User login
Erlotinib Dose Doubled for Smokers With Head/Neck Cancer
PHOENIX – Giving smokers a higher, short-course dose of erlotinib before definitive surgery for squamous cell carcinoma of the head and neck resulted in favorable responses for the first patients evaluated in a small pilot study.
Investigators gave 300 mg of erlotinib (Tarceva) to smokers daily and 150 mg daily to nonsmokers who had a waiting period of more than 14 days before scheduled surgery for head and neck cancer. Seven of the 10 patients evaluated so far had partial responses and 3 had stable disease, according to a poster presented at a head and neck cancer symposium sponsored by the American Society for Radiation Oncology.
The study was based on recent data in non–small cell lung cancer (NSCLC) patients showing that smokers metabolize erlotinib, an epidermal growth factor receptor (EGFR) inhibitor, twice as quickly as do nonsmokers (J. Clin. Oncol. 2009;27:1220-6), said lead author Dr. Mercedes Porosnicu of Wake Forest Baptist Medical Center in Winston Salem, N.C. That study established the maximum tolerated dose of erlotinib at 300 mg daily in NSCLC patients who smoke.
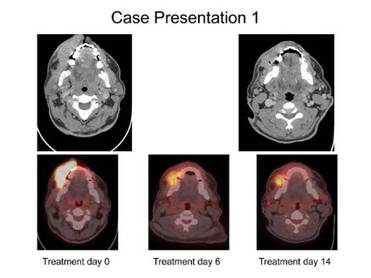
Dr. Poroniscu’s presentation included the case study of a smoker with a very large oral cavity tumor protruding through his lips. He was described as being in significant pain and unable to eat or chew. The first CT scan showed a tumor of at least 8 cm and there was "significant metabolic activity" on PET scan.
"At 6 days of erlotinib treatment, his tumor was obviously smaller and he could chew, eat, and talk. Metabolic activity on PET scan dropped to 44% compared to initial tumor metabolic activity," Dr. Porosnicu said. "At the end of 14 days’ treatment, his tumor was at least 20% smaller, and he had gained 5 pounds. His surgery wasn’t delayed, and the only treatment-related toxicity was a minimal skin rash."

A total of 12 patients have been treated to date, for an average of 18.2 days, she reported. Nine were smokers and three were nonsmokers. All patients, smokers and nonsmokers, tolerated the erlotinib dose well with no serious adverse events and no delays in the scheduled time of surgical intervention. There were no grade 3 or 4 toxicities.
Of 10 evaluable patients (including 8 smokers who received 300 mg), 7 (including 5 smokers) showed a partial response, as defined by at least a 20% reduction in maximum tumor diameter. The other three patients (all smokers) showed stable disease. Two of the 12 treated patients received shorter duration treatment but nonetheless displayed good responses.
Interestingly, all four treated female patients (including one smoker) had good responses, independent of the erlotinib dose received, Dr. Porosnicu said.
Early 18[F]-FDG PET scans taken 4-6 days after the start of neoadjuvant erlotinib showed a decrease in metabolic activity of 2% in maximum standardized uptake value (SUVmax) to 98.75% in patients with stable disease and a decrease to 48.06% in patients with partial response.
"Early changes in the PET scan uptake should be further investigated as a marker predictive of response to EGFR inhibition. This pilot trial will continue to enroll patients," Dr. Porosnicu said.
Erlotinib is approved for indications in non–small cell lung cancer and pancreatic cancer. Head and neck cancer would be an off-label use.
Dr. Porosnicu disclosed that she received financial support for this study from Astellas Pharma.
PHOENIX – Giving smokers a higher, short-course dose of erlotinib before definitive surgery for squamous cell carcinoma of the head and neck resulted in favorable responses for the first patients evaluated in a small pilot study.
Investigators gave 300 mg of erlotinib (Tarceva) to smokers daily and 150 mg daily to nonsmokers who had a waiting period of more than 14 days before scheduled surgery for head and neck cancer. Seven of the 10 patients evaluated so far had partial responses and 3 had stable disease, according to a poster presented at a head and neck cancer symposium sponsored by the American Society for Radiation Oncology.
The study was based on recent data in non–small cell lung cancer (NSCLC) patients showing that smokers metabolize erlotinib, an epidermal growth factor receptor (EGFR) inhibitor, twice as quickly as do nonsmokers (J. Clin. Oncol. 2009;27:1220-6), said lead author Dr. Mercedes Porosnicu of Wake Forest Baptist Medical Center in Winston Salem, N.C. That study established the maximum tolerated dose of erlotinib at 300 mg daily in NSCLC patients who smoke.
Dr. Poroniscu’s presentation included the case study of a smoker with a very large oral cavity tumor protruding through his lips. He was described as being in significant pain and unable to eat or chew. The first CT scan showed a tumor of at least 8 cm and there was "significant metabolic activity" on PET scan.
"At 6 days of erlotinib treatment, his tumor was obviously smaller and he could chew, eat, and talk. Metabolic activity on PET scan dropped to 44% compared to initial tumor metabolic activity," Dr. Porosnicu said. "At the end of 14 days’ treatment, his tumor was at least 20% smaller, and he had gained 5 pounds. His surgery wasn’t delayed, and the only treatment-related toxicity was a minimal skin rash."
A total of 12 patients have been treated to date, for an average of 18.2 days, she reported. Nine were smokers and three were nonsmokers. All patients, smokers and nonsmokers, tolerated the erlotinib dose well with no serious adverse events and no delays in the scheduled time of surgical intervention. There were no grade 3 or 4 toxicities.
Of 10 evaluable patients (including 8 smokers who received 300 mg), 7 (including 5 smokers) showed a partial response, as defined by at least a 20% reduction in maximum tumor diameter. The other three patients (all smokers) showed stable disease. Two of the 12 treated patients received shorter duration treatment but nonetheless displayed good responses.
Interestingly, all four treated female patients (including one smoker) had good responses, independent of the erlotinib dose received, Dr. Porosnicu said.
Early 18[F]-FDG PET scans taken 4-6 days after the start of neoadjuvant erlotinib showed a decrease in metabolic activity of 2% in maximum standardized uptake value (SUVmax) to 98.75% in patients with stable disease and a decrease to 48.06% in patients with partial response.
"Early changes in the PET scan uptake should be further investigated as a marker predictive of response to EGFR inhibition. This pilot trial will continue to enroll patients," Dr. Porosnicu said.
Erlotinib is approved for indications in non–small cell lung cancer and pancreatic cancer. Head and neck cancer would be an off-label use.
Dr. Porosnicu disclosed that she received financial support for this study from Astellas Pharma.
PHOENIX – Giving smokers a higher, short-course dose of erlotinib before definitive surgery for squamous cell carcinoma of the head and neck resulted in favorable responses for the first patients evaluated in a small pilot study.
Investigators gave 300 mg of erlotinib (Tarceva) to smokers daily and 150 mg daily to nonsmokers who had a waiting period of more than 14 days before scheduled surgery for head and neck cancer. Seven of the 10 patients evaluated so far had partial responses and 3 had stable disease, according to a poster presented at a head and neck cancer symposium sponsored by the American Society for Radiation Oncology.
The study was based on recent data in non–small cell lung cancer (NSCLC) patients showing that smokers metabolize erlotinib, an epidermal growth factor receptor (EGFR) inhibitor, twice as quickly as do nonsmokers (J. Clin. Oncol. 2009;27:1220-6), said lead author Dr. Mercedes Porosnicu of Wake Forest Baptist Medical Center in Winston Salem, N.C. That study established the maximum tolerated dose of erlotinib at 300 mg daily in NSCLC patients who smoke.
Dr. Poroniscu’s presentation included the case study of a smoker with a very large oral cavity tumor protruding through his lips. He was described as being in significant pain and unable to eat or chew. The first CT scan showed a tumor of at least 8 cm and there was "significant metabolic activity" on PET scan.
"At 6 days of erlotinib treatment, his tumor was obviously smaller and he could chew, eat, and talk. Metabolic activity on PET scan dropped to 44% compared to initial tumor metabolic activity," Dr. Porosnicu said. "At the end of 14 days’ treatment, his tumor was at least 20% smaller, and he had gained 5 pounds. His surgery wasn’t delayed, and the only treatment-related toxicity was a minimal skin rash."
A total of 12 patients have been treated to date, for an average of 18.2 days, she reported. Nine were smokers and three were nonsmokers. All patients, smokers and nonsmokers, tolerated the erlotinib dose well with no serious adverse events and no delays in the scheduled time of surgical intervention. There were no grade 3 or 4 toxicities.
Of 10 evaluable patients (including 8 smokers who received 300 mg), 7 (including 5 smokers) showed a partial response, as defined by at least a 20% reduction in maximum tumor diameter. The other three patients (all smokers) showed stable disease. Two of the 12 treated patients received shorter duration treatment but nonetheless displayed good responses.
Interestingly, all four treated female patients (including one smoker) had good responses, independent of the erlotinib dose received, Dr. Porosnicu said.
Early 18[F]-FDG PET scans taken 4-6 days after the start of neoadjuvant erlotinib showed a decrease in metabolic activity of 2% in maximum standardized uptake value (SUVmax) to 98.75% in patients with stable disease and a decrease to 48.06% in patients with partial response.
"Early changes in the PET scan uptake should be further investigated as a marker predictive of response to EGFR inhibition. This pilot trial will continue to enroll patients," Dr. Porosnicu said.
Erlotinib is approved for indications in non–small cell lung cancer and pancreatic cancer. Head and neck cancer would be an off-label use.
Dr. Porosnicu disclosed that she received financial support for this study from Astellas Pharma.
FROM A HEAD AND NECK CANCER SYMPOSIUM SPONSORED BY THE AMERICAN SOCIETY FOR RADIATION ONCOLOGY
Major Finding: Of 10 evaluable head and neck cancer patients, 7 (including 5 smokers) showed a partial response, as defined by at least a 20% reduction in maximum tumor diameter.
Data Source: In this small, ongoing pilot study smokers received 300 mg and nonsmokers 150 mg daily of neoadjuvant erlotinib.
Disclosures: Dr. Porosnicu disclosed that she received financial support for this study from Astellas Pharma.
Head/Neck Cancer Treatments Less Effective in HIV Patients
PHOENIX – Definitive radiation therapy with or without chemotherapy was less tolerated and less effective in HIV-positive patients with head and neck squamous cell carcinoma than in HIV-negative patients in a single-institution retrospective study of 71 HIV-positive patients.
"Head and neck squamous cell carcinoma with coexisting HIV remains a challenging clinical problem. ... Due to the advances in highly active antiretroviral therapy (HAART) – which prolongs HIV patients’ survival – the likelihood to develop HIV-related malignancy increases. It is of paramount importance to establish better-tolerated treatment strategies and regimens to improve tolerance, toxicity, and outcomes in this growing patient population," said Dr. Waleed Mourad, a radiation oncologist at Beth Israel Medical Center, New York.
The 71 HIV-positive patients with HNSCC were treated January 1997 through 2010. They had a median age of 34 years at the time of HIV diagnosis (range 25-50 years) with a median 11 years’ duration of seropositivity (6-20 years). Their median age at the time of radiation therapy was 51 years (32-72 years). All but one patient had squamous cell carcinoma, with the other having submandibular salivary duct carcinoma. That patient was treated with definitive surgery and received adjuvant radiation therapy without chemotherapy, Dr. Mourad noted.
Approximately one-third of the patients had cancer of the oropharynx (32%) and larynx (35%), and another 13% had cancer of the oral cavity. Other cancers among the patients included those located in the hypopharynx, nasopharynx, occult primary, and nasal cavity. American Joint Committee on Cancer 7th edition stages I-II, III and IVa/b were 22%, 27%, 51% respectively.
All patients were treated definitively with radiation therapy, with or without chemotherapy (cisplatin, carboplatin, or cetuximab). A total of 50 patients (70%) were on HAART during treatment, with a median CD4 count of 290 (range, 203-1,142). A median dose of 70 Gy (66-70) was delivered to the gross disease; high-risk neck 60-63 Gy; low-risk neck; and lateral retropharyngeal nodes 54 Gy. All fractions were given at the rate of 1.8-2 Gy/fraction. The median duration of treatment was 52 (49-64) days. A total of 12 patients (17%) underwent planned neck dissection for N3 disease.
In all, local control was achieved in 69% (49) and locoregional failure occurred in 31% (22). By site, local control rates were 70% (16) for the oropharynx, 76% (19) for the larynx, 78% (7) for the oral cavity, 0% (of 5) for hypopharynx, 67% (2) for the nasopharynx, 100% (3) for occult primary, 50% (1) for the nasal cavity, and 100% (1) for the submandibular duct.
Thus, locoregional failure rates ranged from 100% (all five patients with hypopharyngeal cancer) to 0 (for the three patients with occult primary cancer and the one with submandibular duct cancer). Seven patients developed second primary cancers, Dr. Mourad reported.
After a median follow up of 47 months (7-140), there were no fatalities related to radiation or chemotherapy. Treatment breaks in excess of 10, 7, and 5 days occurred in 6%, 13%, and 14% of patients, respectively. Acute dysphagia and odynophagia grades 1, 2, and 3 occurred in 31%, 52%, and 17%, respectively. All of the patients experienced dysgeusia, dysphagia, and xerostomia of grades 1-3. Acute desquamation of the skin of grades 1, 2, and 3 occurred in 66%, 20%, and 14%.
One patient was hospitalized for grade 4 mucositis, dysphagia, and fever. Another developed osteoradionecrosis during concurrent chemoradiotherapy. Late dysphagia of grades 1-4 occurred in 46%, 28%, 15%, and 11%. Xerostomia of grades 1-3 occurred in 45%, 32%, and 23%, respectively, he said.
At 4 years, locoregional control was 69% and overall survival 55%. In an interview, Dr. Mourad noted that at his institution, the comparable rates for non-HIV patients were 85%-90% and 75%-85%, respectively.
The median CD4 count prior to chemotherapy was 370, and viral load was undetectable. The CD4 count dropped as chemoradiotherapy progressed to a nadir at 11 weeks, at which point it began to rise again and viral load decreased.
There was a statistically significant relationship between locoregional control and the duration of radiation therapy (P less than .001), and positive trends with weight loss of greater than 10% and absence of second malignancy. However, multivariate analysis did not show any statistically significant relationship because of the relatively small sample size with diverse subsites, Dr. Mourad noted.
"We believe that our data provide important information regarding treatment outcomes for newly diagnosed head and neck cancer with HIV. This is particularly important given the growing population of patients who live with HIV long term because of effective antiretroviral maintenance treatments," Dr. Mourad said in an interview.
Dr. Mourad and his nine coauthors declared that they had no financial disclosures.
PHOENIX – Definitive radiation therapy with or without chemotherapy was less tolerated and less effective in HIV-positive patients with head and neck squamous cell carcinoma than in HIV-negative patients in a single-institution retrospective study of 71 HIV-positive patients.
"Head and neck squamous cell carcinoma with coexisting HIV remains a challenging clinical problem. ... Due to the advances in highly active antiretroviral therapy (HAART) – which prolongs HIV patients’ survival – the likelihood to develop HIV-related malignancy increases. It is of paramount importance to establish better-tolerated treatment strategies and regimens to improve tolerance, toxicity, and outcomes in this growing patient population," said Dr. Waleed Mourad, a radiation oncologist at Beth Israel Medical Center, New York.
The 71 HIV-positive patients with HNSCC were treated January 1997 through 2010. They had a median age of 34 years at the time of HIV diagnosis (range 25-50 years) with a median 11 years’ duration of seropositivity (6-20 years). Their median age at the time of radiation therapy was 51 years (32-72 years). All but one patient had squamous cell carcinoma, with the other having submandibular salivary duct carcinoma. That patient was treated with definitive surgery and received adjuvant radiation therapy without chemotherapy, Dr. Mourad noted.
Approximately one-third of the patients had cancer of the oropharynx (32%) and larynx (35%), and another 13% had cancer of the oral cavity. Other cancers among the patients included those located in the hypopharynx, nasopharynx, occult primary, and nasal cavity. American Joint Committee on Cancer 7th edition stages I-II, III and IVa/b were 22%, 27%, 51% respectively.
All patients were treated definitively with radiation therapy, with or without chemotherapy (cisplatin, carboplatin, or cetuximab). A total of 50 patients (70%) were on HAART during treatment, with a median CD4 count of 290 (range, 203-1,142). A median dose of 70 Gy (66-70) was delivered to the gross disease; high-risk neck 60-63 Gy; low-risk neck; and lateral retropharyngeal nodes 54 Gy. All fractions were given at the rate of 1.8-2 Gy/fraction. The median duration of treatment was 52 (49-64) days. A total of 12 patients (17%) underwent planned neck dissection for N3 disease.
In all, local control was achieved in 69% (49) and locoregional failure occurred in 31% (22). By site, local control rates were 70% (16) for the oropharynx, 76% (19) for the larynx, 78% (7) for the oral cavity, 0% (of 5) for hypopharynx, 67% (2) for the nasopharynx, 100% (3) for occult primary, 50% (1) for the nasal cavity, and 100% (1) for the submandibular duct.
Thus, locoregional failure rates ranged from 100% (all five patients with hypopharyngeal cancer) to 0 (for the three patients with occult primary cancer and the one with submandibular duct cancer). Seven patients developed second primary cancers, Dr. Mourad reported.
After a median follow up of 47 months (7-140), there were no fatalities related to radiation or chemotherapy. Treatment breaks in excess of 10, 7, and 5 days occurred in 6%, 13%, and 14% of patients, respectively. Acute dysphagia and odynophagia grades 1, 2, and 3 occurred in 31%, 52%, and 17%, respectively. All of the patients experienced dysgeusia, dysphagia, and xerostomia of grades 1-3. Acute desquamation of the skin of grades 1, 2, and 3 occurred in 66%, 20%, and 14%.
One patient was hospitalized for grade 4 mucositis, dysphagia, and fever. Another developed osteoradionecrosis during concurrent chemoradiotherapy. Late dysphagia of grades 1-4 occurred in 46%, 28%, 15%, and 11%. Xerostomia of grades 1-3 occurred in 45%, 32%, and 23%, respectively, he said.
At 4 years, locoregional control was 69% and overall survival 55%. In an interview, Dr. Mourad noted that at his institution, the comparable rates for non-HIV patients were 85%-90% and 75%-85%, respectively.
The median CD4 count prior to chemotherapy was 370, and viral load was undetectable. The CD4 count dropped as chemoradiotherapy progressed to a nadir at 11 weeks, at which point it began to rise again and viral load decreased.
There was a statistically significant relationship between locoregional control and the duration of radiation therapy (P less than .001), and positive trends with weight loss of greater than 10% and absence of second malignancy. However, multivariate analysis did not show any statistically significant relationship because of the relatively small sample size with diverse subsites, Dr. Mourad noted.
"We believe that our data provide important information regarding treatment outcomes for newly diagnosed head and neck cancer with HIV. This is particularly important given the growing population of patients who live with HIV long term because of effective antiretroviral maintenance treatments," Dr. Mourad said in an interview.
Dr. Mourad and his nine coauthors declared that they had no financial disclosures.
PHOENIX – Definitive radiation therapy with or without chemotherapy was less tolerated and less effective in HIV-positive patients with head and neck squamous cell carcinoma than in HIV-negative patients in a single-institution retrospective study of 71 HIV-positive patients.
"Head and neck squamous cell carcinoma with coexisting HIV remains a challenging clinical problem. ... Due to the advances in highly active antiretroviral therapy (HAART) – which prolongs HIV patients’ survival – the likelihood to develop HIV-related malignancy increases. It is of paramount importance to establish better-tolerated treatment strategies and regimens to improve tolerance, toxicity, and outcomes in this growing patient population," said Dr. Waleed Mourad, a radiation oncologist at Beth Israel Medical Center, New York.
The 71 HIV-positive patients with HNSCC were treated January 1997 through 2010. They had a median age of 34 years at the time of HIV diagnosis (range 25-50 years) with a median 11 years’ duration of seropositivity (6-20 years). Their median age at the time of radiation therapy was 51 years (32-72 years). All but one patient had squamous cell carcinoma, with the other having submandibular salivary duct carcinoma. That patient was treated with definitive surgery and received adjuvant radiation therapy without chemotherapy, Dr. Mourad noted.
Approximately one-third of the patients had cancer of the oropharynx (32%) and larynx (35%), and another 13% had cancer of the oral cavity. Other cancers among the patients included those located in the hypopharynx, nasopharynx, occult primary, and nasal cavity. American Joint Committee on Cancer 7th edition stages I-II, III and IVa/b were 22%, 27%, 51% respectively.
All patients were treated definitively with radiation therapy, with or without chemotherapy (cisplatin, carboplatin, or cetuximab). A total of 50 patients (70%) were on HAART during treatment, with a median CD4 count of 290 (range, 203-1,142). A median dose of 70 Gy (66-70) was delivered to the gross disease; high-risk neck 60-63 Gy; low-risk neck; and lateral retropharyngeal nodes 54 Gy. All fractions were given at the rate of 1.8-2 Gy/fraction. The median duration of treatment was 52 (49-64) days. A total of 12 patients (17%) underwent planned neck dissection for N3 disease.
In all, local control was achieved in 69% (49) and locoregional failure occurred in 31% (22). By site, local control rates were 70% (16) for the oropharynx, 76% (19) for the larynx, 78% (7) for the oral cavity, 0% (of 5) for hypopharynx, 67% (2) for the nasopharynx, 100% (3) for occult primary, 50% (1) for the nasal cavity, and 100% (1) for the submandibular duct.
Thus, locoregional failure rates ranged from 100% (all five patients with hypopharyngeal cancer) to 0 (for the three patients with occult primary cancer and the one with submandibular duct cancer). Seven patients developed second primary cancers, Dr. Mourad reported.
After a median follow up of 47 months (7-140), there were no fatalities related to radiation or chemotherapy. Treatment breaks in excess of 10, 7, and 5 days occurred in 6%, 13%, and 14% of patients, respectively. Acute dysphagia and odynophagia grades 1, 2, and 3 occurred in 31%, 52%, and 17%, respectively. All of the patients experienced dysgeusia, dysphagia, and xerostomia of grades 1-3. Acute desquamation of the skin of grades 1, 2, and 3 occurred in 66%, 20%, and 14%.
One patient was hospitalized for grade 4 mucositis, dysphagia, and fever. Another developed osteoradionecrosis during concurrent chemoradiotherapy. Late dysphagia of grades 1-4 occurred in 46%, 28%, 15%, and 11%. Xerostomia of grades 1-3 occurred in 45%, 32%, and 23%, respectively, he said.
At 4 years, locoregional control was 69% and overall survival 55%. In an interview, Dr. Mourad noted that at his institution, the comparable rates for non-HIV patients were 85%-90% and 75%-85%, respectively.
The median CD4 count prior to chemotherapy was 370, and viral load was undetectable. The CD4 count dropped as chemoradiotherapy progressed to a nadir at 11 weeks, at which point it began to rise again and viral load decreased.
There was a statistically significant relationship between locoregional control and the duration of radiation therapy (P less than .001), and positive trends with weight loss of greater than 10% and absence of second malignancy. However, multivariate analysis did not show any statistically significant relationship because of the relatively small sample size with diverse subsites, Dr. Mourad noted.
"We believe that our data provide important information regarding treatment outcomes for newly diagnosed head and neck cancer with HIV. This is particularly important given the growing population of patients who live with HIV long term because of effective antiretroviral maintenance treatments," Dr. Mourad said in an interview.
Dr. Mourad and his nine coauthors declared that they had no financial disclosures.
FROM A HEAD AND NECK CANCER SYMPOSIUM BY THE AMERICAN SOCIETY FOR RADIATION ONCOLOGY
Major Finding: At 4 years, locoregional control was 69% and overall survival 55%.
Data Source: The findings come from a single-institution retrospective study of 71 HIV-positive patients with head and neck squamous cell carcinoma.
Disclosures: Dr. Mourad and his nine coauthors declared that they had no financial disclosures.
FDA Turns Down Novel Antidiabetes Drug
Other contenders in a novel class of glucose-lowering agents are waiting in the wings, despite a negative reception by the Food and Drug Administration on dapagliflozin – the first in that class of agents – presumably because of concerns noted by an FDA advisory panel about potential increases in the risk of bladder and breast cancers associated with the drug.
On Jan. 19, the drug’s joint developers, Bristol-Myers Squibb and AstraZeneca, announced that it received a complete response from the FDA that asked for still more clinical data on dapagliflozin. Although the companies offered no specifics about the request, they said in a statement that they are working "closely with the FDA to determine the appropriate next steps for the dapagliflozin application."
Dapagliflozin lowers glucose by selectively inhibiting renal glucose reabsorption via inhibition of sodium-glucose cotransporter 2 (SGLT2). It was developed as an insulin-independent treatment approach for type 2 diabetes mellitus, as an adjunct to diet and exercise, as monotherapy, or in combination with other diabetes drugs. Despite the initial FDA panel vote, interest in the drug persists, as it is believed to address a pathogenic defect that has yet to be addressed in diabetes.
Bristol-Myers Squibb and AstraZeneca submitted data from recently completed and ongoing phase III clinical trials of dapagliflozin in response to an FDA request for clarification on the drug’s cancer and hepatic risks, along with further data on efficacy and safety in special populations, including the elderly, minorities, and patients with moderate renal impairment.
"This data submission constitutes a major amendment to the original new drug application (NDA) for dapagliflozin," Dr. Brian Daniels, senior vice president of global development and medical affairs at Bristol-Myers Squibb, explained in a statement last fall.
In July 2011, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee recommended against its approval in a 9-6 vote. Despite the drug’s associated cardiovascular and weight-loss benefits, panel members were troubled by nine cases each of bladder and breast cancer among dapagliflozin-treated patients, compared with one of each type in control patients. Using these numbers, the FDA calculated risk ratios of 5.08 for the incidence of bladder cancer in dapagliflozin-treated men, compared with controls, and 4.04 for the incidence of breast cancer in women. The agency’s decision to deny marketing approval for dapagliflozin was widely expected.
Nevertheless, the pipeline of SGLT2-based drugs is full. At the European Association for the Study of Diabetes (EASD) meeting in September, data were presented on Boehringer Ingelheim’s empagliflozin, Astellas Pharma’s ipragliflozin, Taisho Pharmaceuticals’ TS-071, and Lexicon Pharmaceuticals’ LX4211, which is a dual inhibitor of both SGLT1 and SGLT2. All of these agents showed that they can successfully lower glucose levels and improve other metabolic parameters, with generally good short-term safety profiles. The largest of the study populations was 495 patients (for empagliflozin), and the longest of the study periods was 16 weeks (for ipragliflozin).
In an interview, Dr. Pablo Lapuerta, senior vice president and chief medical officer at Lexicon, noted that as a dual SGLT1/SGLT2 inhibitor, LX4211 is actually in a distinct class from dapagliflozin.
"This differentiates LX4211 from the SGLT2-specific inhibitors in several ways. For example, in patients with type 2 diabetes, LX4211 has been shown to cause a rapid reduction in blood sugar levels after meals, and an increase in GLP-1 [glucagonlike peptide–1] and the increase in PYY [peptide YY], effects that are associated with SGLT1 inhibition by LX4211 in the gastrointestinal tract. Also, recent studies in healthy subjects have shown that LX4211 substantially decreases postprandial glucose levels without hypoglycemia, and in both diabetic patients and healthy subjects, LX4211 can substantially reduce triglycerides. These results have not been reported for SGLT2-selective inhibitors," he said.
With regard to safety, Dr. Lapuerta noted that the "issue for the FDA advisory committee had to do with the overall benefit/risk profile of dapagliflozin. We believe the solution will involve addressing both benefits and risks. On the benefit side, we believe that LX4211 is a cardiovascular drug, not just a diabetes drug. Dual inhibition of SGLT1/2 with LX4211 offers the potential benefit to combine strong [hemoglobin] A1c reduction with benefits in blood pressure, uric acid, weight loss, and triglycerides. Cardiovascular benefits will be relevant to approval," he said.
"On the risk side, there is the potential that reports of bladder cancer on dapagliflozin reflected an ascertainment bias. We can address this in the LX4211 clinical program by ensuring that we carefully document physician referral patterns and take steps to ensure [that] our studies identify as much as possible new conditions instead of preexisting ones."
Susan Holz, public relations manager at Boehringer Ingelheim Pharmaceuticals, said in an earlier interview, "We are aware of the advisory committee’s concerns with dapagliflozin and are working with the FDA to ensure [that] our filing package for empagliflozin is robust and comprehensive. Phase III trials for empagliflozin are underway, and we are continuing to evaluate the drug’s safety profile." Currently, there are 11 ongoing, multinational, phase III clinical trials, including a large cardiovascular outcomes safety trial, she said.
At the EASD meeting in September, Dr. Michaela Diamant, scientific director of the diabetes center at Free University Medical Center in Amsterdam, commented that SGLT2 inhibitors have "an interesting mechanism that addresses, to a certain extent, a pathogenic defect that has been largely overlooked in diabetes. ... I’m sure there is a huge group of patients who can profit from these novel agents."
Regarding the safety issue, she asked, "If you would have a trial of 2-5 years, would you definitely address causality of cancer? We know that cancer development takes 20 years. It’s very unlikely that the drug caused cancer. We have to do what is feasible. The industry is not going to develop any more of these drugs if they are required to do a trial of 10 years. It’s difficult to tease out [contributors] to the development of cancer," Dr. Diamant continued.
Dr. Diamant has been a board member, advisory panel member, consultant, research support recipient, and/or speakers bureau participant for Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, Abbott, AstraZeneca/BMS, Boehringer Ingelheim, Poxel Pharma, Sanofi-Aventis, Amylin Pharmaceuticals, Novartis, and Takeda.
Sue Sutter of "The Pink Sheet" contributed to this story. "The Pink Sheet" and this publication are both owned by Elsevier.
Other contenders in a novel class of glucose-lowering agents are waiting in the wings, despite a negative reception by the Food and Drug Administration on dapagliflozin – the first in that class of agents – presumably because of concerns noted by an FDA advisory panel about potential increases in the risk of bladder and breast cancers associated with the drug.
On Jan. 19, the drug’s joint developers, Bristol-Myers Squibb and AstraZeneca, announced that it received a complete response from the FDA that asked for still more clinical data on dapagliflozin. Although the companies offered no specifics about the request, they said in a statement that they are working "closely with the FDA to determine the appropriate next steps for the dapagliflozin application."
Dapagliflozin lowers glucose by selectively inhibiting renal glucose reabsorption via inhibition of sodium-glucose cotransporter 2 (SGLT2). It was developed as an insulin-independent treatment approach for type 2 diabetes mellitus, as an adjunct to diet and exercise, as monotherapy, or in combination with other diabetes drugs. Despite the initial FDA panel vote, interest in the drug persists, as it is believed to address a pathogenic defect that has yet to be addressed in diabetes.
Bristol-Myers Squibb and AstraZeneca submitted data from recently completed and ongoing phase III clinical trials of dapagliflozin in response to an FDA request for clarification on the drug’s cancer and hepatic risks, along with further data on efficacy and safety in special populations, including the elderly, minorities, and patients with moderate renal impairment.
"This data submission constitutes a major amendment to the original new drug application (NDA) for dapagliflozin," Dr. Brian Daniels, senior vice president of global development and medical affairs at Bristol-Myers Squibb, explained in a statement last fall.
In July 2011, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee recommended against its approval in a 9-6 vote. Despite the drug’s associated cardiovascular and weight-loss benefits, panel members were troubled by nine cases each of bladder and breast cancer among dapagliflozin-treated patients, compared with one of each type in control patients. Using these numbers, the FDA calculated risk ratios of 5.08 for the incidence of bladder cancer in dapagliflozin-treated men, compared with controls, and 4.04 for the incidence of breast cancer in women. The agency’s decision to deny marketing approval for dapagliflozin was widely expected.
Nevertheless, the pipeline of SGLT2-based drugs is full. At the European Association for the Study of Diabetes (EASD) meeting in September, data were presented on Boehringer Ingelheim’s empagliflozin, Astellas Pharma’s ipragliflozin, Taisho Pharmaceuticals’ TS-071, and Lexicon Pharmaceuticals’ LX4211, which is a dual inhibitor of both SGLT1 and SGLT2. All of these agents showed that they can successfully lower glucose levels and improve other metabolic parameters, with generally good short-term safety profiles. The largest of the study populations was 495 patients (for empagliflozin), and the longest of the study periods was 16 weeks (for ipragliflozin).
In an interview, Dr. Pablo Lapuerta, senior vice president and chief medical officer at Lexicon, noted that as a dual SGLT1/SGLT2 inhibitor, LX4211 is actually in a distinct class from dapagliflozin.
"This differentiates LX4211 from the SGLT2-specific inhibitors in several ways. For example, in patients with type 2 diabetes, LX4211 has been shown to cause a rapid reduction in blood sugar levels after meals, and an increase in GLP-1 [glucagonlike peptide–1] and the increase in PYY [peptide YY], effects that are associated with SGLT1 inhibition by LX4211 in the gastrointestinal tract. Also, recent studies in healthy subjects have shown that LX4211 substantially decreases postprandial glucose levels without hypoglycemia, and in both diabetic patients and healthy subjects, LX4211 can substantially reduce triglycerides. These results have not been reported for SGLT2-selective inhibitors," he said.
With regard to safety, Dr. Lapuerta noted that the "issue for the FDA advisory committee had to do with the overall benefit/risk profile of dapagliflozin. We believe the solution will involve addressing both benefits and risks. On the benefit side, we believe that LX4211 is a cardiovascular drug, not just a diabetes drug. Dual inhibition of SGLT1/2 with LX4211 offers the potential benefit to combine strong [hemoglobin] A1c reduction with benefits in blood pressure, uric acid, weight loss, and triglycerides. Cardiovascular benefits will be relevant to approval," he said.
"On the risk side, there is the potential that reports of bladder cancer on dapagliflozin reflected an ascertainment bias. We can address this in the LX4211 clinical program by ensuring that we carefully document physician referral patterns and take steps to ensure [that] our studies identify as much as possible new conditions instead of preexisting ones."
Susan Holz, public relations manager at Boehringer Ingelheim Pharmaceuticals, said in an earlier interview, "We are aware of the advisory committee’s concerns with dapagliflozin and are working with the FDA to ensure [that] our filing package for empagliflozin is robust and comprehensive. Phase III trials for empagliflozin are underway, and we are continuing to evaluate the drug’s safety profile." Currently, there are 11 ongoing, multinational, phase III clinical trials, including a large cardiovascular outcomes safety trial, she said.
At the EASD meeting in September, Dr. Michaela Diamant, scientific director of the diabetes center at Free University Medical Center in Amsterdam, commented that SGLT2 inhibitors have "an interesting mechanism that addresses, to a certain extent, a pathogenic defect that has been largely overlooked in diabetes. ... I’m sure there is a huge group of patients who can profit from these novel agents."
Regarding the safety issue, she asked, "If you would have a trial of 2-5 years, would you definitely address causality of cancer? We know that cancer development takes 20 years. It’s very unlikely that the drug caused cancer. We have to do what is feasible. The industry is not going to develop any more of these drugs if they are required to do a trial of 10 years. It’s difficult to tease out [contributors] to the development of cancer," Dr. Diamant continued.
Dr. Diamant has been a board member, advisory panel member, consultant, research support recipient, and/or speakers bureau participant for Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, Abbott, AstraZeneca/BMS, Boehringer Ingelheim, Poxel Pharma, Sanofi-Aventis, Amylin Pharmaceuticals, Novartis, and Takeda.
Sue Sutter of "The Pink Sheet" contributed to this story. "The Pink Sheet" and this publication are both owned by Elsevier.
Other contenders in a novel class of glucose-lowering agents are waiting in the wings, despite a negative reception by the Food and Drug Administration on dapagliflozin – the first in that class of agents – presumably because of concerns noted by an FDA advisory panel about potential increases in the risk of bladder and breast cancers associated with the drug.
On Jan. 19, the drug’s joint developers, Bristol-Myers Squibb and AstraZeneca, announced that it received a complete response from the FDA that asked for still more clinical data on dapagliflozin. Although the companies offered no specifics about the request, they said in a statement that they are working "closely with the FDA to determine the appropriate next steps for the dapagliflozin application."
Dapagliflozin lowers glucose by selectively inhibiting renal glucose reabsorption via inhibition of sodium-glucose cotransporter 2 (SGLT2). It was developed as an insulin-independent treatment approach for type 2 diabetes mellitus, as an adjunct to diet and exercise, as monotherapy, or in combination with other diabetes drugs. Despite the initial FDA panel vote, interest in the drug persists, as it is believed to address a pathogenic defect that has yet to be addressed in diabetes.
Bristol-Myers Squibb and AstraZeneca submitted data from recently completed and ongoing phase III clinical trials of dapagliflozin in response to an FDA request for clarification on the drug’s cancer and hepatic risks, along with further data on efficacy and safety in special populations, including the elderly, minorities, and patients with moderate renal impairment.
"This data submission constitutes a major amendment to the original new drug application (NDA) for dapagliflozin," Dr. Brian Daniels, senior vice president of global development and medical affairs at Bristol-Myers Squibb, explained in a statement last fall.
In July 2011, the FDA’s Endocrinologic and Metabolic Drugs Advisory Committee recommended against its approval in a 9-6 vote. Despite the drug’s associated cardiovascular and weight-loss benefits, panel members were troubled by nine cases each of bladder and breast cancer among dapagliflozin-treated patients, compared with one of each type in control patients. Using these numbers, the FDA calculated risk ratios of 5.08 for the incidence of bladder cancer in dapagliflozin-treated men, compared with controls, and 4.04 for the incidence of breast cancer in women. The agency’s decision to deny marketing approval for dapagliflozin was widely expected.
Nevertheless, the pipeline of SGLT2-based drugs is full. At the European Association for the Study of Diabetes (EASD) meeting in September, data were presented on Boehringer Ingelheim’s empagliflozin, Astellas Pharma’s ipragliflozin, Taisho Pharmaceuticals’ TS-071, and Lexicon Pharmaceuticals’ LX4211, which is a dual inhibitor of both SGLT1 and SGLT2. All of these agents showed that they can successfully lower glucose levels and improve other metabolic parameters, with generally good short-term safety profiles. The largest of the study populations was 495 patients (for empagliflozin), and the longest of the study periods was 16 weeks (for ipragliflozin).
In an interview, Dr. Pablo Lapuerta, senior vice president and chief medical officer at Lexicon, noted that as a dual SGLT1/SGLT2 inhibitor, LX4211 is actually in a distinct class from dapagliflozin.
"This differentiates LX4211 from the SGLT2-specific inhibitors in several ways. For example, in patients with type 2 diabetes, LX4211 has been shown to cause a rapid reduction in blood sugar levels after meals, and an increase in GLP-1 [glucagonlike peptide–1] and the increase in PYY [peptide YY], effects that are associated with SGLT1 inhibition by LX4211 in the gastrointestinal tract. Also, recent studies in healthy subjects have shown that LX4211 substantially decreases postprandial glucose levels without hypoglycemia, and in both diabetic patients and healthy subjects, LX4211 can substantially reduce triglycerides. These results have not been reported for SGLT2-selective inhibitors," he said.
With regard to safety, Dr. Lapuerta noted that the "issue for the FDA advisory committee had to do with the overall benefit/risk profile of dapagliflozin. We believe the solution will involve addressing both benefits and risks. On the benefit side, we believe that LX4211 is a cardiovascular drug, not just a diabetes drug. Dual inhibition of SGLT1/2 with LX4211 offers the potential benefit to combine strong [hemoglobin] A1c reduction with benefits in blood pressure, uric acid, weight loss, and triglycerides. Cardiovascular benefits will be relevant to approval," he said.
"On the risk side, there is the potential that reports of bladder cancer on dapagliflozin reflected an ascertainment bias. We can address this in the LX4211 clinical program by ensuring that we carefully document physician referral patterns and take steps to ensure [that] our studies identify as much as possible new conditions instead of preexisting ones."
Susan Holz, public relations manager at Boehringer Ingelheim Pharmaceuticals, said in an earlier interview, "We are aware of the advisory committee’s concerns with dapagliflozin and are working with the FDA to ensure [that] our filing package for empagliflozin is robust and comprehensive. Phase III trials for empagliflozin are underway, and we are continuing to evaluate the drug’s safety profile." Currently, there are 11 ongoing, multinational, phase III clinical trials, including a large cardiovascular outcomes safety trial, she said.
At the EASD meeting in September, Dr. Michaela Diamant, scientific director of the diabetes center at Free University Medical Center in Amsterdam, commented that SGLT2 inhibitors have "an interesting mechanism that addresses, to a certain extent, a pathogenic defect that has been largely overlooked in diabetes. ... I’m sure there is a huge group of patients who can profit from these novel agents."
Regarding the safety issue, she asked, "If you would have a trial of 2-5 years, would you definitely address causality of cancer? We know that cancer development takes 20 years. It’s very unlikely that the drug caused cancer. We have to do what is feasible. The industry is not going to develop any more of these drugs if they are required to do a trial of 10 years. It’s difficult to tease out [contributors] to the development of cancer," Dr. Diamant continued.
Dr. Diamant has been a board member, advisory panel member, consultant, research support recipient, and/or speakers bureau participant for Eli Lilly, Merck Sharp & Dohme, Novo Nordisk, Abbott, AstraZeneca/BMS, Boehringer Ingelheim, Poxel Pharma, Sanofi-Aventis, Amylin Pharmaceuticals, Novartis, and Takeda.
Sue Sutter of "The Pink Sheet" contributed to this story. "The Pink Sheet" and this publication are both owned by Elsevier.
Different Mechanisms May Operate in Postoperative Seizure Recurrence
BALTIMORE – Not all seizure recurrences following epilepsy surgery should be treated in the same way.
Rather, early seizure recurrences may indicate an incomplete resection or inaccurate localization of the epileptic focus, whereas late seizure recurrences are likely due to de novo epileptogenesis. Clinically, this suggests that "patients with early seizure recurrence should be monitored and evaluated for possible reoperation sooner rather than later, while more aggressive medical management may be enough to control seizures in those with late recurrences," Dr. Lara Jehi said at the annual meeting of the American Epilepsy Society.

At 12 years following resective epilepsy surgery of all types, just 45% of patients remain seizure free. For frontal lobectomy in particular, that rate is just 30% (Brain 2007;130:574-84), and for temporal lobectomy the outcome is a little better at 55% (Neurology 2006;66:1938-40). What’s more, that 55% rate has not changed in the past 60 years. "Whether we like it or not, epilepsy surgery is not a magic bullet. ... It doesn’t always work," said Dr. Jehi, a neurologist at the Cleveland Clinic Epilepsy Center, and the head of the Outcomes Research Group there.
But hidden within those statistics is a less-appreciated dichotomy: In the studies just mentioned, the median time of recurrence for all epilepsy surgeries was 4 months. For frontal lobectomy, it was 2 months, and for temporal lobectomy, it was 6.6 months. In all, about half of all failures occurred in the short term, and the rest were spread out over a decade or more, regardless of surgery type. "It’s a common, solid, reproducible observation that reflects two different mechanisms," said Dr. Jehi, who cited an as-yet unpublished study of 1,418 patients that she and her colleagues presented last year at the annual meeting of the American Academy of Neurology.
She noted that a range of factors have been associated with early recurrence in studies of the outcomes of epilepsy surgery. Among 371 patients who underwent anterior temporal lobectomy to treat pharmacoresistant epilepsy, predictors of early recurrence included preoperative seizure frequency, history of generalized tonic-clonic (GTC) seizures, bilateral abnormalities on MRI, use of subdural electrodes, and an epileptiform electroencephalogram at 6 months postoperatively. On the other hand, the only predictor of late recurrence was nonspecific pathology (Neurology 2006;66:1938-40).
In a study of outcomes following failed temporal lobectomy in 68 adult patients, Dr. Jehi and her associates found that there were no early seizure recurrences from foci that were contiguous to the area that had been initially resected, suggesting that early recurrences are likely the result of having "missed the spot," she said (J. Neurosurg. 2010;113:1186-94).
Two other studies by her group also documented a higher rate of early recurrences in "difficult to localize" epilepsies. One examined surgical outcome and prognostic factors of frontal lobe epilepsy surgery in 70 patients (Brain 2007;130:574-84), and the other is a longitudinal study of surgical outcome and its determinants following posterior cortex epilepsy surgery in 57 patients (Epilepsia 2009;50:2040-52).
But in a separate study of 285 patients who were initially seizure free following epilepsy surgery, the presence of preoperative GTC seizures predicted late seizure recurrence among 31 patients with neocortical epilepsy, whereas late age at surgery predicted late recurrence among the remaining 254 with medial temporal lobe epilepsy. Results of MRI and location of surgery were not predictive (Epilepsia 2006;47:567-73).
Dr. Jehi and her group found that there was less risk of intractability with breakthrough seizures that occurred beyond 6 months after temporal lobectomy surgery among 276 patients who had one or more seizures after the immediate postoperative period (Epilepsia 2010;51:994-1003). Her team also determined that late seizure recurrences after frontal lobectomy surgery tended to be milder and less frequent (Brain 2007;130:574-84). These findings suggest a pattern similar to new-onset epilepsy, or "epileptogenesis," she said.
In all, the data suggest that patients with early seizure recurrences need to be investigated as soon as possible for a reoperation via modalities such as video-EEG and repeat brain imaging, and require intense follow-up and management. "In other words, don’t waste much time on switching antiepileptic medications around," Dr. Jehi said in an interview.
On the other hand, patients with late recurrences need more aggressive antiepileptic medication management before another brain surgery is considered. If their seizures subsequently prove to be refractory, brain regions other than the focus of initial resection need to enter into the equation of possible areas in the brain that may be causing seizures, she said.
And, she added, this dichotomy hypothesis "opens the door to investigate antiepileptogenic measures as a tool to improve long-term seizure outcomes after surgery."
Dr. Jehi said that she had no relevant disclosures.
BALTIMORE – Not all seizure recurrences following epilepsy surgery should be treated in the same way.
Rather, early seizure recurrences may indicate an incomplete resection or inaccurate localization of the epileptic focus, whereas late seizure recurrences are likely due to de novo epileptogenesis. Clinically, this suggests that "patients with early seizure recurrence should be monitored and evaluated for possible reoperation sooner rather than later, while more aggressive medical management may be enough to control seizures in those with late recurrences," Dr. Lara Jehi said at the annual meeting of the American Epilepsy Society.
At 12 years following resective epilepsy surgery of all types, just 45% of patients remain seizure free. For frontal lobectomy in particular, that rate is just 30% (Brain 2007;130:574-84), and for temporal lobectomy the outcome is a little better at 55% (Neurology 2006;66:1938-40). What’s more, that 55% rate has not changed in the past 60 years. "Whether we like it or not, epilepsy surgery is not a magic bullet. ... It doesn’t always work," said Dr. Jehi, a neurologist at the Cleveland Clinic Epilepsy Center, and the head of the Outcomes Research Group there.
But hidden within those statistics is a less-appreciated dichotomy: In the studies just mentioned, the median time of recurrence for all epilepsy surgeries was 4 months. For frontal lobectomy, it was 2 months, and for temporal lobectomy, it was 6.6 months. In all, about half of all failures occurred in the short term, and the rest were spread out over a decade or more, regardless of surgery type. "It’s a common, solid, reproducible observation that reflects two different mechanisms," said Dr. Jehi, who cited an as-yet unpublished study of 1,418 patients that she and her colleagues presented last year at the annual meeting of the American Academy of Neurology.
She noted that a range of factors have been associated with early recurrence in studies of the outcomes of epilepsy surgery. Among 371 patients who underwent anterior temporal lobectomy to treat pharmacoresistant epilepsy, predictors of early recurrence included preoperative seizure frequency, history of generalized tonic-clonic (GTC) seizures, bilateral abnormalities on MRI, use of subdural electrodes, and an epileptiform electroencephalogram at 6 months postoperatively. On the other hand, the only predictor of late recurrence was nonspecific pathology (Neurology 2006;66:1938-40).
In a study of outcomes following failed temporal lobectomy in 68 adult patients, Dr. Jehi and her associates found that there were no early seizure recurrences from foci that were contiguous to the area that had been initially resected, suggesting that early recurrences are likely the result of having "missed the spot," she said (J. Neurosurg. 2010;113:1186-94).
Two other studies by her group also documented a higher rate of early recurrences in "difficult to localize" epilepsies. One examined surgical outcome and prognostic factors of frontal lobe epilepsy surgery in 70 patients (Brain 2007;130:574-84), and the other is a longitudinal study of surgical outcome and its determinants following posterior cortex epilepsy surgery in 57 patients (Epilepsia 2009;50:2040-52).
But in a separate study of 285 patients who were initially seizure free following epilepsy surgery, the presence of preoperative GTC seizures predicted late seizure recurrence among 31 patients with neocortical epilepsy, whereas late age at surgery predicted late recurrence among the remaining 254 with medial temporal lobe epilepsy. Results of MRI and location of surgery were not predictive (Epilepsia 2006;47:567-73).
Dr. Jehi and her group found that there was less risk of intractability with breakthrough seizures that occurred beyond 6 months after temporal lobectomy surgery among 276 patients who had one or more seizures after the immediate postoperative period (Epilepsia 2010;51:994-1003). Her team also determined that late seizure recurrences after frontal lobectomy surgery tended to be milder and less frequent (Brain 2007;130:574-84). These findings suggest a pattern similar to new-onset epilepsy, or "epileptogenesis," she said.
In all, the data suggest that patients with early seizure recurrences need to be investigated as soon as possible for a reoperation via modalities such as video-EEG and repeat brain imaging, and require intense follow-up and management. "In other words, don’t waste much time on switching antiepileptic medications around," Dr. Jehi said in an interview.
On the other hand, patients with late recurrences need more aggressive antiepileptic medication management before another brain surgery is considered. If their seizures subsequently prove to be refractory, brain regions other than the focus of initial resection need to enter into the equation of possible areas in the brain that may be causing seizures, she said.
And, she added, this dichotomy hypothesis "opens the door to investigate antiepileptogenic measures as a tool to improve long-term seizure outcomes after surgery."
Dr. Jehi said that she had no relevant disclosures.
BALTIMORE – Not all seizure recurrences following epilepsy surgery should be treated in the same way.
Rather, early seizure recurrences may indicate an incomplete resection or inaccurate localization of the epileptic focus, whereas late seizure recurrences are likely due to de novo epileptogenesis. Clinically, this suggests that "patients with early seizure recurrence should be monitored and evaluated for possible reoperation sooner rather than later, while more aggressive medical management may be enough to control seizures in those with late recurrences," Dr. Lara Jehi said at the annual meeting of the American Epilepsy Society.
At 12 years following resective epilepsy surgery of all types, just 45% of patients remain seizure free. For frontal lobectomy in particular, that rate is just 30% (Brain 2007;130:574-84), and for temporal lobectomy the outcome is a little better at 55% (Neurology 2006;66:1938-40). What’s more, that 55% rate has not changed in the past 60 years. "Whether we like it or not, epilepsy surgery is not a magic bullet. ... It doesn’t always work," said Dr. Jehi, a neurologist at the Cleveland Clinic Epilepsy Center, and the head of the Outcomes Research Group there.
But hidden within those statistics is a less-appreciated dichotomy: In the studies just mentioned, the median time of recurrence for all epilepsy surgeries was 4 months. For frontal lobectomy, it was 2 months, and for temporal lobectomy, it was 6.6 months. In all, about half of all failures occurred in the short term, and the rest were spread out over a decade or more, regardless of surgery type. "It’s a common, solid, reproducible observation that reflects two different mechanisms," said Dr. Jehi, who cited an as-yet unpublished study of 1,418 patients that she and her colleagues presented last year at the annual meeting of the American Academy of Neurology.
She noted that a range of factors have been associated with early recurrence in studies of the outcomes of epilepsy surgery. Among 371 patients who underwent anterior temporal lobectomy to treat pharmacoresistant epilepsy, predictors of early recurrence included preoperative seizure frequency, history of generalized tonic-clonic (GTC) seizures, bilateral abnormalities on MRI, use of subdural electrodes, and an epileptiform electroencephalogram at 6 months postoperatively. On the other hand, the only predictor of late recurrence was nonspecific pathology (Neurology 2006;66:1938-40).
In a study of outcomes following failed temporal lobectomy in 68 adult patients, Dr. Jehi and her associates found that there were no early seizure recurrences from foci that were contiguous to the area that had been initially resected, suggesting that early recurrences are likely the result of having "missed the spot," she said (J. Neurosurg. 2010;113:1186-94).
Two other studies by her group also documented a higher rate of early recurrences in "difficult to localize" epilepsies. One examined surgical outcome and prognostic factors of frontal lobe epilepsy surgery in 70 patients (Brain 2007;130:574-84), and the other is a longitudinal study of surgical outcome and its determinants following posterior cortex epilepsy surgery in 57 patients (Epilepsia 2009;50:2040-52).
But in a separate study of 285 patients who were initially seizure free following epilepsy surgery, the presence of preoperative GTC seizures predicted late seizure recurrence among 31 patients with neocortical epilepsy, whereas late age at surgery predicted late recurrence among the remaining 254 with medial temporal lobe epilepsy. Results of MRI and location of surgery were not predictive (Epilepsia 2006;47:567-73).
Dr. Jehi and her group found that there was less risk of intractability with breakthrough seizures that occurred beyond 6 months after temporal lobectomy surgery among 276 patients who had one or more seizures after the immediate postoperative period (Epilepsia 2010;51:994-1003). Her team also determined that late seizure recurrences after frontal lobectomy surgery tended to be milder and less frequent (Brain 2007;130:574-84). These findings suggest a pattern similar to new-onset epilepsy, or "epileptogenesis," she said.
In all, the data suggest that patients with early seizure recurrences need to be investigated as soon as possible for a reoperation via modalities such as video-EEG and repeat brain imaging, and require intense follow-up and management. "In other words, don’t waste much time on switching antiepileptic medications around," Dr. Jehi said in an interview.
On the other hand, patients with late recurrences need more aggressive antiepileptic medication management before another brain surgery is considered. If their seizures subsequently prove to be refractory, brain regions other than the focus of initial resection need to enter into the equation of possible areas in the brain that may be causing seizures, she said.
And, she added, this dichotomy hypothesis "opens the door to investigate antiepileptogenic measures as a tool to improve long-term seizure outcomes after surgery."
Dr. Jehi said that she had no relevant disclosures.
EXPERT ANALYSIS FROM THE ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
Seizure Increase Not Seen Following Gastric Bypass
BALTIMORE – No notable increases in new-onset seizure disorder or exacerbations of a pre-existing seizure disorder were seen following gastric bypass surgery in a retrospective case series of more than 1,500 patients from the Mayo Clinic.
Reports of new-onset or exacerbated seizure disorders following Roux-en-Y surgery are often posted on epilepsy patient-oriented Web sites such as epilepsy.com, along with reports of other neurologic complications such as Wernicke-Korsakoff syndrome, polyradiculoneuropathy, myelopathy, and optic neuropathy. However, few previous studies have examined a potential connection between gastric bypass and epilepsy, Dr. Richard S. Clemmons and Gregory D. Cascino said in a poster at the annual meeting of the American Epilepsy Society.
A diagnosis of epilepsy pre-existed prior to Roux-en-Y surgery in 12 of 1,542 patients who were operated on at the Mayo Clinic between September 1997 and September 2007. Those patients were selected from a larger group of 1,776 patients because they had more than 1 year of follow-up, had undergone surgery for morbid obesity, and were aged 18 years or older. Despite evidence that gastric bypass surgery might result in decreased absorption of drugs with high proximal absorption or low pH (Am. J. Health Syst. Pharm. 2006;63:1852-7), 8 of these 12 patients had no decrease in drug levels, based on patient report or on serum testing before and after surgery. One patient who did have a low drug level was suspected of poor compliance. None of the 12 had exacerbations of their seizures.
"Based on the limited data here, there was not a decrease in serum drug levels for valproic acid, carbamazepine, or levetiracetam. ... Even patients with significant seizure risk factors did not manifest an exacerbation of seizures," noted Dr. Clemmons and Dr. Cascino, both of whom were affiliated with the division of epilepsy in the department of neurology at the Mayo Clinic, Rochester, Minn., at the time of the study. Dr. Clemmons is currently in private practice in Denver.
Only 5 of the 1,542 patients developed new-onset epilepsy following surgery. Of those, only 3 (1.9% of the total cohort) could be considered to have unprovoked epilepsy. One of the other two patients had a history of meningoencephalitis and had just a single seizure 2 years after surgery that was possibly associated with hypoglycemia. The other one had a seizure in the setting of a stroke 3 months after surgery. None of the five developed intractable epilepsy.
About three-fourths of the patients in the study were female. Their charts were examined for evidence of seizure exacerbation post surgery, defined as an increase in seizure frequency above preoperative baseline where another cause was not identified. Patient questionnaires were used to supplement where data were lacking.
"Based on the reviewed data, there is no clear exacerbation of preexisting seizure disorder following gastric bypass ... Most patients with seizure disorder do well following Roux-en-Y," they concluded.
Dr. Clemmons, who presented the poster at the meeting, stated that he had no financial disclosures.
BALTIMORE – No notable increases in new-onset seizure disorder or exacerbations of a pre-existing seizure disorder were seen following gastric bypass surgery in a retrospective case series of more than 1,500 patients from the Mayo Clinic.
Reports of new-onset or exacerbated seizure disorders following Roux-en-Y surgery are often posted on epilepsy patient-oriented Web sites such as epilepsy.com, along with reports of other neurologic complications such as Wernicke-Korsakoff syndrome, polyradiculoneuropathy, myelopathy, and optic neuropathy. However, few previous studies have examined a potential connection between gastric bypass and epilepsy, Dr. Richard S. Clemmons and Gregory D. Cascino said in a poster at the annual meeting of the American Epilepsy Society.
A diagnosis of epilepsy pre-existed prior to Roux-en-Y surgery in 12 of 1,542 patients who were operated on at the Mayo Clinic between September 1997 and September 2007. Those patients were selected from a larger group of 1,776 patients because they had more than 1 year of follow-up, had undergone surgery for morbid obesity, and were aged 18 years or older. Despite evidence that gastric bypass surgery might result in decreased absorption of drugs with high proximal absorption or low pH (Am. J. Health Syst. Pharm. 2006;63:1852-7), 8 of these 12 patients had no decrease in drug levels, based on patient report or on serum testing before and after surgery. One patient who did have a low drug level was suspected of poor compliance. None of the 12 had exacerbations of their seizures.
"Based on the limited data here, there was not a decrease in serum drug levels for valproic acid, carbamazepine, or levetiracetam. ... Even patients with significant seizure risk factors did not manifest an exacerbation of seizures," noted Dr. Clemmons and Dr. Cascino, both of whom were affiliated with the division of epilepsy in the department of neurology at the Mayo Clinic, Rochester, Minn., at the time of the study. Dr. Clemmons is currently in private practice in Denver.
Only 5 of the 1,542 patients developed new-onset epilepsy following surgery. Of those, only 3 (1.9% of the total cohort) could be considered to have unprovoked epilepsy. One of the other two patients had a history of meningoencephalitis and had just a single seizure 2 years after surgery that was possibly associated with hypoglycemia. The other one had a seizure in the setting of a stroke 3 months after surgery. None of the five developed intractable epilepsy.
About three-fourths of the patients in the study were female. Their charts were examined for evidence of seizure exacerbation post surgery, defined as an increase in seizure frequency above preoperative baseline where another cause was not identified. Patient questionnaires were used to supplement where data were lacking.
"Based on the reviewed data, there is no clear exacerbation of preexisting seizure disorder following gastric bypass ... Most patients with seizure disorder do well following Roux-en-Y," they concluded.
Dr. Clemmons, who presented the poster at the meeting, stated that he had no financial disclosures.
BALTIMORE – No notable increases in new-onset seizure disorder or exacerbations of a pre-existing seizure disorder were seen following gastric bypass surgery in a retrospective case series of more than 1,500 patients from the Mayo Clinic.
Reports of new-onset or exacerbated seizure disorders following Roux-en-Y surgery are often posted on epilepsy patient-oriented Web sites such as epilepsy.com, along with reports of other neurologic complications such as Wernicke-Korsakoff syndrome, polyradiculoneuropathy, myelopathy, and optic neuropathy. However, few previous studies have examined a potential connection between gastric bypass and epilepsy, Dr. Richard S. Clemmons and Gregory D. Cascino said in a poster at the annual meeting of the American Epilepsy Society.
A diagnosis of epilepsy pre-existed prior to Roux-en-Y surgery in 12 of 1,542 patients who were operated on at the Mayo Clinic between September 1997 and September 2007. Those patients were selected from a larger group of 1,776 patients because they had more than 1 year of follow-up, had undergone surgery for morbid obesity, and were aged 18 years or older. Despite evidence that gastric bypass surgery might result in decreased absorption of drugs with high proximal absorption or low pH (Am. J. Health Syst. Pharm. 2006;63:1852-7), 8 of these 12 patients had no decrease in drug levels, based on patient report or on serum testing before and after surgery. One patient who did have a low drug level was suspected of poor compliance. None of the 12 had exacerbations of their seizures.
"Based on the limited data here, there was not a decrease in serum drug levels for valproic acid, carbamazepine, or levetiracetam. ... Even patients with significant seizure risk factors did not manifest an exacerbation of seizures," noted Dr. Clemmons and Dr. Cascino, both of whom were affiliated with the division of epilepsy in the department of neurology at the Mayo Clinic, Rochester, Minn., at the time of the study. Dr. Clemmons is currently in private practice in Denver.
Only 5 of the 1,542 patients developed new-onset epilepsy following surgery. Of those, only 3 (1.9% of the total cohort) could be considered to have unprovoked epilepsy. One of the other two patients had a history of meningoencephalitis and had just a single seizure 2 years after surgery that was possibly associated with hypoglycemia. The other one had a seizure in the setting of a stroke 3 months after surgery. None of the five developed intractable epilepsy.
About three-fourths of the patients in the study were female. Their charts were examined for evidence of seizure exacerbation post surgery, defined as an increase in seizure frequency above preoperative baseline where another cause was not identified. Patient questionnaires were used to supplement where data were lacking.
"Based on the reviewed data, there is no clear exacerbation of preexisting seizure disorder following gastric bypass ... Most patients with seizure disorder do well following Roux-en-Y," they concluded.
Dr. Clemmons, who presented the poster at the meeting, stated that he had no financial disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
Major Finding: Of 1,542 patients who underwent Roux-en-Y gastric bypass surgery, just 5 developed new-onset seizures. Of 12 with pre-existing seizure disorders, none had exacerbations.
Data Source: Retrospective case series of 1,542 patients who underwent Roux-en-Y surgery at the Mayo Clinic between September 1997 and September 2007
Disclosures: Dr. Clemmons has no financial disclosures.
Guideline Focuses on Hyperglycemia Management in Noncritical Hospital Settings
All patients admitted to the hospital in noncritical care settings should have their blood glucose tested, according to a new clinical practice guideline from the Endocrine Society.
The guideline, published in the Journal of Clinical Endocrinology and Metabolism, is designed to complement previous recommendations that focused more on glucose targets, based largely on data from studies conducted in intensive/critical care settings (most recently Diabetes Care [2009;32:1119-31]). This new guideline is focused specifically on glucose management in noncritical settings, with special emphasis on systemic issues such as patient transition between hospital units and from inpatient to outpatient settings, as well as detailed guidance for hospitals on how to create systems and protocols that will ensure optimal patient management and safety (J. Clin. Endocrinol. Metab. 2012;97:16-38).

"This paper is different. It was viewed from the start as something that would be complementary to some of the earlier papers. It was a piece that hadn’t really been focused on. Your patients are more likely not to be in the ICU than in the ICU, so what about glycemic control at all the other times? That’s what a great deal of this statement is about," coauthor Dr. Richard Hellman said in an interview.
"Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline" was developed by an eight-member panel with representatives from the American Diabetes Association, American Heart Association, American Association of Diabetes Educators, European Society of Endocrinology, and the Society of Hospital Medicine. The lead author was Dr. Guillermo E. Umpierrez, professor of medicine at Emory University, and chief of diabetes and endocrinology at Grady Memorial Hospital, both in Atlanta. It was published Jan. 5.
It comprises eight sections, all focused on the noncritical hospital setting: diagnosis and recognition of hyperglycemia and diabetes; monitoring glycemia; glycemic targets; management of hyperglycemia; special situations; recognition and management of hypoglycemia; implementation of a glycemic control program; and patient and professional education. Strong recommendations are given as "we recommend," and weaker ones as "we suggest."
In the first section, assessment of all patients for a history of diabetes on admission is "recommended," while laboratory blood glucose testing on admission for all patients, regardless of prior diagnosis of diabetes, is "suggested." Still, there is strong rationale for it. "There’s abundant data to show that a very large number of people in hospitals have high blood sugars, and that correlates with poorer outcomes. The recommendation to check the glucose is extremely important because it isn’t just for people with a prior diagnosis of diabetes. Some come in with undiagnosed diabetes and people also develop stress hyperglycemia," noted Dr. Hellman, an endocrinologist who is a clinical professor of medicine at the University of Missouri–Kansas City.
Bedside capillary point-of-care (POC) glucose testing is recommended, using monitors that have demonstrated accuracy in acutely ill patients. Despite the acknowledged less-than-optimal accuracy of hand-held devices, the recommendation is based on the need for such testing in order to time glucose measures to match the patient’s nutritional intake and medication regimens. The patients’ personal glucose meters should not be used, and continuous glucose monitors, while "promising," have not been adequately tested in acute care and therefore can’t be recommended for hospital use at this time, Dr. Umpierrez and his associates wrote.
Recommended glycemic targets are the same as in the 2009 guideline: less than 140 mg/dL premeal and less than 180 mg/dL random for the majority of hospitalized patients with noncritical illness, with suggested modification according to clinical status. Lower targets might be considered among those who are able to achieve them without hypoglycemia, while higher targets might be appropriate for those at high risk for hypoglycemia or a limited life expectancy.
Medical nutrition therapy is recommended as a component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia. Meals with consistent amounts of carbohydrate are suggested, to help coordinate doses of rapid-acting insulin to carbohydrate ingestion.
Insulin therapy is recommended as the preferred method for achieving glycemic control in all hospitalized patients with diabetes and hyperglycemia, with the suggestion that oral hypoglycemic agents be discontinued and insulin therapy initiated in patients with type 2 diabetes at the time of admission for acute illness. That advice is based in part on the fact that contraindications to use of many oral agents are present in a high percentage of hospitalized patients. Such contraindications include use of metformin in patients with decompensated heart failure, renal insufficiency, hypoperfusion, or chronic pulmonary disease, and in any patient given intravenous contrast dye, the authors noted.
Scheduled subcutaneous insulin therapy is recommended for all patients, consisting of basal or intermediate-acting insulin once or twice daily in combination with rapid- or short-acting insulin administered before meals in patients who are eating. Prolonged use of sliding-scale therapy should be avoided as the sole method for glycemic control.
Dr. Hellman noted that basal/bolus therapy is a key recommendation of the new guideline. It is based on data from two recent studies led by Dr. Umpierrez, both showing superiority of basal-bolus insulin regimens over sliding scale insulin treatment. One of those studies was done in noncritically ill hospitalized patients with type 2 diabetes (Diabetes Care 2007;30:2181-6), and the other in type 2 patients undergoing general surgery (Diabetes Care 2011;34:256-61).
"Both trials showed that basal/bolus insulin was clearly better than the use of sliding scale–only insulin, which is probably a predominant choice by many physicians, and it is in error. It is wrong," Dr. Hellman said.
At discharge, a preadmission insulin regimen, or oral and noninsulin injectable antidiabetic drugs, can be reinstituted for patients with acceptable preadmission glycemic control and without a contraindication to their continued use. Initiation of insulin administration at least 1 day before discharge is suggested, to allow assessment of the efficacy and safety of this transition. Patients and their caregivers should receive both oral and understandable written instructions for home glycemic management.
Special situations covered in detail in the document include transitions from intravenous to subcutaneous insulin therapy in patients with type 1 and type 2 diabetes, glycemic management of patients who are receiving enteral or parenteral nutrition, perioperative blood glucose control in type 1 and type 2 patients, and management of glucocorticoid-induced diabetes.
For hypoglycemia management, the panel recommends the development of protocols with specific directions for hypoglycemia avoidance and management, implementation of hospital-wide, nurse-initiated hypoglycemia treatment protocols, and implementation of a system for tracking frequency of hypoglycemic events with root cause analysis. The document lists key components of such protocols, and provides suggested nurse-initiated strategies.
Hospitals are advised to provide administrative support for an interdisciplinary steering committee targeting a systems approach to improve care of inpatients with hyperglycemia and diabetes. The establishment of uniform methods for collecting and evaluating POC testing data and insulin use information in hospitals is recommended, as are the provision of accurate devices for glucose measurement at the bedside with ongoing staff competency assessments.
Diabetes self-management education is recommended for patients, including both short-term "survival skills" education in the hospital and referral to community sources for ongoing patient education following discharge. Ongoing staff education is also recommended.
In all, Dr. Hellman commented, the 34-page document is meant to give a broad yet detailed overview of diabetes management in a variety of noncritical hospital settings and for a heterogenous population with hyperglycemia. "There’s a lot of rich information there for clinicians."
Dr. Hellman and Dr. Umpierrez have no financial disclosures, but three other members of the panel declared relationships with manufacturers of diabetes-related products.
All patients admitted to the hospital in noncritical care settings should have their blood glucose tested, according to a new clinical practice guideline from the Endocrine Society.
The guideline, published in the Journal of Clinical Endocrinology and Metabolism, is designed to complement previous recommendations that focused more on glucose targets, based largely on data from studies conducted in intensive/critical care settings (most recently Diabetes Care [2009;32:1119-31]). This new guideline is focused specifically on glucose management in noncritical settings, with special emphasis on systemic issues such as patient transition between hospital units and from inpatient to outpatient settings, as well as detailed guidance for hospitals on how to create systems and protocols that will ensure optimal patient management and safety (J. Clin. Endocrinol. Metab. 2012;97:16-38).
"This paper is different. It was viewed from the start as something that would be complementary to some of the earlier papers. It was a piece that hadn’t really been focused on. Your patients are more likely not to be in the ICU than in the ICU, so what about glycemic control at all the other times? That’s what a great deal of this statement is about," coauthor Dr. Richard Hellman said in an interview.
"Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline" was developed by an eight-member panel with representatives from the American Diabetes Association, American Heart Association, American Association of Diabetes Educators, European Society of Endocrinology, and the Society of Hospital Medicine. The lead author was Dr. Guillermo E. Umpierrez, professor of medicine at Emory University, and chief of diabetes and endocrinology at Grady Memorial Hospital, both in Atlanta. It was published Jan. 5.
It comprises eight sections, all focused on the noncritical hospital setting: diagnosis and recognition of hyperglycemia and diabetes; monitoring glycemia; glycemic targets; management of hyperglycemia; special situations; recognition and management of hypoglycemia; implementation of a glycemic control program; and patient and professional education. Strong recommendations are given as "we recommend," and weaker ones as "we suggest."
In the first section, assessment of all patients for a history of diabetes on admission is "recommended," while laboratory blood glucose testing on admission for all patients, regardless of prior diagnosis of diabetes, is "suggested." Still, there is strong rationale for it. "There’s abundant data to show that a very large number of people in hospitals have high blood sugars, and that correlates with poorer outcomes. The recommendation to check the glucose is extremely important because it isn’t just for people with a prior diagnosis of diabetes. Some come in with undiagnosed diabetes and people also develop stress hyperglycemia," noted Dr. Hellman, an endocrinologist who is a clinical professor of medicine at the University of Missouri–Kansas City.
Bedside capillary point-of-care (POC) glucose testing is recommended, using monitors that have demonstrated accuracy in acutely ill patients. Despite the acknowledged less-than-optimal accuracy of hand-held devices, the recommendation is based on the need for such testing in order to time glucose measures to match the patient’s nutritional intake and medication regimens. The patients’ personal glucose meters should not be used, and continuous glucose monitors, while "promising," have not been adequately tested in acute care and therefore can’t be recommended for hospital use at this time, Dr. Umpierrez and his associates wrote.
Recommended glycemic targets are the same as in the 2009 guideline: less than 140 mg/dL premeal and less than 180 mg/dL random for the majority of hospitalized patients with noncritical illness, with suggested modification according to clinical status. Lower targets might be considered among those who are able to achieve them without hypoglycemia, while higher targets might be appropriate for those at high risk for hypoglycemia or a limited life expectancy.
Medical nutrition therapy is recommended as a component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia. Meals with consistent amounts of carbohydrate are suggested, to help coordinate doses of rapid-acting insulin to carbohydrate ingestion.
Insulin therapy is recommended as the preferred method for achieving glycemic control in all hospitalized patients with diabetes and hyperglycemia, with the suggestion that oral hypoglycemic agents be discontinued and insulin therapy initiated in patients with type 2 diabetes at the time of admission for acute illness. That advice is based in part on the fact that contraindications to use of many oral agents are present in a high percentage of hospitalized patients. Such contraindications include use of metformin in patients with decompensated heart failure, renal insufficiency, hypoperfusion, or chronic pulmonary disease, and in any patient given intravenous contrast dye, the authors noted.
Scheduled subcutaneous insulin therapy is recommended for all patients, consisting of basal or intermediate-acting insulin once or twice daily in combination with rapid- or short-acting insulin administered before meals in patients who are eating. Prolonged use of sliding-scale therapy should be avoided as the sole method for glycemic control.
Dr. Hellman noted that basal/bolus therapy is a key recommendation of the new guideline. It is based on data from two recent studies led by Dr. Umpierrez, both showing superiority of basal-bolus insulin regimens over sliding scale insulin treatment. One of those studies was done in noncritically ill hospitalized patients with type 2 diabetes (Diabetes Care 2007;30:2181-6), and the other in type 2 patients undergoing general surgery (Diabetes Care 2011;34:256-61).
"Both trials showed that basal/bolus insulin was clearly better than the use of sliding scale–only insulin, which is probably a predominant choice by many physicians, and it is in error. It is wrong," Dr. Hellman said.
At discharge, a preadmission insulin regimen, or oral and noninsulin injectable antidiabetic drugs, can be reinstituted for patients with acceptable preadmission glycemic control and without a contraindication to their continued use. Initiation of insulin administration at least 1 day before discharge is suggested, to allow assessment of the efficacy and safety of this transition. Patients and their caregivers should receive both oral and understandable written instructions for home glycemic management.
Special situations covered in detail in the document include transitions from intravenous to subcutaneous insulin therapy in patients with type 1 and type 2 diabetes, glycemic management of patients who are receiving enteral or parenteral nutrition, perioperative blood glucose control in type 1 and type 2 patients, and management of glucocorticoid-induced diabetes.
For hypoglycemia management, the panel recommends the development of protocols with specific directions for hypoglycemia avoidance and management, implementation of hospital-wide, nurse-initiated hypoglycemia treatment protocols, and implementation of a system for tracking frequency of hypoglycemic events with root cause analysis. The document lists key components of such protocols, and provides suggested nurse-initiated strategies.
Hospitals are advised to provide administrative support for an interdisciplinary steering committee targeting a systems approach to improve care of inpatients with hyperglycemia and diabetes. The establishment of uniform methods for collecting and evaluating POC testing data and insulin use information in hospitals is recommended, as are the provision of accurate devices for glucose measurement at the bedside with ongoing staff competency assessments.
Diabetes self-management education is recommended for patients, including both short-term "survival skills" education in the hospital and referral to community sources for ongoing patient education following discharge. Ongoing staff education is also recommended.
In all, Dr. Hellman commented, the 34-page document is meant to give a broad yet detailed overview of diabetes management in a variety of noncritical hospital settings and for a heterogenous population with hyperglycemia. "There’s a lot of rich information there for clinicians."
Dr. Hellman and Dr. Umpierrez have no financial disclosures, but three other members of the panel declared relationships with manufacturers of diabetes-related products.
All patients admitted to the hospital in noncritical care settings should have their blood glucose tested, according to a new clinical practice guideline from the Endocrine Society.
The guideline, published in the Journal of Clinical Endocrinology and Metabolism, is designed to complement previous recommendations that focused more on glucose targets, based largely on data from studies conducted in intensive/critical care settings (most recently Diabetes Care [2009;32:1119-31]). This new guideline is focused specifically on glucose management in noncritical settings, with special emphasis on systemic issues such as patient transition between hospital units and from inpatient to outpatient settings, as well as detailed guidance for hospitals on how to create systems and protocols that will ensure optimal patient management and safety (J. Clin. Endocrinol. Metab. 2012;97:16-38).
"This paper is different. It was viewed from the start as something that would be complementary to some of the earlier papers. It was a piece that hadn’t really been focused on. Your patients are more likely not to be in the ICU than in the ICU, so what about glycemic control at all the other times? That’s what a great deal of this statement is about," coauthor Dr. Richard Hellman said in an interview.
"Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline" was developed by an eight-member panel with representatives from the American Diabetes Association, American Heart Association, American Association of Diabetes Educators, European Society of Endocrinology, and the Society of Hospital Medicine. The lead author was Dr. Guillermo E. Umpierrez, professor of medicine at Emory University, and chief of diabetes and endocrinology at Grady Memorial Hospital, both in Atlanta. It was published Jan. 5.
It comprises eight sections, all focused on the noncritical hospital setting: diagnosis and recognition of hyperglycemia and diabetes; monitoring glycemia; glycemic targets; management of hyperglycemia; special situations; recognition and management of hypoglycemia; implementation of a glycemic control program; and patient and professional education. Strong recommendations are given as "we recommend," and weaker ones as "we suggest."
In the first section, assessment of all patients for a history of diabetes on admission is "recommended," while laboratory blood glucose testing on admission for all patients, regardless of prior diagnosis of diabetes, is "suggested." Still, there is strong rationale for it. "There’s abundant data to show that a very large number of people in hospitals have high blood sugars, and that correlates with poorer outcomes. The recommendation to check the glucose is extremely important because it isn’t just for people with a prior diagnosis of diabetes. Some come in with undiagnosed diabetes and people also develop stress hyperglycemia," noted Dr. Hellman, an endocrinologist who is a clinical professor of medicine at the University of Missouri–Kansas City.
Bedside capillary point-of-care (POC) glucose testing is recommended, using monitors that have demonstrated accuracy in acutely ill patients. Despite the acknowledged less-than-optimal accuracy of hand-held devices, the recommendation is based on the need for such testing in order to time glucose measures to match the patient’s nutritional intake and medication regimens. The patients’ personal glucose meters should not be used, and continuous glucose monitors, while "promising," have not been adequately tested in acute care and therefore can’t be recommended for hospital use at this time, Dr. Umpierrez and his associates wrote.
Recommended glycemic targets are the same as in the 2009 guideline: less than 140 mg/dL premeal and less than 180 mg/dL random for the majority of hospitalized patients with noncritical illness, with suggested modification according to clinical status. Lower targets might be considered among those who are able to achieve them without hypoglycemia, while higher targets might be appropriate for those at high risk for hypoglycemia or a limited life expectancy.
Medical nutrition therapy is recommended as a component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia. Meals with consistent amounts of carbohydrate are suggested, to help coordinate doses of rapid-acting insulin to carbohydrate ingestion.
Insulin therapy is recommended as the preferred method for achieving glycemic control in all hospitalized patients with diabetes and hyperglycemia, with the suggestion that oral hypoglycemic agents be discontinued and insulin therapy initiated in patients with type 2 diabetes at the time of admission for acute illness. That advice is based in part on the fact that contraindications to use of many oral agents are present in a high percentage of hospitalized patients. Such contraindications include use of metformin in patients with decompensated heart failure, renal insufficiency, hypoperfusion, or chronic pulmonary disease, and in any patient given intravenous contrast dye, the authors noted.
Scheduled subcutaneous insulin therapy is recommended for all patients, consisting of basal or intermediate-acting insulin once or twice daily in combination with rapid- or short-acting insulin administered before meals in patients who are eating. Prolonged use of sliding-scale therapy should be avoided as the sole method for glycemic control.
Dr. Hellman noted that basal/bolus therapy is a key recommendation of the new guideline. It is based on data from two recent studies led by Dr. Umpierrez, both showing superiority of basal-bolus insulin regimens over sliding scale insulin treatment. One of those studies was done in noncritically ill hospitalized patients with type 2 diabetes (Diabetes Care 2007;30:2181-6), and the other in type 2 patients undergoing general surgery (Diabetes Care 2011;34:256-61).
"Both trials showed that basal/bolus insulin was clearly better than the use of sliding scale–only insulin, which is probably a predominant choice by many physicians, and it is in error. It is wrong," Dr. Hellman said.
At discharge, a preadmission insulin regimen, or oral and noninsulin injectable antidiabetic drugs, can be reinstituted for patients with acceptable preadmission glycemic control and without a contraindication to their continued use. Initiation of insulin administration at least 1 day before discharge is suggested, to allow assessment of the efficacy and safety of this transition. Patients and their caregivers should receive both oral and understandable written instructions for home glycemic management.
Special situations covered in detail in the document include transitions from intravenous to subcutaneous insulin therapy in patients with type 1 and type 2 diabetes, glycemic management of patients who are receiving enteral or parenteral nutrition, perioperative blood glucose control in type 1 and type 2 patients, and management of glucocorticoid-induced diabetes.
For hypoglycemia management, the panel recommends the development of protocols with specific directions for hypoglycemia avoidance and management, implementation of hospital-wide, nurse-initiated hypoglycemia treatment protocols, and implementation of a system for tracking frequency of hypoglycemic events with root cause analysis. The document lists key components of such protocols, and provides suggested nurse-initiated strategies.
Hospitals are advised to provide administrative support for an interdisciplinary steering committee targeting a systems approach to improve care of inpatients with hyperglycemia and diabetes. The establishment of uniform methods for collecting and evaluating POC testing data and insulin use information in hospitals is recommended, as are the provision of accurate devices for glucose measurement at the bedside with ongoing staff competency assessments.
Diabetes self-management education is recommended for patients, including both short-term "survival skills" education in the hospital and referral to community sources for ongoing patient education following discharge. Ongoing staff education is also recommended.
In all, Dr. Hellman commented, the 34-page document is meant to give a broad yet detailed overview of diabetes management in a variety of noncritical hospital settings and for a heterogenous population with hyperglycemia. "There’s a lot of rich information there for clinicians."
Dr. Hellman and Dr. Umpierrez have no financial disclosures, but three other members of the panel declared relationships with manufacturers of diabetes-related products.
Glucose Testing Suggested for All Inpatients
All patients admitted to the hospital in noncritical care settings should have their blood glucose tested, according to a new clinical practice guideline from the Endocrine Society.
Unlike previous guidelines based largely on data from intensive care and critical care settings, the new guideline focuses on glucose management in noncritical settings, with special emphasis on systemic issues such as patient transition between hospital units and from inpatient to outpatient settings. The guidelines also include detailed guidance for creating systems and protocols to ensure optimal patient management and safety (Diabetes Care [2009;32:1119-31]).
"Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline" was developed by an eight-member panel with representatives from the American Diabetes Association, American Heart Association, American Association of Diabetes Educators, European Society of Endocrinology, and the Society of Hospital Medicine. The lead author was Dr. Guillermo E. Umpierrez, professor of medicine at Emory University, and chief of diabetes and endocrinology at Grady Memorial Hospital, both in Atlanta.
The guideline has eight sections, all focused on the noncritical hospital setting: diagnosis and recognition of hyperglycemia and diabetes, monitoring glycemia, glycemic targets, management of hyperglycemia, special situations, recognition and management of hypoglycemia, implementation of a glycemic control program, and patient and professional education.
The panel’s advice was characterized as "recommended" for items with strong evidence and "suggested" for items with less evidence. In the first of the guideline’s eight sections, the panel recommended all patients be assessed on admission for a history of diabetes and suggested laboratory blood glucose testing on admission for all patients, regardless of prior diagnosis of diabetes.

"There’s abundant data to show that a very large number of people … [are admitted] with undiagnosed diabetes and people also develop stress hyperglycemia" and both conditions affect patient outcomes, Dr. Richard Hellman said in an interview. Dr. Hellman is a coauthor of the guidelines and an endocrinologist who is a clinical professor of medicine at the University of Missouri–Kansas City.
<[stk -3]>While the accuracy of point-of-care testing is not optimal, the panel recommended bedside glucose testing of capillary blood because of the need to time glucose measures to the patient’s nutritional intake and medication regimens. Personal glucose meters should not be used, and continuous glucose monitors while "promising," have not been adequately tested in acute care and therefore can’t be recommended for hospital use at this time, Dr. Umpierrez and his associates wrote.<[etk]>
As in the 2009 guideline that addressed critical care patients, the glycemic targets are less than 140 mg/dL premeal and less than 180 mg/dL random for the majority of hospitalized patients with noncritical illness. Lower targets might be considered among patients who are able to achieve them without hypoglycemia, while higher targets might be appropriate for those at high risk for hypoglycemia and those with a limited life expectancy.
Medical nutrition therapy is recommended as a component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia. Meals with consistent amounts of carbohydrate are suggested to help coordinate dosing of rapid-acting insulin.
Insulin therapy is the preferred method for achieving glycemic control in all hospitalized patients with diabetes and hyperglycemia, the panel said. At admission, they suggested, oral hypoglycemic agents should be discontinued and insulin therapy should be initiated in acutely ill patients with type 2 diabetes. Oral agents are contraindicated in hospitalized patients with decompensated heart failure, renal insufficiency, hypoperfusion, or chronic pulmonary disease, and in any patient given intravenous contrast dye, the authors noted.
<[stk -3]>For patients who are eating, the panel recommended scheduled subcutaneous basal or intermediate-acting insulin once or twice daily in combination with rapid- or short-acting insulin administered before meals. <[etk]>
Prolonged use of sliding-scale therapy should be avoided as the sole method for glycemic control, the panel wrote.
"There’s abundant data to show that a very large number of people [are admitted] with undiagnosed diabetes and people also develop stress hyperglycemia."
<[stk -3]>Two recent studies led by Dr. Umpierrez show basal-bolus insulin regimens to be superior to sliding scale insulin treatment. One of those studies was done in noncritically ill hospitalized patients with type 2 diabetes (Diabetes Care 2007;30:2181-6), and the other was done in type 2 patients undergoing general surgery (Diabetes Care 2011;34:256-61). <[etk]>
Diabetes self-management education is recommended for patients, including both short-term "survival skills" education in the hospital and referral to community sources for ongoing patient education following discharge.
At discharge, the patient’s preadmission regimen – either insulin or oral and noninsulin injectable antidiabetic drugs – can be reinstituted so long as the patient’s preadmission glycemic control was good and there are no contraindications. To assess safety and efficacy, insulin administration should be initiated at least 1 day before discharge. Patients and their caregivers should receive oral and written instructions for home glycemic management.
The guidelines also address transition from intravenous to subcutaneous insulin therapy, glycemic management of patients who are receiving enteral or parenteral nutrition, perioperative blood glucose control, and management of glucocorticoid-induced diabetes.
<[stk -3]>The panel recommended the development of protocols with specific directions for avoiding and managing hypoglycemia as well as the implementation of hospital-wide, nurse-initiated hypoglycemia treatment protocols and a system for tracking with root cause analysis the frequency of hypoglycemic events. The document lists key components of such protocols, and provides suggested nurse-initiated strategies.<[etk]>
<[stk -3]>Hospitals are advised to provide administrative support for an interdisciplinary steering committee targeting a systems approach to improve care of inpatients with hyperglycemia and diabetes. Uniform methods for collecting and evaluating point-of-care testing data and insulin use information in hospitals are recommended, as are the provision of accurate devices for glucose measurement at the bedside with ongoing staff education and competency assessments.
Dr. Hellman and Dr. Umpierrez have no financial disclosures, but three other members of the guideline panel declared relationships with manufacturers of diabetes-related products.
All patients admitted to the hospital in noncritical care settings should have their blood glucose tested, according to a new clinical practice guideline from the Endocrine Society.
Unlike previous guidelines based largely on data from intensive care and critical care settings, the new guideline focuses on glucose management in noncritical settings, with special emphasis on systemic issues such as patient transition between hospital units and from inpatient to outpatient settings. The guidelines also include detailed guidance for creating systems and protocols to ensure optimal patient management and safety (Diabetes Care [2009;32:1119-31]).
"Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline" was developed by an eight-member panel with representatives from the American Diabetes Association, American Heart Association, American Association of Diabetes Educators, European Society of Endocrinology, and the Society of Hospital Medicine. The lead author was Dr. Guillermo E. Umpierrez, professor of medicine at Emory University, and chief of diabetes and endocrinology at Grady Memorial Hospital, both in Atlanta.
The guideline has eight sections, all focused on the noncritical hospital setting: diagnosis and recognition of hyperglycemia and diabetes, monitoring glycemia, glycemic targets, management of hyperglycemia, special situations, recognition and management of hypoglycemia, implementation of a glycemic control program, and patient and professional education.
The panel’s advice was characterized as "recommended" for items with strong evidence and "suggested" for items with less evidence. In the first of the guideline’s eight sections, the panel recommended all patients be assessed on admission for a history of diabetes and suggested laboratory blood glucose testing on admission for all patients, regardless of prior diagnosis of diabetes.
"There’s abundant data to show that a very large number of people … [are admitted] with undiagnosed diabetes and people also develop stress hyperglycemia" and both conditions affect patient outcomes, Dr. Richard Hellman said in an interview. Dr. Hellman is a coauthor of the guidelines and an endocrinologist who is a clinical professor of medicine at the University of Missouri–Kansas City.
<[stk -3]>While the accuracy of point-of-care testing is not optimal, the panel recommended bedside glucose testing of capillary blood because of the need to time glucose measures to the patient’s nutritional intake and medication regimens. Personal glucose meters should not be used, and continuous glucose monitors while "promising," have not been adequately tested in acute care and therefore can’t be recommended for hospital use at this time, Dr. Umpierrez and his associates wrote.<[etk]>
As in the 2009 guideline that addressed critical care patients, the glycemic targets are less than 140 mg/dL premeal and less than 180 mg/dL random for the majority of hospitalized patients with noncritical illness. Lower targets might be considered among patients who are able to achieve them without hypoglycemia, while higher targets might be appropriate for those at high risk for hypoglycemia and those with a limited life expectancy.
Medical nutrition therapy is recommended as a component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia. Meals with consistent amounts of carbohydrate are suggested to help coordinate dosing of rapid-acting insulin.
Insulin therapy is the preferred method for achieving glycemic control in all hospitalized patients with diabetes and hyperglycemia, the panel said. At admission, they suggested, oral hypoglycemic agents should be discontinued and insulin therapy should be initiated in acutely ill patients with type 2 diabetes. Oral agents are contraindicated in hospitalized patients with decompensated heart failure, renal insufficiency, hypoperfusion, or chronic pulmonary disease, and in any patient given intravenous contrast dye, the authors noted.
<[stk -3]>For patients who are eating, the panel recommended scheduled subcutaneous basal or intermediate-acting insulin once or twice daily in combination with rapid- or short-acting insulin administered before meals. <[etk]>
Prolonged use of sliding-scale therapy should be avoided as the sole method for glycemic control, the panel wrote.
"There’s abundant data to show that a very large number of people [are admitted] with undiagnosed diabetes and people also develop stress hyperglycemia."
<[stk -3]>Two recent studies led by Dr. Umpierrez show basal-bolus insulin regimens to be superior to sliding scale insulin treatment. One of those studies was done in noncritically ill hospitalized patients with type 2 diabetes (Diabetes Care 2007;30:2181-6), and the other was done in type 2 patients undergoing general surgery (Diabetes Care 2011;34:256-61). <[etk]>
Diabetes self-management education is recommended for patients, including both short-term "survival skills" education in the hospital and referral to community sources for ongoing patient education following discharge.
At discharge, the patient’s preadmission regimen – either insulin or oral and noninsulin injectable antidiabetic drugs – can be reinstituted so long as the patient’s preadmission glycemic control was good and there are no contraindications. To assess safety and efficacy, insulin administration should be initiated at least 1 day before discharge. Patients and their caregivers should receive oral and written instructions for home glycemic management.
The guidelines also address transition from intravenous to subcutaneous insulin therapy, glycemic management of patients who are receiving enteral or parenteral nutrition, perioperative blood glucose control, and management of glucocorticoid-induced diabetes.
<[stk -3]>The panel recommended the development of protocols with specific directions for avoiding and managing hypoglycemia as well as the implementation of hospital-wide, nurse-initiated hypoglycemia treatment protocols and a system for tracking with root cause analysis the frequency of hypoglycemic events. The document lists key components of such protocols, and provides suggested nurse-initiated strategies.<[etk]>
<[stk -3]>Hospitals are advised to provide administrative support for an interdisciplinary steering committee targeting a systems approach to improve care of inpatients with hyperglycemia and diabetes. Uniform methods for collecting and evaluating point-of-care testing data and insulin use information in hospitals are recommended, as are the provision of accurate devices for glucose measurement at the bedside with ongoing staff education and competency assessments.
Dr. Hellman and Dr. Umpierrez have no financial disclosures, but three other members of the guideline panel declared relationships with manufacturers of diabetes-related products.
All patients admitted to the hospital in noncritical care settings should have their blood glucose tested, according to a new clinical practice guideline from the Endocrine Society.
Unlike previous guidelines based largely on data from intensive care and critical care settings, the new guideline focuses on glucose management in noncritical settings, with special emphasis on systemic issues such as patient transition between hospital units and from inpatient to outpatient settings. The guidelines also include detailed guidance for creating systems and protocols to ensure optimal patient management and safety (Diabetes Care [2009;32:1119-31]).
"Management of Hyperglycemia in Hospitalized Patients in Non-Critical Care Setting: An Endocrine Society Clinical Practice Guideline" was developed by an eight-member panel with representatives from the American Diabetes Association, American Heart Association, American Association of Diabetes Educators, European Society of Endocrinology, and the Society of Hospital Medicine. The lead author was Dr. Guillermo E. Umpierrez, professor of medicine at Emory University, and chief of diabetes and endocrinology at Grady Memorial Hospital, both in Atlanta.
The guideline has eight sections, all focused on the noncritical hospital setting: diagnosis and recognition of hyperglycemia and diabetes, monitoring glycemia, glycemic targets, management of hyperglycemia, special situations, recognition and management of hypoglycemia, implementation of a glycemic control program, and patient and professional education.
The panel’s advice was characterized as "recommended" for items with strong evidence and "suggested" for items with less evidence. In the first of the guideline’s eight sections, the panel recommended all patients be assessed on admission for a history of diabetes and suggested laboratory blood glucose testing on admission for all patients, regardless of prior diagnosis of diabetes.
"There’s abundant data to show that a very large number of people … [are admitted] with undiagnosed diabetes and people also develop stress hyperglycemia" and both conditions affect patient outcomes, Dr. Richard Hellman said in an interview. Dr. Hellman is a coauthor of the guidelines and an endocrinologist who is a clinical professor of medicine at the University of Missouri–Kansas City.
<[stk -3]>While the accuracy of point-of-care testing is not optimal, the panel recommended bedside glucose testing of capillary blood because of the need to time glucose measures to the patient’s nutritional intake and medication regimens. Personal glucose meters should not be used, and continuous glucose monitors while "promising," have not been adequately tested in acute care and therefore can’t be recommended for hospital use at this time, Dr. Umpierrez and his associates wrote.<[etk]>
As in the 2009 guideline that addressed critical care patients, the glycemic targets are less than 140 mg/dL premeal and less than 180 mg/dL random for the majority of hospitalized patients with noncritical illness. Lower targets might be considered among patients who are able to achieve them without hypoglycemia, while higher targets might be appropriate for those at high risk for hypoglycemia and those with a limited life expectancy.
Medical nutrition therapy is recommended as a component of the glycemic management program for all hospitalized patients with diabetes and hyperglycemia. Meals with consistent amounts of carbohydrate are suggested to help coordinate dosing of rapid-acting insulin.
Insulin therapy is the preferred method for achieving glycemic control in all hospitalized patients with diabetes and hyperglycemia, the panel said. At admission, they suggested, oral hypoglycemic agents should be discontinued and insulin therapy should be initiated in acutely ill patients with type 2 diabetes. Oral agents are contraindicated in hospitalized patients with decompensated heart failure, renal insufficiency, hypoperfusion, or chronic pulmonary disease, and in any patient given intravenous contrast dye, the authors noted.
<[stk -3]>For patients who are eating, the panel recommended scheduled subcutaneous basal or intermediate-acting insulin once or twice daily in combination with rapid- or short-acting insulin administered before meals. <[etk]>
Prolonged use of sliding-scale therapy should be avoided as the sole method for glycemic control, the panel wrote.
"There’s abundant data to show that a very large number of people [are admitted] with undiagnosed diabetes and people also develop stress hyperglycemia."
<[stk -3]>Two recent studies led by Dr. Umpierrez show basal-bolus insulin regimens to be superior to sliding scale insulin treatment. One of those studies was done in noncritically ill hospitalized patients with type 2 diabetes (Diabetes Care 2007;30:2181-6), and the other was done in type 2 patients undergoing general surgery (Diabetes Care 2011;34:256-61). <[etk]>
Diabetes self-management education is recommended for patients, including both short-term "survival skills" education in the hospital and referral to community sources for ongoing patient education following discharge.
At discharge, the patient’s preadmission regimen – either insulin or oral and noninsulin injectable antidiabetic drugs – can be reinstituted so long as the patient’s preadmission glycemic control was good and there are no contraindications. To assess safety and efficacy, insulin administration should be initiated at least 1 day before discharge. Patients and their caregivers should receive oral and written instructions for home glycemic management.
The guidelines also address transition from intravenous to subcutaneous insulin therapy, glycemic management of patients who are receiving enteral or parenteral nutrition, perioperative blood glucose control, and management of glucocorticoid-induced diabetes.
<[stk -3]>The panel recommended the development of protocols with specific directions for avoiding and managing hypoglycemia as well as the implementation of hospital-wide, nurse-initiated hypoglycemia treatment protocols and a system for tracking with root cause analysis the frequency of hypoglycemic events. The document lists key components of such protocols, and provides suggested nurse-initiated strategies.<[etk]>
<[stk -3]>Hospitals are advised to provide administrative support for an interdisciplinary steering committee targeting a systems approach to improve care of inpatients with hyperglycemia and diabetes. Uniform methods for collecting and evaluating point-of-care testing data and insulin use information in hospitals are recommended, as are the provision of accurate devices for glucose measurement at the bedside with ongoing staff education and competency assessments.
Dr. Hellman and Dr. Umpierrez have no financial disclosures, but three other members of the guideline panel declared relationships with manufacturers of diabetes-related products.
Levetiracetam Matches Older Antiepileptics for Bone Protection
BALTIMORE – Levetiracetam had effects on bone mineral density and markers of bone turnover that were similar to those seen with the older antiepileptic drugs carbamazepine and sodium valproate in a 12-month, randomized, controlled trial of 84 patients with partial epilepsy.
The finding was counter to the expectation that levetiracetam (Keppra) would have neutral or more benign effects on bone health because of its "cleaner pharmacokinetics – no effect on vitamin D metabolism – and a different mechanism of action," study investigator Dr. Terence J. O’Brien said in an interview. "Most [experts] thought it would be better for bone health. However, there is a previous study in rats that did show effect on bone. ... The clinical message is that neurologists need to monitor bone heath on all their patients chronically treated with AEDs."
Chronic antiepileptic drug use has been associated with increased risk of both bone disease and fracture, as well as weight gain and insulin resistance. It has been hoped that newer antiepileptic drugs with different mechanisms of action would minimize or eliminate these effects. One of these newer agents, levetiracetam, has a novel mechanism of action, binding to the SV2A receptors that interfere with synaptic vesicle exocytosis. It is not hepatically metabolized, so it does not affect hormonal levels.
"The clinical message is that neurologists need to monitor bone heath on all their patients chronically treated with antiepileptic drugs."
"There are plenty of reasons to believe it would have fewer bone and metabolic effects, but this had never been tested before in a randomized, controlled trial," said Dr. O’Brien, a professor of medicine at the University of Melbourne and head of the department of medicine at the Royal Melbourne Hospital.
Of 84 patients randomized to open-label substitution monotherapy with either levetiracetam or carbamazepine or valproate in the KONQUEST trial, 40 levetiracetam patients and 30 carbamazepine/valproate patients completed an assessment at 15 months. Dosing in the trial was flexible, and was increased or decreased by the treating neurologist according to tolerability and seizure control.
Dual energy X-ray absorptiometry (DXA) measurements of areal bone mineral density (aBMD) in the forearm was significantly lower at 15 months in both the levetiracetam and carbamazepine/valproate groups, compared with measurements taken at 3 months, but more so for levetiracetam, with reductions of 1.4% (P less than .001) and 0.96% (P = .015), respectively. Peripheral quantitative CT measurement of trabecular BMD in the radius was also reduced in both groups, by 2.25% (P = .005) with levetiracetam and by 2.9% (P = .001) for the older AEDs. There were no differences from 3-month assessments in aBMD of the lumbar spine or hip in either treatment group.
Markers of bone formation and resorption were among the secondary end points. The bone resorption marker beta C-terminal telopeptide of type 1 collagen was reduced in both treatment groups, by 12.8% (P = .021) with levetiracetam and by 15.6% (P = .028) with carbamazepine/valproate. However, the bone formation marker procollagen type 1 N-terminal propeptide was reduced only with the older AEDs, by 20.9% (P = .008). There were no differences in vitamin D or other markers of calcium homeostasis, Dr. O’Brien said.
Reduction in serum markers of bone turnover suggests reduced bone remodeling with AEDs, "an atypical mechanism for bone loss which warrants further study," he said.
In the interview, he added that the lack of effect on markers of bone formation for levetiracetam may indicate some differences in the mechanism of its effect, or may just have been a lack of power.
The exploratory end points of femoral neck aBMD, total bone area (trabecular), trabecular bone mineral content, and total bone area (cortical) were all significantly reduced in both groups. However, the anthropometric exploratory end points of weight and body mass index were increased only with the older AEDs, by 2.0% (P = .039) and 2.15% (P = .044), respectively.
There are no clear guidelines for bone health monitoring in patients on AEDs. "What we recommend is when you start the drug, [get] a baseline, and then [monitor] every 3-5 years. Vitamin D levels should also be checked and supplemented if deficient," he said in the interview.
A UCB Pharma spokeswoman declined to comment on the findings of KONQUEST. The study was partially funded by the company, but it had no role in its design, data collection, analysis, or interpretation. Dr. O’Brien said that he had no additional disclosures.
BALTIMORE – Levetiracetam had effects on bone mineral density and markers of bone turnover that were similar to those seen with the older antiepileptic drugs carbamazepine and sodium valproate in a 12-month, randomized, controlled trial of 84 patients with partial epilepsy.
The finding was counter to the expectation that levetiracetam (Keppra) would have neutral or more benign effects on bone health because of its "cleaner pharmacokinetics – no effect on vitamin D metabolism – and a different mechanism of action," study investigator Dr. Terence J. O’Brien said in an interview. "Most [experts] thought it would be better for bone health. However, there is a previous study in rats that did show effect on bone. ... The clinical message is that neurologists need to monitor bone heath on all their patients chronically treated with AEDs."
Chronic antiepileptic drug use has been associated with increased risk of both bone disease and fracture, as well as weight gain and insulin resistance. It has been hoped that newer antiepileptic drugs with different mechanisms of action would minimize or eliminate these effects. One of these newer agents, levetiracetam, has a novel mechanism of action, binding to the SV2A receptors that interfere with synaptic vesicle exocytosis. It is not hepatically metabolized, so it does not affect hormonal levels.
"The clinical message is that neurologists need to monitor bone heath on all their patients chronically treated with antiepileptic drugs."
"There are plenty of reasons to believe it would have fewer bone and metabolic effects, but this had never been tested before in a randomized, controlled trial," said Dr. O’Brien, a professor of medicine at the University of Melbourne and head of the department of medicine at the Royal Melbourne Hospital.
Of 84 patients randomized to open-label substitution monotherapy with either levetiracetam or carbamazepine or valproate in the KONQUEST trial, 40 levetiracetam patients and 30 carbamazepine/valproate patients completed an assessment at 15 months. Dosing in the trial was flexible, and was increased or decreased by the treating neurologist according to tolerability and seizure control.
Dual energy X-ray absorptiometry (DXA) measurements of areal bone mineral density (aBMD) in the forearm was significantly lower at 15 months in both the levetiracetam and carbamazepine/valproate groups, compared with measurements taken at 3 months, but more so for levetiracetam, with reductions of 1.4% (P less than .001) and 0.96% (P = .015), respectively. Peripheral quantitative CT measurement of trabecular BMD in the radius was also reduced in both groups, by 2.25% (P = .005) with levetiracetam and by 2.9% (P = .001) for the older AEDs. There were no differences from 3-month assessments in aBMD of the lumbar spine or hip in either treatment group.
Markers of bone formation and resorption were among the secondary end points. The bone resorption marker beta C-terminal telopeptide of type 1 collagen was reduced in both treatment groups, by 12.8% (P = .021) with levetiracetam and by 15.6% (P = .028) with carbamazepine/valproate. However, the bone formation marker procollagen type 1 N-terminal propeptide was reduced only with the older AEDs, by 20.9% (P = .008). There were no differences in vitamin D or other markers of calcium homeostasis, Dr. O’Brien said.
Reduction in serum markers of bone turnover suggests reduced bone remodeling with AEDs, "an atypical mechanism for bone loss which warrants further study," he said.
In the interview, he added that the lack of effect on markers of bone formation for levetiracetam may indicate some differences in the mechanism of its effect, or may just have been a lack of power.
The exploratory end points of femoral neck aBMD, total bone area (trabecular), trabecular bone mineral content, and total bone area (cortical) were all significantly reduced in both groups. However, the anthropometric exploratory end points of weight and body mass index were increased only with the older AEDs, by 2.0% (P = .039) and 2.15% (P = .044), respectively.
There are no clear guidelines for bone health monitoring in patients on AEDs. "What we recommend is when you start the drug, [get] a baseline, and then [monitor] every 3-5 years. Vitamin D levels should also be checked and supplemented if deficient," he said in the interview.
A UCB Pharma spokeswoman declined to comment on the findings of KONQUEST. The study was partially funded by the company, but it had no role in its design, data collection, analysis, or interpretation. Dr. O’Brien said that he had no additional disclosures.
BALTIMORE – Levetiracetam had effects on bone mineral density and markers of bone turnover that were similar to those seen with the older antiepileptic drugs carbamazepine and sodium valproate in a 12-month, randomized, controlled trial of 84 patients with partial epilepsy.
The finding was counter to the expectation that levetiracetam (Keppra) would have neutral or more benign effects on bone health because of its "cleaner pharmacokinetics – no effect on vitamin D metabolism – and a different mechanism of action," study investigator Dr. Terence J. O’Brien said in an interview. "Most [experts] thought it would be better for bone health. However, there is a previous study in rats that did show effect on bone. ... The clinical message is that neurologists need to monitor bone heath on all their patients chronically treated with AEDs."
Chronic antiepileptic drug use has been associated with increased risk of both bone disease and fracture, as well as weight gain and insulin resistance. It has been hoped that newer antiepileptic drugs with different mechanisms of action would minimize or eliminate these effects. One of these newer agents, levetiracetam, has a novel mechanism of action, binding to the SV2A receptors that interfere with synaptic vesicle exocytosis. It is not hepatically metabolized, so it does not affect hormonal levels.
"The clinical message is that neurologists need to monitor bone heath on all their patients chronically treated with antiepileptic drugs."
"There are plenty of reasons to believe it would have fewer bone and metabolic effects, but this had never been tested before in a randomized, controlled trial," said Dr. O’Brien, a professor of medicine at the University of Melbourne and head of the department of medicine at the Royal Melbourne Hospital.
Of 84 patients randomized to open-label substitution monotherapy with either levetiracetam or carbamazepine or valproate in the KONQUEST trial, 40 levetiracetam patients and 30 carbamazepine/valproate patients completed an assessment at 15 months. Dosing in the trial was flexible, and was increased or decreased by the treating neurologist according to tolerability and seizure control.
Dual energy X-ray absorptiometry (DXA) measurements of areal bone mineral density (aBMD) in the forearm was significantly lower at 15 months in both the levetiracetam and carbamazepine/valproate groups, compared with measurements taken at 3 months, but more so for levetiracetam, with reductions of 1.4% (P less than .001) and 0.96% (P = .015), respectively. Peripheral quantitative CT measurement of trabecular BMD in the radius was also reduced in both groups, by 2.25% (P = .005) with levetiracetam and by 2.9% (P = .001) for the older AEDs. There were no differences from 3-month assessments in aBMD of the lumbar spine or hip in either treatment group.
Markers of bone formation and resorption were among the secondary end points. The bone resorption marker beta C-terminal telopeptide of type 1 collagen was reduced in both treatment groups, by 12.8% (P = .021) with levetiracetam and by 15.6% (P = .028) with carbamazepine/valproate. However, the bone formation marker procollagen type 1 N-terminal propeptide was reduced only with the older AEDs, by 20.9% (P = .008). There were no differences in vitamin D or other markers of calcium homeostasis, Dr. O’Brien said.
Reduction in serum markers of bone turnover suggests reduced bone remodeling with AEDs, "an atypical mechanism for bone loss which warrants further study," he said.
In the interview, he added that the lack of effect on markers of bone formation for levetiracetam may indicate some differences in the mechanism of its effect, or may just have been a lack of power.
The exploratory end points of femoral neck aBMD, total bone area (trabecular), trabecular bone mineral content, and total bone area (cortical) were all significantly reduced in both groups. However, the anthropometric exploratory end points of weight and body mass index were increased only with the older AEDs, by 2.0% (P = .039) and 2.15% (P = .044), respectively.
There are no clear guidelines for bone health monitoring in patients on AEDs. "What we recommend is when you start the drug, [get] a baseline, and then [monitor] every 3-5 years. Vitamin D levels should also be checked and supplemented if deficient," he said in the interview.
A UCB Pharma spokeswoman declined to comment on the findings of KONQUEST. The study was partially funded by the company, but it had no role in its design, data collection, analysis, or interpretation. Dr. O’Brien said that he had no additional disclosures.
FROM THE ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
Major Finding: Forearm aBMD was significantly lower at 15 months in both the levetiracetam and carbamazepine/valproate groups, but more so for levetiracetam, with reductions of 1.4% (P less than .001) and 0.96% (P = .015), respectively.
Data Source: Single-center, open-label, randomized study of 84 epilepsy patients.
Disclosures: The study was partially funded by UCB Pharma, but it had no role in its design, data collection, analysis, or interpretation. Dr. O’Brien had no additional disclosures.
Urinary Dysfunction Stands Out on Retigabine's Safety Profile
BALTIMORE – The safety profile for retigabine is generally consistent with that of other antiepileptic drugs, but data from studies in its evaluation process show that it also carries a novel, small increased risk of urinary voiding dysfunction.
At the annual meeting of the American Epilepsy Society Dr. Neil Brickel of GlaxoSmithKline’s clinical safety and pharmacovigilance group in Middlesex, England, reported on the safety of the novel drug in three phase III, randomized, double-blind, placebo-controlled trials, four phase II studies, and six long-term open-label extension studies, totalling 1,365 patients.
Retigabine is the international nonproprietary name of the drug, but it was approved in the United States in June 2011 under the adopted name ezogabine as an adjunctive therapy in adults with partial-onset seizures. It is a first-in-class potassium channel opener manufactured by GlaxoSmithKline and Valeant Pharmaceuticals International, and sold under the brand name Trobalt in Europe and Potiga in the United States.
In all of the studies that Dr. Brickel analyzed, retigabine was evaluated as a second, add-on agent. As of Oct. 2, 2009, 1,217 of the 1,365 patients had been on treatment at least 1 month, 801 for at least 6 months, and 586 for 1 year or longer.
As expected with any antiepileptic drug (AED), the most frequent adverse events involved the central nervous system. The most common in the three pivotal controlled trials were dizziness (23% of retigabine-treated patients vs. 9% of placebo-treated patients) and somnolence (reported by 22% vs. 12%, respectively). The only CNS adverse events that were not dose related were headache (reported by 15% of the retigabine group vs. 16% of the placebo group) and fatigue (by 15% and 6%, respectively). Other adverse events occurring in more than 10% of subjects were confusional state, tremor, and abnormal coordination. For the most part, patients reported these adverse events early on, during the titration phases of the trials, Dr. Brickel said.
Adverse events led to discontinuation in 437 patients (32%) of the total phase II/III study population. Again, these were primarily CNS and dose related. Discontinuations for any event occurred in 11% of the placebo group. Among those taking retigabine, discontinuations occurred in 17% of those assigned to 600 mg, 25% of those assigned to 900 mg, and 31% of those assigned to 1,200 mg. The most common reason for discontinuation was dizziness.
"Two-thirds of patients were able to continue in the study, even with the fixed titration regimen and at the 1,200-mg dose," Dr. Brickel noted.
Serious adverse events (SAEs) were infrequent, and also typically CNS related. In the three pivotal controlled trials, SAEs occurred in 6% of the placebo group and 9% of the retigabine patients. Six of the patients taking retigabine developed a psychotic disorder (five with 1,200 mg, one with 900 mg), compared with none of the placebo patients. Convulsions occurred in 1.2% of the placebo group and in 1.5% of the retigabine patients, across all doses. This finding was not unexpected, considering the underlying epilepsy, he said.
No other SAE was reported in more than two patients in any group. Deaths occurred in three placebo patients and two patients in the retigabine group. One in each group was a sudden death.
In the three pivotal trials, urinary and renal-related adverse events occurred in 17% of retigabine patients, compared with 13% of the placebo-treated patients. In the entire phase II/III study population, 26% of the 1,365 patients reported a urinary adverse event.
However, events related to urinary voiding dysfunction, which have a plausible biological relation to retigabine’s pharmacology, occurred in less than 4% of retigabine-treated patients in the phase III trials alone and in all phase II and III trial populations combined. Urinary hesitation was the most common of these in the entire phase II and III study group, occurring in 3.1%, followed by urinary retention in 1.9%. Catheterization was required in four patients taking retigabine and in one patient on placebo.
"These all occurred in a smaller number of patients and provide a better guide as to how many patents are potentially at risk. It is also important to note that these events were for the most part ‘mild’ in intensity and the patients were able to continue treatment," Dr. Brickel said in an interview.
Dr. Brickel also said that GSK is "communicating these risks to potential prescribers and encouraging them to advise patients of the symptoms relating to difficulty in passing urine that could range from discomfort on bladder emptying, hesitancy, poor flow through to a complete inability to void (acute urinary retention). GSK is keen to proactively manage this."
The study was funded by GSK and Valeant Pharmaceuticals International, and all of the investigators are employees of either company.
BALTIMORE – The safety profile for retigabine is generally consistent with that of other antiepileptic drugs, but data from studies in its evaluation process show that it also carries a novel, small increased risk of urinary voiding dysfunction.
At the annual meeting of the American Epilepsy Society Dr. Neil Brickel of GlaxoSmithKline’s clinical safety and pharmacovigilance group in Middlesex, England, reported on the safety of the novel drug in three phase III, randomized, double-blind, placebo-controlled trials, four phase II studies, and six long-term open-label extension studies, totalling 1,365 patients.
Retigabine is the international nonproprietary name of the drug, but it was approved in the United States in June 2011 under the adopted name ezogabine as an adjunctive therapy in adults with partial-onset seizures. It is a first-in-class potassium channel opener manufactured by GlaxoSmithKline and Valeant Pharmaceuticals International, and sold under the brand name Trobalt in Europe and Potiga in the United States.
In all of the studies that Dr. Brickel analyzed, retigabine was evaluated as a second, add-on agent. As of Oct. 2, 2009, 1,217 of the 1,365 patients had been on treatment at least 1 month, 801 for at least 6 months, and 586 for 1 year or longer.
As expected with any antiepileptic drug (AED), the most frequent adverse events involved the central nervous system. The most common in the three pivotal controlled trials were dizziness (23% of retigabine-treated patients vs. 9% of placebo-treated patients) and somnolence (reported by 22% vs. 12%, respectively). The only CNS adverse events that were not dose related were headache (reported by 15% of the retigabine group vs. 16% of the placebo group) and fatigue (by 15% and 6%, respectively). Other adverse events occurring in more than 10% of subjects were confusional state, tremor, and abnormal coordination. For the most part, patients reported these adverse events early on, during the titration phases of the trials, Dr. Brickel said.
Adverse events led to discontinuation in 437 patients (32%) of the total phase II/III study population. Again, these were primarily CNS and dose related. Discontinuations for any event occurred in 11% of the placebo group. Among those taking retigabine, discontinuations occurred in 17% of those assigned to 600 mg, 25% of those assigned to 900 mg, and 31% of those assigned to 1,200 mg. The most common reason for discontinuation was dizziness.
"Two-thirds of patients were able to continue in the study, even with the fixed titration regimen and at the 1,200-mg dose," Dr. Brickel noted.
Serious adverse events (SAEs) were infrequent, and also typically CNS related. In the three pivotal controlled trials, SAEs occurred in 6% of the placebo group and 9% of the retigabine patients. Six of the patients taking retigabine developed a psychotic disorder (five with 1,200 mg, one with 900 mg), compared with none of the placebo patients. Convulsions occurred in 1.2% of the placebo group and in 1.5% of the retigabine patients, across all doses. This finding was not unexpected, considering the underlying epilepsy, he said.
No other SAE was reported in more than two patients in any group. Deaths occurred in three placebo patients and two patients in the retigabine group. One in each group was a sudden death.
In the three pivotal trials, urinary and renal-related adverse events occurred in 17% of retigabine patients, compared with 13% of the placebo-treated patients. In the entire phase II/III study population, 26% of the 1,365 patients reported a urinary adverse event.
However, events related to urinary voiding dysfunction, which have a plausible biological relation to retigabine’s pharmacology, occurred in less than 4% of retigabine-treated patients in the phase III trials alone and in all phase II and III trial populations combined. Urinary hesitation was the most common of these in the entire phase II and III study group, occurring in 3.1%, followed by urinary retention in 1.9%. Catheterization was required in four patients taking retigabine and in one patient on placebo.
"These all occurred in a smaller number of patients and provide a better guide as to how many patents are potentially at risk. It is also important to note that these events were for the most part ‘mild’ in intensity and the patients were able to continue treatment," Dr. Brickel said in an interview.
Dr. Brickel also said that GSK is "communicating these risks to potential prescribers and encouraging them to advise patients of the symptoms relating to difficulty in passing urine that could range from discomfort on bladder emptying, hesitancy, poor flow through to a complete inability to void (acute urinary retention). GSK is keen to proactively manage this."
The study was funded by GSK and Valeant Pharmaceuticals International, and all of the investigators are employees of either company.
BALTIMORE – The safety profile for retigabine is generally consistent with that of other antiepileptic drugs, but data from studies in its evaluation process show that it also carries a novel, small increased risk of urinary voiding dysfunction.
At the annual meeting of the American Epilepsy Society Dr. Neil Brickel of GlaxoSmithKline’s clinical safety and pharmacovigilance group in Middlesex, England, reported on the safety of the novel drug in three phase III, randomized, double-blind, placebo-controlled trials, four phase II studies, and six long-term open-label extension studies, totalling 1,365 patients.
Retigabine is the international nonproprietary name of the drug, but it was approved in the United States in June 2011 under the adopted name ezogabine as an adjunctive therapy in adults with partial-onset seizures. It is a first-in-class potassium channel opener manufactured by GlaxoSmithKline and Valeant Pharmaceuticals International, and sold under the brand name Trobalt in Europe and Potiga in the United States.
In all of the studies that Dr. Brickel analyzed, retigabine was evaluated as a second, add-on agent. As of Oct. 2, 2009, 1,217 of the 1,365 patients had been on treatment at least 1 month, 801 for at least 6 months, and 586 for 1 year or longer.
As expected with any antiepileptic drug (AED), the most frequent adverse events involved the central nervous system. The most common in the three pivotal controlled trials were dizziness (23% of retigabine-treated patients vs. 9% of placebo-treated patients) and somnolence (reported by 22% vs. 12%, respectively). The only CNS adverse events that were not dose related were headache (reported by 15% of the retigabine group vs. 16% of the placebo group) and fatigue (by 15% and 6%, respectively). Other adverse events occurring in more than 10% of subjects were confusional state, tremor, and abnormal coordination. For the most part, patients reported these adverse events early on, during the titration phases of the trials, Dr. Brickel said.
Adverse events led to discontinuation in 437 patients (32%) of the total phase II/III study population. Again, these were primarily CNS and dose related. Discontinuations for any event occurred in 11% of the placebo group. Among those taking retigabine, discontinuations occurred in 17% of those assigned to 600 mg, 25% of those assigned to 900 mg, and 31% of those assigned to 1,200 mg. The most common reason for discontinuation was dizziness.
"Two-thirds of patients were able to continue in the study, even with the fixed titration regimen and at the 1,200-mg dose," Dr. Brickel noted.
Serious adverse events (SAEs) were infrequent, and also typically CNS related. In the three pivotal controlled trials, SAEs occurred in 6% of the placebo group and 9% of the retigabine patients. Six of the patients taking retigabine developed a psychotic disorder (five with 1,200 mg, one with 900 mg), compared with none of the placebo patients. Convulsions occurred in 1.2% of the placebo group and in 1.5% of the retigabine patients, across all doses. This finding was not unexpected, considering the underlying epilepsy, he said.
No other SAE was reported in more than two patients in any group. Deaths occurred in three placebo patients and two patients in the retigabine group. One in each group was a sudden death.
In the three pivotal trials, urinary and renal-related adverse events occurred in 17% of retigabine patients, compared with 13% of the placebo-treated patients. In the entire phase II/III study population, 26% of the 1,365 patients reported a urinary adverse event.
However, events related to urinary voiding dysfunction, which have a plausible biological relation to retigabine’s pharmacology, occurred in less than 4% of retigabine-treated patients in the phase III trials alone and in all phase II and III trial populations combined. Urinary hesitation was the most common of these in the entire phase II and III study group, occurring in 3.1%, followed by urinary retention in 1.9%. Catheterization was required in four patients taking retigabine and in one patient on placebo.
"These all occurred in a smaller number of patients and provide a better guide as to how many patents are potentially at risk. It is also important to note that these events were for the most part ‘mild’ in intensity and the patients were able to continue treatment," Dr. Brickel said in an interview.
Dr. Brickel also said that GSK is "communicating these risks to potential prescribers and encouraging them to advise patients of the symptoms relating to difficulty in passing urine that could range from discomfort on bladder emptying, hesitancy, poor flow through to a complete inability to void (acute urinary retention). GSK is keen to proactively manage this."
The study was funded by GSK and Valeant Pharmaceuticals International, and all of the investigators are employees of either company.
FROM THE ANNUAL MEETING OF THE AMERICAN EPILEPSY SOCIETY
Major Finding: Urinary hesitation occurred in 3.1% of the entire phase II/III study group, and urinary retention occurred in 1.9%.
Data Source: Safety data collected from three phase III, randomized, double-blind, placebo-controlled trials, as well as from four phase II studies and six long-term open-label extension studies, involving 1,365 patients in all.
Disclosures: The study was funded by GlaxoSmithKline and Valeant Pharmaceuticals International. All of the investigators are employees of either company.
Most Lymphomatoid Papulosis Has Benign Course
LAS VEGAS – Although certain characteristics of lymphomatoid papulosis appear be associated with progression to lymphoma, the majority of patients will have a benign course of disease.
The recurrent papulonodular skin eruption lymphomatoid papulosis (LyP) can be a confusing dermatologic entity because it appears malignant histologically, but it usually follows a clinically benign and indolent course (Arch. Dermatol. 1968;97:23-30). And even the 10%-20% of patients who do progress to lymphoma tend to have less aggressive disease, said Dr. Lawrence E. Gibson, professor of dermatology at the Mayo Clinic in Rochester, Minn. The reasons for this disconnect are not yet known.
"Patients with LyP look like lymphoma under the microscope but have clinically indolent cutaneous disease. ... It is an example of a very important clinical-pathological relationship that really needs to be made to help us understand how to treat patients better," he said.
"The bottom line is most of our patients who have LyP do not go on to have aggressive lymphomas."
To identify which LyP patients are more likely to progress to lymphoma, Dr. Gibson, Dr. Rokea A. el-Azhary, Dr. Aieska de Souza, and their associates conducted a retrospective analysis of 123 patients seen at the Mayo Clinic between 1991 and 2008. The patients were followed for a mean of 4 years (range, 2 months to 14 years). The 65 males and 58 females had a mean age of 47 years (range, 1-83 years), and a mean of 14 lesions (range, 1-100). Most (88%) of the lesions were papules, with a reported mean duration of 5.5 weeks. Pruritis was present in 38% and scar formation in 58%, the researchers reported (J. Am. Acad. Dermatol. 2011 [doi:10.1016/j.jaad.2011.07.012]).
Hematologic malignancies were present in 17 patients (14%). Of those, 10 were cutaneous lymphomas – 8 mycosis fungoides (MF) and 2 anaplastic large-cell lymphomas (ALCL). Hodgkin lymphoma was present in three patients (including the two with ALCL), multiple myeloma or monoclonal gammopathy in three, and myelodysplastic syndrome in one.
"The bottom line is most of our patients who have LyP do not go on to have aggressive lymphomas. They certainly don’t have cytotoxic lymphomas. And if they have lymphoma, they usually have MF. I think that’s somewhat reassuring to us. And for the most part, most of the patients don’t have anything. They have a normal life," Dr. Gibson said at the seminar sponsored by Skin Disease Education Foundation (SDEF).
Of 97 LyP patients for whom original biopsy slides were available, the majority (69) had World Health Organization/European Organization for Research and Treatment of Cancer histologic classification type A, including 35 with immunophenotypic subtype CD8 and 34 with subtype CD4. Another 13 patients had type B lesions (8 CD4, 5 CD8), and 6 had type C, all of which were CD4. The other 9 patients had more than one histologic type (A, B, or C), and/or more than one immunophenotypic subtype (CD4 or CD8). They were designated mixed type.
Clinically, there were no distinguishing features among the subtypes. This finding contrasts with some previous reports that the CD8 subtype might predispose to worse disease outcome (Am. J. Pathol. 1999;155:483-92).
"Our findings indicated that the LyP subtype CD8 does not signify more aggressive disease, a poor prognosis, or an association with malignancy," Dr. Gibson and his colleagues wrote.
Hematologic malignancies were present in 5 of the 9 mixed-type patients (55.5%), compared with 4 of the 34 with A/CD4 (12%), 4 of the 35 A/CD8 (11.5%), 1 of the 8 B/CD4 patients (12.5%), and 1 of the 5 B/CD8 patients (20%). (Two of the 17 malignancies were excluded from analysis because original slides were not available.) The odds ratio for malignancy for the patients with mixed-type LyP versus all other types was a statistically significant 4.33 (P = .03).
In a molecular genetics substudy of 84 LyP lesions from 76 patients, 42 (50%) were positive for clonal T-cell receptor gene rearrangement (TCRGR), 34 (40%) were negative, and 8 (10%) showed equivocal results or had insufficient DNA for analysis. Among the LyP patients who had a hematologic malignancy, 9 of 11 (82%) had positive TCRGR, compared with 30 of 68 (44%) LyP patients without malignancy. That association was also significant, with an odds ratio of 5.7 (P = .02), noted the investigators.
"A positive T-cell receptor gene rearrangement or having more than one type of LyP may have a higher risk of progression to lymphoma, but the evidence is not hard and fast. ... The take-home message is most of these patients do just fine," Dr. Gibson said.
Dr. Gibson stated that he had no relevant financial disclosures or conflicts of interest. SDEF and this news organization are owned by Elsevier.
LAS VEGAS – Although certain characteristics of lymphomatoid papulosis appear be associated with progression to lymphoma, the majority of patients will have a benign course of disease.
The recurrent papulonodular skin eruption lymphomatoid papulosis (LyP) can be a confusing dermatologic entity because it appears malignant histologically, but it usually follows a clinically benign and indolent course (Arch. Dermatol. 1968;97:23-30). And even the 10%-20% of patients who do progress to lymphoma tend to have less aggressive disease, said Dr. Lawrence E. Gibson, professor of dermatology at the Mayo Clinic in Rochester, Minn. The reasons for this disconnect are not yet known.
"Patients with LyP look like lymphoma under the microscope but have clinically indolent cutaneous disease. ... It is an example of a very important clinical-pathological relationship that really needs to be made to help us understand how to treat patients better," he said.
"The bottom line is most of our patients who have LyP do not go on to have aggressive lymphomas."
To identify which LyP patients are more likely to progress to lymphoma, Dr. Gibson, Dr. Rokea A. el-Azhary, Dr. Aieska de Souza, and their associates conducted a retrospective analysis of 123 patients seen at the Mayo Clinic between 1991 and 2008. The patients were followed for a mean of 4 years (range, 2 months to 14 years). The 65 males and 58 females had a mean age of 47 years (range, 1-83 years), and a mean of 14 lesions (range, 1-100). Most (88%) of the lesions were papules, with a reported mean duration of 5.5 weeks. Pruritis was present in 38% and scar formation in 58%, the researchers reported (J. Am. Acad. Dermatol. 2011 [doi:10.1016/j.jaad.2011.07.012]).
Hematologic malignancies were present in 17 patients (14%). Of those, 10 were cutaneous lymphomas – 8 mycosis fungoides (MF) and 2 anaplastic large-cell lymphomas (ALCL). Hodgkin lymphoma was present in three patients (including the two with ALCL), multiple myeloma or monoclonal gammopathy in three, and myelodysplastic syndrome in one.
"The bottom line is most of our patients who have LyP do not go on to have aggressive lymphomas. They certainly don’t have cytotoxic lymphomas. And if they have lymphoma, they usually have MF. I think that’s somewhat reassuring to us. And for the most part, most of the patients don’t have anything. They have a normal life," Dr. Gibson said at the seminar sponsored by Skin Disease Education Foundation (SDEF).
Of 97 LyP patients for whom original biopsy slides were available, the majority (69) had World Health Organization/European Organization for Research and Treatment of Cancer histologic classification type A, including 35 with immunophenotypic subtype CD8 and 34 with subtype CD4. Another 13 patients had type B lesions (8 CD4, 5 CD8), and 6 had type C, all of which were CD4. The other 9 patients had more than one histologic type (A, B, or C), and/or more than one immunophenotypic subtype (CD4 or CD8). They were designated mixed type.
Clinically, there were no distinguishing features among the subtypes. This finding contrasts with some previous reports that the CD8 subtype might predispose to worse disease outcome (Am. J. Pathol. 1999;155:483-92).
"Our findings indicated that the LyP subtype CD8 does not signify more aggressive disease, a poor prognosis, or an association with malignancy," Dr. Gibson and his colleagues wrote.
Hematologic malignancies were present in 5 of the 9 mixed-type patients (55.5%), compared with 4 of the 34 with A/CD4 (12%), 4 of the 35 A/CD8 (11.5%), 1 of the 8 B/CD4 patients (12.5%), and 1 of the 5 B/CD8 patients (20%). (Two of the 17 malignancies were excluded from analysis because original slides were not available.) The odds ratio for malignancy for the patients with mixed-type LyP versus all other types was a statistically significant 4.33 (P = .03).
In a molecular genetics substudy of 84 LyP lesions from 76 patients, 42 (50%) were positive for clonal T-cell receptor gene rearrangement (TCRGR), 34 (40%) were negative, and 8 (10%) showed equivocal results or had insufficient DNA for analysis. Among the LyP patients who had a hematologic malignancy, 9 of 11 (82%) had positive TCRGR, compared with 30 of 68 (44%) LyP patients without malignancy. That association was also significant, with an odds ratio of 5.7 (P = .02), noted the investigators.
"A positive T-cell receptor gene rearrangement or having more than one type of LyP may have a higher risk of progression to lymphoma, but the evidence is not hard and fast. ... The take-home message is most of these patients do just fine," Dr. Gibson said.
Dr. Gibson stated that he had no relevant financial disclosures or conflicts of interest. SDEF and this news organization are owned by Elsevier.
LAS VEGAS – Although certain characteristics of lymphomatoid papulosis appear be associated with progression to lymphoma, the majority of patients will have a benign course of disease.
The recurrent papulonodular skin eruption lymphomatoid papulosis (LyP) can be a confusing dermatologic entity because it appears malignant histologically, but it usually follows a clinically benign and indolent course (Arch. Dermatol. 1968;97:23-30). And even the 10%-20% of patients who do progress to lymphoma tend to have less aggressive disease, said Dr. Lawrence E. Gibson, professor of dermatology at the Mayo Clinic in Rochester, Minn. The reasons for this disconnect are not yet known.
"Patients with LyP look like lymphoma under the microscope but have clinically indolent cutaneous disease. ... It is an example of a very important clinical-pathological relationship that really needs to be made to help us understand how to treat patients better," he said.
"The bottom line is most of our patients who have LyP do not go on to have aggressive lymphomas."
To identify which LyP patients are more likely to progress to lymphoma, Dr. Gibson, Dr. Rokea A. el-Azhary, Dr. Aieska de Souza, and their associates conducted a retrospective analysis of 123 patients seen at the Mayo Clinic between 1991 and 2008. The patients were followed for a mean of 4 years (range, 2 months to 14 years). The 65 males and 58 females had a mean age of 47 years (range, 1-83 years), and a mean of 14 lesions (range, 1-100). Most (88%) of the lesions were papules, with a reported mean duration of 5.5 weeks. Pruritis was present in 38% and scar formation in 58%, the researchers reported (J. Am. Acad. Dermatol. 2011 [doi:10.1016/j.jaad.2011.07.012]).
Hematologic malignancies were present in 17 patients (14%). Of those, 10 were cutaneous lymphomas – 8 mycosis fungoides (MF) and 2 anaplastic large-cell lymphomas (ALCL). Hodgkin lymphoma was present in three patients (including the two with ALCL), multiple myeloma or monoclonal gammopathy in three, and myelodysplastic syndrome in one.
"The bottom line is most of our patients who have LyP do not go on to have aggressive lymphomas. They certainly don’t have cytotoxic lymphomas. And if they have lymphoma, they usually have MF. I think that’s somewhat reassuring to us. And for the most part, most of the patients don’t have anything. They have a normal life," Dr. Gibson said at the seminar sponsored by Skin Disease Education Foundation (SDEF).
Of 97 LyP patients for whom original biopsy slides were available, the majority (69) had World Health Organization/European Organization for Research and Treatment of Cancer histologic classification type A, including 35 with immunophenotypic subtype CD8 and 34 with subtype CD4. Another 13 patients had type B lesions (8 CD4, 5 CD8), and 6 had type C, all of which were CD4. The other 9 patients had more than one histologic type (A, B, or C), and/or more than one immunophenotypic subtype (CD4 or CD8). They were designated mixed type.
Clinically, there were no distinguishing features among the subtypes. This finding contrasts with some previous reports that the CD8 subtype might predispose to worse disease outcome (Am. J. Pathol. 1999;155:483-92).
"Our findings indicated that the LyP subtype CD8 does not signify more aggressive disease, a poor prognosis, or an association with malignancy," Dr. Gibson and his colleagues wrote.
Hematologic malignancies were present in 5 of the 9 mixed-type patients (55.5%), compared with 4 of the 34 with A/CD4 (12%), 4 of the 35 A/CD8 (11.5%), 1 of the 8 B/CD4 patients (12.5%), and 1 of the 5 B/CD8 patients (20%). (Two of the 17 malignancies were excluded from analysis because original slides were not available.) The odds ratio for malignancy for the patients with mixed-type LyP versus all other types was a statistically significant 4.33 (P = .03).
In a molecular genetics substudy of 84 LyP lesions from 76 patients, 42 (50%) were positive for clonal T-cell receptor gene rearrangement (TCRGR), 34 (40%) were negative, and 8 (10%) showed equivocal results or had insufficient DNA for analysis. Among the LyP patients who had a hematologic malignancy, 9 of 11 (82%) had positive TCRGR, compared with 30 of 68 (44%) LyP patients without malignancy. That association was also significant, with an odds ratio of 5.7 (P = .02), noted the investigators.
"A positive T-cell receptor gene rearrangement or having more than one type of LyP may have a higher risk of progression to lymphoma, but the evidence is not hard and fast. ... The take-home message is most of these patients do just fine," Dr. Gibson said.
Dr. Gibson stated that he had no relevant financial disclosures or conflicts of interest. SDEF and this news organization are owned by Elsevier.
FROM THE SDEF LAS VEGAS DERMATOLOGY SEMINAR
Major Finding: Hematologic malignancies were present in 17 patients (14%).
Data Source: Retrospective analysis of 123 LyP patients seen at the Mayo Clinic between 1991 and 2008.
Disclosures: Dr. Gibson has no relevant financial disclosures or conflicts of interest. SDEF and this news organization are owned by Elsevier.