User login
The Official Newspaper of the American Association for Thoracic Surgery
Mean platelet volume higher in DVT patients with PE than without
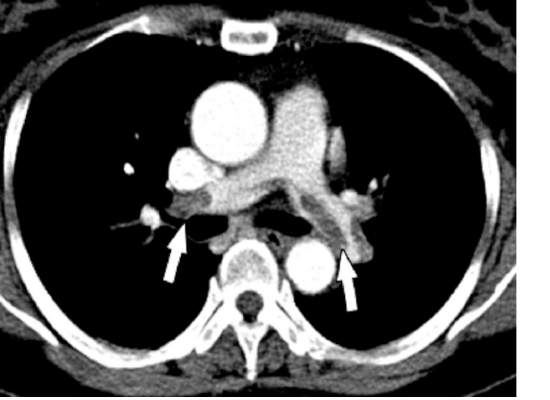
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).

There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).
There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
Mean platelet volume (MPV) has been associated with deep vein thrombosis (DVT), but it also appears to be a potential predictor of the presence of pulmonary embolism (PE), according to a retrospective analysis of patients reported by Dr. Atilla Icli of Ahi Evran University, Kirsehir, Turkey, and his colleagues.
The researchers assessed three groups of patients among those admitted to the emergency department or outpatient clinic of two university hospitals during 2005-2014. The patient study groups consisted of 98 patients with DVT and PE (48 men; mean age, 56.8 years); 97 patients with DVT without PE (48 men; mean age, 54.2 years); and 98 patients admitted with suspicion of DVT, but confirmed to be free of DVT and PE (45 men; mean age, 55.0 years) (Heart Lung Circulation. 2015 Nov;24[11]:1081-6).
There were no statistically significant differences between the groups with regard to sex, age, body mass index, or comorbidities such as hypertension or diabetes. Blood samples were drawn from all patients and assessed for MPV.
MPV was significantly higher in all DVT patients than controls (9.3 femtoliter vs. 7.9 fL; P less than .001) and in DVT patients with PE as compared to DVT patients without PE (9.9 fL vs. 8.7 fL, respectively; P less than .001). A cut-off point was seen where the rate of PE was significantly higher in patients with MPV greater than 9.15 fL, as compared with those with MPV equal to or below 9.15 fL. In addition, the presence of PE in patients with DVT was independently associated with MPV (odds ratio, 22.2; P less than .001).
“Our findings suggest that MPVs are elevated in patients with DVT, and higher MPVs may be associated with this group of patients,” Dr. Icli and his colleagues concluded.
The authors indicated that they had no relevant conflicts.
Read the full study online in Heart, Lung and Circulation.
FROM HEART, LUNG AND CIRCULATION
Idarucizumab approved as first agent to reverse a novel oral anticoagulant
Idarucizumab has been approved by the Food and Drug Administration for reversing the effects of dabigatran, a novel oral anticoagulant.
Specifically, idarucizumab (Praxbind) is intended for use in patients who are taking dabigatran (Pradaxa) during emergency situations when there is a need to reverse its blood-thinning effects, according to an FDA statement. Both drugs are marketed by Boehringer Ingelheim.
“The anticoagulant effects of Pradaxa are important and life-saving for some patients, but there are situations where reversal of the drug’s effects is medically necessary,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research. “Today’s approval offers the medical community an important tool for managing patients taking Pradaxa in emergency or life-threatening situations when bleeding can’t be controlled.”
The decision, released on Oct. 16, was based on efficacy and safety observed in three randomized trials, the largest of which is the ongoing phase III RE-VERSE AD.
Patients were enrolled into two distinct groups in RE-VERSE AD. Group A, with 51 patients, comprised patients on dabigatran experiencing a serious bleeding episode. Group B, with 39 patients, comprised patients on dabigatran who required an urgent surgical procedure. In both, 5 g of idarucizumab solution was administered intravenously. The primary endpoint was maximum percentage reversal of the anticoagulant effect of dabigatran within 4 hours.
In both groups, the median maximum percentage reversal was 100%. Other measures corroborated a rapid and highly effective reversal of anticoagulation. For example, the dilute thrombin time in those who could be evaluated was normalized in 98% of group A and 93% of group B (N Engl J Med. 2015 Aug 6. doi:10.1056/NEJMoa1502000).

Interim results of RE-VERSE AD “show rather convincingly that idarucizumab completely and safely reverses the anticoagulant effects of dabigatran within minutes,” said the lead author, Dr. Charles V. Pollack Jr., chairman of the department of emergency medicine at the University of Pennsylvania, Philadelphia. Dr. Pollack presented the findings at the 2015 International Society of Thrombosis and Haemostatis (ISTH) Congress in June.
Idarucizumab is the first reversal agent for any of the novel oral anticoagulants used as an alternative to warfarin. Unlike warfarin, which can be reversed with vitamin K, the lack of a reversal agent for dabigatran, a direct thrombin inhibitor, and other novel agents, such as rivaroxaban and apixaban, which are direct factor Xa inhibitors, has been a concern for patients who experience unexpected bleeding or face a risk of bleeding because of the need for urgent surgery. The laboratory findings were supported by the clinical findings, according to Dr. Pollack.
“Clinical outcomes were quite good in this multimorbid patient population,” he said. “Restoration of hemostasis as reported by local investigators was achieved in less than 12 hours when assessable, and 92% of the surgical patients were reported to have normal hemostasis at the time of the procedure.”
Idarucizumab was also found safe in this and the two previous randomized studies. In the 237 healthy volunteers evaluated previously, no serious adverse events were reported. In RE-VERSE AD, serious adverse events leading to death included hemorrhagic and thrombotic complications, but there were no off-target side effects, and the deaths occurred in a highly unstable patient population.
“Only one patient experienced a thrombotic complication within 72 hours [of initiating idarucizumab], and that patient had not been restarted on any antithrombotic medications,” Dr. Pollack reported. He noted that no safety concerns arose in patients who were enrolled in the study, but later were found to have normal clotting parameters.
Idarucizumab binds to dabigatran to neutralize its activity. It was given priority review status by the FDA in April 2015. Priority review is now being sought for andexanet, which is a potential reversal agent for the factor Xa inhibitors, according to press releases from the developer, Portola Pharmaceuticals. Idarucizumab and other effective reversal agents – if approved – are expected to increase the utility of novel oral anticoagulants.
The FDA cautioned in its statement that reversing the effect of dabigatran exposes patients to the risk of blood clots and stroke from their underlying disease, and said that the idarucizumab labeling recommends patients resume their anticoagulant therapy as soon as medically appropriate.
Dr. Pollack disclosed that he has financial relationships with Bristol-Myers Squibb, Daiichi-Sankyo, Janssen, and Pfizer. RE-VERSE AD was supported by Boehringer Ingelheim.
Idarucizumab has been approved by the Food and Drug Administration for reversing the effects of dabigatran, a novel oral anticoagulant.
Specifically, idarucizumab (Praxbind) is intended for use in patients who are taking dabigatran (Pradaxa) during emergency situations when there is a need to reverse its blood-thinning effects, according to an FDA statement. Both drugs are marketed by Boehringer Ingelheim.
“The anticoagulant effects of Pradaxa are important and life-saving for some patients, but there are situations where reversal of the drug’s effects is medically necessary,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research. “Today’s approval offers the medical community an important tool for managing patients taking Pradaxa in emergency or life-threatening situations when bleeding can’t be controlled.”
The decision, released on Oct. 16, was based on efficacy and safety observed in three randomized trials, the largest of which is the ongoing phase III RE-VERSE AD.
Patients were enrolled into two distinct groups in RE-VERSE AD. Group A, with 51 patients, comprised patients on dabigatran experiencing a serious bleeding episode. Group B, with 39 patients, comprised patients on dabigatran who required an urgent surgical procedure. In both, 5 g of idarucizumab solution was administered intravenously. The primary endpoint was maximum percentage reversal of the anticoagulant effect of dabigatran within 4 hours.
In both groups, the median maximum percentage reversal was 100%. Other measures corroborated a rapid and highly effective reversal of anticoagulation. For example, the dilute thrombin time in those who could be evaluated was normalized in 98% of group A and 93% of group B (N Engl J Med. 2015 Aug 6. doi:10.1056/NEJMoa1502000).
Interim results of RE-VERSE AD “show rather convincingly that idarucizumab completely and safely reverses the anticoagulant effects of dabigatran within minutes,” said the lead author, Dr. Charles V. Pollack Jr., chairman of the department of emergency medicine at the University of Pennsylvania, Philadelphia. Dr. Pollack presented the findings at the 2015 International Society of Thrombosis and Haemostatis (ISTH) Congress in June.
Idarucizumab is the first reversal agent for any of the novel oral anticoagulants used as an alternative to warfarin. Unlike warfarin, which can be reversed with vitamin K, the lack of a reversal agent for dabigatran, a direct thrombin inhibitor, and other novel agents, such as rivaroxaban and apixaban, which are direct factor Xa inhibitors, has been a concern for patients who experience unexpected bleeding or face a risk of bleeding because of the need for urgent surgery. The laboratory findings were supported by the clinical findings, according to Dr. Pollack.
“Clinical outcomes were quite good in this multimorbid patient population,” he said. “Restoration of hemostasis as reported by local investigators was achieved in less than 12 hours when assessable, and 92% of the surgical patients were reported to have normal hemostasis at the time of the procedure.”
Idarucizumab was also found safe in this and the two previous randomized studies. In the 237 healthy volunteers evaluated previously, no serious adverse events were reported. In RE-VERSE AD, serious adverse events leading to death included hemorrhagic and thrombotic complications, but there were no off-target side effects, and the deaths occurred in a highly unstable patient population.
“Only one patient experienced a thrombotic complication within 72 hours [of initiating idarucizumab], and that patient had not been restarted on any antithrombotic medications,” Dr. Pollack reported. He noted that no safety concerns arose in patients who were enrolled in the study, but later were found to have normal clotting parameters.
Idarucizumab binds to dabigatran to neutralize its activity. It was given priority review status by the FDA in April 2015. Priority review is now being sought for andexanet, which is a potential reversal agent for the factor Xa inhibitors, according to press releases from the developer, Portola Pharmaceuticals. Idarucizumab and other effective reversal agents – if approved – are expected to increase the utility of novel oral anticoagulants.
The FDA cautioned in its statement that reversing the effect of dabigatran exposes patients to the risk of blood clots and stroke from their underlying disease, and said that the idarucizumab labeling recommends patients resume their anticoagulant therapy as soon as medically appropriate.
Dr. Pollack disclosed that he has financial relationships with Bristol-Myers Squibb, Daiichi-Sankyo, Janssen, and Pfizer. RE-VERSE AD was supported by Boehringer Ingelheim.
Idarucizumab has been approved by the Food and Drug Administration for reversing the effects of dabigatran, a novel oral anticoagulant.
Specifically, idarucizumab (Praxbind) is intended for use in patients who are taking dabigatran (Pradaxa) during emergency situations when there is a need to reverse its blood-thinning effects, according to an FDA statement. Both drugs are marketed by Boehringer Ingelheim.
“The anticoagulant effects of Pradaxa are important and life-saving for some patients, but there are situations where reversal of the drug’s effects is medically necessary,” said Dr. Richard Pazdur, director of the Office of Hematology and Oncology Products in the FDA’s Center for Drug Evaluation and Research. “Today’s approval offers the medical community an important tool for managing patients taking Pradaxa in emergency or life-threatening situations when bleeding can’t be controlled.”
The decision, released on Oct. 16, was based on efficacy and safety observed in three randomized trials, the largest of which is the ongoing phase III RE-VERSE AD.
Patients were enrolled into two distinct groups in RE-VERSE AD. Group A, with 51 patients, comprised patients on dabigatran experiencing a serious bleeding episode. Group B, with 39 patients, comprised patients on dabigatran who required an urgent surgical procedure. In both, 5 g of idarucizumab solution was administered intravenously. The primary endpoint was maximum percentage reversal of the anticoagulant effect of dabigatran within 4 hours.
In both groups, the median maximum percentage reversal was 100%. Other measures corroborated a rapid and highly effective reversal of anticoagulation. For example, the dilute thrombin time in those who could be evaluated was normalized in 98% of group A and 93% of group B (N Engl J Med. 2015 Aug 6. doi:10.1056/NEJMoa1502000).
Interim results of RE-VERSE AD “show rather convincingly that idarucizumab completely and safely reverses the anticoagulant effects of dabigatran within minutes,” said the lead author, Dr. Charles V. Pollack Jr., chairman of the department of emergency medicine at the University of Pennsylvania, Philadelphia. Dr. Pollack presented the findings at the 2015 International Society of Thrombosis and Haemostatis (ISTH) Congress in June.
Idarucizumab is the first reversal agent for any of the novel oral anticoagulants used as an alternative to warfarin. Unlike warfarin, which can be reversed with vitamin K, the lack of a reversal agent for dabigatran, a direct thrombin inhibitor, and other novel agents, such as rivaroxaban and apixaban, which are direct factor Xa inhibitors, has been a concern for patients who experience unexpected bleeding or face a risk of bleeding because of the need for urgent surgery. The laboratory findings were supported by the clinical findings, according to Dr. Pollack.
“Clinical outcomes were quite good in this multimorbid patient population,” he said. “Restoration of hemostasis as reported by local investigators was achieved in less than 12 hours when assessable, and 92% of the surgical patients were reported to have normal hemostasis at the time of the procedure.”
Idarucizumab was also found safe in this and the two previous randomized studies. In the 237 healthy volunteers evaluated previously, no serious adverse events were reported. In RE-VERSE AD, serious adverse events leading to death included hemorrhagic and thrombotic complications, but there were no off-target side effects, and the deaths occurred in a highly unstable patient population.
“Only one patient experienced a thrombotic complication within 72 hours [of initiating idarucizumab], and that patient had not been restarted on any antithrombotic medications,” Dr. Pollack reported. He noted that no safety concerns arose in patients who were enrolled in the study, but later were found to have normal clotting parameters.
Idarucizumab binds to dabigatran to neutralize its activity. It was given priority review status by the FDA in April 2015. Priority review is now being sought for andexanet, which is a potential reversal agent for the factor Xa inhibitors, according to press releases from the developer, Portola Pharmaceuticals. Idarucizumab and other effective reversal agents – if approved – are expected to increase the utility of novel oral anticoagulants.
The FDA cautioned in its statement that reversing the effect of dabigatran exposes patients to the risk of blood clots and stroke from their underlying disease, and said that the idarucizumab labeling recommends patients resume their anticoagulant therapy as soon as medically appropriate.
Dr. Pollack disclosed that he has financial relationships with Bristol-Myers Squibb, Daiichi-Sankyo, Janssen, and Pfizer. RE-VERSE AD was supported by Boehringer Ingelheim.
Decline in antibiotic effectiveness could harm surgical, chemotherapy patients
An increase of surgical site infections (SSIs) stemming from pathogens resistant to antibiotic prophylaxis could result in thousands of infection-related deaths in surgical and chemotherapy patients, according to a new study published in the Lancet Infectious Diseases.
A total of 31 published meta-analyses of randomized or quasi–randomized controlled trials were included in the study by Dr. Ramanan Laxminarayan of the Center for Disease Dynamics, Economics & Policy in Washington, and his associates. The researchers surveyed the 10 most common surgeries in which antibiotic prophylaxis provides the greatest benefit. The infection rate in surgical patients receiving prophylaxis was 4.2%, and was 11.1% in patients who did not receive prophylaxis. Relative risk reduction for infection was least in cancer chemotherapy at 35% and greatest in pacemaker implantation at 86%.
Between 38.7% and 50.9% of SSIs and 26.8% of infections after chemotherapy are caused by antibiotic-resistant pathogens. A decrease in prophylaxis effectiveness of 10% would cause 40,000 additional infections and 2,100 additional deaths, while a decrease in effectiveness of 70% would cause 280,000 additional infections and 15,000 additional deaths.
The authors say more data are needed to establish how antibiotic prophylaxis recommendations should be modified in the context of increasing rates of resistance.
In a related comment, Dr. Joshua Wolf from St. Jude Children’s Research Hospital, Memphis, said, “To improve stewardship outcomes, we need more research that focuses on understanding impediments to appropriate antibiotic prescribing, strategies that target these impediments, resources to implement the strategies, and leadership that understands the urgency and complexity of the task. In view of the lack of progress so far, mandatory implementation of these steps could be necessary to achieve notable change.”
Find the full study in the Lancet Infectious Diseases (doi: 10.1016/S1473-3099[15]00270-4).
An increase of surgical site infections (SSIs) stemming from pathogens resistant to antibiotic prophylaxis could result in thousands of infection-related deaths in surgical and chemotherapy patients, according to a new study published in the Lancet Infectious Diseases.
A total of 31 published meta-analyses of randomized or quasi–randomized controlled trials were included in the study by Dr. Ramanan Laxminarayan of the Center for Disease Dynamics, Economics & Policy in Washington, and his associates. The researchers surveyed the 10 most common surgeries in which antibiotic prophylaxis provides the greatest benefit. The infection rate in surgical patients receiving prophylaxis was 4.2%, and was 11.1% in patients who did not receive prophylaxis. Relative risk reduction for infection was least in cancer chemotherapy at 35% and greatest in pacemaker implantation at 86%.
Between 38.7% and 50.9% of SSIs and 26.8% of infections after chemotherapy are caused by antibiotic-resistant pathogens. A decrease in prophylaxis effectiveness of 10% would cause 40,000 additional infections and 2,100 additional deaths, while a decrease in effectiveness of 70% would cause 280,000 additional infections and 15,000 additional deaths.
The authors say more data are needed to establish how antibiotic prophylaxis recommendations should be modified in the context of increasing rates of resistance.
In a related comment, Dr. Joshua Wolf from St. Jude Children’s Research Hospital, Memphis, said, “To improve stewardship outcomes, we need more research that focuses on understanding impediments to appropriate antibiotic prescribing, strategies that target these impediments, resources to implement the strategies, and leadership that understands the urgency and complexity of the task. In view of the lack of progress so far, mandatory implementation of these steps could be necessary to achieve notable change.”
Find the full study in the Lancet Infectious Diseases (doi: 10.1016/S1473-3099[15]00270-4).
An increase of surgical site infections (SSIs) stemming from pathogens resistant to antibiotic prophylaxis could result in thousands of infection-related deaths in surgical and chemotherapy patients, according to a new study published in the Lancet Infectious Diseases.
A total of 31 published meta-analyses of randomized or quasi–randomized controlled trials were included in the study by Dr. Ramanan Laxminarayan of the Center for Disease Dynamics, Economics & Policy in Washington, and his associates. The researchers surveyed the 10 most common surgeries in which antibiotic prophylaxis provides the greatest benefit. The infection rate in surgical patients receiving prophylaxis was 4.2%, and was 11.1% in patients who did not receive prophylaxis. Relative risk reduction for infection was least in cancer chemotherapy at 35% and greatest in pacemaker implantation at 86%.
Between 38.7% and 50.9% of SSIs and 26.8% of infections after chemotherapy are caused by antibiotic-resistant pathogens. A decrease in prophylaxis effectiveness of 10% would cause 40,000 additional infections and 2,100 additional deaths, while a decrease in effectiveness of 70% would cause 280,000 additional infections and 15,000 additional deaths.
The authors say more data are needed to establish how antibiotic prophylaxis recommendations should be modified in the context of increasing rates of resistance.
In a related comment, Dr. Joshua Wolf from St. Jude Children’s Research Hospital, Memphis, said, “To improve stewardship outcomes, we need more research that focuses on understanding impediments to appropriate antibiotic prescribing, strategies that target these impediments, resources to implement the strategies, and leadership that understands the urgency and complexity of the task. In view of the lack of progress so far, mandatory implementation of these steps could be necessary to achieve notable change.”
Find the full study in the Lancet Infectious Diseases (doi: 10.1016/S1473-3099[15]00270-4).
New CPR guide sets compression limits, scratches vasopressin
New guidelines on cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) set upper limits on chest compression rate and depth, add naloxone to the care of suspected opioid abusers, and remove vasopressin from the advanced cardiac life support (ACLS) algorithm.
The American Heart Association published its revised guidelines Oct. 15 in Circulation. The AHA released its previous guidelines in 2010.

“Everyone has a role to play in the chain of survival – from bystanders to dispatchers, emergency responders to health care providers,” Dr. Mark Creager said in a statement. “When everyone knows their role, knows CPR, and works together, we can dramatically improve cardiac arrest victims’ chances of survival,” said Dr. Creager, AHA president and director of the Heart and Vascular Center at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The 2015 guidelines’ new recommendations include the following:
• Resuscitation pathways. The guidelines note that the resuscitation pathways are very different for patients who experience cardiac arrest present in either a hospital setting (IHCA) or out-of-hospital setting (OHCA). In OHCA, the patient depends on lay rescuers to not only recognize the situation but also call for help, initiate CPR, and, if available, administer defibrillation until emergency medical personnel arrive. However, IHCA involves prevention of cardiac arrest and smooth delivery of care in a multidisciplinary setting.
• Layperson CPR. Untrained lay rescuers should provide compression-only CPR for OHCA. Trained lay rescuers who are able to provide rescue breaths should begin CPR with compressions followed by breaths at a ratio of 30 compressions to two breaths. Compression-only CPR is easier to perform for untrained lay rescuers, the guidelines note, and survival rates are similar using CPR with or without rescue breaths in adult cardiac arrest with a cardiac etiology.
• Compression rate and depth. The new guidelines set upper limits on chest compression depth and heart rate, recommending a compression rate of 100-120 compressions per minute with a depth of at least 2 inches, not to exceed 2.4 inches in adults.
• Social media dispatching. Despite limited evidence, the guideline authors said that it may be reasonable for communities to use social media technologies to alert lay rescuers with mobile phones about nearby OHCA cases.
• Naloxone and opioid addiction. Also new to the guidelines is the recommended use of naloxone for patients with suspected or known opioid addiction by appropriately trained lay rescuers or basic life support (BLS) providers.
• CPR training. The guidelines highlight several changes to simplify health care provider training in CPR. For example, trained rescuers can simultaneously perform some tasks to reduce the time to initiate chest compressions. Likewise, in a team of trained rescuers, multiple steps such as activating the emergency response system, chest compression, ventilation, and defibrillator retrieval can be accomplished simultaneously.
• High-quality CPR. Finally, the guidelines focus on emphasizing high-quality CPR with adequate compression rate and depth, complete chest recoil, few interruptions to compressions, and appropriate ventilation.
The guidelines offer several changes to advanced cardiac life support (ACLS). The algorithm was simplified by removing vasopressin, because the authors note that “the combined use of vasopressin and epinephrine offers no advantage to using standard-dose epinephrine in cardiac arrest.”
Likewise, the guidelines note conflicting studies to support the use of lidocaine after return of spontaneous circulation (ROSC). “However, the initiation or continuation of lidocaine may be considered immediately after ROSC from VF/pulseless ventricular tachycardia cardiac arrest,” the guideline authors wrote. Finally, the guidelines highlight updates in post–cardiac arrest care, including a wider range of target temperatures, between 32° C and 36° C, to be maintained for at least 24 hours in comatose adults with ROSC after cardiac arrest. In comparison, the 2010 guidelines called for a target temperature range of 32° C to 34° C for 12-24 hours. The guidelines also detail new updates for acute coronary syndrome, pediatric BLS, pediatric ACLS, and neonatal resuscitation.
As the AHA updates its CPR guidelines, it’s also important for lay rescuers and health providers to update their own training, noted Dr. Clifton Callaway, chair of the AHA’s Emergency Cardiovascular Care (ECC) committee.
“Research shows resuscitation skills can decline within a few months after training – far before the 2-year period in which basic and advanced life support skills are currently evaluated,” cautioned Dr. Callaway, professor of emergency medicine at the University of Pittsburgh. “Frequent training with shorter intervals of basic and advanced cardiovascular life support skills may be helpful for providers who are likely to encounter a cardiac arrest to ensure the patient receives high-quality CPR,” he added.
New guidelines on cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) set upper limits on chest compression rate and depth, add naloxone to the care of suspected opioid abusers, and remove vasopressin from the advanced cardiac life support (ACLS) algorithm.
The American Heart Association published its revised guidelines Oct. 15 in Circulation. The AHA released its previous guidelines in 2010.
“Everyone has a role to play in the chain of survival – from bystanders to dispatchers, emergency responders to health care providers,” Dr. Mark Creager said in a statement. “When everyone knows their role, knows CPR, and works together, we can dramatically improve cardiac arrest victims’ chances of survival,” said Dr. Creager, AHA president and director of the Heart and Vascular Center at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The 2015 guidelines’ new recommendations include the following:
• Resuscitation pathways. The guidelines note that the resuscitation pathways are very different for patients who experience cardiac arrest present in either a hospital setting (IHCA) or out-of-hospital setting (OHCA). In OHCA, the patient depends on lay rescuers to not only recognize the situation but also call for help, initiate CPR, and, if available, administer defibrillation until emergency medical personnel arrive. However, IHCA involves prevention of cardiac arrest and smooth delivery of care in a multidisciplinary setting.
• Layperson CPR. Untrained lay rescuers should provide compression-only CPR for OHCA. Trained lay rescuers who are able to provide rescue breaths should begin CPR with compressions followed by breaths at a ratio of 30 compressions to two breaths. Compression-only CPR is easier to perform for untrained lay rescuers, the guidelines note, and survival rates are similar using CPR with or without rescue breaths in adult cardiac arrest with a cardiac etiology.
• Compression rate and depth. The new guidelines set upper limits on chest compression depth and heart rate, recommending a compression rate of 100-120 compressions per minute with a depth of at least 2 inches, not to exceed 2.4 inches in adults.
• Social media dispatching. Despite limited evidence, the guideline authors said that it may be reasonable for communities to use social media technologies to alert lay rescuers with mobile phones about nearby OHCA cases.
• Naloxone and opioid addiction. Also new to the guidelines is the recommended use of naloxone for patients with suspected or known opioid addiction by appropriately trained lay rescuers or basic life support (BLS) providers.
• CPR training. The guidelines highlight several changes to simplify health care provider training in CPR. For example, trained rescuers can simultaneously perform some tasks to reduce the time to initiate chest compressions. Likewise, in a team of trained rescuers, multiple steps such as activating the emergency response system, chest compression, ventilation, and defibrillator retrieval can be accomplished simultaneously.
• High-quality CPR. Finally, the guidelines focus on emphasizing high-quality CPR with adequate compression rate and depth, complete chest recoil, few interruptions to compressions, and appropriate ventilation.
The guidelines offer several changes to advanced cardiac life support (ACLS). The algorithm was simplified by removing vasopressin, because the authors note that “the combined use of vasopressin and epinephrine offers no advantage to using standard-dose epinephrine in cardiac arrest.”
Likewise, the guidelines note conflicting studies to support the use of lidocaine after return of spontaneous circulation (ROSC). “However, the initiation or continuation of lidocaine may be considered immediately after ROSC from VF/pulseless ventricular tachycardia cardiac arrest,” the guideline authors wrote. Finally, the guidelines highlight updates in post–cardiac arrest care, including a wider range of target temperatures, between 32° C and 36° C, to be maintained for at least 24 hours in comatose adults with ROSC after cardiac arrest. In comparison, the 2010 guidelines called for a target temperature range of 32° C to 34° C for 12-24 hours. The guidelines also detail new updates for acute coronary syndrome, pediatric BLS, pediatric ACLS, and neonatal resuscitation.
As the AHA updates its CPR guidelines, it’s also important for lay rescuers and health providers to update their own training, noted Dr. Clifton Callaway, chair of the AHA’s Emergency Cardiovascular Care (ECC) committee.
“Research shows resuscitation skills can decline within a few months after training – far before the 2-year period in which basic and advanced life support skills are currently evaluated,” cautioned Dr. Callaway, professor of emergency medicine at the University of Pittsburgh. “Frequent training with shorter intervals of basic and advanced cardiovascular life support skills may be helpful for providers who are likely to encounter a cardiac arrest to ensure the patient receives high-quality CPR,” he added.
New guidelines on cardiopulmonary resuscitation (CPR) and emergency cardiovascular care (ECC) set upper limits on chest compression rate and depth, add naloxone to the care of suspected opioid abusers, and remove vasopressin from the advanced cardiac life support (ACLS) algorithm.
The American Heart Association published its revised guidelines Oct. 15 in Circulation. The AHA released its previous guidelines in 2010.
“Everyone has a role to play in the chain of survival – from bystanders to dispatchers, emergency responders to health care providers,” Dr. Mark Creager said in a statement. “When everyone knows their role, knows CPR, and works together, we can dramatically improve cardiac arrest victims’ chances of survival,” said Dr. Creager, AHA president and director of the Heart and Vascular Center at Dartmouth-Hitchcock Medical Center, Lebanon, N.H.
The 2015 guidelines’ new recommendations include the following:
• Resuscitation pathways. The guidelines note that the resuscitation pathways are very different for patients who experience cardiac arrest present in either a hospital setting (IHCA) or out-of-hospital setting (OHCA). In OHCA, the patient depends on lay rescuers to not only recognize the situation but also call for help, initiate CPR, and, if available, administer defibrillation until emergency medical personnel arrive. However, IHCA involves prevention of cardiac arrest and smooth delivery of care in a multidisciplinary setting.
• Layperson CPR. Untrained lay rescuers should provide compression-only CPR for OHCA. Trained lay rescuers who are able to provide rescue breaths should begin CPR with compressions followed by breaths at a ratio of 30 compressions to two breaths. Compression-only CPR is easier to perform for untrained lay rescuers, the guidelines note, and survival rates are similar using CPR with or without rescue breaths in adult cardiac arrest with a cardiac etiology.
• Compression rate and depth. The new guidelines set upper limits on chest compression depth and heart rate, recommending a compression rate of 100-120 compressions per minute with a depth of at least 2 inches, not to exceed 2.4 inches in adults.
• Social media dispatching. Despite limited evidence, the guideline authors said that it may be reasonable for communities to use social media technologies to alert lay rescuers with mobile phones about nearby OHCA cases.
• Naloxone and opioid addiction. Also new to the guidelines is the recommended use of naloxone for patients with suspected or known opioid addiction by appropriately trained lay rescuers or basic life support (BLS) providers.
• CPR training. The guidelines highlight several changes to simplify health care provider training in CPR. For example, trained rescuers can simultaneously perform some tasks to reduce the time to initiate chest compressions. Likewise, in a team of trained rescuers, multiple steps such as activating the emergency response system, chest compression, ventilation, and defibrillator retrieval can be accomplished simultaneously.
• High-quality CPR. Finally, the guidelines focus on emphasizing high-quality CPR with adequate compression rate and depth, complete chest recoil, few interruptions to compressions, and appropriate ventilation.
The guidelines offer several changes to advanced cardiac life support (ACLS). The algorithm was simplified by removing vasopressin, because the authors note that “the combined use of vasopressin and epinephrine offers no advantage to using standard-dose epinephrine in cardiac arrest.”
Likewise, the guidelines note conflicting studies to support the use of lidocaine after return of spontaneous circulation (ROSC). “However, the initiation or continuation of lidocaine may be considered immediately after ROSC from VF/pulseless ventricular tachycardia cardiac arrest,” the guideline authors wrote. Finally, the guidelines highlight updates in post–cardiac arrest care, including a wider range of target temperatures, between 32° C and 36° C, to be maintained for at least 24 hours in comatose adults with ROSC after cardiac arrest. In comparison, the 2010 guidelines called for a target temperature range of 32° C to 34° C for 12-24 hours. The guidelines also detail new updates for acute coronary syndrome, pediatric BLS, pediatric ACLS, and neonatal resuscitation.
As the AHA updates its CPR guidelines, it’s also important for lay rescuers and health providers to update their own training, noted Dr. Clifton Callaway, chair of the AHA’s Emergency Cardiovascular Care (ECC) committee.
“Research shows resuscitation skills can decline within a few months after training – far before the 2-year period in which basic and advanced life support skills are currently evaluated,” cautioned Dr. Callaway, professor of emergency medicine at the University of Pittsburgh. “Frequent training with shorter intervals of basic and advanced cardiovascular life support skills may be helpful for providers who are likely to encounter a cardiac arrest to ensure the patient receives high-quality CPR,” he added.
FROM CIRCULATION

Medical Students: Apply to for an AATS Summer Internship Scholarship
Submissions are open for the AATS Summer Internship Scholarship giving up to 40 successful candidates the opportunity to spend eight weeks during the summer working in the cardiothoracic surgery department of a North American AATS member.
Program Goal
To broaden medical students’ educational experiences and to provide insight into cardiothoracic surgery.
Eligibility
- Candidates must be a North American first- or second-year medical student (as of January 2, 2016).
- Host sponsor (an AATS member) must provide a letter of support/approval.
- Internships must take place at the institution of the host sponsor.
Application
- The application must include no more than a one-page outline, including:
- What the candidate hopes to accomplish during his/her eight week scholarship, specifying the proposed intern’s exposure to CT surgery, including both laboratory and clinical experience.
Selection
- No more than two students from a single institution may receive a scholarship.
- If two students from the same institution are selected, each must have a different host sponsor.
- Award recipients must agree to submit a summary report and evaluation of their experience to AATS within 60 days of internship completion.
Deadline: Friday, January 15, 2015
Submissions are open for the AATS Summer Internship Scholarship giving up to 40 successful candidates the opportunity to spend eight weeks during the summer working in the cardiothoracic surgery department of a North American AATS member.
Program Goal
To broaden medical students’ educational experiences and to provide insight into cardiothoracic surgery.
Eligibility
- Candidates must be a North American first- or second-year medical student (as of January 2, 2016).
- Host sponsor (an AATS member) must provide a letter of support/approval.
- Internships must take place at the institution of the host sponsor.
Application
- The application must include no more than a one-page outline, including:
- What the candidate hopes to accomplish during his/her eight week scholarship, specifying the proposed intern’s exposure to CT surgery, including both laboratory and clinical experience.
Selection
- No more than two students from a single institution may receive a scholarship.
- If two students from the same institution are selected, each must have a different host sponsor.
- Award recipients must agree to submit a summary report and evaluation of their experience to AATS within 60 days of internship completion.
Deadline: Friday, January 15, 2015
Submissions are open for the AATS Summer Internship Scholarship giving up to 40 successful candidates the opportunity to spend eight weeks during the summer working in the cardiothoracic surgery department of a North American AATS member.
Program Goal
To broaden medical students’ educational experiences and to provide insight into cardiothoracic surgery.
Eligibility
- Candidates must be a North American first- or second-year medical student (as of January 2, 2016).
- Host sponsor (an AATS member) must provide a letter of support/approval.
- Internships must take place at the institution of the host sponsor.
Application
- The application must include no more than a one-page outline, including:
- What the candidate hopes to accomplish during his/her eight week scholarship, specifying the proposed intern’s exposure to CT surgery, including both laboratory and clinical experience.
Selection
- No more than two students from a single institution may receive a scholarship.
- If two students from the same institution are selected, each must have a different host sponsor.
- Award recipients must agree to submit a summary report and evaluation of their experience to AATS within 60 days of internship completion.
Deadline: Friday, January 15, 2015
Medical Students, General Surgery Residents & I-6 CT Surgical Residents: Be an AATS Member for a Day
Submissions are open for the AATS Member for a Day program giving up to 30 successful candidates the opportunity to accompany an AATS Member Mentor for portions of the 2016 AATS Annual Meeting.
May 14-18, 2016
Baltimore, MD
Eligibility
Applicants must be North American:
- Medical students
- General surgery residents
- I-6 cardiothoracic residents (within their first three years)
Program Goals
- Offer insight into cardiothoracic surgery.
- Provide an opportunity to network and build relationships within the cardiothoracic surgical community.
Benefits
- Complimentary hotel accommodation for a minimum of three and maximum of four nights at an AATS Annual Meeting hotel.
- A $500 stipend to help offset travel costs.
- An additional $250 stipend to offset the cost of meals.
Deadline: Friday, January 15, 2015
Submissions are open for the AATS Member for a Day program giving up to 30 successful candidates the opportunity to accompany an AATS Member Mentor for portions of the 2016 AATS Annual Meeting.
May 14-18, 2016
Baltimore, MD
Eligibility
Applicants must be North American:
- Medical students
- General surgery residents
- I-6 cardiothoracic residents (within their first three years)
Program Goals
- Offer insight into cardiothoracic surgery.
- Provide an opportunity to network and build relationships within the cardiothoracic surgical community.
Benefits
- Complimentary hotel accommodation for a minimum of three and maximum of four nights at an AATS Annual Meeting hotel.
- A $500 stipend to help offset travel costs.
- An additional $250 stipend to offset the cost of meals.
Deadline: Friday, January 15, 2015
Submissions are open for the AATS Member for a Day program giving up to 30 successful candidates the opportunity to accompany an AATS Member Mentor for portions of the 2016 AATS Annual Meeting.
May 14-18, 2016
Baltimore, MD
Eligibility
Applicants must be North American:
- Medical students
- General surgery residents
- I-6 cardiothoracic residents (within their first three years)
Program Goals
- Offer insight into cardiothoracic surgery.
- Provide an opportunity to network and build relationships within the cardiothoracic surgical community.
Benefits
- Complimentary hotel accommodation for a minimum of three and maximum of four nights at an AATS Annual Meeting hotel.
- A $500 stipend to help offset travel costs.
- An additional $250 stipend to offset the cost of meals.
Deadline: Friday, January 15, 2015

CMS delays Stage 3 meaningful use until 2018, simplifies program
Doctors will have 1 more year – until Jan. 1, 2018 – to comply with Stage 3 meaningful use requirements for electronic health records (EHRs), the Centers for Medicare & Medicaid Services announced.
In its long-awaited final rule, released Oct. 6, CMS also announced simplifications to the program designed to align meaningful use with other incentive programs and shift the overall focus of the programs to make them tools for improving overall health.

The announced changes “will ease the reporting burden for providers, increase simplicity and flexibility, support interoperability and information exchange, and improve patient outcomes,” CMS Acting Principal Deputy Administrator and Chief Medical Officer Patrick Conway noted during an Oct. 6 conference call with the media.
Dr. Conway noted that the final rule reduces the number of objectives from about 20 to 8 to allow doctors to find the measures that are most relevant to their practice. Measures also are better aligned, so that a single measure can allow providers to earn credit across multiple incentive programs.
CMS also explained in a separate fact sheet that it was removing many of the “check box” process measures and enhancing the focus on aspects of patient care, such as clinical decision support, e-prescribing, and information exchange.
The agency also finalized a 90-day reporting period in 2015 for all providers currently active in the meaningful use program. Given that the rule was finalized with fewer than 90 days left in the year, Dr. Conway provided additional clarity regarding the flexibility physicians will have to meet those requirements.
If doctors were using an electronic health record on Oct. 1, 2015, “they actually will not report until the end of February, and if we need to extend that time frame, we would look at that at the end of February 2016,” he said. “So, they still have almost 5 months before the reporting actually occurs.”
Dr. Conway added that even if a provider launched an EHR system after Oct. 1, “the thresholds for the program are not 100%. So, even if they were to deploy it tomorrow [and] use it successfully through the end of the year, they could then report that performance in 2016 and avoid a penalty.”
Providers also can use the exemption process if there have been implementation issues, which CMS reviews on a case-by-case basis.
Stage 2 concerns linger
There was concern that the changes did not go far enough, particularly as they relate to modifications of Stage 2 meaningful use.

“Many of the requirements for Stage 2 proved unattainable,” American College of Cardiology President Kim Allan Williams Sr. said in a statement. “Large numbers of providers either haven’t met them or, after trying and failing, have given up. That is why it is vital that CMS consider participation data from the current stage to see what is working and what isn’t before outlining an upcoming stage.”
By 2018, all providers will have to meet Stage 3 meaningful use requirements, because the earlier stages will no longer be available to help new entrants transition into the program. However, if a provider chooses to adopt the 2018 requirements a year early, they will have only a 90-day reporting requirement.
What about MACRA?
Even with the extended time line, CMS is drawing criticism for progressing with Stage 3.
“We still have some concerns about how the program is going,” Ms. Laura C. Wooster, vice president of public policy at the American Osteopathic Association, said in an interview.
One prime area of concern is the current meaningful use time line’s intersection with the start of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) reforms, which will replace the Medicare Sustainable Growth Rate payment system, Ms. Wooster noted.
“Stage 3 begins voluntarily in 2017 and then is required for all physicians in 2018. MACRA begins in 2019, and electronic health record reporting will still be part of the Merit-Based Incentive Payment System.”

She expressed concern that physicians are going to have to make changes for Stage 3 meaningful use in 2018, only to have to make more changes to account for MACRA a year later.
The American Medical Association expressed similar concerns.
“The AMA recognizes that physicians continue to struggle with the meaningful use program,” AMA President Steven Stack said in a statement. “However, we hope the decision by CMS to leave Stage 3 open to additional comment will allow for further improvements in the program and promote technological innovation that supports patient care,” Dr. Stack added.
Given the changes that will come as a result of MACRA, CMS is taking comments on the final rule to help inform future policy on how it and MACRA will align.
Doctors will have 1 more year – until Jan. 1, 2018 – to comply with Stage 3 meaningful use requirements for electronic health records (EHRs), the Centers for Medicare & Medicaid Services announced.
In its long-awaited final rule, released Oct. 6, CMS also announced simplifications to the program designed to align meaningful use with other incentive programs and shift the overall focus of the programs to make them tools for improving overall health.
The announced changes “will ease the reporting burden for providers, increase simplicity and flexibility, support interoperability and information exchange, and improve patient outcomes,” CMS Acting Principal Deputy Administrator and Chief Medical Officer Patrick Conway noted during an Oct. 6 conference call with the media.
Dr. Conway noted that the final rule reduces the number of objectives from about 20 to 8 to allow doctors to find the measures that are most relevant to their practice. Measures also are better aligned, so that a single measure can allow providers to earn credit across multiple incentive programs.
CMS also explained in a separate fact sheet that it was removing many of the “check box” process measures and enhancing the focus on aspects of patient care, such as clinical decision support, e-prescribing, and information exchange.
The agency also finalized a 90-day reporting period in 2015 for all providers currently active in the meaningful use program. Given that the rule was finalized with fewer than 90 days left in the year, Dr. Conway provided additional clarity regarding the flexibility physicians will have to meet those requirements.
If doctors were using an electronic health record on Oct. 1, 2015, “they actually will not report until the end of February, and if we need to extend that time frame, we would look at that at the end of February 2016,” he said. “So, they still have almost 5 months before the reporting actually occurs.”
Dr. Conway added that even if a provider launched an EHR system after Oct. 1, “the thresholds for the program are not 100%. So, even if they were to deploy it tomorrow [and] use it successfully through the end of the year, they could then report that performance in 2016 and avoid a penalty.”
Providers also can use the exemption process if there have been implementation issues, which CMS reviews on a case-by-case basis.
Stage 2 concerns linger
There was concern that the changes did not go far enough, particularly as they relate to modifications of Stage 2 meaningful use.
“Many of the requirements for Stage 2 proved unattainable,” American College of Cardiology President Kim Allan Williams Sr. said in a statement. “Large numbers of providers either haven’t met them or, after trying and failing, have given up. That is why it is vital that CMS consider participation data from the current stage to see what is working and what isn’t before outlining an upcoming stage.”
By 2018, all providers will have to meet Stage 3 meaningful use requirements, because the earlier stages will no longer be available to help new entrants transition into the program. However, if a provider chooses to adopt the 2018 requirements a year early, they will have only a 90-day reporting requirement.
What about MACRA?
Even with the extended time line, CMS is drawing criticism for progressing with Stage 3.
“We still have some concerns about how the program is going,” Ms. Laura C. Wooster, vice president of public policy at the American Osteopathic Association, said in an interview.
One prime area of concern is the current meaningful use time line’s intersection with the start of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) reforms, which will replace the Medicare Sustainable Growth Rate payment system, Ms. Wooster noted.
“Stage 3 begins voluntarily in 2017 and then is required for all physicians in 2018. MACRA begins in 2019, and electronic health record reporting will still be part of the Merit-Based Incentive Payment System.”
She expressed concern that physicians are going to have to make changes for Stage 3 meaningful use in 2018, only to have to make more changes to account for MACRA a year later.
The American Medical Association expressed similar concerns.
“The AMA recognizes that physicians continue to struggle with the meaningful use program,” AMA President Steven Stack said in a statement. “However, we hope the decision by CMS to leave Stage 3 open to additional comment will allow for further improvements in the program and promote technological innovation that supports patient care,” Dr. Stack added.
Given the changes that will come as a result of MACRA, CMS is taking comments on the final rule to help inform future policy on how it and MACRA will align.
Doctors will have 1 more year – until Jan. 1, 2018 – to comply with Stage 3 meaningful use requirements for electronic health records (EHRs), the Centers for Medicare & Medicaid Services announced.
In its long-awaited final rule, released Oct. 6, CMS also announced simplifications to the program designed to align meaningful use with other incentive programs and shift the overall focus of the programs to make them tools for improving overall health.
The announced changes “will ease the reporting burden for providers, increase simplicity and flexibility, support interoperability and information exchange, and improve patient outcomes,” CMS Acting Principal Deputy Administrator and Chief Medical Officer Patrick Conway noted during an Oct. 6 conference call with the media.
Dr. Conway noted that the final rule reduces the number of objectives from about 20 to 8 to allow doctors to find the measures that are most relevant to their practice. Measures also are better aligned, so that a single measure can allow providers to earn credit across multiple incentive programs.
CMS also explained in a separate fact sheet that it was removing many of the “check box” process measures and enhancing the focus on aspects of patient care, such as clinical decision support, e-prescribing, and information exchange.
The agency also finalized a 90-day reporting period in 2015 for all providers currently active in the meaningful use program. Given that the rule was finalized with fewer than 90 days left in the year, Dr. Conway provided additional clarity regarding the flexibility physicians will have to meet those requirements.
If doctors were using an electronic health record on Oct. 1, 2015, “they actually will not report until the end of February, and if we need to extend that time frame, we would look at that at the end of February 2016,” he said. “So, they still have almost 5 months before the reporting actually occurs.”
Dr. Conway added that even if a provider launched an EHR system after Oct. 1, “the thresholds for the program are not 100%. So, even if they were to deploy it tomorrow [and] use it successfully through the end of the year, they could then report that performance in 2016 and avoid a penalty.”
Providers also can use the exemption process if there have been implementation issues, which CMS reviews on a case-by-case basis.
Stage 2 concerns linger
There was concern that the changes did not go far enough, particularly as they relate to modifications of Stage 2 meaningful use.
“Many of the requirements for Stage 2 proved unattainable,” American College of Cardiology President Kim Allan Williams Sr. said in a statement. “Large numbers of providers either haven’t met them or, after trying and failing, have given up. That is why it is vital that CMS consider participation data from the current stage to see what is working and what isn’t before outlining an upcoming stage.”
By 2018, all providers will have to meet Stage 3 meaningful use requirements, because the earlier stages will no longer be available to help new entrants transition into the program. However, if a provider chooses to adopt the 2018 requirements a year early, they will have only a 90-day reporting requirement.
What about MACRA?
Even with the extended time line, CMS is drawing criticism for progressing with Stage 3.
“We still have some concerns about how the program is going,” Ms. Laura C. Wooster, vice president of public policy at the American Osteopathic Association, said in an interview.
One prime area of concern is the current meaningful use time line’s intersection with the start of the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA) reforms, which will replace the Medicare Sustainable Growth Rate payment system, Ms. Wooster noted.
“Stage 3 begins voluntarily in 2017 and then is required for all physicians in 2018. MACRA begins in 2019, and electronic health record reporting will still be part of the Merit-Based Incentive Payment System.”
She expressed concern that physicians are going to have to make changes for Stage 3 meaningful use in 2018, only to have to make more changes to account for MACRA a year later.
The American Medical Association expressed similar concerns.
“The AMA recognizes that physicians continue to struggle with the meaningful use program,” AMA President Steven Stack said in a statement. “However, we hope the decision by CMS to leave Stage 3 open to additional comment will allow for further improvements in the program and promote technological innovation that supports patient care,” Dr. Stack added.
Given the changes that will come as a result of MACRA, CMS is taking comments on the final rule to help inform future policy on how it and MACRA will align.

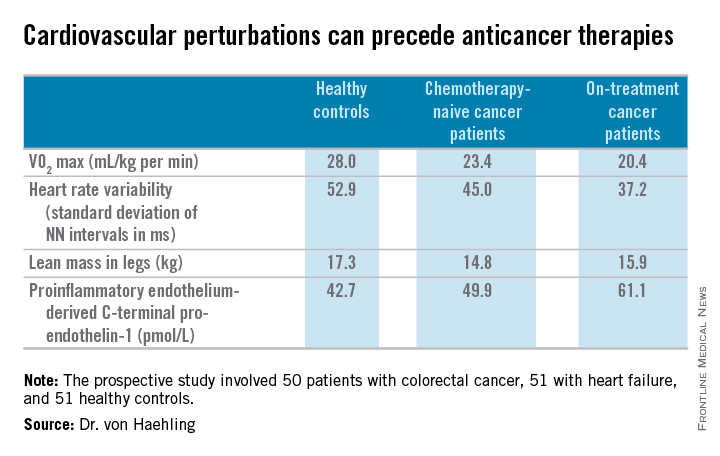
ESC: Cancer itself may cause cardiotoxicity
LONDON – Cancer itself has cardiotoxic effects independent of those caused by chemotherapy, Dr. Stephan von Haehling said at the annual congress of the European Society of Cardiology.
Evidence from both animal and human studies indicates that the malignancy itself may be exerting adverse cardiac effects even before chemotherapy provides an additional hit to the heart, according to Dr. von Haehling, who is a cardiologist at Charity Medical School, Berlin.

“In patients with advanced cancer, significant alterations exist in several markers of cardiovascular perturbation independent of high-dose chemotherapy. So it looks like the cancer is doing something that’s further worsened when chemotherapy starts,” he explained.
Dr. von Haehling and his coinvestigators first demonstrated this phenomenon in a rat model of liver cancer (Eur Heart J. 2014 Apr;35[14]:932-41). The tumor-bearing rats had the classic symptoms of cancer cachexia, including fatigue, impaired exercise capacity, loss of body weight, and dyspnea, as well as progressive wasting of left ventricular mass, even before exposure to chemotherapy. Strikingly, administration of the cardioselective beta-blocker bisoprolol and the aldosterone inhibitor spironolactone reduced left ventricular wasting, curbed cardiac dysfunction, improved a validated measure of rat quality of life, and significantly prolonged rat survival, compared with placebo.
Further exploration of these findings in clinical trials deserves to be a priority in light of the potential quality-of-life benefits for cancer patients, Dr. von Haehling observed.
He and his coworkers followed up the rat study with a prospective study of 50 patients with colorectal cancer, 51 with heart failure, and 51 healthy controls. Of the colorectal cancer patients, 24 underwent echocardiography and other cardiovascular function studies before they went on chemotherapy, while the other 26 did so after starting chemotherapy.
The colorectal cancer patients had a mildly elevated heart rate: an average of 73 beats per minute, compared with 65 bpm in controls and in heart failure patients on beta-blocker therapy. “This is something I see quite often. These patients usually have a mildly elevated heart rate in the range of 80-90 [bpms] or even slightly above,” he said.
Heart rate variability, exercise capacity as measured by treadmill VO2 max testing, and left ventricular ejection fraction were significantly lower in cancer patients than controls, and lower still in the heart failure patients. More interesting were the differences between chemotherapy-naive and on-treatment colorectal cancer patients. Several major determinants of cardiovascular function were impaired in chemotherapy-naive cancer patients, compared with controls, and even more severely impaired in cancer patients on chemotherapy.
For more about current thinking regarding the prevention, monitoring, and treatment of cardiac side effects of anticancer therapies, Dr. von Haehling recommended the multidisciplinary clinical practice guidelines developed by the European Society for Medical Oncology (Ann Oncol. 2012 Oct;23 Suppl 7:vii155-66).
He reported having no financial conflicts regarding his cardio-oncology studies.
LONDON – Cancer itself has cardiotoxic effects independent of those caused by chemotherapy, Dr. Stephan von Haehling said at the annual congress of the European Society of Cardiology.
Evidence from both animal and human studies indicates that the malignancy itself may be exerting adverse cardiac effects even before chemotherapy provides an additional hit to the heart, according to Dr. von Haehling, who is a cardiologist at Charity Medical School, Berlin.
“In patients with advanced cancer, significant alterations exist in several markers of cardiovascular perturbation independent of high-dose chemotherapy. So it looks like the cancer is doing something that’s further worsened when chemotherapy starts,” he explained.
Dr. von Haehling and his coinvestigators first demonstrated this phenomenon in a rat model of liver cancer (Eur Heart J. 2014 Apr;35[14]:932-41). The tumor-bearing rats had the classic symptoms of cancer cachexia, including fatigue, impaired exercise capacity, loss of body weight, and dyspnea, as well as progressive wasting of left ventricular mass, even before exposure to chemotherapy. Strikingly, administration of the cardioselective beta-blocker bisoprolol and the aldosterone inhibitor spironolactone reduced left ventricular wasting, curbed cardiac dysfunction, improved a validated measure of rat quality of life, and significantly prolonged rat survival, compared with placebo.
Further exploration of these findings in clinical trials deserves to be a priority in light of the potential quality-of-life benefits for cancer patients, Dr. von Haehling observed.
He and his coworkers followed up the rat study with a prospective study of 50 patients with colorectal cancer, 51 with heart failure, and 51 healthy controls. Of the colorectal cancer patients, 24 underwent echocardiography and other cardiovascular function studies before they went on chemotherapy, while the other 26 did so after starting chemotherapy.
The colorectal cancer patients had a mildly elevated heart rate: an average of 73 beats per minute, compared with 65 bpm in controls and in heart failure patients on beta-blocker therapy. “This is something I see quite often. These patients usually have a mildly elevated heart rate in the range of 80-90 [bpms] or even slightly above,” he said.
Heart rate variability, exercise capacity as measured by treadmill VO2 max testing, and left ventricular ejection fraction were significantly lower in cancer patients than controls, and lower still in the heart failure patients. More interesting were the differences between chemotherapy-naive and on-treatment colorectal cancer patients. Several major determinants of cardiovascular function were impaired in chemotherapy-naive cancer patients, compared with controls, and even more severely impaired in cancer patients on chemotherapy.
For more about current thinking regarding the prevention, monitoring, and treatment of cardiac side effects of anticancer therapies, Dr. von Haehling recommended the multidisciplinary clinical practice guidelines developed by the European Society for Medical Oncology (Ann Oncol. 2012 Oct;23 Suppl 7:vii155-66).
He reported having no financial conflicts regarding his cardio-oncology studies.
LONDON – Cancer itself has cardiotoxic effects independent of those caused by chemotherapy, Dr. Stephan von Haehling said at the annual congress of the European Society of Cardiology.
Evidence from both animal and human studies indicates that the malignancy itself may be exerting adverse cardiac effects even before chemotherapy provides an additional hit to the heart, according to Dr. von Haehling, who is a cardiologist at Charity Medical School, Berlin.
“In patients with advanced cancer, significant alterations exist in several markers of cardiovascular perturbation independent of high-dose chemotherapy. So it looks like the cancer is doing something that’s further worsened when chemotherapy starts,” he explained.
Dr. von Haehling and his coinvestigators first demonstrated this phenomenon in a rat model of liver cancer (Eur Heart J. 2014 Apr;35[14]:932-41). The tumor-bearing rats had the classic symptoms of cancer cachexia, including fatigue, impaired exercise capacity, loss of body weight, and dyspnea, as well as progressive wasting of left ventricular mass, even before exposure to chemotherapy. Strikingly, administration of the cardioselective beta-blocker bisoprolol and the aldosterone inhibitor spironolactone reduced left ventricular wasting, curbed cardiac dysfunction, improved a validated measure of rat quality of life, and significantly prolonged rat survival, compared with placebo.
Further exploration of these findings in clinical trials deserves to be a priority in light of the potential quality-of-life benefits for cancer patients, Dr. von Haehling observed.
He and his coworkers followed up the rat study with a prospective study of 50 patients with colorectal cancer, 51 with heart failure, and 51 healthy controls. Of the colorectal cancer patients, 24 underwent echocardiography and other cardiovascular function studies before they went on chemotherapy, while the other 26 did so after starting chemotherapy.
The colorectal cancer patients had a mildly elevated heart rate: an average of 73 beats per minute, compared with 65 bpm in controls and in heart failure patients on beta-blocker therapy. “This is something I see quite often. These patients usually have a mildly elevated heart rate in the range of 80-90 [bpms] or even slightly above,” he said.
Heart rate variability, exercise capacity as measured by treadmill VO2 max testing, and left ventricular ejection fraction were significantly lower in cancer patients than controls, and lower still in the heart failure patients. More interesting were the differences between chemotherapy-naive and on-treatment colorectal cancer patients. Several major determinants of cardiovascular function were impaired in chemotherapy-naive cancer patients, compared with controls, and even more severely impaired in cancer patients on chemotherapy.
For more about current thinking regarding the prevention, monitoring, and treatment of cardiac side effects of anticancer therapies, Dr. von Haehling recommended the multidisciplinary clinical practice guidelines developed by the European Society for Medical Oncology (Ann Oncol. 2012 Oct;23 Suppl 7:vii155-66).
He reported having no financial conflicts regarding his cardio-oncology studies.
EXPERT ANALYSIS FROM THE ESC CONGRESS 2015

FDA approves first bioabsorbable-polymer stent
The Food and Drug Administration has approved Synergy, first coronary stent with a bioabsorbable polymer on the U.S. market, Boston Scientific announced.
Synergy is a platinum chrome stent that uses the polymer PLGA as the biodegradable carrier to deliver the antirestenosing agent everolimus. Polymers have been identified as potential contributors to coronary artery restenosis after stent deployment, at least partly due to their contribution to a proinflammatory state.

The new stent, which carries the CE mark and has been in use in several European countries since 2013, was studied in the United States in the pivotal EVOLVE II clinical trial, which was a randomized, multicenter trial of 1,684 patients. That trial met its primary endpoints of noninferiority in safety and efficacy when compared to a drug-eluting stent that used a durable polymer (Circ Cardiovasc Interv. 2015 Apr 8. doi: 10.1161/CIRCINTERVENTIONS.114.002372).
EVOLVE II’s primary efficacy endpoint was a combined measure of cardiac death, myocardial infarction with ischemia from a stented artery, or ischemia-driven target vessel revascularization. The Synergy arm saw 6.7% of patients experiencing one of these events, compared with 6.5% of the durable-polymer stent patients. This difference was not statistically significant.
The primary safety outcome of definite or probable stent thrombosis was seen in three patients with the resorbable polymer stent and in five patients with durable polymer stents. This was also a nonsignificant difference.
In EVOLVE II, procedures using Synergy were slightly more likely to be immediately successful than those using the durable polymer stent, with 98.3% vs. 96.9% immediate success rates.
“I’m very excited to have the next generation of the next generation” of stents available as a choice for patients, Dr. Roxana Mehran, professor of medicine and an interventional cardiologist at Mt. Sinai Hospital in New York, said in an interview. She noted that the data are strong, and expects that this stent will prove to be safe and efficacious. But removing the presumed “bad actor” of the proinflammatory durable polymer, she said, may also afford an opportunity to shorten the duration of antiplatelet therapy (DAPT).
She called for a prospective randomized, controlled trial of a shorter duration of DAPT, emphasizing real-world considerations. “Our patients are real people,” she said. “They might need a colonoscopy, spine surgery, knee surgery, dental implants.” The sooner patients can safely stop DAPT, the better, for the mostly elderly population that will be receiving the stents, she said. “It’s very exciting, but I still think we have a ways to go.”
EVOLVE II was sponsored by Boston Scientific, the manufacturer of Synergy. Dr. Mehran has received honoraria from and has been a consultant to Boston Scientific as well as several other device and drug companies.
On Twitter @karioakes
The Food and Drug Administration has approved Synergy, first coronary stent with a bioabsorbable polymer on the U.S. market, Boston Scientific announced.
Synergy is a platinum chrome stent that uses the polymer PLGA as the biodegradable carrier to deliver the antirestenosing agent everolimus. Polymers have been identified as potential contributors to coronary artery restenosis after stent deployment, at least partly due to their contribution to a proinflammatory state.
The new stent, which carries the CE mark and has been in use in several European countries since 2013, was studied in the United States in the pivotal EVOLVE II clinical trial, which was a randomized, multicenter trial of 1,684 patients. That trial met its primary endpoints of noninferiority in safety and efficacy when compared to a drug-eluting stent that used a durable polymer (Circ Cardiovasc Interv. 2015 Apr 8. doi: 10.1161/CIRCINTERVENTIONS.114.002372).
EVOLVE II’s primary efficacy endpoint was a combined measure of cardiac death, myocardial infarction with ischemia from a stented artery, or ischemia-driven target vessel revascularization. The Synergy arm saw 6.7% of patients experiencing one of these events, compared with 6.5% of the durable-polymer stent patients. This difference was not statistically significant.
The primary safety outcome of definite or probable stent thrombosis was seen in three patients with the resorbable polymer stent and in five patients with durable polymer stents. This was also a nonsignificant difference.
In EVOLVE II, procedures using Synergy were slightly more likely to be immediately successful than those using the durable polymer stent, with 98.3% vs. 96.9% immediate success rates.
“I’m very excited to have the next generation of the next generation” of stents available as a choice for patients, Dr. Roxana Mehran, professor of medicine and an interventional cardiologist at Mt. Sinai Hospital in New York, said in an interview. She noted that the data are strong, and expects that this stent will prove to be safe and efficacious. But removing the presumed “bad actor” of the proinflammatory durable polymer, she said, may also afford an opportunity to shorten the duration of antiplatelet therapy (DAPT).
She called for a prospective randomized, controlled trial of a shorter duration of DAPT, emphasizing real-world considerations. “Our patients are real people,” she said. “They might need a colonoscopy, spine surgery, knee surgery, dental implants.” The sooner patients can safely stop DAPT, the better, for the mostly elderly population that will be receiving the stents, she said. “It’s very exciting, but I still think we have a ways to go.”
EVOLVE II was sponsored by Boston Scientific, the manufacturer of Synergy. Dr. Mehran has received honoraria from and has been a consultant to Boston Scientific as well as several other device and drug companies.
On Twitter @karioakes
The Food and Drug Administration has approved Synergy, first coronary stent with a bioabsorbable polymer on the U.S. market, Boston Scientific announced.
Synergy is a platinum chrome stent that uses the polymer PLGA as the biodegradable carrier to deliver the antirestenosing agent everolimus. Polymers have been identified as potential contributors to coronary artery restenosis after stent deployment, at least partly due to their contribution to a proinflammatory state.
The new stent, which carries the CE mark and has been in use in several European countries since 2013, was studied in the United States in the pivotal EVOLVE II clinical trial, which was a randomized, multicenter trial of 1,684 patients. That trial met its primary endpoints of noninferiority in safety and efficacy when compared to a drug-eluting stent that used a durable polymer (Circ Cardiovasc Interv. 2015 Apr 8. doi: 10.1161/CIRCINTERVENTIONS.114.002372).
EVOLVE II’s primary efficacy endpoint was a combined measure of cardiac death, myocardial infarction with ischemia from a stented artery, or ischemia-driven target vessel revascularization. The Synergy arm saw 6.7% of patients experiencing one of these events, compared with 6.5% of the durable-polymer stent patients. This difference was not statistically significant.
The primary safety outcome of definite or probable stent thrombosis was seen in three patients with the resorbable polymer stent and in five patients with durable polymer stents. This was also a nonsignificant difference.
In EVOLVE II, procedures using Synergy were slightly more likely to be immediately successful than those using the durable polymer stent, with 98.3% vs. 96.9% immediate success rates.
“I’m very excited to have the next generation of the next generation” of stents available as a choice for patients, Dr. Roxana Mehran, professor of medicine and an interventional cardiologist at Mt. Sinai Hospital in New York, said in an interview. She noted that the data are strong, and expects that this stent will prove to be safe and efficacious. But removing the presumed “bad actor” of the proinflammatory durable polymer, she said, may also afford an opportunity to shorten the duration of antiplatelet therapy (DAPT).
She called for a prospective randomized, controlled trial of a shorter duration of DAPT, emphasizing real-world considerations. “Our patients are real people,” she said. “They might need a colonoscopy, spine surgery, knee surgery, dental implants.” The sooner patients can safely stop DAPT, the better, for the mostly elderly population that will be receiving the stents, she said. “It’s very exciting, but I still think we have a ways to go.”
EVOLVE II was sponsored by Boston Scientific, the manufacturer of Synergy. Dr. Mehran has received honoraria from and has been a consultant to Boston Scientific as well as several other device and drug companies.
On Twitter @karioakes

Reattaching intercostals fails to squelch spinal cord ischemia in TAAA repairs
CHICAGO – Intercostal artery reimplantation fails to significantly reduce spinal cord injury following thoracoabdominal aortic aneurysm surgery, results of a large retrospective study show.
“Although there was a small decrease in spinal cord ischemia with ICAR, reattaching the intercostals did not produce a statistically significant reduction in spinal cord ischemia, even in the highest risk patients,” Dr. Charles W. Acher of the University of Wisconsin–Madison, said at the annual meeting of the Midwestern Vascular Surgical Society.
Intercostal artery reimplantation (ICAR) is one of several strategies that have been used to prevent spinal cord ischemia (SCI), paraplegia, and paraparesis that occurs from the interruption of the blood supply to intercostal arteries (ICAs) during thoracoabdominal aortic aneurysm (TAAA) repair.
Surgeons at UW–Madison adopted the ICAR strategy in 2005and now reimplant open ICAs located at T7-L2 in all Type I, II, and III TAAAs, using a previously published technique (J Surg Res. 2009;154:99-104).

Using a prospectively maintained database, the current analysis sought to compare outcomes between 540 patients who had TAAA surgery during 1989-2004 when open ICAs were ligated and 265 patients who had surgery during 2005-2013 with ICAR.The surgical technique for both groups was cross clamp without assisted circulation. The anesthetic technique was also uniform during the study period and included moderate systemic hypothermia (32° - 33° C); spinal fluid drainage (spinal fluid pressure less than 5 mm Hg); naloxone 1 mcg/kg per hour; use of mannitol, methylprednisolone, and barbiturate burst suppression; goal-directed therapy for a mean arterial pressure of 90-100 mm Hg and cardiac index of 2.5 L per minute/meter2; and proactive component blood therapy to avoid anemia, hypovolemia, and hypertension.
Aneurysm extent, acuity, mortality, renal failure, and pulmonary failure were the same in both groups.
The incidence of SCI was similar in all TAAAs at 5.25% without ICAR and 3.4% with ICAR (P = .23) and in the subset of patients with Type I, II, and III aneurysms (8.8% vs. 5.1%; P = .152), Dr. Acher reported on behalf of lead author and his colleague, Dr. Martha M. Wynn.
Interestingly, ICAR patients had more dissections than did the open ICA ligation patients (18% vs. 15%; P = .0016), more previous aortic surgery (47% vs. 31%; P = .0004), and longer renal ischemia time (61 minutes vs. 53 minutes; P = .0001), but had a shorter length of stay (14 days vs. 22 days; P = .0001) and were younger (mean age, 66 years vs. 70 years; P = .0001).
In a multivariate model of all TAAAs, significant predictors of spinal cord ischemia/injury were type II TAAA (odds ratio, 7.59; P = .0001), dissection (OR, 4.25; P = .0015), age as a continuous variable (P = .0085), and acute TAAA (OR, 2.1; P = .0525), Dr. Acher said. Time period of surgery, and therefore ICAR, was not significant (OR, 0.78; P = .55).
ICAR also failed to achieve significance as an SCI predictor in a subanalysis restricted to the highest-risk patients, defined as those having Type II TAAA, dissection, and acute surgery (OR, 0.67; P = .3387).
“Interrupting blood supply to the spinal cord causes spinal cord ischemia that can be mitigated almost entirely by physiologic interventions that increase spinal cord ischemic tolerance and collateral network perfusion during and after surgery,” Dr. Acher said. “Although the cause of SCI in TAAA surgery is anatomic, prevention of the injury is largely physiologic.”
During a discussion of the study, Dr. Acher surprised the audience by saying the findings have not changed current practice at the university. He cited several reasons, observing that there were more dissections in the ICAR group, and most of the ischemia in the ICAR group was delayed, suggesting that more patients could be rescued. In addition, there was a slight downward trend in spinal cord injury and immediate paraplegia with ICAR, however, these were not statistically significant.
“Because of those things, I still think it’s valuable, particularly in patients that are at highest risk, which are the dissections, with lots of open intercostals, but the emphasis should still be on physiologic parameters,” he said. “If you want to salvage patients, that’s the most important thing.
“Even if ICAR were ever shown to be statistically significant in a larger patient population, any role it has in reducing spinal cord injury would be extremely small,” he added in an interview.
The authors reported having no conflicts of interest.
Spinal cord ischemia is a rare but devastating complication of thoracoabdominal aneurysm repair. Crawford and his colleagues documented in 1993 an incidence of spinal cord ischemia (SCI) as high as 30% for extensive thoracoabdominal repairs. Efforts to diminish the risk of SCI were concentrated in identifying and preserving the direct arterial perfusion to the spinal cord from segmental arteries but continued experimental and clinical experience have suggested that multiple factors contribute to SCI.

|
Dr. Luis A. Sanchez |
Some generally accepted principles for minimizing SCI include hypothermia, distal aortic perfusion with atriofemoral bypass or partial cardiopulmonary bypass, cerebrospinal fluid drainage, and avoidance of hemodynamic instability. Reimplantation of intercostal branches has been suggested as an adjunct to these techniques by some investigators with limited data to support its generalized application. More recently, a growing body of evidence supports the concept of a collateral network that can support the perfusion to the spinal cord after interruption of multiple intercostal arteries and the importance of the hypogastric and subclavian arteries as critical branches that perfuse the spinal collateral network.
The retrospective review of the extensive experience at the University of Wisconsin in Madison supports the concept that “physiologic interventions that increase spinal cord tolerance and collateral network perfusion during and after surgery” are more important than the reimplantation of intercostal vessels during this complex procedure, even in patients considered at the highest risk for SCI. Intercostal artery reimplantation failed to achieve significance as an SCI predictor when comparing two large cohorts of patients (540 vs. 265) treated with intercostal ligation vs. reimplantation. Increasingly, available data support the concept of a collateral network that maintains perfusion to the spinal cord after intercostal artery occlusion.
Additional new concepts and techniques including a two-stage approach for extensive thoracoabdominal repair, preliminary occlusion of some segmental arteries, and the use of hybrid and endovascular techniques may further decrease the incidence of SCI by taking advantage of the collateral network and allow some preconditioning of the spinal cord. Fortunately for these challenging patients, significant advances continue to be made to better understand and prevent spinal cord ischemia.
Dr. Luis A. Sanchez is Chief, Section of Vascular Surgery and the Gregorio A. Sicard Distinguished Professor of Surgery and Radiology, Department of Surgery, Washington University in St. Louis.
Spinal cord ischemia is a rare but devastating complication of thoracoabdominal aneurysm repair. Crawford and his colleagues documented in 1993 an incidence of spinal cord ischemia (SCI) as high as 30% for extensive thoracoabdominal repairs. Efforts to diminish the risk of SCI were concentrated in identifying and preserving the direct arterial perfusion to the spinal cord from segmental arteries but continued experimental and clinical experience have suggested that multiple factors contribute to SCI.
|
|
Dr. Luis A. Sanchez |
Some generally accepted principles for minimizing SCI include hypothermia, distal aortic perfusion with atriofemoral bypass or partial cardiopulmonary bypass, cerebrospinal fluid drainage, and avoidance of hemodynamic instability. Reimplantation of intercostal branches has been suggested as an adjunct to these techniques by some investigators with limited data to support its generalized application. More recently, a growing body of evidence supports the concept of a collateral network that can support the perfusion to the spinal cord after interruption of multiple intercostal arteries and the importance of the hypogastric and subclavian arteries as critical branches that perfuse the spinal collateral network.
The retrospective review of the extensive experience at the University of Wisconsin in Madison supports the concept that “physiologic interventions that increase spinal cord tolerance and collateral network perfusion during and after surgery” are more important than the reimplantation of intercostal vessels during this complex procedure, even in patients considered at the highest risk for SCI. Intercostal artery reimplantation failed to achieve significance as an SCI predictor when comparing two large cohorts of patients (540 vs. 265) treated with intercostal ligation vs. reimplantation. Increasingly, available data support the concept of a collateral network that maintains perfusion to the spinal cord after intercostal artery occlusion.
Additional new concepts and techniques including a two-stage approach for extensive thoracoabdominal repair, preliminary occlusion of some segmental arteries, and the use of hybrid and endovascular techniques may further decrease the incidence of SCI by taking advantage of the collateral network and allow some preconditioning of the spinal cord. Fortunately for these challenging patients, significant advances continue to be made to better understand and prevent spinal cord ischemia.
Dr. Luis A. Sanchez is Chief, Section of Vascular Surgery and the Gregorio A. Sicard Distinguished Professor of Surgery and Radiology, Department of Surgery, Washington University in St. Louis.
Spinal cord ischemia is a rare but devastating complication of thoracoabdominal aneurysm repair. Crawford and his colleagues documented in 1993 an incidence of spinal cord ischemia (SCI) as high as 30% for extensive thoracoabdominal repairs. Efforts to diminish the risk of SCI were concentrated in identifying and preserving the direct arterial perfusion to the spinal cord from segmental arteries but continued experimental and clinical experience have suggested that multiple factors contribute to SCI.
|
|
Dr. Luis A. Sanchez |
Some generally accepted principles for minimizing SCI include hypothermia, distal aortic perfusion with atriofemoral bypass or partial cardiopulmonary bypass, cerebrospinal fluid drainage, and avoidance of hemodynamic instability. Reimplantation of intercostal branches has been suggested as an adjunct to these techniques by some investigators with limited data to support its generalized application. More recently, a growing body of evidence supports the concept of a collateral network that can support the perfusion to the spinal cord after interruption of multiple intercostal arteries and the importance of the hypogastric and subclavian arteries as critical branches that perfuse the spinal collateral network.
The retrospective review of the extensive experience at the University of Wisconsin in Madison supports the concept that “physiologic interventions that increase spinal cord tolerance and collateral network perfusion during and after surgery” are more important than the reimplantation of intercostal vessels during this complex procedure, even in patients considered at the highest risk for SCI. Intercostal artery reimplantation failed to achieve significance as an SCI predictor when comparing two large cohorts of patients (540 vs. 265) treated with intercostal ligation vs. reimplantation. Increasingly, available data support the concept of a collateral network that maintains perfusion to the spinal cord after intercostal artery occlusion.
Additional new concepts and techniques including a two-stage approach for extensive thoracoabdominal repair, preliminary occlusion of some segmental arteries, and the use of hybrid and endovascular techniques may further decrease the incidence of SCI by taking advantage of the collateral network and allow some preconditioning of the spinal cord. Fortunately for these challenging patients, significant advances continue to be made to better understand and prevent spinal cord ischemia.
Dr. Luis A. Sanchez is Chief, Section of Vascular Surgery and the Gregorio A. Sicard Distinguished Professor of Surgery and Radiology, Department of Surgery, Washington University in St. Louis.
CHICAGO – Intercostal artery reimplantation fails to significantly reduce spinal cord injury following thoracoabdominal aortic aneurysm surgery, results of a large retrospective study show.
“Although there was a small decrease in spinal cord ischemia with ICAR, reattaching the intercostals did not produce a statistically significant reduction in spinal cord ischemia, even in the highest risk patients,” Dr. Charles W. Acher of the University of Wisconsin–Madison, said at the annual meeting of the Midwestern Vascular Surgical Society.
Intercostal artery reimplantation (ICAR) is one of several strategies that have been used to prevent spinal cord ischemia (SCI), paraplegia, and paraparesis that occurs from the interruption of the blood supply to intercostal arteries (ICAs) during thoracoabdominal aortic aneurysm (TAAA) repair.
Surgeons at UW–Madison adopted the ICAR strategy in 2005and now reimplant open ICAs located at T7-L2 in all Type I, II, and III TAAAs, using a previously published technique (J Surg Res. 2009;154:99-104).
Using a prospectively maintained database, the current analysis sought to compare outcomes between 540 patients who had TAAA surgery during 1989-2004 when open ICAs were ligated and 265 patients who had surgery during 2005-2013 with ICAR.The surgical technique for both groups was cross clamp without assisted circulation. The anesthetic technique was also uniform during the study period and included moderate systemic hypothermia (32° - 33° C); spinal fluid drainage (spinal fluid pressure less than 5 mm Hg); naloxone 1 mcg/kg per hour; use of mannitol, methylprednisolone, and barbiturate burst suppression; goal-directed therapy for a mean arterial pressure of 90-100 mm Hg and cardiac index of 2.5 L per minute/meter2; and proactive component blood therapy to avoid anemia, hypovolemia, and hypertension.
Aneurysm extent, acuity, mortality, renal failure, and pulmonary failure were the same in both groups.
The incidence of SCI was similar in all TAAAs at 5.25% without ICAR and 3.4% with ICAR (P = .23) and in the subset of patients with Type I, II, and III aneurysms (8.8% vs. 5.1%; P = .152), Dr. Acher reported on behalf of lead author and his colleague, Dr. Martha M. Wynn.
Interestingly, ICAR patients had more dissections than did the open ICA ligation patients (18% vs. 15%; P = .0016), more previous aortic surgery (47% vs. 31%; P = .0004), and longer renal ischemia time (61 minutes vs. 53 minutes; P = .0001), but had a shorter length of stay (14 days vs. 22 days; P = .0001) and were younger (mean age, 66 years vs. 70 years; P = .0001).
In a multivariate model of all TAAAs, significant predictors of spinal cord ischemia/injury were type II TAAA (odds ratio, 7.59; P = .0001), dissection (OR, 4.25; P = .0015), age as a continuous variable (P = .0085), and acute TAAA (OR, 2.1; P = .0525), Dr. Acher said. Time period of surgery, and therefore ICAR, was not significant (OR, 0.78; P = .55).
ICAR also failed to achieve significance as an SCI predictor in a subanalysis restricted to the highest-risk patients, defined as those having Type II TAAA, dissection, and acute surgery (OR, 0.67; P = .3387).
“Interrupting blood supply to the spinal cord causes spinal cord ischemia that can be mitigated almost entirely by physiologic interventions that increase spinal cord ischemic tolerance and collateral network perfusion during and after surgery,” Dr. Acher said. “Although the cause of SCI in TAAA surgery is anatomic, prevention of the injury is largely physiologic.”
During a discussion of the study, Dr. Acher surprised the audience by saying the findings have not changed current practice at the university. He cited several reasons, observing that there were more dissections in the ICAR group, and most of the ischemia in the ICAR group was delayed, suggesting that more patients could be rescued. In addition, there was a slight downward trend in spinal cord injury and immediate paraplegia with ICAR, however, these were not statistically significant.
“Because of those things, I still think it’s valuable, particularly in patients that are at highest risk, which are the dissections, with lots of open intercostals, but the emphasis should still be on physiologic parameters,” he said. “If you want to salvage patients, that’s the most important thing.
“Even if ICAR were ever shown to be statistically significant in a larger patient population, any role it has in reducing spinal cord injury would be extremely small,” he added in an interview.
The authors reported having no conflicts of interest.
CHICAGO – Intercostal artery reimplantation fails to significantly reduce spinal cord injury following thoracoabdominal aortic aneurysm surgery, results of a large retrospective study show.
“Although there was a small decrease in spinal cord ischemia with ICAR, reattaching the intercostals did not produce a statistically significant reduction in spinal cord ischemia, even in the highest risk patients,” Dr. Charles W. Acher of the University of Wisconsin–Madison, said at the annual meeting of the Midwestern Vascular Surgical Society.
Intercostal artery reimplantation (ICAR) is one of several strategies that have been used to prevent spinal cord ischemia (SCI), paraplegia, and paraparesis that occurs from the interruption of the blood supply to intercostal arteries (ICAs) during thoracoabdominal aortic aneurysm (TAAA) repair.
Surgeons at UW–Madison adopted the ICAR strategy in 2005and now reimplant open ICAs located at T7-L2 in all Type I, II, and III TAAAs, using a previously published technique (J Surg Res. 2009;154:99-104).
Using a prospectively maintained database, the current analysis sought to compare outcomes between 540 patients who had TAAA surgery during 1989-2004 when open ICAs were ligated and 265 patients who had surgery during 2005-2013 with ICAR.The surgical technique for both groups was cross clamp without assisted circulation. The anesthetic technique was also uniform during the study period and included moderate systemic hypothermia (32° - 33° C); spinal fluid drainage (spinal fluid pressure less than 5 mm Hg); naloxone 1 mcg/kg per hour; use of mannitol, methylprednisolone, and barbiturate burst suppression; goal-directed therapy for a mean arterial pressure of 90-100 mm Hg and cardiac index of 2.5 L per minute/meter2; and proactive component blood therapy to avoid anemia, hypovolemia, and hypertension.
Aneurysm extent, acuity, mortality, renal failure, and pulmonary failure were the same in both groups.
The incidence of SCI was similar in all TAAAs at 5.25% without ICAR and 3.4% with ICAR (P = .23) and in the subset of patients with Type I, II, and III aneurysms (8.8% vs. 5.1%; P = .152), Dr. Acher reported on behalf of lead author and his colleague, Dr. Martha M. Wynn.
Interestingly, ICAR patients had more dissections than did the open ICA ligation patients (18% vs. 15%; P = .0016), more previous aortic surgery (47% vs. 31%; P = .0004), and longer renal ischemia time (61 minutes vs. 53 minutes; P = .0001), but had a shorter length of stay (14 days vs. 22 days; P = .0001) and were younger (mean age, 66 years vs. 70 years; P = .0001).
In a multivariate model of all TAAAs, significant predictors of spinal cord ischemia/injury were type II TAAA (odds ratio, 7.59; P = .0001), dissection (OR, 4.25; P = .0015), age as a continuous variable (P = .0085), and acute TAAA (OR, 2.1; P = .0525), Dr. Acher said. Time period of surgery, and therefore ICAR, was not significant (OR, 0.78; P = .55).
ICAR also failed to achieve significance as an SCI predictor in a subanalysis restricted to the highest-risk patients, defined as those having Type II TAAA, dissection, and acute surgery (OR, 0.67; P = .3387).
“Interrupting blood supply to the spinal cord causes spinal cord ischemia that can be mitigated almost entirely by physiologic interventions that increase spinal cord ischemic tolerance and collateral network perfusion during and after surgery,” Dr. Acher said. “Although the cause of SCI in TAAA surgery is anatomic, prevention of the injury is largely physiologic.”
During a discussion of the study, Dr. Acher surprised the audience by saying the findings have not changed current practice at the university. He cited several reasons, observing that there were more dissections in the ICAR group, and most of the ischemia in the ICAR group was delayed, suggesting that more patients could be rescued. In addition, there was a slight downward trend in spinal cord injury and immediate paraplegia with ICAR, however, these were not statistically significant.
“Because of those things, I still think it’s valuable, particularly in patients that are at highest risk, which are the dissections, with lots of open intercostals, but the emphasis should still be on physiologic parameters,” he said. “If you want to salvage patients, that’s the most important thing.
“Even if ICAR were ever shown to be statistically significant in a larger patient population, any role it has in reducing spinal cord injury would be extremely small,” he added in an interview.
The authors reported having no conflicts of interest.
AT MIDWESTERN VASCULAR 2015
Key clinical point: Intercostal artery reimplantation (ICAR) did not produce a significant reduction in spinal cord ischemia following thoracoabdominal aortic aneurysm repair, even in the highest risk patients.
Major finding: ICAR was not a significant predictor of spinal cord ischemia (OR, 0.78; P = .55).
Data source: Retrospective analysis of 805 patients undergoing TAAA with or without ICAR.
Disclosures: The authors reported having no conflicts of interest.
