User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Children and COVID: Weekly cases rise again, but more slowly
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.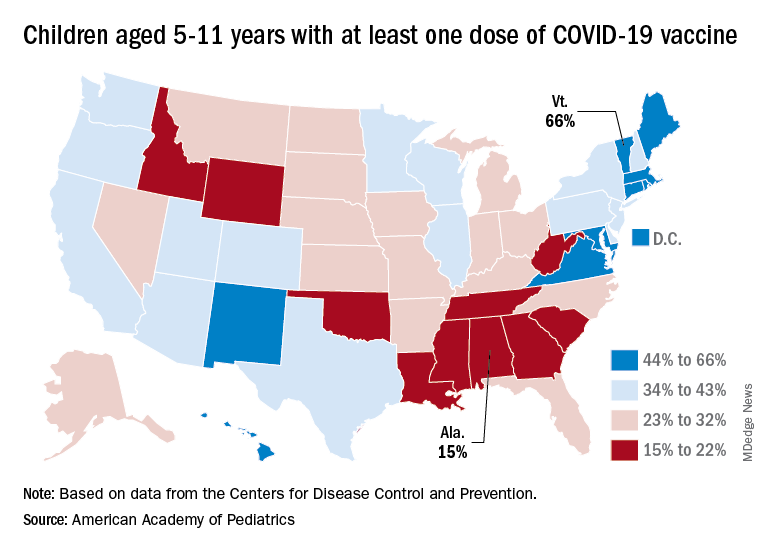
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
New cases of COVID-19 in U.S. children went up for a second consecutive week, but the pace of increase slowed considerably, based on a report from the American Academy of Pediatrics and the Children’s Hospital Association.
The previous week’s count – about 33,000 new COVID cases for April 8-14 – was almost 30% higher than the week before and marked the first rise in incidence after 11 straight weeks of declines, the AAP and CHA said in their weekly COVID-19 report, which is based on data from state and territorial health departments.
The cumulative number of child COVID-19 cases since the start of the pandemic is now over 12.9 million, with children representing 19.0% of cases among all ages. The Centers for Disease Control and Prevention, which uses a different age range for children (0-17 years) than many states, reports corresponding figures of 12.4 million and 17.6%, along with 1,501 deaths.
ED visits show a similar rising trend over recent weeks, as the 7-day average of ED visits with confirmed COVID has crept up from 0.5% in late March/early April to 0.8% on April 22 for children aged 0-11 years, from 0.3% for 0.5% for those aged 12-15, and from 0.3% to 0.6% for 16- and 17-year-olds, based on CDC data.
The daily rate for new admissions for children with confirmed COVID has also moved up slightly, rising from 0.13 per 100,000 population as late as April 13 to 0.15 per 100,000 on April 23. For the number of actual admissions, the latest 7-day (April 17-23) average was 107 in children aged 0-17, compared with 102 for the week of April 10-16, the CDC reported.
Uptake of the COVID vaccine, however, continued to slide since spiking in January. Initial vaccinations for the latest available week (April 14-20) were down to 48,000 from 59,000 the week before in children aged 5-11 years and 35,000 (vs. 47,000) for those aged 12-17. The weekly highs hit 500,000 and 331,000, respectively, during the Omicron surge, the AAP reported based on CDC data.
Among children aged 5-11, the CDC said that 35.0% had received at least one dose of COVID vaccine as of April 25 and that 28.3% are fully vaccinated, with corresponding figures of 68.8% and 58.8% for 12- to 17-year-olds on April 25.
Among the states, the highest vaccination rates generally are found in New England and the lowest in the Southeast. In Alabama, just 15% of children aged 5-11 have received an initial dose of the vaccine, compared with 66% in Vermont, while Wyoming is the lowest (41%) for children aged 12-17 and Massachusetts is the highest (96%), the AAP said in a separate report.
One in four feel fully recovered following COVID-19 hospitalization
One year after hospitalization for COVID-19 only a minority of people feel fully recovered, with being female, obesity, and having had mechanical ventilation in hospital risk factors for not feeling fully recovered.
In the new U.K. study of more than 2,000 patients, presented at this year’s European Congress of Clinical Microbiology & Infectious Diseases (ECCMID 2022), and published in The Lancet Respiratory Medicine, research showed that one in four patients feel fully well again 1 year after hospitalization for COVID-19.
For their study, researchers from the University of Leicester used data from the post-hospitalization COVID-19 (PHOSP-COVID) prospective, longitudinal cohort study, which assessed adults aged 18 years and over who had been hospitalized with COVID-19 across the United Kingdom and subsequently discharged. The researchers assessed the recovery of 2,320 participants discharged from 39 U.K. hospitals between March 7, 2020, and April 18, 2021, who were assessed via patient-reported outcome measures, physical performance, and organ function at 5 months and at 1 year after hospital discharge. Blood samples were taken at the 5-month visit to be analyzed for the presence of various inflammatory proteins.
All participants were assessed at 5 months after discharge and 807 participants (33%) completed both the 5-month and 1-year visits at the time of the analysis. The study is ongoing. The 807 patients were mean age of 59 years, 36% were women, and 28% received invasive mechanical ventilation. The proportion of patients reporting full recovery was similar between 5 months (26%) and 1 year (29%).
Female sex and obesity major risk factors for not recovering
Being female, obese, and having had mechanical ventilation in hospital makes someone 32%, 50%, and 58%, respectively, less likely to feel fully recovered 1 year after COVID-19 hospitalization, the authors said.
“We found female sex and obesity were major risk factors for not recovering at one year,” said the researchers, led by Rachael Evans, PhD, Louise V. Wain, and Christopher E. Brightling, PhD, National Institute for Health Research, Leicester Biomedical Research Centre, University of Leicester.
The authors said fatigue, muscle pain, physically slowing down, poor sleep, and breathlessness were most common ongoing long COVID symptoms. They noted how the total number and range of ongoing symptoms at 1 year was “striking,” positively associated with the severity of long COVID, and emphasizes the “multisystem nature of long COVID.”
Several inflammatory mediators increased
An earlier publication from this study identified four groups or “clusters” of symptom severity at 5 months, which were confirmed by this new study at 1 year, the authors said. They reported that 20% had very severe physical and mental health impairment, 30% had severe physical and mental health impairment, 11% had moderate physical health impairment with cognitive impairment, and 39% had mild mental and physical health impairment.
They added that having obesity, reduced exercise capacity, a greater number of symptoms, and increased levels of C-reactive protein were associated with the “more severe clusters.” In both the very severe and the moderate with cognitive impairment clusters, levels of interleukin-6 (IL-6) were higher when compared with the mild cluster.
“The limited recovery from 5 months to 1 year after hospitalisation in our study across symptoms, mental health, exercise capacity, organ impairment, and quality-of-life is striking,” the researchers noted.
“In our clusters, female sex and obesity were also associated with more severe ongoing health impairments including reduced exercise performance and health-related quality of life at one year,” and suggested that this potentially highlighted a group that “might need higher intensity interventions such as supervised rehabilitation,” they added.
There are no specific therapeutics for long COVID, the researchers said, noting that “effective interventions are urgently required.” The persistent systemic inflammation identified, particularly in those in the very severe and moderate with cognitive impairment clusters, suggested that these groups “might respond to anti-inflammatory strategies,” the authors wrote.
“We found that a minority of participants felt fully recovered 1 year after hospital discharge, with minimal improvement after a 5-month assessment,” they noted.
They added that the findings suggest the need for complex interventions that target both physical and mental health impairments to alleviate symptoms, and that specific therapeutic approaches to manage posttraumatic stress disorder might also be needed. The authors pointed out how “pharmacological and non-pharmacological interventions are urgently needed,” with a “precision-medicine approach with potential treatable traits of systemic inflammation and obesity.”
They said their study highlighted the “urgent need for health-care services to support the large and rapidly increasing patient population in whom a substantial burden of symptoms exist, including reduced exercise capacity and substantially decreased health-related quality of life one year after hospital discharge.”
They warned that without effective treatments, long COVID could become a “highly prevalent new long-term condition.”
A version of this article first appeared on Medscape UK.
One year after hospitalization for COVID-19 only a minority of people feel fully recovered, with being female, obesity, and having had mechanical ventilation in hospital risk factors for not feeling fully recovered.
In the new U.K. study of more than 2,000 patients, presented at this year’s European Congress of Clinical Microbiology & Infectious Diseases (ECCMID 2022), and published in The Lancet Respiratory Medicine, research showed that one in four patients feel fully well again 1 year after hospitalization for COVID-19.
For their study, researchers from the University of Leicester used data from the post-hospitalization COVID-19 (PHOSP-COVID) prospective, longitudinal cohort study, which assessed adults aged 18 years and over who had been hospitalized with COVID-19 across the United Kingdom and subsequently discharged. The researchers assessed the recovery of 2,320 participants discharged from 39 U.K. hospitals between March 7, 2020, and April 18, 2021, who were assessed via patient-reported outcome measures, physical performance, and organ function at 5 months and at 1 year after hospital discharge. Blood samples were taken at the 5-month visit to be analyzed for the presence of various inflammatory proteins.
All participants were assessed at 5 months after discharge and 807 participants (33%) completed both the 5-month and 1-year visits at the time of the analysis. The study is ongoing. The 807 patients were mean age of 59 years, 36% were women, and 28% received invasive mechanical ventilation. The proportion of patients reporting full recovery was similar between 5 months (26%) and 1 year (29%).
Female sex and obesity major risk factors for not recovering
Being female, obese, and having had mechanical ventilation in hospital makes someone 32%, 50%, and 58%, respectively, less likely to feel fully recovered 1 year after COVID-19 hospitalization, the authors said.
“We found female sex and obesity were major risk factors for not recovering at one year,” said the researchers, led by Rachael Evans, PhD, Louise V. Wain, and Christopher E. Brightling, PhD, National Institute for Health Research, Leicester Biomedical Research Centre, University of Leicester.
The authors said fatigue, muscle pain, physically slowing down, poor sleep, and breathlessness were most common ongoing long COVID symptoms. They noted how the total number and range of ongoing symptoms at 1 year was “striking,” positively associated with the severity of long COVID, and emphasizes the “multisystem nature of long COVID.”
Several inflammatory mediators increased
An earlier publication from this study identified four groups or “clusters” of symptom severity at 5 months, which were confirmed by this new study at 1 year, the authors said. They reported that 20% had very severe physical and mental health impairment, 30% had severe physical and mental health impairment, 11% had moderate physical health impairment with cognitive impairment, and 39% had mild mental and physical health impairment.
They added that having obesity, reduced exercise capacity, a greater number of symptoms, and increased levels of C-reactive protein were associated with the “more severe clusters.” In both the very severe and the moderate with cognitive impairment clusters, levels of interleukin-6 (IL-6) were higher when compared with the mild cluster.
“The limited recovery from 5 months to 1 year after hospitalisation in our study across symptoms, mental health, exercise capacity, organ impairment, and quality-of-life is striking,” the researchers noted.
“In our clusters, female sex and obesity were also associated with more severe ongoing health impairments including reduced exercise performance and health-related quality of life at one year,” and suggested that this potentially highlighted a group that “might need higher intensity interventions such as supervised rehabilitation,” they added.
There are no specific therapeutics for long COVID, the researchers said, noting that “effective interventions are urgently required.” The persistent systemic inflammation identified, particularly in those in the very severe and moderate with cognitive impairment clusters, suggested that these groups “might respond to anti-inflammatory strategies,” the authors wrote.
“We found that a minority of participants felt fully recovered 1 year after hospital discharge, with minimal improvement after a 5-month assessment,” they noted.
They added that the findings suggest the need for complex interventions that target both physical and mental health impairments to alleviate symptoms, and that specific therapeutic approaches to manage posttraumatic stress disorder might also be needed. The authors pointed out how “pharmacological and non-pharmacological interventions are urgently needed,” with a “precision-medicine approach with potential treatable traits of systemic inflammation and obesity.”
They said their study highlighted the “urgent need for health-care services to support the large and rapidly increasing patient population in whom a substantial burden of symptoms exist, including reduced exercise capacity and substantially decreased health-related quality of life one year after hospital discharge.”
They warned that without effective treatments, long COVID could become a “highly prevalent new long-term condition.”
A version of this article first appeared on Medscape UK.
One year after hospitalization for COVID-19 only a minority of people feel fully recovered, with being female, obesity, and having had mechanical ventilation in hospital risk factors for not feeling fully recovered.
In the new U.K. study of more than 2,000 patients, presented at this year’s European Congress of Clinical Microbiology & Infectious Diseases (ECCMID 2022), and published in The Lancet Respiratory Medicine, research showed that one in four patients feel fully well again 1 year after hospitalization for COVID-19.
For their study, researchers from the University of Leicester used data from the post-hospitalization COVID-19 (PHOSP-COVID) prospective, longitudinal cohort study, which assessed adults aged 18 years and over who had been hospitalized with COVID-19 across the United Kingdom and subsequently discharged. The researchers assessed the recovery of 2,320 participants discharged from 39 U.K. hospitals between March 7, 2020, and April 18, 2021, who were assessed via patient-reported outcome measures, physical performance, and organ function at 5 months and at 1 year after hospital discharge. Blood samples were taken at the 5-month visit to be analyzed for the presence of various inflammatory proteins.
All participants were assessed at 5 months after discharge and 807 participants (33%) completed both the 5-month and 1-year visits at the time of the analysis. The study is ongoing. The 807 patients were mean age of 59 years, 36% were women, and 28% received invasive mechanical ventilation. The proportion of patients reporting full recovery was similar between 5 months (26%) and 1 year (29%).
Female sex and obesity major risk factors for not recovering
Being female, obese, and having had mechanical ventilation in hospital makes someone 32%, 50%, and 58%, respectively, less likely to feel fully recovered 1 year after COVID-19 hospitalization, the authors said.
“We found female sex and obesity were major risk factors for not recovering at one year,” said the researchers, led by Rachael Evans, PhD, Louise V. Wain, and Christopher E. Brightling, PhD, National Institute for Health Research, Leicester Biomedical Research Centre, University of Leicester.
The authors said fatigue, muscle pain, physically slowing down, poor sleep, and breathlessness were most common ongoing long COVID symptoms. They noted how the total number and range of ongoing symptoms at 1 year was “striking,” positively associated with the severity of long COVID, and emphasizes the “multisystem nature of long COVID.”
Several inflammatory mediators increased
An earlier publication from this study identified four groups or “clusters” of symptom severity at 5 months, which were confirmed by this new study at 1 year, the authors said. They reported that 20% had very severe physical and mental health impairment, 30% had severe physical and mental health impairment, 11% had moderate physical health impairment with cognitive impairment, and 39% had mild mental and physical health impairment.
They added that having obesity, reduced exercise capacity, a greater number of symptoms, and increased levels of C-reactive protein were associated with the “more severe clusters.” In both the very severe and the moderate with cognitive impairment clusters, levels of interleukin-6 (IL-6) were higher when compared with the mild cluster.
“The limited recovery from 5 months to 1 year after hospitalisation in our study across symptoms, mental health, exercise capacity, organ impairment, and quality-of-life is striking,” the researchers noted.
“In our clusters, female sex and obesity were also associated with more severe ongoing health impairments including reduced exercise performance and health-related quality of life at one year,” and suggested that this potentially highlighted a group that “might need higher intensity interventions such as supervised rehabilitation,” they added.
There are no specific therapeutics for long COVID, the researchers said, noting that “effective interventions are urgently required.” The persistent systemic inflammation identified, particularly in those in the very severe and moderate with cognitive impairment clusters, suggested that these groups “might respond to anti-inflammatory strategies,” the authors wrote.
“We found that a minority of participants felt fully recovered 1 year after hospital discharge, with minimal improvement after a 5-month assessment,” they noted.
They added that the findings suggest the need for complex interventions that target both physical and mental health impairments to alleviate symptoms, and that specific therapeutic approaches to manage posttraumatic stress disorder might also be needed. The authors pointed out how “pharmacological and non-pharmacological interventions are urgently needed,” with a “precision-medicine approach with potential treatable traits of systemic inflammation and obesity.”
They said their study highlighted the “urgent need for health-care services to support the large and rapidly increasing patient population in whom a substantial burden of symptoms exist, including reduced exercise capacity and substantially decreased health-related quality of life one year after hospital discharge.”
They warned that without effective treatments, long COVID could become a “highly prevalent new long-term condition.”
A version of this article first appeared on Medscape UK.
FROM THE LANCET RESPIRATORY MEDICINE
2020 presidential election tied to spike in cardiac events
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
The analysis of nearly 6.4 million adults showed that the rate of hospitalization for acute cardiovascular disease (CVD) was 17% higher in the 5 days after the election than in a 5-day period 2 weeks earlier.
The rate of acute myocardial infarction (AMI) was 42% higher, with no significant difference for heart failure or stroke hospital admissions.
“These findings suggest that awareness of the heightened risk of CVD and strategies to mitigate risk during notable political events are needed,” write Matthew T. Mefford, PhD, of Kaiser Permanente Southern California, Pasadena, and colleagues.
The study was published in the April issue of JAMA Network Open.
Stress and the heart
In the American Psychological Association Stress in America 2020 survey conducted roughly 3 months before the 2020 presidential election, 77% of adults cited the future of the country as a substantial source of stress, enhanced by the ongoing COVID-19 pandemic, the authors note. More than two-thirds said the election was a substantial source of stress.
Dr. Mefford and colleagues compared CVD hospitalizations at Kaiser Permanente Southern and Northern California hospitals in the 5-day risk window of Nov. 4-8, 2020, with the control window of Oct. 21-25, 2020.
There were 666 CVD hospitalizations (760.47 per 100,000 person-years [PY]) in the risk window, compared with 569 (647.97 per 100,000 PY) in the control window (rate ratio, 1.17; 95% confidence interval, 1.05-1.31).
There were also significantly more hospitalizations for AMI immediately after the election than before (179 vs. 126 AMI hospitalizations; 204.4 vs. 143.5 per 100,000 PY; RR, 1.42; 95% CI, 1.13-1.79).
There was no significant difference between the risk and control periods for hospitalizations because of stroke or heart failure.
The study also suggests higher rates of acute CVD after the election in older adults, men, and White individuals. Political affiliation was not examined in the study.
“Importantly, results were consistent before and after excluding patients with confirmed COVID-19 infection,” the study team notes.
Yet, the potential influence of COVID-19 stressors on increasing CVD risk cannot be ruled out, they say.
However, COVID-19 stressors occurred over a much longer period and are less likely to explain the transient risks observed in the defined risk and control windows that are in close proximity to the 2020 election, the investigators point out.
There is growing evidence that psychological health contributes to CVD.
Previous studies shown a higher risk for acute CVD around population-wide psychosocial or environmental stressors, but less was known about acute CVD risk in relation to political events.
The researchers note future studies evaluating stress-relieving interventions may be important for understanding the intersection of political events, associated stress, and acute CVD risk.
Partial funding for the study was provided by a grant from the W.K. Kellogg Foundation. The authors have no relevant conflicts of interest.
A version of this article first appeared on Medscape.com.
FROM JAMA NETWORK OPEN
Furosemide seen as safe for preventing newborn lung disease
A medication used to reduce fluid retention can also safely be used to prevent a dangerous lung condition that affects newborns, particularly those born premature, according to a new study.
Furosemide (Lasix) – which can reduce excess fluid in the body caused by heart failure, liver disease, and kidney trouble – is commonly used off-label to prevent bronchopulmonary dysplasia (BPD), a disorder that causes irritation and poor development of lungs in premature infants. But until now, researchers have not studied its safety in this setting.
BPD often affects babies born more than 2 months early and can sometimes result in breathing difficulties into adolescence and young adulthood.
“There are so few drugs that have been tested for newborns, and there are very little data to help neonatologists decide if certain medications are safe and effective,” said Rachel Greenberg, MD, MHS, a neonatologist and member of the Duke Clinical Research Institute, Durham, N.C. “We found there was no greater risk of safety events for newborns given furosemide.”
Dr. Greenberg presented the findings at the 2022 Pediatric Academic Societies meeting in Denver.
For the 28-day randomized controlled trial, Dr. Greenberg and colleagues enrolled 80 preterm newborns, born at less than 29 weeks’ gestation, at 17 centers within the Eunice Kennedy Shriver National Institute of Child Health and Human Development Pediatric Trials Network. Of those, 61 received furosemide and 19 received a placebo.
Although babies given furosemide had more problems with electrolytes – an expected outcome from the use of diuretic medications – the researchers observed no greater risk for more serious issues, namely hearing loss or kidney stones, Dr. Greenberg told this news organization.
“The mechanism here is we know that extra fluid can damage the lungs and can cause you to have to use more respiratory support and more oxygen,” she said. “The thought from a physiological standpoint is using a diuretic can decrease fluid in the lungs and lead to improvements in lung outcomes.”
The researchers did not observe a reduction in BDP or death in babies who received furosemide, but Dr. Greenberg said the study was underpowered to detect such an effect.
“We were not powered to detect a difference in that outcome; the overall objective of this study was always to evaluate safety,” she said. “Of course, we wanted to capture variables that would measure effectiveness as well.
“Because this was a pragmatic trial, we did not limit the amount of fluids that the clinicians could give the participating infants. This could have impacted the effectiveness of furosemide. We would need a different design and larger study to truly determine effectiveness.”
Dr. Greenberg said she hoped the new data will provide greater insight to neonatal providers and help bolster future, more large-scale trials using furosemide in premature infants.
The drug has previously been associated with both kidney stones and ototoxicity, which occurs when medication causes a person to develop hearing or balance problems, said Nicolas Bamat, MD, MSCE, assistant professor of pediatrics at the Perelman School of Medicine, University of Pennsylvania, Philadelphia.
Although the number of children in the latest study was too small to generate any firm conclusions, he said, the trial provides the best data to date on furosemide in premature infants.
The medication is used frequently both on babies at risk of developing BPD and babies who have already reached BPD status. Among newborns with highest risk of dying, furosemide is indeed the “most frequently used pharmacotherapy,” Dr. Bamat said.
“What’s worth noting is that furosemide is an old medication that has been used extensively in the neonatal populations for 40 years, and that is occurring in the absence of data,” Dr. Bamat added. “This is a very important step forward.”
Dr. Greenberg and Dr. Bamat have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A medication used to reduce fluid retention can also safely be used to prevent a dangerous lung condition that affects newborns, particularly those born premature, according to a new study.
Furosemide (Lasix) – which can reduce excess fluid in the body caused by heart failure, liver disease, and kidney trouble – is commonly used off-label to prevent bronchopulmonary dysplasia (BPD), a disorder that causes irritation and poor development of lungs in premature infants. But until now, researchers have not studied its safety in this setting.
BPD often affects babies born more than 2 months early and can sometimes result in breathing difficulties into adolescence and young adulthood.
“There are so few drugs that have been tested for newborns, and there are very little data to help neonatologists decide if certain medications are safe and effective,” said Rachel Greenberg, MD, MHS, a neonatologist and member of the Duke Clinical Research Institute, Durham, N.C. “We found there was no greater risk of safety events for newborns given furosemide.”
Dr. Greenberg presented the findings at the 2022 Pediatric Academic Societies meeting in Denver.
For the 28-day randomized controlled trial, Dr. Greenberg and colleagues enrolled 80 preterm newborns, born at less than 29 weeks’ gestation, at 17 centers within the Eunice Kennedy Shriver National Institute of Child Health and Human Development Pediatric Trials Network. Of those, 61 received furosemide and 19 received a placebo.
Although babies given furosemide had more problems with electrolytes – an expected outcome from the use of diuretic medications – the researchers observed no greater risk for more serious issues, namely hearing loss or kidney stones, Dr. Greenberg told this news organization.
“The mechanism here is we know that extra fluid can damage the lungs and can cause you to have to use more respiratory support and more oxygen,” she said. “The thought from a physiological standpoint is using a diuretic can decrease fluid in the lungs and lead to improvements in lung outcomes.”
The researchers did not observe a reduction in BDP or death in babies who received furosemide, but Dr. Greenberg said the study was underpowered to detect such an effect.
“We were not powered to detect a difference in that outcome; the overall objective of this study was always to evaluate safety,” she said. “Of course, we wanted to capture variables that would measure effectiveness as well.
“Because this was a pragmatic trial, we did not limit the amount of fluids that the clinicians could give the participating infants. This could have impacted the effectiveness of furosemide. We would need a different design and larger study to truly determine effectiveness.”
Dr. Greenberg said she hoped the new data will provide greater insight to neonatal providers and help bolster future, more large-scale trials using furosemide in premature infants.
The drug has previously been associated with both kidney stones and ototoxicity, which occurs when medication causes a person to develop hearing or balance problems, said Nicolas Bamat, MD, MSCE, assistant professor of pediatrics at the Perelman School of Medicine, University of Pennsylvania, Philadelphia.
Although the number of children in the latest study was too small to generate any firm conclusions, he said, the trial provides the best data to date on furosemide in premature infants.
The medication is used frequently both on babies at risk of developing BPD and babies who have already reached BPD status. Among newborns with highest risk of dying, furosemide is indeed the “most frequently used pharmacotherapy,” Dr. Bamat said.
“What’s worth noting is that furosemide is an old medication that has been used extensively in the neonatal populations for 40 years, and that is occurring in the absence of data,” Dr. Bamat added. “This is a very important step forward.”
Dr. Greenberg and Dr. Bamat have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
A medication used to reduce fluid retention can also safely be used to prevent a dangerous lung condition that affects newborns, particularly those born premature, according to a new study.
Furosemide (Lasix) – which can reduce excess fluid in the body caused by heart failure, liver disease, and kidney trouble – is commonly used off-label to prevent bronchopulmonary dysplasia (BPD), a disorder that causes irritation and poor development of lungs in premature infants. But until now, researchers have not studied its safety in this setting.
BPD often affects babies born more than 2 months early and can sometimes result in breathing difficulties into adolescence and young adulthood.
“There are so few drugs that have been tested for newborns, and there are very little data to help neonatologists decide if certain medications are safe and effective,” said Rachel Greenberg, MD, MHS, a neonatologist and member of the Duke Clinical Research Institute, Durham, N.C. “We found there was no greater risk of safety events for newborns given furosemide.”
Dr. Greenberg presented the findings at the 2022 Pediatric Academic Societies meeting in Denver.
For the 28-day randomized controlled trial, Dr. Greenberg and colleagues enrolled 80 preterm newborns, born at less than 29 weeks’ gestation, at 17 centers within the Eunice Kennedy Shriver National Institute of Child Health and Human Development Pediatric Trials Network. Of those, 61 received furosemide and 19 received a placebo.
Although babies given furosemide had more problems with electrolytes – an expected outcome from the use of diuretic medications – the researchers observed no greater risk for more serious issues, namely hearing loss or kidney stones, Dr. Greenberg told this news organization.
“The mechanism here is we know that extra fluid can damage the lungs and can cause you to have to use more respiratory support and more oxygen,” she said. “The thought from a physiological standpoint is using a diuretic can decrease fluid in the lungs and lead to improvements in lung outcomes.”
The researchers did not observe a reduction in BDP or death in babies who received furosemide, but Dr. Greenberg said the study was underpowered to detect such an effect.
“We were not powered to detect a difference in that outcome; the overall objective of this study was always to evaluate safety,” she said. “Of course, we wanted to capture variables that would measure effectiveness as well.
“Because this was a pragmatic trial, we did not limit the amount of fluids that the clinicians could give the participating infants. This could have impacted the effectiveness of furosemide. We would need a different design and larger study to truly determine effectiveness.”
Dr. Greenberg said she hoped the new data will provide greater insight to neonatal providers and help bolster future, more large-scale trials using furosemide in premature infants.
The drug has previously been associated with both kidney stones and ototoxicity, which occurs when medication causes a person to develop hearing or balance problems, said Nicolas Bamat, MD, MSCE, assistant professor of pediatrics at the Perelman School of Medicine, University of Pennsylvania, Philadelphia.
Although the number of children in the latest study was too small to generate any firm conclusions, he said, the trial provides the best data to date on furosemide in premature infants.
The medication is used frequently both on babies at risk of developing BPD and babies who have already reached BPD status. Among newborns with highest risk of dying, furosemide is indeed the “most frequently used pharmacotherapy,” Dr. Bamat said.
“What’s worth noting is that furosemide is an old medication that has been used extensively in the neonatal populations for 40 years, and that is occurring in the absence of data,” Dr. Bamat added. “This is a very important step forward.”
Dr. Greenberg and Dr. Bamat have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM PAS 2022
More antibodies with longer intervals between COVID vaccine doses
An overall ninefold increase in COVID-19 antibody levels can be seen with a longer interval between first and second doses of the Pfizer/BioNTech (BNT162b2) vaccine in people without prior infection, according to data from the U.K. government’s SIREN (SARS-CoV-2 Immunity and Reinfection Evaluation) study.
This interval-dependent antibody level varied by age, with those aged 45-54 years showing an 11-fold increase with a longer dosing interval (greater than 10 weeks vs. 2-4 weeks). People younger than age 25 years showed a 13-fold increase with the longer interval, but participant numbers were low in this sub-group.
Overall antibody levels in infection-naive participants were 1,268.72 Binding Antibody Units (BAU)/mL (1,043.25-1,542.91) in those with a 2-4–week interval, compared with 11,479.73 BAU/mL (10,742.78-12,267.24) (P < .0001), in those with at least a 10-week interval between doses.
The work is the latest analysis from SIREN, which measured antibody levels in the blood from nearly 6,000 health care workers from across the United Kingdom. Study lead Ashley Otter, PhD, technical lead for SIREN serology at the UK Health Security Agency (UKHSA), will present the work on Tuesday at the 2022 European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Lisbon.
In an interview, Dr. Otter noted that, “it is important to remember that antibody levels are only one aspect of the immune response, and in our recent vaccine effectiveness analysis, we found that dosing intervals did not affect protection against infection.”
The study, which appeared in the March issue of the New England Journal of Medicine, also found that after the second dose of vaccine, there was about a 2.5–fold difference in antibody levels between those who had prior infection of 16.052 (14.071-18.312) BAU/mL, compared with 7.050 (6.634-7.491) BAU/mL in infection-naive individuals (P < .0001).
Following the first dose only, antibody levels were up to 10 times higher in participants who were previously infected, compared with infection-naive individuals. This effect lasted up to 8 months and then began to plateau.
Natural infection increased antibody levels
Dr. Otter remarked that, “COVID-19 antibody levels are high in those people who were previously naturally infected and vaccinated, highlighting that vaccination provides an additional benefit to these individuals.”
This news organization asked Charlotte Thålin, PhD, an immunologist from the Karolinska Institute, Stockholm, to comment on the study. Dr. Thålin studies a cohort similar to SIREN, called the Swedish COMMUNITY health care worker cohort. “The new data from the SIREN emphasizes the importance of the number of antigenic exposures and the time interval between them, whether it be exposure through vaccination or exposure through infection.”
“We see similar data in our Swedish COMMUNITY health care worker cohort,” Dr. Thålin continued, “where infection prior to vaccination yields a more than twofold enhancement in antibodies, neutralizing breadth, and T cell responses, and an even larger increase with a longer time interval between infection and vaccination.”
However, she cautioned that they now see a high rate of Omicron vaccine breakthrough infections, and this is also true in people with previous infection and three vaccine doses.
“As we approach a second booster – a fourth vaccine dose – we need to consider that many individuals will have had up to five to six antigen exposures within a short period of time, sometimes within a year,” she pointed out. “This is a whole new scenario, with a lot of different combinations of vaccine and infection-induced immunity. We do not yet know the impact of these frequent immune exposures, and we now need to monitor immune responses following Omicron and booster doses closely.”
SIREN originally aimed to understand how much protection people got after developing a primary infection and why they might become reinfected with COVID-19. Following the rollout of the United Kingdom’s vaccination program, the protective effects of vaccination against COVID-19 were investigated, as well as why some people still become ill after being vaccinated, Dr. Otter explained.
In this latest analysis, Dr. Otter and colleagues assessed anti-spike binding antibodies in serum samples from a total of 5,871 health care workers, with 3,989 after one dose (at least 21 days) and 1,882 after two doses (at least 14 days).
Most participants were women (82.3%), of White ethnicity (87%), and came from across the United Kingdom.
Participants were also categorized into those who had evidence of natural COVID-19 infection (confirmed by a PCR test or assumed because of their antibody profile) or those who were infection-naive. Almost all (> 99%) of those who were infection-naive seroconverted after vaccination.
The primary outcome was anti-spike antibody levels assessed according to dose, previous infection, dosing interval, age, ethnicity, and comorbidities, including immunosuppressive disease such as immune system cancers, rheumatologic disease, chronic respiratory diseases, diabetes, obesity, and chronic neurologic disease.
In the infection-naive group, the mean antibody (anti-S titer) was 75.48 BAU/mL after the first vaccine dose, and this rose to 7,049.76 BAU/mL after the second dose.
The much higher antibody titer with the second dose in infection-naive individuals “is what gives you the most protection, as your antibody titers are at their peak. They then start to gradually wane from this peak,” said Dr. Otter.
In the post-infection group, antibody titers also rose (2,111.08 BAU/mL after first dose and 16,052.39 BAU/mL after second dose), although less so than in the infection-naive group, because of the additional exposure of infection, added Dr. Otter.
Antibody levels also varied according to time elapsed between natural infection and dose 1 of vaccination. With a 3-month interval, antibody levels were 1,970.83 (1,506.01-2,579.1) BAU/mL, compared with 13,759.31 (8,097.78-23,379.09) BAU/mL after a 9-month interval. Antibody levels after one dose in those previously infected are higher than the infection-naive because “previous infection, then vaccination, is likely explained by T-cell expansion upon a boost with a second antigen exposure, and then a maturing memory B-cell response that has been demonstrated up to 6 months,” explained Dr. Otter.
Timing of fourth dose
By March of this year, 86.2% of the U.K. population aged over 12 years had received at least two doses, but with rises in disease prevalence and the spread of variants of concern, further work is ongoing to understand the waning of the immune response, level of protection, and why some individuals develop COVID-19 even when double-vaccinated.
This news organization asked Susanna Dunachie, BMChB, professor of infectious diseases, University of Oxford, U.K., what the interval findings might mean for the timing of the fourth dose of vaccine across the U.K. population.
In the United Kingdom, fourth doses are being given to people who are 75 years and older, residents in care homes for older people, and those with weakened immune systems. “To make decisions about fourth doses for healthy people, we need to see how quickly antibody and T-cell responses drop,” said Ms. Dunachie, who is part of the large SIREN study team but was not involved in the analysis led by Dr. Otter. “Current research suggests that the T-cell response may be better maintained than the antibody response, and less affected by variants like Omicron.”
She explained the balance between antibody and T-cell responses to vaccination. “It is likely that antibodies that neutralize the virus are important for preventing any infection at all, and these unfortunately do fall in time, but T-cell responses are better sustained and help keep people out of [the] hospital,” she said.
Ms. Dunachie added that it was necessary to wait and observe what happens next with SARS-CoV-2 evolution, as well as wait for longer follow-up after the third dose in healthy people. “On current evidence, my estimate is we postpone decisions on fourth doses in healthy people to late summer/autumn.”
A version of this article first appeared on Medscape.com.
An overall ninefold increase in COVID-19 antibody levels can be seen with a longer interval between first and second doses of the Pfizer/BioNTech (BNT162b2) vaccine in people without prior infection, according to data from the U.K. government’s SIREN (SARS-CoV-2 Immunity and Reinfection Evaluation) study.
This interval-dependent antibody level varied by age, with those aged 45-54 years showing an 11-fold increase with a longer dosing interval (greater than 10 weeks vs. 2-4 weeks). People younger than age 25 years showed a 13-fold increase with the longer interval, but participant numbers were low in this sub-group.
Overall antibody levels in infection-naive participants were 1,268.72 Binding Antibody Units (BAU)/mL (1,043.25-1,542.91) in those with a 2-4–week interval, compared with 11,479.73 BAU/mL (10,742.78-12,267.24) (P < .0001), in those with at least a 10-week interval between doses.
The work is the latest analysis from SIREN, which measured antibody levels in the blood from nearly 6,000 health care workers from across the United Kingdom. Study lead Ashley Otter, PhD, technical lead for SIREN serology at the UK Health Security Agency (UKHSA), will present the work on Tuesday at the 2022 European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Lisbon.
In an interview, Dr. Otter noted that, “it is important to remember that antibody levels are only one aspect of the immune response, and in our recent vaccine effectiveness analysis, we found that dosing intervals did not affect protection against infection.”
The study, which appeared in the March issue of the New England Journal of Medicine, also found that after the second dose of vaccine, there was about a 2.5–fold difference in antibody levels between those who had prior infection of 16.052 (14.071-18.312) BAU/mL, compared with 7.050 (6.634-7.491) BAU/mL in infection-naive individuals (P < .0001).
Following the first dose only, antibody levels were up to 10 times higher in participants who were previously infected, compared with infection-naive individuals. This effect lasted up to 8 months and then began to plateau.
Natural infection increased antibody levels
Dr. Otter remarked that, “COVID-19 antibody levels are high in those people who were previously naturally infected and vaccinated, highlighting that vaccination provides an additional benefit to these individuals.”
This news organization asked Charlotte Thålin, PhD, an immunologist from the Karolinska Institute, Stockholm, to comment on the study. Dr. Thålin studies a cohort similar to SIREN, called the Swedish COMMUNITY health care worker cohort. “The new data from the SIREN emphasizes the importance of the number of antigenic exposures and the time interval between them, whether it be exposure through vaccination or exposure through infection.”
“We see similar data in our Swedish COMMUNITY health care worker cohort,” Dr. Thålin continued, “where infection prior to vaccination yields a more than twofold enhancement in antibodies, neutralizing breadth, and T cell responses, and an even larger increase with a longer time interval between infection and vaccination.”
However, she cautioned that they now see a high rate of Omicron vaccine breakthrough infections, and this is also true in people with previous infection and three vaccine doses.
“As we approach a second booster – a fourth vaccine dose – we need to consider that many individuals will have had up to five to six antigen exposures within a short period of time, sometimes within a year,” she pointed out. “This is a whole new scenario, with a lot of different combinations of vaccine and infection-induced immunity. We do not yet know the impact of these frequent immune exposures, and we now need to monitor immune responses following Omicron and booster doses closely.”
SIREN originally aimed to understand how much protection people got after developing a primary infection and why they might become reinfected with COVID-19. Following the rollout of the United Kingdom’s vaccination program, the protective effects of vaccination against COVID-19 were investigated, as well as why some people still become ill after being vaccinated, Dr. Otter explained.
In this latest analysis, Dr. Otter and colleagues assessed anti-spike binding antibodies in serum samples from a total of 5,871 health care workers, with 3,989 after one dose (at least 21 days) and 1,882 after two doses (at least 14 days).
Most participants were women (82.3%), of White ethnicity (87%), and came from across the United Kingdom.
Participants were also categorized into those who had evidence of natural COVID-19 infection (confirmed by a PCR test or assumed because of their antibody profile) or those who were infection-naive. Almost all (> 99%) of those who were infection-naive seroconverted after vaccination.
The primary outcome was anti-spike antibody levels assessed according to dose, previous infection, dosing interval, age, ethnicity, and comorbidities, including immunosuppressive disease such as immune system cancers, rheumatologic disease, chronic respiratory diseases, diabetes, obesity, and chronic neurologic disease.
In the infection-naive group, the mean antibody (anti-S titer) was 75.48 BAU/mL after the first vaccine dose, and this rose to 7,049.76 BAU/mL after the second dose.
The much higher antibody titer with the second dose in infection-naive individuals “is what gives you the most protection, as your antibody titers are at their peak. They then start to gradually wane from this peak,” said Dr. Otter.
In the post-infection group, antibody titers also rose (2,111.08 BAU/mL after first dose and 16,052.39 BAU/mL after second dose), although less so than in the infection-naive group, because of the additional exposure of infection, added Dr. Otter.
Antibody levels also varied according to time elapsed between natural infection and dose 1 of vaccination. With a 3-month interval, antibody levels were 1,970.83 (1,506.01-2,579.1) BAU/mL, compared with 13,759.31 (8,097.78-23,379.09) BAU/mL after a 9-month interval. Antibody levels after one dose in those previously infected are higher than the infection-naive because “previous infection, then vaccination, is likely explained by T-cell expansion upon a boost with a second antigen exposure, and then a maturing memory B-cell response that has been demonstrated up to 6 months,” explained Dr. Otter.
Timing of fourth dose
By March of this year, 86.2% of the U.K. population aged over 12 years had received at least two doses, but with rises in disease prevalence and the spread of variants of concern, further work is ongoing to understand the waning of the immune response, level of protection, and why some individuals develop COVID-19 even when double-vaccinated.
This news organization asked Susanna Dunachie, BMChB, professor of infectious diseases, University of Oxford, U.K., what the interval findings might mean for the timing of the fourth dose of vaccine across the U.K. population.
In the United Kingdom, fourth doses are being given to people who are 75 years and older, residents in care homes for older people, and those with weakened immune systems. “To make decisions about fourth doses for healthy people, we need to see how quickly antibody and T-cell responses drop,” said Ms. Dunachie, who is part of the large SIREN study team but was not involved in the analysis led by Dr. Otter. “Current research suggests that the T-cell response may be better maintained than the antibody response, and less affected by variants like Omicron.”
She explained the balance between antibody and T-cell responses to vaccination. “It is likely that antibodies that neutralize the virus are important for preventing any infection at all, and these unfortunately do fall in time, but T-cell responses are better sustained and help keep people out of [the] hospital,” she said.
Ms. Dunachie added that it was necessary to wait and observe what happens next with SARS-CoV-2 evolution, as well as wait for longer follow-up after the third dose in healthy people. “On current evidence, my estimate is we postpone decisions on fourth doses in healthy people to late summer/autumn.”
A version of this article first appeared on Medscape.com.
An overall ninefold increase in COVID-19 antibody levels can be seen with a longer interval between first and second doses of the Pfizer/BioNTech (BNT162b2) vaccine in people without prior infection, according to data from the U.K. government’s SIREN (SARS-CoV-2 Immunity and Reinfection Evaluation) study.
This interval-dependent antibody level varied by age, with those aged 45-54 years showing an 11-fold increase with a longer dosing interval (greater than 10 weeks vs. 2-4 weeks). People younger than age 25 years showed a 13-fold increase with the longer interval, but participant numbers were low in this sub-group.
Overall antibody levels in infection-naive participants were 1,268.72 Binding Antibody Units (BAU)/mL (1,043.25-1,542.91) in those with a 2-4–week interval, compared with 11,479.73 BAU/mL (10,742.78-12,267.24) (P < .0001), in those with at least a 10-week interval between doses.
The work is the latest analysis from SIREN, which measured antibody levels in the blood from nearly 6,000 health care workers from across the United Kingdom. Study lead Ashley Otter, PhD, technical lead for SIREN serology at the UK Health Security Agency (UKHSA), will present the work on Tuesday at the 2022 European Congress of Clinical Microbiology & Infectious Diseases (ECCMID), Lisbon.
In an interview, Dr. Otter noted that, “it is important to remember that antibody levels are only one aspect of the immune response, and in our recent vaccine effectiveness analysis, we found that dosing intervals did not affect protection against infection.”
The study, which appeared in the March issue of the New England Journal of Medicine, also found that after the second dose of vaccine, there was about a 2.5–fold difference in antibody levels between those who had prior infection of 16.052 (14.071-18.312) BAU/mL, compared with 7.050 (6.634-7.491) BAU/mL in infection-naive individuals (P < .0001).
Following the first dose only, antibody levels were up to 10 times higher in participants who were previously infected, compared with infection-naive individuals. This effect lasted up to 8 months and then began to plateau.
Natural infection increased antibody levels
Dr. Otter remarked that, “COVID-19 antibody levels are high in those people who were previously naturally infected and vaccinated, highlighting that vaccination provides an additional benefit to these individuals.”
This news organization asked Charlotte Thålin, PhD, an immunologist from the Karolinska Institute, Stockholm, to comment on the study. Dr. Thålin studies a cohort similar to SIREN, called the Swedish COMMUNITY health care worker cohort. “The new data from the SIREN emphasizes the importance of the number of antigenic exposures and the time interval between them, whether it be exposure through vaccination or exposure through infection.”
“We see similar data in our Swedish COMMUNITY health care worker cohort,” Dr. Thålin continued, “where infection prior to vaccination yields a more than twofold enhancement in antibodies, neutralizing breadth, and T cell responses, and an even larger increase with a longer time interval between infection and vaccination.”
However, she cautioned that they now see a high rate of Omicron vaccine breakthrough infections, and this is also true in people with previous infection and three vaccine doses.
“As we approach a second booster – a fourth vaccine dose – we need to consider that many individuals will have had up to five to six antigen exposures within a short period of time, sometimes within a year,” she pointed out. “This is a whole new scenario, with a lot of different combinations of vaccine and infection-induced immunity. We do not yet know the impact of these frequent immune exposures, and we now need to monitor immune responses following Omicron and booster doses closely.”
SIREN originally aimed to understand how much protection people got after developing a primary infection and why they might become reinfected with COVID-19. Following the rollout of the United Kingdom’s vaccination program, the protective effects of vaccination against COVID-19 were investigated, as well as why some people still become ill after being vaccinated, Dr. Otter explained.
In this latest analysis, Dr. Otter and colleagues assessed anti-spike binding antibodies in serum samples from a total of 5,871 health care workers, with 3,989 after one dose (at least 21 days) and 1,882 after two doses (at least 14 days).
Most participants were women (82.3%), of White ethnicity (87%), and came from across the United Kingdom.
Participants were also categorized into those who had evidence of natural COVID-19 infection (confirmed by a PCR test or assumed because of their antibody profile) or those who were infection-naive. Almost all (> 99%) of those who were infection-naive seroconverted after vaccination.
The primary outcome was anti-spike antibody levels assessed according to dose, previous infection, dosing interval, age, ethnicity, and comorbidities, including immunosuppressive disease such as immune system cancers, rheumatologic disease, chronic respiratory diseases, diabetes, obesity, and chronic neurologic disease.
In the infection-naive group, the mean antibody (anti-S titer) was 75.48 BAU/mL after the first vaccine dose, and this rose to 7,049.76 BAU/mL after the second dose.
The much higher antibody titer with the second dose in infection-naive individuals “is what gives you the most protection, as your antibody titers are at their peak. They then start to gradually wane from this peak,” said Dr. Otter.
In the post-infection group, antibody titers also rose (2,111.08 BAU/mL after first dose and 16,052.39 BAU/mL after second dose), although less so than in the infection-naive group, because of the additional exposure of infection, added Dr. Otter.
Antibody levels also varied according to time elapsed between natural infection and dose 1 of vaccination. With a 3-month interval, antibody levels were 1,970.83 (1,506.01-2,579.1) BAU/mL, compared with 13,759.31 (8,097.78-23,379.09) BAU/mL after a 9-month interval. Antibody levels after one dose in those previously infected are higher than the infection-naive because “previous infection, then vaccination, is likely explained by T-cell expansion upon a boost with a second antigen exposure, and then a maturing memory B-cell response that has been demonstrated up to 6 months,” explained Dr. Otter.
Timing of fourth dose
By March of this year, 86.2% of the U.K. population aged over 12 years had received at least two doses, but with rises in disease prevalence and the spread of variants of concern, further work is ongoing to understand the waning of the immune response, level of protection, and why some individuals develop COVID-19 even when double-vaccinated.
This news organization asked Susanna Dunachie, BMChB, professor of infectious diseases, University of Oxford, U.K., what the interval findings might mean for the timing of the fourth dose of vaccine across the U.K. population.
In the United Kingdom, fourth doses are being given to people who are 75 years and older, residents in care homes for older people, and those with weakened immune systems. “To make decisions about fourth doses for healthy people, we need to see how quickly antibody and T-cell responses drop,” said Ms. Dunachie, who is part of the large SIREN study team but was not involved in the analysis led by Dr. Otter. “Current research suggests that the T-cell response may be better maintained than the antibody response, and less affected by variants like Omicron.”
She explained the balance between antibody and T-cell responses to vaccination. “It is likely that antibodies that neutralize the virus are important for preventing any infection at all, and these unfortunately do fall in time, but T-cell responses are better sustained and help keep people out of [the] hospital,” she said.
Ms. Dunachie added that it was necessary to wait and observe what happens next with SARS-CoV-2 evolution, as well as wait for longer follow-up after the third dose in healthy people. “On current evidence, my estimate is we postpone decisions on fourth doses in healthy people to late summer/autumn.”
A version of this article first appeared on Medscape.com.
COVID-19 again the third-leading cause of U.S. deaths
the Centers for Disease Control and Prevention said April 22.
About 693,000 people died of heart disease in 2021, with 605,000 dying of cancer and 415,000 of COVID, the CDC said, citing provisional data that might be updated later.
Unintentional injuries were the fourth-leading cause of death, increasing to 219,000 in 2021 from 201,000 in 2020. Influenza and pneumonia dropped out of the top 10 leading causes of death and suicide moved into 10th place.
Overall, about 3,458,697 deaths were reported in the United States in 2021. The age-adjusted death rate was 841.6 deaths per 100,000 people, an increase of 0.7% from 2020. The 2021 death rate was the highest since 2003, the CDC said.
The overall number of COVID deaths in 2021 increased around 20% over 2020, when around 384,000 people died from the virus, the CDC said. COVID deaths in 2021 peaked for the weeks ending Jan. 16 and Sept. 11, following holiday periods.
The demographics of COVID mortality changed slightly, the CDC said in a second report.
Blacks accounted for 13.3% of COVID deaths in 2021 and Hispanics 16.5%, down several percentage points from 2020, the CDC said. Asians made up 3.1% of COVID deaths for 2021, a drop from 3.6% in 2020. White people accounted for 65.2% of COVID deaths in 2021, an increase from 59.6% in 2020.
Non-Hispanic American Indian/Alaskan Native and non-Hispanic Black or African American had the highest overall death rates for COVID, the CDC said.
Breaking the data down by age, the number of COVID deaths among people aged 75 years and older dropped to 178,000 in 2021 from around 207,000 in 2020. The numbers went up in other age groups. Among people aged 65-75, about 101,000 died of COVID in 2021, up from around 76,000 in 2020.
“The results of both studies highlight the need for greater effort to implement effective interventions,” the CDC said in a statement. “We must work to ensure equal treatment in all communities in proportion to their need for effective interventions that can prevent excess COVID-19 deaths.”
Since the pandemic began, about 991,000 people in the United States have died from COVID-related causes, the most among all nations in the world.
A version of this article first appeared on WebMD.com.
the Centers for Disease Control and Prevention said April 22.
About 693,000 people died of heart disease in 2021, with 605,000 dying of cancer and 415,000 of COVID, the CDC said, citing provisional data that might be updated later.
Unintentional injuries were the fourth-leading cause of death, increasing to 219,000 in 2021 from 201,000 in 2020. Influenza and pneumonia dropped out of the top 10 leading causes of death and suicide moved into 10th place.
Overall, about 3,458,697 deaths were reported in the United States in 2021. The age-adjusted death rate was 841.6 deaths per 100,000 people, an increase of 0.7% from 2020. The 2021 death rate was the highest since 2003, the CDC said.
The overall number of COVID deaths in 2021 increased around 20% over 2020, when around 384,000 people died from the virus, the CDC said. COVID deaths in 2021 peaked for the weeks ending Jan. 16 and Sept. 11, following holiday periods.
The demographics of COVID mortality changed slightly, the CDC said in a second report.
Blacks accounted for 13.3% of COVID deaths in 2021 and Hispanics 16.5%, down several percentage points from 2020, the CDC said. Asians made up 3.1% of COVID deaths for 2021, a drop from 3.6% in 2020. White people accounted for 65.2% of COVID deaths in 2021, an increase from 59.6% in 2020.
Non-Hispanic American Indian/Alaskan Native and non-Hispanic Black or African American had the highest overall death rates for COVID, the CDC said.
Breaking the data down by age, the number of COVID deaths among people aged 75 years and older dropped to 178,000 in 2021 from around 207,000 in 2020. The numbers went up in other age groups. Among people aged 65-75, about 101,000 died of COVID in 2021, up from around 76,000 in 2020.
“The results of both studies highlight the need for greater effort to implement effective interventions,” the CDC said in a statement. “We must work to ensure equal treatment in all communities in proportion to their need for effective interventions that can prevent excess COVID-19 deaths.”
Since the pandemic began, about 991,000 people in the United States have died from COVID-related causes, the most among all nations in the world.
A version of this article first appeared on WebMD.com.
the Centers for Disease Control and Prevention said April 22.
About 693,000 people died of heart disease in 2021, with 605,000 dying of cancer and 415,000 of COVID, the CDC said, citing provisional data that might be updated later.
Unintentional injuries were the fourth-leading cause of death, increasing to 219,000 in 2021 from 201,000 in 2020. Influenza and pneumonia dropped out of the top 10 leading causes of death and suicide moved into 10th place.
Overall, about 3,458,697 deaths were reported in the United States in 2021. The age-adjusted death rate was 841.6 deaths per 100,000 people, an increase of 0.7% from 2020. The 2021 death rate was the highest since 2003, the CDC said.
The overall number of COVID deaths in 2021 increased around 20% over 2020, when around 384,000 people died from the virus, the CDC said. COVID deaths in 2021 peaked for the weeks ending Jan. 16 and Sept. 11, following holiday periods.
The demographics of COVID mortality changed slightly, the CDC said in a second report.
Blacks accounted for 13.3% of COVID deaths in 2021 and Hispanics 16.5%, down several percentage points from 2020, the CDC said. Asians made up 3.1% of COVID deaths for 2021, a drop from 3.6% in 2020. White people accounted for 65.2% of COVID deaths in 2021, an increase from 59.6% in 2020.
Non-Hispanic American Indian/Alaskan Native and non-Hispanic Black or African American had the highest overall death rates for COVID, the CDC said.
Breaking the data down by age, the number of COVID deaths among people aged 75 years and older dropped to 178,000 in 2021 from around 207,000 in 2020. The numbers went up in other age groups. Among people aged 65-75, about 101,000 died of COVID in 2021, up from around 76,000 in 2020.
“The results of both studies highlight the need for greater effort to implement effective interventions,” the CDC said in a statement. “We must work to ensure equal treatment in all communities in proportion to their need for effective interventions that can prevent excess COVID-19 deaths.”
Since the pandemic began, about 991,000 people in the United States have died from COVID-related causes, the most among all nations in the world.
A version of this article first appeared on WebMD.com.
FROM THE MMWR
Three in four U.S. doctors are employed by hospitals, corporate entities: Report
Marcus Welby, MD, was a fictitious hometown doctor featured in a TV drama with the same name that was shown on ABC from 1969 to 1976. Played by actor Robert Young, Dr. Welby treated his patients through their bouts with breast cancer, impotence, and Alzheimer’s disease.
, according to a recent report sponsored by the Physicians Advocacy Institute and prepared by consulting firm Avalere Health.
“COVID-19 drove physicians to leave private practice for employment at an even more rapid pace than we’ve seen in recent years, and these trends continued to accelerate in 2021,” Kelly Kenney, chief executive officer of Physicians Advocacy Institute, said in an announcement. “This study underscores the fact that physicians across the nation are facing severe burnout and strain. The pressures of the pandemic forced many independent physicians to make difficult decisions to sell their practices, health insurers, or other corporate entities.”
Corporate entities are defined in the report as health insurers, private equity firms, and umbrella corporate entities that own multiple physician practices.
“The pandemic has been just brutal ... for nurses and physicians who are caring for patients,” Ms. Kenney told this news organization. “Between the financial stress that the pandemic certainly had on practices, because they certainly had little revenue for a while, and then also we know that the stress that physicians have felt mentally, you can’t overstate that.”
More than half of physician practices owned by hospitals, corporate entities
The Physicians Advocacy Institute has tracked changes in physician employment consistently since 2012, said Ms. Kenney. In 2012, 25% of physicians were employed; that has jumped to nearly 74%, which means the past decade has brought a world of change to the nation’s physicians.
“These are essentially small-business people ... and they were primarily trained to care for patients,” said Ms. Kenney, referring to physicians in independent practice. Still, she understands why physicians would seek employment in the face of “the crushing kind of pressure of having to deal with 20 different payers, pay overhead, and keep the lights on [at the practice].”
According to the report, 108,700 physicians left independent practice to enter employment with hospitals or other corporate entities in the 3-year period that ended in 2021. Seventy-six percent of that shift to employed status among physicians has occurred since the start of the COVID-19 pandemic in March 2020.
From a regional perspective, the report found continued growth among employed physicians across all U.S. regions in the last half of 2020. Hospital- or corporate-owned physician practices increased between 28% and 44%, while the percentage of hospital- or corporate-employed physicians increased between 13% and 24%.
Eighty percent of physicians in the Midwest are employed by hospitals or corporations, which leads the rest of the country, per the report. That’s followed by the Northeast, the West, and the South. Overall, the number of physicians working for such entities increased in all regions.
The report revealed that physician employment by corporations such as health insurers and venture capital firms grew from 92,400 in January 2019 to 142,900 in January 2022.
Hospitals and corporate entities acquired 36,200 physician practices (representing 38% growth) between 2019 and 2021, and the majority of these moves occurred since the pandemic’s start, according to the report.
Value-based care, venture capital firms driving change
Ms. Kenney pointed to value-based care as driving much of this activity by hospitals. “We all embrace [value-based payment], because we need to get a handle on cost, and we want better quality [but] those trends tend to favor integrated systems and systems that can handle a lot of risk and populations of patients.”
Still, the moves by private equity firms and health insurers in this space is relatively new, said Ms. Kenney, who added that her organization started tracking this trend 3 years ago. She pointed to a “marked acceleration” in the trend toward employing physicians and the sale of practices in the 18 months following the pandemic’s start; nonhospital corporate entities drove that steep increase, she said.
Ms. Kenney calls for further study and “guardrails” to respond to “that force in the health care system,” referring to the acquisition of practices by entities such as private equity firms. “Are these big [health care] systems going to continue to see patients in underserved areas, rural areas, and Medicaid patients if it doesn’t make sense financially to do so?
“That’s what we’re teeing up with this research,” added Ms. Kenney. “We are providing information that starts some conversations around what we might want to think about in terms of policies to ensure that we don’t impact patients’ access to care.”
The Physicians Advocacy Institute represents more than 170,000 physicians and medical students. Avalere Health used the IQVIA OneKey database for the report. The researchers studied the 3-year period from Jan. 1, 2019, to Jan. 1, 2022.
A version of this article first appeared on Medscape.com.
Marcus Welby, MD, was a fictitious hometown doctor featured in a TV drama with the same name that was shown on ABC from 1969 to 1976. Played by actor Robert Young, Dr. Welby treated his patients through their bouts with breast cancer, impotence, and Alzheimer’s disease.
, according to a recent report sponsored by the Physicians Advocacy Institute and prepared by consulting firm Avalere Health.
“COVID-19 drove physicians to leave private practice for employment at an even more rapid pace than we’ve seen in recent years, and these trends continued to accelerate in 2021,” Kelly Kenney, chief executive officer of Physicians Advocacy Institute, said in an announcement. “This study underscores the fact that physicians across the nation are facing severe burnout and strain. The pressures of the pandemic forced many independent physicians to make difficult decisions to sell their practices, health insurers, or other corporate entities.”
Corporate entities are defined in the report as health insurers, private equity firms, and umbrella corporate entities that own multiple physician practices.
“The pandemic has been just brutal ... for nurses and physicians who are caring for patients,” Ms. Kenney told this news organization. “Between the financial stress that the pandemic certainly had on practices, because they certainly had little revenue for a while, and then also we know that the stress that physicians have felt mentally, you can’t overstate that.”
More than half of physician practices owned by hospitals, corporate entities
The Physicians Advocacy Institute has tracked changes in physician employment consistently since 2012, said Ms. Kenney. In 2012, 25% of physicians were employed; that has jumped to nearly 74%, which means the past decade has brought a world of change to the nation’s physicians.
“These are essentially small-business people ... and they were primarily trained to care for patients,” said Ms. Kenney, referring to physicians in independent practice. Still, she understands why physicians would seek employment in the face of “the crushing kind of pressure of having to deal with 20 different payers, pay overhead, and keep the lights on [at the practice].”
According to the report, 108,700 physicians left independent practice to enter employment with hospitals or other corporate entities in the 3-year period that ended in 2021. Seventy-six percent of that shift to employed status among physicians has occurred since the start of the COVID-19 pandemic in March 2020.
From a regional perspective, the report found continued growth among employed physicians across all U.S. regions in the last half of 2020. Hospital- or corporate-owned physician practices increased between 28% and 44%, while the percentage of hospital- or corporate-employed physicians increased between 13% and 24%.
Eighty percent of physicians in the Midwest are employed by hospitals or corporations, which leads the rest of the country, per the report. That’s followed by the Northeast, the West, and the South. Overall, the number of physicians working for such entities increased in all regions.
The report revealed that physician employment by corporations such as health insurers and venture capital firms grew from 92,400 in January 2019 to 142,900 in January 2022.
Hospitals and corporate entities acquired 36,200 physician practices (representing 38% growth) between 2019 and 2021, and the majority of these moves occurred since the pandemic’s start, according to the report.
Value-based care, venture capital firms driving change
Ms. Kenney pointed to value-based care as driving much of this activity by hospitals. “We all embrace [value-based payment], because we need to get a handle on cost, and we want better quality [but] those trends tend to favor integrated systems and systems that can handle a lot of risk and populations of patients.”
Still, the moves by private equity firms and health insurers in this space is relatively new, said Ms. Kenney, who added that her organization started tracking this trend 3 years ago. She pointed to a “marked acceleration” in the trend toward employing physicians and the sale of practices in the 18 months following the pandemic’s start; nonhospital corporate entities drove that steep increase, she said.
Ms. Kenney calls for further study and “guardrails” to respond to “that force in the health care system,” referring to the acquisition of practices by entities such as private equity firms. “Are these big [health care] systems going to continue to see patients in underserved areas, rural areas, and Medicaid patients if it doesn’t make sense financially to do so?
“That’s what we’re teeing up with this research,” added Ms. Kenney. “We are providing information that starts some conversations around what we might want to think about in terms of policies to ensure that we don’t impact patients’ access to care.”
The Physicians Advocacy Institute represents more than 170,000 physicians and medical students. Avalere Health used the IQVIA OneKey database for the report. The researchers studied the 3-year period from Jan. 1, 2019, to Jan. 1, 2022.
A version of this article first appeared on Medscape.com.
Marcus Welby, MD, was a fictitious hometown doctor featured in a TV drama with the same name that was shown on ABC from 1969 to 1976. Played by actor Robert Young, Dr. Welby treated his patients through their bouts with breast cancer, impotence, and Alzheimer’s disease.
, according to a recent report sponsored by the Physicians Advocacy Institute and prepared by consulting firm Avalere Health.
“COVID-19 drove physicians to leave private practice for employment at an even more rapid pace than we’ve seen in recent years, and these trends continued to accelerate in 2021,” Kelly Kenney, chief executive officer of Physicians Advocacy Institute, said in an announcement. “This study underscores the fact that physicians across the nation are facing severe burnout and strain. The pressures of the pandemic forced many independent physicians to make difficult decisions to sell their practices, health insurers, or other corporate entities.”
Corporate entities are defined in the report as health insurers, private equity firms, and umbrella corporate entities that own multiple physician practices.
“The pandemic has been just brutal ... for nurses and physicians who are caring for patients,” Ms. Kenney told this news organization. “Between the financial stress that the pandemic certainly had on practices, because they certainly had little revenue for a while, and then also we know that the stress that physicians have felt mentally, you can’t overstate that.”
More than half of physician practices owned by hospitals, corporate entities
The Physicians Advocacy Institute has tracked changes in physician employment consistently since 2012, said Ms. Kenney. In 2012, 25% of physicians were employed; that has jumped to nearly 74%, which means the past decade has brought a world of change to the nation’s physicians.
“These are essentially small-business people ... and they were primarily trained to care for patients,” said Ms. Kenney, referring to physicians in independent practice. Still, she understands why physicians would seek employment in the face of “the crushing kind of pressure of having to deal with 20 different payers, pay overhead, and keep the lights on [at the practice].”
According to the report, 108,700 physicians left independent practice to enter employment with hospitals or other corporate entities in the 3-year period that ended in 2021. Seventy-six percent of that shift to employed status among physicians has occurred since the start of the COVID-19 pandemic in March 2020.
From a regional perspective, the report found continued growth among employed physicians across all U.S. regions in the last half of 2020. Hospital- or corporate-owned physician practices increased between 28% and 44%, while the percentage of hospital- or corporate-employed physicians increased between 13% and 24%.
Eighty percent of physicians in the Midwest are employed by hospitals or corporations, which leads the rest of the country, per the report. That’s followed by the Northeast, the West, and the South. Overall, the number of physicians working for such entities increased in all regions.
The report revealed that physician employment by corporations such as health insurers and venture capital firms grew from 92,400 in January 2019 to 142,900 in January 2022.
Hospitals and corporate entities acquired 36,200 physician practices (representing 38% growth) between 2019 and 2021, and the majority of these moves occurred since the pandemic’s start, according to the report.
Value-based care, venture capital firms driving change
Ms. Kenney pointed to value-based care as driving much of this activity by hospitals. “We all embrace [value-based payment], because we need to get a handle on cost, and we want better quality [but] those trends tend to favor integrated systems and systems that can handle a lot of risk and populations of patients.”
Still, the moves by private equity firms and health insurers in this space is relatively new, said Ms. Kenney, who added that her organization started tracking this trend 3 years ago. She pointed to a “marked acceleration” in the trend toward employing physicians and the sale of practices in the 18 months following the pandemic’s start; nonhospital corporate entities drove that steep increase, she said.
Ms. Kenney calls for further study and “guardrails” to respond to “that force in the health care system,” referring to the acquisition of practices by entities such as private equity firms. “Are these big [health care] systems going to continue to see patients in underserved areas, rural areas, and Medicaid patients if it doesn’t make sense financially to do so?
“That’s what we’re teeing up with this research,” added Ms. Kenney. “We are providing information that starts some conversations around what we might want to think about in terms of policies to ensure that we don’t impact patients’ access to care.”
The Physicians Advocacy Institute represents more than 170,000 physicians and medical students. Avalere Health used the IQVIA OneKey database for the report. The researchers studied the 3-year period from Jan. 1, 2019, to Jan. 1, 2022.
A version of this article first appeared on Medscape.com.
Icosapent ethyl’s CV mortality benefit magnified in patients with prior MI
In the placebo-controlled REDUCE-IT trial, icosapent ethyl (IPE) was linked to a significant reduction in major adverse cardiovascular events (MACE) when administered on top of LDL cholesterol control, but a new substudy suggests a greater relative advantage in those with a prior myocardial infarction.
In the study as a whole, IPE (Vascepa, Amarin) was tied to a 20% reduction in CV death (hazard ratio, 0.80; P = .03), but it climbed to a 30% reduction (HR, 0.70; P = .01) in the subgroup with a prior MI, reported a multinational team of investigators led by Prakriti Gaba, MD, a cardiologist at Brigham and Women’s Hospital, Boston.
On the basis of these data, “the imperative to treat patients who have a history of prior MI is even stronger,” said Deepak L. Bhatt, MD, executive director of interventional cardiovascular programs at Brigham and Women’s Hospital.

The principal investigator of REDUCE-IT and a coauthor of this subanalysis, Dr. Bhatt said in an interview, “The significant reduction in cardiovascular mortality, as well as sudden cardiac death and cardiac arrest, really should make physicians strongly consider this therapy in eligible patients.”
The main results of the REDUCE-IT trial were published more than 3 years ago. It enrolled patients with established CV disease or diabetes with additional risk factors who were on a statin and had elevated triglyceride (TG) levels.
A 25% reduction in MACE reported
In those randomized to IPE, there was about a 25% reduction in the primary composite MACE outcome of cardiovascular death, nonfatal MI, nonfatal stroke, revascularization, and unstable angina relative to placebo. About the same relative reduction was achieved in the key secondary endpoint of CV death, nonfatal MI, and nonfatal stroke.
Some guidelines have been changed on the basis of these data. The National Lipid Association, for example, conferred a class 1 recommendation for adding IPE to other appropriate lipid-reducing therapies in any individual 45 years of age or older with atherosclerotic cardiovascular disease.
This new substudy (J Am Coll Cardiol. 2022 Apr 25; doi: 10.1016/j.jacc.2022.02.035), is likely to be influential for those guidelines not yet revised. In the substudy of the prior MI patients, the relative benefit of IPE for the primary and secondary MACE endpoints were of similar magnitude to the overall study population, but events occurred more frequently in the prior-MI subgroup, greatly increasing the statistical power of the advantage.
More MACE in prior MI patients
For example, the primary outcome was observed in 22% of the placebo patients in the overall REDUCE-IT analysis but in 26.1% of those with prior MI, so even though the relative risk reduction remained at about 25%, the statistical strength was a hundred-fold greater (P = .00001 vs. P < .001).
For the key secondary composite MACE endpoint, the relative reduction for those with a prior MI was modestly greater than the study as a whole (HR 0.71 vs. HR. 075) but the statistical strength was again magnified in those with a prior MI (P = .00006 vs. P < .001). In those with a prior MI , the advantage of receiving IPE was similar whether or not there had been a prior revascularization.
The 20% lower rate of all-cause mortality among prior MI patients receiving IPE rather than placebo fell just short of statistical significance (HR, 0.80; P = .054). Ischemic events on IPE were reduced by 35% (P = .0000001) and recurrent MI was reduced by 34% (P = .00009).
In the substudy as well as in the REDUCE-IT trial overall, IPE was well tolerated. A slightly higher rate of atrial fibrillation was reported in both.
The REDUCE-IT substudy evaluated 3,693 patients with a history of MI, representing 45% of the 8,179 patients randomized.
IPE, an ethyl ester of the omega-3 polyunsaturated fatty acid, initially attracted attention for its ability to reduce elevated TG. It was hoped this would address reduce residual risk in patients on maximally reduced LDL cholesterol. However, it is suspected that IPE exerts benefits additive to or independent of TG lowering, according to the authors of the REDUCE-IT substudy. These include attenuation of the inflammatory response, release of nitric oxide, and effects that support stabilization of atherosclerotic plaque.
The investigators reported that the pattern of response supports this theory. In the newly reported substudy, the primary event curves that included nonthrombotic events separated at about 1 year, but even curves for CV death and sudden cardiac death were more delayed.
This delay might be explained “by the slow but steady reduction in plaque volume, mitigation of inflammation, improvements in endothelial function, and membrane stabilization,” according to the authors, who cited studies suggesting each of these effects might not be wholly dependent on TG reductions alone.
Prior TG-lowering studies disappointing
In fact, several studies evaluating other strategies for TG reductions have been disappointing, according to an accompanying editorial (J Am Coll Cardiol. 2022 Apr 25; doi: 10.1016/j.jacc.2022.03.001). For example, the STRENGTH trial did not show clinical benefits despite a slightly greater reduction in TGs than that shown in REDUCE-IT (19% reduction vs. 18.3%).
Overall, the REDUCE-IT trial and the prior-MI REDUCE-IT substudy show that there is targetable residual risk in high risk patients on statin therapy. One of the authors of the editorial that accompanied the prior-MI substudy of REDUCE-IT, William E. Boden, MD, professor of medicine, Boston University, emphasized this point. On the basis of REDUCE-IT, he said he believes that IPE should be considered to have broad indications as an adjunctive treatment to other lipid-lowering strategies.
“My practice centers on optimizing secondary prevention in high-risk patients who have elevated TG levels despite well-controlled LDL levels on statins, ezetimibe, or even PCSK-9 [proprotein convertase subtilisin/kexin type 9] inhibitors,” Dr. Boden said in an interview. Patients with diabetes are notorious for presenting with this profile of dyslipidemia, but he added that “even nondiabetics with prior MI, acute coronary syndrome, or revascularization will benefit from the addition of IPE to high-potency statins.”
Although the American Heart Association and the American College of Cardiology have not yet updated their guidelines to include IPE, Dr. Boden pointed out that the European Society of Cardiology, the Canadian Cardiovascular Society, and the American Diabetes Society have.
Dr. Bhatt added that there is a clear message from REDUCE-IT that IPE addresses residual risk.
Targeting the subgroup of high-risk patients with elevated TGs “is easy” because they are so readily identifiable, according to Dr. Bhatt, but he said it should be used for any patient that meet the entry criteria used for REDUCE-IT.
“The overall results of REDUCE-IT were robustly positive, so I wouldn’t just use it in patients with prior MI,” Dr. Bhatt said.
Dr. Bhatt reports financial relationships with more than 20 pharmaceutical companies, including Amarin, which provided funding for this trial. Dr. Boden reports no potential conflicts of interest.
In the placebo-controlled REDUCE-IT trial, icosapent ethyl (IPE) was linked to a significant reduction in major adverse cardiovascular events (MACE) when administered on top of LDL cholesterol control, but a new substudy suggests a greater relative advantage in those with a prior myocardial infarction.
In the study as a whole, IPE (Vascepa, Amarin) was tied to a 20% reduction in CV death (hazard ratio, 0.80; P = .03), but it climbed to a 30% reduction (HR, 0.70; P = .01) in the subgroup with a prior MI, reported a multinational team of investigators led by Prakriti Gaba, MD, a cardiologist at Brigham and Women’s Hospital, Boston.
On the basis of these data, “the imperative to treat patients who have a history of prior MI is even stronger,” said Deepak L. Bhatt, MD, executive director of interventional cardiovascular programs at Brigham and Women’s Hospital.
The principal investigator of REDUCE-IT and a coauthor of this subanalysis, Dr. Bhatt said in an interview, “The significant reduction in cardiovascular mortality, as well as sudden cardiac death and cardiac arrest, really should make physicians strongly consider this therapy in eligible patients.”
The main results of the REDUCE-IT trial were published more than 3 years ago. It enrolled patients with established CV disease or diabetes with additional risk factors who were on a statin and had elevated triglyceride (TG) levels.
A 25% reduction in MACE reported
In those randomized to IPE, there was about a 25% reduction in the primary composite MACE outcome of cardiovascular death, nonfatal MI, nonfatal stroke, revascularization, and unstable angina relative to placebo. About the same relative reduction was achieved in the key secondary endpoint of CV death, nonfatal MI, and nonfatal stroke.
Some guidelines have been changed on the basis of these data. The National Lipid Association, for example, conferred a class 1 recommendation for adding IPE to other appropriate lipid-reducing therapies in any individual 45 years of age or older with atherosclerotic cardiovascular disease.
This new substudy (J Am Coll Cardiol. 2022 Apr 25; doi: 10.1016/j.jacc.2022.02.035), is likely to be influential for those guidelines not yet revised. In the substudy of the prior MI patients, the relative benefit of IPE for the primary and secondary MACE endpoints were of similar magnitude to the overall study population, but events occurred more frequently in the prior-MI subgroup, greatly increasing the statistical power of the advantage.
More MACE in prior MI patients
For example, the primary outcome was observed in 22% of the placebo patients in the overall REDUCE-IT analysis but in 26.1% of those with prior MI, so even though the relative risk reduction remained at about 25%, the statistical strength was a hundred-fold greater (P = .00001 vs. P < .001).
For the key secondary composite MACE endpoint, the relative reduction for those with a prior MI was modestly greater than the study as a whole (HR 0.71 vs. HR. 075) but the statistical strength was again magnified in those with a prior MI (P = .00006 vs. P < .001). In those with a prior MI , the advantage of receiving IPE was similar whether or not there had been a prior revascularization.
The 20% lower rate of all-cause mortality among prior MI patients receiving IPE rather than placebo fell just short of statistical significance (HR, 0.80; P = .054). Ischemic events on IPE were reduced by 35% (P = .0000001) and recurrent MI was reduced by 34% (P = .00009).
In the substudy as well as in the REDUCE-IT trial overall, IPE was well tolerated. A slightly higher rate of atrial fibrillation was reported in both.
The REDUCE-IT substudy evaluated 3,693 patients with a history of MI, representing 45% of the 8,179 patients randomized.
IPE, an ethyl ester of the omega-3 polyunsaturated fatty acid, initially attracted attention for its ability to reduce elevated TG. It was hoped this would address reduce residual risk in patients on maximally reduced LDL cholesterol. However, it is suspected that IPE exerts benefits additive to or independent of TG lowering, according to the authors of the REDUCE-IT substudy. These include attenuation of the inflammatory response, release of nitric oxide, and effects that support stabilization of atherosclerotic plaque.
The investigators reported that the pattern of response supports this theory. In the newly reported substudy, the primary event curves that included nonthrombotic events separated at about 1 year, but even curves for CV death and sudden cardiac death were more delayed.
This delay might be explained “by the slow but steady reduction in plaque volume, mitigation of inflammation, improvements in endothelial function, and membrane stabilization,” according to the authors, who cited studies suggesting each of these effects might not be wholly dependent on TG reductions alone.
Prior TG-lowering studies disappointing
In fact, several studies evaluating other strategies for TG reductions have been disappointing, according to an accompanying editorial (J Am Coll Cardiol. 2022 Apr 25; doi: 10.1016/j.jacc.2022.03.001). For example, the STRENGTH trial did not show clinical benefits despite a slightly greater reduction in TGs than that shown in REDUCE-IT (19% reduction vs. 18.3%).
Overall, the REDUCE-IT trial and the prior-MI REDUCE-IT substudy show that there is targetable residual risk in high risk patients on statin therapy. One of the authors of the editorial that accompanied the prior-MI substudy of REDUCE-IT, William E. Boden, MD, professor of medicine, Boston University, emphasized this point. On the basis of REDUCE-IT, he said he believes that IPE should be considered to have broad indications as an adjunctive treatment to other lipid-lowering strategies.
“My practice centers on optimizing secondary prevention in high-risk patients who have elevated TG levels despite well-controlled LDL levels on statins, ezetimibe, or even PCSK-9 [proprotein convertase subtilisin/kexin type 9] inhibitors,” Dr. Boden said in an interview. Patients with diabetes are notorious for presenting with this profile of dyslipidemia, but he added that “even nondiabetics with prior MI, acute coronary syndrome, or revascularization will benefit from the addition of IPE to high-potency statins.”
Although the American Heart Association and the American College of Cardiology have not yet updated their guidelines to include IPE, Dr. Boden pointed out that the European Society of Cardiology, the Canadian Cardiovascular Society, and the American Diabetes Society have.
Dr. Bhatt added that there is a clear message from REDUCE-IT that IPE addresses residual risk.
Targeting the subgroup of high-risk patients with elevated TGs “is easy” because they are so readily identifiable, according to Dr. Bhatt, but he said it should be used for any patient that meet the entry criteria used for REDUCE-IT.
“The overall results of REDUCE-IT were robustly positive, so I wouldn’t just use it in patients with prior MI,” Dr. Bhatt said.
Dr. Bhatt reports financial relationships with more than 20 pharmaceutical companies, including Amarin, which provided funding for this trial. Dr. Boden reports no potential conflicts of interest.
In the placebo-controlled REDUCE-IT trial, icosapent ethyl (IPE) was linked to a significant reduction in major adverse cardiovascular events (MACE) when administered on top of LDL cholesterol control, but a new substudy suggests a greater relative advantage in those with a prior myocardial infarction.
In the study as a whole, IPE (Vascepa, Amarin) was tied to a 20% reduction in CV death (hazard ratio, 0.80; P = .03), but it climbed to a 30% reduction (HR, 0.70; P = .01) in the subgroup with a prior MI, reported a multinational team of investigators led by Prakriti Gaba, MD, a cardiologist at Brigham and Women’s Hospital, Boston.
On the basis of these data, “the imperative to treat patients who have a history of prior MI is even stronger,” said Deepak L. Bhatt, MD, executive director of interventional cardiovascular programs at Brigham and Women’s Hospital.
The principal investigator of REDUCE-IT and a coauthor of this subanalysis, Dr. Bhatt said in an interview, “The significant reduction in cardiovascular mortality, as well as sudden cardiac death and cardiac arrest, really should make physicians strongly consider this therapy in eligible patients.”
The main results of the REDUCE-IT trial were published more than 3 years ago. It enrolled patients with established CV disease or diabetes with additional risk factors who were on a statin and had elevated triglyceride (TG) levels.
A 25% reduction in MACE reported
In those randomized to IPE, there was about a 25% reduction in the primary composite MACE outcome of cardiovascular death, nonfatal MI, nonfatal stroke, revascularization, and unstable angina relative to placebo. About the same relative reduction was achieved in the key secondary endpoint of CV death, nonfatal MI, and nonfatal stroke.
Some guidelines have been changed on the basis of these data. The National Lipid Association, for example, conferred a class 1 recommendation for adding IPE to other appropriate lipid-reducing therapies in any individual 45 years of age or older with atherosclerotic cardiovascular disease.
This new substudy (J Am Coll Cardiol. 2022 Apr 25; doi: 10.1016/j.jacc.2022.02.035), is likely to be influential for those guidelines not yet revised. In the substudy of the prior MI patients, the relative benefit of IPE for the primary and secondary MACE endpoints were of similar magnitude to the overall study population, but events occurred more frequently in the prior-MI subgroup, greatly increasing the statistical power of the advantage.
More MACE in prior MI patients
For example, the primary outcome was observed in 22% of the placebo patients in the overall REDUCE-IT analysis but in 26.1% of those with prior MI, so even though the relative risk reduction remained at about 25%, the statistical strength was a hundred-fold greater (P = .00001 vs. P < .001).
For the key secondary composite MACE endpoint, the relative reduction for those with a prior MI was modestly greater than the study as a whole (HR 0.71 vs. HR. 075) but the statistical strength was again magnified in those with a prior MI (P = .00006 vs. P < .001). In those with a prior MI , the advantage of receiving IPE was similar whether or not there had been a prior revascularization.
The 20% lower rate of all-cause mortality among prior MI patients receiving IPE rather than placebo fell just short of statistical significance (HR, 0.80; P = .054). Ischemic events on IPE were reduced by 35% (P = .0000001) and recurrent MI was reduced by 34% (P = .00009).
In the substudy as well as in the REDUCE-IT trial overall, IPE was well tolerated. A slightly higher rate of atrial fibrillation was reported in both.
The REDUCE-IT substudy evaluated 3,693 patients with a history of MI, representing 45% of the 8,179 patients randomized.
IPE, an ethyl ester of the omega-3 polyunsaturated fatty acid, initially attracted attention for its ability to reduce elevated TG. It was hoped this would address reduce residual risk in patients on maximally reduced LDL cholesterol. However, it is suspected that IPE exerts benefits additive to or independent of TG lowering, according to the authors of the REDUCE-IT substudy. These include attenuation of the inflammatory response, release of nitric oxide, and effects that support stabilization of atherosclerotic plaque.
The investigators reported that the pattern of response supports this theory. In the newly reported substudy, the primary event curves that included nonthrombotic events separated at about 1 year, but even curves for CV death and sudden cardiac death were more delayed.
This delay might be explained “by the slow but steady reduction in plaque volume, mitigation of inflammation, improvements in endothelial function, and membrane stabilization,” according to the authors, who cited studies suggesting each of these effects might not be wholly dependent on TG reductions alone.
Prior TG-lowering studies disappointing
In fact, several studies evaluating other strategies for TG reductions have been disappointing, according to an accompanying editorial (J Am Coll Cardiol. 2022 Apr 25; doi: 10.1016/j.jacc.2022.03.001). For example, the STRENGTH trial did not show clinical benefits despite a slightly greater reduction in TGs than that shown in REDUCE-IT (19% reduction vs. 18.3%).
Overall, the REDUCE-IT trial and the prior-MI REDUCE-IT substudy show that there is targetable residual risk in high risk patients on statin therapy. One of the authors of the editorial that accompanied the prior-MI substudy of REDUCE-IT, William E. Boden, MD, professor of medicine, Boston University, emphasized this point. On the basis of REDUCE-IT, he said he believes that IPE should be considered to have broad indications as an adjunctive treatment to other lipid-lowering strategies.
“My practice centers on optimizing secondary prevention in high-risk patients who have elevated TG levels despite well-controlled LDL levels on statins, ezetimibe, or even PCSK-9 [proprotein convertase subtilisin/kexin type 9] inhibitors,” Dr. Boden said in an interview. Patients with diabetes are notorious for presenting with this profile of dyslipidemia, but he added that “even nondiabetics with prior MI, acute coronary syndrome, or revascularization will benefit from the addition of IPE to high-potency statins.”
Although the American Heart Association and the American College of Cardiology have not yet updated their guidelines to include IPE, Dr. Boden pointed out that the European Society of Cardiology, the Canadian Cardiovascular Society, and the American Diabetes Society have.
Dr. Bhatt added that there is a clear message from REDUCE-IT that IPE addresses residual risk.
Targeting the subgroup of high-risk patients with elevated TGs “is easy” because they are so readily identifiable, according to Dr. Bhatt, but he said it should be used for any patient that meet the entry criteria used for REDUCE-IT.
“The overall results of REDUCE-IT were robustly positive, so I wouldn’t just use it in patients with prior MI,” Dr. Bhatt said.
Dr. Bhatt reports financial relationships with more than 20 pharmaceutical companies, including Amarin, which provided funding for this trial. Dr. Boden reports no potential conflicts of interest.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY

Myocarditis higher with Moderna COVID vax in young men
One of the largest studies to date on myocarditis after COVID-19 vaccination confirms an increased risk with both the Pfizer and Moderna vaccines in young men and shows that the risk is higher with the Moderna than with the Pfizer vaccine.
The study also suggests for the first time that in young men 16 to 24 years of age, the risk for myocarditis after vaccination with either the Pfizer or Moderna vaccine is higher than the risk for myocarditis after COVID-19 infection.
The population-based study involved data on 23.1 million residents across four Scandinavian countries – Denmark, Finland, Norway, and Sweden – 74% of whom had received two vaccine doses and 7% of whom had received one dose.
By linking data from high-quality nationwide health registers on COVID-19 vaccination, infection rates, and myocarditis diagnoses, the researchers were able to evaluate the risk for myocarditis by vaccine product, vaccination dose number, sex, and age.
The study was published online in JAMA Cardiology.
The results confirm that the risk for myocarditis after COVID-19 mRNA vaccines is highest in young men 16 to 24 years of age after the second dose.
For men in this age group who received two doses of the same vaccine, data were compatible, with between four and seven excess myocarditis events in 28 days per 100,000 individuals after the second dose of the Pfizer vaccine, and between nine and 28 per 100,000 individuals after the second dose of the Moderna vaccine.
“This is one of the largest studies on this topic to date. The first population studies were in Israel, with 5 million individuals, and looked at just the Pfizer vaccine. We have data on 23 million people from Scandinavia that include both the Pfizer and Moderna vaccines,” senior author Rickard Ljung, MD, Swedish Medical Products Agency, told this news organization.
“We show a clearly higher risk of myocarditis after the Moderna vaccine than after the Pfizer vaccine. This has been suggested before, but our data confirm definitively that the Moderna vaccine has a higher risk of myocarditis than the Pfizer vaccine,” he added.
“In the group at highest risk of myocarditis after COVID vaccination – young men aged 16 to 24 – the Pfizer vaccine shows a five times higher risk of myocarditis versus the unvaccinated cohort, while the Moderna vaccine shows a 15 times higher risk,” Dr. Ljung noted.
After seeing these data, the Swedish regulatory authority is no longer recommending use of the Moderna vaccine for people younger than 30 years, Dr. Ljung said. Similar recommendations have been made in Norway and Finland.
The researchers report that their finding of a higher risk for myocarditis after the Moderna vaccine than after the Pfizer vaccine in young men is in line with data from the Canada, France, the United Kingdom, and the United States. But they point out that, compared with previous studies, the current study had the advantage of data analyzed according to a common protocol from four different countries and that showed similar directions of associations, despite considerable differences in previous COVID-19 infection levels and lockdown policies.
Risk higher with vaccination than infection?
For what is believed to be the first time, the Scandinavian data also suggest a higher risk for myocarditis after COVID-19 vaccination with both the Pfizer and Moderna vaccines than after COVID-19 infection in young men 16 to 24 years.
Although previous studies have shown that males in this age group have the highest risk for myocarditis after vaccination, it has always been suggested that the risk after vaccination is lower than the risk after infection. The Scandinavian data suggest otherwise for this age group.
Dr. Ljung explained that the myocarditis risk after COVID infection is very hard to study.
“It is highly dependent on the testing strategy,” he said. “For example, in the first half of 2020, the only people being tested were those admitted to hospital, so studies would have included the sickest patients and would therefore likely have found a higher rate of myocarditis. But this current Scandinavian dataset only included individuals with a positive COVID test after August 2020, reflecting a broader range of people.”
The researchers found an excess rate of myocarditis of 3.26 per 100,000 individuals within 28 days of a positive COVID-19 test among all males, and 1.37 per 100,000 individuals among males 16 to 24 years of age.
“We show that the risk of myocarditis after COVID infection is lower in younger people and higher in older people, but the opposite is true after COVID vaccination, where the risk of myocarditis is higher in younger people and lower in older people,” Dr. Ljung said.
The study was not able to look at severity of myocarditis but did record length of hospital stay, which was similar in patients who developed myocarditis after vaccination and those in the unvaccinated cohort (4 to 5 days). Deaths were rare, with no deaths in people younger than 40 years.
“I think we can say that in people aged over 40, the risk of myocarditis is greater with infection than with vaccination, but in those under 40, it is not so clear. And our data suggest that for young men aged 16 to 24 years, the risk of myocarditis after COVID vaccination with either the Pfizer or Moderna vaccine is higher than after COVID infection,” Dr. Ljung commented.
Although the Swedish regulatory agency has already stopped recommending use of Moderna vaccine in those younger than 30 years on the basis of these data, Dr. Ljung was reluctant to make any recommendations regarding the use of the Pfizer vaccine in young males, saying it was up to individual public-health agencies to makes these decisions.
But he pointed out that the current study only looked at myocarditis, and COVID infection can result in many other complications that can lead to hospitalization and death, which needs to be taken into account when assessing the risk and benefit of vaccination.
Dr. Ljung noted that the current data only applied to the first two doses of the vaccines; data after booster injections have not been included, although the researchers are looking at that now.
What to advise patients?
In an accompanying Editor’s Note, Ann Marie Navar, MD, University of Texas Southwestern Medical Center, Dallas, who is editor of JAMA Cardiology, and Robert Bonow, MD, Northwestern University Feinberg School of Medicine, Chicago, who is deputy editor of JAMA Cardiology, try to explain how these data can inform the way health care professionals communicate with their patients about vaccination.

They point out the “good news,” that older adults who are at highest risk for COVID-19 complications appear to be at extremely low risk for vaccine-associated myocarditis.
They note that for both men and women older than 40 years, the excess number of cases of myocarditis after vaccination was fewer than two in 100,000 vaccinees across all vaccines studied, and the death toll from COVID-19 in the United States as of March was more than 200 per 100,000 population.
“Given the high rates of morbidity and mortality from COVID-19 infection in older adults and the efficacy of the vaccine in preventing severe infection and death, the benefits of immunization in those older than 40 years clearly outweigh the risks,” the editors say.
But given these data in young men, they suggest that health care professionals consider recommending the Pfizer vaccine over the Moderna vaccine for certain populations, including young men and other individuals for whom concerns about myocarditis present a barrier to immunization.
The editors also point out that although the risk for myocarditis after COVID-19 immunization is real, this low risk must be considered in the context of the overall benefit of the vaccine.
“At the individual level, immunization prevents not only COVID-19-related myocarditis but also severe disease, hospitalization, long-term complications after COVID-19 infection, and death. At the population level, immunization helps to decrease community spread, decrease the chances of new variants emerging, protect people who are immunocompromised, and ensure our health care system can continue to provide for our communities,” they conclude.
Dr. Ljung reports grants from Sanofi Aventis paid to his institution outside the submitted work and personal fees from Pfizer outside the submitted work. Dr. Navar reports personal fees from Pfizer and AstraZeneca, outside the scope of this work.
A version of this article first appeared on Medscape.com.
One of the largest studies to date on myocarditis after COVID-19 vaccination confirms an increased risk with both the Pfizer and Moderna vaccines in young men and shows that the risk is higher with the Moderna than with the Pfizer vaccine.
The study also suggests for the first time that in young men 16 to 24 years of age, the risk for myocarditis after vaccination with either the Pfizer or Moderna vaccine is higher than the risk for myocarditis after COVID-19 infection.
The population-based study involved data on 23.1 million residents across four Scandinavian countries – Denmark, Finland, Norway, and Sweden – 74% of whom had received two vaccine doses and 7% of whom had received one dose.
By linking data from high-quality nationwide health registers on COVID-19 vaccination, infection rates, and myocarditis diagnoses, the researchers were able to evaluate the risk for myocarditis by vaccine product, vaccination dose number, sex, and age.
The study was published online in JAMA Cardiology.
The results confirm that the risk for myocarditis after COVID-19 mRNA vaccines is highest in young men 16 to 24 years of age after the second dose.
For men in this age group who received two doses of the same vaccine, data were compatible, with between four and seven excess myocarditis events in 28 days per 100,000 individuals after the second dose of the Pfizer vaccine, and between nine and 28 per 100,000 individuals after the second dose of the Moderna vaccine.
“This is one of the largest studies on this topic to date. The first population studies were in Israel, with 5 million individuals, and looked at just the Pfizer vaccine. We have data on 23 million people from Scandinavia that include both the Pfizer and Moderna vaccines,” senior author Rickard Ljung, MD, Swedish Medical Products Agency, told this news organization.
“We show a clearly higher risk of myocarditis after the Moderna vaccine than after the Pfizer vaccine. This has been suggested before, but our data confirm definitively that the Moderna vaccine has a higher risk of myocarditis than the Pfizer vaccine,” he added.
“In the group at highest risk of myocarditis after COVID vaccination – young men aged 16 to 24 – the Pfizer vaccine shows a five times higher risk of myocarditis versus the unvaccinated cohort, while the Moderna vaccine shows a 15 times higher risk,” Dr. Ljung noted.
After seeing these data, the Swedish regulatory authority is no longer recommending use of the Moderna vaccine for people younger than 30 years, Dr. Ljung said. Similar recommendations have been made in Norway and Finland.
The researchers report that their finding of a higher risk for myocarditis after the Moderna vaccine than after the Pfizer vaccine in young men is in line with data from the Canada, France, the United Kingdom, and the United States. But they point out that, compared with previous studies, the current study had the advantage of data analyzed according to a common protocol from four different countries and that showed similar directions of associations, despite considerable differences in previous COVID-19 infection levels and lockdown policies.
Risk higher with vaccination than infection?
For what is believed to be the first time, the Scandinavian data also suggest a higher risk for myocarditis after COVID-19 vaccination with both the Pfizer and Moderna vaccines than after COVID-19 infection in young men 16 to 24 years.
Although previous studies have shown that males in this age group have the highest risk for myocarditis after vaccination, it has always been suggested that the risk after vaccination is lower than the risk after infection. The Scandinavian data suggest otherwise for this age group.
Dr. Ljung explained that the myocarditis risk after COVID infection is very hard to study.
“It is highly dependent on the testing strategy,” he said. “For example, in the first half of 2020, the only people being tested were those admitted to hospital, so studies would have included the sickest patients and would therefore likely have found a higher rate of myocarditis. But this current Scandinavian dataset only included individuals with a positive COVID test after August 2020, reflecting a broader range of people.”
The researchers found an excess rate of myocarditis of 3.26 per 100,000 individuals within 28 days of a positive COVID-19 test among all males, and 1.37 per 100,000 individuals among males 16 to 24 years of age.
“We show that the risk of myocarditis after COVID infection is lower in younger people and higher in older people, but the opposite is true after COVID vaccination, where the risk of myocarditis is higher in younger people and lower in older people,” Dr. Ljung said.
The study was not able to look at severity of myocarditis but did record length of hospital stay, which was similar in patients who developed myocarditis after vaccination and those in the unvaccinated cohort (4 to 5 days). Deaths were rare, with no deaths in people younger than 40 years.
“I think we can say that in people aged over 40, the risk of myocarditis is greater with infection than with vaccination, but in those under 40, it is not so clear. And our data suggest that for young men aged 16 to 24 years, the risk of myocarditis after COVID vaccination with either the Pfizer or Moderna vaccine is higher than after COVID infection,” Dr. Ljung commented.
Although the Swedish regulatory agency has already stopped recommending use of Moderna vaccine in those younger than 30 years on the basis of these data, Dr. Ljung was reluctant to make any recommendations regarding the use of the Pfizer vaccine in young males, saying it was up to individual public-health agencies to makes these decisions.
But he pointed out that the current study only looked at myocarditis, and COVID infection can result in many other complications that can lead to hospitalization and death, which needs to be taken into account when assessing the risk and benefit of vaccination.
Dr. Ljung noted that the current data only applied to the first two doses of the vaccines; data after booster injections have not been included, although the researchers are looking at that now.
What to advise patients?
In an accompanying Editor’s Note, Ann Marie Navar, MD, University of Texas Southwestern Medical Center, Dallas, who is editor of JAMA Cardiology, and Robert Bonow, MD, Northwestern University Feinberg School of Medicine, Chicago, who is deputy editor of JAMA Cardiology, try to explain how these data can inform the way health care professionals communicate with their patients about vaccination.
They point out the “good news,” that older adults who are at highest risk for COVID-19 complications appear to be at extremely low risk for vaccine-associated myocarditis.
They note that for both men and women older than 40 years, the excess number of cases of myocarditis after vaccination was fewer than two in 100,000 vaccinees across all vaccines studied, and the death toll from COVID-19 in the United States as of March was more than 200 per 100,000 population.
“Given the high rates of morbidity and mortality from COVID-19 infection in older adults and the efficacy of the vaccine in preventing severe infection and death, the benefits of immunization in those older than 40 years clearly outweigh the risks,” the editors say.
But given these data in young men, they suggest that health care professionals consider recommending the Pfizer vaccine over the Moderna vaccine for certain populations, including young men and other individuals for whom concerns about myocarditis present a barrier to immunization.
The editors also point out that although the risk for myocarditis after COVID-19 immunization is real, this low risk must be considered in the context of the overall benefit of the vaccine.
“At the individual level, immunization prevents not only COVID-19-related myocarditis but also severe disease, hospitalization, long-term complications after COVID-19 infection, and death. At the population level, immunization helps to decrease community spread, decrease the chances of new variants emerging, protect people who are immunocompromised, and ensure our health care system can continue to provide for our communities,” they conclude.
Dr. Ljung reports grants from Sanofi Aventis paid to his institution outside the submitted work and personal fees from Pfizer outside the submitted work. Dr. Navar reports personal fees from Pfizer and AstraZeneca, outside the scope of this work.
A version of this article first appeared on Medscape.com.
One of the largest studies to date on myocarditis after COVID-19 vaccination confirms an increased risk with both the Pfizer and Moderna vaccines in young men and shows that the risk is higher with the Moderna than with the Pfizer vaccine.
The study also suggests for the first time that in young men 16 to 24 years of age, the risk for myocarditis after vaccination with either the Pfizer or Moderna vaccine is higher than the risk for myocarditis after COVID-19 infection.
The population-based study involved data on 23.1 million residents across four Scandinavian countries – Denmark, Finland, Norway, and Sweden – 74% of whom had received two vaccine doses and 7% of whom had received one dose.
By linking data from high-quality nationwide health registers on COVID-19 vaccination, infection rates, and myocarditis diagnoses, the researchers were able to evaluate the risk for myocarditis by vaccine product, vaccination dose number, sex, and age.
The study was published online in JAMA Cardiology.
The results confirm that the risk for myocarditis after COVID-19 mRNA vaccines is highest in young men 16 to 24 years of age after the second dose.
For men in this age group who received two doses of the same vaccine, data were compatible, with between four and seven excess myocarditis events in 28 days per 100,000 individuals after the second dose of the Pfizer vaccine, and between nine and 28 per 100,000 individuals after the second dose of the Moderna vaccine.
“This is one of the largest studies on this topic to date. The first population studies were in Israel, with 5 million individuals, and looked at just the Pfizer vaccine. We have data on 23 million people from Scandinavia that include both the Pfizer and Moderna vaccines,” senior author Rickard Ljung, MD, Swedish Medical Products Agency, told this news organization.
“We show a clearly higher risk of myocarditis after the Moderna vaccine than after the Pfizer vaccine. This has been suggested before, but our data confirm definitively that the Moderna vaccine has a higher risk of myocarditis than the Pfizer vaccine,” he added.
“In the group at highest risk of myocarditis after COVID vaccination – young men aged 16 to 24 – the Pfizer vaccine shows a five times higher risk of myocarditis versus the unvaccinated cohort, while the Moderna vaccine shows a 15 times higher risk,” Dr. Ljung noted.
After seeing these data, the Swedish regulatory authority is no longer recommending use of the Moderna vaccine for people younger than 30 years, Dr. Ljung said. Similar recommendations have been made in Norway and Finland.
The researchers report that their finding of a higher risk for myocarditis after the Moderna vaccine than after the Pfizer vaccine in young men is in line with data from the Canada, France, the United Kingdom, and the United States. But they point out that, compared with previous studies, the current study had the advantage of data analyzed according to a common protocol from four different countries and that showed similar directions of associations, despite considerable differences in previous COVID-19 infection levels and lockdown policies.
Risk higher with vaccination than infection?
For what is believed to be the first time, the Scandinavian data also suggest a higher risk for myocarditis after COVID-19 vaccination with both the Pfizer and Moderna vaccines than after COVID-19 infection in young men 16 to 24 years.
Although previous studies have shown that males in this age group have the highest risk for myocarditis after vaccination, it has always been suggested that the risk after vaccination is lower than the risk after infection. The Scandinavian data suggest otherwise for this age group.
Dr. Ljung explained that the myocarditis risk after COVID infection is very hard to study.
“It is highly dependent on the testing strategy,” he said. “For example, in the first half of 2020, the only people being tested were those admitted to hospital, so studies would have included the sickest patients and would therefore likely have found a higher rate of myocarditis. But this current Scandinavian dataset only included individuals with a positive COVID test after August 2020, reflecting a broader range of people.”
The researchers found an excess rate of myocarditis of 3.26 per 100,000 individuals within 28 days of a positive COVID-19 test among all males, and 1.37 per 100,000 individuals among males 16 to 24 years of age.
“We show that the risk of myocarditis after COVID infection is lower in younger people and higher in older people, but the opposite is true after COVID vaccination, where the risk of myocarditis is higher in younger people and lower in older people,” Dr. Ljung said.
The study was not able to look at severity of myocarditis but did record length of hospital stay, which was similar in patients who developed myocarditis after vaccination and those in the unvaccinated cohort (4 to 5 days). Deaths were rare, with no deaths in people younger than 40 years.
“I think we can say that in people aged over 40, the risk of myocarditis is greater with infection than with vaccination, but in those under 40, it is not so clear. And our data suggest that for young men aged 16 to 24 years, the risk of myocarditis after COVID vaccination with either the Pfizer or Moderna vaccine is higher than after COVID infection,” Dr. Ljung commented.
Although the Swedish regulatory agency has already stopped recommending use of Moderna vaccine in those younger than 30 years on the basis of these data, Dr. Ljung was reluctant to make any recommendations regarding the use of the Pfizer vaccine in young males, saying it was up to individual public-health agencies to makes these decisions.
But he pointed out that the current study only looked at myocarditis, and COVID infection can result in many other complications that can lead to hospitalization and death, which needs to be taken into account when assessing the risk and benefit of vaccination.
Dr. Ljung noted that the current data only applied to the first two doses of the vaccines; data after booster injections have not been included, although the researchers are looking at that now.
What to advise patients?
In an accompanying Editor’s Note, Ann Marie Navar, MD, University of Texas Southwestern Medical Center, Dallas, who is editor of JAMA Cardiology, and Robert Bonow, MD, Northwestern University Feinberg School of Medicine, Chicago, who is deputy editor of JAMA Cardiology, try to explain how these data can inform the way health care professionals communicate with their patients about vaccination.
They point out the “good news,” that older adults who are at highest risk for COVID-19 complications appear to be at extremely low risk for vaccine-associated myocarditis.
They note that for both men and women older than 40 years, the excess number of cases of myocarditis after vaccination was fewer than two in 100,000 vaccinees across all vaccines studied, and the death toll from COVID-19 in the United States as of March was more than 200 per 100,000 population.
“Given the high rates of morbidity and mortality from COVID-19 infection in older adults and the efficacy of the vaccine in preventing severe infection and death, the benefits of immunization in those older than 40 years clearly outweigh the risks,” the editors say.
But given these data in young men, they suggest that health care professionals consider recommending the Pfizer vaccine over the Moderna vaccine for certain populations, including young men and other individuals for whom concerns about myocarditis present a barrier to immunization.
The editors also point out that although the risk for myocarditis after COVID-19 immunization is real, this low risk must be considered in the context of the overall benefit of the vaccine.
“At the individual level, immunization prevents not only COVID-19-related myocarditis but also severe disease, hospitalization, long-term complications after COVID-19 infection, and death. At the population level, immunization helps to decrease community spread, decrease the chances of new variants emerging, protect people who are immunocompromised, and ensure our health care system can continue to provide for our communities,” they conclude.
Dr. Ljung reports grants from Sanofi Aventis paid to his institution outside the submitted work and personal fees from Pfizer outside the submitted work. Dr. Navar reports personal fees from Pfizer and AstraZeneca, outside the scope of this work.
A version of this article first appeared on Medscape.com.
FROM JAMA CARDIOLOGY

Internet intervention improved insomnia in Black women
Data from previous studies suggest that women are up to 40% more likely to experience insomnia disorder compared with men, Eric S. Zhou, PhD, of Harvard Medical School, Boston, and colleagues wrote. The risk is even higher among Black women, but research on tailored treatments for this particular population has been limited.
In their study, published in JAMA Psychiatry, the researchers recruited women with elevated insomnia symptoms who were enrolled in the Black Women’s Health Study, an ongoing national, longitudinal research cohort in the United States. Participants were recruited between October 2019 and June 2020.The participants were randomized to an Internet-delivered behavior intervention (108 women), a stakeholder-informed Internet intervention tailored to Black women (110 women), or non-Internet patient education about sleep (115 women).
The Internet intervention, known as Sleep Healthy Using the Internet (SHUTi), was a 6-session program lasting 45-60 minutes per session and delivered over 6-9 weeks. The program included core elements of cognitive behavioral therapy and took into account information provided by patients about their baseline sleep function, treatment adherence, and sleep progress.
The tailored version of SHUTi for Black women (SHUTi-BWHS) was similar, but included Black actors for video vignettes and the inclusion of content about the cultural and social contexts in which insomnia often occurs for Black women, such while managing neighborhood noise and or living in crowded environments.
A third group received standard patient education material about sleep through a noninteractive website, and served as the control group.
The primary outcome of insomnia severity was measured using the Insomnia Severity Index (ISI), a 0- to 28-point scale. Scores for the ISI are based on responses to seven questions, including some that ask participants to rate the severity of their insomnia symptoms.
Clinically significant improvement in insomnia was defined as a reduction in score of more than 7 points. Patients were assessed at baseline, at 9 weeks, and again at approximately 6 months.
Significantly greater reductions in insomnia severity seen in intervention groups vs. control group
Overall, women randomized to SHUTi or SHUTi-BWHS) reported a significantly greater reduction in insomnia symptoms from baseline to 6 months, compared with the control group (P < .001), with ISI score decreases of 10.0, 9.3, and 3.6, respectively. No statistically significant differences in ISI score changes appeared between the between the SHUTi-BWHS and SHUTi groups.
Also, significantly more women in the SHUTi-BWHS group than in the SHUTi group completed the intervention (78.2% vs. 64.8%).
Treatment response was similar between the SHUTI-BWHS and SHUTi groups; 47.3% and 46.3%, respectively, had a decrease in ISI score of more than 7 points. In addition, 37% of women in the SHUTi-BWHS and 38% of women in the SHUTi groups reached ISI scores of less than 8 points, defined as full resolution of insomnia, by the last follow-up visit.
Both the SHUTi and SHUTi-BWHS interventions had dramatic effects on insomnia, but the increased number of women who completed the intervention in the SHUTi-BWHS group supports the value of tailored intervention, the researchers noted. “Similar to prior SHUTi trials, there was a direct association between the participant’s level of intervention engagement and their improvement in sleep.”
The average age of the participants was 60 years, 62% were single, and 44% had a graduate degree or higher. Approximately 5% were being actively treated for sleep apnea.
The study findings were limited by several factors including the relatively high socioeconomic status of the study participants, lack of data on medical mistrust, and inability to detect smaller differences between SHUTi and SHUTi-BWHS, the researchers noted.
Choose Internet-based CBT first for insomnia
“This was an excellent paper that sought to see the relative efficacy of standard version of Internet-delivered CBT-I [cognitive-behavioral therapy for insomnia] versus a culturally tailored version for Black women,” said Neil Skolnik, MD, professor of family and community medicine at Thomas Jefferson University, Philadelphia, in an interview. “The trial confirmed that, compared with sleep education, which was used as the control, Internet-delivered CBT-I is effective in the treatment of insomnia.”

“These results demonstrate two important things,” said Dr. Skolnik. “The most important is that Internet-delivered CBT-I works, and since it is both safe and effective, should be the first-line therapy for patients who want treatment for insomnia.”
Secondly, “the fact that more people completed culturally tailored versions suggests that, when culturally tailored versions are available, their use is preferable, as it might facilitate a higher proportion of patients being successful in their insomnia treatment,” he added.
The study was supported by the Patient-Centered Outcomes Research Institute. The Black Women’s Health Study is supported by the National Cancer Institute. Dr. Zhou disclosed support from both PCORI and the NCI during the study. Dr. Skolnik, who was not involved in the study, disclosed serving on the advisory board for Idorsia Pharmaceuticals. He is also a member of the editorial advisory board of Family Practice News.
Data from previous studies suggest that women are up to 40% more likely to experience insomnia disorder compared with men, Eric S. Zhou, PhD, of Harvard Medical School, Boston, and colleagues wrote. The risk is even higher among Black women, but research on tailored treatments for this particular population has been limited.
In their study, published in JAMA Psychiatry, the researchers recruited women with elevated insomnia symptoms who were enrolled in the Black Women’s Health Study, an ongoing national, longitudinal research cohort in the United States. Participants were recruited between October 2019 and June 2020.The participants were randomized to an Internet-delivered behavior intervention (108 women), a stakeholder-informed Internet intervention tailored to Black women (110 women), or non-Internet patient education about sleep (115 women).
The Internet intervention, known as Sleep Healthy Using the Internet (SHUTi), was a 6-session program lasting 45-60 minutes per session and delivered over 6-9 weeks. The program included core elements of cognitive behavioral therapy and took into account information provided by patients about their baseline sleep function, treatment adherence, and sleep progress.
The tailored version of SHUTi for Black women (SHUTi-BWHS) was similar, but included Black actors for video vignettes and the inclusion of content about the cultural and social contexts in which insomnia often occurs for Black women, such while managing neighborhood noise and or living in crowded environments.
A third group received standard patient education material about sleep through a noninteractive website, and served as the control group.
The primary outcome of insomnia severity was measured using the Insomnia Severity Index (ISI), a 0- to 28-point scale. Scores for the ISI are based on responses to seven questions, including some that ask participants to rate the severity of their insomnia symptoms.
Clinically significant improvement in insomnia was defined as a reduction in score of more than 7 points. Patients were assessed at baseline, at 9 weeks, and again at approximately 6 months.
Significantly greater reductions in insomnia severity seen in intervention groups vs. control group
Overall, women randomized to SHUTi or SHUTi-BWHS) reported a significantly greater reduction in insomnia symptoms from baseline to 6 months, compared with the control group (P < .001), with ISI score decreases of 10.0, 9.3, and 3.6, respectively. No statistically significant differences in ISI score changes appeared between the between the SHUTi-BWHS and SHUTi groups.
Also, significantly more women in the SHUTi-BWHS group than in the SHUTi group completed the intervention (78.2% vs. 64.8%).
Treatment response was similar between the SHUTI-BWHS and SHUTi groups; 47.3% and 46.3%, respectively, had a decrease in ISI score of more than 7 points. In addition, 37% of women in the SHUTi-BWHS and 38% of women in the SHUTi groups reached ISI scores of less than 8 points, defined as full resolution of insomnia, by the last follow-up visit.
Both the SHUTi and SHUTi-BWHS interventions had dramatic effects on insomnia, but the increased number of women who completed the intervention in the SHUTi-BWHS group supports the value of tailored intervention, the researchers noted. “Similar to prior SHUTi trials, there was a direct association between the participant’s level of intervention engagement and their improvement in sleep.”
The average age of the participants was 60 years, 62% were single, and 44% had a graduate degree or higher. Approximately 5% were being actively treated for sleep apnea.
The study findings were limited by several factors including the relatively high socioeconomic status of the study participants, lack of data on medical mistrust, and inability to detect smaller differences between SHUTi and SHUTi-BWHS, the researchers noted.
Choose Internet-based CBT first for insomnia
“This was an excellent paper that sought to see the relative efficacy of standard version of Internet-delivered CBT-I [cognitive-behavioral therapy for insomnia] versus a culturally tailored version for Black women,” said Neil Skolnik, MD, professor of family and community medicine at Thomas Jefferson University, Philadelphia, in an interview. “The trial confirmed that, compared with sleep education, which was used as the control, Internet-delivered CBT-I is effective in the treatment of insomnia.”
“These results demonstrate two important things,” said Dr. Skolnik. “The most important is that Internet-delivered CBT-I works, and since it is both safe and effective, should be the first-line therapy for patients who want treatment for insomnia.”
Secondly, “the fact that more people completed culturally tailored versions suggests that, when culturally tailored versions are available, their use is preferable, as it might facilitate a higher proportion of patients being successful in their insomnia treatment,” he added.
The study was supported by the Patient-Centered Outcomes Research Institute. The Black Women’s Health Study is supported by the National Cancer Institute. Dr. Zhou disclosed support from both PCORI and the NCI during the study. Dr. Skolnik, who was not involved in the study, disclosed serving on the advisory board for Idorsia Pharmaceuticals. He is also a member of the editorial advisory board of Family Practice News.
Data from previous studies suggest that women are up to 40% more likely to experience insomnia disorder compared with men, Eric S. Zhou, PhD, of Harvard Medical School, Boston, and colleagues wrote. The risk is even higher among Black women, but research on tailored treatments for this particular population has been limited.
In their study, published in JAMA Psychiatry, the researchers recruited women with elevated insomnia symptoms who were enrolled in the Black Women’s Health Study, an ongoing national, longitudinal research cohort in the United States. Participants were recruited between October 2019 and June 2020.The participants were randomized to an Internet-delivered behavior intervention (108 women), a stakeholder-informed Internet intervention tailored to Black women (110 women), or non-Internet patient education about sleep (115 women).
The Internet intervention, known as Sleep Healthy Using the Internet (SHUTi), was a 6-session program lasting 45-60 minutes per session and delivered over 6-9 weeks. The program included core elements of cognitive behavioral therapy and took into account information provided by patients about their baseline sleep function, treatment adherence, and sleep progress.
The tailored version of SHUTi for Black women (SHUTi-BWHS) was similar, but included Black actors for video vignettes and the inclusion of content about the cultural and social contexts in which insomnia often occurs for Black women, such while managing neighborhood noise and or living in crowded environments.
A third group received standard patient education material about sleep through a noninteractive website, and served as the control group.
The primary outcome of insomnia severity was measured using the Insomnia Severity Index (ISI), a 0- to 28-point scale. Scores for the ISI are based on responses to seven questions, including some that ask participants to rate the severity of their insomnia symptoms.
Clinically significant improvement in insomnia was defined as a reduction in score of more than 7 points. Patients were assessed at baseline, at 9 weeks, and again at approximately 6 months.
Significantly greater reductions in insomnia severity seen in intervention groups vs. control group
Overall, women randomized to SHUTi or SHUTi-BWHS) reported a significantly greater reduction in insomnia symptoms from baseline to 6 months, compared with the control group (P < .001), with ISI score decreases of 10.0, 9.3, and 3.6, respectively. No statistically significant differences in ISI score changes appeared between the between the SHUTi-BWHS and SHUTi groups.
Also, significantly more women in the SHUTi-BWHS group than in the SHUTi group completed the intervention (78.2% vs. 64.8%).
Treatment response was similar between the SHUTI-BWHS and SHUTi groups; 47.3% and 46.3%, respectively, had a decrease in ISI score of more than 7 points. In addition, 37% of women in the SHUTi-BWHS and 38% of women in the SHUTi groups reached ISI scores of less than 8 points, defined as full resolution of insomnia, by the last follow-up visit.
Both the SHUTi and SHUTi-BWHS interventions had dramatic effects on insomnia, but the increased number of women who completed the intervention in the SHUTi-BWHS group supports the value of tailored intervention, the researchers noted. “Similar to prior SHUTi trials, there was a direct association between the participant’s level of intervention engagement and their improvement in sleep.”
The average age of the participants was 60 years, 62% were single, and 44% had a graduate degree or higher. Approximately 5% were being actively treated for sleep apnea.
The study findings were limited by several factors including the relatively high socioeconomic status of the study participants, lack of data on medical mistrust, and inability to detect smaller differences between SHUTi and SHUTi-BWHS, the researchers noted.
Choose Internet-based CBT first for insomnia
“This was an excellent paper that sought to see the relative efficacy of standard version of Internet-delivered CBT-I [cognitive-behavioral therapy for insomnia] versus a culturally tailored version for Black women,” said Neil Skolnik, MD, professor of family and community medicine at Thomas Jefferson University, Philadelphia, in an interview. “The trial confirmed that, compared with sleep education, which was used as the control, Internet-delivered CBT-I is effective in the treatment of insomnia.”
“These results demonstrate two important things,” said Dr. Skolnik. “The most important is that Internet-delivered CBT-I works, and since it is both safe and effective, should be the first-line therapy for patients who want treatment for insomnia.”
Secondly, “the fact that more people completed culturally tailored versions suggests that, when culturally tailored versions are available, their use is preferable, as it might facilitate a higher proportion of patients being successful in their insomnia treatment,” he added.
The study was supported by the Patient-Centered Outcomes Research Institute. The Black Women’s Health Study is supported by the National Cancer Institute. Dr. Zhou disclosed support from both PCORI and the NCI during the study. Dr. Skolnik, who was not involved in the study, disclosed serving on the advisory board for Idorsia Pharmaceuticals. He is also a member of the editorial advisory board of Family Practice News.
FROM JAMA PSYCHIATRY