User login
Bringing you the latest news, research and reviews, exclusive interviews, podcasts, quizzes, and more.
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
div[contains(@class, 'main-prefix')]
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
Horse flies (Tabanidae) are hematophagous dipteran insects that feed on the blood of their hosts, including humans.1 Their bites can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers and systemic illness. In this article, we discuss identifying features of horse flies as well as clinical manifestations from bite reactions, symptomatic and emergency management, and strategies for prevention and control.
Morphology and Geographic Distribution
Horse flies, which can grow as large as 30 mm, can be identified by their brown or black bodies and characteristic large heads and proboscises, wing venation, large calypters, pulvilliform empodium between large pulvilli, and lack of bristles on the body.2 Occasionally, their bodies may be gray, yellow, green, or blue, but this is less likely than in the other species of the Tabanidae family. Short hairs are present on the head and thorax. The eyes are large and often patterned, multicolored, and bright, though they also can exhibit shades of dark brown, gray, or black. There is variation in the appearance of male vs female horse flies: females have eyes that are widely spaced apart, while males have eyes that are closer together.2 It is important to note the difference between male and female horseflies, as hematophagy is exhibited only by females.1
Horse flies are found worldwide, with the exception of Hawaii, Greenland, and Iceland.3,4 They are especially prevalent in warm and moist regions, as these conditions are optimal for breeding.3-5 They tend to be active during the day and inactive at night due to a preference for sunlight and warmth.6 Due to this preference, horse flies’ seasonal activity depends on the climate; for many regions, activity persists from summer to early autumn.7
Clinical Manifestations and Treatment
Female horse flies use their mouthparts to pierce the host’s skin, inject saliva, and suck blood. The saliva contains anticoagulant properties. The bites are painful for the host, and various reactions can occur, including large urticarial wheals or papules at the site of the bite. Treatment for these minor cutaneous reactions is largely symptomatic. The bite site should be washed with soap and water; ice can be applied to help reduce inflammation.8 Oral antihistamines may be administered to reduce pruritus and treat urticaria. Topical steroids also can be prescribed for symptomatic relief. Acetaminophen and nonsteroidal anti-inflammatory drugs can be administered for pain control.8
While most cases of horse fly bites are minor, there have been reports of anaphylaxis.9 Horse fly bite–induced anaphylaxis can manifest as generalized itching, urticaria, and angioedema within minutes of being bitten. This may be followed by pharyngeal constriction, shortness of breath, nausea, vomiting, shivers, perspiration, and loss of consciousness.9 Anaphylaxis symptoms should be treated with immediate administration of intramuscular epinephrine.10
Pathogen Transmission, Prevention, and Control
Although horse flies have been found to carry numerous viruses, bacteria, and protozoa that affect other mammals, there is not enough evidence to suggest that they are vectors of transmission for humans for most diseases.11,12 In particular, West Nile virus and Borrelia burgdorferi both have been found in horse flies, but there are no reports of transmission of these diseases to humans through their bites.12
Horse flies, their close cousins deer flies (specifically Chrysops discalis), and ticks are known vectors of Francisella tularensis.13 These bacteria cause tularemia, which can manifest with symptoms such as fever, headache, and malaise. Ulceroglandular tularemia is the most common manifestation, in which the patient develops a cutaneous ulceration at the site of the horse fly bite and exhibits associated tender regional lymphadenopathy.14 Exudative conjunctivitis, exudative pharyngitis, abdominal pain, diarrhea, vomiting, and severe bilateral pneumonia also are common symptoms. The most severe form of tularemia is systemic or typhoidal tularemia, which can manifest with fever, septic shock, and hepatosplenomegaly.14 The current treatment of choice for all forms of tularemia is intravenous gentamicin, with a recommended dosage of 5 mg/kg/d for 7 to 14 days; streptomycin is an acceptable alternative.14-16 Ciprofloxacin is used less commonly and is reserved for milder disease. Incision and drainage of the affected lymph nodes also may be necessary.14 It is important to promptly identify and treat tularemia, as the mortality rate can be as high as 50% for untreated disease, especially in patients with systemic symptoms. Even after treatment, many patients exhibit residual scarring at the site of the ulcer, as well as lung, kidney, and muscle damage.14
It is advised to avoid contact with horse flies due to the range of symptom severity caused by their bites, but avoidance and control can be difficult. Malaise traps, consisting of a tent and polyester netting, can be used to capture the insects.17 Octenol has been shown to be effective for attracting horse flies and can be applied to the trap in order to increase its effectiveness.18 A Manitoba horse fly trap is a modified version of the Malaise trap that contains a suspended dark sphere to further attract horse flies.19 Patients also should be instructed to wear long-sleeved shirts and pants when outdoors in areas with horse flies to avoid contact, and application of DEET (N,N-diethylmeta-toluamide), picaridin, citronella, or geraniol-based repellents also can be effective in reducing exposure.20
Final Thoughts
Horse flies are large, blood‑feeding dipteran insects whose bites usually produce painful local reactions. Although most bites are benign, they rarely can cause anaphylaxis, and certain Tabanidae insects can transmit Francisella tularensis; therefore, clinicians should consider the risk for tularemia infection in patients presenting with horse fly bites and start appropriate antibiotic therapy when indicated. Due to the risks, prevention of bites and reduction of contact with horse flies via protective clothing, repellents, and trapping methods is recommended. Patients should be advised on bite care and to seek urgent care for systemic symptoms or rapidly progressive local signs.
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
- Lucas M, Krolow TK, Riet-Correa F, et al. Diversity and seasonality of horse flies (Diptera: Tabanidae) in Uruguay. Sci Rep. 2020;10:401.
- Chainey JE. Horse‑flies, deer‑flies and clegs (Tabanidae). In: Lane RP, Crosskey RW, eds. Medical Insects and Arachnids. Springer; 1993:310‑332.
- Downes JA. The post‑glacial colonization of the North Atlantic islands. Memoirs of the Entomological Society of Canada. 1988;120(S144):55‑92.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida; April 1, 2014. Accessed September 15, 2023.
- Middlekauff WW, Lane RS. Adult and immature Tabanidae (Diptera) of California. University of California Press. 1980:1‑2.
- Horse flies and deer flies. University of Kentucky. Accessed September 15, 2023. https://entomology.mgcafe.uky.edu/ef511
- Hoover J. Horse flies. LSU College of Agriculture. May 28, 2020. Accessed May 20, 2026. https://www.lsuagcenter.com/profiles/jhoover/articles/page1590683239678
- Powers J, Syed HA, McDowell RH. Insect bites. StatPearls [Internet]. Updated February 15, 2026. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK537235/
- Hemmer W, Focke M, Vieluf D, et al. Anaphylaxis induced by horsefly bites: identification of a 69 kd IgE-binding salivary gland protein from Chrysops spp. (Diptera, Tabanidae) by Western blot analysis. J Allergy Clin Immunol. 1998;101:134-136.
- McLendon K, Sternard BT. Anaphylaxis. StatPearls [Internet]. Updated January 26, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK482124/
- Cheng TC. General Parasitology. Elsevier Science; 2012:660.
- Purdue Medical Entomology. Horse and deer flies. Purdue University. Accessed April 28, 2026. https://extension.entm.purdue.edu/publichealth/diseases/tabanid.html
- US Geological Survey. Tularemia. USGS Publications Warehouse. Accessed April 28, 2026. https://pubs.usgs.gov/circ/1297/report.pdf
- Snowden J, Simonsen KA. Tularemia. StatPearls [Internet]. Updated July 17, 2023. Accessed May 12, 2026. https://www.ncbi.nlm.nih.gov/books/NBK430905/
- Enderlin G, Morales L, Jacobs RF, et al. Streptomycin and alternative agents for the treatment of tularemia: review of the literature. Clin Infect Dis. 1994;19:42-47.
- Balestra A, Bytyci H, Guillod C, et al. A case of ulceroglandular tularemia presenting with lymphadenopathy and an ulcer on a linear morphoea lesion surrounded by erysipelas. Int Med Case Rep J. 2018;11:313-318.
- Malaise R. A new insect‑trap. Entomologisk Tidskrift. 1937;58:148‑160.
- French F, Kline D. l-Octen-3-ol, an effective attractant for Tabanidae (Diptera). J Med Entomol. 1989;26:459-461
- Axtell RC, Edwards TD, Dukes JC. Rigid canopy trap for Tabanidae (Diptera). J Georgia Entomol Soc. 1975;10: 64-67.
- Squitier JM. Deer flies, yellow flies and horse flies. Featured Creatures. University of Florida. April 1, 2014. Accessed May 12, 2026. https://ask.ifas.ufl.edu/publication/IN155
Horse Flies: Identification, Bite Reactions, and Clinical Management
Horse Flies: Identification, Bite Reactions, and Clinical Management
PRACTICE POINTS
- Horse flies (Tabanidae) are hematophagous insects that can cause minor cutaneous reactions (eg, urticaria) or, rarely, severe reactions such as anaphylaxis. They also are vectors of tularemia, which may manifest with cutaneous ulcers or systemic illness.
- Mild reactions are managed symptomatically; anaphylaxis requires epinephrine, and tularemia requires systemic antibiotics such as gentamicin.
- Patients should be counseled on avoidance strategies, including wearing protective clothing and using topical repellents and environmental traps.

Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
Hand dermatitis (HD) is a common dermatologic concern that can impair quality of life, work productivity, and daily functioning.1 Occupational HD is defined as hand eczema caused or worsened by workplace exposures. When caused by work, HD may lead to reduced productivity and even job loss. Subtypes of HD include irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), protein contact dermatitis (PCD), atopic dermatitis (AD), hyperkeratotic HD, and dyshidrotic eczema.2,3
Often caused by wet work, ICD is the most common subtype, whereas PCD—which is caused by immediate hypersensitivity to protein—is less common and usually seen in food service workers.3,4 When HD does not improve with standard treatment, particularly in occupational cases, patch testing is prudent to evaluate for contact allergens. In this article, we review practical considerations for evaluation and management of occupational irritant and allergic HD, highlighting relevant exposures and pearls on workup and management.
Epidemiology of Hand Dermatitis
A 2021 systematic review and meta-analysis of European studies reported a 1-year HD prevalence of 9.1% and a lifetime prevalence of 14.5%.5 Hand dermatitis is most common in women; individuals aged 30 to 39 years; and those who are employed, underscoring the role of workplace exposure.6 High-risk occupations are those involving substantial wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.7 Individuals with a history of AD also are at high risk for HD.8
Hand Dermatitis Subtypes
Irritant Contact Dermatitis—Irritant contact dermatitis, the most common form of occupational HD, is caused by repeated exposure to irritants (eg, water, detergents, cleansers, and soaps) that disrupt the skin barrier.9 Occupations that involve wet work are a major risk factor, associated with a 56% higher likelihood of ICD.8 Wet work involves frequent handwashing, prolonged contact with liquids, or occlusive glove use.9 As a ubiquitous skin irritant, water can penetrate the stratum corneum, impair the skin barrier, and increase sensitization risk. The dorsal hands usually are affected by ICD due to the thinner stratum corneum in this area.9
Allergic Contact Dermatitis—Allergic contact dermatitis should be considered in cases of chronic, recurrent, or treatment-resistant disease. Clinical clues include dermatitis beyond irritant contact sites, recurrent pruritic and vesicular HD, and flares with occupational exposures or materials; however, it can be difficult to distinguish ACD from ICD on clinical presentation alone, as they have many overlapping features. When ACD is suspected, patch testing remains the gold standard for identifying allergens and guiding avoidance strategies, product alternatives, and workplace modifications.
Unique Occupational Considerations
Hairdressers—Hairdressers have an increased risk for HD due to wet work and exposure to sensitizers, with a pooled lifetime prevalence of 38.2% (including ICD, ACD, and occupational cases).10 Notably, frequent shampooing, rinsing, cutting wet hair, handwashing, and glove use increase the risk for ICD. Hairdressers also are exposed to allergens in hair products, including p-phenylenediamine, toluene-2,5-diamine, persulfate salts, glyceryl thioglycolate, preservatives, and fragrances. Occupational exposure to the preservative methylisothiazolinone is high among hairdressers, with a sensitization rate of 10.5% in HD cases.11
It has been reported that hyperkeratotic fissured eczema of the dorsal hands caused by wet work often indicates ICD, whereas pruritic dyshidrotic eczema involving the lateral fingers or palms suggests ACD; however, these conditions can share overlapping features.7 If ACD is suspected, broad patch testing with baseline and hairdresser series, along with specific chemicals that may be encountered in the workplace, is necessary. Management includes allergen avoidance, reduced wet work tasks, use of nitrile gloves with glove changes to mitigate occlusive effects, and skin barrier protection with emollients.
Health Care Workers—Health care workers are vulnerable to HD due to intensive hand hygiene, prolonged glove use, and allergen exposures, with a lifetime prevalence of self-reported HD of 33.4%.12 Common allergens among health care workers include rubber accelerators, most often from rubber gloves.13 Frequent handwashing and glove use can further impair the skin barrier, increasing irritant and sensitization risks.14 In contrast, alcohol-based hand sanitizers containing emollients are less irritating, with prior analyses showing no significant association with HD risk.15,16 Conversely, handwashing 8 to 10 times daily increased HD risk, with a relative risk of 1.51.15
Surgeons and proceduralists face unique risks for HD from preoperative scrubbing with products that can contain potential allergens such as chlorhexidine gluconate, chloroxylenol, povidone-iodine, fragrance, cocamide diethanolamine, lanolin, alkyl glucosides, sodium benzoate, sorbic acid, tocopherol, and propylene glycol.17,18 Subsequent occlusion under glove layers drives ICD and ACD risks, highlighting the importance of patch testing in affected individuals. While patch testing, exposure avoidance, and limited glove use can mitigate HD risk, frequent handwashing can contribute to refractory HD.
Food Service Workers—Food service workers have an increased risk for HD from allergens and irritants. In a retrospective study of patients with occupational food-related HD (N=372), 57% were diagnosed with ICD, 22% with PCD, and 1.8% with ACD.19 Skin barrier disruption from wet work, occlusion from glove use, and contact with food proteins increase HD risk, especially in bakers exposed to flours and grains, which can cause IgE–mediated PCD manifesting with contact urticaria. Protein contact dermatitis is confirmed by prick testing with suspected foods.20 Additionally, exposure to garlic can cause ICD and ACD due to sulfur-containing compounds, particularly allicin and diallyl disulfide.21,22 Pineapple also can trigger ICD associated with bromelain, a proteolytic enzyme that can break down the skin.23 Nickel exposure is another concern, as steel utensils and cookware can release nickel onto the skin of sensitized individuals.24 Rubber accelerator exposure from gloves also contributes to contact allergy and HD among food service workers; vinyl gloves usually are a good alternative in this setting.25 Management of food-related HD involves exposure avoidance, which may affect occupational viability
Construction Workers—Construction workers are at risk for occupational HD due to contact with irritants and sensitizers such as paints, adhesives, asphalt, cement, solvents, and gloves.26 A retrospective analysis of North American Contact Dermatitis Group data identified HD in 37.2% (253/681) of patch-tested construction workers. The most common occupational allergens include potassium dichromate, which can be present in cement and leather items; bisphenol A epoxy resin; cobalt chloride hexahydrate; and the rubber accelerators carba mix and thiuram mix.26 A thorough occupational history should assess materials handled, and patch testing should include common construction-related allergens to inform avoidance strategies. Workplace task modification can reduce exposure, as certain managerial roles in construction work may involve less contact with irritants and sensitizers.26
Nail Technicians—Nail technicians are at risk for HD, especially ACD from acrylate monomers used in nail gels, dips, and acrylics. In a 10-year analysis, around 87.5% (14/16) of nail technicians with contact allergy to methacrylate demonstrated hand involvement.27 Common acrylate monomers include 2-hydroxyethyl methacrylate, 2-hydroxypropyl methacrylate, and ethyl cyanoacrylate. 28 Evaluation requires a detailed occupational history, assessing HD onset relative to exposure, services performed, glove-use practices, and whether symptoms improve away from work. While gloves may appear to reduce exposure, a glove-penetration study showed that acrylate-containing nail products can penetrate commonly used disposable gloves from within seconds to approximately 20 minutes, depending on glove and product type.29 Among available options, nitrile gloves may provide dexterity and allergen avoidance when acrylate exposure is brief, with glove changes required every 15 to 30 minutes.30 Patch testing with 2-hydroxyethyl methacrylate and ethyl cyanoacrylate can identify nail acrylate allergy; however, avoidance can be challenging for nail technicians, as these products often are ubiquitous in their work.
Florists—Florists can develop HD from plant allergens and irritants, particularly tulipalin A and calcium oxalate, with a lifetime prevalence of 19.6%.31 Tulipalin A is a well-documented sensitizer causing ACD among florists exposed to tulip bulbs and other Alstroemeria flowers.32 The term tulip fingers actually was coined to describe ACD caused by tulip bulbs in the European tulip industry.33 Patch testing involves testing for tulipalin A, which may be commercially limited, or tulip plant materials; however, fresh tulips require open testing with small amounts due to higher allergen concentration.32 Additionally, the term daffodil itch describes a type of ICD caused by calcium oxalate crystals in daffodil bulbs and tulip sap.32,34 Diagnosis of plant-related HD requires an occupational history and targeted patch testing, while glove protection and exposure avoidance are essential for improvement.
Evaluation and Management
The workup for HD involves physical examination and medical history, including disease onset, course, and history of AD, along with occupational and exposure history to identify allergens and irritants. Understanding the patient’s tasks and responsibilities and workplace practices along with the materials they handle allows the dermatologist to anticipate relevant allergens for patch testing.
Patch testing should be comprehensive, as baseline screening series alone may miss between 26.3% and 50% of occupationally relevant allergens.35,36 Comprehensive patch testing also should include specialty series and supplemental allergens based on the patient’s clinical history and exposures. Specialty series may include hairdressing, bakery, cosmetics, dental, machinists, and adhesives.37 Gloves also warrant attention, as they may be overlooked as a sensitizer following repeated contact and occlusion. In persistent HD associated with glove use, patch testing should include a rubber accelerator series with relevant allergens, such as thiurams, carbamates, mercaptobenzothiazole, diphenylguanidine, and the patient’s own gloves.38 Latex allergy also should be considered, particularly in immediate-type reactions, and can be evaluated with latex-specific IgE testing.39
Management of HD relies on accurate diagnosis and allergen avoidance, which can be challenging in occupational settings. Structured tools, such as the American Contact Dermatitis Society’s Contact Allergen Management Program (https://www.contactderm.org/ resources/acds-camp), can help identify safe alternatives.
In occupational HD, risk assessment should identify occupational exposures and determine appropriate personal protective equipment while minimizing the risk for HD associated with such equipment. Protective gloves are advised to prevent contact with allergens and irritants. When glove use lasts more than 10 minutes, cotton glove liners may be worn to avoid occlusion and moisture retention.40 For wet work, vinyl gloves are recommended, with regular emollient use to support skin-barrier repair. Overall, gloves should be used when possible, changed regularly, and worn for limited periods of time to prevent ICD.
Work modification may be required to reduce exposure and flares, including task reassignment or substitution of materials containing allergens and irritants. Occupational HD may necessitate workplace accommodations, disability evaluation, medical leave, or even permanent job change. Dermatologists play a crucial role in the medical determination of work relatedness and functional impairment, guiding patients through occupational health, disability, and workers’ compensation when warranted.
Treatments for Occupational HD
Treatment of occupational HD depends on disease severity, chronicity, and avoidance of allergens and irritants in ACD, ICD, and PCD. Foundational management includes regular emollient use, which can even serve as monotherapy in mild occupational HD.40 Corticosteroids are the cornerstone of topical therapy, while calcineurin inhibitors can be used as a steroid-sparing option in milder disease.41 Off-label topical calcipotriol and AD-approved therapies crisaborole and ruxolitinib may be effective. For refractory disease after topical treatments, phototherapy can be considered.40 Biologic and targeted therapies also have emerged as potential treatments. Dupilumab is effective for atopic chronic HD and has demonstrated promise for nonatopic chronic HD.42 Recently, delgocitinib, a topical pan–Janus kinase inhibitor cream, showed clinical efficacy for chronic hand eczema and was approved by the US Food and Drug Administration.43 Off-label use of alternative systemic therapies, including acitretin, cyclosporine, methotrexate, and azathioprine, and other biologics and systemic Janus kinase inhibitors also may treat HD, but larger studies are lacking.40
Our Final Interpretation
Occupational HD is a common skin condition with multiple etiologies. It is important for clinicians to gather a thorough occupational and exposure history to narrow the differential diagnosis, inform patch testing, and guide effective management. In practice, successful treatment depends on screening for and diagnosis of workplace exposures driving disease.
- Agner T, Andersen KE, Brandao FM, et al. Hand eczema severity and quality of life: a cross-sectional, multicentre study of hand eczema patients. Contact Dermatitis. 2008;59:43-47. doi:10.1111 /j.1600-0536.2008.01362.x
- Agner T, Aalto-Korte K, Andersen KE, et al. Classification of hand eczema. J Eur Acad Dermatol Venereol. 2015;29:2417-2422. doi:10.1111 /jdv.13308
- Bissonnette R, Agner T, Molin S, et al. Hand eczema—part 1: epidemiology, pathogenesis, diagnosis, and work-up. J Am Acad Dermatol. 2025;93:1201-1210. doi:10.1016/j.jaad.2024.09.048
- Barbaud A. Mechanism and diagnosis of protein contact dermatitis. Curr Opin Allergy Clin Immunol. 2020;20:117-121. doi:10.1097/ACI.0000000000000621
- Quaade AS, Simonsen AB, Halling AS, et al. Prevalence, incidence, and severity of hand eczema in the general population - a systematic review and meta-analysis. Contact Dermatitis. 2021;84:361-374. doi:10.1111/cod.13804
- Apfelbacher C, Bewley A, Molin S, et al. Prevalence of chronic hand eczema in adults: a cross-sectional survey of over 60 000 respondents from the general population of Canada, France, Germany, Italy, Spain and the UK. Br J Dermatol. 2025;192:1047-1054. doi:10.1093 /bjd/ljaf020
- Weidinger S, Novak N. Hand eczema. Lancet. 2024;404:2476-2486. doi:10.1016/S0140-6736(24)01810-5
- Schütte MG, Tamminga SJ, de Groene GJ, et al. Work-related and personal risk factors for occupational contact dermatitis: a systematic review of the literature with meta-analysis. Contact Dermatitis. 2023;88:171-187. doi:10.1111/cod.14253
- Behroozy A, Keegel TG. Wet-work exposure: a main risk factor for occupational hand dermatitis. Saf Health Work. 2014;5:175-180. doi:10.1016/j.shaw.2014.08.001
- Havmose MS, Kezic S, Uter W, et al. Prevalence and incidence of hand eczema in hairdressers-a systematic review and meta-analysis of the published literature from 2000-2021. Contact Dermatitis. 2022;86:254-265. doi:10.1111/cod.14048
- Uter W, Hallmann S, Gefeller O, et al. Contact allergy to ingredients of hair cosmetics in female hairdressers and female consumers—an update based on IVDK data 2013–2020. Contact Dermatitis. 2023;89:161-170. doi:10.1111/cod.14363
- Yüksel YT, Symanzik C, Christensen MO, et al. Prevalence and incidence of hand eczema in healthcare workers: a systematic review and meta-analysis. Contact Dermatitis. 2024;90:331-342. doi:10.1111 /cod.14489
- Warshaw EM, Schram SE, Maibach HI, et al. Occupation-related contact dermatitis in North American health care workers referred for patch testing: cross-sectional data, 1998 to 2004. Dermatitis. 2008;19:261-274. doi:10.2310/6620.2008.07059
- Hamnerius N, Svedman C, Bergendorff O, et al. Wet work exposure and hand eczema among healthcare workers: a cross-sectional study. Br J Dermatol. 2018;178:452-461. doi:10.1111 /bjd.15813
- Loh EDW, Yew YW. Hand hygiene and hand eczema: a systematic review and meta-analysis. Contact Dermatitis. 2022;87:303-314. doi:10.1111/cod.14133
- Lotfinejad N, Peters A, Tartari E, et al. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect Dis. 2021;21:e209-e221. doi:10.1016/S1473-3099(21)00383-2
- Schlarbaum JP, Hylwa SA. Allergic contact dermatitis to operating room scrubs and disinfectants. Dermat Contact Atopic Occup Drug. 2019;30:363-370. doi:10.1097/DER.0000000000000525
- Rodriguez-Homs LG, Atwater AR. Allergens in medical hand skin cleansers. Dermat Contact Atopic Occup Drug. 2019;30:336-341. doi:10.1097/DER.0000000000000504
- Vester L, Thyssen JP, Menné T, et al. Occupational food-related hand dermatoses seen over a 10-year period. Contact Dermatitis. 2012;66:264-270. doi:10.1111/j.1600-0536.2011.02048.x
- Pesonen M, Koskela K, Aalto-Korte K. Contact urticaria and protein contact dermatitis in the Finnish Register of Occupational Diseases in a period of 12 years. Contact Dermatitis. 2020;83:1-7. doi:10.1111/cod.13547
- McFadden JP, White JML, Basketter DA, et al. Reduced allergy rates in atopic eczema to contact allergens used in both skin products and foods: atopy and the “hapten-atopy hypothesis.” Contact Dermatitis. 2008;58:156-158. doi:10.1111/j.1600-0536.2007.01291.x
- Kao SH, Hsu CH, Su SN, et al. Identification and immunologic characterization of an allergen, alliin lyase, from garlic (Allium sativum). J Allergy Clin Immunol. 2004;113:161-168. doi:10.1016/j.jaci.2003.10.040
- Reddy VB, Lerner EA. Plant cysteine proteases that evoke itch activate protease-activated receptors. Br J Dermatol. 2010;163:532-535. doi:10.1111/j.1365-2133.2010.09862.x
- Silverberg NB, Pelletier JL, Jacob SE, et al; Section on Dermatology, Section on Allergy and Immunology. Nickel allergic contact dermatitis: identification, treatment, and prevention. Pediatrics. 2020;145:e20200628. doi:10.1542/peds.2020-0628
- Clément A, Ferrier le Bouëdec MC, Crépy MN, et al. Hand eczema in glove-wearing patients. Contact Dermatitis. 2023;89:143-152. doi:10.1111/cod.14357
- Reeder MJ, Idrogo-Lam A, Aravamuthan SR, et al. Occupational contact dermatitis in construction workers: a retrospective analysis of the North American Contact Dermatitis Group Data, 2001-2020. Dermat Contact Atopic Occup Drug. 2024;35:467-475. doi:10.1089/derm.2024.0018
- Fisch A, Hamnerius N, Isaksson M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians-a 10-year study. Contact Dermatitis. 2019;81:58-60. doi:10.1111/cod.13216
- Atwater AR, Reeder M. Trends in nail services may cause dermatitis: not your mother’s nail polish. Cutis. 2019;103:315-317.
- Suuronen K, Ylinen K, Heikkilä J, et al. Acrylates in artificial nails— results of product analyses and glove penetration studies. Contact Dermatitis. 2024;90:266-272. doi:10.1111/cod.14474
- Morgado F, Batista M, Gonçalo M. Short exposures and glove protection against (meth)acrylates in nail beauticians-thoughts on a rising concern. Contact Dermatitis. 2019;81:62-63. doi:10.1111 /cod.13222
- Paulsen E, Søgaard J, Andersen KE. Occupational dermatitis in Danish gardeners and greenhouse workers (I). prevalence and possible risk factors. Contact Dermatitis. 1997;37:263-270. doi:10.1111/j.1600-0536.1997.tb02462.x
- Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter–update 2015. J Allergy Clin Immunol Pract. 2015; 3(3 suppl):S1-S39. doi:10.1016/j.jaip.2015.02.009
- Gette MT, Marks JE. Tulip fingers. Arch Dermatol. 1990;126:203-205.
- Bruynzeel DP. Bulb dermatitis. Dermatological problems in the flower bulb industries. Contact Dermatitis. 1997;37:70-77. doi:10.1111/j.1600-0536.1997.tb00042.x
- Nettis E, Marcandrea M, Colanardi MC, et al. Results of standard series patch testing in patients with occupational allergic contact dermatitis. Allergy. 2003;58:1304-1307. doi:10.1046/j.1398-9995.2003.00346.x
- Saripalli YV, Achen F, Belsito DV. The detection of clinically relevant contact allergens using a standard screening tray of twenty-three allergens. J Am Acad Dermatol. 2003;49:65-69. doi:10.1067/mjd.2003.489
- Warshaw EM, Buonomo M, DeKoven JG, et al. Importance of supplemental patch testing beyond a screening series for patients with dermatitis: the North American Contact Dermatitis Group experience. JAMA Dermatol. 2021;157:1456-1465. doi:10.1001/jamadermatol.2021.4314
- Geier J, Lessmann H, Mahler V, et al. Occupational contact allergy caused by rubber gloves--nothing has changed. Contact Dermatitis. 2012;67:149-156. doi:10.1111/j.1600-0536.2012.02139.x
- Toraason M, Sussman G, Biagini R, et al. Latex allergy in the workplace. Toxicol Sci Off J Soc Toxicol. 2000;58:5-14. doi:10.1093/toxsci/58.1.5
- Bissonnette R, Agner T, Taylor JS, et al. Hand eczema-part 2: prevention, management, and treatment. J Am Acad Dermatol. 2025;93:1213-1224. doi:10.1016/j.jaad.2024.09.049
- Schliemann S, Kelterer D, Bauer A, et al. Tacrolimus ointment in the treatment of occupationally induced chronic hand dermatitis. Contact Dermatitis. 2008;58:299-306. doi:10.1111/j.1600-0536.2007.01314.x
- Voorberg AN, Kamphuis E, Christoffers WA, et al. Efficacy and safety of dupilumab in patients with severe chronic hand eczema with inadequate response or intolerance to alitretinoin: a randomized, double-blind, placebo-controlled phase IIb proof-of-concept study. Br J Dermatol. 2023;189:400-409. doi:10.1093/bjd/ljad156
- Gooderham M, Molin S, Bissonnette R, et al. Long-term safety and efficacy of delgocitinib cream for up to 52 weeks in adults with chronic hand eczema: results of the phase 3 open-label extension DELTA 3 trial following the DELTA 1 and 2 trials. J Am Acad Dermatol. 2025;93:95-103. doi:10.1016/j.jaad.2025.03.008
Hand dermatitis (HD) is a common dermatologic concern that can impair quality of life, work productivity, and daily functioning.1 Occupational HD is defined as hand eczema caused or worsened by workplace exposures. When caused by work, HD may lead to reduced productivity and even job loss. Subtypes of HD include irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), protein contact dermatitis (PCD), atopic dermatitis (AD), hyperkeratotic HD, and dyshidrotic eczema.2,3
Often caused by wet work, ICD is the most common subtype, whereas PCD—which is caused by immediate hypersensitivity to protein—is less common and usually seen in food service workers.3,4 When HD does not improve with standard treatment, particularly in occupational cases, patch testing is prudent to evaluate for contact allergens. In this article, we review practical considerations for evaluation and management of occupational irritant and allergic HD, highlighting relevant exposures and pearls on workup and management.
Epidemiology of Hand Dermatitis
A 2021 systematic review and meta-analysis of European studies reported a 1-year HD prevalence of 9.1% and a lifetime prevalence of 14.5%.5 Hand dermatitis is most common in women; individuals aged 30 to 39 years; and those who are employed, underscoring the role of workplace exposure.6 High-risk occupations are those involving substantial wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.7 Individuals with a history of AD also are at high risk for HD.8
Hand Dermatitis Subtypes
Irritant Contact Dermatitis—Irritant contact dermatitis, the most common form of occupational HD, is caused by repeated exposure to irritants (eg, water, detergents, cleansers, and soaps) that disrupt the skin barrier.9 Occupations that involve wet work are a major risk factor, associated with a 56% higher likelihood of ICD.8 Wet work involves frequent handwashing, prolonged contact with liquids, or occlusive glove use.9 As a ubiquitous skin irritant, water can penetrate the stratum corneum, impair the skin barrier, and increase sensitization risk. The dorsal hands usually are affected by ICD due to the thinner stratum corneum in this area.9
Allergic Contact Dermatitis—Allergic contact dermatitis should be considered in cases of chronic, recurrent, or treatment-resistant disease. Clinical clues include dermatitis beyond irritant contact sites, recurrent pruritic and vesicular HD, and flares with occupational exposures or materials; however, it can be difficult to distinguish ACD from ICD on clinical presentation alone, as they have many overlapping features. When ACD is suspected, patch testing remains the gold standard for identifying allergens and guiding avoidance strategies, product alternatives, and workplace modifications.
Unique Occupational Considerations
Hairdressers—Hairdressers have an increased risk for HD due to wet work and exposure to sensitizers, with a pooled lifetime prevalence of 38.2% (including ICD, ACD, and occupational cases).10 Notably, frequent shampooing, rinsing, cutting wet hair, handwashing, and glove use increase the risk for ICD. Hairdressers also are exposed to allergens in hair products, including p-phenylenediamine, toluene-2,5-diamine, persulfate salts, glyceryl thioglycolate, preservatives, and fragrances. Occupational exposure to the preservative methylisothiazolinone is high among hairdressers, with a sensitization rate of 10.5% in HD cases.11
It has been reported that hyperkeratotic fissured eczema of the dorsal hands caused by wet work often indicates ICD, whereas pruritic dyshidrotic eczema involving the lateral fingers or palms suggests ACD; however, these conditions can share overlapping features.7 If ACD is suspected, broad patch testing with baseline and hairdresser series, along with specific chemicals that may be encountered in the workplace, is necessary. Management includes allergen avoidance, reduced wet work tasks, use of nitrile gloves with glove changes to mitigate occlusive effects, and skin barrier protection with emollients.
Health Care Workers—Health care workers are vulnerable to HD due to intensive hand hygiene, prolonged glove use, and allergen exposures, with a lifetime prevalence of self-reported HD of 33.4%.12 Common allergens among health care workers include rubber accelerators, most often from rubber gloves.13 Frequent handwashing and glove use can further impair the skin barrier, increasing irritant and sensitization risks.14 In contrast, alcohol-based hand sanitizers containing emollients are less irritating, with prior analyses showing no significant association with HD risk.15,16 Conversely, handwashing 8 to 10 times daily increased HD risk, with a relative risk of 1.51.15
Surgeons and proceduralists face unique risks for HD from preoperative scrubbing with products that can contain potential allergens such as chlorhexidine gluconate, chloroxylenol, povidone-iodine, fragrance, cocamide diethanolamine, lanolin, alkyl glucosides, sodium benzoate, sorbic acid, tocopherol, and propylene glycol.17,18 Subsequent occlusion under glove layers drives ICD and ACD risks, highlighting the importance of patch testing in affected individuals. While patch testing, exposure avoidance, and limited glove use can mitigate HD risk, frequent handwashing can contribute to refractory HD.
Food Service Workers—Food service workers have an increased risk for HD from allergens and irritants. In a retrospective study of patients with occupational food-related HD (N=372), 57% were diagnosed with ICD, 22% with PCD, and 1.8% with ACD.19 Skin barrier disruption from wet work, occlusion from glove use, and contact with food proteins increase HD risk, especially in bakers exposed to flours and grains, which can cause IgE–mediated PCD manifesting with contact urticaria. Protein contact dermatitis is confirmed by prick testing with suspected foods.20 Additionally, exposure to garlic can cause ICD and ACD due to sulfur-containing compounds, particularly allicin and diallyl disulfide.21,22 Pineapple also can trigger ICD associated with bromelain, a proteolytic enzyme that can break down the skin.23 Nickel exposure is another concern, as steel utensils and cookware can release nickel onto the skin of sensitized individuals.24 Rubber accelerator exposure from gloves also contributes to contact allergy and HD among food service workers; vinyl gloves usually are a good alternative in this setting.25 Management of food-related HD involves exposure avoidance, which may affect occupational viability
Construction Workers—Construction workers are at risk for occupational HD due to contact with irritants and sensitizers such as paints, adhesives, asphalt, cement, solvents, and gloves.26 A retrospective analysis of North American Contact Dermatitis Group data identified HD in 37.2% (253/681) of patch-tested construction workers. The most common occupational allergens include potassium dichromate, which can be present in cement and leather items; bisphenol A epoxy resin; cobalt chloride hexahydrate; and the rubber accelerators carba mix and thiuram mix.26 A thorough occupational history should assess materials handled, and patch testing should include common construction-related allergens to inform avoidance strategies. Workplace task modification can reduce exposure, as certain managerial roles in construction work may involve less contact with irritants and sensitizers.26
Nail Technicians—Nail technicians are at risk for HD, especially ACD from acrylate monomers used in nail gels, dips, and acrylics. In a 10-year analysis, around 87.5% (14/16) of nail technicians with contact allergy to methacrylate demonstrated hand involvement.27 Common acrylate monomers include 2-hydroxyethyl methacrylate, 2-hydroxypropyl methacrylate, and ethyl cyanoacrylate. 28 Evaluation requires a detailed occupational history, assessing HD onset relative to exposure, services performed, glove-use practices, and whether symptoms improve away from work. While gloves may appear to reduce exposure, a glove-penetration study showed that acrylate-containing nail products can penetrate commonly used disposable gloves from within seconds to approximately 20 minutes, depending on glove and product type.29 Among available options, nitrile gloves may provide dexterity and allergen avoidance when acrylate exposure is brief, with glove changes required every 15 to 30 minutes.30 Patch testing with 2-hydroxyethyl methacrylate and ethyl cyanoacrylate can identify nail acrylate allergy; however, avoidance can be challenging for nail technicians, as these products often are ubiquitous in their work.
Florists—Florists can develop HD from plant allergens and irritants, particularly tulipalin A and calcium oxalate, with a lifetime prevalence of 19.6%.31 Tulipalin A is a well-documented sensitizer causing ACD among florists exposed to tulip bulbs and other Alstroemeria flowers.32 The term tulip fingers actually was coined to describe ACD caused by tulip bulbs in the European tulip industry.33 Patch testing involves testing for tulipalin A, which may be commercially limited, or tulip plant materials; however, fresh tulips require open testing with small amounts due to higher allergen concentration.32 Additionally, the term daffodil itch describes a type of ICD caused by calcium oxalate crystals in daffodil bulbs and tulip sap.32,34 Diagnosis of plant-related HD requires an occupational history and targeted patch testing, while glove protection and exposure avoidance are essential for improvement.
Evaluation and Management
The workup for HD involves physical examination and medical history, including disease onset, course, and history of AD, along with occupational and exposure history to identify allergens and irritants. Understanding the patient’s tasks and responsibilities and workplace practices along with the materials they handle allows the dermatologist to anticipate relevant allergens for patch testing.
Patch testing should be comprehensive, as baseline screening series alone may miss between 26.3% and 50% of occupationally relevant allergens.35,36 Comprehensive patch testing also should include specialty series and supplemental allergens based on the patient’s clinical history and exposures. Specialty series may include hairdressing, bakery, cosmetics, dental, machinists, and adhesives.37 Gloves also warrant attention, as they may be overlooked as a sensitizer following repeated contact and occlusion. In persistent HD associated with glove use, patch testing should include a rubber accelerator series with relevant allergens, such as thiurams, carbamates, mercaptobenzothiazole, diphenylguanidine, and the patient’s own gloves.38 Latex allergy also should be considered, particularly in immediate-type reactions, and can be evaluated with latex-specific IgE testing.39
Management of HD relies on accurate diagnosis and allergen avoidance, which can be challenging in occupational settings. Structured tools, such as the American Contact Dermatitis Society’s Contact Allergen Management Program (https://www.contactderm.org/ resources/acds-camp), can help identify safe alternatives.
In occupational HD, risk assessment should identify occupational exposures and determine appropriate personal protective equipment while minimizing the risk for HD associated with such equipment. Protective gloves are advised to prevent contact with allergens and irritants. When glove use lasts more than 10 minutes, cotton glove liners may be worn to avoid occlusion and moisture retention.40 For wet work, vinyl gloves are recommended, with regular emollient use to support skin-barrier repair. Overall, gloves should be used when possible, changed regularly, and worn for limited periods of time to prevent ICD.
Work modification may be required to reduce exposure and flares, including task reassignment or substitution of materials containing allergens and irritants. Occupational HD may necessitate workplace accommodations, disability evaluation, medical leave, or even permanent job change. Dermatologists play a crucial role in the medical determination of work relatedness and functional impairment, guiding patients through occupational health, disability, and workers’ compensation when warranted.
Treatments for Occupational HD
Treatment of occupational HD depends on disease severity, chronicity, and avoidance of allergens and irritants in ACD, ICD, and PCD. Foundational management includes regular emollient use, which can even serve as monotherapy in mild occupational HD.40 Corticosteroids are the cornerstone of topical therapy, while calcineurin inhibitors can be used as a steroid-sparing option in milder disease.41 Off-label topical calcipotriol and AD-approved therapies crisaborole and ruxolitinib may be effective. For refractory disease after topical treatments, phototherapy can be considered.40 Biologic and targeted therapies also have emerged as potential treatments. Dupilumab is effective for atopic chronic HD and has demonstrated promise for nonatopic chronic HD.42 Recently, delgocitinib, a topical pan–Janus kinase inhibitor cream, showed clinical efficacy for chronic hand eczema and was approved by the US Food and Drug Administration.43 Off-label use of alternative systemic therapies, including acitretin, cyclosporine, methotrexate, and azathioprine, and other biologics and systemic Janus kinase inhibitors also may treat HD, but larger studies are lacking.40
Our Final Interpretation
Occupational HD is a common skin condition with multiple etiologies. It is important for clinicians to gather a thorough occupational and exposure history to narrow the differential diagnosis, inform patch testing, and guide effective management. In practice, successful treatment depends on screening for and diagnosis of workplace exposures driving disease.
Hand dermatitis (HD) is a common dermatologic concern that can impair quality of life, work productivity, and daily functioning.1 Occupational HD is defined as hand eczema caused or worsened by workplace exposures. When caused by work, HD may lead to reduced productivity and even job loss. Subtypes of HD include irritant contact dermatitis (ICD), allergic contact dermatitis (ACD), protein contact dermatitis (PCD), atopic dermatitis (AD), hyperkeratotic HD, and dyshidrotic eczema.2,3
Often caused by wet work, ICD is the most common subtype, whereas PCD—which is caused by immediate hypersensitivity to protein—is less common and usually seen in food service workers.3,4 When HD does not improve with standard treatment, particularly in occupational cases, patch testing is prudent to evaluate for contact allergens. In this article, we review practical considerations for evaluation and management of occupational irritant and allergic HD, highlighting relevant exposures and pearls on workup and management.
Epidemiology of Hand Dermatitis
A 2021 systematic review and meta-analysis of European studies reported a 1-year HD prevalence of 9.1% and a lifetime prevalence of 14.5%.5 Hand dermatitis is most common in women; individuals aged 30 to 39 years; and those who are employed, underscoring the role of workplace exposure.6 High-risk occupations are those involving substantial wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.7 Individuals with a history of AD also are at high risk for HD.8
Hand Dermatitis Subtypes
Irritant Contact Dermatitis—Irritant contact dermatitis, the most common form of occupational HD, is caused by repeated exposure to irritants (eg, water, detergents, cleansers, and soaps) that disrupt the skin barrier.9 Occupations that involve wet work are a major risk factor, associated with a 56% higher likelihood of ICD.8 Wet work involves frequent handwashing, prolonged contact with liquids, or occlusive glove use.9 As a ubiquitous skin irritant, water can penetrate the stratum corneum, impair the skin barrier, and increase sensitization risk. The dorsal hands usually are affected by ICD due to the thinner stratum corneum in this area.9
Allergic Contact Dermatitis—Allergic contact dermatitis should be considered in cases of chronic, recurrent, or treatment-resistant disease. Clinical clues include dermatitis beyond irritant contact sites, recurrent pruritic and vesicular HD, and flares with occupational exposures or materials; however, it can be difficult to distinguish ACD from ICD on clinical presentation alone, as they have many overlapping features. When ACD is suspected, patch testing remains the gold standard for identifying allergens and guiding avoidance strategies, product alternatives, and workplace modifications.
Unique Occupational Considerations
Hairdressers—Hairdressers have an increased risk for HD due to wet work and exposure to sensitizers, with a pooled lifetime prevalence of 38.2% (including ICD, ACD, and occupational cases).10 Notably, frequent shampooing, rinsing, cutting wet hair, handwashing, and glove use increase the risk for ICD. Hairdressers also are exposed to allergens in hair products, including p-phenylenediamine, toluene-2,5-diamine, persulfate salts, glyceryl thioglycolate, preservatives, and fragrances. Occupational exposure to the preservative methylisothiazolinone is high among hairdressers, with a sensitization rate of 10.5% in HD cases.11
It has been reported that hyperkeratotic fissured eczema of the dorsal hands caused by wet work often indicates ICD, whereas pruritic dyshidrotic eczema involving the lateral fingers or palms suggests ACD; however, these conditions can share overlapping features.7 If ACD is suspected, broad patch testing with baseline and hairdresser series, along with specific chemicals that may be encountered in the workplace, is necessary. Management includes allergen avoidance, reduced wet work tasks, use of nitrile gloves with glove changes to mitigate occlusive effects, and skin barrier protection with emollients.
Health Care Workers—Health care workers are vulnerable to HD due to intensive hand hygiene, prolonged glove use, and allergen exposures, with a lifetime prevalence of self-reported HD of 33.4%.12 Common allergens among health care workers include rubber accelerators, most often from rubber gloves.13 Frequent handwashing and glove use can further impair the skin barrier, increasing irritant and sensitization risks.14 In contrast, alcohol-based hand sanitizers containing emollients are less irritating, with prior analyses showing no significant association with HD risk.15,16 Conversely, handwashing 8 to 10 times daily increased HD risk, with a relative risk of 1.51.15
Surgeons and proceduralists face unique risks for HD from preoperative scrubbing with products that can contain potential allergens such as chlorhexidine gluconate, chloroxylenol, povidone-iodine, fragrance, cocamide diethanolamine, lanolin, alkyl glucosides, sodium benzoate, sorbic acid, tocopherol, and propylene glycol.17,18 Subsequent occlusion under glove layers drives ICD and ACD risks, highlighting the importance of patch testing in affected individuals. While patch testing, exposure avoidance, and limited glove use can mitigate HD risk, frequent handwashing can contribute to refractory HD.
Food Service Workers—Food service workers have an increased risk for HD from allergens and irritants. In a retrospective study of patients with occupational food-related HD (N=372), 57% were diagnosed with ICD, 22% with PCD, and 1.8% with ACD.19 Skin barrier disruption from wet work, occlusion from glove use, and contact with food proteins increase HD risk, especially in bakers exposed to flours and grains, which can cause IgE–mediated PCD manifesting with contact urticaria. Protein contact dermatitis is confirmed by prick testing with suspected foods.20 Additionally, exposure to garlic can cause ICD and ACD due to sulfur-containing compounds, particularly allicin and diallyl disulfide.21,22 Pineapple also can trigger ICD associated with bromelain, a proteolytic enzyme that can break down the skin.23 Nickel exposure is another concern, as steel utensils and cookware can release nickel onto the skin of sensitized individuals.24 Rubber accelerator exposure from gloves also contributes to contact allergy and HD among food service workers; vinyl gloves usually are a good alternative in this setting.25 Management of food-related HD involves exposure avoidance, which may affect occupational viability
Construction Workers—Construction workers are at risk for occupational HD due to contact with irritants and sensitizers such as paints, adhesives, asphalt, cement, solvents, and gloves.26 A retrospective analysis of North American Contact Dermatitis Group data identified HD in 37.2% (253/681) of patch-tested construction workers. The most common occupational allergens include potassium dichromate, which can be present in cement and leather items; bisphenol A epoxy resin; cobalt chloride hexahydrate; and the rubber accelerators carba mix and thiuram mix.26 A thorough occupational history should assess materials handled, and patch testing should include common construction-related allergens to inform avoidance strategies. Workplace task modification can reduce exposure, as certain managerial roles in construction work may involve less contact with irritants and sensitizers.26
Nail Technicians—Nail technicians are at risk for HD, especially ACD from acrylate monomers used in nail gels, dips, and acrylics. In a 10-year analysis, around 87.5% (14/16) of nail technicians with contact allergy to methacrylate demonstrated hand involvement.27 Common acrylate monomers include 2-hydroxyethyl methacrylate, 2-hydroxypropyl methacrylate, and ethyl cyanoacrylate. 28 Evaluation requires a detailed occupational history, assessing HD onset relative to exposure, services performed, glove-use practices, and whether symptoms improve away from work. While gloves may appear to reduce exposure, a glove-penetration study showed that acrylate-containing nail products can penetrate commonly used disposable gloves from within seconds to approximately 20 minutes, depending on glove and product type.29 Among available options, nitrile gloves may provide dexterity and allergen avoidance when acrylate exposure is brief, with glove changes required every 15 to 30 minutes.30 Patch testing with 2-hydroxyethyl methacrylate and ethyl cyanoacrylate can identify nail acrylate allergy; however, avoidance can be challenging for nail technicians, as these products often are ubiquitous in their work.
Florists—Florists can develop HD from plant allergens and irritants, particularly tulipalin A and calcium oxalate, with a lifetime prevalence of 19.6%.31 Tulipalin A is a well-documented sensitizer causing ACD among florists exposed to tulip bulbs and other Alstroemeria flowers.32 The term tulip fingers actually was coined to describe ACD caused by tulip bulbs in the European tulip industry.33 Patch testing involves testing for tulipalin A, which may be commercially limited, or tulip plant materials; however, fresh tulips require open testing with small amounts due to higher allergen concentration.32 Additionally, the term daffodil itch describes a type of ICD caused by calcium oxalate crystals in daffodil bulbs and tulip sap.32,34 Diagnosis of plant-related HD requires an occupational history and targeted patch testing, while glove protection and exposure avoidance are essential for improvement.
Evaluation and Management
The workup for HD involves physical examination and medical history, including disease onset, course, and history of AD, along with occupational and exposure history to identify allergens and irritants. Understanding the patient’s tasks and responsibilities and workplace practices along with the materials they handle allows the dermatologist to anticipate relevant allergens for patch testing.
Patch testing should be comprehensive, as baseline screening series alone may miss between 26.3% and 50% of occupationally relevant allergens.35,36 Comprehensive patch testing also should include specialty series and supplemental allergens based on the patient’s clinical history and exposures. Specialty series may include hairdressing, bakery, cosmetics, dental, machinists, and adhesives.37 Gloves also warrant attention, as they may be overlooked as a sensitizer following repeated contact and occlusion. In persistent HD associated with glove use, patch testing should include a rubber accelerator series with relevant allergens, such as thiurams, carbamates, mercaptobenzothiazole, diphenylguanidine, and the patient’s own gloves.38 Latex allergy also should be considered, particularly in immediate-type reactions, and can be evaluated with latex-specific IgE testing.39
Management of HD relies on accurate diagnosis and allergen avoidance, which can be challenging in occupational settings. Structured tools, such as the American Contact Dermatitis Society’s Contact Allergen Management Program (https://www.contactderm.org/ resources/acds-camp), can help identify safe alternatives.
In occupational HD, risk assessment should identify occupational exposures and determine appropriate personal protective equipment while minimizing the risk for HD associated with such equipment. Protective gloves are advised to prevent contact with allergens and irritants. When glove use lasts more than 10 minutes, cotton glove liners may be worn to avoid occlusion and moisture retention.40 For wet work, vinyl gloves are recommended, with regular emollient use to support skin-barrier repair. Overall, gloves should be used when possible, changed regularly, and worn for limited periods of time to prevent ICD.
Work modification may be required to reduce exposure and flares, including task reassignment or substitution of materials containing allergens and irritants. Occupational HD may necessitate workplace accommodations, disability evaluation, medical leave, or even permanent job change. Dermatologists play a crucial role in the medical determination of work relatedness and functional impairment, guiding patients through occupational health, disability, and workers’ compensation when warranted.
Treatments for Occupational HD
Treatment of occupational HD depends on disease severity, chronicity, and avoidance of allergens and irritants in ACD, ICD, and PCD. Foundational management includes regular emollient use, which can even serve as monotherapy in mild occupational HD.40 Corticosteroids are the cornerstone of topical therapy, while calcineurin inhibitors can be used as a steroid-sparing option in milder disease.41 Off-label topical calcipotriol and AD-approved therapies crisaborole and ruxolitinib may be effective. For refractory disease after topical treatments, phototherapy can be considered.40 Biologic and targeted therapies also have emerged as potential treatments. Dupilumab is effective for atopic chronic HD and has demonstrated promise for nonatopic chronic HD.42 Recently, delgocitinib, a topical pan–Janus kinase inhibitor cream, showed clinical efficacy for chronic hand eczema and was approved by the US Food and Drug Administration.43 Off-label use of alternative systemic therapies, including acitretin, cyclosporine, methotrexate, and azathioprine, and other biologics and systemic Janus kinase inhibitors also may treat HD, but larger studies are lacking.40
Our Final Interpretation
Occupational HD is a common skin condition with multiple etiologies. It is important for clinicians to gather a thorough occupational and exposure history to narrow the differential diagnosis, inform patch testing, and guide effective management. In practice, successful treatment depends on screening for and diagnosis of workplace exposures driving disease.
- Agner T, Andersen KE, Brandao FM, et al. Hand eczema severity and quality of life: a cross-sectional, multicentre study of hand eczema patients. Contact Dermatitis. 2008;59:43-47. doi:10.1111 /j.1600-0536.2008.01362.x
- Agner T, Aalto-Korte K, Andersen KE, et al. Classification of hand eczema. J Eur Acad Dermatol Venereol. 2015;29:2417-2422. doi:10.1111 /jdv.13308
- Bissonnette R, Agner T, Molin S, et al. Hand eczema—part 1: epidemiology, pathogenesis, diagnosis, and work-up. J Am Acad Dermatol. 2025;93:1201-1210. doi:10.1016/j.jaad.2024.09.048
- Barbaud A. Mechanism and diagnosis of protein contact dermatitis. Curr Opin Allergy Clin Immunol. 2020;20:117-121. doi:10.1097/ACI.0000000000000621
- Quaade AS, Simonsen AB, Halling AS, et al. Prevalence, incidence, and severity of hand eczema in the general population - a systematic review and meta-analysis. Contact Dermatitis. 2021;84:361-374. doi:10.1111/cod.13804
- Apfelbacher C, Bewley A, Molin S, et al. Prevalence of chronic hand eczema in adults: a cross-sectional survey of over 60 000 respondents from the general population of Canada, France, Germany, Italy, Spain and the UK. Br J Dermatol. 2025;192:1047-1054. doi:10.1093 /bjd/ljaf020
- Weidinger S, Novak N. Hand eczema. Lancet. 2024;404:2476-2486. doi:10.1016/S0140-6736(24)01810-5
- Schütte MG, Tamminga SJ, de Groene GJ, et al. Work-related and personal risk factors for occupational contact dermatitis: a systematic review of the literature with meta-analysis. Contact Dermatitis. 2023;88:171-187. doi:10.1111/cod.14253
- Behroozy A, Keegel TG. Wet-work exposure: a main risk factor for occupational hand dermatitis. Saf Health Work. 2014;5:175-180. doi:10.1016/j.shaw.2014.08.001
- Havmose MS, Kezic S, Uter W, et al. Prevalence and incidence of hand eczema in hairdressers-a systematic review and meta-analysis of the published literature from 2000-2021. Contact Dermatitis. 2022;86:254-265. doi:10.1111/cod.14048
- Uter W, Hallmann S, Gefeller O, et al. Contact allergy to ingredients of hair cosmetics in female hairdressers and female consumers—an update based on IVDK data 2013–2020. Contact Dermatitis. 2023;89:161-170. doi:10.1111/cod.14363
- Yüksel YT, Symanzik C, Christensen MO, et al. Prevalence and incidence of hand eczema in healthcare workers: a systematic review and meta-analysis. Contact Dermatitis. 2024;90:331-342. doi:10.1111 /cod.14489
- Warshaw EM, Schram SE, Maibach HI, et al. Occupation-related contact dermatitis in North American health care workers referred for patch testing: cross-sectional data, 1998 to 2004. Dermatitis. 2008;19:261-274. doi:10.2310/6620.2008.07059
- Hamnerius N, Svedman C, Bergendorff O, et al. Wet work exposure and hand eczema among healthcare workers: a cross-sectional study. Br J Dermatol. 2018;178:452-461. doi:10.1111 /bjd.15813
- Loh EDW, Yew YW. Hand hygiene and hand eczema: a systematic review and meta-analysis. Contact Dermatitis. 2022;87:303-314. doi:10.1111/cod.14133
- Lotfinejad N, Peters A, Tartari E, et al. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect Dis. 2021;21:e209-e221. doi:10.1016/S1473-3099(21)00383-2
- Schlarbaum JP, Hylwa SA. Allergic contact dermatitis to operating room scrubs and disinfectants. Dermat Contact Atopic Occup Drug. 2019;30:363-370. doi:10.1097/DER.0000000000000525
- Rodriguez-Homs LG, Atwater AR. Allergens in medical hand skin cleansers. Dermat Contact Atopic Occup Drug. 2019;30:336-341. doi:10.1097/DER.0000000000000504
- Vester L, Thyssen JP, Menné T, et al. Occupational food-related hand dermatoses seen over a 10-year period. Contact Dermatitis. 2012;66:264-270. doi:10.1111/j.1600-0536.2011.02048.x
- Pesonen M, Koskela K, Aalto-Korte K. Contact urticaria and protein contact dermatitis in the Finnish Register of Occupational Diseases in a period of 12 years. Contact Dermatitis. 2020;83:1-7. doi:10.1111/cod.13547
- McFadden JP, White JML, Basketter DA, et al. Reduced allergy rates in atopic eczema to contact allergens used in both skin products and foods: atopy and the “hapten-atopy hypothesis.” Contact Dermatitis. 2008;58:156-158. doi:10.1111/j.1600-0536.2007.01291.x
- Kao SH, Hsu CH, Su SN, et al. Identification and immunologic characterization of an allergen, alliin lyase, from garlic (Allium sativum). J Allergy Clin Immunol. 2004;113:161-168. doi:10.1016/j.jaci.2003.10.040
- Reddy VB, Lerner EA. Plant cysteine proteases that evoke itch activate protease-activated receptors. Br J Dermatol. 2010;163:532-535. doi:10.1111/j.1365-2133.2010.09862.x
- Silverberg NB, Pelletier JL, Jacob SE, et al; Section on Dermatology, Section on Allergy and Immunology. Nickel allergic contact dermatitis: identification, treatment, and prevention. Pediatrics. 2020;145:e20200628. doi:10.1542/peds.2020-0628
- Clément A, Ferrier le Bouëdec MC, Crépy MN, et al. Hand eczema in glove-wearing patients. Contact Dermatitis. 2023;89:143-152. doi:10.1111/cod.14357
- Reeder MJ, Idrogo-Lam A, Aravamuthan SR, et al. Occupational contact dermatitis in construction workers: a retrospective analysis of the North American Contact Dermatitis Group Data, 2001-2020. Dermat Contact Atopic Occup Drug. 2024;35:467-475. doi:10.1089/derm.2024.0018
- Fisch A, Hamnerius N, Isaksson M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians-a 10-year study. Contact Dermatitis. 2019;81:58-60. doi:10.1111/cod.13216
- Atwater AR, Reeder M. Trends in nail services may cause dermatitis: not your mother’s nail polish. Cutis. 2019;103:315-317.
- Suuronen K, Ylinen K, Heikkilä J, et al. Acrylates in artificial nails— results of product analyses and glove penetration studies. Contact Dermatitis. 2024;90:266-272. doi:10.1111/cod.14474
- Morgado F, Batista M, Gonçalo M. Short exposures and glove protection against (meth)acrylates in nail beauticians-thoughts on a rising concern. Contact Dermatitis. 2019;81:62-63. doi:10.1111 /cod.13222
- Paulsen E, Søgaard J, Andersen KE. Occupational dermatitis in Danish gardeners and greenhouse workers (I). prevalence and possible risk factors. Contact Dermatitis. 1997;37:263-270. doi:10.1111/j.1600-0536.1997.tb02462.x
- Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter–update 2015. J Allergy Clin Immunol Pract. 2015; 3(3 suppl):S1-S39. doi:10.1016/j.jaip.2015.02.009
- Gette MT, Marks JE. Tulip fingers. Arch Dermatol. 1990;126:203-205.
- Bruynzeel DP. Bulb dermatitis. Dermatological problems in the flower bulb industries. Contact Dermatitis. 1997;37:70-77. doi:10.1111/j.1600-0536.1997.tb00042.x
- Nettis E, Marcandrea M, Colanardi MC, et al. Results of standard series patch testing in patients with occupational allergic contact dermatitis. Allergy. 2003;58:1304-1307. doi:10.1046/j.1398-9995.2003.00346.x
- Saripalli YV, Achen F, Belsito DV. The detection of clinically relevant contact allergens using a standard screening tray of twenty-three allergens. J Am Acad Dermatol. 2003;49:65-69. doi:10.1067/mjd.2003.489
- Warshaw EM, Buonomo M, DeKoven JG, et al. Importance of supplemental patch testing beyond a screening series for patients with dermatitis: the North American Contact Dermatitis Group experience. JAMA Dermatol. 2021;157:1456-1465. doi:10.1001/jamadermatol.2021.4314
- Geier J, Lessmann H, Mahler V, et al. Occupational contact allergy caused by rubber gloves--nothing has changed. Contact Dermatitis. 2012;67:149-156. doi:10.1111/j.1600-0536.2012.02139.x
- Toraason M, Sussman G, Biagini R, et al. Latex allergy in the workplace. Toxicol Sci Off J Soc Toxicol. 2000;58:5-14. doi:10.1093/toxsci/58.1.5
- Bissonnette R, Agner T, Taylor JS, et al. Hand eczema-part 2: prevention, management, and treatment. J Am Acad Dermatol. 2025;93:1213-1224. doi:10.1016/j.jaad.2024.09.049
- Schliemann S, Kelterer D, Bauer A, et al. Tacrolimus ointment in the treatment of occupationally induced chronic hand dermatitis. Contact Dermatitis. 2008;58:299-306. doi:10.1111/j.1600-0536.2007.01314.x
- Voorberg AN, Kamphuis E, Christoffers WA, et al. Efficacy and safety of dupilumab in patients with severe chronic hand eczema with inadequate response or intolerance to alitretinoin: a randomized, double-blind, placebo-controlled phase IIb proof-of-concept study. Br J Dermatol. 2023;189:400-409. doi:10.1093/bjd/ljad156
- Gooderham M, Molin S, Bissonnette R, et al. Long-term safety and efficacy of delgocitinib cream for up to 52 weeks in adults with chronic hand eczema: results of the phase 3 open-label extension DELTA 3 trial following the DELTA 1 and 2 trials. J Am Acad Dermatol. 2025;93:95-103. doi:10.1016/j.jaad.2025.03.008
- Agner T, Andersen KE, Brandao FM, et al. Hand eczema severity and quality of life: a cross-sectional, multicentre study of hand eczema patients. Contact Dermatitis. 2008;59:43-47. doi:10.1111 /j.1600-0536.2008.01362.x
- Agner T, Aalto-Korte K, Andersen KE, et al. Classification of hand eczema. J Eur Acad Dermatol Venereol. 2015;29:2417-2422. doi:10.1111 /jdv.13308
- Bissonnette R, Agner T, Molin S, et al. Hand eczema—part 1: epidemiology, pathogenesis, diagnosis, and work-up. J Am Acad Dermatol. 2025;93:1201-1210. doi:10.1016/j.jaad.2024.09.048
- Barbaud A. Mechanism and diagnosis of protein contact dermatitis. Curr Opin Allergy Clin Immunol. 2020;20:117-121. doi:10.1097/ACI.0000000000000621
- Quaade AS, Simonsen AB, Halling AS, et al. Prevalence, incidence, and severity of hand eczema in the general population - a systematic review and meta-analysis. Contact Dermatitis. 2021;84:361-374. doi:10.1111/cod.13804
- Apfelbacher C, Bewley A, Molin S, et al. Prevalence of chronic hand eczema in adults: a cross-sectional survey of over 60 000 respondents from the general population of Canada, France, Germany, Italy, Spain and the UK. Br J Dermatol. 2025;192:1047-1054. doi:10.1093 /bjd/ljaf020
- Weidinger S, Novak N. Hand eczema. Lancet. 2024;404:2476-2486. doi:10.1016/S0140-6736(24)01810-5
- Schütte MG, Tamminga SJ, de Groene GJ, et al. Work-related and personal risk factors for occupational contact dermatitis: a systematic review of the literature with meta-analysis. Contact Dermatitis. 2023;88:171-187. doi:10.1111/cod.14253
- Behroozy A, Keegel TG. Wet-work exposure: a main risk factor for occupational hand dermatitis. Saf Health Work. 2014;5:175-180. doi:10.1016/j.shaw.2014.08.001
- Havmose MS, Kezic S, Uter W, et al. Prevalence and incidence of hand eczema in hairdressers-a systematic review and meta-analysis of the published literature from 2000-2021. Contact Dermatitis. 2022;86:254-265. doi:10.1111/cod.14048
- Uter W, Hallmann S, Gefeller O, et al. Contact allergy to ingredients of hair cosmetics in female hairdressers and female consumers—an update based on IVDK data 2013–2020. Contact Dermatitis. 2023;89:161-170. doi:10.1111/cod.14363
- Yüksel YT, Symanzik C, Christensen MO, et al. Prevalence and incidence of hand eczema in healthcare workers: a systematic review and meta-analysis. Contact Dermatitis. 2024;90:331-342. doi:10.1111 /cod.14489
- Warshaw EM, Schram SE, Maibach HI, et al. Occupation-related contact dermatitis in North American health care workers referred for patch testing: cross-sectional data, 1998 to 2004. Dermatitis. 2008;19:261-274. doi:10.2310/6620.2008.07059
- Hamnerius N, Svedman C, Bergendorff O, et al. Wet work exposure and hand eczema among healthcare workers: a cross-sectional study. Br J Dermatol. 2018;178:452-461. doi:10.1111 /bjd.15813
- Loh EDW, Yew YW. Hand hygiene and hand eczema: a systematic review and meta-analysis. Contact Dermatitis. 2022;87:303-314. doi:10.1111/cod.14133
- Lotfinejad N, Peters A, Tartari E, et al. Hand hygiene in health care: 20 years of ongoing advances and perspectives. Lancet Infect Dis. 2021;21:e209-e221. doi:10.1016/S1473-3099(21)00383-2
- Schlarbaum JP, Hylwa SA. Allergic contact dermatitis to operating room scrubs and disinfectants. Dermat Contact Atopic Occup Drug. 2019;30:363-370. doi:10.1097/DER.0000000000000525
- Rodriguez-Homs LG, Atwater AR. Allergens in medical hand skin cleansers. Dermat Contact Atopic Occup Drug. 2019;30:336-341. doi:10.1097/DER.0000000000000504
- Vester L, Thyssen JP, Menné T, et al. Occupational food-related hand dermatoses seen over a 10-year period. Contact Dermatitis. 2012;66:264-270. doi:10.1111/j.1600-0536.2011.02048.x
- Pesonen M, Koskela K, Aalto-Korte K. Contact urticaria and protein contact dermatitis in the Finnish Register of Occupational Diseases in a period of 12 years. Contact Dermatitis. 2020;83:1-7. doi:10.1111/cod.13547
- McFadden JP, White JML, Basketter DA, et al. Reduced allergy rates in atopic eczema to contact allergens used in both skin products and foods: atopy and the “hapten-atopy hypothesis.” Contact Dermatitis. 2008;58:156-158. doi:10.1111/j.1600-0536.2007.01291.x
- Kao SH, Hsu CH, Su SN, et al. Identification and immunologic characterization of an allergen, alliin lyase, from garlic (Allium sativum). J Allergy Clin Immunol. 2004;113:161-168. doi:10.1016/j.jaci.2003.10.040
- Reddy VB, Lerner EA. Plant cysteine proteases that evoke itch activate protease-activated receptors. Br J Dermatol. 2010;163:532-535. doi:10.1111/j.1365-2133.2010.09862.x
- Silverberg NB, Pelletier JL, Jacob SE, et al; Section on Dermatology, Section on Allergy and Immunology. Nickel allergic contact dermatitis: identification, treatment, and prevention. Pediatrics. 2020;145:e20200628. doi:10.1542/peds.2020-0628
- Clément A, Ferrier le Bouëdec MC, Crépy MN, et al. Hand eczema in glove-wearing patients. Contact Dermatitis. 2023;89:143-152. doi:10.1111/cod.14357
- Reeder MJ, Idrogo-Lam A, Aravamuthan SR, et al. Occupational contact dermatitis in construction workers: a retrospective analysis of the North American Contact Dermatitis Group Data, 2001-2020. Dermat Contact Atopic Occup Drug. 2024;35:467-475. doi:10.1089/derm.2024.0018
- Fisch A, Hamnerius N, Isaksson M. Dermatitis and occupational (meth)acrylate contact allergy in nail technicians-a 10-year study. Contact Dermatitis. 2019;81:58-60. doi:10.1111/cod.13216
- Atwater AR, Reeder M. Trends in nail services may cause dermatitis: not your mother’s nail polish. Cutis. 2019;103:315-317.
- Suuronen K, Ylinen K, Heikkilä J, et al. Acrylates in artificial nails— results of product analyses and glove penetration studies. Contact Dermatitis. 2024;90:266-272. doi:10.1111/cod.14474
- Morgado F, Batista M, Gonçalo M. Short exposures and glove protection against (meth)acrylates in nail beauticians-thoughts on a rising concern. Contact Dermatitis. 2019;81:62-63. doi:10.1111 /cod.13222
- Paulsen E, Søgaard J, Andersen KE. Occupational dermatitis in Danish gardeners and greenhouse workers (I). prevalence and possible risk factors. Contact Dermatitis. 1997;37:263-270. doi:10.1111/j.1600-0536.1997.tb02462.x
- Fonacier L, Bernstein DI, Pacheco K, et al. Contact dermatitis: a practice parameter–update 2015. J Allergy Clin Immunol Pract. 2015; 3(3 suppl):S1-S39. doi:10.1016/j.jaip.2015.02.009
- Gette MT, Marks JE. Tulip fingers. Arch Dermatol. 1990;126:203-205.
- Bruynzeel DP. Bulb dermatitis. Dermatological problems in the flower bulb industries. Contact Dermatitis. 1997;37:70-77. doi:10.1111/j.1600-0536.1997.tb00042.x
- Nettis E, Marcandrea M, Colanardi MC, et al. Results of standard series patch testing in patients with occupational allergic contact dermatitis. Allergy. 2003;58:1304-1307. doi:10.1046/j.1398-9995.2003.00346.x
- Saripalli YV, Achen F, Belsito DV. The detection of clinically relevant contact allergens using a standard screening tray of twenty-three allergens. J Am Acad Dermatol. 2003;49:65-69. doi:10.1067/mjd.2003.489
- Warshaw EM, Buonomo M, DeKoven JG, et al. Importance of supplemental patch testing beyond a screening series for patients with dermatitis: the North American Contact Dermatitis Group experience. JAMA Dermatol. 2021;157:1456-1465. doi:10.1001/jamadermatol.2021.4314
- Geier J, Lessmann H, Mahler V, et al. Occupational contact allergy caused by rubber gloves--nothing has changed. Contact Dermatitis. 2012;67:149-156. doi:10.1111/j.1600-0536.2012.02139.x
- Toraason M, Sussman G, Biagini R, et al. Latex allergy in the workplace. Toxicol Sci Off J Soc Toxicol. 2000;58:5-14. doi:10.1093/toxsci/58.1.5
- Bissonnette R, Agner T, Taylor JS, et al. Hand eczema-part 2: prevention, management, and treatment. J Am Acad Dermatol. 2025;93:1213-1224. doi:10.1016/j.jaad.2024.09.049
- Schliemann S, Kelterer D, Bauer A, et al. Tacrolimus ointment in the treatment of occupationally induced chronic hand dermatitis. Contact Dermatitis. 2008;58:299-306. doi:10.1111/j.1600-0536.2007.01314.x
- Voorberg AN, Kamphuis E, Christoffers WA, et al. Efficacy and safety of dupilumab in patients with severe chronic hand eczema with inadequate response or intolerance to alitretinoin: a randomized, double-blind, placebo-controlled phase IIb proof-of-concept study. Br J Dermatol. 2023;189:400-409. doi:10.1093/bjd/ljad156
- Gooderham M, Molin S, Bissonnette R, et al. Long-term safety and efficacy of delgocitinib cream for up to 52 weeks in adults with chronic hand eczema: results of the phase 3 open-label extension DELTA 3 trial following the DELTA 1 and 2 trials. J Am Acad Dermatol. 2025;93:95-103. doi:10.1016/j.jaad.2025.03.008
Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
Getting a Grip on Occupational Hand Dermatitis: Key Considerations for Evaluation and Management
PRACTICE POINTS
- Occupational hand dermatitis (HD) is a common multifactorial disease with a major impact on quality of life, worker safety, and productivity.
- High-risk occupations include those involving wet work, such as hairdressers, beauticians, cleaners, and health care and construction workers.
- A detailed occupational and exposure history is essential for managing occupational HD.

Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
How do social media trends and influencer driven product fads affect the patterns of contact dermatitis you are seeing?
DR. YU: Social media and influencers are huge marketing opportunities for cosmetic and personal care companies and drive consumer demand. One example from a few years ago is slime as a toy for kids. For a period of time, every kid was making slime at home, resulting in high numbers of hand allergic contact dermatitis. Making slime requires a combination of borax (irritant), glue (irritant and allergen), laundry detergent or dish soap (irritant and allergen), and fragrances (irritant and allergen). This fad has been slowing since I cowrote an article on it (doi:10.1111 /pde.13792). More recently, the rise of “Sephora kids” (preteens and adolescents influenced by social media trends promoting multistep skin care and anti-aging products) has raised concerns about contact dermatitis, as many of these products contain ingredients that can disrupt the skin barrier or trigger sensitization in younger patients.
How can products labeled free of fragrances or preservatives still trigger allergic contact dermatitis?
DR. YU: Fragrances are frequently in the top 10 ingredients that cause allergic contact dermatitis in adults and children. For people with sensitive skin, we almost unequivocally recommend fragrance-free products. Now, not all fragrance-free products are truly free of fragrance allergens. Some fragrance chemicals may be used for another purpose (benzyl alcohol as a preservative, for example), so the product can still be fragrance free even though benzyl alcohol has a fragrance. Most products cannot truly be preservative free if they are expected to have a shelf life. One-time-use products do exist and can be preservative free, but they are very rare and very expensive to manufacture and maintain.
Have you seen spikes in reactions from trendy products like CBD-infused creams, botanical serums, or exfoliating acids?
DR. YU: Not yet, but I would not be surprised that this is rising in prevalence. The issue might not be CBD itself; it’s really the other additives in these CBD products that will cause problems. Looking at some CBD products for sale from major retailers, many contain fragrances such as lemongrass oil and botanical extracts such as calendula that have been noted to cause allergic contact dermatitis.
Do certain patient behaviors (eg, layering multiple natural products, frequent product switching, prolonged leave-on use) increase the risk for ACD?
DR. YU: Absolutely possible. The more products you use, the more likely you will develop allergic contact dermatitis due to increased exposure to potential allergens. We know that leave-on products are higher risk than rinse-offs in general. Furthermore, more products used also increase the risk for irritant dermatitis that might break the skin barrier, increasing the odds that someone will develop allergic contact dermatitis. We see this often with facial skin care products where some people might layer on glycolic acid with retinoid acid with vitamin C oil with kojic acid, etc, all leading to irritation on the face.
How do emerging consumer product trends influence your patch-testing approach?
DR. YU: We try to customize our patch-tested allergens to the patient’s rash and symptoms. If it’s a patient with facial dermatitis, for example, we would patch test the patient to a core allergen series (eg, American Contact Dermatitis Society 90, North American Comprehensive 80, North American Contact Dermatitis Group 80) and add on other supplemental panels including cosmetic series if applicable. It is also preferable to patch test for products that are used and/or suspected of causing the rash. For example, if a blush is a suspected cause of dermatitis, we would certainly patch test to that as well. We generally try to encourage the patient to bring in all their products so we can evaluate them for appropriateness for patch testing.
Which consumer-driven ingredients do you now consider high-yield targets for testing?
DR. YU: Fragrances, preservatives, and botanical extracts are all likely causes of allergic contact dermatitis. We are uncovering new allergens all the time, so testing directly to patient products is also important. Just because something has not been reported to be a contact allergen doesn’t mean it can’t become one.
Have you observed any demographic or cultural trends in patients with allergic contact dermatitis related to consumer products?
DR. YU: There are various papers that outline different allergens in adults vs children vs older adults. However, in general, the prevalence of contact dermatitis is very similar across all age groups and distributions. I do think there are definitely gender and cultural variations. Women are more likely to be allergic to nickel, for example, which is more often found in jewelry. However, there really aren’t studies that demonstrate one population is more likely to develop allergic contact dermatitis than others. It really comes down to exposure. For example, neomycin, which is contained in triple antibiotics in the United States and is sold over the counter, is a common allergen here. However, it’s not readily available in other countries, and therefore, neomycin is a rare allergen in those countries.
Looking forward, which emerging consumer trends do you anticipate will create the next wave of contact dermatitis cases?
DR. YU: We have seen an increase in allergic contact dermatitis in the wearables industry, especially in continuous glucose monitors. They are now being sold over the counter so people without diabetes and without a prescription will be able to purchase them from retailers like Amazon or CVS. The adhesives in these glucose monitors have been shown to cause allergic contact dermatitis in a sizeable number of kids and adults. I suspect this problem will continue to increase with increased exposure to the allergens in these adhesives.
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS
Consumer Trends Driving Contact Dermatitis: Insights from JiaDe Yu, MD, MS

Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation
Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation
Practice Gap
Chronic localized granulomatous inflammation can be difficult to manage, particularly when manifesting on the face. Intralesional corticosteroids may lead to atrophy and dyspigmentation and therefore must be used cautiously in cosmetically sensitive areas.1 Surgical removal can lead to recurrence, and systemic agents may carry risks disproportionate to disease burden. Although tumor necrosis factor (TNF) α inhibitors are effective systemically, their localized use in cutaneous granulomatous dermatoses remains underreported.1-3 We describe a technique using intralesional injection of adalimumab to treat chronic refractory cutaneous granulomatous inflammation.
The Technique
A 69-year-old woman presented with a crusted erythematous papule with surrounding inflammation on the left nasal ala of 5 years’ duration (Figure 1). Histopathology demonstrated a localized cutaneous granulomatous process. There was no clinical, radiographic, or laboratory evidence of systemic sarcoidosis. Infectious causes were excluded through negative tissue cultures and special stains, including auramine-rhodamine. Over a 3-month period following initial presentation, the lesion proved refractory to intralesional 5-fluorouracil, intralesional triamcinolone acetonide, pentoxifylline, N-acetylcysteine, and shave excision (Figure 2).
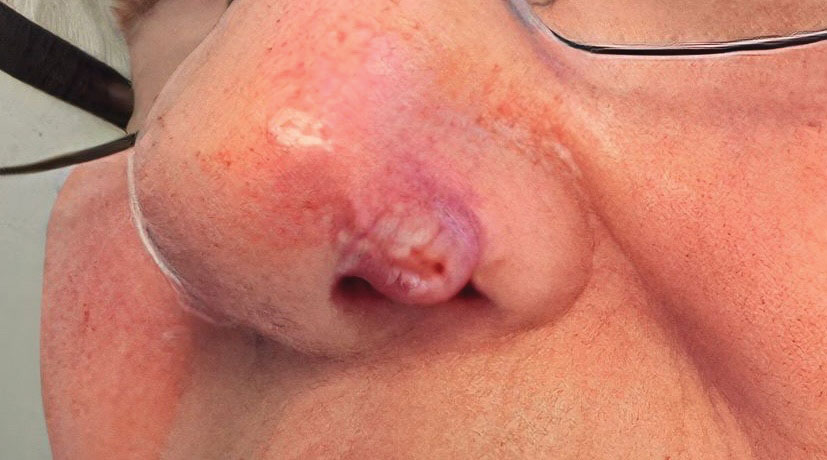

At 3-month follow-up, given the lesion’s persistence despite local and systemic anti-inflammatory approaches and our intent to avoid repeated corticosteroid exposure or more aggressive surgery in a cosmetically sensitive facial site, we attempted treatment with intralesional adalimumab. A 40-mg/0.4-mL dose of adalimumab was withdrawn directly from a prefilled autoinjector and placed into a sterile container, then transferred to a syringe fitted with a 30-gauge needle. Finally, the full 0.4 mL was injected intralesionally (Figure 3) until complete blanching of the lesion was achieved.
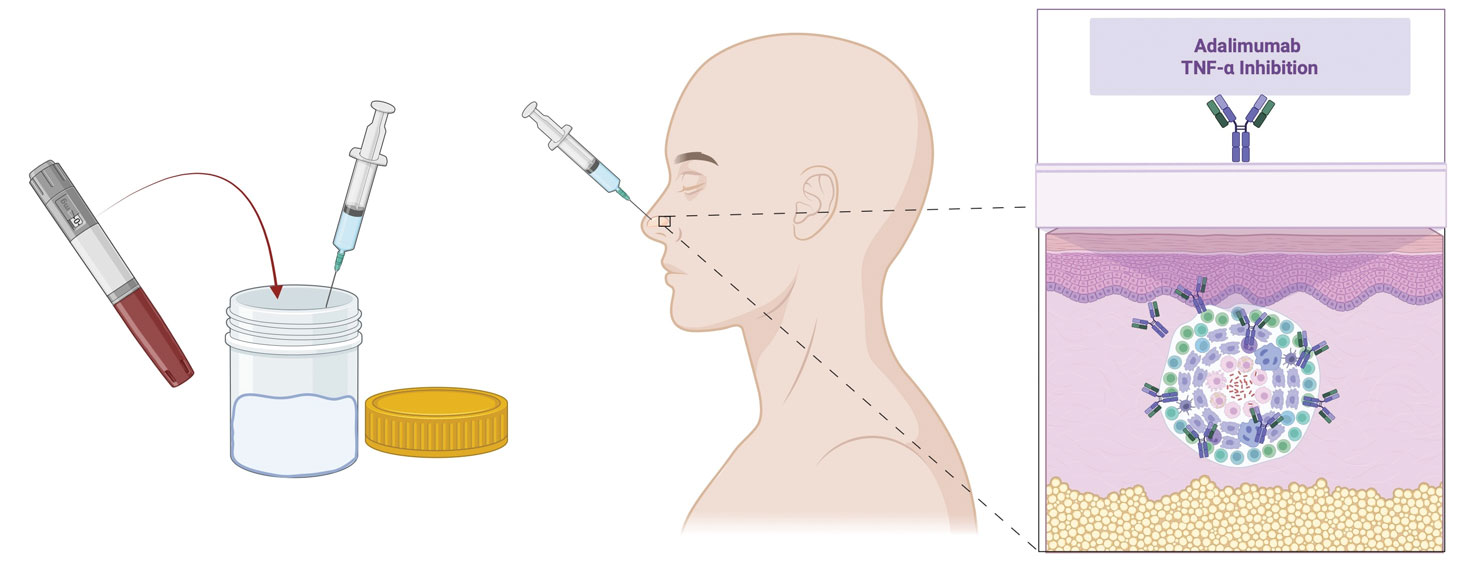
At 1-month follow-up, the lesion demonstrated decreased erythema and crusting (Figure 4A). The patient subsequently underwent 12 adalimumab injections over an 18-month period with marked reduction in size and erythema of the lesion without complications (Figure 4B). In addition, doxycycline 100 mg/d was started 11 months after the first adalimumab injection to address mild residual inflammation (Figure 4C); after 4 months, the dose was reduced to 50 mg/d due to gastrointestinal adverse effects. Doxycycline was maintained for 3 additional months with persistent improvement of the lesion.
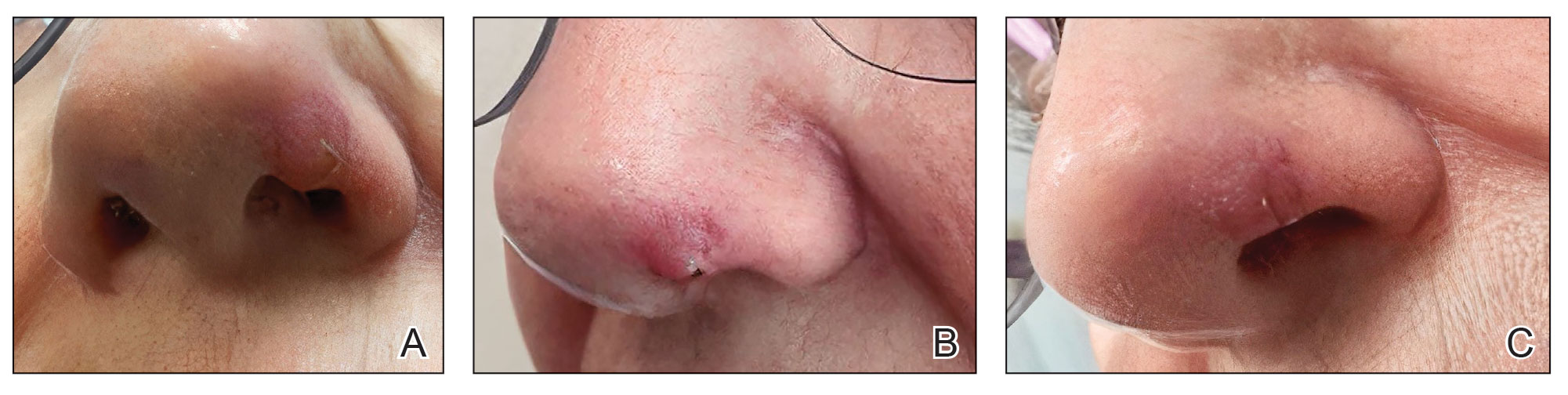
Practice Implication
Intralesional administration of adalimumab may represent a useful therapeutic option for localized refractory granulomatous inflammation, particularly in sensitive areas such as the face, where conventional therapies may be limited by adverse effects or suboptimal response. Localized delivery of TNF-α inhibition directly to the site of inflammation may allow for clinical improvement while minimizing systemic exposure associated with biologic therapy.2 This approach may be particularly advantageous in cases in which repeated intralesional corticosteroid injections raise concern for atrophy or dyspigmentation, or when surgical intervention carries a risk for recurrence or cosmetic morbidity.1,2 Given the established role of TNF-α in granuloma formation and maintenance, intralesional adalimumab provides a biologically plausible targeted therapeutic strategy. Further studies are needed to evaluate the potential applications in other cutaneous granulomatous dermatoses.2,3
- Philips MA, Lynch J, Azmi FH. Ulcerative cutaneous sarcoidosis responding to adalimumab. J Am Acad Dermatol. 2005;53:917. doi:10.1016/j.jaad.2005.02.023
- Balan K, Sagut P, Ederle AC, et al. Cutaneous sarcoidosis treated with intralesional adalimumab. Int J Dermatol. 2025;64:1120-1121. doi:10.1111/ijd.17549
- Dunn C, Whitney Z, Foss M, et al. Intralesional certolizumab for refractory lupus pernio. JAMA Dermatol. 2023;159:890-891. doi:10.1001 /jamadermatol.2023.0987
Practice Gap
Chronic localized granulomatous inflammation can be difficult to manage, particularly when manifesting on the face. Intralesional corticosteroids may lead to atrophy and dyspigmentation and therefore must be used cautiously in cosmetically sensitive areas.1 Surgical removal can lead to recurrence, and systemic agents may carry risks disproportionate to disease burden. Although tumor necrosis factor (TNF) α inhibitors are effective systemically, their localized use in cutaneous granulomatous dermatoses remains underreported.1-3 We describe a technique using intralesional injection of adalimumab to treat chronic refractory cutaneous granulomatous inflammation.
The Technique
A 69-year-old woman presented with a crusted erythematous papule with surrounding inflammation on the left nasal ala of 5 years’ duration (Figure 1). Histopathology demonstrated a localized cutaneous granulomatous process. There was no clinical, radiographic, or laboratory evidence of systemic sarcoidosis. Infectious causes were excluded through negative tissue cultures and special stains, including auramine-rhodamine. Over a 3-month period following initial presentation, the lesion proved refractory to intralesional 5-fluorouracil, intralesional triamcinolone acetonide, pentoxifylline, N-acetylcysteine, and shave excision (Figure 2).
At 3-month follow-up, given the lesion’s persistence despite local and systemic anti-inflammatory approaches and our intent to avoid repeated corticosteroid exposure or more aggressive surgery in a cosmetically sensitive facial site, we attempted treatment with intralesional adalimumab. A 40-mg/0.4-mL dose of adalimumab was withdrawn directly from a prefilled autoinjector and placed into a sterile container, then transferred to a syringe fitted with a 30-gauge needle. Finally, the full 0.4 mL was injected intralesionally (Figure 3) until complete blanching of the lesion was achieved.
At 1-month follow-up, the lesion demonstrated decreased erythema and crusting (Figure 4A). The patient subsequently underwent 12 adalimumab injections over an 18-month period with marked reduction in size and erythema of the lesion without complications (Figure 4B). In addition, doxycycline 100 mg/d was started 11 months after the first adalimumab injection to address mild residual inflammation (Figure 4C); after 4 months, the dose was reduced to 50 mg/d due to gastrointestinal adverse effects. Doxycycline was maintained for 3 additional months with persistent improvement of the lesion.
Practice Implication
Intralesional administration of adalimumab may represent a useful therapeutic option for localized refractory granulomatous inflammation, particularly in sensitive areas such as the face, where conventional therapies may be limited by adverse effects or suboptimal response. Localized delivery of TNF-α inhibition directly to the site of inflammation may allow for clinical improvement while minimizing systemic exposure associated with biologic therapy.2 This approach may be particularly advantageous in cases in which repeated intralesional corticosteroid injections raise concern for atrophy or dyspigmentation, or when surgical intervention carries a risk for recurrence or cosmetic morbidity.1,2 Given the established role of TNF-α in granuloma formation and maintenance, intralesional adalimumab provides a biologically plausible targeted therapeutic strategy. Further studies are needed to evaluate the potential applications in other cutaneous granulomatous dermatoses.2,3
Practice Gap
Chronic localized granulomatous inflammation can be difficult to manage, particularly when manifesting on the face. Intralesional corticosteroids may lead to atrophy and dyspigmentation and therefore must be used cautiously in cosmetically sensitive areas.1 Surgical removal can lead to recurrence, and systemic agents may carry risks disproportionate to disease burden. Although tumor necrosis factor (TNF) α inhibitors are effective systemically, their localized use in cutaneous granulomatous dermatoses remains underreported.1-3 We describe a technique using intralesional injection of adalimumab to treat chronic refractory cutaneous granulomatous inflammation.
The Technique
A 69-year-old woman presented with a crusted erythematous papule with surrounding inflammation on the left nasal ala of 5 years’ duration (Figure 1). Histopathology demonstrated a localized cutaneous granulomatous process. There was no clinical, radiographic, or laboratory evidence of systemic sarcoidosis. Infectious causes were excluded through negative tissue cultures and special stains, including auramine-rhodamine. Over a 3-month period following initial presentation, the lesion proved refractory to intralesional 5-fluorouracil, intralesional triamcinolone acetonide, pentoxifylline, N-acetylcysteine, and shave excision (Figure 2).
At 3-month follow-up, given the lesion’s persistence despite local and systemic anti-inflammatory approaches and our intent to avoid repeated corticosteroid exposure or more aggressive surgery in a cosmetically sensitive facial site, we attempted treatment with intralesional adalimumab. A 40-mg/0.4-mL dose of adalimumab was withdrawn directly from a prefilled autoinjector and placed into a sterile container, then transferred to a syringe fitted with a 30-gauge needle. Finally, the full 0.4 mL was injected intralesionally (Figure 3) until complete blanching of the lesion was achieved.
At 1-month follow-up, the lesion demonstrated decreased erythema and crusting (Figure 4A). The patient subsequently underwent 12 adalimumab injections over an 18-month period with marked reduction in size and erythema of the lesion without complications (Figure 4B). In addition, doxycycline 100 mg/d was started 11 months after the first adalimumab injection to address mild residual inflammation (Figure 4C); after 4 months, the dose was reduced to 50 mg/d due to gastrointestinal adverse effects. Doxycycline was maintained for 3 additional months with persistent improvement of the lesion.
Practice Implication
Intralesional administration of adalimumab may represent a useful therapeutic option for localized refractory granulomatous inflammation, particularly in sensitive areas such as the face, where conventional therapies may be limited by adverse effects or suboptimal response. Localized delivery of TNF-α inhibition directly to the site of inflammation may allow for clinical improvement while minimizing systemic exposure associated with biologic therapy.2 This approach may be particularly advantageous in cases in which repeated intralesional corticosteroid injections raise concern for atrophy or dyspigmentation, or when surgical intervention carries a risk for recurrence or cosmetic morbidity.1,2 Given the established role of TNF-α in granuloma formation and maintenance, intralesional adalimumab provides a biologically plausible targeted therapeutic strategy. Further studies are needed to evaluate the potential applications in other cutaneous granulomatous dermatoses.2,3
- Philips MA, Lynch J, Azmi FH. Ulcerative cutaneous sarcoidosis responding to adalimumab. J Am Acad Dermatol. 2005;53:917. doi:10.1016/j.jaad.2005.02.023
- Balan K, Sagut P, Ederle AC, et al. Cutaneous sarcoidosis treated with intralesional adalimumab. Int J Dermatol. 2025;64:1120-1121. doi:10.1111/ijd.17549
- Dunn C, Whitney Z, Foss M, et al. Intralesional certolizumab for refractory lupus pernio. JAMA Dermatol. 2023;159:890-891. doi:10.1001 /jamadermatol.2023.0987
- Philips MA, Lynch J, Azmi FH. Ulcerative cutaneous sarcoidosis responding to adalimumab. J Am Acad Dermatol. 2005;53:917. doi:10.1016/j.jaad.2005.02.023
- Balan K, Sagut P, Ederle AC, et al. Cutaneous sarcoidosis treated with intralesional adalimumab. Int J Dermatol. 2025;64:1120-1121. doi:10.1111/ijd.17549
- Dunn C, Whitney Z, Foss M, et al. Intralesional certolizumab for refractory lupus pernio. JAMA Dermatol. 2023;159:890-891. doi:10.1001 /jamadermatol.2023.0987
Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation
Using Intralesional Adalimumab for Chronic Refractory Cutaneous Granulomatous Inflammation

Pink Papulonodular Eruption on the Trunk and Arms
Pink Papulonodular Eruption on the Trunk and Arms
THE DIAGNOSIS: Sarcoidlike Reaction
Sarcoidlike reaction (SLR) is a rare cutaneous immune-related adverse event characterized by a multisystem granulomatous reaction indistinguishable from sarcoidosis but temporally associated with a trigger.1 Drug-induced SLR typically involves the mediastinal or hilar lymph nodes, with frequent involvement of the lungs and skin; cutaneous manifestations typically encompass erythematous papulonodular eruptions on the trunk and extremities.1-3 Sarcoidosis predominantly affects middle-aged women of African American or Scandinavian descent; genetic predisposition likely is a contributing factor.4 Unlike sarcoidosis, SLR is linked to various triggers such as medication or malignancy.
Immune checkpoint inhibitors (ICIs), particularly anti–PD-1 agents, have been linked to SLR through overexpression of proinflammatory cytokines, resulting in excessive T-helper 1 cell and macrophage activation and granulomatous eruption; notably, cutaneous immune-related adverse events often are correlated with greater treatment efficacy.5,6 Overall, anticancer therapy–induced SLR is most commonly reported in patients receiving ICIs for melanoma but it also has been described with ICI therapy for other cancers and with chemotherapy for melanoma. 1,3 Although most cases demonstrate both cutaneous and extracutaneous involvement, approximately 13 reported cases have been exclusively cutaneous.1 Recognition of SLR is important because misdiagnosis as true sarcoidosis may prompt unnecessary testing or therapy; furthermore, distinction from tumor progression is critical.3 The lesions can mimic other granulomatous or inflammatory dermatoses, posing a diagnostic challenge.
On histopathology, SLR typically demonstrates well-formed, noncaseating dermal granulomas composed of epithelioid histiocytes and Langhans or foreign-body giant cells, a sparse lymphocytic rim, and few plasma cells.2,4 Immunohistochemistry shows CD68-positive histiocytes predominating within the granulomas. Asteroid and Schaumann bodies occasionally are present.7 Special stains will be negative for microorganisms. Sarcoidosis manifests essentially identically from both a clinical and histopathologic perspective (Figure 1). Temporal association with an offending agent and symptomatic resolution following drug cessation remain the most reliable features for distinguishing SLR from sarcoidosis.7
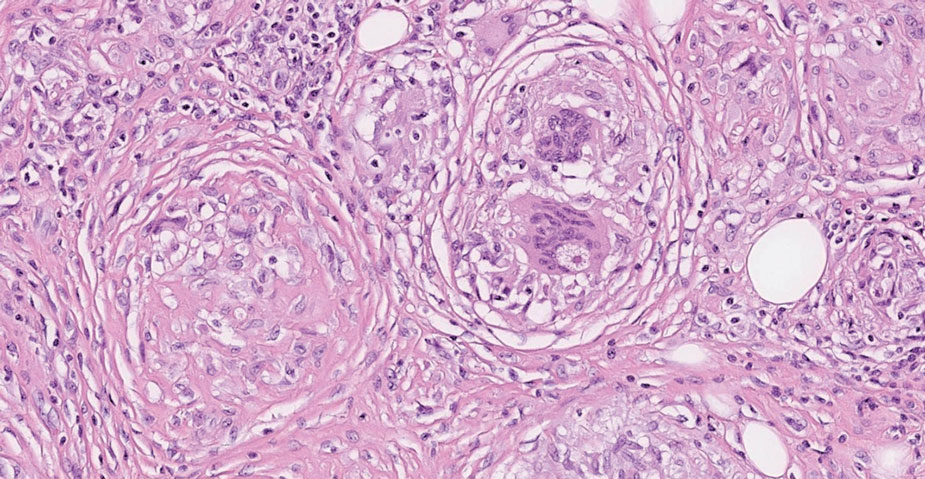
Tuberculoid leprosy is a chronic infectious disease caused by Mycobacterium leprae (found most commonly in tropical regions) and manifesting as localized hypopigmented macules or papules with raised erythematous margins.8 Histopathologically, lesions show well-formed granulomas composed of epithelioid histiocytes and Langhans giant cells without necrosis, surrounded by a prominent lymphocytic rim (Figure 2).9 Rarely, focal caseous necrosis occurs, particularly in involved nerves.10 Hallmark features include enlarged cutaneous nerves surrounded by dermal granulomas and absence of bacilli on special stains; eccrine glands are infrequently involved.9 Standard treatment is 6 months of combination therapy with dapsone and rifampin.
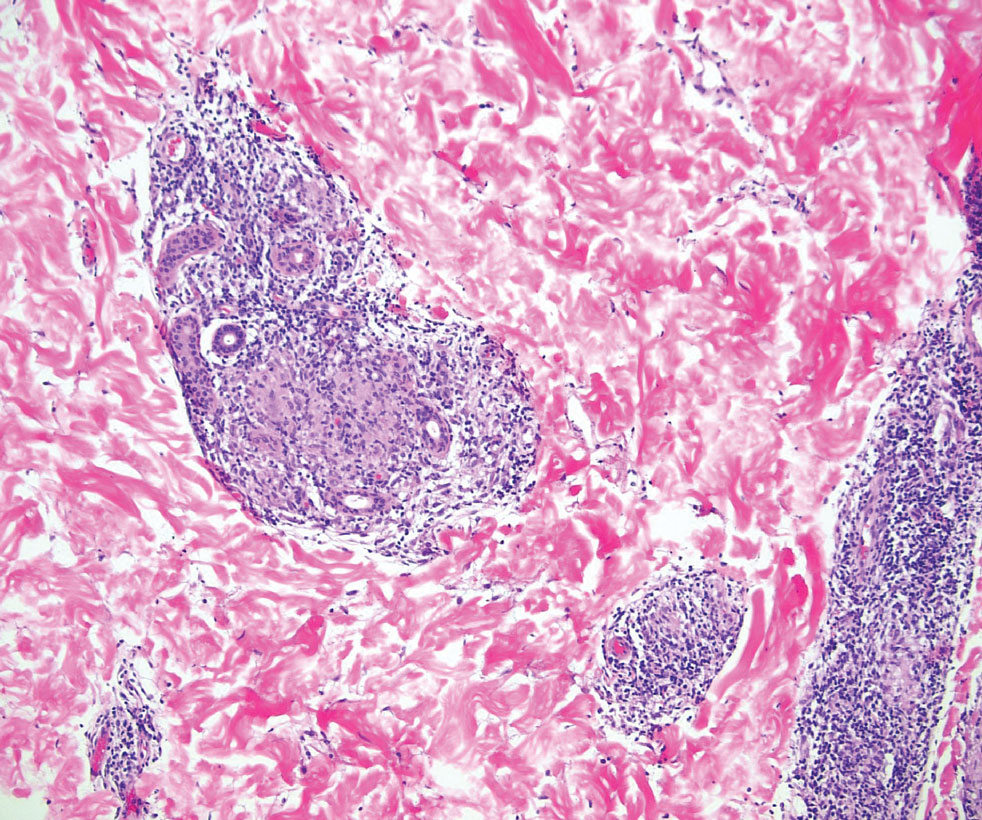
Generalized granuloma annulare is an inflammatory dermatosis manifesting as diffuse erythematous annular papules, classically on the trunk and extremities.11 It predominantly affects individuals in their fifth and sixth decades of life and may be drug induced.2 Histopathology may reveal palisaded granulomas with central necrobiotic collagen, intercalating histiocytes, and interstitial mucin (Figure 3).2 Pathology also may show interstitial histiocytes and lymphocytes intercalating between collagen bundles with increased mucin but absent palisading or necrobiosis or a mixed pattern.2,12 Alcian blue or colloidal iron stains highlight mucin to help distinguish from other granulomatous processes. Multinucleated giant cells are rare. The nonnecrobiotic histologic pattern can mimic sarcoidosis, necessitating clinical correlation for correct diagnosis.13 Certain cases show genetic predisposition, such as HLA-B35, with a relapsing course often requiring combined systemic immunosuppression and phototherapy.14
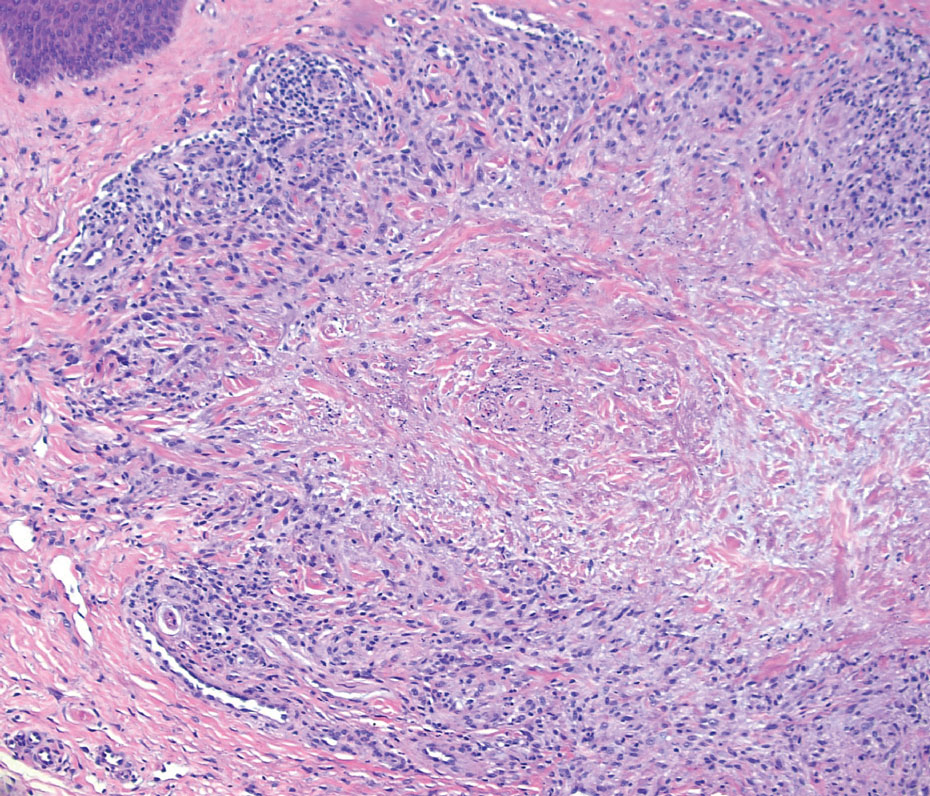
Granulomatosis with polyangiitis is a systemic vasculitis that classically manifests as palpable purpura on the lower extremities, often with ulceration. Localized erythematous papules on the extensor surfaces may occur less commonly.15 Pathogenesis involves antineutrophil cytoplasmic antibodies inducing neutrophil degranulation, release of reactive oxygen species and proinflammatory cytokines, and subsequent endothelial damage.15 Histopathology shows necrotizing granulomatous inflammation and necrotizing vasculitis of small and medium vessels with nuclear debris.15 Poorly formed granulomas containing abundant neutrophils and mixed perivascular inflammatory infiltrates may be seen with or without vasculitis (Figure 4). Systemic features commonly include chronic rhinosinusitis, pauci-immune glomerulonephritis, and pulmonary nodules.15 Pharmacotherapy includes glucocorticoids combined with a glucocorticoid-sparing agent.
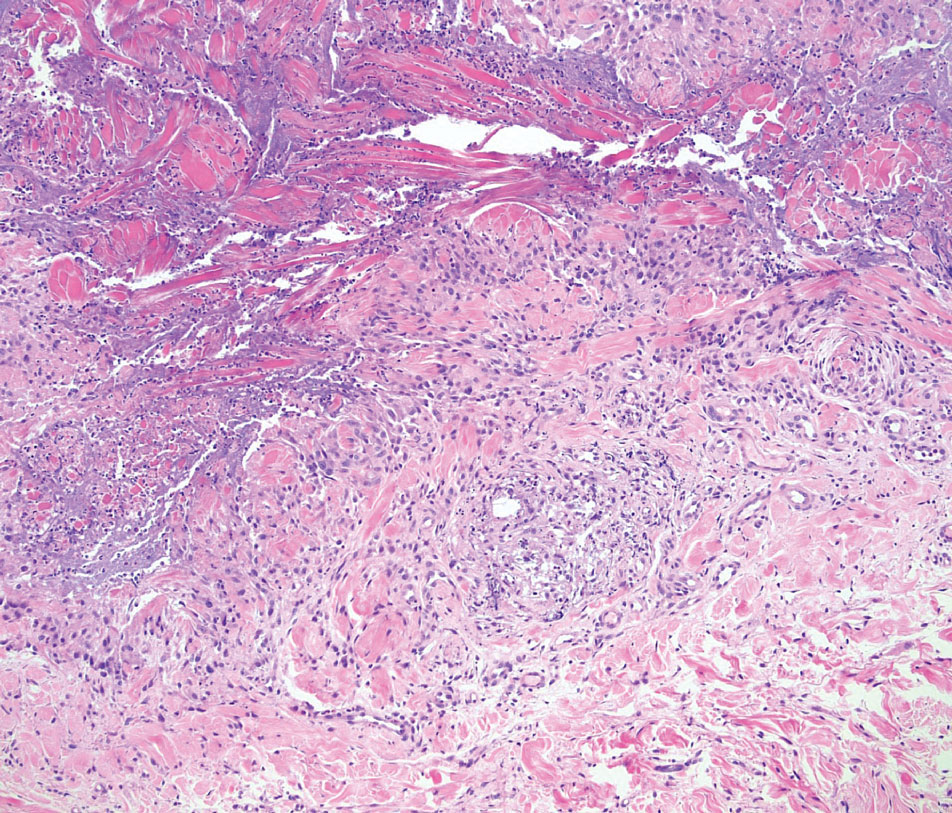
- Mazumder A, Mehrmal S, Chaudhry S. Immunotherapy-induced exclusively cutaneous sarcoid-like reaction. BMJ Case Rep. 2023;16:E252766. doi:10.1136/bcr-2022-252766
- Shah N, Shah M, Drucker AM, et al. Granulomatous cutaneous drug eruptions: a systematic review. Am J Clin Dermatol. 2021;22:39-53. doi:10.1007/s40257-020-00566-4
- Nykaza I, Murciano-Goroff YR, Desilets A, et al. Sarcoid-like reactions in patients treated with checkpoint inhibitors for advanced solid tumors. Oncologist. 2025;30:oyaf017. doi:10.1093/oncolo /oyaf017
- Tana C, Donatiello I, Caputo A, et al. Clinical features, histopathology and differential diagnosis of sarcoidosis. Cells. 2021;11:59. doi:10.3390/cells11010059
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361. doi:10.1007/s40257-017-0336-3
- Diaz-Perez JA, Beveridge MG, Victor TA, et al. Granulomatous and lichenoid dermatitis after IgG4 anti-PD-1 monoclonal antibody therapy for advanced cancer. J Cutan Pathol. 2018;45:434-438. doi:10.1111/cup.13133
- Chopra A, Nautiyal A, Kalkanis A, et al. Drug-induced sarcoidosis-like reactions. Chest. 2018;154:664-677. doi:10.1016 /j.chest.2018.03.056
- Froes LAR Jr, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics. An Bras Dermatol. 2022;97:338-347. doi:10.1016/j.abd.2021.08.006
- Magaña M, Vargas Bornacini MF, Landeta-Sa AP, et al. Lucio phenomenon: a review. Am J Dermatopathol. 2025;47:1-8. doi:10.1097 /DAD.0000000000002833
- Jayalakshmy PS, Prasad PH, Kamala VV, et al. Segmental necrotizing granulomatous neuritis: a rare manifestation of Hansen disease-report of 2 cases. Case Rep Dermatol Med. 2012;2012:758093. doi:10.1155/2012/758093
- Lee JH, Cho S. Resolution of refractory generalized granuloma annulare after treatment with alitretinoin. JAAD Case Rep. 2022;24:38-41. doi:10.1016/j.jdcr.2022.04.006
- Yun JH, Lee JY, Kim MK, et al. Clinical and pathological features of generalized granuloma annulare with their correlation: a retrospective multicenter study in Korea. Ann Dermatol. 2009; 21:113-119. doi:10.5021/ad.2009.21.2.113
- Cohen PR, Carlos CA. Granuloma annulare mimicking sarcoidosis: report of patient with localized granuloma annulare whose skin lesions show 3 clinical morphologies and 2 histology patterns. Am J Dermatopathol. 2015;37:547-550. doi:10.1097/DAD.0000000000000125
- Rankin BD, Haber RM. Familial granuloma annulare: first report of occurrence in a father and daughter and updated review of the literature. JAAD Case Rep. 2021;17:61-64. doi:10.1016 /j.jdcr.2021.09.023
- Rout P, Garlapati P, Qurie A. Granulomatosis with polyangiitis. StatPearls (Internet). Updated August 31, 2024. Accessed May 4, 2026. https://www.ncbi.nlm.nih.gov/books/NBK557827/
THE DIAGNOSIS: Sarcoidlike Reaction
Sarcoidlike reaction (SLR) is a rare cutaneous immune-related adverse event characterized by a multisystem granulomatous reaction indistinguishable from sarcoidosis but temporally associated with a trigger.1 Drug-induced SLR typically involves the mediastinal or hilar lymph nodes, with frequent involvement of the lungs and skin; cutaneous manifestations typically encompass erythematous papulonodular eruptions on the trunk and extremities.1-3 Sarcoidosis predominantly affects middle-aged women of African American or Scandinavian descent; genetic predisposition likely is a contributing factor.4 Unlike sarcoidosis, SLR is linked to various triggers such as medication or malignancy.
Immune checkpoint inhibitors (ICIs), particularly anti–PD-1 agents, have been linked to SLR through overexpression of proinflammatory cytokines, resulting in excessive T-helper 1 cell and macrophage activation and granulomatous eruption; notably, cutaneous immune-related adverse events often are correlated with greater treatment efficacy.5,6 Overall, anticancer therapy–induced SLR is most commonly reported in patients receiving ICIs for melanoma but it also has been described with ICI therapy for other cancers and with chemotherapy for melanoma. 1,3 Although most cases demonstrate both cutaneous and extracutaneous involvement, approximately 13 reported cases have been exclusively cutaneous.1 Recognition of SLR is important because misdiagnosis as true sarcoidosis may prompt unnecessary testing or therapy; furthermore, distinction from tumor progression is critical.3 The lesions can mimic other granulomatous or inflammatory dermatoses, posing a diagnostic challenge.
On histopathology, SLR typically demonstrates well-formed, noncaseating dermal granulomas composed of epithelioid histiocytes and Langhans or foreign-body giant cells, a sparse lymphocytic rim, and few plasma cells.2,4 Immunohistochemistry shows CD68-positive histiocytes predominating within the granulomas. Asteroid and Schaumann bodies occasionally are present.7 Special stains will be negative for microorganisms. Sarcoidosis manifests essentially identically from both a clinical and histopathologic perspective (Figure 1). Temporal association with an offending agent and symptomatic resolution following drug cessation remain the most reliable features for distinguishing SLR from sarcoidosis.7
Tuberculoid leprosy is a chronic infectious disease caused by Mycobacterium leprae (found most commonly in tropical regions) and manifesting as localized hypopigmented macules or papules with raised erythematous margins.8 Histopathologically, lesions show well-formed granulomas composed of epithelioid histiocytes and Langhans giant cells without necrosis, surrounded by a prominent lymphocytic rim (Figure 2).9 Rarely, focal caseous necrosis occurs, particularly in involved nerves.10 Hallmark features include enlarged cutaneous nerves surrounded by dermal granulomas and absence of bacilli on special stains; eccrine glands are infrequently involved.9 Standard treatment is 6 months of combination therapy with dapsone and rifampin.
Generalized granuloma annulare is an inflammatory dermatosis manifesting as diffuse erythematous annular papules, classically on the trunk and extremities.11 It predominantly affects individuals in their fifth and sixth decades of life and may be drug induced.2 Histopathology may reveal palisaded granulomas with central necrobiotic collagen, intercalating histiocytes, and interstitial mucin (Figure 3).2 Pathology also may show interstitial histiocytes and lymphocytes intercalating between collagen bundles with increased mucin but absent palisading or necrobiosis or a mixed pattern.2,12 Alcian blue or colloidal iron stains highlight mucin to help distinguish from other granulomatous processes. Multinucleated giant cells are rare. The nonnecrobiotic histologic pattern can mimic sarcoidosis, necessitating clinical correlation for correct diagnosis.13 Certain cases show genetic predisposition, such as HLA-B35, with a relapsing course often requiring combined systemic immunosuppression and phototherapy.14
Granulomatosis with polyangiitis is a systemic vasculitis that classically manifests as palpable purpura on the lower extremities, often with ulceration. Localized erythematous papules on the extensor surfaces may occur less commonly.15 Pathogenesis involves antineutrophil cytoplasmic antibodies inducing neutrophil degranulation, release of reactive oxygen species and proinflammatory cytokines, and subsequent endothelial damage.15 Histopathology shows necrotizing granulomatous inflammation and necrotizing vasculitis of small and medium vessels with nuclear debris.15 Poorly formed granulomas containing abundant neutrophils and mixed perivascular inflammatory infiltrates may be seen with or without vasculitis (Figure 4). Systemic features commonly include chronic rhinosinusitis, pauci-immune glomerulonephritis, and pulmonary nodules.15 Pharmacotherapy includes glucocorticoids combined with a glucocorticoid-sparing agent.
THE DIAGNOSIS: Sarcoidlike Reaction
Sarcoidlike reaction (SLR) is a rare cutaneous immune-related adverse event characterized by a multisystem granulomatous reaction indistinguishable from sarcoidosis but temporally associated with a trigger.1 Drug-induced SLR typically involves the mediastinal or hilar lymph nodes, with frequent involvement of the lungs and skin; cutaneous manifestations typically encompass erythematous papulonodular eruptions on the trunk and extremities.1-3 Sarcoidosis predominantly affects middle-aged women of African American or Scandinavian descent; genetic predisposition likely is a contributing factor.4 Unlike sarcoidosis, SLR is linked to various triggers such as medication or malignancy.
Immune checkpoint inhibitors (ICIs), particularly anti–PD-1 agents, have been linked to SLR through overexpression of proinflammatory cytokines, resulting in excessive T-helper 1 cell and macrophage activation and granulomatous eruption; notably, cutaneous immune-related adverse events often are correlated with greater treatment efficacy.5,6 Overall, anticancer therapy–induced SLR is most commonly reported in patients receiving ICIs for melanoma but it also has been described with ICI therapy for other cancers and with chemotherapy for melanoma. 1,3 Although most cases demonstrate both cutaneous and extracutaneous involvement, approximately 13 reported cases have been exclusively cutaneous.1 Recognition of SLR is important because misdiagnosis as true sarcoidosis may prompt unnecessary testing or therapy; furthermore, distinction from tumor progression is critical.3 The lesions can mimic other granulomatous or inflammatory dermatoses, posing a diagnostic challenge.
On histopathology, SLR typically demonstrates well-formed, noncaseating dermal granulomas composed of epithelioid histiocytes and Langhans or foreign-body giant cells, a sparse lymphocytic rim, and few plasma cells.2,4 Immunohistochemistry shows CD68-positive histiocytes predominating within the granulomas. Asteroid and Schaumann bodies occasionally are present.7 Special stains will be negative for microorganisms. Sarcoidosis manifests essentially identically from both a clinical and histopathologic perspective (Figure 1). Temporal association with an offending agent and symptomatic resolution following drug cessation remain the most reliable features for distinguishing SLR from sarcoidosis.7
Tuberculoid leprosy is a chronic infectious disease caused by Mycobacterium leprae (found most commonly in tropical regions) and manifesting as localized hypopigmented macules or papules with raised erythematous margins.8 Histopathologically, lesions show well-formed granulomas composed of epithelioid histiocytes and Langhans giant cells without necrosis, surrounded by a prominent lymphocytic rim (Figure 2).9 Rarely, focal caseous necrosis occurs, particularly in involved nerves.10 Hallmark features include enlarged cutaneous nerves surrounded by dermal granulomas and absence of bacilli on special stains; eccrine glands are infrequently involved.9 Standard treatment is 6 months of combination therapy with dapsone and rifampin.
Generalized granuloma annulare is an inflammatory dermatosis manifesting as diffuse erythematous annular papules, classically on the trunk and extremities.11 It predominantly affects individuals in their fifth and sixth decades of life and may be drug induced.2 Histopathology may reveal palisaded granulomas with central necrobiotic collagen, intercalating histiocytes, and interstitial mucin (Figure 3).2 Pathology also may show interstitial histiocytes and lymphocytes intercalating between collagen bundles with increased mucin but absent palisading or necrobiosis or a mixed pattern.2,12 Alcian blue or colloidal iron stains highlight mucin to help distinguish from other granulomatous processes. Multinucleated giant cells are rare. The nonnecrobiotic histologic pattern can mimic sarcoidosis, necessitating clinical correlation for correct diagnosis.13 Certain cases show genetic predisposition, such as HLA-B35, with a relapsing course often requiring combined systemic immunosuppression and phototherapy.14
Granulomatosis with polyangiitis is a systemic vasculitis that classically manifests as palpable purpura on the lower extremities, often with ulceration. Localized erythematous papules on the extensor surfaces may occur less commonly.15 Pathogenesis involves antineutrophil cytoplasmic antibodies inducing neutrophil degranulation, release of reactive oxygen species and proinflammatory cytokines, and subsequent endothelial damage.15 Histopathology shows necrotizing granulomatous inflammation and necrotizing vasculitis of small and medium vessels with nuclear debris.15 Poorly formed granulomas containing abundant neutrophils and mixed perivascular inflammatory infiltrates may be seen with or without vasculitis (Figure 4). Systemic features commonly include chronic rhinosinusitis, pauci-immune glomerulonephritis, and pulmonary nodules.15 Pharmacotherapy includes glucocorticoids combined with a glucocorticoid-sparing agent.
- Mazumder A, Mehrmal S, Chaudhry S. Immunotherapy-induced exclusively cutaneous sarcoid-like reaction. BMJ Case Rep. 2023;16:E252766. doi:10.1136/bcr-2022-252766
- Shah N, Shah M, Drucker AM, et al. Granulomatous cutaneous drug eruptions: a systematic review. Am J Clin Dermatol. 2021;22:39-53. doi:10.1007/s40257-020-00566-4
- Nykaza I, Murciano-Goroff YR, Desilets A, et al. Sarcoid-like reactions in patients treated with checkpoint inhibitors for advanced solid tumors. Oncologist. 2025;30:oyaf017. doi:10.1093/oncolo /oyaf017
- Tana C, Donatiello I, Caputo A, et al. Clinical features, histopathology and differential diagnosis of sarcoidosis. Cells. 2021;11:59. doi:10.3390/cells11010059
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361. doi:10.1007/s40257-017-0336-3
- Diaz-Perez JA, Beveridge MG, Victor TA, et al. Granulomatous and lichenoid dermatitis after IgG4 anti-PD-1 monoclonal antibody therapy for advanced cancer. J Cutan Pathol. 2018;45:434-438. doi:10.1111/cup.13133
- Chopra A, Nautiyal A, Kalkanis A, et al. Drug-induced sarcoidosis-like reactions. Chest. 2018;154:664-677. doi:10.1016 /j.chest.2018.03.056
- Froes LAR Jr, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics. An Bras Dermatol. 2022;97:338-347. doi:10.1016/j.abd.2021.08.006
- Magaña M, Vargas Bornacini MF, Landeta-Sa AP, et al. Lucio phenomenon: a review. Am J Dermatopathol. 2025;47:1-8. doi:10.1097 /DAD.0000000000002833
- Jayalakshmy PS, Prasad PH, Kamala VV, et al. Segmental necrotizing granulomatous neuritis: a rare manifestation of Hansen disease-report of 2 cases. Case Rep Dermatol Med. 2012;2012:758093. doi:10.1155/2012/758093
- Lee JH, Cho S. Resolution of refractory generalized granuloma annulare after treatment with alitretinoin. JAAD Case Rep. 2022;24:38-41. doi:10.1016/j.jdcr.2022.04.006
- Yun JH, Lee JY, Kim MK, et al. Clinical and pathological features of generalized granuloma annulare with their correlation: a retrospective multicenter study in Korea. Ann Dermatol. 2009; 21:113-119. doi:10.5021/ad.2009.21.2.113
- Cohen PR, Carlos CA. Granuloma annulare mimicking sarcoidosis: report of patient with localized granuloma annulare whose skin lesions show 3 clinical morphologies and 2 histology patterns. Am J Dermatopathol. 2015;37:547-550. doi:10.1097/DAD.0000000000000125
- Rankin BD, Haber RM. Familial granuloma annulare: first report of occurrence in a father and daughter and updated review of the literature. JAAD Case Rep. 2021;17:61-64. doi:10.1016 /j.jdcr.2021.09.023
- Rout P, Garlapati P, Qurie A. Granulomatosis with polyangiitis. StatPearls (Internet). Updated August 31, 2024. Accessed May 4, 2026. https://www.ncbi.nlm.nih.gov/books/NBK557827/
- Mazumder A, Mehrmal S, Chaudhry S. Immunotherapy-induced exclusively cutaneous sarcoid-like reaction. BMJ Case Rep. 2023;16:E252766. doi:10.1136/bcr-2022-252766
- Shah N, Shah M, Drucker AM, et al. Granulomatous cutaneous drug eruptions: a systematic review. Am J Clin Dermatol. 2021;22:39-53. doi:10.1007/s40257-020-00566-4
- Nykaza I, Murciano-Goroff YR, Desilets A, et al. Sarcoid-like reactions in patients treated with checkpoint inhibitors for advanced solid tumors. Oncologist. 2025;30:oyaf017. doi:10.1093/oncolo /oyaf017
- Tana C, Donatiello I, Caputo A, et al. Clinical features, histopathology and differential diagnosis of sarcoidosis. Cells. 2021;11:59. doi:10.3390/cells11010059
- Sibaud V. Dermatologic reactions to immune checkpoint inhibitors: skin toxicities and immunotherapy. Am J Clin Dermatol. 2018;19:345-361. doi:10.1007/s40257-017-0336-3
- Diaz-Perez JA, Beveridge MG, Victor TA, et al. Granulomatous and lichenoid dermatitis after IgG4 anti-PD-1 monoclonal antibody therapy for advanced cancer. J Cutan Pathol. 2018;45:434-438. doi:10.1111/cup.13133
- Chopra A, Nautiyal A, Kalkanis A, et al. Drug-induced sarcoidosis-like reactions. Chest. 2018;154:664-677. doi:10.1016 /j.chest.2018.03.056
- Froes LAR Jr, Sotto MN, Trindade MAB. Leprosy: clinical and immunopathological characteristics. An Bras Dermatol. 2022;97:338-347. doi:10.1016/j.abd.2021.08.006
- Magaña M, Vargas Bornacini MF, Landeta-Sa AP, et al. Lucio phenomenon: a review. Am J Dermatopathol. 2025;47:1-8. doi:10.1097 /DAD.0000000000002833
- Jayalakshmy PS, Prasad PH, Kamala VV, et al. Segmental necrotizing granulomatous neuritis: a rare manifestation of Hansen disease-report of 2 cases. Case Rep Dermatol Med. 2012;2012:758093. doi:10.1155/2012/758093
- Lee JH, Cho S. Resolution of refractory generalized granuloma annulare after treatment with alitretinoin. JAAD Case Rep. 2022;24:38-41. doi:10.1016/j.jdcr.2022.04.006
- Yun JH, Lee JY, Kim MK, et al. Clinical and pathological features of generalized granuloma annulare with their correlation: a retrospective multicenter study in Korea. Ann Dermatol. 2009; 21:113-119. doi:10.5021/ad.2009.21.2.113
- Cohen PR, Carlos CA. Granuloma annulare mimicking sarcoidosis: report of patient with localized granuloma annulare whose skin lesions show 3 clinical morphologies and 2 histology patterns. Am J Dermatopathol. 2015;37:547-550. doi:10.1097/DAD.0000000000000125
- Rankin BD, Haber RM. Familial granuloma annulare: first report of occurrence in a father and daughter and updated review of the literature. JAAD Case Rep. 2021;17:61-64. doi:10.1016 /j.jdcr.2021.09.023
- Rout P, Garlapati P, Qurie A. Granulomatosis with polyangiitis. StatPearls (Internet). Updated August 31, 2024. Accessed May 4, 2026. https://www.ncbi.nlm.nih.gov/books/NBK557827/
Pink Papulonodular Eruption on the Trunk and Arms
Pink Papulonodular Eruption on the Trunk and Arms
A 47-year-old man with a history of chronic kidney disease and bilateral clear cell renal cell carcinoma who was undergoing treatment with adjuvant pembrolizumab presented to the dermatology department with a scattered papulonodular eruption of several weeks’ duration. Physical examination revealed pink papules and nodules with coalescing erythema over the trunk and upper extremities, most pronounced on the right elbow (bottom [inset]). A 4-mm punch biopsy demonstrated dermal granulomatous inflammation. Special stains were negative for microorganisms. Computed tomography of the chest revealed a new subpleural nodule and new hilar lymphadenopathy.
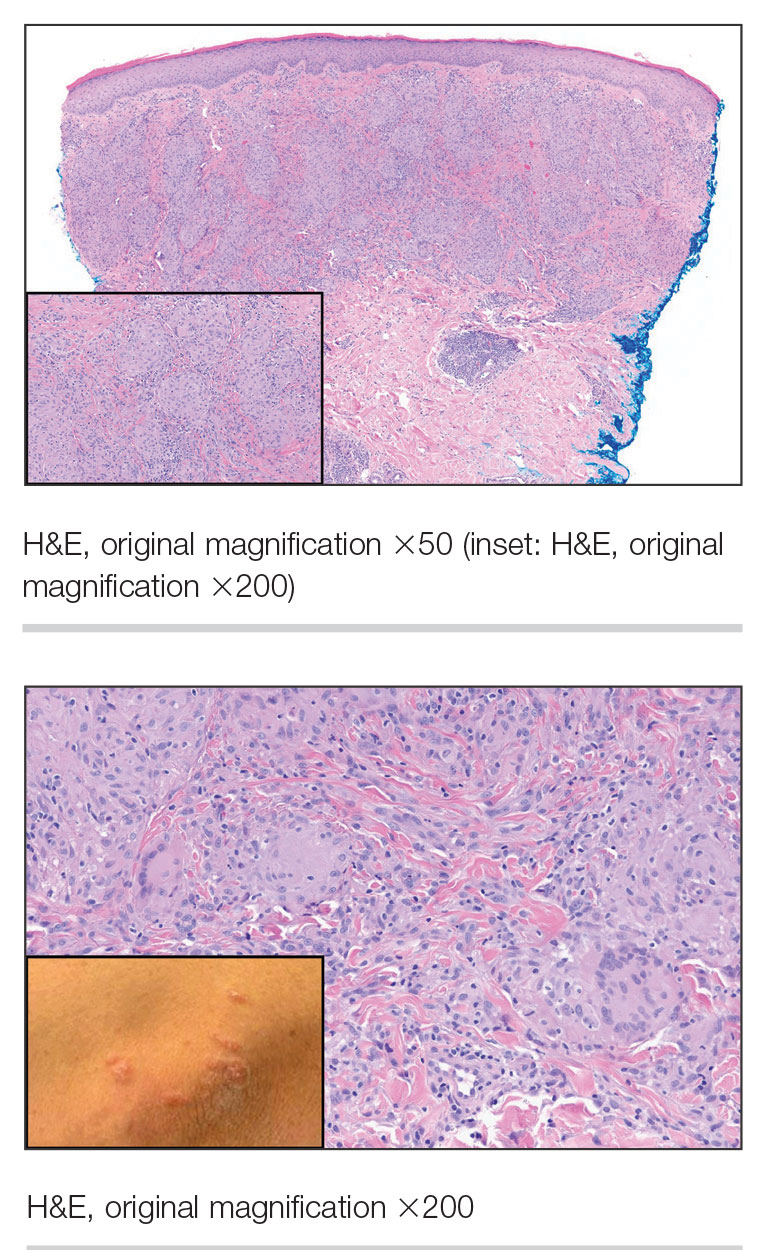

Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
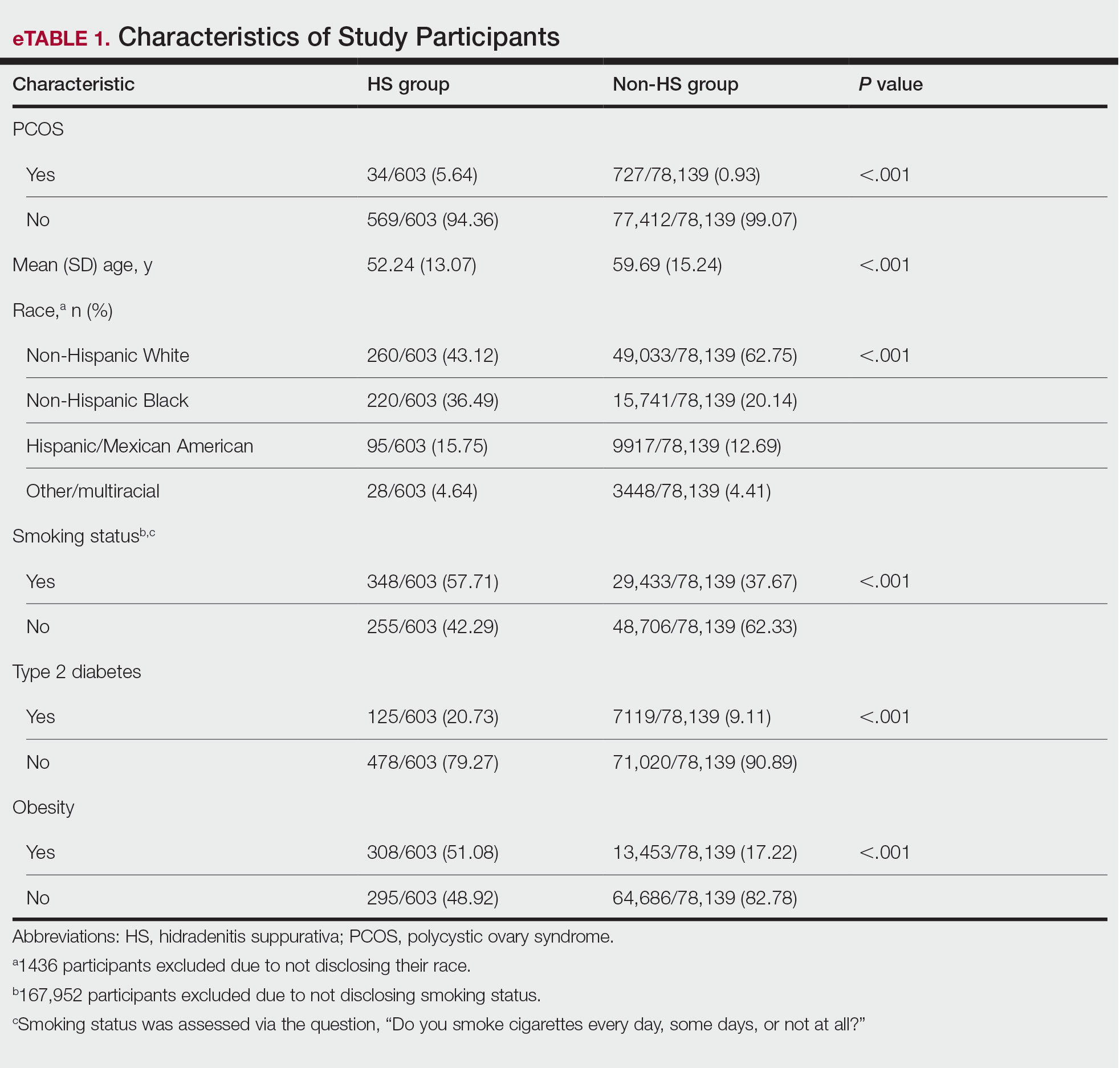
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
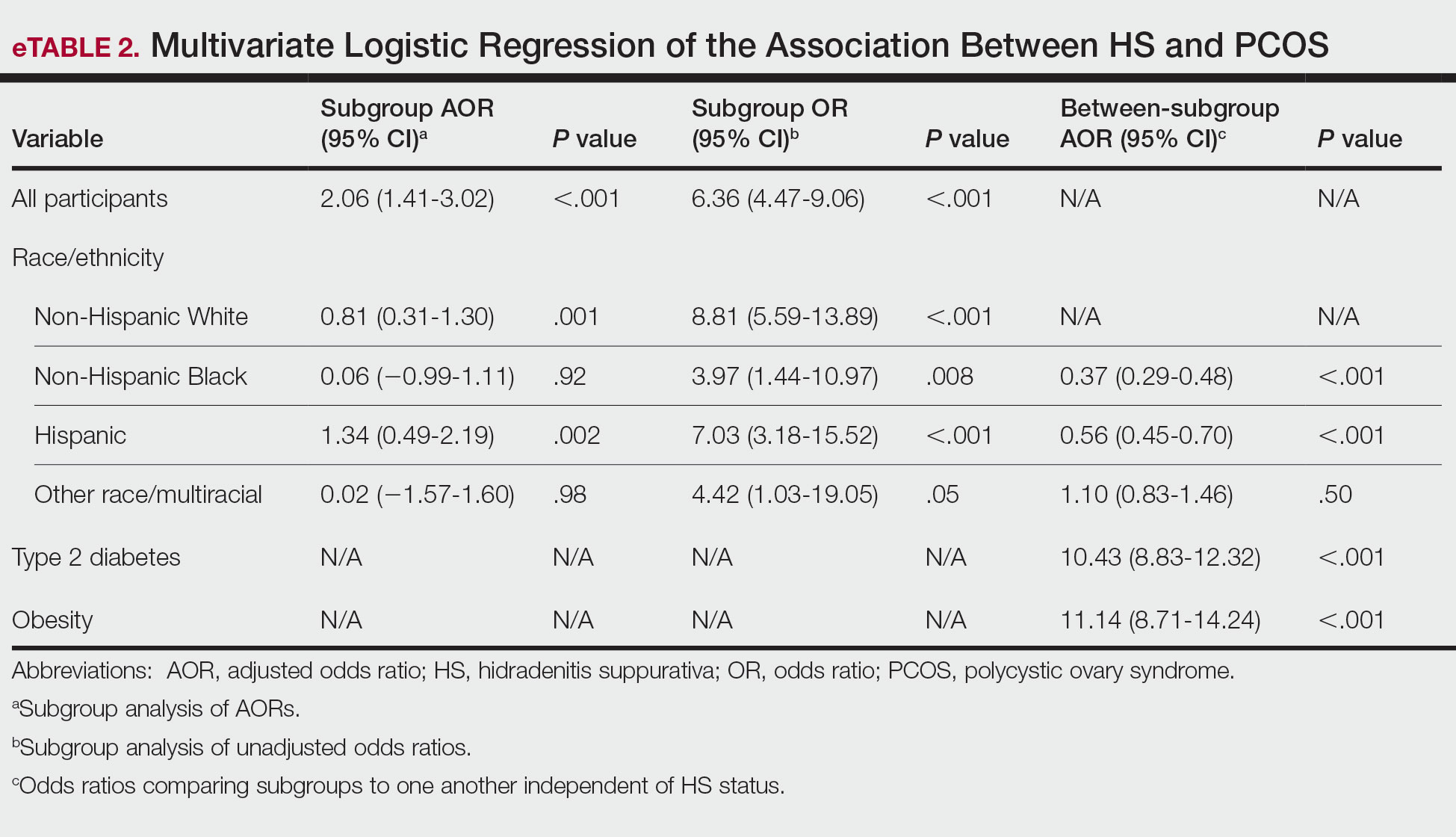
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
Hidradenitis suppurativa (HS) is a chronic inflammatory skin condition characterized by painful nodules, abscesses, scarring, and sinus tracts that commonly manifest in the axillary, inguinal, perianal, and inframammary regions.1 Hidradenitis suppurativa has been associated with several metabolic and cardiovascular comorbidities as well as polycystic ovary syndrome (PCOS)(recently renamed polyendocrine metabolic ovarian syndrome),2,3 a condition characterized by hyperandrogenism, chronic anovulation, and polycystic ovaries.2 Multiple comorbidities of PCOS overlap with those of HS, including type 2 diabetes, cardiovascular disease, and metabolic syndrome.1,3-5 While HS may be associated with PCOS, there is limited literature analyzing the association between these conditions. This study aimed to analyze the association between HS and PCOS using data from the National Institute of Health’s All of Us Research Program database (https://allofus.nih.gov/). While other studies have looked at the association between HS and PCOS, ours is among the first to analyze the relationship between multiple race/ ethnicity groups, which is especially important given racial disparities in HS and comorbid diseases.
Methods
A cross-sectional, population-based study of females included in the All of Us Research Program database was conducted. Patients with HS were identified using the Systematized Nomenclature of Medicine–Clinical Terms (SNOMED CT) code 59393003, while PCOS was identified with the code 237055002. Type 2 diabetes was identified with the following SNOMED CT codes: 44054006, 313436004, 237599002, 199230006, 359642000, and 81531005. Obesity was identified with the following codes: 414916001, 238136002, 190966007, 296526005, 294493008, 238134004, 83911000119104, and 415530009. Male patients and those who did not answer questions regarding sociodemographic variables were excluded from the final analysis. P values were calculated using Pearson χ2 tests. Multivariate logistic regression was used to calculate adjusted odds ratios and unadjusted odds ratios to analyze the association between HS and PCOS while controlling for age, race/ethnicity, smoking status, type 2 diabetes, and obesity. Statistical analyses were conducted using a 95% CI.
Results
The final analysis included 78,742 patients. The prevalence of PCOS was 5.64% in the HS group vs 0.93% in the non-HS group (eTable 1). Individuals with HS had higher rates of smoking cigarettes (57.71% vs 37.67%), obesity (51.08% vs 17.22%), and type 2 diabetes (20.73% vs 9.11%) than individuals without HS, respectively.
Multivariate logistic regression analyses revealed that individuals with HS were 2.06 times more likely to have PCOS after adjusting for sociodemographic variables and comorbidities (95% CI, 1.41-3.02; P<.001). Adjusted subgroup analyses by race/ethnicity did not yield statistically significant results; however, unadjusted analyses revealed that individuals with HS had significantly increased odds of PCOS across all race/ethnicity groups (eTable 2). Interaction terms analysis to determine if the relationship between HS and PCOS differs by race/ ethnicity did not yield statistically significant results. However, independent of HS status, non-Hispanic Black and Hispanic patients were less likely to have PCOS compared to White individuals (adjusted odds ratio, 0.37 and 0.56, respectively; P<.001). Disparities in access to care could have led to underdiagnosis of PCOS among non-Hispanic Black and Hispanic patients. Lastly, individuals with type 2 diabetes were 10.43 times more likely to have PCOS than those without, while patients with obesity were 11.14 times more likely to have PCOS than those without.
Comment
This study demonstrated that females with HS are 2.06 times more likely to have PCOS than those without HS, even after controlling for important sociodemographic variables and comorbidities. While adjusted subgroup analyses did not yield statistically significant results, unadjusted analyses demonstrated increased odds of PCOS in patients with HS across all race/ethnicity groups, suggesting that sociodemographic variables and comorbidities substantially influence the relationship between HS and PCOS; for instance, patients with type 2 diabetes and obesity are approximately 10- to 11-fold more likely to have PCOS than patients without these conditions. Non-Hispanic Black and Hispanic patients were less likely to have PCOS compared with White patients, indicating possible underdiagnosis of PCOS in these populations and highlighting the need for increased PCOS screening. Limitations of this study include the reliance on SNOMED CT codes, which may have led to underdiagnosis of HS or PCOS, as well as the inability to differentiate between mild and severe HS in the database.
Hyperandrogenism is believed to contribute to the pathogenesis of both HS and PCOS, supporting the potential use of antiandrogen therapies, such as spironolactone, in managing both conditions.2,3 Furthermore, oral contraceptives may have a role in managing both conditions. In HS, oral contraceptives help to mitigate flares associated with hormonal changes during menstruation, while in PCOS, they are used to regulate the hormonal cycle and reduce hirsutism.2-4 However, not all women experience menstrual flares of HS, suggesting that variations in HS phenotypes may influence individual responses to hormonal changes.1 Additionally, the considerable overlap in metabolic and cardiovascular comorbidities between HS and PCOS indicates that shared pathomechanisms may contribute to the association between these conditions.1,2 For example, proinflammatory adipokines released in both HS and PCOS may contribute to inflammation, cardiovascular disease, and insulin resistance.3,5
Conclusion
Further research is needed to better understand the shared pathophysiology that links these 2 diseases and to identify targeted approaches for optimizing management and improving patient outcomes. The association between HS and PCOS highlights the importance of screening for metabolic and reproductive comorbidities in patients with HS. Early recognition and management of both HS and PCOS can improve long-term outcomes.
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
- van Straalen KR, Prens EP, Gudjonsson JE. Insights into hidradenitis suppurativa. J Allergy Clin Immunol. 2022;149:1150-1161. doi:10.1016 /j.jaci.2022.02.003
- Choudhari R, Tayade S, Tiwari A, et al. Diagnosis, management, and associated comorbidities of polycystic ovary syndrome: a narrative review. Cureus. 2024;16:e58733. doi:10.7759/cureus.58733
- Abu Rached N, Gambichler T, Dietrich JW, et al. The role of hormones in hidradenitis suppurativa: a systematic review. Int J Mol Sci. 2022;23:15250. doi:10.3390/ijms232315250
- Montero-Vilchez T, Valenzuela-Amigo A, Cuenca-Barrales C, et al. The role of oral contraceptive pills in hidradenitis suppurativa: a cohort study. Life (Basel). 2021;11:697. doi:10.3390/life11070697
- Randeva HS, Tan BK, Weickert MO, et al. Cardiometabolic aspects of the polycystic ovary syndrome. Endocr Rev. 2012;33:812-841. doi:10.1210/er.2012-1003
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
Association Between Hidradenitis Suppurativa and Polycystic Ovary Syndrome
PRACTICE POINTS
- Patients with hidradenitis suppurativa were 2.06 times more likely to have polycystic ovary syndrome (PCOS) than patients without HS after controlling for age, race/ ethnicity, tobacco use, type 2 diabetes, and obesity.
- Non-Hispanic Black and Hispanic patients were less likely than White patients to have a diagnosis of PCOS, potentially reflecting underdiagnosis in these populations.
- Individuals with type 2 diabetes and obesity were 10.43 and 11.14 times more likely, respectively, to have PCOS.

Atopic Dermatitis: New Insights and Expanded Treatment Options
Atopic Dermatitis: New Insights and Expanded Treatment Options
Atopic dermatitis (AD) is a chronic skin condition generally characterized by pruritic and erythematous papules and plaques.1 While AD commonly manifests in childhood, 1 in 4 patients living with AD report adult onset of the disease.2 The clinical presentation and prevalence of AD vary across age groups, skin tones, and racial and ethnic groups. Globally, AD is estimated to have a prevalence of 2.6%; however, rates vary widely by region.1 Morphology and distribution of AD lesions also vary by population; therefore, defining one classic presentation of AD is not sufficient in diverse patient populations.3
Epidemiology
The prevalence of AD ranges from 0.2% to 24.6% worldwide, with higher rates in Africa and Oceania and lower rates in India and Northern and Eastern Europe.1 In the United States, AD affects all racial and ethnic groups; however, prevalence and severity are increased in Black children compared with White children.4 In one prospective cohort study, Hispanic children and non-Hispanic Black children aged 3 years and younger had greater odds of AD persisting into mid childhood (approximately age 7 years) compared with non-Hispanic White children.5,6
Key Clinical Features
Clinical features of AD are heterogeneous and may include differences in color, morphology, and distribution. Brown, hyperpigmented, gray, and/or violaceous plaques may predominate in patients with skin of color (SOC) compared with the erythematous plaques commonly described in lighter skin tones.1,3 Established scoring systems for AD rely on erythema as a key diagnostic feature, but because erythema can be difficult to detect in darker skin tones, disease severity may be underestimated and diagnosis may be delayed in this population.4
Atopic dermatitis in SOC may manifest as lichenoid plaques,7 prurigo nodules,7,8 lichenification,1 and follicular accentuation.9 Lichen planus–like AD is a distinct variant characterized by lichenoid plaques with a predilection for the extensor surfaces and face in patients with darker skin tones1,8 occurring in approximately 9% of patients in one study.10
Other key clinical features of AD in patients with SOC include pityriasis alba,10 increased risk for postinflammatory pigment alteration (including hyperpigmentation and/or hypopigmentation),1 and greater trunk and extensor involvement.1,11
Worth Noting
The scientific landscape for AD has grown rapidly, increasing our understanding of its pathophysiology, treatment, and social impact. Nonsteroidal treatments available for pediatric and adult patients with AD have increased in recent years, including crisaborole (approved for use in those ages ≥3 months), tacrolimus (≥2 years), and pimecrolimus (≥2 years). Injectable options include dupilumab (≥6 months), lebrikizumab (≥12 years), nemolizumab (≥12 years), and tralokinumab (≥12 years). Oral options include abrocitinib (≥12 years) and upadacitinib (≥12 years).12 Topical options include roflumilast 0.15% cream (≥6 years)12 and 0.05% cream (≥2-5 years),13 ruxolitinib 1.5% cream (≥2 years),14 and tapinarof 1% cream (≥2 years).12
For some patients, postinflammatory pigment alteration associated with AD has a higher impact on quality of life than the AD itself.7 In a study of 260 US adults with AD, the emotional impact of pigmentary changes was greatest in Black patients, with 53.3% reporting that pigment changes bothered them “a lot” or “very much.”15
Genome-wide association studies have not identified a single determinant that explains racial and ethnic differences in susceptibility to AD.4 Instead, social determinants of health are thought to play a role in the difference in AD prevalence and severity across groups in the United States.16
Health Disparity Highlight
In an analysis of 20 US metropolitan cities, urban and inner-city residence was associated with approximately 1.7-fold increased odds of AD.4 Among pediatric patients with moderate to severe AD, Black children were more likely to be exposed to tobacco smoke17 and traffic-related air pollution.18 Low socioeconomic status and low income also have been associated with moderate16 and severe19 AD. At the same education level, Black individuals in the United States receive less income than their White counterparts and have markedly less wealth at equivalent incomes.20
In utero exposure to maternal stress is associated with AD.4 Increased IgE levels have been recorded in children who develop AD, with Black children having the highest IgE levels overall compared to other children.18
An analysis of medical records from an urban medical center in Baltimore, Maryland, from 2013 through 2018 showed that Black patients with AD were less likely to receive topical corticosteroids, topical calcineurin inhibitors, a topical phosphodiesterase 4 inhibitor, and a biologic compared to White patients with AD.21
Since the disproportionate burden experienced by patients with AD is not physiologic, it is imperative to address these systemic complexities and address the barriers impacting treatment availability to improve health outcomes for all patients living with AD.
- Kaufman BP, Guttman-Yassky E, Alexis AF. Atopic dermatitis in diverse racial and ethnic groups—variations in epidemiology, genetics, clinical presentation and treatment. Exp Dermatol. 2018;27:340-357.
- Lee HH, Patel KR, Singam V, et al. A systematic review and meta-analysis of the prevalence and phenotype of adult-onset atopic dermatitis. J Am Acad Dermatol. 2019;80:1526-1532.E7.
- Adawi W, Cornman H, Kambala A, et al. Diagnosing atopic dermatitis in skin of color. Dermatol Clin. 2023;41:417-429.
- Narla S, Silverberg JI. Current updates in the epidemiology and comorbidities of atopic dermatitis. Ann Allergy Asthma Immunol. 2025;135:511-520.
- Croce EA, Levy ML, Adamson AS, et al. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol. 2021;148:1104-1111.
- Kim Y, Blomberg M, Rifas-Shiman SL, et al. Racial/ethnic differences in incidence and persistence of childhood atopic dermatitis. J Invest Dermatol. 2019;139:827-834.
- Nomura T, Wu J, Kabashima K, et al. Endophenotypic variations of atopic dermatitis by age, race, and ethnicity. J Allergy Clin Immunol. 2020;8:1840-1852.
- McColl M, Boozalis E, Aguh C, et al. Pruritus in Black skin: unique molecular characteristics and clinical features. J Natl Med Assoc. 2021;114:30-38.
- Silverberg JI, Margolis DJ, Boguniewicz M, et al. Distribution of atopic dermatitis lesions in United States adults. J Eur Acad Dermatol Venereol. 2019;33:1341-1348.
- Summey BT, Bowen SE, Allen HB. Lichen planus-like atopic dermatitis: expanding the differential diagnosis of spongiotic dermatitis. J Cutan Pathol. 2008;35:311-314.
- Odhiambo JA, Williams HC, Clayton TO, et al; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124:1251-1258.E23.
- Gallagher K, Halperin-Goldstein S, Paller AS. New treatments in atopic dermatitis update. Ann Allergy Asthma Immunol. 2025;135:498-510.E10.
- Shaw ML. FDA expands roflumilast use for atopic dermatitis to children aged 2 to 5 years. Am J Managed Care. October 6, 2025. Accessed April 30, 2026. https://www.ajmc.com/view/fda-expands -roflumilast-use-for-atopic-dermatitis-to-children-aged-2-to-5-years
- Eichenfield LF, Stein Gold LF, Simpson EL, et al. Efficacy and safety of ruxolitinib cream in children aged 2 to 11 years with atopic dermatitis: results from TRuE-AD3, a phase 3, randomized double-blind study. J Am Acad of Dermatol. 2025;93:689-698.
- Heath CR, Dosono B, Shi VY, et al. Variability in skin tone changes by race and ethnicity among US adults with atopic dermatitis. Presented at: Skin of Color Update 2024, September 13-15, 2024, New York, NY.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Narla S, Silverberg JI. The role of environmental exposures in atopic dermatitis. Curr Allergy Asthma Rep. 2020;20:74.
- Bauer SJ, Spoer BR, Ehrman R, et al. A systematic review of historic neighborhood redlining and contemporary health outcomes. Public Health. 2025;238:181-187.
- Chung J, Simpson EL. The socioeconomics of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;122:360-366.
- Martinez A, de la Rosa R, Mujahid M, et al. Structural racism and its pathways to asthma and atopic dermatitis. J Allergy Clin Immunol. 2021;148:1112-1120.
- Bell MA, Whang KA, Thomas J, et al. Racial and ethnic disparities in access to emerging and frontline therapies in common dermatological conditions: a cross-sectional study. J Natl Med Assoc. 2020;112:650-653.
Atopic dermatitis (AD) is a chronic skin condition generally characterized by pruritic and erythematous papules and plaques.1 While AD commonly manifests in childhood, 1 in 4 patients living with AD report adult onset of the disease.2 The clinical presentation and prevalence of AD vary across age groups, skin tones, and racial and ethnic groups. Globally, AD is estimated to have a prevalence of 2.6%; however, rates vary widely by region.1 Morphology and distribution of AD lesions also vary by population; therefore, defining one classic presentation of AD is not sufficient in diverse patient populations.3
Epidemiology
The prevalence of AD ranges from 0.2% to 24.6% worldwide, with higher rates in Africa and Oceania and lower rates in India and Northern and Eastern Europe.1 In the United States, AD affects all racial and ethnic groups; however, prevalence and severity are increased in Black children compared with White children.4 In one prospective cohort study, Hispanic children and non-Hispanic Black children aged 3 years and younger had greater odds of AD persisting into mid childhood (approximately age 7 years) compared with non-Hispanic White children.5,6
Key Clinical Features
Clinical features of AD are heterogeneous and may include differences in color, morphology, and distribution. Brown, hyperpigmented, gray, and/or violaceous plaques may predominate in patients with skin of color (SOC) compared with the erythematous plaques commonly described in lighter skin tones.1,3 Established scoring systems for AD rely on erythema as a key diagnostic feature, but because erythema can be difficult to detect in darker skin tones, disease severity may be underestimated and diagnosis may be delayed in this population.4
Atopic dermatitis in SOC may manifest as lichenoid plaques,7 prurigo nodules,7,8 lichenification,1 and follicular accentuation.9 Lichen planus–like AD is a distinct variant characterized by lichenoid plaques with a predilection for the extensor surfaces and face in patients with darker skin tones1,8 occurring in approximately 9% of patients in one study.10
Other key clinical features of AD in patients with SOC include pityriasis alba,10 increased risk for postinflammatory pigment alteration (including hyperpigmentation and/or hypopigmentation),1 and greater trunk and extensor involvement.1,11
Worth Noting
The scientific landscape for AD has grown rapidly, increasing our understanding of its pathophysiology, treatment, and social impact. Nonsteroidal treatments available for pediatric and adult patients with AD have increased in recent years, including crisaborole (approved for use in those ages ≥3 months), tacrolimus (≥2 years), and pimecrolimus (≥2 years). Injectable options include dupilumab (≥6 months), lebrikizumab (≥12 years), nemolizumab (≥12 years), and tralokinumab (≥12 years). Oral options include abrocitinib (≥12 years) and upadacitinib (≥12 years).12 Topical options include roflumilast 0.15% cream (≥6 years)12 and 0.05% cream (≥2-5 years),13 ruxolitinib 1.5% cream (≥2 years),14 and tapinarof 1% cream (≥2 years).12
For some patients, postinflammatory pigment alteration associated with AD has a higher impact on quality of life than the AD itself.7 In a study of 260 US adults with AD, the emotional impact of pigmentary changes was greatest in Black patients, with 53.3% reporting that pigment changes bothered them “a lot” or “very much.”15
Genome-wide association studies have not identified a single determinant that explains racial and ethnic differences in susceptibility to AD.4 Instead, social determinants of health are thought to play a role in the difference in AD prevalence and severity across groups in the United States.16
Health Disparity Highlight
In an analysis of 20 US metropolitan cities, urban and inner-city residence was associated with approximately 1.7-fold increased odds of AD.4 Among pediatric patients with moderate to severe AD, Black children were more likely to be exposed to tobacco smoke17 and traffic-related air pollution.18 Low socioeconomic status and low income also have been associated with moderate16 and severe19 AD. At the same education level, Black individuals in the United States receive less income than their White counterparts and have markedly less wealth at equivalent incomes.20
In utero exposure to maternal stress is associated with AD.4 Increased IgE levels have been recorded in children who develop AD, with Black children having the highest IgE levels overall compared to other children.18
An analysis of medical records from an urban medical center in Baltimore, Maryland, from 2013 through 2018 showed that Black patients with AD were less likely to receive topical corticosteroids, topical calcineurin inhibitors, a topical phosphodiesterase 4 inhibitor, and a biologic compared to White patients with AD.21
Since the disproportionate burden experienced by patients with AD is not physiologic, it is imperative to address these systemic complexities and address the barriers impacting treatment availability to improve health outcomes for all patients living with AD.
Atopic dermatitis (AD) is a chronic skin condition generally characterized by pruritic and erythematous papules and plaques.1 While AD commonly manifests in childhood, 1 in 4 patients living with AD report adult onset of the disease.2 The clinical presentation and prevalence of AD vary across age groups, skin tones, and racial and ethnic groups. Globally, AD is estimated to have a prevalence of 2.6%; however, rates vary widely by region.1 Morphology and distribution of AD lesions also vary by population; therefore, defining one classic presentation of AD is not sufficient in diverse patient populations.3
Epidemiology
The prevalence of AD ranges from 0.2% to 24.6% worldwide, with higher rates in Africa and Oceania and lower rates in India and Northern and Eastern Europe.1 In the United States, AD affects all racial and ethnic groups; however, prevalence and severity are increased in Black children compared with White children.4 In one prospective cohort study, Hispanic children and non-Hispanic Black children aged 3 years and younger had greater odds of AD persisting into mid childhood (approximately age 7 years) compared with non-Hispanic White children.5,6
Key Clinical Features
Clinical features of AD are heterogeneous and may include differences in color, morphology, and distribution. Brown, hyperpigmented, gray, and/or violaceous plaques may predominate in patients with skin of color (SOC) compared with the erythematous plaques commonly described in lighter skin tones.1,3 Established scoring systems for AD rely on erythema as a key diagnostic feature, but because erythema can be difficult to detect in darker skin tones, disease severity may be underestimated and diagnosis may be delayed in this population.4
Atopic dermatitis in SOC may manifest as lichenoid plaques,7 prurigo nodules,7,8 lichenification,1 and follicular accentuation.9 Lichen planus–like AD is a distinct variant characterized by lichenoid plaques with a predilection for the extensor surfaces and face in patients with darker skin tones1,8 occurring in approximately 9% of patients in one study.10
Other key clinical features of AD in patients with SOC include pityriasis alba,10 increased risk for postinflammatory pigment alteration (including hyperpigmentation and/or hypopigmentation),1 and greater trunk and extensor involvement.1,11
Worth Noting
The scientific landscape for AD has grown rapidly, increasing our understanding of its pathophysiology, treatment, and social impact. Nonsteroidal treatments available for pediatric and adult patients with AD have increased in recent years, including crisaborole (approved for use in those ages ≥3 months), tacrolimus (≥2 years), and pimecrolimus (≥2 years). Injectable options include dupilumab (≥6 months), lebrikizumab (≥12 years), nemolizumab (≥12 years), and tralokinumab (≥12 years). Oral options include abrocitinib (≥12 years) and upadacitinib (≥12 years).12 Topical options include roflumilast 0.15% cream (≥6 years)12 and 0.05% cream (≥2-5 years),13 ruxolitinib 1.5% cream (≥2 years),14 and tapinarof 1% cream (≥2 years).12
For some patients, postinflammatory pigment alteration associated with AD has a higher impact on quality of life than the AD itself.7 In a study of 260 US adults with AD, the emotional impact of pigmentary changes was greatest in Black patients, with 53.3% reporting that pigment changes bothered them “a lot” or “very much.”15
Genome-wide association studies have not identified a single determinant that explains racial and ethnic differences in susceptibility to AD.4 Instead, social determinants of health are thought to play a role in the difference in AD prevalence and severity across groups in the United States.16
Health Disparity Highlight
In an analysis of 20 US metropolitan cities, urban and inner-city residence was associated with approximately 1.7-fold increased odds of AD.4 Among pediatric patients with moderate to severe AD, Black children were more likely to be exposed to tobacco smoke17 and traffic-related air pollution.18 Low socioeconomic status and low income also have been associated with moderate16 and severe19 AD. At the same education level, Black individuals in the United States receive less income than their White counterparts and have markedly less wealth at equivalent incomes.20
In utero exposure to maternal stress is associated with AD.4 Increased IgE levels have been recorded in children who develop AD, with Black children having the highest IgE levels overall compared to other children.18
An analysis of medical records from an urban medical center in Baltimore, Maryland, from 2013 through 2018 showed that Black patients with AD were less likely to receive topical corticosteroids, topical calcineurin inhibitors, a topical phosphodiesterase 4 inhibitor, and a biologic compared to White patients with AD.21
Since the disproportionate burden experienced by patients with AD is not physiologic, it is imperative to address these systemic complexities and address the barriers impacting treatment availability to improve health outcomes for all patients living with AD.
- Kaufman BP, Guttman-Yassky E, Alexis AF. Atopic dermatitis in diverse racial and ethnic groups—variations in epidemiology, genetics, clinical presentation and treatment. Exp Dermatol. 2018;27:340-357.
- Lee HH, Patel KR, Singam V, et al. A systematic review and meta-analysis of the prevalence and phenotype of adult-onset atopic dermatitis. J Am Acad Dermatol. 2019;80:1526-1532.E7.
- Adawi W, Cornman H, Kambala A, et al. Diagnosing atopic dermatitis in skin of color. Dermatol Clin. 2023;41:417-429.
- Narla S, Silverberg JI. Current updates in the epidemiology and comorbidities of atopic dermatitis. Ann Allergy Asthma Immunol. 2025;135:511-520.
- Croce EA, Levy ML, Adamson AS, et al. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol. 2021;148:1104-1111.
- Kim Y, Blomberg M, Rifas-Shiman SL, et al. Racial/ethnic differences in incidence and persistence of childhood atopic dermatitis. J Invest Dermatol. 2019;139:827-834.
- Nomura T, Wu J, Kabashima K, et al. Endophenotypic variations of atopic dermatitis by age, race, and ethnicity. J Allergy Clin Immunol. 2020;8:1840-1852.
- McColl M, Boozalis E, Aguh C, et al. Pruritus in Black skin: unique molecular characteristics and clinical features. J Natl Med Assoc. 2021;114:30-38.
- Silverberg JI, Margolis DJ, Boguniewicz M, et al. Distribution of atopic dermatitis lesions in United States adults. J Eur Acad Dermatol Venereol. 2019;33:1341-1348.
- Summey BT, Bowen SE, Allen HB. Lichen planus-like atopic dermatitis: expanding the differential diagnosis of spongiotic dermatitis. J Cutan Pathol. 2008;35:311-314.
- Odhiambo JA, Williams HC, Clayton TO, et al; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124:1251-1258.E23.
- Gallagher K, Halperin-Goldstein S, Paller AS. New treatments in atopic dermatitis update. Ann Allergy Asthma Immunol. 2025;135:498-510.E10.
- Shaw ML. FDA expands roflumilast use for atopic dermatitis to children aged 2 to 5 years. Am J Managed Care. October 6, 2025. Accessed April 30, 2026. https://www.ajmc.com/view/fda-expands -roflumilast-use-for-atopic-dermatitis-to-children-aged-2-to-5-years
- Eichenfield LF, Stein Gold LF, Simpson EL, et al. Efficacy and safety of ruxolitinib cream in children aged 2 to 11 years with atopic dermatitis: results from TRuE-AD3, a phase 3, randomized double-blind study. J Am Acad of Dermatol. 2025;93:689-698.
- Heath CR, Dosono B, Shi VY, et al. Variability in skin tone changes by race and ethnicity among US adults with atopic dermatitis. Presented at: Skin of Color Update 2024, September 13-15, 2024, New York, NY.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Narla S, Silverberg JI. The role of environmental exposures in atopic dermatitis. Curr Allergy Asthma Rep. 2020;20:74.
- Bauer SJ, Spoer BR, Ehrman R, et al. A systematic review of historic neighborhood redlining and contemporary health outcomes. Public Health. 2025;238:181-187.
- Chung J, Simpson EL. The socioeconomics of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;122:360-366.
- Martinez A, de la Rosa R, Mujahid M, et al. Structural racism and its pathways to asthma and atopic dermatitis. J Allergy Clin Immunol. 2021;148:1112-1120.
- Bell MA, Whang KA, Thomas J, et al. Racial and ethnic disparities in access to emerging and frontline therapies in common dermatological conditions: a cross-sectional study. J Natl Med Assoc. 2020;112:650-653.
- Kaufman BP, Guttman-Yassky E, Alexis AF. Atopic dermatitis in diverse racial and ethnic groups—variations in epidemiology, genetics, clinical presentation and treatment. Exp Dermatol. 2018;27:340-357.
- Lee HH, Patel KR, Singam V, et al. A systematic review and meta-analysis of the prevalence and phenotype of adult-onset atopic dermatitis. J Am Acad Dermatol. 2019;80:1526-1532.E7.
- Adawi W, Cornman H, Kambala A, et al. Diagnosing atopic dermatitis in skin of color. Dermatol Clin. 2023;41:417-429.
- Narla S, Silverberg JI. Current updates in the epidemiology and comorbidities of atopic dermatitis. Ann Allergy Asthma Immunol. 2025;135:511-520.
- Croce EA, Levy ML, Adamson AS, et al. Reframing racial and ethnic disparities in atopic dermatitis in Black and Latinx populations. J Allergy Clin Immunol. 2021;148:1104-1111.
- Kim Y, Blomberg M, Rifas-Shiman SL, et al. Racial/ethnic differences in incidence and persistence of childhood atopic dermatitis. J Invest Dermatol. 2019;139:827-834.
- Nomura T, Wu J, Kabashima K, et al. Endophenotypic variations of atopic dermatitis by age, race, and ethnicity. J Allergy Clin Immunol. 2020;8:1840-1852.
- McColl M, Boozalis E, Aguh C, et al. Pruritus in Black skin: unique molecular characteristics and clinical features. J Natl Med Assoc. 2021;114:30-38.
- Silverberg JI, Margolis DJ, Boguniewicz M, et al. Distribution of atopic dermatitis lesions in United States adults. J Eur Acad Dermatol Venereol. 2019;33:1341-1348.
- Summey BT, Bowen SE, Allen HB. Lichen planus-like atopic dermatitis: expanding the differential diagnosis of spongiotic dermatitis. J Cutan Pathol. 2008;35:311-314.
- Odhiambo JA, Williams HC, Clayton TO, et al; ISAAC Phase Three Study Group. Global variations in prevalence of eczema symptoms in children from ISAAC Phase Three. J Allergy Clin Immunol. 2009;124:1251-1258.E23.
- Gallagher K, Halperin-Goldstein S, Paller AS. New treatments in atopic dermatitis update. Ann Allergy Asthma Immunol. 2025;135:498-510.E10.
- Shaw ML. FDA expands roflumilast use for atopic dermatitis to children aged 2 to 5 years. Am J Managed Care. October 6, 2025. Accessed April 30, 2026. https://www.ajmc.com/view/fda-expands -roflumilast-use-for-atopic-dermatitis-to-children-aged-2-to-5-years
- Eichenfield LF, Stein Gold LF, Simpson EL, et al. Efficacy and safety of ruxolitinib cream in children aged 2 to 11 years with atopic dermatitis: results from TRuE-AD3, a phase 3, randomized double-blind study. J Am Acad of Dermatol. 2025;93:689-698.
- Heath CR, Dosono B, Shi VY, et al. Variability in skin tone changes by race and ethnicity among US adults with atopic dermatitis. Presented at: Skin of Color Update 2024, September 13-15, 2024, New York, NY.
- Tackett KJ, Jenkins F, Morrell DS, et al. Structural racism and its influence on the severity of atopic dermatitis in African American children. Pediatr Dermatol. 2020;37:142-146.
- Narla S, Silverberg JI. The role of environmental exposures in atopic dermatitis. Curr Allergy Asthma Rep. 2020;20:74.
- Bauer SJ, Spoer BR, Ehrman R, et al. A systematic review of historic neighborhood redlining and contemporary health outcomes. Public Health. 2025;238:181-187.
- Chung J, Simpson EL. The socioeconomics of atopic dermatitis. Ann Allergy Asthma Immunol. 2019;122:360-366.
- Martinez A, de la Rosa R, Mujahid M, et al. Structural racism and its pathways to asthma and atopic dermatitis. J Allergy Clin Immunol. 2021;148:1112-1120.
- Bell MA, Whang KA, Thomas J, et al. Racial and ethnic disparities in access to emerging and frontline therapies in common dermatological conditions: a cross-sectional study. J Natl Med Assoc. 2020;112:650-653.
Atopic Dermatitis: New Insights and Expanded Treatment Options
Atopic Dermatitis: New Insights and Expanded Treatment Options

Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
The new coding guidelines for evaluation and management services have simplified coding by focusing on medical decision-making (MDM), but practicing clinicians often have questions about how to apply the rules. This article will focus on common mistakes and nuances clarified in communications from the American Medical Association. As before, the highest level of service in 2 of 3 categories—complexity, data, and risk—determine the level of service. Only medically necessary services should be reported, and all reported codes should accurately reflect the services provided.
Key Clarifications to MDM Criteria
Important clarifications that came after the initial distribution of the new coding rules include the following:
- An established problem not at treatment target requiring ongoing MDM counts as moderate complexity in column 1.
- Under the category of risk, prescription drug therapy includes discussion of risks, benefits, and alternatives with a decision to start, stop, or continue a prescription medication; this differs from a simple refill that does not require evaluation, discussion, and shared decision-making.
- Social determinants of health that are medically appropriate to address during the visit are considered moderate under the category of risk. These include issues that directly affect patient management (eg, transportation access, medication affordability, cultural norms, restrictions) and other factors influencing health and well-being (eg, income, education, occupation, environmental change, unemployment, working conditions, social support) when they impact the patient’s condition and inform treatment decisions.
- Independent interpretation of a laboratory test counts as moderate under the category of data; an example would be a biopsy reported as “consistent with lupus erythematosus” in a patient with a heliotrope rash and shawl sign, which may require clinicopathologic correlation and reinterpretation as “diagnostic of dermatomyositis.”
- The decision to perform a 0- or 10-day global procedure on the same date of service as the visit is already bundled in payment for the procedure and should not be reported as a separate service; however, if scheduled for a future date of service, it counts as low under the risk category if the patient has no unique risk factors or moderate if the patient does have unique risk factors that weigh into MDM. In contrast, the decision to perform a 90-day global procedure is reportable even on the same date of service (with modifier 57) and counts as moderate risk without unique risk factors and high with such factors.
Application of MDM Coding in Common Dermatology Encounters
Let’s look at some common scenarios and how they should be coded.
A patient presents with a new lesion of concern. On physical examination, it is a stuck-on keratotic papule with no inflammation, and you reassure them that it is merely a benign seborrheic keratosis. This encounter would be coded as straightforward MDM (level 2, new or established), reflecting the evaluation of a single minor problem.
A patient returns with localized eczema and is doing very well with triamcinolone cream applied as needed, and you simply refill the prescription. This encounter represents low-level MDM (level 3, established), reflecting a single stable problem managed with a simple prescription refill.
A patient presents with psoriasis that has had some response to topical therapy but is clearly not at target, and the patient now reports axial joint stiffness that is much worse in the morning and takes more than 30 minutes to resolve. You discuss risks, benefits, and alternatives; note that the patient already had recent screening for tuberculosis and other infectious diseases; and prescribe a T-helper 17 biologic because of the axial arthritis. This encounter represents moderate-level MDM (level 4, established), reflecting both a problem not at target and a new problem of uncertain prognosis under complexity, as well as shared decision-making to initiate prescription drug therapy under risk. Although review or ordering of 3 laboratory tests would also meet moderate criteria under data, only 2 of the 3 domains are required to establish the level of service.
A patient presents with a severe flare of eczema that requires treatment with cyclosporine. This encounter represents high-level MDM (level 5, established), reflecting a severe exacerbation of an existing condition requiring a high-risk medication with at least quarterly laboratory monitoring and uncertainty regarding long-term therapy needs.
Application of Moderate and High MDM in Dermatology
Many dermatology patients present with multiple problems, and the visit often falls into the moderate category for column 1 (complexity) of MDM (level 4, new or established). Under complexity, moderate could be 2 stable problems, one worsening problem, one new problem of uncertain prognosis, or one problem improved but not at target. Remember that moderate MDM also must be established in a second category, such as risk. Under the risk category, moderate could include prescription drug therapy, addressing a relevant social determinant of health, the decision to perform a 0- or 10-day global procedure not performed on the same date of service with unique patient risk factors, or the decision to perform a 90-day global procedure in a patient with no unique risk factors.
Don’t forget the data category, as it often is relevant to determining the correct level of service. Moderate under the data category includes review or ordering of 3 laboratory tests (a complete metabolic panel is a single laboratory test, and a complete blood count is a single laboratory test), independent interpretation of a laboratory test, or a phone call to another provider caring for the patient with a medically necessary discussion of management (eg, severe eczema in a patient on a calcium channel blocker—you call the primary care physician advising that calcium-channel blockers are the most common cause of eczematous drug eruption and advise a change in therapy). If 2 of the above categories were necessary (eg, order 3 laboratory tests and call the primary care physician), that would count as high MDM under the data category. Remember, 2 categories are required to establish the level of service.
Other examples of high MDM (level 5, new or established) include a new diagnosis with major risk to life or limb plus one of the following: high-risk medication requiring at least quarterly drug monitoring, the decision to perform a 90-day global surgery with documented additional patient risk factors, or the decision to admit to the hospital (eg, new invasive melanoma with excision and decision to perform adjacent tissue transfer in a patient who takes aspirin).
Final Thoughts
Physicians should perform medically necessary services that are in the best interest of their patients. Current coding rules focus on the complexity, risk, and data associated with MDM.
The new coding guidelines for evaluation and management services have simplified coding by focusing on medical decision-making (MDM), but practicing clinicians often have questions about how to apply the rules. This article will focus on common mistakes and nuances clarified in communications from the American Medical Association. As before, the highest level of service in 2 of 3 categories—complexity, data, and risk—determine the level of service. Only medically necessary services should be reported, and all reported codes should accurately reflect the services provided.
Key Clarifications to MDM Criteria
Important clarifications that came after the initial distribution of the new coding rules include the following:
- An established problem not at treatment target requiring ongoing MDM counts as moderate complexity in column 1.
- Under the category of risk, prescription drug therapy includes discussion of risks, benefits, and alternatives with a decision to start, stop, or continue a prescription medication; this differs from a simple refill that does not require evaluation, discussion, and shared decision-making.
- Social determinants of health that are medically appropriate to address during the visit are considered moderate under the category of risk. These include issues that directly affect patient management (eg, transportation access, medication affordability, cultural norms, restrictions) and other factors influencing health and well-being (eg, income, education, occupation, environmental change, unemployment, working conditions, social support) when they impact the patient’s condition and inform treatment decisions.
- Independent interpretation of a laboratory test counts as moderate under the category of data; an example would be a biopsy reported as “consistent with lupus erythematosus” in a patient with a heliotrope rash and shawl sign, which may require clinicopathologic correlation and reinterpretation as “diagnostic of dermatomyositis.”
- The decision to perform a 0- or 10-day global procedure on the same date of service as the visit is already bundled in payment for the procedure and should not be reported as a separate service; however, if scheduled for a future date of service, it counts as low under the risk category if the patient has no unique risk factors or moderate if the patient does have unique risk factors that weigh into MDM. In contrast, the decision to perform a 90-day global procedure is reportable even on the same date of service (with modifier 57) and counts as moderate risk without unique risk factors and high with such factors.
Application of MDM Coding in Common Dermatology Encounters
Let’s look at some common scenarios and how they should be coded.
A patient presents with a new lesion of concern. On physical examination, it is a stuck-on keratotic papule with no inflammation, and you reassure them that it is merely a benign seborrheic keratosis. This encounter would be coded as straightforward MDM (level 2, new or established), reflecting the evaluation of a single minor problem.
A patient returns with localized eczema and is doing very well with triamcinolone cream applied as needed, and you simply refill the prescription. This encounter represents low-level MDM (level 3, established), reflecting a single stable problem managed with a simple prescription refill.
A patient presents with psoriasis that has had some response to topical therapy but is clearly not at target, and the patient now reports axial joint stiffness that is much worse in the morning and takes more than 30 minutes to resolve. You discuss risks, benefits, and alternatives; note that the patient already had recent screening for tuberculosis and other infectious diseases; and prescribe a T-helper 17 biologic because of the axial arthritis. This encounter represents moderate-level MDM (level 4, established), reflecting both a problem not at target and a new problem of uncertain prognosis under complexity, as well as shared decision-making to initiate prescription drug therapy under risk. Although review or ordering of 3 laboratory tests would also meet moderate criteria under data, only 2 of the 3 domains are required to establish the level of service.
A patient presents with a severe flare of eczema that requires treatment with cyclosporine. This encounter represents high-level MDM (level 5, established), reflecting a severe exacerbation of an existing condition requiring a high-risk medication with at least quarterly laboratory monitoring and uncertainty regarding long-term therapy needs.
Application of Moderate and High MDM in Dermatology
Many dermatology patients present with multiple problems, and the visit often falls into the moderate category for column 1 (complexity) of MDM (level 4, new or established). Under complexity, moderate could be 2 stable problems, one worsening problem, one new problem of uncertain prognosis, or one problem improved but not at target. Remember that moderate MDM also must be established in a second category, such as risk. Under the risk category, moderate could include prescription drug therapy, addressing a relevant social determinant of health, the decision to perform a 0- or 10-day global procedure not performed on the same date of service with unique patient risk factors, or the decision to perform a 90-day global procedure in a patient with no unique risk factors.
Don’t forget the data category, as it often is relevant to determining the correct level of service. Moderate under the data category includes review or ordering of 3 laboratory tests (a complete metabolic panel is a single laboratory test, and a complete blood count is a single laboratory test), independent interpretation of a laboratory test, or a phone call to another provider caring for the patient with a medically necessary discussion of management (eg, severe eczema in a patient on a calcium channel blocker—you call the primary care physician advising that calcium-channel blockers are the most common cause of eczematous drug eruption and advise a change in therapy). If 2 of the above categories were necessary (eg, order 3 laboratory tests and call the primary care physician), that would count as high MDM under the data category. Remember, 2 categories are required to establish the level of service.
Other examples of high MDM (level 5, new or established) include a new diagnosis with major risk to life or limb plus one of the following: high-risk medication requiring at least quarterly drug monitoring, the decision to perform a 90-day global surgery with documented additional patient risk factors, or the decision to admit to the hospital (eg, new invasive melanoma with excision and decision to perform adjacent tissue transfer in a patient who takes aspirin).
Final Thoughts
Physicians should perform medically necessary services that are in the best interest of their patients. Current coding rules focus on the complexity, risk, and data associated with MDM.
The new coding guidelines for evaluation and management services have simplified coding by focusing on medical decision-making (MDM), but practicing clinicians often have questions about how to apply the rules. This article will focus on common mistakes and nuances clarified in communications from the American Medical Association. As before, the highest level of service in 2 of 3 categories—complexity, data, and risk—determine the level of service. Only medically necessary services should be reported, and all reported codes should accurately reflect the services provided.
Key Clarifications to MDM Criteria
Important clarifications that came after the initial distribution of the new coding rules include the following:
- An established problem not at treatment target requiring ongoing MDM counts as moderate complexity in column 1.
- Under the category of risk, prescription drug therapy includes discussion of risks, benefits, and alternatives with a decision to start, stop, or continue a prescription medication; this differs from a simple refill that does not require evaluation, discussion, and shared decision-making.
- Social determinants of health that are medically appropriate to address during the visit are considered moderate under the category of risk. These include issues that directly affect patient management (eg, transportation access, medication affordability, cultural norms, restrictions) and other factors influencing health and well-being (eg, income, education, occupation, environmental change, unemployment, working conditions, social support) when they impact the patient’s condition and inform treatment decisions.
- Independent interpretation of a laboratory test counts as moderate under the category of data; an example would be a biopsy reported as “consistent with lupus erythematosus” in a patient with a heliotrope rash and shawl sign, which may require clinicopathologic correlation and reinterpretation as “diagnostic of dermatomyositis.”
- The decision to perform a 0- or 10-day global procedure on the same date of service as the visit is already bundled in payment for the procedure and should not be reported as a separate service; however, if scheduled for a future date of service, it counts as low under the risk category if the patient has no unique risk factors or moderate if the patient does have unique risk factors that weigh into MDM. In contrast, the decision to perform a 90-day global procedure is reportable even on the same date of service (with modifier 57) and counts as moderate risk without unique risk factors and high with such factors.
Application of MDM Coding in Common Dermatology Encounters
Let’s look at some common scenarios and how they should be coded.
A patient presents with a new lesion of concern. On physical examination, it is a stuck-on keratotic papule with no inflammation, and you reassure them that it is merely a benign seborrheic keratosis. This encounter would be coded as straightforward MDM (level 2, new or established), reflecting the evaluation of a single minor problem.
A patient returns with localized eczema and is doing very well with triamcinolone cream applied as needed, and you simply refill the prescription. This encounter represents low-level MDM (level 3, established), reflecting a single stable problem managed with a simple prescription refill.
A patient presents with psoriasis that has had some response to topical therapy but is clearly not at target, and the patient now reports axial joint stiffness that is much worse in the morning and takes more than 30 minutes to resolve. You discuss risks, benefits, and alternatives; note that the patient already had recent screening for tuberculosis and other infectious diseases; and prescribe a T-helper 17 biologic because of the axial arthritis. This encounter represents moderate-level MDM (level 4, established), reflecting both a problem not at target and a new problem of uncertain prognosis under complexity, as well as shared decision-making to initiate prescription drug therapy under risk. Although review or ordering of 3 laboratory tests would also meet moderate criteria under data, only 2 of the 3 domains are required to establish the level of service.
A patient presents with a severe flare of eczema that requires treatment with cyclosporine. This encounter represents high-level MDM (level 5, established), reflecting a severe exacerbation of an existing condition requiring a high-risk medication with at least quarterly laboratory monitoring and uncertainty regarding long-term therapy needs.
Application of Moderate and High MDM in Dermatology
Many dermatology patients present with multiple problems, and the visit often falls into the moderate category for column 1 (complexity) of MDM (level 4, new or established). Under complexity, moderate could be 2 stable problems, one worsening problem, one new problem of uncertain prognosis, or one problem improved but not at target. Remember that moderate MDM also must be established in a second category, such as risk. Under the risk category, moderate could include prescription drug therapy, addressing a relevant social determinant of health, the decision to perform a 0- or 10-day global procedure not performed on the same date of service with unique patient risk factors, or the decision to perform a 90-day global procedure in a patient with no unique risk factors.
Don’t forget the data category, as it often is relevant to determining the correct level of service. Moderate under the data category includes review or ordering of 3 laboratory tests (a complete metabolic panel is a single laboratory test, and a complete blood count is a single laboratory test), independent interpretation of a laboratory test, or a phone call to another provider caring for the patient with a medically necessary discussion of management (eg, severe eczema in a patient on a calcium channel blocker—you call the primary care physician advising that calcium-channel blockers are the most common cause of eczematous drug eruption and advise a change in therapy). If 2 of the above categories were necessary (eg, order 3 laboratory tests and call the primary care physician), that would count as high MDM under the data category. Remember, 2 categories are required to establish the level of service.
Other examples of high MDM (level 5, new or established) include a new diagnosis with major risk to life or limb plus one of the following: high-risk medication requiring at least quarterly drug monitoring, the decision to perform a 90-day global surgery with documented additional patient risk factors, or the decision to admit to the hospital (eg, new invasive melanoma with excision and decision to perform adjacent tissue transfer in a patient who takes aspirin).
Final Thoughts
Physicians should perform medically necessary services that are in the best interest of their patients. Current coding rules focus on the complexity, risk, and data associated with MDM.
Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
Medical Decision-Making in Evaluation and Management Coding: Practical Applications and Key Clarifications
PRACTICE POINTS
- Evaluation and management coding is now based on medical decision-making (MDM), requiring 2 of 3 categories (complexity, data, risk) and strict adherence to medical necessity.
- Moderate MDM includes problems not at target, shared decision-making for prescription therapy (not simple refills), relevant social determinants of health, and independent test interpretation.
- Common errors include misclassifying refills, overlooking the data category, and improperly reporting procedural decisions, especially same-day minor procedures.

Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
Recognizing inflammation in darker skin tones has important implications for diagnosis and management of skin disease, particularly in patients with skin of color.1 In this context, classification systems commonly are used—both in research and clinical practice—to standardize descriptions of skin tone across diverse populations. Fitzpatrick skin type (FST) originally was developed to classify cutaneous response to UV radiation exposure and remains one of the most widely used frameworks in dermatology.2 However, FST often is used beyond its intended purpose as a proxy for differentiating skin color and race.3,4 This mismatch risks obscuring clinically meaningful differences and limiting the accuracy of dermatologic research. Herein, we review the intended use of FST, its limitations in representing skin color and race, and considerations for more accurate characterization of skin pigmentation in clinical practice and research.
Origins and Intended Use of the FST Scale
Fitzpatrick skin type was developed by Thomas B. Fitzpatrick in the 1970s to guide UVA dosing for psoralen plus UVA therapy in patients with psoriasis.5,6 The scale was intended to estimate an individual’s erythematous and pigmentary response to UV exposure.6,7 Early iterations of FST largely were based on lighter skin types, reflecting its initial use in predominantly White populations, which limited representation of the full spectrum of skin tone diversity.5
Clinical, Educational, and Research Limitations of FST
Fitzpatrick skin type now is widely, albeit inaccurately, used in both research and clinical practice as a proxy for skin color and race,7,8 which reflects its ease of use and the lack of standardized alternatives; however, FST does not adequately capture variability in baseline skin pigmentation, undertone, or inflammatory response. These limitations are especially pronounced in phototypes IV to VI, which encompass highly heterogeneous populations. As a result, grouping patients by FST alone to describe skin color and race may obscure important differences and limit meaningful interpretation of clinical and research findings.
Clinically, recognition of dermatologic conditions such as erythema may be more challenging in darker skin tones, in which classic visual cues are less apparent.1,7 Relying on FST to stratify skin color may further compound diagnostic uncertainty by oversimplifying the cutaneous presentation. In addition, treatment decisions, including laser settings and assessment of pigmentary risk, often are guided by FST despite within-group variability.7 Further, educational frameworks that rely heavily on FST may inadequately prepare clinicians to recognize disease across diverse skin tones, contributing to delayed diagnosis and disparities in care in populations with skin of color.
The implications also extend to dermatologic research. Fitzpatrick skin type frequently is used to assess study populations; however, its limited ability to reflect true variation in pigmentation and ethnicity introduces misclassification bias.3,7 The broad FST scale may group heterogeneous populations, obscuring differences in treatment response. As a result, studies relying on FST to represent skin color or race may have reduced generalizability across diverse populations. Importantly, these limitations are not merely conceptual but may contribute to measurable disparities in dermatologic diagnosis and outcomes.
Rethinking Skin Classification Frameworks
Despite these shortcomings, FST remains deeply embedded in dermatology. Its decades-long use has led to widespread familiarity and integration into clinical guidelines, education, and research. At the same time, the absence of a universally accepted alternative has reinforced the continued use of FST as a proxy for skin color and race.
Alternative strategies for characterizing skin pigmentation include objective measures such as spectrophotometry and melanin index assessment.9
Although these approaches may provide more precise quantification of pigmentation, their use may be limited by the need for specialized equipment and reduced feasibility in routine clinical settings. Other proposed approaches incorporate multidimensional factors such as pigmentation, photoreactivity, and genetic ancestry.4 While these techniques represent important advances, none has achieved widespread adoption yet, and each presents challenges related to feasibility and standardization.
In the absence of a single ideal system, a more nuanced approach is needed. Fitzpatrick skin type should be used in the context for which it was designed: estimating UV response. Incorporating additional descriptors, including self-identified race and ethnicity, alongside more detailed assessments of pigmentation may improve the accuracy and relevance of both clinical evaluation and research. Combining FST with more precise and inclusive frameworks represents a pragmatic step toward better reflecting patient diversity.
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
- Taylor SC. Recognizing erythema in skin of color. J Am Acad Dermatol.
- Fitzpatrick TB. The validity and practicality of sun-reactive skin types I through VI. Arch Dermatol. 1988;124:869-871. doi:10.1001 /archderm.124.6.869
- Eilers S, Bach DQ, Gaber R, et al. Accuracy of self-reported Fitzpatrick skin phototype classification in US Hispanic and Latino populations. JAMA Dermatol. 2013;149:797-803. doi:10.1001 /jamadermatol.2013.4091
- Del Bino S, Bernerd F. Variations in skin colour and the biological consequences of ultraviolet radiation exposure. Br J Dermatol. 2013;169(S3):33-40. doi:10.1111/bjd.12529
- Goon P, Banfield C, Bello O, et al. Skin cancers in skin types IV–VI: does the Fitzpatrick scale give a false sense of security? Clin Exp Dermatol. 2022;47:1112-1117. doi:10.1002/ski2.40
- Fitzpatrick TB. Soleil et peau. J Med Asthet. 1975;2:33-34.
- Ware OR, Dawson JE, Shinohara MM, et al. Racial limitations of Fitzpatrick skin type. Cutis. 2020;105:77-80.
- Lester JC, Taylor SC, Chren MM. Under-representation of skin of colour in dermatology images: not just an educational issue. Br J Dermatol. 2019;180:1521-1522. doi:10.1111/bjd.17608
- Fullerton A, Fischer T, Lahti A, et al. Guidelines for measurement of skin colour and erythema. a report from the Standardization Group of the European Society of Contact Dermatitis. Contact Dermatitis. 1996;35:1-10. doi:10.1111/j.1600-0536.1996.tb02242.x
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race
Limitations of Fitzpatrick Skin Type as a Proxy for Skin Color and Race

Exophytic Papule on the Hand
Exophytic Papule on the Hand
THE DIAGNOSIS: Kaposi Sarcoma
Histopathology revealed a serum crust on the surface of the specimen, and the dermis contained compact collections of spindled cells with interspersed erythrocytes (Figure 1). Human herpesvirus 8–stained sections highlighted many lesional cell nuclei (Figure 2). A diagnosis of Kaposi sarcoma (KS) was made based on these findings. The patient expressed interest in surgical excision; however, he was lost to follow-up.
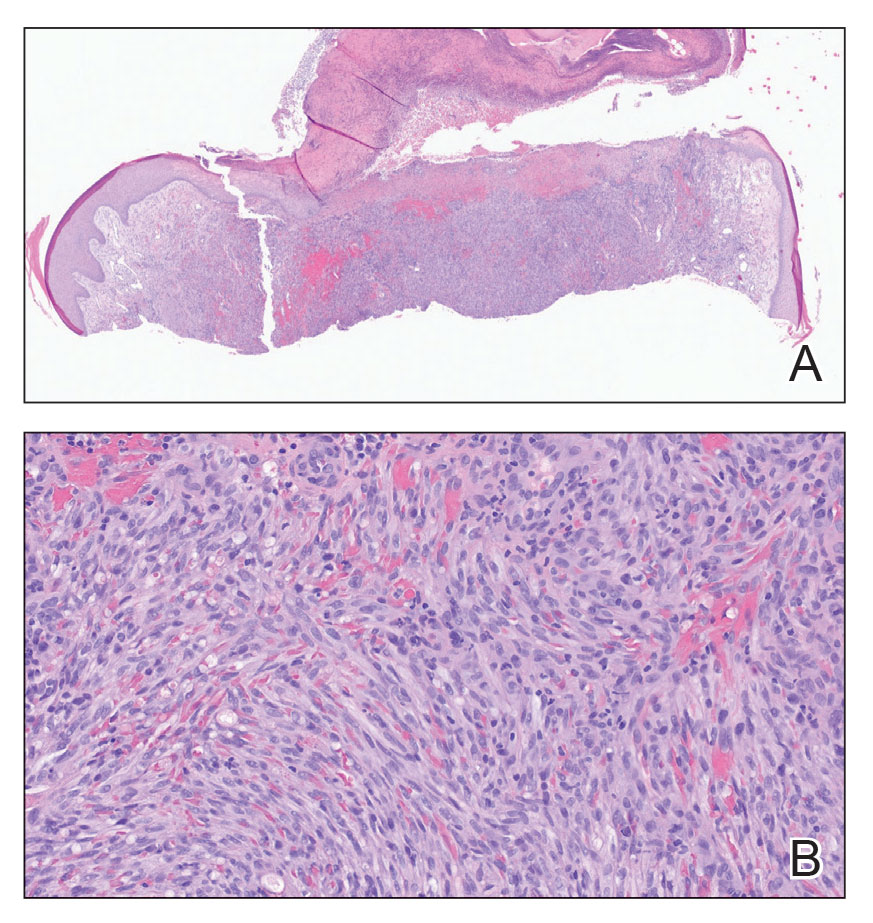
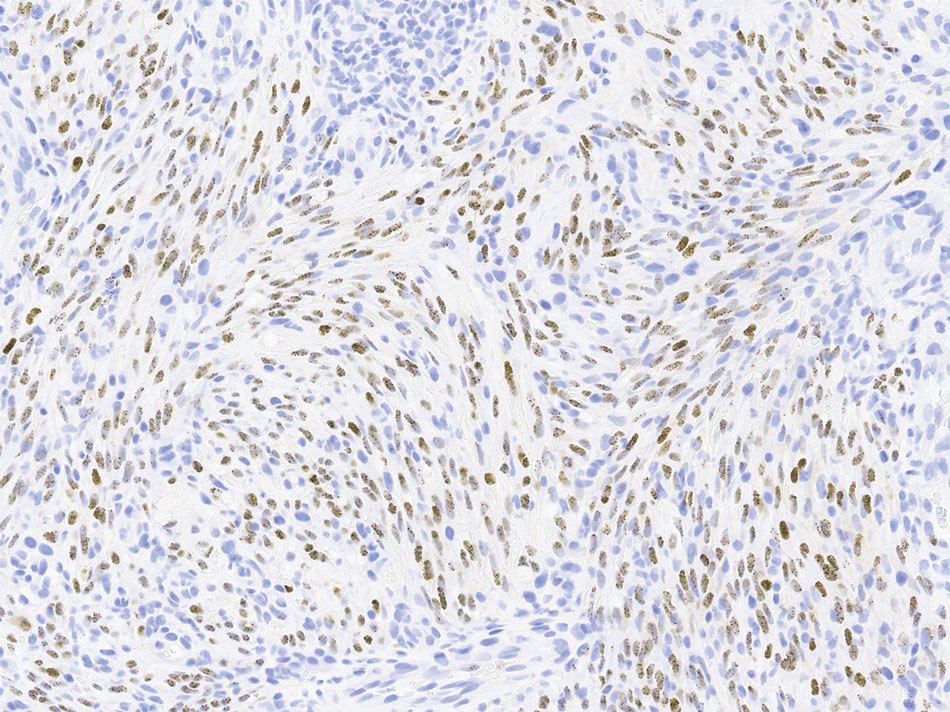
Kaposi sarcoma is an indolent, multifocal, angioproliferative tumor that predominantly affects mucocutaneous sites with less frequent involvement of visceral organs. Kaposi sarcoma is categorized into 4 subtypes: epidemic, iatrogenic, endemic, and classic. Human herpesvirus 8, primarily transmitted through saliva or sexual contact, plays a central role in the pathogenesis of KS, as it drives disease development across all subtypes. The virus causes proliferation of endothelial cells and the formation of angioproliferative lesions characteristic of KS.1
Prevalence is highest in the epidemic subtype, in which patients with advanced HIV and low CD4 T-cell counts may develop KS lesions. Although KS is associated most commonly with HIV, it also has been observed in men who have sex with men regardless of their HIV status.2 Patients undergoing immunosuppressive therapy also may not maintain immune tolerance to previously or newly acquired human herpesvirus 8, leading to the development of iatrogenic KS. This subtype particularly manifests in patients receiving therapy for autoimmune conditions or organ transplants and often only regresses if immunosuppressive therapy is withdrawn.3,4
The endemic and classic subtypes of KS may occur in patients without any known immunocompromise. Endemic KS demonstrates a predilection for pediatric populations in Africa and exhibits less pronounced sex disparity.5 In Uganda and Zimbabwe, endemic KS is the leading cancer in men and the second most frequently occurring cancer in women.6 In contrast, classic KS generally affects older men of Eastern European and Mediterranean descent or Ashkenazi Jewish ancestry. Patients with classic KS generally exhibit a less aggressive disease trajectory relative to other subtypes; however, these patients have a substantial risk for a secondary hematologic malignancy, which may already coexist at the time of diagnosis or emerge subsequently.1,7
Our patient, a native of Eastern Europe, was negative for HIV and was in a monogamous relationship with his wife; therefore, he was likely to have had the classic subtype of KS. As KS is a multifocal disease, lesions may independently emerge at different times and locations on the body. Our patient presented with a new lesion on the hand several years after excision of a similar lesion on the face. Lesions suspicious for KS include slow-growing, painless, red or violaceous patches, nodules, plaques, or patches on the extremities, most commonly manifesting on the feet and ankles. Our differential diagnosis included pyogenic granuloma, amelanotic melanoma, squamous cell carcinoma, and angiosarcoma.
The prognosis in patients with classic KS is favorable, as it often is limited to cutaneous sites and less commonly manifests on visceral organs. Nonetheless, pulmonary and gastrointestinal involvement manifesting as hemoptysis and rectal bleeding, respectively, can occur. This underscores the potential for more serious complications in instances with visceral involvement. Treatment focuses on managing symptoms and preventing growth and progression of individual lesions. Additionally, treatment strategies aim to improve cosmetic outcomes and address any underlying immunosuppression that may exacerbate the condition.8
For most patients, local therapies such as surgical excision, cryotherapy, laser therapy, or intralesional chemotherapy will remove or reduce individual lesions. Patients with widespread cutaneous or extracutaneous disease may require immunomodulatory agents such as interferon α or chemotherapeutic agents such as anthracyclines or paclitaxel.8
Our case highlights the importance of considering risk factors beyond HIV status when including KS as part of the differential diagnosis in patients with atypical vascular lesions. Early recognition enables timely evaluation of potential associated conditions and informs subsequent management decisions.
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Lanternier F, Lebbé C, Schartz N, et al. Kaposi’s sarcoma in HIV-negative men having sex with men. AIDS. 2008;22:1163-1168. doi:10.1097/QAD.0b013e3283031a8a
- Penn I. Kaposi’s sarcoma in transplant recipients. Transplantation. 1997;64:669-673. doi:10.1097/00007890-199709150-00001
- Gallo Marin B, Maymone MBC, El Rayess F, et al. Kaposi sarcoma associated with tofacitinib use in a patient with rheumatoid arthritis. R I Med J (2013). 2023;106:18-20.
- Bishop BN, Lynch DT. Kaposi sarcoma. StatPearls [Internet]. Updated June 5, 2023. Accessed May 15, 2026. https://www.ncbi.nlm .nih.gov/books/NBK534839/
- Dedicoat M, Newton R. Review of the distribution of Kaposi’s sarcoma-associated herpesvirus (KSHV) in Africa in relation to the incidence of Kaposi’s sarcoma. Br J Cancer. 2003;88:1-3. doi:10.1038 /sj.bjc.6600745
- Hiatt KM, Nelson AM, Lichy JH, et al. Classic Kaposi sarcoma in the United States over the last two decades: a clinicopathologic and molecular study of 438 non-HIV-related Kaposi sarcoma patients with comparison to HIV-related Kaposi sarcoma. Mod Pathol. 2008;21:572-582. doi:10.1038/modpathol.2008.15
- Ceccarelli M, Facciolà A, Taibi R, et al. The treatment of Kaposi’s sarcoma: present and future options, a review of the literature. Eur Rev Med Pharmacol Sci. 2019;23:7488-7497. doi:10.26355 /eurrev_201909_18860
THE DIAGNOSIS: Kaposi Sarcoma
Histopathology revealed a serum crust on the surface of the specimen, and the dermis contained compact collections of spindled cells with interspersed erythrocytes (Figure 1). Human herpesvirus 8–stained sections highlighted many lesional cell nuclei (Figure 2). A diagnosis of Kaposi sarcoma (KS) was made based on these findings. The patient expressed interest in surgical excision; however, he was lost to follow-up.
Kaposi sarcoma is an indolent, multifocal, angioproliferative tumor that predominantly affects mucocutaneous sites with less frequent involvement of visceral organs. Kaposi sarcoma is categorized into 4 subtypes: epidemic, iatrogenic, endemic, and classic. Human herpesvirus 8, primarily transmitted through saliva or sexual contact, plays a central role in the pathogenesis of KS, as it drives disease development across all subtypes. The virus causes proliferation of endothelial cells and the formation of angioproliferative lesions characteristic of KS.1
Prevalence is highest in the epidemic subtype, in which patients with advanced HIV and low CD4 T-cell counts may develop KS lesions. Although KS is associated most commonly with HIV, it also has been observed in men who have sex with men regardless of their HIV status.2 Patients undergoing immunosuppressive therapy also may not maintain immune tolerance to previously or newly acquired human herpesvirus 8, leading to the development of iatrogenic KS. This subtype particularly manifests in patients receiving therapy for autoimmune conditions or organ transplants and often only regresses if immunosuppressive therapy is withdrawn.3,4
The endemic and classic subtypes of KS may occur in patients without any known immunocompromise. Endemic KS demonstrates a predilection for pediatric populations in Africa and exhibits less pronounced sex disparity.5 In Uganda and Zimbabwe, endemic KS is the leading cancer in men and the second most frequently occurring cancer in women.6 In contrast, classic KS generally affects older men of Eastern European and Mediterranean descent or Ashkenazi Jewish ancestry. Patients with classic KS generally exhibit a less aggressive disease trajectory relative to other subtypes; however, these patients have a substantial risk for a secondary hematologic malignancy, which may already coexist at the time of diagnosis or emerge subsequently.1,7
Our patient, a native of Eastern Europe, was negative for HIV and was in a monogamous relationship with his wife; therefore, he was likely to have had the classic subtype of KS. As KS is a multifocal disease, lesions may independently emerge at different times and locations on the body. Our patient presented with a new lesion on the hand several years after excision of a similar lesion on the face. Lesions suspicious for KS include slow-growing, painless, red or violaceous patches, nodules, plaques, or patches on the extremities, most commonly manifesting on the feet and ankles. Our differential diagnosis included pyogenic granuloma, amelanotic melanoma, squamous cell carcinoma, and angiosarcoma.
The prognosis in patients with classic KS is favorable, as it often is limited to cutaneous sites and less commonly manifests on visceral organs. Nonetheless, pulmonary and gastrointestinal involvement manifesting as hemoptysis and rectal bleeding, respectively, can occur. This underscores the potential for more serious complications in instances with visceral involvement. Treatment focuses on managing symptoms and preventing growth and progression of individual lesions. Additionally, treatment strategies aim to improve cosmetic outcomes and address any underlying immunosuppression that may exacerbate the condition.8
For most patients, local therapies such as surgical excision, cryotherapy, laser therapy, or intralesional chemotherapy will remove or reduce individual lesions. Patients with widespread cutaneous or extracutaneous disease may require immunomodulatory agents such as interferon α or chemotherapeutic agents such as anthracyclines or paclitaxel.8
Our case highlights the importance of considering risk factors beyond HIV status when including KS as part of the differential diagnosis in patients with atypical vascular lesions. Early recognition enables timely evaluation of potential associated conditions and informs subsequent management decisions.
THE DIAGNOSIS: Kaposi Sarcoma
Histopathology revealed a serum crust on the surface of the specimen, and the dermis contained compact collections of spindled cells with interspersed erythrocytes (Figure 1). Human herpesvirus 8–stained sections highlighted many lesional cell nuclei (Figure 2). A diagnosis of Kaposi sarcoma (KS) was made based on these findings. The patient expressed interest in surgical excision; however, he was lost to follow-up.
Kaposi sarcoma is an indolent, multifocal, angioproliferative tumor that predominantly affects mucocutaneous sites with less frequent involvement of visceral organs. Kaposi sarcoma is categorized into 4 subtypes: epidemic, iatrogenic, endemic, and classic. Human herpesvirus 8, primarily transmitted through saliva or sexual contact, plays a central role in the pathogenesis of KS, as it drives disease development across all subtypes. The virus causes proliferation of endothelial cells and the formation of angioproliferative lesions characteristic of KS.1
Prevalence is highest in the epidemic subtype, in which patients with advanced HIV and low CD4 T-cell counts may develop KS lesions. Although KS is associated most commonly with HIV, it also has been observed in men who have sex with men regardless of their HIV status.2 Patients undergoing immunosuppressive therapy also may not maintain immune tolerance to previously or newly acquired human herpesvirus 8, leading to the development of iatrogenic KS. This subtype particularly manifests in patients receiving therapy for autoimmune conditions or organ transplants and often only regresses if immunosuppressive therapy is withdrawn.3,4
The endemic and classic subtypes of KS may occur in patients without any known immunocompromise. Endemic KS demonstrates a predilection for pediatric populations in Africa and exhibits less pronounced sex disparity.5 In Uganda and Zimbabwe, endemic KS is the leading cancer in men and the second most frequently occurring cancer in women.6 In contrast, classic KS generally affects older men of Eastern European and Mediterranean descent or Ashkenazi Jewish ancestry. Patients with classic KS generally exhibit a less aggressive disease trajectory relative to other subtypes; however, these patients have a substantial risk for a secondary hematologic malignancy, which may already coexist at the time of diagnosis or emerge subsequently.1,7
Our patient, a native of Eastern Europe, was negative for HIV and was in a monogamous relationship with his wife; therefore, he was likely to have had the classic subtype of KS. As KS is a multifocal disease, lesions may independently emerge at different times and locations on the body. Our patient presented with a new lesion on the hand several years after excision of a similar lesion on the face. Lesions suspicious for KS include slow-growing, painless, red or violaceous patches, nodules, plaques, or patches on the extremities, most commonly manifesting on the feet and ankles. Our differential diagnosis included pyogenic granuloma, amelanotic melanoma, squamous cell carcinoma, and angiosarcoma.
The prognosis in patients with classic KS is favorable, as it often is limited to cutaneous sites and less commonly manifests on visceral organs. Nonetheless, pulmonary and gastrointestinal involvement manifesting as hemoptysis and rectal bleeding, respectively, can occur. This underscores the potential for more serious complications in instances with visceral involvement. Treatment focuses on managing symptoms and preventing growth and progression of individual lesions. Additionally, treatment strategies aim to improve cosmetic outcomes and address any underlying immunosuppression that may exacerbate the condition.8
For most patients, local therapies such as surgical excision, cryotherapy, laser therapy, or intralesional chemotherapy will remove or reduce individual lesions. Patients with widespread cutaneous or extracutaneous disease may require immunomodulatory agents such as interferon α or chemotherapeutic agents such as anthracyclines or paclitaxel.8
Our case highlights the importance of considering risk factors beyond HIV status when including KS as part of the differential diagnosis in patients with atypical vascular lesions. Early recognition enables timely evaluation of potential associated conditions and informs subsequent management decisions.
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Lanternier F, Lebbé C, Schartz N, et al. Kaposi’s sarcoma in HIV-negative men having sex with men. AIDS. 2008;22:1163-1168. doi:10.1097/QAD.0b013e3283031a8a
- Penn I. Kaposi’s sarcoma in transplant recipients. Transplantation. 1997;64:669-673. doi:10.1097/00007890-199709150-00001
- Gallo Marin B, Maymone MBC, El Rayess F, et al. Kaposi sarcoma associated with tofacitinib use in a patient with rheumatoid arthritis. R I Med J (2013). 2023;106:18-20.
- Bishop BN, Lynch DT. Kaposi sarcoma. StatPearls [Internet]. Updated June 5, 2023. Accessed May 15, 2026. https://www.ncbi.nlm .nih.gov/books/NBK534839/
- Dedicoat M, Newton R. Review of the distribution of Kaposi’s sarcoma-associated herpesvirus (KSHV) in Africa in relation to the incidence of Kaposi’s sarcoma. Br J Cancer. 2003;88:1-3. doi:10.1038 /sj.bjc.6600745
- Hiatt KM, Nelson AM, Lichy JH, et al. Classic Kaposi sarcoma in the United States over the last two decades: a clinicopathologic and molecular study of 438 non-HIV-related Kaposi sarcoma patients with comparison to HIV-related Kaposi sarcoma. Mod Pathol. 2008;21:572-582. doi:10.1038/modpathol.2008.15
- Ceccarelli M, Facciolà A, Taibi R, et al. The treatment of Kaposi’s sarcoma: present and future options, a review of the literature. Eur Rev Med Pharmacol Sci. 2019;23:7488-7497. doi:10.26355 /eurrev_201909_18860
- Radu O, Pantanowitz L. Kaposi sarcoma. Arch Pathol Lab Med. 2013;137:289-294. doi:10.5858/arpa.2012-0101-RS
- Lanternier F, Lebbé C, Schartz N, et al. Kaposi’s sarcoma in HIV-negative men having sex with men. AIDS. 2008;22:1163-1168. doi:10.1097/QAD.0b013e3283031a8a
- Penn I. Kaposi’s sarcoma in transplant recipients. Transplantation. 1997;64:669-673. doi:10.1097/00007890-199709150-00001
- Gallo Marin B, Maymone MBC, El Rayess F, et al. Kaposi sarcoma associated with tofacitinib use in a patient with rheumatoid arthritis. R I Med J (2013). 2023;106:18-20.
- Bishop BN, Lynch DT. Kaposi sarcoma. StatPearls [Internet]. Updated June 5, 2023. Accessed May 15, 2026. https://www.ncbi.nlm .nih.gov/books/NBK534839/
- Dedicoat M, Newton R. Review of the distribution of Kaposi’s sarcoma-associated herpesvirus (KSHV) in Africa in relation to the incidence of Kaposi’s sarcoma. Br J Cancer. 2003;88:1-3. doi:10.1038 /sj.bjc.6600745
- Hiatt KM, Nelson AM, Lichy JH, et al. Classic Kaposi sarcoma in the United States over the last two decades: a clinicopathologic and molecular study of 438 non-HIV-related Kaposi sarcoma patients with comparison to HIV-related Kaposi sarcoma. Mod Pathol. 2008;21:572-582. doi:10.1038/modpathol.2008.15
- Ceccarelli M, Facciolà A, Taibi R, et al. The treatment of Kaposi’s sarcoma: present and future options, a review of the literature. Eur Rev Med Pharmacol Sci. 2019;23:7488-7497. doi:10.26355 /eurrev_201909_18860
Exophytic Papule on the Hand
Exophytic Papule on the Hand
A man in his 70s with a history of hypertension was admitted to the hospital for symptomatic bradycardia. On the day of admission, he reported a growth on the left second digit of 1 month’s duration, for which dermatology was consulted. The patient said the growth was asymptomatic but occasionally would get caught on objects. He denied any recent fevers, weight loss, or fatigue. He also denied any trauma to the area or other inciting factors. The patient reported there were no lesions anywhere else on the body, but he did mention a similar mass had been excised from his face several years prior. He noted that he had immigrated to the United States from Eastern Europe within the past several years.
Results of laboratory testing at the current presentation, including a basic metabolic panel, complete blood count with differential, hepatic function panel, thyroid-stimulating hormone level, and HIV antigen/antibody testing, were unremarkable. Physical examination revealed a single, well-circumscribed, 6×6–mm, round, red, exophytic papule with a collarette of scale on the volar surface of the left second digit. The skin on both arms was otherwise unremarkable. There was no evidence of lymphadenopathy or mucosal involvement. A shave biopsy of the lesion was performed.

