User login
Daily multivitamins boost memory in older adults: A randomized trial
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. , known as COSMOS (Cocoa Supplement and Multivitamins Outcome Study). This is the second COSMOS trial to show a benefit of multivitamins on memory and cognition. This trial involved a collaboration between Brigham and Columbia University and was published in the American Journal of Clinical Nutrition. I’d like to acknowledge that I am a coauthor of this study, together with Dr. Howard Sesso, who co-leads the main COSMOS trial with me.
Preserving memory and cognitive function is of critical importance to older adults. Nutritional interventions play an important role because we know the brain requires several nutrients for optimal health, and deficiencies in one or more of these nutrients may accelerate cognitive decline. Some of the micronutrients that are known to be important for brain health include vitamin B12, thiamin, other B vitamins, lutein, magnesium, and zinc, among others.
The current trial included 3,500 participants aged 60 or older, looking at performance on a web-based memory test. The multivitamin group did significantly better than the placebo group on memory tests and word recall, a finding that was estimated as the equivalent of slowing age-related memory loss by about 3 years. The benefit was first seen at 1 year and was sustained across the 3 years of the trial.
Intriguingly, in both COSMOS and COSMOS-Web, and the earlier COSMOS-Mind study, which was done in collaboration with Wake Forest, the participants with a history of cardiovascular disease showed the greatest benefits from multivitamins, perhaps due to lower nutrient status. But the basis for this finding needs to be explored further.
A few important caveats need to be emphasized. First, multivitamins and other dietary supplements will never be a substitute for a healthy diet and healthy lifestyle and should not distract from those goals. But multivitamins may have a role as a complementary strategy. Another caveat is that the randomized trials tested recommended dietary allowances and not megadoses of these micronutrients. In fact, randomized trials of high doses of isolated micronutrients have not clearly shown cognitive benefits, and this suggests that more is not necessarily better and may be worse. High doses also may be associated with toxicity, or they may interfere with absorption or bioavailability of other nutrients.
In COSMOS, over the average 3.6 years of follow-up and in the earlier Physicians’ Health Study II, over 1 year of supplementation, multivitamins were found to be safe without any clear risks or safety concerns. A further caveat is that although Centrum Silver was tested in this trial, we would not expect that this is a brand-specific benefit, and other high-quality multivitamin brands would be expected to confer similar benefits. Of course, it’s important to check bottles for quality-control documentation such as the seals of the U.S. Pharmacopeia, National Science Foundation, ConsumerLab.com, and other auditors.
Overall, the finding that a daily multivitamin improved memory and slowed cognitive decline in two separate COSMOS randomized trials is exciting, suggesting that multivitamin supplementation holds promise as a safe, accessible, and affordable approach to protecting cognitive health in older adults. Further research will be needed to understand who is most likely to benefit and the biological mechanisms involved. Expert committees will have to look at the research and decide whether any changes in guidelines are indicated in the future.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School and director of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston. She reported receiving funding/donations from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. , known as COSMOS (Cocoa Supplement and Multivitamins Outcome Study). This is the second COSMOS trial to show a benefit of multivitamins on memory and cognition. This trial involved a collaboration between Brigham and Columbia University and was published in the American Journal of Clinical Nutrition. I’d like to acknowledge that I am a coauthor of this study, together with Dr. Howard Sesso, who co-leads the main COSMOS trial with me.
Preserving memory and cognitive function is of critical importance to older adults. Nutritional interventions play an important role because we know the brain requires several nutrients for optimal health, and deficiencies in one or more of these nutrients may accelerate cognitive decline. Some of the micronutrients that are known to be important for brain health include vitamin B12, thiamin, other B vitamins, lutein, magnesium, and zinc, among others.
The current trial included 3,500 participants aged 60 or older, looking at performance on a web-based memory test. The multivitamin group did significantly better than the placebo group on memory tests and word recall, a finding that was estimated as the equivalent of slowing age-related memory loss by about 3 years. The benefit was first seen at 1 year and was sustained across the 3 years of the trial.
Intriguingly, in both COSMOS and COSMOS-Web, and the earlier COSMOS-Mind study, which was done in collaboration with Wake Forest, the participants with a history of cardiovascular disease showed the greatest benefits from multivitamins, perhaps due to lower nutrient status. But the basis for this finding needs to be explored further.
A few important caveats need to be emphasized. First, multivitamins and other dietary supplements will never be a substitute for a healthy diet and healthy lifestyle and should not distract from those goals. But multivitamins may have a role as a complementary strategy. Another caveat is that the randomized trials tested recommended dietary allowances and not megadoses of these micronutrients. In fact, randomized trials of high doses of isolated micronutrients have not clearly shown cognitive benefits, and this suggests that more is not necessarily better and may be worse. High doses also may be associated with toxicity, or they may interfere with absorption or bioavailability of other nutrients.
In COSMOS, over the average 3.6 years of follow-up and in the earlier Physicians’ Health Study II, over 1 year of supplementation, multivitamins were found to be safe without any clear risks or safety concerns. A further caveat is that although Centrum Silver was tested in this trial, we would not expect that this is a brand-specific benefit, and other high-quality multivitamin brands would be expected to confer similar benefits. Of course, it’s important to check bottles for quality-control documentation such as the seals of the U.S. Pharmacopeia, National Science Foundation, ConsumerLab.com, and other auditors.
Overall, the finding that a daily multivitamin improved memory and slowed cognitive decline in two separate COSMOS randomized trials is exciting, suggesting that multivitamin supplementation holds promise as a safe, accessible, and affordable approach to protecting cognitive health in older adults. Further research will be needed to understand who is most likely to benefit and the biological mechanisms involved. Expert committees will have to look at the research and decide whether any changes in guidelines are indicated in the future.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School and director of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston. She reported receiving funding/donations from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital. , known as COSMOS (Cocoa Supplement and Multivitamins Outcome Study). This is the second COSMOS trial to show a benefit of multivitamins on memory and cognition. This trial involved a collaboration between Brigham and Columbia University and was published in the American Journal of Clinical Nutrition. I’d like to acknowledge that I am a coauthor of this study, together with Dr. Howard Sesso, who co-leads the main COSMOS trial with me.
Preserving memory and cognitive function is of critical importance to older adults. Nutritional interventions play an important role because we know the brain requires several nutrients for optimal health, and deficiencies in one or more of these nutrients may accelerate cognitive decline. Some of the micronutrients that are known to be important for brain health include vitamin B12, thiamin, other B vitamins, lutein, magnesium, and zinc, among others.
The current trial included 3,500 participants aged 60 or older, looking at performance on a web-based memory test. The multivitamin group did significantly better than the placebo group on memory tests and word recall, a finding that was estimated as the equivalent of slowing age-related memory loss by about 3 years. The benefit was first seen at 1 year and was sustained across the 3 years of the trial.
Intriguingly, in both COSMOS and COSMOS-Web, and the earlier COSMOS-Mind study, which was done in collaboration with Wake Forest, the participants with a history of cardiovascular disease showed the greatest benefits from multivitamins, perhaps due to lower nutrient status. But the basis for this finding needs to be explored further.
A few important caveats need to be emphasized. First, multivitamins and other dietary supplements will never be a substitute for a healthy diet and healthy lifestyle and should not distract from those goals. But multivitamins may have a role as a complementary strategy. Another caveat is that the randomized trials tested recommended dietary allowances and not megadoses of these micronutrients. In fact, randomized trials of high doses of isolated micronutrients have not clearly shown cognitive benefits, and this suggests that more is not necessarily better and may be worse. High doses also may be associated with toxicity, or they may interfere with absorption or bioavailability of other nutrients.
In COSMOS, over the average 3.6 years of follow-up and in the earlier Physicians’ Health Study II, over 1 year of supplementation, multivitamins were found to be safe without any clear risks or safety concerns. A further caveat is that although Centrum Silver was tested in this trial, we would not expect that this is a brand-specific benefit, and other high-quality multivitamin brands would be expected to confer similar benefits. Of course, it’s important to check bottles for quality-control documentation such as the seals of the U.S. Pharmacopeia, National Science Foundation, ConsumerLab.com, and other auditors.
Overall, the finding that a daily multivitamin improved memory and slowed cognitive decline in two separate COSMOS randomized trials is exciting, suggesting that multivitamin supplementation holds promise as a safe, accessible, and affordable approach to protecting cognitive health in older adults. Further research will be needed to understand who is most likely to benefit and the biological mechanisms involved. Expert committees will have to look at the research and decide whether any changes in guidelines are indicated in the future.
Dr. Manson is Professor of Medicine and the Michael and Lee Bell Professor of Women’s Health, Harvard Medical School and director of the Division of Preventive Medicine, Brigham and Women’s Hospital, both in Boston. She reported receiving funding/donations from Mars Symbioscience.
A version of this article first appeared on Medscape.com.
The timekeeper
This little fellow greets you at my office. He’s been there for 25 years.
I don’t know where he came from originally. When I started out he was up front with the physician I subleased from and when he retired he passed him on to me (thanks, Fran!).

From the beginning he’s been the first thing I see when I arrive each morning. Because of my suprachiasmatic nucleus kicking me out of bed between 4 and 5 each morning, I’m always the first one in the office and so I update him. At this point he’s as much a part of my morning ritual as coffee and tea. I juggle the cubes to change the day (12 times a year I change the month) and once this is done I don’t think of him again until the next morning.
When I started setting him each morning I didn’t have kids. Now I have three, all grown. Patients, years, drug reps, and even a pandemic have all been marked by the clicking of his cubes when I change them each morning.
Now two-thirds of the way through my career, he’s taken on a different meaning. He’s counting down the days until I walk away and leave neurology in the hands of another generation. I don’t have a date for doing that, nor a plan to do so anytime soon, but sooner or later I’ll be changing his cubes for the last office day of my life as a neurologist.
What will happen to him then? Seems like a strange question to ask about an inanimate object, but after this much time I’ve gotten attached to the little guy. He’s come to symbolize more than just the date – he’s the passage of time. Maybe he’ll stay on a shelf at home, giving me something to do each morning of my retirement. Maybe one of my kids will want him.
Inevitably, he’ll probably end up at a charity store, awaiting a new owner. When that happens I hope he gives them something to pause, smile, and think about each day, like he did with me, as we travel around the sun together.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This little fellow greets you at my office. He’s been there for 25 years.
I don’t know where he came from originally. When I started out he was up front with the physician I subleased from and when he retired he passed him on to me (thanks, Fran!).
From the beginning he’s been the first thing I see when I arrive each morning. Because of my suprachiasmatic nucleus kicking me out of bed between 4 and 5 each morning, I’m always the first one in the office and so I update him. At this point he’s as much a part of my morning ritual as coffee and tea. I juggle the cubes to change the day (12 times a year I change the month) and once this is done I don’t think of him again until the next morning.
When I started setting him each morning I didn’t have kids. Now I have three, all grown. Patients, years, drug reps, and even a pandemic have all been marked by the clicking of his cubes when I change them each morning.
Now two-thirds of the way through my career, he’s taken on a different meaning. He’s counting down the days until I walk away and leave neurology in the hands of another generation. I don’t have a date for doing that, nor a plan to do so anytime soon, but sooner or later I’ll be changing his cubes for the last office day of my life as a neurologist.
What will happen to him then? Seems like a strange question to ask about an inanimate object, but after this much time I’ve gotten attached to the little guy. He’s come to symbolize more than just the date – he’s the passage of time. Maybe he’ll stay on a shelf at home, giving me something to do each morning of my retirement. Maybe one of my kids will want him.
Inevitably, he’ll probably end up at a charity store, awaiting a new owner. When that happens I hope he gives them something to pause, smile, and think about each day, like he did with me, as we travel around the sun together.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
This little fellow greets you at my office. He’s been there for 25 years.
I don’t know where he came from originally. When I started out he was up front with the physician I subleased from and when he retired he passed him on to me (thanks, Fran!).
From the beginning he’s been the first thing I see when I arrive each morning. Because of my suprachiasmatic nucleus kicking me out of bed between 4 and 5 each morning, I’m always the first one in the office and so I update him. At this point he’s as much a part of my morning ritual as coffee and tea. I juggle the cubes to change the day (12 times a year I change the month) and once this is done I don’t think of him again until the next morning.
When I started setting him each morning I didn’t have kids. Now I have three, all grown. Patients, years, drug reps, and even a pandemic have all been marked by the clicking of his cubes when I change them each morning.
Now two-thirds of the way through my career, he’s taken on a different meaning. He’s counting down the days until I walk away and leave neurology in the hands of another generation. I don’t have a date for doing that, nor a plan to do so anytime soon, but sooner or later I’ll be changing his cubes for the last office day of my life as a neurologist.
What will happen to him then? Seems like a strange question to ask about an inanimate object, but after this much time I’ve gotten attached to the little guy. He’s come to symbolize more than just the date – he’s the passage of time. Maybe he’ll stay on a shelf at home, giving me something to do each morning of my retirement. Maybe one of my kids will want him.
Inevitably, he’ll probably end up at a charity store, awaiting a new owner. When that happens I hope he gives them something to pause, smile, and think about each day, like he did with me, as we travel around the sun together.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Did an unfair system help ADAURA win on overall survival?
Barry Bonds and Roger Clemens are two world-class baseball players who played well enough to earn enduring respect and admiration. However, their reputations have been permanently tainted by their use of performance-enhancing drugs. Although they are both undeniably gifted, we’ll never know where their natural talent ended and their unfair advantage began.
The medical oncology version of this scenario played out in front of our eyes at the ASCO 2023 Plenary Session featuring the ADAURA trial. In this case, the unfair advantage was clear: Nearly two-thirds of patients in the control arm did not cross over to a standard-of-care treatment at relapse.
The ADAURA trial tested the value of the third-generation oral EGFR inhibitor osimertinib vs. placebo for up to 3 years in patients with a resected stage IB-IIIA non–small cell lung cancer (NSCLC) harboring an activating EGFR mutation. Initially presented in the ASCO 2020 Plenary Session, the preliminary analysis for ADAURA demonstrated a remarkably favorable improvement in disease-free survival (DFS) in the osimertinib arm, which led to its prompt Food and Drug Administration approval in this setting.
At the time, I was among the more vocal critics of the fanfare around this trial. The DFS improvement was impressive but, in this context, represented a low threshold for FDA approval. We already knew that prior trials of other, less effective adjuvant EGFR inhibitors routinely improved DFS but ultimately failed to improve overall survival.
Although in some cases, a DFS benefit can be sufficient to warrant changing practice, I would argue that overall survival is the most critical endpoint in a curative setting by a wide margin. I would also argue that cost should be a consideration for a drug priced at $440,000 over 3 years in the United States. At the very least, we – patients, oncologists, payers – should want to clarify what we get for $440,000 per patient, especially if that money could be better spent on other things.
Of note, we need to know whether the same overall survival may be achieved in this setting by treating only patients whose disease relapses, avoiding both the cost and toxicity of continuous treatment.
The relevance of this question became even more acute when an updated version of the ADAURA trial showed that the DFS benefit from osimertinib began to erode immediately after patients completed active treatment. Although the DFS benefit remained excellent,
The overall survival data – the critical test in my mind – were presented at the ASCO Plenary Session. The results were highly positive, with a hazard ratio for overall survival of 0.49 and a similar benefit observed across all eligible disease stages.
As with the presentation of the DFS data in 2020, these results were accompanied by adulation during the session and fawning in the media. However, a subset of people in the audience, and on Twitter, voiced a major concern: In the control arm, only 38.5% of the patients whose disease had relapsed (79 of 205) ever received osimertinib.
Post-protocol treatment included reassurances that patients in the control arm were offered crossover to osimertinib, but this only occurred starting in April 2020 and only when the treating investigator requested it.
The fact that only a minority of patients in the control arm ever received osimertinib means that ADAURA is not a trial that tests adjuvant osimertinib to osimertinib at relapse, the prevailing standard of care in the United States and the preferred treatment in this setting, based on NCCN guidelines for patients with relapsed/metastatic EGFR mutation–positive NSCLC since the FDA approval in April 2018.
The change in standard of care in the United States and some other countries did not lead to an amendment in the trial, based on the argument that the trial was designed with DFS as the primary endpoint and that patients in the control arm are effectively off trial at relapse. That means patients would receive their country’s standard of care, which may be below, or different from, the standard in the United States or other parts of the world.
While defensible, others considered the low rate of osimertinib delivery in the control arm a serious flaw in the trial design and arguably an ethical problem.
Given this trial design, it’s important to question whether the trial magnified the difference in overall survival between the two arms compared with the standard of care in countries where adjuvant osimertinib will ultimately be marketed. Although I strongly suspect that the overall survival difference would have been significant without the disparity in access to osimertinib in the control arm, we will never know the magnitude of that difference.
With the current design, the trial demonstrates that osimertinib is associated with improved survival in 100% of patients with EGFR mutation–positive NSCLC who receive the agent vs. 38.5% of patients receiving it at some point after relapse.
At the end of the day, ADAURA followed conventional trial rules, which led to a windfall of accolades at the cost of suboptimal care for many of the patients randomly assigned to the control arm.
We need to decide as an oncology community whether we want to accept a system that confers rewards for stakeholders at the expense of patients enrolled in the trial.
We have developed a system that not only permits but depends on global trials enrolling many patients from countries with staging and off-protocol oncology care below standards of care in other parts of the world – effectively condoning and perpetuating disparities in optimal care globally. I am also saddened that some of the most respected leaders in our field have become upset when I question the ethics of accepting this system, one that I believe we have agency to change.
The question here is not whether osimertinib is a good drug; it is remarkably effective for patients with EGFR mutation–positive NSCLC. The question is how to design trials in a fair and balanced way that doesn’t compromise patient care or ethical standards.
If people think my assessment is too harsh, I openly welcome debate.
Bottom line: The ADAURA trial lays bare deeper problems with clinical trial design, and I would challenge readers to reflect on our clinical trial culture in oncology, which offers a system of rules that rewards denying the best identified care for patients on our clinical trials.
At the very least, should we celebrate these wins without fully acknowledging these problems?
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He reported conflicts of interest with Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly.
A version of this article first appeared on Medscape.com.
Barry Bonds and Roger Clemens are two world-class baseball players who played well enough to earn enduring respect and admiration. However, their reputations have been permanently tainted by their use of performance-enhancing drugs. Although they are both undeniably gifted, we’ll never know where their natural talent ended and their unfair advantage began.
The medical oncology version of this scenario played out in front of our eyes at the ASCO 2023 Plenary Session featuring the ADAURA trial. In this case, the unfair advantage was clear: Nearly two-thirds of patients in the control arm did not cross over to a standard-of-care treatment at relapse.
The ADAURA trial tested the value of the third-generation oral EGFR inhibitor osimertinib vs. placebo for up to 3 years in patients with a resected stage IB-IIIA non–small cell lung cancer (NSCLC) harboring an activating EGFR mutation. Initially presented in the ASCO 2020 Plenary Session, the preliminary analysis for ADAURA demonstrated a remarkably favorable improvement in disease-free survival (DFS) in the osimertinib arm, which led to its prompt Food and Drug Administration approval in this setting.
At the time, I was among the more vocal critics of the fanfare around this trial. The DFS improvement was impressive but, in this context, represented a low threshold for FDA approval. We already knew that prior trials of other, less effective adjuvant EGFR inhibitors routinely improved DFS but ultimately failed to improve overall survival.
Although in some cases, a DFS benefit can be sufficient to warrant changing practice, I would argue that overall survival is the most critical endpoint in a curative setting by a wide margin. I would also argue that cost should be a consideration for a drug priced at $440,000 over 3 years in the United States. At the very least, we – patients, oncologists, payers – should want to clarify what we get for $440,000 per patient, especially if that money could be better spent on other things.
Of note, we need to know whether the same overall survival may be achieved in this setting by treating only patients whose disease relapses, avoiding both the cost and toxicity of continuous treatment.
The relevance of this question became even more acute when an updated version of the ADAURA trial showed that the DFS benefit from osimertinib began to erode immediately after patients completed active treatment. Although the DFS benefit remained excellent,
The overall survival data – the critical test in my mind – were presented at the ASCO Plenary Session. The results were highly positive, with a hazard ratio for overall survival of 0.49 and a similar benefit observed across all eligible disease stages.
As with the presentation of the DFS data in 2020, these results were accompanied by adulation during the session and fawning in the media. However, a subset of people in the audience, and on Twitter, voiced a major concern: In the control arm, only 38.5% of the patients whose disease had relapsed (79 of 205) ever received osimertinib.
Post-protocol treatment included reassurances that patients in the control arm were offered crossover to osimertinib, but this only occurred starting in April 2020 and only when the treating investigator requested it.
The fact that only a minority of patients in the control arm ever received osimertinib means that ADAURA is not a trial that tests adjuvant osimertinib to osimertinib at relapse, the prevailing standard of care in the United States and the preferred treatment in this setting, based on NCCN guidelines for patients with relapsed/metastatic EGFR mutation–positive NSCLC since the FDA approval in April 2018.
The change in standard of care in the United States and some other countries did not lead to an amendment in the trial, based on the argument that the trial was designed with DFS as the primary endpoint and that patients in the control arm are effectively off trial at relapse. That means patients would receive their country’s standard of care, which may be below, or different from, the standard in the United States or other parts of the world.
While defensible, others considered the low rate of osimertinib delivery in the control arm a serious flaw in the trial design and arguably an ethical problem.
Given this trial design, it’s important to question whether the trial magnified the difference in overall survival between the two arms compared with the standard of care in countries where adjuvant osimertinib will ultimately be marketed. Although I strongly suspect that the overall survival difference would have been significant without the disparity in access to osimertinib in the control arm, we will never know the magnitude of that difference.
With the current design, the trial demonstrates that osimertinib is associated with improved survival in 100% of patients with EGFR mutation–positive NSCLC who receive the agent vs. 38.5% of patients receiving it at some point after relapse.
At the end of the day, ADAURA followed conventional trial rules, which led to a windfall of accolades at the cost of suboptimal care for many of the patients randomly assigned to the control arm.
We need to decide as an oncology community whether we want to accept a system that confers rewards for stakeholders at the expense of patients enrolled in the trial.
We have developed a system that not only permits but depends on global trials enrolling many patients from countries with staging and off-protocol oncology care below standards of care in other parts of the world – effectively condoning and perpetuating disparities in optimal care globally. I am also saddened that some of the most respected leaders in our field have become upset when I question the ethics of accepting this system, one that I believe we have agency to change.
The question here is not whether osimertinib is a good drug; it is remarkably effective for patients with EGFR mutation–positive NSCLC. The question is how to design trials in a fair and balanced way that doesn’t compromise patient care or ethical standards.
If people think my assessment is too harsh, I openly welcome debate.
Bottom line: The ADAURA trial lays bare deeper problems with clinical trial design, and I would challenge readers to reflect on our clinical trial culture in oncology, which offers a system of rules that rewards denying the best identified care for patients on our clinical trials.
At the very least, should we celebrate these wins without fully acknowledging these problems?
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He reported conflicts of interest with Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly.
A version of this article first appeared on Medscape.com.
Barry Bonds and Roger Clemens are two world-class baseball players who played well enough to earn enduring respect and admiration. However, their reputations have been permanently tainted by their use of performance-enhancing drugs. Although they are both undeniably gifted, we’ll never know where their natural talent ended and their unfair advantage began.
The medical oncology version of this scenario played out in front of our eyes at the ASCO 2023 Plenary Session featuring the ADAURA trial. In this case, the unfair advantage was clear: Nearly two-thirds of patients in the control arm did not cross over to a standard-of-care treatment at relapse.
The ADAURA trial tested the value of the third-generation oral EGFR inhibitor osimertinib vs. placebo for up to 3 years in patients with a resected stage IB-IIIA non–small cell lung cancer (NSCLC) harboring an activating EGFR mutation. Initially presented in the ASCO 2020 Plenary Session, the preliminary analysis for ADAURA demonstrated a remarkably favorable improvement in disease-free survival (DFS) in the osimertinib arm, which led to its prompt Food and Drug Administration approval in this setting.
At the time, I was among the more vocal critics of the fanfare around this trial. The DFS improvement was impressive but, in this context, represented a low threshold for FDA approval. We already knew that prior trials of other, less effective adjuvant EGFR inhibitors routinely improved DFS but ultimately failed to improve overall survival.
Although in some cases, a DFS benefit can be sufficient to warrant changing practice, I would argue that overall survival is the most critical endpoint in a curative setting by a wide margin. I would also argue that cost should be a consideration for a drug priced at $440,000 over 3 years in the United States. At the very least, we – patients, oncologists, payers – should want to clarify what we get for $440,000 per patient, especially if that money could be better spent on other things.
Of note, we need to know whether the same overall survival may be achieved in this setting by treating only patients whose disease relapses, avoiding both the cost and toxicity of continuous treatment.
The relevance of this question became even more acute when an updated version of the ADAURA trial showed that the DFS benefit from osimertinib began to erode immediately after patients completed active treatment. Although the DFS benefit remained excellent,
The overall survival data – the critical test in my mind – were presented at the ASCO Plenary Session. The results were highly positive, with a hazard ratio for overall survival of 0.49 and a similar benefit observed across all eligible disease stages.
As with the presentation of the DFS data in 2020, these results were accompanied by adulation during the session and fawning in the media. However, a subset of people in the audience, and on Twitter, voiced a major concern: In the control arm, only 38.5% of the patients whose disease had relapsed (79 of 205) ever received osimertinib.
Post-protocol treatment included reassurances that patients in the control arm were offered crossover to osimertinib, but this only occurred starting in April 2020 and only when the treating investigator requested it.
The fact that only a minority of patients in the control arm ever received osimertinib means that ADAURA is not a trial that tests adjuvant osimertinib to osimertinib at relapse, the prevailing standard of care in the United States and the preferred treatment in this setting, based on NCCN guidelines for patients with relapsed/metastatic EGFR mutation–positive NSCLC since the FDA approval in April 2018.
The change in standard of care in the United States and some other countries did not lead to an amendment in the trial, based on the argument that the trial was designed with DFS as the primary endpoint and that patients in the control arm are effectively off trial at relapse. That means patients would receive their country’s standard of care, which may be below, or different from, the standard in the United States or other parts of the world.
While defensible, others considered the low rate of osimertinib delivery in the control arm a serious flaw in the trial design and arguably an ethical problem.
Given this trial design, it’s important to question whether the trial magnified the difference in overall survival between the two arms compared with the standard of care in countries where adjuvant osimertinib will ultimately be marketed. Although I strongly suspect that the overall survival difference would have been significant without the disparity in access to osimertinib in the control arm, we will never know the magnitude of that difference.
With the current design, the trial demonstrates that osimertinib is associated with improved survival in 100% of patients with EGFR mutation–positive NSCLC who receive the agent vs. 38.5% of patients receiving it at some point after relapse.
At the end of the day, ADAURA followed conventional trial rules, which led to a windfall of accolades at the cost of suboptimal care for many of the patients randomly assigned to the control arm.
We need to decide as an oncology community whether we want to accept a system that confers rewards for stakeholders at the expense of patients enrolled in the trial.
We have developed a system that not only permits but depends on global trials enrolling many patients from countries with staging and off-protocol oncology care below standards of care in other parts of the world – effectively condoning and perpetuating disparities in optimal care globally. I am also saddened that some of the most respected leaders in our field have become upset when I question the ethics of accepting this system, one that I believe we have agency to change.
The question here is not whether osimertinib is a good drug; it is remarkably effective for patients with EGFR mutation–positive NSCLC. The question is how to design trials in a fair and balanced way that doesn’t compromise patient care or ethical standards.
If people think my assessment is too harsh, I openly welcome debate.
Bottom line: The ADAURA trial lays bare deeper problems with clinical trial design, and I would challenge readers to reflect on our clinical trial culture in oncology, which offers a system of rules that rewards denying the best identified care for patients on our clinical trials.
At the very least, should we celebrate these wins without fully acknowledging these problems?
Dr. West is clinical associate professor, department of medical oncology, City of Hope Comprehensive Cancer Care, Duarte, Calif. He reported conflicts of interest with Bristol-Myers Squibb, Boehringer Ingelheim, Spectrum, AstraZeneca, Celgene, Genentech/Roche, Pfizer, Merck, and Eli Lilly.
A version of this article first appeared on Medscape.com.
Don’t screen, just listen
A recent study published in the journal Academic Pediatrics suggests that during health maintenance visits clinicians are giving too little attention to their patients’ sleep problems. Using a questionnaire, researchers surveyed patients’ caregivers’ concerns and observations regarding a variety of sleep problems. The investigators then reviewed the clinicians’ documentation of what transpired at the visit and found that while over 90% of the caregivers reported their child had at least one sleep related problem, only 20% of the clinicians documented the problem. And, only 12% documented a management plan regarding the sleep concerns.
I am always bit skeptical about studies that rely on clinicians’ “documentation” because clinicians are busy people and don’t always remember to record things they’ve discussed. You and I know that the lawyers’ dictum “if it wasn’t documented it didn’t happen” is rubbish. However, I still find the basic finding of this study concerning. If we are failing to ask about or even listen to caregivers’ concerns about something as important as sleep, we are missing the boat ... a very large boat.

How could this be happening? First, sleep may have fallen victim to the bloated list of topics that well-intentioned single-issue preventive health advocates have tacked on to the health maintenance visit. It’s a burden that few of us can manage without cutting corners.
However, it is more troubling to me that so many clinicians have chosen sleep as one of those corners to cut. This oversight suggests to me that too many of us have failed to realize from our own observations that sleep is incredibly important to the health of our patients ... and to ourselves.
I will admit that I am extremely sensitive to the importance of sleep. Some might say my sensitivity borders on an obsession. But, the literature is clear and becoming more voluminous every year that sleep is important to the mental health of our patients and their caregivers to things like obesity, to symptoms that suggest an attention-deficit/hyperactivity disorder, to school success, and to migraine ... to name just a few.
It may be that most of us realize the importance of sleep but feel our society has allowed itself to become so sleep deprived that there is little chance we can turn the ship around by spending just a few minutes trying help a family undo their deeply ingrained sleep unfriendly habits.
I am tempted to join those of you who see sleep depravation as a “why bother” issue. But, I’m not ready to throw in the towel. Even simply sharing your observations about the importance of sleep in the whole wellness picture may have an effect.
One of the benefits of retiring in the same community in which I practiced for over 40 years is that at least every month or two I encounter a parent who thanks me for sharing my views on the importance of sleep. They may not recall the little tip or two I gave them, but it seems that urging them to put sleep near the top of their lifestyle priority list has made the difference for them.
If I have failed in getting you to join me in my crusade against sleep deprivation, at least take to heart the most basic message of this study. That is that the investigators found only 20% of clinicians were addressing a concern that 90% of the caregivers shared. It happened to be sleep, but it could have been anything.
The authors of the study suggest that we need to be more assiduous in our screening for sleep problems. On the contrary. You and I know we don’t need more screening. We just need to be better listeners.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
A recent study published in the journal Academic Pediatrics suggests that during health maintenance visits clinicians are giving too little attention to their patients’ sleep problems. Using a questionnaire, researchers surveyed patients’ caregivers’ concerns and observations regarding a variety of sleep problems. The investigators then reviewed the clinicians’ documentation of what transpired at the visit and found that while over 90% of the caregivers reported their child had at least one sleep related problem, only 20% of the clinicians documented the problem. And, only 12% documented a management plan regarding the sleep concerns.
I am always bit skeptical about studies that rely on clinicians’ “documentation” because clinicians are busy people and don’t always remember to record things they’ve discussed. You and I know that the lawyers’ dictum “if it wasn’t documented it didn’t happen” is rubbish. However, I still find the basic finding of this study concerning. If we are failing to ask about or even listen to caregivers’ concerns about something as important as sleep, we are missing the boat ... a very large boat.
How could this be happening? First, sleep may have fallen victim to the bloated list of topics that well-intentioned single-issue preventive health advocates have tacked on to the health maintenance visit. It’s a burden that few of us can manage without cutting corners.
However, it is more troubling to me that so many clinicians have chosen sleep as one of those corners to cut. This oversight suggests to me that too many of us have failed to realize from our own observations that sleep is incredibly important to the health of our patients ... and to ourselves.
I will admit that I am extremely sensitive to the importance of sleep. Some might say my sensitivity borders on an obsession. But, the literature is clear and becoming more voluminous every year that sleep is important to the mental health of our patients and their caregivers to things like obesity, to symptoms that suggest an attention-deficit/hyperactivity disorder, to school success, and to migraine ... to name just a few.
It may be that most of us realize the importance of sleep but feel our society has allowed itself to become so sleep deprived that there is little chance we can turn the ship around by spending just a few minutes trying help a family undo their deeply ingrained sleep unfriendly habits.
I am tempted to join those of you who see sleep depravation as a “why bother” issue. But, I’m not ready to throw in the towel. Even simply sharing your observations about the importance of sleep in the whole wellness picture may have an effect.
One of the benefits of retiring in the same community in which I practiced for over 40 years is that at least every month or two I encounter a parent who thanks me for sharing my views on the importance of sleep. They may not recall the little tip or two I gave them, but it seems that urging them to put sleep near the top of their lifestyle priority list has made the difference for them.
If I have failed in getting you to join me in my crusade against sleep deprivation, at least take to heart the most basic message of this study. That is that the investigators found only 20% of clinicians were addressing a concern that 90% of the caregivers shared. It happened to be sleep, but it could have been anything.
The authors of the study suggest that we need to be more assiduous in our screening for sleep problems. On the contrary. You and I know we don’t need more screening. We just need to be better listeners.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
A recent study published in the journal Academic Pediatrics suggests that during health maintenance visits clinicians are giving too little attention to their patients’ sleep problems. Using a questionnaire, researchers surveyed patients’ caregivers’ concerns and observations regarding a variety of sleep problems. The investigators then reviewed the clinicians’ documentation of what transpired at the visit and found that while over 90% of the caregivers reported their child had at least one sleep related problem, only 20% of the clinicians documented the problem. And, only 12% documented a management plan regarding the sleep concerns.
I am always bit skeptical about studies that rely on clinicians’ “documentation” because clinicians are busy people and don’t always remember to record things they’ve discussed. You and I know that the lawyers’ dictum “if it wasn’t documented it didn’t happen” is rubbish. However, I still find the basic finding of this study concerning. If we are failing to ask about or even listen to caregivers’ concerns about something as important as sleep, we are missing the boat ... a very large boat.
How could this be happening? First, sleep may have fallen victim to the bloated list of topics that well-intentioned single-issue preventive health advocates have tacked on to the health maintenance visit. It’s a burden that few of us can manage without cutting corners.
However, it is more troubling to me that so many clinicians have chosen sleep as one of those corners to cut. This oversight suggests to me that too many of us have failed to realize from our own observations that sleep is incredibly important to the health of our patients ... and to ourselves.
I will admit that I am extremely sensitive to the importance of sleep. Some might say my sensitivity borders on an obsession. But, the literature is clear and becoming more voluminous every year that sleep is important to the mental health of our patients and their caregivers to things like obesity, to symptoms that suggest an attention-deficit/hyperactivity disorder, to school success, and to migraine ... to name just a few.
It may be that most of us realize the importance of sleep but feel our society has allowed itself to become so sleep deprived that there is little chance we can turn the ship around by spending just a few minutes trying help a family undo their deeply ingrained sleep unfriendly habits.
I am tempted to join those of you who see sleep depravation as a “why bother” issue. But, I’m not ready to throw in the towel. Even simply sharing your observations about the importance of sleep in the whole wellness picture may have an effect.
One of the benefits of retiring in the same community in which I practiced for over 40 years is that at least every month or two I encounter a parent who thanks me for sharing my views on the importance of sleep. They may not recall the little tip or two I gave them, but it seems that urging them to put sleep near the top of their lifestyle priority list has made the difference for them.
If I have failed in getting you to join me in my crusade against sleep deprivation, at least take to heart the most basic message of this study. That is that the investigators found only 20% of clinicians were addressing a concern that 90% of the caregivers shared. It happened to be sleep, but it could have been anything.
The authors of the study suggest that we need to be more assiduous in our screening for sleep problems. On the contrary. You and I know we don’t need more screening. We just need to be better listeners.
Dr. Wilkoff practiced primary care pediatrics in Brunswick, Maine, for nearly 40 years. He has authored several books on behavioral pediatrics, including “How to Say No to Your Toddler.” Other than a Littman stethoscope he accepted as a first-year medical student in 1966, Dr. Wilkoff reports having nothing to disclose. Email him at [email protected].
Transplant centers often skip the top spot on the kidney waitlist
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
The idea of rationing medical care is anathema to most doctors. Sure, we acknowledge that the realities of health care costs and insurance companies might limit our options, but there is always a sense that when something is truly, truly needed, we can get it done.
Except in one very particular situation, a situation where rationing of care is the norm. That situation? Organ transplantation.
There is no way around this: More patients need organ transplants than there are organs available to transplant. It is cold, hard arithmetic. No amount of negotiating with an insurance company or engaging in prior authorization can change that.
As a kidney doctor, this issue is close to my heart. There are around 100,000 people on the kidney transplant waiting list in the U.S., with 3,000 new patients being added per month. There are only 25,000 kidney transplants per year. And each year, around 5,000 people die while waiting for a transplant.
A world of scarcity, like the world of kidney transplant, is ripe for bias at best and abuse at worst. It is in part for that reason that the Kidney Allocation System exists. It answers the cold, hard arithmetic of transplant scarcity with the cold, hard arithmetic of a computer algorithm, ranking individuals on the waitlist on a variety of factors to ensure that those who will benefit most from a transplant get it first.
This area is a bit complex but I’ll try to break it down into what you need to know. There are 56 organ procurement organizations (OPOs) in the United States. These are nonprofits with the responsibility to recover organs from deceased donors in their area.
Each of those OPOs maintains a ranked list of those waiting for a kidney transplant. Depending on the OPO, the list may range from a couple hundred people to a couple thousand, but one thing is the same, no matter what: If you are at the top of the list, you should be the next to get a transplant.
Most OPOs have multiple transplant centers in them, and each center is going to prioritize its own patients. If a Yale patient is No. 1 on the list and a kidney offer comes in, it would be a good idea for us to accept, because if we reject the offer, the organ may go to a competing center whose patients is ranked No. 2.
But 11 OPOs around the country are served by only one center. This gives that center huge flexibility to determine who gets what kidney, because if they refuse an offer for whoever is at the top of their list, they can still give the kidney to the second person on their list, or third, or 30th, theoretically.
But in practice, does this phenomenon, known colloquially as “list diving,” actually happen? This manuscript from Sumit Mohan and colleagues suggests that it does, and at rates that are, frankly, eye-popping.
The Columbia team used data from the Scientific Registry of Transplant Recipients to conduct the analysis. The database tracks all aspects of the transplant process, from listing to ranking to, eventually, the transplant itself. With that data, they could determine how often, across these 11 OPOs, the No. 1 person on the list did not get the available kidney.
The answer? Out of 4,668 transplants conducted from 2015 to 2019, the transplant centers skipped their highest-ranked person 3,169 times – 68% of the time.
This graph shows the distribution of where on the list these kidneys went. You can see some centers diving down 100 or 200 places.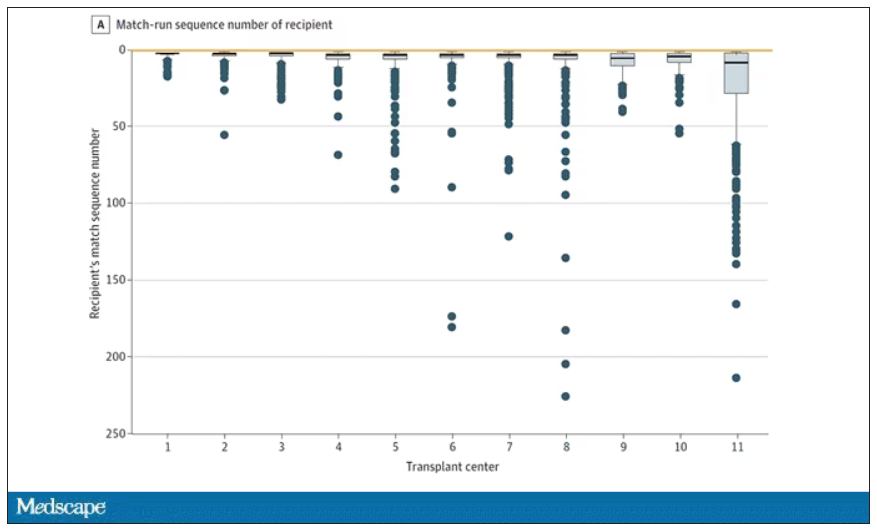
Transplant centers have lists of different lengths, so this graph shows you how far down on the percentage scale the centers dived. You can see centers skipping right to the bottom of their list in some cases.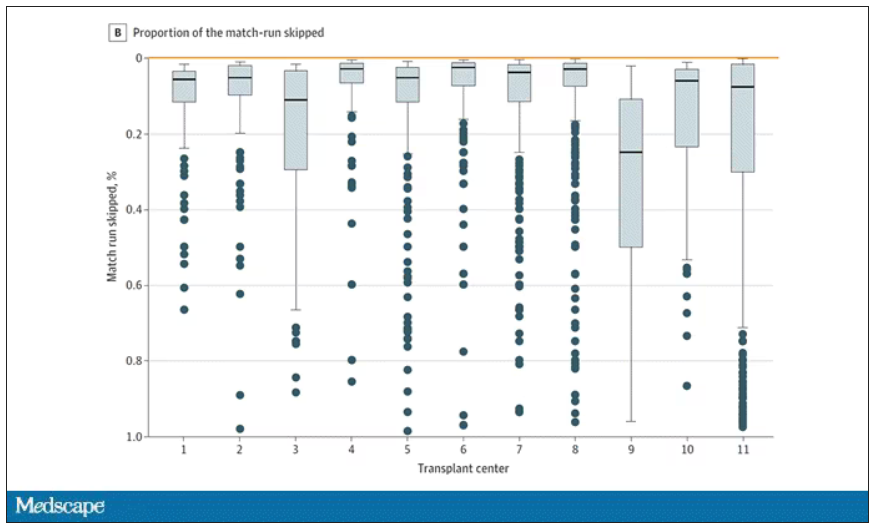
Now, I should make it clear that transplant centers do have legitimate discretion here. Transplant centers may pass up a less-than-perfect kidney for their No. 1 spot, knowing that that individual will get more offers soon, in favor of someone further down the list who will not see an offer for a while. It’s gaming the system a bit, but not, you know, for evil. And the data support this. Top-ranked people who got skipped had received a lower-quality kidney offer than those who did not get skipped. But I will also note that those who were skipped were less likely to be White, less likely to be Hispanic, and more likely to be male. That should raise your eyebrows.
Interestingly, this practice may not be limited to those cases where the OPO has only one transplant center. Conducting the same analysis across all 231 kidney transplant centers in the U.S., the authors found that the top candidate was skipped 76% of the time.
So, what’s going on here? I’m sure that some of this list-skipping is for legitimate medical reasons. And it should be pointed out that recipients have a right to refuse an offer as well – and might be more picky if they know they are at the top of the list. But patient preference was listed as the reason for list diving in only about 14% of cases. The vast majority (65%) of reasons given were based on donor quality. The problem is that donor quality can be quite subjective. And remember, these organs were transplanted eventually so they couldn’t have been that bad.
Putting the data together, though, I can’t shake the sense that centers are using the list more for guidance than as a real mechanism to ensure an equitable allocation system. With all the flexibility that centers have to bypass individuals on the list, the list loses its meaning and its power.
I spoke to one transplant nephrologist who suggested that these data should prompt an investigation by the United Network for Organ Sharing, the body that governs all these OPOs. That may be a necessary step.
I hope there comes a day when this issue is moot, when growing kidneys in the lab – or regenerating one’s own kidneys – is a possibility. But that day is not yet here and we must deal with the scarcity we have. In this world, we need the list to prevent abuse. But the list only works if the list is followed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
The idea of rationing medical care is anathema to most doctors. Sure, we acknowledge that the realities of health care costs and insurance companies might limit our options, but there is always a sense that when something is truly, truly needed, we can get it done.
Except in one very particular situation, a situation where rationing of care is the norm. That situation? Organ transplantation.
There is no way around this: More patients need organ transplants than there are organs available to transplant. It is cold, hard arithmetic. No amount of negotiating with an insurance company or engaging in prior authorization can change that.
As a kidney doctor, this issue is close to my heart. There are around 100,000 people on the kidney transplant waiting list in the U.S., with 3,000 new patients being added per month. There are only 25,000 kidney transplants per year. And each year, around 5,000 people die while waiting for a transplant.
A world of scarcity, like the world of kidney transplant, is ripe for bias at best and abuse at worst. It is in part for that reason that the Kidney Allocation System exists. It answers the cold, hard arithmetic of transplant scarcity with the cold, hard arithmetic of a computer algorithm, ranking individuals on the waitlist on a variety of factors to ensure that those who will benefit most from a transplant get it first.
This area is a bit complex but I’ll try to break it down into what you need to know. There are 56 organ procurement organizations (OPOs) in the United States. These are nonprofits with the responsibility to recover organs from deceased donors in their area.
Each of those OPOs maintains a ranked list of those waiting for a kidney transplant. Depending on the OPO, the list may range from a couple hundred people to a couple thousand, but one thing is the same, no matter what: If you are at the top of the list, you should be the next to get a transplant.
Most OPOs have multiple transplant centers in them, and each center is going to prioritize its own patients. If a Yale patient is No. 1 on the list and a kidney offer comes in, it would be a good idea for us to accept, because if we reject the offer, the organ may go to a competing center whose patients is ranked No. 2.
But 11 OPOs around the country are served by only one center. This gives that center huge flexibility to determine who gets what kidney, because if they refuse an offer for whoever is at the top of their list, they can still give the kidney to the second person on their list, or third, or 30th, theoretically.
But in practice, does this phenomenon, known colloquially as “list diving,” actually happen? This manuscript from Sumit Mohan and colleagues suggests that it does, and at rates that are, frankly, eye-popping.
The Columbia team used data from the Scientific Registry of Transplant Recipients to conduct the analysis. The database tracks all aspects of the transplant process, from listing to ranking to, eventually, the transplant itself. With that data, they could determine how often, across these 11 OPOs, the No. 1 person on the list did not get the available kidney.
The answer? Out of 4,668 transplants conducted from 2015 to 2019, the transplant centers skipped their highest-ranked person 3,169 times – 68% of the time.
This graph shows the distribution of where on the list these kidneys went. You can see some centers diving down 100 or 200 places.
Transplant centers have lists of different lengths, so this graph shows you how far down on the percentage scale the centers dived. You can see centers skipping right to the bottom of their list in some cases.
Now, I should make it clear that transplant centers do have legitimate discretion here. Transplant centers may pass up a less-than-perfect kidney for their No. 1 spot, knowing that that individual will get more offers soon, in favor of someone further down the list who will not see an offer for a while. It’s gaming the system a bit, but not, you know, for evil. And the data support this. Top-ranked people who got skipped had received a lower-quality kidney offer than those who did not get skipped. But I will also note that those who were skipped were less likely to be White, less likely to be Hispanic, and more likely to be male. That should raise your eyebrows.
Interestingly, this practice may not be limited to those cases where the OPO has only one transplant center. Conducting the same analysis across all 231 kidney transplant centers in the U.S., the authors found that the top candidate was skipped 76% of the time.
So, what’s going on here? I’m sure that some of this list-skipping is for legitimate medical reasons. And it should be pointed out that recipients have a right to refuse an offer as well – and might be more picky if they know they are at the top of the list. But patient preference was listed as the reason for list diving in only about 14% of cases. The vast majority (65%) of reasons given were based on donor quality. The problem is that donor quality can be quite subjective. And remember, these organs were transplanted eventually so they couldn’t have been that bad.
Putting the data together, though, I can’t shake the sense that centers are using the list more for guidance than as a real mechanism to ensure an equitable allocation system. With all the flexibility that centers have to bypass individuals on the list, the list loses its meaning and its power.
I spoke to one transplant nephrologist who suggested that these data should prompt an investigation by the United Network for Organ Sharing, the body that governs all these OPOs. That may be a necessary step.
I hope there comes a day when this issue is moot, when growing kidneys in the lab – or regenerating one’s own kidneys – is a possibility. But that day is not yet here and we must deal with the scarcity we have. In this world, we need the list to prevent abuse. But the list only works if the list is followed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
The idea of rationing medical care is anathema to most doctors. Sure, we acknowledge that the realities of health care costs and insurance companies might limit our options, but there is always a sense that when something is truly, truly needed, we can get it done.
Except in one very particular situation, a situation where rationing of care is the norm. That situation? Organ transplantation.
There is no way around this: More patients need organ transplants than there are organs available to transplant. It is cold, hard arithmetic. No amount of negotiating with an insurance company or engaging in prior authorization can change that.
As a kidney doctor, this issue is close to my heart. There are around 100,000 people on the kidney transplant waiting list in the U.S., with 3,000 new patients being added per month. There are only 25,000 kidney transplants per year. And each year, around 5,000 people die while waiting for a transplant.
A world of scarcity, like the world of kidney transplant, is ripe for bias at best and abuse at worst. It is in part for that reason that the Kidney Allocation System exists. It answers the cold, hard arithmetic of transplant scarcity with the cold, hard arithmetic of a computer algorithm, ranking individuals on the waitlist on a variety of factors to ensure that those who will benefit most from a transplant get it first.
This area is a bit complex but I’ll try to break it down into what you need to know. There are 56 organ procurement organizations (OPOs) in the United States. These are nonprofits with the responsibility to recover organs from deceased donors in their area.
Each of those OPOs maintains a ranked list of those waiting for a kidney transplant. Depending on the OPO, the list may range from a couple hundred people to a couple thousand, but one thing is the same, no matter what: If you are at the top of the list, you should be the next to get a transplant.
Most OPOs have multiple transplant centers in them, and each center is going to prioritize its own patients. If a Yale patient is No. 1 on the list and a kidney offer comes in, it would be a good idea for us to accept, because if we reject the offer, the organ may go to a competing center whose patients is ranked No. 2.
But 11 OPOs around the country are served by only one center. This gives that center huge flexibility to determine who gets what kidney, because if they refuse an offer for whoever is at the top of their list, they can still give the kidney to the second person on their list, or third, or 30th, theoretically.
But in practice, does this phenomenon, known colloquially as “list diving,” actually happen? This manuscript from Sumit Mohan and colleagues suggests that it does, and at rates that are, frankly, eye-popping.
The Columbia team used data from the Scientific Registry of Transplant Recipients to conduct the analysis. The database tracks all aspects of the transplant process, from listing to ranking to, eventually, the transplant itself. With that data, they could determine how often, across these 11 OPOs, the No. 1 person on the list did not get the available kidney.
The answer? Out of 4,668 transplants conducted from 2015 to 2019, the transplant centers skipped their highest-ranked person 3,169 times – 68% of the time.
This graph shows the distribution of where on the list these kidneys went. You can see some centers diving down 100 or 200 places.
Transplant centers have lists of different lengths, so this graph shows you how far down on the percentage scale the centers dived. You can see centers skipping right to the bottom of their list in some cases.
Now, I should make it clear that transplant centers do have legitimate discretion here. Transplant centers may pass up a less-than-perfect kidney for their No. 1 spot, knowing that that individual will get more offers soon, in favor of someone further down the list who will not see an offer for a while. It’s gaming the system a bit, but not, you know, for evil. And the data support this. Top-ranked people who got skipped had received a lower-quality kidney offer than those who did not get skipped. But I will also note that those who were skipped were less likely to be White, less likely to be Hispanic, and more likely to be male. That should raise your eyebrows.
Interestingly, this practice may not be limited to those cases where the OPO has only one transplant center. Conducting the same analysis across all 231 kidney transplant centers in the U.S., the authors found that the top candidate was skipped 76% of the time.
So, what’s going on here? I’m sure that some of this list-skipping is for legitimate medical reasons. And it should be pointed out that recipients have a right to refuse an offer as well – and might be more picky if they know they are at the top of the list. But patient preference was listed as the reason for list diving in only about 14% of cases. The vast majority (65%) of reasons given were based on donor quality. The problem is that donor quality can be quite subjective. And remember, these organs were transplanted eventually so they couldn’t have been that bad.
Putting the data together, though, I can’t shake the sense that centers are using the list more for guidance than as a real mechanism to ensure an equitable allocation system. With all the flexibility that centers have to bypass individuals on the list, the list loses its meaning and its power.
I spoke to one transplant nephrologist who suggested that these data should prompt an investigation by the United Network for Organ Sharing, the body that governs all these OPOs. That may be a necessary step.
I hope there comes a day when this issue is moot, when growing kidneys in the lab – or regenerating one’s own kidneys – is a possibility. But that day is not yet here and we must deal with the scarcity we have. In this world, we need the list to prevent abuse. But the list only works if the list is followed.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator, New Haven, Conn. He reported having no conflicts of interest.
A version of this article first appeared on Medscape.com.
How can we make medical training less ‘toxic’?
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Robert D. Glatter, MD: Welcome. I’m Dr. Robert Glatter, medical adviser for Medscape Emergency Medicine. Joining me to discuss ways to address and reform the toxic culture associated with medical training is Dr. Amy Faith Ho, senior vice president of clinical informatics and analytics at Integrative Emergency Services in Dallas. Also joining us is Dr. Júlia Loyola Ferreira, a pediatric surgeon originally from Brazil, now practicing at Montreal Children’s and focused on advocacy for gender equity and patient-centered care.
Welcome to both of you. Thanks so much for joining me.
Amy Faith Ho, MD, MPH: Thanks so much for having us, Rob.
Dr. Glatter: Amy, I noticed a tweet recently where you talked about how your career choice was affected by the toxic environment in medical school, affecting your choice of residency. Can you elaborate on that?
Dr. Ho: In this instance, what we’re talking about is gender, but it can be directed toward any number of other groups as well.
What you’re alluding to is a tweet by Stanford Surgery Group showing the next residency class, and what was really stunning about this residency class was that it was almost all females. And this was something that took off on social media.
When I saw this, I was really brought back to one of my personal experiences that I chose to share, which was basically that, as a medical student, I really wanted to be a surgeon. I’m an emergency medicine doctor now, so you know that didn’t happen.
The story that I was sharing was that when I was a third-year medical student rotating on surgery, we had a male attending who was very well known at that school at the time who basically would take the female medical students, and instead of clinic, he would round us up. He would have us sit around him in the workplace room while everyone else was seeing patients, and he would have you look at news clippings of himself. He would tell you stories about himself, like he was holding court for the ladies.
It was this very weird culture where my takeaway as a med student was like, “Wow, this is kind of abusive patriarchy that is supported,” because everyone knew about it and was complicit. Even though I really liked surgery, this was just one instance and one example of where you see this culture that really resonates into the rest of life that I didn’t really want to be a part of.
I went into emergency medicine and loved it. It’s also highly procedural, and I was very happy with where I was. What was really interesting about this tweet to me, though, is that it really took off and garnered hundreds of thousands of views on a very niche topic, because what was most revealing is that everyone has a story like this.
It is not just surgery. It is definitely not just one specialty and it is not just one school. It is an endemic problem in medicine. Not only does it change the lives of young women, but it also says so much about the complicity and the culture that we have in medicine that many people were upset about just the same way I was.
Medical training experience in other countries vs. the United States
Dr. Glatter: Júlia, I want to hear about your experience in medical school, surgery, and then fellowship training and up to the present, if possible.
Júlia Loyola Ferreira, MD: In Brazil, as in many countries now, women have made up the majority of the medical students since 2010. It’s a more female-friendly environment when you’re going through medical school, and I was lucky enough to do rotations in areas of surgery where people were friendly to women.
I lived in this tiny bubble that also gave me the privilege of not facing some things that I can imagine that people in Brazil in different areas and smaller towns face. In Brazil, people try to not talk about this gender agenda. This is something that’s being talked about outside Brazil. But in Brazil, we are years back. People are not really engaging on this conversation. I thought it was going to be hard for me as a woman, because Brazil has around 20% female surgeons.
I knew it was going to be challenging, but I had no idea how bad it was. When I started and things started happening, the list was big. I have an example of everything that is written about – microaggression, implicit bias, discrimination, harassment.
Every time I would try to speak about it and talk to someone, I would be strongly gaslighted. It was the whole training, the whole 5 years. People would say, “Oh, I don’t think it was like that. I think you were overreacting.” People would come with all these different answers for what I was experiencing, and that was frustrating. That was even harder because I had to cope with everything that was happening and I had no one to turn to. I had no mentors.
When I looked up to women who were in surgery, they would be tougher on us young surgeons than the men and they would tell us that we should not complain because in their time it was even harder. Now, it’s getting better and we are supposed to accept whatever comes.
That was at least a little bit of what I experienced in my training. It was only after I finished and started to do research about it that I really encountered a field of people who would echo what I was trying to say to many people in different hospitals that I attended to.
That was the key for me to get out of that situation of being gaslighted and of not being able to really talk about it. Suddenly, I started to publish things about Brazil that nobody was even writing or studying. That gave me a large amount of responsibility, but also motivation to keep going and to see the change.
Valuing women in medicine
Dr. Glatter: This is a very important point that you’re raising about the environment of women being hard on other women. We know that men can be very difficult on and also judgmental toward their trainees.
Amy, how would you respond to that? Was your experience similar in emergency medicine training?
Dr. Ho: I actually don’t feel like it was. I think what Júlia is alluding to is this “mean girls” idea, of “I went through it and thus you have to go through it.” I think you do see this in many specialties. One of the classic ones we hear about, and I don’t want to speak to it too much because it’s not my specialty, is ob.gyn., where it is a very female-dominant surgery group. There’s almost a hazing level that you hear about in some of the more malignant workplaces.
I think that you speak to two really important things. Number one is the numbers game. As you were saying, Brazil actually has many women. That’s awesome. That’s actually different from the United States, especially for the historic, existing workplace and less so for the medical students and for residents. I think step one is having minorities like women just present and there.
Step two is actually including and valuing them. While I think it’s really easy to move away from the women discussion, because there are women when you look around in medicine, it doesn’t mean that women are actually being heard, that they’re actually being accepted, or that their viewpoints are being listened to. A big part of it is normalizing not only seeing women in medicine but also normalizing the narrative of women in medicine.
It’s not just about motherhood; it’s about things like normalizing talking about advancement, academic promotions, pay, culture, being called things like “too reactive,” “anxious,” or “too assertive.” These are all classic things that we hear about when we talk about women.
That’s why we’re looking to not only conversations like this, but also structured ways for women to discuss being women in medicine. There are many women in medicine groups in emergency medicine, including: Females Working in Emergency Medicine (FemInEM); the American College of Emergency Physicians (ACEP) and Society for Academic Emergency Medicine (SAEM) women’s groups, which are American Association of Women Emergency Physicians (AAWEP) and Academy for Women in Academic Emergency Medicine (AWAEM), respectively; and the American Medical Women’s Association (AMWA), which is the American Medical Association’s offshoot.
All of these groups are geared toward normalizing women in medicine, normalizing the narrative of women in medicine, and then working on mentoring and educating so that we can advance our initiatives.
Gender balance is not gender equity
Dr. Glatter: Amy, you bring up a very critical point that mentoring is sort of the antidote to gender-based discrimination. Júlia had written a paper back in November of 2022 that was published in the Journal of Surgical Research talking exactly about this and how important it is to develop mentoring. Part of her research showed that about 20% of medical students who took the survey, about 1,000 people, had mentors, which was very disturbing.
Dr. Loyola Ferreira: Mentorship is one of the ways of changing the reality about gender-based discrimination. Amy’s comment was very strong and we need to really keep saying it, which is that gender balance is not gender equity.
The idea of having more women is not the same as women being recognized as equals, as able as men, and as valued as men. To change this very long culture of male domination, we need support, and this support comes from mentorship.
Although I didn’t have one, I feel that since I started being a mentor for some students, it changed not only them but myself. It gave me strength to keep going, studying, publishing, and going further with this discussion. I feel like the relationship was as good for them as it is for me. That’s how things change.
Diversity, equity, and inclusion training
Dr. Glatter: We’re talking about the reality of gender equity in terms of the ability to have equal respect, recognition, opportunities, and access. That’s really an important point to realize, and for our audience, to understand that gender equity is not gender balance.
Amy, I want to talk about medical school curriculums. Are there advances that you’re aware of being made at certain schools, programs, even in residencies, to enforce these things and make it a priority?
Dr. Ho: We’re really lucky that, as a culture in the United States, medical training is certainly very geared toward diversity. Some of that is certainly unofficial. Some of that just means when they’re looking at a medical school class or looking at rank lists for residency, that they’re cognizant of the different backgrounds that people have. That’s still a step. That is a step, that we’re at least acknowledging it.
There are multiple medical schools and residencies that have more formal unconscious-bias training or diversity, equity, and inclusion (DEI) training, both of which are excellent not only for us in the workplace but also for our patients. Almost all of us will see patients of highly diverse backgrounds. I think the biggest push is looking toward the criteria that we use for selecting trainees and students into our programs. Historically, it’s been MCAT, GPA, and so on.
We’ve really started to ask the question of, are these sorts of “objective criteria” actually biased in institutional ways? They talk about this all the time where GPAs will bias against students from underrepresented minorities (URM). I think all medical students and residencies have really acknowledged that. Although there are still test cutoffs, we are putting an inquisitive eye to what those mean, why they exist, and what are the other things that we should consider. This is all very heartening from what I’m seeing in medical training.
Dr. Glatter: There’s no formal rating system for DEI curriculums right now, like ranking of this school, or this program has more advanced recognition in terms of DEI?
Dr. Ho: No, but on the flip side, the U.S. News & World Report was classically one of the major rankings for medical schools. What we saw fairly recently was that very high-tier schools like Harvard and University of Chicago pulled out of that ranking because that ranking did not acknowledge the value of diversity. That was an incredible stance for medical schools to take, to say, “Hey, you are not evaluating an important criterion of ours.”
Dr. Glatter: That’s a great point. Júlia, where are we now in Brazil in terms of awareness of DEI and curriculum in schools and training programs?
Dr. Loyola Ferreira: Our reality is not as good as in the U.S., unfortunately. I don’t see much discussion on residency programs or medical schools at the moment. I see many students bringing it out and trying to make their schools engage in that discussion. This is something that is coming from the bottom up and not from the top down. I think it can lead to change as well. It is a step and it’s a beginning. Institutions should take the responsibility of doing this from the beginning. This is something where Brazil is still years behind you guys.
Dr. Glatter: It’s unfortunate, but certainly it’s important to hear that. What about in Canada and certainly your institution, McGill, where you just completed a master’s degree?
Dr. Loyola Ferreira: Canada is very much like the U.S. This is something that is really happening and it’s happening fast. I see, at least at McGill, a large amount of DEI inclusion and everything on this discussion. They have institutional courses for us to do as students, and we are all obliged to do many courses, which I think is really educating, especially for people with different cultures and backgrounds.
Dr. Glatter: Amy, where do you think we are in emergency medicine to look at the other side of it? Comparing surgery with emergency medicine, do you think we’re well advanced in terms of DEI, inclusion criteria, respect, and dignity, or are we really far off?
Dr. Ho: I may be biased, but I think emergency medicine is one of the best in terms of this, and I think there are a couple of reasons for it. One is that we are an inherently team-based organization. The attending, the residents, and the students all work in line with one another. There’s less of a hierarchy.
The same is true for our nurses, pharmacists, techs, and EMS. We all work together as a team. Because of that fairly flat structure, it’s really easy for us to value one another as individuals with our diverse backgrounds. In a way, that’s harder for specialties that are more hierarchical, and I think surgery is certainly one of the most hierarchical.
The second reason why emergency medicine is fairly well off in this is that we’re, by nature, a safety-net specialty. We see patients of all-comers, all walks, all backgrounds. I think we both recognize the value of physician-patient concordance. When we share characteristics with our patients, we recognize that value immediately at the bedside.
It exposes us to so much diversity. I see a refugee one day and the next patient is someone who is incarcerated. The next patient after that is an important businessman in society. That diversity and whiplash in the type of patients that we see back-to-back helps us see the playing field in a really flat, diverse way. Because of that, I think our culture is much better, as is our understanding of the value and importance of diversity not only for our programs, but also for our patients.
Do female doctors have better patient outcomes?
Dr. Glatter: Specialties working together in the emergency department is so important. Building that team and that togetherness is so critical. Júlia, would you agree?
Dr. Loyola Ferreira: Definitely. Something Amy said that is beautiful is that you recognize yourself in these patients. In surgery, we are taught to try to be away from the patients and not to put ourselves in the same position. We are taught to be less engaging, and this is not good. The good thing is when we really have patient-centered care, when we listen to them, and when we are involved with them.
I saw a publication showing that female and male surgeons treating similar patients had the same surgical outcomes. Women are as good as men technically to do surgery and have the same surgical outcomes. However, there is research showing that surgical teams with greater representation of women have improved surgical outcomes because of patient-centered care and the way women conduct bedside attention to patients. And they have better patient experience measures afterward. That is not only from the women who are treating the patients, but the whole environment. Women end up bringing men [into the conversation] and this better improves patient-centered care, and that makes the whole team a better team attending patients. Definitely, we are in the moment of patient experience and satisfaction, and increasing women is a way of achieving better patient satisfaction and experience.
Dr. Ho: There’s much to be said about having female clinicians available for patients. It doesn’t have to be just for female patients, although again, concordance between physicians and patients is certainly beneficial. Besides outcomes benefit, there’s even just a communication benefit. The way that women and men communicate is inherently different. The way women and men experience certain things is also inherently different.
A classic example of this is women who are experiencing a heart attack may not actually have chest pain but present with nausea. As a female who’s sensitive to this, when I see a woman throwing up, I am very attuned to something actually being wrong, knowing that they may not present with classic pain for a syndrome, but actually may be presenting with nausea instead. It doesn’t have to be a woman who takes that knowledge and turns it into something at the bedside. It certainly doesn’t have to, but it is just a natural, easy thing to step into as a female.
While I’m really careful to not step into this “women are better than men” or “men are better than women” argument, there’s something to be said about how the availability of female clinicians for all patients, not just female patients, can have benefit. Again, it’s shown in studies with cardiovascular outcomes and cardiologists, it’s certainly shown in ob.gyn., particularly for underrepresented minorities as well for maternal outcomes of Black mothers. It’s certainly shown again in patient satisfaction, which is concordance.
There is a profound level of research already on this that goes beyond just the idea of stacking the bench and putting more women in there. That’s not the value. We’re not just here to check off the box. We’re here to actually lend some value to our patients and, again, to one another as well.
Dr. Glatter: Absolutely. These are excellent points. The point you make about patient presentation is so vital. The fact that women have nausea sometimes in ACS presentations, the research never was really attentive to this. It was biased. The symptoms that women may have that are not “typical” for ACS weren’t included in patient presentations. Educating everyone about, overall, the types of presentations that we can recognize is vital and important.
Dr. Ho: Yes. It’s worth saying that, when you look at how medicine and research developed, classically, who were the research participants? They were often White men. They were college students who, historically, because women were not allowed to go to college, were men.
I say that not to fault the institution, because that was the culture of our history, but to just say it is okay to question things. It is okay to realize that someone’s presenting outside of the box and that maybe we actually need to reframe what even created the walls of the box in the first place.
Dr. Glatter: Thank you again for joining us. I truly appreciate your insight and expertise.
Dr. Glatter is assistant professor of emergency medicine, department of emergency medicine, Hofstra/Northwell, New York. Dr. Ho is senior vice president of clinical informatics & analytics, department of emergency medicine, Integrative Emergency Services, Dallas. Dr. Loyola Ferreira is a master of science candidate, department of experimental surgery, McGill University, Montreal. They reported that they had no conflicts of interest.
A version of this article first appeared on Medscape.com.
Does weight loss surgery up the risk for bone fractures?
Currently, the two most common types of weight loss surgery performed include sleeve gastrectomy and Roux-en-Y gastric bypass (RYGB). Sleeve gastrectomy involves removing a large portion of the stomach so that its capacity is significantly decreased (to about 20%), reducing the ability to consume large quantities of food. Also, the procedure leads to marked reductions in ghrelin (an appetite-stimulating hormone), and some studies have reported increases in glucagon-like peptide 1 (GLP-1) and peptide YY (PYY), hormones that induce satiety. Gastric bypass involves creating a small stomach pouch and rerouting the small intestine so that it bypasses much of the stomach and also the upper portion of the small intestine. This reduces the amount of food that can be consumed at any time, increases levels of GLP-1 and PYY, and reduces absorption of nutrients with resultant weight loss. Less common bariatric surgeries include gastric banding and biliopancreatic diversion with duodenal switch (BPD-DS). Gastric banding involves placing a ring in the upper portion of the stomach, and the size of the pouch created can be altered by injecting more or less saline through a port inserted under the skin. BPD-DS includes sleeve gastrectomy, resection of a large section of the small intestine, and diversion of the pancreatic and biliary duct to a point below the junction of the ends of the resected gut.
Weight loss surgery is currently recommended for people who have a body mass index greater than or equal to 35 regardless of obesity-related complication and may be considered for those with a BMI greater than or equal to 30. BMI is calculated by dividing the weight (in kilograms) by the height (in meters). In children and adolescents, weight loss surgery should be considered in those with a BMI greater than 120% of the 95th percentile and with a major comorbidity or in those with a BMI greater than 140% of the 95th percentile.
What impact does weight loss surgery have on bone?
Multiple studies in both adults and teenagers have demonstrated that sleeve gastrectomy, RYGB, and BPD-DS (but not gastric banding) are associated with a decrease in bone density, impaired bone structure, and reduced strength estimates over time (Beavers et al; Gagnon, Schafer; Misra, Bredella). The relative risk for fracture after RYGB and BPD-DS is reported to be 1.2-2.3 (that is, 20%-130% more than normal), whereas fracture risk after sleeve gastrectomy is still under study with some conflicting results. Fracture risk starts to increase 2-3 years after surgery and peaks at 5-plus years after surgery. Most of the data for fractures come from studies in adults. With the rising use of weight loss surgery, particularly sleeve gastrectomy, in teenagers, studies are needed to determine fracture risk in this younger age group, who also seem to experience marked reductions in bone density, altered bone structure, and reduced bone strength after bariatric surgery.
What contributes to impaired bone health after weight loss surgery?
The deleterious effect of weight loss surgery on bone appears to be caused by various factors, including the massive and rapid weight loss that occurs after surgery, because body weight has a mechanical loading effect on bone and otherwise promotes bone formation. Weight loss results in mechanical unloading and thus a decrease in bone density. Further, when weight loss occurs, there is loss of both muscle and fat mass, and the reduction in muscle mass is deleterious to bone.
Other possible causes of bone density reduction include reduced absorption of certain nutrients, such as calcium and vitamin D critical for bone mineralization, and alterations in certain hormones that impact bone health. These include increases in parathyroid hormone, which increases bone loss when secreted in excess; increases in PYY (a hormone that reduces bone formation); decreases in ghrelin (a hormone that typically increases bone formation), particularly after sleeve gastrectomy; and decreases in estrone (a kind of estrogen that like other estrogens prevents bone loss). Further, age and gender may modify the bone consequences of surgery as outcomes in postmenopausal women appear to be worse than in younger women and men.
Preventing bone density loss
Given the many benefits of weight loss surgery, what can we do to prevent this decrease in bone density after surgery? It’s important for people undergoing weight loss surgery to be cognizant of this potentially negative outcome and to take appropriate precautions to mitigate this concern.
We should monitor bone density after surgery with the help of dual energy x-ray absorptiometry, starting a few years after surgery, particularly in those who are at greatest risk for fracture, so that we can be proactive about addressing any severe bone loss that warrants pharmacologic intervention.
More general recommendations include optimizing intake of calcium (1,200-1,500 mg/d), vitamin D (2,000-3,000 IUs/d), and protein (60-75 g/d) via diet and/or as supplements and engaging in weight-bearing physical activity because this exerts mechanical loading effects on the skeleton leading to increased bone formation and also increases muscle mass over time, which is beneficial to bone. A progressive resistance training program has been demonstrated to have beneficial effects on bone, and measures should be taken to reduce the risk for falls, which increases after certain kinds of weight loss surgery, such as gastric bypass.
Meeting with a dietitian can help determine any other nutrients that need to be optimized.
Though many hormonal changes after surgery have been linked to reductions in bone density, there are still no recommended hormonal therapies at this time, and more work is required to determine whether specific pharmacologic therapies might help improve bone outcomes after surgery.
Dr. Misra is chief of the division of pediatric endocrinology, Mass General for Children; associate director, Harvard Catalyst Translation and Clinical Research Center; director, Pediatric Endocrine-Sports Endocrine-Neuroendocrine Lab, Mass General Hospital; and professor, department of pediatrics, Harvard Medical School, Boston.
A version of this article originally appeared on Medscape.com.
Currently, the two most common types of weight loss surgery performed include sleeve gastrectomy and Roux-en-Y gastric bypass (RYGB). Sleeve gastrectomy involves removing a large portion of the stomach so that its capacity is significantly decreased (to about 20%), reducing the ability to consume large quantities of food. Also, the procedure leads to marked reductions in ghrelin (an appetite-stimulating hormone), and some studies have reported increases in glucagon-like peptide 1 (GLP-1) and peptide YY (PYY), hormones that induce satiety. Gastric bypass involves creating a small stomach pouch and rerouting the small intestine so that it bypasses much of the stomach and also the upper portion of the small intestine. This reduces the amount of food that can be consumed at any time, increases levels of GLP-1 and PYY, and reduces absorption of nutrients with resultant weight loss. Less common bariatric surgeries include gastric banding and biliopancreatic diversion with duodenal switch (BPD-DS). Gastric banding involves placing a ring in the upper portion of the stomach, and the size of the pouch created can be altered by injecting more or less saline through a port inserted under the skin. BPD-DS includes sleeve gastrectomy, resection of a large section of the small intestine, and diversion of the pancreatic and biliary duct to a point below the junction of the ends of the resected gut.
Weight loss surgery is currently recommended for people who have a body mass index greater than or equal to 35 regardless of obesity-related complication and may be considered for those with a BMI greater than or equal to 30. BMI is calculated by dividing the weight (in kilograms) by the height (in meters). In children and adolescents, weight loss surgery should be considered in those with a BMI greater than 120% of the 95th percentile and with a major comorbidity or in those with a BMI greater than 140% of the 95th percentile.
What impact does weight loss surgery have on bone?
Multiple studies in both adults and teenagers have demonstrated that sleeve gastrectomy, RYGB, and BPD-DS (but not gastric banding) are associated with a decrease in bone density, impaired bone structure, and reduced strength estimates over time (Beavers et al; Gagnon, Schafer; Misra, Bredella). The relative risk for fracture after RYGB and BPD-DS is reported to be 1.2-2.3 (that is, 20%-130% more than normal), whereas fracture risk after sleeve gastrectomy is still under study with some conflicting results. Fracture risk starts to increase 2-3 years after surgery and peaks at 5-plus years after surgery. Most of the data for fractures come from studies in adults. With the rising use of weight loss surgery, particularly sleeve gastrectomy, in teenagers, studies are needed to determine fracture risk in this younger age group, who also seem to experience marked reductions in bone density, altered bone structure, and reduced bone strength after bariatric surgery.
What contributes to impaired bone health after weight loss surgery?
The deleterious effect of weight loss surgery on bone appears to be caused by various factors, including the massive and rapid weight loss that occurs after surgery, because body weight has a mechanical loading effect on bone and otherwise promotes bone formation. Weight loss results in mechanical unloading and thus a decrease in bone density. Further, when weight loss occurs, there is loss of both muscle and fat mass, and the reduction in muscle mass is deleterious to bone.
Other possible causes of bone density reduction include reduced absorption of certain nutrients, such as calcium and vitamin D critical for bone mineralization, and alterations in certain hormones that impact bone health. These include increases in parathyroid hormone, which increases bone loss when secreted in excess; increases in PYY (a hormone that reduces bone formation); decreases in ghrelin (a hormone that typically increases bone formation), particularly after sleeve gastrectomy; and decreases in estrone (a kind of estrogen that like other estrogens prevents bone loss). Further, age and gender may modify the bone consequences of surgery as outcomes in postmenopausal women appear to be worse than in younger women and men.
Preventing bone density loss
Given the many benefits of weight loss surgery, what can we do to prevent this decrease in bone density after surgery? It’s important for people undergoing weight loss surgery to be cognizant of this potentially negative outcome and to take appropriate precautions to mitigate this concern.
We should monitor bone density after surgery with the help of dual energy x-ray absorptiometry, starting a few years after surgery, particularly in those who are at greatest risk for fracture, so that we can be proactive about addressing any severe bone loss that warrants pharmacologic intervention.
More general recommendations include optimizing intake of calcium (1,200-1,500 mg/d), vitamin D (2,000-3,000 IUs/d), and protein (60-75 g/d) via diet and/or as supplements and engaging in weight-bearing physical activity because this exerts mechanical loading effects on the skeleton leading to increased bone formation and also increases muscle mass over time, which is beneficial to bone. A progressive resistance training program has been demonstrated to have beneficial effects on bone, and measures should be taken to reduce the risk for falls, which increases after certain kinds of weight loss surgery, such as gastric bypass.
Meeting with a dietitian can help determine any other nutrients that need to be optimized.
Though many hormonal changes after surgery have been linked to reductions in bone density, there are still no recommended hormonal therapies at this time, and more work is required to determine whether specific pharmacologic therapies might help improve bone outcomes after surgery.
Dr. Misra is chief of the division of pediatric endocrinology, Mass General for Children; associate director, Harvard Catalyst Translation and Clinical Research Center; director, Pediatric Endocrine-Sports Endocrine-Neuroendocrine Lab, Mass General Hospital; and professor, department of pediatrics, Harvard Medical School, Boston.
A version of this article originally appeared on Medscape.com.
Currently, the two most common types of weight loss surgery performed include sleeve gastrectomy and Roux-en-Y gastric bypass (RYGB). Sleeve gastrectomy involves removing a large portion of the stomach so that its capacity is significantly decreased (to about 20%), reducing the ability to consume large quantities of food. Also, the procedure leads to marked reductions in ghrelin (an appetite-stimulating hormone), and some studies have reported increases in glucagon-like peptide 1 (GLP-1) and peptide YY (PYY), hormones that induce satiety. Gastric bypass involves creating a small stomach pouch and rerouting the small intestine so that it bypasses much of the stomach and also the upper portion of the small intestine. This reduces the amount of food that can be consumed at any time, increases levels of GLP-1 and PYY, and reduces absorption of nutrients with resultant weight loss. Less common bariatric surgeries include gastric banding and biliopancreatic diversion with duodenal switch (BPD-DS). Gastric banding involves placing a ring in the upper portion of the stomach, and the size of the pouch created can be altered by injecting more or less saline through a port inserted under the skin. BPD-DS includes sleeve gastrectomy, resection of a large section of the small intestine, and diversion of the pancreatic and biliary duct to a point below the junction of the ends of the resected gut.
Weight loss surgery is currently recommended for people who have a body mass index greater than or equal to 35 regardless of obesity-related complication and may be considered for those with a BMI greater than or equal to 30. BMI is calculated by dividing the weight (in kilograms) by the height (in meters). In children and adolescents, weight loss surgery should be considered in those with a BMI greater than 120% of the 95th percentile and with a major comorbidity or in those with a BMI greater than 140% of the 95th percentile.
What impact does weight loss surgery have on bone?
Multiple studies in both adults and teenagers have demonstrated that sleeve gastrectomy, RYGB, and BPD-DS (but not gastric banding) are associated with a decrease in bone density, impaired bone structure, and reduced strength estimates over time (Beavers et al; Gagnon, Schafer; Misra, Bredella). The relative risk for fracture after RYGB and BPD-DS is reported to be 1.2-2.3 (that is, 20%-130% more than normal), whereas fracture risk after sleeve gastrectomy is still under study with some conflicting results. Fracture risk starts to increase 2-3 years after surgery and peaks at 5-plus years after surgery. Most of the data for fractures come from studies in adults. With the rising use of weight loss surgery, particularly sleeve gastrectomy, in teenagers, studies are needed to determine fracture risk in this younger age group, who also seem to experience marked reductions in bone density, altered bone structure, and reduced bone strength after bariatric surgery.
What contributes to impaired bone health after weight loss surgery?
The deleterious effect of weight loss surgery on bone appears to be caused by various factors, including the massive and rapid weight loss that occurs after surgery, because body weight has a mechanical loading effect on bone and otherwise promotes bone formation. Weight loss results in mechanical unloading and thus a decrease in bone density. Further, when weight loss occurs, there is loss of both muscle and fat mass, and the reduction in muscle mass is deleterious to bone.
Other possible causes of bone density reduction include reduced absorption of certain nutrients, such as calcium and vitamin D critical for bone mineralization, and alterations in certain hormones that impact bone health. These include increases in parathyroid hormone, which increases bone loss when secreted in excess; increases in PYY (a hormone that reduces bone formation); decreases in ghrelin (a hormone that typically increases bone formation), particularly after sleeve gastrectomy; and decreases in estrone (a kind of estrogen that like other estrogens prevents bone loss). Further, age and gender may modify the bone consequences of surgery as outcomes in postmenopausal women appear to be worse than in younger women and men.
Preventing bone density loss
Given the many benefits of weight loss surgery, what can we do to prevent this decrease in bone density after surgery? It’s important for people undergoing weight loss surgery to be cognizant of this potentially negative outcome and to take appropriate precautions to mitigate this concern.
We should monitor bone density after surgery with the help of dual energy x-ray absorptiometry, starting a few years after surgery, particularly in those who are at greatest risk for fracture, so that we can be proactive about addressing any severe bone loss that warrants pharmacologic intervention.
More general recommendations include optimizing intake of calcium (1,200-1,500 mg/d), vitamin D (2,000-3,000 IUs/d), and protein (60-75 g/d) via diet and/or as supplements and engaging in weight-bearing physical activity because this exerts mechanical loading effects on the skeleton leading to increased bone formation and also increases muscle mass over time, which is beneficial to bone. A progressive resistance training program has been demonstrated to have beneficial effects on bone, and measures should be taken to reduce the risk for falls, which increases after certain kinds of weight loss surgery, such as gastric bypass.
Meeting with a dietitian can help determine any other nutrients that need to be optimized.
Though many hormonal changes after surgery have been linked to reductions in bone density, there are still no recommended hormonal therapies at this time, and more work is required to determine whether specific pharmacologic therapies might help improve bone outcomes after surgery.
Dr. Misra is chief of the division of pediatric endocrinology, Mass General for Children; associate director, Harvard Catalyst Translation and Clinical Research Center; director, Pediatric Endocrine-Sports Endocrine-Neuroendocrine Lab, Mass General Hospital; and professor, department of pediatrics, Harvard Medical School, Boston.
A version of this article originally appeared on Medscape.com.
Fibroid characteristics can help us anticipate postpartum hemorrhage
Fibroids, or leiomyomas, are noncancerous monoclonal tumors of the smooth muscle layer of the uterus. Fibroids occur more frequently in Black patients and their prevalence increases with age. The hormonally responsive nature of fibroids, frequently leading to growth with estrogen and progesterone exposure, makes them of particular concern during pregnancy.
Although most patients with fibroids do not have pregnancy complications directly attributable to their fibroids, prior studies have reported several associations, including painful degeneration, early pregnancy loss, preterm birth, placental abruption, malpresentation, and postpartum hemorrhage. Fibroids may predispose to uterine atony and hemorrhage by disrupting or impairing the synchronization and coordination of uterine contractions. Within the current body of literature, it remains less certain whether certain fibroid characteristics are associated with increased hemorrhage risk.
Prior studies evaluating the association between specific fibroid characteristics and postpartum hemorrhage have yielded inconsistent findings. In our study, we evaluated whether certain fibroid characteristics are associated with hemorrhage requiring blood transfusion. Specifically, our goal was to determine whether larger or more numerous fibroids increase the risk of transfusion.

This was a retrospective cohort study spanning 2019-2022. A total of 4,421 patients were included in this study. Fibroid characteristics were collected, including size, number, and location. Fibroid size was classified as small (< 5 cm), medium (5-10 cm), and large (> 10 cm).
In terms of number of fibroids, there was no significant increase in transfusions when comparing one fibroid to multiple fibroids. When assessing fibroid size, however, we did observe a significant incremental increase in rate of transfusions with increasing fibroid size. In terms of fibroid location, patients with fibroids in the lower uterine segment or cervix were about 1.5 times more likely to have hemorrhage requiring transfusion, compared with those without a fibroid in that location.
This study allows practitioners to better risk-stratify patients from the practical perspective of postpartum hemorrhage requiring transfusions. In pregnant patients with fibroids, the specific fibroid characteristics can help us better anticipate clinically significant postpartum hemorrhage. In such patients, it is important to document specific fibroid characteristics, especially the largest fibroid diameter and fibroid location in the lower uterine segment or cervix. This emphasizes the importance of careful sonographic evaluation and consistent documentation of fibroids in pregnant patients.
Our study helps guide more informed counseling and risk stratification in this population, with increasing risk according to fibroid size and location. Patients with high-risk features, that is, medium or large fibroids and those with fibroids located in the lower uterine segment or cervix, should thus receive counseling about their increased risk of hemorrhage. As providers, we can help ameliorate this risk by optimizing hemoglobin levels of those at increased risk prior to delivery, and by ensuring availability of appropriate resources at the time of delivery.
Dr. Yaghoubian is a maternal-fetal medicine fellow at North Shore University Hospital/Long Island Jewish Medical Center in Manhasset, N.Y., and will be joining the faculty at the same institution. Email Dr. Yaghoubian at [email protected].
Fibroids, or leiomyomas, are noncancerous monoclonal tumors of the smooth muscle layer of the uterus. Fibroids occur more frequently in Black patients and their prevalence increases with age. The hormonally responsive nature of fibroids, frequently leading to growth with estrogen and progesterone exposure, makes them of particular concern during pregnancy.
Although most patients with fibroids do not have pregnancy complications directly attributable to their fibroids, prior studies have reported several associations, including painful degeneration, early pregnancy loss, preterm birth, placental abruption, malpresentation, and postpartum hemorrhage. Fibroids may predispose to uterine atony and hemorrhage by disrupting or impairing the synchronization and coordination of uterine contractions. Within the current body of literature, it remains less certain whether certain fibroid characteristics are associated with increased hemorrhage risk.
Prior studies evaluating the association between specific fibroid characteristics and postpartum hemorrhage have yielded inconsistent findings. In our study, we evaluated whether certain fibroid characteristics are associated with hemorrhage requiring blood transfusion. Specifically, our goal was to determine whether larger or more numerous fibroids increase the risk of transfusion.
This was a retrospective cohort study spanning 2019-2022. A total of 4,421 patients were included in this study. Fibroid characteristics were collected, including size, number, and location. Fibroid size was classified as small (< 5 cm), medium (5-10 cm), and large (> 10 cm).
In terms of number of fibroids, there was no significant increase in transfusions when comparing one fibroid to multiple fibroids. When assessing fibroid size, however, we did observe a significant incremental increase in rate of transfusions with increasing fibroid size. In terms of fibroid location, patients with fibroids in the lower uterine segment or cervix were about 1.5 times more likely to have hemorrhage requiring transfusion, compared with those without a fibroid in that location.
This study allows practitioners to better risk-stratify patients from the practical perspective of postpartum hemorrhage requiring transfusions. In pregnant patients with fibroids, the specific fibroid characteristics can help us better anticipate clinically significant postpartum hemorrhage. In such patients, it is important to document specific fibroid characteristics, especially the largest fibroid diameter and fibroid location in the lower uterine segment or cervix. This emphasizes the importance of careful sonographic evaluation and consistent documentation of fibroids in pregnant patients.
Our study helps guide more informed counseling and risk stratification in this population, with increasing risk according to fibroid size and location. Patients with high-risk features, that is, medium or large fibroids and those with fibroids located in the lower uterine segment or cervix, should thus receive counseling about their increased risk of hemorrhage. As providers, we can help ameliorate this risk by optimizing hemoglobin levels of those at increased risk prior to delivery, and by ensuring availability of appropriate resources at the time of delivery.
Dr. Yaghoubian is a maternal-fetal medicine fellow at North Shore University Hospital/Long Island Jewish Medical Center in Manhasset, N.Y., and will be joining the faculty at the same institution. Email Dr. Yaghoubian at [email protected].
Fibroids, or leiomyomas, are noncancerous monoclonal tumors of the smooth muscle layer of the uterus. Fibroids occur more frequently in Black patients and their prevalence increases with age. The hormonally responsive nature of fibroids, frequently leading to growth with estrogen and progesterone exposure, makes them of particular concern during pregnancy.
Although most patients with fibroids do not have pregnancy complications directly attributable to their fibroids, prior studies have reported several associations, including painful degeneration, early pregnancy loss, preterm birth, placental abruption, malpresentation, and postpartum hemorrhage. Fibroids may predispose to uterine atony and hemorrhage by disrupting or impairing the synchronization and coordination of uterine contractions. Within the current body of literature, it remains less certain whether certain fibroid characteristics are associated with increased hemorrhage risk.
Prior studies evaluating the association between specific fibroid characteristics and postpartum hemorrhage have yielded inconsistent findings. In our study, we evaluated whether certain fibroid characteristics are associated with hemorrhage requiring blood transfusion. Specifically, our goal was to determine whether larger or more numerous fibroids increase the risk of transfusion.
This was a retrospective cohort study spanning 2019-2022. A total of 4,421 patients were included in this study. Fibroid characteristics were collected, including size, number, and location. Fibroid size was classified as small (< 5 cm), medium (5-10 cm), and large (> 10 cm).
In terms of number of fibroids, there was no significant increase in transfusions when comparing one fibroid to multiple fibroids. When assessing fibroid size, however, we did observe a significant incremental increase in rate of transfusions with increasing fibroid size. In terms of fibroid location, patients with fibroids in the lower uterine segment or cervix were about 1.5 times more likely to have hemorrhage requiring transfusion, compared with those without a fibroid in that location.
This study allows practitioners to better risk-stratify patients from the practical perspective of postpartum hemorrhage requiring transfusions. In pregnant patients with fibroids, the specific fibroid characteristics can help us better anticipate clinically significant postpartum hemorrhage. In such patients, it is important to document specific fibroid characteristics, especially the largest fibroid diameter and fibroid location in the lower uterine segment or cervix. This emphasizes the importance of careful sonographic evaluation and consistent documentation of fibroids in pregnant patients.
Our study helps guide more informed counseling and risk stratification in this population, with increasing risk according to fibroid size and location. Patients with high-risk features, that is, medium or large fibroids and those with fibroids located in the lower uterine segment or cervix, should thus receive counseling about their increased risk of hemorrhage. As providers, we can help ameliorate this risk by optimizing hemoglobin levels of those at increased risk prior to delivery, and by ensuring availability of appropriate resources at the time of delivery.
Dr. Yaghoubian is a maternal-fetal medicine fellow at North Shore University Hospital/Long Island Jewish Medical Center in Manhasset, N.Y., and will be joining the faculty at the same institution. Email Dr. Yaghoubian at [email protected].
Finding a home in psychiatry: A medical student’s story
Perched on a meditation cushion with the day’s first light creeping up the Himalayan foothills around me, I felt more at ease within myself than I could ever recall over my previous 19 years.

My immersion in daily conversations within the Tibetan monastic community on achieving a more harmonious relationship to our thoughts and feelings awoke a consideration of myself and my inner life in a way that I’d never truly contemplated before. These reflections gave me a vocabulary and a toolkit for navigating my own internal landscape that I have used ever since.
However, upon returning home, I was forced to acknowledge how fortunate I had been, and that these tools and the underlying spirit of inquiry are not commonplace in our society. Despite great strides in shifting views toward mental illness over the past few decades, our public discourse rarely captures the nuances of the mental health crisis that our culture has faced well before COVID-19 catalyzed even greater distress. We all pay the price of this cultural deficit to varying degrees, and I became captivated by the notion that things could be different.
I followed that thread of inquiry through the practices of Buddhist studies, massage therapy, yoga instruction, and refugee aid before coming to psychiatry as the unlikely yet ideal crucible for integrating my experiences in these spaces. Since arriving at medical school, however, my vision of myself as a psychiatrist has changed dramatically as my aspirations have collided with the realities of clinical experience and been tempered by the wisdom of mentors, colleagues, and patients, opening up a space for a deeper appreciation of what psychiatry might offer.
Clinical experience changes perspective
Short on clinical experience, I had previously imagined my future practice primarily as one of mindful listening and finding presence with each patient as a kind ear, supplemented by the ability to prescribe medication. Since then, working with patients has offered me insight into the ways in which my personality, perception, and potential access to a range of affective stances can serve as tools for skillfully developing the therapeutic encounter.
Moreover, “challenging” patients have taught me that my role is not always to offer unbounded empathetic support, but to potentially initiate compassionately tactful confrontation, shifting my sense of my role in the therapeutic relationship.
This is a lofty goal, which might entail modeling the successful navigation of potential ruptures and the subsequent repair of relationships so that they can live more adaptably in the world.
However, while I can support their envisioning of a realistic future for themselves and facilitate their acquisition of the tools needed to get there, my role is significant yet limited. This has been a hard truth to reckon with, but one that’s opened up pathways to greater empathy and a deeper understanding of each patient’s struggles. As a result, my view of pathology as a state has shifted to one of a dynamic process that emerges through the interaction of their genes, environment, life history, pharmacological supplements, psychodynamic tendencies, diet, and more.
Yet, while holding this reality of the complexities of mental illness, clinical decision-making often hinges on making binary choices regarding diagnoses, medications, and criteria for legal determinations. Developing this capacity to simultaneously practice different ways of knowing and sit with uncertainty excites me tremendously, not only equipping me to balance clinical practice with the demands of the modern health care system, but also nourishing the roots of a rich and ethical life.
Psychiatry calls to me for this expectation of sustaining an appropriate tension between uncertainty and decisiveness. It also inspires a deeper dive into the history of the field in order to learn the roots of its theories and perspectives so I can better understand how those inform contemporary practice in ways that are both helpful and harmful.
From individual to community
In tandem with this outer work of learning to appropriately position myself within individual patient relationships, the broader health care system, and the legacy of the field, I’ve also sought to develop a better understanding of how my own history, beliefs, and motivations shape my collaborative efforts.
Through my mindfulness practice and participation in exploratory psychoanalysis, I’ve caught glimpses of my own countertransference investments and opened up space for seeing how patients might experience me as a clinician. This has allowed for tuning in to my own response to them, identifying where in the typology of personality structures our reciprocal experiences might exist, and learning to manage those feelings to ultimately foster empathy through the interaction.
This has shifted my sense of the work from solely mindfully listening and thoughtfully responding to honing deliberate ways of both listening and responding in a way that is directly informed by the person sitting in front of me so I can best support them in creating change.
Given the responsibility inherent to this work, I have treated my medical education as an opportunity to build a foundation for stepping into this role. This has involved going beyond exploring these dynamics within individual clinician-patient relationships and carried over into my experiences with community-based research and program development. It has asked me to recognize the perceptual frames and prioritization of values that I bring to any given project.
This process has sharpened my aim of discovering each community’s understanding of their mental health needs so that I’m not implicitly imposing my own notions of psychological wholeness and “wellness” on others.
Working with San Diego’s Somali and Spanish-speaking populations has helped me to better understand each community’s own conceptualization of their strengths and needs, teaching me how to engage in reciprocal partnerships that honor each of our areas of expertise. Investing myself in medical school curricular reform represents the flip side of this coin, serving as an attempt to better understand my own medical community, how we think about health, and how we can best care for ourselves.
These experiences have offered opportunities to refine my skills in appreciative inquiry, coalition building, navigating institutional dynamics, and initiating and sustaining change within complex systems to carry the lessons of psychiatry beyond explicitly clinical spaces.
Toward integrative care
Ultimately, I view my community-based research and academic program development as outgrowths of my commitment to clinical psychiatry and my desire to learn how to provide people with the tools for changing their relationship to themselves, others, and their communities.
Equipped with formal medical training as the bedrock of this skill set, I have actively sought out opportunities to draw from practices that are outside the scope of the formal curriculum. These range from psychoanalysis and narrative medicine to cultural psychiatry and psychological anthropology, as well as my background in bodywork and mindfulness education. I’m eager to dive more fully into psychiatric practice as I work to integrate these disparate knowledge bases with the biomedical and psychodynamic views of the mind to develop a strengths-based practice that tends to patients’ bodies, minds, and spirits by bringing forth their own knowledge of themselves and their lives as they imagine what could be.
These realizations bring me back to that Himalayan sunrise more than a decade ago. They affirm that my heart lies with traversing disciplines to provide integrative psychiatric care in the community and developing infrastructure that supports these efforts. I’m filled with enthusiasm by the breadth of what psychiatry training offers as I continue expanding my capacity to support patients in this lifelong healing journey.
Alec Terrana is a rising fourth-year medical student at the University of California, San Diego, who intends to apply into psychiatry residency programs. He’s invested in exploring how we can more effectively conceptualize and measure mental health outcomes within San Diego’s Somali and Spanish-speaking communities, as well as advancing mindfulness and compassion training in undergraduate medical education. His professional interests also include implementation science, cultural psychiatry, psychodynamics, and strengthening public mental health infrastructure.
Perched on a meditation cushion with the day’s first light creeping up the Himalayan foothills around me, I felt more at ease within myself than I could ever recall over my previous 19 years.
My immersion in daily conversations within the Tibetan monastic community on achieving a more harmonious relationship to our thoughts and feelings awoke a consideration of myself and my inner life in a way that I’d never truly contemplated before. These reflections gave me a vocabulary and a toolkit for navigating my own internal landscape that I have used ever since.
However, upon returning home, I was forced to acknowledge how fortunate I had been, and that these tools and the underlying spirit of inquiry are not commonplace in our society. Despite great strides in shifting views toward mental illness over the past few decades, our public discourse rarely captures the nuances of the mental health crisis that our culture has faced well before COVID-19 catalyzed even greater distress. We all pay the price of this cultural deficit to varying degrees, and I became captivated by the notion that things could be different.
I followed that thread of inquiry through the practices of Buddhist studies, massage therapy, yoga instruction, and refugee aid before coming to psychiatry as the unlikely yet ideal crucible for integrating my experiences in these spaces. Since arriving at medical school, however, my vision of myself as a psychiatrist has changed dramatically as my aspirations have collided with the realities of clinical experience and been tempered by the wisdom of mentors, colleagues, and patients, opening up a space for a deeper appreciation of what psychiatry might offer.
Clinical experience changes perspective
Short on clinical experience, I had previously imagined my future practice primarily as one of mindful listening and finding presence with each patient as a kind ear, supplemented by the ability to prescribe medication. Since then, working with patients has offered me insight into the ways in which my personality, perception, and potential access to a range of affective stances can serve as tools for skillfully developing the therapeutic encounter.
Moreover, “challenging” patients have taught me that my role is not always to offer unbounded empathetic support, but to potentially initiate compassionately tactful confrontation, shifting my sense of my role in the therapeutic relationship.
This is a lofty goal, which might entail modeling the successful navigation of potential ruptures and the subsequent repair of relationships so that they can live more adaptably in the world.
However, while I can support their envisioning of a realistic future for themselves and facilitate their acquisition of the tools needed to get there, my role is significant yet limited. This has been a hard truth to reckon with, but one that’s opened up pathways to greater empathy and a deeper understanding of each patient’s struggles. As a result, my view of pathology as a state has shifted to one of a dynamic process that emerges through the interaction of their genes, environment, life history, pharmacological supplements, psychodynamic tendencies, diet, and more.
Yet, while holding this reality of the complexities of mental illness, clinical decision-making often hinges on making binary choices regarding diagnoses, medications, and criteria for legal determinations. Developing this capacity to simultaneously practice different ways of knowing and sit with uncertainty excites me tremendously, not only equipping me to balance clinical practice with the demands of the modern health care system, but also nourishing the roots of a rich and ethical life.
Psychiatry calls to me for this expectation of sustaining an appropriate tension between uncertainty and decisiveness. It also inspires a deeper dive into the history of the field in order to learn the roots of its theories and perspectives so I can better understand how those inform contemporary practice in ways that are both helpful and harmful.
From individual to community
In tandem with this outer work of learning to appropriately position myself within individual patient relationships, the broader health care system, and the legacy of the field, I’ve also sought to develop a better understanding of how my own history, beliefs, and motivations shape my collaborative efforts.
Through my mindfulness practice and participation in exploratory psychoanalysis, I’ve caught glimpses of my own countertransference investments and opened up space for seeing how patients might experience me as a clinician. This has allowed for tuning in to my own response to them, identifying where in the typology of personality structures our reciprocal experiences might exist, and learning to manage those feelings to ultimately foster empathy through the interaction.
This has shifted my sense of the work from solely mindfully listening and thoughtfully responding to honing deliberate ways of both listening and responding in a way that is directly informed by the person sitting in front of me so I can best support them in creating change.
Given the responsibility inherent to this work, I have treated my medical education as an opportunity to build a foundation for stepping into this role. This has involved going beyond exploring these dynamics within individual clinician-patient relationships and carried over into my experiences with community-based research and program development. It has asked me to recognize the perceptual frames and prioritization of values that I bring to any given project.
This process has sharpened my aim of discovering each community’s understanding of their mental health needs so that I’m not implicitly imposing my own notions of psychological wholeness and “wellness” on others.
Working with San Diego’s Somali and Spanish-speaking populations has helped me to better understand each community’s own conceptualization of their strengths and needs, teaching me how to engage in reciprocal partnerships that honor each of our areas of expertise. Investing myself in medical school curricular reform represents the flip side of this coin, serving as an attempt to better understand my own medical community, how we think about health, and how we can best care for ourselves.
These experiences have offered opportunities to refine my skills in appreciative inquiry, coalition building, navigating institutional dynamics, and initiating and sustaining change within complex systems to carry the lessons of psychiatry beyond explicitly clinical spaces.
Toward integrative care
Ultimately, I view my community-based research and academic program development as outgrowths of my commitment to clinical psychiatry and my desire to learn how to provide people with the tools for changing their relationship to themselves, others, and their communities.
Equipped with formal medical training as the bedrock of this skill set, I have actively sought out opportunities to draw from practices that are outside the scope of the formal curriculum. These range from psychoanalysis and narrative medicine to cultural psychiatry and psychological anthropology, as well as my background in bodywork and mindfulness education. I’m eager to dive more fully into psychiatric practice as I work to integrate these disparate knowledge bases with the biomedical and psychodynamic views of the mind to develop a strengths-based practice that tends to patients’ bodies, minds, and spirits by bringing forth their own knowledge of themselves and their lives as they imagine what could be.
These realizations bring me back to that Himalayan sunrise more than a decade ago. They affirm that my heart lies with traversing disciplines to provide integrative psychiatric care in the community and developing infrastructure that supports these efforts. I’m filled with enthusiasm by the breadth of what psychiatry training offers as I continue expanding my capacity to support patients in this lifelong healing journey.
Alec Terrana is a rising fourth-year medical student at the University of California, San Diego, who intends to apply into psychiatry residency programs. He’s invested in exploring how we can more effectively conceptualize and measure mental health outcomes within San Diego’s Somali and Spanish-speaking communities, as well as advancing mindfulness and compassion training in undergraduate medical education. His professional interests also include implementation science, cultural psychiatry, psychodynamics, and strengthening public mental health infrastructure.
Perched on a meditation cushion with the day’s first light creeping up the Himalayan foothills around me, I felt more at ease within myself than I could ever recall over my previous 19 years.
My immersion in daily conversations within the Tibetan monastic community on achieving a more harmonious relationship to our thoughts and feelings awoke a consideration of myself and my inner life in a way that I’d never truly contemplated before. These reflections gave me a vocabulary and a toolkit for navigating my own internal landscape that I have used ever since.
However, upon returning home, I was forced to acknowledge how fortunate I had been, and that these tools and the underlying spirit of inquiry are not commonplace in our society. Despite great strides in shifting views toward mental illness over the past few decades, our public discourse rarely captures the nuances of the mental health crisis that our culture has faced well before COVID-19 catalyzed even greater distress. We all pay the price of this cultural deficit to varying degrees, and I became captivated by the notion that things could be different.
I followed that thread of inquiry through the practices of Buddhist studies, massage therapy, yoga instruction, and refugee aid before coming to psychiatry as the unlikely yet ideal crucible for integrating my experiences in these spaces. Since arriving at medical school, however, my vision of myself as a psychiatrist has changed dramatically as my aspirations have collided with the realities of clinical experience and been tempered by the wisdom of mentors, colleagues, and patients, opening up a space for a deeper appreciation of what psychiatry might offer.
Clinical experience changes perspective
Short on clinical experience, I had previously imagined my future practice primarily as one of mindful listening and finding presence with each patient as a kind ear, supplemented by the ability to prescribe medication. Since then, working with patients has offered me insight into the ways in which my personality, perception, and potential access to a range of affective stances can serve as tools for skillfully developing the therapeutic encounter.
Moreover, “challenging” patients have taught me that my role is not always to offer unbounded empathetic support, but to potentially initiate compassionately tactful confrontation, shifting my sense of my role in the therapeutic relationship.
This is a lofty goal, which might entail modeling the successful navigation of potential ruptures and the subsequent repair of relationships so that they can live more adaptably in the world.
However, while I can support their envisioning of a realistic future for themselves and facilitate their acquisition of the tools needed to get there, my role is significant yet limited. This has been a hard truth to reckon with, but one that’s opened up pathways to greater empathy and a deeper understanding of each patient’s struggles. As a result, my view of pathology as a state has shifted to one of a dynamic process that emerges through the interaction of their genes, environment, life history, pharmacological supplements, psychodynamic tendencies, diet, and more.
Yet, while holding this reality of the complexities of mental illness, clinical decision-making often hinges on making binary choices regarding diagnoses, medications, and criteria for legal determinations. Developing this capacity to simultaneously practice different ways of knowing and sit with uncertainty excites me tremendously, not only equipping me to balance clinical practice with the demands of the modern health care system, but also nourishing the roots of a rich and ethical life.
Psychiatry calls to me for this expectation of sustaining an appropriate tension between uncertainty and decisiveness. It also inspires a deeper dive into the history of the field in order to learn the roots of its theories and perspectives so I can better understand how those inform contemporary practice in ways that are both helpful and harmful.
From individual to community
In tandem with this outer work of learning to appropriately position myself within individual patient relationships, the broader health care system, and the legacy of the field, I’ve also sought to develop a better understanding of how my own history, beliefs, and motivations shape my collaborative efforts.
Through my mindfulness practice and participation in exploratory psychoanalysis, I’ve caught glimpses of my own countertransference investments and opened up space for seeing how patients might experience me as a clinician. This has allowed for tuning in to my own response to them, identifying where in the typology of personality structures our reciprocal experiences might exist, and learning to manage those feelings to ultimately foster empathy through the interaction.
This has shifted my sense of the work from solely mindfully listening and thoughtfully responding to honing deliberate ways of both listening and responding in a way that is directly informed by the person sitting in front of me so I can best support them in creating change.
Given the responsibility inherent to this work, I have treated my medical education as an opportunity to build a foundation for stepping into this role. This has involved going beyond exploring these dynamics within individual clinician-patient relationships and carried over into my experiences with community-based research and program development. It has asked me to recognize the perceptual frames and prioritization of values that I bring to any given project.
This process has sharpened my aim of discovering each community’s understanding of their mental health needs so that I’m not implicitly imposing my own notions of psychological wholeness and “wellness” on others.
Working with San Diego’s Somali and Spanish-speaking populations has helped me to better understand each community’s own conceptualization of their strengths and needs, teaching me how to engage in reciprocal partnerships that honor each of our areas of expertise. Investing myself in medical school curricular reform represents the flip side of this coin, serving as an attempt to better understand my own medical community, how we think about health, and how we can best care for ourselves.
These experiences have offered opportunities to refine my skills in appreciative inquiry, coalition building, navigating institutional dynamics, and initiating and sustaining change within complex systems to carry the lessons of psychiatry beyond explicitly clinical spaces.
Toward integrative care
Ultimately, I view my community-based research and academic program development as outgrowths of my commitment to clinical psychiatry and my desire to learn how to provide people with the tools for changing their relationship to themselves, others, and their communities.
Equipped with formal medical training as the bedrock of this skill set, I have actively sought out opportunities to draw from practices that are outside the scope of the formal curriculum. These range from psychoanalysis and narrative medicine to cultural psychiatry and psychological anthropology, as well as my background in bodywork and mindfulness education. I’m eager to dive more fully into psychiatric practice as I work to integrate these disparate knowledge bases with the biomedical and psychodynamic views of the mind to develop a strengths-based practice that tends to patients’ bodies, minds, and spirits by bringing forth their own knowledge of themselves and their lives as they imagine what could be.
These realizations bring me back to that Himalayan sunrise more than a decade ago. They affirm that my heart lies with traversing disciplines to provide integrative psychiatric care in the community and developing infrastructure that supports these efforts. I’m filled with enthusiasm by the breadth of what psychiatry training offers as I continue expanding my capacity to support patients in this lifelong healing journey.
Alec Terrana is a rising fourth-year medical student at the University of California, San Diego, who intends to apply into psychiatry residency programs. He’s invested in exploring how we can more effectively conceptualize and measure mental health outcomes within San Diego’s Somali and Spanish-speaking communities, as well as advancing mindfulness and compassion training in undergraduate medical education. His professional interests also include implementation science, cultural psychiatry, psychodynamics, and strengthening public mental health infrastructure.
What’s in a drug name?
My use of drug names is a mixed bag of terms.
In medical school we learn drugs by their generic names, but it doesn’t take long before we realize that each has both a generic name and one (or more) brand names. I suppose there’s also the chemical names, but no one outside the lab uses those. They’re waaaaay too long.
There is, for better or worse, a lot of variability in this. The purists (almost always academics, or cardiologists, or academic cardiologists) insist on generic names only. In their notes, conversations, presentations, whatever. If you’re a medical student or resident under them, you learn fast not to use the brand name.
After 30 years of doing this ... I don’t care. My notes are a mishmash of both.
Let’s face it, brand names are generally shorter and easier to type, spell, and pronounce than the generic names. I still need to know both, but when I’m writing up a note Keppra is far easier than levetiracetam. And most patients find the brand names a lot easier to say and remember.
An even weirder point, which is my own, is that one of my teaching attendings insisted that we capitalize both generic and brand names while on his rotation. Why? He never explained that, but he was pretty insistent. Now, for whatever reason, the habit has stuck with me. I’m sure the cardiologist down the hall would love to send my notes back, heavily marked up with red ink.
There’s even a weird subdivisions in this: Aspirin is a brand name by Bayer. Shouldn’t it be capitalized in our notes? But it isn’t, and to make things more confusing that varies by country. Why? (if you’re curious, it’s a strange combination of 100-year-old patent claims, generic trademark rulings, and also what country you’re in, whether it was involved in World War I, and, if so, which side. Really).
So the medical lists in my notes are certainly understandable, though aren’t going to score me any points for academic correctness. Not that I care. As a medical Shakespeare might have written, Imitrex, Onzetra, Zembrace, Tosymra, Sumavel, Alsuma, Imigran, Migraitan, and Zecuity ... are still sumatriptan by any other name.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
My use of drug names is a mixed bag of terms.
In medical school we learn drugs by their generic names, but it doesn’t take long before we realize that each has both a generic name and one (or more) brand names. I suppose there’s also the chemical names, but no one outside the lab uses those. They’re waaaaay too long.
There is, for better or worse, a lot of variability in this. The purists (almost always academics, or cardiologists, or academic cardiologists) insist on generic names only. In their notes, conversations, presentations, whatever. If you’re a medical student or resident under them, you learn fast not to use the brand name.
After 30 years of doing this ... I don’t care. My notes are a mishmash of both.
Let’s face it, brand names are generally shorter and easier to type, spell, and pronounce than the generic names. I still need to know both, but when I’m writing up a note Keppra is far easier than levetiracetam. And most patients find the brand names a lot easier to say and remember.
An even weirder point, which is my own, is that one of my teaching attendings insisted that we capitalize both generic and brand names while on his rotation. Why? He never explained that, but he was pretty insistent. Now, for whatever reason, the habit has stuck with me. I’m sure the cardiologist down the hall would love to send my notes back, heavily marked up with red ink.
There’s even a weird subdivisions in this: Aspirin is a brand name by Bayer. Shouldn’t it be capitalized in our notes? But it isn’t, and to make things more confusing that varies by country. Why? (if you’re curious, it’s a strange combination of 100-year-old patent claims, generic trademark rulings, and also what country you’re in, whether it was involved in World War I, and, if so, which side. Really).
So the medical lists in my notes are certainly understandable, though aren’t going to score me any points for academic correctness. Not that I care. As a medical Shakespeare might have written, Imitrex, Onzetra, Zembrace, Tosymra, Sumavel, Alsuma, Imigran, Migraitan, and Zecuity ... are still sumatriptan by any other name.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
My use of drug names is a mixed bag of terms.
In medical school we learn drugs by their generic names, but it doesn’t take long before we realize that each has both a generic name and one (or more) brand names. I suppose there’s also the chemical names, but no one outside the lab uses those. They’re waaaaay too long.
There is, for better or worse, a lot of variability in this. The purists (almost always academics, or cardiologists, or academic cardiologists) insist on generic names only. In their notes, conversations, presentations, whatever. If you’re a medical student or resident under them, you learn fast not to use the brand name.
After 30 years of doing this ... I don’t care. My notes are a mishmash of both.
Let’s face it, brand names are generally shorter and easier to type, spell, and pronounce than the generic names. I still need to know both, but when I’m writing up a note Keppra is far easier than levetiracetam. And most patients find the brand names a lot easier to say and remember.
An even weirder point, which is my own, is that one of my teaching attendings insisted that we capitalize both generic and brand names while on his rotation. Why? He never explained that, but he was pretty insistent. Now, for whatever reason, the habit has stuck with me. I’m sure the cardiologist down the hall would love to send my notes back, heavily marked up with red ink.
There’s even a weird subdivisions in this: Aspirin is a brand name by Bayer. Shouldn’t it be capitalized in our notes? But it isn’t, and to make things more confusing that varies by country. Why? (if you’re curious, it’s a strange combination of 100-year-old patent claims, generic trademark rulings, and also what country you’re in, whether it was involved in World War I, and, if so, which side. Really).
So the medical lists in my notes are certainly understandable, though aren’t going to score me any points for academic correctness. Not that I care. As a medical Shakespeare might have written, Imitrex, Onzetra, Zembrace, Tosymra, Sumavel, Alsuma, Imigran, Migraitan, and Zecuity ... are still sumatriptan by any other name.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.