User login
Alzheimer’s Association to CMS: Ditch restraints on amyloid drugs
In a letter addressed to CMS administrator Chiquita Brooks-LaSure, MPP, the association has asked the agency to remove the requirements for “coverage with evidence development” in its national coverage determination for FDA-approved anti-amyloid monoclonal antibodies.
The CMS coverage restrictions for anti-amyloid drugs were finalized in April on the basis of data available at the time.
Since then, new data from the CLARITY AD trial “clearly demonstrate a meaningful clinical benefit” from the investigational anti-amyloid agent lecanemab (Eisai/Biogen), Robert Egge, chief public policy officer for the Alzheimer’s Association, told this news organization.
The CLARITY AD results were published in the New England Journal of Medicine. Lecanemab is currently under accelerated review at the FDA.
The Alzheimer’s Association’s letter to the CMS includes a joint statement signed by more than 200 AD researchers and experts. All agree that the lecanemab results represent “significant new evidence” that necessitates reconsidering the restrictions on anti-amyloid agents.
“CMS has said it would look at new evidence, and now that evidence is here. We believe CMS recognizes this evidence for lecanemab is stronger than that for many treatments Medicare routinely covers,” Mr. Egge said.
‘No time to waste’
“With the timing of accelerated approvals for both lecanemab and donanemab in the next few months, the Alzheimer’s Association wants to ensure, if approved, that patients can access these treatments,” Mr. Egge noted.
“Because revisions to National Coverage Determinations can be a lengthy process, CMS needs to act quickly to minimize delays. People living with Alzheimer’s disease don’t have time to waste,” he added.
The Alzheimer’s Association estimates that every day, more than 2,000 individuals aged 65 or older may transition from mild dementia due to AD to a more advanced stage of the disease in which they may no longer be eligible for lecanemab and the other anti-amyloid agents currently being tested.
“Each day matters when it comes to slowing the progression of this disease,” Joanne Pike, DrPH, president and incoming chief executive officer for the Alzheimer’s Association, noted in a news release.
“The current CMS policy to severely limit access to these treatments eliminates people’s options, is resulting in continued irreversible disease progression, and contributes to greater health inequities. That’s not acceptable,” Dr. Pike said.
A version of this article first appeared on Medscape.com.
In a letter addressed to CMS administrator Chiquita Brooks-LaSure, MPP, the association has asked the agency to remove the requirements for “coverage with evidence development” in its national coverage determination for FDA-approved anti-amyloid monoclonal antibodies.
The CMS coverage restrictions for anti-amyloid drugs were finalized in April on the basis of data available at the time.
Since then, new data from the CLARITY AD trial “clearly demonstrate a meaningful clinical benefit” from the investigational anti-amyloid agent lecanemab (Eisai/Biogen), Robert Egge, chief public policy officer for the Alzheimer’s Association, told this news organization.
The CLARITY AD results were published in the New England Journal of Medicine. Lecanemab is currently under accelerated review at the FDA.
The Alzheimer’s Association’s letter to the CMS includes a joint statement signed by more than 200 AD researchers and experts. All agree that the lecanemab results represent “significant new evidence” that necessitates reconsidering the restrictions on anti-amyloid agents.
“CMS has said it would look at new evidence, and now that evidence is here. We believe CMS recognizes this evidence for lecanemab is stronger than that for many treatments Medicare routinely covers,” Mr. Egge said.
‘No time to waste’
“With the timing of accelerated approvals for both lecanemab and donanemab in the next few months, the Alzheimer’s Association wants to ensure, if approved, that patients can access these treatments,” Mr. Egge noted.
“Because revisions to National Coverage Determinations can be a lengthy process, CMS needs to act quickly to minimize delays. People living with Alzheimer’s disease don’t have time to waste,” he added.
The Alzheimer’s Association estimates that every day, more than 2,000 individuals aged 65 or older may transition from mild dementia due to AD to a more advanced stage of the disease in which they may no longer be eligible for lecanemab and the other anti-amyloid agents currently being tested.
“Each day matters when it comes to slowing the progression of this disease,” Joanne Pike, DrPH, president and incoming chief executive officer for the Alzheimer’s Association, noted in a news release.
“The current CMS policy to severely limit access to these treatments eliminates people’s options, is resulting in continued irreversible disease progression, and contributes to greater health inequities. That’s not acceptable,” Dr. Pike said.
A version of this article first appeared on Medscape.com.
In a letter addressed to CMS administrator Chiquita Brooks-LaSure, MPP, the association has asked the agency to remove the requirements for “coverage with evidence development” in its national coverage determination for FDA-approved anti-amyloid monoclonal antibodies.
The CMS coverage restrictions for anti-amyloid drugs were finalized in April on the basis of data available at the time.
Since then, new data from the CLARITY AD trial “clearly demonstrate a meaningful clinical benefit” from the investigational anti-amyloid agent lecanemab (Eisai/Biogen), Robert Egge, chief public policy officer for the Alzheimer’s Association, told this news organization.
The CLARITY AD results were published in the New England Journal of Medicine. Lecanemab is currently under accelerated review at the FDA.
The Alzheimer’s Association’s letter to the CMS includes a joint statement signed by more than 200 AD researchers and experts. All agree that the lecanemab results represent “significant new evidence” that necessitates reconsidering the restrictions on anti-amyloid agents.
“CMS has said it would look at new evidence, and now that evidence is here. We believe CMS recognizes this evidence for lecanemab is stronger than that for many treatments Medicare routinely covers,” Mr. Egge said.
‘No time to waste’
“With the timing of accelerated approvals for both lecanemab and donanemab in the next few months, the Alzheimer’s Association wants to ensure, if approved, that patients can access these treatments,” Mr. Egge noted.
“Because revisions to National Coverage Determinations can be a lengthy process, CMS needs to act quickly to minimize delays. People living with Alzheimer’s disease don’t have time to waste,” he added.
The Alzheimer’s Association estimates that every day, more than 2,000 individuals aged 65 or older may transition from mild dementia due to AD to a more advanced stage of the disease in which they may no longer be eligible for lecanemab and the other anti-amyloid agents currently being tested.
“Each day matters when it comes to slowing the progression of this disease,” Joanne Pike, DrPH, president and incoming chief executive officer for the Alzheimer’s Association, noted in a news release.
“The current CMS policy to severely limit access to these treatments eliminates people’s options, is resulting in continued irreversible disease progression, and contributes to greater health inequities. That’s not acceptable,” Dr. Pike said.
A version of this article first appeared on Medscape.com.
A doctor saves a drowning family in a dangerous river
Is There a Doctor in the House? is a new series telling these stories.
I live on the Maumee River in Ohio, about 50 yards from the water. I had an early quit time and came home to meet my wife for lunch. Afterward, I went up to my barn across the main road to tinker around. It was a nice day out, so my wife had opened some windows. Suddenly, she heard screaming from the river. It did not sound like fun.
She ran down to the river’s edge and saw a dad and three boys struggling in the water. She phoned me screaming: “They’re drowning! They’re drowning!” I jumped in my truck and drove up our driveway through the yard right down to the river.
My wife was on the phone with 911 at that point, and I could see them about 75-100 yards out. The dad had two of the boys clinging around his neck. They were going under the water and coming up and going under again. The other boy was just floating nearby, face down, motionless.
I threw my shoes and scrubs off and started to walk towards the water. My wife screamed at me, “You’re not going in there!” I said, “I’m not going to stand here and watch this. It’s not going to happen.”
I’m not a kid anymore, but I was a high school swimmer, and to this day I work out all the time. I felt like I had to try something. So, I went in the water despite my wife yelling and I swam towards them.
What happens when you get in that deep water is that you panic. You can’t hear anyone because of the rapids, and your instinct is to swim back towards where you went in, which is against the current. Unless you’re a very strong swimmer, you’re just wasting your time, swimming in place.
But these guys weren’t trying to go anywhere. Dad was just trying to stay up and keep the boys alive. He was in about 10 feet of water. What they didn’t see or just didn’t know: About 20 yards upstream from that deep water is a little island.
When I got to them, I yelled at the dad to move towards the island, “Go backwards! Go back!” I flipped the boy over who wasn’t moving. He was the oldest of the three, around 10 or 11 years old. When I turned him over, he was blue and wasn’t breathing. I put my fingers on his neck and didn’t feel a pulse.
So, I’m treading water, holding him. I put an arm behind his back and started doing chest compressions on him. I probably did a dozen to 15 compressions – nothing. I thought, I’ve got to get some air in this kid. So, I gave him two deep breaths and then started doing compressions again. I know ACLS and CPR training would say we don’t do that anymore. But I couldn’t just sit there and give up. Shortly after that, he coughed out a large amount of water and started breathing.
The dad and the other two boys had made it to the island. So, I started moving towards it with the boy. It was a few minutes before he regained consciousness. Of course, he was unaware of what had happened. He started to scream, because here’s this strange man holding him. But he was breathing. That’s all I cared about.
When we got to the island, I saw that my neighbor downstream had launched his canoe. He’s a retired gentleman who lives next to me, a very physically fit man. He started rolling as hard as he could towards us, against the stream. I kind of gave him a thumbs up, like, “we’re safe now. We’re standing.” We loaded the kids and the dad in the canoe and made it back against the stream to the parking lot where they went in.
All this took probably 10 or 15 minutes, and by then the paramedics were there. Life Flight had been dispatched up by my barn where there’s room to land. So, they drove up there in the ambulance. The boy I revived was flown to the hospital. The others went in the ambulance.
I know all the ED docs, so I talked to somebody later who, with permission from the family, said they were all doing fine. They were getting x-rays on the boy’s lungs. And then I heard the dad and two boys were released that night. The other boy I worked on was observed overnight and discharged the following morning.
Four or 5 days later, I heard from their pediatrician, who also had permission to share. He sent me a very nice note through Epic that he had seen the boys. Besides some mental trauma, they were all healthy and doing fine.
The family lives in the area and the kids go to school 5 miles from my house. So, the following weekend they came over. It was Father’s Day, which was kind of cool. They brought me some flowers and candy and a card the boys had drawn to thank me.
I learned that the dad had brought the boys to the fishing site. They were horsing around in knee deep water. One of the boys walked off a little way and didn’t realize there was a drop off. He went in, and of course the dad went after him, and the other two followed.
I said to the parents: “Look, things like this happen for a reason. People like your son are saved and go on in this world because they’ve got special things to do. I can’t wait to see what kind of man he becomes.”
Two or 3 months later, it was football season, and I got at a message from the dad saying their son was playing football on Saturday at the school. He wondered if I could drop by. So, I kind of snuck over and watched, but I didn’t go say hi. There’s trauma there, and I didn’t want them to have to relive that.
I’m very fortunate that I exercise every day and I know how to do CPR and swim. And thank God the boy was floating when I got to him, or I never would’ve found him. The Maumee River is known as the “muddy Maumee.” You can’t see anything under the water.
Depending on the time of year, the river can be almost dry or overflowing into the parking lot with the current rushing hard. If it had been like that, I wouldn’t have considered going in. And they wouldn’t they have been there in the first place. They’d have been a mile downstream.
I took a risk. I could have gone out there and had the dad and two other kids jump on top of me. Then we all would have been in trouble. But like I told my wife, I couldn’t stand there and watch it. I’m just not that person.
I think it was also about being a dad myself and having grandkids now. Doctor or no doctor, I felt like I was in reasonably good shape and I had to go in there to help. This dad was trying his butt off, but three little kids is too many. You can’t do that by yourself. They were not going to make it.
I go to the hospital and I save lives as part of my job, and I don’t even come home and talk about it. But this is a whole different thing. Being able to save someone’s life when put in this situation is very gratifying. It’s a tremendous feeling. There’s a reason that young man is here today, and I’ll be watching for great things from him.
A version of this article first appeared on Medscape.com.
Daniel Cassavar, MD, is a cardiologist with ProMedica in Perrysburg, Ohio.
Is There a Doctor in the House? is a new series telling these stories.
I live on the Maumee River in Ohio, about 50 yards from the water. I had an early quit time and came home to meet my wife for lunch. Afterward, I went up to my barn across the main road to tinker around. It was a nice day out, so my wife had opened some windows. Suddenly, she heard screaming from the river. It did not sound like fun.
She ran down to the river’s edge and saw a dad and three boys struggling in the water. She phoned me screaming: “They’re drowning! They’re drowning!” I jumped in my truck and drove up our driveway through the yard right down to the river.
My wife was on the phone with 911 at that point, and I could see them about 75-100 yards out. The dad had two of the boys clinging around his neck. They were going under the water and coming up and going under again. The other boy was just floating nearby, face down, motionless.
I threw my shoes and scrubs off and started to walk towards the water. My wife screamed at me, “You’re not going in there!” I said, “I’m not going to stand here and watch this. It’s not going to happen.”
I’m not a kid anymore, but I was a high school swimmer, and to this day I work out all the time. I felt like I had to try something. So, I went in the water despite my wife yelling and I swam towards them.
What happens when you get in that deep water is that you panic. You can’t hear anyone because of the rapids, and your instinct is to swim back towards where you went in, which is against the current. Unless you’re a very strong swimmer, you’re just wasting your time, swimming in place.
But these guys weren’t trying to go anywhere. Dad was just trying to stay up and keep the boys alive. He was in about 10 feet of water. What they didn’t see or just didn’t know: About 20 yards upstream from that deep water is a little island.
When I got to them, I yelled at the dad to move towards the island, “Go backwards! Go back!” I flipped the boy over who wasn’t moving. He was the oldest of the three, around 10 or 11 years old. When I turned him over, he was blue and wasn’t breathing. I put my fingers on his neck and didn’t feel a pulse.
So, I’m treading water, holding him. I put an arm behind his back and started doing chest compressions on him. I probably did a dozen to 15 compressions – nothing. I thought, I’ve got to get some air in this kid. So, I gave him two deep breaths and then started doing compressions again. I know ACLS and CPR training would say we don’t do that anymore. But I couldn’t just sit there and give up. Shortly after that, he coughed out a large amount of water and started breathing.
The dad and the other two boys had made it to the island. So, I started moving towards it with the boy. It was a few minutes before he regained consciousness. Of course, he was unaware of what had happened. He started to scream, because here’s this strange man holding him. But he was breathing. That’s all I cared about.
When we got to the island, I saw that my neighbor downstream had launched his canoe. He’s a retired gentleman who lives next to me, a very physically fit man. He started rolling as hard as he could towards us, against the stream. I kind of gave him a thumbs up, like, “we’re safe now. We’re standing.” We loaded the kids and the dad in the canoe and made it back against the stream to the parking lot where they went in.
All this took probably 10 or 15 minutes, and by then the paramedics were there. Life Flight had been dispatched up by my barn where there’s room to land. So, they drove up there in the ambulance. The boy I revived was flown to the hospital. The others went in the ambulance.
I know all the ED docs, so I talked to somebody later who, with permission from the family, said they were all doing fine. They were getting x-rays on the boy’s lungs. And then I heard the dad and two boys were released that night. The other boy I worked on was observed overnight and discharged the following morning.
Four or 5 days later, I heard from their pediatrician, who also had permission to share. He sent me a very nice note through Epic that he had seen the boys. Besides some mental trauma, they were all healthy and doing fine.
The family lives in the area and the kids go to school 5 miles from my house. So, the following weekend they came over. It was Father’s Day, which was kind of cool. They brought me some flowers and candy and a card the boys had drawn to thank me.
I learned that the dad had brought the boys to the fishing site. They were horsing around in knee deep water. One of the boys walked off a little way and didn’t realize there was a drop off. He went in, and of course the dad went after him, and the other two followed.
I said to the parents: “Look, things like this happen for a reason. People like your son are saved and go on in this world because they’ve got special things to do. I can’t wait to see what kind of man he becomes.”
Two or 3 months later, it was football season, and I got at a message from the dad saying their son was playing football on Saturday at the school. He wondered if I could drop by. So, I kind of snuck over and watched, but I didn’t go say hi. There’s trauma there, and I didn’t want them to have to relive that.
I’m very fortunate that I exercise every day and I know how to do CPR and swim. And thank God the boy was floating when I got to him, or I never would’ve found him. The Maumee River is known as the “muddy Maumee.” You can’t see anything under the water.
Depending on the time of year, the river can be almost dry or overflowing into the parking lot with the current rushing hard. If it had been like that, I wouldn’t have considered going in. And they wouldn’t they have been there in the first place. They’d have been a mile downstream.
I took a risk. I could have gone out there and had the dad and two other kids jump on top of me. Then we all would have been in trouble. But like I told my wife, I couldn’t stand there and watch it. I’m just not that person.
I think it was also about being a dad myself and having grandkids now. Doctor or no doctor, I felt like I was in reasonably good shape and I had to go in there to help. This dad was trying his butt off, but three little kids is too many. You can’t do that by yourself. They were not going to make it.
I go to the hospital and I save lives as part of my job, and I don’t even come home and talk about it. But this is a whole different thing. Being able to save someone’s life when put in this situation is very gratifying. It’s a tremendous feeling. There’s a reason that young man is here today, and I’ll be watching for great things from him.
A version of this article first appeared on Medscape.com.
Daniel Cassavar, MD, is a cardiologist with ProMedica in Perrysburg, Ohio.
Is There a Doctor in the House? is a new series telling these stories.
I live on the Maumee River in Ohio, about 50 yards from the water. I had an early quit time and came home to meet my wife for lunch. Afterward, I went up to my barn across the main road to tinker around. It was a nice day out, so my wife had opened some windows. Suddenly, she heard screaming from the river. It did not sound like fun.
She ran down to the river’s edge and saw a dad and three boys struggling in the water. She phoned me screaming: “They’re drowning! They’re drowning!” I jumped in my truck and drove up our driveway through the yard right down to the river.
My wife was on the phone with 911 at that point, and I could see them about 75-100 yards out. The dad had two of the boys clinging around his neck. They were going under the water and coming up and going under again. The other boy was just floating nearby, face down, motionless.
I threw my shoes and scrubs off and started to walk towards the water. My wife screamed at me, “You’re not going in there!” I said, “I’m not going to stand here and watch this. It’s not going to happen.”
I’m not a kid anymore, but I was a high school swimmer, and to this day I work out all the time. I felt like I had to try something. So, I went in the water despite my wife yelling and I swam towards them.
What happens when you get in that deep water is that you panic. You can’t hear anyone because of the rapids, and your instinct is to swim back towards where you went in, which is against the current. Unless you’re a very strong swimmer, you’re just wasting your time, swimming in place.
But these guys weren’t trying to go anywhere. Dad was just trying to stay up and keep the boys alive. He was in about 10 feet of water. What they didn’t see or just didn’t know: About 20 yards upstream from that deep water is a little island.
When I got to them, I yelled at the dad to move towards the island, “Go backwards! Go back!” I flipped the boy over who wasn’t moving. He was the oldest of the three, around 10 or 11 years old. When I turned him over, he was blue and wasn’t breathing. I put my fingers on his neck and didn’t feel a pulse.
So, I’m treading water, holding him. I put an arm behind his back and started doing chest compressions on him. I probably did a dozen to 15 compressions – nothing. I thought, I’ve got to get some air in this kid. So, I gave him two deep breaths and then started doing compressions again. I know ACLS and CPR training would say we don’t do that anymore. But I couldn’t just sit there and give up. Shortly after that, he coughed out a large amount of water and started breathing.
The dad and the other two boys had made it to the island. So, I started moving towards it with the boy. It was a few minutes before he regained consciousness. Of course, he was unaware of what had happened. He started to scream, because here’s this strange man holding him. But he was breathing. That’s all I cared about.
When we got to the island, I saw that my neighbor downstream had launched his canoe. He’s a retired gentleman who lives next to me, a very physically fit man. He started rolling as hard as he could towards us, against the stream. I kind of gave him a thumbs up, like, “we’re safe now. We’re standing.” We loaded the kids and the dad in the canoe and made it back against the stream to the parking lot where they went in.
All this took probably 10 or 15 minutes, and by then the paramedics were there. Life Flight had been dispatched up by my barn where there’s room to land. So, they drove up there in the ambulance. The boy I revived was flown to the hospital. The others went in the ambulance.
I know all the ED docs, so I talked to somebody later who, with permission from the family, said they were all doing fine. They were getting x-rays on the boy’s lungs. And then I heard the dad and two boys were released that night. The other boy I worked on was observed overnight and discharged the following morning.
Four or 5 days later, I heard from their pediatrician, who also had permission to share. He sent me a very nice note through Epic that he had seen the boys. Besides some mental trauma, they were all healthy and doing fine.
The family lives in the area and the kids go to school 5 miles from my house. So, the following weekend they came over. It was Father’s Day, which was kind of cool. They brought me some flowers and candy and a card the boys had drawn to thank me.
I learned that the dad had brought the boys to the fishing site. They were horsing around in knee deep water. One of the boys walked off a little way and didn’t realize there was a drop off. He went in, and of course the dad went after him, and the other two followed.
I said to the parents: “Look, things like this happen for a reason. People like your son are saved and go on in this world because they’ve got special things to do. I can’t wait to see what kind of man he becomes.”
Two or 3 months later, it was football season, and I got at a message from the dad saying their son was playing football on Saturday at the school. He wondered if I could drop by. So, I kind of snuck over and watched, but I didn’t go say hi. There’s trauma there, and I didn’t want them to have to relive that.
I’m very fortunate that I exercise every day and I know how to do CPR and swim. And thank God the boy was floating when I got to him, or I never would’ve found him. The Maumee River is known as the “muddy Maumee.” You can’t see anything under the water.
Depending on the time of year, the river can be almost dry or overflowing into the parking lot with the current rushing hard. If it had been like that, I wouldn’t have considered going in. And they wouldn’t they have been there in the first place. They’d have been a mile downstream.
I took a risk. I could have gone out there and had the dad and two other kids jump on top of me. Then we all would have been in trouble. But like I told my wife, I couldn’t stand there and watch it. I’m just not that person.
I think it was also about being a dad myself and having grandkids now. Doctor or no doctor, I felt like I was in reasonably good shape and I had to go in there to help. This dad was trying his butt off, but three little kids is too many. You can’t do that by yourself. They were not going to make it.
I go to the hospital and I save lives as part of my job, and I don’t even come home and talk about it. But this is a whole different thing. Being able to save someone’s life when put in this situation is very gratifying. It’s a tremendous feeling. There’s a reason that young man is here today, and I’ll be watching for great things from him.
A version of this article first appeared on Medscape.com.
Daniel Cassavar, MD, is a cardiologist with ProMedica in Perrysburg, Ohio.
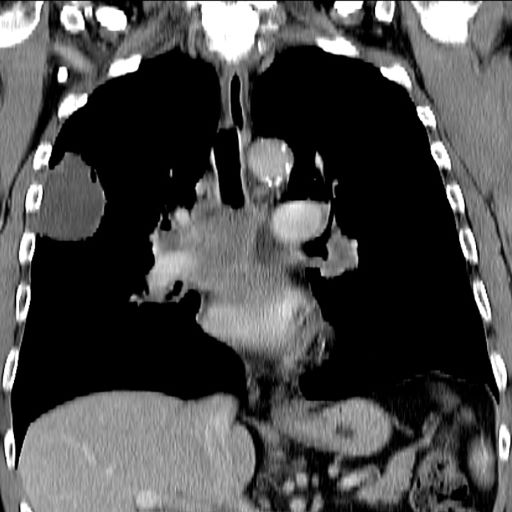
Increasing fatigue and dry cough
This patient's clinical presentation is consistent with a diagnosis of superior vena cava syndrome (SVCS), secondary to SCLC.
SCLC is an aggressive, poorly differentiated, high-grade neuroendocrine carcinoma that accounts for approximately 13%-15% of all new lung cancer cases in the United States. SCLC has a propensity for early dissemination; as such, 80%-85% of patients are diagnosed with extensive disease (ES-SCLC). This is common in heavy smokers. Most SCLC tumors are found in hilar or perihilar areas; <5% present in peripheral locations. In many cases, invasion into the peribronchial tissue and lymph node can be clearly identified, with a typical circumferential spread along the submucosa of the bronchi.
Up to 10% of patients with SCLC develop SVCS, which comprises an array of signs and symptoms that result from the obstruction of blood flow through the thin-walled superior vena cava. Clinical symptoms may include cough, dyspnea, and orthopnea; facial edema and plethora, upper extremity swelling, and venous distension of the chest wall and neck are the most commonly encountered signs. Most cases of SVCS occur in patients with mediastinal tumors, although noncancerous causes (eg, thrombosis and fibrosing mediastinitis) can also give rise to it. The diagnosis of SVCS is usually made clinically and then confirmed with imaging (chest radiography, contrast-enhanced CT, duplex ultrasound, conventional venography, and/or magnetic resonance venography).
Though it was traditionally considered a virtual emergency, patients seldom experience life-threatening complications from SVCS. The goals of treatment are to alleviate the symptoms of SVC obstruction and treat the underlying disease process. Treatment approaches include radiation therapy, chemotherapy, open surgery, and endovenous recanalization; however, patients with clinical SVCS often achieve significant improvement in symptoms from conservative treatment approaches, including elevation of the head of the bed and supplemental oxygen. Systemic chemotherapy can effectively relieve the symptoms of SVCS obstruction, typically within 1-2 weeks of treatment initiation. Up to 80% of patients with SCLC and non-Hodgkin lymphoma may experience complete relief of SVCS symptoms with chemotherapy treatment.
Radiation therapy was once considered the standard approach to the management of SVCS in patients with cancer; however, endovenous recanalization can alleviate symptoms faster than radiation therapy — usually within 72 hours, whereas radiation therapy can take up to 2 weeks to provide relief. Endovascular therapy is also associated with higher efficacy rates than is radiation therapy.
Open surgery plays a limited role in the management of SVC obstruction, although it may be the best approach in select cases.
In cases involving brain edema, decreased cardiac output, or upper airway edema, emergency treatment is indicated.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's clinical presentation is consistent with a diagnosis of superior vena cava syndrome (SVCS), secondary to SCLC.
SCLC is an aggressive, poorly differentiated, high-grade neuroendocrine carcinoma that accounts for approximately 13%-15% of all new lung cancer cases in the United States. SCLC has a propensity for early dissemination; as such, 80%-85% of patients are diagnosed with extensive disease (ES-SCLC). This is common in heavy smokers. Most SCLC tumors are found in hilar or perihilar areas; <5% present in peripheral locations. In many cases, invasion into the peribronchial tissue and lymph node can be clearly identified, with a typical circumferential spread along the submucosa of the bronchi.
Up to 10% of patients with SCLC develop SVCS, which comprises an array of signs and symptoms that result from the obstruction of blood flow through the thin-walled superior vena cava. Clinical symptoms may include cough, dyspnea, and orthopnea; facial edema and plethora, upper extremity swelling, and venous distension of the chest wall and neck are the most commonly encountered signs. Most cases of SVCS occur in patients with mediastinal tumors, although noncancerous causes (eg, thrombosis and fibrosing mediastinitis) can also give rise to it. The diagnosis of SVCS is usually made clinically and then confirmed with imaging (chest radiography, contrast-enhanced CT, duplex ultrasound, conventional venography, and/or magnetic resonance venography).
Though it was traditionally considered a virtual emergency, patients seldom experience life-threatening complications from SVCS. The goals of treatment are to alleviate the symptoms of SVC obstruction and treat the underlying disease process. Treatment approaches include radiation therapy, chemotherapy, open surgery, and endovenous recanalization; however, patients with clinical SVCS often achieve significant improvement in symptoms from conservative treatment approaches, including elevation of the head of the bed and supplemental oxygen. Systemic chemotherapy can effectively relieve the symptoms of SVCS obstruction, typically within 1-2 weeks of treatment initiation. Up to 80% of patients with SCLC and non-Hodgkin lymphoma may experience complete relief of SVCS symptoms with chemotherapy treatment.
Radiation therapy was once considered the standard approach to the management of SVCS in patients with cancer; however, endovenous recanalization can alleviate symptoms faster than radiation therapy — usually within 72 hours, whereas radiation therapy can take up to 2 weeks to provide relief. Endovascular therapy is also associated with higher efficacy rates than is radiation therapy.
Open surgery plays a limited role in the management of SVC obstruction, although it may be the best approach in select cases.
In cases involving brain edema, decreased cardiac output, or upper airway edema, emergency treatment is indicated.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
This patient's clinical presentation is consistent with a diagnosis of superior vena cava syndrome (SVCS), secondary to SCLC.
SCLC is an aggressive, poorly differentiated, high-grade neuroendocrine carcinoma that accounts for approximately 13%-15% of all new lung cancer cases in the United States. SCLC has a propensity for early dissemination; as such, 80%-85% of patients are diagnosed with extensive disease (ES-SCLC). This is common in heavy smokers. Most SCLC tumors are found in hilar or perihilar areas; <5% present in peripheral locations. In many cases, invasion into the peribronchial tissue and lymph node can be clearly identified, with a typical circumferential spread along the submucosa of the bronchi.
Up to 10% of patients with SCLC develop SVCS, which comprises an array of signs and symptoms that result from the obstruction of blood flow through the thin-walled superior vena cava. Clinical symptoms may include cough, dyspnea, and orthopnea; facial edema and plethora, upper extremity swelling, and venous distension of the chest wall and neck are the most commonly encountered signs. Most cases of SVCS occur in patients with mediastinal tumors, although noncancerous causes (eg, thrombosis and fibrosing mediastinitis) can also give rise to it. The diagnosis of SVCS is usually made clinically and then confirmed with imaging (chest radiography, contrast-enhanced CT, duplex ultrasound, conventional venography, and/or magnetic resonance venography).
Though it was traditionally considered a virtual emergency, patients seldom experience life-threatening complications from SVCS. The goals of treatment are to alleviate the symptoms of SVC obstruction and treat the underlying disease process. Treatment approaches include radiation therapy, chemotherapy, open surgery, and endovenous recanalization; however, patients with clinical SVCS often achieve significant improvement in symptoms from conservative treatment approaches, including elevation of the head of the bed and supplemental oxygen. Systemic chemotherapy can effectively relieve the symptoms of SVCS obstruction, typically within 1-2 weeks of treatment initiation. Up to 80% of patients with SCLC and non-Hodgkin lymphoma may experience complete relief of SVCS symptoms with chemotherapy treatment.
Radiation therapy was once considered the standard approach to the management of SVCS in patients with cancer; however, endovenous recanalization can alleviate symptoms faster than radiation therapy — usually within 72 hours, whereas radiation therapy can take up to 2 weeks to provide relief. Endovascular therapy is also associated with higher efficacy rates than is radiation therapy.
Open surgery plays a limited role in the management of SVC obstruction, although it may be the best approach in select cases.
In cases involving brain edema, decreased cardiac output, or upper airway edema, emergency treatment is indicated.
Karl J. D'Silva, MD, Clinical Assistant Professor, Department of Medicine, Tufts University School of Medicine, Boston; Medical Director, Department of Oncology and Hematology, Lahey Hospital and Medical Center, Peabody, Massachusetts.
Karl J. D'Silva, MD, has disclosed no relevant financial relationships.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
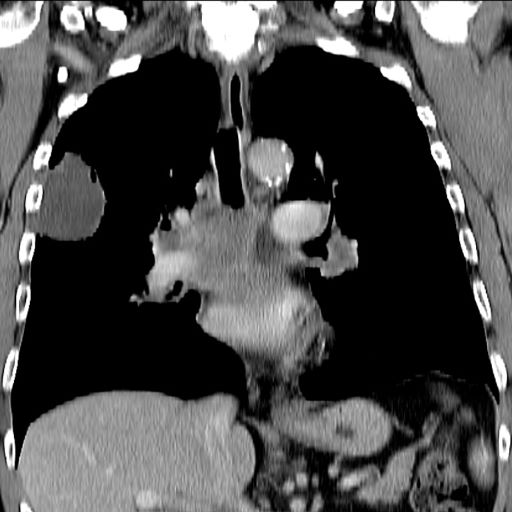
A 66-year-old African American man was diagnosed with small cell lung cancer (SCLC) after the discovery of an endobronchial tumor on bronchoscopy. A biopsy of the tumor was positive for SCLC and CT revealed multiple pulmonary nodules and extensive mediastinal nodal metastases. The patient completed his first cycle of carboplatin-based chemotherapy about 1 month ago. At today's visit, he presents with complaints of worsening symptoms over the past week or so; specifically, he reports increasing fatigue and shortness of breath, a dry cough, light-headedness, difficulty swallowing, and facial swelling. Physical examination reveals facial edema and venous distension of the neck and chest wall; blood pressure is 140/70 mm Hg, respiratory rate is 19 breaths/min, and pulse is 84 beats/min. The patient has a 45-pack-year smoking history and reports having two or three alcoholic drinks per day. His previous medical history is positive for hypertension, which is treated with enalapril 20 mg/day and metoprolol 200 mg/day. Complete blood cell count findings are all within normal range.
Commentary: Early Breast Cancer Treatment Strategies and Acupuncture, January 2023

The risk for disease recurrence, and specifically distant relapse, for women with high-risk early breast cancer highlights the need for novel therapies in this population.2,3 The phase 3 randomized monarchE trial investigated the role of the CDK4/6 inhibitor abemaciclib combined with endocrine therapy vs standard endocrine therapy alone in 5637 patients with high-risk (≥ 4 positive axillary nodes or 1-3 positive nodes and either grade 3 tumor, tumor size ≥ 5 cm or Ki-67 ≥ 20%) hormone receptor–positive/HER2-negative early breast cancer. At a median follow-up of 42 months, the median invasive disease-free survival (iDFS) benefit was sustained with abemaciclib + endocrine therapy vs endocrine therapy alone (HR 0.664; nominal P < .0001); the absolute 4-year iDFS benefit was 6.4% (85.8% in the abemaciclib + endocrine therapy group vs 79.4% in the endocrine therapy–alone group). Furthermore, this effect appeared to deepen over time, as the previous absolute iDFS differences were 2.8% (2 years) and 4.8% (3 years). Abemaciclib was associated with a higher rate of grade 3 or higher adverse events (49.9% vs 16.9%), the most common being neutropenia, leukopenia, and diarrhea (Johnston et al). Although adjuvant palbociclib trials (PALLAS4 and PENELOPE-B5) did not meet their primary endpoint, longer follow-up of monarchE and results from NATALEE with ribociclib are anxiously awaited to further define the role of CDK4/6 inhibitors in this space.
Aromatase inhibitors (AI) are an integral component of treatment for hormone receptor–positive breast cancer for many women. However, joint pain and stiffness associated with these agents can affect compliance. Various management strategies, including trials of alternative AI or endocrine therapies and pharmacologic (duloxetine) and non-pharmacologic (acupuncture,6 exercise) modalities, have been investigated. A randomized trial including 226 women with early-stage breast cancer receiving AI therapy with baseline joint pain (Brief Pain Inventory Worst Pain [BPI-WP] item score of ≥ 3) evaluated whether true acupuncture (TA) provided a sustained reduction in pain symptoms compared with sham acupuncture (SA) or waiting-list control (WC). Acupuncture protocols consisted of 6 weeks of intervention (2 sessions per week) followed by 1 session per week for another 6 weeks. At 52 weeks, mean BPI-WP scores were 1.08 points lower in the TA group compared with the SA group (P = .01) and were 0.99 points lower in the TA group compared with the WC group (P = .03) (Hershman et al). These data support consideration of acupuncture as a mechanism to help maintain patients on aromatase inhibitors, particularly for patients who wish to avoid or have not received benefit from pharmacologic therapy.
Additional References
- Puglisi F, Gerratana L, Lambertini M, et al. Composite risk and benefit from adjuvant dose-dense chemotherapy in hormone receptor-positive breast cancer. NPJ Breast Cancer. 2021;7:82. Doi: 10.1038/s41523-021-00286-w
- Salvo EM, Ramirez AO, Cueto J, et al. Risk of recurrence among patients with HR-positive, HER2-negative, early breast cancer receiving adjuvant endocrine therapy: A systematic review and meta-analysis. Breast. 2021;57:5-17. Doi: 10.1016/j.breast.2021.02.009
- Sheffield KM, Peachey JR, Method M, et al. A real-world US study of recurrence risks using combined clinicopathological features in HR-positive, HER2-negative early breast cancer. Future Oncol.2022;18:2667-2682. Doi: 10.2217/fon-2022-0310
- Mayer EL, Dueck AC, Martin M, et al. Palbociclib with adjuvant endocrine therapy in early breast cancer (PALLAS): Interim analysis of a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2021;22(2):212-222. Doi: Loibl S, Marmé F, Martin M, et al. Palbociclib for residual high-risk invasive HR-positive and HER2-negative early breast cancer-The Penelope-B trial. J Clin Oncol. 2021;39(14):1518-1530. Doi: Liu X, Lu J, Wang G, et al. Acupuncture for arthralgia induced by aromatase inhibitors in patients with breast cancer: A systematic review and meta-analysis. Integr Cancer Ther. 2021;20:1534735420980811. Doi: 10.1177/1534735420980811
The risk for disease recurrence, and specifically distant relapse, for women with high-risk early breast cancer highlights the need for novel therapies in this population.2,3 The phase 3 randomized monarchE trial investigated the role of the CDK4/6 inhibitor abemaciclib combined with endocrine therapy vs standard endocrine therapy alone in 5637 patients with high-risk (≥ 4 positive axillary nodes or 1-3 positive nodes and either grade 3 tumor, tumor size ≥ 5 cm or Ki-67 ≥ 20%) hormone receptor–positive/HER2-negative early breast cancer. At a median follow-up of 42 months, the median invasive disease-free survival (iDFS) benefit was sustained with abemaciclib + endocrine therapy vs endocrine therapy alone (HR 0.664; nominal P < .0001); the absolute 4-year iDFS benefit was 6.4% (85.8% in the abemaciclib + endocrine therapy group vs 79.4% in the endocrine therapy–alone group). Furthermore, this effect appeared to deepen over time, as the previous absolute iDFS differences were 2.8% (2 years) and 4.8% (3 years). Abemaciclib was associated with a higher rate of grade 3 or higher adverse events (49.9% vs 16.9%), the most common being neutropenia, leukopenia, and diarrhea (Johnston et al). Although adjuvant palbociclib trials (PALLAS4 and PENELOPE-B5) did not meet their primary endpoint, longer follow-up of monarchE and results from NATALEE with ribociclib are anxiously awaited to further define the role of CDK4/6 inhibitors in this space.
Aromatase inhibitors (AI) are an integral component of treatment for hormone receptor–positive breast cancer for many women. However, joint pain and stiffness associated with these agents can affect compliance. Various management strategies, including trials of alternative AI or endocrine therapies and pharmacologic (duloxetine) and non-pharmacologic (acupuncture,6 exercise) modalities, have been investigated. A randomized trial including 226 women with early-stage breast cancer receiving AI therapy with baseline joint pain (Brief Pain Inventory Worst Pain [BPI-WP] item score of ≥ 3) evaluated whether true acupuncture (TA) provided a sustained reduction in pain symptoms compared with sham acupuncture (SA) or waiting-list control (WC). Acupuncture protocols consisted of 6 weeks of intervention (2 sessions per week) followed by 1 session per week for another 6 weeks. At 52 weeks, mean BPI-WP scores were 1.08 points lower in the TA group compared with the SA group (P = .01) and were 0.99 points lower in the TA group compared with the WC group (P = .03) (Hershman et al). These data support consideration of acupuncture as a mechanism to help maintain patients on aromatase inhibitors, particularly for patients who wish to avoid or have not received benefit from pharmacologic therapy.
Additional References
- Puglisi F, Gerratana L, Lambertini M, et al. Composite risk and benefit from adjuvant dose-dense chemotherapy in hormone receptor-positive breast cancer. NPJ Breast Cancer. 2021;7:82. Doi: 10.1038/s41523-021-00286-w
- Salvo EM, Ramirez AO, Cueto J, et al. Risk of recurrence among patients with HR-positive, HER2-negative, early breast cancer receiving adjuvant endocrine therapy: A systematic review and meta-analysis. Breast. 2021;57:5-17. Doi: 10.1016/j.breast.2021.02.009
- Sheffield KM, Peachey JR, Method M, et al. A real-world US study of recurrence risks using combined clinicopathological features in HR-positive, HER2-negative early breast cancer. Future Oncol.2022;18:2667-2682. Doi: 10.2217/fon-2022-0310
- Mayer EL, Dueck AC, Martin M, et al. Palbociclib with adjuvant endocrine therapy in early breast cancer (PALLAS): Interim analysis of a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2021;22(2):212-222. Doi: Loibl S, Marmé F, Martin M, et al. Palbociclib for residual high-risk invasive HR-positive and HER2-negative early breast cancer-The Penelope-B trial. J Clin Oncol. 2021;39(14):1518-1530. Doi: Liu X, Lu J, Wang G, et al. Acupuncture for arthralgia induced by aromatase inhibitors in patients with breast cancer: A systematic review and meta-analysis. Integr Cancer Ther. 2021;20:1534735420980811. Doi: 10.1177/1534735420980811
The risk for disease recurrence, and specifically distant relapse, for women with high-risk early breast cancer highlights the need for novel therapies in this population.2,3 The phase 3 randomized monarchE trial investigated the role of the CDK4/6 inhibitor abemaciclib combined with endocrine therapy vs standard endocrine therapy alone in 5637 patients with high-risk (≥ 4 positive axillary nodes or 1-3 positive nodes and either grade 3 tumor, tumor size ≥ 5 cm or Ki-67 ≥ 20%) hormone receptor–positive/HER2-negative early breast cancer. At a median follow-up of 42 months, the median invasive disease-free survival (iDFS) benefit was sustained with abemaciclib + endocrine therapy vs endocrine therapy alone (HR 0.664; nominal P < .0001); the absolute 4-year iDFS benefit was 6.4% (85.8% in the abemaciclib + endocrine therapy group vs 79.4% in the endocrine therapy–alone group). Furthermore, this effect appeared to deepen over time, as the previous absolute iDFS differences were 2.8% (2 years) and 4.8% (3 years). Abemaciclib was associated with a higher rate of grade 3 or higher adverse events (49.9% vs 16.9%), the most common being neutropenia, leukopenia, and diarrhea (Johnston et al). Although adjuvant palbociclib trials (PALLAS4 and PENELOPE-B5) did not meet their primary endpoint, longer follow-up of monarchE and results from NATALEE with ribociclib are anxiously awaited to further define the role of CDK4/6 inhibitors in this space.
Aromatase inhibitors (AI) are an integral component of treatment for hormone receptor–positive breast cancer for many women. However, joint pain and stiffness associated with these agents can affect compliance. Various management strategies, including trials of alternative AI or endocrine therapies and pharmacologic (duloxetine) and non-pharmacologic (acupuncture,6 exercise) modalities, have been investigated. A randomized trial including 226 women with early-stage breast cancer receiving AI therapy with baseline joint pain (Brief Pain Inventory Worst Pain [BPI-WP] item score of ≥ 3) evaluated whether true acupuncture (TA) provided a sustained reduction in pain symptoms compared with sham acupuncture (SA) or waiting-list control (WC). Acupuncture protocols consisted of 6 weeks of intervention (2 sessions per week) followed by 1 session per week for another 6 weeks. At 52 weeks, mean BPI-WP scores were 1.08 points lower in the TA group compared with the SA group (P = .01) and were 0.99 points lower in the TA group compared with the WC group (P = .03) (Hershman et al). These data support consideration of acupuncture as a mechanism to help maintain patients on aromatase inhibitors, particularly for patients who wish to avoid or have not received benefit from pharmacologic therapy.
Additional References
- Puglisi F, Gerratana L, Lambertini M, et al. Composite risk and benefit from adjuvant dose-dense chemotherapy in hormone receptor-positive breast cancer. NPJ Breast Cancer. 2021;7:82. Doi: 10.1038/s41523-021-00286-w
- Salvo EM, Ramirez AO, Cueto J, et al. Risk of recurrence among patients with HR-positive, HER2-negative, early breast cancer receiving adjuvant endocrine therapy: A systematic review and meta-analysis. Breast. 2021;57:5-17. Doi: 10.1016/j.breast.2021.02.009
- Sheffield KM, Peachey JR, Method M, et al. A real-world US study of recurrence risks using combined clinicopathological features in HR-positive, HER2-negative early breast cancer. Future Oncol.2022;18:2667-2682. Doi: 10.2217/fon-2022-0310
- Mayer EL, Dueck AC, Martin M, et al. Palbociclib with adjuvant endocrine therapy in early breast cancer (PALLAS): Interim analysis of a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2021;22(2):212-222. Doi: Loibl S, Marmé F, Martin M, et al. Palbociclib for residual high-risk invasive HR-positive and HER2-negative early breast cancer-The Penelope-B trial. J Clin Oncol. 2021;39(14):1518-1530. Doi: Liu X, Lu J, Wang G, et al. Acupuncture for arthralgia induced by aromatase inhibitors in patients with breast cancer: A systematic review and meta-analysis. Integr Cancer Ther. 2021;20:1534735420980811. Doi: 10.1177/1534735420980811
FMT doesn’t appear to affect weight loss after bariatric surgery
according to results of a randomized controlled trial.
The small study by Perttu Lahtinen, MD, with Päijät-Häme Central Hospital in Lahti, Finland, and colleagues was published online in JAMA Network Open.
Bariatric surgery remains the most effective strategy for treating severe obesity. Yet some patients achieve only minimal weight loss or regain weight after surgery, the researchers noted.
There is much interest in the gut microbiota as a potential target for the treatment of obesity. FMT from a lean donor has shown promise in treating obesity in mouse models (Science. 2013 Sep 6. doi: 10.1126/science.1241214).
The Finnish trial, however, does not support that conclusion.
The study included 41 adults (71% women; mean age, 48.7 years) with severe obesity (mean body mass index, 42.5 kg/m2). Twenty-one received FMT from a lean donor, and 20 received FMT from their own feces (autologous placebo). FMT was administered by gastroscopy into the duodenum 6 months before laparoscopic Roux-en-Y gastric bypass or sleeve gastrectomy. All patients also consumed a very-low-calorie diet approximately 4 weeks before the surgery.
Bariatric surgery led to equal weight reductions for both groups, but there was no additive benefit in terms of weight loss with FMT.
Six months after the administration of FMT, and before the surgery was performed, the percentage of total weight loss, the main outcome, was 4.8% (P < .001) in the FMT group and 4.6% (P = .006) in the placebo group. There was no statistically significant difference between the groups (absolute difference, 0.2%).
At 18 months (12 months after surgery), the percentage of total weight loss was 25.3% (P < .001) in the FMT group and 25.2% (P < .001) in the placebo group – an absolute difference of 0.1%.
The researchers said the main limitation of their study is the small number of patients. Because there were few patients, the study may be inadequate to show possible minor effects of FMT on weight; it’s unclear whether a much larger sample size would have yielded any differences between the groups.
Nonetheless, the study suggests that FMT does not affect weight loss for patients who undergo bariatric surgery, the researchers said.
The study was supported by governmental research grants and the Sigrid Juselius Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to results of a randomized controlled trial.
The small study by Perttu Lahtinen, MD, with Päijät-Häme Central Hospital in Lahti, Finland, and colleagues was published online in JAMA Network Open.
Bariatric surgery remains the most effective strategy for treating severe obesity. Yet some patients achieve only minimal weight loss or regain weight after surgery, the researchers noted.
There is much interest in the gut microbiota as a potential target for the treatment of obesity. FMT from a lean donor has shown promise in treating obesity in mouse models (Science. 2013 Sep 6. doi: 10.1126/science.1241214).
The Finnish trial, however, does not support that conclusion.
The study included 41 adults (71% women; mean age, 48.7 years) with severe obesity (mean body mass index, 42.5 kg/m2). Twenty-one received FMT from a lean donor, and 20 received FMT from their own feces (autologous placebo). FMT was administered by gastroscopy into the duodenum 6 months before laparoscopic Roux-en-Y gastric bypass or sleeve gastrectomy. All patients also consumed a very-low-calorie diet approximately 4 weeks before the surgery.
Bariatric surgery led to equal weight reductions for both groups, but there was no additive benefit in terms of weight loss with FMT.
Six months after the administration of FMT, and before the surgery was performed, the percentage of total weight loss, the main outcome, was 4.8% (P < .001) in the FMT group and 4.6% (P = .006) in the placebo group. There was no statistically significant difference between the groups (absolute difference, 0.2%).
At 18 months (12 months after surgery), the percentage of total weight loss was 25.3% (P < .001) in the FMT group and 25.2% (P < .001) in the placebo group – an absolute difference of 0.1%.
The researchers said the main limitation of their study is the small number of patients. Because there were few patients, the study may be inadequate to show possible minor effects of FMT on weight; it’s unclear whether a much larger sample size would have yielded any differences between the groups.
Nonetheless, the study suggests that FMT does not affect weight loss for patients who undergo bariatric surgery, the researchers said.
The study was supported by governmental research grants and the Sigrid Juselius Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to results of a randomized controlled trial.
The small study by Perttu Lahtinen, MD, with Päijät-Häme Central Hospital in Lahti, Finland, and colleagues was published online in JAMA Network Open.
Bariatric surgery remains the most effective strategy for treating severe obesity. Yet some patients achieve only minimal weight loss or regain weight after surgery, the researchers noted.
There is much interest in the gut microbiota as a potential target for the treatment of obesity. FMT from a lean donor has shown promise in treating obesity in mouse models (Science. 2013 Sep 6. doi: 10.1126/science.1241214).
The Finnish trial, however, does not support that conclusion.
The study included 41 adults (71% women; mean age, 48.7 years) with severe obesity (mean body mass index, 42.5 kg/m2). Twenty-one received FMT from a lean donor, and 20 received FMT from their own feces (autologous placebo). FMT was administered by gastroscopy into the duodenum 6 months before laparoscopic Roux-en-Y gastric bypass or sleeve gastrectomy. All patients also consumed a very-low-calorie diet approximately 4 weeks before the surgery.
Bariatric surgery led to equal weight reductions for both groups, but there was no additive benefit in terms of weight loss with FMT.
Six months after the administration of FMT, and before the surgery was performed, the percentage of total weight loss, the main outcome, was 4.8% (P < .001) in the FMT group and 4.6% (P = .006) in the placebo group. There was no statistically significant difference between the groups (absolute difference, 0.2%).
At 18 months (12 months after surgery), the percentage of total weight loss was 25.3% (P < .001) in the FMT group and 25.2% (P < .001) in the placebo group – an absolute difference of 0.1%.
The researchers said the main limitation of their study is the small number of patients. Because there were few patients, the study may be inadequate to show possible minor effects of FMT on weight; it’s unclear whether a much larger sample size would have yielded any differences between the groups.
Nonetheless, the study suggests that FMT does not affect weight loss for patients who undergo bariatric surgery, the researchers said.
The study was supported by governmental research grants and the Sigrid Juselius Foundation. The authors disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Nonheavy alcohol use associated with liver fibrosis, NASH
according to a new report.
An analysis of current drinkers in the Framingham Heart Study found that a higher number of drinks per week and higher frequency of drinking were associated with increased odds of fibrosis among patients whose consumption fell below the threshold for heavy alcohol use.
“Although the detrimental effects of heavy alcohol use are well accepted, there is no consensus guideline on how to counsel patients about how nonheavy alcohol use may affect liver health,” Brooke Rice, MD, an internal medicine resident at Boston University, said in an interview.
“Current terminology classifies fatty liver disease as either alcoholic or nonalcoholic,” she said. “Our results call this strict categorization into question, suggesting that even nonheavy alcohol use should be considered as a factor contributing to more advanced nonalcoholic fatty liver disease [NAFLD] phenotypes.”
The study was published online in Clinical Gastroenterology and Hepatology.
Analyzing associations
NAFLD and alcohol-related liver disease, which are the most common causes of chronic liver disease worldwide, are histologically identical but distinguished by the presence of significant alcohol use, the study authors wrote.
Heavy alcohol use, based on guidelines from the American Association for the Study of Liver Diseases, is defined as more than 14 drinks per week for women or more than 21 drinks per week for men.
Although heavy alcohol use is consistently associated with cirrhosis and steatohepatitis, studies of nonheavy alcohol use have shown conflicting results, the authors wrote. However, evidence suggests that the pattern of alcohol consumption – particularly increased weekly drinking and binge drinking – may be an important predictor.
Dr. Rice and colleagues conducted a cross-sectional study of 2,629 current drinkers in the Framingham Heart Study who completed alcohol-use questionnaires and vibration-controlled transient elastography between April 2016 and April 2019. They analyzed the association between fibrosis and several alcohol-use measures, including total consumption and drinking patterns, among nonheavy alcohol users whose liver disease would be classified as “nonalcoholic” by current nomenclature.
The research team defined clinically significant fibrosis as a liver stiffness measurement of 8.2 kPa or higher. For at-risk NASH, the researchers used two FibroScan-AST (FAST) score thresholds – greater than 0.35 or 0.67 and higher. They also considered additional metabolic factors such as physical activity, body mass index, blood pressure, glucose measures, and metabolic syndrome.
Participants were asked to estimate the frequency of alcohol use (average number of drinking days per week during the past year) and the usual quantity of alcohol consumed (average number of drinks on a typical drinking day during the past year). Researchers multiplied the figures to estimate the average total number of drinks per week.
Among the 2,629 current drinkers (53% women, 47% men), the average age was 54 years, 7.2% had diabetes, and 26.9% met the criteria for metabolic syndrome. Participants drank about 3 days per week on average with a usual consumption of two drinks per drinking day, averaging a total weekly alcohol consumption of six drinks.
The average liver stiffness measurement was 5.6 kPa, and 8.2% had significant fibrosis.
At the FAST score threshold of 0.67 or greater, 1.9% of participants were likely to have at-risk NASH, with a higher prevalence in those with obesity (4.5%) or diabetes (9.5%). At the FAST score threshold of greater than 0.35, the prevalence of at-risk NASH was 12.4%, which was higher in those with obesity (26.3%) or diabetes (34.4%).
Overall, an increased total number of drinks per week and higher frequency of drinking days were associated with increased odds of fibrosis.
Almost 17.5% of participants engaged in risky weekly drinking, which was defined as 8 or more drinks per week for women and 15 or more drinks per week for men. Risky weekly drinking was also associated with higher odds of fibrosis.
After excluding 158 heavy drinkers, the prevalence of fibrosis was unchanged at 8%, and an increased total of drinks per week remained significantly associated with fibrosis.
In addition, multiple alcohol-use measures were positively associated with a FAST score greater than 0.35 and were similar after excluding heavy alcohol users. These measures include the number of drinks per week, the frequency of drinking days, and binge drinking.
“We showed that nonheavy alcohol use is associated with fibrosis and at-risk NASH, which are both predictors of long-term liver-related morbidity and mortality,” Dr. Rice said.
Implications for patient care
The findings have important implications for both NAFLD clinical trials and patient care, the study authors wrote. For instance, the U.S. Dietary Guidelines for Americans recommend limiting alcohol use to one drink per day for women and two drinks per day for men.
“Our results reinforce the importance of encouraging all patients to reduce alcohol intake as much as possible and to at least adhere to current U.S. Dietary Guidelines recommended limits,” Dr. Rice said. “Almost half of participants in our study consumed in excess of these limits, which strongly associated with at-risk NASH.”
Additional long-term studies are needed to determine the benefits of limiting alcohol consumption to reduce liver-related morbidity and mortality, the authors wrote.
The effect of alcohol consumption on liver health “has been controversial, since some studies have suggested that nonheavy alcohol use can even have some beneficial metabolic effects and has been associated with reduced risk of fatty liver disease, while other studies have found that nonheavy alcohol use is associated with increased risk for liver-related clinical outcomes,” Fredrik Åberg, MD, PhD, a hepatologist and liver transplant specialist at Helsinki University Hospital, said in an interview.
Dr. Åberg wasn’t involved with this study but has researched alcohol consumption and liver disease. Among non–heavy alcohol users, drinking more alcohol per week is associated with increased hospitalization for liver disease, hepatocellular carcinoma, and liver-related death, he and his colleagues have found.
“We concluded that the net effect of non-heavy drinking on the liver is harm,” he said. “Overall, this study by Rice and colleagues supports the recommendation that persons with mild liver disease should reduce their drinking, and persons with severe liver disease (cirrhosis and advanced fibrosis) should abstain from alcohol use.”
The study authors are supported in part by the National Institute of Diabetes and Digestive and Kidney Diseases, a Doris Duke Charitable Foundation Grant, a Gilead Sciences Research Scholars Award, the Boston University Department of Medicine Career Investment Award, and the Boston University Clinical Translational Science Institute. The Framingham Heart Study is supported in part by the National Heart, Lung, and Blood Institute. The authors and Dr. Åberg reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new report.
An analysis of current drinkers in the Framingham Heart Study found that a higher number of drinks per week and higher frequency of drinking were associated with increased odds of fibrosis among patients whose consumption fell below the threshold for heavy alcohol use.
“Although the detrimental effects of heavy alcohol use are well accepted, there is no consensus guideline on how to counsel patients about how nonheavy alcohol use may affect liver health,” Brooke Rice, MD, an internal medicine resident at Boston University, said in an interview.
“Current terminology classifies fatty liver disease as either alcoholic or nonalcoholic,” she said. “Our results call this strict categorization into question, suggesting that even nonheavy alcohol use should be considered as a factor contributing to more advanced nonalcoholic fatty liver disease [NAFLD] phenotypes.”
The study was published online in Clinical Gastroenterology and Hepatology.
Analyzing associations
NAFLD and alcohol-related liver disease, which are the most common causes of chronic liver disease worldwide, are histologically identical but distinguished by the presence of significant alcohol use, the study authors wrote.
Heavy alcohol use, based on guidelines from the American Association for the Study of Liver Diseases, is defined as more than 14 drinks per week for women or more than 21 drinks per week for men.
Although heavy alcohol use is consistently associated with cirrhosis and steatohepatitis, studies of nonheavy alcohol use have shown conflicting results, the authors wrote. However, evidence suggests that the pattern of alcohol consumption – particularly increased weekly drinking and binge drinking – may be an important predictor.
Dr. Rice and colleagues conducted a cross-sectional study of 2,629 current drinkers in the Framingham Heart Study who completed alcohol-use questionnaires and vibration-controlled transient elastography between April 2016 and April 2019. They analyzed the association between fibrosis and several alcohol-use measures, including total consumption and drinking patterns, among nonheavy alcohol users whose liver disease would be classified as “nonalcoholic” by current nomenclature.
The research team defined clinically significant fibrosis as a liver stiffness measurement of 8.2 kPa or higher. For at-risk NASH, the researchers used two FibroScan-AST (FAST) score thresholds – greater than 0.35 or 0.67 and higher. They also considered additional metabolic factors such as physical activity, body mass index, blood pressure, glucose measures, and metabolic syndrome.
Participants were asked to estimate the frequency of alcohol use (average number of drinking days per week during the past year) and the usual quantity of alcohol consumed (average number of drinks on a typical drinking day during the past year). Researchers multiplied the figures to estimate the average total number of drinks per week.
Among the 2,629 current drinkers (53% women, 47% men), the average age was 54 years, 7.2% had diabetes, and 26.9% met the criteria for metabolic syndrome. Participants drank about 3 days per week on average with a usual consumption of two drinks per drinking day, averaging a total weekly alcohol consumption of six drinks.
The average liver stiffness measurement was 5.6 kPa, and 8.2% had significant fibrosis.
At the FAST score threshold of 0.67 or greater, 1.9% of participants were likely to have at-risk NASH, with a higher prevalence in those with obesity (4.5%) or diabetes (9.5%). At the FAST score threshold of greater than 0.35, the prevalence of at-risk NASH was 12.4%, which was higher in those with obesity (26.3%) or diabetes (34.4%).
Overall, an increased total number of drinks per week and higher frequency of drinking days were associated with increased odds of fibrosis.
Almost 17.5% of participants engaged in risky weekly drinking, which was defined as 8 or more drinks per week for women and 15 or more drinks per week for men. Risky weekly drinking was also associated with higher odds of fibrosis.
After excluding 158 heavy drinkers, the prevalence of fibrosis was unchanged at 8%, and an increased total of drinks per week remained significantly associated with fibrosis.
In addition, multiple alcohol-use measures were positively associated with a FAST score greater than 0.35 and were similar after excluding heavy alcohol users. These measures include the number of drinks per week, the frequency of drinking days, and binge drinking.
“We showed that nonheavy alcohol use is associated with fibrosis and at-risk NASH, which are both predictors of long-term liver-related morbidity and mortality,” Dr. Rice said.
Implications for patient care
The findings have important implications for both NAFLD clinical trials and patient care, the study authors wrote. For instance, the U.S. Dietary Guidelines for Americans recommend limiting alcohol use to one drink per day for women and two drinks per day for men.
“Our results reinforce the importance of encouraging all patients to reduce alcohol intake as much as possible and to at least adhere to current U.S. Dietary Guidelines recommended limits,” Dr. Rice said. “Almost half of participants in our study consumed in excess of these limits, which strongly associated with at-risk NASH.”
Additional long-term studies are needed to determine the benefits of limiting alcohol consumption to reduce liver-related morbidity and mortality, the authors wrote.
The effect of alcohol consumption on liver health “has been controversial, since some studies have suggested that nonheavy alcohol use can even have some beneficial metabolic effects and has been associated with reduced risk of fatty liver disease, while other studies have found that nonheavy alcohol use is associated with increased risk for liver-related clinical outcomes,” Fredrik Åberg, MD, PhD, a hepatologist and liver transplant specialist at Helsinki University Hospital, said in an interview.
Dr. Åberg wasn’t involved with this study but has researched alcohol consumption and liver disease. Among non–heavy alcohol users, drinking more alcohol per week is associated with increased hospitalization for liver disease, hepatocellular carcinoma, and liver-related death, he and his colleagues have found.
“We concluded that the net effect of non-heavy drinking on the liver is harm,” he said. “Overall, this study by Rice and colleagues supports the recommendation that persons with mild liver disease should reduce their drinking, and persons with severe liver disease (cirrhosis and advanced fibrosis) should abstain from alcohol use.”
The study authors are supported in part by the National Institute of Diabetes and Digestive and Kidney Diseases, a Doris Duke Charitable Foundation Grant, a Gilead Sciences Research Scholars Award, the Boston University Department of Medicine Career Investment Award, and the Boston University Clinical Translational Science Institute. The Framingham Heart Study is supported in part by the National Heart, Lung, and Blood Institute. The authors and Dr. Åberg reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a new report.
An analysis of current drinkers in the Framingham Heart Study found that a higher number of drinks per week and higher frequency of drinking were associated with increased odds of fibrosis among patients whose consumption fell below the threshold for heavy alcohol use.
“Although the detrimental effects of heavy alcohol use are well accepted, there is no consensus guideline on how to counsel patients about how nonheavy alcohol use may affect liver health,” Brooke Rice, MD, an internal medicine resident at Boston University, said in an interview.
“Current terminology classifies fatty liver disease as either alcoholic or nonalcoholic,” she said. “Our results call this strict categorization into question, suggesting that even nonheavy alcohol use should be considered as a factor contributing to more advanced nonalcoholic fatty liver disease [NAFLD] phenotypes.”
The study was published online in Clinical Gastroenterology and Hepatology.
Analyzing associations
NAFLD and alcohol-related liver disease, which are the most common causes of chronic liver disease worldwide, are histologically identical but distinguished by the presence of significant alcohol use, the study authors wrote.
Heavy alcohol use, based on guidelines from the American Association for the Study of Liver Diseases, is defined as more than 14 drinks per week for women or more than 21 drinks per week for men.
Although heavy alcohol use is consistently associated with cirrhosis and steatohepatitis, studies of nonheavy alcohol use have shown conflicting results, the authors wrote. However, evidence suggests that the pattern of alcohol consumption – particularly increased weekly drinking and binge drinking – may be an important predictor.
Dr. Rice and colleagues conducted a cross-sectional study of 2,629 current drinkers in the Framingham Heart Study who completed alcohol-use questionnaires and vibration-controlled transient elastography between April 2016 and April 2019. They analyzed the association between fibrosis and several alcohol-use measures, including total consumption and drinking patterns, among nonheavy alcohol users whose liver disease would be classified as “nonalcoholic” by current nomenclature.
The research team defined clinically significant fibrosis as a liver stiffness measurement of 8.2 kPa or higher. For at-risk NASH, the researchers used two FibroScan-AST (FAST) score thresholds – greater than 0.35 or 0.67 and higher. They also considered additional metabolic factors such as physical activity, body mass index, blood pressure, glucose measures, and metabolic syndrome.
Participants were asked to estimate the frequency of alcohol use (average number of drinking days per week during the past year) and the usual quantity of alcohol consumed (average number of drinks on a typical drinking day during the past year). Researchers multiplied the figures to estimate the average total number of drinks per week.
Among the 2,629 current drinkers (53% women, 47% men), the average age was 54 years, 7.2% had diabetes, and 26.9% met the criteria for metabolic syndrome. Participants drank about 3 days per week on average with a usual consumption of two drinks per drinking day, averaging a total weekly alcohol consumption of six drinks.
The average liver stiffness measurement was 5.6 kPa, and 8.2% had significant fibrosis.
At the FAST score threshold of 0.67 or greater, 1.9% of participants were likely to have at-risk NASH, with a higher prevalence in those with obesity (4.5%) or diabetes (9.5%). At the FAST score threshold of greater than 0.35, the prevalence of at-risk NASH was 12.4%, which was higher in those with obesity (26.3%) or diabetes (34.4%).
Overall, an increased total number of drinks per week and higher frequency of drinking days were associated with increased odds of fibrosis.
Almost 17.5% of participants engaged in risky weekly drinking, which was defined as 8 or more drinks per week for women and 15 or more drinks per week for men. Risky weekly drinking was also associated with higher odds of fibrosis.
After excluding 158 heavy drinkers, the prevalence of fibrosis was unchanged at 8%, and an increased total of drinks per week remained significantly associated with fibrosis.
In addition, multiple alcohol-use measures were positively associated with a FAST score greater than 0.35 and were similar after excluding heavy alcohol users. These measures include the number of drinks per week, the frequency of drinking days, and binge drinking.
“We showed that nonheavy alcohol use is associated with fibrosis and at-risk NASH, which are both predictors of long-term liver-related morbidity and mortality,” Dr. Rice said.
Implications for patient care
The findings have important implications for both NAFLD clinical trials and patient care, the study authors wrote. For instance, the U.S. Dietary Guidelines for Americans recommend limiting alcohol use to one drink per day for women and two drinks per day for men.
“Our results reinforce the importance of encouraging all patients to reduce alcohol intake as much as possible and to at least adhere to current U.S. Dietary Guidelines recommended limits,” Dr. Rice said. “Almost half of participants in our study consumed in excess of these limits, which strongly associated with at-risk NASH.”
Additional long-term studies are needed to determine the benefits of limiting alcohol consumption to reduce liver-related morbidity and mortality, the authors wrote.
The effect of alcohol consumption on liver health “has been controversial, since some studies have suggested that nonheavy alcohol use can even have some beneficial metabolic effects and has been associated with reduced risk of fatty liver disease, while other studies have found that nonheavy alcohol use is associated with increased risk for liver-related clinical outcomes,” Fredrik Åberg, MD, PhD, a hepatologist and liver transplant specialist at Helsinki University Hospital, said in an interview.
Dr. Åberg wasn’t involved with this study but has researched alcohol consumption and liver disease. Among non–heavy alcohol users, drinking more alcohol per week is associated with increased hospitalization for liver disease, hepatocellular carcinoma, and liver-related death, he and his colleagues have found.
“We concluded that the net effect of non-heavy drinking on the liver is harm,” he said. “Overall, this study by Rice and colleagues supports the recommendation that persons with mild liver disease should reduce their drinking, and persons with severe liver disease (cirrhosis and advanced fibrosis) should abstain from alcohol use.”
The study authors are supported in part by the National Institute of Diabetes and Digestive and Kidney Diseases, a Doris Duke Charitable Foundation Grant, a Gilead Sciences Research Scholars Award, the Boston University Department of Medicine Career Investment Award, and the Boston University Clinical Translational Science Institute. The Framingham Heart Study is supported in part by the National Heart, Lung, and Blood Institute. The authors and Dr. Åberg reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM CLINICAL GASTROENTEROLOGY AND HEPATOLOGY
Lifestyle guidance app may be effective in NASH
After 48 weeks, nonalcoholic fatty liver disease activity scores (NAS) improved in 13 out of 19 patients who used the NASH app developed by CureApp, according to Masaya Sato of the University of Tokyo and colleagues.
If confirmed by a controlled trial, these preliminary results could show promise for digital therapeutics, the researchers stated in an article published in The American Journal of Gastroenterology.
“The widespread use of smartphones, which can process and communicate data in real time, makes them an ideal platform for therapeutic interventions,” they said.
Although lifestyle changes can reduce NASH activity, many patients have difficulty keeping up these changes. Not enough counselors are available to guide patients in healthy practices, and hiring the counselors is expensive, the researchers wrote.
Smartphone applications aimed at instilling healthy behavior have been tried in diabetes, smoking, hypertension, alcoholism, and even cancer, they noted. They wanted to see whether something similar could be done with NASH.
The researchers recruited 19 patients with biopsy-confirmed NASH who consumed no more than moderate amounts of alcohol and had a body mass index (BMI) of at least 25 kg/m2. Their mean age was 52 years, mean BMI was 32, and mean NAS was 5.0.
The patients downloaded the NASH app onto their phones and entered their baseline profile information, including age, gender, diet and exercise practices, and social characteristics. On the basis of this information and daily weight measurements, the system proposed lifestyle improvement programs tailored to each individual. Its chatbot presented them in the form of behavioral goals and lectures from virtual nurses.
While patients used the app for 48 weeks, they also received standard outpatient care for NASH from live physicians, who also promoted the use of the app and provided additional education related to NASH.
The patients underwent liver biopsies within 90 days prior to beginning the study and at the end of 48 weeks. The researchers compared the changes in these patients versus those in a hypothetical control group, which they based on the placebo group in a previous study.
In the patients who used the app, the mean NAS change from baseline to week 48, the main endpoint, was –2.05 (95% confidence interval, –3.00 to –1.11). This result was statistically significant compared with the hypothetical control group, in which the mean change in NAS was –0.7 (P < .001).
In 11 of the patients, NAS decreased by at least 2 points without worsening of liver fibrosis. In eight patients, the researchers observed resolution of steatohepatitis, which they defined as disappearance of hepatocyte ballooning.
In 12 patients with stage F2 or F3 fibrosis, the average stage went from 2.5 to 2.0 (P = .02). No patient with stage F1 fibrosis showed a reduction in fibrosis stage. The scores for steatosis decreased in 11 patients, for lobular inflammation in 9 patients, and for ballooning in 10 patients.
The patients lost an average of 8.3% of their body weight, which was significant, compared with their baseline (P < .001). The patients also notched significant reductions in average serum levels of AST, ALT, gamma-glutamyltransferase, alkaline phosphatase, and triglycerides.
The researchers noted that the lack of a real control group and the small size of the study population limited the importance of their findings. A larger randomized, controlled trial is needed to confirm their results.
During the study, physicians browsed the patients’ data and provided them with feedback about it, the researchers wrote. But the study did not measure the amount of time the physicians spent on this activity.
CureApp founded the study, and one of the authors is a consultant for the company.
A version of this article first appeared on Medscape.com.
After 48 weeks, nonalcoholic fatty liver disease activity scores (NAS) improved in 13 out of 19 patients who used the NASH app developed by CureApp, according to Masaya Sato of the University of Tokyo and colleagues.
If confirmed by a controlled trial, these preliminary results could show promise for digital therapeutics, the researchers stated in an article published in The American Journal of Gastroenterology.
“The widespread use of smartphones, which can process and communicate data in real time, makes them an ideal platform for therapeutic interventions,” they said.
Although lifestyle changes can reduce NASH activity, many patients have difficulty keeping up these changes. Not enough counselors are available to guide patients in healthy practices, and hiring the counselors is expensive, the researchers wrote.
Smartphone applications aimed at instilling healthy behavior have been tried in diabetes, smoking, hypertension, alcoholism, and even cancer, they noted. They wanted to see whether something similar could be done with NASH.
The researchers recruited 19 patients with biopsy-confirmed NASH who consumed no more than moderate amounts of alcohol and had a body mass index (BMI) of at least 25 kg/m2. Their mean age was 52 years, mean BMI was 32, and mean NAS was 5.0.
The patients downloaded the NASH app onto their phones and entered their baseline profile information, including age, gender, diet and exercise practices, and social characteristics. On the basis of this information and daily weight measurements, the system proposed lifestyle improvement programs tailored to each individual. Its chatbot presented them in the form of behavioral goals and lectures from virtual nurses.
While patients used the app for 48 weeks, they also received standard outpatient care for NASH from live physicians, who also promoted the use of the app and provided additional education related to NASH.
The patients underwent liver biopsies within 90 days prior to beginning the study and at the end of 48 weeks. The researchers compared the changes in these patients versus those in a hypothetical control group, which they based on the placebo group in a previous study.
In the patients who used the app, the mean NAS change from baseline to week 48, the main endpoint, was –2.05 (95% confidence interval, –3.00 to –1.11). This result was statistically significant compared with the hypothetical control group, in which the mean change in NAS was –0.7 (P < .001).
In 11 of the patients, NAS decreased by at least 2 points without worsening of liver fibrosis. In eight patients, the researchers observed resolution of steatohepatitis, which they defined as disappearance of hepatocyte ballooning.
In 12 patients with stage F2 or F3 fibrosis, the average stage went from 2.5 to 2.0 (P = .02). No patient with stage F1 fibrosis showed a reduction in fibrosis stage. The scores for steatosis decreased in 11 patients, for lobular inflammation in 9 patients, and for ballooning in 10 patients.
The patients lost an average of 8.3% of their body weight, which was significant, compared with their baseline (P < .001). The patients also notched significant reductions in average serum levels of AST, ALT, gamma-glutamyltransferase, alkaline phosphatase, and triglycerides.
The researchers noted that the lack of a real control group and the small size of the study population limited the importance of their findings. A larger randomized, controlled trial is needed to confirm their results.
During the study, physicians browsed the patients’ data and provided them with feedback about it, the researchers wrote. But the study did not measure the amount of time the physicians spent on this activity.
CureApp founded the study, and one of the authors is a consultant for the company.
A version of this article first appeared on Medscape.com.
After 48 weeks, nonalcoholic fatty liver disease activity scores (NAS) improved in 13 out of 19 patients who used the NASH app developed by CureApp, according to Masaya Sato of the University of Tokyo and colleagues.
If confirmed by a controlled trial, these preliminary results could show promise for digital therapeutics, the researchers stated in an article published in The American Journal of Gastroenterology.
“The widespread use of smartphones, which can process and communicate data in real time, makes them an ideal platform for therapeutic interventions,” they said.
Although lifestyle changes can reduce NASH activity, many patients have difficulty keeping up these changes. Not enough counselors are available to guide patients in healthy practices, and hiring the counselors is expensive, the researchers wrote.
Smartphone applications aimed at instilling healthy behavior have been tried in diabetes, smoking, hypertension, alcoholism, and even cancer, they noted. They wanted to see whether something similar could be done with NASH.
The researchers recruited 19 patients with biopsy-confirmed NASH who consumed no more than moderate amounts of alcohol and had a body mass index (BMI) of at least 25 kg/m2. Their mean age was 52 years, mean BMI was 32, and mean NAS was 5.0.
The patients downloaded the NASH app onto their phones and entered their baseline profile information, including age, gender, diet and exercise practices, and social characteristics. On the basis of this information and daily weight measurements, the system proposed lifestyle improvement programs tailored to each individual. Its chatbot presented them in the form of behavioral goals and lectures from virtual nurses.
While patients used the app for 48 weeks, they also received standard outpatient care for NASH from live physicians, who also promoted the use of the app and provided additional education related to NASH.
The patients underwent liver biopsies within 90 days prior to beginning the study and at the end of 48 weeks. The researchers compared the changes in these patients versus those in a hypothetical control group, which they based on the placebo group in a previous study.
In the patients who used the app, the mean NAS change from baseline to week 48, the main endpoint, was –2.05 (95% confidence interval, –3.00 to –1.11). This result was statistically significant compared with the hypothetical control group, in which the mean change in NAS was –0.7 (P < .001).
In 11 of the patients, NAS decreased by at least 2 points without worsening of liver fibrosis. In eight patients, the researchers observed resolution of steatohepatitis, which they defined as disappearance of hepatocyte ballooning.
In 12 patients with stage F2 or F3 fibrosis, the average stage went from 2.5 to 2.0 (P = .02). No patient with stage F1 fibrosis showed a reduction in fibrosis stage. The scores for steatosis decreased in 11 patients, for lobular inflammation in 9 patients, and for ballooning in 10 patients.
The patients lost an average of 8.3% of their body weight, which was significant, compared with their baseline (P < .001). The patients also notched significant reductions in average serum levels of AST, ALT, gamma-glutamyltransferase, alkaline phosphatase, and triglycerides.
The researchers noted that the lack of a real control group and the small size of the study population limited the importance of their findings. A larger randomized, controlled trial is needed to confirm their results.
During the study, physicians browsed the patients’ data and provided them with feedback about it, the researchers wrote. But the study did not measure the amount of time the physicians spent on this activity.
CureApp founded the study, and one of the authors is a consultant for the company.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF GASTROENTEROLOGY
Endocarditis tied to drug use on the rise, spiked during COVID
A new study provides more evidence that endocarditis associated with drug use is a significant and growing health concern, and further demonstrates that this risk has been exacerbated by the COVID-19 pandemic.
The rate of infective endocarditis among individuals in the United States with opioid or cocaine use disorder increased in the 11-year period 2011 to 2022, with the steepest increase logged during the COVID-19 pandemic (2021-2022), according to the study.
A diagnosis of COVID-19 more than doubled the risk for a new diagnosis of endocarditis in patients with either cocaine (hazard ratio, 2.24) or opioid use disorder (HR, 2.23).
“Our data suggests that, in addition to the major social disruption from the pandemic, including disrupted access to health care, COVID-19 infection itself is a significant risk factor for new diagnosis of endocarditis in drug using populations,” authors Nora Volkow, MD, director of the National Institute on Drug Abuse, and colleagues wrote.
“Drug-using populations, particularly those who use cocaine or opioids, have some of the highest risk for endocarditis, and here we show that having a COVID-19 diagnoses further increases this risk,” they added.
The study was published online in Molecular Psychiatry.
The researchers analyzed electronic health record data collected from January 2011 to August 2022 for more than 109 million people across the United States, including more than 736,000 with an opioid use disorder and more than 379,000 with a cocaine use disorder.
In 2011, there were 4 cases of endocarditis per day for every 1 million people with opioid use disorder. By 2022, the rate had increased to 30 cases per day per 1 million people with opioid use disorder.
For people with cocaine use disorder, cases of endocarditis increased from 5 per 1 million in 2011 to 23 per 1 million in 2022.
Among individuals with cocaine or opioid use disorder, the risk of being hospitalized within 180 days following a diagnosis of endocarditis was higher in those with than without COVID-19 (67.5% vs. 58.7%; HR, 1.21).
The risk of dying within 180 days following new diagnosis of endocarditis was also higher in those with than without COVID-19 (9.2% vs. 8%; HR, 1.16).
The study also showed that Black and Hispanic individuals had a lower risk for COVID-19-associated endocarditis than non-Hispanic White individuals, which is consistent with a higher prevalence of injection drug use in non-Hispanic White populations, compared with Black or Hispanic populations, the researchers pointed out.
Dr. Volkow and colleagues said their findings highlight the need to screen drug users for endocarditis and link them to infectious disease and addiction treatment if they contract COVID-19.
“People with substance use disorder already face major impediments to proper health care due to lack of access and stigma,” Dr. Volkow said in a news release.
“Proven techniques like syringe service programs, which help people avoid infection from reused or shared injection equipment, can help prevent this often fatal and costly condition,” Dr. Volkow added.
The authors said it will also be important to determine exactly how SARS-CoV-2 viral infection exacerbates the risk for endocarditis in drug users.
Support for the study was provided by the National Institute on Aging, National Institute on Alcohol Abuse and Alcoholism, the Clinical and Translational Science Collaborative of Cleveland, and the National Cancer Institute Case Comprehensive Cancer Center. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study provides more evidence that endocarditis associated with drug use is a significant and growing health concern, and further demonstrates that this risk has been exacerbated by the COVID-19 pandemic.
The rate of infective endocarditis among individuals in the United States with opioid or cocaine use disorder increased in the 11-year period 2011 to 2022, with the steepest increase logged during the COVID-19 pandemic (2021-2022), according to the study.
A diagnosis of COVID-19 more than doubled the risk for a new diagnosis of endocarditis in patients with either cocaine (hazard ratio, 2.24) or opioid use disorder (HR, 2.23).
“Our data suggests that, in addition to the major social disruption from the pandemic, including disrupted access to health care, COVID-19 infection itself is a significant risk factor for new diagnosis of endocarditis in drug using populations,” authors Nora Volkow, MD, director of the National Institute on Drug Abuse, and colleagues wrote.
“Drug-using populations, particularly those who use cocaine or opioids, have some of the highest risk for endocarditis, and here we show that having a COVID-19 diagnoses further increases this risk,” they added.
The study was published online in Molecular Psychiatry.
The researchers analyzed electronic health record data collected from January 2011 to August 2022 for more than 109 million people across the United States, including more than 736,000 with an opioid use disorder and more than 379,000 with a cocaine use disorder.
In 2011, there were 4 cases of endocarditis per day for every 1 million people with opioid use disorder. By 2022, the rate had increased to 30 cases per day per 1 million people with opioid use disorder.
For people with cocaine use disorder, cases of endocarditis increased from 5 per 1 million in 2011 to 23 per 1 million in 2022.
Among individuals with cocaine or opioid use disorder, the risk of being hospitalized within 180 days following a diagnosis of endocarditis was higher in those with than without COVID-19 (67.5% vs. 58.7%; HR, 1.21).
The risk of dying within 180 days following new diagnosis of endocarditis was also higher in those with than without COVID-19 (9.2% vs. 8%; HR, 1.16).
The study also showed that Black and Hispanic individuals had a lower risk for COVID-19-associated endocarditis than non-Hispanic White individuals, which is consistent with a higher prevalence of injection drug use in non-Hispanic White populations, compared with Black or Hispanic populations, the researchers pointed out.
Dr. Volkow and colleagues said their findings highlight the need to screen drug users for endocarditis and link them to infectious disease and addiction treatment if they contract COVID-19.
“People with substance use disorder already face major impediments to proper health care due to lack of access and stigma,” Dr. Volkow said in a news release.
“Proven techniques like syringe service programs, which help people avoid infection from reused or shared injection equipment, can help prevent this often fatal and costly condition,” Dr. Volkow added.
The authors said it will also be important to determine exactly how SARS-CoV-2 viral infection exacerbates the risk for endocarditis in drug users.
Support for the study was provided by the National Institute on Aging, National Institute on Alcohol Abuse and Alcoholism, the Clinical and Translational Science Collaborative of Cleveland, and the National Cancer Institute Case Comprehensive Cancer Center. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study provides more evidence that endocarditis associated with drug use is a significant and growing health concern, and further demonstrates that this risk has been exacerbated by the COVID-19 pandemic.
The rate of infective endocarditis among individuals in the United States with opioid or cocaine use disorder increased in the 11-year period 2011 to 2022, with the steepest increase logged during the COVID-19 pandemic (2021-2022), according to the study.
A diagnosis of COVID-19 more than doubled the risk for a new diagnosis of endocarditis in patients with either cocaine (hazard ratio, 2.24) or opioid use disorder (HR, 2.23).
“Our data suggests that, in addition to the major social disruption from the pandemic, including disrupted access to health care, COVID-19 infection itself is a significant risk factor for new diagnosis of endocarditis in drug using populations,” authors Nora Volkow, MD, director of the National Institute on Drug Abuse, and colleagues wrote.
“Drug-using populations, particularly those who use cocaine or opioids, have some of the highest risk for endocarditis, and here we show that having a COVID-19 diagnoses further increases this risk,” they added.
The study was published online in Molecular Psychiatry.
The researchers analyzed electronic health record data collected from January 2011 to August 2022 for more than 109 million people across the United States, including more than 736,000 with an opioid use disorder and more than 379,000 with a cocaine use disorder.
In 2011, there were 4 cases of endocarditis per day for every 1 million people with opioid use disorder. By 2022, the rate had increased to 30 cases per day per 1 million people with opioid use disorder.
For people with cocaine use disorder, cases of endocarditis increased from 5 per 1 million in 2011 to 23 per 1 million in 2022.
Among individuals with cocaine or opioid use disorder, the risk of being hospitalized within 180 days following a diagnosis of endocarditis was higher in those with than without COVID-19 (67.5% vs. 58.7%; HR, 1.21).
The risk of dying within 180 days following new diagnosis of endocarditis was also higher in those with than without COVID-19 (9.2% vs. 8%; HR, 1.16).
The study also showed that Black and Hispanic individuals had a lower risk for COVID-19-associated endocarditis than non-Hispanic White individuals, which is consistent with a higher prevalence of injection drug use in non-Hispanic White populations, compared with Black or Hispanic populations, the researchers pointed out.
Dr. Volkow and colleagues said their findings highlight the need to screen drug users for endocarditis and link them to infectious disease and addiction treatment if they contract COVID-19.
“People with substance use disorder already face major impediments to proper health care due to lack of access and stigma,” Dr. Volkow said in a news release.
“Proven techniques like syringe service programs, which help people avoid infection from reused or shared injection equipment, can help prevent this often fatal and costly condition,” Dr. Volkow added.
The authors said it will also be important to determine exactly how SARS-CoV-2 viral infection exacerbates the risk for endocarditis in drug users.
Support for the study was provided by the National Institute on Aging, National Institute on Alcohol Abuse and Alcoholism, the Clinical and Translational Science Collaborative of Cleveland, and the National Cancer Institute Case Comprehensive Cancer Center. The authors reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM MOLECULAR PSYCHIATRY
A starting point for precision medicine in type 1 diabetes
MADRID – With type 1 diabetes, there can be great differences in terms of epidemiology, genetics, and possible constituent causes, as well as in the course of the disease before and after diagnosis. This point was made evident in the Can We Perform Precision Medicine in T1D? conference.
At the 63rd Congress of the Spanish Society of Endocrinology (SEEN), María José Redondo, MD, PhD, director of research in the division of diabetes and endocrinology at Texas Children’s Hospital Baylor College of Medicine in Houston, noted that delving into this evidence is the “clue” to implementing precision medicine strategies.
“Physiopathologically, there are different forms of type 1 diabetes that must be considered in the therapeutic approach. The objective is to describe this heterogeneity to discover the etiopathogenesis underlying it, so that endotypes can be defined and thus apply precision medicine. This is the paradigm followed by the European Association for the Study of Diabetes (EASD), the American Diabetes Association (ADA), and other organizations,” said Dr. Redondo.
She added that there have been significant advances in knowledge of factors that account for these epidemiologic and genetic variations. “For example, immunological processes appear to be different in children who develop type 1 diabetes at a young age, compared with those who present with the disease later in life.”
Metabolic factors are also involved in the development of type 1 diabetes in adolescents and adults, “and this metabolic heterogeneity is a very important aspect, since we currently use only glucose to diagnose diabetes and especially to classify it as type 1 when other factors should really be measured, such as C-peptide, since it has been seen that people with high levels of this peptide present a process that is closer to type 2 diabetes and have atypical characteristics for type 1 diabetes that are more like type 2 diabetes (obesity, older age, lack of typically genetic factors associated with type 1 diabetes),” noted Dr. Redondo.
Eluding classification
The specialist added that this evidence suggests a need to review the classification of the different types of diabetes. “The current general classification distinguishes type 1 diabetes, type 2 diabetes, gestational diabetes, monogenic (neonatal) diabetes, monogenic diabetes associated with cystic fibrosis, pancreatogenic, steroid-induced, and posttransplantation diabetes. However, in clinical practice, cases that are very difficult to diagnose and classify emerge, such as autoimmune diabetes, type 1 diabetes in people with insulin resistance, positive antibodies for type 2 diabetes, for example, in children with obesity (in which it is not known whether it is type 1 or type 2 diabetes), drug-induced diabetes in cases of insulin resistance, autoimmune type 1 diabetes with persistent C-peptide, or monogenic diabetes in people with obesity.
“Therefore, the current classification does not help to guide prevention or treatment, and the heterogeneity of the pathology is not as clear as we would like. Since, for example, insulin resistance affects both types of diabetes, inflammation exists in both cases, and the genes that give beta cell secretion defects exist in monogenic diabetes and probably in type 2 diabetes as well. It can be argued that type 2 diabetes is like a backdrop to a lot of diabetes that we know of so far and that it interacts with other factors that have happened to the particular person,” said Dr. Redondo.
“Furthermore, it has been shown that metformin can improve insulin resistance and cardiovascular events in patients with type 1 diabetes with obesity. On the other hand, most patients with type 2 diabetes do not need insulin after diagnosis, except for pediatric patients and those with positive antibodies who require insulin quickly. Added to this is the inability to differentiate between responders and nonresponders to immunomodulators in the prevention of type 1 diabetes, all of which highlights that there are pathogenic processes that can appear in different types of diabetes, which is why the current classification leaves out cases that do not clearly fit into a single disease type, while many people with the same diagnosis actually have very different diseases,” she pointed out.
Toward precision diagnostics
“Encapsulating” all these factors is the first step to applying precision medicine in type 1 diabetes, an area, Dr. Redondo explained, in which concrete actions are being carried out. “One of these actions is to determine BMI [body mass index], which has been incorporated into the diabetes prediction strategy that we use in clinical trials, since we know that people with a high BMI, along with other factors, clearly have a different risk. Likewise, we’ve seen that teplizumab could work better in the prevention of type 1 diabetes in individuals with anti-islet antibodies and that people who have the DR4 gene respond better than those who don’t have it and that those with the DR3 gene respond worse.”
Other recent advances along these lines involve the identification of treatments that can delay or even prevent the development of type 1 diabetes in people with positive antibodies, as well as the development of algorithms and models to predict who will develop the disease, thus placing preventive treatments within reach.
“The objective is to use all available information from each individual to understand the etiology and pathogenesis of the disease at a given moment, knowing that changes occur throughout life, and this also applies to other types of diabetes. The next step is to discover and test pathogenesis-focused therapeutic strategies with the most clinical impact in each patient at any given time,” said Dr. Redondo.
Technological tools
The specialist referred to recent advances in diabetes technology, especially semiclosed systems (such as a sensor/pump) that, in her opinion, have radically changed the control of the disease. “However, the main objective is to make type 1 diabetes preventable or reversible in people who have developed it,” she said.
Fernando Gómez-Peralta, MD, PhD, elected coordinator of the Diabetes Department at SEEN and head of the endocrinology and nutrition unit of General Hospital of Segovia, Spain, spoke about these technological advances in his presentation, “Technology and Diabetes: Clinical Experiences,” which was organized in collaboration with the Spanish Diabetes Society.
According to this expert, technological and digital tools are changing the daily lives of people with this disease. “Continuous glucose monitoring and new connected insulin pen and cap systems have increased the benefits for users of treatment with new insulins, for example,” said Dr. Gómez-Peralta.
He explained that most systems make it possible to access complete data regarding glycemic control and the treatment received and to share them with caregivers, professionals, and family members. “Some integrated insulin pump and sensor systems have self-adjusting insulin therapy algorithms that have been shown to greatly increase time-to-target glucose and reduce hypoglycemic events,” he said.
“Regarding glucose monitoring, there are devices with a longer duration (up to 2 weeks) and precision that are characterized by easier use for the patient, avoiding the need for calibration, with annoying capillary blood glucose levels.”
In the case of insulin administration, it is anticipated that in the future, some models will have very interesting features, Dr. Gómez-Peralta said. “Integrated closed-loop glucose sensor and insulin pump systems that have self-adjusting algorithms, regardless of the user, are highly effective and safe, and clearly improve glycemic control.
“For users of insulin injections, connected pens allow the integration of dynamic glucose information with doses, as well as the integration of user support tools for insulin adjustment,” Dr. Gómez-Peralta added.
The specialist stressed that a challenge for the future is to reduce the digital divide so as to increase the capacity and motivation to access these options. “In the coming years, health systems will have to face significant cost so that these systems are made available to all patients, and it is necessary to provide the systems with more material and human resources so that they can be integrated with our endocrinology and diabetes services and units.”
Dr. Redondo and Dr. Gómez-Peralta have disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish edition and a version appeared on Medscape.com.
MADRID – With type 1 diabetes, there can be great differences in terms of epidemiology, genetics, and possible constituent causes, as well as in the course of the disease before and after diagnosis. This point was made evident in the Can We Perform Precision Medicine in T1D? conference.
At the 63rd Congress of the Spanish Society of Endocrinology (SEEN), María José Redondo, MD, PhD, director of research in the division of diabetes and endocrinology at Texas Children’s Hospital Baylor College of Medicine in Houston, noted that delving into this evidence is the “clue” to implementing precision medicine strategies.
“Physiopathologically, there are different forms of type 1 diabetes that must be considered in the therapeutic approach. The objective is to describe this heterogeneity to discover the etiopathogenesis underlying it, so that endotypes can be defined and thus apply precision medicine. This is the paradigm followed by the European Association for the Study of Diabetes (EASD), the American Diabetes Association (ADA), and other organizations,” said Dr. Redondo.
She added that there have been significant advances in knowledge of factors that account for these epidemiologic and genetic variations. “For example, immunological processes appear to be different in children who develop type 1 diabetes at a young age, compared with those who present with the disease later in life.”
Metabolic factors are also involved in the development of type 1 diabetes in adolescents and adults, “and this metabolic heterogeneity is a very important aspect, since we currently use only glucose to diagnose diabetes and especially to classify it as type 1 when other factors should really be measured, such as C-peptide, since it has been seen that people with high levels of this peptide present a process that is closer to type 2 diabetes and have atypical characteristics for type 1 diabetes that are more like type 2 diabetes (obesity, older age, lack of typically genetic factors associated with type 1 diabetes),” noted Dr. Redondo.
Eluding classification
The specialist added that this evidence suggests a need to review the classification of the different types of diabetes. “The current general classification distinguishes type 1 diabetes, type 2 diabetes, gestational diabetes, monogenic (neonatal) diabetes, monogenic diabetes associated with cystic fibrosis, pancreatogenic, steroid-induced, and posttransplantation diabetes. However, in clinical practice, cases that are very difficult to diagnose and classify emerge, such as autoimmune diabetes, type 1 diabetes in people with insulin resistance, positive antibodies for type 2 diabetes, for example, in children with obesity (in which it is not known whether it is type 1 or type 2 diabetes), drug-induced diabetes in cases of insulin resistance, autoimmune type 1 diabetes with persistent C-peptide, or monogenic diabetes in people with obesity.
“Therefore, the current classification does not help to guide prevention or treatment, and the heterogeneity of the pathology is not as clear as we would like. Since, for example, insulin resistance affects both types of diabetes, inflammation exists in both cases, and the genes that give beta cell secretion defects exist in monogenic diabetes and probably in type 2 diabetes as well. It can be argued that type 2 diabetes is like a backdrop to a lot of diabetes that we know of so far and that it interacts with other factors that have happened to the particular person,” said Dr. Redondo.
“Furthermore, it has been shown that metformin can improve insulin resistance and cardiovascular events in patients with type 1 diabetes with obesity. On the other hand, most patients with type 2 diabetes do not need insulin after diagnosis, except for pediatric patients and those with positive antibodies who require insulin quickly. Added to this is the inability to differentiate between responders and nonresponders to immunomodulators in the prevention of type 1 diabetes, all of which highlights that there are pathogenic processes that can appear in different types of diabetes, which is why the current classification leaves out cases that do not clearly fit into a single disease type, while many people with the same diagnosis actually have very different diseases,” she pointed out.
Toward precision diagnostics
“Encapsulating” all these factors is the first step to applying precision medicine in type 1 diabetes, an area, Dr. Redondo explained, in which concrete actions are being carried out. “One of these actions is to determine BMI [body mass index], which has been incorporated into the diabetes prediction strategy that we use in clinical trials, since we know that people with a high BMI, along with other factors, clearly have a different risk. Likewise, we’ve seen that teplizumab could work better in the prevention of type 1 diabetes in individuals with anti-islet antibodies and that people who have the DR4 gene respond better than those who don’t have it and that those with the DR3 gene respond worse.”
Other recent advances along these lines involve the identification of treatments that can delay or even prevent the development of type 1 diabetes in people with positive antibodies, as well as the development of algorithms and models to predict who will develop the disease, thus placing preventive treatments within reach.
“The objective is to use all available information from each individual to understand the etiology and pathogenesis of the disease at a given moment, knowing that changes occur throughout life, and this also applies to other types of diabetes. The next step is to discover and test pathogenesis-focused therapeutic strategies with the most clinical impact in each patient at any given time,” said Dr. Redondo.
Technological tools
The specialist referred to recent advances in diabetes technology, especially semiclosed systems (such as a sensor/pump) that, in her opinion, have radically changed the control of the disease. “However, the main objective is to make type 1 diabetes preventable or reversible in people who have developed it,” she said.
Fernando Gómez-Peralta, MD, PhD, elected coordinator of the Diabetes Department at SEEN and head of the endocrinology and nutrition unit of General Hospital of Segovia, Spain, spoke about these technological advances in his presentation, “Technology and Diabetes: Clinical Experiences,” which was organized in collaboration with the Spanish Diabetes Society.
According to this expert, technological and digital tools are changing the daily lives of people with this disease. “Continuous glucose monitoring and new connected insulin pen and cap systems have increased the benefits for users of treatment with new insulins, for example,” said Dr. Gómez-Peralta.
He explained that most systems make it possible to access complete data regarding glycemic control and the treatment received and to share them with caregivers, professionals, and family members. “Some integrated insulin pump and sensor systems have self-adjusting insulin therapy algorithms that have been shown to greatly increase time-to-target glucose and reduce hypoglycemic events,” he said.
“Regarding glucose monitoring, there are devices with a longer duration (up to 2 weeks) and precision that are characterized by easier use for the patient, avoiding the need for calibration, with annoying capillary blood glucose levels.”
In the case of insulin administration, it is anticipated that in the future, some models will have very interesting features, Dr. Gómez-Peralta said. “Integrated closed-loop glucose sensor and insulin pump systems that have self-adjusting algorithms, regardless of the user, are highly effective and safe, and clearly improve glycemic control.
“For users of insulin injections, connected pens allow the integration of dynamic glucose information with doses, as well as the integration of user support tools for insulin adjustment,” Dr. Gómez-Peralta added.
The specialist stressed that a challenge for the future is to reduce the digital divide so as to increase the capacity and motivation to access these options. “In the coming years, health systems will have to face significant cost so that these systems are made available to all patients, and it is necessary to provide the systems with more material and human resources so that they can be integrated with our endocrinology and diabetes services and units.”
Dr. Redondo and Dr. Gómez-Peralta have disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish edition and a version appeared on Medscape.com.
MADRID – With type 1 diabetes, there can be great differences in terms of epidemiology, genetics, and possible constituent causes, as well as in the course of the disease before and after diagnosis. This point was made evident in the Can We Perform Precision Medicine in T1D? conference.
At the 63rd Congress of the Spanish Society of Endocrinology (SEEN), María José Redondo, MD, PhD, director of research in the division of diabetes and endocrinology at Texas Children’s Hospital Baylor College of Medicine in Houston, noted that delving into this evidence is the “clue” to implementing precision medicine strategies.
“Physiopathologically, there are different forms of type 1 diabetes that must be considered in the therapeutic approach. The objective is to describe this heterogeneity to discover the etiopathogenesis underlying it, so that endotypes can be defined and thus apply precision medicine. This is the paradigm followed by the European Association for the Study of Diabetes (EASD), the American Diabetes Association (ADA), and other organizations,” said Dr. Redondo.
She added that there have been significant advances in knowledge of factors that account for these epidemiologic and genetic variations. “For example, immunological processes appear to be different in children who develop type 1 diabetes at a young age, compared with those who present with the disease later in life.”
Metabolic factors are also involved in the development of type 1 diabetes in adolescents and adults, “and this metabolic heterogeneity is a very important aspect, since we currently use only glucose to diagnose diabetes and especially to classify it as type 1 when other factors should really be measured, such as C-peptide, since it has been seen that people with high levels of this peptide present a process that is closer to type 2 diabetes and have atypical characteristics for type 1 diabetes that are more like type 2 diabetes (obesity, older age, lack of typically genetic factors associated with type 1 diabetes),” noted Dr. Redondo.
Eluding classification
The specialist added that this evidence suggests a need to review the classification of the different types of diabetes. “The current general classification distinguishes type 1 diabetes, type 2 diabetes, gestational diabetes, monogenic (neonatal) diabetes, monogenic diabetes associated with cystic fibrosis, pancreatogenic, steroid-induced, and posttransplantation diabetes. However, in clinical practice, cases that are very difficult to diagnose and classify emerge, such as autoimmune diabetes, type 1 diabetes in people with insulin resistance, positive antibodies for type 2 diabetes, for example, in children with obesity (in which it is not known whether it is type 1 or type 2 diabetes), drug-induced diabetes in cases of insulin resistance, autoimmune type 1 diabetes with persistent C-peptide, or monogenic diabetes in people with obesity.
“Therefore, the current classification does not help to guide prevention or treatment, and the heterogeneity of the pathology is not as clear as we would like. Since, for example, insulin resistance affects both types of diabetes, inflammation exists in both cases, and the genes that give beta cell secretion defects exist in monogenic diabetes and probably in type 2 diabetes as well. It can be argued that type 2 diabetes is like a backdrop to a lot of diabetes that we know of so far and that it interacts with other factors that have happened to the particular person,” said Dr. Redondo.
“Furthermore, it has been shown that metformin can improve insulin resistance and cardiovascular events in patients with type 1 diabetes with obesity. On the other hand, most patients with type 2 diabetes do not need insulin after diagnosis, except for pediatric patients and those with positive antibodies who require insulin quickly. Added to this is the inability to differentiate between responders and nonresponders to immunomodulators in the prevention of type 1 diabetes, all of which highlights that there are pathogenic processes that can appear in different types of diabetes, which is why the current classification leaves out cases that do not clearly fit into a single disease type, while many people with the same diagnosis actually have very different diseases,” she pointed out.
Toward precision diagnostics
“Encapsulating” all these factors is the first step to applying precision medicine in type 1 diabetes, an area, Dr. Redondo explained, in which concrete actions are being carried out. “One of these actions is to determine BMI [body mass index], which has been incorporated into the diabetes prediction strategy that we use in clinical trials, since we know that people with a high BMI, along with other factors, clearly have a different risk. Likewise, we’ve seen that teplizumab could work better in the prevention of type 1 diabetes in individuals with anti-islet antibodies and that people who have the DR4 gene respond better than those who don’t have it and that those with the DR3 gene respond worse.”
Other recent advances along these lines involve the identification of treatments that can delay or even prevent the development of type 1 diabetes in people with positive antibodies, as well as the development of algorithms and models to predict who will develop the disease, thus placing preventive treatments within reach.
“The objective is to use all available information from each individual to understand the etiology and pathogenesis of the disease at a given moment, knowing that changes occur throughout life, and this also applies to other types of diabetes. The next step is to discover and test pathogenesis-focused therapeutic strategies with the most clinical impact in each patient at any given time,” said Dr. Redondo.
Technological tools
The specialist referred to recent advances in diabetes technology, especially semiclosed systems (such as a sensor/pump) that, in her opinion, have radically changed the control of the disease. “However, the main objective is to make type 1 diabetes preventable or reversible in people who have developed it,” she said.
Fernando Gómez-Peralta, MD, PhD, elected coordinator of the Diabetes Department at SEEN and head of the endocrinology and nutrition unit of General Hospital of Segovia, Spain, spoke about these technological advances in his presentation, “Technology and Diabetes: Clinical Experiences,” which was organized in collaboration with the Spanish Diabetes Society.
According to this expert, technological and digital tools are changing the daily lives of people with this disease. “Continuous glucose monitoring and new connected insulin pen and cap systems have increased the benefits for users of treatment with new insulins, for example,” said Dr. Gómez-Peralta.
He explained that most systems make it possible to access complete data regarding glycemic control and the treatment received and to share them with caregivers, professionals, and family members. “Some integrated insulin pump and sensor systems have self-adjusting insulin therapy algorithms that have been shown to greatly increase time-to-target glucose and reduce hypoglycemic events,” he said.
“Regarding glucose monitoring, there are devices with a longer duration (up to 2 weeks) and precision that are characterized by easier use for the patient, avoiding the need for calibration, with annoying capillary blood glucose levels.”
In the case of insulin administration, it is anticipated that in the future, some models will have very interesting features, Dr. Gómez-Peralta said. “Integrated closed-loop glucose sensor and insulin pump systems that have self-adjusting algorithms, regardless of the user, are highly effective and safe, and clearly improve glycemic control.
“For users of insulin injections, connected pens allow the integration of dynamic glucose information with doses, as well as the integration of user support tools for insulin adjustment,” Dr. Gómez-Peralta added.
The specialist stressed that a challenge for the future is to reduce the digital divide so as to increase the capacity and motivation to access these options. “In the coming years, health systems will have to face significant cost so that these systems are made available to all patients, and it is necessary to provide the systems with more material and human resources so that they can be integrated with our endocrinology and diabetes services and units.”
Dr. Redondo and Dr. Gómez-Peralta have disclosed no relevant financial relationships.
This article was translated from the Medscape Spanish edition and a version appeared on Medscape.com.
Lesions on upper arms
The patient is diagnosed with atopic dermatitis (AD) complicated by skin infection.
AD is the most common chronic pruritic inflammatory skin disorder that affects both children and adults. In the United States, up to 18% of children and 7% of adults are affected. Atopic dermatitis is associated with diminished quality of life, including disruption in activities of daily living, sleep disturbance, depression, and anxiety. Moreover, patients with AD have an increased risk for infections. A significantly higher prevalence of cutaneous and systemic infections is seen in patients with AD compared with individuals without AD.
Bacterial infections are common in AD and are usually caused by Staphylococcus aureus. Examples include impetigo, which typically presents with oozing serum that dries, resulting in a honey-crusted appearance surrounded by an erythematous base. Fluid-filled blisters (bullous impetigo) may also be present, which can be mistaken for eczema herpeticum (EH).
Nonpurulent skin and soft tissue infections (SSTIs) include erysipelas and cellulitis. In most cases, these infections begin in a focal skin area but spread rapidly across the affected sites such as the arms, legs, trunk, or face. Signs typically include focal erythema, swelling, warmth, and tenderness; fever and bacteremia may also be present.
Purulent SSTIs present as skin abscesses, involving fluctuant or nonfluctuant nodules or pustules surrounded by an erythematous swelling; the lesions may also be tender and warm. Methicillin-resistant S aureus (MRSA) is a common cause of purulent SSTIs.
Systemic complications of SSTI in AD may include bacteremia, osteomyelitis, septic arthritis, or bursitis; less often, endocarditis and staphylococcal scalded skin syndrome may occur. Clinicians should maintain a high index of suspicion for these complications in patients who present with an ill-looking appearance, lethargy, focal point tenderness of the bone, joint swelling, heart murmur, and widespread desquamation. Persistent elevated inflammatory markers (eg, C-reactive protein or erythrocyte sedimentation rate) should increase the level of suspicion.
Nonbacterial infections can occur concurrently with bacterial skin infections and the two can be difficult to distinguish. For example, EH results from the local spread of herpes simplex virus, which has a predilection for AD lesions. Early during EH, skin lesions appear as superficial clusters of dome‐shaped vesicles and/or small, round, punched‐out erosions. With progression, the lesions may become superficially infected with S aureus and may develop the characteristic honey-colored scale of impetigo.
Factors that contribute to the increased prevalence of infections in AD include skin barrier defects, suppression of cutaneous innate immunity by type 2 inflammation, S aureus colonization, allergen sensitivity, filaggrin loss-of-function mutation, and cutaneous dysbiosis.
Daily skin hydration and moisturization is a fundamental component of treatment for any patient with AD, both to treat the AD and prevent infection. Patients with AD should bathe daily, followed by gentle drying and application of a moisturizer or a prescribed topical medication. Standard topical anti-inflammatory medications, including topical corticosteroids and topical calcineurin inhibitors, improve skin barrier functions and have been reported to decrease S aureus colonization in AD lesions. Similarly, the monoclonal antibody dupilumab has been shown to decrease S aureus colonization and increase microbial diversity.
In the presence of an uncomplicated, nonpurulent skin infection, a beta-lactam antibiotic that covers both S aureus and beta-hemolytic streptococci (eg, cefazolin or cephalexin) may be sufficient, depending on clinical response or culture and in consideration of local epidemiology and resistance patterns. For patients with AD who present with a skin abscess, history of MRSA colonization, close contacts with a history of skin infections, or recent hospitalization, coverage for MRSA should be considered. Acceptable oral options for MRSA skin infections include clindamycin, doxycycline, trimethoprim-sulfamethoxazole, and linezolid, assuming that the isolate is susceptible in vitro. Topical mupirocin ointment can be used for patients with minor, localized skin infections (eg, impetigo).
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient is diagnosed with atopic dermatitis (AD) complicated by skin infection.
AD is the most common chronic pruritic inflammatory skin disorder that affects both children and adults. In the United States, up to 18% of children and 7% of adults are affected. Atopic dermatitis is associated with diminished quality of life, including disruption in activities of daily living, sleep disturbance, depression, and anxiety. Moreover, patients with AD have an increased risk for infections. A significantly higher prevalence of cutaneous and systemic infections is seen in patients with AD compared with individuals without AD.
Bacterial infections are common in AD and are usually caused by Staphylococcus aureus. Examples include impetigo, which typically presents with oozing serum that dries, resulting in a honey-crusted appearance surrounded by an erythematous base. Fluid-filled blisters (bullous impetigo) may also be present, which can be mistaken for eczema herpeticum (EH).
Nonpurulent skin and soft tissue infections (SSTIs) include erysipelas and cellulitis. In most cases, these infections begin in a focal skin area but spread rapidly across the affected sites such as the arms, legs, trunk, or face. Signs typically include focal erythema, swelling, warmth, and tenderness; fever and bacteremia may also be present.
Purulent SSTIs present as skin abscesses, involving fluctuant or nonfluctuant nodules or pustules surrounded by an erythematous swelling; the lesions may also be tender and warm. Methicillin-resistant S aureus (MRSA) is a common cause of purulent SSTIs.
Systemic complications of SSTI in AD may include bacteremia, osteomyelitis, septic arthritis, or bursitis; less often, endocarditis and staphylococcal scalded skin syndrome may occur. Clinicians should maintain a high index of suspicion for these complications in patients who present with an ill-looking appearance, lethargy, focal point tenderness of the bone, joint swelling, heart murmur, and widespread desquamation. Persistent elevated inflammatory markers (eg, C-reactive protein or erythrocyte sedimentation rate) should increase the level of suspicion.
Nonbacterial infections can occur concurrently with bacterial skin infections and the two can be difficult to distinguish. For example, EH results from the local spread of herpes simplex virus, which has a predilection for AD lesions. Early during EH, skin lesions appear as superficial clusters of dome‐shaped vesicles and/or small, round, punched‐out erosions. With progression, the lesions may become superficially infected with S aureus and may develop the characteristic honey-colored scale of impetigo.
Factors that contribute to the increased prevalence of infections in AD include skin barrier defects, suppression of cutaneous innate immunity by type 2 inflammation, S aureus colonization, allergen sensitivity, filaggrin loss-of-function mutation, and cutaneous dysbiosis.
Daily skin hydration and moisturization is a fundamental component of treatment for any patient with AD, both to treat the AD and prevent infection. Patients with AD should bathe daily, followed by gentle drying and application of a moisturizer or a prescribed topical medication. Standard topical anti-inflammatory medications, including topical corticosteroids and topical calcineurin inhibitors, improve skin barrier functions and have been reported to decrease S aureus colonization in AD lesions. Similarly, the monoclonal antibody dupilumab has been shown to decrease S aureus colonization and increase microbial diversity.
In the presence of an uncomplicated, nonpurulent skin infection, a beta-lactam antibiotic that covers both S aureus and beta-hemolytic streptococci (eg, cefazolin or cephalexin) may be sufficient, depending on clinical response or culture and in consideration of local epidemiology and resistance patterns. For patients with AD who present with a skin abscess, history of MRSA colonization, close contacts with a history of skin infections, or recent hospitalization, coverage for MRSA should be considered. Acceptable oral options for MRSA skin infections include clindamycin, doxycycline, trimethoprim-sulfamethoxazole, and linezolid, assuming that the isolate is susceptible in vitro. Topical mupirocin ointment can be used for patients with minor, localized skin infections (eg, impetigo).
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.
The patient is diagnosed with atopic dermatitis (AD) complicated by skin infection.
AD is the most common chronic pruritic inflammatory skin disorder that affects both children and adults. In the United States, up to 18% of children and 7% of adults are affected. Atopic dermatitis is associated with diminished quality of life, including disruption in activities of daily living, sleep disturbance, depression, and anxiety. Moreover, patients with AD have an increased risk for infections. A significantly higher prevalence of cutaneous and systemic infections is seen in patients with AD compared with individuals without AD.
Bacterial infections are common in AD and are usually caused by Staphylococcus aureus. Examples include impetigo, which typically presents with oozing serum that dries, resulting in a honey-crusted appearance surrounded by an erythematous base. Fluid-filled blisters (bullous impetigo) may also be present, which can be mistaken for eczema herpeticum (EH).
Nonpurulent skin and soft tissue infections (SSTIs) include erysipelas and cellulitis. In most cases, these infections begin in a focal skin area but spread rapidly across the affected sites such as the arms, legs, trunk, or face. Signs typically include focal erythema, swelling, warmth, and tenderness; fever and bacteremia may also be present.
Purulent SSTIs present as skin abscesses, involving fluctuant or nonfluctuant nodules or pustules surrounded by an erythematous swelling; the lesions may also be tender and warm. Methicillin-resistant S aureus (MRSA) is a common cause of purulent SSTIs.
Systemic complications of SSTI in AD may include bacteremia, osteomyelitis, septic arthritis, or bursitis; less often, endocarditis and staphylococcal scalded skin syndrome may occur. Clinicians should maintain a high index of suspicion for these complications in patients who present with an ill-looking appearance, lethargy, focal point tenderness of the bone, joint swelling, heart murmur, and widespread desquamation. Persistent elevated inflammatory markers (eg, C-reactive protein or erythrocyte sedimentation rate) should increase the level of suspicion.
Nonbacterial infections can occur concurrently with bacterial skin infections and the two can be difficult to distinguish. For example, EH results from the local spread of herpes simplex virus, which has a predilection for AD lesions. Early during EH, skin lesions appear as superficial clusters of dome‐shaped vesicles and/or small, round, punched‐out erosions. With progression, the lesions may become superficially infected with S aureus and may develop the characteristic honey-colored scale of impetigo.
Factors that contribute to the increased prevalence of infections in AD include skin barrier defects, suppression of cutaneous innate immunity by type 2 inflammation, S aureus colonization, allergen sensitivity, filaggrin loss-of-function mutation, and cutaneous dysbiosis.
Daily skin hydration and moisturization is a fundamental component of treatment for any patient with AD, both to treat the AD and prevent infection. Patients with AD should bathe daily, followed by gentle drying and application of a moisturizer or a prescribed topical medication. Standard topical anti-inflammatory medications, including topical corticosteroids and topical calcineurin inhibitors, improve skin barrier functions and have been reported to decrease S aureus colonization in AD lesions. Similarly, the monoclonal antibody dupilumab has been shown to decrease S aureus colonization and increase microbial diversity.
In the presence of an uncomplicated, nonpurulent skin infection, a beta-lactam antibiotic that covers both S aureus and beta-hemolytic streptococci (eg, cefazolin or cephalexin) may be sufficient, depending on clinical response or culture and in consideration of local epidemiology and resistance patterns. For patients with AD who present with a skin abscess, history of MRSA colonization, close contacts with a history of skin infections, or recent hospitalization, coverage for MRSA should be considered. Acceptable oral options for MRSA skin infections include clindamycin, doxycycline, trimethoprim-sulfamethoxazole, and linezolid, assuming that the isolate is susceptible in vitro. Topical mupirocin ointment can be used for patients with minor, localized skin infections (eg, impetigo).
William D. James, MD, Professor, Department of Dermatology, University of Pennsylvania, Philadelphia.
Disclosure: William D. James, MD, has disclosed the following relevant financial relationships:
Received income in an amount equal to or greater than $250 from: Elsevier.
Image Quizzes are fictional or fictionalized clinical scenarios intended to provide evidence-based educational takeaways.

An 8-year-old girl presents with pruritic lesions on her upper arms. As an infant, the patient was treated for widespread dermatitis with topical steroids and emollients; recently, after a long symptom-free period, she has had multiple bouts of dermatitis on her face, knees, ankles, and elbows. According to the patient's mother, the patient bathes every 2-3 days to not dry out her skin. At the current visit, physical examination reveals scaly patches and plaques with a honey-colored crust surrounded by an erythematous base. No other family members are experiencing symptoms. There is a positive family history for atopy and asthma.
