systematic review and meta-analysis. Fertil Steril. 2021;116:198-207. doi:10.1016/j.fertnstert.2021.01.044.
- Lambertini M, Kroman N, Ameye L, et al. Long-term safety of pregnancy following breast cancer according to estrogen receptor status. J Natl Cancer Inst. 2018;110:426-429. doi:10.1093/jnci/djx206.
- Marklund A, Lundberg FE, Eloranta S, et al. Reproductive outcomes after breast cancer in women with vs without fertility preservation. JAMA Oncol. 2021;7:86-91. doi:10.1001/ jamaoncol.2020.5957.
Marklund A, Lekberg T, Hedayati E, et al. Relapse rates and disease-specific mortality following procedures for fertility preservation at time of breast cancer diagnosis. JAMA Oncol. 2022;8:1438-1446. doi:10.1001/jamaoncol.2022.3677.
EXPERT COMMENTARY
Breast cancer is the most diagnosed cancer among US women after skin cancer.1 As of the end of 2020, 7.8 million women were alive who were diagnosed with breast cancer in the past 5 years, making it the world’s most prevalent cancer. Given the wide reach of breast cancer and the increase in its distant stage by more than 4% per year in women of reproductive age (20–39 years), clinicians are urged to address fertility preservation due to reproductive compromise of gonadotoxic therapies and gonadectomy.2 To predict the risk of infertility following chemotherapy, a Cyclophosphamide Equivalent Dose (CED) calculator can be used. A CED of 4,000 mg/m2 has been associated with a significant risk of infertility.3
In 2012, the American Society for Reproductive Medicine removed the experimental label of oocyte cryopreservation then recently endorsed ovarian cryopreservation, thereby providing acceptable procedures for fertility preservation.4 Gonadotropin-releasing hormone agonist use during chemotherapy, which is used to protect the ovary in premenopausal women against the effects of chemotherapy, has been shown to have inconsistent findings and should not replace the established modalities of oocyte/embryo/ovarian tissue cryopreservation.2,5
Details of the study
While studies have been reassuring that ovarian stimulation for fertility preservation in women with breast cancer does not worsen the prognosis, findings are limited by short-term follow-up.6
The recent study by Marklund and colleagues presented an analysis of breast cancer relapse and mortality following fertility preservation with and without hormonal stimulation. In their prospective cohort study of 425 Swedish women who underwent fertility preservation, the authors categorized patients into 2 groups: oocyte and embryo cryopreservation by ovarian hormonal stimulation and ovarian tissue cryopreservation without hormonal stimulation. The control group included 850 women with breast cancer who did not undergo fertility preservation. The cohort and the control groups were matched on age, calendar period of diagnosis, and region. Three Swedish registers for breast cancer were used to obtain the study cohort, and for each participant, 2 breast cancer patients who were unexposed to fertility preservation were used for comparison. The primary outcome was mortality while the secondary outcome was any event of death due to breast cancer or relapse.
Results. A total of 1,275 women were studied at the time of breast cancer diagnosis. After stratification, which included age, parity at diagnosis, tumor size, number of lymph node metastases, and estrogen receptor status, disease-specific mortality was similar in all categories of women, that is, hormonal fertility preservation, nonhormonal fertility preservation, and controls. In the subcohort of 723 women, the adjusted rate of relapse and disease-specific mortality remained the same among all groups.
Study strengths and limitations
This study prompts several areas of criticism. The follow-up of breast cancer patients was only 5 years, adding to the limitations of short-term monitoring seen in prior studies. The authors also considered a delay in pregnancy attempts following breast cancer treatment of hormonally sensitive cancers of 5 to 10 years. However, the long-term safety of pregnancy following breast cancer has shown a statistically significantly superior disease-free survival (DFS) in patients who became pregnant less than 2 years from diagnosis and no difference in those who became pregnant 2 or more years from diagnosis.7
Only 58 women in the nonhormonal fertility preservation group (ovarian tissue cryopreservation) were studied, which may limit an adequate evaluation although it is not expected to negatively impact breast cancer prognosis. Another area of potential bias was the use of only a subcohort to assess relapse-free survival as opposed to the entire cohort that was used to assess mortality.
Strengths of this study include obligatory reporting to the registry and equal access to anticancer treatment and fertility preservation in Sweden. Ovarian stimulating drugs were examined, as letrozole is often used in breast cancer patients to maintain lower estradiol levels due to aromatase inhibition. Nevertheless, this study did not demonstrate a difference in mortality with or without letrozole use. ●
Marklund and colleagues’ findings revealed no increase of breast cancer relapse and mortality following fertility preservation with or without hormonal stimulation. They also propose a “healthy user effect” whereby a woman who feels healthy may choose to undergo fertility preservation, thereby biasing the outcome by having a better survival.8
Future studies with longer follow-up are needed to address the hormonal impact of fertility preservation, if any, on breast cancer DFS and mortality, as well as to evaluate subsequent pregnancy outcomes, stratified for medication treatment type via the CED calculator. To date, evidence continues to support fertility preservation options that use hormonal ovarian stimulation in breast cancer patients as apparently safe for, at least, up to 5 years of follow-up.
MARK P. TROLICE, MD
Marklund A, Lekberg T, Hedayati E, et al. Relapse rates and disease-specific mortality following procedures for fertility preservation at time of breast cancer diagnosis. JAMA Oncol. 2022;8:1438-1446. doi:10.1001/jamaoncol.2022.3677.
EXPERT COMMENTARY
Breast cancer is the most diagnosed cancer among US women after skin cancer.1 As of the end of 2020, 7.8 million women were alive who were diagnosed with breast cancer in the past 5 years, making it the world’s most prevalent cancer. Given the wide reach of breast cancer and the increase in its distant stage by more than 4% per year in women of reproductive age (20–39 years), clinicians are urged to address fertility preservation due to reproductive compromise of gonadotoxic therapies and gonadectomy.2 To predict the risk of infertility following chemotherapy, a Cyclophosphamide Equivalent Dose (CED) calculator can be used. A CED of 4,000 mg/m2 has been associated with a significant risk of infertility.3
In 2012, the American Society for Reproductive Medicine removed the experimental label of oocyte cryopreservation then recently endorsed ovarian cryopreservation, thereby providing acceptable procedures for fertility preservation.4 Gonadotropin-releasing hormone agonist use during chemotherapy, which is used to protect the ovary in premenopausal women against the effects of chemotherapy, has been shown to have inconsistent findings and should not replace the established modalities of oocyte/embryo/ovarian tissue cryopreservation.2,5
Details of the study
While studies have been reassuring that ovarian stimulation for fertility preservation in women with breast cancer does not worsen the prognosis, findings are limited by short-term follow-up.6
The recent study by Marklund and colleagues presented an analysis of breast cancer relapse and mortality following fertility preservation with and without hormonal stimulation. In their prospective cohort study of 425 Swedish women who underwent fertility preservation, the authors categorized patients into 2 groups: oocyte and embryo cryopreservation by ovarian hormonal stimulation and ovarian tissue cryopreservation without hormonal stimulation. The control group included 850 women with breast cancer who did not undergo fertility preservation. The cohort and the control groups were matched on age, calendar period of diagnosis, and region. Three Swedish registers for breast cancer were used to obtain the study cohort, and for each participant, 2 breast cancer patients who were unexposed to fertility preservation were used for comparison. The primary outcome was mortality while the secondary outcome was any event of death due to breast cancer or relapse.
Results. A total of 1,275 women were studied at the time of breast cancer diagnosis. After stratification, which included age, parity at diagnosis, tumor size, number of lymph node metastases, and estrogen receptor status, disease-specific mortality was similar in all categories of women, that is, hormonal fertility preservation, nonhormonal fertility preservation, and controls. In the subcohort of 723 women, the adjusted rate of relapse and disease-specific mortality remained the same among all groups.
Study strengths and limitations
This study prompts several areas of criticism. The follow-up of breast cancer patients was only 5 years, adding to the limitations of short-term monitoring seen in prior studies. The authors also considered a delay in pregnancy attempts following breast cancer treatment of hormonally sensitive cancers of 5 to 10 years. However, the long-term safety of pregnancy following breast cancer has shown a statistically significantly superior disease-free survival (DFS) in patients who became pregnant less than 2 years from diagnosis and no difference in those who became pregnant 2 or more years from diagnosis.7
Only 58 women in the nonhormonal fertility preservation group (ovarian tissue cryopreservation) were studied, which may limit an adequate evaluation although it is not expected to negatively impact breast cancer prognosis. Another area of potential bias was the use of only a subcohort to assess relapse-free survival as opposed to the entire cohort that was used to assess mortality.
Strengths of this study include obligatory reporting to the registry and equal access to anticancer treatment and fertility preservation in Sweden. Ovarian stimulating drugs were examined, as letrozole is often used in breast cancer patients to maintain lower estradiol levels due to aromatase inhibition. Nevertheless, this study did not demonstrate a difference in mortality with or without letrozole use. ●
Marklund and colleagues’ findings revealed no increase of breast cancer relapse and mortality following fertility preservation with or without hormonal stimulation. They also propose a “healthy user effect” whereby a woman who feels healthy may choose to undergo fertility preservation, thereby biasing the outcome by having a better survival.8
Future studies with longer follow-up are needed to address the hormonal impact of fertility preservation, if any, on breast cancer DFS and mortality, as well as to evaluate subsequent pregnancy outcomes, stratified for medication treatment type via the CED calculator. To date, evidence continues to support fertility preservation options that use hormonal ovarian stimulation in breast cancer patients as apparently safe for, at least, up to 5 years of follow-up.
MARK P. TROLICE, MD
- Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72:524-541. doi:10.3322/caac.21754.
- Oktay K, Harvey BE, Partridge AH, et al. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;1;36:1994-2001. doi:10.1200/JCO.2018.78.1914.
- Fertility Preservation in Pittsburgh. CED calculator. Accessed November 14, 2022. https://fertilitypreservationpittsburgh.org/fertility-resources/fertility-risk-calculator/
- Practice Committee of the American Society for Reproductive Medicine. Fertility preservation in patients undergoing gonadotoxic therapy or gonadectomy: a committee opinion. Fertil Steril. 2019;112:1022-1033. doi:10.1016/j.fertnstert.2019.09.013.
- Blumenfeld Z. Fertility preservation using GnRH agonists: rationale, possible mechanisms, and explanation of controversy. Clin Med Insights Reprod Health. 2019;13: 1179558119870163. doi:10.1177/1179558119870163.
- Beebeejaun Y, Athithan A, Copeland TP, et al. Risk of breast cancer in women treated with ovarian stimulation drugs for infertility: a systematic review and meta-analysis. Fertil Steril. 2021;116:198-207. doi:10.1016/j.fertnstert.2021.01.044.
- Lambertini M, Kroman N, Ameye L, et al. Long-term safety of pregnancy following breast cancer according to estrogen receptor status. J Natl Cancer Inst. 2018;110:426-429. doi:10.1093/jnci/djx206.
- Marklund A, Lundberg FE, Eloranta S, et al. Reproductive outcomes after breast cancer in women with vs without fertility preservation. JAMA Oncol. 2021;7:86-91. doi:10.1001/ jamaoncol.2020.5957.
- Giaquinto AN, Sung H, Miller KD, et al. Breast cancer statistics, 2022. CA Cancer J Clin. 2022;72:524-541. doi:10.3322/caac.21754.
- Oktay K, Harvey BE, Partridge AH, et al. Fertility preservation in patients with cancer: ASCO clinical practice guideline update. J Clin Oncol. 2018;1;36:1994-2001. doi:10.1200/JCO.2018.78.1914.
- Fertility Preservation in Pittsburgh. CED calculator. Accessed November 14, 2022. https://fertilitypreservationpittsburgh.org/fertility-resources/fertility-risk-calculator/
- Practice Committee of the American Society for Reproductive Medicine. Fertility preservation in patients undergoing gonadotoxic therapy or gonadectomy: a committee opinion. Fertil Steril. 2019;112:1022-1033. doi:10.1016/j.fertnstert.2019.09.013.
- Blumenfeld Z. Fertility preservation using GnRH agonists: rationale, possible mechanisms, and explanation of controversy. Clin Med Insights Reprod Health. 2019;13: 1179558119870163. doi:10.1177/1179558119870163.
- Beebeejaun Y, Athithan A, Copeland TP, et al. Risk of breast cancer in women treated with ovarian stimulation drugs for infertility: a systematic review and meta-analysis. Fertil Steril. 2021;116:198-207. doi:10.1016/j.fertnstert.2021.01.044.
- Lambertini M, Kroman N, Ameye L, et al. Long-term safety of pregnancy following breast cancer according to estrogen receptor status. J Natl Cancer Inst. 2018;110:426-429. doi:10.1093/jnci/djx206.
- Marklund A, Lundberg FE, Eloranta S, et al. Reproductive outcomes after breast cancer in women with vs without fertility preservation. JAMA Oncol. 2021;7:86-91. doi:10.1001/ jamaoncol.2020.5957.
Breast conservation safe option in multisite breast cancer
SAN ANTONIO – Women with breast cancer at more than one site can undergo breast-conserving therapy and still have local recurrence rates well under the acceptable threshold of risk, suggest the results of first prospective study of this issue.
The ACOSOG-Z11102 trial involved more than 200 women with primarily endocrine receptor–positive (ER+), human epidermal growth factor receptor 2–negative (HER2-) breast cancer and up to three disease foci, all of whom underwent lumpectomy with nodal staging followed by whole-breast irradiation, then systemic therapy at the oncologist’s discretion.
After 5 years of follow-up, just 3% of women experienced a local recurrence, with none having a local or distant recurrence and one dying of the disease.
The new findings were presented at the San Antonio Breast Cancer Symposium on Dec. 9.
“This study provides important information for clinicians to discuss with patients who have two or three foci of breast cancer in one breast, as it may allow more patients to consider breast-conserving therapy as an option,” said study presenter Judy C. Boughey, MD, chair of the division of breast and melanoma surgical oncology at the Mayo Clinic, Rochester, Minn.
“Lumpectomy with radiation therapy is often preferred to mastectomy, as it is a smaller operation with quicker recovery, resulting in better patient satisfaction and cosmetic outcomes,” Dr. Boughey said in a statement.
“We’ve all been anxiously awaiting the results of this trial,” Andrea V. Barrio, MD, associate attending surgeon, Memorial Sloan Kettering Cancer Center, New York, told this news organization. “We knew that in patients who have a single site tumor in the breast, that outcomes between lumpectomy and mastectomy are the same ... But none of those trials have enrolled women with multiple sites.”
“There were no prospective data out there telling us that doing two lumpectomies in the breast was safe, so a lot of times, women were getting mastectomy for these multiple tumors, even if women had two small tumors in the breast and could easily undergo a lumpectomy with a good cosmetic result,” she said.
“So this data provides very strong evidence that we can begin treating women with small tumors in the breast who can undergo lumpectomy with a good cosmetic results without needing a mastectomy,” Dr. Barrio continued. “From a long-term quality of life standpoint, this is a big deal for women moving forward who really want to keep their breasts.”
Dr. Barrio did highlight, however, that “not everybody routinely does MRI” in women with breast cancer, including her institution, although generally she feels that “our standard imaging has gotten better,” with screening ultrasound identifying more lesions than previously.
She also believes that the numbers of women in the study who did not receive MRI are too small to “draw any definitive conclusions.
“Personally, when I have a patient with multisite disease and I’m going to keep their breasts, that to me is one indication that I would consider an MRI, to make sure that I wasn’t missing intervening disease between the two sites – that there wasn’t something else that would change my mind about doing a two-site lumpectomy,” Dr. Barrio said.
Linda M. Pak, MD, a breast cancer surgeon and surgical oncologist at NYU Langone’s Breast Cancer Center, New York, who was not involved in the study, said that the new study provides “importation information regarding the oncologic safety” of lumpectomy.
These results are “exciting to see, as they provide important information that breast-conserving surgery is safe in these patients, and that we can now share the results of this study with patients when we discuss with them their surgical options.
“I hope this will make more breast surgeons and patients comfortable with this approach and that it will increase the use of breast conservation among these patients,” Dr. Pak said.
Study details
In recent years, there has been increased diagnosis of multiple foci of ipsilateral breast cancer, Dr. Boughey said in her presentation. “This is both as a result of improvements in screening imaging, as well as diagnostic imaging and an increased use of preoperative breast MRI.”
Although historical, retrospective studies have shown high rates of local regional recurrences with breast-conserving therapy in women with more than one foci of breast cancer, more recent analyses have indicated that the approach is associated with “acceptable” recurrence rates.
This, Dr. Boughey explained, is due not only to improvements in breast imaging but also to better pathologic margin assessment, and improved systematic and radiation therapy.
Nevertheless, “most patients who present with two or three sites of cancer in one breast are recommended to undergo a mastectomy,” she noted.
To examine the safety of breast-conserving therapy in such patients, the team conducted a single-arm, phase 2 trial in women at least 40 years of age who had two or three foci of breast cancer, of which at least one site was invasive disease.
“While a randomized trial design would have provided stronger data, we felt that accrual to such a design would be problematic, as many patients and surgeons would not be willing to randomize,” Dr. Boughey explained.
Participants were required to have at least 2 cm of normal tissue between the lesions and disease in no more than two quadrants of the breast. They could have node-negative or N1 disease.
Women were excluded if they had foci > 5 cm on imaging; had bilateral breast cancer; had known BRCA1/2 mutations; had had prior ipsilateral breast cancer; or had received neoadjuvant therapy.
All women in the trial underwent lumpectomy with nodal staging, with adjuvant chemotherapy at the physician’s discretion, followed by whole-breast irradiation, with regional nodal irradiation again at the physician’s discretion. This was followed by systemic therapy, at the discretion of the medical oncologist.
The women were then followed up every 6 months until 5 years after the completion of whole-breast irradiation.
Details of the results
Dr. Boughey said that previously presented data from this study revealed that 67.6% of women achieved a margin-negative excision in a single operation, whereas 7.1% converted to mastectomy. The cosmetic outcome was rated as good or excellent at 2 years by 70.6% of women.
For the current analysis, a total of 204 women were evaluable, who had a median age of 61.1 years. Just over half (59.3%) had T1 stage disease, and 95.6% were node-negative. The majority (83.5%) had ER+/HER2- breast cancer, whereas 5.0% had ER-/HER2- disease and 11.5% had HER2+ positive tumors.
Adjuvant chemotherapy was given to 28.9% of women, whereas 89.7% of those with ER+ disease received adjuvant endocrine therapy.
The primary outcome was local recurrence rate at 5 years, which had a prespecified acceptable rate of less than 8%.
Dr. Boughey showed that, in their series, the 5-year recurrence rate was just 3.1% (95% confidence interval [CI], 1.3%-6.4%), which was “well below” the predefined “clinically significantly threshold.” This involved four cases in the ipsilateral breast, one in the skin, and one in the chest wall.
In addition to the six women with local regional recurrence, six developed contralateral breast cancer and four patients developed distant disease. There were no cases of local and distant recurrence. There were three non–breast cancer primary cancers: one gastric, one lung, and one ovarian.
Eight women died during follow-up; only one of the deaths was related to breast cancer.
Dr. Boughey explained that the small number of local recurrences was too small to identify predictive factors via multivariate analysis.
However, univariate analysis indicated that there were numerical but nonsignificant associations between local recurrence and pathologic stage T2-3 disease, pathologic nodal involvement, and surgical margins just under the negative threshold.
Among the 10 cases of ER–/HER2– breast cancer, there was one local recurrence, giving a 5-year rate of 10.0% vs. 2.6% for women with ER+/HER2– disease.
To examine the role of MRI, Dr. Boughey highlighted that although the imaging modality was initially a requirement for study entry, an amendment to the protocol in 2015 allowed 15 women who had not had MRI to take part.
The local recurrence rate in women who had undergone MRI was 1.7% vs. 22.6% in those who had not, for a hazard ratio of 13.5 (P = .002).
“While this was statistically significant, we need to bear in mind that this was a secondary unplanned analysis,” Dr. Boughey underlined.
Next, the team analyzed the impact of adjuvant endocrine therapy in the 195 women with at least one ER+ lesion, finding that it was associated with a 5-year recurrence rate of 1.9% vs. 12.5% in those who did not receive endocrine therapy, for a hazard ratio of 7.7 (P = .025).
Dr. Boughey highlighted that the study is limited by being single-arm and having only a small subset of patients without preoperative MRI, with HER2+ or ER–/HER2– disease, and with three foci of disease.
She also emphasized that “there is concern that the 5-year follow up on this protocol may be shorter than needed,” especially in women with ER+ disease.
The study was supported by the National Institutes of Health. Dr. Boughey declared relationships with Eli Lilly and Company, Symbiosis Pharma, CairnSurgical, UpToDate, and PeerView.
A version of this article first appeared on Medscape.com.
SAN ANTONIO – Women with breast cancer at more than one site can undergo breast-conserving therapy and still have local recurrence rates well under the acceptable threshold of risk, suggest the results of first prospective study of this issue.
The ACOSOG-Z11102 trial involved more than 200 women with primarily endocrine receptor–positive (ER+), human epidermal growth factor receptor 2–negative (HER2-) breast cancer and up to three disease foci, all of whom underwent lumpectomy with nodal staging followed by whole-breast irradiation, then systemic therapy at the oncologist’s discretion.
After 5 years of follow-up, just 3% of women experienced a local recurrence, with none having a local or distant recurrence and one dying of the disease.
The new findings were presented at the San Antonio Breast Cancer Symposium on Dec. 9.
“This study provides important information for clinicians to discuss with patients who have two or three foci of breast cancer in one breast, as it may allow more patients to consider breast-conserving therapy as an option,” said study presenter Judy C. Boughey, MD, chair of the division of breast and melanoma surgical oncology at the Mayo Clinic, Rochester, Minn.
“Lumpectomy with radiation therapy is often preferred to mastectomy, as it is a smaller operation with quicker recovery, resulting in better patient satisfaction and cosmetic outcomes,” Dr. Boughey said in a statement.
“We’ve all been anxiously awaiting the results of this trial,” Andrea V. Barrio, MD, associate attending surgeon, Memorial Sloan Kettering Cancer Center, New York, told this news organization. “We knew that in patients who have a single site tumor in the breast, that outcomes between lumpectomy and mastectomy are the same ... But none of those trials have enrolled women with multiple sites.”
“There were no prospective data out there telling us that doing two lumpectomies in the breast was safe, so a lot of times, women were getting mastectomy for these multiple tumors, even if women had two small tumors in the breast and could easily undergo a lumpectomy with a good cosmetic result,” she said.
“So this data provides very strong evidence that we can begin treating women with small tumors in the breast who can undergo lumpectomy with a good cosmetic results without needing a mastectomy,” Dr. Barrio continued. “From a long-term quality of life standpoint, this is a big deal for women moving forward who really want to keep their breasts.”
Dr. Barrio did highlight, however, that “not everybody routinely does MRI” in women with breast cancer, including her institution, although generally she feels that “our standard imaging has gotten better,” with screening ultrasound identifying more lesions than previously.
She also believes that the numbers of women in the study who did not receive MRI are too small to “draw any definitive conclusions.
“Personally, when I have a patient with multisite disease and I’m going to keep their breasts, that to me is one indication that I would consider an MRI, to make sure that I wasn’t missing intervening disease between the two sites – that there wasn’t something else that would change my mind about doing a two-site lumpectomy,” Dr. Barrio said.
Linda M. Pak, MD, a breast cancer surgeon and surgical oncologist at NYU Langone’s Breast Cancer Center, New York, who was not involved in the study, said that the new study provides “importation information regarding the oncologic safety” of lumpectomy.
These results are “exciting to see, as they provide important information that breast-conserving surgery is safe in these patients, and that we can now share the results of this study with patients when we discuss with them their surgical options.
“I hope this will make more breast surgeons and patients comfortable with this approach and that it will increase the use of breast conservation among these patients,” Dr. Pak said.
Study details
In recent years, there has been increased diagnosis of multiple foci of ipsilateral breast cancer, Dr. Boughey said in her presentation. “This is both as a result of improvements in screening imaging, as well as diagnostic imaging and an increased use of preoperative breast MRI.”
Although historical, retrospective studies have shown high rates of local regional recurrences with breast-conserving therapy in women with more than one foci of breast cancer, more recent analyses have indicated that the approach is associated with “acceptable” recurrence rates.
This, Dr. Boughey explained, is due not only to improvements in breast imaging but also to better pathologic margin assessment, and improved systematic and radiation therapy.
Nevertheless, “most patients who present with two or three sites of cancer in one breast are recommended to undergo a mastectomy,” she noted.
To examine the safety of breast-conserving therapy in such patients, the team conducted a single-arm, phase 2 trial in women at least 40 years of age who had two or three foci of breast cancer, of which at least one site was invasive disease.
“While a randomized trial design would have provided stronger data, we felt that accrual to such a design would be problematic, as many patients and surgeons would not be willing to randomize,” Dr. Boughey explained.
Participants were required to have at least 2 cm of normal tissue between the lesions and disease in no more than two quadrants of the breast. They could have node-negative or N1 disease.
Women were excluded if they had foci > 5 cm on imaging; had bilateral breast cancer; had known BRCA1/2 mutations; had had prior ipsilateral breast cancer; or had received neoadjuvant therapy.
All women in the trial underwent lumpectomy with nodal staging, with adjuvant chemotherapy at the physician’s discretion, followed by whole-breast irradiation, with regional nodal irradiation again at the physician’s discretion. This was followed by systemic therapy, at the discretion of the medical oncologist.
The women were then followed up every 6 months until 5 years after the completion of whole-breast irradiation.
Details of the results
Dr. Boughey said that previously presented data from this study revealed that 67.6% of women achieved a margin-negative excision in a single operation, whereas 7.1% converted to mastectomy. The cosmetic outcome was rated as good or excellent at 2 years by 70.6% of women.
For the current analysis, a total of 204 women were evaluable, who had a median age of 61.1 years. Just over half (59.3%) had T1 stage disease, and 95.6% were node-negative. The majority (83.5%) had ER+/HER2- breast cancer, whereas 5.0% had ER-/HER2- disease and 11.5% had HER2+ positive tumors.
Adjuvant chemotherapy was given to 28.9% of women, whereas 89.7% of those with ER+ disease received adjuvant endocrine therapy.
The primary outcome was local recurrence rate at 5 years, which had a prespecified acceptable rate of less than 8%.
Dr. Boughey showed that, in their series, the 5-year recurrence rate was just 3.1% (95% confidence interval [CI], 1.3%-6.4%), which was “well below” the predefined “clinically significantly threshold.” This involved four cases in the ipsilateral breast, one in the skin, and one in the chest wall.
In addition to the six women with local regional recurrence, six developed contralateral breast cancer and four patients developed distant disease. There were no cases of local and distant recurrence. There were three non–breast cancer primary cancers: one gastric, one lung, and one ovarian.
Eight women died during follow-up; only one of the deaths was related to breast cancer.
Dr. Boughey explained that the small number of local recurrences was too small to identify predictive factors via multivariate analysis.
However, univariate analysis indicated that there were numerical but nonsignificant associations between local recurrence and pathologic stage T2-3 disease, pathologic nodal involvement, and surgical margins just under the negative threshold.
Among the 10 cases of ER–/HER2– breast cancer, there was one local recurrence, giving a 5-year rate of 10.0% vs. 2.6% for women with ER+/HER2– disease.
To examine the role of MRI, Dr. Boughey highlighted that although the imaging modality was initially a requirement for study entry, an amendment to the protocol in 2015 allowed 15 women who had not had MRI to take part.
The local recurrence rate in women who had undergone MRI was 1.7% vs. 22.6% in those who had not, for a hazard ratio of 13.5 (P = .002).
“While this was statistically significant, we need to bear in mind that this was a secondary unplanned analysis,” Dr. Boughey underlined.
Next, the team analyzed the impact of adjuvant endocrine therapy in the 195 women with at least one ER+ lesion, finding that it was associated with a 5-year recurrence rate of 1.9% vs. 12.5% in those who did not receive endocrine therapy, for a hazard ratio of 7.7 (P = .025).
Dr. Boughey highlighted that the study is limited by being single-arm and having only a small subset of patients without preoperative MRI, with HER2+ or ER–/HER2– disease, and with three foci of disease.
She also emphasized that “there is concern that the 5-year follow up on this protocol may be shorter than needed,” especially in women with ER+ disease.
The study was supported by the National Institutes of Health. Dr. Boughey declared relationships with Eli Lilly and Company, Symbiosis Pharma, CairnSurgical, UpToDate, and PeerView.
A version of this article first appeared on Medscape.com.
SAN ANTONIO – Women with breast cancer at more than one site can undergo breast-conserving therapy and still have local recurrence rates well under the acceptable threshold of risk, suggest the results of first prospective study of this issue.
The ACOSOG-Z11102 trial involved more than 200 women with primarily endocrine receptor–positive (ER+), human epidermal growth factor receptor 2–negative (HER2-) breast cancer and up to three disease foci, all of whom underwent lumpectomy with nodal staging followed by whole-breast irradiation, then systemic therapy at the oncologist’s discretion.
After 5 years of follow-up, just 3% of women experienced a local recurrence, with none having a local or distant recurrence and one dying of the disease.
The new findings were presented at the San Antonio Breast Cancer Symposium on Dec. 9.
“This study provides important information for clinicians to discuss with patients who have two or three foci of breast cancer in one breast, as it may allow more patients to consider breast-conserving therapy as an option,” said study presenter Judy C. Boughey, MD, chair of the division of breast and melanoma surgical oncology at the Mayo Clinic, Rochester, Minn.
“Lumpectomy with radiation therapy is often preferred to mastectomy, as it is a smaller operation with quicker recovery, resulting in better patient satisfaction and cosmetic outcomes,” Dr. Boughey said in a statement.
“We’ve all been anxiously awaiting the results of this trial,” Andrea V. Barrio, MD, associate attending surgeon, Memorial Sloan Kettering Cancer Center, New York, told this news organization. “We knew that in patients who have a single site tumor in the breast, that outcomes between lumpectomy and mastectomy are the same ... But none of those trials have enrolled women with multiple sites.”
“There were no prospective data out there telling us that doing two lumpectomies in the breast was safe, so a lot of times, women were getting mastectomy for these multiple tumors, even if women had two small tumors in the breast and could easily undergo a lumpectomy with a good cosmetic result,” she said.
“So this data provides very strong evidence that we can begin treating women with small tumors in the breast who can undergo lumpectomy with a good cosmetic results without needing a mastectomy,” Dr. Barrio continued. “From a long-term quality of life standpoint, this is a big deal for women moving forward who really want to keep their breasts.”
Dr. Barrio did highlight, however, that “not everybody routinely does MRI” in women with breast cancer, including her institution, although generally she feels that “our standard imaging has gotten better,” with screening ultrasound identifying more lesions than previously.
She also believes that the numbers of women in the study who did not receive MRI are too small to “draw any definitive conclusions.
“Personally, when I have a patient with multisite disease and I’m going to keep their breasts, that to me is one indication that I would consider an MRI, to make sure that I wasn’t missing intervening disease between the two sites – that there wasn’t something else that would change my mind about doing a two-site lumpectomy,” Dr. Barrio said.
Linda M. Pak, MD, a breast cancer surgeon and surgical oncologist at NYU Langone’s Breast Cancer Center, New York, who was not involved in the study, said that the new study provides “importation information regarding the oncologic safety” of lumpectomy.
These results are “exciting to see, as they provide important information that breast-conserving surgery is safe in these patients, and that we can now share the results of this study with patients when we discuss with them their surgical options.
“I hope this will make more breast surgeons and patients comfortable with this approach and that it will increase the use of breast conservation among these patients,” Dr. Pak said.
Study details
In recent years, there has been increased diagnosis of multiple foci of ipsilateral breast cancer, Dr. Boughey said in her presentation. “This is both as a result of improvements in screening imaging, as well as diagnostic imaging and an increased use of preoperative breast MRI.”
Although historical, retrospective studies have shown high rates of local regional recurrences with breast-conserving therapy in women with more than one foci of breast cancer, more recent analyses have indicated that the approach is associated with “acceptable” recurrence rates.
This, Dr. Boughey explained, is due not only to improvements in breast imaging but also to better pathologic margin assessment, and improved systematic and radiation therapy.
Nevertheless, “most patients who present with two or three sites of cancer in one breast are recommended to undergo a mastectomy,” she noted.
To examine the safety of breast-conserving therapy in such patients, the team conducted a single-arm, phase 2 trial in women at least 40 years of age who had two or three foci of breast cancer, of which at least one site was invasive disease.
“While a randomized trial design would have provided stronger data, we felt that accrual to such a design would be problematic, as many patients and surgeons would not be willing to randomize,” Dr. Boughey explained.
Participants were required to have at least 2 cm of normal tissue between the lesions and disease in no more than two quadrants of the breast. They could have node-negative or N1 disease.
Women were excluded if they had foci > 5 cm on imaging; had bilateral breast cancer; had known BRCA1/2 mutations; had had prior ipsilateral breast cancer; or had received neoadjuvant therapy.
All women in the trial underwent lumpectomy with nodal staging, with adjuvant chemotherapy at the physician’s discretion, followed by whole-breast irradiation, with regional nodal irradiation again at the physician’s discretion. This was followed by systemic therapy, at the discretion of the medical oncologist.
The women were then followed up every 6 months until 5 years after the completion of whole-breast irradiation.
Details of the results
Dr. Boughey said that previously presented data from this study revealed that 67.6% of women achieved a margin-negative excision in a single operation, whereas 7.1% converted to mastectomy. The cosmetic outcome was rated as good or excellent at 2 years by 70.6% of women.
For the current analysis, a total of 204 women were evaluable, who had a median age of 61.1 years. Just over half (59.3%) had T1 stage disease, and 95.6% were node-negative. The majority (83.5%) had ER+/HER2- breast cancer, whereas 5.0% had ER-/HER2- disease and 11.5% had HER2+ positive tumors.
Adjuvant chemotherapy was given to 28.9% of women, whereas 89.7% of those with ER+ disease received adjuvant endocrine therapy.
The primary outcome was local recurrence rate at 5 years, which had a prespecified acceptable rate of less than 8%.
Dr. Boughey showed that, in their series, the 5-year recurrence rate was just 3.1% (95% confidence interval [CI], 1.3%-6.4%), which was “well below” the predefined “clinically significantly threshold.” This involved four cases in the ipsilateral breast, one in the skin, and one in the chest wall.
In addition to the six women with local regional recurrence, six developed contralateral breast cancer and four patients developed distant disease. There were no cases of local and distant recurrence. There were three non–breast cancer primary cancers: one gastric, one lung, and one ovarian.
Eight women died during follow-up; only one of the deaths was related to breast cancer.
Dr. Boughey explained that the small number of local recurrences was too small to identify predictive factors via multivariate analysis.
However, univariate analysis indicated that there were numerical but nonsignificant associations between local recurrence and pathologic stage T2-3 disease, pathologic nodal involvement, and surgical margins just under the negative threshold.
Among the 10 cases of ER–/HER2– breast cancer, there was one local recurrence, giving a 5-year rate of 10.0% vs. 2.6% for women with ER+/HER2– disease.
To examine the role of MRI, Dr. Boughey highlighted that although the imaging modality was initially a requirement for study entry, an amendment to the protocol in 2015 allowed 15 women who had not had MRI to take part.
The local recurrence rate in women who had undergone MRI was 1.7% vs. 22.6% in those who had not, for a hazard ratio of 13.5 (P = .002).
“While this was statistically significant, we need to bear in mind that this was a secondary unplanned analysis,” Dr. Boughey underlined.
Next, the team analyzed the impact of adjuvant endocrine therapy in the 195 women with at least one ER+ lesion, finding that it was associated with a 5-year recurrence rate of 1.9% vs. 12.5% in those who did not receive endocrine therapy, for a hazard ratio of 7.7 (P = .025).
Dr. Boughey highlighted that the study is limited by being single-arm and having only a small subset of patients without preoperative MRI, with HER2+ or ER–/HER2– disease, and with three foci of disease.
She also emphasized that “there is concern that the 5-year follow up on this protocol may be shorter than needed,” especially in women with ER+ disease.
The study was supported by the National Institutes of Health. Dr. Boughey declared relationships with Eli Lilly and Company, Symbiosis Pharma, CairnSurgical, UpToDate, and PeerView.
A version of this article first appeared on Medscape.com.
AT SABCS 2022
Mindfulness, exercise strike out in memory trial
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
We are coming to the end of the year, which always makes me think about getting older. Much like the search for the fountain of youth, many promising leads have ultimately led to dead ends. And yet, I had high hopes for a trial that focused on two cornerstones of wellness – exercise and mindfulness – to address the subjective loss of memory that comes with aging. Alas, meditation and exercise do not appear to be the fountain of youth.
I’m talking about this study, appearing in JAMA, known as the MEDEX trial.
It’s a clever design: a 2 x 2 factorial randomized trial where participants could be randomized to a mindfulness intervention, an exercise intervention, both, or neither.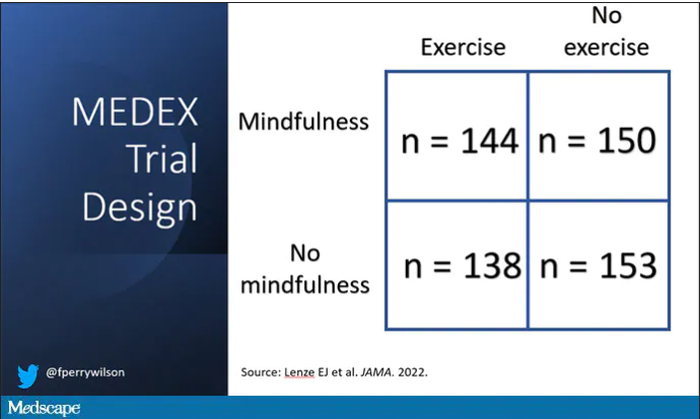
In this manner, you can test multiple hypotheses exploiting a shared control group. Or as a mentor of mine used to say, you get two trials for the price of one and a half.
The participants were older adults, aged 65-84, living in the community. They had to be relatively sedentary at baseline and not engaging in mindfulness practices. They had to subjectively report some memory or concentration issues but had to be cognitively intact, based on a standard dementia screening test. In other words, these are your average older people who are worried that they aren’t as sharp as they used to be.
The interventions themselves were fairly intense. The exercise group had instructor-led sessions for 90 minutes twice a week for the first 6 months of the study, once a week thereafter. And participants were encouraged to exercise at home such that they had a total of 300 minutes of weekly exercise.
The mindfulness program was characterized by eight weekly classes of 2.5 hours each as well as a half-day retreat to teach the tenets of mindfulness and meditation, with monthly refreshers thereafter. Participants were instructed to meditate for 60 minutes a day in addition to the classes.
For the 144 people who were randomized to both meditation and exercise, this trial amounted to something of a part-time job. So you might think that adherence to the interventions was low, but apparently that’s not the case. Attendance to the mindfulness classes was over 90%, and over 80% for the exercise classes. And diary-based reporting of home efforts was also pretty good.
The control group wasn’t left to their own devices. Recognizing that the community aspect of exercise or mindfulness classes might convey a benefit independent of the actual exercise or mindfulness, the control group met on a similar schedule to discuss health education, but no mention of exercise or mindfulness occurred in that setting.
The primary outcome was change in memory and executive function scores across a battery of neuropsychologic testing, but the story is told in just a few pictures.
Memory scores improved in all three groups – mindfulness, exercise, and health education – over time. Cognitive composite score improved in all three groups similarly. There was no synergistic effect of mindfulness and exercise either. Basically, everyone got a bit better.
But the study did way more than look at scores on tests. Researchers used MRI to measure brain anatomic outcomes as well. And the surprising thing is that virtually none of these outcomes were different between the groups either.
Hippocampal volume decreased a bit in all the groups. Dorsolateral prefrontal cortex volume was flat. There was no change in scores measuring tasks of daily living.
When you see negative results like this, right away you worry that the intervention wasn’t properly delivered. Were these people really exercising and meditating? Well, the authors showed that individuals randomized to exercise, at least, had less sleep latency, greater aerobic fitness, and greater strength. So we know something was happening.
They then asked, would the people in the exercise group with the greatest changes in those physiologic parameters show some improvement in cognitive parameters? In other words, we know you were exercising because you got stronger and are sleeping better; is your memory better? The answer? Surprisingly, still no. Even in that honestly somewhat cherry-picked group, the interventions had no effect.
Could it be that the control was inappropriate, that the “health education” intervention was actually so helpful that it obscured the benefits of exercise and meditation? After all, cognitive scores did improve in all groups. The authors doubt it. They say they think the improvement in cognitive scores reflects the fact that patients had learned a bit about how to take the tests. This is pretty common in the neuropsychiatric literature.
So here we are and I just want to say, well, shoot. This is not the result I wanted. And I think the reason I’m so disappointed is because aging and the loss of cognitive faculties that comes with aging are just sort of scary. We are all looking for some control over that fear, and how nice it would be to be able to tell ourselves not to worry – that we won’t have those problems as we get older because we exercise, or meditate, or drink red wine, or don’t drink wine, or whatever. And while I have no doubt that staying healthier physically will keep you healthier mentally, it may take more than one simple thing to move the needle.
Dr. Wilson is associate professor, department of medicine, and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
We are coming to the end of the year, which always makes me think about getting older. Much like the search for the fountain of youth, many promising leads have ultimately led to dead ends. And yet, I had high hopes for a trial that focused on two cornerstones of wellness – exercise and mindfulness – to address the subjective loss of memory that comes with aging. Alas, meditation and exercise do not appear to be the fountain of youth.
I’m talking about this study, appearing in JAMA, known as the MEDEX trial.
It’s a clever design: a 2 x 2 factorial randomized trial where participants could be randomized to a mindfulness intervention, an exercise intervention, both, or neither.
In this manner, you can test multiple hypotheses exploiting a shared control group. Or as a mentor of mine used to say, you get two trials for the price of one and a half.
The participants were older adults, aged 65-84, living in the community. They had to be relatively sedentary at baseline and not engaging in mindfulness practices. They had to subjectively report some memory or concentration issues but had to be cognitively intact, based on a standard dementia screening test. In other words, these are your average older people who are worried that they aren’t as sharp as they used to be.
The interventions themselves were fairly intense. The exercise group had instructor-led sessions for 90 minutes twice a week for the first 6 months of the study, once a week thereafter. And participants were encouraged to exercise at home such that they had a total of 300 minutes of weekly exercise.
The mindfulness program was characterized by eight weekly classes of 2.5 hours each as well as a half-day retreat to teach the tenets of mindfulness and meditation, with monthly refreshers thereafter. Participants were instructed to meditate for 60 minutes a day in addition to the classes.
For the 144 people who were randomized to both meditation and exercise, this trial amounted to something of a part-time job. So you might think that adherence to the interventions was low, but apparently that’s not the case. Attendance to the mindfulness classes was over 90%, and over 80% for the exercise classes. And diary-based reporting of home efforts was also pretty good.
The control group wasn’t left to their own devices. Recognizing that the community aspect of exercise or mindfulness classes might convey a benefit independent of the actual exercise or mindfulness, the control group met on a similar schedule to discuss health education, but no mention of exercise or mindfulness occurred in that setting.
The primary outcome was change in memory and executive function scores across a battery of neuropsychologic testing, but the story is told in just a few pictures.
Memory scores improved in all three groups – mindfulness, exercise, and health education – over time. Cognitive composite score improved in all three groups similarly. There was no synergistic effect of mindfulness and exercise either. Basically, everyone got a bit better.
But the study did way more than look at scores on tests. Researchers used MRI to measure brain anatomic outcomes as well. And the surprising thing is that virtually none of these outcomes were different between the groups either.
Hippocampal volume decreased a bit in all the groups. Dorsolateral prefrontal cortex volume was flat. There was no change in scores measuring tasks of daily living.
When you see negative results like this, right away you worry that the intervention wasn’t properly delivered. Were these people really exercising and meditating? Well, the authors showed that individuals randomized to exercise, at least, had less sleep latency, greater aerobic fitness, and greater strength. So we know something was happening.
They then asked, would the people in the exercise group with the greatest changes in those physiologic parameters show some improvement in cognitive parameters? In other words, we know you were exercising because you got stronger and are sleeping better; is your memory better? The answer? Surprisingly, still no. Even in that honestly somewhat cherry-picked group, the interventions had no effect.
Could it be that the control was inappropriate, that the “health education” intervention was actually so helpful that it obscured the benefits of exercise and meditation? After all, cognitive scores did improve in all groups. The authors doubt it. They say they think the improvement in cognitive scores reflects the fact that patients had learned a bit about how to take the tests. This is pretty common in the neuropsychiatric literature.
So here we are and I just want to say, well, shoot. This is not the result I wanted. And I think the reason I’m so disappointed is because aging and the loss of cognitive faculties that comes with aging are just sort of scary. We are all looking for some control over that fear, and how nice it would be to be able to tell ourselves not to worry – that we won’t have those problems as we get older because we exercise, or meditate, or drink red wine, or don’t drink wine, or whatever. And while I have no doubt that staying healthier physically will keep you healthier mentally, it may take more than one simple thing to move the needle.
Dr. Wilson is associate professor, department of medicine, and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr. F. Perry Wilson of the Yale School of Medicine.
We are coming to the end of the year, which always makes me think about getting older. Much like the search for the fountain of youth, many promising leads have ultimately led to dead ends. And yet, I had high hopes for a trial that focused on two cornerstones of wellness – exercise and mindfulness – to address the subjective loss of memory that comes with aging. Alas, meditation and exercise do not appear to be the fountain of youth.
I’m talking about this study, appearing in JAMA, known as the MEDEX trial.
It’s a clever design: a 2 x 2 factorial randomized trial where participants could be randomized to a mindfulness intervention, an exercise intervention, both, or neither.
In this manner, you can test multiple hypotheses exploiting a shared control group. Or as a mentor of mine used to say, you get two trials for the price of one and a half.
The participants were older adults, aged 65-84, living in the community. They had to be relatively sedentary at baseline and not engaging in mindfulness practices. They had to subjectively report some memory or concentration issues but had to be cognitively intact, based on a standard dementia screening test. In other words, these are your average older people who are worried that they aren’t as sharp as they used to be.
The interventions themselves were fairly intense. The exercise group had instructor-led sessions for 90 minutes twice a week for the first 6 months of the study, once a week thereafter. And participants were encouraged to exercise at home such that they had a total of 300 minutes of weekly exercise.
The mindfulness program was characterized by eight weekly classes of 2.5 hours each as well as a half-day retreat to teach the tenets of mindfulness and meditation, with monthly refreshers thereafter. Participants were instructed to meditate for 60 minutes a day in addition to the classes.
For the 144 people who were randomized to both meditation and exercise, this trial amounted to something of a part-time job. So you might think that adherence to the interventions was low, but apparently that’s not the case. Attendance to the mindfulness classes was over 90%, and over 80% for the exercise classes. And diary-based reporting of home efforts was also pretty good.
The control group wasn’t left to their own devices. Recognizing that the community aspect of exercise or mindfulness classes might convey a benefit independent of the actual exercise or mindfulness, the control group met on a similar schedule to discuss health education, but no mention of exercise or mindfulness occurred in that setting.
The primary outcome was change in memory and executive function scores across a battery of neuropsychologic testing, but the story is told in just a few pictures.
Memory scores improved in all three groups – mindfulness, exercise, and health education – over time. Cognitive composite score improved in all three groups similarly. There was no synergistic effect of mindfulness and exercise either. Basically, everyone got a bit better.
But the study did way more than look at scores on tests. Researchers used MRI to measure brain anatomic outcomes as well. And the surprising thing is that virtually none of these outcomes were different between the groups either.
Hippocampal volume decreased a bit in all the groups. Dorsolateral prefrontal cortex volume was flat. There was no change in scores measuring tasks of daily living.
When you see negative results like this, right away you worry that the intervention wasn’t properly delivered. Were these people really exercising and meditating? Well, the authors showed that individuals randomized to exercise, at least, had less sleep latency, greater aerobic fitness, and greater strength. So we know something was happening.
They then asked, would the people in the exercise group with the greatest changes in those physiologic parameters show some improvement in cognitive parameters? In other words, we know you were exercising because you got stronger and are sleeping better; is your memory better? The answer? Surprisingly, still no. Even in that honestly somewhat cherry-picked group, the interventions had no effect.
Could it be that the control was inappropriate, that the “health education” intervention was actually so helpful that it obscured the benefits of exercise and meditation? After all, cognitive scores did improve in all groups. The authors doubt it. They say they think the improvement in cognitive scores reflects the fact that patients had learned a bit about how to take the tests. This is pretty common in the neuropsychiatric literature.
So here we are and I just want to say, well, shoot. This is not the result I wanted. And I think the reason I’m so disappointed is because aging and the loss of cognitive faculties that comes with aging are just sort of scary. We are all looking for some control over that fear, and how nice it would be to be able to tell ourselves not to worry – that we won’t have those problems as we get older because we exercise, or meditate, or drink red wine, or don’t drink wine, or whatever. And while I have no doubt that staying healthier physically will keep you healthier mentally, it may take more than one simple thing to move the needle.
Dr. Wilson is associate professor, department of medicine, and director of the Clinical and Translational Research Accelerator at Yale University, New Haven, Conn. He reported no conflicts of interest.
A version of this article first appeared on Medscape.com.
Patient With Severe Headache After IV Immunoglobulin
A 35-year-old woman with a history of hypothyroidism and idiopathic small fiber autonomic and sensory neuropathy presented to the emergency department (ED) 48 hours after IV immunoglobulin (IG) infusion with a severe headache, nausea, neck stiffness, photophobia, and episodes of intense positional eye pressure. The patient reported previous episodes of headaches post-IVIG infusion but not nearly as severe. On ED arrival, the patient was afebrile with vital signs within normal limits. Initial laboratory results were notable for levels within reference range parameters: 5.9 × 109/L white blood cell (WBC) count, 13.3 g/dL hemoglobin, 38.7% hematocrit, and 279 × 109/L platelet count; there were no abnormal urinalysis findings, and she was negative for human chorionic gonadotropin.
Due to the patient’s symptoms concerning for an acute intracranial process, a brain computed tomography (CT) without contrast was ordered. The CT demonstrated no intracranial abnormalities, but the patient’s symptoms continued to worsen. The patient was started on IV fluids and 1 g IV acetaminophen and underwent a lumbar puncture (LP). Her opening pressure was elevated at 29 cm H2O (reference range, 6-20 cm), and the fluid was notably clear. During the LP, 25 mL of cerebrospinal fluid (CSF) was collected for laboratory analysis to include a polymerase chain reaction (PCR) panel and cultures, and a closing pressure of 12 cm H2O was recorded at the end of the procedure with the patient reporting some relief of pressure. The patient was admitted to the medicine ward for further workup and observations.The patient’s meningitis/encephalitis PCR panel detected no pathogens in the CSF, but her WBC count was 84 × 109/L (reference range, 4-11) with 30 segmented neutrophils (reference range, 0-6) and red blood cell count of 24 (reference range, 0-1); her normal glucose at 60 mg/dL (reference range, 40-70) and protein of 33 mg/dL (reference range, 15-45) were within normal parameters. Brain magnetic resonance images with and without contrast was inconsistent with any acute intracranial pathology to include subarachnoid hemorrhage or central nervous system neoplasm (Figure 1). Bacterial and fungal cultures were negative.
- What is your diagnosis?
- How would you treat this patient?
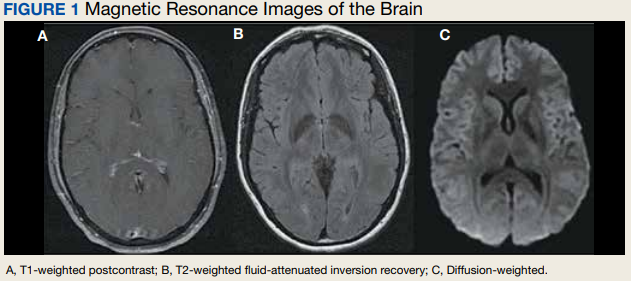
Discussion
Aseptic meningitis presents with a typical clinical picture of meningitis to include headache, stiffened neck, and photophobia. In the event of negative CSF bacterial and fungal cultures and negative viral PCR, a diagnosis of aseptic meningitis is considered.1 Though the differential for aseptic meningitis is broad, in the immunocompetent patient, the most common etiology of aseptic meningitis in the United States is by far viral, and specifically, enterovirus (50.9%). It is less commonly caused by herpes simplex virus (8.3%), varicella zoster virus, and finally, the mosquito-borne St. Louis encephalitis and West Nile viruses typically acquired in the summer or early fall months. Other infectious agents that can present with aseptic meningitis are spirochetes (Lyme disease and syphilis), tuberculous meningitis, fungal infections (cryptococcal meningitis), and other bacterial infections that have a negative culture.
The patient’s history, physical examination, vital signs, imaging, and lumbar puncture findings were most concerning for drug-induced aseptic meningitis (DIAM) secondary to her recent IVIG infusion. An algorithm can be used to work through the diagnostic approach (Figure 2).3,4 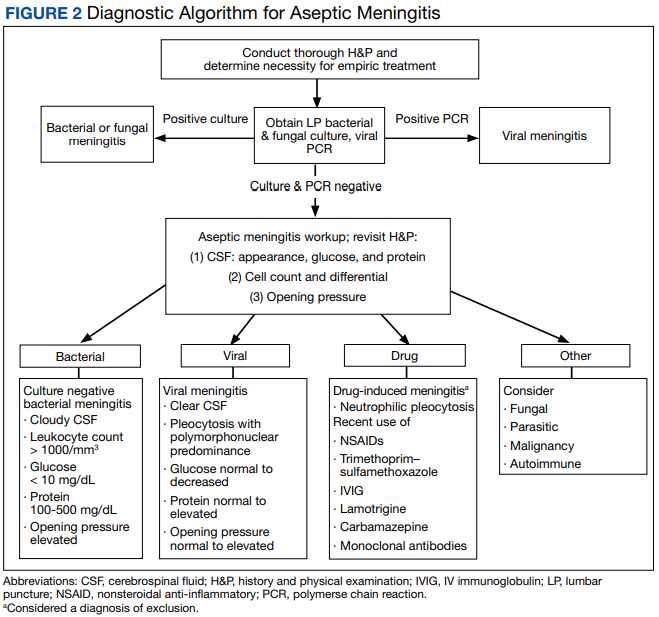
Immediate and delayed adverse reactions to IVIG are known risks for IVIG therapy. About 1% to 15% of patients who receive IVIG will experience mild immediate reactions to the infusion.6 These immediate reactions include fever (78.6%), acrocyanosis (71.4%), rash (64.3%), headache (57.1%), shortness of breath (42.8%), hypotension (35.7%), and chest pain (21.4%).
IVIG is an increasingly used biologic pharmacologic agent used for a variety of medical conditions. This can be attributed to its multifaceted properties and ability to fight infection when given as replacement therapy and provide immunomodulation in conjunction with its more well-known anti-inflammatory properties.8 The number of conditions that can potentially benefit from IVIG is so vast that the American Academy of Allergy, Asthma and Immunology had to divide the indication for IVIG therapy into definitely beneficial, probably beneficial, may provide benefit, and unlikely to provide benefit categories.8
Conclusions
We encourage heightened clinical suspicion of DIAM in patients who have recently undergone IVIG infusion and present with meningeal signs (stiff neck, headache, photophobia, and ear/eye pressure) without any evidence of infection on physical examination or laboratory results. With such, we hope to improve clinician suspicion, detection, as well as patient education and outcomes in cases of DIAM.
1. Kareva L, Mironska K, Stavric K, Hasani A. Adverse reactions to intravenous immunoglobulins—our experience. Open Access Maced J Med Sci. 2018;6(12):2359-2362. doi:10.3889/oamjms.2018.513
2. Mount HR, Boyle SD. Aseptic and bacterial meningitis: evaluation, treatment, and prevention. Am Fam Physician. 2017;96(5):314-322.
3. Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician. 2003;68(6):1103-1108.
4. Connolly KJ, Hammer SM. The acute aseptic meningitis syndrome. Infect Dis Clin North Am. 1990;4(4):599-622.
5. Jolles S, Sewell WA, Leighton C. Drug-induced aseptic meningitis: diagnosis and management. Drug Saf. 2000;22(3):215-226. doi:10.2165/00002018-200022030-00005
6. Yelehe-Okouma M, Czmil-Garon J, Pape E, Petitpain N, Gillet P. Drug-induced aseptic meningitis: a mini-review. Fundam Clin Pharmacol. 2018;32(3):252-260. doi:10.1111/fcp.12349
7. Kepa L, Oczko-Grzesik B, Stolarz W, Sobala-Szczygiel B. Drug-induced aseptic meningitis in suspected central nervous system infections. J Clin Neurosci. 2005;12(5):562-564. doi:10.1016/j.jocn.2004.08.024
8. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3S):S1-S46. doi:10.1016/j.jaci.2016.09.023
9. Kaarthigeyan K, Burli VV. Aseptic meningitis following intravenous immunoglobulin therapy of common variable immunodeficiency. J Pediatr Neurosci. 2011;6(2):160-161. doi:10.4103/1817-1745.92858
A 35-year-old woman with a history of hypothyroidism and idiopathic small fiber autonomic and sensory neuropathy presented to the emergency department (ED) 48 hours after IV immunoglobulin (IG) infusion with a severe headache, nausea, neck stiffness, photophobia, and episodes of intense positional eye pressure. The patient reported previous episodes of headaches post-IVIG infusion but not nearly as severe. On ED arrival, the patient was afebrile with vital signs within normal limits. Initial laboratory results were notable for levels within reference range parameters: 5.9 × 109/L white blood cell (WBC) count, 13.3 g/dL hemoglobin, 38.7% hematocrit, and 279 × 109/L platelet count; there were no abnormal urinalysis findings, and she was negative for human chorionic gonadotropin.
Due to the patient’s symptoms concerning for an acute intracranial process, a brain computed tomography (CT) without contrast was ordered. The CT demonstrated no intracranial abnormalities, but the patient’s symptoms continued to worsen. The patient was started on IV fluids and 1 g IV acetaminophen and underwent a lumbar puncture (LP). Her opening pressure was elevated at 29 cm H2O (reference range, 6-20 cm), and the fluid was notably clear. During the LP, 25 mL of cerebrospinal fluid (CSF) was collected for laboratory analysis to include a polymerase chain reaction (PCR) panel and cultures, and a closing pressure of 12 cm H2O was recorded at the end of the procedure with the patient reporting some relief of pressure. The patient was admitted to the medicine ward for further workup and observations.The patient’s meningitis/encephalitis PCR panel detected no pathogens in the CSF, but her WBC count was 84 × 109/L (reference range, 4-11) with 30 segmented neutrophils (reference range, 0-6) and red blood cell count of 24 (reference range, 0-1); her normal glucose at 60 mg/dL (reference range, 40-70) and protein of 33 mg/dL (reference range, 15-45) were within normal parameters. Brain magnetic resonance images with and without contrast was inconsistent with any acute intracranial pathology to include subarachnoid hemorrhage or central nervous system neoplasm (Figure 1). Bacterial and fungal cultures were negative.
- What is your diagnosis?
- How would you treat this patient?
Discussion
Aseptic meningitis presents with a typical clinical picture of meningitis to include headache, stiffened neck, and photophobia. In the event of negative CSF bacterial and fungal cultures and negative viral PCR, a diagnosis of aseptic meningitis is considered.1 Though the differential for aseptic meningitis is broad, in the immunocompetent patient, the most common etiology of aseptic meningitis in the United States is by far viral, and specifically, enterovirus (50.9%). It is less commonly caused by herpes simplex virus (8.3%), varicella zoster virus, and finally, the mosquito-borne St. Louis encephalitis and West Nile viruses typically acquired in the summer or early fall months. Other infectious agents that can present with aseptic meningitis are spirochetes (Lyme disease and syphilis), tuberculous meningitis, fungal infections (cryptococcal meningitis), and other bacterial infections that have a negative culture.
The patient’s history, physical examination, vital signs, imaging, and lumbar puncture findings were most concerning for drug-induced aseptic meningitis (DIAM) secondary to her recent IVIG infusion. An algorithm can be used to work through the diagnostic approach (Figure 2).3,4
Immediate and delayed adverse reactions to IVIG are known risks for IVIG therapy. About 1% to 15% of patients who receive IVIG will experience mild immediate reactions to the infusion.6 These immediate reactions include fever (78.6%), acrocyanosis (71.4%), rash (64.3%), headache (57.1%), shortness of breath (42.8%), hypotension (35.7%), and chest pain (21.4%).
IVIG is an increasingly used biologic pharmacologic agent used for a variety of medical conditions. This can be attributed to its multifaceted properties and ability to fight infection when given as replacement therapy and provide immunomodulation in conjunction with its more well-known anti-inflammatory properties.8 The number of conditions that can potentially benefit from IVIG is so vast that the American Academy of Allergy, Asthma and Immunology had to divide the indication for IVIG therapy into definitely beneficial, probably beneficial, may provide benefit, and unlikely to provide benefit categories.8
Conclusions
We encourage heightened clinical suspicion of DIAM in patients who have recently undergone IVIG infusion and present with meningeal signs (stiff neck, headache, photophobia, and ear/eye pressure) without any evidence of infection on physical examination or laboratory results. With such, we hope to improve clinician suspicion, detection, as well as patient education and outcomes in cases of DIAM.
A 35-year-old woman with a history of hypothyroidism and idiopathic small fiber autonomic and sensory neuropathy presented to the emergency department (ED) 48 hours after IV immunoglobulin (IG) infusion with a severe headache, nausea, neck stiffness, photophobia, and episodes of intense positional eye pressure. The patient reported previous episodes of headaches post-IVIG infusion but not nearly as severe. On ED arrival, the patient was afebrile with vital signs within normal limits. Initial laboratory results were notable for levels within reference range parameters: 5.9 × 109/L white blood cell (WBC) count, 13.3 g/dL hemoglobin, 38.7% hematocrit, and 279 × 109/L platelet count; there were no abnormal urinalysis findings, and she was negative for human chorionic gonadotropin.
Due to the patient’s symptoms concerning for an acute intracranial process, a brain computed tomography (CT) without contrast was ordered. The CT demonstrated no intracranial abnormalities, but the patient’s symptoms continued to worsen. The patient was started on IV fluids and 1 g IV acetaminophen and underwent a lumbar puncture (LP). Her opening pressure was elevated at 29 cm H2O (reference range, 6-20 cm), and the fluid was notably clear. During the LP, 25 mL of cerebrospinal fluid (CSF) was collected for laboratory analysis to include a polymerase chain reaction (PCR) panel and cultures, and a closing pressure of 12 cm H2O was recorded at the end of the procedure with the patient reporting some relief of pressure. The patient was admitted to the medicine ward for further workup and observations.The patient’s meningitis/encephalitis PCR panel detected no pathogens in the CSF, but her WBC count was 84 × 109/L (reference range, 4-11) with 30 segmented neutrophils (reference range, 0-6) and red blood cell count of 24 (reference range, 0-1); her normal glucose at 60 mg/dL (reference range, 40-70) and protein of 33 mg/dL (reference range, 15-45) were within normal parameters. Brain magnetic resonance images with and without contrast was inconsistent with any acute intracranial pathology to include subarachnoid hemorrhage or central nervous system neoplasm (Figure 1). Bacterial and fungal cultures were negative.
- What is your diagnosis?
- How would you treat this patient?
Discussion
Aseptic meningitis presents with a typical clinical picture of meningitis to include headache, stiffened neck, and photophobia. In the event of negative CSF bacterial and fungal cultures and negative viral PCR, a diagnosis of aseptic meningitis is considered.1 Though the differential for aseptic meningitis is broad, in the immunocompetent patient, the most common etiology of aseptic meningitis in the United States is by far viral, and specifically, enterovirus (50.9%). It is less commonly caused by herpes simplex virus (8.3%), varicella zoster virus, and finally, the mosquito-borne St. Louis encephalitis and West Nile viruses typically acquired in the summer or early fall months. Other infectious agents that can present with aseptic meningitis are spirochetes (Lyme disease and syphilis), tuberculous meningitis, fungal infections (cryptococcal meningitis), and other bacterial infections that have a negative culture.
The patient’s history, physical examination, vital signs, imaging, and lumbar puncture findings were most concerning for drug-induced aseptic meningitis (DIAM) secondary to her recent IVIG infusion. An algorithm can be used to work through the diagnostic approach (Figure 2).3,4
Immediate and delayed adverse reactions to IVIG are known risks for IVIG therapy. About 1% to 15% of patients who receive IVIG will experience mild immediate reactions to the infusion.6 These immediate reactions include fever (78.6%), acrocyanosis (71.4%), rash (64.3%), headache (57.1%), shortness of breath (42.8%), hypotension (35.7%), and chest pain (21.4%).
IVIG is an increasingly used biologic pharmacologic agent used for a variety of medical conditions. This can be attributed to its multifaceted properties and ability to fight infection when given as replacement therapy and provide immunomodulation in conjunction with its more well-known anti-inflammatory properties.8 The number of conditions that can potentially benefit from IVIG is so vast that the American Academy of Allergy, Asthma and Immunology had to divide the indication for IVIG therapy into definitely beneficial, probably beneficial, may provide benefit, and unlikely to provide benefit categories.8
Conclusions
We encourage heightened clinical suspicion of DIAM in patients who have recently undergone IVIG infusion and present with meningeal signs (stiff neck, headache, photophobia, and ear/eye pressure) without any evidence of infection on physical examination or laboratory results. With such, we hope to improve clinician suspicion, detection, as well as patient education and outcomes in cases of DIAM.
1. Kareva L, Mironska K, Stavric K, Hasani A. Adverse reactions to intravenous immunoglobulins—our experience. Open Access Maced J Med Sci. 2018;6(12):2359-2362. doi:10.3889/oamjms.2018.513
2. Mount HR, Boyle SD. Aseptic and bacterial meningitis: evaluation, treatment, and prevention. Am Fam Physician. 2017;96(5):314-322.
3. Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician. 2003;68(6):1103-1108.
4. Connolly KJ, Hammer SM. The acute aseptic meningitis syndrome. Infect Dis Clin North Am. 1990;4(4):599-622.
5. Jolles S, Sewell WA, Leighton C. Drug-induced aseptic meningitis: diagnosis and management. Drug Saf. 2000;22(3):215-226. doi:10.2165/00002018-200022030-00005
6. Yelehe-Okouma M, Czmil-Garon J, Pape E, Petitpain N, Gillet P. Drug-induced aseptic meningitis: a mini-review. Fundam Clin Pharmacol. 2018;32(3):252-260. doi:10.1111/fcp.12349
7. Kepa L, Oczko-Grzesik B, Stolarz W, Sobala-Szczygiel B. Drug-induced aseptic meningitis in suspected central nervous system infections. J Clin Neurosci. 2005;12(5):562-564. doi:10.1016/j.jocn.2004.08.024
8. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3S):S1-S46. doi:10.1016/j.jaci.2016.09.023
9. Kaarthigeyan K, Burli VV. Aseptic meningitis following intravenous immunoglobulin therapy of common variable immunodeficiency. J Pediatr Neurosci. 2011;6(2):160-161. doi:10.4103/1817-1745.92858
1. Kareva L, Mironska K, Stavric K, Hasani A. Adverse reactions to intravenous immunoglobulins—our experience. Open Access Maced J Med Sci. 2018;6(12):2359-2362. doi:10.3889/oamjms.2018.513
2. Mount HR, Boyle SD. Aseptic and bacterial meningitis: evaluation, treatment, and prevention. Am Fam Physician. 2017;96(5):314-322.
3. Seehusen DA, Reeves MM, Fomin DA. Cerebrospinal fluid analysis. Am Fam Physician. 2003;68(6):1103-1108.
4. Connolly KJ, Hammer SM. The acute aseptic meningitis syndrome. Infect Dis Clin North Am. 1990;4(4):599-622.
5. Jolles S, Sewell WA, Leighton C. Drug-induced aseptic meningitis: diagnosis and management. Drug Saf. 2000;22(3):215-226. doi:10.2165/00002018-200022030-00005
6. Yelehe-Okouma M, Czmil-Garon J, Pape E, Petitpain N, Gillet P. Drug-induced aseptic meningitis: a mini-review. Fundam Clin Pharmacol. 2018;32(3):252-260. doi:10.1111/fcp.12349
7. Kepa L, Oczko-Grzesik B, Stolarz W, Sobala-Szczygiel B. Drug-induced aseptic meningitis in suspected central nervous system infections. J Clin Neurosci. 2005;12(5):562-564. doi:10.1016/j.jocn.2004.08.024
8. Perez EE, Orange JS, Bonilla F, et al. Update on the use of immunoglobulin in human disease: a review of evidence. J Allergy Clin Immunol. 2017;139(3S):S1-S46. doi:10.1016/j.jaci.2016.09.023
9. Kaarthigeyan K, Burli VV. Aseptic meningitis following intravenous immunoglobulin therapy of common variable immunodeficiency. J Pediatr Neurosci. 2011;6(2):160-161. doi:10.4103/1817-1745.92858