User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Children and COVID: Severe illness rising as vaccination effort stalls
, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
After new child cases jumped by 22% during the week of July 15-21, the two successive weeks have produced increases of 3.9% (July 22-29) and 1.2% (July 30-Aug. 4). The latest weekly count from all states and territories still reporting was 96,599, the AAP and CHA said in their weekly COVID report, noting that several states have stopped reporting child cases and that others are reporting every other week.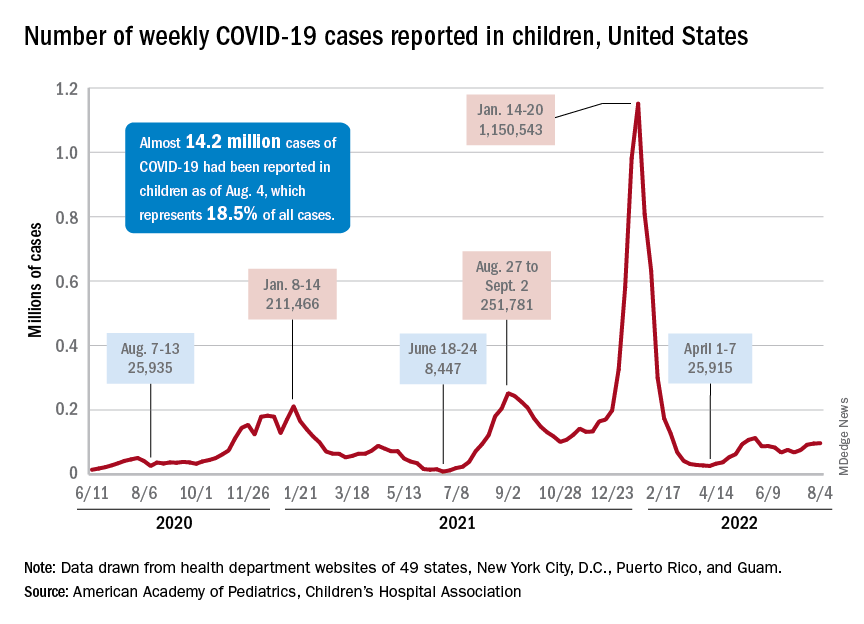
The deceleration in new cases, however, does not apply to emergency department visits and hospital admissions. The proportion of ED visits with diagnosed COVID rose steadily throughout June and July, as 7-day averages went from 2.6% on June 1 to 6.3% on July 31 for children aged 0-11 years, from 2.1% to 3.1% for children aged 12-15, and from 2.4% to 3.5% for 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
The rate of new admissions with confirmed COVID, which reached 0.46 per 100,000 population for children aged 0-17 years on July 30, has more than tripled since early April, when it had fallen to 0.13 per 100,000 in the wake of the Omicron surge, the CDC reported on its COVID Data Tracker.
A smaller but more detailed sample of children from the COVID-19–Associated Hospitalization Network (COVID-NET), which covers nearly 100 counties in 14 states, indicates that the increase in new admissions is occurring almost entirely among children aged 0-4 years, who had a rate of 5.6 per 100,000 for the week of July 17-23, compared with 0.8 per 100,000 for 5- to 11-year-olds and 1.5 per 100,000 for those aged 12-17, the CDC said.
Vaccine’s summer rollout gets lukewarm reception
As a group, children aged 0-4 years have not exactly flocked to the COVID-19 vaccine. As of Aug. 2 – about 6 weeks since the vaccine was authorized for children aged 6 months to 4 years – just 3.8% of those eligible had received at least one dose. Among children aged 5-11 the corresponding number on Aug. 2 was 37.4%, and for those aged 12-17 years it was 70.3%, the CDC data show.
That 3.8% of children aged less than 5 years represents almost 756,000 initial doses. That compares with over 6 million children aged 5-11 years who had received at least one dose through the first 6 weeks of their vaccination experience and over 5 million children aged 12-15, according to the COVID Data Tracker.
, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
After new child cases jumped by 22% during the week of July 15-21, the two successive weeks have produced increases of 3.9% (July 22-29) and 1.2% (July 30-Aug. 4). The latest weekly count from all states and territories still reporting was 96,599, the AAP and CHA said in their weekly COVID report, noting that several states have stopped reporting child cases and that others are reporting every other week.
The deceleration in new cases, however, does not apply to emergency department visits and hospital admissions. The proportion of ED visits with diagnosed COVID rose steadily throughout June and July, as 7-day averages went from 2.6% on June 1 to 6.3% on July 31 for children aged 0-11 years, from 2.1% to 3.1% for children aged 12-15, and from 2.4% to 3.5% for 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
The rate of new admissions with confirmed COVID, which reached 0.46 per 100,000 population for children aged 0-17 years on July 30, has more than tripled since early April, when it had fallen to 0.13 per 100,000 in the wake of the Omicron surge, the CDC reported on its COVID Data Tracker.
A smaller but more detailed sample of children from the COVID-19–Associated Hospitalization Network (COVID-NET), which covers nearly 100 counties in 14 states, indicates that the increase in new admissions is occurring almost entirely among children aged 0-4 years, who had a rate of 5.6 per 100,000 for the week of July 17-23, compared with 0.8 per 100,000 for 5- to 11-year-olds and 1.5 per 100,000 for those aged 12-17, the CDC said.
Vaccine’s summer rollout gets lukewarm reception
As a group, children aged 0-4 years have not exactly flocked to the COVID-19 vaccine. As of Aug. 2 – about 6 weeks since the vaccine was authorized for children aged 6 months to 4 years – just 3.8% of those eligible had received at least one dose. Among children aged 5-11 the corresponding number on Aug. 2 was 37.4%, and for those aged 12-17 years it was 70.3%, the CDC data show.
That 3.8% of children aged less than 5 years represents almost 756,000 initial doses. That compares with over 6 million children aged 5-11 years who had received at least one dose through the first 6 weeks of their vaccination experience and over 5 million children aged 12-15, according to the COVID Data Tracker.
, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
After new child cases jumped by 22% during the week of July 15-21, the two successive weeks have produced increases of 3.9% (July 22-29) and 1.2% (July 30-Aug. 4). The latest weekly count from all states and territories still reporting was 96,599, the AAP and CHA said in their weekly COVID report, noting that several states have stopped reporting child cases and that others are reporting every other week.
The deceleration in new cases, however, does not apply to emergency department visits and hospital admissions. The proportion of ED visits with diagnosed COVID rose steadily throughout June and July, as 7-day averages went from 2.6% on June 1 to 6.3% on July 31 for children aged 0-11 years, from 2.1% to 3.1% for children aged 12-15, and from 2.4% to 3.5% for 16- to 17-year-olds, according to data from the Centers for Disease Control and Prevention.
The rate of new admissions with confirmed COVID, which reached 0.46 per 100,000 population for children aged 0-17 years on July 30, has more than tripled since early April, when it had fallen to 0.13 per 100,000 in the wake of the Omicron surge, the CDC reported on its COVID Data Tracker.
A smaller but more detailed sample of children from the COVID-19–Associated Hospitalization Network (COVID-NET), which covers nearly 100 counties in 14 states, indicates that the increase in new admissions is occurring almost entirely among children aged 0-4 years, who had a rate of 5.6 per 100,000 for the week of July 17-23, compared with 0.8 per 100,000 for 5- to 11-year-olds and 1.5 per 100,000 for those aged 12-17, the CDC said.
Vaccine’s summer rollout gets lukewarm reception
As a group, children aged 0-4 years have not exactly flocked to the COVID-19 vaccine. As of Aug. 2 – about 6 weeks since the vaccine was authorized for children aged 6 months to 4 years – just 3.8% of those eligible had received at least one dose. Among children aged 5-11 the corresponding number on Aug. 2 was 37.4%, and for those aged 12-17 years it was 70.3%, the CDC data show.
That 3.8% of children aged less than 5 years represents almost 756,000 initial doses. That compares with over 6 million children aged 5-11 years who had received at least one dose through the first 6 weeks of their vaccination experience and over 5 million children aged 12-15, according to the COVID Data Tracker.
Updates on treatment/prevention of VTE in cancer patients
Updated clinical practice guidelines for the treatment and prevention of venous thromboembolism for patients with cancer, including those with cancer and COVID-19, have been released by the International Initiative on Thrombosis and Cancer (ITAC), an academic working group of VTE experts.
“Because patients with cancer have a baseline increased risk of VTE, compared with patients without cancer, the combination of both COVID-19 and cancer – and its effect on VTE risk and treatment – is of concern,” said the authors, led by Dominique Farge, MD, PhD, Nord Universite de Paris.
they added.
The new guidelines were published online in The Lancet Oncology.
“Cancer-associated VTE remains an important clinical problem, associated with increased morbidity and mortality,” Dr. Farge and colleagues observed.
“The ITAC guidelines’ companion free web-based mobile application will assist the practicing clinician with decision making at various levels to provide optimal care of patients with cancer to treat and prevent VTE,” they emphasized. More information is available at itaccme.com.
Cancer patients with COVID
The new section of the guidelines notes that the treatment and prevention of VTE for cancer patients infected with SARS-CoV-2 remain the same as for patients without COVID.
Whether or not cancer patients with COVID-19 are hospitalized, have been discharged, or are ambulatory, they should be assessed for the risk of VTE, as should any other patient. For cancer patients with COVID-19 who are hospitalized, pharmacologic prophylaxis should be given at the same dose and anticoagulant type as for hospitalized cancer patients who do not have COVID-19.
Following discharge, VTE prophylaxis is not advised for cancer patients infected with SARS-CoV-2, and routine primary pharmacologic prophylaxis of VTE for ambulatory patients with COVID-19 is also not recommended, the authors noted.
Initial treatment of established VTE
Initial treatment of established VTE for up to 10 days of anticoagulation should include low-molecular-weight heparin (LMWH) when creatinine clearance is at least 30 mL/min.
“A regimen of LMWH, taken once per day, is recommended unless a twice-per-day regimen is required because of patients’ characteristics,” the authors noted. These characteristics include a high risk of bleeding, moderate renal failure, and the need for technical intervention, including surgery.
If a twice-a-day regimen is required, only enoxaparin at a dose of 1 mg/kg twice daily can be used, the authors cautioned.
For patients with a low risk of gastrointestinal or genitourinary bleeding, rivaroxaban (Xarelto) or apixaban (Eliquis) can be given in the first 10 days, as well as edoxaban (Lixiana). The latter should be started after at least 5 days of parenteral anticoagulation, provided creatinine clearance is at least 30 mL/min.
“Unfractionated heparin as well as fondaparinux (GlaxoSmithKline) can be also used for the initial treatment of established VTE when LMWH or direct oral anticoagulants are contraindicated,” Dr. Farge and colleagues wrote.
Thrombolysis can be considered on a case-by-case basis, although physicians must pay attention to specific contraindications, especially bleeding risk.
“In the initial treatment of VTE, inferior vena cava filters might be considered when anticoagulant treatment is contraindicated or, in the case of pulmonary embolism, when recurrence occurs under optimal anticoagulation,” the authors noted.
Maintenance VTE treatment
For maintenance therapy, which the authors define as early maintenance for up to 6 months and long-term maintenance beyond 6 months, they point out that LMWHs are preferred over vitamin K antagonists for the treatment of VTE when the creatinine clearance is again at least 30 mL/min.
Any of the direct oral anticoagulants (DOAs) – edoxaban, rivaroxaban, or apixaban – is also recommended for the same patients, provided there is no risk of inducing a strong drug-drug interaction or GI absorption is impaired.
However, the DOAs should be used with caution for patients with GI malignancies, especially upper GI cancers, because data show there is an increased risk of GI bleeding with both edoxaban and rivaroxaban.
“LMWH or direct oral anticoagulants should be used for a minimum of 6 months to treat established VTE in patients with cancer,” the authors wrote.
“After 6 months, termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists) should be based on individual evaluation of the benefit-risk ratio,” they added.
Treatment of VTE recurrence
The guideline authors explain that three options can be considered in the event of VTE recurrence. These include an increase in the LMWH dose by 20%-25%, or a switch to a DOA, or, if patients are taking a DOA, a switch to an LMWH. If the patient is taking a vitamin K antagonist, it can be switched to either an LMWH or a DOA.
For treatment of catheter-related thrombosis, anticoagulant treatment is recommended for a minimum of 3 months and as long as the central venous catheter is in place. In this setting, the LMWHs are recommended.
The central venous catheter can be kept in place if it is functional, well positioned, and is not infected, provided there is good resolution of symptoms under close surveillance while anticoagulants are being administered.
In surgically treated patients, the LMWH, given once a day, to patients with a serum creatinine concentration of at least 30 mL/min can be used to prevent VTE. Alternatively, VTE can be prevented by the use low-dose unfractionated heparin, given three times a day.
“Pharmacological prophylaxis should be started 2-12 h preoperatively and continued for at least 7–10 days,” Dr. Farge and colleagues advised. In this setting, there is insufficient evidence to support the use of fondaparinux or a DOA as an alternative to an LMWH for the prophylaxis of postoperative VTE. “Use of the highest prophylactic dose of LMWH to prevent postoperative VTE in patients with cancer is recommended,” the authors advised.
Furthermore, extended prophylaxis of at least 4 weeks with LMWH is advised to prevent postoperative VTE after major abdominal or pelvic surgery. Mechanical methods are not recommended except when pharmacologic methods are contraindicated. Inferior vena cava filters are also not recommended for routine prophylaxis.
Patients with reduced mobility
For medically treated hospitalized patients with cancer whose mobility is reduced, the authors recommend prophylaxis with either an LMWH or fondaparinux, provided their creatinine clearance is at least 30 mL/min. These patients can also be treated with unfractionated heparin, they add.
In contrast, DOAs are not recommended – at least not routinely – in this setting, the authors cautioned. Primary pharmacologic prophylaxis of VTE with either LMWH or DOAs – either rivaroxaban or apixaban – is indicated in ambulatory patients with locally advanced or metastatic pancreatic cancer who are receiving systemic anticancer therapy, provided they are at low risk of bleeding.
However, primary pharmacologic prophylaxis with LMWH is not recommended outside of a clinical trial for patients with locally advanced or metastatic lung cancer who are undergoing systemic anticancer therapy, even for patients who are at low risk of bleeding.
For ambulatory patients who are receiving systemic anticancer therapy and who are at intermediate risk of VTE, primary prophylaxis with rivaroxaban or apixaban is recommended for those with myeloma who are receiving immunomodulatory therapy plus steroids or other systemic therapies.
In this setting, oral anticoagulants should consist of a vitamin K antagonist, given at low or therapeutic doses, or apixaban, given at prophylactic doses. Alternatively, LMWH, given at prophylactic doses, or low-dose aspirin, given at a dose of 100 mg/day, can be used.
Catheter-related thrombosis
Use of anticoagulation for routine prophylaxis of catheter-related thrombosis is not recommended. Catheters should be inserted on the right side in the jugular vein, and the distal extremity of the central catheter should be located at the junction of the superior vena cava and the right atrium. “In patients requiring central venous catheters, we suggest the use of implanted ports over peripheral inserted central catheter lines,” the authors noted.
The authors described a number of unique situations regarding the treatment of VTE. These situations include patients with a brain tumor, for whom treatment of established VTE should favor either LMWH or a DOA. The authors also recommended the use of LMWH or unfractionated heparin, started postoperatively, for the prevention of VTE for patients undergoing neurosurgery.
In contrast, pharmacologic prophylaxis of VTE in medically treated patients with a brain tumor who are not undergoing neurosurgery is not recommended. “In the presence of severe renal failure...we suggest using unfractionated heparin followed by early vitamin K antagonists (possibly from day 1) or LMWH adjusted to anti-Xa concentration of the treatment of established VTE,” Dr. Farge and colleagues wrote.
Anticoagulant treatment is also recommended for a minimum of 3 months for children with symptomatic catheter-related thrombosis and as long as the central venous catheter is in place. For children with acute lymphoblastic leukemia who are undergoing induction chemotherapy, LMWH is also recommended as thromboprophylaxis.
For children who require a central venous catheter, the authors suggested that physicians use implanted ports over peripherally inserted central lines.
A version of this article first appeared on Medscape.com.
Updated clinical practice guidelines for the treatment and prevention of venous thromboembolism for patients with cancer, including those with cancer and COVID-19, have been released by the International Initiative on Thrombosis and Cancer (ITAC), an academic working group of VTE experts.
“Because patients with cancer have a baseline increased risk of VTE, compared with patients without cancer, the combination of both COVID-19 and cancer – and its effect on VTE risk and treatment – is of concern,” said the authors, led by Dominique Farge, MD, PhD, Nord Universite de Paris.
they added.
The new guidelines were published online in The Lancet Oncology.
“Cancer-associated VTE remains an important clinical problem, associated with increased morbidity and mortality,” Dr. Farge and colleagues observed.
“The ITAC guidelines’ companion free web-based mobile application will assist the practicing clinician with decision making at various levels to provide optimal care of patients with cancer to treat and prevent VTE,” they emphasized. More information is available at itaccme.com.
Cancer patients with COVID
The new section of the guidelines notes that the treatment and prevention of VTE for cancer patients infected with SARS-CoV-2 remain the same as for patients without COVID.
Whether or not cancer patients with COVID-19 are hospitalized, have been discharged, or are ambulatory, they should be assessed for the risk of VTE, as should any other patient. For cancer patients with COVID-19 who are hospitalized, pharmacologic prophylaxis should be given at the same dose and anticoagulant type as for hospitalized cancer patients who do not have COVID-19.
Following discharge, VTE prophylaxis is not advised for cancer patients infected with SARS-CoV-2, and routine primary pharmacologic prophylaxis of VTE for ambulatory patients with COVID-19 is also not recommended, the authors noted.
Initial treatment of established VTE
Initial treatment of established VTE for up to 10 days of anticoagulation should include low-molecular-weight heparin (LMWH) when creatinine clearance is at least 30 mL/min.
“A regimen of LMWH, taken once per day, is recommended unless a twice-per-day regimen is required because of patients’ characteristics,” the authors noted. These characteristics include a high risk of bleeding, moderate renal failure, and the need for technical intervention, including surgery.
If a twice-a-day regimen is required, only enoxaparin at a dose of 1 mg/kg twice daily can be used, the authors cautioned.
For patients with a low risk of gastrointestinal or genitourinary bleeding, rivaroxaban (Xarelto) or apixaban (Eliquis) can be given in the first 10 days, as well as edoxaban (Lixiana). The latter should be started after at least 5 days of parenteral anticoagulation, provided creatinine clearance is at least 30 mL/min.
“Unfractionated heparin as well as fondaparinux (GlaxoSmithKline) can be also used for the initial treatment of established VTE when LMWH or direct oral anticoagulants are contraindicated,” Dr. Farge and colleagues wrote.
Thrombolysis can be considered on a case-by-case basis, although physicians must pay attention to specific contraindications, especially bleeding risk.
“In the initial treatment of VTE, inferior vena cava filters might be considered when anticoagulant treatment is contraindicated or, in the case of pulmonary embolism, when recurrence occurs under optimal anticoagulation,” the authors noted.
Maintenance VTE treatment
For maintenance therapy, which the authors define as early maintenance for up to 6 months and long-term maintenance beyond 6 months, they point out that LMWHs are preferred over vitamin K antagonists for the treatment of VTE when the creatinine clearance is again at least 30 mL/min.
Any of the direct oral anticoagulants (DOAs) – edoxaban, rivaroxaban, or apixaban – is also recommended for the same patients, provided there is no risk of inducing a strong drug-drug interaction or GI absorption is impaired.
However, the DOAs should be used with caution for patients with GI malignancies, especially upper GI cancers, because data show there is an increased risk of GI bleeding with both edoxaban and rivaroxaban.
“LMWH or direct oral anticoagulants should be used for a minimum of 6 months to treat established VTE in patients with cancer,” the authors wrote.
“After 6 months, termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists) should be based on individual evaluation of the benefit-risk ratio,” they added.
Treatment of VTE recurrence
The guideline authors explain that three options can be considered in the event of VTE recurrence. These include an increase in the LMWH dose by 20%-25%, or a switch to a DOA, or, if patients are taking a DOA, a switch to an LMWH. If the patient is taking a vitamin K antagonist, it can be switched to either an LMWH or a DOA.
For treatment of catheter-related thrombosis, anticoagulant treatment is recommended for a minimum of 3 months and as long as the central venous catheter is in place. In this setting, the LMWHs are recommended.
The central venous catheter can be kept in place if it is functional, well positioned, and is not infected, provided there is good resolution of symptoms under close surveillance while anticoagulants are being administered.
In surgically treated patients, the LMWH, given once a day, to patients with a serum creatinine concentration of at least 30 mL/min can be used to prevent VTE. Alternatively, VTE can be prevented by the use low-dose unfractionated heparin, given three times a day.
“Pharmacological prophylaxis should be started 2-12 h preoperatively and continued for at least 7–10 days,” Dr. Farge and colleagues advised. In this setting, there is insufficient evidence to support the use of fondaparinux or a DOA as an alternative to an LMWH for the prophylaxis of postoperative VTE. “Use of the highest prophylactic dose of LMWH to prevent postoperative VTE in patients with cancer is recommended,” the authors advised.
Furthermore, extended prophylaxis of at least 4 weeks with LMWH is advised to prevent postoperative VTE after major abdominal or pelvic surgery. Mechanical methods are not recommended except when pharmacologic methods are contraindicated. Inferior vena cava filters are also not recommended for routine prophylaxis.
Patients with reduced mobility
For medically treated hospitalized patients with cancer whose mobility is reduced, the authors recommend prophylaxis with either an LMWH or fondaparinux, provided their creatinine clearance is at least 30 mL/min. These patients can also be treated with unfractionated heparin, they add.
In contrast, DOAs are not recommended – at least not routinely – in this setting, the authors cautioned. Primary pharmacologic prophylaxis of VTE with either LMWH or DOAs – either rivaroxaban or apixaban – is indicated in ambulatory patients with locally advanced or metastatic pancreatic cancer who are receiving systemic anticancer therapy, provided they are at low risk of bleeding.
However, primary pharmacologic prophylaxis with LMWH is not recommended outside of a clinical trial for patients with locally advanced or metastatic lung cancer who are undergoing systemic anticancer therapy, even for patients who are at low risk of bleeding.
For ambulatory patients who are receiving systemic anticancer therapy and who are at intermediate risk of VTE, primary prophylaxis with rivaroxaban or apixaban is recommended for those with myeloma who are receiving immunomodulatory therapy plus steroids or other systemic therapies.
In this setting, oral anticoagulants should consist of a vitamin K antagonist, given at low or therapeutic doses, or apixaban, given at prophylactic doses. Alternatively, LMWH, given at prophylactic doses, or low-dose aspirin, given at a dose of 100 mg/day, can be used.
Catheter-related thrombosis
Use of anticoagulation for routine prophylaxis of catheter-related thrombosis is not recommended. Catheters should be inserted on the right side in the jugular vein, and the distal extremity of the central catheter should be located at the junction of the superior vena cava and the right atrium. “In patients requiring central venous catheters, we suggest the use of implanted ports over peripheral inserted central catheter lines,” the authors noted.
The authors described a number of unique situations regarding the treatment of VTE. These situations include patients with a brain tumor, for whom treatment of established VTE should favor either LMWH or a DOA. The authors also recommended the use of LMWH or unfractionated heparin, started postoperatively, for the prevention of VTE for patients undergoing neurosurgery.
In contrast, pharmacologic prophylaxis of VTE in medically treated patients with a brain tumor who are not undergoing neurosurgery is not recommended. “In the presence of severe renal failure...we suggest using unfractionated heparin followed by early vitamin K antagonists (possibly from day 1) or LMWH adjusted to anti-Xa concentration of the treatment of established VTE,” Dr. Farge and colleagues wrote.
Anticoagulant treatment is also recommended for a minimum of 3 months for children with symptomatic catheter-related thrombosis and as long as the central venous catheter is in place. For children with acute lymphoblastic leukemia who are undergoing induction chemotherapy, LMWH is also recommended as thromboprophylaxis.
For children who require a central venous catheter, the authors suggested that physicians use implanted ports over peripherally inserted central lines.
A version of this article first appeared on Medscape.com.
Updated clinical practice guidelines for the treatment and prevention of venous thromboembolism for patients with cancer, including those with cancer and COVID-19, have been released by the International Initiative on Thrombosis and Cancer (ITAC), an academic working group of VTE experts.
“Because patients with cancer have a baseline increased risk of VTE, compared with patients without cancer, the combination of both COVID-19 and cancer – and its effect on VTE risk and treatment – is of concern,” said the authors, led by Dominique Farge, MD, PhD, Nord Universite de Paris.
they added.
The new guidelines were published online in The Lancet Oncology.
“Cancer-associated VTE remains an important clinical problem, associated with increased morbidity and mortality,” Dr. Farge and colleagues observed.
“The ITAC guidelines’ companion free web-based mobile application will assist the practicing clinician with decision making at various levels to provide optimal care of patients with cancer to treat and prevent VTE,” they emphasized. More information is available at itaccme.com.
Cancer patients with COVID
The new section of the guidelines notes that the treatment and prevention of VTE for cancer patients infected with SARS-CoV-2 remain the same as for patients without COVID.
Whether or not cancer patients with COVID-19 are hospitalized, have been discharged, or are ambulatory, they should be assessed for the risk of VTE, as should any other patient. For cancer patients with COVID-19 who are hospitalized, pharmacologic prophylaxis should be given at the same dose and anticoagulant type as for hospitalized cancer patients who do not have COVID-19.
Following discharge, VTE prophylaxis is not advised for cancer patients infected with SARS-CoV-2, and routine primary pharmacologic prophylaxis of VTE for ambulatory patients with COVID-19 is also not recommended, the authors noted.
Initial treatment of established VTE
Initial treatment of established VTE for up to 10 days of anticoagulation should include low-molecular-weight heparin (LMWH) when creatinine clearance is at least 30 mL/min.
“A regimen of LMWH, taken once per day, is recommended unless a twice-per-day regimen is required because of patients’ characteristics,” the authors noted. These characteristics include a high risk of bleeding, moderate renal failure, and the need for technical intervention, including surgery.
If a twice-a-day regimen is required, only enoxaparin at a dose of 1 mg/kg twice daily can be used, the authors cautioned.
For patients with a low risk of gastrointestinal or genitourinary bleeding, rivaroxaban (Xarelto) or apixaban (Eliquis) can be given in the first 10 days, as well as edoxaban (Lixiana). The latter should be started after at least 5 days of parenteral anticoagulation, provided creatinine clearance is at least 30 mL/min.
“Unfractionated heparin as well as fondaparinux (GlaxoSmithKline) can be also used for the initial treatment of established VTE when LMWH or direct oral anticoagulants are contraindicated,” Dr. Farge and colleagues wrote.
Thrombolysis can be considered on a case-by-case basis, although physicians must pay attention to specific contraindications, especially bleeding risk.
“In the initial treatment of VTE, inferior vena cava filters might be considered when anticoagulant treatment is contraindicated or, in the case of pulmonary embolism, when recurrence occurs under optimal anticoagulation,” the authors noted.
Maintenance VTE treatment
For maintenance therapy, which the authors define as early maintenance for up to 6 months and long-term maintenance beyond 6 months, they point out that LMWHs are preferred over vitamin K antagonists for the treatment of VTE when the creatinine clearance is again at least 30 mL/min.
Any of the direct oral anticoagulants (DOAs) – edoxaban, rivaroxaban, or apixaban – is also recommended for the same patients, provided there is no risk of inducing a strong drug-drug interaction or GI absorption is impaired.
However, the DOAs should be used with caution for patients with GI malignancies, especially upper GI cancers, because data show there is an increased risk of GI bleeding with both edoxaban and rivaroxaban.
“LMWH or direct oral anticoagulants should be used for a minimum of 6 months to treat established VTE in patients with cancer,” the authors wrote.
“After 6 months, termination or continuation of anticoagulation (LMWH, direct oral anticoagulants, or vitamin K antagonists) should be based on individual evaluation of the benefit-risk ratio,” they added.
Treatment of VTE recurrence
The guideline authors explain that three options can be considered in the event of VTE recurrence. These include an increase in the LMWH dose by 20%-25%, or a switch to a DOA, or, if patients are taking a DOA, a switch to an LMWH. If the patient is taking a vitamin K antagonist, it can be switched to either an LMWH or a DOA.
For treatment of catheter-related thrombosis, anticoagulant treatment is recommended for a minimum of 3 months and as long as the central venous catheter is in place. In this setting, the LMWHs are recommended.
The central venous catheter can be kept in place if it is functional, well positioned, and is not infected, provided there is good resolution of symptoms under close surveillance while anticoagulants are being administered.
In surgically treated patients, the LMWH, given once a day, to patients with a serum creatinine concentration of at least 30 mL/min can be used to prevent VTE. Alternatively, VTE can be prevented by the use low-dose unfractionated heparin, given three times a day.
“Pharmacological prophylaxis should be started 2-12 h preoperatively and continued for at least 7–10 days,” Dr. Farge and colleagues advised. In this setting, there is insufficient evidence to support the use of fondaparinux or a DOA as an alternative to an LMWH for the prophylaxis of postoperative VTE. “Use of the highest prophylactic dose of LMWH to prevent postoperative VTE in patients with cancer is recommended,” the authors advised.
Furthermore, extended prophylaxis of at least 4 weeks with LMWH is advised to prevent postoperative VTE after major abdominal or pelvic surgery. Mechanical methods are not recommended except when pharmacologic methods are contraindicated. Inferior vena cava filters are also not recommended for routine prophylaxis.
Patients with reduced mobility
For medically treated hospitalized patients with cancer whose mobility is reduced, the authors recommend prophylaxis with either an LMWH or fondaparinux, provided their creatinine clearance is at least 30 mL/min. These patients can also be treated with unfractionated heparin, they add.
In contrast, DOAs are not recommended – at least not routinely – in this setting, the authors cautioned. Primary pharmacologic prophylaxis of VTE with either LMWH or DOAs – either rivaroxaban or apixaban – is indicated in ambulatory patients with locally advanced or metastatic pancreatic cancer who are receiving systemic anticancer therapy, provided they are at low risk of bleeding.
However, primary pharmacologic prophylaxis with LMWH is not recommended outside of a clinical trial for patients with locally advanced or metastatic lung cancer who are undergoing systemic anticancer therapy, even for patients who are at low risk of bleeding.
For ambulatory patients who are receiving systemic anticancer therapy and who are at intermediate risk of VTE, primary prophylaxis with rivaroxaban or apixaban is recommended for those with myeloma who are receiving immunomodulatory therapy plus steroids or other systemic therapies.
In this setting, oral anticoagulants should consist of a vitamin K antagonist, given at low or therapeutic doses, or apixaban, given at prophylactic doses. Alternatively, LMWH, given at prophylactic doses, or low-dose aspirin, given at a dose of 100 mg/day, can be used.
Catheter-related thrombosis
Use of anticoagulation for routine prophylaxis of catheter-related thrombosis is not recommended. Catheters should be inserted on the right side in the jugular vein, and the distal extremity of the central catheter should be located at the junction of the superior vena cava and the right atrium. “In patients requiring central venous catheters, we suggest the use of implanted ports over peripheral inserted central catheter lines,” the authors noted.
The authors described a number of unique situations regarding the treatment of VTE. These situations include patients with a brain tumor, for whom treatment of established VTE should favor either LMWH or a DOA. The authors also recommended the use of LMWH or unfractionated heparin, started postoperatively, for the prevention of VTE for patients undergoing neurosurgery.
In contrast, pharmacologic prophylaxis of VTE in medically treated patients with a brain tumor who are not undergoing neurosurgery is not recommended. “In the presence of severe renal failure...we suggest using unfractionated heparin followed by early vitamin K antagonists (possibly from day 1) or LMWH adjusted to anti-Xa concentration of the treatment of established VTE,” Dr. Farge and colleagues wrote.
Anticoagulant treatment is also recommended for a minimum of 3 months for children with symptomatic catheter-related thrombosis and as long as the central venous catheter is in place. For children with acute lymphoblastic leukemia who are undergoing induction chemotherapy, LMWH is also recommended as thromboprophylaxis.
For children who require a central venous catheter, the authors suggested that physicians use implanted ports over peripherally inserted central lines.
A version of this article first appeared on Medscape.com.
FROM THE LANCET ONCOLOGY
Mysterious cases of illness with an unusual cause
So begins the search for evidence.
No relations or common journeys
Between March and July 2021, cases of the bacterial infectious disease sprang up in Georgia, Kansas, Minnesota, and Texas, with the disease being fatal for two of those affected. Usually, cases of melioidosis occur in the United States after traveling to regions where the pathogen is prevalent. However, none of the patients had undertaken any previous international travel.
When the genomes of the bacterial strains (Burkholderia pseudomallei) were sequenced, they showed a high level of concordance, suggesting a common source of infection. The bacterial strain is similar to those that are found in Southeast Asia above all. An imported product from there was taken into consideration as the trigger.
The Centers for Disease Control and Prevention examined blood samples from the patients, as well as samples from the soil, water, food, and household items around their homes.
Aroma spray as a trigger
In October, the cause of the melioidosis was finally identified in the house of the patient from Georgia: an aromatherapy spray. The genetic fingerprint of the bacterial strain matched with that from the other patients. The common trigger was thus discovered.
The contaminated spray, with a lavender-chamomile scent for room fragrancing, was sold between February and October in some branches of Walmart, as well as in their online store. The product was therefore recalled and it was checked whether the ingredients were also being used in other products.
The CDC requested physicians to also take melioidosis into account if they were presented with acute bacterial infections that did not respond to normal antibiotics and to inquire whether the affected room spray had been used.
More information about melioidosis
Melioidosis is an infectious disease affecting humans and animals. The trigger is the bacteria B pseudomallei. The disease appears predominantly in tropical regions, especially in Southeast Asia and northern Australia.
Transmission
The bacteria can be found in contaminated water and soil. It is disseminated between humans and animals through direct contact with the infectious source, such as through inhaling dust particles or water droplets, or through consuming contaminated water or food. Human-to-human transmission is extremely rare. Recently however, tropical saltwater fish were identified as potential carriers.
Symptoms
Melioidosis has a wide range of symptoms, which can lead to its being confused with other diseases such as tuberculosis or other forms of pneumonia. There are different forms of the disease, each with different symptoms.
- Localized infection: localized pain and swelling, fever, ulceration, and abscess.
- Pulmonary infection: cough, chest pain, high fever, headaches, and loss of appetite
- Bacteremia: fever, headaches, breathing problems, stomach discomfort, joint pain, and disorientation.
- Disseminated infection: fever, weight loss, stomach or chest pain, muscle or joint pain, headaches, central nervous system infections, and epileptic seizures.
The incubation time is not clearly defined and can be from 1 day to several years; however, the symptoms mostly emerge 2-4 weeks after exposure. The risk factors include diabetes, high alcohol consumption, chronic pulmonary or kidney disease, and immunodeficiencies.
Diagnosis based on the symptoms is often difficult since the clinical picture is similar to other, more common conditions.
Therapy
If the melioidosis is identified as such, it can be treated with only mildly effective antibiotics, since it has a natural resistance to many commonly used antibiotics. The type of infection and the course of treatment also affects the long-term outcome. Without treatment, 90% of the infections have a fatal outcome. With appropriate treatment, the mortality rate still lies at 40%.
Therapy generally begins with intravenous antibiotic therapy for at least 2-8 weeks (ceftazidime or meropenem). Oral antibiotic therapy then follows for 3-6 months (trimethoprim-sulfamethoxazole or amoxicillin/clavulanic acid). If the patient is allergic to penicillin, alternative antibiotics can be used.
Use as a bioweapon
The CDC classifies B. pseudomallei as a potential pathogen for biological attack (class-B candidate). The agency lists the potential reasons for use as a bioweapon as:
- The pathogen can be found naturally in certain regions.
- The triggered disease can take a serious course and ultimately be fatal without appropriate therapy.
- In the past, the United States has used similar pathogens in wars as bioweapons.
In a potential attack, the pathogen could be spread through air, water, or food, and by doing so, many people would be exposed. Any contact with the bacteria can result in melioidosis. As the bacteria cannot be seen, smelled, or tasted, the biological attack would not be recognized for some time. A certain amount of time can also pass until the pathogen is identified, once fever and respiratory diseases have developed.
In such an emergency, the CDC would collaborate with other federal and local authorities to supply specialized testing laboratories and provide the public with information.
This content was translated from Coliquio. A version appeared on Medscape.com.
So begins the search for evidence.
No relations or common journeys
Between March and July 2021, cases of the bacterial infectious disease sprang up in Georgia, Kansas, Minnesota, and Texas, with the disease being fatal for two of those affected. Usually, cases of melioidosis occur in the United States after traveling to regions where the pathogen is prevalent. However, none of the patients had undertaken any previous international travel.
When the genomes of the bacterial strains (Burkholderia pseudomallei) were sequenced, they showed a high level of concordance, suggesting a common source of infection. The bacterial strain is similar to those that are found in Southeast Asia above all. An imported product from there was taken into consideration as the trigger.
The Centers for Disease Control and Prevention examined blood samples from the patients, as well as samples from the soil, water, food, and household items around their homes.
Aroma spray as a trigger
In October, the cause of the melioidosis was finally identified in the house of the patient from Georgia: an aromatherapy spray. The genetic fingerprint of the bacterial strain matched with that from the other patients. The common trigger was thus discovered.
The contaminated spray, with a lavender-chamomile scent for room fragrancing, was sold between February and October in some branches of Walmart, as well as in their online store. The product was therefore recalled and it was checked whether the ingredients were also being used in other products.
The CDC requested physicians to also take melioidosis into account if they were presented with acute bacterial infections that did not respond to normal antibiotics and to inquire whether the affected room spray had been used.
More information about melioidosis
Melioidosis is an infectious disease affecting humans and animals. The trigger is the bacteria B pseudomallei. The disease appears predominantly in tropical regions, especially in Southeast Asia and northern Australia.
Transmission
The bacteria can be found in contaminated water and soil. It is disseminated between humans and animals through direct contact with the infectious source, such as through inhaling dust particles or water droplets, or through consuming contaminated water or food. Human-to-human transmission is extremely rare. Recently however, tropical saltwater fish were identified as potential carriers.
Symptoms
Melioidosis has a wide range of symptoms, which can lead to its being confused with other diseases such as tuberculosis or other forms of pneumonia. There are different forms of the disease, each with different symptoms.
- Localized infection: localized pain and swelling, fever, ulceration, and abscess.
- Pulmonary infection: cough, chest pain, high fever, headaches, and loss of appetite
- Bacteremia: fever, headaches, breathing problems, stomach discomfort, joint pain, and disorientation.
- Disseminated infection: fever, weight loss, stomach or chest pain, muscle or joint pain, headaches, central nervous system infections, and epileptic seizures.
The incubation time is not clearly defined and can be from 1 day to several years; however, the symptoms mostly emerge 2-4 weeks after exposure. The risk factors include diabetes, high alcohol consumption, chronic pulmonary or kidney disease, and immunodeficiencies.
Diagnosis based on the symptoms is often difficult since the clinical picture is similar to other, more common conditions.
Therapy
If the melioidosis is identified as such, it can be treated with only mildly effective antibiotics, since it has a natural resistance to many commonly used antibiotics. The type of infection and the course of treatment also affects the long-term outcome. Without treatment, 90% of the infections have a fatal outcome. With appropriate treatment, the mortality rate still lies at 40%.
Therapy generally begins with intravenous antibiotic therapy for at least 2-8 weeks (ceftazidime or meropenem). Oral antibiotic therapy then follows for 3-6 months (trimethoprim-sulfamethoxazole or amoxicillin/clavulanic acid). If the patient is allergic to penicillin, alternative antibiotics can be used.
Use as a bioweapon
The CDC classifies B. pseudomallei as a potential pathogen for biological attack (class-B candidate). The agency lists the potential reasons for use as a bioweapon as:
- The pathogen can be found naturally in certain regions.
- The triggered disease can take a serious course and ultimately be fatal without appropriate therapy.
- In the past, the United States has used similar pathogens in wars as bioweapons.
In a potential attack, the pathogen could be spread through air, water, or food, and by doing so, many people would be exposed. Any contact with the bacteria can result in melioidosis. As the bacteria cannot be seen, smelled, or tasted, the biological attack would not be recognized for some time. A certain amount of time can also pass until the pathogen is identified, once fever and respiratory diseases have developed.
In such an emergency, the CDC would collaborate with other federal and local authorities to supply specialized testing laboratories and provide the public with information.
This content was translated from Coliquio. A version appeared on Medscape.com.
So begins the search for evidence.
No relations or common journeys
Between March and July 2021, cases of the bacterial infectious disease sprang up in Georgia, Kansas, Minnesota, and Texas, with the disease being fatal for two of those affected. Usually, cases of melioidosis occur in the United States after traveling to regions where the pathogen is prevalent. However, none of the patients had undertaken any previous international travel.
When the genomes of the bacterial strains (Burkholderia pseudomallei) were sequenced, they showed a high level of concordance, suggesting a common source of infection. The bacterial strain is similar to those that are found in Southeast Asia above all. An imported product from there was taken into consideration as the trigger.
The Centers for Disease Control and Prevention examined blood samples from the patients, as well as samples from the soil, water, food, and household items around their homes.
Aroma spray as a trigger
In October, the cause of the melioidosis was finally identified in the house of the patient from Georgia: an aromatherapy spray. The genetic fingerprint of the bacterial strain matched with that from the other patients. The common trigger was thus discovered.
The contaminated spray, with a lavender-chamomile scent for room fragrancing, was sold between February and October in some branches of Walmart, as well as in their online store. The product was therefore recalled and it was checked whether the ingredients were also being used in other products.
The CDC requested physicians to also take melioidosis into account if they were presented with acute bacterial infections that did not respond to normal antibiotics and to inquire whether the affected room spray had been used.
More information about melioidosis
Melioidosis is an infectious disease affecting humans and animals. The trigger is the bacteria B pseudomallei. The disease appears predominantly in tropical regions, especially in Southeast Asia and northern Australia.
Transmission
The bacteria can be found in contaminated water and soil. It is disseminated between humans and animals through direct contact with the infectious source, such as through inhaling dust particles or water droplets, or through consuming contaminated water or food. Human-to-human transmission is extremely rare. Recently however, tropical saltwater fish were identified as potential carriers.
Symptoms
Melioidosis has a wide range of symptoms, which can lead to its being confused with other diseases such as tuberculosis or other forms of pneumonia. There are different forms of the disease, each with different symptoms.
- Localized infection: localized pain and swelling, fever, ulceration, and abscess.
- Pulmonary infection: cough, chest pain, high fever, headaches, and loss of appetite
- Bacteremia: fever, headaches, breathing problems, stomach discomfort, joint pain, and disorientation.
- Disseminated infection: fever, weight loss, stomach or chest pain, muscle or joint pain, headaches, central nervous system infections, and epileptic seizures.
The incubation time is not clearly defined and can be from 1 day to several years; however, the symptoms mostly emerge 2-4 weeks after exposure. The risk factors include diabetes, high alcohol consumption, chronic pulmonary or kidney disease, and immunodeficiencies.
Diagnosis based on the symptoms is often difficult since the clinical picture is similar to other, more common conditions.
Therapy
If the melioidosis is identified as such, it can be treated with only mildly effective antibiotics, since it has a natural resistance to many commonly used antibiotics. The type of infection and the course of treatment also affects the long-term outcome. Without treatment, 90% of the infections have a fatal outcome. With appropriate treatment, the mortality rate still lies at 40%.
Therapy generally begins with intravenous antibiotic therapy for at least 2-8 weeks (ceftazidime or meropenem). Oral antibiotic therapy then follows for 3-6 months (trimethoprim-sulfamethoxazole or amoxicillin/clavulanic acid). If the patient is allergic to penicillin, alternative antibiotics can be used.
Use as a bioweapon
The CDC classifies B. pseudomallei as a potential pathogen for biological attack (class-B candidate). The agency lists the potential reasons for use as a bioweapon as:
- The pathogen can be found naturally in certain regions.
- The triggered disease can take a serious course and ultimately be fatal without appropriate therapy.
- In the past, the United States has used similar pathogens in wars as bioweapons.
In a potential attack, the pathogen could be spread through air, water, or food, and by doing so, many people would be exposed. Any contact with the bacteria can result in melioidosis. As the bacteria cannot be seen, smelled, or tasted, the biological attack would not be recognized for some time. A certain amount of time can also pass until the pathogen is identified, once fever and respiratory diseases have developed.
In such an emergency, the CDC would collaborate with other federal and local authorities to supply specialized testing laboratories and provide the public with information.
This content was translated from Coliquio. A version appeared on Medscape.com.
How well do vaccines protect against long COVID?
New York City veterinarian Erin Kulick used to be a weekend warrior. Only 2½ years ago, the 38-year-old new mother played ultimate Frisbee and flag football with friends. She went for regular 30-minute runs to burn off stress.
Now, Dr. Kulick is usually so exhausted, she can’t walk nonstop for 15 minutes. She recently tried to take her 4-year-old son, Cooper, to the American Museum of Natural History for his first visit, but ended up on a bench outside the museum, sobbing in the rain, because she couldn’t even get through the first hurdle of standing in line. “I just wanted to be there with my kid,” she said.
Dr. Kulick got sick with COVID-19 at the start of the pandemic in March 2020, 9 months before the first vaccine would be approved. Now she is among the estimated one in five infected Americans, or 19%, whose symptoms developed into long COVID.
Dr. Kulick also is now vaccinated and boosted. Had a vaccine been available sooner, could it have protected her from long COVID?
Evidence is starting to show it’s likely.
“The best way not to have long COVID is not to have COVID at all,” said Leora Horwitz, MD, a professor of population health and medicine at New York University. “To the extent that vaccination can prevent you from getting COVID at all, then it helps to reduce long COVID.”
And People with more serious initial illness appear more likely to have prolonged symptoms, but those with milder disease can certainly get it, too.
“You’re more likely to have long COVID with more severe disease, and we have ample evidence that vaccination reduces the severity of disease,” Dr. Horwitz said. “We also now have quite a lot of evidence that vaccination does reduce your risk of long COVID – probably because it reduces your risk of severe disease.”
There is little consensus about how much vaccines can lower the risk of long-term COVID symptoms, but several studies suggest that number lies anywhere from 15% to more than 80%.
That might seem like a big variation, but infectious disease experts argue that trying to interpret the gap isn’t as important as noticing what’s consistent across all these studies: “Vaccines do offer some protection, but it’s incomplete,” said Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs St. Louis Health Care System. Dr. Al-Aly, who has led several large studies on long COVID, said focusing on the fact that vaccines do offer some protection is a much better public health message than looking at the different levels of risk.
“Vaccines do a miraculous job for what they were designed to do,” said Dr. Al-Aly. “Vaccines were designed to reduce the risk of hospitalization ... and for that, vaccines are still holding up, even with all the changes in the virus.”
Still, Elena Azzolini, MD, PhD, head of the Humanitas Research Hospital’s vaccination center in Milan, thinks some studies may have underestimated the level of long COVID protection from vaccines because of limits in the study methods, such as not including enough women, who are more affected by long COVID. Her recent study, which looked at 2,560 health care professionals working in nine Italian centers from March 2020 to April 2022, focused on the risk for healthy women and men in their 20s to their 70s.
In the paper, Dr. Azzolini and associates reported that two or three doses of vaccine reduced the risk of hospitalization from COVID-19 from 42% among those who are unvaccinated to 16%-17%. In other words, they found unvaccinated people in the study were nearly three times as likely to have serious symptoms for longer than 4 weeks.
But Dr. Azzolini and Dr. Al-Aly still say that, even for the vaccinated, as long as COVID is around, masks are necessary. That’s because current vaccines don’t do enough to reduce transmission, said Dr. Al-Aly. “The only way that can really help [stop] transmission is covering our nose and mouth with a mask.”
How vaccinations affect people who already have long COVID
Some long COVID patients have said they got better after they get boosted, while some say they’re getting worse, said Dr. Horwitz, who is also a lead investigator at the National Institutes of Health’s flagship RECOVER program, a 4-year research project to study long COVID across the United States. (The NIH is still recruiting volunteers for these studies, which are also open to people who have never had COVID.)
One study published in the British Medical Journal analyzed survey data of more than 28,000 people infected with COVID in the United Kingdom and found a 13% reduction in long-term symptoms after a first dose of the vaccine, although it was unclear from the data if the improvement was sustained.
A second dose was associated with another 8% improvement over a 2-month period. “It’s reassuring that we see an average modest improvement in symptoms, not an average worsening in symptoms,” said Daniel Ayoubkhani, principal statistician at the U.K. Office for National Statistics and lead author of the study. Of course, the experience will differ among different people.
“It doesn’t appear that vaccination is the silver bullet that’s going to eradicate long COVID,” he said, but evidence from multiple studies suggests vaccines may help people with long-term symptoms.
Akiko Iwasaki, PhD, an immunobiologist at Yale University, New Haven, Conn., told a White House summit in July that one of the best ways to prevent long COVID is to develop the next generation of vaccines that also prevent milder cases by blocking transmission in the first place.
Back in New York, Dr. Kulick is now triple vaccinated. She’s due for a fourth dose soon but admits she’s “terrified every time” that she’s going to get sicker.
In her Facebook support group for long COVID, she reads that most people with prolonged symptoms handle it well. She has also noticed some of her symptoms eased after her first two doses of vaccine.
Since being diagnosed, Dr. Kulick learned she has a genetic condition, Ehlers-Danlos syndrome, which affects connective tissues that support skin, joints, organs, and blood vessels, and which her doctors say may have made her more prone to long COVID. She’s also being screened for autoimmune diseases, but for now, the only relief she has found has come from long COVID physical therapy, changes to her diet, and integrative medicine.
Dr. Kulick is still trying to figure out how she can get better while keeping her long hours at her veterinary job – and her health benefits. She is thankful her husband is a devoted caregiver to their son and a professional jazz musician with a schedule that allows for some flexibility.
“But it’s really hard when every week feels like I’ve run a marathon,” she said. “I can barely make it through.”
A version of this article first appeared on WebMD.com.
New York City veterinarian Erin Kulick used to be a weekend warrior. Only 2½ years ago, the 38-year-old new mother played ultimate Frisbee and flag football with friends. She went for regular 30-minute runs to burn off stress.
Now, Dr. Kulick is usually so exhausted, she can’t walk nonstop for 15 minutes. She recently tried to take her 4-year-old son, Cooper, to the American Museum of Natural History for his first visit, but ended up on a bench outside the museum, sobbing in the rain, because she couldn’t even get through the first hurdle of standing in line. “I just wanted to be there with my kid,” she said.
Dr. Kulick got sick with COVID-19 at the start of the pandemic in March 2020, 9 months before the first vaccine would be approved. Now she is among the estimated one in five infected Americans, or 19%, whose symptoms developed into long COVID.
Dr. Kulick also is now vaccinated and boosted. Had a vaccine been available sooner, could it have protected her from long COVID?
Evidence is starting to show it’s likely.
“The best way not to have long COVID is not to have COVID at all,” said Leora Horwitz, MD, a professor of population health and medicine at New York University. “To the extent that vaccination can prevent you from getting COVID at all, then it helps to reduce long COVID.”
And People with more serious initial illness appear more likely to have prolonged symptoms, but those with milder disease can certainly get it, too.
“You’re more likely to have long COVID with more severe disease, and we have ample evidence that vaccination reduces the severity of disease,” Dr. Horwitz said. “We also now have quite a lot of evidence that vaccination does reduce your risk of long COVID – probably because it reduces your risk of severe disease.”
There is little consensus about how much vaccines can lower the risk of long-term COVID symptoms, but several studies suggest that number lies anywhere from 15% to more than 80%.
That might seem like a big variation, but infectious disease experts argue that trying to interpret the gap isn’t as important as noticing what’s consistent across all these studies: “Vaccines do offer some protection, but it’s incomplete,” said Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs St. Louis Health Care System. Dr. Al-Aly, who has led several large studies on long COVID, said focusing on the fact that vaccines do offer some protection is a much better public health message than looking at the different levels of risk.
“Vaccines do a miraculous job for what they were designed to do,” said Dr. Al-Aly. “Vaccines were designed to reduce the risk of hospitalization ... and for that, vaccines are still holding up, even with all the changes in the virus.”
Still, Elena Azzolini, MD, PhD, head of the Humanitas Research Hospital’s vaccination center in Milan, thinks some studies may have underestimated the level of long COVID protection from vaccines because of limits in the study methods, such as not including enough women, who are more affected by long COVID. Her recent study, which looked at 2,560 health care professionals working in nine Italian centers from March 2020 to April 2022, focused on the risk for healthy women and men in their 20s to their 70s.
In the paper, Dr. Azzolini and associates reported that two or three doses of vaccine reduced the risk of hospitalization from COVID-19 from 42% among those who are unvaccinated to 16%-17%. In other words, they found unvaccinated people in the study were nearly three times as likely to have serious symptoms for longer than 4 weeks.
But Dr. Azzolini and Dr. Al-Aly still say that, even for the vaccinated, as long as COVID is around, masks are necessary. That’s because current vaccines don’t do enough to reduce transmission, said Dr. Al-Aly. “The only way that can really help [stop] transmission is covering our nose and mouth with a mask.”
How vaccinations affect people who already have long COVID
Some long COVID patients have said they got better after they get boosted, while some say they’re getting worse, said Dr. Horwitz, who is also a lead investigator at the National Institutes of Health’s flagship RECOVER program, a 4-year research project to study long COVID across the United States. (The NIH is still recruiting volunteers for these studies, which are also open to people who have never had COVID.)
One study published in the British Medical Journal analyzed survey data of more than 28,000 people infected with COVID in the United Kingdom and found a 13% reduction in long-term symptoms after a first dose of the vaccine, although it was unclear from the data if the improvement was sustained.
A second dose was associated with another 8% improvement over a 2-month period. “It’s reassuring that we see an average modest improvement in symptoms, not an average worsening in symptoms,” said Daniel Ayoubkhani, principal statistician at the U.K. Office for National Statistics and lead author of the study. Of course, the experience will differ among different people.
“It doesn’t appear that vaccination is the silver bullet that’s going to eradicate long COVID,” he said, but evidence from multiple studies suggests vaccines may help people with long-term symptoms.
Akiko Iwasaki, PhD, an immunobiologist at Yale University, New Haven, Conn., told a White House summit in July that one of the best ways to prevent long COVID is to develop the next generation of vaccines that also prevent milder cases by blocking transmission in the first place.
Back in New York, Dr. Kulick is now triple vaccinated. She’s due for a fourth dose soon but admits she’s “terrified every time” that she’s going to get sicker.
In her Facebook support group for long COVID, she reads that most people with prolonged symptoms handle it well. She has also noticed some of her symptoms eased after her first two doses of vaccine.
Since being diagnosed, Dr. Kulick learned she has a genetic condition, Ehlers-Danlos syndrome, which affects connective tissues that support skin, joints, organs, and blood vessels, and which her doctors say may have made her more prone to long COVID. She’s also being screened for autoimmune diseases, but for now, the only relief she has found has come from long COVID physical therapy, changes to her diet, and integrative medicine.
Dr. Kulick is still trying to figure out how she can get better while keeping her long hours at her veterinary job – and her health benefits. She is thankful her husband is a devoted caregiver to their son and a professional jazz musician with a schedule that allows for some flexibility.
“But it’s really hard when every week feels like I’ve run a marathon,” she said. “I can barely make it through.”
A version of this article first appeared on WebMD.com.
New York City veterinarian Erin Kulick used to be a weekend warrior. Only 2½ years ago, the 38-year-old new mother played ultimate Frisbee and flag football with friends. She went for regular 30-minute runs to burn off stress.
Now, Dr. Kulick is usually so exhausted, she can’t walk nonstop for 15 minutes. She recently tried to take her 4-year-old son, Cooper, to the American Museum of Natural History for his first visit, but ended up on a bench outside the museum, sobbing in the rain, because she couldn’t even get through the first hurdle of standing in line. “I just wanted to be there with my kid,” she said.
Dr. Kulick got sick with COVID-19 at the start of the pandemic in March 2020, 9 months before the first vaccine would be approved. Now she is among the estimated one in five infected Americans, or 19%, whose symptoms developed into long COVID.
Dr. Kulick also is now vaccinated and boosted. Had a vaccine been available sooner, could it have protected her from long COVID?
Evidence is starting to show it’s likely.
“The best way not to have long COVID is not to have COVID at all,” said Leora Horwitz, MD, a professor of population health and medicine at New York University. “To the extent that vaccination can prevent you from getting COVID at all, then it helps to reduce long COVID.”
And People with more serious initial illness appear more likely to have prolonged symptoms, but those with milder disease can certainly get it, too.
“You’re more likely to have long COVID with more severe disease, and we have ample evidence that vaccination reduces the severity of disease,” Dr. Horwitz said. “We also now have quite a lot of evidence that vaccination does reduce your risk of long COVID – probably because it reduces your risk of severe disease.”
There is little consensus about how much vaccines can lower the risk of long-term COVID symptoms, but several studies suggest that number lies anywhere from 15% to more than 80%.
That might seem like a big variation, but infectious disease experts argue that trying to interpret the gap isn’t as important as noticing what’s consistent across all these studies: “Vaccines do offer some protection, but it’s incomplete,” said Ziyad Al-Aly, MD, chief of research and development at the Veterans Affairs St. Louis Health Care System. Dr. Al-Aly, who has led several large studies on long COVID, said focusing on the fact that vaccines do offer some protection is a much better public health message than looking at the different levels of risk.
“Vaccines do a miraculous job for what they were designed to do,” said Dr. Al-Aly. “Vaccines were designed to reduce the risk of hospitalization ... and for that, vaccines are still holding up, even with all the changes in the virus.”
Still, Elena Azzolini, MD, PhD, head of the Humanitas Research Hospital’s vaccination center in Milan, thinks some studies may have underestimated the level of long COVID protection from vaccines because of limits in the study methods, such as not including enough women, who are more affected by long COVID. Her recent study, which looked at 2,560 health care professionals working in nine Italian centers from March 2020 to April 2022, focused on the risk for healthy women and men in their 20s to their 70s.
In the paper, Dr. Azzolini and associates reported that two or three doses of vaccine reduced the risk of hospitalization from COVID-19 from 42% among those who are unvaccinated to 16%-17%. In other words, they found unvaccinated people in the study were nearly three times as likely to have serious symptoms for longer than 4 weeks.
But Dr. Azzolini and Dr. Al-Aly still say that, even for the vaccinated, as long as COVID is around, masks are necessary. That’s because current vaccines don’t do enough to reduce transmission, said Dr. Al-Aly. “The only way that can really help [stop] transmission is covering our nose and mouth with a mask.”
How vaccinations affect people who already have long COVID
Some long COVID patients have said they got better after they get boosted, while some say they’re getting worse, said Dr. Horwitz, who is also a lead investigator at the National Institutes of Health’s flagship RECOVER program, a 4-year research project to study long COVID across the United States. (The NIH is still recruiting volunteers for these studies, which are also open to people who have never had COVID.)
One study published in the British Medical Journal analyzed survey data of more than 28,000 people infected with COVID in the United Kingdom and found a 13% reduction in long-term symptoms after a first dose of the vaccine, although it was unclear from the data if the improvement was sustained.
A second dose was associated with another 8% improvement over a 2-month period. “It’s reassuring that we see an average modest improvement in symptoms, not an average worsening in symptoms,” said Daniel Ayoubkhani, principal statistician at the U.K. Office for National Statistics and lead author of the study. Of course, the experience will differ among different people.
“It doesn’t appear that vaccination is the silver bullet that’s going to eradicate long COVID,” he said, but evidence from multiple studies suggests vaccines may help people with long-term symptoms.
Akiko Iwasaki, PhD, an immunobiologist at Yale University, New Haven, Conn., told a White House summit in July that one of the best ways to prevent long COVID is to develop the next generation of vaccines that also prevent milder cases by blocking transmission in the first place.
Back in New York, Dr. Kulick is now triple vaccinated. She’s due for a fourth dose soon but admits she’s “terrified every time” that she’s going to get sicker.
In her Facebook support group for long COVID, she reads that most people with prolonged symptoms handle it well. She has also noticed some of her symptoms eased after her first two doses of vaccine.
Since being diagnosed, Dr. Kulick learned she has a genetic condition, Ehlers-Danlos syndrome, which affects connective tissues that support skin, joints, organs, and blood vessels, and which her doctors say may have made her more prone to long COVID. She’s also being screened for autoimmune diseases, but for now, the only relief she has found has come from long COVID physical therapy, changes to her diet, and integrative medicine.
Dr. Kulick is still trying to figure out how she can get better while keeping her long hours at her veterinary job – and her health benefits. She is thankful her husband is a devoted caregiver to their son and a professional jazz musician with a schedule that allows for some flexibility.
“But it’s really hard when every week feels like I’ve run a marathon,” she said. “I can barely make it through.”
A version of this article first appeared on WebMD.com.
ACR makes changes to adult, pediatric vaccinations guidance
Patients with rheumatic and musculoskeletal diseases may need additional vaccines or different versions of vaccines they were not previously recommended to receive, according to updated guidelines from the American College of Rheumatology (ACR) on vaccinations for these patients. The new guidelines pertain to routine vaccinations for adults and children and are based on the most current evidence. They include recommendations on whether to hold certain medications before or after vaccination. They do not include recommendations regarding COVID-19 vaccines.
For guidance on COVID-19 vaccine timing and frequency, the ACR directs physicians to the CDC’s recommendations for people with mild or severe immunosuppression and the ACR’s previous clinical guidance summary on the topic, last revised in February 2022. The recommendations in the new guidance differ from ACR’s guidance on COVID-19 vaccines on whether and when to hold immunosuppressive medications when patients receive nonlive vaccines. The new guidelines now align more closely with those of EULAR, the Infectious Diseases Society of America, and the CDC’s recommendations for human papillomavirus (HPV), pneumococcal, and shingles vaccines.
Vaccinations in this population are particularly important because “a leading cause of morbidity and mortality in those with rheumatic diseases is infections, due to the detrimental impact immunosuppression has on the ability for the patient to properly clear the pathogen,” Alfred Kim, MD, PhD, professor of rheumatology at Washington University, St. Louis, told this news organization. While immunosuppressive medications are the most common reason patients with these conditions may have impaired immune function, “some of our patients with autoimmune disease also have a preexisting immunodeficiency that can inherently blunt immune responses to either infection or vaccination,” Dr. Kim explained.
“The authors of the guidelines have done a really nice job of making distinct recommendations based on the mechanism of action of various immunosuppressive medications,” Dr. Kim said. “This helps simplify the process of deciding the timing of vaccination for the health provider, especially for those on multiple immunosuppressives who represent an important proportion of our patients with rheumatic diseases.”
The main change to the guidelines for children, aside from those related to flu vaccination, is in regard to rotavirus vaccination for infants exposed to tumor necrosis factor (TNF) inhibitors or rituximab in utero. Infants prenatally exposed to rituximab should not receive the rotavirus vaccine until they are older than 6 months. Those exposed prenatally to TNF inhibitors should receive the rotavirus vaccine on time, according to the CDC schedule for all infants.

The new rotavirus recommendations follow data showing that immune responses to rotavirus are blunted in those with infliximab exposure, according to Dr. Kim.
“Thus, this poses a serious theoretical risk in newborns with mothers on [a TNF inhibitor] of ineffective clearance of rotavirus infections,” Dr. Kim said in an interview. “While rotavirus infections are quite common with typically self-limiting disease, sometimes requiring hydration to counteract diarrhea-induced dehydration, this can become severe in these newborns that have [a TNF inhibitor] in their system.”
For adults, the ACR issued the following expanded indications for four vaccines for patients currently taking immunosuppressive medication:
- Patients aged 18 and older should receive the recombinant zoster vaccine against shingles.
- For patients aged 27-44 who weren’t previously vaccinated against HPV, the HPV vaccine is “conditionally recommended.”
- Patients younger than 65 should receive the pneumococcal vaccine.
- Patients aged 19-64 are conditionally recommended to receive the high-dose or adjuvanted flu vaccine rather than the regular-dose flu vaccine.
The guidelines also conditionally recommend that all patients aged 65 and older who have rheumatic or musculoskeletal diseases receive the high-dose or adjuvanted flu vaccine, regardless of whether they are taking immunosuppressive medication. Another new conditional recommendation is to give multiple vaccinations to patients on the same day, rather than give individual vaccines on different days.
The guidelines make conditional recommendations regarding flu and nonlive attenuated vaccines for those taking methotrexate, rituximab, or glucocorticoids. Methotrexate should be held for 2 weeks after flu vaccination as long as disease activity allows it, but patients who are taking methotrexate should continue taking it for any other nonlive attenuated vaccinations.
“Non-rheumatology providers, such as general pediatricians and internists, are encouraged to give the influenza vaccination and then consult with the patient’s rheumatology provider about holding methotrexate to avoid a missed vaccination opportunity,” the guidelines state.
Patients taking rituximab should receive the flu vaccine on schedule and continue taking rituximab. However, for these patients, the guidelines recommend to “delay any subsequent rituximab dosing for at least two weeks after influenza vaccination if disease activity allows.”
“Because of the relatively short time period between the rollout of the influenza vaccine and its season, we can’t always wait to time the B-cell depletion dosage,” Dr. Kim said. “Also, it is not always easy to synchronize the patient’s B-cell depletion dosing schedule to the influenza vaccine rollout. Thus, we now just recommend getting the influenza vaccine regardless of the patient’s last B-cell depletion dosage despite its known strong attenuation of optimal immune responses.”
For other nonlive attenuated vaccines, providers should time vaccination for when the next rituximab dose is due and then hold the drug for at least 2 weeks thereafter, providing time for the B cells to mount a response before rituximab depletes B cells again.
Patients taking less than 20 mg of prednisone daily should still receive the flu vaccine and other nonlive attenuated vaccines. Those taking 20 mg or more of prednisone each day should still receive the flu vaccine, but other vaccines should be deferred until their dose of glucocorticoids has been tapered down to less than 20 mg daily.
Patients taking all other immunosuppressive medications should continue taking them for the flu vaccine and other nonlive attenuated vaccinations, but it is conditionally recommended that live attenuated vaccines be deferred. For any patient with a rheumatic and musculoskeletal disease, regardless of disease activity, it is conditionally recommended that all routine nonlive attenuated vaccines be administered.
For live attenuated virus vaccines, the ACR provides a chart on which immunosuppressive medications to hold and for how long. Glucocorticoids, methotrexate, azathioprine, leflunomide, mycophenolate mofetil, calcineurin inhibitors, and oral cyclophosphamide should all be held 4 weeks before and 4 weeks after administration of a live attenuated vaccine. For those taking JAK inhibitors, the medication should be halted 1 week before administration of a live vaccine and should continue to be withheld for 4 weeks after.
For most other biologics, the ACR recommends holding the medication for one dosing interval before the live vaccine and 4 weeks thereafter. The main exception is rituximab, which should be held for 6 months before a live vaccine and then for 4 more weeks thereafter.
For patients receiving intravenous immunoglobulin, the drug should be held for 8-11 months before they are administered a live attenuated vaccine, depending on the dosage, and then 4 weeks after vaccination, regardless of dosage.
To reassure people with rheumatic disease who may have anxiety or concerns about receiving immunizations, whether taking immunosuppressive medication or not, Dr. Kim said it’s important to provide lots of education to patients.
“Fear and emotion have replaced facts, and data as a leading factor in decision-making, as seen with COVID-19,” Dr. Kim said. “The reality is that a small minority of people will have any issues with most vaccines, which include disease flares, adverse events, or acquisition of an autoimmune disease. We are not saying there is zero risk, rather, that the risk is quite small. This is where shared decision-making between the health care provider and the patient must be done effectively to enable the patient to properly weigh risk versus benefit.”
Dr. Kim has relationships with GlaxoSmithKline, Aurinia Pharmaceuticals, Kypha, Pfizer, Alexion Pharmaceuticals, AstraZeneca, Exagen Diagnostics, and Foghorn Therapeutics.
A version of this article first appeared on Medscape.com.
Patients with rheumatic and musculoskeletal diseases may need additional vaccines or different versions of vaccines they were not previously recommended to receive, according to updated guidelines from the American College of Rheumatology (ACR) on vaccinations for these patients. The new guidelines pertain to routine vaccinations for adults and children and are based on the most current evidence. They include recommendations on whether to hold certain medications before or after vaccination. They do not include recommendations regarding COVID-19 vaccines.
For guidance on COVID-19 vaccine timing and frequency, the ACR directs physicians to the CDC’s recommendations for people with mild or severe immunosuppression and the ACR’s previous clinical guidance summary on the topic, last revised in February 2022. The recommendations in the new guidance differ from ACR’s guidance on COVID-19 vaccines on whether and when to hold immunosuppressive medications when patients receive nonlive vaccines. The new guidelines now align more closely with those of EULAR, the Infectious Diseases Society of America, and the CDC’s recommendations for human papillomavirus (HPV), pneumococcal, and shingles vaccines.
Vaccinations in this population are particularly important because “a leading cause of morbidity and mortality in those with rheumatic diseases is infections, due to the detrimental impact immunosuppression has on the ability for the patient to properly clear the pathogen,” Alfred Kim, MD, PhD, professor of rheumatology at Washington University, St. Louis, told this news organization. While immunosuppressive medications are the most common reason patients with these conditions may have impaired immune function, “some of our patients with autoimmune disease also have a preexisting immunodeficiency that can inherently blunt immune responses to either infection or vaccination,” Dr. Kim explained.
“The authors of the guidelines have done a really nice job of making distinct recommendations based on the mechanism of action of various immunosuppressive medications,” Dr. Kim said. “This helps simplify the process of deciding the timing of vaccination for the health provider, especially for those on multiple immunosuppressives who represent an important proportion of our patients with rheumatic diseases.”
The main change to the guidelines for children, aside from those related to flu vaccination, is in regard to rotavirus vaccination for infants exposed to tumor necrosis factor (TNF) inhibitors or rituximab in utero. Infants prenatally exposed to rituximab should not receive the rotavirus vaccine until they are older than 6 months. Those exposed prenatally to TNF inhibitors should receive the rotavirus vaccine on time, according to the CDC schedule for all infants.
The new rotavirus recommendations follow data showing that immune responses to rotavirus are blunted in those with infliximab exposure, according to Dr. Kim.
“Thus, this poses a serious theoretical risk in newborns with mothers on [a TNF inhibitor] of ineffective clearance of rotavirus infections,” Dr. Kim said in an interview. “While rotavirus infections are quite common with typically self-limiting disease, sometimes requiring hydration to counteract diarrhea-induced dehydration, this can become severe in these newborns that have [a TNF inhibitor] in their system.”
For adults, the ACR issued the following expanded indications for four vaccines for patients currently taking immunosuppressive medication:
- Patients aged 18 and older should receive the recombinant zoster vaccine against shingles.
- For patients aged 27-44 who weren’t previously vaccinated against HPV, the HPV vaccine is “conditionally recommended.”
- Patients younger than 65 should receive the pneumococcal vaccine.
- Patients aged 19-64 are conditionally recommended to receive the high-dose or adjuvanted flu vaccine rather than the regular-dose flu vaccine.
The guidelines also conditionally recommend that all patients aged 65 and older who have rheumatic or musculoskeletal diseases receive the high-dose or adjuvanted flu vaccine, regardless of whether they are taking immunosuppressive medication. Another new conditional recommendation is to give multiple vaccinations to patients on the same day, rather than give individual vaccines on different days.
The guidelines make conditional recommendations regarding flu and nonlive attenuated vaccines for those taking methotrexate, rituximab, or glucocorticoids. Methotrexate should be held for 2 weeks after flu vaccination as long as disease activity allows it, but patients who are taking methotrexate should continue taking it for any other nonlive attenuated vaccinations.
“Non-rheumatology providers, such as general pediatricians and internists, are encouraged to give the influenza vaccination and then consult with the patient’s rheumatology provider about holding methotrexate to avoid a missed vaccination opportunity,” the guidelines state.
Patients taking rituximab should receive the flu vaccine on schedule and continue taking rituximab. However, for these patients, the guidelines recommend to “delay any subsequent rituximab dosing for at least two weeks after influenza vaccination if disease activity allows.”
“Because of the relatively short time period between the rollout of the influenza vaccine and its season, we can’t always wait to time the B-cell depletion dosage,” Dr. Kim said. “Also, it is not always easy to synchronize the patient’s B-cell depletion dosing schedule to the influenza vaccine rollout. Thus, we now just recommend getting the influenza vaccine regardless of the patient’s last B-cell depletion dosage despite its known strong attenuation of optimal immune responses.”
For other nonlive attenuated vaccines, providers should time vaccination for when the next rituximab dose is due and then hold the drug for at least 2 weeks thereafter, providing time for the B cells to mount a response before rituximab depletes B cells again.
Patients taking less than 20 mg of prednisone daily should still receive the flu vaccine and other nonlive attenuated vaccines. Those taking 20 mg or more of prednisone each day should still receive the flu vaccine, but other vaccines should be deferred until their dose of glucocorticoids has been tapered down to less than 20 mg daily.
Patients taking all other immunosuppressive medications should continue taking them for the flu vaccine and other nonlive attenuated vaccinations, but it is conditionally recommended that live attenuated vaccines be deferred. For any patient with a rheumatic and musculoskeletal disease, regardless of disease activity, it is conditionally recommended that all routine nonlive attenuated vaccines be administered.
For live attenuated virus vaccines, the ACR provides a chart on which immunosuppressive medications to hold and for how long. Glucocorticoids, methotrexate, azathioprine, leflunomide, mycophenolate mofetil, calcineurin inhibitors, and oral cyclophosphamide should all be held 4 weeks before and 4 weeks after administration of a live attenuated vaccine. For those taking JAK inhibitors, the medication should be halted 1 week before administration of a live vaccine and should continue to be withheld for 4 weeks after.
For most other biologics, the ACR recommends holding the medication for one dosing interval before the live vaccine and 4 weeks thereafter. The main exception is rituximab, which should be held for 6 months before a live vaccine and then for 4 more weeks thereafter.
For patients receiving intravenous immunoglobulin, the drug should be held for 8-11 months before they are administered a live attenuated vaccine, depending on the dosage, and then 4 weeks after vaccination, regardless of dosage.
To reassure people with rheumatic disease who may have anxiety or concerns about receiving immunizations, whether taking immunosuppressive medication or not, Dr. Kim said it’s important to provide lots of education to patients.
“Fear and emotion have replaced facts, and data as a leading factor in decision-making, as seen with COVID-19,” Dr. Kim said. “The reality is that a small minority of people will have any issues with most vaccines, which include disease flares, adverse events, or acquisition of an autoimmune disease. We are not saying there is zero risk, rather, that the risk is quite small. This is where shared decision-making between the health care provider and the patient must be done effectively to enable the patient to properly weigh risk versus benefit.”
Dr. Kim has relationships with GlaxoSmithKline, Aurinia Pharmaceuticals, Kypha, Pfizer, Alexion Pharmaceuticals, AstraZeneca, Exagen Diagnostics, and Foghorn Therapeutics.
A version of this article first appeared on Medscape.com.
Patients with rheumatic and musculoskeletal diseases may need additional vaccines or different versions of vaccines they were not previously recommended to receive, according to updated guidelines from the American College of Rheumatology (ACR) on vaccinations for these patients. The new guidelines pertain to routine vaccinations for adults and children and are based on the most current evidence. They include recommendations on whether to hold certain medications before or after vaccination. They do not include recommendations regarding COVID-19 vaccines.
For guidance on COVID-19 vaccine timing and frequency, the ACR directs physicians to the CDC’s recommendations for people with mild or severe immunosuppression and the ACR’s previous clinical guidance summary on the topic, last revised in February 2022. The recommendations in the new guidance differ from ACR’s guidance on COVID-19 vaccines on whether and when to hold immunosuppressive medications when patients receive nonlive vaccines. The new guidelines now align more closely with those of EULAR, the Infectious Diseases Society of America, and the CDC’s recommendations for human papillomavirus (HPV), pneumococcal, and shingles vaccines.
Vaccinations in this population are particularly important because “a leading cause of morbidity and mortality in those with rheumatic diseases is infections, due to the detrimental impact immunosuppression has on the ability for the patient to properly clear the pathogen,” Alfred Kim, MD, PhD, professor of rheumatology at Washington University, St. Louis, told this news organization. While immunosuppressive medications are the most common reason patients with these conditions may have impaired immune function, “some of our patients with autoimmune disease also have a preexisting immunodeficiency that can inherently blunt immune responses to either infection or vaccination,” Dr. Kim explained.
“The authors of the guidelines have done a really nice job of making distinct recommendations based on the mechanism of action of various immunosuppressive medications,” Dr. Kim said. “This helps simplify the process of deciding the timing of vaccination for the health provider, especially for those on multiple immunosuppressives who represent an important proportion of our patients with rheumatic diseases.”
The main change to the guidelines for children, aside from those related to flu vaccination, is in regard to rotavirus vaccination for infants exposed to tumor necrosis factor (TNF) inhibitors or rituximab in utero. Infants prenatally exposed to rituximab should not receive the rotavirus vaccine until they are older than 6 months. Those exposed prenatally to TNF inhibitors should receive the rotavirus vaccine on time, according to the CDC schedule for all infants.
The new rotavirus recommendations follow data showing that immune responses to rotavirus are blunted in those with infliximab exposure, according to Dr. Kim.
“Thus, this poses a serious theoretical risk in newborns with mothers on [a TNF inhibitor] of ineffective clearance of rotavirus infections,” Dr. Kim said in an interview. “While rotavirus infections are quite common with typically self-limiting disease, sometimes requiring hydration to counteract diarrhea-induced dehydration, this can become severe in these newborns that have [a TNF inhibitor] in their system.”
For adults, the ACR issued the following expanded indications for four vaccines for patients currently taking immunosuppressive medication:
- Patients aged 18 and older should receive the recombinant zoster vaccine against shingles.
- For patients aged 27-44 who weren’t previously vaccinated against HPV, the HPV vaccine is “conditionally recommended.”
- Patients younger than 65 should receive the pneumococcal vaccine.
- Patients aged 19-64 are conditionally recommended to receive the high-dose or adjuvanted flu vaccine rather than the regular-dose flu vaccine.
The guidelines also conditionally recommend that all patients aged 65 and older who have rheumatic or musculoskeletal diseases receive the high-dose or adjuvanted flu vaccine, regardless of whether they are taking immunosuppressive medication. Another new conditional recommendation is to give multiple vaccinations to patients on the same day, rather than give individual vaccines on different days.
The guidelines make conditional recommendations regarding flu and nonlive attenuated vaccines for those taking methotrexate, rituximab, or glucocorticoids. Methotrexate should be held for 2 weeks after flu vaccination as long as disease activity allows it, but patients who are taking methotrexate should continue taking it for any other nonlive attenuated vaccinations.
“Non-rheumatology providers, such as general pediatricians and internists, are encouraged to give the influenza vaccination and then consult with the patient’s rheumatology provider about holding methotrexate to avoid a missed vaccination opportunity,” the guidelines state.
Patients taking rituximab should receive the flu vaccine on schedule and continue taking rituximab. However, for these patients, the guidelines recommend to “delay any subsequent rituximab dosing for at least two weeks after influenza vaccination if disease activity allows.”
“Because of the relatively short time period between the rollout of the influenza vaccine and its season, we can’t always wait to time the B-cell depletion dosage,” Dr. Kim said. “Also, it is not always easy to synchronize the patient’s B-cell depletion dosing schedule to the influenza vaccine rollout. Thus, we now just recommend getting the influenza vaccine regardless of the patient’s last B-cell depletion dosage despite its known strong attenuation of optimal immune responses.”
For other nonlive attenuated vaccines, providers should time vaccination for when the next rituximab dose is due and then hold the drug for at least 2 weeks thereafter, providing time for the B cells to mount a response before rituximab depletes B cells again.
Patients taking less than 20 mg of prednisone daily should still receive the flu vaccine and other nonlive attenuated vaccines. Those taking 20 mg or more of prednisone each day should still receive the flu vaccine, but other vaccines should be deferred until their dose of glucocorticoids has been tapered down to less than 20 mg daily.
Patients taking all other immunosuppressive medications should continue taking them for the flu vaccine and other nonlive attenuated vaccinations, but it is conditionally recommended that live attenuated vaccines be deferred. For any patient with a rheumatic and musculoskeletal disease, regardless of disease activity, it is conditionally recommended that all routine nonlive attenuated vaccines be administered.
For live attenuated virus vaccines, the ACR provides a chart on which immunosuppressive medications to hold and for how long. Glucocorticoids, methotrexate, azathioprine, leflunomide, mycophenolate mofetil, calcineurin inhibitors, and oral cyclophosphamide should all be held 4 weeks before and 4 weeks after administration of a live attenuated vaccine. For those taking JAK inhibitors, the medication should be halted 1 week before administration of a live vaccine and should continue to be withheld for 4 weeks after.
For most other biologics, the ACR recommends holding the medication for one dosing interval before the live vaccine and 4 weeks thereafter. The main exception is rituximab, which should be held for 6 months before a live vaccine and then for 4 more weeks thereafter.
For patients receiving intravenous immunoglobulin, the drug should be held for 8-11 months before they are administered a live attenuated vaccine, depending on the dosage, and then 4 weeks after vaccination, regardless of dosage.
To reassure people with rheumatic disease who may have anxiety or concerns about receiving immunizations, whether taking immunosuppressive medication or not, Dr. Kim said it’s important to provide lots of education to patients.
“Fear and emotion have replaced facts, and data as a leading factor in decision-making, as seen with COVID-19,” Dr. Kim said. “The reality is that a small minority of people will have any issues with most vaccines, which include disease flares, adverse events, or acquisition of an autoimmune disease. We are not saying there is zero risk, rather, that the risk is quite small. This is where shared decision-making between the health care provider and the patient must be done effectively to enable the patient to properly weigh risk versus benefit.”
Dr. Kim has relationships with GlaxoSmithKline, Aurinia Pharmaceuticals, Kypha, Pfizer, Alexion Pharmaceuticals, AstraZeneca, Exagen Diagnostics, and Foghorn Therapeutics.
A version of this article first appeared on Medscape.com.
Clinicians can help people with severe ME/CFS, even unseen
People who are severely ill with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are often too sick to leave home, but clinicians can still support them in many ways, experts say.
Approximately 250,000 people in the United Kingdom (0.2%-0.4%) have ME/CFS – where it’s called “ME.” As many as 2.5 million in the United States have it. Those numbers are expected to dramatically increase with the addition of people with long COVID. An estimated 25% of patients with the condition are so severely impaired that they are housebound or bedbound to the point where they’re unable to attend medical office visits. There are very few data about them because they’re typically unable to participate in studies.
Speaking at the annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (IACFS/ME), patient advocate Helen Baxter, of the U.K. charity 25% ME Group, presented a case series of five patients bedbound with ME/CFS who became severely malnourished because of delays in the placement of feeding tubes. The delays occurred because it was not recognized that the patients were unable to eat. The inability to eat may be due to a variety of factors, including gastrointestinal dysfunction, dysphagia, nausea, or lack of sufficient energy to eat or drink.
A report of those cases was included in a special issue of Healthcare, devoted to the topic of severe and very severe ME/CFS. The issue, which was published in April 2021, included 25 articles on the pathophysiology of severe ME/CFS, ways that clinicians can support patients who are too sick to make office visits, and psychosocial aspects of the condition that result from physical debilitation.
Two additional articles by specialist physicians aim to counter the skepticism about ME/CFS that has long persisted among some in the medical community.
“ME/CFS is under-researched and has historically received insufficient funding for research, particularly when compared to other chronic conditions, such as multiple sclerosis. And most of the research that has been done about it has focused on patients who are able to attend clinics. Patients with severe ME/CFS have largely been excluded from research due to the severity of their illness and are often described as ‘hard to reach.’ Consequently, research into severe ME is very limited,” Ms. Baxter said.
Asked to comment, Lucinda Bateman, MD, founder and director of the Bateman Horne Center, Salt Lake City, told this news organization, “It’s a big gap, even in the knowledgeable community. The research is totally skewed towards people who can get up and go participate in research. ... I don’t think most clinicians have any idea how sick people can get with ME/CFS.”
Cardiopulmonary exercise testing (CPET), which is commonly used in research, is intended to elicit objective biomarker responses. Such testing, which is considered the gold standard for determining disability, is impossible for the most severely ill patients with ME/CFS and is potentially harmful to these patients because of the hallmark postexertional malaise (PEM) phenomenon, Dr. Bateman noted.
“If we want to use CPET for research, we have to remember that it harms people to some degree and that we’re only studying the people who aren’t as sick. ... It’s one of the reasons I’ve been aggressively pursuing medical education about orthostatic testing, because it’s a clear objective marker, not as deleterious, and potentially leads to treatment options,” she said.
Misdiagnosis, treatment delays led to life-threatening malnutrition
The five patients that Ms. Baxter presented had become severely malnourished and dehydrated. There was evidence of clinical inertia for each of them.
“All were judged to have anorexia nervosa, and psychiatrists were involved, which was an added delay to starting tube feeding. ... In each case, the doctors resorted to making inappropriate psychological diagnoses without positive evidence of psychopathology, failing to recognize the significance of the malnutrition,” Ms. Baxter said. (Urgent tube feeding would have been warranted even had anorexia nervosa been the correct diagnosis, she pointed out.)
Once the problem was finally recognized, “all participants saw an improvement in their situation following the allocation of a home enteral nutrition dietician.”
At the IACFS/ME conference, Ms. Baxter described the painstaking methods used for gathering information, which were described in the same journal. These involved a combination of online, telephone, and text communications with patients or their caregivers. Efforts were made to avoid overtaxing the patients and triggering PEM.
“An early warning system needs to be put in place for patients with severe ME so that when they or their representatives become aware of the development of problems with oral intake, prompt action is taken, and tube feeding started, thereby avoiding undernutrition in patients with very severe ME,” Ms. Baxter and colleagues write.
Indeed, coauthor and semiretired pediatric ME/CFS specialist physician Nigel Speight, of Durham, United Kingdom, said in an interview, “In most of my patients, I used tube feeding early simply to avoid using unnecessary energy and causing stress to the patient.”
Dr. Speight added, “Patients can also die from sheer weakness leading to lack of respiratory drive. Also, and very understandably, some commit suicide.”
Caring for the patient with severe or very severe ME/CFS
Appearing in the special issue is an article entitled, “Caring for the Patient with Severe or Very Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome”. It was authored by a multidisciplinary group led by Jose G. Montoya, MD, of the Jack S. Remington Laboratory for Specialty Diagnostics, Palo Alto Medical Foundation, Calif.
In that article, four levels of severity are defined: mild, moderate, severe, and very severe. Included in the “severe” category are patients who are mostly homebound and whose activities of daily living are limited. They may have severe cognitive difficulties. Patients in the “very severe” caregory are bedbound and are unable to care for themselves.
Clinical features include more extreme versions of the core ME/CFS criteria: profound fatigue/weakness, PEM, unrefreshing sleep, orthostatic intolerance, and cognitive impairment. Additional symptoms in those with severe/very severe ME can include extreme hypersensitivity to light, sound, touch, and/or odors. Even small amounts of physical, mental, emotional, and orthostatic stressors can trigger PEM and increased weakness.
The authors recommend a “patient-centered, collaborative approach that is grounded in compassion and respect for the patient in all interactions,” and they provide lists of steps providers can take. These include seeing patients at home if possible and considerations regarding that care, such as partnering with the patient’s caregivers and other health care providers, who may include physical and occupational therapists, home health nurses, and social workers who understand the condition. Home visits by optometrists or ophthalmologists and dentists may be required.
Documenting limitations in activities of daily living is particularly important for helping patients to obtain homecare and disability benefits, Dr. Montoya and colleagues say.
Clinicians should investigate any medical problems that may be amenable to treatment, including orthostatic intolerance, pain, sleep difficulties, comorbidities, or gastrointestinal problems. For patients with pain, bloating, and diarrhea who are found on assessment to have mast cell activation disorder (MCAD), a trial of sodium cromoglicate may be tried, Ms. Baxter told this news organization.
Nonmedical problems that may be contributing to the patient’s morbidity should also be assessed, including a lack of caretaking, social services, transportation, food, and/or supportive devices, such as wheelchairs, bedpans, feeding tubes, and catheters.
The article provides additional detailed recommendations regarding pharmacologic treatments, follow-up visits – in-person or virtual – and hospitalization, as well as recommendations for energy conservation and management.
A section titled Practical Considerations for Busy Providers includes advice to be aware of any regulatory or insurance requirements for providing home visits and to maximize reimbursement by diagnosing any comorbidities, such as postural orthostatic tachycardia syndrome, Ehlers-Danlos syndrome, or MCAD.
Dr. Speight, who authored an article in the special issue on the management of ME in children, called the article by Dr. Montoya and colleagues “absolutely excellent,” and added his own advice, which included not “overinvestigating to cover your back but at the expense of causing stress to the patient” and considering a trial of immunoglobulin.
Importantly, Dr. Speight stressed, “avoid referral to psychiatrists unless specifically indicated for additional psychiatric morbidity; in which case, make clear that the psychiatrist accepts [that the] basic illness is medical.”
He also advised that clinicians stop using the term “chronic fatigue syndrome” because it suggests the illness is mild and/or psychosomatic. “Maybe the United States should embrace the term ME once and for all,” he said.
Dr. Baxter, Dr. Speight, and Dr. Montoya have disclosed no relevant financial relationships. Dr. Bateman is conducting research for Terra Biological.
A version of this article first appeared on Medscape.com.
People who are severely ill with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are often too sick to leave home, but clinicians can still support them in many ways, experts say.
Approximately 250,000 people in the United Kingdom (0.2%-0.4%) have ME/CFS – where it’s called “ME.” As many as 2.5 million in the United States have it. Those numbers are expected to dramatically increase with the addition of people with long COVID. An estimated 25% of patients with the condition are so severely impaired that they are housebound or bedbound to the point where they’re unable to attend medical office visits. There are very few data about them because they’re typically unable to participate in studies.
Speaking at the annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (IACFS/ME), patient advocate Helen Baxter, of the U.K. charity 25% ME Group, presented a case series of five patients bedbound with ME/CFS who became severely malnourished because of delays in the placement of feeding tubes. The delays occurred because it was not recognized that the patients were unable to eat. The inability to eat may be due to a variety of factors, including gastrointestinal dysfunction, dysphagia, nausea, or lack of sufficient energy to eat or drink.
A report of those cases was included in a special issue of Healthcare, devoted to the topic of severe and very severe ME/CFS. The issue, which was published in April 2021, included 25 articles on the pathophysiology of severe ME/CFS, ways that clinicians can support patients who are too sick to make office visits, and psychosocial aspects of the condition that result from physical debilitation.
Two additional articles by specialist physicians aim to counter the skepticism about ME/CFS that has long persisted among some in the medical community.
“ME/CFS is under-researched and has historically received insufficient funding for research, particularly when compared to other chronic conditions, such as multiple sclerosis. And most of the research that has been done about it has focused on patients who are able to attend clinics. Patients with severe ME/CFS have largely been excluded from research due to the severity of their illness and are often described as ‘hard to reach.’ Consequently, research into severe ME is very limited,” Ms. Baxter said.
Asked to comment, Lucinda Bateman, MD, founder and director of the Bateman Horne Center, Salt Lake City, told this news organization, “It’s a big gap, even in the knowledgeable community. The research is totally skewed towards people who can get up and go participate in research. ... I don’t think most clinicians have any idea how sick people can get with ME/CFS.”
Cardiopulmonary exercise testing (CPET), which is commonly used in research, is intended to elicit objective biomarker responses. Such testing, which is considered the gold standard for determining disability, is impossible for the most severely ill patients with ME/CFS and is potentially harmful to these patients because of the hallmark postexertional malaise (PEM) phenomenon, Dr. Bateman noted.
“If we want to use CPET for research, we have to remember that it harms people to some degree and that we’re only studying the people who aren’t as sick. ... It’s one of the reasons I’ve been aggressively pursuing medical education about orthostatic testing, because it’s a clear objective marker, not as deleterious, and potentially leads to treatment options,” she said.
Misdiagnosis, treatment delays led to life-threatening malnutrition
The five patients that Ms. Baxter presented had become severely malnourished and dehydrated. There was evidence of clinical inertia for each of them.
“All were judged to have anorexia nervosa, and psychiatrists were involved, which was an added delay to starting tube feeding. ... In each case, the doctors resorted to making inappropriate psychological diagnoses without positive evidence of psychopathology, failing to recognize the significance of the malnutrition,” Ms. Baxter said. (Urgent tube feeding would have been warranted even had anorexia nervosa been the correct diagnosis, she pointed out.)
Once the problem was finally recognized, “all participants saw an improvement in their situation following the allocation of a home enteral nutrition dietician.”
At the IACFS/ME conference, Ms. Baxter described the painstaking methods used for gathering information, which were described in the same journal. These involved a combination of online, telephone, and text communications with patients or their caregivers. Efforts were made to avoid overtaxing the patients and triggering PEM.
“An early warning system needs to be put in place for patients with severe ME so that when they or their representatives become aware of the development of problems with oral intake, prompt action is taken, and tube feeding started, thereby avoiding undernutrition in patients with very severe ME,” Ms. Baxter and colleagues write.
Indeed, coauthor and semiretired pediatric ME/CFS specialist physician Nigel Speight, of Durham, United Kingdom, said in an interview, “In most of my patients, I used tube feeding early simply to avoid using unnecessary energy and causing stress to the patient.”
Dr. Speight added, “Patients can also die from sheer weakness leading to lack of respiratory drive. Also, and very understandably, some commit suicide.”
Caring for the patient with severe or very severe ME/CFS
Appearing in the special issue is an article entitled, “Caring for the Patient with Severe or Very Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome”. It was authored by a multidisciplinary group led by Jose G. Montoya, MD, of the Jack S. Remington Laboratory for Specialty Diagnostics, Palo Alto Medical Foundation, Calif.
In that article, four levels of severity are defined: mild, moderate, severe, and very severe. Included in the “severe” category are patients who are mostly homebound and whose activities of daily living are limited. They may have severe cognitive difficulties. Patients in the “very severe” caregory are bedbound and are unable to care for themselves.
Clinical features include more extreme versions of the core ME/CFS criteria: profound fatigue/weakness, PEM, unrefreshing sleep, orthostatic intolerance, and cognitive impairment. Additional symptoms in those with severe/very severe ME can include extreme hypersensitivity to light, sound, touch, and/or odors. Even small amounts of physical, mental, emotional, and orthostatic stressors can trigger PEM and increased weakness.
The authors recommend a “patient-centered, collaborative approach that is grounded in compassion and respect for the patient in all interactions,” and they provide lists of steps providers can take. These include seeing patients at home if possible and considerations regarding that care, such as partnering with the patient’s caregivers and other health care providers, who may include physical and occupational therapists, home health nurses, and social workers who understand the condition. Home visits by optometrists or ophthalmologists and dentists may be required.
Documenting limitations in activities of daily living is particularly important for helping patients to obtain homecare and disability benefits, Dr. Montoya and colleagues say.
Clinicians should investigate any medical problems that may be amenable to treatment, including orthostatic intolerance, pain, sleep difficulties, comorbidities, or gastrointestinal problems. For patients with pain, bloating, and diarrhea who are found on assessment to have mast cell activation disorder (MCAD), a trial of sodium cromoglicate may be tried, Ms. Baxter told this news organization.
Nonmedical problems that may be contributing to the patient’s morbidity should also be assessed, including a lack of caretaking, social services, transportation, food, and/or supportive devices, such as wheelchairs, bedpans, feeding tubes, and catheters.
The article provides additional detailed recommendations regarding pharmacologic treatments, follow-up visits – in-person or virtual – and hospitalization, as well as recommendations for energy conservation and management.
A section titled Practical Considerations for Busy Providers includes advice to be aware of any regulatory or insurance requirements for providing home visits and to maximize reimbursement by diagnosing any comorbidities, such as postural orthostatic tachycardia syndrome, Ehlers-Danlos syndrome, or MCAD.
Dr. Speight, who authored an article in the special issue on the management of ME in children, called the article by Dr. Montoya and colleagues “absolutely excellent,” and added his own advice, which included not “overinvestigating to cover your back but at the expense of causing stress to the patient” and considering a trial of immunoglobulin.
Importantly, Dr. Speight stressed, “avoid referral to psychiatrists unless specifically indicated for additional psychiatric morbidity; in which case, make clear that the psychiatrist accepts [that the] basic illness is medical.”
He also advised that clinicians stop using the term “chronic fatigue syndrome” because it suggests the illness is mild and/or psychosomatic. “Maybe the United States should embrace the term ME once and for all,” he said.
Dr. Baxter, Dr. Speight, and Dr. Montoya have disclosed no relevant financial relationships. Dr. Bateman is conducting research for Terra Biological.
A version of this article first appeared on Medscape.com.
People who are severely ill with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are often too sick to leave home, but clinicians can still support them in many ways, experts say.
Approximately 250,000 people in the United Kingdom (0.2%-0.4%) have ME/CFS – where it’s called “ME.” As many as 2.5 million in the United States have it. Those numbers are expected to dramatically increase with the addition of people with long COVID. An estimated 25% of patients with the condition are so severely impaired that they are housebound or bedbound to the point where they’re unable to attend medical office visits. There are very few data about them because they’re typically unable to participate in studies.
Speaking at the annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (IACFS/ME), patient advocate Helen Baxter, of the U.K. charity 25% ME Group, presented a case series of five patients bedbound with ME/CFS who became severely malnourished because of delays in the placement of feeding tubes. The delays occurred because it was not recognized that the patients were unable to eat. The inability to eat may be due to a variety of factors, including gastrointestinal dysfunction, dysphagia, nausea, or lack of sufficient energy to eat or drink.
A report of those cases was included in a special issue of Healthcare, devoted to the topic of severe and very severe ME/CFS. The issue, which was published in April 2021, included 25 articles on the pathophysiology of severe ME/CFS, ways that clinicians can support patients who are too sick to make office visits, and psychosocial aspects of the condition that result from physical debilitation.
Two additional articles by specialist physicians aim to counter the skepticism about ME/CFS that has long persisted among some in the medical community.
“ME/CFS is under-researched and has historically received insufficient funding for research, particularly when compared to other chronic conditions, such as multiple sclerosis. And most of the research that has been done about it has focused on patients who are able to attend clinics. Patients with severe ME/CFS have largely been excluded from research due to the severity of their illness and are often described as ‘hard to reach.’ Consequently, research into severe ME is very limited,” Ms. Baxter said.
Asked to comment, Lucinda Bateman, MD, founder and director of the Bateman Horne Center, Salt Lake City, told this news organization, “It’s a big gap, even in the knowledgeable community. The research is totally skewed towards people who can get up and go participate in research. ... I don’t think most clinicians have any idea how sick people can get with ME/CFS.”
Cardiopulmonary exercise testing (CPET), which is commonly used in research, is intended to elicit objective biomarker responses. Such testing, which is considered the gold standard for determining disability, is impossible for the most severely ill patients with ME/CFS and is potentially harmful to these patients because of the hallmark postexertional malaise (PEM) phenomenon, Dr. Bateman noted.
“If we want to use CPET for research, we have to remember that it harms people to some degree and that we’re only studying the people who aren’t as sick. ... It’s one of the reasons I’ve been aggressively pursuing medical education about orthostatic testing, because it’s a clear objective marker, not as deleterious, and potentially leads to treatment options,” she said.
Misdiagnosis, treatment delays led to life-threatening malnutrition
The five patients that Ms. Baxter presented had become severely malnourished and dehydrated. There was evidence of clinical inertia for each of them.
“All were judged to have anorexia nervosa, and psychiatrists were involved, which was an added delay to starting tube feeding. ... In each case, the doctors resorted to making inappropriate psychological diagnoses without positive evidence of psychopathology, failing to recognize the significance of the malnutrition,” Ms. Baxter said. (Urgent tube feeding would have been warranted even had anorexia nervosa been the correct diagnosis, she pointed out.)
Once the problem was finally recognized, “all participants saw an improvement in their situation following the allocation of a home enteral nutrition dietician.”
At the IACFS/ME conference, Ms. Baxter described the painstaking methods used for gathering information, which were described in the same journal. These involved a combination of online, telephone, and text communications with patients or their caregivers. Efforts were made to avoid overtaxing the patients and triggering PEM.
“An early warning system needs to be put in place for patients with severe ME so that when they or their representatives become aware of the development of problems with oral intake, prompt action is taken, and tube feeding started, thereby avoiding undernutrition in patients with very severe ME,” Ms. Baxter and colleagues write.
Indeed, coauthor and semiretired pediatric ME/CFS specialist physician Nigel Speight, of Durham, United Kingdom, said in an interview, “In most of my patients, I used tube feeding early simply to avoid using unnecessary energy and causing stress to the patient.”
Dr. Speight added, “Patients can also die from sheer weakness leading to lack of respiratory drive. Also, and very understandably, some commit suicide.”
Caring for the patient with severe or very severe ME/CFS
Appearing in the special issue is an article entitled, “Caring for the Patient with Severe or Very Severe Myalgic Encephalomyelitis/Chronic Fatigue Syndrome”. It was authored by a multidisciplinary group led by Jose G. Montoya, MD, of the Jack S. Remington Laboratory for Specialty Diagnostics, Palo Alto Medical Foundation, Calif.
In that article, four levels of severity are defined: mild, moderate, severe, and very severe. Included in the “severe” category are patients who are mostly homebound and whose activities of daily living are limited. They may have severe cognitive difficulties. Patients in the “very severe” caregory are bedbound and are unable to care for themselves.
Clinical features include more extreme versions of the core ME/CFS criteria: profound fatigue/weakness, PEM, unrefreshing sleep, orthostatic intolerance, and cognitive impairment. Additional symptoms in those with severe/very severe ME can include extreme hypersensitivity to light, sound, touch, and/or odors. Even small amounts of physical, mental, emotional, and orthostatic stressors can trigger PEM and increased weakness.
The authors recommend a “patient-centered, collaborative approach that is grounded in compassion and respect for the patient in all interactions,” and they provide lists of steps providers can take. These include seeing patients at home if possible and considerations regarding that care, such as partnering with the patient’s caregivers and other health care providers, who may include physical and occupational therapists, home health nurses, and social workers who understand the condition. Home visits by optometrists or ophthalmologists and dentists may be required.
Documenting limitations in activities of daily living is particularly important for helping patients to obtain homecare and disability benefits, Dr. Montoya and colleagues say.
Clinicians should investigate any medical problems that may be amenable to treatment, including orthostatic intolerance, pain, sleep difficulties, comorbidities, or gastrointestinal problems. For patients with pain, bloating, and diarrhea who are found on assessment to have mast cell activation disorder (MCAD), a trial of sodium cromoglicate may be tried, Ms. Baxter told this news organization.
Nonmedical problems that may be contributing to the patient’s morbidity should also be assessed, including a lack of caretaking, social services, transportation, food, and/or supportive devices, such as wheelchairs, bedpans, feeding tubes, and catheters.
The article provides additional detailed recommendations regarding pharmacologic treatments, follow-up visits – in-person or virtual – and hospitalization, as well as recommendations for energy conservation and management.
A section titled Practical Considerations for Busy Providers includes advice to be aware of any regulatory or insurance requirements for providing home visits and to maximize reimbursement by diagnosing any comorbidities, such as postural orthostatic tachycardia syndrome, Ehlers-Danlos syndrome, or MCAD.
Dr. Speight, who authored an article in the special issue on the management of ME in children, called the article by Dr. Montoya and colleagues “absolutely excellent,” and added his own advice, which included not “overinvestigating to cover your back but at the expense of causing stress to the patient” and considering a trial of immunoglobulin.
Importantly, Dr. Speight stressed, “avoid referral to psychiatrists unless specifically indicated for additional psychiatric morbidity; in which case, make clear that the psychiatrist accepts [that the] basic illness is medical.”
He also advised that clinicians stop using the term “chronic fatigue syndrome” because it suggests the illness is mild and/or psychosomatic. “Maybe the United States should embrace the term ME once and for all,” he said.
Dr. Baxter, Dr. Speight, and Dr. Montoya have disclosed no relevant financial relationships. Dr. Bateman is conducting research for Terra Biological.
A version of this article first appeared on Medscape.com.
FROM IACFS/ME 2022
HCV reinfection uncommon among people who inject drugs
The findings, which are based on prospective data from 13 countries, including the United States, and were published in Annals of Internal Medicine (2022 Aug 8. doi: 10.7326/M21-4119), should encourage physicians to treat HCV in people with a history of injection drug use, said lead author Jason Grebely, PhD. They should also pressure payers to lift reimbursement restrictions on the same population.

“Direct-acting antiviral medications for HCV infection are safe and effective among people receiving OAT and people with recent injecting-drug use,” the investigators wrote. “Concerns remain, however, that HCV reinfection may reduce the benefits of cure among people who inject drugs and compromise HCV elimination efforts.”
They explored these concerns through a 3-year extension of the phase 3 CO-STAR trial that evaluated elbasvir and grazoprevir in people consistently taking OAT. Participants in the CO-STAR trial, which had a 96% sustained virologic response rate among those who completed therapy, could elect to participate in the present study, offering a prospective look at long-term reinfection.
Out of 296 participants in the CO-STAR trial, 286 were evaluable for reinfection and 199 enrolled in the present extension. The majority were White (79.4%) and male (75.9%), with most taking methadone (79%), followed by buprenorphine (20%). At 6 months, 40 out of 191 respondents (21%) reported injection-drug use in the previous month. At the 3-year mark, 26 out of 142 respondents (18%) disclosed injection-drug use in the previous month.
For all participants in the CO-STAR trial, the overall rate of reinfection at 3 years was 1.7 per 100 person-years (95% confidence interval, 0.8-3.0), which is lower than the rate reported in systematic reviews (3.8 per 100 person-years), according to the investigators.
In the extension analysis, the 3-year reinfection rate was lower still, at 1.2 per 100 person-years. The rate was slightly higher among people who reported injection-drug use in the previous month (1.9 per 100 person-years), and slightly lower among those who did not report injection-drug use in the prior month (0.5 per 100 person-years). More pronounced differences in reinfection were observed among participants who shared needles (6.4 per 100 person-years), versus those who didn’t share needles (1.5 per 100 person years).
Low reinfection rate may help facilitate removal of reimbursement restrictions
“Most of the reinfections in this study occurred within 24 weeks of completing treatment, suggesting that this is a key period for optimizing treatment of opioid use disorder and for providing access to needle and syringe programs that have documented benefits in preventing HCV transmission,” the investigators wrote.
This is one of the largest observational studies of its kind to date, bolstered by “excellent study retention” and a “well-characterized cohort,” with findings that should prompt real-world action, said Dr. Grebely, who is head of the hepatitis C and drug use group in the viral hepatitis clinical research program at the Kirby Institute, University of New South Wales, Sydney.
“Given that reinfection has often been cited ... by some providers as a reason for not offering treatment to people receiving OAT, the low reinfection rate in this study will be incredibly important for guiding practice and ensuring therapy is not withheld from this group,” Dr. Grebely said in an interview. “In terms of policy implications, these data may also help to facilitate the removal of reimbursement restrictions based on recent drug/alcohol use criteria that are in place among many payers in the United States.”
More research needed to determine optimal intervention strategies
Carl Latkin, PhD, professor and vice chair of the department of health, behavior, and society at Johns Hopkins University, Baltimore, called the present publication a “great article and well-done study with long-term follow-up.”
Dr. Latkin, who investigates biobehavioral interventions for disadvantaged communities, said the reported rate of reinfection is “very low among a group of current and former injectors.”
Affirming Dr. Grebely’s call for supportive practices by physicians and payers, Dr. Latkin said: “The study highlights the importance of improving access to medication for opioid use disorder. This level of treatment adherence in this group is much higher than for many other medications. Given these data, it would be difficult for payers to have a rational reason for blanket restrictions for HCV treatment among people who use drugs.”
Dr. Latkin explained that “it isn’t simply injection drug use per se” that drives HCV reinfection; instead, he cited social factors, such as lack of housing, as well as withdrawal symptoms, especially among those without access to medications for opioid use disorder (MOUD).
Dr. Latkin and Grebely also agreed that more research is needed to determine optimal intervention strategies.
Dr. Grebely called for one to enhance HCV testing and linkage to care, a topic he covered in a recent review article (Lancet Gastroenterol Hepatol. 2022 May;7[5]:426-45.).
Dr. Latkin said that, while it’s clear that “syringe services programs, accessible HCV treatment, and MOUD are needed,” it is unclear how much coverage is necessary for a given population.
Findings support critical nature of needle and syringe exchange programs
Sarah M. Kattakuzhy, MD, an associate professor in the division of clinical care & research at the Institute of Human Virology, University of Maryland, Baltimore, agreed that the findings “support the critical nature of needle and syringe exchange programs.”

“As most cities in the United States fall well below the high coverage needle and syringe program threshold required to maximally prevent disease transmission, the study serves as a push toward an evidence-based harm reduction policy,” she said.
Dr. Kattakuzhy he added that the study “supports the need to longitudinally engage individuals after HCV treatment to monitor reinfection risk behaviors and test for reinfection,” she continued.
When it came to translating all the data to populations in the United States, she offered a more guarded view.
“Critically, the study population included only individuals who were engaged with OAT and adherent for 3 or more months, selecting to a population of individuals with high adherence and engagement in care,” Dr. Kattakuzhy said in an interview. “As such, the study findings are not applicable to other cross sections of the drug-using community, including individuals not engaged in OAT, and cohorts with higher rates of ongoing injection drug use. Furthermore, there are known genetic impacts on spontaneous clearance, and emerging data on the immunology of reinfection.
“Studies with a focus on less engaged, higher-risk, and minority populations with active drug use are required to answer the remaining questions in HCV reinfection,” she said.
The study was supported by Merck, the Australian Government Department of Health, and the Australian National Health and Medical Research Council. Dr. Grebely disclosed receiving funding from Cepheid, the manufacturer of the Xpert HCV assay. The other investigators disclosed additional relationships with Gilead, AbbVie, Cepheid, and others. Dr. Latkin and Dr. Kattakuzhy disclosed no relevant conflicts of interest.
The findings, which are based on prospective data from 13 countries, including the United States, and were published in Annals of Internal Medicine (2022 Aug 8. doi: 10.7326/M21-4119), should encourage physicians to treat HCV in people with a history of injection drug use, said lead author Jason Grebely, PhD. They should also pressure payers to lift reimbursement restrictions on the same population.
“Direct-acting antiviral medications for HCV infection are safe and effective among people receiving OAT and people with recent injecting-drug use,” the investigators wrote. “Concerns remain, however, that HCV reinfection may reduce the benefits of cure among people who inject drugs and compromise HCV elimination efforts.”
They explored these concerns through a 3-year extension of the phase 3 CO-STAR trial that evaluated elbasvir and grazoprevir in people consistently taking OAT. Participants in the CO-STAR trial, which had a 96% sustained virologic response rate among those who completed therapy, could elect to participate in the present study, offering a prospective look at long-term reinfection.
Out of 296 participants in the CO-STAR trial, 286 were evaluable for reinfection and 199 enrolled in the present extension. The majority were White (79.4%) and male (75.9%), with most taking methadone (79%), followed by buprenorphine (20%). At 6 months, 40 out of 191 respondents (21%) reported injection-drug use in the previous month. At the 3-year mark, 26 out of 142 respondents (18%) disclosed injection-drug use in the previous month.
For all participants in the CO-STAR trial, the overall rate of reinfection at 3 years was 1.7 per 100 person-years (95% confidence interval, 0.8-3.0), which is lower than the rate reported in systematic reviews (3.8 per 100 person-years), according to the investigators.
In the extension analysis, the 3-year reinfection rate was lower still, at 1.2 per 100 person-years. The rate was slightly higher among people who reported injection-drug use in the previous month (1.9 per 100 person-years), and slightly lower among those who did not report injection-drug use in the prior month (0.5 per 100 person-years). More pronounced differences in reinfection were observed among participants who shared needles (6.4 per 100 person-years), versus those who didn’t share needles (1.5 per 100 person years).
Low reinfection rate may help facilitate removal of reimbursement restrictions
“Most of the reinfections in this study occurred within 24 weeks of completing treatment, suggesting that this is a key period for optimizing treatment of opioid use disorder and for providing access to needle and syringe programs that have documented benefits in preventing HCV transmission,” the investigators wrote.
This is one of the largest observational studies of its kind to date, bolstered by “excellent study retention” and a “well-characterized cohort,” with findings that should prompt real-world action, said Dr. Grebely, who is head of the hepatitis C and drug use group in the viral hepatitis clinical research program at the Kirby Institute, University of New South Wales, Sydney.
“Given that reinfection has often been cited ... by some providers as a reason for not offering treatment to people receiving OAT, the low reinfection rate in this study will be incredibly important for guiding practice and ensuring therapy is not withheld from this group,” Dr. Grebely said in an interview. “In terms of policy implications, these data may also help to facilitate the removal of reimbursement restrictions based on recent drug/alcohol use criteria that are in place among many payers in the United States.”
More research needed to determine optimal intervention strategies
Carl Latkin, PhD, professor and vice chair of the department of health, behavior, and society at Johns Hopkins University, Baltimore, called the present publication a “great article and well-done study with long-term follow-up.”
Dr. Latkin, who investigates biobehavioral interventions for disadvantaged communities, said the reported rate of reinfection is “very low among a group of current and former injectors.”
Affirming Dr. Grebely’s call for supportive practices by physicians and payers, Dr. Latkin said: “The study highlights the importance of improving access to medication for opioid use disorder. This level of treatment adherence in this group is much higher than for many other medications. Given these data, it would be difficult for payers to have a rational reason for blanket restrictions for HCV treatment among people who use drugs.”
Dr. Latkin explained that “it isn’t simply injection drug use per se” that drives HCV reinfection; instead, he cited social factors, such as lack of housing, as well as withdrawal symptoms, especially among those without access to medications for opioid use disorder (MOUD).
Dr. Latkin and Grebely also agreed that more research is needed to determine optimal intervention strategies.
Dr. Grebely called for one to enhance HCV testing and linkage to care, a topic he covered in a recent review article (Lancet Gastroenterol Hepatol. 2022 May;7[5]:426-45.).
Dr. Latkin said that, while it’s clear that “syringe services programs, accessible HCV treatment, and MOUD are needed,” it is unclear how much coverage is necessary for a given population.
Findings support critical nature of needle and syringe exchange programs
Sarah M. Kattakuzhy, MD, an associate professor in the division of clinical care & research at the Institute of Human Virology, University of Maryland, Baltimore, agreed that the findings “support the critical nature of needle and syringe exchange programs.”
“As most cities in the United States fall well below the high coverage needle and syringe program threshold required to maximally prevent disease transmission, the study serves as a push toward an evidence-based harm reduction policy,” she said.
Dr. Kattakuzhy he added that the study “supports the need to longitudinally engage individuals after HCV treatment to monitor reinfection risk behaviors and test for reinfection,” she continued.
When it came to translating all the data to populations in the United States, she offered a more guarded view.
“Critically, the study population included only individuals who were engaged with OAT and adherent for 3 or more months, selecting to a population of individuals with high adherence and engagement in care,” Dr. Kattakuzhy said in an interview. “As such, the study findings are not applicable to other cross sections of the drug-using community, including individuals not engaged in OAT, and cohorts with higher rates of ongoing injection drug use. Furthermore, there are known genetic impacts on spontaneous clearance, and emerging data on the immunology of reinfection.
“Studies with a focus on less engaged, higher-risk, and minority populations with active drug use are required to answer the remaining questions in HCV reinfection,” she said.
The study was supported by Merck, the Australian Government Department of Health, and the Australian National Health and Medical Research Council. Dr. Grebely disclosed receiving funding from Cepheid, the manufacturer of the Xpert HCV assay. The other investigators disclosed additional relationships with Gilead, AbbVie, Cepheid, and others. Dr. Latkin and Dr. Kattakuzhy disclosed no relevant conflicts of interest.
The findings, which are based on prospective data from 13 countries, including the United States, and were published in Annals of Internal Medicine (2022 Aug 8. doi: 10.7326/M21-4119), should encourage physicians to treat HCV in people with a history of injection drug use, said lead author Jason Grebely, PhD. They should also pressure payers to lift reimbursement restrictions on the same population.
“Direct-acting antiviral medications for HCV infection are safe and effective among people receiving OAT and people with recent injecting-drug use,” the investigators wrote. “Concerns remain, however, that HCV reinfection may reduce the benefits of cure among people who inject drugs and compromise HCV elimination efforts.”
They explored these concerns through a 3-year extension of the phase 3 CO-STAR trial that evaluated elbasvir and grazoprevir in people consistently taking OAT. Participants in the CO-STAR trial, which had a 96% sustained virologic response rate among those who completed therapy, could elect to participate in the present study, offering a prospective look at long-term reinfection.
Out of 296 participants in the CO-STAR trial, 286 were evaluable for reinfection and 199 enrolled in the present extension. The majority were White (79.4%) and male (75.9%), with most taking methadone (79%), followed by buprenorphine (20%). At 6 months, 40 out of 191 respondents (21%) reported injection-drug use in the previous month. At the 3-year mark, 26 out of 142 respondents (18%) disclosed injection-drug use in the previous month.
For all participants in the CO-STAR trial, the overall rate of reinfection at 3 years was 1.7 per 100 person-years (95% confidence interval, 0.8-3.0), which is lower than the rate reported in systematic reviews (3.8 per 100 person-years), according to the investigators.
In the extension analysis, the 3-year reinfection rate was lower still, at 1.2 per 100 person-years. The rate was slightly higher among people who reported injection-drug use in the previous month (1.9 per 100 person-years), and slightly lower among those who did not report injection-drug use in the prior month (0.5 per 100 person-years). More pronounced differences in reinfection were observed among participants who shared needles (6.4 per 100 person-years), versus those who didn’t share needles (1.5 per 100 person years).
Low reinfection rate may help facilitate removal of reimbursement restrictions
“Most of the reinfections in this study occurred within 24 weeks of completing treatment, suggesting that this is a key period for optimizing treatment of opioid use disorder and for providing access to needle and syringe programs that have documented benefits in preventing HCV transmission,” the investigators wrote.
This is one of the largest observational studies of its kind to date, bolstered by “excellent study retention” and a “well-characterized cohort,” with findings that should prompt real-world action, said Dr. Grebely, who is head of the hepatitis C and drug use group in the viral hepatitis clinical research program at the Kirby Institute, University of New South Wales, Sydney.
“Given that reinfection has often been cited ... by some providers as a reason for not offering treatment to people receiving OAT, the low reinfection rate in this study will be incredibly important for guiding practice and ensuring therapy is not withheld from this group,” Dr. Grebely said in an interview. “In terms of policy implications, these data may also help to facilitate the removal of reimbursement restrictions based on recent drug/alcohol use criteria that are in place among many payers in the United States.”
More research needed to determine optimal intervention strategies
Carl Latkin, PhD, professor and vice chair of the department of health, behavior, and society at Johns Hopkins University, Baltimore, called the present publication a “great article and well-done study with long-term follow-up.”
Dr. Latkin, who investigates biobehavioral interventions for disadvantaged communities, said the reported rate of reinfection is “very low among a group of current and former injectors.”
Affirming Dr. Grebely’s call for supportive practices by physicians and payers, Dr. Latkin said: “The study highlights the importance of improving access to medication for opioid use disorder. This level of treatment adherence in this group is much higher than for many other medications. Given these data, it would be difficult for payers to have a rational reason for blanket restrictions for HCV treatment among people who use drugs.”
Dr. Latkin explained that “it isn’t simply injection drug use per se” that drives HCV reinfection; instead, he cited social factors, such as lack of housing, as well as withdrawal symptoms, especially among those without access to medications for opioid use disorder (MOUD).
Dr. Latkin and Grebely also agreed that more research is needed to determine optimal intervention strategies.
Dr. Grebely called for one to enhance HCV testing and linkage to care, a topic he covered in a recent review article (Lancet Gastroenterol Hepatol. 2022 May;7[5]:426-45.).
Dr. Latkin said that, while it’s clear that “syringe services programs, accessible HCV treatment, and MOUD are needed,” it is unclear how much coverage is necessary for a given population.
Findings support critical nature of needle and syringe exchange programs
Sarah M. Kattakuzhy, MD, an associate professor in the division of clinical care & research at the Institute of Human Virology, University of Maryland, Baltimore, agreed that the findings “support the critical nature of needle and syringe exchange programs.”
“As most cities in the United States fall well below the high coverage needle and syringe program threshold required to maximally prevent disease transmission, the study serves as a push toward an evidence-based harm reduction policy,” she said.
Dr. Kattakuzhy he added that the study “supports the need to longitudinally engage individuals after HCV treatment to monitor reinfection risk behaviors and test for reinfection,” she continued.
When it came to translating all the data to populations in the United States, she offered a more guarded view.
“Critically, the study population included only individuals who were engaged with OAT and adherent for 3 or more months, selecting to a population of individuals with high adherence and engagement in care,” Dr. Kattakuzhy said in an interview. “As such, the study findings are not applicable to other cross sections of the drug-using community, including individuals not engaged in OAT, and cohorts with higher rates of ongoing injection drug use. Furthermore, there are known genetic impacts on spontaneous clearance, and emerging data on the immunology of reinfection.
“Studies with a focus on less engaged, higher-risk, and minority populations with active drug use are required to answer the remaining questions in HCV reinfection,” she said.
The study was supported by Merck, the Australian Government Department of Health, and the Australian National Health and Medical Research Council. Dr. Grebely disclosed receiving funding from Cepheid, the manufacturer of the Xpert HCV assay. The other investigators disclosed additional relationships with Gilead, AbbVie, Cepheid, and others. Dr. Latkin and Dr. Kattakuzhy disclosed no relevant conflicts of interest.
FROM ANNALS OF INTERNAL MEDICINE
Increasing data link ME/CFS, long COVID, and dysautonomia
At the virtual annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (IACFSME), speakers presented data showing similar pathophysiologic abnormalities in people with systemic symptoms associated with ME/CFS who had a prior SARS-CoV-2 infection and those who did not, including individuals whose illness preceded the COVID-19 pandemic.
Core clinical diagnostic criteria for ME/CFS established by the Institute of Medicine in 2015 include substantial decrement in functioning for 6 months or longer, postexertional malaise, or a worsening of symptoms following even minor exertion (often described by patients as “crashes”), unrefreshing sleep, and cognitive dysfunction and/or orthostatic intolerance that are frequent and severe.
Long COVID has been defined in several different ways using different terminology. The U.S. Centers for Disease Control and Prevention, for example, defines “post-COVID conditions” as those continuing four or more weeks beyond first symptoms. The World Health Organization’s clinical case definition of “post COVID-19 condition” includes otherwise unexplained symptoms 3 months from COVID-19 onset and lasting longer than 2 months.
Both ME/CFS and long COVID commonly involve numerous symptoms beyond the defining ones, affecting nearly every organ system in the body, including systemic, neurocognitive, endocrine, cardiovascular, pulmonary, musculoskeletal, and gastrointestinal, with wide variation among individuals. Autonomic dysfunction is common to both conditions, particularly postural orthostatic tachycardia syndrome (POTS).
“My way of understanding these illnesses is that they’re not just multisystem illnesses, but all these interactive systems that lean on each other are dysregulated. … I would say that a very common underlying mediator of both ME/CFS and long COVID is autonomic dysfunction, and it presents as POTS,” Nancy Klimas, MD, director of the Institute for Neuro-Immune Medicine at Nova Southeastern University, Fort Lauderdale, Fla., told this news organization.
Dr. Klimas, who is also director of Clinical Immunology Research at the Miami Veterans Affairs Medical Center, added that “if basic bioenergetics are disrupted and in an oxidative-stress state [then] they have downregulated energy production at the cellular level, which seems to be the case in ME/CFS and now in long COVID.”
New ICD-10 codes better characterize the syndromes
New ICD-10 codes for 2023, being implemented on Oct. 1, will enable clinicians to better document all of these interrelated conditions.
Under the existing G93.3, Postviral and related fatigue syndromes, there will now be:
- G93.31 – Postviral fatigue syndrome.
- G93.32 – Myalgic encephalomyelitis/chronic fatigue syndrome (and the separate terms).
- G93.39 – Other postinfection and related fatigue syndromes.
The old R53.82, “Chronic fatigue, unspecified” code now excludes all of the above conditions.
The additional code U09.9 for “post COVID-19 condition, unspecified,” may also be used if applicable.
In addition, a new code for POTS, G90.A, which wasn’t previously mentioned in ICD-10, may also be used starting Oct. 1.
Lucinda Bateman, MD, founder and director of the Bateman Horne Center, Salt Lake City, advises using all applicable codes for a given patient. “If a patient came into my office with long COVID and met criteria for ME/CFS, we would code both, and also any other syndrome criteria that they may meet, such as POTS or fibromyalgia.
“If people use the codes appropriately, then you can understand the overlap better. It increases the likelihood of reimbursement, creates a more accurate medical record for the patient, and provides them with a better tool should they require disability benefits.”
Dr. Bateman advises in-office orthostatic evaluation for all patients with this symptom constellation, using a passive standing evaluation such as the 10-minute NASA Lean test.
“Clinicians should take the time to do orthostatic testing in these patients because it provides objective markers and will help lead us to potential interventions to help improve people’s function.”
The Bateman Horne center offers clinician resources on management of ME/CFS and related conditions.
How common is ME/CFS after COVID-19?
According to one published meta-analysis, the global prevalence of “post-acute sequelae of SARS-CoV-2,” defined by any symptom, is about 43% of patients overall following infection, and 49% at 120 days. Fatigue was the most commonly reported symptom, followed by memory problems. As of March 22, the World Health Organization estimated that there have been more than 470 million COVID-19 cases, which would give a figure of about 200 million people who are experiencing a wide range of long-COVID symptoms.
On the final day of the IACFSME conference, Luis Nacul, MD, of the University of British Columbia, Vancouver, presented several sets of data from his group and others aiming to determine the proportion of individuals who develop symptoms suggestive of ME/CFS following a COVID-19 infection.
Among a cohort of 88 adults hospitalized with confirmed SARS-CoV-2 infections during the first pandemic wave in 2020 and followed up in the respiratory clinic, rates of reported generalized fatigue were 67% at 3 months and 59.5% at 6 months. Substantial fatigue (that is, present most days and affecting activity levels) were reported by 16% at 3 months and 7% at 6 months. “This should represent in principle the maximum prevalence of cases who would meet the criteria for ME/CFS,” Dr. Nacul said.
Baseline age was indirectly associated with fatigue at 3 and 6 months, while the number of comorbidities a patient had was directly associated. Comorbidities also predicted severe fatigue at 3 months, but the numbers were too small for assessment at 6 months.
Studies involving nonhospitalized patients suggested lower rates. One meta-analysis showed 1-year rates of fatigue in 32% and cognitive impairment in 22%. Another showed very similar rates, reporting fatigue in 28% and memory/concentration difficulties in 18%-19%.
Dr. Nacul cautioned that these figures are likely overestimates since many of the study populations are taken from respiratory or long-COVID clinics. “The evidence on ‘post-COVID fatigue syndrome’ or ME/CFS following COVID is still evolving. There is a huge need for studies looking more closely at cases meeting well-defined ME/CFS criteria. This unfortunately hasn’t been done for most studies.”
Immune system dysfunction appears to underlie many cases
In a keynote address during the conference, Akiko Iwasaki, PhD, of Yale University, New Haven, Conn., pointed out that long COVID and ME/CFS are among many unexplained postacute infection syndromes associated with a long list of viral pathogens, including Ebola, the prior SARS viruses, Epstein-Barr virus, and Dengue, as well as nonviral pathogens such as Coxiella burnetii (Q fever syndrome) and Borrelia (posttreatment Lyme disease syndrome).
Dr. Iwasaki cited a recent Nature Medicine review article that she coauthored on this topic with an ME/CFS patient, noting: “We really need to understand why some people are failing to recover from these types of diseases.”
Emerging evidence supports four different hypotheses regarding pathogenesis: viral reservoir/viral pathogen-associated molecular pattern molecules, autoimmunity, dysbiosis/viral reactivation, and tissue damage
“Right now, it’s too early to exclude or make any conclusions about these. We need to have an open mind to dissect these various possibilities,” she said.
Two speakers reported findings of immune dysregulation in both ME/CFS and long COVID. Wakiro Sato, MD, PhD, of the National Center of Neurology and Psychiatry, Tokyo, reported that anti–G-protein coupled receptor antibodies were found in 33 (55%) of 60 patients with long COVID, and more than 40% had peripheral immune cell profile abnormalities. These findings were similar to those found in patients with ME/CFS, published by Sato’s team (Brain Behav Immun. 2021 Mar 29. doi: 10.1016/j.bbi.2021.03.023) and other researchers in Germany.
Liisa K. Selin, MD, PhD, professor of pathology at the University of Massachusetts, Worcester, presented data for an analysis of peripheral blood mononuclear cells from 26 donors with ME/CFS (8 with long COVID) and 24 healthy controls. In both patient groups, they found altered expression of inflammatory markers and decreases in CD8 T-cell number and function. The patients with long COVID showed evidence of sustained activation of both T-cell populations with increased CD38 and HLA-DR, associated with a compensatory increased frequency of activated CD4+CD8+ T cells.
“These results are consistent with immune dysregulation associated with overactivation and exhaustion of CD8 T cells, as observed in chronic viral infections and tumor environments,” Dr. Selin said.
ME/CFS and long COVID ‘frighteningly similar, if not identical’
Data for a different system derangement in long COVID and ME/CFS, the pathophysiology of exercise intolerance, were presented in another keynote talk by David M. Systrom, MD, a pulmonary and critical care medicine specialist at Brigham and Women’s Hospital and director of the Massachusetts General Hospital cardiopulmonary laboratory, both in Boston. He has conducted invasive cardiopulmonary exercise testing in patients with ME/CFS and patients with long COVID.
Previously, Dr. Systrom and his team found that patients with ME/CFS have distinct defects in both ventricular filling pressure and oxygen extraction from the muscles. Neither of those are features of deconditioning, which is often blamed for exercise intolerance in people with ME/CFS. Rather, the major defect in deconditioning is decreased stroke volume and cardiac output. In ME/CFS patients, he found supranormal pulmonary blood flow, compared with VO2 max, suggesting peripheral left-to-right shunting.
In addition, Dr. Systrom and colleagues found that a large proportion of ME/CFS patients with these peripheral vascular defects also have biopsy-demonstrated small-fiber neuropathy, suggesting that acute exercise intolerance is related to underlying autonomic nervous system dysfunction.
In Dr. Systrom and colleagues’ long COVID study, invasive cardiopulmonary exercise testing in 10 patients who had recovered from COVID-19 at least 6 months prior and did not have cardiopulmonary disease had significantly revealed reduced peak exercise aerobic capacity (VO2 max), compared with 10 age- and sex-matched controls. The reduction in peak VO2 was associated with impaired systemic oxygen extraction, compared with the controls, despite a preserved peak cardiac index.
The long-COVID patients also showed greater ventilatory inefficiency, which “is entirely related to hyperventilation, not intrinsic lung disease,” Dr. Systrom said, adding that while there may be subsets of patients with interstitial lung disease after acute respiratory distress syndrome, these patients didn’t have that. “This for all the world looks like ME/CFS. We think they are frighteningly similar, if not identical,” Dr. Systrom said.
In a third study for which Dr. Systrom was a coauthor, published in Annals of Neurology, multisystem involvement was found in nine patients following mild COVID-19 infection, using standardized autonomic assessments including Valsalva maneuver, sudomotor and tilt tests, and skin biopsies for small-fiber neuropathy. The findings included cerebrovascular dysregulation with persistent cerebral arteriolar vasoconstriction, small-fiber neuropathy and related dysautonomia, respiratory dysregulation, and chronic inflammation.
Dr. Systrom’s conclusion: “Dyspnea and hyperventilation are common in ME/CFS and long COVID and there is significant overlap with POTS.”
Dr. Bateman disclosed that she is conducting research for Terra Biological. Dr. Systrom said he is conducting research for Astellas.
A version of this article first appeared on Medscape.com.
At the virtual annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (IACFSME), speakers presented data showing similar pathophysiologic abnormalities in people with systemic symptoms associated with ME/CFS who had a prior SARS-CoV-2 infection and those who did not, including individuals whose illness preceded the COVID-19 pandemic.
Core clinical diagnostic criteria for ME/CFS established by the Institute of Medicine in 2015 include substantial decrement in functioning for 6 months or longer, postexertional malaise, or a worsening of symptoms following even minor exertion (often described by patients as “crashes”), unrefreshing sleep, and cognitive dysfunction and/or orthostatic intolerance that are frequent and severe.
Long COVID has been defined in several different ways using different terminology. The U.S. Centers for Disease Control and Prevention, for example, defines “post-COVID conditions” as those continuing four or more weeks beyond first symptoms. The World Health Organization’s clinical case definition of “post COVID-19 condition” includes otherwise unexplained symptoms 3 months from COVID-19 onset and lasting longer than 2 months.
Both ME/CFS and long COVID commonly involve numerous symptoms beyond the defining ones, affecting nearly every organ system in the body, including systemic, neurocognitive, endocrine, cardiovascular, pulmonary, musculoskeletal, and gastrointestinal, with wide variation among individuals. Autonomic dysfunction is common to both conditions, particularly postural orthostatic tachycardia syndrome (POTS).
“My way of understanding these illnesses is that they’re not just multisystem illnesses, but all these interactive systems that lean on each other are dysregulated. … I would say that a very common underlying mediator of both ME/CFS and long COVID is autonomic dysfunction, and it presents as POTS,” Nancy Klimas, MD, director of the Institute for Neuro-Immune Medicine at Nova Southeastern University, Fort Lauderdale, Fla., told this news organization.
Dr. Klimas, who is also director of Clinical Immunology Research at the Miami Veterans Affairs Medical Center, added that “if basic bioenergetics are disrupted and in an oxidative-stress state [then] they have downregulated energy production at the cellular level, which seems to be the case in ME/CFS and now in long COVID.”
New ICD-10 codes better characterize the syndromes
New ICD-10 codes for 2023, being implemented on Oct. 1, will enable clinicians to better document all of these interrelated conditions.
Under the existing G93.3, Postviral and related fatigue syndromes, there will now be:
- G93.31 – Postviral fatigue syndrome.
- G93.32 – Myalgic encephalomyelitis/chronic fatigue syndrome (and the separate terms).
- G93.39 – Other postinfection and related fatigue syndromes.
The old R53.82, “Chronic fatigue, unspecified” code now excludes all of the above conditions.
The additional code U09.9 for “post COVID-19 condition, unspecified,” may also be used if applicable.
In addition, a new code for POTS, G90.A, which wasn’t previously mentioned in ICD-10, may also be used starting Oct. 1.
Lucinda Bateman, MD, founder and director of the Bateman Horne Center, Salt Lake City, advises using all applicable codes for a given patient. “If a patient came into my office with long COVID and met criteria for ME/CFS, we would code both, and also any other syndrome criteria that they may meet, such as POTS or fibromyalgia.
“If people use the codes appropriately, then you can understand the overlap better. It increases the likelihood of reimbursement, creates a more accurate medical record for the patient, and provides them with a better tool should they require disability benefits.”
Dr. Bateman advises in-office orthostatic evaluation for all patients with this symptom constellation, using a passive standing evaluation such as the 10-minute NASA Lean test.
“Clinicians should take the time to do orthostatic testing in these patients because it provides objective markers and will help lead us to potential interventions to help improve people’s function.”
The Bateman Horne center offers clinician resources on management of ME/CFS and related conditions.
How common is ME/CFS after COVID-19?
According to one published meta-analysis, the global prevalence of “post-acute sequelae of SARS-CoV-2,” defined by any symptom, is about 43% of patients overall following infection, and 49% at 120 days. Fatigue was the most commonly reported symptom, followed by memory problems. As of March 22, the World Health Organization estimated that there have been more than 470 million COVID-19 cases, which would give a figure of about 200 million people who are experiencing a wide range of long-COVID symptoms.
On the final day of the IACFSME conference, Luis Nacul, MD, of the University of British Columbia, Vancouver, presented several sets of data from his group and others aiming to determine the proportion of individuals who develop symptoms suggestive of ME/CFS following a COVID-19 infection.
Among a cohort of 88 adults hospitalized with confirmed SARS-CoV-2 infections during the first pandemic wave in 2020 and followed up in the respiratory clinic, rates of reported generalized fatigue were 67% at 3 months and 59.5% at 6 months. Substantial fatigue (that is, present most days and affecting activity levels) were reported by 16% at 3 months and 7% at 6 months. “This should represent in principle the maximum prevalence of cases who would meet the criteria for ME/CFS,” Dr. Nacul said.
Baseline age was indirectly associated with fatigue at 3 and 6 months, while the number of comorbidities a patient had was directly associated. Comorbidities also predicted severe fatigue at 3 months, but the numbers were too small for assessment at 6 months.
Studies involving nonhospitalized patients suggested lower rates. One meta-analysis showed 1-year rates of fatigue in 32% and cognitive impairment in 22%. Another showed very similar rates, reporting fatigue in 28% and memory/concentration difficulties in 18%-19%.
Dr. Nacul cautioned that these figures are likely overestimates since many of the study populations are taken from respiratory or long-COVID clinics. “The evidence on ‘post-COVID fatigue syndrome’ or ME/CFS following COVID is still evolving. There is a huge need for studies looking more closely at cases meeting well-defined ME/CFS criteria. This unfortunately hasn’t been done for most studies.”
Immune system dysfunction appears to underlie many cases
In a keynote address during the conference, Akiko Iwasaki, PhD, of Yale University, New Haven, Conn., pointed out that long COVID and ME/CFS are among many unexplained postacute infection syndromes associated with a long list of viral pathogens, including Ebola, the prior SARS viruses, Epstein-Barr virus, and Dengue, as well as nonviral pathogens such as Coxiella burnetii (Q fever syndrome) and Borrelia (posttreatment Lyme disease syndrome).
Dr. Iwasaki cited a recent Nature Medicine review article that she coauthored on this topic with an ME/CFS patient, noting: “We really need to understand why some people are failing to recover from these types of diseases.”
Emerging evidence supports four different hypotheses regarding pathogenesis: viral reservoir/viral pathogen-associated molecular pattern molecules, autoimmunity, dysbiosis/viral reactivation, and tissue damage
“Right now, it’s too early to exclude or make any conclusions about these. We need to have an open mind to dissect these various possibilities,” she said.
Two speakers reported findings of immune dysregulation in both ME/CFS and long COVID. Wakiro Sato, MD, PhD, of the National Center of Neurology and Psychiatry, Tokyo, reported that anti–G-protein coupled receptor antibodies were found in 33 (55%) of 60 patients with long COVID, and more than 40% had peripheral immune cell profile abnormalities. These findings were similar to those found in patients with ME/CFS, published by Sato’s team (Brain Behav Immun. 2021 Mar 29. doi: 10.1016/j.bbi.2021.03.023) and other researchers in Germany.
Liisa K. Selin, MD, PhD, professor of pathology at the University of Massachusetts, Worcester, presented data for an analysis of peripheral blood mononuclear cells from 26 donors with ME/CFS (8 with long COVID) and 24 healthy controls. In both patient groups, they found altered expression of inflammatory markers and decreases in CD8 T-cell number and function. The patients with long COVID showed evidence of sustained activation of both T-cell populations with increased CD38 and HLA-DR, associated with a compensatory increased frequency of activated CD4+CD8+ T cells.
“These results are consistent with immune dysregulation associated with overactivation and exhaustion of CD8 T cells, as observed in chronic viral infections and tumor environments,” Dr. Selin said.
ME/CFS and long COVID ‘frighteningly similar, if not identical’
Data for a different system derangement in long COVID and ME/CFS, the pathophysiology of exercise intolerance, were presented in another keynote talk by David M. Systrom, MD, a pulmonary and critical care medicine specialist at Brigham and Women’s Hospital and director of the Massachusetts General Hospital cardiopulmonary laboratory, both in Boston. He has conducted invasive cardiopulmonary exercise testing in patients with ME/CFS and patients with long COVID.
Previously, Dr. Systrom and his team found that patients with ME/CFS have distinct defects in both ventricular filling pressure and oxygen extraction from the muscles. Neither of those are features of deconditioning, which is often blamed for exercise intolerance in people with ME/CFS. Rather, the major defect in deconditioning is decreased stroke volume and cardiac output. In ME/CFS patients, he found supranormal pulmonary blood flow, compared with VO2 max, suggesting peripheral left-to-right shunting.
In addition, Dr. Systrom and colleagues found that a large proportion of ME/CFS patients with these peripheral vascular defects also have biopsy-demonstrated small-fiber neuropathy, suggesting that acute exercise intolerance is related to underlying autonomic nervous system dysfunction.
In Dr. Systrom and colleagues’ long COVID study, invasive cardiopulmonary exercise testing in 10 patients who had recovered from COVID-19 at least 6 months prior and did not have cardiopulmonary disease had significantly revealed reduced peak exercise aerobic capacity (VO2 max), compared with 10 age- and sex-matched controls. The reduction in peak VO2 was associated with impaired systemic oxygen extraction, compared with the controls, despite a preserved peak cardiac index.
The long-COVID patients also showed greater ventilatory inefficiency, which “is entirely related to hyperventilation, not intrinsic lung disease,” Dr. Systrom said, adding that while there may be subsets of patients with interstitial lung disease after acute respiratory distress syndrome, these patients didn’t have that. “This for all the world looks like ME/CFS. We think they are frighteningly similar, if not identical,” Dr. Systrom said.
In a third study for which Dr. Systrom was a coauthor, published in Annals of Neurology, multisystem involvement was found in nine patients following mild COVID-19 infection, using standardized autonomic assessments including Valsalva maneuver, sudomotor and tilt tests, and skin biopsies for small-fiber neuropathy. The findings included cerebrovascular dysregulation with persistent cerebral arteriolar vasoconstriction, small-fiber neuropathy and related dysautonomia, respiratory dysregulation, and chronic inflammation.
Dr. Systrom’s conclusion: “Dyspnea and hyperventilation are common in ME/CFS and long COVID and there is significant overlap with POTS.”
Dr. Bateman disclosed that she is conducting research for Terra Biological. Dr. Systrom said he is conducting research for Astellas.
A version of this article first appeared on Medscape.com.
At the virtual annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis (IACFSME), speakers presented data showing similar pathophysiologic abnormalities in people with systemic symptoms associated with ME/CFS who had a prior SARS-CoV-2 infection and those who did not, including individuals whose illness preceded the COVID-19 pandemic.
Core clinical diagnostic criteria for ME/CFS established by the Institute of Medicine in 2015 include substantial decrement in functioning for 6 months or longer, postexertional malaise, or a worsening of symptoms following even minor exertion (often described by patients as “crashes”), unrefreshing sleep, and cognitive dysfunction and/or orthostatic intolerance that are frequent and severe.
Long COVID has been defined in several different ways using different terminology. The U.S. Centers for Disease Control and Prevention, for example, defines “post-COVID conditions” as those continuing four or more weeks beyond first symptoms. The World Health Organization’s clinical case definition of “post COVID-19 condition” includes otherwise unexplained symptoms 3 months from COVID-19 onset and lasting longer than 2 months.
Both ME/CFS and long COVID commonly involve numerous symptoms beyond the defining ones, affecting nearly every organ system in the body, including systemic, neurocognitive, endocrine, cardiovascular, pulmonary, musculoskeletal, and gastrointestinal, with wide variation among individuals. Autonomic dysfunction is common to both conditions, particularly postural orthostatic tachycardia syndrome (POTS).
“My way of understanding these illnesses is that they’re not just multisystem illnesses, but all these interactive systems that lean on each other are dysregulated. … I would say that a very common underlying mediator of both ME/CFS and long COVID is autonomic dysfunction, and it presents as POTS,” Nancy Klimas, MD, director of the Institute for Neuro-Immune Medicine at Nova Southeastern University, Fort Lauderdale, Fla., told this news organization.
Dr. Klimas, who is also director of Clinical Immunology Research at the Miami Veterans Affairs Medical Center, added that “if basic bioenergetics are disrupted and in an oxidative-stress state [then] they have downregulated energy production at the cellular level, which seems to be the case in ME/CFS and now in long COVID.”
New ICD-10 codes better characterize the syndromes
New ICD-10 codes for 2023, being implemented on Oct. 1, will enable clinicians to better document all of these interrelated conditions.
Under the existing G93.3, Postviral and related fatigue syndromes, there will now be:
- G93.31 – Postviral fatigue syndrome.
- G93.32 – Myalgic encephalomyelitis/chronic fatigue syndrome (and the separate terms).
- G93.39 – Other postinfection and related fatigue syndromes.
The old R53.82, “Chronic fatigue, unspecified” code now excludes all of the above conditions.
The additional code U09.9 for “post COVID-19 condition, unspecified,” may also be used if applicable.
In addition, a new code for POTS, G90.A, which wasn’t previously mentioned in ICD-10, may also be used starting Oct. 1.
Lucinda Bateman, MD, founder and director of the Bateman Horne Center, Salt Lake City, advises using all applicable codes for a given patient. “If a patient came into my office with long COVID and met criteria for ME/CFS, we would code both, and also any other syndrome criteria that they may meet, such as POTS or fibromyalgia.
“If people use the codes appropriately, then you can understand the overlap better. It increases the likelihood of reimbursement, creates a more accurate medical record for the patient, and provides them with a better tool should they require disability benefits.”
Dr. Bateman advises in-office orthostatic evaluation for all patients with this symptom constellation, using a passive standing evaluation such as the 10-minute NASA Lean test.
“Clinicians should take the time to do orthostatic testing in these patients because it provides objective markers and will help lead us to potential interventions to help improve people’s function.”
The Bateman Horne center offers clinician resources on management of ME/CFS and related conditions.
How common is ME/CFS after COVID-19?
According to one published meta-analysis, the global prevalence of “post-acute sequelae of SARS-CoV-2,” defined by any symptom, is about 43% of patients overall following infection, and 49% at 120 days. Fatigue was the most commonly reported symptom, followed by memory problems. As of March 22, the World Health Organization estimated that there have been more than 470 million COVID-19 cases, which would give a figure of about 200 million people who are experiencing a wide range of long-COVID symptoms.
On the final day of the IACFSME conference, Luis Nacul, MD, of the University of British Columbia, Vancouver, presented several sets of data from his group and others aiming to determine the proportion of individuals who develop symptoms suggestive of ME/CFS following a COVID-19 infection.
Among a cohort of 88 adults hospitalized with confirmed SARS-CoV-2 infections during the first pandemic wave in 2020 and followed up in the respiratory clinic, rates of reported generalized fatigue were 67% at 3 months and 59.5% at 6 months. Substantial fatigue (that is, present most days and affecting activity levels) were reported by 16% at 3 months and 7% at 6 months. “This should represent in principle the maximum prevalence of cases who would meet the criteria for ME/CFS,” Dr. Nacul said.
Baseline age was indirectly associated with fatigue at 3 and 6 months, while the number of comorbidities a patient had was directly associated. Comorbidities also predicted severe fatigue at 3 months, but the numbers were too small for assessment at 6 months.
Studies involving nonhospitalized patients suggested lower rates. One meta-analysis showed 1-year rates of fatigue in 32% and cognitive impairment in 22%. Another showed very similar rates, reporting fatigue in 28% and memory/concentration difficulties in 18%-19%.
Dr. Nacul cautioned that these figures are likely overestimates since many of the study populations are taken from respiratory or long-COVID clinics. “The evidence on ‘post-COVID fatigue syndrome’ or ME/CFS following COVID is still evolving. There is a huge need for studies looking more closely at cases meeting well-defined ME/CFS criteria. This unfortunately hasn’t been done for most studies.”
Immune system dysfunction appears to underlie many cases
In a keynote address during the conference, Akiko Iwasaki, PhD, of Yale University, New Haven, Conn., pointed out that long COVID and ME/CFS are among many unexplained postacute infection syndromes associated with a long list of viral pathogens, including Ebola, the prior SARS viruses, Epstein-Barr virus, and Dengue, as well as nonviral pathogens such as Coxiella burnetii (Q fever syndrome) and Borrelia (posttreatment Lyme disease syndrome).
Dr. Iwasaki cited a recent Nature Medicine review article that she coauthored on this topic with an ME/CFS patient, noting: “We really need to understand why some people are failing to recover from these types of diseases.”
Emerging evidence supports four different hypotheses regarding pathogenesis: viral reservoir/viral pathogen-associated molecular pattern molecules, autoimmunity, dysbiosis/viral reactivation, and tissue damage
“Right now, it’s too early to exclude or make any conclusions about these. We need to have an open mind to dissect these various possibilities,” she said.
Two speakers reported findings of immune dysregulation in both ME/CFS and long COVID. Wakiro Sato, MD, PhD, of the National Center of Neurology and Psychiatry, Tokyo, reported that anti–G-protein coupled receptor antibodies were found in 33 (55%) of 60 patients with long COVID, and more than 40% had peripheral immune cell profile abnormalities. These findings were similar to those found in patients with ME/CFS, published by Sato’s team (Brain Behav Immun. 2021 Mar 29. doi: 10.1016/j.bbi.2021.03.023) and other researchers in Germany.
Liisa K. Selin, MD, PhD, professor of pathology at the University of Massachusetts, Worcester, presented data for an analysis of peripheral blood mononuclear cells from 26 donors with ME/CFS (8 with long COVID) and 24 healthy controls. In both patient groups, they found altered expression of inflammatory markers and decreases in CD8 T-cell number and function. The patients with long COVID showed evidence of sustained activation of both T-cell populations with increased CD38 and HLA-DR, associated with a compensatory increased frequency of activated CD4+CD8+ T cells.
“These results are consistent with immune dysregulation associated with overactivation and exhaustion of CD8 T cells, as observed in chronic viral infections and tumor environments,” Dr. Selin said.
ME/CFS and long COVID ‘frighteningly similar, if not identical’
Data for a different system derangement in long COVID and ME/CFS, the pathophysiology of exercise intolerance, were presented in another keynote talk by David M. Systrom, MD, a pulmonary and critical care medicine specialist at Brigham and Women’s Hospital and director of the Massachusetts General Hospital cardiopulmonary laboratory, both in Boston. He has conducted invasive cardiopulmonary exercise testing in patients with ME/CFS and patients with long COVID.
Previously, Dr. Systrom and his team found that patients with ME/CFS have distinct defects in both ventricular filling pressure and oxygen extraction from the muscles. Neither of those are features of deconditioning, which is often blamed for exercise intolerance in people with ME/CFS. Rather, the major defect in deconditioning is decreased stroke volume and cardiac output. In ME/CFS patients, he found supranormal pulmonary blood flow, compared with VO2 max, suggesting peripheral left-to-right shunting.
In addition, Dr. Systrom and colleagues found that a large proportion of ME/CFS patients with these peripheral vascular defects also have biopsy-demonstrated small-fiber neuropathy, suggesting that acute exercise intolerance is related to underlying autonomic nervous system dysfunction.
In Dr. Systrom and colleagues’ long COVID study, invasive cardiopulmonary exercise testing in 10 patients who had recovered from COVID-19 at least 6 months prior and did not have cardiopulmonary disease had significantly revealed reduced peak exercise aerobic capacity (VO2 max), compared with 10 age- and sex-matched controls. The reduction in peak VO2 was associated with impaired systemic oxygen extraction, compared with the controls, despite a preserved peak cardiac index.
The long-COVID patients also showed greater ventilatory inefficiency, which “is entirely related to hyperventilation, not intrinsic lung disease,” Dr. Systrom said, adding that while there may be subsets of patients with interstitial lung disease after acute respiratory distress syndrome, these patients didn’t have that. “This for all the world looks like ME/CFS. We think they are frighteningly similar, if not identical,” Dr. Systrom said.
In a third study for which Dr. Systrom was a coauthor, published in Annals of Neurology, multisystem involvement was found in nine patients following mild COVID-19 infection, using standardized autonomic assessments including Valsalva maneuver, sudomotor and tilt tests, and skin biopsies for small-fiber neuropathy. The findings included cerebrovascular dysregulation with persistent cerebral arteriolar vasoconstriction, small-fiber neuropathy and related dysautonomia, respiratory dysregulation, and chronic inflammation.
Dr. Systrom’s conclusion: “Dyspnea and hyperventilation are common in ME/CFS and long COVID and there is significant overlap with POTS.”
Dr. Bateman disclosed that she is conducting research for Terra Biological. Dr. Systrom said he is conducting research for Astellas.
A version of this article first appeared on Medscape.com.
FROM IACFSME 2022
Treatments explored to ease postviral symptoms of ME/CFS and long COVID
A variety of treatments, most already commercially available, are under investigation for treating the constellation of overlapping symptoms associated with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), “long COVID,” and dysautonomia.
At the virtual annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, speakers presented data for a variety of approaches to ease symptoms common across postviral conditions, such as extreme fatigue, postexertional malaise (“crash”), cognitive dysfunction (“brain fog”), orthostatic intolerance including postural orthostatic tachycardia syndrome (POTS), and chronic pain. Most of the modalities are already commercially available for other indications, although some are costly and not covered by payers for these conditions.
“ ... In the past, patients were told ‘you have chronic fatigue syndrome but there’s nothing we can do for it.’ That certainly is not the case. There aren’t cures, but there are many management techniques to improve symptoms,” Charles W. Lapp, MD, medical director of the Hunter-Hopkins Center, Charlotte, N.C., said in an interview.
A current mainstay of treatment for ME/CFS – including that triggered by COVID-19 – is activity pacing, in which patients learn to stay within their “energy envelopes” in order to avoid postexertional malaise, a worsening of all symptoms with exertion. The use of “graded exercise” is no longer recommended, per U.K. and U.S. guidelines.
Data for the following approaches were presented at the IACFS/ME conference:
Pyridostigmine (mestinon, others)
Pyridostigmine, an acetylcholinesterase inhibitor, is approved for the treatment of muscle weakness resulting from myasthenia gravis and is available in generic form. It has previously been shown to produce significant improvement in both symptom burden and heart rate response in POTS.
At the IACFS/ME conference, David M. Systrom, MD, a pulmonary and critical care medicine specialist at Brigham and Women’s Hospital and director of the Massachusetts General Hospital Cardiopulmonary laboratory, both in Boston, summarized his group’s study in patients with ME/CFS using pyridostigmine as both a potential treatment for improving exercise capacity and a proof-of-concept that neurovascular dysregulation underlies exertional intolerance in the condition.
A total of 45 patients were randomized to 60 mg oral pyridostigmine or placebo after an invasive cardiopulmonary exercise test, and a second test performed 50 minutes later. Peak VO2 increased after pyridostigmine but decreased after placebo (+13.3 mL/min vs. –40.2 mL/min, P < .05). Cardiac output and right atrial pressure were also significantly improved with pyridostigmine and worse with placebo.
“We suggest that treatable neurovascular dysregulation underlies acute exercise intolerance in ME/CFS. ... Pyridostigmine may be a useful repurposed off-label treatment [for] a subset of patients with exercise intolerance,” Dr. Systrom said.
Asked to comment, Dr. Lapp said: “We’ve used Mestinon for years because it helps with POTS and also with neurally mediated hypotension. Systrom is taking it to a new level because he’s shown that it increases preload to the heart.” However, he noted that it’s unclear whether the drug will help patients who don’t have POTS specifically. On the other hand, patients rarely experience side effects from the drug.
Since the generic tablets come only in 60-mg doses, and the starting dose is 30 mg three times a day, he advised cutting the tablets in half during titration up to 60 mg three times a day.
Oxaloacetate (benaGene)
David Lyons Kaufman, MD, of the Center for Complex Diseases, Mountain View, Calif., summarized data from his group’s recently published open-label, nonrandomized, “proof-of-concept” study on use of the commercially available nutritional supplement anhydrous enol-oxaloacetate for treating mental and physical fatigue in 76 patients with longstanding ME/CFS and 43 with long-COVID fatigue.
Oxaloacetate is a major step in the Krebs cycle within the mitochondria that are depleted in patients with ME/CFS. It is also an energy metabolite that has multiple effects in cells and mitochondria, Dr. Kaufman explained.
Doses ranging from 500 mg twice daily up to 1,000 mg three times a day were given for 6 weeks. Up to 33% of the patients with ME/CFS and up to 46.8% of the long-COVID group achieved clinical efficacy as measured by physical and mental fatigue scores, compared with just 5.9% of historical ME/CFS controls. All doses showed highly significant improvements.
The only adverse effects were occasional dyspepsia, which was avoided by taking the supplement with food, and insomnia, resolved by having them dose at breakfast and lunch, Dr. Kaufman said.
Following those preliminary data, there is now an ongoing 90-day, randomized, placebo-controlled clinical trial of 80 patients with ME/CFS using 2,000 mg anhydrous enol-oxaloacetate per day. Endpoints include multiple objective measures.
“We have a health care crisis with long COVID, and we’ve had this smoldering crisis with ME/CFS for decades that’s never been addressed. ME/CFS and long COVID, if not identical, are certainly overlapping. ... We have to pursue these translational medicine pilot studies as rapidly as possible,” Dr. Kaufman remarked.
Dr. Lapp told this news organization that it makes sense to use constituents of the Krebs cycle to improve mitochondrial function, but the problem with oxaloacetate is its cost. Dr. Kaufman mentioned that based on the preliminary trial, the therapeutic “sweet spot” appeared to be 1,000 mg twice daily. The manufacturer’s website lists the price for a single bottle of 30 250-mg capsules at $49, or $42 if purchased via a monthly subscription.
“It’s a benign drug, and it’s over the counter. I would give it to any patient who’s got a big wallet,” Dr. Lapp quipped, adding: “If they’ve got the money, they can order it tonight.”
Inspiritol
Inspiritol is an investigational “nebulized, inhaled, multimechanism medication designed to treat the major symptoms of respiratory distress with antioxidant, anti-inflammatory, and broad-spectrum antiviral and antibacterial properties. Inspiritol is composed of both endogenously produced and naturally occurring, well-tolerated biochemicals,” according to the company website.
The hypothesis, Liisa K. Selin, MD, PhD, professor of pathology at the University of Massachusetts, Worcester, said at the meeting, is that “ME/CFS and long COVID-19 result from an aberrant response to an immunological trigger like infection, which results in a permanently dysregulated immune system as a result of overactivation of CD8 T cells and subsequent exhaustion.”
Inspiritol, containing five antioxidants, acts as an immune modulator to reverse the CD8 T cell exhaustion and improve symptoms. Administration by inhaler delivers it directly to the brain from the lung. It was originally designed for use in chronic obstructive pulmonary disease and asthma and has shown efficacy for acute COVID-19, Dr. Selin said.
In a preliminary study, four patients with ME/CFS and five with long COVID have been treated with Inspiritol for 2-15 months, and all have self-reported improved symptoms. Cough has been the only reported side effect.
The company is pursuing an Investigational New Drug Application for the product with the Food and Drug Administration and has several patents pending. Dr. Lapp called Inspiritol “very interesting,” and said that reversal of CD8 “exhaustion” also would appear to be a promising approach. However, he noted, “the problem is that we don’t know what’s in it.”
Stellate ganglion block
Injection of local anesthetic near the stellate ganglion to block activity of the entire cervical sympathetic chain has been used for nearly a century to treat a variety of sympathetically mediated conditions, including complex regional pain syndrome (CRPS), shingles, and phantom-limb pain. More recently, it has been used in a variety of other conditions, including PTSD, Raynaud’s disease, menopausal hot flashes, and hyperhidrosis.
Insurance companies typically cover it for CRPS, neuropathic upper-extremity pain, hyperhidrosis, and Raynaud’s, said Luke Liu, MD, an anesthesiologist who is founder and chief executive officer of Alaska-based pain management company Neuroversion.
Deborah Duricka, PhD, also with Neuroversion, presented results from a now-published case series of 11 patients with long COVID who underwent stellate ganglion block by a board-certified anesthesiologist, first on one side at the level of C6, then on the contralateral side the following day.
Clinically meaningful benefits were seen in at least five of the patients in fatigue, memory problems, problems concentrating, rapid heartbeat, orthostatic intolerance, sleep problems, postexertional malaise, anxiety, and depression.
The hypothetical mechanism, she said, is that “sympathetic block prevents sympathetically driven vasoconstriction in carotid and vertebral arteries.”
Dr. Liu presented another case series of five patients with ME/CFS who underwent the procedure with ultrasound guidance, again on one side and the other side the next day. All had upper-limb autonomic issues such as Raynaud’s and/or neuropathic pain that had been refractory to more conventional treatments.
All five patients reported improvements in symptoms of ME/CFS, including energy level, cognition, pain, and postexertional malaise. One patient reported “feeling well for the first time in decades.” However, that patient relapsed after a mild viral illness 3.5 months after treatment. Some of the patients have required further treatments.
Dr. Lapp commented that, although the procedure is generally safe when performed by an experienced clinician, “Any time you do an injection like that, there’s a high risk that you could nick an artery or a vein or hit an essential nerve in the neck. That’s why it has to be done under fluoroscopy or ultrasound.”
He said he’s had a few patients undergo the procedure, mostly for CRPS, and they seem to have benefited from it. “It might increase cerebral blood flow and preload to the heart, so it might decrease ME/CFS symptoms and help with POTS as well.”
Nonetheless, Dr. Lapp said he wouldn’t consider stellate ganglion block as first-line treatment for ME/CFS or long COVID. “I think it would be for the treatment-resistant patient, when you’ve gone through all the treatments that we know and addressed all the comorbidities and they’re still not getting better.”
But, he added, it is a standard procedure. “Any pain clinic can do a stellate block.”
Transcutaneous auricular vagus nerve stimulation
Nicola Clague-Baker, PhD, a physiotherapist at the University of Liverpool (England), presented findings from an international survey of people with ME/CFS regarding their experience with transcutaneous auricular vagus nerve stimulation (taVNS) to manage their autonomic symptoms. The technique involves stimulation of the autonomic nervous system via the vagus nerve using electrodes applied to part of the ear. The theory is that the technique stimulates the parasympathetic nervous system and improves autonomic balance.
Two small previous trials showing benefit of vagus nerve stimulation for people with ME/CFS used more invasive and less comfortable methods of applying the stimulation rather than to the ear, Dr. Clague-Baker and colleagues noted in a poster. It has also been used successfully in treating POTS, another conference speaker noted.
A total of 131 people with ME/CFS (called simply “ME” in the United Kingdom) responded to a survey advertised on social media and websites. The majority (60%) were from the United Kingdom while the rest were from Europe, Australia, and North America. Most were female, and slightly more than half had lived with ME for 10 or more years.
The majority (72%) were still using taVNS, while 28% had stopped using it. Only 9% had used the modality for longer than a year. Respondents identified more than 30 benefits in symptoms and activities, with improvements in postexertional malaise (39%) and brain fog (37%) being the most common. One reported significant reduction in constipation.
However, respondents also mentioned more than 20 short- and long-term negatives, including headaches (15%) and long-term irritation at the site (9%). One participant reported a “big improvement in neuropathic pain, but not so much for muscles and joints.”
Overall, 80% reported that they would continue using taVNS and 67% said they would recommend it to others with ME, and 56% said that the system was mildly to very beneficial.
Dr. Lapp noted that several types of transcutaneous electrical nerve stimulation units with ear clips are sold online, and he’s seen them work well for migraine treatment. However, he cautioned that some patients have had side effects from the treatment, such as headaches and dizziness. “It’s putting an electrical current through your brain. In my mind, it’s another last-ditch measure.”
Dr. Lapp reported no financial disclosures.
A version of this article first appeared on Medscape.com.
A variety of treatments, most already commercially available, are under investigation for treating the constellation of overlapping symptoms associated with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), “long COVID,” and dysautonomia.
At the virtual annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, speakers presented data for a variety of approaches to ease symptoms common across postviral conditions, such as extreme fatigue, postexertional malaise (“crash”), cognitive dysfunction (“brain fog”), orthostatic intolerance including postural orthostatic tachycardia syndrome (POTS), and chronic pain. Most of the modalities are already commercially available for other indications, although some are costly and not covered by payers for these conditions.
“ ... In the past, patients were told ‘you have chronic fatigue syndrome but there’s nothing we can do for it.’ That certainly is not the case. There aren’t cures, but there are many management techniques to improve symptoms,” Charles W. Lapp, MD, medical director of the Hunter-Hopkins Center, Charlotte, N.C., said in an interview.
A current mainstay of treatment for ME/CFS – including that triggered by COVID-19 – is activity pacing, in which patients learn to stay within their “energy envelopes” in order to avoid postexertional malaise, a worsening of all symptoms with exertion. The use of “graded exercise” is no longer recommended, per U.K. and U.S. guidelines.
Data for the following approaches were presented at the IACFS/ME conference:
Pyridostigmine (mestinon, others)
Pyridostigmine, an acetylcholinesterase inhibitor, is approved for the treatment of muscle weakness resulting from myasthenia gravis and is available in generic form. It has previously been shown to produce significant improvement in both symptom burden and heart rate response in POTS.
At the IACFS/ME conference, David M. Systrom, MD, a pulmonary and critical care medicine specialist at Brigham and Women’s Hospital and director of the Massachusetts General Hospital Cardiopulmonary laboratory, both in Boston, summarized his group’s study in patients with ME/CFS using pyridostigmine as both a potential treatment for improving exercise capacity and a proof-of-concept that neurovascular dysregulation underlies exertional intolerance in the condition.
A total of 45 patients were randomized to 60 mg oral pyridostigmine or placebo after an invasive cardiopulmonary exercise test, and a second test performed 50 minutes later. Peak VO2 increased after pyridostigmine but decreased after placebo (+13.3 mL/min vs. –40.2 mL/min, P < .05). Cardiac output and right atrial pressure were also significantly improved with pyridostigmine and worse with placebo.
“We suggest that treatable neurovascular dysregulation underlies acute exercise intolerance in ME/CFS. ... Pyridostigmine may be a useful repurposed off-label treatment [for] a subset of patients with exercise intolerance,” Dr. Systrom said.
Asked to comment, Dr. Lapp said: “We’ve used Mestinon for years because it helps with POTS and also with neurally mediated hypotension. Systrom is taking it to a new level because he’s shown that it increases preload to the heart.” However, he noted that it’s unclear whether the drug will help patients who don’t have POTS specifically. On the other hand, patients rarely experience side effects from the drug.
Since the generic tablets come only in 60-mg doses, and the starting dose is 30 mg three times a day, he advised cutting the tablets in half during titration up to 60 mg three times a day.
Oxaloacetate (benaGene)
David Lyons Kaufman, MD, of the Center for Complex Diseases, Mountain View, Calif., summarized data from his group’s recently published open-label, nonrandomized, “proof-of-concept” study on use of the commercially available nutritional supplement anhydrous enol-oxaloacetate for treating mental and physical fatigue in 76 patients with longstanding ME/CFS and 43 with long-COVID fatigue.
Oxaloacetate is a major step in the Krebs cycle within the mitochondria that are depleted in patients with ME/CFS. It is also an energy metabolite that has multiple effects in cells and mitochondria, Dr. Kaufman explained.
Doses ranging from 500 mg twice daily up to 1,000 mg three times a day were given for 6 weeks. Up to 33% of the patients with ME/CFS and up to 46.8% of the long-COVID group achieved clinical efficacy as measured by physical and mental fatigue scores, compared with just 5.9% of historical ME/CFS controls. All doses showed highly significant improvements.
The only adverse effects were occasional dyspepsia, which was avoided by taking the supplement with food, and insomnia, resolved by having them dose at breakfast and lunch, Dr. Kaufman said.
Following those preliminary data, there is now an ongoing 90-day, randomized, placebo-controlled clinical trial of 80 patients with ME/CFS using 2,000 mg anhydrous enol-oxaloacetate per day. Endpoints include multiple objective measures.
“We have a health care crisis with long COVID, and we’ve had this smoldering crisis with ME/CFS for decades that’s never been addressed. ME/CFS and long COVID, if not identical, are certainly overlapping. ... We have to pursue these translational medicine pilot studies as rapidly as possible,” Dr. Kaufman remarked.
Dr. Lapp told this news organization that it makes sense to use constituents of the Krebs cycle to improve mitochondrial function, but the problem with oxaloacetate is its cost. Dr. Kaufman mentioned that based on the preliminary trial, the therapeutic “sweet spot” appeared to be 1,000 mg twice daily. The manufacturer’s website lists the price for a single bottle of 30 250-mg capsules at $49, or $42 if purchased via a monthly subscription.
“It’s a benign drug, and it’s over the counter. I would give it to any patient who’s got a big wallet,” Dr. Lapp quipped, adding: “If they’ve got the money, they can order it tonight.”
Inspiritol
Inspiritol is an investigational “nebulized, inhaled, multimechanism medication designed to treat the major symptoms of respiratory distress with antioxidant, anti-inflammatory, and broad-spectrum antiviral and antibacterial properties. Inspiritol is composed of both endogenously produced and naturally occurring, well-tolerated biochemicals,” according to the company website.
The hypothesis, Liisa K. Selin, MD, PhD, professor of pathology at the University of Massachusetts, Worcester, said at the meeting, is that “ME/CFS and long COVID-19 result from an aberrant response to an immunological trigger like infection, which results in a permanently dysregulated immune system as a result of overactivation of CD8 T cells and subsequent exhaustion.”
Inspiritol, containing five antioxidants, acts as an immune modulator to reverse the CD8 T cell exhaustion and improve symptoms. Administration by inhaler delivers it directly to the brain from the lung. It was originally designed for use in chronic obstructive pulmonary disease and asthma and has shown efficacy for acute COVID-19, Dr. Selin said.
In a preliminary study, four patients with ME/CFS and five with long COVID have been treated with Inspiritol for 2-15 months, and all have self-reported improved symptoms. Cough has been the only reported side effect.
The company is pursuing an Investigational New Drug Application for the product with the Food and Drug Administration and has several patents pending. Dr. Lapp called Inspiritol “very interesting,” and said that reversal of CD8 “exhaustion” also would appear to be a promising approach. However, he noted, “the problem is that we don’t know what’s in it.”
Stellate ganglion block
Injection of local anesthetic near the stellate ganglion to block activity of the entire cervical sympathetic chain has been used for nearly a century to treat a variety of sympathetically mediated conditions, including complex regional pain syndrome (CRPS), shingles, and phantom-limb pain. More recently, it has been used in a variety of other conditions, including PTSD, Raynaud’s disease, menopausal hot flashes, and hyperhidrosis.
Insurance companies typically cover it for CRPS, neuropathic upper-extremity pain, hyperhidrosis, and Raynaud’s, said Luke Liu, MD, an anesthesiologist who is founder and chief executive officer of Alaska-based pain management company Neuroversion.
Deborah Duricka, PhD, also with Neuroversion, presented results from a now-published case series of 11 patients with long COVID who underwent stellate ganglion block by a board-certified anesthesiologist, first on one side at the level of C6, then on the contralateral side the following day.
Clinically meaningful benefits were seen in at least five of the patients in fatigue, memory problems, problems concentrating, rapid heartbeat, orthostatic intolerance, sleep problems, postexertional malaise, anxiety, and depression.
The hypothetical mechanism, she said, is that “sympathetic block prevents sympathetically driven vasoconstriction in carotid and vertebral arteries.”
Dr. Liu presented another case series of five patients with ME/CFS who underwent the procedure with ultrasound guidance, again on one side and the other side the next day. All had upper-limb autonomic issues such as Raynaud’s and/or neuropathic pain that had been refractory to more conventional treatments.
All five patients reported improvements in symptoms of ME/CFS, including energy level, cognition, pain, and postexertional malaise. One patient reported “feeling well for the first time in decades.” However, that patient relapsed after a mild viral illness 3.5 months after treatment. Some of the patients have required further treatments.
Dr. Lapp commented that, although the procedure is generally safe when performed by an experienced clinician, “Any time you do an injection like that, there’s a high risk that you could nick an artery or a vein or hit an essential nerve in the neck. That’s why it has to be done under fluoroscopy or ultrasound.”
He said he’s had a few patients undergo the procedure, mostly for CRPS, and they seem to have benefited from it. “It might increase cerebral blood flow and preload to the heart, so it might decrease ME/CFS symptoms and help with POTS as well.”
Nonetheless, Dr. Lapp said he wouldn’t consider stellate ganglion block as first-line treatment for ME/CFS or long COVID. “I think it would be for the treatment-resistant patient, when you’ve gone through all the treatments that we know and addressed all the comorbidities and they’re still not getting better.”
But, he added, it is a standard procedure. “Any pain clinic can do a stellate block.”
Transcutaneous auricular vagus nerve stimulation
Nicola Clague-Baker, PhD, a physiotherapist at the University of Liverpool (England), presented findings from an international survey of people with ME/CFS regarding their experience with transcutaneous auricular vagus nerve stimulation (taVNS) to manage their autonomic symptoms. The technique involves stimulation of the autonomic nervous system via the vagus nerve using electrodes applied to part of the ear. The theory is that the technique stimulates the parasympathetic nervous system and improves autonomic balance.
Two small previous trials showing benefit of vagus nerve stimulation for people with ME/CFS used more invasive and less comfortable methods of applying the stimulation rather than to the ear, Dr. Clague-Baker and colleagues noted in a poster. It has also been used successfully in treating POTS, another conference speaker noted.
A total of 131 people with ME/CFS (called simply “ME” in the United Kingdom) responded to a survey advertised on social media and websites. The majority (60%) were from the United Kingdom while the rest were from Europe, Australia, and North America. Most were female, and slightly more than half had lived with ME for 10 or more years.
The majority (72%) were still using taVNS, while 28% had stopped using it. Only 9% had used the modality for longer than a year. Respondents identified more than 30 benefits in symptoms and activities, with improvements in postexertional malaise (39%) and brain fog (37%) being the most common. One reported significant reduction in constipation.
However, respondents also mentioned more than 20 short- and long-term negatives, including headaches (15%) and long-term irritation at the site (9%). One participant reported a “big improvement in neuropathic pain, but not so much for muscles and joints.”
Overall, 80% reported that they would continue using taVNS and 67% said they would recommend it to others with ME, and 56% said that the system was mildly to very beneficial.
Dr. Lapp noted that several types of transcutaneous electrical nerve stimulation units with ear clips are sold online, and he’s seen them work well for migraine treatment. However, he cautioned that some patients have had side effects from the treatment, such as headaches and dizziness. “It’s putting an electrical current through your brain. In my mind, it’s another last-ditch measure.”
Dr. Lapp reported no financial disclosures.
A version of this article first appeared on Medscape.com.
A variety of treatments, most already commercially available, are under investigation for treating the constellation of overlapping symptoms associated with myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS), “long COVID,” and dysautonomia.
At the virtual annual meeting of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, speakers presented data for a variety of approaches to ease symptoms common across postviral conditions, such as extreme fatigue, postexertional malaise (“crash”), cognitive dysfunction (“brain fog”), orthostatic intolerance including postural orthostatic tachycardia syndrome (POTS), and chronic pain. Most of the modalities are already commercially available for other indications, although some are costly and not covered by payers for these conditions.
“ ... In the past, patients were told ‘you have chronic fatigue syndrome but there’s nothing we can do for it.’ That certainly is not the case. There aren’t cures, but there are many management techniques to improve symptoms,” Charles W. Lapp, MD, medical director of the Hunter-Hopkins Center, Charlotte, N.C., said in an interview.
A current mainstay of treatment for ME/CFS – including that triggered by COVID-19 – is activity pacing, in which patients learn to stay within their “energy envelopes” in order to avoid postexertional malaise, a worsening of all symptoms with exertion. The use of “graded exercise” is no longer recommended, per U.K. and U.S. guidelines.
Data for the following approaches were presented at the IACFS/ME conference:
Pyridostigmine (mestinon, others)
Pyridostigmine, an acetylcholinesterase inhibitor, is approved for the treatment of muscle weakness resulting from myasthenia gravis and is available in generic form. It has previously been shown to produce significant improvement in both symptom burden and heart rate response in POTS.
At the IACFS/ME conference, David M. Systrom, MD, a pulmonary and critical care medicine specialist at Brigham and Women’s Hospital and director of the Massachusetts General Hospital Cardiopulmonary laboratory, both in Boston, summarized his group’s study in patients with ME/CFS using pyridostigmine as both a potential treatment for improving exercise capacity and a proof-of-concept that neurovascular dysregulation underlies exertional intolerance in the condition.
A total of 45 patients were randomized to 60 mg oral pyridostigmine or placebo after an invasive cardiopulmonary exercise test, and a second test performed 50 minutes later. Peak VO2 increased after pyridostigmine but decreased after placebo (+13.3 mL/min vs. –40.2 mL/min, P < .05). Cardiac output and right atrial pressure were also significantly improved with pyridostigmine and worse with placebo.
“We suggest that treatable neurovascular dysregulation underlies acute exercise intolerance in ME/CFS. ... Pyridostigmine may be a useful repurposed off-label treatment [for] a subset of patients with exercise intolerance,” Dr. Systrom said.
Asked to comment, Dr. Lapp said: “We’ve used Mestinon for years because it helps with POTS and also with neurally mediated hypotension. Systrom is taking it to a new level because he’s shown that it increases preload to the heart.” However, he noted that it’s unclear whether the drug will help patients who don’t have POTS specifically. On the other hand, patients rarely experience side effects from the drug.
Since the generic tablets come only in 60-mg doses, and the starting dose is 30 mg three times a day, he advised cutting the tablets in half during titration up to 60 mg three times a day.
Oxaloacetate (benaGene)
David Lyons Kaufman, MD, of the Center for Complex Diseases, Mountain View, Calif., summarized data from his group’s recently published open-label, nonrandomized, “proof-of-concept” study on use of the commercially available nutritional supplement anhydrous enol-oxaloacetate for treating mental and physical fatigue in 76 patients with longstanding ME/CFS and 43 with long-COVID fatigue.
Oxaloacetate is a major step in the Krebs cycle within the mitochondria that are depleted in patients with ME/CFS. It is also an energy metabolite that has multiple effects in cells and mitochondria, Dr. Kaufman explained.
Doses ranging from 500 mg twice daily up to 1,000 mg three times a day were given for 6 weeks. Up to 33% of the patients with ME/CFS and up to 46.8% of the long-COVID group achieved clinical efficacy as measured by physical and mental fatigue scores, compared with just 5.9% of historical ME/CFS controls. All doses showed highly significant improvements.
The only adverse effects were occasional dyspepsia, which was avoided by taking the supplement with food, and insomnia, resolved by having them dose at breakfast and lunch, Dr. Kaufman said.
Following those preliminary data, there is now an ongoing 90-day, randomized, placebo-controlled clinical trial of 80 patients with ME/CFS using 2,000 mg anhydrous enol-oxaloacetate per day. Endpoints include multiple objective measures.
“We have a health care crisis with long COVID, and we’ve had this smoldering crisis with ME/CFS for decades that’s never been addressed. ME/CFS and long COVID, if not identical, are certainly overlapping. ... We have to pursue these translational medicine pilot studies as rapidly as possible,” Dr. Kaufman remarked.
Dr. Lapp told this news organization that it makes sense to use constituents of the Krebs cycle to improve mitochondrial function, but the problem with oxaloacetate is its cost. Dr. Kaufman mentioned that based on the preliminary trial, the therapeutic “sweet spot” appeared to be 1,000 mg twice daily. The manufacturer’s website lists the price for a single bottle of 30 250-mg capsules at $49, or $42 if purchased via a monthly subscription.
“It’s a benign drug, and it’s over the counter. I would give it to any patient who’s got a big wallet,” Dr. Lapp quipped, adding: “If they’ve got the money, they can order it tonight.”
Inspiritol
Inspiritol is an investigational “nebulized, inhaled, multimechanism medication designed to treat the major symptoms of respiratory distress with antioxidant, anti-inflammatory, and broad-spectrum antiviral and antibacterial properties. Inspiritol is composed of both endogenously produced and naturally occurring, well-tolerated biochemicals,” according to the company website.
The hypothesis, Liisa K. Selin, MD, PhD, professor of pathology at the University of Massachusetts, Worcester, said at the meeting, is that “ME/CFS and long COVID-19 result from an aberrant response to an immunological trigger like infection, which results in a permanently dysregulated immune system as a result of overactivation of CD8 T cells and subsequent exhaustion.”
Inspiritol, containing five antioxidants, acts as an immune modulator to reverse the CD8 T cell exhaustion and improve symptoms. Administration by inhaler delivers it directly to the brain from the lung. It was originally designed for use in chronic obstructive pulmonary disease and asthma and has shown efficacy for acute COVID-19, Dr. Selin said.
In a preliminary study, four patients with ME/CFS and five with long COVID have been treated with Inspiritol for 2-15 months, and all have self-reported improved symptoms. Cough has been the only reported side effect.
The company is pursuing an Investigational New Drug Application for the product with the Food and Drug Administration and has several patents pending. Dr. Lapp called Inspiritol “very interesting,” and said that reversal of CD8 “exhaustion” also would appear to be a promising approach. However, he noted, “the problem is that we don’t know what’s in it.”
Stellate ganglion block
Injection of local anesthetic near the stellate ganglion to block activity of the entire cervical sympathetic chain has been used for nearly a century to treat a variety of sympathetically mediated conditions, including complex regional pain syndrome (CRPS), shingles, and phantom-limb pain. More recently, it has been used in a variety of other conditions, including PTSD, Raynaud’s disease, menopausal hot flashes, and hyperhidrosis.
Insurance companies typically cover it for CRPS, neuropathic upper-extremity pain, hyperhidrosis, and Raynaud’s, said Luke Liu, MD, an anesthesiologist who is founder and chief executive officer of Alaska-based pain management company Neuroversion.
Deborah Duricka, PhD, also with Neuroversion, presented results from a now-published case series of 11 patients with long COVID who underwent stellate ganglion block by a board-certified anesthesiologist, first on one side at the level of C6, then on the contralateral side the following day.
Clinically meaningful benefits were seen in at least five of the patients in fatigue, memory problems, problems concentrating, rapid heartbeat, orthostatic intolerance, sleep problems, postexertional malaise, anxiety, and depression.
The hypothetical mechanism, she said, is that “sympathetic block prevents sympathetically driven vasoconstriction in carotid and vertebral arteries.”
Dr. Liu presented another case series of five patients with ME/CFS who underwent the procedure with ultrasound guidance, again on one side and the other side the next day. All had upper-limb autonomic issues such as Raynaud’s and/or neuropathic pain that had been refractory to more conventional treatments.
All five patients reported improvements in symptoms of ME/CFS, including energy level, cognition, pain, and postexertional malaise. One patient reported “feeling well for the first time in decades.” However, that patient relapsed after a mild viral illness 3.5 months after treatment. Some of the patients have required further treatments.
Dr. Lapp commented that, although the procedure is generally safe when performed by an experienced clinician, “Any time you do an injection like that, there’s a high risk that you could nick an artery or a vein or hit an essential nerve in the neck. That’s why it has to be done under fluoroscopy or ultrasound.”
He said he’s had a few patients undergo the procedure, mostly for CRPS, and they seem to have benefited from it. “It might increase cerebral blood flow and preload to the heart, so it might decrease ME/CFS symptoms and help with POTS as well.”
Nonetheless, Dr. Lapp said he wouldn’t consider stellate ganglion block as first-line treatment for ME/CFS or long COVID. “I think it would be for the treatment-resistant patient, when you’ve gone through all the treatments that we know and addressed all the comorbidities and they’re still not getting better.”
But, he added, it is a standard procedure. “Any pain clinic can do a stellate block.”
Transcutaneous auricular vagus nerve stimulation
Nicola Clague-Baker, PhD, a physiotherapist at the University of Liverpool (England), presented findings from an international survey of people with ME/CFS regarding their experience with transcutaneous auricular vagus nerve stimulation (taVNS) to manage their autonomic symptoms. The technique involves stimulation of the autonomic nervous system via the vagus nerve using electrodes applied to part of the ear. The theory is that the technique stimulates the parasympathetic nervous system and improves autonomic balance.
Two small previous trials showing benefit of vagus nerve stimulation for people with ME/CFS used more invasive and less comfortable methods of applying the stimulation rather than to the ear, Dr. Clague-Baker and colleagues noted in a poster. It has also been used successfully in treating POTS, another conference speaker noted.
A total of 131 people with ME/CFS (called simply “ME” in the United Kingdom) responded to a survey advertised on social media and websites. The majority (60%) were from the United Kingdom while the rest were from Europe, Australia, and North America. Most were female, and slightly more than half had lived with ME for 10 or more years.
The majority (72%) were still using taVNS, while 28% had stopped using it. Only 9% had used the modality for longer than a year. Respondents identified more than 30 benefits in symptoms and activities, with improvements in postexertional malaise (39%) and brain fog (37%) being the most common. One reported significant reduction in constipation.
However, respondents also mentioned more than 20 short- and long-term negatives, including headaches (15%) and long-term irritation at the site (9%). One participant reported a “big improvement in neuropathic pain, but not so much for muscles and joints.”
Overall, 80% reported that they would continue using taVNS and 67% said they would recommend it to others with ME, and 56% said that the system was mildly to very beneficial.
Dr. Lapp noted that several types of transcutaneous electrical nerve stimulation units with ear clips are sold online, and he’s seen them work well for migraine treatment. However, he cautioned that some patients have had side effects from the treatment, such as headaches and dizziness. “It’s putting an electrical current through your brain. In my mind, it’s another last-ditch measure.”
Dr. Lapp reported no financial disclosures.
A version of this article first appeared on Medscape.com.
FROM IACFSME 2022
Antibiotic-resistant bacteria emerging in community settings
A new study from the Centers for Disease Control and Prevention found that
Traditionally, CRE has been thought of as a nosocomial infection, acquired in a hospital or other health care facility (nursing home, long-term acute care hospital, dialysis center, etc.). This is the first population-level study to show otherwise, with fully 10% of the CRE isolates found to be community acquired.
CREs are a group of multidrug-resistant bacteria considered an urgent health threat by the CDC because they can rapidly spread between patients, especially those who are most seriously ill and vulnerable, and because they are so difficult to treat. These patients often require treatment with toxic antibiotics, such as colistin, and carry a high mortality rate – up to 50% in some studies.
Overall, 30% of CREs carry a carbapenemase – an enzyme that can make them resistant to carbapenem antibiotics. The genes for this are readily transferable between bacteria and help account for their spread in hospitals.
But in this study, published in the American Journal of Infection Control, of the 12 isolates that underwent whole-genome sequencing, 42% of the CA-CRE isolates carried the carbapenemase gene. Lead author Sandra Bulens, MPH, a health scientist in the CDC’s division of health care quality promotion, said in an interview, “The findings highlight the potential for CP-CRE to move from health care settings into the community. The fact that 5 of the 12 isolates harbored a carbapenemase gene introduces new challenges for controlling spread of CP-CRE.”
CDC researchers analyzed data from eight U.S. metropolitan areas between 2012 and 2015 as part of the CDC’s Emerging Infections Program (EIP) health care–associated infections – community interface activity, which conducts surveillance for CRE and other drug-resistant gram-negative bacteria. Cases of CA-CRE were compared with HCA-CRE, with 1499 cases in 1,194 case-patients being analyzed. Though Klebsiella pneumoniae was the most common isolate, there were some differences between metropolitan areas.
The incidence of CRE cases per 100,000 population was 2.96 (95% confidence interval, 2.81-3.11) overall and 0.29 (95% CI, 0.25-0.25) for CA-CRE. Most CA-CRE cases were in White persons (73%) and women (84%). Urine cultures were the source of 98% of all CA-CRE cases, compared with 86% of HCA-CRE cases (P < .001). Though small numbers, the numbers of patients with CA-CRE without apparent underlying medical condition (n = 51; 37%) was greater when compared with patients with HCA-CRE (n = 36; 3%; P < .001).
Asked for independent comment, Lance Price, PhD, of George Washington University and the founding director of GW’s Antibiotic Resistance Action Center, Washington, said, “what’s striking about these data is that: ‘Who is the front line, at least in the United States for CRE?’ It’s women, older women. ... At some point, we have to frame drug resistance as a women’s health issue.”
Dr. Price noted that the 10% of patients with CA-CRE acquired it in the community. “I would argue that probably none of them had any idea, because there’s this silent community epidemic,” he said. “It’s asymptomatic carriage and transmission in the community. Somebody can be this walking reservoir of these really dangerous bacteria and have no idea.”
This is an increasingly serious problem for women, Dr. Price said, because, “with a community-acquired bladder infection, you’re going to call your doctor or go to an urgent care, and they’re not going to test you. They’re going to guess what you have, and they’re going to prescribe an antibiotic, and that antibiotic is going to fail. So then your bladder infection continues, and then you wait a few more days, and you start to get flank pain and kidney infection. ... If you start getting a fever, they might admit you. They are going to start treating you immediately, and they might miss it because you’ve got this organism that’s resistant to all the best antibiotics. ... The gateway to the blood is the UTI.”
Because of such empiric treatment and increasing resistance, the risk for treatment failure is quite high, especially for older women. Ms. Bulens, however, said that, “[although] 10% of CRE were in persons without health care risk factors, the proportion of all UTIs in this population that are CRE is going to be very, very small.”
This study involved cultures from 2012 to 2015. Before the pandemic, from 2012 to 2017, U.S. deaths from antibiotic resistance fell by 18% overall and by 30% in hospitals.
But in the first year of the COVID-19 pandemic, there was a 15% increase in infections and deaths from antibiotic-resistant (AMR), hospital-acquired bacteria. In 2020, 29,400 patients died from AMR infections. There was a 78% increase in carbapenem-resistant Acinetobacter baumannii health care–associated infections, a 35% increase in carbapenem-resistant Enterobacterales, and 32% increases in both multidrug-resistant Pseudomonas aeruginosa and extended-spectrum beta-lactamase–producing Enterobacterales. Aside from gram-negative bacteria, methicillin-resistant Staphylococcus aureus rose 13%, and Candida auris rose 60%. But owing to limited surveillance, recent sound figures are lacking.
Ms. Bulens and Dr. Price reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study from the Centers for Disease Control and Prevention found that
Traditionally, CRE has been thought of as a nosocomial infection, acquired in a hospital or other health care facility (nursing home, long-term acute care hospital, dialysis center, etc.). This is the first population-level study to show otherwise, with fully 10% of the CRE isolates found to be community acquired.
CREs are a group of multidrug-resistant bacteria considered an urgent health threat by the CDC because they can rapidly spread between patients, especially those who are most seriously ill and vulnerable, and because they are so difficult to treat. These patients often require treatment with toxic antibiotics, such as colistin, and carry a high mortality rate – up to 50% in some studies.
Overall, 30% of CREs carry a carbapenemase – an enzyme that can make them resistant to carbapenem antibiotics. The genes for this are readily transferable between bacteria and help account for their spread in hospitals.
But in this study, published in the American Journal of Infection Control, of the 12 isolates that underwent whole-genome sequencing, 42% of the CA-CRE isolates carried the carbapenemase gene. Lead author Sandra Bulens, MPH, a health scientist in the CDC’s division of health care quality promotion, said in an interview, “The findings highlight the potential for CP-CRE to move from health care settings into the community. The fact that 5 of the 12 isolates harbored a carbapenemase gene introduces new challenges for controlling spread of CP-CRE.”
CDC researchers analyzed data from eight U.S. metropolitan areas between 2012 and 2015 as part of the CDC’s Emerging Infections Program (EIP) health care–associated infections – community interface activity, which conducts surveillance for CRE and other drug-resistant gram-negative bacteria. Cases of CA-CRE were compared with HCA-CRE, with 1499 cases in 1,194 case-patients being analyzed. Though Klebsiella pneumoniae was the most common isolate, there were some differences between metropolitan areas.
The incidence of CRE cases per 100,000 population was 2.96 (95% confidence interval, 2.81-3.11) overall and 0.29 (95% CI, 0.25-0.25) for CA-CRE. Most CA-CRE cases were in White persons (73%) and women (84%). Urine cultures were the source of 98% of all CA-CRE cases, compared with 86% of HCA-CRE cases (P < .001). Though small numbers, the numbers of patients with CA-CRE without apparent underlying medical condition (n = 51; 37%) was greater when compared with patients with HCA-CRE (n = 36; 3%; P < .001).
Asked for independent comment, Lance Price, PhD, of George Washington University and the founding director of GW’s Antibiotic Resistance Action Center, Washington, said, “what’s striking about these data is that: ‘Who is the front line, at least in the United States for CRE?’ It’s women, older women. ... At some point, we have to frame drug resistance as a women’s health issue.”
Dr. Price noted that the 10% of patients with CA-CRE acquired it in the community. “I would argue that probably none of them had any idea, because there’s this silent community epidemic,” he said. “It’s asymptomatic carriage and transmission in the community. Somebody can be this walking reservoir of these really dangerous bacteria and have no idea.”
This is an increasingly serious problem for women, Dr. Price said, because, “with a community-acquired bladder infection, you’re going to call your doctor or go to an urgent care, and they’re not going to test you. They’re going to guess what you have, and they’re going to prescribe an antibiotic, and that antibiotic is going to fail. So then your bladder infection continues, and then you wait a few more days, and you start to get flank pain and kidney infection. ... If you start getting a fever, they might admit you. They are going to start treating you immediately, and they might miss it because you’ve got this organism that’s resistant to all the best antibiotics. ... The gateway to the blood is the UTI.”
Because of such empiric treatment and increasing resistance, the risk for treatment failure is quite high, especially for older women. Ms. Bulens, however, said that, “[although] 10% of CRE were in persons without health care risk factors, the proportion of all UTIs in this population that are CRE is going to be very, very small.”
This study involved cultures from 2012 to 2015. Before the pandemic, from 2012 to 2017, U.S. deaths from antibiotic resistance fell by 18% overall and by 30% in hospitals.
But in the first year of the COVID-19 pandemic, there was a 15% increase in infections and deaths from antibiotic-resistant (AMR), hospital-acquired bacteria. In 2020, 29,400 patients died from AMR infections. There was a 78% increase in carbapenem-resistant Acinetobacter baumannii health care–associated infections, a 35% increase in carbapenem-resistant Enterobacterales, and 32% increases in both multidrug-resistant Pseudomonas aeruginosa and extended-spectrum beta-lactamase–producing Enterobacterales. Aside from gram-negative bacteria, methicillin-resistant Staphylococcus aureus rose 13%, and Candida auris rose 60%. But owing to limited surveillance, recent sound figures are lacking.
Ms. Bulens and Dr. Price reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A new study from the Centers for Disease Control and Prevention found that
Traditionally, CRE has been thought of as a nosocomial infection, acquired in a hospital or other health care facility (nursing home, long-term acute care hospital, dialysis center, etc.). This is the first population-level study to show otherwise, with fully 10% of the CRE isolates found to be community acquired.
CREs are a group of multidrug-resistant bacteria considered an urgent health threat by the CDC because they can rapidly spread between patients, especially those who are most seriously ill and vulnerable, and because they are so difficult to treat. These patients often require treatment with toxic antibiotics, such as colistin, and carry a high mortality rate – up to 50% in some studies.
Overall, 30% of CREs carry a carbapenemase – an enzyme that can make them resistant to carbapenem antibiotics. The genes for this are readily transferable between bacteria and help account for their spread in hospitals.
But in this study, published in the American Journal of Infection Control, of the 12 isolates that underwent whole-genome sequencing, 42% of the CA-CRE isolates carried the carbapenemase gene. Lead author Sandra Bulens, MPH, a health scientist in the CDC’s division of health care quality promotion, said in an interview, “The findings highlight the potential for CP-CRE to move from health care settings into the community. The fact that 5 of the 12 isolates harbored a carbapenemase gene introduces new challenges for controlling spread of CP-CRE.”
CDC researchers analyzed data from eight U.S. metropolitan areas between 2012 and 2015 as part of the CDC’s Emerging Infections Program (EIP) health care–associated infections – community interface activity, which conducts surveillance for CRE and other drug-resistant gram-negative bacteria. Cases of CA-CRE were compared with HCA-CRE, with 1499 cases in 1,194 case-patients being analyzed. Though Klebsiella pneumoniae was the most common isolate, there were some differences between metropolitan areas.
The incidence of CRE cases per 100,000 population was 2.96 (95% confidence interval, 2.81-3.11) overall and 0.29 (95% CI, 0.25-0.25) for CA-CRE. Most CA-CRE cases were in White persons (73%) and women (84%). Urine cultures were the source of 98% of all CA-CRE cases, compared with 86% of HCA-CRE cases (P < .001). Though small numbers, the numbers of patients with CA-CRE without apparent underlying medical condition (n = 51; 37%) was greater when compared with patients with HCA-CRE (n = 36; 3%; P < .001).
Asked for independent comment, Lance Price, PhD, of George Washington University and the founding director of GW’s Antibiotic Resistance Action Center, Washington, said, “what’s striking about these data is that: ‘Who is the front line, at least in the United States for CRE?’ It’s women, older women. ... At some point, we have to frame drug resistance as a women’s health issue.”
Dr. Price noted that the 10% of patients with CA-CRE acquired it in the community. “I would argue that probably none of them had any idea, because there’s this silent community epidemic,” he said. “It’s asymptomatic carriage and transmission in the community. Somebody can be this walking reservoir of these really dangerous bacteria and have no idea.”
This is an increasingly serious problem for women, Dr. Price said, because, “with a community-acquired bladder infection, you’re going to call your doctor or go to an urgent care, and they’re not going to test you. They’re going to guess what you have, and they’re going to prescribe an antibiotic, and that antibiotic is going to fail. So then your bladder infection continues, and then you wait a few more days, and you start to get flank pain and kidney infection. ... If you start getting a fever, they might admit you. They are going to start treating you immediately, and they might miss it because you’ve got this organism that’s resistant to all the best antibiotics. ... The gateway to the blood is the UTI.”
Because of such empiric treatment and increasing resistance, the risk for treatment failure is quite high, especially for older women. Ms. Bulens, however, said that, “[although] 10% of CRE were in persons without health care risk factors, the proportion of all UTIs in this population that are CRE is going to be very, very small.”
This study involved cultures from 2012 to 2015. Before the pandemic, from 2012 to 2017, U.S. deaths from antibiotic resistance fell by 18% overall and by 30% in hospitals.
But in the first year of the COVID-19 pandemic, there was a 15% increase in infections and deaths from antibiotic-resistant (AMR), hospital-acquired bacteria. In 2020, 29,400 patients died from AMR infections. There was a 78% increase in carbapenem-resistant Acinetobacter baumannii health care–associated infections, a 35% increase in carbapenem-resistant Enterobacterales, and 32% increases in both multidrug-resistant Pseudomonas aeruginosa and extended-spectrum beta-lactamase–producing Enterobacterales. Aside from gram-negative bacteria, methicillin-resistant Staphylococcus aureus rose 13%, and Candida auris rose 60%. But owing to limited surveillance, recent sound figures are lacking.
Ms. Bulens and Dr. Price reported no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF INFECTION CONTROL