User login
For trichotillomania, try behavioral therapy before drugs
NEW YORK – Behavioral therapy is generally a more effective way than prescribing medications to help children with trichotillomania – especially if the symptoms are not too severe.
While adults with the disorder seem to improve with some antidepressants and neuroleptics, children and teens do not reap nearly the same benefit, Dr. Barbara J. Coffey said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.

"A lovely randomized study showed that even little children did very well with behavioral therapy," said Dr. Coffey, director of the Institute for Tourette and Tic Disorders at New York University Langone Medical Center. "The concern was that they might not respond as well as [with] older children but, in fact, they did – and maybe even did a little bit better."
Treatment decisions should be based on symptom severity, she said. A couple of scales have been created to assess that in youngsters, including the Trichotillomania Scale for Children. It characterizes symptoms according to both distress and impairment (interference with relationships, school, and grooming routines) and severity (frequency, duration, number of hairs pulled, and controllability).
The Massachusetts General Hospital Hairpulling Scale is a seven-item self-report with a severity rating of 0-4. The Milwaukee Inventory for Styles of Trichotillomania–Child Version is another self-report, this one containing 36 items. The U.S. National Institute of Mental Health Trichotillomania Severity Scale, however, might be the most useful for small children. This tool, which contains a semistructured interview, also is used as an assessment tool in many clinical trials.
For children with mild symptoms, without distress or impairment, "simple behavioral interventions and monitoring may be all that’s needed," Dr. Coffey said.
This includes using strategies that make it just a little harder to physically grasp and pull hairs, such as placing small Band-Aids on fingertips, wearing gloves, or putting on a hat. Parents can help by making sure that the interventions are consistent and giving lots of praise when the child abstains from pulling.
For moderate symptoms, habit reversal therapy is a better choice. "The first few days of treatment are designed to help the child develop an awareness of the circumstances and triggers for pulling, and the sensations or urges that are involved," she said. "We are trying to develop an awareness of the premonitory urge."
The second phase of therapy focuses on developing competing behaviors. "We want them to engage in a behavior that is physically incompatible with pulling – like making a fist, playing with a stress ball, or sitting on their hands. They’re instructed to do this behavior for 1 full minute, so they can learn to tolerate the uncomfortable sensation that drives them to pull."
If the symptoms do not improve, or if they get worse, medication might be looked at as an add-on treatment. The first choice is usually an antidepressant or a neuroleptic, Dr. Coffey said.
Clomipramine probably have a little more positive data behind it than do selective serotonin reuptake inhibitors (SSRIs). A 2007 meta-analysis examined seven studies that included 157 adults who were treated with clomipramine, SSRIs, and behavioral interventions. "Habit reversal therapy was superior to clomipramine. Clomipramine was superior to placebo and to SSRIs. But SSRIs were not superior to placebo. So our usual toolbox of medications that we might use for an obsessive compulsive disorder failed to show efficacy."
Since behavioral therapy is more effective than medical therapy, it is very important to keep these strategies on board when adding any drugs, Dr. Coffey stressed.
N-acetylcysteine, a glutamate modulator, also is being used as an add-on treatment. A few studies have suggested a benefit, but the most recent, published last year, was "a big disappointment," she said. That study randomized 39 children aged 8-17 years to the compound or to placebo for 12 weeks (J. Am Acad. Child Adolesc. Psychiatry 2013;52:231-40).
"The good news is that both groups improved, and there were no real adverse effects," she said. "The bad news is that while both groups improved, there was no significant difference between the active and the placebo groups."
N-acetylcysteine reduces glutamate in glial cells and synapses, and promotes the production of glutathione, the body’s most powerful antioxidant. In adults, it’s been shown to benefit people who have addictions to cocaine and other drugs that activate opioid receptors.
"I still do use it sometimes," Dr. Coffey said. "I believe there are some children who are helped by it." She said the medication is over the counter and has virtually no side effects.
Dr. Coffey disclosed that she is on the advisory boards of Eli Lilly, Jazz Pharmaceuticals, and Novartis. She has received research support from Boehringer Ingelheim, Bristol-Myers Squibb, CatalystPharma, Eli Lilly, Otsuka Pharmaceutical, and Shire. She is on the speakers bureau for Quintiles.
NEW YORK – Behavioral therapy is generally a more effective way than prescribing medications to help children with trichotillomania – especially if the symptoms are not too severe.
While adults with the disorder seem to improve with some antidepressants and neuroleptics, children and teens do not reap nearly the same benefit, Dr. Barbara J. Coffey said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
"A lovely randomized study showed that even little children did very well with behavioral therapy," said Dr. Coffey, director of the Institute for Tourette and Tic Disorders at New York University Langone Medical Center. "The concern was that they might not respond as well as [with] older children but, in fact, they did – and maybe even did a little bit better."
Treatment decisions should be based on symptom severity, she said. A couple of scales have been created to assess that in youngsters, including the Trichotillomania Scale for Children. It characterizes symptoms according to both distress and impairment (interference with relationships, school, and grooming routines) and severity (frequency, duration, number of hairs pulled, and controllability).
The Massachusetts General Hospital Hairpulling Scale is a seven-item self-report with a severity rating of 0-4. The Milwaukee Inventory for Styles of Trichotillomania–Child Version is another self-report, this one containing 36 items. The U.S. National Institute of Mental Health Trichotillomania Severity Scale, however, might be the most useful for small children. This tool, which contains a semistructured interview, also is used as an assessment tool in many clinical trials.
For children with mild symptoms, without distress or impairment, "simple behavioral interventions and monitoring may be all that’s needed," Dr. Coffey said.
This includes using strategies that make it just a little harder to physically grasp and pull hairs, such as placing small Band-Aids on fingertips, wearing gloves, or putting on a hat. Parents can help by making sure that the interventions are consistent and giving lots of praise when the child abstains from pulling.
For moderate symptoms, habit reversal therapy is a better choice. "The first few days of treatment are designed to help the child develop an awareness of the circumstances and triggers for pulling, and the sensations or urges that are involved," she said. "We are trying to develop an awareness of the premonitory urge."
The second phase of therapy focuses on developing competing behaviors. "We want them to engage in a behavior that is physically incompatible with pulling – like making a fist, playing with a stress ball, or sitting on their hands. They’re instructed to do this behavior for 1 full minute, so they can learn to tolerate the uncomfortable sensation that drives them to pull."
If the symptoms do not improve, or if they get worse, medication might be looked at as an add-on treatment. The first choice is usually an antidepressant or a neuroleptic, Dr. Coffey said.
Clomipramine probably have a little more positive data behind it than do selective serotonin reuptake inhibitors (SSRIs). A 2007 meta-analysis examined seven studies that included 157 adults who were treated with clomipramine, SSRIs, and behavioral interventions. "Habit reversal therapy was superior to clomipramine. Clomipramine was superior to placebo and to SSRIs. But SSRIs were not superior to placebo. So our usual toolbox of medications that we might use for an obsessive compulsive disorder failed to show efficacy."
Since behavioral therapy is more effective than medical therapy, it is very important to keep these strategies on board when adding any drugs, Dr. Coffey stressed.
N-acetylcysteine, a glutamate modulator, also is being used as an add-on treatment. A few studies have suggested a benefit, but the most recent, published last year, was "a big disappointment," she said. That study randomized 39 children aged 8-17 years to the compound or to placebo for 12 weeks (J. Am Acad. Child Adolesc. Psychiatry 2013;52:231-40).
"The good news is that both groups improved, and there were no real adverse effects," she said. "The bad news is that while both groups improved, there was no significant difference between the active and the placebo groups."
N-acetylcysteine reduces glutamate in glial cells and synapses, and promotes the production of glutathione, the body’s most powerful antioxidant. In adults, it’s been shown to benefit people who have addictions to cocaine and other drugs that activate opioid receptors.
"I still do use it sometimes," Dr. Coffey said. "I believe there are some children who are helped by it." She said the medication is over the counter and has virtually no side effects.
Dr. Coffey disclosed that she is on the advisory boards of Eli Lilly, Jazz Pharmaceuticals, and Novartis. She has received research support from Boehringer Ingelheim, Bristol-Myers Squibb, CatalystPharma, Eli Lilly, Otsuka Pharmaceutical, and Shire. She is on the speakers bureau for Quintiles.
NEW YORK – Behavioral therapy is generally a more effective way than prescribing medications to help children with trichotillomania – especially if the symptoms are not too severe.
While adults with the disorder seem to improve with some antidepressants and neuroleptics, children and teens do not reap nearly the same benefit, Dr. Barbara J. Coffey said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
"A lovely randomized study showed that even little children did very well with behavioral therapy," said Dr. Coffey, director of the Institute for Tourette and Tic Disorders at New York University Langone Medical Center. "The concern was that they might not respond as well as [with] older children but, in fact, they did – and maybe even did a little bit better."
Treatment decisions should be based on symptom severity, she said. A couple of scales have been created to assess that in youngsters, including the Trichotillomania Scale for Children. It characterizes symptoms according to both distress and impairment (interference with relationships, school, and grooming routines) and severity (frequency, duration, number of hairs pulled, and controllability).
The Massachusetts General Hospital Hairpulling Scale is a seven-item self-report with a severity rating of 0-4. The Milwaukee Inventory for Styles of Trichotillomania–Child Version is another self-report, this one containing 36 items. The U.S. National Institute of Mental Health Trichotillomania Severity Scale, however, might be the most useful for small children. This tool, which contains a semistructured interview, also is used as an assessment tool in many clinical trials.
For children with mild symptoms, without distress or impairment, "simple behavioral interventions and monitoring may be all that’s needed," Dr. Coffey said.
This includes using strategies that make it just a little harder to physically grasp and pull hairs, such as placing small Band-Aids on fingertips, wearing gloves, or putting on a hat. Parents can help by making sure that the interventions are consistent and giving lots of praise when the child abstains from pulling.
For moderate symptoms, habit reversal therapy is a better choice. "The first few days of treatment are designed to help the child develop an awareness of the circumstances and triggers for pulling, and the sensations or urges that are involved," she said. "We are trying to develop an awareness of the premonitory urge."
The second phase of therapy focuses on developing competing behaviors. "We want them to engage in a behavior that is physically incompatible with pulling – like making a fist, playing with a stress ball, or sitting on their hands. They’re instructed to do this behavior for 1 full minute, so they can learn to tolerate the uncomfortable sensation that drives them to pull."
If the symptoms do not improve, or if they get worse, medication might be looked at as an add-on treatment. The first choice is usually an antidepressant or a neuroleptic, Dr. Coffey said.
Clomipramine probably have a little more positive data behind it than do selective serotonin reuptake inhibitors (SSRIs). A 2007 meta-analysis examined seven studies that included 157 adults who were treated with clomipramine, SSRIs, and behavioral interventions. "Habit reversal therapy was superior to clomipramine. Clomipramine was superior to placebo and to SSRIs. But SSRIs were not superior to placebo. So our usual toolbox of medications that we might use for an obsessive compulsive disorder failed to show efficacy."
Since behavioral therapy is more effective than medical therapy, it is very important to keep these strategies on board when adding any drugs, Dr. Coffey stressed.
N-acetylcysteine, a glutamate modulator, also is being used as an add-on treatment. A few studies have suggested a benefit, but the most recent, published last year, was "a big disappointment," she said. That study randomized 39 children aged 8-17 years to the compound or to placebo for 12 weeks (J. Am Acad. Child Adolesc. Psychiatry 2013;52:231-40).
"The good news is that both groups improved, and there were no real adverse effects," she said. "The bad news is that while both groups improved, there was no significant difference between the active and the placebo groups."
N-acetylcysteine reduces glutamate in glial cells and synapses, and promotes the production of glutathione, the body’s most powerful antioxidant. In adults, it’s been shown to benefit people who have addictions to cocaine and other drugs that activate opioid receptors.
"I still do use it sometimes," Dr. Coffey said. "I believe there are some children who are helped by it." She said the medication is over the counter and has virtually no side effects.
Dr. Coffey disclosed that she is on the advisory boards of Eli Lilly, Jazz Pharmaceuticals, and Novartis. She has received research support from Boehringer Ingelheim, Bristol-Myers Squibb, CatalystPharma, Eli Lilly, Otsuka Pharmaceutical, and Shire. She is on the speakers bureau for Quintiles.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE

Drug therapy for children with autism: No magic bullets yet
NEW YORK – Neither approved nor investigational drugs seem to have much of an effect on the core symptoms of autism.
Medications that help psychiatric conditions in children with otherwise normal development don’t seem to work as well for children who have autism spectrum disorders (ASDs), Dr. Jean A. Frazier said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
"The effects seem to be maximized at lower doses than in typically developing youth, and the medications are often much less well tolerated," said Dr. Frazier, a professor of psychiatry at the University of Massachusetts, Worcester.
"If you do try them, the old axiom, ‘Start low, go slow,’ certainly applies."
Because there’s nothing that reliably ameliorates the core symptoms, clinicians and parents focus on treating the behavioral symptoms. Aggression, irritability, and self-injury; hyperactivity and anxiety; and sleep problems not only disrupt family life, but they also can endanger the child. A major cause of death among children with ASDs is "bolting" and falling into a neighbor’s swimming pool, or being hit by a car, Dr. Frazier said.

Risperidone and aripiprazole are approved by the Food and Drug Administration for the treatment of aggression and irritability. But the other commonly used medications, including selective serotonin reuptake inhibitors (SSRIs), atypical antipsychotics, and stimulants are used off label and supported by limited evidence, much of which is based on adult studies.
Risperidone is "pretty effective for reducing tantrums and self-injury," with stable gains over time, Dr. Frazier said. However, it’s associated with "huge weight gain." In its two pivotal trials, children taking risperidone gained an average of 5.6 kg over 6 months – about twice as much as investigators anticipated. This must be balanced with the fact that relapse will occur if treatment stops.
Aripiprazole also was effective in its two pivotal studies, but those were of short duration, she said. Both of the drugs are supported by A-level evidence – the highest grade.
Methylphenidate is used off label and is supported by B-level evidence. In two randomized, placebo-controlled studies, it was superior to placebo, but again, the studies were short and had small numbers enrolled. One of them reported very high levels of "intolerable side effects," including agitation, mood changes, and movement disorders. Divalproex sodium, lamotrigine, and naltrexone have much less supporting evidence.
SSRIs are used off label for repetitive behaviors. All of the evidence behind their use is based on adult studies, Dr. Frazier said. Case series of fluoxetine, quetiapine, and citalopram in children show "promise," but that promise hasn’t been confirmed in large randomized trials. In a recent pediatric citalopram study, many children showed increased energy, hyperactivity, decreased concentration, stereotypic behaviors, gastrointestinal issues, and dry skin.
A Cochrane review published last August found no evidence that SSRIs are of clinical benefit for children with ASDs and, it said "there is emerging evidence of harm" (Cochrane Database Syst. Rev. 2013;8).
The lack of SSRI effectiveness in children with autism spectrum disorders could be related to developmental differences in the serotonin uptake receptors, compared with normally developing children, Dr. Frazier added.
There are also few pediatric studies looking at medical therapy for sleep disorders in ASD. Melatonin is of interest in this arena. "Several recent randomized controlled trials of melatonin have been encouraging. They used up to 6 mg/night. It’s relatively benign, with almost no side effects."
Research continues, Dr. Frazier said. Gamma-aminobutyric acid and glutamate are being pursued as targets. Bumetanide is a loop diuretic used to treat heart failure – it also potentiates the action of gamma-aminobutyric acid. A recent study included 60 children with autism or Asperger’s disorder (Transl. Psychiatry 2012;2:e202). It showed significant improvements in the Childhood Autism Rating Scale and Clinical Global Impression score, but no changes relative to placebo on the Autism Diagnostic Observation Schedule.
Tetrahydrobiopterin is an essential co-factor for several metabolic pathways involved in the production of neurotransmitters. The most recent study randomized 46 children to tetrahydrobiopterin or placebo for 16 weeks (J. Child Adolesc. Psychopharmacol. 2013;23:320-8). There were no improvements on the CGI scales – the primary endpoints – but significant improvements were found in measures of language, social responsiveness, and aberrant and adaptive behavior.
"However, I caution you about taking these studies too much to heart, because they need to be replicated in larger groups," Dr. Frazier said.
Dr. Frazier reported receiving grant funding from GlaxoSmithKline, Hoffmann-La Roche, Neuren Pharmaceuticals, Pfizer, and Seaside Therapeutics.
NEW YORK – Neither approved nor investigational drugs seem to have much of an effect on the core symptoms of autism.
Medications that help psychiatric conditions in children with otherwise normal development don’t seem to work as well for children who have autism spectrum disorders (ASDs), Dr. Jean A. Frazier said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
"The effects seem to be maximized at lower doses than in typically developing youth, and the medications are often much less well tolerated," said Dr. Frazier, a professor of psychiatry at the University of Massachusetts, Worcester.
"If you do try them, the old axiom, ‘Start low, go slow,’ certainly applies."
Because there’s nothing that reliably ameliorates the core symptoms, clinicians and parents focus on treating the behavioral symptoms. Aggression, irritability, and self-injury; hyperactivity and anxiety; and sleep problems not only disrupt family life, but they also can endanger the child. A major cause of death among children with ASDs is "bolting" and falling into a neighbor’s swimming pool, or being hit by a car, Dr. Frazier said.
Risperidone and aripiprazole are approved by the Food and Drug Administration for the treatment of aggression and irritability. But the other commonly used medications, including selective serotonin reuptake inhibitors (SSRIs), atypical antipsychotics, and stimulants are used off label and supported by limited evidence, much of which is based on adult studies.
Risperidone is "pretty effective for reducing tantrums and self-injury," with stable gains over time, Dr. Frazier said. However, it’s associated with "huge weight gain." In its two pivotal trials, children taking risperidone gained an average of 5.6 kg over 6 months – about twice as much as investigators anticipated. This must be balanced with the fact that relapse will occur if treatment stops.
Aripiprazole also was effective in its two pivotal studies, but those were of short duration, she said. Both of the drugs are supported by A-level evidence – the highest grade.
Methylphenidate is used off label and is supported by B-level evidence. In two randomized, placebo-controlled studies, it was superior to placebo, but again, the studies were short and had small numbers enrolled. One of them reported very high levels of "intolerable side effects," including agitation, mood changes, and movement disorders. Divalproex sodium, lamotrigine, and naltrexone have much less supporting evidence.
SSRIs are used off label for repetitive behaviors. All of the evidence behind their use is based on adult studies, Dr. Frazier said. Case series of fluoxetine, quetiapine, and citalopram in children show "promise," but that promise hasn’t been confirmed in large randomized trials. In a recent pediatric citalopram study, many children showed increased energy, hyperactivity, decreased concentration, stereotypic behaviors, gastrointestinal issues, and dry skin.
A Cochrane review published last August found no evidence that SSRIs are of clinical benefit for children with ASDs and, it said "there is emerging evidence of harm" (Cochrane Database Syst. Rev. 2013;8).
The lack of SSRI effectiveness in children with autism spectrum disorders could be related to developmental differences in the serotonin uptake receptors, compared with normally developing children, Dr. Frazier added.
There are also few pediatric studies looking at medical therapy for sleep disorders in ASD. Melatonin is of interest in this arena. "Several recent randomized controlled trials of melatonin have been encouraging. They used up to 6 mg/night. It’s relatively benign, with almost no side effects."
Research continues, Dr. Frazier said. Gamma-aminobutyric acid and glutamate are being pursued as targets. Bumetanide is a loop diuretic used to treat heart failure – it also potentiates the action of gamma-aminobutyric acid. A recent study included 60 children with autism or Asperger’s disorder (Transl. Psychiatry 2012;2:e202). It showed significant improvements in the Childhood Autism Rating Scale and Clinical Global Impression score, but no changes relative to placebo on the Autism Diagnostic Observation Schedule.
Tetrahydrobiopterin is an essential co-factor for several metabolic pathways involved in the production of neurotransmitters. The most recent study randomized 46 children to tetrahydrobiopterin or placebo for 16 weeks (J. Child Adolesc. Psychopharmacol. 2013;23:320-8). There were no improvements on the CGI scales – the primary endpoints – but significant improvements were found in measures of language, social responsiveness, and aberrant and adaptive behavior.
"However, I caution you about taking these studies too much to heart, because they need to be replicated in larger groups," Dr. Frazier said.
Dr. Frazier reported receiving grant funding from GlaxoSmithKline, Hoffmann-La Roche, Neuren Pharmaceuticals, Pfizer, and Seaside Therapeutics.
NEW YORK – Neither approved nor investigational drugs seem to have much of an effect on the core symptoms of autism.
Medications that help psychiatric conditions in children with otherwise normal development don’t seem to work as well for children who have autism spectrum disorders (ASDs), Dr. Jean A. Frazier said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
"The effects seem to be maximized at lower doses than in typically developing youth, and the medications are often much less well tolerated," said Dr. Frazier, a professor of psychiatry at the University of Massachusetts, Worcester.
"If you do try them, the old axiom, ‘Start low, go slow,’ certainly applies."
Because there’s nothing that reliably ameliorates the core symptoms, clinicians and parents focus on treating the behavioral symptoms. Aggression, irritability, and self-injury; hyperactivity and anxiety; and sleep problems not only disrupt family life, but they also can endanger the child. A major cause of death among children with ASDs is "bolting" and falling into a neighbor’s swimming pool, or being hit by a car, Dr. Frazier said.
Risperidone and aripiprazole are approved by the Food and Drug Administration for the treatment of aggression and irritability. But the other commonly used medications, including selective serotonin reuptake inhibitors (SSRIs), atypical antipsychotics, and stimulants are used off label and supported by limited evidence, much of which is based on adult studies.
Risperidone is "pretty effective for reducing tantrums and self-injury," with stable gains over time, Dr. Frazier said. However, it’s associated with "huge weight gain." In its two pivotal trials, children taking risperidone gained an average of 5.6 kg over 6 months – about twice as much as investigators anticipated. This must be balanced with the fact that relapse will occur if treatment stops.
Aripiprazole also was effective in its two pivotal studies, but those were of short duration, she said. Both of the drugs are supported by A-level evidence – the highest grade.
Methylphenidate is used off label and is supported by B-level evidence. In two randomized, placebo-controlled studies, it was superior to placebo, but again, the studies were short and had small numbers enrolled. One of them reported very high levels of "intolerable side effects," including agitation, mood changes, and movement disorders. Divalproex sodium, lamotrigine, and naltrexone have much less supporting evidence.
SSRIs are used off label for repetitive behaviors. All of the evidence behind their use is based on adult studies, Dr. Frazier said. Case series of fluoxetine, quetiapine, and citalopram in children show "promise," but that promise hasn’t been confirmed in large randomized trials. In a recent pediatric citalopram study, many children showed increased energy, hyperactivity, decreased concentration, stereotypic behaviors, gastrointestinal issues, and dry skin.
A Cochrane review published last August found no evidence that SSRIs are of clinical benefit for children with ASDs and, it said "there is emerging evidence of harm" (Cochrane Database Syst. Rev. 2013;8).
The lack of SSRI effectiveness in children with autism spectrum disorders could be related to developmental differences in the serotonin uptake receptors, compared with normally developing children, Dr. Frazier added.
There are also few pediatric studies looking at medical therapy for sleep disorders in ASD. Melatonin is of interest in this arena. "Several recent randomized controlled trials of melatonin have been encouraging. They used up to 6 mg/night. It’s relatively benign, with almost no side effects."
Research continues, Dr. Frazier said. Gamma-aminobutyric acid and glutamate are being pursued as targets. Bumetanide is a loop diuretic used to treat heart failure – it also potentiates the action of gamma-aminobutyric acid. A recent study included 60 children with autism or Asperger’s disorder (Transl. Psychiatry 2012;2:e202). It showed significant improvements in the Childhood Autism Rating Scale and Clinical Global Impression score, but no changes relative to placebo on the Autism Diagnostic Observation Schedule.
Tetrahydrobiopterin is an essential co-factor for several metabolic pathways involved in the production of neurotransmitters. The most recent study randomized 46 children to tetrahydrobiopterin or placebo for 16 weeks (J. Child Adolesc. Psychopharmacol. 2013;23:320-8). There were no improvements on the CGI scales – the primary endpoints – but significant improvements were found in measures of language, social responsiveness, and aberrant and adaptive behavior.
"However, I caution you about taking these studies too much to heart, because they need to be replicated in larger groups," Dr. Frazier said.
Dr. Frazier reported receiving grant funding from GlaxoSmithKline, Hoffmann-La Roche, Neuren Pharmaceuticals, Pfizer, and Seaside Therapeutics.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE

When ADHD doesn’t improve, check medication adherence first
NEW YORK – Assessing nonresponsiveness to attention-deficit/hyperactivity disorder treatment requires a bit of detective work, according to Dr. Laurence L. Greenhill.
The reason can be as simple as a little kid not being able to swallow a big pill, or as complex as a dysfunctional family dynamic that interferes with medication adherence. But once the problem is rooted out and addressed, most refractory patients can experience a good response, Dr. Greenhill said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
Since primary care physicians usually continue to manage children who respond to ADHD medications, psychiatrists are usually the ones who see nonresponders, said Dr. Greenhill, a child and adolescent psychiatrist at the New York Psychiatric Institute.
Medication nonadherence, the most common cause of a failure to improve, can arise from numerous situations.

On the simple side, it might be a matter of finding the right form of medication; a liquid or sprinkle capsule might be much easier for a child to take than a pill. And not all pills are created equally easy to take.
"For example, [the osmotic controlled release oral delivery system methylphenidate] just went off patent, and generics are now available. But some of these generics are much bigger. In fact, one of the 18-mg pills is twice as large as the patent medicine, and lots of kids can’t swallow it," he said.
The ADHD medication guide published by Long Island Jewish Hospital can be a helpful tool when working with parents on this issue. It lists all the Food and Drug Administration–approved medications for ADHD, with full-size photographs of each capsule, tablet, or pill.
Some generics are not pharmacokinetically or pharmacodynamically identical to the original formulation, Dr. Greenhill noted. Although the drug has to be molecularly identical and dose identical, "the ascending dose curve and duration of action need not be matched." Some generic formulations do fall into this problematic category. "For this reason, I try to encourage parents to get the brand," said Dr. Greenhill, adding that he has no financial interest in any of the drugs.
Medication nonadherence also can be attributable to uncomfortable or even intolerable side effects. These can include gastrointestinal issues, trouble sleeping, lack of appetite, restlessness, irritability, and "feeling fidgety."
Dosage adjustments or a medication change might be in order. For appetite issues, recommend giving the medication after meals, and reassure parents it’s OK to let a child eat later in the evening, when hunger may return.
It’s important to get the child’s growth records from the pediatrician, and plot height and weight curves every 6 months. If there’s a consistent fall-off, consider lowering the dose or changing to another drug.
Contrary to widely held belief, stimulants don’t pose significant cardiac risks to most children. A baseline electrocardiogram is really only necessary for a child who has a family history of sudden cardiac death or a personal history of syncope or cardiac abnormalities. Blood pressure and pulse should be monitored at every visit.
Melatonin is worth a try for youngsters whose ADHD meds interfere with good sleep, Dr. Greenhill said.
"I would start at 1 mg/night and work up," he said. "Starting at a high dose can actually shut off the naturally occurring melatonin. Plasma levels peak about an hour after taking it, so timing is important. I usually start with it about 3 hours before the scheduled sleeping time and then adjust."
Family dynamics also can play a big role in medication nonadherence. "ADHD families are often poor at scheduling activities, sometimes to the extent that parents are the ones who forget to give the medication. They also might not have a clear idea of how to give it, and just leave it on the kitchen table, making it the child’s responsibility to take it every day.
"If this is a child who can’t remember to bring homework back from school, then how is he going to remember to stay on schedule with medication?"
If it’s clear that parents are having difficulty in this area, the simplest thing to do is send the medicine to school and ask the nurse to administer it. Switching to a long-acting form might help, too, since it’s just easier to remember to take one pill than to take two.
The ADHD Parents Medication Guide is a great resource that can be used to get parents actively involved with the child’s drug therapy, Dr. Greenhill said. Developed by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, the online guide is designed to help families and physicians work together to make the best decisions about a child’s care.
Dr. Greenhill is on the advisory board of Quotient, which manufactures an ADHD testing system, and is a consultant for the Health Information Technology Lab.
NEW YORK – Assessing nonresponsiveness to attention-deficit/hyperactivity disorder treatment requires a bit of detective work, according to Dr. Laurence L. Greenhill.
The reason can be as simple as a little kid not being able to swallow a big pill, or as complex as a dysfunctional family dynamic that interferes with medication adherence. But once the problem is rooted out and addressed, most refractory patients can experience a good response, Dr. Greenhill said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
Since primary care physicians usually continue to manage children who respond to ADHD medications, psychiatrists are usually the ones who see nonresponders, said Dr. Greenhill, a child and adolescent psychiatrist at the New York Psychiatric Institute.
Medication nonadherence, the most common cause of a failure to improve, can arise from numerous situations.
On the simple side, it might be a matter of finding the right form of medication; a liquid or sprinkle capsule might be much easier for a child to take than a pill. And not all pills are created equally easy to take.
"For example, [the osmotic controlled release oral delivery system methylphenidate] just went off patent, and generics are now available. But some of these generics are much bigger. In fact, one of the 18-mg pills is twice as large as the patent medicine, and lots of kids can’t swallow it," he said.
The ADHD medication guide published by Long Island Jewish Hospital can be a helpful tool when working with parents on this issue. It lists all the Food and Drug Administration–approved medications for ADHD, with full-size photographs of each capsule, tablet, or pill.
Some generics are not pharmacokinetically or pharmacodynamically identical to the original formulation, Dr. Greenhill noted. Although the drug has to be molecularly identical and dose identical, "the ascending dose curve and duration of action need not be matched." Some generic formulations do fall into this problematic category. "For this reason, I try to encourage parents to get the brand," said Dr. Greenhill, adding that he has no financial interest in any of the drugs.
Medication nonadherence also can be attributable to uncomfortable or even intolerable side effects. These can include gastrointestinal issues, trouble sleeping, lack of appetite, restlessness, irritability, and "feeling fidgety."
Dosage adjustments or a medication change might be in order. For appetite issues, recommend giving the medication after meals, and reassure parents it’s OK to let a child eat later in the evening, when hunger may return.
It’s important to get the child’s growth records from the pediatrician, and plot height and weight curves every 6 months. If there’s a consistent fall-off, consider lowering the dose or changing to another drug.
Contrary to widely held belief, stimulants don’t pose significant cardiac risks to most children. A baseline electrocardiogram is really only necessary for a child who has a family history of sudden cardiac death or a personal history of syncope or cardiac abnormalities. Blood pressure and pulse should be monitored at every visit.
Melatonin is worth a try for youngsters whose ADHD meds interfere with good sleep, Dr. Greenhill said.
"I would start at 1 mg/night and work up," he said. "Starting at a high dose can actually shut off the naturally occurring melatonin. Plasma levels peak about an hour after taking it, so timing is important. I usually start with it about 3 hours before the scheduled sleeping time and then adjust."
Family dynamics also can play a big role in medication nonadherence. "ADHD families are often poor at scheduling activities, sometimes to the extent that parents are the ones who forget to give the medication. They also might not have a clear idea of how to give it, and just leave it on the kitchen table, making it the child’s responsibility to take it every day.
"If this is a child who can’t remember to bring homework back from school, then how is he going to remember to stay on schedule with medication?"
If it’s clear that parents are having difficulty in this area, the simplest thing to do is send the medicine to school and ask the nurse to administer it. Switching to a long-acting form might help, too, since it’s just easier to remember to take one pill than to take two.
The ADHD Parents Medication Guide is a great resource that can be used to get parents actively involved with the child’s drug therapy, Dr. Greenhill said. Developed by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, the online guide is designed to help families and physicians work together to make the best decisions about a child’s care.
Dr. Greenhill is on the advisory board of Quotient, which manufactures an ADHD testing system, and is a consultant for the Health Information Technology Lab.
NEW YORK – Assessing nonresponsiveness to attention-deficit/hyperactivity disorder treatment requires a bit of detective work, according to Dr. Laurence L. Greenhill.
The reason can be as simple as a little kid not being able to swallow a big pill, or as complex as a dysfunctional family dynamic that interferes with medication adherence. But once the problem is rooted out and addressed, most refractory patients can experience a good response, Dr. Greenhill said at a psychopharmacology update held by the American Academy of Child and Adolescent Psychiatry.
Since primary care physicians usually continue to manage children who respond to ADHD medications, psychiatrists are usually the ones who see nonresponders, said Dr. Greenhill, a child and adolescent psychiatrist at the New York Psychiatric Institute.
Medication nonadherence, the most common cause of a failure to improve, can arise from numerous situations.
On the simple side, it might be a matter of finding the right form of medication; a liquid or sprinkle capsule might be much easier for a child to take than a pill. And not all pills are created equally easy to take.
"For example, [the osmotic controlled release oral delivery system methylphenidate] just went off patent, and generics are now available. But some of these generics are much bigger. In fact, one of the 18-mg pills is twice as large as the patent medicine, and lots of kids can’t swallow it," he said.
The ADHD medication guide published by Long Island Jewish Hospital can be a helpful tool when working with parents on this issue. It lists all the Food and Drug Administration–approved medications for ADHD, with full-size photographs of each capsule, tablet, or pill.
Some generics are not pharmacokinetically or pharmacodynamically identical to the original formulation, Dr. Greenhill noted. Although the drug has to be molecularly identical and dose identical, "the ascending dose curve and duration of action need not be matched." Some generic formulations do fall into this problematic category. "For this reason, I try to encourage parents to get the brand," said Dr. Greenhill, adding that he has no financial interest in any of the drugs.
Medication nonadherence also can be attributable to uncomfortable or even intolerable side effects. These can include gastrointestinal issues, trouble sleeping, lack of appetite, restlessness, irritability, and "feeling fidgety."
Dosage adjustments or a medication change might be in order. For appetite issues, recommend giving the medication after meals, and reassure parents it’s OK to let a child eat later in the evening, when hunger may return.
It’s important to get the child’s growth records from the pediatrician, and plot height and weight curves every 6 months. If there’s a consistent fall-off, consider lowering the dose or changing to another drug.
Contrary to widely held belief, stimulants don’t pose significant cardiac risks to most children. A baseline electrocardiogram is really only necessary for a child who has a family history of sudden cardiac death or a personal history of syncope or cardiac abnormalities. Blood pressure and pulse should be monitored at every visit.
Melatonin is worth a try for youngsters whose ADHD meds interfere with good sleep, Dr. Greenhill said.
"I would start at 1 mg/night and work up," he said. "Starting at a high dose can actually shut off the naturally occurring melatonin. Plasma levels peak about an hour after taking it, so timing is important. I usually start with it about 3 hours before the scheduled sleeping time and then adjust."
Family dynamics also can play a big role in medication nonadherence. "ADHD families are often poor at scheduling activities, sometimes to the extent that parents are the ones who forget to give the medication. They also might not have a clear idea of how to give it, and just leave it on the kitchen table, making it the child’s responsibility to take it every day.
"If this is a child who can’t remember to bring homework back from school, then how is he going to remember to stay on schedule with medication?"
If it’s clear that parents are having difficulty in this area, the simplest thing to do is send the medicine to school and ask the nurse to administer it. Switching to a long-acting form might help, too, since it’s just easier to remember to take one pill than to take two.
The ADHD Parents Medication Guide is a great resource that can be used to get parents actively involved with the child’s drug therapy, Dr. Greenhill said. Developed by the American Psychiatric Association and the American Academy of Child and Adolescent Psychiatry, the online guide is designed to help families and physicians work together to make the best decisions about a child’s care.
Dr. Greenhill is on the advisory board of Quotient, which manufactures an ADHD testing system, and is a consultant for the Health Information Technology Lab.
EXPERT ANALYSIS FROM THE PSYCHOPHARMACOLOGY UPDATE INSTITUTE

Oseltamivir suspension back in production
Manufacturing delays that led to a nationwide shortage of oseltamivir oral suspension have been resolved, according to a spokeswoman for Genentech, which makes the drug.
"We now anticipate having sufficient supply of both the liquid and capsule forms ... to meet demand for this flu season," Tara Iannuccillo said in an interview.
Ms. Iannuccillo said that distributors who supply the product to retail pharmacies now have access to it. However, she added, "Given the widespread flu activity in 35 states nationally, there may be some instances where a local pharmacy may not have the liquid formulation in stock."
There are no shortages of the oseltamivir capsules, which are available in 30 mg, 45 mg, and 75 mg. Patients older than 1 year can be dosed correctly using the 30 mg and 45 mg capsules, according to the Food and Drug Administration.
"For those patients who cannot swallow capsules, the capsules can be opened and the contents may be mixed with chocolate syrup or some other thick, sweet liquid," FDA noted.
Alternatively, a suspension can be compounded using the 75-mg oseltamivir capsules. The instructions are on the package insert, and also available on Genetech’s website.
Manufacturing delays that led to a nationwide shortage of oseltamivir oral suspension have been resolved, according to a spokeswoman for Genentech, which makes the drug.
"We now anticipate having sufficient supply of both the liquid and capsule forms ... to meet demand for this flu season," Tara Iannuccillo said in an interview.
Ms. Iannuccillo said that distributors who supply the product to retail pharmacies now have access to it. However, she added, "Given the widespread flu activity in 35 states nationally, there may be some instances where a local pharmacy may not have the liquid formulation in stock."
There are no shortages of the oseltamivir capsules, which are available in 30 mg, 45 mg, and 75 mg. Patients older than 1 year can be dosed correctly using the 30 mg and 45 mg capsules, according to the Food and Drug Administration.
"For those patients who cannot swallow capsules, the capsules can be opened and the contents may be mixed with chocolate syrup or some other thick, sweet liquid," FDA noted.
Alternatively, a suspension can be compounded using the 75-mg oseltamivir capsules. The instructions are on the package insert, and also available on Genetech’s website.
Manufacturing delays that led to a nationwide shortage of oseltamivir oral suspension have been resolved, according to a spokeswoman for Genentech, which makes the drug.
"We now anticipate having sufficient supply of both the liquid and capsule forms ... to meet demand for this flu season," Tara Iannuccillo said in an interview.
Ms. Iannuccillo said that distributors who supply the product to retail pharmacies now have access to it. However, she added, "Given the widespread flu activity in 35 states nationally, there may be some instances where a local pharmacy may not have the liquid formulation in stock."
There are no shortages of the oseltamivir capsules, which are available in 30 mg, 45 mg, and 75 mg. Patients older than 1 year can be dosed correctly using the 30 mg and 45 mg capsules, according to the Food and Drug Administration.
"For those patients who cannot swallow capsules, the capsules can be opened and the contents may be mixed with chocolate syrup or some other thick, sweet liquid," FDA noted.
Alternatively, a suspension can be compounded using the 75-mg oseltamivir capsules. The instructions are on the package insert, and also available on Genetech’s website.
Triple-antiviral therapy achieves 94% response without interferon, ribavirin
Both a 12-week and a 24-week regimen of three oral antiviral drugs achieved sustained viral remissions at 12 weeks in up to 94% of treatment-naive patients with genotype 1 hepatitis C virus infections.
The three oral antivirals included daclatasvir, an NS5A replication complex inhibitor; asunaprevir, an NS3 protease inhibitor; and BMS-791325, an investigational selective non-nucleoside polymerase inhibitor. A key point of the study is its proof that short-duration treatment – even without interferon or ribavirin – can result in sustained remission, Dr. Gregory T. Everson and his colleagues wrote in the February issue of Gastroenterology (doi.org/10.1053/j.gastro.2013.10.057). "Shorter treatment durations are preferable because they may improve patient compliance. In this study, treatment periods of both 12 and 24 weeks yielded high SVR (sustained viral remission) rates, suggesting no advantage for extending treatment duration to 24 weeks."
Source: American Gastroenterological Association
Further, the triple-antiviral combination apparently controlled viral replication without using interferon or ribavirin, thus avoiding their side effects. The current regimen for treatment-naive patients with genotype 1 hepatitis C virus infections calls for a 48-week treatment with peginterferon and ribavirin with telaprevir or boceprevir.
"Ribavirin contributes to anemia and it is teratogenic; thus, effective treatments without ribavirin are desirable," wrote Dr. Everson of the University of Colorado, Denver, and his coauthors. "This interferon- and ribavirin-free regimen did not alter hemoglobin levels in a clinically meaningfully manner, as evidenced by no grade 1 or higher hemoglobin reductions and no adverse events of anemia."
Dr. Everson and his colleagues gave the regimen for periods of 12 and 24 weeks and with two different doses of BMS-791325, resulting in a four-way randomized study. Groups 1 and 2 were treated for 12 weeks with the combination of daclatasvir 60 mg once daily, asunaprevir 200 mg twice daily, and BMS-791325 (twice daily 75 mg or 150 mg). Groups 3 and 4 had exactly the same two-treatment regimen, but took the drugs for 24 weeks. After treatment, there was a 48-week follow-up period.
Among the 66 patients in the study, the average age was about 50 years old, and the mean HCV-RNA level was 6 log10 IU/mL. Most (75%) had HCV genotype 1a; the rest had 1b. All were treatment naive. Four patients withdrew before the study’s end; none of the withdrawals were for adverse events.
In groups 1 and 2 (75 mg BMS-791325, twice daily for 12 and 24 weeks), the viral load decreased rapidly. By week 4, all of these patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
In groups 3 and 4 (150 mg BMS-791325, twice daily for 12 or 24 weeks), HCV-RNA levels also fell rapidly in the first month, By week 4, all of those in the 12-week group and all but one in the 24-week group had levels of less than 25 IU/mL, which were sustained through the end of treatment. In the intent-to-treat analysis, 91% overall had an HCV-RNA load of less than 25 IU/mL by the end of treatment.
Overall, there were three treatment failures: one each in groups 3 and 4 had viral breakthrough, and one in group 4 experienced a relapse at week 4.
Both breakthrough patients were given peginterferon-alfa/ribavirin in addition to the direct-acting antivirals. After 16 weeks, one discontinued treatment because of interferon-related cerebral vasoconstriction. That patient had an undetectable HCV-RNA level at the end of treatment, but relapsed by post treatment week 4. The other patient had a sustained viral response.
The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
This critical proof-of-concept study demonstrates that a combination of three direct-acting antivirals (an NS5A inhibitor + NS3PI + NNPI) without ribavirin can achieve sustained viral response at 12 weeks at rates of 94% in a genotype 1 treatment-naive (TN) population. The data are a foundation for multiple large, randomized, phase III trials using this regimen in TN patients, treatment failure, cirrhosis, HIV coinfection, and other genotypes, and thus, it is important to the development of interferon- and ribavirin-free therapies for HCV.
The authors have selected a TN population without advanced fibrosis for this regimen so far, and it remains to be seen whether these high sustained viral remission (SVR) rates can be duplicated in cirrhosis and those with prior treatment failure. It may also show reduced efficacy when studied in more difficult-to-treat patients such as with protease inhibitor failure, HIV coinfection, and other genotypes. However, the importance of this study is that the lack of efficacy seen in genotype 1a with the dual therapy published in 2012 was successfully overcome simply by adding an non-nucleoside polymerase inhibitor (N. Engl. J. Med. 2012;366:216-24). The implications may extend to other interferon-free, direct-acting antiviral regimens in development. An NS5B nucleotide polymerase inhibitor may not be required for the backbone of therapy, as it appears to be the based on sofosbuvir studies (N. Engl. J. Med. 2013;368:34-44; 1878-87). Rather, a best-in-class drug, here daclatasvir for the NS5A class, may be added to two other relatively weak compounds and still have greater than 90% SVR rates as an interferon-free regimen.
This would pave the way for many compounds to be competitive without the nucleotide polymerase inhibitor backbone regimen, in both genotype 1a and 1b patients. However, with the promise of a 12-week regimen of sofosbuvir and ledipasvir as a single, fixed-dose combination for all patient types (Gilead Sciences press release, Dec. 18, 2013: "Gilead announces SVR12 rates from three phase III studies evaluating once-daily fixed-dose combination of sofosbuvir and ledipasvir for genotype 1 hepatitis C patients"), a competitor would need to show similar efficacy and tolerability. Even if not proven in all patient populations, this would lead to a price competitive market that would provide the patient, physician, and payer with multiple choices. Although this may not be as important in the United States, it will be critical to many resource-limited countries where price will be a primary constraint.
Dr. Paul Pockros is director, Liver Disease Center Scripps Clinic, and clinical director of research, Scripps Translational Science Institute, both in La Jolla, Calif. He does research, speaks, and consults for Bristol-Myers Squibb, Gilead, Genetech, and Janssen. He also does research and consults for Boehringer Ingelheim and Novartis.
This critical proof-of-concept study demonstrates that a combination of three direct-acting antivirals (an NS5A inhibitor + NS3PI + NNPI) without ribavirin can achieve sustained viral response at 12 weeks at rates of 94% in a genotype 1 treatment-naive (TN) population. The data are a foundation for multiple large, randomized, phase III trials using this regimen in TN patients, treatment failure, cirrhosis, HIV coinfection, and other genotypes, and thus, it is important to the development of interferon- and ribavirin-free therapies for HCV.
The authors have selected a TN population without advanced fibrosis for this regimen so far, and it remains to be seen whether these high sustained viral remission (SVR) rates can be duplicated in cirrhosis and those with prior treatment failure. It may also show reduced efficacy when studied in more difficult-to-treat patients such as with protease inhibitor failure, HIV coinfection, and other genotypes. However, the importance of this study is that the lack of efficacy seen in genotype 1a with the dual therapy published in 2012 was successfully overcome simply by adding an non-nucleoside polymerase inhibitor (N. Engl. J. Med. 2012;366:216-24). The implications may extend to other interferon-free, direct-acting antiviral regimens in development. An NS5B nucleotide polymerase inhibitor may not be required for the backbone of therapy, as it appears to be the based on sofosbuvir studies (N. Engl. J. Med. 2013;368:34-44; 1878-87). Rather, a best-in-class drug, here daclatasvir for the NS5A class, may be added to two other relatively weak compounds and still have greater than 90% SVR rates as an interferon-free regimen.
This would pave the way for many compounds to be competitive without the nucleotide polymerase inhibitor backbone regimen, in both genotype 1a and 1b patients. However, with the promise of a 12-week regimen of sofosbuvir and ledipasvir as a single, fixed-dose combination for all patient types (Gilead Sciences press release, Dec. 18, 2013: "Gilead announces SVR12 rates from three phase III studies evaluating once-daily fixed-dose combination of sofosbuvir and ledipasvir for genotype 1 hepatitis C patients"), a competitor would need to show similar efficacy and tolerability. Even if not proven in all patient populations, this would lead to a price competitive market that would provide the patient, physician, and payer with multiple choices. Although this may not be as important in the United States, it will be critical to many resource-limited countries where price will be a primary constraint.
Dr. Paul Pockros is director, Liver Disease Center Scripps Clinic, and clinical director of research, Scripps Translational Science Institute, both in La Jolla, Calif. He does research, speaks, and consults for Bristol-Myers Squibb, Gilead, Genetech, and Janssen. He also does research and consults for Boehringer Ingelheim and Novartis.
This critical proof-of-concept study demonstrates that a combination of three direct-acting antivirals (an NS5A inhibitor + NS3PI + NNPI) without ribavirin can achieve sustained viral response at 12 weeks at rates of 94% in a genotype 1 treatment-naive (TN) population. The data are a foundation for multiple large, randomized, phase III trials using this regimen in TN patients, treatment failure, cirrhosis, HIV coinfection, and other genotypes, and thus, it is important to the development of interferon- and ribavirin-free therapies for HCV.
The authors have selected a TN population without advanced fibrosis for this regimen so far, and it remains to be seen whether these high sustained viral remission (SVR) rates can be duplicated in cirrhosis and those with prior treatment failure. It may also show reduced efficacy when studied in more difficult-to-treat patients such as with protease inhibitor failure, HIV coinfection, and other genotypes. However, the importance of this study is that the lack of efficacy seen in genotype 1a with the dual therapy published in 2012 was successfully overcome simply by adding an non-nucleoside polymerase inhibitor (N. Engl. J. Med. 2012;366:216-24). The implications may extend to other interferon-free, direct-acting antiviral regimens in development. An NS5B nucleotide polymerase inhibitor may not be required for the backbone of therapy, as it appears to be the based on sofosbuvir studies (N. Engl. J. Med. 2013;368:34-44; 1878-87). Rather, a best-in-class drug, here daclatasvir for the NS5A class, may be added to two other relatively weak compounds and still have greater than 90% SVR rates as an interferon-free regimen.
This would pave the way for many compounds to be competitive without the nucleotide polymerase inhibitor backbone regimen, in both genotype 1a and 1b patients. However, with the promise of a 12-week regimen of sofosbuvir and ledipasvir as a single, fixed-dose combination for all patient types (Gilead Sciences press release, Dec. 18, 2013: "Gilead announces SVR12 rates from three phase III studies evaluating once-daily fixed-dose combination of sofosbuvir and ledipasvir for genotype 1 hepatitis C patients"), a competitor would need to show similar efficacy and tolerability. Even if not proven in all patient populations, this would lead to a price competitive market that would provide the patient, physician, and payer with multiple choices. Although this may not be as important in the United States, it will be critical to many resource-limited countries where price will be a primary constraint.
Dr. Paul Pockros is director, Liver Disease Center Scripps Clinic, and clinical director of research, Scripps Translational Science Institute, both in La Jolla, Calif. He does research, speaks, and consults for Bristol-Myers Squibb, Gilead, Genetech, and Janssen. He also does research and consults for Boehringer Ingelheim and Novartis.
Both a 12-week and a 24-week regimen of three oral antiviral drugs achieved sustained viral remissions at 12 weeks in up to 94% of treatment-naive patients with genotype 1 hepatitis C virus infections.
The three oral antivirals included daclatasvir, an NS5A replication complex inhibitor; asunaprevir, an NS3 protease inhibitor; and BMS-791325, an investigational selective non-nucleoside polymerase inhibitor. A key point of the study is its proof that short-duration treatment – even without interferon or ribavirin – can result in sustained remission, Dr. Gregory T. Everson and his colleagues wrote in the February issue of Gastroenterology (doi.org/10.1053/j.gastro.2013.10.057). "Shorter treatment durations are preferable because they may improve patient compliance. In this study, treatment periods of both 12 and 24 weeks yielded high SVR (sustained viral remission) rates, suggesting no advantage for extending treatment duration to 24 weeks."
Source: American Gastroenterological Association
Further, the triple-antiviral combination apparently controlled viral replication without using interferon or ribavirin, thus avoiding their side effects. The current regimen for treatment-naive patients with genotype 1 hepatitis C virus infections calls for a 48-week treatment with peginterferon and ribavirin with telaprevir or boceprevir.
"Ribavirin contributes to anemia and it is teratogenic; thus, effective treatments without ribavirin are desirable," wrote Dr. Everson of the University of Colorado, Denver, and his coauthors. "This interferon- and ribavirin-free regimen did not alter hemoglobin levels in a clinically meaningfully manner, as evidenced by no grade 1 or higher hemoglobin reductions and no adverse events of anemia."
Dr. Everson and his colleagues gave the regimen for periods of 12 and 24 weeks and with two different doses of BMS-791325, resulting in a four-way randomized study. Groups 1 and 2 were treated for 12 weeks with the combination of daclatasvir 60 mg once daily, asunaprevir 200 mg twice daily, and BMS-791325 (twice daily 75 mg or 150 mg). Groups 3 and 4 had exactly the same two-treatment regimen, but took the drugs for 24 weeks. After treatment, there was a 48-week follow-up period.
Among the 66 patients in the study, the average age was about 50 years old, and the mean HCV-RNA level was 6 log10 IU/mL. Most (75%) had HCV genotype 1a; the rest had 1b. All were treatment naive. Four patients withdrew before the study’s end; none of the withdrawals were for adverse events.
In groups 1 and 2 (75 mg BMS-791325, twice daily for 12 and 24 weeks), the viral load decreased rapidly. By week 4, all of these patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
In groups 3 and 4 (150 mg BMS-791325, twice daily for 12 or 24 weeks), HCV-RNA levels also fell rapidly in the first month, By week 4, all of those in the 12-week group and all but one in the 24-week group had levels of less than 25 IU/mL, which were sustained through the end of treatment. In the intent-to-treat analysis, 91% overall had an HCV-RNA load of less than 25 IU/mL by the end of treatment.
Overall, there were three treatment failures: one each in groups 3 and 4 had viral breakthrough, and one in group 4 experienced a relapse at week 4.
Both breakthrough patients were given peginterferon-alfa/ribavirin in addition to the direct-acting antivirals. After 16 weeks, one discontinued treatment because of interferon-related cerebral vasoconstriction. That patient had an undetectable HCV-RNA level at the end of treatment, but relapsed by post treatment week 4. The other patient had a sustained viral response.
The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
Both a 12-week and a 24-week regimen of three oral antiviral drugs achieved sustained viral remissions at 12 weeks in up to 94% of treatment-naive patients with genotype 1 hepatitis C virus infections.
The three oral antivirals included daclatasvir, an NS5A replication complex inhibitor; asunaprevir, an NS3 protease inhibitor; and BMS-791325, an investigational selective non-nucleoside polymerase inhibitor. A key point of the study is its proof that short-duration treatment – even without interferon or ribavirin – can result in sustained remission, Dr. Gregory T. Everson and his colleagues wrote in the February issue of Gastroenterology (doi.org/10.1053/j.gastro.2013.10.057). "Shorter treatment durations are preferable because they may improve patient compliance. In this study, treatment periods of both 12 and 24 weeks yielded high SVR (sustained viral remission) rates, suggesting no advantage for extending treatment duration to 24 weeks."
Source: American Gastroenterological Association
Further, the triple-antiviral combination apparently controlled viral replication without using interferon or ribavirin, thus avoiding their side effects. The current regimen for treatment-naive patients with genotype 1 hepatitis C virus infections calls for a 48-week treatment with peginterferon and ribavirin with telaprevir or boceprevir.
"Ribavirin contributes to anemia and it is teratogenic; thus, effective treatments without ribavirin are desirable," wrote Dr. Everson of the University of Colorado, Denver, and his coauthors. "This interferon- and ribavirin-free regimen did not alter hemoglobin levels in a clinically meaningfully manner, as evidenced by no grade 1 or higher hemoglobin reductions and no adverse events of anemia."
Dr. Everson and his colleagues gave the regimen for periods of 12 and 24 weeks and with two different doses of BMS-791325, resulting in a four-way randomized study. Groups 1 and 2 were treated for 12 weeks with the combination of daclatasvir 60 mg once daily, asunaprevir 200 mg twice daily, and BMS-791325 (twice daily 75 mg or 150 mg). Groups 3 and 4 had exactly the same two-treatment regimen, but took the drugs for 24 weeks. After treatment, there was a 48-week follow-up period.
Among the 66 patients in the study, the average age was about 50 years old, and the mean HCV-RNA level was 6 log10 IU/mL. Most (75%) had HCV genotype 1a; the rest had 1b. All were treatment naive. Four patients withdrew before the study’s end; none of the withdrawals were for adverse events.
In groups 1 and 2 (75 mg BMS-791325, twice daily for 12 and 24 weeks), the viral load decreased rapidly. By week 4, all of these patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
In groups 3 and 4 (150 mg BMS-791325, twice daily for 12 or 24 weeks), HCV-RNA levels also fell rapidly in the first month, By week 4, all of those in the 12-week group and all but one in the 24-week group had levels of less than 25 IU/mL, which were sustained through the end of treatment. In the intent-to-treat analysis, 91% overall had an HCV-RNA load of less than 25 IU/mL by the end of treatment.
Overall, there were three treatment failures: one each in groups 3 and 4 had viral breakthrough, and one in group 4 experienced a relapse at week 4.
Both breakthrough patients were given peginterferon-alfa/ribavirin in addition to the direct-acting antivirals. After 16 weeks, one discontinued treatment because of interferon-related cerebral vasoconstriction. That patient had an undetectable HCV-RNA level at the end of treatment, but relapsed by post treatment week 4. The other patient had a sustained viral response.
The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
Major finding: By week 4, patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
Data source: A trial of 66 treatment-naive patients randomized to one of four antiviral regimens that differed by dose of BMS-791325, an investigational selective non-nucleoside polymerase inhibitor.
Disclosures: The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers Squibb. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
Two-thirds of women with uterine pathology got pregnant after combined procedure
NATIONAL HARBOR, MD. – More than two-thirds of 30 women with infertility related to uterine pathology achieved pregnancy after a single surgery that combined both hysteroscopy and laparoscopy, a study showed.
"After treatment, many of these patients can achieve pregnancy spontaneously without the use of assisted reproductive technology, and significant cost savings are achieved if the procedures are done at the same time," said Dr. Chris J. Allphin, a gynecologist at the Eastern Idaho Regional Medical Center, Idaho Falls.
The single procedure cost an average of $15,000 less than having sequential procedures.
Dr. Allphin reported a retrospective study of 30 patients treated since 2007 for infertility due to ultrasound-confirmed uterine pathology; 13 women had a uterine septum and 17 had leiomyomata.
Two surgeons simultaneously performed the procedures. Septae were diagnosed laparoscopically and treated with hysteroscopic metroplasty. Leiomyomata were diagnosed laparoscopically and treated with either a hysteroscopic or laparoscopic myomectomy.
Of the 30 patients, 21 women (70%) became pregnant and 5 women conceived twice. Fourteen pregnancies (66%) – including one set of twins – were conceived without assisted reproduction techniques. Four were the result of intrauterine insemination. There were seven in vitro fertilization pregnancies, Dr. Allphin reported at the meeting sponsored by AAGL.
Younger women achieved the best pregnancy rates, with 82% of those younger than 35 years conceiving. The rate was 62% among those aged 35-40 years and 60% in those older than 40 years.
The average cost of having the laparoscopy and hysteroscopy at different admissions is $38,256. The average cost of the dual procedure at a single admission was $23,185. "Thirty patients having the dual procedure saved the system $450,000," according to Dr. Allphin.
Of the nine patients who did not conceive, two had no antral follicles at return to the fertility specialist, two had attempted one in vitro fertilization cycle and then discontinued treatment, one had two intrauterine insemination cycles and then discontinued treatment, three continue to go through in vitro fertilization cycles, and one has postponed trying to conceive.
Dr. Allphin said he had no relevant financial disclosures.
NATIONAL HARBOR, MD. – More than two-thirds of 30 women with infertility related to uterine pathology achieved pregnancy after a single surgery that combined both hysteroscopy and laparoscopy, a study showed.
"After treatment, many of these patients can achieve pregnancy spontaneously without the use of assisted reproductive technology, and significant cost savings are achieved if the procedures are done at the same time," said Dr. Chris J. Allphin, a gynecologist at the Eastern Idaho Regional Medical Center, Idaho Falls.
The single procedure cost an average of $15,000 less than having sequential procedures.
Dr. Allphin reported a retrospective study of 30 patients treated since 2007 for infertility due to ultrasound-confirmed uterine pathology; 13 women had a uterine septum and 17 had leiomyomata.
Two surgeons simultaneously performed the procedures. Septae were diagnosed laparoscopically and treated with hysteroscopic metroplasty. Leiomyomata were diagnosed laparoscopically and treated with either a hysteroscopic or laparoscopic myomectomy.
Of the 30 patients, 21 women (70%) became pregnant and 5 women conceived twice. Fourteen pregnancies (66%) – including one set of twins – were conceived without assisted reproduction techniques. Four were the result of intrauterine insemination. There were seven in vitro fertilization pregnancies, Dr. Allphin reported at the meeting sponsored by AAGL.
Younger women achieved the best pregnancy rates, with 82% of those younger than 35 years conceiving. The rate was 62% among those aged 35-40 years and 60% in those older than 40 years.
The average cost of having the laparoscopy and hysteroscopy at different admissions is $38,256. The average cost of the dual procedure at a single admission was $23,185. "Thirty patients having the dual procedure saved the system $450,000," according to Dr. Allphin.
Of the nine patients who did not conceive, two had no antral follicles at return to the fertility specialist, two had attempted one in vitro fertilization cycle and then discontinued treatment, one had two intrauterine insemination cycles and then discontinued treatment, three continue to go through in vitro fertilization cycles, and one has postponed trying to conceive.
Dr. Allphin said he had no relevant financial disclosures.
NATIONAL HARBOR, MD. – More than two-thirds of 30 women with infertility related to uterine pathology achieved pregnancy after a single surgery that combined both hysteroscopy and laparoscopy, a study showed.
"After treatment, many of these patients can achieve pregnancy spontaneously without the use of assisted reproductive technology, and significant cost savings are achieved if the procedures are done at the same time," said Dr. Chris J. Allphin, a gynecologist at the Eastern Idaho Regional Medical Center, Idaho Falls.
The single procedure cost an average of $15,000 less than having sequential procedures.
Dr. Allphin reported a retrospective study of 30 patients treated since 2007 for infertility due to ultrasound-confirmed uterine pathology; 13 women had a uterine septum and 17 had leiomyomata.
Two surgeons simultaneously performed the procedures. Septae were diagnosed laparoscopically and treated with hysteroscopic metroplasty. Leiomyomata were diagnosed laparoscopically and treated with either a hysteroscopic or laparoscopic myomectomy.
Of the 30 patients, 21 women (70%) became pregnant and 5 women conceived twice. Fourteen pregnancies (66%) – including one set of twins – were conceived without assisted reproduction techniques. Four were the result of intrauterine insemination. There were seven in vitro fertilization pregnancies, Dr. Allphin reported at the meeting sponsored by AAGL.
Younger women achieved the best pregnancy rates, with 82% of those younger than 35 years conceiving. The rate was 62% among those aged 35-40 years and 60% in those older than 40 years.
The average cost of having the laparoscopy and hysteroscopy at different admissions is $38,256. The average cost of the dual procedure at a single admission was $23,185. "Thirty patients having the dual procedure saved the system $450,000," according to Dr. Allphin.
Of the nine patients who did not conceive, two had no antral follicles at return to the fertility specialist, two had attempted one in vitro fertilization cycle and then discontinued treatment, one had two intrauterine insemination cycles and then discontinued treatment, three continue to go through in vitro fertilization cycles, and one has postponed trying to conceive.
Dr. Allphin said he had no relevant financial disclosures.
AT THE AAGL GLOBAL CONGRESS
Major finding: Fourteen pregnancies (66%) – including one set of twins – were conceived without assisted reproduction techniques.
Data source: A retrospective study of 30 patients.
Disclosures: Dr. Allphin said he had no relevant financial disclosures.
Anti-CCP antibodies associated with increased mortality in RA
Postmenopausal women with rheumatoid arthritis were almost three times more likely to die over a 10-year period than were those who did not have the disease in a subanalysis of participants in the Women’s Health Initiative study.
Using stored serum from Women’s Health Initiative (WHI) subjects, investigators found that the increased risk was mostly attributable to women with anti-cyclic citrullinated peptide (anti-CCP) antibodies – a marker used to identify those in the sample who probably had true rheumatoid arthritis (RA). This finding stayed significant even when the analysis controlled for the use of disease-modifying antirheumatic drugs (DMARDs), and also in several models that controlled for health and lifestyle risk factors, Dr. Lewis H. Kuller and his colleagues reported in Arthritis & Rheumatism.
"The increased risk of death for anti-CCP positive women was not explained by age, rheumatoid factor positivity, ANA [antinuclear antibody] positivity, or DMARD use," wrote Dr. Kuller of the University of Pittsburgh and his coauthors (Arthritis Rheum. 2014 Dec. 23 [doi:10.1002/art.38268]).

"Traditional risk factors (e.g., smoking, diabetes), kidney disease, joint pain, health status or [white blood cell] count also did not statistically explain the increased risk for anti-CCP-positivity, despite their independent associations with higher mortality," they said.
The study focused on 9,988 women from the WHI, all of whom self-reported having RA at baseline or at follow-up visits. To further refine the sample, the investigators defined probable RA as the presence of anti-CCP antibodies, with or without the use of DMARDs (8% of the sample), or the absence of anti-CCP antibodies reported with DMARD use (7%). Thus, a total of 1,029 women were considered to have probable RA. The remainder of the sample probably had osteoarthritis, the authors suggested.
The mortality analysis further considered the timing of RA onset by whether it was reported at baseline or during follow-up.
During the 10-year study period, 13% of the group died, including 14% of those with RA at baseline and follow-up, 16% of those with RA only at baseline, and 10% of those who reported it only at follow-up. The median times to death were 8 years for those with baseline RA, 7 years for those with baseline and follow-up RA, and 6 years for those with RA at follow-up.
Women with anti-CCP antibodies had the highest age-adjusted death rate (19 per 1,000 person-years), followed by those who did not have anti-CCP antibodies but were taking DMARDs (18 per 1,000 person-years) and those who probably did not have RA (no antibodies and no DMARDS; 10 per 1,000 person-years).
ANA positivity occurred in 16% of the women, but two-thirds of them were negative for anti-CCP and rheumatoid factor and "therefore probably did not have clinical RA." Age-adjusted death rates were lower for ANA-positive women than for anti-CCP–positive and rheumatoid factor–positive women and were not higher for anti-CPP–positive women with or without rheumatoid factor, or for anti-CPP–negative women with rheumatoid factor. This suggested to the investigators that "anti-CCP positivity rather than rheumatoid factor positivity was the correlate of increased death rates."
Mortality was similar for those using DMARDs and those not using them, and for the use of methotrexate, compared with other DMARDs.
There were no between-group differences in causes of death, which were most frequently cardiovascular disease and cancers. Smoking, diabetes, less physical activity, poor overall health, and a history of coronary heart disease all increased the death rate among those with anti-CCP antibodies. About a quarter of those with the antibodies reported poor health status, with a death rate four times higher than those who probably didn’t have RA and who also said they had excellent health.
Joint pain in the 4 weeks before the baseline interview was another indicator of mortality. Among all antibody-positive women, those who reported severe pain were twice as likely to die during the follow-up as were those who reported no pain or mild pain. Additionally, among all women with severe joint pain, the death rates were significantly higher for those with the antibodies (35.5 per 1,000 person-years) than for those who reported RA but were antibody negative (17.2 per 1,000 person-years), those who reported arthritis but not RA (12.1 per 1,000 person-years), and those who reported no arthritis (11.4 per 1,000 person-years).
In a multivariate, age-adjusted model, anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio [HR], 2.8) than were women without RA. The risk was also significantly elevated in anti-CCP–positive women who weren’t taking DMARDs (HR, 2.2) and for those who were anti-CCP–negative but who used DMARDs (HR, 1.8).
The study was funded by the National Heart, Lung, and Blood Institute. No financial disclosures were listed.
Postmenopausal women with rheumatoid arthritis were almost three times more likely to die over a 10-year period than were those who did not have the disease in a subanalysis of participants in the Women’s Health Initiative study.
Using stored serum from Women’s Health Initiative (WHI) subjects, investigators found that the increased risk was mostly attributable to women with anti-cyclic citrullinated peptide (anti-CCP) antibodies – a marker used to identify those in the sample who probably had true rheumatoid arthritis (RA). This finding stayed significant even when the analysis controlled for the use of disease-modifying antirheumatic drugs (DMARDs), and also in several models that controlled for health and lifestyle risk factors, Dr. Lewis H. Kuller and his colleagues reported in Arthritis & Rheumatism.
"The increased risk of death for anti-CCP positive women was not explained by age, rheumatoid factor positivity, ANA [antinuclear antibody] positivity, or DMARD use," wrote Dr. Kuller of the University of Pittsburgh and his coauthors (Arthritis Rheum. 2014 Dec. 23 [doi:10.1002/art.38268]).
"Traditional risk factors (e.g., smoking, diabetes), kidney disease, joint pain, health status or [white blood cell] count also did not statistically explain the increased risk for anti-CCP-positivity, despite their independent associations with higher mortality," they said.
The study focused on 9,988 women from the WHI, all of whom self-reported having RA at baseline or at follow-up visits. To further refine the sample, the investigators defined probable RA as the presence of anti-CCP antibodies, with or without the use of DMARDs (8% of the sample), or the absence of anti-CCP antibodies reported with DMARD use (7%). Thus, a total of 1,029 women were considered to have probable RA. The remainder of the sample probably had osteoarthritis, the authors suggested.
The mortality analysis further considered the timing of RA onset by whether it was reported at baseline or during follow-up.
During the 10-year study period, 13% of the group died, including 14% of those with RA at baseline and follow-up, 16% of those with RA only at baseline, and 10% of those who reported it only at follow-up. The median times to death were 8 years for those with baseline RA, 7 years for those with baseline and follow-up RA, and 6 years for those with RA at follow-up.
Women with anti-CCP antibodies had the highest age-adjusted death rate (19 per 1,000 person-years), followed by those who did not have anti-CCP antibodies but were taking DMARDs (18 per 1,000 person-years) and those who probably did not have RA (no antibodies and no DMARDS; 10 per 1,000 person-years).
ANA positivity occurred in 16% of the women, but two-thirds of them were negative for anti-CCP and rheumatoid factor and "therefore probably did not have clinical RA." Age-adjusted death rates were lower for ANA-positive women than for anti-CCP–positive and rheumatoid factor–positive women and were not higher for anti-CPP–positive women with or without rheumatoid factor, or for anti-CPP–negative women with rheumatoid factor. This suggested to the investigators that "anti-CCP positivity rather than rheumatoid factor positivity was the correlate of increased death rates."
Mortality was similar for those using DMARDs and those not using them, and for the use of methotrexate, compared with other DMARDs.
There were no between-group differences in causes of death, which were most frequently cardiovascular disease and cancers. Smoking, diabetes, less physical activity, poor overall health, and a history of coronary heart disease all increased the death rate among those with anti-CCP antibodies. About a quarter of those with the antibodies reported poor health status, with a death rate four times higher than those who probably didn’t have RA and who also said they had excellent health.
Joint pain in the 4 weeks before the baseline interview was another indicator of mortality. Among all antibody-positive women, those who reported severe pain were twice as likely to die during the follow-up as were those who reported no pain or mild pain. Additionally, among all women with severe joint pain, the death rates were significantly higher for those with the antibodies (35.5 per 1,000 person-years) than for those who reported RA but were antibody negative (17.2 per 1,000 person-years), those who reported arthritis but not RA (12.1 per 1,000 person-years), and those who reported no arthritis (11.4 per 1,000 person-years).
In a multivariate, age-adjusted model, anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio [HR], 2.8) than were women without RA. The risk was also significantly elevated in anti-CCP–positive women who weren’t taking DMARDs (HR, 2.2) and for those who were anti-CCP–negative but who used DMARDs (HR, 1.8).
The study was funded by the National Heart, Lung, and Blood Institute. No financial disclosures were listed.
Postmenopausal women with rheumatoid arthritis were almost three times more likely to die over a 10-year period than were those who did not have the disease in a subanalysis of participants in the Women’s Health Initiative study.
Using stored serum from Women’s Health Initiative (WHI) subjects, investigators found that the increased risk was mostly attributable to women with anti-cyclic citrullinated peptide (anti-CCP) antibodies – a marker used to identify those in the sample who probably had true rheumatoid arthritis (RA). This finding stayed significant even when the analysis controlled for the use of disease-modifying antirheumatic drugs (DMARDs), and also in several models that controlled for health and lifestyle risk factors, Dr. Lewis H. Kuller and his colleagues reported in Arthritis & Rheumatism.
"The increased risk of death for anti-CCP positive women was not explained by age, rheumatoid factor positivity, ANA [antinuclear antibody] positivity, or DMARD use," wrote Dr. Kuller of the University of Pittsburgh and his coauthors (Arthritis Rheum. 2014 Dec. 23 [doi:10.1002/art.38268]).
"Traditional risk factors (e.g., smoking, diabetes), kidney disease, joint pain, health status or [white blood cell] count also did not statistically explain the increased risk for anti-CCP-positivity, despite their independent associations with higher mortality," they said.
The study focused on 9,988 women from the WHI, all of whom self-reported having RA at baseline or at follow-up visits. To further refine the sample, the investigators defined probable RA as the presence of anti-CCP antibodies, with or without the use of DMARDs (8% of the sample), or the absence of anti-CCP antibodies reported with DMARD use (7%). Thus, a total of 1,029 women were considered to have probable RA. The remainder of the sample probably had osteoarthritis, the authors suggested.
The mortality analysis further considered the timing of RA onset by whether it was reported at baseline or during follow-up.
During the 10-year study period, 13% of the group died, including 14% of those with RA at baseline and follow-up, 16% of those with RA only at baseline, and 10% of those who reported it only at follow-up. The median times to death were 8 years for those with baseline RA, 7 years for those with baseline and follow-up RA, and 6 years for those with RA at follow-up.
Women with anti-CCP antibodies had the highest age-adjusted death rate (19 per 1,000 person-years), followed by those who did not have anti-CCP antibodies but were taking DMARDs (18 per 1,000 person-years) and those who probably did not have RA (no antibodies and no DMARDS; 10 per 1,000 person-years).
ANA positivity occurred in 16% of the women, but two-thirds of them were negative for anti-CCP and rheumatoid factor and "therefore probably did not have clinical RA." Age-adjusted death rates were lower for ANA-positive women than for anti-CCP–positive and rheumatoid factor–positive women and were not higher for anti-CPP–positive women with or without rheumatoid factor, or for anti-CPP–negative women with rheumatoid factor. This suggested to the investigators that "anti-CCP positivity rather than rheumatoid factor positivity was the correlate of increased death rates."
Mortality was similar for those using DMARDs and those not using them, and for the use of methotrexate, compared with other DMARDs.
There were no between-group differences in causes of death, which were most frequently cardiovascular disease and cancers. Smoking, diabetes, less physical activity, poor overall health, and a history of coronary heart disease all increased the death rate among those with anti-CCP antibodies. About a quarter of those with the antibodies reported poor health status, with a death rate four times higher than those who probably didn’t have RA and who also said they had excellent health.
Joint pain in the 4 weeks before the baseline interview was another indicator of mortality. Among all antibody-positive women, those who reported severe pain were twice as likely to die during the follow-up as were those who reported no pain or mild pain. Additionally, among all women with severe joint pain, the death rates were significantly higher for those with the antibodies (35.5 per 1,000 person-years) than for those who reported RA but were antibody negative (17.2 per 1,000 person-years), those who reported arthritis but not RA (12.1 per 1,000 person-years), and those who reported no arthritis (11.4 per 1,000 person-years).
In a multivariate, age-adjusted model, anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio [HR], 2.8) than were women without RA. The risk was also significantly elevated in anti-CCP–positive women who weren’t taking DMARDs (HR, 2.2) and for those who were anti-CCP–negative but who used DMARDs (HR, 1.8).
The study was funded by the National Heart, Lung, and Blood Institute. No financial disclosures were listed.
FROM ARTHRITIS & RHEUMATISM
Major finding: Anti-CCP–positive women using DMARDs were almost three times more likely to die (hazard ratio, 2.8) than were women without RA in a multivariate, age-adjusted model.
Data source: The study involved 9,988 women who had been in the Women’s Health Initiative and reported RA at baseline or at follow-up visits.
Disclosures: The study was sponsored by the National Heart, Lung, and Blood Institutes. No financial disclosures were listed.

Revascularization saves limbs and dollars in elderly patients
In older, frailer patients, limb revascularization appeared to preserve both limbs and ambulation longer – and cost less – than either amputation or a program of local wound care.
Although these patients had worse clinical outcomes than did healthy patients who had revascularization, the benefits were still evident, Dr. Neal R. Barshes and his colleagues wrote in the January issue of Annals of Vascular Surgery (Ann. Vasc. Surg. 2014;28:10-17).

"We believe that major amputation should be reserved for patients who develop life-threatening foot infections that cannot be controlled with foot drainage or minor amputations and subsequent palliative wound care," wrote Dr. Barshes of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and his coauthors.
The team conducted a clinical outcomes and cost model that ran 1,000 simulated trials of 1,000 patients each. The clinical parameters were drawn from the landmark MOVIE (Model to Optimize Healthcare Value in Ischemic Extremities) study. The study was modified to simulate a patient population older than 80 years, or who had undergone a prior major amputation of the contralateral lower limb, as these two groups have poorer postoperative outcomes than the usual population undergoing revascularization for lower limb ischemia.
The analysis examined outcomes associated with six procedures:
• Primary amputation.
• Local wound care.
• Surgical revascularization followed if needed by surgical revision.
• Surgical revascularization followed if needed by endovascular revision.
• Initial endovascular revascularization followed if needed by surgical revision.
• Endovascular revascularization followed if needed by endovascular revision.

Analysis revealed that primary amputation was the least clinically beneficial and the most expensive procedure, with no limb salvage, a median ambulatory period of 1.5 years, and a total 10-year cost of $185,955. Much of the cost was for nursing and long-term care due to loss of functional independence.
Wound care also produced less desirable outcomes. The median 5-year limb salvage rate was 28%, with a median limb salvage period of about 1.5 years. The median ambulatory period was less than 1 year, and the median total cost, $129,651.
Surgical bypass with either surgical or endovascular revision produced a limb salvage rate of 80%, with a median salvage time of 3 years and a median ambulatory period of 2.4 years. With surgical revision, the median total cost was $113,944; with endovascular revision, it was $110,910.
Endovascular revascularization followed by surgical revision produced a 5-year limb salvage rate of 80%, with a median limb salvage period of about 3 years and a median of 2.4 ambulatory years. The median total cost was $108,794.
Endovascular revascularization with endovascular revision produced a 5-year limb salvage rate of 80.5%, with a median salvage period of 3 years and a median ambulatory period of 2.5 years. This was the least expensive strategy, with a median total cost of $104,118.
These outcomes were much worse than those seen in the population of younger, healthier patients, the researchers said. The median 10-year cost for revascularization was up to $35,000 more. The clinical outcomes of the older population were also worse, with a 3-year period of limb preservation compared with more than 4 years in a healthier population, and about 2.5 ambulatory years compared with 4.6 years.
"In spite of these findings, revascularization still appears to be the most cost-effective alternative to wound care and primary amputation," the team noted. In fact, the less-healthy population actually stands to gain relatively more than the healthier one.
"In other words, the difference in outcomes between revascularization and either local wound care or primary amputation is much larger in this marginal population and therefore more likely to produce cost savings. The situation is akin to performing carotid endarterectomy early after a completed stroke – although the absolute risk of perioperative stroke is higher than when delayed for 6 weeks, the risk reduction of early carotid endarterectomy is significant compared with late carotid endarterectomy."
The research was initially presented at the annual winter meeting of the Peripheral Vascular Surgery Society. The paper did not note any potential financial conflicts of interest or the study’s sponsor.
Dr. Barshes and colleagues suggest that an aggressive approach to limb revascularization, both endovascular and open bypass, may be appropriate and cost effective in older, frailer patients.
What Dr. Barshes has found is that in a simulated model trial, ill patients did worse with primary amputation due to increased cost for long-term care and nursing care secondary to loss of functional independence. Amputation in this elderly, frail population clearly is associated with the majority of patients requiring long-term care. The question is, how long can the independence be maintained with either endovascular or open revascularization methods, as well as the frequency of re-intervention necessary?
They found in the model that revascularization produced a median limb salvage time of 3 years, and a median ambulatory period of 2.4 years. The need for revision did not significantly change these time frames, but did result in increased cost to the system. They do note that these findings were significantly worse than for healthier vascular patients. However, even with their worst-case scenario for revascularization, the cost to the system was decreased by about $72,000 per patient over a 10-year time period.
Certainly, in today's era of cost-effective care, it is incumbent upon all of us, as health care providers, to further examine these types of issues. However, the studies necessary are not necessarily easy to perform. We must take into account not only the costs of the actual procedures and hospital stays, which are relatively easy to determine, but also the costs of rehabilitation, outpatient nursing care, wound care, and long-term care for those with loss of functional independence. Even this type of study does not assess all aspects that are important, including how much it is worth to maintain a limb and functional independence per year for each patient. What is not so easy to do is to put a value on limb salvage.
In this day of outcomes assessment, hopefully we will be able to cull out the factors that may impact upon our decisions to re-intervene for critical limb ischemia, versus offering amputation when the patient presents with inadequate perfusion to the limb after initial attempts at limb salvage.
Dr. Linda Harris is an ACS Fellow and division chief, vascular surgery, State University of New York at Buffalo. She has no disclosures.
Dr. Barshes and colleagues suggest that an aggressive approach to limb revascularization, both endovascular and open bypass, may be appropriate and cost effective in older, frailer patients.
What Dr. Barshes has found is that in a simulated model trial, ill patients did worse with primary amputation due to increased cost for long-term care and nursing care secondary to loss of functional independence. Amputation in this elderly, frail population clearly is associated with the majority of patients requiring long-term care. The question is, how long can the independence be maintained with either endovascular or open revascularization methods, as well as the frequency of re-intervention necessary?
They found in the model that revascularization produced a median limb salvage time of 3 years, and a median ambulatory period of 2.4 years. The need for revision did not significantly change these time frames, but did result in increased cost to the system. They do note that these findings were significantly worse than for healthier vascular patients. However, even with their worst-case scenario for revascularization, the cost to the system was decreased by about $72,000 per patient over a 10-year time period.
Certainly, in today's era of cost-effective care, it is incumbent upon all of us, as health care providers, to further examine these types of issues. However, the studies necessary are not necessarily easy to perform. We must take into account not only the costs of the actual procedures and hospital stays, which are relatively easy to determine, but also the costs of rehabilitation, outpatient nursing care, wound care, and long-term care for those with loss of functional independence. Even this type of study does not assess all aspects that are important, including how much it is worth to maintain a limb and functional independence per year for each patient. What is not so easy to do is to put a value on limb salvage.
In this day of outcomes assessment, hopefully we will be able to cull out the factors that may impact upon our decisions to re-intervene for critical limb ischemia, versus offering amputation when the patient presents with inadequate perfusion to the limb after initial attempts at limb salvage.
Dr. Linda Harris is an ACS Fellow and division chief, vascular surgery, State University of New York at Buffalo. She has no disclosures.
Dr. Barshes and colleagues suggest that an aggressive approach to limb revascularization, both endovascular and open bypass, may be appropriate and cost effective in older, frailer patients.
What Dr. Barshes has found is that in a simulated model trial, ill patients did worse with primary amputation due to increased cost for long-term care and nursing care secondary to loss of functional independence. Amputation in this elderly, frail population clearly is associated with the majority of patients requiring long-term care. The question is, how long can the independence be maintained with either endovascular or open revascularization methods, as well as the frequency of re-intervention necessary?
They found in the model that revascularization produced a median limb salvage time of 3 years, and a median ambulatory period of 2.4 years. The need for revision did not significantly change these time frames, but did result in increased cost to the system. They do note that these findings were significantly worse than for healthier vascular patients. However, even with their worst-case scenario for revascularization, the cost to the system was decreased by about $72,000 per patient over a 10-year time period.
Certainly, in today's era of cost-effective care, it is incumbent upon all of us, as health care providers, to further examine these types of issues. However, the studies necessary are not necessarily easy to perform. We must take into account not only the costs of the actual procedures and hospital stays, which are relatively easy to determine, but also the costs of rehabilitation, outpatient nursing care, wound care, and long-term care for those with loss of functional independence. Even this type of study does not assess all aspects that are important, including how much it is worth to maintain a limb and functional independence per year for each patient. What is not so easy to do is to put a value on limb salvage.
In this day of outcomes assessment, hopefully we will be able to cull out the factors that may impact upon our decisions to re-intervene for critical limb ischemia, versus offering amputation when the patient presents with inadequate perfusion to the limb after initial attempts at limb salvage.
Dr. Linda Harris is an ACS Fellow and division chief, vascular surgery, State University of New York at Buffalo. She has no disclosures.
In older, frailer patients, limb revascularization appeared to preserve both limbs and ambulation longer – and cost less – than either amputation or a program of local wound care.
Although these patients had worse clinical outcomes than did healthy patients who had revascularization, the benefits were still evident, Dr. Neal R. Barshes and his colleagues wrote in the January issue of Annals of Vascular Surgery (Ann. Vasc. Surg. 2014;28:10-17).
"We believe that major amputation should be reserved for patients who develop life-threatening foot infections that cannot be controlled with foot drainage or minor amputations and subsequent palliative wound care," wrote Dr. Barshes of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and his coauthors.
The team conducted a clinical outcomes and cost model that ran 1,000 simulated trials of 1,000 patients each. The clinical parameters were drawn from the landmark MOVIE (Model to Optimize Healthcare Value in Ischemic Extremities) study. The study was modified to simulate a patient population older than 80 years, or who had undergone a prior major amputation of the contralateral lower limb, as these two groups have poorer postoperative outcomes than the usual population undergoing revascularization for lower limb ischemia.
The analysis examined outcomes associated with six procedures:
• Primary amputation.
• Local wound care.
• Surgical revascularization followed if needed by surgical revision.
• Surgical revascularization followed if needed by endovascular revision.
• Initial endovascular revascularization followed if needed by surgical revision.
• Endovascular revascularization followed if needed by endovascular revision.
Analysis revealed that primary amputation was the least clinically beneficial and the most expensive procedure, with no limb salvage, a median ambulatory period of 1.5 years, and a total 10-year cost of $185,955. Much of the cost was for nursing and long-term care due to loss of functional independence.
Wound care also produced less desirable outcomes. The median 5-year limb salvage rate was 28%, with a median limb salvage period of about 1.5 years. The median ambulatory period was less than 1 year, and the median total cost, $129,651.
Surgical bypass with either surgical or endovascular revision produced a limb salvage rate of 80%, with a median salvage time of 3 years and a median ambulatory period of 2.4 years. With surgical revision, the median total cost was $113,944; with endovascular revision, it was $110,910.
Endovascular revascularization followed by surgical revision produced a 5-year limb salvage rate of 80%, with a median limb salvage period of about 3 years and a median of 2.4 ambulatory years. The median total cost was $108,794.
Endovascular revascularization with endovascular revision produced a 5-year limb salvage rate of 80.5%, with a median salvage period of 3 years and a median ambulatory period of 2.5 years. This was the least expensive strategy, with a median total cost of $104,118.
These outcomes were much worse than those seen in the population of younger, healthier patients, the researchers said. The median 10-year cost for revascularization was up to $35,000 more. The clinical outcomes of the older population were also worse, with a 3-year period of limb preservation compared with more than 4 years in a healthier population, and about 2.5 ambulatory years compared with 4.6 years.
"In spite of these findings, revascularization still appears to be the most cost-effective alternative to wound care and primary amputation," the team noted. In fact, the less-healthy population actually stands to gain relatively more than the healthier one.
"In other words, the difference in outcomes between revascularization and either local wound care or primary amputation is much larger in this marginal population and therefore more likely to produce cost savings. The situation is akin to performing carotid endarterectomy early after a completed stroke – although the absolute risk of perioperative stroke is higher than when delayed for 6 weeks, the risk reduction of early carotid endarterectomy is significant compared with late carotid endarterectomy."
The research was initially presented at the annual winter meeting of the Peripheral Vascular Surgery Society. The paper did not note any potential financial conflicts of interest or the study’s sponsor.
In older, frailer patients, limb revascularization appeared to preserve both limbs and ambulation longer – and cost less – than either amputation or a program of local wound care.
Although these patients had worse clinical outcomes than did healthy patients who had revascularization, the benefits were still evident, Dr. Neal R. Barshes and his colleagues wrote in the January issue of Annals of Vascular Surgery (Ann. Vasc. Surg. 2014;28:10-17).
"We believe that major amputation should be reserved for patients who develop life-threatening foot infections that cannot be controlled with foot drainage or minor amputations and subsequent palliative wound care," wrote Dr. Barshes of the Michael E. DeBakey Veterans Affairs Medical Center, Houston, and his coauthors.
The team conducted a clinical outcomes and cost model that ran 1,000 simulated trials of 1,000 patients each. The clinical parameters were drawn from the landmark MOVIE (Model to Optimize Healthcare Value in Ischemic Extremities) study. The study was modified to simulate a patient population older than 80 years, or who had undergone a prior major amputation of the contralateral lower limb, as these two groups have poorer postoperative outcomes than the usual population undergoing revascularization for lower limb ischemia.
The analysis examined outcomes associated with six procedures:
• Primary amputation.
• Local wound care.
• Surgical revascularization followed if needed by surgical revision.
• Surgical revascularization followed if needed by endovascular revision.
• Initial endovascular revascularization followed if needed by surgical revision.
• Endovascular revascularization followed if needed by endovascular revision.
Analysis revealed that primary amputation was the least clinically beneficial and the most expensive procedure, with no limb salvage, a median ambulatory period of 1.5 years, and a total 10-year cost of $185,955. Much of the cost was for nursing and long-term care due to loss of functional independence.
Wound care also produced less desirable outcomes. The median 5-year limb salvage rate was 28%, with a median limb salvage period of about 1.5 years. The median ambulatory period was less than 1 year, and the median total cost, $129,651.
Surgical bypass with either surgical or endovascular revision produced a limb salvage rate of 80%, with a median salvage time of 3 years and a median ambulatory period of 2.4 years. With surgical revision, the median total cost was $113,944; with endovascular revision, it was $110,910.
Endovascular revascularization followed by surgical revision produced a 5-year limb salvage rate of 80%, with a median limb salvage period of about 3 years and a median of 2.4 ambulatory years. The median total cost was $108,794.
Endovascular revascularization with endovascular revision produced a 5-year limb salvage rate of 80.5%, with a median salvage period of 3 years and a median ambulatory period of 2.5 years. This was the least expensive strategy, with a median total cost of $104,118.
These outcomes were much worse than those seen in the population of younger, healthier patients, the researchers said. The median 10-year cost for revascularization was up to $35,000 more. The clinical outcomes of the older population were also worse, with a 3-year period of limb preservation compared with more than 4 years in a healthier population, and about 2.5 ambulatory years compared with 4.6 years.
"In spite of these findings, revascularization still appears to be the most cost-effective alternative to wound care and primary amputation," the team noted. In fact, the less-healthy population actually stands to gain relatively more than the healthier one.
"In other words, the difference in outcomes between revascularization and either local wound care or primary amputation is much larger in this marginal population and therefore more likely to produce cost savings. The situation is akin to performing carotid endarterectomy early after a completed stroke – although the absolute risk of perioperative stroke is higher than when delayed for 6 weeks, the risk reduction of early carotid endarterectomy is significant compared with late carotid endarterectomy."
The research was initially presented at the annual winter meeting of the Peripheral Vascular Surgery Society. The paper did not note any potential financial conflicts of interest or the study’s sponsor.
FROM ANNALS OF VASCULAR SURGERY
Major finding: In older, more frail patients, lower limb revascularization cost up to $90,000 less over 10 years, and yielded better clinical outcomes, than did primary amputation.
Data source: The clinical and cost outcomes model simulated 1,000 trials of 1,000 patients each.
Disclosures: The paper did not note any potential financial conflicts of interest or the study’s sponsor.
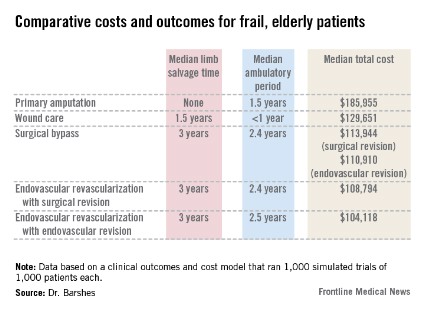
Triple-antiviral therapy achieves 94% response without interferon, ribavirin
Both a 12-week and a 24-week regimen of three oral antiviral drugs achieved sustained viral remissions at 12 weeks in up to 94% of treatment-naive patients with genotype 1 hepatitis C virus infections.
The three oral antivirals included daclatasvir, an NS5A replication complex inhibitor; asunaprevir, an NS3 protease inhibitor; and BMS-791325, an investigational selective non-nucleoside polymerase inhibitor. A key point of the study is its proof that short-duration treatment – even without interferon or ribavirin – can result in sustained remission, Dr. Gregory T. Everson and his colleagues wrote in the February issue of Gastroenterology (doi.org/10.1053/j.gastro.2013.10.057). "Shorter treatment durations are preferable because they may improve patient compliance. In this study, treatment periods of both 12 and 24 weeks yielded high SVR (sustained viral remission) rates, suggesting no advantage for extending treatment duration to 24 weeks."
Source: American Gastroenterological Association
Further, the triple-antiviral combination apparently controlled viral replication without using interferon or ribavirin, thus avoiding their side effects. The current regimen for treatment-naive patients with genotype 1 hepatitis C virus infections calls for a 48-week treatment with peginterferon and ribavirin with telaprevir or boceprevir.
"Ribavirin contributes to anemia and it is teratogenic; thus, effective treatments without ribavirin are desirable," wrote Dr. Everson of the University of Colorado, Denver, and his coauthors. "This interferon- and ribavirin-free regimen did not alter hemoglobin levels in a clinically meaningfully manner, as evidenced by no grade 1 or higher hemoglobin reductions and no adverse events of anemia."
Dr. Everson and his colleagues gave the regimen for periods of 12 and 24 weeks and with two different doses of BMS-791325, resulting in a four-way randomized study. Groups 1 and 2 were treated for 12 weeks with the combination of daclatasvir 60 mg once daily, asunaprevir 200 mg twice daily, and BMS-791325 (twice daily 75 mg or 150 mg). Groups 3 and 4 had exactly the same two-treatment regimen, but took the drugs for 24 weeks. After treatment, there was a 48-week follow-up period.
Among the 66 patients in the study, the average age was about 50 years old, and the mean HCV-RNA level was 6 log10 IU/mL. Most (75%) had HCV genotype 1a; the rest had 1b. All were treatment naive. Four patients withdrew before the study’s end; none of the withdrawals were for adverse events.
In groups 1 and 2 (75 mg BMS-791325, twice daily for 12 and 24 weeks), the viral load decreased rapidly. By week 4, all of these patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
In groups 3 and 4 (150 mg BMS-791325, twice daily for 12 or 24 weeks), HCV-RNA levels also fell rapidly in the first month, By week 4, all of those in the 12-week group and all but one in the 24-week group had levels of less than 25 IU/mL, which were sustained through the end of treatment. In the intent-to-treat analysis, 91% overall had an HCV-RNA load of less than 25 IU/mL by the end of treatment.
Overall, there were three treatment failures: one each in groups 3 and 4 had viral breakthrough, and one in group 4 experienced a relapse at week 4.
Both breakthrough patients were given peginterferon-alfa/ribavirin in addition to the direct-acting antivirals. After 16 weeks, one discontinued treatment because of interferon-related cerebral vasoconstriction. That patient had an undetectable HCV-RNA level at the end of treatment, but relapsed by post treatment week 4. The other patient had a sustained viral response.
The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
This critical proof-of-concept study demonstrates that a combination of three direct-acting antivirals (an NS5A inhibitor + NS3PI + NNPI) without ribavirin can achieve sustained viral response at 12 weeks at rates of 94% in a genotype 1 treatment-naive (TN) population. The data are a foundation for multiple large, randomized, phase III trials using this regimen in TN patients, treatment failure, cirrhosis, HIV coinfection, and other genotypes, and thus, it is important to the development of interferon- and ribavirin-free therapies for HCV.
The authors have selected a TN population without advanced fibrosis for this regimen so far, and it remains to be seen whether these high sustained viral remission (SVR) rates can be duplicated in cirrhosis and those with prior treatment failure. It may also show reduced efficacy when studied in more difficult-to-treat patients such as with protease inhibitor failure, HIV coinfection, and other genotypes. However, the importance of this study is that the lack of efficacy seen in genotype 1a with the dual therapy published in 2012 was successfully overcome simply by adding an non-nucleoside polymerase inhibitor (N. Engl. J. Med. 2012;366:216-24). The implications may extend to other interferon-free, direct-acting antiviral regimens in development. An NS5B nucleotide polymerase inhibitor may not be required for the backbone of therapy, as it appears to be the based on sofosbuvir studies (N. Engl. J. Med. 2013;368:34-44; 1878-87). Rather, a best-in-class drug, here daclatasvir for the NS5A class, may be added to two other relatively weak compounds and still have greater than 90% SVR rates as an interferon-free regimen.
This would pave the way for many compounds to be competitive without the nucleotide polymerase inhibitor backbone regimen, in both genotype 1a and 1b patients. However, with the promise of a 12-week regimen of sofosbuvir and ledipasvir as a single, fixed-dose combination for all patient types (Gilead Sciences press release, Dec. 18, 2013: "Gilead announces SVR12 rates from three phase III studies evaluating once-daily fixed-dose combination of sofosbuvir and ledipasvir for genotype 1 hepatitis C patients"), a competitor would need to show similar efficacy and tolerability. Even if not proven in all patient populations, this would lead to a price competitive market that would provide the patient, physician, and payer with multiple choices. Although this may not be as important in the United States, it will be critical to many resource-limited countries where price will be a primary constraint.
Dr. Paul Pockros is director, Liver Disease Center Scripps Clinic, and clinical director of research, Scripps Translational Science Institute, both in La Jolla, Calif. He does research, speaks, and consults for Bristol-Myers Squibb, Gilead, Genetech, and Janssen. He also does research and consults for Boehringer Ingelheim and Novartis.
This critical proof-of-concept study demonstrates that a combination of three direct-acting antivirals (an NS5A inhibitor + NS3PI + NNPI) without ribavirin can achieve sustained viral response at 12 weeks at rates of 94% in a genotype 1 treatment-naive (TN) population. The data are a foundation for multiple large, randomized, phase III trials using this regimen in TN patients, treatment failure, cirrhosis, HIV coinfection, and other genotypes, and thus, it is important to the development of interferon- and ribavirin-free therapies for HCV.
The authors have selected a TN population without advanced fibrosis for this regimen so far, and it remains to be seen whether these high sustained viral remission (SVR) rates can be duplicated in cirrhosis and those with prior treatment failure. It may also show reduced efficacy when studied in more difficult-to-treat patients such as with protease inhibitor failure, HIV coinfection, and other genotypes. However, the importance of this study is that the lack of efficacy seen in genotype 1a with the dual therapy published in 2012 was successfully overcome simply by adding an non-nucleoside polymerase inhibitor (N. Engl. J. Med. 2012;366:216-24). The implications may extend to other interferon-free, direct-acting antiviral regimens in development. An NS5B nucleotide polymerase inhibitor may not be required for the backbone of therapy, as it appears to be the based on sofosbuvir studies (N. Engl. J. Med. 2013;368:34-44; 1878-87). Rather, a best-in-class drug, here daclatasvir for the NS5A class, may be added to two other relatively weak compounds and still have greater than 90% SVR rates as an interferon-free regimen.
This would pave the way for many compounds to be competitive without the nucleotide polymerase inhibitor backbone regimen, in both genotype 1a and 1b patients. However, with the promise of a 12-week regimen of sofosbuvir and ledipasvir as a single, fixed-dose combination for all patient types (Gilead Sciences press release, Dec. 18, 2013: "Gilead announces SVR12 rates from three phase III studies evaluating once-daily fixed-dose combination of sofosbuvir and ledipasvir for genotype 1 hepatitis C patients"), a competitor would need to show similar efficacy and tolerability. Even if not proven in all patient populations, this would lead to a price competitive market that would provide the patient, physician, and payer with multiple choices. Although this may not be as important in the United States, it will be critical to many resource-limited countries where price will be a primary constraint.
Dr. Paul Pockros is director, Liver Disease Center Scripps Clinic, and clinical director of research, Scripps Translational Science Institute, both in La Jolla, Calif. He does research, speaks, and consults for Bristol-Myers Squibb, Gilead, Genetech, and Janssen. He also does research and consults for Boehringer Ingelheim and Novartis.
This critical proof-of-concept study demonstrates that a combination of three direct-acting antivirals (an NS5A inhibitor + NS3PI + NNPI) without ribavirin can achieve sustained viral response at 12 weeks at rates of 94% in a genotype 1 treatment-naive (TN) population. The data are a foundation for multiple large, randomized, phase III trials using this regimen in TN patients, treatment failure, cirrhosis, HIV coinfection, and other genotypes, and thus, it is important to the development of interferon- and ribavirin-free therapies for HCV.
The authors have selected a TN population without advanced fibrosis for this regimen so far, and it remains to be seen whether these high sustained viral remission (SVR) rates can be duplicated in cirrhosis and those with prior treatment failure. It may also show reduced efficacy when studied in more difficult-to-treat patients such as with protease inhibitor failure, HIV coinfection, and other genotypes. However, the importance of this study is that the lack of efficacy seen in genotype 1a with the dual therapy published in 2012 was successfully overcome simply by adding an non-nucleoside polymerase inhibitor (N. Engl. J. Med. 2012;366:216-24). The implications may extend to other interferon-free, direct-acting antiviral regimens in development. An NS5B nucleotide polymerase inhibitor may not be required for the backbone of therapy, as it appears to be the based on sofosbuvir studies (N. Engl. J. Med. 2013;368:34-44; 1878-87). Rather, a best-in-class drug, here daclatasvir for the NS5A class, may be added to two other relatively weak compounds and still have greater than 90% SVR rates as an interferon-free regimen.
This would pave the way for many compounds to be competitive without the nucleotide polymerase inhibitor backbone regimen, in both genotype 1a and 1b patients. However, with the promise of a 12-week regimen of sofosbuvir and ledipasvir as a single, fixed-dose combination for all patient types (Gilead Sciences press release, Dec. 18, 2013: "Gilead announces SVR12 rates from three phase III studies evaluating once-daily fixed-dose combination of sofosbuvir and ledipasvir for genotype 1 hepatitis C patients"), a competitor would need to show similar efficacy and tolerability. Even if not proven in all patient populations, this would lead to a price competitive market that would provide the patient, physician, and payer with multiple choices. Although this may not be as important in the United States, it will be critical to many resource-limited countries where price will be a primary constraint.
Dr. Paul Pockros is director, Liver Disease Center Scripps Clinic, and clinical director of research, Scripps Translational Science Institute, both in La Jolla, Calif. He does research, speaks, and consults for Bristol-Myers Squibb, Gilead, Genetech, and Janssen. He also does research and consults for Boehringer Ingelheim and Novartis.
Both a 12-week and a 24-week regimen of three oral antiviral drugs achieved sustained viral remissions at 12 weeks in up to 94% of treatment-naive patients with genotype 1 hepatitis C virus infections.
The three oral antivirals included daclatasvir, an NS5A replication complex inhibitor; asunaprevir, an NS3 protease inhibitor; and BMS-791325, an investigational selective non-nucleoside polymerase inhibitor. A key point of the study is its proof that short-duration treatment – even without interferon or ribavirin – can result in sustained remission, Dr. Gregory T. Everson and his colleagues wrote in the February issue of Gastroenterology (doi.org/10.1053/j.gastro.2013.10.057). "Shorter treatment durations are preferable because they may improve patient compliance. In this study, treatment periods of both 12 and 24 weeks yielded high SVR (sustained viral remission) rates, suggesting no advantage for extending treatment duration to 24 weeks."
Source: American Gastroenterological Association
Further, the triple-antiviral combination apparently controlled viral replication without using interferon or ribavirin, thus avoiding their side effects. The current regimen for treatment-naive patients with genotype 1 hepatitis C virus infections calls for a 48-week treatment with peginterferon and ribavirin with telaprevir or boceprevir.
"Ribavirin contributes to anemia and it is teratogenic; thus, effective treatments without ribavirin are desirable," wrote Dr. Everson of the University of Colorado, Denver, and his coauthors. "This interferon- and ribavirin-free regimen did not alter hemoglobin levels in a clinically meaningfully manner, as evidenced by no grade 1 or higher hemoglobin reductions and no adverse events of anemia."
Dr. Everson and his colleagues gave the regimen for periods of 12 and 24 weeks and with two different doses of BMS-791325, resulting in a four-way randomized study. Groups 1 and 2 were treated for 12 weeks with the combination of daclatasvir 60 mg once daily, asunaprevir 200 mg twice daily, and BMS-791325 (twice daily 75 mg or 150 mg). Groups 3 and 4 had exactly the same two-treatment regimen, but took the drugs for 24 weeks. After treatment, there was a 48-week follow-up period.
Among the 66 patients in the study, the average age was about 50 years old, and the mean HCV-RNA level was 6 log10 IU/mL. Most (75%) had HCV genotype 1a; the rest had 1b. All were treatment naive. Four patients withdrew before the study’s end; none of the withdrawals were for adverse events.
In groups 1 and 2 (75 mg BMS-791325, twice daily for 12 and 24 weeks), the viral load decreased rapidly. By week 4, all of these patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
In groups 3 and 4 (150 mg BMS-791325, twice daily for 12 or 24 weeks), HCV-RNA levels also fell rapidly in the first month, By week 4, all of those in the 12-week group and all but one in the 24-week group had levels of less than 25 IU/mL, which were sustained through the end of treatment. In the intent-to-treat analysis, 91% overall had an HCV-RNA load of less than 25 IU/mL by the end of treatment.
Overall, there were three treatment failures: one each in groups 3 and 4 had viral breakthrough, and one in group 4 experienced a relapse at week 4.
Both breakthrough patients were given peginterferon-alfa/ribavirin in addition to the direct-acting antivirals. After 16 weeks, one discontinued treatment because of interferon-related cerebral vasoconstriction. That patient had an undetectable HCV-RNA level at the end of treatment, but relapsed by post treatment week 4. The other patient had a sustained viral response.
The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
Both a 12-week and a 24-week regimen of three oral antiviral drugs achieved sustained viral remissions at 12 weeks in up to 94% of treatment-naive patients with genotype 1 hepatitis C virus infections.
The three oral antivirals included daclatasvir, an NS5A replication complex inhibitor; asunaprevir, an NS3 protease inhibitor; and BMS-791325, an investigational selective non-nucleoside polymerase inhibitor. A key point of the study is its proof that short-duration treatment – even without interferon or ribavirin – can result in sustained remission, Dr. Gregory T. Everson and his colleagues wrote in the February issue of Gastroenterology (doi.org/10.1053/j.gastro.2013.10.057). "Shorter treatment durations are preferable because they may improve patient compliance. In this study, treatment periods of both 12 and 24 weeks yielded high SVR (sustained viral remission) rates, suggesting no advantage for extending treatment duration to 24 weeks."
Source: American Gastroenterological Association
Further, the triple-antiviral combination apparently controlled viral replication without using interferon or ribavirin, thus avoiding their side effects. The current regimen for treatment-naive patients with genotype 1 hepatitis C virus infections calls for a 48-week treatment with peginterferon and ribavirin with telaprevir or boceprevir.
"Ribavirin contributes to anemia and it is teratogenic; thus, effective treatments without ribavirin are desirable," wrote Dr. Everson of the University of Colorado, Denver, and his coauthors. "This interferon- and ribavirin-free regimen did not alter hemoglobin levels in a clinically meaningfully manner, as evidenced by no grade 1 or higher hemoglobin reductions and no adverse events of anemia."
Dr. Everson and his colleagues gave the regimen for periods of 12 and 24 weeks and with two different doses of BMS-791325, resulting in a four-way randomized study. Groups 1 and 2 were treated for 12 weeks with the combination of daclatasvir 60 mg once daily, asunaprevir 200 mg twice daily, and BMS-791325 (twice daily 75 mg or 150 mg). Groups 3 and 4 had exactly the same two-treatment regimen, but took the drugs for 24 weeks. After treatment, there was a 48-week follow-up period.
Among the 66 patients in the study, the average age was about 50 years old, and the mean HCV-RNA level was 6 log10 IU/mL. Most (75%) had HCV genotype 1a; the rest had 1b. All were treatment naive. Four patients withdrew before the study’s end; none of the withdrawals were for adverse events.
In groups 1 and 2 (75 mg BMS-791325, twice daily for 12 and 24 weeks), the viral load decreased rapidly. By week 4, all of these patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
In groups 3 and 4 (150 mg BMS-791325, twice daily for 12 or 24 weeks), HCV-RNA levels also fell rapidly in the first month, By week 4, all of those in the 12-week group and all but one in the 24-week group had levels of less than 25 IU/mL, which were sustained through the end of treatment. In the intent-to-treat analysis, 91% overall had an HCV-RNA load of less than 25 IU/mL by the end of treatment.
Overall, there were three treatment failures: one each in groups 3 and 4 had viral breakthrough, and one in group 4 experienced a relapse at week 4.
Both breakthrough patients were given peginterferon-alfa/ribavirin in addition to the direct-acting antivirals. After 16 weeks, one discontinued treatment because of interferon-related cerebral vasoconstriction. That patient had an undetectable HCV-RNA level at the end of treatment, but relapsed by post treatment week 4. The other patient had a sustained viral response.
The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
Major finding: By week 4, patients achieved a HCV-RNA level of less than 25 IU/mL; 97% maintained that level through the end of treatment. In a modified intent-to-treat analysis, 94% achieved a sustained viral response by week 12.
Data source: A trial of 66 treatment-naive patients randomized to one of four antiviral regimens that differed by dose of BMS-791325, an investigational selective non-nucleoside polymerase inhibitor.
Disclosures: The study was sponsored by Bristol-Myers Squibb. Dr. Everson listed financial and research relationships with numerous pharmaceutical companies, including Bristol-Myers Squibb. His coauthors also declared relationships with numerous drug manufacturers, including Bristol-Myers.
Vitamin E may slow functional decline in Alzheimer’s
High-dose vitamin E significantly slowed functional decline over 2 years in a population of patients with mild-moderate Alzheimer’s disease.
Compared with placebo, 2,000 IU daily of vitamin E reduced progression by 19% per year, Dr. Maurice W. Dysken and his colleagues wrote in the January issue of the Journal of the American Medical Association (JAMA 2014;311:33-44 [doi:10.1001/jama.2013.28283]).
Patients who took vitamin E scored about 3 units higher on a measure of daily function, wrote Dr. Dysken of the Minneapolis Veterans Affairs Health Care System. "A loss of this magnitude could translate into either the complete loss of being able to dress or bathe independently, or losing independence on any three different activities of daily living."
Vitamin E also proved better than memantine at delaying progression, although the difference was not statistically significant. But paradoxically, the combination of vitamin E and memantine was significantly less helpful than either intervention alone.
The 4-year study randomized 613 patients with mild-moderate Alzheimer’s into four treatment groups: placebo, 2,000 IU/day of vitamin E, 20 mg/day memantine, a combination of both, or placebo.
The primary outcome was change on the Alzheimer’s Disease Cooperative Study/Activities of Daily Living Inventory (ADCS-ADL). Secondary endpoints included the Alzheimer’s Disease Assessment Scale-cognitive (ADAS-Cog), the Mini Mental State Examination (MMSE), the Neuropsychiatric Index (NPI), and the Caregiver Activity Survey (CAS), a measure of the time caregivers spend assisting Alzheimer’s patients.
The patients were a mean of 79 years old; 97% were men. About half had at least one apolipoprotein E4 allele. The mean baseline score on the ADCS-ADL was 57 on a scale of 0-78, with lower numbers representing worse function.
The final analysis contained data on 561 patents. The dropout rate was similar between the groups; most of it was from death during the study. Only three withdrew from medication-related adverse events.
The mean follow-up time was just over 2 years. The mean decline on the ADCS-ADL from baseline was 3.15 units less than the decline in the placebo group. "The treatment effect translates into a clinically meaningful delay in progression in the [vitamin E group] of 6.2 months," the investigators wrote. "A delay in progression was sustained throughout most of the trial, with delays at 1, 2, 3, and 4 years of 10.6, 8.7, 9.3, and 1.8 months, respectively."
The placebo group also declined more than both the memantine and combination groups, but those differences were not statistically significant.
However, there was a significant negative treatment interaction between vitamin E and memantine, with patients who took the combination performing worse than patients taking either of the interventions alone.
There were no between-group differences in the rate of cognitive decline or neuropsychiatric symptoms. Patients in the vitamin E group did require about 2 hours less of caregiver time per day, compared with those on memantine, but that difference was not statistically significant, with a confidence interval of 0.63-3.71.
Despite being statistically nonsignificant, the authors said the reduction in caregiver time was clinically meaningful and could have "a major effect on informal and direct medical costs. ... The loss of the ability to perform ADLs is associated not only with increased caregiver burden, but also with nursing home placement," the investigators noted.
Any "infection or infestation" was the only category of adverse events reported significantly more commonly in both the memantine and combination groups. The most common, occurring in at least 5% more of treated than placebo patients, were falls, bleeding, pneumonia, and urinary tract infections.
Annual mortality was similar between the groups: 7% for the vitamin E group, 11% for the memantine group, and 9% for both the combination and placebo groups. This finding is in contrast to a 2005 meta-analysis that found a significant mortality increase associated with vitamin E doses exceeding 400 IU/day (Ann. Intern. Med. 2005;142:37-46).
The meta-analysis included only one Alzheimer’s study, the authors noted. In it, all-cause mortality was lower in the vitamin E groups, compared with the other treatment groups.
The finding of a "rather robust" treatment effect is confusing, given the results of previous studies of vitamin E in Alzheimer’s patients – especially in light of a 2005 trial in patients with mild cognitive impairment, Dr. Richard Caselli, professor of neurology and associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic in Scottsdale, Ariz., said in an interview.
That trial, part of the Alzheimer’s Disease Cooperative Study, randomized patients to 2,000 IU/day vitamin E, donepezil, or placebo. The overall rate of progression to Alzheimer’s was 16% per year, and there were no differences between either active group and the placebo group.
"I expect some will suggest that the difference in disease stage may matter, but there seems to be a growing and now large consensus that earlier intervention is better, so why would we expect later intervention with an agent of proven nonbenefit earlier to be effective later? I am actually puzzled that anyone is even still studying this."
The study by Dr. Dysken and his colleagues was funded by the Veterans Affairs Cooperative Studies Program. The authors noted multiple financial disclosures, including many with pharmaceutical companies.
This study contains both potentially good and bad news for Alzheimer’s disease therapy, Dr. Denis Evans and his coauthors wrote in an accompanying editorial (JAMA 2014;311:29-30).
"For memantine therapy in this context, the trial results are not encouraging," wrote Dr. Evans. "Use in individuals with milder AD may be widespread, despite little evidence suggesting the agent is beneficial at this level of disease severity. This trial ... does not provide any new data to support its use."
For vitamin E, however, the results are more intriguing, especially in light of findings from prior studies.
"A previous trial among individuals with moderate to severe AD found delayed disease progression with 2,000 IU/day of [vitamin E] both alone and in combination with selegiline (N. Engl. J. Med. 1997;336:1216-22). The results of a trial of vitamin E therapy among people with mild cognitive impairment were null, however, as were the results of trials examining the effects of vitamin E on cognitive function among people with normal cognition."
The study begs three questions, Dr. Evans noted. First, is the use of functional ability a more sensitive measure of AD progression than cognition, which showed no improvement?
Second, why did the secondary measures of caregiver time and dependence not confirm the primary finding of a slower functional decline?
Third, how would vitamin E work to delay decline in Alzheimer’s? "Much attention is focused on its antioxidant properties, but this mechanism is not specific for AD," Dr. Evans wrote.
"Although these considerations do not lessen the significance of the difference found between the group randomized to vitamin E and the group randomized to placebo for the primary outcome, this difference would have been more convincing if also supported by parallel improvements in the relevant secondary outcomes and by a vitamin E mechanism of action more specific to AD."
Dr. Evans is the Alla V. and Solomon Jesmer Professor of Medicine at Rush Medical Center, Chicago. He had no commercial financial disclosures. A coauthor, Dr. Martha Clare Morris, reported receiving consultant fees from Nutrispective.
This study contains both potentially good and bad news for Alzheimer’s disease therapy, Dr. Denis Evans and his coauthors wrote in an accompanying editorial (JAMA 2014;311:29-30).
"For memantine therapy in this context, the trial results are not encouraging," wrote Dr. Evans. "Use in individuals with milder AD may be widespread, despite little evidence suggesting the agent is beneficial at this level of disease severity. This trial ... does not provide any new data to support its use."
For vitamin E, however, the results are more intriguing, especially in light of findings from prior studies.
"A previous trial among individuals with moderate to severe AD found delayed disease progression with 2,000 IU/day of [vitamin E] both alone and in combination with selegiline (N. Engl. J. Med. 1997;336:1216-22). The results of a trial of vitamin E therapy among people with mild cognitive impairment were null, however, as were the results of trials examining the effects of vitamin E on cognitive function among people with normal cognition."
The study begs three questions, Dr. Evans noted. First, is the use of functional ability a more sensitive measure of AD progression than cognition, which showed no improvement?
Second, why did the secondary measures of caregiver time and dependence not confirm the primary finding of a slower functional decline?
Third, how would vitamin E work to delay decline in Alzheimer’s? "Much attention is focused on its antioxidant properties, but this mechanism is not specific for AD," Dr. Evans wrote.
"Although these considerations do not lessen the significance of the difference found between the group randomized to vitamin E and the group randomized to placebo for the primary outcome, this difference would have been more convincing if also supported by parallel improvements in the relevant secondary outcomes and by a vitamin E mechanism of action more specific to AD."
Dr. Evans is the Alla V. and Solomon Jesmer Professor of Medicine at Rush Medical Center, Chicago. He had no commercial financial disclosures. A coauthor, Dr. Martha Clare Morris, reported receiving consultant fees from Nutrispective.
This study contains both potentially good and bad news for Alzheimer’s disease therapy, Dr. Denis Evans and his coauthors wrote in an accompanying editorial (JAMA 2014;311:29-30).
"For memantine therapy in this context, the trial results are not encouraging," wrote Dr. Evans. "Use in individuals with milder AD may be widespread, despite little evidence suggesting the agent is beneficial at this level of disease severity. This trial ... does not provide any new data to support its use."
For vitamin E, however, the results are more intriguing, especially in light of findings from prior studies.
"A previous trial among individuals with moderate to severe AD found delayed disease progression with 2,000 IU/day of [vitamin E] both alone and in combination with selegiline (N. Engl. J. Med. 1997;336:1216-22). The results of a trial of vitamin E therapy among people with mild cognitive impairment were null, however, as were the results of trials examining the effects of vitamin E on cognitive function among people with normal cognition."
The study begs three questions, Dr. Evans noted. First, is the use of functional ability a more sensitive measure of AD progression than cognition, which showed no improvement?
Second, why did the secondary measures of caregiver time and dependence not confirm the primary finding of a slower functional decline?
Third, how would vitamin E work to delay decline in Alzheimer’s? "Much attention is focused on its antioxidant properties, but this mechanism is not specific for AD," Dr. Evans wrote.
"Although these considerations do not lessen the significance of the difference found between the group randomized to vitamin E and the group randomized to placebo for the primary outcome, this difference would have been more convincing if also supported by parallel improvements in the relevant secondary outcomes and by a vitamin E mechanism of action more specific to AD."
Dr. Evans is the Alla V. and Solomon Jesmer Professor of Medicine at Rush Medical Center, Chicago. He had no commercial financial disclosures. A coauthor, Dr. Martha Clare Morris, reported receiving consultant fees from Nutrispective.
High-dose vitamin E significantly slowed functional decline over 2 years in a population of patients with mild-moderate Alzheimer’s disease.
Compared with placebo, 2,000 IU daily of vitamin E reduced progression by 19% per year, Dr. Maurice W. Dysken and his colleagues wrote in the January issue of the Journal of the American Medical Association (JAMA 2014;311:33-44 [doi:10.1001/jama.2013.28283]).
Patients who took vitamin E scored about 3 units higher on a measure of daily function, wrote Dr. Dysken of the Minneapolis Veterans Affairs Health Care System. "A loss of this magnitude could translate into either the complete loss of being able to dress or bathe independently, or losing independence on any three different activities of daily living."
Vitamin E also proved better than memantine at delaying progression, although the difference was not statistically significant. But paradoxically, the combination of vitamin E and memantine was significantly less helpful than either intervention alone.
The 4-year study randomized 613 patients with mild-moderate Alzheimer’s into four treatment groups: placebo, 2,000 IU/day of vitamin E, 20 mg/day memantine, a combination of both, or placebo.
The primary outcome was change on the Alzheimer’s Disease Cooperative Study/Activities of Daily Living Inventory (ADCS-ADL). Secondary endpoints included the Alzheimer’s Disease Assessment Scale-cognitive (ADAS-Cog), the Mini Mental State Examination (MMSE), the Neuropsychiatric Index (NPI), and the Caregiver Activity Survey (CAS), a measure of the time caregivers spend assisting Alzheimer’s patients.
The patients were a mean of 79 years old; 97% were men. About half had at least one apolipoprotein E4 allele. The mean baseline score on the ADCS-ADL was 57 on a scale of 0-78, with lower numbers representing worse function.
The final analysis contained data on 561 patents. The dropout rate was similar between the groups; most of it was from death during the study. Only three withdrew from medication-related adverse events.
The mean follow-up time was just over 2 years. The mean decline on the ADCS-ADL from baseline was 3.15 units less than the decline in the placebo group. "The treatment effect translates into a clinically meaningful delay in progression in the [vitamin E group] of 6.2 months," the investigators wrote. "A delay in progression was sustained throughout most of the trial, with delays at 1, 2, 3, and 4 years of 10.6, 8.7, 9.3, and 1.8 months, respectively."
The placebo group also declined more than both the memantine and combination groups, but those differences were not statistically significant.
However, there was a significant negative treatment interaction between vitamin E and memantine, with patients who took the combination performing worse than patients taking either of the interventions alone.
There were no between-group differences in the rate of cognitive decline or neuropsychiatric symptoms. Patients in the vitamin E group did require about 2 hours less of caregiver time per day, compared with those on memantine, but that difference was not statistically significant, with a confidence interval of 0.63-3.71.
Despite being statistically nonsignificant, the authors said the reduction in caregiver time was clinically meaningful and could have "a major effect on informal and direct medical costs. ... The loss of the ability to perform ADLs is associated not only with increased caregiver burden, but also with nursing home placement," the investigators noted.
Any "infection or infestation" was the only category of adverse events reported significantly more commonly in both the memantine and combination groups. The most common, occurring in at least 5% more of treated than placebo patients, were falls, bleeding, pneumonia, and urinary tract infections.
Annual mortality was similar between the groups: 7% for the vitamin E group, 11% for the memantine group, and 9% for both the combination and placebo groups. This finding is in contrast to a 2005 meta-analysis that found a significant mortality increase associated with vitamin E doses exceeding 400 IU/day (Ann. Intern. Med. 2005;142:37-46).
The meta-analysis included only one Alzheimer’s study, the authors noted. In it, all-cause mortality was lower in the vitamin E groups, compared with the other treatment groups.
The finding of a "rather robust" treatment effect is confusing, given the results of previous studies of vitamin E in Alzheimer’s patients – especially in light of a 2005 trial in patients with mild cognitive impairment, Dr. Richard Caselli, professor of neurology and associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic in Scottsdale, Ariz., said in an interview.
That trial, part of the Alzheimer’s Disease Cooperative Study, randomized patients to 2,000 IU/day vitamin E, donepezil, or placebo. The overall rate of progression to Alzheimer’s was 16% per year, and there were no differences between either active group and the placebo group.
"I expect some will suggest that the difference in disease stage may matter, but there seems to be a growing and now large consensus that earlier intervention is better, so why would we expect later intervention with an agent of proven nonbenefit earlier to be effective later? I am actually puzzled that anyone is even still studying this."
The study by Dr. Dysken and his colleagues was funded by the Veterans Affairs Cooperative Studies Program. The authors noted multiple financial disclosures, including many with pharmaceutical companies.
High-dose vitamin E significantly slowed functional decline over 2 years in a population of patients with mild-moderate Alzheimer’s disease.
Compared with placebo, 2,000 IU daily of vitamin E reduced progression by 19% per year, Dr. Maurice W. Dysken and his colleagues wrote in the January issue of the Journal of the American Medical Association (JAMA 2014;311:33-44 [doi:10.1001/jama.2013.28283]).
Patients who took vitamin E scored about 3 units higher on a measure of daily function, wrote Dr. Dysken of the Minneapolis Veterans Affairs Health Care System. "A loss of this magnitude could translate into either the complete loss of being able to dress or bathe independently, or losing independence on any three different activities of daily living."
Vitamin E also proved better than memantine at delaying progression, although the difference was not statistically significant. But paradoxically, the combination of vitamin E and memantine was significantly less helpful than either intervention alone.
The 4-year study randomized 613 patients with mild-moderate Alzheimer’s into four treatment groups: placebo, 2,000 IU/day of vitamin E, 20 mg/day memantine, a combination of both, or placebo.
The primary outcome was change on the Alzheimer’s Disease Cooperative Study/Activities of Daily Living Inventory (ADCS-ADL). Secondary endpoints included the Alzheimer’s Disease Assessment Scale-cognitive (ADAS-Cog), the Mini Mental State Examination (MMSE), the Neuropsychiatric Index (NPI), and the Caregiver Activity Survey (CAS), a measure of the time caregivers spend assisting Alzheimer’s patients.
The patients were a mean of 79 years old; 97% were men. About half had at least one apolipoprotein E4 allele. The mean baseline score on the ADCS-ADL was 57 on a scale of 0-78, with lower numbers representing worse function.
The final analysis contained data on 561 patents. The dropout rate was similar between the groups; most of it was from death during the study. Only three withdrew from medication-related adverse events.
The mean follow-up time was just over 2 years. The mean decline on the ADCS-ADL from baseline was 3.15 units less than the decline in the placebo group. "The treatment effect translates into a clinically meaningful delay in progression in the [vitamin E group] of 6.2 months," the investigators wrote. "A delay in progression was sustained throughout most of the trial, with delays at 1, 2, 3, and 4 years of 10.6, 8.7, 9.3, and 1.8 months, respectively."
The placebo group also declined more than both the memantine and combination groups, but those differences were not statistically significant.
However, there was a significant negative treatment interaction between vitamin E and memantine, with patients who took the combination performing worse than patients taking either of the interventions alone.
There were no between-group differences in the rate of cognitive decline or neuropsychiatric symptoms. Patients in the vitamin E group did require about 2 hours less of caregiver time per day, compared with those on memantine, but that difference was not statistically significant, with a confidence interval of 0.63-3.71.
Despite being statistically nonsignificant, the authors said the reduction in caregiver time was clinically meaningful and could have "a major effect on informal and direct medical costs. ... The loss of the ability to perform ADLs is associated not only with increased caregiver burden, but also with nursing home placement," the investigators noted.
Any "infection or infestation" was the only category of adverse events reported significantly more commonly in both the memantine and combination groups. The most common, occurring in at least 5% more of treated than placebo patients, were falls, bleeding, pneumonia, and urinary tract infections.
Annual mortality was similar between the groups: 7% for the vitamin E group, 11% for the memantine group, and 9% for both the combination and placebo groups. This finding is in contrast to a 2005 meta-analysis that found a significant mortality increase associated with vitamin E doses exceeding 400 IU/day (Ann. Intern. Med. 2005;142:37-46).
The meta-analysis included only one Alzheimer’s study, the authors noted. In it, all-cause mortality was lower in the vitamin E groups, compared with the other treatment groups.
The finding of a "rather robust" treatment effect is confusing, given the results of previous studies of vitamin E in Alzheimer’s patients – especially in light of a 2005 trial in patients with mild cognitive impairment, Dr. Richard Caselli, professor of neurology and associate director and clinical core director of the Alzheimer’s Disease Center at the Mayo Clinic in Scottsdale, Ariz., said in an interview.
That trial, part of the Alzheimer’s Disease Cooperative Study, randomized patients to 2,000 IU/day vitamin E, donepezil, or placebo. The overall rate of progression to Alzheimer’s was 16% per year, and there were no differences between either active group and the placebo group.
"I expect some will suggest that the difference in disease stage may matter, but there seems to be a growing and now large consensus that earlier intervention is better, so why would we expect later intervention with an agent of proven nonbenefit earlier to be effective later? I am actually puzzled that anyone is even still studying this."
The study by Dr. Dysken and his colleagues was funded by the Veterans Affairs Cooperative Studies Program. The authors noted multiple financial disclosures, including many with pharmaceutical companies.
Major finding: Compared with placebo, 2,000 IU/day of vitamin E was associated with a significantly 19% slowing of functional decline in patients with mild-moderate Alzheimer’s disease.
Data source: The randomized, placebo-controlled study comprising 613 patients
Disclosures: The study was sponsored by the Veterans Affairs Cooperative Studies Program. The authors noted multiple financial disclosures, including many with pharmaceutical companies.