User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Pneumonia decision tool reduces death in ED patients
a 3-year, pragmatic, cluster-controlled study shows.
“We designed the ePNa specifically to require minimal input from the clinician so everything it does is already in the electronic medical record,” Nathan Dean, MD, University of Utah, Salt Lake City, told this news organization.
“So it’s actually putting the guideline recommendations into effect for physicians so that they can make better decisions by having all this information – it’s a comprehensive best practice kind of tool where best practices are likely to make the biggest difference for patients with a high severity of illness,” he added.
The study was published online in the American Journal of Respiratory and Critical Care Medicine.
Guideline-based tool
The ePNa makes use of pneumonia guidelines of 2007 and 2019 from the American Thoracic Society/Infectious Disease Society of America. The system was deployed into six geographic clusters of 16 Intermountain hospital EDs at 2-month intervals between December 2017 and November 2018. Simultaneous deployment was impractical, as implementation of the tool takes education, monitoring, and feedback that can be facilitated by focusing on only a few hospitals at a time.
The decision support tool gathers key patient indicators including age, fever, oxygen saturation, vital signs, and laboratory and chest imaging results to offer recommendations on care, including appropriate antibiotic therapy, microbiology studies, and whether a given patient should be sent to the intensive care unit, admitted to hospital, or may safely be discharged home.
Investigators analyzed a total of 6,848 patients, of whom 4,536 were managed for pneumonia before the ePNa was deployed and 2,312 after deployment.
The median age of patients was 67 years (interquartile range, 50-79 years). Roughly half were female and almost all were White. “Observed 30-day all-cause mortality including both outpatients and inpatients was 8.6% before deployment versus 4.8% after deployment of ePNa,” Dr. Dean and colleagues reported.
Adjusted for severity of illness, the odds ratio for lower mortality post-ePNa launch was 0.62 (95% confidence interval, 0.49-0.79; P < .0010) “and lower morality was consistent across hospital clusters.”
Compared with patients who were discharged home, reductions in mortality were greatest in patients who were directly admitted to ICUs from the ED (OR, 0.32; 95% CI, 0.14-0.77; P = .01). The OR for patients admitted to the medical floor was 0.53 (95% CI, 0.25-1.1; P = .09), which did not reach statistical significance.
Dr. Dean explained that the reductions in mortality were seen among those with the most severe illness, in whom best practices would benefit the most. In contrast, patients who are sent home on an antibiotic are at low risk for mortality while patients admitted to the medical floor may well have another, more lethal illness from which they end up dying, rather than simple pneumonia.
“For me, this was a clear demonstration that these best practices made the biggest difference in patients who were sick and who did not have any underlying disease that was going to kill them anyway,” he emphasized. On the other hand, both 30-day mortality and 7-day secondary hospital admission were higher among patients the tool recommended for hospital ward admission but who were discharged home from the ED.
“This was an unexpected finding,” Dr. Dean observed. However, as he explained, the authors reviewed 25% of randomly selected patients who fell into this subgroup and discovered that the ePNa tool was used in only about 20% of patients – “so doctors did not use the tool in the majority of this group.”
In addition, some of these patients declined hospital admission, so the doctors may have recommended that they be admitted but the patients said no. “The hypothesis here is that if they had been admitted to the hospital, they may have had a lower mortality risk,” Dr. Dean said.
Noticeable changes
Another noticeable change following the introduction of the ePNa tool was that guideline-concordant antibiotic prescribing increased in the 8 hours after patients presented to the ED, from 79.5% prior to the tool’s launch to 87.9%, again after adjusting for pneumonia severity (P < .001). Use of broad-spectrum antibiotics was not significantly different between the two treatment intervals, but administration of antibiotics active against methicillin-resistant Staphylococcus aureus dropped significantly between the two treatment intervals (P < .001). And the mean time from admission to the ED to the first antibiotic taken was slightly faster, improving from 159.4 minutes (95% CI, 156.9-161.9 minutes) prior to the ePNa launch to 150.9 minutes (95% CI, 144.1-157.8) post deployment (P < .001).
“Overall outpatient disposition for treatment of pneumonia from the emergency department increased from 29.2% before ePNa to 46.9% [post ePNA],” the authors noted, while a similar increase was observed in patients for whom ePNA recommended outpatient care – from 49.2% pre-ePNA to 66.6% after ePNA.
Both hospital ward admission and admission to the ICU decreased after ePNa had been introduced. Despite a significant increase in the percentage of patients being discharged home, neither 7-day secondary hospital admission nor severity-adjusted, 30-day mortality were significantly different before versus after the introduction of ePNa, the authors stressed.
A limitation of the study was that the trial was confined to a single health care system in one region of the United States with a patient population that may differ from that in other regions.
Reason for its success
Asked to comment on the findings, Adam Balls, MD, emergency department chair, Intermountain Medical Center, Murray, Utah, suggested that the reason the ePNa tool has been so successful at improving care for pneumonia patients is that it puts the guidelines directly into the hands of individual providers and tells them what’s going on. (Dr. Balls was not involved in the study.) “The tool allows us to take into consideration various clinical features – a patient’s oxygen requirements and whether or not they had prior complicated pneumonias that required additional antibiotics, for example – and then it makes the best determination for not only the disposition for that patient but antibiotic treatment as well,” he said in an interview.
This then allows physicians to either appropriately discharge less severely ill patients and admit those who are more ill – “and in general, just do a better job of treating pneumonia with this tool,” Dr. Balls said. He himself uses the decision support tool when attending to his own patients with pneumonia, as he feels that the tool really does make his care of these patients better. “There is a disparity around how we treat pneumonia in the U.S.
“Clinicians sometimes have a bias or a preference for certain antibiotics and we may not be appropriately treating these patients with broad-spectrum antibiotics or are perhaps using antibiotics that are not as effective based on an individual patient scenario so this is definitely a user-friendly tool that hopefully can be deployed throughout other health care systems to improve the treatment of pneumonia overall,” Dr. Balls emphasized.
A version of this article first appeared on Medscape.com.
a 3-year, pragmatic, cluster-controlled study shows.
“We designed the ePNa specifically to require minimal input from the clinician so everything it does is already in the electronic medical record,” Nathan Dean, MD, University of Utah, Salt Lake City, told this news organization.
“So it’s actually putting the guideline recommendations into effect for physicians so that they can make better decisions by having all this information – it’s a comprehensive best practice kind of tool where best practices are likely to make the biggest difference for patients with a high severity of illness,” he added.
The study was published online in the American Journal of Respiratory and Critical Care Medicine.
Guideline-based tool
The ePNa makes use of pneumonia guidelines of 2007 and 2019 from the American Thoracic Society/Infectious Disease Society of America. The system was deployed into six geographic clusters of 16 Intermountain hospital EDs at 2-month intervals between December 2017 and November 2018. Simultaneous deployment was impractical, as implementation of the tool takes education, monitoring, and feedback that can be facilitated by focusing on only a few hospitals at a time.
The decision support tool gathers key patient indicators including age, fever, oxygen saturation, vital signs, and laboratory and chest imaging results to offer recommendations on care, including appropriate antibiotic therapy, microbiology studies, and whether a given patient should be sent to the intensive care unit, admitted to hospital, or may safely be discharged home.
Investigators analyzed a total of 6,848 patients, of whom 4,536 were managed for pneumonia before the ePNa was deployed and 2,312 after deployment.
The median age of patients was 67 years (interquartile range, 50-79 years). Roughly half were female and almost all were White. “Observed 30-day all-cause mortality including both outpatients and inpatients was 8.6% before deployment versus 4.8% after deployment of ePNa,” Dr. Dean and colleagues reported.
Adjusted for severity of illness, the odds ratio for lower mortality post-ePNa launch was 0.62 (95% confidence interval, 0.49-0.79; P < .0010) “and lower morality was consistent across hospital clusters.”
Compared with patients who were discharged home, reductions in mortality were greatest in patients who were directly admitted to ICUs from the ED (OR, 0.32; 95% CI, 0.14-0.77; P = .01). The OR for patients admitted to the medical floor was 0.53 (95% CI, 0.25-1.1; P = .09), which did not reach statistical significance.
Dr. Dean explained that the reductions in mortality were seen among those with the most severe illness, in whom best practices would benefit the most. In contrast, patients who are sent home on an antibiotic are at low risk for mortality while patients admitted to the medical floor may well have another, more lethal illness from which they end up dying, rather than simple pneumonia.
“For me, this was a clear demonstration that these best practices made the biggest difference in patients who were sick and who did not have any underlying disease that was going to kill them anyway,” he emphasized. On the other hand, both 30-day mortality and 7-day secondary hospital admission were higher among patients the tool recommended for hospital ward admission but who were discharged home from the ED.
“This was an unexpected finding,” Dr. Dean observed. However, as he explained, the authors reviewed 25% of randomly selected patients who fell into this subgroup and discovered that the ePNa tool was used in only about 20% of patients – “so doctors did not use the tool in the majority of this group.”
In addition, some of these patients declined hospital admission, so the doctors may have recommended that they be admitted but the patients said no. “The hypothesis here is that if they had been admitted to the hospital, they may have had a lower mortality risk,” Dr. Dean said.
Noticeable changes
Another noticeable change following the introduction of the ePNa tool was that guideline-concordant antibiotic prescribing increased in the 8 hours after patients presented to the ED, from 79.5% prior to the tool’s launch to 87.9%, again after adjusting for pneumonia severity (P < .001). Use of broad-spectrum antibiotics was not significantly different between the two treatment intervals, but administration of antibiotics active against methicillin-resistant Staphylococcus aureus dropped significantly between the two treatment intervals (P < .001). And the mean time from admission to the ED to the first antibiotic taken was slightly faster, improving from 159.4 minutes (95% CI, 156.9-161.9 minutes) prior to the ePNa launch to 150.9 minutes (95% CI, 144.1-157.8) post deployment (P < .001).
“Overall outpatient disposition for treatment of pneumonia from the emergency department increased from 29.2% before ePNa to 46.9% [post ePNA],” the authors noted, while a similar increase was observed in patients for whom ePNA recommended outpatient care – from 49.2% pre-ePNA to 66.6% after ePNA.
Both hospital ward admission and admission to the ICU decreased after ePNa had been introduced. Despite a significant increase in the percentage of patients being discharged home, neither 7-day secondary hospital admission nor severity-adjusted, 30-day mortality were significantly different before versus after the introduction of ePNa, the authors stressed.
A limitation of the study was that the trial was confined to a single health care system in one region of the United States with a patient population that may differ from that in other regions.
Reason for its success
Asked to comment on the findings, Adam Balls, MD, emergency department chair, Intermountain Medical Center, Murray, Utah, suggested that the reason the ePNa tool has been so successful at improving care for pneumonia patients is that it puts the guidelines directly into the hands of individual providers and tells them what’s going on. (Dr. Balls was not involved in the study.) “The tool allows us to take into consideration various clinical features – a patient’s oxygen requirements and whether or not they had prior complicated pneumonias that required additional antibiotics, for example – and then it makes the best determination for not only the disposition for that patient but antibiotic treatment as well,” he said in an interview.
This then allows physicians to either appropriately discharge less severely ill patients and admit those who are more ill – “and in general, just do a better job of treating pneumonia with this tool,” Dr. Balls said. He himself uses the decision support tool when attending to his own patients with pneumonia, as he feels that the tool really does make his care of these patients better. “There is a disparity around how we treat pneumonia in the U.S.
“Clinicians sometimes have a bias or a preference for certain antibiotics and we may not be appropriately treating these patients with broad-spectrum antibiotics or are perhaps using antibiotics that are not as effective based on an individual patient scenario so this is definitely a user-friendly tool that hopefully can be deployed throughout other health care systems to improve the treatment of pneumonia overall,” Dr. Balls emphasized.
A version of this article first appeared on Medscape.com.
a 3-year, pragmatic, cluster-controlled study shows.
“We designed the ePNa specifically to require minimal input from the clinician so everything it does is already in the electronic medical record,” Nathan Dean, MD, University of Utah, Salt Lake City, told this news organization.
“So it’s actually putting the guideline recommendations into effect for physicians so that they can make better decisions by having all this information – it’s a comprehensive best practice kind of tool where best practices are likely to make the biggest difference for patients with a high severity of illness,” he added.
The study was published online in the American Journal of Respiratory and Critical Care Medicine.
Guideline-based tool
The ePNa makes use of pneumonia guidelines of 2007 and 2019 from the American Thoracic Society/Infectious Disease Society of America. The system was deployed into six geographic clusters of 16 Intermountain hospital EDs at 2-month intervals between December 2017 and November 2018. Simultaneous deployment was impractical, as implementation of the tool takes education, monitoring, and feedback that can be facilitated by focusing on only a few hospitals at a time.
The decision support tool gathers key patient indicators including age, fever, oxygen saturation, vital signs, and laboratory and chest imaging results to offer recommendations on care, including appropriate antibiotic therapy, microbiology studies, and whether a given patient should be sent to the intensive care unit, admitted to hospital, or may safely be discharged home.
Investigators analyzed a total of 6,848 patients, of whom 4,536 were managed for pneumonia before the ePNa was deployed and 2,312 after deployment.
The median age of patients was 67 years (interquartile range, 50-79 years). Roughly half were female and almost all were White. “Observed 30-day all-cause mortality including both outpatients and inpatients was 8.6% before deployment versus 4.8% after deployment of ePNa,” Dr. Dean and colleagues reported.
Adjusted for severity of illness, the odds ratio for lower mortality post-ePNa launch was 0.62 (95% confidence interval, 0.49-0.79; P < .0010) “and lower morality was consistent across hospital clusters.”
Compared with patients who were discharged home, reductions in mortality were greatest in patients who were directly admitted to ICUs from the ED (OR, 0.32; 95% CI, 0.14-0.77; P = .01). The OR for patients admitted to the medical floor was 0.53 (95% CI, 0.25-1.1; P = .09), which did not reach statistical significance.
Dr. Dean explained that the reductions in mortality were seen among those with the most severe illness, in whom best practices would benefit the most. In contrast, patients who are sent home on an antibiotic are at low risk for mortality while patients admitted to the medical floor may well have another, more lethal illness from which they end up dying, rather than simple pneumonia.
“For me, this was a clear demonstration that these best practices made the biggest difference in patients who were sick and who did not have any underlying disease that was going to kill them anyway,” he emphasized. On the other hand, both 30-day mortality and 7-day secondary hospital admission were higher among patients the tool recommended for hospital ward admission but who were discharged home from the ED.
“This was an unexpected finding,” Dr. Dean observed. However, as he explained, the authors reviewed 25% of randomly selected patients who fell into this subgroup and discovered that the ePNa tool was used in only about 20% of patients – “so doctors did not use the tool in the majority of this group.”
In addition, some of these patients declined hospital admission, so the doctors may have recommended that they be admitted but the patients said no. “The hypothesis here is that if they had been admitted to the hospital, they may have had a lower mortality risk,” Dr. Dean said.
Noticeable changes
Another noticeable change following the introduction of the ePNa tool was that guideline-concordant antibiotic prescribing increased in the 8 hours after patients presented to the ED, from 79.5% prior to the tool’s launch to 87.9%, again after adjusting for pneumonia severity (P < .001). Use of broad-spectrum antibiotics was not significantly different between the two treatment intervals, but administration of antibiotics active against methicillin-resistant Staphylococcus aureus dropped significantly between the two treatment intervals (P < .001). And the mean time from admission to the ED to the first antibiotic taken was slightly faster, improving from 159.4 minutes (95% CI, 156.9-161.9 minutes) prior to the ePNa launch to 150.9 minutes (95% CI, 144.1-157.8) post deployment (P < .001).
“Overall outpatient disposition for treatment of pneumonia from the emergency department increased from 29.2% before ePNa to 46.9% [post ePNA],” the authors noted, while a similar increase was observed in patients for whom ePNA recommended outpatient care – from 49.2% pre-ePNA to 66.6% after ePNA.
Both hospital ward admission and admission to the ICU decreased after ePNa had been introduced. Despite a significant increase in the percentage of patients being discharged home, neither 7-day secondary hospital admission nor severity-adjusted, 30-day mortality were significantly different before versus after the introduction of ePNa, the authors stressed.
A limitation of the study was that the trial was confined to a single health care system in one region of the United States with a patient population that may differ from that in other regions.
Reason for its success
Asked to comment on the findings, Adam Balls, MD, emergency department chair, Intermountain Medical Center, Murray, Utah, suggested that the reason the ePNa tool has been so successful at improving care for pneumonia patients is that it puts the guidelines directly into the hands of individual providers and tells them what’s going on. (Dr. Balls was not involved in the study.) “The tool allows us to take into consideration various clinical features – a patient’s oxygen requirements and whether or not they had prior complicated pneumonias that required additional antibiotics, for example – and then it makes the best determination for not only the disposition for that patient but antibiotic treatment as well,” he said in an interview.
This then allows physicians to either appropriately discharge less severely ill patients and admit those who are more ill – “and in general, just do a better job of treating pneumonia with this tool,” Dr. Balls said. He himself uses the decision support tool when attending to his own patients with pneumonia, as he feels that the tool really does make his care of these patients better. “There is a disparity around how we treat pneumonia in the U.S.
“Clinicians sometimes have a bias or a preference for certain antibiotics and we may not be appropriately treating these patients with broad-spectrum antibiotics or are perhaps using antibiotics that are not as effective based on an individual patient scenario so this is definitely a user-friendly tool that hopefully can be deployed throughout other health care systems to improve the treatment of pneumonia overall,” Dr. Balls emphasized.
A version of this article first appeared on Medscape.com.
FROM THE AMERICAN JOURNAL OF RESPIRATORY AND CRITICAL CARE MEDICINE
‘Profound implications’: COVID ups diabetes risk 40% a year later
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
COVID-19 infection appears to significantly raise the risk for diabetes by about 40% at 1 year, indicate new data from a very large Veterans Administration population.
“If patients have a prior history of COVID-19, that’s a risk factor for diabetes and they should certainly be screened for diabetes,” study coauthor Ziyad Al-Aly, MD, a nephrologist and chief of research and development at VA St. Louis Health Care, told this news organization.
“It’s still premature to make guidelines. I think we have to process the data landscape to understand what this all really means, but it’s really, really clear that all these roads are pointing in one direction, that COVID-19 increases the risk of diabetes up to a year later. The risk is small but not negligible,” he said.
The database includes over 8 million people and 180,000 with a prior COVID-19 diagnosis. Significantly increased diabetes risks compared to those not infected ranging from 31% to more than double were found in an analysis of subgroups based on diabetes risk score, body mass index, age, race, prediabetes status, and deprivation level, even after adjustment for confounding factors.
There was a gradient of diabetes risk by COVID-19 severity – i.e., whether patients had not been hospitalized, had been hospitalized, or stayed in intensive care – but a significant excess diabetes burden was seen even among those with “mild” COVID-19. The diabetes risk was also elevated compared to both contemporary and historical controls.
The study was published March 21 in The Lancet Diabetes & Endocrinology, by Yan Xie, MPH, also of VA St Louis Health Care, along with Dr. Al-Aly.
The data align with those from another study just published from a nationwide German primary care database. That study was smaller and of shorter duration than the new VA study but consistent, said Dr. Al-Aly, a clinical epidemiologist at Washington University, St. Louis.
Millions more with new diabetes as late manifestation of COVID-19
“Millions of people in the U.S. have had COVID-19, so this is going to translate to literally millions more people with new-onset diabetes. Better to identify them early so they can be adequately treated,” Dr. Al-Aly said in an interview.
“The long-term implications of SARS-CoV-2 infection increasing diabetes risk are profound,” Venkat Narayan, MD, and Lisa R. Staimez, PhD, both of the Rollins School of Public Health and Emory Global Diabetes Research Center at Emory University, Atlanta, said in an accompanying editorial.
“With large and growing numbers of people worldwide infected with SARS-CoV-2 (434,154,739 cumulative cases by Feb. 28, 2022), any COVID-19-related increases in diabetes incidence could lead to unprecedented cases of diabetes worldwide – wreaking havoc on already over-stretched and under-resourced clinical and public health systems globally, with devastating tolls in terms of deaths and suffering,” they added.
Medscape Medical News contributor Eric Topol MD, of Scripps Research Institute, La Jolla, Calif., agrees. He said these new data “are most profound. The researchers found a 40% increase in diabetes that wasn’t present at 1 month after COVID-19 but at 1 year, it was. Some kind of late manifestation is happening here.”
Dr. Al-Aly told this news organization that the mechanisms for the association are unknown and likely to be heterogeneous. Among the people who already had risk factors for type 2 diabetes, such as obesity or metabolic syndrome, SARS-CoV-2 could simply accelerate that process and “put them over the edge” to overt diabetes.
However, for those without diabetes risk factors, “COVID-19 with all the inflammation it provokes in the body could be leading to de novo disease.” (Diabetes status was ascertained by ICD-10 codes and only about 0.70% of the total were recorded as type 1 diabetes. But, since autoantibody testing wasn’t routinely conducted, it’s unknown how many of the cases may have been type 1 misclassified as type 2, Dr. Al-Aly acknowledged.)
Diabetes risk significantly increased after COVID-19 in all analyses
The analysis included 181,280 patients in the U.S. Department of Veterans Affairs health care database with a COVID-19 diagnosis who survived for at least 30 days afterward during March 2020 through Sept. 30, 2021, with 4,118,441 contemporary controls without COVID-19 seen during 2019, and a historical control group of 4,286,911 people seen at the VA in 2017. Average follow-up was about a year.
Compared with the contemporary controls, the COVID-19 group had an excess diabetes burden of 13.46 per 1,000 person-years with a hazard ratio of 1.40. They had an increased 12.35 per 1,000 person-year risk for incident use of glucose-lowering medications, with a hazard ratio of 1.85. Similar results were seen with the historical controls.
Subgroup analyses showed an increased risk for diabetes following COVID-19 infection by age (≤ 65 years and > 65 years), race (White and Black), sex (male and female), BMI categories (> 18.5 to ≤ 25 kg/m², > 25 to ≤ 30 kg/m², and > 30 kg/m²), and area deprivation index quartiles. The increased risk was also seen across diabetes risk score quartiles.
Notably, COVID-19 significantly elevated the diabetes risk by 59% even for the subgroup with BMI between 18 and 25 kg/m², and by 38% among those with the lowest diabetes risk score quartile.
The COVID-19 population included 162,096 who were not hospitalized, 15,078 hospitalized, and 4,106 admitted to intensive care. Here, the hazard ratios for diabetes compared to the contemporary controls were 1.25, 2.73, and 3.76, respectively, all significant.
Dr. Al-Aly said that his group is now further analyzing the VA data for other outcomes including cardiovascular disease and kidney disease, as well as the now well-documented long COVID symptoms including fatigue, pain, and neurocognitive dysfunction.
They’re also investigating the impact of the COVID-19 vaccine to see whether the risks are mitigated in the case of breakthrough infections: “We’re doing a broad systematic assessment. The next paper will be more comprehensive.”
Dr. Narayan and Dr. Staimez wrote: “The potential connection between COVID-19 and diabetes highlights that infectious diseases (eg, SARS-CoV-2) and chronic diseases (eg, diabetes) cannot be viewed in siloes. When we emerge out of the pandemic, the much-neglected non-communicable diseases, such as type 2 diabetes, will continue their relentless trajectory, possibly in an accelerated manner, as the leading burdens of global health.”
Dr. Al-Aly declared support from the U.S. Department of Veterans Affairs for the submitted work. He has received consultation fees from Gilead Sciences and funding (unrelated to this work) from Tonix Pharmaceuticals. He is a member of the board of directors for Veterans Research and Education Foundation of Saint Louis, associate editor for the Journal of the American Society of Nephrology, and a member of multiple editorial boards. Dr. Narayan and Dr. Staimez have received support from the National Institutes of Health.
A version of this article first appeared on Medscape.com.
FROM THE LANCET DIABETES & ENDOCRINOLOGY
Pfizer recalls BP drugs because of potential carcinogen
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
Pfizer is voluntarily recalling some antihypertensive medications because of unacceptable levels of a potential carcinogen, the company announced.
The affected products are quinapril HCI/hydrochlorothiazide (Accuretic) tablets that Pfizer distributes, and two authorized generics, quinapril plus hydrochlorothiazide and quinapril HCI/hydrochlorothiazide, distributed by Greenstone. The drugs have been withdrawn because of the presence of nitrosamine, N-nitroso-quinapril.
“Although long-term ingestion of N-nitroso-quinapril may be associated with a potential increased cancer risk in humans, there is no immediate risk to patients taking this medication,” Pfizer said in a news release.
The tablets are indicated for the treatment of hypertension. Patients currently taking the products are asked to consult with their doctor about alternative treatment options.
To date, there have been no reports of adverse events related to the recall, the company said.
In all, Pfizer is recalling six lots of Accuretic tablets (two at 10 mg/12.5 mg, three at 20 mg/12.5 mg, and one at 20 mg/25 mg), one lot of quinapril plus hydrochlorothiazide 20-mg/25-mg tablets, and four lots of quinapril HCl/ hydrochlorothiazide tablets (three at 20 mg/12.5 mg and one at 20 mg/25 mg)
The recalled tablets were sold in 90-count bottles distributed in the United States and Puerto Rico between November 2019 and March 2022. Product codes and lot numbers of the recalled medications are listed on the Pfizer website.
Patients who are taking this product should consult with their health care provider or pharmacy to determine if they have the affected product. Those with the affected tablets should contact claims management firm Sedgwick by phone at 888-843-0247 Monday through Friday from 8 a.m. to 5 p.m. ET for instructions on how to return their product and obtain reimbursement.
Health care providers with medical questions regarding the recall can contact Pfizer by telephone at 800-438-1985, option 3, Monday through Friday 8 a.m. to 9 p.m. ET.
Providers should report adverse reactions or quality problems they experience using these tablets to Pfizer either by telephone at 800-438-1985, option 1, by regular mail or by fax, or to the Food and Drug Administration’s MedWatch program.
A version of this article first appeared on Medscape.com.
As a nurse faces prison for a deadly error, her colleagues worry: Could I be next?
Four years ago, inside the most prestigious hospital in Tennessee, nurse RaDonda Vaught withdrew a vial from an electronic medication cabinet, administered the drug to a patient, and somehow overlooked signs of a terrible and deadly mistake.
The patient was supposed to get Versed, a sedative intended to calm her before being scanned in a large, MRI-like machine. But Ms. Vaught accidentally grabbed vecuronium, a powerful paralyzer, which stopped the patient’s breathing and left her brain-dead before the error was discovered.
Ms. Vaught, 38, admitted her mistake at a Tennessee Board of Nursing hearing last year, saying she became “complacent” in her job and “distracted” by a trainee while operating the computerized medication cabinet. She did not shirk responsibility for the error, but she said the blame was not hers alone.
“I know the reason this patient is no longer here is because of me,” Ms. Vaught said, starting to cry. “There won’t ever be a day that goes by that I don’t think about what I did.”
If Ms. Vaught’s story followed the path of most medical errors, it would have been over hours later, when the Board of Nursing revoked her RN license and almost certainly ended her nursing career. But Ms. Vaught’s case is different: This week she goes on trial in Nashville on criminal charges of reckless homicide and felony abuse of an impaired adult for the killing of Charlene Murphey, a 75-year-old patient who died at Vanderbilt University Medical Center on Dec. 27, 2017.
Prosecutors do not allege in their court filings that Ms. Vaught intended to hurt Ms. Murphey or was impaired by any substance when she made the mistake, so Fatal errors are generally handled by licensing boards and civil courts. And experts say prosecutions like Ms. Vaught’s loom large for a profession terrified of the criminalization of such mistakes — especially because her case hinges on an automated system for dispensing drugs that many nurses use every day.
The Nashville district attorney’s office declined to discuss Ms. Vaught’s trial. Ms. Vaught’s lawyer, Peter Strianse, did not respond to requests for comment. Vanderbilt University Medical Center has repeatedly declined to comment on Ms. Vaught’s trial or its procedures.
Ms. Vaught’s trial will be followed by nurses nationwide, many of whom worry a conviction may set a precedent even as the coronavirus pandemic leaves countless nurses exhausted, demoralized, and likely more prone to error.
Janie Harvey Garner, a St. Louis registered nurse and founder of Show Me Your Stethoscope, a nursing group with more than 600,000 members on Facebook, said the group has closely watched Ms. Vaught’s case for years out of concern for her fate — and their own.
Ms. Garner said most nurses know all too well the pressures that contribute to such an error: long hours, crowded hospitals, imperfect protocols, and the inevitable creep of complacency in a job with daily life-or-death stakes.
Ms. Garner said she once switched powerful medications just as Ms. Vaught did and caught her mistake only in a last-minute triple-check.
“In response to a story like this one, there are two kinds of nurses,” Ms. Garner said. “You have the nurses who assume they would never make a mistake like that, and usually it’s because they don’t realize they could. And the second kind are the ones who know this could happen, any day, no matter how careful they are. This could be me. I could be RaDonda.”
As the trial begins, the Nashville DA’s prosecutors will argue that Ms. Vaught’s error was anything but a common mistake any nurse could make. Prosecutors will say she ignored a cascade of warnings that led to the deadly error.
The case hinges on the nurse’s use of an electronic medication cabinet, a computerized device that dispenses a range of drugs. According to documents filed in the case, Ms. Vaught initially tried to withdraw Versed from a cabinet by typing “VE” into its search function without realizing she should have been looking for its generic name, midazolam. When the cabinet did not produce Versed, Ms. Vaught triggered an “override” that unlocked a much larger swath of medications, then searched for “VE” again. This time, the cabinet offered vecuronium.
Ms. Vaught then overlooked or bypassed at least five warnings or pop-ups saying she was withdrawing a paralyzing medication, documents state. She also did not recognize that Versed is a liquid but vecuronium is a powder that must be mixed into liquid, documents state.
Finally, just before injecting the vecuronium, Ms. Vaught stuck a syringe into the vial, which would have required her to “look directly” at a bottle cap that read “Warning: Paralyzing Agent,” the DA’s documents state.
The DA’s office points to this override as central to Ms. Vaught’s reckless homicide charge. Ms. Vaught acknowledges she performed an override on the cabinet. But she and others say overrides are a normal operating procedure used daily at hospitals.
While testifying before the nursing board last year, foreshadowing her defense in the upcoming trial, Ms. Vaught said at the time of Ms. Murphey’s death that Vanderbilt was instructing nurses to use overrides to overcome cabinet delays and constant technical problems caused by an ongoing overhaul of the hospital’s electronic health records system.
Ms. Murphey’s care alone required at least 20 cabinet overrides in just three days, Ms. Vaught said.
“Overriding was something we did as part of our practice every day,” Ms. Vaught said. “You couldn’t get a bag of fluids for a patient without using an override function.”
Overrides are common outside of Vanderbilt too, according to experts following Ms. Vaught’s case.
Michael Cohen, president emeritus of the Institute for Safe Medication Practices, and Lorie Brown, past president of the American Association of Nurse Attorneys, each said it is common for nurses to use an override to obtain medication in a hospital.
Mr. Cohen and Ms. Brown stressed that even with an override it should not have been so easy to access vecuronium.
“This is a medication that you should never, ever, be able to override to,” Ms. Brown said. “It’s probably the most dangerous medication out there.”
Mr. Cohen said that in response to Ms. Vaught’s case, manufacturers of medication cabinets modified the devices’ software to require up to five letters to be typed when searching for drugs during an override, but not all hospitals have implemented this safeguard. Two years after Ms. Vaught’s error, Mr. Cohen’s organization documented a “strikingly similar” incident in which another nurse swapped Versed with another drug, verapamil, while using an override and searching with just the first few letters. That incident did not result in a patient’s death or criminal prosecution, Mr. Cohen said.
Maureen Shawn Kennedy, the editor-in-chief emerita of the American Journal of Nursing, wrote in 2019 that Ms. Vaught’s case was “every nurse’s nightmare.”
In the pandemic, she said, this is truer than ever.
“We know that the more patients a nurse has, the more room there is for errors,” Ms. Kennedy said. “We know that when nurses work longer shifts, there is more room for errors. So I think nurses get very concerned because they know this could be them.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Four years ago, inside the most prestigious hospital in Tennessee, nurse RaDonda Vaught withdrew a vial from an electronic medication cabinet, administered the drug to a patient, and somehow overlooked signs of a terrible and deadly mistake.
The patient was supposed to get Versed, a sedative intended to calm her before being scanned in a large, MRI-like machine. But Ms. Vaught accidentally grabbed vecuronium, a powerful paralyzer, which stopped the patient’s breathing and left her brain-dead before the error was discovered.
Ms. Vaught, 38, admitted her mistake at a Tennessee Board of Nursing hearing last year, saying she became “complacent” in her job and “distracted” by a trainee while operating the computerized medication cabinet. She did not shirk responsibility for the error, but she said the blame was not hers alone.
“I know the reason this patient is no longer here is because of me,” Ms. Vaught said, starting to cry. “There won’t ever be a day that goes by that I don’t think about what I did.”
If Ms. Vaught’s story followed the path of most medical errors, it would have been over hours later, when the Board of Nursing revoked her RN license and almost certainly ended her nursing career. But Ms. Vaught’s case is different: This week she goes on trial in Nashville on criminal charges of reckless homicide and felony abuse of an impaired adult for the killing of Charlene Murphey, a 75-year-old patient who died at Vanderbilt University Medical Center on Dec. 27, 2017.
Prosecutors do not allege in their court filings that Ms. Vaught intended to hurt Ms. Murphey or was impaired by any substance when she made the mistake, so Fatal errors are generally handled by licensing boards and civil courts. And experts say prosecutions like Ms. Vaught’s loom large for a profession terrified of the criminalization of such mistakes — especially because her case hinges on an automated system for dispensing drugs that many nurses use every day.
The Nashville district attorney’s office declined to discuss Ms. Vaught’s trial. Ms. Vaught’s lawyer, Peter Strianse, did not respond to requests for comment. Vanderbilt University Medical Center has repeatedly declined to comment on Ms. Vaught’s trial or its procedures.
Ms. Vaught’s trial will be followed by nurses nationwide, many of whom worry a conviction may set a precedent even as the coronavirus pandemic leaves countless nurses exhausted, demoralized, and likely more prone to error.
Janie Harvey Garner, a St. Louis registered nurse and founder of Show Me Your Stethoscope, a nursing group with more than 600,000 members on Facebook, said the group has closely watched Ms. Vaught’s case for years out of concern for her fate — and their own.
Ms. Garner said most nurses know all too well the pressures that contribute to such an error: long hours, crowded hospitals, imperfect protocols, and the inevitable creep of complacency in a job with daily life-or-death stakes.
Ms. Garner said she once switched powerful medications just as Ms. Vaught did and caught her mistake only in a last-minute triple-check.
“In response to a story like this one, there are two kinds of nurses,” Ms. Garner said. “You have the nurses who assume they would never make a mistake like that, and usually it’s because they don’t realize they could. And the second kind are the ones who know this could happen, any day, no matter how careful they are. This could be me. I could be RaDonda.”
As the trial begins, the Nashville DA’s prosecutors will argue that Ms. Vaught’s error was anything but a common mistake any nurse could make. Prosecutors will say she ignored a cascade of warnings that led to the deadly error.
The case hinges on the nurse’s use of an electronic medication cabinet, a computerized device that dispenses a range of drugs. According to documents filed in the case, Ms. Vaught initially tried to withdraw Versed from a cabinet by typing “VE” into its search function without realizing she should have been looking for its generic name, midazolam. When the cabinet did not produce Versed, Ms. Vaught triggered an “override” that unlocked a much larger swath of medications, then searched for “VE” again. This time, the cabinet offered vecuronium.
Ms. Vaught then overlooked or bypassed at least five warnings or pop-ups saying she was withdrawing a paralyzing medication, documents state. She also did not recognize that Versed is a liquid but vecuronium is a powder that must be mixed into liquid, documents state.
Finally, just before injecting the vecuronium, Ms. Vaught stuck a syringe into the vial, which would have required her to “look directly” at a bottle cap that read “Warning: Paralyzing Agent,” the DA’s documents state.
The DA’s office points to this override as central to Ms. Vaught’s reckless homicide charge. Ms. Vaught acknowledges she performed an override on the cabinet. But she and others say overrides are a normal operating procedure used daily at hospitals.
While testifying before the nursing board last year, foreshadowing her defense in the upcoming trial, Ms. Vaught said at the time of Ms. Murphey’s death that Vanderbilt was instructing nurses to use overrides to overcome cabinet delays and constant technical problems caused by an ongoing overhaul of the hospital’s electronic health records system.
Ms. Murphey’s care alone required at least 20 cabinet overrides in just three days, Ms. Vaught said.
“Overriding was something we did as part of our practice every day,” Ms. Vaught said. “You couldn’t get a bag of fluids for a patient without using an override function.”
Overrides are common outside of Vanderbilt too, according to experts following Ms. Vaught’s case.
Michael Cohen, president emeritus of the Institute for Safe Medication Practices, and Lorie Brown, past president of the American Association of Nurse Attorneys, each said it is common for nurses to use an override to obtain medication in a hospital.
Mr. Cohen and Ms. Brown stressed that even with an override it should not have been so easy to access vecuronium.
“This is a medication that you should never, ever, be able to override to,” Ms. Brown said. “It’s probably the most dangerous medication out there.”
Mr. Cohen said that in response to Ms. Vaught’s case, manufacturers of medication cabinets modified the devices’ software to require up to five letters to be typed when searching for drugs during an override, but not all hospitals have implemented this safeguard. Two years after Ms. Vaught’s error, Mr. Cohen’s organization documented a “strikingly similar” incident in which another nurse swapped Versed with another drug, verapamil, while using an override and searching with just the first few letters. That incident did not result in a patient’s death or criminal prosecution, Mr. Cohen said.
Maureen Shawn Kennedy, the editor-in-chief emerita of the American Journal of Nursing, wrote in 2019 that Ms. Vaught’s case was “every nurse’s nightmare.”
In the pandemic, she said, this is truer than ever.
“We know that the more patients a nurse has, the more room there is for errors,” Ms. Kennedy said. “We know that when nurses work longer shifts, there is more room for errors. So I think nurses get very concerned because they know this could be them.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Four years ago, inside the most prestigious hospital in Tennessee, nurse RaDonda Vaught withdrew a vial from an electronic medication cabinet, administered the drug to a patient, and somehow overlooked signs of a terrible and deadly mistake.
The patient was supposed to get Versed, a sedative intended to calm her before being scanned in a large, MRI-like machine. But Ms. Vaught accidentally grabbed vecuronium, a powerful paralyzer, which stopped the patient’s breathing and left her brain-dead before the error was discovered.
Ms. Vaught, 38, admitted her mistake at a Tennessee Board of Nursing hearing last year, saying she became “complacent” in her job and “distracted” by a trainee while operating the computerized medication cabinet. She did not shirk responsibility for the error, but she said the blame was not hers alone.
“I know the reason this patient is no longer here is because of me,” Ms. Vaught said, starting to cry. “There won’t ever be a day that goes by that I don’t think about what I did.”
If Ms. Vaught’s story followed the path of most medical errors, it would have been over hours later, when the Board of Nursing revoked her RN license and almost certainly ended her nursing career. But Ms. Vaught’s case is different: This week she goes on trial in Nashville on criminal charges of reckless homicide and felony abuse of an impaired adult for the killing of Charlene Murphey, a 75-year-old patient who died at Vanderbilt University Medical Center on Dec. 27, 2017.
Prosecutors do not allege in their court filings that Ms. Vaught intended to hurt Ms. Murphey or was impaired by any substance when she made the mistake, so Fatal errors are generally handled by licensing boards and civil courts. And experts say prosecutions like Ms. Vaught’s loom large for a profession terrified of the criminalization of such mistakes — especially because her case hinges on an automated system for dispensing drugs that many nurses use every day.
The Nashville district attorney’s office declined to discuss Ms. Vaught’s trial. Ms. Vaught’s lawyer, Peter Strianse, did not respond to requests for comment. Vanderbilt University Medical Center has repeatedly declined to comment on Ms. Vaught’s trial or its procedures.
Ms. Vaught’s trial will be followed by nurses nationwide, many of whom worry a conviction may set a precedent even as the coronavirus pandemic leaves countless nurses exhausted, demoralized, and likely more prone to error.
Janie Harvey Garner, a St. Louis registered nurse and founder of Show Me Your Stethoscope, a nursing group with more than 600,000 members on Facebook, said the group has closely watched Ms. Vaught’s case for years out of concern for her fate — and their own.
Ms. Garner said most nurses know all too well the pressures that contribute to such an error: long hours, crowded hospitals, imperfect protocols, and the inevitable creep of complacency in a job with daily life-or-death stakes.
Ms. Garner said she once switched powerful medications just as Ms. Vaught did and caught her mistake only in a last-minute triple-check.
“In response to a story like this one, there are two kinds of nurses,” Ms. Garner said. “You have the nurses who assume they would never make a mistake like that, and usually it’s because they don’t realize they could. And the second kind are the ones who know this could happen, any day, no matter how careful they are. This could be me. I could be RaDonda.”
As the trial begins, the Nashville DA’s prosecutors will argue that Ms. Vaught’s error was anything but a common mistake any nurse could make. Prosecutors will say she ignored a cascade of warnings that led to the deadly error.
The case hinges on the nurse’s use of an electronic medication cabinet, a computerized device that dispenses a range of drugs. According to documents filed in the case, Ms. Vaught initially tried to withdraw Versed from a cabinet by typing “VE” into its search function without realizing she should have been looking for its generic name, midazolam. When the cabinet did not produce Versed, Ms. Vaught triggered an “override” that unlocked a much larger swath of medications, then searched for “VE” again. This time, the cabinet offered vecuronium.
Ms. Vaught then overlooked or bypassed at least five warnings or pop-ups saying she was withdrawing a paralyzing medication, documents state. She also did not recognize that Versed is a liquid but vecuronium is a powder that must be mixed into liquid, documents state.
Finally, just before injecting the vecuronium, Ms. Vaught stuck a syringe into the vial, which would have required her to “look directly” at a bottle cap that read “Warning: Paralyzing Agent,” the DA’s documents state.
The DA’s office points to this override as central to Ms. Vaught’s reckless homicide charge. Ms. Vaught acknowledges she performed an override on the cabinet. But she and others say overrides are a normal operating procedure used daily at hospitals.
While testifying before the nursing board last year, foreshadowing her defense in the upcoming trial, Ms. Vaught said at the time of Ms. Murphey’s death that Vanderbilt was instructing nurses to use overrides to overcome cabinet delays and constant technical problems caused by an ongoing overhaul of the hospital’s electronic health records system.
Ms. Murphey’s care alone required at least 20 cabinet overrides in just three days, Ms. Vaught said.
“Overriding was something we did as part of our practice every day,” Ms. Vaught said. “You couldn’t get a bag of fluids for a patient without using an override function.”
Overrides are common outside of Vanderbilt too, according to experts following Ms. Vaught’s case.
Michael Cohen, president emeritus of the Institute for Safe Medication Practices, and Lorie Brown, past president of the American Association of Nurse Attorneys, each said it is common for nurses to use an override to obtain medication in a hospital.
Mr. Cohen and Ms. Brown stressed that even with an override it should not have been so easy to access vecuronium.
“This is a medication that you should never, ever, be able to override to,” Ms. Brown said. “It’s probably the most dangerous medication out there.”
Mr. Cohen said that in response to Ms. Vaught’s case, manufacturers of medication cabinets modified the devices’ software to require up to five letters to be typed when searching for drugs during an override, but not all hospitals have implemented this safeguard. Two years after Ms. Vaught’s error, Mr. Cohen’s organization documented a “strikingly similar” incident in which another nurse swapped Versed with another drug, verapamil, while using an override and searching with just the first few letters. That incident did not result in a patient’s death or criminal prosecution, Mr. Cohen said.
Maureen Shawn Kennedy, the editor-in-chief emerita of the American Journal of Nursing, wrote in 2019 that Ms. Vaught’s case was “every nurse’s nightmare.”
In the pandemic, she said, this is truer than ever.
“We know that the more patients a nurse has, the more room there is for errors,” Ms. Kennedy said. “We know that when nurses work longer shifts, there is more room for errors. So I think nurses get very concerned because they know this could be them.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Children and COVID: CDC gives perspective on hospitalizations
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.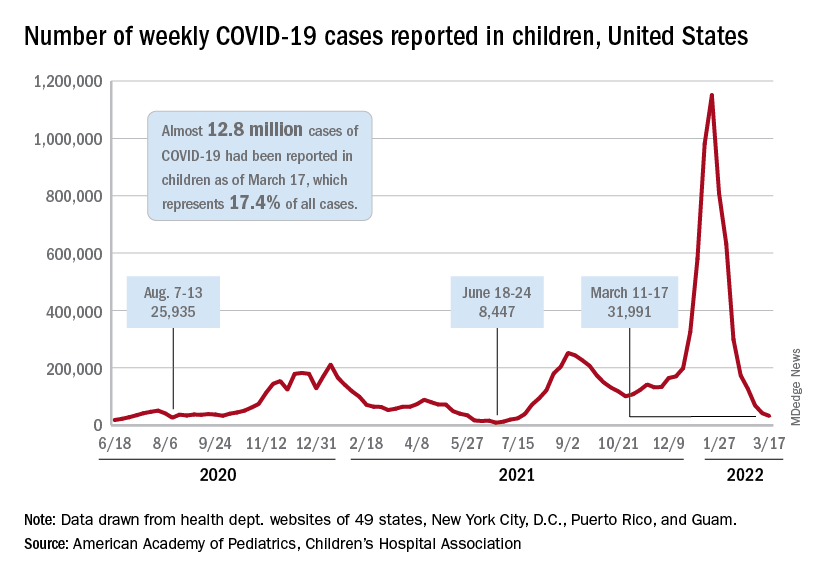
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
New COVID-19 cases in children fell by 23% as the latest weekly count dropped to its lowest level since July of 2021, based on data from the American Academy of Pediatrics and the Children’s Hospital Association.
, when the early stages of the Delta surge led to 23,551 cases, the AAP and CHA said in their weekly COVID report.
The two organizations put the total number of cases at nearly 12.8 million from the start of the pandemic to March 17, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention puts the cumulative number of COVID-19 cases at almost 12.0 million as of March 21, or 17.5% of the nationwide total.
COVID-related hospitalizations also continue to fall, and two new studies from the CDC put children’s experiences during the Omicron surge and the larger pandemic into perspective.
One study showed that hospitalization rates for children aged 4 years and younger during the Omicron surge were five times higher than at the peak of the Delta surge, with the highest rates occurring in infants under 6 months of age. That report was based on the CDC’s COVID-19–Associated Hospitalization Surveillance Network (COVID-NET), which covers 99 counties across 14 states (MMWR. 2022 March 18;71[11]:429-36).
The second study compared child hospitalizations during 1 year of the COVID pandemic (Oct. 1, 2020, to Sept. 30, 2021) with three influenza seasons (2017-2018 through 2019-2020). The pre-Omicron hospitalization rate for those under age 18 years, 48.2 per 100,000 children, was higher than any of the three flu seasons: 33.5 per 100,000 in 2017-2018, 33.8 in 2018-2019, and 41.7 for 2019-2020, the investigators said in a medRxiv preprint.
Most of the increased COVID burden fell on adolescents aged 12-17, they said. The COVID hospitalization rate for that age group was 59.9 per 100,000, versus 12.2-14.1 for influenza, while children aged 5-11 had a COVID-related rate of 25.0 and flu-related rates of 24.3-31.7, and those aged 0-4 had rates of 66.8 for COVID and 70.9-91.5 for the flu, Miranda J. Delahoy of the CDC’s COVID-19 Response Team and associates reported.
Mild COVID-19 infection linked to later type 2 diabetes
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
People who recover from a mild case of COVID-19 appear to have an increased risk for subsequent new-onset type 2 diabetes but not other types of diabetes, new data suggest.
“If confirmed, the results of the present study indicate that diabetes screening in individuals who have recovered from even mild COVID-19 should be recommended,” say Wolfgang Rathmann, MD, of the Leibniz Center for Diabetes Research at Heinrich Heine University, Düsseldorf, Germany, and colleagues.
The findings, from a nationwide primary care database in Germany, were recently published in Diabetologia.
These primary care data align with those from other studies of more seriously ill patients with COVID-19 that found increased rates of type 2 diabetes diagnoses in the subsequent months following illness, they point out.
“COVID-19 infection may lead to diabetes by upregulation of the immune system after remission, which may induce pancreatic beta-cell dysfunction and insulin resistance, or patients may have been at risk for developing diabetes due to having obesity or prediabetes, and the stress COVID-19 put on their bodies sped it up,” said Dr. Rathmann in a press release.
However, because the patients with COVID-19 in the study were only followed for about 3 months, “further follow-up is needed to understand whether type 2 diabetes after mild COVID-19 is just temporary and can be reversed after they have fully recovered or whether it leads to a chronic condition,” he noted.
Increase in type 2 diabetes 3 months after mild COVID-19
The retrospective cohort analysis was performed using data from the Disease Analyzer, a representative panel of 1,171 physician practices in Germany, from March 2020 to January 2021, with follow-up through July 2021.
Individuals with a history of COVID-19 or diabetes and those taking corticosteroids within 30 days after the index dates were excluded.
A total of 35,865 patients with confirmed SARS-CoV-2 infection were propensity score-matched on a one-to-one basis for sex, age, health insurance, and comorbidities with those who had acute respiratory tract infections (controls) but were COVID-19 negative. Median follow-up was 119 days for the COVID-19 group and 161 days for controls.
There was a 28% increased risk of type 2 diabetes for those who had COVID-19 versus controls (15.8 per 1,000 person-years vs. 12.3 per 1,000 person-years, respectively, which was significantly different, and an incidence rate ratio of 1.28).
The incidence of other types of diabetes or unspecified diabetes for the COVID-19 and control groups did not differ significantly (4.3 per 1,000 person-years vs. 3.7 per 1,000 person-years; IRR, 1.17).
Similar findings were seen in sensitivity analyses by glucose-lowering medication prescriptions and by ICD-10 codes.
Although type 2 diabetes is not likely to be a problem for the vast majority of people who have mild COVID-19, the authors recommend that anyone who has recovered from COVID-19 be aware of the warning signs and symptoms such as fatigue, frequent urination, and increased thirst, and seek treatment right away.
CoviDiab registry tracking type 1 and type 2 diabetes
Over the course of the pandemic, there have been conflicting data on whether COVID-19 induces or reveals a propensity for type 1 and type 2 diabetes.
The CoviDiab global registry is tracking this and will include diabetes type for adults and children.
The aim is to have “as many as possible cases of new-onset diabetes for which we can have also a minimum set of clinical data including type of diabetes and A1c,” coprincipal investigator Francesco Rubino, MD, of King’s College London, previously told this news organization.
“By looking at this information we can infer whether a role of COVID-19 in triggering diabetes is clinically plausible – or not – and what type of diabetes is most frequently associated with COVID-19.”
Rubino said that the CoviDiab team is approaching the data with the assumption that, at least in adults diagnosed with type 2 diabetes, the explanation might be that the person already had undiagnosed diabetes or the hyperglycemia may be stress-induced and temporary.
The German Diabetes Center is funded by the German Federal Ministry of Health and the Ministry of Culture and Science of the State of North Rhine-Westphalia. Dr. Rathmann has reported receiving consulting fees for attending educational sessions or advisory boards for AstraZeneca, Boehringer Ingelheim, and Novo Nordisk and institutional research grants from Novo Nordisk outside of the topic of the current work.
A version of this article first appeared on Medscape.com.
FROM DIABETOLOGIA
U.S. health officials tracking COVID-19 increase in U.K.
according to NPR.
Daily cases counts have increased 38% in the past week, according to the latest data from the U.K. Health Security Agency. Hospitalizations are up about 25% as well.
“Over the last year or so, what happens in the U.K. usually happens here a few weeks later,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, told NPR.
“And right now, the U.K. is seeing somewhat of a rebound in cases,” he said.
Health officials in the United Kingdom have noted the latest increase is likely due to the contagious BA.2 Omicron subvariant, the recent loosening of coronavirus restrictions, and waning immunity from vaccinations and infections.
“All three of those factors we have here in the United States,” Dr. Fauci said. “So I would not be surprised if, in the next few weeks, we see either a plateauing … of cases or even [the curve] rebounds and slightly goes up.”
Right now, COVID-19 cases in the United Stastes have dropped to their lowest levels since July 2021, according to the latest Centers for Disease Control and Prevention data, with fewer than 30,000 daily cases. At the same time, the rate of decline in cases has slowed significantly and is beginning to plateau.
Public health experts are also pointing to wastewater surveillance data that shows an uptick in viral activity across the country. The CDC’s wastewater dashboard indicates that about 35% of sites that monitor wastewater are seeing an increase, with consistent growth in Florida, Rhode Island, and West Virginia.
“The power of wastewater surveillance is that it’s an early warning system,” Amy Kirby, the program lead for the CDC’s National Wastewater Surveillance System, told NPR.
“We are seeing evidence of increases in some communities across the country,” she said. “What looked like noise at the beginning of the week is starting to look like a true signal here at the end of the week.”
The wastewater system doesn’t distinguish between Omicron and subvariants such as BA.2. However, other CDC data has found an increase in BA.2 cases in the United States, making up about a quarter of new COVID-19 cases.
The BA.2 variant has roughly doubled each week for the last month, which means it could become the dominant coronavirus strain in the United States in coming weeks, according to USA Today. Cases appear to be spreading more quickly in the Northeast and West, making up about 39% of cases in New York and New Jersey last week.
BA.2 also accounts for nearly 39% of cases across the Northeast, including Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island and Vermont, USA Today reported. In the West, which includes Arizona, California and Nevada, the subvariant makes up about 28% of new cases. In the upper West, which includes Alaska, Oregon and Washington, about 26% of cases are BA.2.
The good news is that BA.2 “doesn’t seem to evade our vaccines or immunity any more than the prior Omicron [variant]. And it doesn’t seem to lead to any more increased severity of disease,” Rochelle Walensky, MD, the CDC director, told NPR’s Morning Edition on March 18.
The effects of BA.2 will likely depend on the immunity profile in the United States, including how long it’s been since someone was vaccinated, boosted, or recovered from an infection, she said.
Health officials are watching other countries with BA.2 increases, such as Germany, Italy, and the Netherlands. Many European countries have been reporting an uptick but not implementing major restrictions or shutdowns, USA Today reported.
The BA.2 variant likely won’t lead to a major surge in severe disease or strict COVID-19 measures, Dr. Fauci told NPR, but some coronavirus protocols may need to be implemented again if cases grow dramatically.
“We must be ready to pivot and, if necessary, to go back to stricter mitigation with regard to masks,” he said.
A version of this article first appeared on WebMD.com.
according to NPR.
Daily cases counts have increased 38% in the past week, according to the latest data from the U.K. Health Security Agency. Hospitalizations are up about 25% as well.
“Over the last year or so, what happens in the U.K. usually happens here a few weeks later,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, told NPR.
“And right now, the U.K. is seeing somewhat of a rebound in cases,” he said.
Health officials in the United Kingdom have noted the latest increase is likely due to the contagious BA.2 Omicron subvariant, the recent loosening of coronavirus restrictions, and waning immunity from vaccinations and infections.
“All three of those factors we have here in the United States,” Dr. Fauci said. “So I would not be surprised if, in the next few weeks, we see either a plateauing … of cases or even [the curve] rebounds and slightly goes up.”
Right now, COVID-19 cases in the United Stastes have dropped to their lowest levels since July 2021, according to the latest Centers for Disease Control and Prevention data, with fewer than 30,000 daily cases. At the same time, the rate of decline in cases has slowed significantly and is beginning to plateau.
Public health experts are also pointing to wastewater surveillance data that shows an uptick in viral activity across the country. The CDC’s wastewater dashboard indicates that about 35% of sites that monitor wastewater are seeing an increase, with consistent growth in Florida, Rhode Island, and West Virginia.
“The power of wastewater surveillance is that it’s an early warning system,” Amy Kirby, the program lead for the CDC’s National Wastewater Surveillance System, told NPR.
“We are seeing evidence of increases in some communities across the country,” she said. “What looked like noise at the beginning of the week is starting to look like a true signal here at the end of the week.”
The wastewater system doesn’t distinguish between Omicron and subvariants such as BA.2. However, other CDC data has found an increase in BA.2 cases in the United States, making up about a quarter of new COVID-19 cases.
The BA.2 variant has roughly doubled each week for the last month, which means it could become the dominant coronavirus strain in the United States in coming weeks, according to USA Today. Cases appear to be spreading more quickly in the Northeast and West, making up about 39% of cases in New York and New Jersey last week.
BA.2 also accounts for nearly 39% of cases across the Northeast, including Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island and Vermont, USA Today reported. In the West, which includes Arizona, California and Nevada, the subvariant makes up about 28% of new cases. In the upper West, which includes Alaska, Oregon and Washington, about 26% of cases are BA.2.
The good news is that BA.2 “doesn’t seem to evade our vaccines or immunity any more than the prior Omicron [variant]. And it doesn’t seem to lead to any more increased severity of disease,” Rochelle Walensky, MD, the CDC director, told NPR’s Morning Edition on March 18.
The effects of BA.2 will likely depend on the immunity profile in the United States, including how long it’s been since someone was vaccinated, boosted, or recovered from an infection, she said.
Health officials are watching other countries with BA.2 increases, such as Germany, Italy, and the Netherlands. Many European countries have been reporting an uptick but not implementing major restrictions or shutdowns, USA Today reported.
The BA.2 variant likely won’t lead to a major surge in severe disease or strict COVID-19 measures, Dr. Fauci told NPR, but some coronavirus protocols may need to be implemented again if cases grow dramatically.
“We must be ready to pivot and, if necessary, to go back to stricter mitigation with regard to masks,” he said.
A version of this article first appeared on WebMD.com.
according to NPR.
Daily cases counts have increased 38% in the past week, according to the latest data from the U.K. Health Security Agency. Hospitalizations are up about 25% as well.
“Over the last year or so, what happens in the U.K. usually happens here a few weeks later,” Anthony S. Fauci, MD, director of the National Institute of Allergy and Infectious Diseases, told NPR.
“And right now, the U.K. is seeing somewhat of a rebound in cases,” he said.
Health officials in the United Kingdom have noted the latest increase is likely due to the contagious BA.2 Omicron subvariant, the recent loosening of coronavirus restrictions, and waning immunity from vaccinations and infections.
“All three of those factors we have here in the United States,” Dr. Fauci said. “So I would not be surprised if, in the next few weeks, we see either a plateauing … of cases or even [the curve] rebounds and slightly goes up.”
Right now, COVID-19 cases in the United Stastes have dropped to their lowest levels since July 2021, according to the latest Centers for Disease Control and Prevention data, with fewer than 30,000 daily cases. At the same time, the rate of decline in cases has slowed significantly and is beginning to plateau.
Public health experts are also pointing to wastewater surveillance data that shows an uptick in viral activity across the country. The CDC’s wastewater dashboard indicates that about 35% of sites that monitor wastewater are seeing an increase, with consistent growth in Florida, Rhode Island, and West Virginia.
“The power of wastewater surveillance is that it’s an early warning system,” Amy Kirby, the program lead for the CDC’s National Wastewater Surveillance System, told NPR.
“We are seeing evidence of increases in some communities across the country,” she said. “What looked like noise at the beginning of the week is starting to look like a true signal here at the end of the week.”
The wastewater system doesn’t distinguish between Omicron and subvariants such as BA.2. However, other CDC data has found an increase in BA.2 cases in the United States, making up about a quarter of new COVID-19 cases.
The BA.2 variant has roughly doubled each week for the last month, which means it could become the dominant coronavirus strain in the United States in coming weeks, according to USA Today. Cases appear to be spreading more quickly in the Northeast and West, making up about 39% of cases in New York and New Jersey last week.
BA.2 also accounts for nearly 39% of cases across the Northeast, including Connecticut, Maine, Massachusetts, New Hampshire, Rhode Island and Vermont, USA Today reported. In the West, which includes Arizona, California and Nevada, the subvariant makes up about 28% of new cases. In the upper West, which includes Alaska, Oregon and Washington, about 26% of cases are BA.2.
The good news is that BA.2 “doesn’t seem to evade our vaccines or immunity any more than the prior Omicron [variant]. And it doesn’t seem to lead to any more increased severity of disease,” Rochelle Walensky, MD, the CDC director, told NPR’s Morning Edition on March 18.
The effects of BA.2 will likely depend on the immunity profile in the United States, including how long it’s been since someone was vaccinated, boosted, or recovered from an infection, she said.
Health officials are watching other countries with BA.2 increases, such as Germany, Italy, and the Netherlands. Many European countries have been reporting an uptick but not implementing major restrictions or shutdowns, USA Today reported.
The BA.2 variant likely won’t lead to a major surge in severe disease or strict COVID-19 measures, Dr. Fauci told NPR, but some coronavirus protocols may need to be implemented again if cases grow dramatically.
“We must be ready to pivot and, if necessary, to go back to stricter mitigation with regard to masks,” he said.
A version of this article first appeared on WebMD.com.
Empagliflozin scores topline win in EMPA-KIDNEY trial
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.

In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.
In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
Researchers running the EMPA-KIDNEY trial that’s been testing the safety and efficacy of the SGLT2 inhibitor empagliflozin (Jardiance) in about 6,600 patients with chronic kidney disease (CKD) announced on March 16 that they had stopped the trial early because of positive efficacy that met the study’s prespecified threshold for early termination.
EMPA-KIDNEY is the third major trial of an agent from the sodium-glucose cotransport 2 (SGLT2) inhibitor class tested in patients with CKD to be stopped early because of positive results that met a prespecified termination rule.
In 2020, the DAPA-CKD trial of dapagliflozin (Farxiga) stopped early, after a median follow-up of 2.4 years, because of positive efficacy results. In 2019, the same thing happened in the CREDENCE trial of canagliflozin (Invokana), with the unexpected halt coming after a median follow-up of 2.62 years.
The announcement about EMPA-KIDNEY did not include information on median follow-up, but enrollment into the trial ran from May 2019 to April 2021, which means that the longest that enrolled patients could have been in the study was about 2.85 years.
The primary efficacy endpoint in EMPA-KIDNEY was a composite of a sustained decline in estimated glomerular filtration rate (eGFR) to less than 10 mL/min/1.73 m2, renal death, a sustained decline of at least 40% in eGFR from baseline, or cardiovascular death. The announcement of the trial’s early termination provided no details on the efficacy results.
EMPA-KIDNEY enrolled a wider range of patients
EMPA-KIDNEY expands the scope of types of patients with CKD now shown to benefit from treatment with an SGLT2 inhibitor. CREDENCE tested canagliflozin only in patients with type 2 diabetes and diabetic nephropathy, and in DAPA-CKD, two-thirds of enrolled patients had type 2 diabetes, and all had CKD. In EMPA-KIDNEY, 46% of the 6,609 enrolled patients had diabetes (including a very small number with type 1 diabetes).
Another departure from prior studies of an SGLT2 inhibitor for patients selected primarily for having CKD was that in EMPA-KIDNEY, 20% of patients did not have albuminuria, and for 34%, eGFR at entry was less than 30 mL/min/1.73 m2, with all enrolled patients required to have an eGFR at entry of greater than or equal to 20 mL/min/1.73 m2. Average eGFR in EMPA-KIDNEY was about 38 mL/min/1.73 m2. To be included in the trial, patients were not required to have albuminuria, except those whose eGFR was greater than or equal to 45 mL/min/1.73 m2.
In DAPA-CKD, the minimum eGFR at entry had to be greater than or equal to 25 mL/min/1.73 m2, and roughly 14% of enrolled patients had an eGFR of less than 30 mL/min/1.73 m2. The average eGFR in DAPA-CKD was about 43 mL/min/1.73 m2. In addition, all patients had at least microalbuminuria, with a minimum urinary albumin-to-creatinine ratio of 200. In CREDENCE, the minimum eGFR for enrollment was 30 mL/min/1.73 m2, and the average eGFR was about 56 mL/min/1.73 m2. All patients in CREDENCE had to have macroalbuminuria, with a urinary albumin-to-creatinine ratio of more than 300.
According to the researchers who designed EMPA-KIDNEY, the trial enrollment criteria aimed to include adults with CKD “who are frequently seen in practice but were under-represented in previous SGLT2 inhibitor trials.”
Indications for empagliflozin are expanding
The success of empagliflozin in EMPA-KIDNEY follows its positive results in both the EMPEROR-Reduced and EMPEROR-Preserved trials, which collectively proved the efficacy of the agent for patients with heart failure regardless of their left ventricular ejection fraction and regardless of whether they also had diabetes.
These results led the U.S. Food and Drug Administration to recently expand the labeled indication for empagliflozin to all patients with heart failure. Empagliflozin also has labeled indications for glycemic control in patients with type 2 diabetes and to reduce the risk of cardiovascular death in adults with type 2 diabetes and established cardiovascular disease.
As of today, empagliflozin has no labeled indication for treating patients with CKD. Dapagliflozin received that indication in April 2021, and canagliflozin received an indication for treating patients with type 2 diabetes, diabetic nephropathy, and albuminuria in September 2019.
EMPA-KIDNEY is sponsored by Boehringer Ingelheim and Lilly, the two companies that jointly market empagliflozin (Jardiance).
A version of this article first appeared on Medscape.com.
New ACC guidance on cardiovascular consequences of COVID-19
The American College of Cardiology has issued an expert consensus clinical guidance document for the evaluation and management of adults with key cardiovascular consequences of COVID-19.
The document makes recommendations on how to evaluate and manage COVID-associated myocarditis and long COVID and gives advice on resumption of exercise following COVID-19 infection.
The clinical guidance was published online March 16 in the Journal of the American College of Cardiology.
“The best means to diagnose and treat myocarditis and long COVID following SARS-CoV-2 infection continues to evolve,” said Ty Gluckman, MD, MHA, cochair of the expert consensus decision pathway. “This document attempts to provide key recommendations for how to evaluate and manage adults with these conditions, including guidance for safe return to play for both competitive and noncompetitive athletes.”
The authors of the guidance note that COVID-19 can be associated with various abnormalities in cardiac testing and a wide range of cardiovascular complications. For some patients, cardiac symptoms such as chest pain, shortness of breath, fatigue, and palpitations persist, lasting months after the initial illness, and evidence of myocardial injury has also been observed in both symptomatic and asymptomatic individuals, as well as after receipt of the COVID-19 mRNA vaccine.
“For clinicians treating these individuals, a growing number of questions exist related to evaluation and management of these conditions, as well as safe resumption of physical activity,” they say. This report is intended to provide practical guidance on these issues.
Myocarditis
The report states that myocarditis has been recognized as a rare but serious complication of SARS-CoV-2 infection as well as COVID-19 mRNA vaccination.
It defines myocarditis as: 1.cardiac symptoms such as chest pain, dyspnea, palpitations, or syncope; 2. elevated cardiac troponin; and 3. abnormal electrocardiographic, echocardiographic, cardiac MRI, and/or histopathologic findings on biopsy.
The document makes the following recommendations in regard to COVID-related myocarditis:
When there is increased suspicion for cardiac involvement with COVID-19, initial testing should consist of an ECG, measurement of cardiac troponin, and an echocardiogram. Cardiology consultation is recommended for those with a rising cardiac troponin and/or echocardiographic abnormalities. Cardiac MRI is recommended in hemodynamically stable patients with suspected myocarditis.
Hospitalization is recommended for patients with definite myocarditis, ideally at an advanced heart failure center. Patients with fulminant myocarditis should be managed at centers with an expertise in advanced heart failure, mechanical circulatory support, and other advanced therapies.
Patients with myocarditis and COVID-19 pneumonia (with an ongoing need for supplemental oxygen) should be treated with corticosteroids. For patients with suspected pericardial involvement, treatment with NSAIDs, colchicine, and/or prednisone is reasonable. Intravenous corticosteroids may be considered in those with suspected or confirmed COVID-19 myocarditis with hemodynamic compromise or MIS-A (multisystem inflammatory syndrome in adults). Empiric use of corticosteroids may also be considered in those with biopsy evidence of severe myocardial infiltrates or fulminant myocarditis, balanced against infection risk.
As appropriate, guideline-directed medical therapy for heart failure should be initiated and continued after discharge.
The document notes that myocarditis following COVID-19 mRNA vaccination is rare, with highest rates seen in young males after the second vaccine dose. As of May 22, 2021, the U.S. Vaccine Adverse Event Reporting System noted rates of 40.6 cases per million after the second vaccine dose among male individuals aged 12-29 years and 2.4 cases per million among male individuals aged 30 and older. Corresponding rates in female individuals were 4.2 and 1 cases per million, respectively.
But the report says that COVID-19 vaccination is associated with “a very favorable benefit-to-risk ratio” for all age and sex groups evaluated thus far.
In general, vaccine-associated myocarditis should be diagnosed, categorized, and treated in a manner analogous to myocarditis following SARS-CoV-2 infection, the guidance advises.
Long COVID
The document refers to long COVID as postacute sequelae of SARS-CoV-2 infection (PASC), and reports that this condition is experienced by up to 10%-30% of infected individuals. It is defined by a constellation of new, returning, or persistent health problems experienced by individuals 4 or more weeks after COVID-19 infection.
Although individuals with this condition may experience wide-ranging symptoms, the symptoms that draw increased attention to the cardiovascular system include tachycardia, exercise intolerance, chest pain, and shortness of breath.
Nicole Bhave, MD, cochair of the expert consensus decision pathway, says: “There appears to be a ‘downward spiral’ for long-COVID patients. Fatigue and decreased exercise capacity lead to diminished activity and bed rest, in turn leading to worsening symptoms and decreased quality of life.” She adds that “the writing committee recommends a basic cardiopulmonary evaluation performed up front to determine if further specialty care and formalized medical therapy is needed for these patients.”
The authors propose two terms to better understand potential etiologies for those with cardiovascular symptoms:
PASC-CVD, or PASC-cardiovascular disease, refers to a broad group of cardiovascular conditions (including myocarditis) that manifest at least 4 weeks after COVID-19 infection.
PASC-CVS, or PASC-cardiovascular syndrome, includes a wide range of cardiovascular symptoms without objective evidence of cardiovascular disease following standard diagnostic testing.
The document makes the following recommendations for the management of PASC-CVD and PASC-CVS.
For patients with cardiovascular symptoms and suspected PASC, the authors suggest that a reasonable initial testing approach includes basic laboratory testing, including cardiac troponin, an ECG, an echocardiogram, an ambulatory rhythm monitor, chest imaging, and/or pulmonary function tests.
Cardiology consultation is recommended for patients with PASC who have abnormal cardiac test results, known cardiovascular disease with new or worsening symptoms, documented cardiac complications during SARS-CoV-2 infection, and/or persistent cardiopulmonary symptoms that are not otherwise explained.
Recumbent or semirecumbent exercise (for example, rowing, swimming, or cycling) is recommended initially for PASC-CVS patients with tachycardia, exercise/orthostatic intolerance, and/or deconditioning, with transition to upright exercise as orthostatic intolerance improves. Exercise duration should also be short (5-10 minutes/day) initially, with gradual increases as functional capacity improves.
Salt and fluid loading represent nonpharmacologic interventions that may provide symptomatic relief for patients with tachycardia, palpitations, and/or orthostatic hypotension.
Beta-blockers, nondihydropyridine calcium-channel blockers, ivabradine, fludrocortisone, and midodrine may be used empirically as well.
Return to play for athletes
The authors note that concerns about possible cardiac injury after COVID-19 fueled early apprehension regarding the safety of competitive sports for athletes recovering from the infection.
But they say that subsequent data from large registries have demonstrated an overall low prevalence of clinical myocarditis, without a rise in the rate of adverse cardiac events. Based on this, updated guidance is provided with a practical, evidence-based framework to guide resumption of athletics and intense exercise training.
They make the following recommendations:
- For athletes recovering from COVID-19 with ongoing cardiopulmonary symptoms (chest pain, shortness of breath, palpitations, lightheadedness) or those requiring hospitalization with increased suspicion for cardiac involvement, further evaluation with triad testing – an ECG, measurement of cardiac troponin, and an echocardiogram – should be performed.
- For those with abnormal test results, further evaluation with cardiac MRI should be considered. Individuals diagnosed with clinical myocarditis should abstain from exercise for 3-6 months.
- Cardiac testing is not recommended for asymptomatic individuals following COVID-19 infection. Individuals should abstain from training for 3 days to ensure that symptoms do not develop.
- For those with mild or moderate noncardiopulmonary symptoms (fever, lethargy, muscle aches), training may resume after symptom resolution.
- For those with remote infection (≥3 months) without ongoing cardiopulmonary symptoms, a gradual increase in exercise is recommended without the need for cardiac testing.
Based on the low prevalence of myocarditis observed in competitive athletes with COVID-19, the authors note that these recommendations can be reasonably applied to high-school athletes (aged 14 and older) along with adult recreational exercise enthusiasts.
Future study is needed, however, to better understand how long cardiac abnormalities persist following COVID-19 infection and the role of exercise training in long COVID.
The authors conclude that the current guidance is intended to help clinicians understand not only when testing may be warranted, but also when it is not.
“Given that it reflects the current state of knowledge through early 2022, it is anticipated that recommendations will change over time as our understanding evolves,” they say.
The 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19: Myocarditis, Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), and Return to Play will be discussed in a session at the American College of Cardiology’s annual scientific session meeting in Washington in April.
A version of this article first appeared on Medscape.com.
The American College of Cardiology has issued an expert consensus clinical guidance document for the evaluation and management of adults with key cardiovascular consequences of COVID-19.
The document makes recommendations on how to evaluate and manage COVID-associated myocarditis and long COVID and gives advice on resumption of exercise following COVID-19 infection.
The clinical guidance was published online March 16 in the Journal of the American College of Cardiology.
“The best means to diagnose and treat myocarditis and long COVID following SARS-CoV-2 infection continues to evolve,” said Ty Gluckman, MD, MHA, cochair of the expert consensus decision pathway. “This document attempts to provide key recommendations for how to evaluate and manage adults with these conditions, including guidance for safe return to play for both competitive and noncompetitive athletes.”
The authors of the guidance note that COVID-19 can be associated with various abnormalities in cardiac testing and a wide range of cardiovascular complications. For some patients, cardiac symptoms such as chest pain, shortness of breath, fatigue, and palpitations persist, lasting months after the initial illness, and evidence of myocardial injury has also been observed in both symptomatic and asymptomatic individuals, as well as after receipt of the COVID-19 mRNA vaccine.
“For clinicians treating these individuals, a growing number of questions exist related to evaluation and management of these conditions, as well as safe resumption of physical activity,” they say. This report is intended to provide practical guidance on these issues.
Myocarditis
The report states that myocarditis has been recognized as a rare but serious complication of SARS-CoV-2 infection as well as COVID-19 mRNA vaccination.
It defines myocarditis as: 1.cardiac symptoms such as chest pain, dyspnea, palpitations, or syncope; 2. elevated cardiac troponin; and 3. abnormal electrocardiographic, echocardiographic, cardiac MRI, and/or histopathologic findings on biopsy.
The document makes the following recommendations in regard to COVID-related myocarditis:
When there is increased suspicion for cardiac involvement with COVID-19, initial testing should consist of an ECG, measurement of cardiac troponin, and an echocardiogram. Cardiology consultation is recommended for those with a rising cardiac troponin and/or echocardiographic abnormalities. Cardiac MRI is recommended in hemodynamically stable patients with suspected myocarditis.
Hospitalization is recommended for patients with definite myocarditis, ideally at an advanced heart failure center. Patients with fulminant myocarditis should be managed at centers with an expertise in advanced heart failure, mechanical circulatory support, and other advanced therapies.
Patients with myocarditis and COVID-19 pneumonia (with an ongoing need for supplemental oxygen) should be treated with corticosteroids. For patients with suspected pericardial involvement, treatment with NSAIDs, colchicine, and/or prednisone is reasonable. Intravenous corticosteroids may be considered in those with suspected or confirmed COVID-19 myocarditis with hemodynamic compromise or MIS-A (multisystem inflammatory syndrome in adults). Empiric use of corticosteroids may also be considered in those with biopsy evidence of severe myocardial infiltrates or fulminant myocarditis, balanced against infection risk.
As appropriate, guideline-directed medical therapy for heart failure should be initiated and continued after discharge.
The document notes that myocarditis following COVID-19 mRNA vaccination is rare, with highest rates seen in young males after the second vaccine dose. As of May 22, 2021, the U.S. Vaccine Adverse Event Reporting System noted rates of 40.6 cases per million after the second vaccine dose among male individuals aged 12-29 years and 2.4 cases per million among male individuals aged 30 and older. Corresponding rates in female individuals were 4.2 and 1 cases per million, respectively.
But the report says that COVID-19 vaccination is associated with “a very favorable benefit-to-risk ratio” for all age and sex groups evaluated thus far.
In general, vaccine-associated myocarditis should be diagnosed, categorized, and treated in a manner analogous to myocarditis following SARS-CoV-2 infection, the guidance advises.
Long COVID
The document refers to long COVID as postacute sequelae of SARS-CoV-2 infection (PASC), and reports that this condition is experienced by up to 10%-30% of infected individuals. It is defined by a constellation of new, returning, or persistent health problems experienced by individuals 4 or more weeks after COVID-19 infection.
Although individuals with this condition may experience wide-ranging symptoms, the symptoms that draw increased attention to the cardiovascular system include tachycardia, exercise intolerance, chest pain, and shortness of breath.
Nicole Bhave, MD, cochair of the expert consensus decision pathway, says: “There appears to be a ‘downward spiral’ for long-COVID patients. Fatigue and decreased exercise capacity lead to diminished activity and bed rest, in turn leading to worsening symptoms and decreased quality of life.” She adds that “the writing committee recommends a basic cardiopulmonary evaluation performed up front to determine if further specialty care and formalized medical therapy is needed for these patients.”
The authors propose two terms to better understand potential etiologies for those with cardiovascular symptoms:
PASC-CVD, or PASC-cardiovascular disease, refers to a broad group of cardiovascular conditions (including myocarditis) that manifest at least 4 weeks after COVID-19 infection.
PASC-CVS, or PASC-cardiovascular syndrome, includes a wide range of cardiovascular symptoms without objective evidence of cardiovascular disease following standard diagnostic testing.
The document makes the following recommendations for the management of PASC-CVD and PASC-CVS.
For patients with cardiovascular symptoms and suspected PASC, the authors suggest that a reasonable initial testing approach includes basic laboratory testing, including cardiac troponin, an ECG, an echocardiogram, an ambulatory rhythm monitor, chest imaging, and/or pulmonary function tests.
Cardiology consultation is recommended for patients with PASC who have abnormal cardiac test results, known cardiovascular disease with new or worsening symptoms, documented cardiac complications during SARS-CoV-2 infection, and/or persistent cardiopulmonary symptoms that are not otherwise explained.
Recumbent or semirecumbent exercise (for example, rowing, swimming, or cycling) is recommended initially for PASC-CVS patients with tachycardia, exercise/orthostatic intolerance, and/or deconditioning, with transition to upright exercise as orthostatic intolerance improves. Exercise duration should also be short (5-10 minutes/day) initially, with gradual increases as functional capacity improves.
Salt and fluid loading represent nonpharmacologic interventions that may provide symptomatic relief for patients with tachycardia, palpitations, and/or orthostatic hypotension.
Beta-blockers, nondihydropyridine calcium-channel blockers, ivabradine, fludrocortisone, and midodrine may be used empirically as well.
Return to play for athletes
The authors note that concerns about possible cardiac injury after COVID-19 fueled early apprehension regarding the safety of competitive sports for athletes recovering from the infection.
But they say that subsequent data from large registries have demonstrated an overall low prevalence of clinical myocarditis, without a rise in the rate of adverse cardiac events. Based on this, updated guidance is provided with a practical, evidence-based framework to guide resumption of athletics and intense exercise training.
They make the following recommendations:
- For athletes recovering from COVID-19 with ongoing cardiopulmonary symptoms (chest pain, shortness of breath, palpitations, lightheadedness) or those requiring hospitalization with increased suspicion for cardiac involvement, further evaluation with triad testing – an ECG, measurement of cardiac troponin, and an echocardiogram – should be performed.
- For those with abnormal test results, further evaluation with cardiac MRI should be considered. Individuals diagnosed with clinical myocarditis should abstain from exercise for 3-6 months.
- Cardiac testing is not recommended for asymptomatic individuals following COVID-19 infection. Individuals should abstain from training for 3 days to ensure that symptoms do not develop.
- For those with mild or moderate noncardiopulmonary symptoms (fever, lethargy, muscle aches), training may resume after symptom resolution.
- For those with remote infection (≥3 months) without ongoing cardiopulmonary symptoms, a gradual increase in exercise is recommended without the need for cardiac testing.
Based on the low prevalence of myocarditis observed in competitive athletes with COVID-19, the authors note that these recommendations can be reasonably applied to high-school athletes (aged 14 and older) along with adult recreational exercise enthusiasts.
Future study is needed, however, to better understand how long cardiac abnormalities persist following COVID-19 infection and the role of exercise training in long COVID.
The authors conclude that the current guidance is intended to help clinicians understand not only when testing may be warranted, but also when it is not.
“Given that it reflects the current state of knowledge through early 2022, it is anticipated that recommendations will change over time as our understanding evolves,” they say.
The 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19: Myocarditis, Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), and Return to Play will be discussed in a session at the American College of Cardiology’s annual scientific session meeting in Washington in April.
A version of this article first appeared on Medscape.com.
The American College of Cardiology has issued an expert consensus clinical guidance document for the evaluation and management of adults with key cardiovascular consequences of COVID-19.
The document makes recommendations on how to evaluate and manage COVID-associated myocarditis and long COVID and gives advice on resumption of exercise following COVID-19 infection.
The clinical guidance was published online March 16 in the Journal of the American College of Cardiology.
“The best means to diagnose and treat myocarditis and long COVID following SARS-CoV-2 infection continues to evolve,” said Ty Gluckman, MD, MHA, cochair of the expert consensus decision pathway. “This document attempts to provide key recommendations for how to evaluate and manage adults with these conditions, including guidance for safe return to play for both competitive and noncompetitive athletes.”
The authors of the guidance note that COVID-19 can be associated with various abnormalities in cardiac testing and a wide range of cardiovascular complications. For some patients, cardiac symptoms such as chest pain, shortness of breath, fatigue, and palpitations persist, lasting months after the initial illness, and evidence of myocardial injury has also been observed in both symptomatic and asymptomatic individuals, as well as after receipt of the COVID-19 mRNA vaccine.
“For clinicians treating these individuals, a growing number of questions exist related to evaluation and management of these conditions, as well as safe resumption of physical activity,” they say. This report is intended to provide practical guidance on these issues.
Myocarditis
The report states that myocarditis has been recognized as a rare but serious complication of SARS-CoV-2 infection as well as COVID-19 mRNA vaccination.
It defines myocarditis as: 1.cardiac symptoms such as chest pain, dyspnea, palpitations, or syncope; 2. elevated cardiac troponin; and 3. abnormal electrocardiographic, echocardiographic, cardiac MRI, and/or histopathologic findings on biopsy.
The document makes the following recommendations in regard to COVID-related myocarditis:
When there is increased suspicion for cardiac involvement with COVID-19, initial testing should consist of an ECG, measurement of cardiac troponin, and an echocardiogram. Cardiology consultation is recommended for those with a rising cardiac troponin and/or echocardiographic abnormalities. Cardiac MRI is recommended in hemodynamically stable patients with suspected myocarditis.
Hospitalization is recommended for patients with definite myocarditis, ideally at an advanced heart failure center. Patients with fulminant myocarditis should be managed at centers with an expertise in advanced heart failure, mechanical circulatory support, and other advanced therapies.
Patients with myocarditis and COVID-19 pneumonia (with an ongoing need for supplemental oxygen) should be treated with corticosteroids. For patients with suspected pericardial involvement, treatment with NSAIDs, colchicine, and/or prednisone is reasonable. Intravenous corticosteroids may be considered in those with suspected or confirmed COVID-19 myocarditis with hemodynamic compromise or MIS-A (multisystem inflammatory syndrome in adults). Empiric use of corticosteroids may also be considered in those with biopsy evidence of severe myocardial infiltrates or fulminant myocarditis, balanced against infection risk.
As appropriate, guideline-directed medical therapy for heart failure should be initiated and continued after discharge.
The document notes that myocarditis following COVID-19 mRNA vaccination is rare, with highest rates seen in young males after the second vaccine dose. As of May 22, 2021, the U.S. Vaccine Adverse Event Reporting System noted rates of 40.6 cases per million after the second vaccine dose among male individuals aged 12-29 years and 2.4 cases per million among male individuals aged 30 and older. Corresponding rates in female individuals were 4.2 and 1 cases per million, respectively.
But the report says that COVID-19 vaccination is associated with “a very favorable benefit-to-risk ratio” for all age and sex groups evaluated thus far.
In general, vaccine-associated myocarditis should be diagnosed, categorized, and treated in a manner analogous to myocarditis following SARS-CoV-2 infection, the guidance advises.
Long COVID
The document refers to long COVID as postacute sequelae of SARS-CoV-2 infection (PASC), and reports that this condition is experienced by up to 10%-30% of infected individuals. It is defined by a constellation of new, returning, or persistent health problems experienced by individuals 4 or more weeks after COVID-19 infection.
Although individuals with this condition may experience wide-ranging symptoms, the symptoms that draw increased attention to the cardiovascular system include tachycardia, exercise intolerance, chest pain, and shortness of breath.
Nicole Bhave, MD, cochair of the expert consensus decision pathway, says: “There appears to be a ‘downward spiral’ for long-COVID patients. Fatigue and decreased exercise capacity lead to diminished activity and bed rest, in turn leading to worsening symptoms and decreased quality of life.” She adds that “the writing committee recommends a basic cardiopulmonary evaluation performed up front to determine if further specialty care and formalized medical therapy is needed for these patients.”
The authors propose two terms to better understand potential etiologies for those with cardiovascular symptoms:
PASC-CVD, or PASC-cardiovascular disease, refers to a broad group of cardiovascular conditions (including myocarditis) that manifest at least 4 weeks after COVID-19 infection.
PASC-CVS, or PASC-cardiovascular syndrome, includes a wide range of cardiovascular symptoms without objective evidence of cardiovascular disease following standard diagnostic testing.
The document makes the following recommendations for the management of PASC-CVD and PASC-CVS.
For patients with cardiovascular symptoms and suspected PASC, the authors suggest that a reasonable initial testing approach includes basic laboratory testing, including cardiac troponin, an ECG, an echocardiogram, an ambulatory rhythm monitor, chest imaging, and/or pulmonary function tests.
Cardiology consultation is recommended for patients with PASC who have abnormal cardiac test results, known cardiovascular disease with new or worsening symptoms, documented cardiac complications during SARS-CoV-2 infection, and/or persistent cardiopulmonary symptoms that are not otherwise explained.
Recumbent or semirecumbent exercise (for example, rowing, swimming, or cycling) is recommended initially for PASC-CVS patients with tachycardia, exercise/orthostatic intolerance, and/or deconditioning, with transition to upright exercise as orthostatic intolerance improves. Exercise duration should also be short (5-10 minutes/day) initially, with gradual increases as functional capacity improves.
Salt and fluid loading represent nonpharmacologic interventions that may provide symptomatic relief for patients with tachycardia, palpitations, and/or orthostatic hypotension.
Beta-blockers, nondihydropyridine calcium-channel blockers, ivabradine, fludrocortisone, and midodrine may be used empirically as well.
Return to play for athletes
The authors note that concerns about possible cardiac injury after COVID-19 fueled early apprehension regarding the safety of competitive sports for athletes recovering from the infection.
But they say that subsequent data from large registries have demonstrated an overall low prevalence of clinical myocarditis, without a rise in the rate of adverse cardiac events. Based on this, updated guidance is provided with a practical, evidence-based framework to guide resumption of athletics and intense exercise training.
They make the following recommendations:
- For athletes recovering from COVID-19 with ongoing cardiopulmonary symptoms (chest pain, shortness of breath, palpitations, lightheadedness) or those requiring hospitalization with increased suspicion for cardiac involvement, further evaluation with triad testing – an ECG, measurement of cardiac troponin, and an echocardiogram – should be performed.
- For those with abnormal test results, further evaluation with cardiac MRI should be considered. Individuals diagnosed with clinical myocarditis should abstain from exercise for 3-6 months.
- Cardiac testing is not recommended for asymptomatic individuals following COVID-19 infection. Individuals should abstain from training for 3 days to ensure that symptoms do not develop.
- For those with mild or moderate noncardiopulmonary symptoms (fever, lethargy, muscle aches), training may resume after symptom resolution.
- For those with remote infection (≥3 months) without ongoing cardiopulmonary symptoms, a gradual increase in exercise is recommended without the need for cardiac testing.
Based on the low prevalence of myocarditis observed in competitive athletes with COVID-19, the authors note that these recommendations can be reasonably applied to high-school athletes (aged 14 and older) along with adult recreational exercise enthusiasts.
Future study is needed, however, to better understand how long cardiac abnormalities persist following COVID-19 infection and the role of exercise training in long COVID.
The authors conclude that the current guidance is intended to help clinicians understand not only when testing may be warranted, but also when it is not.
“Given that it reflects the current state of knowledge through early 2022, it is anticipated that recommendations will change over time as our understanding evolves,” they say.
The 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19: Myocarditis, Post-Acute Sequelae of SARS-CoV-2 Infection (PASC), and Return to Play will be discussed in a session at the American College of Cardiology’s annual scientific session meeting in Washington in April.
A version of this article first appeared on Medscape.com.
Is cancer testing going to the dogs? Nope, ants
The oncologist’s new best friend
We know that dogs have very sensitive noses. They can track criminals and missing persons and sniff out drugs and bombs. They can even detect cancer cells … after months of training.
And then there are ants.
Cancer cells produce volatile organic compounds (VOCs), which can be sniffed out by dogs and other animals with sufficiently sophisticated olfactory senses. A group of French investigators decided to find out if Formica fusca is such an animal.
First, they placed breast cancer cells and healthy cells in a petri dish. The sample of cancer cells, however, included a sugary treat. “Over successive trials, the ants got quicker and quicker at finding the treat, indicating that they had learned to recognize the VOCs produced by the cancerous cells, using these as a beacon to guide their way to the sugary delight,” according to IFL Science.
When the researchers removed the treat, the ants still went straight for the cancer cells. Then they removed the healthy cells and substituted another type of breast cancer cell, with just one type getting the treat. They went for the cancer cells with the treat, “indicating that they were capable of distinguishing between the different cancer types based on the unique pattern of VOCs emitted by each one,” IFL Science explained.
It’s just another chapter in the eternal struggle between dogs and ants. Dogs need months of training to learn to detect cancer cells; ants can do it in 30 minutes. Over the course of a dog’s training, Fido eats more food than 10,000 ants combined. (Okay, we’re guessing here, but it’s got to be a pretty big number, right?)
Then there’s the warm and fuzzy factor. Just look at that picture. Who wouldn’t want a cutie like that curling up in the bed next to you?
Console War II: Battle of the Twitter users
Video games can be a lot of fun, provided you’re not playing something like Rock Simulator. Or Surgeon Simulator. Or Surgeon Simulator 2. Yes, those are all real games. But calling yourself a video gamer invites a certain negative connotation, and nowhere can that be better exemplified than the increasingly ridiculous console war.
For those who don’t know their video game history, back in the early 90s Nintendo and Sega were the main video game console makers. Nintendo had Mario, Sega had Sonic, and everyone had an opinion on which was best. With Sega now but a shell of its former self and Nintendo viewed as too “casual” for the true gaming connoisseur, today’s battle pits Playstation against Xbox, and fans of both consoles spend their time trying to one-up each other in increasingly silly online arguments.
That brings us nicely to a Twitter user named “Shreeveera,” who is very vocal about his love of Playstation and hatred of the Xbox. Importantly, for LOTME purposes, Shreeveera identified himself as a doctor on his profile, and in the middle of an argument, Xbox enthusiasts called his credentials into question.
At this point, most people would recognize that there are very few noteworthy console-exclusive video games in today’s world and that any argument about consoles essentially comes down to which console design you like or which company you find less distasteful, and they would step away from the Twitter argument. Shreeveera is not most people, and he decided the next logical move was to post a video of himself and an anesthetized patient about to undergo a laparoscopic cholecystectomy.
This move did prove that he was indeed a doctor, but the ethics of posting such a video with a patient in the room is a bit dubious at best. Since Shreeveera also listed the hospital he worked at, numerous Twitter users review bombed the hospital with one-star reviews. Shreeveera’s fate is unknown, but he did take down the video and removed “doctor by profession” from his profile. He also made a second video asking Twitter to stop trying to ruin his life. We’re sure that’ll go well. Twitter is known for being completely fair and reasonable.
Use your words to gain power
We live in the age of the emoji. The use of emojis in texts and emails is basically the new shorthand. It’s a fun and easy way to chat with people close to us, but a new study shows that it doesn’t help in a business setting. In fact, it may do a little damage.

The use of images such as emojis in communication or logos can make a person seem less powerful than someone who opts for written words, according to Elinor Amit, PhD, of Tel Aviv University and associates.
Participants in their study were asked to imagine shopping with a person wearing a T-shirt. Half were then shown the logo of the Red Sox baseball team and half saw the words “Red Sox.” In another scenario, they were asked to imagine attending a retreat of a company called Lotus. Then half were shown an employee wearing a shirt with an image of lotus flower and half saw the verbal logo “Lotus.” In both scenarios, the individuals wearing shirts with images were seen as less powerful than the people who wore shirts with words on them.
Why is that? In a Eurekalert statement, Dr. Amit said that “visual messages are often interpreted as a signal for desire for social proximity.” In a world with COVID-19, that could give anyone pause.
That desire for more social proximity, in turn, equals a suggested loss of power because research shows that people who want to be around other people more are less powerful than people who don’t.
With the reduced social proximity we have these days, we may want to keep things cool and lighthearted, especially in work emails with people who we’ve never met. It may be, however, that using your words to say thank you in the multitude of emails you respond to on a regular basis is better than that thumbs-up emoji. Nobody will think less of you.
Should Daylight Savings Time still be a thing?
This past week, we just experienced the spring-forward portion of Daylight Savings Time, which took an hour of sleep away from us all. Some of us may still be struggling to find our footing with the time change, but at least it’s still sunny out at 7 pm. For those who don’t really see the point of changing the clocks twice a year, there are actually some good reasons to do so.

Sen. Marco Rubio, sponsor of a bill to make the time change permanent, put it simply: “If we can get this passed, we don’t have to do this stupidity anymore.” Message received, apparently, since the measure just passed unanimously in the Senate.
It’s not clear if President Biden will approve it, though, because there’s a lot that comes into play: economic needs, seasonal depression, and safety.
“I know this is not the most important issue confronting America, but it’s one of those issues where there’s a lot of agreement,” Sen. Rubio said.
Not total agreement, though. The National Association of Convenience Stores is opposed to the bill, and Reuters noted that one witness at a recent hearing said the time change “is like living in the wrong time zone for almost eight months out of the year.”
Many people, however, seem to be leaning toward the permanent spring-forward as it gives businesses a longer window to provide entertainment in the evenings and kids are able to play outside longer after school.
Honestly, we’re leaning toward whichever one can reduce seasonal depression.
The oncologist’s new best friend
We know that dogs have very sensitive noses. They can track criminals and missing persons and sniff out drugs and bombs. They can even detect cancer cells … after months of training.
And then there are ants.
Cancer cells produce volatile organic compounds (VOCs), which can be sniffed out by dogs and other animals with sufficiently sophisticated olfactory senses. A group of French investigators decided to find out if Formica fusca is such an animal.
First, they placed breast cancer cells and healthy cells in a petri dish. The sample of cancer cells, however, included a sugary treat. “Over successive trials, the ants got quicker and quicker at finding the treat, indicating that they had learned to recognize the VOCs produced by the cancerous cells, using these as a beacon to guide their way to the sugary delight,” according to IFL Science.
When the researchers removed the treat, the ants still went straight for the cancer cells. Then they removed the healthy cells and substituted another type of breast cancer cell, with just one type getting the treat. They went for the cancer cells with the treat, “indicating that they were capable of distinguishing between the different cancer types based on the unique pattern of VOCs emitted by each one,” IFL Science explained.
It’s just another chapter in the eternal struggle between dogs and ants. Dogs need months of training to learn to detect cancer cells; ants can do it in 30 minutes. Over the course of a dog’s training, Fido eats more food than 10,000 ants combined. (Okay, we’re guessing here, but it’s got to be a pretty big number, right?)
Then there’s the warm and fuzzy factor. Just look at that picture. Who wouldn’t want a cutie like that curling up in the bed next to you?
Console War II: Battle of the Twitter users
Video games can be a lot of fun, provided you’re not playing something like Rock Simulator. Or Surgeon Simulator. Or Surgeon Simulator 2. Yes, those are all real games. But calling yourself a video gamer invites a certain negative connotation, and nowhere can that be better exemplified than the increasingly ridiculous console war.
For those who don’t know their video game history, back in the early 90s Nintendo and Sega were the main video game console makers. Nintendo had Mario, Sega had Sonic, and everyone had an opinion on which was best. With Sega now but a shell of its former self and Nintendo viewed as too “casual” for the true gaming connoisseur, today’s battle pits Playstation against Xbox, and fans of both consoles spend their time trying to one-up each other in increasingly silly online arguments.
That brings us nicely to a Twitter user named “Shreeveera,” who is very vocal about his love of Playstation and hatred of the Xbox. Importantly, for LOTME purposes, Shreeveera identified himself as a doctor on his profile, and in the middle of an argument, Xbox enthusiasts called his credentials into question.
At this point, most people would recognize that there are very few noteworthy console-exclusive video games in today’s world and that any argument about consoles essentially comes down to which console design you like or which company you find less distasteful, and they would step away from the Twitter argument. Shreeveera is not most people, and he decided the next logical move was to post a video of himself and an anesthetized patient about to undergo a laparoscopic cholecystectomy.
This move did prove that he was indeed a doctor, but the ethics of posting such a video with a patient in the room is a bit dubious at best. Since Shreeveera also listed the hospital he worked at, numerous Twitter users review bombed the hospital with one-star reviews. Shreeveera’s fate is unknown, but he did take down the video and removed “doctor by profession” from his profile. He also made a second video asking Twitter to stop trying to ruin his life. We’re sure that’ll go well. Twitter is known for being completely fair and reasonable.
Use your words to gain power
We live in the age of the emoji. The use of emojis in texts and emails is basically the new shorthand. It’s a fun and easy way to chat with people close to us, but a new study shows that it doesn’t help in a business setting. In fact, it may do a little damage.
The use of images such as emojis in communication or logos can make a person seem less powerful than someone who opts for written words, according to Elinor Amit, PhD, of Tel Aviv University and associates.
Participants in their study were asked to imagine shopping with a person wearing a T-shirt. Half were then shown the logo of the Red Sox baseball team and half saw the words “Red Sox.” In another scenario, they were asked to imagine attending a retreat of a company called Lotus. Then half were shown an employee wearing a shirt with an image of lotus flower and half saw the verbal logo “Lotus.” In both scenarios, the individuals wearing shirts with images were seen as less powerful than the people who wore shirts with words on them.
Why is that? In a Eurekalert statement, Dr. Amit said that “visual messages are often interpreted as a signal for desire for social proximity.” In a world with COVID-19, that could give anyone pause.
That desire for more social proximity, in turn, equals a suggested loss of power because research shows that people who want to be around other people more are less powerful than people who don’t.
With the reduced social proximity we have these days, we may want to keep things cool and lighthearted, especially in work emails with people who we’ve never met. It may be, however, that using your words to say thank you in the multitude of emails you respond to on a regular basis is better than that thumbs-up emoji. Nobody will think less of you.
Should Daylight Savings Time still be a thing?
This past week, we just experienced the spring-forward portion of Daylight Savings Time, which took an hour of sleep away from us all. Some of us may still be struggling to find our footing with the time change, but at least it’s still sunny out at 7 pm. For those who don’t really see the point of changing the clocks twice a year, there are actually some good reasons to do so.
Sen. Marco Rubio, sponsor of a bill to make the time change permanent, put it simply: “If we can get this passed, we don’t have to do this stupidity anymore.” Message received, apparently, since the measure just passed unanimously in the Senate.
It’s not clear if President Biden will approve it, though, because there’s a lot that comes into play: economic needs, seasonal depression, and safety.
“I know this is not the most important issue confronting America, but it’s one of those issues where there’s a lot of agreement,” Sen. Rubio said.
Not total agreement, though. The National Association of Convenience Stores is opposed to the bill, and Reuters noted that one witness at a recent hearing said the time change “is like living in the wrong time zone for almost eight months out of the year.”
Many people, however, seem to be leaning toward the permanent spring-forward as it gives businesses a longer window to provide entertainment in the evenings and kids are able to play outside longer after school.
Honestly, we’re leaning toward whichever one can reduce seasonal depression.
The oncologist’s new best friend
We know that dogs have very sensitive noses. They can track criminals and missing persons and sniff out drugs and bombs. They can even detect cancer cells … after months of training.
And then there are ants.
Cancer cells produce volatile organic compounds (VOCs), which can be sniffed out by dogs and other animals with sufficiently sophisticated olfactory senses. A group of French investigators decided to find out if Formica fusca is such an animal.
First, they placed breast cancer cells and healthy cells in a petri dish. The sample of cancer cells, however, included a sugary treat. “Over successive trials, the ants got quicker and quicker at finding the treat, indicating that they had learned to recognize the VOCs produced by the cancerous cells, using these as a beacon to guide their way to the sugary delight,” according to IFL Science.
When the researchers removed the treat, the ants still went straight for the cancer cells. Then they removed the healthy cells and substituted another type of breast cancer cell, with just one type getting the treat. They went for the cancer cells with the treat, “indicating that they were capable of distinguishing between the different cancer types based on the unique pattern of VOCs emitted by each one,” IFL Science explained.
It’s just another chapter in the eternal struggle between dogs and ants. Dogs need months of training to learn to detect cancer cells; ants can do it in 30 minutes. Over the course of a dog’s training, Fido eats more food than 10,000 ants combined. (Okay, we’re guessing here, but it’s got to be a pretty big number, right?)
Then there’s the warm and fuzzy factor. Just look at that picture. Who wouldn’t want a cutie like that curling up in the bed next to you?
Console War II: Battle of the Twitter users
Video games can be a lot of fun, provided you’re not playing something like Rock Simulator. Or Surgeon Simulator. Or Surgeon Simulator 2. Yes, those are all real games. But calling yourself a video gamer invites a certain negative connotation, and nowhere can that be better exemplified than the increasingly ridiculous console war.
For those who don’t know their video game history, back in the early 90s Nintendo and Sega were the main video game console makers. Nintendo had Mario, Sega had Sonic, and everyone had an opinion on which was best. With Sega now but a shell of its former self and Nintendo viewed as too “casual” for the true gaming connoisseur, today’s battle pits Playstation against Xbox, and fans of both consoles spend their time trying to one-up each other in increasingly silly online arguments.
That brings us nicely to a Twitter user named “Shreeveera,” who is very vocal about his love of Playstation and hatred of the Xbox. Importantly, for LOTME purposes, Shreeveera identified himself as a doctor on his profile, and in the middle of an argument, Xbox enthusiasts called his credentials into question.
At this point, most people would recognize that there are very few noteworthy console-exclusive video games in today’s world and that any argument about consoles essentially comes down to which console design you like or which company you find less distasteful, and they would step away from the Twitter argument. Shreeveera is not most people, and he decided the next logical move was to post a video of himself and an anesthetized patient about to undergo a laparoscopic cholecystectomy.
This move did prove that he was indeed a doctor, but the ethics of posting such a video with a patient in the room is a bit dubious at best. Since Shreeveera also listed the hospital he worked at, numerous Twitter users review bombed the hospital with one-star reviews. Shreeveera’s fate is unknown, but he did take down the video and removed “doctor by profession” from his profile. He also made a second video asking Twitter to stop trying to ruin his life. We’re sure that’ll go well. Twitter is known for being completely fair and reasonable.
Use your words to gain power
We live in the age of the emoji. The use of emojis in texts and emails is basically the new shorthand. It’s a fun and easy way to chat with people close to us, but a new study shows that it doesn’t help in a business setting. In fact, it may do a little damage.
The use of images such as emojis in communication or logos can make a person seem less powerful than someone who opts for written words, according to Elinor Amit, PhD, of Tel Aviv University and associates.
Participants in their study were asked to imagine shopping with a person wearing a T-shirt. Half were then shown the logo of the Red Sox baseball team and half saw the words “Red Sox.” In another scenario, they were asked to imagine attending a retreat of a company called Lotus. Then half were shown an employee wearing a shirt with an image of lotus flower and half saw the verbal logo “Lotus.” In both scenarios, the individuals wearing shirts with images were seen as less powerful than the people who wore shirts with words on them.
Why is that? In a Eurekalert statement, Dr. Amit said that “visual messages are often interpreted as a signal for desire for social proximity.” In a world with COVID-19, that could give anyone pause.
That desire for more social proximity, in turn, equals a suggested loss of power because research shows that people who want to be around other people more are less powerful than people who don’t.
With the reduced social proximity we have these days, we may want to keep things cool and lighthearted, especially in work emails with people who we’ve never met. It may be, however, that using your words to say thank you in the multitude of emails you respond to on a regular basis is better than that thumbs-up emoji. Nobody will think less of you.
Should Daylight Savings Time still be a thing?
This past week, we just experienced the spring-forward portion of Daylight Savings Time, which took an hour of sleep away from us all. Some of us may still be struggling to find our footing with the time change, but at least it’s still sunny out at 7 pm. For those who don’t really see the point of changing the clocks twice a year, there are actually some good reasons to do so.
Sen. Marco Rubio, sponsor of a bill to make the time change permanent, put it simply: “If we can get this passed, we don’t have to do this stupidity anymore.” Message received, apparently, since the measure just passed unanimously in the Senate.
It’s not clear if President Biden will approve it, though, because there’s a lot that comes into play: economic needs, seasonal depression, and safety.
“I know this is not the most important issue confronting America, but it’s one of those issues where there’s a lot of agreement,” Sen. Rubio said.
Not total agreement, though. The National Association of Convenience Stores is opposed to the bill, and Reuters noted that one witness at a recent hearing said the time change “is like living in the wrong time zone for almost eight months out of the year.”
Many people, however, seem to be leaning toward the permanent spring-forward as it gives businesses a longer window to provide entertainment in the evenings and kids are able to play outside longer after school.
Honestly, we’re leaning toward whichever one can reduce seasonal depression.