User login
Clinical Endocrinology News is an independent news source that provides endocrinologists with timely and relevant news and commentary about clinical developments and the impact of health care policy on the endocrinologist's practice. Specialty topics include Diabetes, Lipid & Metabolic Disorders Menopause, Obesity, Osteoporosis, Pediatric Endocrinology, Pituitary, Thyroid & Adrenal Disorders, and Reproductive Endocrinology. Featured content includes Commentaries, Implementin Health Reform, Law & Medicine, and In the Loop, the blog of Clinical Endocrinology News. Clinical Endocrinology News is owned by Frontline Medical Communications.
addict
addicted
addicting
addiction
adult sites
alcohol
antibody
ass
attorney
audit
auditor
babies
babpa
baby
ban
banned
banning
best
bisexual
bitch
bleach
blog
blow job
bondage
boobs
booty
buy
cannabis
certificate
certification
certified
cheap
cheapest
class action
cocaine
cock
counterfeit drug
crack
crap
crime
criminal
cunt
curable
cure
dangerous
dangers
dead
deadly
death
defend
defended
depedent
dependence
dependent
detergent
dick
die
dildo
drug abuse
drug recall
dying
fag
fake
fatal
fatalities
fatality
free
fuck
gangs
gingivitis
guns
hardcore
herbal
herbs
heroin
herpes
home remedies
homo
horny
hypersensitivity
hypoglycemia treatment
illegal drug use
illegal use of prescription
incest
infant
infants
job
ketoacidosis
kill
killer
killing
kinky
law suit
lawsuit
lawyer
lesbian
marijuana
medicine for hypoglycemia
murder
naked
natural
newborn
nigger
noise
nude
nudity
orgy
over the counter
overdosage
overdose
overdosed
overdosing
penis
pimp
pistol
porn
porno
pornographic
pornography
prison
profanity
purchase
purchasing
pussy
queer
rape
rapist
recall
recreational drug
rob
robberies
sale
sales
sex
sexual
shit
shoot
slut
slutty
stole
stolen
store
sue
suicidal
suicide
supplements
supply company
theft
thief
thieves
tit
toddler
toddlers
toxic
toxin
tragedy
treating dka
treating hypoglycemia
treatment for hypoglycemia
vagina
violence
whore
withdrawal
without prescription
section[contains(@class, 'nav-hidden')]
footer[@id='footer']
div[contains(@class, 'pane-pub-article-imn')]
div[contains(@class, 'pane-pub-home-imn')]
div[contains(@class, 'pane-pub-topic-imn')]
div[contains(@class, 'panel-panel-inner')]
div[contains(@class, 'pane-node-field-article-topics')]
section[contains(@class, 'footer-nav-section-wrapper')]
Statin misinformation on social media flagged by AI
Using artificial intelligence to analyze large amounts of information from social media platforms generated some novel insights into public perceptions about statins, results of a new study show.
The study, which used AI to analyze discussions about statins on the social media platform Reddit, corroborated previously documented reasons for statin hesitancy, including adverse effect profiles and general disenfranchisement with health care.
But it also found novel points of discourse, including linking statins to COVID-19 outcomes and the role of cholesterol, statins, and the ketogenic diet.
“We used AI to tell us what is being discussed about statins on social media and to quantify the information in topics that people think are important,” senior study author Fatima Rodriguez, MD, MPH, Stanford (Calif.) University School of Medicine, said in an interview.
“Some of the themes were surprising to us. While we expected discussion on side effects, we were surprised to see so much discussion refuting the idea that increased levels of LDL were detrimental. There were also a large amount of posts on statin use being correlated to COVID outcomes. Our findings show how widespread this misinformation is,” she said.
“As a preventative cardiologist, I spend a lot of my time trying to get patients to take statins, but patients often rely on social media for information, and this can contain a lot of misinformation. People tend to be more honest on online forums than they are in the doctor’s office, so they are probably asking the questions and having discussions on subjects they really care about. So, understanding what is being discussed on social media is very valuable information for us as clinicians.”
The study was published online in JAMA Network Open.
The researchers analyzed all statin-related discussions on Reddit that were dated between Jan. 1, 2009, and July 12, 2022. Statin- and cholesterol-focused communities were identified to create a list of statin-related discussions. An AI pipeline was developed to cluster these discussions into specific topics and overarching thematic groups.
A total of 10,233 unique statin-related discussions and 5,188 unique authors were identified. A total of 100 discussion topics were identified and classified into six overarching thematic groups: (1) ketogenic diets, diabetes, supplements, and statins; (2) statin adverse effects; (3) statin hesitancy; (4) clinical trial appraisals; (5) pharmaceutical industry bias and statins; and (6) red yeast rice and statins.
Several examples of statin-related misinformation were identified, including distrust of the hypothesis that LDL-C has a causal association with heart disease. Discussions included quotes such as, “I think LDL is pretty much irrelevant. Your HDL and triglycerides are far more important.”
Other topics suggested that certain natural supplements would be an acceptable alternative to statins. Quotes included: “Red yeast rice is a statin basically, by the way,” and “statins are basically mycotoxins and deplete you of fat-soluble nutrients, like coQ10, vit D, K, A and E, and in all likelihood through these depletions worsen cardiovascular health.”
The researchers also looked at temporal trends and found that these sorts of discussions have increased over time.
One of the common themes identified was using the ketogenic diet phenomenon as an argument against increased cholesterol levels being bad for health.
Dr. Rodriguez elaborated: “People think the ketogenic diet is healthy as they lose weight on it. And as it can be associated with a small increase in LDL cholesterol, there was a lot of opinion that this meant increasing LDL was a good thing.”
The researchers also conducted a sentiment analysis, which designated topics as positive, negative, or neutral with regard to statins.
“We found that almost no topic was positive. Everything was either neutral or negative. This is pretty consistent with what we are seeing around hesitancy in clinical practice, but you would think that maybe a few people may have a positive view on statins,” Dr. Rodriguez commented.
“One of the problems with statins and lowering cholesterol is that it takes a long time to see a benefit, but this misinformation will result in some people not taking their medication,” she added.
Dr. Rodriguez noted that in this study AI is augmenting, not replacing, what clinicians and researchers do. “But it is a valuable tool to scan a large volume of information, and we have shown here it can generate new insights that we may not have thought of. It’s important to know what’s out there so we can try and combat it.”
She pointed out that patients don’t read the medical literature showing the benefits of statins but rather rely on social media for their information.
“We need to understand all sorts of patient engagement and use the same tools to combat this misinformation. We have a responsibility to try and stop dangerous and false information from being propagated,” she commented.
“These drugs are clearly not dangerous when used in line with clinical guidelines, and they have been proven to have multiple benefits again and again, but we don’t see those kinds of discussions in the community at all. We as clinicians need to use social media and AI to give out the right information. This could start to combat all the misinformation out there.”
A version of this article first appeared on Medscape.com.
Using artificial intelligence to analyze large amounts of information from social media platforms generated some novel insights into public perceptions about statins, results of a new study show.
The study, which used AI to analyze discussions about statins on the social media platform Reddit, corroborated previously documented reasons for statin hesitancy, including adverse effect profiles and general disenfranchisement with health care.
But it also found novel points of discourse, including linking statins to COVID-19 outcomes and the role of cholesterol, statins, and the ketogenic diet.
“We used AI to tell us what is being discussed about statins on social media and to quantify the information in topics that people think are important,” senior study author Fatima Rodriguez, MD, MPH, Stanford (Calif.) University School of Medicine, said in an interview.
“Some of the themes were surprising to us. While we expected discussion on side effects, we were surprised to see so much discussion refuting the idea that increased levels of LDL were detrimental. There were also a large amount of posts on statin use being correlated to COVID outcomes. Our findings show how widespread this misinformation is,” she said.
“As a preventative cardiologist, I spend a lot of my time trying to get patients to take statins, but patients often rely on social media for information, and this can contain a lot of misinformation. People tend to be more honest on online forums than they are in the doctor’s office, so they are probably asking the questions and having discussions on subjects they really care about. So, understanding what is being discussed on social media is very valuable information for us as clinicians.”
The study was published online in JAMA Network Open.
The researchers analyzed all statin-related discussions on Reddit that were dated between Jan. 1, 2009, and July 12, 2022. Statin- and cholesterol-focused communities were identified to create a list of statin-related discussions. An AI pipeline was developed to cluster these discussions into specific topics and overarching thematic groups.
A total of 10,233 unique statin-related discussions and 5,188 unique authors were identified. A total of 100 discussion topics were identified and classified into six overarching thematic groups: (1) ketogenic diets, diabetes, supplements, and statins; (2) statin adverse effects; (3) statin hesitancy; (4) clinical trial appraisals; (5) pharmaceutical industry bias and statins; and (6) red yeast rice and statins.
Several examples of statin-related misinformation were identified, including distrust of the hypothesis that LDL-C has a causal association with heart disease. Discussions included quotes such as, “I think LDL is pretty much irrelevant. Your HDL and triglycerides are far more important.”
Other topics suggested that certain natural supplements would be an acceptable alternative to statins. Quotes included: “Red yeast rice is a statin basically, by the way,” and “statins are basically mycotoxins and deplete you of fat-soluble nutrients, like coQ10, vit D, K, A and E, and in all likelihood through these depletions worsen cardiovascular health.”
The researchers also looked at temporal trends and found that these sorts of discussions have increased over time.
One of the common themes identified was using the ketogenic diet phenomenon as an argument against increased cholesterol levels being bad for health.
Dr. Rodriguez elaborated: “People think the ketogenic diet is healthy as they lose weight on it. And as it can be associated with a small increase in LDL cholesterol, there was a lot of opinion that this meant increasing LDL was a good thing.”
The researchers also conducted a sentiment analysis, which designated topics as positive, negative, or neutral with regard to statins.
“We found that almost no topic was positive. Everything was either neutral or negative. This is pretty consistent with what we are seeing around hesitancy in clinical practice, but you would think that maybe a few people may have a positive view on statins,” Dr. Rodriguez commented.
“One of the problems with statins and lowering cholesterol is that it takes a long time to see a benefit, but this misinformation will result in some people not taking their medication,” she added.
Dr. Rodriguez noted that in this study AI is augmenting, not replacing, what clinicians and researchers do. “But it is a valuable tool to scan a large volume of information, and we have shown here it can generate new insights that we may not have thought of. It’s important to know what’s out there so we can try and combat it.”
She pointed out that patients don’t read the medical literature showing the benefits of statins but rather rely on social media for their information.
“We need to understand all sorts of patient engagement and use the same tools to combat this misinformation. We have a responsibility to try and stop dangerous and false information from being propagated,” she commented.
“These drugs are clearly not dangerous when used in line with clinical guidelines, and they have been proven to have multiple benefits again and again, but we don’t see those kinds of discussions in the community at all. We as clinicians need to use social media and AI to give out the right information. This could start to combat all the misinformation out there.”
A version of this article first appeared on Medscape.com.
Using artificial intelligence to analyze large amounts of information from social media platforms generated some novel insights into public perceptions about statins, results of a new study show.
The study, which used AI to analyze discussions about statins on the social media platform Reddit, corroborated previously documented reasons for statin hesitancy, including adverse effect profiles and general disenfranchisement with health care.
But it also found novel points of discourse, including linking statins to COVID-19 outcomes and the role of cholesterol, statins, and the ketogenic diet.
“We used AI to tell us what is being discussed about statins on social media and to quantify the information in topics that people think are important,” senior study author Fatima Rodriguez, MD, MPH, Stanford (Calif.) University School of Medicine, said in an interview.
“Some of the themes were surprising to us. While we expected discussion on side effects, we were surprised to see so much discussion refuting the idea that increased levels of LDL were detrimental. There were also a large amount of posts on statin use being correlated to COVID outcomes. Our findings show how widespread this misinformation is,” she said.
“As a preventative cardiologist, I spend a lot of my time trying to get patients to take statins, but patients often rely on social media for information, and this can contain a lot of misinformation. People tend to be more honest on online forums than they are in the doctor’s office, so they are probably asking the questions and having discussions on subjects they really care about. So, understanding what is being discussed on social media is very valuable information for us as clinicians.”
The study was published online in JAMA Network Open.
The researchers analyzed all statin-related discussions on Reddit that were dated between Jan. 1, 2009, and July 12, 2022. Statin- and cholesterol-focused communities were identified to create a list of statin-related discussions. An AI pipeline was developed to cluster these discussions into specific topics and overarching thematic groups.
A total of 10,233 unique statin-related discussions and 5,188 unique authors were identified. A total of 100 discussion topics were identified and classified into six overarching thematic groups: (1) ketogenic diets, diabetes, supplements, and statins; (2) statin adverse effects; (3) statin hesitancy; (4) clinical trial appraisals; (5) pharmaceutical industry bias and statins; and (6) red yeast rice and statins.
Several examples of statin-related misinformation were identified, including distrust of the hypothesis that LDL-C has a causal association with heart disease. Discussions included quotes such as, “I think LDL is pretty much irrelevant. Your HDL and triglycerides are far more important.”
Other topics suggested that certain natural supplements would be an acceptable alternative to statins. Quotes included: “Red yeast rice is a statin basically, by the way,” and “statins are basically mycotoxins and deplete you of fat-soluble nutrients, like coQ10, vit D, K, A and E, and in all likelihood through these depletions worsen cardiovascular health.”
The researchers also looked at temporal trends and found that these sorts of discussions have increased over time.
One of the common themes identified was using the ketogenic diet phenomenon as an argument against increased cholesterol levels being bad for health.
Dr. Rodriguez elaborated: “People think the ketogenic diet is healthy as they lose weight on it. And as it can be associated with a small increase in LDL cholesterol, there was a lot of opinion that this meant increasing LDL was a good thing.”
The researchers also conducted a sentiment analysis, which designated topics as positive, negative, or neutral with regard to statins.
“We found that almost no topic was positive. Everything was either neutral or negative. This is pretty consistent with what we are seeing around hesitancy in clinical practice, but you would think that maybe a few people may have a positive view on statins,” Dr. Rodriguez commented.
“One of the problems with statins and lowering cholesterol is that it takes a long time to see a benefit, but this misinformation will result in some people not taking their medication,” she added.
Dr. Rodriguez noted that in this study AI is augmenting, not replacing, what clinicians and researchers do. “But it is a valuable tool to scan a large volume of information, and we have shown here it can generate new insights that we may not have thought of. It’s important to know what’s out there so we can try and combat it.”
She pointed out that patients don’t read the medical literature showing the benefits of statins but rather rely on social media for their information.
“We need to understand all sorts of patient engagement and use the same tools to combat this misinformation. We have a responsibility to try and stop dangerous and false information from being propagated,” she commented.
“These drugs are clearly not dangerous when used in line with clinical guidelines, and they have been proven to have multiple benefits again and again, but we don’t see those kinds of discussions in the community at all. We as clinicians need to use social media and AI to give out the right information. This could start to combat all the misinformation out there.”
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Study shows higher obesity-related cancer mortality in areas with more fast food
based on data from a new cross-sectional study of more than 3,000 communities.
Although increased healthy eating has been associated with reduced risk of obesity and with reduced cancer incidence and mortality, access to healthier eating remains a challenge in communities with less access to grocery stores and healthy food options (food deserts) and/or easy access to convenience stores and fast food (food swamps), Malcolm Seth Bevel, PhD, of the Medical College of Georgia, Augusta, and colleagues, wrote in their paper, published in JAMA Oncology.
In addition, data on the association between food deserts and swamps and obesity-related cancer mortality are limited, they said.
“We felt that the study was important given the fact that obesity is an epidemic in the United States, and multiple factors contribute to obesity, especially adverse food environments,” Dr. Bevel said in an interview. “Also, I lived in these areas my whole life, and saw how it affected underserved populations. There was a story that needed to be told, so we’re telling it,” he said in an interview.
In a study, the researchers analyzed food access and cancer mortality data from 3,038 counties across the United States. The food access data came from the U.S. Department of Agriculture Food Environment Atlas (FEA) for the years 2012, 2014, 2015, 2017, and 2020. Data on obesity-related cancer mortality came from the Centers for Disease Control and Prevention for the years from 2010 to 2020.
Food desert scores were calculated through data from the FEA, and food swamp scores were based on the ratio of fast-food restaurants and convenience stores to grocery stores and farmers markets in a modification of the Retail Food Environment Index score.
The researchers used an age-adjusted, multiple regression model to determine the association between food desert and food swamp scores and obesity-related cancer mortality rates. Higher food swamp and food desert scores (defined as 20.0 to 58.0 or higher) were used to classify counties as having fewer healthy food resources. The primary outcome was obesity-related cancer mortality, defined as high or low (71.8 or higher per 100,000 individuals and less than 71.8 per 100,000 individuals, respectively).
Overall, high rates of obesity-related cancer mortality were 77% more likely in the counties that met the criteria for high food swamp scores (adjusted odds ratio 1.77). In addition, researchers found a positive dose-response relationship among three levels of both food desert scores and food swamp scores and obesity-related cancer mortality.
A total of 758 counties had obesity-related cancer mortality rates in the highest quartile. Compared to counties with low rates of obesity-related cancer mortality, counties with high rates of obesity-related cancer mortality also had a higher percentage of non-Hispanic Black residents (3.26% vs. 1.77%), higher percentage of adults older than 65 years (15.71% vs. 15.40%), higher rates of adult obesity (33.0% vs. 32.10%), and higher rates of adult diabetes (12.50% vs. 10.70%).
Possible explanations for the results include the lack of interest in grocery stores in neighborhoods with a population with a lower socioeconomic status, which can create a food desert, the researchers wrote in their discussion. “Coupled with the increasing growth rate of fast-food restaurants in recent years and the intentional advertisement of unhealthy foods in urban neighborhoods with [people of lower income], the food desert may transform into a food swamp,” they said.
The findings were limited by several factors including the study design, which did not allow for showing a causal association of food deserts and food swamps with obesity-related cancer mortality, the researchers noted. Other limitations included the use of groups rather than individuals, the potential misclassification of food stores, and the use of county-level data on race, ethnicity, and income, they wrote.
The results indicate that “food swamps appear to be a growing epidemic across the U.S., likely because of systemic issues, and should draw concern and conversation from local and state officials,” the researchers concluded.
Community-level investments can benefit individual health
Dr. Bevel said he was not surprised by the findings, as he has seen firsthand the lack of healthy food options and growth of unhealthy food options, especially for certain populations in certain communities. “Typically, these are people who have lower socioeconomic status, primarily non-Hispanic Black or African American or Hispanic American,” he said “I have watched people have to choose between getting fruits/vegetables versus their medications or running to fast food places to feed their families. What is truly surprising is that we’re not talking about people’s lived environment enough for my taste,” he said.
“I hope that our data and results can inform local and state policymakers to truly invest in all communities, such as funding for community gardens, and realize that adverse food environments, including the barriers in navigating these environments, have significant consequences on real people,” said Dr. Bevel. “Also, I hope that the results can help clinicians realize that a patient’s lived environment can truly affect their obesity and/or obesity-related cancer status; being cognizant of that is the first step in holistic, comprehensive care,” he said.
“One role that oncologists might be able to play in improving patients’ access to healthier food is to create and/or implement healthy lifestyle programs with gardening components to combat the poorest food environments that their patients likely reside in,” said Dr. Bevel. Clinicians also could consider the innovative approach of “food prescriptions” to help reduce the effects of deprived, built environments, he noted.
Looking ahead, next steps for research include determining the severity of association between food swamps and obesity-related cancer by varying factors such as cancer type, and examining any potential racial disparities between people living in these environments and obesity-related cancer, Dr. Bevel added.
Data provide foundation for multilevel interventions
The current study findings “raise a clarion call to elevate the discussion on food availability and access to ensure an equitable emphasis on both the importance of lifestyle factors and the upstream structural, economic, and environmental contexts that shape these behaviors at the individual level,” Karriem S. Watson, DHSc, MS, MPH, of the National Institutes of Health, Bethesda, Md., and Angela Odoms-Young, PhD, of Cornell University, Ithaca, N.Y., wrote in an accompanying editorial.
The findings provide a foundation for studies of obesity-related cancer outcomes that take the community environment into consideration, they added.
The causes of both obesity and cancer are complex, and the study findings suggest that the links between unhealthy food environments and obesity-related cancer may go beyond dietary consumption alone and extend to social and psychological factors, the editorialists noted.
“Whether dealing with the lack of access to healthy foods or an overabundance of unhealthy food, there is a critical need to develop additional research that explores the associations between obesity-related cancer mortality and food inequities,” they concluded.
The study received no outside funding. The researchers and the editorialists had no financial conflicts to disclose.
based on data from a new cross-sectional study of more than 3,000 communities.
Although increased healthy eating has been associated with reduced risk of obesity and with reduced cancer incidence and mortality, access to healthier eating remains a challenge in communities with less access to grocery stores and healthy food options (food deserts) and/or easy access to convenience stores and fast food (food swamps), Malcolm Seth Bevel, PhD, of the Medical College of Georgia, Augusta, and colleagues, wrote in their paper, published in JAMA Oncology.
In addition, data on the association between food deserts and swamps and obesity-related cancer mortality are limited, they said.
“We felt that the study was important given the fact that obesity is an epidemic in the United States, and multiple factors contribute to obesity, especially adverse food environments,” Dr. Bevel said in an interview. “Also, I lived in these areas my whole life, and saw how it affected underserved populations. There was a story that needed to be told, so we’re telling it,” he said in an interview.
In a study, the researchers analyzed food access and cancer mortality data from 3,038 counties across the United States. The food access data came from the U.S. Department of Agriculture Food Environment Atlas (FEA) for the years 2012, 2014, 2015, 2017, and 2020. Data on obesity-related cancer mortality came from the Centers for Disease Control and Prevention for the years from 2010 to 2020.
Food desert scores were calculated through data from the FEA, and food swamp scores were based on the ratio of fast-food restaurants and convenience stores to grocery stores and farmers markets in a modification of the Retail Food Environment Index score.
The researchers used an age-adjusted, multiple regression model to determine the association between food desert and food swamp scores and obesity-related cancer mortality rates. Higher food swamp and food desert scores (defined as 20.0 to 58.0 or higher) were used to classify counties as having fewer healthy food resources. The primary outcome was obesity-related cancer mortality, defined as high or low (71.8 or higher per 100,000 individuals and less than 71.8 per 100,000 individuals, respectively).
Overall, high rates of obesity-related cancer mortality were 77% more likely in the counties that met the criteria for high food swamp scores (adjusted odds ratio 1.77). In addition, researchers found a positive dose-response relationship among three levels of both food desert scores and food swamp scores and obesity-related cancer mortality.
A total of 758 counties had obesity-related cancer mortality rates in the highest quartile. Compared to counties with low rates of obesity-related cancer mortality, counties with high rates of obesity-related cancer mortality also had a higher percentage of non-Hispanic Black residents (3.26% vs. 1.77%), higher percentage of adults older than 65 years (15.71% vs. 15.40%), higher rates of adult obesity (33.0% vs. 32.10%), and higher rates of adult diabetes (12.50% vs. 10.70%).
Possible explanations for the results include the lack of interest in grocery stores in neighborhoods with a population with a lower socioeconomic status, which can create a food desert, the researchers wrote in their discussion. “Coupled with the increasing growth rate of fast-food restaurants in recent years and the intentional advertisement of unhealthy foods in urban neighborhoods with [people of lower income], the food desert may transform into a food swamp,” they said.
The findings were limited by several factors including the study design, which did not allow for showing a causal association of food deserts and food swamps with obesity-related cancer mortality, the researchers noted. Other limitations included the use of groups rather than individuals, the potential misclassification of food stores, and the use of county-level data on race, ethnicity, and income, they wrote.
The results indicate that “food swamps appear to be a growing epidemic across the U.S., likely because of systemic issues, and should draw concern and conversation from local and state officials,” the researchers concluded.
Community-level investments can benefit individual health
Dr. Bevel said he was not surprised by the findings, as he has seen firsthand the lack of healthy food options and growth of unhealthy food options, especially for certain populations in certain communities. “Typically, these are people who have lower socioeconomic status, primarily non-Hispanic Black or African American or Hispanic American,” he said “I have watched people have to choose between getting fruits/vegetables versus their medications or running to fast food places to feed their families. What is truly surprising is that we’re not talking about people’s lived environment enough for my taste,” he said.
“I hope that our data and results can inform local and state policymakers to truly invest in all communities, such as funding for community gardens, and realize that adverse food environments, including the barriers in navigating these environments, have significant consequences on real people,” said Dr. Bevel. “Also, I hope that the results can help clinicians realize that a patient’s lived environment can truly affect their obesity and/or obesity-related cancer status; being cognizant of that is the first step in holistic, comprehensive care,” he said.
“One role that oncologists might be able to play in improving patients’ access to healthier food is to create and/or implement healthy lifestyle programs with gardening components to combat the poorest food environments that their patients likely reside in,” said Dr. Bevel. Clinicians also could consider the innovative approach of “food prescriptions” to help reduce the effects of deprived, built environments, he noted.
Looking ahead, next steps for research include determining the severity of association between food swamps and obesity-related cancer by varying factors such as cancer type, and examining any potential racial disparities between people living in these environments and obesity-related cancer, Dr. Bevel added.
Data provide foundation for multilevel interventions
The current study findings “raise a clarion call to elevate the discussion on food availability and access to ensure an equitable emphasis on both the importance of lifestyle factors and the upstream structural, economic, and environmental contexts that shape these behaviors at the individual level,” Karriem S. Watson, DHSc, MS, MPH, of the National Institutes of Health, Bethesda, Md., and Angela Odoms-Young, PhD, of Cornell University, Ithaca, N.Y., wrote in an accompanying editorial.
The findings provide a foundation for studies of obesity-related cancer outcomes that take the community environment into consideration, they added.
The causes of both obesity and cancer are complex, and the study findings suggest that the links between unhealthy food environments and obesity-related cancer may go beyond dietary consumption alone and extend to social and psychological factors, the editorialists noted.
“Whether dealing with the lack of access to healthy foods or an overabundance of unhealthy food, there is a critical need to develop additional research that explores the associations between obesity-related cancer mortality and food inequities,” they concluded.
The study received no outside funding. The researchers and the editorialists had no financial conflicts to disclose.
based on data from a new cross-sectional study of more than 3,000 communities.
Although increased healthy eating has been associated with reduced risk of obesity and with reduced cancer incidence and mortality, access to healthier eating remains a challenge in communities with less access to grocery stores and healthy food options (food deserts) and/or easy access to convenience stores and fast food (food swamps), Malcolm Seth Bevel, PhD, of the Medical College of Georgia, Augusta, and colleagues, wrote in their paper, published in JAMA Oncology.
In addition, data on the association between food deserts and swamps and obesity-related cancer mortality are limited, they said.
“We felt that the study was important given the fact that obesity is an epidemic in the United States, and multiple factors contribute to obesity, especially adverse food environments,” Dr. Bevel said in an interview. “Also, I lived in these areas my whole life, and saw how it affected underserved populations. There was a story that needed to be told, so we’re telling it,” he said in an interview.
In a study, the researchers analyzed food access and cancer mortality data from 3,038 counties across the United States. The food access data came from the U.S. Department of Agriculture Food Environment Atlas (FEA) for the years 2012, 2014, 2015, 2017, and 2020. Data on obesity-related cancer mortality came from the Centers for Disease Control and Prevention for the years from 2010 to 2020.
Food desert scores were calculated through data from the FEA, and food swamp scores were based on the ratio of fast-food restaurants and convenience stores to grocery stores and farmers markets in a modification of the Retail Food Environment Index score.
The researchers used an age-adjusted, multiple regression model to determine the association between food desert and food swamp scores and obesity-related cancer mortality rates. Higher food swamp and food desert scores (defined as 20.0 to 58.0 or higher) were used to classify counties as having fewer healthy food resources. The primary outcome was obesity-related cancer mortality, defined as high or low (71.8 or higher per 100,000 individuals and less than 71.8 per 100,000 individuals, respectively).
Overall, high rates of obesity-related cancer mortality were 77% more likely in the counties that met the criteria for high food swamp scores (adjusted odds ratio 1.77). In addition, researchers found a positive dose-response relationship among three levels of both food desert scores and food swamp scores and obesity-related cancer mortality.
A total of 758 counties had obesity-related cancer mortality rates in the highest quartile. Compared to counties with low rates of obesity-related cancer mortality, counties with high rates of obesity-related cancer mortality also had a higher percentage of non-Hispanic Black residents (3.26% vs. 1.77%), higher percentage of adults older than 65 years (15.71% vs. 15.40%), higher rates of adult obesity (33.0% vs. 32.10%), and higher rates of adult diabetes (12.50% vs. 10.70%).
Possible explanations for the results include the lack of interest in grocery stores in neighborhoods with a population with a lower socioeconomic status, which can create a food desert, the researchers wrote in their discussion. “Coupled with the increasing growth rate of fast-food restaurants in recent years and the intentional advertisement of unhealthy foods in urban neighborhoods with [people of lower income], the food desert may transform into a food swamp,” they said.
The findings were limited by several factors including the study design, which did not allow for showing a causal association of food deserts and food swamps with obesity-related cancer mortality, the researchers noted. Other limitations included the use of groups rather than individuals, the potential misclassification of food stores, and the use of county-level data on race, ethnicity, and income, they wrote.
The results indicate that “food swamps appear to be a growing epidemic across the U.S., likely because of systemic issues, and should draw concern and conversation from local and state officials,” the researchers concluded.
Community-level investments can benefit individual health
Dr. Bevel said he was not surprised by the findings, as he has seen firsthand the lack of healthy food options and growth of unhealthy food options, especially for certain populations in certain communities. “Typically, these are people who have lower socioeconomic status, primarily non-Hispanic Black or African American or Hispanic American,” he said “I have watched people have to choose between getting fruits/vegetables versus their medications or running to fast food places to feed their families. What is truly surprising is that we’re not talking about people’s lived environment enough for my taste,” he said.
“I hope that our data and results can inform local and state policymakers to truly invest in all communities, such as funding for community gardens, and realize that adverse food environments, including the barriers in navigating these environments, have significant consequences on real people,” said Dr. Bevel. “Also, I hope that the results can help clinicians realize that a patient’s lived environment can truly affect their obesity and/or obesity-related cancer status; being cognizant of that is the first step in holistic, comprehensive care,” he said.
“One role that oncologists might be able to play in improving patients’ access to healthier food is to create and/or implement healthy lifestyle programs with gardening components to combat the poorest food environments that their patients likely reside in,” said Dr. Bevel. Clinicians also could consider the innovative approach of “food prescriptions” to help reduce the effects of deprived, built environments, he noted.
Looking ahead, next steps for research include determining the severity of association between food swamps and obesity-related cancer by varying factors such as cancer type, and examining any potential racial disparities between people living in these environments and obesity-related cancer, Dr. Bevel added.
Data provide foundation for multilevel interventions
The current study findings “raise a clarion call to elevate the discussion on food availability and access to ensure an equitable emphasis on both the importance of lifestyle factors and the upstream structural, economic, and environmental contexts that shape these behaviors at the individual level,” Karriem S. Watson, DHSc, MS, MPH, of the National Institutes of Health, Bethesda, Md., and Angela Odoms-Young, PhD, of Cornell University, Ithaca, N.Y., wrote in an accompanying editorial.
The findings provide a foundation for studies of obesity-related cancer outcomes that take the community environment into consideration, they added.
The causes of both obesity and cancer are complex, and the study findings suggest that the links between unhealthy food environments and obesity-related cancer may go beyond dietary consumption alone and extend to social and psychological factors, the editorialists noted.
“Whether dealing with the lack of access to healthy foods or an overabundance of unhealthy food, there is a critical need to develop additional research that explores the associations between obesity-related cancer mortality and food inequities,” they concluded.
The study received no outside funding. The researchers and the editorialists had no financial conflicts to disclose.
FROM JAMA ONCOLOGY
Expert discusses which diets are best, based on the evidence
according to a speaker at the annual meeting of the American College of Physicians.
“Evidence from studies can help clinicians and their patients develop a successful dietary management plan and achieve optimal health,” said internist Michelle Hauser, MD, clinical associate professor at Stanford (Calif.) University. She also discussed evidence-based techniques to support patients in maintaining dietary modifications.
Predominantly plant‐based diets
Popular predominantly plant‐based diets include a Mediterranean diet, healthy vegetarian diet, predominantly whole-food plant‐based (WFPB) diet, and a dietary approach to stop hypertension (DASH).
The DASH diet was originally designed to help patients manage their blood pressure, but evidence suggests that it also can help adults with obesity lose weight. In contrast to the DASH diet, the Mediterranean diet is not low-fat and not very restrictive. Yet the evidence suggests that the Mediterranean diet is not only helpful for losing weight but also can reduce the risk of various chronic diseases, including obesity, type 2 diabetes, cardiovascular disease (CVD), and cancer, Dr. Hauser said. In addition, data suggest that the Mediterranean diet may reduce the risk of all-cause mortality and lower the levels of cholesterol.
“I like to highlight all these protective effects to my patients, because even if their goal is to lose weight, knowing that hard work pays off in additional ways can keep them motivated,” Dr. Hauser stated.
A healthy vegetarian diet and a WFPB diet are similar, and both are helpful in weight loss and management of total cholesterol and LDL‐C levels. Furthermore, healthy vegetarian and WFPB diets may reduce the risk of type 2 diabetes, CVD, and some cancers. Cohort study data suggest that progressively more vegetarian diets are associated with lower BMIs.
“My interpretation of these data is that predominantly plant-based diets rich in whole foods are healthful and can be done in a way that is sustainable for most,” said Dr. Hauser. However, this generally requires a lot of support at the outset to address gaps in knowledge, skills, and other potential barriers.
For example, she referred one obese patient at risk of diabetes and cardiovascular disease to a registered dietitian to develop a dietary plan. The patient also attended a behavioral medicine weight management program to learn strategies such as using smaller plates, and his family attended a healthy cooking class together to improve meal planning and cooking skills.
Time‐restricted feeding
There are numerous variations of time-restricted feeding, commonly referred to as intermittent fasting, but the principles are similar – limiting food intake to a specific window of time each day or week.
Although some studies have shown that time-restricted feeding may help patients reduce adiposity and improve lipid markers, most studies comparing time-restricted feeding to a calorie-restricted diet have shown little to no difference in weight-related outcomes, Dr. Hauser said.
These data suggest that time-restricted feeding may help patients with weight loss only if time restriction helps them reduce calorie intake. She also warned that time-restrictive feeding might cause late-night cravings and might not be helpful in individuals prone to food cravings.
Low‐carbohydrate and ketogenic diets
Losing muscle mass can prevent some people from dieting, but evidence suggests that a high-fat, very low-carbohydrate diet – also called a ketogenic diet – may help patients reduce weight and fat mass while preserving fat‐free mass, Dr. Hauser said.
The evidence regarding the usefulness of a low-carbohydrate (non-keto) diet is less clear because most studies compared it to a low-fat diet, and these two diets might lead to a similar extent of weight loss.
Rating the level of scientific evidence behind different diet options
Nutrition studies do no provide the same level of evidence as drug studies, said Dr. Hauser, because it is easier to conduct a randomized controlled trial of a drug versus placebo. Diets have many more variables, and it also takes much longer to observe most outcomes of a dietary change.
In addition, clinical trials of dietary interventions are typically short and focus on disease markers such as serum lipids and hemoglobin A1c levels. To obtain reliable information on the usefulness of a diet, researchers need to collect detailed health and lifestyle information from hundreds of thousands of people over several decades, which is not always feasible. “This is why meta-analyses of pooled dietary study data are more likely to yield dependable findings,” she noted.
Getting to know patients is essential to help them maintain diet modifications
When developing a diet plan for a patient, it is important to consider the sustainability of a dietary pattern. “The benefits of any healthy dietary change will only last as long as they can be maintained,” said Dr. Hauser. “Counseling someone on choosing an appropriate long-term dietary pattern requires getting to know them – taste preferences, food traditions, barriers, facilitators, food access, and time and cost restrictions.”
In an interview after the session, David Bittleman, MD, an internist at Veterans Affairs San Diego Health Care System, agreed that getting to know patients is essential for successfully advising them on diet.
“I always start developing a diet plan by trying to find out what [a patient’s] diet is like and what their goals are. I need to know what they are already doing in order to make suggestions about what they can do to make their diet healthier,” he said.
When asked about her approach to supporting patients in the long term, Dr. Hauser said that she recommends sequential, gradual changes. Dr. Hauser added that she suggests her patients prioritize implementing dietary changes that they are confident they can maintain.
Dr. Hauser and Dr. Bittleman report no relevant financial relationships.
according to a speaker at the annual meeting of the American College of Physicians.
“Evidence from studies can help clinicians and their patients develop a successful dietary management plan and achieve optimal health,” said internist Michelle Hauser, MD, clinical associate professor at Stanford (Calif.) University. She also discussed evidence-based techniques to support patients in maintaining dietary modifications.
Predominantly plant‐based diets
Popular predominantly plant‐based diets include a Mediterranean diet, healthy vegetarian diet, predominantly whole-food plant‐based (WFPB) diet, and a dietary approach to stop hypertension (DASH).
The DASH diet was originally designed to help patients manage their blood pressure, but evidence suggests that it also can help adults with obesity lose weight. In contrast to the DASH diet, the Mediterranean diet is not low-fat and not very restrictive. Yet the evidence suggests that the Mediterranean diet is not only helpful for losing weight but also can reduce the risk of various chronic diseases, including obesity, type 2 diabetes, cardiovascular disease (CVD), and cancer, Dr. Hauser said. In addition, data suggest that the Mediterranean diet may reduce the risk of all-cause mortality and lower the levels of cholesterol.
“I like to highlight all these protective effects to my patients, because even if their goal is to lose weight, knowing that hard work pays off in additional ways can keep them motivated,” Dr. Hauser stated.
A healthy vegetarian diet and a WFPB diet are similar, and both are helpful in weight loss and management of total cholesterol and LDL‐C levels. Furthermore, healthy vegetarian and WFPB diets may reduce the risk of type 2 diabetes, CVD, and some cancers. Cohort study data suggest that progressively more vegetarian diets are associated with lower BMIs.
“My interpretation of these data is that predominantly plant-based diets rich in whole foods are healthful and can be done in a way that is sustainable for most,” said Dr. Hauser. However, this generally requires a lot of support at the outset to address gaps in knowledge, skills, and other potential barriers.
For example, she referred one obese patient at risk of diabetes and cardiovascular disease to a registered dietitian to develop a dietary plan. The patient also attended a behavioral medicine weight management program to learn strategies such as using smaller plates, and his family attended a healthy cooking class together to improve meal planning and cooking skills.
Time‐restricted feeding
There are numerous variations of time-restricted feeding, commonly referred to as intermittent fasting, but the principles are similar – limiting food intake to a specific window of time each day or week.
Although some studies have shown that time-restricted feeding may help patients reduce adiposity and improve lipid markers, most studies comparing time-restricted feeding to a calorie-restricted diet have shown little to no difference in weight-related outcomes, Dr. Hauser said.
These data suggest that time-restricted feeding may help patients with weight loss only if time restriction helps them reduce calorie intake. She also warned that time-restrictive feeding might cause late-night cravings and might not be helpful in individuals prone to food cravings.
Low‐carbohydrate and ketogenic diets
Losing muscle mass can prevent some people from dieting, but evidence suggests that a high-fat, very low-carbohydrate diet – also called a ketogenic diet – may help patients reduce weight and fat mass while preserving fat‐free mass, Dr. Hauser said.
The evidence regarding the usefulness of a low-carbohydrate (non-keto) diet is less clear because most studies compared it to a low-fat diet, and these two diets might lead to a similar extent of weight loss.
Rating the level of scientific evidence behind different diet options
Nutrition studies do no provide the same level of evidence as drug studies, said Dr. Hauser, because it is easier to conduct a randomized controlled trial of a drug versus placebo. Diets have many more variables, and it also takes much longer to observe most outcomes of a dietary change.
In addition, clinical trials of dietary interventions are typically short and focus on disease markers such as serum lipids and hemoglobin A1c levels. To obtain reliable information on the usefulness of a diet, researchers need to collect detailed health and lifestyle information from hundreds of thousands of people over several decades, which is not always feasible. “This is why meta-analyses of pooled dietary study data are more likely to yield dependable findings,” she noted.
Getting to know patients is essential to help them maintain diet modifications
When developing a diet plan for a patient, it is important to consider the sustainability of a dietary pattern. “The benefits of any healthy dietary change will only last as long as they can be maintained,” said Dr. Hauser. “Counseling someone on choosing an appropriate long-term dietary pattern requires getting to know them – taste preferences, food traditions, barriers, facilitators, food access, and time and cost restrictions.”
In an interview after the session, David Bittleman, MD, an internist at Veterans Affairs San Diego Health Care System, agreed that getting to know patients is essential for successfully advising them on diet.
“I always start developing a diet plan by trying to find out what [a patient’s] diet is like and what their goals are. I need to know what they are already doing in order to make suggestions about what they can do to make their diet healthier,” he said.
When asked about her approach to supporting patients in the long term, Dr. Hauser said that she recommends sequential, gradual changes. Dr. Hauser added that she suggests her patients prioritize implementing dietary changes that they are confident they can maintain.
Dr. Hauser and Dr. Bittleman report no relevant financial relationships.
according to a speaker at the annual meeting of the American College of Physicians.
“Evidence from studies can help clinicians and their patients develop a successful dietary management plan and achieve optimal health,” said internist Michelle Hauser, MD, clinical associate professor at Stanford (Calif.) University. She also discussed evidence-based techniques to support patients in maintaining dietary modifications.
Predominantly plant‐based diets
Popular predominantly plant‐based diets include a Mediterranean diet, healthy vegetarian diet, predominantly whole-food plant‐based (WFPB) diet, and a dietary approach to stop hypertension (DASH).
The DASH diet was originally designed to help patients manage their blood pressure, but evidence suggests that it also can help adults with obesity lose weight. In contrast to the DASH diet, the Mediterranean diet is not low-fat and not very restrictive. Yet the evidence suggests that the Mediterranean diet is not only helpful for losing weight but also can reduce the risk of various chronic diseases, including obesity, type 2 diabetes, cardiovascular disease (CVD), and cancer, Dr. Hauser said. In addition, data suggest that the Mediterranean diet may reduce the risk of all-cause mortality and lower the levels of cholesterol.
“I like to highlight all these protective effects to my patients, because even if their goal is to lose weight, knowing that hard work pays off in additional ways can keep them motivated,” Dr. Hauser stated.
A healthy vegetarian diet and a WFPB diet are similar, and both are helpful in weight loss and management of total cholesterol and LDL‐C levels. Furthermore, healthy vegetarian and WFPB diets may reduce the risk of type 2 diabetes, CVD, and some cancers. Cohort study data suggest that progressively more vegetarian diets are associated with lower BMIs.
“My interpretation of these data is that predominantly plant-based diets rich in whole foods are healthful and can be done in a way that is sustainable for most,” said Dr. Hauser. However, this generally requires a lot of support at the outset to address gaps in knowledge, skills, and other potential barriers.
For example, she referred one obese patient at risk of diabetes and cardiovascular disease to a registered dietitian to develop a dietary plan. The patient also attended a behavioral medicine weight management program to learn strategies such as using smaller plates, and his family attended a healthy cooking class together to improve meal planning and cooking skills.
Time‐restricted feeding
There are numerous variations of time-restricted feeding, commonly referred to as intermittent fasting, but the principles are similar – limiting food intake to a specific window of time each day or week.
Although some studies have shown that time-restricted feeding may help patients reduce adiposity and improve lipid markers, most studies comparing time-restricted feeding to a calorie-restricted diet have shown little to no difference in weight-related outcomes, Dr. Hauser said.
These data suggest that time-restricted feeding may help patients with weight loss only if time restriction helps them reduce calorie intake. She also warned that time-restrictive feeding might cause late-night cravings and might not be helpful in individuals prone to food cravings.
Low‐carbohydrate and ketogenic diets
Losing muscle mass can prevent some people from dieting, but evidence suggests that a high-fat, very low-carbohydrate diet – also called a ketogenic diet – may help patients reduce weight and fat mass while preserving fat‐free mass, Dr. Hauser said.
The evidence regarding the usefulness of a low-carbohydrate (non-keto) diet is less clear because most studies compared it to a low-fat diet, and these two diets might lead to a similar extent of weight loss.
Rating the level of scientific evidence behind different diet options
Nutrition studies do no provide the same level of evidence as drug studies, said Dr. Hauser, because it is easier to conduct a randomized controlled trial of a drug versus placebo. Diets have many more variables, and it also takes much longer to observe most outcomes of a dietary change.
In addition, clinical trials of dietary interventions are typically short and focus on disease markers such as serum lipids and hemoglobin A1c levels. To obtain reliable information on the usefulness of a diet, researchers need to collect detailed health and lifestyle information from hundreds of thousands of people over several decades, which is not always feasible. “This is why meta-analyses of pooled dietary study data are more likely to yield dependable findings,” she noted.
Getting to know patients is essential to help them maintain diet modifications
When developing a diet plan for a patient, it is important to consider the sustainability of a dietary pattern. “The benefits of any healthy dietary change will only last as long as they can be maintained,” said Dr. Hauser. “Counseling someone on choosing an appropriate long-term dietary pattern requires getting to know them – taste preferences, food traditions, barriers, facilitators, food access, and time and cost restrictions.”
In an interview after the session, David Bittleman, MD, an internist at Veterans Affairs San Diego Health Care System, agreed that getting to know patients is essential for successfully advising them on diet.
“I always start developing a diet plan by trying to find out what [a patient’s] diet is like and what their goals are. I need to know what they are already doing in order to make suggestions about what they can do to make their diet healthier,” he said.
When asked about her approach to supporting patients in the long term, Dr. Hauser said that she recommends sequential, gradual changes. Dr. Hauser added that she suggests her patients prioritize implementing dietary changes that they are confident they can maintain.
Dr. Hauser and Dr. Bittleman report no relevant financial relationships.
AT INTERNAL MEDICINE 2023
Should CGM be used for those without diabetes?
Dallas Waldon doesn’t have diabetes, but she says she benefits from continuous glucose monitoring (CGM). “I’m a huge fan of CGMs and used them before, during, and after my pregnancy, [up to] 6 months postpartum, I’m down 11 pounds from my prepregnancy weight,” said Ms. Waldon, a manager for a land-buying company who lives in El Dorado, Calif.
“CGMs bring a certain level of accountability to what you’re eating. You can’t pretend you didn’t eat that cookie while making the kids’ lunch, or that the latte you had was ‘just coffee,’ ” she said. “You have the hard numbers to answer to, and that makes you think twice before putting anything in your mouth.”
Ms. Waldon is not alone. Although CGMs are typically used by people with type 1 diabetes, and increasingly those with type 2 diabetes, some endocrinologists say they are seeing an increased demand for CGM use from individuals who don’t have diabetes.
This allows users to monitor the glucose level and see how eating and exercise affects it. The companies claim that CGM use will help motivate individuals to eat better and maximize their exercise, and therefore consequently lose weight.
These lifestyle programs typically offer users the FreeStyle Libre (Abbott Laboratories). It uses a coin-sized sensor, generally worn on the upper arm, which lasts 14 days and measures glucose in the interstitial fluid. Users can read their glucose levels via an app on their smartphones as many times a day as they want. The FreeStyle Libre is worn by many people with diabetes and is a simple CGM to use, said Anne Peters, MD, professor of clinical medicine, University of Southern California, Los Angeles.
This growing demand for CGM use among healthy people is driven by an increasing “fascination” for monitoring every bodily function, as can be seen by the popularity of smart devices such as Fitbits and Apple watches, Dr. Peters added. These devices allow users to see their heart rates, review their sleep patterns, and monitor their pulses in real time; a CGM is an extension of that by providing up-to-the-minute glucose monitoring.
‘Everyone wants a CGM’
“Everyone wants a CGM,” Dr. Peters said, noting that even family members of her patients with diabetes are asking for them. She admits that their use can be effective for those who are prediabetic so they can see their glycemic responses to food. For instance, someone who typically eats oatmeal for breakfast may see their blood glucose increase, meaning they might want to lower their carbs.
David Klonoff, MD, medical director of the Diabetes Research Institute, Mills-Peninsula Medical Center, San Mateo, Calif., agrees that there has been an increase in use by people who don’t have diabetes as CGMs offer information they wouldn’t otherwise have access to “without having to prick themselves many times.”
People are using CGMs to monitor how high their blood glucose rises after eating certain foods, the length of time it takes to reach peak levels, and how quickly levels drop, he added. Elite athletes are using CGMs to ensure that they are consuming enough calories to avoid hypoglycemia, Dr. Klonoff said.
David T. Ahn, MD, program director at the Mary & Dick Allen Diabetes Center at Hoag Hospital in Newport Beach, Calif., also believes that the devices can provide useful information. “I find that CGM helps people learn a lot about nutrition and how lifestyle choices like food, activity, and stress impact their own physiology,” he stated.

“For example, comparing glucose spikes after different [types of] meals can deepen people’s understanding of carbohydrates vs. protein, or high glycemic index foods vs. low glycemic index foods,” he continued. “In addition, if a patient chooses to follow a very low-carbohydrate diet and/or an intermittent fasting diet, a CGM can be a powerful tool to measure consistency with that lifestyle choice.”
And for a person without diabetes, wearing a CGM provides a way to have personalized information on other physiologic measures, part of the quantified self movement where users log and track their blood pressure, urine output, and oxygen saturation, among other things, Dr. Klonoff said.
But does knowing all this result in behavioral changes?
Dr. Ahn isn’t sure. “For many people, being able to see glucose excursions throughout the day and after meals can be extremely educational and motivating. But much like the Fitbit or Apple Watch, simply wearing [a CGM] ... does not translate to behavior change. The CGM data patterns in someone without diabetes can start to become predictable over time, leading to a drop-off in utility/adherence after the initial education period,” he said.
Dr. Peters said she too isn’t convinced about the long-term worth of CGM in promoting or sustaining behavioral change, as the “novelty” of tracking may wear off after a few months.
And there’s no scientific proof that CGM use in those without diabetes has any impact.
“While there are many programs that offer coaching with CGM data, we need more studies to determine if this leads to improved outcomes like weight loss and prevention, or delay in the development of diabetes,” said Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, FADCES, FCCP, director of education and training in diabetes technology at Cleveland Clinic Diabetes Center.

A 2019 study published in the Journal of Clinical Endocrinology and Metabolism found that the blood glucose of individuals without diabetes using a CGM was in the “ideal” range between 70 mg/dL and 140 mg/dL 96% of the time. “Their glucose was beautifully controlled,” said Dr. Peters, who was one of the study authors.
Currently there aren’t any studies evaluating patterns among healthy individuals wearing CGMs, Dr. Klonoff noted, but he predicts that those studies will be done in the future to examine metabolic patterns that might contribute to someone developing prediabetes or diabetes.
“More data are needed from studies that focus on individuals at risk for diabetes to better understand the role of CGM in these cases, and how to best interpret and utilize the results,” said Fida Bacha, MD, a diabetes and endocrinology specialist and associate professor of pediatrics at Baylor College of Medicine in Houston.
“If clear metrics are identified to predict the progression to diabetes, then this would be worthwhile for early detection and prevention of the disease,” Dr. Bacha said.
Are CGMs too expensive, and can the information overwhelm some?
The biggest obstacle to many people using CGM is cost. “The main downside of using a CGM without diabetes is cost, since insurance won’t usually cover a CGM if the patient does not have diabetes,” said Marilyn Tan, MD, FACE, chief of the Endocrine Clinic, Stanford Health Clinic, Palo Alto, Calif. “Even for patients with diabetes but not on insulin, CGM coverage can be challenging, as out-of-pocket costs for CGM are variable.”
The lifestyle companies mentioned above charge $139-$399 per month, which covers two CGM sensors, each one good for 14 days. Users need to subscribe to a plan for service and delivery. Additional services such as nutrition counseling may be available at an additional cost. Because CGMs in the United States require a prescription, these companies offer web screening and access to a web-based provider.
If healthy patients feel that the informational value of CGMs is worth the money, then they shouldn’t be discouraged, the experts believe.
“There’s little risk of harm with wearing a CGM,” Dr. Tan said, although she acknowledges that “[t]oo much information can also be overwhelming for some individuals.”
Users need to consult with their clinicians to ensure they understand the readings, Dr. Peters said. “You have to tell them not to overreact if the device reads low [glucose] or not to freak out if they get an alarm.” A high glucose reading, indicating hyperglycemia, can be caused by a steroid injection, or older people may experience a postprandial high after eating, she added. “They need to talk to their healthcare provider to interpret the data especially if they are out of [the ideal glucose] range.”
Dr. Klonoff agreed that there is a risk of people trying to “medicalize” too much information. “If you have a fever, you don’t have to go to a doctor to know you have an infection,” he said.
And the point, he added, is not to obsess over the individual numbers but to look for patterns particularly as predictors of metabolic syndrome. If a patient’s glucose is primarily in range, he or she wouldn’t necessarily worry about diabetes. But if it’s out of range more than 10% of the time, it might mean that patient is at risk for diabetes. “It might be time to counsel the patient to eat healthier and exercise more,” he said. “It’s never wrong to steer people to a healthier lifestyle.”
But another issue is whether the numbers from CGMs are entirely accurate in people without diabetes. A 2020 study published in the American Journal of Clinical Nutrition had 16 adults without diabetes wear both the Dexcom G4 Platinum CGM and Abbott FreeStyle Libre Pro for 28 days.
Researchers found that mean postprandial glucose was higher with the Dexcom than with the Abbott system, suggesting that “postprandial glycemic excursions were somewhat inconsistent between the CGMs.” The authors concluded that it may be too early to personalize meal recommendations via CGM.
Dr. Isaacs said perhaps the happy medium is for those without diabetes to just use CGMs occasionally. “It’s ... unclear [if] the right [use] of CGM needs to be continuous or if periodic use, such as once every 3 months, is enough for benefits,” she concluded.
A version of this article first appeared on Medscape.com.
Dallas Waldon doesn’t have diabetes, but she says she benefits from continuous glucose monitoring (CGM). “I’m a huge fan of CGMs and used them before, during, and after my pregnancy, [up to] 6 months postpartum, I’m down 11 pounds from my prepregnancy weight,” said Ms. Waldon, a manager for a land-buying company who lives in El Dorado, Calif.
“CGMs bring a certain level of accountability to what you’re eating. You can’t pretend you didn’t eat that cookie while making the kids’ lunch, or that the latte you had was ‘just coffee,’ ” she said. “You have the hard numbers to answer to, and that makes you think twice before putting anything in your mouth.”
Ms. Waldon is not alone. Although CGMs are typically used by people with type 1 diabetes, and increasingly those with type 2 diabetes, some endocrinologists say they are seeing an increased demand for CGM use from individuals who don’t have diabetes.
This allows users to monitor the glucose level and see how eating and exercise affects it. The companies claim that CGM use will help motivate individuals to eat better and maximize their exercise, and therefore consequently lose weight.
These lifestyle programs typically offer users the FreeStyle Libre (Abbott Laboratories). It uses a coin-sized sensor, generally worn on the upper arm, which lasts 14 days and measures glucose in the interstitial fluid. Users can read their glucose levels via an app on their smartphones as many times a day as they want. The FreeStyle Libre is worn by many people with diabetes and is a simple CGM to use, said Anne Peters, MD, professor of clinical medicine, University of Southern California, Los Angeles.
This growing demand for CGM use among healthy people is driven by an increasing “fascination” for monitoring every bodily function, as can be seen by the popularity of smart devices such as Fitbits and Apple watches, Dr. Peters added. These devices allow users to see their heart rates, review their sleep patterns, and monitor their pulses in real time; a CGM is an extension of that by providing up-to-the-minute glucose monitoring.
‘Everyone wants a CGM’
“Everyone wants a CGM,” Dr. Peters said, noting that even family members of her patients with diabetes are asking for them. She admits that their use can be effective for those who are prediabetic so they can see their glycemic responses to food. For instance, someone who typically eats oatmeal for breakfast may see their blood glucose increase, meaning they might want to lower their carbs.
David Klonoff, MD, medical director of the Diabetes Research Institute, Mills-Peninsula Medical Center, San Mateo, Calif., agrees that there has been an increase in use by people who don’t have diabetes as CGMs offer information they wouldn’t otherwise have access to “without having to prick themselves many times.”
People are using CGMs to monitor how high their blood glucose rises after eating certain foods, the length of time it takes to reach peak levels, and how quickly levels drop, he added. Elite athletes are using CGMs to ensure that they are consuming enough calories to avoid hypoglycemia, Dr. Klonoff said.
David T. Ahn, MD, program director at the Mary & Dick Allen Diabetes Center at Hoag Hospital in Newport Beach, Calif., also believes that the devices can provide useful information. “I find that CGM helps people learn a lot about nutrition and how lifestyle choices like food, activity, and stress impact their own physiology,” he stated.
“For example, comparing glucose spikes after different [types of] meals can deepen people’s understanding of carbohydrates vs. protein, or high glycemic index foods vs. low glycemic index foods,” he continued. “In addition, if a patient chooses to follow a very low-carbohydrate diet and/or an intermittent fasting diet, a CGM can be a powerful tool to measure consistency with that lifestyle choice.”
And for a person without diabetes, wearing a CGM provides a way to have personalized information on other physiologic measures, part of the quantified self movement where users log and track their blood pressure, urine output, and oxygen saturation, among other things, Dr. Klonoff said.
But does knowing all this result in behavioral changes?
Dr. Ahn isn’t sure. “For many people, being able to see glucose excursions throughout the day and after meals can be extremely educational and motivating. But much like the Fitbit or Apple Watch, simply wearing [a CGM] ... does not translate to behavior change. The CGM data patterns in someone without diabetes can start to become predictable over time, leading to a drop-off in utility/adherence after the initial education period,” he said.
Dr. Peters said she too isn’t convinced about the long-term worth of CGM in promoting or sustaining behavioral change, as the “novelty” of tracking may wear off after a few months.
And there’s no scientific proof that CGM use in those without diabetes has any impact.
“While there are many programs that offer coaching with CGM data, we need more studies to determine if this leads to improved outcomes like weight loss and prevention, or delay in the development of diabetes,” said Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, FADCES, FCCP, director of education and training in diabetes technology at Cleveland Clinic Diabetes Center.
A 2019 study published in the Journal of Clinical Endocrinology and Metabolism found that the blood glucose of individuals without diabetes using a CGM was in the “ideal” range between 70 mg/dL and 140 mg/dL 96% of the time. “Their glucose was beautifully controlled,” said Dr. Peters, who was one of the study authors.
Currently there aren’t any studies evaluating patterns among healthy individuals wearing CGMs, Dr. Klonoff noted, but he predicts that those studies will be done in the future to examine metabolic patterns that might contribute to someone developing prediabetes or diabetes.
“More data are needed from studies that focus on individuals at risk for diabetes to better understand the role of CGM in these cases, and how to best interpret and utilize the results,” said Fida Bacha, MD, a diabetes and endocrinology specialist and associate professor of pediatrics at Baylor College of Medicine in Houston.
“If clear metrics are identified to predict the progression to diabetes, then this would be worthwhile for early detection and prevention of the disease,” Dr. Bacha said.
Are CGMs too expensive, and can the information overwhelm some?
The biggest obstacle to many people using CGM is cost. “The main downside of using a CGM without diabetes is cost, since insurance won’t usually cover a CGM if the patient does not have diabetes,” said Marilyn Tan, MD, FACE, chief of the Endocrine Clinic, Stanford Health Clinic, Palo Alto, Calif. “Even for patients with diabetes but not on insulin, CGM coverage can be challenging, as out-of-pocket costs for CGM are variable.”
The lifestyle companies mentioned above charge $139-$399 per month, which covers two CGM sensors, each one good for 14 days. Users need to subscribe to a plan for service and delivery. Additional services such as nutrition counseling may be available at an additional cost. Because CGMs in the United States require a prescription, these companies offer web screening and access to a web-based provider.
If healthy patients feel that the informational value of CGMs is worth the money, then they shouldn’t be discouraged, the experts believe.
“There’s little risk of harm with wearing a CGM,” Dr. Tan said, although she acknowledges that “[t]oo much information can also be overwhelming for some individuals.”
Users need to consult with their clinicians to ensure they understand the readings, Dr. Peters said. “You have to tell them not to overreact if the device reads low [glucose] or not to freak out if they get an alarm.” A high glucose reading, indicating hyperglycemia, can be caused by a steroid injection, or older people may experience a postprandial high after eating, she added. “They need to talk to their healthcare provider to interpret the data especially if they are out of [the ideal glucose] range.”
Dr. Klonoff agreed that there is a risk of people trying to “medicalize” too much information. “If you have a fever, you don’t have to go to a doctor to know you have an infection,” he said.
And the point, he added, is not to obsess over the individual numbers but to look for patterns particularly as predictors of metabolic syndrome. If a patient’s glucose is primarily in range, he or she wouldn’t necessarily worry about diabetes. But if it’s out of range more than 10% of the time, it might mean that patient is at risk for diabetes. “It might be time to counsel the patient to eat healthier and exercise more,” he said. “It’s never wrong to steer people to a healthier lifestyle.”
But another issue is whether the numbers from CGMs are entirely accurate in people without diabetes. A 2020 study published in the American Journal of Clinical Nutrition had 16 adults without diabetes wear both the Dexcom G4 Platinum CGM and Abbott FreeStyle Libre Pro for 28 days.
Researchers found that mean postprandial glucose was higher with the Dexcom than with the Abbott system, suggesting that “postprandial glycemic excursions were somewhat inconsistent between the CGMs.” The authors concluded that it may be too early to personalize meal recommendations via CGM.
Dr. Isaacs said perhaps the happy medium is for those without diabetes to just use CGMs occasionally. “It’s ... unclear [if] the right [use] of CGM needs to be continuous or if periodic use, such as once every 3 months, is enough for benefits,” she concluded.
A version of this article first appeared on Medscape.com.
Dallas Waldon doesn’t have diabetes, but she says she benefits from continuous glucose monitoring (CGM). “I’m a huge fan of CGMs and used them before, during, and after my pregnancy, [up to] 6 months postpartum, I’m down 11 pounds from my prepregnancy weight,” said Ms. Waldon, a manager for a land-buying company who lives in El Dorado, Calif.
“CGMs bring a certain level of accountability to what you’re eating. You can’t pretend you didn’t eat that cookie while making the kids’ lunch, or that the latte you had was ‘just coffee,’ ” she said. “You have the hard numbers to answer to, and that makes you think twice before putting anything in your mouth.”
Ms. Waldon is not alone. Although CGMs are typically used by people with type 1 diabetes, and increasingly those with type 2 diabetes, some endocrinologists say they are seeing an increased demand for CGM use from individuals who don’t have diabetes.
This allows users to monitor the glucose level and see how eating and exercise affects it. The companies claim that CGM use will help motivate individuals to eat better and maximize their exercise, and therefore consequently lose weight.
These lifestyle programs typically offer users the FreeStyle Libre (Abbott Laboratories). It uses a coin-sized sensor, generally worn on the upper arm, which lasts 14 days and measures glucose in the interstitial fluid. Users can read their glucose levels via an app on their smartphones as many times a day as they want. The FreeStyle Libre is worn by many people with diabetes and is a simple CGM to use, said Anne Peters, MD, professor of clinical medicine, University of Southern California, Los Angeles.
This growing demand for CGM use among healthy people is driven by an increasing “fascination” for monitoring every bodily function, as can be seen by the popularity of smart devices such as Fitbits and Apple watches, Dr. Peters added. These devices allow users to see their heart rates, review their sleep patterns, and monitor their pulses in real time; a CGM is an extension of that by providing up-to-the-minute glucose monitoring.
‘Everyone wants a CGM’
“Everyone wants a CGM,” Dr. Peters said, noting that even family members of her patients with diabetes are asking for them. She admits that their use can be effective for those who are prediabetic so they can see their glycemic responses to food. For instance, someone who typically eats oatmeal for breakfast may see their blood glucose increase, meaning they might want to lower their carbs.
David Klonoff, MD, medical director of the Diabetes Research Institute, Mills-Peninsula Medical Center, San Mateo, Calif., agrees that there has been an increase in use by people who don’t have diabetes as CGMs offer information they wouldn’t otherwise have access to “without having to prick themselves many times.”
People are using CGMs to monitor how high their blood glucose rises after eating certain foods, the length of time it takes to reach peak levels, and how quickly levels drop, he added. Elite athletes are using CGMs to ensure that they are consuming enough calories to avoid hypoglycemia, Dr. Klonoff said.
David T. Ahn, MD, program director at the Mary & Dick Allen Diabetes Center at Hoag Hospital in Newport Beach, Calif., also believes that the devices can provide useful information. “I find that CGM helps people learn a lot about nutrition and how lifestyle choices like food, activity, and stress impact their own physiology,” he stated.
“For example, comparing glucose spikes after different [types of] meals can deepen people’s understanding of carbohydrates vs. protein, or high glycemic index foods vs. low glycemic index foods,” he continued. “In addition, if a patient chooses to follow a very low-carbohydrate diet and/or an intermittent fasting diet, a CGM can be a powerful tool to measure consistency with that lifestyle choice.”
And for a person without diabetes, wearing a CGM provides a way to have personalized information on other physiologic measures, part of the quantified self movement where users log and track their blood pressure, urine output, and oxygen saturation, among other things, Dr. Klonoff said.
But does knowing all this result in behavioral changes?
Dr. Ahn isn’t sure. “For many people, being able to see glucose excursions throughout the day and after meals can be extremely educational and motivating. But much like the Fitbit or Apple Watch, simply wearing [a CGM] ... does not translate to behavior change. The CGM data patterns in someone without diabetes can start to become predictable over time, leading to a drop-off in utility/adherence after the initial education period,” he said.
Dr. Peters said she too isn’t convinced about the long-term worth of CGM in promoting or sustaining behavioral change, as the “novelty” of tracking may wear off after a few months.
And there’s no scientific proof that CGM use in those without diabetes has any impact.
“While there are many programs that offer coaching with CGM data, we need more studies to determine if this leads to improved outcomes like weight loss and prevention, or delay in the development of diabetes,” said Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, FADCES, FCCP, director of education and training in diabetes technology at Cleveland Clinic Diabetes Center.
A 2019 study published in the Journal of Clinical Endocrinology and Metabolism found that the blood glucose of individuals without diabetes using a CGM was in the “ideal” range between 70 mg/dL and 140 mg/dL 96% of the time. “Their glucose was beautifully controlled,” said Dr. Peters, who was one of the study authors.
Currently there aren’t any studies evaluating patterns among healthy individuals wearing CGMs, Dr. Klonoff noted, but he predicts that those studies will be done in the future to examine metabolic patterns that might contribute to someone developing prediabetes or diabetes.
“More data are needed from studies that focus on individuals at risk for diabetes to better understand the role of CGM in these cases, and how to best interpret and utilize the results,” said Fida Bacha, MD, a diabetes and endocrinology specialist and associate professor of pediatrics at Baylor College of Medicine in Houston.
“If clear metrics are identified to predict the progression to diabetes, then this would be worthwhile for early detection and prevention of the disease,” Dr. Bacha said.
Are CGMs too expensive, and can the information overwhelm some?
The biggest obstacle to many people using CGM is cost. “The main downside of using a CGM without diabetes is cost, since insurance won’t usually cover a CGM if the patient does not have diabetes,” said Marilyn Tan, MD, FACE, chief of the Endocrine Clinic, Stanford Health Clinic, Palo Alto, Calif. “Even for patients with diabetes but not on insulin, CGM coverage can be challenging, as out-of-pocket costs for CGM are variable.”
The lifestyle companies mentioned above charge $139-$399 per month, which covers two CGM sensors, each one good for 14 days. Users need to subscribe to a plan for service and delivery. Additional services such as nutrition counseling may be available at an additional cost. Because CGMs in the United States require a prescription, these companies offer web screening and access to a web-based provider.
If healthy patients feel that the informational value of CGMs is worth the money, then they shouldn’t be discouraged, the experts believe.
“There’s little risk of harm with wearing a CGM,” Dr. Tan said, although she acknowledges that “[t]oo much information can also be overwhelming for some individuals.”
Users need to consult with their clinicians to ensure they understand the readings, Dr. Peters said. “You have to tell them not to overreact if the device reads low [glucose] or not to freak out if they get an alarm.” A high glucose reading, indicating hyperglycemia, can be caused by a steroid injection, or older people may experience a postprandial high after eating, she added. “They need to talk to their healthcare provider to interpret the data especially if they are out of [the ideal glucose] range.”
Dr. Klonoff agreed that there is a risk of people trying to “medicalize” too much information. “If you have a fever, you don’t have to go to a doctor to know you have an infection,” he said.
And the point, he added, is not to obsess over the individual numbers but to look for patterns particularly as predictors of metabolic syndrome. If a patient’s glucose is primarily in range, he or she wouldn’t necessarily worry about diabetes. But if it’s out of range more than 10% of the time, it might mean that patient is at risk for diabetes. “It might be time to counsel the patient to eat healthier and exercise more,” he said. “It’s never wrong to steer people to a healthier lifestyle.”
But another issue is whether the numbers from CGMs are entirely accurate in people without diabetes. A 2020 study published in the American Journal of Clinical Nutrition had 16 adults without diabetes wear both the Dexcom G4 Platinum CGM and Abbott FreeStyle Libre Pro for 28 days.
Researchers found that mean postprandial glucose was higher with the Dexcom than with the Abbott system, suggesting that “postprandial glycemic excursions were somewhat inconsistent between the CGMs.” The authors concluded that it may be too early to personalize meal recommendations via CGM.
Dr. Isaacs said perhaps the happy medium is for those without diabetes to just use CGMs occasionally. “It’s ... unclear [if] the right [use] of CGM needs to be continuous or if periodic use, such as once every 3 months, is enough for benefits,” she concluded.
A version of this article first appeared on Medscape.com.
Statins tied to lower stroke risk in atrial fibrillation
Among patients with atrial fibrillation (AFib), initiation of statins soon after diagnosis was protective against stroke and related vascular events, and longer duration of use was associated with greater protection, a new cohort study shows.
Statin use was associated with lower risks of ischemic stroke or systemic embolism, hemorrhagic stroke, and transient ischemic attack (TIA), regardless of whether patients were also taking anticoagulant medications.
Lead author Jiayi Huang, a PhD student at Hong Kong University at Shenzhen (China) Hospital, concluded that the study’s findings support the use of statins to prevent stroke for patients with new-onset AFib.
“The findings have important clinical implications, particularly given that in atrial fibrillation, patients’ ischemic strokes are often fatal or disabling and have a high risk of recurrence,” she said.
The results were presented in a moderated poster session at the European Heart Rhythm Association 2023 Congress.
Widely prescribed
Anticoagulant drugs are prescribed to lower the fivefold increased risk of stroke among individuals with AFib, compared with those without AFib, but the therapy does not eliminate the higher risk, Ms. Huang explained. And although statins are widely prescribed to reduce the likelihood of myocardial infarction and stroke, “the benefit of statins for stroke prevention in patients with atrial fibrillation has been unclear.”
Ms. Huang and colleagues analyzed data from 51,472 patients newly diagnosed with AFib between 2010 and 2018. The population was divided into statin users (n = 11,866), defined as patients who had taken statins for at least 19 consecutive days in the first year after AFib diagnosis, and statin nonusers (n = 39,606), based on whether they were prescribed statin therapy after their first diagnosis of AFib.
The median age of the cohort was 74.9 years, and 47.7% were women. The investigators used statistical methods to balance baseline covariates between the two groups.
The primary outcomes were ischemic stroke or systemic embolism, hemorrhagic stroke, and TIA. Median follow-up was 5.1 years.
Statin use was associated with a significantly lower risk of all outcomes, compared with nonuse. Statin users had a 17% reduced risk of ischemic stroke or systemic embolism, a 7% reduced risk of hemorrhagic stroke, and a 15% rate of reduced risk of TIA, Ms. Huang reported.
“We also found long-term statin use was associated with greater protection than short-term use,” she said. For statin use of 6 years or longer, in comparison with use of 3 months to 2 years, the risk of ischemic stroke or systemic embolism was lowered by 43%; for hemorrhagic stroke, it was lowered by 44%, and for TIA, it was lowered by 42%.
These associations were consistent regardless of whether patients used anticoagulant medications or the type of anticoagulant.
Oussama Wazni, MD, MBA, section head of cardiac electrophysiology and pacing at the Cleveland Clinic, was a moderator of the poster session at which Ms. Huang presented her study. In an interview, he called the study “very important.”
“The message should be that all patients who have atrial fibrillation should be checked for cholesterol levels, and we should consider placing them on statins,” he said. “Is there an opportunity? Probably there is, and that’s why we’re seeing this effect in this group of patients.”
When asked about a possible mechanism by which statins produced the effects seen in the study, he pointed to LDL cholesterol lowering and possibly an effect on inflammation. “If a patient had a carotid atheroma, for example, maybe it helped with that,” he said. Previous work has shown that inflammation is related to or is associated with higher risk of thrombogenic effects, including MI or stroke.
It may be a bit less clear how statins reduced the incidence of hemorrhagic strokes, but Dr. Wazni proposed that some strokes could have started as an ischemic stroke “and then had hemorrhagic conversion, so we don’t have the granularity in here to know whether that was the case or not.”
Given the fact that the effect was stronger the longer a patient had been taking a statin, Dr. Wazni said that if a patient is tolerating the drug well, there should be no reason to discontinue it, regardless of age.
He said the study provides “welcome data and evidence because it’s pointing in the right direction,” but prospective studies would be useful “so that we can see what is driving what. Otherwise, this is just an association.”
The study was supported by Sanming Project Shenzhen. Ms. Huang and Dr. Wazni disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among patients with atrial fibrillation (AFib), initiation of statins soon after diagnosis was protective against stroke and related vascular events, and longer duration of use was associated with greater protection, a new cohort study shows.
Statin use was associated with lower risks of ischemic stroke or systemic embolism, hemorrhagic stroke, and transient ischemic attack (TIA), regardless of whether patients were also taking anticoagulant medications.
Lead author Jiayi Huang, a PhD student at Hong Kong University at Shenzhen (China) Hospital, concluded that the study’s findings support the use of statins to prevent stroke for patients with new-onset AFib.
“The findings have important clinical implications, particularly given that in atrial fibrillation, patients’ ischemic strokes are often fatal or disabling and have a high risk of recurrence,” she said.
The results were presented in a moderated poster session at the European Heart Rhythm Association 2023 Congress.
Widely prescribed
Anticoagulant drugs are prescribed to lower the fivefold increased risk of stroke among individuals with AFib, compared with those without AFib, but the therapy does not eliminate the higher risk, Ms. Huang explained. And although statins are widely prescribed to reduce the likelihood of myocardial infarction and stroke, “the benefit of statins for stroke prevention in patients with atrial fibrillation has been unclear.”
Ms. Huang and colleagues analyzed data from 51,472 patients newly diagnosed with AFib between 2010 and 2018. The population was divided into statin users (n = 11,866), defined as patients who had taken statins for at least 19 consecutive days in the first year after AFib diagnosis, and statin nonusers (n = 39,606), based on whether they were prescribed statin therapy after their first diagnosis of AFib.
The median age of the cohort was 74.9 years, and 47.7% were women. The investigators used statistical methods to balance baseline covariates between the two groups.
The primary outcomes were ischemic stroke or systemic embolism, hemorrhagic stroke, and TIA. Median follow-up was 5.1 years.
Statin use was associated with a significantly lower risk of all outcomes, compared with nonuse. Statin users had a 17% reduced risk of ischemic stroke or systemic embolism, a 7% reduced risk of hemorrhagic stroke, and a 15% rate of reduced risk of TIA, Ms. Huang reported.
“We also found long-term statin use was associated with greater protection than short-term use,” she said. For statin use of 6 years or longer, in comparison with use of 3 months to 2 years, the risk of ischemic stroke or systemic embolism was lowered by 43%; for hemorrhagic stroke, it was lowered by 44%, and for TIA, it was lowered by 42%.
These associations were consistent regardless of whether patients used anticoagulant medications or the type of anticoagulant.
Oussama Wazni, MD, MBA, section head of cardiac electrophysiology and pacing at the Cleveland Clinic, was a moderator of the poster session at which Ms. Huang presented her study. In an interview, he called the study “very important.”
“The message should be that all patients who have atrial fibrillation should be checked for cholesterol levels, and we should consider placing them on statins,” he said. “Is there an opportunity? Probably there is, and that’s why we’re seeing this effect in this group of patients.”
When asked about a possible mechanism by which statins produced the effects seen in the study, he pointed to LDL cholesterol lowering and possibly an effect on inflammation. “If a patient had a carotid atheroma, for example, maybe it helped with that,” he said. Previous work has shown that inflammation is related to or is associated with higher risk of thrombogenic effects, including MI or stroke.
It may be a bit less clear how statins reduced the incidence of hemorrhagic strokes, but Dr. Wazni proposed that some strokes could have started as an ischemic stroke “and then had hemorrhagic conversion, so we don’t have the granularity in here to know whether that was the case or not.”
Given the fact that the effect was stronger the longer a patient had been taking a statin, Dr. Wazni said that if a patient is tolerating the drug well, there should be no reason to discontinue it, regardless of age.
He said the study provides “welcome data and evidence because it’s pointing in the right direction,” but prospective studies would be useful “so that we can see what is driving what. Otherwise, this is just an association.”
The study was supported by Sanming Project Shenzhen. Ms. Huang and Dr. Wazni disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Among patients with atrial fibrillation (AFib), initiation of statins soon after diagnosis was protective against stroke and related vascular events, and longer duration of use was associated with greater protection, a new cohort study shows.
Statin use was associated with lower risks of ischemic stroke or systemic embolism, hemorrhagic stroke, and transient ischemic attack (TIA), regardless of whether patients were also taking anticoagulant medications.
Lead author Jiayi Huang, a PhD student at Hong Kong University at Shenzhen (China) Hospital, concluded that the study’s findings support the use of statins to prevent stroke for patients with new-onset AFib.
“The findings have important clinical implications, particularly given that in atrial fibrillation, patients’ ischemic strokes are often fatal or disabling and have a high risk of recurrence,” she said.
The results were presented in a moderated poster session at the European Heart Rhythm Association 2023 Congress.
Widely prescribed
Anticoagulant drugs are prescribed to lower the fivefold increased risk of stroke among individuals with AFib, compared with those without AFib, but the therapy does not eliminate the higher risk, Ms. Huang explained. And although statins are widely prescribed to reduce the likelihood of myocardial infarction and stroke, “the benefit of statins for stroke prevention in patients with atrial fibrillation has been unclear.”
Ms. Huang and colleagues analyzed data from 51,472 patients newly diagnosed with AFib between 2010 and 2018. The population was divided into statin users (n = 11,866), defined as patients who had taken statins for at least 19 consecutive days in the first year after AFib diagnosis, and statin nonusers (n = 39,606), based on whether they were prescribed statin therapy after their first diagnosis of AFib.
The median age of the cohort was 74.9 years, and 47.7% were women. The investigators used statistical methods to balance baseline covariates between the two groups.
The primary outcomes were ischemic stroke or systemic embolism, hemorrhagic stroke, and TIA. Median follow-up was 5.1 years.
Statin use was associated with a significantly lower risk of all outcomes, compared with nonuse. Statin users had a 17% reduced risk of ischemic stroke or systemic embolism, a 7% reduced risk of hemorrhagic stroke, and a 15% rate of reduced risk of TIA, Ms. Huang reported.
“We also found long-term statin use was associated with greater protection than short-term use,” she said. For statin use of 6 years or longer, in comparison with use of 3 months to 2 years, the risk of ischemic stroke or systemic embolism was lowered by 43%; for hemorrhagic stroke, it was lowered by 44%, and for TIA, it was lowered by 42%.
These associations were consistent regardless of whether patients used anticoagulant medications or the type of anticoagulant.
Oussama Wazni, MD, MBA, section head of cardiac electrophysiology and pacing at the Cleveland Clinic, was a moderator of the poster session at which Ms. Huang presented her study. In an interview, he called the study “very important.”
“The message should be that all patients who have atrial fibrillation should be checked for cholesterol levels, and we should consider placing them on statins,” he said. “Is there an opportunity? Probably there is, and that’s why we’re seeing this effect in this group of patients.”
When asked about a possible mechanism by which statins produced the effects seen in the study, he pointed to LDL cholesterol lowering and possibly an effect on inflammation. “If a patient had a carotid atheroma, for example, maybe it helped with that,” he said. Previous work has shown that inflammation is related to or is associated with higher risk of thrombogenic effects, including MI or stroke.
It may be a bit less clear how statins reduced the incidence of hemorrhagic strokes, but Dr. Wazni proposed that some strokes could have started as an ischemic stroke “and then had hemorrhagic conversion, so we don’t have the granularity in here to know whether that was the case or not.”
Given the fact that the effect was stronger the longer a patient had been taking a statin, Dr. Wazni said that if a patient is tolerating the drug well, there should be no reason to discontinue it, regardless of age.
He said the study provides “welcome data and evidence because it’s pointing in the right direction,” but prospective studies would be useful “so that we can see what is driving what. Otherwise, this is just an association.”
The study was supported by Sanming Project Shenzhen. Ms. Huang and Dr. Wazni disclosed no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM EHRA 2023
Lifestyle med experts tell how to deprescribe diabetes meds
Nine lifestyle medicine practitioners describe how they safely and effectively deprescribe glucose-lowering medications after patients demonstrate a reduced need for such medications following lifestyle changes.
The report by Michael D. Bradley, PharmD, and colleagues was recently published as a feature article in Clinical Diabetes.
“Lifestyle medicine uses an evidence-based lifestyle therapeutic approach to treat lifestyle-related chronic disease,” they wrote, and it includes “a whole-food, predominantly plant-based eating plan, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connection.”
“Medication deprescribing,” senior author Micaela C. Karlsen, PhD, said in an email, “is a planned and supervised process of dose reduction or discontinuation of a medication that may be causing harm, or no longer providing benefit to a patient.”
According to the authors, the article “is the first account published of the medication de-escalation methods used by lifestyle medicine providers when patients demonstrate a decreased need for pharmacotherapy.” It “supports the feasibility of de-escalating glucose-lowering medications in this context and provides pilot data on protocols from individual practitioners experienced in deprescribing glucose-lowering medications.”
The study was not designed to cover deprescribing glucose-lowering medications following weight loss and diabetes remission after bariatric surgery.
“A key takeaway [from the current study] for general practitioners and endocrinologists is that, while deprescribing is already known to be beneficial to reduce polypharmacy, it may be appropriate following lifestyle interventions,” said Dr. Karlsen, who is senior director of the American College of Lifestyle Medicine in Chesterfield, Md.
“The protocols presented can serve as a model for how to do so,” she continued.
The American Diabetes Association and the American Association of Clinical Endocrinology recommend lifestyle optimization as part of medical care for type 2 diabetes.
According to the ACLM, “remission of type 2 diabetes should be a clinical goal and may be achieved with a whole-food, plant-based dietary pattern coupled with moderate exercise,” the researchers noted.
“Remission,” they wrote, “can be defined as attainment of a [hemoglobin] A1c less than 6.5% for at least 3 months with no surgery, devices, or active pharmacologic therapy for the specific purpose of lowering blood glucose.”
In ACLM’s recent expert consensus statement on dietary interventions for type 2 diabetes remission, which was also endorsed by AACE, supported by the Academy of Nutrition and Dietetics, and cosponsored by the Endocrine Society, panel members agreed that remission is a realistic and achievable goal for some adults with type 2 diabetes, and a high-intensity dietary intervention can result in remission, Dr. Karlsen said.
To avoid hypoglycemia when deprescribing antiglycemic drugs, medications known to cause hypoglycemia – notably sulfonylurea and insulin – are often deprescribed first, she noted.
“Our biggest hope,” she said, “is that [type 2 diabetes] remission may come to the forefront as a clinical goal in treatment and that other organizations will more strongly emphasize lifestyle in standards of care.”
“We hope that clinicians reading this paper will be made aware that de-escalation of glucose-lowering medications is feasible, is a desirable outcome, and can be necessary in a lifestyle medicine context,” she added.
Further research is needed to prospectively track the likelihood of type 2 diabetes remission, factors that predict successful remission, and decision-making protocols followed by practitioners, Dr. Karlsen said.
Deprescribing antiglycemic meds in lifestyle medicine
Researchers at the Bruyère Research Institute, Ottawa, and Université de Montréal provide algorithms for deprescribing antihyperglycemic medications specifically for older individuals.
In the current study, the authors conducted individual, 30-minute to 1-hour interviews with nine lifestyle medicine practitioners to document their protocols for deprescribing glucose-lowering medications after lifestyle interventions with a goal of potential type 2 diabetes remission.
Three practitioners reported medication deprescribing in an intensive therapeutic lifestyle program (longer, more frequent treatment with greater monitoring). The others provide deprescribing in a nonintensive program (similar to primary care practice) or both.
Deprescribing is necessary when using intensive therapeutic lifestyle change, as substantial and rapid drops in glucose levels aren’t adjusted for, the authors noted.
Most practitioners work with a team of allied health care providers.
During the deprescribing process, most protocols require that patients get a basic or comprehensive metabolic panel of blood tests, with variations in laboratory tests for A1c, C-peptide, and renal function.
Most practitioners recommend a target blood glucose less than 120 mg/dL for further deprescribing.
Currently, there is no clinical guidance for use of continuous glucose monitoring (CGM) during medication de-escalation, the authors note.
Most practitioners reported they consider patient expenses associated with CGM and third-party payor coverage in their decision-making.
Most practitioners prefer to deprescribe sulfonylureas, insulin, and other medications known to cause hypoglycemia first.
Conversely, most prefer to defer deprescribing medications that have demonstrated cardiovascular and/or renal benefits (that is, glucagonlike peptide–1 receptor agonists and sodium-glucose cotransporter 2 inhibitors), as well as those with a less severe adverse effect profile (that is, metformin and GLP-1 receptor agonists) until after other medications are deprescribed.
The study was funded by the Ardmore Institute of Health. The authors reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Nine lifestyle medicine practitioners describe how they safely and effectively deprescribe glucose-lowering medications after patients demonstrate a reduced need for such medications following lifestyle changes.
The report by Michael D. Bradley, PharmD, and colleagues was recently published as a feature article in Clinical Diabetes.
“Lifestyle medicine uses an evidence-based lifestyle therapeutic approach to treat lifestyle-related chronic disease,” they wrote, and it includes “a whole-food, predominantly plant-based eating plan, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connection.”
“Medication deprescribing,” senior author Micaela C. Karlsen, PhD, said in an email, “is a planned and supervised process of dose reduction or discontinuation of a medication that may be causing harm, or no longer providing benefit to a patient.”
According to the authors, the article “is the first account published of the medication de-escalation methods used by lifestyle medicine providers when patients demonstrate a decreased need for pharmacotherapy.” It “supports the feasibility of de-escalating glucose-lowering medications in this context and provides pilot data on protocols from individual practitioners experienced in deprescribing glucose-lowering medications.”
The study was not designed to cover deprescribing glucose-lowering medications following weight loss and diabetes remission after bariatric surgery.
“A key takeaway [from the current study] for general practitioners and endocrinologists is that, while deprescribing is already known to be beneficial to reduce polypharmacy, it may be appropriate following lifestyle interventions,” said Dr. Karlsen, who is senior director of the American College of Lifestyle Medicine in Chesterfield, Md.
“The protocols presented can serve as a model for how to do so,” she continued.
The American Diabetes Association and the American Association of Clinical Endocrinology recommend lifestyle optimization as part of medical care for type 2 diabetes.
According to the ACLM, “remission of type 2 diabetes should be a clinical goal and may be achieved with a whole-food, plant-based dietary pattern coupled with moderate exercise,” the researchers noted.
“Remission,” they wrote, “can be defined as attainment of a [hemoglobin] A1c less than 6.5% for at least 3 months with no surgery, devices, or active pharmacologic therapy for the specific purpose of lowering blood glucose.”
In ACLM’s recent expert consensus statement on dietary interventions for type 2 diabetes remission, which was also endorsed by AACE, supported by the Academy of Nutrition and Dietetics, and cosponsored by the Endocrine Society, panel members agreed that remission is a realistic and achievable goal for some adults with type 2 diabetes, and a high-intensity dietary intervention can result in remission, Dr. Karlsen said.
To avoid hypoglycemia when deprescribing antiglycemic drugs, medications known to cause hypoglycemia – notably sulfonylurea and insulin – are often deprescribed first, she noted.
“Our biggest hope,” she said, “is that [type 2 diabetes] remission may come to the forefront as a clinical goal in treatment and that other organizations will more strongly emphasize lifestyle in standards of care.”
“We hope that clinicians reading this paper will be made aware that de-escalation of glucose-lowering medications is feasible, is a desirable outcome, and can be necessary in a lifestyle medicine context,” she added.
Further research is needed to prospectively track the likelihood of type 2 diabetes remission, factors that predict successful remission, and decision-making protocols followed by practitioners, Dr. Karlsen said.
Deprescribing antiglycemic meds in lifestyle medicine
Researchers at the Bruyère Research Institute, Ottawa, and Université de Montréal provide algorithms for deprescribing antihyperglycemic medications specifically for older individuals.
In the current study, the authors conducted individual, 30-minute to 1-hour interviews with nine lifestyle medicine practitioners to document their protocols for deprescribing glucose-lowering medications after lifestyle interventions with a goal of potential type 2 diabetes remission.
Three practitioners reported medication deprescribing in an intensive therapeutic lifestyle program (longer, more frequent treatment with greater monitoring). The others provide deprescribing in a nonintensive program (similar to primary care practice) or both.
Deprescribing is necessary when using intensive therapeutic lifestyle change, as substantial and rapid drops in glucose levels aren’t adjusted for, the authors noted.
Most practitioners work with a team of allied health care providers.
During the deprescribing process, most protocols require that patients get a basic or comprehensive metabolic panel of blood tests, with variations in laboratory tests for A1c, C-peptide, and renal function.
Most practitioners recommend a target blood glucose less than 120 mg/dL for further deprescribing.
Currently, there is no clinical guidance for use of continuous glucose monitoring (CGM) during medication de-escalation, the authors note.
Most practitioners reported they consider patient expenses associated with CGM and third-party payor coverage in their decision-making.
Most practitioners prefer to deprescribe sulfonylureas, insulin, and other medications known to cause hypoglycemia first.
Conversely, most prefer to defer deprescribing medications that have demonstrated cardiovascular and/or renal benefits (that is, glucagonlike peptide–1 receptor agonists and sodium-glucose cotransporter 2 inhibitors), as well as those with a less severe adverse effect profile (that is, metformin and GLP-1 receptor agonists) until after other medications are deprescribed.
The study was funded by the Ardmore Institute of Health. The authors reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
Nine lifestyle medicine practitioners describe how they safely and effectively deprescribe glucose-lowering medications after patients demonstrate a reduced need for such medications following lifestyle changes.
The report by Michael D. Bradley, PharmD, and colleagues was recently published as a feature article in Clinical Diabetes.
“Lifestyle medicine uses an evidence-based lifestyle therapeutic approach to treat lifestyle-related chronic disease,” they wrote, and it includes “a whole-food, predominantly plant-based eating plan, regular physical activity, restorative sleep, stress management, avoidance of risky substances, and positive social connection.”
“Medication deprescribing,” senior author Micaela C. Karlsen, PhD, said in an email, “is a planned and supervised process of dose reduction or discontinuation of a medication that may be causing harm, or no longer providing benefit to a patient.”
According to the authors, the article “is the first account published of the medication de-escalation methods used by lifestyle medicine providers when patients demonstrate a decreased need for pharmacotherapy.” It “supports the feasibility of de-escalating glucose-lowering medications in this context and provides pilot data on protocols from individual practitioners experienced in deprescribing glucose-lowering medications.”
The study was not designed to cover deprescribing glucose-lowering medications following weight loss and diabetes remission after bariatric surgery.
“A key takeaway [from the current study] for general practitioners and endocrinologists is that, while deprescribing is already known to be beneficial to reduce polypharmacy, it may be appropriate following lifestyle interventions,” said Dr. Karlsen, who is senior director of the American College of Lifestyle Medicine in Chesterfield, Md.
“The protocols presented can serve as a model for how to do so,” she continued.
The American Diabetes Association and the American Association of Clinical Endocrinology recommend lifestyle optimization as part of medical care for type 2 diabetes.
According to the ACLM, “remission of type 2 diabetes should be a clinical goal and may be achieved with a whole-food, plant-based dietary pattern coupled with moderate exercise,” the researchers noted.
“Remission,” they wrote, “can be defined as attainment of a [hemoglobin] A1c less than 6.5% for at least 3 months with no surgery, devices, or active pharmacologic therapy for the specific purpose of lowering blood glucose.”
In ACLM’s recent expert consensus statement on dietary interventions for type 2 diabetes remission, which was also endorsed by AACE, supported by the Academy of Nutrition and Dietetics, and cosponsored by the Endocrine Society, panel members agreed that remission is a realistic and achievable goal for some adults with type 2 diabetes, and a high-intensity dietary intervention can result in remission, Dr. Karlsen said.
To avoid hypoglycemia when deprescribing antiglycemic drugs, medications known to cause hypoglycemia – notably sulfonylurea and insulin – are often deprescribed first, she noted.
“Our biggest hope,” she said, “is that [type 2 diabetes] remission may come to the forefront as a clinical goal in treatment and that other organizations will more strongly emphasize lifestyle in standards of care.”
“We hope that clinicians reading this paper will be made aware that de-escalation of glucose-lowering medications is feasible, is a desirable outcome, and can be necessary in a lifestyle medicine context,” she added.
Further research is needed to prospectively track the likelihood of type 2 diabetes remission, factors that predict successful remission, and decision-making protocols followed by practitioners, Dr. Karlsen said.
Deprescribing antiglycemic meds in lifestyle medicine
Researchers at the Bruyère Research Institute, Ottawa, and Université de Montréal provide algorithms for deprescribing antihyperglycemic medications specifically for older individuals.
In the current study, the authors conducted individual, 30-minute to 1-hour interviews with nine lifestyle medicine practitioners to document their protocols for deprescribing glucose-lowering medications after lifestyle interventions with a goal of potential type 2 diabetes remission.
Three practitioners reported medication deprescribing in an intensive therapeutic lifestyle program (longer, more frequent treatment with greater monitoring). The others provide deprescribing in a nonintensive program (similar to primary care practice) or both.
Deprescribing is necessary when using intensive therapeutic lifestyle change, as substantial and rapid drops in glucose levels aren’t adjusted for, the authors noted.
Most practitioners work with a team of allied health care providers.
During the deprescribing process, most protocols require that patients get a basic or comprehensive metabolic panel of blood tests, with variations in laboratory tests for A1c, C-peptide, and renal function.
Most practitioners recommend a target blood glucose less than 120 mg/dL for further deprescribing.
Currently, there is no clinical guidance for use of continuous glucose monitoring (CGM) during medication de-escalation, the authors note.
Most practitioners reported they consider patient expenses associated with CGM and third-party payor coverage in their decision-making.
Most practitioners prefer to deprescribe sulfonylureas, insulin, and other medications known to cause hypoglycemia first.
Conversely, most prefer to defer deprescribing medications that have demonstrated cardiovascular and/or renal benefits (that is, glucagonlike peptide–1 receptor agonists and sodium-glucose cotransporter 2 inhibitors), as well as those with a less severe adverse effect profile (that is, metformin and GLP-1 receptor agonists) until after other medications are deprescribed.
The study was funded by the Ardmore Institute of Health. The authors reported no relevant financial relationships.
A version of this article originally appeared on Medscape.com.
FROM CLINICAL DIABETES
Medical-level empathy? Yup, ChatGPT can fake that
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?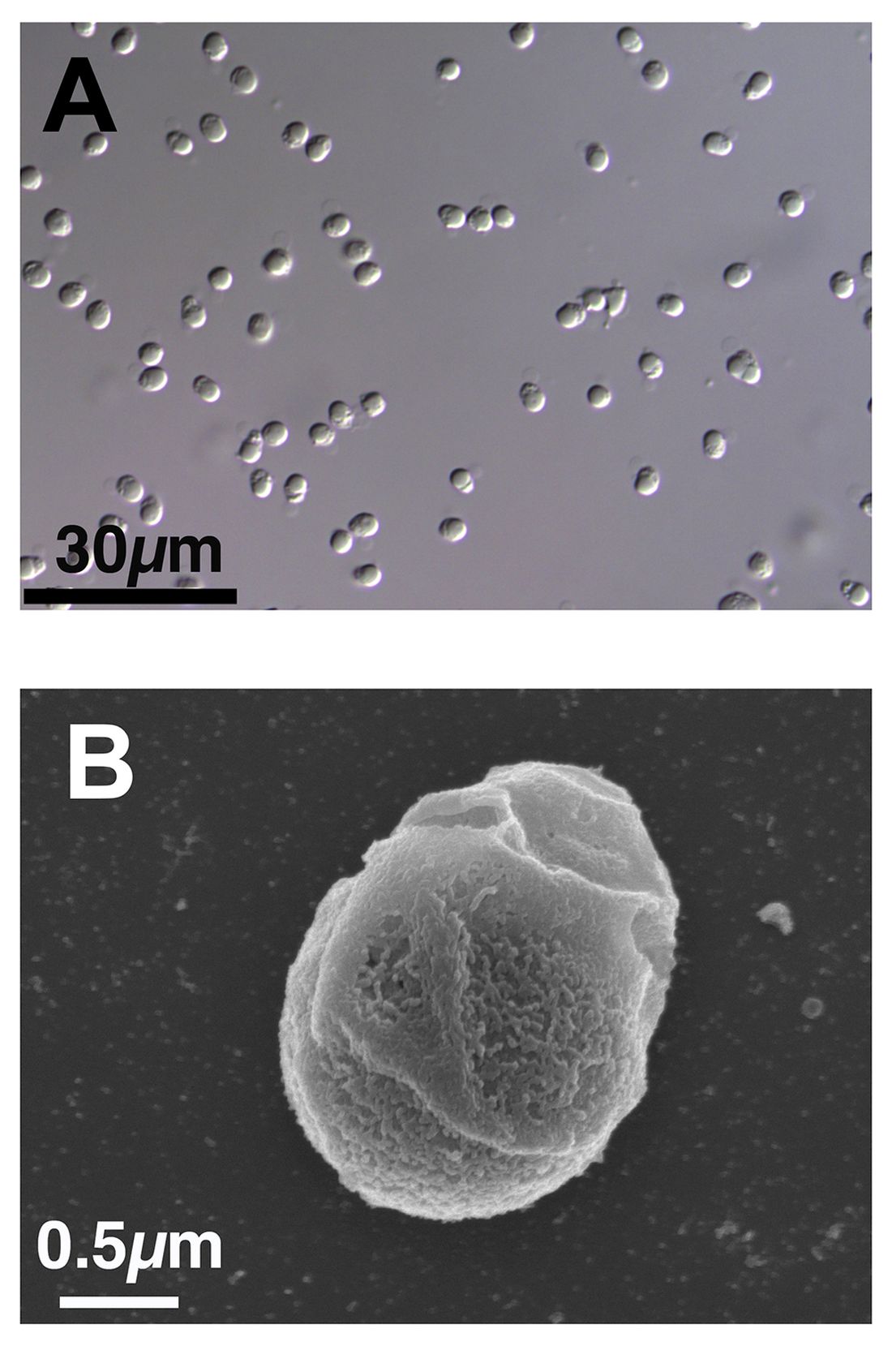
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
Caution: Robotic uprisings in the rearview mirror are closer than they appear
ChatGPT. If you’ve been even in the proximity of the Internet lately, you may have heard of it. It’s quite an incredible piece of technology, an artificial intelligence that really could up-end a lot of industries. And lest doctors believe they’re safe from robotic replacement, consider this: ChatGPT took a test commonly used as a study resource by ophthalmologists and scored a 46%. Obviously, that’s not a passing grade. Job safe, right?
A month later, the researchers tried again. This time, ChatGPT got a 58%. Still not passing, and ChatGPT did especially poorly on ophthalmology specialty questions (it got 80% of general medicine questions right), but still, the jump in quality after just a month is ... concerning. It’s not like an AI will forget things. That score can only go up, and it’ll go up faster than you think.
“Sure, the robot is smart,” the doctors out there are thinking, “but how can an AI compete with human compassion, understanding, and bedside manner?”
And they’d be right. When it comes to bedside manner, there’s no competition between man and bot. ChatGPT is already winning.
In another study, researchers sampled nearly 200 questions from the subreddit r/AskDocs, which received verified physician responses. The researchers fed ChatGPT the questions – without the doctor’s answer – and a panel of health care professionals evaluated both the human doctor and ChatGPT in terms of quality and empathy.
Perhaps not surprisingly, the robot did better when it came to quality, providing a high-quality response 79% of the time, versus 22% for the human. But empathy? It was a bloodbath. ChatGPT provided an empathetic or very empathetic response 45% of the time, while humans could only do so 4.6% of the time. So much for bedside manner.
The researchers were suspiciously quick to note that ChatGPT isn’t a legitimate replacement for physicians, but could represent a tool to better provide care for patients. But let’s be honest, given ChatGPT’s quick advancement, how long before some intrepid stockholder says: “Hey, instead of paying doctors, why don’t we just use the free robot instead?” We give it a week. Or 11 minutes.
This week, on ‘As the sperm turns’
We’ve got a lot of spermy ground to cover, so let’s get right to it, starting with the small and working our way up.
We’re all pretty familiar with the basic structure of a sperm cell, yes? Bulbous head that contains all the important genetic information and a tail-like flagellum to propel it to its ultimate destination. Not much to work with there, you’d think, but what if Mother Nature, who clearly has a robust sense of humor, had something else in mind?
We present exhibit A, Paramormyorps kingsleyae, also known as the electric elephantfish, which happens to be the only known vertebrate species with tailless sperm. Sounds crazy to us, too, but Jason Gallant, PhD, of
Michigan State University, Lansing, has a theory: “A general notion in biology is that sperm are cheap, and eggs are expensive – but these fish may be telling us that sperm are more expensive than we might think. They could be saving energy by cutting back on sperm tails.”
He and his team think that finding the gene that turns off development of the flagellum in the elephant fish could benefit humans, specifically those with a genetic disorder called primary ciliary dyskinesia, whose lack of normally functioning cilia and flagella leads to chronic respiratory infection, abnormally positioned organs, fluid on the brain, and infertility.
And that – with “that” being infertility – brings us to exhibit B, a 41-year-old Dutch man named Jonathan Meijer who clearly has too much time on his hands.
A court in the Netherlands recently ordered him, and not for the first time, to stop donating sperm to fertility clinics after it was discovered that he had fathered between 500 and 600 children around the world. He had been banned from donating to Dutch clinics in 2017, at which point he had already fathered 100 children, but managed a workaround by donating internationally and online, sometimes using another name.
The judge ordered Mr. Meijer to contact all of the clinics abroad and ask them to destroy any of his sperm they still had in stock and threatened to fine him over $100,000 for each future violation.
Okay, so here’s the thing. We have been, um, let’s call it ... warned, about the evils of tastelessness in journalism, so we’re going to do what Mr. Meijer should have done and abstain. And we can last for longer than 11 minutes.
The realm of lost luggage and lost sleep
It may be convenient to live near an airport if you’re a frequent flyer, but it really doesn’t help your sleep numbers.
The first look at how such a common sound affects sleep duration showed that people exposed to even 45 decibels of airplane noise were less likely to get the 7-9 hours of sleep needed for healthy functioning, investigators said in Environmental Health Perspectives.
How loud is 45 dB exactly? A normal conversation is about 50 dB, while a whisper is 30 dB, to give you an idea. Airplane noise at 45 dB? You might not even notice it amongst the other noises in daily life.
The researchers looked at data from about 35,000 participants in the Nurses’ Health Study who live around 90 major U.S. airports. They examined plane noise every 5 years between 1995 and 2005, focusing on estimates of nighttime and daytime levels. Short sleep was most common among the nurses who lived on the West Coast, near major cargo airports or large bodies of water, and also among those who reported no hearing loss.
The investigators noted, however, that there was no consistent association between airplane noise and quality of sleep and stopped short of making any policy recommendations. Still, sleep is a very important, yet slept-on (pun intended) factor for our overall health, so it’s good to know if anything has the potential to cause disruption.
10 popular diets for heart health ranked
An evidence-based analysis of 10 popular dietary patterns shows that some promote heart health better than others.
A new American Heart Association scientific statement concludes that the Mediterranean, Dietary Approach to Stop Hypertension (DASH), pescatarian, and vegetarian eating patterns most strongly align with heart-healthy eating guidelines issued by the AHA in 2021, whereas the popular paleolithic (paleo) and ketogenic (keto) diets fall short.
“The good news for the public and their clinicians is that there are several dietary patterns that allow for substantial flexibility for following a heart healthy diet – DASH, Mediterranean, vegetarian,” writing-group chair Christopher Gardner, PhD, with Stanford (Calif.) University, told this news organization.

“However, some of the popular diets – particularly paleo and keto – are so strictly restrictive of specific food groups that when these diets are followed as intended by their proponents, they are not aligned with the scientific evidence for a heart-healthy diet,” Dr. Gardner said.
The statement was published online in Circulation.
A tool for clinicians
“The number of different, popular dietary patterns has proliferated in recent years, and the amount of misinformation about them on social media has reached critical levels,” Dr. Gardner said in a news release.
“The public – and even many health care professionals – may rightfully be confused about heart-healthy eating, and they may feel that they don’t have the time or the training to evaluate the different diets. We hope this statement serves as a tool for clinicians and the public to understand which diets promote good cardiometabolic health,” he noted.
The writing group rated on a scale of 1-100 how well 10 popular diets or eating patterns align with AHA dietary advice for heart-healthy eating.
That advice includes consuming a wide variety of fruits and vegetables; choosing mostly whole grains instead of refined grains; using liquid plant oils rather than tropical oils; eating healthy sources of protein, such as from plants, seafood, or lean meats; minimizing added sugars and salt; limiting alcohol; choosing minimally processed foods instead of ultraprocessed foods; and following this guidance wherever food is prepared or consumed.
The 10 diets/dietary patterns were DASH, Mediterranean-style, pescatarian, ovo-lacto vegetarian, vegan, low-fat, very low–fat, low-carbohydrate, paleo, and very low–carbohydrate/keto patterns.
The diets were divided into four tiers on the basis of their scores, which ranged from a low of 31 to a high of 100.
Only the DASH eating plan got a perfect score of 100. This eating pattern is low in salt, added sugar, tropical oil, alcohol, and processed foods and high in nonstarchy vegetables, fruits, whole grains, and legumes. Proteins are mostly plant-based, such as legumes, beans, or nuts, along with fish or seafood, lean poultry and meats, and low-fat or fat-free dairy products.
The Mediterranean eating pattern achieved a slightly lower score of 89 because unlike DASH, it allows for moderate alcohol consumption and does not address added salt.
The other two top tier eating patterns were pescatarian, with a score of 92, and vegetarian, with a score of 86.
“If implemented as intended, the top-tier dietary patterns align best with the American Heart Association’s guidance and may be adapted to respect cultural practices, food preferences and budgets to enable people to always eat this way, for the long term,” Dr. Gardner said in the release.
Vegan and low-fat diets (each with a score of 78) fell into the second tier.
Though these diets emphasize fruits, vegetables, whole grains, legumes, and nuts while limiting alcohol and added sugars, the vegan diet is so restrictive that it could be challenging to follow long-term or when eating out and may increase the risk for vitamin B12 deficiency, which can lead to anemia, the writing group notes.
There also are concerns that low-fat diets treat all fats equally, whereas the AHA guidance calls for replacing saturated fats with healthier fats, they point out.
The third tier includes the very low–fat diet (score 72) and low-carb diet (score 64), whereas the paleo and very low–carb/keto diets fall into the fourth tier, with the lowest scores of 53 and 31, respectively.
Dr. Gardner said that it’s important to note that all 10 diet patterns “share four positive characteristics: more veggies, more whole foods, less added sugars, less refined grains.”
“These are all areas for which Americans have substantial room for improvement, and these are all things that we could work on together. Progress across these aspects would make a large difference in the heart-healthiness of the U.S. diet,” he told this news organization.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Council on Lifestyle and Cardiometabolic Health, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, and the Council on Peripheral Vascular Disease.
A version of this article first appeared on Medscape.com.
An evidence-based analysis of 10 popular dietary patterns shows that some promote heart health better than others.
A new American Heart Association scientific statement concludes that the Mediterranean, Dietary Approach to Stop Hypertension (DASH), pescatarian, and vegetarian eating patterns most strongly align with heart-healthy eating guidelines issued by the AHA in 2021, whereas the popular paleolithic (paleo) and ketogenic (keto) diets fall short.
“The good news for the public and their clinicians is that there are several dietary patterns that allow for substantial flexibility for following a heart healthy diet – DASH, Mediterranean, vegetarian,” writing-group chair Christopher Gardner, PhD, with Stanford (Calif.) University, told this news organization.
“However, some of the popular diets – particularly paleo and keto – are so strictly restrictive of specific food groups that when these diets are followed as intended by their proponents, they are not aligned with the scientific evidence for a heart-healthy diet,” Dr. Gardner said.
The statement was published online in Circulation.
A tool for clinicians
“The number of different, popular dietary patterns has proliferated in recent years, and the amount of misinformation about them on social media has reached critical levels,” Dr. Gardner said in a news release.
“The public – and even many health care professionals – may rightfully be confused about heart-healthy eating, and they may feel that they don’t have the time or the training to evaluate the different diets. We hope this statement serves as a tool for clinicians and the public to understand which diets promote good cardiometabolic health,” he noted.
The writing group rated on a scale of 1-100 how well 10 popular diets or eating patterns align with AHA dietary advice for heart-healthy eating.
That advice includes consuming a wide variety of fruits and vegetables; choosing mostly whole grains instead of refined grains; using liquid plant oils rather than tropical oils; eating healthy sources of protein, such as from plants, seafood, or lean meats; minimizing added sugars and salt; limiting alcohol; choosing minimally processed foods instead of ultraprocessed foods; and following this guidance wherever food is prepared or consumed.
The 10 diets/dietary patterns were DASH, Mediterranean-style, pescatarian, ovo-lacto vegetarian, vegan, low-fat, very low–fat, low-carbohydrate, paleo, and very low–carbohydrate/keto patterns.
The diets were divided into four tiers on the basis of their scores, which ranged from a low of 31 to a high of 100.
Only the DASH eating plan got a perfect score of 100. This eating pattern is low in salt, added sugar, tropical oil, alcohol, and processed foods and high in nonstarchy vegetables, fruits, whole grains, and legumes. Proteins are mostly plant-based, such as legumes, beans, or nuts, along with fish or seafood, lean poultry and meats, and low-fat or fat-free dairy products.
The Mediterranean eating pattern achieved a slightly lower score of 89 because unlike DASH, it allows for moderate alcohol consumption and does not address added salt.
The other two top tier eating patterns were pescatarian, with a score of 92, and vegetarian, with a score of 86.
“If implemented as intended, the top-tier dietary patterns align best with the American Heart Association’s guidance and may be adapted to respect cultural practices, food preferences and budgets to enable people to always eat this way, for the long term,” Dr. Gardner said in the release.
Vegan and low-fat diets (each with a score of 78) fell into the second tier.
Though these diets emphasize fruits, vegetables, whole grains, legumes, and nuts while limiting alcohol and added sugars, the vegan diet is so restrictive that it could be challenging to follow long-term or when eating out and may increase the risk for vitamin B12 deficiency, which can lead to anemia, the writing group notes.
There also are concerns that low-fat diets treat all fats equally, whereas the AHA guidance calls for replacing saturated fats with healthier fats, they point out.
The third tier includes the very low–fat diet (score 72) and low-carb diet (score 64), whereas the paleo and very low–carb/keto diets fall into the fourth tier, with the lowest scores of 53 and 31, respectively.
Dr. Gardner said that it’s important to note that all 10 diet patterns “share four positive characteristics: more veggies, more whole foods, less added sugars, less refined grains.”
“These are all areas for which Americans have substantial room for improvement, and these are all things that we could work on together. Progress across these aspects would make a large difference in the heart-healthiness of the U.S. diet,” he told this news organization.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Council on Lifestyle and Cardiometabolic Health, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, and the Council on Peripheral Vascular Disease.
A version of this article first appeared on Medscape.com.
An evidence-based analysis of 10 popular dietary patterns shows that some promote heart health better than others.
A new American Heart Association scientific statement concludes that the Mediterranean, Dietary Approach to Stop Hypertension (DASH), pescatarian, and vegetarian eating patterns most strongly align with heart-healthy eating guidelines issued by the AHA in 2021, whereas the popular paleolithic (paleo) and ketogenic (keto) diets fall short.
“The good news for the public and their clinicians is that there are several dietary patterns that allow for substantial flexibility for following a heart healthy diet – DASH, Mediterranean, vegetarian,” writing-group chair Christopher Gardner, PhD, with Stanford (Calif.) University, told this news organization.
“However, some of the popular diets – particularly paleo and keto – are so strictly restrictive of specific food groups that when these diets are followed as intended by their proponents, they are not aligned with the scientific evidence for a heart-healthy diet,” Dr. Gardner said.
The statement was published online in Circulation.
A tool for clinicians
“The number of different, popular dietary patterns has proliferated in recent years, and the amount of misinformation about them on social media has reached critical levels,” Dr. Gardner said in a news release.
“The public – and even many health care professionals – may rightfully be confused about heart-healthy eating, and they may feel that they don’t have the time or the training to evaluate the different diets. We hope this statement serves as a tool for clinicians and the public to understand which diets promote good cardiometabolic health,” he noted.
The writing group rated on a scale of 1-100 how well 10 popular diets or eating patterns align with AHA dietary advice for heart-healthy eating.
That advice includes consuming a wide variety of fruits and vegetables; choosing mostly whole grains instead of refined grains; using liquid plant oils rather than tropical oils; eating healthy sources of protein, such as from plants, seafood, or lean meats; minimizing added sugars and salt; limiting alcohol; choosing minimally processed foods instead of ultraprocessed foods; and following this guidance wherever food is prepared or consumed.
The 10 diets/dietary patterns were DASH, Mediterranean-style, pescatarian, ovo-lacto vegetarian, vegan, low-fat, very low–fat, low-carbohydrate, paleo, and very low–carbohydrate/keto patterns.
The diets were divided into four tiers on the basis of their scores, which ranged from a low of 31 to a high of 100.
Only the DASH eating plan got a perfect score of 100. This eating pattern is low in salt, added sugar, tropical oil, alcohol, and processed foods and high in nonstarchy vegetables, fruits, whole grains, and legumes. Proteins are mostly plant-based, such as legumes, beans, or nuts, along with fish or seafood, lean poultry and meats, and low-fat or fat-free dairy products.
The Mediterranean eating pattern achieved a slightly lower score of 89 because unlike DASH, it allows for moderate alcohol consumption and does not address added salt.
The other two top tier eating patterns were pescatarian, with a score of 92, and vegetarian, with a score of 86.
“If implemented as intended, the top-tier dietary patterns align best with the American Heart Association’s guidance and may be adapted to respect cultural practices, food preferences and budgets to enable people to always eat this way, for the long term,” Dr. Gardner said in the release.
Vegan and low-fat diets (each with a score of 78) fell into the second tier.
Though these diets emphasize fruits, vegetables, whole grains, legumes, and nuts while limiting alcohol and added sugars, the vegan diet is so restrictive that it could be challenging to follow long-term or when eating out and may increase the risk for vitamin B12 deficiency, which can lead to anemia, the writing group notes.
There also are concerns that low-fat diets treat all fats equally, whereas the AHA guidance calls for replacing saturated fats with healthier fats, they point out.
The third tier includes the very low–fat diet (score 72) and low-carb diet (score 64), whereas the paleo and very low–carb/keto diets fall into the fourth tier, with the lowest scores of 53 and 31, respectively.
Dr. Gardner said that it’s important to note that all 10 diet patterns “share four positive characteristics: more veggies, more whole foods, less added sugars, less refined grains.”
“These are all areas for which Americans have substantial room for improvement, and these are all things that we could work on together. Progress across these aspects would make a large difference in the heart-healthiness of the U.S. diet,” he told this news organization.
This scientific statement was prepared by the volunteer writing group on behalf of the AHA Council on Lifestyle and Cardiometabolic Health, the Council on Cardiovascular and Stroke Nursing, the Council on Hypertension, and the Council on Peripheral Vascular Disease.
A version of this article first appeared on Medscape.com.
Medications provide best risk-to-benefit ratio for weight loss, says expert
Lifestyle changes result in the least weight loss and may be safest, while surgery provides the most weight loss and has the greatest risk. Antiobesity medications, especially the newer ones used in combination with lifestyle changes, can provide significant and sustained weight loss with manageable side effects, said Daniel Bessesen, MD, a professor in the endocrinology, diabetes, and metabolism at University of Colorado at Denver, Aurora.
New and more effective antiobesity medications have given internists more potential options to discuss with their patients, Dr. Bessesen said. He reviewed the pros and cons of the different options.
Medications are indicated for patients with a body mass index greater than 30, including those with a weight-related comorbidity, Dr. Bessesen said. The average weight loss is 5%-15% over 3-6 months but may vary greatly. Insurance often does not cover the medication costs.
Older FDA-approved antiobesity medications
Phentermine is the most widely prescribed antiobesity medication, partly because it is the only option most people can afford out of pocket. Dr. Bessesen presented recent data showing that long-term use of phentermine was associated with greater weight loss and that patients continuously taking phentermine for 24 months lost 7.5% of their weight.
Phentermine suppresses appetite by increasing norepinephrine production. Dr. Bessesen warned that internists should be careful when prescribing it to patients with mental conditions, because it acts as a stimulant. Early studies raised concerns about the risk of cardiovascular disease (CVD) in patients taking phentermine. However, analysis of data from over 13,000 individuals showed no evidence of a relationship between phentermine exposure and CVD events.
“These data provide some reassurance that it could be used in patients with CVD risk,” he noted. Phentermine can also be combined with topiramate extended release, a combination that provides greater efficacy (up to 10% weight loss) with fewer side effects. However, this combination is less effective in patients with diabetes than in those without.
Additional treatment options included orlistat and naltrexone sustained release/bupropion SR. Orlistat is a good treatment alternative for patients with constipation and is the safest option among older anti-obesity medications, whereas naltrexone SR/bupropion SR may be useful in patients with food cravings. However, there is more variability in the individual-level benefit from these agents compared to phentermine and phentermine/topiramate ER, Dr. Bessesen said.
Newer anti‐obesity medications
Liraglutide, an agent used for the management of type 2 diabetes, has recently been approved for weight loss. Liraglutide causes moderate weight loss, and it may reduce the risk of CVD. However, there are tolerability issues, such as nausea and other risks, and Dr. Bessesen advises internists to “start at low doses and increase slowly.”
Semaglutide is the newest and most effective antiobesity drug approved by the Food and Drug Administration, providing sustained weight loss of 8% for up to 48 weeks after starting treatment. Although its efficacy is lower in patients with diabetes, Dr. Bessesen noted that “this is common for antiobesity agents, and clinicians should not refrain from prescribing it in this population.”
Setmelanotide is another new medication approved for chronic weight management in patients with monogenic obesity. This medication can be considered for patients with early-onset severe obesity with abnormal feeding behavior.
Commenting on barriers to access to new antiobesity medications, Dr. Bessesen said that “the high cost of these medications is a substantial problem, but as more companies become involved and products are on the market for a longer period of time, I am hopeful that prices will come down.”
Emerging antiobesity medications
Dr. Bessesen presented recent phase 3 data showing that treatment with tirzepatide provided sustained chronic loss and improved cardiometabolic measures with no diet. Tirzepatide, which targets receptors for glucagonlike peptide–1 and glucose-dependent insulinotropic polypeptide, is used for the management of type 2 diabetes and is expected to be reviewed soon by the FDA for its use in weight management.
A semaglutide/cagrilintide combination may also provide a new treatment option for patients with obesity. In a phase 1b trial, semaglutide/cagrilintide treatment resulted in up to 17% weight loss in patients with obesity who were otherwise healthy; however, phase 2 and 3 data are needed to confirm its efficacy.
A ‘holistic approach’
When deciding whether to prescribe antiobesity medications, Dr. Bessesen noted that medications are better than exercise alone. Factors to consider when deciding whether to prescribe drugs, as well as which ones, include costs, local regulatory guidelines, requirement for long-term use, and patient comorbidities.
He also stated that lifestyle changes, such as adopting healthy nutrition and exercising regularly, are also important and can enhance weight loss when combined with medications.
Richele Corrado, DO, MPH, agreed that lifestyle management in combination with medications may provide greater weight loss than each of these interventions alone.
“If you look at the data, exercise doesn’t help you lose much weight,” said Dr. Corrado, a staff internist and obesity medicine specialist at Walter Reed National Military Medical Center in Bethesda, Md., who spoke at the same session. She added that she has many patients who struggle to lose weight despite having a healthy lifestyle. “It’s important to discuss with these patients about medications and surgery.”
Dr. Bessesen noted that management of mental health and emotional well-being should also be an integral part of obesity management. “Treatment for obesity may be more successful when underlying psychological conditions such as depression, childhood sexual trauma, or anxiety are addressed and treated,” he said.
Dr. Bessesen was involved in the study of the efficacy of semaglutide/cagrilintide. He does not have any financial conflicts with the companies that make other mentioned medications. He has received research grants or contracts from Novo Nordisk, honoraria from Novo Nordisk, and consultantship from Eli Lilly. Dr. Corrado reported no relevant financial conflicts.
Lifestyle changes result in the least weight loss and may be safest, while surgery provides the most weight loss and has the greatest risk. Antiobesity medications, especially the newer ones used in combination with lifestyle changes, can provide significant and sustained weight loss with manageable side effects, said Daniel Bessesen, MD, a professor in the endocrinology, diabetes, and metabolism at University of Colorado at Denver, Aurora.
New and more effective antiobesity medications have given internists more potential options to discuss with their patients, Dr. Bessesen said. He reviewed the pros and cons of the different options.
Medications are indicated for patients with a body mass index greater than 30, including those with a weight-related comorbidity, Dr. Bessesen said. The average weight loss is 5%-15% over 3-6 months but may vary greatly. Insurance often does not cover the medication costs.
Older FDA-approved antiobesity medications
Phentermine is the most widely prescribed antiobesity medication, partly because it is the only option most people can afford out of pocket. Dr. Bessesen presented recent data showing that long-term use of phentermine was associated with greater weight loss and that patients continuously taking phentermine for 24 months lost 7.5% of their weight.
Phentermine suppresses appetite by increasing norepinephrine production. Dr. Bessesen warned that internists should be careful when prescribing it to patients with mental conditions, because it acts as a stimulant. Early studies raised concerns about the risk of cardiovascular disease (CVD) in patients taking phentermine. However, analysis of data from over 13,000 individuals showed no evidence of a relationship between phentermine exposure and CVD events.
“These data provide some reassurance that it could be used in patients with CVD risk,” he noted. Phentermine can also be combined with topiramate extended release, a combination that provides greater efficacy (up to 10% weight loss) with fewer side effects. However, this combination is less effective in patients with diabetes than in those without.
Additional treatment options included orlistat and naltrexone sustained release/bupropion SR. Orlistat is a good treatment alternative for patients with constipation and is the safest option among older anti-obesity medications, whereas naltrexone SR/bupropion SR may be useful in patients with food cravings. However, there is more variability in the individual-level benefit from these agents compared to phentermine and phentermine/topiramate ER, Dr. Bessesen said.
Newer anti‐obesity medications
Liraglutide, an agent used for the management of type 2 diabetes, has recently been approved for weight loss. Liraglutide causes moderate weight loss, and it may reduce the risk of CVD. However, there are tolerability issues, such as nausea and other risks, and Dr. Bessesen advises internists to “start at low doses and increase slowly.”
Semaglutide is the newest and most effective antiobesity drug approved by the Food and Drug Administration, providing sustained weight loss of 8% for up to 48 weeks after starting treatment. Although its efficacy is lower in patients with diabetes, Dr. Bessesen noted that “this is common for antiobesity agents, and clinicians should not refrain from prescribing it in this population.”
Setmelanotide is another new medication approved for chronic weight management in patients with monogenic obesity. This medication can be considered for patients with early-onset severe obesity with abnormal feeding behavior.
Commenting on barriers to access to new antiobesity medications, Dr. Bessesen said that “the high cost of these medications is a substantial problem, but as more companies become involved and products are on the market for a longer period of time, I am hopeful that prices will come down.”
Emerging antiobesity medications
Dr. Bessesen presented recent phase 3 data showing that treatment with tirzepatide provided sustained chronic loss and improved cardiometabolic measures with no diet. Tirzepatide, which targets receptors for glucagonlike peptide–1 and glucose-dependent insulinotropic polypeptide, is used for the management of type 2 diabetes and is expected to be reviewed soon by the FDA for its use in weight management.
A semaglutide/cagrilintide combination may also provide a new treatment option for patients with obesity. In a phase 1b trial, semaglutide/cagrilintide treatment resulted in up to 17% weight loss in patients with obesity who were otherwise healthy; however, phase 2 and 3 data are needed to confirm its efficacy.
A ‘holistic approach’
When deciding whether to prescribe antiobesity medications, Dr. Bessesen noted that medications are better than exercise alone. Factors to consider when deciding whether to prescribe drugs, as well as which ones, include costs, local regulatory guidelines, requirement for long-term use, and patient comorbidities.
He also stated that lifestyle changes, such as adopting healthy nutrition and exercising regularly, are also important and can enhance weight loss when combined with medications.
Richele Corrado, DO, MPH, agreed that lifestyle management in combination with medications may provide greater weight loss than each of these interventions alone.
“If you look at the data, exercise doesn’t help you lose much weight,” said Dr. Corrado, a staff internist and obesity medicine specialist at Walter Reed National Military Medical Center in Bethesda, Md., who spoke at the same session. She added that she has many patients who struggle to lose weight despite having a healthy lifestyle. “It’s important to discuss with these patients about medications and surgery.”
Dr. Bessesen noted that management of mental health and emotional well-being should also be an integral part of obesity management. “Treatment for obesity may be more successful when underlying psychological conditions such as depression, childhood sexual trauma, or anxiety are addressed and treated,” he said.
Dr. Bessesen was involved in the study of the efficacy of semaglutide/cagrilintide. He does not have any financial conflicts with the companies that make other mentioned medications. He has received research grants or contracts from Novo Nordisk, honoraria from Novo Nordisk, and consultantship from Eli Lilly. Dr. Corrado reported no relevant financial conflicts.
Lifestyle changes result in the least weight loss and may be safest, while surgery provides the most weight loss and has the greatest risk. Antiobesity medications, especially the newer ones used in combination with lifestyle changes, can provide significant and sustained weight loss with manageable side effects, said Daniel Bessesen, MD, a professor in the endocrinology, diabetes, and metabolism at University of Colorado at Denver, Aurora.
New and more effective antiobesity medications have given internists more potential options to discuss with their patients, Dr. Bessesen said. He reviewed the pros and cons of the different options.
Medications are indicated for patients with a body mass index greater than 30, including those with a weight-related comorbidity, Dr. Bessesen said. The average weight loss is 5%-15% over 3-6 months but may vary greatly. Insurance often does not cover the medication costs.
Older FDA-approved antiobesity medications
Phentermine is the most widely prescribed antiobesity medication, partly because it is the only option most people can afford out of pocket. Dr. Bessesen presented recent data showing that long-term use of phentermine was associated with greater weight loss and that patients continuously taking phentermine for 24 months lost 7.5% of their weight.
Phentermine suppresses appetite by increasing norepinephrine production. Dr. Bessesen warned that internists should be careful when prescribing it to patients with mental conditions, because it acts as a stimulant. Early studies raised concerns about the risk of cardiovascular disease (CVD) in patients taking phentermine. However, analysis of data from over 13,000 individuals showed no evidence of a relationship between phentermine exposure and CVD events.
“These data provide some reassurance that it could be used in patients with CVD risk,” he noted. Phentermine can also be combined with topiramate extended release, a combination that provides greater efficacy (up to 10% weight loss) with fewer side effects. However, this combination is less effective in patients with diabetes than in those without.
Additional treatment options included orlistat and naltrexone sustained release/bupropion SR. Orlistat is a good treatment alternative for patients with constipation and is the safest option among older anti-obesity medications, whereas naltrexone SR/bupropion SR may be useful in patients with food cravings. However, there is more variability in the individual-level benefit from these agents compared to phentermine and phentermine/topiramate ER, Dr. Bessesen said.
Newer anti‐obesity medications
Liraglutide, an agent used for the management of type 2 diabetes, has recently been approved for weight loss. Liraglutide causes moderate weight loss, and it may reduce the risk of CVD. However, there are tolerability issues, such as nausea and other risks, and Dr. Bessesen advises internists to “start at low doses and increase slowly.”
Semaglutide is the newest and most effective antiobesity drug approved by the Food and Drug Administration, providing sustained weight loss of 8% for up to 48 weeks after starting treatment. Although its efficacy is lower in patients with diabetes, Dr. Bessesen noted that “this is common for antiobesity agents, and clinicians should not refrain from prescribing it in this population.”
Setmelanotide is another new medication approved for chronic weight management in patients with monogenic obesity. This medication can be considered for patients with early-onset severe obesity with abnormal feeding behavior.
Commenting on barriers to access to new antiobesity medications, Dr. Bessesen said that “the high cost of these medications is a substantial problem, but as more companies become involved and products are on the market for a longer period of time, I am hopeful that prices will come down.”
Emerging antiobesity medications
Dr. Bessesen presented recent phase 3 data showing that treatment with tirzepatide provided sustained chronic loss and improved cardiometabolic measures with no diet. Tirzepatide, which targets receptors for glucagonlike peptide–1 and glucose-dependent insulinotropic polypeptide, is used for the management of type 2 diabetes and is expected to be reviewed soon by the FDA for its use in weight management.
A semaglutide/cagrilintide combination may also provide a new treatment option for patients with obesity. In a phase 1b trial, semaglutide/cagrilintide treatment resulted in up to 17% weight loss in patients with obesity who were otherwise healthy; however, phase 2 and 3 data are needed to confirm its efficacy.
A ‘holistic approach’
When deciding whether to prescribe antiobesity medications, Dr. Bessesen noted that medications are better than exercise alone. Factors to consider when deciding whether to prescribe drugs, as well as which ones, include costs, local regulatory guidelines, requirement for long-term use, and patient comorbidities.
He also stated that lifestyle changes, such as adopting healthy nutrition and exercising regularly, are also important and can enhance weight loss when combined with medications.
Richele Corrado, DO, MPH, agreed that lifestyle management in combination with medications may provide greater weight loss than each of these interventions alone.
“If you look at the data, exercise doesn’t help you lose much weight,” said Dr. Corrado, a staff internist and obesity medicine specialist at Walter Reed National Military Medical Center in Bethesda, Md., who spoke at the same session. She added that she has many patients who struggle to lose weight despite having a healthy lifestyle. “It’s important to discuss with these patients about medications and surgery.”
Dr. Bessesen noted that management of mental health and emotional well-being should also be an integral part of obesity management. “Treatment for obesity may be more successful when underlying psychological conditions such as depression, childhood sexual trauma, or anxiety are addressed and treated,” he said.
Dr. Bessesen was involved in the study of the efficacy of semaglutide/cagrilintide. He does not have any financial conflicts with the companies that make other mentioned medications. He has received research grants or contracts from Novo Nordisk, honoraria from Novo Nordisk, and consultantship from Eli Lilly. Dr. Corrado reported no relevant financial conflicts.
AT INTERNAL MEDICINE 2023
Lose weight, gain huge debt: N.Y. provider has sued more than 300 patients who had bariatric surgery
Seven months after Lahavah Wallace’s weight-loss operation, a New York bariatric surgery practice sued her, accusing her of “intentionally” failing to pay nearly $18,000 of her bill.
Long Island Minimally Invasive Surgery, which does business as the New York Bariatric Group, went on to accuse Ms. Wallace of “embezzlement,” alleging she kept insurance payments that should have been turned over to the practice.
Ms. Wallace denies the allegations, which the bariatric practice has leveled against patients in hundreds of debt-collection lawsuits filed over the past 4 years, court records in New York state show.
In about 60 cases, the lawsuits demanded $100,000 or more from patients. Some patients were found liable for tens of thousands of dollars in interest charges or wound up shackled with debt that could take a decade or more to shake. Others are facing the likely prospect of six-figure financial penalties, court records show.
Backed by a major private equity firm, the bariatric practice spends millions each year on advertisements featuring patients who have dropped 100 pounds or more after bariatric procedures, sometimes having had a portion of their stomachs removed. The ads have run on TV, online, and on New York City subway posters.
The online ads, often showcasing the slogan “Stop obesity for life,” appealed to Ms. Wallace, who lives in Brooklyn and works as a legal assistant for the state of New York. She said she turned over checks from her insurer to the bariatric group and was stunned when the medical practice hauled her into court citing an “out-of-network payment agreement” she had signed before her surgery.
“I really didn’t know what I was signing,” Ms. Wallace told KFF Health News. “I didn’t pay enough attention.”
Shawn Garber, MD, a bariatric surgeon who founded the practice in 2000 on Long Island and serves as its CEO, said that “prior to rendering services” his office staff advises patients of the costs and their responsibility to pay the bill.
The bariatric group has cited these out-of-network payment agreements in at least 300 lawsuits filed against patients from January 2019 to 2022 demanding nearly $19 million to cover medical bills, interest charges, and attorney’s fees, a KFF Health News review of New York state court records found.
Danny De Voe, a partner at Sahn Ward Braff Koblenz law firm in Uniondale, N.Y., who filed many of those suits, declined to comment, citing attorney-client privilege.
In most cases, the medical practice had agreed to accept an insurance company’s out-of-network rate as full payment for its services – with caveats, according to court filings.
In the agreements they signed, patients promised to pay any coinsurance, meeting any deductible, and pass on to the medical practice any reimbursement checks they received from their health plans within 7 days.
KFF Health News found – while legal fees and other costs can layer on thousands more.
Elisabeth Benjamin, a lawyer with the Community Service Society of New York, said conflicts can arise when insurers send checks to pay for out-of-network medical services to patients rather than reimbursing a medical provider directly.
“We would prefer to see regulators step in and stop that practice,” she said, adding it “causes tension between providers and patients.”
That’s certainly true for Ms. Wallace. The surgery practice sued her in August 2022demanding $17,981 in fees it said remained unpaid after her January 2022 laparoscopic sleeve gastrectomy, an operation in which much of the stomach is removed to assist weight loss.
The lawsuit also tacked on a demand for $5,993 in attorney’s fees, court records show.
The suit alleges Ms. Wallace signed the contract even though she “had no intention” of paying her bills. The complaint goes on to accuse her of “committing embezzlement” by “willfully, intentionally, deliberately and maliciously” depositing checks from her health plan into her personal account.
The suit doesn’t include details to substantiate these claims, and Ms. Wallace said in her court response they are not true. Ms. Wallace said she turned over checks for the charges.
“They billed the insurance for everything they possibly could,” Ms. Wallace said.
In September, Ms. Wallace filed for bankruptcy, hoping to discharge the bariatric care debt along with about $4,700 in unrelated credit card charges.
The medical practice fired back in November by filing an “adversary complaint” in her Brooklyn bankruptcy court proceeding that argues her medical debt should not be forgiven because Ms. Wallace committed fraud.
The adversary complaint, which is pending in the bankruptcy case, accuses Ms. Wallace of “fraudulently” inducing the surgery center to perform “elective medical procedures” without requiring payment up front.
Both the harsh wording and claims of wrongdoing have infuriated Ms. Wallace and her attorney, Jacob Silver, of Brooklyn.
Mr. Silver wants the medical practice to turn over records of the payments received from Ms. Wallace. “There is no fraud here,” he said. “This is frivolous. We are taking a no-settlement position.”
Gaining debt
Few patients sued by the bariatric practice mount a defense in court and those who do fight often lose, court records show.
The medical practice won default judgments totaling nearly $6 million in about 90 of the 300 cases in the sample reviewed by KFF Health News. Default judgments are entered when the defendant fails to respond.
Many cases either are pending, or it is not clear from court filings how they were resolved.
Some patients tried to argue that the fees were too high or that they didn’t understand going in how much they could owe. One woman, trying to push back against a demand for more than $100,000, said in a legal filing that she “was given numerous papers to sign without anyone of the staff members explaining to me what it actually meant.” Another patient, who was sued for more than $40,000, wrote: “I don’t have the means to pay this bill.”
Among the cases described in court records:
- A Westchester County, N.Y., woman was sued for $102,556 and settled for $72,000 in May 2021. She agreed to pay $7,500 upon signing the settlement and $500 a month from September 2021 to May 2032.
- A Peekskill, N.Y., woman in a December 2019 judgment was held liable for $384,092, which included $94,047 in interest.
- A Newburgh, N.Y., man was sued in 2021 for $252,309 in medical bills, 12% interest, and $84,103 in attorneys’ fees. The case is pending.
Robert Cohen, a longtime attorney for the bariatric practice, testified in a November 2021 hearing that the lawyers take “a contingency fee of one-third of our recovery” in these cases. In that case, Mr. Cohen had requested $13,578 based on his contingency fee arrangement. He testified that he spent 7.3 hours on the case and that his customary billing rate was $475 per hour, which came to $3,467.50. The judge awarded the lower amount, according to a transcript of the hearing.
Teresa LaMasters, MD, president of the American Society for Metabolic and Bariatric Surgery, said suing patients for large sums “is not a common practice” among bariatric surgeons.
“This is not what the vast majority in the field would espouse,” she said.
But Dr. Garber, the NYBG’s chief executive, suggested patients deserve blame.
“These lawsuits stem from these patients stealing the insurance money rather than forwarding it onto NYBG as they are morally and contractually obligated to do,” Dr. Garber wrote in an email to KFF Health News.
Dr. Garber added: “The issue is not with what we bill, but rather with the fact that the insurance companies refuse to send payment directly to us.”
‘A kooky system’
Defense attorneys argue that many patients don’t fully comprehend the perils of failing to pay on time – for whatever reason.
In a few cases, patients admitted pocketing checks they were obligated to turn over to the medical practice. But for the most part, court records don’t specify how many such checks were issued and for what amounts – or whether the patient improperly cashed them.
“It’s a kooky system,” said Paul Brite, an attorney who has faced off against the bariatric practice in court.
“You sign these documents that could cost you tons of money. It shouldn’t be that way,” he said. “This can ruin their financial life.”
New York lawmakers have acted to limit the damage from medical debt, including “surprise bills.”
In November, Democratic Gov. Kathy Hochul signed legislation that prohibits health care providers from slapping liens on a primary residence or garnishing wages.
But contracts with onerous repayment terms represent an “evolving area of law” and an alarming “new twist” on concerns over medical debt, said Ms. Benjamin, the community service society lawyer.
She said contract “accelerator clauses” that trigger severe penalties if patients miss payments should not be permitted for medical debt.
“If you default, the full amount is due,” she said. “This is really a bummer.”
‘Fair market value’
The debt collection lawsuits argue that weight-loss patients had agreed to pay “fair market value” for services – and the doctors are only trying to secure money they are due.
But some prices far exceed typical insurance payments for obesity treatments across the country, according to a medical billing data registry. Surgeons performed about 200,000 bariatric operations in 2020, according to the bariatric surgery society.
Ms. Wallace, the Brooklyn legal assistant, was billed $60,500 for her lap sleeve gastrectomy, though how much her insurance actually paid remains to be hashed out in court.
Michael Arrigo, a California medical billing expert at No World Borders, called the prices “outrageous” and “unreasonable and, in fact, likely unconscionable.”
“I disagree that these are fair market charges,” he said.
Dr. LaMasters called the gastrectomy price billed to Ms. Wallace “really expensive” and “a severe outlier.” While charges vary by region, she quoted a typical price of around $22,000.
Dr. Garber said NYBG “bills at usual and customary rates” determined by Fair Health, a New York City-based repository of insurance claims data. Fair Health “sets these rates based upon the acceptable price for our geographic location,” he said.
But Rachel Kent, Fair Health’s senior director of marketing, told KFF Health News that the group “does not set rates, nor determine or take any position on what constitutes ‘usual and customary rates.’ ” Instead, it reports the prices providers are charging in a given area.
Overall, Fair Health data shows huge price variations even in adjacent ZIP codes in the metro area. In Long Island’s Roslyn Heights neighborhood, where NYBG is based, Fair Health lists the out-of-network price charged by providers in the area as $60,500, the figure Ms. Wallace was billed.
But in several other New York City–area ZIP codes the price charged for the gastrectomy procedure hovers around $20,000, according to the data bank. The price in Manhattan is $17,500, for instance, according to Fair Health.
Nationwide, the average cost in 2021 for bariatric surgery done in a hospital was $32,868, according to a KFF analysis of health insurance claims.
Private equity arrives
Dr. Garber said in a court affidavit in May 2022 that he founded the bariatric practice “with a singular focus: providing safe, effective care to patients suffering from obesity and its resulting complications.”
Under his leadership, the practice has “developed into New York’s elite institution for obesity treatment,” Dr. Garber said. He said the group’s surgeons are “highly sought after to train other bariatric surgeons throughout the country and are active in the development of new, cutting-edge bariatric surgery techniques.”
In 2017, Dr. Garber and partners agreed on a business plan to help spur growth and “attract private equity investment,” according to the affidavit.
They formed a separate company to handle the bariatric practice’s business side. Known as management services organizations, such companies provide a way for private equity investors to circumvent laws in some states that prohibit nonphysicians from owning a stake in a medical practice.
In August 2019, the private equity firm Sentinel Capital Partners bought 65% of the MSO for $156.5 million, according to Dr. Garber’s affidavit. The management company is now known as New You Bariatric Group. The private equity firm did not respond to requests for comment.
Dr. Garber, in a September 2021 American Society for Metabolic and Bariatric Surgery webinar viewable online, said the weight-loss practice spends $6 million a year on media and marketing directly to patients – and is on a roll. Nationally, bariatric surgery is growing 6% annually, he said. NYBG boasts two dozen offices in the tri-state area of New York, New Jersey, and Connecticut and is poised to expand into more states.
“Since private equity, we’ve been growing at 30%-40% year over year,” Dr. Garber said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Seven months after Lahavah Wallace’s weight-loss operation, a New York bariatric surgery practice sued her, accusing her of “intentionally” failing to pay nearly $18,000 of her bill.
Long Island Minimally Invasive Surgery, which does business as the New York Bariatric Group, went on to accuse Ms. Wallace of “embezzlement,” alleging she kept insurance payments that should have been turned over to the practice.
Ms. Wallace denies the allegations, which the bariatric practice has leveled against patients in hundreds of debt-collection lawsuits filed over the past 4 years, court records in New York state show.
In about 60 cases, the lawsuits demanded $100,000 or more from patients. Some patients were found liable for tens of thousands of dollars in interest charges or wound up shackled with debt that could take a decade or more to shake. Others are facing the likely prospect of six-figure financial penalties, court records show.
Backed by a major private equity firm, the bariatric practice spends millions each year on advertisements featuring patients who have dropped 100 pounds or more after bariatric procedures, sometimes having had a portion of their stomachs removed. The ads have run on TV, online, and on New York City subway posters.
The online ads, often showcasing the slogan “Stop obesity for life,” appealed to Ms. Wallace, who lives in Brooklyn and works as a legal assistant for the state of New York. She said she turned over checks from her insurer to the bariatric group and was stunned when the medical practice hauled her into court citing an “out-of-network payment agreement” she had signed before her surgery.
“I really didn’t know what I was signing,” Ms. Wallace told KFF Health News. “I didn’t pay enough attention.”
Shawn Garber, MD, a bariatric surgeon who founded the practice in 2000 on Long Island and serves as its CEO, said that “prior to rendering services” his office staff advises patients of the costs and their responsibility to pay the bill.
The bariatric group has cited these out-of-network payment agreements in at least 300 lawsuits filed against patients from January 2019 to 2022 demanding nearly $19 million to cover medical bills, interest charges, and attorney’s fees, a KFF Health News review of New York state court records found.
Danny De Voe, a partner at Sahn Ward Braff Koblenz law firm in Uniondale, N.Y., who filed many of those suits, declined to comment, citing attorney-client privilege.
In most cases, the medical practice had agreed to accept an insurance company’s out-of-network rate as full payment for its services – with caveats, according to court filings.
In the agreements they signed, patients promised to pay any coinsurance, meeting any deductible, and pass on to the medical practice any reimbursement checks they received from their health plans within 7 days.
KFF Health News found – while legal fees and other costs can layer on thousands more.
Elisabeth Benjamin, a lawyer with the Community Service Society of New York, said conflicts can arise when insurers send checks to pay for out-of-network medical services to patients rather than reimbursing a medical provider directly.
“We would prefer to see regulators step in and stop that practice,” she said, adding it “causes tension between providers and patients.”
That’s certainly true for Ms. Wallace. The surgery practice sued her in August 2022demanding $17,981 in fees it said remained unpaid after her January 2022 laparoscopic sleeve gastrectomy, an operation in which much of the stomach is removed to assist weight loss.
The lawsuit also tacked on a demand for $5,993 in attorney’s fees, court records show.
The suit alleges Ms. Wallace signed the contract even though she “had no intention” of paying her bills. The complaint goes on to accuse her of “committing embezzlement” by “willfully, intentionally, deliberately and maliciously” depositing checks from her health plan into her personal account.
The suit doesn’t include details to substantiate these claims, and Ms. Wallace said in her court response they are not true. Ms. Wallace said she turned over checks for the charges.
“They billed the insurance for everything they possibly could,” Ms. Wallace said.
In September, Ms. Wallace filed for bankruptcy, hoping to discharge the bariatric care debt along with about $4,700 in unrelated credit card charges.
The medical practice fired back in November by filing an “adversary complaint” in her Brooklyn bankruptcy court proceeding that argues her medical debt should not be forgiven because Ms. Wallace committed fraud.
The adversary complaint, which is pending in the bankruptcy case, accuses Ms. Wallace of “fraudulently” inducing the surgery center to perform “elective medical procedures” without requiring payment up front.
Both the harsh wording and claims of wrongdoing have infuriated Ms. Wallace and her attorney, Jacob Silver, of Brooklyn.
Mr. Silver wants the medical practice to turn over records of the payments received from Ms. Wallace. “There is no fraud here,” he said. “This is frivolous. We are taking a no-settlement position.”
Gaining debt
Few patients sued by the bariatric practice mount a defense in court and those who do fight often lose, court records show.
The medical practice won default judgments totaling nearly $6 million in about 90 of the 300 cases in the sample reviewed by KFF Health News. Default judgments are entered when the defendant fails to respond.
Many cases either are pending, or it is not clear from court filings how they were resolved.
Some patients tried to argue that the fees were too high or that they didn’t understand going in how much they could owe. One woman, trying to push back against a demand for more than $100,000, said in a legal filing that she “was given numerous papers to sign without anyone of the staff members explaining to me what it actually meant.” Another patient, who was sued for more than $40,000, wrote: “I don’t have the means to pay this bill.”
Among the cases described in court records:
- A Westchester County, N.Y., woman was sued for $102,556 and settled for $72,000 in May 2021. She agreed to pay $7,500 upon signing the settlement and $500 a month from September 2021 to May 2032.
- A Peekskill, N.Y., woman in a December 2019 judgment was held liable for $384,092, which included $94,047 in interest.
- A Newburgh, N.Y., man was sued in 2021 for $252,309 in medical bills, 12% interest, and $84,103 in attorneys’ fees. The case is pending.
Robert Cohen, a longtime attorney for the bariatric practice, testified in a November 2021 hearing that the lawyers take “a contingency fee of one-third of our recovery” in these cases. In that case, Mr. Cohen had requested $13,578 based on his contingency fee arrangement. He testified that he spent 7.3 hours on the case and that his customary billing rate was $475 per hour, which came to $3,467.50. The judge awarded the lower amount, according to a transcript of the hearing.
Teresa LaMasters, MD, president of the American Society for Metabolic and Bariatric Surgery, said suing patients for large sums “is not a common practice” among bariatric surgeons.
“This is not what the vast majority in the field would espouse,” she said.
But Dr. Garber, the NYBG’s chief executive, suggested patients deserve blame.
“These lawsuits stem from these patients stealing the insurance money rather than forwarding it onto NYBG as they are morally and contractually obligated to do,” Dr. Garber wrote in an email to KFF Health News.
Dr. Garber added: “The issue is not with what we bill, but rather with the fact that the insurance companies refuse to send payment directly to us.”
‘A kooky system’
Defense attorneys argue that many patients don’t fully comprehend the perils of failing to pay on time – for whatever reason.
In a few cases, patients admitted pocketing checks they were obligated to turn over to the medical practice. But for the most part, court records don’t specify how many such checks were issued and for what amounts – or whether the patient improperly cashed them.
“It’s a kooky system,” said Paul Brite, an attorney who has faced off against the bariatric practice in court.
“You sign these documents that could cost you tons of money. It shouldn’t be that way,” he said. “This can ruin their financial life.”
New York lawmakers have acted to limit the damage from medical debt, including “surprise bills.”
In November, Democratic Gov. Kathy Hochul signed legislation that prohibits health care providers from slapping liens on a primary residence or garnishing wages.
But contracts with onerous repayment terms represent an “evolving area of law” and an alarming “new twist” on concerns over medical debt, said Ms. Benjamin, the community service society lawyer.
She said contract “accelerator clauses” that trigger severe penalties if patients miss payments should not be permitted for medical debt.
“If you default, the full amount is due,” she said. “This is really a bummer.”
‘Fair market value’
The debt collection lawsuits argue that weight-loss patients had agreed to pay “fair market value” for services – and the doctors are only trying to secure money they are due.
But some prices far exceed typical insurance payments for obesity treatments across the country, according to a medical billing data registry. Surgeons performed about 200,000 bariatric operations in 2020, according to the bariatric surgery society.
Ms. Wallace, the Brooklyn legal assistant, was billed $60,500 for her lap sleeve gastrectomy, though how much her insurance actually paid remains to be hashed out in court.
Michael Arrigo, a California medical billing expert at No World Borders, called the prices “outrageous” and “unreasonable and, in fact, likely unconscionable.”
“I disagree that these are fair market charges,” he said.
Dr. LaMasters called the gastrectomy price billed to Ms. Wallace “really expensive” and “a severe outlier.” While charges vary by region, she quoted a typical price of around $22,000.
Dr. Garber said NYBG “bills at usual and customary rates” determined by Fair Health, a New York City-based repository of insurance claims data. Fair Health “sets these rates based upon the acceptable price for our geographic location,” he said.
But Rachel Kent, Fair Health’s senior director of marketing, told KFF Health News that the group “does not set rates, nor determine or take any position on what constitutes ‘usual and customary rates.’ ” Instead, it reports the prices providers are charging in a given area.
Overall, Fair Health data shows huge price variations even in adjacent ZIP codes in the metro area. In Long Island’s Roslyn Heights neighborhood, where NYBG is based, Fair Health lists the out-of-network price charged by providers in the area as $60,500, the figure Ms. Wallace was billed.
But in several other New York City–area ZIP codes the price charged for the gastrectomy procedure hovers around $20,000, according to the data bank. The price in Manhattan is $17,500, for instance, according to Fair Health.
Nationwide, the average cost in 2021 for bariatric surgery done in a hospital was $32,868, according to a KFF analysis of health insurance claims.
Private equity arrives
Dr. Garber said in a court affidavit in May 2022 that he founded the bariatric practice “with a singular focus: providing safe, effective care to patients suffering from obesity and its resulting complications.”
Under his leadership, the practice has “developed into New York’s elite institution for obesity treatment,” Dr. Garber said. He said the group’s surgeons are “highly sought after to train other bariatric surgeons throughout the country and are active in the development of new, cutting-edge bariatric surgery techniques.”
In 2017, Dr. Garber and partners agreed on a business plan to help spur growth and “attract private equity investment,” according to the affidavit.
They formed a separate company to handle the bariatric practice’s business side. Known as management services organizations, such companies provide a way for private equity investors to circumvent laws in some states that prohibit nonphysicians from owning a stake in a medical practice.
In August 2019, the private equity firm Sentinel Capital Partners bought 65% of the MSO for $156.5 million, according to Dr. Garber’s affidavit. The management company is now known as New You Bariatric Group. The private equity firm did not respond to requests for comment.
Dr. Garber, in a September 2021 American Society for Metabolic and Bariatric Surgery webinar viewable online, said the weight-loss practice spends $6 million a year on media and marketing directly to patients – and is on a roll. Nationally, bariatric surgery is growing 6% annually, he said. NYBG boasts two dozen offices in the tri-state area of New York, New Jersey, and Connecticut and is poised to expand into more states.
“Since private equity, we’ve been growing at 30%-40% year over year,” Dr. Garber said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Seven months after Lahavah Wallace’s weight-loss operation, a New York bariatric surgery practice sued her, accusing her of “intentionally” failing to pay nearly $18,000 of her bill.
Long Island Minimally Invasive Surgery, which does business as the New York Bariatric Group, went on to accuse Ms. Wallace of “embezzlement,” alleging she kept insurance payments that should have been turned over to the practice.
Ms. Wallace denies the allegations, which the bariatric practice has leveled against patients in hundreds of debt-collection lawsuits filed over the past 4 years, court records in New York state show.
In about 60 cases, the lawsuits demanded $100,000 or more from patients. Some patients were found liable for tens of thousands of dollars in interest charges or wound up shackled with debt that could take a decade or more to shake. Others are facing the likely prospect of six-figure financial penalties, court records show.
Backed by a major private equity firm, the bariatric practice spends millions each year on advertisements featuring patients who have dropped 100 pounds or more after bariatric procedures, sometimes having had a portion of their stomachs removed. The ads have run on TV, online, and on New York City subway posters.
The online ads, often showcasing the slogan “Stop obesity for life,” appealed to Ms. Wallace, who lives in Brooklyn and works as a legal assistant for the state of New York. She said she turned over checks from her insurer to the bariatric group and was stunned when the medical practice hauled her into court citing an “out-of-network payment agreement” she had signed before her surgery.
“I really didn’t know what I was signing,” Ms. Wallace told KFF Health News. “I didn’t pay enough attention.”
Shawn Garber, MD, a bariatric surgeon who founded the practice in 2000 on Long Island and serves as its CEO, said that “prior to rendering services” his office staff advises patients of the costs and their responsibility to pay the bill.
The bariatric group has cited these out-of-network payment agreements in at least 300 lawsuits filed against patients from January 2019 to 2022 demanding nearly $19 million to cover medical bills, interest charges, and attorney’s fees, a KFF Health News review of New York state court records found.
Danny De Voe, a partner at Sahn Ward Braff Koblenz law firm in Uniondale, N.Y., who filed many of those suits, declined to comment, citing attorney-client privilege.
In most cases, the medical practice had agreed to accept an insurance company’s out-of-network rate as full payment for its services – with caveats, according to court filings.
In the agreements they signed, patients promised to pay any coinsurance, meeting any deductible, and pass on to the medical practice any reimbursement checks they received from their health plans within 7 days.
KFF Health News found – while legal fees and other costs can layer on thousands more.
Elisabeth Benjamin, a lawyer with the Community Service Society of New York, said conflicts can arise when insurers send checks to pay for out-of-network medical services to patients rather than reimbursing a medical provider directly.
“We would prefer to see regulators step in and stop that practice,” she said, adding it “causes tension between providers and patients.”
That’s certainly true for Ms. Wallace. The surgery practice sued her in August 2022demanding $17,981 in fees it said remained unpaid after her January 2022 laparoscopic sleeve gastrectomy, an operation in which much of the stomach is removed to assist weight loss.
The lawsuit also tacked on a demand for $5,993 in attorney’s fees, court records show.
The suit alleges Ms. Wallace signed the contract even though she “had no intention” of paying her bills. The complaint goes on to accuse her of “committing embezzlement” by “willfully, intentionally, deliberately and maliciously” depositing checks from her health plan into her personal account.
The suit doesn’t include details to substantiate these claims, and Ms. Wallace said in her court response they are not true. Ms. Wallace said she turned over checks for the charges.
“They billed the insurance for everything they possibly could,” Ms. Wallace said.
In September, Ms. Wallace filed for bankruptcy, hoping to discharge the bariatric care debt along with about $4,700 in unrelated credit card charges.
The medical practice fired back in November by filing an “adversary complaint” in her Brooklyn bankruptcy court proceeding that argues her medical debt should not be forgiven because Ms. Wallace committed fraud.
The adversary complaint, which is pending in the bankruptcy case, accuses Ms. Wallace of “fraudulently” inducing the surgery center to perform “elective medical procedures” without requiring payment up front.
Both the harsh wording and claims of wrongdoing have infuriated Ms. Wallace and her attorney, Jacob Silver, of Brooklyn.
Mr. Silver wants the medical practice to turn over records of the payments received from Ms. Wallace. “There is no fraud here,” he said. “This is frivolous. We are taking a no-settlement position.”
Gaining debt
Few patients sued by the bariatric practice mount a defense in court and those who do fight often lose, court records show.
The medical practice won default judgments totaling nearly $6 million in about 90 of the 300 cases in the sample reviewed by KFF Health News. Default judgments are entered when the defendant fails to respond.
Many cases either are pending, or it is not clear from court filings how they were resolved.
Some patients tried to argue that the fees were too high or that they didn’t understand going in how much they could owe. One woman, trying to push back against a demand for more than $100,000, said in a legal filing that she “was given numerous papers to sign without anyone of the staff members explaining to me what it actually meant.” Another patient, who was sued for more than $40,000, wrote: “I don’t have the means to pay this bill.”
Among the cases described in court records:
- A Westchester County, N.Y., woman was sued for $102,556 and settled for $72,000 in May 2021. She agreed to pay $7,500 upon signing the settlement and $500 a month from September 2021 to May 2032.
- A Peekskill, N.Y., woman in a December 2019 judgment was held liable for $384,092, which included $94,047 in interest.
- A Newburgh, N.Y., man was sued in 2021 for $252,309 in medical bills, 12% interest, and $84,103 in attorneys’ fees. The case is pending.
Robert Cohen, a longtime attorney for the bariatric practice, testified in a November 2021 hearing that the lawyers take “a contingency fee of one-third of our recovery” in these cases. In that case, Mr. Cohen had requested $13,578 based on his contingency fee arrangement. He testified that he spent 7.3 hours on the case and that his customary billing rate was $475 per hour, which came to $3,467.50. The judge awarded the lower amount, according to a transcript of the hearing.
Teresa LaMasters, MD, president of the American Society for Metabolic and Bariatric Surgery, said suing patients for large sums “is not a common practice” among bariatric surgeons.
“This is not what the vast majority in the field would espouse,” she said.
But Dr. Garber, the NYBG’s chief executive, suggested patients deserve blame.
“These lawsuits stem from these patients stealing the insurance money rather than forwarding it onto NYBG as they are morally and contractually obligated to do,” Dr. Garber wrote in an email to KFF Health News.
Dr. Garber added: “The issue is not with what we bill, but rather with the fact that the insurance companies refuse to send payment directly to us.”
‘A kooky system’
Defense attorneys argue that many patients don’t fully comprehend the perils of failing to pay on time – for whatever reason.
In a few cases, patients admitted pocketing checks they were obligated to turn over to the medical practice. But for the most part, court records don’t specify how many such checks were issued and for what amounts – or whether the patient improperly cashed them.
“It’s a kooky system,” said Paul Brite, an attorney who has faced off against the bariatric practice in court.
“You sign these documents that could cost you tons of money. It shouldn’t be that way,” he said. “This can ruin their financial life.”
New York lawmakers have acted to limit the damage from medical debt, including “surprise bills.”
In November, Democratic Gov. Kathy Hochul signed legislation that prohibits health care providers from slapping liens on a primary residence or garnishing wages.
But contracts with onerous repayment terms represent an “evolving area of law” and an alarming “new twist” on concerns over medical debt, said Ms. Benjamin, the community service society lawyer.
She said contract “accelerator clauses” that trigger severe penalties if patients miss payments should not be permitted for medical debt.
“If you default, the full amount is due,” she said. “This is really a bummer.”
‘Fair market value’
The debt collection lawsuits argue that weight-loss patients had agreed to pay “fair market value” for services – and the doctors are only trying to secure money they are due.
But some prices far exceed typical insurance payments for obesity treatments across the country, according to a medical billing data registry. Surgeons performed about 200,000 bariatric operations in 2020, according to the bariatric surgery society.
Ms. Wallace, the Brooklyn legal assistant, was billed $60,500 for her lap sleeve gastrectomy, though how much her insurance actually paid remains to be hashed out in court.
Michael Arrigo, a California medical billing expert at No World Borders, called the prices “outrageous” and “unreasonable and, in fact, likely unconscionable.”
“I disagree that these are fair market charges,” he said.
Dr. LaMasters called the gastrectomy price billed to Ms. Wallace “really expensive” and “a severe outlier.” While charges vary by region, she quoted a typical price of around $22,000.
Dr. Garber said NYBG “bills at usual and customary rates” determined by Fair Health, a New York City-based repository of insurance claims data. Fair Health “sets these rates based upon the acceptable price for our geographic location,” he said.
But Rachel Kent, Fair Health’s senior director of marketing, told KFF Health News that the group “does not set rates, nor determine or take any position on what constitutes ‘usual and customary rates.’ ” Instead, it reports the prices providers are charging in a given area.
Overall, Fair Health data shows huge price variations even in adjacent ZIP codes in the metro area. In Long Island’s Roslyn Heights neighborhood, where NYBG is based, Fair Health lists the out-of-network price charged by providers in the area as $60,500, the figure Ms. Wallace was billed.
But in several other New York City–area ZIP codes the price charged for the gastrectomy procedure hovers around $20,000, according to the data bank. The price in Manhattan is $17,500, for instance, according to Fair Health.
Nationwide, the average cost in 2021 for bariatric surgery done in a hospital was $32,868, according to a KFF analysis of health insurance claims.
Private equity arrives
Dr. Garber said in a court affidavit in May 2022 that he founded the bariatric practice “with a singular focus: providing safe, effective care to patients suffering from obesity and its resulting complications.”
Under his leadership, the practice has “developed into New York’s elite institution for obesity treatment,” Dr. Garber said. He said the group’s surgeons are “highly sought after to train other bariatric surgeons throughout the country and are active in the development of new, cutting-edge bariatric surgery techniques.”
In 2017, Dr. Garber and partners agreed on a business plan to help spur growth and “attract private equity investment,” according to the affidavit.
They formed a separate company to handle the bariatric practice’s business side. Known as management services organizations, such companies provide a way for private equity investors to circumvent laws in some states that prohibit nonphysicians from owning a stake in a medical practice.
In August 2019, the private equity firm Sentinel Capital Partners bought 65% of the MSO for $156.5 million, according to Dr. Garber’s affidavit. The management company is now known as New You Bariatric Group. The private equity firm did not respond to requests for comment.
Dr. Garber, in a September 2021 American Society for Metabolic and Bariatric Surgery webinar viewable online, said the weight-loss practice spends $6 million a year on media and marketing directly to patients – and is on a roll. Nationally, bariatric surgery is growing 6% annually, he said. NYBG boasts two dozen offices in the tri-state area of New York, New Jersey, and Connecticut and is poised to expand into more states.
“Since private equity, we’ve been growing at 30%-40% year over year,” Dr. Garber said.
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.