User login
The Official Newspaper of the American Association for Thoracic Surgery
Submit Abstracts & Videos for AATS Aortic Symposium 2016
Abstract and video submissions are now open for AATS Aortic Symposium 2016.
May 12-13, 2016
Sheraton New York Times Square Hotel
New York, NY, USA
Course Directors
Joseph S. Coselli
Steven L. Lansman
Co-Directors
Joseph E. Bavaria
Nicholas T. Kouchoukos
G. Chad Hughes
David Spielvogel
Thoralf M. Sundt, III
Lars G. Svensson
Submission of Abstracts & Videos
Specific instructions for abstract/video submission
Submit original work to include BOTH of the following:
- Abstract (maximum of 200 words), accompanied by
- PowerPointpresentation of the material (maximum of 12 slides)
OR
- Abstract (maximum of 200 words), accompanied by
- Video (maximum of five minutes, for the Presentation On Demand (POD) system ONLY and must be narrated in English)
Submission Categories:
- Aortic Root
- Descending/Thoracoabdominal Aorta
- Endoluminal Prostheses
- Natural History/ Follow-up
- Spinal Cord Protection
- Trauma
- Other
Deadline: Monday, December 14, 2015 11:59 pm (EDT)
Abstract and video submissions are now open for AATS Aortic Symposium 2016.
May 12-13, 2016
Sheraton New York Times Square Hotel
New York, NY, USA
Course Directors
Joseph S. Coselli
Steven L. Lansman
Co-Directors
Joseph E. Bavaria
Nicholas T. Kouchoukos
G. Chad Hughes
David Spielvogel
Thoralf M. Sundt, III
Lars G. Svensson
Submission of Abstracts & Videos
Specific instructions for abstract/video submission
Submit original work to include BOTH of the following:
- Abstract (maximum of 200 words), accompanied by
- PowerPointpresentation of the material (maximum of 12 slides)
OR
- Abstract (maximum of 200 words), accompanied by
- Video (maximum of five minutes, for the Presentation On Demand (POD) system ONLY and must be narrated in English)
Submission Categories:
- Aortic Root
- Descending/Thoracoabdominal Aorta
- Endoluminal Prostheses
- Natural History/ Follow-up
- Spinal Cord Protection
- Trauma
- Other
Deadline: Monday, December 14, 2015 11:59 pm (EDT)
Abstract and video submissions are now open for AATS Aortic Symposium 2016.
May 12-13, 2016
Sheraton New York Times Square Hotel
New York, NY, USA
Course Directors
Joseph S. Coselli
Steven L. Lansman
Co-Directors
Joseph E. Bavaria
Nicholas T. Kouchoukos
G. Chad Hughes
David Spielvogel
Thoralf M. Sundt, III
Lars G. Svensson
Submission of Abstracts & Videos
Specific instructions for abstract/video submission
Submit original work to include BOTH of the following:
- Abstract (maximum of 200 words), accompanied by
- PowerPointpresentation of the material (maximum of 12 slides)
OR
- Abstract (maximum of 200 words), accompanied by
- Video (maximum of five minutes, for the Presentation On Demand (POD) system ONLY and must be narrated in English)
Submission Categories:
- Aortic Root
- Descending/Thoracoabdominal Aorta
- Endoluminal Prostheses
- Natural History/ Follow-up
- Spinal Cord Protection
- Trauma
- Other
Deadline: Monday, December 14, 2015 11:59 pm (EDT)

Call for Abstracts & Videos for 96th AATS Annual Meeting
Submissions are now open for abstracts and case videos for the AATS Annual Meeting.
Presentation Types
- Regular Session (Plenary and Simultaneous Sessions)
- Laboratory Research Fora (Cardiac Surgery and General Thoracic Surgery)
- Emerging Technologies and Techniques Forum
- C. Walton Lillehei Resident Forum
- Case Videos
Plenary and Simultaneous Session Abstracts may be submitted for the following categories
- Adult Cardiac
- Congenital
- General Thoracic
- Perioperative Care
Case Videos may be submitted for the following categories
- Adult Cardiac
- Congenital
- General Thoracic
Waiver of mandatory manuscript submission for publication in the Journal of Thoracic and Cardiovascular Surgery may be requested at the time of submission.
Deadline: Monday, October 19, 2014 at 11:59 p.m. EDT
Submissions are now open for abstracts and case videos for the AATS Annual Meeting.
Presentation Types
- Regular Session (Plenary and Simultaneous Sessions)
- Laboratory Research Fora (Cardiac Surgery and General Thoracic Surgery)
- Emerging Technologies and Techniques Forum
- C. Walton Lillehei Resident Forum
- Case Videos
Plenary and Simultaneous Session Abstracts may be submitted for the following categories
- Adult Cardiac
- Congenital
- General Thoracic
- Perioperative Care
Case Videos may be submitted for the following categories
- Adult Cardiac
- Congenital
- General Thoracic
Waiver of mandatory manuscript submission for publication in the Journal of Thoracic and Cardiovascular Surgery may be requested at the time of submission.
Deadline: Monday, October 19, 2014 at 11:59 p.m. EDT
Submissions are now open for abstracts and case videos for the AATS Annual Meeting.
Presentation Types
- Regular Session (Plenary and Simultaneous Sessions)
- Laboratory Research Fora (Cardiac Surgery and General Thoracic Surgery)
- Emerging Technologies and Techniques Forum
- C. Walton Lillehei Resident Forum
- Case Videos
Plenary and Simultaneous Session Abstracts may be submitted for the following categories
- Adult Cardiac
- Congenital
- General Thoracic
- Perioperative Care
Case Videos may be submitted for the following categories
- Adult Cardiac
- Congenital
- General Thoracic
Waiver of mandatory manuscript submission for publication in the Journal of Thoracic and Cardiovascular Surgery may be requested at the time of submission.
Deadline: Monday, October 19, 2014 at 11:59 p.m. EDT
Focus on Thoracic Surgery: Technical Challenges and Complications
October 23-24, 2015
Seaport Hotel & World Trade Center
Boston, MA
Overview
Complications remain one of the major challenges in treating patients. The 2015 Focus on Thoracic Surgery meeting will concentrate on the intraoperative challenges and management of complications facing thoracic surgeons in treating lung and esophageal cancers. This year’s course is particularly aimed at operating surgeons who are active and seek to learn innovative solutions to clinical problems during surgery.
This course will display new advanced diagnosis and prompt management approaches, allowing attendees to understand and readily translate them into daily practice. This two-day conference will have a faculty of experts in the field who are leaders in the application of new technologies in surgical management. It will combine informational sessions, panel discussions and complex case presentations.
Focus on Thoracic Surgery is a must for surgeons who specialize in the treatment of lung and esophageal cancers and want to enhance their skills so they can overcome challenges and complications in their surgical practices.
Session Highlights
- Intraoperative Challenges during Thoracoscopic Lobectomy
- Intraoperative Challenges during Extended Pulmonary Resections
- Managing Complications after Pneumonectomy
- Intraoperative Challenges during Complex Esophageal Surgery
- Intraoperative Challenges during Esophagectomy
- Managing Complications after Esophageal Resection
- Intraoperative Challenges in Airway Surgery
- Complex Case Presentations
Hotel rooms are limited!
Register/Reserve Accommodations
Program Directors
G. Alec Patterson
David J. Sugarbaker
Program Committee Members
Thomas A. D’Amico
Shaf Keshavjee
James D. Luketich
Bryan F. Meyers
Scott J. Swanson
October 23-24, 2015
Seaport Hotel & World Trade Center
Boston, MA
Overview
Complications remain one of the major challenges in treating patients. The 2015 Focus on Thoracic Surgery meeting will concentrate on the intraoperative challenges and management of complications facing thoracic surgeons in treating lung and esophageal cancers. This year’s course is particularly aimed at operating surgeons who are active and seek to learn innovative solutions to clinical problems during surgery.
This course will display new advanced diagnosis and prompt management approaches, allowing attendees to understand and readily translate them into daily practice. This two-day conference will have a faculty of experts in the field who are leaders in the application of new technologies in surgical management. It will combine informational sessions, panel discussions and complex case presentations.
Focus on Thoracic Surgery is a must for surgeons who specialize in the treatment of lung and esophageal cancers and want to enhance their skills so they can overcome challenges and complications in their surgical practices.
Session Highlights
- Intraoperative Challenges during Thoracoscopic Lobectomy
- Intraoperative Challenges during Extended Pulmonary Resections
- Managing Complications after Pneumonectomy
- Intraoperative Challenges during Complex Esophageal Surgery
- Intraoperative Challenges during Esophagectomy
- Managing Complications after Esophageal Resection
- Intraoperative Challenges in Airway Surgery
- Complex Case Presentations
Hotel rooms are limited!
Register/Reserve Accommodations
Program Directors
G. Alec Patterson
David J. Sugarbaker
Program Committee Members
Thomas A. D’Amico
Shaf Keshavjee
James D. Luketich
Bryan F. Meyers
Scott J. Swanson
October 23-24, 2015
Seaport Hotel & World Trade Center
Boston, MA
Overview
Complications remain one of the major challenges in treating patients. The 2015 Focus on Thoracic Surgery meeting will concentrate on the intraoperative challenges and management of complications facing thoracic surgeons in treating lung and esophageal cancers. This year’s course is particularly aimed at operating surgeons who are active and seek to learn innovative solutions to clinical problems during surgery.
This course will display new advanced diagnosis and prompt management approaches, allowing attendees to understand and readily translate them into daily practice. This two-day conference will have a faculty of experts in the field who are leaders in the application of new technologies in surgical management. It will combine informational sessions, panel discussions and complex case presentations.
Focus on Thoracic Surgery is a must for surgeons who specialize in the treatment of lung and esophageal cancers and want to enhance their skills so they can overcome challenges and complications in their surgical practices.
Session Highlights
- Intraoperative Challenges during Thoracoscopic Lobectomy
- Intraoperative Challenges during Extended Pulmonary Resections
- Managing Complications after Pneumonectomy
- Intraoperative Challenges during Complex Esophageal Surgery
- Intraoperative Challenges during Esophagectomy
- Managing Complications after Esophageal Resection
- Intraoperative Challenges in Airway Surgery
- Complex Case Presentations
Hotel rooms are limited!
Register/Reserve Accommodations
Program Directors
G. Alec Patterson
David J. Sugarbaker
Program Committee Members
Thomas A. D’Amico
Shaf Keshavjee
James D. Luketich
Bryan F. Meyers
Scott J. Swanson

Honor Our Mentors: Support the Marc R. de Leval and F. Griffith Pearson Fellowships
In 2013, the AATS Graham Foundation created the Honoring Our Mentors Fellowship Program to recognize prominent cardiothoracic and thoracic surgeons who have demonstrated longstanding leadership and dedication throughout their careers in both their clinical practices and their commitment to training the future generation.
This month, the AATS Graham Foundation is pleased to announce that its two Honoring Our Mentors fellowships will be accepting applications.
Marc R. de Leval Fellowship
About: Currently, there is only limited funding available for North American surgeons to receive specified training at international congenital heart surgery centers. Launching this fall, the de Leval Fellowship will give young North American trainees and early career congenital heart surgeons the opportunity to spend four (4) to six (6) weeks studying congenital CT surgery techniques at UK/European institutions. One fellow will be selected each year to receive a $5,000 award to help cover travel and living costs while abroad.
F. Griffith Pearson Fellowship
About: Created in 2013, the Pearson Fellowship supports surgeons who have finished their residencies to advance their clinical thoracic techniques at a North American host institution. Each fellow receives $3,500 to defray living expenses during four (4) to six (6) weeks of training. The first two awardees were named in 2014.
Invest in future cardiothoracic surgeons by making a contribution to one or both of these fellowships.
Or contact Kaylee Meredith, Project Coordinator, via email or phone: 1-978-927-8330.
In 2013, the AATS Graham Foundation created the Honoring Our Mentors Fellowship Program to recognize prominent cardiothoracic and thoracic surgeons who have demonstrated longstanding leadership and dedication throughout their careers in both their clinical practices and their commitment to training the future generation.
This month, the AATS Graham Foundation is pleased to announce that its two Honoring Our Mentors fellowships will be accepting applications.
Marc R. de Leval Fellowship
About: Currently, there is only limited funding available for North American surgeons to receive specified training at international congenital heart surgery centers. Launching this fall, the de Leval Fellowship will give young North American trainees and early career congenital heart surgeons the opportunity to spend four (4) to six (6) weeks studying congenital CT surgery techniques at UK/European institutions. One fellow will be selected each year to receive a $5,000 award to help cover travel and living costs while abroad.
F. Griffith Pearson Fellowship
About: Created in 2013, the Pearson Fellowship supports surgeons who have finished their residencies to advance their clinical thoracic techniques at a North American host institution. Each fellow receives $3,500 to defray living expenses during four (4) to six (6) weeks of training. The first two awardees were named in 2014.
Invest in future cardiothoracic surgeons by making a contribution to one or both of these fellowships.
Or contact Kaylee Meredith, Project Coordinator, via email or phone: 1-978-927-8330.
In 2013, the AATS Graham Foundation created the Honoring Our Mentors Fellowship Program to recognize prominent cardiothoracic and thoracic surgeons who have demonstrated longstanding leadership and dedication throughout their careers in both their clinical practices and their commitment to training the future generation.
This month, the AATS Graham Foundation is pleased to announce that its two Honoring Our Mentors fellowships will be accepting applications.
Marc R. de Leval Fellowship
About: Currently, there is only limited funding available for North American surgeons to receive specified training at international congenital heart surgery centers. Launching this fall, the de Leval Fellowship will give young North American trainees and early career congenital heart surgeons the opportunity to spend four (4) to six (6) weeks studying congenital CT surgery techniques at UK/European institutions. One fellow will be selected each year to receive a $5,000 award to help cover travel and living costs while abroad.
F. Griffith Pearson Fellowship
About: Created in 2013, the Pearson Fellowship supports surgeons who have finished their residencies to advance their clinical thoracic techniques at a North American host institution. Each fellow receives $3,500 to defray living expenses during four (4) to six (6) weeks of training. The first two awardees were named in 2014.
Invest in future cardiothoracic surgeons by making a contribution to one or both of these fellowships.
Or contact Kaylee Meredith, Project Coordinator, via email or phone: 1-978-927-8330.
Invest in the Future: Support the AATS Graham Foundation
The AATS Graham Foundation is dedicated to providing surgeons with the opportunity to hone and update their knowledge and skills. Every day, CT surgeons change the lives of your patients. And every day, young men and women are choosing CT surgery as a career. Be part of the Foundation’s Annual Pursuit of Excellence Campaign and invest in future generations of cardiothoracic surgeons.
Over the past three years, the Foundation has quadrupled its programming and is determined to continue providing educational and research opportunities for surgeons — benefitting the next generation of physicians and patients, alike.
The Annual Pursuit of Excellence Campaign helps underwrite our many educational and research programs and will allow us to expand them in the future thanks to generous contributions from individuals and industry partners.
We invite you to take a moment to visit the Foundation’s website and make a commitment to our work.
One hundred percent (100%) of your individual contribution will go to support AATS Graham Foundation programs, and you may designate the entirety of your gift to a particular program of interest.
Join us in investing in the future of cardiothoracic surgery. Become a new Foundation donor. If you’re already a supporter, please renew your commitment. Contributions received by December 31st will afford U.S. tax benefits for the 2015 calendar year.
For more information, contact Luiza Pellerin, Development Officer, via email or phone: 1-978-927-8330.
The AATS Graham Foundation is dedicated to providing surgeons with the opportunity to hone and update their knowledge and skills. Every day, CT surgeons change the lives of your patients. And every day, young men and women are choosing CT surgery as a career. Be part of the Foundation’s Annual Pursuit of Excellence Campaign and invest in future generations of cardiothoracic surgeons.
Over the past three years, the Foundation has quadrupled its programming and is determined to continue providing educational and research opportunities for surgeons — benefitting the next generation of physicians and patients, alike.
The Annual Pursuit of Excellence Campaign helps underwrite our many educational and research programs and will allow us to expand them in the future thanks to generous contributions from individuals and industry partners.
We invite you to take a moment to visit the Foundation’s website and make a commitment to our work.
One hundred percent (100%) of your individual contribution will go to support AATS Graham Foundation programs, and you may designate the entirety of your gift to a particular program of interest.
Join us in investing in the future of cardiothoracic surgery. Become a new Foundation donor. If you’re already a supporter, please renew your commitment. Contributions received by December 31st will afford U.S. tax benefits for the 2015 calendar year.
For more information, contact Luiza Pellerin, Development Officer, via email or phone: 1-978-927-8330.
The AATS Graham Foundation is dedicated to providing surgeons with the opportunity to hone and update their knowledge and skills. Every day, CT surgeons change the lives of your patients. And every day, young men and women are choosing CT surgery as a career. Be part of the Foundation’s Annual Pursuit of Excellence Campaign and invest in future generations of cardiothoracic surgeons.
Over the past three years, the Foundation has quadrupled its programming and is determined to continue providing educational and research opportunities for surgeons — benefitting the next generation of physicians and patients, alike.
The Annual Pursuit of Excellence Campaign helps underwrite our many educational and research programs and will allow us to expand them in the future thanks to generous contributions from individuals and industry partners.
We invite you to take a moment to visit the Foundation’s website and make a commitment to our work.
One hundred percent (100%) of your individual contribution will go to support AATS Graham Foundation programs, and you may designate the entirety of your gift to a particular program of interest.
Join us in investing in the future of cardiothoracic surgery. Become a new Foundation donor. If you’re already a supporter, please renew your commitment. Contributions received by December 31st will afford U.S. tax benefits for the 2015 calendar year.
For more information, contact Luiza Pellerin, Development Officer, via email or phone: 1-978-927-8330.
‘Minimalist’ TAVR has short learning curve
As a “minimalist” approach to transcatheter aortic valve replacement – known as MA-TAVR – gains in popularity at high-volume centers, questions persist about the surgeon’s learning curve. A small series of MA-TAVR cases at Emory University in Atlanta has shown that the leaning curve may be like the TAVR approach itself: minimal.
Dr. Hanna Jensen and her associates reported on 151 consecutive patients who had MA-TAVR in the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.078). They previously reported their findings at the annual meeting of the American Association for Thoracic Surgery in April in Seattle.
This study builds on an Emory study last year that reported the minimalist approach to TAVR cost about $10,000 less per patient than the standard transfemoral approach (JACC Cardiovasc Interv. 2014;7:898-904).
The operation the study authors evaluated is performed in the catheterization laboratory rather than the operating room, as in traditional TAVR. Both approaches use a femoral approach, but where traditional TAVR requires general anesthesia and transesophageal echocardiography (TEE), MA-TAVR uses local anesthesia, minimal conscious sedation, and transthoracic echocardiography (TTE).
The study authors acknowledged concerns that TTE may underestimate the severity of paravalvular leak after the procedure when compared with TEE. Their protocol relies on preoperative TTE and CT scans, or three-dimensional TEE if the case warrants it, to ensure optimal sizing of the transcatheter valve before the operation. “If any concerns arise, our threshold is low to perform intraoperative balloon-sizing,” Dr. Jensen and her coauthors said. They also use TTE, along with a root-angiogram after valve deployment, and invasively measure the aortic regurgitation index before and after deployment.
Most study patients were high-risk surgical candidates with a median Society of Thoracic Surgeons Predicted Risk of Mortality (STS PROM) score of 10%. The overall major stroke rate was 3.3%, while major vascular complications occurred in 3% of patients and the greater-than-mild paravalvular leak rate was 7%.
The study retrospectively evaluated 151 consecutive patients who were divided into three groups at different time points: May 2012 to January 2013, February to August 2013, and September 2013 to July 2014. Complications were similar among all three groups, but the third group had shorter hospital stays and less time in the intensive care unit (ICU).
The first group received only the first-generation SAPIEN valve system; use of the second-generation SAPIEN XT valve increased in latter two groups. The SAPIEN XT valve is available in 23, 26, or 29 mm, but the 29-mm size was not available in the first-generation SAPIEN implant.
A subgroup analysis looked at patients who were discharged within 48 hours of the operation or more than 48 hours afterward. The early-discharge patients had lower STS PROM scores (8.3% vs. 10.3%) and lower rates of diabetes (31% vs. 49%). They also had less need for postoperative pacemakers and less frequent rehospitalization. “This implies that in selected MA-TAVR patients early discharge is feasible and safe, but larger studies are required to identify the optimal profile of patients who can be sent home within the first two postoperative days,” Dr. Jensen and her colleagues said.
Early in the MA-TAVR protocol all patients were sent to the ICU. As the care team gained more experience with the procedure, the protocol changed to send all patients to a regular telemetry floor after surgery unless they had vascular issues or potential need for a pacemaker. The decreasing need for ICU “was the only indication of an institutional learning curve that was discovered, and demonstrated improved resource utilization over time,” the investigators said.
They encouraged other centers to pursue MA-TAVR. “As experience grows, we believe that this procedure can be done with less or no ICU support leading to a shorter hospital stay and improved resource utilization,” Dr. Jensen and her coauthors concluded. They called for further studies to determine the characteristics that make a patient most suitable for a short-admission MA-TAVR procedure.
Study coauthors Dr. Vasilis Babaliaros, Dr. Vinod Thourani, Amy Simone, and Patricia Keegan are research consultants with Edwards Lifesciences. The rest of the authors had no disclosures.
Calling this report an “early milestone in the relentless simplification” of transcatheter aortic valve replacement (TAVR), Dr. Craig Smith of Columbia University Medical Center/New York Presbyterian Hospital, wrote in his invited commentary that it nonetheless leaves a few questions unanswered – and may leave surgeons seeing their role in TAVR marginalized as the procedure moves from the operating room to the catheterization lab (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.082). .

|
Dr. Craig Smith |
One unanswered question revolves around the use of conscious sedation and transthoracic echocardiography (TTE) for the minimalist approach (MA), rather than general anesthesia and transesophageal echocardiography (TEE) of the traditional transfemoral approach. “MA requires reliance on [TTE] for assessment of paravalvular leak, and since TTE can’t be compared to TEE in the same patients and still be MA, the merits of this trade-off cannot be assessed in this population,” he said.
Further, he said that the study data do not conclusively link MA to early discharge because the early discharge patients had lower Society of Thoracic Surgery scores.
Another important unanswered question is whether endocarditis is more frequent in TAVR when it’s performed outside the operating room.
“While I suspect the answer will be ‘yes,’ this question will be left dangling until large numbers have been done in hybrid cath labs, because the frequency will be low, and because the forces propelling a ‘cath lab’ alternative to surgical or transcatheter valve replacement done in an operating room will be too powerful to retard on a hunch,” Dr. Smith wrote. “What will the departure of TAVR from operating rooms mean for the role of the surgeon? That is for surgeons to determine. Stay involved, or say goodbye!”
Calling this report an “early milestone in the relentless simplification” of transcatheter aortic valve replacement (TAVR), Dr. Craig Smith of Columbia University Medical Center/New York Presbyterian Hospital, wrote in his invited commentary that it nonetheless leaves a few questions unanswered – and may leave surgeons seeing their role in TAVR marginalized as the procedure moves from the operating room to the catheterization lab (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.082). .
|
|
Dr. Craig Smith |
One unanswered question revolves around the use of conscious sedation and transthoracic echocardiography (TTE) for the minimalist approach (MA), rather than general anesthesia and transesophageal echocardiography (TEE) of the traditional transfemoral approach. “MA requires reliance on [TTE] for assessment of paravalvular leak, and since TTE can’t be compared to TEE in the same patients and still be MA, the merits of this trade-off cannot be assessed in this population,” he said.
Further, he said that the study data do not conclusively link MA to early discharge because the early discharge patients had lower Society of Thoracic Surgery scores.
Another important unanswered question is whether endocarditis is more frequent in TAVR when it’s performed outside the operating room.
“While I suspect the answer will be ‘yes,’ this question will be left dangling until large numbers have been done in hybrid cath labs, because the frequency will be low, and because the forces propelling a ‘cath lab’ alternative to surgical or transcatheter valve replacement done in an operating room will be too powerful to retard on a hunch,” Dr. Smith wrote. “What will the departure of TAVR from operating rooms mean for the role of the surgeon? That is for surgeons to determine. Stay involved, or say goodbye!”
Calling this report an “early milestone in the relentless simplification” of transcatheter aortic valve replacement (TAVR), Dr. Craig Smith of Columbia University Medical Center/New York Presbyterian Hospital, wrote in his invited commentary that it nonetheless leaves a few questions unanswered – and may leave surgeons seeing their role in TAVR marginalized as the procedure moves from the operating room to the catheterization lab (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.082). .
|
|
Dr. Craig Smith |
One unanswered question revolves around the use of conscious sedation and transthoracic echocardiography (TTE) for the minimalist approach (MA), rather than general anesthesia and transesophageal echocardiography (TEE) of the traditional transfemoral approach. “MA requires reliance on [TTE] for assessment of paravalvular leak, and since TTE can’t be compared to TEE in the same patients and still be MA, the merits of this trade-off cannot be assessed in this population,” he said.
Further, he said that the study data do not conclusively link MA to early discharge because the early discharge patients had lower Society of Thoracic Surgery scores.
Another important unanswered question is whether endocarditis is more frequent in TAVR when it’s performed outside the operating room.
“While I suspect the answer will be ‘yes,’ this question will be left dangling until large numbers have been done in hybrid cath labs, because the frequency will be low, and because the forces propelling a ‘cath lab’ alternative to surgical or transcatheter valve replacement done in an operating room will be too powerful to retard on a hunch,” Dr. Smith wrote. “What will the departure of TAVR from operating rooms mean for the role of the surgeon? That is for surgeons to determine. Stay involved, or say goodbye!”
As a “minimalist” approach to transcatheter aortic valve replacement – known as MA-TAVR – gains in popularity at high-volume centers, questions persist about the surgeon’s learning curve. A small series of MA-TAVR cases at Emory University in Atlanta has shown that the leaning curve may be like the TAVR approach itself: minimal.
Dr. Hanna Jensen and her associates reported on 151 consecutive patients who had MA-TAVR in the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.078). They previously reported their findings at the annual meeting of the American Association for Thoracic Surgery in April in Seattle.
This study builds on an Emory study last year that reported the minimalist approach to TAVR cost about $10,000 less per patient than the standard transfemoral approach (JACC Cardiovasc Interv. 2014;7:898-904).
The operation the study authors evaluated is performed in the catheterization laboratory rather than the operating room, as in traditional TAVR. Both approaches use a femoral approach, but where traditional TAVR requires general anesthesia and transesophageal echocardiography (TEE), MA-TAVR uses local anesthesia, minimal conscious sedation, and transthoracic echocardiography (TTE).
The study authors acknowledged concerns that TTE may underestimate the severity of paravalvular leak after the procedure when compared with TEE. Their protocol relies on preoperative TTE and CT scans, or three-dimensional TEE if the case warrants it, to ensure optimal sizing of the transcatheter valve before the operation. “If any concerns arise, our threshold is low to perform intraoperative balloon-sizing,” Dr. Jensen and her coauthors said. They also use TTE, along with a root-angiogram after valve deployment, and invasively measure the aortic regurgitation index before and after deployment.
Most study patients were high-risk surgical candidates with a median Society of Thoracic Surgeons Predicted Risk of Mortality (STS PROM) score of 10%. The overall major stroke rate was 3.3%, while major vascular complications occurred in 3% of patients and the greater-than-mild paravalvular leak rate was 7%.
The study retrospectively evaluated 151 consecutive patients who were divided into three groups at different time points: May 2012 to January 2013, February to August 2013, and September 2013 to July 2014. Complications were similar among all three groups, but the third group had shorter hospital stays and less time in the intensive care unit (ICU).
The first group received only the first-generation SAPIEN valve system; use of the second-generation SAPIEN XT valve increased in latter two groups. The SAPIEN XT valve is available in 23, 26, or 29 mm, but the 29-mm size was not available in the first-generation SAPIEN implant.
A subgroup analysis looked at patients who were discharged within 48 hours of the operation or more than 48 hours afterward. The early-discharge patients had lower STS PROM scores (8.3% vs. 10.3%) and lower rates of diabetes (31% vs. 49%). They also had less need for postoperative pacemakers and less frequent rehospitalization. “This implies that in selected MA-TAVR patients early discharge is feasible and safe, but larger studies are required to identify the optimal profile of patients who can be sent home within the first two postoperative days,” Dr. Jensen and her colleagues said.
Early in the MA-TAVR protocol all patients were sent to the ICU. As the care team gained more experience with the procedure, the protocol changed to send all patients to a regular telemetry floor after surgery unless they had vascular issues or potential need for a pacemaker. The decreasing need for ICU “was the only indication of an institutional learning curve that was discovered, and demonstrated improved resource utilization over time,” the investigators said.
They encouraged other centers to pursue MA-TAVR. “As experience grows, we believe that this procedure can be done with less or no ICU support leading to a shorter hospital stay and improved resource utilization,” Dr. Jensen and her coauthors concluded. They called for further studies to determine the characteristics that make a patient most suitable for a short-admission MA-TAVR procedure.
Study coauthors Dr. Vasilis Babaliaros, Dr. Vinod Thourani, Amy Simone, and Patricia Keegan are research consultants with Edwards Lifesciences. The rest of the authors had no disclosures.
As a “minimalist” approach to transcatheter aortic valve replacement – known as MA-TAVR – gains in popularity at high-volume centers, questions persist about the surgeon’s learning curve. A small series of MA-TAVR cases at Emory University in Atlanta has shown that the leaning curve may be like the TAVR approach itself: minimal.
Dr. Hanna Jensen and her associates reported on 151 consecutive patients who had MA-TAVR in the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015. doi: 10.1016/j.jtcvs.2015.07.078). They previously reported their findings at the annual meeting of the American Association for Thoracic Surgery in April in Seattle.
This study builds on an Emory study last year that reported the minimalist approach to TAVR cost about $10,000 less per patient than the standard transfemoral approach (JACC Cardiovasc Interv. 2014;7:898-904).
The operation the study authors evaluated is performed in the catheterization laboratory rather than the operating room, as in traditional TAVR. Both approaches use a femoral approach, but where traditional TAVR requires general anesthesia and transesophageal echocardiography (TEE), MA-TAVR uses local anesthesia, minimal conscious sedation, and transthoracic echocardiography (TTE).
The study authors acknowledged concerns that TTE may underestimate the severity of paravalvular leak after the procedure when compared with TEE. Their protocol relies on preoperative TTE and CT scans, or three-dimensional TEE if the case warrants it, to ensure optimal sizing of the transcatheter valve before the operation. “If any concerns arise, our threshold is low to perform intraoperative balloon-sizing,” Dr. Jensen and her coauthors said. They also use TTE, along with a root-angiogram after valve deployment, and invasively measure the aortic regurgitation index before and after deployment.
Most study patients were high-risk surgical candidates with a median Society of Thoracic Surgeons Predicted Risk of Mortality (STS PROM) score of 10%. The overall major stroke rate was 3.3%, while major vascular complications occurred in 3% of patients and the greater-than-mild paravalvular leak rate was 7%.
The study retrospectively evaluated 151 consecutive patients who were divided into three groups at different time points: May 2012 to January 2013, February to August 2013, and September 2013 to July 2014. Complications were similar among all three groups, but the third group had shorter hospital stays and less time in the intensive care unit (ICU).
The first group received only the first-generation SAPIEN valve system; use of the second-generation SAPIEN XT valve increased in latter two groups. The SAPIEN XT valve is available in 23, 26, or 29 mm, but the 29-mm size was not available in the first-generation SAPIEN implant.
A subgroup analysis looked at patients who were discharged within 48 hours of the operation or more than 48 hours afterward. The early-discharge patients had lower STS PROM scores (8.3% vs. 10.3%) and lower rates of diabetes (31% vs. 49%). They also had less need for postoperative pacemakers and less frequent rehospitalization. “This implies that in selected MA-TAVR patients early discharge is feasible and safe, but larger studies are required to identify the optimal profile of patients who can be sent home within the first two postoperative days,” Dr. Jensen and her colleagues said.
Early in the MA-TAVR protocol all patients were sent to the ICU. As the care team gained more experience with the procedure, the protocol changed to send all patients to a regular telemetry floor after surgery unless they had vascular issues or potential need for a pacemaker. The decreasing need for ICU “was the only indication of an institutional learning curve that was discovered, and demonstrated improved resource utilization over time,” the investigators said.
They encouraged other centers to pursue MA-TAVR. “As experience grows, we believe that this procedure can be done with less or no ICU support leading to a shorter hospital stay and improved resource utilization,” Dr. Jensen and her coauthors concluded. They called for further studies to determine the characteristics that make a patient most suitable for a short-admission MA-TAVR procedure.
Study coauthors Dr. Vasilis Babaliaros, Dr. Vinod Thourani, Amy Simone, and Patricia Keegan are research consultants with Edwards Lifesciences. The rest of the authors had no disclosures.
FROM THE JOURNAL OF THORACIC AND CARDIOVASCULAR SURGERY
Key clinical point: A minimalist approach to transcatheter aortic valve replacement (MA-TAVR) is feasible with acceptable outcomes.
Major finding: Transition to MA-TAVR in a high-volume center had a relatively small learning curve.
Data source: A review of 151 consecutive patients who had MA-TAVR at Emory University between May 2012 and July 2014.
Disclosures: Study coauthors Dr. Vasilis Babaliaros, Dr. Vinod Thourani, Amy Simone, and Patricia Keegan are research consultants with Edwards Lifesciences. The rest of the authors had no disclosures.
HFSA: In heart failure, beta-blocker dosage trumps heart rate
NATIONAL HARBOR, MD. – In beta-blocker treatment of heart failure, dose matters; heart rate, not so much.
When using beta-blockers to treat patients with heart failure and reduced ejection fraction, administering a high, evidence-backed dosage of the drug had much more beneficial impact than did getting patients to a low heart rate, according to a post hoc analysis of data from more than 2,000 patients.
The finding provides new evidence supporting “titrating the beta-blocker to evidence-based, high dosages of a beta-blocker and not holding back,” Mona Fiuzat, Ph.D., said in an interview at the annual scientific meeting of the Heart Failure Society of America. “It’s not just lowering the heart rate; there is something else, other mechanisms [of beta-blocker effects] that may be of greater benefit” to patients beyond heart-rate reduction when patients they receive the full dosage of beta-blocker treatment that had been shown effective in the randomized trials run about 2 decades ago.
“The point of our report is that if you have [heart failure with reduced ejection fraction] patients on a beta-blocker, they will be better off by increasing the dose” to the target level rather than by adding an additional, non–beta-blocker drug, such as ivabradine (Corlanor), to further reduce heart rate, said Dr. Fiuzat, a clinical pharmacologist and heart-failure researcher at Duke University in Durham, N.C. In the trial that enrolled the 2,320 patients included in the current analysis, half the patients were not on their target beta-blocker dosage.
Some clinicians are too heart-rate focused, she said. “Our results show that there is added benefit from using the full beta-blocker dosage even when the patient’s heart rate is already low.”
The analysis run by Dr. Fiuzat and her associates used data collected in HF-ACTION (Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training), a randomized, controlled study that assessed the impact of exercise training on patients with heart failure with reduced ejection fraction (JAMA 2009 Apr 8;301[14]:1439-50). All patients received usual care (and the intervention group also received exercise training), which meant they were on whichever beta-blocker and dosage their individual physician prescribed.
The current analysis converted these baseline dosages into carvedilol (Coreg) equivalents and identified the dosage levels as either low, defined as a daily carvedilol equivalent of less than 25 mg/day, or high, a daily equivalent of at least 25 mg/day. The analysis also categorized heart rate at baseline into a high rate defined as at least 70 beats/min, and a low rate of less than 70 beats/min. At entry, 71% of patients were on a high beta-blocker dosage (although in many cases not their full, ideal dosage), and 52% of patients had a high heart rate.
The new analysis showed that after a median follow-up of 2.5 years, the rate of all-cause death and all-cause hospitalization was significantly higher among patients who entered the study on a low beta-blocker dosage and with a high heart rate compared with patients in the other three groups: low dosage/low heart rate, high dosage/high heart rate, and high dosage/low heart rate. In addition, the results showed that a high beta-blocker dosage at baseline mitigated the impact of a high heart rate; patients in this subgroup had outcomes comparable to those of patients on a high beta-blocker dosage with a low heart rate.
In an analysis that adjusted for baseline differences in several clinical and demographic variables, patients on a high beta-blocker dosage had a statistically significant 13% reduced rate of all-cause death or all-cause hospitalization compared with patients on a low-dosage beta-blocker. In contrast, baseline heart rate had no statistically significant impact on outcomes, Dr. Fiuzat and her associates reported in an article published online concurrently with the presentation of the results at the meeting by one of Dr. Fiuzat’s colleagues (JACC: Heart Failure 2015. doi: 10.1016/j.jchf.2015.09.002]).
On Twitter @mitchelzoler
NATIONAL HARBOR, MD. – In beta-blocker treatment of heart failure, dose matters; heart rate, not so much.
When using beta-blockers to treat patients with heart failure and reduced ejection fraction, administering a high, evidence-backed dosage of the drug had much more beneficial impact than did getting patients to a low heart rate, according to a post hoc analysis of data from more than 2,000 patients.
The finding provides new evidence supporting “titrating the beta-blocker to evidence-based, high dosages of a beta-blocker and not holding back,” Mona Fiuzat, Ph.D., said in an interview at the annual scientific meeting of the Heart Failure Society of America. “It’s not just lowering the heart rate; there is something else, other mechanisms [of beta-blocker effects] that may be of greater benefit” to patients beyond heart-rate reduction when patients they receive the full dosage of beta-blocker treatment that had been shown effective in the randomized trials run about 2 decades ago.
“The point of our report is that if you have [heart failure with reduced ejection fraction] patients on a beta-blocker, they will be better off by increasing the dose” to the target level rather than by adding an additional, non–beta-blocker drug, such as ivabradine (Corlanor), to further reduce heart rate, said Dr. Fiuzat, a clinical pharmacologist and heart-failure researcher at Duke University in Durham, N.C. In the trial that enrolled the 2,320 patients included in the current analysis, half the patients were not on their target beta-blocker dosage.
Some clinicians are too heart-rate focused, she said. “Our results show that there is added benefit from using the full beta-blocker dosage even when the patient’s heart rate is already low.”
The analysis run by Dr. Fiuzat and her associates used data collected in HF-ACTION (Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training), a randomized, controlled study that assessed the impact of exercise training on patients with heart failure with reduced ejection fraction (JAMA 2009 Apr 8;301[14]:1439-50). All patients received usual care (and the intervention group also received exercise training), which meant they were on whichever beta-blocker and dosage their individual physician prescribed.
The current analysis converted these baseline dosages into carvedilol (Coreg) equivalents and identified the dosage levels as either low, defined as a daily carvedilol equivalent of less than 25 mg/day, or high, a daily equivalent of at least 25 mg/day. The analysis also categorized heart rate at baseline into a high rate defined as at least 70 beats/min, and a low rate of less than 70 beats/min. At entry, 71% of patients were on a high beta-blocker dosage (although in many cases not their full, ideal dosage), and 52% of patients had a high heart rate.
The new analysis showed that after a median follow-up of 2.5 years, the rate of all-cause death and all-cause hospitalization was significantly higher among patients who entered the study on a low beta-blocker dosage and with a high heart rate compared with patients in the other three groups: low dosage/low heart rate, high dosage/high heart rate, and high dosage/low heart rate. In addition, the results showed that a high beta-blocker dosage at baseline mitigated the impact of a high heart rate; patients in this subgroup had outcomes comparable to those of patients on a high beta-blocker dosage with a low heart rate.
In an analysis that adjusted for baseline differences in several clinical and demographic variables, patients on a high beta-blocker dosage had a statistically significant 13% reduced rate of all-cause death or all-cause hospitalization compared with patients on a low-dosage beta-blocker. In contrast, baseline heart rate had no statistically significant impact on outcomes, Dr. Fiuzat and her associates reported in an article published online concurrently with the presentation of the results at the meeting by one of Dr. Fiuzat’s colleagues (JACC: Heart Failure 2015. doi: 10.1016/j.jchf.2015.09.002]).
On Twitter @mitchelzoler
NATIONAL HARBOR, MD. – In beta-blocker treatment of heart failure, dose matters; heart rate, not so much.
When using beta-blockers to treat patients with heart failure and reduced ejection fraction, administering a high, evidence-backed dosage of the drug had much more beneficial impact than did getting patients to a low heart rate, according to a post hoc analysis of data from more than 2,000 patients.
The finding provides new evidence supporting “titrating the beta-blocker to evidence-based, high dosages of a beta-blocker and not holding back,” Mona Fiuzat, Ph.D., said in an interview at the annual scientific meeting of the Heart Failure Society of America. “It’s not just lowering the heart rate; there is something else, other mechanisms [of beta-blocker effects] that may be of greater benefit” to patients beyond heart-rate reduction when patients they receive the full dosage of beta-blocker treatment that had been shown effective in the randomized trials run about 2 decades ago.
“The point of our report is that if you have [heart failure with reduced ejection fraction] patients on a beta-blocker, they will be better off by increasing the dose” to the target level rather than by adding an additional, non–beta-blocker drug, such as ivabradine (Corlanor), to further reduce heart rate, said Dr. Fiuzat, a clinical pharmacologist and heart-failure researcher at Duke University in Durham, N.C. In the trial that enrolled the 2,320 patients included in the current analysis, half the patients were not on their target beta-blocker dosage.
Some clinicians are too heart-rate focused, she said. “Our results show that there is added benefit from using the full beta-blocker dosage even when the patient’s heart rate is already low.”
The analysis run by Dr. Fiuzat and her associates used data collected in HF-ACTION (Heart Failure: A Controlled Trial Investigating Outcomes of Exercise Training), a randomized, controlled study that assessed the impact of exercise training on patients with heart failure with reduced ejection fraction (JAMA 2009 Apr 8;301[14]:1439-50). All patients received usual care (and the intervention group also received exercise training), which meant they were on whichever beta-blocker and dosage their individual physician prescribed.
The current analysis converted these baseline dosages into carvedilol (Coreg) equivalents and identified the dosage levels as either low, defined as a daily carvedilol equivalent of less than 25 mg/day, or high, a daily equivalent of at least 25 mg/day. The analysis also categorized heart rate at baseline into a high rate defined as at least 70 beats/min, and a low rate of less than 70 beats/min. At entry, 71% of patients were on a high beta-blocker dosage (although in many cases not their full, ideal dosage), and 52% of patients had a high heart rate.
The new analysis showed that after a median follow-up of 2.5 years, the rate of all-cause death and all-cause hospitalization was significantly higher among patients who entered the study on a low beta-blocker dosage and with a high heart rate compared with patients in the other three groups: low dosage/low heart rate, high dosage/high heart rate, and high dosage/low heart rate. In addition, the results showed that a high beta-blocker dosage at baseline mitigated the impact of a high heart rate; patients in this subgroup had outcomes comparable to those of patients on a high beta-blocker dosage with a low heart rate.
In an analysis that adjusted for baseline differences in several clinical and demographic variables, patients on a high beta-blocker dosage had a statistically significant 13% reduced rate of all-cause death or all-cause hospitalization compared with patients on a low-dosage beta-blocker. In contrast, baseline heart rate had no statistically significant impact on outcomes, Dr. Fiuzat and her associates reported in an article published online concurrently with the presentation of the results at the meeting by one of Dr. Fiuzat’s colleagues (JACC: Heart Failure 2015. doi: 10.1016/j.jchf.2015.09.002]).
On Twitter @mitchelzoler
AT THE HFSA ANNUAL SCIENTIFIC MEETING
Key clinical point: High-dose beta-blockers produced significantly better outcomes than did low-dose beta-blockers, while heart rate had no significant impact.
Major finding: Patients on high beta-blocker dosage had a significant 13% reduced rate of bad outcomes compared with low-dosage patients.
Data source: A post hoc analysis of data from the HF-ACTION trial, which enrolled 2,331 patients with heart failure and reduced ejection fraction.
Disclosures: Dr. Fiuzat had no disclosures.
HFSA: Next-generation LVAD meets survival goal
NATIONAL HARBOR, MD. – A next-generation left-ventricular assist device, the HeartMate 3, gave a solid debut performance in an uncontrolled series of the first 50 recipients, which was designed to gain the device CE mark approval in Europe.
In this study, run at 10 sites in Australia, Austria, Canada, Czech Republic, Germany, and Kazakhstan, the new-design left ventricular assist device (LVAD) numerically surpassed the study’s prespecified primary endpoint with 6-month recipient survival of 92%. This bested the target survival rate of 88% that the trial’s designers derived from the survival rate among 50 matched patients who had received a LVAD during 2012-2014 and had entered the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), Dr. Ivan Netuka said at the annual meeting of the Heart Failure Society of America.

Other notable findings of the HeartMate 3’s performance in the first 50 patients followed for 6 months were no pump malfunctions, no thrombosis within the pump, and no evidence of hemolysis, said Dr. Netuka, deputy director of cardiovascular surgery at IKEM hospital in Prague.
HeartMate 3 features several improvements over the HeartMate II model, such as a fully magnetically levitated rotor designed to eliminate friction and wear within the pump. The device also is engineered to produce an artificial pulse of 30 beats per minute, and it can deliver a wide blood-flow range of 2-10 L/min. Larger and consistent pump gaps are designed to reduced shear stress on blood components.
The study enrolled patients during June-November 2014 with NYHA class IIIB or IV heart failure and stage D heart failure, with a left ventricular ejection fraction of 25% or less. The 50 patients averaged 59 years of age and 90% were men; they were divided about equally between patients who received the device as a bridge to transplant and those who received the LVAD as destination therapy.
During 6 months of follow-up, two patients received a heart transplant. Twenty-one (42%) of the enrolled patients classified as INTERMACS patient profile 3, 20 (40%) as profile 4, and 5 (10%) as profile 2 patients, with the remaining four patients falling into other profile levels. Twenty-one patients had concomitant heart surgery when they received their LVAD, usually valve replacement. All patients received warfarin treatment and aspirin following device placement. Dr. Netuka and his associates calculated an expected 6-month survival of 78% for the enrolled patients without LVAD intervention.
The four deaths included a patient who died from cardiac arrest following a stroke on day 19 – a complication judged attributable to the device-placement procedure, a patient with circulatory failure on day 48, a suicide on day 113, and a patient with multiorgan failure on day 144.
After 6 months of follow-up, notable adverse events included bleeding in 19 patients (38%) – including gastrointestinal bleeds in 4 patients (8%) – strokes in 6 patients (12%), and infections in 18 patients (36%). Most of the adverse events occurred in the first 7 days following LVAD placement. Three of the six strokes were judged procedure associated, Dr. Netuka said.
Following device placement, patients showed improvements in their NYHA class and quality of life; their 6-minute walk distance improved by an average of 231 m.
The HeartMate 3 device is currently undergoing U.S. assessment in comparison to HeartMate II prior to submission to the Food and Drug Administration. The randomized trial, known as MOMENTUM 3, plans to enroll 1,028 patients with completion scheduled for 2018.
The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.
On Twitter @mitchelzoler
It is extremely exciting to see this next-generation left ventricular assist device move forward, but it is important not to overinterpret the findings because the number of patients treated was relatively small and, as a result, the findings are limited by very wide confidence limits.

|
| Mitchel L. Zoler/Frontline Medical News Dr. Marvin A. Konstam |
The HeartMate 3 device probably represents an important advance beyond currently available technology. Its attractive features include full magnetic levitation of the rotor, production of an artificial pulse, and the ability to deliver a wide range of blood-flow rates. These features may improve performance and could have favorable effects on thrombus and stroke rates.
The device clearly achieved its primary performance goal of 88% 6-month survival. The INTERMACS profiles of the enrolled patients included 40% of patients with profile 4 and 10% with profile 2. This does not exactly mimic the typical U.S. population receiving these devices, which recently had 15% of patients with a level 4 profile and 36% of patients with more severe disease at level 2. I applaud the decision to include patients who received their devices as destination therapy as well as patients who received it as a bridge to transplant.
The technologic advances that this new device represents are a step in the right direction, and the results provide a green light for further assessment. I look forward to seeing results from the U.S. randomized trial.
Dr. Marvin A. Konstam is professor and chief physician executive of the CardioVascular Center at Tufts Medical Center in Boston. He made these comments as designated discussant for Dr. Netuka’s report. Dr. Konstam has been a consultant to Merck, Novartis, Amgen, Johnson & Johnson, Arbor, Mast, and Cardioxyl.
It is extremely exciting to see this next-generation left ventricular assist device move forward, but it is important not to overinterpret the findings because the number of patients treated was relatively small and, as a result, the findings are limited by very wide confidence limits.
|
|
| Mitchel L. Zoler/Frontline Medical News Dr. Marvin A. Konstam |
The HeartMate 3 device probably represents an important advance beyond currently available technology. Its attractive features include full magnetic levitation of the rotor, production of an artificial pulse, and the ability to deliver a wide range of blood-flow rates. These features may improve performance and could have favorable effects on thrombus and stroke rates.
The device clearly achieved its primary performance goal of 88% 6-month survival. The INTERMACS profiles of the enrolled patients included 40% of patients with profile 4 and 10% with profile 2. This does not exactly mimic the typical U.S. population receiving these devices, which recently had 15% of patients with a level 4 profile and 36% of patients with more severe disease at level 2. I applaud the decision to include patients who received their devices as destination therapy as well as patients who received it as a bridge to transplant.
The technologic advances that this new device represents are a step in the right direction, and the results provide a green light for further assessment. I look forward to seeing results from the U.S. randomized trial.
Dr. Marvin A. Konstam is professor and chief physician executive of the CardioVascular Center at Tufts Medical Center in Boston. He made these comments as designated discussant for Dr. Netuka’s report. Dr. Konstam has been a consultant to Merck, Novartis, Amgen, Johnson & Johnson, Arbor, Mast, and Cardioxyl.
It is extremely exciting to see this next-generation left ventricular assist device move forward, but it is important not to overinterpret the findings because the number of patients treated was relatively small and, as a result, the findings are limited by very wide confidence limits.
|
|
| Mitchel L. Zoler/Frontline Medical News Dr. Marvin A. Konstam |
The HeartMate 3 device probably represents an important advance beyond currently available technology. Its attractive features include full magnetic levitation of the rotor, production of an artificial pulse, and the ability to deliver a wide range of blood-flow rates. These features may improve performance and could have favorable effects on thrombus and stroke rates.
The device clearly achieved its primary performance goal of 88% 6-month survival. The INTERMACS profiles of the enrolled patients included 40% of patients with profile 4 and 10% with profile 2. This does not exactly mimic the typical U.S. population receiving these devices, which recently had 15% of patients with a level 4 profile and 36% of patients with more severe disease at level 2. I applaud the decision to include patients who received their devices as destination therapy as well as patients who received it as a bridge to transplant.
The technologic advances that this new device represents are a step in the right direction, and the results provide a green light for further assessment. I look forward to seeing results from the U.S. randomized trial.
Dr. Marvin A. Konstam is professor and chief physician executive of the CardioVascular Center at Tufts Medical Center in Boston. He made these comments as designated discussant for Dr. Netuka’s report. Dr. Konstam has been a consultant to Merck, Novartis, Amgen, Johnson & Johnson, Arbor, Mast, and Cardioxyl.
NATIONAL HARBOR, MD. – A next-generation left-ventricular assist device, the HeartMate 3, gave a solid debut performance in an uncontrolled series of the first 50 recipients, which was designed to gain the device CE mark approval in Europe.
In this study, run at 10 sites in Australia, Austria, Canada, Czech Republic, Germany, and Kazakhstan, the new-design left ventricular assist device (LVAD) numerically surpassed the study’s prespecified primary endpoint with 6-month recipient survival of 92%. This bested the target survival rate of 88% that the trial’s designers derived from the survival rate among 50 matched patients who had received a LVAD during 2012-2014 and had entered the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), Dr. Ivan Netuka said at the annual meeting of the Heart Failure Society of America.
Other notable findings of the HeartMate 3’s performance in the first 50 patients followed for 6 months were no pump malfunctions, no thrombosis within the pump, and no evidence of hemolysis, said Dr. Netuka, deputy director of cardiovascular surgery at IKEM hospital in Prague.
HeartMate 3 features several improvements over the HeartMate II model, such as a fully magnetically levitated rotor designed to eliminate friction and wear within the pump. The device also is engineered to produce an artificial pulse of 30 beats per minute, and it can deliver a wide blood-flow range of 2-10 L/min. Larger and consistent pump gaps are designed to reduced shear stress on blood components.
The study enrolled patients during June-November 2014 with NYHA class IIIB or IV heart failure and stage D heart failure, with a left ventricular ejection fraction of 25% or less. The 50 patients averaged 59 years of age and 90% were men; they were divided about equally between patients who received the device as a bridge to transplant and those who received the LVAD as destination therapy.
During 6 months of follow-up, two patients received a heart transplant. Twenty-one (42%) of the enrolled patients classified as INTERMACS patient profile 3, 20 (40%) as profile 4, and 5 (10%) as profile 2 patients, with the remaining four patients falling into other profile levels. Twenty-one patients had concomitant heart surgery when they received their LVAD, usually valve replacement. All patients received warfarin treatment and aspirin following device placement. Dr. Netuka and his associates calculated an expected 6-month survival of 78% for the enrolled patients without LVAD intervention.
The four deaths included a patient who died from cardiac arrest following a stroke on day 19 – a complication judged attributable to the device-placement procedure, a patient with circulatory failure on day 48, a suicide on day 113, and a patient with multiorgan failure on day 144.
After 6 months of follow-up, notable adverse events included bleeding in 19 patients (38%) – including gastrointestinal bleeds in 4 patients (8%) – strokes in 6 patients (12%), and infections in 18 patients (36%). Most of the adverse events occurred in the first 7 days following LVAD placement. Three of the six strokes were judged procedure associated, Dr. Netuka said.
Following device placement, patients showed improvements in their NYHA class and quality of life; their 6-minute walk distance improved by an average of 231 m.
The HeartMate 3 device is currently undergoing U.S. assessment in comparison to HeartMate II prior to submission to the Food and Drug Administration. The randomized trial, known as MOMENTUM 3, plans to enroll 1,028 patients with completion scheduled for 2018.
The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.
On Twitter @mitchelzoler
NATIONAL HARBOR, MD. – A next-generation left-ventricular assist device, the HeartMate 3, gave a solid debut performance in an uncontrolled series of the first 50 recipients, which was designed to gain the device CE mark approval in Europe.
In this study, run at 10 sites in Australia, Austria, Canada, Czech Republic, Germany, and Kazakhstan, the new-design left ventricular assist device (LVAD) numerically surpassed the study’s prespecified primary endpoint with 6-month recipient survival of 92%. This bested the target survival rate of 88% that the trial’s designers derived from the survival rate among 50 matched patients who had received a LVAD during 2012-2014 and had entered the Interagency Registry for Mechanically Assisted Circulatory Support (INTERMACS), Dr. Ivan Netuka said at the annual meeting of the Heart Failure Society of America.
Other notable findings of the HeartMate 3’s performance in the first 50 patients followed for 6 months were no pump malfunctions, no thrombosis within the pump, and no evidence of hemolysis, said Dr. Netuka, deputy director of cardiovascular surgery at IKEM hospital in Prague.
HeartMate 3 features several improvements over the HeartMate II model, such as a fully magnetically levitated rotor designed to eliminate friction and wear within the pump. The device also is engineered to produce an artificial pulse of 30 beats per minute, and it can deliver a wide blood-flow range of 2-10 L/min. Larger and consistent pump gaps are designed to reduced shear stress on blood components.
The study enrolled patients during June-November 2014 with NYHA class IIIB or IV heart failure and stage D heart failure, with a left ventricular ejection fraction of 25% or less. The 50 patients averaged 59 years of age and 90% were men; they were divided about equally between patients who received the device as a bridge to transplant and those who received the LVAD as destination therapy.
During 6 months of follow-up, two patients received a heart transplant. Twenty-one (42%) of the enrolled patients classified as INTERMACS patient profile 3, 20 (40%) as profile 4, and 5 (10%) as profile 2 patients, with the remaining four patients falling into other profile levels. Twenty-one patients had concomitant heart surgery when they received their LVAD, usually valve replacement. All patients received warfarin treatment and aspirin following device placement. Dr. Netuka and his associates calculated an expected 6-month survival of 78% for the enrolled patients without LVAD intervention.
The four deaths included a patient who died from cardiac arrest following a stroke on day 19 – a complication judged attributable to the device-placement procedure, a patient with circulatory failure on day 48, a suicide on day 113, and a patient with multiorgan failure on day 144.
After 6 months of follow-up, notable adverse events included bleeding in 19 patients (38%) – including gastrointestinal bleeds in 4 patients (8%) – strokes in 6 patients (12%), and infections in 18 patients (36%). Most of the adverse events occurred in the first 7 days following LVAD placement. Three of the six strokes were judged procedure associated, Dr. Netuka said.
Following device placement, patients showed improvements in their NYHA class and quality of life; their 6-minute walk distance improved by an average of 231 m.
The HeartMate 3 device is currently undergoing U.S. assessment in comparison to HeartMate II prior to submission to the Food and Drug Administration. The randomized trial, known as MOMENTUM 3, plans to enroll 1,028 patients with completion scheduled for 2018.
The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.
On Twitter @mitchelzoler
AT THE HFSA ANNUAL SCIENTIFIC MEETING
Key clinical point: A next-generation left ventricular assist device, HeartMate 3, met its 6-month survival goal to receive CE mark approval in Europe.
Major finding: The advanced heart failure patients who received the HeartMate 3 LVAD had a 92% survival rate after 6 months.
Data source: A prospective series of 50 patients enrolled at 10 centers in six countries.
Disclosures: The study was sponsored by Thoratec, which is developing the HeartMate 3 device. Dr. Netuka is a speaker for and consultant to Thoratec.

Mentoring that takes it up a notch
Everything seems to be extreme nowadays – “Extreme Makeover: Home Edition,” “Extreme Weight Loss,” even “Extreme Fishing” and “Extreme Couponing” – so it was only a matter of time that extreme came to cardiothoracic surgery.
Dr. Michael K. Pasque of Washington University in St. Louis explored “Extreme Mentoring in Cardiothoracic Surgery” in his commentary published online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 doi: 10.1016/j.jtcvs.2015.04.056).
Meaningful mentoring “carries with it considerable responsibility. Extreme mentoring comes only at a price – it is going to cost us,” Dr. Pasque wrote, calling on academic cardiothoracic surgical mentors to perform a self-appraisal of their commitment and mentoring skills. He even developed a self-appraisal checklist that involves 37 different markers in four different categories: general; goals, pathways, and meetings; milestone timelines and taking action; and clinical assistance.
The first step in extreme mentoring for the academic cardiothoracic surgeon is to focus exclusively on the mentee. “As cardiothoracic surgeons, we are used to having the attention focused on us,” Dr. Pasque noted, but mentoring is different: the “energy of our relationship” must focus on the mentee.
The next step involves an objective assessment of the mentee. “If we are to throw our support wholeheartedly behind our mentee, we must genuinely believe in them,” he said. This assessment leads to setting goals for the mentee. “My formula is to honestly estimate the surgical, research, teaching and academic life goals that are both desired by and within reach of our mentee – and then double them,” he said. “We must set very aggressive goals for our mentee.”
Achieving those goals involves directing mentees to the right pathway and then helping them stay on that pathway despite obstacles. “When their progress through these barriers is discussed – and that should be often – then ours should be the voice that reminds them that despite the momentary setbacks, the goals we have set are going to happen,” Dr. Pasque said.
The process involves frequent “and substantive” meetings between mentor and mentee and establishing timelines for achieving milestones and goals. The mentor must back up what happens in those meetings with action – both overt, like assisting them in surgery or introducing them to influential colleagues, and covert in ways the mentee may never know about.
One “clandestine” operation involves the mentor keeping an updated list of 10 individuals who have the most to offer the mentee, “especially in areas in which we have limited or no influence,” and habitually following up with them. The mentor must be willing to “pick a fight” so the mentee doesn’t get left behind on call while senior colleagues attend meetings.
“We must be the senior voice that speaks up for them,” Dr. Pasque wrote. “They need to attend these meetings, even if it is we who must stay behind in their place.”
The mentoring process involves being across the operating room table from them at key milestones in their surgical development and being on-call 24/7 for the mentee. That may seem like extreme handholding to some critics, but Dr. Pasque said that letting a patient suffer or die is inexcusable. “Our first priority is always the patient’s well-being.”
The mentor must show respect to the mentee and practice “extreme encouragement,” especially in the operating room. “There is something magical about being told you are a good surgeon,” he said. “You become one.” This isn’t about falsely building up the mentee, but instilling the confidence to act on the patient’s behalf. The mentee will face enough doubters. “We must be the voice that assures them otherwise,” he said.
Teaching leadership also is key for the mentor. Mentors teach leadership by modeling it. “The best leaders are always those who place the needs of others above their own,” Dr. Pasque pointed out, harkening back to putting the focus on the mentee. “We can’t teach them to put the needs of others above their own without putting their needs about ours.”
Ultimately, the mentor’s greatest desire should be that the mentee exceeds them, “that they make everyone forget about us,” Dr. Pasque said. That would be the “crowning achievement” that would make the mentor “most unforgettable.”
Dr. Pasque had no disclosures.
Everything seems to be extreme nowadays – “Extreme Makeover: Home Edition,” “Extreme Weight Loss,” even “Extreme Fishing” and “Extreme Couponing” – so it was only a matter of time that extreme came to cardiothoracic surgery.
Dr. Michael K. Pasque of Washington University in St. Louis explored “Extreme Mentoring in Cardiothoracic Surgery” in his commentary published online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 doi: 10.1016/j.jtcvs.2015.04.056).
Meaningful mentoring “carries with it considerable responsibility. Extreme mentoring comes only at a price – it is going to cost us,” Dr. Pasque wrote, calling on academic cardiothoracic surgical mentors to perform a self-appraisal of their commitment and mentoring skills. He even developed a self-appraisal checklist that involves 37 different markers in four different categories: general; goals, pathways, and meetings; milestone timelines and taking action; and clinical assistance.
The first step in extreme mentoring for the academic cardiothoracic surgeon is to focus exclusively on the mentee. “As cardiothoracic surgeons, we are used to having the attention focused on us,” Dr. Pasque noted, but mentoring is different: the “energy of our relationship” must focus on the mentee.
The next step involves an objective assessment of the mentee. “If we are to throw our support wholeheartedly behind our mentee, we must genuinely believe in them,” he said. This assessment leads to setting goals for the mentee. “My formula is to honestly estimate the surgical, research, teaching and academic life goals that are both desired by and within reach of our mentee – and then double them,” he said. “We must set very aggressive goals for our mentee.”
Achieving those goals involves directing mentees to the right pathway and then helping them stay on that pathway despite obstacles. “When their progress through these barriers is discussed – and that should be often – then ours should be the voice that reminds them that despite the momentary setbacks, the goals we have set are going to happen,” Dr. Pasque said.
The process involves frequent “and substantive” meetings between mentor and mentee and establishing timelines for achieving milestones and goals. The mentor must back up what happens in those meetings with action – both overt, like assisting them in surgery or introducing them to influential colleagues, and covert in ways the mentee may never know about.
One “clandestine” operation involves the mentor keeping an updated list of 10 individuals who have the most to offer the mentee, “especially in areas in which we have limited or no influence,” and habitually following up with them. The mentor must be willing to “pick a fight” so the mentee doesn’t get left behind on call while senior colleagues attend meetings.
“We must be the senior voice that speaks up for them,” Dr. Pasque wrote. “They need to attend these meetings, even if it is we who must stay behind in their place.”
The mentoring process involves being across the operating room table from them at key milestones in their surgical development and being on-call 24/7 for the mentee. That may seem like extreme handholding to some critics, but Dr. Pasque said that letting a patient suffer or die is inexcusable. “Our first priority is always the patient’s well-being.”
The mentor must show respect to the mentee and practice “extreme encouragement,” especially in the operating room. “There is something magical about being told you are a good surgeon,” he said. “You become one.” This isn’t about falsely building up the mentee, but instilling the confidence to act on the patient’s behalf. The mentee will face enough doubters. “We must be the voice that assures them otherwise,” he said.
Teaching leadership also is key for the mentor. Mentors teach leadership by modeling it. “The best leaders are always those who place the needs of others above their own,” Dr. Pasque pointed out, harkening back to putting the focus on the mentee. “We can’t teach them to put the needs of others above their own without putting their needs about ours.”
Ultimately, the mentor’s greatest desire should be that the mentee exceeds them, “that they make everyone forget about us,” Dr. Pasque said. That would be the “crowning achievement” that would make the mentor “most unforgettable.”
Dr. Pasque had no disclosures.
Everything seems to be extreme nowadays – “Extreme Makeover: Home Edition,” “Extreme Weight Loss,” even “Extreme Fishing” and “Extreme Couponing” – so it was only a matter of time that extreme came to cardiothoracic surgery.
Dr. Michael K. Pasque of Washington University in St. Louis explored “Extreme Mentoring in Cardiothoracic Surgery” in his commentary published online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (J Thorac Cardiovasc Surg. 2015 doi: 10.1016/j.jtcvs.2015.04.056).
Meaningful mentoring “carries with it considerable responsibility. Extreme mentoring comes only at a price – it is going to cost us,” Dr. Pasque wrote, calling on academic cardiothoracic surgical mentors to perform a self-appraisal of their commitment and mentoring skills. He even developed a self-appraisal checklist that involves 37 different markers in four different categories: general; goals, pathways, and meetings; milestone timelines and taking action; and clinical assistance.
The first step in extreme mentoring for the academic cardiothoracic surgeon is to focus exclusively on the mentee. “As cardiothoracic surgeons, we are used to having the attention focused on us,” Dr. Pasque noted, but mentoring is different: the “energy of our relationship” must focus on the mentee.
The next step involves an objective assessment of the mentee. “If we are to throw our support wholeheartedly behind our mentee, we must genuinely believe in them,” he said. This assessment leads to setting goals for the mentee. “My formula is to honestly estimate the surgical, research, teaching and academic life goals that are both desired by and within reach of our mentee – and then double them,” he said. “We must set very aggressive goals for our mentee.”
Achieving those goals involves directing mentees to the right pathway and then helping them stay on that pathway despite obstacles. “When their progress through these barriers is discussed – and that should be often – then ours should be the voice that reminds them that despite the momentary setbacks, the goals we have set are going to happen,” Dr. Pasque said.
The process involves frequent “and substantive” meetings between mentor and mentee and establishing timelines for achieving milestones and goals. The mentor must back up what happens in those meetings with action – both overt, like assisting them in surgery or introducing them to influential colleagues, and covert in ways the mentee may never know about.
One “clandestine” operation involves the mentor keeping an updated list of 10 individuals who have the most to offer the mentee, “especially in areas in which we have limited or no influence,” and habitually following up with them. The mentor must be willing to “pick a fight” so the mentee doesn’t get left behind on call while senior colleagues attend meetings.
“We must be the senior voice that speaks up for them,” Dr. Pasque wrote. “They need to attend these meetings, even if it is we who must stay behind in their place.”
The mentoring process involves being across the operating room table from them at key milestones in their surgical development and being on-call 24/7 for the mentee. That may seem like extreme handholding to some critics, but Dr. Pasque said that letting a patient suffer or die is inexcusable. “Our first priority is always the patient’s well-being.”
The mentor must show respect to the mentee and practice “extreme encouragement,” especially in the operating room. “There is something magical about being told you are a good surgeon,” he said. “You become one.” This isn’t about falsely building up the mentee, but instilling the confidence to act on the patient’s behalf. The mentee will face enough doubters. “We must be the voice that assures them otherwise,” he said.
Teaching leadership also is key for the mentor. Mentors teach leadership by modeling it. “The best leaders are always those who place the needs of others above their own,” Dr. Pasque pointed out, harkening back to putting the focus on the mentee. “We can’t teach them to put the needs of others above their own without putting their needs about ours.”
Ultimately, the mentor’s greatest desire should be that the mentee exceeds them, “that they make everyone forget about us,” Dr. Pasque said. That would be the “crowning achievement” that would make the mentor “most unforgettable.”
Dr. Pasque had no disclosures.
Is Skip N2 metastasis its own category?
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
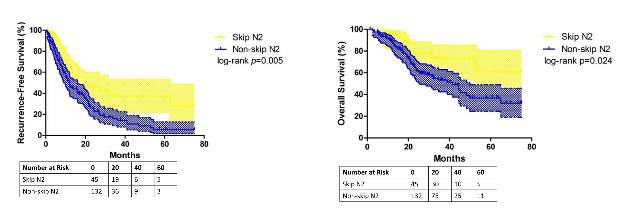
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
“Perhaps the most interesting aspect of the study by Chen and colleagues is the novel observation that skip metastases seem to correlate with acinar histological subtype of lung adenocarcinoma,” Dr. Valerie Rusch of Memorial Sloan Kettering Cancer Center, New York, said in her invited commentary (J Thorac Cardiovasc Surg. 2015 May 8 [doi: 10.1016/j.jtcvs.2015.04.051]) .
“This nicely performed study adds to the evidence that [non–small cell lung cancer) with skip metastases are a distinct subset of stage IIIa disease,” she said.
Dr. Rusch noted that when the International Association for the Study of Lung Cancer (IASLC) revised its lung cancer staging system in 2007 (J Thorac Oncol. 2007;2:603-12), a report for which she served as lead author, it considered giving non–small cell lung cancer with skip metastases its own category. However, the authors decided not to do so because of the small numbers of patients who fall into the category.
In the updated histological classification for adenocarcinoma in 2011 from IASLC, along with the American Thoracic Society and European Respiratory Society (J Thorac Oncol. 2011;6[2]:244-85) , papillary and acinar-predominant adenocarcinomas appear to be associated with similar outcomes. However, the Fudan (Shanghai) University researchers suggest “that there may be some important differences between the two subtypes,” Dr. Rusch said.
Because the study population was so small, the results cannot be considered “definitive,” Dr. Rusch said. “In this era of increasingly high throughput molecular medicine, future, much larger-scale analyses are needed to prove or refute these initial results.”
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
So-called “skip metastasis” of lung cancer to the lymph nodes – when the cancer “skips” over the N1 bronchopulmonary or hilar stage to N2 ipsilateral mediastinal metastasis – may be associated with distinct histological characteristics that can further help understand its association with longer survival and better prognosis in advanced resectable lung adenocarcinoma, according to a small study from China.
Researchers at Fudan (Shanghai ) University Cancer Center published their findings online ahead of print for the October issue of the Journal of Thoracic and Cardiovascular Surgery (2015 July 6 [doi: 10.1016/j.jtcvs.2015.03.067]). In all, they enrolled 177 patients with N2 adenocarcinoma, 45 (25.4%) of whom had skip N2 metastasis.
They reported that patients with skip metastasis had considerably better 5-year recurrence-free survival rates of 37.4% vs. 5.7% and better overall survival rates of 60.7% vs. 32.1% when compared with those with non-skip involvement.
“There are distinct differences in clinicopathological features and prognosis in patients with or without skip N2 metastasis,” Dr. Haiquan Chen and his colleagues said. “Considering the results of our study, subclassifications of mediastinal lymph nodes metastases would have potential clinical significance for patients with lung adenocarcinoma.”
Dr. Chen and his colleagues sought to identify specific histological features that characterized the association between skip N2 metastasis and adenocarcinoma subtypes and prognosis. “Skip N2 patients have more cases that are acinar adenocarcinoma subtype, well differentiated and located in the right lung than [do] non-skip patients,” they said.
In fact, they found the predictive value of skip N2 was more significant in patients with right-lung disease, with 5-year recurrence-free survival of 36.6% vs. 0% and overall survival of 57.2% vs. 28% in non–right-lung lesions. They also reported that tumor size of 3 cm or smaller in skip N2 was associated with significantly improved survival rates – 43% vs. 6.7% recurrence-free survival and 74.6% vs. 27.6% for overall survival, compared with patients with larger tumors.
The skip N2 lung adenocarcinoma patients had “remarkably lower incidence” of vascular invasion of the lymph nodes, Dr. Chen and his coauthors wrote. Skip N2 patients also had lower, but not statistically significant, rates of pleural invasion. The Fudan University researchers also reported that the incidence of non-skip N2 metastasis was “significantly high” in patients with papillary-predominant subtype.
“Considering our results, skip N2 should not be recognized as [a] predictor for better survival in all lung adenocarcinoma cases, but in [a] more specific group of patients,” Dr. Chen and his coauthors said.
A multivariate analysis confirmed the predictive significance of skip N2 for recurrence-free survival, but not so much for overall survival. Single N2 metastasis was also an independent predictor for better recurrence-free and overall survival, Dr. Chen and his colleagues said.
The study received funding from the Key Construction Program of the National “985” Project, Ministry of Science and Technology of China; the National Natural Science Foundation of China; the Science and Technology Commission of Shanghai Municipality; and Shanghai Hospital Development Center.
The authors had no disclosures.
Key clinical point: Skip N2 metastases in resectable lung cancer have distinct histological characteristics from non-skip N2 disease.
Major finding: A subset of patients with skip N2 metastasis had higher rates of acinar adenocarcinoma subtype and right-lung disease.
Data source: Retrospective analysis of 177 patients with lung adenocarcinoma and N2 metastasis
Disclosures: The study received funding from the government of China and Shanghai Municipality as well as Shanghai Hospital Development Center. The authors have no relationships to disclose.