User login
How mental health care would look under a Trump vs. Biden administration
The COVID-19 pandemic is one of the most pressing public health challenges the United States has ever faced, and the resulting financial ruin and social isolation are creating a mental health pandemic that will continue well after COVID-19 lockdowns end. To understand which presidential candidate would best lead the mental health recovery, we identified three of the most critical issues in mental health and compared the plans of the two candidates.
Fighting the opioid epidemic

Over the last several years, the opioid epidemic has devastated American families and communities. Prior to the pandemic, drug overdoses were the leading cause of death for American adults under 50 years of age. The effects of COVID-19–enabled overdose deaths to rise even higher. Multiple elements of the pandemic – isolation, unemployment, and increased anxiety and depression – make those struggling with substance use even more vulnerable, and immediate and comprehensive action is needed to address this national tragedy.
Donald J. Trump: President Trump has been vocal and active in addressing this problem since he took office. One of the Trump administration’s successes is launching the Opioid and Drug Abuse Commission and rolling out a five-point strategy built around improving services, data, research, overdose-reversing drugs, and pain management. Last year, the Trump administration funded $10 billion over 5 years to combat both the opioid epidemic and mental health issues by building upon the 21st Century CURES Act. However, in this same budget, the administration proposed cutting funding by $600 million for SAMHSA, the Substance Abuse and Mental Health Services Administration, which is the top government agency for addressing and providing care for substance use.
President Trump also created an assistant secretary for mental health and substance use position in the Department of Health & Human Services, and appointed Elinore F. McCance-Katz, MD, PhD, a psychiatrist with a strong track record on fighting opioid abuse in Rhode Island, to the post.
Joe Biden: Former Vice President Biden emphasizes that substance use is “a disease of the brain,” refuting the long-held misconception that addiction is an issue of willpower. This stigmatization is very personal given that his own son Hunter reportedly suffered through mental health and substance use issues since his teenage years. However, Biden also had a major role in pushing forward the federal “war on drugs,” including his role in crafting the “Len Bias law.”

Mr. Biden has since released a multifaceted plan for reducing substance use, aiming to make prevention and treatment services more available through a $125 billion federal investment. There are also measures to hold pharmaceutical companies accountable for triggering the crisis, stop the flow of fentanyl to the United States, and restrict incentive payments from manufacturers to doctors so as to limit the dosing and usage of powerful opioids.
Accessing health care
One of the main dividing lines in this election has been the battle to either gut or build upon the Affordable Care Act (ACA). This will have deep ramifications on people’s access to health mental health services. Since COVID-19 started, more than 50% of Americans have reported worsening mental health. This makes it crucial that each candidate’s mental health plan is judged by how they would expand access to insurance, address unenforced parity laws, and protect those who have a mental health disorder as a preexisting condition.
Mr. Trump: Following a failed Senate vote to repeal this law, the Trump administration took a piecemeal approach to dismantling the ACA that included removing the individual mandate, enabling states to introduce Medicaid work requirements, and reducing cost-sharing subsidies to insurers.
If a re-elected Trump administration pursued a complete repeal of the ACA law, many individuals with previous access to mental health and substance abuse treatment via Medicaid expansion may lose access altogether. In addition, key mechanisms aimed at making sure that mental health services are covered by private health plans may be lost, which could undermine policies to address opioids and suicide. On the other hand, the Trump administration’s move during the pandemic to expand telemedicine services has also expanded access to mental health services.
Mr. Biden: Mr. Biden’s plan would build upon the ACA by working to achieve parity between the treatment of mental health and physical health. The ACA itself strengthened the Mental Health Parity and Addiction Equity Act (federal parity law), which Mr. Biden championed as vice president, by mandating that all private insurance cover mental health and substance abuse treatment. This act still exempts some health plans, such as larger employers; and many insurers have used loopholes in the policy to illegally deny what could be life-saving coverage.
It follows that those who can afford Mr. Biden’s proposed public option Medicare buy-in would receive more comprehensive mental health benefits. He also says he would invest in school and college mental health professionals, an important opportunity for early intervention given 75% of lifetime mental illness starts by age 24 years. While Mr. Biden has not stated a specific plan for addressing minority groups, whose mental health has been disproportionately affected by COVID-19, he has acknowledged that this unmet need should be targeted.
Addressing suicide
More than 3,000 Americans attempt suicide every day. Suicide is the second leading cause of death for America’s youth and one of the top 10 leading causes of death across the population. Numerous strategies are necessary to address suicide, but one of the most decisive is gun control. Gun violence is inextricably tied to suicide: States where gun prevalence is higher see about four times the number of suicides because of guns, whereas nonfirearm suicide rates are the same as those seen elsewhere. In 2017, of the nearly 40,000 people who died of gun violence, 60% were attributable to suicides. Since the pandemic started, there have been increases in reported suicidal thoughts and a nearly 1,000% increase in use of the national crisis hotline. This is especially concerning given the uptick during the pandemic of gun purchases; as of September, more guns have been purchased this year than any year before.
Mr. Trump: Prior to coronavirus, the Trump administration was unwilling to enact gun control legislation. In early 2017, Mr. Trump removed an Obama-era bill that would have expanded the background check database. It would have added those deemed legally unfit to handle their own funds and those who received Social Security funds for mental health reasons. During the lockdown, the administration made an advisory ruling declaring gun shops as essential businesses that states should keep open.
Mr. Biden: The former vice president has a history of supporting gun control measures in his time as a senator and vice president. In the Senate, Mr. Biden supported both the Brady handgun bill in 1993 and a ban on assault weapons in 1994. As vice president, he was tasked by President Obama to push for a renewed assault weapons ban and a background check bill (Manchin-Toomey bill).
During his 2020 presidential campaign, Mr. Biden has suggested creating universal background checks and reinstating bans on assault rifle sales. He has said that he is also open to having a federal buyback program for assault rifles from gun owners.
Why this matters
The winner of the 2020 election will lead an electorate that is reeling from the health, economic, and social consequences COVID-19. The next administration needs to act swiftly to address the mental health pandemic and have a keen awareness of what is ahead. As Americans make their voting decision, consider who has the best plans not only to contain the virus but also the mental health crises that are ravaging our nation.
Dr. Vasan is a clinical assistant professor of psychiatry at Stanford (Calif.) University, where she is founder and executive director of Brainstorm: The Stanford Lab for Mental Health Innovation. She also serves as chief medical officer of Real, and chair of the American Psychiatric Association Committee on Innovation. Dr. Vasan has no conflicts of interest. Mr. Agbafe is a fellow at Stanford Brainstorm and a first-year medical student at the University of Michigan, Ann Arbor. He has no conflicts of interest. Ms. Li is a policy intern at Stanford Brainstorm and an undergraduate student in the department of economics at the University of California, Berkeley. She has no conflicts of interest.
The COVID-19 pandemic is one of the most pressing public health challenges the United States has ever faced, and the resulting financial ruin and social isolation are creating a mental health pandemic that will continue well after COVID-19 lockdowns end. To understand which presidential candidate would best lead the mental health recovery, we identified three of the most critical issues in mental health and compared the plans of the two candidates.
Fighting the opioid epidemic
Over the last several years, the opioid epidemic has devastated American families and communities. Prior to the pandemic, drug overdoses were the leading cause of death for American adults under 50 years of age. The effects of COVID-19–enabled overdose deaths to rise even higher. Multiple elements of the pandemic – isolation, unemployment, and increased anxiety and depression – make those struggling with substance use even more vulnerable, and immediate and comprehensive action is needed to address this national tragedy.
Donald J. Trump: President Trump has been vocal and active in addressing this problem since he took office. One of the Trump administration’s successes is launching the Opioid and Drug Abuse Commission and rolling out a five-point strategy built around improving services, data, research, overdose-reversing drugs, and pain management. Last year, the Trump administration funded $10 billion over 5 years to combat both the opioid epidemic and mental health issues by building upon the 21st Century CURES Act. However, in this same budget, the administration proposed cutting funding by $600 million for SAMHSA, the Substance Abuse and Mental Health Services Administration, which is the top government agency for addressing and providing care for substance use.
President Trump also created an assistant secretary for mental health and substance use position in the Department of Health & Human Services, and appointed Elinore F. McCance-Katz, MD, PhD, a psychiatrist with a strong track record on fighting opioid abuse in Rhode Island, to the post.
Joe Biden: Former Vice President Biden emphasizes that substance use is “a disease of the brain,” refuting the long-held misconception that addiction is an issue of willpower. This stigmatization is very personal given that his own son Hunter reportedly suffered through mental health and substance use issues since his teenage years. However, Biden also had a major role in pushing forward the federal “war on drugs,” including his role in crafting the “Len Bias law.”
Mr. Biden has since released a multifaceted plan for reducing substance use, aiming to make prevention and treatment services more available through a $125 billion federal investment. There are also measures to hold pharmaceutical companies accountable for triggering the crisis, stop the flow of fentanyl to the United States, and restrict incentive payments from manufacturers to doctors so as to limit the dosing and usage of powerful opioids.
Accessing health care
One of the main dividing lines in this election has been the battle to either gut or build upon the Affordable Care Act (ACA). This will have deep ramifications on people’s access to health mental health services. Since COVID-19 started, more than 50% of Americans have reported worsening mental health. This makes it crucial that each candidate’s mental health plan is judged by how they would expand access to insurance, address unenforced parity laws, and protect those who have a mental health disorder as a preexisting condition.
Mr. Trump: Following a failed Senate vote to repeal this law, the Trump administration took a piecemeal approach to dismantling the ACA that included removing the individual mandate, enabling states to introduce Medicaid work requirements, and reducing cost-sharing subsidies to insurers.
If a re-elected Trump administration pursued a complete repeal of the ACA law, many individuals with previous access to mental health and substance abuse treatment via Medicaid expansion may lose access altogether. In addition, key mechanisms aimed at making sure that mental health services are covered by private health plans may be lost, which could undermine policies to address opioids and suicide. On the other hand, the Trump administration’s move during the pandemic to expand telemedicine services has also expanded access to mental health services.
Mr. Biden: Mr. Biden’s plan would build upon the ACA by working to achieve parity between the treatment of mental health and physical health. The ACA itself strengthened the Mental Health Parity and Addiction Equity Act (federal parity law), which Mr. Biden championed as vice president, by mandating that all private insurance cover mental health and substance abuse treatment. This act still exempts some health plans, such as larger employers; and many insurers have used loopholes in the policy to illegally deny what could be life-saving coverage.
It follows that those who can afford Mr. Biden’s proposed public option Medicare buy-in would receive more comprehensive mental health benefits. He also says he would invest in school and college mental health professionals, an important opportunity for early intervention given 75% of lifetime mental illness starts by age 24 years. While Mr. Biden has not stated a specific plan for addressing minority groups, whose mental health has been disproportionately affected by COVID-19, he has acknowledged that this unmet need should be targeted.
Addressing suicide
More than 3,000 Americans attempt suicide every day. Suicide is the second leading cause of death for America’s youth and one of the top 10 leading causes of death across the population. Numerous strategies are necessary to address suicide, but one of the most decisive is gun control. Gun violence is inextricably tied to suicide: States where gun prevalence is higher see about four times the number of suicides because of guns, whereas nonfirearm suicide rates are the same as those seen elsewhere. In 2017, of the nearly 40,000 people who died of gun violence, 60% were attributable to suicides. Since the pandemic started, there have been increases in reported suicidal thoughts and a nearly 1,000% increase in use of the national crisis hotline. This is especially concerning given the uptick during the pandemic of gun purchases; as of September, more guns have been purchased this year than any year before.
Mr. Trump: Prior to coronavirus, the Trump administration was unwilling to enact gun control legislation. In early 2017, Mr. Trump removed an Obama-era bill that would have expanded the background check database. It would have added those deemed legally unfit to handle their own funds and those who received Social Security funds for mental health reasons. During the lockdown, the administration made an advisory ruling declaring gun shops as essential businesses that states should keep open.
Mr. Biden: The former vice president has a history of supporting gun control measures in his time as a senator and vice president. In the Senate, Mr. Biden supported both the Brady handgun bill in 1993 and a ban on assault weapons in 1994. As vice president, he was tasked by President Obama to push for a renewed assault weapons ban and a background check bill (Manchin-Toomey bill).
During his 2020 presidential campaign, Mr. Biden has suggested creating universal background checks and reinstating bans on assault rifle sales. He has said that he is also open to having a federal buyback program for assault rifles from gun owners.
Why this matters
The winner of the 2020 election will lead an electorate that is reeling from the health, economic, and social consequences COVID-19. The next administration needs to act swiftly to address the mental health pandemic and have a keen awareness of what is ahead. As Americans make their voting decision, consider who has the best plans not only to contain the virus but also the mental health crises that are ravaging our nation.
Dr. Vasan is a clinical assistant professor of psychiatry at Stanford (Calif.) University, where she is founder and executive director of Brainstorm: The Stanford Lab for Mental Health Innovation. She also serves as chief medical officer of Real, and chair of the American Psychiatric Association Committee on Innovation. Dr. Vasan has no conflicts of interest. Mr. Agbafe is a fellow at Stanford Brainstorm and a first-year medical student at the University of Michigan, Ann Arbor. He has no conflicts of interest. Ms. Li is a policy intern at Stanford Brainstorm and an undergraduate student in the department of economics at the University of California, Berkeley. She has no conflicts of interest.
The COVID-19 pandemic is one of the most pressing public health challenges the United States has ever faced, and the resulting financial ruin and social isolation are creating a mental health pandemic that will continue well after COVID-19 lockdowns end. To understand which presidential candidate would best lead the mental health recovery, we identified three of the most critical issues in mental health and compared the plans of the two candidates.
Fighting the opioid epidemic
Over the last several years, the opioid epidemic has devastated American families and communities. Prior to the pandemic, drug overdoses were the leading cause of death for American adults under 50 years of age. The effects of COVID-19–enabled overdose deaths to rise even higher. Multiple elements of the pandemic – isolation, unemployment, and increased anxiety and depression – make those struggling with substance use even more vulnerable, and immediate and comprehensive action is needed to address this national tragedy.
Donald J. Trump: President Trump has been vocal and active in addressing this problem since he took office. One of the Trump administration’s successes is launching the Opioid and Drug Abuse Commission and rolling out a five-point strategy built around improving services, data, research, overdose-reversing drugs, and pain management. Last year, the Trump administration funded $10 billion over 5 years to combat both the opioid epidemic and mental health issues by building upon the 21st Century CURES Act. However, in this same budget, the administration proposed cutting funding by $600 million for SAMHSA, the Substance Abuse and Mental Health Services Administration, which is the top government agency for addressing and providing care for substance use.
President Trump also created an assistant secretary for mental health and substance use position in the Department of Health & Human Services, and appointed Elinore F. McCance-Katz, MD, PhD, a psychiatrist with a strong track record on fighting opioid abuse in Rhode Island, to the post.
Joe Biden: Former Vice President Biden emphasizes that substance use is “a disease of the brain,” refuting the long-held misconception that addiction is an issue of willpower. This stigmatization is very personal given that his own son Hunter reportedly suffered through mental health and substance use issues since his teenage years. However, Biden also had a major role in pushing forward the federal “war on drugs,” including his role in crafting the “Len Bias law.”
Mr. Biden has since released a multifaceted plan for reducing substance use, aiming to make prevention and treatment services more available through a $125 billion federal investment. There are also measures to hold pharmaceutical companies accountable for triggering the crisis, stop the flow of fentanyl to the United States, and restrict incentive payments from manufacturers to doctors so as to limit the dosing and usage of powerful opioids.
Accessing health care
One of the main dividing lines in this election has been the battle to either gut or build upon the Affordable Care Act (ACA). This will have deep ramifications on people’s access to health mental health services. Since COVID-19 started, more than 50% of Americans have reported worsening mental health. This makes it crucial that each candidate’s mental health plan is judged by how they would expand access to insurance, address unenforced parity laws, and protect those who have a mental health disorder as a preexisting condition.
Mr. Trump: Following a failed Senate vote to repeal this law, the Trump administration took a piecemeal approach to dismantling the ACA that included removing the individual mandate, enabling states to introduce Medicaid work requirements, and reducing cost-sharing subsidies to insurers.
If a re-elected Trump administration pursued a complete repeal of the ACA law, many individuals with previous access to mental health and substance abuse treatment via Medicaid expansion may lose access altogether. In addition, key mechanisms aimed at making sure that mental health services are covered by private health plans may be lost, which could undermine policies to address opioids and suicide. On the other hand, the Trump administration’s move during the pandemic to expand telemedicine services has also expanded access to mental health services.
Mr. Biden: Mr. Biden’s plan would build upon the ACA by working to achieve parity between the treatment of mental health and physical health. The ACA itself strengthened the Mental Health Parity and Addiction Equity Act (federal parity law), which Mr. Biden championed as vice president, by mandating that all private insurance cover mental health and substance abuse treatment. This act still exempts some health plans, such as larger employers; and many insurers have used loopholes in the policy to illegally deny what could be life-saving coverage.
It follows that those who can afford Mr. Biden’s proposed public option Medicare buy-in would receive more comprehensive mental health benefits. He also says he would invest in school and college mental health professionals, an important opportunity for early intervention given 75% of lifetime mental illness starts by age 24 years. While Mr. Biden has not stated a specific plan for addressing minority groups, whose mental health has been disproportionately affected by COVID-19, he has acknowledged that this unmet need should be targeted.
Addressing suicide
More than 3,000 Americans attempt suicide every day. Suicide is the second leading cause of death for America’s youth and one of the top 10 leading causes of death across the population. Numerous strategies are necessary to address suicide, but one of the most decisive is gun control. Gun violence is inextricably tied to suicide: States where gun prevalence is higher see about four times the number of suicides because of guns, whereas nonfirearm suicide rates are the same as those seen elsewhere. In 2017, of the nearly 40,000 people who died of gun violence, 60% were attributable to suicides. Since the pandemic started, there have been increases in reported suicidal thoughts and a nearly 1,000% increase in use of the national crisis hotline. This is especially concerning given the uptick during the pandemic of gun purchases; as of September, more guns have been purchased this year than any year before.
Mr. Trump: Prior to coronavirus, the Trump administration was unwilling to enact gun control legislation. In early 2017, Mr. Trump removed an Obama-era bill that would have expanded the background check database. It would have added those deemed legally unfit to handle their own funds and those who received Social Security funds for mental health reasons. During the lockdown, the administration made an advisory ruling declaring gun shops as essential businesses that states should keep open.
Mr. Biden: The former vice president has a history of supporting gun control measures in his time as a senator and vice president. In the Senate, Mr. Biden supported both the Brady handgun bill in 1993 and a ban on assault weapons in 1994. As vice president, he was tasked by President Obama to push for a renewed assault weapons ban and a background check bill (Manchin-Toomey bill).
During his 2020 presidential campaign, Mr. Biden has suggested creating universal background checks and reinstating bans on assault rifle sales. He has said that he is also open to having a federal buyback program for assault rifles from gun owners.
Why this matters
The winner of the 2020 election will lead an electorate that is reeling from the health, economic, and social consequences COVID-19. The next administration needs to act swiftly to address the mental health pandemic and have a keen awareness of what is ahead. As Americans make their voting decision, consider who has the best plans not only to contain the virus but also the mental health crises that are ravaging our nation.
Dr. Vasan is a clinical assistant professor of psychiatry at Stanford (Calif.) University, where she is founder and executive director of Brainstorm: The Stanford Lab for Mental Health Innovation. She also serves as chief medical officer of Real, and chair of the American Psychiatric Association Committee on Innovation. Dr. Vasan has no conflicts of interest. Mr. Agbafe is a fellow at Stanford Brainstorm and a first-year medical student at the University of Michigan, Ann Arbor. He has no conflicts of interest. Ms. Li is a policy intern at Stanford Brainstorm and an undergraduate student in the department of economics at the University of California, Berkeley. She has no conflicts of interest.
Understand the legal implications of telehealth medicine
Telehealth has been steadily gaining mainstream use throughout the last decade, but the practice was recently shoved, almost overnight, into the forefront of the health care profession. Telehealth is now used more frequently by medical groups and physicians than ever before. General reports before the COVID-19 pandemic approximated 90% of health care organizations used or planned to use telehealth in the future. This future may already be a reality, with a McKinsey & Company report estimating that physicians saw 50-175 times more patients over telehealth platforms since the pandemic’s start.1
In general, telehealth includes use of electronic communication and information technologies to deliver long-distance or remote health care. A physician’s use of telemedicine (clinical services) is one of the most common uses, but the industry also includes other professionals, such as pharmacists and nurses.

Telehealth platforms can be used to monitor, diagnose, treat, and counsel patients successfully. It works best for reading images, follow-up care, outpatient care, and long-term care. However, telemedicine is inappropriate for urgent issues, diagnosing underlying health conditions, or any practice where the standard of care would require a physical exam. There is potential liability for decision making without a proper physical exam.

There are many advantages to telehealth over more traditional health care options. Some of these advantages include:
- Increased access to health care.
- Increased access to medical specialists in small and rural communities.
- Improved long-term care from the comfort of patients’ homes.
- Improved platforms to document patient care outside regular business hours.
But along with these benefits, telehealth carries the disadvantage of potential increased liability. This increased liability could stem from:
- Breached standards of care.
- Inadequate or improper licensing.
- Limited care options.
- Decision making without a proper physical exam.
- Increased informed consent requirements.
- Restricted prescription access.
Before expanding any practice into telemedicine, awareness of potential legal issues is crucial.
Standard of care
Currently, telehealth laws and regulations vary significantly from state to state. But one rule is consistent across the board – that the standard of care for practicing medicine through telemedicine is identical to the standard of care required for practicing medicine during physical practice. It still requires the appropriate examination, testing, labs, imaging, and consultations that any in-person diagnosis needs. For physicians, it also includes supervising nonphysician clinicians, where state law requires supervision.
The American Telemedicine Association currently determines the primary governing standards and guidelines for telemedicine. These can help physicians understand best practices in meeting the standard of care through telemedicine. The American Gastroenterological Association provides coding guidelines and other resources to help physicians with telehealth and e-visits. Other professional societies, such as the American College of Radiology and the American Academy of Dermatology, offer guidelines specific to their medical specialties’ standards of care. These standards still vary from state to state, so medical professionals must be aware of any differences before treating patients in multiple states.
Licensing
Licensing is one of telemedicine’s most confusing legal issues. All states require a license to practice medicine (traditional or telehealth) within their borders. Without that license, practicing medicine in the state is a crime. On top of being criminal, unlicensed practice can affect insurance, liability, billing, and malpractice coverage. When in a brick-and-mortar clinic, a physician’s confidence in practicing within the licensed jurisdiction is easy. Now, the distinction is not so clear. Patients and physicians no longer have to be in the same room, city, or even state, meaning there could be unknown conflicting laws between the two locations. With rare exceptions, standards of care are based on the patient’s location, not the physician’s location. This increases the risk of practicing without being correctly licensed to higher than ever.
Because licensing is a significant roadblock in providing telemedicine, efforts are underway to make the process simpler and more streamlined. The Federation of State Medical Boards developed the Interstate Medical Licensure Compact (IMLC).2 This can qualify physicians to practice medicine across state lines within the compact so long as they meet specific eligibility requirements. The IMLC creates a fast-track option for physicians to fill out one application and receive licenses from multiple states at once. Currently, the compact includes 32 states, the District of Columbia, and Guam.3
Informed consent
Telemedicine health care still requires informed consent from patients. In fact, in some states, the requirements for care provided through telehealth are actually stricter than requirements for informed consent obtained in person.
Most informed consent laws require physicians to cover the risks and benefits of a recommended course of treatment and all feasible and reasonable material alternatives. On top of this traditional informed consent, physicians must get additional consent to receive care over a telehealth platform. This unique requirement explains what telehealth is, possible risks and expected benefits, and security measures used to protect patient information. States vary regarding when verbal consent is sufficient, and when written consent is required.
Prescriptions
Telemedicine is still a relatively new industry, and few legal opinions specifically address telemedicine malpractice. However, prescribing medication based on telemedicine information is among the few issues the courts have addressed. A 2008 decision found that a physician review of patient questionnaires submitted over the Internet was insufficient to prescribe medication without a physical examination determining patient health.4 This cautious approach stemmed from telehealth’s early concern about the absence of patient-physician relationships and potential online pharmacy abuse. Since this decision, many states require an “in-person” visit with a patient before prescribing medication. The definition of what qualifies as an in-person visit varies from state to state – some still consider the use of real-time, audiovisual conferencing sufficient.
The law is still evolving for prescriptions. Some states don’t allow any prescriptions, while others allow physicians to prescribe their patients’ medications as part of an appropriate treatment plan according to their professional discretion. Almost every state prohibits the prescription of controlled substances based on telemedicine.
Conclusion
Telemedicine is becoming an increasingly significant part of both physician-patient relationships and the broader health care industry. Used appropriately, it can be an incredibly effective method of care for physicians and patients. Physicians should learn the laws governing telemedicine in every state they want to practice and continue to stay current on any changes. The Center for Connected Health Policy offers a report, updated semiannually, to help physicians stay up to date on their state laws. These efforts will help prevent physicians from exposure to liability and medical malpractice claims.
Mr. Hyde is a partner at Younker Hyde Macfarlane, a law firm that focuses on prosecuting medical malpractice claims on behalf of injured patients. Ms. Johnson is an associate attorney with the firm. You can find them at YHMLaw.com.
References
1. Bestsennyy O, Harris A, Rost J. Telehealth: A quarter-trillion-dollar post-COVID-19 reality? Mckinsey & Company, May 29, 2020.
2. FSMB: Draft Interstate Compact for Physician Licensure Nears Completion, 2014.
3. Interstate Medical Licensure Compact: U.S. State Participation in the Compact.
4. See, Low Cost Pharm., Inc. v. Ariz. State Bd. Of Pharm, 2008 Ariz. App. Unpub. LEXIS 790, referencing conclusion of Arizona Medical Board.
Telehealth has been steadily gaining mainstream use throughout the last decade, but the practice was recently shoved, almost overnight, into the forefront of the health care profession. Telehealth is now used more frequently by medical groups and physicians than ever before. General reports before the COVID-19 pandemic approximated 90% of health care organizations used or planned to use telehealth in the future. This future may already be a reality, with a McKinsey & Company report estimating that physicians saw 50-175 times more patients over telehealth platforms since the pandemic’s start.1
In general, telehealth includes use of electronic communication and information technologies to deliver long-distance or remote health care. A physician’s use of telemedicine (clinical services) is one of the most common uses, but the industry also includes other professionals, such as pharmacists and nurses.
Telehealth platforms can be used to monitor, diagnose, treat, and counsel patients successfully. It works best for reading images, follow-up care, outpatient care, and long-term care. However, telemedicine is inappropriate for urgent issues, diagnosing underlying health conditions, or any practice where the standard of care would require a physical exam. There is potential liability for decision making without a proper physical exam.
There are many advantages to telehealth over more traditional health care options. Some of these advantages include:
- Increased access to health care.
- Increased access to medical specialists in small and rural communities.
- Improved long-term care from the comfort of patients’ homes.
- Improved platforms to document patient care outside regular business hours.
But along with these benefits, telehealth carries the disadvantage of potential increased liability. This increased liability could stem from:
- Breached standards of care.
- Inadequate or improper licensing.
- Limited care options.
- Decision making without a proper physical exam.
- Increased informed consent requirements.
- Restricted prescription access.
Before expanding any practice into telemedicine, awareness of potential legal issues is crucial.
Standard of care
Currently, telehealth laws and regulations vary significantly from state to state. But one rule is consistent across the board – that the standard of care for practicing medicine through telemedicine is identical to the standard of care required for practicing medicine during physical practice. It still requires the appropriate examination, testing, labs, imaging, and consultations that any in-person diagnosis needs. For physicians, it also includes supervising nonphysician clinicians, where state law requires supervision.
The American Telemedicine Association currently determines the primary governing standards and guidelines for telemedicine. These can help physicians understand best practices in meeting the standard of care through telemedicine. The American Gastroenterological Association provides coding guidelines and other resources to help physicians with telehealth and e-visits. Other professional societies, such as the American College of Radiology and the American Academy of Dermatology, offer guidelines specific to their medical specialties’ standards of care. These standards still vary from state to state, so medical professionals must be aware of any differences before treating patients in multiple states.
Licensing
Licensing is one of telemedicine’s most confusing legal issues. All states require a license to practice medicine (traditional or telehealth) within their borders. Without that license, practicing medicine in the state is a crime. On top of being criminal, unlicensed practice can affect insurance, liability, billing, and malpractice coverage. When in a brick-and-mortar clinic, a physician’s confidence in practicing within the licensed jurisdiction is easy. Now, the distinction is not so clear. Patients and physicians no longer have to be in the same room, city, or even state, meaning there could be unknown conflicting laws between the two locations. With rare exceptions, standards of care are based on the patient’s location, not the physician’s location. This increases the risk of practicing without being correctly licensed to higher than ever.
Because licensing is a significant roadblock in providing telemedicine, efforts are underway to make the process simpler and more streamlined. The Federation of State Medical Boards developed the Interstate Medical Licensure Compact (IMLC).2 This can qualify physicians to practice medicine across state lines within the compact so long as they meet specific eligibility requirements. The IMLC creates a fast-track option for physicians to fill out one application and receive licenses from multiple states at once. Currently, the compact includes 32 states, the District of Columbia, and Guam.3
Informed consent
Telemedicine health care still requires informed consent from patients. In fact, in some states, the requirements for care provided through telehealth are actually stricter than requirements for informed consent obtained in person.
Most informed consent laws require physicians to cover the risks and benefits of a recommended course of treatment and all feasible and reasonable material alternatives. On top of this traditional informed consent, physicians must get additional consent to receive care over a telehealth platform. This unique requirement explains what telehealth is, possible risks and expected benefits, and security measures used to protect patient information. States vary regarding when verbal consent is sufficient, and when written consent is required.
Prescriptions
Telemedicine is still a relatively new industry, and few legal opinions specifically address telemedicine malpractice. However, prescribing medication based on telemedicine information is among the few issues the courts have addressed. A 2008 decision found that a physician review of patient questionnaires submitted over the Internet was insufficient to prescribe medication without a physical examination determining patient health.4 This cautious approach stemmed from telehealth’s early concern about the absence of patient-physician relationships and potential online pharmacy abuse. Since this decision, many states require an “in-person” visit with a patient before prescribing medication. The definition of what qualifies as an in-person visit varies from state to state – some still consider the use of real-time, audiovisual conferencing sufficient.
The law is still evolving for prescriptions. Some states don’t allow any prescriptions, while others allow physicians to prescribe their patients’ medications as part of an appropriate treatment plan according to their professional discretion. Almost every state prohibits the prescription of controlled substances based on telemedicine.
Conclusion
Telemedicine is becoming an increasingly significant part of both physician-patient relationships and the broader health care industry. Used appropriately, it can be an incredibly effective method of care for physicians and patients. Physicians should learn the laws governing telemedicine in every state they want to practice and continue to stay current on any changes. The Center for Connected Health Policy offers a report, updated semiannually, to help physicians stay up to date on their state laws. These efforts will help prevent physicians from exposure to liability and medical malpractice claims.
Mr. Hyde is a partner at Younker Hyde Macfarlane, a law firm that focuses on prosecuting medical malpractice claims on behalf of injured patients. Ms. Johnson is an associate attorney with the firm. You can find them at YHMLaw.com.
References
1. Bestsennyy O, Harris A, Rost J. Telehealth: A quarter-trillion-dollar post-COVID-19 reality? Mckinsey & Company, May 29, 2020.
2. FSMB: Draft Interstate Compact for Physician Licensure Nears Completion, 2014.
3. Interstate Medical Licensure Compact: U.S. State Participation in the Compact.
4. See, Low Cost Pharm., Inc. v. Ariz. State Bd. Of Pharm, 2008 Ariz. App. Unpub. LEXIS 790, referencing conclusion of Arizona Medical Board.
Telehealth has been steadily gaining mainstream use throughout the last decade, but the practice was recently shoved, almost overnight, into the forefront of the health care profession. Telehealth is now used more frequently by medical groups and physicians than ever before. General reports before the COVID-19 pandemic approximated 90% of health care organizations used or planned to use telehealth in the future. This future may already be a reality, with a McKinsey & Company report estimating that physicians saw 50-175 times more patients over telehealth platforms since the pandemic’s start.1
In general, telehealth includes use of electronic communication and information technologies to deliver long-distance or remote health care. A physician’s use of telemedicine (clinical services) is one of the most common uses, but the industry also includes other professionals, such as pharmacists and nurses.
Telehealth platforms can be used to monitor, diagnose, treat, and counsel patients successfully. It works best for reading images, follow-up care, outpatient care, and long-term care. However, telemedicine is inappropriate for urgent issues, diagnosing underlying health conditions, or any practice where the standard of care would require a physical exam. There is potential liability for decision making without a proper physical exam.
There are many advantages to telehealth over more traditional health care options. Some of these advantages include:
- Increased access to health care.
- Increased access to medical specialists in small and rural communities.
- Improved long-term care from the comfort of patients’ homes.
- Improved platforms to document patient care outside regular business hours.
But along with these benefits, telehealth carries the disadvantage of potential increased liability. This increased liability could stem from:
- Breached standards of care.
- Inadequate or improper licensing.
- Limited care options.
- Decision making without a proper physical exam.
- Increased informed consent requirements.
- Restricted prescription access.
Before expanding any practice into telemedicine, awareness of potential legal issues is crucial.
Standard of care
Currently, telehealth laws and regulations vary significantly from state to state. But one rule is consistent across the board – that the standard of care for practicing medicine through telemedicine is identical to the standard of care required for practicing medicine during physical practice. It still requires the appropriate examination, testing, labs, imaging, and consultations that any in-person diagnosis needs. For physicians, it also includes supervising nonphysician clinicians, where state law requires supervision.
The American Telemedicine Association currently determines the primary governing standards and guidelines for telemedicine. These can help physicians understand best practices in meeting the standard of care through telemedicine. The American Gastroenterological Association provides coding guidelines and other resources to help physicians with telehealth and e-visits. Other professional societies, such as the American College of Radiology and the American Academy of Dermatology, offer guidelines specific to their medical specialties’ standards of care. These standards still vary from state to state, so medical professionals must be aware of any differences before treating patients in multiple states.
Licensing
Licensing is one of telemedicine’s most confusing legal issues. All states require a license to practice medicine (traditional or telehealth) within their borders. Without that license, practicing medicine in the state is a crime. On top of being criminal, unlicensed practice can affect insurance, liability, billing, and malpractice coverage. When in a brick-and-mortar clinic, a physician’s confidence in practicing within the licensed jurisdiction is easy. Now, the distinction is not so clear. Patients and physicians no longer have to be in the same room, city, or even state, meaning there could be unknown conflicting laws between the two locations. With rare exceptions, standards of care are based on the patient’s location, not the physician’s location. This increases the risk of practicing without being correctly licensed to higher than ever.
Because licensing is a significant roadblock in providing telemedicine, efforts are underway to make the process simpler and more streamlined. The Federation of State Medical Boards developed the Interstate Medical Licensure Compact (IMLC).2 This can qualify physicians to practice medicine across state lines within the compact so long as they meet specific eligibility requirements. The IMLC creates a fast-track option for physicians to fill out one application and receive licenses from multiple states at once. Currently, the compact includes 32 states, the District of Columbia, and Guam.3
Informed consent
Telemedicine health care still requires informed consent from patients. In fact, in some states, the requirements for care provided through telehealth are actually stricter than requirements for informed consent obtained in person.
Most informed consent laws require physicians to cover the risks and benefits of a recommended course of treatment and all feasible and reasonable material alternatives. On top of this traditional informed consent, physicians must get additional consent to receive care over a telehealth platform. This unique requirement explains what telehealth is, possible risks and expected benefits, and security measures used to protect patient information. States vary regarding when verbal consent is sufficient, and when written consent is required.
Prescriptions
Telemedicine is still a relatively new industry, and few legal opinions specifically address telemedicine malpractice. However, prescribing medication based on telemedicine information is among the few issues the courts have addressed. A 2008 decision found that a physician review of patient questionnaires submitted over the Internet was insufficient to prescribe medication without a physical examination determining patient health.4 This cautious approach stemmed from telehealth’s early concern about the absence of patient-physician relationships and potential online pharmacy abuse. Since this decision, many states require an “in-person” visit with a patient before prescribing medication. The definition of what qualifies as an in-person visit varies from state to state – some still consider the use of real-time, audiovisual conferencing sufficient.
The law is still evolving for prescriptions. Some states don’t allow any prescriptions, while others allow physicians to prescribe their patients’ medications as part of an appropriate treatment plan according to their professional discretion. Almost every state prohibits the prescription of controlled substances based on telemedicine.
Conclusion
Telemedicine is becoming an increasingly significant part of both physician-patient relationships and the broader health care industry. Used appropriately, it can be an incredibly effective method of care for physicians and patients. Physicians should learn the laws governing telemedicine in every state they want to practice and continue to stay current on any changes. The Center for Connected Health Policy offers a report, updated semiannually, to help physicians stay up to date on their state laws. These efforts will help prevent physicians from exposure to liability and medical malpractice claims.
Mr. Hyde is a partner at Younker Hyde Macfarlane, a law firm that focuses on prosecuting medical malpractice claims on behalf of injured patients. Ms. Johnson is an associate attorney with the firm. You can find them at YHMLaw.com.
References
1. Bestsennyy O, Harris A, Rost J. Telehealth: A quarter-trillion-dollar post-COVID-19 reality? Mckinsey & Company, May 29, 2020.
2. FSMB: Draft Interstate Compact for Physician Licensure Nears Completion, 2014.
3. Interstate Medical Licensure Compact: U.S. State Participation in the Compact.
4. See, Low Cost Pharm., Inc. v. Ariz. State Bd. Of Pharm, 2008 Ariz. App. Unpub. LEXIS 790, referencing conclusion of Arizona Medical Board.
Is ketamine living up to the promise for depression?
After years of dormancy, psychiatric drug development is showing signs of life. There is the novel antipsychotic lumateperone, recently approved for adults with schizophrenia. Brexanolone was approved last year for postpartum depression. And perhaps generating the most attention lately among psychiatrists – and people with depression – is the use of ketamine and esketamine for depression.

Columbia psychiatrist J. John Mann, MD, a professor of translational neuroscience and a mood disorder specialist, has been involved in several notable studies of ketamine in patients with depression. He and his colleagues’ recent research efforts include a randomized study into ketamine’s ability to reduce suicidal thoughts in bipolar depression and an MRI analysis illuminating the role that dosing plays in antidepressant effects.
Dr. Sederer: Nearly 20 million people in this country alone suffer from clinical depression every year. That means they have a functional impairment in addition to their suffering and are at risk of taking their own lives. Depression is a very prevalent, painful, and disabling condition. The psychopharmacologic treatments we’ve had have been more or less the same for the past 20 or 30 years.

We’ve asked Dr. Mann to … talk to us about ketamine and its nasal preparation esketamine, which is a novel psychopharmacologic treatment. Dr. Mann, please tell us about ketamine, its utility, and the yet-to-be-answered questions.
Dr. Mann: Ketamine and esketamine, which is a component of ketamine itself, is different from traditional antidepressant medications in three fundamental ways.
The first is that it acts very quickly. Traditional antidepressants take 4, 6, 8 weeks to work. This means that the patient has to put up with a great deal of suffering while waiting for a response. And the probability of the medication working isn’t that high. About 50%-70% of individuals will respond eventually at the end of this ride. But ketamine, when it works, does so in 2 hours. That’s a totally different timescale.
The second aspect is that, when it does work, it often works very robustly, even though it’s a quick-acting antidepressant. The patient often quickly feels distinctly better.
Very often when you’re using traditional antidepressants, it takes a while for the improvement to reach the point that the patient is confident that they are clearly better, and too often that does not happen.
Dr. Sederer: As the treating doctor, you’re trying to keep that patient’s hope alive, even though we don’t have substantial evidence that they’re going to respond.
Dr. Mann: Exactly. One of the difficulties of keeping patients on track with traditional antidepressants is that, after the first dose or two, they have all the side effects and yet no benefit has emerged. In many ways patients sometimes feel that they’re going backwards. They have all of their depression plus the side effects of the medication.
But with ketamine, it’s rather different. You come in, you have the treatment, and many patients feel improved in a couple of hours. And not just a bit improved, but in many cases distinctly improved.
It’s very important for clinicians to appreciate that ketamine will work in patients who have a classically described treatment-resistant depression, meaning they’ve tried several other types of antidepressant medications that haven’t worked.
A prerequisite for treatment with ketamine is that they have had a number of treatment failures. The labeling for the intranasal esketamine states that you should try the other antidepressants first and then use this if they don’t work. The fact that ketamine can work even when the other medications have failed is a huge advantage.
Dr. Sederer: There is another feature of ketamine, in that it also has a pronounced benefit for suicidal ideation, which your research has reported on.
Dr. Mann: Yes, we’ve learned over the years that depression and suicidality are in some ways comorbid conditions. That both have to be addressed in order to keep somebody alive so that they can respond to treatment.
That’s a very important point. If the patient is suffering from depression and the antidepressant takes weeks to work, they may lose hope during that time. They may become overwhelmed by the suicidal ideation, no longer able to control or resist the impulse to take their life. A lot of the management is therefore to try to help support the patient (and family) so that these thoughts never become too compelling. Often we have to consider hospitalization to protect these patients so that they can stay alive long enough for the antidepressant to work. But ketamine not only has this very rapid effect for their depression, it also has a partly independent effect on suicidal ideation that is equally rapid and robust, which can render the patient safer.
Dr. Sederer: In other words, it’s effective and rapidly so for depression, with a bonus of reducing suicidality? This sounds almost too good to be true.
Dr. Mann: There are some limitations that we have to keep in mind. One limitation is that a single administration of ketamine will produce this robust improvement but it will only persist for most people for 5-7 days.
Dr. Sederer: Is the same duration true for scheduling the next treatment as well?
Dr. Mann: Yes, it is. The patient will gradually begin to deteriorate if you do not repeat the treatment. But as we showed in our randomized controlled clinical study, with ketamine for suicidal ideation, if you continue to deliver the medication, you can sustain the benefit.
Dr. Sederer: Can a person receive both ketamine and a conventional antidepressant at the same time?
Dr. Mann: Yes. In this study, half of the patients were actually continued on their previous medication while we added the ketamine on top of that. It worked very well.
In practice, people use two approaches. One approach used by most ketamine clinics is to give six doses of ketamine at a frequency of about two per week. Then they will reduce the frequency down to once a week for a few more doses and then once a month.
Dr. Sederer:: And this is a ketamine infusion?
Dr. Mann: Yes, this generally has been a ketamine infusion. This approach seems to work quite well. But that may not be necessary.
Another strategy is to give one, two, or three doses of ketamine. If the patient doesn’t respond robustly to two or three doses, they’re not going to respond to subsequent doses.
Dr. Sederer: So, initial responses are a predictor of future response?
Dr. Mann: Exactly. Now, if they haven’t done well with two or three doses, then you’ve got to use other treatments. But if they do well with the two or three, then you’ve got a choice: You can either complete the treatment course with ketamine and then continue them on antidepressant medications, or simply treat them with ketamine alone. What we tend to do is to treat with only antidepressant medications after a small number of ketamine treatments. We also use ketamine as a kind of “rescue medication” if they relapse into severe depression, though this is true for only a minority of patients.
Dr. Sederer: One of the things that we’ve learned is that antidepressants have a very beneficial effect for some people, but then they wear out and the person starts to relapse. Should ketamine be studied as an intervention for people who are no longer responding to the antidepressant(s) that they are on?
Dr. Mann: We do not really know the answer to that question. My experience treating very seriously ill patients is that sometimes the ketamine will work very well the first time or the second time but then in the future, if you try to use it as a rescue medication, it might not work that well. There is some clinical experience that suggests that that may be true for some people. But we have no idea about the frequency or timing with which this might happen. That’s all uncertain.
Moreover, most of our control clinical trial data come from either one dose of ketamine or from a few trials where people have received multiple doses of ketamine, followed by a bit of a taper. But there are very, very few of those types of studies. We’re still learning about the use of this medication.
Dr. Sederer: Importantly, you referenced the side effects of antidepressants. What are the side effects and risks of ketamine?
Dr. Mann: We know a lot more about the immediate short-term side effects of a single dose or a few doses of ketamine. Most people will get a kind of tripping experience. They’ll feel a bit unreal, or their circumstances or experiences of the world feel a bit distorted.
Some patients develop strange ideas. Most patients don’t enjoy those symptoms, even though I know ketamine is used as a party drug, and so on and so forth.
Dr. Sederer: It seems that the context is what matters.
Dr. Mann: Yes. And in a clinic context, most patients simply don’t enjoy these types of dissociative experiences, but they put up with them. They’re not severe, in general.
Dr. Sederer: Is part of the preparation of the patient telling them that this may happen?
Dr. Mann: Yes. We try to explain the potential for these symptoms and that most people get them. These side effects almost invariably terminate with the cessation of the administration.
Dr. Sederer: What’s the typical duration of the infusion you use?
Dr. Mann: Traditionally, infusion is 40 minutes and always in a clinic setting.
Dr. Sederer: And that’s because of the concern that a patient may have these symptoms?
Dr. Mann: Exactly. They may have dissociative effects that they’re disturbed by, and we need to monitor that. They’re probably going to remain under observation in the clinic for about the same amount of time because it takes about the same time for these effects to wear off.
The other consideration is that some people get a little nausea. In our experience with the intravenous ketamine, there’s also a problematic side effect that their blood pressure will be slightly raised. Therefore, it’s good to know that the person’s blood pressure is under control before they begin the treatments and that you’re monitoring it during administration.
Dr. Sederer: What are the differences you’re discovering between esketamine and ketamine?
Dr. Mann: It is a bit different. We’ve just completed a very important National Institutes of Health–funded clinical trial here at Columbia showing that with esketamine or ketamine itself, the dose and the blood levels are very closely related to the robustness of the clinical response.
When you give a drug intravenously, you give a very reliable dose. When you give the drug over 40 minutes, you’re spreading the dose administration over a period of time so that it doesn’t peak very high. The side effects appear to be proportional to the peak dose.
When you give it intranasally, you give the drug over a much shorter period of time. Even if you use more than one intranasal administration to give the whole dose, it’s still a relatively shorter time, compared with the 40 minutes.
Dr. Sederer: This means that to get the equivalent dose intranasally, the patient is going to have to experience a higher peak. Can you predict that those patients who are treated intranasally are going to have more side effects?
Dr. Mann: Right. And that should be explained to the patient. You will not need an intravenous line inserted, which some people might find highly appealing and advantageous, but you will probably have more side effects.
Also, in general, intranasal absorption of drugs is more variable. The predictability of the blood level and, therefore, the degree of antidepressant effect is not as good intranasally as intravenously.
Now, all of this is anecdotal clinical experience, based on theoretical pharmacology, because nobody has actually done a head-to-head control comparison.
Dr. Sederer: What about the cost of both of these preparations?
Dr. Mann: There is a bit of a range in pricing between ketamine clinics around the country. It’s always important to find out what they charge per administration. And then it makes a difference whether you have two or three administrations versus six plus further tapered administration. Clearly, the cost can vary a great deal.
Dr. Sederer: But it’s generally not covered by insurance, so most people are paying out of pocket.
Dr. Mann: Yes. The intranasal ketamine is still in negotiation at the moment, but it should be resolved before it’s fully marketed.
Dr. Sederer: Ketamine is used for major depression. Does it have utility in bipolar depression?
Dr. Mann: We and some others have done initial studies in bipolar depression. In our view, it’s probably going to be as effective in bipolar disorder as it is in major depressive disorder, unipolar depression.
We haven’t seen any manic episodes triggered, but we don’t give repeated doses. We allow research patients to stay on anticonvulsants or mood stabilizers, so that’s helpful. Generally, people with bipolar disorder who come for ketamine treatment for their depression are coming on a mood stabilizer, because that and perhaps other conventional antidepressants have not proven to be effective. So, I think that ketamine plus mood stabilizers seems to be very promising.
Dr. Sederer: I want to return to the antisuicidal properties that you had previously mentioned. I heard from a colleague about a patient who had been admitted to a psychiatric inpatient unit. The patient was in her 20s; she did not have major depression but was persistently suicidal, constantly trying to hurt herself in any way she could. But that seemed to be more a product of borderline personality disorder, with its impulsive and self-destructive problems.
In the end, they tried intranasal ketamine. The response was, just as you described, robust. Her self-injurious behavior dropped in a very pronounced way within a day or two. But she then did require administrations a couple of times a week in order to keep that suicidality at bay.
Based on that example, I’m wondering whether there is an application here for people who are suicidal yet who may not have features of major depression or bipolar depression.
Dr. Mann: It’s a very interesting suggestion for which we have no data-based answer. However, we have a clue from the study that we published in the American Journal of Psychiatry and have since published further analyses on.
The reasons that people die by suicide, or make suicide attempts, are not entirely attributable to the fact that they suffer from a mood disorder.
Dr. Sederer: Yes, because only a minority of individuals with a mood disorder ever make suicide attempts. But there is a subgroup at risk.
Dr. Mann: Here at Columbia, we’ve promulgated the stress-diathesis model for suicidal behavior. A stressor could be external life events, but the internal stressor would be something like an acute episode of depression.
But predisposition also plays an important role, which has several elements to it. One is decision-making. These are patients with a propensity to go for a short-term, quick relief. In other words, a patient would be seeking immediate relief rather than waiting for the delayed improvement from an antidepressant. They’re more prone to act on the pain of the depression and terminate their lives – to try to end their pain – rather than wait and hope that, in time, there’s a chance that the antidepressant will work.
Dr. Sederer: What else do you want to share with our viewers about this medication and how it’s used?
Dr. Mann: My goal in treating patients is to try to use the least amount of medication possible. We do not really know yet the long-term safety of ketamine treatment.
It’s been used for many decades in anesthesia, but people don’t get repeated anesthetic doses of ketamine. And higher doses of ketamine given repeatedly have been shown in preclinical studies to produce little lesions in the brain, which is not good. But we’re using much lower doses.
As we potentially move into a time when we could be giving multiple doses of ketamine to patients, we should remember that we need to be cautious about that. If we don’t need to give them more doses, we shouldn’t. We should know that there is a potential downside that we don’t fully understand yet to giving ketamine repeatedly.
And that’s aside from its abuse potential. We know that people have employed ketamine for physical and emotional pain, and when they administer it themselves, they tend to get dependent on it. In a clinic setting it’s given in a very formal and structured fashion, a bit like the administration of opioids. In that setting, it is much safer and the risk for abuse and diversion is minimized. But we need to remember that this drug does have abuse potential and perhaps not yet fully measurable neurotoxic effects.
Dr. Sederer: If physicians, nurses, and other professional clinicians want to learn more about this medication, what are the accurate, reliable sources of information to which you suggest they turn?
Dr. Mann: The National Institute of Mental Health’s website offers good and reliable information for patients and their families. It is an unbiased, scientific, and thoughtful source of information, and better than just trolling the Internet for information.
People are much more sophisticated now than they were 20 years ago in these matters, and scientific papers are much more accessible to the public. Reading papers in recognized journals is also a useful way to gain information.
For example, one of the major papers that we published in the American Journal of Psychiatry is available to anybody on the Internet to read. So, I encourage people to make their own inquiries and talk to more than one doctor. Informed patients and families are the best partners a doctor can ever have. We encourage that in all of our patients.
Dr. Sederer: I want to thank you very much, Dr. Mann, for your work in this area and for joining us here at Medscape and Columbia Psychiatry to teach us so much about what is truly a novel psychopharmacologic agent, yet one where we still have a lot more to learn.
A version of this article originally appeared on Medscape.com.
After years of dormancy, psychiatric drug development is showing signs of life. There is the novel antipsychotic lumateperone, recently approved for adults with schizophrenia. Brexanolone was approved last year for postpartum depression. And perhaps generating the most attention lately among psychiatrists – and people with depression – is the use of ketamine and esketamine for depression.
Columbia psychiatrist J. John Mann, MD, a professor of translational neuroscience and a mood disorder specialist, has been involved in several notable studies of ketamine in patients with depression. He and his colleagues’ recent research efforts include a randomized study into ketamine’s ability to reduce suicidal thoughts in bipolar depression and an MRI analysis illuminating the role that dosing plays in antidepressant effects.
Dr. Sederer: Nearly 20 million people in this country alone suffer from clinical depression every year. That means they have a functional impairment in addition to their suffering and are at risk of taking their own lives. Depression is a very prevalent, painful, and disabling condition. The psychopharmacologic treatments we’ve had have been more or less the same for the past 20 or 30 years.
We’ve asked Dr. Mann to … talk to us about ketamine and its nasal preparation esketamine, which is a novel psychopharmacologic treatment. Dr. Mann, please tell us about ketamine, its utility, and the yet-to-be-answered questions.
Dr. Mann: Ketamine and esketamine, which is a component of ketamine itself, is different from traditional antidepressant medications in three fundamental ways.
The first is that it acts very quickly. Traditional antidepressants take 4, 6, 8 weeks to work. This means that the patient has to put up with a great deal of suffering while waiting for a response. And the probability of the medication working isn’t that high. About 50%-70% of individuals will respond eventually at the end of this ride. But ketamine, when it works, does so in 2 hours. That’s a totally different timescale.
The second aspect is that, when it does work, it often works very robustly, even though it’s a quick-acting antidepressant. The patient often quickly feels distinctly better.
Very often when you’re using traditional antidepressants, it takes a while for the improvement to reach the point that the patient is confident that they are clearly better, and too often that does not happen.
Dr. Sederer: As the treating doctor, you’re trying to keep that patient’s hope alive, even though we don’t have substantial evidence that they’re going to respond.
Dr. Mann: Exactly. One of the difficulties of keeping patients on track with traditional antidepressants is that, after the first dose or two, they have all the side effects and yet no benefit has emerged. In many ways patients sometimes feel that they’re going backwards. They have all of their depression plus the side effects of the medication.
But with ketamine, it’s rather different. You come in, you have the treatment, and many patients feel improved in a couple of hours. And not just a bit improved, but in many cases distinctly improved.
It’s very important for clinicians to appreciate that ketamine will work in patients who have a classically described treatment-resistant depression, meaning they’ve tried several other types of antidepressant medications that haven’t worked.
A prerequisite for treatment with ketamine is that they have had a number of treatment failures. The labeling for the intranasal esketamine states that you should try the other antidepressants first and then use this if they don’t work. The fact that ketamine can work even when the other medications have failed is a huge advantage.
Dr. Sederer: There is another feature of ketamine, in that it also has a pronounced benefit for suicidal ideation, which your research has reported on.
Dr. Mann: Yes, we’ve learned over the years that depression and suicidality are in some ways comorbid conditions. That both have to be addressed in order to keep somebody alive so that they can respond to treatment.
That’s a very important point. If the patient is suffering from depression and the antidepressant takes weeks to work, they may lose hope during that time. They may become overwhelmed by the suicidal ideation, no longer able to control or resist the impulse to take their life. A lot of the management is therefore to try to help support the patient (and family) so that these thoughts never become too compelling. Often we have to consider hospitalization to protect these patients so that they can stay alive long enough for the antidepressant to work. But ketamine not only has this very rapid effect for their depression, it also has a partly independent effect on suicidal ideation that is equally rapid and robust, which can render the patient safer.
Dr. Sederer: In other words, it’s effective and rapidly so for depression, with a bonus of reducing suicidality? This sounds almost too good to be true.
Dr. Mann: There are some limitations that we have to keep in mind. One limitation is that a single administration of ketamine will produce this robust improvement but it will only persist for most people for 5-7 days.
Dr. Sederer: Is the same duration true for scheduling the next treatment as well?
Dr. Mann: Yes, it is. The patient will gradually begin to deteriorate if you do not repeat the treatment. But as we showed in our randomized controlled clinical study, with ketamine for suicidal ideation, if you continue to deliver the medication, you can sustain the benefit.
Dr. Sederer: Can a person receive both ketamine and a conventional antidepressant at the same time?
Dr. Mann: Yes. In this study, half of the patients were actually continued on their previous medication while we added the ketamine on top of that. It worked very well.
In practice, people use two approaches. One approach used by most ketamine clinics is to give six doses of ketamine at a frequency of about two per week. Then they will reduce the frequency down to once a week for a few more doses and then once a month.
Dr. Sederer:: And this is a ketamine infusion?
Dr. Mann: Yes, this generally has been a ketamine infusion. This approach seems to work quite well. But that may not be necessary.
Another strategy is to give one, two, or three doses of ketamine. If the patient doesn’t respond robustly to two or three doses, they’re not going to respond to subsequent doses.
Dr. Sederer: So, initial responses are a predictor of future response?
Dr. Mann: Exactly. Now, if they haven’t done well with two or three doses, then you’ve got to use other treatments. But if they do well with the two or three, then you’ve got a choice: You can either complete the treatment course with ketamine and then continue them on antidepressant medications, or simply treat them with ketamine alone. What we tend to do is to treat with only antidepressant medications after a small number of ketamine treatments. We also use ketamine as a kind of “rescue medication” if they relapse into severe depression, though this is true for only a minority of patients.
Dr. Sederer: One of the things that we’ve learned is that antidepressants have a very beneficial effect for some people, but then they wear out and the person starts to relapse. Should ketamine be studied as an intervention for people who are no longer responding to the antidepressant(s) that they are on?
Dr. Mann: We do not really know the answer to that question. My experience treating very seriously ill patients is that sometimes the ketamine will work very well the first time or the second time but then in the future, if you try to use it as a rescue medication, it might not work that well. There is some clinical experience that suggests that that may be true for some people. But we have no idea about the frequency or timing with which this might happen. That’s all uncertain.
Moreover, most of our control clinical trial data come from either one dose of ketamine or from a few trials where people have received multiple doses of ketamine, followed by a bit of a taper. But there are very, very few of those types of studies. We’re still learning about the use of this medication.
Dr. Sederer: Importantly, you referenced the side effects of antidepressants. What are the side effects and risks of ketamine?
Dr. Mann: We know a lot more about the immediate short-term side effects of a single dose or a few doses of ketamine. Most people will get a kind of tripping experience. They’ll feel a bit unreal, or their circumstances or experiences of the world feel a bit distorted.
Some patients develop strange ideas. Most patients don’t enjoy those symptoms, even though I know ketamine is used as a party drug, and so on and so forth.
Dr. Sederer: It seems that the context is what matters.
Dr. Mann: Yes. And in a clinic context, most patients simply don’t enjoy these types of dissociative experiences, but they put up with them. They’re not severe, in general.
Dr. Sederer: Is part of the preparation of the patient telling them that this may happen?
Dr. Mann: Yes. We try to explain the potential for these symptoms and that most people get them. These side effects almost invariably terminate with the cessation of the administration.
Dr. Sederer: What’s the typical duration of the infusion you use?
Dr. Mann: Traditionally, infusion is 40 minutes and always in a clinic setting.
Dr. Sederer: And that’s because of the concern that a patient may have these symptoms?
Dr. Mann: Exactly. They may have dissociative effects that they’re disturbed by, and we need to monitor that. They’re probably going to remain under observation in the clinic for about the same amount of time because it takes about the same time for these effects to wear off.
The other consideration is that some people get a little nausea. In our experience with the intravenous ketamine, there’s also a problematic side effect that their blood pressure will be slightly raised. Therefore, it’s good to know that the person’s blood pressure is under control before they begin the treatments and that you’re monitoring it during administration.
Dr. Sederer: What are the differences you’re discovering between esketamine and ketamine?
Dr. Mann: It is a bit different. We’ve just completed a very important National Institutes of Health–funded clinical trial here at Columbia showing that with esketamine or ketamine itself, the dose and the blood levels are very closely related to the robustness of the clinical response.
When you give a drug intravenously, you give a very reliable dose. When you give the drug over 40 minutes, you’re spreading the dose administration over a period of time so that it doesn’t peak very high. The side effects appear to be proportional to the peak dose.
When you give it intranasally, you give the drug over a much shorter period of time. Even if you use more than one intranasal administration to give the whole dose, it’s still a relatively shorter time, compared with the 40 minutes.
Dr. Sederer: This means that to get the equivalent dose intranasally, the patient is going to have to experience a higher peak. Can you predict that those patients who are treated intranasally are going to have more side effects?
Dr. Mann: Right. And that should be explained to the patient. You will not need an intravenous line inserted, which some people might find highly appealing and advantageous, but you will probably have more side effects.
Also, in general, intranasal absorption of drugs is more variable. The predictability of the blood level and, therefore, the degree of antidepressant effect is not as good intranasally as intravenously.
Now, all of this is anecdotal clinical experience, based on theoretical pharmacology, because nobody has actually done a head-to-head control comparison.
Dr. Sederer: What about the cost of both of these preparations?
Dr. Mann: There is a bit of a range in pricing between ketamine clinics around the country. It’s always important to find out what they charge per administration. And then it makes a difference whether you have two or three administrations versus six plus further tapered administration. Clearly, the cost can vary a great deal.
Dr. Sederer: But it’s generally not covered by insurance, so most people are paying out of pocket.
Dr. Mann: Yes. The intranasal ketamine is still in negotiation at the moment, but it should be resolved before it’s fully marketed.
Dr. Sederer: Ketamine is used for major depression. Does it have utility in bipolar depression?
Dr. Mann: We and some others have done initial studies in bipolar depression. In our view, it’s probably going to be as effective in bipolar disorder as it is in major depressive disorder, unipolar depression.
We haven’t seen any manic episodes triggered, but we don’t give repeated doses. We allow research patients to stay on anticonvulsants or mood stabilizers, so that’s helpful. Generally, people with bipolar disorder who come for ketamine treatment for their depression are coming on a mood stabilizer, because that and perhaps other conventional antidepressants have not proven to be effective. So, I think that ketamine plus mood stabilizers seems to be very promising.
Dr. Sederer: I want to return to the antisuicidal properties that you had previously mentioned. I heard from a colleague about a patient who had been admitted to a psychiatric inpatient unit. The patient was in her 20s; she did not have major depression but was persistently suicidal, constantly trying to hurt herself in any way she could. But that seemed to be more a product of borderline personality disorder, with its impulsive and self-destructive problems.
In the end, they tried intranasal ketamine. The response was, just as you described, robust. Her self-injurious behavior dropped in a very pronounced way within a day or two. But she then did require administrations a couple of times a week in order to keep that suicidality at bay.
Based on that example, I’m wondering whether there is an application here for people who are suicidal yet who may not have features of major depression or bipolar depression.
Dr. Mann: It’s a very interesting suggestion for which we have no data-based answer. However, we have a clue from the study that we published in the American Journal of Psychiatry and have since published further analyses on.
The reasons that people die by suicide, or make suicide attempts, are not entirely attributable to the fact that they suffer from a mood disorder.
Dr. Sederer: Yes, because only a minority of individuals with a mood disorder ever make suicide attempts. But there is a subgroup at risk.
Dr. Mann: Here at Columbia, we’ve promulgated the stress-diathesis model for suicidal behavior. A stressor could be external life events, but the internal stressor would be something like an acute episode of depression.
But predisposition also plays an important role, which has several elements to it. One is decision-making. These are patients with a propensity to go for a short-term, quick relief. In other words, a patient would be seeking immediate relief rather than waiting for the delayed improvement from an antidepressant. They’re more prone to act on the pain of the depression and terminate their lives – to try to end their pain – rather than wait and hope that, in time, there’s a chance that the antidepressant will work.
Dr. Sederer: What else do you want to share with our viewers about this medication and how it’s used?
Dr. Mann: My goal in treating patients is to try to use the least amount of medication possible. We do not really know yet the long-term safety of ketamine treatment.
It’s been used for many decades in anesthesia, but people don’t get repeated anesthetic doses of ketamine. And higher doses of ketamine given repeatedly have been shown in preclinical studies to produce little lesions in the brain, which is not good. But we’re using much lower doses.
As we potentially move into a time when we could be giving multiple doses of ketamine to patients, we should remember that we need to be cautious about that. If we don’t need to give them more doses, we shouldn’t. We should know that there is a potential downside that we don’t fully understand yet to giving ketamine repeatedly.
And that’s aside from its abuse potential. We know that people have employed ketamine for physical and emotional pain, and when they administer it themselves, they tend to get dependent on it. In a clinic setting it’s given in a very formal and structured fashion, a bit like the administration of opioids. In that setting, it is much safer and the risk for abuse and diversion is minimized. But we need to remember that this drug does have abuse potential and perhaps not yet fully measurable neurotoxic effects.
Dr. Sederer: If physicians, nurses, and other professional clinicians want to learn more about this medication, what are the accurate, reliable sources of information to which you suggest they turn?
Dr. Mann: The National Institute of Mental Health’s website offers good and reliable information for patients and their families. It is an unbiased, scientific, and thoughtful source of information, and better than just trolling the Internet for information.
People are much more sophisticated now than they were 20 years ago in these matters, and scientific papers are much more accessible to the public. Reading papers in recognized journals is also a useful way to gain information.
For example, one of the major papers that we published in the American Journal of Psychiatry is available to anybody on the Internet to read. So, I encourage people to make their own inquiries and talk to more than one doctor. Informed patients and families are the best partners a doctor can ever have. We encourage that in all of our patients.
Dr. Sederer: I want to thank you very much, Dr. Mann, for your work in this area and for joining us here at Medscape and Columbia Psychiatry to teach us so much about what is truly a novel psychopharmacologic agent, yet one where we still have a lot more to learn.
A version of this article originally appeared on Medscape.com.
After years of dormancy, psychiatric drug development is showing signs of life. There is the novel antipsychotic lumateperone, recently approved for adults with schizophrenia. Brexanolone was approved last year for postpartum depression. And perhaps generating the most attention lately among psychiatrists – and people with depression – is the use of ketamine and esketamine for depression.
Columbia psychiatrist J. John Mann, MD, a professor of translational neuroscience and a mood disorder specialist, has been involved in several notable studies of ketamine in patients with depression. He and his colleagues’ recent research efforts include a randomized study into ketamine’s ability to reduce suicidal thoughts in bipolar depression and an MRI analysis illuminating the role that dosing plays in antidepressant effects.
Dr. Sederer: Nearly 20 million people in this country alone suffer from clinical depression every year. That means they have a functional impairment in addition to their suffering and are at risk of taking their own lives. Depression is a very prevalent, painful, and disabling condition. The psychopharmacologic treatments we’ve had have been more or less the same for the past 20 or 30 years.
We’ve asked Dr. Mann to … talk to us about ketamine and its nasal preparation esketamine, which is a novel psychopharmacologic treatment. Dr. Mann, please tell us about ketamine, its utility, and the yet-to-be-answered questions.
Dr. Mann: Ketamine and esketamine, which is a component of ketamine itself, is different from traditional antidepressant medications in three fundamental ways.
The first is that it acts very quickly. Traditional antidepressants take 4, 6, 8 weeks to work. This means that the patient has to put up with a great deal of suffering while waiting for a response. And the probability of the medication working isn’t that high. About 50%-70% of individuals will respond eventually at the end of this ride. But ketamine, when it works, does so in 2 hours. That’s a totally different timescale.
The second aspect is that, when it does work, it often works very robustly, even though it’s a quick-acting antidepressant. The patient often quickly feels distinctly better.
Very often when you’re using traditional antidepressants, it takes a while for the improvement to reach the point that the patient is confident that they are clearly better, and too often that does not happen.
Dr. Sederer: As the treating doctor, you’re trying to keep that patient’s hope alive, even though we don’t have substantial evidence that they’re going to respond.
Dr. Mann: Exactly. One of the difficulties of keeping patients on track with traditional antidepressants is that, after the first dose or two, they have all the side effects and yet no benefit has emerged. In many ways patients sometimes feel that they’re going backwards. They have all of their depression plus the side effects of the medication.
But with ketamine, it’s rather different. You come in, you have the treatment, and many patients feel improved in a couple of hours. And not just a bit improved, but in many cases distinctly improved.
It’s very important for clinicians to appreciate that ketamine will work in patients who have a classically described treatment-resistant depression, meaning they’ve tried several other types of antidepressant medications that haven’t worked.
A prerequisite for treatment with ketamine is that they have had a number of treatment failures. The labeling for the intranasal esketamine states that you should try the other antidepressants first and then use this if they don’t work. The fact that ketamine can work even when the other medications have failed is a huge advantage.
Dr. Sederer: There is another feature of ketamine, in that it also has a pronounced benefit for suicidal ideation, which your research has reported on.
Dr. Mann: Yes, we’ve learned over the years that depression and suicidality are in some ways comorbid conditions. That both have to be addressed in order to keep somebody alive so that they can respond to treatment.
That’s a very important point. If the patient is suffering from depression and the antidepressant takes weeks to work, they may lose hope during that time. They may become overwhelmed by the suicidal ideation, no longer able to control or resist the impulse to take their life. A lot of the management is therefore to try to help support the patient (and family) so that these thoughts never become too compelling. Often we have to consider hospitalization to protect these patients so that they can stay alive long enough for the antidepressant to work. But ketamine not only has this very rapid effect for their depression, it also has a partly independent effect on suicidal ideation that is equally rapid and robust, which can render the patient safer.
Dr. Sederer: In other words, it’s effective and rapidly so for depression, with a bonus of reducing suicidality? This sounds almost too good to be true.
Dr. Mann: There are some limitations that we have to keep in mind. One limitation is that a single administration of ketamine will produce this robust improvement but it will only persist for most people for 5-7 days.
Dr. Sederer: Is the same duration true for scheduling the next treatment as well?
Dr. Mann: Yes, it is. The patient will gradually begin to deteriorate if you do not repeat the treatment. But as we showed in our randomized controlled clinical study, with ketamine for suicidal ideation, if you continue to deliver the medication, you can sustain the benefit.
Dr. Sederer: Can a person receive both ketamine and a conventional antidepressant at the same time?
Dr. Mann: Yes. In this study, half of the patients were actually continued on their previous medication while we added the ketamine on top of that. It worked very well.
In practice, people use two approaches. One approach used by most ketamine clinics is to give six doses of ketamine at a frequency of about two per week. Then they will reduce the frequency down to once a week for a few more doses and then once a month.
Dr. Sederer:: And this is a ketamine infusion?
Dr. Mann: Yes, this generally has been a ketamine infusion. This approach seems to work quite well. But that may not be necessary.
Another strategy is to give one, two, or three doses of ketamine. If the patient doesn’t respond robustly to two or three doses, they’re not going to respond to subsequent doses.
Dr. Sederer: So, initial responses are a predictor of future response?
Dr. Mann: Exactly. Now, if they haven’t done well with two or three doses, then you’ve got to use other treatments. But if they do well with the two or three, then you’ve got a choice: You can either complete the treatment course with ketamine and then continue them on antidepressant medications, or simply treat them with ketamine alone. What we tend to do is to treat with only antidepressant medications after a small number of ketamine treatments. We also use ketamine as a kind of “rescue medication” if they relapse into severe depression, though this is true for only a minority of patients.
Dr. Sederer: One of the things that we’ve learned is that antidepressants have a very beneficial effect for some people, but then they wear out and the person starts to relapse. Should ketamine be studied as an intervention for people who are no longer responding to the antidepressant(s) that they are on?
Dr. Mann: We do not really know the answer to that question. My experience treating very seriously ill patients is that sometimes the ketamine will work very well the first time or the second time but then in the future, if you try to use it as a rescue medication, it might not work that well. There is some clinical experience that suggests that that may be true for some people. But we have no idea about the frequency or timing with which this might happen. That’s all uncertain.
Moreover, most of our control clinical trial data come from either one dose of ketamine or from a few trials where people have received multiple doses of ketamine, followed by a bit of a taper. But there are very, very few of those types of studies. We’re still learning about the use of this medication.
Dr. Sederer: Importantly, you referenced the side effects of antidepressants. What are the side effects and risks of ketamine?
Dr. Mann: We know a lot more about the immediate short-term side effects of a single dose or a few doses of ketamine. Most people will get a kind of tripping experience. They’ll feel a bit unreal, or their circumstances or experiences of the world feel a bit distorted.
Some patients develop strange ideas. Most patients don’t enjoy those symptoms, even though I know ketamine is used as a party drug, and so on and so forth.
Dr. Sederer: It seems that the context is what matters.
Dr. Mann: Yes. And in a clinic context, most patients simply don’t enjoy these types of dissociative experiences, but they put up with them. They’re not severe, in general.
Dr. Sederer: Is part of the preparation of the patient telling them that this may happen?
Dr. Mann: Yes. We try to explain the potential for these symptoms and that most people get them. These side effects almost invariably terminate with the cessation of the administration.
Dr. Sederer: What’s the typical duration of the infusion you use?
Dr. Mann: Traditionally, infusion is 40 minutes and always in a clinic setting.
Dr. Sederer: And that’s because of the concern that a patient may have these symptoms?
Dr. Mann: Exactly. They may have dissociative effects that they’re disturbed by, and we need to monitor that. They’re probably going to remain under observation in the clinic for about the same amount of time because it takes about the same time for these effects to wear off.
The other consideration is that some people get a little nausea. In our experience with the intravenous ketamine, there’s also a problematic side effect that their blood pressure will be slightly raised. Therefore, it’s good to know that the person’s blood pressure is under control before they begin the treatments and that you’re monitoring it during administration.
Dr. Sederer: What are the differences you’re discovering between esketamine and ketamine?
Dr. Mann: It is a bit different. We’ve just completed a very important National Institutes of Health–funded clinical trial here at Columbia showing that with esketamine or ketamine itself, the dose and the blood levels are very closely related to the robustness of the clinical response.
When you give a drug intravenously, you give a very reliable dose. When you give the drug over 40 minutes, you’re spreading the dose administration over a period of time so that it doesn’t peak very high. The side effects appear to be proportional to the peak dose.
When you give it intranasally, you give the drug over a much shorter period of time. Even if you use more than one intranasal administration to give the whole dose, it’s still a relatively shorter time, compared with the 40 minutes.
Dr. Sederer: This means that to get the equivalent dose intranasally, the patient is going to have to experience a higher peak. Can you predict that those patients who are treated intranasally are going to have more side effects?
Dr. Mann: Right. And that should be explained to the patient. You will not need an intravenous line inserted, which some people might find highly appealing and advantageous, but you will probably have more side effects.
Also, in general, intranasal absorption of drugs is more variable. The predictability of the blood level and, therefore, the degree of antidepressant effect is not as good intranasally as intravenously.
Now, all of this is anecdotal clinical experience, based on theoretical pharmacology, because nobody has actually done a head-to-head control comparison.
Dr. Sederer: What about the cost of both of these preparations?
Dr. Mann: There is a bit of a range in pricing between ketamine clinics around the country. It’s always important to find out what they charge per administration. And then it makes a difference whether you have two or three administrations versus six plus further tapered administration. Clearly, the cost can vary a great deal.
Dr. Sederer: But it’s generally not covered by insurance, so most people are paying out of pocket.
Dr. Mann: Yes. The intranasal ketamine is still in negotiation at the moment, but it should be resolved before it’s fully marketed.
Dr. Sederer: Ketamine is used for major depression. Does it have utility in bipolar depression?
Dr. Mann: We and some others have done initial studies in bipolar depression. In our view, it’s probably going to be as effective in bipolar disorder as it is in major depressive disorder, unipolar depression.
We haven’t seen any manic episodes triggered, but we don’t give repeated doses. We allow research patients to stay on anticonvulsants or mood stabilizers, so that’s helpful. Generally, people with bipolar disorder who come for ketamine treatment for their depression are coming on a mood stabilizer, because that and perhaps other conventional antidepressants have not proven to be effective. So, I think that ketamine plus mood stabilizers seems to be very promising.
Dr. Sederer: I want to return to the antisuicidal properties that you had previously mentioned. I heard from a colleague about a patient who had been admitted to a psychiatric inpatient unit. The patient was in her 20s; she did not have major depression but was persistently suicidal, constantly trying to hurt herself in any way she could. But that seemed to be more a product of borderline personality disorder, with its impulsive and self-destructive problems.
In the end, they tried intranasal ketamine. The response was, just as you described, robust. Her self-injurious behavior dropped in a very pronounced way within a day or two. But she then did require administrations a couple of times a week in order to keep that suicidality at bay.
Based on that example, I’m wondering whether there is an application here for people who are suicidal yet who may not have features of major depression or bipolar depression.
Dr. Mann: It’s a very interesting suggestion for which we have no data-based answer. However, we have a clue from the study that we published in the American Journal of Psychiatry and have since published further analyses on.
The reasons that people die by suicide, or make suicide attempts, are not entirely attributable to the fact that they suffer from a mood disorder.
Dr. Sederer: Yes, because only a minority of individuals with a mood disorder ever make suicide attempts. But there is a subgroup at risk.
Dr. Mann: Here at Columbia, we’ve promulgated the stress-diathesis model for suicidal behavior. A stressor could be external life events, but the internal stressor would be something like an acute episode of depression.
But predisposition also plays an important role, which has several elements to it. One is decision-making. These are patients with a propensity to go for a short-term, quick relief. In other words, a patient would be seeking immediate relief rather than waiting for the delayed improvement from an antidepressant. They’re more prone to act on the pain of the depression and terminate their lives – to try to end their pain – rather than wait and hope that, in time, there’s a chance that the antidepressant will work.
Dr. Sederer: What else do you want to share with our viewers about this medication and how it’s used?
Dr. Mann: My goal in treating patients is to try to use the least amount of medication possible. We do not really know yet the long-term safety of ketamine treatment.
It’s been used for many decades in anesthesia, but people don’t get repeated anesthetic doses of ketamine. And higher doses of ketamine given repeatedly have been shown in preclinical studies to produce little lesions in the brain, which is not good. But we’re using much lower doses.
As we potentially move into a time when we could be giving multiple doses of ketamine to patients, we should remember that we need to be cautious about that. If we don’t need to give them more doses, we shouldn’t. We should know that there is a potential downside that we don’t fully understand yet to giving ketamine repeatedly.
And that’s aside from its abuse potential. We know that people have employed ketamine for physical and emotional pain, and when they administer it themselves, they tend to get dependent on it. In a clinic setting it’s given in a very formal and structured fashion, a bit like the administration of opioids. In that setting, it is much safer and the risk for abuse and diversion is minimized. But we need to remember that this drug does have abuse potential and perhaps not yet fully measurable neurotoxic effects.
Dr. Sederer: If physicians, nurses, and other professional clinicians want to learn more about this medication, what are the accurate, reliable sources of information to which you suggest they turn?
Dr. Mann: The National Institute of Mental Health’s website offers good and reliable information for patients and their families. It is an unbiased, scientific, and thoughtful source of information, and better than just trolling the Internet for information.
People are much more sophisticated now than they were 20 years ago in these matters, and scientific papers are much more accessible to the public. Reading papers in recognized journals is also a useful way to gain information.
For example, one of the major papers that we published in the American Journal of Psychiatry is available to anybody on the Internet to read. So, I encourage people to make their own inquiries and talk to more than one doctor. Informed patients and families are the best partners a doctor can ever have. We encourage that in all of our patients.
Dr. Sederer: I want to thank you very much, Dr. Mann, for your work in this area and for joining us here at Medscape and Columbia Psychiatry to teach us so much about what is truly a novel psychopharmacologic agent, yet one where we still have a lot more to learn.
A version of this article originally appeared on Medscape.com.
Web-based interviews, financial planning in a pandemic, and more
Dear colleagues,
I’m excited to introduce the November issue of The New Gastroenterologist – the last edition of 2020 features a fantastic line-up of articles! As the year comes to a close, we reflect on what has certainly been an interesting year, defined by a set of unique challenges we have faced as a nation and as a specialty.

The fellowship recruitment season is one that has looked starkly different as interviews have converted to a virtual format. Dr. Wissam Khan, Dr. Nada Al Masalmeh, Dr. Stephanie Judd, and Dr. Diane Levine (Wayne State University) compile a helpful list of tips and tricks on proper interview etiquette in the new era of web-based interviews.
Financial planning in the face of a pandemic is a formidable task – Jonathan Tudor (Fidelity Investments) offers valuable advice for gastroenterologists on how to remain secure in your finances even in uncertain circumstances.
This quarter’s “In Focus” feature, written by Dr. Yutaka Tomizawa (University of Washington), is a comprehensive piece elucidating the role of gastroenterologists in the management of gastric cancer. The article reviews the individual risk factors that exist for gastric cancer and provides guidance on how to stratify patients accordingly, which is critical in the ethnically diverse population of the United States.
Keeping a procedure log during fellowship can seem daunting and cumbersome, but it is important. Dr. Houman Rezaizadeh (University of Connecticut) shares his program’s experience with the AGA Procedure Log, a convenient online tracking tool, which can provide accurate and secure documentation of endoscopic procedures performed throughout fellowship.
Dr. Nazia Hasan (North Bay Health Care) and Dr. Allison Schulman (University of Michigan) broach an incredibly important topic: the paucity of women in interventional endoscopy. Dr. Hasan and Dr. Shulman candidly discuss the barriers women face in pursuing this subspecialty and offer practical solutions on how to approach these challenges – a piece that will surely resonate with many young gastroenterologists.
We wrap up our first year of TNG’s ethics series with two cases discussing the utilization of cannabis therapy in inflammatory bowel disease (IBD). Dr. Jami Kinnucan (University of Michigan) and Dr. Arun Swaminath (Lenox Hill Hospital) systematically review existing data on the efficacy of cannabis use in IBD, the risks associated with therapy, and legal implications for both physicians and patients.
Also in this issue is a high-yield clinical review on the endoscopic drainage of pancreatic fluid collections by Dr. Robert Moran and Dr. Joseph Elmunzer (Medical University of South Carolina). Dr. Manol Jovani (Johns Hopkins) teaches us about confounding – a critical concept to keep in mind when evaluating any manuscript. Lastly, our DHPA Private Practice Perspectives article, written by Dr. Mehul Lalani (US Digestive), reviews how quality measures and initiatives are tracked and implemented in private practice.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor in Chief
Assistant Professor of Medicine, University of Chicago, Section of Gastroenterology, Hepatology & Nutrition
Dear colleagues,
I’m excited to introduce the November issue of The New Gastroenterologist – the last edition of 2020 features a fantastic line-up of articles! As the year comes to a close, we reflect on what has certainly been an interesting year, defined by a set of unique challenges we have faced as a nation and as a specialty.
The fellowship recruitment season is one that has looked starkly different as interviews have converted to a virtual format. Dr. Wissam Khan, Dr. Nada Al Masalmeh, Dr. Stephanie Judd, and Dr. Diane Levine (Wayne State University) compile a helpful list of tips and tricks on proper interview etiquette in the new era of web-based interviews.
Financial planning in the face of a pandemic is a formidable task – Jonathan Tudor (Fidelity Investments) offers valuable advice for gastroenterologists on how to remain secure in your finances even in uncertain circumstances.
This quarter’s “In Focus” feature, written by Dr. Yutaka Tomizawa (University of Washington), is a comprehensive piece elucidating the role of gastroenterologists in the management of gastric cancer. The article reviews the individual risk factors that exist for gastric cancer and provides guidance on how to stratify patients accordingly, which is critical in the ethnically diverse population of the United States.
Keeping a procedure log during fellowship can seem daunting and cumbersome, but it is important. Dr. Houman Rezaizadeh (University of Connecticut) shares his program’s experience with the AGA Procedure Log, a convenient online tracking tool, which can provide accurate and secure documentation of endoscopic procedures performed throughout fellowship.
Dr. Nazia Hasan (North Bay Health Care) and Dr. Allison Schulman (University of Michigan) broach an incredibly important topic: the paucity of women in interventional endoscopy. Dr. Hasan and Dr. Shulman candidly discuss the barriers women face in pursuing this subspecialty and offer practical solutions on how to approach these challenges – a piece that will surely resonate with many young gastroenterologists.
We wrap up our first year of TNG’s ethics series with two cases discussing the utilization of cannabis therapy in inflammatory bowel disease (IBD). Dr. Jami Kinnucan (University of Michigan) and Dr. Arun Swaminath (Lenox Hill Hospital) systematically review existing data on the efficacy of cannabis use in IBD, the risks associated with therapy, and legal implications for both physicians and patients.
Also in this issue is a high-yield clinical review on the endoscopic drainage of pancreatic fluid collections by Dr. Robert Moran and Dr. Joseph Elmunzer (Medical University of South Carolina). Dr. Manol Jovani (Johns Hopkins) teaches us about confounding – a critical concept to keep in mind when evaluating any manuscript. Lastly, our DHPA Private Practice Perspectives article, written by Dr. Mehul Lalani (US Digestive), reviews how quality measures and initiatives are tracked and implemented in private practice.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor in Chief
Assistant Professor of Medicine, University of Chicago, Section of Gastroenterology, Hepatology & Nutrition
Dear colleagues,
I’m excited to introduce the November issue of The New Gastroenterologist – the last edition of 2020 features a fantastic line-up of articles! As the year comes to a close, we reflect on what has certainly been an interesting year, defined by a set of unique challenges we have faced as a nation and as a specialty.
The fellowship recruitment season is one that has looked starkly different as interviews have converted to a virtual format. Dr. Wissam Khan, Dr. Nada Al Masalmeh, Dr. Stephanie Judd, and Dr. Diane Levine (Wayne State University) compile a helpful list of tips and tricks on proper interview etiquette in the new era of web-based interviews.
Financial planning in the face of a pandemic is a formidable task – Jonathan Tudor (Fidelity Investments) offers valuable advice for gastroenterologists on how to remain secure in your finances even in uncertain circumstances.
This quarter’s “In Focus” feature, written by Dr. Yutaka Tomizawa (University of Washington), is a comprehensive piece elucidating the role of gastroenterologists in the management of gastric cancer. The article reviews the individual risk factors that exist for gastric cancer and provides guidance on how to stratify patients accordingly, which is critical in the ethnically diverse population of the United States.
Keeping a procedure log during fellowship can seem daunting and cumbersome, but it is important. Dr. Houman Rezaizadeh (University of Connecticut) shares his program’s experience with the AGA Procedure Log, a convenient online tracking tool, which can provide accurate and secure documentation of endoscopic procedures performed throughout fellowship.
Dr. Nazia Hasan (North Bay Health Care) and Dr. Allison Schulman (University of Michigan) broach an incredibly important topic: the paucity of women in interventional endoscopy. Dr. Hasan and Dr. Shulman candidly discuss the barriers women face in pursuing this subspecialty and offer practical solutions on how to approach these challenges – a piece that will surely resonate with many young gastroenterologists.
We wrap up our first year of TNG’s ethics series with two cases discussing the utilization of cannabis therapy in inflammatory bowel disease (IBD). Dr. Jami Kinnucan (University of Michigan) and Dr. Arun Swaminath (Lenox Hill Hospital) systematically review existing data on the efficacy of cannabis use in IBD, the risks associated with therapy, and legal implications for both physicians and patients.
Also in this issue is a high-yield clinical review on the endoscopic drainage of pancreatic fluid collections by Dr. Robert Moran and Dr. Joseph Elmunzer (Medical University of South Carolina). Dr. Manol Jovani (Johns Hopkins) teaches us about confounding – a critical concept to keep in mind when evaluating any manuscript. Lastly, our DHPA Private Practice Perspectives article, written by Dr. Mehul Lalani (US Digestive), reviews how quality measures and initiatives are tracked and implemented in private practice.
If you have interest in contributing or have ideas for future TNG topics, please contact me ([email protected]), or Ryan Farrell ([email protected]), managing editor of TNG.
Stay well,
Vijaya L. Rao, MD
Editor in Chief
Assistant Professor of Medicine, University of Chicago, Section of Gastroenterology, Hepatology & Nutrition
Disruption of postpandemic world will precipitate innovation
When this editorial is published, we will know the results of the national election (hopefully) and whether there will be a smooth transition of power. We should know whether the Affordable Care Act will remain intact, and we will have indications about the impact of a COVID/flu combination. Health care will never be the same.

According to a recent Medscape survey, 62% of U.S. physicians saw a reduction of monthly income (12% saw a reduction of over 70%) in the first 6 months of this year. Almost a third of the physician workforce is contemplating retirement earlier than anticipated. As worrisome, according to a JAMA article (Aug 4, 2020;324:510-3) the United States saw a 35% increase in excess deaths because of non-COVID etiologies, an indication of health care deferral and avoidance. We all are scrambling to catch up and accommodate an enormous demand.
We are witnessing a “K” shaped recovery for both individuals and GI practices. If your health care is covered by Medicare, you own a mortgage-free home and your wealth is based on a balanced equity/bond portfolio, then all of your assets increased in value compared to last year’s peak valuations. For the other 90% of Americans, the recovery is modest, neutral, or more often nonexistent. Gastroenterologists who work in academic centers or large health systems did not lose income this year and were protected by billion-dollar credit lines and cash-on-hand accounts from robust days available to these entities. Independent practices (critically dependent on monthly cash flow) were decimated, furthering the trend towards consolidation, retirement, and acquisitions. With the new CMS E/M valuations we will see further reduction in procedural reimbursement.
However, disruption always precipitates innovation. Challenges are great but opportunities are clearly evident for those willing to risk.
John I. Allen, MD, MBA, AGAF
Editor in Chief
When this editorial is published, we will know the results of the national election (hopefully) and whether there will be a smooth transition of power. We should know whether the Affordable Care Act will remain intact, and we will have indications about the impact of a COVID/flu combination. Health care will never be the same.
According to a recent Medscape survey, 62% of U.S. physicians saw a reduction of monthly income (12% saw a reduction of over 70%) in the first 6 months of this year. Almost a third of the physician workforce is contemplating retirement earlier than anticipated. As worrisome, according to a JAMA article (Aug 4, 2020;324:510-3) the United States saw a 35% increase in excess deaths because of non-COVID etiologies, an indication of health care deferral and avoidance. We all are scrambling to catch up and accommodate an enormous demand.
We are witnessing a “K” shaped recovery for both individuals and GI practices. If your health care is covered by Medicare, you own a mortgage-free home and your wealth is based on a balanced equity/bond portfolio, then all of your assets increased in value compared to last year’s peak valuations. For the other 90% of Americans, the recovery is modest, neutral, or more often nonexistent. Gastroenterologists who work in academic centers or large health systems did not lose income this year and were protected by billion-dollar credit lines and cash-on-hand accounts from robust days available to these entities. Independent practices (critically dependent on monthly cash flow) were decimated, furthering the trend towards consolidation, retirement, and acquisitions. With the new CMS E/M valuations we will see further reduction in procedural reimbursement.
However, disruption always precipitates innovation. Challenges are great but opportunities are clearly evident for those willing to risk.
John I. Allen, MD, MBA, AGAF
Editor in Chief
When this editorial is published, we will know the results of the national election (hopefully) and whether there will be a smooth transition of power. We should know whether the Affordable Care Act will remain intact, and we will have indications about the impact of a COVID/flu combination. Health care will never be the same.
According to a recent Medscape survey, 62% of U.S. physicians saw a reduction of monthly income (12% saw a reduction of over 70%) in the first 6 months of this year. Almost a third of the physician workforce is contemplating retirement earlier than anticipated. As worrisome, according to a JAMA article (Aug 4, 2020;324:510-3) the United States saw a 35% increase in excess deaths because of non-COVID etiologies, an indication of health care deferral and avoidance. We all are scrambling to catch up and accommodate an enormous demand.
We are witnessing a “K” shaped recovery for both individuals and GI practices. If your health care is covered by Medicare, you own a mortgage-free home and your wealth is based on a balanced equity/bond portfolio, then all of your assets increased in value compared to last year’s peak valuations. For the other 90% of Americans, the recovery is modest, neutral, or more often nonexistent. Gastroenterologists who work in academic centers or large health systems did not lose income this year and were protected by billion-dollar credit lines and cash-on-hand accounts from robust days available to these entities. Independent practices (critically dependent on monthly cash flow) were decimated, furthering the trend towards consolidation, retirement, and acquisitions. With the new CMS E/M valuations we will see further reduction in procedural reimbursement.
However, disruption always precipitates innovation. Challenges are great but opportunities are clearly evident for those willing to risk.
John I. Allen, MD, MBA, AGAF
Editor in Chief
Adenomyosis: An update on imaging, medical, and surgical treatment
Adenomyosis is a benign disorder, present in 20%-35% of women and characterized by the presence of endometrial glands and stroma within the myometrium. The ectopic endometrial tissue appears to cause hypertrophy in the myometrium, resulting in an enlarged globular uterus.

Adenomyosis may present as diffuse or focal involvement within the uterus. When the focal lesion appears to be well defined, it is referred to as an adenomyoma. It is not encapsulated like a fibroid. There may be involvement of the junctional zone of the myometrium – the area between the subendometrial myometrium and the outer myometrium. While the pathogenesis of adenomyosis is unknown, two rigorous theories exist: endomyometrial invagination of the endometrium and de novo from Müllerian rests.
For this installment of the Master Class in Gynecologic Surgery, I have enlisted Keith B. Isaacson, MD, to discuss the clinical presentation, diagnosis, and medical and surgical treatment of adenomyosis.
Dr. Isaacson is the director of minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, Newton, Mass., and associate professor of obstetrics and gynecology at Harvard Medical School, Boston. He is currently in practice specializing in minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, where he is the director of the AAGL Fellowship in Minimally Invasive Gynecologic Surgery. Dr. Isaacson is a past president of both the AAGL and the Society of Reproductive Surgeons, as well as a published clinical researcher and surgical innovator.
It is a true honor to welcome Dr. Isaacson to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is professor of obstetrics & gynecology in the Department of Clinical Sciences, Rosalind Franklin University, North Chicago, and director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, both in Illinois. Dr. Miller reported that he has no relevant disclosures. Email him at [email protected].
Adenomyosis is a benign disorder, present in 20%-35% of women and characterized by the presence of endometrial glands and stroma within the myometrium. The ectopic endometrial tissue appears to cause hypertrophy in the myometrium, resulting in an enlarged globular uterus.
Adenomyosis may present as diffuse or focal involvement within the uterus. When the focal lesion appears to be well defined, it is referred to as an adenomyoma. It is not encapsulated like a fibroid. There may be involvement of the junctional zone of the myometrium – the area between the subendometrial myometrium and the outer myometrium. While the pathogenesis of adenomyosis is unknown, two rigorous theories exist: endomyometrial invagination of the endometrium and de novo from Müllerian rests.
For this installment of the Master Class in Gynecologic Surgery, I have enlisted Keith B. Isaacson, MD, to discuss the clinical presentation, diagnosis, and medical and surgical treatment of adenomyosis.
Dr. Isaacson is the director of minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, Newton, Mass., and associate professor of obstetrics and gynecology at Harvard Medical School, Boston. He is currently in practice specializing in minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, where he is the director of the AAGL Fellowship in Minimally Invasive Gynecologic Surgery. Dr. Isaacson is a past president of both the AAGL and the Society of Reproductive Surgeons, as well as a published clinical researcher and surgical innovator.
It is a true honor to welcome Dr. Isaacson to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is professor of obstetrics & gynecology in the Department of Clinical Sciences, Rosalind Franklin University, North Chicago, and director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, both in Illinois. Dr. Miller reported that he has no relevant disclosures. Email him at [email protected].
Adenomyosis is a benign disorder, present in 20%-35% of women and characterized by the presence of endometrial glands and stroma within the myometrium. The ectopic endometrial tissue appears to cause hypertrophy in the myometrium, resulting in an enlarged globular uterus.
Adenomyosis may present as diffuse or focal involvement within the uterus. When the focal lesion appears to be well defined, it is referred to as an adenomyoma. It is not encapsulated like a fibroid. There may be involvement of the junctional zone of the myometrium – the area between the subendometrial myometrium and the outer myometrium. While the pathogenesis of adenomyosis is unknown, two rigorous theories exist: endomyometrial invagination of the endometrium and de novo from Müllerian rests.
For this installment of the Master Class in Gynecologic Surgery, I have enlisted Keith B. Isaacson, MD, to discuss the clinical presentation, diagnosis, and medical and surgical treatment of adenomyosis.
Dr. Isaacson is the director of minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, Newton, Mass., and associate professor of obstetrics and gynecology at Harvard Medical School, Boston. He is currently in practice specializing in minimally invasive gynecologic surgery and infertility at Newton-Wellesley Hospital, where he is the director of the AAGL Fellowship in Minimally Invasive Gynecologic Surgery. Dr. Isaacson is a past president of both the AAGL and the Society of Reproductive Surgeons, as well as a published clinical researcher and surgical innovator.
It is a true honor to welcome Dr. Isaacson to this edition of the Master Class in Gynecologic Surgery.
Dr. Miller is professor of obstetrics & gynecology in the Department of Clinical Sciences, Rosalind Franklin University, North Chicago, and director of minimally invasive gynecologic surgery at Advocate Lutheran General Hospital, Park Ridge, both in Illinois. Dr. Miller reported that he has no relevant disclosures. Email him at [email protected].

Adenomyosis: While a last resort, surgery remains an option
Adenomyosis causing severe dysmenorrhea, dyspareunia, and heavy menstrual bleeding has been thought to affect primarily multiparous women in their mid- to late 40s. Often women who experience pain and heavy bleeding will tolerate their symptoms until they are done with childbearing, at which point they often go on to have a hysterectomy to relieve them of these symptoms. Tissue histology obtained at the time of hysterectomy confirms the diagnosis of adenomyosis.

Because the diagnosis is made at the time of hysterectomy, the published incidence and prevalence of adenomyosis is more a reflection of a risk for hysterectomy and not for the disease itself. MRI has been used to evaluate the junctional zone in patients with symptoms of endometriosis. This screen tool is an expensive one, however, and has not been used extensively to evaluate women with symptoms of adenomyosis who are not candidates for a hysterectomy.
Ultrasound studies
Over the past 5-7 years, numerous studies have been performed that demonstrate ultrasound changes consistent with adenomyosis within the uterus. These changes include asymmetry and heterogeneity of the anterior and posterior myometrium, cystic lesions in the myometrium, ultrasound striations, and streaking and irregular junctional zone thickening seen on 3-D scans.
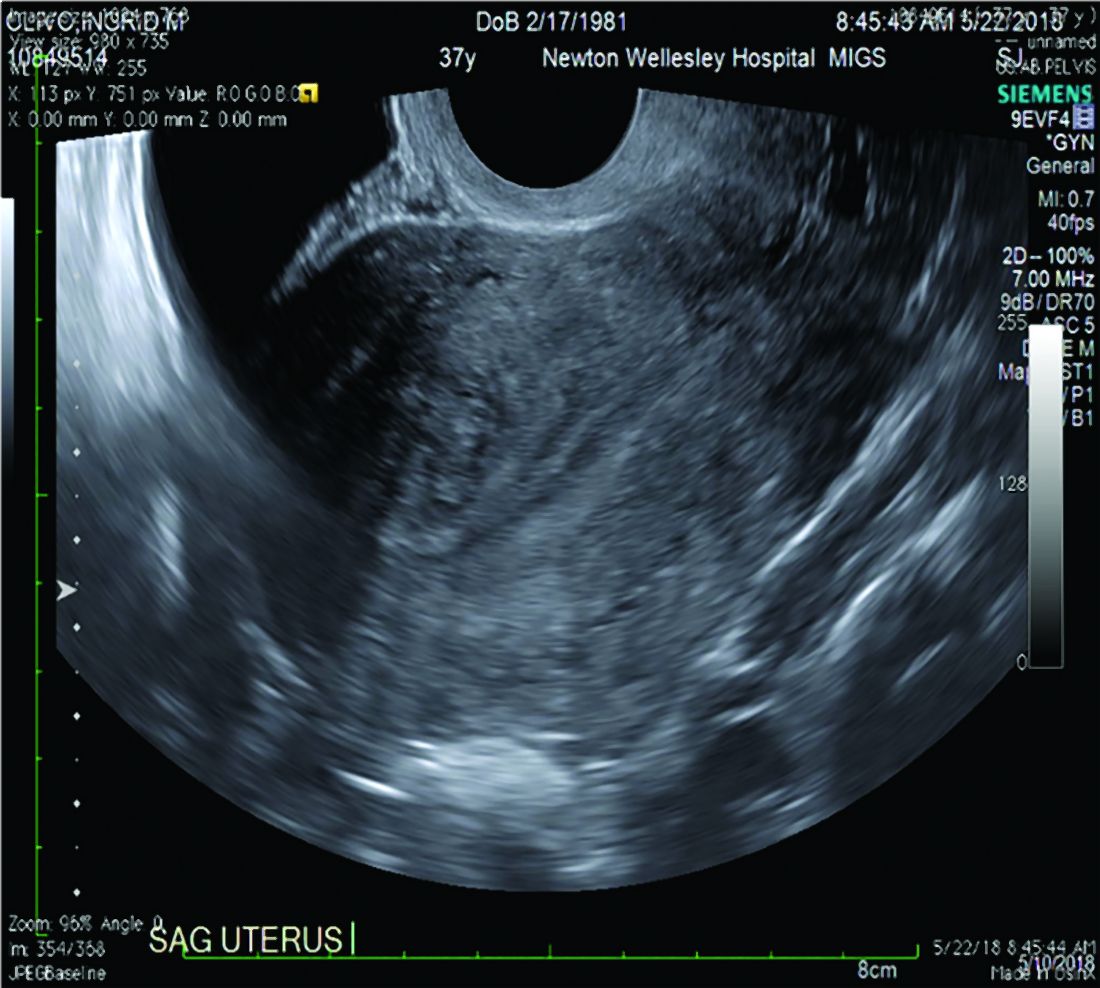
Our newfound ability to demonstrate changes consistent with adenomyosis by ultrasound – a tool that is much less expensive than MRI and more available to patients – means that we can and should consider adenomyosis in patients suffering from dysmenorrhea, heavy menstrual bleeding, back pain, dyspareunia, and infertility – regardless of the patient’s age.
In the last 5 years, adenomyosis has been increasingly recognized as a disorder affecting women of all reproductive ages, including teenagers whose dysmenorrhea disrupts their education and young women undergoing infertility evaluations. In one study, 12% of adolescent girls and young women aged 14–20 years lost days of school or work each month because of dysmenorrhea.1 This disruption is not “normal.”
Several meta-analyses have also demonstrated that ultrasound and MRI changes consistent with adenomyosis can affect embryo implantation rates in women undergoing in vitro fertilization. The implantation rates can be as low as one half the expected rate without adenomyosis. Additionally, adenomyosis has been shown to increase the risk of miscarriage and preterm delivery.2,3
The clinicians who order and carefully look at the ultrasound themselves, rather than rely on the radiologist to make the diagnosis, will be able to see the changes consistent with adenomyosis. Over time – I anticipate the next several years – a standardized radiologic definition for adenomyosis will evolve, and radiologists will become more familiar with these changes. In the meantime, our patients should not have missed diagnoses.
Considerations for surgery
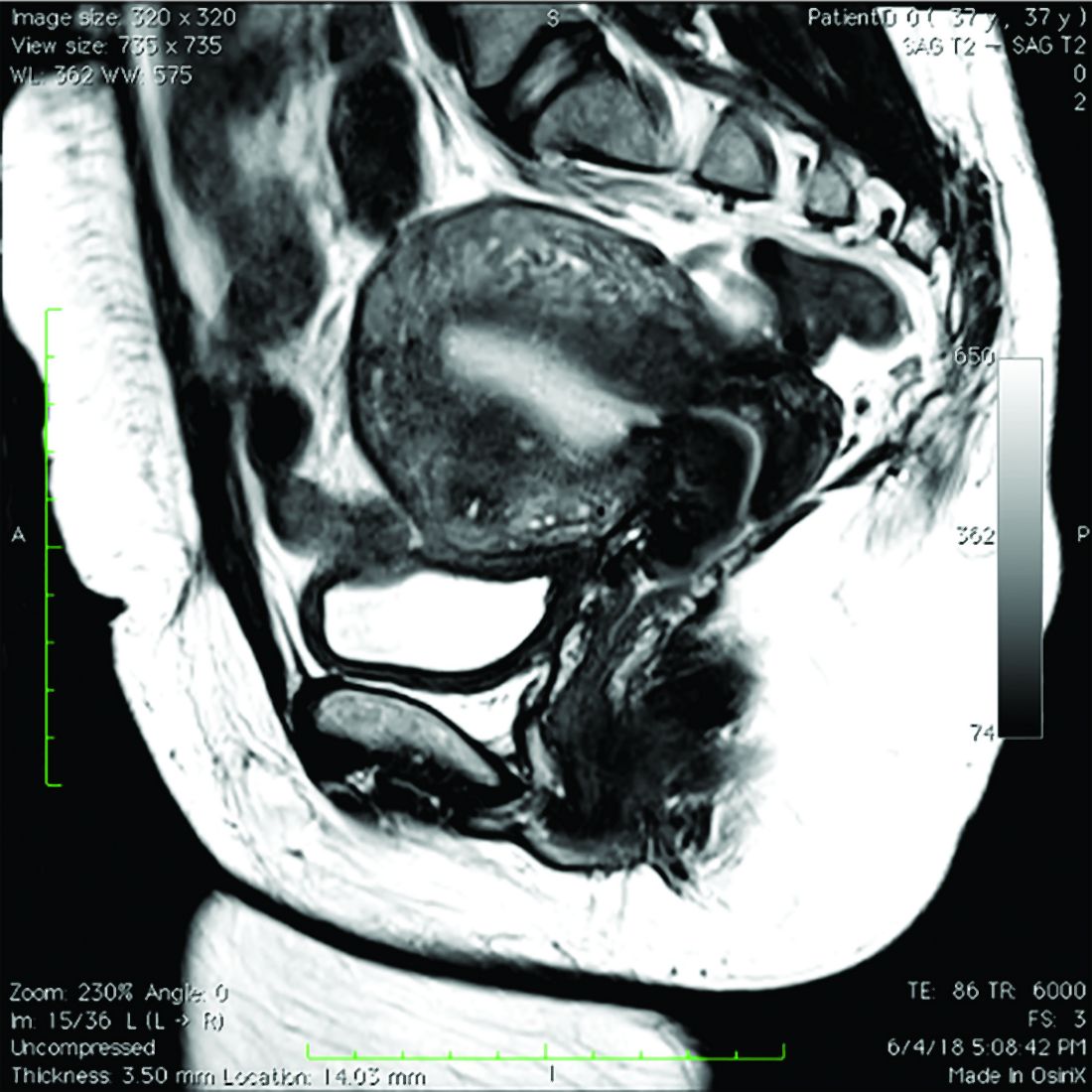
For the majority of younger patients who are not trying to conceive but want to maintain their fertility, medical treatment with oral contraceptives, progestins, or the levonorgestrel-releasing intrauterine device (Mirena) will relieve symptoms. The Mirena IUD has been found in studies of 6-36 months’ treatment duration to decrease the size of the uterus by 25%4 and improve dysmenorrhea and menorrhagia with a low profile of adverse effects in most women.
The Mirena IUD should be considered as a first-line therapy for all women with heavy menstrual bleeding and dyspareunia who want to preserve their fertility.
Patients who do not respond to or cannot tolerate medical therapy, and do not want to preserve their fertility, may consider hysterectomy, long regarded as the preferred method of treatment. Endometrial ablation can also be considered in those who no longer desire to preserve fertility and are experiencing heavy menstrual bleeding. Those with extensive adenomyosis, however, often experience poor results with endometrial ablation and may ultimately require hysterectomy. Endometrial ablation has a history of a high failure rate in women younger than 45 years old.
Patients with adenomyosis who wish to preserve their fertility and cannot tolerate or are unresponsive to hormonal therapy, or those with infertility thought to be caused by adenomyosis, should consider these three management options:
- Do nothing. The embryo implantation rate is not zero with adenomyosis, and we have no data on the number of patients who conceive with adenomyotic changes detected by MRI or ultrasound.
- Pretreat with a GnRH agonist for 2-3 months prior to a frozen embryo transfer (FET). Suppressing the disease prior to an FET seems to increase the implantation rate to what is expected for that patient given her age and other fertility factors.3 While this approach is often successful, an estimated 15%-20% of patients are unable to tolerate GnRH agonist treatment because of its side effects.
- Seek surgical resection of adenomyosis. Unlike uterine fibroids, adenomyosis has no pseudocapsule. When resecting the disease via laparotomy, laparoscopy, or hysteroscopy, the process is more of a debulking procedure. Surgical resection should be reserved for those who cannot tolerate hormonal suppression or have failed the other two options.
Surgical approaches
Surgical excision can be challenging because adenomyosis burrows its way through the muscle, is often diffuse, and cannot necessarily be resected with clean margins as can a fibroid. Yet, as demonstrated in a systematic review of 27 observational studies of conservative surgery for adenomyosis – 10 prospective and 17 retrospective studies with a total of almost 1,400 patients and all with adenomyosis confirmed histopathologically – surgery can improve pain, menorrhagia, and adenomyosis-related infertility in a significant number of cases.5
Disease may be resected through laparotomy, laparoscopy, or as we are currently doing with focal disease that is close to the endometrium, hysteroscopy. The type of surgery will depend on the location and characteristics of the disease, and on the surgeon’s skills. The principles are the same with all three approaches: to remove as much diseased tissue – and preserve as much healthy myometrial tissue – as possible and to reconstruct the uterine wall so that it maintains its integrity and can sustain a pregnancy.
The open approach known as the Osada procedure, after Hisao Osada, MD, PhD, in Tokyo, is well described in the literature, with a relatively large number of cases reported in prospective studies. Dr. Osada performs a radical adenomyosis excision with a triple flap method of uterine wall reconstruction. The uterus is bisected in the mid-sagittal plane all the way down through the adenomyosis until the uterine cavity is reached. Excision of the adenomyotic tissue is guided by palpation with the index finger, and a myometrial thickness of 1 cm from the serosa and the endometrium is preserved.
The endometrium is closed, and the myometrial defect is closed with a triple flap method that avoids overlapping suture lines. On one side of the uterus, the myometrium and serosa are sutured in the antero-posterior plane. The seromuscular layer of the opposite side of the uterine wall is then brought over the first seromuscular suture line.6
Others, such as Grigoris H. Grimbizis, MD, PhD, in Greece, have used a laparoscopic approach and closed the myometrium in layers similar to those of a myomectomy.7 There are no comparative trials that demonstrate one technique is superior to the other.
While there are no textbook techniques published for resecting adenomyotic tissue laparoscopically or hysteroscopically from the normal myometrium, there are some general principals the surgeon should keep in mind. Adenomyosis is defined as the presence of endometrial glands and stroma within myometrium, but biopsy studies have demonstrated that there are relatively few glands and stroma within the diseased tissue. Mostly, the adenomyotic tissue we encounter comprises smooth muscle hyperplasia and fibrosis.
Since there is no pseudocapsule surrounding adenomyotic tissue, the visual cue for the cytoreductive procedure is the presence of normal-appearing myometrium. The normal myometrium can be delineated by palpation with laparoscopic instruments or hysteroscopic loops as it clearly feels less fibrotic and firm than the adenomyotic tissue. For this reason, the adenomyotic tissue is removed in a piecemeal fashion until normal tissue is encountered. (This same philosophy can be applied to removing fibrotic, glandular, or cystic tissue hysteroscopically.)
If the disease involves the inner myometrium, it should resected as this may be very important to restoring normal uterine contractions needed for embryo implantation and development, even if it means entering the cavity laparoscopically.
Hysteroscopically, there is no ability to suture a myometrial defect. This limitation is concerning because the adenomyosis is thought to invade the myometrium and not displace it as seen with monoclonal uterine fibroids. There are no case reports of uterine rupture after hysteroscopic resection of adenomyosis, but the number of cases reported with this type of resection in general is very small.
Laparoscopically, the myometrial defect should be repaired similarly to a myomectomy defect. Chromic or polydioxanone (PDS) suture is appropriate. We have used 2-0 PDS V-loc and a 2-3 layer closure in our laparoscopic cases.
Diffuse adenomyosis can involve the entire anterior or posterior wall of the uterus or both. The surgeon should not attempt to remove all of the disease in this situation and must leave enough tissue, even diseased, to allow for structural integrity during pregnancy. Uterine rupture has not been reported in all published case series and studies, but overall, it is a concern with surgical excision of adenomyosis. An analysis of over 2,000 cases of adenomyomectomies reported worldwide since 1990 shows a uterine rupture rate in the 6% rate, with a pregnancy rate ranging from 7%-72%.8
When the disease is focal and close to the endometrium, as opposed to diffuse and affecting the entire back wall of the uterus, hysteroscopic excision may be an appropriate, less invasive approach.
One of the patients for whom we’ve taken this approach was a 37-year-old patient who presented with a history of six miscarriages, a negative work-up for recurrent pregnancy loss, an enlarged uterus, 8 years of heavy menstrual bleeding, and only mild dysmenorrhea. She had undergone in vitro fertilization with failed embryo transfers but normal genetic screens of the embryos. She was referred with a suspicion of fibroids. An MRI and ultrasound showed heterogeneous myometrium adjacent to the endometrium. This tissue was resected using a bipolar loop electrode until normal myometrium was encountered.
Hysteroscopic resections are currently described in the literature through case reports rather than larger prospective or retrospective studies, and much more research is needed to demonstrate the efficacy and safety of this approach.
At this point in time, while surgery to excise adenomyosis is a last resort and best methods are deliberated, it is still important to appreciate that surgery is an option. Continued infertility is not the only choice, nor is hysterectomy.
References
1. J Pediatr Adolesc Gynecol 2014;27:258-65.
2. Minerva Ginecol. 2018 Jun;70(3):295-302.
3. Fertil Steril. 2017;108(3):483-490.e3.
4. Am J Obstet Gynecol. 2008;198(4):373.e1-7.
5. J. Minim Invasive Gynecol. 2018 Feb;25:265-76.
6. Reproductive BioMed Online. 2011 Jan;22(1):94-9.
7. Fertil Steril. 2014 Feb;101(2):472-87.
8. Fertil Steril. 2018 Mar;109(3):406-17.
Adenomyosis causing severe dysmenorrhea, dyspareunia, and heavy menstrual bleeding has been thought to affect primarily multiparous women in their mid- to late 40s. Often women who experience pain and heavy bleeding will tolerate their symptoms until they are done with childbearing, at which point they often go on to have a hysterectomy to relieve them of these symptoms. Tissue histology obtained at the time of hysterectomy confirms the diagnosis of adenomyosis.
Because the diagnosis is made at the time of hysterectomy, the published incidence and prevalence of adenomyosis is more a reflection of a risk for hysterectomy and not for the disease itself. MRI has been used to evaluate the junctional zone in patients with symptoms of endometriosis. This screen tool is an expensive one, however, and has not been used extensively to evaluate women with symptoms of adenomyosis who are not candidates for a hysterectomy.
Ultrasound studies
Over the past 5-7 years, numerous studies have been performed that demonstrate ultrasound changes consistent with adenomyosis within the uterus. These changes include asymmetry and heterogeneity of the anterior and posterior myometrium, cystic lesions in the myometrium, ultrasound striations, and streaking and irregular junctional zone thickening seen on 3-D scans.
Our newfound ability to demonstrate changes consistent with adenomyosis by ultrasound – a tool that is much less expensive than MRI and more available to patients – means that we can and should consider adenomyosis in patients suffering from dysmenorrhea, heavy menstrual bleeding, back pain, dyspareunia, and infertility – regardless of the patient’s age.
In the last 5 years, adenomyosis has been increasingly recognized as a disorder affecting women of all reproductive ages, including teenagers whose dysmenorrhea disrupts their education and young women undergoing infertility evaluations. In one study, 12% of adolescent girls and young women aged 14–20 years lost days of school or work each month because of dysmenorrhea.1 This disruption is not “normal.”
Several meta-analyses have also demonstrated that ultrasound and MRI changes consistent with adenomyosis can affect embryo implantation rates in women undergoing in vitro fertilization. The implantation rates can be as low as one half the expected rate without adenomyosis. Additionally, adenomyosis has been shown to increase the risk of miscarriage and preterm delivery.2,3
The clinicians who order and carefully look at the ultrasound themselves, rather than rely on the radiologist to make the diagnosis, will be able to see the changes consistent with adenomyosis. Over time – I anticipate the next several years – a standardized radiologic definition for adenomyosis will evolve, and radiologists will become more familiar with these changes. In the meantime, our patients should not have missed diagnoses.
Considerations for surgery
For the majority of younger patients who are not trying to conceive but want to maintain their fertility, medical treatment with oral contraceptives, progestins, or the levonorgestrel-releasing intrauterine device (Mirena) will relieve symptoms. The Mirena IUD has been found in studies of 6-36 months’ treatment duration to decrease the size of the uterus by 25%4 and improve dysmenorrhea and menorrhagia with a low profile of adverse effects in most women.
The Mirena IUD should be considered as a first-line therapy for all women with heavy menstrual bleeding and dyspareunia who want to preserve their fertility.
Patients who do not respond to or cannot tolerate medical therapy, and do not want to preserve their fertility, may consider hysterectomy, long regarded as the preferred method of treatment. Endometrial ablation can also be considered in those who no longer desire to preserve fertility and are experiencing heavy menstrual bleeding. Those with extensive adenomyosis, however, often experience poor results with endometrial ablation and may ultimately require hysterectomy. Endometrial ablation has a history of a high failure rate in women younger than 45 years old.
Patients with adenomyosis who wish to preserve their fertility and cannot tolerate or are unresponsive to hormonal therapy, or those with infertility thought to be caused by adenomyosis, should consider these three management options:
- Do nothing. The embryo implantation rate is not zero with adenomyosis, and we have no data on the number of patients who conceive with adenomyotic changes detected by MRI or ultrasound.
- Pretreat with a GnRH agonist for 2-3 months prior to a frozen embryo transfer (FET). Suppressing the disease prior to an FET seems to increase the implantation rate to what is expected for that patient given her age and other fertility factors.3 While this approach is often successful, an estimated 15%-20% of patients are unable to tolerate GnRH agonist treatment because of its side effects.
- Seek surgical resection of adenomyosis. Unlike uterine fibroids, adenomyosis has no pseudocapsule. When resecting the disease via laparotomy, laparoscopy, or hysteroscopy, the process is more of a debulking procedure. Surgical resection should be reserved for those who cannot tolerate hormonal suppression or have failed the other two options.
Surgical approaches
Surgical excision can be challenging because adenomyosis burrows its way through the muscle, is often diffuse, and cannot necessarily be resected with clean margins as can a fibroid. Yet, as demonstrated in a systematic review of 27 observational studies of conservative surgery for adenomyosis – 10 prospective and 17 retrospective studies with a total of almost 1,400 patients and all with adenomyosis confirmed histopathologically – surgery can improve pain, menorrhagia, and adenomyosis-related infertility in a significant number of cases.5
Disease may be resected through laparotomy, laparoscopy, or as we are currently doing with focal disease that is close to the endometrium, hysteroscopy. The type of surgery will depend on the location and characteristics of the disease, and on the surgeon’s skills. The principles are the same with all three approaches: to remove as much diseased tissue – and preserve as much healthy myometrial tissue – as possible and to reconstruct the uterine wall so that it maintains its integrity and can sustain a pregnancy.
The open approach known as the Osada procedure, after Hisao Osada, MD, PhD, in Tokyo, is well described in the literature, with a relatively large number of cases reported in prospective studies. Dr. Osada performs a radical adenomyosis excision with a triple flap method of uterine wall reconstruction. The uterus is bisected in the mid-sagittal plane all the way down through the adenomyosis until the uterine cavity is reached. Excision of the adenomyotic tissue is guided by palpation with the index finger, and a myometrial thickness of 1 cm from the serosa and the endometrium is preserved.
The endometrium is closed, and the myometrial defect is closed with a triple flap method that avoids overlapping suture lines. On one side of the uterus, the myometrium and serosa are sutured in the antero-posterior plane. The seromuscular layer of the opposite side of the uterine wall is then brought over the first seromuscular suture line.6
Others, such as Grigoris H. Grimbizis, MD, PhD, in Greece, have used a laparoscopic approach and closed the myometrium in layers similar to those of a myomectomy.7 There are no comparative trials that demonstrate one technique is superior to the other.
While there are no textbook techniques published for resecting adenomyotic tissue laparoscopically or hysteroscopically from the normal myometrium, there are some general principals the surgeon should keep in mind. Adenomyosis is defined as the presence of endometrial glands and stroma within myometrium, but biopsy studies have demonstrated that there are relatively few glands and stroma within the diseased tissue. Mostly, the adenomyotic tissue we encounter comprises smooth muscle hyperplasia and fibrosis.
Since there is no pseudocapsule surrounding adenomyotic tissue, the visual cue for the cytoreductive procedure is the presence of normal-appearing myometrium. The normal myometrium can be delineated by palpation with laparoscopic instruments or hysteroscopic loops as it clearly feels less fibrotic and firm than the adenomyotic tissue. For this reason, the adenomyotic tissue is removed in a piecemeal fashion until normal tissue is encountered. (This same philosophy can be applied to removing fibrotic, glandular, or cystic tissue hysteroscopically.)
If the disease involves the inner myometrium, it should resected as this may be very important to restoring normal uterine contractions needed for embryo implantation and development, even if it means entering the cavity laparoscopically.
Hysteroscopically, there is no ability to suture a myometrial defect. This limitation is concerning because the adenomyosis is thought to invade the myometrium and not displace it as seen with monoclonal uterine fibroids. There are no case reports of uterine rupture after hysteroscopic resection of adenomyosis, but the number of cases reported with this type of resection in general is very small.
Laparoscopically, the myometrial defect should be repaired similarly to a myomectomy defect. Chromic or polydioxanone (PDS) suture is appropriate. We have used 2-0 PDS V-loc and a 2-3 layer closure in our laparoscopic cases.
Diffuse adenomyosis can involve the entire anterior or posterior wall of the uterus or both. The surgeon should not attempt to remove all of the disease in this situation and must leave enough tissue, even diseased, to allow for structural integrity during pregnancy. Uterine rupture has not been reported in all published case series and studies, but overall, it is a concern with surgical excision of adenomyosis. An analysis of over 2,000 cases of adenomyomectomies reported worldwide since 1990 shows a uterine rupture rate in the 6% rate, with a pregnancy rate ranging from 7%-72%.8
When the disease is focal and close to the endometrium, as opposed to diffuse and affecting the entire back wall of the uterus, hysteroscopic excision may be an appropriate, less invasive approach.
One of the patients for whom we’ve taken this approach was a 37-year-old patient who presented with a history of six miscarriages, a negative work-up for recurrent pregnancy loss, an enlarged uterus, 8 years of heavy menstrual bleeding, and only mild dysmenorrhea. She had undergone in vitro fertilization with failed embryo transfers but normal genetic screens of the embryos. She was referred with a suspicion of fibroids. An MRI and ultrasound showed heterogeneous myometrium adjacent to the endometrium. This tissue was resected using a bipolar loop electrode until normal myometrium was encountered.
Hysteroscopic resections are currently described in the literature through case reports rather than larger prospective or retrospective studies, and much more research is needed to demonstrate the efficacy and safety of this approach.
At this point in time, while surgery to excise adenomyosis is a last resort and best methods are deliberated, it is still important to appreciate that surgery is an option. Continued infertility is not the only choice, nor is hysterectomy.
References
1. J Pediatr Adolesc Gynecol 2014;27:258-65.
2. Minerva Ginecol. 2018 Jun;70(3):295-302.
3. Fertil Steril. 2017;108(3):483-490.e3.
4. Am J Obstet Gynecol. 2008;198(4):373.e1-7.
5. J. Minim Invasive Gynecol. 2018 Feb;25:265-76.
6. Reproductive BioMed Online. 2011 Jan;22(1):94-9.
7. Fertil Steril. 2014 Feb;101(2):472-87.
8. Fertil Steril. 2018 Mar;109(3):406-17.
Adenomyosis causing severe dysmenorrhea, dyspareunia, and heavy menstrual bleeding has been thought to affect primarily multiparous women in their mid- to late 40s. Often women who experience pain and heavy bleeding will tolerate their symptoms until they are done with childbearing, at which point they often go on to have a hysterectomy to relieve them of these symptoms. Tissue histology obtained at the time of hysterectomy confirms the diagnosis of adenomyosis.
Because the diagnosis is made at the time of hysterectomy, the published incidence and prevalence of adenomyosis is more a reflection of a risk for hysterectomy and not for the disease itself. MRI has been used to evaluate the junctional zone in patients with symptoms of endometriosis. This screen tool is an expensive one, however, and has not been used extensively to evaluate women with symptoms of adenomyosis who are not candidates for a hysterectomy.
Ultrasound studies
Over the past 5-7 years, numerous studies have been performed that demonstrate ultrasound changes consistent with adenomyosis within the uterus. These changes include asymmetry and heterogeneity of the anterior and posterior myometrium, cystic lesions in the myometrium, ultrasound striations, and streaking and irregular junctional zone thickening seen on 3-D scans.
Our newfound ability to demonstrate changes consistent with adenomyosis by ultrasound – a tool that is much less expensive than MRI and more available to patients – means that we can and should consider adenomyosis in patients suffering from dysmenorrhea, heavy menstrual bleeding, back pain, dyspareunia, and infertility – regardless of the patient’s age.
In the last 5 years, adenomyosis has been increasingly recognized as a disorder affecting women of all reproductive ages, including teenagers whose dysmenorrhea disrupts their education and young women undergoing infertility evaluations. In one study, 12% of adolescent girls and young women aged 14–20 years lost days of school or work each month because of dysmenorrhea.1 This disruption is not “normal.”
Several meta-analyses have also demonstrated that ultrasound and MRI changes consistent with adenomyosis can affect embryo implantation rates in women undergoing in vitro fertilization. The implantation rates can be as low as one half the expected rate without adenomyosis. Additionally, adenomyosis has been shown to increase the risk of miscarriage and preterm delivery.2,3
The clinicians who order and carefully look at the ultrasound themselves, rather than rely on the radiologist to make the diagnosis, will be able to see the changes consistent with adenomyosis. Over time – I anticipate the next several years – a standardized radiologic definition for adenomyosis will evolve, and radiologists will become more familiar with these changes. In the meantime, our patients should not have missed diagnoses.
Considerations for surgery
For the majority of younger patients who are not trying to conceive but want to maintain their fertility, medical treatment with oral contraceptives, progestins, or the levonorgestrel-releasing intrauterine device (Mirena) will relieve symptoms. The Mirena IUD has been found in studies of 6-36 months’ treatment duration to decrease the size of the uterus by 25%4 and improve dysmenorrhea and menorrhagia with a low profile of adverse effects in most women.
The Mirena IUD should be considered as a first-line therapy for all women with heavy menstrual bleeding and dyspareunia who want to preserve their fertility.
Patients who do not respond to or cannot tolerate medical therapy, and do not want to preserve their fertility, may consider hysterectomy, long regarded as the preferred method of treatment. Endometrial ablation can also be considered in those who no longer desire to preserve fertility and are experiencing heavy menstrual bleeding. Those with extensive adenomyosis, however, often experience poor results with endometrial ablation and may ultimately require hysterectomy. Endometrial ablation has a history of a high failure rate in women younger than 45 years old.
Patients with adenomyosis who wish to preserve their fertility and cannot tolerate or are unresponsive to hormonal therapy, or those with infertility thought to be caused by adenomyosis, should consider these three management options:
- Do nothing. The embryo implantation rate is not zero with adenomyosis, and we have no data on the number of patients who conceive with adenomyotic changes detected by MRI or ultrasound.
- Pretreat with a GnRH agonist for 2-3 months prior to a frozen embryo transfer (FET). Suppressing the disease prior to an FET seems to increase the implantation rate to what is expected for that patient given her age and other fertility factors.3 While this approach is often successful, an estimated 15%-20% of patients are unable to tolerate GnRH agonist treatment because of its side effects.
- Seek surgical resection of adenomyosis. Unlike uterine fibroids, adenomyosis has no pseudocapsule. When resecting the disease via laparotomy, laparoscopy, or hysteroscopy, the process is more of a debulking procedure. Surgical resection should be reserved for those who cannot tolerate hormonal suppression or have failed the other two options.
Surgical approaches
Surgical excision can be challenging because adenomyosis burrows its way through the muscle, is often diffuse, and cannot necessarily be resected with clean margins as can a fibroid. Yet, as demonstrated in a systematic review of 27 observational studies of conservative surgery for adenomyosis – 10 prospective and 17 retrospective studies with a total of almost 1,400 patients and all with adenomyosis confirmed histopathologically – surgery can improve pain, menorrhagia, and adenomyosis-related infertility in a significant number of cases.5
Disease may be resected through laparotomy, laparoscopy, or as we are currently doing with focal disease that is close to the endometrium, hysteroscopy. The type of surgery will depend on the location and characteristics of the disease, and on the surgeon’s skills. The principles are the same with all three approaches: to remove as much diseased tissue – and preserve as much healthy myometrial tissue – as possible and to reconstruct the uterine wall so that it maintains its integrity and can sustain a pregnancy.
The open approach known as the Osada procedure, after Hisao Osada, MD, PhD, in Tokyo, is well described in the literature, with a relatively large number of cases reported in prospective studies. Dr. Osada performs a radical adenomyosis excision with a triple flap method of uterine wall reconstruction. The uterus is bisected in the mid-sagittal plane all the way down through the adenomyosis until the uterine cavity is reached. Excision of the adenomyotic tissue is guided by palpation with the index finger, and a myometrial thickness of 1 cm from the serosa and the endometrium is preserved.
The endometrium is closed, and the myometrial defect is closed with a triple flap method that avoids overlapping suture lines. On one side of the uterus, the myometrium and serosa are sutured in the antero-posterior plane. The seromuscular layer of the opposite side of the uterine wall is then brought over the first seromuscular suture line.6
Others, such as Grigoris H. Grimbizis, MD, PhD, in Greece, have used a laparoscopic approach and closed the myometrium in layers similar to those of a myomectomy.7 There are no comparative trials that demonstrate one technique is superior to the other.
While there are no textbook techniques published for resecting adenomyotic tissue laparoscopically or hysteroscopically from the normal myometrium, there are some general principals the surgeon should keep in mind. Adenomyosis is defined as the presence of endometrial glands and stroma within myometrium, but biopsy studies have demonstrated that there are relatively few glands and stroma within the diseased tissue. Mostly, the adenomyotic tissue we encounter comprises smooth muscle hyperplasia and fibrosis.
Since there is no pseudocapsule surrounding adenomyotic tissue, the visual cue for the cytoreductive procedure is the presence of normal-appearing myometrium. The normal myometrium can be delineated by palpation with laparoscopic instruments or hysteroscopic loops as it clearly feels less fibrotic and firm than the adenomyotic tissue. For this reason, the adenomyotic tissue is removed in a piecemeal fashion until normal tissue is encountered. (This same philosophy can be applied to removing fibrotic, glandular, or cystic tissue hysteroscopically.)
If the disease involves the inner myometrium, it should resected as this may be very important to restoring normal uterine contractions needed for embryo implantation and development, even if it means entering the cavity laparoscopically.
Hysteroscopically, there is no ability to suture a myometrial defect. This limitation is concerning because the adenomyosis is thought to invade the myometrium and not displace it as seen with monoclonal uterine fibroids. There are no case reports of uterine rupture after hysteroscopic resection of adenomyosis, but the number of cases reported with this type of resection in general is very small.
Laparoscopically, the myometrial defect should be repaired similarly to a myomectomy defect. Chromic or polydioxanone (PDS) suture is appropriate. We have used 2-0 PDS V-loc and a 2-3 layer closure in our laparoscopic cases.
Diffuse adenomyosis can involve the entire anterior or posterior wall of the uterus or both. The surgeon should not attempt to remove all of the disease in this situation and must leave enough tissue, even diseased, to allow for structural integrity during pregnancy. Uterine rupture has not been reported in all published case series and studies, but overall, it is a concern with surgical excision of adenomyosis. An analysis of over 2,000 cases of adenomyomectomies reported worldwide since 1990 shows a uterine rupture rate in the 6% rate, with a pregnancy rate ranging from 7%-72%.8
When the disease is focal and close to the endometrium, as opposed to diffuse and affecting the entire back wall of the uterus, hysteroscopic excision may be an appropriate, less invasive approach.
One of the patients for whom we’ve taken this approach was a 37-year-old patient who presented with a history of six miscarriages, a negative work-up for recurrent pregnancy loss, an enlarged uterus, 8 years of heavy menstrual bleeding, and only mild dysmenorrhea. She had undergone in vitro fertilization with failed embryo transfers but normal genetic screens of the embryos. She was referred with a suspicion of fibroids. An MRI and ultrasound showed heterogeneous myometrium adjacent to the endometrium. This tissue was resected using a bipolar loop electrode until normal myometrium was encountered.
Hysteroscopic resections are currently described in the literature through case reports rather than larger prospective or retrospective studies, and much more research is needed to demonstrate the efficacy and safety of this approach.
At this point in time, while surgery to excise adenomyosis is a last resort and best methods are deliberated, it is still important to appreciate that surgery is an option. Continued infertility is not the only choice, nor is hysterectomy.
References
1. J Pediatr Adolesc Gynecol 2014;27:258-65.
2. Minerva Ginecol. 2018 Jun;70(3):295-302.
3. Fertil Steril. 2017;108(3):483-490.e3.
4. Am J Obstet Gynecol. 2008;198(4):373.e1-7.
5. J. Minim Invasive Gynecol. 2018 Feb;25:265-76.
6. Reproductive BioMed Online. 2011 Jan;22(1):94-9.
7. Fertil Steril. 2014 Feb;101(2):472-87.
8. Fertil Steril. 2018 Mar;109(3):406-17.
Chronic abdominal pain: What to do when a patient presents with it
She reports the pain is about a 7 out of 10, located in the right upper quadrant. The pain does not worsen with food and not relieved with bowel movements. She has no nausea or vomiting. She reports that the pain worsens when she is sitting or standing and is relieved by lying down. Her past medical history includes having had a cholecystectomy in 2016, having hypertension, and having type 2 diabetes mellitus.

The patient’s medications include metformin, lisinopril, and empagliflozin. Her blood pressure was 130/70, and her pulse was 80. An abdominal exam of her found tenderness to palpation in the right upper quadrant, and no rebound tenderness. Her labs found a white blood cell count of 5.4, a hematocrit of 44%, an erythrocyte sedimentation rate of 13, a C-reactive protein of 1.0, a bilirubin of .8, an alkaline phosphatase of 100, an aspartate aminotransferase of 30, and an alanine transaminase of 22.
What is the most appropriate next step?
A) Right side up oblique ultrasound.
B) Abdominal CT scan.
C) Upper endoscopy.
D) More detailed physical exam.
The correct answer here is D, a more detailed physical exam is needed. Given the positional nature of this patient’s abdominal pain, an evaluation for an abdominal wall cause is appropriate.
Abdominal wall pain as a cause of chronic abdominal pain is rarely considered, but it really should be. Costanza and colleagues looked at 2,709 patients referred to gastroenterologists for chronic abdominal pain.1 Chronic abdominal wall pain was diagnosed in 137 patients, with the diagnosis unchanged in 97% of these patients after 4 years. Most of the patients were women (four to one), and the diagnosis was almost always unsuspected by the referring physician. Physical exam was helpful in suggesting the diagnosis of abdominal wall pain.
The use of Carnett sign can be helpful. A positive Carnett sign is when abdominal pain increases or remains unchanged with tensing abdomen or when the examiner palpates the tensed abdomen. Thompson and colleagues looked at the outcome of 72 patients with undiagnosed abdominal pain and a positive Carnett sign.2 Despite multiple diagnostic tests and surgeries done on these patients, very few of them had serious underlying pathology.
Thompson and Frances published another study looking at 120 patients presenting to an ED with undiagnosed abdominal pain.3 Twenty-four of the patients had positive abdominal wall tenderness on exam, and of those, only 1 had intra-abdominal pathology.
In another study, 158 patients admitted to the hospital with abdominal pain were evaluated for the presence of abdominal wall pain.4 Fifty-three patients were diagnosed with appendicitis, and 5 had abdominal wall tenderness on exam. Thirty-eight patients had other intra-abdominal pathology, and none of those had abdominal wall tenderness on exam. Of the 67 patients in the study who had nonspecific abdominal pain, 19 had abdominal wall tenderness on exam.
Most physicians do not include evaluation for abdominal wall tenderness as part of their evaluation of patients with abdominal pain. I think looking for this is helpful and, if positive, may lead to a diagnosis, as well as reduce the likelihood of intra-abdominal diagnoses.
What can we do in regard to therapy for patients with an abdominal wall source of pain?
Many patients with abdominal wall pain have anterior cutaneous nerve entrapment syndrome (ACNES). Patient’s with this often have discrete areas of tenderness on exam, often on the lateral edge of the rectus sheath, frequently on the right side of the abdomen. Anesthetic injection at the point of tenderness provides immediate relief for patients with ACNES, and is helpful in confirming the diagnosis.
Boelens and colleagues did injections in 48 patients suspected of having ACNE, randomizing half to receive lidocaine and half to receive saline placebo.5The majority of the patients receiving lidocaine (54%) had a response, compared with 17% of placebo patients (P less than .007).
Greenbaum and colleagues studied 79 patients with chronic abdominal wall pain.6 In this study, 72 of 79 patients had greater than 50% pain relief with anesthetic injection and were followed for a mean of almost 14 months. Only four of these patients ended up having a visceral cause of pain.
Can using injections help pain from ACNES longer term?
Koop and colleagues looked at all published studies in regards to both immediate and longer-term pain relief with injections.7 Both lidocaine injections and injections with lidocaine plus steroids led to long-term pain relief (40%-50% of patients with multiple lidocaine injections and up to 80% with lidocaine plus steroid injections). I think that injections are certainly worth a try in patients with chronic abdominal wall pain.
Pearl
Consider chronic abdominal wall pain in your differential diagnoses for patients with chronic abdominal pain, and use Carnett sign to help with diagnosis.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Costanza CD et al. Clin Gastroenterol Hepatol. 2004 May;2(5):395-9.
2. Thomson WH et al. Br J Surg. 1991 Feb;78(2):223-5.
3. Thomson H, Francis DM. Lancet. 1977 Nov 19;2(8047):1053-4.
4. Gray DW et al. Ann R Coll Surg Engl. 1988 Jul;70(4):233-4.
5. Boelens OB et al. Br J Surg. 2013 Jan;100(2):217-21.
6. Greenbaum DS et al. Dig Dis Sci. 1994 Sep;39(9):1935-41.
7. Koop H et al. Dtsch Arztebl Int. 2016 Jan 29;113(4):51-7.
She reports the pain is about a 7 out of 10, located in the right upper quadrant. The pain does not worsen with food and not relieved with bowel movements. She has no nausea or vomiting. She reports that the pain worsens when she is sitting or standing and is relieved by lying down. Her past medical history includes having had a cholecystectomy in 2016, having hypertension, and having type 2 diabetes mellitus.
The patient’s medications include metformin, lisinopril, and empagliflozin. Her blood pressure was 130/70, and her pulse was 80. An abdominal exam of her found tenderness to palpation in the right upper quadrant, and no rebound tenderness. Her labs found a white blood cell count of 5.4, a hematocrit of 44%, an erythrocyte sedimentation rate of 13, a C-reactive protein of 1.0, a bilirubin of .8, an alkaline phosphatase of 100, an aspartate aminotransferase of 30, and an alanine transaminase of 22.
What is the most appropriate next step?
A) Right side up oblique ultrasound.
B) Abdominal CT scan.
C) Upper endoscopy.
D) More detailed physical exam.
The correct answer here is D, a more detailed physical exam is needed. Given the positional nature of this patient’s abdominal pain, an evaluation for an abdominal wall cause is appropriate.
Abdominal wall pain as a cause of chronic abdominal pain is rarely considered, but it really should be. Costanza and colleagues looked at 2,709 patients referred to gastroenterologists for chronic abdominal pain.1 Chronic abdominal wall pain was diagnosed in 137 patients, with the diagnosis unchanged in 97% of these patients after 4 years. Most of the patients were women (four to one), and the diagnosis was almost always unsuspected by the referring physician. Physical exam was helpful in suggesting the diagnosis of abdominal wall pain.
The use of Carnett sign can be helpful. A positive Carnett sign is when abdominal pain increases or remains unchanged with tensing abdomen or when the examiner palpates the tensed abdomen. Thompson and colleagues looked at the outcome of 72 patients with undiagnosed abdominal pain and a positive Carnett sign.2 Despite multiple diagnostic tests and surgeries done on these patients, very few of them had serious underlying pathology.
Thompson and Frances published another study looking at 120 patients presenting to an ED with undiagnosed abdominal pain.3 Twenty-four of the patients had positive abdominal wall tenderness on exam, and of those, only 1 had intra-abdominal pathology.
In another study, 158 patients admitted to the hospital with abdominal pain were evaluated for the presence of abdominal wall pain.4 Fifty-three patients were diagnosed with appendicitis, and 5 had abdominal wall tenderness on exam. Thirty-eight patients had other intra-abdominal pathology, and none of those had abdominal wall tenderness on exam. Of the 67 patients in the study who had nonspecific abdominal pain, 19 had abdominal wall tenderness on exam.
Most physicians do not include evaluation for abdominal wall tenderness as part of their evaluation of patients with abdominal pain. I think looking for this is helpful and, if positive, may lead to a diagnosis, as well as reduce the likelihood of intra-abdominal diagnoses.
What can we do in regard to therapy for patients with an abdominal wall source of pain?
Many patients with abdominal wall pain have anterior cutaneous nerve entrapment syndrome (ACNES). Patient’s with this often have discrete areas of tenderness on exam, often on the lateral edge of the rectus sheath, frequently on the right side of the abdomen. Anesthetic injection at the point of tenderness provides immediate relief for patients with ACNES, and is helpful in confirming the diagnosis.
Boelens and colleagues did injections in 48 patients suspected of having ACNE, randomizing half to receive lidocaine and half to receive saline placebo.5The majority of the patients receiving lidocaine (54%) had a response, compared with 17% of placebo patients (P less than .007).
Greenbaum and colleagues studied 79 patients with chronic abdominal wall pain.6 In this study, 72 of 79 patients had greater than 50% pain relief with anesthetic injection and were followed for a mean of almost 14 months. Only four of these patients ended up having a visceral cause of pain.
Can using injections help pain from ACNES longer term?
Koop and colleagues looked at all published studies in regards to both immediate and longer-term pain relief with injections.7 Both lidocaine injections and injections with lidocaine plus steroids led to long-term pain relief (40%-50% of patients with multiple lidocaine injections and up to 80% with lidocaine plus steroid injections). I think that injections are certainly worth a try in patients with chronic abdominal wall pain.
Pearl
Consider chronic abdominal wall pain in your differential diagnoses for patients with chronic abdominal pain, and use Carnett sign to help with diagnosis.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Costanza CD et al. Clin Gastroenterol Hepatol. 2004 May;2(5):395-9.
2. Thomson WH et al. Br J Surg. 1991 Feb;78(2):223-5.
3. Thomson H, Francis DM. Lancet. 1977 Nov 19;2(8047):1053-4.
4. Gray DW et al. Ann R Coll Surg Engl. 1988 Jul;70(4):233-4.
5. Boelens OB et al. Br J Surg. 2013 Jan;100(2):217-21.
6. Greenbaum DS et al. Dig Dis Sci. 1994 Sep;39(9):1935-41.
7. Koop H et al. Dtsch Arztebl Int. 2016 Jan 29;113(4):51-7.
She reports the pain is about a 7 out of 10, located in the right upper quadrant. The pain does not worsen with food and not relieved with bowel movements. She has no nausea or vomiting. She reports that the pain worsens when she is sitting or standing and is relieved by lying down. Her past medical history includes having had a cholecystectomy in 2016, having hypertension, and having type 2 diabetes mellitus.
The patient’s medications include metformin, lisinopril, and empagliflozin. Her blood pressure was 130/70, and her pulse was 80. An abdominal exam of her found tenderness to palpation in the right upper quadrant, and no rebound tenderness. Her labs found a white blood cell count of 5.4, a hematocrit of 44%, an erythrocyte sedimentation rate of 13, a C-reactive protein of 1.0, a bilirubin of .8, an alkaline phosphatase of 100, an aspartate aminotransferase of 30, and an alanine transaminase of 22.
What is the most appropriate next step?
A) Right side up oblique ultrasound.
B) Abdominal CT scan.
C) Upper endoscopy.
D) More detailed physical exam.
The correct answer here is D, a more detailed physical exam is needed. Given the positional nature of this patient’s abdominal pain, an evaluation for an abdominal wall cause is appropriate.
Abdominal wall pain as a cause of chronic abdominal pain is rarely considered, but it really should be. Costanza and colleagues looked at 2,709 patients referred to gastroenterologists for chronic abdominal pain.1 Chronic abdominal wall pain was diagnosed in 137 patients, with the diagnosis unchanged in 97% of these patients after 4 years. Most of the patients were women (four to one), and the diagnosis was almost always unsuspected by the referring physician. Physical exam was helpful in suggesting the diagnosis of abdominal wall pain.
The use of Carnett sign can be helpful. A positive Carnett sign is when abdominal pain increases or remains unchanged with tensing abdomen or when the examiner palpates the tensed abdomen. Thompson and colleagues looked at the outcome of 72 patients with undiagnosed abdominal pain and a positive Carnett sign.2 Despite multiple diagnostic tests and surgeries done on these patients, very few of them had serious underlying pathology.
Thompson and Frances published another study looking at 120 patients presenting to an ED with undiagnosed abdominal pain.3 Twenty-four of the patients had positive abdominal wall tenderness on exam, and of those, only 1 had intra-abdominal pathology.
In another study, 158 patients admitted to the hospital with abdominal pain were evaluated for the presence of abdominal wall pain.4 Fifty-three patients were diagnosed with appendicitis, and 5 had abdominal wall tenderness on exam. Thirty-eight patients had other intra-abdominal pathology, and none of those had abdominal wall tenderness on exam. Of the 67 patients in the study who had nonspecific abdominal pain, 19 had abdominal wall tenderness on exam.
Most physicians do not include evaluation for abdominal wall tenderness as part of their evaluation of patients with abdominal pain. I think looking for this is helpful and, if positive, may lead to a diagnosis, as well as reduce the likelihood of intra-abdominal diagnoses.
What can we do in regard to therapy for patients with an abdominal wall source of pain?
Many patients with abdominal wall pain have anterior cutaneous nerve entrapment syndrome (ACNES). Patient’s with this often have discrete areas of tenderness on exam, often on the lateral edge of the rectus sheath, frequently on the right side of the abdomen. Anesthetic injection at the point of tenderness provides immediate relief for patients with ACNES, and is helpful in confirming the diagnosis.
Boelens and colleagues did injections in 48 patients suspected of having ACNE, randomizing half to receive lidocaine and half to receive saline placebo.5The majority of the patients receiving lidocaine (54%) had a response, compared with 17% of placebo patients (P less than .007).
Greenbaum and colleagues studied 79 patients with chronic abdominal wall pain.6 In this study, 72 of 79 patients had greater than 50% pain relief with anesthetic injection and were followed for a mean of almost 14 months. Only four of these patients ended up having a visceral cause of pain.
Can using injections help pain from ACNES longer term?
Koop and colleagues looked at all published studies in regards to both immediate and longer-term pain relief with injections.7 Both lidocaine injections and injections with lidocaine plus steroids led to long-term pain relief (40%-50% of patients with multiple lidocaine injections and up to 80% with lidocaine plus steroid injections). I think that injections are certainly worth a try in patients with chronic abdominal wall pain.
Pearl
Consider chronic abdominal wall pain in your differential diagnoses for patients with chronic abdominal pain, and use Carnett sign to help with diagnosis.
Dr. Paauw is professor of medicine in the division of general internal medicine at the University of Washington, Seattle, and serves as third-year medical student clerkship director at the University of Washington. He is a member of the editorial advisory board of Internal Medicine News. Dr. Paauw has no conflicts to disclose. Contact him at [email protected].
References
1. Costanza CD et al. Clin Gastroenterol Hepatol. 2004 May;2(5):395-9.
2. Thomson WH et al. Br J Surg. 1991 Feb;78(2):223-5.
3. Thomson H, Francis DM. Lancet. 1977 Nov 19;2(8047):1053-4.
4. Gray DW et al. Ann R Coll Surg Engl. 1988 Jul;70(4):233-4.
5. Boelens OB et al. Br J Surg. 2013 Jan;100(2):217-21.
6. Greenbaum DS et al. Dig Dis Sci. 1994 Sep;39(9):1935-41.
7. Koop H et al. Dtsch Arztebl Int. 2016 Jan 29;113(4):51-7.
Is the troll tracker crying wolf?
I’m a big believer in my state’s Prescription Monitoring Program (PMP), perhaps more commonly known as the troll tracker. The ability to quickly access a patient’s controlled prescription records across pharmacies has been enormously helpful in my everyday practice. I rely on it and check it often.

With it I can see if my patients are getting the same drug from other prescribers, pharmacy-shopping, or carrying out other concerning activities. The database helpfully sends me emails alerting me to such conflicts, so I can take prompt action on them.
Unfortunately, the threshold for such emails has gradually crept lower, to where I now get maybe 10 a week.
A lady to whom I gave two Valium tablets to get her through a lumbar spine MRI also got 20 Percocet for the same back pain from her internist … and I get an alert email.
A long-established patient for whom I’ve been prescribing Ativan and Tramadol for years, fills them both every month … and I get an alert email every month (and I’m the only prescriber who has written for him in the last 10 years).
A patient who suffered a painful vertebral fracture, got 10 Norco in the ED, follows with up with me 5 days later, and I write her for 20 more … and I get an email.
Now, I understand what the program is trying to do – and wholeheartedly agree with it – but the problem is that the more email warnings I get the less likely I am to have time to investigate each one. It’s like the boy who cried “wolf!” In fact, it’s probably been over a year since a warning email from the PMP told me something I didn’t already know.
Granted, these emails are sent by a computer, following a rigid set of parameters to do so. The machine doesn’t know I’m aware of the situation, or keep track of case nuances, or even notice that I’m the only prescriber of all the medications involved. It just does what it’s set to do. And the warnings all make it clear that they’re just warnings, and that the treatment is still left to physician’s discretion.
Arizona currently has roughly 18,000 practicing physicians. Granted, not all of them are routinely prescribing controlled agents, but I’d guess at least two-thirds of them are. So it’s safe to assume at least 12,000 doctors here are receiving email warnings with varying degrees of frequency.
At some point, with all the other tasks and hats your average doctor goes through in a day, too many of these warnings – the vast majority of them meaningless – become part of the background noise.
There are only so many hours in a day to see patients, write notes, send prescriptions, review tests, return calls, fill out forms, and all the other things that are part of our days. Having to log into the PMP website to see what’s up every time you get an email from them, especially when the last 20 (or more) warnings that you received were meaningless, gets pushed farther and farther onto the back burner. So when a real warning shows up, it may not got noticed much at all.
Like I said, I believe in and routinely use the state PMP. But it may be time to take a second look at the criteria under which its email warning system operates.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m a big believer in my state’s Prescription Monitoring Program (PMP), perhaps more commonly known as the troll tracker. The ability to quickly access a patient’s controlled prescription records across pharmacies has been enormously helpful in my everyday practice. I rely on it and check it often.
With it I can see if my patients are getting the same drug from other prescribers, pharmacy-shopping, or carrying out other concerning activities. The database helpfully sends me emails alerting me to such conflicts, so I can take prompt action on them.
Unfortunately, the threshold for such emails has gradually crept lower, to where I now get maybe 10 a week.
A lady to whom I gave two Valium tablets to get her through a lumbar spine MRI also got 20 Percocet for the same back pain from her internist … and I get an alert email.
A long-established patient for whom I’ve been prescribing Ativan and Tramadol for years, fills them both every month … and I get an alert email every month (and I’m the only prescriber who has written for him in the last 10 years).
A patient who suffered a painful vertebral fracture, got 10 Norco in the ED, follows with up with me 5 days later, and I write her for 20 more … and I get an email.
Now, I understand what the program is trying to do – and wholeheartedly agree with it – but the problem is that the more email warnings I get the less likely I am to have time to investigate each one. It’s like the boy who cried “wolf!” In fact, it’s probably been over a year since a warning email from the PMP told me something I didn’t already know.
Granted, these emails are sent by a computer, following a rigid set of parameters to do so. The machine doesn’t know I’m aware of the situation, or keep track of case nuances, or even notice that I’m the only prescriber of all the medications involved. It just does what it’s set to do. And the warnings all make it clear that they’re just warnings, and that the treatment is still left to physician’s discretion.
Arizona currently has roughly 18,000 practicing physicians. Granted, not all of them are routinely prescribing controlled agents, but I’d guess at least two-thirds of them are. So it’s safe to assume at least 12,000 doctors here are receiving email warnings with varying degrees of frequency.
At some point, with all the other tasks and hats your average doctor goes through in a day, too many of these warnings – the vast majority of them meaningless – become part of the background noise.
There are only so many hours in a day to see patients, write notes, send prescriptions, review tests, return calls, fill out forms, and all the other things that are part of our days. Having to log into the PMP website to see what’s up every time you get an email from them, especially when the last 20 (or more) warnings that you received were meaningless, gets pushed farther and farther onto the back burner. So when a real warning shows up, it may not got noticed much at all.
Like I said, I believe in and routinely use the state PMP. But it may be time to take a second look at the criteria under which its email warning system operates.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
I’m a big believer in my state’s Prescription Monitoring Program (PMP), perhaps more commonly known as the troll tracker. The ability to quickly access a patient’s controlled prescription records across pharmacies has been enormously helpful in my everyday practice. I rely on it and check it often.
With it I can see if my patients are getting the same drug from other prescribers, pharmacy-shopping, or carrying out other concerning activities. The database helpfully sends me emails alerting me to such conflicts, so I can take prompt action on them.
Unfortunately, the threshold for such emails has gradually crept lower, to where I now get maybe 10 a week.
A lady to whom I gave two Valium tablets to get her through a lumbar spine MRI also got 20 Percocet for the same back pain from her internist … and I get an alert email.
A long-established patient for whom I’ve been prescribing Ativan and Tramadol for years, fills them both every month … and I get an alert email every month (and I’m the only prescriber who has written for him in the last 10 years).
A patient who suffered a painful vertebral fracture, got 10 Norco in the ED, follows with up with me 5 days later, and I write her for 20 more … and I get an email.
Now, I understand what the program is trying to do – and wholeheartedly agree with it – but the problem is that the more email warnings I get the less likely I am to have time to investigate each one. It’s like the boy who cried “wolf!” In fact, it’s probably been over a year since a warning email from the PMP told me something I didn’t already know.
Granted, these emails are sent by a computer, following a rigid set of parameters to do so. The machine doesn’t know I’m aware of the situation, or keep track of case nuances, or even notice that I’m the only prescriber of all the medications involved. It just does what it’s set to do. And the warnings all make it clear that they’re just warnings, and that the treatment is still left to physician’s discretion.
Arizona currently has roughly 18,000 practicing physicians. Granted, not all of them are routinely prescribing controlled agents, but I’d guess at least two-thirds of them are. So it’s safe to assume at least 12,000 doctors here are receiving email warnings with varying degrees of frequency.
At some point, with all the other tasks and hats your average doctor goes through in a day, too many of these warnings – the vast majority of them meaningless – become part of the background noise.
There are only so many hours in a day to see patients, write notes, send prescriptions, review tests, return calls, fill out forms, and all the other things that are part of our days. Having to log into the PMP website to see what’s up every time you get an email from them, especially when the last 20 (or more) warnings that you received were meaningless, gets pushed farther and farther onto the back burner. So when a real warning shows up, it may not got noticed much at all.
Like I said, I believe in and routinely use the state PMP. But it may be time to take a second look at the criteria under which its email warning system operates.
Dr. Block has a solo neurology practice in Scottsdale, Ariz.
Are uterine manipulators safe for gynecologic cancer surgery?
Over the past 4 decades there has been increasing use of minimally invasive surgery (MIS) for gynecologic cancer, particularly endometrial and cervical cancers. Uterine manipulators are a device inserted into the uterine cavity during MIS approaches to aid in directing the uterus within the pelvis, facilitating access to the uterine blood supply, defining the cardinal ligaments, lateralizing the ureters, and delineating the cervicovaginal junction. However, concerns have been raised regarding whether these devices are safe to use when the uterine corpus or cervix contains cancer.

In 2018, the LACC trial was published and demonstrated decreased survival for patients with cervical cancer who had undergone radical hysterectomy via a minimally invasive route.1 Several hypotheses were proposed to explain this finding including possible tumor disruption from use of a uterine manipulator. Regrettably, this study did not document manipulator use, and therefore its influence on outcomes could not be measured. However, since that time there has been honed interest into the potential negative influence of uterine manipulators on endometrial and cervical cancer surgery.
Uterine manipulators typically are inserted through the uterine cervix and reside in the endometrial cavity. It is often an inflated balloon which stabilizes the device within the cavity. Hypotheses for how they may contribute to the spread of malignancy include the massage of endometrial tumor from the pressure of the inflated balloon, facilitation of tumor dissemination through cervical lymphatics or vasculature as the manipulator traverses or punctures a cervical cancer, and possibly perforation of the uterine cavity during placement of the manipulator, and in doing so, contaminating the peritoneal cavity with endometrial or cervical cancer cells that have been dragged through with the device.
Interestingly, uterine manipulator placement is not the only time during which endometrial or cervical cancers may be disturbed prior to resection. Many diagnostic procedures such as cervical excisional procedures (loop electrosurgical excision procedure and conizations) or hysteroscopic resections cause significant intentional disruption of tumor. In the case of hysteroscopy for endometrial cancer, endometrial cancer cells have been detected in the peritoneal washings of endometrial cancer patients who have undergone this procedure, however, no worse outcomes have been associated when hysteroscopy was included as part of the diagnostic work-up, suggesting that more than simply efflux into the peritoneal cavity is necessary for those tumor cells to have metastatic potential.2
Indeed the data is mixed regarding oncologic outcomes with uterine manipulator use, especially for endometrial cancer. In one recent study the outcomes of 951 patients with endometrial cancer from seven Italian centers were evaluated.3 There was no difference in recurrence rates or disease-specific survival between the 579 patients in whom manipulators were used and the 372 patients in which surgery was performed without manipulators. More recently a Spanish study reported retrospectively on 2,661 patients at 15 centers and determined that use of a uterine manipulator (two-thirds of the cohort) was associated with a hazard ratio of 1.74 (95% confidence interval, 1.07-2.83) for risk of death.4 Unfortunately, in this study there were substantial differences between sites that used manipulators and those that did not. Additionally, while one would expect different patterns of recurrence if the manipulator was introducing a unique mechanism for metastasis, this was not observed between the manipulator and nonmanipulator arms. Finally, the groups were intrinsically different with respect to important risk factors such as lymphovascular space invasion, which might have contributed to the observed outcomes. It is important to recognize that, in both the LAP-2 and LACE trials, minimally invasive hysterectomy for endometrial cancer had been shown to have noninferior survival outcomes, compared with open hysterectomy.5,6 While these large randomized, controlled trials did not capture uterine manipulator usage, presumably it was utilized in at least some or most cases, and without apparent significant negative effect.
In cervical cancer, there is more competing data raising concern regarding manipulator use. The SUCCOR study was completed in 2020 and included a retrospective evaluation of 1,272 patients who had undergone open or MIS radical hysterectomy for early stage cervical cancer across 126 European centers during 2013-2014.7 They were able to evaluate for variables, such as uterine manipulator use. While they found that recurrence was higher for patients who had MIS hysterectomy, the HR (2.07) was similar to the HR for recurrence (2.76) among those who had uterine manipulator use. Conversely, the hazard ratio for recurrence following MIS radical hysterectomy without a manipulator was comparable with the superior rates seen with open surgery. This study was retrospective and therefore is largely hypothesis generating, however it does raise the question of whether the technique of MIS radical hysterectomy can be performed safely if particular steps, such as avoidance of a uterine manipulator, are followed. We await definitive results from prospective trials to determine this.
As mentioned earlier, the uterine manipulator is an important safety and feasibility tool for MIS hysterectomy. When not utilized, surgeons may need to add additional ports and instrumentation to maneuver the uterus and may have difficulty completing hysterectomy via a MIS approach for obese patients. There are additional urologic safety concerns when uterine elevation and cervicovaginal delineation is missing. Therefore, While the wealth of prospective data suggests that manipulators are most likely safe in hysterectomy for endometrial cancer, they should be avoided if a minimally invasive approach to cervical cancer is employed.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest to report. Email her at [email protected].
References
1. N Engl J Med. 2018 Nov 15. doi: 10.1056/NEJMoa1806395.
2. Fertil Steril. 2011 Oct. doi: 10.1016/j.fertnstert.2011.07.1146.
3. Am J Obstet Gynecol. 2017 Jun. doi: 10.1016/j.ajog.2017.01.027.
4. Am J Obstet Gynecol. 2020 Jul 18. doi: 10.1016/j.ajog.2020.07.025.
5. J Clin Oncol. 2009 Nov 10. doi: 10.1200/JCO.2009.22.3248.
6. JAMA. 2017 Mar 28. doi: 10.1001/jama.2017.2068.
7. Int J Gynecol Cancer. 2020. doi: 10.1136/ijgc-2020-001506.
Over the past 4 decades there has been increasing use of minimally invasive surgery (MIS) for gynecologic cancer, particularly endometrial and cervical cancers. Uterine manipulators are a device inserted into the uterine cavity during MIS approaches to aid in directing the uterus within the pelvis, facilitating access to the uterine blood supply, defining the cardinal ligaments, lateralizing the ureters, and delineating the cervicovaginal junction. However, concerns have been raised regarding whether these devices are safe to use when the uterine corpus or cervix contains cancer.
In 2018, the LACC trial was published and demonstrated decreased survival for patients with cervical cancer who had undergone radical hysterectomy via a minimally invasive route.1 Several hypotheses were proposed to explain this finding including possible tumor disruption from use of a uterine manipulator. Regrettably, this study did not document manipulator use, and therefore its influence on outcomes could not be measured. However, since that time there has been honed interest into the potential negative influence of uterine manipulators on endometrial and cervical cancer surgery.
Uterine manipulators typically are inserted through the uterine cervix and reside in the endometrial cavity. It is often an inflated balloon which stabilizes the device within the cavity. Hypotheses for how they may contribute to the spread of malignancy include the massage of endometrial tumor from the pressure of the inflated balloon, facilitation of tumor dissemination through cervical lymphatics or vasculature as the manipulator traverses or punctures a cervical cancer, and possibly perforation of the uterine cavity during placement of the manipulator, and in doing so, contaminating the peritoneal cavity with endometrial or cervical cancer cells that have been dragged through with the device.
Interestingly, uterine manipulator placement is not the only time during which endometrial or cervical cancers may be disturbed prior to resection. Many diagnostic procedures such as cervical excisional procedures (loop electrosurgical excision procedure and conizations) or hysteroscopic resections cause significant intentional disruption of tumor. In the case of hysteroscopy for endometrial cancer, endometrial cancer cells have been detected in the peritoneal washings of endometrial cancer patients who have undergone this procedure, however, no worse outcomes have been associated when hysteroscopy was included as part of the diagnostic work-up, suggesting that more than simply efflux into the peritoneal cavity is necessary for those tumor cells to have metastatic potential.2
Indeed the data is mixed regarding oncologic outcomes with uterine manipulator use, especially for endometrial cancer. In one recent study the outcomes of 951 patients with endometrial cancer from seven Italian centers were evaluated.3 There was no difference in recurrence rates or disease-specific survival between the 579 patients in whom manipulators were used and the 372 patients in which surgery was performed without manipulators. More recently a Spanish study reported retrospectively on 2,661 patients at 15 centers and determined that use of a uterine manipulator (two-thirds of the cohort) was associated with a hazard ratio of 1.74 (95% confidence interval, 1.07-2.83) for risk of death.4 Unfortunately, in this study there were substantial differences between sites that used manipulators and those that did not. Additionally, while one would expect different patterns of recurrence if the manipulator was introducing a unique mechanism for metastasis, this was not observed between the manipulator and nonmanipulator arms. Finally, the groups were intrinsically different with respect to important risk factors such as lymphovascular space invasion, which might have contributed to the observed outcomes. It is important to recognize that, in both the LAP-2 and LACE trials, minimally invasive hysterectomy for endometrial cancer had been shown to have noninferior survival outcomes, compared with open hysterectomy.5,6 While these large randomized, controlled trials did not capture uterine manipulator usage, presumably it was utilized in at least some or most cases, and without apparent significant negative effect.
In cervical cancer, there is more competing data raising concern regarding manipulator use. The SUCCOR study was completed in 2020 and included a retrospective evaluation of 1,272 patients who had undergone open or MIS radical hysterectomy for early stage cervical cancer across 126 European centers during 2013-2014.7 They were able to evaluate for variables, such as uterine manipulator use. While they found that recurrence was higher for patients who had MIS hysterectomy, the HR (2.07) was similar to the HR for recurrence (2.76) among those who had uterine manipulator use. Conversely, the hazard ratio for recurrence following MIS radical hysterectomy without a manipulator was comparable with the superior rates seen with open surgery. This study was retrospective and therefore is largely hypothesis generating, however it does raise the question of whether the technique of MIS radical hysterectomy can be performed safely if particular steps, such as avoidance of a uterine manipulator, are followed. We await definitive results from prospective trials to determine this.
As mentioned earlier, the uterine manipulator is an important safety and feasibility tool for MIS hysterectomy. When not utilized, surgeons may need to add additional ports and instrumentation to maneuver the uterus and may have difficulty completing hysterectomy via a MIS approach for obese patients. There are additional urologic safety concerns when uterine elevation and cervicovaginal delineation is missing. Therefore, While the wealth of prospective data suggests that manipulators are most likely safe in hysterectomy for endometrial cancer, they should be avoided if a minimally invasive approach to cervical cancer is employed.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest to report. Email her at [email protected].
References
1. N Engl J Med. 2018 Nov 15. doi: 10.1056/NEJMoa1806395.
2. Fertil Steril. 2011 Oct. doi: 10.1016/j.fertnstert.2011.07.1146.
3. Am J Obstet Gynecol. 2017 Jun. doi: 10.1016/j.ajog.2017.01.027.
4. Am J Obstet Gynecol. 2020 Jul 18. doi: 10.1016/j.ajog.2020.07.025.
5. J Clin Oncol. 2009 Nov 10. doi: 10.1200/JCO.2009.22.3248.
6. JAMA. 2017 Mar 28. doi: 10.1001/jama.2017.2068.
7. Int J Gynecol Cancer. 2020. doi: 10.1136/ijgc-2020-001506.
Over the past 4 decades there has been increasing use of minimally invasive surgery (MIS) for gynecologic cancer, particularly endometrial and cervical cancers. Uterine manipulators are a device inserted into the uterine cavity during MIS approaches to aid in directing the uterus within the pelvis, facilitating access to the uterine blood supply, defining the cardinal ligaments, lateralizing the ureters, and delineating the cervicovaginal junction. However, concerns have been raised regarding whether these devices are safe to use when the uterine corpus or cervix contains cancer.
In 2018, the LACC trial was published and demonstrated decreased survival for patients with cervical cancer who had undergone radical hysterectomy via a minimally invasive route.1 Several hypotheses were proposed to explain this finding including possible tumor disruption from use of a uterine manipulator. Regrettably, this study did not document manipulator use, and therefore its influence on outcomes could not be measured. However, since that time there has been honed interest into the potential negative influence of uterine manipulators on endometrial and cervical cancer surgery.
Uterine manipulators typically are inserted through the uterine cervix and reside in the endometrial cavity. It is often an inflated balloon which stabilizes the device within the cavity. Hypotheses for how they may contribute to the spread of malignancy include the massage of endometrial tumor from the pressure of the inflated balloon, facilitation of tumor dissemination through cervical lymphatics or vasculature as the manipulator traverses or punctures a cervical cancer, and possibly perforation of the uterine cavity during placement of the manipulator, and in doing so, contaminating the peritoneal cavity with endometrial or cervical cancer cells that have been dragged through with the device.
Interestingly, uterine manipulator placement is not the only time during which endometrial or cervical cancers may be disturbed prior to resection. Many diagnostic procedures such as cervical excisional procedures (loop electrosurgical excision procedure and conizations) or hysteroscopic resections cause significant intentional disruption of tumor. In the case of hysteroscopy for endometrial cancer, endometrial cancer cells have been detected in the peritoneal washings of endometrial cancer patients who have undergone this procedure, however, no worse outcomes have been associated when hysteroscopy was included as part of the diagnostic work-up, suggesting that more than simply efflux into the peritoneal cavity is necessary for those tumor cells to have metastatic potential.2
Indeed the data is mixed regarding oncologic outcomes with uterine manipulator use, especially for endometrial cancer. In one recent study the outcomes of 951 patients with endometrial cancer from seven Italian centers were evaluated.3 There was no difference in recurrence rates or disease-specific survival between the 579 patients in whom manipulators were used and the 372 patients in which surgery was performed without manipulators. More recently a Spanish study reported retrospectively on 2,661 patients at 15 centers and determined that use of a uterine manipulator (two-thirds of the cohort) was associated with a hazard ratio of 1.74 (95% confidence interval, 1.07-2.83) for risk of death.4 Unfortunately, in this study there were substantial differences between sites that used manipulators and those that did not. Additionally, while one would expect different patterns of recurrence if the manipulator was introducing a unique mechanism for metastasis, this was not observed between the manipulator and nonmanipulator arms. Finally, the groups were intrinsically different with respect to important risk factors such as lymphovascular space invasion, which might have contributed to the observed outcomes. It is important to recognize that, in both the LAP-2 and LACE trials, minimally invasive hysterectomy for endometrial cancer had been shown to have noninferior survival outcomes, compared with open hysterectomy.5,6 While these large randomized, controlled trials did not capture uterine manipulator usage, presumably it was utilized in at least some or most cases, and without apparent significant negative effect.
In cervical cancer, there is more competing data raising concern regarding manipulator use. The SUCCOR study was completed in 2020 and included a retrospective evaluation of 1,272 patients who had undergone open or MIS radical hysterectomy for early stage cervical cancer across 126 European centers during 2013-2014.7 They were able to evaluate for variables, such as uterine manipulator use. While they found that recurrence was higher for patients who had MIS hysterectomy, the HR (2.07) was similar to the HR for recurrence (2.76) among those who had uterine manipulator use. Conversely, the hazard ratio for recurrence following MIS radical hysterectomy without a manipulator was comparable with the superior rates seen with open surgery. This study was retrospective and therefore is largely hypothesis generating, however it does raise the question of whether the technique of MIS radical hysterectomy can be performed safely if particular steps, such as avoidance of a uterine manipulator, are followed. We await definitive results from prospective trials to determine this.
As mentioned earlier, the uterine manipulator is an important safety and feasibility tool for MIS hysterectomy. When not utilized, surgeons may need to add additional ports and instrumentation to maneuver the uterus and may have difficulty completing hysterectomy via a MIS approach for obese patients. There are additional urologic safety concerns when uterine elevation and cervicovaginal delineation is missing. Therefore, While the wealth of prospective data suggests that manipulators are most likely safe in hysterectomy for endometrial cancer, they should be avoided if a minimally invasive approach to cervical cancer is employed.
Dr. Rossi is assistant professor in the division of gynecologic oncology at the University of North Carolina at Chapel Hill. She has no conflicts of interest to report. Email her at [email protected].
References
1. N Engl J Med. 2018 Nov 15. doi: 10.1056/NEJMoa1806395.
2. Fertil Steril. 2011 Oct. doi: 10.1016/j.fertnstert.2011.07.1146.
3. Am J Obstet Gynecol. 2017 Jun. doi: 10.1016/j.ajog.2017.01.027.
4. Am J Obstet Gynecol. 2020 Jul 18. doi: 10.1016/j.ajog.2020.07.025.
5. J Clin Oncol. 2009 Nov 10. doi: 10.1200/JCO.2009.22.3248.
6. JAMA. 2017 Mar 28. doi: 10.1001/jama.2017.2068.
7. Int J Gynecol Cancer. 2020. doi: 10.1136/ijgc-2020-001506.