User login
Official news magazine of the Society of Hospital Medicine
Copyright by Society of Hospital Medicine or related companies. All rights reserved. ISSN 1553-085X
nav[contains(@class, 'nav-ce-stack nav-ce-stack__large-screen')]
header[@id='header']
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
div[contains(@class, 'pane-pub-article-hospitalist')]

Do you want to become a hospitalist leader?
Learn how or even whether you should
Have you ever thought you could be a leader, in your hospitalist group, in hospital administration, or at another institution? The reasons to seek a leadership role as a hospitalist are many, but there are also many drawbacks. According to hospitalists who have reached high rungs on the leadership ladder, you will need a blend of desire, enthusiasm, education, and experience if you want to succeed in leadership.
The right reasons
“People who make good leaders have a sense of purpose and want to make a difference,” said Eric Howell, MD, MHM, CEO of the Society of Hospital Medicine, and former chief of medical units at Johns Hopkins Bayview in Baltimore. “I think most hospitalists have that sense of wanting to help patients and society, so that’s a strong mission in itself. Just by training and the very design of our health care system, hospitalists are often natural leaders, and in leadership roles, because they run teams of clinicians and train medical students.”
Danielle Scheurer, MD, SFHM, chief quality officer and professor of medicine at the Medical University of South Carolina, and current president of SHM, said some hospitalists end up in leadership roles almost by accident – because there is a leadership “void” in the health system where they work, and no one else wants to step up. Others disconnect from the leadership track and are happy to simply be part of a team.
“If you are yearning to make a difference and that’s your motivation then you will find leadership is more fulfilling than difficult,” she said. “But if you take a leadership role to fill a void or think you just want to take some nonclinical time, it’s probably not a good idea. Some people think administrative leadership is easier than being a hospitalist, but it is not. Leadership should not be about getting away from something else. It should be a thoughtful career move, and if it is, being a leader can be meaningful and fulfilling.”
Nancy Spector, MD, the vice dean for faculty and executive director of the Executive Leadership in Academic Medicine program at Drexel University College of Medicine in Philadelphia, said a willingness to fail is vital for a leader. “You have to be open to successes, yes, but also to making mistakes,” she said. “It’s about honing the skills that leadership requires and be open to development and change.”
Kierstin Cates Kennedy, MD, SFHM, chief of hospital medicine at the University of Alabama at Birmingham, said that a hospitalist fresh out of residency will gain insight into whether leadership is the right path by acquiring a deeper understanding of how health care institutions work.

“When you are new to the hospital, you see how things work, how people interact with each other, and learn the politics,” she said. “One of the easiest ways to do it is get involved in a committee and be a part of meetings. You can have some input and get exposure to other leaders and they can learn more about you. Once you get an organizational understanding under your belt, then you can start taking on projects to gain even more understanding.”
Still up for it?
If you think you have the commitment and desire for leadership as an early career hospitalist, how would you continue down the leadership path?
“A great way is to find a person you want to be like, who could be a mentor. Find a successful leader that you admire, and one who is willing to guide you,” Dr. Howell said. “Books are helpful as well, and I still find I’m learning today – I have a list that includes Drive by Daniel Pink and Good to Great by Jim Collins. There are Malcolm Gladwell books that also have terrific knowledge to impart.”
Mark W. Shen, MD, SFHM, associate professor at Dell Medical School at the University of Texas at Austin and former president of St. Louis Children’s Hospital, said potential hospitalist leaders must be aware of their fellow clinicians.
“Pay attention to the needs of the hospitalist group as they are articulated by the lead hospitalist, the administration, and the patients,” he said. “There are so many activities that come up on a day-in, day-out basis. You should jump in and volunteer to take the lead on some of those activities. Leading your peers is often one of the most challenging parts of leadership. I think taking on even just a small activity like, say, working on a clinical pathway for the group, will result in a lot of preparation for future leadership roles.”
An example of an early career activity that Dr. Shen felt was valuable to future leaders was helping in the development of a hospitalist core curriculum. “We would use the core curriculum to educate students and residents coming through our rotation and have some degree of commonality or standardization,” he said. “So even though I wasn’t an explicit leader of the hospitalist group at the time, I’d say that helping develop the core curriculum aided me in understanding what leadership was all about.”
Getting started in a leadership role, Dr. Spector said, can be helped by embracing a knowledge of the business of medicine. “Business and finance are a reality you shouldn’t avoid,” she said. “Another way to learn is to partner with your local administrators or whoever is running your division or your department. There are business managers and business partners in every institution, and you can learn a great deal from them. It’s important to network and get to know people because we’re a people business, and opportunity comes when people know who you are.”
Dr. Howell noted that advocating for yourself is sometimes hard, and it can be a red flag in some circumstances, but you should tell your bosses where you want to go professionally.
“You can say that you want to grow professionally, and let’s face it, there are naturally-inclined leaders. We all need to be transparent in goal paths,” he said. “But if you want a leadership role for power, money, and prestige then you’re not applying the right thinking. If you want to help others and you have a mission you believe in, then communicate that to your bosses.”
Dr. Scheurer believes choosing between clinical and administrative leadership is not so clear cut, because in the health care setting they tend to morph into each other. “Many times clinicians will end up taking on a leadership role that has a significant administrative component to it,” she said. “I do think if clinicians make a career move and get the right training then they can be exemplary leaders in health care, but I do worry a little about clinicians going into leadership roles without any formal training. They are usually well-intentioned but that’s not enough. It’s not any different than medical training. If you want to be a good leader you need training to develop your skills, and a lot of those skills do not come naturally or easily. We thrust good clinicians into leadership roles because they are good clinicians, but if they don’t have the right skills, being a leader can be a problem.”
How do leaders improve?
If you have made it to a leadership position, and have been in that role for a while, you might start to feel you are stuck in your growth trajectory. If so, how do you continue to improve?
According to Dr. Kennedy, whether you are looking to get into leadership or want to improve, focusing on emotional intelligence is important. “A book like Emotional Intelligence 2.0 by Travis Bradbury is a great introduction,” she said. “With my leadership team, we did a book club where we read Primal Leadership, which is focused on emotional intelligence and on aspects like setting a culture.”
Dr. Howell said that to grow as a leader, be careful what you say no to. “I used to talk about having a tag line that was ‘just say yes,’” he said. “At least try to say yes most of the time because it opens up opportunities and shows you are looking to do more, not less.”
Also, Dr. Howell recommends that leaders look for tools that minimize blind spots and get information from staff through survey assessments. “Get the input of others on your strengths and weaknesses,” he said. “Nurses, doctors, and sometimes patients can give you good information that will help you grow as a leader. Don’t be afraid of feedback.”
Never stop learning
Dr. Scheurer said it is important to recognize that you are never finished learning when you are a leader.
“See leadership as a continuous learning journey. You can never be too good of a leader in medicine,” she said. “Never stop learning, because the field keeps changing and you have to constantly learn and find pleasure in that learning. You should look at leadership the same way. A lot of leadership theories change with the times and you should always try to get good advice. You don’t take every piece of advice – just like in medicine when you read an article and you try to apply it to patients in your practice. Take some advice, leave some advice, and develop a leadership style that is genuine and authentic.”
Dr. Kennedy believes that a hospitalist’s leadership potential may be limited if you see continued learning as a chore, rather than an opportunity.
“If you resent it learning about leadership, then is it really for you?” she asked. “I find myself reading on the topic or talking about it, and it’s fun. How do you make an environment work better, how do you inspire people, how do you help them grow? These are some of the most important questions leaders face. Isn’t it fun if you can find some answers?”
Learn how or even whether you should
Learn how or even whether you should
Have you ever thought you could be a leader, in your hospitalist group, in hospital administration, or at another institution? The reasons to seek a leadership role as a hospitalist are many, but there are also many drawbacks. According to hospitalists who have reached high rungs on the leadership ladder, you will need a blend of desire, enthusiasm, education, and experience if you want to succeed in leadership.
The right reasons
“People who make good leaders have a sense of purpose and want to make a difference,” said Eric Howell, MD, MHM, CEO of the Society of Hospital Medicine, and former chief of medical units at Johns Hopkins Bayview in Baltimore. “I think most hospitalists have that sense of wanting to help patients and society, so that’s a strong mission in itself. Just by training and the very design of our health care system, hospitalists are often natural leaders, and in leadership roles, because they run teams of clinicians and train medical students.”
Danielle Scheurer, MD, SFHM, chief quality officer and professor of medicine at the Medical University of South Carolina, and current president of SHM, said some hospitalists end up in leadership roles almost by accident – because there is a leadership “void” in the health system where they work, and no one else wants to step up. Others disconnect from the leadership track and are happy to simply be part of a team.
“If you are yearning to make a difference and that’s your motivation then you will find leadership is more fulfilling than difficult,” she said. “But if you take a leadership role to fill a void or think you just want to take some nonclinical time, it’s probably not a good idea. Some people think administrative leadership is easier than being a hospitalist, but it is not. Leadership should not be about getting away from something else. It should be a thoughtful career move, and if it is, being a leader can be meaningful and fulfilling.”
Nancy Spector, MD, the vice dean for faculty and executive director of the Executive Leadership in Academic Medicine program at Drexel University College of Medicine in Philadelphia, said a willingness to fail is vital for a leader. “You have to be open to successes, yes, but also to making mistakes,” she said. “It’s about honing the skills that leadership requires and be open to development and change.”
Kierstin Cates Kennedy, MD, SFHM, chief of hospital medicine at the University of Alabama at Birmingham, said that a hospitalist fresh out of residency will gain insight into whether leadership is the right path by acquiring a deeper understanding of how health care institutions work.
“When you are new to the hospital, you see how things work, how people interact with each other, and learn the politics,” she said. “One of the easiest ways to do it is get involved in a committee and be a part of meetings. You can have some input and get exposure to other leaders and they can learn more about you. Once you get an organizational understanding under your belt, then you can start taking on projects to gain even more understanding.”
Still up for it?
If you think you have the commitment and desire for leadership as an early career hospitalist, how would you continue down the leadership path?
“A great way is to find a person you want to be like, who could be a mentor. Find a successful leader that you admire, and one who is willing to guide you,” Dr. Howell said. “Books are helpful as well, and I still find I’m learning today – I have a list that includes Drive by Daniel Pink and Good to Great by Jim Collins. There are Malcolm Gladwell books that also have terrific knowledge to impart.”
Mark W. Shen, MD, SFHM, associate professor at Dell Medical School at the University of Texas at Austin and former president of St. Louis Children’s Hospital, said potential hospitalist leaders must be aware of their fellow clinicians.
“Pay attention to the needs of the hospitalist group as they are articulated by the lead hospitalist, the administration, and the patients,” he said. “There are so many activities that come up on a day-in, day-out basis. You should jump in and volunteer to take the lead on some of those activities. Leading your peers is often one of the most challenging parts of leadership. I think taking on even just a small activity like, say, working on a clinical pathway for the group, will result in a lot of preparation for future leadership roles.”
An example of an early career activity that Dr. Shen felt was valuable to future leaders was helping in the development of a hospitalist core curriculum. “We would use the core curriculum to educate students and residents coming through our rotation and have some degree of commonality or standardization,” he said. “So even though I wasn’t an explicit leader of the hospitalist group at the time, I’d say that helping develop the core curriculum aided me in understanding what leadership was all about.”
Getting started in a leadership role, Dr. Spector said, can be helped by embracing a knowledge of the business of medicine. “Business and finance are a reality you shouldn’t avoid,” she said. “Another way to learn is to partner with your local administrators or whoever is running your division or your department. There are business managers and business partners in every institution, and you can learn a great deal from them. It’s important to network and get to know people because we’re a people business, and opportunity comes when people know who you are.”
Dr. Howell noted that advocating for yourself is sometimes hard, and it can be a red flag in some circumstances, but you should tell your bosses where you want to go professionally.
“You can say that you want to grow professionally, and let’s face it, there are naturally-inclined leaders. We all need to be transparent in goal paths,” he said. “But if you want a leadership role for power, money, and prestige then you’re not applying the right thinking. If you want to help others and you have a mission you believe in, then communicate that to your bosses.”
Dr. Scheurer believes choosing between clinical and administrative leadership is not so clear cut, because in the health care setting they tend to morph into each other. “Many times clinicians will end up taking on a leadership role that has a significant administrative component to it,” she said. “I do think if clinicians make a career move and get the right training then they can be exemplary leaders in health care, but I do worry a little about clinicians going into leadership roles without any formal training. They are usually well-intentioned but that’s not enough. It’s not any different than medical training. If you want to be a good leader you need training to develop your skills, and a lot of those skills do not come naturally or easily. We thrust good clinicians into leadership roles because they are good clinicians, but if they don’t have the right skills, being a leader can be a problem.”
How do leaders improve?
If you have made it to a leadership position, and have been in that role for a while, you might start to feel you are stuck in your growth trajectory. If so, how do you continue to improve?
According to Dr. Kennedy, whether you are looking to get into leadership or want to improve, focusing on emotional intelligence is important. “A book like Emotional Intelligence 2.0 by Travis Bradbury is a great introduction,” she said. “With my leadership team, we did a book club where we read Primal Leadership, which is focused on emotional intelligence and on aspects like setting a culture.”
Dr. Howell said that to grow as a leader, be careful what you say no to. “I used to talk about having a tag line that was ‘just say yes,’” he said. “At least try to say yes most of the time because it opens up opportunities and shows you are looking to do more, not less.”
Also, Dr. Howell recommends that leaders look for tools that minimize blind spots and get information from staff through survey assessments. “Get the input of others on your strengths and weaknesses,” he said. “Nurses, doctors, and sometimes patients can give you good information that will help you grow as a leader. Don’t be afraid of feedback.”
Never stop learning
Dr. Scheurer said it is important to recognize that you are never finished learning when you are a leader.
“See leadership as a continuous learning journey. You can never be too good of a leader in medicine,” she said. “Never stop learning, because the field keeps changing and you have to constantly learn and find pleasure in that learning. You should look at leadership the same way. A lot of leadership theories change with the times and you should always try to get good advice. You don’t take every piece of advice – just like in medicine when you read an article and you try to apply it to patients in your practice. Take some advice, leave some advice, and develop a leadership style that is genuine and authentic.”
Dr. Kennedy believes that a hospitalist’s leadership potential may be limited if you see continued learning as a chore, rather than an opportunity.
“If you resent it learning about leadership, then is it really for you?” she asked. “I find myself reading on the topic or talking about it, and it’s fun. How do you make an environment work better, how do you inspire people, how do you help them grow? These are some of the most important questions leaders face. Isn’t it fun if you can find some answers?”
Have you ever thought you could be a leader, in your hospitalist group, in hospital administration, or at another institution? The reasons to seek a leadership role as a hospitalist are many, but there are also many drawbacks. According to hospitalists who have reached high rungs on the leadership ladder, you will need a blend of desire, enthusiasm, education, and experience if you want to succeed in leadership.
The right reasons
“People who make good leaders have a sense of purpose and want to make a difference,” said Eric Howell, MD, MHM, CEO of the Society of Hospital Medicine, and former chief of medical units at Johns Hopkins Bayview in Baltimore. “I think most hospitalists have that sense of wanting to help patients and society, so that’s a strong mission in itself. Just by training and the very design of our health care system, hospitalists are often natural leaders, and in leadership roles, because they run teams of clinicians and train medical students.”
Danielle Scheurer, MD, SFHM, chief quality officer and professor of medicine at the Medical University of South Carolina, and current president of SHM, said some hospitalists end up in leadership roles almost by accident – because there is a leadership “void” in the health system where they work, and no one else wants to step up. Others disconnect from the leadership track and are happy to simply be part of a team.
“If you are yearning to make a difference and that’s your motivation then you will find leadership is more fulfilling than difficult,” she said. “But if you take a leadership role to fill a void or think you just want to take some nonclinical time, it’s probably not a good idea. Some people think administrative leadership is easier than being a hospitalist, but it is not. Leadership should not be about getting away from something else. It should be a thoughtful career move, and if it is, being a leader can be meaningful and fulfilling.”
Nancy Spector, MD, the vice dean for faculty and executive director of the Executive Leadership in Academic Medicine program at Drexel University College of Medicine in Philadelphia, said a willingness to fail is vital for a leader. “You have to be open to successes, yes, but also to making mistakes,” she said. “It’s about honing the skills that leadership requires and be open to development and change.”
Kierstin Cates Kennedy, MD, SFHM, chief of hospital medicine at the University of Alabama at Birmingham, said that a hospitalist fresh out of residency will gain insight into whether leadership is the right path by acquiring a deeper understanding of how health care institutions work.
“When you are new to the hospital, you see how things work, how people interact with each other, and learn the politics,” she said. “One of the easiest ways to do it is get involved in a committee and be a part of meetings. You can have some input and get exposure to other leaders and they can learn more about you. Once you get an organizational understanding under your belt, then you can start taking on projects to gain even more understanding.”
Still up for it?
If you think you have the commitment and desire for leadership as an early career hospitalist, how would you continue down the leadership path?
“A great way is to find a person you want to be like, who could be a mentor. Find a successful leader that you admire, and one who is willing to guide you,” Dr. Howell said. “Books are helpful as well, and I still find I’m learning today – I have a list that includes Drive by Daniel Pink and Good to Great by Jim Collins. There are Malcolm Gladwell books that also have terrific knowledge to impart.”
Mark W. Shen, MD, SFHM, associate professor at Dell Medical School at the University of Texas at Austin and former president of St. Louis Children’s Hospital, said potential hospitalist leaders must be aware of their fellow clinicians.
“Pay attention to the needs of the hospitalist group as they are articulated by the lead hospitalist, the administration, and the patients,” he said. “There are so many activities that come up on a day-in, day-out basis. You should jump in and volunteer to take the lead on some of those activities. Leading your peers is often one of the most challenging parts of leadership. I think taking on even just a small activity like, say, working on a clinical pathway for the group, will result in a lot of preparation for future leadership roles.”
An example of an early career activity that Dr. Shen felt was valuable to future leaders was helping in the development of a hospitalist core curriculum. “We would use the core curriculum to educate students and residents coming through our rotation and have some degree of commonality or standardization,” he said. “So even though I wasn’t an explicit leader of the hospitalist group at the time, I’d say that helping develop the core curriculum aided me in understanding what leadership was all about.”
Getting started in a leadership role, Dr. Spector said, can be helped by embracing a knowledge of the business of medicine. “Business and finance are a reality you shouldn’t avoid,” she said. “Another way to learn is to partner with your local administrators or whoever is running your division or your department. There are business managers and business partners in every institution, and you can learn a great deal from them. It’s important to network and get to know people because we’re a people business, and opportunity comes when people know who you are.”
Dr. Howell noted that advocating for yourself is sometimes hard, and it can be a red flag in some circumstances, but you should tell your bosses where you want to go professionally.
“You can say that you want to grow professionally, and let’s face it, there are naturally-inclined leaders. We all need to be transparent in goal paths,” he said. “But if you want a leadership role for power, money, and prestige then you’re not applying the right thinking. If you want to help others and you have a mission you believe in, then communicate that to your bosses.”
Dr. Scheurer believes choosing between clinical and administrative leadership is not so clear cut, because in the health care setting they tend to morph into each other. “Many times clinicians will end up taking on a leadership role that has a significant administrative component to it,” she said. “I do think if clinicians make a career move and get the right training then they can be exemplary leaders in health care, but I do worry a little about clinicians going into leadership roles without any formal training. They are usually well-intentioned but that’s not enough. It’s not any different than medical training. If you want to be a good leader you need training to develop your skills, and a lot of those skills do not come naturally or easily. We thrust good clinicians into leadership roles because they are good clinicians, but if they don’t have the right skills, being a leader can be a problem.”
How do leaders improve?
If you have made it to a leadership position, and have been in that role for a while, you might start to feel you are stuck in your growth trajectory. If so, how do you continue to improve?
According to Dr. Kennedy, whether you are looking to get into leadership or want to improve, focusing on emotional intelligence is important. “A book like Emotional Intelligence 2.0 by Travis Bradbury is a great introduction,” she said. “With my leadership team, we did a book club where we read Primal Leadership, which is focused on emotional intelligence and on aspects like setting a culture.”
Dr. Howell said that to grow as a leader, be careful what you say no to. “I used to talk about having a tag line that was ‘just say yes,’” he said. “At least try to say yes most of the time because it opens up opportunities and shows you are looking to do more, not less.”
Also, Dr. Howell recommends that leaders look for tools that minimize blind spots and get information from staff through survey assessments. “Get the input of others on your strengths and weaknesses,” he said. “Nurses, doctors, and sometimes patients can give you good information that will help you grow as a leader. Don’t be afraid of feedback.”
Never stop learning
Dr. Scheurer said it is important to recognize that you are never finished learning when you are a leader.
“See leadership as a continuous learning journey. You can never be too good of a leader in medicine,” she said. “Never stop learning, because the field keeps changing and you have to constantly learn and find pleasure in that learning. You should look at leadership the same way. A lot of leadership theories change with the times and you should always try to get good advice. You don’t take every piece of advice – just like in medicine when you read an article and you try to apply it to patients in your practice. Take some advice, leave some advice, and develop a leadership style that is genuine and authentic.”
Dr. Kennedy believes that a hospitalist’s leadership potential may be limited if you see continued learning as a chore, rather than an opportunity.
“If you resent it learning about leadership, then is it really for you?” she asked. “I find myself reading on the topic or talking about it, and it’s fun. How do you make an environment work better, how do you inspire people, how do you help them grow? These are some of the most important questions leaders face. Isn’t it fun if you can find some answers?”
The skill set of the ‘pluripotent’ hospitalist
Editor’s note: National Hospitalist Day occurs the first Thursday in March annually, and serves to celebrate the fastest growing specialty in modern medicine and hospitalists’ enduring contributions to the evolving health care landscape. On National Hospitalist Day in 2021, SHM convened a virtual roundtable with a diverse group of hospitalists to discuss skill set, wellness, and other key issues for hospitalists. To listen to the entire roundtable discussion, visit this Explore The Space podcast episode.
A hospitalist isn’t just a physician who happens to work in a hospital. They are medical professionals with a robust skill set that they use both inside and outside the hospital setting. But what skill sets do hospitalists need to become successful in their careers? And what skill sets does a “pluripotent” hospitalist need in their armamentarium?

These were the issues discussed by participants of a virtual roundtable discussion on National Hospitalist Day – March 4, 2021 – as part of a joint effort of the Society of Hospital Medicine and the Explore the Space podcast.
Maylyn S. Martinez, MD, clinician-researcher and clinical associate at the University of Chicago, sees her hospitalist and research skill sets as two “buckets” of skills she can sort through, with diagnostic, knowledge-based care coordination, and interpersonal skills as lanes where she can focus and improve. “I’m always trying to work in, and sharpen, and find ways to get better at something in each of those every day,” she said.
For Anika Kumar, MD, FHM, pediatric editor of the Hospitalist and clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine, much of her work is focused on problem solving. “I approach that as: ‘How do I come up with my differential diagnosis, and how do I diagnose the patient?’ I think that the lanes are a little bit different, but there is some overlap.”

Adaptability is another important part of the skill set for the hospitalist, Ndidi Unaka, MD, MEd, associate professor in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center, said during the discussion. “I think we all really value teamwork, and we take on the role of being the coordinator and making sure things are getting done in a seamless and thoughtful manner. Communicating with families, communicating with our research team, communicating with primary care physicians. I think that is something we’re very used to doing, and I think we do it well. I think we don’t shy away from difficult conversations with consultants. And I think that’s what makes being a hospitalist so amazing.”
Achieving wellness as a hospitalist
Another topic discussed during the roundtable was “comprehensive care for the hospitalist” and how they can achieve a sense of wellness for themselves. Gurpreet Dhaliwal, MD, clinician-educator and professor of medicine at the University of California, San Francisco, said long-term satisfaction in one’s career is less about compensation and more about autonomy, mastery, and purpose.

“Autonomy is shrinking a little bit in health care. But if we connect to our purpose – ‘what are we doing here and how do we connect?’ – it’s either learning about patients and their stories, being with a team of people that you work with, that really builds that purpose,” he said.
Regarding mastery, there’s “tremendous joy if you’re in an environment where people value your mastery, whether it is working in a team or communicating or diagnosing or doing a procedure. If you think of setting up the work environment and those things are in place, I think a lot of wellness can actually happen at work, even though another component, of course, is balancing your life outside of work,” Dr. Dhaliwal said.
This may seem out of reach during COVID-19, but wellness is still achievable during the pandemic, Dr. Martinez said. Her time is spent 75% as a researcher and 25% as a clinician, which is her ideal balance. “I enjoy doing my research, doing my own statistics and writing grants and just learning about this problem that I’ve developed an interest in,” she said. “I just think that’s an important piece for people to focus on as far as health care for the hospitalist, is that there’s no no-one-size-fits-all, that’s for sure.”

Dr. Kumar noted that her clinical time gives her energy for nonclinical work. “I love my clinical time. It’s one of my favorite things that I do,” she said. Although she is tired at the end of the week, “I feel like I am not only giving back to my patients and my team, but I’m also giving back to myself and reminding myself why it is I do what I do every day,” she said.
Wellness for Dr. Unaka meant remembering what drew her to medicine. “It was definitely the opportunity to build strong relationships with patients and families,” she said. While these encounters can sometimes be heavy and stay with a hospitalist, “the fact that we’re in it with them is something that gives a lot of us purpose. I think that when I reflect on all of those things, I’m so happy that I’m in the role that I am.”
Unique skills during COVID-19
Mark Shapiro, MD, hospitalist and host of the roundtable and the Explore the Space podcast, also asked the panelists what skills they unexpectedly leveraged during the pandemic. Communication – with colleagues and with the community they serve – was a universal answer among the panelists.
“I learned – really from seeing some of our senior leaders here do it so well – the importance of being visible, particularly at a time when people were not together and more isolated,” Dr. Unaka said. “I think being able to be visible when you can, in order to deliver really complicated or tough news or communicate about uncertainty, for instance. Being here for our residents – many of our interns moved here sight unseen. I think they needed to feel like they had some sense of normalcy and a sense of community. I really learned how important it was to be visible, and available, and how important the little things mattered.”
Dr. Martinez said that worrying about her patients with COVID-19 in the hospital and the uncertainty around the disease kept her up at night. “I think we always have a hard time leaving work at work and getting a good night’s sleep. I just could not let go of worrying about these patients and having terrible insomnia, trying to leave work at work and I couldn’t – even after they were discharged.”

Dr. Shapiro said the skill he most needed to work on during the pandemic was his courage. “I remember the first time I took care of COVID patients. I was scared. I have no problems saying that out loud. That was a scary experience.”
The demeanor of the nurses on his unit, who had already seen patients with COVID-19, helped ground him during those moments and gave him the courage to move forward. “They’d already been doing it and they were the same. Same affect, same jokes, same everything,” he said. “That actually really helped, and I’ve leaned on that every time I’ve been back on our COVID service.”
Importance of mental health
The COVID-19 pandemic has also shined a light on the importance of mental health. “I think it is important to acknowledge that as hospitalists who have been out on the bleeding edge for a year, mental health is critically important, and we know that we face shortages in that space for the public at large and also for our profession,” Dr. Shapiro said.
When asked about what mental health and self-care looks like for her, Dr. Kumar referenced the need for exercise, meditation, and yoga. “My mental health was better knowing that the people closest to me – whether they be colleagues or friends or family – their mental health was also in a good place and they were also in a good place. And that helped to build me up,” she said.
Dr. Unaka called attention to the stigma around mental health, particularly among physicians, and the lack of resources to address the issue. “It’s a real problem,” she said. “I think it’s at a point where we as a profession need to advocate on behalf of each other and on behalf of our trainees. And honestly, I think we need to view mental health as just ‘health’ and stop separating it out in order for us to move to a place where people feel like they can access what they need without feeling shame about it.”
Editor’s note: National Hospitalist Day occurs the first Thursday in March annually, and serves to celebrate the fastest growing specialty in modern medicine and hospitalists’ enduring contributions to the evolving health care landscape. On National Hospitalist Day in 2021, SHM convened a virtual roundtable with a diverse group of hospitalists to discuss skill set, wellness, and other key issues for hospitalists. To listen to the entire roundtable discussion, visit this Explore The Space podcast episode.
A hospitalist isn’t just a physician who happens to work in a hospital. They are medical professionals with a robust skill set that they use both inside and outside the hospital setting. But what skill sets do hospitalists need to become successful in their careers? And what skill sets does a “pluripotent” hospitalist need in their armamentarium?
These were the issues discussed by participants of a virtual roundtable discussion on National Hospitalist Day – March 4, 2021 – as part of a joint effort of the Society of Hospital Medicine and the Explore the Space podcast.
Maylyn S. Martinez, MD, clinician-researcher and clinical associate at the University of Chicago, sees her hospitalist and research skill sets as two “buckets” of skills she can sort through, with diagnostic, knowledge-based care coordination, and interpersonal skills as lanes where she can focus and improve. “I’m always trying to work in, and sharpen, and find ways to get better at something in each of those every day,” she said.
For Anika Kumar, MD, FHM, pediatric editor of the Hospitalist and clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine, much of her work is focused on problem solving. “I approach that as: ‘How do I come up with my differential diagnosis, and how do I diagnose the patient?’ I think that the lanes are a little bit different, but there is some overlap.”
Adaptability is another important part of the skill set for the hospitalist, Ndidi Unaka, MD, MEd, associate professor in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center, said during the discussion. “I think we all really value teamwork, and we take on the role of being the coordinator and making sure things are getting done in a seamless and thoughtful manner. Communicating with families, communicating with our research team, communicating with primary care physicians. I think that is something we’re very used to doing, and I think we do it well. I think we don’t shy away from difficult conversations with consultants. And I think that’s what makes being a hospitalist so amazing.”
Achieving wellness as a hospitalist
Another topic discussed during the roundtable was “comprehensive care for the hospitalist” and how they can achieve a sense of wellness for themselves. Gurpreet Dhaliwal, MD, clinician-educator and professor of medicine at the University of California, San Francisco, said long-term satisfaction in one’s career is less about compensation and more about autonomy, mastery, and purpose.
“Autonomy is shrinking a little bit in health care. But if we connect to our purpose – ‘what are we doing here and how do we connect?’ – it’s either learning about patients and their stories, being with a team of people that you work with, that really builds that purpose,” he said.
Regarding mastery, there’s “tremendous joy if you’re in an environment where people value your mastery, whether it is working in a team or communicating or diagnosing or doing a procedure. If you think of setting up the work environment and those things are in place, I think a lot of wellness can actually happen at work, even though another component, of course, is balancing your life outside of work,” Dr. Dhaliwal said.
This may seem out of reach during COVID-19, but wellness is still achievable during the pandemic, Dr. Martinez said. Her time is spent 75% as a researcher and 25% as a clinician, which is her ideal balance. “I enjoy doing my research, doing my own statistics and writing grants and just learning about this problem that I’ve developed an interest in,” she said. “I just think that’s an important piece for people to focus on as far as health care for the hospitalist, is that there’s no no-one-size-fits-all, that’s for sure.”
Dr. Kumar noted that her clinical time gives her energy for nonclinical work. “I love my clinical time. It’s one of my favorite things that I do,” she said. Although she is tired at the end of the week, “I feel like I am not only giving back to my patients and my team, but I’m also giving back to myself and reminding myself why it is I do what I do every day,” she said.
Wellness for Dr. Unaka meant remembering what drew her to medicine. “It was definitely the opportunity to build strong relationships with patients and families,” she said. While these encounters can sometimes be heavy and stay with a hospitalist, “the fact that we’re in it with them is something that gives a lot of us purpose. I think that when I reflect on all of those things, I’m so happy that I’m in the role that I am.”
Unique skills during COVID-19
Mark Shapiro, MD, hospitalist and host of the roundtable and the Explore the Space podcast, also asked the panelists what skills they unexpectedly leveraged during the pandemic. Communication – with colleagues and with the community they serve – was a universal answer among the panelists.
“I learned – really from seeing some of our senior leaders here do it so well – the importance of being visible, particularly at a time when people were not together and more isolated,” Dr. Unaka said. “I think being able to be visible when you can, in order to deliver really complicated or tough news or communicate about uncertainty, for instance. Being here for our residents – many of our interns moved here sight unseen. I think they needed to feel like they had some sense of normalcy and a sense of community. I really learned how important it was to be visible, and available, and how important the little things mattered.”
Dr. Martinez said that worrying about her patients with COVID-19 in the hospital and the uncertainty around the disease kept her up at night. “I think we always have a hard time leaving work at work and getting a good night’s sleep. I just could not let go of worrying about these patients and having terrible insomnia, trying to leave work at work and I couldn’t – even after they were discharged.”
Dr. Shapiro said the skill he most needed to work on during the pandemic was his courage. “I remember the first time I took care of COVID patients. I was scared. I have no problems saying that out loud. That was a scary experience.”
The demeanor of the nurses on his unit, who had already seen patients with COVID-19, helped ground him during those moments and gave him the courage to move forward. “They’d already been doing it and they were the same. Same affect, same jokes, same everything,” he said. “That actually really helped, and I’ve leaned on that every time I’ve been back on our COVID service.”
Importance of mental health
The COVID-19 pandemic has also shined a light on the importance of mental health. “I think it is important to acknowledge that as hospitalists who have been out on the bleeding edge for a year, mental health is critically important, and we know that we face shortages in that space for the public at large and also for our profession,” Dr. Shapiro said.
When asked about what mental health and self-care looks like for her, Dr. Kumar referenced the need for exercise, meditation, and yoga. “My mental health was better knowing that the people closest to me – whether they be colleagues or friends or family – their mental health was also in a good place and they were also in a good place. And that helped to build me up,” she said.
Dr. Unaka called attention to the stigma around mental health, particularly among physicians, and the lack of resources to address the issue. “It’s a real problem,” she said. “I think it’s at a point where we as a profession need to advocate on behalf of each other and on behalf of our trainees. And honestly, I think we need to view mental health as just ‘health’ and stop separating it out in order for us to move to a place where people feel like they can access what they need without feeling shame about it.”
Editor’s note: National Hospitalist Day occurs the first Thursday in March annually, and serves to celebrate the fastest growing specialty in modern medicine and hospitalists’ enduring contributions to the evolving health care landscape. On National Hospitalist Day in 2021, SHM convened a virtual roundtable with a diverse group of hospitalists to discuss skill set, wellness, and other key issues for hospitalists. To listen to the entire roundtable discussion, visit this Explore The Space podcast episode.
A hospitalist isn’t just a physician who happens to work in a hospital. They are medical professionals with a robust skill set that they use both inside and outside the hospital setting. But what skill sets do hospitalists need to become successful in their careers? And what skill sets does a “pluripotent” hospitalist need in their armamentarium?
These were the issues discussed by participants of a virtual roundtable discussion on National Hospitalist Day – March 4, 2021 – as part of a joint effort of the Society of Hospital Medicine and the Explore the Space podcast.
Maylyn S. Martinez, MD, clinician-researcher and clinical associate at the University of Chicago, sees her hospitalist and research skill sets as two “buckets” of skills she can sort through, with diagnostic, knowledge-based care coordination, and interpersonal skills as lanes where she can focus and improve. “I’m always trying to work in, and sharpen, and find ways to get better at something in each of those every day,” she said.
For Anika Kumar, MD, FHM, pediatric editor of the Hospitalist and clinical assistant professor of pediatrics at the Cleveland Clinic Lerner College of Medicine, much of her work is focused on problem solving. “I approach that as: ‘How do I come up with my differential diagnosis, and how do I diagnose the patient?’ I think that the lanes are a little bit different, but there is some overlap.”
Adaptability is another important part of the skill set for the hospitalist, Ndidi Unaka, MD, MEd, associate professor in the division of hospital medicine at Cincinnati Children’s Hospital Medical Center, said during the discussion. “I think we all really value teamwork, and we take on the role of being the coordinator and making sure things are getting done in a seamless and thoughtful manner. Communicating with families, communicating with our research team, communicating with primary care physicians. I think that is something we’re very used to doing, and I think we do it well. I think we don’t shy away from difficult conversations with consultants. And I think that’s what makes being a hospitalist so amazing.”
Achieving wellness as a hospitalist
Another topic discussed during the roundtable was “comprehensive care for the hospitalist” and how they can achieve a sense of wellness for themselves. Gurpreet Dhaliwal, MD, clinician-educator and professor of medicine at the University of California, San Francisco, said long-term satisfaction in one’s career is less about compensation and more about autonomy, mastery, and purpose.
“Autonomy is shrinking a little bit in health care. But if we connect to our purpose – ‘what are we doing here and how do we connect?’ – it’s either learning about patients and their stories, being with a team of people that you work with, that really builds that purpose,” he said.
Regarding mastery, there’s “tremendous joy if you’re in an environment where people value your mastery, whether it is working in a team or communicating or diagnosing or doing a procedure. If you think of setting up the work environment and those things are in place, I think a lot of wellness can actually happen at work, even though another component, of course, is balancing your life outside of work,” Dr. Dhaliwal said.
This may seem out of reach during COVID-19, but wellness is still achievable during the pandemic, Dr. Martinez said. Her time is spent 75% as a researcher and 25% as a clinician, which is her ideal balance. “I enjoy doing my research, doing my own statistics and writing grants and just learning about this problem that I’ve developed an interest in,” she said. “I just think that’s an important piece for people to focus on as far as health care for the hospitalist, is that there’s no no-one-size-fits-all, that’s for sure.”
Dr. Kumar noted that her clinical time gives her energy for nonclinical work. “I love my clinical time. It’s one of my favorite things that I do,” she said. Although she is tired at the end of the week, “I feel like I am not only giving back to my patients and my team, but I’m also giving back to myself and reminding myself why it is I do what I do every day,” she said.
Wellness for Dr. Unaka meant remembering what drew her to medicine. “It was definitely the opportunity to build strong relationships with patients and families,” she said. While these encounters can sometimes be heavy and stay with a hospitalist, “the fact that we’re in it with them is something that gives a lot of us purpose. I think that when I reflect on all of those things, I’m so happy that I’m in the role that I am.”
Unique skills during COVID-19
Mark Shapiro, MD, hospitalist and host of the roundtable and the Explore the Space podcast, also asked the panelists what skills they unexpectedly leveraged during the pandemic. Communication – with colleagues and with the community they serve – was a universal answer among the panelists.
“I learned – really from seeing some of our senior leaders here do it so well – the importance of being visible, particularly at a time when people were not together and more isolated,” Dr. Unaka said. “I think being able to be visible when you can, in order to deliver really complicated or tough news or communicate about uncertainty, for instance. Being here for our residents – many of our interns moved here sight unseen. I think they needed to feel like they had some sense of normalcy and a sense of community. I really learned how important it was to be visible, and available, and how important the little things mattered.”
Dr. Martinez said that worrying about her patients with COVID-19 in the hospital and the uncertainty around the disease kept her up at night. “I think we always have a hard time leaving work at work and getting a good night’s sleep. I just could not let go of worrying about these patients and having terrible insomnia, trying to leave work at work and I couldn’t – even after they were discharged.”
Dr. Shapiro said the skill he most needed to work on during the pandemic was his courage. “I remember the first time I took care of COVID patients. I was scared. I have no problems saying that out loud. That was a scary experience.”
The demeanor of the nurses on his unit, who had already seen patients with COVID-19, helped ground him during those moments and gave him the courage to move forward. “They’d already been doing it and they were the same. Same affect, same jokes, same everything,” he said. “That actually really helped, and I’ve leaned on that every time I’ve been back on our COVID service.”
Importance of mental health
The COVID-19 pandemic has also shined a light on the importance of mental health. “I think it is important to acknowledge that as hospitalists who have been out on the bleeding edge for a year, mental health is critically important, and we know that we face shortages in that space for the public at large and also for our profession,” Dr. Shapiro said.
When asked about what mental health and self-care looks like for her, Dr. Kumar referenced the need for exercise, meditation, and yoga. “My mental health was better knowing that the people closest to me – whether they be colleagues or friends or family – their mental health was also in a good place and they were also in a good place. And that helped to build me up,” she said.
Dr. Unaka called attention to the stigma around mental health, particularly among physicians, and the lack of resources to address the issue. “It’s a real problem,” she said. “I think it’s at a point where we as a profession need to advocate on behalf of each other and on behalf of our trainees. And honestly, I think we need to view mental health as just ‘health’ and stop separating it out in order for us to move to a place where people feel like they can access what they need without feeling shame about it.”
Colchicine before PCI for acute MI fails to improve major outcomes
In a placebo-controlled randomized trial, a preprocedural dose of colchicine administered immediately before percutaneous coronary intervention (PCI) for an acute ST-segment elevated myocardial infarction (STEMI) did not reduce the no-reflow phenomenon or improve outcomes.
No-reflow, in which insufficient myocardial perfusion is present even though the coronary artery appears patent, was the primary outcome, and the proportion of patients experiencing this event was exactly the same (14.4%) in the colchicine and placebo groups, reported Yaser Jenab, MD, at CRT 2021 sponsored by MedStar Heart & Vascular Institute.
The hypothesis that colchicine would offer benefit in this setting was largely based on the Colchicine Cardiovascular Outcomes Trial (COLCOT). In that study, colchicine was associated with a 23% reduction in risk for major adverse cardiovascular events (MACE) relative to placebo when administered within 30 days after a myocardial infarction (hazard ratio, 0.77; P = .02).
The benefit in that trial was attributed to an anti-inflammatory effect, according to Dr. Jenab, associate professor of cardiology at Tehran (Iran) Heart Center. In particular as it relates to vascular disease, he cited experimental studies associating colchicine with a reduction in neutrophil activation and adherence to vascular endothelium.
The rationale for a preprocedural approach to colchicine was supplied by a subsequent time-to-treatment COLCOT analysis. In this study, MACE risk reduction for colchicine climbed to 48% (HR 0.52) for those treated within 3 days of the MI but largely disappeared (HR 0.96) if treatment was started at least 8 days post MI.
PodCAST-PCI trial
In the preprocedural study, called the PodCAST-PCI trial, 321 acute STEMI patients were randomized. Patients received a 1-mg dose of oral colchicine or placebo at the time PCI was scheduled. Another dose of colchicine (0.5 mg) or placebo was administered 1 hour after the procedure.
Of secondary outcomes, which included MACE at 1 month and 1 year, ST-segment resolution at 1 month, and change in inflammatory markers at 1 month, none were significant. Few even trended for significance.
For MACE, which included cardiac death, stroke, nonfatal MI, new hospitalization due to heart failure, or target vessel revascularization, the rates were lower in the colchicine group at 1 month (4.3% vs. 7.5%) and 1 year (9.3% vs. 11.2%), but neither approached significance.
For ST-segment resolution, the proportions were generally comparable among the colchicine and placebo groups, respectively, for the proportion below 50% (18.6% vs. 23.1%), between 50% and 70% (16.8% vs. 15.6%), and above 70% (64.6% vs. 61.3%).
The average troponin levels were nonsignificantly lower at 6 hours (1,847 vs. 2,883 ng/mL) in the colchicine group but higher at 48 hours (1,197 vs. 1,147 ng/mL). The average C-reactive protein (CRP) levels at 48 hours were nonsignificantly lower on colchicine (176.5 vs. 244.5 mg/L).
There were no significant differences in postprocedural perfusion, as measured with TIMI blood flow, or in the rate of stent thrombosis, which occurred in roughly 3% of each group of patients.
The small sample size was one limitation of this study, Dr. Jenab acknowledged. For this and other reasons, he cautioned that these data are not definitive and do not preclude a benefit on clinical outcomes in a study with a larger size, a different design, or different dosing.
Timing might be the issue
However, even if colchicine has a potential benefit in this setting, timing might be a major obstacle, according to Binata Shah, MD, associate director of research for the Cardiac Catheterization Laboratory at New York University.

“We have learned from our rheumatology colleagues that peak plasma levels of colchicine are not achieved for at least 1 hour after the full loading dose,” Dr. Shah said. “With us moving so quickly in a primary PCI setting, it is hard to imagine that colchicine would have had time to really kick in and exert its anti-inflammatory effect.”
Indeed, the problem might be worse than reaching the peak plasma level.
“Even though peak plasma levels occur as early as 1 hour after a full loading dose, we see that it takes about 24 hours to really see the effects translate downstream into more systemic inflammatory markers such as CRP and interleukin-6,” she added. If lowering these signals of inflammation is predictive of benefit, than this might be the biggest obstacle to benefit from colchicine in an urgent treatment setting.
Dr. Jenab and Dr. Shah reported no potential conflicts of interest.
In a placebo-controlled randomized trial, a preprocedural dose of colchicine administered immediately before percutaneous coronary intervention (PCI) for an acute ST-segment elevated myocardial infarction (STEMI) did not reduce the no-reflow phenomenon or improve outcomes.
No-reflow, in which insufficient myocardial perfusion is present even though the coronary artery appears patent, was the primary outcome, and the proportion of patients experiencing this event was exactly the same (14.4%) in the colchicine and placebo groups, reported Yaser Jenab, MD, at CRT 2021 sponsored by MedStar Heart & Vascular Institute.
The hypothesis that colchicine would offer benefit in this setting was largely based on the Colchicine Cardiovascular Outcomes Trial (COLCOT). In that study, colchicine was associated with a 23% reduction in risk for major adverse cardiovascular events (MACE) relative to placebo when administered within 30 days after a myocardial infarction (hazard ratio, 0.77; P = .02).
The benefit in that trial was attributed to an anti-inflammatory effect, according to Dr. Jenab, associate professor of cardiology at Tehran (Iran) Heart Center. In particular as it relates to vascular disease, he cited experimental studies associating colchicine with a reduction in neutrophil activation and adherence to vascular endothelium.
The rationale for a preprocedural approach to colchicine was supplied by a subsequent time-to-treatment COLCOT analysis. In this study, MACE risk reduction for colchicine climbed to 48% (HR 0.52) for those treated within 3 days of the MI but largely disappeared (HR 0.96) if treatment was started at least 8 days post MI.
PodCAST-PCI trial
In the preprocedural study, called the PodCAST-PCI trial, 321 acute STEMI patients were randomized. Patients received a 1-mg dose of oral colchicine or placebo at the time PCI was scheduled. Another dose of colchicine (0.5 mg) or placebo was administered 1 hour after the procedure.
Of secondary outcomes, which included MACE at 1 month and 1 year, ST-segment resolution at 1 month, and change in inflammatory markers at 1 month, none were significant. Few even trended for significance.
For MACE, which included cardiac death, stroke, nonfatal MI, new hospitalization due to heart failure, or target vessel revascularization, the rates were lower in the colchicine group at 1 month (4.3% vs. 7.5%) and 1 year (9.3% vs. 11.2%), but neither approached significance.
For ST-segment resolution, the proportions were generally comparable among the colchicine and placebo groups, respectively, for the proportion below 50% (18.6% vs. 23.1%), between 50% and 70% (16.8% vs. 15.6%), and above 70% (64.6% vs. 61.3%).
The average troponin levels were nonsignificantly lower at 6 hours (1,847 vs. 2,883 ng/mL) in the colchicine group but higher at 48 hours (1,197 vs. 1,147 ng/mL). The average C-reactive protein (CRP) levels at 48 hours were nonsignificantly lower on colchicine (176.5 vs. 244.5 mg/L).
There were no significant differences in postprocedural perfusion, as measured with TIMI blood flow, or in the rate of stent thrombosis, which occurred in roughly 3% of each group of patients.
The small sample size was one limitation of this study, Dr. Jenab acknowledged. For this and other reasons, he cautioned that these data are not definitive and do not preclude a benefit on clinical outcomes in a study with a larger size, a different design, or different dosing.
Timing might be the issue
However, even if colchicine has a potential benefit in this setting, timing might be a major obstacle, according to Binata Shah, MD, associate director of research for the Cardiac Catheterization Laboratory at New York University.
“We have learned from our rheumatology colleagues that peak plasma levels of colchicine are not achieved for at least 1 hour after the full loading dose,” Dr. Shah said. “With us moving so quickly in a primary PCI setting, it is hard to imagine that colchicine would have had time to really kick in and exert its anti-inflammatory effect.”
Indeed, the problem might be worse than reaching the peak plasma level.
“Even though peak plasma levels occur as early as 1 hour after a full loading dose, we see that it takes about 24 hours to really see the effects translate downstream into more systemic inflammatory markers such as CRP and interleukin-6,” she added. If lowering these signals of inflammation is predictive of benefit, than this might be the biggest obstacle to benefit from colchicine in an urgent treatment setting.
Dr. Jenab and Dr. Shah reported no potential conflicts of interest.
In a placebo-controlled randomized trial, a preprocedural dose of colchicine administered immediately before percutaneous coronary intervention (PCI) for an acute ST-segment elevated myocardial infarction (STEMI) did not reduce the no-reflow phenomenon or improve outcomes.
No-reflow, in which insufficient myocardial perfusion is present even though the coronary artery appears patent, was the primary outcome, and the proportion of patients experiencing this event was exactly the same (14.4%) in the colchicine and placebo groups, reported Yaser Jenab, MD, at CRT 2021 sponsored by MedStar Heart & Vascular Institute.
The hypothesis that colchicine would offer benefit in this setting was largely based on the Colchicine Cardiovascular Outcomes Trial (COLCOT). In that study, colchicine was associated with a 23% reduction in risk for major adverse cardiovascular events (MACE) relative to placebo when administered within 30 days after a myocardial infarction (hazard ratio, 0.77; P = .02).
The benefit in that trial was attributed to an anti-inflammatory effect, according to Dr. Jenab, associate professor of cardiology at Tehran (Iran) Heart Center. In particular as it relates to vascular disease, he cited experimental studies associating colchicine with a reduction in neutrophil activation and adherence to vascular endothelium.
The rationale for a preprocedural approach to colchicine was supplied by a subsequent time-to-treatment COLCOT analysis. In this study, MACE risk reduction for colchicine climbed to 48% (HR 0.52) for those treated within 3 days of the MI but largely disappeared (HR 0.96) if treatment was started at least 8 days post MI.
PodCAST-PCI trial
In the preprocedural study, called the PodCAST-PCI trial, 321 acute STEMI patients were randomized. Patients received a 1-mg dose of oral colchicine or placebo at the time PCI was scheduled. Another dose of colchicine (0.5 mg) or placebo was administered 1 hour after the procedure.
Of secondary outcomes, which included MACE at 1 month and 1 year, ST-segment resolution at 1 month, and change in inflammatory markers at 1 month, none were significant. Few even trended for significance.
For MACE, which included cardiac death, stroke, nonfatal MI, new hospitalization due to heart failure, or target vessel revascularization, the rates were lower in the colchicine group at 1 month (4.3% vs. 7.5%) and 1 year (9.3% vs. 11.2%), but neither approached significance.
For ST-segment resolution, the proportions were generally comparable among the colchicine and placebo groups, respectively, for the proportion below 50% (18.6% vs. 23.1%), between 50% and 70% (16.8% vs. 15.6%), and above 70% (64.6% vs. 61.3%).
The average troponin levels were nonsignificantly lower at 6 hours (1,847 vs. 2,883 ng/mL) in the colchicine group but higher at 48 hours (1,197 vs. 1,147 ng/mL). The average C-reactive protein (CRP) levels at 48 hours were nonsignificantly lower on colchicine (176.5 vs. 244.5 mg/L).
There were no significant differences in postprocedural perfusion, as measured with TIMI blood flow, or in the rate of stent thrombosis, which occurred in roughly 3% of each group of patients.
The small sample size was one limitation of this study, Dr. Jenab acknowledged. For this and other reasons, he cautioned that these data are not definitive and do not preclude a benefit on clinical outcomes in a study with a larger size, a different design, or different dosing.
Timing might be the issue
However, even if colchicine has a potential benefit in this setting, timing might be a major obstacle, according to Binata Shah, MD, associate director of research for the Cardiac Catheterization Laboratory at New York University.
“We have learned from our rheumatology colleagues that peak plasma levels of colchicine are not achieved for at least 1 hour after the full loading dose,” Dr. Shah said. “With us moving so quickly in a primary PCI setting, it is hard to imagine that colchicine would have had time to really kick in and exert its anti-inflammatory effect.”
Indeed, the problem might be worse than reaching the peak plasma level.
“Even though peak plasma levels occur as early as 1 hour after a full loading dose, we see that it takes about 24 hours to really see the effects translate downstream into more systemic inflammatory markers such as CRP and interleukin-6,” she added. If lowering these signals of inflammation is predictive of benefit, than this might be the biggest obstacle to benefit from colchicine in an urgent treatment setting.
Dr. Jenab and Dr. Shah reported no potential conflicts of interest.
FROM CRT 2021
Virtual is the new real
Why did we fall short on maximizing telehealth’s value in the COVID-19 pandemic?
The COVID-19 pandemic catalyzed the transformation of Internet-based, remotely accessible innovative technologies. Internet-based customer service delivery technology was rapidly adopted and utilized by several services industries, but health care systems in most of the countries across the world faced unique challenges in adopting the technology for the delivery of health care services. The health care ecosystem of the United States was not immune to such challenges, and several significant barriers surfaced while the pandemic was underway.

Complexly structured, fragmented, unprepared, and overly burnt-out health systems in the United States arguably have fallen short of maximizing the value of telehealth in delivering safe, easily accessible, comprehensive, and cost-effective health care services. In this essay, we examine the reasons for such a suboptimal performance and discuss a few important strategies that may be useful in maximizing the value of telehealth value in several, appropriate health care services.
Hospitals and telehealth
Are hospitalists preparing ourselves “not to see” patients in a hospital-based health care delivery setting? If you have not yet started yet, now may be the right time! Yes, a certain percentage of doctor-patient encounters in hospital settings will remain virtual forever.
A well-established telehealth infrastructure is rarely found in most U.S. hospitals, although the COVID-19 pandemic has unexpectedly boosted the rapid growth of telehealth in the country.1 Public health emergency declarations in the United States in the face of the COVID-19 crisis have facilitated two important initiatives to restore health care delivery amidst formal and informal lockdowns that brought states to a grinding halt. These extend from expansion of virtual services, including telehealth, virtual check-ins, and e-visits, to the decision by the Department of Health & Human Services Office of Civil Rights to exercise enforcement discretion and waive penalties for the use of relatively inexpensive, non–public-facing mobile and other audiovisual technology tools.2
Hospital-based care in the United States taps nearly 33% of national health expenditure. An additional 30% of national health expenditure that is related to physicians, prescriptions, and other facilities is indirectly influenced by care delivered at health care facilities.3 Studies show that about 20% of ED visits could potentially be avoided via virtual urgent care offerings.4 A rapidly changing health care ecosystem is proving formidable for most hospital systems, and a test for their resilience and agility. Not just the implementation of telehealth is challenging, but getting it right is the key success factor.
Hospital-based telehealth
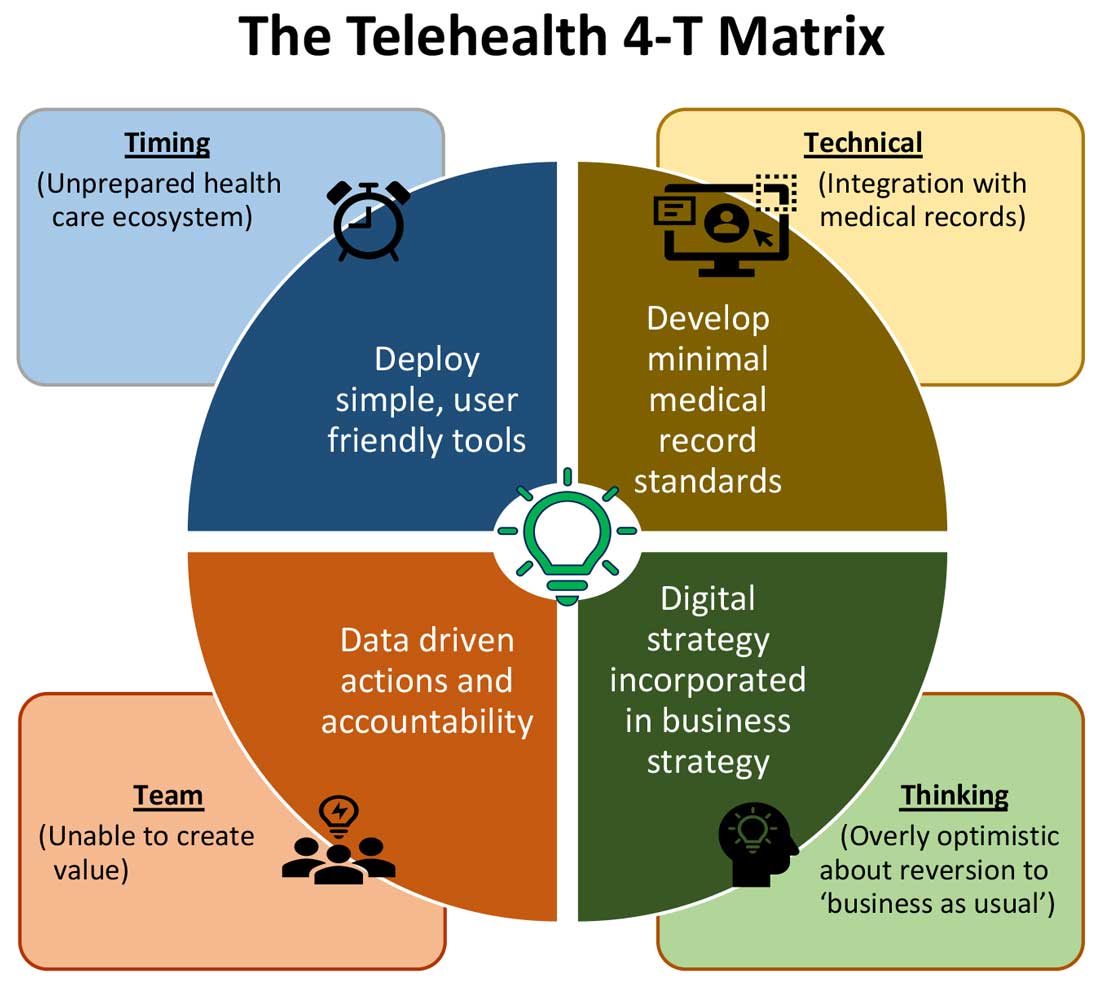
Expansion of telehealth coverage by the Centers for Medicare & Medicaid Services and most commercial payers did not quite ride the pandemic-induced momentum across the care continuum. Hospitals are lagging far behind ambulatory care in implementing telehealth. As illustrated in the “4-T Matrix” (see graphic) we would like to examine four key reasons for such a sluggish initial uptake and try to propose four important strategies that may help us to maximize the value created by telehealth technologies.
1. Timing
The health care system has always lagged far behind other service industries in terms of technology adaptation. Because of the unique nature of health care services, face-to-face interaction supersedes all other forms of communication. A rapidly evolving pandemic was not matched by simultaneous technology education for patients and providers. The enormous choice of hard-to-navigate telehealth tools; time and labor-intensive implementation; and uncertainty around payer, policy, and regulatory expectations might have precluded providers from the rapid adoption of telehealth in the hospital setting. Patients’ specific characteristics, such as the absence of technology-centered education, information, age, comorbidities, lack of technical literacy, and dependency on caregivers contributed to the suboptimal response from patients and families.
Deploying simple, ubiquitous, user-friendly, and technologically less challenging telehealth solutions may be a better approach to increase the adoption of such solutions by providers and patients. Hospitals need to develop and distribute telehealth user guides in all possible modes of communication. Provider-centric in-service sessions, workshops, and live support by “superuser teams” often work well in reducing end-user resistance.
2. Technical
Current electronic medical records vary widely in their features and offerings, and their ability to interact with third-party software and platforms. Dissatisfaction of end users with EMRs is well known, as is their likely relationship to burnout. Recent research continues to show a strong relationship between EMR usability and the odds of burnout among physicians.5 In the current climate, administrators and health informaticists have the responsibility to avoid adding increased burdens to end users.

Another issue is the limited connectivity in many remote/rural areas that would impact implementation of telehealth platforms. Studies indicate that 33% of rural Americans lack access to high-speed broadband Internet to support video visits.6 The recent successful implementation of telehealth across 530 providers in 75 ambulatory practices operated by Munson Healthcare, a rural health system in northern Michigan, sheds light on the technology’s enormous potential in providing safe access to rural populations.6,7
Privacy and safety of patient data is of paramount importance. According to a national poll on healthy aging by the University of Michigan in May 2019, targeting older adults, 47% of survey responders expressed difficulty using technology and 49% of survey responders were concerned about privacy.8 Use of certification and other tools offered by the Office of the National Coordinator for Health Information Technology would help reassure users, and the ability to capture and share images between providers would be of immense benefit in facilitating e-consults.
The need of the hour is redesigned work flow, to help providers adopt and use virtual care/telehealth efficiently. Work flow redesign must be coupled with technological advances to allow seamless integration of third-party telehealth platforms into existing EMR systems or built directly into EMRs. Use of quality metrics and analytical tools specific to telehealth would help measure the technology’s impact on patient care, outcomes, and end-user/provider experience.
3. Teams and training
Outcomes of health care interventions are often determined by the effectiveness of teams. Irrespective of how robust health care systems may have been initially, rapidly spreading infectious diseases like COVID-19 can quickly derail the system, bringing the workforce and patients to a breaking point.5 Decentralized, uncoordinated, and siloed efforts by individual teams across the care continuum were contributing factors for the partial success of telehealth care delivery pathways. The hospital systems with telehealth-ready teams at the start of the COVID-19 pandemic were so rare that the knowledge and technical training opportunities for innovators grew severalfold during the pandemic.

As per the American Medical Association, telehealth success is massively dependent on building the right team. Core, leadership, advisory, and implementation teams comprised of clinical representatives, end users, administrative personnel, executive members of the organization, technical experts, and payment/policy experts should be put together before implementing a telehealth strategy.9 Seamless integration of hospital-based care with ambulatory care via a telehealth platform is only complete when care managers are trained and deployed to fulfill the needs of a diverse group of patients. Deriving overall value from telehealth is only possible when there is a skill development, training and mentoring team put in place.
4. Thinking
In most U.S. hospitals, inpatient health care is equally distributed between nonprocedure and procedure-based services. Hospitals resorted to suspension of nonemergent procedures to mitigate the risk of spreading COVID-19. This was further compounded by many patients’ self-selection to defer care, an abrupt reduction in the influx of patients from the referral base because of suboptimally operating ambulatory care services, leading to low hospital occupancy.
Hospitals across the nation have gone through a massive short-term financial crunch and unfavorable cash-flow forecast, which prompted a paradoxical work-force reduction. While some argue that it may be akin to strategic myopia, the authors believed that such a response is strategically imperative to keep the hospital afloat. It is reasonable to attribute the paucity of innovation to constrained resources, and health systems are simply staying overly optimistic about “weathering the storm” and reverting soon to “business as usual.” The technological framework necessary for deploying a telehealth solution often comes with a price. Financially challenged hospital systems rarely exercise any capital-intensive activities. By contrast, telehealth adoption by ambulatory care can result in quicker resumption of patient care in community settings. A lack of operational and infrastructure synchrony between ambulatory and in-hospital systems has failed to capture telehealth-driven inpatient volume. For example, direct admissions from ambulatory telehealth referrals was a missed opportunity in several places. Referrals for labs, diagnostic tests, and other allied services could have helped hospitals offset their fixed costs. Similarly, work flows related to discharge and postdischarge follow up rarely embrace telehealth tools or telehealth care pathways. A brisk change in the health care ecosystem is partly responsible for this.
Digital strategy needs to be incorporated into business strategy. For the reasons already discussed, telehealth technology is not a “nice to have” anymore, but a “must have.” At present, providers are of the opinion that about 20% of their patient services can be delivered via a telehealth platform. Similar trends are observed among patients, as a new modality of access to care is increasingly beneficial to them. Telehealth must be incorporated in standardized hospital work flows. Use of telehealth for preoperative clearance will greatly minimize same-day surgery cancellations. Given the potential shortage in resources, telehealth adoption for inpatient consultations will help systems conserve personal protective equipment, minimize the risk of staff exposure to COVID-19, and improve efficiency.
Digital strategy also prompts the reengineering of care delivery.10 Excessive and unused physical capacity can be converted into digital care hubs. Health maintenance, prevention, health promotion, health education, and chronic disease management not only can serve a variety of patient groups but can also help address the “last-mile problem” in health care. A successful digital strategy usually has three important components – Commitment: Hospital leadership is committed to include digital transformation as a strategic objective; Cost: Digital strategy is added as a line item in the budget; and Control: Measurable metrics are put in place to monitor the performance, impact, and influence of the digital strategy.
Conclusion
For decades, most U.S. health systems occupied the periphery of technological transformation when compared to the rest of the service industry. While most health systems took a heroic approach to the adoption of telehealth during COVID-19, despite being unprepared, the need for a systematic telehealth deployment is far from being adequately fulfilled. The COVID-19 pandemic brought permanent changes to several business disciplines globally. Given the impact of the pandemic on the health and overall wellbeing of American society, the U.S. health care industry must leave no stone unturned in its quest for transformation.
Dr. Lingisetty is a hospitalist and physician executive at Baptist Health System, Little Rock, Ark, and is cofounder/president of SHM’s Arkansas chapter. Dr. Prasad is medical director of care management and a hospitalist at Advocate Aurora Health in Milwaukee. He is cochair of SHM’s IT Special Interest Group, sits on the HQPS committee, and is president of SHM’s Wisconsin chapter. Dr. Palabindala is the medical director, utilization management, and physician advisory services at the University of Mississippi Medical Center and an associate professor of medicine and academic hospitalist at the University of Mississippi, both in Jackson.
References
1. Finnegan M. “Telehealth booms amid COVID-19 crisis.” Computerworld. 2020 Apr 27. www.computerworld.com/article/3540315/telehealth-booms-amid-covid-19-crisis-virtual-care-is-here-to-stay.html. Accessed 2020 Sep 12.
2. Department of Health & Human Services. “OCR Announces Notification of Enforcement Discretion for Telehealth Remote Communications During the COVID-19 Nationwide Public Health Emergency.” 2020 Mar 17. www.hhs.gov/about/news/2020/03/17/ocr-announces-notification-of-enforcement-discretion-for-telehealth-remote-communications-during-the-covid-19.html. Accessed 2020 Sep 12.
3. National Center for Health Statistics. “Health Expenditures.” www.cdc.gov/nchs/fastats/health-expenditures.htm. Accessed 2020 Sep 12.
4. Bestsennyy O et al. “Telehealth: A post–COVID-19 reality?” McKinsey & Company. 2020 May 29. www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality. Accessed 2020 Sep 12.
5. Melnick ER et al. The Association Between Perceived Electronic Health Record Usability and Professional Burnout Among U.S. Physicians. Mayo Clin Proc. 2020 March;95(3):476-87.
6. Hirko KA et al. Telehealth in response to the COVID-19 pandemic: Implications for rural health disparities. J Am Med Inform Assoc. 2020 Nov;27(11):1816-8. .
7. American Academy of Family Physicians. “Study Examines Telehealth, Rural Disparities in Pandemic.” 2020 July 30. www.aafp.org/news/practice-professional-issues/20200730ruraltelehealth.html. Accessed 2020 Dec 15.
8. Kurlander J et al. “Virtual Visits: Telehealth and Older Adults.” National Poll on Healthy Aging. 2019 Oct. hdl.handle.net/2027.42/151376.
9. American Medical Association. Telehealth Implementation Playbook. 2019. www.ama-assn.org/system/files/2020-04/ama-telehealth-implementation-playbook.pdf.
10. Smith AC et al. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020 Jun;26(5):309-13.
Why did we fall short on maximizing telehealth’s value in the COVID-19 pandemic?
Why did we fall short on maximizing telehealth’s value in the COVID-19 pandemic?
The COVID-19 pandemic catalyzed the transformation of Internet-based, remotely accessible innovative technologies. Internet-based customer service delivery technology was rapidly adopted and utilized by several services industries, but health care systems in most of the countries across the world faced unique challenges in adopting the technology for the delivery of health care services. The health care ecosystem of the United States was not immune to such challenges, and several significant barriers surfaced while the pandemic was underway.
Complexly structured, fragmented, unprepared, and overly burnt-out health systems in the United States arguably have fallen short of maximizing the value of telehealth in delivering safe, easily accessible, comprehensive, and cost-effective health care services. In this essay, we examine the reasons for such a suboptimal performance and discuss a few important strategies that may be useful in maximizing the value of telehealth value in several, appropriate health care services.
Hospitals and telehealth
Are hospitalists preparing ourselves “not to see” patients in a hospital-based health care delivery setting? If you have not yet started yet, now may be the right time! Yes, a certain percentage of doctor-patient encounters in hospital settings will remain virtual forever.
A well-established telehealth infrastructure is rarely found in most U.S. hospitals, although the COVID-19 pandemic has unexpectedly boosted the rapid growth of telehealth in the country.1 Public health emergency declarations in the United States in the face of the COVID-19 crisis have facilitated two important initiatives to restore health care delivery amidst formal and informal lockdowns that brought states to a grinding halt. These extend from expansion of virtual services, including telehealth, virtual check-ins, and e-visits, to the decision by the Department of Health & Human Services Office of Civil Rights to exercise enforcement discretion and waive penalties for the use of relatively inexpensive, non–public-facing mobile and other audiovisual technology tools.2
Hospital-based care in the United States taps nearly 33% of national health expenditure. An additional 30% of national health expenditure that is related to physicians, prescriptions, and other facilities is indirectly influenced by care delivered at health care facilities.3 Studies show that about 20% of ED visits could potentially be avoided via virtual urgent care offerings.4 A rapidly changing health care ecosystem is proving formidable for most hospital systems, and a test for their resilience and agility. Not just the implementation of telehealth is challenging, but getting it right is the key success factor.
Hospital-based telehealth
Expansion of telehealth coverage by the Centers for Medicare & Medicaid Services and most commercial payers did not quite ride the pandemic-induced momentum across the care continuum. Hospitals are lagging far behind ambulatory care in implementing telehealth. As illustrated in the “4-T Matrix” (see graphic) we would like to examine four key reasons for such a sluggish initial uptake and try to propose four important strategies that may help us to maximize the value created by telehealth technologies.
1. Timing
The health care system has always lagged far behind other service industries in terms of technology adaptation. Because of the unique nature of health care services, face-to-face interaction supersedes all other forms of communication. A rapidly evolving pandemic was not matched by simultaneous technology education for patients and providers. The enormous choice of hard-to-navigate telehealth tools; time and labor-intensive implementation; and uncertainty around payer, policy, and regulatory expectations might have precluded providers from the rapid adoption of telehealth in the hospital setting. Patients’ specific characteristics, such as the absence of technology-centered education, information, age, comorbidities, lack of technical literacy, and dependency on caregivers contributed to the suboptimal response from patients and families.
Deploying simple, ubiquitous, user-friendly, and technologically less challenging telehealth solutions may be a better approach to increase the adoption of such solutions by providers and patients. Hospitals need to develop and distribute telehealth user guides in all possible modes of communication. Provider-centric in-service sessions, workshops, and live support by “superuser teams” often work well in reducing end-user resistance.
2. Technical
Current electronic medical records vary widely in their features and offerings, and their ability to interact with third-party software and platforms. Dissatisfaction of end users with EMRs is well known, as is their likely relationship to burnout. Recent research continues to show a strong relationship between EMR usability and the odds of burnout among physicians.5 In the current climate, administrators and health informaticists have the responsibility to avoid adding increased burdens to end users.
Another issue is the limited connectivity in many remote/rural areas that would impact implementation of telehealth platforms. Studies indicate that 33% of rural Americans lack access to high-speed broadband Internet to support video visits.6 The recent successful implementation of telehealth across 530 providers in 75 ambulatory practices operated by Munson Healthcare, a rural health system in northern Michigan, sheds light on the technology’s enormous potential in providing safe access to rural populations.6,7
Privacy and safety of patient data is of paramount importance. According to a national poll on healthy aging by the University of Michigan in May 2019, targeting older adults, 47% of survey responders expressed difficulty using technology and 49% of survey responders were concerned about privacy.8 Use of certification and other tools offered by the Office of the National Coordinator for Health Information Technology would help reassure users, and the ability to capture and share images between providers would be of immense benefit in facilitating e-consults.
The need of the hour is redesigned work flow, to help providers adopt and use virtual care/telehealth efficiently. Work flow redesign must be coupled with technological advances to allow seamless integration of third-party telehealth platforms into existing EMR systems or built directly into EMRs. Use of quality metrics and analytical tools specific to telehealth would help measure the technology’s impact on patient care, outcomes, and end-user/provider experience.
3. Teams and training
Outcomes of health care interventions are often determined by the effectiveness of teams. Irrespective of how robust health care systems may have been initially, rapidly spreading infectious diseases like COVID-19 can quickly derail the system, bringing the workforce and patients to a breaking point.5 Decentralized, uncoordinated, and siloed efforts by individual teams across the care continuum were contributing factors for the partial success of telehealth care delivery pathways. The hospital systems with telehealth-ready teams at the start of the COVID-19 pandemic were so rare that the knowledge and technical training opportunities for innovators grew severalfold during the pandemic.
As per the American Medical Association, telehealth success is massively dependent on building the right team. Core, leadership, advisory, and implementation teams comprised of clinical representatives, end users, administrative personnel, executive members of the organization, technical experts, and payment/policy experts should be put together before implementing a telehealth strategy.9 Seamless integration of hospital-based care with ambulatory care via a telehealth platform is only complete when care managers are trained and deployed to fulfill the needs of a diverse group of patients. Deriving overall value from telehealth is only possible when there is a skill development, training and mentoring team put in place.
4. Thinking
In most U.S. hospitals, inpatient health care is equally distributed between nonprocedure and procedure-based services. Hospitals resorted to suspension of nonemergent procedures to mitigate the risk of spreading COVID-19. This was further compounded by many patients’ self-selection to defer care, an abrupt reduction in the influx of patients from the referral base because of suboptimally operating ambulatory care services, leading to low hospital occupancy.
Hospitals across the nation have gone through a massive short-term financial crunch and unfavorable cash-flow forecast, which prompted a paradoxical work-force reduction. While some argue that it may be akin to strategic myopia, the authors believed that such a response is strategically imperative to keep the hospital afloat. It is reasonable to attribute the paucity of innovation to constrained resources, and health systems are simply staying overly optimistic about “weathering the storm” and reverting soon to “business as usual.” The technological framework necessary for deploying a telehealth solution often comes with a price. Financially challenged hospital systems rarely exercise any capital-intensive activities. By contrast, telehealth adoption by ambulatory care can result in quicker resumption of patient care in community settings. A lack of operational and infrastructure synchrony between ambulatory and in-hospital systems has failed to capture telehealth-driven inpatient volume. For example, direct admissions from ambulatory telehealth referrals was a missed opportunity in several places. Referrals for labs, diagnostic tests, and other allied services could have helped hospitals offset their fixed costs. Similarly, work flows related to discharge and postdischarge follow up rarely embrace telehealth tools or telehealth care pathways. A brisk change in the health care ecosystem is partly responsible for this.
Digital strategy needs to be incorporated into business strategy. For the reasons already discussed, telehealth technology is not a “nice to have” anymore, but a “must have.” At present, providers are of the opinion that about 20% of their patient services can be delivered via a telehealth platform. Similar trends are observed among patients, as a new modality of access to care is increasingly beneficial to them. Telehealth must be incorporated in standardized hospital work flows. Use of telehealth for preoperative clearance will greatly minimize same-day surgery cancellations. Given the potential shortage in resources, telehealth adoption for inpatient consultations will help systems conserve personal protective equipment, minimize the risk of staff exposure to COVID-19, and improve efficiency.
Digital strategy also prompts the reengineering of care delivery.10 Excessive and unused physical capacity can be converted into digital care hubs. Health maintenance, prevention, health promotion, health education, and chronic disease management not only can serve a variety of patient groups but can also help address the “last-mile problem” in health care. A successful digital strategy usually has three important components – Commitment: Hospital leadership is committed to include digital transformation as a strategic objective; Cost: Digital strategy is added as a line item in the budget; and Control: Measurable metrics are put in place to monitor the performance, impact, and influence of the digital strategy.
Conclusion
For decades, most U.S. health systems occupied the periphery of technological transformation when compared to the rest of the service industry. While most health systems took a heroic approach to the adoption of telehealth during COVID-19, despite being unprepared, the need for a systematic telehealth deployment is far from being adequately fulfilled. The COVID-19 pandemic brought permanent changes to several business disciplines globally. Given the impact of the pandemic on the health and overall wellbeing of American society, the U.S. health care industry must leave no stone unturned in its quest for transformation.
Dr. Lingisetty is a hospitalist and physician executive at Baptist Health System, Little Rock, Ark, and is cofounder/president of SHM’s Arkansas chapter. Dr. Prasad is medical director of care management and a hospitalist at Advocate Aurora Health in Milwaukee. He is cochair of SHM’s IT Special Interest Group, sits on the HQPS committee, and is president of SHM’s Wisconsin chapter. Dr. Palabindala is the medical director, utilization management, and physician advisory services at the University of Mississippi Medical Center and an associate professor of medicine and academic hospitalist at the University of Mississippi, both in Jackson.
References
1. Finnegan M. “Telehealth booms amid COVID-19 crisis.” Computerworld. 2020 Apr 27. www.computerworld.com/article/3540315/telehealth-booms-amid-covid-19-crisis-virtual-care-is-here-to-stay.html. Accessed 2020 Sep 12.
2. Department of Health & Human Services. “OCR Announces Notification of Enforcement Discretion for Telehealth Remote Communications During the COVID-19 Nationwide Public Health Emergency.” 2020 Mar 17. www.hhs.gov/about/news/2020/03/17/ocr-announces-notification-of-enforcement-discretion-for-telehealth-remote-communications-during-the-covid-19.html. Accessed 2020 Sep 12.
3. National Center for Health Statistics. “Health Expenditures.” www.cdc.gov/nchs/fastats/health-expenditures.htm. Accessed 2020 Sep 12.
4. Bestsennyy O et al. “Telehealth: A post–COVID-19 reality?” McKinsey & Company. 2020 May 29. www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality. Accessed 2020 Sep 12.
5. Melnick ER et al. The Association Between Perceived Electronic Health Record Usability and Professional Burnout Among U.S. Physicians. Mayo Clin Proc. 2020 March;95(3):476-87.
6. Hirko KA et al. Telehealth in response to the COVID-19 pandemic: Implications for rural health disparities. J Am Med Inform Assoc. 2020 Nov;27(11):1816-8. .
7. American Academy of Family Physicians. “Study Examines Telehealth, Rural Disparities in Pandemic.” 2020 July 30. www.aafp.org/news/practice-professional-issues/20200730ruraltelehealth.html. Accessed 2020 Dec 15.
8. Kurlander J et al. “Virtual Visits: Telehealth and Older Adults.” National Poll on Healthy Aging. 2019 Oct. hdl.handle.net/2027.42/151376.
9. American Medical Association. Telehealth Implementation Playbook. 2019. www.ama-assn.org/system/files/2020-04/ama-telehealth-implementation-playbook.pdf.
10. Smith AC et al. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020 Jun;26(5):309-13.
The COVID-19 pandemic catalyzed the transformation of Internet-based, remotely accessible innovative technologies. Internet-based customer service delivery technology was rapidly adopted and utilized by several services industries, but health care systems in most of the countries across the world faced unique challenges in adopting the technology for the delivery of health care services. The health care ecosystem of the United States was not immune to such challenges, and several significant barriers surfaced while the pandemic was underway.
Complexly structured, fragmented, unprepared, and overly burnt-out health systems in the United States arguably have fallen short of maximizing the value of telehealth in delivering safe, easily accessible, comprehensive, and cost-effective health care services. In this essay, we examine the reasons for such a suboptimal performance and discuss a few important strategies that may be useful in maximizing the value of telehealth value in several, appropriate health care services.
Hospitals and telehealth
Are hospitalists preparing ourselves “not to see” patients in a hospital-based health care delivery setting? If you have not yet started yet, now may be the right time! Yes, a certain percentage of doctor-patient encounters in hospital settings will remain virtual forever.
A well-established telehealth infrastructure is rarely found in most U.S. hospitals, although the COVID-19 pandemic has unexpectedly boosted the rapid growth of telehealth in the country.1 Public health emergency declarations in the United States in the face of the COVID-19 crisis have facilitated two important initiatives to restore health care delivery amidst formal and informal lockdowns that brought states to a grinding halt. These extend from expansion of virtual services, including telehealth, virtual check-ins, and e-visits, to the decision by the Department of Health & Human Services Office of Civil Rights to exercise enforcement discretion and waive penalties for the use of relatively inexpensive, non–public-facing mobile and other audiovisual technology tools.2
Hospital-based care in the United States taps nearly 33% of national health expenditure. An additional 30% of national health expenditure that is related to physicians, prescriptions, and other facilities is indirectly influenced by care delivered at health care facilities.3 Studies show that about 20% of ED visits could potentially be avoided via virtual urgent care offerings.4 A rapidly changing health care ecosystem is proving formidable for most hospital systems, and a test for their resilience and agility. Not just the implementation of telehealth is challenging, but getting it right is the key success factor.
Hospital-based telehealth
Expansion of telehealth coverage by the Centers for Medicare & Medicaid Services and most commercial payers did not quite ride the pandemic-induced momentum across the care continuum. Hospitals are lagging far behind ambulatory care in implementing telehealth. As illustrated in the “4-T Matrix” (see graphic) we would like to examine four key reasons for such a sluggish initial uptake and try to propose four important strategies that may help us to maximize the value created by telehealth technologies.
1. Timing
The health care system has always lagged far behind other service industries in terms of technology adaptation. Because of the unique nature of health care services, face-to-face interaction supersedes all other forms of communication. A rapidly evolving pandemic was not matched by simultaneous technology education for patients and providers. The enormous choice of hard-to-navigate telehealth tools; time and labor-intensive implementation; and uncertainty around payer, policy, and regulatory expectations might have precluded providers from the rapid adoption of telehealth in the hospital setting. Patients’ specific characteristics, such as the absence of technology-centered education, information, age, comorbidities, lack of technical literacy, and dependency on caregivers contributed to the suboptimal response from patients and families.
Deploying simple, ubiquitous, user-friendly, and technologically less challenging telehealth solutions may be a better approach to increase the adoption of such solutions by providers and patients. Hospitals need to develop and distribute telehealth user guides in all possible modes of communication. Provider-centric in-service sessions, workshops, and live support by “superuser teams” often work well in reducing end-user resistance.
2. Technical
Current electronic medical records vary widely in their features and offerings, and their ability to interact with third-party software and platforms. Dissatisfaction of end users with EMRs is well known, as is their likely relationship to burnout. Recent research continues to show a strong relationship between EMR usability and the odds of burnout among physicians.5 In the current climate, administrators and health informaticists have the responsibility to avoid adding increased burdens to end users.
Another issue is the limited connectivity in many remote/rural areas that would impact implementation of telehealth platforms. Studies indicate that 33% of rural Americans lack access to high-speed broadband Internet to support video visits.6 The recent successful implementation of telehealth across 530 providers in 75 ambulatory practices operated by Munson Healthcare, a rural health system in northern Michigan, sheds light on the technology’s enormous potential in providing safe access to rural populations.6,7
Privacy and safety of patient data is of paramount importance. According to a national poll on healthy aging by the University of Michigan in May 2019, targeting older adults, 47% of survey responders expressed difficulty using technology and 49% of survey responders were concerned about privacy.8 Use of certification and other tools offered by the Office of the National Coordinator for Health Information Technology would help reassure users, and the ability to capture and share images between providers would be of immense benefit in facilitating e-consults.
The need of the hour is redesigned work flow, to help providers adopt and use virtual care/telehealth efficiently. Work flow redesign must be coupled with technological advances to allow seamless integration of third-party telehealth platforms into existing EMR systems or built directly into EMRs. Use of quality metrics and analytical tools specific to telehealth would help measure the technology’s impact on patient care, outcomes, and end-user/provider experience.
3. Teams and training
Outcomes of health care interventions are often determined by the effectiveness of teams. Irrespective of how robust health care systems may have been initially, rapidly spreading infectious diseases like COVID-19 can quickly derail the system, bringing the workforce and patients to a breaking point.5 Decentralized, uncoordinated, and siloed efforts by individual teams across the care continuum were contributing factors for the partial success of telehealth care delivery pathways. The hospital systems with telehealth-ready teams at the start of the COVID-19 pandemic were so rare that the knowledge and technical training opportunities for innovators grew severalfold during the pandemic.
As per the American Medical Association, telehealth success is massively dependent on building the right team. Core, leadership, advisory, and implementation teams comprised of clinical representatives, end users, administrative personnel, executive members of the organization, technical experts, and payment/policy experts should be put together before implementing a telehealth strategy.9 Seamless integration of hospital-based care with ambulatory care via a telehealth platform is only complete when care managers are trained and deployed to fulfill the needs of a diverse group of patients. Deriving overall value from telehealth is only possible when there is a skill development, training and mentoring team put in place.
4. Thinking
In most U.S. hospitals, inpatient health care is equally distributed between nonprocedure and procedure-based services. Hospitals resorted to suspension of nonemergent procedures to mitigate the risk of spreading COVID-19. This was further compounded by many patients’ self-selection to defer care, an abrupt reduction in the influx of patients from the referral base because of suboptimally operating ambulatory care services, leading to low hospital occupancy.
Hospitals across the nation have gone through a massive short-term financial crunch and unfavorable cash-flow forecast, which prompted a paradoxical work-force reduction. While some argue that it may be akin to strategic myopia, the authors believed that such a response is strategically imperative to keep the hospital afloat. It is reasonable to attribute the paucity of innovation to constrained resources, and health systems are simply staying overly optimistic about “weathering the storm” and reverting soon to “business as usual.” The technological framework necessary for deploying a telehealth solution often comes with a price. Financially challenged hospital systems rarely exercise any capital-intensive activities. By contrast, telehealth adoption by ambulatory care can result in quicker resumption of patient care in community settings. A lack of operational and infrastructure synchrony between ambulatory and in-hospital systems has failed to capture telehealth-driven inpatient volume. For example, direct admissions from ambulatory telehealth referrals was a missed opportunity in several places. Referrals for labs, diagnostic tests, and other allied services could have helped hospitals offset their fixed costs. Similarly, work flows related to discharge and postdischarge follow up rarely embrace telehealth tools or telehealth care pathways. A brisk change in the health care ecosystem is partly responsible for this.
Digital strategy needs to be incorporated into business strategy. For the reasons already discussed, telehealth technology is not a “nice to have” anymore, but a “must have.” At present, providers are of the opinion that about 20% of their patient services can be delivered via a telehealth platform. Similar trends are observed among patients, as a new modality of access to care is increasingly beneficial to them. Telehealth must be incorporated in standardized hospital work flows. Use of telehealth for preoperative clearance will greatly minimize same-day surgery cancellations. Given the potential shortage in resources, telehealth adoption for inpatient consultations will help systems conserve personal protective equipment, minimize the risk of staff exposure to COVID-19, and improve efficiency.
Digital strategy also prompts the reengineering of care delivery.10 Excessive and unused physical capacity can be converted into digital care hubs. Health maintenance, prevention, health promotion, health education, and chronic disease management not only can serve a variety of patient groups but can also help address the “last-mile problem” in health care. A successful digital strategy usually has three important components – Commitment: Hospital leadership is committed to include digital transformation as a strategic objective; Cost: Digital strategy is added as a line item in the budget; and Control: Measurable metrics are put in place to monitor the performance, impact, and influence of the digital strategy.
Conclusion
For decades, most U.S. health systems occupied the periphery of technological transformation when compared to the rest of the service industry. While most health systems took a heroic approach to the adoption of telehealth during COVID-19, despite being unprepared, the need for a systematic telehealth deployment is far from being adequately fulfilled. The COVID-19 pandemic brought permanent changes to several business disciplines globally. Given the impact of the pandemic on the health and overall wellbeing of American society, the U.S. health care industry must leave no stone unturned in its quest for transformation.
Dr. Lingisetty is a hospitalist and physician executive at Baptist Health System, Little Rock, Ark, and is cofounder/president of SHM’s Arkansas chapter. Dr. Prasad is medical director of care management and a hospitalist at Advocate Aurora Health in Milwaukee. He is cochair of SHM’s IT Special Interest Group, sits on the HQPS committee, and is president of SHM’s Wisconsin chapter. Dr. Palabindala is the medical director, utilization management, and physician advisory services at the University of Mississippi Medical Center and an associate professor of medicine and academic hospitalist at the University of Mississippi, both in Jackson.
References
1. Finnegan M. “Telehealth booms amid COVID-19 crisis.” Computerworld. 2020 Apr 27. www.computerworld.com/article/3540315/telehealth-booms-amid-covid-19-crisis-virtual-care-is-here-to-stay.html. Accessed 2020 Sep 12.
2. Department of Health & Human Services. “OCR Announces Notification of Enforcement Discretion for Telehealth Remote Communications During the COVID-19 Nationwide Public Health Emergency.” 2020 Mar 17. www.hhs.gov/about/news/2020/03/17/ocr-announces-notification-of-enforcement-discretion-for-telehealth-remote-communications-during-the-covid-19.html. Accessed 2020 Sep 12.
3. National Center for Health Statistics. “Health Expenditures.” www.cdc.gov/nchs/fastats/health-expenditures.htm. Accessed 2020 Sep 12.
4. Bestsennyy O et al. “Telehealth: A post–COVID-19 reality?” McKinsey & Company. 2020 May 29. www.mckinsey.com/industries/healthcare-systems-and-services/our-insights/telehealth-a-quarter-trillion-dollar-post-covid-19-reality. Accessed 2020 Sep 12.
5. Melnick ER et al. The Association Between Perceived Electronic Health Record Usability and Professional Burnout Among U.S. Physicians. Mayo Clin Proc. 2020 March;95(3):476-87.
6. Hirko KA et al. Telehealth in response to the COVID-19 pandemic: Implications for rural health disparities. J Am Med Inform Assoc. 2020 Nov;27(11):1816-8. .
7. American Academy of Family Physicians. “Study Examines Telehealth, Rural Disparities in Pandemic.” 2020 July 30. www.aafp.org/news/practice-professional-issues/20200730ruraltelehealth.html. Accessed 2020 Dec 15.
8. Kurlander J et al. “Virtual Visits: Telehealth and Older Adults.” National Poll on Healthy Aging. 2019 Oct. hdl.handle.net/2027.42/151376.
9. American Medical Association. Telehealth Implementation Playbook. 2019. www.ama-assn.org/system/files/2020-04/ama-telehealth-implementation-playbook.pdf.
10. Smith AC et al. Telehealth for global emergencies: Implications for coronavirus disease 2019 (COVID-19). J Telemed Telecare. 2020 Jun;26(5):309-13.
Decline in child COVID-19 cases picks up after 2-week slowdown
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.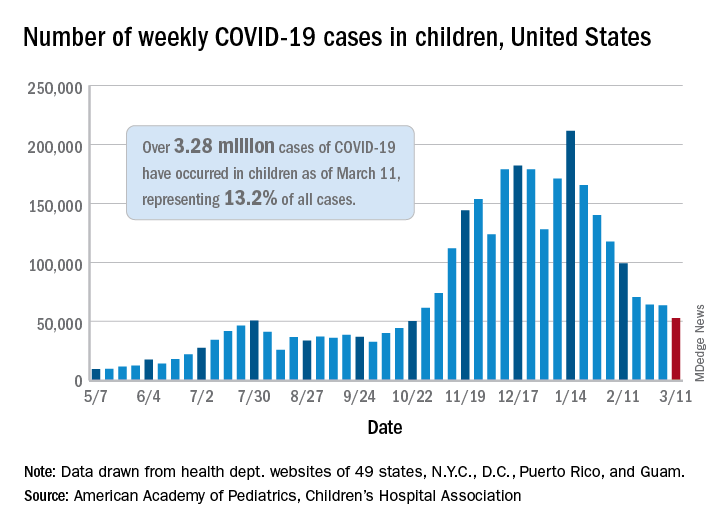
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
, according to data gathered by the American Academy of Pediatrics and the Children’s Hospital Association.
From Feb. 19 to March 4, the drop in new cases averaged just 5% each week, compared with 13.3% per week over the 5-week period from Jan. 15 to Feb. 18. For the week of March 5-11, a total of 52,695 COVID-19 cases were reported in children, down from 63,562 the previous week and the lowest number since late October, based on data from 49 states (excluding New York), the District of Columbia, New York City, Puerto Rico, and Guam.
In those jurisdictions, 3.28 million children have been infected with SARS-CoV-2, representing 13.2% of all cases since the beginning of the pandemic. The cumulative rate of COVID-19 has now risen to 4,364 cases per 100,000 children nationally, with state rates ranging from 1,062 per 100,000 in Hawaii to 8,692 per 100,000 in North Dakota, the AAP and CHA said in their weekly COVID-19 report.
Hospitalization data are more limited – 24 states and New York City – but continue to show that serious illness is much less common in younger individuals: Children represent just 1.9% of all hospitalizations, and only 0.8% of the children who have been infected were hospitalized. Neither rate has changed since early February, the AAP and CHA said.
The number of deaths in children, however, rose from 253 to 266, the largest 1-week increase since early February in the 43 states (along with New York City, Puerto Rico, and Guam) that are tracking mortality data by age, the AAP and CHA reported.
Among those 46 jurisdictions, there are 10 (9 states and the District of Columbia) that have not yet reported a COVID-19–related child death, while Texas has almost twice as many deaths, 47, as the next state, Arizona, which has 24. Meanwhile, California’s total of 452,000 cases is almost 2½ times higher than the 183,000 recorded by Illinois, according to the report.
‘Major update’ of BP guidance for kidney disease; treat to 120 mm Hg
The new 2021 Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline for blood pressure management for adults with chronic kidney disease (CKD) who are not receiving dialysis advises treating to a target systolic blood pressure of less than 120 mm Hg, provided measurements are “standardized” and that blood pressure is “measured properly.”
This blood pressure target – largely based on evidence from the Systolic Blood Pressure Intervention Trial (SPRINT) – represents “a major update” from the 2012 KDIGO guideline, which advised clinicians to treat to a target blood pressure of less than or equal to 130/80 mm Hg for patients with albuminuria or less than or equal to 140/90 mm Hg for patients without albuminuria.
The new goal is also lower than the less than 130/80 mm Hg target in the 2017 American College of Cardiology/American Heart Association guideline.
In a study of the public health implications of the guideline, Kathryn Foti, PhD, and colleagues determined that 70% of U.S. adults with CKD would now be eligible for treatment to lower blood pressure, as opposed to 50% under the previous KDIGO guideline and 56% under the ACC/AHA guideline.
“This is a major update of an influential set of guidelines for chronic kidney disease patients” at a time when blood pressure control is worsening in the United States, Dr. Foti, a postdoctoral researcher in the department of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, said in a statement from her institution.
The 2021 KDIGO blood pressure guideline and executive summary and the public health implications study are published online in Kidney International.
First, ‘take blood pressure well’
The cochair of the new KDIGO guidelines, Alfred K. Cheung, MD, from the University of Utah, Salt Lake City, said in an interview that the guideline has “two important points.”
First, “take that blood pressure well,” he said. “That has a lot to do with patient preparation rather than any fancy instrument,” he emphasized.
Second, the guideline proposes a systolic blood pressure target of less than 120 mm Hg for most people with CKD not receiving dialysis, except for children and kidney transplant recipients. This target is “contingent on ‘standardized’ blood pressure measurement.”
The document provides a checklist for obtaining a standardized blood pressure measurement, adapted from the 2017 ACC/AHA blood pressure guidelines. It starts with the patient relaxed and sitting on a chair for more than 5 minutes.
In contrast to this measurement, a “routine” or “casual” office blood pressure measurement could be off by plus or minus 10 mm Hg, Dr. Cheung noted.
In a typical scenario, he continued, a patient cannot find a place to park, rushes into the clinic, and has his or her blood pressure checked right away, which would provide a “totally unreliable” reading. Adding a “fudge factor” (correction factor) would not provide an accurate reading.
Clinicians “would not settle for a potassium measurement that is 5.0 mmol/L plus or minus a few decimal points” to guide treatment, he pointed out.
Second, target 120, properly measured
“The very first chapter of the guidelines is devoted to blood pressure measurement, because we recognize if we’re going to do 120 [mm Hg] – the emphasis is on 120 measured properly – so we try to drive that point home,” Tara I. Chang, MD, guideline second author and a coauthor of the public health implications study, pointed out in an interview.
“There are a lot of other things that we base clinical decisions on where we really require some degree of precision, and blood pressure is important enough that to us it’s kind of in the same boat,” said Dr. Chang, from Stanford (Calif.) University.
“In SPRINT, people were randomized to less than less than 120 vs. less than 140 (they weren’t randomized to <130),” she noted.
“The recommendation should be widely adopted in clinical practice,” the guideline authors write, “since accurate measurements will ensure that proper guidance is being applied to the management of BP, as it is to the management of other risk factors.”
Still need individual treatment
Nevertheless, patients still need individualized treatment, the document stresses. “Not every patient with CKD will be appropriate to target to less than 120,” Dr. Chang said. However, “we want people to at least consider less than 120,” she added, to avoid therapeutic inertia.
“If you take the blood pressure in a standardized manner – such as in the ACCORD trial and in the SPRINT trial – even patients over 75 years old, or people over 80 years old, they have very little side effects,” Dr. Cheung noted.
“In the overall cohort,” he continued, “they do not have a significant increase in serious adverse events, do not have adverse events of postural hypotension, syncope, bradycardia, injurious falls – so people are worried about it, but it’s not borne out by the data.
“That said, I have two cautions,” Dr. Cheung noted. “One. If you drop somebody’s blood pressure rapidly over a week, you may be more likely to get in trouble. If you drop the blood pressure gradually over several weeks, several months, you’re much less likely to get into trouble.”
“Two. If the patient is old, you know the patient has carotid stenosis and already has postural dizziness, you may not want to try on that patient – but just because the patient is old is not the reason not to target 120.”
ACE inhibitors and ARBs beneficial in albuminuria, underused
“How do you get to less than 120? The short answer is, use whatever medications you need to – there is no necessarily right cocktail,” Dr. Chang said.
“We’ve known that angiotensin-converting enzyme (ACE) inhibitors and ARBs [angiotensin II receptor blockers] are beneficial in patients with CKD and in particular those with heavier albuminuria,” she continued. “We’ve known this for over 20 years.”
Yet, the study identified underutilization – “a persistent gap, just like blood pressure control and awareness,” she noted. “We’re just not making much headway.
“We are not recommending ACE inhibitors or ARBs for all the patients,” Dr. Cheung clarified. “If you are diabetic and have heavy proteinuria, that’s when the use of ACE inhibitors and ARBs are most indicated.”
Public health implications
SPRINT showed that treating to a systolic blood pressure of less than 120 mm Hg vs. less than 140 mm Hg reduced the risk for cardiovascular disease by 25% and all-cause mortality by 27% for participants with and those without CKD, Dr. Foti and colleagues stress.
They aimed to estimate how the new guideline would affect (1) the number of U.S. patients with CKD who would be eligible for blood pressure lowering treatment, and (2) the proportion of those with albuminuria who would be eligible for an ACE inhibitor or an ARB.
The researchers analyzed data from 1,699 adults with CKD (estimated glomerular filtration rate, 15-59 mL/min/1.73 m2 or a urinary albumin-to-creatinine ratio of ≥30 mg/g) who participated in the 2015-2018 National Health and Nutrition Examination Survey.
Both the 2021 and 2012 KDIGO guidelines recommend that patients with albuminuria and blood pressure higher than the target value who are not kidney transplant recipients should be treated with an ACE inhibitor or an ARB.
On the basis of the new target, 78% of patients with CKD and albuminuria were eligible for ACE inhibitor/ARB treatment by the 2021 KDIGO guideline, compared with 71% by the 2012 KDIGO guideline. However, only 39% were taking one of these drugs.
These findings show that “with the new guideline and with the lower blood pressure target, you potentially have an even larger pool of people who have blood pressure that’s not under control, and a potential larger group of people who may benefit from ACE inhibitors and ARBs,” Dr. Chang said.
“Our paper is not the only one to show that we haven’t made a whole lot of progress,” she said, “and now that the bar has been lowered, there [have] to be some renewed efforts on controlling blood pressure, because we know that blood pressure control is such an important risk factor for cardiovascular outcomes.”
Dr. Foti is supported by an NIH/National Heart, Lung, and Blood Institute grant. Dr. Cheung has received consultancy fees from Amgen, Bard, Boehringer Ingelheim, Calliditas, Tricida, and UpToDate, and grant/research support from the National Institutes of Health for SPRINT (monies paid to institution). Dr. Chang has received consultancy fees from Bayer, Gilead, Janssen Research and Development, Novo Nordisk, Tricida, and Vascular Dynamics; grant/research support from AstraZeneca and Satellite Healthcare (monies paid to institution), the NIH, and the American Heart Association; is on advisory boards for AstraZeneca and Fresenius Medical Care Renal Therapies Group; and has received workshop honoraria from Fresenius. Disclosures of relevant financial relationships of the other authors are listed in the original articles.
A version of this article first appeared on Medscape.com.
The new 2021 Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline for blood pressure management for adults with chronic kidney disease (CKD) who are not receiving dialysis advises treating to a target systolic blood pressure of less than 120 mm Hg, provided measurements are “standardized” and that blood pressure is “measured properly.”
This blood pressure target – largely based on evidence from the Systolic Blood Pressure Intervention Trial (SPRINT) – represents “a major update” from the 2012 KDIGO guideline, which advised clinicians to treat to a target blood pressure of less than or equal to 130/80 mm Hg for patients with albuminuria or less than or equal to 140/90 mm Hg for patients without albuminuria.
The new goal is also lower than the less than 130/80 mm Hg target in the 2017 American College of Cardiology/American Heart Association guideline.
In a study of the public health implications of the guideline, Kathryn Foti, PhD, and colleagues determined that 70% of U.S. adults with CKD would now be eligible for treatment to lower blood pressure, as opposed to 50% under the previous KDIGO guideline and 56% under the ACC/AHA guideline.
“This is a major update of an influential set of guidelines for chronic kidney disease patients” at a time when blood pressure control is worsening in the United States, Dr. Foti, a postdoctoral researcher in the department of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, said in a statement from her institution.
The 2021 KDIGO blood pressure guideline and executive summary and the public health implications study are published online in Kidney International.
First, ‘take blood pressure well’
The cochair of the new KDIGO guidelines, Alfred K. Cheung, MD, from the University of Utah, Salt Lake City, said in an interview that the guideline has “two important points.”
First, “take that blood pressure well,” he said. “That has a lot to do with patient preparation rather than any fancy instrument,” he emphasized.
Second, the guideline proposes a systolic blood pressure target of less than 120 mm Hg for most people with CKD not receiving dialysis, except for children and kidney transplant recipients. This target is “contingent on ‘standardized’ blood pressure measurement.”
The document provides a checklist for obtaining a standardized blood pressure measurement, adapted from the 2017 ACC/AHA blood pressure guidelines. It starts with the patient relaxed and sitting on a chair for more than 5 minutes.
In contrast to this measurement, a “routine” or “casual” office blood pressure measurement could be off by plus or minus 10 mm Hg, Dr. Cheung noted.
In a typical scenario, he continued, a patient cannot find a place to park, rushes into the clinic, and has his or her blood pressure checked right away, which would provide a “totally unreliable” reading. Adding a “fudge factor” (correction factor) would not provide an accurate reading.
Clinicians “would not settle for a potassium measurement that is 5.0 mmol/L plus or minus a few decimal points” to guide treatment, he pointed out.
Second, target 120, properly measured
“The very first chapter of the guidelines is devoted to blood pressure measurement, because we recognize if we’re going to do 120 [mm Hg] – the emphasis is on 120 measured properly – so we try to drive that point home,” Tara I. Chang, MD, guideline second author and a coauthor of the public health implications study, pointed out in an interview.
“There are a lot of other things that we base clinical decisions on where we really require some degree of precision, and blood pressure is important enough that to us it’s kind of in the same boat,” said Dr. Chang, from Stanford (Calif.) University.
“In SPRINT, people were randomized to less than less than 120 vs. less than 140 (they weren’t randomized to <130),” she noted.
“The recommendation should be widely adopted in clinical practice,” the guideline authors write, “since accurate measurements will ensure that proper guidance is being applied to the management of BP, as it is to the management of other risk factors.”
Still need individual treatment
Nevertheless, patients still need individualized treatment, the document stresses. “Not every patient with CKD will be appropriate to target to less than 120,” Dr. Chang said. However, “we want people to at least consider less than 120,” she added, to avoid therapeutic inertia.
“If you take the blood pressure in a standardized manner – such as in the ACCORD trial and in the SPRINT trial – even patients over 75 years old, or people over 80 years old, they have very little side effects,” Dr. Cheung noted.
“In the overall cohort,” he continued, “they do not have a significant increase in serious adverse events, do not have adverse events of postural hypotension, syncope, bradycardia, injurious falls – so people are worried about it, but it’s not borne out by the data.
“That said, I have two cautions,” Dr. Cheung noted. “One. If you drop somebody’s blood pressure rapidly over a week, you may be more likely to get in trouble. If you drop the blood pressure gradually over several weeks, several months, you’re much less likely to get into trouble.”
“Two. If the patient is old, you know the patient has carotid stenosis and already has postural dizziness, you may not want to try on that patient – but just because the patient is old is not the reason not to target 120.”
ACE inhibitors and ARBs beneficial in albuminuria, underused
“How do you get to less than 120? The short answer is, use whatever medications you need to – there is no necessarily right cocktail,” Dr. Chang said.
“We’ve known that angiotensin-converting enzyme (ACE) inhibitors and ARBs [angiotensin II receptor blockers] are beneficial in patients with CKD and in particular those with heavier albuminuria,” she continued. “We’ve known this for over 20 years.”
Yet, the study identified underutilization – “a persistent gap, just like blood pressure control and awareness,” she noted. “We’re just not making much headway.
“We are not recommending ACE inhibitors or ARBs for all the patients,” Dr. Cheung clarified. “If you are diabetic and have heavy proteinuria, that’s when the use of ACE inhibitors and ARBs are most indicated.”
Public health implications
SPRINT showed that treating to a systolic blood pressure of less than 120 mm Hg vs. less than 140 mm Hg reduced the risk for cardiovascular disease by 25% and all-cause mortality by 27% for participants with and those without CKD, Dr. Foti and colleagues stress.
They aimed to estimate how the new guideline would affect (1) the number of U.S. patients with CKD who would be eligible for blood pressure lowering treatment, and (2) the proportion of those with albuminuria who would be eligible for an ACE inhibitor or an ARB.
The researchers analyzed data from 1,699 adults with CKD (estimated glomerular filtration rate, 15-59 mL/min/1.73 m2 or a urinary albumin-to-creatinine ratio of ≥30 mg/g) who participated in the 2015-2018 National Health and Nutrition Examination Survey.
Both the 2021 and 2012 KDIGO guidelines recommend that patients with albuminuria and blood pressure higher than the target value who are not kidney transplant recipients should be treated with an ACE inhibitor or an ARB.
On the basis of the new target, 78% of patients with CKD and albuminuria were eligible for ACE inhibitor/ARB treatment by the 2021 KDIGO guideline, compared with 71% by the 2012 KDIGO guideline. However, only 39% were taking one of these drugs.
These findings show that “with the new guideline and with the lower blood pressure target, you potentially have an even larger pool of people who have blood pressure that’s not under control, and a potential larger group of people who may benefit from ACE inhibitors and ARBs,” Dr. Chang said.
“Our paper is not the only one to show that we haven’t made a whole lot of progress,” she said, “and now that the bar has been lowered, there [have] to be some renewed efforts on controlling blood pressure, because we know that blood pressure control is such an important risk factor for cardiovascular outcomes.”
Dr. Foti is supported by an NIH/National Heart, Lung, and Blood Institute grant. Dr. Cheung has received consultancy fees from Amgen, Bard, Boehringer Ingelheim, Calliditas, Tricida, and UpToDate, and grant/research support from the National Institutes of Health for SPRINT (monies paid to institution). Dr. Chang has received consultancy fees from Bayer, Gilead, Janssen Research and Development, Novo Nordisk, Tricida, and Vascular Dynamics; grant/research support from AstraZeneca and Satellite Healthcare (monies paid to institution), the NIH, and the American Heart Association; is on advisory boards for AstraZeneca and Fresenius Medical Care Renal Therapies Group; and has received workshop honoraria from Fresenius. Disclosures of relevant financial relationships of the other authors are listed in the original articles.
A version of this article first appeared on Medscape.com.
The new 2021 Kidney Disease: Improving Global Outcomes (KDIGO) clinical practice guideline for blood pressure management for adults with chronic kidney disease (CKD) who are not receiving dialysis advises treating to a target systolic blood pressure of less than 120 mm Hg, provided measurements are “standardized” and that blood pressure is “measured properly.”
This blood pressure target – largely based on evidence from the Systolic Blood Pressure Intervention Trial (SPRINT) – represents “a major update” from the 2012 KDIGO guideline, which advised clinicians to treat to a target blood pressure of less than or equal to 130/80 mm Hg for patients with albuminuria or less than or equal to 140/90 mm Hg for patients without albuminuria.
The new goal is also lower than the less than 130/80 mm Hg target in the 2017 American College of Cardiology/American Heart Association guideline.
In a study of the public health implications of the guideline, Kathryn Foti, PhD, and colleagues determined that 70% of U.S. adults with CKD would now be eligible for treatment to lower blood pressure, as opposed to 50% under the previous KDIGO guideline and 56% under the ACC/AHA guideline.
“This is a major update of an influential set of guidelines for chronic kidney disease patients” at a time when blood pressure control is worsening in the United States, Dr. Foti, a postdoctoral researcher in the department of epidemiology at Johns Hopkins Bloomberg School of Public Health, Baltimore, said in a statement from her institution.
The 2021 KDIGO blood pressure guideline and executive summary and the public health implications study are published online in Kidney International.
First, ‘take blood pressure well’
The cochair of the new KDIGO guidelines, Alfred K. Cheung, MD, from the University of Utah, Salt Lake City, said in an interview that the guideline has “two important points.”
First, “take that blood pressure well,” he said. “That has a lot to do with patient preparation rather than any fancy instrument,” he emphasized.
Second, the guideline proposes a systolic blood pressure target of less than 120 mm Hg for most people with CKD not receiving dialysis, except for children and kidney transplant recipients. This target is “contingent on ‘standardized’ blood pressure measurement.”
The document provides a checklist for obtaining a standardized blood pressure measurement, adapted from the 2017 ACC/AHA blood pressure guidelines. It starts with the patient relaxed and sitting on a chair for more than 5 minutes.
In contrast to this measurement, a “routine” or “casual” office blood pressure measurement could be off by plus or minus 10 mm Hg, Dr. Cheung noted.
In a typical scenario, he continued, a patient cannot find a place to park, rushes into the clinic, and has his or her blood pressure checked right away, which would provide a “totally unreliable” reading. Adding a “fudge factor” (correction factor) would not provide an accurate reading.
Clinicians “would not settle for a potassium measurement that is 5.0 mmol/L plus or minus a few decimal points” to guide treatment, he pointed out.
Second, target 120, properly measured
“The very first chapter of the guidelines is devoted to blood pressure measurement, because we recognize if we’re going to do 120 [mm Hg] – the emphasis is on 120 measured properly – so we try to drive that point home,” Tara I. Chang, MD, guideline second author and a coauthor of the public health implications study, pointed out in an interview.
“There are a lot of other things that we base clinical decisions on where we really require some degree of precision, and blood pressure is important enough that to us it’s kind of in the same boat,” said Dr. Chang, from Stanford (Calif.) University.
“In SPRINT, people were randomized to less than less than 120 vs. less than 140 (they weren’t randomized to <130),” she noted.
“The recommendation should be widely adopted in clinical practice,” the guideline authors write, “since accurate measurements will ensure that proper guidance is being applied to the management of BP, as it is to the management of other risk factors.”
Still need individual treatment
Nevertheless, patients still need individualized treatment, the document stresses. “Not every patient with CKD will be appropriate to target to less than 120,” Dr. Chang said. However, “we want people to at least consider less than 120,” she added, to avoid therapeutic inertia.
“If you take the blood pressure in a standardized manner – such as in the ACCORD trial and in the SPRINT trial – even patients over 75 years old, or people over 80 years old, they have very little side effects,” Dr. Cheung noted.
“In the overall cohort,” he continued, “they do not have a significant increase in serious adverse events, do not have adverse events of postural hypotension, syncope, bradycardia, injurious falls – so people are worried about it, but it’s not borne out by the data.
“That said, I have two cautions,” Dr. Cheung noted. “One. If you drop somebody’s blood pressure rapidly over a week, you may be more likely to get in trouble. If you drop the blood pressure gradually over several weeks, several months, you’re much less likely to get into trouble.”
“Two. If the patient is old, you know the patient has carotid stenosis and already has postural dizziness, you may not want to try on that patient – but just because the patient is old is not the reason not to target 120.”
ACE inhibitors and ARBs beneficial in albuminuria, underused
“How do you get to less than 120? The short answer is, use whatever medications you need to – there is no necessarily right cocktail,” Dr. Chang said.
“We’ve known that angiotensin-converting enzyme (ACE) inhibitors and ARBs [angiotensin II receptor blockers] are beneficial in patients with CKD and in particular those with heavier albuminuria,” she continued. “We’ve known this for over 20 years.”
Yet, the study identified underutilization – “a persistent gap, just like blood pressure control and awareness,” she noted. “We’re just not making much headway.
“We are not recommending ACE inhibitors or ARBs for all the patients,” Dr. Cheung clarified. “If you are diabetic and have heavy proteinuria, that’s when the use of ACE inhibitors and ARBs are most indicated.”
Public health implications
SPRINT showed that treating to a systolic blood pressure of less than 120 mm Hg vs. less than 140 mm Hg reduced the risk for cardiovascular disease by 25% and all-cause mortality by 27% for participants with and those without CKD, Dr. Foti and colleagues stress.
They aimed to estimate how the new guideline would affect (1) the number of U.S. patients with CKD who would be eligible for blood pressure lowering treatment, and (2) the proportion of those with albuminuria who would be eligible for an ACE inhibitor or an ARB.
The researchers analyzed data from 1,699 adults with CKD (estimated glomerular filtration rate, 15-59 mL/min/1.73 m2 or a urinary albumin-to-creatinine ratio of ≥30 mg/g) who participated in the 2015-2018 National Health and Nutrition Examination Survey.
Both the 2021 and 2012 KDIGO guidelines recommend that patients with albuminuria and blood pressure higher than the target value who are not kidney transplant recipients should be treated with an ACE inhibitor or an ARB.
On the basis of the new target, 78% of patients with CKD and albuminuria were eligible for ACE inhibitor/ARB treatment by the 2021 KDIGO guideline, compared with 71% by the 2012 KDIGO guideline. However, only 39% were taking one of these drugs.
These findings show that “with the new guideline and with the lower blood pressure target, you potentially have an even larger pool of people who have blood pressure that’s not under control, and a potential larger group of people who may benefit from ACE inhibitors and ARBs,” Dr. Chang said.
“Our paper is not the only one to show that we haven’t made a whole lot of progress,” she said, “and now that the bar has been lowered, there [have] to be some renewed efforts on controlling blood pressure, because we know that blood pressure control is such an important risk factor for cardiovascular outcomes.”
Dr. Foti is supported by an NIH/National Heart, Lung, and Blood Institute grant. Dr. Cheung has received consultancy fees from Amgen, Bard, Boehringer Ingelheim, Calliditas, Tricida, and UpToDate, and grant/research support from the National Institutes of Health for SPRINT (monies paid to institution). Dr. Chang has received consultancy fees from Bayer, Gilead, Janssen Research and Development, Novo Nordisk, Tricida, and Vascular Dynamics; grant/research support from AstraZeneca and Satellite Healthcare (monies paid to institution), the NIH, and the American Heart Association; is on advisory boards for AstraZeneca and Fresenius Medical Care Renal Therapies Group; and has received workshop honoraria from Fresenius. Disclosures of relevant financial relationships of the other authors are listed in the original articles.
A version of this article first appeared on Medscape.com.
Hospitalist movers and shakers – March 2021
Vivek H. Murthy, MD, was named by President Joe Biden as his selection for Surgeon General of the United States. Dr. Murthy filled the same role from 2014-17 during President Barack Obama’s administration.

Dr. Murthy was a hospitalist and an instructor at Brigham and Women’s Hospital at Harvard Medical School prior to becoming surgeon general the first time. He also is the founder of Doctors for America.
David Tupponce, MD, recently was named the new president of Allegheny Health Network’s Grove City (Pa.) Medical Center. He takes over for interim president Allan Klapper, MD, who filled the position since August 2020.
Dr. Tupponce comes to Grove City Medical Center after a successful tenure as president of Central Maine Medical Center (Lewiston, Maine), where he grew its physician group and fine-tuned the hospital quality program. Prior to that, he was chief executive officer at Tenet Healthcare’s Abrazo Scottsdale (Ariz.) Campus and CEO at Paradise Valley Hospital (Phoenix, Ariz.).

Dr. Tupponce is familiar with western Pennsylvania, having earned a master’s degree in medical management from Carnegie Mellon University in Pittsburgh. He also was chief resident at the University of Pittsburgh Medical Center.
Malcolm Mar Fan, MD, has been elevated to medical director of the Hospitalist Group at Evangelical Community Hospital (Lewisburg, Pa.). In the newly established position, Dr. Mar Fan will oversee all operations for the facility’s hospitalist program.
Dr. Mar Fan has been a hospitalist at Evangelical since 2014 after completing his internist residency at Albert Einstein Medical Center in Philadelphia. He has played a major role on Evangelical’s Peri-operative Glucose Management Committee and its Informatics Committee for Impatient and Outpatient Electronic Health Records.
Lyon County (Kansas) recently announced that Ladun Oyenuga, MD, has been appointed as public health officer for the county. She began her tenure on January 1.
Dr. Oyenuga is a hospitalist at Newman Regional Health (Emporia, Kan.). She is a native of Nigeria and did her residency at Harlem (N.Y.) Hospital Center. She has been with Newman since 2017.
Cherese Mari Laulhere BirthCare Center (Long Beach, Calif.) recently announced the addition of an OB hospitalist program at Miller Children’s & Women’s Hospital. OB hospitalists, or laborists, care for women with obstetrical issues while in the hospital.
At Cherese Mari Laulhere, OB hospitalists will be on hand 24 hours a day to assist patients’ OB/GYNs or to fill in if the personal physician cannot get to the hospital quickly.
Hospitalists at Nationwide Children’s (Columbus, Ohio) are now providing care for children who are hospitalized at Adena Regional Medical Center (Chillicothe, Ohio).
It is an expansion of an ongoing partnership between the two hospitals. Adena and Nationwide Children’s have been working together in helping to care for children in the south central and southern Ohio region since 2011. Nationwide Children’s hospitalists will round in special care and the well-baby nursery at Adena, as well as provide education programs for Adena providers and staff.
MultiCare Health System (Tacoma, Wash.) has announced that it will expand its hospitalist program partnership with Sound Physicians, also based in Tacoma, to create a region-wide, cohesive group of providers. The goal is to help ensure efficient management of inpatient populations as a region instead of at the individual hospital level, and will allow MultiCare to implement standard tools, processes and regionwide best practices.
The hospitalist programs at Tacoma General Hospital, Allenmore Hospital and Covington Medical Center will transition to Sound Physicians on April 5, 2021. Sound hospitalists are already working at three other MultiCare facilities – Tacoma General Hospital, Allenmore Hospital, and Covington Medical Center.
Vivek H. Murthy, MD, was named by President Joe Biden as his selection for Surgeon General of the United States. Dr. Murthy filled the same role from 2014-17 during President Barack Obama’s administration.
Dr. Murthy was a hospitalist and an instructor at Brigham and Women’s Hospital at Harvard Medical School prior to becoming surgeon general the first time. He also is the founder of Doctors for America.
David Tupponce, MD, recently was named the new president of Allegheny Health Network’s Grove City (Pa.) Medical Center. He takes over for interim president Allan Klapper, MD, who filled the position since August 2020.
Dr. Tupponce comes to Grove City Medical Center after a successful tenure as president of Central Maine Medical Center (Lewiston, Maine), where he grew its physician group and fine-tuned the hospital quality program. Prior to that, he was chief executive officer at Tenet Healthcare’s Abrazo Scottsdale (Ariz.) Campus and CEO at Paradise Valley Hospital (Phoenix, Ariz.).
Dr. Tupponce is familiar with western Pennsylvania, having earned a master’s degree in medical management from Carnegie Mellon University in Pittsburgh. He also was chief resident at the University of Pittsburgh Medical Center.
Malcolm Mar Fan, MD, has been elevated to medical director of the Hospitalist Group at Evangelical Community Hospital (Lewisburg, Pa.). In the newly established position, Dr. Mar Fan will oversee all operations for the facility’s hospitalist program.
Dr. Mar Fan has been a hospitalist at Evangelical since 2014 after completing his internist residency at Albert Einstein Medical Center in Philadelphia. He has played a major role on Evangelical’s Peri-operative Glucose Management Committee and its Informatics Committee for Impatient and Outpatient Electronic Health Records.
Lyon County (Kansas) recently announced that Ladun Oyenuga, MD, has been appointed as public health officer for the county. She began her tenure on January 1.
Dr. Oyenuga is a hospitalist at Newman Regional Health (Emporia, Kan.). She is a native of Nigeria and did her residency at Harlem (N.Y.) Hospital Center. She has been with Newman since 2017.
Cherese Mari Laulhere BirthCare Center (Long Beach, Calif.) recently announced the addition of an OB hospitalist program at Miller Children’s & Women’s Hospital. OB hospitalists, or laborists, care for women with obstetrical issues while in the hospital.
At Cherese Mari Laulhere, OB hospitalists will be on hand 24 hours a day to assist patients’ OB/GYNs or to fill in if the personal physician cannot get to the hospital quickly.
Hospitalists at Nationwide Children’s (Columbus, Ohio) are now providing care for children who are hospitalized at Adena Regional Medical Center (Chillicothe, Ohio).
It is an expansion of an ongoing partnership between the two hospitals. Adena and Nationwide Children’s have been working together in helping to care for children in the south central and southern Ohio region since 2011. Nationwide Children’s hospitalists will round in special care and the well-baby nursery at Adena, as well as provide education programs for Adena providers and staff.
MultiCare Health System (Tacoma, Wash.) has announced that it will expand its hospitalist program partnership with Sound Physicians, also based in Tacoma, to create a region-wide, cohesive group of providers. The goal is to help ensure efficient management of inpatient populations as a region instead of at the individual hospital level, and will allow MultiCare to implement standard tools, processes and regionwide best practices.
The hospitalist programs at Tacoma General Hospital, Allenmore Hospital and Covington Medical Center will transition to Sound Physicians on April 5, 2021. Sound hospitalists are already working at three other MultiCare facilities – Tacoma General Hospital, Allenmore Hospital, and Covington Medical Center.
Vivek H. Murthy, MD, was named by President Joe Biden as his selection for Surgeon General of the United States. Dr. Murthy filled the same role from 2014-17 during President Barack Obama’s administration.
Dr. Murthy was a hospitalist and an instructor at Brigham and Women’s Hospital at Harvard Medical School prior to becoming surgeon general the first time. He also is the founder of Doctors for America.
David Tupponce, MD, recently was named the new president of Allegheny Health Network’s Grove City (Pa.) Medical Center. He takes over for interim president Allan Klapper, MD, who filled the position since August 2020.
Dr. Tupponce comes to Grove City Medical Center after a successful tenure as president of Central Maine Medical Center (Lewiston, Maine), where he grew its physician group and fine-tuned the hospital quality program. Prior to that, he was chief executive officer at Tenet Healthcare’s Abrazo Scottsdale (Ariz.) Campus and CEO at Paradise Valley Hospital (Phoenix, Ariz.).
Dr. Tupponce is familiar with western Pennsylvania, having earned a master’s degree in medical management from Carnegie Mellon University in Pittsburgh. He also was chief resident at the University of Pittsburgh Medical Center.
Malcolm Mar Fan, MD, has been elevated to medical director of the Hospitalist Group at Evangelical Community Hospital (Lewisburg, Pa.). In the newly established position, Dr. Mar Fan will oversee all operations for the facility’s hospitalist program.
Dr. Mar Fan has been a hospitalist at Evangelical since 2014 after completing his internist residency at Albert Einstein Medical Center in Philadelphia. He has played a major role on Evangelical’s Peri-operative Glucose Management Committee and its Informatics Committee for Impatient and Outpatient Electronic Health Records.
Lyon County (Kansas) recently announced that Ladun Oyenuga, MD, has been appointed as public health officer for the county. She began her tenure on January 1.
Dr. Oyenuga is a hospitalist at Newman Regional Health (Emporia, Kan.). She is a native of Nigeria and did her residency at Harlem (N.Y.) Hospital Center. She has been with Newman since 2017.
Cherese Mari Laulhere BirthCare Center (Long Beach, Calif.) recently announced the addition of an OB hospitalist program at Miller Children’s & Women’s Hospital. OB hospitalists, or laborists, care for women with obstetrical issues while in the hospital.
At Cherese Mari Laulhere, OB hospitalists will be on hand 24 hours a day to assist patients’ OB/GYNs or to fill in if the personal physician cannot get to the hospital quickly.
Hospitalists at Nationwide Children’s (Columbus, Ohio) are now providing care for children who are hospitalized at Adena Regional Medical Center (Chillicothe, Ohio).
It is an expansion of an ongoing partnership between the two hospitals. Adena and Nationwide Children’s have been working together in helping to care for children in the south central and southern Ohio region since 2011. Nationwide Children’s hospitalists will round in special care and the well-baby nursery at Adena, as well as provide education programs for Adena providers and staff.
MultiCare Health System (Tacoma, Wash.) has announced that it will expand its hospitalist program partnership with Sound Physicians, also based in Tacoma, to create a region-wide, cohesive group of providers. The goal is to help ensure efficient management of inpatient populations as a region instead of at the individual hospital level, and will allow MultiCare to implement standard tools, processes and regionwide best practices.
The hospitalist programs at Tacoma General Hospital, Allenmore Hospital and Covington Medical Center will transition to Sound Physicians on April 5, 2021. Sound hospitalists are already working at three other MultiCare facilities – Tacoma General Hospital, Allenmore Hospital, and Covington Medical Center.
First pill for COVID-19 could be ready by year’s end
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.

Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.
Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
New pills to treat patients with COVID-19 are currently in midstage clinical trials and, if successful, could be ready by the end of the year.
Only one treatment – remdesivir (Veklury) – has been fully approved by the U.S. Food and Drug Administration for patients in the hospital and it must be administered intravenously.
Hopes for a day when patients with COVID-19 can take a pill to rid their bodies of the virus got a boost when early trial results were presented at a medical conference.
Interim phase 2 results for the oral experimental COVID-19 drug molnupiravir, designed to do for patients with COVID-19 what oseltamivir (Tamiflu) can do for patients with the flu, were presented at the Conference on Retroviruses and Opportunistic Infections 2021 Annual Meeting, as reported by this news organization.
In the small study, the pill significantly reduced infectious virus in patients who were symptomatic and had tested positive for COVID-19 during the previous 4 days but were not hospitalized.
After 5 days of treatment, no participants who received molnupiravir had detectable virus, whereas 24% who received placebo did.
Two other oral agents are being developed by RedHill Biopharma: one for severe COVID-19 infection for hospitalized patients and one for patients at home with mild infection.
The first, opaganib (Yeliva), proceeded to a phase 2/3 global trial for hospitalized patients after the company announced top-line safety and efficacy data in December. In phase 2, the drug was shown to be safe in patients requiring oxygen and effectively reduced the need for oxygen by the end of the treatment period.
A key feature is that it is both an antiviral and an anti-inflammatory, Gilead Raday, RedHill’s chief operating officer, said in an interview. Data are expected midyear on its performance in 464 patients. The drug is being tested on top of remdesivir or in addition to dexamethasone.
The second, upamostat (RHB-107), is currently undergoing a phase 2/3 trial in the United States and is being investigated for use in nonhospitalized COVID-19 patients.
“I would expect data to be available in the second half of this year,” Mr. Raday said.
Upamostat is a novel serine protease inhibitor expected to be effective against emerging variants because it targets human cell factors involved in viral entry, according to the company.
Other drugs are being investigated in trials that are in earlier stages.
Urgent need for oral agents
Infectious disease specialists are watching the move toward a COVID-19 pill enthusiastically.
“We badly need an oral treatment option for COVID,” said Sarah Doernberg, MD, an infectious disease specialist from the University of California, San Francisco.
“It’s a real gap in our armamentarium for COVID in outpatient treatment, which is where most who contract COVID-19 will seek care,” she said in an interview.
Although some studies have shown the benefit of monoclonal antibodies for prevention and early treatment, there are major logistical issues because all the current options require IV administration, she explained.
“If we had a pill to treat early COVID, especially in high-risk patients, it would fill a gap,” she said, noting that a pill could help people get better faster and prevent hospital stays.
Studies of molnupiravir suggest that it decreases viral shedding in the first few days after COVID infection, Dr. Doernberg reported.
There is excitement around the drug, but it will be important to see whether the results translate into fewer people requiring hospital admission and whether people feel better faster.
“I want to see the clinical data,” Dr. Doernberg said.
She will also be watching for the upamostat and opaganib results in the coming weeks.
“If these drugs are successful, I think it’s possible we could use them – maybe under an emergency use authorization – this year,” she said.
Once antiviral pills are a viable option for COVID-19 treatment, questions will arise about their use, she said.
One question is whether patients who are getting remdesivir in the hospital and are ready to leave after 5 days should continue treatment with antiviral pills at home.
Another is whether the pills – if they are shown to be effective – will be helpful for COVID post exposure. That use would be important for people who do not have COVID-19 but who are in close contact with someone who does, such as a member of their household.
“We have that model,” Dr. Doernberg said. “We know that oseltamivir can be used for postexposure prophylaxis and can help to prevent development of clinical disease.”
But she cautioned that a challenge with COVID is that people are contagious very early. A pill would need to come with the ability to test for COVID-19 early and get patients linked to care immediately.
“Those are not small challenges,” she said.
Vaccines alone won’t end the COVID threat
Treatments are part of the “belt-and-suspenders” approach, along with vaccines to combat COVID-19, Dr. Doernberg said.
“We’re not going to eradicate COVID,” she said. “We’re still going to need treatments for people who either don’t respond to the vaccine or haven’t gotten the vaccine or developed disease despite the vaccine.”
Oral formulations are desperately needed, agreed Kenneth Johnson, PhD, professor of molecular biosciences at the University of Texas at Austin.
Right now, remdesivir treatments involve patients being hooked up to an IV for 30-120 minutes each day for 5 days. And the cost of a 5-day course of remdesivir ranges from $2340 to $3120 in the United States.
“We’re hoping we can come up with something that is a little bit easier to administer, and without as many concerns for toxic side effects,” he said.
Dr. Johnson’s team at UT-Austin recently made a key discovery about the way remdesivir stops the replication of viral RNA.
The understanding of where the virus starts to replicate in the infection chain of events and how and where it reacts with remdesivir might lead to the development of better, more concentrated pill forms of antivirals in the future, with fewer toxicities, he said.
The team used a lab dish to recreate the step-by-step process that occurs when a patient who is infected with SARS-CoV-2 receives remdesivir.
The discovery was published online in Molecular Cell in January and will be printed in the April issue of the journal.
The discovery won’t lead to an effective COVID-19 pill for our current crisis, but will be important for the next generation of drugs needed to deal with future coronaviruses, Dr. Johnson explained.
And there will be other coronaviruses, he said, noting that this one is the third in 20 years to jump from animals to humans. “It’s just a matter of time,” he said.
A version of this article first appeared on Medscape.com.
SHM Fellowship Class of 2021
The Society of Hospital Medicine has announced its 2021 class of Master Fellows, Senior Fellows, and Fellows in Hospital Medicine.
All Fellowship classes are listed in alphabetical order.
Master Fellows Class of 2021
Nasim Afsar, MD, MBA, MHM
Shaun D. Frost, MD, MHM
Jeffrey L. Schnipper, MD, MPH, MHM
Senior Fellows Class of 2021
Akindele Adaramola, MD, MPH, SFHM
Ramesh Adhikari, MD, SFHM
Pankaj Agrawal, MD, SFHM
Robert L. Anderson, MD, SFHM
Glenda B. Atilano, MD, SFHM
Bi A. Awosika, MD, FACP, SFHM
David N. Aymond, MD, SFHM
Paula Bailey, MD, SFHM
Amit B. Bansal, MD, MBA, SFHM
Jamie K. Bartley, DO, FACP, SFHM
Stephen J. Behnke, MD, SFHM
Christina A. Beyer, MD, SFHM
Vinil K. Bhuma, MD, SFHM
John P. Biebelhausen, MD, MBA, SFHM
Matthew T. Calestino, MD, FACP, SFHM
Domingo Caparas Jr., MD, FAAFP, SFHM
Darren Caudill, DO, FACP, SFHM
Julie M. Cernanec, MD, FAAP, SFHM
Will Cushing, PA-C, SFHM
Douglas A. Dodds II, MD, FAAP, SFHM
Coley B. Duncan, MD, CPE, MMM, SFHM
Noah Finkel, MD, SFHM
Justin Glasgow, MD, PhD, SFHM
Taylor Goot, MD, SFHM
Craig G. Gunderson, MD, SFHM
Alan Hall, MD, SFHM
Vivian Hamlett, MD, SFHM
Kathrin Harrington, MD, SFHM
Hossan Hassan, MD, SFHM
Anand D. Hongalgi, MD, FACP, SFHM
Akshata Hopkins, MD, FAAP, SFHM
Neelima Kamineni, MD, SFHM
Sudheer R. Kantharajpur, MBBS, MD, MHA, SFHM
Prakash Karki, MD, SFHM
Susrutha Kotwal, MD, SFHM
Ethan Kuperman, MD, SFHM
Rumman A. Langah, MD, FACP, SFHM
Sean LaVine, MD, FACP, SFHM
Don S. Lee, MD, FACP, SFHM
Charmaine A. Lewis, MD, MPH, CLHM, SFHM
Rishi Likhi, MD, SFHM
Lenny Lopez, MD, MPH, SFHM
Anthony Macchiavelli, MD, SFHM
Brian McGillen, MD, FACP, SFHM
Parth H. Mehta, MBBS, MD, MPH, SFHM
Anuj Mehta, MBBS, MD, MBA, SFHM
Prem Nair, MD, FACP, SFHM
Don J. Neer, MD, FACP, SFHM
Shyam Odeti, MD, FAAFP, SFHM
Amy T. O’Linn, DO, SFHM
Mihir Patel, MD, FACP, MBA, MPH, SFHM
Kimberly S. Pedram, MD, FACP, SFHM
Thomas Pineo, DO, SFHM
Mauricio Pinto, MD, SFHM
Lakmali C. Ranathunga, MBBS, SFHM
Matthew Reuter, MD, SFHM
Erik P. Rufa, MD, SFHM
Dipali Ruby Sahoo, DO, MBA, SFHM
Chady Sarraf, MD, SFHM
Suchita S. Sata, MD, SFHM
Klint Schwenk, MD, FAAP, MBA, SFHM
Aaron M. Sebach, CRNP, DNP, MBA, PhD, SFHM
Kevin Sowti, MD, MBA, SFHM
Joseph G. Surber, DO, FAAFP, SFHM
Bright Thilagar, MD, SFHM
Thomas S. Trawick Jr., MD, SFHM
Rehman Usmani, MD, SFHM
Arash Velayati, MD, SFHM
Jose A. Ventura, MD, FAAFP, SFHM
Andre Wajner, MD, PhD, SFHM
Phillip D. Warr, MD, SFHM
Virginia E. Watson, MD, SFHM
Kristin R. Wise, MD, SFHM
Elham A. Yousef, MD, FACP, MBA, MSc, SFHM
Fellows Class of 2021
Elizabeth M. Aarons, MD, FHM
Suhail A. Abbasi, MD, FACP, FHM
Waqas Adeel, MD, FHM
Rajender K. Agarwal, MD, MBA, MPH, FHM
Khaalisha Ajala, MD, MBA, FHM
Faraz S. Alam, MD, FHM
Amee Amin, MD, FHM
Muhammad W. Amir, MD, FACP, FHM
Saba Asad, MD, FHM
Logan Atkins, MD, FHM
Navneet Attri, MD, FHM
Jennifer Barnett, PA, FHM
Karyn Baum, MD, FHM
Prabhjot Bedi, MD, FHM
Nicolle R. Benz, DO, FHM
Ricky Bhimani, MD, FHM
Elizabeth Blankenship, PA-C, FHM
Rahul Borsadia, MD, FHM
Kalpana Chalasani, MD, FHM
Rani Chikkanna, MD, FHM
Venu Chippa, MBBS, MD, FHM
Lisa M. Coontz, FNP, FHM
Christie Crawford, MD, FHM
Rene Daniel, MD, PhD, FHM
Elda Dede, FHM
Radha Denmark, CNP, FHM
Alvine N. Nwehla Desamours, PA-C, FHM
Satyendra Dhar, MD, FHM
Manuel Jose Diaz, MD, FHM
Tiffany Egbe, MD, FHM
Chinwe Egbo, MD, FHM
Mohammad A. Farkhondehpour, MD, FACP, FHM
Shaheen Faruque, MBBS, FHM
Chris W. Fellin, MD, FACP, FHM
Juan Carlos Fuentes-Rosales, MD, FACP, MPH, FHM
Evelyn W. Gathecha, MD, FHM
Benjamin P. Geisler, MD, FACP, MPH, FHM
Matthew George, MD, FHM
Sonia George, DO, FHM
Mirna Giordano, MD, FHM
Rebecca Gomez, MD, FHM
David Gonzales, MD, FHM
Maria A. Guevara Hernandez, MD, FACP, FHM
Shubhra Gupta, MBBS, FHM
Rohini Harvey, MD, FHM
Allison Heinen, DO, FHM
Hollie L. Hurner, PA-C, FHM
Doug Hutcheon, MD, FHM
Varalakshmi Janamanchi, MD, FHM
Brian Keegan, MD, FACP, FHM
Qasim Khalil, MD, FHM
Irfana Khan, MD, FHM
Muhammad O. Khan, MD, FAAFP, MBA, FHM
Smita Kohli, MD, FHM
Julie Kolinski, MD, FAAP, FHM
Ewa Kontny, MD, FHM
Sungmi Lian, MD, FHM
Brian Lichtenstein, MD, FHM
Fernando Madero Gorostieta, MD, FHM
Vipul Mahajan, MD, FACP, FHM
Neetu Mahendraker, MD, FHM
Victoria McCurry, MD, FHM
Bridget McGrath, PA-C, FHM
Evan Meadors, MD, FHM
Kapil Mehta, MD, FACP, MBA, FHM
Waseem Mohamed, MD, FHM
Ernest Murray, MD, FHM
Murali K. Nagubandi, MD, FHM
Jessica Nave Allen, MD, FHM
Peter Nwafor, MD, FACP, FHM
Ike Anthony Nwaobi, MBBS, MBA, FHM
Olugbenga B. Ojo, MD, FACP, MBA, FHM
Jacqueline Okere, MD, FHM
Ifedolapo S. Olanrewaju, MD, MBchB, FHM
Mobolaji Olulade, MD, FHM
Elizabeth H. Papetti, MBA, FHM
Love Patel, MBBS, FHM
Kamakshya P. Patra, MD, MMM, FHM
Charles Pizanis, MD, FHM
Rajat Prakash, MD, FHM
Chris Pribula, MD, FHM
Michael Puchaev, MD, FHM
Ryan Punsalan, MD, FHM
Bhavya Rajanna, MD, FHM
Miguel A. Ramirez, MD, FHM
Raymund Ramirez, MD, FHM
Sandeep Randhawa, MBBS, FHM
Rohit Rattan, MD, FHM
Denisha Powell Rawlings, MD, FHM
Praveen K. Reddy, MD, MPH, FHM
Michael Ree, DO, MPH, FHM
Patrick Rendon, MD, FHM
David J. Rizk, MD, FAAFP, MBA, FHM
Michael Roberts, MD, FHM
Edwin Rosas, MD, FHM
Devjit Roy, MD, FHM
Sabyasachi Roy, MD, FHM
Paul Sandroni, CMPE, MSM, FHM
Vijairam Selvaraj, MD, MPH, FHM
Megha Shah, MD, MMM, FHM
Edie Shen, MD, FHM
Gurpinder Singh, MD, FACP, FHM
Vishwas A. Singh, MD, FHM
Karen Slatkovsky, MD, FHM
Sean M. Snyder, MD, FHM
Jaclyn Spiegel, MD, FHM
Dale Stapler Jr., MD, FHM
Christina E. Stovall, MD, FHM
Daniel Suders, DO, FHM
Clayton Swalstad, CMPE, MSM, FHM
Harshil Swaminarayan, MD, FHM
Keniesha Thompson, MD, FHM
Tet Toe, MD, FACP, FHM
Christine Tsai, MD, FHM
Ajay Vaikuntam, MD, FHM
Valerie Vaughn, MD, FHM
Jane N. Wainaina, FACP, MBchB, FHM
Neshahthari Wijeyakuhan, MD, FACP, FHM
Chia-Shing Yang, MD, FHM
Jennifer Zagursky, MD, FHM
The Society of Hospital Medicine has announced its 2021 class of Master Fellows, Senior Fellows, and Fellows in Hospital Medicine.
All Fellowship classes are listed in alphabetical order.
Master Fellows Class of 2021
Nasim Afsar, MD, MBA, MHM
Shaun D. Frost, MD, MHM
Jeffrey L. Schnipper, MD, MPH, MHM
Senior Fellows Class of 2021
Akindele Adaramola, MD, MPH, SFHM
Ramesh Adhikari, MD, SFHM
Pankaj Agrawal, MD, SFHM
Robert L. Anderson, MD, SFHM
Glenda B. Atilano, MD, SFHM
Bi A. Awosika, MD, FACP, SFHM
David N. Aymond, MD, SFHM
Paula Bailey, MD, SFHM
Amit B. Bansal, MD, MBA, SFHM
Jamie K. Bartley, DO, FACP, SFHM
Stephen J. Behnke, MD, SFHM
Christina A. Beyer, MD, SFHM
Vinil K. Bhuma, MD, SFHM
John P. Biebelhausen, MD, MBA, SFHM
Matthew T. Calestino, MD, FACP, SFHM
Domingo Caparas Jr., MD, FAAFP, SFHM
Darren Caudill, DO, FACP, SFHM
Julie M. Cernanec, MD, FAAP, SFHM
Will Cushing, PA-C, SFHM
Douglas A. Dodds II, MD, FAAP, SFHM
Coley B. Duncan, MD, CPE, MMM, SFHM
Noah Finkel, MD, SFHM
Justin Glasgow, MD, PhD, SFHM
Taylor Goot, MD, SFHM
Craig G. Gunderson, MD, SFHM
Alan Hall, MD, SFHM
Vivian Hamlett, MD, SFHM
Kathrin Harrington, MD, SFHM
Hossan Hassan, MD, SFHM
Anand D. Hongalgi, MD, FACP, SFHM
Akshata Hopkins, MD, FAAP, SFHM
Neelima Kamineni, MD, SFHM
Sudheer R. Kantharajpur, MBBS, MD, MHA, SFHM
Prakash Karki, MD, SFHM
Susrutha Kotwal, MD, SFHM
Ethan Kuperman, MD, SFHM
Rumman A. Langah, MD, FACP, SFHM
Sean LaVine, MD, FACP, SFHM
Don S. Lee, MD, FACP, SFHM
Charmaine A. Lewis, MD, MPH, CLHM, SFHM
Rishi Likhi, MD, SFHM
Lenny Lopez, MD, MPH, SFHM
Anthony Macchiavelli, MD, SFHM
Brian McGillen, MD, FACP, SFHM
Parth H. Mehta, MBBS, MD, MPH, SFHM
Anuj Mehta, MBBS, MD, MBA, SFHM
Prem Nair, MD, FACP, SFHM
Don J. Neer, MD, FACP, SFHM
Shyam Odeti, MD, FAAFP, SFHM
Amy T. O’Linn, DO, SFHM
Mihir Patel, MD, FACP, MBA, MPH, SFHM
Kimberly S. Pedram, MD, FACP, SFHM
Thomas Pineo, DO, SFHM
Mauricio Pinto, MD, SFHM
Lakmali C. Ranathunga, MBBS, SFHM
Matthew Reuter, MD, SFHM
Erik P. Rufa, MD, SFHM
Dipali Ruby Sahoo, DO, MBA, SFHM
Chady Sarraf, MD, SFHM
Suchita S. Sata, MD, SFHM
Klint Schwenk, MD, FAAP, MBA, SFHM
Aaron M. Sebach, CRNP, DNP, MBA, PhD, SFHM
Kevin Sowti, MD, MBA, SFHM
Joseph G. Surber, DO, FAAFP, SFHM
Bright Thilagar, MD, SFHM
Thomas S. Trawick Jr., MD, SFHM
Rehman Usmani, MD, SFHM
Arash Velayati, MD, SFHM
Jose A. Ventura, MD, FAAFP, SFHM
Andre Wajner, MD, PhD, SFHM
Phillip D. Warr, MD, SFHM
Virginia E. Watson, MD, SFHM
Kristin R. Wise, MD, SFHM
Elham A. Yousef, MD, FACP, MBA, MSc, SFHM
Fellows Class of 2021
Elizabeth M. Aarons, MD, FHM
Suhail A. Abbasi, MD, FACP, FHM
Waqas Adeel, MD, FHM
Rajender K. Agarwal, MD, MBA, MPH, FHM
Khaalisha Ajala, MD, MBA, FHM
Faraz S. Alam, MD, FHM
Amee Amin, MD, FHM
Muhammad W. Amir, MD, FACP, FHM
Saba Asad, MD, FHM
Logan Atkins, MD, FHM
Navneet Attri, MD, FHM
Jennifer Barnett, PA, FHM
Karyn Baum, MD, FHM
Prabhjot Bedi, MD, FHM
Nicolle R. Benz, DO, FHM
Ricky Bhimani, MD, FHM
Elizabeth Blankenship, PA-C, FHM
Rahul Borsadia, MD, FHM
Kalpana Chalasani, MD, FHM
Rani Chikkanna, MD, FHM
Venu Chippa, MBBS, MD, FHM
Lisa M. Coontz, FNP, FHM
Christie Crawford, MD, FHM
Rene Daniel, MD, PhD, FHM
Elda Dede, FHM
Radha Denmark, CNP, FHM
Alvine N. Nwehla Desamours, PA-C, FHM
Satyendra Dhar, MD, FHM
Manuel Jose Diaz, MD, FHM
Tiffany Egbe, MD, FHM
Chinwe Egbo, MD, FHM
Mohammad A. Farkhondehpour, MD, FACP, FHM
Shaheen Faruque, MBBS, FHM
Chris W. Fellin, MD, FACP, FHM
Juan Carlos Fuentes-Rosales, MD, FACP, MPH, FHM
Evelyn W. Gathecha, MD, FHM
Benjamin P. Geisler, MD, FACP, MPH, FHM
Matthew George, MD, FHM
Sonia George, DO, FHM
Mirna Giordano, MD, FHM
Rebecca Gomez, MD, FHM
David Gonzales, MD, FHM
Maria A. Guevara Hernandez, MD, FACP, FHM
Shubhra Gupta, MBBS, FHM
Rohini Harvey, MD, FHM
Allison Heinen, DO, FHM
Hollie L. Hurner, PA-C, FHM
Doug Hutcheon, MD, FHM
Varalakshmi Janamanchi, MD, FHM
Brian Keegan, MD, FACP, FHM
Qasim Khalil, MD, FHM
Irfana Khan, MD, FHM
Muhammad O. Khan, MD, FAAFP, MBA, FHM
Smita Kohli, MD, FHM
Julie Kolinski, MD, FAAP, FHM
Ewa Kontny, MD, FHM
Sungmi Lian, MD, FHM
Brian Lichtenstein, MD, FHM
Fernando Madero Gorostieta, MD, FHM
Vipul Mahajan, MD, FACP, FHM
Neetu Mahendraker, MD, FHM
Victoria McCurry, MD, FHM
Bridget McGrath, PA-C, FHM
Evan Meadors, MD, FHM
Kapil Mehta, MD, FACP, MBA, FHM
Waseem Mohamed, MD, FHM
Ernest Murray, MD, FHM
Murali K. Nagubandi, MD, FHM
Jessica Nave Allen, MD, FHM
Peter Nwafor, MD, FACP, FHM
Ike Anthony Nwaobi, MBBS, MBA, FHM
Olugbenga B. Ojo, MD, FACP, MBA, FHM
Jacqueline Okere, MD, FHM
Ifedolapo S. Olanrewaju, MD, MBchB, FHM
Mobolaji Olulade, MD, FHM
Elizabeth H. Papetti, MBA, FHM
Love Patel, MBBS, FHM
Kamakshya P. Patra, MD, MMM, FHM
Charles Pizanis, MD, FHM
Rajat Prakash, MD, FHM
Chris Pribula, MD, FHM
Michael Puchaev, MD, FHM
Ryan Punsalan, MD, FHM
Bhavya Rajanna, MD, FHM
Miguel A. Ramirez, MD, FHM
Raymund Ramirez, MD, FHM
Sandeep Randhawa, MBBS, FHM
Rohit Rattan, MD, FHM
Denisha Powell Rawlings, MD, FHM
Praveen K. Reddy, MD, MPH, FHM
Michael Ree, DO, MPH, FHM
Patrick Rendon, MD, FHM
David J. Rizk, MD, FAAFP, MBA, FHM
Michael Roberts, MD, FHM
Edwin Rosas, MD, FHM
Devjit Roy, MD, FHM
Sabyasachi Roy, MD, FHM
Paul Sandroni, CMPE, MSM, FHM
Vijairam Selvaraj, MD, MPH, FHM
Megha Shah, MD, MMM, FHM
Edie Shen, MD, FHM
Gurpinder Singh, MD, FACP, FHM
Vishwas A. Singh, MD, FHM
Karen Slatkovsky, MD, FHM
Sean M. Snyder, MD, FHM
Jaclyn Spiegel, MD, FHM
Dale Stapler Jr., MD, FHM
Christina E. Stovall, MD, FHM
Daniel Suders, DO, FHM
Clayton Swalstad, CMPE, MSM, FHM
Harshil Swaminarayan, MD, FHM
Keniesha Thompson, MD, FHM
Tet Toe, MD, FACP, FHM
Christine Tsai, MD, FHM
Ajay Vaikuntam, MD, FHM
Valerie Vaughn, MD, FHM
Jane N. Wainaina, FACP, MBchB, FHM
Neshahthari Wijeyakuhan, MD, FACP, FHM
Chia-Shing Yang, MD, FHM
Jennifer Zagursky, MD, FHM
The Society of Hospital Medicine has announced its 2021 class of Master Fellows, Senior Fellows, and Fellows in Hospital Medicine.
All Fellowship classes are listed in alphabetical order.
Master Fellows Class of 2021
Nasim Afsar, MD, MBA, MHM
Shaun D. Frost, MD, MHM
Jeffrey L. Schnipper, MD, MPH, MHM
Senior Fellows Class of 2021
Akindele Adaramola, MD, MPH, SFHM
Ramesh Adhikari, MD, SFHM
Pankaj Agrawal, MD, SFHM
Robert L. Anderson, MD, SFHM
Glenda B. Atilano, MD, SFHM
Bi A. Awosika, MD, FACP, SFHM
David N. Aymond, MD, SFHM
Paula Bailey, MD, SFHM
Amit B. Bansal, MD, MBA, SFHM
Jamie K. Bartley, DO, FACP, SFHM
Stephen J. Behnke, MD, SFHM
Christina A. Beyer, MD, SFHM
Vinil K. Bhuma, MD, SFHM
John P. Biebelhausen, MD, MBA, SFHM
Matthew T. Calestino, MD, FACP, SFHM
Domingo Caparas Jr., MD, FAAFP, SFHM
Darren Caudill, DO, FACP, SFHM
Julie M. Cernanec, MD, FAAP, SFHM
Will Cushing, PA-C, SFHM
Douglas A. Dodds II, MD, FAAP, SFHM
Coley B. Duncan, MD, CPE, MMM, SFHM
Noah Finkel, MD, SFHM
Justin Glasgow, MD, PhD, SFHM
Taylor Goot, MD, SFHM
Craig G. Gunderson, MD, SFHM
Alan Hall, MD, SFHM
Vivian Hamlett, MD, SFHM
Kathrin Harrington, MD, SFHM
Hossan Hassan, MD, SFHM
Anand D. Hongalgi, MD, FACP, SFHM
Akshata Hopkins, MD, FAAP, SFHM
Neelima Kamineni, MD, SFHM
Sudheer R. Kantharajpur, MBBS, MD, MHA, SFHM
Prakash Karki, MD, SFHM
Susrutha Kotwal, MD, SFHM
Ethan Kuperman, MD, SFHM
Rumman A. Langah, MD, FACP, SFHM
Sean LaVine, MD, FACP, SFHM
Don S. Lee, MD, FACP, SFHM
Charmaine A. Lewis, MD, MPH, CLHM, SFHM
Rishi Likhi, MD, SFHM
Lenny Lopez, MD, MPH, SFHM
Anthony Macchiavelli, MD, SFHM
Brian McGillen, MD, FACP, SFHM
Parth H. Mehta, MBBS, MD, MPH, SFHM
Anuj Mehta, MBBS, MD, MBA, SFHM
Prem Nair, MD, FACP, SFHM
Don J. Neer, MD, FACP, SFHM
Shyam Odeti, MD, FAAFP, SFHM
Amy T. O’Linn, DO, SFHM
Mihir Patel, MD, FACP, MBA, MPH, SFHM
Kimberly S. Pedram, MD, FACP, SFHM
Thomas Pineo, DO, SFHM
Mauricio Pinto, MD, SFHM
Lakmali C. Ranathunga, MBBS, SFHM
Matthew Reuter, MD, SFHM
Erik P. Rufa, MD, SFHM
Dipali Ruby Sahoo, DO, MBA, SFHM
Chady Sarraf, MD, SFHM
Suchita S. Sata, MD, SFHM
Klint Schwenk, MD, FAAP, MBA, SFHM
Aaron M. Sebach, CRNP, DNP, MBA, PhD, SFHM
Kevin Sowti, MD, MBA, SFHM
Joseph G. Surber, DO, FAAFP, SFHM
Bright Thilagar, MD, SFHM
Thomas S. Trawick Jr., MD, SFHM
Rehman Usmani, MD, SFHM
Arash Velayati, MD, SFHM
Jose A. Ventura, MD, FAAFP, SFHM
Andre Wajner, MD, PhD, SFHM
Phillip D. Warr, MD, SFHM
Virginia E. Watson, MD, SFHM
Kristin R. Wise, MD, SFHM
Elham A. Yousef, MD, FACP, MBA, MSc, SFHM
Fellows Class of 2021
Elizabeth M. Aarons, MD, FHM
Suhail A. Abbasi, MD, FACP, FHM
Waqas Adeel, MD, FHM
Rajender K. Agarwal, MD, MBA, MPH, FHM
Khaalisha Ajala, MD, MBA, FHM
Faraz S. Alam, MD, FHM
Amee Amin, MD, FHM
Muhammad W. Amir, MD, FACP, FHM
Saba Asad, MD, FHM
Logan Atkins, MD, FHM
Navneet Attri, MD, FHM
Jennifer Barnett, PA, FHM
Karyn Baum, MD, FHM
Prabhjot Bedi, MD, FHM
Nicolle R. Benz, DO, FHM
Ricky Bhimani, MD, FHM
Elizabeth Blankenship, PA-C, FHM
Rahul Borsadia, MD, FHM
Kalpana Chalasani, MD, FHM
Rani Chikkanna, MD, FHM
Venu Chippa, MBBS, MD, FHM
Lisa M. Coontz, FNP, FHM
Christie Crawford, MD, FHM
Rene Daniel, MD, PhD, FHM
Elda Dede, FHM
Radha Denmark, CNP, FHM
Alvine N. Nwehla Desamours, PA-C, FHM
Satyendra Dhar, MD, FHM
Manuel Jose Diaz, MD, FHM
Tiffany Egbe, MD, FHM
Chinwe Egbo, MD, FHM
Mohammad A. Farkhondehpour, MD, FACP, FHM
Shaheen Faruque, MBBS, FHM
Chris W. Fellin, MD, FACP, FHM
Juan Carlos Fuentes-Rosales, MD, FACP, MPH, FHM
Evelyn W. Gathecha, MD, FHM
Benjamin P. Geisler, MD, FACP, MPH, FHM
Matthew George, MD, FHM
Sonia George, DO, FHM
Mirna Giordano, MD, FHM
Rebecca Gomez, MD, FHM
David Gonzales, MD, FHM
Maria A. Guevara Hernandez, MD, FACP, FHM
Shubhra Gupta, MBBS, FHM
Rohini Harvey, MD, FHM
Allison Heinen, DO, FHM
Hollie L. Hurner, PA-C, FHM
Doug Hutcheon, MD, FHM
Varalakshmi Janamanchi, MD, FHM
Brian Keegan, MD, FACP, FHM
Qasim Khalil, MD, FHM
Irfana Khan, MD, FHM
Muhammad O. Khan, MD, FAAFP, MBA, FHM
Smita Kohli, MD, FHM
Julie Kolinski, MD, FAAP, FHM
Ewa Kontny, MD, FHM
Sungmi Lian, MD, FHM
Brian Lichtenstein, MD, FHM
Fernando Madero Gorostieta, MD, FHM
Vipul Mahajan, MD, FACP, FHM
Neetu Mahendraker, MD, FHM
Victoria McCurry, MD, FHM
Bridget McGrath, PA-C, FHM
Evan Meadors, MD, FHM
Kapil Mehta, MD, FACP, MBA, FHM
Waseem Mohamed, MD, FHM
Ernest Murray, MD, FHM
Murali K. Nagubandi, MD, FHM
Jessica Nave Allen, MD, FHM
Peter Nwafor, MD, FACP, FHM
Ike Anthony Nwaobi, MBBS, MBA, FHM
Olugbenga B. Ojo, MD, FACP, MBA, FHM
Jacqueline Okere, MD, FHM
Ifedolapo S. Olanrewaju, MD, MBchB, FHM
Mobolaji Olulade, MD, FHM
Elizabeth H. Papetti, MBA, FHM
Love Patel, MBBS, FHM
Kamakshya P. Patra, MD, MMM, FHM
Charles Pizanis, MD, FHM
Rajat Prakash, MD, FHM
Chris Pribula, MD, FHM
Michael Puchaev, MD, FHM
Ryan Punsalan, MD, FHM
Bhavya Rajanna, MD, FHM
Miguel A. Ramirez, MD, FHM
Raymund Ramirez, MD, FHM
Sandeep Randhawa, MBBS, FHM
Rohit Rattan, MD, FHM
Denisha Powell Rawlings, MD, FHM
Praveen K. Reddy, MD, MPH, FHM
Michael Ree, DO, MPH, FHM
Patrick Rendon, MD, FHM
David J. Rizk, MD, FAAFP, MBA, FHM
Michael Roberts, MD, FHM
Edwin Rosas, MD, FHM
Devjit Roy, MD, FHM
Sabyasachi Roy, MD, FHM
Paul Sandroni, CMPE, MSM, FHM
Vijairam Selvaraj, MD, MPH, FHM
Megha Shah, MD, MMM, FHM
Edie Shen, MD, FHM
Gurpinder Singh, MD, FACP, FHM
Vishwas A. Singh, MD, FHM
Karen Slatkovsky, MD, FHM
Sean M. Snyder, MD, FHM
Jaclyn Spiegel, MD, FHM
Dale Stapler Jr., MD, FHM
Christina E. Stovall, MD, FHM
Daniel Suders, DO, FHM
Clayton Swalstad, CMPE, MSM, FHM
Harshil Swaminarayan, MD, FHM
Keniesha Thompson, MD, FHM
Tet Toe, MD, FACP, FHM
Christine Tsai, MD, FHM
Ajay Vaikuntam, MD, FHM
Valerie Vaughn, MD, FHM
Jane N. Wainaina, FACP, MBchB, FHM
Neshahthari Wijeyakuhan, MD, FACP, FHM
Chia-Shing Yang, MD, FHM
Jennifer Zagursky, MD, FHM
Don’t discontinue osteoporosis meds for COVID-19 vaccines, expert guidance says
COVID-19 vaccines are safe and effective for patients taking osteoporosis medications, according to joint guidance from six endocrine and osteoporosis societies and foundations.

They noted, though, that some timing modifications with certain medications should be considered to help distinguish between adverse events from the medication versus the vaccine.
The American Society for Bone and Mineral Research “is an international organization, so we brought together our sister societies that have a vested interested in bone health. Vaccination is happening worldwide, and we wanted to present a united front and united recommendations about how to handle osteoporosis medications appropriately during vaccination,” said Suzanne Jan De Beur, MD, who is president of ASBMR and an associate professor of medicine at Johns Hopkins University, Baltimore.
There has been quite a lot of concern from the community about vaccine and medications, from both physicians and patients wondering whether treatments and vaccines should occur in a certain order, and whether there should be a time gap between the two, said Dr. Jan De Beur. “There was a dearth of information about the best practices for osteoporosis treatment management during vaccination, and we didn’t want people missing their opportunity for a vaccine, and we also didn’t want them unnecessarily delaying their osteoporosis treatment.”
There is no evidence that osteoporosis therapies affect the risk or severity of COVID-19 disease, nor do they appear to change the disease course. Osteoporosis itself does not appear associated with increased risk of infection or severe outcomes, so patients with osteoporosis do not need to be prioritized for vaccination based on that condition alone.
There is no evidence that osteoporosis therapies affect the safety or efficacy of vaccination, but given that vaccine availability is currently inconsistent, patients may need to make temporary changes to their osteoporosis regimens to ensure they can receive vaccine when it is available, such as ensuring a delay between medication and vaccination injections.
A key reason for a delay between injectable or infusion medications and a vaccine is to distinguish between adverse events that could occur, so that an adverse reaction to vaccine isn’t mistaken for an adverse reaction to a drug. Nevertheless, the real world is messy. Dr. Jan De Beur noted a recent patient who arrived at her clinic for an injectable treatment who had just received a COVID-19 vaccination that morning. “We decided to put the injection in the other arm, rather than reschedule the person and put them through the risk of coming back. We could distinguish between injection-site reactions, at least,” she said.
No changes should be made to general bone health therapies, such as calcium and vitamin D supplementation, weight-bearing exercises, and maintenance of a balanced diet.
The guidance includes some recommendations for specific osteoporosis medications.
- Oral bisphosphonates: Alendronate, risedronate, and ibandronate should be continued.
- Intravenous bisphosphonates: a 7-day interval (4-day minimum) is recommended between intravenous bisphosphonate (zoledronic acid and ibandronate) infusion and COVID-19 vaccination in order to distinguish potential autoimmune or inflammatory reactions that could be attributable to either intravenous bisphosphonate or the vaccine.
- Denosumab: There should be a 4- to 7-day delay between denosumab infusion and COVID-19 vaccination to account for injection-site reactions. Another option is to have denosumab injected into the contralateral arm or another site like the abdomen or upper thigh, if spacing the injections is not possible. In any case, denosumab injections should be performed within 7 months of the previous dose.
- Teriparatide and abaloparatide should be continued.
- Romosozumab: There should be a 4- to 7-day delay between a romosozumab injection and COVID-19 vaccine, or romosozumab can be injected in the abdomen (with the exception of a 2-inch area around the naval) or thigh if spacing is not possible.
- Raloxifene should be continued in patients receiving COVID-19 vaccination.
Guidance signatories include ASBMR, the American Association of Clinical Endocrinology, the Endocrine Society, the European Calcified Tissue Society, the National Osteoporosis Foundation, and the International Osteoporosis Foundation.
Dr. Jan De Beur has no relevant financial disclosures.
COVID-19 vaccines are safe and effective for patients taking osteoporosis medications, according to joint guidance from six endocrine and osteoporosis societies and foundations.
They noted, though, that some timing modifications with certain medications should be considered to help distinguish between adverse events from the medication versus the vaccine.
The American Society for Bone and Mineral Research “is an international organization, so we brought together our sister societies that have a vested interested in bone health. Vaccination is happening worldwide, and we wanted to present a united front and united recommendations about how to handle osteoporosis medications appropriately during vaccination,” said Suzanne Jan De Beur, MD, who is president of ASBMR and an associate professor of medicine at Johns Hopkins University, Baltimore.
There has been quite a lot of concern from the community about vaccine and medications, from both physicians and patients wondering whether treatments and vaccines should occur in a certain order, and whether there should be a time gap between the two, said Dr. Jan De Beur. “There was a dearth of information about the best practices for osteoporosis treatment management during vaccination, and we didn’t want people missing their opportunity for a vaccine, and we also didn’t want them unnecessarily delaying their osteoporosis treatment.”
There is no evidence that osteoporosis therapies affect the risk or severity of COVID-19 disease, nor do they appear to change the disease course. Osteoporosis itself does not appear associated with increased risk of infection or severe outcomes, so patients with osteoporosis do not need to be prioritized for vaccination based on that condition alone.
There is no evidence that osteoporosis therapies affect the safety or efficacy of vaccination, but given that vaccine availability is currently inconsistent, patients may need to make temporary changes to their osteoporosis regimens to ensure they can receive vaccine when it is available, such as ensuring a delay between medication and vaccination injections.
A key reason for a delay between injectable or infusion medications and a vaccine is to distinguish between adverse events that could occur, so that an adverse reaction to vaccine isn’t mistaken for an adverse reaction to a drug. Nevertheless, the real world is messy. Dr. Jan De Beur noted a recent patient who arrived at her clinic for an injectable treatment who had just received a COVID-19 vaccination that morning. “We decided to put the injection in the other arm, rather than reschedule the person and put them through the risk of coming back. We could distinguish between injection-site reactions, at least,” she said.
No changes should be made to general bone health therapies, such as calcium and vitamin D supplementation, weight-bearing exercises, and maintenance of a balanced diet.
The guidance includes some recommendations for specific osteoporosis medications.
- Oral bisphosphonates: Alendronate, risedronate, and ibandronate should be continued.
- Intravenous bisphosphonates: a 7-day interval (4-day minimum) is recommended between intravenous bisphosphonate (zoledronic acid and ibandronate) infusion and COVID-19 vaccination in order to distinguish potential autoimmune or inflammatory reactions that could be attributable to either intravenous bisphosphonate or the vaccine.
- Denosumab: There should be a 4- to 7-day delay between denosumab infusion and COVID-19 vaccination to account for injection-site reactions. Another option is to have denosumab injected into the contralateral arm or another site like the abdomen or upper thigh, if spacing the injections is not possible. In any case, denosumab injections should be performed within 7 months of the previous dose.
- Teriparatide and abaloparatide should be continued.
- Romosozumab: There should be a 4- to 7-day delay between a romosozumab injection and COVID-19 vaccine, or romosozumab can be injected in the abdomen (with the exception of a 2-inch area around the naval) or thigh if spacing is not possible.
- Raloxifene should be continued in patients receiving COVID-19 vaccination.
Guidance signatories include ASBMR, the American Association of Clinical Endocrinology, the Endocrine Society, the European Calcified Tissue Society, the National Osteoporosis Foundation, and the International Osteoporosis Foundation.
Dr. Jan De Beur has no relevant financial disclosures.
COVID-19 vaccines are safe and effective for patients taking osteoporosis medications, according to joint guidance from six endocrine and osteoporosis societies and foundations.
They noted, though, that some timing modifications with certain medications should be considered to help distinguish between adverse events from the medication versus the vaccine.
The American Society for Bone and Mineral Research “is an international organization, so we brought together our sister societies that have a vested interested in bone health. Vaccination is happening worldwide, and we wanted to present a united front and united recommendations about how to handle osteoporosis medications appropriately during vaccination,” said Suzanne Jan De Beur, MD, who is president of ASBMR and an associate professor of medicine at Johns Hopkins University, Baltimore.
There has been quite a lot of concern from the community about vaccine and medications, from both physicians and patients wondering whether treatments and vaccines should occur in a certain order, and whether there should be a time gap between the two, said Dr. Jan De Beur. “There was a dearth of information about the best practices for osteoporosis treatment management during vaccination, and we didn’t want people missing their opportunity for a vaccine, and we also didn’t want them unnecessarily delaying their osteoporosis treatment.”
There is no evidence that osteoporosis therapies affect the risk or severity of COVID-19 disease, nor do they appear to change the disease course. Osteoporosis itself does not appear associated with increased risk of infection or severe outcomes, so patients with osteoporosis do not need to be prioritized for vaccination based on that condition alone.
There is no evidence that osteoporosis therapies affect the safety or efficacy of vaccination, but given that vaccine availability is currently inconsistent, patients may need to make temporary changes to their osteoporosis regimens to ensure they can receive vaccine when it is available, such as ensuring a delay between medication and vaccination injections.
A key reason for a delay between injectable or infusion medications and a vaccine is to distinguish between adverse events that could occur, so that an adverse reaction to vaccine isn’t mistaken for an adverse reaction to a drug. Nevertheless, the real world is messy. Dr. Jan De Beur noted a recent patient who arrived at her clinic for an injectable treatment who had just received a COVID-19 vaccination that morning. “We decided to put the injection in the other arm, rather than reschedule the person and put them through the risk of coming back. We could distinguish between injection-site reactions, at least,” she said.
No changes should be made to general bone health therapies, such as calcium and vitamin D supplementation, weight-bearing exercises, and maintenance of a balanced diet.
The guidance includes some recommendations for specific osteoporosis medications.
- Oral bisphosphonates: Alendronate, risedronate, and ibandronate should be continued.
- Intravenous bisphosphonates: a 7-day interval (4-day minimum) is recommended between intravenous bisphosphonate (zoledronic acid and ibandronate) infusion and COVID-19 vaccination in order to distinguish potential autoimmune or inflammatory reactions that could be attributable to either intravenous bisphosphonate or the vaccine.
- Denosumab: There should be a 4- to 7-day delay between denosumab infusion and COVID-19 vaccination to account for injection-site reactions. Another option is to have denosumab injected into the contralateral arm or another site like the abdomen or upper thigh, if spacing the injections is not possible. In any case, denosumab injections should be performed within 7 months of the previous dose.
- Teriparatide and abaloparatide should be continued.
- Romosozumab: There should be a 4- to 7-day delay between a romosozumab injection and COVID-19 vaccine, or romosozumab can be injected in the abdomen (with the exception of a 2-inch area around the naval) or thigh if spacing is not possible.
- Raloxifene should be continued in patients receiving COVID-19 vaccination.
Guidance signatories include ASBMR, the American Association of Clinical Endocrinology, the Endocrine Society, the European Calcified Tissue Society, the National Osteoporosis Foundation, and the International Osteoporosis Foundation.
Dr. Jan De Beur has no relevant financial disclosures.