User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Sewage as our salvation: Tracking COVID-19
“The sewer is the conscience of the city. Everything there converges and confronts everything else. In that livid spot there are shades, but there are no longer any secrets.” Victor Hugo – “Les Miserables”
To get a sense of the prevalence of COVID-19 in a community you need to test hundreds to thousands of people. This is difficult, resource intensive, and requires cooperation for testing among people both with and without symptoms.

In various locations from China to medieval London, there have been attempts to utilize human excrement for the betterment of mankind, from employing it as fertilizer to processing it to make gunpowder. Such attempts did not always work as planned. The use of sewage for fertilizer in Europe and the United States in the 1840s and 1850s led to the spread of waterborne diseases, including cholera and typhoid. As the importance of sanitary elimination of human waste became ever clearer, ideas and technology for our modern system of sewage management evolved. We have since advanced a great deal, so that all industrialized nations now have a well-developed system for clean water entry, as well as sewage treatment and disposal. Nonetheless, there remains a nagging question of whether human waste could be used for something productive.1
In the early 2000s, SCIM was developed as a technique to assess population-level human health and disease. In SCIM, untreated sewage is tested for a chemical of interest which reflects a health parameter for a community. Chemicals of interest and usage rates can be calculated for substances as varied as opioids, tobacco, pesticides, and even nonnutritive sweeteners. For instance, relative opioid use can be calculated over time for a given “sewershed” or sewage catchment area. The calculation of community-wide exposure to substances as a means of getting real-time data on shifts of usage without having to collect and collate data from thousands of individuals has been termed wastewater-based epidemiology.
We use urine and stool testing in so many other areas, such as urinalysis, urine drug testing, urine Legionella antigen testing, and stool testing for common pathogens. What a rich source of information is present in the combination of urine and stool that collectively make up sewage! With the average volume of urine per adult being approximately 1 liter daily (and with urine calculated to be approximately 1% of wastewater), accurate analytic techniques can estimate per capita exposure to different substances. Applications of wastewater-based epidemiology have included tracking community prevalence of enteric viral infections, opioid and tobacco use, and many other indicators of health and disease.2
Given the enormous work in the field over the last 2 decades and that SARS-CoV-2 RNA has been detected in feces of both symptomatic and asymptomatic patients, it was only a short conceptual step for those familiar with sewage epidemiology to consider adapting it to assess the prevalence of COVID-19 in a community.
An elegant study collected untreated sewage from southeast Queensland, Australia. The sewage was processed, concentrated, and then tested with reverse transcriptase polymerase chain reaction analysis for SARS-CoV-2 RNA. The number of RNA copies was then entered into an equation that included the population served by the sewage encatchment area, as well as the measured liters of wastewater and grams of feces per day. This provided an estimate of the number of persons infected in the community, and the researchers were able to show reasonable agreement between the numbers estimated by sewage analysis and that found in traditional clinical testing.3,4
The promise of wastewater-based epidemiology is large. Early research indicates that quantification of viral particles in sewage can be accurately assessed and correlated with the prevalence of the infection in the community. Such levels can then be used to track infection rates of COVID-19 over time, as well as to compare the relative rates in different communities.
Our sewage may hold the answer to accurately and easily tracking COVID-19, and ultimately help us gain a better hold on this disease.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Follow him on Twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
References
1. History of water supply and sanitation. Wikipedia, https://en.wikipedia.org/wiki/History_of_water_supply_and_sanitation.
2. Daughton C. Monitoring wastewater for assessing community health: Sewage Chemical-Information Mining (SCIM). Sci Total Environ. 2017 Nov 29. doi: 10.1016/j.scitotenv.2017.11.102.
3. Ahmed W et al. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: A proof of concept for the wastewater surveillance of COVID-19 in the community. Sci Total Environ. 2020 Apr 18. doi: doi.org/10.1016/j.scitotenv.2020.138764.
4. Daughton C. The international imperative to rapidly and inexpensively monitor community-wide COVID-19 infection status and trends. Sci Total Environ. 2020 Mar 23. doi: 10.1016/j.scitotenv.2020.138149.
“The sewer is the conscience of the city. Everything there converges and confronts everything else. In that livid spot there are shades, but there are no longer any secrets.” Victor Hugo – “Les Miserables”
To get a sense of the prevalence of COVID-19 in a community you need to test hundreds to thousands of people. This is difficult, resource intensive, and requires cooperation for testing among people both with and without symptoms.
In various locations from China to medieval London, there have been attempts to utilize human excrement for the betterment of mankind, from employing it as fertilizer to processing it to make gunpowder. Such attempts did not always work as planned. The use of sewage for fertilizer in Europe and the United States in the 1840s and 1850s led to the spread of waterborne diseases, including cholera and typhoid. As the importance of sanitary elimination of human waste became ever clearer, ideas and technology for our modern system of sewage management evolved. We have since advanced a great deal, so that all industrialized nations now have a well-developed system for clean water entry, as well as sewage treatment and disposal. Nonetheless, there remains a nagging question of whether human waste could be used for something productive.1
In the early 2000s, SCIM was developed as a technique to assess population-level human health and disease. In SCIM, untreated sewage is tested for a chemical of interest which reflects a health parameter for a community. Chemicals of interest and usage rates can be calculated for substances as varied as opioids, tobacco, pesticides, and even nonnutritive sweeteners. For instance, relative opioid use can be calculated over time for a given “sewershed” or sewage catchment area. The calculation of community-wide exposure to substances as a means of getting real-time data on shifts of usage without having to collect and collate data from thousands of individuals has been termed wastewater-based epidemiology.
We use urine and stool testing in so many other areas, such as urinalysis, urine drug testing, urine Legionella antigen testing, and stool testing for common pathogens. What a rich source of information is present in the combination of urine and stool that collectively make up sewage! With the average volume of urine per adult being approximately 1 liter daily (and with urine calculated to be approximately 1% of wastewater), accurate analytic techniques can estimate per capita exposure to different substances. Applications of wastewater-based epidemiology have included tracking community prevalence of enteric viral infections, opioid and tobacco use, and many other indicators of health and disease.2
Given the enormous work in the field over the last 2 decades and that SARS-CoV-2 RNA has been detected in feces of both symptomatic and asymptomatic patients, it was only a short conceptual step for those familiar with sewage epidemiology to consider adapting it to assess the prevalence of COVID-19 in a community.
An elegant study collected untreated sewage from southeast Queensland, Australia. The sewage was processed, concentrated, and then tested with reverse transcriptase polymerase chain reaction analysis for SARS-CoV-2 RNA. The number of RNA copies was then entered into an equation that included the population served by the sewage encatchment area, as well as the measured liters of wastewater and grams of feces per day. This provided an estimate of the number of persons infected in the community, and the researchers were able to show reasonable agreement between the numbers estimated by sewage analysis and that found in traditional clinical testing.3,4
The promise of wastewater-based epidemiology is large. Early research indicates that quantification of viral particles in sewage can be accurately assessed and correlated with the prevalence of the infection in the community. Such levels can then be used to track infection rates of COVID-19 over time, as well as to compare the relative rates in different communities.
Our sewage may hold the answer to accurately and easily tracking COVID-19, and ultimately help us gain a better hold on this disease.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Follow him on Twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
References
1. History of water supply and sanitation. Wikipedia, https://en.wikipedia.org/wiki/History_of_water_supply_and_sanitation.
2. Daughton C. Monitoring wastewater for assessing community health: Sewage Chemical-Information Mining (SCIM). Sci Total Environ. 2017 Nov 29. doi: 10.1016/j.scitotenv.2017.11.102.
3. Ahmed W et al. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: A proof of concept for the wastewater surveillance of COVID-19 in the community. Sci Total Environ. 2020 Apr 18. doi: doi.org/10.1016/j.scitotenv.2020.138764.
4. Daughton C. The international imperative to rapidly and inexpensively monitor community-wide COVID-19 infection status and trends. Sci Total Environ. 2020 Mar 23. doi: 10.1016/j.scitotenv.2020.138149.
“The sewer is the conscience of the city. Everything there converges and confronts everything else. In that livid spot there are shades, but there are no longer any secrets.” Victor Hugo – “Les Miserables”
To get a sense of the prevalence of COVID-19 in a community you need to test hundreds to thousands of people. This is difficult, resource intensive, and requires cooperation for testing among people both with and without symptoms.
In various locations from China to medieval London, there have been attempts to utilize human excrement for the betterment of mankind, from employing it as fertilizer to processing it to make gunpowder. Such attempts did not always work as planned. The use of sewage for fertilizer in Europe and the United States in the 1840s and 1850s led to the spread of waterborne diseases, including cholera and typhoid. As the importance of sanitary elimination of human waste became ever clearer, ideas and technology for our modern system of sewage management evolved. We have since advanced a great deal, so that all industrialized nations now have a well-developed system for clean water entry, as well as sewage treatment and disposal. Nonetheless, there remains a nagging question of whether human waste could be used for something productive.1
In the early 2000s, SCIM was developed as a technique to assess population-level human health and disease. In SCIM, untreated sewage is tested for a chemical of interest which reflects a health parameter for a community. Chemicals of interest and usage rates can be calculated for substances as varied as opioids, tobacco, pesticides, and even nonnutritive sweeteners. For instance, relative opioid use can be calculated over time for a given “sewershed” or sewage catchment area. The calculation of community-wide exposure to substances as a means of getting real-time data on shifts of usage without having to collect and collate data from thousands of individuals has been termed wastewater-based epidemiology.
We use urine and stool testing in so many other areas, such as urinalysis, urine drug testing, urine Legionella antigen testing, and stool testing for common pathogens. What a rich source of information is present in the combination of urine and stool that collectively make up sewage! With the average volume of urine per adult being approximately 1 liter daily (and with urine calculated to be approximately 1% of wastewater), accurate analytic techniques can estimate per capita exposure to different substances. Applications of wastewater-based epidemiology have included tracking community prevalence of enteric viral infections, opioid and tobacco use, and many other indicators of health and disease.2
Given the enormous work in the field over the last 2 decades and that SARS-CoV-2 RNA has been detected in feces of both symptomatic and asymptomatic patients, it was only a short conceptual step for those familiar with sewage epidemiology to consider adapting it to assess the prevalence of COVID-19 in a community.
An elegant study collected untreated sewage from southeast Queensland, Australia. The sewage was processed, concentrated, and then tested with reverse transcriptase polymerase chain reaction analysis for SARS-CoV-2 RNA. The number of RNA copies was then entered into an equation that included the population served by the sewage encatchment area, as well as the measured liters of wastewater and grams of feces per day. This provided an estimate of the number of persons infected in the community, and the researchers were able to show reasonable agreement between the numbers estimated by sewage analysis and that found in traditional clinical testing.3,4
The promise of wastewater-based epidemiology is large. Early research indicates that quantification of viral particles in sewage can be accurately assessed and correlated with the prevalence of the infection in the community. Such levels can then be used to track infection rates of COVID-19 over time, as well as to compare the relative rates in different communities.
Our sewage may hold the answer to accurately and easily tracking COVID-19, and ultimately help us gain a better hold on this disease.
Dr. Notte is a family physician and chief medical officer of Abington (Pa.) Hospital–Jefferson Health. Follow him on Twitter (@doctornotte). Dr. Skolnik is professor of family and community medicine at Sidney Kimmel Medical College, Philadelphia, and associate director of the family medicine residency program at Abington (Pa.) Hospital–Jefferson Health. They have no conflicts related to the content of this piece.
References
1. History of water supply and sanitation. Wikipedia, https://en.wikipedia.org/wiki/History_of_water_supply_and_sanitation.
2. Daughton C. Monitoring wastewater for assessing community health: Sewage Chemical-Information Mining (SCIM). Sci Total Environ. 2017 Nov 29. doi: 10.1016/j.scitotenv.2017.11.102.
3. Ahmed W et al. First confirmed detection of SARS-CoV-2 in untreated wastewater in Australia: A proof of concept for the wastewater surveillance of COVID-19 in the community. Sci Total Environ. 2020 Apr 18. doi: doi.org/10.1016/j.scitotenv.2020.138764.
4. Daughton C. The international imperative to rapidly and inexpensively monitor community-wide COVID-19 infection status and trends. Sci Total Environ. 2020 Mar 23. doi: 10.1016/j.scitotenv.2020.138149.
Behind the mask
Bicycling has always been part of who I am because it offered me the freedom to explore as a preteen. As an adult I have always been a bicycle commuter and a very visible part of the community as I pedal around town to do my errands. But, I didn’t always wear a helmet ... because well, I just didn’t. I saw the helmet as a nuisance with very little benefit to myself. Eventually, when bike races required helmets I bought one just for the competitions. Until one day about 30 years ago when the mother of a child I was seeing in the office said, “Dr. Wilkoff, you know as an influential member of this community, particularly its children, you should be wearing a helmet.” My wife had been badgering me for years but this woman’s courage to speak up embarrassed me into changing my ways.

For some, maybe many, people, wearing a mask during the COVID-19 pandemic is a nuisance and an assault on their independence just as I viewed a bicycle helmet. Initially there was some information being circulated that any mask less robust than a N-95 had very little if any effect, either as protection or as way to decrease spread. I certainly had my doubts about the value of mask other than as a statement of solidarity. However, we are now learning that masks can serve an important role along with social distancing in a comprehensive community effort to minimize contagion.
In light of this new information, why are there are still people who won’t wear a mask? It may be that they are receiving their news filtered through a lens that discredits science. But, it is more likely the result of the same mindset that permeates the anti-vaccine faction that the common good is less important than personal freedom to follow their beliefs.
Do we have any tools at our disposal to increase the number of folks wearing masks? Based on our experience with attempts to convince those who are anti-vaccine, education will be ineffective in shifting the focus from personal freedom to a commitment to the welfare of the community at large. Shaming might be effective, but it runs the risk of igniting conflicts and further widening the gaps in our society. Some establishments have been effective in simply saying “no mask, no entry,” but this runs the same risk of creating friction depending on the community and the situation.
The ship may have already sailed on our best opportunity to achieve community compliance when the leaders of our national government have chosen to ignore their obligation to set an example by refusing to wear masks. I fear that the wedge has already been set and the widening of the gap between those who see their responsibility to the community at large and those who do not will continue to grow.
I am fortunate to live in a town whose residents look out for each other and have relied on local leaders to set an example in the absence of leadership on a national level.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Bicycling has always been part of who I am because it offered me the freedom to explore as a preteen. As an adult I have always been a bicycle commuter and a very visible part of the community as I pedal around town to do my errands. But, I didn’t always wear a helmet ... because well, I just didn’t. I saw the helmet as a nuisance with very little benefit to myself. Eventually, when bike races required helmets I bought one just for the competitions. Until one day about 30 years ago when the mother of a child I was seeing in the office said, “Dr. Wilkoff, you know as an influential member of this community, particularly its children, you should be wearing a helmet.” My wife had been badgering me for years but this woman’s courage to speak up embarrassed me into changing my ways.
For some, maybe many, people, wearing a mask during the COVID-19 pandemic is a nuisance and an assault on their independence just as I viewed a bicycle helmet. Initially there was some information being circulated that any mask less robust than a N-95 had very little if any effect, either as protection or as way to decrease spread. I certainly had my doubts about the value of mask other than as a statement of solidarity. However, we are now learning that masks can serve an important role along with social distancing in a comprehensive community effort to minimize contagion.
In light of this new information, why are there are still people who won’t wear a mask? It may be that they are receiving their news filtered through a lens that discredits science. But, it is more likely the result of the same mindset that permeates the anti-vaccine faction that the common good is less important than personal freedom to follow their beliefs.
Do we have any tools at our disposal to increase the number of folks wearing masks? Based on our experience with attempts to convince those who are anti-vaccine, education will be ineffective in shifting the focus from personal freedom to a commitment to the welfare of the community at large. Shaming might be effective, but it runs the risk of igniting conflicts and further widening the gaps in our society. Some establishments have been effective in simply saying “no mask, no entry,” but this runs the same risk of creating friction depending on the community and the situation.
The ship may have already sailed on our best opportunity to achieve community compliance when the leaders of our national government have chosen to ignore their obligation to set an example by refusing to wear masks. I fear that the wedge has already been set and the widening of the gap between those who see their responsibility to the community at large and those who do not will continue to grow.
I am fortunate to live in a town whose residents look out for each other and have relied on local leaders to set an example in the absence of leadership on a national level.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
Bicycling has always been part of who I am because it offered me the freedom to explore as a preteen. As an adult I have always been a bicycle commuter and a very visible part of the community as I pedal around town to do my errands. But, I didn’t always wear a helmet ... because well, I just didn’t. I saw the helmet as a nuisance with very little benefit to myself. Eventually, when bike races required helmets I bought one just for the competitions. Until one day about 30 years ago when the mother of a child I was seeing in the office said, “Dr. Wilkoff, you know as an influential member of this community, particularly its children, you should be wearing a helmet.” My wife had been badgering me for years but this woman’s courage to speak up embarrassed me into changing my ways.
For some, maybe many, people, wearing a mask during the COVID-19 pandemic is a nuisance and an assault on their independence just as I viewed a bicycle helmet. Initially there was some information being circulated that any mask less robust than a N-95 had very little if any effect, either as protection or as way to decrease spread. I certainly had my doubts about the value of mask other than as a statement of solidarity. However, we are now learning that masks can serve an important role along with social distancing in a comprehensive community effort to minimize contagion.
In light of this new information, why are there are still people who won’t wear a mask? It may be that they are receiving their news filtered through a lens that discredits science. But, it is more likely the result of the same mindset that permeates the anti-vaccine faction that the common good is less important than personal freedom to follow their beliefs.
Do we have any tools at our disposal to increase the number of folks wearing masks? Based on our experience with attempts to convince those who are anti-vaccine, education will be ineffective in shifting the focus from personal freedom to a commitment to the welfare of the community at large. Shaming might be effective, but it runs the risk of igniting conflicts and further widening the gaps in our society. Some establishments have been effective in simply saying “no mask, no entry,” but this runs the same risk of creating friction depending on the community and the situation.
The ship may have already sailed on our best opportunity to achieve community compliance when the leaders of our national government have chosen to ignore their obligation to set an example by refusing to wear masks. I fear that the wedge has already been set and the widening of the gap between those who see their responsibility to the community at large and those who do not will continue to grow.
I am fortunate to live in a town whose residents look out for each other and have relied on local leaders to set an example in the absence of leadership on a national level.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Email him at [email protected].
In remission for 10 years: Long-term toxicity data on CAR T cells
When a patient with cancer hears there isn’t much left that doctors can do, it always stays fresh in the mind.
Doug Olson was first diagnosed with chronic lymphocytic leukemia (CLL) over 20 years ago, in 1996. For several years, his doctors used the watch-and-wait approach. But then his cancer progressed and needed treatment. By 2010, it had mutated so much that it no longer responded to standard therapy.
He was rapidly running out of options. Back then, the only treatment left was a bone marrow transplant. Without one, his doctors said, he would have 1 or 2 years left to live.
“I was really trying to avoid a bone marrow transplant. You’re playing your last card if that doesn’t work. It’s a pretty rough procedure,” Olson told Medscape Medical News.
Looking back, Olson counts himself as lucky – for being in the right place, at the right time, with the right doctor. His oncologist was David Porter, MD, the principal investigator on a trial at the University of Pennsylvania that was investigating a brand new approach to treating cancer: chimeric antigen receptor (CAR) T-cell therapy.
CAR T-cell therapy uses a patient’s own T cells engineered to express a receptor that targets proteins on cancer cells. CAR T cells are considered “living drugs” because they expand inside the body and stick around for years – maybe for a lifetime – to fight the cancer if it tries to come back.
“I was certainly intrigued by the approach. It had worked in mice, and it was the sort of thing that looked like it would work,” Olson recalled.
Science is not a foreign language to Olson. He holds a PhD in medicinal chemistry, spent most of his career in the in vitro diagnostics industry, and currently acts as chief executive officer of Buhlmann Diagnostics Corp.
So he read the clinical protocol for the first in-human trial of CAR T cells and agreed to become patient number two.
Olson’s T cells were harvested, engineered to attack the CD19 antigen found on malignant and normal B lymphocytes, and then were expanded into millions in the lab. After undergoing preconditioning with chemotherapy to minimize rejection and boost the CAR T cells’ expansion inside the body, he received several infusions of the new therapy over the course of 3 days.
Nothing really happened for 2 weeks. Then he developed severe flu-like symptoms – so bad that he was hospitalized.
Ironically, getting sick was a sign that the CAR T cells were working. Olson was experiencing one of the main short-term effects of CAR T-cell therapy: cytokine release syndrome. Symptoms include extremely high fevers and dangerous drops in blood pressure that can potentially cause end-organ damage.
In the early trials of these products, some patients experienced such a severe reaction that they needed intensive care, and some died. With increasing clinical experience, doctors have learned to control the reaction with the use of steroids and interleukein-6 inhibitors such as tocilizumab (Actemra).
Fortunately for Olson, the reaction passed, and he was eventually discharged.
Then the “aha moment” happened. Four weeks after receiving the CAR T cells, Olson found out that he was cancer free.
“It still gives me shivers,” he said. “Dr Porter said, ‘Your bone marrow’s completely free. We just can’t find a cancer cell anywhere.’ “
The remission has lasted, and it is now 10 years later.
Balancing long-term risks vs benefits
Long-term data have been accumulating for these novel therapies since Olson’s treatment in 2010. This is particularly important for CAR T-cell therapy, because of its longevity. Because these are living cells and are expected to persist in the body for years, there is great interest in longer-term data, especially the risks for toxicity.
The FDA requires clinical follow-up for at least 15 years for patients treated with CAR T-cell therapy or any other genetically modified cells.
So far, most of the experience with CAR T cells comes from anti-CD19-directed therapy, which has shown “remarkable” remission rates in the 50% to 85% range, said Nirali Shah, MD, head of the hematologic malignancies section of the Pediatric Oncology Branch at the National Cancer Institute (NCI).
The most recent results presented at this year’s annual meeting of the American Society of Clinical Oncology support earlier efficacy data, she noted. In the longest follow-up to date, researchers reported remissions lasting over 9 years in patients with relapsed/refractory B-cell lymphoma or CLL treated with Kite›s axicaptagene cilleucel (Yescarta), one of two anti-CD19-directed CAR T-cell therapies approved by the FDA in 2017 (the other is Novartis’ tisagenlecleucel [Kymriah]).
This study included 43 patients and showed an overall remission rate of 76%. Complete remission was achieved in 54% of patients, and 22% had partial remission.
The other focus is long-term safety. Although some of the long-term adverse effects are known and are manageable, others fall into the theoretical realm. In early May 2020, the NCI held a multidisciplinary virtual conference on CAR T-cell therapy «to encourage collaborative research about the subacute and potentially long-term toxicity profile of these treatments.»
“We know just a little at this point about late- and long-term effects of CAR-T therapy, because we are relatively early in the era of CAR T cells,” said Merav Bar, MD, from the Fred Hutchinson Cancer Research Center in Seattle, Washington.
B-cell aplasia and risk for new infections
What is known is that B-cell aplasia represents the most common long-term adverse effect of CAR T-cell therapy. B-cell aplasia results when anti-CD19 CAR-T therapy wipes out healthy B cells as well as the malignant ones responsible for leukemia/lymphoma.
As major players in the immune system, B cells are a key defense against viruses. So B-cell aplasia represents a very specific type of immunosuppression. It is generally less severe than immunosuppression that occurs after organ transplant, which hits the immune system pretty much across the board and carries a much higher risk for infection.
The main concern is what happens when someone with B-cell aplasia encounters a new pathogen, such as SARS-CoV-2.
After infection, B cells generate memory cells, which are not killed off by anti-CD19 therapy and that stick around for life. So a patient such as Olson would still make antibodies that fight infections they experienced before receiving CAR-T therapy, such as childhood chickenpox. But now they are unable to make new memory cells, so these patients receive monthly immunoglobulin infusions to protect against pathogens they have not previously encountered.
Olson takes this in stride and says he isn’t overly worried about COVID-19. He follows the recommended precautions for a man his age. He wears a mask, washes his hands frequently, and tries to maintain social distancing. But he doesn’t stay locked up in his New Hampshire home.
“I took the attitude when I was diagnosed with cancer that I’m going to live my life,” he said. “Quality of life to me is more important than quantity.”
Neuropsychiatric toxicity
Another problem is the possibility of neuropsychiatric toxicity. Past studies have reported a wide range of such toxicities associated with CAR T-cell therapy, including seizures and hallucinations. Most have occurred early in the course of treatment and appear to be short-lived and reversible. However, there remain questions about long-term neuropsychiatric problems.
In a long-term study of 40 patients with relapsed/refractory CLL, non-Hodgkin lymphoma, and ALL, nearly half of patients (47.5%, 19/40) self-reported at least one clinically meaningful negative neuropsychiatric outcome (anxiety, depression, or cognitive difficulty) 1 to 5 years after anti-CD19 CAR T-cell therapy. In addition, 37.5% (15/40) self-reported cognitive difficulties.
“Patients with more severe neurotoxicity showed a trend for more cognitive difficulties afterwards,» said Bar, senior author of the study.
However, teasing out the role that CAR T-cell therapy plays in these problems poses a challenge. All of these patients had been heavily pretreated with previous cancer therapy, which has also been associated with neuropsychiatric problems.
“So far, we don’t know what caused it,” Bar said. “Nevertheless, people need to pay attention to neuropsychiatric symptoms in CAR T-cell therapy. It is important to continue to monitor these patients for these issues.”
Graft-vs-host disease
Another potential problem is graft-vs-host disease (GVHD). This is not uncommon after hematopoietic stem cell transplants. It develops when the donor T cells view antigens on healthy recipient cells as foreign and attack them.
For patients who are treated with CAR T cells, GVHD is mostly a concern among individuals who have previously had a transplant and who are already at increased risk for it.
In a study of late effects among 86 adults treated with anti-CD19 CAR T cells for relapsed/refractory non-Hodgkin lymphoma, Bar and colleagues found that GVHD occurred only among patients who had received a previous donor stem cell transplant. Of these, 20% (3/15) developed GVHD about 28 months after CAR-T therapy.
“The data for CAR T cells causing GVHD really hasn’t shown that it’s a huge problem, although we have seen it and are continuing to monitor for it,” the NCI’s Shah commented to Medscape Medical News.
Other Long-term Adverse Effects
A range of other long-term adverse effects have been reported with CAR-T therapy, including prolonged cytopenias (reduced mature blood cells), myelodysplasia (bone marrow failure), and second malignancies.
In the study with the longest follow-up to date, 16% (7/43) of patients developed second malignancies, which is comparable to data from Bar’s study in Seattle (15%, 13/86). The researchers in this study consider this rate to be no higher than expected: these patients had already received extensive chemotherapy, which increases the risk for other cancers, they point out.
However, this brings up theoretical concerns about the long-term effects of gene modification. CAR T cells are engineered using retroviruses (mainly lentiviruses), which randomly insert the CAR genes into the host genome. Doing so may cause mutations that could promote cancer. These lentiviruses also carry the theoretical risk of becoming capable of viral replication once inside the body.
To address these concerns, viruses used to engineer CAR T cells go through comprehensive safety testing. After therapy, patients are checked every few months during the first year and annually after that.
So far, there have been no reports of cancers associated with CAR T-cell therapy.
“Any type of cancer is a very theoretical risk,” Bar told Medscape Medical News. «Most likely the malignancies in our study were related to prior treatment that the patients received. None of them had any evidence of replication-competent lentivirus, or any other evidence that the malignancies were related to the CAR T cells.»
Another theoretical concern is the possibility of new-onset autoimmune disease, although, once again, no cases have been reported so far.
“We think of it as a theoretic possibility. Whenever you jack up the immune system, autoimmune disease is a potential risk,” said Carl June, MD, director of the Center for Cellular Immunotherapies at the University of Pennsylvania.
June was the co–principal investigator of the trial in which Olson participated. He is also the inventor on patents for CAR T cells licensed by the University of Pennsylvania to Novartis and Tmunity and is a scientific founder with equity in Tmunity.
Still, autoimmunity could occur, and scientists are looking out for it.
“We are continuing to be vigilant in our monitoring for autoimmune disease,” Shah added. “We’ve been doing CAR T-cell therapy since 2012, and I think we have yet to see true autoimmunity beyond GVHD.”
Future directions
In the 10 years since Olson received CAR T-cell therapy, an entire industry has sprung up. Over 100 companies worldwide are now developing CAR T-cell therapies targeting various antigens. These therapies are directed at about 60 different tumor types, including solid tumors. Nearly 200 clinical trials are underway, though most are still in early stages: as of September 2019, only 5% had reached phase 3.
Clinical data show promising results for CAR T-cell therapy directed against CD22 (overexpressed on ALL cells), and BCMA (found on almost all multiple myeloma cells). Yet questions remain as to whether CAR T cells will be as effective if they target antigens other than CD19 or cells other than B lymphocytes. One of the biggest research questions is whether they will be effective against solid tumors.
One research avenue being watched with great interest is the development of universal CAR T cells. So far, such products are at very early stages of development (phase 1 trials), but they are attractive because of the potential advantages they offer over bespoke CAR T cells. Automating the process holds the promise of immediate availability, standardizing production, expanding access, and lowering costs. And because the T cells for this universal product come from healthy donors, they may function better than T cells that have been battered and bruised by past cancer treatments, or even the cancer itself.
However, precisely because they are developed from healthy donor T cells, universal CAR T cells may pose increased risk for GVHD. Scientists are trying to get around this problem by engineering universal CAR T cells that lack the T-cell receptor involved in GVHD.
There are also other concerns. Nature has a penchant for mutation. Engineering CAR T cells without T-cell receptors means the body may no longer detect or reject a universal CAR T cell if it goes rogue. Also, gene insertion in universal CAR-T therapy is targeted rather than random (as in bespoke CAR T cells), which could create off-target effects. Both issues create a theoretical risk of such products inducing an untreatable CAR T-cell therapy–associated cancer.
“The theoretic risk with universal cells is that their safety profile may not be as good for long term,” June commented.
Hope for the future
From that first trial in which June and Porter used CAR T cells, two of three patients they treated are still alive 10 years later.
Olson is one of these two, and he still undergoes monitoring every 3 months to check for relapse. So far, none of his tests have shown signs of his cancer returning.
After going into remission, Doug spent the next 6 to 9 months regaining his health and strength.
“I figured if I had this amazing treatment that saved my life, I had an obligation to stay alive,” he said. “I’d better not die of something like a heart attack!”
He took up long distance running and has completed six half marathons. He became involved in the Leukemia and Lymphoma Society, participating in fund-raising and helping newly diagnosed patients. Over the years, he has also given talks for researchers, people with cancer, and healthcare providers.
Doug is now 73. Today, he marvels at how rapidly the CAR-T field has progressed.
“Twenty years ago, if you had cancer, your prospects weren’t nearly as good as these days. In 2010, people still didn’t believe in CAR T-cell therapy,” he said. “My goal always in telling my story is a message of hope.”
This article first appeared on Medscape.com.
When a patient with cancer hears there isn’t much left that doctors can do, it always stays fresh in the mind.
Doug Olson was first diagnosed with chronic lymphocytic leukemia (CLL) over 20 years ago, in 1996. For several years, his doctors used the watch-and-wait approach. But then his cancer progressed and needed treatment. By 2010, it had mutated so much that it no longer responded to standard therapy.
He was rapidly running out of options. Back then, the only treatment left was a bone marrow transplant. Without one, his doctors said, he would have 1 or 2 years left to live.
“I was really trying to avoid a bone marrow transplant. You’re playing your last card if that doesn’t work. It’s a pretty rough procedure,” Olson told Medscape Medical News.
Looking back, Olson counts himself as lucky – for being in the right place, at the right time, with the right doctor. His oncologist was David Porter, MD, the principal investigator on a trial at the University of Pennsylvania that was investigating a brand new approach to treating cancer: chimeric antigen receptor (CAR) T-cell therapy.
CAR T-cell therapy uses a patient’s own T cells engineered to express a receptor that targets proteins on cancer cells. CAR T cells are considered “living drugs” because they expand inside the body and stick around for years – maybe for a lifetime – to fight the cancer if it tries to come back.
“I was certainly intrigued by the approach. It had worked in mice, and it was the sort of thing that looked like it would work,” Olson recalled.
Science is not a foreign language to Olson. He holds a PhD in medicinal chemistry, spent most of his career in the in vitro diagnostics industry, and currently acts as chief executive officer of Buhlmann Diagnostics Corp.
So he read the clinical protocol for the first in-human trial of CAR T cells and agreed to become patient number two.
Olson’s T cells were harvested, engineered to attack the CD19 antigen found on malignant and normal B lymphocytes, and then were expanded into millions in the lab. After undergoing preconditioning with chemotherapy to minimize rejection and boost the CAR T cells’ expansion inside the body, he received several infusions of the new therapy over the course of 3 days.
Nothing really happened for 2 weeks. Then he developed severe flu-like symptoms – so bad that he was hospitalized.
Ironically, getting sick was a sign that the CAR T cells were working. Olson was experiencing one of the main short-term effects of CAR T-cell therapy: cytokine release syndrome. Symptoms include extremely high fevers and dangerous drops in blood pressure that can potentially cause end-organ damage.
In the early trials of these products, some patients experienced such a severe reaction that they needed intensive care, and some died. With increasing clinical experience, doctors have learned to control the reaction with the use of steroids and interleukein-6 inhibitors such as tocilizumab (Actemra).
Fortunately for Olson, the reaction passed, and he was eventually discharged.
Then the “aha moment” happened. Four weeks after receiving the CAR T cells, Olson found out that he was cancer free.
“It still gives me shivers,” he said. “Dr Porter said, ‘Your bone marrow’s completely free. We just can’t find a cancer cell anywhere.’ “
The remission has lasted, and it is now 10 years later.
Balancing long-term risks vs benefits
Long-term data have been accumulating for these novel therapies since Olson’s treatment in 2010. This is particularly important for CAR T-cell therapy, because of its longevity. Because these are living cells and are expected to persist in the body for years, there is great interest in longer-term data, especially the risks for toxicity.
The FDA requires clinical follow-up for at least 15 years for patients treated with CAR T-cell therapy or any other genetically modified cells.
So far, most of the experience with CAR T cells comes from anti-CD19-directed therapy, which has shown “remarkable” remission rates in the 50% to 85% range, said Nirali Shah, MD, head of the hematologic malignancies section of the Pediatric Oncology Branch at the National Cancer Institute (NCI).
The most recent results presented at this year’s annual meeting of the American Society of Clinical Oncology support earlier efficacy data, she noted. In the longest follow-up to date, researchers reported remissions lasting over 9 years in patients with relapsed/refractory B-cell lymphoma or CLL treated with Kite›s axicaptagene cilleucel (Yescarta), one of two anti-CD19-directed CAR T-cell therapies approved by the FDA in 2017 (the other is Novartis’ tisagenlecleucel [Kymriah]).
This study included 43 patients and showed an overall remission rate of 76%. Complete remission was achieved in 54% of patients, and 22% had partial remission.
The other focus is long-term safety. Although some of the long-term adverse effects are known and are manageable, others fall into the theoretical realm. In early May 2020, the NCI held a multidisciplinary virtual conference on CAR T-cell therapy «to encourage collaborative research about the subacute and potentially long-term toxicity profile of these treatments.»
“We know just a little at this point about late- and long-term effects of CAR-T therapy, because we are relatively early in the era of CAR T cells,” said Merav Bar, MD, from the Fred Hutchinson Cancer Research Center in Seattle, Washington.
B-cell aplasia and risk for new infections
What is known is that B-cell aplasia represents the most common long-term adverse effect of CAR T-cell therapy. B-cell aplasia results when anti-CD19 CAR-T therapy wipes out healthy B cells as well as the malignant ones responsible for leukemia/lymphoma.
As major players in the immune system, B cells are a key defense against viruses. So B-cell aplasia represents a very specific type of immunosuppression. It is generally less severe than immunosuppression that occurs after organ transplant, which hits the immune system pretty much across the board and carries a much higher risk for infection.
The main concern is what happens when someone with B-cell aplasia encounters a new pathogen, such as SARS-CoV-2.
After infection, B cells generate memory cells, which are not killed off by anti-CD19 therapy and that stick around for life. So a patient such as Olson would still make antibodies that fight infections they experienced before receiving CAR-T therapy, such as childhood chickenpox. But now they are unable to make new memory cells, so these patients receive monthly immunoglobulin infusions to protect against pathogens they have not previously encountered.
Olson takes this in stride and says he isn’t overly worried about COVID-19. He follows the recommended precautions for a man his age. He wears a mask, washes his hands frequently, and tries to maintain social distancing. But he doesn’t stay locked up in his New Hampshire home.
“I took the attitude when I was diagnosed with cancer that I’m going to live my life,” he said. “Quality of life to me is more important than quantity.”
Neuropsychiatric toxicity
Another problem is the possibility of neuropsychiatric toxicity. Past studies have reported a wide range of such toxicities associated with CAR T-cell therapy, including seizures and hallucinations. Most have occurred early in the course of treatment and appear to be short-lived and reversible. However, there remain questions about long-term neuropsychiatric problems.
In a long-term study of 40 patients with relapsed/refractory CLL, non-Hodgkin lymphoma, and ALL, nearly half of patients (47.5%, 19/40) self-reported at least one clinically meaningful negative neuropsychiatric outcome (anxiety, depression, or cognitive difficulty) 1 to 5 years after anti-CD19 CAR T-cell therapy. In addition, 37.5% (15/40) self-reported cognitive difficulties.
“Patients with more severe neurotoxicity showed a trend for more cognitive difficulties afterwards,» said Bar, senior author of the study.
However, teasing out the role that CAR T-cell therapy plays in these problems poses a challenge. All of these patients had been heavily pretreated with previous cancer therapy, which has also been associated with neuropsychiatric problems.
“So far, we don’t know what caused it,” Bar said. “Nevertheless, people need to pay attention to neuropsychiatric symptoms in CAR T-cell therapy. It is important to continue to monitor these patients for these issues.”
Graft-vs-host disease
Another potential problem is graft-vs-host disease (GVHD). This is not uncommon after hematopoietic stem cell transplants. It develops when the donor T cells view antigens on healthy recipient cells as foreign and attack them.
For patients who are treated with CAR T cells, GVHD is mostly a concern among individuals who have previously had a transplant and who are already at increased risk for it.
In a study of late effects among 86 adults treated with anti-CD19 CAR T cells for relapsed/refractory non-Hodgkin lymphoma, Bar and colleagues found that GVHD occurred only among patients who had received a previous donor stem cell transplant. Of these, 20% (3/15) developed GVHD about 28 months after CAR-T therapy.
“The data for CAR T cells causing GVHD really hasn’t shown that it’s a huge problem, although we have seen it and are continuing to monitor for it,” the NCI’s Shah commented to Medscape Medical News.
Other Long-term Adverse Effects
A range of other long-term adverse effects have been reported with CAR-T therapy, including prolonged cytopenias (reduced mature blood cells), myelodysplasia (bone marrow failure), and second malignancies.
In the study with the longest follow-up to date, 16% (7/43) of patients developed second malignancies, which is comparable to data from Bar’s study in Seattle (15%, 13/86). The researchers in this study consider this rate to be no higher than expected: these patients had already received extensive chemotherapy, which increases the risk for other cancers, they point out.
However, this brings up theoretical concerns about the long-term effects of gene modification. CAR T cells are engineered using retroviruses (mainly lentiviruses), which randomly insert the CAR genes into the host genome. Doing so may cause mutations that could promote cancer. These lentiviruses also carry the theoretical risk of becoming capable of viral replication once inside the body.
To address these concerns, viruses used to engineer CAR T cells go through comprehensive safety testing. After therapy, patients are checked every few months during the first year and annually after that.
So far, there have been no reports of cancers associated with CAR T-cell therapy.
“Any type of cancer is a very theoretical risk,” Bar told Medscape Medical News. «Most likely the malignancies in our study were related to prior treatment that the patients received. None of them had any evidence of replication-competent lentivirus, or any other evidence that the malignancies were related to the CAR T cells.»
Another theoretical concern is the possibility of new-onset autoimmune disease, although, once again, no cases have been reported so far.
“We think of it as a theoretic possibility. Whenever you jack up the immune system, autoimmune disease is a potential risk,” said Carl June, MD, director of the Center for Cellular Immunotherapies at the University of Pennsylvania.
June was the co–principal investigator of the trial in which Olson participated. He is also the inventor on patents for CAR T cells licensed by the University of Pennsylvania to Novartis and Tmunity and is a scientific founder with equity in Tmunity.
Still, autoimmunity could occur, and scientists are looking out for it.
“We are continuing to be vigilant in our monitoring for autoimmune disease,” Shah added. “We’ve been doing CAR T-cell therapy since 2012, and I think we have yet to see true autoimmunity beyond GVHD.”
Future directions
In the 10 years since Olson received CAR T-cell therapy, an entire industry has sprung up. Over 100 companies worldwide are now developing CAR T-cell therapies targeting various antigens. These therapies are directed at about 60 different tumor types, including solid tumors. Nearly 200 clinical trials are underway, though most are still in early stages: as of September 2019, only 5% had reached phase 3.
Clinical data show promising results for CAR T-cell therapy directed against CD22 (overexpressed on ALL cells), and BCMA (found on almost all multiple myeloma cells). Yet questions remain as to whether CAR T cells will be as effective if they target antigens other than CD19 or cells other than B lymphocytes. One of the biggest research questions is whether they will be effective against solid tumors.
One research avenue being watched with great interest is the development of universal CAR T cells. So far, such products are at very early stages of development (phase 1 trials), but they are attractive because of the potential advantages they offer over bespoke CAR T cells. Automating the process holds the promise of immediate availability, standardizing production, expanding access, and lowering costs. And because the T cells for this universal product come from healthy donors, they may function better than T cells that have been battered and bruised by past cancer treatments, or even the cancer itself.
However, precisely because they are developed from healthy donor T cells, universal CAR T cells may pose increased risk for GVHD. Scientists are trying to get around this problem by engineering universal CAR T cells that lack the T-cell receptor involved in GVHD.
There are also other concerns. Nature has a penchant for mutation. Engineering CAR T cells without T-cell receptors means the body may no longer detect or reject a universal CAR T cell if it goes rogue. Also, gene insertion in universal CAR-T therapy is targeted rather than random (as in bespoke CAR T cells), which could create off-target effects. Both issues create a theoretical risk of such products inducing an untreatable CAR T-cell therapy–associated cancer.
“The theoretic risk with universal cells is that their safety profile may not be as good for long term,” June commented.
Hope for the future
From that first trial in which June and Porter used CAR T cells, two of three patients they treated are still alive 10 years later.
Olson is one of these two, and he still undergoes monitoring every 3 months to check for relapse. So far, none of his tests have shown signs of his cancer returning.
After going into remission, Doug spent the next 6 to 9 months regaining his health and strength.
“I figured if I had this amazing treatment that saved my life, I had an obligation to stay alive,” he said. “I’d better not die of something like a heart attack!”
He took up long distance running and has completed six half marathons. He became involved in the Leukemia and Lymphoma Society, participating in fund-raising and helping newly diagnosed patients. Over the years, he has also given talks for researchers, people with cancer, and healthcare providers.
Doug is now 73. Today, he marvels at how rapidly the CAR-T field has progressed.
“Twenty years ago, if you had cancer, your prospects weren’t nearly as good as these days. In 2010, people still didn’t believe in CAR T-cell therapy,” he said. “My goal always in telling my story is a message of hope.”
This article first appeared on Medscape.com.
When a patient with cancer hears there isn’t much left that doctors can do, it always stays fresh in the mind.
Doug Olson was first diagnosed with chronic lymphocytic leukemia (CLL) over 20 years ago, in 1996. For several years, his doctors used the watch-and-wait approach. But then his cancer progressed and needed treatment. By 2010, it had mutated so much that it no longer responded to standard therapy.
He was rapidly running out of options. Back then, the only treatment left was a bone marrow transplant. Without one, his doctors said, he would have 1 or 2 years left to live.
“I was really trying to avoid a bone marrow transplant. You’re playing your last card if that doesn’t work. It’s a pretty rough procedure,” Olson told Medscape Medical News.
Looking back, Olson counts himself as lucky – for being in the right place, at the right time, with the right doctor. His oncologist was David Porter, MD, the principal investigator on a trial at the University of Pennsylvania that was investigating a brand new approach to treating cancer: chimeric antigen receptor (CAR) T-cell therapy.
CAR T-cell therapy uses a patient’s own T cells engineered to express a receptor that targets proteins on cancer cells. CAR T cells are considered “living drugs” because they expand inside the body and stick around for years – maybe for a lifetime – to fight the cancer if it tries to come back.
“I was certainly intrigued by the approach. It had worked in mice, and it was the sort of thing that looked like it would work,” Olson recalled.
Science is not a foreign language to Olson. He holds a PhD in medicinal chemistry, spent most of his career in the in vitro diagnostics industry, and currently acts as chief executive officer of Buhlmann Diagnostics Corp.
So he read the clinical protocol for the first in-human trial of CAR T cells and agreed to become patient number two.
Olson’s T cells were harvested, engineered to attack the CD19 antigen found on malignant and normal B lymphocytes, and then were expanded into millions in the lab. After undergoing preconditioning with chemotherapy to minimize rejection and boost the CAR T cells’ expansion inside the body, he received several infusions of the new therapy over the course of 3 days.
Nothing really happened for 2 weeks. Then he developed severe flu-like symptoms – so bad that he was hospitalized.
Ironically, getting sick was a sign that the CAR T cells were working. Olson was experiencing one of the main short-term effects of CAR T-cell therapy: cytokine release syndrome. Symptoms include extremely high fevers and dangerous drops in blood pressure that can potentially cause end-organ damage.
In the early trials of these products, some patients experienced such a severe reaction that they needed intensive care, and some died. With increasing clinical experience, doctors have learned to control the reaction with the use of steroids and interleukein-6 inhibitors such as tocilizumab (Actemra).
Fortunately for Olson, the reaction passed, and he was eventually discharged.
Then the “aha moment” happened. Four weeks after receiving the CAR T cells, Olson found out that he was cancer free.
“It still gives me shivers,” he said. “Dr Porter said, ‘Your bone marrow’s completely free. We just can’t find a cancer cell anywhere.’ “
The remission has lasted, and it is now 10 years later.
Balancing long-term risks vs benefits
Long-term data have been accumulating for these novel therapies since Olson’s treatment in 2010. This is particularly important for CAR T-cell therapy, because of its longevity. Because these are living cells and are expected to persist in the body for years, there is great interest in longer-term data, especially the risks for toxicity.
The FDA requires clinical follow-up for at least 15 years for patients treated with CAR T-cell therapy or any other genetically modified cells.
So far, most of the experience with CAR T cells comes from anti-CD19-directed therapy, which has shown “remarkable” remission rates in the 50% to 85% range, said Nirali Shah, MD, head of the hematologic malignancies section of the Pediatric Oncology Branch at the National Cancer Institute (NCI).
The most recent results presented at this year’s annual meeting of the American Society of Clinical Oncology support earlier efficacy data, she noted. In the longest follow-up to date, researchers reported remissions lasting over 9 years in patients with relapsed/refractory B-cell lymphoma or CLL treated with Kite›s axicaptagene cilleucel (Yescarta), one of two anti-CD19-directed CAR T-cell therapies approved by the FDA in 2017 (the other is Novartis’ tisagenlecleucel [Kymriah]).
This study included 43 patients and showed an overall remission rate of 76%. Complete remission was achieved in 54% of patients, and 22% had partial remission.
The other focus is long-term safety. Although some of the long-term adverse effects are known and are manageable, others fall into the theoretical realm. In early May 2020, the NCI held a multidisciplinary virtual conference on CAR T-cell therapy «to encourage collaborative research about the subacute and potentially long-term toxicity profile of these treatments.»
“We know just a little at this point about late- and long-term effects of CAR-T therapy, because we are relatively early in the era of CAR T cells,” said Merav Bar, MD, from the Fred Hutchinson Cancer Research Center in Seattle, Washington.
B-cell aplasia and risk for new infections
What is known is that B-cell aplasia represents the most common long-term adverse effect of CAR T-cell therapy. B-cell aplasia results when anti-CD19 CAR-T therapy wipes out healthy B cells as well as the malignant ones responsible for leukemia/lymphoma.
As major players in the immune system, B cells are a key defense against viruses. So B-cell aplasia represents a very specific type of immunosuppression. It is generally less severe than immunosuppression that occurs after organ transplant, which hits the immune system pretty much across the board and carries a much higher risk for infection.
The main concern is what happens when someone with B-cell aplasia encounters a new pathogen, such as SARS-CoV-2.
After infection, B cells generate memory cells, which are not killed off by anti-CD19 therapy and that stick around for life. So a patient such as Olson would still make antibodies that fight infections they experienced before receiving CAR-T therapy, such as childhood chickenpox. But now they are unable to make new memory cells, so these patients receive monthly immunoglobulin infusions to protect against pathogens they have not previously encountered.
Olson takes this in stride and says he isn’t overly worried about COVID-19. He follows the recommended precautions for a man his age. He wears a mask, washes his hands frequently, and tries to maintain social distancing. But he doesn’t stay locked up in his New Hampshire home.
“I took the attitude when I was diagnosed with cancer that I’m going to live my life,” he said. “Quality of life to me is more important than quantity.”
Neuropsychiatric toxicity
Another problem is the possibility of neuropsychiatric toxicity. Past studies have reported a wide range of such toxicities associated with CAR T-cell therapy, including seizures and hallucinations. Most have occurred early in the course of treatment and appear to be short-lived and reversible. However, there remain questions about long-term neuropsychiatric problems.
In a long-term study of 40 patients with relapsed/refractory CLL, non-Hodgkin lymphoma, and ALL, nearly half of patients (47.5%, 19/40) self-reported at least one clinically meaningful negative neuropsychiatric outcome (anxiety, depression, or cognitive difficulty) 1 to 5 years after anti-CD19 CAR T-cell therapy. In addition, 37.5% (15/40) self-reported cognitive difficulties.
“Patients with more severe neurotoxicity showed a trend for more cognitive difficulties afterwards,» said Bar, senior author of the study.
However, teasing out the role that CAR T-cell therapy plays in these problems poses a challenge. All of these patients had been heavily pretreated with previous cancer therapy, which has also been associated with neuropsychiatric problems.
“So far, we don’t know what caused it,” Bar said. “Nevertheless, people need to pay attention to neuropsychiatric symptoms in CAR T-cell therapy. It is important to continue to monitor these patients for these issues.”
Graft-vs-host disease
Another potential problem is graft-vs-host disease (GVHD). This is not uncommon after hematopoietic stem cell transplants. It develops when the donor T cells view antigens on healthy recipient cells as foreign and attack them.
For patients who are treated with CAR T cells, GVHD is mostly a concern among individuals who have previously had a transplant and who are already at increased risk for it.
In a study of late effects among 86 adults treated with anti-CD19 CAR T cells for relapsed/refractory non-Hodgkin lymphoma, Bar and colleagues found that GVHD occurred only among patients who had received a previous donor stem cell transplant. Of these, 20% (3/15) developed GVHD about 28 months after CAR-T therapy.
“The data for CAR T cells causing GVHD really hasn’t shown that it’s a huge problem, although we have seen it and are continuing to monitor for it,” the NCI’s Shah commented to Medscape Medical News.
Other Long-term Adverse Effects
A range of other long-term adverse effects have been reported with CAR-T therapy, including prolonged cytopenias (reduced mature blood cells), myelodysplasia (bone marrow failure), and second malignancies.
In the study with the longest follow-up to date, 16% (7/43) of patients developed second malignancies, which is comparable to data from Bar’s study in Seattle (15%, 13/86). The researchers in this study consider this rate to be no higher than expected: these patients had already received extensive chemotherapy, which increases the risk for other cancers, they point out.
However, this brings up theoretical concerns about the long-term effects of gene modification. CAR T cells are engineered using retroviruses (mainly lentiviruses), which randomly insert the CAR genes into the host genome. Doing so may cause mutations that could promote cancer. These lentiviruses also carry the theoretical risk of becoming capable of viral replication once inside the body.
To address these concerns, viruses used to engineer CAR T cells go through comprehensive safety testing. After therapy, patients are checked every few months during the first year and annually after that.
So far, there have been no reports of cancers associated with CAR T-cell therapy.
“Any type of cancer is a very theoretical risk,” Bar told Medscape Medical News. «Most likely the malignancies in our study were related to prior treatment that the patients received. None of them had any evidence of replication-competent lentivirus, or any other evidence that the malignancies were related to the CAR T cells.»
Another theoretical concern is the possibility of new-onset autoimmune disease, although, once again, no cases have been reported so far.
“We think of it as a theoretic possibility. Whenever you jack up the immune system, autoimmune disease is a potential risk,” said Carl June, MD, director of the Center for Cellular Immunotherapies at the University of Pennsylvania.
June was the co–principal investigator of the trial in which Olson participated. He is also the inventor on patents for CAR T cells licensed by the University of Pennsylvania to Novartis and Tmunity and is a scientific founder with equity in Tmunity.
Still, autoimmunity could occur, and scientists are looking out for it.
“We are continuing to be vigilant in our monitoring for autoimmune disease,” Shah added. “We’ve been doing CAR T-cell therapy since 2012, and I think we have yet to see true autoimmunity beyond GVHD.”
Future directions
In the 10 years since Olson received CAR T-cell therapy, an entire industry has sprung up. Over 100 companies worldwide are now developing CAR T-cell therapies targeting various antigens. These therapies are directed at about 60 different tumor types, including solid tumors. Nearly 200 clinical trials are underway, though most are still in early stages: as of September 2019, only 5% had reached phase 3.
Clinical data show promising results for CAR T-cell therapy directed against CD22 (overexpressed on ALL cells), and BCMA (found on almost all multiple myeloma cells). Yet questions remain as to whether CAR T cells will be as effective if they target antigens other than CD19 or cells other than B lymphocytes. One of the biggest research questions is whether they will be effective against solid tumors.
One research avenue being watched with great interest is the development of universal CAR T cells. So far, such products are at very early stages of development (phase 1 trials), but they are attractive because of the potential advantages they offer over bespoke CAR T cells. Automating the process holds the promise of immediate availability, standardizing production, expanding access, and lowering costs. And because the T cells for this universal product come from healthy donors, they may function better than T cells that have been battered and bruised by past cancer treatments, or even the cancer itself.
However, precisely because they are developed from healthy donor T cells, universal CAR T cells may pose increased risk for GVHD. Scientists are trying to get around this problem by engineering universal CAR T cells that lack the T-cell receptor involved in GVHD.
There are also other concerns. Nature has a penchant for mutation. Engineering CAR T cells without T-cell receptors means the body may no longer detect or reject a universal CAR T cell if it goes rogue. Also, gene insertion in universal CAR-T therapy is targeted rather than random (as in bespoke CAR T cells), which could create off-target effects. Both issues create a theoretical risk of such products inducing an untreatable CAR T-cell therapy–associated cancer.
“The theoretic risk with universal cells is that their safety profile may not be as good for long term,” June commented.
Hope for the future
From that first trial in which June and Porter used CAR T cells, two of three patients they treated are still alive 10 years later.
Olson is one of these two, and he still undergoes monitoring every 3 months to check for relapse. So far, none of his tests have shown signs of his cancer returning.
After going into remission, Doug spent the next 6 to 9 months regaining his health and strength.
“I figured if I had this amazing treatment that saved my life, I had an obligation to stay alive,” he said. “I’d better not die of something like a heart attack!”
He took up long distance running and has completed six half marathons. He became involved in the Leukemia and Lymphoma Society, participating in fund-raising and helping newly diagnosed patients. Over the years, he has also given talks for researchers, people with cancer, and healthcare providers.
Doug is now 73. Today, he marvels at how rapidly the CAR-T field has progressed.
“Twenty years ago, if you had cancer, your prospects weren’t nearly as good as these days. In 2010, people still didn’t believe in CAR T-cell therapy,” he said. “My goal always in telling my story is a message of hope.”
This article first appeared on Medscape.com.
Socioeconomic status key factor in CPAP adherence in older adults
The benefits of continuous positive airway pressure therapy for patients with obstructive sleep apnea are well documented, but it only works if patients can adhere to the therapy.
A large national study of older Medicare patients with obstructive sleep apnea (OSA) has identified lower socioeconomic status and comorbidities as independent risk factors for nonadherence to continuous positive airway pressure (CPAP) therapy.
“[The] present results represent the largest study to date of rates and predictors of CPAP adherence among older adults in the United States. In our national sample of Medicare beneficiaries, adherence rates were generally lower than previously reported in smaller, clinic-based studies,” Emerson M. Wickwire, PhD, of the Sleep Disorders Center and division of pulmonary and critical care medicine at the University of Maryland, Baltimore, and colleagues wrote in Sleep.
Dr. Wickwire and colleagues estimated CPAP machine adherence using a 5% sample of Medicare claims data, identifying 3,229 Medicare beneficiaries with OSA who began CPAP therapy between 2009 and 2011. Individuals in the sample were aged at least 65 years with a new diagnosis of OSA, 88.1% of beneficiaries were white, and 52.3% were male.
The researchers applied objective adherence criteria set by the Centers for Medicare & Medicaid Services, which defines CPAP adherence as a patient using CPAP for at least 4 hours on 70% of nights, or CPAP use for 21 of 30 consecutive days within 90 days after beginning therapy.
Using CPAP machine charges as a measure of who adhered to therapy, they found 1,420 of 3,229 individuals (44%) achieved adherence under these criteria, which included making 13 monthly payments during their CPAP machine’s “rent-to-own” period. Partial adherence was found in 997 individuals (30.9%) who made between 4-12 payments on their CPAP machine, while 812 individuals (25.2%) made 4 payments or fewer on their CPAP machines, which the researchers classified as nonadherence. Nonadherers tended to be slightly younger (mean, 72.5 years vs. 79.2 years; P < .001) and had a higher number of comorbidities (35.2% vs. 30.4%; P = .002), compared with individuals with high adherence. Anxiety (odds ratio, 1.34; 95% confidence interval, 1.12-1.61), anemia (OR, 1.16; 95% CI, 1.02-1.32), fibromyalgia (OR, 1.19; 95% CI, 1.03-1.38), traumatic brain injury (OR, 1.58; 95% CI, 1.21-2.07), and Medicaid eligibility (OR, 1.48; 95% CI, 1.24-1.75) were all independently associated with lower CPAP adherence. Medicaid eligibility was considered an indicator of lower socioeconomic status.

Krishna M. Sundar, MD, FCCP, director at the Sleep-Wake Center in the University of Utah pulmonary division in Salt Lake City and CHEST Physician editorial board member, said in an interview that studies have shown early signs of adherence within the first few weeks are an important indicator of overall adherence to CPAP therapy. However, the use of CPAP machine payments in the study by Dr. Wickwire and colleagues was a novel way to track adherence.
Some of the issues with nonadherence may be related to challenges in using the technology, but it is the clinician’s role to communicate with patients about the effectiveness of CPAP and identifying reasons for nonadherence while also attempting to tease out the subtle socioeconomic factors related to nonadherence, Dr. Sundar noted. “We need to alter our practice to make sure that we communicate with these patients and better understand what are the social factors in getting the CPAP or utilizing CPAP, and also following these patients more closely, especially in the first month of starting CPAP therapy.
“Just because somebody has severe sleep apnea and other comorbid conditions does not mean that they’re going to wear the CPAP,” he said. “So, the fact that socioeconomic factors play an equal if not more important role in terms of predicting CPAP adherence. That is an important takeaway.”

Octavian C. Ioachimescu, MD, FCCP, of Emory University, Atlanta, and the Atlanta Veteran Affairs Administration and CHEST Physician editorial board member, said in an interview that the study raises a major question of what is next. “What can we offer to these patients, and what is the real-world compliance to that ‘next-best’ modality?” Dr. Ioachimescu said. “What are the outcomes of these individuals in the point-of-care environment, or ‘real world?’ ”
The analysis by the authors adds the perspective of a “real-world depiction of clinical care for patients with OSA,” Dr. Ioachimescu said. “One major lesson of such an analysis is that the health care goal setting that is referential to initial, randomized, well-controlled studies on highly selected patient populations need to be reassessed periodically from the point of view of actual results in the clinics.”
Clinicians may need to borrow ideas from other therapeutic fields to help improve patient adherence, he said. “[W]e may be able to develop and implement in the future peer involvement, behavioral and cognitive approaches, motivational enhancement interventions, as well as elements of acceptance and commitment techniques, all in the larger context of more integrated and in the same time individualized approaches to therapy.”
The investigators concluded that, “relative to Medicare-only beneficiaries, those eligible for both Medicare and Medicaid were significantly less likely to adhere to CPAP. Future research should seek to develop a deeper understanding of the mechanisms through which [socioeconomic status] and other social determinants impact patient experience throughout the OSA diagnostic and treatment process, including receiving, acclimating, and adhering to CPAP therapy.”
Dr. Sundar concurred with this assessment and said more research is needed on factors impacting adherence such as poverty, homelessness, and home support systems. “It’s not just coordinating with the patient. Clearly, more work is needed in understanding the social aspects of CPAP adherence.”
This study was funded in part by an investigator-initiated grant provided by ResMed to Dr. Wickmire’s institution, the University of Maryland, Baltimore. Dr. Wickmire reported being a scientific consultant to DayZz, Eisai, Merck, and Purdue and holds shares in WellTap. Dr. Oldstone is a ResMed employee and shareholder. Dr. Sundar reported being a cofounder of Hypnoscure, which creates software for population management of sleep apnea, and an investigator in trials where ResMed and Respironics devices were used. Dr. Ioachimescu reported no relevant financial disclosures.
SOURCE: Wickwire EM et al. Sleep. 2020 Jun 23. doi: 10.1093/sleep/zsaa122.
The benefits of continuous positive airway pressure therapy for patients with obstructive sleep apnea are well documented, but it only works if patients can adhere to the therapy.
A large national study of older Medicare patients with obstructive sleep apnea (OSA) has identified lower socioeconomic status and comorbidities as independent risk factors for nonadherence to continuous positive airway pressure (CPAP) therapy.
“[The] present results represent the largest study to date of rates and predictors of CPAP adherence among older adults in the United States. In our national sample of Medicare beneficiaries, adherence rates were generally lower than previously reported in smaller, clinic-based studies,” Emerson M. Wickwire, PhD, of the Sleep Disorders Center and division of pulmonary and critical care medicine at the University of Maryland, Baltimore, and colleagues wrote in Sleep.
Dr. Wickwire and colleagues estimated CPAP machine adherence using a 5% sample of Medicare claims data, identifying 3,229 Medicare beneficiaries with OSA who began CPAP therapy between 2009 and 2011. Individuals in the sample were aged at least 65 years with a new diagnosis of OSA, 88.1% of beneficiaries were white, and 52.3% were male.
The researchers applied objective adherence criteria set by the Centers for Medicare & Medicaid Services, which defines CPAP adherence as a patient using CPAP for at least 4 hours on 70% of nights, or CPAP use for 21 of 30 consecutive days within 90 days after beginning therapy.
Using CPAP machine charges as a measure of who adhered to therapy, they found 1,420 of 3,229 individuals (44%) achieved adherence under these criteria, which included making 13 monthly payments during their CPAP machine’s “rent-to-own” period. Partial adherence was found in 997 individuals (30.9%) who made between 4-12 payments on their CPAP machine, while 812 individuals (25.2%) made 4 payments or fewer on their CPAP machines, which the researchers classified as nonadherence. Nonadherers tended to be slightly younger (mean, 72.5 years vs. 79.2 years; P < .001) and had a higher number of comorbidities (35.2% vs. 30.4%; P = .002), compared with individuals with high adherence. Anxiety (odds ratio, 1.34; 95% confidence interval, 1.12-1.61), anemia (OR, 1.16; 95% CI, 1.02-1.32), fibromyalgia (OR, 1.19; 95% CI, 1.03-1.38), traumatic brain injury (OR, 1.58; 95% CI, 1.21-2.07), and Medicaid eligibility (OR, 1.48; 95% CI, 1.24-1.75) were all independently associated with lower CPAP adherence. Medicaid eligibility was considered an indicator of lower socioeconomic status.
Krishna M. Sundar, MD, FCCP, director at the Sleep-Wake Center in the University of Utah pulmonary division in Salt Lake City and CHEST Physician editorial board member, said in an interview that studies have shown early signs of adherence within the first few weeks are an important indicator of overall adherence to CPAP therapy. However, the use of CPAP machine payments in the study by Dr. Wickwire and colleagues was a novel way to track adherence.
Some of the issues with nonadherence may be related to challenges in using the technology, but it is the clinician’s role to communicate with patients about the effectiveness of CPAP and identifying reasons for nonadherence while also attempting to tease out the subtle socioeconomic factors related to nonadherence, Dr. Sundar noted. “We need to alter our practice to make sure that we communicate with these patients and better understand what are the social factors in getting the CPAP or utilizing CPAP, and also following these patients more closely, especially in the first month of starting CPAP therapy.
“Just because somebody has severe sleep apnea and other comorbid conditions does not mean that they’re going to wear the CPAP,” he said. “So, the fact that socioeconomic factors play an equal if not more important role in terms of predicting CPAP adherence. That is an important takeaway.”
Octavian C. Ioachimescu, MD, FCCP, of Emory University, Atlanta, and the Atlanta Veteran Affairs Administration and CHEST Physician editorial board member, said in an interview that the study raises a major question of what is next. “What can we offer to these patients, and what is the real-world compliance to that ‘next-best’ modality?” Dr. Ioachimescu said. “What are the outcomes of these individuals in the point-of-care environment, or ‘real world?’ ”
The analysis by the authors adds the perspective of a “real-world depiction of clinical care for patients with OSA,” Dr. Ioachimescu said. “One major lesson of such an analysis is that the health care goal setting that is referential to initial, randomized, well-controlled studies on highly selected patient populations need to be reassessed periodically from the point of view of actual results in the clinics.”
Clinicians may need to borrow ideas from other therapeutic fields to help improve patient adherence, he said. “[W]e may be able to develop and implement in the future peer involvement, behavioral and cognitive approaches, motivational enhancement interventions, as well as elements of acceptance and commitment techniques, all in the larger context of more integrated and in the same time individualized approaches to therapy.”
The investigators concluded that, “relative to Medicare-only beneficiaries, those eligible for both Medicare and Medicaid were significantly less likely to adhere to CPAP. Future research should seek to develop a deeper understanding of the mechanisms through which [socioeconomic status] and other social determinants impact patient experience throughout the OSA diagnostic and treatment process, including receiving, acclimating, and adhering to CPAP therapy.”
Dr. Sundar concurred with this assessment and said more research is needed on factors impacting adherence such as poverty, homelessness, and home support systems. “It’s not just coordinating with the patient. Clearly, more work is needed in understanding the social aspects of CPAP adherence.”
This study was funded in part by an investigator-initiated grant provided by ResMed to Dr. Wickmire’s institution, the University of Maryland, Baltimore. Dr. Wickmire reported being a scientific consultant to DayZz, Eisai, Merck, and Purdue and holds shares in WellTap. Dr. Oldstone is a ResMed employee and shareholder. Dr. Sundar reported being a cofounder of Hypnoscure, which creates software for population management of sleep apnea, and an investigator in trials where ResMed and Respironics devices were used. Dr. Ioachimescu reported no relevant financial disclosures.
SOURCE: Wickwire EM et al. Sleep. 2020 Jun 23. doi: 10.1093/sleep/zsaa122.
The benefits of continuous positive airway pressure therapy for patients with obstructive sleep apnea are well documented, but it only works if patients can adhere to the therapy.
A large national study of older Medicare patients with obstructive sleep apnea (OSA) has identified lower socioeconomic status and comorbidities as independent risk factors for nonadherence to continuous positive airway pressure (CPAP) therapy.
“[The] present results represent the largest study to date of rates and predictors of CPAP adherence among older adults in the United States. In our national sample of Medicare beneficiaries, adherence rates were generally lower than previously reported in smaller, clinic-based studies,” Emerson M. Wickwire, PhD, of the Sleep Disorders Center and division of pulmonary and critical care medicine at the University of Maryland, Baltimore, and colleagues wrote in Sleep.
Dr. Wickwire and colleagues estimated CPAP machine adherence using a 5% sample of Medicare claims data, identifying 3,229 Medicare beneficiaries with OSA who began CPAP therapy between 2009 and 2011. Individuals in the sample were aged at least 65 years with a new diagnosis of OSA, 88.1% of beneficiaries were white, and 52.3% were male.
The researchers applied objective adherence criteria set by the Centers for Medicare & Medicaid Services, which defines CPAP adherence as a patient using CPAP for at least 4 hours on 70% of nights, or CPAP use for 21 of 30 consecutive days within 90 days after beginning therapy.
Using CPAP machine charges as a measure of who adhered to therapy, they found 1,420 of 3,229 individuals (44%) achieved adherence under these criteria, which included making 13 monthly payments during their CPAP machine’s “rent-to-own” period. Partial adherence was found in 997 individuals (30.9%) who made between 4-12 payments on their CPAP machine, while 812 individuals (25.2%) made 4 payments or fewer on their CPAP machines, which the researchers classified as nonadherence. Nonadherers tended to be slightly younger (mean, 72.5 years vs. 79.2 years; P < .001) and had a higher number of comorbidities (35.2% vs. 30.4%; P = .002), compared with individuals with high adherence. Anxiety (odds ratio, 1.34; 95% confidence interval, 1.12-1.61), anemia (OR, 1.16; 95% CI, 1.02-1.32), fibromyalgia (OR, 1.19; 95% CI, 1.03-1.38), traumatic brain injury (OR, 1.58; 95% CI, 1.21-2.07), and Medicaid eligibility (OR, 1.48; 95% CI, 1.24-1.75) were all independently associated with lower CPAP adherence. Medicaid eligibility was considered an indicator of lower socioeconomic status.
Krishna M. Sundar, MD, FCCP, director at the Sleep-Wake Center in the University of Utah pulmonary division in Salt Lake City and CHEST Physician editorial board member, said in an interview that studies have shown early signs of adherence within the first few weeks are an important indicator of overall adherence to CPAP therapy. However, the use of CPAP machine payments in the study by Dr. Wickwire and colleagues was a novel way to track adherence.
Some of the issues with nonadherence may be related to challenges in using the technology, but it is the clinician’s role to communicate with patients about the effectiveness of CPAP and identifying reasons for nonadherence while also attempting to tease out the subtle socioeconomic factors related to nonadherence, Dr. Sundar noted. “We need to alter our practice to make sure that we communicate with these patients and better understand what are the social factors in getting the CPAP or utilizing CPAP, and also following these patients more closely, especially in the first month of starting CPAP therapy.
“Just because somebody has severe sleep apnea and other comorbid conditions does not mean that they’re going to wear the CPAP,” he said. “So, the fact that socioeconomic factors play an equal if not more important role in terms of predicting CPAP adherence. That is an important takeaway.”
Octavian C. Ioachimescu, MD, FCCP, of Emory University, Atlanta, and the Atlanta Veteran Affairs Administration and CHEST Physician editorial board member, said in an interview that the study raises a major question of what is next. “What can we offer to these patients, and what is the real-world compliance to that ‘next-best’ modality?” Dr. Ioachimescu said. “What are the outcomes of these individuals in the point-of-care environment, or ‘real world?’ ”
The analysis by the authors adds the perspective of a “real-world depiction of clinical care for patients with OSA,” Dr. Ioachimescu said. “One major lesson of such an analysis is that the health care goal setting that is referential to initial, randomized, well-controlled studies on highly selected patient populations need to be reassessed periodically from the point of view of actual results in the clinics.”
Clinicians may need to borrow ideas from other therapeutic fields to help improve patient adherence, he said. “[W]e may be able to develop and implement in the future peer involvement, behavioral and cognitive approaches, motivational enhancement interventions, as well as elements of acceptance and commitment techniques, all in the larger context of more integrated and in the same time individualized approaches to therapy.”
The investigators concluded that, “relative to Medicare-only beneficiaries, those eligible for both Medicare and Medicaid were significantly less likely to adhere to CPAP. Future research should seek to develop a deeper understanding of the mechanisms through which [socioeconomic status] and other social determinants impact patient experience throughout the OSA diagnostic and treatment process, including receiving, acclimating, and adhering to CPAP therapy.”
Dr. Sundar concurred with this assessment and said more research is needed on factors impacting adherence such as poverty, homelessness, and home support systems. “It’s not just coordinating with the patient. Clearly, more work is needed in understanding the social aspects of CPAP adherence.”
This study was funded in part by an investigator-initiated grant provided by ResMed to Dr. Wickmire’s institution, the University of Maryland, Baltimore. Dr. Wickmire reported being a scientific consultant to DayZz, Eisai, Merck, and Purdue and holds shares in WellTap. Dr. Oldstone is a ResMed employee and shareholder. Dr. Sundar reported being a cofounder of Hypnoscure, which creates software for population management of sleep apnea, and an investigator in trials where ResMed and Respironics devices were used. Dr. Ioachimescu reported no relevant financial disclosures.
SOURCE: Wickwire EM et al. Sleep. 2020 Jun 23. doi: 10.1093/sleep/zsaa122.
FROM SLEEP
CMS to broaden transcatheter mitral valve repair coverage, and change its name
The first order of business in the long-awaited, recently released Centers for Medicare & Medicaid Services (CMS) proposed national coverage decision (NCD) for transcatheter mitral valve repair (TMVR) was to get rid of its familiar moniker.
The document tosses the term TMVR in favor of transcatheter edge-to-edge repair (TEER) “to more precisely define the treatment addressed in this NCD” and differentiate it from other therapies that repair or replace the mitral valve.
(In an off-the-cuff Twitter poll launched right after the CMS document’s release, 80.3% of respondents answered that they “hate” the new acronym and the remainder said they “love” it; those two were the poll’s only choices.)
The NCD proposal goes on to say that CMS coverage of TEER would expand to include treatment of symptomatic moderate-to-severe or severe functional mitral regurgitation (MR) when used with maximally tolerated guideline-directed medical therapy.
The proposed NCD has been expected since March 2019 when the US Food and Drug Administration (FDA) approved the MitraClip (Abbott Vascular) for secondary functional MR. Medicare has covered MitraClip for primary degenerative MR since 2014.
Abbott announced in October 2019 that it would ramp up production of the MitraClip, which is currently the only FDA-approved TEER device.
Further specifications
Even as the new proposed NCD would add CMS coverage for functional MR, it would also decline a coverage statement for degenerative MR. Instead, it proposes to leave such coverage decisions to local Medical Administrative Contractors (MACs), given a relatively low incidence of clip intervention for degenerative MR. Less than 1% of the Medicare population undergo TEER of the mitral valve for that indication, the document says.
“The MACs are structured to be able to take into account local patient, physician, and institutional factors, which are especially important when overall prevalence is very low.”
The proposal also emphasizes that patients undergoing such covered TEER procedures be “under the care of a heart failure physician specialist experienced in the care and treatment of mitral valve disease,» with additional care provided by a heart team that includes a cardiac surgeon, interventional cardiologist, interventional echocardiographer.
The new document is generally consistent with a Consensus Statement from the American Association for Thoracic Surgery, the American College of Cardiology (ACC), the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons published in December 2019 and covered then by theheart.org / Medscape Cardiology.
In anticipation the CMS coverage proposal, the ACC earlier this year published a Focused Update of the 2017 Expert Consensus Decision Pathway on the Management of Mitral Regurgitation to reflect new evidence in the field, mainly the recent clinical trial data on functional MR from the MITRA-FR and COAPT trials.
“The proposed criteria are nicely guided by the multisociety consensus document, which sought to foster optimal patient outcomes while also maintaining access to TEER,” Sammy Elmariah, MD, MPH, from Massachusetts General Hospital in Boston, commented by email.
“These criteria, in conjunction with results of the COAPT trial, establish TEER as the standard of care for patients with symptomatic functional MR despite guideline-directed medical therapy who do not possess an alternative indication for cardiac surgery,” said Elmariah, a coauthor on both the Consensus Statement and the Focused Update.
The proposed NCD seems “reasonable,” cardiothoracic surgeon Michael J. Reardon, MD, Houston Methodist Hospital, said by email. But he thought there might be some objections to the requirement for TEER centers to have a surgery program with a minimum annual volume for mitral-valve surgeries.
The proposed NCD says a hospital must have “a surgical program that performs ≥25 total mitral valve surgical procedures for severe MR per year, of which at least 10 must be mitral valve repairs.”
“There is a very definite relationship between mitral valve surgery volume and surgical outcomes and between TEER volume and TEER outcomes, but no real relationship between mitral valve surgery volumes and TEER outcomes,” Reardon said. “A mitral valve surgery program is important, but how many cases do you need to be able to start and run a TEER program?”
Edwards Lifesciences is currently testing its own device for TEER: the PASCAL transcatheter mitral valve repair system. Early findings from the company’s ongoing CLASP IID trial, a head-to-head comparison of Pascal and MitraClip, are expected in December 2023.
CMS is seeking comments on the proposed national coverage determination, and will render a final decision within 60 days of the end of the 30-day public comment period.
Elmariah discloses receiving research grants from the American Heart Association, the National Institutes of Health, Edwards Lifesciences, Svelte Medical, and Medtronic, and consulting fees from AstraZeneca. Reardon recently reported no relevant conflicts of interest.
This article first appeared on Medscape.com.
The first order of business in the long-awaited, recently released Centers for Medicare & Medicaid Services (CMS) proposed national coverage decision (NCD) for transcatheter mitral valve repair (TMVR) was to get rid of its familiar moniker.
The document tosses the term TMVR in favor of transcatheter edge-to-edge repair (TEER) “to more precisely define the treatment addressed in this NCD” and differentiate it from other therapies that repair or replace the mitral valve.
(In an off-the-cuff Twitter poll launched right after the CMS document’s release, 80.3% of respondents answered that they “hate” the new acronym and the remainder said they “love” it; those two were the poll’s only choices.)
The NCD proposal goes on to say that CMS coverage of TEER would expand to include treatment of symptomatic moderate-to-severe or severe functional mitral regurgitation (MR) when used with maximally tolerated guideline-directed medical therapy.
The proposed NCD has been expected since March 2019 when the US Food and Drug Administration (FDA) approved the MitraClip (Abbott Vascular) for secondary functional MR. Medicare has covered MitraClip for primary degenerative MR since 2014.
Abbott announced in October 2019 that it would ramp up production of the MitraClip, which is currently the only FDA-approved TEER device.
Further specifications
Even as the new proposed NCD would add CMS coverage for functional MR, it would also decline a coverage statement for degenerative MR. Instead, it proposes to leave such coverage decisions to local Medical Administrative Contractors (MACs), given a relatively low incidence of clip intervention for degenerative MR. Less than 1% of the Medicare population undergo TEER of the mitral valve for that indication, the document says.
“The MACs are structured to be able to take into account local patient, physician, and institutional factors, which are especially important when overall prevalence is very low.”
The proposal also emphasizes that patients undergoing such covered TEER procedures be “under the care of a heart failure physician specialist experienced in the care and treatment of mitral valve disease,» with additional care provided by a heart team that includes a cardiac surgeon, interventional cardiologist, interventional echocardiographer.
The new document is generally consistent with a Consensus Statement from the American Association for Thoracic Surgery, the American College of Cardiology (ACC), the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons published in December 2019 and covered then by theheart.org / Medscape Cardiology.
In anticipation the CMS coverage proposal, the ACC earlier this year published a Focused Update of the 2017 Expert Consensus Decision Pathway on the Management of Mitral Regurgitation to reflect new evidence in the field, mainly the recent clinical trial data on functional MR from the MITRA-FR and COAPT trials.
“The proposed criteria are nicely guided by the multisociety consensus document, which sought to foster optimal patient outcomes while also maintaining access to TEER,” Sammy Elmariah, MD, MPH, from Massachusetts General Hospital in Boston, commented by email.
“These criteria, in conjunction with results of the COAPT trial, establish TEER as the standard of care for patients with symptomatic functional MR despite guideline-directed medical therapy who do not possess an alternative indication for cardiac surgery,” said Elmariah, a coauthor on both the Consensus Statement and the Focused Update.
The proposed NCD seems “reasonable,” cardiothoracic surgeon Michael J. Reardon, MD, Houston Methodist Hospital, said by email. But he thought there might be some objections to the requirement for TEER centers to have a surgery program with a minimum annual volume for mitral-valve surgeries.
The proposed NCD says a hospital must have “a surgical program that performs ≥25 total mitral valve surgical procedures for severe MR per year, of which at least 10 must be mitral valve repairs.”
“There is a very definite relationship between mitral valve surgery volume and surgical outcomes and between TEER volume and TEER outcomes, but no real relationship between mitral valve surgery volumes and TEER outcomes,” Reardon said. “A mitral valve surgery program is important, but how many cases do you need to be able to start and run a TEER program?”
Edwards Lifesciences is currently testing its own device for TEER: the PASCAL transcatheter mitral valve repair system. Early findings from the company’s ongoing CLASP IID trial, a head-to-head comparison of Pascal and MitraClip, are expected in December 2023.
CMS is seeking comments on the proposed national coverage determination, and will render a final decision within 60 days of the end of the 30-day public comment period.
Elmariah discloses receiving research grants from the American Heart Association, the National Institutes of Health, Edwards Lifesciences, Svelte Medical, and Medtronic, and consulting fees from AstraZeneca. Reardon recently reported no relevant conflicts of interest.
This article first appeared on Medscape.com.
The first order of business in the long-awaited, recently released Centers for Medicare & Medicaid Services (CMS) proposed national coverage decision (NCD) for transcatheter mitral valve repair (TMVR) was to get rid of its familiar moniker.
The document tosses the term TMVR in favor of transcatheter edge-to-edge repair (TEER) “to more precisely define the treatment addressed in this NCD” and differentiate it from other therapies that repair or replace the mitral valve.
(In an off-the-cuff Twitter poll launched right after the CMS document’s release, 80.3% of respondents answered that they “hate” the new acronym and the remainder said they “love” it; those two were the poll’s only choices.)
The NCD proposal goes on to say that CMS coverage of TEER would expand to include treatment of symptomatic moderate-to-severe or severe functional mitral regurgitation (MR) when used with maximally tolerated guideline-directed medical therapy.
The proposed NCD has been expected since March 2019 when the US Food and Drug Administration (FDA) approved the MitraClip (Abbott Vascular) for secondary functional MR. Medicare has covered MitraClip for primary degenerative MR since 2014.
Abbott announced in October 2019 that it would ramp up production of the MitraClip, which is currently the only FDA-approved TEER device.
Further specifications
Even as the new proposed NCD would add CMS coverage for functional MR, it would also decline a coverage statement for degenerative MR. Instead, it proposes to leave such coverage decisions to local Medical Administrative Contractors (MACs), given a relatively low incidence of clip intervention for degenerative MR. Less than 1% of the Medicare population undergo TEER of the mitral valve for that indication, the document says.
“The MACs are structured to be able to take into account local patient, physician, and institutional factors, which are especially important when overall prevalence is very low.”
The proposal also emphasizes that patients undergoing such covered TEER procedures be “under the care of a heart failure physician specialist experienced in the care and treatment of mitral valve disease,» with additional care provided by a heart team that includes a cardiac surgeon, interventional cardiologist, interventional echocardiographer.
The new document is generally consistent with a Consensus Statement from the American Association for Thoracic Surgery, the American College of Cardiology (ACC), the Society for Cardiovascular Angiography and Interventions, and the Society of Thoracic Surgeons published in December 2019 and covered then by theheart.org / Medscape Cardiology.
In anticipation the CMS coverage proposal, the ACC earlier this year published a Focused Update of the 2017 Expert Consensus Decision Pathway on the Management of Mitral Regurgitation to reflect new evidence in the field, mainly the recent clinical trial data on functional MR from the MITRA-FR and COAPT trials.
“The proposed criteria are nicely guided by the multisociety consensus document, which sought to foster optimal patient outcomes while also maintaining access to TEER,” Sammy Elmariah, MD, MPH, from Massachusetts General Hospital in Boston, commented by email.
“These criteria, in conjunction with results of the COAPT trial, establish TEER as the standard of care for patients with symptomatic functional MR despite guideline-directed medical therapy who do not possess an alternative indication for cardiac surgery,” said Elmariah, a coauthor on both the Consensus Statement and the Focused Update.
The proposed NCD seems “reasonable,” cardiothoracic surgeon Michael J. Reardon, MD, Houston Methodist Hospital, said by email. But he thought there might be some objections to the requirement for TEER centers to have a surgery program with a minimum annual volume for mitral-valve surgeries.
The proposed NCD says a hospital must have “a surgical program that performs ≥25 total mitral valve surgical procedures for severe MR per year, of which at least 10 must be mitral valve repairs.”
“There is a very definite relationship between mitral valve surgery volume and surgical outcomes and between TEER volume and TEER outcomes, but no real relationship between mitral valve surgery volumes and TEER outcomes,” Reardon said. “A mitral valve surgery program is important, but how many cases do you need to be able to start and run a TEER program?”
Edwards Lifesciences is currently testing its own device for TEER: the PASCAL transcatheter mitral valve repair system. Early findings from the company’s ongoing CLASP IID trial, a head-to-head comparison of Pascal and MitraClip, are expected in December 2023.
CMS is seeking comments on the proposed national coverage determination, and will render a final decision within 60 days of the end of the 30-day public comment period.
Elmariah discloses receiving research grants from the American Heart Association, the National Institutes of Health, Edwards Lifesciences, Svelte Medical, and Medtronic, and consulting fees from AstraZeneca. Reardon recently reported no relevant conflicts of interest.
This article first appeared on Medscape.com.
Oxford coronavirus vaccine ‘triggers immune response’
The early stage results, published in The Lancet, found that the candidate vaccine, known as ChAdOx1 nCoV-19, provoked a T-cell response peaking 14 days after vaccination, and an antibody response within 28 days.
Andrew Pollard, chief investigator on the study, and professor of pediatric infection and immunity at Oxford University, described the results as “encouraging”. He told a briefing convened by the Science Media Centre on Monday that it was “a really important milestone on the path to the development of the vaccine”.
In the Commons, the Health Secretary, Matt Hancock, hailed the results for taking us “one step closer to finding a vaccine that can potentially save lives, all around the world”.
The trial, which has so far involved 1,077 healthy adults, caused minor side effects when compared with a control group given a meningitis vaccine. Fatigue and headache were the most commonly reported reactions.
However, there were no serious adverse events from the vaccine, the researchers said.
‘Still a long way to go’
Sarah Gilbert, lead researcher of the vaccine development program, and professor of vaccinology at Oxford, cautioned that there was still a long way to go before the team could confirm that the vaccine could protect against developing COVID-19.
“The difficulty that we have, and that all vaccine developers have in trying to make a vaccine against this particular virus, is that we don’t know how strong that immune response needs to be,” she said.
“So, we can’t say just by looking at immune responses whether this is going to protect people or not. And the only way we’re going to find out is by doing the large phase 3 trials and wait for people to be infected as part of that trial before we know if the vaccine can work.”
The authors noted some limitations to their findings. They said more research was needed to confirm their results in different groups of people – including older age groups, those with other health conditions, and in ethnically and geographically diverse populations.
A notable result of the trial was that participants given a second dose of the vaccine appeared to display a stronger immune response, a finding that had influenced plans to “look at two dose regimes as well as one dose regimes in the phase 3 trial”, Prof Adrian Hill, director of Oxford’s Jenner Institute, confirmed.
ChAdOx1 nCoV-19 is made from a weakened version of an adenovirus that causes infections in chimpanzees. The virus has been genetically modified so that it cannot grow in humans.
On Monday, the government announced that it had struck a deal with AstraZeneca for access to 100 million doses of the Oxford vaccine, in addition to millions of doses of other promising candidate vaccines.
Expert reaction to the findings
The Medical Research Council helped to fund the trial. Executive Chair Professor Fiona Watt commented: “It is truly remarkable how fast this vaccine has progressed, with our support, through early clinical trials, and it is very encouraging that it shows no safety concerns and evokes strong immune responses.
“There is a lot that we don’t yet know about immunity to the virus that causes COVID-19. However, it seems that both antibody and T cell immunity are important, and this vaccine triggers both responses. The much anticipated next milestone will be the results of the larger trials that are happening now to find out if the vaccine will protect people from the virus.”
Jonathan Ball, professor of molecular virology at the University of Nottingham, told the SMC: “The results of the Oxford chimp adenovirus vaccine candidate show that the vaccine is able to generate antibodies and T cells in humans and these persisted for several weeks. Whilst encouraging there is still a long way to go before we can herald the arrival of a successful coronavirus vaccine.
“It is unclear whether the levels of immunity can protect against infection – that’s what the larger ongoing phase III trials are designed to test. Nor do we know if this vaccine can protect those most vulnerable to severe COVID-19 disease.”
Stephen Evans, professor of pharmacoepidemiology at the London School of Hygiene and Tropical Medicine, commented: “For the vaccine to be really useful, we not only need the larger studies conducted where COVID-19 is still occurring at a high rate, but we need to be reasonably sure that the protection lasts for a considerable time.”
He said it was also vital that people older than 55 were included in later trials.
Richard Torbett, chief executive of the Association of the British Pharmaceutical Industry, said: “Developing a vaccine is an incredibly difficult challenge; the fact that there are multiple candidates in development is hopefully a sign that the hard work will ultimately pay off.
“But we must be patient. Proving that a vaccine is safe and effective is a long process and we could still be many months away.”
This article first appeared on Medscape.com.
The early stage results, published in The Lancet, found that the candidate vaccine, known as ChAdOx1 nCoV-19, provoked a T-cell response peaking 14 days after vaccination, and an antibody response within 28 days.
Andrew Pollard, chief investigator on the study, and professor of pediatric infection and immunity at Oxford University, described the results as “encouraging”. He told a briefing convened by the Science Media Centre on Monday that it was “a really important milestone on the path to the development of the vaccine”.
In the Commons, the Health Secretary, Matt Hancock, hailed the results for taking us “one step closer to finding a vaccine that can potentially save lives, all around the world”.
The trial, which has so far involved 1,077 healthy adults, caused minor side effects when compared with a control group given a meningitis vaccine. Fatigue and headache were the most commonly reported reactions.
However, there were no serious adverse events from the vaccine, the researchers said.
‘Still a long way to go’
Sarah Gilbert, lead researcher of the vaccine development program, and professor of vaccinology at Oxford, cautioned that there was still a long way to go before the team could confirm that the vaccine could protect against developing COVID-19.
“The difficulty that we have, and that all vaccine developers have in trying to make a vaccine against this particular virus, is that we don’t know how strong that immune response needs to be,” she said.
“So, we can’t say just by looking at immune responses whether this is going to protect people or not. And the only way we’re going to find out is by doing the large phase 3 trials and wait for people to be infected as part of that trial before we know if the vaccine can work.”
The authors noted some limitations to their findings. They said more research was needed to confirm their results in different groups of people – including older age groups, those with other health conditions, and in ethnically and geographically diverse populations.
A notable result of the trial was that participants given a second dose of the vaccine appeared to display a stronger immune response, a finding that had influenced plans to “look at two dose regimes as well as one dose regimes in the phase 3 trial”, Prof Adrian Hill, director of Oxford’s Jenner Institute, confirmed.
ChAdOx1 nCoV-19 is made from a weakened version of an adenovirus that causes infections in chimpanzees. The virus has been genetically modified so that it cannot grow in humans.
On Monday, the government announced that it had struck a deal with AstraZeneca for access to 100 million doses of the Oxford vaccine, in addition to millions of doses of other promising candidate vaccines.
Expert reaction to the findings
The Medical Research Council helped to fund the trial. Executive Chair Professor Fiona Watt commented: “It is truly remarkable how fast this vaccine has progressed, with our support, through early clinical trials, and it is very encouraging that it shows no safety concerns and evokes strong immune responses.
“There is a lot that we don’t yet know about immunity to the virus that causes COVID-19. However, it seems that both antibody and T cell immunity are important, and this vaccine triggers both responses. The much anticipated next milestone will be the results of the larger trials that are happening now to find out if the vaccine will protect people from the virus.”
Jonathan Ball, professor of molecular virology at the University of Nottingham, told the SMC: “The results of the Oxford chimp adenovirus vaccine candidate show that the vaccine is able to generate antibodies and T cells in humans and these persisted for several weeks. Whilst encouraging there is still a long way to go before we can herald the arrival of a successful coronavirus vaccine.
“It is unclear whether the levels of immunity can protect against infection – that’s what the larger ongoing phase III trials are designed to test. Nor do we know if this vaccine can protect those most vulnerable to severe COVID-19 disease.”
Stephen Evans, professor of pharmacoepidemiology at the London School of Hygiene and Tropical Medicine, commented: “For the vaccine to be really useful, we not only need the larger studies conducted where COVID-19 is still occurring at a high rate, but we need to be reasonably sure that the protection lasts for a considerable time.”
He said it was also vital that people older than 55 were included in later trials.
Richard Torbett, chief executive of the Association of the British Pharmaceutical Industry, said: “Developing a vaccine is an incredibly difficult challenge; the fact that there are multiple candidates in development is hopefully a sign that the hard work will ultimately pay off.
“But we must be patient. Proving that a vaccine is safe and effective is a long process and we could still be many months away.”
This article first appeared on Medscape.com.
The early stage results, published in The Lancet, found that the candidate vaccine, known as ChAdOx1 nCoV-19, provoked a T-cell response peaking 14 days after vaccination, and an antibody response within 28 days.
Andrew Pollard, chief investigator on the study, and professor of pediatric infection and immunity at Oxford University, described the results as “encouraging”. He told a briefing convened by the Science Media Centre on Monday that it was “a really important milestone on the path to the development of the vaccine”.
In the Commons, the Health Secretary, Matt Hancock, hailed the results for taking us “one step closer to finding a vaccine that can potentially save lives, all around the world”.
The trial, which has so far involved 1,077 healthy adults, caused minor side effects when compared with a control group given a meningitis vaccine. Fatigue and headache were the most commonly reported reactions.
However, there were no serious adverse events from the vaccine, the researchers said.
‘Still a long way to go’
Sarah Gilbert, lead researcher of the vaccine development program, and professor of vaccinology at Oxford, cautioned that there was still a long way to go before the team could confirm that the vaccine could protect against developing COVID-19.
“The difficulty that we have, and that all vaccine developers have in trying to make a vaccine against this particular virus, is that we don’t know how strong that immune response needs to be,” she said.
“So, we can’t say just by looking at immune responses whether this is going to protect people or not. And the only way we’re going to find out is by doing the large phase 3 trials and wait for people to be infected as part of that trial before we know if the vaccine can work.”
The authors noted some limitations to their findings. They said more research was needed to confirm their results in different groups of people – including older age groups, those with other health conditions, and in ethnically and geographically diverse populations.
A notable result of the trial was that participants given a second dose of the vaccine appeared to display a stronger immune response, a finding that had influenced plans to “look at two dose regimes as well as one dose regimes in the phase 3 trial”, Prof Adrian Hill, director of Oxford’s Jenner Institute, confirmed.
ChAdOx1 nCoV-19 is made from a weakened version of an adenovirus that causes infections in chimpanzees. The virus has been genetically modified so that it cannot grow in humans.
On Monday, the government announced that it had struck a deal with AstraZeneca for access to 100 million doses of the Oxford vaccine, in addition to millions of doses of other promising candidate vaccines.
Expert reaction to the findings
The Medical Research Council helped to fund the trial. Executive Chair Professor Fiona Watt commented: “It is truly remarkable how fast this vaccine has progressed, with our support, through early clinical trials, and it is very encouraging that it shows no safety concerns and evokes strong immune responses.
“There is a lot that we don’t yet know about immunity to the virus that causes COVID-19. However, it seems that both antibody and T cell immunity are important, and this vaccine triggers both responses. The much anticipated next milestone will be the results of the larger trials that are happening now to find out if the vaccine will protect people from the virus.”
Jonathan Ball, professor of molecular virology at the University of Nottingham, told the SMC: “The results of the Oxford chimp adenovirus vaccine candidate show that the vaccine is able to generate antibodies and T cells in humans and these persisted for several weeks. Whilst encouraging there is still a long way to go before we can herald the arrival of a successful coronavirus vaccine.
“It is unclear whether the levels of immunity can protect against infection – that’s what the larger ongoing phase III trials are designed to test. Nor do we know if this vaccine can protect those most vulnerable to severe COVID-19 disease.”
Stephen Evans, professor of pharmacoepidemiology at the London School of Hygiene and Tropical Medicine, commented: “For the vaccine to be really useful, we not only need the larger studies conducted where COVID-19 is still occurring at a high rate, but we need to be reasonably sure that the protection lasts for a considerable time.”
He said it was also vital that people older than 55 were included in later trials.
Richard Torbett, chief executive of the Association of the British Pharmaceutical Industry, said: “Developing a vaccine is an incredibly difficult challenge; the fact that there are multiple candidates in development is hopefully a sign that the hard work will ultimately pay off.
“But we must be patient. Proving that a vaccine is safe and effective is a long process and we could still be many months away.”
This article first appeared on Medscape.com.
COVID vaccine tested in people shows early promise
the company says in a news release.
Researchers also reported some side effects in the 45 people in the phase I study, but no significant safety issues, the news release says.
The vaccine is among hundreds being tested worldwide in an effort to halt the pandemic that has killed nearly 600,000 worldwide.
A researcher testing the vaccine called the results encouraging but cautioned more study is needed. “Importantly, the vaccine resulted in a robust immune response,” Evan Anderson, MD, principal investigator for the trial at Emory University, says in a news release. Emory and Kaiser Permanente Washington Health Research Institute were the two sites for the study.
The company is already testing the vaccine in a larger group of people, known as a phase II trial. It plans to begin phase III trials in late July. Phase III trials involve testing the vaccine on an even larger group and are the final step before FDA approval.
The study results are published in The New England Journal of Medicine. The study was led by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health.
Moderna’s vaccine uses messenger RNA, also called mRNA. It carries the instruction for making the spike protein, a key protein on the surface of the virus that allows it to enter cells when a person is infected. After it’s injected, it goes to the immune cells and instructs them to make copies of the spike protein, acting as if the cells have been infected with the actual coronavirus. This allows other immune cells to develop immunity.
In the study, participants were divided into three groups of 15 people each. All groups received two vaccinations 28 days apart. Each group received a different strength of the vaccine – either 25, 100, or 250 micrograms.
Every person in the study developed antibodies that can block the infection. Most commonly reported side effects after the second vaccination in the 100-microgram group were fatigue, chills, headache, and muscle pains, ranging from mild to moderately severe.
The phase II study has 300 heathy adults ages 18-55, along with another 300 ages 55 and older
Moderna says it hopes to include about 30,000 participants at the 100-microgram dose level in the U.S. for the phase III trial. The estimated start date is July 27.
This article first appeared on WebMD.com.
the company says in a news release.
Researchers also reported some side effects in the 45 people in the phase I study, but no significant safety issues, the news release says.
The vaccine is among hundreds being tested worldwide in an effort to halt the pandemic that has killed nearly 600,000 worldwide.
A researcher testing the vaccine called the results encouraging but cautioned more study is needed. “Importantly, the vaccine resulted in a robust immune response,” Evan Anderson, MD, principal investigator for the trial at Emory University, says in a news release. Emory and Kaiser Permanente Washington Health Research Institute were the two sites for the study.
The company is already testing the vaccine in a larger group of people, known as a phase II trial. It plans to begin phase III trials in late July. Phase III trials involve testing the vaccine on an even larger group and are the final step before FDA approval.
The study results are published in The New England Journal of Medicine. The study was led by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health.
Moderna’s vaccine uses messenger RNA, also called mRNA. It carries the instruction for making the spike protein, a key protein on the surface of the virus that allows it to enter cells when a person is infected. After it’s injected, it goes to the immune cells and instructs them to make copies of the spike protein, acting as if the cells have been infected with the actual coronavirus. This allows other immune cells to develop immunity.
In the study, participants were divided into three groups of 15 people each. All groups received two vaccinations 28 days apart. Each group received a different strength of the vaccine – either 25, 100, or 250 micrograms.
Every person in the study developed antibodies that can block the infection. Most commonly reported side effects after the second vaccination in the 100-microgram group were fatigue, chills, headache, and muscle pains, ranging from mild to moderately severe.
The phase II study has 300 heathy adults ages 18-55, along with another 300 ages 55 and older
Moderna says it hopes to include about 30,000 participants at the 100-microgram dose level in the U.S. for the phase III trial. The estimated start date is July 27.
This article first appeared on WebMD.com.
the company says in a news release.
Researchers also reported some side effects in the 45 people in the phase I study, but no significant safety issues, the news release says.
The vaccine is among hundreds being tested worldwide in an effort to halt the pandemic that has killed nearly 600,000 worldwide.
A researcher testing the vaccine called the results encouraging but cautioned more study is needed. “Importantly, the vaccine resulted in a robust immune response,” Evan Anderson, MD, principal investigator for the trial at Emory University, says in a news release. Emory and Kaiser Permanente Washington Health Research Institute were the two sites for the study.
The company is already testing the vaccine in a larger group of people, known as a phase II trial. It plans to begin phase III trials in late July. Phase III trials involve testing the vaccine on an even larger group and are the final step before FDA approval.
The study results are published in The New England Journal of Medicine. The study was led by the National Institute of Allergy and Infectious Diseases of the National Institutes of Health.
Moderna’s vaccine uses messenger RNA, also called mRNA. It carries the instruction for making the spike protein, a key protein on the surface of the virus that allows it to enter cells when a person is infected. After it’s injected, it goes to the immune cells and instructs them to make copies of the spike protein, acting as if the cells have been infected with the actual coronavirus. This allows other immune cells to develop immunity.
In the study, participants were divided into three groups of 15 people each. All groups received two vaccinations 28 days apart. Each group received a different strength of the vaccine – either 25, 100, or 250 micrograms.
Every person in the study developed antibodies that can block the infection. Most commonly reported side effects after the second vaccination in the 100-microgram group were fatigue, chills, headache, and muscle pains, ranging from mild to moderately severe.
The phase II study has 300 heathy adults ages 18-55, along with another 300 ages 55 and older
Moderna says it hopes to include about 30,000 participants at the 100-microgram dose level in the U.S. for the phase III trial. The estimated start date is July 27.
This article first appeared on WebMD.com.
Even mild obesity raises severe COVID-19 risks
People with a body mass index of 30 kg/m2 or above are at significantly increased risk for severe COVID-19, while a BMI of 35 and higher dramatically increases the risk for death, new research suggests.
The data, from nearly 500 patients hospitalized with COVID-19 in March and April 2020, were published in the European Journal of Endocrinology by Matteo Rottoli, MD, of the Alma Mater Studiorum, University of Bologna (Italy), and colleagues.
The data support the recent change by the Centers for Disease Control and Prevention to lower the cutoff for categorizing a person at increased risk from COVID-19 from a BMI of 40 down to 30. However, in the United Kingdom, the National Health Service still lists only a BMI of 40 or above as placing a person at “moderate risk (clinically vulnerable).”
“This finding calls for prevention and treatment strategies to reduce the risk of infection and hospitalization in patients with relevant degrees of obesity, supporting a revision of the BMI cutoff of 40 kg/m2, which was proposed as an independent risk factor for an adverse outcome of COVID-19 in the ... guidelines for social distancing in the United Kingdom: It may be appropriate to include patients with BMI >30 among those at higher risk for COVID-19 severe progression,” the authors wrote.
The study included 482 adults admitted with confirmed COVID-19 to a single Italian hospital between March 1 and April 20, 2020. Of those, 41.9% had a BMI of less than 25 (normal weight), 36.5% had a BMI of 25-29.9 (overweight), and 21.6% had BMI of at least 30 (obese). Of the obese group, 20 (4.1%) had BMIs of at least 35, while 18 patients (3.7%) had BMIs of less than 20 (underweight).
Among those with obesity, 51.9% experienced respiratory failure, 36.4% were admitted to the ICU, 25% required mechanical ventilation, and 29.8% died within 30 days of symptom onset.
Patients with BMIs of at least 30 had significantly increased risks for respiratory failure (odds ratio, 2.48; P = .001), ICU admission (OR, 5.28; P < .001), and death (2.35, P = .017), compared with those with lower BMIs. Within the group classified as obese, the risks of respiratory failure and ICU admission were higher, with BMIs of 30-34.9 (OR, 2.32; P = .004 and OR, 4.96; P < .001, respectively) and for BMIs of at least 35 (OR, 3.24; P = .019 and OR, 6.58; P < .001, respectively).
The risk of death was significantly higher among patients with a BMI of at least 35 (OR, 12.1; P < .001).
Every 1-unit increase in BMI was significantly associated with all outcomes, but there was no significant difference in any outcome between the 25-29.9 BMI category and normal weight. In all models, the BMI cutoff for increased risk was 30.
The authors reported no disclosures.
SOURCE: Rottoli M et al. Eur J Endocrinol. 2020 Jul 1. doi: 10.1530/EJE-20-054.
People with a body mass index of 30 kg/m2 or above are at significantly increased risk for severe COVID-19, while a BMI of 35 and higher dramatically increases the risk for death, new research suggests.
The data, from nearly 500 patients hospitalized with COVID-19 in March and April 2020, were published in the European Journal of Endocrinology by Matteo Rottoli, MD, of the Alma Mater Studiorum, University of Bologna (Italy), and colleagues.
The data support the recent change by the Centers for Disease Control and Prevention to lower the cutoff for categorizing a person at increased risk from COVID-19 from a BMI of 40 down to 30. However, in the United Kingdom, the National Health Service still lists only a BMI of 40 or above as placing a person at “moderate risk (clinically vulnerable).”
“This finding calls for prevention and treatment strategies to reduce the risk of infection and hospitalization in patients with relevant degrees of obesity, supporting a revision of the BMI cutoff of 40 kg/m2, which was proposed as an independent risk factor for an adverse outcome of COVID-19 in the ... guidelines for social distancing in the United Kingdom: It may be appropriate to include patients with BMI >30 among those at higher risk for COVID-19 severe progression,” the authors wrote.
The study included 482 adults admitted with confirmed COVID-19 to a single Italian hospital between March 1 and April 20, 2020. Of those, 41.9% had a BMI of less than 25 (normal weight), 36.5% had a BMI of 25-29.9 (overweight), and 21.6% had BMI of at least 30 (obese). Of the obese group, 20 (4.1%) had BMIs of at least 35, while 18 patients (3.7%) had BMIs of less than 20 (underweight).
Among those with obesity, 51.9% experienced respiratory failure, 36.4% were admitted to the ICU, 25% required mechanical ventilation, and 29.8% died within 30 days of symptom onset.
Patients with BMIs of at least 30 had significantly increased risks for respiratory failure (odds ratio, 2.48; P = .001), ICU admission (OR, 5.28; P < .001), and death (2.35, P = .017), compared with those with lower BMIs. Within the group classified as obese, the risks of respiratory failure and ICU admission were higher, with BMIs of 30-34.9 (OR, 2.32; P = .004 and OR, 4.96; P < .001, respectively) and for BMIs of at least 35 (OR, 3.24; P = .019 and OR, 6.58; P < .001, respectively).
The risk of death was significantly higher among patients with a BMI of at least 35 (OR, 12.1; P < .001).
Every 1-unit increase in BMI was significantly associated with all outcomes, but there was no significant difference in any outcome between the 25-29.9 BMI category and normal weight. In all models, the BMI cutoff for increased risk was 30.
The authors reported no disclosures.
SOURCE: Rottoli M et al. Eur J Endocrinol. 2020 Jul 1. doi: 10.1530/EJE-20-054.
People with a body mass index of 30 kg/m2 or above are at significantly increased risk for severe COVID-19, while a BMI of 35 and higher dramatically increases the risk for death, new research suggests.
The data, from nearly 500 patients hospitalized with COVID-19 in March and April 2020, were published in the European Journal of Endocrinology by Matteo Rottoli, MD, of the Alma Mater Studiorum, University of Bologna (Italy), and colleagues.
The data support the recent change by the Centers for Disease Control and Prevention to lower the cutoff for categorizing a person at increased risk from COVID-19 from a BMI of 40 down to 30. However, in the United Kingdom, the National Health Service still lists only a BMI of 40 or above as placing a person at “moderate risk (clinically vulnerable).”
“This finding calls for prevention and treatment strategies to reduce the risk of infection and hospitalization in patients with relevant degrees of obesity, supporting a revision of the BMI cutoff of 40 kg/m2, which was proposed as an independent risk factor for an adverse outcome of COVID-19 in the ... guidelines for social distancing in the United Kingdom: It may be appropriate to include patients with BMI >30 among those at higher risk for COVID-19 severe progression,” the authors wrote.
The study included 482 adults admitted with confirmed COVID-19 to a single Italian hospital between March 1 and April 20, 2020. Of those, 41.9% had a BMI of less than 25 (normal weight), 36.5% had a BMI of 25-29.9 (overweight), and 21.6% had BMI of at least 30 (obese). Of the obese group, 20 (4.1%) had BMIs of at least 35, while 18 patients (3.7%) had BMIs of less than 20 (underweight).
Among those with obesity, 51.9% experienced respiratory failure, 36.4% were admitted to the ICU, 25% required mechanical ventilation, and 29.8% died within 30 days of symptom onset.
Patients with BMIs of at least 30 had significantly increased risks for respiratory failure (odds ratio, 2.48; P = .001), ICU admission (OR, 5.28; P < .001), and death (2.35, P = .017), compared with those with lower BMIs. Within the group classified as obese, the risks of respiratory failure and ICU admission were higher, with BMIs of 30-34.9 (OR, 2.32; P = .004 and OR, 4.96; P < .001, respectively) and for BMIs of at least 35 (OR, 3.24; P = .019 and OR, 6.58; P < .001, respectively).
The risk of death was significantly higher among patients with a BMI of at least 35 (OR, 12.1; P < .001).
Every 1-unit increase in BMI was significantly associated with all outcomes, but there was no significant difference in any outcome between the 25-29.9 BMI category and normal weight. In all models, the BMI cutoff for increased risk was 30.
The authors reported no disclosures.
SOURCE: Rottoli M et al. Eur J Endocrinol. 2020 Jul 1. doi: 10.1530/EJE-20-054.
FROM THE EUROPEAN JOURNAL OF ENDOCRINOLOGY
Consider adverse childhood experiences during the pandemic
We live in historic times. A worldwide pandemic is surging in the United States, with millions infected and the world’s highest death rate. Many of our hospitals are overwhelmed. Schools have been closed for months. Businesses are struggling, and unemployment is at record levels. The murder of George Floyd unleashed an outpouring of grief and rage over police brutality and structural racism.

It is ironic that this age of adversity emerged at the same time that efforts to assess and address childhood adversity are gaining momentum. The effects of adverse childhood experiences (ACEs) have been well known for decades, but only recently have efforts at universal screening been initiated in primary care offices around the country. The multiple crises we face have made this work more pressing than ever. And
While there has long been awareness, especially among pediatricians, of the social determinants of health, it was only 1995 when Robert F. Anda, MD, and Vincent J. Felitti, MD, set about studying over 13,000 adult patients at Kaiser Permanente to understand the relationship between childhood trauma and chronic health problems in adulthood. In 1998 they published the results of this landmark study, establishing that childhood trauma was common and that it predicted chronic diseases and psychosocial problems in adulthood1.
They detailed 10 specific ACEs, and a patient’s ACE score was determined by how many of these experiences they had before they turned 18 years: neglect (emotional or physical), abuse (emotional, physical or sexual), and household dysfunction (parental divorce, incarceration of a parent, domestic violence, parental mental illness, or parental substance abuse). They found that more than half of adults studied had a score of at least 1, and 6% had scores of 4 or more. Those adults with an ACE score of 4 or more are twice as likely to be obese, twice as likely to smoke, and seven times as likely to abuse alcohol as the rest of the population. They are 4 times as likely to have emphysema, 5 times as likely to have depression, and 12 times as likely to attempt suicide. They have higher rates of heart disease, autoimmune disorders, and cancer. Those with ACE scores of 6 or more have their life expectancy shortened by an average of 20 years.

The value of knowing about these risk factors would seem self-evident; it would inform a patient’s health care from screening for cancer or heart disease, referral for mild depressive symptoms, and counseling about alcohol consumption. But this research did not lead to the establishment of routine screening for childhood adversity in primary care practices. There are multiple reasons for this, including growing pressure on physician time and discomfort with starting conversations about potentially traumatic material. But perhaps the greatest obstacle has been uncertainty about what to offer patients who screened in. What is the treatment for a high ACE score?
Even without treatments, we have learned much about childhood adversity since Dr. Anda and Dr. Felitti published their landmark study. Other more chronic adverse childhood experiences also contribute to adult health risk, such as poverty, homelessness, discrimination, community violence, parental chronic illness, or disability or placement in foster care. Having a high ACE score does not only affect health in adulthood. Children with an ACE score of 4 are 2 times as likely to have asthma2,3 and allergies3, 2 times as likely to be obese4, 3 times as likely to have headaches3 and dental problems5,6, 4 times as likely to have depression7,8, 5 times as likely to have ADHD8,9, 7 times as likely to have high rates of school absenteeism3 and aggression10, and over 30 times as likely to have learning or behavioral problems at school4. There is a growing body of knowledge about how chronic, severe stress in childhood affects can lead to pathological alterations in neuroendocrine and immune function. But this has not led to any concrete treatments that may be preventive or reparative.
Movement toward expanding screening nonetheless has accelerated. In California, Nadine Burke-Harris, MD, a pediatrician who studied ACEs and children’s health was named the state’s first Surgeon General in 2019 and spearheaded an effort to make screening for ACEs easier. Starting in 2020, MediCal will pay for annual screenings, and the state is offering training and resources on how to screen and what to do with the information to help patients and families.

The coronavirus pandemic has only highlighted the risks of childhood adversity. The burden of infection and mortality has been borne disproportionately by people of color and those with multiple chronic medical conditions (obesity, cardiovascular disease, diabetes, etc.). While viruses do not discriminate, they are more likely to infect those with higher risk of exposure and to kill those who are physiologically vulnerable.
And the pandemic increases the risk for adversity for today’s children and families. When children cannot attend school, financially vulnerable parents may have to choose between supervising them or feeding them. Families who suddenly are all in a small apartment together without school or other outside supports may be at higher risk for domestic violence and child abuse. Unemployment and financial uncertainty will increase the rates of substance abuse and depression amongst parents. And the serious illness or death of a parent will be a more common event for children in the year ahead. One of these risk factors may increase the likelihood of others.
Beyond the obvious need for substantial policy changes focused on housing, education, and health care, And resilience can build on itself, as children face subsequent challenges with the support of caring connected adults.
The critical first step is asking. Then listen calmly and supportively, normalizing for parents and children how common these experiences are. Explain how they affect health and well-being. Explain that adversity and its consequences are not their fault. Then educate them about what is in their control: the skills they can practice to buffer against the consequences of adversity and build resilience. They sound simple, but still require effort and work. And the pandemic has created some difficulty (social distancing) and opportunity (more family time, fewer school demands).
Sleep
Help parents establish and protect consistent, restful sleep for their children. They can set a consistent bedtime and a calm routine, with screens all off at least 30 minutes before sleep and reading before sleep. Restful sleep is physiologically and psychologically protective to everyone in a family.
Movement
Beyond directly improving physical health, establishing habits of exercise – especially outside – every day can effectively manage ongoing stress, build skills of self-regulation, and help with sleep.
Find out what parents and their children like to do together (walking the dog, shooting hoops, even dancing) and help them devise ways to create family routines around exercise.
Nutrition
Food should be a source of pleasure, but stress can make food into a source of comfort or escape. Help parents to create realistic ways to consistently offer healthy family meals and discourage unhealthy habits.
Even small changes like water instead of soda can help, and there are nutritional and emotional benefits to eating a healthy breakfast or dinner together as a family.
Connections
Nourishing social connections are protective. Help parents think about protecting time to spend with their children for talking, playing games, or even singing.
They should support their children’s connections to other caring adults, through community organizations (church, community centers, or sports), and they should know who their children’s reliable friends are. Parents will benefit from these supports for themselves, which in turn will benefit the full family.
Self-awareness
Activities that cultivate mindfulness are protective. Parents can simply ask how their children are feeling, physically or emotionally, and be able to bear it when it is uncomfortable. Work towards nonjudgmental awareness of how they are feeling. Learning what is relaxing or recharging for them (exercise, music, a hot bath, a good book, time with a friend) will protect against defaulting into maladaptive coping such as escape, numbing, or avoidance.
Of course, if you learn about symptoms that suggest PTSD, depression, or addiction, you should help your patient connect with effective treatment. The difficulty of referring to a mental health provider does not mean you should not try and bring as many people onto the team and into the orbit of the child and family at risk. It may be easier to access some therapy given the new availability of telemedicine visits across many more systems of care. Although the heaviest burdens of adversity are not being borne equally, the fact that adversity is currently a shared experience makes this a moment of promise.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Dr. Swick and Dr. Jellinek had no relevant financial disclosures. Email them at [email protected].
References
1. Am J Prev Med. 1998 May;14(4):245-58.
2. Ann Allergy Asthma Immunol. 2015;114: 379-84.
3. BMC Public Health. 2018. doi: 10.1186/s12889-018-5699-8.
4. Child Abuse Negl. 2011 Jun;35(6):408-13.
5. Community Dent Oral Epidemiol. 2015;43:193-9.
6. Community Dent Oral Epidemiol. 2018 Oct;46(5): 442-8.
7. Pediatrics 2016 Apr. doi: 10.1542/peds.2015-4016.
8. Matern Child Health J. 2016 Apr. doi: 10.1007/s10995-015-1915-7.
9. Acad Pediatr. 2017 May-Jun. doi: 10.1016/j.acap.2016.08.013.
10. Pediatrics. 2010 Apr. doi: 10.1542/peds.2009-0597.
This article was updated 7/27/2020.
We live in historic times. A worldwide pandemic is surging in the United States, with millions infected and the world’s highest death rate. Many of our hospitals are overwhelmed. Schools have been closed for months. Businesses are struggling, and unemployment is at record levels. The murder of George Floyd unleashed an outpouring of grief and rage over police brutality and structural racism.
It is ironic that this age of adversity emerged at the same time that efforts to assess and address childhood adversity are gaining momentum. The effects of adverse childhood experiences (ACEs) have been well known for decades, but only recently have efforts at universal screening been initiated in primary care offices around the country. The multiple crises we face have made this work more pressing than ever. And
While there has long been awareness, especially among pediatricians, of the social determinants of health, it was only 1995 when Robert F. Anda, MD, and Vincent J. Felitti, MD, set about studying over 13,000 adult patients at Kaiser Permanente to understand the relationship between childhood trauma and chronic health problems in adulthood. In 1998 they published the results of this landmark study, establishing that childhood trauma was common and that it predicted chronic diseases and psychosocial problems in adulthood1.
They detailed 10 specific ACEs, and a patient’s ACE score was determined by how many of these experiences they had before they turned 18 years: neglect (emotional or physical), abuse (emotional, physical or sexual), and household dysfunction (parental divorce, incarceration of a parent, domestic violence, parental mental illness, or parental substance abuse). They found that more than half of adults studied had a score of at least 1, and 6% had scores of 4 or more. Those adults with an ACE score of 4 or more are twice as likely to be obese, twice as likely to smoke, and seven times as likely to abuse alcohol as the rest of the population. They are 4 times as likely to have emphysema, 5 times as likely to have depression, and 12 times as likely to attempt suicide. They have higher rates of heart disease, autoimmune disorders, and cancer. Those with ACE scores of 6 or more have their life expectancy shortened by an average of 20 years.
The value of knowing about these risk factors would seem self-evident; it would inform a patient’s health care from screening for cancer or heart disease, referral for mild depressive symptoms, and counseling about alcohol consumption. But this research did not lead to the establishment of routine screening for childhood adversity in primary care practices. There are multiple reasons for this, including growing pressure on physician time and discomfort with starting conversations about potentially traumatic material. But perhaps the greatest obstacle has been uncertainty about what to offer patients who screened in. What is the treatment for a high ACE score?
Even without treatments, we have learned much about childhood adversity since Dr. Anda and Dr. Felitti published their landmark study. Other more chronic adverse childhood experiences also contribute to adult health risk, such as poverty, homelessness, discrimination, community violence, parental chronic illness, or disability or placement in foster care. Having a high ACE score does not only affect health in adulthood. Children with an ACE score of 4 are 2 times as likely to have asthma2,3 and allergies3, 2 times as likely to be obese4, 3 times as likely to have headaches3 and dental problems5,6, 4 times as likely to have depression7,8, 5 times as likely to have ADHD8,9, 7 times as likely to have high rates of school absenteeism3 and aggression10, and over 30 times as likely to have learning or behavioral problems at school4. There is a growing body of knowledge about how chronic, severe stress in childhood affects can lead to pathological alterations in neuroendocrine and immune function. But this has not led to any concrete treatments that may be preventive or reparative.
Movement toward expanding screening nonetheless has accelerated. In California, Nadine Burke-Harris, MD, a pediatrician who studied ACEs and children’s health was named the state’s first Surgeon General in 2019 and spearheaded an effort to make screening for ACEs easier. Starting in 2020, MediCal will pay for annual screenings, and the state is offering training and resources on how to screen and what to do with the information to help patients and families.
The coronavirus pandemic has only highlighted the risks of childhood adversity. The burden of infection and mortality has been borne disproportionately by people of color and those with multiple chronic medical conditions (obesity, cardiovascular disease, diabetes, etc.). While viruses do not discriminate, they are more likely to infect those with higher risk of exposure and to kill those who are physiologically vulnerable.
And the pandemic increases the risk for adversity for today’s children and families. When children cannot attend school, financially vulnerable parents may have to choose between supervising them or feeding them. Families who suddenly are all in a small apartment together without school or other outside supports may be at higher risk for domestic violence and child abuse. Unemployment and financial uncertainty will increase the rates of substance abuse and depression amongst parents. And the serious illness or death of a parent will be a more common event for children in the year ahead. One of these risk factors may increase the likelihood of others.
Beyond the obvious need for substantial policy changes focused on housing, education, and health care, And resilience can build on itself, as children face subsequent challenges with the support of caring connected adults.
The critical first step is asking. Then listen calmly and supportively, normalizing for parents and children how common these experiences are. Explain how they affect health and well-being. Explain that adversity and its consequences are not their fault. Then educate them about what is in their control: the skills they can practice to buffer against the consequences of adversity and build resilience. They sound simple, but still require effort and work. And the pandemic has created some difficulty (social distancing) and opportunity (more family time, fewer school demands).
Sleep
Help parents establish and protect consistent, restful sleep for their children. They can set a consistent bedtime and a calm routine, with screens all off at least 30 minutes before sleep and reading before sleep. Restful sleep is physiologically and psychologically protective to everyone in a family.
Movement
Beyond directly improving physical health, establishing habits of exercise – especially outside – every day can effectively manage ongoing stress, build skills of self-regulation, and help with sleep.
Find out what parents and their children like to do together (walking the dog, shooting hoops, even dancing) and help them devise ways to create family routines around exercise.
Nutrition
Food should be a source of pleasure, but stress can make food into a source of comfort or escape. Help parents to create realistic ways to consistently offer healthy family meals and discourage unhealthy habits.
Even small changes like water instead of soda can help, and there are nutritional and emotional benefits to eating a healthy breakfast or dinner together as a family.
Connections
Nourishing social connections are protective. Help parents think about protecting time to spend with their children for talking, playing games, or even singing.
They should support their children’s connections to other caring adults, through community organizations (church, community centers, or sports), and they should know who their children’s reliable friends are. Parents will benefit from these supports for themselves, which in turn will benefit the full family.
Self-awareness
Activities that cultivate mindfulness are protective. Parents can simply ask how their children are feeling, physically or emotionally, and be able to bear it when it is uncomfortable. Work towards nonjudgmental awareness of how they are feeling. Learning what is relaxing or recharging for them (exercise, music, a hot bath, a good book, time with a friend) will protect against defaulting into maladaptive coping such as escape, numbing, or avoidance.
Of course, if you learn about symptoms that suggest PTSD, depression, or addiction, you should help your patient connect with effective treatment. The difficulty of referring to a mental health provider does not mean you should not try and bring as many people onto the team and into the orbit of the child and family at risk. It may be easier to access some therapy given the new availability of telemedicine visits across many more systems of care. Although the heaviest burdens of adversity are not being borne equally, the fact that adversity is currently a shared experience makes this a moment of promise.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Dr. Swick and Dr. Jellinek had no relevant financial disclosures. Email them at [email protected].
References
1. Am J Prev Med. 1998 May;14(4):245-58.
2. Ann Allergy Asthma Immunol. 2015;114: 379-84.
3. BMC Public Health. 2018. doi: 10.1186/s12889-018-5699-8.
4. Child Abuse Negl. 2011 Jun;35(6):408-13.
5. Community Dent Oral Epidemiol. 2015;43:193-9.
6. Community Dent Oral Epidemiol. 2018 Oct;46(5): 442-8.
7. Pediatrics 2016 Apr. doi: 10.1542/peds.2015-4016.
8. Matern Child Health J. 2016 Apr. doi: 10.1007/s10995-015-1915-7.
9. Acad Pediatr. 2017 May-Jun. doi: 10.1016/j.acap.2016.08.013.
10. Pediatrics. 2010 Apr. doi: 10.1542/peds.2009-0597.
This article was updated 7/27/2020.
We live in historic times. A worldwide pandemic is surging in the United States, with millions infected and the world’s highest death rate. Many of our hospitals are overwhelmed. Schools have been closed for months. Businesses are struggling, and unemployment is at record levels. The murder of George Floyd unleashed an outpouring of grief and rage over police brutality and structural racism.
It is ironic that this age of adversity emerged at the same time that efforts to assess and address childhood adversity are gaining momentum. The effects of adverse childhood experiences (ACEs) have been well known for decades, but only recently have efforts at universal screening been initiated in primary care offices around the country. The multiple crises we face have made this work more pressing than ever. And
While there has long been awareness, especially among pediatricians, of the social determinants of health, it was only 1995 when Robert F. Anda, MD, and Vincent J. Felitti, MD, set about studying over 13,000 adult patients at Kaiser Permanente to understand the relationship between childhood trauma and chronic health problems in adulthood. In 1998 they published the results of this landmark study, establishing that childhood trauma was common and that it predicted chronic diseases and psychosocial problems in adulthood1.
They detailed 10 specific ACEs, and a patient’s ACE score was determined by how many of these experiences they had before they turned 18 years: neglect (emotional or physical), abuse (emotional, physical or sexual), and household dysfunction (parental divorce, incarceration of a parent, domestic violence, parental mental illness, or parental substance abuse). They found that more than half of adults studied had a score of at least 1, and 6% had scores of 4 or more. Those adults with an ACE score of 4 or more are twice as likely to be obese, twice as likely to smoke, and seven times as likely to abuse alcohol as the rest of the population. They are 4 times as likely to have emphysema, 5 times as likely to have depression, and 12 times as likely to attempt suicide. They have higher rates of heart disease, autoimmune disorders, and cancer. Those with ACE scores of 6 or more have their life expectancy shortened by an average of 20 years.
The value of knowing about these risk factors would seem self-evident; it would inform a patient’s health care from screening for cancer or heart disease, referral for mild depressive symptoms, and counseling about alcohol consumption. But this research did not lead to the establishment of routine screening for childhood adversity in primary care practices. There are multiple reasons for this, including growing pressure on physician time and discomfort with starting conversations about potentially traumatic material. But perhaps the greatest obstacle has been uncertainty about what to offer patients who screened in. What is the treatment for a high ACE score?
Even without treatments, we have learned much about childhood adversity since Dr. Anda and Dr. Felitti published their landmark study. Other more chronic adverse childhood experiences also contribute to adult health risk, such as poverty, homelessness, discrimination, community violence, parental chronic illness, or disability or placement in foster care. Having a high ACE score does not only affect health in adulthood. Children with an ACE score of 4 are 2 times as likely to have asthma2,3 and allergies3, 2 times as likely to be obese4, 3 times as likely to have headaches3 and dental problems5,6, 4 times as likely to have depression7,8, 5 times as likely to have ADHD8,9, 7 times as likely to have high rates of school absenteeism3 and aggression10, and over 30 times as likely to have learning or behavioral problems at school4. There is a growing body of knowledge about how chronic, severe stress in childhood affects can lead to pathological alterations in neuroendocrine and immune function. But this has not led to any concrete treatments that may be preventive or reparative.
Movement toward expanding screening nonetheless has accelerated. In California, Nadine Burke-Harris, MD, a pediatrician who studied ACEs and children’s health was named the state’s first Surgeon General in 2019 and spearheaded an effort to make screening for ACEs easier. Starting in 2020, MediCal will pay for annual screenings, and the state is offering training and resources on how to screen and what to do with the information to help patients and families.
The coronavirus pandemic has only highlighted the risks of childhood adversity. The burden of infection and mortality has been borne disproportionately by people of color and those with multiple chronic medical conditions (obesity, cardiovascular disease, diabetes, etc.). While viruses do not discriminate, they are more likely to infect those with higher risk of exposure and to kill those who are physiologically vulnerable.
And the pandemic increases the risk for adversity for today’s children and families. When children cannot attend school, financially vulnerable parents may have to choose between supervising them or feeding them. Families who suddenly are all in a small apartment together without school or other outside supports may be at higher risk for domestic violence and child abuse. Unemployment and financial uncertainty will increase the rates of substance abuse and depression amongst parents. And the serious illness or death of a parent will be a more common event for children in the year ahead. One of these risk factors may increase the likelihood of others.
Beyond the obvious need for substantial policy changes focused on housing, education, and health care, And resilience can build on itself, as children face subsequent challenges with the support of caring connected adults.
The critical first step is asking. Then listen calmly and supportively, normalizing for parents and children how common these experiences are. Explain how they affect health and well-being. Explain that adversity and its consequences are not their fault. Then educate them about what is in their control: the skills they can practice to buffer against the consequences of adversity and build resilience. They sound simple, but still require effort and work. And the pandemic has created some difficulty (social distancing) and opportunity (more family time, fewer school demands).
Sleep
Help parents establish and protect consistent, restful sleep for their children. They can set a consistent bedtime and a calm routine, with screens all off at least 30 minutes before sleep and reading before sleep. Restful sleep is physiologically and psychologically protective to everyone in a family.
Movement
Beyond directly improving physical health, establishing habits of exercise – especially outside – every day can effectively manage ongoing stress, build skills of self-regulation, and help with sleep.
Find out what parents and their children like to do together (walking the dog, shooting hoops, even dancing) and help them devise ways to create family routines around exercise.
Nutrition
Food should be a source of pleasure, but stress can make food into a source of comfort or escape. Help parents to create realistic ways to consistently offer healthy family meals and discourage unhealthy habits.
Even small changes like water instead of soda can help, and there are nutritional and emotional benefits to eating a healthy breakfast or dinner together as a family.
Connections
Nourishing social connections are protective. Help parents think about protecting time to spend with their children for talking, playing games, or even singing.
They should support their children’s connections to other caring adults, through community organizations (church, community centers, or sports), and they should know who their children’s reliable friends are. Parents will benefit from these supports for themselves, which in turn will benefit the full family.
Self-awareness
Activities that cultivate mindfulness are protective. Parents can simply ask how their children are feeling, physically or emotionally, and be able to bear it when it is uncomfortable. Work towards nonjudgmental awareness of how they are feeling. Learning what is relaxing or recharging for them (exercise, music, a hot bath, a good book, time with a friend) will protect against defaulting into maladaptive coping such as escape, numbing, or avoidance.
Of course, if you learn about symptoms that suggest PTSD, depression, or addiction, you should help your patient connect with effective treatment. The difficulty of referring to a mental health provider does not mean you should not try and bring as many people onto the team and into the orbit of the child and family at risk. It may be easier to access some therapy given the new availability of telemedicine visits across many more systems of care. Although the heaviest burdens of adversity are not being borne equally, the fact that adversity is currently a shared experience makes this a moment of promise.
Dr. Swick is physician in chief at Ohana, Center for Child and Adolescent Behavioral Health, Community Hospital of the Monterey (Calif.) Peninsula. Dr. Jellinek is professor emeritus of psychiatry and pediatrics, Harvard Medical School, Boston. Dr. Swick and Dr. Jellinek had no relevant financial disclosures. Email them at [email protected].
References
1. Am J Prev Med. 1998 May;14(4):245-58.
2. Ann Allergy Asthma Immunol. 2015;114: 379-84.
3. BMC Public Health. 2018. doi: 10.1186/s12889-018-5699-8.
4. Child Abuse Negl. 2011 Jun;35(6):408-13.
5. Community Dent Oral Epidemiol. 2015;43:193-9.
6. Community Dent Oral Epidemiol. 2018 Oct;46(5): 442-8.
7. Pediatrics 2016 Apr. doi: 10.1542/peds.2015-4016.
8. Matern Child Health J. 2016 Apr. doi: 10.1007/s10995-015-1915-7.
9. Acad Pediatr. 2017 May-Jun. doi: 10.1016/j.acap.2016.08.013.
10. Pediatrics. 2010 Apr. doi: 10.1542/peds.2009-0597.
This article was updated 7/27/2020.
Some women use prescription opioids during pregnancy
and almost a third of those women did not receive counseling from a provider on the effects of opioids on their unborn children, according to analysis from the Centers for Disease Control and Prevention.
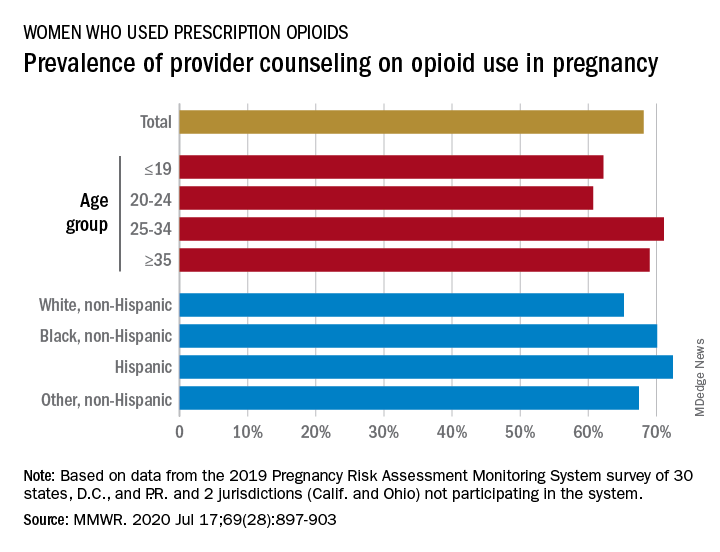
Data from the Pregnancy Risk Assessment Monitoring System 2019 survey show that 7% of the nearly 21,000 respondents reported using an opioid pain reliever during pregnancy, considerably lower than the fill rates of 14%-22% seen in studies of pharmacy dispensing, Jean Y. Ko, PhD, and associates at the CDC said in the Morbidity and Mortality Weekly Report.
In the current analysis, opioid use during pregnancy varied by age – the rate was highest, 10%, in those aged 19 years and under and dropped as age increased to 6% among those aged 35 and older – and by race/ethnicity – 9% of black women reported use, compared with 7% of Hispanics, 6% of whites, and 7% of all others, the investigators reported.
Use of prescription opioids was significantly higher for two specific groups. Women who smoked cigarettes during the last 3 months of their pregnancy had a 16% rate of opioid use, and those with depression during pregnancy had a rate of 13%, they said.
Physicians caring for pregnant women should seek to identify and address substance use and misuse, and mental health conditions such as depression, history of trauma, posttraumatic stress disorder, and anxiety, the CDC researchers pointed out.
The CDC and the American College of Obstetricians and Gynecologists both recommend that caregivers and patients also need to “discuss and carefully weigh risks and benefits when considering initiation of opioid therapy for chronic pain during pregnancy,” Dr. Ko and associates wrote.
That sort of counseling, however, was not always offered: 32% of the women with self-reported prescription opioid use during their pregnancy said that they had not been counseled about the drugs’ effect on an infant. Some variation was seen by age or race/ethnicity, but the differences were not significant, the researchers reported.
“Opioid prescribing consistent with clinical practice guidelines can ensure that patients, particularly those who are pregnant, have access to safer, more effective chronic pain treatment and reduce the number of persons at risk for opioid misuse, opioid use disorder, and overdose,” the investigators concluded.
Survey data from 32 jurisdictions (30 states, along with the District of Columbia and Puerto Rico) that participate in the monitoring system were included in the analysis, as were data from California and Ohio, which do not participate. All of the respondents had a live birth in the preceding 2-6 months, the researchers explained.
SOURCE: Ko JY et al. MMWR. 2020 Jul 17;69(28):897-903.
and almost a third of those women did not receive counseling from a provider on the effects of opioids on their unborn children, according to analysis from the Centers for Disease Control and Prevention.
Data from the Pregnancy Risk Assessment Monitoring System 2019 survey show that 7% of the nearly 21,000 respondents reported using an opioid pain reliever during pregnancy, considerably lower than the fill rates of 14%-22% seen in studies of pharmacy dispensing, Jean Y. Ko, PhD, and associates at the CDC said in the Morbidity and Mortality Weekly Report.
In the current analysis, opioid use during pregnancy varied by age – the rate was highest, 10%, in those aged 19 years and under and dropped as age increased to 6% among those aged 35 and older – and by race/ethnicity – 9% of black women reported use, compared with 7% of Hispanics, 6% of whites, and 7% of all others, the investigators reported.
Use of prescription opioids was significantly higher for two specific groups. Women who smoked cigarettes during the last 3 months of their pregnancy had a 16% rate of opioid use, and those with depression during pregnancy had a rate of 13%, they said.
Physicians caring for pregnant women should seek to identify and address substance use and misuse, and mental health conditions such as depression, history of trauma, posttraumatic stress disorder, and anxiety, the CDC researchers pointed out.
The CDC and the American College of Obstetricians and Gynecologists both recommend that caregivers and patients also need to “discuss and carefully weigh risks and benefits when considering initiation of opioid therapy for chronic pain during pregnancy,” Dr. Ko and associates wrote.
That sort of counseling, however, was not always offered: 32% of the women with self-reported prescription opioid use during their pregnancy said that they had not been counseled about the drugs’ effect on an infant. Some variation was seen by age or race/ethnicity, but the differences were not significant, the researchers reported.
“Opioid prescribing consistent with clinical practice guidelines can ensure that patients, particularly those who are pregnant, have access to safer, more effective chronic pain treatment and reduce the number of persons at risk for opioid misuse, opioid use disorder, and overdose,” the investigators concluded.
Survey data from 32 jurisdictions (30 states, along with the District of Columbia and Puerto Rico) that participate in the monitoring system were included in the analysis, as were data from California and Ohio, which do not participate. All of the respondents had a live birth in the preceding 2-6 months, the researchers explained.
SOURCE: Ko JY et al. MMWR. 2020 Jul 17;69(28):897-903.
and almost a third of those women did not receive counseling from a provider on the effects of opioids on their unborn children, according to analysis from the Centers for Disease Control and Prevention.
Data from the Pregnancy Risk Assessment Monitoring System 2019 survey show that 7% of the nearly 21,000 respondents reported using an opioid pain reliever during pregnancy, considerably lower than the fill rates of 14%-22% seen in studies of pharmacy dispensing, Jean Y. Ko, PhD, and associates at the CDC said in the Morbidity and Mortality Weekly Report.
In the current analysis, opioid use during pregnancy varied by age – the rate was highest, 10%, in those aged 19 years and under and dropped as age increased to 6% among those aged 35 and older – and by race/ethnicity – 9% of black women reported use, compared with 7% of Hispanics, 6% of whites, and 7% of all others, the investigators reported.
Use of prescription opioids was significantly higher for two specific groups. Women who smoked cigarettes during the last 3 months of their pregnancy had a 16% rate of opioid use, and those with depression during pregnancy had a rate of 13%, they said.
Physicians caring for pregnant women should seek to identify and address substance use and misuse, and mental health conditions such as depression, history of trauma, posttraumatic stress disorder, and anxiety, the CDC researchers pointed out.
The CDC and the American College of Obstetricians and Gynecologists both recommend that caregivers and patients also need to “discuss and carefully weigh risks and benefits when considering initiation of opioid therapy for chronic pain during pregnancy,” Dr. Ko and associates wrote.
That sort of counseling, however, was not always offered: 32% of the women with self-reported prescription opioid use during their pregnancy said that they had not been counseled about the drugs’ effect on an infant. Some variation was seen by age or race/ethnicity, but the differences were not significant, the researchers reported.
“Opioid prescribing consistent with clinical practice guidelines can ensure that patients, particularly those who are pregnant, have access to safer, more effective chronic pain treatment and reduce the number of persons at risk for opioid misuse, opioid use disorder, and overdose,” the investigators concluded.
Survey data from 32 jurisdictions (30 states, along with the District of Columbia and Puerto Rico) that participate in the monitoring system were included in the analysis, as were data from California and Ohio, which do not participate. All of the respondents had a live birth in the preceding 2-6 months, the researchers explained.
SOURCE: Ko JY et al. MMWR. 2020 Jul 17;69(28):897-903.
FROM MMWR