User login
EHR Report: Take your medicine!
“Drugs don’t work in patients who don’t take them.”
–C. Everett Koop, M.D.
While it would be hard to imagine accountable care organizations being able to get the data they need to manage care without electronic health records, and EHRs are critical as payment has evolved to emphasize the outcomes of treatment, one area remains the holy grail of disease management: how to get patients to take the medications that are prescribed.
Poor adherence to medications is a critical issue in the management of chronic disease. The causes for suboptimal adherence are numerous, including the cost of medications, patient-physician communication, patient education, motivation, and simple forgetfulness.

Approximately 1.5 billion prescriptions, at a cost of more than $250 billion, are dispensed each year in the United States. A large body of evidence supports the use of these medications. For patients with diabetes, for instance, correct medication use can lower blood sugar, blood pressure, and cholesterol, and by so doing, decrease morbidity and mortality from both microvascular and macrovascular disease.
The act of taking medications is influenced by many factors, and all of these factors come together at a point in time when patients are not directly engaged with the health care system. It is at that moment that patients remember and decide whether to take their medications.
Numerous studies show that individuals often do not take their medicines as prescribed. Adherence rates for medications for chronic disease show that patients on average take only about 50% of prescribed doses. For patients with diabetes, the average adherence rate is about 70%, with rates ranging in different studies from 31% to 87%.
When patients do not take their medications correctly, there can be severe consequences. Poor medication adherence can lead to poorer clinical outcomes, including increased hospitalizations. One large dataset of more than 56,000 individuals with type 2 diabetes covered by employer-sponsored health insurance showed that increased adherence to medications significantly reduced hospitalizations and emergency department visits. When adherence rates increased, the hospitalization rate fell 23%, and the rate of emergency department visits decreased 46%, resulting in significant cost savings for the health system.1
In response to this issue, many strategies have emerged. We now regularly get correspondence from insurance companies alerting us to nonadherence of individual patients. This information tends to be of little benefit, because the information is received long after the decision to take or not take the medication is made. Our response in the office to our patients is generally to remind them to take their medications, which is not much different from the discussion we have with them without that information.
Recently, a new set of apps for smartphones and tablets has emerged to help patients organize their approach to taking medications. Examples of some of these apps include Care4Today, Dosecast, Medisafe, MedSimple, MyMedREc, MyMeds, and OnTimeRx. Most of these apps allow a patient to put in their medication schedule and are organized to provide reminders when it is time to take medications.
The problem with reminders, of course, is that they don’t always happen at a time when it is convenient for a person to take their medications. For example, if your app reminds you to take your medicines at 9 p.m. each night, and you are at the movies on a Saturday night, you may extinguish the reminder and not remember to take the medications when you get home.
Many of the apps also track adherence rates so that patients can see how well they are doing in taking their medications. The results are often startling to patients, and it is hoped that such information would encourage more effort in taking medications.
One problem with many of the apps currently available is that they essentially function as sophisticated alarm clocks. They do not get at some of the fundamental reasons that people do not take their medications, which would require more behavioral input.
In fact, a recent article in the American Journal of Preventive Medicine looked at 166 medication adherence apps and concluded that current apps contained little in the way of evidence-based behavioral change techniques that have been shown to help change behavior. In fact, only about one-third of apps contained any feedback on behavior at all.2
While adherence apps still have a way to go, they can be helpful, and many contain interesting, novel features. Some allow the patient to input the name of a medication by scanning the name from the medication’s pill bottle. Some have the ability not only to remind a patient to take a medication, but also to text that patient’s caregiver (or parent, in the case of a teenager) if the medication is not taken.
While not perfect, these adherence apps are worth learning more about. They may be helpful additions to our efforts to achieve the best outcomes for our patients by helping them to actually take the medications that we so carefully prescribe.
References
1. Encinosa, W.E.; Bernard, D.; Dor, A. Does prescription drug adherence reduce hospitalizations and costs? The case of diabetes. Advances in Health Economics and Health Services Research 22, pp. 151-73, 2010 (AHRQ Publication No. 11-R008).
2. Am J Prev Med. 2015 Nov 17. pii: S0749-3797(15)00637-6. doi: 10.1016/j.amepre.2015.09.034.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
“Drugs don’t work in patients who don’t take them.”
–C. Everett Koop, M.D.
While it would be hard to imagine accountable care organizations being able to get the data they need to manage care without electronic health records, and EHRs are critical as payment has evolved to emphasize the outcomes of treatment, one area remains the holy grail of disease management: how to get patients to take the medications that are prescribed.
Poor adherence to medications is a critical issue in the management of chronic disease. The causes for suboptimal adherence are numerous, including the cost of medications, patient-physician communication, patient education, motivation, and simple forgetfulness.
Approximately 1.5 billion prescriptions, at a cost of more than $250 billion, are dispensed each year in the United States. A large body of evidence supports the use of these medications. For patients with diabetes, for instance, correct medication use can lower blood sugar, blood pressure, and cholesterol, and by so doing, decrease morbidity and mortality from both microvascular and macrovascular disease.
The act of taking medications is influenced by many factors, and all of these factors come together at a point in time when patients are not directly engaged with the health care system. It is at that moment that patients remember and decide whether to take their medications.
Numerous studies show that individuals often do not take their medicines as prescribed. Adherence rates for medications for chronic disease show that patients on average take only about 50% of prescribed doses. For patients with diabetes, the average adherence rate is about 70%, with rates ranging in different studies from 31% to 87%.
When patients do not take their medications correctly, there can be severe consequences. Poor medication adherence can lead to poorer clinical outcomes, including increased hospitalizations. One large dataset of more than 56,000 individuals with type 2 diabetes covered by employer-sponsored health insurance showed that increased adherence to medications significantly reduced hospitalizations and emergency department visits. When adherence rates increased, the hospitalization rate fell 23%, and the rate of emergency department visits decreased 46%, resulting in significant cost savings for the health system.1
In response to this issue, many strategies have emerged. We now regularly get correspondence from insurance companies alerting us to nonadherence of individual patients. This information tends to be of little benefit, because the information is received long after the decision to take or not take the medication is made. Our response in the office to our patients is generally to remind them to take their medications, which is not much different from the discussion we have with them without that information.
Recently, a new set of apps for smartphones and tablets has emerged to help patients organize their approach to taking medications. Examples of some of these apps include Care4Today, Dosecast, Medisafe, MedSimple, MyMedREc, MyMeds, and OnTimeRx. Most of these apps allow a patient to put in their medication schedule and are organized to provide reminders when it is time to take medications.
The problem with reminders, of course, is that they don’t always happen at a time when it is convenient for a person to take their medications. For example, if your app reminds you to take your medicines at 9 p.m. each night, and you are at the movies on a Saturday night, you may extinguish the reminder and not remember to take the medications when you get home.
Many of the apps also track adherence rates so that patients can see how well they are doing in taking their medications. The results are often startling to patients, and it is hoped that such information would encourage more effort in taking medications.
One problem with many of the apps currently available is that they essentially function as sophisticated alarm clocks. They do not get at some of the fundamental reasons that people do not take their medications, which would require more behavioral input.
In fact, a recent article in the American Journal of Preventive Medicine looked at 166 medication adherence apps and concluded that current apps contained little in the way of evidence-based behavioral change techniques that have been shown to help change behavior. In fact, only about one-third of apps contained any feedback on behavior at all.2
While adherence apps still have a way to go, they can be helpful, and many contain interesting, novel features. Some allow the patient to input the name of a medication by scanning the name from the medication’s pill bottle. Some have the ability not only to remind a patient to take a medication, but also to text that patient’s caregiver (or parent, in the case of a teenager) if the medication is not taken.
While not perfect, these adherence apps are worth learning more about. They may be helpful additions to our efforts to achieve the best outcomes for our patients by helping them to actually take the medications that we so carefully prescribe.
References
1. Encinosa, W.E.; Bernard, D.; Dor, A. Does prescription drug adherence reduce hospitalizations and costs? The case of diabetes. Advances in Health Economics and Health Services Research 22, pp. 151-73, 2010 (AHRQ Publication No. 11-R008).
2. Am J Prev Med. 2015 Nov 17. pii: S0749-3797(15)00637-6. doi: 10.1016/j.amepre.2015.09.034.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
“Drugs don’t work in patients who don’t take them.”
–C. Everett Koop, M.D.
While it would be hard to imagine accountable care organizations being able to get the data they need to manage care without electronic health records, and EHRs are critical as payment has evolved to emphasize the outcomes of treatment, one area remains the holy grail of disease management: how to get patients to take the medications that are prescribed.
Poor adherence to medications is a critical issue in the management of chronic disease. The causes for suboptimal adherence are numerous, including the cost of medications, patient-physician communication, patient education, motivation, and simple forgetfulness.
Approximately 1.5 billion prescriptions, at a cost of more than $250 billion, are dispensed each year in the United States. A large body of evidence supports the use of these medications. For patients with diabetes, for instance, correct medication use can lower blood sugar, blood pressure, and cholesterol, and by so doing, decrease morbidity and mortality from both microvascular and macrovascular disease.
The act of taking medications is influenced by many factors, and all of these factors come together at a point in time when patients are not directly engaged with the health care system. It is at that moment that patients remember and decide whether to take their medications.
Numerous studies show that individuals often do not take their medicines as prescribed. Adherence rates for medications for chronic disease show that patients on average take only about 50% of prescribed doses. For patients with diabetes, the average adherence rate is about 70%, with rates ranging in different studies from 31% to 87%.
When patients do not take their medications correctly, there can be severe consequences. Poor medication adherence can lead to poorer clinical outcomes, including increased hospitalizations. One large dataset of more than 56,000 individuals with type 2 diabetes covered by employer-sponsored health insurance showed that increased adherence to medications significantly reduced hospitalizations and emergency department visits. When adherence rates increased, the hospitalization rate fell 23%, and the rate of emergency department visits decreased 46%, resulting in significant cost savings for the health system.1
In response to this issue, many strategies have emerged. We now regularly get correspondence from insurance companies alerting us to nonadherence of individual patients. This information tends to be of little benefit, because the information is received long after the decision to take or not take the medication is made. Our response in the office to our patients is generally to remind them to take their medications, which is not much different from the discussion we have with them without that information.
Recently, a new set of apps for smartphones and tablets has emerged to help patients organize their approach to taking medications. Examples of some of these apps include Care4Today, Dosecast, Medisafe, MedSimple, MyMedREc, MyMeds, and OnTimeRx. Most of these apps allow a patient to put in their medication schedule and are organized to provide reminders when it is time to take medications.
The problem with reminders, of course, is that they don’t always happen at a time when it is convenient for a person to take their medications. For example, if your app reminds you to take your medicines at 9 p.m. each night, and you are at the movies on a Saturday night, you may extinguish the reminder and not remember to take the medications when you get home.
Many of the apps also track adherence rates so that patients can see how well they are doing in taking their medications. The results are often startling to patients, and it is hoped that such information would encourage more effort in taking medications.
One problem with many of the apps currently available is that they essentially function as sophisticated alarm clocks. They do not get at some of the fundamental reasons that people do not take their medications, which would require more behavioral input.
In fact, a recent article in the American Journal of Preventive Medicine looked at 166 medication adherence apps and concluded that current apps contained little in the way of evidence-based behavioral change techniques that have been shown to help change behavior. In fact, only about one-third of apps contained any feedback on behavior at all.2
While adherence apps still have a way to go, they can be helpful, and many contain interesting, novel features. Some allow the patient to input the name of a medication by scanning the name from the medication’s pill bottle. Some have the ability not only to remind a patient to take a medication, but also to text that patient’s caregiver (or parent, in the case of a teenager) if the medication is not taken.
While not perfect, these adherence apps are worth learning more about. They may be helpful additions to our efforts to achieve the best outcomes for our patients by helping them to actually take the medications that we so carefully prescribe.
References
1. Encinosa, W.E.; Bernard, D.; Dor, A. Does prescription drug adherence reduce hospitalizations and costs? The case of diabetes. Advances in Health Economics and Health Services Research 22, pp. 151-73, 2010 (AHRQ Publication No. 11-R008).
2. Am J Prev Med. 2015 Nov 17. pii: S0749-3797(15)00637-6. doi: 10.1016/j.amepre.2015.09.034.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.

Binge drinking in adolescents
Binge drinking is a common problem in adolescents as well as adults. In a 2013 survey, 60 million Americans, representing 22% of the population, 12 years of age and older engaged in binge drinking in the previous month. Among those 12-20 years of age, 14%, or one in seven, reported binge drinking. Depending on the survey, between one-third and one-half of all high school students currently drink alcohol. Among young people who drink, a higher proportion drink heavily than among adult drinkers. For teenagers who drink, 28%-60% report binge drinking. Among high school seniors, 1 in 10 report drinking more than 10 drinks in a row. The predominant liquor consumed by 13- to 20-year-olds is vodka (44% ), whereas beer is consumed by less than one-third of respondents. Underage drinkers typically get alcohol from adults of legal drinking age, and frequently drink in their own home or that of a friend. Clearly, this is an important, underappreciated problem that warrants clinical attention.
Background
Binge drinking is defined by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) as the pattern of drinking required to bring the blood alcohol concentration (BAC) to 0.08% or greater. For adolescents, the required amount of alcohol to achieve the same BAC is thought to be less than the amount required for adults. Binge drinking for adults has traditionally been defined as more than five drinks over a 2-hour period for men or more than four drinks over 2 hours for women. Different cutoffs have been suggested for youth in several studies but were not clearly defined for this analysis.

Implications
Alcohol consumption in adolescents is associated with adverse events, and this is only exacerbated by binge drinking. These events include, but are not limited to, engaging in higher-risk behaviors, such as impaired driving or being the passenger in a vehicle with an impaired driver; an increased risk of suicide or attempted suicide; and an increased risk of nonautomobile accidents that can lead to severe injury or drowning. Adolescents who start drinking before the age of 15 years are four times as likely to develop alcohol dependence as people who start drinking after 20 years of age. In addition, adolescents who engage in binge drinking have an increased rate of high-risk sexual activity, which may result in a sexually transmitted infection as well as an unplanned pregnancy. Adolescents who continue to imbibe during pregnancy risk the development of fetal alcohol spectrum disorder. Finally, adolescent binge drinkers are subject to the immediate effects of alcohol, including hangover, blackout, and alcohol poisoning.
Guidance for the provider
The AAP recommends screening every adolescent for substance abuse, but if time constraints exist, alcohol abuse only (Pediatrics. 2015;136[3]:e718-26). The AAP has set up specific screening questions that are based upon the age group of the patient:
For elementary school students (ages 9-11) the following questions are appropriate:
• Do you have any friends who drank beer, wine, or any alcoholic drink in the past year?
• How about you? Have you ever had more than a few sips of beer, wine, or any drink with alcohol?
For patients in middle school (ages 11-14):
• Do you have any friends who drank beer, wine, or any alcohol-containing drink in the past year?
• How about you? Over the past year, how many days have you had where you’ve had more than a few sips of beer, wine, or any other alcohol?
For patients in high school (ages 14-18):
• Over the past year, how many days have you had where you’ve had more than a few sips of beer, wine, or any other alcohol?
• If your friends drink, how many drinks do they usually drink on an occasion?
The above questions help to risk stratify patients into three groups: low, moderate, and high risk. The guidelines do not make a recommendation on how to use these questions to risk stratify the patients. Low-risk patients receive brief counseling. Moderate-risk patients receive more intensive counseling as well as motivational interviewing. Motivational interviewing delivered over the course of one or more sessions has been found to be effective in reducing consumption of alcohol. Lastly, the high-risk group is given motivational interviewing, as well as possible referral.
The bottom line
Alcohol abuse in adolescents can have significant detrimental effects, both short and long term. The AAP recommends screening every adolescent for alcohol abuse and, if time permits, for other drug abuse as well, in order to prevent the morbidity and mortality associated with these substances. Interventions can range from brief counseling to motivational interviewing of adolescents at risk and finally referral to substance abuse specialists in the highest-risk groups
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Dr. Kiriakov is a second-year resident in the Abington-Jefferson Family Medicine Residency Program in Abington.
Binge drinking is a common problem in adolescents as well as adults. In a 2013 survey, 60 million Americans, representing 22% of the population, 12 years of age and older engaged in binge drinking in the previous month. Among those 12-20 years of age, 14%, or one in seven, reported binge drinking. Depending on the survey, between one-third and one-half of all high school students currently drink alcohol. Among young people who drink, a higher proportion drink heavily than among adult drinkers. For teenagers who drink, 28%-60% report binge drinking. Among high school seniors, 1 in 10 report drinking more than 10 drinks in a row. The predominant liquor consumed by 13- to 20-year-olds is vodka (44% ), whereas beer is consumed by less than one-third of respondents. Underage drinkers typically get alcohol from adults of legal drinking age, and frequently drink in their own home or that of a friend. Clearly, this is an important, underappreciated problem that warrants clinical attention.
Background
Binge drinking is defined by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) as the pattern of drinking required to bring the blood alcohol concentration (BAC) to 0.08% or greater. For adolescents, the required amount of alcohol to achieve the same BAC is thought to be less than the amount required for adults. Binge drinking for adults has traditionally been defined as more than five drinks over a 2-hour period for men or more than four drinks over 2 hours for women. Different cutoffs have been suggested for youth in several studies but were not clearly defined for this analysis.
Implications
Alcohol consumption in adolescents is associated with adverse events, and this is only exacerbated by binge drinking. These events include, but are not limited to, engaging in higher-risk behaviors, such as impaired driving or being the passenger in a vehicle with an impaired driver; an increased risk of suicide or attempted suicide; and an increased risk of nonautomobile accidents that can lead to severe injury or drowning. Adolescents who start drinking before the age of 15 years are four times as likely to develop alcohol dependence as people who start drinking after 20 years of age. In addition, adolescents who engage in binge drinking have an increased rate of high-risk sexual activity, which may result in a sexually transmitted infection as well as an unplanned pregnancy. Adolescents who continue to imbibe during pregnancy risk the development of fetal alcohol spectrum disorder. Finally, adolescent binge drinkers are subject to the immediate effects of alcohol, including hangover, blackout, and alcohol poisoning.
Guidance for the provider
The AAP recommends screening every adolescent for substance abuse, but if time constraints exist, alcohol abuse only (Pediatrics. 2015;136[3]:e718-26). The AAP has set up specific screening questions that are based upon the age group of the patient:
For elementary school students (ages 9-11) the following questions are appropriate:
• Do you have any friends who drank beer, wine, or any alcoholic drink in the past year?
• How about you? Have you ever had more than a few sips of beer, wine, or any drink with alcohol?
For patients in middle school (ages 11-14):
• Do you have any friends who drank beer, wine, or any alcohol-containing drink in the past year?
• How about you? Over the past year, how many days have you had where you’ve had more than a few sips of beer, wine, or any other alcohol?
For patients in high school (ages 14-18):
• Over the past year, how many days have you had where you’ve had more than a few sips of beer, wine, or any other alcohol?
• If your friends drink, how many drinks do they usually drink on an occasion?
The above questions help to risk stratify patients into three groups: low, moderate, and high risk. The guidelines do not make a recommendation on how to use these questions to risk stratify the patients. Low-risk patients receive brief counseling. Moderate-risk patients receive more intensive counseling as well as motivational interviewing. Motivational interviewing delivered over the course of one or more sessions has been found to be effective in reducing consumption of alcohol. Lastly, the high-risk group is given motivational interviewing, as well as possible referral.
The bottom line
Alcohol abuse in adolescents can have significant detrimental effects, both short and long term. The AAP recommends screening every adolescent for alcohol abuse and, if time permits, for other drug abuse as well, in order to prevent the morbidity and mortality associated with these substances. Interventions can range from brief counseling to motivational interviewing of adolescents at risk and finally referral to substance abuse specialists in the highest-risk groups
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Dr. Kiriakov is a second-year resident in the Abington-Jefferson Family Medicine Residency Program in Abington.
Binge drinking is a common problem in adolescents as well as adults. In a 2013 survey, 60 million Americans, representing 22% of the population, 12 years of age and older engaged in binge drinking in the previous month. Among those 12-20 years of age, 14%, or one in seven, reported binge drinking. Depending on the survey, between one-third and one-half of all high school students currently drink alcohol. Among young people who drink, a higher proportion drink heavily than among adult drinkers. For teenagers who drink, 28%-60% report binge drinking. Among high school seniors, 1 in 10 report drinking more than 10 drinks in a row. The predominant liquor consumed by 13- to 20-year-olds is vodka (44% ), whereas beer is consumed by less than one-third of respondents. Underage drinkers typically get alcohol from adults of legal drinking age, and frequently drink in their own home or that of a friend. Clearly, this is an important, underappreciated problem that warrants clinical attention.
Background
Binge drinking is defined by the National Institute on Alcohol Abuse and Alcoholism (NIAAA) as the pattern of drinking required to bring the blood alcohol concentration (BAC) to 0.08% or greater. For adolescents, the required amount of alcohol to achieve the same BAC is thought to be less than the amount required for adults. Binge drinking for adults has traditionally been defined as more than five drinks over a 2-hour period for men or more than four drinks over 2 hours for women. Different cutoffs have been suggested for youth in several studies but were not clearly defined for this analysis.
Implications
Alcohol consumption in adolescents is associated with adverse events, and this is only exacerbated by binge drinking. These events include, but are not limited to, engaging in higher-risk behaviors, such as impaired driving or being the passenger in a vehicle with an impaired driver; an increased risk of suicide or attempted suicide; and an increased risk of nonautomobile accidents that can lead to severe injury or drowning. Adolescents who start drinking before the age of 15 years are four times as likely to develop alcohol dependence as people who start drinking after 20 years of age. In addition, adolescents who engage in binge drinking have an increased rate of high-risk sexual activity, which may result in a sexually transmitted infection as well as an unplanned pregnancy. Adolescents who continue to imbibe during pregnancy risk the development of fetal alcohol spectrum disorder. Finally, adolescent binge drinkers are subject to the immediate effects of alcohol, including hangover, blackout, and alcohol poisoning.
Guidance for the provider
The AAP recommends screening every adolescent for substance abuse, but if time constraints exist, alcohol abuse only (Pediatrics. 2015;136[3]:e718-26). The AAP has set up specific screening questions that are based upon the age group of the patient:
For elementary school students (ages 9-11) the following questions are appropriate:
• Do you have any friends who drank beer, wine, or any alcoholic drink in the past year?
• How about you? Have you ever had more than a few sips of beer, wine, or any drink with alcohol?
For patients in middle school (ages 11-14):
• Do you have any friends who drank beer, wine, or any alcohol-containing drink in the past year?
• How about you? Over the past year, how many days have you had where you’ve had more than a few sips of beer, wine, or any other alcohol?
For patients in high school (ages 14-18):
• Over the past year, how many days have you had where you’ve had more than a few sips of beer, wine, or any other alcohol?
• If your friends drink, how many drinks do they usually drink on an occasion?
The above questions help to risk stratify patients into three groups: low, moderate, and high risk. The guidelines do not make a recommendation on how to use these questions to risk stratify the patients. Low-risk patients receive brief counseling. Moderate-risk patients receive more intensive counseling as well as motivational interviewing. Motivational interviewing delivered over the course of one or more sessions has been found to be effective in reducing consumption of alcohol. Lastly, the high-risk group is given motivational interviewing, as well as possible referral.
The bottom line
Alcohol abuse in adolescents can have significant detrimental effects, both short and long term. The AAP recommends screening every adolescent for alcohol abuse and, if time permits, for other drug abuse as well, in order to prevent the morbidity and mortality associated with these substances. Interventions can range from brief counseling to motivational interviewing of adolescents at risk and finally referral to substance abuse specialists in the highest-risk groups
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia. Dr. Kiriakov is a second-year resident in the Abington-Jefferson Family Medicine Residency Program in Abington.

Baby, back back back it up
As many young physicians might recognize, the title of today’s column is from a song by Prince Royce featuring Jennifer Lopez and Pitbull. This article, though, is about what we believe is likely an urgent matter for many of our readers – the issue of appropriately backing up information that resides on their personal computers. We were prompted to write about this after a colleague came to one of us in a panic after losing all of the information on her meticulously performed, but poorly conceived backup. For years she has been developing and storing her lectures on a flash drive, and every month she has been backing up her flash drive to her personal computer. She even set a reminder in her calendar to make sure that she perform those backups each and every month. Unfortunately, she lost her flash drive, and even more unfortunately discovered that what she thought were copies of files on her computer were actually only shortcuts to the files on her now-missing flash drive. All her files were gone.

We are going to organize our discussion in three parts: First, we want to convince you of the importance of making backups, essentially informational life insurance. Unlike life insurance, however, you have a pretty good chance of using your backups at some point over the next 10 years. Second, we are going to discuss locally based backups, and then lastly, we’ll cover cloud-based backups. This may seem like an incredibly dull topic to some, but we anticipate receiving emails of thanks over many years for the knowledge and actions that come out of today’s column.
Hard drive failure rates, derived from data published by companies that professionally manage large numbers of hard drives, is about 3%-5% in the first year. This remains at about 3% per year for the next 2-3 years, and then can go up to 10% or more per year as hard drives continue to age. That means that over a 4-year period, 15%-20% of hard drives are likely to fail.1,2 This fact underscores the importance of backing up your data, because there is a good chance that over time, loss of data will happen to you.
One strategy is to back up to an external drive. The drive can be either a flash drive if you have less than 128 GB to store, or a traditional external hard drive – a very affordable option for memory up to 4 TB (4,000 GB). There are many excellent external hard drives and flash drives from which to choose, but you also need to have backup software that will take the information from your personal computer and place it in an organized manner on your external drive. Many drives now come bundled with backup software. An example of such a drive is the Western Digital My Passport Elite. If the hard drive you have does not already have backup software, there are lots of good choices out there. Backup software solutions include Time Machine (built into all Mac Computers), and many software choices for PCs.3
While the speed of backup and recovery is fast – often just a few hours – there are two main issues that make external drives suboptimal as your main backup strategy. The first is that most people simply don’t remember to plug their external drive into their computer regularly; months and sometimes years can go by without backing up your files. The second issue, which is usually not considered, is that the hard drive usually sits on your desk next to your computer. Therefore, if there is a fire, a flood, an electrical surge, or even a simple spill on your desk, you may lose both your main files and your backup in one fell swoop. For this reason, if you choose to use an external drive as your backup method, you should back up to two different external drives and keep one drive in your office and one at home.
The best method of backup, and the one we recommend to everyone, eliminates the major disadvantages of local backups. This method is cloud-based backup. For cloud-based backup, you purchase a subscription with an annual fee, then you download software from the backup vendor to your computer. It usually takes about 15 minutes to set up the software by selecting the file folders that you would like to back up, then the software does the rest. The first backup can take a long time, typically a few days, as the speed of the backup is limited by the speed of your Internet connection. After that first time, though, backups don’t take long because they back up only the files that have changed since the previous backup.
The main advantages to cloud-based solutions is that once it has been set up, the software ensures that incremental backups occur automatically every time your computer is connected to the Internet. In addition, since the cloud backups are off-site, you are protected from an adverse occurrence taking out your backup drive and your computer when they are sitting next to each other on your desk. In addition, most cloud backup services also allow you to access your file from any computer or smartphone for access where and when you need the files.
So, let us end where we began, with lyrics from the music video, with which we agree, “Word of advice: Want a happy life … Back it up one more time.”
References
1. http://www.extremetech.com/computing/170748-how-long-do-hard-drives-actually-live-for
2. http://www.pcworld.com/article/131168/article.html
3. The Best Backup Software at http://www.pcmag.com/article2/0,2817,2278661,00.asp
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
As many young physicians might recognize, the title of today’s column is from a song by Prince Royce featuring Jennifer Lopez and Pitbull. This article, though, is about what we believe is likely an urgent matter for many of our readers – the issue of appropriately backing up information that resides on their personal computers. We were prompted to write about this after a colleague came to one of us in a panic after losing all of the information on her meticulously performed, but poorly conceived backup. For years she has been developing and storing her lectures on a flash drive, and every month she has been backing up her flash drive to her personal computer. She even set a reminder in her calendar to make sure that she perform those backups each and every month. Unfortunately, she lost her flash drive, and even more unfortunately discovered that what she thought were copies of files on her computer were actually only shortcuts to the files on her now-missing flash drive. All her files were gone.
We are going to organize our discussion in three parts: First, we want to convince you of the importance of making backups, essentially informational life insurance. Unlike life insurance, however, you have a pretty good chance of using your backups at some point over the next 10 years. Second, we are going to discuss locally based backups, and then lastly, we’ll cover cloud-based backups. This may seem like an incredibly dull topic to some, but we anticipate receiving emails of thanks over many years for the knowledge and actions that come out of today’s column.
Hard drive failure rates, derived from data published by companies that professionally manage large numbers of hard drives, is about 3%-5% in the first year. This remains at about 3% per year for the next 2-3 years, and then can go up to 10% or more per year as hard drives continue to age. That means that over a 4-year period, 15%-20% of hard drives are likely to fail.1,2 This fact underscores the importance of backing up your data, because there is a good chance that over time, loss of data will happen to you.
One strategy is to back up to an external drive. The drive can be either a flash drive if you have less than 128 GB to store, or a traditional external hard drive – a very affordable option for memory up to 4 TB (4,000 GB). There are many excellent external hard drives and flash drives from which to choose, but you also need to have backup software that will take the information from your personal computer and place it in an organized manner on your external drive. Many drives now come bundled with backup software. An example of such a drive is the Western Digital My Passport Elite. If the hard drive you have does not already have backup software, there are lots of good choices out there. Backup software solutions include Time Machine (built into all Mac Computers), and many software choices for PCs.3
While the speed of backup and recovery is fast – often just a few hours – there are two main issues that make external drives suboptimal as your main backup strategy. The first is that most people simply don’t remember to plug their external drive into their computer regularly; months and sometimes years can go by without backing up your files. The second issue, which is usually not considered, is that the hard drive usually sits on your desk next to your computer. Therefore, if there is a fire, a flood, an electrical surge, or even a simple spill on your desk, you may lose both your main files and your backup in one fell swoop. For this reason, if you choose to use an external drive as your backup method, you should back up to two different external drives and keep one drive in your office and one at home.
The best method of backup, and the one we recommend to everyone, eliminates the major disadvantages of local backups. This method is cloud-based backup. For cloud-based backup, you purchase a subscription with an annual fee, then you download software from the backup vendor to your computer. It usually takes about 15 minutes to set up the software by selecting the file folders that you would like to back up, then the software does the rest. The first backup can take a long time, typically a few days, as the speed of the backup is limited by the speed of your Internet connection. After that first time, though, backups don’t take long because they back up only the files that have changed since the previous backup.
The main advantages to cloud-based solutions is that once it has been set up, the software ensures that incremental backups occur automatically every time your computer is connected to the Internet. In addition, since the cloud backups are off-site, you are protected from an adverse occurrence taking out your backup drive and your computer when they are sitting next to each other on your desk. In addition, most cloud backup services also allow you to access your file from any computer or smartphone for access where and when you need the files.
So, let us end where we began, with lyrics from the music video, with which we agree, “Word of advice: Want a happy life … Back it up one more time.”
References
1. http://www.extremetech.com/computing/170748-how-long-do-hard-drives-actually-live-for
2. http://www.pcworld.com/article/131168/article.html
3. The Best Backup Software at http://www.pcmag.com/article2/0,2817,2278661,00.asp
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
As many young physicians might recognize, the title of today’s column is from a song by Prince Royce featuring Jennifer Lopez and Pitbull. This article, though, is about what we believe is likely an urgent matter for many of our readers – the issue of appropriately backing up information that resides on their personal computers. We were prompted to write about this after a colleague came to one of us in a panic after losing all of the information on her meticulously performed, but poorly conceived backup. For years she has been developing and storing her lectures on a flash drive, and every month she has been backing up her flash drive to her personal computer. She even set a reminder in her calendar to make sure that she perform those backups each and every month. Unfortunately, she lost her flash drive, and even more unfortunately discovered that what she thought were copies of files on her computer were actually only shortcuts to the files on her now-missing flash drive. All her files were gone.
We are going to organize our discussion in three parts: First, we want to convince you of the importance of making backups, essentially informational life insurance. Unlike life insurance, however, you have a pretty good chance of using your backups at some point over the next 10 years. Second, we are going to discuss locally based backups, and then lastly, we’ll cover cloud-based backups. This may seem like an incredibly dull topic to some, but we anticipate receiving emails of thanks over many years for the knowledge and actions that come out of today’s column.
Hard drive failure rates, derived from data published by companies that professionally manage large numbers of hard drives, is about 3%-5% in the first year. This remains at about 3% per year for the next 2-3 years, and then can go up to 10% or more per year as hard drives continue to age. That means that over a 4-year period, 15%-20% of hard drives are likely to fail.1,2 This fact underscores the importance of backing up your data, because there is a good chance that over time, loss of data will happen to you.
One strategy is to back up to an external drive. The drive can be either a flash drive if you have less than 128 GB to store, or a traditional external hard drive – a very affordable option for memory up to 4 TB (4,000 GB). There are many excellent external hard drives and flash drives from which to choose, but you also need to have backup software that will take the information from your personal computer and place it in an organized manner on your external drive. Many drives now come bundled with backup software. An example of such a drive is the Western Digital My Passport Elite. If the hard drive you have does not already have backup software, there are lots of good choices out there. Backup software solutions include Time Machine (built into all Mac Computers), and many software choices for PCs.3
While the speed of backup and recovery is fast – often just a few hours – there are two main issues that make external drives suboptimal as your main backup strategy. The first is that most people simply don’t remember to plug their external drive into their computer regularly; months and sometimes years can go by without backing up your files. The second issue, which is usually not considered, is that the hard drive usually sits on your desk next to your computer. Therefore, if there is a fire, a flood, an electrical surge, or even a simple spill on your desk, you may lose both your main files and your backup in one fell swoop. For this reason, if you choose to use an external drive as your backup method, you should back up to two different external drives and keep one drive in your office and one at home.
The best method of backup, and the one we recommend to everyone, eliminates the major disadvantages of local backups. This method is cloud-based backup. For cloud-based backup, you purchase a subscription with an annual fee, then you download software from the backup vendor to your computer. It usually takes about 15 minutes to set up the software by selecting the file folders that you would like to back up, then the software does the rest. The first backup can take a long time, typically a few days, as the speed of the backup is limited by the speed of your Internet connection. After that first time, though, backups don’t take long because they back up only the files that have changed since the previous backup.
The main advantages to cloud-based solutions is that once it has been set up, the software ensures that incremental backups occur automatically every time your computer is connected to the Internet. In addition, since the cloud backups are off-site, you are protected from an adverse occurrence taking out your backup drive and your computer when they are sitting next to each other on your desk. In addition, most cloud backup services also allow you to access your file from any computer or smartphone for access where and when you need the files.
So, let us end where we began, with lyrics from the music video, with which we agree, “Word of advice: Want a happy life … Back it up one more time.”
References
1. http://www.extremetech.com/computing/170748-how-long-do-hard-drives-actually-live-for
2. http://www.pcworld.com/article/131168/article.html
3. The Best Backup Software at http://www.pcmag.com/article2/0,2817,2278661,00.asp
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.

Clinical Guidelines: USPSTF guidelines for treatment of tobacco dependence (2015)
Tobacco use is the leading cause of preventable early death in the United States as well as a major risk factor for cardiovascular disease, many cancers, COPD, and type 2 diabetes. Approximately 18% of the U.S. population currently smokes, leading to 480,000 premature deaths each year, accounting for almost one in five deaths. The U.S. Preventive Services Task Force (USPSTF) 2015 guidelines update the 2009 guidelines and include recent data on the use of behavioral interventions, tobacco cessation pharmacotherapies, and electronic nicotine delivery systems (ENDS) in pregnant and nonpregnant adults.
Behavioral interventions
Minimal and intensive behavioral interventions (BI) have both been found to increase tobacco abstinence rates, and there is a dose-response relationship between the intensity of BI and tobacco abstinence rates. The types of counseling studied included in-person, group, and telephone sessions primarily provided by physicians, advanced practice professionals, nurses, cessation counselors, or social workers. Even brief (less than 20 minutes in one visit) physician advice interventions help improve cessation rates, while longer physician interventions are more effective, with a dose-response relationship between the intensity and frequency of counseling and cessation rates. If possible, several sessions should be provided. Cessation training can be done effectively by physicians, nurses, psychologists, social workers, and counselors. There is high degree of certainty that the net benefit of behavioral interventions in the treatment of tobacco dependence is substantial.

FDA-approved pharmacotherapies
The only pharmacotherapies currently approved for use in the treatment of tobacco dependence in nonpregnant adults are nicotine replacement therapies (NRT: transdermal patches, gum, lozenges, nasal spray, or inhalers), bupropion SR, and varenicline. The efficacy of pharmacotherapy is substantial. For NRT, cessation rates are 10% in control groups vs. 17% in NRT groups. For bupropion SR,cessation rates are 11% in the control groups and 19% among those using bupropion SR. For varenicline, it is 12% in control groups and 28% in the varenicline groups. The use of multiple types of nicotine replacement therapy is more effective than use of a single type (cessation rates 21% vs. 16%, respectively). Some studies suggest that the combination of NRT and bupropion SR is similar in efficacy to NRT alone but superior to bupropion SR alone. In total, the USPSTF concluded with a high degree of certainty that the net benefit of pharmacotherapy in the treatment of tobacco dependence is substantial.
Side effects of NRT include an increased risk for minor cardiovascular adverse events (tachycardia), but no significant increase in major cardiovascular adverse events or mortality. Findings from studies of bupropion SR use showed mixed evidence for cardiovascular adverse events, with some trials finding a decreased risk for cardiovascular adverse events and others showing increased risk for such events (with borderline clinical significance). Despite the presence of a black-box warning about serious neuropsychiatric events in users of bupropion SR, the task force’s review found no significant increase in serious psychiatric events. Varenicline data suggested no significant increase in cardiovascular adverse events (minor or major). The data about serious neuropsychiatric events in patients using varenicline were insufficient to draw conclusions, though evidence suggested this may be an issue.
Combination of behavioral and pharmacotherapies
There is convincing evidence that combination therapy with BI and FDA-approved pharmacotherapies is superior to either intervention alone. Studies have compared nicotine replacement therapy alone to BI plus NRT with abstinence rates of 18% and 21%. The Task Force concluded (with a high degree of certainty) that the net benefit of providing combined interventions for smoking cessation is substantial.
Pregnant women
The task force found insufficient evidence to support the use of pharmacotherapy in pregnancy. There were few data available regarding the benefits or harms (maternal or fetal) of the use of these therapies in pregnancy.
Electronic nicotine delivery systems
There is insufficient evidence to support the use of electronic nicotine delivery symptoms (ENDS, so-called “e-cigarettes”) in the treatment of tobacco dependence. There have been only two randomized controlled trials (RCTs) of these devices that were rated as “fair quality.” One of these studies suggested an increased risk for serious adverse events with ENDS compared to nicotine patch, but no increase in total adverse events. No data were available surrounding the potentially harmful ingredients in ENDS. As for efficacy, of the two RCTs reviewed, one showed higher abstinence rates at 12 months while the larger study found no significant difference in abstinence rates at 6 months.
Bottom line
The 2015 recommendations are:
1. Ask all adults (pregnant and nonpregnant) about tobacco use.
2. Advise all smokers to cease tobacco use.
3. Offer behavioral interventions and FDA-approved pharmacotherapies to all nonpregnant adults.
4. Offer behavioral interventions alone to pregnant women.
5. There is insufficient evidence currently to support the use of tobacco cessation pharmacotherapy in pregnancy.
6. There is insufficient evidence currently to support the use of electronic nicotine delivery systems in adults.
Reference
Siu AL. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163[8]:622-34.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Lent is a second-year resident in the program.
Tobacco use is the leading cause of preventable early death in the United States as well as a major risk factor for cardiovascular disease, many cancers, COPD, and type 2 diabetes. Approximately 18% of the U.S. population currently smokes, leading to 480,000 premature deaths each year, accounting for almost one in five deaths. The U.S. Preventive Services Task Force (USPSTF) 2015 guidelines update the 2009 guidelines and include recent data on the use of behavioral interventions, tobacco cessation pharmacotherapies, and electronic nicotine delivery systems (ENDS) in pregnant and nonpregnant adults.
Behavioral interventions
Minimal and intensive behavioral interventions (BI) have both been found to increase tobacco abstinence rates, and there is a dose-response relationship between the intensity of BI and tobacco abstinence rates. The types of counseling studied included in-person, group, and telephone sessions primarily provided by physicians, advanced practice professionals, nurses, cessation counselors, or social workers. Even brief (less than 20 minutes in one visit) physician advice interventions help improve cessation rates, while longer physician interventions are more effective, with a dose-response relationship between the intensity and frequency of counseling and cessation rates. If possible, several sessions should be provided. Cessation training can be done effectively by physicians, nurses, psychologists, social workers, and counselors. There is high degree of certainty that the net benefit of behavioral interventions in the treatment of tobacco dependence is substantial.
FDA-approved pharmacotherapies
The only pharmacotherapies currently approved for use in the treatment of tobacco dependence in nonpregnant adults are nicotine replacement therapies (NRT: transdermal patches, gum, lozenges, nasal spray, or inhalers), bupropion SR, and varenicline. The efficacy of pharmacotherapy is substantial. For NRT, cessation rates are 10% in control groups vs. 17% in NRT groups. For bupropion SR,cessation rates are 11% in the control groups and 19% among those using bupropion SR. For varenicline, it is 12% in control groups and 28% in the varenicline groups. The use of multiple types of nicotine replacement therapy is more effective than use of a single type (cessation rates 21% vs. 16%, respectively). Some studies suggest that the combination of NRT and bupropion SR is similar in efficacy to NRT alone but superior to bupropion SR alone. In total, the USPSTF concluded with a high degree of certainty that the net benefit of pharmacotherapy in the treatment of tobacco dependence is substantial.
Side effects of NRT include an increased risk for minor cardiovascular adverse events (tachycardia), but no significant increase in major cardiovascular adverse events or mortality. Findings from studies of bupropion SR use showed mixed evidence for cardiovascular adverse events, with some trials finding a decreased risk for cardiovascular adverse events and others showing increased risk for such events (with borderline clinical significance). Despite the presence of a black-box warning about serious neuropsychiatric events in users of bupropion SR, the task force’s review found no significant increase in serious psychiatric events. Varenicline data suggested no significant increase in cardiovascular adverse events (minor or major). The data about serious neuropsychiatric events in patients using varenicline were insufficient to draw conclusions, though evidence suggested this may be an issue.
Combination of behavioral and pharmacotherapies
There is convincing evidence that combination therapy with BI and FDA-approved pharmacotherapies is superior to either intervention alone. Studies have compared nicotine replacement therapy alone to BI plus NRT with abstinence rates of 18% and 21%. The Task Force concluded (with a high degree of certainty) that the net benefit of providing combined interventions for smoking cessation is substantial.
Pregnant women
The task force found insufficient evidence to support the use of pharmacotherapy in pregnancy. There were few data available regarding the benefits or harms (maternal or fetal) of the use of these therapies in pregnancy.
Electronic nicotine delivery systems
There is insufficient evidence to support the use of electronic nicotine delivery symptoms (ENDS, so-called “e-cigarettes”) in the treatment of tobacco dependence. There have been only two randomized controlled trials (RCTs) of these devices that were rated as “fair quality.” One of these studies suggested an increased risk for serious adverse events with ENDS compared to nicotine patch, but no increase in total adverse events. No data were available surrounding the potentially harmful ingredients in ENDS. As for efficacy, of the two RCTs reviewed, one showed higher abstinence rates at 12 months while the larger study found no significant difference in abstinence rates at 6 months.
Bottom line
The 2015 recommendations are:
1. Ask all adults (pregnant and nonpregnant) about tobacco use.
2. Advise all smokers to cease tobacco use.
3. Offer behavioral interventions and FDA-approved pharmacotherapies to all nonpregnant adults.
4. Offer behavioral interventions alone to pregnant women.
5. There is insufficient evidence currently to support the use of tobacco cessation pharmacotherapy in pregnancy.
6. There is insufficient evidence currently to support the use of electronic nicotine delivery systems in adults.
Reference
Siu AL. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163[8]:622-34.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Lent is a second-year resident in the program.
Tobacco use is the leading cause of preventable early death in the United States as well as a major risk factor for cardiovascular disease, many cancers, COPD, and type 2 diabetes. Approximately 18% of the U.S. population currently smokes, leading to 480,000 premature deaths each year, accounting for almost one in five deaths. The U.S. Preventive Services Task Force (USPSTF) 2015 guidelines update the 2009 guidelines and include recent data on the use of behavioral interventions, tobacco cessation pharmacotherapies, and electronic nicotine delivery systems (ENDS) in pregnant and nonpregnant adults.
Behavioral interventions
Minimal and intensive behavioral interventions (BI) have both been found to increase tobacco abstinence rates, and there is a dose-response relationship between the intensity of BI and tobacco abstinence rates. The types of counseling studied included in-person, group, and telephone sessions primarily provided by physicians, advanced practice professionals, nurses, cessation counselors, or social workers. Even brief (less than 20 minutes in one visit) physician advice interventions help improve cessation rates, while longer physician interventions are more effective, with a dose-response relationship between the intensity and frequency of counseling and cessation rates. If possible, several sessions should be provided. Cessation training can be done effectively by physicians, nurses, psychologists, social workers, and counselors. There is high degree of certainty that the net benefit of behavioral interventions in the treatment of tobacco dependence is substantial.
FDA-approved pharmacotherapies
The only pharmacotherapies currently approved for use in the treatment of tobacco dependence in nonpregnant adults are nicotine replacement therapies (NRT: transdermal patches, gum, lozenges, nasal spray, or inhalers), bupropion SR, and varenicline. The efficacy of pharmacotherapy is substantial. For NRT, cessation rates are 10% in control groups vs. 17% in NRT groups. For bupropion SR,cessation rates are 11% in the control groups and 19% among those using bupropion SR. For varenicline, it is 12% in control groups and 28% in the varenicline groups. The use of multiple types of nicotine replacement therapy is more effective than use of a single type (cessation rates 21% vs. 16%, respectively). Some studies suggest that the combination of NRT and bupropion SR is similar in efficacy to NRT alone but superior to bupropion SR alone. In total, the USPSTF concluded with a high degree of certainty that the net benefit of pharmacotherapy in the treatment of tobacco dependence is substantial.
Side effects of NRT include an increased risk for minor cardiovascular adverse events (tachycardia), but no significant increase in major cardiovascular adverse events or mortality. Findings from studies of bupropion SR use showed mixed evidence for cardiovascular adverse events, with some trials finding a decreased risk for cardiovascular adverse events and others showing increased risk for such events (with borderline clinical significance). Despite the presence of a black-box warning about serious neuropsychiatric events in users of bupropion SR, the task force’s review found no significant increase in serious psychiatric events. Varenicline data suggested no significant increase in cardiovascular adverse events (minor or major). The data about serious neuropsychiatric events in patients using varenicline were insufficient to draw conclusions, though evidence suggested this may be an issue.
Combination of behavioral and pharmacotherapies
There is convincing evidence that combination therapy with BI and FDA-approved pharmacotherapies is superior to either intervention alone. Studies have compared nicotine replacement therapy alone to BI plus NRT with abstinence rates of 18% and 21%. The Task Force concluded (with a high degree of certainty) that the net benefit of providing combined interventions for smoking cessation is substantial.
Pregnant women
The task force found insufficient evidence to support the use of pharmacotherapy in pregnancy. There were few data available regarding the benefits or harms (maternal or fetal) of the use of these therapies in pregnancy.
Electronic nicotine delivery systems
There is insufficient evidence to support the use of electronic nicotine delivery symptoms (ENDS, so-called “e-cigarettes”) in the treatment of tobacco dependence. There have been only two randomized controlled trials (RCTs) of these devices that were rated as “fair quality.” One of these studies suggested an increased risk for serious adverse events with ENDS compared to nicotine patch, but no increase in total adverse events. No data were available surrounding the potentially harmful ingredients in ENDS. As for efficacy, of the two RCTs reviewed, one showed higher abstinence rates at 12 months while the larger study found no significant difference in abstinence rates at 6 months.
Bottom line
The 2015 recommendations are:
1. Ask all adults (pregnant and nonpregnant) about tobacco use.
2. Advise all smokers to cease tobacco use.
3. Offer behavioral interventions and FDA-approved pharmacotherapies to all nonpregnant adults.
4. Offer behavioral interventions alone to pregnant women.
5. There is insufficient evidence currently to support the use of tobacco cessation pharmacotherapy in pregnancy.
6. There is insufficient evidence currently to support the use of electronic nicotine delivery systems in adults.
Reference
Siu AL. Behavioral and Pharmacotherapy Interventions for Tobacco Smoking Cessation in Adults, Including Pregnant Women: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015;163[8]:622-34.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Lent is a second-year resident in the program.

The scribe in the room and the scribe in the sky
A core feature of all electronic health records is the necessity of data input into discrete fields in the chart. This is most frequently accomplished by a combination of typing the information that is needed and selecting, by clicking, the discrete information that is required, such as specific diagnoses and lab and radiology studies. The need to efficiently and effectively input a large amount of information has presented perhaps the greatest challenge of going digital for many physicians, particularly those over 40 years of age who do not type very well.
A number of innovative solutions are now available to address this issue, none perfect, and all offering alternatives to traditional means of documentation. We will briefly review three of these alternative methods, along with some thoughts about the advantages and disadvantages of each method. Let us also say that a challenge for all the methods we will discuss is the cost of the methods, and an advantage that all these assistive technologies offer is the ability for physicians to save time and lessen aggravation. Proponents of all strategies that charge money to save physicians time state that the time saved is equal to revenue earned seeing more patients, which in turn more than pays for the cost of the solution.
Transcription software, the most popular of which is Dragon, has been available for quite some time. This software can accurately transcribe the physician’s dictated notes into the appropriate section of the EHR. Many of the most popular EHRs now have the ability to have speech recognition fully integrated into the workflow of documentation of the EHR. The benefit of transcription software is that the physician directly determines what is going to be documented in the chart and retains complete control of the note. The disadvantage is that the physician still takes time organizing the note and inputting data.
To address the issue of the physician’s needing to take time to input information into the EHR, some practices have begun to use medical “scribes” in the form of a person who is in the room during the visit and is trained to write a note as the doctor sees the patient. The scribe will also order labs and x-rays as requested by the physician. An advantage of the scribe is that the physician can focus on the patient and does not need to navigate the EHR or worry about inputting data at all. In addition, feedback is usually given to the scribe on an ongoing basis so the scribe learns the preferences of the physician. The disadvantage is that the scribe is in the room during the visit, which can be awkward for patients, particularly if sensitive information is being shared about psychological problems, family planning, STDs, or any of many other issues that are routinely discussed at primary care office visits.
Finally, a California company, Augmedix, is trying to blend a 20th-century concept with 21st-century technology, seeing and paying attention to patients while doing electronic documentation. We want to disclose that we have no personal or financial interests in the company. Augmedix is essentially a scribe service with a modern twist. The physician wears a small head-mounted computer that includes a microphone, camera, and transparent display. This allows visual and auditory data from the patient visit to be transmitted to a scribe (a real, live human) located remotely in one of Augmedix’s data centers. The scribe is “logged in” to a copy of the physician’s electronic record and documents the visit in the appropriate place in the chart. This occurs in real time, so when the physician is finished seeing the patient, the note is complete and ready to be signed off. The benefit here is that there is no additional person in the room during the visit, yet just as when a scribe is in the room, the physician does not have to deal with negotiating the complexities of input into the EHR. In addition, through a feature the company calls “concierge service,” Augmedix scribes have the ability to display data to the physician upon request. For example, if the provider says “show me the blood pressure from our last visit” or “bring up Mrs. Smith’s x-ray results,” the scribe can send the requested information right to the tiny display on the headset. This allows the clinician to be “untethered” from the computer.
The concept raises a number of technical and philosophical questions. Foremost among these questions is that of privacy. Pelu Tran, president, CCO, and cofounder, explained that the technology is completely secure and compliant with all privacy laws. The data feeds transmitted through the headset are encrypted and are not permanently stored on any of Augmedix’s servers. Once the documentation is complete, the information is destroyed. HIPAA laws allow for this arrangement in the same way other transcription services are allowed. One disadvantage is likely to be cost, but Mr. Tran states that internal data show that a typical primary care physician can have about one to three additional patient visits per day using this tool and that the added revenue from seeing more patients should cover the cost of the service. Another potential disadvantage is a question of whether the note will reflect the ideas of the physician versus becoming a transcript of the visit, including the important as well as extraneous information that might be difficult to wade through when looking back at a note.
As for us, we are still typing our notes into the EHR, for now. We remain intrigued by the range of approaches that are beginning to appear, offering options for solutions that improve the quality of physicians’ lives with attention to maintaining and improving the physician-patient relationship.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
A core feature of all electronic health records is the necessity of data input into discrete fields in the chart. This is most frequently accomplished by a combination of typing the information that is needed and selecting, by clicking, the discrete information that is required, such as specific diagnoses and lab and radiology studies. The need to efficiently and effectively input a large amount of information has presented perhaps the greatest challenge of going digital for many physicians, particularly those over 40 years of age who do not type very well.
A number of innovative solutions are now available to address this issue, none perfect, and all offering alternatives to traditional means of documentation. We will briefly review three of these alternative methods, along with some thoughts about the advantages and disadvantages of each method. Let us also say that a challenge for all the methods we will discuss is the cost of the methods, and an advantage that all these assistive technologies offer is the ability for physicians to save time and lessen aggravation. Proponents of all strategies that charge money to save physicians time state that the time saved is equal to revenue earned seeing more patients, which in turn more than pays for the cost of the solution.
Transcription software, the most popular of which is Dragon, has been available for quite some time. This software can accurately transcribe the physician’s dictated notes into the appropriate section of the EHR. Many of the most popular EHRs now have the ability to have speech recognition fully integrated into the workflow of documentation of the EHR. The benefit of transcription software is that the physician directly determines what is going to be documented in the chart and retains complete control of the note. The disadvantage is that the physician still takes time organizing the note and inputting data.
To address the issue of the physician’s needing to take time to input information into the EHR, some practices have begun to use medical “scribes” in the form of a person who is in the room during the visit and is trained to write a note as the doctor sees the patient. The scribe will also order labs and x-rays as requested by the physician. An advantage of the scribe is that the physician can focus on the patient and does not need to navigate the EHR or worry about inputting data at all. In addition, feedback is usually given to the scribe on an ongoing basis so the scribe learns the preferences of the physician. The disadvantage is that the scribe is in the room during the visit, which can be awkward for patients, particularly if sensitive information is being shared about psychological problems, family planning, STDs, or any of many other issues that are routinely discussed at primary care office visits.
Finally, a California company, Augmedix, is trying to blend a 20th-century concept with 21st-century technology, seeing and paying attention to patients while doing electronic documentation. We want to disclose that we have no personal or financial interests in the company. Augmedix is essentially a scribe service with a modern twist. The physician wears a small head-mounted computer that includes a microphone, camera, and transparent display. This allows visual and auditory data from the patient visit to be transmitted to a scribe (a real, live human) located remotely in one of Augmedix’s data centers. The scribe is “logged in” to a copy of the physician’s electronic record and documents the visit in the appropriate place in the chart. This occurs in real time, so when the physician is finished seeing the patient, the note is complete and ready to be signed off. The benefit here is that there is no additional person in the room during the visit, yet just as when a scribe is in the room, the physician does not have to deal with negotiating the complexities of input into the EHR. In addition, through a feature the company calls “concierge service,” Augmedix scribes have the ability to display data to the physician upon request. For example, if the provider says “show me the blood pressure from our last visit” or “bring up Mrs. Smith’s x-ray results,” the scribe can send the requested information right to the tiny display on the headset. This allows the clinician to be “untethered” from the computer.
The concept raises a number of technical and philosophical questions. Foremost among these questions is that of privacy. Pelu Tran, president, CCO, and cofounder, explained that the technology is completely secure and compliant with all privacy laws. The data feeds transmitted through the headset are encrypted and are not permanently stored on any of Augmedix’s servers. Once the documentation is complete, the information is destroyed. HIPAA laws allow for this arrangement in the same way other transcription services are allowed. One disadvantage is likely to be cost, but Mr. Tran states that internal data show that a typical primary care physician can have about one to three additional patient visits per day using this tool and that the added revenue from seeing more patients should cover the cost of the service. Another potential disadvantage is a question of whether the note will reflect the ideas of the physician versus becoming a transcript of the visit, including the important as well as extraneous information that might be difficult to wade through when looking back at a note.
As for us, we are still typing our notes into the EHR, for now. We remain intrigued by the range of approaches that are beginning to appear, offering options for solutions that improve the quality of physicians’ lives with attention to maintaining and improving the physician-patient relationship.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
A core feature of all electronic health records is the necessity of data input into discrete fields in the chart. This is most frequently accomplished by a combination of typing the information that is needed and selecting, by clicking, the discrete information that is required, such as specific diagnoses and lab and radiology studies. The need to efficiently and effectively input a large amount of information has presented perhaps the greatest challenge of going digital for many physicians, particularly those over 40 years of age who do not type very well.
A number of innovative solutions are now available to address this issue, none perfect, and all offering alternatives to traditional means of documentation. We will briefly review three of these alternative methods, along with some thoughts about the advantages and disadvantages of each method. Let us also say that a challenge for all the methods we will discuss is the cost of the methods, and an advantage that all these assistive technologies offer is the ability for physicians to save time and lessen aggravation. Proponents of all strategies that charge money to save physicians time state that the time saved is equal to revenue earned seeing more patients, which in turn more than pays for the cost of the solution.
Transcription software, the most popular of which is Dragon, has been available for quite some time. This software can accurately transcribe the physician’s dictated notes into the appropriate section of the EHR. Many of the most popular EHRs now have the ability to have speech recognition fully integrated into the workflow of documentation of the EHR. The benefit of transcription software is that the physician directly determines what is going to be documented in the chart and retains complete control of the note. The disadvantage is that the physician still takes time organizing the note and inputting data.
To address the issue of the physician’s needing to take time to input information into the EHR, some practices have begun to use medical “scribes” in the form of a person who is in the room during the visit and is trained to write a note as the doctor sees the patient. The scribe will also order labs and x-rays as requested by the physician. An advantage of the scribe is that the physician can focus on the patient and does not need to navigate the EHR or worry about inputting data at all. In addition, feedback is usually given to the scribe on an ongoing basis so the scribe learns the preferences of the physician. The disadvantage is that the scribe is in the room during the visit, which can be awkward for patients, particularly if sensitive information is being shared about psychological problems, family planning, STDs, or any of many other issues that are routinely discussed at primary care office visits.
Finally, a California company, Augmedix, is trying to blend a 20th-century concept with 21st-century technology, seeing and paying attention to patients while doing electronic documentation. We want to disclose that we have no personal or financial interests in the company. Augmedix is essentially a scribe service with a modern twist. The physician wears a small head-mounted computer that includes a microphone, camera, and transparent display. This allows visual and auditory data from the patient visit to be transmitted to a scribe (a real, live human) located remotely in one of Augmedix’s data centers. The scribe is “logged in” to a copy of the physician’s electronic record and documents the visit in the appropriate place in the chart. This occurs in real time, so when the physician is finished seeing the patient, the note is complete and ready to be signed off. The benefit here is that there is no additional person in the room during the visit, yet just as when a scribe is in the room, the physician does not have to deal with negotiating the complexities of input into the EHR. In addition, through a feature the company calls “concierge service,” Augmedix scribes have the ability to display data to the physician upon request. For example, if the provider says “show me the blood pressure from our last visit” or “bring up Mrs. Smith’s x-ray results,” the scribe can send the requested information right to the tiny display on the headset. This allows the clinician to be “untethered” from the computer.
The concept raises a number of technical and philosophical questions. Foremost among these questions is that of privacy. Pelu Tran, president, CCO, and cofounder, explained that the technology is completely secure and compliant with all privacy laws. The data feeds transmitted through the headset are encrypted and are not permanently stored on any of Augmedix’s servers. Once the documentation is complete, the information is destroyed. HIPAA laws allow for this arrangement in the same way other transcription services are allowed. One disadvantage is likely to be cost, but Mr. Tran states that internal data show that a typical primary care physician can have about one to three additional patient visits per day using this tool and that the added revenue from seeing more patients should cover the cost of the service. Another potential disadvantage is a question of whether the note will reflect the ideas of the physician versus becoming a transcript of the visit, including the important as well as extraneous information that might be difficult to wade through when looking back at a note.
As for us, we are still typing our notes into the EHR, for now. We remain intrigued by the range of approaches that are beginning to appear, offering options for solutions that improve the quality of physicians’ lives with attention to maintaining and improving the physician-patient relationship.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.

Updates in Pediatrics
TALKING OUT CHILDHOOD OBESITY
Resnicow K, McMaster F, Bocian A, et al. Motivational interviewing and dietary counseling for obesity in primary care: an RCT. Pediatrics. 2015;135(4):649-657.
Counseling parents of overweight children using motivational interviewing from both health care providers and registered dietitians can significantly improve BMI, according to a study of 42 practices in the Pediatric Research in Office Settings Network of the American Academy of Pediatrics.
Researchers randomly assigned parents of overweight children, ages 2 through 8, to one of three groups: (1) usual care, (2) four provider-delivered motivational interviewing sessions over two years, or (3) four provider-delivered motivational interviewing sessions plus six sessions with a registered dietitian over two years. At study end, BMI percentile and change in BMI for the different groups were as follows:
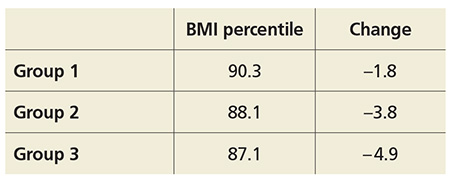
COMMENTARY
The results of this study are exciting. Motivational interviewing is a technique in which the practitioner asks questions of a patient and allows the patient to discover his/her own conclusions about the topic. By so doing, the patient is more engaged in the discussion and is less resistant to input. This technique, with excellent evidence of effectiveness in the area of drug and alcohol abuse, has been shown to facilitate effective behavioral change in many areas and is recommended by the American Heart Association for behavioral change in adults.1,2 This is an exciting paper demonstrating evidence-based efficacy in addressing childhood obesity—a critical health issue—and is worth trying in the office.
1. Rubak S, Sandbaek A, Lauritzen T, Christensen B. Motivational interviewing: a systematic review and meta-analysis. Br J Gen Pract. 2005;55(513):305-312.
2. Spring B, Ockene JK, Gidding SS, et al; American Heart Association Behavior Change Committee of the Council on Epidemiology and Prevention, Council on Lifestyle and Cardiometabolic Health, Council for High Blood Pressure Research, and Council on Cardiovascular and Stroke Nursing. Better population health through behavior change in adults: a call to action. Circulation. 2013;128(19):2169-2176. doi: 10.1161/01.cir.0000435173.25936.e1.
Continue for long-acting reversible contraception among teens >>
LONG-ACTING REVERSIBLE CONTRACEPTION AMONG TEENS
Romero L, Pazol K, Warner L, et al. Vital signs: trends in use of long-acting reversible contraception among teens aged 15-19 years seeking contraceptive services – United States, 2005-2013. MMWR Morb Mortal Wkly Rep. 2015;64(13):363-369.
Efforts to improve teen access to long-acting reversible contraception (LARC) have increased use of these methods, according to a CDC review of services provided at Title X National Family Planning Program centers. The report found
• LARC rates among teen patients increased from 0.4% in 2005 to 7.2% in 2013.
• In 2013, 2.8% of those seeking contraception used IUDs and 4.3% used implants.
• Among Title X patients, 7.6% of 18- and 19-year-olds used LARC, compared with 6.5% of 15- to 17-year-olds.
• Rates of LARC were lowest in Mississippi (0.7%) and highest in Colorado (25.8%).
COMMENTARY
LARCs, which include IUD and implantable hormonal contraceptive devices, require no effort for adherence on the part of the user; once in place, they are effective without further action. Current CDC guidelines on contraceptive use clearly recommend LARC for teenagers based on the efficacy and safety.1 LARCs are favored for teenagers because poor compliance has yielded suboptimal effectiveness of oral contraceptives and condoms in teenagers, who often forget to take their birth control pills or don’t use condoms when they should. Many clinicians have been slow to recommend LARCs in teenagers based on safety concerns related to adverse experience with IUDs 20 to 30 years ago. According to CDC guidelines, IUDs and implantable contraceptive devices now have robust safety data, and this article shows that they are being increasingly made available to teenagers who need them.
1. Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. US Selected Practice Recommendations for Contraceptive Use, 2013: adapted from the World Health Organization selected practice recommendations for contraceptive use, 2nd edition. MMWR Recomm Rep. 2013;62(RR-05):1-60.
Continue to testing for celiac in pediatric rheumatology patients >>
TESTING FOR CELIAC IN PEDIATRIC RHEUMATOLOGY PATIENTS
Sherman Y, Karanicolas R, DiMarco B, et al. Unrecognized celiac disease in children presenting for rheumatology evaluation. Pediatrics. 2015; [Epub ahead of print].
Children presenting for rheumatology evaluation should be screened for celiac disease, according to a review of 2,125 pediatric patients who were screened for celiac as part of the standard initial serologic evaluation.
Researchers identified 36 new cases of celiac disease (2.0% prevalence rate). The most common presenting complaints among these patients were myalgia, arthralgia, and rash. Less frequent complaints included gastrointestinal complaints of abdominal pain, nausea, and diarrhea.
After initiating a gluten-free diet, all of the patients with celiac disease reported improvement or complete resolution of musculoskeletal symptoms.
COMMENTARY
Celiac disease has a prevalence of 0.5% to 1% in the US and can present with a range of symptoms that include diarrhea, abdominal discomfort, and weight loss. In addition to these typical symptoms, celiac disease can cause a wide range of systemic symptoms, including osteopenia, abnormal liver function tests, anemia, neurologic symptoms, and general malaise and fatigue.1 This study suggests that celiac testing be considered in children presenting with rheumatologic symptoms, including myalgia, arthralgia, and rash.
1. Presutti RJ, Cangemi JR, Cassidy HD, et al. Celiac disease. Am Fam Physician. 2007;76(12):1795-1802, 1809-1810.
Continue for educating parents about antibiotic use >>
EDUCATING PARENTS ABOUT ANTIBIOTIC USE
Vaz LE, Kleinman KP, Lakoma MD, et al. Prevalence of parental misconceptions about antibiotic use. Pediatrics. 2015;136:221-231.
Misperceptions about antibiotic use persist and continue to be more prevalent among parents of Medicaid-insured children, according to a study of 1,500 Massachusetts parents.
Investigators examined antibiotic-related knowledge and attitudes among both Medicaid-insured and private-insured parents and found
• Fewer Medicaid parents answered questions correctly, except for one regarding bronchitis.
• Medicaid patients were more likely to request unnecessary antibiotics.
• More parents in 2013 understood that green nasal discharge did not require antibiotics than in 2000.
• Medicaid-insured parents were younger, less likely to be white, and had less education than those commercially insured.
COMMENTARY
Decreasing the unnecessary use of antibiotics for viral infections is an important component of decreasing the development of antibiotic-resistant organisms. An important driver of clinician use of antibiotics is patients’ expectations for antibiotics. This study shows that much work remains to be done in changing patient expectations, which is not surprising to any practicing clinician. This study also suggests that the expectation for antibiotics is greater among those individuals with Medicaid insurance, which suggests that an opportunity exists for Medicaid insurance plans to do targeted patient education on this issue—which should improve patient outcomes, decrease cost from use of unneeded antibiotics, and decrease the development of antibiotic-resistant organisms.
Continue for newborn pulmonary hypertension and maternal antidepressant use >>
NEWBORN PULMONARY HYPERTENSION AND MATERNAL ANTIDEPRESSANT USE
Huybrechts KF, Bateman BT, Palmsten K, et al. Antidepressant use late in pregnancy and risk of persistent pulmonary hypertension of the newborn. JAMA. 2015;313(21):2142-2151.
Taking antidepressants during late pregnancy may increase the risk for persistent pulmonary hypertension of the newborn (PPHN), according to a nested cohort study of more than 3.7 million pregnant women in the 2000-2010 Medicaid Analytic eXtract.
Investigators compared offspring of mothers who used selective serotonin reuptake inhibitors (SSRIs) or non-SSRI monotherapy in the last 90 days of pregnancy to those who did not and found 3.4% of women filled at least one prescription for antidepressants late in pregnancy, primarily SSRIs.
Rates and odds ratios (ORs) of PPHN stratified by use and type of antidepressant were as follows:
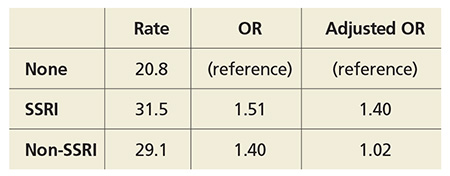
The study authors note the absolute risk is small, and the increased risk is more modest than previous studies found.
COMMENTARY
Depression affects more than 12% of pregnancies and has important consequences, including increased risk for suicide, preterm birth, poor fetal growth, and impaired fetal and infant development.1 PPHN is a serious condition that can require intubation and can be fatal in 10% to 20% of cases. This study adds to the conflicting data suggesting that SSRI use in pregnancy can lead to an increase in this rare condition. The decision to use an antidepressant during pregnancy is a difficult one, because depression has serious consequences but so, potentially, does treatment. The treatment of depression during pregnancy requires thoughtful, informed discussion between patient and provider.
1. Stewart DE. Clinical practice. Depression during pregnancy. N Engl J Med. 2011;365(17):1605-1611. doi:10.1056/NEJMcp1102730.
Continue for new infant vaccine treats 6 diseases >>
NEW INFANT VACCINE TREATS 6 DISEASES
Marshall GS, Adams GL, Leonardi ML, et al. Immunogenicity, safety, and tolerability of a hexavalent vaccine in infants. Pediatrics. 2015:136(2):323-332.
The safety and immunogenicity of DTaP5-IPV-Hib-HepB fully liquid investigational hexavalent vaccine are comparable with the analogous licensed component vaccines and provide a new combination vaccine option aligned with the recommended US infant immunization schedule, according to a phase III study of 1,465 participants. Overall, 981 healthy infants were vaccinated in group 1 with the hexavalent vaccine and 484 in group 2 with the analogous licensed component vaccines.
The study found
• Immune responses in group 1 to all antigens contained in the vaccine one month after dose 3 were essentially noninferior to those in group 2.
• Adverse event rates after any dose were similar in both groups.
COMMENTARY
Vaccine administration has led to many diseases, including Haemophilus influenzae type b, polio, and measles, becoming quite rare. As we have recently seen with the resurgence of measles, continued vigilance and high immunization rates are important in ensuring that these diseases remain rare. The development of a hexavalent vaccine is another step in making immunization easier for clinicians to administer and for patients to accept.
Continue for treating infants with bronchiolitis >>
TREATING INFANTS WITH BRONCHIOLITIS
Silver AH, Esteban-Cruciani N, Azzarone G, et al. 3% hypertonic saline versus normal saline in inpatient bronchiolitis: a randomized controlled trial. Pediatrics. 2015;136:1036-1043.
Infants hospitalized with bronchiolitis saw no difference in length of stay or seven-day readmission rates when treated with nebulized 3% hypertonic saline (HS) compared with nebulized normal saline (NS), according to a randomized, controlled study of 227 infants who were younger than 12 months when admitted. Patients received either 4 mL nebulized 3% HS (113 infants) or 4 mL 0.9% NS (114 infants) every four hours from enrollment until hospital discharge. Researchers found
• Median length of stay of HS and NS groups was 2.1 days vs 2.1 days, respectively.
• Seven-day readmission rates for HS and NS groups were 4.3% vs 3.1%, respectively.
• Clinical worsening events were similar between groups.
COMMENTARY
Bronchiolitis, the most common lower respiratory tract infection in infants, is usually due to a viral infection, most often respiratory syncytial virus, and can cause disease that ranges in severity from mild to life-threatening. Infants with bronchiolitis typically present with rhinitis, tachypnea, wheezing, and cough, and occasionally crackles and use of accessory muscles. While many medications are used, supportive care and monitoring are the mainstays of therapy. Maintaining pulse above 90% is important, using supplemental oxygen when needed to achieve this. Alpha-adrenergic and beta-adrenergic bronchodilators are often used; though the evidence suggests that they are not usually helpful, they can be tried and continued if they appear to help. Systemic steroids are often used, but they too lack evidence of efficacy.1 This study shows that hypertonic saline can now join the list of interventions used with evidence of a lack of efficacy.
1. Diagnosis and management of bronchiolitis. Subcommittee on diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774-1793. doi:10.1542/peds.2006-2223.
Continue for azithromycin and preschool children >>
AZITHROMYCIN AND PRESCHOOL CHILDREN: CAN ANTIBIOTICS LESSEN ONSET OF SEVERE LRTIs?
Bacharier LB, Guilbert TW, Mauger DT, et al. Early administration of azithromycin and prevention of severe lower respiratory tract illnesses in preschool children with a history of such illnesses: a randomized clinical trial. JAMA. 2015;314(19):2034-2044.
The use of azithromycin early during an apparent respiratory tract illness (RTI) reduced the likelihood of severe lower RTI (LRTI) among young children with a history of recurrent severe LRTI, compared with placebo, according to a study of 607 children ages 12 to 71 months. Participants were randomized in a 1:1 ratio to receive either azithromycin (12 mg/kg/d for 5 d) or matching placebo at the start of an RTI. Researchers found
• A total of 937 treated RTIs were experienced by 443 children, including 92 severe LRTIs (azithromycin group, 35; placebo group, 57).
• Azithromycin significantly reduced the risk for progression to severe LRTI relative to placebo (HR, 0.64).
• Induction of azithromycin-resistant organisms and adverse events were infrequent.
COMMENTARY
Recurrent episodes of severe wheezing with RTI are an important and common occurrence, affecting up to 15% to 20% of children prior to age 6.1 LRTI was defined in this study as RTI that required the use of additional rescue medication. The current approach to RTI is to try to minimize the use of antibiotics unless an infection is clearly bacterial in origin, and to treat severe LRTI when it occurs. The results of this trial suggest that in children at high risk for severe LRTI, identified by their episodes of recurrent wheezing, early treatment of RTI with azithromycin may decrease the development of severe LRTI by more than 35%—an important result. It is important to recognize that this study does not suggest treating all RTIs with antibiotics, but rather that the use of a macrolide antibiotic may be considered, perhaps, in the select group of children similar to those studied, with a history of recurrent wheezing with previous RTIs.
1. Ly NP, Gold DR, Weiss ST, Celedón JC. Recurrent wheeze in early childhood and asthma among children at risk for atopy. Pediatrics. 2006;117(6):e1132-e1138.
TALKING OUT CHILDHOOD OBESITY
Resnicow K, McMaster F, Bocian A, et al. Motivational interviewing and dietary counseling for obesity in primary care: an RCT. Pediatrics. 2015;135(4):649-657.
Counseling parents of overweight children using motivational interviewing from both health care providers and registered dietitians can significantly improve BMI, according to a study of 42 practices in the Pediatric Research in Office Settings Network of the American Academy of Pediatrics.
Researchers randomly assigned parents of overweight children, ages 2 through 8, to one of three groups: (1) usual care, (2) four provider-delivered motivational interviewing sessions over two years, or (3) four provider-delivered motivational interviewing sessions plus six sessions with a registered dietitian over two years. At study end, BMI percentile and change in BMI for the different groups were as follows:
COMMENTARY
The results of this study are exciting. Motivational interviewing is a technique in which the practitioner asks questions of a patient and allows the patient to discover his/her own conclusions about the topic. By so doing, the patient is more engaged in the discussion and is less resistant to input. This technique, with excellent evidence of effectiveness in the area of drug and alcohol abuse, has been shown to facilitate effective behavioral change in many areas and is recommended by the American Heart Association for behavioral change in adults.1,2 This is an exciting paper demonstrating evidence-based efficacy in addressing childhood obesity—a critical health issue—and is worth trying in the office.
1. Rubak S, Sandbaek A, Lauritzen T, Christensen B. Motivational interviewing: a systematic review and meta-analysis. Br J Gen Pract. 2005;55(513):305-312.
2. Spring B, Ockene JK, Gidding SS, et al; American Heart Association Behavior Change Committee of the Council on Epidemiology and Prevention, Council on Lifestyle and Cardiometabolic Health, Council for High Blood Pressure Research, and Council on Cardiovascular and Stroke Nursing. Better population health through behavior change in adults: a call to action. Circulation. 2013;128(19):2169-2176. doi: 10.1161/01.cir.0000435173.25936.e1.
Continue for long-acting reversible contraception among teens >>
LONG-ACTING REVERSIBLE CONTRACEPTION AMONG TEENS
Romero L, Pazol K, Warner L, et al. Vital signs: trends in use of long-acting reversible contraception among teens aged 15-19 years seeking contraceptive services – United States, 2005-2013. MMWR Morb Mortal Wkly Rep. 2015;64(13):363-369.
Efforts to improve teen access to long-acting reversible contraception (LARC) have increased use of these methods, according to a CDC review of services provided at Title X National Family Planning Program centers. The report found
• LARC rates among teen patients increased from 0.4% in 2005 to 7.2% in 2013.
• In 2013, 2.8% of those seeking contraception used IUDs and 4.3% used implants.
• Among Title X patients, 7.6% of 18- and 19-year-olds used LARC, compared with 6.5% of 15- to 17-year-olds.
• Rates of LARC were lowest in Mississippi (0.7%) and highest in Colorado (25.8%).
COMMENTARY
LARCs, which include IUD and implantable hormonal contraceptive devices, require no effort for adherence on the part of the user; once in place, they are effective without further action. Current CDC guidelines on contraceptive use clearly recommend LARC for teenagers based on the efficacy and safety.1 LARCs are favored for teenagers because poor compliance has yielded suboptimal effectiveness of oral contraceptives and condoms in teenagers, who often forget to take their birth control pills or don’t use condoms when they should. Many clinicians have been slow to recommend LARCs in teenagers based on safety concerns related to adverse experience with IUDs 20 to 30 years ago. According to CDC guidelines, IUDs and implantable contraceptive devices now have robust safety data, and this article shows that they are being increasingly made available to teenagers who need them.
1. Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. US Selected Practice Recommendations for Contraceptive Use, 2013: adapted from the World Health Organization selected practice recommendations for contraceptive use, 2nd edition. MMWR Recomm Rep. 2013;62(RR-05):1-60.
Continue to testing for celiac in pediatric rheumatology patients >>
TESTING FOR CELIAC IN PEDIATRIC RHEUMATOLOGY PATIENTS
Sherman Y, Karanicolas R, DiMarco B, et al. Unrecognized celiac disease in children presenting for rheumatology evaluation. Pediatrics. 2015; [Epub ahead of print].
Children presenting for rheumatology evaluation should be screened for celiac disease, according to a review of 2,125 pediatric patients who were screened for celiac as part of the standard initial serologic evaluation.
Researchers identified 36 new cases of celiac disease (2.0% prevalence rate). The most common presenting complaints among these patients were myalgia, arthralgia, and rash. Less frequent complaints included gastrointestinal complaints of abdominal pain, nausea, and diarrhea.
After initiating a gluten-free diet, all of the patients with celiac disease reported improvement or complete resolution of musculoskeletal symptoms.
COMMENTARY
Celiac disease has a prevalence of 0.5% to 1% in the US and can present with a range of symptoms that include diarrhea, abdominal discomfort, and weight loss. In addition to these typical symptoms, celiac disease can cause a wide range of systemic symptoms, including osteopenia, abnormal liver function tests, anemia, neurologic symptoms, and general malaise and fatigue.1 This study suggests that celiac testing be considered in children presenting with rheumatologic symptoms, including myalgia, arthralgia, and rash.
1. Presutti RJ, Cangemi JR, Cassidy HD, et al. Celiac disease. Am Fam Physician. 2007;76(12):1795-1802, 1809-1810.
Continue for educating parents about antibiotic use >>
EDUCATING PARENTS ABOUT ANTIBIOTIC USE
Vaz LE, Kleinman KP, Lakoma MD, et al. Prevalence of parental misconceptions about antibiotic use. Pediatrics. 2015;136:221-231.
Misperceptions about antibiotic use persist and continue to be more prevalent among parents of Medicaid-insured children, according to a study of 1,500 Massachusetts parents.
Investigators examined antibiotic-related knowledge and attitudes among both Medicaid-insured and private-insured parents and found
• Fewer Medicaid parents answered questions correctly, except for one regarding bronchitis.
• Medicaid patients were more likely to request unnecessary antibiotics.
• More parents in 2013 understood that green nasal discharge did not require antibiotics than in 2000.
• Medicaid-insured parents were younger, less likely to be white, and had less education than those commercially insured.
COMMENTARY
Decreasing the unnecessary use of antibiotics for viral infections is an important component of decreasing the development of antibiotic-resistant organisms. An important driver of clinician use of antibiotics is patients’ expectations for antibiotics. This study shows that much work remains to be done in changing patient expectations, which is not surprising to any practicing clinician. This study also suggests that the expectation for antibiotics is greater among those individuals with Medicaid insurance, which suggests that an opportunity exists for Medicaid insurance plans to do targeted patient education on this issue—which should improve patient outcomes, decrease cost from use of unneeded antibiotics, and decrease the development of antibiotic-resistant organisms.
Continue for newborn pulmonary hypertension and maternal antidepressant use >>
NEWBORN PULMONARY HYPERTENSION AND MATERNAL ANTIDEPRESSANT USE
Huybrechts KF, Bateman BT, Palmsten K, et al. Antidepressant use late in pregnancy and risk of persistent pulmonary hypertension of the newborn. JAMA. 2015;313(21):2142-2151.
Taking antidepressants during late pregnancy may increase the risk for persistent pulmonary hypertension of the newborn (PPHN), according to a nested cohort study of more than 3.7 million pregnant women in the 2000-2010 Medicaid Analytic eXtract.
Investigators compared offspring of mothers who used selective serotonin reuptake inhibitors (SSRIs) or non-SSRI monotherapy in the last 90 days of pregnancy to those who did not and found 3.4% of women filled at least one prescription for antidepressants late in pregnancy, primarily SSRIs.
Rates and odds ratios (ORs) of PPHN stratified by use and type of antidepressant were as follows:
The study authors note the absolute risk is small, and the increased risk is more modest than previous studies found.
COMMENTARY
Depression affects more than 12% of pregnancies and has important consequences, including increased risk for suicide, preterm birth, poor fetal growth, and impaired fetal and infant development.1 PPHN is a serious condition that can require intubation and can be fatal in 10% to 20% of cases. This study adds to the conflicting data suggesting that SSRI use in pregnancy can lead to an increase in this rare condition. The decision to use an antidepressant during pregnancy is a difficult one, because depression has serious consequences but so, potentially, does treatment. The treatment of depression during pregnancy requires thoughtful, informed discussion between patient and provider.
1. Stewart DE. Clinical practice. Depression during pregnancy. N Engl J Med. 2011;365(17):1605-1611. doi:10.1056/NEJMcp1102730.
Continue for new infant vaccine treats 6 diseases >>
NEW INFANT VACCINE TREATS 6 DISEASES
Marshall GS, Adams GL, Leonardi ML, et al. Immunogenicity, safety, and tolerability of a hexavalent vaccine in infants. Pediatrics. 2015:136(2):323-332.
The safety and immunogenicity of DTaP5-IPV-Hib-HepB fully liquid investigational hexavalent vaccine are comparable with the analogous licensed component vaccines and provide a new combination vaccine option aligned with the recommended US infant immunization schedule, according to a phase III study of 1,465 participants. Overall, 981 healthy infants were vaccinated in group 1 with the hexavalent vaccine and 484 in group 2 with the analogous licensed component vaccines.
The study found
• Immune responses in group 1 to all antigens contained in the vaccine one month after dose 3 were essentially noninferior to those in group 2.
• Adverse event rates after any dose were similar in both groups.
COMMENTARY
Vaccine administration has led to many diseases, including Haemophilus influenzae type b, polio, and measles, becoming quite rare. As we have recently seen with the resurgence of measles, continued vigilance and high immunization rates are important in ensuring that these diseases remain rare. The development of a hexavalent vaccine is another step in making immunization easier for clinicians to administer and for patients to accept.
Continue for treating infants with bronchiolitis >>
TREATING INFANTS WITH BRONCHIOLITIS
Silver AH, Esteban-Cruciani N, Azzarone G, et al. 3% hypertonic saline versus normal saline in inpatient bronchiolitis: a randomized controlled trial. Pediatrics. 2015;136:1036-1043.
Infants hospitalized with bronchiolitis saw no difference in length of stay or seven-day readmission rates when treated with nebulized 3% hypertonic saline (HS) compared with nebulized normal saline (NS), according to a randomized, controlled study of 227 infants who were younger than 12 months when admitted. Patients received either 4 mL nebulized 3% HS (113 infants) or 4 mL 0.9% NS (114 infants) every four hours from enrollment until hospital discharge. Researchers found
• Median length of stay of HS and NS groups was 2.1 days vs 2.1 days, respectively.
• Seven-day readmission rates for HS and NS groups were 4.3% vs 3.1%, respectively.
• Clinical worsening events were similar between groups.
COMMENTARY
Bronchiolitis, the most common lower respiratory tract infection in infants, is usually due to a viral infection, most often respiratory syncytial virus, and can cause disease that ranges in severity from mild to life-threatening. Infants with bronchiolitis typically present with rhinitis, tachypnea, wheezing, and cough, and occasionally crackles and use of accessory muscles. While many medications are used, supportive care and monitoring are the mainstays of therapy. Maintaining pulse above 90% is important, using supplemental oxygen when needed to achieve this. Alpha-adrenergic and beta-adrenergic bronchodilators are often used; though the evidence suggests that they are not usually helpful, they can be tried and continued if they appear to help. Systemic steroids are often used, but they too lack evidence of efficacy.1 This study shows that hypertonic saline can now join the list of interventions used with evidence of a lack of efficacy.
1. Diagnosis and management of bronchiolitis. Subcommittee on diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774-1793. doi:10.1542/peds.2006-2223.
Continue for azithromycin and preschool children >>
AZITHROMYCIN AND PRESCHOOL CHILDREN: CAN ANTIBIOTICS LESSEN ONSET OF SEVERE LRTIs?
Bacharier LB, Guilbert TW, Mauger DT, et al. Early administration of azithromycin and prevention of severe lower respiratory tract illnesses in preschool children with a history of such illnesses: a randomized clinical trial. JAMA. 2015;314(19):2034-2044.
The use of azithromycin early during an apparent respiratory tract illness (RTI) reduced the likelihood of severe lower RTI (LRTI) among young children with a history of recurrent severe LRTI, compared with placebo, according to a study of 607 children ages 12 to 71 months. Participants were randomized in a 1:1 ratio to receive either azithromycin (12 mg/kg/d for 5 d) or matching placebo at the start of an RTI. Researchers found
• A total of 937 treated RTIs were experienced by 443 children, including 92 severe LRTIs (azithromycin group, 35; placebo group, 57).
• Azithromycin significantly reduced the risk for progression to severe LRTI relative to placebo (HR, 0.64).
• Induction of azithromycin-resistant organisms and adverse events were infrequent.
COMMENTARY
Recurrent episodes of severe wheezing with RTI are an important and common occurrence, affecting up to 15% to 20% of children prior to age 6.1 LRTI was defined in this study as RTI that required the use of additional rescue medication. The current approach to RTI is to try to minimize the use of antibiotics unless an infection is clearly bacterial in origin, and to treat severe LRTI when it occurs. The results of this trial suggest that in children at high risk for severe LRTI, identified by their episodes of recurrent wheezing, early treatment of RTI with azithromycin may decrease the development of severe LRTI by more than 35%—an important result. It is important to recognize that this study does not suggest treating all RTIs with antibiotics, but rather that the use of a macrolide antibiotic may be considered, perhaps, in the select group of children similar to those studied, with a history of recurrent wheezing with previous RTIs.
1. Ly NP, Gold DR, Weiss ST, Celedón JC. Recurrent wheeze in early childhood and asthma among children at risk for atopy. Pediatrics. 2006;117(6):e1132-e1138.
TALKING OUT CHILDHOOD OBESITY
Resnicow K, McMaster F, Bocian A, et al. Motivational interviewing and dietary counseling for obesity in primary care: an RCT. Pediatrics. 2015;135(4):649-657.
Counseling parents of overweight children using motivational interviewing from both health care providers and registered dietitians can significantly improve BMI, according to a study of 42 practices in the Pediatric Research in Office Settings Network of the American Academy of Pediatrics.
Researchers randomly assigned parents of overweight children, ages 2 through 8, to one of three groups: (1) usual care, (2) four provider-delivered motivational interviewing sessions over two years, or (3) four provider-delivered motivational interviewing sessions plus six sessions with a registered dietitian over two years. At study end, BMI percentile and change in BMI for the different groups were as follows:
COMMENTARY
The results of this study are exciting. Motivational interviewing is a technique in which the practitioner asks questions of a patient and allows the patient to discover his/her own conclusions about the topic. By so doing, the patient is more engaged in the discussion and is less resistant to input. This technique, with excellent evidence of effectiveness in the area of drug and alcohol abuse, has been shown to facilitate effective behavioral change in many areas and is recommended by the American Heart Association for behavioral change in adults.1,2 This is an exciting paper demonstrating evidence-based efficacy in addressing childhood obesity—a critical health issue—and is worth trying in the office.
1. Rubak S, Sandbaek A, Lauritzen T, Christensen B. Motivational interviewing: a systematic review and meta-analysis. Br J Gen Pract. 2005;55(513):305-312.
2. Spring B, Ockene JK, Gidding SS, et al; American Heart Association Behavior Change Committee of the Council on Epidemiology and Prevention, Council on Lifestyle and Cardiometabolic Health, Council for High Blood Pressure Research, and Council on Cardiovascular and Stroke Nursing. Better population health through behavior change in adults: a call to action. Circulation. 2013;128(19):2169-2176. doi: 10.1161/01.cir.0000435173.25936.e1.
Continue for long-acting reversible contraception among teens >>
LONG-ACTING REVERSIBLE CONTRACEPTION AMONG TEENS
Romero L, Pazol K, Warner L, et al. Vital signs: trends in use of long-acting reversible contraception among teens aged 15-19 years seeking contraceptive services – United States, 2005-2013. MMWR Morb Mortal Wkly Rep. 2015;64(13):363-369.
Efforts to improve teen access to long-acting reversible contraception (LARC) have increased use of these methods, according to a CDC review of services provided at Title X National Family Planning Program centers. The report found
• LARC rates among teen patients increased from 0.4% in 2005 to 7.2% in 2013.
• In 2013, 2.8% of those seeking contraception used IUDs and 4.3% used implants.
• Among Title X patients, 7.6% of 18- and 19-year-olds used LARC, compared with 6.5% of 15- to 17-year-olds.
• Rates of LARC were lowest in Mississippi (0.7%) and highest in Colorado (25.8%).
COMMENTARY
LARCs, which include IUD and implantable hormonal contraceptive devices, require no effort for adherence on the part of the user; once in place, they are effective without further action. Current CDC guidelines on contraceptive use clearly recommend LARC for teenagers based on the efficacy and safety.1 LARCs are favored for teenagers because poor compliance has yielded suboptimal effectiveness of oral contraceptives and condoms in teenagers, who often forget to take their birth control pills or don’t use condoms when they should. Many clinicians have been slow to recommend LARCs in teenagers based on safety concerns related to adverse experience with IUDs 20 to 30 years ago. According to CDC guidelines, IUDs and implantable contraceptive devices now have robust safety data, and this article shows that they are being increasingly made available to teenagers who need them.
1. Division of Reproductive Health, National Center for Chronic Disease Prevention and Health Promotion, CDC. US Selected Practice Recommendations for Contraceptive Use, 2013: adapted from the World Health Organization selected practice recommendations for contraceptive use, 2nd edition. MMWR Recomm Rep. 2013;62(RR-05):1-60.
Continue to testing for celiac in pediatric rheumatology patients >>
TESTING FOR CELIAC IN PEDIATRIC RHEUMATOLOGY PATIENTS
Sherman Y, Karanicolas R, DiMarco B, et al. Unrecognized celiac disease in children presenting for rheumatology evaluation. Pediatrics. 2015; [Epub ahead of print].
Children presenting for rheumatology evaluation should be screened for celiac disease, according to a review of 2,125 pediatric patients who were screened for celiac as part of the standard initial serologic evaluation.
Researchers identified 36 new cases of celiac disease (2.0% prevalence rate). The most common presenting complaints among these patients were myalgia, arthralgia, and rash. Less frequent complaints included gastrointestinal complaints of abdominal pain, nausea, and diarrhea.
After initiating a gluten-free diet, all of the patients with celiac disease reported improvement or complete resolution of musculoskeletal symptoms.
COMMENTARY
Celiac disease has a prevalence of 0.5% to 1% in the US and can present with a range of symptoms that include diarrhea, abdominal discomfort, and weight loss. In addition to these typical symptoms, celiac disease can cause a wide range of systemic symptoms, including osteopenia, abnormal liver function tests, anemia, neurologic symptoms, and general malaise and fatigue.1 This study suggests that celiac testing be considered in children presenting with rheumatologic symptoms, including myalgia, arthralgia, and rash.
1. Presutti RJ, Cangemi JR, Cassidy HD, et al. Celiac disease. Am Fam Physician. 2007;76(12):1795-1802, 1809-1810.
Continue for educating parents about antibiotic use >>
EDUCATING PARENTS ABOUT ANTIBIOTIC USE
Vaz LE, Kleinman KP, Lakoma MD, et al. Prevalence of parental misconceptions about antibiotic use. Pediatrics. 2015;136:221-231.
Misperceptions about antibiotic use persist and continue to be more prevalent among parents of Medicaid-insured children, according to a study of 1,500 Massachusetts parents.
Investigators examined antibiotic-related knowledge and attitudes among both Medicaid-insured and private-insured parents and found
• Fewer Medicaid parents answered questions correctly, except for one regarding bronchitis.
• Medicaid patients were more likely to request unnecessary antibiotics.
• More parents in 2013 understood that green nasal discharge did not require antibiotics than in 2000.
• Medicaid-insured parents were younger, less likely to be white, and had less education than those commercially insured.
COMMENTARY
Decreasing the unnecessary use of antibiotics for viral infections is an important component of decreasing the development of antibiotic-resistant organisms. An important driver of clinician use of antibiotics is patients’ expectations for antibiotics. This study shows that much work remains to be done in changing patient expectations, which is not surprising to any practicing clinician. This study also suggests that the expectation for antibiotics is greater among those individuals with Medicaid insurance, which suggests that an opportunity exists for Medicaid insurance plans to do targeted patient education on this issue—which should improve patient outcomes, decrease cost from use of unneeded antibiotics, and decrease the development of antibiotic-resistant organisms.
Continue for newborn pulmonary hypertension and maternal antidepressant use >>
NEWBORN PULMONARY HYPERTENSION AND MATERNAL ANTIDEPRESSANT USE
Huybrechts KF, Bateman BT, Palmsten K, et al. Antidepressant use late in pregnancy and risk of persistent pulmonary hypertension of the newborn. JAMA. 2015;313(21):2142-2151.
Taking antidepressants during late pregnancy may increase the risk for persistent pulmonary hypertension of the newborn (PPHN), according to a nested cohort study of more than 3.7 million pregnant women in the 2000-2010 Medicaid Analytic eXtract.
Investigators compared offspring of mothers who used selective serotonin reuptake inhibitors (SSRIs) or non-SSRI monotherapy in the last 90 days of pregnancy to those who did not and found 3.4% of women filled at least one prescription for antidepressants late in pregnancy, primarily SSRIs.
Rates and odds ratios (ORs) of PPHN stratified by use and type of antidepressant were as follows:
The study authors note the absolute risk is small, and the increased risk is more modest than previous studies found.
COMMENTARY
Depression affects more than 12% of pregnancies and has important consequences, including increased risk for suicide, preterm birth, poor fetal growth, and impaired fetal and infant development.1 PPHN is a serious condition that can require intubation and can be fatal in 10% to 20% of cases. This study adds to the conflicting data suggesting that SSRI use in pregnancy can lead to an increase in this rare condition. The decision to use an antidepressant during pregnancy is a difficult one, because depression has serious consequences but so, potentially, does treatment. The treatment of depression during pregnancy requires thoughtful, informed discussion between patient and provider.
1. Stewart DE. Clinical practice. Depression during pregnancy. N Engl J Med. 2011;365(17):1605-1611. doi:10.1056/NEJMcp1102730.
Continue for new infant vaccine treats 6 diseases >>
NEW INFANT VACCINE TREATS 6 DISEASES
Marshall GS, Adams GL, Leonardi ML, et al. Immunogenicity, safety, and tolerability of a hexavalent vaccine in infants. Pediatrics. 2015:136(2):323-332.
The safety and immunogenicity of DTaP5-IPV-Hib-HepB fully liquid investigational hexavalent vaccine are comparable with the analogous licensed component vaccines and provide a new combination vaccine option aligned with the recommended US infant immunization schedule, according to a phase III study of 1,465 participants. Overall, 981 healthy infants were vaccinated in group 1 with the hexavalent vaccine and 484 in group 2 with the analogous licensed component vaccines.
The study found
• Immune responses in group 1 to all antigens contained in the vaccine one month after dose 3 were essentially noninferior to those in group 2.
• Adverse event rates after any dose were similar in both groups.
COMMENTARY
Vaccine administration has led to many diseases, including Haemophilus influenzae type b, polio, and measles, becoming quite rare. As we have recently seen with the resurgence of measles, continued vigilance and high immunization rates are important in ensuring that these diseases remain rare. The development of a hexavalent vaccine is another step in making immunization easier for clinicians to administer and for patients to accept.
Continue for treating infants with bronchiolitis >>
TREATING INFANTS WITH BRONCHIOLITIS
Silver AH, Esteban-Cruciani N, Azzarone G, et al. 3% hypertonic saline versus normal saline in inpatient bronchiolitis: a randomized controlled trial. Pediatrics. 2015;136:1036-1043.
Infants hospitalized with bronchiolitis saw no difference in length of stay or seven-day readmission rates when treated with nebulized 3% hypertonic saline (HS) compared with nebulized normal saline (NS), according to a randomized, controlled study of 227 infants who were younger than 12 months when admitted. Patients received either 4 mL nebulized 3% HS (113 infants) or 4 mL 0.9% NS (114 infants) every four hours from enrollment until hospital discharge. Researchers found
• Median length of stay of HS and NS groups was 2.1 days vs 2.1 days, respectively.
• Seven-day readmission rates for HS and NS groups were 4.3% vs 3.1%, respectively.
• Clinical worsening events were similar between groups.
COMMENTARY
Bronchiolitis, the most common lower respiratory tract infection in infants, is usually due to a viral infection, most often respiratory syncytial virus, and can cause disease that ranges in severity from mild to life-threatening. Infants with bronchiolitis typically present with rhinitis, tachypnea, wheezing, and cough, and occasionally crackles and use of accessory muscles. While many medications are used, supportive care and monitoring are the mainstays of therapy. Maintaining pulse above 90% is important, using supplemental oxygen when needed to achieve this. Alpha-adrenergic and beta-adrenergic bronchodilators are often used; though the evidence suggests that they are not usually helpful, they can be tried and continued if they appear to help. Systemic steroids are often used, but they too lack evidence of efficacy.1 This study shows that hypertonic saline can now join the list of interventions used with evidence of a lack of efficacy.
1. Diagnosis and management of bronchiolitis. Subcommittee on diagnosis and management of bronchiolitis. Pediatrics. 2006;118(4):1774-1793. doi:10.1542/peds.2006-2223.
Continue for azithromycin and preschool children >>
AZITHROMYCIN AND PRESCHOOL CHILDREN: CAN ANTIBIOTICS LESSEN ONSET OF SEVERE LRTIs?
Bacharier LB, Guilbert TW, Mauger DT, et al. Early administration of azithromycin and prevention of severe lower respiratory tract illnesses in preschool children with a history of such illnesses: a randomized clinical trial. JAMA. 2015;314(19):2034-2044.
The use of azithromycin early during an apparent respiratory tract illness (RTI) reduced the likelihood of severe lower RTI (LRTI) among young children with a history of recurrent severe LRTI, compared with placebo, according to a study of 607 children ages 12 to 71 months. Participants were randomized in a 1:1 ratio to receive either azithromycin (12 mg/kg/d for 5 d) or matching placebo at the start of an RTI. Researchers found
• A total of 937 treated RTIs were experienced by 443 children, including 92 severe LRTIs (azithromycin group, 35; placebo group, 57).
• Azithromycin significantly reduced the risk for progression to severe LRTI relative to placebo (HR, 0.64).
• Induction of azithromycin-resistant organisms and adverse events were infrequent.
COMMENTARY
Recurrent episodes of severe wheezing with RTI are an important and common occurrence, affecting up to 15% to 20% of children prior to age 6.1 LRTI was defined in this study as RTI that required the use of additional rescue medication. The current approach to RTI is to try to minimize the use of antibiotics unless an infection is clearly bacterial in origin, and to treat severe LRTI when it occurs. The results of this trial suggest that in children at high risk for severe LRTI, identified by their episodes of recurrent wheezing, early treatment of RTI with azithromycin may decrease the development of severe LRTI by more than 35%—an important result. It is important to recognize that this study does not suggest treating all RTIs with antibiotics, but rather that the use of a macrolide antibiotic may be considered, perhaps, in the select group of children similar to those studied, with a history of recurrent wheezing with previous RTIs.
1. Ly NP, Gold DR, Weiss ST, Celedón JC. Recurrent wheeze in early childhood and asthma among children at risk for atopy. Pediatrics. 2006;117(6):e1132-e1138.
Stroke Risk
ALCOHOL CONSUMPTION AND STROKE RISK IN MIDLIFE
Jones SB, Loehr L, Avery CL, et al. Midlife alcohol consumption and the risk of stroke in the Atherosclerosis Risk in Communities study. Stroke. 2015;46(11):3124-3130.
Light-to-moderate alcohol consumption at midlife was not associated with reduced stroke risk compared with abstention over 20 years of follow-up in a study of 12,433 never and current drinkers ages 45 to 65. An increased risk for both stroke and intracerebral hemorrhage (ICH) was observed with heavier consumption, as well as moderate intake for ICH. There were 773 ischemic strokes and 81 ICH incidents over follow-up. Study details included
• For ICH, light and moderate alcohol consumption was not associated with incidence (hazard ratios [HRs], 0.98, 1.06, 0.84).
• Heavier drinking was associated with a 31% increased rate relative to abstention (HR, 1.31).
• For ICH, moderate to heavy (HR, 1.99), but not light, consumption increased incidence.
Continue for spicy foods and mortality >>
SPICY FOODS AND MORTALITY
Lv J, Qi L, Yu C, et al. Consumption of spicy foods and total and cause specific mortality: population based cohort study. BMJ. 2015;351:h3942.
Consumption of spicy foods was inversely associated with total and certain cause-specific mortality, independent of other risk factors for death (eg, cancer, heart disease, and stroke), according to a population-based cohort study of 199,293 men and 288,082 women ages 30 to 79 in China. Specifically:
• Spicy food consumption showed highly consistent inverse associations with total mortality among both men and women.
• Compared with those who ate spicy foods less than once per week, adjusted hazard ratios for death were 0.90, 0.86, and 0.86 for those who ate spicy food on one or two; three to five; or six or seven days per week.
• A 14% relative risk reduction in total mortality was shown among those who consumed spicy foods on six or seven days per week.
COMMENTARY
This is the type of study that I look forward to and use as an argument to defend my eating habits. Previous studies have shown that chocolate consumption decreases blood pressure and mortality.1-3 Pistachio consumption has been associated with beneficial effects on glucose metabolism and insulin resistance.4 This study makes me think of suggesting to a local restaurant a new health food, based on the evidence, that I would suggest they call the “Skolnik Meal”: a spicy, chocolate pistachio taco.
1. Taubert D, Roesen R, Lehmann C, et al. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide. JAMA. 2007;298(1):49-60.
2. Taubert D, Roesen R, Schomig E. Effect of cocoa and tea intake on blood pressure: a meta-analysis. Arch Intern Med. 2007;167(7):626-634.
3. Buijsse B, Feskens EJM, Kok FJ, Kromhout D. Cocoa intake, blood pressure, and cardiovascular mortality: the Zutphen Elderly Study. Arch Intern Med. 2006;166:411-417.
4. Hernandez-Alonso P, Salas-Salvado J, Baldrich-Mora M, et al. Beneficial effect of pistachio consumption on glucose metabolism, insulin resistance, inflammation, and related metabolic risk markers: a randomized clinical trial. Diabetes Care. 2014;37:1–8.
Continue for FDA warns of heart attack and stroke risk of NSAIDs >>
FDA WARNS OF HEART ATTACK AND STROKE RISK OF NSAIDs
FDA Drug Safety Communication: FDA strengthens warning that non-aspirin nonsteroidal anti-inflammatory drugs (NSAIDs) can cause heart attacks or strokes. www.fda.gov/Drugs/DrugSafety/ucm451800.htm. Accessed November 19, 2015.
The FDA has added heart attack and stroke warnings to OTC nonaspirin NSAIDs. The warning is similar to that added to prescription NSAIDs in 2005.
People who have cardiovascular disease, particularly those who recently had a heart attack or cardiac bypass surgery, are at the greatest risk for cardiovascular adverse events associated with NSAIDs, according to the FDA announcement.
While people who have already had a heart attack are most vulnerable for having another or for dying of heart attack–related causes if treated with NSAIDs, everyone may be at risk—even those without an underlying risk for CVD.
COMMENTARY
This new statement was based on a comprehensive review of observational studies and clinical trials published since the FDA boxed warning appeared in 2005. The primary changes reflect that the risk for heart attack or stroke can occur as early as the first few weeks of using an NSAID, and the risk increases with longer use and higher doses. The estimates of the level of increased risk range from 10% to more than 50%, depending on the medication and the doses studied. The relative increase in risk is similar for patients with and without heart disease, but of course the likelihood of an adverse event is higher in patients with existent heart disease because of the increased prevalence of cardiovascular outcomes. NSAIDs also increase the risk for congestive heart failure.
Continue for childhood arterial ischemic stroke triggers >>
CHILDHOOD ARTERIAL ISCHEMIC STROKE TRIGGERS
Fullerton HJ, Hills NK, Elkind MS, et al. Infection, vaccination, and childhood arterial ischemic stroke: Results of the VIPS study. Neurology. 2015; 85(17):1459-1466.
Infection may act as a trigger for childhood arterial ischemic stroke (AIS), while routine vaccinations appear protective, according to a study of 355 patients (ages 29 days to 18 years) with AIS and 354 controls. Researchers found:
• Infection in the week prior to stroke was reported in 18% of cases versus 3% of controls, conferring a 6.3-fold increased risk for AIS.
• Upper respiratory infections were the most common.
• Prevalence of preceding infection was similar across arteriopathic, cardioembolic, and idiopathic stroke types.
• Use of vasoactive cold medications was similarly low in both groups.
• Children with some/few/no vaccinations were at higher stroke risk than those receiving all or most immunizations.
• In an age-adjusted model, independent risk factors for AIS included infection in the prior week, undervaccination, black race (compared to white), and rural residence.
Continue for comparing stroke risk scores for patients with AF >>
COMPARING STROKE RISK SCORES FOR PATIENTS WITH AF
van den Ham HA, Klungel OH, Singer DE, et al. Comparative performance of ATRIA, CHADS2, and CHA2DS2-VASc risk scores predicting stroke in patients with atrial fibrillation: results from a national primary care database. J Am Coll Cardiol. 2015;66(17):1851-1859.
The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) risk score more accurately identified patients with atrial fibrillation (AF) who were at low risk for stroke than did the CHA2DS2-VASc score, which assigned the same patients to higher-risk categories, in a study of 60,594 patients with AF. Researchers found:
• Event rates for moderate- and high-risk categories for CHA2DS2-VASc were lower than those of the ATRIA and CHADS2.
• Age and previous stroke most strongly predicted ischemic stroke.
• C statistics for the full point scores were 0.70 for the ATRIA risk score, 0.68 for CHADS2, and 0.68 for CHA2DS2-VASc risk score.
• Net reclassification improvement was 0.23 for the ATRIA compared with CHA2DS2-VASc.
• Reclassifying patients with very low stroke risk and AF could prevent overuse of anticoagulants.
Continue for risk of thromboembolism after ICH: Is resumption of warfarin therapy safe? >>
RISK OF THROMBOEMBOLISM AFTER ICH: IS RESUMPTION OF WARFARIN THERAPY SAFE?
Witt DM, Clark NP, Martinez K, et al. Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for intracranial hemorrhage. Thromb Res. 2015;136(5):1040-1044.
Patients resuming warfarin therapy following warfarin-associated intracranial hemorrhage (ICH) appeared not to be at increased risk for recurrent ICH but instead tended toward reduced thrombosis and all-cause mortality in a cohort study of 160 individuals discharged from the hospital following warfarin-related index of ICH. In the study, 33.8% of patients resumed warfarin therapy and 66.2% did not. Researchers found:
• Recurrent ICH occurred in a numerically greater, but statistically nonsignificant, proportion of patients who did not resume warfarin therapy (7.6% vs 3.7%).
• Patients who did not resume warfarin had three-fold higher (12.3% vs 3.7%) and approximately two-fold higher (31.3% vs. 18.5%) rates of thrombosis and all-cause mortality during follow-up.
Continue for lipid lowering drugs and stroke risk >>
LIPID LOWERING DRUGS AND STROKE RISK
Alpérovitch A, Kurth T, Bertrand M, et al. Primary prevention with lipid lowering drugs and long term risk of vascular events in older people: population based cohort study. BMJ. 2015;350:h2335.
Statins and fibrates may reduce stroke risk by 30% in older adults with no history of vascular events, according to a population-based cohort study of 7,484 patients.
In a random sample of community-dwelling adults ages 65 and older, investigators calculated hazard ratios for use of any lipid-lowering drug, and for statin and fibrates separately, and found:
• Users of lipid-lowering drugs were at decreased risk for stroke compared with nonusers (hazard ratio [HR], 0.66).
• Statin users were at similarly decreased risk (HR, 0.68).
• Fibrate users were also at decreased risk (HR, 0.66).
• There was no association between lipid-lowering drug use and coronary heart disease (HR, 1.12).
COMMENTARY
This study supports the use of LDL cholesterol–lowering medication as primary prevention in older individuals to reduce the risk for stroke. The mean age in this study was 74. Previously, the PROSPER study—the only randomized study of older individuals with high vascular risk—showed that pravastatin reduced the risk for coronary disease but not for stroke.1 This study gives support that lowering cholesterol in older patients with elevated cholesterol can decrease their risk for stroke.
1. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk for vascular disease (PROSPER). Lancet. 2002;360;1623-1630.
Continue for metabolic syndrome and diabetes in stroke recurrence >>
METABOLIC SYNDROME AND DIABETES IN STROKE RECURRENCE
Zhu S, McClure LA, Lau H, et al. Recurrent vascular events in lacunar stroke patients with metabolic syndrome and/or diabetes. Neurology. 2015 Aug 21. [Epub ahead of print]
Metabolic syndrome (METS) and diabetes mellitus (DM) were significant comorbid conditions in lacunar stroke patients, and they were associated with stroke recurrence, according to a study of 3,020 patients with lacunar strokes. Researchers found:
• 25% of patients had METS only, 6% had DM only, 32% had both conditions, and 37% had neither.
• Over a median 3.8 years of follow-up, there were 274 recurrent strokes and 74 myocardial infarctions (MIs).
• Among 240 recurrent ischemic strokes, 56% were lacunar.
• The hazard ratios for any recurrent stroke (HR, 1.7) or lacunar stroke (HR, 2.4) were significantly higher for those with concurrent METS and DM than for those who had neither.
• Risk for incident MI was higher in patients with DM (HR, 2.8) or concurrent DM and METS (HR, 2.6).
ALCOHOL CONSUMPTION AND STROKE RISK IN MIDLIFE
Jones SB, Loehr L, Avery CL, et al. Midlife alcohol consumption and the risk of stroke in the Atherosclerosis Risk in Communities study. Stroke. 2015;46(11):3124-3130.
Light-to-moderate alcohol consumption at midlife was not associated with reduced stroke risk compared with abstention over 20 years of follow-up in a study of 12,433 never and current drinkers ages 45 to 65. An increased risk for both stroke and intracerebral hemorrhage (ICH) was observed with heavier consumption, as well as moderate intake for ICH. There were 773 ischemic strokes and 81 ICH incidents over follow-up. Study details included
• For ICH, light and moderate alcohol consumption was not associated with incidence (hazard ratios [HRs], 0.98, 1.06, 0.84).
• Heavier drinking was associated with a 31% increased rate relative to abstention (HR, 1.31).
• For ICH, moderate to heavy (HR, 1.99), but not light, consumption increased incidence.
Continue for spicy foods and mortality >>
SPICY FOODS AND MORTALITY
Lv J, Qi L, Yu C, et al. Consumption of spicy foods and total and cause specific mortality: population based cohort study. BMJ. 2015;351:h3942.
Consumption of spicy foods was inversely associated with total and certain cause-specific mortality, independent of other risk factors for death (eg, cancer, heart disease, and stroke), according to a population-based cohort study of 199,293 men and 288,082 women ages 30 to 79 in China. Specifically:
• Spicy food consumption showed highly consistent inverse associations with total mortality among both men and women.
• Compared with those who ate spicy foods less than once per week, adjusted hazard ratios for death were 0.90, 0.86, and 0.86 for those who ate spicy food on one or two; three to five; or six or seven days per week.
• A 14% relative risk reduction in total mortality was shown among those who consumed spicy foods on six or seven days per week.
COMMENTARY
This is the type of study that I look forward to and use as an argument to defend my eating habits. Previous studies have shown that chocolate consumption decreases blood pressure and mortality.1-3 Pistachio consumption has been associated with beneficial effects on glucose metabolism and insulin resistance.4 This study makes me think of suggesting to a local restaurant a new health food, based on the evidence, that I would suggest they call the “Skolnik Meal”: a spicy, chocolate pistachio taco.
1. Taubert D, Roesen R, Lehmann C, et al. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide. JAMA. 2007;298(1):49-60.
2. Taubert D, Roesen R, Schomig E. Effect of cocoa and tea intake on blood pressure: a meta-analysis. Arch Intern Med. 2007;167(7):626-634.
3. Buijsse B, Feskens EJM, Kok FJ, Kromhout D. Cocoa intake, blood pressure, and cardiovascular mortality: the Zutphen Elderly Study. Arch Intern Med. 2006;166:411-417.
4. Hernandez-Alonso P, Salas-Salvado J, Baldrich-Mora M, et al. Beneficial effect of pistachio consumption on glucose metabolism, insulin resistance, inflammation, and related metabolic risk markers: a randomized clinical trial. Diabetes Care. 2014;37:1–8.
Continue for FDA warns of heart attack and stroke risk of NSAIDs >>
FDA WARNS OF HEART ATTACK AND STROKE RISK OF NSAIDs
FDA Drug Safety Communication: FDA strengthens warning that non-aspirin nonsteroidal anti-inflammatory drugs (NSAIDs) can cause heart attacks or strokes. www.fda.gov/Drugs/DrugSafety/ucm451800.htm. Accessed November 19, 2015.
The FDA has added heart attack and stroke warnings to OTC nonaspirin NSAIDs. The warning is similar to that added to prescription NSAIDs in 2005.
People who have cardiovascular disease, particularly those who recently had a heart attack or cardiac bypass surgery, are at the greatest risk for cardiovascular adverse events associated with NSAIDs, according to the FDA announcement.
While people who have already had a heart attack are most vulnerable for having another or for dying of heart attack–related causes if treated with NSAIDs, everyone may be at risk—even those without an underlying risk for CVD.
COMMENTARY
This new statement was based on a comprehensive review of observational studies and clinical trials published since the FDA boxed warning appeared in 2005. The primary changes reflect that the risk for heart attack or stroke can occur as early as the first few weeks of using an NSAID, and the risk increases with longer use and higher doses. The estimates of the level of increased risk range from 10% to more than 50%, depending on the medication and the doses studied. The relative increase in risk is similar for patients with and without heart disease, but of course the likelihood of an adverse event is higher in patients with existent heart disease because of the increased prevalence of cardiovascular outcomes. NSAIDs also increase the risk for congestive heart failure.
Continue for childhood arterial ischemic stroke triggers >>
CHILDHOOD ARTERIAL ISCHEMIC STROKE TRIGGERS
Fullerton HJ, Hills NK, Elkind MS, et al. Infection, vaccination, and childhood arterial ischemic stroke: Results of the VIPS study. Neurology. 2015; 85(17):1459-1466.
Infection may act as a trigger for childhood arterial ischemic stroke (AIS), while routine vaccinations appear protective, according to a study of 355 patients (ages 29 days to 18 years) with AIS and 354 controls. Researchers found:
• Infection in the week prior to stroke was reported in 18% of cases versus 3% of controls, conferring a 6.3-fold increased risk for AIS.
• Upper respiratory infections were the most common.
• Prevalence of preceding infection was similar across arteriopathic, cardioembolic, and idiopathic stroke types.
• Use of vasoactive cold medications was similarly low in both groups.
• Children with some/few/no vaccinations were at higher stroke risk than those receiving all or most immunizations.
• In an age-adjusted model, independent risk factors for AIS included infection in the prior week, undervaccination, black race (compared to white), and rural residence.
Continue for comparing stroke risk scores for patients with AF >>
COMPARING STROKE RISK SCORES FOR PATIENTS WITH AF
van den Ham HA, Klungel OH, Singer DE, et al. Comparative performance of ATRIA, CHADS2, and CHA2DS2-VASc risk scores predicting stroke in patients with atrial fibrillation: results from a national primary care database. J Am Coll Cardiol. 2015;66(17):1851-1859.
The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) risk score more accurately identified patients with atrial fibrillation (AF) who were at low risk for stroke than did the CHA2DS2-VASc score, which assigned the same patients to higher-risk categories, in a study of 60,594 patients with AF. Researchers found:
• Event rates for moderate- and high-risk categories for CHA2DS2-VASc were lower than those of the ATRIA and CHADS2.
• Age and previous stroke most strongly predicted ischemic stroke.
• C statistics for the full point scores were 0.70 for the ATRIA risk score, 0.68 for CHADS2, and 0.68 for CHA2DS2-VASc risk score.
• Net reclassification improvement was 0.23 for the ATRIA compared with CHA2DS2-VASc.
• Reclassifying patients with very low stroke risk and AF could prevent overuse of anticoagulants.
Continue for risk of thromboembolism after ICH: Is resumption of warfarin therapy safe? >>
RISK OF THROMBOEMBOLISM AFTER ICH: IS RESUMPTION OF WARFARIN THERAPY SAFE?
Witt DM, Clark NP, Martinez K, et al. Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for intracranial hemorrhage. Thromb Res. 2015;136(5):1040-1044.
Patients resuming warfarin therapy following warfarin-associated intracranial hemorrhage (ICH) appeared not to be at increased risk for recurrent ICH but instead tended toward reduced thrombosis and all-cause mortality in a cohort study of 160 individuals discharged from the hospital following warfarin-related index of ICH. In the study, 33.8% of patients resumed warfarin therapy and 66.2% did not. Researchers found:
• Recurrent ICH occurred in a numerically greater, but statistically nonsignificant, proportion of patients who did not resume warfarin therapy (7.6% vs 3.7%).
• Patients who did not resume warfarin had three-fold higher (12.3% vs 3.7%) and approximately two-fold higher (31.3% vs. 18.5%) rates of thrombosis and all-cause mortality during follow-up.
Continue for lipid lowering drugs and stroke risk >>
LIPID LOWERING DRUGS AND STROKE RISK
Alpérovitch A, Kurth T, Bertrand M, et al. Primary prevention with lipid lowering drugs and long term risk of vascular events in older people: population based cohort study. BMJ. 2015;350:h2335.
Statins and fibrates may reduce stroke risk by 30% in older adults with no history of vascular events, according to a population-based cohort study of 7,484 patients.
In a random sample of community-dwelling adults ages 65 and older, investigators calculated hazard ratios for use of any lipid-lowering drug, and for statin and fibrates separately, and found:
• Users of lipid-lowering drugs were at decreased risk for stroke compared with nonusers (hazard ratio [HR], 0.66).
• Statin users were at similarly decreased risk (HR, 0.68).
• Fibrate users were also at decreased risk (HR, 0.66).
• There was no association between lipid-lowering drug use and coronary heart disease (HR, 1.12).
COMMENTARY
This study supports the use of LDL cholesterol–lowering medication as primary prevention in older individuals to reduce the risk for stroke. The mean age in this study was 74. Previously, the PROSPER study—the only randomized study of older individuals with high vascular risk—showed that pravastatin reduced the risk for coronary disease but not for stroke.1 This study gives support that lowering cholesterol in older patients with elevated cholesterol can decrease their risk for stroke.
1. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk for vascular disease (PROSPER). Lancet. 2002;360;1623-1630.
Continue for metabolic syndrome and diabetes in stroke recurrence >>
METABOLIC SYNDROME AND DIABETES IN STROKE RECURRENCE
Zhu S, McClure LA, Lau H, et al. Recurrent vascular events in lacunar stroke patients with metabolic syndrome and/or diabetes. Neurology. 2015 Aug 21. [Epub ahead of print]
Metabolic syndrome (METS) and diabetes mellitus (DM) were significant comorbid conditions in lacunar stroke patients, and they were associated with stroke recurrence, according to a study of 3,020 patients with lacunar strokes. Researchers found:
• 25% of patients had METS only, 6% had DM only, 32% had both conditions, and 37% had neither.
• Over a median 3.8 years of follow-up, there were 274 recurrent strokes and 74 myocardial infarctions (MIs).
• Among 240 recurrent ischemic strokes, 56% were lacunar.
• The hazard ratios for any recurrent stroke (HR, 1.7) or lacunar stroke (HR, 2.4) were significantly higher for those with concurrent METS and DM than for those who had neither.
• Risk for incident MI was higher in patients with DM (HR, 2.8) or concurrent DM and METS (HR, 2.6).
ALCOHOL CONSUMPTION AND STROKE RISK IN MIDLIFE
Jones SB, Loehr L, Avery CL, et al. Midlife alcohol consumption and the risk of stroke in the Atherosclerosis Risk in Communities study. Stroke. 2015;46(11):3124-3130.
Light-to-moderate alcohol consumption at midlife was not associated with reduced stroke risk compared with abstention over 20 years of follow-up in a study of 12,433 never and current drinkers ages 45 to 65. An increased risk for both stroke and intracerebral hemorrhage (ICH) was observed with heavier consumption, as well as moderate intake for ICH. There were 773 ischemic strokes and 81 ICH incidents over follow-up. Study details included
• For ICH, light and moderate alcohol consumption was not associated with incidence (hazard ratios [HRs], 0.98, 1.06, 0.84).
• Heavier drinking was associated with a 31% increased rate relative to abstention (HR, 1.31).
• For ICH, moderate to heavy (HR, 1.99), but not light, consumption increased incidence.
Continue for spicy foods and mortality >>
SPICY FOODS AND MORTALITY
Lv J, Qi L, Yu C, et al. Consumption of spicy foods and total and cause specific mortality: population based cohort study. BMJ. 2015;351:h3942.
Consumption of spicy foods was inversely associated with total and certain cause-specific mortality, independent of other risk factors for death (eg, cancer, heart disease, and stroke), according to a population-based cohort study of 199,293 men and 288,082 women ages 30 to 79 in China. Specifically:
• Spicy food consumption showed highly consistent inverse associations with total mortality among both men and women.
• Compared with those who ate spicy foods less than once per week, adjusted hazard ratios for death were 0.90, 0.86, and 0.86 for those who ate spicy food on one or two; three to five; or six or seven days per week.
• A 14% relative risk reduction in total mortality was shown among those who consumed spicy foods on six or seven days per week.
COMMENTARY
This is the type of study that I look forward to and use as an argument to defend my eating habits. Previous studies have shown that chocolate consumption decreases blood pressure and mortality.1-3 Pistachio consumption has been associated with beneficial effects on glucose metabolism and insulin resistance.4 This study makes me think of suggesting to a local restaurant a new health food, based on the evidence, that I would suggest they call the “Skolnik Meal”: a spicy, chocolate pistachio taco.
1. Taubert D, Roesen R, Lehmann C, et al. Effects of low habitual cocoa intake on blood pressure and bioactive nitric oxide. JAMA. 2007;298(1):49-60.
2. Taubert D, Roesen R, Schomig E. Effect of cocoa and tea intake on blood pressure: a meta-analysis. Arch Intern Med. 2007;167(7):626-634.
3. Buijsse B, Feskens EJM, Kok FJ, Kromhout D. Cocoa intake, blood pressure, and cardiovascular mortality: the Zutphen Elderly Study. Arch Intern Med. 2006;166:411-417.
4. Hernandez-Alonso P, Salas-Salvado J, Baldrich-Mora M, et al. Beneficial effect of pistachio consumption on glucose metabolism, insulin resistance, inflammation, and related metabolic risk markers: a randomized clinical trial. Diabetes Care. 2014;37:1–8.
Continue for FDA warns of heart attack and stroke risk of NSAIDs >>
FDA WARNS OF HEART ATTACK AND STROKE RISK OF NSAIDs
FDA Drug Safety Communication: FDA strengthens warning that non-aspirin nonsteroidal anti-inflammatory drugs (NSAIDs) can cause heart attacks or strokes. www.fda.gov/Drugs/DrugSafety/ucm451800.htm. Accessed November 19, 2015.
The FDA has added heart attack and stroke warnings to OTC nonaspirin NSAIDs. The warning is similar to that added to prescription NSAIDs in 2005.
People who have cardiovascular disease, particularly those who recently had a heart attack or cardiac bypass surgery, are at the greatest risk for cardiovascular adverse events associated with NSAIDs, according to the FDA announcement.
While people who have already had a heart attack are most vulnerable for having another or for dying of heart attack–related causes if treated with NSAIDs, everyone may be at risk—even those without an underlying risk for CVD.
COMMENTARY
This new statement was based on a comprehensive review of observational studies and clinical trials published since the FDA boxed warning appeared in 2005. The primary changes reflect that the risk for heart attack or stroke can occur as early as the first few weeks of using an NSAID, and the risk increases with longer use and higher doses. The estimates of the level of increased risk range from 10% to more than 50%, depending on the medication and the doses studied. The relative increase in risk is similar for patients with and without heart disease, but of course the likelihood of an adverse event is higher in patients with existent heart disease because of the increased prevalence of cardiovascular outcomes. NSAIDs also increase the risk for congestive heart failure.
Continue for childhood arterial ischemic stroke triggers >>
CHILDHOOD ARTERIAL ISCHEMIC STROKE TRIGGERS
Fullerton HJ, Hills NK, Elkind MS, et al. Infection, vaccination, and childhood arterial ischemic stroke: Results of the VIPS study. Neurology. 2015; 85(17):1459-1466.
Infection may act as a trigger for childhood arterial ischemic stroke (AIS), while routine vaccinations appear protective, according to a study of 355 patients (ages 29 days to 18 years) with AIS and 354 controls. Researchers found:
• Infection in the week prior to stroke was reported in 18% of cases versus 3% of controls, conferring a 6.3-fold increased risk for AIS.
• Upper respiratory infections were the most common.
• Prevalence of preceding infection was similar across arteriopathic, cardioembolic, and idiopathic stroke types.
• Use of vasoactive cold medications was similarly low in both groups.
• Children with some/few/no vaccinations were at higher stroke risk than those receiving all or most immunizations.
• In an age-adjusted model, independent risk factors for AIS included infection in the prior week, undervaccination, black race (compared to white), and rural residence.
Continue for comparing stroke risk scores for patients with AF >>
COMPARING STROKE RISK SCORES FOR PATIENTS WITH AF
van den Ham HA, Klungel OH, Singer DE, et al. Comparative performance of ATRIA, CHADS2, and CHA2DS2-VASc risk scores predicting stroke in patients with atrial fibrillation: results from a national primary care database. J Am Coll Cardiol. 2015;66(17):1851-1859.
The Anticoagulation and Risk Factors in Atrial Fibrillation (ATRIA) risk score more accurately identified patients with atrial fibrillation (AF) who were at low risk for stroke than did the CHA2DS2-VASc score, which assigned the same patients to higher-risk categories, in a study of 60,594 patients with AF. Researchers found:
• Event rates for moderate- and high-risk categories for CHA2DS2-VASc were lower than those of the ATRIA and CHADS2.
• Age and previous stroke most strongly predicted ischemic stroke.
• C statistics for the full point scores were 0.70 for the ATRIA risk score, 0.68 for CHADS2, and 0.68 for CHA2DS2-VASc risk score.
• Net reclassification improvement was 0.23 for the ATRIA compared with CHA2DS2-VASc.
• Reclassifying patients with very low stroke risk and AF could prevent overuse of anticoagulants.
Continue for risk of thromboembolism after ICH: Is resumption of warfarin therapy safe? >>
RISK OF THROMBOEMBOLISM AFTER ICH: IS RESUMPTION OF WARFARIN THERAPY SAFE?
Witt DM, Clark NP, Martinez K, et al. Risk of thromboembolism, recurrent hemorrhage, and death after warfarin therapy interruption for intracranial hemorrhage. Thromb Res. 2015;136(5):1040-1044.
Patients resuming warfarin therapy following warfarin-associated intracranial hemorrhage (ICH) appeared not to be at increased risk for recurrent ICH but instead tended toward reduced thrombosis and all-cause mortality in a cohort study of 160 individuals discharged from the hospital following warfarin-related index of ICH. In the study, 33.8% of patients resumed warfarin therapy and 66.2% did not. Researchers found:
• Recurrent ICH occurred in a numerically greater, but statistically nonsignificant, proportion of patients who did not resume warfarin therapy (7.6% vs 3.7%).
• Patients who did not resume warfarin had three-fold higher (12.3% vs 3.7%) and approximately two-fold higher (31.3% vs. 18.5%) rates of thrombosis and all-cause mortality during follow-up.
Continue for lipid lowering drugs and stroke risk >>
LIPID LOWERING DRUGS AND STROKE RISK
Alpérovitch A, Kurth T, Bertrand M, et al. Primary prevention with lipid lowering drugs and long term risk of vascular events in older people: population based cohort study. BMJ. 2015;350:h2335.
Statins and fibrates may reduce stroke risk by 30% in older adults with no history of vascular events, according to a population-based cohort study of 7,484 patients.
In a random sample of community-dwelling adults ages 65 and older, investigators calculated hazard ratios for use of any lipid-lowering drug, and for statin and fibrates separately, and found:
• Users of lipid-lowering drugs were at decreased risk for stroke compared with nonusers (hazard ratio [HR], 0.66).
• Statin users were at similarly decreased risk (HR, 0.68).
• Fibrate users were also at decreased risk (HR, 0.66).
• There was no association between lipid-lowering drug use and coronary heart disease (HR, 1.12).
COMMENTARY
This study supports the use of LDL cholesterol–lowering medication as primary prevention in older individuals to reduce the risk for stroke. The mean age in this study was 74. Previously, the PROSPER study—the only randomized study of older individuals with high vascular risk—showed that pravastatin reduced the risk for coronary disease but not for stroke.1 This study gives support that lowering cholesterol in older patients with elevated cholesterol can decrease their risk for stroke.
1. Shepherd J, Blauw GJ, Murphy MB, et al. Pravastatin in elderly individuals at risk for vascular disease (PROSPER). Lancet. 2002;360;1623-1630.
Continue for metabolic syndrome and diabetes in stroke recurrence >>
METABOLIC SYNDROME AND DIABETES IN STROKE RECURRENCE
Zhu S, McClure LA, Lau H, et al. Recurrent vascular events in lacunar stroke patients with metabolic syndrome and/or diabetes. Neurology. 2015 Aug 21. [Epub ahead of print]
Metabolic syndrome (METS) and diabetes mellitus (DM) were significant comorbid conditions in lacunar stroke patients, and they were associated with stroke recurrence, according to a study of 3,020 patients with lacunar strokes. Researchers found:
• 25% of patients had METS only, 6% had DM only, 32% had both conditions, and 37% had neither.
• Over a median 3.8 years of follow-up, there were 274 recurrent strokes and 74 myocardial infarctions (MIs).
• Among 240 recurrent ischemic strokes, 56% were lacunar.
• The hazard ratios for any recurrent stroke (HR, 1.7) or lacunar stroke (HR, 2.4) were significantly higher for those with concurrent METS and DM than for those who had neither.
• Risk for incident MI was higher in patients with DM (HR, 2.8) or concurrent DM and METS (HR, 2.6).
American Cancer Society recommendations for breast cancer screening
Breast cancer is the most common cancer in women and ranks second, after lung cancer, as a cause of cancer-related death in women.
In the United States alone, an estimated 231,840 women will be diagnosed with breast cancer in 2015. Largely as a result of screening mammography and early detection, associated mortality has been steadily declining since 1990. Still, the American Cancer Society has estimated that 40,290 U.S. women will die of breast cancer in 2015.

Specific recommendations for breast cancer screening vary significantly between two major guidelines: the U.S. Preventive Services Task Force (USPSTF) and the American Cancer Society (ACS). In 2003, the ACS recommended annual screening with mammography for women beginning at age 40, stopping only when a woman’s health would preclude her from cancer treatment. Furthermore, the ACS recommended a clinical breast examination (CBE) at least every 3 years for women in their 20s and 30s and then annually starting at age 40. Current USPSTF guidelines recommend mammograms biennially from age 50 to age 74, finding insufficient evidence to recommend CBE.
Gaps between these two organizations are shrinking, however, as the ACS released its new 2015 guidelines, updating the 2003 recommendations for breast cancer screening for women at average risk. The ACS defined average risk broadly: women without a personal history of breast cancer, a confirmed or suspected genetic mutation known to increase risk of breast cancer (e.g., BRCA), or a history of previous radiotherapy to the chest at a young age. These guidelines include the following recommendations:
1. Women with an average risk of breast cancer should undergo regular screening mammography starting at age 45 years. (Strong Recommendation)
1a. Women aged 45-54 years should be screening annually. (Qualified Recommendation)
1b. Women 55 years and older should transition to biennial screening or have the opportunity to continue screening annually. (Qualified Recommendation)
1c. Women should have the opportunity to begin annual screening between the ages of 40 and 44 years. (Qualified Recommendation)
2. Women should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer. (Qualified Recommendation)
3. The ACS does not recommend CBE for breast cancer screening among average-risk women at any age. (Qualified Recommendation)
These new guidelines bring the USPSTF and ACS recommendation closer to one another; they provide a clear step toward consensus. Both guidelines now agree that for average-risk women who are younger than 45 years, the harms of screening mammography likely outweigh the benefits. They are also consistent in their position that for women older than 55 years, biennial mammography is likely to provide the best balance of benefits to harms. Finally, they both recommend decisions to be individualized to reflect a woman’s preferences and her underlying risk of breast cancer.
Differences between the two guidelines originate from several methodological decisions made by the group responsible for the new ACS guidelines. In addition to randomized controlled trials and mathematic modeling, the group reviewed and utilized results from recent observational studies. The group also decided to analyze the benefits and harms of mammography using 5-year age groups, rather than the conventional 10 years. Also, it assessed annual vs. biennial screening, finding that the proportion of tumors that were stage IIB or higher and larger than 15 mm was greater for premenopausal women undergoing biennial screening but not for postmenopausal women.
Several messages are worth emphasizing as clinicians continue to review these new guidelines and decide whether or not to incorporate them into practice. First, thanks to breakthroughs in breast cancer treatment, the majority of women who are diagnosed with breast cancer will do well regardless of whether their cancer was found by mammography. Evidence from randomized trials of women in their 40s and 50s suggests that screening mammography only decreases breast cancer mortality by approximately 15%. Thus, about 85% of women in their 40s and 50s who die of breast cancer would have died regardless of mammography screening. Furthermore, because of the low risk of breast cancer for women in their 40s, this relative benefit of 15% translates to a small absolute benefit of around 5 of 10,000 women likely to have a breast cancer death prevented by mammography. Obviously the absolute benefit is higher for women with an increased risk of breast cancer, highlighting the importance of identifying higher-risk women. The lifetime risk of dying from breast cancer with no screening is 2.7%. Using the screening guidelines of the USPSTF that risk decreases to 2% with a total of 13 mammograms by 74 years of age. Using the new screening guidelines from the ACS, the calculated risk of dying from breast cancer is 1.8%-1.9% with 20 mammograms by 74 years of age. This is a significant departure from the 35 mammograms that were recommended by the older 2003 ACS guidelines.
Bottom line
The American Cancer Society has released a 2015 update to its breast cancer screening guidelines for women at average risk. The new guidelines recommend against clinical breast exams and in favor of annual mammograms between ages 45 and 54 years, followed by biennial mammograms starting at age 55 years and ending when life expectancy is less than 10 years. These guidelines also allow for patient preference or clinical judgment to opt in for annual mammography from 40 to 44 years of age and to continue with annual screening beyond age 55.
References
1. Keating NL, Pace LE. New guidelines for breast cancer screening in U.S. women. JAMA. 2015;314(15)1658.
2. Kerlikowske K. Progress toward consensus on breast cancer screening guidelines and reducing screening harms. JAMA Intern Med. 2015 Oct 20. doi:10.1001/jamainternmed.2015.6466.
3. Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk. JAMA. 2015;314(15):1599-614. doi:10/1001/jama.2015.12783.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Lyons is a third-year resident in the program.
Breast cancer is the most common cancer in women and ranks second, after lung cancer, as a cause of cancer-related death in women.
In the United States alone, an estimated 231,840 women will be diagnosed with breast cancer in 2015. Largely as a result of screening mammography and early detection, associated mortality has been steadily declining since 1990. Still, the American Cancer Society has estimated that 40,290 U.S. women will die of breast cancer in 2015.
Specific recommendations for breast cancer screening vary significantly between two major guidelines: the U.S. Preventive Services Task Force (USPSTF) and the American Cancer Society (ACS). In 2003, the ACS recommended annual screening with mammography for women beginning at age 40, stopping only when a woman’s health would preclude her from cancer treatment. Furthermore, the ACS recommended a clinical breast examination (CBE) at least every 3 years for women in their 20s and 30s and then annually starting at age 40. Current USPSTF guidelines recommend mammograms biennially from age 50 to age 74, finding insufficient evidence to recommend CBE.
Gaps between these two organizations are shrinking, however, as the ACS released its new 2015 guidelines, updating the 2003 recommendations for breast cancer screening for women at average risk. The ACS defined average risk broadly: women without a personal history of breast cancer, a confirmed or suspected genetic mutation known to increase risk of breast cancer (e.g., BRCA), or a history of previous radiotherapy to the chest at a young age. These guidelines include the following recommendations:
1. Women with an average risk of breast cancer should undergo regular screening mammography starting at age 45 years. (Strong Recommendation)
1a. Women aged 45-54 years should be screening annually. (Qualified Recommendation)
1b. Women 55 years and older should transition to biennial screening or have the opportunity to continue screening annually. (Qualified Recommendation)
1c. Women should have the opportunity to begin annual screening between the ages of 40 and 44 years. (Qualified Recommendation)
2. Women should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer. (Qualified Recommendation)
3. The ACS does not recommend CBE for breast cancer screening among average-risk women at any age. (Qualified Recommendation)
These new guidelines bring the USPSTF and ACS recommendation closer to one another; they provide a clear step toward consensus. Both guidelines now agree that for average-risk women who are younger than 45 years, the harms of screening mammography likely outweigh the benefits. They are also consistent in their position that for women older than 55 years, biennial mammography is likely to provide the best balance of benefits to harms. Finally, they both recommend decisions to be individualized to reflect a woman’s preferences and her underlying risk of breast cancer.
Differences between the two guidelines originate from several methodological decisions made by the group responsible for the new ACS guidelines. In addition to randomized controlled trials and mathematic modeling, the group reviewed and utilized results from recent observational studies. The group also decided to analyze the benefits and harms of mammography using 5-year age groups, rather than the conventional 10 years. Also, it assessed annual vs. biennial screening, finding that the proportion of tumors that were stage IIB or higher and larger than 15 mm was greater for premenopausal women undergoing biennial screening but not for postmenopausal women.
Several messages are worth emphasizing as clinicians continue to review these new guidelines and decide whether or not to incorporate them into practice. First, thanks to breakthroughs in breast cancer treatment, the majority of women who are diagnosed with breast cancer will do well regardless of whether their cancer was found by mammography. Evidence from randomized trials of women in their 40s and 50s suggests that screening mammography only decreases breast cancer mortality by approximately 15%. Thus, about 85% of women in their 40s and 50s who die of breast cancer would have died regardless of mammography screening. Furthermore, because of the low risk of breast cancer for women in their 40s, this relative benefit of 15% translates to a small absolute benefit of around 5 of 10,000 women likely to have a breast cancer death prevented by mammography. Obviously the absolute benefit is higher for women with an increased risk of breast cancer, highlighting the importance of identifying higher-risk women. The lifetime risk of dying from breast cancer with no screening is 2.7%. Using the screening guidelines of the USPSTF that risk decreases to 2% with a total of 13 mammograms by 74 years of age. Using the new screening guidelines from the ACS, the calculated risk of dying from breast cancer is 1.8%-1.9% with 20 mammograms by 74 years of age. This is a significant departure from the 35 mammograms that were recommended by the older 2003 ACS guidelines.
Bottom line
The American Cancer Society has released a 2015 update to its breast cancer screening guidelines for women at average risk. The new guidelines recommend against clinical breast exams and in favor of annual mammograms between ages 45 and 54 years, followed by biennial mammograms starting at age 55 years and ending when life expectancy is less than 10 years. These guidelines also allow for patient preference or clinical judgment to opt in for annual mammography from 40 to 44 years of age and to continue with annual screening beyond age 55.
References
1. Keating NL, Pace LE. New guidelines for breast cancer screening in U.S. women. JAMA. 2015;314(15)1658.
2. Kerlikowske K. Progress toward consensus on breast cancer screening guidelines and reducing screening harms. JAMA Intern Med. 2015 Oct 20. doi:10.1001/jamainternmed.2015.6466.
3. Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk. JAMA. 2015;314(15):1599-614. doi:10/1001/jama.2015.12783.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Lyons is a third-year resident in the program.
Breast cancer is the most common cancer in women and ranks second, after lung cancer, as a cause of cancer-related death in women.
In the United States alone, an estimated 231,840 women will be diagnosed with breast cancer in 2015. Largely as a result of screening mammography and early detection, associated mortality has been steadily declining since 1990. Still, the American Cancer Society has estimated that 40,290 U.S. women will die of breast cancer in 2015.
Specific recommendations for breast cancer screening vary significantly between two major guidelines: the U.S. Preventive Services Task Force (USPSTF) and the American Cancer Society (ACS). In 2003, the ACS recommended annual screening with mammography for women beginning at age 40, stopping only when a woman’s health would preclude her from cancer treatment. Furthermore, the ACS recommended a clinical breast examination (CBE) at least every 3 years for women in their 20s and 30s and then annually starting at age 40. Current USPSTF guidelines recommend mammograms biennially from age 50 to age 74, finding insufficient evidence to recommend CBE.
Gaps between these two organizations are shrinking, however, as the ACS released its new 2015 guidelines, updating the 2003 recommendations for breast cancer screening for women at average risk. The ACS defined average risk broadly: women without a personal history of breast cancer, a confirmed or suspected genetic mutation known to increase risk of breast cancer (e.g., BRCA), or a history of previous radiotherapy to the chest at a young age. These guidelines include the following recommendations:
1. Women with an average risk of breast cancer should undergo regular screening mammography starting at age 45 years. (Strong Recommendation)
1a. Women aged 45-54 years should be screening annually. (Qualified Recommendation)
1b. Women 55 years and older should transition to biennial screening or have the opportunity to continue screening annually. (Qualified Recommendation)
1c. Women should have the opportunity to begin annual screening between the ages of 40 and 44 years. (Qualified Recommendation)
2. Women should continue screening mammography as long as their overall health is good and they have a life expectancy of 10 years or longer. (Qualified Recommendation)
3. The ACS does not recommend CBE for breast cancer screening among average-risk women at any age. (Qualified Recommendation)
These new guidelines bring the USPSTF and ACS recommendation closer to one another; they provide a clear step toward consensus. Both guidelines now agree that for average-risk women who are younger than 45 years, the harms of screening mammography likely outweigh the benefits. They are also consistent in their position that for women older than 55 years, biennial mammography is likely to provide the best balance of benefits to harms. Finally, they both recommend decisions to be individualized to reflect a woman’s preferences and her underlying risk of breast cancer.
Differences between the two guidelines originate from several methodological decisions made by the group responsible for the new ACS guidelines. In addition to randomized controlled trials and mathematic modeling, the group reviewed and utilized results from recent observational studies. The group also decided to analyze the benefits and harms of mammography using 5-year age groups, rather than the conventional 10 years. Also, it assessed annual vs. biennial screening, finding that the proportion of tumors that were stage IIB or higher and larger than 15 mm was greater for premenopausal women undergoing biennial screening but not for postmenopausal women.
Several messages are worth emphasizing as clinicians continue to review these new guidelines and decide whether or not to incorporate them into practice. First, thanks to breakthroughs in breast cancer treatment, the majority of women who are diagnosed with breast cancer will do well regardless of whether their cancer was found by mammography. Evidence from randomized trials of women in their 40s and 50s suggests that screening mammography only decreases breast cancer mortality by approximately 15%. Thus, about 85% of women in their 40s and 50s who die of breast cancer would have died regardless of mammography screening. Furthermore, because of the low risk of breast cancer for women in their 40s, this relative benefit of 15% translates to a small absolute benefit of around 5 of 10,000 women likely to have a breast cancer death prevented by mammography. Obviously the absolute benefit is higher for women with an increased risk of breast cancer, highlighting the importance of identifying higher-risk women. The lifetime risk of dying from breast cancer with no screening is 2.7%. Using the screening guidelines of the USPSTF that risk decreases to 2% with a total of 13 mammograms by 74 years of age. Using the new screening guidelines from the ACS, the calculated risk of dying from breast cancer is 1.8%-1.9% with 20 mammograms by 74 years of age. This is a significant departure from the 35 mammograms that were recommended by the older 2003 ACS guidelines.
Bottom line
The American Cancer Society has released a 2015 update to its breast cancer screening guidelines for women at average risk. The new guidelines recommend against clinical breast exams and in favor of annual mammograms between ages 45 and 54 years, followed by biennial mammograms starting at age 55 years and ending when life expectancy is less than 10 years. These guidelines also allow for patient preference or clinical judgment to opt in for annual mammography from 40 to 44 years of age and to continue with annual screening beyond age 55.
References
1. Keating NL, Pace LE. New guidelines for breast cancer screening in U.S. women. JAMA. 2015;314(15)1658.
2. Kerlikowske K. Progress toward consensus on breast cancer screening guidelines and reducing screening harms. JAMA Intern Med. 2015 Oct 20. doi:10.1001/jamainternmed.2015.6466.
3. Oeffinger KC, Fontham ETH, Etzioni R, et al. Breast cancer screening for women at average risk. JAMA. 2015;314(15):1599-614. doi:10/1001/jama.2015.12783.
Dr. Skolnik is associate director of the family medicine residency program at Abington (Pa.) Memorial Hospital. Dr. Lyons is a third-year resident in the program.

Aunt Tillie and electronic health records
I’m lost, but I’m making record time.
– A pilot, somewhere over the Pacific Ocean
The other day I was reading the printout of an electronic medical record of a patient transferred to our practice. The record reminded me a lot of my Aunt Tillie. Aunt Tillie was the aunt whom everyone would avoid at family gatherings when I was young because the minute she started talking you could be sure of two things: first, that it would be a long time till she stopped talking, and second, that most of what she had to say simply was not relevant to what anyone was interested in hearing. She was interested in what she was interested in and seemed to care little about the needs of anyone else in the room.
The patient in question was 32 years old and had gone to an emergency room for headache and chest pain. Headache and chest pain can be challenging problems, but there are still certain things in both the history and on physical exam that are relevant and informative. It was hard to find those things in this medical record. After a relatively short history of present illness (HPI) that said my patient had presented with 1 day of headache and chest pain. The HPI on this record took up less than three lines. The assessment scales went on for over two pages. When we see records like this, driven by a system that desires to document every question or scale that every possible insurer might be looking for on every possible patient, we fear that common sense has died.

Among the extraneous information in the EHR was a Morse Fall Scale score. The Morse scale and point system were carefully laid out with the actions to be taken at various levels of risk, from bed in the lowest position to when to use skid-proof slipper socks. Then the Braden Scale for Predicting Pressure Sore Risk was recorded, followed by the Domestic Violence Score, complete with indication of whether the patient was under immediate threat and whether police, social services, and mental health professionals were notified. There also was a pain assessment that was filled out with an area indicating that the patient and her family were instructed to tell someone if her level of pain changed. Seriously. The pain assessment scale was located right after the suicide risk assessment and the depression scale, presumably because if the depression assessment occurred any later in the visit the patient might have scored higher out of desperation.
The death of common sense is neither pretty nor fast. As we fill out scales that answer neither evidence-based preventive health interventions nor meet the current needs of the patient, we have become concerned that we, as physicians, have chosen a path that seems to be the clearest – including all possible questions on all possible patients – but is actually fraught with peril.
We have become so concerned about not missing any potential source of reimbursement and protecting ourselves from any source of liability that our visits take longer and our focus has become distracted from the real problems that patients bring to us. By so doing we end up not accomplishing our goal of maximizing reimbursement because we move slower through our visits, filling out information that is not meaningful to either patient or physician. We also do not protect ourselves from liability when we are distracted by the need to fill out irrelevant information and are subsequently left with less time to get through the important parts of our visit, leaving us to take a less detailed history than we might otherwise have performed.
In 1995, Phillip K. Howard wrote a book about the legal system, The Death of Common Sense (Random House). In it, he argues that the desire to have clear rules that allow uniformity in the operation of law has resulted in a system that is inefficient and “precludes the exercise of judgment.” Mr. Howard argues that, no matter how detailed, laws cannot anticipate all of society’s needs. He goes on to state that “law can’t think, and so law must be entrusted to humans and they must take responsibility for their interpretation of it.”
We find a similar case to what Mr. Howard described to be occurring in medicine today. Patients present as individuals, with complex problems that require well-trained clinicians who can prioritize among the many concerns and determine which algorithms of diagnosis and treatment are appropriate to a given visit on a given day. When each visit follows a rote format, no visit follows the format that best serves the patient.
The argument that each visit is unique is not an argument for chaos in the organization of our visits and record – the visits need to be organized and recorded in a standard fashion. It is, rather, recognition that patients typically present with atypical symptoms and that all patients and visits are different from one another. To provide excellent medical care requires that well-trained clinicians make choices about what should be addressed at any given visit and that our charts and electronic record systems must be driven by patient needs and outcomes, not checkboxes derived from potential needs that are divorced from common sense for the visit at hand.
As we reflect further on this issue, we have come to the conclusion that the difference between our EHR systems and Aunt Tillie is that, when Thanksgiving came, we could avoid Aunt Tillie.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
I’m lost, but I’m making record time.
– A pilot, somewhere over the Pacific Ocean
The other day I was reading the printout of an electronic medical record of a patient transferred to our practice. The record reminded me a lot of my Aunt Tillie. Aunt Tillie was the aunt whom everyone would avoid at family gatherings when I was young because the minute she started talking you could be sure of two things: first, that it would be a long time till she stopped talking, and second, that most of what she had to say simply was not relevant to what anyone was interested in hearing. She was interested in what she was interested in and seemed to care little about the needs of anyone else in the room.
The patient in question was 32 years old and had gone to an emergency room for headache and chest pain. Headache and chest pain can be challenging problems, but there are still certain things in both the history and on physical exam that are relevant and informative. It was hard to find those things in this medical record. After a relatively short history of present illness (HPI) that said my patient had presented with 1 day of headache and chest pain. The HPI on this record took up less than three lines. The assessment scales went on for over two pages. When we see records like this, driven by a system that desires to document every question or scale that every possible insurer might be looking for on every possible patient, we fear that common sense has died.
Among the extraneous information in the EHR was a Morse Fall Scale score. The Morse scale and point system were carefully laid out with the actions to be taken at various levels of risk, from bed in the lowest position to when to use skid-proof slipper socks. Then the Braden Scale for Predicting Pressure Sore Risk was recorded, followed by the Domestic Violence Score, complete with indication of whether the patient was under immediate threat and whether police, social services, and mental health professionals were notified. There also was a pain assessment that was filled out with an area indicating that the patient and her family were instructed to tell someone if her level of pain changed. Seriously. The pain assessment scale was located right after the suicide risk assessment and the depression scale, presumably because if the depression assessment occurred any later in the visit the patient might have scored higher out of desperation.
The death of common sense is neither pretty nor fast. As we fill out scales that answer neither evidence-based preventive health interventions nor meet the current needs of the patient, we have become concerned that we, as physicians, have chosen a path that seems to be the clearest – including all possible questions on all possible patients – but is actually fraught with peril.
We have become so concerned about not missing any potential source of reimbursement and protecting ourselves from any source of liability that our visits take longer and our focus has become distracted from the real problems that patients bring to us. By so doing we end up not accomplishing our goal of maximizing reimbursement because we move slower through our visits, filling out information that is not meaningful to either patient or physician. We also do not protect ourselves from liability when we are distracted by the need to fill out irrelevant information and are subsequently left with less time to get through the important parts of our visit, leaving us to take a less detailed history than we might otherwise have performed.
In 1995, Phillip K. Howard wrote a book about the legal system, The Death of Common Sense (Random House). In it, he argues that the desire to have clear rules that allow uniformity in the operation of law has resulted in a system that is inefficient and “precludes the exercise of judgment.” Mr. Howard argues that, no matter how detailed, laws cannot anticipate all of society’s needs. He goes on to state that “law can’t think, and so law must be entrusted to humans and they must take responsibility for their interpretation of it.”
We find a similar case to what Mr. Howard described to be occurring in medicine today. Patients present as individuals, with complex problems that require well-trained clinicians who can prioritize among the many concerns and determine which algorithms of diagnosis and treatment are appropriate to a given visit on a given day. When each visit follows a rote format, no visit follows the format that best serves the patient.
The argument that each visit is unique is not an argument for chaos in the organization of our visits and record – the visits need to be organized and recorded in a standard fashion. It is, rather, recognition that patients typically present with atypical symptoms and that all patients and visits are different from one another. To provide excellent medical care requires that well-trained clinicians make choices about what should be addressed at any given visit and that our charts and electronic record systems must be driven by patient needs and outcomes, not checkboxes derived from potential needs that are divorced from common sense for the visit at hand.
As we reflect further on this issue, we have come to the conclusion that the difference between our EHR systems and Aunt Tillie is that, when Thanksgiving came, we could avoid Aunt Tillie.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.
I’m lost, but I’m making record time.
– A pilot, somewhere over the Pacific Ocean
The other day I was reading the printout of an electronic medical record of a patient transferred to our practice. The record reminded me a lot of my Aunt Tillie. Aunt Tillie was the aunt whom everyone would avoid at family gatherings when I was young because the minute she started talking you could be sure of two things: first, that it would be a long time till she stopped talking, and second, that most of what she had to say simply was not relevant to what anyone was interested in hearing. She was interested in what she was interested in and seemed to care little about the needs of anyone else in the room.
The patient in question was 32 years old and had gone to an emergency room for headache and chest pain. Headache and chest pain can be challenging problems, but there are still certain things in both the history and on physical exam that are relevant and informative. It was hard to find those things in this medical record. After a relatively short history of present illness (HPI) that said my patient had presented with 1 day of headache and chest pain. The HPI on this record took up less than three lines. The assessment scales went on for over two pages. When we see records like this, driven by a system that desires to document every question or scale that every possible insurer might be looking for on every possible patient, we fear that common sense has died.
Among the extraneous information in the EHR was a Morse Fall Scale score. The Morse scale and point system were carefully laid out with the actions to be taken at various levels of risk, from bed in the lowest position to when to use skid-proof slipper socks. Then the Braden Scale for Predicting Pressure Sore Risk was recorded, followed by the Domestic Violence Score, complete with indication of whether the patient was under immediate threat and whether police, social services, and mental health professionals were notified. There also was a pain assessment that was filled out with an area indicating that the patient and her family were instructed to tell someone if her level of pain changed. Seriously. The pain assessment scale was located right after the suicide risk assessment and the depression scale, presumably because if the depression assessment occurred any later in the visit the patient might have scored higher out of desperation.
The death of common sense is neither pretty nor fast. As we fill out scales that answer neither evidence-based preventive health interventions nor meet the current needs of the patient, we have become concerned that we, as physicians, have chosen a path that seems to be the clearest – including all possible questions on all possible patients – but is actually fraught with peril.
We have become so concerned about not missing any potential source of reimbursement and protecting ourselves from any source of liability that our visits take longer and our focus has become distracted from the real problems that patients bring to us. By so doing we end up not accomplishing our goal of maximizing reimbursement because we move slower through our visits, filling out information that is not meaningful to either patient or physician. We also do not protect ourselves from liability when we are distracted by the need to fill out irrelevant information and are subsequently left with less time to get through the important parts of our visit, leaving us to take a less detailed history than we might otherwise have performed.
In 1995, Phillip K. Howard wrote a book about the legal system, The Death of Common Sense (Random House). In it, he argues that the desire to have clear rules that allow uniformity in the operation of law has resulted in a system that is inefficient and “precludes the exercise of judgment.” Mr. Howard argues that, no matter how detailed, laws cannot anticipate all of society’s needs. He goes on to state that “law can’t think, and so law must be entrusted to humans and they must take responsibility for their interpretation of it.”
We find a similar case to what Mr. Howard described to be occurring in medicine today. Patients present as individuals, with complex problems that require well-trained clinicians who can prioritize among the many concerns and determine which algorithms of diagnosis and treatment are appropriate to a given visit on a given day. When each visit follows a rote format, no visit follows the format that best serves the patient.
The argument that each visit is unique is not an argument for chaos in the organization of our visits and record – the visits need to be organized and recorded in a standard fashion. It is, rather, recognition that patients typically present with atypical symptoms and that all patients and visits are different from one another. To provide excellent medical care requires that well-trained clinicians make choices about what should be addressed at any given visit and that our charts and electronic record systems must be driven by patient needs and outcomes, not checkboxes derived from potential needs that are divorced from common sense for the visit at hand.
As we reflect further on this issue, we have come to the conclusion that the difference between our EHR systems and Aunt Tillie is that, when Thanksgiving came, we could avoid Aunt Tillie.
Dr. Notte is a family physician and clinical informaticist for Abington (Pa.) Memorial Hospital. He is a partner in EHR Practice Consultants, a firm that aids physicians in adopting electronic health records. Dr. Skolnik is associate director of the family medicine residency program at Abington Memorial Hospital and professor of family and community medicine at Temple University in Philadelphia.

Latest Clinical Guidelines
IN THIS ARTICLE
• ACP: Telemedicine in Primary Care Settings
• AAP: Binge Drinking Among Adolescents
• Management of Primary Immunodeficiency
• Atopic Dermatitis in Children
• Obesity Treatment in Primary Care
• Management of Chronic Kidney Disease
ACP: TELEMEDICINE IN PRIMARY CARE SETTINGS
Daniel H, Sulmasy, LS. Policy recommendations to guide the use of telemedicine in primary care settings: an American College of Physicians position paper. Ann Intern Med. [Epub ahead of print September 8, 2015]. doi:10.7326/M15-0498.
The American College of Physicians (ACP) has issued policy recommendations to guide the use of telemedicine in primary care settings, along with clinician considerations for those who use telemedicine and policy recommendations on the practice and reimbursement of telemedicine. ACP’s position is that telemedicine can potentially be a beneficial and important part of the future of health care delivery; however, it also stresses the importance of balancing the benefits of telemedicine against the potential risks for patients. Among the ACP position statements and recommendations are:
• ACP believes that a valid patient-provider relationship must be established for a professionally responsible telemedicine service to take place.
• ACP recommends the telehealth activities address the needs of all patients without disenfranchising financially disadvantaged populations or those with low literacy or low technologic literacy.
ACP believes that clinicians should use their professional judgment about whether the use of telemedicine is appropriate for a patient.
COMMENTARY
The issue of professional judgment about when it is sufficient to see a patient using a digital interface will ultimately determine the safety and effectiveness of telemedicine. It is a mode of health care delivery that was nonexistent just a few years ago and now has an estimated annual growth rate of 20% per year, with an expected 7 million visits per year by 2018. The potential advantages include health savings, convenience, and the potential to deliver specialized services to people who might otherwise not have access to them. In addition, the use of telemedicine as a part of case-management and patient follow-up has shown promise. In this era of ever-changing technologies, we need to embrace new modes of care with skeptical open arms and be honest about the potential benefits as well as the risks.
Continue for AAP: Binge drinking among adolescents >>
AAP: BINGE DRINKING AMONG ADOLESCENTS
Siqueira L, Smith VC; Committee on Substance Abuse. Binge drinking (clinical report). Pediatrics. 2015;136(3):e718-e726. doi: 10.1542/peds.2015-2337.
A clinical report released by the American Academy of Pediatrics (AAP) details alcohol abuse by children and adolescents in the United States and offers guidance and recommendations to combat this high-risk behavior. The report states that among youth who drink, the proportion that drinks heavily is higher than among adult drinkers.
Among those who drink, binge drinking increases from approximately 50% in those ages 12 to 14 to 72% among those ages 18 to 20. Alcohol use is also associated with the leading causes of death and serious injury in this age-group, including motor vehicle accidents, homicides, and suicides. Recommendations offered in the report include
• In the office setting, provide programs designed to deliver messages about binge-drinking prevention to parents.
• Ask adolescents about alcohol use during office visits.
• Encourage schools to adopt preventive measures, including school-based health education programs.
COMMENTARY
Binge drinking in adults is defined as consumption of five or more alcoholic drinks in a two-hour period for men and four or more drinks for women. The number of drinks that qualifies as binge drinking in teenagers is slightly less and varies by age.
Using a 30-day time period, 14% of adolescents (1 out of 7) reported binge drinking. When teenagers drink alcohol, they tend to binge drink. Of students who consume alcohol, two-thirds report binge drinking, and 10% report having drunk 10 or more drinks in a row.
It is important to address this problem with parents and youth beginning at about age 9, as the change in attitudes toward drinking appears to begin between ages 9 and 12. It is also important to remind parents, supported by good evidence, that the message they send to their children about alcohol is the most important influence on teenage and young adult decisions about drinking.1
1. Turrisi R, Mallett KA, Cleveland MJ, et al. Evaluation of timing and dosage of a parent-based intervention to minimize college students’ alcohol consumption. J Stud Alcohol Drugs. 2013;74(1):30-40.
Continue for management of primary immunodeficiency >>
MANAGEMENT OF PRIMARY IMMUNODEFICIENCY
Bonilla FA, Khan DA, Ballas ZK, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. [Epub ahead of print September 11, 2015]. doi: 10.1016/j.jaci.2015.04.049.
This practice parameter is intended to provide practical guidance on the clinical recognition and diagnosis of primary immunodeficiency (PIDD), along with general principles on management of these disorders. Highlights include
• PIDD has a prevalence of 1:2,000 children.
• PIDD is subdivided into humoral or antibody deficiencies and combined immunodeficiency.
• Initial evaluation is guided by the clinical presentation, and screening tests are applied and followed by advanced tests, ensuring efficient and thorough evaluation of mechanisms of immune dysfunction that underlie the clinical presentation.
• Diagnosis and therapy should be guided overall or performed in consultation with persons and centers with knowledge and experience diagnosing and treating a broad range of immunodeficiencies.
COMMENTARY
Clinicians should be aware of PIDD in order to refer appropriate patients on to an allergist/immunologist for further evaluation. While many different types of PIDD exist, they generally present with recurrent or severe infections or infections by unusual organisms. For example, approximately a quarter of patients older than 2 with invasive pneumococcal disease have an identifiable PIDD. This is a group of disorders that, while rare, is helpful to be aware of and to refer on for further evaluation when indicated.
Continue for atopic dermatitis in children >>
ATOPIC DERMATITIS IN CHILDREN
Eichenfield LF, Boguniewicz M, Simpson EL, et al. Translating atopic dermatitis management guidelines into practice for primary care providers. Pediatrics. [Epub ahead of print August 3, 2015]. doi: 10.1542/peds.2014-3678.
Treatment guidelines for atopic dermatitis (AD) in children, designed specifically for use by pediatricians and other primary care providers, include basic management such as skin care, antiseptic measures, and trigger avoidance, to be used regardless of AD severity, according to a roundtable discussion to address challenges in AD management. Recommendations for the primary care provider include
• The diagnosis of eczema is a clinical one, based on a chronic or relapsing course of a pruritic dermatitis consisting of erythematous papules or patches of scaling and/or excoriated skin.
• Basic management is important and should include skin hydration with an appropriate moisturizer, use of diluted bleach baths, trigger avoidance, and acute treatment for flares.
• Treatment of acute flares is managed with topical corticosteroids, using a more potent topical steroid initially and then deescalating therapy to a less potent agent after a few days to weeks.
For patients with moderate-to-severe eczema, maintenance therapy for flare-prone areas should be applied regularly or at first sign of a flare-up. Recommended agents include tacrolimus or pimecrolimus (topical calcineurin inhibitors) or medium- or low-potency topical corticosteroids (avoiding medium-potency topical steroids on the face), depending on the severity of eczema.
COMMENTARY
Eczema affects about 12% of US children (ages 0 to 17 years), most of whom have mild disease and are well taken care of by primary care providers. This article provides clear guidance for treatment of a disease that we see quite frequently. Use of diluted bleach baths or washes is an underappreciated approach, and I suspect the clear recommendation for it, based on very good evidence, will lead to a helpful addition to many clinicians’ standard approach.
Continue for obesity treatment in primary care >>
OBESITY TREATMENT IN PRIMARY CARE
Fitzpatrick SL, Wischenka D, Appelhans BM, et al. An evidence-based guide for obesity treatment in primary care. Am J Med. [Epub ahead of print July 31, 2015]. doi: 10.1016/j.amjmed.2015.07.015.
A new evidence-based guideline from the Society of Behavioral Medicine for obesity management and treatment in primary care is based on the “5As” counseling framework (assess, advise, agree, assist, and arrange). The guide recommends building a multidisciplinary team that helps patients lose weight and maintain their weight loss by
• Addressing patients’ psychosocial issues and medical and psychiatric comorbidities associated with obesity treatment failure
• Delivering intensive counseling consisting of goal setting, self-monitoring, and problem solving
• Connecting patients with community resources to assist them in making healthy lifestyle changes.
COMMENTARY
Combating obesity is the critical health issue of the next decade. Currently, two-thirds of the adult population is either overweight or obese, and if the current trend continues, diabetes, one of the most important consequences of obesity, will develop in one out of three Americans born today. Clinicians are generally good at accomplishing the first and second of the three “As”: assessing and advising.1 The challenge for most of us in busy office practices is in assisting patients with the development of specific, concrete goals using specific, concrete behaviors, and then, when appropriate, arranging for referral to nutritionists, personal trainers, and multicomponent programs to help patients accomplish the agreed-upon goals.
1. Spring B, Ockene JK, Gidding SS, et al. Better population health through behavior change in adults. Circulation. 2013;128:2169-2176.
Continue for management of CKD >>
MANAGEMENT OF CKD
Vassalotti JA, Centor R, Turner BJ, et al; US Kidney Disease Outcomes Quality Initiative. A practical approach to detection and management of chronic kidney disease for the primary care clinician. Am J Med. [Epub ahead of print September 25, 2015]. doi: 10.1016/j.amjmed.2015.08.025.
This guideline was developed for the primary care provider to guide assessment and care of chronic kidney disease (CKD). Recommendations include
• Assessment of estimated glomerular filtration rate (GFR) and albuminuria should be performed for persons with diabetes and/or hypertension but is not recommended for the general population.
• Prevention of CKD progression requires blood pressure < 140/90 mm Hg, use of ACE inhibitors or angiotensin receptor blockers (ARB) for patients with albuminuria and hypertension, A1C < 7% for patients with diabetes, and correction of CKD-associated metabolic acidosis.
• Nephrotoxic drugs (eg, NSAIDs) should be avoided, and providers should be aware to use reduced doses of medications that are renally excreted, such as insulin, many antibiotics, and some statins.
The ultimate goal of CKD management is to prevent disease progression, minimize complications, and promote quality of life.
COMMENTARY
More than 10% of the US population has CKD, defined as a GFR < 60 mL/min/1.73 m2 and/or albumin-creatinine ratio > 30 mg/g. Both GFR and albuminuria independently predict progression of CKD. Control of blood pressure and A1C and use of an ACE inhibitor or an ARB are well-appreciated methods of slowing CKD progression. What is not as well appreciated is that treatment with ACE inhibitors or ARBs remains renal protective even with GFR < 30. Also important is the use of oral alkali therapy to maintain normal serum bicarbonate levels, which may slow CKD progression. When bicarbonate levels decrease to < 22 mmol/L, sodium bicarbonate (650 mg tid) should be added to raise the bicarbonate level above 22 mmol/L. For patients with severe CKD, referral to a nephrologist is appropriate.
IN THIS ARTICLE
• ACP: Telemedicine in Primary Care Settings
• AAP: Binge Drinking Among Adolescents
• Management of Primary Immunodeficiency
• Atopic Dermatitis in Children
• Obesity Treatment in Primary Care
• Management of Chronic Kidney Disease
ACP: TELEMEDICINE IN PRIMARY CARE SETTINGS
Daniel H, Sulmasy, LS. Policy recommendations to guide the use of telemedicine in primary care settings: an American College of Physicians position paper. Ann Intern Med. [Epub ahead of print September 8, 2015]. doi:10.7326/M15-0498.
The American College of Physicians (ACP) has issued policy recommendations to guide the use of telemedicine in primary care settings, along with clinician considerations for those who use telemedicine and policy recommendations on the practice and reimbursement of telemedicine. ACP’s position is that telemedicine can potentially be a beneficial and important part of the future of health care delivery; however, it also stresses the importance of balancing the benefits of telemedicine against the potential risks for patients. Among the ACP position statements and recommendations are:
• ACP believes that a valid patient-provider relationship must be established for a professionally responsible telemedicine service to take place.
• ACP recommends the telehealth activities address the needs of all patients without disenfranchising financially disadvantaged populations or those with low literacy or low technologic literacy.
ACP believes that clinicians should use their professional judgment about whether the use of telemedicine is appropriate for a patient.
COMMENTARY
The issue of professional judgment about when it is sufficient to see a patient using a digital interface will ultimately determine the safety and effectiveness of telemedicine. It is a mode of health care delivery that was nonexistent just a few years ago and now has an estimated annual growth rate of 20% per year, with an expected 7 million visits per year by 2018. The potential advantages include health savings, convenience, and the potential to deliver specialized services to people who might otherwise not have access to them. In addition, the use of telemedicine as a part of case-management and patient follow-up has shown promise. In this era of ever-changing technologies, we need to embrace new modes of care with skeptical open arms and be honest about the potential benefits as well as the risks.
Continue for AAP: Binge drinking among adolescents >>
AAP: BINGE DRINKING AMONG ADOLESCENTS
Siqueira L, Smith VC; Committee on Substance Abuse. Binge drinking (clinical report). Pediatrics. 2015;136(3):e718-e726. doi: 10.1542/peds.2015-2337.
A clinical report released by the American Academy of Pediatrics (AAP) details alcohol abuse by children and adolescents in the United States and offers guidance and recommendations to combat this high-risk behavior. The report states that among youth who drink, the proportion that drinks heavily is higher than among adult drinkers.
Among those who drink, binge drinking increases from approximately 50% in those ages 12 to 14 to 72% among those ages 18 to 20. Alcohol use is also associated with the leading causes of death and serious injury in this age-group, including motor vehicle accidents, homicides, and suicides. Recommendations offered in the report include
• In the office setting, provide programs designed to deliver messages about binge-drinking prevention to parents.
• Ask adolescents about alcohol use during office visits.
• Encourage schools to adopt preventive measures, including school-based health education programs.
COMMENTARY
Binge drinking in adults is defined as consumption of five or more alcoholic drinks in a two-hour period for men and four or more drinks for women. The number of drinks that qualifies as binge drinking in teenagers is slightly less and varies by age.
Using a 30-day time period, 14% of adolescents (1 out of 7) reported binge drinking. When teenagers drink alcohol, they tend to binge drink. Of students who consume alcohol, two-thirds report binge drinking, and 10% report having drunk 10 or more drinks in a row.
It is important to address this problem with parents and youth beginning at about age 9, as the change in attitudes toward drinking appears to begin between ages 9 and 12. It is also important to remind parents, supported by good evidence, that the message they send to their children about alcohol is the most important influence on teenage and young adult decisions about drinking.1
1. Turrisi R, Mallett KA, Cleveland MJ, et al. Evaluation of timing and dosage of a parent-based intervention to minimize college students’ alcohol consumption. J Stud Alcohol Drugs. 2013;74(1):30-40.
Continue for management of primary immunodeficiency >>
MANAGEMENT OF PRIMARY IMMUNODEFICIENCY
Bonilla FA, Khan DA, Ballas ZK, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. [Epub ahead of print September 11, 2015]. doi: 10.1016/j.jaci.2015.04.049.
This practice parameter is intended to provide practical guidance on the clinical recognition and diagnosis of primary immunodeficiency (PIDD), along with general principles on management of these disorders. Highlights include
• PIDD has a prevalence of 1:2,000 children.
• PIDD is subdivided into humoral or antibody deficiencies and combined immunodeficiency.
• Initial evaluation is guided by the clinical presentation, and screening tests are applied and followed by advanced tests, ensuring efficient and thorough evaluation of mechanisms of immune dysfunction that underlie the clinical presentation.
• Diagnosis and therapy should be guided overall or performed in consultation with persons and centers with knowledge and experience diagnosing and treating a broad range of immunodeficiencies.
COMMENTARY
Clinicians should be aware of PIDD in order to refer appropriate patients on to an allergist/immunologist for further evaluation. While many different types of PIDD exist, they generally present with recurrent or severe infections or infections by unusual organisms. For example, approximately a quarter of patients older than 2 with invasive pneumococcal disease have an identifiable PIDD. This is a group of disorders that, while rare, is helpful to be aware of and to refer on for further evaluation when indicated.
Continue for atopic dermatitis in children >>
ATOPIC DERMATITIS IN CHILDREN
Eichenfield LF, Boguniewicz M, Simpson EL, et al. Translating atopic dermatitis management guidelines into practice for primary care providers. Pediatrics. [Epub ahead of print August 3, 2015]. doi: 10.1542/peds.2014-3678.
Treatment guidelines for atopic dermatitis (AD) in children, designed specifically for use by pediatricians and other primary care providers, include basic management such as skin care, antiseptic measures, and trigger avoidance, to be used regardless of AD severity, according to a roundtable discussion to address challenges in AD management. Recommendations for the primary care provider include
• The diagnosis of eczema is a clinical one, based on a chronic or relapsing course of a pruritic dermatitis consisting of erythematous papules or patches of scaling and/or excoriated skin.
• Basic management is important and should include skin hydration with an appropriate moisturizer, use of diluted bleach baths, trigger avoidance, and acute treatment for flares.
• Treatment of acute flares is managed with topical corticosteroids, using a more potent topical steroid initially and then deescalating therapy to a less potent agent after a few days to weeks.
For patients with moderate-to-severe eczema, maintenance therapy for flare-prone areas should be applied regularly or at first sign of a flare-up. Recommended agents include tacrolimus or pimecrolimus (topical calcineurin inhibitors) or medium- or low-potency topical corticosteroids (avoiding medium-potency topical steroids on the face), depending on the severity of eczema.
COMMENTARY
Eczema affects about 12% of US children (ages 0 to 17 years), most of whom have mild disease and are well taken care of by primary care providers. This article provides clear guidance for treatment of a disease that we see quite frequently. Use of diluted bleach baths or washes is an underappreciated approach, and I suspect the clear recommendation for it, based on very good evidence, will lead to a helpful addition to many clinicians’ standard approach.
Continue for obesity treatment in primary care >>
OBESITY TREATMENT IN PRIMARY CARE
Fitzpatrick SL, Wischenka D, Appelhans BM, et al. An evidence-based guide for obesity treatment in primary care. Am J Med. [Epub ahead of print July 31, 2015]. doi: 10.1016/j.amjmed.2015.07.015.
A new evidence-based guideline from the Society of Behavioral Medicine for obesity management and treatment in primary care is based on the “5As” counseling framework (assess, advise, agree, assist, and arrange). The guide recommends building a multidisciplinary team that helps patients lose weight and maintain their weight loss by
• Addressing patients’ psychosocial issues and medical and psychiatric comorbidities associated with obesity treatment failure
• Delivering intensive counseling consisting of goal setting, self-monitoring, and problem solving
• Connecting patients with community resources to assist them in making healthy lifestyle changes.
COMMENTARY
Combating obesity is the critical health issue of the next decade. Currently, two-thirds of the adult population is either overweight or obese, and if the current trend continues, diabetes, one of the most important consequences of obesity, will develop in one out of three Americans born today. Clinicians are generally good at accomplishing the first and second of the three “As”: assessing and advising.1 The challenge for most of us in busy office practices is in assisting patients with the development of specific, concrete goals using specific, concrete behaviors, and then, when appropriate, arranging for referral to nutritionists, personal trainers, and multicomponent programs to help patients accomplish the agreed-upon goals.
1. Spring B, Ockene JK, Gidding SS, et al. Better population health through behavior change in adults. Circulation. 2013;128:2169-2176.
Continue for management of CKD >>
MANAGEMENT OF CKD
Vassalotti JA, Centor R, Turner BJ, et al; US Kidney Disease Outcomes Quality Initiative. A practical approach to detection and management of chronic kidney disease for the primary care clinician. Am J Med. [Epub ahead of print September 25, 2015]. doi: 10.1016/j.amjmed.2015.08.025.
This guideline was developed for the primary care provider to guide assessment and care of chronic kidney disease (CKD). Recommendations include
• Assessment of estimated glomerular filtration rate (GFR) and albuminuria should be performed for persons with diabetes and/or hypertension but is not recommended for the general population.
• Prevention of CKD progression requires blood pressure < 140/90 mm Hg, use of ACE inhibitors or angiotensin receptor blockers (ARB) for patients with albuminuria and hypertension, A1C < 7% for patients with diabetes, and correction of CKD-associated metabolic acidosis.
• Nephrotoxic drugs (eg, NSAIDs) should be avoided, and providers should be aware to use reduced doses of medications that are renally excreted, such as insulin, many antibiotics, and some statins.
The ultimate goal of CKD management is to prevent disease progression, minimize complications, and promote quality of life.
COMMENTARY
More than 10% of the US population has CKD, defined as a GFR < 60 mL/min/1.73 m2 and/or albumin-creatinine ratio > 30 mg/g. Both GFR and albuminuria independently predict progression of CKD. Control of blood pressure and A1C and use of an ACE inhibitor or an ARB are well-appreciated methods of slowing CKD progression. What is not as well appreciated is that treatment with ACE inhibitors or ARBs remains renal protective even with GFR < 30. Also important is the use of oral alkali therapy to maintain normal serum bicarbonate levels, which may slow CKD progression. When bicarbonate levels decrease to < 22 mmol/L, sodium bicarbonate (650 mg tid) should be added to raise the bicarbonate level above 22 mmol/L. For patients with severe CKD, referral to a nephrologist is appropriate.
IN THIS ARTICLE
• ACP: Telemedicine in Primary Care Settings
• AAP: Binge Drinking Among Adolescents
• Management of Primary Immunodeficiency
• Atopic Dermatitis in Children
• Obesity Treatment in Primary Care
• Management of Chronic Kidney Disease
ACP: TELEMEDICINE IN PRIMARY CARE SETTINGS
Daniel H, Sulmasy, LS. Policy recommendations to guide the use of telemedicine in primary care settings: an American College of Physicians position paper. Ann Intern Med. [Epub ahead of print September 8, 2015]. doi:10.7326/M15-0498.
The American College of Physicians (ACP) has issued policy recommendations to guide the use of telemedicine in primary care settings, along with clinician considerations for those who use telemedicine and policy recommendations on the practice and reimbursement of telemedicine. ACP’s position is that telemedicine can potentially be a beneficial and important part of the future of health care delivery; however, it also stresses the importance of balancing the benefits of telemedicine against the potential risks for patients. Among the ACP position statements and recommendations are:
• ACP believes that a valid patient-provider relationship must be established for a professionally responsible telemedicine service to take place.
• ACP recommends the telehealth activities address the needs of all patients without disenfranchising financially disadvantaged populations or those with low literacy or low technologic literacy.
ACP believes that clinicians should use their professional judgment about whether the use of telemedicine is appropriate for a patient.
COMMENTARY
The issue of professional judgment about when it is sufficient to see a patient using a digital interface will ultimately determine the safety and effectiveness of telemedicine. It is a mode of health care delivery that was nonexistent just a few years ago and now has an estimated annual growth rate of 20% per year, with an expected 7 million visits per year by 2018. The potential advantages include health savings, convenience, and the potential to deliver specialized services to people who might otherwise not have access to them. In addition, the use of telemedicine as a part of case-management and patient follow-up has shown promise. In this era of ever-changing technologies, we need to embrace new modes of care with skeptical open arms and be honest about the potential benefits as well as the risks.
Continue for AAP: Binge drinking among adolescents >>
AAP: BINGE DRINKING AMONG ADOLESCENTS
Siqueira L, Smith VC; Committee on Substance Abuse. Binge drinking (clinical report). Pediatrics. 2015;136(3):e718-e726. doi: 10.1542/peds.2015-2337.
A clinical report released by the American Academy of Pediatrics (AAP) details alcohol abuse by children and adolescents in the United States and offers guidance and recommendations to combat this high-risk behavior. The report states that among youth who drink, the proportion that drinks heavily is higher than among adult drinkers.
Among those who drink, binge drinking increases from approximately 50% in those ages 12 to 14 to 72% among those ages 18 to 20. Alcohol use is also associated with the leading causes of death and serious injury in this age-group, including motor vehicle accidents, homicides, and suicides. Recommendations offered in the report include
• In the office setting, provide programs designed to deliver messages about binge-drinking prevention to parents.
• Ask adolescents about alcohol use during office visits.
• Encourage schools to adopt preventive measures, including school-based health education programs.
COMMENTARY
Binge drinking in adults is defined as consumption of five or more alcoholic drinks in a two-hour period for men and four or more drinks for women. The number of drinks that qualifies as binge drinking in teenagers is slightly less and varies by age.
Using a 30-day time period, 14% of adolescents (1 out of 7) reported binge drinking. When teenagers drink alcohol, they tend to binge drink. Of students who consume alcohol, two-thirds report binge drinking, and 10% report having drunk 10 or more drinks in a row.
It is important to address this problem with parents and youth beginning at about age 9, as the change in attitudes toward drinking appears to begin between ages 9 and 12. It is also important to remind parents, supported by good evidence, that the message they send to their children about alcohol is the most important influence on teenage and young adult decisions about drinking.1
1. Turrisi R, Mallett KA, Cleveland MJ, et al. Evaluation of timing and dosage of a parent-based intervention to minimize college students’ alcohol consumption. J Stud Alcohol Drugs. 2013;74(1):30-40.
Continue for management of primary immunodeficiency >>
MANAGEMENT OF PRIMARY IMMUNODEFICIENCY
Bonilla FA, Khan DA, Ballas ZK, et al. Practice parameter for the diagnosis and management of primary immunodeficiency. J Allergy Clin Immunol. [Epub ahead of print September 11, 2015]. doi: 10.1016/j.jaci.2015.04.049.
This practice parameter is intended to provide practical guidance on the clinical recognition and diagnosis of primary immunodeficiency (PIDD), along with general principles on management of these disorders. Highlights include
• PIDD has a prevalence of 1:2,000 children.
• PIDD is subdivided into humoral or antibody deficiencies and combined immunodeficiency.
• Initial evaluation is guided by the clinical presentation, and screening tests are applied and followed by advanced tests, ensuring efficient and thorough evaluation of mechanisms of immune dysfunction that underlie the clinical presentation.
• Diagnosis and therapy should be guided overall or performed in consultation with persons and centers with knowledge and experience diagnosing and treating a broad range of immunodeficiencies.
COMMENTARY
Clinicians should be aware of PIDD in order to refer appropriate patients on to an allergist/immunologist for further evaluation. While many different types of PIDD exist, they generally present with recurrent or severe infections or infections by unusual organisms. For example, approximately a quarter of patients older than 2 with invasive pneumococcal disease have an identifiable PIDD. This is a group of disorders that, while rare, is helpful to be aware of and to refer on for further evaluation when indicated.
Continue for atopic dermatitis in children >>
ATOPIC DERMATITIS IN CHILDREN
Eichenfield LF, Boguniewicz M, Simpson EL, et al. Translating atopic dermatitis management guidelines into practice for primary care providers. Pediatrics. [Epub ahead of print August 3, 2015]. doi: 10.1542/peds.2014-3678.
Treatment guidelines for atopic dermatitis (AD) in children, designed specifically for use by pediatricians and other primary care providers, include basic management such as skin care, antiseptic measures, and trigger avoidance, to be used regardless of AD severity, according to a roundtable discussion to address challenges in AD management. Recommendations for the primary care provider include
• The diagnosis of eczema is a clinical one, based on a chronic or relapsing course of a pruritic dermatitis consisting of erythematous papules or patches of scaling and/or excoriated skin.
• Basic management is important and should include skin hydration with an appropriate moisturizer, use of diluted bleach baths, trigger avoidance, and acute treatment for flares.
• Treatment of acute flares is managed with topical corticosteroids, using a more potent topical steroid initially and then deescalating therapy to a less potent agent after a few days to weeks.
For patients with moderate-to-severe eczema, maintenance therapy for flare-prone areas should be applied regularly or at first sign of a flare-up. Recommended agents include tacrolimus or pimecrolimus (topical calcineurin inhibitors) or medium- or low-potency topical corticosteroids (avoiding medium-potency topical steroids on the face), depending on the severity of eczema.
COMMENTARY
Eczema affects about 12% of US children (ages 0 to 17 years), most of whom have mild disease and are well taken care of by primary care providers. This article provides clear guidance for treatment of a disease that we see quite frequently. Use of diluted bleach baths or washes is an underappreciated approach, and I suspect the clear recommendation for it, based on very good evidence, will lead to a helpful addition to many clinicians’ standard approach.
Continue for obesity treatment in primary care >>
OBESITY TREATMENT IN PRIMARY CARE
Fitzpatrick SL, Wischenka D, Appelhans BM, et al. An evidence-based guide for obesity treatment in primary care. Am J Med. [Epub ahead of print July 31, 2015]. doi: 10.1016/j.amjmed.2015.07.015.
A new evidence-based guideline from the Society of Behavioral Medicine for obesity management and treatment in primary care is based on the “5As” counseling framework (assess, advise, agree, assist, and arrange). The guide recommends building a multidisciplinary team that helps patients lose weight and maintain their weight loss by
• Addressing patients’ psychosocial issues and medical and psychiatric comorbidities associated with obesity treatment failure
• Delivering intensive counseling consisting of goal setting, self-monitoring, and problem solving
• Connecting patients with community resources to assist them in making healthy lifestyle changes.
COMMENTARY
Combating obesity is the critical health issue of the next decade. Currently, two-thirds of the adult population is either overweight or obese, and if the current trend continues, diabetes, one of the most important consequences of obesity, will develop in one out of three Americans born today. Clinicians are generally good at accomplishing the first and second of the three “As”: assessing and advising.1 The challenge for most of us in busy office practices is in assisting patients with the development of specific, concrete goals using specific, concrete behaviors, and then, when appropriate, arranging for referral to nutritionists, personal trainers, and multicomponent programs to help patients accomplish the agreed-upon goals.
1. Spring B, Ockene JK, Gidding SS, et al. Better population health through behavior change in adults. Circulation. 2013;128:2169-2176.
Continue for management of CKD >>
MANAGEMENT OF CKD
Vassalotti JA, Centor R, Turner BJ, et al; US Kidney Disease Outcomes Quality Initiative. A practical approach to detection and management of chronic kidney disease for the primary care clinician. Am J Med. [Epub ahead of print September 25, 2015]. doi: 10.1016/j.amjmed.2015.08.025.
This guideline was developed for the primary care provider to guide assessment and care of chronic kidney disease (CKD). Recommendations include
• Assessment of estimated glomerular filtration rate (GFR) and albuminuria should be performed for persons with diabetes and/or hypertension but is not recommended for the general population.
• Prevention of CKD progression requires blood pressure < 140/90 mm Hg, use of ACE inhibitors or angiotensin receptor blockers (ARB) for patients with albuminuria and hypertension, A1C < 7% for patients with diabetes, and correction of CKD-associated metabolic acidosis.
• Nephrotoxic drugs (eg, NSAIDs) should be avoided, and providers should be aware to use reduced doses of medications that are renally excreted, such as insulin, many antibiotics, and some statins.
The ultimate goal of CKD management is to prevent disease progression, minimize complications, and promote quality of life.
COMMENTARY
More than 10% of the US population has CKD, defined as a GFR < 60 mL/min/1.73 m2 and/or albumin-creatinine ratio > 30 mg/g. Both GFR and albuminuria independently predict progression of CKD. Control of blood pressure and A1C and use of an ACE inhibitor or an ARB are well-appreciated methods of slowing CKD progression. What is not as well appreciated is that treatment with ACE inhibitors or ARBs remains renal protective even with GFR < 30. Also important is the use of oral alkali therapy to maintain normal serum bicarbonate levels, which may slow CKD progression. When bicarbonate levels decrease to < 22 mmol/L, sodium bicarbonate (650 mg tid) should be added to raise the bicarbonate level above 22 mmol/L. For patients with severe CKD, referral to a nephrologist is appropriate.