User login
-
div[contains(@class, 'header__large-screen')]
div[contains(@class, 'read-next-article')]
div[contains(@class, 'main-prefix')]
div[contains(@class, 'nav-primary')]
nav[contains(@class, 'nav-primary')]
section[contains(@class, 'footer-nav-section-wrapper')]
footer[@id='footer']
section[contains(@class, 'nav-hidden')]
div[contains(@class, 'ce-card-content')]
nav[contains(@class, 'nav-ce-stack')]
div[contains(@class, 'view-medstat-quiz-listing-panes')]
div[contains(@class, 'pane-article-sidebar-latest-news')]
Which drug best reduces sleepiness in patients with OSA?
Solriamfetol who have residual daytime sleepiness after conventional treatment, according to a systematic review and meta-analysis.
In a systematic review of 14 trials that included more than 3,000 patients, solriamfetol was associated with improvements of 3.85 points on the Epworth Sleepiness Scale (ESS) score, compared with placebo.
“We found that solriamfetol is almost twice as effective as modafinil-armodafinil – the cheaper, older option – in improving the ESS score and much more effective at improving the Maintenance of Wakefulness Test (MWT),” study author Tyler Pitre, MD, an internal medicine physician at McMaster University, Hamilton, Ont., said in an interview.
The findings were published online in Annals of Internal Medicine.
High-certainty evidence
The analysis included 3,085 adults with excessive daytime sleepiness (EDS) who were receiving or were eligible for conventional OSA treatment such as positive airway pressure. Participants were randomly assigned to either placebo or any EDS pharmacotherapy (armodafinil, modafinil, solriamfetol, or pitolisant). The primary outcomes of the analysis were change in ESS and MWT. Secondary outcomes were drug-related adverse events.

The trials had a median follow-up time of 4 weeks. The meta-analysis showed that solriamfetol improves ESS to a greater extent than placebo (high certainty), armodafinil-modafinil and pitolisant (moderate certainty). Compared with placebo, the mean difference in ESS scores for solriamfetol, armodafinil-modafinil, and pitolisant was –3.85, –2.25, and –2.78, respectively.
The analysis yielded high-certainty evidence that solriamfetol and armodafinil-modafinil improved MWT, compared with placebo. The former was “probably superior,” while pitolisant “may have little to no effect on MWT, compared with placebo,” write the authors. The standardized mean difference in MWT scores, compared with placebo, was 0.90 for solriamfetol and 0.41 for armodafinil-modafinil. “Solriamfetol is probably superior to armodafinil-modafinil in improving MWT (SMD, 0.49),” say the authors.
Compared with placebo, armodafinil-modafinil probably increases the risk for discontinuation due to adverse events (relative risk, 2.01), and solriamfetol may increase the risk for discontinuation (RR, 2.04), according to the authors. Pitolisant “may have little to no effect on drug discontinuations due to adverse events,” write the authors.
Although solriamfetol may have led to more discontinuations than armodafinil-modafinil, “we did not find convincing evidence of serious adverse events, albeit with very short-term follow-up,” they add.
The most common side effects for all interventions were headaches, insomnia, and anxiety. Headaches were most likely with armodafinil-modafinil (RR, 1.87), and insomnia was most likely with pitolisant (RR, 7.25).
“Although solriamfetol appears most effective, comorbid hypertension and costs may be barriers to its use,” say the researchers. “Furthermore, there are potentially effective candidate therapies such as methylphenidate, atomoxetine, or caffeine, which have not been examined in randomized clinical trials.”
Although EDS is reported in 40%-58% of patients with OSA and can persist in 6%-18% despite PAP therapy, most non-sleep specialists may not be aware of pharmacologic options, said Dr. Pitre. “I have not seen a study that looks at the prescribing habits of physicians for this condition, but I suspect that primary care physicians are not prescribing modafinil-armodafinil frequently for this and less so for solriamfetol,” he said. “I hope this paper builds awareness of this condition and also informs clinicians on the options available to patients, as well as common side effects to counsel them on before starting treatment.”
Dr. Pitre was surprised at the magnitude of solriamfetol’s superiority to modafinil-armodafinil but cautioned that solriamfetol has been shown to increase blood pressure in higher doses. It therefore must be prescribed carefully, “especially to a population of patients who often have comorbid hypertension,” he said.
Some limitations of the analysis were that all trials were conducted in high-income countries (most commonly the United States). Moreover, 77% of participants were White, and 71% were male.
Beneficial adjunctive therapy
Commenting on the findings, Sogol Javaheri, MD, MPH, who was not involved in the research, said that they confirm those of prior studies and are “consistent with what my colleagues and I experience in our clinical practices.”
Dr. Javaheri is associate program director of the sleep medicine fellowship at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, both in Boston.
While sleep medicine specialists are more likely than others to prescribe these medications, “any clinician may use these medications, ideally if they have ruled out other potential reversible causes of EDS,” said Dr. Javaheri. “The medications do not treat the underlying cause, which is why it’s important to use them as an adjunct to conventional therapy that actually treats the underlying sleep disorder and to rule out additional potential causes of sleepiness that are treatable.”
These potential causes might include insufficient sleep (less than 7 hours per night), untreated anemia, and incompletely treated sleep disorders, she explained. In sleep medicine, modafinil is usually the treatment of choice because of its lower cost, but it may reduce the efficacy of hormonal contraception. Solriamfetol, however, does not. “Additionally, I look forward to validation of pitolisant for treatment of EDS in OSA patients, as it is not a controlled substance and may benefit patients with a history of substance abuse or who may be at higher risk of addiction,” said Dr. Javaheri.
The study was conducted without outside funding. Dr. Pitre and Dr. Javaheri report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Solriamfetol who have residual daytime sleepiness after conventional treatment, according to a systematic review and meta-analysis.
In a systematic review of 14 trials that included more than 3,000 patients, solriamfetol was associated with improvements of 3.85 points on the Epworth Sleepiness Scale (ESS) score, compared with placebo.
“We found that solriamfetol is almost twice as effective as modafinil-armodafinil – the cheaper, older option – in improving the ESS score and much more effective at improving the Maintenance of Wakefulness Test (MWT),” study author Tyler Pitre, MD, an internal medicine physician at McMaster University, Hamilton, Ont., said in an interview.
The findings were published online in Annals of Internal Medicine.
High-certainty evidence
The analysis included 3,085 adults with excessive daytime sleepiness (EDS) who were receiving or were eligible for conventional OSA treatment such as positive airway pressure. Participants were randomly assigned to either placebo or any EDS pharmacotherapy (armodafinil, modafinil, solriamfetol, or pitolisant). The primary outcomes of the analysis were change in ESS and MWT. Secondary outcomes were drug-related adverse events.
The trials had a median follow-up time of 4 weeks. The meta-analysis showed that solriamfetol improves ESS to a greater extent than placebo (high certainty), armodafinil-modafinil and pitolisant (moderate certainty). Compared with placebo, the mean difference in ESS scores for solriamfetol, armodafinil-modafinil, and pitolisant was –3.85, –2.25, and –2.78, respectively.
The analysis yielded high-certainty evidence that solriamfetol and armodafinil-modafinil improved MWT, compared with placebo. The former was “probably superior,” while pitolisant “may have little to no effect on MWT, compared with placebo,” write the authors. The standardized mean difference in MWT scores, compared with placebo, was 0.90 for solriamfetol and 0.41 for armodafinil-modafinil. “Solriamfetol is probably superior to armodafinil-modafinil in improving MWT (SMD, 0.49),” say the authors.
Compared with placebo, armodafinil-modafinil probably increases the risk for discontinuation due to adverse events (relative risk, 2.01), and solriamfetol may increase the risk for discontinuation (RR, 2.04), according to the authors. Pitolisant “may have little to no effect on drug discontinuations due to adverse events,” write the authors.
Although solriamfetol may have led to more discontinuations than armodafinil-modafinil, “we did not find convincing evidence of serious adverse events, albeit with very short-term follow-up,” they add.
The most common side effects for all interventions were headaches, insomnia, and anxiety. Headaches were most likely with armodafinil-modafinil (RR, 1.87), and insomnia was most likely with pitolisant (RR, 7.25).
“Although solriamfetol appears most effective, comorbid hypertension and costs may be barriers to its use,” say the researchers. “Furthermore, there are potentially effective candidate therapies such as methylphenidate, atomoxetine, or caffeine, which have not been examined in randomized clinical trials.”
Although EDS is reported in 40%-58% of patients with OSA and can persist in 6%-18% despite PAP therapy, most non-sleep specialists may not be aware of pharmacologic options, said Dr. Pitre. “I have not seen a study that looks at the prescribing habits of physicians for this condition, but I suspect that primary care physicians are not prescribing modafinil-armodafinil frequently for this and less so for solriamfetol,” he said. “I hope this paper builds awareness of this condition and also informs clinicians on the options available to patients, as well as common side effects to counsel them on before starting treatment.”
Dr. Pitre was surprised at the magnitude of solriamfetol’s superiority to modafinil-armodafinil but cautioned that solriamfetol has been shown to increase blood pressure in higher doses. It therefore must be prescribed carefully, “especially to a population of patients who often have comorbid hypertension,” he said.
Some limitations of the analysis were that all trials were conducted in high-income countries (most commonly the United States). Moreover, 77% of participants were White, and 71% were male.
Beneficial adjunctive therapy
Commenting on the findings, Sogol Javaheri, MD, MPH, who was not involved in the research, said that they confirm those of prior studies and are “consistent with what my colleagues and I experience in our clinical practices.”
Dr. Javaheri is associate program director of the sleep medicine fellowship at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, both in Boston.
While sleep medicine specialists are more likely than others to prescribe these medications, “any clinician may use these medications, ideally if they have ruled out other potential reversible causes of EDS,” said Dr. Javaheri. “The medications do not treat the underlying cause, which is why it’s important to use them as an adjunct to conventional therapy that actually treats the underlying sleep disorder and to rule out additional potential causes of sleepiness that are treatable.”
These potential causes might include insufficient sleep (less than 7 hours per night), untreated anemia, and incompletely treated sleep disorders, she explained. In sleep medicine, modafinil is usually the treatment of choice because of its lower cost, but it may reduce the efficacy of hormonal contraception. Solriamfetol, however, does not. “Additionally, I look forward to validation of pitolisant for treatment of EDS in OSA patients, as it is not a controlled substance and may benefit patients with a history of substance abuse or who may be at higher risk of addiction,” said Dr. Javaheri.
The study was conducted without outside funding. Dr. Pitre and Dr. Javaheri report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Solriamfetol who have residual daytime sleepiness after conventional treatment, according to a systematic review and meta-analysis.
In a systematic review of 14 trials that included more than 3,000 patients, solriamfetol was associated with improvements of 3.85 points on the Epworth Sleepiness Scale (ESS) score, compared with placebo.
“We found that solriamfetol is almost twice as effective as modafinil-armodafinil – the cheaper, older option – in improving the ESS score and much more effective at improving the Maintenance of Wakefulness Test (MWT),” study author Tyler Pitre, MD, an internal medicine physician at McMaster University, Hamilton, Ont., said in an interview.
The findings were published online in Annals of Internal Medicine.
High-certainty evidence
The analysis included 3,085 adults with excessive daytime sleepiness (EDS) who were receiving or were eligible for conventional OSA treatment such as positive airway pressure. Participants were randomly assigned to either placebo or any EDS pharmacotherapy (armodafinil, modafinil, solriamfetol, or pitolisant). The primary outcomes of the analysis were change in ESS and MWT. Secondary outcomes were drug-related adverse events.
The trials had a median follow-up time of 4 weeks. The meta-analysis showed that solriamfetol improves ESS to a greater extent than placebo (high certainty), armodafinil-modafinil and pitolisant (moderate certainty). Compared with placebo, the mean difference in ESS scores for solriamfetol, armodafinil-modafinil, and pitolisant was –3.85, –2.25, and –2.78, respectively.
The analysis yielded high-certainty evidence that solriamfetol and armodafinil-modafinil improved MWT, compared with placebo. The former was “probably superior,” while pitolisant “may have little to no effect on MWT, compared with placebo,” write the authors. The standardized mean difference in MWT scores, compared with placebo, was 0.90 for solriamfetol and 0.41 for armodafinil-modafinil. “Solriamfetol is probably superior to armodafinil-modafinil in improving MWT (SMD, 0.49),” say the authors.
Compared with placebo, armodafinil-modafinil probably increases the risk for discontinuation due to adverse events (relative risk, 2.01), and solriamfetol may increase the risk for discontinuation (RR, 2.04), according to the authors. Pitolisant “may have little to no effect on drug discontinuations due to adverse events,” write the authors.
Although solriamfetol may have led to more discontinuations than armodafinil-modafinil, “we did not find convincing evidence of serious adverse events, albeit with very short-term follow-up,” they add.
The most common side effects for all interventions were headaches, insomnia, and anxiety. Headaches were most likely with armodafinil-modafinil (RR, 1.87), and insomnia was most likely with pitolisant (RR, 7.25).
“Although solriamfetol appears most effective, comorbid hypertension and costs may be barriers to its use,” say the researchers. “Furthermore, there are potentially effective candidate therapies such as methylphenidate, atomoxetine, or caffeine, which have not been examined in randomized clinical trials.”
Although EDS is reported in 40%-58% of patients with OSA and can persist in 6%-18% despite PAP therapy, most non-sleep specialists may not be aware of pharmacologic options, said Dr. Pitre. “I have not seen a study that looks at the prescribing habits of physicians for this condition, but I suspect that primary care physicians are not prescribing modafinil-armodafinil frequently for this and less so for solriamfetol,” he said. “I hope this paper builds awareness of this condition and also informs clinicians on the options available to patients, as well as common side effects to counsel them on before starting treatment.”
Dr. Pitre was surprised at the magnitude of solriamfetol’s superiority to modafinil-armodafinil but cautioned that solriamfetol has been shown to increase blood pressure in higher doses. It therefore must be prescribed carefully, “especially to a population of patients who often have comorbid hypertension,” he said.
Some limitations of the analysis were that all trials were conducted in high-income countries (most commonly the United States). Moreover, 77% of participants were White, and 71% were male.
Beneficial adjunctive therapy
Commenting on the findings, Sogol Javaheri, MD, MPH, who was not involved in the research, said that they confirm those of prior studies and are “consistent with what my colleagues and I experience in our clinical practices.”
Dr. Javaheri is associate program director of the sleep medicine fellowship at Brigham and Women’s Hospital and assistant professor of medicine at Harvard Medical School, both in Boston.
While sleep medicine specialists are more likely than others to prescribe these medications, “any clinician may use these medications, ideally if they have ruled out other potential reversible causes of EDS,” said Dr. Javaheri. “The medications do not treat the underlying cause, which is why it’s important to use them as an adjunct to conventional therapy that actually treats the underlying sleep disorder and to rule out additional potential causes of sleepiness that are treatable.”
These potential causes might include insufficient sleep (less than 7 hours per night), untreated anemia, and incompletely treated sleep disorders, she explained. In sleep medicine, modafinil is usually the treatment of choice because of its lower cost, but it may reduce the efficacy of hormonal contraception. Solriamfetol, however, does not. “Additionally, I look forward to validation of pitolisant for treatment of EDS in OSA patients, as it is not a controlled substance and may benefit patients with a history of substance abuse or who may be at higher risk of addiction,” said Dr. Javaheri.
The study was conducted without outside funding. Dr. Pitre and Dr. Javaheri report no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
AI at the office: Are clinicians prepared?
AURORA, COLO. – Artificial Intelligence has arrived at medical offices, whether or not clinicians feel ready for it.
AI might result in more accurate, efficient, and cost-effective care. But it’s possible it could cause harm. That’s according to Benjamin Collins, MD, at Vanderbilt University Medical Center, Nashville, Tenn., who spoke on the subject at the annual meeting of the Society of General Internal Medicine.
Understanding the nuances of AI is even more important because of the quick development of the algorithms.
“When I submitted this workshop, there was no ChatGPT,” said Dr. Collins, referring to Chat Generative Pre-trained Transformer, a recently released natural language processing model. “A lot has already changed.”
Biased data
Biased data are perhaps the biggest pitfall of AI algorithms, Dr. Collins said. If garbage data go in, garbage predictions come out.
If the dataset that trains the algorithm underrepresents a particular gender or ethnic group, for example, the algorithm may not respond accurately to prompts. When an AI tool compounds existing inequalities related to socioeconomic status, ethnicity, or sexual orientation, the algorithm is biased, according to Harvard researchers.
“People often assume that artificial intelligence is free of bias due to the use of scientific processes and its development,” he said. “But whatever flaws exist in data collection and old data can lead to poor representation or underrepresentation in the data used to train the AI tool.”
Racial minorities are underrepresented in studies; therefore, data input into an AI tool might skew results for these patients.
The Framingham Heart Study, for example, which began in 1948, examined heart disease in mainly White participants. The findings from the study resulted in the creation of a sex-specific algorithm that was used to estimate the 10-year cardiovascular risk of a patient. While the cardiovascular risk score was accurate for White persons, it was less accurate for Black patients.
A study published in Science in 2019 revealed bias in an algorithm that used health care costs as a proxy for health needs. Because less money was spent on Black patients who had the same level of need as their White counterparts, the output inaccurately showed that Black patients were healthier and thus did not require extra care.
Developers can also be a source of bias, inasmuch as AI often reflects preexisting human biases, Dr. Collins said.
“Algorithmic bias presents a clear risk of harm that clinicians must play against the benefits of using AI,” Dr. Collins said. “That risk of harm is often disproportionately distributed to marginalized populations.”
As clinicians use AI algorithms to diagnose and detect disease, predict outcomes, and guide treatment, trouble comes when those algorithms perform well for some patients and poorly for others. This gap can exacerbate existing disparities in health care outcomes.
Dr. Collins advised clinicians to push to find out what data were used to train AI algorithms to determine how bias could have influenced the model and whether the developers risk-adjusted for bias. If the training data are not available, clinicians should ask their employers and AI developers to know more about the system.
Clinicians may face the so-called black box phenomenon, which occurs when developers cannot or will not explain what data went into an AI model, Dr. Collins said.
According to Stanford (Calif.) University, AI must be trained on large datasets of images that have been annotated by human experts. Those datasets can cost millions of dollars to create, meaning corporations often fund them and do not always share the data publicly.
Some groups, such as Stanford’s Center for Artificial Intelligence in Medicine and Imaging, are working to acquire annotated datasets so researchers who train AI models can know where the data came from.
Paul Haidet, MD, MPH, an internist at Penn State College of Medicine, Hershey, sees the technology as a tool that requires careful handling.
“It takes a while to learn how to use a stethoscope, and AI is like that,” Dr. Haidet said. “The thing about AI, though, is that it can be just dropped into a system and no one knows how it works.”
Dr. Haidet said he likes knowing how the sausage is made, something AI developers are often reticent to make known.
“If you’re just putting blind faith in a tool, that’s scary,” Dr. Haidet said.
Transparency and ‘explainability’
The ability to explain what goes into tools is essential to maintaining trust in the health care system, Dr. Collins said.
“Part of knowing how much trust to place in the system is the transparency of those systems and the ability to audit how well the algorithm is performing,” Dr. Collins said. “The system should also regularly report to users the level of certainty with which it is providing an output rather than providing a simple binary output.”
Dr. Collins recommends that providers develop an understanding of the limits of AI regulations as well, which might including learning how the system was approved and how it is monitored.
“The FDA has oversight over some applications of AI and health care for software as a medical device, but there’s currently no dedicated process to evaluate the systems for the presence of bias,” Dr. Collins said. “The gaps in regulation leave the door open for the use of AI in clinical care that contain significant biases.”
Dr. Haidet likened AI tools to the Global Positioning System: A good GPS system will let users see alternate routes, opt out of toll roads or highways, and will highlight why routes have changed. But users need to understand how to read the map so they can tell when something seems amiss.
Dr. Collins and Dr. Haidet report no relevant financial relationships
A version of this article first appeared on Medscape.com.
AURORA, COLO. – Artificial Intelligence has arrived at medical offices, whether or not clinicians feel ready for it.
AI might result in more accurate, efficient, and cost-effective care. But it’s possible it could cause harm. That’s according to Benjamin Collins, MD, at Vanderbilt University Medical Center, Nashville, Tenn., who spoke on the subject at the annual meeting of the Society of General Internal Medicine.
Understanding the nuances of AI is even more important because of the quick development of the algorithms.
“When I submitted this workshop, there was no ChatGPT,” said Dr. Collins, referring to Chat Generative Pre-trained Transformer, a recently released natural language processing model. “A lot has already changed.”
Biased data
Biased data are perhaps the biggest pitfall of AI algorithms, Dr. Collins said. If garbage data go in, garbage predictions come out.
If the dataset that trains the algorithm underrepresents a particular gender or ethnic group, for example, the algorithm may not respond accurately to prompts. When an AI tool compounds existing inequalities related to socioeconomic status, ethnicity, or sexual orientation, the algorithm is biased, according to Harvard researchers.
“People often assume that artificial intelligence is free of bias due to the use of scientific processes and its development,” he said. “But whatever flaws exist in data collection and old data can lead to poor representation or underrepresentation in the data used to train the AI tool.”
Racial minorities are underrepresented in studies; therefore, data input into an AI tool might skew results for these patients.
The Framingham Heart Study, for example, which began in 1948, examined heart disease in mainly White participants. The findings from the study resulted in the creation of a sex-specific algorithm that was used to estimate the 10-year cardiovascular risk of a patient. While the cardiovascular risk score was accurate for White persons, it was less accurate for Black patients.
A study published in Science in 2019 revealed bias in an algorithm that used health care costs as a proxy for health needs. Because less money was spent on Black patients who had the same level of need as their White counterparts, the output inaccurately showed that Black patients were healthier and thus did not require extra care.
Developers can also be a source of bias, inasmuch as AI often reflects preexisting human biases, Dr. Collins said.
“Algorithmic bias presents a clear risk of harm that clinicians must play against the benefits of using AI,” Dr. Collins said. “That risk of harm is often disproportionately distributed to marginalized populations.”
As clinicians use AI algorithms to diagnose and detect disease, predict outcomes, and guide treatment, trouble comes when those algorithms perform well for some patients and poorly for others. This gap can exacerbate existing disparities in health care outcomes.
Dr. Collins advised clinicians to push to find out what data were used to train AI algorithms to determine how bias could have influenced the model and whether the developers risk-adjusted for bias. If the training data are not available, clinicians should ask their employers and AI developers to know more about the system.
Clinicians may face the so-called black box phenomenon, which occurs when developers cannot or will not explain what data went into an AI model, Dr. Collins said.
According to Stanford (Calif.) University, AI must be trained on large datasets of images that have been annotated by human experts. Those datasets can cost millions of dollars to create, meaning corporations often fund them and do not always share the data publicly.
Some groups, such as Stanford’s Center for Artificial Intelligence in Medicine and Imaging, are working to acquire annotated datasets so researchers who train AI models can know where the data came from.
Paul Haidet, MD, MPH, an internist at Penn State College of Medicine, Hershey, sees the technology as a tool that requires careful handling.
“It takes a while to learn how to use a stethoscope, and AI is like that,” Dr. Haidet said. “The thing about AI, though, is that it can be just dropped into a system and no one knows how it works.”
Dr. Haidet said he likes knowing how the sausage is made, something AI developers are often reticent to make known.
“If you’re just putting blind faith in a tool, that’s scary,” Dr. Haidet said.
Transparency and ‘explainability’
The ability to explain what goes into tools is essential to maintaining trust in the health care system, Dr. Collins said.
“Part of knowing how much trust to place in the system is the transparency of those systems and the ability to audit how well the algorithm is performing,” Dr. Collins said. “The system should also regularly report to users the level of certainty with which it is providing an output rather than providing a simple binary output.”
Dr. Collins recommends that providers develop an understanding of the limits of AI regulations as well, which might including learning how the system was approved and how it is monitored.
“The FDA has oversight over some applications of AI and health care for software as a medical device, but there’s currently no dedicated process to evaluate the systems for the presence of bias,” Dr. Collins said. “The gaps in regulation leave the door open for the use of AI in clinical care that contain significant biases.”
Dr. Haidet likened AI tools to the Global Positioning System: A good GPS system will let users see alternate routes, opt out of toll roads or highways, and will highlight why routes have changed. But users need to understand how to read the map so they can tell when something seems amiss.
Dr. Collins and Dr. Haidet report no relevant financial relationships
A version of this article first appeared on Medscape.com.
AURORA, COLO. – Artificial Intelligence has arrived at medical offices, whether or not clinicians feel ready for it.
AI might result in more accurate, efficient, and cost-effective care. But it’s possible it could cause harm. That’s according to Benjamin Collins, MD, at Vanderbilt University Medical Center, Nashville, Tenn., who spoke on the subject at the annual meeting of the Society of General Internal Medicine.
Understanding the nuances of AI is even more important because of the quick development of the algorithms.
“When I submitted this workshop, there was no ChatGPT,” said Dr. Collins, referring to Chat Generative Pre-trained Transformer, a recently released natural language processing model. “A lot has already changed.”
Biased data
Biased data are perhaps the biggest pitfall of AI algorithms, Dr. Collins said. If garbage data go in, garbage predictions come out.
If the dataset that trains the algorithm underrepresents a particular gender or ethnic group, for example, the algorithm may not respond accurately to prompts. When an AI tool compounds existing inequalities related to socioeconomic status, ethnicity, or sexual orientation, the algorithm is biased, according to Harvard researchers.
“People often assume that artificial intelligence is free of bias due to the use of scientific processes and its development,” he said. “But whatever flaws exist in data collection and old data can lead to poor representation or underrepresentation in the data used to train the AI tool.”
Racial minorities are underrepresented in studies; therefore, data input into an AI tool might skew results for these patients.
The Framingham Heart Study, for example, which began in 1948, examined heart disease in mainly White participants. The findings from the study resulted in the creation of a sex-specific algorithm that was used to estimate the 10-year cardiovascular risk of a patient. While the cardiovascular risk score was accurate for White persons, it was less accurate for Black patients.
A study published in Science in 2019 revealed bias in an algorithm that used health care costs as a proxy for health needs. Because less money was spent on Black patients who had the same level of need as their White counterparts, the output inaccurately showed that Black patients were healthier and thus did not require extra care.
Developers can also be a source of bias, inasmuch as AI often reflects preexisting human biases, Dr. Collins said.
“Algorithmic bias presents a clear risk of harm that clinicians must play against the benefits of using AI,” Dr. Collins said. “That risk of harm is often disproportionately distributed to marginalized populations.”
As clinicians use AI algorithms to diagnose and detect disease, predict outcomes, and guide treatment, trouble comes when those algorithms perform well for some patients and poorly for others. This gap can exacerbate existing disparities in health care outcomes.
Dr. Collins advised clinicians to push to find out what data were used to train AI algorithms to determine how bias could have influenced the model and whether the developers risk-adjusted for bias. If the training data are not available, clinicians should ask their employers and AI developers to know more about the system.
Clinicians may face the so-called black box phenomenon, which occurs when developers cannot or will not explain what data went into an AI model, Dr. Collins said.
According to Stanford (Calif.) University, AI must be trained on large datasets of images that have been annotated by human experts. Those datasets can cost millions of dollars to create, meaning corporations often fund them and do not always share the data publicly.
Some groups, such as Stanford’s Center for Artificial Intelligence in Medicine and Imaging, are working to acquire annotated datasets so researchers who train AI models can know where the data came from.
Paul Haidet, MD, MPH, an internist at Penn State College of Medicine, Hershey, sees the technology as a tool that requires careful handling.
“It takes a while to learn how to use a stethoscope, and AI is like that,” Dr. Haidet said. “The thing about AI, though, is that it can be just dropped into a system and no one knows how it works.”
Dr. Haidet said he likes knowing how the sausage is made, something AI developers are often reticent to make known.
“If you’re just putting blind faith in a tool, that’s scary,” Dr. Haidet said.
Transparency and ‘explainability’
The ability to explain what goes into tools is essential to maintaining trust in the health care system, Dr. Collins said.
“Part of knowing how much trust to place in the system is the transparency of those systems and the ability to audit how well the algorithm is performing,” Dr. Collins said. “The system should also regularly report to users the level of certainty with which it is providing an output rather than providing a simple binary output.”
Dr. Collins recommends that providers develop an understanding of the limits of AI regulations as well, which might including learning how the system was approved and how it is monitored.
“The FDA has oversight over some applications of AI and health care for software as a medical device, but there’s currently no dedicated process to evaluate the systems for the presence of bias,” Dr. Collins said. “The gaps in regulation leave the door open for the use of AI in clinical care that contain significant biases.”
Dr. Haidet likened AI tools to the Global Positioning System: A good GPS system will let users see alternate routes, opt out of toll roads or highways, and will highlight why routes have changed. But users need to understand how to read the map so they can tell when something seems amiss.
Dr. Collins and Dr. Haidet report no relevant financial relationships
A version of this article first appeared on Medscape.com.
AT SGIM 2023
Review supports continued mask-wearing in health care visits
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
The study said one reason people should wear masks to medical settings is because “health care personnel are notorious for coming to work while ill.” Transmission from patient to staff and staff to patient is still possible, but rare, when both are masked.
The review authors reported no conflicts of interest. Dr. Palmore has received grants from the NIH, Rigel, Gilead, and AbbVie, and Dr. Henderson is a past president of the Society for Healthcare Epidemiology of America.
A version of this article first appeared on WebMD.com.
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
The study said one reason people should wear masks to medical settings is because “health care personnel are notorious for coming to work while ill.” Transmission from patient to staff and staff to patient is still possible, but rare, when both are masked.
The review authors reported no conflicts of interest. Dr. Palmore has received grants from the NIH, Rigel, Gilead, and AbbVie, and Dr. Henderson is a past president of the Society for Healthcare Epidemiology of America.
A version of this article first appeared on WebMD.com.
A new study urges people to continue wearing protective masks in medical settings, even though the U.S. public health emergency declaration around COVID-19 has expired.
Masks continue to lower the risk of catching the virus during medical visits, according to the study, published in Annals of Internal Medicine. And there was not much difference between wearing surgical masks and N95 respirators in health care settings.
The researchers reviewed 3 randomized trials and 21 observational studies to compare the effectiveness of those and cloth masks in reducing COVID-19 transmission.
Tara N. Palmore, MD, of George Washington University, Washington, and David K. Henderson, MD, of the National Institutes of Health, Bethesda, Md., wrote in an opinion article accompanying the study.
“In our enthusiasm to return to the appearance and feeling of normalcy, and as institutions decide which mitigation strategies to discontinue, we strongly advocate not discarding this important lesson learned for the sake of our patients’ safety,” Dr. Palmore and Dr. Henderson wrote.
Surgical masks limit the spread of aerosols and droplets from people who have the flu, coronaviruses or other respiratory viruses, CNN reported. And while masks are not 100% effective, they substantially lower the amount of virus put into the air via coughing and talking.
The study said one reason people should wear masks to medical settings is because “health care personnel are notorious for coming to work while ill.” Transmission from patient to staff and staff to patient is still possible, but rare, when both are masked.
The review authors reported no conflicts of interest. Dr. Palmore has received grants from the NIH, Rigel, Gilead, and AbbVie, and Dr. Henderson is a past president of the Society for Healthcare Epidemiology of America.
A version of this article first appeared on WebMD.com.
FROM ANNALS OF INTERNAL MEDICINE
COVID emergency over, but hundreds are still dying weekly
Traci Sikes’s older sister Debbie had survived several health setbacks in life – a heart attack, a cancer diagnosis, and a couple of botched surgeries for a bad back. But by early 2023, the 68-year-old from Brownwood, Tex., was in remission from lymphoma, feeling stronger, and celebrating a birthday for one of her 11 beloved grandchildren.
Then Debbie caught COVID-19. Less than 2 months later, in March, she died of severe lung damage caused by the coronavirus.
Traci was able to make the trip from her home in Washington state to Texas to be with Debbie before she died. She was grateful that she arrived while her sister was still lucid and to hear her sister’s last word – “love” – spoken to one of her grandchildren before she took her final breath.
“My sister was wonderful,” Sikes said. “And she shouldn’t be gone.”
Just 6 months after President Joe Biden declared last fall that “the pandemic is over,” Just as both the World Health Organization and U.S. government recently ended the 3-year-old coronavirus public health emergency, COVID is still killing more than 100 people every day in the U.S., according to the CDC, and amid widespread efforts to move on and drop protective measures, the country’s most vulnerable people are still at significant risk.
The prevailing attitude that we need to learn to live with the current level of risk feels like a “slap in the face,” for COVID grievers who have already paid the price,” said Sabila Khan, who cofounded a Facebook group for COVID loss support, which now has more than 14,000 members.
It also minimizes the continuing loss of life and that so many people are still dying traumatic and unnecessary deaths, she said.
“It feels like it’s been brushed aside,” she said. “Like, ‘It’s business as usual. It’s over. Take off your mask.’ My family and I are still masked, and we’re probably the only ones masked in any given room.”
The abandoning of protective measures also fails to recognize the ongoing and catastrophic risks of long COVID and the experiences of an estimated 26 million people in the U.S. living with long COVID.
“It’s been drummed into us that death is the only serious outcome [of the virus] and we still haven’t made enough space for the idea that long COVID is a very serious outcome,” said David Putrino, PhD, director of rehabilitation innovation for the Mount Sinai Health System in New York, who has helped care for thousands of patients with long COVID.
Historic drop in life expectancy
More than 1.1 million Americans have died from COVID over the past 3 years, and experts say the official numbers are likely underestimated because of errors in death certificate reporting. Although deaths have waned from earlier in the pandemic, the disease has become the fourth leading cause of death in the United States after heart disease, cancer, and “unintentional injury” such as drug overdoses.
What makes these deaths all the more tragic is that COVID is a preventable disease, said Carla Sevin, MD, a critical care doctor and director of the Pulmonary Patient Care Center at Vanderbilt University Medical Center in Nashville, Tenn. Masking, available vaccines, and social distancing have all been shown to significantly lower the risk of spreading and catching the virus. New drugs have also made it possible for infected people to survive COVID.
“It’s possible to not spread COVID,” she said. “It’s possible to protect yourself against COVID. It’s possible to treat COVID. And we’re doing all of those things imperfectly.”
By the end of 2021, Americans overall were dying 3 years sooner, on average, than they were before the pandemic, with life expectancy dropping from 79 years to 76 years, the largest decline in a century.
Globally, the COVID death toll is nearing 7 million. Across all ages, on average, each person who died passed away 10 years younger than they otherwise would have. That’s tens of millions of years wiped away.
As U.S. surgeon and health researcher Atul Gawande, MD, put it in a New York Times essay about the pandemic response: “Human development has been pushed into reverse.”
What is an acceptable threshold of death?
In the United States, more than 80% of deaths from the disease have been in people age 65 and older. Underlying medical conditions and disabilities also raise the risk of severe illness and dying from COVID.
The virus is also disproportionately killing Black, Hispanic, and Indigenous people and those with less access to health care. Racialized groups are dying from COVID at younger ages. COVID advocates and Americans who’ve lost loved ones to the disease say our willingness to accept these facts and the current mortality rate amounts to health-based discrimination.
“Would politicians be approaching this differently had it mostly affected rich white people?” Ms. Khan said.
Ms. Khan’s dad, Shafqat, was an advocate and community organizer for Pakistani immigrants. After contracting COVID, he was rushed to a hospital near his daughter’s Jersey City, N.J., home from a rehab facility where he was being treated for an aggressive form of Parkinson’s disease. For the 8 days her father was in the hospital, she and other family members couldn’t visit him, and he wasn’t even well enough to talk on the phone. He died from COVID in April 2020.
“My father was an extraordinary person who did so much good and he died alone, terrified in a hospital,” she said. “I can’t even wrap my head around that and how he deserved more. No one deserves that.”
At Vanderbilt University Medical Center, where she works as a critical care doctor, COVID deaths are now different from those in the early days of the pandemic, Dr. Sevin said. Most patients now in the intensive care unit are older and immunocompromised – and they tend to blend in more with others in the intensive care unit. That makes the impact of COVID even more hidden and easily ignored.
“It’s easy not to value somebody who’s an invisible number you don’t know,” she said. “You don’t see them writing their will and talking to their best friend. You don’t see the tears rolling down their face because they know what’s going to happen to them and they’re going to asphyxiate to death.”
One COVID patient who died recently in Dr. Sevin’s ICU ward was an older woman who had no living relatives. “She was very, very lonely, and we would always stand outside the door on rounds, and she would motion for us to come in, but we had to then all gown up,” Dr. Sevin said. “It just breaks your heart that people are still having to go through it.”
Dr. Sevin finds it frustrating that so many of the measures that public health officials fought so hard for over the last 3 years – including masking guidelines, government-funded vaccine clinics, and access to potentially life-saving antiviral medications – are now going away because of the lifting of the pandemic emergency declaration.
What makes matters worse, she said, is that public consciousness about taking precautions to protect others is starting to disappear in favor of an “all or nothing attitude” about the continued risks.
“Like either I’m going to stay home and be a hermit, or I’m going to just throw caution to the wind and go to bars and let people yell in my face,” she said. “We learned some hard lessons, and I wish we could hold onto those.”
Americans like Traci Sikes who’ve lost loved ones and health care workers on the front lines say it is particularly frustrating that so many people are framing the current response to the risks of COVID as “personal choice” over responsibility to others, as well as a sense of fatalism and lack of urgent care.
“Why does nobody seem to be angry about this?” Ms. Sikes said. “People talk about COVID like it’s just another thing to die from. But my sister didn’t have to die from it at all.”
A version of this article first appeared on WebMD.com.
Traci Sikes’s older sister Debbie had survived several health setbacks in life – a heart attack, a cancer diagnosis, and a couple of botched surgeries for a bad back. But by early 2023, the 68-year-old from Brownwood, Tex., was in remission from lymphoma, feeling stronger, and celebrating a birthday for one of her 11 beloved grandchildren.
Then Debbie caught COVID-19. Less than 2 months later, in March, she died of severe lung damage caused by the coronavirus.
Traci was able to make the trip from her home in Washington state to Texas to be with Debbie before she died. She was grateful that she arrived while her sister was still lucid and to hear her sister’s last word – “love” – spoken to one of her grandchildren before she took her final breath.
“My sister was wonderful,” Sikes said. “And she shouldn’t be gone.”
Just 6 months after President Joe Biden declared last fall that “the pandemic is over,” Just as both the World Health Organization and U.S. government recently ended the 3-year-old coronavirus public health emergency, COVID is still killing more than 100 people every day in the U.S., according to the CDC, and amid widespread efforts to move on and drop protective measures, the country’s most vulnerable people are still at significant risk.
The prevailing attitude that we need to learn to live with the current level of risk feels like a “slap in the face,” for COVID grievers who have already paid the price,” said Sabila Khan, who cofounded a Facebook group for COVID loss support, which now has more than 14,000 members.
It also minimizes the continuing loss of life and that so many people are still dying traumatic and unnecessary deaths, she said.
“It feels like it’s been brushed aside,” she said. “Like, ‘It’s business as usual. It’s over. Take off your mask.’ My family and I are still masked, and we’re probably the only ones masked in any given room.”
The abandoning of protective measures also fails to recognize the ongoing and catastrophic risks of long COVID and the experiences of an estimated 26 million people in the U.S. living with long COVID.
“It’s been drummed into us that death is the only serious outcome [of the virus] and we still haven’t made enough space for the idea that long COVID is a very serious outcome,” said David Putrino, PhD, director of rehabilitation innovation for the Mount Sinai Health System in New York, who has helped care for thousands of patients with long COVID.
Historic drop in life expectancy
More than 1.1 million Americans have died from COVID over the past 3 years, and experts say the official numbers are likely underestimated because of errors in death certificate reporting. Although deaths have waned from earlier in the pandemic, the disease has become the fourth leading cause of death in the United States after heart disease, cancer, and “unintentional injury” such as drug overdoses.
What makes these deaths all the more tragic is that COVID is a preventable disease, said Carla Sevin, MD, a critical care doctor and director of the Pulmonary Patient Care Center at Vanderbilt University Medical Center in Nashville, Tenn. Masking, available vaccines, and social distancing have all been shown to significantly lower the risk of spreading and catching the virus. New drugs have also made it possible for infected people to survive COVID.
“It’s possible to not spread COVID,” she said. “It’s possible to protect yourself against COVID. It’s possible to treat COVID. And we’re doing all of those things imperfectly.”
By the end of 2021, Americans overall were dying 3 years sooner, on average, than they were before the pandemic, with life expectancy dropping from 79 years to 76 years, the largest decline in a century.
Globally, the COVID death toll is nearing 7 million. Across all ages, on average, each person who died passed away 10 years younger than they otherwise would have. That’s tens of millions of years wiped away.
As U.S. surgeon and health researcher Atul Gawande, MD, put it in a New York Times essay about the pandemic response: “Human development has been pushed into reverse.”
What is an acceptable threshold of death?
In the United States, more than 80% of deaths from the disease have been in people age 65 and older. Underlying medical conditions and disabilities also raise the risk of severe illness and dying from COVID.
The virus is also disproportionately killing Black, Hispanic, and Indigenous people and those with less access to health care. Racialized groups are dying from COVID at younger ages. COVID advocates and Americans who’ve lost loved ones to the disease say our willingness to accept these facts and the current mortality rate amounts to health-based discrimination.
“Would politicians be approaching this differently had it mostly affected rich white people?” Ms. Khan said.
Ms. Khan’s dad, Shafqat, was an advocate and community organizer for Pakistani immigrants. After contracting COVID, he was rushed to a hospital near his daughter’s Jersey City, N.J., home from a rehab facility where he was being treated for an aggressive form of Parkinson’s disease. For the 8 days her father was in the hospital, she and other family members couldn’t visit him, and he wasn’t even well enough to talk on the phone. He died from COVID in April 2020.
“My father was an extraordinary person who did so much good and he died alone, terrified in a hospital,” she said. “I can’t even wrap my head around that and how he deserved more. No one deserves that.”
At Vanderbilt University Medical Center, where she works as a critical care doctor, COVID deaths are now different from those in the early days of the pandemic, Dr. Sevin said. Most patients now in the intensive care unit are older and immunocompromised – and they tend to blend in more with others in the intensive care unit. That makes the impact of COVID even more hidden and easily ignored.
“It’s easy not to value somebody who’s an invisible number you don’t know,” she said. “You don’t see them writing their will and talking to their best friend. You don’t see the tears rolling down their face because they know what’s going to happen to them and they’re going to asphyxiate to death.”
One COVID patient who died recently in Dr. Sevin’s ICU ward was an older woman who had no living relatives. “She was very, very lonely, and we would always stand outside the door on rounds, and she would motion for us to come in, but we had to then all gown up,” Dr. Sevin said. “It just breaks your heart that people are still having to go through it.”
Dr. Sevin finds it frustrating that so many of the measures that public health officials fought so hard for over the last 3 years – including masking guidelines, government-funded vaccine clinics, and access to potentially life-saving antiviral medications – are now going away because of the lifting of the pandemic emergency declaration.
What makes matters worse, she said, is that public consciousness about taking precautions to protect others is starting to disappear in favor of an “all or nothing attitude” about the continued risks.
“Like either I’m going to stay home and be a hermit, or I’m going to just throw caution to the wind and go to bars and let people yell in my face,” she said. “We learned some hard lessons, and I wish we could hold onto those.”
Americans like Traci Sikes who’ve lost loved ones and health care workers on the front lines say it is particularly frustrating that so many people are framing the current response to the risks of COVID as “personal choice” over responsibility to others, as well as a sense of fatalism and lack of urgent care.
“Why does nobody seem to be angry about this?” Ms. Sikes said. “People talk about COVID like it’s just another thing to die from. But my sister didn’t have to die from it at all.”
A version of this article first appeared on WebMD.com.
Traci Sikes’s older sister Debbie had survived several health setbacks in life – a heart attack, a cancer diagnosis, and a couple of botched surgeries for a bad back. But by early 2023, the 68-year-old from Brownwood, Tex., was in remission from lymphoma, feeling stronger, and celebrating a birthday for one of her 11 beloved grandchildren.
Then Debbie caught COVID-19. Less than 2 months later, in March, she died of severe lung damage caused by the coronavirus.
Traci was able to make the trip from her home in Washington state to Texas to be with Debbie before she died. She was grateful that she arrived while her sister was still lucid and to hear her sister’s last word – “love” – spoken to one of her grandchildren before she took her final breath.
“My sister was wonderful,” Sikes said. “And she shouldn’t be gone.”
Just 6 months after President Joe Biden declared last fall that “the pandemic is over,” Just as both the World Health Organization and U.S. government recently ended the 3-year-old coronavirus public health emergency, COVID is still killing more than 100 people every day in the U.S., according to the CDC, and amid widespread efforts to move on and drop protective measures, the country’s most vulnerable people are still at significant risk.
The prevailing attitude that we need to learn to live with the current level of risk feels like a “slap in the face,” for COVID grievers who have already paid the price,” said Sabila Khan, who cofounded a Facebook group for COVID loss support, which now has more than 14,000 members.
It also minimizes the continuing loss of life and that so many people are still dying traumatic and unnecessary deaths, she said.
“It feels like it’s been brushed aside,” she said. “Like, ‘It’s business as usual. It’s over. Take off your mask.’ My family and I are still masked, and we’re probably the only ones masked in any given room.”
The abandoning of protective measures also fails to recognize the ongoing and catastrophic risks of long COVID and the experiences of an estimated 26 million people in the U.S. living with long COVID.
“It’s been drummed into us that death is the only serious outcome [of the virus] and we still haven’t made enough space for the idea that long COVID is a very serious outcome,” said David Putrino, PhD, director of rehabilitation innovation for the Mount Sinai Health System in New York, who has helped care for thousands of patients with long COVID.
Historic drop in life expectancy
More than 1.1 million Americans have died from COVID over the past 3 years, and experts say the official numbers are likely underestimated because of errors in death certificate reporting. Although deaths have waned from earlier in the pandemic, the disease has become the fourth leading cause of death in the United States after heart disease, cancer, and “unintentional injury” such as drug overdoses.
What makes these deaths all the more tragic is that COVID is a preventable disease, said Carla Sevin, MD, a critical care doctor and director of the Pulmonary Patient Care Center at Vanderbilt University Medical Center in Nashville, Tenn. Masking, available vaccines, and social distancing have all been shown to significantly lower the risk of spreading and catching the virus. New drugs have also made it possible for infected people to survive COVID.
“It’s possible to not spread COVID,” she said. “It’s possible to protect yourself against COVID. It’s possible to treat COVID. And we’re doing all of those things imperfectly.”
By the end of 2021, Americans overall were dying 3 years sooner, on average, than they were before the pandemic, with life expectancy dropping from 79 years to 76 years, the largest decline in a century.
Globally, the COVID death toll is nearing 7 million. Across all ages, on average, each person who died passed away 10 years younger than they otherwise would have. That’s tens of millions of years wiped away.
As U.S. surgeon and health researcher Atul Gawande, MD, put it in a New York Times essay about the pandemic response: “Human development has been pushed into reverse.”
What is an acceptable threshold of death?
In the United States, more than 80% of deaths from the disease have been in people age 65 and older. Underlying medical conditions and disabilities also raise the risk of severe illness and dying from COVID.
The virus is also disproportionately killing Black, Hispanic, and Indigenous people and those with less access to health care. Racialized groups are dying from COVID at younger ages. COVID advocates and Americans who’ve lost loved ones to the disease say our willingness to accept these facts and the current mortality rate amounts to health-based discrimination.
“Would politicians be approaching this differently had it mostly affected rich white people?” Ms. Khan said.
Ms. Khan’s dad, Shafqat, was an advocate and community organizer for Pakistani immigrants. After contracting COVID, he was rushed to a hospital near his daughter’s Jersey City, N.J., home from a rehab facility where he was being treated for an aggressive form of Parkinson’s disease. For the 8 days her father was in the hospital, she and other family members couldn’t visit him, and he wasn’t even well enough to talk on the phone. He died from COVID in April 2020.
“My father was an extraordinary person who did so much good and he died alone, terrified in a hospital,” she said. “I can’t even wrap my head around that and how he deserved more. No one deserves that.”
At Vanderbilt University Medical Center, where she works as a critical care doctor, COVID deaths are now different from those in the early days of the pandemic, Dr. Sevin said. Most patients now in the intensive care unit are older and immunocompromised – and they tend to blend in more with others in the intensive care unit. That makes the impact of COVID even more hidden and easily ignored.
“It’s easy not to value somebody who’s an invisible number you don’t know,” she said. “You don’t see them writing their will and talking to their best friend. You don’t see the tears rolling down their face because they know what’s going to happen to them and they’re going to asphyxiate to death.”
One COVID patient who died recently in Dr. Sevin’s ICU ward was an older woman who had no living relatives. “She was very, very lonely, and we would always stand outside the door on rounds, and she would motion for us to come in, but we had to then all gown up,” Dr. Sevin said. “It just breaks your heart that people are still having to go through it.”
Dr. Sevin finds it frustrating that so many of the measures that public health officials fought so hard for over the last 3 years – including masking guidelines, government-funded vaccine clinics, and access to potentially life-saving antiviral medications – are now going away because of the lifting of the pandemic emergency declaration.
What makes matters worse, she said, is that public consciousness about taking precautions to protect others is starting to disappear in favor of an “all or nothing attitude” about the continued risks.
“Like either I’m going to stay home and be a hermit, or I’m going to just throw caution to the wind and go to bars and let people yell in my face,” she said. “We learned some hard lessons, and I wish we could hold onto those.”
Americans like Traci Sikes who’ve lost loved ones and health care workers on the front lines say it is particularly frustrating that so many people are framing the current response to the risks of COVID as “personal choice” over responsibility to others, as well as a sense of fatalism and lack of urgent care.
“Why does nobody seem to be angry about this?” Ms. Sikes said. “People talk about COVID like it’s just another thing to die from. But my sister didn’t have to die from it at all.”
A version of this article first appeared on WebMD.com.
CDC cuts back hospital data reporting on COVID
When the federal government’s public health emergency (PHE) ended on May 11, the Centers for Disease Control and Prevention scaled back the amount of COVID-related data that it had required hospitals to collect and report during the previous 3 years. The CDC had to do this, an agency spokesman said in an interview, because “CDC’s authorizations to collect certain types of public health data” expired with the PHE.
The CDC insists that it will have enough data to keep up with the virus, which repeatedly defied scientists’ expectations during the course of the pandemic. But some experts have doubts about whether this will turn out to be the case.
While the COVID pandemic is subsiding and transitioning to an endemic phase, many things about the coronavirus are still not understood, noted Marisa Eisenberg, PhD, associate professor of epidemiology at the University of Michigan, Ann Arbor.
“COVID is here to stay, and it ebbs and flows but is staying at fairly consistent levels across the country,” she said in an interview. “Meanwhile, we haven’t established a regular seasonality for COVID that we see for most other respiratory illnesses. We’re still seeing pretty rapidly invading new waves of variants. With flu and other respiratory illnesses, you often see a particular variant in each season. There’s an established pattern. For COVID, that’s still shifting.”
Similarly, Sam Scarpino, PhD, a public health expert at Northeastern University, Boston, told the New York Times: “The CDC is shuffling COVID into the deck of infectious diseases that we’re satisfied living with. One thousand deaths a week is just unacceptable.”
William Schaffner, MD, a professor of preventive medicine and health policy at Vanderbilt University Medical Center, Nashville, Tenn., said in an interview that “how we deal with influenza is something of a template or a model for what the CDC is trying to get to with COVID.” It’s not practical for physicians and hospitals to report every flu case, and the same is now true for COVID. However, “we’re still asking for data on people who are hospitalized with COVID to be reported. That will give us a measure of the major public health impact.”
Dr. Eisenberg doesn’t fully subscribe to this notion. “COVID and influenza are both respiratory illnesses, and our initial pandemic response was based on playbooks that we’d built for potential flu pandemics. But COVID is not the flu. We still have to grapple with the fact that it’s killing a lot more people than the flu does. So maybe it’s a template, but not a perfect one.”
What data is being deleted
The CDC is now requiring hospitals to submit COVID-related data weekly, rather than daily, as it previously had. In addition, the agency has cut the number of data elements that hospitals must report from 62 to 44. Among the data fields that are now optional for hospitals to report are the numbers of hospitalized children with suspected or lab-confirmed COVID; hospitalized and ventilated COVID patients; adults in the ICU with suspected or lab-confirmed COVID; adult and pediatric admissions with suspected COVID; COVID-related emergency department visits; and inpatients with hospital-acquired COVID.
Although widely feared by health care workers and the public, hospital-acquired COVID has never been a major factor in the pandemic, Dr. Schaffner said. “So why ask for something that’s actually not so critical? Let’s keep the emphasis on rapid, accurate reporting of people who are hospitalized because of this disease.”
Akin Demehin, senior director for quality and patient safety policy for the American Hospital Association, agreed that the rate of hospital-acquired COVID cases “has been very low throughout the pandemic.” That was one reason why CDC made this measure optional.
Dr. Eisenberg concurred with this view. “We worried about [hospital-acquired COVID] a lot, and then, because people were very careful, it wasn’t as much of a problem as we feared it would be.” But she added a note of caution: “Masking and other [preventive guidelines] are shifting in hospitals, so it will be interesting to see whether that affects things.”
CDC justifies its new policy
To put the hospital data reporting changes in context, it’s important to know that CDC will no longer directly track community levels of COVID and the percentage of tests that come back positive for COVID, which until now were used to measure transmission rates. (Laboratories no longer have to report these test data, whether they are in hospitals or in the community.) To track death rates, CDC will rely on the National Vital Statistics System, which is accurate but lags other kinds of surveillance by 2-3 weeks, according to the New York Times.
In a recent MMWR report, CDC defended its new COVID surveillance system, saying: “Weekly COVID-19 hospital admission levels and the percentage of all COVID-19–associated deaths will be primary surveillance indicators. Emergency department visits and percentage of positive SARS-CoV-2 laboratory test results will help detect early changes in trends. Genomic surveillance will continue to help identify and monitor SARS-CoV-2 variants.”
Clarifying the latter point, CDC said that national genomic surveillance, along with wastewater surveillance, will continue to be used to estimate COVID variant proportions. Dr. Eisenberg stressed the importance of genomic surveillance at the hundreds of sites that CDC now maintains across the country. But currently, many of these sites are only monitoring the level of COVID.
CDC also observed that COVID-19 hospital admission levels have been shown to be “concordant” with community levels of SARS-CoV-2 infection. Therefore, rates of COVID-associated admissions and the percentages of positive test results, COVID ED visits, and COVID deaths are “suitable and timely indicators of trends in COVID-19 activity and severity.”
Ready to shift to voluntary reporting?
In a news release, AHA praised the “streamlining” of CDC requirements for data reporting but said that it hoped that mandatory reporting would be phased out as soon as possible.
The association noted that this would require action by the Centers for Medicare & Medicaid Services. CMS now enforces the CDC requirements with a “condition of participation” (COP) provision, by which noncompliant hospitals could be excluded from Medicare. CMS has extended this COP to April 30, 2024, although it could choose to ask the Secretary of Health and Human Services to terminate it earlier.
If mandatory reporting were repealed, would most hospitals still report on the key COVID metrics? Mr. Demehin noted that before CMS implemented its COP, hospitals reported COVID data voluntarily, “and the participation rate was well over 90%. So setting up a mechanism similar to that is something we’ve encouraged CMS to consider.”
Dr. Eisenberg is skeptical. While bigger hospitals with more resources might continue reporting voluntarily, she said, safety-net hospitals in underserved areas might not, because they are especially short staffed. “Then you have disparities in which hospitals will report.”
Vaccinations: The sleeping dragon
COVID continues to ravage the nation. According to CDC statistics, there were 1,109 deaths from COVID in the U.S. in the week ending May 6, and total deaths have hit 1.13 million. There were 1,333 new COVID-related hospital admissions, and 7,261 people were in the hospital because of COVID.
Another eye-catching number: Only 16.9% of the U.S. population has received an updated COVID vaccine booster. Dr. Schaffner thinks that this is what we should really keep our eye on. While the combination of vaccinations and widespread SARS-CoV-2 infections has conferred herd immunity on most Americans, he said it’s temporary. “Whether your immunity comes from the virus and recovery from disease or from the vaccines, that immunity will wane over time. Unless we keep our vaccination rate up, we may see more future cases. We’ll have to see how that works out. But I’m nervous about that, because people do appear to be nonchalant.”
A version of this article first appeared on Medscape.com.
When the federal government’s public health emergency (PHE) ended on May 11, the Centers for Disease Control and Prevention scaled back the amount of COVID-related data that it had required hospitals to collect and report during the previous 3 years. The CDC had to do this, an agency spokesman said in an interview, because “CDC’s authorizations to collect certain types of public health data” expired with the PHE.
The CDC insists that it will have enough data to keep up with the virus, which repeatedly defied scientists’ expectations during the course of the pandemic. But some experts have doubts about whether this will turn out to be the case.
While the COVID pandemic is subsiding and transitioning to an endemic phase, many things about the coronavirus are still not understood, noted Marisa Eisenberg, PhD, associate professor of epidemiology at the University of Michigan, Ann Arbor.
“COVID is here to stay, and it ebbs and flows but is staying at fairly consistent levels across the country,” she said in an interview. “Meanwhile, we haven’t established a regular seasonality for COVID that we see for most other respiratory illnesses. We’re still seeing pretty rapidly invading new waves of variants. With flu and other respiratory illnesses, you often see a particular variant in each season. There’s an established pattern. For COVID, that’s still shifting.”
Similarly, Sam Scarpino, PhD, a public health expert at Northeastern University, Boston, told the New York Times: “The CDC is shuffling COVID into the deck of infectious diseases that we’re satisfied living with. One thousand deaths a week is just unacceptable.”
William Schaffner, MD, a professor of preventive medicine and health policy at Vanderbilt University Medical Center, Nashville, Tenn., said in an interview that “how we deal with influenza is something of a template or a model for what the CDC is trying to get to with COVID.” It’s not practical for physicians and hospitals to report every flu case, and the same is now true for COVID. However, “we’re still asking for data on people who are hospitalized with COVID to be reported. That will give us a measure of the major public health impact.”
Dr. Eisenberg doesn’t fully subscribe to this notion. “COVID and influenza are both respiratory illnesses, and our initial pandemic response was based on playbooks that we’d built for potential flu pandemics. But COVID is not the flu. We still have to grapple with the fact that it’s killing a lot more people than the flu does. So maybe it’s a template, but not a perfect one.”
What data is being deleted
The CDC is now requiring hospitals to submit COVID-related data weekly, rather than daily, as it previously had. In addition, the agency has cut the number of data elements that hospitals must report from 62 to 44. Among the data fields that are now optional for hospitals to report are the numbers of hospitalized children with suspected or lab-confirmed COVID; hospitalized and ventilated COVID patients; adults in the ICU with suspected or lab-confirmed COVID; adult and pediatric admissions with suspected COVID; COVID-related emergency department visits; and inpatients with hospital-acquired COVID.
Although widely feared by health care workers and the public, hospital-acquired COVID has never been a major factor in the pandemic, Dr. Schaffner said. “So why ask for something that’s actually not so critical? Let’s keep the emphasis on rapid, accurate reporting of people who are hospitalized because of this disease.”
Akin Demehin, senior director for quality and patient safety policy for the American Hospital Association, agreed that the rate of hospital-acquired COVID cases “has been very low throughout the pandemic.” That was one reason why CDC made this measure optional.
Dr. Eisenberg concurred with this view. “We worried about [hospital-acquired COVID] a lot, and then, because people were very careful, it wasn’t as much of a problem as we feared it would be.” But she added a note of caution: “Masking and other [preventive guidelines] are shifting in hospitals, so it will be interesting to see whether that affects things.”
CDC justifies its new policy
To put the hospital data reporting changes in context, it’s important to know that CDC will no longer directly track community levels of COVID and the percentage of tests that come back positive for COVID, which until now were used to measure transmission rates. (Laboratories no longer have to report these test data, whether they are in hospitals or in the community.) To track death rates, CDC will rely on the National Vital Statistics System, which is accurate but lags other kinds of surveillance by 2-3 weeks, according to the New York Times.
In a recent MMWR report, CDC defended its new COVID surveillance system, saying: “Weekly COVID-19 hospital admission levels and the percentage of all COVID-19–associated deaths will be primary surveillance indicators. Emergency department visits and percentage of positive SARS-CoV-2 laboratory test results will help detect early changes in trends. Genomic surveillance will continue to help identify and monitor SARS-CoV-2 variants.”
Clarifying the latter point, CDC said that national genomic surveillance, along with wastewater surveillance, will continue to be used to estimate COVID variant proportions. Dr. Eisenberg stressed the importance of genomic surveillance at the hundreds of sites that CDC now maintains across the country. But currently, many of these sites are only monitoring the level of COVID.
CDC also observed that COVID-19 hospital admission levels have been shown to be “concordant” with community levels of SARS-CoV-2 infection. Therefore, rates of COVID-associated admissions and the percentages of positive test results, COVID ED visits, and COVID deaths are “suitable and timely indicators of trends in COVID-19 activity and severity.”
Ready to shift to voluntary reporting?
In a news release, AHA praised the “streamlining” of CDC requirements for data reporting but said that it hoped that mandatory reporting would be phased out as soon as possible.
The association noted that this would require action by the Centers for Medicare & Medicaid Services. CMS now enforces the CDC requirements with a “condition of participation” (COP) provision, by which noncompliant hospitals could be excluded from Medicare. CMS has extended this COP to April 30, 2024, although it could choose to ask the Secretary of Health and Human Services to terminate it earlier.
If mandatory reporting were repealed, would most hospitals still report on the key COVID metrics? Mr. Demehin noted that before CMS implemented its COP, hospitals reported COVID data voluntarily, “and the participation rate was well over 90%. So setting up a mechanism similar to that is something we’ve encouraged CMS to consider.”
Dr. Eisenberg is skeptical. While bigger hospitals with more resources might continue reporting voluntarily, she said, safety-net hospitals in underserved areas might not, because they are especially short staffed. “Then you have disparities in which hospitals will report.”
Vaccinations: The sleeping dragon
COVID continues to ravage the nation. According to CDC statistics, there were 1,109 deaths from COVID in the U.S. in the week ending May 6, and total deaths have hit 1.13 million. There were 1,333 new COVID-related hospital admissions, and 7,261 people were in the hospital because of COVID.
Another eye-catching number: Only 16.9% of the U.S. population has received an updated COVID vaccine booster. Dr. Schaffner thinks that this is what we should really keep our eye on. While the combination of vaccinations and widespread SARS-CoV-2 infections has conferred herd immunity on most Americans, he said it’s temporary. “Whether your immunity comes from the virus and recovery from disease or from the vaccines, that immunity will wane over time. Unless we keep our vaccination rate up, we may see more future cases. We’ll have to see how that works out. But I’m nervous about that, because people do appear to be nonchalant.”
A version of this article first appeared on Medscape.com.
When the federal government’s public health emergency (PHE) ended on May 11, the Centers for Disease Control and Prevention scaled back the amount of COVID-related data that it had required hospitals to collect and report during the previous 3 years. The CDC had to do this, an agency spokesman said in an interview, because “CDC’s authorizations to collect certain types of public health data” expired with the PHE.
The CDC insists that it will have enough data to keep up with the virus, which repeatedly defied scientists’ expectations during the course of the pandemic. But some experts have doubts about whether this will turn out to be the case.
While the COVID pandemic is subsiding and transitioning to an endemic phase, many things about the coronavirus are still not understood, noted Marisa Eisenberg, PhD, associate professor of epidemiology at the University of Michigan, Ann Arbor.
“COVID is here to stay, and it ebbs and flows but is staying at fairly consistent levels across the country,” she said in an interview. “Meanwhile, we haven’t established a regular seasonality for COVID that we see for most other respiratory illnesses. We’re still seeing pretty rapidly invading new waves of variants. With flu and other respiratory illnesses, you often see a particular variant in each season. There’s an established pattern. For COVID, that’s still shifting.”
Similarly, Sam Scarpino, PhD, a public health expert at Northeastern University, Boston, told the New York Times: “The CDC is shuffling COVID into the deck of infectious diseases that we’re satisfied living with. One thousand deaths a week is just unacceptable.”
William Schaffner, MD, a professor of preventive medicine and health policy at Vanderbilt University Medical Center, Nashville, Tenn., said in an interview that “how we deal with influenza is something of a template or a model for what the CDC is trying to get to with COVID.” It’s not practical for physicians and hospitals to report every flu case, and the same is now true for COVID. However, “we’re still asking for data on people who are hospitalized with COVID to be reported. That will give us a measure of the major public health impact.”
Dr. Eisenberg doesn’t fully subscribe to this notion. “COVID and influenza are both respiratory illnesses, and our initial pandemic response was based on playbooks that we’d built for potential flu pandemics. But COVID is not the flu. We still have to grapple with the fact that it’s killing a lot more people than the flu does. So maybe it’s a template, but not a perfect one.”
What data is being deleted
The CDC is now requiring hospitals to submit COVID-related data weekly, rather than daily, as it previously had. In addition, the agency has cut the number of data elements that hospitals must report from 62 to 44. Among the data fields that are now optional for hospitals to report are the numbers of hospitalized children with suspected or lab-confirmed COVID; hospitalized and ventilated COVID patients; adults in the ICU with suspected or lab-confirmed COVID; adult and pediatric admissions with suspected COVID; COVID-related emergency department visits; and inpatients with hospital-acquired COVID.
Although widely feared by health care workers and the public, hospital-acquired COVID has never been a major factor in the pandemic, Dr. Schaffner said. “So why ask for something that’s actually not so critical? Let’s keep the emphasis on rapid, accurate reporting of people who are hospitalized because of this disease.”
Akin Demehin, senior director for quality and patient safety policy for the American Hospital Association, agreed that the rate of hospital-acquired COVID cases “has been very low throughout the pandemic.” That was one reason why CDC made this measure optional.
Dr. Eisenberg concurred with this view. “We worried about [hospital-acquired COVID] a lot, and then, because people were very careful, it wasn’t as much of a problem as we feared it would be.” But she added a note of caution: “Masking and other [preventive guidelines] are shifting in hospitals, so it will be interesting to see whether that affects things.”
CDC justifies its new policy
To put the hospital data reporting changes in context, it’s important to know that CDC will no longer directly track community levels of COVID and the percentage of tests that come back positive for COVID, which until now were used to measure transmission rates. (Laboratories no longer have to report these test data, whether they are in hospitals or in the community.) To track death rates, CDC will rely on the National Vital Statistics System, which is accurate but lags other kinds of surveillance by 2-3 weeks, according to the New York Times.
In a recent MMWR report, CDC defended its new COVID surveillance system, saying: “Weekly COVID-19 hospital admission levels and the percentage of all COVID-19–associated deaths will be primary surveillance indicators. Emergency department visits and percentage of positive SARS-CoV-2 laboratory test results will help detect early changes in trends. Genomic surveillance will continue to help identify and monitor SARS-CoV-2 variants.”
Clarifying the latter point, CDC said that national genomic surveillance, along with wastewater surveillance, will continue to be used to estimate COVID variant proportions. Dr. Eisenberg stressed the importance of genomic surveillance at the hundreds of sites that CDC now maintains across the country. But currently, many of these sites are only monitoring the level of COVID.
CDC also observed that COVID-19 hospital admission levels have been shown to be “concordant” with community levels of SARS-CoV-2 infection. Therefore, rates of COVID-associated admissions and the percentages of positive test results, COVID ED visits, and COVID deaths are “suitable and timely indicators of trends in COVID-19 activity and severity.”
Ready to shift to voluntary reporting?
In a news release, AHA praised the “streamlining” of CDC requirements for data reporting but said that it hoped that mandatory reporting would be phased out as soon as possible.
The association noted that this would require action by the Centers for Medicare & Medicaid Services. CMS now enforces the CDC requirements with a “condition of participation” (COP) provision, by which noncompliant hospitals could be excluded from Medicare. CMS has extended this COP to April 30, 2024, although it could choose to ask the Secretary of Health and Human Services to terminate it earlier.
If mandatory reporting were repealed, would most hospitals still report on the key COVID metrics? Mr. Demehin noted that before CMS implemented its COP, hospitals reported COVID data voluntarily, “and the participation rate was well over 90%. So setting up a mechanism similar to that is something we’ve encouraged CMS to consider.”
Dr. Eisenberg is skeptical. While bigger hospitals with more resources might continue reporting voluntarily, she said, safety-net hospitals in underserved areas might not, because they are especially short staffed. “Then you have disparities in which hospitals will report.”
Vaccinations: The sleeping dragon
COVID continues to ravage the nation. According to CDC statistics, there were 1,109 deaths from COVID in the U.S. in the week ending May 6, and total deaths have hit 1.13 million. There were 1,333 new COVID-related hospital admissions, and 7,261 people were in the hospital because of COVID.
Another eye-catching number: Only 16.9% of the U.S. population has received an updated COVID vaccine booster. Dr. Schaffner thinks that this is what we should really keep our eye on. While the combination of vaccinations and widespread SARS-CoV-2 infections has conferred herd immunity on most Americans, he said it’s temporary. “Whether your immunity comes from the virus and recovery from disease or from the vaccines, that immunity will wane over time. Unless we keep our vaccination rate up, we may see more future cases. We’ll have to see how that works out. But I’m nervous about that, because people do appear to be nonchalant.”
A version of this article first appeared on Medscape.com.
How providers are adjusting to clinical care post PHE
The first day of seeing patients without a mask was, for Sterling Ransone Jr., MD, “unsettling.”
“I can’t tell you how weird it was the first day that I walked down the hall from my office to where my exam rooms are, to not have a mask on after 3 years of the habit,” said Dr. Ransone, a family physician in Deltaville, Va., and board chair of the American Academy of Family Physicians.
The White House recently lifted the public health emergency order that overhauled the way health care providers operated and advised patients over the past 3 years.
For Dr. Ransone, this transition entails getting used to his bare face, reminding patients of the latest and varying symptoms of the virus, and parting ways with sick patients if they refuse to wear a mask.
As states, hospitals, and health care systems around the country relax their mask mandates for care providers, clinicians will have to fall back on their own policies that patients with potential symptoms mask up.
“Now that it’s up to our offices, we have to have a little bit more backbone,” Dr. Ransone said. “If they’re not willing to follow a health-related policy that will protect the vulnerable, we will not see them. And so for us, it’s been pretty straightforward.”
Despite the policy, Dr. Ransone has cared for patients who don’t disclose they are feeling sick until he enters the room.
“And I wasn’t masked,” Dr. Ransone said. So, “I will wear masks for the rest of the day just to try to protect the rest of my patients in case I was exposed.”
Masks are optional for both patients and staff at the University of Maryland Medical System, but Niharika Khanna, MD, MBBS, said she still wears one with her patients, and her office advises staff to do the same. If patients are experiencing respiratory symptoms, like a cough, they are asked to wear one.
“When the patient first walks up to you, you have no idea what they have,” Dr. Khanna said.
Dr. Khanna is especially mindful of immunocompromised patients who have cancer, and Dr. Ransone cares for several patients who have received kidney transplants and are on potent immunosuppressive drugs.
“I know they’re appreciating our efforts to protect them, and I think the other patients are realizing that it’s a wise thing to do,” Dr. Ransone said.
Some patients have anxiety about the end of masking in doctor offices, but others have been excited about interacting more with their care teams, according to William Dahut, MD, chief scientific officer for the American Cancer Society. Many clinicians will advise their most immunocompromised patients the same as they did prior to the COVID-19 pandemic.
“There’s always been guidelines that oncologists have given to patients who are immunocompromised – we always told them to avoid crowded places, crowded scenes, be outside more than inside,” Dr. Dahut said. “Those general recommendations will continue.”
The AAFP supports masking to limit COVID’s spread, but the “most important thing people can do is to get vaccinated,” Tochi Iroku-Malize, MD, MPH, MBA, president of the AAFP, said.
But the accessibility of vaccinations is also shifting.
Testing shifts
The government will continue to provide free COVID-19 vaccines because it still has supplies on hand. When this stock runs out, commercial insurance providers will be required to cover the immunizations, as they are considered preventive, but people without insurance will have to pay out of pocket.
The AAFP is pushing the Biden administration and Congress to keep the purchase price of those vaccines low enough that clinicians can keep them in stock, according to Dr. Iroku-Malize. Once the federal government transitions COVID-19 vaccines to the commercial market – as early as later in 2023 – it may pose some challenges for providers.
“If the price of the vaccines is too high, physician practices may struggle to make the upfront investment in COVID-19 vaccines,” Dr. Iroku-Malize said. “Patients often prefer to receive vaccine counseling and administration from their usual source of primary care, like their family physician.”
The federal government has also said it still has a supply of treatments for the public to access for free, but has not revealed how much it has on hand or given a timeline for the transition to the private market.
COVID-19 tests, meanwhile, are no longer covered because of the end of the public health emergency, and cost about $45 per kit on average, according to an analysis by the Kaiser Family Foundation.
Pediatrician Lisa Costello, MD, MPH, knows that price point will be a challenge for some families she cares for at West Virginia University Medicine Children’s Hospital in Morgantown. Many still ask her where they can access free tests.
“Testing if you’re a higher risk person is something we need to ensure that people continue to be educated about,” Dr. Costello said.
She’s hopeful that COVID-19 vaccines and treatments such as Paxlovid will stay free in the coming months so patients can continue to easily access them.
Future of telehealth
Relaxed regulations of prescribing controlled substances via telehealth and across state lines allowed clinicians to treat patients near and far during the pandemic. But many providers were worried about a proposal from the Drug Enforcement Administration to clamp down on the prescribing of controlled substances via telehealth, according to A. Mark Fendrick, MD, an internal medicine physician at the University of Michigan, Ann Arbor.
“We were all panicking about what was going to happen to what is for many clinicians a very valuable policy,” Dr. Fendrick said of the telehealth flexibilities introduced during COVID-19.
The DEA, after getting 38,000 comments on their proposed regulations, pulled back on that plan, delaying the cliff until November.
Dr. Fendrick said that telehealth has allowed clinicians to reach patients who have historically faced barriers to care, such as lacking transportation.
“The benefits of that outweigh the potential harms,” he said. “Every policy you make that tightens access because you want to decrease the untoward and unfortunate outcomes will also decrease access to clinical indications.”
The AAFP said it hopes for clear guidance from the DEA in the coming months on what the new telehealth landscape for prescribing will look like.
Medicaid changes
About half of the patients who see Dr. Khanna have insurance through Medicaid.
During the public health emergency, states were not allowed to remove anyone from Medicaid, regardless of whether they no longer qualified for the program or not. But a law passed by Congress last year requires states to once again check Medicaid eligibility. As many as 15 million people could lose their Medicaid coverage.
That could affect the treatments Dr. Khanna recommends for her patients who get kicked off because those who become uninsured or transition to private insurance will have to pay more out of pocket. Maryland will start removals in June.
“When you have an uninsured patient versus Medicaid, it’s a huge difference in what you can ask the patient to do – the medications you can provide, the testing you can provide,” Dr. Khanna said.
States were authorized to remove people from Medicaid as of April 1, with Arkansas, New Hampshire, and South Dakota starting right away. But many states are just now getting the review process going. About a dozen states, including Indiana, Ohio, Utah, and West Virginia, started removing people in May 2023.
Uninsurance rates hit record lows across the United States during the pandemic. Keeping Americans on health insurance is a top priority for the AAFP, Dr. Iroku-Malize said. “We know health care coverage disruptions prevent people from seeking and accessing the care they need.”
Many people who are removed from Medicaid will be eligible for health insurance through employers, or through the Affordable Care Act’s private marketplace. But premiums and deductibles are often higher in these plans, which studies have shown result in patients delaying medical visits and not filling prescriptions or receiving treatment.
Staying mindful
Hospitals that receive federal funds will still have to report COVID-19 test results to the Centers for Medicare & Medicaid Services through 2024, although private labs will no longer be obligated to do so. The Centers for Disease Control and Prevention will also continue to monitor virus levels in communities through wastewater. But some states will no longer collect data.
Gone are the days when clinicians and others would watch for daily totals of case counts with the type of fervor typically reserved for live scoring updates during sports games, according to Dr. Costello.
“We just have to be mindful of the numbers that might be coming in,” Dr. Costello said.
Dr. Ransone, however, cautioned that clinicians not become complacent. In early May, Dr. Ransone saw two patients with conjunctivitis, what patients thought was simply pink eye – a symptom of the latest COVID-19 variant. Both patients told him it wasn’t possible they had COVID-19 because they didn’t have coughs.
“I don’t want to see physician offices fall into that trap that it’s over and be a potential nidus for infection for other patients,” Dr. Ransone said. “It’s incumbent upon us to remind people of the current symptoms so that folks will know when they need to wear a mask when they’re around their grandmother.”
The move away from universal masking in the office has benefits. Many of his older patients have difficulty hearing and had used lip reading to help understand him, he said. During the pandemic, masks got in the way of that form of communication. Now they can see his mouth again and better decipher what he says.
“Being able to have that face-to-face contact, without a mask intervening, has been really beneficial for a lot of my older patients,” he said.
A version of this article first appeared on Medscape.com.
The first day of seeing patients without a mask was, for Sterling Ransone Jr., MD, “unsettling.”
“I can’t tell you how weird it was the first day that I walked down the hall from my office to where my exam rooms are, to not have a mask on after 3 years of the habit,” said Dr. Ransone, a family physician in Deltaville, Va., and board chair of the American Academy of Family Physicians.
The White House recently lifted the public health emergency order that overhauled the way health care providers operated and advised patients over the past 3 years.
For Dr. Ransone, this transition entails getting used to his bare face, reminding patients of the latest and varying symptoms of the virus, and parting ways with sick patients if they refuse to wear a mask.
As states, hospitals, and health care systems around the country relax their mask mandates for care providers, clinicians will have to fall back on their own policies that patients with potential symptoms mask up.
“Now that it’s up to our offices, we have to have a little bit more backbone,” Dr. Ransone said. “If they’re not willing to follow a health-related policy that will protect the vulnerable, we will not see them. And so for us, it’s been pretty straightforward.”
Despite the policy, Dr. Ransone has cared for patients who don’t disclose they are feeling sick until he enters the room.
“And I wasn’t masked,” Dr. Ransone said. So, “I will wear masks for the rest of the day just to try to protect the rest of my patients in case I was exposed.”
Masks are optional for both patients and staff at the University of Maryland Medical System, but Niharika Khanna, MD, MBBS, said she still wears one with her patients, and her office advises staff to do the same. If patients are experiencing respiratory symptoms, like a cough, they are asked to wear one.
“When the patient first walks up to you, you have no idea what they have,” Dr. Khanna said.
Dr. Khanna is especially mindful of immunocompromised patients who have cancer, and Dr. Ransone cares for several patients who have received kidney transplants and are on potent immunosuppressive drugs.
“I know they’re appreciating our efforts to protect them, and I think the other patients are realizing that it’s a wise thing to do,” Dr. Ransone said.
Some patients have anxiety about the end of masking in doctor offices, but others have been excited about interacting more with their care teams, according to William Dahut, MD, chief scientific officer for the American Cancer Society. Many clinicians will advise their most immunocompromised patients the same as they did prior to the COVID-19 pandemic.
“There’s always been guidelines that oncologists have given to patients who are immunocompromised – we always told them to avoid crowded places, crowded scenes, be outside more than inside,” Dr. Dahut said. “Those general recommendations will continue.”
The AAFP supports masking to limit COVID’s spread, but the “most important thing people can do is to get vaccinated,” Tochi Iroku-Malize, MD, MPH, MBA, president of the AAFP, said.
But the accessibility of vaccinations is also shifting.
Testing shifts
The government will continue to provide free COVID-19 vaccines because it still has supplies on hand. When this stock runs out, commercial insurance providers will be required to cover the immunizations, as they are considered preventive, but people without insurance will have to pay out of pocket.
The AAFP is pushing the Biden administration and Congress to keep the purchase price of those vaccines low enough that clinicians can keep them in stock, according to Dr. Iroku-Malize. Once the federal government transitions COVID-19 vaccines to the commercial market – as early as later in 2023 – it may pose some challenges for providers.
“If the price of the vaccines is too high, physician practices may struggle to make the upfront investment in COVID-19 vaccines,” Dr. Iroku-Malize said. “Patients often prefer to receive vaccine counseling and administration from their usual source of primary care, like their family physician.”
The federal government has also said it still has a supply of treatments for the public to access for free, but has not revealed how much it has on hand or given a timeline for the transition to the private market.
COVID-19 tests, meanwhile, are no longer covered because of the end of the public health emergency, and cost about $45 per kit on average, according to an analysis by the Kaiser Family Foundation.
Pediatrician Lisa Costello, MD, MPH, knows that price point will be a challenge for some families she cares for at West Virginia University Medicine Children’s Hospital in Morgantown. Many still ask her where they can access free tests.
“Testing if you’re a higher risk person is something we need to ensure that people continue to be educated about,” Dr. Costello said.
She’s hopeful that COVID-19 vaccines and treatments such as Paxlovid will stay free in the coming months so patients can continue to easily access them.
Future of telehealth
Relaxed regulations of prescribing controlled substances via telehealth and across state lines allowed clinicians to treat patients near and far during the pandemic. But many providers were worried about a proposal from the Drug Enforcement Administration to clamp down on the prescribing of controlled substances via telehealth, according to A. Mark Fendrick, MD, an internal medicine physician at the University of Michigan, Ann Arbor.
“We were all panicking about what was going to happen to what is for many clinicians a very valuable policy,” Dr. Fendrick said of the telehealth flexibilities introduced during COVID-19.
The DEA, after getting 38,000 comments on their proposed regulations, pulled back on that plan, delaying the cliff until November.
Dr. Fendrick said that telehealth has allowed clinicians to reach patients who have historically faced barriers to care, such as lacking transportation.
“The benefits of that outweigh the potential harms,” he said. “Every policy you make that tightens access because you want to decrease the untoward and unfortunate outcomes will also decrease access to clinical indications.”
The AAFP said it hopes for clear guidance from the DEA in the coming months on what the new telehealth landscape for prescribing will look like.
Medicaid changes
About half of the patients who see Dr. Khanna have insurance through Medicaid.
During the public health emergency, states were not allowed to remove anyone from Medicaid, regardless of whether they no longer qualified for the program or not. But a law passed by Congress last year requires states to once again check Medicaid eligibility. As many as 15 million people could lose their Medicaid coverage.
That could affect the treatments Dr. Khanna recommends for her patients who get kicked off because those who become uninsured or transition to private insurance will have to pay more out of pocket. Maryland will start removals in June.
“When you have an uninsured patient versus Medicaid, it’s a huge difference in what you can ask the patient to do – the medications you can provide, the testing you can provide,” Dr. Khanna said.
States were authorized to remove people from Medicaid as of April 1, with Arkansas, New Hampshire, and South Dakota starting right away. But many states are just now getting the review process going. About a dozen states, including Indiana, Ohio, Utah, and West Virginia, started removing people in May 2023.
Uninsurance rates hit record lows across the United States during the pandemic. Keeping Americans on health insurance is a top priority for the AAFP, Dr. Iroku-Malize said. “We know health care coverage disruptions prevent people from seeking and accessing the care they need.”
Many people who are removed from Medicaid will be eligible for health insurance through employers, or through the Affordable Care Act’s private marketplace. But premiums and deductibles are often higher in these plans, which studies have shown result in patients delaying medical visits and not filling prescriptions or receiving treatment.
Staying mindful
Hospitals that receive federal funds will still have to report COVID-19 test results to the Centers for Medicare & Medicaid Services through 2024, although private labs will no longer be obligated to do so. The Centers for Disease Control and Prevention will also continue to monitor virus levels in communities through wastewater. But some states will no longer collect data.
Gone are the days when clinicians and others would watch for daily totals of case counts with the type of fervor typically reserved for live scoring updates during sports games, according to Dr. Costello.
“We just have to be mindful of the numbers that might be coming in,” Dr. Costello said.
Dr. Ransone, however, cautioned that clinicians not become complacent. In early May, Dr. Ransone saw two patients with conjunctivitis, what patients thought was simply pink eye – a symptom of the latest COVID-19 variant. Both patients told him it wasn’t possible they had COVID-19 because they didn’t have coughs.
“I don’t want to see physician offices fall into that trap that it’s over and be a potential nidus for infection for other patients,” Dr. Ransone said. “It’s incumbent upon us to remind people of the current symptoms so that folks will know when they need to wear a mask when they’re around their grandmother.”
The move away from universal masking in the office has benefits. Many of his older patients have difficulty hearing and had used lip reading to help understand him, he said. During the pandemic, masks got in the way of that form of communication. Now they can see his mouth again and better decipher what he says.
“Being able to have that face-to-face contact, without a mask intervening, has been really beneficial for a lot of my older patients,” he said.
A version of this article first appeared on Medscape.com.
The first day of seeing patients without a mask was, for Sterling Ransone Jr., MD, “unsettling.”
“I can’t tell you how weird it was the first day that I walked down the hall from my office to where my exam rooms are, to not have a mask on after 3 years of the habit,” said Dr. Ransone, a family physician in Deltaville, Va., and board chair of the American Academy of Family Physicians.
The White House recently lifted the public health emergency order that overhauled the way health care providers operated and advised patients over the past 3 years.
For Dr. Ransone, this transition entails getting used to his bare face, reminding patients of the latest and varying symptoms of the virus, and parting ways with sick patients if they refuse to wear a mask.
As states, hospitals, and health care systems around the country relax their mask mandates for care providers, clinicians will have to fall back on their own policies that patients with potential symptoms mask up.
“Now that it’s up to our offices, we have to have a little bit more backbone,” Dr. Ransone said. “If they’re not willing to follow a health-related policy that will protect the vulnerable, we will not see them. And so for us, it’s been pretty straightforward.”
Despite the policy, Dr. Ransone has cared for patients who don’t disclose they are feeling sick until he enters the room.
“And I wasn’t masked,” Dr. Ransone said. So, “I will wear masks for the rest of the day just to try to protect the rest of my patients in case I was exposed.”
Masks are optional for both patients and staff at the University of Maryland Medical System, but Niharika Khanna, MD, MBBS, said she still wears one with her patients, and her office advises staff to do the same. If patients are experiencing respiratory symptoms, like a cough, they are asked to wear one.
“When the patient first walks up to you, you have no idea what they have,” Dr. Khanna said.
Dr. Khanna is especially mindful of immunocompromised patients who have cancer, and Dr. Ransone cares for several patients who have received kidney transplants and are on potent immunosuppressive drugs.
“I know they’re appreciating our efforts to protect them, and I think the other patients are realizing that it’s a wise thing to do,” Dr. Ransone said.
Some patients have anxiety about the end of masking in doctor offices, but others have been excited about interacting more with their care teams, according to William Dahut, MD, chief scientific officer for the American Cancer Society. Many clinicians will advise their most immunocompromised patients the same as they did prior to the COVID-19 pandemic.
“There’s always been guidelines that oncologists have given to patients who are immunocompromised – we always told them to avoid crowded places, crowded scenes, be outside more than inside,” Dr. Dahut said. “Those general recommendations will continue.”
The AAFP supports masking to limit COVID’s spread, but the “most important thing people can do is to get vaccinated,” Tochi Iroku-Malize, MD, MPH, MBA, president of the AAFP, said.
But the accessibility of vaccinations is also shifting.
Testing shifts
The government will continue to provide free COVID-19 vaccines because it still has supplies on hand. When this stock runs out, commercial insurance providers will be required to cover the immunizations, as they are considered preventive, but people without insurance will have to pay out of pocket.
The AAFP is pushing the Biden administration and Congress to keep the purchase price of those vaccines low enough that clinicians can keep them in stock, according to Dr. Iroku-Malize. Once the federal government transitions COVID-19 vaccines to the commercial market – as early as later in 2023 – it may pose some challenges for providers.
“If the price of the vaccines is too high, physician practices may struggle to make the upfront investment in COVID-19 vaccines,” Dr. Iroku-Malize said. “Patients often prefer to receive vaccine counseling and administration from their usual source of primary care, like their family physician.”
The federal government has also said it still has a supply of treatments for the public to access for free, but has not revealed how much it has on hand or given a timeline for the transition to the private market.
COVID-19 tests, meanwhile, are no longer covered because of the end of the public health emergency, and cost about $45 per kit on average, according to an analysis by the Kaiser Family Foundation.
Pediatrician Lisa Costello, MD, MPH, knows that price point will be a challenge for some families she cares for at West Virginia University Medicine Children’s Hospital in Morgantown. Many still ask her where they can access free tests.
“Testing if you’re a higher risk person is something we need to ensure that people continue to be educated about,” Dr. Costello said.
She’s hopeful that COVID-19 vaccines and treatments such as Paxlovid will stay free in the coming months so patients can continue to easily access them.
Future of telehealth
Relaxed regulations of prescribing controlled substances via telehealth and across state lines allowed clinicians to treat patients near and far during the pandemic. But many providers were worried about a proposal from the Drug Enforcement Administration to clamp down on the prescribing of controlled substances via telehealth, according to A. Mark Fendrick, MD, an internal medicine physician at the University of Michigan, Ann Arbor.
“We were all panicking about what was going to happen to what is for many clinicians a very valuable policy,” Dr. Fendrick said of the telehealth flexibilities introduced during COVID-19.
The DEA, after getting 38,000 comments on their proposed regulations, pulled back on that plan, delaying the cliff until November.
Dr. Fendrick said that telehealth has allowed clinicians to reach patients who have historically faced barriers to care, such as lacking transportation.
“The benefits of that outweigh the potential harms,” he said. “Every policy you make that tightens access because you want to decrease the untoward and unfortunate outcomes will also decrease access to clinical indications.”
The AAFP said it hopes for clear guidance from the DEA in the coming months on what the new telehealth landscape for prescribing will look like.
Medicaid changes
About half of the patients who see Dr. Khanna have insurance through Medicaid.
During the public health emergency, states were not allowed to remove anyone from Medicaid, regardless of whether they no longer qualified for the program or not. But a law passed by Congress last year requires states to once again check Medicaid eligibility. As many as 15 million people could lose their Medicaid coverage.
That could affect the treatments Dr. Khanna recommends for her patients who get kicked off because those who become uninsured or transition to private insurance will have to pay more out of pocket. Maryland will start removals in June.
“When you have an uninsured patient versus Medicaid, it’s a huge difference in what you can ask the patient to do – the medications you can provide, the testing you can provide,” Dr. Khanna said.
States were authorized to remove people from Medicaid as of April 1, with Arkansas, New Hampshire, and South Dakota starting right away. But many states are just now getting the review process going. About a dozen states, including Indiana, Ohio, Utah, and West Virginia, started removing people in May 2023.
Uninsurance rates hit record lows across the United States during the pandemic. Keeping Americans on health insurance is a top priority for the AAFP, Dr. Iroku-Malize said. “We know health care coverage disruptions prevent people from seeking and accessing the care they need.”
Many people who are removed from Medicaid will be eligible for health insurance through employers, or through the Affordable Care Act’s private marketplace. But premiums and deductibles are often higher in these plans, which studies have shown result in patients delaying medical visits and not filling prescriptions or receiving treatment.
Staying mindful
Hospitals that receive federal funds will still have to report COVID-19 test results to the Centers for Medicare & Medicaid Services through 2024, although private labs will no longer be obligated to do so. The Centers for Disease Control and Prevention will also continue to monitor virus levels in communities through wastewater. But some states will no longer collect data.
Gone are the days when clinicians and others would watch for daily totals of case counts with the type of fervor typically reserved for live scoring updates during sports games, according to Dr. Costello.
“We just have to be mindful of the numbers that might be coming in,” Dr. Costello said.
Dr. Ransone, however, cautioned that clinicians not become complacent. In early May, Dr. Ransone saw two patients with conjunctivitis, what patients thought was simply pink eye – a symptom of the latest COVID-19 variant. Both patients told him it wasn’t possible they had COVID-19 because they didn’t have coughs.
“I don’t want to see physician offices fall into that trap that it’s over and be a potential nidus for infection for other patients,” Dr. Ransone said. “It’s incumbent upon us to remind people of the current symptoms so that folks will know when they need to wear a mask when they’re around their grandmother.”
The move away from universal masking in the office has benefits. Many of his older patients have difficulty hearing and had used lip reading to help understand him, he said. During the pandemic, masks got in the way of that form of communication. Now they can see his mouth again and better decipher what he says.
“Being able to have that face-to-face contact, without a mask intervening, has been really beneficial for a lot of my older patients,” he said.
A version of this article first appeared on Medscape.com.
The antimicrobial peptide that even Pharma can love
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.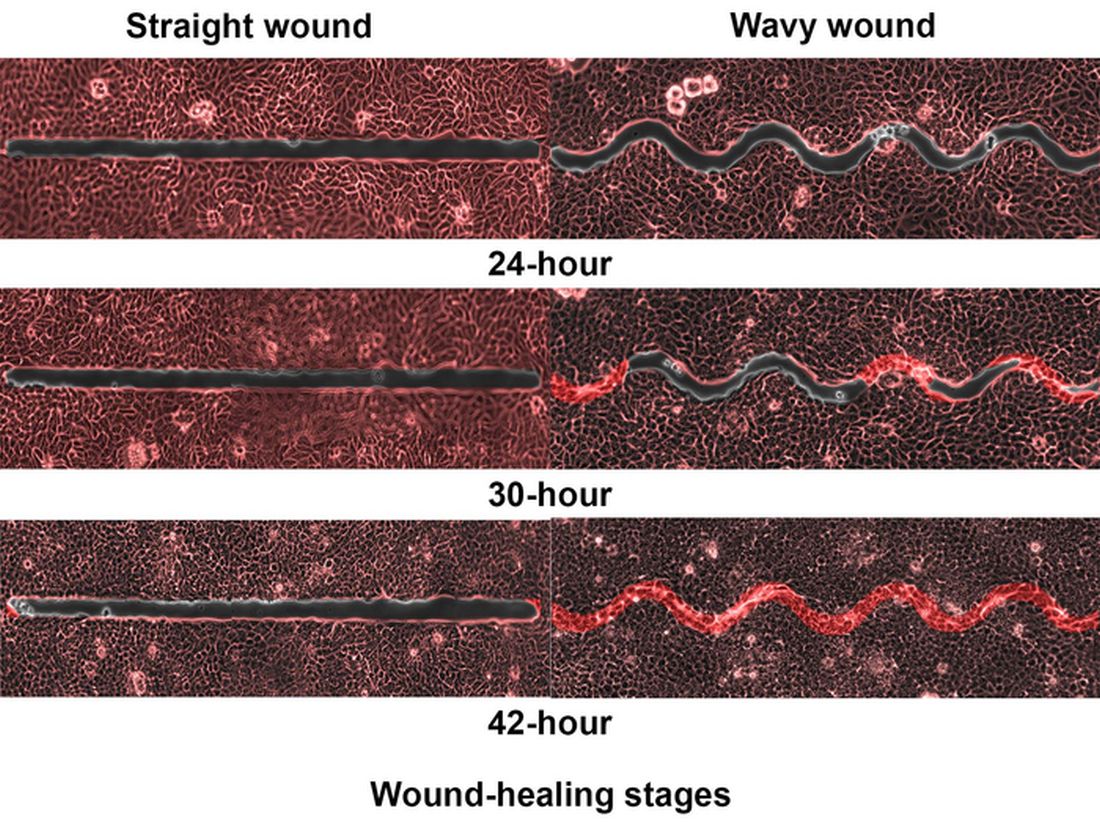
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fastest peptide north, south, east, aaaaand west of the Pecos
Bacterial infections are supposed to be simple. You get infected, you get an antibiotic to treat it. Easy. Some bacteria, though, don’t play by the rules. Those antibiotics may kill 99.9% of germs, but what about the 0.1% that gets left behind? With their fallen comrades out of the way, the accidentally drug resistant species are free to inherit the Earth.
Antibiotic resistance is thus a major concern for the medical community. Naturally, anything that prevents doctors from successfully curing sick people is a priority. Unless you’re a major pharmaceutical company that has been loath to develop new drugs that can beat antibiotic-resistant bacteria. Blah blah, time and money, blah blah, long time between development and market application, blah blah, no profit. We all know the story with pharmaceutical companies.
Research from other sources has continued, however, and Brazilian scientists recently published research involving a peptide known as plantaricin 149. This peptide, derived from the bacterium Lactobacillus plantarum, has been known for nearly 30 years to have antibacterial properties. Pln149 in its natural state, though, is not particularly efficient at bacteria-killing. Fortunately, we have science and technology on our side.
The researchers synthesized 20 analogs of Pln149, of which Pln149-PEP20 had the best results. The elegantly named compound is less than half the size of the original peptide, less toxic, and far better at killing any and all drug-resistant bacteria the researchers threw at it. How much better? Pln149-PEP20 started killing bacteria less than an hour after being introduced in lab trials.
The research is just in its early days – just because something is less toxic doesn’t necessarily mean you want to go and help yourself to it – but we can only hope that those lovely pharmaceutical companies deign to look down upon us and actually develop a drug utilizing Pln149-PEP20 to, you know, actually help sick people, instead of trying to build monopolies or avoiding paying billions in taxes. Yeah, we couldn’t keep a straight face through that last sentence either.
Speed healing: The wavy wound gets the swirl
Did you know that wavy wounds heal faster than straight wounds? Well, we didn’t, but apparently quite a few people did, because somebody has been trying to figure out why wavy wounds heal faster than straight ones. Do the surgeons know about this? How about you dermatologists? Wavy over straight? We’re the media. We’re supposed to report this kind of stuff. Maybe hit us with a tweet next time you do something important, or push a TikTok our way, okay?
You could be more like the investigators at Nanyang Technological University in Singapore, who figured out the why and then released a statement about it.
They created synthetic wounds – some straight, some wavy – in micropatterned hydrogel substrates that mimicked human skin. Then they used an advanced optical technique known as particle image velocimetry to measure fluid flow and learn how cells moved to close the wound gaps.
The wavy wounds “induced more complex collective cell movements, such as a swirly, vortex-like motion,” according to the written statement from NTU Singapore. In the straight wounds, cell movements paralleled the wound front, “moving in straight lines like a marching band,” they pointed out, unlike some researchers who never call us unless they need money.
Complex epithelial cell movements are better, it turns out. Over an observation period of 64 hours the NTU team found that the healing efficiency of wavy gaps – measured by the area covered by the cells over time – is nearly five times faster than straight gaps.
The complex motion “enabled cells to quickly connect with similar cells on the opposite site of the wound edge, forming a bridge and closing the wavy wound gaps faster than straight gaps,” explained lead author Xu Hongmei, a doctoral student at NTU’s School of Mechanical and Aerospace Engineering, who seems to have time to toss out a tumblr or two to keep the press informed.
As for the rest of you, would it kill you to pick up a phone once in a while? Maybe let a journalist know that you’re still alive? We have feelings too, you know, and we worry.
A little Jekyll, a little Hyde, and a little shop of horrors
More “Little Shop of Horrors” references are coming, so be prepared.
We begin with Triphyophyllum peltatum. This woody vine is of great interest to medical and pharmaceutical researchers because its constituents have shown promise against pancreatic cancer and leukemia cells, among others, along with the pathogens that cause malaria and other diseases. There is another side, however. T. peltatum also has a tendency to turn into a realistic Audrey II when deprived.
No, of course they’re not craving human flesh, but it does become … carnivorous in its appetite.
T. peltatum, native to the West African tropics and not found in a New York florist shop, has the unique ability to change its diet and development based on the environmental circumstances. For some unknown reason, the leaves would develop adhesive traps in the form of sticky drops that capture insect prey. The plant is notoriously hard to grow, however, so no one could study the transformation under lab conditions. Until now.
A group of German scientists “exposed the plant to different stress factors, including deficiencies of various nutrients, and studied how it responded to each,” said Dr. Traud Winkelmann of Leibniz University Hannover. “Only in one case were we able to observe the formation of traps: in the case of a lack of phosphorus.”
Well, there you have it: phosphorus. We need it for healthy bones and teeth, which this plant doesn’t have to worry about, unlike its Tony Award–nominated counterpart. The investigators hope that their findings could lead to “future molecular analyses that will help understand the origins of carnivory,” but we’re guessing that a certain singing alien species will be left out of that research.
Fatigue is a monster for patients with pulmonary disease
If you’re looking for it, you’ll find fatigue almost everywhere. It’s so common that it hides in plain sight, never dealt with because it’s present for good reason: the inevitable consequence of age, whatever disease you’re treating, poor lifestyle choices, and the daily grind of twenty-first–century life. Its impact is so ubiquitous and pernicious that it’s considered acceptable.
Is it though? After all, fatigue can be debilitating. Not every symptom is worthy of a chronic syndrome bearing its name. Furthermore, what if its relationship to the disease you’re treating is bidirectional?
Outside of sleep medicine, I see little focus on fatigue among pulmonologists. This despite the existing data on fatigue related to sarcoidosis, chronic obstructive pulmonary disease (COPD), and interstitial lung disease. Even when we do pay it lip service, “addressing” fatigue or sleep is essentially a euphemism for ordering a sleep study.
As with fatigue, if you look for obstructive sleep apnea, it’ll be there, although with OSA, it’s related to the incredibly low, nonevidence-based threshold the American Academy of Sleep Medicine has established for making the diagnosis. With continuous positive airway pressure (CPAP) in hand, the patient has a new disease to worry about and a difficult behavioral change (wearing, cleaning, and resupplying their CPAP equipment) to make. Too often, the CPAP isn’t used – or is – and the fatigue persists. But it’s okay, because we followed somebody’s guideline.
The American Thoracic Society just published a research statement on cancer-related fatigue. It is comprehensive and highlights the high prevalence and poor recognition of cancer-related fatigue. The authors note that among cancers, those of the lung are associated with a higher comorbid disease burden, older age, and cigarette smoking. All these factors make patients with lung cancer particularly prone to fatigue. Interactions between these factors, lung cancer histology, and specific chemotherapy regimens are poorly understood. True to its title, the “research statement” serves more as a call to action than an evidence-based blueprint for diagnosis and management.
The cancer-related fatigue data that does exist suggests treatment starts with recognition followed by a focus on sleep, exercise, and nutrition. This should surprise no one. The data on fatigue in general (not specific to cancer-related fatigue) shows that although fatigue is not synonymous with poor quality or insufficient sleep, sleep is usually a major factor. The cancer-related conditions affecting sleep include anxiety, depression, insufficient sleep, insomnia, medication side effects, and OSA. The intersecting web is complex, but across underlying conditions (cancer or otherwise), the quickest most efficient method for mitigating fatigue is optimizing sleep.
Exercise and nutrition are also important. Again, across disease processes (interstitial lung disease, COPD, lung cancer, and so on), no drug comes close to aerobic exercise for reducing symptoms, including fatigue. If an exercise prescription could be delivered in pill-form, it’d be a blockbuster. But it can’t be, and the ATS lung cancer–related fatigue research statement nicely outlines the evidence for increased activity levels and the barriers to obtaining support and compliance. As is the case with exercise, support for improving nutrition is limited by cost, access, and patient education.
Perhaps most importantly, sleep, exercise, and nutrition require time for counseling and a behavior change for the physician and patient. Both are in short supply, and commitment is always ephemeral. Incentivization could perhaps be re-structured, but the ATS document notes this will be challenging. With respect to pulmonary rehabilitation (about 50% of patients with lung cancer have comorbid COPD), for example, reimbursement is poor, which serves as a disincentive. Their suggestions? Early integration and repeated introduction to rehabilitation and exercise concepts. Sounds great.
In summary, in my opinion, fatigue doesn’t receive the attention level commensurate with its impact. It’s easy to understand why, but I’m glad the ATS is highlighting the problem. Unbeknownst to me, multiple cancer guidelines already recommend screening for fatigue. The recent sarcoidosis treatment guideline published by the European Respiratory Society dedicated a PICO (Patients, Intervention, Comparison, Outcomes) to the topic and recommended exercise (pulmonary rehabilitation). That said, consensus statements on COPD mention it only in passing in relation to severe disease and end-of-life care, and idiopathic pulmonary fibrosis guidelines ignore it entirely. So, recognition is improving, but we’ve got ways to go.

Dr. Holley is professor of medicine at Uniformed Services University, Bethesda, Md., and a pulmonary/sleep and critical care medicine physician at MedStar Washington Hospital Center in Washington. He disclosed ties with Metapharm, CHEST College, and WebMD.
A version of this article originally appeared on Medscape.com.
If you’re looking for it, you’ll find fatigue almost everywhere. It’s so common that it hides in plain sight, never dealt with because it’s present for good reason: the inevitable consequence of age, whatever disease you’re treating, poor lifestyle choices, and the daily grind of twenty-first–century life. Its impact is so ubiquitous and pernicious that it’s considered acceptable.
Is it though? After all, fatigue can be debilitating. Not every symptom is worthy of a chronic syndrome bearing its name. Furthermore, what if its relationship to the disease you’re treating is bidirectional?
Outside of sleep medicine, I see little focus on fatigue among pulmonologists. This despite the existing data on fatigue related to sarcoidosis, chronic obstructive pulmonary disease (COPD), and interstitial lung disease. Even when we do pay it lip service, “addressing” fatigue or sleep is essentially a euphemism for ordering a sleep study.
As with fatigue, if you look for obstructive sleep apnea, it’ll be there, although with OSA, it’s related to the incredibly low, nonevidence-based threshold the American Academy of Sleep Medicine has established for making the diagnosis. With continuous positive airway pressure (CPAP) in hand, the patient has a new disease to worry about and a difficult behavioral change (wearing, cleaning, and resupplying their CPAP equipment) to make. Too often, the CPAP isn’t used – or is – and the fatigue persists. But it’s okay, because we followed somebody’s guideline.
The American Thoracic Society just published a research statement on cancer-related fatigue. It is comprehensive and highlights the high prevalence and poor recognition of cancer-related fatigue. The authors note that among cancers, those of the lung are associated with a higher comorbid disease burden, older age, and cigarette smoking. All these factors make patients with lung cancer particularly prone to fatigue. Interactions between these factors, lung cancer histology, and specific chemotherapy regimens are poorly understood. True to its title, the “research statement” serves more as a call to action than an evidence-based blueprint for diagnosis and management.
The cancer-related fatigue data that does exist suggests treatment starts with recognition followed by a focus on sleep, exercise, and nutrition. This should surprise no one. The data on fatigue in general (not specific to cancer-related fatigue) shows that although fatigue is not synonymous with poor quality or insufficient sleep, sleep is usually a major factor. The cancer-related conditions affecting sleep include anxiety, depression, insufficient sleep, insomnia, medication side effects, and OSA. The intersecting web is complex, but across underlying conditions (cancer or otherwise), the quickest most efficient method for mitigating fatigue is optimizing sleep.
Exercise and nutrition are also important. Again, across disease processes (interstitial lung disease, COPD, lung cancer, and so on), no drug comes close to aerobic exercise for reducing symptoms, including fatigue. If an exercise prescription could be delivered in pill-form, it’d be a blockbuster. But it can’t be, and the ATS lung cancer–related fatigue research statement nicely outlines the evidence for increased activity levels and the barriers to obtaining support and compliance. As is the case with exercise, support for improving nutrition is limited by cost, access, and patient education.
Perhaps most importantly, sleep, exercise, and nutrition require time for counseling and a behavior change for the physician and patient. Both are in short supply, and commitment is always ephemeral. Incentivization could perhaps be re-structured, but the ATS document notes this will be challenging. With respect to pulmonary rehabilitation (about 50% of patients with lung cancer have comorbid COPD), for example, reimbursement is poor, which serves as a disincentive. Their suggestions? Early integration and repeated introduction to rehabilitation and exercise concepts. Sounds great.
In summary, in my opinion, fatigue doesn’t receive the attention level commensurate with its impact. It’s easy to understand why, but I’m glad the ATS is highlighting the problem. Unbeknownst to me, multiple cancer guidelines already recommend screening for fatigue. The recent sarcoidosis treatment guideline published by the European Respiratory Society dedicated a PICO (Patients, Intervention, Comparison, Outcomes) to the topic and recommended exercise (pulmonary rehabilitation). That said, consensus statements on COPD mention it only in passing in relation to severe disease and end-of-life care, and idiopathic pulmonary fibrosis guidelines ignore it entirely. So, recognition is improving, but we’ve got ways to go.
Dr. Holley is professor of medicine at Uniformed Services University, Bethesda, Md., and a pulmonary/sleep and critical care medicine physician at MedStar Washington Hospital Center in Washington. He disclosed ties with Metapharm, CHEST College, and WebMD.
A version of this article originally appeared on Medscape.com.
If you’re looking for it, you’ll find fatigue almost everywhere. It’s so common that it hides in plain sight, never dealt with because it’s present for good reason: the inevitable consequence of age, whatever disease you’re treating, poor lifestyle choices, and the daily grind of twenty-first–century life. Its impact is so ubiquitous and pernicious that it’s considered acceptable.
Is it though? After all, fatigue can be debilitating. Not every symptom is worthy of a chronic syndrome bearing its name. Furthermore, what if its relationship to the disease you’re treating is bidirectional?
Outside of sleep medicine, I see little focus on fatigue among pulmonologists. This despite the existing data on fatigue related to sarcoidosis, chronic obstructive pulmonary disease (COPD), and interstitial lung disease. Even when we do pay it lip service, “addressing” fatigue or sleep is essentially a euphemism for ordering a sleep study.
As with fatigue, if you look for obstructive sleep apnea, it’ll be there, although with OSA, it’s related to the incredibly low, nonevidence-based threshold the American Academy of Sleep Medicine has established for making the diagnosis. With continuous positive airway pressure (CPAP) in hand, the patient has a new disease to worry about and a difficult behavioral change (wearing, cleaning, and resupplying their CPAP equipment) to make. Too often, the CPAP isn’t used – or is – and the fatigue persists. But it’s okay, because we followed somebody’s guideline.
The American Thoracic Society just published a research statement on cancer-related fatigue. It is comprehensive and highlights the high prevalence and poor recognition of cancer-related fatigue. The authors note that among cancers, those of the lung are associated with a higher comorbid disease burden, older age, and cigarette smoking. All these factors make patients with lung cancer particularly prone to fatigue. Interactions between these factors, lung cancer histology, and specific chemotherapy regimens are poorly understood. True to its title, the “research statement” serves more as a call to action than an evidence-based blueprint for diagnosis and management.
The cancer-related fatigue data that does exist suggests treatment starts with recognition followed by a focus on sleep, exercise, and nutrition. This should surprise no one. The data on fatigue in general (not specific to cancer-related fatigue) shows that although fatigue is not synonymous with poor quality or insufficient sleep, sleep is usually a major factor. The cancer-related conditions affecting sleep include anxiety, depression, insufficient sleep, insomnia, medication side effects, and OSA. The intersecting web is complex, but across underlying conditions (cancer or otherwise), the quickest most efficient method for mitigating fatigue is optimizing sleep.
Exercise and nutrition are also important. Again, across disease processes (interstitial lung disease, COPD, lung cancer, and so on), no drug comes close to aerobic exercise for reducing symptoms, including fatigue. If an exercise prescription could be delivered in pill-form, it’d be a blockbuster. But it can’t be, and the ATS lung cancer–related fatigue research statement nicely outlines the evidence for increased activity levels and the barriers to obtaining support and compliance. As is the case with exercise, support for improving nutrition is limited by cost, access, and patient education.
Perhaps most importantly, sleep, exercise, and nutrition require time for counseling and a behavior change for the physician and patient. Both are in short supply, and commitment is always ephemeral. Incentivization could perhaps be re-structured, but the ATS document notes this will be challenging. With respect to pulmonary rehabilitation (about 50% of patients with lung cancer have comorbid COPD), for example, reimbursement is poor, which serves as a disincentive. Their suggestions? Early integration and repeated introduction to rehabilitation and exercise concepts. Sounds great.
In summary, in my opinion, fatigue doesn’t receive the attention level commensurate with its impact. It’s easy to understand why, but I’m glad the ATS is highlighting the problem. Unbeknownst to me, multiple cancer guidelines already recommend screening for fatigue. The recent sarcoidosis treatment guideline published by the European Respiratory Society dedicated a PICO (Patients, Intervention, Comparison, Outcomes) to the topic and recommended exercise (pulmonary rehabilitation). That said, consensus statements on COPD mention it only in passing in relation to severe disease and end-of-life care, and idiopathic pulmonary fibrosis guidelines ignore it entirely. So, recognition is improving, but we’ve got ways to go.
Dr. Holley is professor of medicine at Uniformed Services University, Bethesda, Md., and a pulmonary/sleep and critical care medicine physician at MedStar Washington Hospital Center in Washington. He disclosed ties with Metapharm, CHEST College, and WebMD.
A version of this article originally appeared on Medscape.com.
Number of cancer survivors with functional limitations doubled in 20 years
Vishal Patel, BS, a student at the Dell Medical School at The University of Texas at Austin, and colleagues identified 51,258 cancer survivors from the National Health Interview Survey, representing a weighted population of approximately 178.8 million from 1999 to 2018.
Most survivors were women (60.2%) and were at least 65 years old (55.4%). In 1999, 3.6 million weighted survivors reported functional limitation. In 2018, the number increased to 8.2 million, a 2.25-fold increase.
The number of survivors who reported no limitations also increased, but not by as much. That group grew 1.34-fold during the study period.
For context, “the 70% prevalence of functional limitation among survivors in 2018 is nearly twice that of the general population,” the authors wrote.
Patients surveyed on function
Functional limitation was defined as “self-reported difficulty performing any of 12 routine physical or social activities without assistance.” Examples of the activities included difficulty sitting for more than 2 hours, difficulty participating in social activities or difficulty pushing or pulling an object the size of a living room chair.
Over the 2 decades analyzed, the adjusted prevalence of functional limitation was highest among survivors of pancreatic cancer (80.3%) and lung cancer (76.5%). Prevalence was lowest for survivors of melanoma (62.2%), breast (61.8%) and prostate (59.5%) cancers.
Not just a result of living longer
Mr. Patel told this publication that one assumption people might make when they read these results is that people are just living longer with cancer and losing functional ability accordingly.
“But, in fact, we found that the youngest [– those less than 65 years–] actually contributed to this trend more than the oldest people, which means it’s not just [happening], because people are getting older,” he said.
Hispanic and Black individuals had disproportionately higher increases in functional limitation; percentage point increases over the 2 decades were 19.5 for Black people, 25.1 for Hispanic people and 12.5 for White people. There may be a couple of reasons for that, Mr. Patel noted.
Those who are Black or Hispanic tend to have less access to cancer survivorship care for reasons including insurance status and historic health care inequities, he noted.
“The other potential reason is that they have had less access to cancer care historically. And if, 20 years ago Black and Hispanic individuals didn’t have access to some chemotherapies, and now they do, maybe it’s the increased access to care that’s causing these functional limitations. Because chemotherapy can sometimes be very toxic. It may be sort of a catch-up toxicity,” he said.
Quality of life beyond survivorship
Mr. Patel said the results seem to call for building on improved survival rates by tracking and improving function.
“It’s good to celebrate that there are more survivors. But now that we can keep people alive longer, maybe we can shift gears to improving their quality of life,” he said.
The more-than-doubling of functional limitations over 2 decades “is a very sobering trend,” he noted, while pointing out that the functional limitations applied to 8 million people in the United States – people whose needs are not being met.
There’s no sign of the trend stopping, he continued. “We saw no downward trend, only an upward trend.”
Increasingly, including functionality as an endpoint in cancer trials, in addition to improvements in mortality, is one place to start, he added.
“Our findings suggest an urgent need for care teams to understand and address function, for researchers to evaluate function as a core outcome in trials, and for health systems and policy makers to reimagine survivorship care, recognizing the burden of cancer and its treatment on physical, psychosocial, and cognitive function,” the authors wrote in their paper. Limitations of the study include the potential for recall bias, lack of cancer staging or treatment information, and the subjective perception of function.
A coauthor reported personal fees from Astellas, AstraZeneca, AAA, Blue Earth, Janssen, Lantheus, Myovant, Myriad Genetics, Novartis, Telix, and Sanofi, as well as grants from Pfizer and Bayer during the conduct of the study. No other disclosures were reported.
Vishal Patel, BS, a student at the Dell Medical School at The University of Texas at Austin, and colleagues identified 51,258 cancer survivors from the National Health Interview Survey, representing a weighted population of approximately 178.8 million from 1999 to 2018.
Most survivors were women (60.2%) and were at least 65 years old (55.4%). In 1999, 3.6 million weighted survivors reported functional limitation. In 2018, the number increased to 8.2 million, a 2.25-fold increase.
The number of survivors who reported no limitations also increased, but not by as much. That group grew 1.34-fold during the study period.
For context, “the 70% prevalence of functional limitation among survivors in 2018 is nearly twice that of the general population,” the authors wrote.
Patients surveyed on function
Functional limitation was defined as “self-reported difficulty performing any of 12 routine physical or social activities without assistance.” Examples of the activities included difficulty sitting for more than 2 hours, difficulty participating in social activities or difficulty pushing or pulling an object the size of a living room chair.
Over the 2 decades analyzed, the adjusted prevalence of functional limitation was highest among survivors of pancreatic cancer (80.3%) and lung cancer (76.5%). Prevalence was lowest for survivors of melanoma (62.2%), breast (61.8%) and prostate (59.5%) cancers.
Not just a result of living longer
Mr. Patel told this publication that one assumption people might make when they read these results is that people are just living longer with cancer and losing functional ability accordingly.
“But, in fact, we found that the youngest [– those less than 65 years–] actually contributed to this trend more than the oldest people, which means it’s not just [happening], because people are getting older,” he said.
Hispanic and Black individuals had disproportionately higher increases in functional limitation; percentage point increases over the 2 decades were 19.5 for Black people, 25.1 for Hispanic people and 12.5 for White people. There may be a couple of reasons for that, Mr. Patel noted.
Those who are Black or Hispanic tend to have less access to cancer survivorship care for reasons including insurance status and historic health care inequities, he noted.
“The other potential reason is that they have had less access to cancer care historically. And if, 20 years ago Black and Hispanic individuals didn’t have access to some chemotherapies, and now they do, maybe it’s the increased access to care that’s causing these functional limitations. Because chemotherapy can sometimes be very toxic. It may be sort of a catch-up toxicity,” he said.
Quality of life beyond survivorship
Mr. Patel said the results seem to call for building on improved survival rates by tracking and improving function.
“It’s good to celebrate that there are more survivors. But now that we can keep people alive longer, maybe we can shift gears to improving their quality of life,” he said.
The more-than-doubling of functional limitations over 2 decades “is a very sobering trend,” he noted, while pointing out that the functional limitations applied to 8 million people in the United States – people whose needs are not being met.
There’s no sign of the trend stopping, he continued. “We saw no downward trend, only an upward trend.”
Increasingly, including functionality as an endpoint in cancer trials, in addition to improvements in mortality, is one place to start, he added.
“Our findings suggest an urgent need for care teams to understand and address function, for researchers to evaluate function as a core outcome in trials, and for health systems and policy makers to reimagine survivorship care, recognizing the burden of cancer and its treatment on physical, psychosocial, and cognitive function,” the authors wrote in their paper. Limitations of the study include the potential for recall bias, lack of cancer staging or treatment information, and the subjective perception of function.
A coauthor reported personal fees from Astellas, AstraZeneca, AAA, Blue Earth, Janssen, Lantheus, Myovant, Myriad Genetics, Novartis, Telix, and Sanofi, as well as grants from Pfizer and Bayer during the conduct of the study. No other disclosures were reported.
Vishal Patel, BS, a student at the Dell Medical School at The University of Texas at Austin, and colleagues identified 51,258 cancer survivors from the National Health Interview Survey, representing a weighted population of approximately 178.8 million from 1999 to 2018.
Most survivors were women (60.2%) and were at least 65 years old (55.4%). In 1999, 3.6 million weighted survivors reported functional limitation. In 2018, the number increased to 8.2 million, a 2.25-fold increase.
The number of survivors who reported no limitations also increased, but not by as much. That group grew 1.34-fold during the study period.
For context, “the 70% prevalence of functional limitation among survivors in 2018 is nearly twice that of the general population,” the authors wrote.
Patients surveyed on function
Functional limitation was defined as “self-reported difficulty performing any of 12 routine physical or social activities without assistance.” Examples of the activities included difficulty sitting for more than 2 hours, difficulty participating in social activities or difficulty pushing or pulling an object the size of a living room chair.
Over the 2 decades analyzed, the adjusted prevalence of functional limitation was highest among survivors of pancreatic cancer (80.3%) and lung cancer (76.5%). Prevalence was lowest for survivors of melanoma (62.2%), breast (61.8%) and prostate (59.5%) cancers.
Not just a result of living longer
Mr. Patel told this publication that one assumption people might make when they read these results is that people are just living longer with cancer and losing functional ability accordingly.
“But, in fact, we found that the youngest [– those less than 65 years–] actually contributed to this trend more than the oldest people, which means it’s not just [happening], because people are getting older,” he said.
Hispanic and Black individuals had disproportionately higher increases in functional limitation; percentage point increases over the 2 decades were 19.5 for Black people, 25.1 for Hispanic people and 12.5 for White people. There may be a couple of reasons for that, Mr. Patel noted.
Those who are Black or Hispanic tend to have less access to cancer survivorship care for reasons including insurance status and historic health care inequities, he noted.
“The other potential reason is that they have had less access to cancer care historically. And if, 20 years ago Black and Hispanic individuals didn’t have access to some chemotherapies, and now they do, maybe it’s the increased access to care that’s causing these functional limitations. Because chemotherapy can sometimes be very toxic. It may be sort of a catch-up toxicity,” he said.
Quality of life beyond survivorship
Mr. Patel said the results seem to call for building on improved survival rates by tracking and improving function.
“It’s good to celebrate that there are more survivors. But now that we can keep people alive longer, maybe we can shift gears to improving their quality of life,” he said.
The more-than-doubling of functional limitations over 2 decades “is a very sobering trend,” he noted, while pointing out that the functional limitations applied to 8 million people in the United States – people whose needs are not being met.
There’s no sign of the trend stopping, he continued. “We saw no downward trend, only an upward trend.”
Increasingly, including functionality as an endpoint in cancer trials, in addition to improvements in mortality, is one place to start, he added.
“Our findings suggest an urgent need for care teams to understand and address function, for researchers to evaluate function as a core outcome in trials, and for health systems and policy makers to reimagine survivorship care, recognizing the burden of cancer and its treatment on physical, psychosocial, and cognitive function,” the authors wrote in their paper. Limitations of the study include the potential for recall bias, lack of cancer staging or treatment information, and the subjective perception of function.
A coauthor reported personal fees from Astellas, AstraZeneca, AAA, Blue Earth, Janssen, Lantheus, Myovant, Myriad Genetics, Novartis, Telix, and Sanofi, as well as grants from Pfizer and Bayer during the conduct of the study. No other disclosures were reported.
FROM JAMA ONCOLOGY
Medical students gain momentum in effort to ban legacy admissions
, which they say offer preferential treatment to applicants based on their association with donors or alumni.
While an estimated 25% of public colleges and universities still use legacy admissions, a growing list of top medical schools have moved away from the practice over the last decade, including Johns Hopkins University, Baltimore, and Tufts University, Medford, Mass.
Legacy admissions contradict schools’ more inclusive policies, Senila Yasmin, MPH, a second-year medical student at Tufts University, said in an interview. While Tufts maintains legacy admissions for its undergraduate applicants, the medical school stopped the practice in 2021, said Ms. Yasmin, a member of a student group that lobbied against the school’s legacy preferences.
Describing herself as a low-income, first-generation Muslim-Pakistani American, Ms. Yasmin wants to use her experience at Tufts to improve accessibility for students like herself.
As a member of the American Medical Association (AMA) Medical Student Section, she coauthored a resolution stating that legacy admissions go against the AMA’s strategic plan to advance racial justice and health equity. The Student Section passed the resolution in November, and in June, the AMA House of Delegates will vote on whether to adopt the policy.
Along with a Supreme Court decision that could strike down race-conscious college admissions, an AMA policy could convince medical schools to rethink legacy admissions and how to maintain diverse student bodies. In June, the court is expected to issue a decision in the Students for Fair Admissions lawsuit against Harvard University, Cambridge, Mass., and the University of North Carolina, Chapel Hill, which alleges that considering race in holistic admissions constitutes racial discrimination and violates the Equal Protection Clause.
Opponents of legacy admissions, like Ms. Yasmin, say it penalizes students from racial minorities and lower socioeconomic backgrounds, hampering a fair and equitable admissions process that attracts diverse medical school admissions.
Diversity of medical applicants
Diversity in medical schools continued to increase last year with more Black, Hispanic, and female students applying and enrolling, according to a recent report by the Association of American Medical Colleges (AAMC). However, universities often include nonacademic criteria in their admission assessments to improve educational access for underrepresented minorities.
Medical schools carefully consider each applicant’s background “to yield a diverse class of students,” Geoffrey Young, PhD, AAMC’s senior director of transforming the health care workforce, told this news organization.
Some schools, such as Morehouse School of Medicine, Atlanta, the University of Virginia School of Medicine, Charlottesville, and the University of Arizona College of Medicine, Tucson, perform a thorough review of candidates while offering admissions practices designed specifically for legacy applicants. The schools assert that legacy designation doesn’t factor into the student’s likelihood of acceptance.
The arrangement may show that schools want to commit to equity and fairness but have trouble moving away from entrenched traditions, two professors from Penn State College of Medicine, Hershey, Pa., who sit on separate medical admissions subcommittees, wrote last year in Bioethics Today.
Legislation may hasten legacies’ end
In December, Ms. Yasmin and a group of Massachusetts Medical Society student-members presented another resolution to the state medical society, which adopted it.
The society’s new policy opposes the use of legacy status in medical school admissions and supports mechanisms to eliminate its inclusion from the application process, Theodore Calianos II, MD, FACS, president of the Massachusetts Medical Society, said in an interview.
“Legacy preferences limit racial and socioeconomic diversity on campuses, so we asked, ‘What can we do so that everyone has equal access to medical education?’ It is exciting to see the students and young physicians – the future of medicine – become involved in policymaking.”
Proposed laws may also hasten the end of legacy admissions. Last year, the U.S. Senate began considering a bill prohibiting colleges receiving federal financial aid from giving preferential treatment to students based on their relations to donors or alumni. However, the bill allows the Department of Education to make exceptions for institutions serving historically underrepresented groups.
The New York State Senate and the New York State Assembly also are reviewing bills that ban legacy and early admissions policies at public and private universities. Connecticut announced similar legislation last year. Massachusetts legislators are considering two bills: one that would ban the practice at the state’s public universities and another that would require all schools using legacy status to pay a “public service fee” equal to a percentage of its endowment. Colleges with endowment assets exceeding $2 billion must pay at least $2 million, according to the bill’s text.
At schools like Harvard, whose endowment surpasses $50 billion, the option to pay the penalty will make the law moot, Michael Walls, DO, MPH, president of the American Medical Student Association (AMSA), said in an interview. “Smaller schools wouldn’t be able to afford the fine and are less likely to be doing [legacy admissions] anyway,” he said. “The schools that want to continue doing it could just pay the fine.”
Dr. Walls said AMSA supports race-conscious admissions processes and anything that increases fairness for medical school applicants. “Whatever [fair] means is up for interpretation, but it would be great to eliminate legacy admissions,” he said.
A version of this article originally appeared on Medscape.com.
, which they say offer preferential treatment to applicants based on their association with donors or alumni.
While an estimated 25% of public colleges and universities still use legacy admissions, a growing list of top medical schools have moved away from the practice over the last decade, including Johns Hopkins University, Baltimore, and Tufts University, Medford, Mass.
Legacy admissions contradict schools’ more inclusive policies, Senila Yasmin, MPH, a second-year medical student at Tufts University, said in an interview. While Tufts maintains legacy admissions for its undergraduate applicants, the medical school stopped the practice in 2021, said Ms. Yasmin, a member of a student group that lobbied against the school’s legacy preferences.
Describing herself as a low-income, first-generation Muslim-Pakistani American, Ms. Yasmin wants to use her experience at Tufts to improve accessibility for students like herself.
As a member of the American Medical Association (AMA) Medical Student Section, she coauthored a resolution stating that legacy admissions go against the AMA’s strategic plan to advance racial justice and health equity. The Student Section passed the resolution in November, and in June, the AMA House of Delegates will vote on whether to adopt the policy.
Along with a Supreme Court decision that could strike down race-conscious college admissions, an AMA policy could convince medical schools to rethink legacy admissions and how to maintain diverse student bodies. In June, the court is expected to issue a decision in the Students for Fair Admissions lawsuit against Harvard University, Cambridge, Mass., and the University of North Carolina, Chapel Hill, which alleges that considering race in holistic admissions constitutes racial discrimination and violates the Equal Protection Clause.
Opponents of legacy admissions, like Ms. Yasmin, say it penalizes students from racial minorities and lower socioeconomic backgrounds, hampering a fair and equitable admissions process that attracts diverse medical school admissions.
Diversity of medical applicants
Diversity in medical schools continued to increase last year with more Black, Hispanic, and female students applying and enrolling, according to a recent report by the Association of American Medical Colleges (AAMC). However, universities often include nonacademic criteria in their admission assessments to improve educational access for underrepresented minorities.
Medical schools carefully consider each applicant’s background “to yield a diverse class of students,” Geoffrey Young, PhD, AAMC’s senior director of transforming the health care workforce, told this news organization.
Some schools, such as Morehouse School of Medicine, Atlanta, the University of Virginia School of Medicine, Charlottesville, and the University of Arizona College of Medicine, Tucson, perform a thorough review of candidates while offering admissions practices designed specifically for legacy applicants. The schools assert that legacy designation doesn’t factor into the student’s likelihood of acceptance.
The arrangement may show that schools want to commit to equity and fairness but have trouble moving away from entrenched traditions, two professors from Penn State College of Medicine, Hershey, Pa., who sit on separate medical admissions subcommittees, wrote last year in Bioethics Today.
Legislation may hasten legacies’ end
In December, Ms. Yasmin and a group of Massachusetts Medical Society student-members presented another resolution to the state medical society, which adopted it.
The society’s new policy opposes the use of legacy status in medical school admissions and supports mechanisms to eliminate its inclusion from the application process, Theodore Calianos II, MD, FACS, president of the Massachusetts Medical Society, said in an interview.
“Legacy preferences limit racial and socioeconomic diversity on campuses, so we asked, ‘What can we do so that everyone has equal access to medical education?’ It is exciting to see the students and young physicians – the future of medicine – become involved in policymaking.”
Proposed laws may also hasten the end of legacy admissions. Last year, the U.S. Senate began considering a bill prohibiting colleges receiving federal financial aid from giving preferential treatment to students based on their relations to donors or alumni. However, the bill allows the Department of Education to make exceptions for institutions serving historically underrepresented groups.
The New York State Senate and the New York State Assembly also are reviewing bills that ban legacy and early admissions policies at public and private universities. Connecticut announced similar legislation last year. Massachusetts legislators are considering two bills: one that would ban the practice at the state’s public universities and another that would require all schools using legacy status to pay a “public service fee” equal to a percentage of its endowment. Colleges with endowment assets exceeding $2 billion must pay at least $2 million, according to the bill’s text.
At schools like Harvard, whose endowment surpasses $50 billion, the option to pay the penalty will make the law moot, Michael Walls, DO, MPH, president of the American Medical Student Association (AMSA), said in an interview. “Smaller schools wouldn’t be able to afford the fine and are less likely to be doing [legacy admissions] anyway,” he said. “The schools that want to continue doing it could just pay the fine.”
Dr. Walls said AMSA supports race-conscious admissions processes and anything that increases fairness for medical school applicants. “Whatever [fair] means is up for interpretation, but it would be great to eliminate legacy admissions,” he said.
A version of this article originally appeared on Medscape.com.
, which they say offer preferential treatment to applicants based on their association with donors or alumni.
While an estimated 25% of public colleges and universities still use legacy admissions, a growing list of top medical schools have moved away from the practice over the last decade, including Johns Hopkins University, Baltimore, and Tufts University, Medford, Mass.
Legacy admissions contradict schools’ more inclusive policies, Senila Yasmin, MPH, a second-year medical student at Tufts University, said in an interview. While Tufts maintains legacy admissions for its undergraduate applicants, the medical school stopped the practice in 2021, said Ms. Yasmin, a member of a student group that lobbied against the school’s legacy preferences.
Describing herself as a low-income, first-generation Muslim-Pakistani American, Ms. Yasmin wants to use her experience at Tufts to improve accessibility for students like herself.
As a member of the American Medical Association (AMA) Medical Student Section, she coauthored a resolution stating that legacy admissions go against the AMA’s strategic plan to advance racial justice and health equity. The Student Section passed the resolution in November, and in June, the AMA House of Delegates will vote on whether to adopt the policy.
Along with a Supreme Court decision that could strike down race-conscious college admissions, an AMA policy could convince medical schools to rethink legacy admissions and how to maintain diverse student bodies. In June, the court is expected to issue a decision in the Students for Fair Admissions lawsuit against Harvard University, Cambridge, Mass., and the University of North Carolina, Chapel Hill, which alleges that considering race in holistic admissions constitutes racial discrimination and violates the Equal Protection Clause.
Opponents of legacy admissions, like Ms. Yasmin, say it penalizes students from racial minorities and lower socioeconomic backgrounds, hampering a fair and equitable admissions process that attracts diverse medical school admissions.
Diversity of medical applicants
Diversity in medical schools continued to increase last year with more Black, Hispanic, and female students applying and enrolling, according to a recent report by the Association of American Medical Colleges (AAMC). However, universities often include nonacademic criteria in their admission assessments to improve educational access for underrepresented minorities.
Medical schools carefully consider each applicant’s background “to yield a diverse class of students,” Geoffrey Young, PhD, AAMC’s senior director of transforming the health care workforce, told this news organization.
Some schools, such as Morehouse School of Medicine, Atlanta, the University of Virginia School of Medicine, Charlottesville, and the University of Arizona College of Medicine, Tucson, perform a thorough review of candidates while offering admissions practices designed specifically for legacy applicants. The schools assert that legacy designation doesn’t factor into the student’s likelihood of acceptance.
The arrangement may show that schools want to commit to equity and fairness but have trouble moving away from entrenched traditions, two professors from Penn State College of Medicine, Hershey, Pa., who sit on separate medical admissions subcommittees, wrote last year in Bioethics Today.
Legislation may hasten legacies’ end
In December, Ms. Yasmin and a group of Massachusetts Medical Society student-members presented another resolution to the state medical society, which adopted it.
The society’s new policy opposes the use of legacy status in medical school admissions and supports mechanisms to eliminate its inclusion from the application process, Theodore Calianos II, MD, FACS, president of the Massachusetts Medical Society, said in an interview.
“Legacy preferences limit racial and socioeconomic diversity on campuses, so we asked, ‘What can we do so that everyone has equal access to medical education?’ It is exciting to see the students and young physicians – the future of medicine – become involved in policymaking.”
Proposed laws may also hasten the end of legacy admissions. Last year, the U.S. Senate began considering a bill prohibiting colleges receiving federal financial aid from giving preferential treatment to students based on their relations to donors or alumni. However, the bill allows the Department of Education to make exceptions for institutions serving historically underrepresented groups.
The New York State Senate and the New York State Assembly also are reviewing bills that ban legacy and early admissions policies at public and private universities. Connecticut announced similar legislation last year. Massachusetts legislators are considering two bills: one that would ban the practice at the state’s public universities and another that would require all schools using legacy status to pay a “public service fee” equal to a percentage of its endowment. Colleges with endowment assets exceeding $2 billion must pay at least $2 million, according to the bill’s text.
At schools like Harvard, whose endowment surpasses $50 billion, the option to pay the penalty will make the law moot, Michael Walls, DO, MPH, president of the American Medical Student Association (AMSA), said in an interview. “Smaller schools wouldn’t be able to afford the fine and are less likely to be doing [legacy admissions] anyway,” he said. “The schools that want to continue doing it could just pay the fine.”
Dr. Walls said AMSA supports race-conscious admissions processes and anything that increases fairness for medical school applicants. “Whatever [fair] means is up for interpretation, but it would be great to eliminate legacy admissions,” he said.
A version of this article originally appeared on Medscape.com.