User login
Cardiology News is an independent news source that provides cardiologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on cardiology and the cardiologist's practice. Cardiology News Digital Network is the online destination and multimedia properties of Cardiology News, the independent news publication for cardiologists. Cardiology news is the leading source of news and commentary about clinical developments in cardiology as well as health care policy and regulations that affect the cardiologist's practice. Cardiology News Digital Network is owned by Frontline Medical Communications.
Vaccine rollout on track, expect 300 million doses through March: Feds
If the initial success of the Pfizer-BioNTech rollout continues, and emergency use authorization (EAU) is granted to Moderna and Johnson & Johnson vaccines in development, Operation Warp Speed officials expect to have 300 million doses of COVID-19 vaccines to distribute across the United States between now and March 31.
The initial rollout remains on track, said Alex Azar, US Department of Health and Human Services (HHS) secretary, during a media briefing today. “We continue to have good news to report. As of today, shipments of vaccine will have been delivered to every delivery site identified by public health jurisdictions for our first wave of shipments.”
Anomalies in shipments to California and Alabama arose when temperature monitors showed the Pfizer vaccine dropped lower than the recommended -80 ºC (-112 °F). These vaccine trays remained on delivery trucks and were returned to Pfizer for prompt replacement, said Operation Warp Speed Chief Operating Officer Gen. Gustave F. Perna.
Azar estimated another 2 million doses of the Pfizer vaccine will be available next week. “And if the Moderna vaccine is authorized by the FDA in the coming days, we have allocated nearly 5.9 million doses of that product.”
The Moderna vaccine data released this week look promising, said Moncef Slaoui, PhD, Operation Warp Speed chief scientific adviser. “In the short term, I expect the protection to be quite significant.”
The findings in the first 2 weeks after the first dose show up to 65% protection, he said, and predicted the second-dose efficacy data will be coming in the next few weeks.
Enrollment in the phase 3 Johnson & Johnson trial with nearly 44,000 participants is expected to end December 17. Initial efficacy results are anticipated by early January, with more complete efficacy numbers by late January, Slaoui said.
The AstraZeneca COVID-19 vaccine trial also is underway with enrollment continuing. “We expect accruement to end in late December or early next year, with first results expected probably in February,” Slaoui said.
Antibody treatments underutilized
The media briefing also addressed COVID-19 therapeutics. Azar reported low uptake of available antibody therapies. “I want to remind Americans that there are two authorized antibody treatments that Operation Warp Speed has supported. They can help prevent hospitalization in those patients with the highest risk for severe disease.”
The higher-risk group includes those who are 65 and older and people with comorbid conditions that put them at increased risk for COVID-19 hospitalization.
The federal government allocated more than 330,000 doses of these treatments and many states have product available, Azar said.
Slaoui agreed, saying there is a “disappointing level of usage of monoclonal antibody therapy in hospitals. We look forward to that improving.”
Up to 3 billion vaccine doses possible
“We now have more than 900 million doses of the vaccine we have contracted delivery for,” Azar said. The government has options to increase that to a total of 3 billion doses.
In addition to the 100 million Pfizer vaccine doses and 100 million Moderna doses already ordered, the government just took an option for another 100 million Moderna doses for the second quarter of 2021. Operation Warp Speed officials are negotiating with Pfizer for additional product as well.
Azar added that there are 100 million doses of the Johnson & Johnson vaccine in active production and expects AstraZeneca can provide 300 million doses of their product.
With the possibility of three or more vaccine products and with 330 million Americans, minus the 70 million or so children under age 16, “we believe we will actually have surplus supplies,” Azar said. Plans are to take the US surplus vaccine and surplus manufacturing capacity “and use that for the benefit of the world community.”
This article first appeared on Medscape.com.
If the initial success of the Pfizer-BioNTech rollout continues, and emergency use authorization (EAU) is granted to Moderna and Johnson & Johnson vaccines in development, Operation Warp Speed officials expect to have 300 million doses of COVID-19 vaccines to distribute across the United States between now and March 31.
The initial rollout remains on track, said Alex Azar, US Department of Health and Human Services (HHS) secretary, during a media briefing today. “We continue to have good news to report. As of today, shipments of vaccine will have been delivered to every delivery site identified by public health jurisdictions for our first wave of shipments.”
Anomalies in shipments to California and Alabama arose when temperature monitors showed the Pfizer vaccine dropped lower than the recommended -80 ºC (-112 °F). These vaccine trays remained on delivery trucks and were returned to Pfizer for prompt replacement, said Operation Warp Speed Chief Operating Officer Gen. Gustave F. Perna.
Azar estimated another 2 million doses of the Pfizer vaccine will be available next week. “And if the Moderna vaccine is authorized by the FDA in the coming days, we have allocated nearly 5.9 million doses of that product.”
The Moderna vaccine data released this week look promising, said Moncef Slaoui, PhD, Operation Warp Speed chief scientific adviser. “In the short term, I expect the protection to be quite significant.”
The findings in the first 2 weeks after the first dose show up to 65% protection, he said, and predicted the second-dose efficacy data will be coming in the next few weeks.
Enrollment in the phase 3 Johnson & Johnson trial with nearly 44,000 participants is expected to end December 17. Initial efficacy results are anticipated by early January, with more complete efficacy numbers by late January, Slaoui said.
The AstraZeneca COVID-19 vaccine trial also is underway with enrollment continuing. “We expect accruement to end in late December or early next year, with first results expected probably in February,” Slaoui said.
Antibody treatments underutilized
The media briefing also addressed COVID-19 therapeutics. Azar reported low uptake of available antibody therapies. “I want to remind Americans that there are two authorized antibody treatments that Operation Warp Speed has supported. They can help prevent hospitalization in those patients with the highest risk for severe disease.”
The higher-risk group includes those who are 65 and older and people with comorbid conditions that put them at increased risk for COVID-19 hospitalization.
The federal government allocated more than 330,000 doses of these treatments and many states have product available, Azar said.
Slaoui agreed, saying there is a “disappointing level of usage of monoclonal antibody therapy in hospitals. We look forward to that improving.”
Up to 3 billion vaccine doses possible
“We now have more than 900 million doses of the vaccine we have contracted delivery for,” Azar said. The government has options to increase that to a total of 3 billion doses.
In addition to the 100 million Pfizer vaccine doses and 100 million Moderna doses already ordered, the government just took an option for another 100 million Moderna doses for the second quarter of 2021. Operation Warp Speed officials are negotiating with Pfizer for additional product as well.
Azar added that there are 100 million doses of the Johnson & Johnson vaccine in active production and expects AstraZeneca can provide 300 million doses of their product.
With the possibility of three or more vaccine products and with 330 million Americans, minus the 70 million or so children under age 16, “we believe we will actually have surplus supplies,” Azar said. Plans are to take the US surplus vaccine and surplus manufacturing capacity “and use that for the benefit of the world community.”
This article first appeared on Medscape.com.
If the initial success of the Pfizer-BioNTech rollout continues, and emergency use authorization (EAU) is granted to Moderna and Johnson & Johnson vaccines in development, Operation Warp Speed officials expect to have 300 million doses of COVID-19 vaccines to distribute across the United States between now and March 31.
The initial rollout remains on track, said Alex Azar, US Department of Health and Human Services (HHS) secretary, during a media briefing today. “We continue to have good news to report. As of today, shipments of vaccine will have been delivered to every delivery site identified by public health jurisdictions for our first wave of shipments.”
Anomalies in shipments to California and Alabama arose when temperature monitors showed the Pfizer vaccine dropped lower than the recommended -80 ºC (-112 °F). These vaccine trays remained on delivery trucks and were returned to Pfizer for prompt replacement, said Operation Warp Speed Chief Operating Officer Gen. Gustave F. Perna.
Azar estimated another 2 million doses of the Pfizer vaccine will be available next week. “And if the Moderna vaccine is authorized by the FDA in the coming days, we have allocated nearly 5.9 million doses of that product.”
The Moderna vaccine data released this week look promising, said Moncef Slaoui, PhD, Operation Warp Speed chief scientific adviser. “In the short term, I expect the protection to be quite significant.”
The findings in the first 2 weeks after the first dose show up to 65% protection, he said, and predicted the second-dose efficacy data will be coming in the next few weeks.
Enrollment in the phase 3 Johnson & Johnson trial with nearly 44,000 participants is expected to end December 17. Initial efficacy results are anticipated by early January, with more complete efficacy numbers by late January, Slaoui said.
The AstraZeneca COVID-19 vaccine trial also is underway with enrollment continuing. “We expect accruement to end in late December or early next year, with first results expected probably in February,” Slaoui said.
Antibody treatments underutilized
The media briefing also addressed COVID-19 therapeutics. Azar reported low uptake of available antibody therapies. “I want to remind Americans that there are two authorized antibody treatments that Operation Warp Speed has supported. They can help prevent hospitalization in those patients with the highest risk for severe disease.”
The higher-risk group includes those who are 65 and older and people with comorbid conditions that put them at increased risk for COVID-19 hospitalization.
The federal government allocated more than 330,000 doses of these treatments and many states have product available, Azar said.
Slaoui agreed, saying there is a “disappointing level of usage of monoclonal antibody therapy in hospitals. We look forward to that improving.”
Up to 3 billion vaccine doses possible
“We now have more than 900 million doses of the vaccine we have contracted delivery for,” Azar said. The government has options to increase that to a total of 3 billion doses.
In addition to the 100 million Pfizer vaccine doses and 100 million Moderna doses already ordered, the government just took an option for another 100 million Moderna doses for the second quarter of 2021. Operation Warp Speed officials are negotiating with Pfizer for additional product as well.
Azar added that there are 100 million doses of the Johnson & Johnson vaccine in active production and expects AstraZeneca can provide 300 million doses of their product.
With the possibility of three or more vaccine products and with 330 million Americans, minus the 70 million or so children under age 16, “we believe we will actually have surplus supplies,” Azar said. Plans are to take the US surplus vaccine and surplus manufacturing capacity “and use that for the benefit of the world community.”
This article first appeared on Medscape.com.
Urgent recall for Penumbra JET 7 Xtra Flex reperfusion catheters
“All users should stop using this device, and facilities should remove these devices from inventory,” the recall notice, posted on the U.S. Food and Drug Administration website, advises.
The recall covers the JET 7 Xtra Flex catheter, which was cleared for use in June 2019, and the JET 7MAX configuration (which includes the JET 7 Xtra Flex catheter and MAX delivery device), which was cleared in February of this year.
The recall does not apply to the Penumbra JET 7 reperfusion catheter with standard tip.
The FDA says it has received over 200 medical device reports (MDRs) associated with the JET 7 Xtra Flex catheter, including reports of deaths, serious injuries, and malfunctions.
Twenty of these MDRs describe 14 unique patient deaths. Other MDRs describe serious patient injury, such as vessel damage, hemorrhage, and cerebral infarction.
Device malfunctions described in the reports include ballooning, expansion, rupture, breakage or complete separation, and exposure of internal support coils near the distal tip region of the JET 7 Xtra Flex catheter.
According to the FDA, bench testing by the manufacturer, in which the catheter distal tip is plugged and pressurized to failure, indicates that the JET 7 Xtra Flex catheter is not able to withstand the same burst pressures to failure as the manufacturer’s other large-bore aspiration catheters used to remove thrombus for patients with acute ischemic stroke.
Penumbra’s urgent medical device recall letter advises health care providers and facilities to remove and quarantine all unused devices covered by this recall, to complete the product identification and return form, and to return all products to Penumbra in accordance with instructions provided.
For questions regarding this recall, contact Penumbra customer service by phone at 888-272-4606 or by email at [email protected].
A version of this article first appeared on Medscape.com.
“All users should stop using this device, and facilities should remove these devices from inventory,” the recall notice, posted on the U.S. Food and Drug Administration website, advises.
The recall covers the JET 7 Xtra Flex catheter, which was cleared for use in June 2019, and the JET 7MAX configuration (which includes the JET 7 Xtra Flex catheter and MAX delivery device), which was cleared in February of this year.
The recall does not apply to the Penumbra JET 7 reperfusion catheter with standard tip.
The FDA says it has received over 200 medical device reports (MDRs) associated with the JET 7 Xtra Flex catheter, including reports of deaths, serious injuries, and malfunctions.
Twenty of these MDRs describe 14 unique patient deaths. Other MDRs describe serious patient injury, such as vessel damage, hemorrhage, and cerebral infarction.
Device malfunctions described in the reports include ballooning, expansion, rupture, breakage or complete separation, and exposure of internal support coils near the distal tip region of the JET 7 Xtra Flex catheter.
According to the FDA, bench testing by the manufacturer, in which the catheter distal tip is plugged and pressurized to failure, indicates that the JET 7 Xtra Flex catheter is not able to withstand the same burst pressures to failure as the manufacturer’s other large-bore aspiration catheters used to remove thrombus for patients with acute ischemic stroke.
Penumbra’s urgent medical device recall letter advises health care providers and facilities to remove and quarantine all unused devices covered by this recall, to complete the product identification and return form, and to return all products to Penumbra in accordance with instructions provided.
For questions regarding this recall, contact Penumbra customer service by phone at 888-272-4606 or by email at [email protected].
A version of this article first appeared on Medscape.com.
“All users should stop using this device, and facilities should remove these devices from inventory,” the recall notice, posted on the U.S. Food and Drug Administration website, advises.
The recall covers the JET 7 Xtra Flex catheter, which was cleared for use in June 2019, and the JET 7MAX configuration (which includes the JET 7 Xtra Flex catheter and MAX delivery device), which was cleared in February of this year.
The recall does not apply to the Penumbra JET 7 reperfusion catheter with standard tip.
The FDA says it has received over 200 medical device reports (MDRs) associated with the JET 7 Xtra Flex catheter, including reports of deaths, serious injuries, and malfunctions.
Twenty of these MDRs describe 14 unique patient deaths. Other MDRs describe serious patient injury, such as vessel damage, hemorrhage, and cerebral infarction.
Device malfunctions described in the reports include ballooning, expansion, rupture, breakage or complete separation, and exposure of internal support coils near the distal tip region of the JET 7 Xtra Flex catheter.
According to the FDA, bench testing by the manufacturer, in which the catheter distal tip is plugged and pressurized to failure, indicates that the JET 7 Xtra Flex catheter is not able to withstand the same burst pressures to failure as the manufacturer’s other large-bore aspiration catheters used to remove thrombus for patients with acute ischemic stroke.
Penumbra’s urgent medical device recall letter advises health care providers and facilities to remove and quarantine all unused devices covered by this recall, to complete the product identification and return form, and to return all products to Penumbra in accordance with instructions provided.
For questions regarding this recall, contact Penumbra customer service by phone at 888-272-4606 or by email at [email protected].
A version of this article first appeared on Medscape.com.
COVID-19 ranks as a leading cause of death in United States
Adults over age 45 were more likely to die from COVID-19 than car crashes, respiratory diseases, drug overdoses, and suicide. And those over age 55 faced even higher rates of dying because of the coronavirus.
“The current exponential increase in COVID-19 is reaching a calamitous scale in the U.S.,” the authors wrote. “Putting these numbers in perspective may be difficult.”
Population health researchers at Virginia Commonwealth University put COVID-19 deaths into context by comparing this year’s numbers to the leading causes of death for March through October 2018, sorting by age.
By October 2020, COVID-19 had become the third leading cause of death overall for those between the ages of 45 and 84 years, following after heart disease and cancer. For those over age 85, COVID-19 was the second leading cause of death, surpassing cancer and following behind heart disease.
For people aged 35-44 years, COVID-19 surpassed car crashes and respiratory diseases and was slightly lower than suicide, heart disease, and cancer. For those under age 35, drug overdoses, suicide, and car crashes remained the leading causes of death.
Importantly, the authors wrote, death rates for the two leading causes – heart disease and cancer – are about 1,700 and 1,600 per day, respectively. COVID-19 deaths have surpassed these numbers individually throughout December and, on Wednesday, beat them combined. More than 3,400 deaths were reported, according to the COVID Tracking Project, marking an all-time high that continues to increase. Hospitalizations were also at a new high, with more than 113,000 COVID-19 patients in hospitals across the country, and another 232,000 new cases were reported.
“With COVID-19 mortality rates now exceeding these thresholds, this infectious disease has become deadlier than heart disease and cancer,” the authors wrote. “Its lethality may increase further as transmission increases with holiday travel and gatherings and with the intensified indoor exposure that winter brings.”
The reported number of COVID-19 deaths is likely a 20% underestimate, they wrote, attributable to delays in reporting and an increase in non–COVID-19 deaths that were undetected and untreated because of pandemic-related disruptions. Since the coronavirus is communicable and spreads easily, COVID-19 deaths are particularly unique and worrying, they said.
“Individuals who die from homicide or cancer do not transmit the risk of morbidity and mortality to those nearby,” they wrote. “Every COVID-19 death signals the possibility of more deaths among close contacts.”
The fall surge in cases and deaths is widespread nationally, as compared to the spring, with hot spots on both coasts and in rural areas, according to an accompanying editorial in JAMA from public health researchers at the Harvard T.H. Chan School of Public Health, Boston. People of color have faced twice the death rate as well, with one in 875 Black people and one in 925 Indigenous people dying from COVID-19, as compared with one in 1,625 White people.
“The year 2020 ends with COVID-19 massively surging, as it was in the spring, to be the leading cause of death,” they wrote. “The accelerating numbers of deaths fall far short of fully capturing each devastating human story: Every death represents untold loss for countless families.”
Vaccines offer hope, they said, but won’t prevent the upcoming increase in COVID-19 hospitalizations and deaths this winter. In 2021, containing the pandemic will require national coordination, resources to help overwhelmed health care workers, new support for state and local public health officials, a stimulus package for schools and businesses, and financial aid for people on the brink of eviction. The country needs federal coordination of testing, contact tracing, personal protective equipment, travel precautions, and a face mask mandate, they wrote.
“Ending this crisis will require not only further advances in treatment but also unprecedented commitment to all aspects of prevention, vaccination, and public health,” they wrote. “Only by doing so can future years see this illness revert back to the unfamiliar and unknown condition it once was.”
This article first appeared on WebMD.com.
Adults over age 45 were more likely to die from COVID-19 than car crashes, respiratory diseases, drug overdoses, and suicide. And those over age 55 faced even higher rates of dying because of the coronavirus.
“The current exponential increase in COVID-19 is reaching a calamitous scale in the U.S.,” the authors wrote. “Putting these numbers in perspective may be difficult.”
Population health researchers at Virginia Commonwealth University put COVID-19 deaths into context by comparing this year’s numbers to the leading causes of death for March through October 2018, sorting by age.
By October 2020, COVID-19 had become the third leading cause of death overall for those between the ages of 45 and 84 years, following after heart disease and cancer. For those over age 85, COVID-19 was the second leading cause of death, surpassing cancer and following behind heart disease.
For people aged 35-44 years, COVID-19 surpassed car crashes and respiratory diseases and was slightly lower than suicide, heart disease, and cancer. For those under age 35, drug overdoses, suicide, and car crashes remained the leading causes of death.
Importantly, the authors wrote, death rates for the two leading causes – heart disease and cancer – are about 1,700 and 1,600 per day, respectively. COVID-19 deaths have surpassed these numbers individually throughout December and, on Wednesday, beat them combined. More than 3,400 deaths were reported, according to the COVID Tracking Project, marking an all-time high that continues to increase. Hospitalizations were also at a new high, with more than 113,000 COVID-19 patients in hospitals across the country, and another 232,000 new cases were reported.
“With COVID-19 mortality rates now exceeding these thresholds, this infectious disease has become deadlier than heart disease and cancer,” the authors wrote. “Its lethality may increase further as transmission increases with holiday travel and gatherings and with the intensified indoor exposure that winter brings.”
The reported number of COVID-19 deaths is likely a 20% underestimate, they wrote, attributable to delays in reporting and an increase in non–COVID-19 deaths that were undetected and untreated because of pandemic-related disruptions. Since the coronavirus is communicable and spreads easily, COVID-19 deaths are particularly unique and worrying, they said.
“Individuals who die from homicide or cancer do not transmit the risk of morbidity and mortality to those nearby,” they wrote. “Every COVID-19 death signals the possibility of more deaths among close contacts.”
The fall surge in cases and deaths is widespread nationally, as compared to the spring, with hot spots on both coasts and in rural areas, according to an accompanying editorial in JAMA from public health researchers at the Harvard T.H. Chan School of Public Health, Boston. People of color have faced twice the death rate as well, with one in 875 Black people and one in 925 Indigenous people dying from COVID-19, as compared with one in 1,625 White people.
“The year 2020 ends with COVID-19 massively surging, as it was in the spring, to be the leading cause of death,” they wrote. “The accelerating numbers of deaths fall far short of fully capturing each devastating human story: Every death represents untold loss for countless families.”
Vaccines offer hope, they said, but won’t prevent the upcoming increase in COVID-19 hospitalizations and deaths this winter. In 2021, containing the pandemic will require national coordination, resources to help overwhelmed health care workers, new support for state and local public health officials, a stimulus package for schools and businesses, and financial aid for people on the brink of eviction. The country needs federal coordination of testing, contact tracing, personal protective equipment, travel precautions, and a face mask mandate, they wrote.
“Ending this crisis will require not only further advances in treatment but also unprecedented commitment to all aspects of prevention, vaccination, and public health,” they wrote. “Only by doing so can future years see this illness revert back to the unfamiliar and unknown condition it once was.”
This article first appeared on WebMD.com.
Adults over age 45 were more likely to die from COVID-19 than car crashes, respiratory diseases, drug overdoses, and suicide. And those over age 55 faced even higher rates of dying because of the coronavirus.
“The current exponential increase in COVID-19 is reaching a calamitous scale in the U.S.,” the authors wrote. “Putting these numbers in perspective may be difficult.”
Population health researchers at Virginia Commonwealth University put COVID-19 deaths into context by comparing this year’s numbers to the leading causes of death for March through October 2018, sorting by age.
By October 2020, COVID-19 had become the third leading cause of death overall for those between the ages of 45 and 84 years, following after heart disease and cancer. For those over age 85, COVID-19 was the second leading cause of death, surpassing cancer and following behind heart disease.
For people aged 35-44 years, COVID-19 surpassed car crashes and respiratory diseases and was slightly lower than suicide, heart disease, and cancer. For those under age 35, drug overdoses, suicide, and car crashes remained the leading causes of death.
Importantly, the authors wrote, death rates for the two leading causes – heart disease and cancer – are about 1,700 and 1,600 per day, respectively. COVID-19 deaths have surpassed these numbers individually throughout December and, on Wednesday, beat them combined. More than 3,400 deaths were reported, according to the COVID Tracking Project, marking an all-time high that continues to increase. Hospitalizations were also at a new high, with more than 113,000 COVID-19 patients in hospitals across the country, and another 232,000 new cases were reported.
“With COVID-19 mortality rates now exceeding these thresholds, this infectious disease has become deadlier than heart disease and cancer,” the authors wrote. “Its lethality may increase further as transmission increases with holiday travel and gatherings and with the intensified indoor exposure that winter brings.”
The reported number of COVID-19 deaths is likely a 20% underestimate, they wrote, attributable to delays in reporting and an increase in non–COVID-19 deaths that were undetected and untreated because of pandemic-related disruptions. Since the coronavirus is communicable and spreads easily, COVID-19 deaths are particularly unique and worrying, they said.
“Individuals who die from homicide or cancer do not transmit the risk of morbidity and mortality to those nearby,” they wrote. “Every COVID-19 death signals the possibility of more deaths among close contacts.”
The fall surge in cases and deaths is widespread nationally, as compared to the spring, with hot spots on both coasts and in rural areas, according to an accompanying editorial in JAMA from public health researchers at the Harvard T.H. Chan School of Public Health, Boston. People of color have faced twice the death rate as well, with one in 875 Black people and one in 925 Indigenous people dying from COVID-19, as compared with one in 1,625 White people.
“The year 2020 ends with COVID-19 massively surging, as it was in the spring, to be the leading cause of death,” they wrote. “The accelerating numbers of deaths fall far short of fully capturing each devastating human story: Every death represents untold loss for countless families.”
Vaccines offer hope, they said, but won’t prevent the upcoming increase in COVID-19 hospitalizations and deaths this winter. In 2021, containing the pandemic will require national coordination, resources to help overwhelmed health care workers, new support for state and local public health officials, a stimulus package for schools and businesses, and financial aid for people on the brink of eviction. The country needs federal coordination of testing, contact tracing, personal protective equipment, travel precautions, and a face mask mandate, they wrote.
“Ending this crisis will require not only further advances in treatment but also unprecedented commitment to all aspects of prevention, vaccination, and public health,” they wrote. “Only by doing so can future years see this illness revert back to the unfamiliar and unknown condition it once was.”
This article first appeared on WebMD.com.
Ambulatory BP monitoring reliability questioned for HTN diagnosis
Although guidelines generally recommend ambulatory over home blood pressure monitoring for diagnosing hypertension, new research questions home BP monitoring’s role as second fiddle.
One week of home BP monitoring (HBPM) was more reliable than one 24-hour ambulatory BP or nine mercury readings across three office visits among younger, untreated participants in the Improving the Detection of Hypertension study.
The reliability coefficients were 0.938, 0.846, and 0.894 for systolic BP and 0.918, 0.843, and 0.847 for diastolic BP, respectively.
Further, HBPM had the strongest association with left ventricular mass index (LVMI), a predictor of adverse cardiovascular events, according to researchers led by Joseph E. Schwartz, PhD, Stony Brook (N.Y.) University and Columbia University Irving Medical Center, New York.
The association with LVMI also remained after multivariate adjustment and after correcting for regression dilution bias, indicating the results were not a result of differences in the number of readings, they write in the study, published online in the Journal of the American College of Cardiology.
Whenever patients have an elevated blood pressure for the first time or even borderline elevated BP, guidelines recommend clinicians request a 24-hour ambulatory recording or home monitoring, Dr. Schwartz said in an interview. “I think this has the potential, for that purpose, to put ambulatory blood pressure monitoring out of business, even though that’s what I’ve done for 30 years.”
Previous studies have shown that home and ambulatory BP monitoring (ABPM) correlate more strongly with target-organ damage and cardiovascular outcomes than office BP, but head-to-head outcomes trials of the two techniques are lacking. A recent systematic review also found scant evidence supporting one approach over the other for predicting cardiovascular events or mortality.
An accompanying editorial notes that ABPM is largely unavailable to primary care physicians in the United States and poorly reimbursed. “Thus the demonstration that HBPM is more reliable and associates more closely with LVMI than ABPM, if confirmed, would carry the potential to change clinical practice,” wrote Robert M. Carey, MD, University of Virginia Health System in Charlottesville, and Thomas H. Marwick, MBBS, PhD, MPH, Baker Heart and Diabetes Institute, Melbourne.
In a comment, ABPM proponent Raymond R. Townsend, MD, said, “Honestly, it may be that we’ll need to act on this. I’m not quite ready to do that and change my practice patterns but, on the other hand, I can’t sweep this under the rug.”
He noted that it’s ironic the study is coauthored by the late Thomas Pickering, MD, a maven of ABPM who coined the term “white-coat hypertension” and pointed out masked hypertension.
That said, “it raised the bar on ambulatory blood pressure monitoring: Is it really worth our public health dollars? So I think it’s a very good call to arms,” said Dr. Townsend, who directs the hypertension program at the University of Pennsylvania, Philadelphia.
Ambulatory BP monitoring has long been considered the preferred method but, from a cost standpoint, HBPM is more attractive because the devices can be used more than once and track more than one person in a household, he said. The Center for Medicare Management also has a code in the 2020 bundle to reimburse physicians $15 for training patients and has a monthly charge for communicating with those filing regularly. “You’re not going to get rich doing monitoring of home BP, but at least the government is recognizing we are moving more and more to the home base in terms of our managing common conditions like blood pressure.”
One of the attractions of ABPM is the ability to do every half hour to every hour nocturnal pressures, but at least one home monitor, manufactured by Microlife, has added a nocturnal feature, Dr. Townsend noted. “So that’s just one more incoming against the ABPM defenses about why ABPMs are still better.”
The study enrolled a community-based sample of 408 participants who had office BP assessed at three visits (three readings per visit) using a mercury sphygmomanometer, a BpTRU (VSM MedTech) automated oscillometric device, and a home-validated Omron Healthcare oscillometric device.
After 5 minutes of in-office training and receipt of a reference sheet, participants also completed 3 weeks of HBPM with the Omron device as well as two 24-hour ambulatory measurements (Spacelabs Healthcare, Model 90207). Cardiovascular evaluations, including two-dimensional echocardiograms, were performed during the fifth office visit.
The 400 participants who completed all five visits had a mean age of 41 years, mean LVMI of 79.3 g/m2, and mean office systolic BP ranging from 116.0 to 117.2 mm Hg and diastolic BP from 75.6 to 76.5 mm Hg.
Both before and after correction for regression dilution bias, home systolic and diastolic BP were more highly correlated with LVMI than 24-hour ambulatory or office mercury readings. The corrected correlations for systolic BP were 0.501, 0.430, and 0.389, respectively.
After multivariable adjustment including office and 24-hour ambulatory BP, 10 mm Hg higher systolic and diastolic home BP were associated with 5.07 g/m2 (P = .001) and 3.92 g/m2 (P = .07) higher LVMI, respectively. After adjustment for home BP, however, neither systolic or diastolic office BP nor ambulatory BP was associated with LVMI.
Dr. Townsend and editorialists Dr. Carey and Dr. Marwick pointed out the study included a younger population in whom just 30% to 50% would have been classified as having hypertension by the 2017 American College of Cardiology/American Heart Association guidelines, which Dr. Carey helped to pen.
“These people are young and older people have a different kind of blood pressure driven more by the stiffness in their circulation and less by the resistance to blood flow that you find more characteristic in younger people,” Dr. Townsend observed.
“I don’t know that you can extrapolate the findings from this study in healthy, younger untreated people to older, perhaps sicker, and more diabetic people where the real action is and where the endpoints like heart attack, death, and stroke actually occur,” he said.
The results suggest measurement of resting daytime BP may be relatively more important than dynamic daytime and/or nocturnal parameters in predicting subclinical cardiac target organ damage, but this requires further study, Dr. Carey and Dr. Marwick noted.
Commenting further, they wrote that the results suggest “HBPM could be especially important for detecting elevated BP and hypertension early in life, when adults are relatively healthy, but those with hypertension have a high lifetime risk of CVD.”
Dr. Schwartz acknowledged the study didn’t include the typical hypertensive patient but said it goes to the central question of whether the risk associated with blood pressure is because of the heart’s cumulative exposure over its lifetime and, thus, best measured with multiple readings taken under a variety of circumstances or with readings taken only at rest.
“I’ve been posing that question at a conceptual level for 15 years, never in print, and this paper is the first hint, at least with respect to the left ventricular mass index … that getting a better measure of resting blood pressure is more important for controlling risk than the heart’s cumulative exposure to blood pressure, as measured by ambulatory,” he said.
The Improving the Detection of Hypertension study was supported by a grant from the National Heart, Lung, and Blood Institute of the National Institutes of Health. The authors disclosed no relevant financial relationships. Dr. Townsend reported receiving royalties as a writer for UpToDate and serving as an unpaid reviewer for ValidateBP.org. Dr. Carey is principal investigator and project director of a NIH R01 and P01 grant, respectively; vice chair of the 2017 ACC/AHA hypertension guideline writing committee; and chair of the AHA Resistant Hypertension Scientific Statement writing committee. Dr. Marwick disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Although guidelines generally recommend ambulatory over home blood pressure monitoring for diagnosing hypertension, new research questions home BP monitoring’s role as second fiddle.
One week of home BP monitoring (HBPM) was more reliable than one 24-hour ambulatory BP or nine mercury readings across three office visits among younger, untreated participants in the Improving the Detection of Hypertension study.
The reliability coefficients were 0.938, 0.846, and 0.894 for systolic BP and 0.918, 0.843, and 0.847 for diastolic BP, respectively.
Further, HBPM had the strongest association with left ventricular mass index (LVMI), a predictor of adverse cardiovascular events, according to researchers led by Joseph E. Schwartz, PhD, Stony Brook (N.Y.) University and Columbia University Irving Medical Center, New York.
The association with LVMI also remained after multivariate adjustment and after correcting for regression dilution bias, indicating the results were not a result of differences in the number of readings, they write in the study, published online in the Journal of the American College of Cardiology.
Whenever patients have an elevated blood pressure for the first time or even borderline elevated BP, guidelines recommend clinicians request a 24-hour ambulatory recording or home monitoring, Dr. Schwartz said in an interview. “I think this has the potential, for that purpose, to put ambulatory blood pressure monitoring out of business, even though that’s what I’ve done for 30 years.”
Previous studies have shown that home and ambulatory BP monitoring (ABPM) correlate more strongly with target-organ damage and cardiovascular outcomes than office BP, but head-to-head outcomes trials of the two techniques are lacking. A recent systematic review also found scant evidence supporting one approach over the other for predicting cardiovascular events or mortality.
An accompanying editorial notes that ABPM is largely unavailable to primary care physicians in the United States and poorly reimbursed. “Thus the demonstration that HBPM is more reliable and associates more closely with LVMI than ABPM, if confirmed, would carry the potential to change clinical practice,” wrote Robert M. Carey, MD, University of Virginia Health System in Charlottesville, and Thomas H. Marwick, MBBS, PhD, MPH, Baker Heart and Diabetes Institute, Melbourne.
In a comment, ABPM proponent Raymond R. Townsend, MD, said, “Honestly, it may be that we’ll need to act on this. I’m not quite ready to do that and change my practice patterns but, on the other hand, I can’t sweep this under the rug.”
He noted that it’s ironic the study is coauthored by the late Thomas Pickering, MD, a maven of ABPM who coined the term “white-coat hypertension” and pointed out masked hypertension.
That said, “it raised the bar on ambulatory blood pressure monitoring: Is it really worth our public health dollars? So I think it’s a very good call to arms,” said Dr. Townsend, who directs the hypertension program at the University of Pennsylvania, Philadelphia.
Ambulatory BP monitoring has long been considered the preferred method but, from a cost standpoint, HBPM is more attractive because the devices can be used more than once and track more than one person in a household, he said. The Center for Medicare Management also has a code in the 2020 bundle to reimburse physicians $15 for training patients and has a monthly charge for communicating with those filing regularly. “You’re not going to get rich doing monitoring of home BP, but at least the government is recognizing we are moving more and more to the home base in terms of our managing common conditions like blood pressure.”
One of the attractions of ABPM is the ability to do every half hour to every hour nocturnal pressures, but at least one home monitor, manufactured by Microlife, has added a nocturnal feature, Dr. Townsend noted. “So that’s just one more incoming against the ABPM defenses about why ABPMs are still better.”
The study enrolled a community-based sample of 408 participants who had office BP assessed at three visits (three readings per visit) using a mercury sphygmomanometer, a BpTRU (VSM MedTech) automated oscillometric device, and a home-validated Omron Healthcare oscillometric device.
After 5 minutes of in-office training and receipt of a reference sheet, participants also completed 3 weeks of HBPM with the Omron device as well as two 24-hour ambulatory measurements (Spacelabs Healthcare, Model 90207). Cardiovascular evaluations, including two-dimensional echocardiograms, were performed during the fifth office visit.
The 400 participants who completed all five visits had a mean age of 41 years, mean LVMI of 79.3 g/m2, and mean office systolic BP ranging from 116.0 to 117.2 mm Hg and diastolic BP from 75.6 to 76.5 mm Hg.
Both before and after correction for regression dilution bias, home systolic and diastolic BP were more highly correlated with LVMI than 24-hour ambulatory or office mercury readings. The corrected correlations for systolic BP were 0.501, 0.430, and 0.389, respectively.
After multivariable adjustment including office and 24-hour ambulatory BP, 10 mm Hg higher systolic and diastolic home BP were associated with 5.07 g/m2 (P = .001) and 3.92 g/m2 (P = .07) higher LVMI, respectively. After adjustment for home BP, however, neither systolic or diastolic office BP nor ambulatory BP was associated with LVMI.
Dr. Townsend and editorialists Dr. Carey and Dr. Marwick pointed out the study included a younger population in whom just 30% to 50% would have been classified as having hypertension by the 2017 American College of Cardiology/American Heart Association guidelines, which Dr. Carey helped to pen.
“These people are young and older people have a different kind of blood pressure driven more by the stiffness in their circulation and less by the resistance to blood flow that you find more characteristic in younger people,” Dr. Townsend observed.
“I don’t know that you can extrapolate the findings from this study in healthy, younger untreated people to older, perhaps sicker, and more diabetic people where the real action is and where the endpoints like heart attack, death, and stroke actually occur,” he said.
The results suggest measurement of resting daytime BP may be relatively more important than dynamic daytime and/or nocturnal parameters in predicting subclinical cardiac target organ damage, but this requires further study, Dr. Carey and Dr. Marwick noted.
Commenting further, they wrote that the results suggest “HBPM could be especially important for detecting elevated BP and hypertension early in life, when adults are relatively healthy, but those with hypertension have a high lifetime risk of CVD.”
Dr. Schwartz acknowledged the study didn’t include the typical hypertensive patient but said it goes to the central question of whether the risk associated with blood pressure is because of the heart’s cumulative exposure over its lifetime and, thus, best measured with multiple readings taken under a variety of circumstances or with readings taken only at rest.
“I’ve been posing that question at a conceptual level for 15 years, never in print, and this paper is the first hint, at least with respect to the left ventricular mass index … that getting a better measure of resting blood pressure is more important for controlling risk than the heart’s cumulative exposure to blood pressure, as measured by ambulatory,” he said.
The Improving the Detection of Hypertension study was supported by a grant from the National Heart, Lung, and Blood Institute of the National Institutes of Health. The authors disclosed no relevant financial relationships. Dr. Townsend reported receiving royalties as a writer for UpToDate and serving as an unpaid reviewer for ValidateBP.org. Dr. Carey is principal investigator and project director of a NIH R01 and P01 grant, respectively; vice chair of the 2017 ACC/AHA hypertension guideline writing committee; and chair of the AHA Resistant Hypertension Scientific Statement writing committee. Dr. Marwick disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Although guidelines generally recommend ambulatory over home blood pressure monitoring for diagnosing hypertension, new research questions home BP monitoring’s role as second fiddle.
One week of home BP monitoring (HBPM) was more reliable than one 24-hour ambulatory BP or nine mercury readings across three office visits among younger, untreated participants in the Improving the Detection of Hypertension study.
The reliability coefficients were 0.938, 0.846, and 0.894 for systolic BP and 0.918, 0.843, and 0.847 for diastolic BP, respectively.
Further, HBPM had the strongest association with left ventricular mass index (LVMI), a predictor of adverse cardiovascular events, according to researchers led by Joseph E. Schwartz, PhD, Stony Brook (N.Y.) University and Columbia University Irving Medical Center, New York.
The association with LVMI also remained after multivariate adjustment and after correcting for regression dilution bias, indicating the results were not a result of differences in the number of readings, they write in the study, published online in the Journal of the American College of Cardiology.
Whenever patients have an elevated blood pressure for the first time or even borderline elevated BP, guidelines recommend clinicians request a 24-hour ambulatory recording or home monitoring, Dr. Schwartz said in an interview. “I think this has the potential, for that purpose, to put ambulatory blood pressure monitoring out of business, even though that’s what I’ve done for 30 years.”
Previous studies have shown that home and ambulatory BP monitoring (ABPM) correlate more strongly with target-organ damage and cardiovascular outcomes than office BP, but head-to-head outcomes trials of the two techniques are lacking. A recent systematic review also found scant evidence supporting one approach over the other for predicting cardiovascular events or mortality.
An accompanying editorial notes that ABPM is largely unavailable to primary care physicians in the United States and poorly reimbursed. “Thus the demonstration that HBPM is more reliable and associates more closely with LVMI than ABPM, if confirmed, would carry the potential to change clinical practice,” wrote Robert M. Carey, MD, University of Virginia Health System in Charlottesville, and Thomas H. Marwick, MBBS, PhD, MPH, Baker Heart and Diabetes Institute, Melbourne.
In a comment, ABPM proponent Raymond R. Townsend, MD, said, “Honestly, it may be that we’ll need to act on this. I’m not quite ready to do that and change my practice patterns but, on the other hand, I can’t sweep this under the rug.”
He noted that it’s ironic the study is coauthored by the late Thomas Pickering, MD, a maven of ABPM who coined the term “white-coat hypertension” and pointed out masked hypertension.
That said, “it raised the bar on ambulatory blood pressure monitoring: Is it really worth our public health dollars? So I think it’s a very good call to arms,” said Dr. Townsend, who directs the hypertension program at the University of Pennsylvania, Philadelphia.
Ambulatory BP monitoring has long been considered the preferred method but, from a cost standpoint, HBPM is more attractive because the devices can be used more than once and track more than one person in a household, he said. The Center for Medicare Management also has a code in the 2020 bundle to reimburse physicians $15 for training patients and has a monthly charge for communicating with those filing regularly. “You’re not going to get rich doing monitoring of home BP, but at least the government is recognizing we are moving more and more to the home base in terms of our managing common conditions like blood pressure.”
One of the attractions of ABPM is the ability to do every half hour to every hour nocturnal pressures, but at least one home monitor, manufactured by Microlife, has added a nocturnal feature, Dr. Townsend noted. “So that’s just one more incoming against the ABPM defenses about why ABPMs are still better.”
The study enrolled a community-based sample of 408 participants who had office BP assessed at three visits (three readings per visit) using a mercury sphygmomanometer, a BpTRU (VSM MedTech) automated oscillometric device, and a home-validated Omron Healthcare oscillometric device.
After 5 minutes of in-office training and receipt of a reference sheet, participants also completed 3 weeks of HBPM with the Omron device as well as two 24-hour ambulatory measurements (Spacelabs Healthcare, Model 90207). Cardiovascular evaluations, including two-dimensional echocardiograms, were performed during the fifth office visit.
The 400 participants who completed all five visits had a mean age of 41 years, mean LVMI of 79.3 g/m2, and mean office systolic BP ranging from 116.0 to 117.2 mm Hg and diastolic BP from 75.6 to 76.5 mm Hg.
Both before and after correction for regression dilution bias, home systolic and diastolic BP were more highly correlated with LVMI than 24-hour ambulatory or office mercury readings. The corrected correlations for systolic BP were 0.501, 0.430, and 0.389, respectively.
After multivariable adjustment including office and 24-hour ambulatory BP, 10 mm Hg higher systolic and diastolic home BP were associated with 5.07 g/m2 (P = .001) and 3.92 g/m2 (P = .07) higher LVMI, respectively. After adjustment for home BP, however, neither systolic or diastolic office BP nor ambulatory BP was associated with LVMI.
Dr. Townsend and editorialists Dr. Carey and Dr. Marwick pointed out the study included a younger population in whom just 30% to 50% would have been classified as having hypertension by the 2017 American College of Cardiology/American Heart Association guidelines, which Dr. Carey helped to pen.
“These people are young and older people have a different kind of blood pressure driven more by the stiffness in their circulation and less by the resistance to blood flow that you find more characteristic in younger people,” Dr. Townsend observed.
“I don’t know that you can extrapolate the findings from this study in healthy, younger untreated people to older, perhaps sicker, and more diabetic people where the real action is and where the endpoints like heart attack, death, and stroke actually occur,” he said.
The results suggest measurement of resting daytime BP may be relatively more important than dynamic daytime and/or nocturnal parameters in predicting subclinical cardiac target organ damage, but this requires further study, Dr. Carey and Dr. Marwick noted.
Commenting further, they wrote that the results suggest “HBPM could be especially important for detecting elevated BP and hypertension early in life, when adults are relatively healthy, but those with hypertension have a high lifetime risk of CVD.”
Dr. Schwartz acknowledged the study didn’t include the typical hypertensive patient but said it goes to the central question of whether the risk associated with blood pressure is because of the heart’s cumulative exposure over its lifetime and, thus, best measured with multiple readings taken under a variety of circumstances or with readings taken only at rest.
“I’ve been posing that question at a conceptual level for 15 years, never in print, and this paper is the first hint, at least with respect to the left ventricular mass index … that getting a better measure of resting blood pressure is more important for controlling risk than the heart’s cumulative exposure to blood pressure, as measured by ambulatory,” he said.
The Improving the Detection of Hypertension study was supported by a grant from the National Heart, Lung, and Blood Institute of the National Institutes of Health. The authors disclosed no relevant financial relationships. Dr. Townsend reported receiving royalties as a writer for UpToDate and serving as an unpaid reviewer for ValidateBP.org. Dr. Carey is principal investigator and project director of a NIH R01 and P01 grant, respectively; vice chair of the 2017 ACC/AHA hypertension guideline writing committee; and chair of the AHA Resistant Hypertension Scientific Statement writing committee. Dr. Marwick disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
COVID-19 vaccines: Safe for immunocompromised patients?
Coronavirus vaccines have become a reality, as they are now being approved and authorized for use in a growing number of countries including the United States. The U.S. Food and Drug Administration has just issued emergency authorization for the use of the COVID-19 vaccine produced by Pfizer and BioNTech. Close behind is the vaccine developed by Moderna, which has also applied to the FDA for emergency authorization.

The efficacy of a two-dose administration of the vaccine has been pegged at 95.0%, and the FDA has said that the 95% credible interval for the vaccine efficacy was 90.3%-97.6%. But as with many initial clinical trials, whether for drugs or vaccines, not all populations were represented in the trial cohort, including individuals who are immunocompromised. At the current time, it is largely unknown how safe or effective the vaccine may be in this large population, many of whom are at high risk for serious COVID-19 complications.
At a special session held during the recent annual meeting of the American Society of Hematology, Anthony Fauci, MD, the nation’s leading infectious disease expert, said that individuals with compromised immune systems, whether because of chemotherapy or a bone marrow transplant, should plan to be vaccinated when the opportunity arises.

In response to a question from ASH President Stephanie J. Lee, MD, of the Fred Hutchinson Cancer Center, Seattle, Dr. Fauci emphasized that, despite being excluded from clinical trials, this population should get vaccinated. “I think we should recommend that they get vaccinated,” he said. “I mean, it is clear that, if you are on immunosuppressive agents, history tells us that you’re not going to have as robust a response as if you had an intact immune system that was not being compromised. But some degree of immunity is better than no degree of immunity.”
That does seem to be the consensus among experts who spoke in interviews: that as long as these are not live attenuated vaccines, they hold no specific risk to an immunocompromised patient, other than any factors specific to the individual that could be a contraindication.
“Patients, family members, friends, and work contacts should be encouraged to receive the vaccine,” said William Stohl, MD, PhD, chief of the division of rheumatology at the University of Southern California, Los Angeles. “Clinicians should advise patients to obtain the vaccine sooner rather than later.”
Kevin C. Wang, MD, PhD, of the department of dermatology at Stanford (Calif.) University, agreed. “I am 100% with Dr. Fauci. Everyone should get the vaccine, even if it may not be as effective,” he said. “I would treat it exactly like the flu vaccines that we recommend folks get every year.”
Dr. Wang noted that he couldn’t think of any contraindications unless the immunosuppressed patients have a history of severe allergic reactions to prior vaccinations. “But I would even say patients with history of cancer, upon recommendation of their oncologists, are likely to be suitable candidates for the vaccine,” he added. “I would say clinicians should approach counseling the same way they counsel patients for the flu vaccine, and as far as I know, there are no concerns for systemic drugs commonly used in dermatology patients.”
However, guidance has not yet been issued from either the FDA or the Centers for Disease Control and Prevention regarding the use of the vaccine in immunocompromised individuals. Given the lack of data, the FDA has said that “it will be something that providers will need to consider on an individual basis,” and that individuals should consult with physicians to weigh the potential benefits and potential risks.
The CDC’s Advisory Committee on Immunization Practices has said that clinicians need more guidance on whether to use the vaccine in pregnant or breastfeeding women, the immunocompromised, or those who have a history of allergies. The CDC itself has not yet released its formal guidance on vaccine use.
COVID-19 vaccines
Vaccines typically require years of research and testing before reaching the clinic, but this year researchers embarked on a global effort to develop safe and effective coronavirus vaccines in record time. Both the Pfizer/BioNTech and Moderna vaccines have only a few months of phase 3 clinical trial data, so much remains unknown about them, including their duration of effect and any long-term safety signals. In addition to excluding immunocompromised individuals, the clinical trials did not include children or pregnant women, so data are lacking for several population subgroups.
But these will not be the only vaccines available, as the pipeline is already becoming crowded. U.S. clinical trial data from a vaccine jointly being developed by Oxford-AstraZeneca, could potentially be ready, along with a request for FDA emergency use authorization, by late January 2021.
In addition, China and Russia have released vaccines, and there are currently 61 vaccines being investigated in clinical trials and at least 85 preclinical products under active investigation.
The vaccine candidates are using both conventional and novel mechanisms of action to elicit an immune response in patients. Conventional methods include attenuated inactivated (killed) virus and recombinant viral protein vaccines to develop immunity. Novel approaches include replication-deficient, adenovirus vector-based vaccines that contain the viral protein, and mRNA-based vaccines, such as the Pfizer and Moderna vaccines, that encode for a SARS-CoV-2 spike protein.
“The special vaccine concern for immunocompromised individuals is introduction of a live virus,” Dr. Stohl said. “Neither the Moderna nor Pfizer vaccines are live viruses, so there should be no special contraindication for such individuals.”
Live vaccine should be avoided in immunocompromised patients, and currently, live SARS-CoV-2 vaccines are only being developed in India and Turkey.
It is not unusual for vaccine trials to begin with cohorts that exclude participants with various health conditions, including those who are immunocompromised. These groups are generally then evaluated in phase 4 trials, or postmarketing surveillance. While the precise number of immunosuppressed adults in the United States is not known, the numbers are believed to be rising because of increased life expectancy among immunosuppressed adults as a result of advances in treatment and new and wider indications for therapies that can affect the immune system.
According to data from the 2013 National Health Interview Survey, an estimated 2.7% of U.S. adults are immunosuppressed. This population covers a broad array of health conditions and medical specialties; people living with inflammatory or autoimmune conditions, such as inflammatory rheumatic diseases (rheumatoid arthritis, axial spondyloarthritis, lupus); inflammatory bowel disease (Crohn’s disease and ulcerative colitis); psoriasis; multiple sclerosis; organ transplant recipients; patients undergoing chemotherapy; and life-long immunosuppression attributable to HIV infection.
As the vaccines begin to roll out and become available, how should clinicians advise their patients, in the absence of any clinical trial data?
Risk vs. benefit
Gilaad Kaplan, MD, MPH, a gastroenterologist and professor of medicine at the University of Calgary (Alta.), noted that the inflammatory bowel disease (IBD) community has dealt with tremendous anxiety during the pandemic because many are immunocompromised because of the medications they use to treat their disease.
“For example, many patients with IBD are on biologics like anti-TNF [tumor necrosis factor] therapies, which are also used in other immune-mediated inflammatory diseases such as rheumatoid arthritis,” he said. “Understandably, individuals with IBD on immunosuppressive medications are concerned about the risk of severe complications due to COVID-19.”
The entire IBD community, along with the world, celebrated the announcement that multiple vaccines are protective against SARS-CoV-2, he noted. “Vaccines offer the potential to reduce the spread of COVID-19, allowing society to revert back to normalcy,” Dr. Kaplan said. “Moreover, for vulnerable populations, including those who are immunocompromised, vaccines offer the potential to directly protect them from the morbidity and mortality associated with COVID-19.”
That said, even though the news of vaccines are extremely promising, some cautions must be raised regarding their use in immunocompromised populations, such as persons with IBD. “The current trials, to my knowledge, did not include immunocompromised individuals and thus, we can only extrapolate from what we know from other trials of different vaccines,” he explained. “We know from prior vaccines studies that the immune response following vaccination is less robust in those who are immunocompromised as compared to a healthy control population.”
Dr. Kaplan also pointed to recent reports of allergic reactions that have been reported in healthy individuals. “We don’t know whether side effects, like allergic reactions, may be different in unstudied populations,” he said. “Thus, the medical and scientific community should prioritize clinical studies of safety and effectiveness of COVID-19 vaccines in immunocompromised populations.”
So, what does this mean for an individual with an immune-mediated inflammatory disease like Crohn’s disease or ulcerative colitis who is immunocompromised? Dr. Kaplan explained that it is a balance between the potential harm of being infected with COVID-19 and the uncertainty of receiving a vaccine in an understudied population. For those who are highly susceptible to dying from COVID-19, such as an older adult with IBD, or someone who faces high exposure, such as a health care worker, the potential protection of the vaccine greatly outweighs the uncertainty.
“However, for individuals who are at otherwise lower risk – for example, young and able to work from home – then waiting a few extra months for postmarketing surveillance studies in immunocompromised populations may be a reasonable approach, as long as these individuals are taking great care to avoid infection,” he said.
No waiting needed
Joel M. Gelfand, MD, MSCE, professor of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, feels that the newly approved vaccine should be safe for most of his patients.

“Patients with psoriatic disease should get the mRNA-based COVID-19 vaccine as soon as possible based on eligibility as determined by the CDC and local public health officials,” he said. “It is not a live vaccine, and therefore patients on biologics or other immune-modulating or immune-suppressing treatment can receive it.”
However, the impact of psoriasis treatment on immune response to the mRNA-based vaccines is not known. Dr. Gelfand noted that, extrapolating from the vaccine literature, there is some evidence that methotrexate reduces response to the influenza vaccine. “However, the clinical significance of this finding is not clear,” he said. “Since the mRNA vaccine needs to be taken twice, a few weeks apart, I do not recommend interrupting or delaying treatment for psoriatic disease while undergoing vaccination for COVID-19.”
Given the reports of allergic reactions, he added that it is advisable for patients with a history of life-threatening allergic reactions such as anaphylaxis or who have been advised to carry an epinephrine autoinjector, to talk with their health care provider to determine if COVID-19 vaccination is medically appropriate.
The National Psoriasis Foundation has issued guidance on COVID-19, explained Steven R. Feldman, MD, PhD, professor of dermatology, pathology, and social sciences & health policy at Wake Forest University, Winston-Salem, N.C., who is also a member of the committee that is working on those guidelines and keeping them up to date. “We are in the process of updating the guidelines with information on COVID vaccines,” he said.

He agreed that there are no contraindications for psoriasis patients to receive the vaccine, regardless of whether they are on immunosuppressive treatment, even though definitive data are lacking. “Fortunately, there’s a lot of good data coming out of Italy that patients with psoriasis on biologics do not appear to be at increased risk of getting COVID or of having worse outcomes from COVID,” he said.
Patients are going to ask about the vaccines, and when counseling them, clinicians should discuss the available data, the residual uncertainty, and patients’ concerns should be considered, Dr. Feldman explained. “There may be some concern that steroids and cyclosporine would reduce the effectiveness of vaccines, but there is no concern that any of the drugs would cause increased risk from nonlive vaccines.”
He added that there is evidence that “patients on biologics who receive nonlive vaccines do develop antibody responses and are immunized.”
Boosting efficacy
Even prior to making their announcement, the American College of Rheumatology had said that they would endorse the vaccine for all patients, explained rheumatologist Brett Smith, DO, from Blount Memorial Physicians Group and East Tennessee Children’s Hospital, Alcoa. “The vaccine is safe for all patients, but the problem may be that it’s not as effective,” he said. “But we don’t know that because it hasn’t been tested.”
With other vaccines, biologic medicines are held for 2 weeks before and afterwards, to get the best response. “But some patients don’t want to stop the medication,” Dr. Smith said. “They are afraid that their symptoms will return.”
As for counseling patients as to whether they should receive this vaccine, he explained that he typically doesn’t try to sway patients one way or another until they are really high risk. “When I counsel, it really depends on the individual situation. And for this vaccine, we have to be open to the fact that many people have already made up their mind.”
There are a lot of questions regarding the vaccine. One is the short time frame of development. “Vaccines typically take 6-10 years to come on the market, and this one is now available after a 3-month study,” Dr. Smith said. “Some have already decided that it’s too new for them.”
The process is also new, and patients need to understand that it doesn’t contain an active virus and “you can’t catch coronavirus from it.”
Dr. Smith also explained that, because the vaccine may be less effective in a person using biologic therapies, there is currently no information available on repeat vaccination. “These are all unanswered questions,” he said. “If the antibodies wane in a short time, can we be revaccinated and in what time frame? We just don’t know that yet.”
Marcelo Bonomi, MD, a medical oncologist from The Ohio State University Comprehensive Cancer Center, Columbus, explained that one way to ensure a more optimal response to the vaccine would be to wait until the patient has finished chemotherapy.* “The vaccine can be offered at that time, and in the meantime, they can take other steps to avoid infection,” he said. “If they are very immunosuppressed, it isn’t worth trying to give the vaccine.”
Cancer patients should be encouraged to stay as healthy as possible, and to wear masks and social distance. “It’s a comprehensive approach. Eat healthy, avoid alcohol and tobacco, and exercise. [These things] will help boost the immune system,” Dr. Bonomi said. “Family members should be encouraged to get vaccinated, which will help them avoid infection and exposing the patient.”
Jim Boonyaratanakornkit, MD, PhD, an infectious disease specialist who cares for cancer patients at the Fred Hutchinson Cancer Research Center, agreed. “Giving a vaccine right after a transplant is a futile endeavor,” he said. “We need to wait 6 months to have an immune response.”
He pointed out there may be a continuing higher number of cases, with high levels peaking in Washington in February and March. “Close friends and family should be vaccinated if possible,” he said, “which will help interrupt transmission.”
The vaccines are using new platforms that are totally different, and there is no clear data as to how long the antibodies will persist. “We know that they last for at least 4 months,” said Dr. Boonyaratanakornkit. “We don’t know what level of antibody will protect them from COVID-19 infection. Current studies are being conducted, but we don’t have that information for anyone yet.”
*Correction, 1/7/21: An earlier version of this article misattributed quotes from Dr. Marcelo Bonomi.
Coronavirus vaccines have become a reality, as they are now being approved and authorized for use in a growing number of countries including the United States. The U.S. Food and Drug Administration has just issued emergency authorization for the use of the COVID-19 vaccine produced by Pfizer and BioNTech. Close behind is the vaccine developed by Moderna, which has also applied to the FDA for emergency authorization.
The efficacy of a two-dose administration of the vaccine has been pegged at 95.0%, and the FDA has said that the 95% credible interval for the vaccine efficacy was 90.3%-97.6%. But as with many initial clinical trials, whether for drugs or vaccines, not all populations were represented in the trial cohort, including individuals who are immunocompromised. At the current time, it is largely unknown how safe or effective the vaccine may be in this large population, many of whom are at high risk for serious COVID-19 complications.
At a special session held during the recent annual meeting of the American Society of Hematology, Anthony Fauci, MD, the nation’s leading infectious disease expert, said that individuals with compromised immune systems, whether because of chemotherapy or a bone marrow transplant, should plan to be vaccinated when the opportunity arises.
In response to a question from ASH President Stephanie J. Lee, MD, of the Fred Hutchinson Cancer Center, Seattle, Dr. Fauci emphasized that, despite being excluded from clinical trials, this population should get vaccinated. “I think we should recommend that they get vaccinated,” he said. “I mean, it is clear that, if you are on immunosuppressive agents, history tells us that you’re not going to have as robust a response as if you had an intact immune system that was not being compromised. But some degree of immunity is better than no degree of immunity.”
That does seem to be the consensus among experts who spoke in interviews: that as long as these are not live attenuated vaccines, they hold no specific risk to an immunocompromised patient, other than any factors specific to the individual that could be a contraindication.
“Patients, family members, friends, and work contacts should be encouraged to receive the vaccine,” said William Stohl, MD, PhD, chief of the division of rheumatology at the University of Southern California, Los Angeles. “Clinicians should advise patients to obtain the vaccine sooner rather than later.”
Kevin C. Wang, MD, PhD, of the department of dermatology at Stanford (Calif.) University, agreed. “I am 100% with Dr. Fauci. Everyone should get the vaccine, even if it may not be as effective,” he said. “I would treat it exactly like the flu vaccines that we recommend folks get every year.”
Dr. Wang noted that he couldn’t think of any contraindications unless the immunosuppressed patients have a history of severe allergic reactions to prior vaccinations. “But I would even say patients with history of cancer, upon recommendation of their oncologists, are likely to be suitable candidates for the vaccine,” he added. “I would say clinicians should approach counseling the same way they counsel patients for the flu vaccine, and as far as I know, there are no concerns for systemic drugs commonly used in dermatology patients.”
However, guidance has not yet been issued from either the FDA or the Centers for Disease Control and Prevention regarding the use of the vaccine in immunocompromised individuals. Given the lack of data, the FDA has said that “it will be something that providers will need to consider on an individual basis,” and that individuals should consult with physicians to weigh the potential benefits and potential risks.
The CDC’s Advisory Committee on Immunization Practices has said that clinicians need more guidance on whether to use the vaccine in pregnant or breastfeeding women, the immunocompromised, or those who have a history of allergies. The CDC itself has not yet released its formal guidance on vaccine use.
COVID-19 vaccines
Vaccines typically require years of research and testing before reaching the clinic, but this year researchers embarked on a global effort to develop safe and effective coronavirus vaccines in record time. Both the Pfizer/BioNTech and Moderna vaccines have only a few months of phase 3 clinical trial data, so much remains unknown about them, including their duration of effect and any long-term safety signals. In addition to excluding immunocompromised individuals, the clinical trials did not include children or pregnant women, so data are lacking for several population subgroups.
But these will not be the only vaccines available, as the pipeline is already becoming crowded. U.S. clinical trial data from a vaccine jointly being developed by Oxford-AstraZeneca, could potentially be ready, along with a request for FDA emergency use authorization, by late January 2021.
In addition, China and Russia have released vaccines, and there are currently 61 vaccines being investigated in clinical trials and at least 85 preclinical products under active investigation.
The vaccine candidates are using both conventional and novel mechanisms of action to elicit an immune response in patients. Conventional methods include attenuated inactivated (killed) virus and recombinant viral protein vaccines to develop immunity. Novel approaches include replication-deficient, adenovirus vector-based vaccines that contain the viral protein, and mRNA-based vaccines, such as the Pfizer and Moderna vaccines, that encode for a SARS-CoV-2 spike protein.
“The special vaccine concern for immunocompromised individuals is introduction of a live virus,” Dr. Stohl said. “Neither the Moderna nor Pfizer vaccines are live viruses, so there should be no special contraindication for such individuals.”
Live vaccine should be avoided in immunocompromised patients, and currently, live SARS-CoV-2 vaccines are only being developed in India and Turkey.
It is not unusual for vaccine trials to begin with cohorts that exclude participants with various health conditions, including those who are immunocompromised. These groups are generally then evaluated in phase 4 trials, or postmarketing surveillance. While the precise number of immunosuppressed adults in the United States is not known, the numbers are believed to be rising because of increased life expectancy among immunosuppressed adults as a result of advances in treatment and new and wider indications for therapies that can affect the immune system.
According to data from the 2013 National Health Interview Survey, an estimated 2.7% of U.S. adults are immunosuppressed. This population covers a broad array of health conditions and medical specialties; people living with inflammatory or autoimmune conditions, such as inflammatory rheumatic diseases (rheumatoid arthritis, axial spondyloarthritis, lupus); inflammatory bowel disease (Crohn’s disease and ulcerative colitis); psoriasis; multiple sclerosis; organ transplant recipients; patients undergoing chemotherapy; and life-long immunosuppression attributable to HIV infection.
As the vaccines begin to roll out and become available, how should clinicians advise their patients, in the absence of any clinical trial data?
Risk vs. benefit
Gilaad Kaplan, MD, MPH, a gastroenterologist and professor of medicine at the University of Calgary (Alta.), noted that the inflammatory bowel disease (IBD) community has dealt with tremendous anxiety during the pandemic because many are immunocompromised because of the medications they use to treat their disease.
“For example, many patients with IBD are on biologics like anti-TNF [tumor necrosis factor] therapies, which are also used in other immune-mediated inflammatory diseases such as rheumatoid arthritis,” he said. “Understandably, individuals with IBD on immunosuppressive medications are concerned about the risk of severe complications due to COVID-19.”
The entire IBD community, along with the world, celebrated the announcement that multiple vaccines are protective against SARS-CoV-2, he noted. “Vaccines offer the potential to reduce the spread of COVID-19, allowing society to revert back to normalcy,” Dr. Kaplan said. “Moreover, for vulnerable populations, including those who are immunocompromised, vaccines offer the potential to directly protect them from the morbidity and mortality associated with COVID-19.”
That said, even though the news of vaccines are extremely promising, some cautions must be raised regarding their use in immunocompromised populations, such as persons with IBD. “The current trials, to my knowledge, did not include immunocompromised individuals and thus, we can only extrapolate from what we know from other trials of different vaccines,” he explained. “We know from prior vaccines studies that the immune response following vaccination is less robust in those who are immunocompromised as compared to a healthy control population.”
Dr. Kaplan also pointed to recent reports of allergic reactions that have been reported in healthy individuals. “We don’t know whether side effects, like allergic reactions, may be different in unstudied populations,” he said. “Thus, the medical and scientific community should prioritize clinical studies of safety and effectiveness of COVID-19 vaccines in immunocompromised populations.”
So, what does this mean for an individual with an immune-mediated inflammatory disease like Crohn’s disease or ulcerative colitis who is immunocompromised? Dr. Kaplan explained that it is a balance between the potential harm of being infected with COVID-19 and the uncertainty of receiving a vaccine in an understudied population. For those who are highly susceptible to dying from COVID-19, such as an older adult with IBD, or someone who faces high exposure, such as a health care worker, the potential protection of the vaccine greatly outweighs the uncertainty.
“However, for individuals who are at otherwise lower risk – for example, young and able to work from home – then waiting a few extra months for postmarketing surveillance studies in immunocompromised populations may be a reasonable approach, as long as these individuals are taking great care to avoid infection,” he said.
No waiting needed
Joel M. Gelfand, MD, MSCE, professor of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, feels that the newly approved vaccine should be safe for most of his patients.
“Patients with psoriatic disease should get the mRNA-based COVID-19 vaccine as soon as possible based on eligibility as determined by the CDC and local public health officials,” he said. “It is not a live vaccine, and therefore patients on biologics or other immune-modulating or immune-suppressing treatment can receive it.”
However, the impact of psoriasis treatment on immune response to the mRNA-based vaccines is not known. Dr. Gelfand noted that, extrapolating from the vaccine literature, there is some evidence that methotrexate reduces response to the influenza vaccine. “However, the clinical significance of this finding is not clear,” he said. “Since the mRNA vaccine needs to be taken twice, a few weeks apart, I do not recommend interrupting or delaying treatment for psoriatic disease while undergoing vaccination for COVID-19.”
Given the reports of allergic reactions, he added that it is advisable for patients with a history of life-threatening allergic reactions such as anaphylaxis or who have been advised to carry an epinephrine autoinjector, to talk with their health care provider to determine if COVID-19 vaccination is medically appropriate.
The National Psoriasis Foundation has issued guidance on COVID-19, explained Steven R. Feldman, MD, PhD, professor of dermatology, pathology, and social sciences & health policy at Wake Forest University, Winston-Salem, N.C., who is also a member of the committee that is working on those guidelines and keeping them up to date. “We are in the process of updating the guidelines with information on COVID vaccines,” he said.
He agreed that there are no contraindications for psoriasis patients to receive the vaccine, regardless of whether they are on immunosuppressive treatment, even though definitive data are lacking. “Fortunately, there’s a lot of good data coming out of Italy that patients with psoriasis on biologics do not appear to be at increased risk of getting COVID or of having worse outcomes from COVID,” he said.
Patients are going to ask about the vaccines, and when counseling them, clinicians should discuss the available data, the residual uncertainty, and patients’ concerns should be considered, Dr. Feldman explained. “There may be some concern that steroids and cyclosporine would reduce the effectiveness of vaccines, but there is no concern that any of the drugs would cause increased risk from nonlive vaccines.”
He added that there is evidence that “patients on biologics who receive nonlive vaccines do develop antibody responses and are immunized.”
Boosting efficacy
Even prior to making their announcement, the American College of Rheumatology had said that they would endorse the vaccine for all patients, explained rheumatologist Brett Smith, DO, from Blount Memorial Physicians Group and East Tennessee Children’s Hospital, Alcoa. “The vaccine is safe for all patients, but the problem may be that it’s not as effective,” he said. “But we don’t know that because it hasn’t been tested.”
With other vaccines, biologic medicines are held for 2 weeks before and afterwards, to get the best response. “But some patients don’t want to stop the medication,” Dr. Smith said. “They are afraid that their symptoms will return.”
As for counseling patients as to whether they should receive this vaccine, he explained that he typically doesn’t try to sway patients one way or another until they are really high risk. “When I counsel, it really depends on the individual situation. And for this vaccine, we have to be open to the fact that many people have already made up their mind.”
There are a lot of questions regarding the vaccine. One is the short time frame of development. “Vaccines typically take 6-10 years to come on the market, and this one is now available after a 3-month study,” Dr. Smith said. “Some have already decided that it’s too new for them.”
The process is also new, and patients need to understand that it doesn’t contain an active virus and “you can’t catch coronavirus from it.”
Dr. Smith also explained that, because the vaccine may be less effective in a person using biologic therapies, there is currently no information available on repeat vaccination. “These are all unanswered questions,” he said. “If the antibodies wane in a short time, can we be revaccinated and in what time frame? We just don’t know that yet.”
Marcelo Bonomi, MD, a medical oncologist from The Ohio State University Comprehensive Cancer Center, Columbus, explained that one way to ensure a more optimal response to the vaccine would be to wait until the patient has finished chemotherapy.* “The vaccine can be offered at that time, and in the meantime, they can take other steps to avoid infection,” he said. “If they are very immunosuppressed, it isn’t worth trying to give the vaccine.”
Cancer patients should be encouraged to stay as healthy as possible, and to wear masks and social distance. “It’s a comprehensive approach. Eat healthy, avoid alcohol and tobacco, and exercise. [These things] will help boost the immune system,” Dr. Bonomi said. “Family members should be encouraged to get vaccinated, which will help them avoid infection and exposing the patient.”
Jim Boonyaratanakornkit, MD, PhD, an infectious disease specialist who cares for cancer patients at the Fred Hutchinson Cancer Research Center, agreed. “Giving a vaccine right after a transplant is a futile endeavor,” he said. “We need to wait 6 months to have an immune response.”
He pointed out there may be a continuing higher number of cases, with high levels peaking in Washington in February and March. “Close friends and family should be vaccinated if possible,” he said, “which will help interrupt transmission.”
The vaccines are using new platforms that are totally different, and there is no clear data as to how long the antibodies will persist. “We know that they last for at least 4 months,” said Dr. Boonyaratanakornkit. “We don’t know what level of antibody will protect them from COVID-19 infection. Current studies are being conducted, but we don’t have that information for anyone yet.”
*Correction, 1/7/21: An earlier version of this article misattributed quotes from Dr. Marcelo Bonomi.
Coronavirus vaccines have become a reality, as they are now being approved and authorized for use in a growing number of countries including the United States. The U.S. Food and Drug Administration has just issued emergency authorization for the use of the COVID-19 vaccine produced by Pfizer and BioNTech. Close behind is the vaccine developed by Moderna, which has also applied to the FDA for emergency authorization.
The efficacy of a two-dose administration of the vaccine has been pegged at 95.0%, and the FDA has said that the 95% credible interval for the vaccine efficacy was 90.3%-97.6%. But as with many initial clinical trials, whether for drugs or vaccines, not all populations were represented in the trial cohort, including individuals who are immunocompromised. At the current time, it is largely unknown how safe or effective the vaccine may be in this large population, many of whom are at high risk for serious COVID-19 complications.
At a special session held during the recent annual meeting of the American Society of Hematology, Anthony Fauci, MD, the nation’s leading infectious disease expert, said that individuals with compromised immune systems, whether because of chemotherapy or a bone marrow transplant, should plan to be vaccinated when the opportunity arises.
In response to a question from ASH President Stephanie J. Lee, MD, of the Fred Hutchinson Cancer Center, Seattle, Dr. Fauci emphasized that, despite being excluded from clinical trials, this population should get vaccinated. “I think we should recommend that they get vaccinated,” he said. “I mean, it is clear that, if you are on immunosuppressive agents, history tells us that you’re not going to have as robust a response as if you had an intact immune system that was not being compromised. But some degree of immunity is better than no degree of immunity.”
That does seem to be the consensus among experts who spoke in interviews: that as long as these are not live attenuated vaccines, they hold no specific risk to an immunocompromised patient, other than any factors specific to the individual that could be a contraindication.
“Patients, family members, friends, and work contacts should be encouraged to receive the vaccine,” said William Stohl, MD, PhD, chief of the division of rheumatology at the University of Southern California, Los Angeles. “Clinicians should advise patients to obtain the vaccine sooner rather than later.”
Kevin C. Wang, MD, PhD, of the department of dermatology at Stanford (Calif.) University, agreed. “I am 100% with Dr. Fauci. Everyone should get the vaccine, even if it may not be as effective,” he said. “I would treat it exactly like the flu vaccines that we recommend folks get every year.”
Dr. Wang noted that he couldn’t think of any contraindications unless the immunosuppressed patients have a history of severe allergic reactions to prior vaccinations. “But I would even say patients with history of cancer, upon recommendation of their oncologists, are likely to be suitable candidates for the vaccine,” he added. “I would say clinicians should approach counseling the same way they counsel patients for the flu vaccine, and as far as I know, there are no concerns for systemic drugs commonly used in dermatology patients.”
However, guidance has not yet been issued from either the FDA or the Centers for Disease Control and Prevention regarding the use of the vaccine in immunocompromised individuals. Given the lack of data, the FDA has said that “it will be something that providers will need to consider on an individual basis,” and that individuals should consult with physicians to weigh the potential benefits and potential risks.
The CDC’s Advisory Committee on Immunization Practices has said that clinicians need more guidance on whether to use the vaccine in pregnant or breastfeeding women, the immunocompromised, or those who have a history of allergies. The CDC itself has not yet released its formal guidance on vaccine use.
COVID-19 vaccines
Vaccines typically require years of research and testing before reaching the clinic, but this year researchers embarked on a global effort to develop safe and effective coronavirus vaccines in record time. Both the Pfizer/BioNTech and Moderna vaccines have only a few months of phase 3 clinical trial data, so much remains unknown about them, including their duration of effect and any long-term safety signals. In addition to excluding immunocompromised individuals, the clinical trials did not include children or pregnant women, so data are lacking for several population subgroups.
But these will not be the only vaccines available, as the pipeline is already becoming crowded. U.S. clinical trial data from a vaccine jointly being developed by Oxford-AstraZeneca, could potentially be ready, along with a request for FDA emergency use authorization, by late January 2021.
In addition, China and Russia have released vaccines, and there are currently 61 vaccines being investigated in clinical trials and at least 85 preclinical products under active investigation.
The vaccine candidates are using both conventional and novel mechanisms of action to elicit an immune response in patients. Conventional methods include attenuated inactivated (killed) virus and recombinant viral protein vaccines to develop immunity. Novel approaches include replication-deficient, adenovirus vector-based vaccines that contain the viral protein, and mRNA-based vaccines, such as the Pfizer and Moderna vaccines, that encode for a SARS-CoV-2 spike protein.
“The special vaccine concern for immunocompromised individuals is introduction of a live virus,” Dr. Stohl said. “Neither the Moderna nor Pfizer vaccines are live viruses, so there should be no special contraindication for such individuals.”
Live vaccine should be avoided in immunocompromised patients, and currently, live SARS-CoV-2 vaccines are only being developed in India and Turkey.
It is not unusual for vaccine trials to begin with cohorts that exclude participants with various health conditions, including those who are immunocompromised. These groups are generally then evaluated in phase 4 trials, or postmarketing surveillance. While the precise number of immunosuppressed adults in the United States is not known, the numbers are believed to be rising because of increased life expectancy among immunosuppressed adults as a result of advances in treatment and new and wider indications for therapies that can affect the immune system.
According to data from the 2013 National Health Interview Survey, an estimated 2.7% of U.S. adults are immunosuppressed. This population covers a broad array of health conditions and medical specialties; people living with inflammatory or autoimmune conditions, such as inflammatory rheumatic diseases (rheumatoid arthritis, axial spondyloarthritis, lupus); inflammatory bowel disease (Crohn’s disease and ulcerative colitis); psoriasis; multiple sclerosis; organ transplant recipients; patients undergoing chemotherapy; and life-long immunosuppression attributable to HIV infection.
As the vaccines begin to roll out and become available, how should clinicians advise their patients, in the absence of any clinical trial data?
Risk vs. benefit
Gilaad Kaplan, MD, MPH, a gastroenterologist and professor of medicine at the University of Calgary (Alta.), noted that the inflammatory bowel disease (IBD) community has dealt with tremendous anxiety during the pandemic because many are immunocompromised because of the medications they use to treat their disease.
“For example, many patients with IBD are on biologics like anti-TNF [tumor necrosis factor] therapies, which are also used in other immune-mediated inflammatory diseases such as rheumatoid arthritis,” he said. “Understandably, individuals with IBD on immunosuppressive medications are concerned about the risk of severe complications due to COVID-19.”
The entire IBD community, along with the world, celebrated the announcement that multiple vaccines are protective against SARS-CoV-2, he noted. “Vaccines offer the potential to reduce the spread of COVID-19, allowing society to revert back to normalcy,” Dr. Kaplan said. “Moreover, for vulnerable populations, including those who are immunocompromised, vaccines offer the potential to directly protect them from the morbidity and mortality associated with COVID-19.”
That said, even though the news of vaccines are extremely promising, some cautions must be raised regarding their use in immunocompromised populations, such as persons with IBD. “The current trials, to my knowledge, did not include immunocompromised individuals and thus, we can only extrapolate from what we know from other trials of different vaccines,” he explained. “We know from prior vaccines studies that the immune response following vaccination is less robust in those who are immunocompromised as compared to a healthy control population.”
Dr. Kaplan also pointed to recent reports of allergic reactions that have been reported in healthy individuals. “We don’t know whether side effects, like allergic reactions, may be different in unstudied populations,” he said. “Thus, the medical and scientific community should prioritize clinical studies of safety and effectiveness of COVID-19 vaccines in immunocompromised populations.”
So, what does this mean for an individual with an immune-mediated inflammatory disease like Crohn’s disease or ulcerative colitis who is immunocompromised? Dr. Kaplan explained that it is a balance between the potential harm of being infected with COVID-19 and the uncertainty of receiving a vaccine in an understudied population. For those who are highly susceptible to dying from COVID-19, such as an older adult with IBD, or someone who faces high exposure, such as a health care worker, the potential protection of the vaccine greatly outweighs the uncertainty.
“However, for individuals who are at otherwise lower risk – for example, young and able to work from home – then waiting a few extra months for postmarketing surveillance studies in immunocompromised populations may be a reasonable approach, as long as these individuals are taking great care to avoid infection,” he said.
No waiting needed
Joel M. Gelfand, MD, MSCE, professor of dermatology and epidemiology at the University of Pennsylvania, Philadelphia, feels that the newly approved vaccine should be safe for most of his patients.
“Patients with psoriatic disease should get the mRNA-based COVID-19 vaccine as soon as possible based on eligibility as determined by the CDC and local public health officials,” he said. “It is not a live vaccine, and therefore patients on biologics or other immune-modulating or immune-suppressing treatment can receive it.”
However, the impact of psoriasis treatment on immune response to the mRNA-based vaccines is not known. Dr. Gelfand noted that, extrapolating from the vaccine literature, there is some evidence that methotrexate reduces response to the influenza vaccine. “However, the clinical significance of this finding is not clear,” he said. “Since the mRNA vaccine needs to be taken twice, a few weeks apart, I do not recommend interrupting or delaying treatment for psoriatic disease while undergoing vaccination for COVID-19.”
Given the reports of allergic reactions, he added that it is advisable for patients with a history of life-threatening allergic reactions such as anaphylaxis or who have been advised to carry an epinephrine autoinjector, to talk with their health care provider to determine if COVID-19 vaccination is medically appropriate.
The National Psoriasis Foundation has issued guidance on COVID-19, explained Steven R. Feldman, MD, PhD, professor of dermatology, pathology, and social sciences & health policy at Wake Forest University, Winston-Salem, N.C., who is also a member of the committee that is working on those guidelines and keeping them up to date. “We are in the process of updating the guidelines with information on COVID vaccines,” he said.
He agreed that there are no contraindications for psoriasis patients to receive the vaccine, regardless of whether they are on immunosuppressive treatment, even though definitive data are lacking. “Fortunately, there’s a lot of good data coming out of Italy that patients with psoriasis on biologics do not appear to be at increased risk of getting COVID or of having worse outcomes from COVID,” he said.
Patients are going to ask about the vaccines, and when counseling them, clinicians should discuss the available data, the residual uncertainty, and patients’ concerns should be considered, Dr. Feldman explained. “There may be some concern that steroids and cyclosporine would reduce the effectiveness of vaccines, but there is no concern that any of the drugs would cause increased risk from nonlive vaccines.”
He added that there is evidence that “patients on biologics who receive nonlive vaccines do develop antibody responses and are immunized.”
Boosting efficacy
Even prior to making their announcement, the American College of Rheumatology had said that they would endorse the vaccine for all patients, explained rheumatologist Brett Smith, DO, from Blount Memorial Physicians Group and East Tennessee Children’s Hospital, Alcoa. “The vaccine is safe for all patients, but the problem may be that it’s not as effective,” he said. “But we don’t know that because it hasn’t been tested.”
With other vaccines, biologic medicines are held for 2 weeks before and afterwards, to get the best response. “But some patients don’t want to stop the medication,” Dr. Smith said. “They are afraid that their symptoms will return.”
As for counseling patients as to whether they should receive this vaccine, he explained that he typically doesn’t try to sway patients one way or another until they are really high risk. “When I counsel, it really depends on the individual situation. And for this vaccine, we have to be open to the fact that many people have already made up their mind.”
There are a lot of questions regarding the vaccine. One is the short time frame of development. “Vaccines typically take 6-10 years to come on the market, and this one is now available after a 3-month study,” Dr. Smith said. “Some have already decided that it’s too new for them.”
The process is also new, and patients need to understand that it doesn’t contain an active virus and “you can’t catch coronavirus from it.”
Dr. Smith also explained that, because the vaccine may be less effective in a person using biologic therapies, there is currently no information available on repeat vaccination. “These are all unanswered questions,” he said. “If the antibodies wane in a short time, can we be revaccinated and in what time frame? We just don’t know that yet.”
Marcelo Bonomi, MD, a medical oncologist from The Ohio State University Comprehensive Cancer Center, Columbus, explained that one way to ensure a more optimal response to the vaccine would be to wait until the patient has finished chemotherapy.* “The vaccine can be offered at that time, and in the meantime, they can take other steps to avoid infection,” he said. “If they are very immunosuppressed, it isn’t worth trying to give the vaccine.”
Cancer patients should be encouraged to stay as healthy as possible, and to wear masks and social distance. “It’s a comprehensive approach. Eat healthy, avoid alcohol and tobacco, and exercise. [These things] will help boost the immune system,” Dr. Bonomi said. “Family members should be encouraged to get vaccinated, which will help them avoid infection and exposing the patient.”
Jim Boonyaratanakornkit, MD, PhD, an infectious disease specialist who cares for cancer patients at the Fred Hutchinson Cancer Research Center, agreed. “Giving a vaccine right after a transplant is a futile endeavor,” he said. “We need to wait 6 months to have an immune response.”
He pointed out there may be a continuing higher number of cases, with high levels peaking in Washington in February and March. “Close friends and family should be vaccinated if possible,” he said, “which will help interrupt transmission.”
The vaccines are using new platforms that are totally different, and there is no clear data as to how long the antibodies will persist. “We know that they last for at least 4 months,” said Dr. Boonyaratanakornkit. “We don’t know what level of antibody will protect them from COVID-19 infection. Current studies are being conducted, but we don’t have that information for anyone yet.”
*Correction, 1/7/21: An earlier version of this article misattributed quotes from Dr. Marcelo Bonomi.
FDA clears first OTC rapid at-home COVID diagnostic test
The Food and Drug Administration has issued an emergency-use authorization (EUA) for the first COVID-19 diagnostic test that can be completed at home without a prescription.
Authorization of the Ellume COVID-19 Home Test is “a major milestone in diagnostic testing for COVID-19,” FDA Commissioner Stephen M. Hahn, MD, said in a news release.
“By authorizing a test for over-the-counter use, the FDA allows it to be sold in places like drug stores, where a patient can buy it, swab their nose, run the test, and find out their results in as little as 20 minutes,” said Dr. Hahn.
The Ellume COVID-19 Home Test is a rapid antigen test that detects fragments of the SARS-CoV-2 virus from a nasal swab sample taken from anyone aged 2 years and older, including those not showing any symptoms.
In testing, the Ellume COVID-19 Home Test correctly identified 96% of positive samples and 100% of negative samples in individuals with symptoms.
In people without symptoms, the test correctly identified 91% of positive samples and 96% of negative samples, the FDA said.
The test includes a sterile nasal swab, a dropper, processing fluid, and a Bluetooth-connected analyzer for use with an app on the user’s smartphone. The sample is analyzed and results are automatically transmitted to the user’s smartphone.
“The Ellume COVID-19 home test’s core technology combines ultra-sensitive optics, electronics, and proprietary software to leverage best-in-class digital immunoassay technology with next-generation multi-quantum dot fluorescence technology,” the company said in a news release.
The mobile app requires individuals to input their ZIP code and date of birth, with optional fields including name and email address. The app automatically reports the results as appropriate to public health authorities to monitor disease prevalence.
Ellume expects to produce more than 3 million tests in January 2021. The company said the test will cost around $30.
FDA authorization of this first fully at-home nonprescription COVID-19 diagnostic test follows last month’s EUA for the first prescription COVID-19 test for home use, as reported this news organization.
Since the start of the pandemic, the FDA has authorized more than 225 diagnostic tests for COVID-19, including more than 25 tests that allow for home collection of samples, which are then sent to a lab for testing.
“As we continue to authorize additional tests for home use, we are helping expand Americans’ access to testing, reducing the burden on laboratories and test supplies, and giving Americans more testing options from the comfort and safety of their own homes,” Dr. Hahn said.
“This test, like other antigen tests, is less sensitive and less specific than typical molecular tests run in a lab,” said Jeffrey Shuren, MD, JD, director of FDA’s Center for Devices and Radiological Health, in the release. “However, the fact that it can be used completely at home and return results quickly means that it can play an important role in response to the pandemic.”
As with other antigen tests, a small percentage of positive and negative results from the Ellume test may be false. In patients without symptoms, positive results should be treated as presumptively positive until confirmed by another test as soon as possible, the FDA advised.
This is especially true if there are fewer infections in a particular community, as false-positive results can be more common when antigen tests are used in populations where there is a low prevalence of COVID-19, the agency said.
Because all tests can give false-negative and false-positive results, individuals with positive results should self-isolate and seek additional care from their health care provider.
Individuals who test negative and have symptoms of COVID-19 should follow up with their health care provider, as negative results don’t preclude an individual from SARS-CoV-2 infection.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has issued an emergency-use authorization (EUA) for the first COVID-19 diagnostic test that can be completed at home without a prescription.
Authorization of the Ellume COVID-19 Home Test is “a major milestone in diagnostic testing for COVID-19,” FDA Commissioner Stephen M. Hahn, MD, said in a news release.
“By authorizing a test for over-the-counter use, the FDA allows it to be sold in places like drug stores, where a patient can buy it, swab their nose, run the test, and find out their results in as little as 20 minutes,” said Dr. Hahn.
The Ellume COVID-19 Home Test is a rapid antigen test that detects fragments of the SARS-CoV-2 virus from a nasal swab sample taken from anyone aged 2 years and older, including those not showing any symptoms.
In testing, the Ellume COVID-19 Home Test correctly identified 96% of positive samples and 100% of negative samples in individuals with symptoms.
In people without symptoms, the test correctly identified 91% of positive samples and 96% of negative samples, the FDA said.
The test includes a sterile nasal swab, a dropper, processing fluid, and a Bluetooth-connected analyzer for use with an app on the user’s smartphone. The sample is analyzed and results are automatically transmitted to the user’s smartphone.
“The Ellume COVID-19 home test’s core technology combines ultra-sensitive optics, electronics, and proprietary software to leverage best-in-class digital immunoassay technology with next-generation multi-quantum dot fluorescence technology,” the company said in a news release.
The mobile app requires individuals to input their ZIP code and date of birth, with optional fields including name and email address. The app automatically reports the results as appropriate to public health authorities to monitor disease prevalence.
Ellume expects to produce more than 3 million tests in January 2021. The company said the test will cost around $30.
FDA authorization of this first fully at-home nonprescription COVID-19 diagnostic test follows last month’s EUA for the first prescription COVID-19 test for home use, as reported this news organization.
Since the start of the pandemic, the FDA has authorized more than 225 diagnostic tests for COVID-19, including more than 25 tests that allow for home collection of samples, which are then sent to a lab for testing.
“As we continue to authorize additional tests for home use, we are helping expand Americans’ access to testing, reducing the burden on laboratories and test supplies, and giving Americans more testing options from the comfort and safety of their own homes,” Dr. Hahn said.
“This test, like other antigen tests, is less sensitive and less specific than typical molecular tests run in a lab,” said Jeffrey Shuren, MD, JD, director of FDA’s Center for Devices and Radiological Health, in the release. “However, the fact that it can be used completely at home and return results quickly means that it can play an important role in response to the pandemic.”
As with other antigen tests, a small percentage of positive and negative results from the Ellume test may be false. In patients without symptoms, positive results should be treated as presumptively positive until confirmed by another test as soon as possible, the FDA advised.
This is especially true if there are fewer infections in a particular community, as false-positive results can be more common when antigen tests are used in populations where there is a low prevalence of COVID-19, the agency said.
Because all tests can give false-negative and false-positive results, individuals with positive results should self-isolate and seek additional care from their health care provider.
Individuals who test negative and have symptoms of COVID-19 should follow up with their health care provider, as negative results don’t preclude an individual from SARS-CoV-2 infection.
A version of this article first appeared on Medscape.com.
The Food and Drug Administration has issued an emergency-use authorization (EUA) for the first COVID-19 diagnostic test that can be completed at home without a prescription.
Authorization of the Ellume COVID-19 Home Test is “a major milestone in diagnostic testing for COVID-19,” FDA Commissioner Stephen M. Hahn, MD, said in a news release.
“By authorizing a test for over-the-counter use, the FDA allows it to be sold in places like drug stores, where a patient can buy it, swab their nose, run the test, and find out their results in as little as 20 minutes,” said Dr. Hahn.
The Ellume COVID-19 Home Test is a rapid antigen test that detects fragments of the SARS-CoV-2 virus from a nasal swab sample taken from anyone aged 2 years and older, including those not showing any symptoms.
In testing, the Ellume COVID-19 Home Test correctly identified 96% of positive samples and 100% of negative samples in individuals with symptoms.
In people without symptoms, the test correctly identified 91% of positive samples and 96% of negative samples, the FDA said.
The test includes a sterile nasal swab, a dropper, processing fluid, and a Bluetooth-connected analyzer for use with an app on the user’s smartphone. The sample is analyzed and results are automatically transmitted to the user’s smartphone.
“The Ellume COVID-19 home test’s core technology combines ultra-sensitive optics, electronics, and proprietary software to leverage best-in-class digital immunoassay technology with next-generation multi-quantum dot fluorescence technology,” the company said in a news release.
The mobile app requires individuals to input their ZIP code and date of birth, with optional fields including name and email address. The app automatically reports the results as appropriate to public health authorities to monitor disease prevalence.
Ellume expects to produce more than 3 million tests in January 2021. The company said the test will cost around $30.
FDA authorization of this first fully at-home nonprescription COVID-19 diagnostic test follows last month’s EUA for the first prescription COVID-19 test for home use, as reported this news organization.
Since the start of the pandemic, the FDA has authorized more than 225 diagnostic tests for COVID-19, including more than 25 tests that allow for home collection of samples, which are then sent to a lab for testing.
“As we continue to authorize additional tests for home use, we are helping expand Americans’ access to testing, reducing the burden on laboratories and test supplies, and giving Americans more testing options from the comfort and safety of their own homes,” Dr. Hahn said.
“This test, like other antigen tests, is less sensitive and less specific than typical molecular tests run in a lab,” said Jeffrey Shuren, MD, JD, director of FDA’s Center for Devices and Radiological Health, in the release. “However, the fact that it can be used completely at home and return results quickly means that it can play an important role in response to the pandemic.”
As with other antigen tests, a small percentage of positive and negative results from the Ellume test may be false. In patients without symptoms, positive results should be treated as presumptively positive until confirmed by another test as soon as possible, the FDA advised.
This is especially true if there are fewer infections in a particular community, as false-positive results can be more common when antigen tests are used in populations where there is a low prevalence of COVID-19, the agency said.
Because all tests can give false-negative and false-positive results, individuals with positive results should self-isolate and seek additional care from their health care provider.
Individuals who test negative and have symptoms of COVID-19 should follow up with their health care provider, as negative results don’t preclude an individual from SARS-CoV-2 infection.
A version of this article first appeared on Medscape.com.
Six big changes coming for office-visit coding
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to [email protected].
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
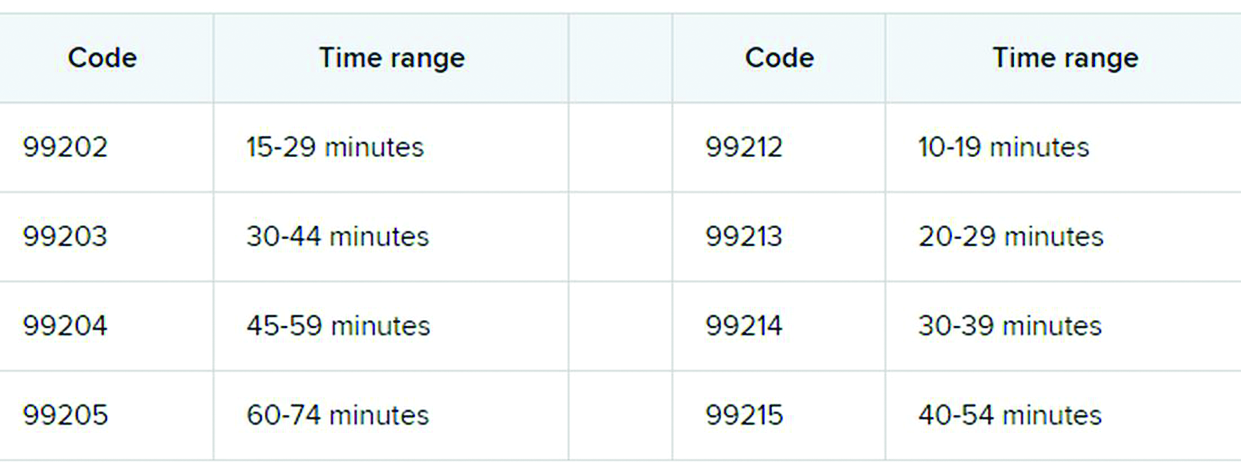
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to [email protected].
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
Betsy Nicoletti, MS, a nationally recognized coding expert, will take your coding questions via email and provide guidance on how to code properly to maximize reimbursement. Have a question about coding? Send it to [email protected].
thanks to the American Medical Association.
The first major changes to the definitions for E/M services will be in effect as of Jan. 1, 2021, with all payers expected to adopt these new guidelines. In particular, the AMA has revised the definitions for E/M codes 99202-99215 in the Current Procedural Terminology (CPT) 2021 codebook. The existing guidelines were developed in 1995 and 1997 and remain in effect for all other E/M services determined by history, exam, and medical decision-making (MDM).
What do the new changes mean to you? In 2021, for new and established office and other outpatient services reported with codes 99202-99215, a clinician may select the code on the basis of time or MDM.
There are three elements in MDM, and two of three are required. These elements are the number and complexity of problems addressed, amount and/or complexity of data to be reviewed and analyzed, and risk of complications and/or morbidity or mortality of patient management.
Make sure you familiarize yourself with these six big changes. It may take a bit of time to integrate these new processes into your daily routine, but wrapping your head around them as soon as possible can help boost your bottom line:
1. History and exam don’t count toward level of service
Physicians, advanced practice registered nurses, and physician assistants won’t use history or exam to select what level of code to bill for office visits 99202-99215, as they did in the past. They need only document a medically appropriate history and exam. The history may be obtained by staff members and reviewed by the billing practitioner.
While specific history and exam requirements disappear for office visit codes, they remain for all other types of visits, selected on the basis of history, exam, and MDM, such as hospital services, nursing facility services, and home and domiciliary care. So, say goodbye to “all other systems reviewed and negative” in office notes, but keep it handy for those other E/M codes.
2. All time spent caring for the patient on a particular day counts
This includes all time spent on the day of service, including preparing to see the patient, seeing the patient, phone calls or other work done after the visit (if not billed with a care management or other CPT code), and documenting in the medical record. The AMA developed new guidelines for using time for office and other outpatient services. For codes 99202-99215, count all of the face-to-face and non–face-to-face time spent by the billing clinician on the day of the visit. Counseling does not need to be more than 50% of the total time.
Do not include any staff time or time spent on any days before or after the visit. This allows clinicians to capture the work when a significant amount of it takes place before or after the visit with the patient, and to bill for it on the day of the visit.
According to the 2021 CPT codebook, physician or other qualified health care professional time includes the following activities:
- Preparing to see the patient (e.g., review of tests).
- Obtaining and/or reviewing separately obtained history.
- Performing a medically appropriate examination and/or evaluation.
- Counseling and educating the patient/family/caregiver.
- Ordering medications, tests, or procedures.
- Referring and communicating with other health care professionals (when not separately reported).
- Documenting clinical information in the electronic or other health record.
- Independently interpreting results (not separately reported) and communicating results to the patient/family/caregiver.
- Care coordination (not separately reported).
3. Soon to be gone: ‘new to the examiner’ and ‘workup planned’
The current guidelines don’t differentiate between a new problem to the clinician or an established problem to the clinician. So it doesn’t matter whether you’re hearing about a particular problem for the first time or the fifth time. The new office and outpatient services guidelines define problems only as they relate to the patient. For example, when selecting a level of service, a chronic problem with a mild exacerbation is the same level whether it’s the primary care physician seeing the patient for the 10th time to help manage her diabetes or the endocrinologist seeing the patient for the first time.
In the current guidelines (1995 and 1997), additional weight is given in selecting the level of MDM for a problem that’s new to the examiner with a workup planned, yet when the diagnostic test couldn’t be completed at the visit. This concept is gone from element of number and complexity of new problems. Ordering diagnostic tests is part of the second element, the amount and/or complexity of data to be reviewed.
4. Different guidelines if you need a history from a parent or other source
The new guidelines recognize the additional work required by the clinician when the patient is unable to give a history or when the practitioner doesn’t find the history to be reliable.
For example, in the case of a baby or child who is unable to give a history, the parent counts as an “independent historian,” according to the new guidelines. Likewise, for a patient with dementia, the caregiver counts as a historian. Note, however, that the criteria is not met simply because the patient is accompanied by another person. The additional weight in selecting the level of service is based on the patient being unable to give a reliable history.
Bottom line: In cases where patients are unable to communicate clearly, physicians or other providers should document the necessity of getting a complete history and who provided it.
5. A new spin on social determinants of health (SDoH)
In the risk of morbidity and/or mortality element, conditions described as “social determinants of health” are considered moderate complexity. SDoH are social and environmental factors that affect a patient’s health and medical outcomes. These include homelessness, inability to afford medications, food insecurity, and occupational exposure to risk factors. These circumstances are reported with codes in categories Z55-Z65.
In the past, physicians often documented this information in their office notes but rarely added a diagnosis code that described the patient’s situation. The ICD-10-CM code set includes codes that describe these factors. Using them allows the practice to track patients who have increased needs, and it communicates to payers the complexity of caring for these patients.
6. Risks related to surgery are defined
The current guidelines assign different levels of risk to minor and major surgery. They also include differentiation for “minor surgery with no identified risk factors,” “minor surgery with identified risk factors,” “elective major surgery with no identified risk factors,” and “elective major surgery with identified risk factors.” The old guidelines didn’t state whether the risk factors pertained to the patient – such as smoking, heart disease, or high body mass index – or to the procedure itself.
The new guidelines specifically say that it’s both. In the risk column, “decision regarding minor surgery with identified patient or procedure risk factors” and “decision regarding elective major surgery without patient or procedure risk factors” are both considered moderate. “Decision regarding elective major surgery with identified patient or procedure risk factors” and “decision regarding emergency major surgery” are in the high complexity column for risk.
Keep in mind that two of three elements are required: the number and complexity of problems, amount of data, and morbidity/mortality risk. Risk of morbidity/mortality alone doesn’t count as the basis for selecting the code. Of course, when surgeons see this, they ask, “What major procedures don’t have identified risk factors?”
Note, too, that these new CPT guidelines do not define the terms “minor” and “major” surgery. For payment reasons related to the postop period, the Centers for Medicare & Medicaid Services defines minor surgery as a procedure with 0-10 global days and a major surgery as a procedure with 90 global days. However, there are many procedures with 0 global days (endoscopy, cardiac catheterization) that are not minor procedures. Hopefully, the AMA will clarify this in 2021.
What’s the take-away for clinicians?
There are sure to be shifts in coding patterns based on these new guidelines. Some specialties will find that not being able to select a service based on history and exam alone will lower the level of service for which they can bill. Some practices, on the other hand, will be able to code for more high-level visits, without the need for a complete review of systems or a comprehensive exam.
The biggest challenge will be for practices that provide services both in the hospital and in the office, because they’ll have to use both sets of guidelines, depending on which type of service they’re performing.
For more details on what’s coming your way beginning on New Year’s Day, you may want to read the 16-page AMA document .
A version of this article first appeared on Medscape.com.
FDA panel supports expanded HF role for sacubitril/valsartan
UPDATED DECEMBER 17
A panel of federal advisers on Tuesday effectively backed a bid to expand approval of sacubitril/valsartan for use in a form of heart failure for which there is not yet an approved medication.

The U.S. Food and Drug Administration asked its Cardiovascular and Renal Drugs Advisory Committee to broadly consider whether new analyses of data from the PARAGON-HF trial, combined with other information, could support use of sacubitril/valsartan (Entresto, Novartis) in heart failure with preserved ejection fraction (HFpEF).
The advisory committee voted 12-1 on this question, which can be seen as a marker for an expanded approval: “Does PARAGON-HF, perhaps supported by previous studies, provide sufficient evidence to support any indication?”
The dissenting vote was cast by the panel’s chairperson, Julia B. Lewis, MD, a professor of medicine from Vanderbilt University. In explaining her vote, Dr. Lewis cited concerns about expanding use of the drug, which has a potential for hypotension. But she noted that the rest of the panelists were “impressed by the totality of the evidence” presented, including a willingness to take a new look at the PARAGON-HF trial. This study was perceived at first pass as having failed to prove a benefit for people with HFpEF.
The 2019 initial unveiling of the PARAGON-HF results had dampened hopes for an evidence-based drug therapy for HFpEF. Patients treated with the first-of-its-kind renin-angiotensin system (RAS) inhibitor, compared with those who received standard valsartan, had 13% fewer heart failure hospitalizations or cardiovascular (CV) deaths over an average of about 3 years, but the difference missed significance at a P value of .059.
“Everybody agreed that the P value of .05 was not written in stone,” Dr. Lewis said in summarizing the panelists’ views on the voting question.
At the FDA’s request, the panel also addressed several other questions without voting on them. The agency asked the panel to describe the patient population for whom an expanded approval would be appropriate. The FDA initially approved sacubitril/valsartan in 2015 to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic heart failure (NYHA Class II-IV) and reduced ejection fraction.
Novartis in April submitted an application to the FDA, seeking to expand the use of sacubitril/valsartan from the currently approved indication for the treatment of chronic heart failure (CHF) patients with reduced ejection fraction (HFrEF) to include what the company terms “the adjacent population of patients with preserved ejection fraction (HFpEF) who have a left ventricular ejection fraction (LVEF) below normal.” The American Society of Echocardiography and European Association of Cardiovascular Imaging define normal LVEF and normal range (±2 standard deviations) as 62% (range, 52%-72%) in men and 64% (range, 54%-74%) in women, Novartis said in its briefing materials for the meeting.
FDA panelist Christopher M. O’Connor, MD, for example, suggested that an expanded approval could allow for use of sacubitril/valsartan for the reduction of heart failure or hospitalization in patients with mildly reduced ejection fraction as defined by greater than 45% through 55%. FDA panelist C. Noel Bairey Merz, MD, director of the Barbra Streisand Women’s Heart Center at Cedars-Sinai Medical Center in Los Angeles, suggested extending this to 57% to acknowledge the higher threshold for women.
Another FDA panelist, Steven E. Nissen, MD, of the Cleveland Clinic, argued against use of imprecise terms in defining an expanded patient population for sacubitril/valsartan. If used in the right patient population, the drug could provide a benefit for people who have active heart failure with symptoms, including preventing hospitalizations and renal disease, he said.
“If you are symptomatic with a syndrome that’s consistent with heart failure and you have an ejection fraction below the lower limits of normal, I believe it’s in the public interest for you to get sacubitril/valsartan,” Dr. Nissen said.
The FDA usually follows the advice of its panels, but is not obligated to. But in this case, the agency staff were clearly seeking a path for an expanded approval of sacubitril/valsartan.
Challenging a standard
The FDA had encouraged Novartis to submit the supplementary application for the HFpEF indication and even suggested some of the post-hoc analyses, the agency staff said in a briefing document for the meeting.
PARAGON-HF illustrated some of the agency’s concerns about missed opportunities in general in large research trials. Some events of interest in studies may be miscounted due to a lack of information such as a requirement for the presence of physical examination findings that are not documented in the patient’s dossier, the FDA staff said.
“We would like to consider giving ‘partial credit’ to events based on the level of evidence provided, e.g., use of an ordinal variable rather than a dichotomous ‘yes’ or ‘no,’ ” the staff said in the briefing document.
At the panel meeting, Norman Stockbridge, MD, PhD, director of the Division of Cardiology and Nephrology in the FDA’s Center for Drug Evaluation and Research, told the panelists there is no basis in law for setting a P value of .05 as the benchmark on whether to declare a trial a success or failure.
“I wanted to take a few minutes and make sure that you on the committee understands what flexibility you have in addressing the case study in question,” Dr. Stockbridge said at the start of the meeting.
He then reviewed cases where the FDA had approved claims for cardiac medicines that had not shown desired results in key tests. These include approval of enalapril for use in asymptomatic left ventricular dysfunction on the basis of the SOLVD-Prevention trial, approval of digoxin for heart failure on the basis of the DIG study, and approval of carvedilol for reduced ejection fraction following myocardial infarction on
the basis of the CAPRICORN study, Dr. Stockbridge said.
In reviewing the data for sacubitril/valsartan, FDA staff noted a similarity between investigator-reported and adjudicated results, Stockbridge said.
“This suggested that there were events that did not need all evidentiary criteria as qualified events, but likely were nonetheless,” he said. “This is an example of dichotomization of events being wasteful of information.”
Post-hoc exploratory analyses in PARAGON-HF were able to meet the commonly used standard, according to the FDA briefing document. Among the key findings of these analyses were:
- An analysis of investigator-reported events for the primary composite endpoint of total hospitalizations for heart failure (HHF) and cardiovascular (CV) death demonstrated a rate ratio (RR) of 0.84 (95% confidence interval 0.74- 0.97; P = .01).
- Investigator-reported events added 226 and 290 HHF events but decreased CV death by 56 and 58 events in the sacubitril/valsartan and valsartan arms, respectively. Hence, a net 170 and 232 events were added to the clinical endpoint committee–reported primary composite endpoint leading to a P value of .01, without a significant change in RR.
- Analysis of investigator-reported expanded primary composite endpoint events including total HHF, urgent HF visits, and CV death demonstrated a RR of 0.83 (95% CI, 0.73-0.95; P = .006. There were 136 and 173 investigator-reported urgent HF events in sacubitril/valsartan and valsartan arms, respectively.
Opening a floodgate?
Cynthia L. Chauhan, MSW, of Wichita, Kansas, who served as the consumer representative on the panel, questioned whether a decision to revisit the data on PARAGON-HF might lead drugmakers to seek to repurpose other failed trials.
“Are we opening any kind of floodgate for other researchers to go back and see this is an invitation to try to, for want of a better term, back-door their way into some approvals?” Ms. Chauhan asked.
Dr. Nissen assured her that this concern was valid and would be considered. The goal would be to allow some flexibility in cases that merit further consideration, while preventing companies from data mining until they find some evidence to support an FDA application, he said.
Re-analyzing trials “should be done carefully, conservatively, and only when it really is compelling that the public interest supports it,” Dr. Nissen stressed.
Panelists reported no conflicts of interest related to the topic of the meeting.
UPDATED DECEMBER 17
A panel of federal advisers on Tuesday effectively backed a bid to expand approval of sacubitril/valsartan for use in a form of heart failure for which there is not yet an approved medication.
The U.S. Food and Drug Administration asked its Cardiovascular and Renal Drugs Advisory Committee to broadly consider whether new analyses of data from the PARAGON-HF trial, combined with other information, could support use of sacubitril/valsartan (Entresto, Novartis) in heart failure with preserved ejection fraction (HFpEF).
The advisory committee voted 12-1 on this question, which can be seen as a marker for an expanded approval: “Does PARAGON-HF, perhaps supported by previous studies, provide sufficient evidence to support any indication?”
The dissenting vote was cast by the panel’s chairperson, Julia B. Lewis, MD, a professor of medicine from Vanderbilt University. In explaining her vote, Dr. Lewis cited concerns about expanding use of the drug, which has a potential for hypotension. But she noted that the rest of the panelists were “impressed by the totality of the evidence” presented, including a willingness to take a new look at the PARAGON-HF trial. This study was perceived at first pass as having failed to prove a benefit for people with HFpEF.
The 2019 initial unveiling of the PARAGON-HF results had dampened hopes for an evidence-based drug therapy for HFpEF. Patients treated with the first-of-its-kind renin-angiotensin system (RAS) inhibitor, compared with those who received standard valsartan, had 13% fewer heart failure hospitalizations or cardiovascular (CV) deaths over an average of about 3 years, but the difference missed significance at a P value of .059.
“Everybody agreed that the P value of .05 was not written in stone,” Dr. Lewis said in summarizing the panelists’ views on the voting question.
At the FDA’s request, the panel also addressed several other questions without voting on them. The agency asked the panel to describe the patient population for whom an expanded approval would be appropriate. The FDA initially approved sacubitril/valsartan in 2015 to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic heart failure (NYHA Class II-IV) and reduced ejection fraction.
Novartis in April submitted an application to the FDA, seeking to expand the use of sacubitril/valsartan from the currently approved indication for the treatment of chronic heart failure (CHF) patients with reduced ejection fraction (HFrEF) to include what the company terms “the adjacent population of patients with preserved ejection fraction (HFpEF) who have a left ventricular ejection fraction (LVEF) below normal.” The American Society of Echocardiography and European Association of Cardiovascular Imaging define normal LVEF and normal range (±2 standard deviations) as 62% (range, 52%-72%) in men and 64% (range, 54%-74%) in women, Novartis said in its briefing materials for the meeting.
FDA panelist Christopher M. O’Connor, MD, for example, suggested that an expanded approval could allow for use of sacubitril/valsartan for the reduction of heart failure or hospitalization in patients with mildly reduced ejection fraction as defined by greater than 45% through 55%. FDA panelist C. Noel Bairey Merz, MD, director of the Barbra Streisand Women’s Heart Center at Cedars-Sinai Medical Center in Los Angeles, suggested extending this to 57% to acknowledge the higher threshold for women.
Another FDA panelist, Steven E. Nissen, MD, of the Cleveland Clinic, argued against use of imprecise terms in defining an expanded patient population for sacubitril/valsartan. If used in the right patient population, the drug could provide a benefit for people who have active heart failure with symptoms, including preventing hospitalizations and renal disease, he said.
“If you are symptomatic with a syndrome that’s consistent with heart failure and you have an ejection fraction below the lower limits of normal, I believe it’s in the public interest for you to get sacubitril/valsartan,” Dr. Nissen said.
The FDA usually follows the advice of its panels, but is not obligated to. But in this case, the agency staff were clearly seeking a path for an expanded approval of sacubitril/valsartan.
Challenging a standard
The FDA had encouraged Novartis to submit the supplementary application for the HFpEF indication and even suggested some of the post-hoc analyses, the agency staff said in a briefing document for the meeting.
PARAGON-HF illustrated some of the agency’s concerns about missed opportunities in general in large research trials. Some events of interest in studies may be miscounted due to a lack of information such as a requirement for the presence of physical examination findings that are not documented in the patient’s dossier, the FDA staff said.
“We would like to consider giving ‘partial credit’ to events based on the level of evidence provided, e.g., use of an ordinal variable rather than a dichotomous ‘yes’ or ‘no,’ ” the staff said in the briefing document.
At the panel meeting, Norman Stockbridge, MD, PhD, director of the Division of Cardiology and Nephrology in the FDA’s Center for Drug Evaluation and Research, told the panelists there is no basis in law for setting a P value of .05 as the benchmark on whether to declare a trial a success or failure.
“I wanted to take a few minutes and make sure that you on the committee understands what flexibility you have in addressing the case study in question,” Dr. Stockbridge said at the start of the meeting.
He then reviewed cases where the FDA had approved claims for cardiac medicines that had not shown desired results in key tests. These include approval of enalapril for use in asymptomatic left ventricular dysfunction on the basis of the SOLVD-Prevention trial, approval of digoxin for heart failure on the basis of the DIG study, and approval of carvedilol for reduced ejection fraction following myocardial infarction on
the basis of the CAPRICORN study, Dr. Stockbridge said.
In reviewing the data for sacubitril/valsartan, FDA staff noted a similarity between investigator-reported and adjudicated results, Stockbridge said.
“This suggested that there were events that did not need all evidentiary criteria as qualified events, but likely were nonetheless,” he said. “This is an example of dichotomization of events being wasteful of information.”
Post-hoc exploratory analyses in PARAGON-HF were able to meet the commonly used standard, according to the FDA briefing document. Among the key findings of these analyses were:
- An analysis of investigator-reported events for the primary composite endpoint of total hospitalizations for heart failure (HHF) and cardiovascular (CV) death demonstrated a rate ratio (RR) of 0.84 (95% confidence interval 0.74- 0.97; P = .01).
- Investigator-reported events added 226 and 290 HHF events but decreased CV death by 56 and 58 events in the sacubitril/valsartan and valsartan arms, respectively. Hence, a net 170 and 232 events were added to the clinical endpoint committee–reported primary composite endpoint leading to a P value of .01, without a significant change in RR.
- Analysis of investigator-reported expanded primary composite endpoint events including total HHF, urgent HF visits, and CV death demonstrated a RR of 0.83 (95% CI, 0.73-0.95; P = .006. There were 136 and 173 investigator-reported urgent HF events in sacubitril/valsartan and valsartan arms, respectively.
Opening a floodgate?
Cynthia L. Chauhan, MSW, of Wichita, Kansas, who served as the consumer representative on the panel, questioned whether a decision to revisit the data on PARAGON-HF might lead drugmakers to seek to repurpose other failed trials.
“Are we opening any kind of floodgate for other researchers to go back and see this is an invitation to try to, for want of a better term, back-door their way into some approvals?” Ms. Chauhan asked.
Dr. Nissen assured her that this concern was valid and would be considered. The goal would be to allow some flexibility in cases that merit further consideration, while preventing companies from data mining until they find some evidence to support an FDA application, he said.
Re-analyzing trials “should be done carefully, conservatively, and only when it really is compelling that the public interest supports it,” Dr. Nissen stressed.
Panelists reported no conflicts of interest related to the topic of the meeting.
UPDATED DECEMBER 17
A panel of federal advisers on Tuesday effectively backed a bid to expand approval of sacubitril/valsartan for use in a form of heart failure for which there is not yet an approved medication.
The U.S. Food and Drug Administration asked its Cardiovascular and Renal Drugs Advisory Committee to broadly consider whether new analyses of data from the PARAGON-HF trial, combined with other information, could support use of sacubitril/valsartan (Entresto, Novartis) in heart failure with preserved ejection fraction (HFpEF).
The advisory committee voted 12-1 on this question, which can be seen as a marker for an expanded approval: “Does PARAGON-HF, perhaps supported by previous studies, provide sufficient evidence to support any indication?”
The dissenting vote was cast by the panel’s chairperson, Julia B. Lewis, MD, a professor of medicine from Vanderbilt University. In explaining her vote, Dr. Lewis cited concerns about expanding use of the drug, which has a potential for hypotension. But she noted that the rest of the panelists were “impressed by the totality of the evidence” presented, including a willingness to take a new look at the PARAGON-HF trial. This study was perceived at first pass as having failed to prove a benefit for people with HFpEF.
The 2019 initial unveiling of the PARAGON-HF results had dampened hopes for an evidence-based drug therapy for HFpEF. Patients treated with the first-of-its-kind renin-angiotensin system (RAS) inhibitor, compared with those who received standard valsartan, had 13% fewer heart failure hospitalizations or cardiovascular (CV) deaths over an average of about 3 years, but the difference missed significance at a P value of .059.
“Everybody agreed that the P value of .05 was not written in stone,” Dr. Lewis said in summarizing the panelists’ views on the voting question.
At the FDA’s request, the panel also addressed several other questions without voting on them. The agency asked the panel to describe the patient population for whom an expanded approval would be appropriate. The FDA initially approved sacubitril/valsartan in 2015 to reduce the risk of cardiovascular death and hospitalization for heart failure in patients with chronic heart failure (NYHA Class II-IV) and reduced ejection fraction.
Novartis in April submitted an application to the FDA, seeking to expand the use of sacubitril/valsartan from the currently approved indication for the treatment of chronic heart failure (CHF) patients with reduced ejection fraction (HFrEF) to include what the company terms “the adjacent population of patients with preserved ejection fraction (HFpEF) who have a left ventricular ejection fraction (LVEF) below normal.” The American Society of Echocardiography and European Association of Cardiovascular Imaging define normal LVEF and normal range (±2 standard deviations) as 62% (range, 52%-72%) in men and 64% (range, 54%-74%) in women, Novartis said in its briefing materials for the meeting.
FDA panelist Christopher M. O’Connor, MD, for example, suggested that an expanded approval could allow for use of sacubitril/valsartan for the reduction of heart failure or hospitalization in patients with mildly reduced ejection fraction as defined by greater than 45% through 55%. FDA panelist C. Noel Bairey Merz, MD, director of the Barbra Streisand Women’s Heart Center at Cedars-Sinai Medical Center in Los Angeles, suggested extending this to 57% to acknowledge the higher threshold for women.
Another FDA panelist, Steven E. Nissen, MD, of the Cleveland Clinic, argued against use of imprecise terms in defining an expanded patient population for sacubitril/valsartan. If used in the right patient population, the drug could provide a benefit for people who have active heart failure with symptoms, including preventing hospitalizations and renal disease, he said.
“If you are symptomatic with a syndrome that’s consistent with heart failure and you have an ejection fraction below the lower limits of normal, I believe it’s in the public interest for you to get sacubitril/valsartan,” Dr. Nissen said.
The FDA usually follows the advice of its panels, but is not obligated to. But in this case, the agency staff were clearly seeking a path for an expanded approval of sacubitril/valsartan.
Challenging a standard
The FDA had encouraged Novartis to submit the supplementary application for the HFpEF indication and even suggested some of the post-hoc analyses, the agency staff said in a briefing document for the meeting.
PARAGON-HF illustrated some of the agency’s concerns about missed opportunities in general in large research trials. Some events of interest in studies may be miscounted due to a lack of information such as a requirement for the presence of physical examination findings that are not documented in the patient’s dossier, the FDA staff said.
“We would like to consider giving ‘partial credit’ to events based on the level of evidence provided, e.g., use of an ordinal variable rather than a dichotomous ‘yes’ or ‘no,’ ” the staff said in the briefing document.
At the panel meeting, Norman Stockbridge, MD, PhD, director of the Division of Cardiology and Nephrology in the FDA’s Center for Drug Evaluation and Research, told the panelists there is no basis in law for setting a P value of .05 as the benchmark on whether to declare a trial a success or failure.
“I wanted to take a few minutes and make sure that you on the committee understands what flexibility you have in addressing the case study in question,” Dr. Stockbridge said at the start of the meeting.
He then reviewed cases where the FDA had approved claims for cardiac medicines that had not shown desired results in key tests. These include approval of enalapril for use in asymptomatic left ventricular dysfunction on the basis of the SOLVD-Prevention trial, approval of digoxin for heart failure on the basis of the DIG study, and approval of carvedilol for reduced ejection fraction following myocardial infarction on
the basis of the CAPRICORN study, Dr. Stockbridge said.
In reviewing the data for sacubitril/valsartan, FDA staff noted a similarity between investigator-reported and adjudicated results, Stockbridge said.
“This suggested that there were events that did not need all evidentiary criteria as qualified events, but likely were nonetheless,” he said. “This is an example of dichotomization of events being wasteful of information.”
Post-hoc exploratory analyses in PARAGON-HF were able to meet the commonly used standard, according to the FDA briefing document. Among the key findings of these analyses were:
- An analysis of investigator-reported events for the primary composite endpoint of total hospitalizations for heart failure (HHF) and cardiovascular (CV) death demonstrated a rate ratio (RR) of 0.84 (95% confidence interval 0.74- 0.97; P = .01).
- Investigator-reported events added 226 and 290 HHF events but decreased CV death by 56 and 58 events in the sacubitril/valsartan and valsartan arms, respectively. Hence, a net 170 and 232 events were added to the clinical endpoint committee–reported primary composite endpoint leading to a P value of .01, without a significant change in RR.
- Analysis of investigator-reported expanded primary composite endpoint events including total HHF, urgent HF visits, and CV death demonstrated a RR of 0.83 (95% CI, 0.73-0.95; P = .006. There were 136 and 173 investigator-reported urgent HF events in sacubitril/valsartan and valsartan arms, respectively.
Opening a floodgate?
Cynthia L. Chauhan, MSW, of Wichita, Kansas, who served as the consumer representative on the panel, questioned whether a decision to revisit the data on PARAGON-HF might lead drugmakers to seek to repurpose other failed trials.
“Are we opening any kind of floodgate for other researchers to go back and see this is an invitation to try to, for want of a better term, back-door their way into some approvals?” Ms. Chauhan asked.
Dr. Nissen assured her that this concern was valid and would be considered. The goal would be to allow some flexibility in cases that merit further consideration, while preventing companies from data mining until they find some evidence to support an FDA application, he said.
Re-analyzing trials “should be done carefully, conservatively, and only when it really is compelling that the public interest supports it,” Dr. Nissen stressed.
Panelists reported no conflicts of interest related to the topic of the meeting.
Endocrine-disrupting plastics pose growing health threat
Many types of plastics pose an unrecognized threat to human health by leaching endocrine-disrupting chemicals, and a new report from the Endocrine Society and the International Pollutants Elimination Network presents their dangers and risks.

Written in a consumer-friendly form designed to guide public interest groups and policy makers, the report also can be used by clinicians to inform discussions with patients about the potential dangers of plastics and how they can reduce their exposure to endocrine-disrupting chemicals.
The report, Plastics, EDCs, & Health, defines endocrine-disrupting chemicals (EDCs) as “an exogenous chemical, or mixture of chemicals, that interferes with any aspect of hormone action.” Hormones in the body must be released at specific times, and therefore interference with their normal activity can have profound effects on health in areas including growth and reproductive development, according to the report.
The available data show “more and more information about the different chemicals and the different effects they are having,” said lead author, Jodi Flaws, PhD, of the University of Illinois at Urbana-Champaign, in a virtual press conference accompanying the release of the report.
Although numerous EDCs have been identified, a recent study suggested that many potentially dangerous chemical additives remain unknown because they are identified as confidential or simply not well described, the report authors said. In addition, creation of more plastic products will likely lead to increased exposure to EDCs and make health problems worse, said report coauthor Pauliina Damdimopoulou, PhD, of the Karolinska Institutet in Stockholm.
Lesser-known EDCs populate consumer products
Most consumers are aware of bisphenol A and phthalates as known EDCs, said Dr. Flaws, but the report identifies other lesser-known EDCs including per- and polyfluoroalkyl substances (PFAS), dioxins, flame retardants, and UV stabilizers.
For example, PFAS have been used for decades in a range of consumer products including stain resistant clothes, fast food wrappers, carpet and furniture treatments, cookware, and firefighting foams, according to the report. Consequently, PFAS have become common in many water sources including surface water, drinking water, and ground water because of how they are disposed. “Consumption of fish and other aquatic creatures caught in waterways contaminated with PFAS also poses heightened risks due to bioaccumulation of persistent chemicals in these animals,” the report authors noted. Human exposures to PFAS have been documented in urine, serum, plasma, placenta, umbilical cord, breast milk, and fetal tissues, they added.
Brominated flame retardants are another lesser-known EDC highlighted in the report. These chemical additives are used in plastics such as electronics cases to reduce the spread of fire, as well as in furniture foam and other building materials, the authors wrote. UV stabilizers, which also have been linked to health problems, often are used in manufacturing cars and other machinery.
Microplastics create large risk
Microplastics, defined as plastic particles less than 5 mm in diameter, are another source of exposure to EDCs that is not well publicized, according to the report. Plastic waste disposal often leads to the release of microplastics, which can infiltrate soil and water. Plastic waste is often dumped or burned; outdoor burning of plastic causes emission of dioxins into the air and ground.
“Not only do microplastics contain endogenous chemical additives, which are not bound to the microplastic and can leach out of the microplastic and expose the population, they can also bind and accumulate toxic chemicals from the surrounding environment such as sea water and sediment,” the report authors said.
Recycling is not an easy answer, either. Often more chemicals are created and released during the process of using plastics to make other plastics, according to the report.
Overall, more awareness of the potential for increased exposure to EDCs and support of strategies to seek out alternatives to hazardous chemicals is needed at the global level, the authors wrote. For example, the European Union has proposed a chemicals strategy that includes improved classification of EDCs and banning identified EDCs in consumer products.
New data support ongoing dangers
“It was important to produce the report at this time because several new studies came out on the effects of EDCs from plastics on human health,” Dr. Flaws said in an interview. “Further, there was not previously a single source that brought together all the information in a manner that was targeted towards the public, policy makers, and others,” she said.
Dr. Flaws said that what has surprised her most in the recent research is the fact that plastics contain such a range of chemicals and EDCs.
“A good take-home message [from the report] is that plastics can contain endocrine-disrupting chemicals that can interfere with normal hormones and lead to adverse health outcomes,” she said. “I suggest limiting the use of plastics as much as possible. I know this is very hard to do, so if someone needs to use plastic, they should not heat food or drink in plastic containers,” she emphasized. Individuals also can limit reuse of plastics over and over,” she said. “Heating and repeated use/washing often causes plastics to leach EDCs into food and drink that we then get into our bodies.”
Additional research is needed to understand the mechanisms by which EDCs from plastics cause damage, Dr. Flaws emphasized. “Given that it is not possible to eliminate plastics at this time, if we understood mechanisms of action, we could develop ways to prevent toxicity or treat EDC-induced adverse health outcomes,” she said. “We also need research designed to develop plastics or ‘green materials’ that do not contain endocrine disruptors and do not cause health problems or damage the environment,” she noted.
The report was produced as a joint effort of the Endocrine Society and International Pollutants Elimination Network. The report authors had no financial conflicts to disclose.
Many types of plastics pose an unrecognized threat to human health by leaching endocrine-disrupting chemicals, and a new report from the Endocrine Society and the International Pollutants Elimination Network presents their dangers and risks.
Written in a consumer-friendly form designed to guide public interest groups and policy makers, the report also can be used by clinicians to inform discussions with patients about the potential dangers of plastics and how they can reduce their exposure to endocrine-disrupting chemicals.
The report, Plastics, EDCs, & Health, defines endocrine-disrupting chemicals (EDCs) as “an exogenous chemical, or mixture of chemicals, that interferes with any aspect of hormone action.” Hormones in the body must be released at specific times, and therefore interference with their normal activity can have profound effects on health in areas including growth and reproductive development, according to the report.
The available data show “more and more information about the different chemicals and the different effects they are having,” said lead author, Jodi Flaws, PhD, of the University of Illinois at Urbana-Champaign, in a virtual press conference accompanying the release of the report.
Although numerous EDCs have been identified, a recent study suggested that many potentially dangerous chemical additives remain unknown because they are identified as confidential or simply not well described, the report authors said. In addition, creation of more plastic products will likely lead to increased exposure to EDCs and make health problems worse, said report coauthor Pauliina Damdimopoulou, PhD, of the Karolinska Institutet in Stockholm.
Lesser-known EDCs populate consumer products
Most consumers are aware of bisphenol A and phthalates as known EDCs, said Dr. Flaws, but the report identifies other lesser-known EDCs including per- and polyfluoroalkyl substances (PFAS), dioxins, flame retardants, and UV stabilizers.
For example, PFAS have been used for decades in a range of consumer products including stain resistant clothes, fast food wrappers, carpet and furniture treatments, cookware, and firefighting foams, according to the report. Consequently, PFAS have become common in many water sources including surface water, drinking water, and ground water because of how they are disposed. “Consumption of fish and other aquatic creatures caught in waterways contaminated with PFAS also poses heightened risks due to bioaccumulation of persistent chemicals in these animals,” the report authors noted. Human exposures to PFAS have been documented in urine, serum, plasma, placenta, umbilical cord, breast milk, and fetal tissues, they added.
Brominated flame retardants are another lesser-known EDC highlighted in the report. These chemical additives are used in plastics such as electronics cases to reduce the spread of fire, as well as in furniture foam and other building materials, the authors wrote. UV stabilizers, which also have been linked to health problems, often are used in manufacturing cars and other machinery.
Microplastics create large risk
Microplastics, defined as plastic particles less than 5 mm in diameter, are another source of exposure to EDCs that is not well publicized, according to the report. Plastic waste disposal often leads to the release of microplastics, which can infiltrate soil and water. Plastic waste is often dumped or burned; outdoor burning of plastic causes emission of dioxins into the air and ground.
“Not only do microplastics contain endogenous chemical additives, which are not bound to the microplastic and can leach out of the microplastic and expose the population, they can also bind and accumulate toxic chemicals from the surrounding environment such as sea water and sediment,” the report authors said.
Recycling is not an easy answer, either. Often more chemicals are created and released during the process of using plastics to make other plastics, according to the report.
Overall, more awareness of the potential for increased exposure to EDCs and support of strategies to seek out alternatives to hazardous chemicals is needed at the global level, the authors wrote. For example, the European Union has proposed a chemicals strategy that includes improved classification of EDCs and banning identified EDCs in consumer products.
New data support ongoing dangers
“It was important to produce the report at this time because several new studies came out on the effects of EDCs from plastics on human health,” Dr. Flaws said in an interview. “Further, there was not previously a single source that brought together all the information in a manner that was targeted towards the public, policy makers, and others,” she said.
Dr. Flaws said that what has surprised her most in the recent research is the fact that plastics contain such a range of chemicals and EDCs.
“A good take-home message [from the report] is that plastics can contain endocrine-disrupting chemicals that can interfere with normal hormones and lead to adverse health outcomes,” she said. “I suggest limiting the use of plastics as much as possible. I know this is very hard to do, so if someone needs to use plastic, they should not heat food or drink in plastic containers,” she emphasized. Individuals also can limit reuse of plastics over and over,” she said. “Heating and repeated use/washing often causes plastics to leach EDCs into food and drink that we then get into our bodies.”
Additional research is needed to understand the mechanisms by which EDCs from plastics cause damage, Dr. Flaws emphasized. “Given that it is not possible to eliminate plastics at this time, if we understood mechanisms of action, we could develop ways to prevent toxicity or treat EDC-induced adverse health outcomes,” she said. “We also need research designed to develop plastics or ‘green materials’ that do not contain endocrine disruptors and do not cause health problems or damage the environment,” she noted.
The report was produced as a joint effort of the Endocrine Society and International Pollutants Elimination Network. The report authors had no financial conflicts to disclose.
Many types of plastics pose an unrecognized threat to human health by leaching endocrine-disrupting chemicals, and a new report from the Endocrine Society and the International Pollutants Elimination Network presents their dangers and risks.
Written in a consumer-friendly form designed to guide public interest groups and policy makers, the report also can be used by clinicians to inform discussions with patients about the potential dangers of plastics and how they can reduce their exposure to endocrine-disrupting chemicals.
The report, Plastics, EDCs, & Health, defines endocrine-disrupting chemicals (EDCs) as “an exogenous chemical, or mixture of chemicals, that interferes with any aspect of hormone action.” Hormones in the body must be released at specific times, and therefore interference with their normal activity can have profound effects on health in areas including growth and reproductive development, according to the report.
The available data show “more and more information about the different chemicals and the different effects they are having,” said lead author, Jodi Flaws, PhD, of the University of Illinois at Urbana-Champaign, in a virtual press conference accompanying the release of the report.
Although numerous EDCs have been identified, a recent study suggested that many potentially dangerous chemical additives remain unknown because they are identified as confidential or simply not well described, the report authors said. In addition, creation of more plastic products will likely lead to increased exposure to EDCs and make health problems worse, said report coauthor Pauliina Damdimopoulou, PhD, of the Karolinska Institutet in Stockholm.
Lesser-known EDCs populate consumer products
Most consumers are aware of bisphenol A and phthalates as known EDCs, said Dr. Flaws, but the report identifies other lesser-known EDCs including per- and polyfluoroalkyl substances (PFAS), dioxins, flame retardants, and UV stabilizers.
For example, PFAS have been used for decades in a range of consumer products including stain resistant clothes, fast food wrappers, carpet and furniture treatments, cookware, and firefighting foams, according to the report. Consequently, PFAS have become common in many water sources including surface water, drinking water, and ground water because of how they are disposed. “Consumption of fish and other aquatic creatures caught in waterways contaminated with PFAS also poses heightened risks due to bioaccumulation of persistent chemicals in these animals,” the report authors noted. Human exposures to PFAS have been documented in urine, serum, plasma, placenta, umbilical cord, breast milk, and fetal tissues, they added.
Brominated flame retardants are another lesser-known EDC highlighted in the report. These chemical additives are used in plastics such as electronics cases to reduce the spread of fire, as well as in furniture foam and other building materials, the authors wrote. UV stabilizers, which also have been linked to health problems, often are used in manufacturing cars and other machinery.
Microplastics create large risk
Microplastics, defined as plastic particles less than 5 mm in diameter, are another source of exposure to EDCs that is not well publicized, according to the report. Plastic waste disposal often leads to the release of microplastics, which can infiltrate soil and water. Plastic waste is often dumped or burned; outdoor burning of plastic causes emission of dioxins into the air and ground.
“Not only do microplastics contain endogenous chemical additives, which are not bound to the microplastic and can leach out of the microplastic and expose the population, they can also bind and accumulate toxic chemicals from the surrounding environment such as sea water and sediment,” the report authors said.
Recycling is not an easy answer, either. Often more chemicals are created and released during the process of using plastics to make other plastics, according to the report.
Overall, more awareness of the potential for increased exposure to EDCs and support of strategies to seek out alternatives to hazardous chemicals is needed at the global level, the authors wrote. For example, the European Union has proposed a chemicals strategy that includes improved classification of EDCs and banning identified EDCs in consumer products.
New data support ongoing dangers
“It was important to produce the report at this time because several new studies came out on the effects of EDCs from plastics on human health,” Dr. Flaws said in an interview. “Further, there was not previously a single source that brought together all the information in a manner that was targeted towards the public, policy makers, and others,” she said.
Dr. Flaws said that what has surprised her most in the recent research is the fact that plastics contain such a range of chemicals and EDCs.
“A good take-home message [from the report] is that plastics can contain endocrine-disrupting chemicals that can interfere with normal hormones and lead to adverse health outcomes,” she said. “I suggest limiting the use of plastics as much as possible. I know this is very hard to do, so if someone needs to use plastic, they should not heat food or drink in plastic containers,” she emphasized. Individuals also can limit reuse of plastics over and over,” she said. “Heating and repeated use/washing often causes plastics to leach EDCs into food and drink that we then get into our bodies.”
Additional research is needed to understand the mechanisms by which EDCs from plastics cause damage, Dr. Flaws emphasized. “Given that it is not possible to eliminate plastics at this time, if we understood mechanisms of action, we could develop ways to prevent toxicity or treat EDC-induced adverse health outcomes,” she said. “We also need research designed to develop plastics or ‘green materials’ that do not contain endocrine disruptors and do not cause health problems or damage the environment,” she noted.
The report was produced as a joint effort of the Endocrine Society and International Pollutants Elimination Network. The report authors had no financial conflicts to disclose.
COVID-related harm to HCWs must be tracked more rigorously: NAS panel
A panel of scientific experts is urging the nation to do more to track morbidity and mortality among health care workers (HCWs), given the large and disproportionate number who have been infected with or died from SARS-CoV-2.
The National Academies of Sciences, Engineering, and Medicine’s Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats issued a 10-page “rapid expert consultation” on what is known about deaths and mental health problems among HCWs associated with the COVID-19 pandemic and how to protect workers.
“The absence of a uniform national framework and inconsistent requirements across states for collecting, recording, and reporting HCW mortality and morbidity data associated with COVID-19 impairs anyone’s ability to make comparisons, do combined analyses, or draw conclusions about the scale of the problem,” says the panel in the report.
Mental health, in particular, needs to be examined, it says. Although the data are still limited, the prevalence of burnout and suicide “points to a serious concern,” according to the report.
“As with mortality due to COVID-19, there are currently no national systems nor reporting standards for morbidity measures related to the pandemic, such as mental health status, provider well-being, and other psychological effects on HCWs,” the report says.
A more robust national system that collected data on circumstances and interventions that may raise or lower risk, as well as on where the infection occurred, “would support the adoption of effective mitigation strategies,” says the report. It would also facilitate epidemiologic studies on risk factors, such as face-to-face contact with COVID-19 patients and the availability and use of personal protective equipment (PPE). Studies could also examine the impact of institutional requirements for masking.
Studies have consistently shown that universal mask wearing and access to appropriate PPE support the physical safety and mental health of HCWs, says the report.
Track scale of crisis
The committee cited many gaps in the current system. The Occupational Safety and Health Administration, for instance, doesn’t count deaths from occupationally acquired infection. Many states don’t report COVID-19 deaths by profession. The Centers for Disease Control and Prevention (CDC) relies on case report forms from local health departments for all COVID-19 cases, which typically are lacking in specifics, such as occupation or job setting, says the committee’s report.
As of Nov. 3, the CDC had reported 786 deaths among HCWs that were attributable to COVID-19 – a far lower number than other sources have reported.
The committee notes that much could be done immediately. A National Academy of Medicine panel on clinician well-being and resilience in August recommended that the CDC establish a national epidemiologic tracking program to measure HCWs’ well-being, assess the acute and long-term effects of COVID-19 on those workers, and report on the outcomes of interventions.
Such a program “is needed to comprehensively acknowledge the scale of the COVID-19 crisis and protect the health care workforce that is already stretched to the breaking point in many locations,” the committee says in its report.
A version of this article originally appeared on Medscape.com.
A panel of scientific experts is urging the nation to do more to track morbidity and mortality among health care workers (HCWs), given the large and disproportionate number who have been infected with or died from SARS-CoV-2.
The National Academies of Sciences, Engineering, and Medicine’s Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats issued a 10-page “rapid expert consultation” on what is known about deaths and mental health problems among HCWs associated with the COVID-19 pandemic and how to protect workers.
“The absence of a uniform national framework and inconsistent requirements across states for collecting, recording, and reporting HCW mortality and morbidity data associated with COVID-19 impairs anyone’s ability to make comparisons, do combined analyses, or draw conclusions about the scale of the problem,” says the panel in the report.
Mental health, in particular, needs to be examined, it says. Although the data are still limited, the prevalence of burnout and suicide “points to a serious concern,” according to the report.
“As with mortality due to COVID-19, there are currently no national systems nor reporting standards for morbidity measures related to the pandemic, such as mental health status, provider well-being, and other psychological effects on HCWs,” the report says.
A more robust national system that collected data on circumstances and interventions that may raise or lower risk, as well as on where the infection occurred, “would support the adoption of effective mitigation strategies,” says the report. It would also facilitate epidemiologic studies on risk factors, such as face-to-face contact with COVID-19 patients and the availability and use of personal protective equipment (PPE). Studies could also examine the impact of institutional requirements for masking.
Studies have consistently shown that universal mask wearing and access to appropriate PPE support the physical safety and mental health of HCWs, says the report.
Track scale of crisis
The committee cited many gaps in the current system. The Occupational Safety and Health Administration, for instance, doesn’t count deaths from occupationally acquired infection. Many states don’t report COVID-19 deaths by profession. The Centers for Disease Control and Prevention (CDC) relies on case report forms from local health departments for all COVID-19 cases, which typically are lacking in specifics, such as occupation or job setting, says the committee’s report.
As of Nov. 3, the CDC had reported 786 deaths among HCWs that were attributable to COVID-19 – a far lower number than other sources have reported.
The committee notes that much could be done immediately. A National Academy of Medicine panel on clinician well-being and resilience in August recommended that the CDC establish a national epidemiologic tracking program to measure HCWs’ well-being, assess the acute and long-term effects of COVID-19 on those workers, and report on the outcomes of interventions.
Such a program “is needed to comprehensively acknowledge the scale of the COVID-19 crisis and protect the health care workforce that is already stretched to the breaking point in many locations,” the committee says in its report.
A version of this article originally appeared on Medscape.com.
A panel of scientific experts is urging the nation to do more to track morbidity and mortality among health care workers (HCWs), given the large and disproportionate number who have been infected with or died from SARS-CoV-2.
The National Academies of Sciences, Engineering, and Medicine’s Standing Committee on Emerging Infectious Diseases and 21st Century Health Threats issued a 10-page “rapid expert consultation” on what is known about deaths and mental health problems among HCWs associated with the COVID-19 pandemic and how to protect workers.
“The absence of a uniform national framework and inconsistent requirements across states for collecting, recording, and reporting HCW mortality and morbidity data associated with COVID-19 impairs anyone’s ability to make comparisons, do combined analyses, or draw conclusions about the scale of the problem,” says the panel in the report.
Mental health, in particular, needs to be examined, it says. Although the data are still limited, the prevalence of burnout and suicide “points to a serious concern,” according to the report.
“As with mortality due to COVID-19, there are currently no national systems nor reporting standards for morbidity measures related to the pandemic, such as mental health status, provider well-being, and other psychological effects on HCWs,” the report says.
A more robust national system that collected data on circumstances and interventions that may raise or lower risk, as well as on where the infection occurred, “would support the adoption of effective mitigation strategies,” says the report. It would also facilitate epidemiologic studies on risk factors, such as face-to-face contact with COVID-19 patients and the availability and use of personal protective equipment (PPE). Studies could also examine the impact of institutional requirements for masking.
Studies have consistently shown that universal mask wearing and access to appropriate PPE support the physical safety and mental health of HCWs, says the report.
Track scale of crisis
The committee cited many gaps in the current system. The Occupational Safety and Health Administration, for instance, doesn’t count deaths from occupationally acquired infection. Many states don’t report COVID-19 deaths by profession. The Centers for Disease Control and Prevention (CDC) relies on case report forms from local health departments for all COVID-19 cases, which typically are lacking in specifics, such as occupation or job setting, says the committee’s report.
As of Nov. 3, the CDC had reported 786 deaths among HCWs that were attributable to COVID-19 – a far lower number than other sources have reported.
The committee notes that much could be done immediately. A National Academy of Medicine panel on clinician well-being and resilience in August recommended that the CDC establish a national epidemiologic tracking program to measure HCWs’ well-being, assess the acute and long-term effects of COVID-19 on those workers, and report on the outcomes of interventions.
Such a program “is needed to comprehensively acknowledge the scale of the COVID-19 crisis and protect the health care workforce that is already stretched to the breaking point in many locations,” the committee says in its report.
A version of this article originally appeared on Medscape.com.