User login
Mastectomy may not be necessary for young breast cancer patients
Mastectomies among younger women with nonmetastatic invasive breast cancer may not always be necessary, according to a new study that shows survival outcomes are similar to those of women who had a lumpectomy.
“A lot of times, there’s this assumption that removal of the entire breast is going to prevent cancer from returning in that breast. That makes complete sense, it’s intuitive, so I think a lot of patients are surprised to find that less extensive surgery provides the same overall survival as a really extensive surgery,” said Christine Pestana, MD, a fellow in breast surgical oncology with the Atrium Health Levine Cancer Institute, Charlotte, N.C. Dr. Pestana presented the study at the annual meeting of the American Society of Breast Surgeons earlier this year.
In fact, it has been well-demonstrated among women over age 50 with breast cancer that lumpectomy and mastectomy result in similar outcomes, but efforts to show similar efficacy by analyzing data from randomized trials have been limited by small numbers of women under 40, said the study’s lead author Lejla Hadzikadic-Gusic, MD, who is codirector of the Sandra Levine Young Women’s Breast Cancer Program at Atrium Health. “We’ve done a lot of research since the 1970s to be able to keep a woman’s breasts and just treat her for breast cancer. It’s nice to be able to say the same thing for younger women,” said Dr. Hadzikadic-Gusic, in an interview.
The researchers drew from the Young Women’s Database from the Levine Cancer Institute. The analysis included data from nearly 600 women treated between 2010 and 2018.
The increasing frequency of mastectomies in younger women may be traceable, in part, to high-profile cases of celebrities who have had mastectomies after an early breast cancer diagnosis, with Angelina Jolie being among the most known of examples. But Ms. Jolie had the procedure proactively without a cancer diagnosis because she carried the BRCA1 mutation, which increases breast cancer risk. That information was often lost in press coverage, which can lead to confusion among young women with breast cancer, according to Dr. Hadzikadic-Gusic. “What we’re trying to do is have this data help us educate our patients,” she said.
It’s also important for physicians to help guide patients through these decisions, and family history is a key factor. Dr. Pestana encourages primary care providers to explore family history to help understand cancer risks. “It’s not just breast cancer. It’s also ovarian cancer, colon cancer, prostate cancer. Those all have associations with different genetic mutations. If we start asking those questions, we may be able to identify patients who potentially could have that mutation, refer them to a geneticist, have them tested,” she said.
All of the 591 patients in the study were under age 40, with a median age of 37, and the median follow-up was 67 months. Twelve percent of patients died; 53.3% of patients were HR+/HER2–, 20.8% were HR+/HER2+, 19.3% were triple negative, and 6.6% were HR–/HER2+. There was no association between type of surgery and mortality.
The study was funded by the Levine Family Cancer Institute. Dr. Pestana and Dr. Hadzikadic-Gusic have no relevant financial disclosures.
Mastectomies among younger women with nonmetastatic invasive breast cancer may not always be necessary, according to a new study that shows survival outcomes are similar to those of women who had a lumpectomy.
“A lot of times, there’s this assumption that removal of the entire breast is going to prevent cancer from returning in that breast. That makes complete sense, it’s intuitive, so I think a lot of patients are surprised to find that less extensive surgery provides the same overall survival as a really extensive surgery,” said Christine Pestana, MD, a fellow in breast surgical oncology with the Atrium Health Levine Cancer Institute, Charlotte, N.C. Dr. Pestana presented the study at the annual meeting of the American Society of Breast Surgeons earlier this year.
In fact, it has been well-demonstrated among women over age 50 with breast cancer that lumpectomy and mastectomy result in similar outcomes, but efforts to show similar efficacy by analyzing data from randomized trials have been limited by small numbers of women under 40, said the study’s lead author Lejla Hadzikadic-Gusic, MD, who is codirector of the Sandra Levine Young Women’s Breast Cancer Program at Atrium Health. “We’ve done a lot of research since the 1970s to be able to keep a woman’s breasts and just treat her for breast cancer. It’s nice to be able to say the same thing for younger women,” said Dr. Hadzikadic-Gusic, in an interview.
The researchers drew from the Young Women’s Database from the Levine Cancer Institute. The analysis included data from nearly 600 women treated between 2010 and 2018.
The increasing frequency of mastectomies in younger women may be traceable, in part, to high-profile cases of celebrities who have had mastectomies after an early breast cancer diagnosis, with Angelina Jolie being among the most known of examples. But Ms. Jolie had the procedure proactively without a cancer diagnosis because she carried the BRCA1 mutation, which increases breast cancer risk. That information was often lost in press coverage, which can lead to confusion among young women with breast cancer, according to Dr. Hadzikadic-Gusic. “What we’re trying to do is have this data help us educate our patients,” she said.
It’s also important for physicians to help guide patients through these decisions, and family history is a key factor. Dr. Pestana encourages primary care providers to explore family history to help understand cancer risks. “It’s not just breast cancer. It’s also ovarian cancer, colon cancer, prostate cancer. Those all have associations with different genetic mutations. If we start asking those questions, we may be able to identify patients who potentially could have that mutation, refer them to a geneticist, have them tested,” she said.
All of the 591 patients in the study were under age 40, with a median age of 37, and the median follow-up was 67 months. Twelve percent of patients died; 53.3% of patients were HR+/HER2–, 20.8% were HR+/HER2+, 19.3% were triple negative, and 6.6% were HR–/HER2+. There was no association between type of surgery and mortality.
The study was funded by the Levine Family Cancer Institute. Dr. Pestana and Dr. Hadzikadic-Gusic have no relevant financial disclosures.
Mastectomies among younger women with nonmetastatic invasive breast cancer may not always be necessary, according to a new study that shows survival outcomes are similar to those of women who had a lumpectomy.
“A lot of times, there’s this assumption that removal of the entire breast is going to prevent cancer from returning in that breast. That makes complete sense, it’s intuitive, so I think a lot of patients are surprised to find that less extensive surgery provides the same overall survival as a really extensive surgery,” said Christine Pestana, MD, a fellow in breast surgical oncology with the Atrium Health Levine Cancer Institute, Charlotte, N.C. Dr. Pestana presented the study at the annual meeting of the American Society of Breast Surgeons earlier this year.
In fact, it has been well-demonstrated among women over age 50 with breast cancer that lumpectomy and mastectomy result in similar outcomes, but efforts to show similar efficacy by analyzing data from randomized trials have been limited by small numbers of women under 40, said the study’s lead author Lejla Hadzikadic-Gusic, MD, who is codirector of the Sandra Levine Young Women’s Breast Cancer Program at Atrium Health. “We’ve done a lot of research since the 1970s to be able to keep a woman’s breasts and just treat her for breast cancer. It’s nice to be able to say the same thing for younger women,” said Dr. Hadzikadic-Gusic, in an interview.
The researchers drew from the Young Women’s Database from the Levine Cancer Institute. The analysis included data from nearly 600 women treated between 2010 and 2018.
The increasing frequency of mastectomies in younger women may be traceable, in part, to high-profile cases of celebrities who have had mastectomies after an early breast cancer diagnosis, with Angelina Jolie being among the most known of examples. But Ms. Jolie had the procedure proactively without a cancer diagnosis because she carried the BRCA1 mutation, which increases breast cancer risk. That information was often lost in press coverage, which can lead to confusion among young women with breast cancer, according to Dr. Hadzikadic-Gusic. “What we’re trying to do is have this data help us educate our patients,” she said.
It’s also important for physicians to help guide patients through these decisions, and family history is a key factor. Dr. Pestana encourages primary care providers to explore family history to help understand cancer risks. “It’s not just breast cancer. It’s also ovarian cancer, colon cancer, prostate cancer. Those all have associations with different genetic mutations. If we start asking those questions, we may be able to identify patients who potentially could have that mutation, refer them to a geneticist, have them tested,” she said.
All of the 591 patients in the study were under age 40, with a median age of 37, and the median follow-up was 67 months. Twelve percent of patients died; 53.3% of patients were HR+/HER2–, 20.8% were HR+/HER2+, 19.3% were triple negative, and 6.6% were HR–/HER2+. There was no association between type of surgery and mortality.
The study was funded by the Levine Family Cancer Institute. Dr. Pestana and Dr. Hadzikadic-Gusic have no relevant financial disclosures.
FROM ASBS 2022
Using anti-inflammatory drugs may prolong back pain
A new study questions the conventional wisdom of using steroids and anti-inflammatory drugs like ibuprofen to treat low back pain if exercise and other nondrug therapies don’t work right away.
Those medications offer relief from acute pain but may actually increase a person’s chances of developing chronic pain, said the investigators for a study published in Science Translational Medicine. The study results indicate that
“For many decades it’s been standard medical practice to treat pain with anti-inflammatory drugs,” Jeffrey Mogil, PhD, a psychology professor at McGill University, Montreal, said in a school news release. “But we found that this short-term fix could lead to longer-term problems.”
Researchers looked at low back pain because it’s so common, with 25% of U.S. adults saying they had low back pain in the previous 3 months, according to the Centers for Disease Control and Prevention. Acute back pain is defined as lasting less than 4 weeks while chronic back pain lasts more than 12 weeks.
By examining blood samples, researchers discovered that people whose low back pain was resolved had high inflammation driven by neutrophils, a type of white blood cell that helps the body fight infection, the study said.
“Neutrophils dominate the early stages of inflammation and set the stage for repair of tissue damage. Inflammation occurs for a reason, and it looks like it’s dangerous to interfere with it,” Dr. Mogil said in the news release.
The research team found that blocking neutrophils in mice prolonged pain in the animals up to 10-fold. Pain also was prolonged when the mice were given anti-inflammatory drugs and steroids, the news release says.
McGill University said other studies support the findings. The school cited an analysis of 500,000 people in the United Kingdom. The analysis found that those taking anti-inflammatory drugs for pain were more likely to have pain 2 to 10 years later.
While saying the study suggests it’s time to reconsider how pain is treated, the researchers called for clinical trials on humans, not just observations of people with low back pain.
Experts warned about accepting the results without further investigation.
“It’s intriguing but requires further study,” Steven J. Atlas, MD, director of the Primary Care Research & Quality Improvement Network at Massachusetts General Hospital, Boston, told The New York Times.
A version of this article first appeared on WebMD.com.
A new study questions the conventional wisdom of using steroids and anti-inflammatory drugs like ibuprofen to treat low back pain if exercise and other nondrug therapies don’t work right away.
Those medications offer relief from acute pain but may actually increase a person’s chances of developing chronic pain, said the investigators for a study published in Science Translational Medicine. The study results indicate that
“For many decades it’s been standard medical practice to treat pain with anti-inflammatory drugs,” Jeffrey Mogil, PhD, a psychology professor at McGill University, Montreal, said in a school news release. “But we found that this short-term fix could lead to longer-term problems.”
Researchers looked at low back pain because it’s so common, with 25% of U.S. adults saying they had low back pain in the previous 3 months, according to the Centers for Disease Control and Prevention. Acute back pain is defined as lasting less than 4 weeks while chronic back pain lasts more than 12 weeks.
By examining blood samples, researchers discovered that people whose low back pain was resolved had high inflammation driven by neutrophils, a type of white blood cell that helps the body fight infection, the study said.
“Neutrophils dominate the early stages of inflammation and set the stage for repair of tissue damage. Inflammation occurs for a reason, and it looks like it’s dangerous to interfere with it,” Dr. Mogil said in the news release.
The research team found that blocking neutrophils in mice prolonged pain in the animals up to 10-fold. Pain also was prolonged when the mice were given anti-inflammatory drugs and steroids, the news release says.
McGill University said other studies support the findings. The school cited an analysis of 500,000 people in the United Kingdom. The analysis found that those taking anti-inflammatory drugs for pain were more likely to have pain 2 to 10 years later.
While saying the study suggests it’s time to reconsider how pain is treated, the researchers called for clinical trials on humans, not just observations of people with low back pain.
Experts warned about accepting the results without further investigation.
“It’s intriguing but requires further study,” Steven J. Atlas, MD, director of the Primary Care Research & Quality Improvement Network at Massachusetts General Hospital, Boston, told The New York Times.
A version of this article first appeared on WebMD.com.
A new study questions the conventional wisdom of using steroids and anti-inflammatory drugs like ibuprofen to treat low back pain if exercise and other nondrug therapies don’t work right away.
Those medications offer relief from acute pain but may actually increase a person’s chances of developing chronic pain, said the investigators for a study published in Science Translational Medicine. The study results indicate that
“For many decades it’s been standard medical practice to treat pain with anti-inflammatory drugs,” Jeffrey Mogil, PhD, a psychology professor at McGill University, Montreal, said in a school news release. “But we found that this short-term fix could lead to longer-term problems.”
Researchers looked at low back pain because it’s so common, with 25% of U.S. adults saying they had low back pain in the previous 3 months, according to the Centers for Disease Control and Prevention. Acute back pain is defined as lasting less than 4 weeks while chronic back pain lasts more than 12 weeks.
By examining blood samples, researchers discovered that people whose low back pain was resolved had high inflammation driven by neutrophils, a type of white blood cell that helps the body fight infection, the study said.
“Neutrophils dominate the early stages of inflammation and set the stage for repair of tissue damage. Inflammation occurs for a reason, and it looks like it’s dangerous to interfere with it,” Dr. Mogil said in the news release.
The research team found that blocking neutrophils in mice prolonged pain in the animals up to 10-fold. Pain also was prolonged when the mice were given anti-inflammatory drugs and steroids, the news release says.
McGill University said other studies support the findings. The school cited an analysis of 500,000 people in the United Kingdom. The analysis found that those taking anti-inflammatory drugs for pain were more likely to have pain 2 to 10 years later.
While saying the study suggests it’s time to reconsider how pain is treated, the researchers called for clinical trials on humans, not just observations of people with low back pain.
Experts warned about accepting the results without further investigation.
“It’s intriguing but requires further study,” Steven J. Atlas, MD, director of the Primary Care Research & Quality Improvement Network at Massachusetts General Hospital, Boston, told The New York Times.
A version of this article first appeared on WebMD.com.
FROM SCIENCE TRANSLATIONAL MEDICINE
Tirzepatide (Mounjaro) approved for type 2 diabetes
The “twincretin” era for treating patients with type 2 diabetes has begun, with the Food and Drug Administration’s approval of tirzepatide for this indication on May 13, making it the first approved agent that works as a dual agonist for the two principal human incretins.
Tirzepatide represents “an important advance in the treatment of type 2 diabetes,” the FDA’s Patrick Archdeacon, MD, associate director of the division of diabetes, lipid disorders, and obesity, said in a statement released by the agency.
That advance is based on tirzepatide’s engineering, which gives it agonist properties for both the glucagonlike peptide–1 (GLP-1) receptor, as well as the glucose-dependent insulinotropic polypeptide (GIP). Several agents are already approved for U.S. use from the class with single-agonist activity on the GLP-1 receptor, including semaglutide (Ozempic for treating patients with type 2 diabetes; Wegovy for weight loss).
The FDA’s approved label includes all three dosages of tirzepatide that underwent testing in the pivotal trials: 5 mg, 10 mg, and 15 mg, each delivered by subcutaneous injection once a week. Also approved was the 2.5-mg/week dose used when starting a patient on the agent. Gradual up-titration appears to minimize possible gastrointestinal adverse effects during initial tirzepatide use.
Tirzepatide, which will be marketed by Lilly as Mounjaro, will hit the U.S. market with much anticipation, based on results from five pivotal trials, all reported during the past year or so, that established the drug’s unprecedented efficacy for reducing hemoglobin A1c levels as well as triggering significant weight loss in most patients with a generally benign safety profile.
‘Impressive’ effects
The effects from tirzepatide on A1c and weight seen in these studies was “impressive, and will likely drive use of this agent,” commented Carol H. Wysham, MD, an endocrinologist at the MultiCare Rockwood Clinic in Spokane, Wash.

Tirzepatide received good notices in several editorials that accompanied the published reports of the pivotal trials. The first of these, a commentary from two U.K.-based endocrinologists, said that “tirzepatide appears to represent an advancement over current GLP-1 analogues, providing enhanced glycemic and weight benefits without an added penalty in terms of gastrointestinal adverse effects.”
The pivotal trials included head-to-head comparisons between tirzepatide and a 1.0-mg/week dose of semaglutide, as well as comparisons with each of two long-acting insulin analogs, insulin glargine (Lantus) and insulin degludec (Tresiba).
“These are the most important comparators,” Dr. Wysham said.
“Tirzepatide was appropriately compared with the best-in-class and most effective glucose-lowering agents currently available,” said Ildiko Lingvay, MD, an endocrinologist and professor at the University of Texas Southwestern Medical Center in Dallas.

“Given its outstanding efficacy at both lowering glucose and weight, I expect tirzepatide to have quick uptake among patients with diabetes,” Dr. Lingvay said. “The only limiting factor will be cost,” she added in an interview, highlighting the major stumbling block that could limit tirzepatide’s uptake.
“As with any new medication, access will be the biggest barrier to uptake,” agreed Alice Y.Y. Cheng, MD, an endocrinologist at the University of Toronto.
Lingering uncertainties
The timing of the comparison with semaglutide leaves some unanswered questions. The SURPASS-2 trial compared the three primary tirzepatide regimens (5 mg, 10 mg, and 15 mg/week) with a 1.0-mg/week dose of semaglutide, which was at the time the only approved dosage of semaglutide for patients with type 2 diabetes. Since then, a 2.0-mg/week dosage of semaglutide (Ozempic) received U.S. approval for treating patients with type 2 diabetes, and a 2.4-mg/week dosage (Wegovy) received an FDA nod for treating people with obesity.
The lack of head-to-head data for tirzepatide against the 2.0-mg/week dose of semaglutide “leaves a clinical gap,” said Dr. Cheng. Tirzepatide “represents an advance over semaglutide at the 1-mg/week dose, but we do not know for sure compared to the higher dose.”
Another important limitation for tirzepatide right now is that the agent’s obligatory cardiovascular outcome trial, SURPASS CVOT, with about 12,500 enrolled patients, will not have findings out until about 2025, leaving uncertainty until then about tirzepatide’s cardiovascular effects.
“We are missing the cardiovascular outcome data – very important data will come” from that trial, noted Dr. Wysham. “There will be some reluctance to use the agent in high-risk patients until we see the results.”
Given tirzepatide’s proven efficacy so far, the missing cardiovascular results “are not a limitation for most patients, but for patients with preexisting cardiovascular disease I will continue to use agents with proven benefits until the SURPASS CVOT results come out,” Dr. Lingvay said.
And then there is the cost issue, something that Lilly had not yet publicly addressed at the time that the FDA announced its decision.
An analysis of cost effectiveness published by the U.S. Institute for Clinical and Economic Review in February 2022 concluded that tirzepatide had a better impact on patient quality of life, compared with 1.0 mg/week semaglutide for treating patients with type 2 diabetes, which gave it a modest pricing cushion, compared with semaglutide of about $5,500 per quality-adjusted life-year gained. But the researchers who prepared the report admitted that tirzepatide’s cost-effectiveness was hard to estimate without knowing the drug’s actual price.
Dr. Wysham has financial ties to AstraZeneca, Abbott, Boehringer Ingelheim, Intercept, Janssen, Mylan, Novo Nordisk, and Sanofi. Dr. Lingvay has dies to Lilly, Novo Nordisk, Sanofi, Boehringer Ingelheim, Merck, Pfizer, and Mylan, Intarcia, MannKind, Valeritas, and several other drug and device makers.
A version of this article first appeared on Medscape.com.
The “twincretin” era for treating patients with type 2 diabetes has begun, with the Food and Drug Administration’s approval of tirzepatide for this indication on May 13, making it the first approved agent that works as a dual agonist for the two principal human incretins.
Tirzepatide represents “an important advance in the treatment of type 2 diabetes,” the FDA’s Patrick Archdeacon, MD, associate director of the division of diabetes, lipid disorders, and obesity, said in a statement released by the agency.
That advance is based on tirzepatide’s engineering, which gives it agonist properties for both the glucagonlike peptide–1 (GLP-1) receptor, as well as the glucose-dependent insulinotropic polypeptide (GIP). Several agents are already approved for U.S. use from the class with single-agonist activity on the GLP-1 receptor, including semaglutide (Ozempic for treating patients with type 2 diabetes; Wegovy for weight loss).
The FDA’s approved label includes all three dosages of tirzepatide that underwent testing in the pivotal trials: 5 mg, 10 mg, and 15 mg, each delivered by subcutaneous injection once a week. Also approved was the 2.5-mg/week dose used when starting a patient on the agent. Gradual up-titration appears to minimize possible gastrointestinal adverse effects during initial tirzepatide use.
Tirzepatide, which will be marketed by Lilly as Mounjaro, will hit the U.S. market with much anticipation, based on results from five pivotal trials, all reported during the past year or so, that established the drug’s unprecedented efficacy for reducing hemoglobin A1c levels as well as triggering significant weight loss in most patients with a generally benign safety profile.
‘Impressive’ effects
The effects from tirzepatide on A1c and weight seen in these studies was “impressive, and will likely drive use of this agent,” commented Carol H. Wysham, MD, an endocrinologist at the MultiCare Rockwood Clinic in Spokane, Wash.
Tirzepatide received good notices in several editorials that accompanied the published reports of the pivotal trials. The first of these, a commentary from two U.K.-based endocrinologists, said that “tirzepatide appears to represent an advancement over current GLP-1 analogues, providing enhanced glycemic and weight benefits without an added penalty in terms of gastrointestinal adverse effects.”
The pivotal trials included head-to-head comparisons between tirzepatide and a 1.0-mg/week dose of semaglutide, as well as comparisons with each of two long-acting insulin analogs, insulin glargine (Lantus) and insulin degludec (Tresiba).
“These are the most important comparators,” Dr. Wysham said.
“Tirzepatide was appropriately compared with the best-in-class and most effective glucose-lowering agents currently available,” said Ildiko Lingvay, MD, an endocrinologist and professor at the University of Texas Southwestern Medical Center in Dallas.
“Given its outstanding efficacy at both lowering glucose and weight, I expect tirzepatide to have quick uptake among patients with diabetes,” Dr. Lingvay said. “The only limiting factor will be cost,” she added in an interview, highlighting the major stumbling block that could limit tirzepatide’s uptake.
“As with any new medication, access will be the biggest barrier to uptake,” agreed Alice Y.Y. Cheng, MD, an endocrinologist at the University of Toronto.
Lingering uncertainties
The timing of the comparison with semaglutide leaves some unanswered questions. The SURPASS-2 trial compared the three primary tirzepatide regimens (5 mg, 10 mg, and 15 mg/week) with a 1.0-mg/week dose of semaglutide, which was at the time the only approved dosage of semaglutide for patients with type 2 diabetes. Since then, a 2.0-mg/week dosage of semaglutide (Ozempic) received U.S. approval for treating patients with type 2 diabetes, and a 2.4-mg/week dosage (Wegovy) received an FDA nod for treating people with obesity.
The lack of head-to-head data for tirzepatide against the 2.0-mg/week dose of semaglutide “leaves a clinical gap,” said Dr. Cheng. Tirzepatide “represents an advance over semaglutide at the 1-mg/week dose, but we do not know for sure compared to the higher dose.”
Another important limitation for tirzepatide right now is that the agent’s obligatory cardiovascular outcome trial, SURPASS CVOT, with about 12,500 enrolled patients, will not have findings out until about 2025, leaving uncertainty until then about tirzepatide’s cardiovascular effects.
“We are missing the cardiovascular outcome data – very important data will come” from that trial, noted Dr. Wysham. “There will be some reluctance to use the agent in high-risk patients until we see the results.”
Given tirzepatide’s proven efficacy so far, the missing cardiovascular results “are not a limitation for most patients, but for patients with preexisting cardiovascular disease I will continue to use agents with proven benefits until the SURPASS CVOT results come out,” Dr. Lingvay said.
And then there is the cost issue, something that Lilly had not yet publicly addressed at the time that the FDA announced its decision.
An analysis of cost effectiveness published by the U.S. Institute for Clinical and Economic Review in February 2022 concluded that tirzepatide had a better impact on patient quality of life, compared with 1.0 mg/week semaglutide for treating patients with type 2 diabetes, which gave it a modest pricing cushion, compared with semaglutide of about $5,500 per quality-adjusted life-year gained. But the researchers who prepared the report admitted that tirzepatide’s cost-effectiveness was hard to estimate without knowing the drug’s actual price.
Dr. Wysham has financial ties to AstraZeneca, Abbott, Boehringer Ingelheim, Intercept, Janssen, Mylan, Novo Nordisk, and Sanofi. Dr. Lingvay has dies to Lilly, Novo Nordisk, Sanofi, Boehringer Ingelheim, Merck, Pfizer, and Mylan, Intarcia, MannKind, Valeritas, and several other drug and device makers.
A version of this article first appeared on Medscape.com.
The “twincretin” era for treating patients with type 2 diabetes has begun, with the Food and Drug Administration’s approval of tirzepatide for this indication on May 13, making it the first approved agent that works as a dual agonist for the two principal human incretins.
Tirzepatide represents “an important advance in the treatment of type 2 diabetes,” the FDA’s Patrick Archdeacon, MD, associate director of the division of diabetes, lipid disorders, and obesity, said in a statement released by the agency.
That advance is based on tirzepatide’s engineering, which gives it agonist properties for both the glucagonlike peptide–1 (GLP-1) receptor, as well as the glucose-dependent insulinotropic polypeptide (GIP). Several agents are already approved for U.S. use from the class with single-agonist activity on the GLP-1 receptor, including semaglutide (Ozempic for treating patients with type 2 diabetes; Wegovy for weight loss).
The FDA’s approved label includes all three dosages of tirzepatide that underwent testing in the pivotal trials: 5 mg, 10 mg, and 15 mg, each delivered by subcutaneous injection once a week. Also approved was the 2.5-mg/week dose used when starting a patient on the agent. Gradual up-titration appears to minimize possible gastrointestinal adverse effects during initial tirzepatide use.
Tirzepatide, which will be marketed by Lilly as Mounjaro, will hit the U.S. market with much anticipation, based on results from five pivotal trials, all reported during the past year or so, that established the drug’s unprecedented efficacy for reducing hemoglobin A1c levels as well as triggering significant weight loss in most patients with a generally benign safety profile.
‘Impressive’ effects
The effects from tirzepatide on A1c and weight seen in these studies was “impressive, and will likely drive use of this agent,” commented Carol H. Wysham, MD, an endocrinologist at the MultiCare Rockwood Clinic in Spokane, Wash.
Tirzepatide received good notices in several editorials that accompanied the published reports of the pivotal trials. The first of these, a commentary from two U.K.-based endocrinologists, said that “tirzepatide appears to represent an advancement over current GLP-1 analogues, providing enhanced glycemic and weight benefits without an added penalty in terms of gastrointestinal adverse effects.”
The pivotal trials included head-to-head comparisons between tirzepatide and a 1.0-mg/week dose of semaglutide, as well as comparisons with each of two long-acting insulin analogs, insulin glargine (Lantus) and insulin degludec (Tresiba).
“These are the most important comparators,” Dr. Wysham said.
“Tirzepatide was appropriately compared with the best-in-class and most effective glucose-lowering agents currently available,” said Ildiko Lingvay, MD, an endocrinologist and professor at the University of Texas Southwestern Medical Center in Dallas.
“Given its outstanding efficacy at both lowering glucose and weight, I expect tirzepatide to have quick uptake among patients with diabetes,” Dr. Lingvay said. “The only limiting factor will be cost,” she added in an interview, highlighting the major stumbling block that could limit tirzepatide’s uptake.
“As with any new medication, access will be the biggest barrier to uptake,” agreed Alice Y.Y. Cheng, MD, an endocrinologist at the University of Toronto.
Lingering uncertainties
The timing of the comparison with semaglutide leaves some unanswered questions. The SURPASS-2 trial compared the three primary tirzepatide regimens (5 mg, 10 mg, and 15 mg/week) with a 1.0-mg/week dose of semaglutide, which was at the time the only approved dosage of semaglutide for patients with type 2 diabetes. Since then, a 2.0-mg/week dosage of semaglutide (Ozempic) received U.S. approval for treating patients with type 2 diabetes, and a 2.4-mg/week dosage (Wegovy) received an FDA nod for treating people with obesity.
The lack of head-to-head data for tirzepatide against the 2.0-mg/week dose of semaglutide “leaves a clinical gap,” said Dr. Cheng. Tirzepatide “represents an advance over semaglutide at the 1-mg/week dose, but we do not know for sure compared to the higher dose.”
Another important limitation for tirzepatide right now is that the agent’s obligatory cardiovascular outcome trial, SURPASS CVOT, with about 12,500 enrolled patients, will not have findings out until about 2025, leaving uncertainty until then about tirzepatide’s cardiovascular effects.
“We are missing the cardiovascular outcome data – very important data will come” from that trial, noted Dr. Wysham. “There will be some reluctance to use the agent in high-risk patients until we see the results.”
Given tirzepatide’s proven efficacy so far, the missing cardiovascular results “are not a limitation for most patients, but for patients with preexisting cardiovascular disease I will continue to use agents with proven benefits until the SURPASS CVOT results come out,” Dr. Lingvay said.
And then there is the cost issue, something that Lilly had not yet publicly addressed at the time that the FDA announced its decision.
An analysis of cost effectiveness published by the U.S. Institute for Clinical and Economic Review in February 2022 concluded that tirzepatide had a better impact on patient quality of life, compared with 1.0 mg/week semaglutide for treating patients with type 2 diabetes, which gave it a modest pricing cushion, compared with semaglutide of about $5,500 per quality-adjusted life-year gained. But the researchers who prepared the report admitted that tirzepatide’s cost-effectiveness was hard to estimate without knowing the drug’s actual price.
Dr. Wysham has financial ties to AstraZeneca, Abbott, Boehringer Ingelheim, Intercept, Janssen, Mylan, Novo Nordisk, and Sanofi. Dr. Lingvay has dies to Lilly, Novo Nordisk, Sanofi, Boehringer Ingelheim, Merck, Pfizer, and Mylan, Intarcia, MannKind, Valeritas, and several other drug and device makers.
A version of this article first appeared on Medscape.com.
Study shows link between dairy consumption and cancer
A relationship between consumption of dairy products and risk of various cancers has been intensively investigated in the past but yielded inconclusive or conflicting results.
The study, by researchers from Oxford University’s department of population health, and Peking University and the Chinese Academy of Medical Sciences in Beijing, used data from the China Kadoorie Biobank Study, a long-term prospective study involving more than over 510,000 participants recruited from 10 geographically diverse areas across China, including both rural and urban regions. They compared this to data from the UK biobank.
Subjects were 59% female, 41% male, aged 30-79 years, and had no history of cancer at recruitment between 2004 and 2008. Food questionnaires were completed at the outset and participants followed for an average of 11 years, using national cancer and death registries and health insurance records to identify new cancer diagnoses, including both fatal and nonfatal events.
Participants were categorized into three groups according to how often they consumed dairy products (primarily milk):
- Regular consumers (at least once a week): 20.4% of the cohort.
- Monthly consumers: 11.1%.
- Nonconsumers who never or rarely consumed dairy products: 68.5%.
Average dairy consumption was 37.9 g/day overall and 80.8 g/day among regular consumers. This compares with an average consumption of around 300 g/day in participants in the UK Biobank cohort.
Over the course of the study, 29,277 new cancer cases were recorded, including 6,282 lung, 2,582 female breast, 3,577 stomach, 3,350 colorectal, and 3,191 liver cancer cases.
Analyses correlating cases with consumption took into account a range of other factors potentially affecting cancer risk, including age, sex, region, family history of cancer, socioeconomic status (education and income), lifestyle factors (alcohol intake, smoking, physical activity, soy consumption, and fresh fruit intake), body mass index, chronic hepatitis B virus infection, and female reproductive factors.
Higher dairy intakes linked with risk of liver and breast cancers
Results revealed that higher regular dairy intake was associated with significantly higher risks of liver cancer and female breast cancer, both common types of cancer in China. Analyses indicated that for each 50-g/day intake, the risks increased by 12% and 17%, respectively.
There was also an increase in total cancer diagnoses, and an increased risk of lymphoma, though this was not statistically significant after correction for confounders. No association was found between dairy products and colorectal cancer, prostate cancer, or any other site-specific cancer.
The research, published in BMC Medicine, is the first major study to investigate dairy consumption and cancer risk in Chinese adults. The results conflict with previous studies on Western populations, which have suggested that dairy products may be associated with a lower risk of colorectal cancer and a higher risk of prostate cancer but have found no clear link for breast or other types of cancer.
Lead researchers Maria Kakkoura, PhD, MSc, and associate professor Huaidong Du, MD, PhD, told this news organization that, although they don’t know the reason for the difference, “there is clear evidence that colorectal cancer has a different incidence pattern in China, compared with Western countries. Other risk factors, like adiposity, may have a stronger effect on the risk of colorectal cancer in Western countries than in China.” Notably, the mean body mass index in the study population was around 23 kg/m2, they said – by contrast in the United Kingdom it is 27.6 kg/m2.
Effects not necessarily causal
Ian Givens, PhD, professor of food chain nutrition at the University of Reading (England), said the study was “potentially very important for Chinese people, if it can be confirmed that dairy products affect the risk of breast and/or liver cancer differently in Chinese subjects to those in Western Societies, especially as dairy consumption in China is much lower than in most Western diets.”
He added: “As always it needs to be kept in mind that this type of study can only establish associations with disease risk, not cause.”
Dr. Kakkoura, nutritional epidemiologist at Oxford (England) University’s department of population health, said: “This was the first major study to investigate the link between dairy products and cancer risk in a Chinese population. Further studies are needed to validate these current findings, establish if these associations are causal, and investigate the potential underlying mechanisms involved.”
The researchers said that, while the results do not prove causation, “there are several plausible biological mechanisms that may explain these associations.” They pointed to higher dairy consumption potentially increasing levels of insulinlike growth factor-I, known to promote cell proliferation and associated with higher risks of several types of cancer.
In addition, estrogen and progesterone present in cows’ milk may play a role in increasing breast cancer risk, whilst saturated and trans-fatty acids from dairy products may increase the risk of liver cancer. As many Chinese people are lactase deficient, dairy products may also be broken down into products that affect cancer risk.
No justification for dietary change
Confounding factors may also have influenced the results, commented Duane Mellor, PhD, RD, RNutr, registered dietitian and senior teaching fellow at Aston University, Birmingham, England. “Those in the study who consumed dairy were more likely to live in cities and have other health conditions, including cardiovascular disease and diabetes – although some of these factors were considered in the analysis, not all of these covariates were, which could influence the findings.
“In my view this study alone does not provide strong evidence that reducing dairy intake would reduce cancer risk.”
He added: “Although the paper suggests a 12% increased relative risk for female breast cancer, this does not equate to 12 more cases per 100 individuals – in absolute terms this would be more like 1 or 2 cases per 1,000 people.”
Similarly, Kevin McConway, PhD, emeritus professor of applied statistics at the Open University, Milton Keynes, England, said: “An issue is that there were many differences between the people that consumed different amounts of dairy products, apart from their difference in dairy consumption. For instance, of those who never or rarely consumed dairy products, fewer than a third lived in urban areas, but of regular dairy consumers (at least once a week), 83% lived in urban areas. Regular consumers were considerably more likely to be well educated than those who never or rarely consumed dairy products, and there were other differences too.
“So if, as the researchers found, a greater proportion of the regular consumers than of the never or rare consumers had a cancer diagnosis, that could have been because of their different dairy consumption, or it could have been (in part or entirely) because of the different places they lived, or their different education levels, or any of the other factors on which the groups differed.
“One can never be sure that all the relevant factors have been adjusted for. That’s why the researchers rightly say that these results can’t establish whether the associations between dairy consumption and the risks of some cancers, that they found, are there because the dairy consumption differences change the cancer risks in a cause-and-effect way. They might, or they might not.”
He cautioned: “I don’t think anyone should decide to change their individual diet solely because of the results of this new study.”
Commenting on the study, Fiona Osgun, senior health information manager at Cancer Research UK, London, told this news organization: “This early-stage study found an association between dairy consumption and the risks of certain cancers, but that doesn’t mean that they’re causing them or that people need to avoid dairy. Dairy products can be part of a healthy balanced diet and, in the U.K., the Food Standards Agency regulates them to make sure they’re safe. There’s good evidence that dairy reduces the risk of bowel cancer, but no clear evidence for other cancer types, and this is no different for people who are lactose intolerant.”
A version of this article first appeared on Medscape UK.
A relationship between consumption of dairy products and risk of various cancers has been intensively investigated in the past but yielded inconclusive or conflicting results.
The study, by researchers from Oxford University’s department of population health, and Peking University and the Chinese Academy of Medical Sciences in Beijing, used data from the China Kadoorie Biobank Study, a long-term prospective study involving more than over 510,000 participants recruited from 10 geographically diverse areas across China, including both rural and urban regions. They compared this to data from the UK biobank.
Subjects were 59% female, 41% male, aged 30-79 years, and had no history of cancer at recruitment between 2004 and 2008. Food questionnaires were completed at the outset and participants followed for an average of 11 years, using national cancer and death registries and health insurance records to identify new cancer diagnoses, including both fatal and nonfatal events.
Participants were categorized into three groups according to how often they consumed dairy products (primarily milk):
- Regular consumers (at least once a week): 20.4% of the cohort.
- Monthly consumers: 11.1%.
- Nonconsumers who never or rarely consumed dairy products: 68.5%.
Average dairy consumption was 37.9 g/day overall and 80.8 g/day among regular consumers. This compares with an average consumption of around 300 g/day in participants in the UK Biobank cohort.
Over the course of the study, 29,277 new cancer cases were recorded, including 6,282 lung, 2,582 female breast, 3,577 stomach, 3,350 colorectal, and 3,191 liver cancer cases.
Analyses correlating cases with consumption took into account a range of other factors potentially affecting cancer risk, including age, sex, region, family history of cancer, socioeconomic status (education and income), lifestyle factors (alcohol intake, smoking, physical activity, soy consumption, and fresh fruit intake), body mass index, chronic hepatitis B virus infection, and female reproductive factors.
Higher dairy intakes linked with risk of liver and breast cancers
Results revealed that higher regular dairy intake was associated with significantly higher risks of liver cancer and female breast cancer, both common types of cancer in China. Analyses indicated that for each 50-g/day intake, the risks increased by 12% and 17%, respectively.
There was also an increase in total cancer diagnoses, and an increased risk of lymphoma, though this was not statistically significant after correction for confounders. No association was found between dairy products and colorectal cancer, prostate cancer, or any other site-specific cancer.
The research, published in BMC Medicine, is the first major study to investigate dairy consumption and cancer risk in Chinese adults. The results conflict with previous studies on Western populations, which have suggested that dairy products may be associated with a lower risk of colorectal cancer and a higher risk of prostate cancer but have found no clear link for breast or other types of cancer.
Lead researchers Maria Kakkoura, PhD, MSc, and associate professor Huaidong Du, MD, PhD, told this news organization that, although they don’t know the reason for the difference, “there is clear evidence that colorectal cancer has a different incidence pattern in China, compared with Western countries. Other risk factors, like adiposity, may have a stronger effect on the risk of colorectal cancer in Western countries than in China.” Notably, the mean body mass index in the study population was around 23 kg/m2, they said – by contrast in the United Kingdom it is 27.6 kg/m2.
Effects not necessarily causal
Ian Givens, PhD, professor of food chain nutrition at the University of Reading (England), said the study was “potentially very important for Chinese people, if it can be confirmed that dairy products affect the risk of breast and/or liver cancer differently in Chinese subjects to those in Western Societies, especially as dairy consumption in China is much lower than in most Western diets.”
He added: “As always it needs to be kept in mind that this type of study can only establish associations with disease risk, not cause.”
Dr. Kakkoura, nutritional epidemiologist at Oxford (England) University’s department of population health, said: “This was the first major study to investigate the link between dairy products and cancer risk in a Chinese population. Further studies are needed to validate these current findings, establish if these associations are causal, and investigate the potential underlying mechanisms involved.”
The researchers said that, while the results do not prove causation, “there are several plausible biological mechanisms that may explain these associations.” They pointed to higher dairy consumption potentially increasing levels of insulinlike growth factor-I, known to promote cell proliferation and associated with higher risks of several types of cancer.
In addition, estrogen and progesterone present in cows’ milk may play a role in increasing breast cancer risk, whilst saturated and trans-fatty acids from dairy products may increase the risk of liver cancer. As many Chinese people are lactase deficient, dairy products may also be broken down into products that affect cancer risk.
No justification for dietary change
Confounding factors may also have influenced the results, commented Duane Mellor, PhD, RD, RNutr, registered dietitian and senior teaching fellow at Aston University, Birmingham, England. “Those in the study who consumed dairy were more likely to live in cities and have other health conditions, including cardiovascular disease and diabetes – although some of these factors were considered in the analysis, not all of these covariates were, which could influence the findings.
“In my view this study alone does not provide strong evidence that reducing dairy intake would reduce cancer risk.”
He added: “Although the paper suggests a 12% increased relative risk for female breast cancer, this does not equate to 12 more cases per 100 individuals – in absolute terms this would be more like 1 or 2 cases per 1,000 people.”
Similarly, Kevin McConway, PhD, emeritus professor of applied statistics at the Open University, Milton Keynes, England, said: “An issue is that there were many differences between the people that consumed different amounts of dairy products, apart from their difference in dairy consumption. For instance, of those who never or rarely consumed dairy products, fewer than a third lived in urban areas, but of regular dairy consumers (at least once a week), 83% lived in urban areas. Regular consumers were considerably more likely to be well educated than those who never or rarely consumed dairy products, and there were other differences too.
“So if, as the researchers found, a greater proportion of the regular consumers than of the never or rare consumers had a cancer diagnosis, that could have been because of their different dairy consumption, or it could have been (in part or entirely) because of the different places they lived, or their different education levels, or any of the other factors on which the groups differed.
“One can never be sure that all the relevant factors have been adjusted for. That’s why the researchers rightly say that these results can’t establish whether the associations between dairy consumption and the risks of some cancers, that they found, are there because the dairy consumption differences change the cancer risks in a cause-and-effect way. They might, or they might not.”
He cautioned: “I don’t think anyone should decide to change their individual diet solely because of the results of this new study.”
Commenting on the study, Fiona Osgun, senior health information manager at Cancer Research UK, London, told this news organization: “This early-stage study found an association between dairy consumption and the risks of certain cancers, but that doesn’t mean that they’re causing them or that people need to avoid dairy. Dairy products can be part of a healthy balanced diet and, in the U.K., the Food Standards Agency regulates them to make sure they’re safe. There’s good evidence that dairy reduces the risk of bowel cancer, but no clear evidence for other cancer types, and this is no different for people who are lactose intolerant.”
A version of this article first appeared on Medscape UK.
A relationship between consumption of dairy products and risk of various cancers has been intensively investigated in the past but yielded inconclusive or conflicting results.
The study, by researchers from Oxford University’s department of population health, and Peking University and the Chinese Academy of Medical Sciences in Beijing, used data from the China Kadoorie Biobank Study, a long-term prospective study involving more than over 510,000 participants recruited from 10 geographically diverse areas across China, including both rural and urban regions. They compared this to data from the UK biobank.
Subjects were 59% female, 41% male, aged 30-79 years, and had no history of cancer at recruitment between 2004 and 2008. Food questionnaires were completed at the outset and participants followed for an average of 11 years, using national cancer and death registries and health insurance records to identify new cancer diagnoses, including both fatal and nonfatal events.
Participants were categorized into three groups according to how often they consumed dairy products (primarily milk):
- Regular consumers (at least once a week): 20.4% of the cohort.
- Monthly consumers: 11.1%.
- Nonconsumers who never or rarely consumed dairy products: 68.5%.
Average dairy consumption was 37.9 g/day overall and 80.8 g/day among regular consumers. This compares with an average consumption of around 300 g/day in participants in the UK Biobank cohort.
Over the course of the study, 29,277 new cancer cases were recorded, including 6,282 lung, 2,582 female breast, 3,577 stomach, 3,350 colorectal, and 3,191 liver cancer cases.
Analyses correlating cases with consumption took into account a range of other factors potentially affecting cancer risk, including age, sex, region, family history of cancer, socioeconomic status (education and income), lifestyle factors (alcohol intake, smoking, physical activity, soy consumption, and fresh fruit intake), body mass index, chronic hepatitis B virus infection, and female reproductive factors.
Higher dairy intakes linked with risk of liver and breast cancers
Results revealed that higher regular dairy intake was associated with significantly higher risks of liver cancer and female breast cancer, both common types of cancer in China. Analyses indicated that for each 50-g/day intake, the risks increased by 12% and 17%, respectively.
There was also an increase in total cancer diagnoses, and an increased risk of lymphoma, though this was not statistically significant after correction for confounders. No association was found between dairy products and colorectal cancer, prostate cancer, or any other site-specific cancer.
The research, published in BMC Medicine, is the first major study to investigate dairy consumption and cancer risk in Chinese adults. The results conflict with previous studies on Western populations, which have suggested that dairy products may be associated with a lower risk of colorectal cancer and a higher risk of prostate cancer but have found no clear link for breast or other types of cancer.
Lead researchers Maria Kakkoura, PhD, MSc, and associate professor Huaidong Du, MD, PhD, told this news organization that, although they don’t know the reason for the difference, “there is clear evidence that colorectal cancer has a different incidence pattern in China, compared with Western countries. Other risk factors, like adiposity, may have a stronger effect on the risk of colorectal cancer in Western countries than in China.” Notably, the mean body mass index in the study population was around 23 kg/m2, they said – by contrast in the United Kingdom it is 27.6 kg/m2.
Effects not necessarily causal
Ian Givens, PhD, professor of food chain nutrition at the University of Reading (England), said the study was “potentially very important for Chinese people, if it can be confirmed that dairy products affect the risk of breast and/or liver cancer differently in Chinese subjects to those in Western Societies, especially as dairy consumption in China is much lower than in most Western diets.”
He added: “As always it needs to be kept in mind that this type of study can only establish associations with disease risk, not cause.”
Dr. Kakkoura, nutritional epidemiologist at Oxford (England) University’s department of population health, said: “This was the first major study to investigate the link between dairy products and cancer risk in a Chinese population. Further studies are needed to validate these current findings, establish if these associations are causal, and investigate the potential underlying mechanisms involved.”
The researchers said that, while the results do not prove causation, “there are several plausible biological mechanisms that may explain these associations.” They pointed to higher dairy consumption potentially increasing levels of insulinlike growth factor-I, known to promote cell proliferation and associated with higher risks of several types of cancer.
In addition, estrogen and progesterone present in cows’ milk may play a role in increasing breast cancer risk, whilst saturated and trans-fatty acids from dairy products may increase the risk of liver cancer. As many Chinese people are lactase deficient, dairy products may also be broken down into products that affect cancer risk.
No justification for dietary change
Confounding factors may also have influenced the results, commented Duane Mellor, PhD, RD, RNutr, registered dietitian and senior teaching fellow at Aston University, Birmingham, England. “Those in the study who consumed dairy were more likely to live in cities and have other health conditions, including cardiovascular disease and diabetes – although some of these factors were considered in the analysis, not all of these covariates were, which could influence the findings.
“In my view this study alone does not provide strong evidence that reducing dairy intake would reduce cancer risk.”
He added: “Although the paper suggests a 12% increased relative risk for female breast cancer, this does not equate to 12 more cases per 100 individuals – in absolute terms this would be more like 1 or 2 cases per 1,000 people.”
Similarly, Kevin McConway, PhD, emeritus professor of applied statistics at the Open University, Milton Keynes, England, said: “An issue is that there were many differences between the people that consumed different amounts of dairy products, apart from their difference in dairy consumption. For instance, of those who never or rarely consumed dairy products, fewer than a third lived in urban areas, but of regular dairy consumers (at least once a week), 83% lived in urban areas. Regular consumers were considerably more likely to be well educated than those who never or rarely consumed dairy products, and there were other differences too.
“So if, as the researchers found, a greater proportion of the regular consumers than of the never or rare consumers had a cancer diagnosis, that could have been because of their different dairy consumption, or it could have been (in part or entirely) because of the different places they lived, or their different education levels, or any of the other factors on which the groups differed.
“One can never be sure that all the relevant factors have been adjusted for. That’s why the researchers rightly say that these results can’t establish whether the associations between dairy consumption and the risks of some cancers, that they found, are there because the dairy consumption differences change the cancer risks in a cause-and-effect way. They might, or they might not.”
He cautioned: “I don’t think anyone should decide to change their individual diet solely because of the results of this new study.”
Commenting on the study, Fiona Osgun, senior health information manager at Cancer Research UK, London, told this news organization: “This early-stage study found an association between dairy consumption and the risks of certain cancers, but that doesn’t mean that they’re causing them or that people need to avoid dairy. Dairy products can be part of a healthy balanced diet and, in the U.K., the Food Standards Agency regulates them to make sure they’re safe. There’s good evidence that dairy reduces the risk of bowel cancer, but no clear evidence for other cancer types, and this is no different for people who are lactose intolerant.”
A version of this article first appeared on Medscape UK.
FROM BMC MEDICINE
Exenatide linked to less hyperglycemia after stroke
Treatment with the diabetes drug exenatide was associated with a significant decrease in hyperglycemia in acute stroke patients, a new study shows.
The research could offer clinicians an alternative to insulin therapy to treat hyperglycemia and reduce glucose levels, which are elevated in up to 60% of stroke patients and associated with worse outcomes after stroke.
“Use of these diabetes drugs to control glucose in acute stroke has enormous potential,” said lead researcher Christopher Bladin, PhD, professor of neurology at Monash University and Eastern Health Clinical School, Australia.
The findings were presented at the European Stroke Organisation Conference (ESOC) 2022 annual meeting in Lyon, France.
A better fix than insulin?
Hyperglycemia is common in stroke patients, including those who have no prior history of diabetes. Among stroke patients with normal blood glucose upon admission, about 30% will develop hyperglycemia within 48 hours of stroke onset.
Previous research suggests that hyperglycemia is a poor prognostic factor in patients with stroke and may reduce the efficacy of reperfusion therapies such as thrombolysis and mechanical thrombectomy.
“We’ve been looking for different ways of treating hyperglycemia for quite some time, and one of the obvious ways is to use insulin therapy,” Dr. Bladin said. “But as we’ve seen from multiple studies, insulin therapy is difficult.”
Insulin treatment is resource-heavy, significantly increases the risk for hypoglycemia, and some studies suggest the therapy isn’t associated with better outcomes.
An advantage to a GLP-1 agonist-like exenatide, Dr. Bladin added, is that it’s glucose-dependent. As the glucose level falls, the drug’s efficacy diminishes. It is delivered via an autoinjector and easy to administer.
A case for more study
To study exenatide’s efficacy in reducing hyperglycemia and improving neurologic outcomes, researchers developed the phase 2, international, multicenter, randomized controlled TEXAIS trial.
The study enrolled 350 patients following an ischemic stroke. Within 9 hours of stroke onset, patients received either standard care or a subcutaneous injection of 5 mg of exenatide twice daily for 5 days.
On admission, 42% of patients had hyperglycemia, defined as blood glucose > 7.0 mmol/L.
The study’s primary outcome was at least an 8-point improvement in National Institutes of Health Stroke Scale (NIHSS) score by 7 days after treatment with exenatide. Although there was a trend toward better scores with exenatide, the score was not significantly different between groups (56.7% with standard care versus 61.2% with exenatide; adjusted odds ratio, 1.22; P = .38).
However, when the researchers examined hyperglycemia frequency, they found significantly lower incidence in patients treated with exenatide (P = .002).
There were no cases of hypoglycemia in either group, and only 4% of the study group reported nausea or vomiting.
“Clearly exenatide is having some benefit in terms of keeping glucose under control, reducing hyperglycemia,” Dr. Bladin said. “It certainly lends itself to a larger phase 3 study which can look at this more completely.”
Value to clinicians
Commenting on the findings, Yvonne Chun, PhD, honorary senior clinical lecturer at University of Edinburgh, noted that, even though the study didn’t find a significant association with improved neurological outcomes, the reduced risk for hypoglycemia makes exenatide an attractive alternative to insulin therapy in stroke patients.
“The results are of value to clinicians, as exenatide could potentially be a safer medication to administer than an insulin infusion in acute stroke patients with hyperglycemia,” Dr. Chun said. “There is less risk of hypoglycemia with exenatide compared to standard care.”
However, Dr. Chun noted that more study is needed before exenatide can replace standard care. Dr. Bladin agrees and would like to pursue a phase 3 trial with a modified design to answer questions raised by Dr. Chun and others.
“The next phase could consider changing the primary outcome to an ordinal shift analysis on modified Rankin Scale – a very commonly used primary outcome in stroke clinical trials to assess improvement in disability,” Dr. Chun said. “The primary outcome used in the presented trial – an 8-point improvement on NIHSS – seemed too ambitious and does not inform disability of the patient post stroke.”
Dr. Bladin said he would also like to see the next phase enroll more patients, examine a higher dose of exenatide, and include better stratification of patients with a history of diabetes. Such a trial could yield findings demonstrating the drug’s effectiveness at reducing hyperglycemia and improving outcomes after stroke, he said.
“I can see the day patients will come in with acute stroke, and as they’re coming into the emergency department, they’ll simply get their shot of exenatide because we know it’s safe to use, and it doesn’t cause hypoglycemia,” Dr. Bladin said. “And from the moment that patient arrives the glucose control is underway.”
Dr. Bladin and Dr. Chun reported no relevant financial relationships. Study funding was not disclosed.
A version of this article first appeared on Medscape.com.
Treatment with the diabetes drug exenatide was associated with a significant decrease in hyperglycemia in acute stroke patients, a new study shows.
The research could offer clinicians an alternative to insulin therapy to treat hyperglycemia and reduce glucose levels, which are elevated in up to 60% of stroke patients and associated with worse outcomes after stroke.
“Use of these diabetes drugs to control glucose in acute stroke has enormous potential,” said lead researcher Christopher Bladin, PhD, professor of neurology at Monash University and Eastern Health Clinical School, Australia.
The findings were presented at the European Stroke Organisation Conference (ESOC) 2022 annual meeting in Lyon, France.
A better fix than insulin?
Hyperglycemia is common in stroke patients, including those who have no prior history of diabetes. Among stroke patients with normal blood glucose upon admission, about 30% will develop hyperglycemia within 48 hours of stroke onset.
Previous research suggests that hyperglycemia is a poor prognostic factor in patients with stroke and may reduce the efficacy of reperfusion therapies such as thrombolysis and mechanical thrombectomy.
“We’ve been looking for different ways of treating hyperglycemia for quite some time, and one of the obvious ways is to use insulin therapy,” Dr. Bladin said. “But as we’ve seen from multiple studies, insulin therapy is difficult.”
Insulin treatment is resource-heavy, significantly increases the risk for hypoglycemia, and some studies suggest the therapy isn’t associated with better outcomes.
An advantage to a GLP-1 agonist-like exenatide, Dr. Bladin added, is that it’s glucose-dependent. As the glucose level falls, the drug’s efficacy diminishes. It is delivered via an autoinjector and easy to administer.
A case for more study
To study exenatide’s efficacy in reducing hyperglycemia and improving neurologic outcomes, researchers developed the phase 2, international, multicenter, randomized controlled TEXAIS trial.
The study enrolled 350 patients following an ischemic stroke. Within 9 hours of stroke onset, patients received either standard care or a subcutaneous injection of 5 mg of exenatide twice daily for 5 days.
On admission, 42% of patients had hyperglycemia, defined as blood glucose > 7.0 mmol/L.
The study’s primary outcome was at least an 8-point improvement in National Institutes of Health Stroke Scale (NIHSS) score by 7 days after treatment with exenatide. Although there was a trend toward better scores with exenatide, the score was not significantly different between groups (56.7% with standard care versus 61.2% with exenatide; adjusted odds ratio, 1.22; P = .38).
However, when the researchers examined hyperglycemia frequency, they found significantly lower incidence in patients treated with exenatide (P = .002).
There were no cases of hypoglycemia in either group, and only 4% of the study group reported nausea or vomiting.
“Clearly exenatide is having some benefit in terms of keeping glucose under control, reducing hyperglycemia,” Dr. Bladin said. “It certainly lends itself to a larger phase 3 study which can look at this more completely.”
Value to clinicians
Commenting on the findings, Yvonne Chun, PhD, honorary senior clinical lecturer at University of Edinburgh, noted that, even though the study didn’t find a significant association with improved neurological outcomes, the reduced risk for hypoglycemia makes exenatide an attractive alternative to insulin therapy in stroke patients.
“The results are of value to clinicians, as exenatide could potentially be a safer medication to administer than an insulin infusion in acute stroke patients with hyperglycemia,” Dr. Chun said. “There is less risk of hypoglycemia with exenatide compared to standard care.”
However, Dr. Chun noted that more study is needed before exenatide can replace standard care. Dr. Bladin agrees and would like to pursue a phase 3 trial with a modified design to answer questions raised by Dr. Chun and others.
“The next phase could consider changing the primary outcome to an ordinal shift analysis on modified Rankin Scale – a very commonly used primary outcome in stroke clinical trials to assess improvement in disability,” Dr. Chun said. “The primary outcome used in the presented trial – an 8-point improvement on NIHSS – seemed too ambitious and does not inform disability of the patient post stroke.”
Dr. Bladin said he would also like to see the next phase enroll more patients, examine a higher dose of exenatide, and include better stratification of patients with a history of diabetes. Such a trial could yield findings demonstrating the drug’s effectiveness at reducing hyperglycemia and improving outcomes after stroke, he said.
“I can see the day patients will come in with acute stroke, and as they’re coming into the emergency department, they’ll simply get their shot of exenatide because we know it’s safe to use, and it doesn’t cause hypoglycemia,” Dr. Bladin said. “And from the moment that patient arrives the glucose control is underway.”
Dr. Bladin and Dr. Chun reported no relevant financial relationships. Study funding was not disclosed.
A version of this article first appeared on Medscape.com.
Treatment with the diabetes drug exenatide was associated with a significant decrease in hyperglycemia in acute stroke patients, a new study shows.
The research could offer clinicians an alternative to insulin therapy to treat hyperglycemia and reduce glucose levels, which are elevated in up to 60% of stroke patients and associated with worse outcomes after stroke.
“Use of these diabetes drugs to control glucose in acute stroke has enormous potential,” said lead researcher Christopher Bladin, PhD, professor of neurology at Monash University and Eastern Health Clinical School, Australia.
The findings were presented at the European Stroke Organisation Conference (ESOC) 2022 annual meeting in Lyon, France.
A better fix than insulin?
Hyperglycemia is common in stroke patients, including those who have no prior history of diabetes. Among stroke patients with normal blood glucose upon admission, about 30% will develop hyperglycemia within 48 hours of stroke onset.
Previous research suggests that hyperglycemia is a poor prognostic factor in patients with stroke and may reduce the efficacy of reperfusion therapies such as thrombolysis and mechanical thrombectomy.
“We’ve been looking for different ways of treating hyperglycemia for quite some time, and one of the obvious ways is to use insulin therapy,” Dr. Bladin said. “But as we’ve seen from multiple studies, insulin therapy is difficult.”
Insulin treatment is resource-heavy, significantly increases the risk for hypoglycemia, and some studies suggest the therapy isn’t associated with better outcomes.
An advantage to a GLP-1 agonist-like exenatide, Dr. Bladin added, is that it’s glucose-dependent. As the glucose level falls, the drug’s efficacy diminishes. It is delivered via an autoinjector and easy to administer.
A case for more study
To study exenatide’s efficacy in reducing hyperglycemia and improving neurologic outcomes, researchers developed the phase 2, international, multicenter, randomized controlled TEXAIS trial.
The study enrolled 350 patients following an ischemic stroke. Within 9 hours of stroke onset, patients received either standard care or a subcutaneous injection of 5 mg of exenatide twice daily for 5 days.
On admission, 42% of patients had hyperglycemia, defined as blood glucose > 7.0 mmol/L.
The study’s primary outcome was at least an 8-point improvement in National Institutes of Health Stroke Scale (NIHSS) score by 7 days after treatment with exenatide. Although there was a trend toward better scores with exenatide, the score was not significantly different between groups (56.7% with standard care versus 61.2% with exenatide; adjusted odds ratio, 1.22; P = .38).
However, when the researchers examined hyperglycemia frequency, they found significantly lower incidence in patients treated with exenatide (P = .002).
There were no cases of hypoglycemia in either group, and only 4% of the study group reported nausea or vomiting.
“Clearly exenatide is having some benefit in terms of keeping glucose under control, reducing hyperglycemia,” Dr. Bladin said. “It certainly lends itself to a larger phase 3 study which can look at this more completely.”
Value to clinicians
Commenting on the findings, Yvonne Chun, PhD, honorary senior clinical lecturer at University of Edinburgh, noted that, even though the study didn’t find a significant association with improved neurological outcomes, the reduced risk for hypoglycemia makes exenatide an attractive alternative to insulin therapy in stroke patients.
“The results are of value to clinicians, as exenatide could potentially be a safer medication to administer than an insulin infusion in acute stroke patients with hyperglycemia,” Dr. Chun said. “There is less risk of hypoglycemia with exenatide compared to standard care.”
However, Dr. Chun noted that more study is needed before exenatide can replace standard care. Dr. Bladin agrees and would like to pursue a phase 3 trial with a modified design to answer questions raised by Dr. Chun and others.
“The next phase could consider changing the primary outcome to an ordinal shift analysis on modified Rankin Scale – a very commonly used primary outcome in stroke clinical trials to assess improvement in disability,” Dr. Chun said. “The primary outcome used in the presented trial – an 8-point improvement on NIHSS – seemed too ambitious and does not inform disability of the patient post stroke.”
Dr. Bladin said he would also like to see the next phase enroll more patients, examine a higher dose of exenatide, and include better stratification of patients with a history of diabetes. Such a trial could yield findings demonstrating the drug’s effectiveness at reducing hyperglycemia and improving outcomes after stroke, he said.
“I can see the day patients will come in with acute stroke, and as they’re coming into the emergency department, they’ll simply get their shot of exenatide because we know it’s safe to use, and it doesn’t cause hypoglycemia,” Dr. Bladin said. “And from the moment that patient arrives the glucose control is underway.”
Dr. Bladin and Dr. Chun reported no relevant financial relationships. Study funding was not disclosed.
A version of this article first appeared on Medscape.com.
FROM ESOC 2022
Grit your teeth for a lesser-known complication of diabetes
Type 2 diabetes was associated with a 20% increased risk of tooth loss after adjusting for multiple other risk factors in a meta-analysis of 22 recent observational studies from around the world.
The risk of tooth loss with type 2 diabetes (versus no diabetes) ranged from 15% higher in cross-sectional studies to 29% higher in cohort studies to five times higher in case-control studies.
“For diabetes, there are various known complications that are considered in [patient] treatment and management, including neuropathy, nephropathy, cardiovascular [disease] and hypertension, and kidney disease,” senior author Abdolhalim Rajabi, PhD, told this news organization in an email.
“However, a chronic complication of this disease, which may be less noticeable and less tangible, is missing teeth, which can also exacerbate other complications in patients with diabetes,” Dr. Rajabi, a biostatistician at Golestan University of Medical Sciences, Gorgan, Iran, continued.
The meta-analysis showed that “physicians should pay attention to [dental health] in the management and control of diabetic patients,” he summarized.
The analysis by Amir Reza Ahmadian, DDS, dean of the Faculty of Dentistry, Golestan University of Medical Sciences, and colleagues was recently published in BMC Endocrine Disorders.
“Our study is the first comprehensive meta-analysis about the association between [type 2 diabetes] and tooth loss,” Dr. Ahmadian and colleagues write. It summarizes articles in dentistry and medicine about “an important question:” the relationship between type 2 diabetes and tooth loss.
Nevertheless, “large-scale prospective studies are needed to validate the current results in the future,” they conclude.
Oral complications of diabetes
Diabetes increases the risk of oral disease directly by a gingival inflammatory response and indirectly by decreased saliva production due to antidiabetic medications.
Oral complications arising from this include dry mouth, tooth decay, and periodontal disease (gum disease). The latter ranges from gingivitis (gum inflammation) to severe periodontal disease (periodontitis) that can lead to tooth loss, the authors explain.
About a third of people with diabetes have severe periodontal disease, and the American Diabetes Association estimates that one in five cases of tooth loss in adults is related to diabetes.
Tooth loss has decreased over the past decades but is still a major health problem and is associated with poorer quality of life as well as risk of cardiovascular disease, hypertension, stroke, and cancer.
Previous studies and meta-analyses of the relationship between type 2 diabetes and tooth loss have reported inconsistent findings, and they did not include several more recent studies.
Therefore, Dr. Ahmadian and colleagues performed a meta-analysis of 13 cross-sectional, six cohort, and three case-control studies that investigated the link between type 2 diabetes and tooth loss published from 2007 to 2021.
Eleven studies were from North and South America: Brazil (2), Columbia (1), Mexico (2), and the United States (6). Seven studies were from Europe: Belgium (1), Finland (2), France (1), Germany (2), and Portugal (1). Four studies were from the Middle East and Asia: Saudi Arabia (1), South Korea (1), Thailand (1), and Yemen (1).
Diabetes was diagnosed based on glucose or A1c levels in half the studies and based on self-report in the other studies. Most studies investigated any tooth loss (16 studies) and the rest only considered loss of five or more teeth.
The meta-analysis included 677,532 patients, ranging from 60 to 379,021 patients per study. Most studies (77%) were judged to be of moderate or high quality.
The studies adjusted for confounders, including age, sex, place of residence, education, lifestyle factors (smoking, alcohol consumption, physical activity), use of medications and vitamin supplements, and health insurance.
Overall, after adjusting for confounders, participants with type 2 diabetes had a significantly (20%) greater risk of tooth loss than participants without diabetes (adjusted odds ratio, 1.20; P < 0.001).
The association persisted in the different study types. The risk of tooth loss was highest in the case-control studies (OR, 5.10), but was also significantly higher in the cohort (OR, 1.29) and cross-sectional studies (OR, 1.15).
The association “was also present in other subgroups, including ... method of diagnosing type 2 diabetes, continent, study quality, and number of tooth loss,” the researchers write.
“This event seems to be in line with what has been reported in other epidemiologic studies, as several cases have supported the link between diabetes, periodontal disease, and tooth decay,” which “are two common reasons for the endpoint of the tooth loss parameter,” they note.
The researchers did not find any publication bias. However, most of the studies were cross-sectional, so they cannot determine a causal relationship between diabetes and tooth loss.
The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Type 2 diabetes was associated with a 20% increased risk of tooth loss after adjusting for multiple other risk factors in a meta-analysis of 22 recent observational studies from around the world.
The risk of tooth loss with type 2 diabetes (versus no diabetes) ranged from 15% higher in cross-sectional studies to 29% higher in cohort studies to five times higher in case-control studies.
“For diabetes, there are various known complications that are considered in [patient] treatment and management, including neuropathy, nephropathy, cardiovascular [disease] and hypertension, and kidney disease,” senior author Abdolhalim Rajabi, PhD, told this news organization in an email.
“However, a chronic complication of this disease, which may be less noticeable and less tangible, is missing teeth, which can also exacerbate other complications in patients with diabetes,” Dr. Rajabi, a biostatistician at Golestan University of Medical Sciences, Gorgan, Iran, continued.
The meta-analysis showed that “physicians should pay attention to [dental health] in the management and control of diabetic patients,” he summarized.
The analysis by Amir Reza Ahmadian, DDS, dean of the Faculty of Dentistry, Golestan University of Medical Sciences, and colleagues was recently published in BMC Endocrine Disorders.
“Our study is the first comprehensive meta-analysis about the association between [type 2 diabetes] and tooth loss,” Dr. Ahmadian and colleagues write. It summarizes articles in dentistry and medicine about “an important question:” the relationship between type 2 diabetes and tooth loss.
Nevertheless, “large-scale prospective studies are needed to validate the current results in the future,” they conclude.
Oral complications of diabetes
Diabetes increases the risk of oral disease directly by a gingival inflammatory response and indirectly by decreased saliva production due to antidiabetic medications.
Oral complications arising from this include dry mouth, tooth decay, and periodontal disease (gum disease). The latter ranges from gingivitis (gum inflammation) to severe periodontal disease (periodontitis) that can lead to tooth loss, the authors explain.
About a third of people with diabetes have severe periodontal disease, and the American Diabetes Association estimates that one in five cases of tooth loss in adults is related to diabetes.
Tooth loss has decreased over the past decades but is still a major health problem and is associated with poorer quality of life as well as risk of cardiovascular disease, hypertension, stroke, and cancer.
Previous studies and meta-analyses of the relationship between type 2 diabetes and tooth loss have reported inconsistent findings, and they did not include several more recent studies.
Therefore, Dr. Ahmadian and colleagues performed a meta-analysis of 13 cross-sectional, six cohort, and three case-control studies that investigated the link between type 2 diabetes and tooth loss published from 2007 to 2021.
Eleven studies were from North and South America: Brazil (2), Columbia (1), Mexico (2), and the United States (6). Seven studies were from Europe: Belgium (1), Finland (2), France (1), Germany (2), and Portugal (1). Four studies were from the Middle East and Asia: Saudi Arabia (1), South Korea (1), Thailand (1), and Yemen (1).
Diabetes was diagnosed based on glucose or A1c levels in half the studies and based on self-report in the other studies. Most studies investigated any tooth loss (16 studies) and the rest only considered loss of five or more teeth.
The meta-analysis included 677,532 patients, ranging from 60 to 379,021 patients per study. Most studies (77%) were judged to be of moderate or high quality.
The studies adjusted for confounders, including age, sex, place of residence, education, lifestyle factors (smoking, alcohol consumption, physical activity), use of medications and vitamin supplements, and health insurance.
Overall, after adjusting for confounders, participants with type 2 diabetes had a significantly (20%) greater risk of tooth loss than participants without diabetes (adjusted odds ratio, 1.20; P < 0.001).
The association persisted in the different study types. The risk of tooth loss was highest in the case-control studies (OR, 5.10), but was also significantly higher in the cohort (OR, 1.29) and cross-sectional studies (OR, 1.15).
The association “was also present in other subgroups, including ... method of diagnosing type 2 diabetes, continent, study quality, and number of tooth loss,” the researchers write.
“This event seems to be in line with what has been reported in other epidemiologic studies, as several cases have supported the link between diabetes, periodontal disease, and tooth decay,” which “are two common reasons for the endpoint of the tooth loss parameter,” they note.
The researchers did not find any publication bias. However, most of the studies were cross-sectional, so they cannot determine a causal relationship between diabetes and tooth loss.
The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
Type 2 diabetes was associated with a 20% increased risk of tooth loss after adjusting for multiple other risk factors in a meta-analysis of 22 recent observational studies from around the world.
The risk of tooth loss with type 2 diabetes (versus no diabetes) ranged from 15% higher in cross-sectional studies to 29% higher in cohort studies to five times higher in case-control studies.
“For diabetes, there are various known complications that are considered in [patient] treatment and management, including neuropathy, nephropathy, cardiovascular [disease] and hypertension, and kidney disease,” senior author Abdolhalim Rajabi, PhD, told this news organization in an email.
“However, a chronic complication of this disease, which may be less noticeable and less tangible, is missing teeth, which can also exacerbate other complications in patients with diabetes,” Dr. Rajabi, a biostatistician at Golestan University of Medical Sciences, Gorgan, Iran, continued.
The meta-analysis showed that “physicians should pay attention to [dental health] in the management and control of diabetic patients,” he summarized.
The analysis by Amir Reza Ahmadian, DDS, dean of the Faculty of Dentistry, Golestan University of Medical Sciences, and colleagues was recently published in BMC Endocrine Disorders.
“Our study is the first comprehensive meta-analysis about the association between [type 2 diabetes] and tooth loss,” Dr. Ahmadian and colleagues write. It summarizes articles in dentistry and medicine about “an important question:” the relationship between type 2 diabetes and tooth loss.
Nevertheless, “large-scale prospective studies are needed to validate the current results in the future,” they conclude.
Oral complications of diabetes
Diabetes increases the risk of oral disease directly by a gingival inflammatory response and indirectly by decreased saliva production due to antidiabetic medications.
Oral complications arising from this include dry mouth, tooth decay, and periodontal disease (gum disease). The latter ranges from gingivitis (gum inflammation) to severe periodontal disease (periodontitis) that can lead to tooth loss, the authors explain.
About a third of people with diabetes have severe periodontal disease, and the American Diabetes Association estimates that one in five cases of tooth loss in adults is related to diabetes.
Tooth loss has decreased over the past decades but is still a major health problem and is associated with poorer quality of life as well as risk of cardiovascular disease, hypertension, stroke, and cancer.
Previous studies and meta-analyses of the relationship between type 2 diabetes and tooth loss have reported inconsistent findings, and they did not include several more recent studies.
Therefore, Dr. Ahmadian and colleagues performed a meta-analysis of 13 cross-sectional, six cohort, and three case-control studies that investigated the link between type 2 diabetes and tooth loss published from 2007 to 2021.
Eleven studies were from North and South America: Brazil (2), Columbia (1), Mexico (2), and the United States (6). Seven studies were from Europe: Belgium (1), Finland (2), France (1), Germany (2), and Portugal (1). Four studies were from the Middle East and Asia: Saudi Arabia (1), South Korea (1), Thailand (1), and Yemen (1).
Diabetes was diagnosed based on glucose or A1c levels in half the studies and based on self-report in the other studies. Most studies investigated any tooth loss (16 studies) and the rest only considered loss of five or more teeth.
The meta-analysis included 677,532 patients, ranging from 60 to 379,021 patients per study. Most studies (77%) were judged to be of moderate or high quality.
The studies adjusted for confounders, including age, sex, place of residence, education, lifestyle factors (smoking, alcohol consumption, physical activity), use of medications and vitamin supplements, and health insurance.
Overall, after adjusting for confounders, participants with type 2 diabetes had a significantly (20%) greater risk of tooth loss than participants without diabetes (adjusted odds ratio, 1.20; P < 0.001).
The association persisted in the different study types. The risk of tooth loss was highest in the case-control studies (OR, 5.10), but was also significantly higher in the cohort (OR, 1.29) and cross-sectional studies (OR, 1.15).
The association “was also present in other subgroups, including ... method of diagnosing type 2 diabetes, continent, study quality, and number of tooth loss,” the researchers write.
“This event seems to be in line with what has been reported in other epidemiologic studies, as several cases have supported the link between diabetes, periodontal disease, and tooth decay,” which “are two common reasons for the endpoint of the tooth loss parameter,” they note.
The researchers did not find any publication bias. However, most of the studies were cross-sectional, so they cannot determine a causal relationship between diabetes and tooth loss.
The authors have reported no relevant financial disclosures.
A version of this article first appeared on Medscape.com.
FROM BMJ ENDOCRINE DISORDERS
Twenty years and counting: Tamoxifen’s lasting improvement in breast cancer
The study was a secondary analysis of women with estrogen receptor (ER)-positive HER2-negative breast cancer who were treated between 1976 and 1996 in Sweden.
“Our findings suggest a significant long-term tamoxifen treatment benefit among patients with larger tumors, lymph node-negative tumors, PR-positive tumors, and Ki-67 low tumors,” according to Huma Dar, a doctoral candidate at Karolinska Institute, Stockholm, who authored the study.
The analysis found that patients with tumor size T1c, grade 2, lymph node-negative, PR-positive, and Ki-67-low tumors significantly benefited from treatment with tamoxifen for 20 years. And, for patients with tumor size T2-3, benefited significantly after 10 years of treatment with tamoxifen.
It is known that breast cancer patients with ER-positive tumors have a greater risk of distant recurrence – cancer spreading to tissues and organs far from the original tumor site. The selective estrogen receptor modulator tamoxifen, when used as an adjuvant therapy, has been shown to reduce the risk of tumor recurrence and increase survival in patients with ER-positive breast cancer, but not all patients benefit from this therapy.
To examine the long-term benefit of tamoxifen, Ms. Dar and colleagues analyzed data from randomized clinical trials of tamoxifen that took place in Stockholm between 1976 and 1997. The study included 1,242 patients with ER-positive/HER2-negative breast cancer and included a 20-year follow-up. Researchers looked at the relationship between tumor characteristics – including size, grade, lymph node status, the presence of progesterone receptor (PR), and levels of Ki-67, a protein linked with cell proliferation – and patient outcomes.
In a related study published last year in JAMA Network Open, Ms. Dar and colleagues examined the long-term effects of tamoxifen in patients with low risk, postmenopausal, and lymph-node negative cancer. They found that patients with larger tumors, lower tumor grade and PR-positive tumors appeared to significantly benefit from tamoxifen treatment for up to 25 years. The team has since extended that work by looking at pre- and postmenopausal as well as low- and high-risk patients, Ms. Dar said.
“We believe that our findings together with other study findings are important to understand the lifetime risk for patients diagnosed with breast cancer,” Ms. Dar said. “One potential clinical implication is related to tamoxifen benefit, which in our study we don’t see for patients with the smallest tumors.” She said that more studies are needed to confirm this result.
A limitation of this study is that clinical recommendations for disease management and treatment have changed since the initiation of the clinical trials. “The STO-trials were performed before aromatase inhibitors or ovarian function suppression became one of the recommended treatment options for ER-positive breast cancer, and when the duration of tamoxifen therapy was shorter than current recommendations,” Ms. Dar said.
The study was funded by the Swedish Research Council, Swedish Research Council for Health, Working life and Welfare, The Gösta Milton Donation Fund, and Swedish Cancer Society. The authors had no relevant disclosures.
The study was a secondary analysis of women with estrogen receptor (ER)-positive HER2-negative breast cancer who were treated between 1976 and 1996 in Sweden.
“Our findings suggest a significant long-term tamoxifen treatment benefit among patients with larger tumors, lymph node-negative tumors, PR-positive tumors, and Ki-67 low tumors,” according to Huma Dar, a doctoral candidate at Karolinska Institute, Stockholm, who authored the study.
The analysis found that patients with tumor size T1c, grade 2, lymph node-negative, PR-positive, and Ki-67-low tumors significantly benefited from treatment with tamoxifen for 20 years. And, for patients with tumor size T2-3, benefited significantly after 10 years of treatment with tamoxifen.
It is known that breast cancer patients with ER-positive tumors have a greater risk of distant recurrence – cancer spreading to tissues and organs far from the original tumor site. The selective estrogen receptor modulator tamoxifen, when used as an adjuvant therapy, has been shown to reduce the risk of tumor recurrence and increase survival in patients with ER-positive breast cancer, but not all patients benefit from this therapy.
To examine the long-term benefit of tamoxifen, Ms. Dar and colleagues analyzed data from randomized clinical trials of tamoxifen that took place in Stockholm between 1976 and 1997. The study included 1,242 patients with ER-positive/HER2-negative breast cancer and included a 20-year follow-up. Researchers looked at the relationship between tumor characteristics – including size, grade, lymph node status, the presence of progesterone receptor (PR), and levels of Ki-67, a protein linked with cell proliferation – and patient outcomes.
In a related study published last year in JAMA Network Open, Ms. Dar and colleagues examined the long-term effects of tamoxifen in patients with low risk, postmenopausal, and lymph-node negative cancer. They found that patients with larger tumors, lower tumor grade and PR-positive tumors appeared to significantly benefit from tamoxifen treatment for up to 25 years. The team has since extended that work by looking at pre- and postmenopausal as well as low- and high-risk patients, Ms. Dar said.
“We believe that our findings together with other study findings are important to understand the lifetime risk for patients diagnosed with breast cancer,” Ms. Dar said. “One potential clinical implication is related to tamoxifen benefit, which in our study we don’t see for patients with the smallest tumors.” She said that more studies are needed to confirm this result.
A limitation of this study is that clinical recommendations for disease management and treatment have changed since the initiation of the clinical trials. “The STO-trials were performed before aromatase inhibitors or ovarian function suppression became one of the recommended treatment options for ER-positive breast cancer, and when the duration of tamoxifen therapy was shorter than current recommendations,” Ms. Dar said.
The study was funded by the Swedish Research Council, Swedish Research Council for Health, Working life and Welfare, The Gösta Milton Donation Fund, and Swedish Cancer Society. The authors had no relevant disclosures.
The study was a secondary analysis of women with estrogen receptor (ER)-positive HER2-negative breast cancer who were treated between 1976 and 1996 in Sweden.
“Our findings suggest a significant long-term tamoxifen treatment benefit among patients with larger tumors, lymph node-negative tumors, PR-positive tumors, and Ki-67 low tumors,” according to Huma Dar, a doctoral candidate at Karolinska Institute, Stockholm, who authored the study.
The analysis found that patients with tumor size T1c, grade 2, lymph node-negative, PR-positive, and Ki-67-low tumors significantly benefited from treatment with tamoxifen for 20 years. And, for patients with tumor size T2-3, benefited significantly after 10 years of treatment with tamoxifen.
It is known that breast cancer patients with ER-positive tumors have a greater risk of distant recurrence – cancer spreading to tissues and organs far from the original tumor site. The selective estrogen receptor modulator tamoxifen, when used as an adjuvant therapy, has been shown to reduce the risk of tumor recurrence and increase survival in patients with ER-positive breast cancer, but not all patients benefit from this therapy.
To examine the long-term benefit of tamoxifen, Ms. Dar and colleagues analyzed data from randomized clinical trials of tamoxifen that took place in Stockholm between 1976 and 1997. The study included 1,242 patients with ER-positive/HER2-negative breast cancer and included a 20-year follow-up. Researchers looked at the relationship between tumor characteristics – including size, grade, lymph node status, the presence of progesterone receptor (PR), and levels of Ki-67, a protein linked with cell proliferation – and patient outcomes.
In a related study published last year in JAMA Network Open, Ms. Dar and colleagues examined the long-term effects of tamoxifen in patients with low risk, postmenopausal, and lymph-node negative cancer. They found that patients with larger tumors, lower tumor grade and PR-positive tumors appeared to significantly benefit from tamoxifen treatment for up to 25 years. The team has since extended that work by looking at pre- and postmenopausal as well as low- and high-risk patients, Ms. Dar said.
“We believe that our findings together with other study findings are important to understand the lifetime risk for patients diagnosed with breast cancer,” Ms. Dar said. “One potential clinical implication is related to tamoxifen benefit, which in our study we don’t see for patients with the smallest tumors.” She said that more studies are needed to confirm this result.
A limitation of this study is that clinical recommendations for disease management and treatment have changed since the initiation of the clinical trials. “The STO-trials were performed before aromatase inhibitors or ovarian function suppression became one of the recommended treatment options for ER-positive breast cancer, and when the duration of tamoxifen therapy was shorter than current recommendations,” Ms. Dar said.
The study was funded by the Swedish Research Council, Swedish Research Council for Health, Working life and Welfare, The Gösta Milton Donation Fund, and Swedish Cancer Society. The authors had no relevant disclosures.
FROM ESMO 2022
Uninformed breast cancer patients are making treatment decisions
and are making uninformed treatment decisions, according to results of a study presented this month at ESMO Breast Cancer 2022, an annual meeting of the European Society for Medical Oncology.
The standard of care for women diagnosed with DCIS includes surgery with or without radiotherapy – even low-risk patients who are increasingly being steered toward active surveillance with annual mammograms. But few patients understand their diagnosis well enough to make informed decisions about treatment, according to a study led by Ellen Engelhardt, PhD, a postdoctoral fellow at The Netherlands Cancer Institute, Amsterdam.
“You’re not able to really have an informed preference until you understand the choices,” she said.
Dr. Engelhardt and colleagues surveyed 200 patients (mean age 59 years) from the LORD study, which is currently underway at The Netherlands Cancer Institute. The women were asked to complete a survey before treatment decisions were made. Their objective was to determine how knowledgeable patients were about DCIS. They found that only 34% of women answered four out of seven questions correctly: 19% of patients believed that DCIS could metastasize to organs other than the breast; 31% did not realize DCIS could progress to invasive breast cancer if left untreated; 79% thought DCIS could always be seen on mammograms; and, 93% said that progression could always be detected before it becomes “too extensive.” Knowledge of DCIS was found not to be associated with patient education level.
Susie X. Sun, MD, FACS, a breast surgeon at the University of Texas MD Anderson Cancer Center, Houston, said the findings clearly highlight a disconnect in communication between doctor and patient.
“I was surprised, because this clearly demonstrates there is a disconnect between what patients are being told by their providers and what is being perceived. It really shows us that we need to do a better job of making sure that our patients understand the information they’re given,” she said.
Dr. Sun, who was not involved in the study, said that DCIS needs to be explained well to patients. When they receive a diagnosis, often all they hear is, “I have breast cancer. It is really important for us to stress to patients how DCIS is different from invasive breast cancer,” she said.
The “Management of Low-risk (grade I and II) DCIS (LORD)” study is one of three studies comparing active surveillance to surgery (with or without radiotherapy).
A limitation of the study presented at ESMO Breast Cancer is that it remains unclear why patients answered questions incorrectly. Was information never communicated to them? Or, did they mishear or misunderstand the doctor? In future studies, Dr. Engelhardt and her colleagues plan to record and analyze audio tapes of consultations to determine where the communication disconnect lies.
Dr. Engelhardt did not disclose any conflicts associated with this work.
and are making uninformed treatment decisions, according to results of a study presented this month at ESMO Breast Cancer 2022, an annual meeting of the European Society for Medical Oncology.
The standard of care for women diagnosed with DCIS includes surgery with or without radiotherapy – even low-risk patients who are increasingly being steered toward active surveillance with annual mammograms. But few patients understand their diagnosis well enough to make informed decisions about treatment, according to a study led by Ellen Engelhardt, PhD, a postdoctoral fellow at The Netherlands Cancer Institute, Amsterdam.
“You’re not able to really have an informed preference until you understand the choices,” she said.
Dr. Engelhardt and colleagues surveyed 200 patients (mean age 59 years) from the LORD study, which is currently underway at The Netherlands Cancer Institute. The women were asked to complete a survey before treatment decisions were made. Their objective was to determine how knowledgeable patients were about DCIS. They found that only 34% of women answered four out of seven questions correctly: 19% of patients believed that DCIS could metastasize to organs other than the breast; 31% did not realize DCIS could progress to invasive breast cancer if left untreated; 79% thought DCIS could always be seen on mammograms; and, 93% said that progression could always be detected before it becomes “too extensive.” Knowledge of DCIS was found not to be associated with patient education level.
Susie X. Sun, MD, FACS, a breast surgeon at the University of Texas MD Anderson Cancer Center, Houston, said the findings clearly highlight a disconnect in communication between doctor and patient.
“I was surprised, because this clearly demonstrates there is a disconnect between what patients are being told by their providers and what is being perceived. It really shows us that we need to do a better job of making sure that our patients understand the information they’re given,” she said.
Dr. Sun, who was not involved in the study, said that DCIS needs to be explained well to patients. When they receive a diagnosis, often all they hear is, “I have breast cancer. It is really important for us to stress to patients how DCIS is different from invasive breast cancer,” she said.
The “Management of Low-risk (grade I and II) DCIS (LORD)” study is one of three studies comparing active surveillance to surgery (with or without radiotherapy).
A limitation of the study presented at ESMO Breast Cancer is that it remains unclear why patients answered questions incorrectly. Was information never communicated to them? Or, did they mishear or misunderstand the doctor? In future studies, Dr. Engelhardt and her colleagues plan to record and analyze audio tapes of consultations to determine where the communication disconnect lies.
Dr. Engelhardt did not disclose any conflicts associated with this work.
and are making uninformed treatment decisions, according to results of a study presented this month at ESMO Breast Cancer 2022, an annual meeting of the European Society for Medical Oncology.
The standard of care for women diagnosed with DCIS includes surgery with or without radiotherapy – even low-risk patients who are increasingly being steered toward active surveillance with annual mammograms. But few patients understand their diagnosis well enough to make informed decisions about treatment, according to a study led by Ellen Engelhardt, PhD, a postdoctoral fellow at The Netherlands Cancer Institute, Amsterdam.
“You’re not able to really have an informed preference until you understand the choices,” she said.
Dr. Engelhardt and colleagues surveyed 200 patients (mean age 59 years) from the LORD study, which is currently underway at The Netherlands Cancer Institute. The women were asked to complete a survey before treatment decisions were made. Their objective was to determine how knowledgeable patients were about DCIS. They found that only 34% of women answered four out of seven questions correctly: 19% of patients believed that DCIS could metastasize to organs other than the breast; 31% did not realize DCIS could progress to invasive breast cancer if left untreated; 79% thought DCIS could always be seen on mammograms; and, 93% said that progression could always be detected before it becomes “too extensive.” Knowledge of DCIS was found not to be associated with patient education level.
Susie X. Sun, MD, FACS, a breast surgeon at the University of Texas MD Anderson Cancer Center, Houston, said the findings clearly highlight a disconnect in communication between doctor and patient.
“I was surprised, because this clearly demonstrates there is a disconnect between what patients are being told by their providers and what is being perceived. It really shows us that we need to do a better job of making sure that our patients understand the information they’re given,” she said.
Dr. Sun, who was not involved in the study, said that DCIS needs to be explained well to patients. When they receive a diagnosis, often all they hear is, “I have breast cancer. It is really important for us to stress to patients how DCIS is different from invasive breast cancer,” she said.
The “Management of Low-risk (grade I and II) DCIS (LORD)” study is one of three studies comparing active surveillance to surgery (with or without radiotherapy).
A limitation of the study presented at ESMO Breast Cancer is that it remains unclear why patients answered questions incorrectly. Was information never communicated to them? Or, did they mishear or misunderstand the doctor? In future studies, Dr. Engelhardt and her colleagues plan to record and analyze audio tapes of consultations to determine where the communication disconnect lies.
Dr. Engelhardt did not disclose any conflicts associated with this work.
FROM ESMO 2022
Skull Base Regeneration During Treatment With Chemoradiation for Nasopharyngeal Carcinoma: A Case Report
Nasopharyngeal carcinoma (NPC) differs from other head and neck (H&N) cancers in its epidemiology and treatment. Unlike other H&N cancers, NPC has a distinct geographical distribution with a much higher incidence in endemic areas, such as southern China, than in areas where it is relatively uncommon, such as the United States.1 The etiology of NPC varies based on the geographical distribution, with Epstein-Barr virus (EBV) thought to be the primary etiologic agent in endemic areas. On the other hand, in North America 2 additional subsets of NPC have been identified: human papillomavirus (HPV)–positive/EBV-negative and HPV-negative/EBV-negative.2,3 NPC arises from the epithelial lining of the nasopharynx, often in the fossa of Rosenmuller, and is the most seen tumor in the nasopharynx.4 NPC is less surgically accessible than other H&N cancers, and surgery to the nasopharynx poses more risks given the proximity of critical surrounding structures. NPC is radiosensitive, and therefore radiotherapy (RT), in combination with chemotherapy for locally advanced tumors, has become the mainstay of treatment for nonmetastatic NPC.4
NPC often presents with an asymptomatic neck mass or with symptoms of epistaxis, nasal obstruction, and otitis media.5 Advanced cases of NPC can present with direct extension into the skull base, paranasal sinuses, and orbit, as well as involvement of cranial nerves. Radiation planning for tumors of the nasopharynx is complicated by the need to deliver an adequate dose to the tumor while limiting dose and toxicity to nearby critical structures such as the brainstem, optic chiasm, eyes, spinal cord (SC), temporal lobes, and cochleae. Achieving an adequate dose to nasopharyngeal primary tumors is especially complicated for T4 tumors invading the skull base with intracranial extension, in direct contact with these critical structures (Table 1).
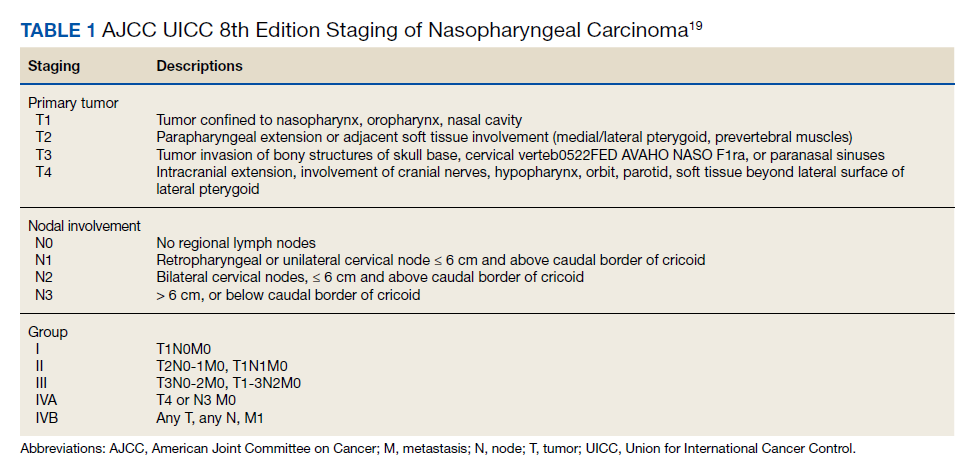
Skull base invasion is a poor prognostic factor, predicting for an increased risk of locoregional recurrence and worse overall survival. Furthermore, the extent of skull base invasion in NPC affects overall prognosis, with cranial nerve involvement and intracranial extension predictive for worse outcomes.5 Depending on the extent of destruction, a bony defect along the skull base could develop with tumor shrinkage during RT, resulting in complications such as cerebrospinal fluid leaks, herniation, and atlantoaxial instability.6
There is a paucity of literature on the ability of bone to regenerate during or after RT for cases of NPC with skull base destruction. To our knowledge, nothing has been published detailing the extent of bony regeneration that can occur during treatment itself, as the tumor regresses and poses a threat of a skull base defect. Here we present a case of T4 HPV-positive/EBV-negative NPC with intracranial extension and describe the RT planning methods leading to prolonged local control, limited toxicities, and bony regeneration of the skull base during treatment.
Case Presentation
A 34-year-old male patient with no previous medical history presented to the emergency department with worsening diplopia, nasal obstruction, facial pain, and neck stiffness. The patient reported a 3 pack-year smoking history with recent smoking cessation. His physical examination was notable for a right abducens nerve palsy and an ulcerated nasopharyngeal mass on endoscopy.
Computed tomography (CT) scan revealed a 7-cm mass in the nasopharynx, eroding through the skull base with destruction and replacement of the clivus by tumor. Also noted was erosion of the petrous apices, carotid canals, sella turcica, dens, and the bilateral occipital condyles. There was intracranial extension with replacement of portions of the cavernous sinuses as well as mass effect on the prepontine cistern. Additional brain imaging studies, including magnetic resonance imaging (MRI) and positron emission tomography (PET) scans, were obtained for completion of the staging workup. The MRI correlated with the findings noted on CT and demonstrated involvement of Meckel cave, foramen ovale, foramen rotundum, Dorello canal, and the hypoglossal canals. No cervical lymphadenopathy or distant metastases were noted on imaging. Pathology from biopsy revealed poorly differentiated squamous cell carcinoma, EBV-negative, strongly p16-positive, HPV-16 positive, and P53-negative.
The H&N multidisciplinary tumor board recommended concurrent chemoradiation for this stage IVA (T4N0M0) EBV-negative, HPV-positive, Word Health Organization type I NPC (Table 2). The patient underwent CT simulation for RT planning, and both tumor volumes and critical normal structures were contoured. The goal was to deliver 70 Gy to the gross tumor. However, given the inability to deliver this dose while meeting the SC dose tolerance of < 45 Gy, a 2-Gy fraction was removed. Therefore, 34 fractions of 2 Gy were delivered to the tumor volume for a total dose of 68 Gy. Weekly cisplatin, at a dose of 40 mg/m2, was administered concurrently with RT.
RT planning was complicated by the tumor’s contact with the brainstem and upper cervical SC, as well as proximity of the tumor to the optic apparatus. The patient underwent 2 replanning CT scans at 26 Gy and 44 Gy to evaluate for tumor shrinkage. These CT scans demonstrated shrinkage of the tumor away from critical neural structures, allowing the treatment volume to be reduced away from these structures in order to achieve required dose tolerances (brainstem < 54 Gy, optic nerves and chiasm < 50 Gy, SC < 45 Gy for this case). The replanning CT scan at 44 Gy, 5 weeks after treatment initiation, demonstrated that dramatic tumor shrinkage had occurred early in treatment, with separation of the remaining tumor from the area of the SC and brainstem with which it was initially in contact (Figure 1). This improvement allowed for shrinkage of the high-dose radiation field away from these critical neural structures.
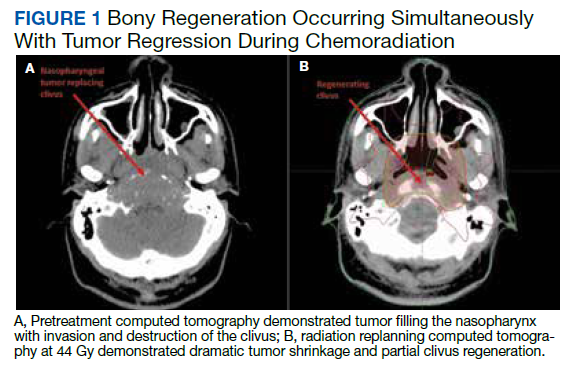
Baseline destruction of the skull base by tumor raised concern for craniospinal instability with tumor response. The patient was evaluated by neurosurgery before the start of RT, and the recommendation was for reimaging during treatment and close follow-up of the patient’s symptoms to determine whether surgical fixation would be indicated during or after treatment. The patient underwent a replanning CT scan at 44 Gy, 5 weeks after treatment initiation, that demonstrated impressive bony regeneration occurring during chemoradiation. New bone formation was noted in the region of the clivus and bilateral occipital condyles, which had been absent on CT prior to treatment initiation. Another CT at 54 Gy demonstrated further ossification of the clivus and bilateral occipital condyles, and bony regeneration occurring rapidly during chemoradiation. The posttreatment CT 3 months after completion of chemoradiation demonstrated complete skull base regeneration, maintaining stability of this area and precluding the need for neurosurgical intervention (Figure 2).
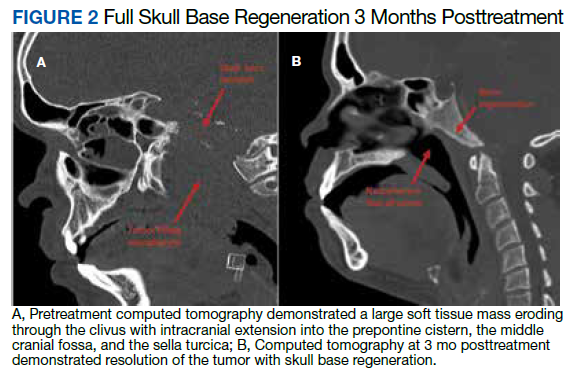
During RT,
The patient had no evidence of disease at 5 years posttreatment. After completing treatment, the patient experienced ongoing intermittent nasal congestion and occasional aural fullness. He experienced an early decay of several teeth starting 1 year after completion of RT, and he continues to visit his dentist for management. He experienced no other treatment-related toxicities. In particular, he has exhibited no signs of neurologic toxicity to date.
Discussion
RT for NPC is complicated by the proximity of these tumors to critical surrounding neural structures. It is challenging to achieve the required dose constraints to surrounding neural tissues while delivering the usual 70-Gy dose to the gross tumor, especially when the tumor comes into direct contact with these structures.
This case provides an example of response-adapted RT using imaging during treatment to shrink the high-dose target as the tumor shrinks away from critical surrounding structures.7 This strategy permits delivery of the maximum dose to the tumor while minimizing radiation dose, and therefore risk of toxicity, to normal surrounding structures. While it is typical to deliver 70 Gy to the full extent of tumor involvement for H&N tumors, this was not possible in this case as the tumor was in contact with the brainstem and upper cervical SC. Delivering the full 70 Gy to these areas of tumor would have placed this patient at substantial risk of brainstem and/or SC toxicity. This report demonstrates that response-adapted RT with shrinking fields can allow for tumor control while avoiding toxicity to critical neural structures for cases of locally advanced NPC in which tumor is abutting these structures.
Bony regeneration of the skull base following RT has been reported in the literature, but in limited reviews. Early reports used plain radiography to follow changes. Unger and colleagues demonstrated the regeneration of bone using skull radiographs 4 to 6 months after completion of RT for NPC.8 More recent literature details the ability of bone to regenerate after RT based on CT findings. Fang and colleagues reported on 90 cases of NPC with skull base destruction, with 63% having bony regeneration on posttreatment CT.9 Most of the patients in Fang’s report had bony regeneration within 1 year of treatment, and in general, bony regeneration became more evident on imaging with longer follow-up. Of note, local control was significantly greater in patients with regeneration vs persistent destruction (77% vs 21%, P < .001). On multivariate analysis, complete tumor response was significantly associated with bony regeneration; other factors such as age, sex, radiation dose, and chemotherapy were not significantly associated with the likelihood of bony regeneration.
Our report details a nasopharyngeal tumor that destroyed the skull base with no intact bony barrier. In such cases, concern arises regarding craniospinal instability with tumor regression if there is not simultaneous bone regeneration. Tumor invasion of the skull base and C1-2 vertebral bodies and complications from treatment of such tumor extent can lead to symptoms of craniospinal instability, including pain, difficulty with neck range of motion, and loss of strength and sensation in the upper and lower extremities.10 A case report of a woman treated with chemoradiation for a plasmacytoma of the skull base detailed her posttreatment presentation with quadriparesis resulting from craniospinal instability after tumor regression.11 Such instability is generally treated surgically, and during this woman’s surgery, there was an injury to the right vertebral artery, although this did not cause any additional neurologic deficits.
RT leads to hypocellularity, hypovascularity, and hypoxia of treated tissues, resulting in a reduced ability for growth and healing. Studies demonstrate that irradiated bone contains fewer osteoblast cells and osteocytes than unirradiated bone, resulting in reduced regenerative capacity.12,13 Furthermore, the reconstruction of bony defects resulting after cancer treatment has been shown to be difficult and associated with a high risk of complications.14 Given the impaired ability of irradiated bone to regenerate, studies have evaluated the use of growth factors and gene therapy to promote bone formation after treatment.15 Bone marrow stem cells have been shown to reverse radiation-induced cellular depletion and to increase osteocyte counts in animal studies.12 Further, overexpression of miR-34a, a tumor suppressor involved in tissue development, has been shown to improve osteoblastic differentiation of irradiated bone marrow stem cells and promote bone regeneration in vitro and in animal studies.13 While several techniques are being studied in vitro and in animal studies to promote bony regeneration after RT, there is a lack of data on use of these techniques in humans with cancer.
With our case, there was great uncertainty related to the ability of bone to regenerate during treatment and concern regarding consequences of formation of a skull base defect during treatment. CT imaging revealed bony regeneration of the central skull base and clivus, as well as occipital condyles, that occurred throughout the RT course. There was clear evidence of bone regeneration on the replanning CT obtained 5 weeks after treatment initiation. To our knowledge, this is the first report to demonstrate rapid bony regeneration during RT, thereby maintaining the integrity of the skull base and precluding the need for neurosurgical intervention. Moving forward, imaging should be considered during treatment for patients with tumor-related destruction of the skull base and upper cervical spine to evaluate the extent of bony regeneration during treatment and estimate the potential risk of craniocervical instability. Further studies with imaging during treatment are needed for more information on the likelihood of bony regeneration and factors that correlate with bony regeneration during treatment. As in other reports, our case demonstrates that bony regeneration may predict complete response to RT.9
Our patient’s tumor was HPV-positive and EBV-negative. In the US, the rate of HPV-positive NPC is 35%.16 However, HPV-positive NPC is much less common in endemic areas. A recent study from China of 1,328 patients with NPC revealed a 6.4% rate of HPV-positive/EBV-negative cases.17 In that study, patients with HPV-positive/EBV-negative tumors had improved survival compared to patients whose tumors were HPV-negative/EBV-positive. Another study suggests that the impact of HPV in NPC varies according to race, with HPV-positivity predicting for improved outcomes in East Asian patients and worse outcomes in White patients.17 A study from the University of Michigan suggests that both HPV-positive/EBV-negative and HPV-negative/EBV-negative NPC are associated with worse overall survival and locoregional control than EBV-positive NPC.2 Overall, the prognostic role of HPV in NPC remains unclear given conflicting information in the literature and the lack of large population studies.18
Conclusions
There is a paucity of literature on bony regeneration in patients with skull base destruction from advanced NPC, and in particular, the ability of skull base regeneration to occur during treatment simultaneous with tumor regression. Our patient had HPV-positive/EBV-negative NPC, but it is unclear how this subtype affected his prognosis. Factors such as tumor histology, radiosensitivity with rapid tumor regression, and young age may have all contributed to the rapidity of bone regeneration in our patient. This case report demonstrates that an impressive tumor response to chemoradiation with simultaneous bony regeneration is possible among patients presenting with tumor destruction of the skull base, precluding the need for neurosurgical intervention.
1. Chang ET, Adami HO. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol Biomarkers Prev. 2006;15(10):1765-1777. doi:10.1158/1055-9965.EPI-06-0353
2. Stenmark MH, McHugh JB, Schipper M, et al. Nonendemic HPV-positive nasopharyngeal carcinoma: association with poor prognosis. Int J Radiat Oncol Biol Phys. 2014;88(3):580-588. doi:10.1016/j.ijrobp.2013.11.246
3. Maxwell JH, Kumar B, Feng FY, et al. HPV-positive/p16-positive/EBV-negative nasopharyngeal carcinoma in white North Americans. Head Neck. 2010;32(5):562-567. doi:10.1002/hed.21216
4. Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64-80. doi:10.1016/S0140-6736(19)30956-0
5. Roh JL, Sung MW, Kim KH, et al.. Nasopharyngeal carcinoma with skull base invasion: a necessity of staging subdivision. Am J Otolaryngol. 2004;25(1):26-32. doi:10.1016/j.amjoto.2003.09.011
6. Orr RD, Salo PT. Atlantoaxial instability complicating radiation therapy for recurrent nasopharyngeal carcinoma. A case report. Spine. 1998;23(11):1280-1282. doi:10.1097/00007632-199806010-00021
7. Morgan HE, Sher DJ. Adaptive radiotherapy for head and neck cancer. Cancers Head Neck. 2020;5:1. doi:10.1186/s41199-019-0046-z
8. Unger JD, Chiang LC, Unger GF. Apparent reformation of the base of the skull following radiotherapy for nasopharyngeal carcinoma. Radiology. 1978;126(3):779-782. doi:10.1148/126.3.779
9. Fang FM, Leung SW, Wang CJ, et al. Computed tomography findings of bony regeneration after radiotherapy for nasopharyngeal carcinoma with skull base destruction: implications for local control. Int J Radiat Oncol Biol Phys. 1999;44(2):305-309. doi:10.1016/s0360-3016(99)00004-8
10. Tiruchelvarayan R, Lee KA, Ng I. Surgery for atlanto-axial (C1-2) involvement or instability in nasopharyngeal carcinoma patients. Singapore Med J. 2012;53(6):416-421.
11. Samprón N, Arrazola M, Urculo E. Skull-base plasmacytoma with craniocervical instability [in Spanish]. Neurocirugia (Astur). 2009;20(5):478-483.
12. Zheutlin AR, Deshpande SS, Nelson NS, et al. Bone marrow stem cells assuage radiation-induced damage in a murine model of distraction osteogenesis: a histomorphometric evaluation. Cytotherapy. 2016;18(5):664-672. doi:10.1016/j.jcyt.2016.01.013
13. Liu H, Dong Y, Feng X, et al. miR-34a promotes bone regeneration in irradiated bone defects by enhancing osteoblast differentiation of mesenchymal stromal cells in rats. Stem Cell Res Ther. 2019;10(1):180. doi:10.1186/s13287-019-1285-y
14. Holzapfel BM, Wagner F, Martine LC, et al. Tissue engineering and regenerative medicine in musculoskeletal oncology. Cancer Metastasis Rev. 2016;35(3):475-487. doi:10.1007/s10555-016-9635-z
15. Hu WW, Ward BB, Wang Z, Krebsbach PH. Bone regeneration in defects compromised by radiotherapy. J Dent Res. 2010;89(1):77-81. doi:10.1177/0022034509352151
16. Wotman M, Oh EJ, Ahn S, Kraus D, Constantino P, Tham T. HPV status in patients with nasopharyngeal carcinoma in the United States: a SEER database study. Am J Otolaryngol. 2019;40(5):705-710. doi:10.1016/j.amjoto.2019.06.00717. Huang WB, Chan JYW, Liu DL. Human papillomavirus and World Health Organization type III nasopharyngeal carcinoma: multicenter study from an endemic area in Southern China. Cancer. 2018;124(3):530-536. doi:10.1002/cncr.31031.
18. Verma V, Simone CB 2nd, Lin C. Human papillomavirus and nasopharyngeal cancer. Head Neck. 2018;40(4):696-706. doi:10.1002/hed.24978
19. Lee AWM, Lydiatt WM, Colevas AD, et al. Nasopharynx. In: Amin MB, ed. AJCC Cancer Staging Manual. 8th ed. Springer; 2017:103.
20. Barnes L, Eveson JW, Reichart P, Sidransky D, eds. Pathology and genetics of head and neck tumors. In: World Health Organization Classification of Tumours. IARC Press; 2005.
Nasopharyngeal carcinoma (NPC) differs from other head and neck (H&N) cancers in its epidemiology and treatment. Unlike other H&N cancers, NPC has a distinct geographical distribution with a much higher incidence in endemic areas, such as southern China, than in areas where it is relatively uncommon, such as the United States.1 The etiology of NPC varies based on the geographical distribution, with Epstein-Barr virus (EBV) thought to be the primary etiologic agent in endemic areas. On the other hand, in North America 2 additional subsets of NPC have been identified: human papillomavirus (HPV)–positive/EBV-negative and HPV-negative/EBV-negative.2,3 NPC arises from the epithelial lining of the nasopharynx, often in the fossa of Rosenmuller, and is the most seen tumor in the nasopharynx.4 NPC is less surgically accessible than other H&N cancers, and surgery to the nasopharynx poses more risks given the proximity of critical surrounding structures. NPC is radiosensitive, and therefore radiotherapy (RT), in combination with chemotherapy for locally advanced tumors, has become the mainstay of treatment for nonmetastatic NPC.4
NPC often presents with an asymptomatic neck mass or with symptoms of epistaxis, nasal obstruction, and otitis media.5 Advanced cases of NPC can present with direct extension into the skull base, paranasal sinuses, and orbit, as well as involvement of cranial nerves. Radiation planning for tumors of the nasopharynx is complicated by the need to deliver an adequate dose to the tumor while limiting dose and toxicity to nearby critical structures such as the brainstem, optic chiasm, eyes, spinal cord (SC), temporal lobes, and cochleae. Achieving an adequate dose to nasopharyngeal primary tumors is especially complicated for T4 tumors invading the skull base with intracranial extension, in direct contact with these critical structures (Table 1).
Skull base invasion is a poor prognostic factor, predicting for an increased risk of locoregional recurrence and worse overall survival. Furthermore, the extent of skull base invasion in NPC affects overall prognosis, with cranial nerve involvement and intracranial extension predictive for worse outcomes.5 Depending on the extent of destruction, a bony defect along the skull base could develop with tumor shrinkage during RT, resulting in complications such as cerebrospinal fluid leaks, herniation, and atlantoaxial instability.6
There is a paucity of literature on the ability of bone to regenerate during or after RT for cases of NPC with skull base destruction. To our knowledge, nothing has been published detailing the extent of bony regeneration that can occur during treatment itself, as the tumor regresses and poses a threat of a skull base defect. Here we present a case of T4 HPV-positive/EBV-negative NPC with intracranial extension and describe the RT planning methods leading to prolonged local control, limited toxicities, and bony regeneration of the skull base during treatment.
Case Presentation
A 34-year-old male patient with no previous medical history presented to the emergency department with worsening diplopia, nasal obstruction, facial pain, and neck stiffness. The patient reported a 3 pack-year smoking history with recent smoking cessation. His physical examination was notable for a right abducens nerve palsy and an ulcerated nasopharyngeal mass on endoscopy.
Computed tomography (CT) scan revealed a 7-cm mass in the nasopharynx, eroding through the skull base with destruction and replacement of the clivus by tumor. Also noted was erosion of the petrous apices, carotid canals, sella turcica, dens, and the bilateral occipital condyles. There was intracranial extension with replacement of portions of the cavernous sinuses as well as mass effect on the prepontine cistern. Additional brain imaging studies, including magnetic resonance imaging (MRI) and positron emission tomography (PET) scans, were obtained for completion of the staging workup. The MRI correlated with the findings noted on CT and demonstrated involvement of Meckel cave, foramen ovale, foramen rotundum, Dorello canal, and the hypoglossal canals. No cervical lymphadenopathy or distant metastases were noted on imaging. Pathology from biopsy revealed poorly differentiated squamous cell carcinoma, EBV-negative, strongly p16-positive, HPV-16 positive, and P53-negative.
The H&N multidisciplinary tumor board recommended concurrent chemoradiation for this stage IVA (T4N0M0) EBV-negative, HPV-positive, Word Health Organization type I NPC (Table 2). The patient underwent CT simulation for RT planning, and both tumor volumes and critical normal structures were contoured. The goal was to deliver 70 Gy to the gross tumor. However, given the inability to deliver this dose while meeting the SC dose tolerance of < 45 Gy, a 2-Gy fraction was removed. Therefore, 34 fractions of 2 Gy were delivered to the tumor volume for a total dose of 68 Gy. Weekly cisplatin, at a dose of 40 mg/m2, was administered concurrently with RT.
RT planning was complicated by the tumor’s contact with the brainstem and upper cervical SC, as well as proximity of the tumor to the optic apparatus. The patient underwent 2 replanning CT scans at 26 Gy and 44 Gy to evaluate for tumor shrinkage. These CT scans demonstrated shrinkage of the tumor away from critical neural structures, allowing the treatment volume to be reduced away from these structures in order to achieve required dose tolerances (brainstem < 54 Gy, optic nerves and chiasm < 50 Gy, SC < 45 Gy for this case). The replanning CT scan at 44 Gy, 5 weeks after treatment initiation, demonstrated that dramatic tumor shrinkage had occurred early in treatment, with separation of the remaining tumor from the area of the SC and brainstem with which it was initially in contact (Figure 1). This improvement allowed for shrinkage of the high-dose radiation field away from these critical neural structures.
Baseline destruction of the skull base by tumor raised concern for craniospinal instability with tumor response. The patient was evaluated by neurosurgery before the start of RT, and the recommendation was for reimaging during treatment and close follow-up of the patient’s symptoms to determine whether surgical fixation would be indicated during or after treatment. The patient underwent a replanning CT scan at 44 Gy, 5 weeks after treatment initiation, that demonstrated impressive bony regeneration occurring during chemoradiation. New bone formation was noted in the region of the clivus and bilateral occipital condyles, which had been absent on CT prior to treatment initiation. Another CT at 54 Gy demonstrated further ossification of the clivus and bilateral occipital condyles, and bony regeneration occurring rapidly during chemoradiation. The posttreatment CT 3 months after completion of chemoradiation demonstrated complete skull base regeneration, maintaining stability of this area and precluding the need for neurosurgical intervention (Figure 2).
During RT,
The patient had no evidence of disease at 5 years posttreatment. After completing treatment, the patient experienced ongoing intermittent nasal congestion and occasional aural fullness. He experienced an early decay of several teeth starting 1 year after completion of RT, and he continues to visit his dentist for management. He experienced no other treatment-related toxicities. In particular, he has exhibited no signs of neurologic toxicity to date.
Discussion
RT for NPC is complicated by the proximity of these tumors to critical surrounding neural structures. It is challenging to achieve the required dose constraints to surrounding neural tissues while delivering the usual 70-Gy dose to the gross tumor, especially when the tumor comes into direct contact with these structures.
This case provides an example of response-adapted RT using imaging during treatment to shrink the high-dose target as the tumor shrinks away from critical surrounding structures.7 This strategy permits delivery of the maximum dose to the tumor while minimizing radiation dose, and therefore risk of toxicity, to normal surrounding structures. While it is typical to deliver 70 Gy to the full extent of tumor involvement for H&N tumors, this was not possible in this case as the tumor was in contact with the brainstem and upper cervical SC. Delivering the full 70 Gy to these areas of tumor would have placed this patient at substantial risk of brainstem and/or SC toxicity. This report demonstrates that response-adapted RT with shrinking fields can allow for tumor control while avoiding toxicity to critical neural structures for cases of locally advanced NPC in which tumor is abutting these structures.
Bony regeneration of the skull base following RT has been reported in the literature, but in limited reviews. Early reports used plain radiography to follow changes. Unger and colleagues demonstrated the regeneration of bone using skull radiographs 4 to 6 months after completion of RT for NPC.8 More recent literature details the ability of bone to regenerate after RT based on CT findings. Fang and colleagues reported on 90 cases of NPC with skull base destruction, with 63% having bony regeneration on posttreatment CT.9 Most of the patients in Fang’s report had bony regeneration within 1 year of treatment, and in general, bony regeneration became more evident on imaging with longer follow-up. Of note, local control was significantly greater in patients with regeneration vs persistent destruction (77% vs 21%, P < .001). On multivariate analysis, complete tumor response was significantly associated with bony regeneration; other factors such as age, sex, radiation dose, and chemotherapy were not significantly associated with the likelihood of bony regeneration.
Our report details a nasopharyngeal tumor that destroyed the skull base with no intact bony barrier. In such cases, concern arises regarding craniospinal instability with tumor regression if there is not simultaneous bone regeneration. Tumor invasion of the skull base and C1-2 vertebral bodies and complications from treatment of such tumor extent can lead to symptoms of craniospinal instability, including pain, difficulty with neck range of motion, and loss of strength and sensation in the upper and lower extremities.10 A case report of a woman treated with chemoradiation for a plasmacytoma of the skull base detailed her posttreatment presentation with quadriparesis resulting from craniospinal instability after tumor regression.11 Such instability is generally treated surgically, and during this woman’s surgery, there was an injury to the right vertebral artery, although this did not cause any additional neurologic deficits.
RT leads to hypocellularity, hypovascularity, and hypoxia of treated tissues, resulting in a reduced ability for growth and healing. Studies demonstrate that irradiated bone contains fewer osteoblast cells and osteocytes than unirradiated bone, resulting in reduced regenerative capacity.12,13 Furthermore, the reconstruction of bony defects resulting after cancer treatment has been shown to be difficult and associated with a high risk of complications.14 Given the impaired ability of irradiated bone to regenerate, studies have evaluated the use of growth factors and gene therapy to promote bone formation after treatment.15 Bone marrow stem cells have been shown to reverse radiation-induced cellular depletion and to increase osteocyte counts in animal studies.12 Further, overexpression of miR-34a, a tumor suppressor involved in tissue development, has been shown to improve osteoblastic differentiation of irradiated bone marrow stem cells and promote bone regeneration in vitro and in animal studies.13 While several techniques are being studied in vitro and in animal studies to promote bony regeneration after RT, there is a lack of data on use of these techniques in humans with cancer.
With our case, there was great uncertainty related to the ability of bone to regenerate during treatment and concern regarding consequences of formation of a skull base defect during treatment. CT imaging revealed bony regeneration of the central skull base and clivus, as well as occipital condyles, that occurred throughout the RT course. There was clear evidence of bone regeneration on the replanning CT obtained 5 weeks after treatment initiation. To our knowledge, this is the first report to demonstrate rapid bony regeneration during RT, thereby maintaining the integrity of the skull base and precluding the need for neurosurgical intervention. Moving forward, imaging should be considered during treatment for patients with tumor-related destruction of the skull base and upper cervical spine to evaluate the extent of bony regeneration during treatment and estimate the potential risk of craniocervical instability. Further studies with imaging during treatment are needed for more information on the likelihood of bony regeneration and factors that correlate with bony regeneration during treatment. As in other reports, our case demonstrates that bony regeneration may predict complete response to RT.9
Our patient’s tumor was HPV-positive and EBV-negative. In the US, the rate of HPV-positive NPC is 35%.16 However, HPV-positive NPC is much less common in endemic areas. A recent study from China of 1,328 patients with NPC revealed a 6.4% rate of HPV-positive/EBV-negative cases.17 In that study, patients with HPV-positive/EBV-negative tumors had improved survival compared to patients whose tumors were HPV-negative/EBV-positive. Another study suggests that the impact of HPV in NPC varies according to race, with HPV-positivity predicting for improved outcomes in East Asian patients and worse outcomes in White patients.17 A study from the University of Michigan suggests that both HPV-positive/EBV-negative and HPV-negative/EBV-negative NPC are associated with worse overall survival and locoregional control than EBV-positive NPC.2 Overall, the prognostic role of HPV in NPC remains unclear given conflicting information in the literature and the lack of large population studies.18
Conclusions
There is a paucity of literature on bony regeneration in patients with skull base destruction from advanced NPC, and in particular, the ability of skull base regeneration to occur during treatment simultaneous with tumor regression. Our patient had HPV-positive/EBV-negative NPC, but it is unclear how this subtype affected his prognosis. Factors such as tumor histology, radiosensitivity with rapid tumor regression, and young age may have all contributed to the rapidity of bone regeneration in our patient. This case report demonstrates that an impressive tumor response to chemoradiation with simultaneous bony regeneration is possible among patients presenting with tumor destruction of the skull base, precluding the need for neurosurgical intervention.
Nasopharyngeal carcinoma (NPC) differs from other head and neck (H&N) cancers in its epidemiology and treatment. Unlike other H&N cancers, NPC has a distinct geographical distribution with a much higher incidence in endemic areas, such as southern China, than in areas where it is relatively uncommon, such as the United States.1 The etiology of NPC varies based on the geographical distribution, with Epstein-Barr virus (EBV) thought to be the primary etiologic agent in endemic areas. On the other hand, in North America 2 additional subsets of NPC have been identified: human papillomavirus (HPV)–positive/EBV-negative and HPV-negative/EBV-negative.2,3 NPC arises from the epithelial lining of the nasopharynx, often in the fossa of Rosenmuller, and is the most seen tumor in the nasopharynx.4 NPC is less surgically accessible than other H&N cancers, and surgery to the nasopharynx poses more risks given the proximity of critical surrounding structures. NPC is radiosensitive, and therefore radiotherapy (RT), in combination with chemotherapy for locally advanced tumors, has become the mainstay of treatment for nonmetastatic NPC.4
NPC often presents with an asymptomatic neck mass or with symptoms of epistaxis, nasal obstruction, and otitis media.5 Advanced cases of NPC can present with direct extension into the skull base, paranasal sinuses, and orbit, as well as involvement of cranial nerves. Radiation planning for tumors of the nasopharynx is complicated by the need to deliver an adequate dose to the tumor while limiting dose and toxicity to nearby critical structures such as the brainstem, optic chiasm, eyes, spinal cord (SC), temporal lobes, and cochleae. Achieving an adequate dose to nasopharyngeal primary tumors is especially complicated for T4 tumors invading the skull base with intracranial extension, in direct contact with these critical structures (Table 1).
Skull base invasion is a poor prognostic factor, predicting for an increased risk of locoregional recurrence and worse overall survival. Furthermore, the extent of skull base invasion in NPC affects overall prognosis, with cranial nerve involvement and intracranial extension predictive for worse outcomes.5 Depending on the extent of destruction, a bony defect along the skull base could develop with tumor shrinkage during RT, resulting in complications such as cerebrospinal fluid leaks, herniation, and atlantoaxial instability.6
There is a paucity of literature on the ability of bone to regenerate during or after RT for cases of NPC with skull base destruction. To our knowledge, nothing has been published detailing the extent of bony regeneration that can occur during treatment itself, as the tumor regresses and poses a threat of a skull base defect. Here we present a case of T4 HPV-positive/EBV-negative NPC with intracranial extension and describe the RT planning methods leading to prolonged local control, limited toxicities, and bony regeneration of the skull base during treatment.
Case Presentation
A 34-year-old male patient with no previous medical history presented to the emergency department with worsening diplopia, nasal obstruction, facial pain, and neck stiffness. The patient reported a 3 pack-year smoking history with recent smoking cessation. His physical examination was notable for a right abducens nerve palsy and an ulcerated nasopharyngeal mass on endoscopy.
Computed tomography (CT) scan revealed a 7-cm mass in the nasopharynx, eroding through the skull base with destruction and replacement of the clivus by tumor. Also noted was erosion of the petrous apices, carotid canals, sella turcica, dens, and the bilateral occipital condyles. There was intracranial extension with replacement of portions of the cavernous sinuses as well as mass effect on the prepontine cistern. Additional brain imaging studies, including magnetic resonance imaging (MRI) and positron emission tomography (PET) scans, were obtained for completion of the staging workup. The MRI correlated with the findings noted on CT and demonstrated involvement of Meckel cave, foramen ovale, foramen rotundum, Dorello canal, and the hypoglossal canals. No cervical lymphadenopathy or distant metastases were noted on imaging. Pathology from biopsy revealed poorly differentiated squamous cell carcinoma, EBV-negative, strongly p16-positive, HPV-16 positive, and P53-negative.
The H&N multidisciplinary tumor board recommended concurrent chemoradiation for this stage IVA (T4N0M0) EBV-negative, HPV-positive, Word Health Organization type I NPC (Table 2). The patient underwent CT simulation for RT planning, and both tumor volumes and critical normal structures were contoured. The goal was to deliver 70 Gy to the gross tumor. However, given the inability to deliver this dose while meeting the SC dose tolerance of < 45 Gy, a 2-Gy fraction was removed. Therefore, 34 fractions of 2 Gy were delivered to the tumor volume for a total dose of 68 Gy. Weekly cisplatin, at a dose of 40 mg/m2, was administered concurrently with RT.
RT planning was complicated by the tumor’s contact with the brainstem and upper cervical SC, as well as proximity of the tumor to the optic apparatus. The patient underwent 2 replanning CT scans at 26 Gy and 44 Gy to evaluate for tumor shrinkage. These CT scans demonstrated shrinkage of the tumor away from critical neural structures, allowing the treatment volume to be reduced away from these structures in order to achieve required dose tolerances (brainstem < 54 Gy, optic nerves and chiasm < 50 Gy, SC < 45 Gy for this case). The replanning CT scan at 44 Gy, 5 weeks after treatment initiation, demonstrated that dramatic tumor shrinkage had occurred early in treatment, with separation of the remaining tumor from the area of the SC and brainstem with which it was initially in contact (Figure 1). This improvement allowed for shrinkage of the high-dose radiation field away from these critical neural structures.
Baseline destruction of the skull base by tumor raised concern for craniospinal instability with tumor response. The patient was evaluated by neurosurgery before the start of RT, and the recommendation was for reimaging during treatment and close follow-up of the patient’s symptoms to determine whether surgical fixation would be indicated during or after treatment. The patient underwent a replanning CT scan at 44 Gy, 5 weeks after treatment initiation, that demonstrated impressive bony regeneration occurring during chemoradiation. New bone formation was noted in the region of the clivus and bilateral occipital condyles, which had been absent on CT prior to treatment initiation. Another CT at 54 Gy demonstrated further ossification of the clivus and bilateral occipital condyles, and bony regeneration occurring rapidly during chemoradiation. The posttreatment CT 3 months after completion of chemoradiation demonstrated complete skull base regeneration, maintaining stability of this area and precluding the need for neurosurgical intervention (Figure 2).
During RT,
The patient had no evidence of disease at 5 years posttreatment. After completing treatment, the patient experienced ongoing intermittent nasal congestion and occasional aural fullness. He experienced an early decay of several teeth starting 1 year after completion of RT, and he continues to visit his dentist for management. He experienced no other treatment-related toxicities. In particular, he has exhibited no signs of neurologic toxicity to date.
Discussion
RT for NPC is complicated by the proximity of these tumors to critical surrounding neural structures. It is challenging to achieve the required dose constraints to surrounding neural tissues while delivering the usual 70-Gy dose to the gross tumor, especially when the tumor comes into direct contact with these structures.
This case provides an example of response-adapted RT using imaging during treatment to shrink the high-dose target as the tumor shrinks away from critical surrounding structures.7 This strategy permits delivery of the maximum dose to the tumor while minimizing radiation dose, and therefore risk of toxicity, to normal surrounding structures. While it is typical to deliver 70 Gy to the full extent of tumor involvement for H&N tumors, this was not possible in this case as the tumor was in contact with the brainstem and upper cervical SC. Delivering the full 70 Gy to these areas of tumor would have placed this patient at substantial risk of brainstem and/or SC toxicity. This report demonstrates that response-adapted RT with shrinking fields can allow for tumor control while avoiding toxicity to critical neural structures for cases of locally advanced NPC in which tumor is abutting these structures.
Bony regeneration of the skull base following RT has been reported in the literature, but in limited reviews. Early reports used plain radiography to follow changes. Unger and colleagues demonstrated the regeneration of bone using skull radiographs 4 to 6 months after completion of RT for NPC.8 More recent literature details the ability of bone to regenerate after RT based on CT findings. Fang and colleagues reported on 90 cases of NPC with skull base destruction, with 63% having bony regeneration on posttreatment CT.9 Most of the patients in Fang’s report had bony regeneration within 1 year of treatment, and in general, bony regeneration became more evident on imaging with longer follow-up. Of note, local control was significantly greater in patients with regeneration vs persistent destruction (77% vs 21%, P < .001). On multivariate analysis, complete tumor response was significantly associated with bony regeneration; other factors such as age, sex, radiation dose, and chemotherapy were not significantly associated with the likelihood of bony regeneration.
Our report details a nasopharyngeal tumor that destroyed the skull base with no intact bony barrier. In such cases, concern arises regarding craniospinal instability with tumor regression if there is not simultaneous bone regeneration. Tumor invasion of the skull base and C1-2 vertebral bodies and complications from treatment of such tumor extent can lead to symptoms of craniospinal instability, including pain, difficulty with neck range of motion, and loss of strength and sensation in the upper and lower extremities.10 A case report of a woman treated with chemoradiation for a plasmacytoma of the skull base detailed her posttreatment presentation with quadriparesis resulting from craniospinal instability after tumor regression.11 Such instability is generally treated surgically, and during this woman’s surgery, there was an injury to the right vertebral artery, although this did not cause any additional neurologic deficits.
RT leads to hypocellularity, hypovascularity, and hypoxia of treated tissues, resulting in a reduced ability for growth and healing. Studies demonstrate that irradiated bone contains fewer osteoblast cells and osteocytes than unirradiated bone, resulting in reduced regenerative capacity.12,13 Furthermore, the reconstruction of bony defects resulting after cancer treatment has been shown to be difficult and associated with a high risk of complications.14 Given the impaired ability of irradiated bone to regenerate, studies have evaluated the use of growth factors and gene therapy to promote bone formation after treatment.15 Bone marrow stem cells have been shown to reverse radiation-induced cellular depletion and to increase osteocyte counts in animal studies.12 Further, overexpression of miR-34a, a tumor suppressor involved in tissue development, has been shown to improve osteoblastic differentiation of irradiated bone marrow stem cells and promote bone regeneration in vitro and in animal studies.13 While several techniques are being studied in vitro and in animal studies to promote bony regeneration after RT, there is a lack of data on use of these techniques in humans with cancer.
With our case, there was great uncertainty related to the ability of bone to regenerate during treatment and concern regarding consequences of formation of a skull base defect during treatment. CT imaging revealed bony regeneration of the central skull base and clivus, as well as occipital condyles, that occurred throughout the RT course. There was clear evidence of bone regeneration on the replanning CT obtained 5 weeks after treatment initiation. To our knowledge, this is the first report to demonstrate rapid bony regeneration during RT, thereby maintaining the integrity of the skull base and precluding the need for neurosurgical intervention. Moving forward, imaging should be considered during treatment for patients with tumor-related destruction of the skull base and upper cervical spine to evaluate the extent of bony regeneration during treatment and estimate the potential risk of craniocervical instability. Further studies with imaging during treatment are needed for more information on the likelihood of bony regeneration and factors that correlate with bony regeneration during treatment. As in other reports, our case demonstrates that bony regeneration may predict complete response to RT.9
Our patient’s tumor was HPV-positive and EBV-negative. In the US, the rate of HPV-positive NPC is 35%.16 However, HPV-positive NPC is much less common in endemic areas. A recent study from China of 1,328 patients with NPC revealed a 6.4% rate of HPV-positive/EBV-negative cases.17 In that study, patients with HPV-positive/EBV-negative tumors had improved survival compared to patients whose tumors were HPV-negative/EBV-positive. Another study suggests that the impact of HPV in NPC varies according to race, with HPV-positivity predicting for improved outcomes in East Asian patients and worse outcomes in White patients.17 A study from the University of Michigan suggests that both HPV-positive/EBV-negative and HPV-negative/EBV-negative NPC are associated with worse overall survival and locoregional control than EBV-positive NPC.2 Overall, the prognostic role of HPV in NPC remains unclear given conflicting information in the literature and the lack of large population studies.18
Conclusions
There is a paucity of literature on bony regeneration in patients with skull base destruction from advanced NPC, and in particular, the ability of skull base regeneration to occur during treatment simultaneous with tumor regression. Our patient had HPV-positive/EBV-negative NPC, but it is unclear how this subtype affected his prognosis. Factors such as tumor histology, radiosensitivity with rapid tumor regression, and young age may have all contributed to the rapidity of bone regeneration in our patient. This case report demonstrates that an impressive tumor response to chemoradiation with simultaneous bony regeneration is possible among patients presenting with tumor destruction of the skull base, precluding the need for neurosurgical intervention.
1. Chang ET, Adami HO. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol Biomarkers Prev. 2006;15(10):1765-1777. doi:10.1158/1055-9965.EPI-06-0353
2. Stenmark MH, McHugh JB, Schipper M, et al. Nonendemic HPV-positive nasopharyngeal carcinoma: association with poor prognosis. Int J Radiat Oncol Biol Phys. 2014;88(3):580-588. doi:10.1016/j.ijrobp.2013.11.246
3. Maxwell JH, Kumar B, Feng FY, et al. HPV-positive/p16-positive/EBV-negative nasopharyngeal carcinoma in white North Americans. Head Neck. 2010;32(5):562-567. doi:10.1002/hed.21216
4. Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64-80. doi:10.1016/S0140-6736(19)30956-0
5. Roh JL, Sung MW, Kim KH, et al.. Nasopharyngeal carcinoma with skull base invasion: a necessity of staging subdivision. Am J Otolaryngol. 2004;25(1):26-32. doi:10.1016/j.amjoto.2003.09.011
6. Orr RD, Salo PT. Atlantoaxial instability complicating radiation therapy for recurrent nasopharyngeal carcinoma. A case report. Spine. 1998;23(11):1280-1282. doi:10.1097/00007632-199806010-00021
7. Morgan HE, Sher DJ. Adaptive radiotherapy for head and neck cancer. Cancers Head Neck. 2020;5:1. doi:10.1186/s41199-019-0046-z
8. Unger JD, Chiang LC, Unger GF. Apparent reformation of the base of the skull following radiotherapy for nasopharyngeal carcinoma. Radiology. 1978;126(3):779-782. doi:10.1148/126.3.779
9. Fang FM, Leung SW, Wang CJ, et al. Computed tomography findings of bony regeneration after radiotherapy for nasopharyngeal carcinoma with skull base destruction: implications for local control. Int J Radiat Oncol Biol Phys. 1999;44(2):305-309. doi:10.1016/s0360-3016(99)00004-8
10. Tiruchelvarayan R, Lee KA, Ng I. Surgery for atlanto-axial (C1-2) involvement or instability in nasopharyngeal carcinoma patients. Singapore Med J. 2012;53(6):416-421.
11. Samprón N, Arrazola M, Urculo E. Skull-base plasmacytoma with craniocervical instability [in Spanish]. Neurocirugia (Astur). 2009;20(5):478-483.
12. Zheutlin AR, Deshpande SS, Nelson NS, et al. Bone marrow stem cells assuage radiation-induced damage in a murine model of distraction osteogenesis: a histomorphometric evaluation. Cytotherapy. 2016;18(5):664-672. doi:10.1016/j.jcyt.2016.01.013
13. Liu H, Dong Y, Feng X, et al. miR-34a promotes bone regeneration in irradiated bone defects by enhancing osteoblast differentiation of mesenchymal stromal cells in rats. Stem Cell Res Ther. 2019;10(1):180. doi:10.1186/s13287-019-1285-y
14. Holzapfel BM, Wagner F, Martine LC, et al. Tissue engineering and regenerative medicine in musculoskeletal oncology. Cancer Metastasis Rev. 2016;35(3):475-487. doi:10.1007/s10555-016-9635-z
15. Hu WW, Ward BB, Wang Z, Krebsbach PH. Bone regeneration in defects compromised by radiotherapy. J Dent Res. 2010;89(1):77-81. doi:10.1177/0022034509352151
16. Wotman M, Oh EJ, Ahn S, Kraus D, Constantino P, Tham T. HPV status in patients with nasopharyngeal carcinoma in the United States: a SEER database study. Am J Otolaryngol. 2019;40(5):705-710. doi:10.1016/j.amjoto.2019.06.00717. Huang WB, Chan JYW, Liu DL. Human papillomavirus and World Health Organization type III nasopharyngeal carcinoma: multicenter study from an endemic area in Southern China. Cancer. 2018;124(3):530-536. doi:10.1002/cncr.31031.
18. Verma V, Simone CB 2nd, Lin C. Human papillomavirus and nasopharyngeal cancer. Head Neck. 2018;40(4):696-706. doi:10.1002/hed.24978
19. Lee AWM, Lydiatt WM, Colevas AD, et al. Nasopharynx. In: Amin MB, ed. AJCC Cancer Staging Manual. 8th ed. Springer; 2017:103.
20. Barnes L, Eveson JW, Reichart P, Sidransky D, eds. Pathology and genetics of head and neck tumors. In: World Health Organization Classification of Tumours. IARC Press; 2005.
1. Chang ET, Adami HO. The enigmatic epidemiology of nasopharyngeal carcinoma. Cancer Epidemiol Biomarkers Prev. 2006;15(10):1765-1777. doi:10.1158/1055-9965.EPI-06-0353
2. Stenmark MH, McHugh JB, Schipper M, et al. Nonendemic HPV-positive nasopharyngeal carcinoma: association with poor prognosis. Int J Radiat Oncol Biol Phys. 2014;88(3):580-588. doi:10.1016/j.ijrobp.2013.11.246
3. Maxwell JH, Kumar B, Feng FY, et al. HPV-positive/p16-positive/EBV-negative nasopharyngeal carcinoma in white North Americans. Head Neck. 2010;32(5):562-567. doi:10.1002/hed.21216
4. Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64-80. doi:10.1016/S0140-6736(19)30956-0
5. Roh JL, Sung MW, Kim KH, et al.. Nasopharyngeal carcinoma with skull base invasion: a necessity of staging subdivision. Am J Otolaryngol. 2004;25(1):26-32. doi:10.1016/j.amjoto.2003.09.011
6. Orr RD, Salo PT. Atlantoaxial instability complicating radiation therapy for recurrent nasopharyngeal carcinoma. A case report. Spine. 1998;23(11):1280-1282. doi:10.1097/00007632-199806010-00021
7. Morgan HE, Sher DJ. Adaptive radiotherapy for head and neck cancer. Cancers Head Neck. 2020;5:1. doi:10.1186/s41199-019-0046-z
8. Unger JD, Chiang LC, Unger GF. Apparent reformation of the base of the skull following radiotherapy for nasopharyngeal carcinoma. Radiology. 1978;126(3):779-782. doi:10.1148/126.3.779
9. Fang FM, Leung SW, Wang CJ, et al. Computed tomography findings of bony regeneration after radiotherapy for nasopharyngeal carcinoma with skull base destruction: implications for local control. Int J Radiat Oncol Biol Phys. 1999;44(2):305-309. doi:10.1016/s0360-3016(99)00004-8
10. Tiruchelvarayan R, Lee KA, Ng I. Surgery for atlanto-axial (C1-2) involvement or instability in nasopharyngeal carcinoma patients. Singapore Med J. 2012;53(6):416-421.
11. Samprón N, Arrazola M, Urculo E. Skull-base plasmacytoma with craniocervical instability [in Spanish]. Neurocirugia (Astur). 2009;20(5):478-483.
12. Zheutlin AR, Deshpande SS, Nelson NS, et al. Bone marrow stem cells assuage radiation-induced damage in a murine model of distraction osteogenesis: a histomorphometric evaluation. Cytotherapy. 2016;18(5):664-672. doi:10.1016/j.jcyt.2016.01.013
13. Liu H, Dong Y, Feng X, et al. miR-34a promotes bone regeneration in irradiated bone defects by enhancing osteoblast differentiation of mesenchymal stromal cells in rats. Stem Cell Res Ther. 2019;10(1):180. doi:10.1186/s13287-019-1285-y
14. Holzapfel BM, Wagner F, Martine LC, et al. Tissue engineering and regenerative medicine in musculoskeletal oncology. Cancer Metastasis Rev. 2016;35(3):475-487. doi:10.1007/s10555-016-9635-z
15. Hu WW, Ward BB, Wang Z, Krebsbach PH. Bone regeneration in defects compromised by radiotherapy. J Dent Res. 2010;89(1):77-81. doi:10.1177/0022034509352151
16. Wotman M, Oh EJ, Ahn S, Kraus D, Constantino P, Tham T. HPV status in patients with nasopharyngeal carcinoma in the United States: a SEER database study. Am J Otolaryngol. 2019;40(5):705-710. doi:10.1016/j.amjoto.2019.06.00717. Huang WB, Chan JYW, Liu DL. Human papillomavirus and World Health Organization type III nasopharyngeal carcinoma: multicenter study from an endemic area in Southern China. Cancer. 2018;124(3):530-536. doi:10.1002/cncr.31031.
18. Verma V, Simone CB 2nd, Lin C. Human papillomavirus and nasopharyngeal cancer. Head Neck. 2018;40(4):696-706. doi:10.1002/hed.24978
19. Lee AWM, Lydiatt WM, Colevas AD, et al. Nasopharynx. In: Amin MB, ed. AJCC Cancer Staging Manual. 8th ed. Springer; 2017:103.
20. Barnes L, Eveson JW, Reichart P, Sidransky D, eds. Pathology and genetics of head and neck tumors. In: World Health Organization Classification of Tumours. IARC Press; 2005.
Screening for diabetes at normal BMIs could cut racial disparities
Use of race-based diabetes screening thresholds could reduce the disparity that arises from current screening guidelines in the United States, new research suggests.
In August 2021, the U.S. Preventive Services Task Force (USPSTF) lowered the recommended age for type 2 diabetes screening from 40 to 35 years among people with a body mass index of 25 kg/m2 or greater.
However, the diabetes rate among ethnic minorities aged 35-70 years in the United States is not just higher overall but, in certain populations, also occurs more frequently at a younger age and at lower BMIs, the new study indicates.
Among people with a BMI below 25 kg/m2, the diabetes prevalence is two to four times higher among Asian, Black, and Hispanic Americans than among the U.S. White population.
And the authors of the new study, led by Rahul Aggarwal, MD, predict that if screening begins at age 35 years, the BMI cut-off equivalent to 25 kg/m2 for White Americans would be 18.5 kg/m2 for Hispanic and Black Americans and 20 kg/m2 for Asian Americans.
“While diabetes has often been thought of as a disease that primarily affects adults with overweight or [obesity], our findings suggest that normal-weight adults in minority groups have surprisingly high rates of diabetes,” Dr. Aggarwal, senior resident physician in internal medicine at Harvard Medical School, Boston, told this news organization.
“Assessing diabetes risks in certain racial/ethnic groups will be necessary, even if these adults do not have overweight or [obesity],” he added.
Not screening in this way “is a missed opportunity for early intervention,” he noted.
And both the authors and an editorialist stress that the issue isn’t just theoretical.
“USPSTF recommendations influence what payers choose to cover, which in turn determines access to preventative services ... Addressing the staggering inequities in diabetes outcomes will require substantial investments in diabetes prevention and treatment, but making screening more equitable is a good place to start,” said senior author Dhruv S. Kazi, MD, of the Smith Center for Outcomes Research in Cardiology and director of the Cardiac Critical Care Unit at Beth Israel, Boston.
Screen minorities at a younger age if current BMI threshold kept
In their study, based on data from the National Health and Nutrition Examination Survey (NHANES) for 2011-2018, Dr. Aggarwal and colleagues also calculated that, if the BMI threshold is kept at 25 kg/m2, then the equivalent age cut-offs for Asian, Black, and Hispanic Americans would be 23, 21, and 25 years, respectively, compared with 35 years for White Americans.
The findings were published online in the Annals of Internal Medicine.
The prevalence of diabetes in those aged 35-70 years in the NHANES population was 17.3% for Asian Americans and 12.5% for those who were White (odds ratio, 1.51 vs. Whites). Among Black Americans and Mexican Americans, the prevalence was 20.7% and 20.6%, respectively, almost twice the prevalence in Whites (OR, 1.85 and 1.80). For other Hispanic Americans, the prevalence was 16.4% (OR, 1.37 vs. Whites). All of those differences were significant, compared with White Americans.
Undiagnosed diabetes was also significantly more common among minority populations, at 27.6%, 22.8%, 21.2%, and 23.5% for Asian, Black, Mexican, and other Hispanic Americans, respectively, versus 12.5% for White Americans.
‘The time has come for USPSTF to offer more concrete guidance’
“While there is more work to be done on carefully examining the long-term risk–benefit trade-off of various diabetes screening, I believe the time has come for USPSTF to offer more concrete guidance on the use of lower thresholds for screening higher-risk individuals,” Dr. Kazi told this news organization.
The author of an accompanying editorial agrees, noting that in a recent commentary the USPSTF, itself, “acknowledged the persistent inequalities across the screening-to-treatment continuum that result in racial/ethnic health disparities in the United States.”
And the USPSTF “emphasized the need to improve systems of care to ensure equitable and consistent delivery of high-quality preventive and treatment services, with special attention to racial/ethnic groups who may experience worse health outcomes,” continues Quyen Ngo-Metzger, MD, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, California.
For other conditions, including cancer, cardiovascular disease, and infectious disease, the USPSTF already recommends risk-based preventive services.
“To address the current inequity in diabetes screening, the USPSTF should apply the same consideration to its diabetes screening recommendation,” she notes.
‘Implementation will require an eye for pragmatism’
Asked about how this recommendation might be carried out in the real world, Dr. Aggarwal said in an interview that, because all three minority groups with normal weight had similar diabetes risk profiles to White adults with overweight, “one way for clinicians to easily implement these findings is by screening all Asian, Black, and Hispanic adults ages 35-70 years with normal weight for diabetes, similarly to how all White adults ages 35-70 years with overweight are currently recommended for screening.”
Dr. Kazi said: “I believe that implementation will require an eye for pragmatism,” noting that another option would be to have screening algorithms embedded in the electronic health record to flag individuals who qualify.
In any case, “the simplicity of the current one-size-fits-all approach is alluring, but it is profoundly inequitable. The more I look at the empiric evidence on diabetes burden in our communities, the more the status quo becomes untenable.”
However, Dr. Kazi also noted, “the benefit of any screening program relates to what we do with the information. The key is to ensure that folks identified as having diabetes – or better still prediabetes – receive timely lifestyle and pharmacological interventions to avert its long-term complications.”
This study was supported by institutional funds from the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology. Dr. Aggarwal, Dr. Kazi, and Dr. Ngo-Metzger have reported no relevant relationships.
A version of this article first appeared on Medscape.com.
Use of race-based diabetes screening thresholds could reduce the disparity that arises from current screening guidelines in the United States, new research suggests.
In August 2021, the U.S. Preventive Services Task Force (USPSTF) lowered the recommended age for type 2 diabetes screening from 40 to 35 years among people with a body mass index of 25 kg/m2 or greater.
However, the diabetes rate among ethnic minorities aged 35-70 years in the United States is not just higher overall but, in certain populations, also occurs more frequently at a younger age and at lower BMIs, the new study indicates.
Among people with a BMI below 25 kg/m2, the diabetes prevalence is two to four times higher among Asian, Black, and Hispanic Americans than among the U.S. White population.
And the authors of the new study, led by Rahul Aggarwal, MD, predict that if screening begins at age 35 years, the BMI cut-off equivalent to 25 kg/m2 for White Americans would be 18.5 kg/m2 for Hispanic and Black Americans and 20 kg/m2 for Asian Americans.
“While diabetes has often been thought of as a disease that primarily affects adults with overweight or [obesity], our findings suggest that normal-weight adults in minority groups have surprisingly high rates of diabetes,” Dr. Aggarwal, senior resident physician in internal medicine at Harvard Medical School, Boston, told this news organization.
“Assessing diabetes risks in certain racial/ethnic groups will be necessary, even if these adults do not have overweight or [obesity],” he added.
Not screening in this way “is a missed opportunity for early intervention,” he noted.
And both the authors and an editorialist stress that the issue isn’t just theoretical.
“USPSTF recommendations influence what payers choose to cover, which in turn determines access to preventative services ... Addressing the staggering inequities in diabetes outcomes will require substantial investments in diabetes prevention and treatment, but making screening more equitable is a good place to start,” said senior author Dhruv S. Kazi, MD, of the Smith Center for Outcomes Research in Cardiology and director of the Cardiac Critical Care Unit at Beth Israel, Boston.
Screen minorities at a younger age if current BMI threshold kept
In their study, based on data from the National Health and Nutrition Examination Survey (NHANES) for 2011-2018, Dr. Aggarwal and colleagues also calculated that, if the BMI threshold is kept at 25 kg/m2, then the equivalent age cut-offs for Asian, Black, and Hispanic Americans would be 23, 21, and 25 years, respectively, compared with 35 years for White Americans.
The findings were published online in the Annals of Internal Medicine.
The prevalence of diabetes in those aged 35-70 years in the NHANES population was 17.3% for Asian Americans and 12.5% for those who were White (odds ratio, 1.51 vs. Whites). Among Black Americans and Mexican Americans, the prevalence was 20.7% and 20.6%, respectively, almost twice the prevalence in Whites (OR, 1.85 and 1.80). For other Hispanic Americans, the prevalence was 16.4% (OR, 1.37 vs. Whites). All of those differences were significant, compared with White Americans.
Undiagnosed diabetes was also significantly more common among minority populations, at 27.6%, 22.8%, 21.2%, and 23.5% for Asian, Black, Mexican, and other Hispanic Americans, respectively, versus 12.5% for White Americans.
‘The time has come for USPSTF to offer more concrete guidance’
“While there is more work to be done on carefully examining the long-term risk–benefit trade-off of various diabetes screening, I believe the time has come for USPSTF to offer more concrete guidance on the use of lower thresholds for screening higher-risk individuals,” Dr. Kazi told this news organization.
The author of an accompanying editorial agrees, noting that in a recent commentary the USPSTF, itself, “acknowledged the persistent inequalities across the screening-to-treatment continuum that result in racial/ethnic health disparities in the United States.”
And the USPSTF “emphasized the need to improve systems of care to ensure equitable and consistent delivery of high-quality preventive and treatment services, with special attention to racial/ethnic groups who may experience worse health outcomes,” continues Quyen Ngo-Metzger, MD, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, California.
For other conditions, including cancer, cardiovascular disease, and infectious disease, the USPSTF already recommends risk-based preventive services.
“To address the current inequity in diabetes screening, the USPSTF should apply the same consideration to its diabetes screening recommendation,” she notes.
‘Implementation will require an eye for pragmatism’
Asked about how this recommendation might be carried out in the real world, Dr. Aggarwal said in an interview that, because all three minority groups with normal weight had similar diabetes risk profiles to White adults with overweight, “one way for clinicians to easily implement these findings is by screening all Asian, Black, and Hispanic adults ages 35-70 years with normal weight for diabetes, similarly to how all White adults ages 35-70 years with overweight are currently recommended for screening.”
Dr. Kazi said: “I believe that implementation will require an eye for pragmatism,” noting that another option would be to have screening algorithms embedded in the electronic health record to flag individuals who qualify.
In any case, “the simplicity of the current one-size-fits-all approach is alluring, but it is profoundly inequitable. The more I look at the empiric evidence on diabetes burden in our communities, the more the status quo becomes untenable.”
However, Dr. Kazi also noted, “the benefit of any screening program relates to what we do with the information. The key is to ensure that folks identified as having diabetes – or better still prediabetes – receive timely lifestyle and pharmacological interventions to avert its long-term complications.”
This study was supported by institutional funds from the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology. Dr. Aggarwal, Dr. Kazi, and Dr. Ngo-Metzger have reported no relevant relationships.
A version of this article first appeared on Medscape.com.
Use of race-based diabetes screening thresholds could reduce the disparity that arises from current screening guidelines in the United States, new research suggests.
In August 2021, the U.S. Preventive Services Task Force (USPSTF) lowered the recommended age for type 2 diabetes screening from 40 to 35 years among people with a body mass index of 25 kg/m2 or greater.
However, the diabetes rate among ethnic minorities aged 35-70 years in the United States is not just higher overall but, in certain populations, also occurs more frequently at a younger age and at lower BMIs, the new study indicates.
Among people with a BMI below 25 kg/m2, the diabetes prevalence is two to four times higher among Asian, Black, and Hispanic Americans than among the U.S. White population.
And the authors of the new study, led by Rahul Aggarwal, MD, predict that if screening begins at age 35 years, the BMI cut-off equivalent to 25 kg/m2 for White Americans would be 18.5 kg/m2 for Hispanic and Black Americans and 20 kg/m2 for Asian Americans.
“While diabetes has often been thought of as a disease that primarily affects adults with overweight or [obesity], our findings suggest that normal-weight adults in minority groups have surprisingly high rates of diabetes,” Dr. Aggarwal, senior resident physician in internal medicine at Harvard Medical School, Boston, told this news organization.
“Assessing diabetes risks in certain racial/ethnic groups will be necessary, even if these adults do not have overweight or [obesity],” he added.
Not screening in this way “is a missed opportunity for early intervention,” he noted.
And both the authors and an editorialist stress that the issue isn’t just theoretical.
“USPSTF recommendations influence what payers choose to cover, which in turn determines access to preventative services ... Addressing the staggering inequities in diabetes outcomes will require substantial investments in diabetes prevention and treatment, but making screening more equitable is a good place to start,” said senior author Dhruv S. Kazi, MD, of the Smith Center for Outcomes Research in Cardiology and director of the Cardiac Critical Care Unit at Beth Israel, Boston.
Screen minorities at a younger age if current BMI threshold kept
In their study, based on data from the National Health and Nutrition Examination Survey (NHANES) for 2011-2018, Dr. Aggarwal and colleagues also calculated that, if the BMI threshold is kept at 25 kg/m2, then the equivalent age cut-offs for Asian, Black, and Hispanic Americans would be 23, 21, and 25 years, respectively, compared with 35 years for White Americans.
The findings were published online in the Annals of Internal Medicine.
The prevalence of diabetes in those aged 35-70 years in the NHANES population was 17.3% for Asian Americans and 12.5% for those who were White (odds ratio, 1.51 vs. Whites). Among Black Americans and Mexican Americans, the prevalence was 20.7% and 20.6%, respectively, almost twice the prevalence in Whites (OR, 1.85 and 1.80). For other Hispanic Americans, the prevalence was 16.4% (OR, 1.37 vs. Whites). All of those differences were significant, compared with White Americans.
Undiagnosed diabetes was also significantly more common among minority populations, at 27.6%, 22.8%, 21.2%, and 23.5% for Asian, Black, Mexican, and other Hispanic Americans, respectively, versus 12.5% for White Americans.
‘The time has come for USPSTF to offer more concrete guidance’
“While there is more work to be done on carefully examining the long-term risk–benefit trade-off of various diabetes screening, I believe the time has come for USPSTF to offer more concrete guidance on the use of lower thresholds for screening higher-risk individuals,” Dr. Kazi told this news organization.
The author of an accompanying editorial agrees, noting that in a recent commentary the USPSTF, itself, “acknowledged the persistent inequalities across the screening-to-treatment continuum that result in racial/ethnic health disparities in the United States.”
And the USPSTF “emphasized the need to improve systems of care to ensure equitable and consistent delivery of high-quality preventive and treatment services, with special attention to racial/ethnic groups who may experience worse health outcomes,” continues Quyen Ngo-Metzger, MD, Kaiser Permanente Bernard J. Tyson School of Medicine, Pasadena, California.
For other conditions, including cancer, cardiovascular disease, and infectious disease, the USPSTF already recommends risk-based preventive services.
“To address the current inequity in diabetes screening, the USPSTF should apply the same consideration to its diabetes screening recommendation,” she notes.
‘Implementation will require an eye for pragmatism’
Asked about how this recommendation might be carried out in the real world, Dr. Aggarwal said in an interview that, because all three minority groups with normal weight had similar diabetes risk profiles to White adults with overweight, “one way for clinicians to easily implement these findings is by screening all Asian, Black, and Hispanic adults ages 35-70 years with normal weight for diabetes, similarly to how all White adults ages 35-70 years with overweight are currently recommended for screening.”
Dr. Kazi said: “I believe that implementation will require an eye for pragmatism,” noting that another option would be to have screening algorithms embedded in the electronic health record to flag individuals who qualify.
In any case, “the simplicity of the current one-size-fits-all approach is alluring, but it is profoundly inequitable. The more I look at the empiric evidence on diabetes burden in our communities, the more the status quo becomes untenable.”
However, Dr. Kazi also noted, “the benefit of any screening program relates to what we do with the information. The key is to ensure that folks identified as having diabetes – or better still prediabetes – receive timely lifestyle and pharmacological interventions to avert its long-term complications.”
This study was supported by institutional funds from the Richard A. and Susan F. Smith Center for Outcomes Research in Cardiology. Dr. Aggarwal, Dr. Kazi, and Dr. Ngo-Metzger have reported no relevant relationships.
A version of this article first appeared on Medscape.com.