User login
Richard Franki is the associate editor who writes and creates graphs. He started with the company in 1987, when it was known as the International Medical News Group. In his years as a journalist, Richard has worked for Cap Cities/ABC, Disney, Harcourt, Elsevier, Quadrant, Frontline, and Internet Brands. In the 1990s, he was a contributor to the ill-fated Indications column, predecessor of Livin' on the MDedge.
U.S. infant mortality continued slow decline in 2017
according to data released Aug. 1 by the National Center for Health Statistics, based on data from the National Vital Statistics System.
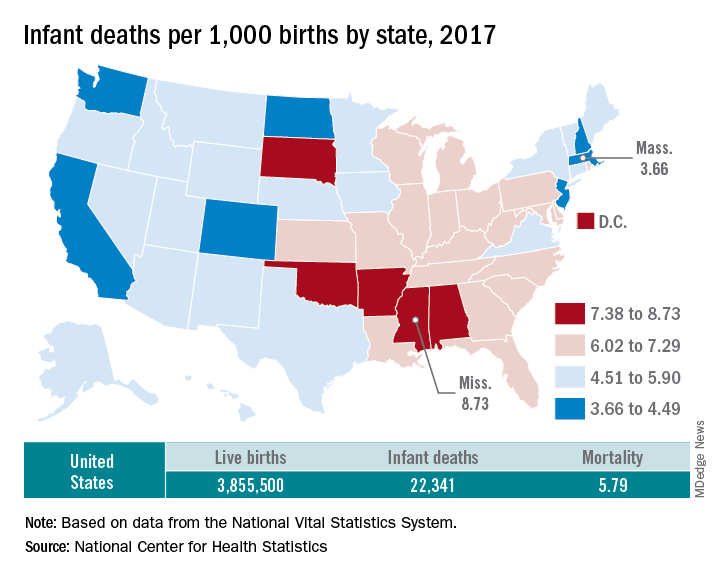
The rate for 2017 was 5.79 deaths per 1,000 live births, which was not statistically different from the rate of 5.87 in 2016, the National Center for Health Statistics said in a new report. Neonatal and postneonatal mortality – 3.85 and 1.94 per 1,000, respectively – both showed the same nonsignificant drop from 2016 to 2017.
About two-thirds of the infants who died in 2017 were children born preterm (less than 37 weeks’ gestation), the NCHS said, and “the mortality rate for infants born before 28 weeks of gestation [389.4 per 1,000] was 183 times the rate for term infants” born at 37-41 weeks.
Rates at the state level in 2017 ranged from a low of 3.66 deaths/1,000 live births in Massachusetts to a high of 8.73/1,000 in Mississippi. Washington (3.88) was the only other state with a rate below 4.0, while Arkansas (8.10) was the only other state above 8.0 (The District of Columbia had a rate of 8.16.). Infant mortality was significantly lower than the national rate in 11 states and significantly higher in 15 states and D.C., according to the report.
Overall, in 2017, 3,855,500 live births occurred, with 22,341 infants having died before the age of 1 year, data from the National Vital Statistics System’s linked birth/infant death file show. In 1995, the first year that the linked file was available, the corresponding numbers were 3,899,589 births and 29,505 deaths, for a rate of 7.57 deaths/1,000 live births.
according to data released Aug. 1 by the National Center for Health Statistics, based on data from the National Vital Statistics System.
The rate for 2017 was 5.79 deaths per 1,000 live births, which was not statistically different from the rate of 5.87 in 2016, the National Center for Health Statistics said in a new report. Neonatal and postneonatal mortality – 3.85 and 1.94 per 1,000, respectively – both showed the same nonsignificant drop from 2016 to 2017.
About two-thirds of the infants who died in 2017 were children born preterm (less than 37 weeks’ gestation), the NCHS said, and “the mortality rate for infants born before 28 weeks of gestation [389.4 per 1,000] was 183 times the rate for term infants” born at 37-41 weeks.
Rates at the state level in 2017 ranged from a low of 3.66 deaths/1,000 live births in Massachusetts to a high of 8.73/1,000 in Mississippi. Washington (3.88) was the only other state with a rate below 4.0, while Arkansas (8.10) was the only other state above 8.0 (The District of Columbia had a rate of 8.16.). Infant mortality was significantly lower than the national rate in 11 states and significantly higher in 15 states and D.C., according to the report.
Overall, in 2017, 3,855,500 live births occurred, with 22,341 infants having died before the age of 1 year, data from the National Vital Statistics System’s linked birth/infant death file show. In 1995, the first year that the linked file was available, the corresponding numbers were 3,899,589 births and 29,505 deaths, for a rate of 7.57 deaths/1,000 live births.
according to data released Aug. 1 by the National Center for Health Statistics, based on data from the National Vital Statistics System.
The rate for 2017 was 5.79 deaths per 1,000 live births, which was not statistically different from the rate of 5.87 in 2016, the National Center for Health Statistics said in a new report. Neonatal and postneonatal mortality – 3.85 and 1.94 per 1,000, respectively – both showed the same nonsignificant drop from 2016 to 2017.
About two-thirds of the infants who died in 2017 were children born preterm (less than 37 weeks’ gestation), the NCHS said, and “the mortality rate for infants born before 28 weeks of gestation [389.4 per 1,000] was 183 times the rate for term infants” born at 37-41 weeks.
Rates at the state level in 2017 ranged from a low of 3.66 deaths/1,000 live births in Massachusetts to a high of 8.73/1,000 in Mississippi. Washington (3.88) was the only other state with a rate below 4.0, while Arkansas (8.10) was the only other state above 8.0 (The District of Columbia had a rate of 8.16.). Infant mortality was significantly lower than the national rate in 11 states and significantly higher in 15 states and D.C., according to the report.
Overall, in 2017, 3,855,500 live births occurred, with 22,341 infants having died before the age of 1 year, data from the National Vital Statistics System’s linked birth/infant death file show. In 1995, the first year that the linked file was available, the corresponding numbers were 3,899,589 births and 29,505 deaths, for a rate of 7.57 deaths/1,000 live births.
Predatory journals and HULLK’s prostate
The incredible HULLK
HULLK TYPE OF RNA THAT CONTROLS GROWTH OF PROSTATE CANCER CELLS. HULLK IS STRONGEST RNA THERE IS. HULLK SMASH CANCER!
Is everyone’s favorite not-so-jolly green giant the key to crushing prostate cancer? Not exactly: HULLK is a noncoding type of RNA. Which means, instead of coding a protein, it helps regulate cellular processes.
Cancer researchers from the University of Virginia found there was more HULLK in tumors from patients with advanced prostate cancer. They also found that decreasing the incredible RNA slows tumor cell growth.
In other words, we need a little more Bruce Banner, a little less HULLK.
The scientists who identified HULLK are hopeful that it can function as a biomarker and a therapeutic target in the future, and could be an integral discovery on the way to curing prostate cancer. HULLK LIKE.
Trading places with Sigmund Freud
Sometimes, it can be helpful to talk to someone about your problems. We’re not really going out on a limb here. That is, after all, pretty much the basis of psychotherapy.

But what if that someone else was really you, disguised as Sigmund Freud?
That was the premise for a recent study involving body swapping and immersive virtual reality. The investigators scanned each subject to create a 3D avatar that functioned as an online representation and moved as he or she moved during the experiment. In virtual reality, the subject’s avatar sat across a table from Sigmund Freud, who was the variable element in the study.
For the control group, Freud responded with prescripted questions and comments about the subject’s problem. The other group, however, was able to swap virtual bodies and respond to their own bodies as Freud. In other words, they could have a conversation with themselves, but it looked like they were talking to Freud.
A week after the virtual conversations, more than 80% of those in the body-swapping group experienced some sort of change with respect to their problem, compared with less than 50% of controls.
“We found that those in the body-swapping group got better knowledge, understanding, control, and new ideas about their problem, compared to the control group,” one of the investigators said.
We’re just wondering about their choice of Freud. It kind of makes sense, because that was his line of work; but would another person have been even more helpful?
How about Dr. Phil? Or maybe Oprah? Seems like Dwayne “the Rock” Johnson is everywhere else, so why not virtual reality? It would be hard to go wrong with some type of Kardashian, right?
Cue the ‘Jaws’ music
Doctors with freshly written studies beware, for you are not alone. Lurking in the undergrowth, stalking your every move, are the predatory journals. They’ve come for you. And they pose a danger not only to you, but to the entire field of medical literature.

However, there’s no need to fear, as you have a guide through the great Serengeti of the publication process: a new guideline on avoiding predatory journals from the American Medical Writers Association, European Medical Writers Association, and International Society for Medical Publication Professionals.
According to the guideline, some telltale characteristics of these journals include a lack of information, poorly made websites, a lack of indexing in a recognized system, promises of unrealistically quick peer review, and an insatiable thirst for your blood. We may have made that last one up.
The guideline authors call for all medical authors to conduct research while submitting to journals, and only submit to those journals that conduct a full peer review process and that genuinely seek to contribute to medical literature.
Failure to do so may result in a damaged reputation, being unwittingly appointed to an editorial board, losing your paper, or having your liver eaten by an eagle day after day until Hercules finally frees you from your torture.
We may have made that one up as well.
The incredible HULLK
HULLK TYPE OF RNA THAT CONTROLS GROWTH OF PROSTATE CANCER CELLS. HULLK IS STRONGEST RNA THERE IS. HULLK SMASH CANCER!
Is everyone’s favorite not-so-jolly green giant the key to crushing prostate cancer? Not exactly: HULLK is a noncoding type of RNA. Which means, instead of coding a protein, it helps regulate cellular processes.
Cancer researchers from the University of Virginia found there was more HULLK in tumors from patients with advanced prostate cancer. They also found that decreasing the incredible RNA slows tumor cell growth.
In other words, we need a little more Bruce Banner, a little less HULLK.
The scientists who identified HULLK are hopeful that it can function as a biomarker and a therapeutic target in the future, and could be an integral discovery on the way to curing prostate cancer. HULLK LIKE.
Trading places with Sigmund Freud
Sometimes, it can be helpful to talk to someone about your problems. We’re not really going out on a limb here. That is, after all, pretty much the basis of psychotherapy.
But what if that someone else was really you, disguised as Sigmund Freud?
That was the premise for a recent study involving body swapping and immersive virtual reality. The investigators scanned each subject to create a 3D avatar that functioned as an online representation and moved as he or she moved during the experiment. In virtual reality, the subject’s avatar sat across a table from Sigmund Freud, who was the variable element in the study.
For the control group, Freud responded with prescripted questions and comments about the subject’s problem. The other group, however, was able to swap virtual bodies and respond to their own bodies as Freud. In other words, they could have a conversation with themselves, but it looked like they were talking to Freud.
A week after the virtual conversations, more than 80% of those in the body-swapping group experienced some sort of change with respect to their problem, compared with less than 50% of controls.
“We found that those in the body-swapping group got better knowledge, understanding, control, and new ideas about their problem, compared to the control group,” one of the investigators said.
We’re just wondering about their choice of Freud. It kind of makes sense, because that was his line of work; but would another person have been even more helpful?
How about Dr. Phil? Or maybe Oprah? Seems like Dwayne “the Rock” Johnson is everywhere else, so why not virtual reality? It would be hard to go wrong with some type of Kardashian, right?
Cue the ‘Jaws’ music
Doctors with freshly written studies beware, for you are not alone. Lurking in the undergrowth, stalking your every move, are the predatory journals. They’ve come for you. And they pose a danger not only to you, but to the entire field of medical literature.
However, there’s no need to fear, as you have a guide through the great Serengeti of the publication process: a new guideline on avoiding predatory journals from the American Medical Writers Association, European Medical Writers Association, and International Society for Medical Publication Professionals.
According to the guideline, some telltale characteristics of these journals include a lack of information, poorly made websites, a lack of indexing in a recognized system, promises of unrealistically quick peer review, and an insatiable thirst for your blood. We may have made that last one up.
The guideline authors call for all medical authors to conduct research while submitting to journals, and only submit to those journals that conduct a full peer review process and that genuinely seek to contribute to medical literature.
Failure to do so may result in a damaged reputation, being unwittingly appointed to an editorial board, losing your paper, or having your liver eaten by an eagle day after day until Hercules finally frees you from your torture.
We may have made that one up as well.
The incredible HULLK
HULLK TYPE OF RNA THAT CONTROLS GROWTH OF PROSTATE CANCER CELLS. HULLK IS STRONGEST RNA THERE IS. HULLK SMASH CANCER!
Is everyone’s favorite not-so-jolly green giant the key to crushing prostate cancer? Not exactly: HULLK is a noncoding type of RNA. Which means, instead of coding a protein, it helps regulate cellular processes.
Cancer researchers from the University of Virginia found there was more HULLK in tumors from patients with advanced prostate cancer. They also found that decreasing the incredible RNA slows tumor cell growth.
In other words, we need a little more Bruce Banner, a little less HULLK.
The scientists who identified HULLK are hopeful that it can function as a biomarker and a therapeutic target in the future, and could be an integral discovery on the way to curing prostate cancer. HULLK LIKE.
Trading places with Sigmund Freud
Sometimes, it can be helpful to talk to someone about your problems. We’re not really going out on a limb here. That is, after all, pretty much the basis of psychotherapy.
But what if that someone else was really you, disguised as Sigmund Freud?
That was the premise for a recent study involving body swapping and immersive virtual reality. The investigators scanned each subject to create a 3D avatar that functioned as an online representation and moved as he or she moved during the experiment. In virtual reality, the subject’s avatar sat across a table from Sigmund Freud, who was the variable element in the study.
For the control group, Freud responded with prescripted questions and comments about the subject’s problem. The other group, however, was able to swap virtual bodies and respond to their own bodies as Freud. In other words, they could have a conversation with themselves, but it looked like they were talking to Freud.
A week after the virtual conversations, more than 80% of those in the body-swapping group experienced some sort of change with respect to their problem, compared with less than 50% of controls.
“We found that those in the body-swapping group got better knowledge, understanding, control, and new ideas about their problem, compared to the control group,” one of the investigators said.
We’re just wondering about their choice of Freud. It kind of makes sense, because that was his line of work; but would another person have been even more helpful?
How about Dr. Phil? Or maybe Oprah? Seems like Dwayne “the Rock” Johnson is everywhere else, so why not virtual reality? It would be hard to go wrong with some type of Kardashian, right?
Cue the ‘Jaws’ music
Doctors with freshly written studies beware, for you are not alone. Lurking in the undergrowth, stalking your every move, are the predatory journals. They’ve come for you. And they pose a danger not only to you, but to the entire field of medical literature.
However, there’s no need to fear, as you have a guide through the great Serengeti of the publication process: a new guideline on avoiding predatory journals from the American Medical Writers Association, European Medical Writers Association, and International Society for Medical Publication Professionals.
According to the guideline, some telltale characteristics of these journals include a lack of information, poorly made websites, a lack of indexing in a recognized system, promises of unrealistically quick peer review, and an insatiable thirst for your blood. We may have made that last one up.
The guideline authors call for all medical authors to conduct research while submitting to journals, and only submit to those journals that conduct a full peer review process and that genuinely seek to contribute to medical literature.
Failure to do so may result in a damaged reputation, being unwittingly appointed to an editorial board, losing your paper, or having your liver eaten by an eagle day after day until Hercules finally frees you from your torture.
We may have made that one up as well.
Mayo Clinic takes honors as top hospital
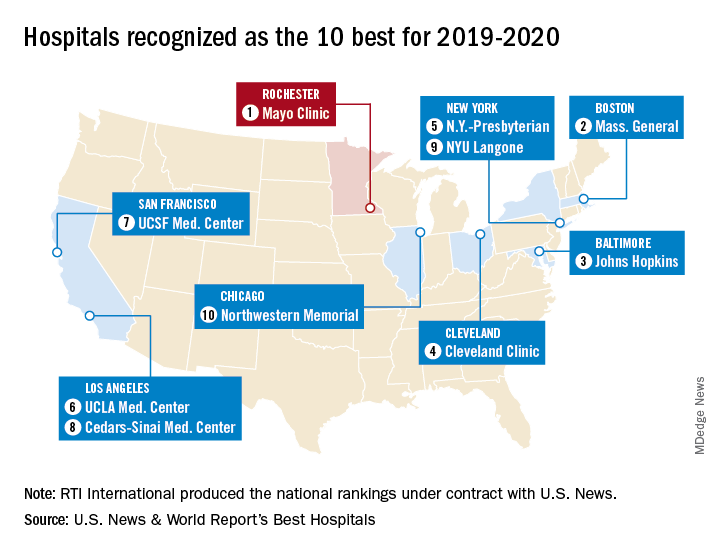
The Rochester, Minn., hospital has now been No. 1 on the U.S. News Honor Roll for 4 consecutive years. The last institution to head the list before that streak, Massachusetts General Hospital in Boston, was second this year, followed by Johns Hopkins Hospital in Baltimore, the Cleveland Clinic, and New York-Presbyterian Hospital–Columbia and Cornell in New York, U.S. News reported July 30.
The Mayo Clinic finished first in five of the 16 specialties used in the evaluation process – diabetes and endocrinology; ear, nose, and throat; gastroenterology and GI surgery; urology; and nephrology – and had a total of 13 top-five rankings. Massachusetts General had one first place in psychiatry and six total top fives, while Johns Hopkins, despite its lower overall ranking, had three top rankings – geriatrics, neurology and neurosurgery, and rheumatology – and nine top fives, the U.S. News data show.
This year’s 30th edition of the rankings involved 4,653 community inpatient hospitals, of which 1,447 received a “High Performing” rating in at least one of the nine procedures and conditions assessed and 165 were nationally ranked (top 50) in at least one of the 16 specialties. Twelve specialties are ranked largely on objective data, with the three most recent years of an annual expert opinion survey of specialized physicians also factored in. The other four specialties are ranked based entirely on the survey of expert opinion.
The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
The Rochester, Minn., hospital has now been No. 1 on the U.S. News Honor Roll for 4 consecutive years. The last institution to head the list before that streak, Massachusetts General Hospital in Boston, was second this year, followed by Johns Hopkins Hospital in Baltimore, the Cleveland Clinic, and New York-Presbyterian Hospital–Columbia and Cornell in New York, U.S. News reported July 30.
The Mayo Clinic finished first in five of the 16 specialties used in the evaluation process – diabetes and endocrinology; ear, nose, and throat; gastroenterology and GI surgery; urology; and nephrology – and had a total of 13 top-five rankings. Massachusetts General had one first place in psychiatry and six total top fives, while Johns Hopkins, despite its lower overall ranking, had three top rankings – geriatrics, neurology and neurosurgery, and rheumatology – and nine top fives, the U.S. News data show.
This year’s 30th edition of the rankings involved 4,653 community inpatient hospitals, of which 1,447 received a “High Performing” rating in at least one of the nine procedures and conditions assessed and 165 were nationally ranked (top 50) in at least one of the 16 specialties. Twelve specialties are ranked largely on objective data, with the three most recent years of an annual expert opinion survey of specialized physicians also factored in. The other four specialties are ranked based entirely on the survey of expert opinion.
The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
The Rochester, Minn., hospital has now been No. 1 on the U.S. News Honor Roll for 4 consecutive years. The last institution to head the list before that streak, Massachusetts General Hospital in Boston, was second this year, followed by Johns Hopkins Hospital in Baltimore, the Cleveland Clinic, and New York-Presbyterian Hospital–Columbia and Cornell in New York, U.S. News reported July 30.
The Mayo Clinic finished first in five of the 16 specialties used in the evaluation process – diabetes and endocrinology; ear, nose, and throat; gastroenterology and GI surgery; urology; and nephrology – and had a total of 13 top-five rankings. Massachusetts General had one first place in psychiatry and six total top fives, while Johns Hopkins, despite its lower overall ranking, had three top rankings – geriatrics, neurology and neurosurgery, and rheumatology – and nine top fives, the U.S. News data show.
This year’s 30th edition of the rankings involved 4,653 community inpatient hospitals, of which 1,447 received a “High Performing” rating in at least one of the nine procedures and conditions assessed and 165 were nationally ranked (top 50) in at least one of the 16 specialties. Twelve specialties are ranked largely on objective data, with the three most recent years of an annual expert opinion survey of specialized physicians also factored in. The other four specialties are ranked based entirely on the survey of expert opinion.
The research organization RTI International conducted the physician survey and produced the Best Hospitals methodology and national rankings under contract with U.S. News.
Washington State removes exemption for MMR vaccine
Washington state parents may no longer cite personal or philosophical objections to refuse the MMR vaccine for their children, effective July 28, according to the state’s department of health.
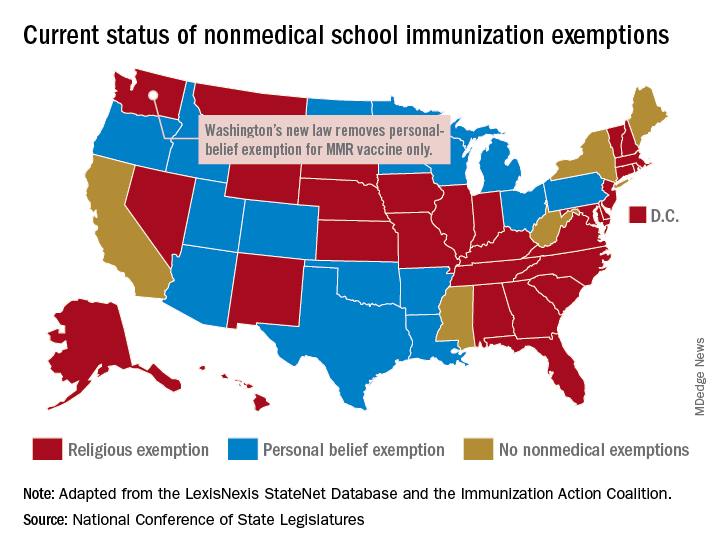
“In Washington state we believe in our doctors. We believe in our nurses. We believe in our educators. We believe in science and we love our children,” Gov. Jay Inslee (D) said when he signed the bill into law on May 10. “And that is why in Washington State, we are against measles.”
The new law applies only to the MMR vaccine and “does not change religious and medical exemption laws. Children who have one of these types of exemptions on file are not affected by the new law,” the health department said.
Washington is one of 45 states that allows religious exemptions from school immunization requirements, according to the National Conference of State Legislatures, which also reported that 15 of those states allow personal-belief exemptions.
The five states that do not allow any form of nonmedical exemption are California, Maine, Mississippi, New York, and West Virginia.
Washington state parents may no longer cite personal or philosophical objections to refuse the MMR vaccine for their children, effective July 28, according to the state’s department of health.
“In Washington state we believe in our doctors. We believe in our nurses. We believe in our educators. We believe in science and we love our children,” Gov. Jay Inslee (D) said when he signed the bill into law on May 10. “And that is why in Washington State, we are against measles.”
The new law applies only to the MMR vaccine and “does not change religious and medical exemption laws. Children who have one of these types of exemptions on file are not affected by the new law,” the health department said.
Washington is one of 45 states that allows religious exemptions from school immunization requirements, according to the National Conference of State Legislatures, which also reported that 15 of those states allow personal-belief exemptions.
The five states that do not allow any form of nonmedical exemption are California, Maine, Mississippi, New York, and West Virginia.
Washington state parents may no longer cite personal or philosophical objections to refuse the MMR vaccine for their children, effective July 28, according to the state’s department of health.
“In Washington state we believe in our doctors. We believe in our nurses. We believe in our educators. We believe in science and we love our children,” Gov. Jay Inslee (D) said when he signed the bill into law on May 10. “And that is why in Washington State, we are against measles.”
The new law applies only to the MMR vaccine and “does not change religious and medical exemption laws. Children who have one of these types of exemptions on file are not affected by the new law,” the health department said.
Washington is one of 45 states that allows religious exemptions from school immunization requirements, according to the National Conference of State Legislatures, which also reported that 15 of those states allow personal-belief exemptions.
The five states that do not allow any form of nonmedical exemption are California, Maine, Mississippi, New York, and West Virginia.
Prescriptions for cough, cold medicine dropping for children
with evidence suggesting replacement by off-label antihistamines, according to analysis of two national databases.
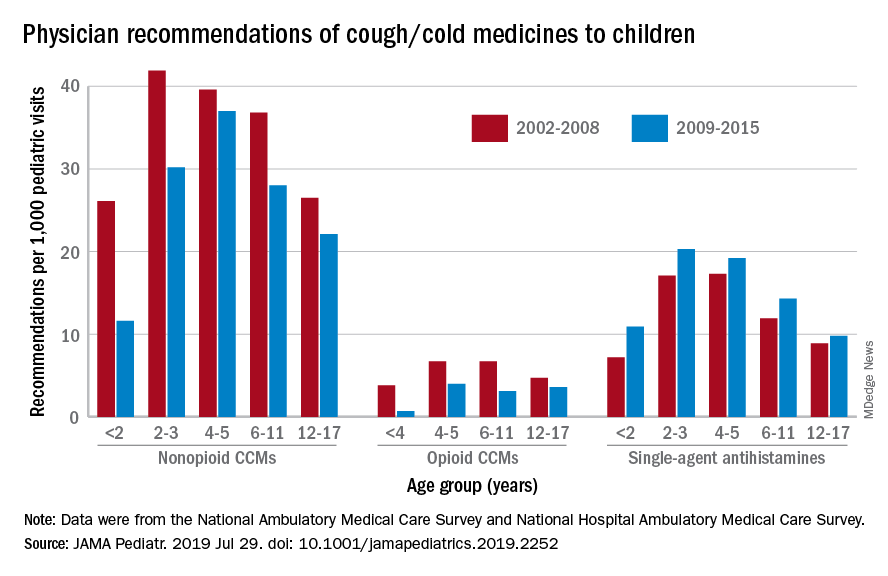
Compared with older children, declines in both opioid and nonopioid cold and cough medicine (CCM) use “appeared to accelerate in children younger than 2 years … and among children younger than 6 years for opioid-containing CCM” after the Food and Drug Administration’s 2008 public health advisory on use of OTC forms of CCM, Daniel B. Horton, MD, of the Robert Wood Johnson Medical School, New Brunswick, N.J., and his associates wrote in JAMA Pediatrics.
Meanwhile, recommendations for single-agent antihistamines rose – for some age groups significantly – over the 14-year study period, which was divided into two eras: 2002-2008 and 2009-2015.
When the two eras were compared, trends for decreased use of CCM in children under 2 years of age (nonopioid) and under 4 years (opioid) approached – both were P = .05 – but did not quite reach the less than .05 considered statistically significant. Adjusted odds ratios for the other age groups were further off the mark. For antihistamines, the upward trend between the two eras was significant for children aged under 2 years, 2-3 years, and 6-11 years, Dr. Horton and associates reported.
The two youngest groups, under 2 years and 2-3, were combined for the opioid CCM analyses to avoid a population under 30, which would have yielded unreliable estimates. The investigators used data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, with the sample representing 3.1 billion pediatric visits from 2002 to 2015.
Dr. Horton is supported by an award from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The investigators reported no disclosures relevant to this study.
SOURCE: Horton DB et al. JAMA Pediatr. 2019 Jul 29. doi: 10.1001/jamapediatrics.2019.2252.
with evidence suggesting replacement by off-label antihistamines, according to analysis of two national databases.
Compared with older children, declines in both opioid and nonopioid cold and cough medicine (CCM) use “appeared to accelerate in children younger than 2 years … and among children younger than 6 years for opioid-containing CCM” after the Food and Drug Administration’s 2008 public health advisory on use of OTC forms of CCM, Daniel B. Horton, MD, of the Robert Wood Johnson Medical School, New Brunswick, N.J., and his associates wrote in JAMA Pediatrics.
Meanwhile, recommendations for single-agent antihistamines rose – for some age groups significantly – over the 14-year study period, which was divided into two eras: 2002-2008 and 2009-2015.
When the two eras were compared, trends for decreased use of CCM in children under 2 years of age (nonopioid) and under 4 years (opioid) approached – both were P = .05 – but did not quite reach the less than .05 considered statistically significant. Adjusted odds ratios for the other age groups were further off the mark. For antihistamines, the upward trend between the two eras was significant for children aged under 2 years, 2-3 years, and 6-11 years, Dr. Horton and associates reported.
The two youngest groups, under 2 years and 2-3, were combined for the opioid CCM analyses to avoid a population under 30, which would have yielded unreliable estimates. The investigators used data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, with the sample representing 3.1 billion pediatric visits from 2002 to 2015.
Dr. Horton is supported by an award from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The investigators reported no disclosures relevant to this study.
SOURCE: Horton DB et al. JAMA Pediatr. 2019 Jul 29. doi: 10.1001/jamapediatrics.2019.2252.
with evidence suggesting replacement by off-label antihistamines, according to analysis of two national databases.
Compared with older children, declines in both opioid and nonopioid cold and cough medicine (CCM) use “appeared to accelerate in children younger than 2 years … and among children younger than 6 years for opioid-containing CCM” after the Food and Drug Administration’s 2008 public health advisory on use of OTC forms of CCM, Daniel B. Horton, MD, of the Robert Wood Johnson Medical School, New Brunswick, N.J., and his associates wrote in JAMA Pediatrics.
Meanwhile, recommendations for single-agent antihistamines rose – for some age groups significantly – over the 14-year study period, which was divided into two eras: 2002-2008 and 2009-2015.
When the two eras were compared, trends for decreased use of CCM in children under 2 years of age (nonopioid) and under 4 years (opioid) approached – both were P = .05 – but did not quite reach the less than .05 considered statistically significant. Adjusted odds ratios for the other age groups were further off the mark. For antihistamines, the upward trend between the two eras was significant for children aged under 2 years, 2-3 years, and 6-11 years, Dr. Horton and associates reported.
The two youngest groups, under 2 years and 2-3, were combined for the opioid CCM analyses to avoid a population under 30, which would have yielded unreliable estimates. The investigators used data from the National Ambulatory Medical Care Survey and the National Hospital Ambulatory Medical Care Survey, with the sample representing 3.1 billion pediatric visits from 2002 to 2015.
Dr. Horton is supported by an award from the National Institute of Arthritis and Musculoskeletal and Skin Diseases. The investigators reported no disclosures relevant to this study.
SOURCE: Horton DB et al. JAMA Pediatr. 2019 Jul 29. doi: 10.1001/jamapediatrics.2019.2252.
FROM JAMA PEDIATRICS
Postpartum care: State scorecard for Medicaid enrollees
Timely postpartum care for Medicaid enrollees varies considerably, ranging from 17% to 74% among the states, according to the Centers for Medicare & Medicaid Services.
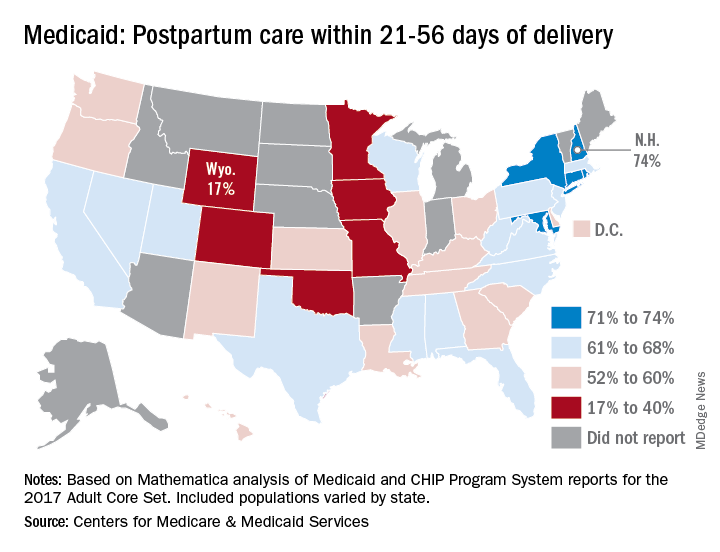
A national median of 60% of women saw a health care provider within 21-56 days of their delivery, CMS reported in its Medicaid and Children’s Health Insurance Program Scorecard.
“Medicaid is the largest payer for maternity care in the United States. The program has an important role to play in improving maternal and perinatal health outcomes,” the CMS noted.
New Hampshire’s rate of 74% was the highest of any state, just edging out Maryland and Rhode Island, each at 73%. The only other states over 70% were Connecticut and New York, which both reported rates of 71%, scorecard data show.
In Wyoming, the state with the lowest rate, 17% of Medicaid enrollees received timely postpartum care. The other four states with rates below 40% were Oklahoma (22%), Colorado (35%), Iowa (37%), and Missouri (38%), the CMS said after a recent refresh of data in the scorecard.
“The included populations … can vary by state. For example, some states report data on certain populations such as those covered under managed care but not those covered under fee for service. This variation in data and calculation methods can affect measure performance and comparisons between states,” the CMS said.
The scorecard is based on Mathematica analysis of Medicaid and CHIP Program System reports for the 2017 Adult Core Set, and the measurement period was Nov. 6, 2015, to Nov. 5, 2016. Twelve states did not report data on postpartum care to the CMS.
“More and more states are voluntarily reporting their health outcomes in the scorecard, and the new data is leading us into an era of increased transparency and accountability, so that together we can improve the quality of care we give to the vulnerable Americans that depend on this vital program,” CMS Administrator Seema Verma said in a written statement.
Timely postpartum care for Medicaid enrollees varies considerably, ranging from 17% to 74% among the states, according to the Centers for Medicare & Medicaid Services.
A national median of 60% of women saw a health care provider within 21-56 days of their delivery, CMS reported in its Medicaid and Children’s Health Insurance Program Scorecard.
“Medicaid is the largest payer for maternity care in the United States. The program has an important role to play in improving maternal and perinatal health outcomes,” the CMS noted.
New Hampshire’s rate of 74% was the highest of any state, just edging out Maryland and Rhode Island, each at 73%. The only other states over 70% were Connecticut and New York, which both reported rates of 71%, scorecard data show.
In Wyoming, the state with the lowest rate, 17% of Medicaid enrollees received timely postpartum care. The other four states with rates below 40% were Oklahoma (22%), Colorado (35%), Iowa (37%), and Missouri (38%), the CMS said after a recent refresh of data in the scorecard.
“The included populations … can vary by state. For example, some states report data on certain populations such as those covered under managed care but not those covered under fee for service. This variation in data and calculation methods can affect measure performance and comparisons between states,” the CMS said.
The scorecard is based on Mathematica analysis of Medicaid and CHIP Program System reports for the 2017 Adult Core Set, and the measurement period was Nov. 6, 2015, to Nov. 5, 2016. Twelve states did not report data on postpartum care to the CMS.
“More and more states are voluntarily reporting their health outcomes in the scorecard, and the new data is leading us into an era of increased transparency and accountability, so that together we can improve the quality of care we give to the vulnerable Americans that depend on this vital program,” CMS Administrator Seema Verma said in a written statement.
Timely postpartum care for Medicaid enrollees varies considerably, ranging from 17% to 74% among the states, according to the Centers for Medicare & Medicaid Services.
A national median of 60% of women saw a health care provider within 21-56 days of their delivery, CMS reported in its Medicaid and Children’s Health Insurance Program Scorecard.
“Medicaid is the largest payer for maternity care in the United States. The program has an important role to play in improving maternal and perinatal health outcomes,” the CMS noted.
New Hampshire’s rate of 74% was the highest of any state, just edging out Maryland and Rhode Island, each at 73%. The only other states over 70% were Connecticut and New York, which both reported rates of 71%, scorecard data show.
In Wyoming, the state with the lowest rate, 17% of Medicaid enrollees received timely postpartum care. The other four states with rates below 40% were Oklahoma (22%), Colorado (35%), Iowa (37%), and Missouri (38%), the CMS said after a recent refresh of data in the scorecard.
“The included populations … can vary by state. For example, some states report data on certain populations such as those covered under managed care but not those covered under fee for service. This variation in data and calculation methods can affect measure performance and comparisons between states,” the CMS said.
The scorecard is based on Mathematica analysis of Medicaid and CHIP Program System reports for the 2017 Adult Core Set, and the measurement period was Nov. 6, 2015, to Nov. 5, 2016. Twelve states did not report data on postpartum care to the CMS.
“More and more states are voluntarily reporting their health outcomes in the scorecard, and the new data is leading us into an era of increased transparency and accountability, so that together we can improve the quality of care we give to the vulnerable Americans that depend on this vital program,” CMS Administrator Seema Verma said in a written statement.
Robust microbiota, cat dominance, and a nice Martian red
Aesop’s infant fecal microbiotas

There once was a city baby who visited his Amish country cousin. (Actually, this study involved two groups of five babies each; but for our purposes, one child will do.)
Amish baby served a simple meal, and the two relations talked of an odd experience they had shared.
City baby said that one day, a group of scientists from The Ohio State University visited his home in Wooster, where he had no known contact with livestock. The scientists asked if they could have some of city baby’s poop so they could examine his microbiome. Amish baby said that scientists also had visited her rural home, where the family raised goats and pigs, and asked for some of her poop.
Amish baby said that there was “an abundance of beneficial bacteria” in her gut, as the researchers had put it, that wasn’t found in city baby’s gut. The reason, the scientists told Amish baby, was her “exposure to the livestock and the fact that the Amish tend to live a relatively less-sanitized lifestyle than most other Americans.”
City baby frowned and pulled out his smartphone. After some quick Googling, he found a written statement from the study’s co-lead author, Zhongtang Yu of Ohio State’s Food Innovation Center: “Good hygiene is important, but from the perspective of our immune systems, a sanitized environment robs our immune systems of the opportunity to be educated by microbes. Too clean is not necessarily a good thing.”
City baby became a little sad, so Amish baby tried to comfort him. But then his Uber showed up, and he had to go home.
The Red (wine) Planet
The first astronauts who make the long voyage to Mars will face many health challenges. The hostility of space itself. Years of isolation cooped up inside a tiny metal can. Potentially lethal doses of radiation.
Comparatively speaking, the degrading effects of the Red Planet’s lighter gravity on the human body seem almost trivial. But the weakening of both bone and muscle is a serious problem; luckily, it’s a problem that seems to have a solution. Just bring some wine along.
Specifically, red wine.
According to a study undertaken by researchers in Boston, resveratrol – a chemical found in red wine with anti-inflammatory, antioxidant, and antidiabetic effects – may stave off the musculoskeletal degradation effects of lighter gravity.
Rats placed in an environment simulating Mars’s lighter gravity that received resveratrol had significantly greater limb grip force, muscle weight, myofiber size, and muscle composition protection than did rats placed in Mars-like gravity that did not receive the chemical.
While some muscle atrophy did occur, the results were definitely impressive, and the researchers noted that a greater dose may further improve results.
We eagerly await the first fateful words when the first Mars expedition touches down: “Tranquility Base here, the commander’s gotten into the wine cellar again. Give us a few minutes to sober him up.”
The purrrrfect pet

There’s more than one way to pet a cat, but what’s the very best way? Cats are notoriously fickle – one second they could be enjoying a nice back rub and the next, you’ve been eviscerated. How do you avoid this fate when you’re just trying to bond with Mittens? Science has your answer.
A surprising amount of studies are done on domestic cats (surprising to this dog lover, anyway). Unlike man’s best friend, domestic cats display only a slight genetic divergence from their ancestors, which means they still have strong wildcat instincts. That’s right, your precious Snowball knows she’s actually a lion. It might be best not to dissuade her of this notion.
Cats vary widely in whether they like being touched or not. Many cats simply tolerate their humans in order to receive food – although a tolerant cat is not always a happy cat. The best way to pet your cat is to let them be in control. A study on the human-cat relationship found that the most successful interactions happened when the cat initiated. Basically, just wait until your cat pets you. As any cat parent will tell you, they don’t own a cat – the cat owns them.
Aesop’s infant fecal microbiotas
There once was a city baby who visited his Amish country cousin. (Actually, this study involved two groups of five babies each; but for our purposes, one child will do.)
Amish baby served a simple meal, and the two relations talked of an odd experience they had shared.
City baby said that one day, a group of scientists from The Ohio State University visited his home in Wooster, where he had no known contact with livestock. The scientists asked if they could have some of city baby’s poop so they could examine his microbiome. Amish baby said that scientists also had visited her rural home, where the family raised goats and pigs, and asked for some of her poop.
Amish baby said that there was “an abundance of beneficial bacteria” in her gut, as the researchers had put it, that wasn’t found in city baby’s gut. The reason, the scientists told Amish baby, was her “exposure to the livestock and the fact that the Amish tend to live a relatively less-sanitized lifestyle than most other Americans.”
City baby frowned and pulled out his smartphone. After some quick Googling, he found a written statement from the study’s co-lead author, Zhongtang Yu of Ohio State’s Food Innovation Center: “Good hygiene is important, but from the perspective of our immune systems, a sanitized environment robs our immune systems of the opportunity to be educated by microbes. Too clean is not necessarily a good thing.”
City baby became a little sad, so Amish baby tried to comfort him. But then his Uber showed up, and he had to go home.
The Red (wine) Planet
The first astronauts who make the long voyage to Mars will face many health challenges. The hostility of space itself. Years of isolation cooped up inside a tiny metal can. Potentially lethal doses of radiation.
Comparatively speaking, the degrading effects of the Red Planet’s lighter gravity on the human body seem almost trivial. But the weakening of both bone and muscle is a serious problem; luckily, it’s a problem that seems to have a solution. Just bring some wine along.
Specifically, red wine.
According to a study undertaken by researchers in Boston, resveratrol – a chemical found in red wine with anti-inflammatory, antioxidant, and antidiabetic effects – may stave off the musculoskeletal degradation effects of lighter gravity.
Rats placed in an environment simulating Mars’s lighter gravity that received resveratrol had significantly greater limb grip force, muscle weight, myofiber size, and muscle composition protection than did rats placed in Mars-like gravity that did not receive the chemical.
While some muscle atrophy did occur, the results were definitely impressive, and the researchers noted that a greater dose may further improve results.
We eagerly await the first fateful words when the first Mars expedition touches down: “Tranquility Base here, the commander’s gotten into the wine cellar again. Give us a few minutes to sober him up.”
The purrrrfect pet
There’s more than one way to pet a cat, but what’s the very best way? Cats are notoriously fickle – one second they could be enjoying a nice back rub and the next, you’ve been eviscerated. How do you avoid this fate when you’re just trying to bond with Mittens? Science has your answer.
A surprising amount of studies are done on domestic cats (surprising to this dog lover, anyway). Unlike man’s best friend, domestic cats display only a slight genetic divergence from their ancestors, which means they still have strong wildcat instincts. That’s right, your precious Snowball knows she’s actually a lion. It might be best not to dissuade her of this notion.
Cats vary widely in whether they like being touched or not. Many cats simply tolerate their humans in order to receive food – although a tolerant cat is not always a happy cat. The best way to pet your cat is to let them be in control. A study on the human-cat relationship found that the most successful interactions happened when the cat initiated. Basically, just wait until your cat pets you. As any cat parent will tell you, they don’t own a cat – the cat owns them.
Aesop’s infant fecal microbiotas
There once was a city baby who visited his Amish country cousin. (Actually, this study involved two groups of five babies each; but for our purposes, one child will do.)
Amish baby served a simple meal, and the two relations talked of an odd experience they had shared.
City baby said that one day, a group of scientists from The Ohio State University visited his home in Wooster, where he had no known contact with livestock. The scientists asked if they could have some of city baby’s poop so they could examine his microbiome. Amish baby said that scientists also had visited her rural home, where the family raised goats and pigs, and asked for some of her poop.
Amish baby said that there was “an abundance of beneficial bacteria” in her gut, as the researchers had put it, that wasn’t found in city baby’s gut. The reason, the scientists told Amish baby, was her “exposure to the livestock and the fact that the Amish tend to live a relatively less-sanitized lifestyle than most other Americans.”
City baby frowned and pulled out his smartphone. After some quick Googling, he found a written statement from the study’s co-lead author, Zhongtang Yu of Ohio State’s Food Innovation Center: “Good hygiene is important, but from the perspective of our immune systems, a sanitized environment robs our immune systems of the opportunity to be educated by microbes. Too clean is not necessarily a good thing.”
City baby became a little sad, so Amish baby tried to comfort him. But then his Uber showed up, and he had to go home.
The Red (wine) Planet
The first astronauts who make the long voyage to Mars will face many health challenges. The hostility of space itself. Years of isolation cooped up inside a tiny metal can. Potentially lethal doses of radiation.
Comparatively speaking, the degrading effects of the Red Planet’s lighter gravity on the human body seem almost trivial. But the weakening of both bone and muscle is a serious problem; luckily, it’s a problem that seems to have a solution. Just bring some wine along.
Specifically, red wine.
According to a study undertaken by researchers in Boston, resveratrol – a chemical found in red wine with anti-inflammatory, antioxidant, and antidiabetic effects – may stave off the musculoskeletal degradation effects of lighter gravity.
Rats placed in an environment simulating Mars’s lighter gravity that received resveratrol had significantly greater limb grip force, muscle weight, myofiber size, and muscle composition protection than did rats placed in Mars-like gravity that did not receive the chemical.
While some muscle atrophy did occur, the results were definitely impressive, and the researchers noted that a greater dose may further improve results.
We eagerly await the first fateful words when the first Mars expedition touches down: “Tranquility Base here, the commander’s gotten into the wine cellar again. Give us a few minutes to sober him up.”
The purrrrfect pet
There’s more than one way to pet a cat, but what’s the very best way? Cats are notoriously fickle – one second they could be enjoying a nice back rub and the next, you’ve been eviscerated. How do you avoid this fate when you’re just trying to bond with Mittens? Science has your answer.
A surprising amount of studies are done on domestic cats (surprising to this dog lover, anyway). Unlike man’s best friend, domestic cats display only a slight genetic divergence from their ancestors, which means they still have strong wildcat instincts. That’s right, your precious Snowball knows she’s actually a lion. It might be best not to dissuade her of this notion.
Cats vary widely in whether they like being touched or not. Many cats simply tolerate their humans in order to receive food – although a tolerant cat is not always a happy cat. The best way to pet your cat is to let them be in control. A study on the human-cat relationship found that the most successful interactions happened when the cat initiated. Basically, just wait until your cat pets you. As any cat parent will tell you, they don’t own a cat – the cat owns them.
Follow-up after mental illness admission: State scorecard
Follow-up rates after hospitalization for mental illness varied considerably among the states, ranging from 38% to 89% in 2016, according to the Centers for Medicare & Medicaid Services.
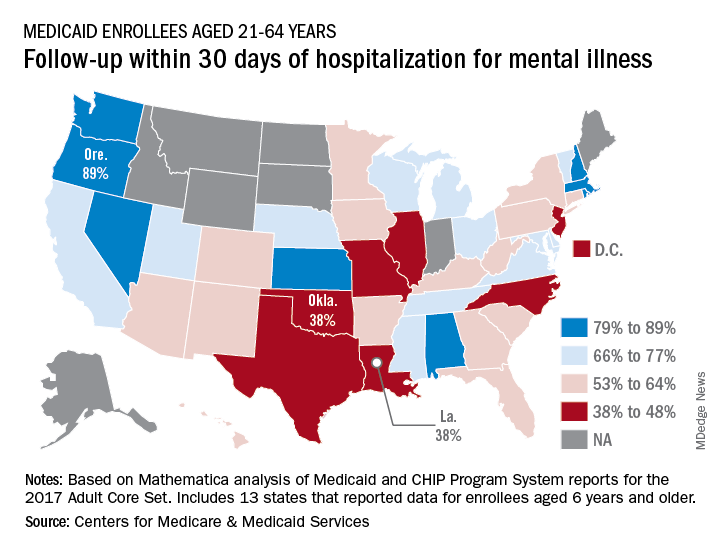
All that variation added up to a national median of 64% of Medicaid enrollees who saw a mental health clinician within 30 days of discharge, CMS reported in its Medicaid and Children’s Health Insurance Program Scorecard.
The other states in the top five were Nevada (85%), Rhode Island (82%), and New Hampshire (80%), scoreboard data show.
In Louisiana and Oklahoma, the states with the lowest rate, only 38% of Medicaid enrollees had a follow-up visit within 30 days of their discharge. The next three rungs on the follow-up ladder were occupied by New Jersey (43%), Illinois (44%), and North Carolina (44%), the CMS said after a recent refresh of data in the scorecard.
“Everyone – whether you are a beneficiary, taxpayer, or lawmaker – deserves to understand the performance of our nation’s largest health coverage programs and often the largest state expenses,” CMS Administrator Seema Verma said in a written statement. “More and more states are voluntarily reporting their health outcomes in the scorecard, and the new data is leading us into an era of increased transparency and accountability, so that together we can improve the quality of care we give to the vulnerable Americans that depend on this vital program.”
Data for this measure “reflect state reporting for Medicaid enrollees ages 21 to 64” years, the CMS noted, but eight states did not report at all. A total of 13 states reported on enrollees aged 6 years and older, 2 states reported results for those aged 21 and older, and 1 state reported data for ages 6-64.
“The included populations … can vary by state. For example, some states report data on certain populations such as those covered under managed care but not those covered under fee for service. This variation in data can affect measure performance and comparisons between states,” the CMS said.
Follow-up rates after hospitalization for mental illness varied considerably among the states, ranging from 38% to 89% in 2016, according to the Centers for Medicare & Medicaid Services.
All that variation added up to a national median of 64% of Medicaid enrollees who saw a mental health clinician within 30 days of discharge, CMS reported in its Medicaid and Children’s Health Insurance Program Scorecard.
The other states in the top five were Nevada (85%), Rhode Island (82%), and New Hampshire (80%), scoreboard data show.
In Louisiana and Oklahoma, the states with the lowest rate, only 38% of Medicaid enrollees had a follow-up visit within 30 days of their discharge. The next three rungs on the follow-up ladder were occupied by New Jersey (43%), Illinois (44%), and North Carolina (44%), the CMS said after a recent refresh of data in the scorecard.
“Everyone – whether you are a beneficiary, taxpayer, or lawmaker – deserves to understand the performance of our nation’s largest health coverage programs and often the largest state expenses,” CMS Administrator Seema Verma said in a written statement. “More and more states are voluntarily reporting their health outcomes in the scorecard, and the new data is leading us into an era of increased transparency and accountability, so that together we can improve the quality of care we give to the vulnerable Americans that depend on this vital program.”
Data for this measure “reflect state reporting for Medicaid enrollees ages 21 to 64” years, the CMS noted, but eight states did not report at all. A total of 13 states reported on enrollees aged 6 years and older, 2 states reported results for those aged 21 and older, and 1 state reported data for ages 6-64.
“The included populations … can vary by state. For example, some states report data on certain populations such as those covered under managed care but not those covered under fee for service. This variation in data can affect measure performance and comparisons between states,” the CMS said.
Follow-up rates after hospitalization for mental illness varied considerably among the states, ranging from 38% to 89% in 2016, according to the Centers for Medicare & Medicaid Services.
All that variation added up to a national median of 64% of Medicaid enrollees who saw a mental health clinician within 30 days of discharge, CMS reported in its Medicaid and Children’s Health Insurance Program Scorecard.
The other states in the top five were Nevada (85%), Rhode Island (82%), and New Hampshire (80%), scoreboard data show.
In Louisiana and Oklahoma, the states with the lowest rate, only 38% of Medicaid enrollees had a follow-up visit within 30 days of their discharge. The next three rungs on the follow-up ladder were occupied by New Jersey (43%), Illinois (44%), and North Carolina (44%), the CMS said after a recent refresh of data in the scorecard.
“Everyone – whether you are a beneficiary, taxpayer, or lawmaker – deserves to understand the performance of our nation’s largest health coverage programs and often the largest state expenses,” CMS Administrator Seema Verma said in a written statement. “More and more states are voluntarily reporting their health outcomes in the scorecard, and the new data is leading us into an era of increased transparency and accountability, so that together we can improve the quality of care we give to the vulnerable Americans that depend on this vital program.”
Data for this measure “reflect state reporting for Medicaid enrollees ages 21 to 64” years, the CMS noted, but eight states did not report at all. A total of 13 states reported on enrollees aged 6 years and older, 2 states reported results for those aged 21 and older, and 1 state reported data for ages 6-64.
“The included populations … can vary by state. For example, some states report data on certain populations such as those covered under managed care but not those covered under fee for service. This variation in data can affect measure performance and comparisons between states,” the CMS said.
New measles outbreaks reported in Los Angeles and El Paso
according to the Centers for Disease Control and Prevention.
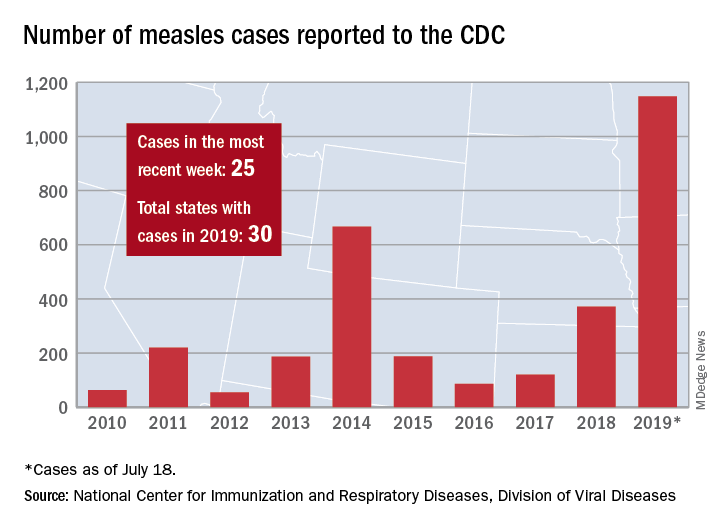
The total number of confirmed cases of measles in the United States is now up to 1,148 for the year, which is 25 more than the previous week, the CDC said on July 22. The highest 1-week total for the year was the 90 cases reported during the week of April 11.
The number of outbreaks is back up to five as California returned to the list after a 1-week absence and El Paso, Tex., made its first appearance of the year. The current outbreak in California – the state’s fifth – is occurring in Los Angeles, which is now up to 16 total cases in 2019. El Paso just reported its fourth case on July 17, and the city’s health department noted that “it had been more than 25 years since El Paso saw its last case of measles before these four recent cases.” Outbreaks also are ongoing in Rockland County, N.Y.; New York City; and three counties in Washington State.
States that joined the ranks of the measles-infected during this most recent reporting week were Alaska and Ohio, which brings the total number to 30 for the year, the CDC said.
The Alaska Department of Health and Social Services said that it “has confirmed a single case of measles in an unvaccinated teenager from the Kenai Peninsula who recently traveled out of state to Arizona via Seattle.” The Ohio case is a “young adult from Stark County [who] recently traveled to a state with confirmed measles cases,” according to the state’s health department.
according to the Centers for Disease Control and Prevention.
The total number of confirmed cases of measles in the United States is now up to 1,148 for the year, which is 25 more than the previous week, the CDC said on July 22. The highest 1-week total for the year was the 90 cases reported during the week of April 11.
The number of outbreaks is back up to five as California returned to the list after a 1-week absence and El Paso, Tex., made its first appearance of the year. The current outbreak in California – the state’s fifth – is occurring in Los Angeles, which is now up to 16 total cases in 2019. El Paso just reported its fourth case on July 17, and the city’s health department noted that “it had been more than 25 years since El Paso saw its last case of measles before these four recent cases.” Outbreaks also are ongoing in Rockland County, N.Y.; New York City; and three counties in Washington State.
States that joined the ranks of the measles-infected during this most recent reporting week were Alaska and Ohio, which brings the total number to 30 for the year, the CDC said.
The Alaska Department of Health and Social Services said that it “has confirmed a single case of measles in an unvaccinated teenager from the Kenai Peninsula who recently traveled out of state to Arizona via Seattle.” The Ohio case is a “young adult from Stark County [who] recently traveled to a state with confirmed measles cases,” according to the state’s health department.
according to the Centers for Disease Control and Prevention.
The total number of confirmed cases of measles in the United States is now up to 1,148 for the year, which is 25 more than the previous week, the CDC said on July 22. The highest 1-week total for the year was the 90 cases reported during the week of April 11.
The number of outbreaks is back up to five as California returned to the list after a 1-week absence and El Paso, Tex., made its first appearance of the year. The current outbreak in California – the state’s fifth – is occurring in Los Angeles, which is now up to 16 total cases in 2019. El Paso just reported its fourth case on July 17, and the city’s health department noted that “it had been more than 25 years since El Paso saw its last case of measles before these four recent cases.” Outbreaks also are ongoing in Rockland County, N.Y.; New York City; and three counties in Washington State.
States that joined the ranks of the measles-infected during this most recent reporting week were Alaska and Ohio, which brings the total number to 30 for the year, the CDC said.
The Alaska Department of Health and Social Services said that it “has confirmed a single case of measles in an unvaccinated teenager from the Kenai Peninsula who recently traveled out of state to Arizona via Seattle.” The Ohio case is a “young adult from Stark County [who] recently traveled to a state with confirmed measles cases,” according to the state’s health department.
Smoking-cessation attempts changed little over 7-year span
according to the Centers for Disease Control and Prevention.

The median percentage of adult smokers who tried to quit cigarettes over the past year went from 64.9% in 2011 to 65.4% in 2017, CDC investigators reported in the Morbidity and Mortality Weekly Report, but the rate has gone down since 2014, when it reached 66.9%.
“The limited progress in increasing quit attempts … together with the variation in quit attempt prevalence among states, underscores the importance of enhanced efforts to motivate and help smokers to quit,” wrote Kimp Walton, MS, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion and associates.
State-specific trends in quit-attempt rates reflected the national situation. The prevalence of past-year cessation attempts went up significantly in four states (Kansas, Louisiana, Virginia, and West Virginia) from 2011 to 2017, went down significantly in two states (New York and Tennessee), and did not change significantly in the other 44 states and the District of Columbia, they wrote.
In 2017, cigarette smokers in Connecticut were the most likely to have tried to quit in the past year, with a rate of 71.6%. The only other places with rates greater than 70% were Delaware, D.C., New Jersey, and Texas. The lowest quit-attempt rate that year, 58.6%, belonged to Wisconsin, with Iowa and Missouri the only other states under 60%, the investigators reported based on data from annual Behavioral Risk Factor Surveillance System surveys.
“Because most smokers make multiple quit attempts before succeeding, as many as 30 on average, tobacco dependence is viewed as a chronic, relapsing condition that requires repeated intervention. Smokers should be encouraged to keep trying to quit until they succeed, and health care providers should be encouraged to keep supporting smokers until they quit,” investigators wrote.
SOURCE: Walton K et al. MMWR. 2019 Jul 19;68(28):621-6.
according to the Centers for Disease Control and Prevention.
The median percentage of adult smokers who tried to quit cigarettes over the past year went from 64.9% in 2011 to 65.4% in 2017, CDC investigators reported in the Morbidity and Mortality Weekly Report, but the rate has gone down since 2014, when it reached 66.9%.
“The limited progress in increasing quit attempts … together with the variation in quit attempt prevalence among states, underscores the importance of enhanced efforts to motivate and help smokers to quit,” wrote Kimp Walton, MS, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion and associates.
State-specific trends in quit-attempt rates reflected the national situation. The prevalence of past-year cessation attempts went up significantly in four states (Kansas, Louisiana, Virginia, and West Virginia) from 2011 to 2017, went down significantly in two states (New York and Tennessee), and did not change significantly in the other 44 states and the District of Columbia, they wrote.
In 2017, cigarette smokers in Connecticut were the most likely to have tried to quit in the past year, with a rate of 71.6%. The only other places with rates greater than 70% were Delaware, D.C., New Jersey, and Texas. The lowest quit-attempt rate that year, 58.6%, belonged to Wisconsin, with Iowa and Missouri the only other states under 60%, the investigators reported based on data from annual Behavioral Risk Factor Surveillance System surveys.
“Because most smokers make multiple quit attempts before succeeding, as many as 30 on average, tobacco dependence is viewed as a chronic, relapsing condition that requires repeated intervention. Smokers should be encouraged to keep trying to quit until they succeed, and health care providers should be encouraged to keep supporting smokers until they quit,” investigators wrote.
SOURCE: Walton K et al. MMWR. 2019 Jul 19;68(28):621-6.
according to the Centers for Disease Control and Prevention.
The median percentage of adult smokers who tried to quit cigarettes over the past year went from 64.9% in 2011 to 65.4% in 2017, CDC investigators reported in the Morbidity and Mortality Weekly Report, but the rate has gone down since 2014, when it reached 66.9%.
“The limited progress in increasing quit attempts … together with the variation in quit attempt prevalence among states, underscores the importance of enhanced efforts to motivate and help smokers to quit,” wrote Kimp Walton, MS, of the CDC’s National Center for Chronic Disease Prevention and Health Promotion and associates.
State-specific trends in quit-attempt rates reflected the national situation. The prevalence of past-year cessation attempts went up significantly in four states (Kansas, Louisiana, Virginia, and West Virginia) from 2011 to 2017, went down significantly in two states (New York and Tennessee), and did not change significantly in the other 44 states and the District of Columbia, they wrote.
In 2017, cigarette smokers in Connecticut were the most likely to have tried to quit in the past year, with a rate of 71.6%. The only other places with rates greater than 70% were Delaware, D.C., New Jersey, and Texas. The lowest quit-attempt rate that year, 58.6%, belonged to Wisconsin, with Iowa and Missouri the only other states under 60%, the investigators reported based on data from annual Behavioral Risk Factor Surveillance System surveys.
“Because most smokers make multiple quit attempts before succeeding, as many as 30 on average, tobacco dependence is viewed as a chronic, relapsing condition that requires repeated intervention. Smokers should be encouraged to keep trying to quit until they succeed, and health care providers should be encouraged to keep supporting smokers until they quit,” investigators wrote.
SOURCE: Walton K et al. MMWR. 2019 Jul 19;68(28):621-6.
FROM MMWR