User login
The Journal of Clinical Outcomes Management® is an independent, peer-reviewed journal offering evidence-based, practical information for improving the quality, safety, and value of health care.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Children and COVID: New cases climb slowly but steadily
The current sustained increase in COVID-19 has brought the total number of cases in children to over 13 million since the start of the pandemic, according to the American Academy of Pediatrics and the Children’s Hospital Association.
, when cases dropped to their lowest point since last summer. The cumulative number of cases in children is 13,052,988, which accounts for 19.0% of all cases reported in the United States, the AAP and CHA said in their weekly COVID-19 report.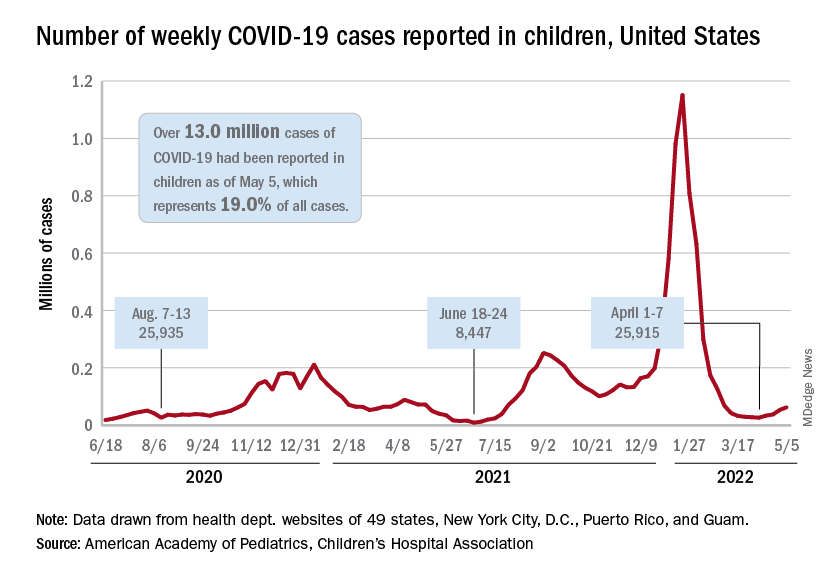
Other measures of incidence show the same steady rise. The rate of new admissions of children aged 0-17 with confirmed COVID-19, which had dipped as low as 0.13 per 100,000 population on April 11, was up to 0.19 per 100,000 on May 6, and the 7-day average for total admissions was 136 per day for May 1-7, compared with 118 for the last week of April, according to the Centers for Disease Control and Prevention.
At the state level, new admission rates for May 6 show wide variation, even regionally. Rhode Island came in with a 0.00 per 100,000 on that day, while Vermont recorded 0.88 admissions per 100,000, the highest of any state and lower only than the District of Columbia’s 1.23 per 100,000. Connecticut (0.45) and Massachusetts (0.33) also were in the highest group (see map), while Maine was in the lowest, CDC data show.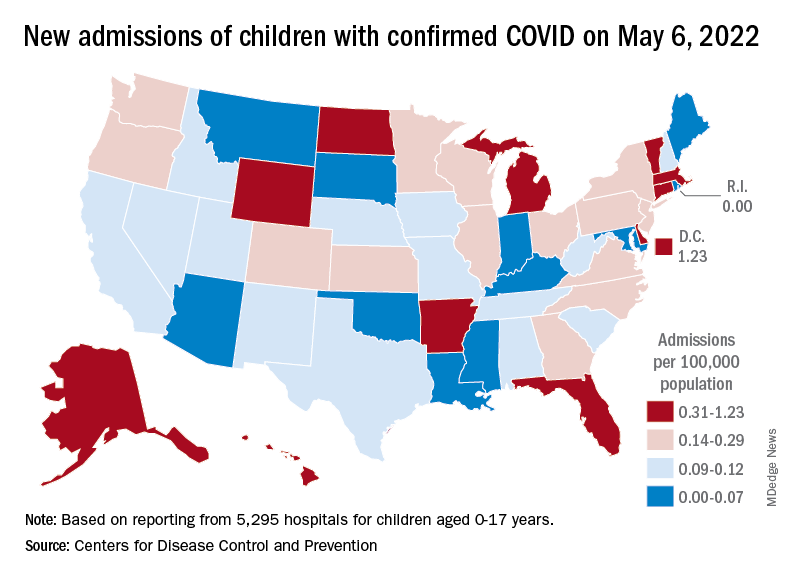
Nationally, emergency department visits also have been rising over the last month or so. Children aged 0-11 years, who were down to a 7-day average of 0.5% of ED visits with diagnosed COVID-19 in early April, saw that number rise to 1.4% on May 5. Children aged 12-15 years went from a rate of 0.3% in late March to the current 1.2%, as did 16- to 17-year-olds, the CDC said on its COVID Data Tracker.
The vaccination effort, meanwhile, continues to lose steam, at least among children who are currently eligible. Initial vaccinations in those aged 5-11 slipped to their lowest-ever 1-week total, 47,000 for April 28 to May 4, while children aged 16-17 continued a long-term slide that has the weekly count down to just 29,000, the AAP said in its weekly vaccination report.
Here’s how those latest recipients changed the populations of vaccinated children in the last week: 35.4% of all 5- to 11-year-olds had received at least one dose as of May 4, compared with 35.3% on April 27, with increases from 67.4% to 67.5% for 12- to 15-year-olds and 72.7% to 72.8% among those aged 16-17, the CDC reported.
The current sustained increase in COVID-19 has brought the total number of cases in children to over 13 million since the start of the pandemic, according to the American Academy of Pediatrics and the Children’s Hospital Association.
, when cases dropped to their lowest point since last summer. The cumulative number of cases in children is 13,052,988, which accounts for 19.0% of all cases reported in the United States, the AAP and CHA said in their weekly COVID-19 report.
Other measures of incidence show the same steady rise. The rate of new admissions of children aged 0-17 with confirmed COVID-19, which had dipped as low as 0.13 per 100,000 population on April 11, was up to 0.19 per 100,000 on May 6, and the 7-day average for total admissions was 136 per day for May 1-7, compared with 118 for the last week of April, according to the Centers for Disease Control and Prevention.
At the state level, new admission rates for May 6 show wide variation, even regionally. Rhode Island came in with a 0.00 per 100,000 on that day, while Vermont recorded 0.88 admissions per 100,000, the highest of any state and lower only than the District of Columbia’s 1.23 per 100,000. Connecticut (0.45) and Massachusetts (0.33) also were in the highest group (see map), while Maine was in the lowest, CDC data show.
Nationally, emergency department visits also have been rising over the last month or so. Children aged 0-11 years, who were down to a 7-day average of 0.5% of ED visits with diagnosed COVID-19 in early April, saw that number rise to 1.4% on May 5. Children aged 12-15 years went from a rate of 0.3% in late March to the current 1.2%, as did 16- to 17-year-olds, the CDC said on its COVID Data Tracker.
The vaccination effort, meanwhile, continues to lose steam, at least among children who are currently eligible. Initial vaccinations in those aged 5-11 slipped to their lowest-ever 1-week total, 47,000 for April 28 to May 4, while children aged 16-17 continued a long-term slide that has the weekly count down to just 29,000, the AAP said in its weekly vaccination report.
Here’s how those latest recipients changed the populations of vaccinated children in the last week: 35.4% of all 5- to 11-year-olds had received at least one dose as of May 4, compared with 35.3% on April 27, with increases from 67.4% to 67.5% for 12- to 15-year-olds and 72.7% to 72.8% among those aged 16-17, the CDC reported.
The current sustained increase in COVID-19 has brought the total number of cases in children to over 13 million since the start of the pandemic, according to the American Academy of Pediatrics and the Children’s Hospital Association.
, when cases dropped to their lowest point since last summer. The cumulative number of cases in children is 13,052,988, which accounts for 19.0% of all cases reported in the United States, the AAP and CHA said in their weekly COVID-19 report.
Other measures of incidence show the same steady rise. The rate of new admissions of children aged 0-17 with confirmed COVID-19, which had dipped as low as 0.13 per 100,000 population on April 11, was up to 0.19 per 100,000 on May 6, and the 7-day average for total admissions was 136 per day for May 1-7, compared with 118 for the last week of April, according to the Centers for Disease Control and Prevention.
At the state level, new admission rates for May 6 show wide variation, even regionally. Rhode Island came in with a 0.00 per 100,000 on that day, while Vermont recorded 0.88 admissions per 100,000, the highest of any state and lower only than the District of Columbia’s 1.23 per 100,000. Connecticut (0.45) and Massachusetts (0.33) also were in the highest group (see map), while Maine was in the lowest, CDC data show.
Nationally, emergency department visits also have been rising over the last month or so. Children aged 0-11 years, who were down to a 7-day average of 0.5% of ED visits with diagnosed COVID-19 in early April, saw that number rise to 1.4% on May 5. Children aged 12-15 years went from a rate of 0.3% in late March to the current 1.2%, as did 16- to 17-year-olds, the CDC said on its COVID Data Tracker.
The vaccination effort, meanwhile, continues to lose steam, at least among children who are currently eligible. Initial vaccinations in those aged 5-11 slipped to their lowest-ever 1-week total, 47,000 for April 28 to May 4, while children aged 16-17 continued a long-term slide that has the weekly count down to just 29,000, the AAP said in its weekly vaccination report.
Here’s how those latest recipients changed the populations of vaccinated children in the last week: 35.4% of all 5- to 11-year-olds had received at least one dose as of May 4, compared with 35.3% on April 27, with increases from 67.4% to 67.5% for 12- to 15-year-olds and 72.7% to 72.8% among those aged 16-17, the CDC reported.
My choice? Unvaccinated pose outsize risk to vaccinated
according to a mathematical modeling study.
The study, which simulated patterns of infection among vaccinated and unvaccinated populations, showed that, as the populations mixed less, attack rates decreased among vaccinated people (from 15% to 10%) and increased among unvaccinated people (from 62% to 79%). The unvaccinated increasingly became the source of infection, however.
“When the vaccinated and unvaccinated mix, indirect protection is conferred upon the unvaccinated by the buffering effect of vaccinated individuals, and by contrast, risk in the vaccinated goes up,” lead author David Fisman, MD, professor of epidemiology at the University of Toronto, told this news organization.
As the groups mix less and less, the size of the epidemic increases among the unvaccinated and decreases among the vaccinated. “But the impact of the unvaccinated on risk in the vaccinated is disproportionate to the numbers of contacts between the two groups,” said Dr. Fisman.
The study was published online in the Canadian Medical Association Journal.
Relative contributions to risk
The researchers used a model of a respiratory viral disease “similar to SARS-CoV-2 infection with Delta variant.” They included reproduction values to capture the dynamics of the Omicron variant, which was emerging at the time. In the study, vaccines ranged in effectiveness from 40% to 80%. The study incorporated various levels of mixing between a partially vaccinated and an unvaccinated population. The mixing ranged from random mixing to like-with-like mixing (“assortativity”). There were three possible “compartments” of people in the model: those considered susceptible to infection, those considered infected and infectious, and those considered immune because of recovery.
The model showed that, as mixing between the vaccinated and the unvaccinated populations increased, case numbers rose, “with cases in the unvaccinated subpopulation accounting for a substantial proportion of infections.” However, as mixing between the populations decreased, the final attack rate decreased among vaccinated people, but the relative “contribution of risk to vaccinated people caused by infection acquired from contact with unvaccinated people ... increased.”
When the vaccination rate was increased in the model, case numbers among the vaccinated declined “as expected, owing to indirect protective effects,” the researchers noted. But this also “further increased the relative contribution to risk in vaccinated people by those who were unvaccinated.”
Self-regarding risk?
The findings show that “choices made by people who forgo vaccination contribute disproportionately to risk among those who do get vaccinated,” the researchers wrote. “Although risk associated with avoiding vaccination during a virulent pandemic accrues chiefly to those who are unvaccinated, the choice of some individuals to refuse vaccination is likely to affect the health and safety of vaccinated people in a manner disproportionate to the fraction of unvaccinated people in the population.”
The fact that like-with-like mixing cannot mitigate the risk to vaccinated people “undermines the assertion that vaccine choice is best left to the individual and supports strong public actions aimed at enhancing vaccine uptake and limiting access to public spaces for unvaccinated people,” they wrote.
Mandates and passports
“Our model provides support for vaccine mandates and passports during epidemics, such that vaccination is required for people to take part in nonessential activities,” said Dr. Fisman. The choice to not be vaccinated against COVID-19 should not be considered “self-regarding,” he added. “Risk is self-regarding when it only impacts the person engaging in the activity. Something like smoking cigarettes (alone, without others around) creates a lot of risk over time, but if nobody is breathing your secondhand smoke, you’re only creating risk for yourself. By contrast, we regulate, in Ontario, your right to smoke in public indoor spaces such as restaurants, because once other people are around, the risk isn’t self-regarding anymore. You’re creating risk for others.”
The authors also noted that the risks created by the unvaccinated extend beyond those of infection by “creating a risk that those around them may not be able to obtain the care they need.” They recommended that considerations of equity and justice for people who do choose to be vaccinated, as well as those who choose not to be, need to be included in formulating vaccination policy.
Illuminating the discussion
Asked to comment on the study, Matthew Oughton, MD, assistant professor of medicine at McGill University, Montreal, said: “It is easy to dismiss a mathematical model as a series of assumptions that leads to an implausible conclusion. ... However, they can serve to illustrate and, to an extent, quantify the results of complex interactions, and this study does just that.” Dr. Oughton was not involved in the research.
During the past 2 years, the scientific press and the general press have often discussed the individual and collective effects of disease-prevention methods, including nonpharmaceutical interventions. “Models like this can help illuminate those discussions by highlighting important consequences of preventive measures,” said Dr. Oughton, who also works in the division of infectious diseases at the Jewish General Hospital, Montreal.
It’s worth noting that the authors modeled vaccine effectiveness against all infection, “rather than the generally greater and more durable effects we have seen for vaccines in prevention of severe infection,” said Dr. Oughton. He added that the authors did not include the effect of vaccination in reducing forward transmission. “Inclusion of this effect would presumably have reduced overall infectious burden in mixed populations and increased the difference between groups at lower levels of mixing between populations.”
The research was supported by a grant from the Canadian Institutes of Health Research. Dr. Fisman has served on advisory boards related to influenza and SARS-CoV-2 vaccines for Seqirus, Pfizer, AstraZeneca, and Sanofi-Pasteur Vaccines and has served as a legal expert on issues related to COVID-19 epidemiology for the Elementary Teachers Federation of Ontario and the Registered Nurses Association of Ontario. Dr. Oughton disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a mathematical modeling study.
The study, which simulated patterns of infection among vaccinated and unvaccinated populations, showed that, as the populations mixed less, attack rates decreased among vaccinated people (from 15% to 10%) and increased among unvaccinated people (from 62% to 79%). The unvaccinated increasingly became the source of infection, however.
“When the vaccinated and unvaccinated mix, indirect protection is conferred upon the unvaccinated by the buffering effect of vaccinated individuals, and by contrast, risk in the vaccinated goes up,” lead author David Fisman, MD, professor of epidemiology at the University of Toronto, told this news organization.
As the groups mix less and less, the size of the epidemic increases among the unvaccinated and decreases among the vaccinated. “But the impact of the unvaccinated on risk in the vaccinated is disproportionate to the numbers of contacts between the two groups,” said Dr. Fisman.
The study was published online in the Canadian Medical Association Journal.
Relative contributions to risk
The researchers used a model of a respiratory viral disease “similar to SARS-CoV-2 infection with Delta variant.” They included reproduction values to capture the dynamics of the Omicron variant, which was emerging at the time. In the study, vaccines ranged in effectiveness from 40% to 80%. The study incorporated various levels of mixing between a partially vaccinated and an unvaccinated population. The mixing ranged from random mixing to like-with-like mixing (“assortativity”). There were three possible “compartments” of people in the model: those considered susceptible to infection, those considered infected and infectious, and those considered immune because of recovery.
The model showed that, as mixing between the vaccinated and the unvaccinated populations increased, case numbers rose, “with cases in the unvaccinated subpopulation accounting for a substantial proportion of infections.” However, as mixing between the populations decreased, the final attack rate decreased among vaccinated people, but the relative “contribution of risk to vaccinated people caused by infection acquired from contact with unvaccinated people ... increased.”
When the vaccination rate was increased in the model, case numbers among the vaccinated declined “as expected, owing to indirect protective effects,” the researchers noted. But this also “further increased the relative contribution to risk in vaccinated people by those who were unvaccinated.”
Self-regarding risk?
The findings show that “choices made by people who forgo vaccination contribute disproportionately to risk among those who do get vaccinated,” the researchers wrote. “Although risk associated with avoiding vaccination during a virulent pandemic accrues chiefly to those who are unvaccinated, the choice of some individuals to refuse vaccination is likely to affect the health and safety of vaccinated people in a manner disproportionate to the fraction of unvaccinated people in the population.”
The fact that like-with-like mixing cannot mitigate the risk to vaccinated people “undermines the assertion that vaccine choice is best left to the individual and supports strong public actions aimed at enhancing vaccine uptake and limiting access to public spaces for unvaccinated people,” they wrote.
Mandates and passports
“Our model provides support for vaccine mandates and passports during epidemics, such that vaccination is required for people to take part in nonessential activities,” said Dr. Fisman. The choice to not be vaccinated against COVID-19 should not be considered “self-regarding,” he added. “Risk is self-regarding when it only impacts the person engaging in the activity. Something like smoking cigarettes (alone, without others around) creates a lot of risk over time, but if nobody is breathing your secondhand smoke, you’re only creating risk for yourself. By contrast, we regulate, in Ontario, your right to smoke in public indoor spaces such as restaurants, because once other people are around, the risk isn’t self-regarding anymore. You’re creating risk for others.”
The authors also noted that the risks created by the unvaccinated extend beyond those of infection by “creating a risk that those around them may not be able to obtain the care they need.” They recommended that considerations of equity and justice for people who do choose to be vaccinated, as well as those who choose not to be, need to be included in formulating vaccination policy.
Illuminating the discussion
Asked to comment on the study, Matthew Oughton, MD, assistant professor of medicine at McGill University, Montreal, said: “It is easy to dismiss a mathematical model as a series of assumptions that leads to an implausible conclusion. ... However, they can serve to illustrate and, to an extent, quantify the results of complex interactions, and this study does just that.” Dr. Oughton was not involved in the research.
During the past 2 years, the scientific press and the general press have often discussed the individual and collective effects of disease-prevention methods, including nonpharmaceutical interventions. “Models like this can help illuminate those discussions by highlighting important consequences of preventive measures,” said Dr. Oughton, who also works in the division of infectious diseases at the Jewish General Hospital, Montreal.
It’s worth noting that the authors modeled vaccine effectiveness against all infection, “rather than the generally greater and more durable effects we have seen for vaccines in prevention of severe infection,” said Dr. Oughton. He added that the authors did not include the effect of vaccination in reducing forward transmission. “Inclusion of this effect would presumably have reduced overall infectious burden in mixed populations and increased the difference between groups at lower levels of mixing between populations.”
The research was supported by a grant from the Canadian Institutes of Health Research. Dr. Fisman has served on advisory boards related to influenza and SARS-CoV-2 vaccines for Seqirus, Pfizer, AstraZeneca, and Sanofi-Pasteur Vaccines and has served as a legal expert on issues related to COVID-19 epidemiology for the Elementary Teachers Federation of Ontario and the Registered Nurses Association of Ontario. Dr. Oughton disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
according to a mathematical modeling study.
The study, which simulated patterns of infection among vaccinated and unvaccinated populations, showed that, as the populations mixed less, attack rates decreased among vaccinated people (from 15% to 10%) and increased among unvaccinated people (from 62% to 79%). The unvaccinated increasingly became the source of infection, however.
“When the vaccinated and unvaccinated mix, indirect protection is conferred upon the unvaccinated by the buffering effect of vaccinated individuals, and by contrast, risk in the vaccinated goes up,” lead author David Fisman, MD, professor of epidemiology at the University of Toronto, told this news organization.
As the groups mix less and less, the size of the epidemic increases among the unvaccinated and decreases among the vaccinated. “But the impact of the unvaccinated on risk in the vaccinated is disproportionate to the numbers of contacts between the two groups,” said Dr. Fisman.
The study was published online in the Canadian Medical Association Journal.
Relative contributions to risk
The researchers used a model of a respiratory viral disease “similar to SARS-CoV-2 infection with Delta variant.” They included reproduction values to capture the dynamics of the Omicron variant, which was emerging at the time. In the study, vaccines ranged in effectiveness from 40% to 80%. The study incorporated various levels of mixing between a partially vaccinated and an unvaccinated population. The mixing ranged from random mixing to like-with-like mixing (“assortativity”). There were three possible “compartments” of people in the model: those considered susceptible to infection, those considered infected and infectious, and those considered immune because of recovery.
The model showed that, as mixing between the vaccinated and the unvaccinated populations increased, case numbers rose, “with cases in the unvaccinated subpopulation accounting for a substantial proportion of infections.” However, as mixing between the populations decreased, the final attack rate decreased among vaccinated people, but the relative “contribution of risk to vaccinated people caused by infection acquired from contact with unvaccinated people ... increased.”
When the vaccination rate was increased in the model, case numbers among the vaccinated declined “as expected, owing to indirect protective effects,” the researchers noted. But this also “further increased the relative contribution to risk in vaccinated people by those who were unvaccinated.”
Self-regarding risk?
The findings show that “choices made by people who forgo vaccination contribute disproportionately to risk among those who do get vaccinated,” the researchers wrote. “Although risk associated with avoiding vaccination during a virulent pandemic accrues chiefly to those who are unvaccinated, the choice of some individuals to refuse vaccination is likely to affect the health and safety of vaccinated people in a manner disproportionate to the fraction of unvaccinated people in the population.”
The fact that like-with-like mixing cannot mitigate the risk to vaccinated people “undermines the assertion that vaccine choice is best left to the individual and supports strong public actions aimed at enhancing vaccine uptake and limiting access to public spaces for unvaccinated people,” they wrote.
Mandates and passports
“Our model provides support for vaccine mandates and passports during epidemics, such that vaccination is required for people to take part in nonessential activities,” said Dr. Fisman. The choice to not be vaccinated against COVID-19 should not be considered “self-regarding,” he added. “Risk is self-regarding when it only impacts the person engaging in the activity. Something like smoking cigarettes (alone, without others around) creates a lot of risk over time, but if nobody is breathing your secondhand smoke, you’re only creating risk for yourself. By contrast, we regulate, in Ontario, your right to smoke in public indoor spaces such as restaurants, because once other people are around, the risk isn’t self-regarding anymore. You’re creating risk for others.”
The authors also noted that the risks created by the unvaccinated extend beyond those of infection by “creating a risk that those around them may not be able to obtain the care they need.” They recommended that considerations of equity and justice for people who do choose to be vaccinated, as well as those who choose not to be, need to be included in formulating vaccination policy.
Illuminating the discussion
Asked to comment on the study, Matthew Oughton, MD, assistant professor of medicine at McGill University, Montreal, said: “It is easy to dismiss a mathematical model as a series of assumptions that leads to an implausible conclusion. ... However, they can serve to illustrate and, to an extent, quantify the results of complex interactions, and this study does just that.” Dr. Oughton was not involved in the research.
During the past 2 years, the scientific press and the general press have often discussed the individual and collective effects of disease-prevention methods, including nonpharmaceutical interventions. “Models like this can help illuminate those discussions by highlighting important consequences of preventive measures,” said Dr. Oughton, who also works in the division of infectious diseases at the Jewish General Hospital, Montreal.
It’s worth noting that the authors modeled vaccine effectiveness against all infection, “rather than the generally greater and more durable effects we have seen for vaccines in prevention of severe infection,” said Dr. Oughton. He added that the authors did not include the effect of vaccination in reducing forward transmission. “Inclusion of this effect would presumably have reduced overall infectious burden in mixed populations and increased the difference between groups at lower levels of mixing between populations.”
The research was supported by a grant from the Canadian Institutes of Health Research. Dr. Fisman has served on advisory boards related to influenza and SARS-CoV-2 vaccines for Seqirus, Pfizer, AstraZeneca, and Sanofi-Pasteur Vaccines and has served as a legal expert on issues related to COVID-19 epidemiology for the Elementary Teachers Federation of Ontario and the Registered Nurses Association of Ontario. Dr. Oughton disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE CANADIAN MEDICAL ASSOCIATION JOURNAL
Hospital factors tied to lower maternal morbidity
A new study of hospitals in New York City suggests ways to reduce severe maternal morbidity (SMM). The researchers interviewed health care professionals in four institutions with low performance and four with high performance, and identified various themes associated with good performance.
“Our results raise the hypothesis that hospital learning collaboratives focused on optimizing organizational practices and policies, increasing clinician and staff awareness and education on maternal health disparities, and addressing structural racism may be important tools for improving equity in maternal outcomes,” the authors wrote in the study, published in Obstetrics & Gynecology.
The researchers conducted 50 semistructured interviews with health care professionals at lower-performing and higher-performing New York City hospitals, which were selected based on risk-adjusted morbidity metrics. The interviews explored various topics, including structural characteristics like staffing, organizational characteristics like culture and communication, labor and delivery practices such as teamwork and use of evidence-based practices, and racial and ethnic disparities.
The analysis revealed six broad areas that were stronger in high-performing hospitals: day-to-day involvement of leadership in quality activities, an emphasis on standards and standardized care, good communication and teamwork between nurses and physicians, good staffing and supervision among physicians and nurses, sharing of performance data with health care workers, and acknowledgment of the existence of racial and ethnic disparities and that bias can cause treatment differences.
“I think this qualitative approach is an important lens to pair with the quantitative approach. With such variability in severe maternal morbidity between hospitals in New York, it is not enough to just look at the quantitative data. To understand how to improve you must examine structures and processes. The structures, which are the physical and organizational characteristics in health care, and the process, which is how health care is delivered,” Veronica Gillispie-Bell, MD, wrote in a comment. Dr. Gillispie-Bell is medical director at Louisiana Perinatal Quality Collaborative and the Pregnancy-Associated Mortality Review for the Louisiana Department of Health.
“We know that high reliability organizations are those who are preoccupied with quality and safety. That means accountability from leadership (structure) and stability in standardization of care (processes). However, none of this matters if you do not have a culture that promotes safety. Based on the key findings of the high-performing hospitals, there was a culture that promoted safety and quality evidenced in the nurse-physician communication and the transparency around data through a lens of equity,” wrote Dr. Gillispie-Bell.
She noted that the study should encourage low-performing hospitals, since it illustrates avenues for improvement. Her personal experience reflects that, though she said that hospitals need help. The Louisiana Perinatal Quality Collaborative addressed severe maternal morbidity at birthing centers by implementing evidence-based best practices for management of hypertension and hemorrhage along with health equity measures. The team conducted coaching calls, in-person learning sessions, and in-person visits through a “Listening Tour.”
The result was a 35% reduction in hemorrhage overall and a reduction of 49% in hemorrhage in Black women, as well as hypertension by 12% overall between August 2018 and May 2020. Not all the news was good, as Black women still had an increase in severe maternal morbidity, possibly because of the COVID epidemic, since it is a risk factor for hypertension during pregnancy and infection rates are higher among Black individuals. “We need support for state based perinatal quality collaboratives to do this work and we need accountability as we are now seeing from metrics being implemented by [the Centers for Medicare & Medicaid Services]. Hospitals need to stratify their data by race and ethnicity to see where there are disparities in their outcomes,” said Dr. Gillispie-Bell.
The improvements are needed, given that the United States has the highest rates of maternal mortality and morbidity among developed countries, “most of which is preventable, and we have significant inequities by race and ethnicity,” said Laurie Zephyrin, MD, vice president for advancing health equity at the Commonwealth Fund. The question becomes how to effect change, and “there’s a lot happening in the policy space. Some of this policy change is directed at expanding insurance coverage, including more opportunities, including funding for community health workers and doulas, and thinking about how to incorporate midwives. There’s also work around how do we actually improve the care delivered by our health system.” Dr. Zephyrin added that the Department of Health & Human Services has contracted with the health improvement company Premier to use data and best-practices to improve maternal health.
The new work has the potential to be complementary to such approaches. “It provides some structure around how to approach some of the solutions, none of which I think is rocket science. It’s just something that needs to be focused on more intentionally,” said Dr. Zephyrin.
For example, the report found that high-performing hospitals had leaders who collaborated with frontline clinicians to share performance data, and this occurred in person, at departmental quality meetings, and during grand rounds. In contrast, staff in low-performing hospitals did not mention data feedback and some said that their institution made little effort to communicate performance metrics to frontline staff.
“One of the key lessons from the pandemic is that we need to have better data, and we need to have data around race and ethnicity to be able to understand the impact on marginalized communities. This study highlights that there’s more to be done around data to ensure that we can truly move the needle on advancing health equity,” said Dr. Zephyrin.
The researchers also found that clinicians in low-performing institutions did not acknowledge the presence of structural racism or differences in care associated with race or ethnicity. When they acknowledge differences in care, they attributed them to factors outside of the hospital’s control, such as patients not seeking out health care or not maintaining a healthy weight. Clinicians at high-performing hospitals were more likely to explicitly mention racism and bias and acknowledged that these factors could contribute to differences in care.
Dr. Gillispie-Bell and Dr. Zephyrin have no relevant financial disclosures.
A new study of hospitals in New York City suggests ways to reduce severe maternal morbidity (SMM). The researchers interviewed health care professionals in four institutions with low performance and four with high performance, and identified various themes associated with good performance.
“Our results raise the hypothesis that hospital learning collaboratives focused on optimizing organizational practices and policies, increasing clinician and staff awareness and education on maternal health disparities, and addressing structural racism may be important tools for improving equity in maternal outcomes,” the authors wrote in the study, published in Obstetrics & Gynecology.
The researchers conducted 50 semistructured interviews with health care professionals at lower-performing and higher-performing New York City hospitals, which were selected based on risk-adjusted morbidity metrics. The interviews explored various topics, including structural characteristics like staffing, organizational characteristics like culture and communication, labor and delivery practices such as teamwork and use of evidence-based practices, and racial and ethnic disparities.
The analysis revealed six broad areas that were stronger in high-performing hospitals: day-to-day involvement of leadership in quality activities, an emphasis on standards and standardized care, good communication and teamwork between nurses and physicians, good staffing and supervision among physicians and nurses, sharing of performance data with health care workers, and acknowledgment of the existence of racial and ethnic disparities and that bias can cause treatment differences.
“I think this qualitative approach is an important lens to pair with the quantitative approach. With such variability in severe maternal morbidity between hospitals in New York, it is not enough to just look at the quantitative data. To understand how to improve you must examine structures and processes. The structures, which are the physical and organizational characteristics in health care, and the process, which is how health care is delivered,” Veronica Gillispie-Bell, MD, wrote in a comment. Dr. Gillispie-Bell is medical director at Louisiana Perinatal Quality Collaborative and the Pregnancy-Associated Mortality Review for the Louisiana Department of Health.
“We know that high reliability organizations are those who are preoccupied with quality and safety. That means accountability from leadership (structure) and stability in standardization of care (processes). However, none of this matters if you do not have a culture that promotes safety. Based on the key findings of the high-performing hospitals, there was a culture that promoted safety and quality evidenced in the nurse-physician communication and the transparency around data through a lens of equity,” wrote Dr. Gillispie-Bell.
She noted that the study should encourage low-performing hospitals, since it illustrates avenues for improvement. Her personal experience reflects that, though she said that hospitals need help. The Louisiana Perinatal Quality Collaborative addressed severe maternal morbidity at birthing centers by implementing evidence-based best practices for management of hypertension and hemorrhage along with health equity measures. The team conducted coaching calls, in-person learning sessions, and in-person visits through a “Listening Tour.”
The result was a 35% reduction in hemorrhage overall and a reduction of 49% in hemorrhage in Black women, as well as hypertension by 12% overall between August 2018 and May 2020. Not all the news was good, as Black women still had an increase in severe maternal morbidity, possibly because of the COVID epidemic, since it is a risk factor for hypertension during pregnancy and infection rates are higher among Black individuals. “We need support for state based perinatal quality collaboratives to do this work and we need accountability as we are now seeing from metrics being implemented by [the Centers for Medicare & Medicaid Services]. Hospitals need to stratify their data by race and ethnicity to see where there are disparities in their outcomes,” said Dr. Gillispie-Bell.
The improvements are needed, given that the United States has the highest rates of maternal mortality and morbidity among developed countries, “most of which is preventable, and we have significant inequities by race and ethnicity,” said Laurie Zephyrin, MD, vice president for advancing health equity at the Commonwealth Fund. The question becomes how to effect change, and “there’s a lot happening in the policy space. Some of this policy change is directed at expanding insurance coverage, including more opportunities, including funding for community health workers and doulas, and thinking about how to incorporate midwives. There’s also work around how do we actually improve the care delivered by our health system.” Dr. Zephyrin added that the Department of Health & Human Services has contracted with the health improvement company Premier to use data and best-practices to improve maternal health.
The new work has the potential to be complementary to such approaches. “It provides some structure around how to approach some of the solutions, none of which I think is rocket science. It’s just something that needs to be focused on more intentionally,” said Dr. Zephyrin.
For example, the report found that high-performing hospitals had leaders who collaborated with frontline clinicians to share performance data, and this occurred in person, at departmental quality meetings, and during grand rounds. In contrast, staff in low-performing hospitals did not mention data feedback and some said that their institution made little effort to communicate performance metrics to frontline staff.
“One of the key lessons from the pandemic is that we need to have better data, and we need to have data around race and ethnicity to be able to understand the impact on marginalized communities. This study highlights that there’s more to be done around data to ensure that we can truly move the needle on advancing health equity,” said Dr. Zephyrin.
The researchers also found that clinicians in low-performing institutions did not acknowledge the presence of structural racism or differences in care associated with race or ethnicity. When they acknowledge differences in care, they attributed them to factors outside of the hospital’s control, such as patients not seeking out health care or not maintaining a healthy weight. Clinicians at high-performing hospitals were more likely to explicitly mention racism and bias and acknowledged that these factors could contribute to differences in care.
Dr. Gillispie-Bell and Dr. Zephyrin have no relevant financial disclosures.
A new study of hospitals in New York City suggests ways to reduce severe maternal morbidity (SMM). The researchers interviewed health care professionals in four institutions with low performance and four with high performance, and identified various themes associated with good performance.
“Our results raise the hypothesis that hospital learning collaboratives focused on optimizing organizational practices and policies, increasing clinician and staff awareness and education on maternal health disparities, and addressing structural racism may be important tools for improving equity in maternal outcomes,” the authors wrote in the study, published in Obstetrics & Gynecology.
The researchers conducted 50 semistructured interviews with health care professionals at lower-performing and higher-performing New York City hospitals, which were selected based on risk-adjusted morbidity metrics. The interviews explored various topics, including structural characteristics like staffing, organizational characteristics like culture and communication, labor and delivery practices such as teamwork and use of evidence-based practices, and racial and ethnic disparities.
The analysis revealed six broad areas that were stronger in high-performing hospitals: day-to-day involvement of leadership in quality activities, an emphasis on standards and standardized care, good communication and teamwork between nurses and physicians, good staffing and supervision among physicians and nurses, sharing of performance data with health care workers, and acknowledgment of the existence of racial and ethnic disparities and that bias can cause treatment differences.
“I think this qualitative approach is an important lens to pair with the quantitative approach. With such variability in severe maternal morbidity between hospitals in New York, it is not enough to just look at the quantitative data. To understand how to improve you must examine structures and processes. The structures, which are the physical and organizational characteristics in health care, and the process, which is how health care is delivered,” Veronica Gillispie-Bell, MD, wrote in a comment. Dr. Gillispie-Bell is medical director at Louisiana Perinatal Quality Collaborative and the Pregnancy-Associated Mortality Review for the Louisiana Department of Health.
“We know that high reliability organizations are those who are preoccupied with quality and safety. That means accountability from leadership (structure) and stability in standardization of care (processes). However, none of this matters if you do not have a culture that promotes safety. Based on the key findings of the high-performing hospitals, there was a culture that promoted safety and quality evidenced in the nurse-physician communication and the transparency around data through a lens of equity,” wrote Dr. Gillispie-Bell.
She noted that the study should encourage low-performing hospitals, since it illustrates avenues for improvement. Her personal experience reflects that, though she said that hospitals need help. The Louisiana Perinatal Quality Collaborative addressed severe maternal morbidity at birthing centers by implementing evidence-based best practices for management of hypertension and hemorrhage along with health equity measures. The team conducted coaching calls, in-person learning sessions, and in-person visits through a “Listening Tour.”
The result was a 35% reduction in hemorrhage overall and a reduction of 49% in hemorrhage in Black women, as well as hypertension by 12% overall between August 2018 and May 2020. Not all the news was good, as Black women still had an increase in severe maternal morbidity, possibly because of the COVID epidemic, since it is a risk factor for hypertension during pregnancy and infection rates are higher among Black individuals. “We need support for state based perinatal quality collaboratives to do this work and we need accountability as we are now seeing from metrics being implemented by [the Centers for Medicare & Medicaid Services]. Hospitals need to stratify their data by race and ethnicity to see where there are disparities in their outcomes,” said Dr. Gillispie-Bell.
The improvements are needed, given that the United States has the highest rates of maternal mortality and morbidity among developed countries, “most of which is preventable, and we have significant inequities by race and ethnicity,” said Laurie Zephyrin, MD, vice president for advancing health equity at the Commonwealth Fund. The question becomes how to effect change, and “there’s a lot happening in the policy space. Some of this policy change is directed at expanding insurance coverage, including more opportunities, including funding for community health workers and doulas, and thinking about how to incorporate midwives. There’s also work around how do we actually improve the care delivered by our health system.” Dr. Zephyrin added that the Department of Health & Human Services has contracted with the health improvement company Premier to use data and best-practices to improve maternal health.
The new work has the potential to be complementary to such approaches. “It provides some structure around how to approach some of the solutions, none of which I think is rocket science. It’s just something that needs to be focused on more intentionally,” said Dr. Zephyrin.
For example, the report found that high-performing hospitals had leaders who collaborated with frontline clinicians to share performance data, and this occurred in person, at departmental quality meetings, and during grand rounds. In contrast, staff in low-performing hospitals did not mention data feedback and some said that their institution made little effort to communicate performance metrics to frontline staff.
“One of the key lessons from the pandemic is that we need to have better data, and we need to have data around race and ethnicity to be able to understand the impact on marginalized communities. This study highlights that there’s more to be done around data to ensure that we can truly move the needle on advancing health equity,” said Dr. Zephyrin.
The researchers also found that clinicians in low-performing institutions did not acknowledge the presence of structural racism or differences in care associated with race or ethnicity. When they acknowledge differences in care, they attributed them to factors outside of the hospital’s control, such as patients not seeking out health care or not maintaining a healthy weight. Clinicians at high-performing hospitals were more likely to explicitly mention racism and bias and acknowledged that these factors could contribute to differences in care.
Dr. Gillispie-Bell and Dr. Zephyrin have no relevant financial disclosures.
FROM OBSTETRICS & GYNECOLOGY
CDC predicts a rise in COVID-19 hospitalizations and deaths in coming weeks
, according to a national forecast used by the Centers for Disease Control and Prevention.
The national model also predicts that about 5,000 deaths will occur over the next two weeks, with Ohio, New Jersey, and New York projected to see the largest totals of daily deaths in upcoming weeks.
The numbers follow several weeks of steady increases in infections across the country. More than 67,000 new cases are being reported daily, according to the data tracker from The New York Times, marking a 59% increase in the past two weeks.
In the Northeast, infection rates have risen by nearly 65%. In the New York and New Jersey region, infection rates are up about 55% in the past two weeks.
Hospitalizations have already begun to climb as well, with about 19,000 COVID-19 patients hospitalized nationwide and 1,725 in intensive care, according to the latest data from the Department of Health and Human Services. In the last week, hospital admissions have jumped by 20%, and emergency department visits are up by 18%.
The CDC forecast shows that 42 states and territories will see increases in hospital admissions during the next two weeks. Florida, Minnesota, New York, and Wisconsin will see some of the largest increases.
On average, more than 2,200 COVID-19 patients are entering the hospital each day, which has increased about 20% in the last week, according to ABC News. This also marks the highest number of COVID-19 patients needing hospital care since mid-March.
Public health officials have cited several factors for the increase in cases, such as states lifting mask mandates and other safety restrictions, ABC News reported. Highly contagious Omicron subvariants, such as BA.2 and BA.2.12.1, continue to spread in the United States and escape immunity from previous infections.
The BA.2 subvariant accounts for 62% of new national cases, according to the latest CDC data. The BA.2.12.1 subvariant makes up about 36% of new cases across the United States but 62% in the New York area.
A version of this article first appeared on WebMD.com.
, according to a national forecast used by the Centers for Disease Control and Prevention.
The national model also predicts that about 5,000 deaths will occur over the next two weeks, with Ohio, New Jersey, and New York projected to see the largest totals of daily deaths in upcoming weeks.
The numbers follow several weeks of steady increases in infections across the country. More than 67,000 new cases are being reported daily, according to the data tracker from The New York Times, marking a 59% increase in the past two weeks.
In the Northeast, infection rates have risen by nearly 65%. In the New York and New Jersey region, infection rates are up about 55% in the past two weeks.
Hospitalizations have already begun to climb as well, with about 19,000 COVID-19 patients hospitalized nationwide and 1,725 in intensive care, according to the latest data from the Department of Health and Human Services. In the last week, hospital admissions have jumped by 20%, and emergency department visits are up by 18%.
The CDC forecast shows that 42 states and territories will see increases in hospital admissions during the next two weeks. Florida, Minnesota, New York, and Wisconsin will see some of the largest increases.
On average, more than 2,200 COVID-19 patients are entering the hospital each day, which has increased about 20% in the last week, according to ABC News. This also marks the highest number of COVID-19 patients needing hospital care since mid-March.
Public health officials have cited several factors for the increase in cases, such as states lifting mask mandates and other safety restrictions, ABC News reported. Highly contagious Omicron subvariants, such as BA.2 and BA.2.12.1, continue to spread in the United States and escape immunity from previous infections.
The BA.2 subvariant accounts for 62% of new national cases, according to the latest CDC data. The BA.2.12.1 subvariant makes up about 36% of new cases across the United States but 62% in the New York area.
A version of this article first appeared on WebMD.com.
, according to a national forecast used by the Centers for Disease Control and Prevention.
The national model also predicts that about 5,000 deaths will occur over the next two weeks, with Ohio, New Jersey, and New York projected to see the largest totals of daily deaths in upcoming weeks.
The numbers follow several weeks of steady increases in infections across the country. More than 67,000 new cases are being reported daily, according to the data tracker from The New York Times, marking a 59% increase in the past two weeks.
In the Northeast, infection rates have risen by nearly 65%. In the New York and New Jersey region, infection rates are up about 55% in the past two weeks.
Hospitalizations have already begun to climb as well, with about 19,000 COVID-19 patients hospitalized nationwide and 1,725 in intensive care, according to the latest data from the Department of Health and Human Services. In the last week, hospital admissions have jumped by 20%, and emergency department visits are up by 18%.
The CDC forecast shows that 42 states and territories will see increases in hospital admissions during the next two weeks. Florida, Minnesota, New York, and Wisconsin will see some of the largest increases.
On average, more than 2,200 COVID-19 patients are entering the hospital each day, which has increased about 20% in the last week, according to ABC News. This also marks the highest number of COVID-19 patients needing hospital care since mid-March.
Public health officials have cited several factors for the increase in cases, such as states lifting mask mandates and other safety restrictions, ABC News reported. Highly contagious Omicron subvariants, such as BA.2 and BA.2.12.1, continue to spread in the United States and escape immunity from previous infections.
The BA.2 subvariant accounts for 62% of new national cases, according to the latest CDC data. The BA.2.12.1 subvariant makes up about 36% of new cases across the United States but 62% in the New York area.
A version of this article first appeared on WebMD.com.
‘Bane of my existence:’ The burden of Medicare Advantage denials
, a recent analysis suggests.
The report from the Office of Inspector General (OIG) of the U.S. Department of Health & Human Services found that 13% of prior authorization denials were for service requests, which included cancer care, that met Medicare coverage rules and 18% of payment denials were for claims that met Medicare coverage and MAO billing rules, delaying or halting payments for services that clinicians had provided.
MAO denials are the “bane of my existence,” said Michael Buckstein, MD, PhD, a radiation oncologist at Mount Sinai Hospital in New York.
“Working at a large hospital in a metropolitan city, we spend enormous and increasing amounts of time on prior approvals and we get denials quite frequently, which certainly can lead to delays in treatment,” said Dr. Buckstein, who reviewed the OIG report for this news organization.
According to Dr. Buckstein, once a claim is denied, staff must spend time filing and scheduling an appeal, and if the appeal is denied in a physician peer-to-peer review, staff could face secondary and tertiary appeals. “We have been living with this frustration for a long time,” Dr. Buckstein said.
Widespread and persistent problems
Medicare Advantage plans, which are approved by the Centers for Medicare & Medicaid Services but run by private companies, continue to grow in popularity.
In 2021, 26.4 million Medicare beneficiaries (42%) were enrolled in a Medicare Advantage plan, and by 2030, about 51% of all Medicare beneficiaries will be enrolled, according to estimates from the Kaiser Family Foundation.
“Although MAOs approve the vast majority of prior authorization requests and provider payment requests, MAOs also deny millions of requests each year,” the OIG wrote. “CMS’s annual audits of MAOs have highlighted widespread and persistent problems related to inappropriate denials of services and payment.”
In the current report, the OIG reviewed case files for 247 denials of prior authorization requests and 183 payment denials issued by 15 of the largest MAOs during 1 week in June of 2019.
The authors found that 13% of prior authorization denials occurred for service requests that met Medicare coverage rules, meaning these services would likely have been approved had the patient been enrolled in traditional Medicare.
The most prominent service types among these denials included imaging services, stays in postacute facilities, and injections.
In one case, for example, the MAO stated that a beneficiary would need to wait at least 1 year for a follow-up MRI because the size of the patient’s adrenal lesion (< 2 cm) was too small to warrant follow-up before 1 year. However, this restriction is not included in Medicare coverage rules. And an OIG physician panel found that the documentation in the original request demonstrated that the MRI was medically necessary to determine whether the lesion seen on an earlier CT scan was malignant.
Upon appeal, the MAO reversed its original denial.
Among the payment requests that MAOs denied, almost one in five were for claims that met Medicare coverage and billing rules, which delayed or prevented payments for services already delivered. Most payment denials were caused by human error during manual claims-processing reviews and system processing errors, the OIG report found.
In one case, for example, a MAO denied payment for radiation treatment for a patient with a tumor on the pancreas, incorrectly claiming that no prior authorization had been submitted for the service. However, the physician subsequently provided a screenshot demonstrating that the MAO had granted prior authorization for the billed claim, and the MAO reversed the denial.
Most of these prior authorization denial reversals occurred because of an appeal filed by the beneficiary or the provider, which can take weeks.
In one case, an MAO denied a request for a CT scan of the chest and pelvis for a beneficiary with endometrial cancer. It took 5 weeks for the provider to get the denial reversed. The OIG panel determined that the original request included sufficient documentation to demonstrate the CT was needed to assess the stage of the cancer and determine the appropriate course of treatment.
These denials and reversals not only waste time but may also cause harm. In a 2021 American Medical Association survey, 34% of physicians reported that prior authorization led to a serious adverse event for a patient in their care, including hospitalization, medical intervention to prevent permanent impairment, and even disability or death.
Almost 90% of the physicians surveyed described the burden associated with prior authorizations as ‘high’ or ‘extremely high.’ More specifically, physicians and their staff spend nearly 2 days a week on prior authorizations and 40% of physicians have staff who work exclusively on prior authorizations.
“It’s just not the way medicine should be practiced, especially for cancer patients who are very vulnerable and want rapid care,” Dr. Buckstein said.
Time for action
Weighing in on the OIG report, Robert E. Wailes, MD, president of the California Medical Association, noted that “it has become common practice for health insurance companies to create obstacles for patients in hopes of not having to pay for essential healthcare.”
The reason for these obstacles is simple, he said: “Fewer procedures performed translates to larger insurance company profits.”
America’s Health Insurance Plans (AHIP) defended prior authorization, saying it is “an important patient safety, cost-saving, and waste-prevention tool.”
The group also called out the OIG review for its “extraordinarily small” sample of 247 prior authorization requests over 1 week.
“Drawing far-reaching conclusions based on a very small sample of data and misleading headlines is not a productive way to improve our healthcare system for patients,” the AHIP statement reads.
But, according to Anna Schwamlein Howard, who works on policy development at the American Cancer Society Cancer Action Network, the recent OIG report is in line with previous OIG reports.
And, Ms. Howard emphasized, the current report and others like it “highlight the need for CMS to utilize its audit authority and ensure that beneficiaries have access to medically necessary treatments, particularly cancer treatments.”
Along those lines, the OIG report recommends that the CMS should issue new guidance on the appropriate use of MAO clinical criteria in medical necessity reviews, update its audit protocols to address issues identified in the report, and direct MAOs to take additional steps to identify and address vulnerabilities that can lead to manual review and system errors.
In a statement, the CMS said it is committed to oversight and enforcement of the requirements of the Medicare Advantage program and agreed with the OIG recommendations.
“Lawmakers must act now to place patient needs before corporate profits and simplify by streamlining prior authorization processes,” Dr. Wailes said.
The ACS recently released a paper on this topic entitled, “The Medicare Appeals Process: Reforms Needed to Ensure Beneficiary Access.”
A version of this article first appeared on Medscape.com.
, a recent analysis suggests.
The report from the Office of Inspector General (OIG) of the U.S. Department of Health & Human Services found that 13% of prior authorization denials were for service requests, which included cancer care, that met Medicare coverage rules and 18% of payment denials were for claims that met Medicare coverage and MAO billing rules, delaying or halting payments for services that clinicians had provided.
MAO denials are the “bane of my existence,” said Michael Buckstein, MD, PhD, a radiation oncologist at Mount Sinai Hospital in New York.
“Working at a large hospital in a metropolitan city, we spend enormous and increasing amounts of time on prior approvals and we get denials quite frequently, which certainly can lead to delays in treatment,” said Dr. Buckstein, who reviewed the OIG report for this news organization.
According to Dr. Buckstein, once a claim is denied, staff must spend time filing and scheduling an appeal, and if the appeal is denied in a physician peer-to-peer review, staff could face secondary and tertiary appeals. “We have been living with this frustration for a long time,” Dr. Buckstein said.
Widespread and persistent problems
Medicare Advantage plans, which are approved by the Centers for Medicare & Medicaid Services but run by private companies, continue to grow in popularity.
In 2021, 26.4 million Medicare beneficiaries (42%) were enrolled in a Medicare Advantage plan, and by 2030, about 51% of all Medicare beneficiaries will be enrolled, according to estimates from the Kaiser Family Foundation.
“Although MAOs approve the vast majority of prior authorization requests and provider payment requests, MAOs also deny millions of requests each year,” the OIG wrote. “CMS’s annual audits of MAOs have highlighted widespread and persistent problems related to inappropriate denials of services and payment.”
In the current report, the OIG reviewed case files for 247 denials of prior authorization requests and 183 payment denials issued by 15 of the largest MAOs during 1 week in June of 2019.
The authors found that 13% of prior authorization denials occurred for service requests that met Medicare coverage rules, meaning these services would likely have been approved had the patient been enrolled in traditional Medicare.
The most prominent service types among these denials included imaging services, stays in postacute facilities, and injections.
In one case, for example, the MAO stated that a beneficiary would need to wait at least 1 year for a follow-up MRI because the size of the patient’s adrenal lesion (< 2 cm) was too small to warrant follow-up before 1 year. However, this restriction is not included in Medicare coverage rules. And an OIG physician panel found that the documentation in the original request demonstrated that the MRI was medically necessary to determine whether the lesion seen on an earlier CT scan was malignant.
Upon appeal, the MAO reversed its original denial.
Among the payment requests that MAOs denied, almost one in five were for claims that met Medicare coverage and billing rules, which delayed or prevented payments for services already delivered. Most payment denials were caused by human error during manual claims-processing reviews and system processing errors, the OIG report found.
In one case, for example, a MAO denied payment for radiation treatment for a patient with a tumor on the pancreas, incorrectly claiming that no prior authorization had been submitted for the service. However, the physician subsequently provided a screenshot demonstrating that the MAO had granted prior authorization for the billed claim, and the MAO reversed the denial.
Most of these prior authorization denial reversals occurred because of an appeal filed by the beneficiary or the provider, which can take weeks.
In one case, an MAO denied a request for a CT scan of the chest and pelvis for a beneficiary with endometrial cancer. It took 5 weeks for the provider to get the denial reversed. The OIG panel determined that the original request included sufficient documentation to demonstrate the CT was needed to assess the stage of the cancer and determine the appropriate course of treatment.
These denials and reversals not only waste time but may also cause harm. In a 2021 American Medical Association survey, 34% of physicians reported that prior authorization led to a serious adverse event for a patient in their care, including hospitalization, medical intervention to prevent permanent impairment, and even disability or death.
Almost 90% of the physicians surveyed described the burden associated with prior authorizations as ‘high’ or ‘extremely high.’ More specifically, physicians and their staff spend nearly 2 days a week on prior authorizations and 40% of physicians have staff who work exclusively on prior authorizations.
“It’s just not the way medicine should be practiced, especially for cancer patients who are very vulnerable and want rapid care,” Dr. Buckstein said.
Time for action
Weighing in on the OIG report, Robert E. Wailes, MD, president of the California Medical Association, noted that “it has become common practice for health insurance companies to create obstacles for patients in hopes of not having to pay for essential healthcare.”
The reason for these obstacles is simple, he said: “Fewer procedures performed translates to larger insurance company profits.”
America’s Health Insurance Plans (AHIP) defended prior authorization, saying it is “an important patient safety, cost-saving, and waste-prevention tool.”
The group also called out the OIG review for its “extraordinarily small” sample of 247 prior authorization requests over 1 week.
“Drawing far-reaching conclusions based on a very small sample of data and misleading headlines is not a productive way to improve our healthcare system for patients,” the AHIP statement reads.
But, according to Anna Schwamlein Howard, who works on policy development at the American Cancer Society Cancer Action Network, the recent OIG report is in line with previous OIG reports.
And, Ms. Howard emphasized, the current report and others like it “highlight the need for CMS to utilize its audit authority and ensure that beneficiaries have access to medically necessary treatments, particularly cancer treatments.”
Along those lines, the OIG report recommends that the CMS should issue new guidance on the appropriate use of MAO clinical criteria in medical necessity reviews, update its audit protocols to address issues identified in the report, and direct MAOs to take additional steps to identify and address vulnerabilities that can lead to manual review and system errors.
In a statement, the CMS said it is committed to oversight and enforcement of the requirements of the Medicare Advantage program and agreed with the OIG recommendations.
“Lawmakers must act now to place patient needs before corporate profits and simplify by streamlining prior authorization processes,” Dr. Wailes said.
The ACS recently released a paper on this topic entitled, “The Medicare Appeals Process: Reforms Needed to Ensure Beneficiary Access.”
A version of this article first appeared on Medscape.com.
, a recent analysis suggests.
The report from the Office of Inspector General (OIG) of the U.S. Department of Health & Human Services found that 13% of prior authorization denials were for service requests, which included cancer care, that met Medicare coverage rules and 18% of payment denials were for claims that met Medicare coverage and MAO billing rules, delaying or halting payments for services that clinicians had provided.
MAO denials are the “bane of my existence,” said Michael Buckstein, MD, PhD, a radiation oncologist at Mount Sinai Hospital in New York.
“Working at a large hospital in a metropolitan city, we spend enormous and increasing amounts of time on prior approvals and we get denials quite frequently, which certainly can lead to delays in treatment,” said Dr. Buckstein, who reviewed the OIG report for this news organization.
According to Dr. Buckstein, once a claim is denied, staff must spend time filing and scheduling an appeal, and if the appeal is denied in a physician peer-to-peer review, staff could face secondary and tertiary appeals. “We have been living with this frustration for a long time,” Dr. Buckstein said.
Widespread and persistent problems
Medicare Advantage plans, which are approved by the Centers for Medicare & Medicaid Services but run by private companies, continue to grow in popularity.
In 2021, 26.4 million Medicare beneficiaries (42%) were enrolled in a Medicare Advantage plan, and by 2030, about 51% of all Medicare beneficiaries will be enrolled, according to estimates from the Kaiser Family Foundation.
“Although MAOs approve the vast majority of prior authorization requests and provider payment requests, MAOs also deny millions of requests each year,” the OIG wrote. “CMS’s annual audits of MAOs have highlighted widespread and persistent problems related to inappropriate denials of services and payment.”
In the current report, the OIG reviewed case files for 247 denials of prior authorization requests and 183 payment denials issued by 15 of the largest MAOs during 1 week in June of 2019.
The authors found that 13% of prior authorization denials occurred for service requests that met Medicare coverage rules, meaning these services would likely have been approved had the patient been enrolled in traditional Medicare.
The most prominent service types among these denials included imaging services, stays in postacute facilities, and injections.
In one case, for example, the MAO stated that a beneficiary would need to wait at least 1 year for a follow-up MRI because the size of the patient’s adrenal lesion (< 2 cm) was too small to warrant follow-up before 1 year. However, this restriction is not included in Medicare coverage rules. And an OIG physician panel found that the documentation in the original request demonstrated that the MRI was medically necessary to determine whether the lesion seen on an earlier CT scan was malignant.
Upon appeal, the MAO reversed its original denial.
Among the payment requests that MAOs denied, almost one in five were for claims that met Medicare coverage and billing rules, which delayed or prevented payments for services already delivered. Most payment denials were caused by human error during manual claims-processing reviews and system processing errors, the OIG report found.
In one case, for example, a MAO denied payment for radiation treatment for a patient with a tumor on the pancreas, incorrectly claiming that no prior authorization had been submitted for the service. However, the physician subsequently provided a screenshot demonstrating that the MAO had granted prior authorization for the billed claim, and the MAO reversed the denial.
Most of these prior authorization denial reversals occurred because of an appeal filed by the beneficiary or the provider, which can take weeks.
In one case, an MAO denied a request for a CT scan of the chest and pelvis for a beneficiary with endometrial cancer. It took 5 weeks for the provider to get the denial reversed. The OIG panel determined that the original request included sufficient documentation to demonstrate the CT was needed to assess the stage of the cancer and determine the appropriate course of treatment.
These denials and reversals not only waste time but may also cause harm. In a 2021 American Medical Association survey, 34% of physicians reported that prior authorization led to a serious adverse event for a patient in their care, including hospitalization, medical intervention to prevent permanent impairment, and even disability or death.
Almost 90% of the physicians surveyed described the burden associated with prior authorizations as ‘high’ or ‘extremely high.’ More specifically, physicians and their staff spend nearly 2 days a week on prior authorizations and 40% of physicians have staff who work exclusively on prior authorizations.
“It’s just not the way medicine should be practiced, especially for cancer patients who are very vulnerable and want rapid care,” Dr. Buckstein said.
Time for action
Weighing in on the OIG report, Robert E. Wailes, MD, president of the California Medical Association, noted that “it has become common practice for health insurance companies to create obstacles for patients in hopes of not having to pay for essential healthcare.”
The reason for these obstacles is simple, he said: “Fewer procedures performed translates to larger insurance company profits.”
America’s Health Insurance Plans (AHIP) defended prior authorization, saying it is “an important patient safety, cost-saving, and waste-prevention tool.”
The group also called out the OIG review for its “extraordinarily small” sample of 247 prior authorization requests over 1 week.
“Drawing far-reaching conclusions based on a very small sample of data and misleading headlines is not a productive way to improve our healthcare system for patients,” the AHIP statement reads.
But, according to Anna Schwamlein Howard, who works on policy development at the American Cancer Society Cancer Action Network, the recent OIG report is in line with previous OIG reports.
And, Ms. Howard emphasized, the current report and others like it “highlight the need for CMS to utilize its audit authority and ensure that beneficiaries have access to medically necessary treatments, particularly cancer treatments.”
Along those lines, the OIG report recommends that the CMS should issue new guidance on the appropriate use of MAO clinical criteria in medical necessity reviews, update its audit protocols to address issues identified in the report, and direct MAOs to take additional steps to identify and address vulnerabilities that can lead to manual review and system errors.
In a statement, the CMS said it is committed to oversight and enforcement of the requirements of the Medicare Advantage program and agreed with the OIG recommendations.
“Lawmakers must act now to place patient needs before corporate profits and simplify by streamlining prior authorization processes,” Dr. Wailes said.
The ACS recently released a paper on this topic entitled, “The Medicare Appeals Process: Reforms Needed to Ensure Beneficiary Access.”
A version of this article first appeared on Medscape.com.
Screening for diabetes at normal BMIs could cut racial disparities
Use of race-based diabetes screening thresholds could reduce the disparity that arises from current screening guidelines in the United States, new research suggests.
In August 2021, the U.S. Preventive Services Task Force (USPSTF) lowered the recommended age for type 2 diabetes screening from 40 to 35 years among people with a body mass index of 25 kg/m2 or greater.
However, the diabetes rate among ethnic minorities aged 35-70 years in the United States is not just higher overall but, in certain populations, also occurs more frequently at a younger age and at lower BMIs, the new study indicates.
Among people with a BMI below 25 kg/m2, the diabetes prevalence is two to four times higher among Asian, Black, and Hispanic Americans than among the U.S. White population.
And the authors of the new study, led by Rahul Aggarwal, MD, predict that if screening begins at age 35 years, the BMI cut-off equivalent to 25 kg/m2 for White Americans would be 18.5 kg/m2 for Hispanic and Black Americans and 20 kg/m2 for Asian Americans.
“While diabetes has often been thought of as a disease that primarily affects adults with overweight or [obesity], our findings suggest that normal-weight adults in minority groups have surprisingly high rates of diabetes,” Dr. Aggarwal, senior resident physician in internal medicine at Harvard Medical School, Boston, told this news organization.
“Assessing diabetes risks in certain racial/ethnic groups will be necessary, even if these adults do not have overweight or [obesity],” he added.
Not screening in this way “is a missed opportunity for early intervention,” he noted.
And both the authors and an editorialist stress that the issue isn’t just theoretical.
“USPSTF recommendations influence what payers choose to cover, which in turn determines access to preventative services ... Addressing the staggering inequities in diabetes outcomes will require substantial investments in diabetes prevention and treatment, but making screening more equitable is a good place to start,” said senior author Dhruv S. Kazi, MD, of the Smith Center for Outcomes Research in Cardiology and director of the Cardiac Critical Care Unit at Beth Israel, Boston.
Screen minorities at a younger age if current BMI threshold kept
In their study, based on data from the National Health and Nutrition Examination Survey (NHANES) for 2011-2018, Dr. Aggarwal and colleagues also calculated that, if the BMI threshold is kept at 25 kg/m2, then the equivalent age cut-offs for Asian, Black, and Hispanic Americans would be 23, 21, and 25 years, respectively, compared with 35 years for White Americans.
The findings were published online in the Annals of Internal Medicine.
The prevalence of diabetes in those aged 35-70 years in the NHANES population was 17.3% for Asian Americans and 12.5% for those who were White (odds ratio, 1.51 vs. Whites). Among Black Americans and Mexican Americans, the prevalence was 20.7% and 20.6%, respectively, almost twice the prevalence in Whites (OR, 1.85 and 1.80). For other Hispanic Americans, the prevalence was 16.4% (OR, 1.37 vs. Whites). All of those differences were significant, compared with White Americans.
Undiagnosed diabetes was also significantly more common among minority populations, at 27.6%, 22.8%, 21.2%, and 23.5% for Asian, Black, Mexican, and other Hispanic Americans, respectively, versus 12.5% for White Americans.
‘The time has come for USPSTF to offer more concrete guidance’
“While there is more work to be done on carefully examining the long-term risk–benefit trade-off of various diabetes screening, I believe the time has come for USPSTF to offer more concrete guidance on the use of lower thresholds for screening higher-risk individuals,” Dr. Kazi told this news organization.
The author of an accompanying editorial agrees, noting that in a recent commentary the USPSTF, itself, “acknowledged the persistent inequalities across the screening-to-treatment continuum that result in racial/ethnic health disparities in the United States.”
And the USPSTF “emphasized the need to improve systems of care to ensure equitable and consistent delivery of high-quality preventive and treatment services, with special attention to racial/ethnic groups who may experience worse health outcomes,” continues Quyen Ngo-Metzger, MD, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, California.
For other conditions, including cancer, cardiovascular disease, and infectious disease, the USPSTF already recommends risk-based preventive services.
“To address the current inequity in diabetes screening, the USPSTF should apply the same consideration to its diabetes screening recommendation,” she notes.
‘Implementation will require an eye for pragmatism’
Asked about how this recommendation might be carried out in the real world, Dr. Aggarwal said in an interview that, because all three minority groups with normal weight had similar diabetes risk profiles to White adults with overweight, “one way for clinicians to easily implement these findings is by screening all Asian, Black, and Hispanic adults ages 35-70 years with normal weight for diabetes, similarly to how all White adults ages 35-70 years with overweight are currently recommended for screening.”
Dr. Kazi said: “I believe that implementation will require an eye for pragmatism,” noting that another option would be to have screening algorithms embedded in the electronic health record to flag individuals who qualify.
In any case, “the simplicity of the current one-size-fits-all approach is alluring, but it is profoundly inequitable. The more I look at the empiric evidence on diabetes burden in our communities, the more the status quo becomes untenable.”
However, Dr. Kazi also noted, “the benefit of any screening program relates to what we do with the information. The key is to ensure that folks identified as having diabetes – or better still prediabetes – receive timely lifestyle and pharmacological interventions to avert its long-term complications.”
This study was supported by institutional funds from the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology. Dr. Aggarwal, Dr. Kazi, and Dr. Ngo-Metzger have reported no relevant relationships.
A version of this article first appeared on Medscape.com.
Use of race-based diabetes screening thresholds could reduce the disparity that arises from current screening guidelines in the United States, new research suggests.
In August 2021, the U.S. Preventive Services Task Force (USPSTF) lowered the recommended age for type 2 diabetes screening from 40 to 35 years among people with a body mass index of 25 kg/m2 or greater.
However, the diabetes rate among ethnic minorities aged 35-70 years in the United States is not just higher overall but, in certain populations, also occurs more frequently at a younger age and at lower BMIs, the new study indicates.
Among people with a BMI below 25 kg/m2, the diabetes prevalence is two to four times higher among Asian, Black, and Hispanic Americans than among the U.S. White population.
And the authors of the new study, led by Rahul Aggarwal, MD, predict that if screening begins at age 35 years, the BMI cut-off equivalent to 25 kg/m2 for White Americans would be 18.5 kg/m2 for Hispanic and Black Americans and 20 kg/m2 for Asian Americans.
“While diabetes has often been thought of as a disease that primarily affects adults with overweight or [obesity], our findings suggest that normal-weight adults in minority groups have surprisingly high rates of diabetes,” Dr. Aggarwal, senior resident physician in internal medicine at Harvard Medical School, Boston, told this news organization.
“Assessing diabetes risks in certain racial/ethnic groups will be necessary, even if these adults do not have overweight or [obesity],” he added.
Not screening in this way “is a missed opportunity for early intervention,” he noted.
And both the authors and an editorialist stress that the issue isn’t just theoretical.
“USPSTF recommendations influence what payers choose to cover, which in turn determines access to preventative services ... Addressing the staggering inequities in diabetes outcomes will require substantial investments in diabetes prevention and treatment, but making screening more equitable is a good place to start,” said senior author Dhruv S. Kazi, MD, of the Smith Center for Outcomes Research in Cardiology and director of the Cardiac Critical Care Unit at Beth Israel, Boston.
Screen minorities at a younger age if current BMI threshold kept
In their study, based on data from the National Health and Nutrition Examination Survey (NHANES) for 2011-2018, Dr. Aggarwal and colleagues also calculated that, if the BMI threshold is kept at 25 kg/m2, then the equivalent age cut-offs for Asian, Black, and Hispanic Americans would be 23, 21, and 25 years, respectively, compared with 35 years for White Americans.
The findings were published online in the Annals of Internal Medicine.
The prevalence of diabetes in those aged 35-70 years in the NHANES population was 17.3% for Asian Americans and 12.5% for those who were White (odds ratio, 1.51 vs. Whites). Among Black Americans and Mexican Americans, the prevalence was 20.7% and 20.6%, respectively, almost twice the prevalence in Whites (OR, 1.85 and 1.80). For other Hispanic Americans, the prevalence was 16.4% (OR, 1.37 vs. Whites). All of those differences were significant, compared with White Americans.
Undiagnosed diabetes was also significantly more common among minority populations, at 27.6%, 22.8%, 21.2%, and 23.5% for Asian, Black, Mexican, and other Hispanic Americans, respectively, versus 12.5% for White Americans.
‘The time has come for USPSTF to offer more concrete guidance’
“While there is more work to be done on carefully examining the long-term risk–benefit trade-off of various diabetes screening, I believe the time has come for USPSTF to offer more concrete guidance on the use of lower thresholds for screening higher-risk individuals,” Dr. Kazi told this news organization.
The author of an accompanying editorial agrees, noting that in a recent commentary the USPSTF, itself, “acknowledged the persistent inequalities across the screening-to-treatment continuum that result in racial/ethnic health disparities in the United States.”
And the USPSTF “emphasized the need to improve systems of care to ensure equitable and consistent delivery of high-quality preventive and treatment services, with special attention to racial/ethnic groups who may experience worse health outcomes,” continues Quyen Ngo-Metzger, MD, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, California.
For other conditions, including cancer, cardiovascular disease, and infectious disease, the USPSTF already recommends risk-based preventive services.
“To address the current inequity in diabetes screening, the USPSTF should apply the same consideration to its diabetes screening recommendation,” she notes.
‘Implementation will require an eye for pragmatism’
Asked about how this recommendation might be carried out in the real world, Dr. Aggarwal said in an interview that, because all three minority groups with normal weight had similar diabetes risk profiles to White adults with overweight, “one way for clinicians to easily implement these findings is by screening all Asian, Black, and Hispanic adults ages 35-70 years with normal weight for diabetes, similarly to how all White adults ages 35-70 years with overweight are currently recommended for screening.”
Dr. Kazi said: “I believe that implementation will require an eye for pragmatism,” noting that another option would be to have screening algorithms embedded in the electronic health record to flag individuals who qualify.
In any case, “the simplicity of the current one-size-fits-all approach is alluring, but it is profoundly inequitable. The more I look at the empiric evidence on diabetes burden in our communities, the more the status quo becomes untenable.”
However, Dr. Kazi also noted, “the benefit of any screening program relates to what we do with the information. The key is to ensure that folks identified as having diabetes – or better still prediabetes – receive timely lifestyle and pharmacological interventions to avert its long-term complications.”
This study was supported by institutional funds from the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology. Dr. Aggarwal, Dr. Kazi, and Dr. Ngo-Metzger have reported no relevant relationships.
A version of this article first appeared on Medscape.com.
Use of race-based diabetes screening thresholds could reduce the disparity that arises from current screening guidelines in the United States, new research suggests.
In August 2021, the U.S. Preventive Services Task Force (USPSTF) lowered the recommended age for type 2 diabetes screening from 40 to 35 years among people with a body mass index of 25 kg/m2 or greater.
However, the diabetes rate among ethnic minorities aged 35-70 years in the United States is not just higher overall but, in certain populations, also occurs more frequently at a younger age and at lower BMIs, the new study indicates.
Among people with a BMI below 25 kg/m2, the diabetes prevalence is two to four times higher among Asian, Black, and Hispanic Americans than among the U.S. White population.
And the authors of the new study, led by Rahul Aggarwal, MD, predict that if screening begins at age 35 years, the BMI cut-off equivalent to 25 kg/m2 for White Americans would be 18.5 kg/m2 for Hispanic and Black Americans and 20 kg/m2 for Asian Americans.
“While diabetes has often been thought of as a disease that primarily affects adults with overweight or [obesity], our findings suggest that normal-weight adults in minority groups have surprisingly high rates of diabetes,” Dr. Aggarwal, senior resident physician in internal medicine at Harvard Medical School, Boston, told this news organization.
“Assessing diabetes risks in certain racial/ethnic groups will be necessary, even if these adults do not have overweight or [obesity],” he added.
Not screening in this way “is a missed opportunity for early intervention,” he noted.
And both the authors and an editorialist stress that the issue isn’t just theoretical.
“USPSTF recommendations influence what payers choose to cover, which in turn determines access to preventative services ... Addressing the staggering inequities in diabetes outcomes will require substantial investments in diabetes prevention and treatment, but making screening more equitable is a good place to start,” said senior author Dhruv S. Kazi, MD, of the Smith Center for Outcomes Research in Cardiology and director of the Cardiac Critical Care Unit at Beth Israel, Boston.
Screen minorities at a younger age if current BMI threshold kept
In their study, based on data from the National Health and Nutrition Examination Survey (NHANES) for 2011-2018, Dr. Aggarwal and colleagues also calculated that, if the BMI threshold is kept at 25 kg/m2, then the equivalent age cut-offs for Asian, Black, and Hispanic Americans would be 23, 21, and 25 years, respectively, compared with 35 years for White Americans.
The findings were published online in the Annals of Internal Medicine.
The prevalence of diabetes in those aged 35-70 years in the NHANES population was 17.3% for Asian Americans and 12.5% for those who were White (odds ratio, 1.51 vs. Whites). Among Black Americans and Mexican Americans, the prevalence was 20.7% and 20.6%, respectively, almost twice the prevalence in Whites (OR, 1.85 and 1.80). For other Hispanic Americans, the prevalence was 16.4% (OR, 1.37 vs. Whites). All of those differences were significant, compared with White Americans.
Undiagnosed diabetes was also significantly more common among minority populations, at 27.6%, 22.8%, 21.2%, and 23.5% for Asian, Black, Mexican, and other Hispanic Americans, respectively, versus 12.5% for White Americans.
‘The time has come for USPSTF to offer more concrete guidance’
“While there is more work to be done on carefully examining the long-term risk–benefit trade-off of various diabetes screening, I believe the time has come for USPSTF to offer more concrete guidance on the use of lower thresholds for screening higher-risk individuals,” Dr. Kazi told this news organization.
The author of an accompanying editorial agrees, noting that in a recent commentary the USPSTF, itself, “acknowledged the persistent inequalities across the screening-to-treatment continuum that result in racial/ethnic health disparities in the United States.”
And the USPSTF “emphasized the need to improve systems of care to ensure equitable and consistent delivery of high-quality preventive and treatment services, with special attention to racial/ethnic groups who may experience worse health outcomes,” continues Quyen Ngo-Metzger, MD, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, California.
For other conditions, including cancer, cardiovascular disease, and infectious disease, the USPSTF already recommends risk-based preventive services.
“To address the current inequity in diabetes screening, the USPSTF should apply the same consideration to its diabetes screening recommendation,” she notes.
‘Implementation will require an eye for pragmatism’
Asked about how this recommendation might be carried out in the real world, Dr. Aggarwal said in an interview that, because all three minority groups with normal weight had similar diabetes risk profiles to White adults with overweight, “one way for clinicians to easily implement these findings is by screening all Asian, Black, and Hispanic adults ages 35-70 years with normal weight for diabetes, similarly to how all White adults ages 35-70 years with overweight are currently recommended for screening.”
Dr. Kazi said: “I believe that implementation will require an eye for pragmatism,” noting that another option would be to have screening algorithms embedded in the electronic health record to flag individuals who qualify.
In any case, “the simplicity of the current one-size-fits-all approach is alluring, but it is profoundly inequitable. The more I look at the empiric evidence on diabetes burden in our communities, the more the status quo becomes untenable.”
However, Dr. Kazi also noted, “the benefit of any screening program relates to what we do with the information. The key is to ensure that folks identified as having diabetes – or better still prediabetes – receive timely lifestyle and pharmacological interventions to avert its long-term complications.”
This study was supported by institutional funds from the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology. Dr. Aggarwal, Dr. Kazi, and Dr. Ngo-Metzger have reported no relevant relationships.
A version of this article first appeared on Medscape.com.
More selective antibiotic shows promise for C. diff. infection
An investigational, novel oral antibiotic with greater selectivity than vancomycin, metronidazole, and even fidaxomicin may offer improved protection of healthy gut bacteria during the treatment of Clostridium difficile infection (CDI), according to ongoing research.
“CDI treatment has historically been dominated by metronidazole and vancomycin,” said Katherine Johnson, DO, from the Western Infectious Disease Consultants, P.C., Denver. However, these broad-spectrum drugs negatively affect healthy bacteria in the gut and increase the risk of CDI recurrence.
This is also a problem for drugs in the CDI antibiotic pipeline: Many candidate drugs have failed because of their broad-spectrum activity, she added during a session at the Peggy Lillis Foundation 2022 National C. diff. Advocacy Summit.
“An ideal CDI therapy would be a very narrow-spectrum antibiotic that has a minimal effect on normal gut bacteria,” she said.
Dr. Johnson is currently working on a phase 2 clinical trial that is evaluating the novel antibiotic, dubbed CRS3123, for the treatment of primary CDI and first-recurrence CDI. The investigational agent targets and inhibits a form of the methionyl tRNA synthetase enzyme, which is strictly required for protein biosynthesis in C. diff. and is therefore an ideal target for treatment of primary and recurrent CDI.
In her session, Dr. Johnson reported that CRS3123 inhibits the damaging toxins produced by C. diff., potentially resulting in more rapid symptom resolution. Additionally, owing to its novel mode of action, no strains are currently resistant to CRS3123.
She presented findings from an animal study that showed that CRS3123 was superior to vancomycin in terms of prolonging survival. She also presented findings from phase 1 clinical trials that showed that most adverse events (AEs) associated with CRS3123 were mild. No serious AEs were reported.
A ‘huge infectious burden’
If successful in further research, CRS3123 could offer significant value to patients with C. diff., especially those with recurrent infection, given the sometimes extreme clinical, quality-of-life, and economic burdens associated with CDI.
“CDI is a huge infectious burden to the U.S. health care system and globally has been listed by the Centers for Disease Control and Prevention as an urgent threat,” Byron Vaughn, MD, from the University of Minnesota, told this news organization.
“Despite a number of antibiotic stewardship and infection control and prevention efforts, we haven’t seen much of a change in the incidence of CDI,” he said. He said that the risk of recurrence can be as high as 30%.
While oral vancomycin is effective for treating C. diff., Dr. Vaughn noted that the antibiotic lacks selectivity and destroys healthy gut bacteria, resulting in substantial dysbiosis. “Dysbiosis is really the key to getting recurrent C. diff.,” he explained, “because if you have healthy gut bacteria, you will inherently resist CDI.”
Dr. Vaughn stated that his center is in the startup phase for being a site for a clinical trial of CRS3123. The hope is that CRS3123, because its spectrum is narrower than that of fidaxomicin and vancomycin, doesn’t induce intestinal dysbiosis. “It really just treats the C. diff. and leaves every other bug alone so that your gut bacteria can recover while the C. diff. is being treated,” he said. “And then when you stop CRS3123, you have healthy gut bacteria already present to prevent recurrence.”
If this is confirmed in large-scale trials, there could be a “dramatic decrease” in the rates of recurrent C. diff., said Dr. Vaughn.
Aside from the potential clinical impact, the economic implications of a novel selective antibiotic that preserves healthy gut bacteria could be significant, he added. “Depending on exactly what population you’re looking at, probably about a third of the cost of C. diff. is actually attributable to recurrence. That’s a huge economic burden that could be improved.”
Dr. Johnson is an employee of Crestone, which is developing CRS3123. Dr. Vaughn reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An investigational, novel oral antibiotic with greater selectivity than vancomycin, metronidazole, and even fidaxomicin may offer improved protection of healthy gut bacteria during the treatment of Clostridium difficile infection (CDI), according to ongoing research.
“CDI treatment has historically been dominated by metronidazole and vancomycin,” said Katherine Johnson, DO, from the Western Infectious Disease Consultants, P.C., Denver. However, these broad-spectrum drugs negatively affect healthy bacteria in the gut and increase the risk of CDI recurrence.
This is also a problem for drugs in the CDI antibiotic pipeline: Many candidate drugs have failed because of their broad-spectrum activity, she added during a session at the Peggy Lillis Foundation 2022 National C. diff. Advocacy Summit.
“An ideal CDI therapy would be a very narrow-spectrum antibiotic that has a minimal effect on normal gut bacteria,” she said.
Dr. Johnson is currently working on a phase 2 clinical trial that is evaluating the novel antibiotic, dubbed CRS3123, for the treatment of primary CDI and first-recurrence CDI. The investigational agent targets and inhibits a form of the methionyl tRNA synthetase enzyme, which is strictly required for protein biosynthesis in C. diff. and is therefore an ideal target for treatment of primary and recurrent CDI.
In her session, Dr. Johnson reported that CRS3123 inhibits the damaging toxins produced by C. diff., potentially resulting in more rapid symptom resolution. Additionally, owing to its novel mode of action, no strains are currently resistant to CRS3123.
She presented findings from an animal study that showed that CRS3123 was superior to vancomycin in terms of prolonging survival. She also presented findings from phase 1 clinical trials that showed that most adverse events (AEs) associated with CRS3123 were mild. No serious AEs were reported.
A ‘huge infectious burden’
If successful in further research, CRS3123 could offer significant value to patients with C. diff., especially those with recurrent infection, given the sometimes extreme clinical, quality-of-life, and economic burdens associated with CDI.
“CDI is a huge infectious burden to the U.S. health care system and globally has been listed by the Centers for Disease Control and Prevention as an urgent threat,” Byron Vaughn, MD, from the University of Minnesota, told this news organization.
“Despite a number of antibiotic stewardship and infection control and prevention efforts, we haven’t seen much of a change in the incidence of CDI,” he said. He said that the risk of recurrence can be as high as 30%.
While oral vancomycin is effective for treating C. diff., Dr. Vaughn noted that the antibiotic lacks selectivity and destroys healthy gut bacteria, resulting in substantial dysbiosis. “Dysbiosis is really the key to getting recurrent C. diff.,” he explained, “because if you have healthy gut bacteria, you will inherently resist CDI.”
Dr. Vaughn stated that his center is in the startup phase for being a site for a clinical trial of CRS3123. The hope is that CRS3123, because its spectrum is narrower than that of fidaxomicin and vancomycin, doesn’t induce intestinal dysbiosis. “It really just treats the C. diff. and leaves every other bug alone so that your gut bacteria can recover while the C. diff. is being treated,” he said. “And then when you stop CRS3123, you have healthy gut bacteria already present to prevent recurrence.”
If this is confirmed in large-scale trials, there could be a “dramatic decrease” in the rates of recurrent C. diff., said Dr. Vaughn.
Aside from the potential clinical impact, the economic implications of a novel selective antibiotic that preserves healthy gut bacteria could be significant, he added. “Depending on exactly what population you’re looking at, probably about a third of the cost of C. diff. is actually attributable to recurrence. That’s a huge economic burden that could be improved.”
Dr. Johnson is an employee of Crestone, which is developing CRS3123. Dr. Vaughn reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
An investigational, novel oral antibiotic with greater selectivity than vancomycin, metronidazole, and even fidaxomicin may offer improved protection of healthy gut bacteria during the treatment of Clostridium difficile infection (CDI), according to ongoing research.
“CDI treatment has historically been dominated by metronidazole and vancomycin,” said Katherine Johnson, DO, from the Western Infectious Disease Consultants, P.C., Denver. However, these broad-spectrum drugs negatively affect healthy bacteria in the gut and increase the risk of CDI recurrence.
This is also a problem for drugs in the CDI antibiotic pipeline: Many candidate drugs have failed because of their broad-spectrum activity, she added during a session at the Peggy Lillis Foundation 2022 National C. diff. Advocacy Summit.
“An ideal CDI therapy would be a very narrow-spectrum antibiotic that has a minimal effect on normal gut bacteria,” she said.
Dr. Johnson is currently working on a phase 2 clinical trial that is evaluating the novel antibiotic, dubbed CRS3123, for the treatment of primary CDI and first-recurrence CDI. The investigational agent targets and inhibits a form of the methionyl tRNA synthetase enzyme, which is strictly required for protein biosynthesis in C. diff. and is therefore an ideal target for treatment of primary and recurrent CDI.
In her session, Dr. Johnson reported that CRS3123 inhibits the damaging toxins produced by C. diff., potentially resulting in more rapid symptom resolution. Additionally, owing to its novel mode of action, no strains are currently resistant to CRS3123.
She presented findings from an animal study that showed that CRS3123 was superior to vancomycin in terms of prolonging survival. She also presented findings from phase 1 clinical trials that showed that most adverse events (AEs) associated with CRS3123 were mild. No serious AEs were reported.
A ‘huge infectious burden’
If successful in further research, CRS3123 could offer significant value to patients with C. diff., especially those with recurrent infection, given the sometimes extreme clinical, quality-of-life, and economic burdens associated with CDI.
“CDI is a huge infectious burden to the U.S. health care system and globally has been listed by the Centers for Disease Control and Prevention as an urgent threat,” Byron Vaughn, MD, from the University of Minnesota, told this news organization.
“Despite a number of antibiotic stewardship and infection control and prevention efforts, we haven’t seen much of a change in the incidence of CDI,” he said. He said that the risk of recurrence can be as high as 30%.
While oral vancomycin is effective for treating C. diff., Dr. Vaughn noted that the antibiotic lacks selectivity and destroys healthy gut bacteria, resulting in substantial dysbiosis. “Dysbiosis is really the key to getting recurrent C. diff.,” he explained, “because if you have healthy gut bacteria, you will inherently resist CDI.”
Dr. Vaughn stated that his center is in the startup phase for being a site for a clinical trial of CRS3123. The hope is that CRS3123, because its spectrum is narrower than that of fidaxomicin and vancomycin, doesn’t induce intestinal dysbiosis. “It really just treats the C. diff. and leaves every other bug alone so that your gut bacteria can recover while the C. diff. is being treated,” he said. “And then when you stop CRS3123, you have healthy gut bacteria already present to prevent recurrence.”
If this is confirmed in large-scale trials, there could be a “dramatic decrease” in the rates of recurrent C. diff., said Dr. Vaughn.
Aside from the potential clinical impact, the economic implications of a novel selective antibiotic that preserves healthy gut bacteria could be significant, he added. “Depending on exactly what population you’re looking at, probably about a third of the cost of C. diff. is actually attributable to recurrence. That’s a huge economic burden that could be improved.”
Dr. Johnson is an employee of Crestone, which is developing CRS3123. Dr. Vaughn reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The importance of toxin testing in C. difficile infection: Understanding the results
Clostridioides difficile infection is often confirmed through toxin testing, yet toxin tests alone may not be sufficient for diagnosing and guiding treatment decisions for patients with CDI.
“The presence of a toxigenic strain does not always equal disease,” said David Lyerly, PhD, during a session on C. difficile toxin testing at the Peggy Lillis Foundation 2022 National C. diff Advocacy Summit.
Dr. Lyerly, the chief science officer at Techlab, explained that exotoxins A and B are produced by specific strains of C. difficile and are involved in infections, but some patients who test positive for these toxins by polymerase chain reaction or other tests do not have CDI or they are not appropriate candidates for CDI treatment.
Several studies conducted during the past decade, however, support the importance of toxin detection. Some research has suggested that toxin-positive patients tend to have more clinically severe disease than those who test negative, he noted.
Although its use is limited when it is used alone, toxin testing is needed to confirm a CDI diagnosis and to ensure antibiotic stewardship, Dr. Lyerly said.
He suggested that, in addition to toxin testing, there is a need for molecular measures and other improved diagnostics to identify candidates most likely to benefit from CDI treatment.
“Because we generally detect toxin genes instead of toxin proteins, you can identify persons colonized with toxigenic C. difficile who do not actually have CDI,” Kevin W. Garey, PharmD, from the University of Houston, said in an interview.
Dr. Garey added that a person could likewise have low levels of toxins that aren’t detected by toxin tests but could still have CDI.
“Given this, better diagnostics that incorporate active toxin production and your body’s response to those toxins are needed,” he said, especially since C. difficile toxins are responsible for disease sequelae, including gastroenteritis, colonic perforation, sepsis, and death.
Toxin testing a ‘controversial area’
“C. difficile toxin testing has been a controversial area for almost a decade or more,” Shruti K. Gohil, MD, from University of California, Irvine, Health Epidemiology and Infection Prevention, said in an interview.
Dr. Gohil noted that toxin testing is a better test for clinical C. difficile colitis but by itself can miss C. difficile. “So, we are in this conundrum nationally,” she said.
“Many facilities will use a double- or triple-test strategy to make sure that you have a true C. difficile case mandating the use of antibiotics,” she explained. “The reason we test specifically with the enzyme immunoassay or toxin test is to know whether or not you have real C. difficile that’s actively producing the toxin for colitis.”
A patient with C. difficile who has been treated and is in recovery may still test positive on a C. difficile toxin test, added Dr. Gohil. “It would be great if we had a test that could really judge an active, clinical C. difficile infection. This [test] would help in identifying the right patients who need treatment and would also be able to tell if a patient has been cleared of C. difficile.”
Dr. Lyerly is an employee of Techlab. Dr. Garey and Dr. Gohil reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Clostridioides difficile infection is often confirmed through toxin testing, yet toxin tests alone may not be sufficient for diagnosing and guiding treatment decisions for patients with CDI.
“The presence of a toxigenic strain does not always equal disease,” said David Lyerly, PhD, during a session on C. difficile toxin testing at the Peggy Lillis Foundation 2022 National C. diff Advocacy Summit.
Dr. Lyerly, the chief science officer at Techlab, explained that exotoxins A and B are produced by specific strains of C. difficile and are involved in infections, but some patients who test positive for these toxins by polymerase chain reaction or other tests do not have CDI or they are not appropriate candidates for CDI treatment.
Several studies conducted during the past decade, however, support the importance of toxin detection. Some research has suggested that toxin-positive patients tend to have more clinically severe disease than those who test negative, he noted.
Although its use is limited when it is used alone, toxin testing is needed to confirm a CDI diagnosis and to ensure antibiotic stewardship, Dr. Lyerly said.
He suggested that, in addition to toxin testing, there is a need for molecular measures and other improved diagnostics to identify candidates most likely to benefit from CDI treatment.
“Because we generally detect toxin genes instead of toxin proteins, you can identify persons colonized with toxigenic C. difficile who do not actually have CDI,” Kevin W. Garey, PharmD, from the University of Houston, said in an interview.
Dr. Garey added that a person could likewise have low levels of toxins that aren’t detected by toxin tests but could still have CDI.
“Given this, better diagnostics that incorporate active toxin production and your body’s response to those toxins are needed,” he said, especially since C. difficile toxins are responsible for disease sequelae, including gastroenteritis, colonic perforation, sepsis, and death.
Toxin testing a ‘controversial area’
“C. difficile toxin testing has been a controversial area for almost a decade or more,” Shruti K. Gohil, MD, from University of California, Irvine, Health Epidemiology and Infection Prevention, said in an interview.
Dr. Gohil noted that toxin testing is a better test for clinical C. difficile colitis but by itself can miss C. difficile. “So, we are in this conundrum nationally,” she said.
“Many facilities will use a double- or triple-test strategy to make sure that you have a true C. difficile case mandating the use of antibiotics,” she explained. “The reason we test specifically with the enzyme immunoassay or toxin test is to know whether or not you have real C. difficile that’s actively producing the toxin for colitis.”
A patient with C. difficile who has been treated and is in recovery may still test positive on a C. difficile toxin test, added Dr. Gohil. “It would be great if we had a test that could really judge an active, clinical C. difficile infection. This [test] would help in identifying the right patients who need treatment and would also be able to tell if a patient has been cleared of C. difficile.”
Dr. Lyerly is an employee of Techlab. Dr. Garey and Dr. Gohil reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Clostridioides difficile infection is often confirmed through toxin testing, yet toxin tests alone may not be sufficient for diagnosing and guiding treatment decisions for patients with CDI.
“The presence of a toxigenic strain does not always equal disease,” said David Lyerly, PhD, during a session on C. difficile toxin testing at the Peggy Lillis Foundation 2022 National C. diff Advocacy Summit.
Dr. Lyerly, the chief science officer at Techlab, explained that exotoxins A and B are produced by specific strains of C. difficile and are involved in infections, but some patients who test positive for these toxins by polymerase chain reaction or other tests do not have CDI or they are not appropriate candidates for CDI treatment.
Several studies conducted during the past decade, however, support the importance of toxin detection. Some research has suggested that toxin-positive patients tend to have more clinically severe disease than those who test negative, he noted.
Although its use is limited when it is used alone, toxin testing is needed to confirm a CDI diagnosis and to ensure antibiotic stewardship, Dr. Lyerly said.
He suggested that, in addition to toxin testing, there is a need for molecular measures and other improved diagnostics to identify candidates most likely to benefit from CDI treatment.
“Because we generally detect toxin genes instead of toxin proteins, you can identify persons colonized with toxigenic C. difficile who do not actually have CDI,” Kevin W. Garey, PharmD, from the University of Houston, said in an interview.
Dr. Garey added that a person could likewise have low levels of toxins that aren’t detected by toxin tests but could still have CDI.
“Given this, better diagnostics that incorporate active toxin production and your body’s response to those toxins are needed,” he said, especially since C. difficile toxins are responsible for disease sequelae, including gastroenteritis, colonic perforation, sepsis, and death.
Toxin testing a ‘controversial area’
“C. difficile toxin testing has been a controversial area for almost a decade or more,” Shruti K. Gohil, MD, from University of California, Irvine, Health Epidemiology and Infection Prevention, said in an interview.
Dr. Gohil noted that toxin testing is a better test for clinical C. difficile colitis but by itself can miss C. difficile. “So, we are in this conundrum nationally,” she said.
“Many facilities will use a double- or triple-test strategy to make sure that you have a true C. difficile case mandating the use of antibiotics,” she explained. “The reason we test specifically with the enzyme immunoassay or toxin test is to know whether or not you have real C. difficile that’s actively producing the toxin for colitis.”
A patient with C. difficile who has been treated and is in recovery may still test positive on a C. difficile toxin test, added Dr. Gohil. “It would be great if we had a test that could really judge an active, clinical C. difficile infection. This [test] would help in identifying the right patients who need treatment and would also be able to tell if a patient has been cleared of C. difficile.”
Dr. Lyerly is an employee of Techlab. Dr. Garey and Dr. Gohil reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Early-onset colon cancer projected to double by 2030
from 7.9 to 12.9 cases in 2015 per 100,000 people. The reason for the increase isn’t well understood.
The findings were highlighted in a recent review article published online in the New England Journal of Medicine. “It’s a national phenomenon and it’s also occurring in other parts of the developed world. We’re used to seeing mostly older people who have this diagnosis. Now we’re seeing a lot of younger people with this disease. It’s rather alarming,” said author Frank Sinicrope, MD, a medical oncologist with Mayo Clinic, Rochester, Minn.
The trend contrasts with a decline in later-onset CRC likely attributable to increases in screening. As a result of the two trends, but especially the increased number of early-onset cases, the median age of diagnosis dropped from 72 in the early 2000s to 66 today.
“Although patients with early-onset colorectal cancer are more likely to have a hereditary syndrome than those who have later-onset disease, most cases are sporadic, with no identifiable cause. Furthermore, somatic mutational profiling of early-onset colorectal cancers has not revealed previously unidentified or actionable alterations to inform our understanding of the pathogenesis of these cancers or to guide treatment,” he wrote in the review.
“Early-onset colorectal cancers are most commonly detected in the rectum, followed by the distal colon; more than 70% of early-onset colorectal cancers are in the left colon at presentation,” he wrote in the review. Younger patients tend to be unfamiliar with CRC symptoms, which are often mistaken for benign conditions.
“We’ve moved the screening age down to 45, but that still is not going to capture a lot of these patients,” Dr. Sinicrope said. He estimates that 25% of rectal cancers and 10%-12% of colon cancers diagnosed in the next 10 years will be early onset.
Although the direct cause of the increased incidence isn’t clear, Dr. Sinicrope suggested it may reflect changing dietary habits and rising obesity among adolescents. “The sugar-containing beverages, the processed sugar and a lot of red meat in the diet and refined grains … reflect changes in the diet over the last 50 years. We may now be seeing the end result of many of these dietary changes that have occurred,” he said, calling for a greater emphasis on plant-based diets, which promote a healthier gut microbiome that may reduce CRC risk. Western-style diets can change the gut microbiome leading to inflammation which increases the risk of CRC.
Most patients with early CRC present with advanced disease in the left colon. And, pathogenic germline variants are present in one in six patients – half of which are associated with Lynch syndrome which increases the risk for CRC.
Dr. Sinicrope highlighted the need for more risk-based intervention, which in turn requires a better knowledge of family history.
“We need to do better job to risk stratify, and that will help us figure out who’s best to target our screening efforts toward,” Dr. Sinicrope said. He pointed out guidelines from the U.S. Multi-Society Task Force on Colorectal Cancer and the American Cancer Society that can help physicians identify patients who might benefit from earlier screening. The American Cancer Society recommends that CRC screening be conducted at 45 years for average-risk individuals.
“The best screening test is the one that the patient will do,” Dr. Sinicrope said.
from 7.9 to 12.9 cases in 2015 per 100,000 people. The reason for the increase isn’t well understood.
The findings were highlighted in a recent review article published online in the New England Journal of Medicine. “It’s a national phenomenon and it’s also occurring in other parts of the developed world. We’re used to seeing mostly older people who have this diagnosis. Now we’re seeing a lot of younger people with this disease. It’s rather alarming,” said author Frank Sinicrope, MD, a medical oncologist with Mayo Clinic, Rochester, Minn.
The trend contrasts with a decline in later-onset CRC likely attributable to increases in screening. As a result of the two trends, but especially the increased number of early-onset cases, the median age of diagnosis dropped from 72 in the early 2000s to 66 today.
“Although patients with early-onset colorectal cancer are more likely to have a hereditary syndrome than those who have later-onset disease, most cases are sporadic, with no identifiable cause. Furthermore, somatic mutational profiling of early-onset colorectal cancers has not revealed previously unidentified or actionable alterations to inform our understanding of the pathogenesis of these cancers or to guide treatment,” he wrote in the review.
“Early-onset colorectal cancers are most commonly detected in the rectum, followed by the distal colon; more than 70% of early-onset colorectal cancers are in the left colon at presentation,” he wrote in the review. Younger patients tend to be unfamiliar with CRC symptoms, which are often mistaken for benign conditions.
“We’ve moved the screening age down to 45, but that still is not going to capture a lot of these patients,” Dr. Sinicrope said. He estimates that 25% of rectal cancers and 10%-12% of colon cancers diagnosed in the next 10 years will be early onset.
Although the direct cause of the increased incidence isn’t clear, Dr. Sinicrope suggested it may reflect changing dietary habits and rising obesity among adolescents. “The sugar-containing beverages, the processed sugar and a lot of red meat in the diet and refined grains … reflect changes in the diet over the last 50 years. We may now be seeing the end result of many of these dietary changes that have occurred,” he said, calling for a greater emphasis on plant-based diets, which promote a healthier gut microbiome that may reduce CRC risk. Western-style diets can change the gut microbiome leading to inflammation which increases the risk of CRC.
Most patients with early CRC present with advanced disease in the left colon. And, pathogenic germline variants are present in one in six patients – half of which are associated with Lynch syndrome which increases the risk for CRC.
Dr. Sinicrope highlighted the need for more risk-based intervention, which in turn requires a better knowledge of family history.
“We need to do better job to risk stratify, and that will help us figure out who’s best to target our screening efforts toward,” Dr. Sinicrope said. He pointed out guidelines from the U.S. Multi-Society Task Force on Colorectal Cancer and the American Cancer Society that can help physicians identify patients who might benefit from earlier screening. The American Cancer Society recommends that CRC screening be conducted at 45 years for average-risk individuals.
“The best screening test is the one that the patient will do,” Dr. Sinicrope said.
from 7.9 to 12.9 cases in 2015 per 100,000 people. The reason for the increase isn’t well understood.
The findings were highlighted in a recent review article published online in the New England Journal of Medicine. “It’s a national phenomenon and it’s also occurring in other parts of the developed world. We’re used to seeing mostly older people who have this diagnosis. Now we’re seeing a lot of younger people with this disease. It’s rather alarming,” said author Frank Sinicrope, MD, a medical oncologist with Mayo Clinic, Rochester, Minn.
The trend contrasts with a decline in later-onset CRC likely attributable to increases in screening. As a result of the two trends, but especially the increased number of early-onset cases, the median age of diagnosis dropped from 72 in the early 2000s to 66 today.
“Although patients with early-onset colorectal cancer are more likely to have a hereditary syndrome than those who have later-onset disease, most cases are sporadic, with no identifiable cause. Furthermore, somatic mutational profiling of early-onset colorectal cancers has not revealed previously unidentified or actionable alterations to inform our understanding of the pathogenesis of these cancers or to guide treatment,” he wrote in the review.
“Early-onset colorectal cancers are most commonly detected in the rectum, followed by the distal colon; more than 70% of early-onset colorectal cancers are in the left colon at presentation,” he wrote in the review. Younger patients tend to be unfamiliar with CRC symptoms, which are often mistaken for benign conditions.
“We’ve moved the screening age down to 45, but that still is not going to capture a lot of these patients,” Dr. Sinicrope said. He estimates that 25% of rectal cancers and 10%-12% of colon cancers diagnosed in the next 10 years will be early onset.
Although the direct cause of the increased incidence isn’t clear, Dr. Sinicrope suggested it may reflect changing dietary habits and rising obesity among adolescents. “The sugar-containing beverages, the processed sugar and a lot of red meat in the diet and refined grains … reflect changes in the diet over the last 50 years. We may now be seeing the end result of many of these dietary changes that have occurred,” he said, calling for a greater emphasis on plant-based diets, which promote a healthier gut microbiome that may reduce CRC risk. Western-style diets can change the gut microbiome leading to inflammation which increases the risk of CRC.
Most patients with early CRC present with advanced disease in the left colon. And, pathogenic germline variants are present in one in six patients – half of which are associated with Lynch syndrome which increases the risk for CRC.
Dr. Sinicrope highlighted the need for more risk-based intervention, which in turn requires a better knowledge of family history.
“We need to do better job to risk stratify, and that will help us figure out who’s best to target our screening efforts toward,” Dr. Sinicrope said. He pointed out guidelines from the U.S. Multi-Society Task Force on Colorectal Cancer and the American Cancer Society that can help physicians identify patients who might benefit from earlier screening. The American Cancer Society recommends that CRC screening be conducted at 45 years for average-risk individuals.
“The best screening test is the one that the patient will do,” Dr. Sinicrope said.
FROM NEW ENGLAND JOURNAL OF MEDICINE
Head and neck cancer patients recommend 11 needed improvements in health care
HNC has a high burden of treatment-related adverse events, along with frequent trouble with speech, swallowing, facial disfigurement, and psychological distress.
Among cancer patients, “they have the highest rates of emergency department use and hospitalization during treatment. They also have the highest rates of psychological distress. We have some Ontario data that shows they’ve got the highest rates of suicide and self-harm. So I think this is a really special population that we need to support,” Christopher Noel, MD, PhD, said in an interview. Dr. Noel was the lead author of the study, which was published in JAMA Otolaryngology – Head & Neck Surgery.
These issues can strongly affect quality of life, and even patient outcomes. “Even a 1-day interruption in treatment has been shown to impact oncologic outcomes. This is a very big issue whether you’re a surgeon, a medical oncologist, or a radiation oncologist,” said Dr. Noel, who is a resident physician at the University of Toronto.
He advocates that physicians interview patients and review the results in a structured way and then act on it. “If we just rely on patient [provided] communication, we’re going to miss about 50% of patient symptoms,” he said.
The researchers aimed for the patient’s perspective on treatment. “What is the patient’s perception of going through head neck cancer and their treatment, and managing their symptoms at home? And where do they think that we could do better?” Dr. Noel asked.
The most pressing issue was that patients felt their emotional and informational needs often were not met. That challenge is even harder for patients who have trouble communicating, which in turn makes them more prone to isolation and loneliness. Many felt that they had to get the information on their own. “They wanted it to be a more effortless process,” said Dr. Noel.
He described one patient with oropharynx cancer who was able to talk to people about her grief over her diagnosis, but treatment led to her throat becoming swollen and she lost the ability to communicate. “She felt very isolated and lonely. She really highlighted the emotional and psychosocial barriers in cancer care. Her treatment inherently leaves her feeling very isolated and lonely, and she had such a hard time connecting with a psychotherapist,” Dr. Noel said.
Another common issue revolved around efforts to communicate about symptoms and adverse effects of treatment. Resources often aren’t available on evenings or weekends, and it can take time for a nurse to call them back. Patients wanted to see more modern approaches, such as use of email or apps.
The patients in the study recommended 11 health care improvements.
- 1. Nurse navigator teams should have hours extended to evenings and weekends.
- 2. Patient communication methods should be expanded, using methods like email or apps.
- 3. HNC resources should be more broadly disseminated.
- 4. Education and information approaches should be individualized to the patient.
- 5. All HNC patients should be offered psychological resources.
- 6. Mental health needs should be assessed repeatedly throughout treatment and extended care.
- 7. Physicians should recognize the added symptom burden often faced by patients who travel extensively for treatment.
- 8. Partners and caregivers should be included as part of the treatment team.
- 9. Share symptom data with patients, which can improve engagement.
- 10. Review symptom scores and act on them regularly.
- 11. A member of the care team should be identified to oversee symptom management.
Dr. Noel had no relevant financial disclosures.
HNC has a high burden of treatment-related adverse events, along with frequent trouble with speech, swallowing, facial disfigurement, and psychological distress.
Among cancer patients, “they have the highest rates of emergency department use and hospitalization during treatment. They also have the highest rates of psychological distress. We have some Ontario data that shows they’ve got the highest rates of suicide and self-harm. So I think this is a really special population that we need to support,” Christopher Noel, MD, PhD, said in an interview. Dr. Noel was the lead author of the study, which was published in JAMA Otolaryngology – Head & Neck Surgery.
These issues can strongly affect quality of life, and even patient outcomes. “Even a 1-day interruption in treatment has been shown to impact oncologic outcomes. This is a very big issue whether you’re a surgeon, a medical oncologist, or a radiation oncologist,” said Dr. Noel, who is a resident physician at the University of Toronto.
He advocates that physicians interview patients and review the results in a structured way and then act on it. “If we just rely on patient [provided] communication, we’re going to miss about 50% of patient symptoms,” he said.
The researchers aimed for the patient’s perspective on treatment. “What is the patient’s perception of going through head neck cancer and their treatment, and managing their symptoms at home? And where do they think that we could do better?” Dr. Noel asked.
The most pressing issue was that patients felt their emotional and informational needs often were not met. That challenge is even harder for patients who have trouble communicating, which in turn makes them more prone to isolation and loneliness. Many felt that they had to get the information on their own. “They wanted it to be a more effortless process,” said Dr. Noel.
He described one patient with oropharynx cancer who was able to talk to people about her grief over her diagnosis, but treatment led to her throat becoming swollen and she lost the ability to communicate. “She felt very isolated and lonely. She really highlighted the emotional and psychosocial barriers in cancer care. Her treatment inherently leaves her feeling very isolated and lonely, and she had such a hard time connecting with a psychotherapist,” Dr. Noel said.
Another common issue revolved around efforts to communicate about symptoms and adverse effects of treatment. Resources often aren’t available on evenings or weekends, and it can take time for a nurse to call them back. Patients wanted to see more modern approaches, such as use of email or apps.
The patients in the study recommended 11 health care improvements.
- 1. Nurse navigator teams should have hours extended to evenings and weekends.
- 2. Patient communication methods should be expanded, using methods like email or apps.
- 3. HNC resources should be more broadly disseminated.
- 4. Education and information approaches should be individualized to the patient.
- 5. All HNC patients should be offered psychological resources.
- 6. Mental health needs should be assessed repeatedly throughout treatment and extended care.
- 7. Physicians should recognize the added symptom burden often faced by patients who travel extensively for treatment.
- 8. Partners and caregivers should be included as part of the treatment team.
- 9. Share symptom data with patients, which can improve engagement.
- 10. Review symptom scores and act on them regularly.
- 11. A member of the care team should be identified to oversee symptom management.
Dr. Noel had no relevant financial disclosures.
HNC has a high burden of treatment-related adverse events, along with frequent trouble with speech, swallowing, facial disfigurement, and psychological distress.
Among cancer patients, “they have the highest rates of emergency department use and hospitalization during treatment. They also have the highest rates of psychological distress. We have some Ontario data that shows they’ve got the highest rates of suicide and self-harm. So I think this is a really special population that we need to support,” Christopher Noel, MD, PhD, said in an interview. Dr. Noel was the lead author of the study, which was published in JAMA Otolaryngology – Head & Neck Surgery.
These issues can strongly affect quality of life, and even patient outcomes. “Even a 1-day interruption in treatment has been shown to impact oncologic outcomes. This is a very big issue whether you’re a surgeon, a medical oncologist, or a radiation oncologist,” said Dr. Noel, who is a resident physician at the University of Toronto.
He advocates that physicians interview patients and review the results in a structured way and then act on it. “If we just rely on patient [provided] communication, we’re going to miss about 50% of patient symptoms,” he said.
The researchers aimed for the patient’s perspective on treatment. “What is the patient’s perception of going through head neck cancer and their treatment, and managing their symptoms at home? And where do they think that we could do better?” Dr. Noel asked.
The most pressing issue was that patients felt their emotional and informational needs often were not met. That challenge is even harder for patients who have trouble communicating, which in turn makes them more prone to isolation and loneliness. Many felt that they had to get the information on their own. “They wanted it to be a more effortless process,” said Dr. Noel.
He described one patient with oropharynx cancer who was able to talk to people about her grief over her diagnosis, but treatment led to her throat becoming swollen and she lost the ability to communicate. “She felt very isolated and lonely. She really highlighted the emotional and psychosocial barriers in cancer care. Her treatment inherently leaves her feeling very isolated and lonely, and she had such a hard time connecting with a psychotherapist,” Dr. Noel said.
Another common issue revolved around efforts to communicate about symptoms and adverse effects of treatment. Resources often aren’t available on evenings or weekends, and it can take time for a nurse to call them back. Patients wanted to see more modern approaches, such as use of email or apps.
The patients in the study recommended 11 health care improvements.
- 1. Nurse navigator teams should have hours extended to evenings and weekends.
- 2. Patient communication methods should be expanded, using methods like email or apps.
- 3. HNC resources should be more broadly disseminated.
- 4. Education and information approaches should be individualized to the patient.
- 5. All HNC patients should be offered psychological resources.
- 6. Mental health needs should be assessed repeatedly throughout treatment and extended care.
- 7. Physicians should recognize the added symptom burden often faced by patients who travel extensively for treatment.
- 8. Partners and caregivers should be included as part of the treatment team.
- 9. Share symptom data with patients, which can improve engagement.
- 10. Review symptom scores and act on them regularly.
- 11. A member of the care team should be identified to oversee symptom management.
Dr. Noel had no relevant financial disclosures.
FROM JAMA OTOLARYNGOLOGY – HEAD & NECK SURGERY