User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
‘Profound implications’: COVID ups diabetes risk 40% a year later
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
Sit-to-stand BP spike tied to CV events in young adults
A sudden drop in blood pressure when standing is a common and concerning problem in elderly hypertensive people. Now, research suggests a large BP swing in the opposite direction on standing may be equally concerning in younger hypertensive people.
Young and middle-aged adults with a systolic BP response to standing greater than 6.5 mm Hg had almost double the risk of major adverse cardiovascular events (MACE) during follow-up, compared with other participants.
An exaggerated BP response remained an independent predictor of MACE, even after adjusting for traditional risk factors, including 24-hour BP (hazard ratio, 1.94; 95% confidence interval, 1.10 to 3.44), the study showed.
“The clinical implication is important, because now doctors measure blood pressure in young people in the upright posture, but what we say is it must be measured also while standing,” said Paolo Palatini, MD, a professor of internal medicine at the University of Padova, Italy, who led the study.
Previous studies have found that an exaggerated BP response to standing is a predictor of future hypertension, CV events, and mortality, particularly in older patients, but few prognostic data exist in those who are young to middle age, he noted.
The study, published in Hypertension, included 1,207 participants ages 18-45 years with untreated stage 1 hypertension (systolic BP 140-159 mm Hg or diastolic BP 90-100 mm Hg) in the prospective multicenter HARVEST study that began in Italy in 1990. The average age at enrollment was 33 years.
BP was measured at two visits 2 weeks apart, with each visit including three supine measurements taken after the patient had lain down for a minimum of 5 minutes, followed by three standing measurements taken 1 minute apart.
Based on the average of standing-lying BP differences during the two visits, participants were then classified as having a normal or exaggerated (top decile, lower limit > 6.5 mm Hg) systolic BP response to standing.
The 120 participants classified as “hyper-reactors” averaged an 11.4 mm Hg systolic BP increase upon standing, whereas the rest of the participants averaged a 3.8 mm Hg fall in systolic BP upon standing.
At their initial visit, hyper-reactors were more likely to be smokers (32.1% vs. 19.9%) and coffee drinkers (81.7% vs. 73%) and to have ambulatory hypertension (90.8% vs. 76.4%).
They were, however, no more likely to have a family history of cardiovascular events and had a lower supine systolic BP (140.5 mm Hg vs. 146.0 mm Hg), lower total cholesterol (4.93 mmol/L vs. 5.13 mmol/L), and higher HDL cholesterol (1.42 mmol/L vs. 1.35 mmol/L).
Age, sex, and body mass index were similar between the two groups, as was BP variability, nocturnal BP dip, and the frequency of extreme dippers. Participants with a normal systolic BP response were more likely to be treated for hypertension during follow-up (81.7% vs. 69.7%; P = .003).
In 630 participants who had catecholamines measured from 24-hour urine samples, the epinephrine/creatinine ratio was higher in hyper-reactors than normal responders (118.4 nmol/mol vs. 77.0 nmol/mol; P = .005).
During a median follow-up of 17.3 years, there were 105 major cardiovascular events, broadly defined to include acute coronary syndromes (48), any stroke (13), heart failure requiring hospitalization (3), aortic aneurysms (3), peripheral vascular disease (6), chronic kidney disease (12), and permanent atrial fibrillation (20).
The near doubling of MACE risk among hyper-reactors remained when atrial fibrillation was excluded and when 24-hour ambulatory systolic BP was included in the model, the author reported.
The results are in line with previous studies, indicating that hyper-reactors to standing have normal sympathetic activity at rest but an increased sympathetic response to stressors, observed Dr. Palatini and colleagues. This neurohumoral overshoot seems to be peculiar to young adults, whereas vascular stiffness seems to be the driving mechanism of orthostatic hypertension in older adults.
If a young person’s BP spikes upon standing, “then you have to treat them according to the average of the lying and the standing pressure,” Dr. Palatini said. “In these people, blood pressure should be treated earlier than in the past.”
“The study is important because it identified a new marker for hypertension that is easily evaluated in clinical practice,” Nieca Goldberg, MD, medical director of the Atria Institute, New York, and an associate professor of medicine at New York University Grossman School of Medicine, commented via email.
She noted that standing blood pressures are usually not taken as part of a medical visit and, in fact, seated blood pressures are often taken incorrectly while the patient is seated on the exam table rather than with their feet on the floor and using the proper cuff size.
“By incorporating standing BP, we will improve our diagnosis for hypertension, and with interventions such as diet and exercise, salt reduction, and medication when indicated, lower risk for heart attack, stroke, heart failure, [and] kidney and eye disease,” said Dr. Goldberg, who is also a spokesperson for the American Heart Association.
“The biggest barrier is that office visits are limited to 15 minutes, and not enough time is spent on the vital signs,” she noted. “We need changes to the health care system that value our ability to diagnose BP and take the time to counsel patients and explain treatment options.”
Limitations of the present study are that 72.7% of participants were men and all were White, Dr. Palatini said. Future work is also needed to create a uniform definition of BP hyper-reactivity to standing, possibly based on risk estimates, for inclusion in future hypertension guidelines.
The study was funded by the Association 18 Maggio 1370 in Italy. The authors have disclosed no relevant financial relationships. Dr. Goldberg reported being a spokesperson for the American Heart Association.
A version of this article first appeared on Medscape.com.
A sudden drop in blood pressure when standing is a common and concerning problem in elderly hypertensive people. Now, research suggests a large BP swing in the opposite direction on standing may be equally concerning in younger hypertensive people.
Young and middle-aged adults with a systolic BP response to standing greater than 6.5 mm Hg had almost double the risk of major adverse cardiovascular events (MACE) during follow-up, compared with other participants.
An exaggerated BP response remained an independent predictor of MACE, even after adjusting for traditional risk factors, including 24-hour BP (hazard ratio, 1.94; 95% confidence interval, 1.10 to 3.44), the study showed.
“The clinical implication is important, because now doctors measure blood pressure in young people in the upright posture, but what we say is it must be measured also while standing,” said Paolo Palatini, MD, a professor of internal medicine at the University of Padova, Italy, who led the study.
Previous studies have found that an exaggerated BP response to standing is a predictor of future hypertension, CV events, and mortality, particularly in older patients, but few prognostic data exist in those who are young to middle age, he noted.
The study, published in Hypertension, included 1,207 participants ages 18-45 years with untreated stage 1 hypertension (systolic BP 140-159 mm Hg or diastolic BP 90-100 mm Hg) in the prospective multicenter HARVEST study that began in Italy in 1990. The average age at enrollment was 33 years.
BP was measured at two visits 2 weeks apart, with each visit including three supine measurements taken after the patient had lain down for a minimum of 5 minutes, followed by three standing measurements taken 1 minute apart.
Based on the average of standing-lying BP differences during the two visits, participants were then classified as having a normal or exaggerated (top decile, lower limit > 6.5 mm Hg) systolic BP response to standing.
The 120 participants classified as “hyper-reactors” averaged an 11.4 mm Hg systolic BP increase upon standing, whereas the rest of the participants averaged a 3.8 mm Hg fall in systolic BP upon standing.
At their initial visit, hyper-reactors were more likely to be smokers (32.1% vs. 19.9%) and coffee drinkers (81.7% vs. 73%) and to have ambulatory hypertension (90.8% vs. 76.4%).
They were, however, no more likely to have a family history of cardiovascular events and had a lower supine systolic BP (140.5 mm Hg vs. 146.0 mm Hg), lower total cholesterol (4.93 mmol/L vs. 5.13 mmol/L), and higher HDL cholesterol (1.42 mmol/L vs. 1.35 mmol/L).
Age, sex, and body mass index were similar between the two groups, as was BP variability, nocturnal BP dip, and the frequency of extreme dippers. Participants with a normal systolic BP response were more likely to be treated for hypertension during follow-up (81.7% vs. 69.7%; P = .003).
In 630 participants who had catecholamines measured from 24-hour urine samples, the epinephrine/creatinine ratio was higher in hyper-reactors than normal responders (118.4 nmol/mol vs. 77.0 nmol/mol; P = .005).
During a median follow-up of 17.3 years, there were 105 major cardiovascular events, broadly defined to include acute coronary syndromes (48), any stroke (13), heart failure requiring hospitalization (3), aortic aneurysms (3), peripheral vascular disease (6), chronic kidney disease (12), and permanent atrial fibrillation (20).
The near doubling of MACE risk among hyper-reactors remained when atrial fibrillation was excluded and when 24-hour ambulatory systolic BP was included in the model, the author reported.
The results are in line with previous studies, indicating that hyper-reactors to standing have normal sympathetic activity at rest but an increased sympathetic response to stressors, observed Dr. Palatini and colleagues. This neurohumoral overshoot seems to be peculiar to young adults, whereas vascular stiffness seems to be the driving mechanism of orthostatic hypertension in older adults.
If a young person’s BP spikes upon standing, “then you have to treat them according to the average of the lying and the standing pressure,” Dr. Palatini said. “In these people, blood pressure should be treated earlier than in the past.”
“The study is important because it identified a new marker for hypertension that is easily evaluated in clinical practice,” Nieca Goldberg, MD, medical director of the Atria Institute, New York, and an associate professor of medicine at New York University Grossman School of Medicine, commented via email.
She noted that standing blood pressures are usually not taken as part of a medical visit and, in fact, seated blood pressures are often taken incorrectly while the patient is seated on the exam table rather than with their feet on the floor and using the proper cuff size.
“By incorporating standing BP, we will improve our diagnosis for hypertension, and with interventions such as diet and exercise, salt reduction, and medication when indicated, lower risk for heart attack, stroke, heart failure, [and] kidney and eye disease,” said Dr. Goldberg, who is also a spokesperson for the American Heart Association.
“The biggest barrier is that office visits are limited to 15 minutes, and not enough time is spent on the vital signs,” she noted. “We need changes to the health care system that value our ability to diagnose BP and take the time to counsel patients and explain treatment options.”
Limitations of the present study are that 72.7% of participants were men and all were White, Dr. Palatini said. Future work is also needed to create a uniform definition of BP hyper-reactivity to standing, possibly based on risk estimates, for inclusion in future hypertension guidelines.
The study was funded by the Association 18 Maggio 1370 in Italy. The authors have disclosed no relevant financial relationships. Dr. Goldberg reported being a spokesperson for the American Heart Association.
A version of this article first appeared on Medscape.com.
A sudden drop in blood pressure when standing is a common and concerning problem in elderly hypertensive people. Now, research suggests a large BP swing in the opposite direction on standing may be equally concerning in younger hypertensive people.
Young and middle-aged adults with a systolic BP response to standing greater than 6.5 mm Hg had almost double the risk of major adverse cardiovascular events (MACE) during follow-up, compared with other participants.
An exaggerated BP response remained an independent predictor of MACE, even after adjusting for traditional risk factors, including 24-hour BP (hazard ratio, 1.94; 95% confidence interval, 1.10 to 3.44), the study showed.
“The clinical implication is important, because now doctors measure blood pressure in young people in the upright posture, but what we say is it must be measured also while standing,” said Paolo Palatini, MD, a professor of internal medicine at the University of Padova, Italy, who led the study.
Previous studies have found that an exaggerated BP response to standing is a predictor of future hypertension, CV events, and mortality, particularly in older patients, but few prognostic data exist in those who are young to middle age, he noted.
The study, published in Hypertension, included 1,207 participants ages 18-45 years with untreated stage 1 hypertension (systolic BP 140-159 mm Hg or diastolic BP 90-100 mm Hg) in the prospective multicenter HARVEST study that began in Italy in 1990. The average age at enrollment was 33 years.
BP was measured at two visits 2 weeks apart, with each visit including three supine measurements taken after the patient had lain down for a minimum of 5 minutes, followed by three standing measurements taken 1 minute apart.
Based on the average of standing-lying BP differences during the two visits, participants were then classified as having a normal or exaggerated (top decile, lower limit > 6.5 mm Hg) systolic BP response to standing.
The 120 participants classified as “hyper-reactors” averaged an 11.4 mm Hg systolic BP increase upon standing, whereas the rest of the participants averaged a 3.8 mm Hg fall in systolic BP upon standing.
At their initial visit, hyper-reactors were more likely to be smokers (32.1% vs. 19.9%) and coffee drinkers (81.7% vs. 73%) and to have ambulatory hypertension (90.8% vs. 76.4%).
They were, however, no more likely to have a family history of cardiovascular events and had a lower supine systolic BP (140.5 mm Hg vs. 146.0 mm Hg), lower total cholesterol (4.93 mmol/L vs. 5.13 mmol/L), and higher HDL cholesterol (1.42 mmol/L vs. 1.35 mmol/L).
Age, sex, and body mass index were similar between the two groups, as was BP variability, nocturnal BP dip, and the frequency of extreme dippers. Participants with a normal systolic BP response were more likely to be treated for hypertension during follow-up (81.7% vs. 69.7%; P = .003).
In 630 participants who had catecholamines measured from 24-hour urine samples, the epinephrine/creatinine ratio was higher in hyper-reactors than normal responders (118.4 nmol/mol vs. 77.0 nmol/mol; P = .005).
During a median follow-up of 17.3 years, there were 105 major cardiovascular events, broadly defined to include acute coronary syndromes (48), any stroke (13), heart failure requiring hospitalization (3), aortic aneurysms (3), peripheral vascular disease (6), chronic kidney disease (12), and permanent atrial fibrillation (20).
The near doubling of MACE risk among hyper-reactors remained when atrial fibrillation was excluded and when 24-hour ambulatory systolic BP was included in the model, the author reported.
The results are in line with previous studies, indicating that hyper-reactors to standing have normal sympathetic activity at rest but an increased sympathetic response to stressors, observed Dr. Palatini and colleagues. This neurohumoral overshoot seems to be peculiar to young adults, whereas vascular stiffness seems to be the driving mechanism of orthostatic hypertension in older adults.
If a young person’s BP spikes upon standing, “then you have to treat them according to the average of the lying and the standing pressure,” Dr. Palatini said. “In these people, blood pressure should be treated earlier than in the past.”
“The study is important because it identified a new marker for hypertension that is easily evaluated in clinical practice,” Nieca Goldberg, MD, medical director of the Atria Institute, New York, and an associate professor of medicine at New York University Grossman School of Medicine, commented via email.
She noted that standing blood pressures are usually not taken as part of a medical visit and, in fact, seated blood pressures are often taken incorrectly while the patient is seated on the exam table rather than with their feet on the floor and using the proper cuff size.
“By incorporating standing BP, we will improve our diagnosis for hypertension, and with interventions such as diet and exercise, salt reduction, and medication when indicated, lower risk for heart attack, stroke, heart failure, [and] kidney and eye disease,” said Dr. Goldberg, who is also a spokesperson for the American Heart Association.
“The biggest barrier is that office visits are limited to 15 minutes, and not enough time is spent on the vital signs,” she noted. “We need changes to the health care system that value our ability to diagnose BP and take the time to counsel patients and explain treatment options.”
Limitations of the present study are that 72.7% of participants were men and all were White, Dr. Palatini said. Future work is also needed to create a uniform definition of BP hyper-reactivity to standing, possibly based on risk estimates, for inclusion in future hypertension guidelines.
The study was funded by the Association 18 Maggio 1370 in Italy. The authors have disclosed no relevant financial relationships. Dr. Goldberg reported being a spokesperson for the American Heart Association.
A version of this article first appeared on Medscape.com.
Pfizer recalls BP drugs because of potential carcinogen
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Complex surgery 10 times more likely with some ovarian tumors
according to a report at the Society of Gynecologic Oncology annual meeting.
Investigators found that women with those features, compared with those without them, are 10 times more likely to have a high-complexity surgery and almost 27 times more likely to have something other than a complete (RD0) resection.
The findings speak to a common dilemma in advanced ovarian cancer, whether women should have surgery or chemotherapy first. Part of the decision hinges on the likelihood of surgical success, explained lead investigator Diogo Torres, MD, a gynecologic oncologist at Ochsner Health in New Orleans.
He and his team concluded that “preoperative CT imaging combined with tumor molecular subtyping can identify a subset of women for whom successful primary surgery is unlikely. Preoperative tumor sampling may be useful in advanced [ovarian cancer] to better triage these cases to alternative approaches.”
For years “we’ve been trying to figure out” how best to make the call between primary debulking and neoadjuvant chemotherapy, said Pamela T. Soliman, MD, MPH,a gynecologic oncologist at the University of Texas MD Anderson Cancer Center, Houston, who discussed the abstract at the meeting.
Imaging alone or CA-125 are often used to make the decision, but they’re unreliable. Diagnostic laparoscopy is accurate, but it isn’t used much, she said.
What’s unique about Dr. Torres’s approach is that, by including tumor subtype, it incorporates tumor biology. It makes sense because his team previously found that women with mesenchymal (MES) tumors are more likely than those with other subtypes to have upper abdominal and miliary disease.
The approach needs validation in a larger study, but “I really commend” the team “for incorporating biology into the decision-making because it is clearly a step in the right direction,” Dr. Soliman said.
The study included 129 women who underwent primary debulking surgery for stage 3c or 4 high-grade serous ovarian cancer; 46x women (36%) had MES tumors according to RNA profiling of surgical specimens.
Preoperative CTs were reviewed to assess diaphragmatic disease; gastrohepatic/portahepatis lesions; root of superior mesenteric artery involvement; presence of moderate to severe ascites; intrahepatic lesions, and diffuse peritoneal thickening greater than 4 mm.
Fifty-nine women (46%) were classified as “CT high,” meaning that they had two or more of those findings. Women with no more than one were categorized as “CT low.”
Patients with MES tumors and CT-high disease had the lowest rates of complete resections, 8% versus 46% for the entire cohort and 72% for non-MES, CT-low women. MES, CT-high women were also the most likely to have high-complexity surgery (81% versus 35% in the non-MES, CT-low group).
Adjusting for age, stage, and American Society of Anesthesiologists score, the odds of high-complexity surgery were 9.53 times higher and the odds of something less than a complete resection were 26.73 times greater in MES, CT-high patients, compared with non-MES, CT-low women.
“Further studies are needed to evaluate and validate this model using preoperative biopsy specimens” instead of surgical specimens, the investigators said.
No funding was reported for the work. Dr. Torres didn’t have any disclosures. Dr. Soliman is an adviser for Eisai and Amgen, a consultant for Medscape, and receives research funding from Novartis and Incyte.
according to a report at the Society of Gynecologic Oncology annual meeting.
Investigators found that women with those features, compared with those without them, are 10 times more likely to have a high-complexity surgery and almost 27 times more likely to have something other than a complete (RD0) resection.
The findings speak to a common dilemma in advanced ovarian cancer, whether women should have surgery or chemotherapy first. Part of the decision hinges on the likelihood of surgical success, explained lead investigator Diogo Torres, MD, a gynecologic oncologist at Ochsner Health in New Orleans.
He and his team concluded that “preoperative CT imaging combined with tumor molecular subtyping can identify a subset of women for whom successful primary surgery is unlikely. Preoperative tumor sampling may be useful in advanced [ovarian cancer] to better triage these cases to alternative approaches.”
For years “we’ve been trying to figure out” how best to make the call between primary debulking and neoadjuvant chemotherapy, said Pamela T. Soliman, MD, MPH,a gynecologic oncologist at the University of Texas MD Anderson Cancer Center, Houston, who discussed the abstract at the meeting.
Imaging alone or CA-125 are often used to make the decision, but they’re unreliable. Diagnostic laparoscopy is accurate, but it isn’t used much, she said.
What’s unique about Dr. Torres’s approach is that, by including tumor subtype, it incorporates tumor biology. It makes sense because his team previously found that women with mesenchymal (MES) tumors are more likely than those with other subtypes to have upper abdominal and miliary disease.
The approach needs validation in a larger study, but “I really commend” the team “for incorporating biology into the decision-making because it is clearly a step in the right direction,” Dr. Soliman said.
The study included 129 women who underwent primary debulking surgery for stage 3c or 4 high-grade serous ovarian cancer; 46x women (36%) had MES tumors according to RNA profiling of surgical specimens.
Preoperative CTs were reviewed to assess diaphragmatic disease; gastrohepatic/portahepatis lesions; root of superior mesenteric artery involvement; presence of moderate to severe ascites; intrahepatic lesions, and diffuse peritoneal thickening greater than 4 mm.
Fifty-nine women (46%) were classified as “CT high,” meaning that they had two or more of those findings. Women with no more than one were categorized as “CT low.”
Patients with MES tumors and CT-high disease had the lowest rates of complete resections, 8% versus 46% for the entire cohort and 72% for non-MES, CT-low women. MES, CT-high women were also the most likely to have high-complexity surgery (81% versus 35% in the non-MES, CT-low group).
Adjusting for age, stage, and American Society of Anesthesiologists score, the odds of high-complexity surgery were 9.53 times higher and the odds of something less than a complete resection were 26.73 times greater in MES, CT-high patients, compared with non-MES, CT-low women.
“Further studies are needed to evaluate and validate this model using preoperative biopsy specimens” instead of surgical specimens, the investigators said.
No funding was reported for the work. Dr. Torres didn’t have any disclosures. Dr. Soliman is an adviser for Eisai and Amgen, a consultant for Medscape, and receives research funding from Novartis and Incyte.
according to a report at the Society of Gynecologic Oncology annual meeting.
Investigators found that women with those features, compared with those without them, are 10 times more likely to have a high-complexity surgery and almost 27 times more likely to have something other than a complete (RD0) resection.
The findings speak to a common dilemma in advanced ovarian cancer, whether women should have surgery or chemotherapy first. Part of the decision hinges on the likelihood of surgical success, explained lead investigator Diogo Torres, MD, a gynecologic oncologist at Ochsner Health in New Orleans.
He and his team concluded that “preoperative CT imaging combined with tumor molecular subtyping can identify a subset of women for whom successful primary surgery is unlikely. Preoperative tumor sampling may be useful in advanced [ovarian cancer] to better triage these cases to alternative approaches.”
For years “we’ve been trying to figure out” how best to make the call between primary debulking and neoadjuvant chemotherapy, said Pamela T. Soliman, MD, MPH,a gynecologic oncologist at the University of Texas MD Anderson Cancer Center, Houston, who discussed the abstract at the meeting.
Imaging alone or CA-125 are often used to make the decision, but they’re unreliable. Diagnostic laparoscopy is accurate, but it isn’t used much, she said.
What’s unique about Dr. Torres’s approach is that, by including tumor subtype, it incorporates tumor biology. It makes sense because his team previously found that women with mesenchymal (MES) tumors are more likely than those with other subtypes to have upper abdominal and miliary disease.
The approach needs validation in a larger study, but “I really commend” the team “for incorporating biology into the decision-making because it is clearly a step in the right direction,” Dr. Soliman said.
The study included 129 women who underwent primary debulking surgery for stage 3c or 4 high-grade serous ovarian cancer; 46x women (36%) had MES tumors according to RNA profiling of surgical specimens.
Preoperative CTs were reviewed to assess diaphragmatic disease; gastrohepatic/portahepatis lesions; root of superior mesenteric artery involvement; presence of moderate to severe ascites; intrahepatic lesions, and diffuse peritoneal thickening greater than 4 mm.
Fifty-nine women (46%) were classified as “CT high,” meaning that they had two or more of those findings. Women with no more than one were categorized as “CT low.”
Patients with MES tumors and CT-high disease had the lowest rates of complete resections, 8% versus 46% for the entire cohort and 72% for non-MES, CT-low women. MES, CT-high women were also the most likely to have high-complexity surgery (81% versus 35% in the non-MES, CT-low group).
Adjusting for age, stage, and American Society of Anesthesiologists score, the odds of high-complexity surgery were 9.53 times higher and the odds of something less than a complete resection were 26.73 times greater in MES, CT-high patients, compared with non-MES, CT-low women.
“Further studies are needed to evaluate and validate this model using preoperative biopsy specimens” instead of surgical specimens, the investigators said.
No funding was reported for the work. Dr. Torres didn’t have any disclosures. Dr. Soliman is an adviser for Eisai and Amgen, a consultant for Medscape, and receives research funding from Novartis and Incyte.
FROM SGO 2022
Are ‘antibiotic diets’ good practice?
Antibiotics are among the most commonly prescribed medications in both outpatient and hospital settings. Global efforts at curbing antibiotic-resistant strains have prompted clinicians to pursue better stewardship, whereby they limit their prescribing of such medications to those who truly need them.
Yet there’s another possible means of addressing antibiotic resistance – using dietary interventions to reduce the gastrointestinal complaints that so often accompany the use of antibiotics: vomiting, nausea, diarrhea, bloating/indigestion, abdominal pain, and loss of appetite. Far from being a mere nuisance, these complications can have major ramifications.
“Often [these side effects] will result in people stopping an antibiotic they need or taking a second- or third-generation one, which potentially causes even more problems with resistance,” explained Daniel J. Merenstein, MD, a professor of family medicine at Georgetown University, Washington, who has conducted multiple trials on antibiotic stewardship and probiotics.
And it’s not just clinicians who would like to find a way around these common complaints. On lifestyle blogs such as Livestrong and Goop, medical news websites, and via academic institutions, patients can learn how the right probiotic supplement or certain fermented or high-fiber foods, for example, might spare them the upset stomach that often accompanies a course of antibiotics.
Yet according to experts in the field, there are notable questions to be answered about whether there’s evidence to support this approach.
The cost of GI discomfort
Pinpointing the exact manner by which antibiotics upend GI tracts is a complex task, according to Gail Cresci, PhD, RD, a microbiome researcher in the department of pediatric gastroenterology, hepatology, and nutrition and director of nutrition research at the Cleveland Clinic.
“A lot of different mechanisms can go awry,” Dr. Cresci said. “But normally, the good microbes are there to help keep the balance, so when that balance is gone, the pathogens can take over and lead to this disruption.”
According to Lynne V. McFarland, PhD, a recently retired infectious disease epidemiologist who now serves as a private consultant, such complications can have substantial ramifications for patients and health care systems.
“If you’re an inpatient and develop antibiotic-associated diarrhea, it usually increases the length of stay from 8 to 20 days. It also increases the cost of care. And small children who have this can get severely dehydrated, which can become life threatening.”
Proponents of probiotics
Several of the researchers who were interviewed believe there’s convincing evidence supporting probiotics for the treatment of common antibiotic-related GI complaints. In many instances, they were involved in the studies themselves.
During Dr. McFarland’s 4-decade career in probiotics research, she has participated in early animal studies with strains such as Saccharomyces boulardii and was involved in meta-analyses of their role in Clostridioides difficile infection and associated diarrhea and even as a potential GI intervention for COVID-19 patients (Antibiotics (Basel). 2021 Apr 9;10(4):408).
In mouse model studies from 2013 and 2018, Dr. Cresci and colleagues showed that the probiotic strains Lactobacillus GG and Faecalibacterium prausnitzii reduced the structural gut changes that lead to antibiotic-associated diarrhea and minimized the risk of C. difficile infection.
In a 2021 randomized controlled trial led by Merenstein, healthy participants were given a trial of amoxicillin/clavulanate (days 1-7) in conjunction with either yogurt containing the probiotic Bifidobacterium animalis subsp lactis BB-12 or control yogurt (days 1-14). After assessing feces samples over a 30-day period, they found that those who received the probiotic yogurt had a significantly smaller decrease in short-chain fatty acid levels and a more stable taxonomic microbiota profile than control persons.
Dr. Merenstein said that, on the basis of results such as these and others, he’s comfortable being relatively definitive about the value of probiotics.
“I believe it’s close to standard of care that if you’re prescribing antibiotics, especially for more than 7 days, you really need to put people on probiotics that have been studied, simply because the evidence is robust enough now,” he said.
Even for proponents, there are caveats
However, all the researchers recommending the use of probiotics did so with caveats. First and foremost, they advise clinicians that the term “probiotics” is an imprecise catchall and is essentially meaningless.
“A lot of products label themselves as probiotic. It’s a great marketing scheme, but many of the products out there aren’t really probiotics; they’re not proven with randomized control trials and don’t have the scientific background,” said Dr. McFarland. “We’ve found that the efficacy is extremely strain specific and disease specific. A strain may work for one disease and not work for another.”
In 2018, Dr. McFarland coauthored an evidence-based practical guide to help clinicians and patients identify the specific strain that works in certain indications. Dr. Cresci recommends that clinicians consult websites such as Probiotics.org or the National Institutes of Health’s database to find the strains that have been proven to work in well-designed clinical trials.
There was also agreement that, to date, the most robust data support probiotics for the treatment of antibiotic-associated diarrhea.
Although the optimal timing of probiotics is a subject of debate, most proponents agreed that the general rule is “the sooner the better.”
Dr. McFarland recommended incorporating probiotics within 24 hours of starting an antibiotic “because the damage done to your GI tract microbiome is pretty quick, and the probiotics work best if they’re established before major disruption occurs.” She added that patients should continue taking probiotics for 2-8 weeks after stopping antibiotics.
“It takes a long time for your normal flora to get restored,” she said. “It’s best to cover your bases.”
For others, the evidence is not definitive
Opinions on the value of probiotics to combat antibiotic-related GI side effects are divergent, though.
“I would not recommend the routine use of probiotics, and certainly not in the prevention of C. difficile or antibiotic-related diarrhea,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk. “I think the evidence does not support that, and I stand strongly on that recommendation.”
Dr. Johnson cited the 2020 guidelines from the American Gastroenterological Association, which offer only a conditional recommendation for the use of specific probiotics and only in preventing antibiotic-associated C. difficile infection.
Geoffrey A. Preidis, MD, PhD, an assistant professor of pediatrics in the section of gastroenterology, hepatology, and nutrition at Baylor College of Medicine, Houston, served as a coauthor of the AGA’s guidelines. He noted that after reviewing 39 published trials of approximately 10,000 patients given probiotics while receiving antibiotics, the authors “did find some evidence that specific probiotics might decrease the risk of C. difficile diarrhea, but the quality of that evidence was low.”
Dr. Preidis attributed this to the lack of well-designed multicenter trials that can isolate the effects of certain strains and determine their benefit in this application.
“The majority of published trials have not reported safety data as rigorously as these data are reported in pharmaceutical trials, so the risk of side effects could be higher than we think,” said Dr. Preidis. “As living microbes, probiotics can move from the intestines into the bloodstream, causing sepsis. Contamination in the manufacturing process has been reported. There might be other long-term effects that we are not yet aware of.”
When asked to characterize the available data on probiotics, Dr. Johnson replied, “I’d generally label it, ‘caveat emptor.’ ”
Dr. McFarland agreed that the field would benefit from better-designed studies and called out meta-analyses that pool outcomes with various strains for particular criticism.
“When researchers do that, it’s no longer valid and shouldn’t have been published, in my opinion,” she told this news organization.
‘Antibiotic diets’ as a possible approach
A compromise between the two sides may be the so-called antibiotic diet. The theory behind such diets is that foods and beverages with biome-boosting properties may be a risk-free intervention that patients can adopt to alleviate antibiotic-related side effects.
“You want your diet to include more soluble fibers to help support the good bacteria, particularly when you’re taking antibiotics,” said Dr. Cresci. “You can get this through eating fresh fruits and vegetables, whole grains, and foods that have more prebiotic, like potatoes. You can also eat fermented food, such as kefir, kombucha, kimchi, and yogurt, so you’re adding more beneficial bacteria into your intestinal tract.”
There is ample published evidence that such foods can boost microbiome diversity and decrease inflammation, including a July 2021 study in Cell. However, the protection this may confer while taking antibiotics isn’t known. Establishing a clear role for the efficacy of such interventions is made additionally difficult by the well-established limitations of conducting dietary clinical trials.
Dr. Merenstein said that there is no compelling evidence that antibiotic-related complications can be offset by changing what goes onto our dinner plates. He joked: “We can’t say, ‘Here’s amoxicillin for your ear infection, now make sure you increase your fermented food, fiber, and water.’ ”
Dr. Johnson said he’s intrigued by studies of prebiotics – fibers that boost beneficial bacteria in the GI system.
“I would love to have more findings about prebiotic identification; that is, things we could do in a healthy way to keep the gut balanced while it’s subject to a change with antibiotics,” he said. “We’re just not there yet.”
Dr. Johnson added that he generally recommends that patients taking antibiotics eat “a bland diet, avoiding things that may have been provocative in the past.”
If patients are already enjoying foods with microbiome-boosting reputations, Dr. Johnson sees “very little downside to continuing that [while on antibiotics].” However, he noted that the period in which you’re taking antibiotics isn’t ideal for trying new foods, given the lack of experience with how the gut bacteria will react.
There are data about foods to avoid while taking antibiotics, which generally fall in line with common dietary knowledge. Many patients may know not to drink grapefruit juice with certain medications, but it’s worth a reminder. Certain antibiotics may also require delaying or avoiding dairy products, although this does not apply to yogurt.
A fiber-deficient diet can aggravate microbiota collapse following antibiotics. In a 2020 study, researchers showed that people on a high-fat diet who were using antibiotics were 8.6 times more likely to have preinflammatory bowel disease than those eating low-fat foods and who had no recent history of antibiotic use. Mouse model data from the same study indicated that poor diet and antibiotics may have worked in conjunction to reduce oxygen in the gut.
Dr. McFarland noted that building a healthy microbiome is a lifelong pursuit and that several factors (for example, environmental or genetic) are out of individuals’ hands. The general public might want a quick fix – ironically, one of the main drivers behind their requesting and receiving antibiotics when they’re not indicated – but it’s likely not available to them.
“You can’t eat one salad and suddenly have a healthy gut, unfortunately.”
A version of this article first appeared on Medscape.com.
Antibiotics are among the most commonly prescribed medications in both outpatient and hospital settings. Global efforts at curbing antibiotic-resistant strains have prompted clinicians to pursue better stewardship, whereby they limit their prescribing of such medications to those who truly need them.
Yet there’s another possible means of addressing antibiotic resistance – using dietary interventions to reduce the gastrointestinal complaints that so often accompany the use of antibiotics: vomiting, nausea, diarrhea, bloating/indigestion, abdominal pain, and loss of appetite. Far from being a mere nuisance, these complications can have major ramifications.
“Often [these side effects] will result in people stopping an antibiotic they need or taking a second- or third-generation one, which potentially causes even more problems with resistance,” explained Daniel J. Merenstein, MD, a professor of family medicine at Georgetown University, Washington, who has conducted multiple trials on antibiotic stewardship and probiotics.
And it’s not just clinicians who would like to find a way around these common complaints. On lifestyle blogs such as Livestrong and Goop, medical news websites, and via academic institutions, patients can learn how the right probiotic supplement or certain fermented or high-fiber foods, for example, might spare them the upset stomach that often accompanies a course of antibiotics.
Yet according to experts in the field, there are notable questions to be answered about whether there’s evidence to support this approach.
The cost of GI discomfort
Pinpointing the exact manner by which antibiotics upend GI tracts is a complex task, according to Gail Cresci, PhD, RD, a microbiome researcher in the department of pediatric gastroenterology, hepatology, and nutrition and director of nutrition research at the Cleveland Clinic.
“A lot of different mechanisms can go awry,” Dr. Cresci said. “But normally, the good microbes are there to help keep the balance, so when that balance is gone, the pathogens can take over and lead to this disruption.”
According to Lynne V. McFarland, PhD, a recently retired infectious disease epidemiologist who now serves as a private consultant, such complications can have substantial ramifications for patients and health care systems.
“If you’re an inpatient and develop antibiotic-associated diarrhea, it usually increases the length of stay from 8 to 20 days. It also increases the cost of care. And small children who have this can get severely dehydrated, which can become life threatening.”
Proponents of probiotics
Several of the researchers who were interviewed believe there’s convincing evidence supporting probiotics for the treatment of common antibiotic-related GI complaints. In many instances, they were involved in the studies themselves.
During Dr. McFarland’s 4-decade career in probiotics research, she has participated in early animal studies with strains such as Saccharomyces boulardii and was involved in meta-analyses of their role in Clostridioides difficile infection and associated diarrhea and even as a potential GI intervention for COVID-19 patients (Antibiotics (Basel). 2021 Apr 9;10(4):408).
In mouse model studies from 2013 and 2018, Dr. Cresci and colleagues showed that the probiotic strains Lactobacillus GG and Faecalibacterium prausnitzii reduced the structural gut changes that lead to antibiotic-associated diarrhea and minimized the risk of C. difficile infection.
In a 2021 randomized controlled trial led by Merenstein, healthy participants were given a trial of amoxicillin/clavulanate (days 1-7) in conjunction with either yogurt containing the probiotic Bifidobacterium animalis subsp lactis BB-12 or control yogurt (days 1-14). After assessing feces samples over a 30-day period, they found that those who received the probiotic yogurt had a significantly smaller decrease in short-chain fatty acid levels and a more stable taxonomic microbiota profile than control persons.
Dr. Merenstein said that, on the basis of results such as these and others, he’s comfortable being relatively definitive about the value of probiotics.
“I believe it’s close to standard of care that if you’re prescribing antibiotics, especially for more than 7 days, you really need to put people on probiotics that have been studied, simply because the evidence is robust enough now,” he said.
Even for proponents, there are caveats
However, all the researchers recommending the use of probiotics did so with caveats. First and foremost, they advise clinicians that the term “probiotics” is an imprecise catchall and is essentially meaningless.
“A lot of products label themselves as probiotic. It’s a great marketing scheme, but many of the products out there aren’t really probiotics; they’re not proven with randomized control trials and don’t have the scientific background,” said Dr. McFarland. “We’ve found that the efficacy is extremely strain specific and disease specific. A strain may work for one disease and not work for another.”
In 2018, Dr. McFarland coauthored an evidence-based practical guide to help clinicians and patients identify the specific strain that works in certain indications. Dr. Cresci recommends that clinicians consult websites such as Probiotics.org or the National Institutes of Health’s database to find the strains that have been proven to work in well-designed clinical trials.
There was also agreement that, to date, the most robust data support probiotics for the treatment of antibiotic-associated diarrhea.
Although the optimal timing of probiotics is a subject of debate, most proponents agreed that the general rule is “the sooner the better.”
Dr. McFarland recommended incorporating probiotics within 24 hours of starting an antibiotic “because the damage done to your GI tract microbiome is pretty quick, and the probiotics work best if they’re established before major disruption occurs.” She added that patients should continue taking probiotics for 2-8 weeks after stopping antibiotics.
“It takes a long time for your normal flora to get restored,” she said. “It’s best to cover your bases.”
For others, the evidence is not definitive
Opinions on the value of probiotics to combat antibiotic-related GI side effects are divergent, though.
“I would not recommend the routine use of probiotics, and certainly not in the prevention of C. difficile or antibiotic-related diarrhea,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk. “I think the evidence does not support that, and I stand strongly on that recommendation.”
Dr. Johnson cited the 2020 guidelines from the American Gastroenterological Association, which offer only a conditional recommendation for the use of specific probiotics and only in preventing antibiotic-associated C. difficile infection.
Geoffrey A. Preidis, MD, PhD, an assistant professor of pediatrics in the section of gastroenterology, hepatology, and nutrition at Baylor College of Medicine, Houston, served as a coauthor of the AGA’s guidelines. He noted that after reviewing 39 published trials of approximately 10,000 patients given probiotics while receiving antibiotics, the authors “did find some evidence that specific probiotics might decrease the risk of C. difficile diarrhea, but the quality of that evidence was low.”
Dr. Preidis attributed this to the lack of well-designed multicenter trials that can isolate the effects of certain strains and determine their benefit in this application.
“The majority of published trials have not reported safety data as rigorously as these data are reported in pharmaceutical trials, so the risk of side effects could be higher than we think,” said Dr. Preidis. “As living microbes, probiotics can move from the intestines into the bloodstream, causing sepsis. Contamination in the manufacturing process has been reported. There might be other long-term effects that we are not yet aware of.”
When asked to characterize the available data on probiotics, Dr. Johnson replied, “I’d generally label it, ‘caveat emptor.’ ”
Dr. McFarland agreed that the field would benefit from better-designed studies and called out meta-analyses that pool outcomes with various strains for particular criticism.
“When researchers do that, it’s no longer valid and shouldn’t have been published, in my opinion,” she told this news organization.
‘Antibiotic diets’ as a possible approach
A compromise between the two sides may be the so-called antibiotic diet. The theory behind such diets is that foods and beverages with biome-boosting properties may be a risk-free intervention that patients can adopt to alleviate antibiotic-related side effects.
“You want your diet to include more soluble fibers to help support the good bacteria, particularly when you’re taking antibiotics,” said Dr. Cresci. “You can get this through eating fresh fruits and vegetables, whole grains, and foods that have more prebiotic, like potatoes. You can also eat fermented food, such as kefir, kombucha, kimchi, and yogurt, so you’re adding more beneficial bacteria into your intestinal tract.”
There is ample published evidence that such foods can boost microbiome diversity and decrease inflammation, including a July 2021 study in Cell. However, the protection this may confer while taking antibiotics isn’t known. Establishing a clear role for the efficacy of such interventions is made additionally difficult by the well-established limitations of conducting dietary clinical trials.
Dr. Merenstein said that there is no compelling evidence that antibiotic-related complications can be offset by changing what goes onto our dinner plates. He joked: “We can’t say, ‘Here’s amoxicillin for your ear infection, now make sure you increase your fermented food, fiber, and water.’ ”
Dr. Johnson said he’s intrigued by studies of prebiotics – fibers that boost beneficial bacteria in the GI system.
“I would love to have more findings about prebiotic identification; that is, things we could do in a healthy way to keep the gut balanced while it’s subject to a change with antibiotics,” he said. “We’re just not there yet.”
Dr. Johnson added that he generally recommends that patients taking antibiotics eat “a bland diet, avoiding things that may have been provocative in the past.”
If patients are already enjoying foods with microbiome-boosting reputations, Dr. Johnson sees “very little downside to continuing that [while on antibiotics].” However, he noted that the period in which you’re taking antibiotics isn’t ideal for trying new foods, given the lack of experience with how the gut bacteria will react.
There are data about foods to avoid while taking antibiotics, which generally fall in line with common dietary knowledge. Many patients may know not to drink grapefruit juice with certain medications, but it’s worth a reminder. Certain antibiotics may also require delaying or avoiding dairy products, although this does not apply to yogurt.
A fiber-deficient diet can aggravate microbiota collapse following antibiotics. In a 2020 study, researchers showed that people on a high-fat diet who were using antibiotics were 8.6 times more likely to have preinflammatory bowel disease than those eating low-fat foods and who had no recent history of antibiotic use. Mouse model data from the same study indicated that poor diet and antibiotics may have worked in conjunction to reduce oxygen in the gut.
Dr. McFarland noted that building a healthy microbiome is a lifelong pursuit and that several factors (for example, environmental or genetic) are out of individuals’ hands. The general public might want a quick fix – ironically, one of the main drivers behind their requesting and receiving antibiotics when they’re not indicated – but it’s likely not available to them.
“You can’t eat one salad and suddenly have a healthy gut, unfortunately.”
A version of this article first appeared on Medscape.com.
Antibiotics are among the most commonly prescribed medications in both outpatient and hospital settings. Global efforts at curbing antibiotic-resistant strains have prompted clinicians to pursue better stewardship, whereby they limit their prescribing of such medications to those who truly need them.
Yet there’s another possible means of addressing antibiotic resistance – using dietary interventions to reduce the gastrointestinal complaints that so often accompany the use of antibiotics: vomiting, nausea, diarrhea, bloating/indigestion, abdominal pain, and loss of appetite. Far from being a mere nuisance, these complications can have major ramifications.
“Often [these side effects] will result in people stopping an antibiotic they need or taking a second- or third-generation one, which potentially causes even more problems with resistance,” explained Daniel J. Merenstein, MD, a professor of family medicine at Georgetown University, Washington, who has conducted multiple trials on antibiotic stewardship and probiotics.
And it’s not just clinicians who would like to find a way around these common complaints. On lifestyle blogs such as Livestrong and Goop, medical news websites, and via academic institutions, patients can learn how the right probiotic supplement or certain fermented or high-fiber foods, for example, might spare them the upset stomach that often accompanies a course of antibiotics.
Yet according to experts in the field, there are notable questions to be answered about whether there’s evidence to support this approach.
The cost of GI discomfort
Pinpointing the exact manner by which antibiotics upend GI tracts is a complex task, according to Gail Cresci, PhD, RD, a microbiome researcher in the department of pediatric gastroenterology, hepatology, and nutrition and director of nutrition research at the Cleveland Clinic.
“A lot of different mechanisms can go awry,” Dr. Cresci said. “But normally, the good microbes are there to help keep the balance, so when that balance is gone, the pathogens can take over and lead to this disruption.”
According to Lynne V. McFarland, PhD, a recently retired infectious disease epidemiologist who now serves as a private consultant, such complications can have substantial ramifications for patients and health care systems.
“If you’re an inpatient and develop antibiotic-associated diarrhea, it usually increases the length of stay from 8 to 20 days. It also increases the cost of care. And small children who have this can get severely dehydrated, which can become life threatening.”
Proponents of probiotics
Several of the researchers who were interviewed believe there’s convincing evidence supporting probiotics for the treatment of common antibiotic-related GI complaints. In many instances, they were involved in the studies themselves.
During Dr. McFarland’s 4-decade career in probiotics research, she has participated in early animal studies with strains such as Saccharomyces boulardii and was involved in meta-analyses of their role in Clostridioides difficile infection and associated diarrhea and even as a potential GI intervention for COVID-19 patients (Antibiotics (Basel). 2021 Apr 9;10(4):408).
In mouse model studies from 2013 and 2018, Dr. Cresci and colleagues showed that the probiotic strains Lactobacillus GG and Faecalibacterium prausnitzii reduced the structural gut changes that lead to antibiotic-associated diarrhea and minimized the risk of C. difficile infection.
In a 2021 randomized controlled trial led by Merenstein, healthy participants were given a trial of amoxicillin/clavulanate (days 1-7) in conjunction with either yogurt containing the probiotic Bifidobacterium animalis subsp lactis BB-12 or control yogurt (days 1-14). After assessing feces samples over a 30-day period, they found that those who received the probiotic yogurt had a significantly smaller decrease in short-chain fatty acid levels and a more stable taxonomic microbiota profile than control persons.
Dr. Merenstein said that, on the basis of results such as these and others, he’s comfortable being relatively definitive about the value of probiotics.
“I believe it’s close to standard of care that if you’re prescribing antibiotics, especially for more than 7 days, you really need to put people on probiotics that have been studied, simply because the evidence is robust enough now,” he said.
Even for proponents, there are caveats
However, all the researchers recommending the use of probiotics did so with caveats. First and foremost, they advise clinicians that the term “probiotics” is an imprecise catchall and is essentially meaningless.
“A lot of products label themselves as probiotic. It’s a great marketing scheme, but many of the products out there aren’t really probiotics; they’re not proven with randomized control trials and don’t have the scientific background,” said Dr. McFarland. “We’ve found that the efficacy is extremely strain specific and disease specific. A strain may work for one disease and not work for another.”
In 2018, Dr. McFarland coauthored an evidence-based practical guide to help clinicians and patients identify the specific strain that works in certain indications. Dr. Cresci recommends that clinicians consult websites such as Probiotics.org or the National Institutes of Health’s database to find the strains that have been proven to work in well-designed clinical trials.
There was also agreement that, to date, the most robust data support probiotics for the treatment of antibiotic-associated diarrhea.
Although the optimal timing of probiotics is a subject of debate, most proponents agreed that the general rule is “the sooner the better.”
Dr. McFarland recommended incorporating probiotics within 24 hours of starting an antibiotic “because the damage done to your GI tract microbiome is pretty quick, and the probiotics work best if they’re established before major disruption occurs.” She added that patients should continue taking probiotics for 2-8 weeks after stopping antibiotics.
“It takes a long time for your normal flora to get restored,” she said. “It’s best to cover your bases.”
For others, the evidence is not definitive
Opinions on the value of probiotics to combat antibiotic-related GI side effects are divergent, though.
“I would not recommend the routine use of probiotics, and certainly not in the prevention of C. difficile or antibiotic-related diarrhea,” said David A. Johnson, MD, professor of medicine and chief of gastroenterology at Eastern Virginia Medical School, Norfolk. “I think the evidence does not support that, and I stand strongly on that recommendation.”
Dr. Johnson cited the 2020 guidelines from the American Gastroenterological Association, which offer only a conditional recommendation for the use of specific probiotics and only in preventing antibiotic-associated C. difficile infection.
Geoffrey A. Preidis, MD, PhD, an assistant professor of pediatrics in the section of gastroenterology, hepatology, and nutrition at Baylor College of Medicine, Houston, served as a coauthor of the AGA’s guidelines. He noted that after reviewing 39 published trials of approximately 10,000 patients given probiotics while receiving antibiotics, the authors “did find some evidence that specific probiotics might decrease the risk of C. difficile diarrhea, but the quality of that evidence was low.”
Dr. Preidis attributed this to the lack of well-designed multicenter trials that can isolate the effects of certain strains and determine their benefit in this application.
“The majority of published trials have not reported safety data as rigorously as these data are reported in pharmaceutical trials, so the risk of side effects could be higher than we think,” said Dr. Preidis. “As living microbes, probiotics can move from the intestines into the bloodstream, causing sepsis. Contamination in the manufacturing process has been reported. There might be other long-term effects that we are not yet aware of.”
When asked to characterize the available data on probiotics, Dr. Johnson replied, “I’d generally label it, ‘caveat emptor.’ ”
Dr. McFarland agreed that the field would benefit from better-designed studies and called out meta-analyses that pool outcomes with various strains for particular criticism.
“When researchers do that, it’s no longer valid and shouldn’t have been published, in my opinion,” she told this news organization.
‘Antibiotic diets’ as a possible approach
A compromise between the two sides may be the so-called antibiotic diet. The theory behind such diets is that foods and beverages with biome-boosting properties may be a risk-free intervention that patients can adopt to alleviate antibiotic-related side effects.
“You want your diet to include more soluble fibers to help support the good bacteria, particularly when you’re taking antibiotics,” said Dr. Cresci. “You can get this through eating fresh fruits and vegetables, whole grains, and foods that have more prebiotic, like potatoes. You can also eat fermented food, such as kefir, kombucha, kimchi, and yogurt, so you’re adding more beneficial bacteria into your intestinal tract.”
There is ample published evidence that such foods can boost microbiome diversity and decrease inflammation, including a July 2021 study in Cell. However, the protection this may confer while taking antibiotics isn’t known. Establishing a clear role for the efficacy of such interventions is made additionally difficult by the well-established limitations of conducting dietary clinical trials.
Dr. Merenstein said that there is no compelling evidence that antibiotic-related complications can be offset by changing what goes onto our dinner plates. He joked: “We can’t say, ‘Here’s amoxicillin for your ear infection, now make sure you increase your fermented food, fiber, and water.’ ”
Dr. Johnson said he’s intrigued by studies of prebiotics – fibers that boost beneficial bacteria in the GI system.
“I would love to have more findings about prebiotic identification; that is, things we could do in a healthy way to keep the gut balanced while it’s subject to a change with antibiotics,” he said. “We’re just not there yet.”
Dr. Johnson added that he generally recommends that patients taking antibiotics eat “a bland diet, avoiding things that may have been provocative in the past.”
If patients are already enjoying foods with microbiome-boosting reputations, Dr. Johnson sees “very little downside to continuing that [while on antibiotics].” However, he noted that the period in which you’re taking antibiotics isn’t ideal for trying new foods, given the lack of experience with how the gut bacteria will react.
There are data about foods to avoid while taking antibiotics, which generally fall in line with common dietary knowledge. Many patients may know not to drink grapefruit juice with certain medications, but it’s worth a reminder. Certain antibiotics may also require delaying or avoiding dairy products, although this does not apply to yogurt.
A fiber-deficient diet can aggravate microbiota collapse following antibiotics. In a 2020 study, researchers showed that people on a high-fat diet who were using antibiotics were 8.6 times more likely to have preinflammatory bowel disease than those eating low-fat foods and who had no recent history of antibiotic use. Mouse model data from the same study indicated that poor diet and antibiotics may have worked in conjunction to reduce oxygen in the gut.
Dr. McFarland noted that building a healthy microbiome is a lifelong pursuit and that several factors (for example, environmental or genetic) are out of individuals’ hands. The general public might want a quick fix – ironically, one of the main drivers behind their requesting and receiving antibiotics when they’re not indicated – but it’s likely not available to them.
“You can’t eat one salad and suddenly have a healthy gut, unfortunately.”
A version of this article first appeared on Medscape.com.
Children and COVID: CDC gives perspective on hospitalizations
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.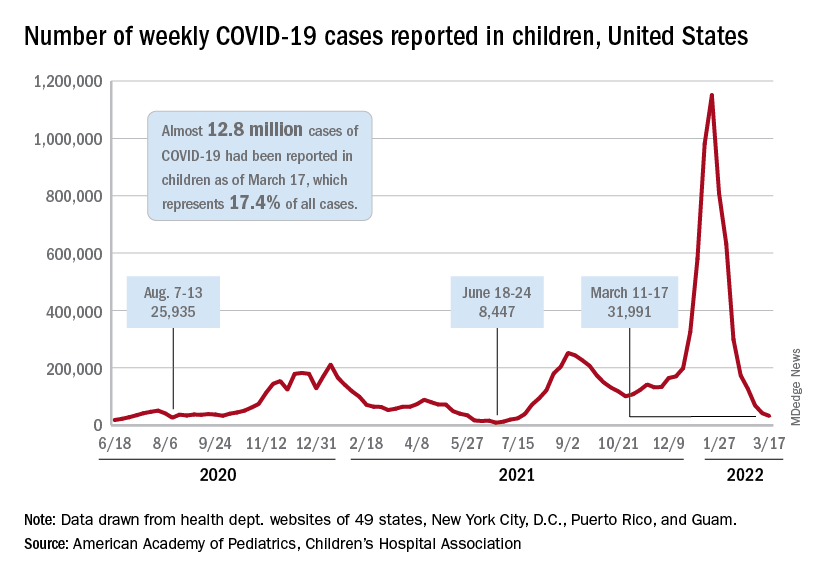
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
Racial disparities seen in pediatric postoperative mortality rates
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
Among Black and White children, higher socioeconomic status (SES) was associated with lower pediatric postoperative mortality, according to a cohort study published in JAMA Network Open. However, this association was not equitable when comparing Black and White children.
The results showed that postoperative mortality rates were significantly higher in Black children in the highest income category, compared with White children in the same category.
“[We] assessed whether increasing family SES is associated with lower pediatric postoperative mortality and, if so, whether this association is equitable among Black and White children,” Brittany L. Willer, MD, of Nationwide Children’s Hospital in Columbus, Ohio, and colleagues wrote.
The researchers retrospectively analyzed data from 51 pediatric tertiary care hospitals apart of the Children’s Hospital Association Pediatric Health Information System. The cohort included children younger than 18 years who underwent inpatient surgical procedures between January 2004 and December 2020.
The exposures of interest were race and parental income quartile; the primary endpoint was risk-adjusted in-hospital mortality rates by race and parental income quartile.
Results
The study cohort included 1,378,111 participants, including 248,464 (18.0%) Black and 1,129,647 (82.0%) White children, respectively.
The overall mortality rate was 1.2%, and rates decreased as income quartile increased (1.4% in quartile 1 [lowest income]; 1.3% in quartile 2; 1.0% in quartile 3; and 0.9% in quartile 4 [highest income]; P < .001).
Among participants in the three lowest income quartiles, Black children had 33% greater odds of postoperative death versus White children (adjusted odds ratio, 1.33; 95% confidence interval, 1.27-1.39; P < .001). This difference persisted in children in the highest income quartile (aOR, 1.39; 95% CI, 1.25-1.54; P < .001).
In addition, postoperative mortality rates in Black children in the highest income quartile (1.30%; 95% CI, 1.19%-1.42%) were similar to those of White children in the lowest income quartile (1.20%; 95% CI, 1.16%-1.25%).
“These findings suggest that increasing family SES did not provide equitable advantage to Black, compared with White children, and interventions that target socioeconomic inequities alone may not fully address persistent racial disparities in pediatric postoperative mortality,” wrote Dr. Willer and colleagues. “A multifaceted approach that includes dismantling of socioeconomic barriers, equitable availability of comprehensive pediatric surgical care, and personalized care for children of all races is needed.”
The researchers acknowledged that a potential limitation of the study was the use of zip code–level median household income as a proxy for family SES.
A perspective
In an interview, Timothy Joos, MD, a Seattle internist and pediatrician in private practice, said “there is a fair dose of racism and classism inside all of us – recognizing and coming to terms with it are steps toward improving equity issues.
“As providers, we have to remind ourselves to give our most prompt and thorough care to the patients with the most acute and severe illnesses,” Dr. Joos said. “As organizations, we have to pursue feedback from all our clients, but with special outreach to those that are used to not having their voices heard.”
No funding sources were reported. The authors reported no relevant disclosures. Dr. Joos is a member of the Pediatric News editorial advisory board but had no other disclosures.
FROM JAMA NETWORK OPEN
New guidance on cannabis use for treatment-resistant epilepsy
A recent review article draws from existing clinical trials and clinical experience in New South Wales, Australia, to fill this gap with interim guidance for both pediatric and adult patients. The article was published in the British Journal of Clinical Pharmacology.
The only current U.S. guidelines are from the American Academy of Neurology’s position statement on the use of medical cannabis for neurologic disorders and the American Epilepsy Society’s position statement on cannabis as a treatment for epileptic seizures. The AAN statement “highlights the current evidence, which currently only supports [Food and Drug Administration]–approved CBD [cannabidiol] (Epidiolex) for specific epilepsy syndromes,” said Daniel Freedman, DO, an assistant professor of neurology at the University of Texas at Austin and coauthor of the AAN’s position statement.
“Rescheduling marijuana will enable researchers to study CBD, THC [tetrahydrocannabinol], and other cannabinoids in high-quality studies so that we can better understand what works and for which conditions,” said Dr. Freedman, who was not involved in the Australian guidance document. He noted that little consensus exists because little evidence exists outside the handful of trials for Epidiolex.
“There are some patients with epilepsy that can benefit from high-quality, pharmaceutical-grade CBD products,” Dr. Freedman said. “These patients need to be carefully identified by a neurologist or epileptologist and prescribed a legal, safe, quality-controlled, and FDA-regulated product.”
Appropriate patient populations
Drug-resistant epilepsy, defined as failure of two appropriate antiseizure medications, affects an estimated one third of people with epilepsy, the new guideline notes. Though many over-the-counter products are available at dispensaries in the 33 U.S. states that allow use of cannabis for medical purposes, Epidiolex (cannabidiol) is the only FDA-approved drug for epilepsy that contains a substance derived from cannabis and the only one for which evidence from randomized, controlled trials exists.
Dr. Freedman notes that hemp-derived CBD oils are classified differently in the United States than marijuana-derived CBD oil, including Epidiolex, and are loosely regulated supplements or food additives commonly seen, for example at gas station.
“The point I drive home to patients is that you wouldn’t get your antibiotics from a gas station, so please don’t get your seizure medication from there,” Dr. Freedman said. “Studies have been done on ‘over-the-counter’ CBD oils and shown that they have variable quality, sometimes no detectable CBD, and sometimes other chemicals added like THC.”
Studies of Epidiolex showed that cannabidiol more effectively reduced seizure frequency than placebo for pediatric patients with Dravet syndrome (42% reduction) and for pediatric and adult patients with Lennox-Gastaut syndrome (39% reduction) or tuberous sclerosis complex (49% reduction). Efficacy was similar across dosing from 10-50 mg/kg per day, but higher doses involved higher rates of serious adverse events.
No reliable evidence in humans exists for THC or other cannabinoids in treating epilepsy.
The Australian guidance recommends limiting cannabis treatment to patients with severe drug-resistant epilepsy; a diagnosis of Dravet syndrome, Lennox-Gastaut syndrome, or tuberous sclerosis complex; and previous treatment with four approved antiseizure medications and/or the ketogenic diet, epilepsy surgery, or neurostimulator. The authors provide specific criteria for each of these conditions and then address exceptional cases that may be considered outside that criteria, such as patients under 2 years old, severe epilepsy with extended or repeated hospitalization or ICU admission, or a dangerous seizure type. The review also includes a detailed list of exclusion criteria for CBD medicine use.
The authors advised a thorough consent process before prescribing any cannabinoids, including therapeutic goals and stopping criteria; the lack of evidence available on dosing, efficacy, and side effects; and the potential for dependence or withdrawal. Consent discussions should also note whether the products are unregistered and not covered by external payers (anything other than Epidiolex currently), any activity restrictions, and any implications for occupational drug screening.
Considerations for unapproved cannabinoids
The authors note several factors to consider if prescribing or recommending a nonapproved, nonregulated cannabis medicine, including the ”differences between registered plant-derived cannabis medicines, synthetic cannabis medicines, and unregistered hemp-derived products.” Epidiolex is plant derived while other cannabis-derived medications (Marinol, Syndos, and Cesamet) that have been approved for nonepilepsy conditions, such as nausea associated with chemotherapy, are synthetic.
The guidance document notes several reasons to use a regulated medication instead of an unregulated product:
- Manufacturing processes can differ for unregulated products, including inconsistency in batches and unknown shelf life.
- Quality control processes, including risk of impurities, are much better with regulated products, which also have a system in place for safety recalls.
- More scientific evidence is available for regulated products.
- Safety surveillance reporting is more robust and standardized for regulated products whereas adverse event reporting is less reliable for unregulated products.
- Nonregulated products are rarely covered by insurance or other reimbursement.
Legal considerations will also vary by jurisdiction. ”Right now in the U.S. we have a confused legality where state level programs are still technically illegal at the federal level and I imagine there are some quality differences amongst dispensaries and states,” Dr. Freedman said. “Whenever there is disagreement between state and federal laws, this creates tension for our patients.” He noted, for example, that a patient using a CBD product that contains THC may, even if legal in their state, be confiscated by the Transportation Security Administration at an airport since it is not FDA approved and is not legal, according to the Drug Enforcement Agency.
The authors noted that inadequate data on long-term CBD use and data on neurodevelopmental effects of THC in children, teens, and young adults means THC products should be contraindicated for these age groups. (Epidiolex has less than 2% THC.) Drug interactions should also be considered, particularly for clobazam, CYP3A4 inhibitors or inducers (including St. John’s wort), digoxin, or a mechanistic target of rapamycin inhibitor.
Dr. Freedman said that most neurologists are comfortable prescribing Epidiolex since it has FDA approval while prescribing unapproved products varies more in the field. “Now that many states have compassionate use programs for medical marijuana, some neurologists do this as well,” Dr. Freedman said. Patients often ask about unregulated CBD or CBD+THC products because they’re seen as “natural and therefore better than manufactured pharmaceuticals.”
“I think this is the naturalistic fallacy at work and try to educate my patients on that since our only high-level data to show marijuana products work for epilepsy comes from a pharmaceutical company,” Dr. Freedman said. “My reasons for hesitating on compassionate use are that there is often THC, with variable amounts of concentration, and we know that THC can harm the developing pediatric brain.”
Dosing and adverse effects
Pediatric and adult dosing differences need to be considered, and “patient response (efficacy and toxicity) to these medications varies widely,” the authors noted. They advised getting serum transaminases (ALT and AST) and total bilirubin levels before beginning treatment. All patients should begin Epidiolex at a low dose, such as 2-5 mg/kg per day of CBD in two divided doses, the authors advise, and titrate slowly while monitoring for side effects (no more than 5 mg/kg per day per week). The current dosing range for CBD is 5-20 mg/kg per day in two divided doses, with higher rates involving more risk of adverse events.
“Note that some cannabinoids auto-inhibit their own metabolism and some have active metabolites with longer half-lives,” the authors wrote. “Therefore, dose or frequency may need to be reduced over time, unless tolerance occurs.” These doses, specific to Epidiolex, “cannot necessarily be applied to other oral CBD formulations or other types of epilepsy.” This guidance also does not apply to inhaled or transdermal routes of administration.
The most common adverse events were sleepiness – which occurred in up to 60% of trial participants – as well as diarrhea, decreases in appetite and weight, and drug interactions. Risk of hepatotoxicity means there’s a need to monitor liver function and adjust dosing for patients with moderate or severe hepatic impairment. “Other short-term side effects reported only with THC-containing cannabinoid compounds include increased risk of cardiac and cerebrovascular events, anxiety and psychosis risk, dependency, and withdrawal,” the authors wrote.
Though no withdrawal syndrome has been linked to stopping CBD, the authors suggested decreasing the dose by 10% every 2 days if stopping is not urgent.
“The key points to this issue are that CBD and all marijuana products need to be safe and regulated,” Dr. Freedman said. “Any claims about them need to be backed by high-quality evidence looking at that specific product for that specific condition.”
Dr. Freedman noted the need for children to receive treatment from clinicians with expertise in their specific condition since many other evidence-based treatments exist even for patients with epilepsy syndromes that are difficult to treat, such as other medications, surgery, and specialized diets.
“We need to fix the inconsistent regulation between over-the-counter CBD products, state dispensaries, and federal laws,” Dr. Freedman added. “Any medicine being used to treat children should be held to the same FDA standard of safety and efficacy.”
Dr. Freedman and the authors had no conflicts of interest. No external funding was noted.
A recent review article draws from existing clinical trials and clinical experience in New South Wales, Australia, to fill this gap with interim guidance for both pediatric and adult patients. The article was published in the British Journal of Clinical Pharmacology.
The only current U.S. guidelines are from the American Academy of Neurology’s position statement on the use of medical cannabis for neurologic disorders and the American Epilepsy Society’s position statement on cannabis as a treatment for epileptic seizures. The AAN statement “highlights the current evidence, which currently only supports [Food and Drug Administration]–approved CBD [cannabidiol] (Epidiolex) for specific epilepsy syndromes,” said Daniel Freedman, DO, an assistant professor of neurology at the University of Texas at Austin and coauthor of the AAN’s position statement.
“Rescheduling marijuana will enable researchers to study CBD, THC [tetrahydrocannabinol], and other cannabinoids in high-quality studies so that we can better understand what works and for which conditions,” said Dr. Freedman, who was not involved in the Australian guidance document. He noted that little consensus exists because little evidence exists outside the handful of trials for Epidiolex.
“There are some patients with epilepsy that can benefit from high-quality, pharmaceutical-grade CBD products,” Dr. Freedman said. “These patients need to be carefully identified by a neurologist or epileptologist and prescribed a legal, safe, quality-controlled, and FDA-regulated product.”
Appropriate patient populations
Drug-resistant epilepsy, defined as failure of two appropriate antiseizure medications, affects an estimated one third of people with epilepsy, the new guideline notes. Though many over-the-counter products are available at dispensaries in the 33 U.S. states that allow use of cannabis for medical purposes, Epidiolex (cannabidiol) is the only FDA-approved drug for epilepsy that contains a substance derived from cannabis and the only one for which evidence from randomized, controlled trials exists.
Dr. Freedman notes that hemp-derived CBD oils are classified differently in the United States than marijuana-derived CBD oil, including Epidiolex, and are loosely regulated supplements or food additives commonly seen, for example at gas station.
“The point I drive home to patients is that you wouldn’t get your antibiotics from a gas station, so please don’t get your seizure medication from there,” Dr. Freedman said. “Studies have been done on ‘over-the-counter’ CBD oils and shown that they have variable quality, sometimes no detectable CBD, and sometimes other chemicals added like THC.”
Studies of Epidiolex showed that cannabidiol more effectively reduced seizure frequency than placebo for pediatric patients with Dravet syndrome (42% reduction) and for pediatric and adult patients with Lennox-Gastaut syndrome (39% reduction) or tuberous sclerosis complex (49% reduction). Efficacy was similar across dosing from 10-50 mg/kg per day, but higher doses involved higher rates of serious adverse events.
No reliable evidence in humans exists for THC or other cannabinoids in treating epilepsy.
The Australian guidance recommends limiting cannabis treatment to patients with severe drug-resistant epilepsy; a diagnosis of Dravet syndrome, Lennox-Gastaut syndrome, or tuberous sclerosis complex; and previous treatment with four approved antiseizure medications and/or the ketogenic diet, epilepsy surgery, or neurostimulator. The authors provide specific criteria for each of these conditions and then address exceptional cases that may be considered outside that criteria, such as patients under 2 years old, severe epilepsy with extended or repeated hospitalization or ICU admission, or a dangerous seizure type. The review also includes a detailed list of exclusion criteria for CBD medicine use.
The authors advised a thorough consent process before prescribing any cannabinoids, including therapeutic goals and stopping criteria; the lack of evidence available on dosing, efficacy, and side effects; and the potential for dependence or withdrawal. Consent discussions should also note whether the products are unregistered and not covered by external payers (anything other than Epidiolex currently), any activity restrictions, and any implications for occupational drug screening.
Considerations for unapproved cannabinoids
The authors note several factors to consider if prescribing or recommending a nonapproved, nonregulated cannabis medicine, including the ”differences between registered plant-derived cannabis medicines, synthetic cannabis medicines, and unregistered hemp-derived products.” Epidiolex is plant derived while other cannabis-derived medications (Marinol, Syndos, and Cesamet) that have been approved for nonepilepsy conditions, such as nausea associated with chemotherapy, are synthetic.
The guidance document notes several reasons to use a regulated medication instead of an unregulated product:
- Manufacturing processes can differ for unregulated products, including inconsistency in batches and unknown shelf life.
- Quality control processes, including risk of impurities, are much better with regulated products, which also have a system in place for safety recalls.
- More scientific evidence is available for regulated products.
- Safety surveillance reporting is more robust and standardized for regulated products whereas adverse event reporting is less reliable for unregulated products.
- Nonregulated products are rarely covered by insurance or other reimbursement.
Legal considerations will also vary by jurisdiction. ”Right now in the U.S. we have a confused legality where state level programs are still technically illegal at the federal level and I imagine there are some quality differences amongst dispensaries and states,” Dr. Freedman said. “Whenever there is disagreement between state and federal laws, this creates tension for our patients.” He noted, for example, that a patient using a CBD product that contains THC may, even if legal in their state, be confiscated by the Transportation Security Administration at an airport since it is not FDA approved and is not legal, according to the Drug Enforcement Agency.
The authors noted that inadequate data on long-term CBD use and data on neurodevelopmental effects of THC in children, teens, and young adults means THC products should be contraindicated for these age groups. (Epidiolex has less than 2% THC.) Drug interactions should also be considered, particularly for clobazam, CYP3A4 inhibitors or inducers (including St. John’s wort), digoxin, or a mechanistic target of rapamycin inhibitor.
Dr. Freedman said that most neurologists are comfortable prescribing Epidiolex since it has FDA approval while prescribing unapproved products varies more in the field. “Now that many states have compassionate use programs for medical marijuana, some neurologists do this as well,” Dr. Freedman said. Patients often ask about unregulated CBD or CBD+THC products because they’re seen as “natural and therefore better than manufactured pharmaceuticals.”
“I think this is the naturalistic fallacy at work and try to educate my patients on that since our only high-level data to show marijuana products work for epilepsy comes from a pharmaceutical company,” Dr. Freedman said. “My reasons for hesitating on compassionate use are that there is often THC, with variable amounts of concentration, and we know that THC can harm the developing pediatric brain.”
Dosing and adverse effects
Pediatric and adult dosing differences need to be considered, and “patient response (efficacy and toxicity) to these medications varies widely,” the authors noted. They advised getting serum transaminases (ALT and AST) and total bilirubin levels before beginning treatment. All patients should begin Epidiolex at a low dose, such as 2-5 mg/kg per day of CBD in two divided doses, the authors advise, and titrate slowly while monitoring for side effects (no more than 5 mg/kg per day per week). The current dosing range for CBD is 5-20 mg/kg per day in two divided doses, with higher rates involving more risk of adverse events.
“Note that some cannabinoids auto-inhibit their own metabolism and some have active metabolites with longer half-lives,” the authors wrote. “Therefore, dose or frequency may need to be reduced over time, unless tolerance occurs.” These doses, specific to Epidiolex, “cannot necessarily be applied to other oral CBD formulations or other types of epilepsy.” This guidance also does not apply to inhaled or transdermal routes of administration.
The most common adverse events were sleepiness – which occurred in up to 60% of trial participants – as well as diarrhea, decreases in appetite and weight, and drug interactions. Risk of hepatotoxicity means there’s a need to monitor liver function and adjust dosing for patients with moderate or severe hepatic impairment. “Other short-term side effects reported only with THC-containing cannabinoid compounds include increased risk of cardiac and cerebrovascular events, anxiety and psychosis risk, dependency, and withdrawal,” the authors wrote.
Though no withdrawal syndrome has been linked to stopping CBD, the authors suggested decreasing the dose by 10% every 2 days if stopping is not urgent.
“The key points to this issue are that CBD and all marijuana products need to be safe and regulated,” Dr. Freedman said. “Any claims about them need to be backed by high-quality evidence looking at that specific product for that specific condition.”
Dr. Freedman noted the need for children to receive treatment from clinicians with expertise in their specific condition since many other evidence-based treatments exist even for patients with epilepsy syndromes that are difficult to treat, such as other medications, surgery, and specialized diets.
“We need to fix the inconsistent regulation between over-the-counter CBD products, state dispensaries, and federal laws,” Dr. Freedman added. “Any medicine being used to treat children should be held to the same FDA standard of safety and efficacy.”
Dr. Freedman and the authors had no conflicts of interest. No external funding was noted.
A recent review article draws from existing clinical trials and clinical experience in New South Wales, Australia, to fill this gap with interim guidance for both pediatric and adult patients. The article was published in the British Journal of Clinical Pharmacology.
The only current U.S. guidelines are from the American Academy of Neurology’s position statement on the use of medical cannabis for neurologic disorders and the American Epilepsy Society’s position statement on cannabis as a treatment for epileptic seizures. The AAN statement “highlights the current evidence, which currently only supports [Food and Drug Administration]–approved CBD [cannabidiol] (Epidiolex) for specific epilepsy syndromes,” said Daniel Freedman, DO, an assistant professor of neurology at the University of Texas at Austin and coauthor of the AAN’s position statement.
“Rescheduling marijuana will enable researchers to study CBD, THC [tetrahydrocannabinol], and other cannabinoids in high-quality studies so that we can better understand what works and for which conditions,” said Dr. Freedman, who was not involved in the Australian guidance document. He noted that little consensus exists because little evidence exists outside the handful of trials for Epidiolex.
“There are some patients with epilepsy that can benefit from high-quality, pharmaceutical-grade CBD products,” Dr. Freedman said. “These patients need to be carefully identified by a neurologist or epileptologist and prescribed a legal, safe, quality-controlled, and FDA-regulated product.”
Appropriate patient populations
Drug-resistant epilepsy, defined as failure of two appropriate antiseizure medications, affects an estimated one third of people with epilepsy, the new guideline notes. Though many over-the-counter products are available at dispensaries in the 33 U.S. states that allow use of cannabis for medical purposes, Epidiolex (cannabidiol) is the only FDA-approved drug for epilepsy that contains a substance derived from cannabis and the only one for which evidence from randomized, controlled trials exists.
Dr. Freedman notes that hemp-derived CBD oils are classified differently in the United States than marijuana-derived CBD oil, including Epidiolex, and are loosely regulated supplements or food additives commonly seen, for example at gas station.
“The point I drive home to patients is that you wouldn’t get your antibiotics from a gas station, so please don’t get your seizure medication from there,” Dr. Freedman said. “Studies have been done on ‘over-the-counter’ CBD oils and shown that they have variable quality, sometimes no detectable CBD, and sometimes other chemicals added like THC.”
Studies of Epidiolex showed that cannabidiol more effectively reduced seizure frequency than placebo for pediatric patients with Dravet syndrome (42% reduction) and for pediatric and adult patients with Lennox-Gastaut syndrome (39% reduction) or tuberous sclerosis complex (49% reduction). Efficacy was similar across dosing from 10-50 mg/kg per day, but higher doses involved higher rates of serious adverse events.
No reliable evidence in humans exists for THC or other cannabinoids in treating epilepsy.
The Australian guidance recommends limiting cannabis treatment to patients with severe drug-resistant epilepsy; a diagnosis of Dravet syndrome, Lennox-Gastaut syndrome, or tuberous sclerosis complex; and previous treatment with four approved antiseizure medications and/or the ketogenic diet, epilepsy surgery, or neurostimulator. The authors provide specific criteria for each of these conditions and then address exceptional cases that may be considered outside that criteria, such as patients under 2 years old, severe epilepsy with extended or repeated hospitalization or ICU admission, or a dangerous seizure type. The review also includes a detailed list of exclusion criteria for CBD medicine use.
The authors advised a thorough consent process before prescribing any cannabinoids, including therapeutic goals and stopping criteria; the lack of evidence available on dosing, efficacy, and side effects; and the potential for dependence or withdrawal. Consent discussions should also note whether the products are unregistered and not covered by external payers (anything other than Epidiolex currently), any activity restrictions, and any implications for occupational drug screening.
Considerations for unapproved cannabinoids
The authors note several factors to consider if prescribing or recommending a nonapproved, nonregulated cannabis medicine, including the ”differences between registered plant-derived cannabis medicines, synthetic cannabis medicines, and unregistered hemp-derived products.” Epidiolex is plant derived while other cannabis-derived medications (Marinol, Syndos, and Cesamet) that have been approved for nonepilepsy conditions, such as nausea associated with chemotherapy, are synthetic.
The guidance document notes several reasons to use a regulated medication instead of an unregulated product:
- Manufacturing processes can differ for unregulated products, including inconsistency in batches and unknown shelf life.
- Quality control processes, including risk of impurities, are much better with regulated products, which also have a system in place for safety recalls.
- More scientific evidence is available for regulated products.
- Safety surveillance reporting is more robust and standardized for regulated products whereas adverse event reporting is less reliable for unregulated products.
- Nonregulated products are rarely covered by insurance or other reimbursement.
Legal considerations will also vary by jurisdiction. ”Right now in the U.S. we have a confused legality where state level programs are still technically illegal at the federal level and I imagine there are some quality differences amongst dispensaries and states,” Dr. Freedman said. “Whenever there is disagreement between state and federal laws, this creates tension for our patients.” He noted, for example, that a patient using a CBD product that contains THC may, even if legal in their state, be confiscated by the Transportation Security Administration at an airport since it is not FDA approved and is not legal, according to the Drug Enforcement Agency.
The authors noted that inadequate data on long-term CBD use and data on neurodevelopmental effects of THC in children, teens, and young adults means THC products should be contraindicated for these age groups. (Epidiolex has less than 2% THC.) Drug interactions should also be considered, particularly for clobazam, CYP3A4 inhibitors or inducers (including St. John’s wort), digoxin, or a mechanistic target of rapamycin inhibitor.
Dr. Freedman said that most neurologists are comfortable prescribing Epidiolex since it has FDA approval while prescribing unapproved products varies more in the field. “Now that many states have compassionate use programs for medical marijuana, some neurologists do this as well,” Dr. Freedman said. Patients often ask about unregulated CBD or CBD+THC products because they’re seen as “natural and therefore better than manufactured pharmaceuticals.”
“I think this is the naturalistic fallacy at work and try to educate my patients on that since our only high-level data to show marijuana products work for epilepsy comes from a pharmaceutical company,” Dr. Freedman said. “My reasons for hesitating on compassionate use are that there is often THC, with variable amounts of concentration, and we know that THC can harm the developing pediatric brain.”
Dosing and adverse effects
Pediatric and adult dosing differences need to be considered, and “patient response (efficacy and toxicity) to these medications varies widely,” the authors noted. They advised getting serum transaminases (ALT and AST) and total bilirubin levels before beginning treatment. All patients should begin Epidiolex at a low dose, such as 2-5 mg/kg per day of CBD in two divided doses, the authors advise, and titrate slowly while monitoring for side effects (no more than 5 mg/kg per day per week). The current dosing range for CBD is 5-20 mg/kg per day in two divided doses, with higher rates involving more risk of adverse events.
“Note that some cannabinoids auto-inhibit their own metabolism and some have active metabolites with longer half-lives,” the authors wrote. “Therefore, dose or frequency may need to be reduced over time, unless tolerance occurs.” These doses, specific to Epidiolex, “cannot necessarily be applied to other oral CBD formulations or other types of epilepsy.” This guidance also does not apply to inhaled or transdermal routes of administration.
The most common adverse events were sleepiness – which occurred in up to 60% of trial participants – as well as diarrhea, decreases in appetite and weight, and drug interactions. Risk of hepatotoxicity means there’s a need to monitor liver function and adjust dosing for patients with moderate or severe hepatic impairment. “Other short-term side effects reported only with THC-containing cannabinoid compounds include increased risk of cardiac and cerebrovascular events, anxiety and psychosis risk, dependency, and withdrawal,” the authors wrote.
Though no withdrawal syndrome has been linked to stopping CBD, the authors suggested decreasing the dose by 10% every 2 days if stopping is not urgent.
“The key points to this issue are that CBD and all marijuana products need to be safe and regulated,” Dr. Freedman said. “Any claims about them need to be backed by high-quality evidence looking at that specific product for that specific condition.”
Dr. Freedman noted the need for children to receive treatment from clinicians with expertise in their specific condition since many other evidence-based treatments exist even for patients with epilepsy syndromes that are difficult to treat, such as other medications, surgery, and specialized diets.
“We need to fix the inconsistent regulation between over-the-counter CBD products, state dispensaries, and federal laws,” Dr. Freedman added. “Any medicine being used to treat children should be held to the same FDA standard of safety and efficacy.”
Dr. Freedman and the authors had no conflicts of interest. No external funding was noted.
FROM THE BRITISH JOURNAL OF CLINICAL PHARMACOLOGY
Intermittent fasting good for weight loss, at least short term
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The health benefits of intermittent fasting are slowly being clarified as more evidence continues to emerge, say the authors of a new review of 21 studies. Initial findings suggest that fasting might be effective for mild to moderate weight loss for certain groups of people, at least in the short term.
And data so far at least dispel the myth that “people are going to feel weak and not be able to concentrate during fasting,” lead researcher Krista A. Varady, PhD, professor of nutrition in the University of Illinois at Chicago, noted in a press release from her university.
“We’ve shown it is the opposite,” she said. “They actually have a better ability to concentrate.”
Yet much longer-term data are needed on issues such as safety, Dr. Varady and colleagues note in their review in Nature Reviews: Endocrinology .
The trials so far have only been conducted in adults – generally with overweight or obesity and sometimes hypertension, dyslipidemia, and/or diabetes – but some have been performed in those of normal weight.
Dr. Varady and colleague recommend that those with type 1 diabetes, type 2 diabetes, or other comorbidities, or patients who need to take medications with meals at certain times of the day, should seek clinical supervision when considering intermittent fasting.
And currently, based on existing evidence, intermittent fasting is contraindicated for children under age 12 and those who have a history of an eating disorder or a body mass index <18.5 kg/m2. Opinions vary about the safety of supervised fasting in adolescents with obesity. Also, safety has not been evaluated in those older than age 70, and in women who are pregnant or lactating.
‘A few studies’ show 3%-8% weight loss over 2-3 months
Despite the recent surge in the popularity of intermittent fasting, “only a few studies have examined the health benefits of these diets in humans,” Dr. Varady and coauthors emphasize.
They identified 21 clinical trials of three types of intermittent fasting strategies:
Alternate day fasting (alternating between consuming 0-500 kcal on “fasting” days, followed by unlimited food on “feasting” days), six trials.
5:2 diet (“feasting” on 5 days and “fasting” on 2 days), seven trials.
Time-restricted eating (eating during a 4- to 8- hour window), nine trials.
The trials were short (mostly 5-12 weeks long) and small (10-150 participants), and mostly conducted in the United States.
They found these strategies can all produce a mild to moderate 3%-8% weight loss during 8-12 weeks, similar to that attained with a calorie-restricted diet.
Some studies found that patients had improvements in blood pressure, LDL cholesterol, triglycerides, insulin resistance, and hemoglobin A1c.
These weight-loss strategies produced few gastrointestinal, neurological, hormonal, or metabolic adverse effects; “however, as adverse outcomes are not regularly assessed in human trials of fasting, definitive conclusions regarding the safety of these diets are difficult to draw at present,” the researchers caution.
Practical advice, great anecdotes
Typically, 1-2 weeks of adjustment is needed when individuals start intermittent fasting, the researchers say.
While following this eating pattern, patients should be encouraged to consume plenty of fruits, vegetables, and whole grains to boost their fiber and micronutrient intake.
On fasting days, they should consume at least 50 g of lean protein to help control hunger and prevent excessive loss of lean mass. On those days, alcohol is permitted but not recommended. Energy drinks and coffee or tea without sugar, milk, or cream are allowed, and diet soda should be limited to two servings a day because it can increase sugar cravings.
Ideally, clinicians should regularly assess patients for adverse effects during the first 3 months of intermittent fasting. They should also monitor patients for deficiencies in vitamin D, vitamin B12, and electrolytes, as well as for changes in medications for blood pressure, lipids, and glucose that may be needed if patients lose weight.
Patients who reach their weight-loss goals and wish to stop intermittent fasting need to transition to a weight-maintenance program, possibly by increasing energy intake on fasting days to 1,000-1,200 kcal/day or widening the eating window to 12 hours in time-restricted eating.
“I get lots of emails from people saying that they have been on the diet for 10-15 years, and it reversed their type 2 diabetes, and they lost 60 pounds, and it was the only diet they could stick to,” Dr. Varady noted.
“That is always nice to hear, but we really do need long-term data to see if people can do intermittent fasting for the long term,” she reiterated.
The review was funded by the National Institute of Diabetes and Digestive and Kidney Diseases. Dr. Varady received author fees from the Hachette Book Group for the book, “The Every Other Day Diet.” The other authors have declared no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NATURE REVIEWS: ENDOCRINOLOGY
Mild COVID-19 infection linked to later type 2 diabetes
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA