User login
Transition to Tenecteplase From t-PA for Acute Ischemic Stroke at Walter Reed National Military Medical Center
Tissue plasminogen activator (t-PA) has been the standard IV thrombolytic used in acute ischemic stroke treatment since its US Food and Drug Administration (FDA) approval in 1995. Trials have established this drug’s efficacy in the treatment of acute ischemic stroke and the appropriate patient population for therapy.1-3 Published guidelines and experiences have made clear that a written protocol with extensive personnel training is important to deliver this care properly.4
Tenecteplase has been available for use in the treatment of acute myocardial infarction (MI) and studied in acute ischemic strokes since 2000. Recent large multicenter trials have suggested tenecteplase may work better than t-PA in the recanalization of large vessel occlusions (LVOs) and have provided guidance on proper dosing in acute ischemic stroke victims.5-8 Compared with t-PA, tenecteplase has a longer half-life, is more fibrin specific (causing less coagulopathy), and is more resistant to endogenous plasminogen activator inhibitor.9,10 Using tenecteplase for acute ischemic stroke is simpler as a single dose bolus rather than a bolus followed by a 1-hour infusion with t-PA. Immediate mechanical thrombectomy for LVO is less complicated without the 1-hour t-PA infusion.5,6 Tenecteplase use also allows for nonthrombectomy hospitals to accelerate transfer times for patients who need thrombectomy following thrombolysis by eliminating the need for critical care nurse–staffed ambulances for interfacility transfer.11 Tenecteplase also is cheaper: Tenecteplase costs $3748 per vial, whereas t-PA costs $5800 per vial equating to roughly a $2000 savings per patient.12,13 Finally, the pharmacy formulary is simplified by using a single thrombolytic agent for both cardiac and neurologic emergencies.
Tenecteplase does have some drawbacks to consider. Currently, tenecteplase is not approved by the FDA for the indication of acute ischemic stroke, though the drug is endorsed by the American Heart Association stroke guidelines of 2019 as an alternative to t-PA.14 There is no stroke-specific preparation of the drug, leading to potential dosing errors. Therefore, a systematic process to safely transition from t-PA to tenecteplase for acute ischemic stroke was undertaken at Walter Reed National Military Medical Center (WRNMMC) in Bethesda, Maryland. Here, we report the process required in making a complex switch in thrombolytic medication along with the potential benefits of making this transition.
OBSERVATIONS
The process to implement tenecteplase required extensive training and education for staff physicians, nurses, pharmacists, radiologists, trainees, and the rapid response team. Our institution administered IV thrombolytic drugs up to 25 times annually to acute ischemic stroke victims, meaning we had to train personnel extensively and repeatedly.
In preparation for the transition to tenecteplase, hospital leadership gathered staff for multidisciplinary administrative meetings that included neurology, emergency medicine, intensive care, pharmacy, radiology, and nursing departments. The purpose of these meetings was to establish a standard operating procedure (SOP) to ensure a safe transition. This process began in May 2020 and involved regular meetings to draft and revise our SOP. Additionally, several leadership and training sessions were held over a 6-month period. Stroke boxes were developed that contained the required evaluation tools, consent forms, medications (tenecteplase and treatments for known complications), dosing cards, and instructions. Final approval of the updated acute ischemic stroke hospital policy was obtained in November 2020 and signed by the above departments.
All inclusion and exclusion criteria were determined to be the same for tenecteplase as they were for t-PA with the notable exception that the WAKE-UP trial protocol would not be supported until further evidence became available.9 The results of the WAKE-UP trial had previously been used at WRNMMC to justify administration of t-PA in patients who awoke with symptoms of acute ischemic stroke, the last known well was unclear or > 4.5 hours, and for whom a magnetic resonance imaging (MRI) of the brain could be obtained rapidly. Based on the WAKE-UP trial, if the MRI scan of the brain in these patients demonstrated restricted diffusion without fluid attenuated inversion recovery (FLAIR) signal changes (diffusion-weighted [DWI]-FLAIR mismatch sign), this indicated that the stroke had likely occurred recently, and it was safe to administer t-PA. This allowed for administration of t-PA outside the standard treatment window of 4.5 hours from last known well, especially in the cases of patients who awoke with symptoms.
Since safety data are not yet available for the use of tenecteplase in this fashion, the WAKE-UP trial protocol was not used as an inclusion criterion. The informed consent form was modified, and the following scenarios were outlined: (1) If the patient or surrogate is immediately available to consent, paper consent will be documented with the additional note that tenecteplase is being used off-label; and (2) If the patient cannot consent and a surrogate is not immediately available, the medicine will be used emergently as long as the neurology resident and attending physicians agree.15
Risk mitigation was considered carefully. The stroke box described above is stocked and maintained by the pharmacy as we have transitioned to using designated pharmacists for the storage and preparation of tenecteplase. We highly recommend the use of designated pharmacists or emergency department pharmacists in this manner to avoid dosing errors.7,16 Since the current pharmacy-provided tenecteplase bottle contains twice the maximum dose indicated for ischemic stroke, only a 5 mL syringe is included in the stroke box to ensure a maximum dose of 25 mg is drawn up after reconstitution. Dosing card charts were made like existing dosing card charts for t-PA to quickly calculate the 0.25 mg/kg dose. In training, the difference in dosing in ischemic stroke was emphasized. Finally, pharmacy has taken responsibility for dosing the medication during stroke codes.
Any medical personnel at WRNMMC can initiate a stroke code by sending a page to the neurology consult service (Figure). 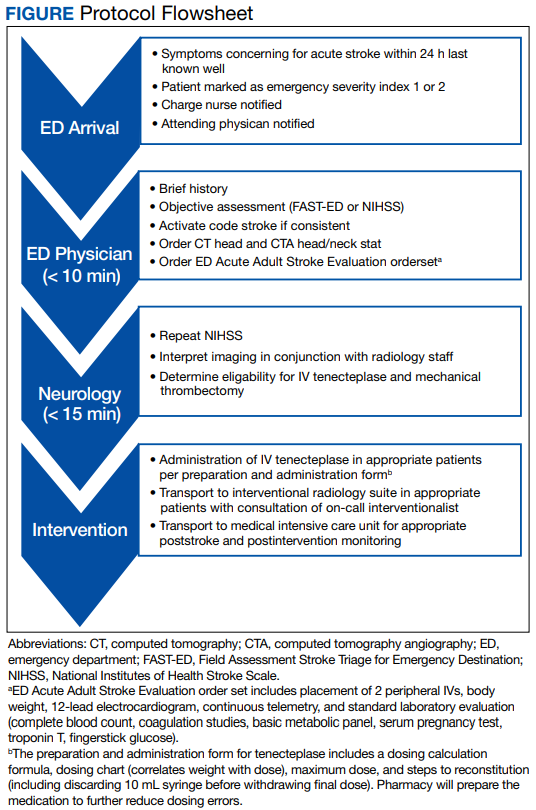
TRANSITION AND RESULTS
From November 2020 to December 2021, 10 patients have been treated in total at WRNMMC (Table). 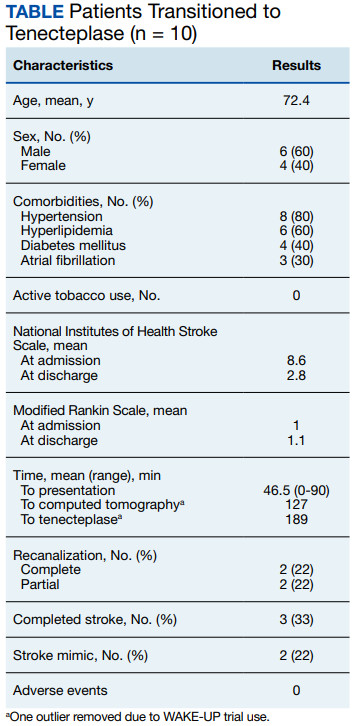
CONCLUSIONS
The available evidence supports the transition from t-PA to tenecteplase for acute ischemic stroke. The successful transition required months of preparation involving multidisciplinary meetings between neurology, nursing, pharmacy, radiology, rapid response teams, critical care, and emergency medicine departments. Safeguards must be implemented to avoid a tenecteplase dosing error that can lead to potentially life-threatening adverse effects. The results at WRNMMC thus far are promising for safety and efficacy. Several process improvements are planned: a hospital-wide overhead page will accompany the direct page to neurology; other team members, including radiology and pharmacy, will be included on the acute stroke alert; and a stroke-specific paging application will be implemented to better track real-time stroke metrics and improve flow. These measures mirror processes that are occurring in institutions that treat acute stroke patients.
1. Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375(9727):1695-1703. doi:10.1016/S0140-6736(10)60491-6
2. National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581- 1587. doi:10.1056/NEJM199512143332401
3. Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363(9411):768-774. doi:10.1016/S0140-6736(04)15692-4
4. Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(3):870-947. doi:10.1161/STR.0b013e318284056a
5. Campbell B, Mitchell P, Churilov L, et al. Tenecteplase versus alteplase before thrombectomy for ischemic stroke. N Engl J Med. 2018;378(17):1573-1582. doi:10.1056/nejmoa1716405
6. Yang P, Zhang Y, Zhang L, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke. N Engl J Med. 2020;382(21):1981-1993. doi:10.1056/NEJMoa2001123
7. Menon BK, Buck BH, Singh N, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, noninferiority trial. Lancet. 2022;400(10347):161-169. doi:10.1016/S0140-6736(22)01054-6
8. Campbell BCV, Mitchell PJ, Churilov L, et al. Effect of intravenous tenecteplase dose on cerebral reperfusion before thrombectomy in patients with large vessel occlusion ischemic stroke: the EXTEND-IA TNK part 2 randomized clinical trial. JAMA. 2020;323(13):1257- 1265. doi:10.1001/jama.2020.1511
9. Warach SJ, Dula AN, Milling TJ Jr. Tenecteplase thrombolysis for acute ischemic stroke. Stroke. 2020;51(11):3440- 3451. doi:10.1161/STROKEAHA.120.029749
10. Huang X, Moreton FC, Kalladka D, et al. Coagulation and fibrinolytic activity of tenecteplase and alteplase in acute ischemic stroke. Stroke. 2015;46(12):3543-3546. doi:10.1161/STROKEAHA.115.011290
11. Burgos AM, Saver JL. Evidence that tenecteplase is noninferior to alteplase for acute ischemic stroke: meta-analysis of 5 randomized trials. Stroke. 2019;50(8):2156-2162. doi:10.1161/STROKEAHA.119.025080
12. Potla N, Ganti L. Tenecteplase vs. alteplase for acute ischemic stroke: a systematic review. Int J Emerg Med. 2022;15(1). doi:10.1186/s12245-021-00399-w
13. Warach SJ, Winegar A, Ottenbacher A, Miller C, Gibson D. Abstract WMP52: reduced hospital costs for ischemic stroke treated with tenecteplase. Stroke. 2022;53(suppl 1):AWMP52. doi:10.1161/str.53.suppl_1.WMP52
14. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi:10.1161/str.0000000000000211
15. Faris H, Dewar B, Dowlatshahi D, et al. Ethical justification for deferral of consent in the AcT trial for acute ischemic stroke. Stroke. 2022;53(7):2420-2423. doi:10.1161/strokeaha.122.038760
16. Kvistad CE, Næss H, Helleberg BH, et al. Tenecteplase versus alteplase for the management of acute ischaemic stroke in Norway (NOR-TEST 2, part A): a phase 3, randomised, open-label, blinded endpoint, non-inferiority trial. Lancet Neurol. 2022;21(6):511-519. doi:10.1016/S1474-4422(22)00124-7
Tissue plasminogen activator (t-PA) has been the standard IV thrombolytic used in acute ischemic stroke treatment since its US Food and Drug Administration (FDA) approval in 1995. Trials have established this drug’s efficacy in the treatment of acute ischemic stroke and the appropriate patient population for therapy.1-3 Published guidelines and experiences have made clear that a written protocol with extensive personnel training is important to deliver this care properly.4
Tenecteplase has been available for use in the treatment of acute myocardial infarction (MI) and studied in acute ischemic strokes since 2000. Recent large multicenter trials have suggested tenecteplase may work better than t-PA in the recanalization of large vessel occlusions (LVOs) and have provided guidance on proper dosing in acute ischemic stroke victims.5-8 Compared with t-PA, tenecteplase has a longer half-life, is more fibrin specific (causing less coagulopathy), and is more resistant to endogenous plasminogen activator inhibitor.9,10 Using tenecteplase for acute ischemic stroke is simpler as a single dose bolus rather than a bolus followed by a 1-hour infusion with t-PA. Immediate mechanical thrombectomy for LVO is less complicated without the 1-hour t-PA infusion.5,6 Tenecteplase use also allows for nonthrombectomy hospitals to accelerate transfer times for patients who need thrombectomy following thrombolysis by eliminating the need for critical care nurse–staffed ambulances for interfacility transfer.11 Tenecteplase also is cheaper: Tenecteplase costs $3748 per vial, whereas t-PA costs $5800 per vial equating to roughly a $2000 savings per patient.12,13 Finally, the pharmacy formulary is simplified by using a single thrombolytic agent for both cardiac and neurologic emergencies.
Tenecteplase does have some drawbacks to consider. Currently, tenecteplase is not approved by the FDA for the indication of acute ischemic stroke, though the drug is endorsed by the American Heart Association stroke guidelines of 2019 as an alternative to t-PA.14 There is no stroke-specific preparation of the drug, leading to potential dosing errors. Therefore, a systematic process to safely transition from t-PA to tenecteplase for acute ischemic stroke was undertaken at Walter Reed National Military Medical Center (WRNMMC) in Bethesda, Maryland. Here, we report the process required in making a complex switch in thrombolytic medication along with the potential benefits of making this transition.
OBSERVATIONS
The process to implement tenecteplase required extensive training and education for staff physicians, nurses, pharmacists, radiologists, trainees, and the rapid response team. Our institution administered IV thrombolytic drugs up to 25 times annually to acute ischemic stroke victims, meaning we had to train personnel extensively and repeatedly.
In preparation for the transition to tenecteplase, hospital leadership gathered staff for multidisciplinary administrative meetings that included neurology, emergency medicine, intensive care, pharmacy, radiology, and nursing departments. The purpose of these meetings was to establish a standard operating procedure (SOP) to ensure a safe transition. This process began in May 2020 and involved regular meetings to draft and revise our SOP. Additionally, several leadership and training sessions were held over a 6-month period. Stroke boxes were developed that contained the required evaluation tools, consent forms, medications (tenecteplase and treatments for known complications), dosing cards, and instructions. Final approval of the updated acute ischemic stroke hospital policy was obtained in November 2020 and signed by the above departments.
All inclusion and exclusion criteria were determined to be the same for tenecteplase as they were for t-PA with the notable exception that the WAKE-UP trial protocol would not be supported until further evidence became available.9 The results of the WAKE-UP trial had previously been used at WRNMMC to justify administration of t-PA in patients who awoke with symptoms of acute ischemic stroke, the last known well was unclear or > 4.5 hours, and for whom a magnetic resonance imaging (MRI) of the brain could be obtained rapidly. Based on the WAKE-UP trial, if the MRI scan of the brain in these patients demonstrated restricted diffusion without fluid attenuated inversion recovery (FLAIR) signal changes (diffusion-weighted [DWI]-FLAIR mismatch sign), this indicated that the stroke had likely occurred recently, and it was safe to administer t-PA. This allowed for administration of t-PA outside the standard treatment window of 4.5 hours from last known well, especially in the cases of patients who awoke with symptoms.
Since safety data are not yet available for the use of tenecteplase in this fashion, the WAKE-UP trial protocol was not used as an inclusion criterion. The informed consent form was modified, and the following scenarios were outlined: (1) If the patient or surrogate is immediately available to consent, paper consent will be documented with the additional note that tenecteplase is being used off-label; and (2) If the patient cannot consent and a surrogate is not immediately available, the medicine will be used emergently as long as the neurology resident and attending physicians agree.15
Risk mitigation was considered carefully. The stroke box described above is stocked and maintained by the pharmacy as we have transitioned to using designated pharmacists for the storage and preparation of tenecteplase. We highly recommend the use of designated pharmacists or emergency department pharmacists in this manner to avoid dosing errors.7,16 Since the current pharmacy-provided tenecteplase bottle contains twice the maximum dose indicated for ischemic stroke, only a 5 mL syringe is included in the stroke box to ensure a maximum dose of 25 mg is drawn up after reconstitution. Dosing card charts were made like existing dosing card charts for t-PA to quickly calculate the 0.25 mg/kg dose. In training, the difference in dosing in ischemic stroke was emphasized. Finally, pharmacy has taken responsibility for dosing the medication during stroke codes.
Any medical personnel at WRNMMC can initiate a stroke code by sending a page to the neurology consult service (Figure).
TRANSITION AND RESULTS
From November 2020 to December 2021, 10 patients have been treated in total at WRNMMC (Table).
CONCLUSIONS
The available evidence supports the transition from t-PA to tenecteplase for acute ischemic stroke. The successful transition required months of preparation involving multidisciplinary meetings between neurology, nursing, pharmacy, radiology, rapid response teams, critical care, and emergency medicine departments. Safeguards must be implemented to avoid a tenecteplase dosing error that can lead to potentially life-threatening adverse effects. The results at WRNMMC thus far are promising for safety and efficacy. Several process improvements are planned: a hospital-wide overhead page will accompany the direct page to neurology; other team members, including radiology and pharmacy, will be included on the acute stroke alert; and a stroke-specific paging application will be implemented to better track real-time stroke metrics and improve flow. These measures mirror processes that are occurring in institutions that treat acute stroke patients.
Tissue plasminogen activator (t-PA) has been the standard IV thrombolytic used in acute ischemic stroke treatment since its US Food and Drug Administration (FDA) approval in 1995. Trials have established this drug’s efficacy in the treatment of acute ischemic stroke and the appropriate patient population for therapy.1-3 Published guidelines and experiences have made clear that a written protocol with extensive personnel training is important to deliver this care properly.4
Tenecteplase has been available for use in the treatment of acute myocardial infarction (MI) and studied in acute ischemic strokes since 2000. Recent large multicenter trials have suggested tenecteplase may work better than t-PA in the recanalization of large vessel occlusions (LVOs) and have provided guidance on proper dosing in acute ischemic stroke victims.5-8 Compared with t-PA, tenecteplase has a longer half-life, is more fibrin specific (causing less coagulopathy), and is more resistant to endogenous plasminogen activator inhibitor.9,10 Using tenecteplase for acute ischemic stroke is simpler as a single dose bolus rather than a bolus followed by a 1-hour infusion with t-PA. Immediate mechanical thrombectomy for LVO is less complicated without the 1-hour t-PA infusion.5,6 Tenecteplase use also allows for nonthrombectomy hospitals to accelerate transfer times for patients who need thrombectomy following thrombolysis by eliminating the need for critical care nurse–staffed ambulances for interfacility transfer.11 Tenecteplase also is cheaper: Tenecteplase costs $3748 per vial, whereas t-PA costs $5800 per vial equating to roughly a $2000 savings per patient.12,13 Finally, the pharmacy formulary is simplified by using a single thrombolytic agent for both cardiac and neurologic emergencies.
Tenecteplase does have some drawbacks to consider. Currently, tenecteplase is not approved by the FDA for the indication of acute ischemic stroke, though the drug is endorsed by the American Heart Association stroke guidelines of 2019 as an alternative to t-PA.14 There is no stroke-specific preparation of the drug, leading to potential dosing errors. Therefore, a systematic process to safely transition from t-PA to tenecteplase for acute ischemic stroke was undertaken at Walter Reed National Military Medical Center (WRNMMC) in Bethesda, Maryland. Here, we report the process required in making a complex switch in thrombolytic medication along with the potential benefits of making this transition.
OBSERVATIONS
The process to implement tenecteplase required extensive training and education for staff physicians, nurses, pharmacists, radiologists, trainees, and the rapid response team. Our institution administered IV thrombolytic drugs up to 25 times annually to acute ischemic stroke victims, meaning we had to train personnel extensively and repeatedly.
In preparation for the transition to tenecteplase, hospital leadership gathered staff for multidisciplinary administrative meetings that included neurology, emergency medicine, intensive care, pharmacy, radiology, and nursing departments. The purpose of these meetings was to establish a standard operating procedure (SOP) to ensure a safe transition. This process began in May 2020 and involved regular meetings to draft and revise our SOP. Additionally, several leadership and training sessions were held over a 6-month period. Stroke boxes were developed that contained the required evaluation tools, consent forms, medications (tenecteplase and treatments for known complications), dosing cards, and instructions. Final approval of the updated acute ischemic stroke hospital policy was obtained in November 2020 and signed by the above departments.
All inclusion and exclusion criteria were determined to be the same for tenecteplase as they were for t-PA with the notable exception that the WAKE-UP trial protocol would not be supported until further evidence became available.9 The results of the WAKE-UP trial had previously been used at WRNMMC to justify administration of t-PA in patients who awoke with symptoms of acute ischemic stroke, the last known well was unclear or > 4.5 hours, and for whom a magnetic resonance imaging (MRI) of the brain could be obtained rapidly. Based on the WAKE-UP trial, if the MRI scan of the brain in these patients demonstrated restricted diffusion without fluid attenuated inversion recovery (FLAIR) signal changes (diffusion-weighted [DWI]-FLAIR mismatch sign), this indicated that the stroke had likely occurred recently, and it was safe to administer t-PA. This allowed for administration of t-PA outside the standard treatment window of 4.5 hours from last known well, especially in the cases of patients who awoke with symptoms.
Since safety data are not yet available for the use of tenecteplase in this fashion, the WAKE-UP trial protocol was not used as an inclusion criterion. The informed consent form was modified, and the following scenarios were outlined: (1) If the patient or surrogate is immediately available to consent, paper consent will be documented with the additional note that tenecteplase is being used off-label; and (2) If the patient cannot consent and a surrogate is not immediately available, the medicine will be used emergently as long as the neurology resident and attending physicians agree.15
Risk mitigation was considered carefully. The stroke box described above is stocked and maintained by the pharmacy as we have transitioned to using designated pharmacists for the storage and preparation of tenecteplase. We highly recommend the use of designated pharmacists or emergency department pharmacists in this manner to avoid dosing errors.7,16 Since the current pharmacy-provided tenecteplase bottle contains twice the maximum dose indicated for ischemic stroke, only a 5 mL syringe is included in the stroke box to ensure a maximum dose of 25 mg is drawn up after reconstitution. Dosing card charts were made like existing dosing card charts for t-PA to quickly calculate the 0.25 mg/kg dose. In training, the difference in dosing in ischemic stroke was emphasized. Finally, pharmacy has taken responsibility for dosing the medication during stroke codes.
Any medical personnel at WRNMMC can initiate a stroke code by sending a page to the neurology consult service (Figure).
TRANSITION AND RESULTS
From November 2020 to December 2021, 10 patients have been treated in total at WRNMMC (Table).
CONCLUSIONS
The available evidence supports the transition from t-PA to tenecteplase for acute ischemic stroke. The successful transition required months of preparation involving multidisciplinary meetings between neurology, nursing, pharmacy, radiology, rapid response teams, critical care, and emergency medicine departments. Safeguards must be implemented to avoid a tenecteplase dosing error that can lead to potentially life-threatening adverse effects. The results at WRNMMC thus far are promising for safety and efficacy. Several process improvements are planned: a hospital-wide overhead page will accompany the direct page to neurology; other team members, including radiology and pharmacy, will be included on the acute stroke alert; and a stroke-specific paging application will be implemented to better track real-time stroke metrics and improve flow. These measures mirror processes that are occurring in institutions that treat acute stroke patients.
1. Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375(9727):1695-1703. doi:10.1016/S0140-6736(10)60491-6
2. National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581- 1587. doi:10.1056/NEJM199512143332401
3. Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363(9411):768-774. doi:10.1016/S0140-6736(04)15692-4
4. Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(3):870-947. doi:10.1161/STR.0b013e318284056a
5. Campbell B, Mitchell P, Churilov L, et al. Tenecteplase versus alteplase before thrombectomy for ischemic stroke. N Engl J Med. 2018;378(17):1573-1582. doi:10.1056/nejmoa1716405
6. Yang P, Zhang Y, Zhang L, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke. N Engl J Med. 2020;382(21):1981-1993. doi:10.1056/NEJMoa2001123
7. Menon BK, Buck BH, Singh N, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, noninferiority trial. Lancet. 2022;400(10347):161-169. doi:10.1016/S0140-6736(22)01054-6
8. Campbell BCV, Mitchell PJ, Churilov L, et al. Effect of intravenous tenecteplase dose on cerebral reperfusion before thrombectomy in patients with large vessel occlusion ischemic stroke: the EXTEND-IA TNK part 2 randomized clinical trial. JAMA. 2020;323(13):1257- 1265. doi:10.1001/jama.2020.1511
9. Warach SJ, Dula AN, Milling TJ Jr. Tenecteplase thrombolysis for acute ischemic stroke. Stroke. 2020;51(11):3440- 3451. doi:10.1161/STROKEAHA.120.029749
10. Huang X, Moreton FC, Kalladka D, et al. Coagulation and fibrinolytic activity of tenecteplase and alteplase in acute ischemic stroke. Stroke. 2015;46(12):3543-3546. doi:10.1161/STROKEAHA.115.011290
11. Burgos AM, Saver JL. Evidence that tenecteplase is noninferior to alteplase for acute ischemic stroke: meta-analysis of 5 randomized trials. Stroke. 2019;50(8):2156-2162. doi:10.1161/STROKEAHA.119.025080
12. Potla N, Ganti L. Tenecteplase vs. alteplase for acute ischemic stroke: a systematic review. Int J Emerg Med. 2022;15(1). doi:10.1186/s12245-021-00399-w
13. Warach SJ, Winegar A, Ottenbacher A, Miller C, Gibson D. Abstract WMP52: reduced hospital costs for ischemic stroke treated with tenecteplase. Stroke. 2022;53(suppl 1):AWMP52. doi:10.1161/str.53.suppl_1.WMP52
14. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi:10.1161/str.0000000000000211
15. Faris H, Dewar B, Dowlatshahi D, et al. Ethical justification for deferral of consent in the AcT trial for acute ischemic stroke. Stroke. 2022;53(7):2420-2423. doi:10.1161/strokeaha.122.038760
16. Kvistad CE, Næss H, Helleberg BH, et al. Tenecteplase versus alteplase for the management of acute ischaemic stroke in Norway (NOR-TEST 2, part A): a phase 3, randomised, open-label, blinded endpoint, non-inferiority trial. Lancet Neurol. 2022;21(6):511-519. doi:10.1016/S1474-4422(22)00124-7
1. Lees KR, Bluhmki E, von Kummer R, et al. Time to treatment with intravenous alteplase and outcome in stroke: an updated pooled analysis of ECASS, ATLANTIS, NINDS, and EPITHET trials. Lancet. 2010;375(9727):1695-1703. doi:10.1016/S0140-6736(10)60491-6
2. National Institute of Neurological Disorders and Stroke rt-PA Stroke Study Group. Tissue plasminogen activator for acute ischemic stroke. N Engl J Med. 1995;333(24):1581- 1587. doi:10.1056/NEJM199512143332401
3. Hacke W, Donnan G, Fieschi C, et al. Association of outcome with early stroke treatment: pooled analysis of ATLANTIS, ECASS, and NINDS rt-PA stroke trials. Lancet. 2004;363(9411):768-774. doi:10.1016/S0140-6736(04)15692-4
4. Jauch EC, Saver JL, Adams HP Jr, et al. Guidelines for the early management of patients with acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2013;44(3):870-947. doi:10.1161/STR.0b013e318284056a
5. Campbell B, Mitchell P, Churilov L, et al. Tenecteplase versus alteplase before thrombectomy for ischemic stroke. N Engl J Med. 2018;378(17):1573-1582. doi:10.1056/nejmoa1716405
6. Yang P, Zhang Y, Zhang L, et al. Endovascular thrombectomy with or without intravenous alteplase in acute stroke. N Engl J Med. 2020;382(21):1981-1993. doi:10.1056/NEJMoa2001123
7. Menon BK, Buck BH, Singh N, et al. Intravenous tenecteplase compared with alteplase for acute ischaemic stroke in Canada (AcT): a pragmatic, multicentre, open-label, registry-linked, randomised, controlled, noninferiority trial. Lancet. 2022;400(10347):161-169. doi:10.1016/S0140-6736(22)01054-6
8. Campbell BCV, Mitchell PJ, Churilov L, et al. Effect of intravenous tenecteplase dose on cerebral reperfusion before thrombectomy in patients with large vessel occlusion ischemic stroke: the EXTEND-IA TNK part 2 randomized clinical trial. JAMA. 2020;323(13):1257- 1265. doi:10.1001/jama.2020.1511
9. Warach SJ, Dula AN, Milling TJ Jr. Tenecteplase thrombolysis for acute ischemic stroke. Stroke. 2020;51(11):3440- 3451. doi:10.1161/STROKEAHA.120.029749
10. Huang X, Moreton FC, Kalladka D, et al. Coagulation and fibrinolytic activity of tenecteplase and alteplase in acute ischemic stroke. Stroke. 2015;46(12):3543-3546. doi:10.1161/STROKEAHA.115.011290
11. Burgos AM, Saver JL. Evidence that tenecteplase is noninferior to alteplase for acute ischemic stroke: meta-analysis of 5 randomized trials. Stroke. 2019;50(8):2156-2162. doi:10.1161/STROKEAHA.119.025080
12. Potla N, Ganti L. Tenecteplase vs. alteplase for acute ischemic stroke: a systematic review. Int J Emerg Med. 2022;15(1). doi:10.1186/s12245-021-00399-w
13. Warach SJ, Winegar A, Ottenbacher A, Miller C, Gibson D. Abstract WMP52: reduced hospital costs for ischemic stroke treated with tenecteplase. Stroke. 2022;53(suppl 1):AWMP52. doi:10.1161/str.53.suppl_1.WMP52
14. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association. Stroke. 2019;50(12):e344-e418. doi:10.1161/str.0000000000000211
15. Faris H, Dewar B, Dowlatshahi D, et al. Ethical justification for deferral of consent in the AcT trial for acute ischemic stroke. Stroke. 2022;53(7):2420-2423. doi:10.1161/strokeaha.122.038760
16. Kvistad CE, Næss H, Helleberg BH, et al. Tenecteplase versus alteplase for the management of acute ischaemic stroke in Norway (NOR-TEST 2, part A): a phase 3, randomised, open-label, blinded endpoint, non-inferiority trial. Lancet Neurol. 2022;21(6):511-519. doi:10.1016/S1474-4422(22)00124-7
Warfarin best for thrombotic antiphospholipid syndrome?
Patients with thrombotic antiphospholipid syndrome are better treated with a vitamin K antagonist, such as warfarin, rather than a direct oral anticoagulant (DOAC), a new systematic review and meta-analysis suggests.
“Our study is showing that in randomized controlled trials in patients with thrombotic antiphospholipid syndrome, the risk of arterial thrombotic events, particularly stroke, is significantly increased with DOACs vs. vitamin K antagonists,” senior author, Behnood Bikdeli, MD, Brigham and Women’s Hospital, Boston, told this news organization. “These results probably suggest that DOACs are not the optimal regimen for patients with thrombotic antiphospholipid syndrome.”
The study was published online in the Journal of the American College of Cardiology.
Autoimmune disorder
Thrombotic antiphospholipid syndrome is a systemic autoimmune disorder characterized by recurrent arterial and/or venous thrombotic events.
Dr. Bikdeli estimates that antiphospholipid syndrome is the cause of 50,000-100,000 strokes, 100,000 cases of myocardial infarction, and 30,000 cases of deep vein thrombosis every year.
“It is a serious condition, and these are a high-risk and complex group of patients,” he said.
The standard treatment has been anticoagulation with a vitamin K antagonist such as warfarin. “But this is a cumbersome treatment, with many drug interactions and the need for INR [International Normalized Ratio] monitoring, which can be difficult to manage in patients with antiphospholipid syndrome as there can sometimes be falsely abnormal numbers,” Dr. Bikdeli noted. “Because of these challenges, it looked very promising to explore the use of DOACs in this population.”
Four main randomized trials have been conducted to investigate the use of DOACs in antiphospholipid syndrome – three with rivaroxaban and one with apixaban. “These trials were all quite small and, while they did not show definite results, some of them suggested nonsignificant findings of slightly worse outcomes for DOACs vs. vitamin K antagonists. But there is a lot of uncertainty, and it is difficult to look at subgroups in such small trials,” Dr. Bikdeli said. “There are many questions remaining about whether we should use DOACs in patients with antiphospholipid syndrome and, if so, which particular subgroups.”
The authors therefore performed a systematic review and meta-analysis of randomized controlled trials that compared DOACs with vitamin K antagonists in patients with antiphospholipid syndrome. They also contacted the principal investigators of the trials to obtain additional unpublished aggregate level data on specific subgroups.
Four open-label randomized controlled trials involving 472 patients were included in the meta-analysis.
Overall, the use of DOACs, compared with vitamin K antagonists, was associated with increased odds of subsequent arterial thrombotic events (odds ratio, 5.43; P < .001), especially stroke.
The odds of subsequent venous thrombotic events or major bleeding were not significantly different between the two groups. Most findings were consistent within subgroups.
“Our results show that use of DOACs vs. vitamin K antagonists is associated with increased risk of arterial thrombotic events – a risk that is primarily driven by a significant increase in the risk of stroke,” Dr. Bikdeli commented.
When looking at subgroups of interest, it was previously thought that DOACs may not be so effective in the so-called “triple-positive” antiphospholipid patients. These patients have three different types of antibodies and have the highest risk of thrombosis, Dr. Bikdeli noted.
“But one of the interesting findings of our study is that the results are actually consistent in women vs. men and in people who have triple-positive antibodies and those who had double- or single-positive antibodies,” he said. “Our analyses did not show effect modification by antibody subgroups. They suggest similar trends towards worse outcomes in all subgroups.”
“From these results, I would be similarly concerned to use DOACs even if someone has double-positive or single-positive antiphospholipid antibodies,” he added.
Dr. Bikdeli said he would still recommend shared decision-making with patients. “If I have a patient who has thrombotic antiphospholipid syndrome, I would share my reservation about DOACs, but there are multiple factors that come into decision-making. If someone has difficulty with checking INRs, we may make an informed choice and still use a DOAC, but patients need to know that there is likely an excess risk of subsequent arterial events with DOACs, compared with a vitamin K antagonist.”
He noted that it is still not completely clear on the situation for people with single-positive antiphospholipid syndrome or the type of antibody that is present. It is also possible that a higher dose of DOAC could be more effective, a strategy that is being investigated in a separate randomized trial currently ongoing.
“But for routine practice I would have concerns about using DOACs in antiphospholipid syndrome patients in general,” he said. “For triple positive there is more data and greater concern, but I wouldn’t give a pass for a double- or single-positive patient either.”
The reason why DOACs would be less effective than vitamin K antagonists in antiphospholipid syndrome is not known.
“That is the million-dollar question,” Dr. Bikdeli commented. “DOACs have been such helpful drugs for many patients and clinicians as well. But we have seen that they are not optimal in a series of scenarios now – patients with mechanical heart valves, patients with rheumatic [atrial fibrillaton], and now patients with thrombotic antiphospholipid syndrome.”
One hypothesis is that these patients have some more components of inflammation and are more prone to blood clots, and because vitamin K antagonists work at several parts of the coagulation cascade, they might be more successful, compared with the more targeted DOAC therapy. “But I think we need more studies to fully understand this,” he said.
‘Important implications’
In an accompanying editorial,Mark A. Crowther, MD, McMaster University, Hamilton, Ont., and Aubrey E. Jones, PharmD, and Daniel M. Witt, PharmD, both of the University of Utah College of Pharmacy, Salt Lake City, say that: “As the quality of the evidence was rated ‘high’ for the arterial thrombosis outcome and ‘moderate’ for the venous thrombosis and bleeding outcomes, these results should lead to a revision of evidence-based guidelines to recommend against using DOACs as an option for most patients with thrombotic antiphospholipid syndrome.”
They add that this recommendation for vitamin K antagonists also applies to patients previously thought to be at lower risk from antiphospholipid syndrome – including those with only one or two positive serological tests and those with only prior venous thrombosis.
The editorialists point out that this will have important implications, particularly for the accurate diagnosis of antiphospholipid syndrome, including confirmation and documentation of positive laboratory tests at least 12 weeks after the initial positive test.
They recommend that while awaiting confirmatory testing, patients with suspected antiphospholipid syndrome should avoid DOACs, and that “strong consideration” should be given to switching essentially all antiphospholipid syndrome patients currently receiving DOACs to vitamin K antagonists.
Dr. Bikdeli is a consulting expert, on behalf of the plaintiff, for litigation related to two specific brand models of IVC filters and is supported by the Scott Schoen and Nancy Adams IGNITE Award from the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and a Career Development Award from the American Heart Association and VIVA Physicians. Dr. Crowther has received personal funding from AstraZeneca, Precision Biologics, Hemostasis Reference Laboratories, Syneos Health, Bayer, Pfizer, and CSL Behring; and holds the Leo Pharma Chair in Thromboembolism Research, which is endowed at McMaster University. Dr. Jones is supported by a career development award from the National Heart, Lung, and Blood Institute; and Dr. Witt is supported by grant funding from the Agency for Healthcare Research and Quality.
A version of this article first appeared on Medscape.com.
Patients with thrombotic antiphospholipid syndrome are better treated with a vitamin K antagonist, such as warfarin, rather than a direct oral anticoagulant (DOAC), a new systematic review and meta-analysis suggests.
“Our study is showing that in randomized controlled trials in patients with thrombotic antiphospholipid syndrome, the risk of arterial thrombotic events, particularly stroke, is significantly increased with DOACs vs. vitamin K antagonists,” senior author, Behnood Bikdeli, MD, Brigham and Women’s Hospital, Boston, told this news organization. “These results probably suggest that DOACs are not the optimal regimen for patients with thrombotic antiphospholipid syndrome.”
The study was published online in the Journal of the American College of Cardiology.
Autoimmune disorder
Thrombotic antiphospholipid syndrome is a systemic autoimmune disorder characterized by recurrent arterial and/or venous thrombotic events.
Dr. Bikdeli estimates that antiphospholipid syndrome is the cause of 50,000-100,000 strokes, 100,000 cases of myocardial infarction, and 30,000 cases of deep vein thrombosis every year.
“It is a serious condition, and these are a high-risk and complex group of patients,” he said.
The standard treatment has been anticoagulation with a vitamin K antagonist such as warfarin. “But this is a cumbersome treatment, with many drug interactions and the need for INR [International Normalized Ratio] monitoring, which can be difficult to manage in patients with antiphospholipid syndrome as there can sometimes be falsely abnormal numbers,” Dr. Bikdeli noted. “Because of these challenges, it looked very promising to explore the use of DOACs in this population.”
Four main randomized trials have been conducted to investigate the use of DOACs in antiphospholipid syndrome – three with rivaroxaban and one with apixaban. “These trials were all quite small and, while they did not show definite results, some of them suggested nonsignificant findings of slightly worse outcomes for DOACs vs. vitamin K antagonists. But there is a lot of uncertainty, and it is difficult to look at subgroups in such small trials,” Dr. Bikdeli said. “There are many questions remaining about whether we should use DOACs in patients with antiphospholipid syndrome and, if so, which particular subgroups.”
The authors therefore performed a systematic review and meta-analysis of randomized controlled trials that compared DOACs with vitamin K antagonists in patients with antiphospholipid syndrome. They also contacted the principal investigators of the trials to obtain additional unpublished aggregate level data on specific subgroups.
Four open-label randomized controlled trials involving 472 patients were included in the meta-analysis.
Overall, the use of DOACs, compared with vitamin K antagonists, was associated with increased odds of subsequent arterial thrombotic events (odds ratio, 5.43; P < .001), especially stroke.
The odds of subsequent venous thrombotic events or major bleeding were not significantly different between the two groups. Most findings were consistent within subgroups.
“Our results show that use of DOACs vs. vitamin K antagonists is associated with increased risk of arterial thrombotic events – a risk that is primarily driven by a significant increase in the risk of stroke,” Dr. Bikdeli commented.
When looking at subgroups of interest, it was previously thought that DOACs may not be so effective in the so-called “triple-positive” antiphospholipid patients. These patients have three different types of antibodies and have the highest risk of thrombosis, Dr. Bikdeli noted.
“But one of the interesting findings of our study is that the results are actually consistent in women vs. men and in people who have triple-positive antibodies and those who had double- or single-positive antibodies,” he said. “Our analyses did not show effect modification by antibody subgroups. They suggest similar trends towards worse outcomes in all subgroups.”
“From these results, I would be similarly concerned to use DOACs even if someone has double-positive or single-positive antiphospholipid antibodies,” he added.
Dr. Bikdeli said he would still recommend shared decision-making with patients. “If I have a patient who has thrombotic antiphospholipid syndrome, I would share my reservation about DOACs, but there are multiple factors that come into decision-making. If someone has difficulty with checking INRs, we may make an informed choice and still use a DOAC, but patients need to know that there is likely an excess risk of subsequent arterial events with DOACs, compared with a vitamin K antagonist.”
He noted that it is still not completely clear on the situation for people with single-positive antiphospholipid syndrome or the type of antibody that is present. It is also possible that a higher dose of DOAC could be more effective, a strategy that is being investigated in a separate randomized trial currently ongoing.
“But for routine practice I would have concerns about using DOACs in antiphospholipid syndrome patients in general,” he said. “For triple positive there is more data and greater concern, but I wouldn’t give a pass for a double- or single-positive patient either.”
The reason why DOACs would be less effective than vitamin K antagonists in antiphospholipid syndrome is not known.
“That is the million-dollar question,” Dr. Bikdeli commented. “DOACs have been such helpful drugs for many patients and clinicians as well. But we have seen that they are not optimal in a series of scenarios now – patients with mechanical heart valves, patients with rheumatic [atrial fibrillaton], and now patients with thrombotic antiphospholipid syndrome.”
One hypothesis is that these patients have some more components of inflammation and are more prone to blood clots, and because vitamin K antagonists work at several parts of the coagulation cascade, they might be more successful, compared with the more targeted DOAC therapy. “But I think we need more studies to fully understand this,” he said.
‘Important implications’
In an accompanying editorial,Mark A. Crowther, MD, McMaster University, Hamilton, Ont., and Aubrey E. Jones, PharmD, and Daniel M. Witt, PharmD, both of the University of Utah College of Pharmacy, Salt Lake City, say that: “As the quality of the evidence was rated ‘high’ for the arterial thrombosis outcome and ‘moderate’ for the venous thrombosis and bleeding outcomes, these results should lead to a revision of evidence-based guidelines to recommend against using DOACs as an option for most patients with thrombotic antiphospholipid syndrome.”
They add that this recommendation for vitamin K antagonists also applies to patients previously thought to be at lower risk from antiphospholipid syndrome – including those with only one or two positive serological tests and those with only prior venous thrombosis.
The editorialists point out that this will have important implications, particularly for the accurate diagnosis of antiphospholipid syndrome, including confirmation and documentation of positive laboratory tests at least 12 weeks after the initial positive test.
They recommend that while awaiting confirmatory testing, patients with suspected antiphospholipid syndrome should avoid DOACs, and that “strong consideration” should be given to switching essentially all antiphospholipid syndrome patients currently receiving DOACs to vitamin K antagonists.
Dr. Bikdeli is a consulting expert, on behalf of the plaintiff, for litigation related to two specific brand models of IVC filters and is supported by the Scott Schoen and Nancy Adams IGNITE Award from the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and a Career Development Award from the American Heart Association and VIVA Physicians. Dr. Crowther has received personal funding from AstraZeneca, Precision Biologics, Hemostasis Reference Laboratories, Syneos Health, Bayer, Pfizer, and CSL Behring; and holds the Leo Pharma Chair in Thromboembolism Research, which is endowed at McMaster University. Dr. Jones is supported by a career development award from the National Heart, Lung, and Blood Institute; and Dr. Witt is supported by grant funding from the Agency for Healthcare Research and Quality.
A version of this article first appeared on Medscape.com.
Patients with thrombotic antiphospholipid syndrome are better treated with a vitamin K antagonist, such as warfarin, rather than a direct oral anticoagulant (DOAC), a new systematic review and meta-analysis suggests.
“Our study is showing that in randomized controlled trials in patients with thrombotic antiphospholipid syndrome, the risk of arterial thrombotic events, particularly stroke, is significantly increased with DOACs vs. vitamin K antagonists,” senior author, Behnood Bikdeli, MD, Brigham and Women’s Hospital, Boston, told this news organization. “These results probably suggest that DOACs are not the optimal regimen for patients with thrombotic antiphospholipid syndrome.”
The study was published online in the Journal of the American College of Cardiology.
Autoimmune disorder
Thrombotic antiphospholipid syndrome is a systemic autoimmune disorder characterized by recurrent arterial and/or venous thrombotic events.
Dr. Bikdeli estimates that antiphospholipid syndrome is the cause of 50,000-100,000 strokes, 100,000 cases of myocardial infarction, and 30,000 cases of deep vein thrombosis every year.
“It is a serious condition, and these are a high-risk and complex group of patients,” he said.
The standard treatment has been anticoagulation with a vitamin K antagonist such as warfarin. “But this is a cumbersome treatment, with many drug interactions and the need for INR [International Normalized Ratio] monitoring, which can be difficult to manage in patients with antiphospholipid syndrome as there can sometimes be falsely abnormal numbers,” Dr. Bikdeli noted. “Because of these challenges, it looked very promising to explore the use of DOACs in this population.”
Four main randomized trials have been conducted to investigate the use of DOACs in antiphospholipid syndrome – three with rivaroxaban and one with apixaban. “These trials were all quite small and, while they did not show definite results, some of them suggested nonsignificant findings of slightly worse outcomes for DOACs vs. vitamin K antagonists. But there is a lot of uncertainty, and it is difficult to look at subgroups in such small trials,” Dr. Bikdeli said. “There are many questions remaining about whether we should use DOACs in patients with antiphospholipid syndrome and, if so, which particular subgroups.”
The authors therefore performed a systematic review and meta-analysis of randomized controlled trials that compared DOACs with vitamin K antagonists in patients with antiphospholipid syndrome. They also contacted the principal investigators of the trials to obtain additional unpublished aggregate level data on specific subgroups.
Four open-label randomized controlled trials involving 472 patients were included in the meta-analysis.
Overall, the use of DOACs, compared with vitamin K antagonists, was associated with increased odds of subsequent arterial thrombotic events (odds ratio, 5.43; P < .001), especially stroke.
The odds of subsequent venous thrombotic events or major bleeding were not significantly different between the two groups. Most findings were consistent within subgroups.
“Our results show that use of DOACs vs. vitamin K antagonists is associated with increased risk of arterial thrombotic events – a risk that is primarily driven by a significant increase in the risk of stroke,” Dr. Bikdeli commented.
When looking at subgroups of interest, it was previously thought that DOACs may not be so effective in the so-called “triple-positive” antiphospholipid patients. These patients have three different types of antibodies and have the highest risk of thrombosis, Dr. Bikdeli noted.
“But one of the interesting findings of our study is that the results are actually consistent in women vs. men and in people who have triple-positive antibodies and those who had double- or single-positive antibodies,” he said. “Our analyses did not show effect modification by antibody subgroups. They suggest similar trends towards worse outcomes in all subgroups.”
“From these results, I would be similarly concerned to use DOACs even if someone has double-positive or single-positive antiphospholipid antibodies,” he added.
Dr. Bikdeli said he would still recommend shared decision-making with patients. “If I have a patient who has thrombotic antiphospholipid syndrome, I would share my reservation about DOACs, but there are multiple factors that come into decision-making. If someone has difficulty with checking INRs, we may make an informed choice and still use a DOAC, but patients need to know that there is likely an excess risk of subsequent arterial events with DOACs, compared with a vitamin K antagonist.”
He noted that it is still not completely clear on the situation for people with single-positive antiphospholipid syndrome or the type of antibody that is present. It is also possible that a higher dose of DOAC could be more effective, a strategy that is being investigated in a separate randomized trial currently ongoing.
“But for routine practice I would have concerns about using DOACs in antiphospholipid syndrome patients in general,” he said. “For triple positive there is more data and greater concern, but I wouldn’t give a pass for a double- or single-positive patient either.”
The reason why DOACs would be less effective than vitamin K antagonists in antiphospholipid syndrome is not known.
“That is the million-dollar question,” Dr. Bikdeli commented. “DOACs have been such helpful drugs for many patients and clinicians as well. But we have seen that they are not optimal in a series of scenarios now – patients with mechanical heart valves, patients with rheumatic [atrial fibrillaton], and now patients with thrombotic antiphospholipid syndrome.”
One hypothesis is that these patients have some more components of inflammation and are more prone to blood clots, and because vitamin K antagonists work at several parts of the coagulation cascade, they might be more successful, compared with the more targeted DOAC therapy. “But I think we need more studies to fully understand this,” he said.
‘Important implications’
In an accompanying editorial,Mark A. Crowther, MD, McMaster University, Hamilton, Ont., and Aubrey E. Jones, PharmD, and Daniel M. Witt, PharmD, both of the University of Utah College of Pharmacy, Salt Lake City, say that: “As the quality of the evidence was rated ‘high’ for the arterial thrombosis outcome and ‘moderate’ for the venous thrombosis and bleeding outcomes, these results should lead to a revision of evidence-based guidelines to recommend against using DOACs as an option for most patients with thrombotic antiphospholipid syndrome.”
They add that this recommendation for vitamin K antagonists also applies to patients previously thought to be at lower risk from antiphospholipid syndrome – including those with only one or two positive serological tests and those with only prior venous thrombosis.
The editorialists point out that this will have important implications, particularly for the accurate diagnosis of antiphospholipid syndrome, including confirmation and documentation of positive laboratory tests at least 12 weeks after the initial positive test.
They recommend that while awaiting confirmatory testing, patients with suspected antiphospholipid syndrome should avoid DOACs, and that “strong consideration” should be given to switching essentially all antiphospholipid syndrome patients currently receiving DOACs to vitamin K antagonists.
Dr. Bikdeli is a consulting expert, on behalf of the plaintiff, for litigation related to two specific brand models of IVC filters and is supported by the Scott Schoen and Nancy Adams IGNITE Award from the Mary Horrigan Connors Center for Women’s Health and Gender Biology at Brigham and Women’s Hospital and a Career Development Award from the American Heart Association and VIVA Physicians. Dr. Crowther has received personal funding from AstraZeneca, Precision Biologics, Hemostasis Reference Laboratories, Syneos Health, Bayer, Pfizer, and CSL Behring; and holds the Leo Pharma Chair in Thromboembolism Research, which is endowed at McMaster University. Dr. Jones is supported by a career development award from the National Heart, Lung, and Blood Institute; and Dr. Witt is supported by grant funding from the Agency for Healthcare Research and Quality.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY
Atrial fibrillation: Sex differences and modifiable risk factors
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
This transcript has been edited for clarity.
Hello. This is Dr. JoAnn Manson, professor of medicine at Harvard Medical School and Brigham and Women’s Hospital.
We looked at these questions in our vitamin D and omega-3 trial VITAL in an ancillary study called VITAL Rhythm, led by Dr. Christine Albert at Cedars-Sinai. And this particular project was led by Dr. Hasan Siddiqi at Vanderbilt.
As you know, AF is the most common arrhythmia in the world, and it’s burgeoning in numbers, primarily because of the aging of the population. It’s also a major cause of stroke, heart failure, and cardiovascular mortality. Although women are known to have lower rates of AF than men, they’re also known to have a higher risk for cardiovascular complications and sequelae, such as higher risk for stroke and CVD mortality. Therefore, we thought that understanding sex differences in risk and modifiable risk factors for AF that could reduce the burden of disease would be important.
It’s known that greater height is a risk factor for AF, but the extent to which it explains the differences in AF risk between men and women isn’t really known. So we looked at these questions in the VITAL cohort. VITAL has more than 25,000 participants. It’s a large, diverse, nationwide cohort. About 51% are women, and all are aged 50 years or older, with a mean age of 67. All were free of known clinical cardiovascular disease at the start of the study.
AF reports were confirmed by medical records and also supplemented by Medicare CMS linkage for fuller ascertainment of outcomes. We had 900 incident cases of AF in the study, and we did see that women were less likely to be diagnosed with AF. They had a 32% lower risk – strongly statistically significant compared with men, with a P < .001. Women were also more likely to be symptomatic: About 77% of women vs. 63% of men had symptoms prior to or at diagnosis.
It was very interesting that adjustment for height eliminated the lower risk for AF in women compared with men. After accounting for height, there was not only no reduction in risk for AF among the women, there was actually a reversal of the association so that there was a slightly higher risk for AF in the women. Other risk factors for AF in the cohort included older age, higher body mass index, hypertension, and higher consumption of alcohol. We did not see an association between diabetes and higher risk for AF. We also saw no clear association with physical activity, although very strenuous physical activity has been linked to AF in some other studies.
We looked at the interventions of vitamin D (2,000 IU/day) and omega-3 fatty acids (460 mg/day of EPA and 380 mg/day of DHA) and found no association with AF, although some other studies have seen increased risk for AF with higher doses of the marine omega-3s > 1 g/day and certainly at doses of 4 g/day. So overall, the findings highlight the fact that many of the risk factors for AF do seem to be modifiable, and it is really important to identify and try to reduce these risk factors in order to reduce the burden of AF. This may be particularly important in women because women are more likely to have stroke and cardiovascular mortality in these adverse cardiovascular outcomes.
A version of this article first appeared on Medscape.com.
Is thrombolysis safe for stroke patients on DOACs?
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
, a new study has found.
The study, the largest ever regarding the safety of thrombolysis in patients on DOACs, actually found a lower rate of sICH among patients taking DOACs than among those not taking anticoagulants.
“Thrombolysis is a backbone therapy in stroke, but the large population of patients who take DOACs are currently excluded from this treatment because DOAC use is a contraindication to treatment with thrombolysis. This is based on the presumption of an increased risk of sICH, but data to support or refute this presumption are lacking,” said senior author David J. Seiffge, MD, Bern University Hospital, Switzerland.
“Our results suggest that current guidelines need to be revised to remove the absolute contraindication of thrombolysis in patients on DOACs. The guidelines need to be more liberal on the use of thrombolysis in these patients,” he added.
“This study provides the basis for extending vital thrombolysis treatment to this substantial population of patients who take DOACs,” Dr. Seiffge said.
He estimates that 1 of every 6 stroke patients are taking a DOAC and that 1% to 2% of patients taking DOACs have a stroke each year. “As millions of patients are on DOACs, this is a large number of people who are not getting potentially life-saving thrombolysis therapy.”
Dr. Seiffge comments: “In our hospital we see at least one stroke patient on DOACs every day. It is a very frequent scenario. With this new data, we believe many of these patients could now benefit from thrombolysis without an increased bleeding risk.”
The study was published online in JAMA Neurology.
An international investigation
While thrombolysis is currently contraindicated for patients taking DOACs, some clinicians still administer thrombolysis to these patients. Different selection strategies are used, including the use of DOAC reversal agents prior to thrombolysis or the selection of patients with low anticoagulant activity, the authors noted.
The current study involved an international collaboration. The investigators compared the risk of sICH among patients who had recently taken DOACs and who underwent thrombolysis as treatment for acute ischemic stroke with the risk among control stroke patients who underwent thrombolysis but who had not been taking DOACs.
Potential contributing centers were identified by a systematic search of the literature based on published studies on the use of thrombolysis for patients who had recently taken DOACs or prospective stroke registries that may include patients who had recently taken DOACs.
The study included 832 patients from 64 centers worldwide who were confirmed to have taken a DOAC within 48 hours of receiving thrombolysis for acute ischemic stroke. The comparison group was made up of 32,375 patients who had experienced ischemic stroke that was treated with thrombolysis but who had received no prior anticoagulation therapy.
Compared with control patients, patients who had recently taken DOACs were older; the incidence of hypertension among them was higher; they had a higher degree of prestroke disability; they were less likely to be smokers; the time from symptom onset to treatment was longer; they had experienced more severe stroke; and they were more likely to have a large-vessel occlusion.
Of the patients taking DOACs, 30.3% received DOAC reversal prior to thrombolysis. For 27.0%, DOAC plasma levels were measured. The remainder were treated with thrombolysis without either of these selection methods.
Results showed that the unadjusted rate of sICH was 2.5% among patients taking DOACs, compared with 4.1% among control patients who were not taking anticoagulants.
After adjustment for stroke severity and other baseline sICH predictors, patients who had recently taken DOACs and who received thrombolysis had lower odds of developing sICH (adjusted odds ratio, 0.57; 95% confidence interval, 0.36-0.92; P = .02).
There was no difference between the selection strategies, and results were consistent in different sensitivity analyses.
The secondary outcome of any ICH occurred in 18.0% in patients taking DOACs, compared with 17.4% among control patients who used no anticoagulants. After adjustment, there was no difference in the odds for any ICH between the groups (aOR, 1.18; 95% CI, 0.95-1.45; P = .14).
The unadjusted rate of functional independence was 45% among patients taking DOACs, compared with 57% among control patients. After adjustment, patients who had recently taken DOACs and who underwent thrombolysis had numerically higher odds of being functionally independent than control patients, although this difference did not reach statistical significance (aOR, 1.13; 95% CI, 0.94-1.36; P = .20).
The association of DOAC therapy with lower odds of sICH remained when mechanical thrombectomy, large-vessel occlusion, or concomitant antiplatelet therapy was added to the model.
“This is by far the largest study to look at this issue of thrombolytic use in patients on DOACs, and we did not find any group on DOACs that had an excess ICH rate with thrombolysis,” Dr. Seiffge said,
He explained that receiving warfarin was at one time an absolute contraindication for thrombolysis, but after a 2014 study suggested that the risk was not increased for patients with an international normalized ratio below 117, this was downgraded to a relative contraindication.
“We think our study is comparable and should lead to a guideline change,” Dr. Seiffge commented.
“A relative contraindication allows clinicians the space to make a considered decision on an individual basis,” he added.
Dr. Seiffge said that at his hospital, local guidelines regarding this issue have already been changed on the basis of these data, and use of DOACs is now considered a relative contraindication.
“International guidelines can take years to update, so in the meantime, I think other centers will also go ahead with a more liberal approach. There are always some centers that are ahead of the guidelines,” he added.
Although the lower risk of sICH seen in patients who have recently used DOACs seems counterintuitive at first glance, there could be a pathophysiologic explanation for this finding, the authors suggest.
They point out that thrombin inhibition, either directly or via the coagulation cascade, might be protective against the occurrence of sICH.
“Anticoagulants may allow the clot to respond better to thrombolysis – the clot is not as solid and is easier to recanalize. This leads to smaller strokes and a lower bleeding risk. Thrombin generation is also a major driver for blood brain barrier breakdown. DOACs reduce thrombin generation, so reduce blood brain barrier breakdown and reduce bleeding,” Dr. Seiffge explained. “But these are hypotheses,” he added.
Study ‘meaningfully advances the field’
In an accompanying editorial, Eva A. Mistry, MBBS, University of Cincinnati, said the current study “meaningfully advances the field” and provides an estimation of safety of intravenous thrombolysis among patients who have taken DOACs within 48 hours of hospital admission.
She lists strengths of the study as inclusion of a large number of patients across several geographically diverse institutions with heterogeneous standard practices for thrombolysis with recent DOAC use and narrow confidence intervals regarding observed rates of sICH.
“Further, the upper bound of this confidence interval for the DOAC group is below 4%, which is a welcome result and provides supportive data for clinicians who already practice thrombolysis for patients with recent DOAC ingestion,” Dr. Mistry adds.
However, she points out several study limitations, which she says limit immediate, widespread clinical applicability.
These include use of a nonconcurrent control population, which included patients from centers that did not contribute to the DOAC group and the inclusion of Asian patients who likely received a lower thrombolytic dose.
Dr. Seiffge noted that the researchers did adjust for Asian patients but not for the thrombolytic dosage. “I personally do not think this affects the results, as Asian patients have a lower dosage because they have a higher bleeding risk. The lower bleeding risk with DOACs was seen in all continents.”
Dr. Mistry also suggests that the DOAC group itself is prone to selection bias from preferential thrombolysis of patients receiving DOAC who are at lower risk of sICH.
But Dr. Seiffge argued: “I think, actually, the opposite is true. The DOAC patients were older, had more severe comorbidities, and an increased bleeding risk.”
Dr. Mistry concluded, “Despite the limitations of the study design and enrolled population, these data may be used by clinicians to make individualized decisions regarding thrombolysis among patients with recent DOAC use. Importantly, this study lays the foundation for prospective, well-powered studies that definitively determine the safety of thrombolysis in this population.”
The study was supported by a grant from the Bangerter-Rhyner Foundation. Dr. Seiffge received grants from Bangerter Rhyner Foundation during the conduct of the study and personal fees from Bayer, Alexion, and VarmX outside the submitted work. Dr. Mistry receives grant funding from the National Institute of Neurological Disorders and Stroke and serves as a consultant for RAPID AI.
A version of this article first appeared on Medscape.com.
From JAMA Neurology
Statins tied to lower ICH risk regardless of bleed location
A new study has provided further reassurance on questions about the risk of intracerebral hemorrhage (ICH) with statins.
The Danish case-control study, which compared statin use in 2,164 case patients with ICH and in 86,255 matched control persons, found that current statin use was associated with a lower risk of having a first ICH and that the risk was further reduced with longer duration of statin use.
The study also showed that statin use was linked to a lower risk of ICH in the more superficial lobar areas of the brain and in the deeper, nonlobar locations. There was no difference in the magnitude of risk reduction between the two locations.
“Although this study is observational, I feel these data are strong, and the results are reassuring. It certainly does not suggest any increased risk of ICH with statins,” senior author David Gaist, PhD, Odense University Hospital, Denmark, said in an interview.
“On the contrary, it indicates a lower risk, which seems to be independent of the location of the bleed.”
The study was published online in Neurology.
The authors note that statins effectively reduce the occurrence of cardiovascular events and ischemic stroke in high-risk populations, but early randomized trials raised concerns of an increased risk of ICH among statin users who have a history of stroke.
Subsequent observational studies, including four meta-analyses, included patients with and those without prior stroke. The results were inconsistent, although most found no increase in bleeding. More recent studies have found a lower risk of ICH among statin users; the risk was inversely associated with the duration and intensity of statin treatment.
However, the researchers point out that few studies have assessed the association between statin use and the location of ICH. Hemorrhages that occur in the lobar region of the brain and those that occur in the nonlobar areas can have different pathophysiologies. Arteriolosclerosis, which is strongly associated with hypertension, is a common histologic finding in patients with ICH, regardless of hemorrhage location, while cerebral amyloid angiopathy (CAA) is associated with lobar but not nonlobar ICH.
The current study was conducted to look more closely at the relationship between statin use and hematoma location as a reflection of differences in the underlying pathophysiologies of lobar versus nonlobar ICH.
The researchers used Danish registries to identify all first-ever cases of spontaneous ICH that occurred between 2009 and 2018 in persons older than 55 years in the Southern Denmark region. Patients with traumatic ICH or ICH related to vascular malformations and tumors were excluded.
These cases were verified through medical records. ICH diagnoses were classified as having a lobar or nonlobar location, and patients were matched for age, sex, and calendar year to general population control persons. The nationwide prescription registry was also analyzed to ascertain use of statins and other medications.
The study included 989 patients with lobar ICH who were matched to 39,500 control persons and 1,175 patients with nonlobar ICH who were matched to 46,755 control persons.
Results showed that current statin use was associated with a 16%-17% relative reduction in ICH risk. There was no difference with respect to ICH location.
For lobar ICH, statin use showed an adjusted odds ratio of 0.83 (95% confidence interval, 0.70-0.98); for nonlobar ICH, the adjusted odds ratio was 0.84 (95% CI, 0.72-0.98).
Longer duration of statin use was associated with a greater reduction in risk of ICH; use for more than 5 years was associated with a relative reduction of ICH of 33%-38%, again with no difference with regard to ICH location.
For lobar ICH, statin use for more than 5 years showed an adjusted odds ratio of 0.67 (95% CI, 0.51-0.87); and for nonlobar ICH, the adjusted odds ratio was 0.62 (95% CI, 0.48-0.80).
“We suspected that statins may have more of an effect in reducing nonlobar ICH, as this type is considered to be more associated with arteriosclerosis, compared with lobar ICH,” Dr. Gaist explained. “But we didn’t find that. We found that taking statins was associated with a similar reduction in risk of both lobar and nonlobar ICH.”
Although amyloid angiopathy can contribute to lobar ICH, arteriosclerosis is still involved in the majority of cases, he noted. He cited a recent population-based U.K. study that showed that while histologically verified CAA was present in 58% of patients with a lobar ICH, most also had evidence of arteriosclerosis, with only 13% having isolated CAA pathology.
“If statins exert their effect on reducing ICH by reducing arteriosclerosis, which is likely, then this observation of arteriosclerosis pathology being prevalent in both lobar and nonlobar ICH locations would explain our results,” Dr. Gaist commented.
“Strengths of our study include the large numbers involved and the fact that the patients are unselected. We tried to find everyone who had had a first ICH in a well-defined region of Denmark, so issues of selection are less of a concern than in some other studies,” he noted.
He also pointed out that all the ICH diagnoses were verified from medical records and that in a substudy, brain scans were evaluated, with investigators masked to clinical data to evaluate the location and characteristics of the hematoma. In addition, data on statin use were collected prospectively from a nationwide prescription registry.
Interaction with antihypertensives, anticoagulants?
Other results from the study suggest a possible interaction between statin use and antihypertensive and anticoagulant drugs.
Data showed that the lower ICH risk was restricted to patients who received statins and antihypertensive drugs concurrently. Conversely, only patients who were not concurrently taking anticoagulants had a lower risk of ICH in association with statin use.
Dr. Gaist suggested that the lack of a reduction in ICH with statins among patients taking anticoagulants could be because the increased risk of ICH with anticoagulants was stronger than the reduced risk with statins.
Regarding the fact that the reduced risk of ICH with statins was only observed among individuals who were also taking antihypertensive medication, Dr. Gaist noted that because hypertension is such an important risk factor for ICH, “it may be that to get the true benefit of statins, patients have to have their hypertension controlled.”
However, an alternative explanation could that the finding is a result of “healthy adherer” bias, in which people who take antihypertensive medication and follow a healthy lifestyle as advised would be more likely to take statins.
“The observational nature of our study does not allow us to determine the extent to which associations are causal,” the authors say.
Dr. Gaist also noted that an important caveat in this study is that they focused on individuals who had had a first ICH.
“This data does not inform us about those who have already had an ICH and are taking statins. But we are planning to look at this in our next study,” he said.
The study was funded by the Novo Nordisk Foundation. Dr. Gaist has received speaker honorarium from Bristol-Myers Squibb and Pfizer unrelated to this work.
A version of this article first appeared on Medscape.com.
A new study has provided further reassurance on questions about the risk of intracerebral hemorrhage (ICH) with statins.
The Danish case-control study, which compared statin use in 2,164 case patients with ICH and in 86,255 matched control persons, found that current statin use was associated with a lower risk of having a first ICH and that the risk was further reduced with longer duration of statin use.
The study also showed that statin use was linked to a lower risk of ICH in the more superficial lobar areas of the brain and in the deeper, nonlobar locations. There was no difference in the magnitude of risk reduction between the two locations.
“Although this study is observational, I feel these data are strong, and the results are reassuring. It certainly does not suggest any increased risk of ICH with statins,” senior author David Gaist, PhD, Odense University Hospital, Denmark, said in an interview.
“On the contrary, it indicates a lower risk, which seems to be independent of the location of the bleed.”
The study was published online in Neurology.
The authors note that statins effectively reduce the occurrence of cardiovascular events and ischemic stroke in high-risk populations, but early randomized trials raised concerns of an increased risk of ICH among statin users who have a history of stroke.
Subsequent observational studies, including four meta-analyses, included patients with and those without prior stroke. The results were inconsistent, although most found no increase in bleeding. More recent studies have found a lower risk of ICH among statin users; the risk was inversely associated with the duration and intensity of statin treatment.
However, the researchers point out that few studies have assessed the association between statin use and the location of ICH. Hemorrhages that occur in the lobar region of the brain and those that occur in the nonlobar areas can have different pathophysiologies. Arteriolosclerosis, which is strongly associated with hypertension, is a common histologic finding in patients with ICH, regardless of hemorrhage location, while cerebral amyloid angiopathy (CAA) is associated with lobar but not nonlobar ICH.
The current study was conducted to look more closely at the relationship between statin use and hematoma location as a reflection of differences in the underlying pathophysiologies of lobar versus nonlobar ICH.
The researchers used Danish registries to identify all first-ever cases of spontaneous ICH that occurred between 2009 and 2018 in persons older than 55 years in the Southern Denmark region. Patients with traumatic ICH or ICH related to vascular malformations and tumors were excluded.
These cases were verified through medical records. ICH diagnoses were classified as having a lobar or nonlobar location, and patients were matched for age, sex, and calendar year to general population control persons. The nationwide prescription registry was also analyzed to ascertain use of statins and other medications.
The study included 989 patients with lobar ICH who were matched to 39,500 control persons and 1,175 patients with nonlobar ICH who were matched to 46,755 control persons.
Results showed that current statin use was associated with a 16%-17% relative reduction in ICH risk. There was no difference with respect to ICH location.
For lobar ICH, statin use showed an adjusted odds ratio of 0.83 (95% confidence interval, 0.70-0.98); for nonlobar ICH, the adjusted odds ratio was 0.84 (95% CI, 0.72-0.98).
Longer duration of statin use was associated with a greater reduction in risk of ICH; use for more than 5 years was associated with a relative reduction of ICH of 33%-38%, again with no difference with regard to ICH location.
For lobar ICH, statin use for more than 5 years showed an adjusted odds ratio of 0.67 (95% CI, 0.51-0.87); and for nonlobar ICH, the adjusted odds ratio was 0.62 (95% CI, 0.48-0.80).
“We suspected that statins may have more of an effect in reducing nonlobar ICH, as this type is considered to be more associated with arteriosclerosis, compared with lobar ICH,” Dr. Gaist explained. “But we didn’t find that. We found that taking statins was associated with a similar reduction in risk of both lobar and nonlobar ICH.”
Although amyloid angiopathy can contribute to lobar ICH, arteriosclerosis is still involved in the majority of cases, he noted. He cited a recent population-based U.K. study that showed that while histologically verified CAA was present in 58% of patients with a lobar ICH, most also had evidence of arteriosclerosis, with only 13% having isolated CAA pathology.
“If statins exert their effect on reducing ICH by reducing arteriosclerosis, which is likely, then this observation of arteriosclerosis pathology being prevalent in both lobar and nonlobar ICH locations would explain our results,” Dr. Gaist commented.
“Strengths of our study include the large numbers involved and the fact that the patients are unselected. We tried to find everyone who had had a first ICH in a well-defined region of Denmark, so issues of selection are less of a concern than in some other studies,” he noted.
He also pointed out that all the ICH diagnoses were verified from medical records and that in a substudy, brain scans were evaluated, with investigators masked to clinical data to evaluate the location and characteristics of the hematoma. In addition, data on statin use were collected prospectively from a nationwide prescription registry.
Interaction with antihypertensives, anticoagulants?
Other results from the study suggest a possible interaction between statin use and antihypertensive and anticoagulant drugs.
Data showed that the lower ICH risk was restricted to patients who received statins and antihypertensive drugs concurrently. Conversely, only patients who were not concurrently taking anticoagulants had a lower risk of ICH in association with statin use.
Dr. Gaist suggested that the lack of a reduction in ICH with statins among patients taking anticoagulants could be because the increased risk of ICH with anticoagulants was stronger than the reduced risk with statins.
Regarding the fact that the reduced risk of ICH with statins was only observed among individuals who were also taking antihypertensive medication, Dr. Gaist noted that because hypertension is such an important risk factor for ICH, “it may be that to get the true benefit of statins, patients have to have their hypertension controlled.”
However, an alternative explanation could that the finding is a result of “healthy adherer” bias, in which people who take antihypertensive medication and follow a healthy lifestyle as advised would be more likely to take statins.
“The observational nature of our study does not allow us to determine the extent to which associations are causal,” the authors say.
Dr. Gaist also noted that an important caveat in this study is that they focused on individuals who had had a first ICH.
“This data does not inform us about those who have already had an ICH and are taking statins. But we are planning to look at this in our next study,” he said.
The study was funded by the Novo Nordisk Foundation. Dr. Gaist has received speaker honorarium from Bristol-Myers Squibb and Pfizer unrelated to this work.
A version of this article first appeared on Medscape.com.
A new study has provided further reassurance on questions about the risk of intracerebral hemorrhage (ICH) with statins.
The Danish case-control study, which compared statin use in 2,164 case patients with ICH and in 86,255 matched control persons, found that current statin use was associated with a lower risk of having a first ICH and that the risk was further reduced with longer duration of statin use.
The study also showed that statin use was linked to a lower risk of ICH in the more superficial lobar areas of the brain and in the deeper, nonlobar locations. There was no difference in the magnitude of risk reduction between the two locations.
“Although this study is observational, I feel these data are strong, and the results are reassuring. It certainly does not suggest any increased risk of ICH with statins,” senior author David Gaist, PhD, Odense University Hospital, Denmark, said in an interview.
“On the contrary, it indicates a lower risk, which seems to be independent of the location of the bleed.”
The study was published online in Neurology.
The authors note that statins effectively reduce the occurrence of cardiovascular events and ischemic stroke in high-risk populations, but early randomized trials raised concerns of an increased risk of ICH among statin users who have a history of stroke.
Subsequent observational studies, including four meta-analyses, included patients with and those without prior stroke. The results were inconsistent, although most found no increase in bleeding. More recent studies have found a lower risk of ICH among statin users; the risk was inversely associated with the duration and intensity of statin treatment.
However, the researchers point out that few studies have assessed the association between statin use and the location of ICH. Hemorrhages that occur in the lobar region of the brain and those that occur in the nonlobar areas can have different pathophysiologies. Arteriolosclerosis, which is strongly associated with hypertension, is a common histologic finding in patients with ICH, regardless of hemorrhage location, while cerebral amyloid angiopathy (CAA) is associated with lobar but not nonlobar ICH.
The current study was conducted to look more closely at the relationship between statin use and hematoma location as a reflection of differences in the underlying pathophysiologies of lobar versus nonlobar ICH.
The researchers used Danish registries to identify all first-ever cases of spontaneous ICH that occurred between 2009 and 2018 in persons older than 55 years in the Southern Denmark region. Patients with traumatic ICH or ICH related to vascular malformations and tumors were excluded.
These cases were verified through medical records. ICH diagnoses were classified as having a lobar or nonlobar location, and patients were matched for age, sex, and calendar year to general population control persons. The nationwide prescription registry was also analyzed to ascertain use of statins and other medications.
The study included 989 patients with lobar ICH who were matched to 39,500 control persons and 1,175 patients with nonlobar ICH who were matched to 46,755 control persons.
Results showed that current statin use was associated with a 16%-17% relative reduction in ICH risk. There was no difference with respect to ICH location.
For lobar ICH, statin use showed an adjusted odds ratio of 0.83 (95% confidence interval, 0.70-0.98); for nonlobar ICH, the adjusted odds ratio was 0.84 (95% CI, 0.72-0.98).
Longer duration of statin use was associated with a greater reduction in risk of ICH; use for more than 5 years was associated with a relative reduction of ICH of 33%-38%, again with no difference with regard to ICH location.
For lobar ICH, statin use for more than 5 years showed an adjusted odds ratio of 0.67 (95% CI, 0.51-0.87); and for nonlobar ICH, the adjusted odds ratio was 0.62 (95% CI, 0.48-0.80).
“We suspected that statins may have more of an effect in reducing nonlobar ICH, as this type is considered to be more associated with arteriosclerosis, compared with lobar ICH,” Dr. Gaist explained. “But we didn’t find that. We found that taking statins was associated with a similar reduction in risk of both lobar and nonlobar ICH.”
Although amyloid angiopathy can contribute to lobar ICH, arteriosclerosis is still involved in the majority of cases, he noted. He cited a recent population-based U.K. study that showed that while histologically verified CAA was present in 58% of patients with a lobar ICH, most also had evidence of arteriosclerosis, with only 13% having isolated CAA pathology.
“If statins exert their effect on reducing ICH by reducing arteriosclerosis, which is likely, then this observation of arteriosclerosis pathology being prevalent in both lobar and nonlobar ICH locations would explain our results,” Dr. Gaist commented.
“Strengths of our study include the large numbers involved and the fact that the patients are unselected. We tried to find everyone who had had a first ICH in a well-defined region of Denmark, so issues of selection are less of a concern than in some other studies,” he noted.
He also pointed out that all the ICH diagnoses were verified from medical records and that in a substudy, brain scans were evaluated, with investigators masked to clinical data to evaluate the location and characteristics of the hematoma. In addition, data on statin use were collected prospectively from a nationwide prescription registry.
Interaction with antihypertensives, anticoagulants?
Other results from the study suggest a possible interaction between statin use and antihypertensive and anticoagulant drugs.
Data showed that the lower ICH risk was restricted to patients who received statins and antihypertensive drugs concurrently. Conversely, only patients who were not concurrently taking anticoagulants had a lower risk of ICH in association with statin use.
Dr. Gaist suggested that the lack of a reduction in ICH with statins among patients taking anticoagulants could be because the increased risk of ICH with anticoagulants was stronger than the reduced risk with statins.
Regarding the fact that the reduced risk of ICH with statins was only observed among individuals who were also taking antihypertensive medication, Dr. Gaist noted that because hypertension is such an important risk factor for ICH, “it may be that to get the true benefit of statins, patients have to have their hypertension controlled.”
However, an alternative explanation could that the finding is a result of “healthy adherer” bias, in which people who take antihypertensive medication and follow a healthy lifestyle as advised would be more likely to take statins.
“The observational nature of our study does not allow us to determine the extent to which associations are causal,” the authors say.
Dr. Gaist also noted that an important caveat in this study is that they focused on individuals who had had a first ICH.
“This data does not inform us about those who have already had an ICH and are taking statins. But we are planning to look at this in our next study,” he said.
The study was funded by the Novo Nordisk Foundation. Dr. Gaist has received speaker honorarium from Bristol-Myers Squibb and Pfizer unrelated to this work.
A version of this article first appeared on Medscape.com.
Stroke management: A 30-year retrospective
In 1993, managing patients with stroke had long remained an elusive and somewhat intimidating task for the neurological world. Previous efforts to treat the condition had produced more frustration than success, leaving clinicians and patients alike in despair for a solution. However, some successes in treating coronary thrombosis during that era rejuvenated researchers’ efforts to crack the code. An international team of researchers had studied a Streptococcus derivative (streptokinase) and others had begun to study a natural substance termed tissue plasminogen activator (tPA) as thrombolytic agents to lyse coronary clots and to treat pulmonary embolism. The adverse event of excessive bleeding found in Australian studies done on streptokinase intervention in patients with stroke prompted researchers to contemplate use of tPA in stroke management.
A group of German, Japanese, and American investigators began to research thrombolysis in acute stroke patients during the mid-1980s.

“What was unique is that patients had a CT scan followed by a catheter angiogram,” said Louis Caplan, MD, a senior member of the division of cerebrovascular disease at Beth Israel Deaconess Medical Center, Boston, professor of neurology at Harvard Medical School, Boston, and founder of the Harvard Stroke Registry at Beth Israel Deaconess Medical Center.
“If they had a blocked vessel, they got the drug, delivered either intravenously or intra-arterially.”
The process involved keeping the catheter open after drug administration to determine whether the vessel had opened or remained occluded. The researchers learned which blocked vessels opened when the drug was given intravenously and which required direct introduction of the drug into the clots.
A group of investigators in the United States funded by the National Institute of Neurological Disease and Stroke then performed a randomized therapeutic trial of intravenous tPA given within 90 minutes and 180 minutes after stroke symptom onset. The study was reported in the New England Journal of Medicine. Soon thereafter, in 1995, the Food and Drug Administration approved the use of tPA following the inclusion and exclusion rules used in the NINDS trial.
After the FDA approved tPA in 1995, stroke management was never the same.
tPA was just one factor in optimizing stroke management
Despite the major therapeutic breakthrough with tPA’s approval, it took the clinics, hospitals, and other acute care systems a while to catch up. “Neurologists and hospitals weren’t ready for acute stroke intervention and proper stroke management in the mid-90s,” Dr. Caplan recalled. “At the time, stroke wasn’t at the forefront of treatment, general neurologists weren’t trained, and there weren’t enough stroke neurologists.”
The preparation and training deficit was further exacerbated by low reimbursement for services. As a result, only about 5% of patients who were eligible for acute stroke management were treated with tPA.
According to Dr. Caplan, during the next 15-20 years, the accumulation of stroke data from MRI and CT vascular imaging clarified further which patients, with what extent of infarction, with which blocked vessels, would be good candidates for treatment.
More patients received interventional treatment using catheters directed into the area of clotting in attempt to remove the blockages. In addition, information regarding intervention at different periods (10-16 hours, up to 24 hours) and conditions (for example, patients with varying degrees of disability, infarct) were tested.
Eventually, hospitals became more attuned to emergency stroke treatment. More neurologists became trained, more stroke centers emerged, and clinicians enjoyed the benefit of technological advancements that allowed them to explore perfusion.
While decentralized care enhances outcomes in stroke management, more progress is needed
As of early 2023, stroke is one of the leading emergency diagnoses, and patients have access to primary and secondary stroke centers that are sprinkled throughout the United States. As impressive as the feat may seem, health care systems still have major strides to make to truly optimize therapy and outcomes in this patient population.
For example, location and access remain important issues. Secondary centers are typically located in large, metropolitan areas. While an urban location makes a primary center geographically more accessible to a larger patient population, traffic frequently hinders door-to-door access.
In the case of rural centers, distance can retard access, but they also face the challenges of how to route patients – especially patients who require more specialized care offered by secondary centers. Fortunately, primary centers have some ways to help better support their patients.
“One thing that happened is that primary centers made agreements with secondary centers via telemedicine to determine whether patients should be treated at the primary center or whether they should be routed to the higher-level center. These arrangements were termed ‘spoke and wheel,’ ” Dr. Caplan told this publication.
However, not all patients who are candidates for transport to a secondary center are able to be transported. In such cases, primary centers can use telemedicine to collaborate with secondary centers for support.
Logistics aside, perhaps today’s greatest challenge for clinicians is ensuring their patients and families receive education to increase their awareness of stroke centers as an important option for treatment and outcome optimization. Many patients and their loved ones do not realize that these centers exist or how to utilize them if and when the time comes.
Right now, some cities have stroke ambulances staffed with physicians to treat patients in the field. This decentralized model helps address access burdens such as door-to-needle delays and transportation while improving survival and recovery. Dr. Caplan said these services are available in Munich, and in a few select U.S. cities such as Cleveland and Houston, which helped pioneer the concept.
Better access in the future?
Looking ahead, Dr. Caplan seems optimistic about how stroke management will continue to evolve. Many cities will have stroke ambulances to provide on-site care, while stroke institutions will improve their cross-collaborative efforts to support their patient populations.
At the crux of cross-collaboration lies enhanced communication between peripheral and urban hospitals.
“Peripheral and urban hospitals and state organizations will engage in smoother integration to figure out when to take patient to the bigger hospitals,” Dr. Caplan said. “I also believe we will see greater emphasis on rehabilitation and recovery.”
As promising as the future looks, only time will tell.
In 1993, managing patients with stroke had long remained an elusive and somewhat intimidating task for the neurological world. Previous efforts to treat the condition had produced more frustration than success, leaving clinicians and patients alike in despair for a solution. However, some successes in treating coronary thrombosis during that era rejuvenated researchers’ efforts to crack the code. An international team of researchers had studied a Streptococcus derivative (streptokinase) and others had begun to study a natural substance termed tissue plasminogen activator (tPA) as thrombolytic agents to lyse coronary clots and to treat pulmonary embolism. The adverse event of excessive bleeding found in Australian studies done on streptokinase intervention in patients with stroke prompted researchers to contemplate use of tPA in stroke management.
A group of German, Japanese, and American investigators began to research thrombolysis in acute stroke patients during the mid-1980s.
“What was unique is that patients had a CT scan followed by a catheter angiogram,” said Louis Caplan, MD, a senior member of the division of cerebrovascular disease at Beth Israel Deaconess Medical Center, Boston, professor of neurology at Harvard Medical School, Boston, and founder of the Harvard Stroke Registry at Beth Israel Deaconess Medical Center.
“If they had a blocked vessel, they got the drug, delivered either intravenously or intra-arterially.”
The process involved keeping the catheter open after drug administration to determine whether the vessel had opened or remained occluded. The researchers learned which blocked vessels opened when the drug was given intravenously and which required direct introduction of the drug into the clots.
A group of investigators in the United States funded by the National Institute of Neurological Disease and Stroke then performed a randomized therapeutic trial of intravenous tPA given within 90 minutes and 180 minutes after stroke symptom onset. The study was reported in the New England Journal of Medicine. Soon thereafter, in 1995, the Food and Drug Administration approved the use of tPA following the inclusion and exclusion rules used in the NINDS trial.
After the FDA approved tPA in 1995, stroke management was never the same.
tPA was just one factor in optimizing stroke management
Despite the major therapeutic breakthrough with tPA’s approval, it took the clinics, hospitals, and other acute care systems a while to catch up. “Neurologists and hospitals weren’t ready for acute stroke intervention and proper stroke management in the mid-90s,” Dr. Caplan recalled. “At the time, stroke wasn’t at the forefront of treatment, general neurologists weren’t trained, and there weren’t enough stroke neurologists.”
The preparation and training deficit was further exacerbated by low reimbursement for services. As a result, only about 5% of patients who were eligible for acute stroke management were treated with tPA.
According to Dr. Caplan, during the next 15-20 years, the accumulation of stroke data from MRI and CT vascular imaging clarified further which patients, with what extent of infarction, with which blocked vessels, would be good candidates for treatment.
More patients received interventional treatment using catheters directed into the area of clotting in attempt to remove the blockages. In addition, information regarding intervention at different periods (10-16 hours, up to 24 hours) and conditions (for example, patients with varying degrees of disability, infarct) were tested.
Eventually, hospitals became more attuned to emergency stroke treatment. More neurologists became trained, more stroke centers emerged, and clinicians enjoyed the benefit of technological advancements that allowed them to explore perfusion.
While decentralized care enhances outcomes in stroke management, more progress is needed
As of early 2023, stroke is one of the leading emergency diagnoses, and patients have access to primary and secondary stroke centers that are sprinkled throughout the United States. As impressive as the feat may seem, health care systems still have major strides to make to truly optimize therapy and outcomes in this patient population.
For example, location and access remain important issues. Secondary centers are typically located in large, metropolitan areas. While an urban location makes a primary center geographically more accessible to a larger patient population, traffic frequently hinders door-to-door access.
In the case of rural centers, distance can retard access, but they also face the challenges of how to route patients – especially patients who require more specialized care offered by secondary centers. Fortunately, primary centers have some ways to help better support their patients.
“One thing that happened is that primary centers made agreements with secondary centers via telemedicine to determine whether patients should be treated at the primary center or whether they should be routed to the higher-level center. These arrangements were termed ‘spoke and wheel,’ ” Dr. Caplan told this publication.
However, not all patients who are candidates for transport to a secondary center are able to be transported. In such cases, primary centers can use telemedicine to collaborate with secondary centers for support.
Logistics aside, perhaps today’s greatest challenge for clinicians is ensuring their patients and families receive education to increase their awareness of stroke centers as an important option for treatment and outcome optimization. Many patients and their loved ones do not realize that these centers exist or how to utilize them if and when the time comes.
Right now, some cities have stroke ambulances staffed with physicians to treat patients in the field. This decentralized model helps address access burdens such as door-to-needle delays and transportation while improving survival and recovery. Dr. Caplan said these services are available in Munich, and in a few select U.S. cities such as Cleveland and Houston, which helped pioneer the concept.
Better access in the future?
Looking ahead, Dr. Caplan seems optimistic about how stroke management will continue to evolve. Many cities will have stroke ambulances to provide on-site care, while stroke institutions will improve their cross-collaborative efforts to support their patient populations.
At the crux of cross-collaboration lies enhanced communication between peripheral and urban hospitals.
“Peripheral and urban hospitals and state organizations will engage in smoother integration to figure out when to take patient to the bigger hospitals,” Dr. Caplan said. “I also believe we will see greater emphasis on rehabilitation and recovery.”
As promising as the future looks, only time will tell.
In 1993, managing patients with stroke had long remained an elusive and somewhat intimidating task for the neurological world. Previous efforts to treat the condition had produced more frustration than success, leaving clinicians and patients alike in despair for a solution. However, some successes in treating coronary thrombosis during that era rejuvenated researchers’ efforts to crack the code. An international team of researchers had studied a Streptococcus derivative (streptokinase) and others had begun to study a natural substance termed tissue plasminogen activator (tPA) as thrombolytic agents to lyse coronary clots and to treat pulmonary embolism. The adverse event of excessive bleeding found in Australian studies done on streptokinase intervention in patients with stroke prompted researchers to contemplate use of tPA in stroke management.
A group of German, Japanese, and American investigators began to research thrombolysis in acute stroke patients during the mid-1980s.
“What was unique is that patients had a CT scan followed by a catheter angiogram,” said Louis Caplan, MD, a senior member of the division of cerebrovascular disease at Beth Israel Deaconess Medical Center, Boston, professor of neurology at Harvard Medical School, Boston, and founder of the Harvard Stroke Registry at Beth Israel Deaconess Medical Center.
“If they had a blocked vessel, they got the drug, delivered either intravenously or intra-arterially.”
The process involved keeping the catheter open after drug administration to determine whether the vessel had opened or remained occluded. The researchers learned which blocked vessels opened when the drug was given intravenously and which required direct introduction of the drug into the clots.
A group of investigators in the United States funded by the National Institute of Neurological Disease and Stroke then performed a randomized therapeutic trial of intravenous tPA given within 90 minutes and 180 minutes after stroke symptom onset. The study was reported in the New England Journal of Medicine. Soon thereafter, in 1995, the Food and Drug Administration approved the use of tPA following the inclusion and exclusion rules used in the NINDS trial.
After the FDA approved tPA in 1995, stroke management was never the same.
tPA was just one factor in optimizing stroke management
Despite the major therapeutic breakthrough with tPA’s approval, it took the clinics, hospitals, and other acute care systems a while to catch up. “Neurologists and hospitals weren’t ready for acute stroke intervention and proper stroke management in the mid-90s,” Dr. Caplan recalled. “At the time, stroke wasn’t at the forefront of treatment, general neurologists weren’t trained, and there weren’t enough stroke neurologists.”
The preparation and training deficit was further exacerbated by low reimbursement for services. As a result, only about 5% of patients who were eligible for acute stroke management were treated with tPA.
According to Dr. Caplan, during the next 15-20 years, the accumulation of stroke data from MRI and CT vascular imaging clarified further which patients, with what extent of infarction, with which blocked vessels, would be good candidates for treatment.
More patients received interventional treatment using catheters directed into the area of clotting in attempt to remove the blockages. In addition, information regarding intervention at different periods (10-16 hours, up to 24 hours) and conditions (for example, patients with varying degrees of disability, infarct) were tested.
Eventually, hospitals became more attuned to emergency stroke treatment. More neurologists became trained, more stroke centers emerged, and clinicians enjoyed the benefit of technological advancements that allowed them to explore perfusion.
While decentralized care enhances outcomes in stroke management, more progress is needed
As of early 2023, stroke is one of the leading emergency diagnoses, and patients have access to primary and secondary stroke centers that are sprinkled throughout the United States. As impressive as the feat may seem, health care systems still have major strides to make to truly optimize therapy and outcomes in this patient population.
For example, location and access remain important issues. Secondary centers are typically located in large, metropolitan areas. While an urban location makes a primary center geographically more accessible to a larger patient population, traffic frequently hinders door-to-door access.
In the case of rural centers, distance can retard access, but they also face the challenges of how to route patients – especially patients who require more specialized care offered by secondary centers. Fortunately, primary centers have some ways to help better support their patients.
“One thing that happened is that primary centers made agreements with secondary centers via telemedicine to determine whether patients should be treated at the primary center or whether they should be routed to the higher-level center. These arrangements were termed ‘spoke and wheel,’ ” Dr. Caplan told this publication.
However, not all patients who are candidates for transport to a secondary center are able to be transported. In such cases, primary centers can use telemedicine to collaborate with secondary centers for support.
Logistics aside, perhaps today’s greatest challenge for clinicians is ensuring their patients and families receive education to increase their awareness of stroke centers as an important option for treatment and outcome optimization. Many patients and their loved ones do not realize that these centers exist or how to utilize them if and when the time comes.
Right now, some cities have stroke ambulances staffed with physicians to treat patients in the field. This decentralized model helps address access burdens such as door-to-needle delays and transportation while improving survival and recovery. Dr. Caplan said these services are available in Munich, and in a few select U.S. cities such as Cleveland and Houston, which helped pioneer the concept.
Better access in the future?
Looking ahead, Dr. Caplan seems optimistic about how stroke management will continue to evolve. Many cities will have stroke ambulances to provide on-site care, while stroke institutions will improve their cross-collaborative efforts to support their patient populations.
At the crux of cross-collaboration lies enhanced communication between peripheral and urban hospitals.
“Peripheral and urban hospitals and state organizations will engage in smoother integration to figure out when to take patient to the bigger hospitals,” Dr. Caplan said. “I also believe we will see greater emphasis on rehabilitation and recovery.”
As promising as the future looks, only time will tell.
High drug costs exclude most neurology patients from cutting-edge treatment
, new research shows.
“Our study of people with neurologic conditions found that fewer than 20% were being treated with new medications,” study author Brian C. Callaghan, MD, with University of Michigan Health in Ann Arbor, said in a statement.
“For new, high-cost medications that have similar effectiveness to older drugs, limited use is likely appropriate. However, future studies are needed to look into whether the high costs are barriers to those new medications that can really make a difference for people living with neurologic disease,” Dr. Callaghan said.
The study was published online in Neurology.
Most expensive drugs
Using insurance claims data, the investigators compared the utilization and costs of new-to-market drugs from 2014 to 2018 with those for existing guideline-supported medications for treating 11 neurologic conditions.
The new drugs included:
- erenumab, fremanezumab, and galcanezumab for migraine.
- ocrelizumab and peginterferon beta-1a for multiple sclerosis (MS).
- pimavanserin and safinamide for Parkinson’s disease.
- droxidopa for orthostatic hypertension.
- eculizumab for myasthenia gravis (MG).
- edaravone for amyotrophic lateral sclerosis (ALS).
- deutetrabenazine and valbenazine for Huntington’s disease and tardive dyskinesia.
- patisiran and inotersen for transthyretin amyloidosis (ATTR).
- eteplirsen and deflazacort for Duchenne disease.
- nusinersen for spinal muscular atrophy (SMA).
Utilization of new drugs was modest – they accounted for one in five prescriptions for every condition except tardive dyskinesia (32% for valbenazine), the researchers noted.
Mean out-of-pocket costs were significantly higher for the new medications, although there was large variability among individual drugs.
The two most expensive drugs were edaravone, for ALS, with a mean out-of-pocket cost of $713 for a 30-day supply, and eculizumab, for MG, which costs $91 per month.
“For new-to-market medications, the distribution of out-of-pocket costs were highly variable and the trends over time were unpredictable compared with existing guideline-supported medications,” the authors reported.
They noted that potential reasons for low utilization of newer agents include delay in provider uptake and prescriber and/or patient avoidance because of high cost.
Given that most of the new neurologic agents offer little advantage compared with existing treatments – exceptions being new drugs for SMA and ATTR – drug costs should be a key consideration in prescribing decisions, Dr. Callaghan and colleagues concluded.
One limitation of the study is that follow-up time was short for some of the recently approved medications. Another limitation is that the number of people in the study who had rare diseases was small.
Revolution in neurotherapeutics
“We are living in a time when new treatments bring hope to people with neurologic diseases and disorders,” Orly Avitzur, MD, president of the American Academy of Neurology, said in a statement.
“However, even existing prescription medication can be expensive and drug prices continue to rise. In order for neurologists to provide people with the highest quality care, it is imperative that new drugs are accessible and affordable to the people who need them,” Dr. Avitzur added.
Writing in a linked editorial, A. Gordon Smith, MD, professor and chair, department of neurology, Virginia Commonwealth University, Richmond, said there is a revolution in neurotherapeutics, with particularly robust growth in new drug approvals for orphan diseases (those affecting < 200,000 Americans).
“This study adds to a growing literature indicating rising drug prices are a threat to the health care system. No matter how effective a disease-modifying therapy may be, if a patient cannot afford the cost, it doesn’t work,” Dr. Smith wrote.
He added that neurologists must be “diligent in assessing for financial toxicity and appropriately tailor individual treatment recommendations. We must insist on development of point-of-care tools to accurately estimate each patient’s potential financial toxicity including RTBT [real-time benefit tools].
“Neurologists’ primary obligation is to the individual patient, but we are also compelled to support access to high-quality care for all people, which requires advocacy for appropriate policy reforms to ensure value based and fair drug pricing and treatment success,” Dr. Smith added.
The study was funded by the American Academy of Neurology Health Services Research Subcommittee. Dr. Callaghan consults for a PCORI grant, DynaMed, receives research support from the American Academy of Neurology, and performs medical/legal consultations, including consultations for the Vaccine Injury Compensation Program. Dr. Smith has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
“Our study of people with neurologic conditions found that fewer than 20% were being treated with new medications,” study author Brian C. Callaghan, MD, with University of Michigan Health in Ann Arbor, said in a statement.
“For new, high-cost medications that have similar effectiveness to older drugs, limited use is likely appropriate. However, future studies are needed to look into whether the high costs are barriers to those new medications that can really make a difference for people living with neurologic disease,” Dr. Callaghan said.
The study was published online in Neurology.
Most expensive drugs
Using insurance claims data, the investigators compared the utilization and costs of new-to-market drugs from 2014 to 2018 with those for existing guideline-supported medications for treating 11 neurologic conditions.
The new drugs included:
- erenumab, fremanezumab, and galcanezumab for migraine.
- ocrelizumab and peginterferon beta-1a for multiple sclerosis (MS).
- pimavanserin and safinamide for Parkinson’s disease.
- droxidopa for orthostatic hypertension.
- eculizumab for myasthenia gravis (MG).
- edaravone for amyotrophic lateral sclerosis (ALS).
- deutetrabenazine and valbenazine for Huntington’s disease and tardive dyskinesia.
- patisiran and inotersen for transthyretin amyloidosis (ATTR).
- eteplirsen and deflazacort for Duchenne disease.
- nusinersen for spinal muscular atrophy (SMA).
Utilization of new drugs was modest – they accounted for one in five prescriptions for every condition except tardive dyskinesia (32% for valbenazine), the researchers noted.
Mean out-of-pocket costs were significantly higher for the new medications, although there was large variability among individual drugs.
The two most expensive drugs were edaravone, for ALS, with a mean out-of-pocket cost of $713 for a 30-day supply, and eculizumab, for MG, which costs $91 per month.
“For new-to-market medications, the distribution of out-of-pocket costs were highly variable and the trends over time were unpredictable compared with existing guideline-supported medications,” the authors reported.
They noted that potential reasons for low utilization of newer agents include delay in provider uptake and prescriber and/or patient avoidance because of high cost.
Given that most of the new neurologic agents offer little advantage compared with existing treatments – exceptions being new drugs for SMA and ATTR – drug costs should be a key consideration in prescribing decisions, Dr. Callaghan and colleagues concluded.
One limitation of the study is that follow-up time was short for some of the recently approved medications. Another limitation is that the number of people in the study who had rare diseases was small.
Revolution in neurotherapeutics
“We are living in a time when new treatments bring hope to people with neurologic diseases and disorders,” Orly Avitzur, MD, president of the American Academy of Neurology, said in a statement.
“However, even existing prescription medication can be expensive and drug prices continue to rise. In order for neurologists to provide people with the highest quality care, it is imperative that new drugs are accessible and affordable to the people who need them,” Dr. Avitzur added.
Writing in a linked editorial, A. Gordon Smith, MD, professor and chair, department of neurology, Virginia Commonwealth University, Richmond, said there is a revolution in neurotherapeutics, with particularly robust growth in new drug approvals for orphan diseases (those affecting < 200,000 Americans).
“This study adds to a growing literature indicating rising drug prices are a threat to the health care system. No matter how effective a disease-modifying therapy may be, if a patient cannot afford the cost, it doesn’t work,” Dr. Smith wrote.
He added that neurologists must be “diligent in assessing for financial toxicity and appropriately tailor individual treatment recommendations. We must insist on development of point-of-care tools to accurately estimate each patient’s potential financial toxicity including RTBT [real-time benefit tools].
“Neurologists’ primary obligation is to the individual patient, but we are also compelled to support access to high-quality care for all people, which requires advocacy for appropriate policy reforms to ensure value based and fair drug pricing and treatment success,” Dr. Smith added.
The study was funded by the American Academy of Neurology Health Services Research Subcommittee. Dr. Callaghan consults for a PCORI grant, DynaMed, receives research support from the American Academy of Neurology, and performs medical/legal consultations, including consultations for the Vaccine Injury Compensation Program. Dr. Smith has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, new research shows.
“Our study of people with neurologic conditions found that fewer than 20% were being treated with new medications,” study author Brian C. Callaghan, MD, with University of Michigan Health in Ann Arbor, said in a statement.
“For new, high-cost medications that have similar effectiveness to older drugs, limited use is likely appropriate. However, future studies are needed to look into whether the high costs are barriers to those new medications that can really make a difference for people living with neurologic disease,” Dr. Callaghan said.
The study was published online in Neurology.
Most expensive drugs
Using insurance claims data, the investigators compared the utilization and costs of new-to-market drugs from 2014 to 2018 with those for existing guideline-supported medications for treating 11 neurologic conditions.
The new drugs included:
- erenumab, fremanezumab, and galcanezumab for migraine.
- ocrelizumab and peginterferon beta-1a for multiple sclerosis (MS).
- pimavanserin and safinamide for Parkinson’s disease.
- droxidopa for orthostatic hypertension.
- eculizumab for myasthenia gravis (MG).
- edaravone for amyotrophic lateral sclerosis (ALS).
- deutetrabenazine and valbenazine for Huntington’s disease and tardive dyskinesia.
- patisiran and inotersen for transthyretin amyloidosis (ATTR).
- eteplirsen and deflazacort for Duchenne disease.
- nusinersen for spinal muscular atrophy (SMA).
Utilization of new drugs was modest – they accounted for one in five prescriptions for every condition except tardive dyskinesia (32% for valbenazine), the researchers noted.
Mean out-of-pocket costs were significantly higher for the new medications, although there was large variability among individual drugs.
The two most expensive drugs were edaravone, for ALS, with a mean out-of-pocket cost of $713 for a 30-day supply, and eculizumab, for MG, which costs $91 per month.
“For new-to-market medications, the distribution of out-of-pocket costs were highly variable and the trends over time were unpredictable compared with existing guideline-supported medications,” the authors reported.
They noted that potential reasons for low utilization of newer agents include delay in provider uptake and prescriber and/or patient avoidance because of high cost.
Given that most of the new neurologic agents offer little advantage compared with existing treatments – exceptions being new drugs for SMA and ATTR – drug costs should be a key consideration in prescribing decisions, Dr. Callaghan and colleagues concluded.
One limitation of the study is that follow-up time was short for some of the recently approved medications. Another limitation is that the number of people in the study who had rare diseases was small.
Revolution in neurotherapeutics
“We are living in a time when new treatments bring hope to people with neurologic diseases and disorders,” Orly Avitzur, MD, president of the American Academy of Neurology, said in a statement.
“However, even existing prescription medication can be expensive and drug prices continue to rise. In order for neurologists to provide people with the highest quality care, it is imperative that new drugs are accessible and affordable to the people who need them,” Dr. Avitzur added.
Writing in a linked editorial, A. Gordon Smith, MD, professor and chair, department of neurology, Virginia Commonwealth University, Richmond, said there is a revolution in neurotherapeutics, with particularly robust growth in new drug approvals for orphan diseases (those affecting < 200,000 Americans).
“This study adds to a growing literature indicating rising drug prices are a threat to the health care system. No matter how effective a disease-modifying therapy may be, if a patient cannot afford the cost, it doesn’t work,” Dr. Smith wrote.
He added that neurologists must be “diligent in assessing for financial toxicity and appropriately tailor individual treatment recommendations. We must insist on development of point-of-care tools to accurately estimate each patient’s potential financial toxicity including RTBT [real-time benefit tools].
“Neurologists’ primary obligation is to the individual patient, but we are also compelled to support access to high-quality care for all people, which requires advocacy for appropriate policy reforms to ensure value based and fair drug pricing and treatment success,” Dr. Smith added.
The study was funded by the American Academy of Neurology Health Services Research Subcommittee. Dr. Callaghan consults for a PCORI grant, DynaMed, receives research support from the American Academy of Neurology, and performs medical/legal consultations, including consultations for the Vaccine Injury Compensation Program. Dr. Smith has disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM NEUROLOGY
Consider quality of life, comorbidities in hidradenitis suppurativa
LAS VEGAS – , Robert G. Micheletti, MD, said in a presentation at MedscapeLive’s annual Las Vegas Dermatology Seminar.

For patients with HS, “the quality-of-life impact is profound, greater than any other systematically studied dermatologic condition,” said Dr. Micheletti, associate professor of dermatology at the Hospital of the University of Pennsylavnia, and chief of hospital dermatology, and chief of dermatology at Pennsylvania Hospital, Philadelphia.
Two key aspects of quality of life that affect HS patients are sexual health and overall pain, he said. The female-to-male ratio of HS is approximately 3:1, and data show that approximately 40% of female HS patients experience fertility issues and have unaddressed questions about HS and pregnancy, said Dr. Micheletti. Additionally, data from a systematic review showed that 50%-60% of patients with HS reported sexual dysfunction. Impaired sexual function is also associated with both overall impaired quality of life ratings and the presence of mood disorders, he noted.

Pain also has a significant impact on quality of life for HS patients. When these patients present in an emergency department, 70% report severe pain, and approximately 60% receive opioids, said Dr. Micheletti.
Data from a 2021 study showed that HS patients are significantly more likely to receive opioids compared with controls, and also more likely to be diagnosed with opioid use disorder than controls, especially if they are seen by nondermatologists, he noted.
For acute pain, Dr. Micheletti recommended starting with acetaminophen 500 mg every 4 to 6 hours as needed, and topical nonsteroidal anti-inflammatory drugs (NSAIDs). “It still makes sense to do topical care,” said Dr. Micheletti, but he added that he also prescribes medications for anxiety for these patients.
Patients with increased pain severity or refractory disease may benefit from systemic NSAIDs, or intralesional triamcinolone, he noted. Incision and draining of abscesses may provide temporary symptomatic relief, but keep in mind that lesions will recur, he noted.
For the most severe cases, Dr. Micheletti advised adding tramadol as a first-line opioid, or another short-acting opioid for breakthrough pain.
To manage patients with HS who have chronic pain, Dr. Micheletti recommended starting with HS disease–directed therapy, but also screening for pain severity and psychological comorbidities.
His strategies in these cases include nonpharmacological pain management in the form of physical therapy, wound care, and behavioral health. His algorithm for nociceptive pain is NSAIDs with or without acetaminophen; duloxetine or nortriptyline are other options. For neuropathic pain, gabapentin and/or duloxetine are top choices, but pregabalin, venlafaxine, and nortriptyline are on the list as well.
Topical NSAIDs or topical lidocaine may serve as add-ons to systemic therapy in more severe cases, or as first-line therapy for milder chronic pain, Dr. Micheletti noted. Patients who have failed treatment with at least two pharmacologic agents, suffer medically refractory HS with debilitating pain, or use opioids on an ongoing basis should be referred to a pain management specialist, he said.
Don’t forget lifestyle
Although data on the impact of diet on patients with HS are limited, “we know anecdotally that dairy and refined carbohydrates are associated with exacerbations,” said Dr. Micheletti.
In addition, many patients use complementary medicine “and they aren’t always telling us,” he emphasized. Smoking is prevalent among patients with HS, and is a risk factor for the disease in general, and for more severe and refractory disease, he added. Consequently, screening for tobacco smoking is recommended for patients with HS not only because of the impact on disease, but because it is a potentially modifiable cardiovascular risk factor, he explained.
Consider comorbidities
Cardiovascular disease is among several comorbidities associated with HS, said Dr. Micheletti. HS foundations in the United States and Canada recently published evidence-based recommendations for comorbidity screening. The recommendations included screening for 19 specific comorbidities: acne, dissecting cellulitis, pilonidal disease, pyoderma gangrenosum, depression, anxiety, suicide, smoking, substance abuse, polycystic ovary syndrome, obesity, dyslipidemia, diabetes mellitus, metabolic syndrome, hypertension, cardiovascular disease, inflammatory bowel disease, spondyloarthritis, and sexual dysfunction.
Dr. Micheletti highlighted cardiovascular comorbidities, and noted the association between HS and modifiable cardiovascular risk factors: smoking, obesity, diabetes mellitus, and dyslipidemia. “HS is also independently associated with cardiovascular disease leading to myocardial infarction, stroke, cardiovascular-associated death, and all-cause mortality compared to controls,” he said. Studies show an incidence rate ratio of 1.53 for major adverse cardiovascular events in patients with HS compared with controls, with the highest relative risk among those aged 18-29 years, he added.
Medical management
Depending on the patient, medical management of HS may involve antibiotics, hormonal agents, and biologics, said Dr. Micheletti. Some of the most commonly used antibiotic regimens for HS are those recommended in treatment guidelines, including doxycycline and a clindamycin/rifampin combination, he said. However, the use of trimethoprim-sulfamethoxazole or ciprofloxacin has been associated with increased antibiotic resistance and is not supported by available evidence, he noted.
Hormonal therapies may help some women with HS, said Dr. Micheletti. Options include spironolactone, metformin, or estrogen-containing hormonal contraceptives, he said.
When it comes to biologics, only 33% of HS patients meet criteria for their use (Hurley stage II or III, moderate or severe HS), he noted. However, research suggests “a huge gap” in the use of anti-TNF therapy even among patients for whom it is recommended, he said.
Of the TNF-alpha inhibitors, data on adalimumab, which is FDA-approved for HS, are the most recent. Adalimumab “is our gold standard biologic and our gateway biologic, for HS at this time,” Dr. Micheletti said.
However, those who respond to adalimumab “can continue to do better, but they can wax and wane and flare,” he cautioned. Infliximab, while not approved for HS, has been studied in patients with HS and is prescribed by some providers. Although no comparative studies have been done for infliximab versus adalimumab, “anecdotally, response to infliximab tends to be better, and it is the most effective biologic in common use for severe HS,” he noted.
Dr. Micheletti’s top treatment recommendations for using biologics start with considering biosimilars. Most patients on biosimilars do fine, but some patients who previously responded to infliximab will unpredictably lose efficacy or have reactions when switched to a biosimilar, he said.
Patients on biologics also may experience waning efficacy in the wake of an immune response stimulated by foreign antibodies, said Dr. Micheletti. “Anti-drug antibody formation is more likely to occur when treatment is interrupted,” he noted. Minimize the risk of antibody formation by paying attention to adherence issues and dosing frequency, he advised.
If patients fail both adalimumab and infliximab, Dr. Micheletti tells them not to lose hope, and that treatment is a trial-and-error process that may involve more than one therapy. Other biologics in active use for HS include ustekinumab, anakinra, secukinumab, brodalumab, golimumab, and JAK inhibitors, any of which might be effective in any given patient, he said.
Surgical solutions
For HS patients with chronic, recurring inflammation and drainage associated with a sinus tract, surgical deroofing may the best treatment option, Dr. Micheletti said. “Deroofing involves the use of a probe to trace the extent of the subcutaneous tract, followed by incision and removal of the tract ‘roof,’ ’’ he explained. The deroofing procedure involves local anesthesia and has a low morbidity rate, as well as a low recurrence rate and high levels of patient satisfaction, he said.
“The acute role for surgery is to remove active foci of inflammation and relieve pain,” which is achieved more effectively with deroofing, said Dr. Micheletti. By contrast, incision and drainage is associated with an almost 100% recurrence rate, he added.
When planning elective surgery for HS, Dr. Micheletti noted that holding infliximab for less than 4 weeks does not affect postoperative infection rates in patients with rheumatoid arthritis, and a recent randomized, controlled trial showed that adalimumab can be continued safely through HS surgeries.
In fact, “continuing TNF inhibitors through elective surgery does not increase infection risk and results in better disease control,” and dermatologists should work with surgery to balance infection and disease flare concerns in HS patients, he said.
Dr. Micheletti disclosed serving as a consultant or advisor for Adaptimmune and Vertex, and research funding from Amgen and Cabaletta Bio. MedscapeLive and this news organization are owned by the same parent company.
LAS VEGAS – , Robert G. Micheletti, MD, said in a presentation at MedscapeLive’s annual Las Vegas Dermatology Seminar.
For patients with HS, “the quality-of-life impact is profound, greater than any other systematically studied dermatologic condition,” said Dr. Micheletti, associate professor of dermatology at the Hospital of the University of Pennsylavnia, and chief of hospital dermatology, and chief of dermatology at Pennsylvania Hospital, Philadelphia.
Two key aspects of quality of life that affect HS patients are sexual health and overall pain, he said. The female-to-male ratio of HS is approximately 3:1, and data show that approximately 40% of female HS patients experience fertility issues and have unaddressed questions about HS and pregnancy, said Dr. Micheletti. Additionally, data from a systematic review showed that 50%-60% of patients with HS reported sexual dysfunction. Impaired sexual function is also associated with both overall impaired quality of life ratings and the presence of mood disorders, he noted.
Pain also has a significant impact on quality of life for HS patients. When these patients present in an emergency department, 70% report severe pain, and approximately 60% receive opioids, said Dr. Micheletti.
Data from a 2021 study showed that HS patients are significantly more likely to receive opioids compared with controls, and also more likely to be diagnosed with opioid use disorder than controls, especially if they are seen by nondermatologists, he noted.
For acute pain, Dr. Micheletti recommended starting with acetaminophen 500 mg every 4 to 6 hours as needed, and topical nonsteroidal anti-inflammatory drugs (NSAIDs). “It still makes sense to do topical care,” said Dr. Micheletti, but he added that he also prescribes medications for anxiety for these patients.
Patients with increased pain severity or refractory disease may benefit from systemic NSAIDs, or intralesional triamcinolone, he noted. Incision and draining of abscesses may provide temporary symptomatic relief, but keep in mind that lesions will recur, he noted.
For the most severe cases, Dr. Micheletti advised adding tramadol as a first-line opioid, or another short-acting opioid for breakthrough pain.
To manage patients with HS who have chronic pain, Dr. Micheletti recommended starting with HS disease–directed therapy, but also screening for pain severity and psychological comorbidities.
His strategies in these cases include nonpharmacological pain management in the form of physical therapy, wound care, and behavioral health. His algorithm for nociceptive pain is NSAIDs with or without acetaminophen; duloxetine or nortriptyline are other options. For neuropathic pain, gabapentin and/or duloxetine are top choices, but pregabalin, venlafaxine, and nortriptyline are on the list as well.
Topical NSAIDs or topical lidocaine may serve as add-ons to systemic therapy in more severe cases, or as first-line therapy for milder chronic pain, Dr. Micheletti noted. Patients who have failed treatment with at least two pharmacologic agents, suffer medically refractory HS with debilitating pain, or use opioids on an ongoing basis should be referred to a pain management specialist, he said.
Don’t forget lifestyle
Although data on the impact of diet on patients with HS are limited, “we know anecdotally that dairy and refined carbohydrates are associated with exacerbations,” said Dr. Micheletti.
In addition, many patients use complementary medicine “and they aren’t always telling us,” he emphasized. Smoking is prevalent among patients with HS, and is a risk factor for the disease in general, and for more severe and refractory disease, he added. Consequently, screening for tobacco smoking is recommended for patients with HS not only because of the impact on disease, but because it is a potentially modifiable cardiovascular risk factor, he explained.
Consider comorbidities
Cardiovascular disease is among several comorbidities associated with HS, said Dr. Micheletti. HS foundations in the United States and Canada recently published evidence-based recommendations for comorbidity screening. The recommendations included screening for 19 specific comorbidities: acne, dissecting cellulitis, pilonidal disease, pyoderma gangrenosum, depression, anxiety, suicide, smoking, substance abuse, polycystic ovary syndrome, obesity, dyslipidemia, diabetes mellitus, metabolic syndrome, hypertension, cardiovascular disease, inflammatory bowel disease, spondyloarthritis, and sexual dysfunction.
Dr. Micheletti highlighted cardiovascular comorbidities, and noted the association between HS and modifiable cardiovascular risk factors: smoking, obesity, diabetes mellitus, and dyslipidemia. “HS is also independently associated with cardiovascular disease leading to myocardial infarction, stroke, cardiovascular-associated death, and all-cause mortality compared to controls,” he said. Studies show an incidence rate ratio of 1.53 for major adverse cardiovascular events in patients with HS compared with controls, with the highest relative risk among those aged 18-29 years, he added.
Medical management
Depending on the patient, medical management of HS may involve antibiotics, hormonal agents, and biologics, said Dr. Micheletti. Some of the most commonly used antibiotic regimens for HS are those recommended in treatment guidelines, including doxycycline and a clindamycin/rifampin combination, he said. However, the use of trimethoprim-sulfamethoxazole or ciprofloxacin has been associated with increased antibiotic resistance and is not supported by available evidence, he noted.
Hormonal therapies may help some women with HS, said Dr. Micheletti. Options include spironolactone, metformin, or estrogen-containing hormonal contraceptives, he said.
When it comes to biologics, only 33% of HS patients meet criteria for their use (Hurley stage II or III, moderate or severe HS), he noted. However, research suggests “a huge gap” in the use of anti-TNF therapy even among patients for whom it is recommended, he said.
Of the TNF-alpha inhibitors, data on adalimumab, which is FDA-approved for HS, are the most recent. Adalimumab “is our gold standard biologic and our gateway biologic, for HS at this time,” Dr. Micheletti said.
However, those who respond to adalimumab “can continue to do better, but they can wax and wane and flare,” he cautioned. Infliximab, while not approved for HS, has been studied in patients with HS and is prescribed by some providers. Although no comparative studies have been done for infliximab versus adalimumab, “anecdotally, response to infliximab tends to be better, and it is the most effective biologic in common use for severe HS,” he noted.
Dr. Micheletti’s top treatment recommendations for using biologics start with considering biosimilars. Most patients on biosimilars do fine, but some patients who previously responded to infliximab will unpredictably lose efficacy or have reactions when switched to a biosimilar, he said.
Patients on biologics also may experience waning efficacy in the wake of an immune response stimulated by foreign antibodies, said Dr. Micheletti. “Anti-drug antibody formation is more likely to occur when treatment is interrupted,” he noted. Minimize the risk of antibody formation by paying attention to adherence issues and dosing frequency, he advised.
If patients fail both adalimumab and infliximab, Dr. Micheletti tells them not to lose hope, and that treatment is a trial-and-error process that may involve more than one therapy. Other biologics in active use for HS include ustekinumab, anakinra, secukinumab, brodalumab, golimumab, and JAK inhibitors, any of which might be effective in any given patient, he said.
Surgical solutions
For HS patients with chronic, recurring inflammation and drainage associated with a sinus tract, surgical deroofing may the best treatment option, Dr. Micheletti said. “Deroofing involves the use of a probe to trace the extent of the subcutaneous tract, followed by incision and removal of the tract ‘roof,’ ’’ he explained. The deroofing procedure involves local anesthesia and has a low morbidity rate, as well as a low recurrence rate and high levels of patient satisfaction, he said.
“The acute role for surgery is to remove active foci of inflammation and relieve pain,” which is achieved more effectively with deroofing, said Dr. Micheletti. By contrast, incision and drainage is associated with an almost 100% recurrence rate, he added.
When planning elective surgery for HS, Dr. Micheletti noted that holding infliximab for less than 4 weeks does not affect postoperative infection rates in patients with rheumatoid arthritis, and a recent randomized, controlled trial showed that adalimumab can be continued safely through HS surgeries.
In fact, “continuing TNF inhibitors through elective surgery does not increase infection risk and results in better disease control,” and dermatologists should work with surgery to balance infection and disease flare concerns in HS patients, he said.
Dr. Micheletti disclosed serving as a consultant or advisor for Adaptimmune and Vertex, and research funding from Amgen and Cabaletta Bio. MedscapeLive and this news organization are owned by the same parent company.
LAS VEGAS – , Robert G. Micheletti, MD, said in a presentation at MedscapeLive’s annual Las Vegas Dermatology Seminar.
For patients with HS, “the quality-of-life impact is profound, greater than any other systematically studied dermatologic condition,” said Dr. Micheletti, associate professor of dermatology at the Hospital of the University of Pennsylavnia, and chief of hospital dermatology, and chief of dermatology at Pennsylvania Hospital, Philadelphia.
Two key aspects of quality of life that affect HS patients are sexual health and overall pain, he said. The female-to-male ratio of HS is approximately 3:1, and data show that approximately 40% of female HS patients experience fertility issues and have unaddressed questions about HS and pregnancy, said Dr. Micheletti. Additionally, data from a systematic review showed that 50%-60% of patients with HS reported sexual dysfunction. Impaired sexual function is also associated with both overall impaired quality of life ratings and the presence of mood disorders, he noted.
Pain also has a significant impact on quality of life for HS patients. When these patients present in an emergency department, 70% report severe pain, and approximately 60% receive opioids, said Dr. Micheletti.
Data from a 2021 study showed that HS patients are significantly more likely to receive opioids compared with controls, and also more likely to be diagnosed with opioid use disorder than controls, especially if they are seen by nondermatologists, he noted.
For acute pain, Dr. Micheletti recommended starting with acetaminophen 500 mg every 4 to 6 hours as needed, and topical nonsteroidal anti-inflammatory drugs (NSAIDs). “It still makes sense to do topical care,” said Dr. Micheletti, but he added that he also prescribes medications for anxiety for these patients.
Patients with increased pain severity or refractory disease may benefit from systemic NSAIDs, or intralesional triamcinolone, he noted. Incision and draining of abscesses may provide temporary symptomatic relief, but keep in mind that lesions will recur, he noted.
For the most severe cases, Dr. Micheletti advised adding tramadol as a first-line opioid, or another short-acting opioid for breakthrough pain.
To manage patients with HS who have chronic pain, Dr. Micheletti recommended starting with HS disease–directed therapy, but also screening for pain severity and psychological comorbidities.
His strategies in these cases include nonpharmacological pain management in the form of physical therapy, wound care, and behavioral health. His algorithm for nociceptive pain is NSAIDs with or without acetaminophen; duloxetine or nortriptyline are other options. For neuropathic pain, gabapentin and/or duloxetine are top choices, but pregabalin, venlafaxine, and nortriptyline are on the list as well.
Topical NSAIDs or topical lidocaine may serve as add-ons to systemic therapy in more severe cases, or as first-line therapy for milder chronic pain, Dr. Micheletti noted. Patients who have failed treatment with at least two pharmacologic agents, suffer medically refractory HS with debilitating pain, or use opioids on an ongoing basis should be referred to a pain management specialist, he said.
Don’t forget lifestyle
Although data on the impact of diet on patients with HS are limited, “we know anecdotally that dairy and refined carbohydrates are associated with exacerbations,” said Dr. Micheletti.
In addition, many patients use complementary medicine “and they aren’t always telling us,” he emphasized. Smoking is prevalent among patients with HS, and is a risk factor for the disease in general, and for more severe and refractory disease, he added. Consequently, screening for tobacco smoking is recommended for patients with HS not only because of the impact on disease, but because it is a potentially modifiable cardiovascular risk factor, he explained.
Consider comorbidities
Cardiovascular disease is among several comorbidities associated with HS, said Dr. Micheletti. HS foundations in the United States and Canada recently published evidence-based recommendations for comorbidity screening. The recommendations included screening for 19 specific comorbidities: acne, dissecting cellulitis, pilonidal disease, pyoderma gangrenosum, depression, anxiety, suicide, smoking, substance abuse, polycystic ovary syndrome, obesity, dyslipidemia, diabetes mellitus, metabolic syndrome, hypertension, cardiovascular disease, inflammatory bowel disease, spondyloarthritis, and sexual dysfunction.
Dr. Micheletti highlighted cardiovascular comorbidities, and noted the association between HS and modifiable cardiovascular risk factors: smoking, obesity, diabetes mellitus, and dyslipidemia. “HS is also independently associated with cardiovascular disease leading to myocardial infarction, stroke, cardiovascular-associated death, and all-cause mortality compared to controls,” he said. Studies show an incidence rate ratio of 1.53 for major adverse cardiovascular events in patients with HS compared with controls, with the highest relative risk among those aged 18-29 years, he added.
Medical management
Depending on the patient, medical management of HS may involve antibiotics, hormonal agents, and biologics, said Dr. Micheletti. Some of the most commonly used antibiotic regimens for HS are those recommended in treatment guidelines, including doxycycline and a clindamycin/rifampin combination, he said. However, the use of trimethoprim-sulfamethoxazole or ciprofloxacin has been associated with increased antibiotic resistance and is not supported by available evidence, he noted.
Hormonal therapies may help some women with HS, said Dr. Micheletti. Options include spironolactone, metformin, or estrogen-containing hormonal contraceptives, he said.
When it comes to biologics, only 33% of HS patients meet criteria for their use (Hurley stage II or III, moderate or severe HS), he noted. However, research suggests “a huge gap” in the use of anti-TNF therapy even among patients for whom it is recommended, he said.
Of the TNF-alpha inhibitors, data on adalimumab, which is FDA-approved for HS, are the most recent. Adalimumab “is our gold standard biologic and our gateway biologic, for HS at this time,” Dr. Micheletti said.
However, those who respond to adalimumab “can continue to do better, but they can wax and wane and flare,” he cautioned. Infliximab, while not approved for HS, has been studied in patients with HS and is prescribed by some providers. Although no comparative studies have been done for infliximab versus adalimumab, “anecdotally, response to infliximab tends to be better, and it is the most effective biologic in common use for severe HS,” he noted.
Dr. Micheletti’s top treatment recommendations for using biologics start with considering biosimilars. Most patients on biosimilars do fine, but some patients who previously responded to infliximab will unpredictably lose efficacy or have reactions when switched to a biosimilar, he said.
Patients on biologics also may experience waning efficacy in the wake of an immune response stimulated by foreign antibodies, said Dr. Micheletti. “Anti-drug antibody formation is more likely to occur when treatment is interrupted,” he noted. Minimize the risk of antibody formation by paying attention to adherence issues and dosing frequency, he advised.
If patients fail both adalimumab and infliximab, Dr. Micheletti tells them not to lose hope, and that treatment is a trial-and-error process that may involve more than one therapy. Other biologics in active use for HS include ustekinumab, anakinra, secukinumab, brodalumab, golimumab, and JAK inhibitors, any of which might be effective in any given patient, he said.
Surgical solutions
For HS patients with chronic, recurring inflammation and drainage associated with a sinus tract, surgical deroofing may the best treatment option, Dr. Micheletti said. “Deroofing involves the use of a probe to trace the extent of the subcutaneous tract, followed by incision and removal of the tract ‘roof,’ ’’ he explained. The deroofing procedure involves local anesthesia and has a low morbidity rate, as well as a low recurrence rate and high levels of patient satisfaction, he said.
“The acute role for surgery is to remove active foci of inflammation and relieve pain,” which is achieved more effectively with deroofing, said Dr. Micheletti. By contrast, incision and drainage is associated with an almost 100% recurrence rate, he added.
When planning elective surgery for HS, Dr. Micheletti noted that holding infliximab for less than 4 weeks does not affect postoperative infection rates in patients with rheumatoid arthritis, and a recent randomized, controlled trial showed that adalimumab can be continued safely through HS surgeries.
In fact, “continuing TNF inhibitors through elective surgery does not increase infection risk and results in better disease control,” and dermatologists should work with surgery to balance infection and disease flare concerns in HS patients, he said.
Dr. Micheletti disclosed serving as a consultant or advisor for Adaptimmune and Vertex, and research funding from Amgen and Cabaletta Bio. MedscapeLive and this news organization are owned by the same parent company.
AT INNOVATIONS IN DERMATOLOGY
Single chest x-ray could predict 10-year CVD risk
who presented the results of their deep-learning model at the annual meeting of the Radiological Society of North America.
Current American College of Cardiologists and American Heart Association guidelines recommend estimating 10-year risk of major adverse cardiovascular events (MACE) to determine whether a patient should receive statins to help prevent atherosclerotic cardiovascular disease (ASCVD). Statins are recommended for patients with a 10-year risk of 7.5% or higher, the authors noted.
The current ASCVD risk score is determined with nine factors: age, sex, race, systolic blood pressure, hypertension treatment, smoking, type 2 diabetes, and a lipid panel.
Not all data points available in EHR
But not all of those data points may be available through the electronic health record, “which makes novel and easier approaches for population-wide screening desirable,” said lead researcher Jakob Weiss, MD, a radiologist affiliated with the Cardiovascular Imaging Research Center at Massachusetts General Hospital and the AI in medicine program at the Brigham and Women’s Hospital in Boston.
Chest x-ray images, on the other hand, are commonly available. The images carry rich information beyond diagnostic data but have not been used in this type of prediction model because AI models have been lacking, Dr. Weiss said.
The researchers trained a deep-learning model with single chest x-rays only.
They used 147,497 chest x-rays from 40,643 participants in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial, a multicenter, randomized controlled trial designed and sponsored by the National Cancer Institute.
Dr. Weiss acknowledged that the population used to train the model was heavily White and that should be a consideration in validating the model.
They compared their model’s ability to predict 10-year ASCVD risk with the standard ACC/AHA model.
“Based on a single chest radiograph image, deep learning can predict the risk of future cardiovascular events independent of cardiovascular risk factors and with similar performance to the established and guideline-recommended ASCVD risk score,” Dr. Weiss said.
Tested against independent group
They tested the model against an independent group of 11,430 outpatients (average age, 60 years; 42.9% male) who underwent a routine outpatient chest x-ray at Mass General Brigham and were potentially eligible to receive statins.
Of those 11,430 patients, 1,096 (9.6%) had a major adverse cardiac event over the median follow-up of 10.3 years.
There was a significant association of CXR-CVD risk and MACE among patients eligible to receive statins, the researchers found (hazard ratio, 2.03; 95% confidence interval, 1.81-2.30; P < .001), which remained significant after adjusting for cardiovascular risk factors (adjusted HR, 1.63; 95% CI, 1.43-1.86; P < .001).
Some of the variables were missing in the standard model, but in a subgroup of 2,401 patients, all the variables were available.
They calculated ASCVD risk in that subgroup using the standard model and the CXR model and found that the performance was similar (c-statistic, 0.64 vs. 0.65; P = .48) to the ASCVD risk score (aHR, 1.58; 95% CI, 1.20-2.09; P = .001).
Ritu R. Gill MD, MPH, associate professor of radiology at Harvard Medical School in Boston, who was not part of the study, said in an interview that “the predictive algorithm is promising and potentially translatable and could enhance the annual medical checkup in a select population.
“The algorithm was developed using the PLCO cohort with radiographs, which are likely subjects in the lung cancer screening arm,” she said. “This cohort would be at high risk of cardiovascular diseases, as smoking is a known risk factor for atherosclerotic disease, and therefore the results are expected.
“The algorithm needs to be validated in an independent database with inclusion of subjects with younger age groups and adjusted for gender and racial diversity,” Gill said.
David Cho, MD, a cardiologist at the University of California, Los Angeles, who also was not part of the study, said in an interview that “this work is a great example of AI being able to detect clinically relevant outcomes with a widely used and low-cost screening test.
“The volume of data needed to train these models is already out there,” Dr. Cho said. “It just needs to be mined.”
He noted that this tool, if validated in randomized trials, could help determine risk among patients living in places where access to specialized cardiac care is limited.
Dr. Weiss and Dr. Cho disclosed no relevant financial relationships. Dr. Gill has received research support from Cannon Inc and consultant fees from Imbio and WorldCare.
A version of this article first appeared on Medscape.com.
who presented the results of their deep-learning model at the annual meeting of the Radiological Society of North America.
Current American College of Cardiologists and American Heart Association guidelines recommend estimating 10-year risk of major adverse cardiovascular events (MACE) to determine whether a patient should receive statins to help prevent atherosclerotic cardiovascular disease (ASCVD). Statins are recommended for patients with a 10-year risk of 7.5% or higher, the authors noted.
The current ASCVD risk score is determined with nine factors: age, sex, race, systolic blood pressure, hypertension treatment, smoking, type 2 diabetes, and a lipid panel.
Not all data points available in EHR
But not all of those data points may be available through the electronic health record, “which makes novel and easier approaches for population-wide screening desirable,” said lead researcher Jakob Weiss, MD, a radiologist affiliated with the Cardiovascular Imaging Research Center at Massachusetts General Hospital and the AI in medicine program at the Brigham and Women’s Hospital in Boston.
Chest x-ray images, on the other hand, are commonly available. The images carry rich information beyond diagnostic data but have not been used in this type of prediction model because AI models have been lacking, Dr. Weiss said.
The researchers trained a deep-learning model with single chest x-rays only.
They used 147,497 chest x-rays from 40,643 participants in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial, a multicenter, randomized controlled trial designed and sponsored by the National Cancer Institute.
Dr. Weiss acknowledged that the population used to train the model was heavily White and that should be a consideration in validating the model.
They compared their model’s ability to predict 10-year ASCVD risk with the standard ACC/AHA model.
“Based on a single chest radiograph image, deep learning can predict the risk of future cardiovascular events independent of cardiovascular risk factors and with similar performance to the established and guideline-recommended ASCVD risk score,” Dr. Weiss said.
Tested against independent group
They tested the model against an independent group of 11,430 outpatients (average age, 60 years; 42.9% male) who underwent a routine outpatient chest x-ray at Mass General Brigham and were potentially eligible to receive statins.
Of those 11,430 patients, 1,096 (9.6%) had a major adverse cardiac event over the median follow-up of 10.3 years.
There was a significant association of CXR-CVD risk and MACE among patients eligible to receive statins, the researchers found (hazard ratio, 2.03; 95% confidence interval, 1.81-2.30; P < .001), which remained significant after adjusting for cardiovascular risk factors (adjusted HR, 1.63; 95% CI, 1.43-1.86; P < .001).
Some of the variables were missing in the standard model, but in a subgroup of 2,401 patients, all the variables were available.
They calculated ASCVD risk in that subgroup using the standard model and the CXR model and found that the performance was similar (c-statistic, 0.64 vs. 0.65; P = .48) to the ASCVD risk score (aHR, 1.58; 95% CI, 1.20-2.09; P = .001).
Ritu R. Gill MD, MPH, associate professor of radiology at Harvard Medical School in Boston, who was not part of the study, said in an interview that “the predictive algorithm is promising and potentially translatable and could enhance the annual medical checkup in a select population.
“The algorithm was developed using the PLCO cohort with radiographs, which are likely subjects in the lung cancer screening arm,” she said. “This cohort would be at high risk of cardiovascular diseases, as smoking is a known risk factor for atherosclerotic disease, and therefore the results are expected.
“The algorithm needs to be validated in an independent database with inclusion of subjects with younger age groups and adjusted for gender and racial diversity,” Gill said.
David Cho, MD, a cardiologist at the University of California, Los Angeles, who also was not part of the study, said in an interview that “this work is a great example of AI being able to detect clinically relevant outcomes with a widely used and low-cost screening test.
“The volume of data needed to train these models is already out there,” Dr. Cho said. “It just needs to be mined.”
He noted that this tool, if validated in randomized trials, could help determine risk among patients living in places where access to specialized cardiac care is limited.
Dr. Weiss and Dr. Cho disclosed no relevant financial relationships. Dr. Gill has received research support from Cannon Inc and consultant fees from Imbio and WorldCare.
A version of this article first appeared on Medscape.com.
who presented the results of their deep-learning model at the annual meeting of the Radiological Society of North America.
Current American College of Cardiologists and American Heart Association guidelines recommend estimating 10-year risk of major adverse cardiovascular events (MACE) to determine whether a patient should receive statins to help prevent atherosclerotic cardiovascular disease (ASCVD). Statins are recommended for patients with a 10-year risk of 7.5% or higher, the authors noted.
The current ASCVD risk score is determined with nine factors: age, sex, race, systolic blood pressure, hypertension treatment, smoking, type 2 diabetes, and a lipid panel.
Not all data points available in EHR
But not all of those data points may be available through the electronic health record, “which makes novel and easier approaches for population-wide screening desirable,” said lead researcher Jakob Weiss, MD, a radiologist affiliated with the Cardiovascular Imaging Research Center at Massachusetts General Hospital and the AI in medicine program at the Brigham and Women’s Hospital in Boston.
Chest x-ray images, on the other hand, are commonly available. The images carry rich information beyond diagnostic data but have not been used in this type of prediction model because AI models have been lacking, Dr. Weiss said.
The researchers trained a deep-learning model with single chest x-rays only.
They used 147,497 chest x-rays from 40,643 participants in the Prostate, Lung, Colorectal, and Ovarian Cancer (PLCO) Screening Trial, a multicenter, randomized controlled trial designed and sponsored by the National Cancer Institute.
Dr. Weiss acknowledged that the population used to train the model was heavily White and that should be a consideration in validating the model.
They compared their model’s ability to predict 10-year ASCVD risk with the standard ACC/AHA model.
“Based on a single chest radiograph image, deep learning can predict the risk of future cardiovascular events independent of cardiovascular risk factors and with similar performance to the established and guideline-recommended ASCVD risk score,” Dr. Weiss said.
Tested against independent group
They tested the model against an independent group of 11,430 outpatients (average age, 60 years; 42.9% male) who underwent a routine outpatient chest x-ray at Mass General Brigham and were potentially eligible to receive statins.
Of those 11,430 patients, 1,096 (9.6%) had a major adverse cardiac event over the median follow-up of 10.3 years.
There was a significant association of CXR-CVD risk and MACE among patients eligible to receive statins, the researchers found (hazard ratio, 2.03; 95% confidence interval, 1.81-2.30; P < .001), which remained significant after adjusting for cardiovascular risk factors (adjusted HR, 1.63; 95% CI, 1.43-1.86; P < .001).
Some of the variables were missing in the standard model, but in a subgroup of 2,401 patients, all the variables were available.
They calculated ASCVD risk in that subgroup using the standard model and the CXR model and found that the performance was similar (c-statistic, 0.64 vs. 0.65; P = .48) to the ASCVD risk score (aHR, 1.58; 95% CI, 1.20-2.09; P = .001).
Ritu R. Gill MD, MPH, associate professor of radiology at Harvard Medical School in Boston, who was not part of the study, said in an interview that “the predictive algorithm is promising and potentially translatable and could enhance the annual medical checkup in a select population.
“The algorithm was developed using the PLCO cohort with radiographs, which are likely subjects in the lung cancer screening arm,” she said. “This cohort would be at high risk of cardiovascular diseases, as smoking is a known risk factor for atherosclerotic disease, and therefore the results are expected.
“The algorithm needs to be validated in an independent database with inclusion of subjects with younger age groups and adjusted for gender and racial diversity,” Gill said.
David Cho, MD, a cardiologist at the University of California, Los Angeles, who also was not part of the study, said in an interview that “this work is a great example of AI being able to detect clinically relevant outcomes with a widely used and low-cost screening test.
“The volume of data needed to train these models is already out there,” Dr. Cho said. “It just needs to be mined.”
He noted that this tool, if validated in randomized trials, could help determine risk among patients living in places where access to specialized cardiac care is limited.
Dr. Weiss and Dr. Cho disclosed no relevant financial relationships. Dr. Gill has received research support from Cannon Inc and consultant fees from Imbio and WorldCare.
A version of this article first appeared on Medscape.com.
AT RSNA 2022
Advancing health equity in neurology is essential to patient care
Black and Latinx older adults are up to three times as likely to develop Alzheimer’s disease than non-Latinx White adults and tend to experience onset at a younger age with more severe symptoms, according to Monica Rivera-Mindt, PhD, a professor of psychology at Fordham University and the Icahn School of Medicine at Mount Sinai, New York. Looking ahead, that means by 2030, nearly 40% of the 8.4 million Americans affected by Alzheimer’s disease will be Black and/or Latinx, she said. These facts were among the stark disparities in health care outcomes Dr. Rivera-Mindt discussed in her presentation on brain health equity at the 2022 annual meeting of the American Neurological Association.
Dr. Rivera-Mindt’s presentation opened the ANA’s plenary session on health disparities and inequities. The plenary, “Advancing Neurologic Equity: Challenges and Paths Forward,” did not simply enumerate racial and ethnic disparities that exist with various neurological conditions. Rather it went beyond the discussion of what disparities exist into understanding the roots of them as well as tips, tools, and resources that can aid clinicians in addressing or ameliorating them.
Roy Hamilton, MD, an associate professor of neurology and physical medicine and rehabilitation at the University of Pennsylvania, Philadelphia, said. “If clinicians are unaware of these disparities or don’t have any sense of how to start to address or think about them, then they’re really missing out on an important component of their education as persons who take care of patients with brain disorders.”
Dr. Hamilton, who organized the plenary, noted that awareness of these disparities is crucial to comprehensively caring for patients.
Missed opportunities
“We’re talking about disadvantages that are structural and large scale, but those disadvantages play themselves out in the individual encounter,” Dr. Hamilton said. “When physicians see patients, they have to treat the whole patient in front of them,” which means being aware of the risks and factors that could affect a patient’s clinical presentation. “Being aware of disparities has practical impacts on physician judgment,” he said.
For example, recent research in multiple sclerosis (MS) has highlighted how clinicians may be missing diagnosis of this condition in non-White populations because the condition has been regarded for so long as a “White person’s” disease, Dr. Hamilton said. In non-White patients exhibiting MS symptoms, then, clinicians may have been less likely to consider MS as a possibility, thereby delaying diagnosis and treatment.
Those patterns may partly explain why the mortality rate for MS is greater in Black patients, who also show more rapid neurodegeneration than White patients with MS, Lilyana Amezcua, MD, an associate professor of neurology at the University of Southern California, Los Angeles, reported in the plenary’s second presentation.
Transgender issues
The third session, presented by Nicole Rosendale, MD, an assistant professor of neurology at the University of California, San Francisco, and director of the San Francisco General Hospital neurology inpatient services, examined disparities in neurology within the LGBTQ+ community through representative case studies and then offered specific ways that neurologists could make their practices more inclusive and equitable for sexual and gender minorities.
Her first case study was a 52-year-old man who presented with new-onset seizures, right hemiparesis, and aphasia. A brain biopsy consistent with adenocarcinoma eventually led his physician to discover he had metastatic breast cancer. It turned out the man was transgender and, despite a family history of breast cancer, hadn’t been advised to get breast cancer screenings.
“Breast cancer was not initially on the differential as no one had identified that the patient was transmasculine,” Dr. Rosendale said. A major challenge to providing care to transgender patients is a dearth of data on risks and screening recommendations. Another barrier is low knowledge of LGBTQ+ health among neurologists, Dr. Rosendale said while sharing findings from her 2019 study on the topic and calling for more research in LGBTQ+ populations.
Dr. Rosendale’s second case study dealt with a nonbinary patient who suffered from debilitating headaches for decades, first because they lacked access to health insurance and then because negative experiences with providers dissuaded them from seeking care. In data from the Center for American Progress she shared, 8% of LGB respondents and 22% of transgender respondents said they had avoided or delayed care because of fear of discrimination or mistreatment.
“So it’s not only access but also what experiences people are having when they go in and whether they’re actually even getting access to care or being taken care of,” Dr. Rosendale said. Other findings from the CAP found that:
- 8% of LGB patients and 29% of transgender patients reported having a clinician refuse to see them.
- 6% of LGB patients and 12% of transgender patients reported that a clinician refused to give them health care.
- 9% of LGB patients and 21% of transgender patients experienced harsh or abusive language during a health care experience.
- 7% of LGB patients and nearly a third (29%) of transgender patients experienced unwanted physical contact, such as fondling or sexual assault.
Reducing the disparities
Adys Mendizabal, MD, an assistant professor of neurology at the Institute of Society and Genetics at the University of California, Los Angeles, who attended the presentation, was grateful to see how the various lectures enriched the discussion beyond stating the fact of racial/ethnic disparities and dug into the nuances on how to think about and address these disparities. She particularly appreciated discussion about the need to go out of the way to recruit diverse patient populations for clinical trials while also providing them care.
“It is definitely complicated, but it’s not impossible for an individual neurologist or an individual department to do something to reduce some of the disparities,” Dr. Mendizabal said. “It starts with just knowing that they exist and being aware of some of the things that may be impacting care for a particular patient.”
Tools to counter disparity
In the final presentation, Amy Kind, MD, PhD, the associate dean for social health sciences and programs at the University of Wisconsin–Madison, rounded out the discussion by exploring social determinants of health and their influence on outcomes.
“Social determinants impact brain health, and brain health is not distributed equally,” Dr. Kind told attendees. “We have known this for decades, yet disparities persist.”
Dr. Kind described the “exposome,” a “measure of all the exposures of an individual in a lifetime and how those exposures relate to health,” according to the CDC, and then introduced a tool clinicians can use to better understand social determinants of health in specific geographic areas. The Neighborhood Atlas, which Dr. Kind described in the New England Journal of Medicine in 2018, measures 17 social determinants across small population-sensitive areas and provides an area deprivation index. A high area deprivation index is linked to a range of negative outcomes, including reshopitalization, later diagnoses, less comprehensive diagnostic evaluation, increased risk of postsurgical complications, and decreased life expectancy.
“One of the things that really stood out to me about Dr. Kind’s discussion of the use of the area deprivation index was the fact that understanding and quantifying these kinds of risks and exposures is the vehicle for creating the kinds of social changes, including policy changes, that will actually lead to addressing and mitigating some of these lifelong risks and exposures,” Dr. Hamilton said. “It is implausible to think that a specific group of people would be genetically more susceptible to basically every disease that we know,” he added. “It makes much more sense to think that groups of individuals have been subjected systematically to conditions that impair health in a variety of ways.”
Not just race, ethnicity, sex, and gender
Following the four presentations from researchers in health inequities was an Emerging Scholar presentation in which Jay B. Lusk, an MD/MBA candidate at Duke University, Durham, N.C., shared new research findings on the role of neighborhood disadvantage in predicting mortality from coma, stroke, and other neurologic conditions. His findings revealed that living in a neighborhood with greater deprivation substantially increased risk of mortality even after accounting for individual wealth and demographics.
Maria Eugenia Diaz-Ortiz, PhD, of the department of neurology, University of Pennsylvania, Philadelphia, said she found the five presentations to be an excellent introduction to people like herself who are in the earlier stages of learning about health equity research.
“I think they introduced various important concepts and frameworks and provided tools for people who don’t know about them,” Dr. Diaz-Ortiz said. “Then they asked important questions and provided some solutions to them.”
Dr. Diaz-Ortiz also appreciated seemingly minor but actually important details in how the speakers presented themselves, such as Dr. Rivera-Mindt opening with a land acknowledgment and her disclosures of “positionality.” The former recognized the traditional Native American custodians of the land on which she lives and works, and the latter revealed details about her as an individual – such as being the Afro-Latinx daughter of immigrants yet being cisgender, able-bodied, and U.S.-born – that show where she falls on the axis of adversity and axis of privilege.
Implications for research
The biggest takeaway for Dr. Diaz-Ortiz, however, came from the first Q&A session when someone asked how to increase underrepresented populations in dementia research. Dr. Rivera-Mindt described her experience engaging these communities by employing “community-based participatory research practices, which involves making yourself a part of the community and making the community active participants in the research,” Dr. Diaz-Ortiz said. “It’s an evidence-based approach that has been shown to increase participation in research not only in her work but in the work of others.”
Preaching to the choir
Dr. Diaz-Ortiz was pleased overall with the plenary but disappointed in its placement at the end of the meeting, when attendance is always lower as attendees head home.
“The people who stayed were people who already know and recognize the value of health equity work, so I think that was a missed opportunity where the session could have been included on day one or two to boost attendance and also to educate like a broader group of neurologists,” Dr. Diaz-Ortiz said in an interview.
Dr. Mendizabal felt similarly, appreciating the plenary but noting it was “definitely overdue” and that it should not be the last session. Instead, sessions on health equity should be as easy as possible to attend to bring in larger audiences. “Perhaps having that session on a Saturday or Sunday would have a higher likelihood of greater attendance than on a Tuesday,” she said. That said, Dr. Mendizabal also noticed that greater attention to health care disparities was woven into many other sessions throughout the conference, which is “the best way of addressing health equity instead of trying to just designate a session,” she said.
Dr. Mendizabal hopes that plenaries like this one and the weaving of health equity issues into presentations throughout neurology conferences continue.
“After the racial reckoning in 2020, there was a big impetus and a big wave of energy in addressing health disparities in the field, and I hope that that momentum is not starting to wane,” Dr. Mendizabal said. “It’s important because not talking about is not going to make this issue go away.”
Dr. Hamilton agreed that it is important that the conversation continue and that physicians recognize the importance of understanding health care disparities and determinants of health, regardless of where they fall on the political spectrum or whether they choose to get involved in policy or advocacy.
“Irrespective of whether you think race or ethnicity or socioeconomic status are political issues or not, it is the case that you’re obligated to have an objective understanding of the factors that contribute to your patient’s health and as points of intervention,” Dr. Hamilton said. “So even if you don’t want to sit down and jot off that email to your senator, you still have to take these factors into account when you’re treating the person who’s sitting right in front of you, and that’s not political. That’s the promise of being a physician.”
Dr. Amezcua has received personal compensation for consulting, speaking, or serving on steering committees or advisory boards for Biogen Idec, Novartis, Genentech, and EMD Serono, and she has received research support from Biogen Idec and Bristol Myers Squibb Foundation. Dr. Kind reported support from the Alzheimer’s Association. Dr. Diaz-Ortiz is coinventor of a provisional patent submitted by the University of Pennsylvania that relates to a potential therapeutic in Parkinson’s disease. Mr. Lusk reported fellowship support from American Heart Association and travel support from the American Neurological Association. No other speakers or sources had relevant disclosures.
Black and Latinx older adults are up to three times as likely to develop Alzheimer’s disease than non-Latinx White adults and tend to experience onset at a younger age with more severe symptoms, according to Monica Rivera-Mindt, PhD, a professor of psychology at Fordham University and the Icahn School of Medicine at Mount Sinai, New York. Looking ahead, that means by 2030, nearly 40% of the 8.4 million Americans affected by Alzheimer’s disease will be Black and/or Latinx, she said. These facts were among the stark disparities in health care outcomes Dr. Rivera-Mindt discussed in her presentation on brain health equity at the 2022 annual meeting of the American Neurological Association.
Dr. Rivera-Mindt’s presentation opened the ANA’s plenary session on health disparities and inequities. The plenary, “Advancing Neurologic Equity: Challenges and Paths Forward,” did not simply enumerate racial and ethnic disparities that exist with various neurological conditions. Rather it went beyond the discussion of what disparities exist into understanding the roots of them as well as tips, tools, and resources that can aid clinicians in addressing or ameliorating them.
Roy Hamilton, MD, an associate professor of neurology and physical medicine and rehabilitation at the University of Pennsylvania, Philadelphia, said. “If clinicians are unaware of these disparities or don’t have any sense of how to start to address or think about them, then they’re really missing out on an important component of their education as persons who take care of patients with brain disorders.”
Dr. Hamilton, who organized the plenary, noted that awareness of these disparities is crucial to comprehensively caring for patients.
Missed opportunities
“We’re talking about disadvantages that are structural and large scale, but those disadvantages play themselves out in the individual encounter,” Dr. Hamilton said. “When physicians see patients, they have to treat the whole patient in front of them,” which means being aware of the risks and factors that could affect a patient’s clinical presentation. “Being aware of disparities has practical impacts on physician judgment,” he said.
For example, recent research in multiple sclerosis (MS) has highlighted how clinicians may be missing diagnosis of this condition in non-White populations because the condition has been regarded for so long as a “White person’s” disease, Dr. Hamilton said. In non-White patients exhibiting MS symptoms, then, clinicians may have been less likely to consider MS as a possibility, thereby delaying diagnosis and treatment.
Those patterns may partly explain why the mortality rate for MS is greater in Black patients, who also show more rapid neurodegeneration than White patients with MS, Lilyana Amezcua, MD, an associate professor of neurology at the University of Southern California, Los Angeles, reported in the plenary’s second presentation.
Transgender issues
The third session, presented by Nicole Rosendale, MD, an assistant professor of neurology at the University of California, San Francisco, and director of the San Francisco General Hospital neurology inpatient services, examined disparities in neurology within the LGBTQ+ community through representative case studies and then offered specific ways that neurologists could make their practices more inclusive and equitable for sexual and gender minorities.
Her first case study was a 52-year-old man who presented with new-onset seizures, right hemiparesis, and aphasia. A brain biopsy consistent with adenocarcinoma eventually led his physician to discover he had metastatic breast cancer. It turned out the man was transgender and, despite a family history of breast cancer, hadn’t been advised to get breast cancer screenings.
“Breast cancer was not initially on the differential as no one had identified that the patient was transmasculine,” Dr. Rosendale said. A major challenge to providing care to transgender patients is a dearth of data on risks and screening recommendations. Another barrier is low knowledge of LGBTQ+ health among neurologists, Dr. Rosendale said while sharing findings from her 2019 study on the topic and calling for more research in LGBTQ+ populations.
Dr. Rosendale’s second case study dealt with a nonbinary patient who suffered from debilitating headaches for decades, first because they lacked access to health insurance and then because negative experiences with providers dissuaded them from seeking care. In data from the Center for American Progress she shared, 8% of LGB respondents and 22% of transgender respondents said they had avoided or delayed care because of fear of discrimination or mistreatment.
“So it’s not only access but also what experiences people are having when they go in and whether they’re actually even getting access to care or being taken care of,” Dr. Rosendale said. Other findings from the CAP found that:
- 8% of LGB patients and 29% of transgender patients reported having a clinician refuse to see them.
- 6% of LGB patients and 12% of transgender patients reported that a clinician refused to give them health care.
- 9% of LGB patients and 21% of transgender patients experienced harsh or abusive language during a health care experience.
- 7% of LGB patients and nearly a third (29%) of transgender patients experienced unwanted physical contact, such as fondling or sexual assault.
Reducing the disparities
Adys Mendizabal, MD, an assistant professor of neurology at the Institute of Society and Genetics at the University of California, Los Angeles, who attended the presentation, was grateful to see how the various lectures enriched the discussion beyond stating the fact of racial/ethnic disparities and dug into the nuances on how to think about and address these disparities. She particularly appreciated discussion about the need to go out of the way to recruit diverse patient populations for clinical trials while also providing them care.
“It is definitely complicated, but it’s not impossible for an individual neurologist or an individual department to do something to reduce some of the disparities,” Dr. Mendizabal said. “It starts with just knowing that they exist and being aware of some of the things that may be impacting care for a particular patient.”
Tools to counter disparity
In the final presentation, Amy Kind, MD, PhD, the associate dean for social health sciences and programs at the University of Wisconsin–Madison, rounded out the discussion by exploring social determinants of health and their influence on outcomes.
“Social determinants impact brain health, and brain health is not distributed equally,” Dr. Kind told attendees. “We have known this for decades, yet disparities persist.”
Dr. Kind described the “exposome,” a “measure of all the exposures of an individual in a lifetime and how those exposures relate to health,” according to the CDC, and then introduced a tool clinicians can use to better understand social determinants of health in specific geographic areas. The Neighborhood Atlas, which Dr. Kind described in the New England Journal of Medicine in 2018, measures 17 social determinants across small population-sensitive areas and provides an area deprivation index. A high area deprivation index is linked to a range of negative outcomes, including reshopitalization, later diagnoses, less comprehensive diagnostic evaluation, increased risk of postsurgical complications, and decreased life expectancy.
“One of the things that really stood out to me about Dr. Kind’s discussion of the use of the area deprivation index was the fact that understanding and quantifying these kinds of risks and exposures is the vehicle for creating the kinds of social changes, including policy changes, that will actually lead to addressing and mitigating some of these lifelong risks and exposures,” Dr. Hamilton said. “It is implausible to think that a specific group of people would be genetically more susceptible to basically every disease that we know,” he added. “It makes much more sense to think that groups of individuals have been subjected systematically to conditions that impair health in a variety of ways.”
Not just race, ethnicity, sex, and gender
Following the four presentations from researchers in health inequities was an Emerging Scholar presentation in which Jay B. Lusk, an MD/MBA candidate at Duke University, Durham, N.C., shared new research findings on the role of neighborhood disadvantage in predicting mortality from coma, stroke, and other neurologic conditions. His findings revealed that living in a neighborhood with greater deprivation substantially increased risk of mortality even after accounting for individual wealth and demographics.
Maria Eugenia Diaz-Ortiz, PhD, of the department of neurology, University of Pennsylvania, Philadelphia, said she found the five presentations to be an excellent introduction to people like herself who are in the earlier stages of learning about health equity research.
“I think they introduced various important concepts and frameworks and provided tools for people who don’t know about them,” Dr. Diaz-Ortiz said. “Then they asked important questions and provided some solutions to them.”
Dr. Diaz-Ortiz also appreciated seemingly minor but actually important details in how the speakers presented themselves, such as Dr. Rivera-Mindt opening with a land acknowledgment and her disclosures of “positionality.” The former recognized the traditional Native American custodians of the land on which she lives and works, and the latter revealed details about her as an individual – such as being the Afro-Latinx daughter of immigrants yet being cisgender, able-bodied, and U.S.-born – that show where she falls on the axis of adversity and axis of privilege.
Implications for research
The biggest takeaway for Dr. Diaz-Ortiz, however, came from the first Q&A session when someone asked how to increase underrepresented populations in dementia research. Dr. Rivera-Mindt described her experience engaging these communities by employing “community-based participatory research practices, which involves making yourself a part of the community and making the community active participants in the research,” Dr. Diaz-Ortiz said. “It’s an evidence-based approach that has been shown to increase participation in research not only in her work but in the work of others.”
Preaching to the choir
Dr. Diaz-Ortiz was pleased overall with the plenary but disappointed in its placement at the end of the meeting, when attendance is always lower as attendees head home.
“The people who stayed were people who already know and recognize the value of health equity work, so I think that was a missed opportunity where the session could have been included on day one or two to boost attendance and also to educate like a broader group of neurologists,” Dr. Diaz-Ortiz said in an interview.
Dr. Mendizabal felt similarly, appreciating the plenary but noting it was “definitely overdue” and that it should not be the last session. Instead, sessions on health equity should be as easy as possible to attend to bring in larger audiences. “Perhaps having that session on a Saturday or Sunday would have a higher likelihood of greater attendance than on a Tuesday,” she said. That said, Dr. Mendizabal also noticed that greater attention to health care disparities was woven into many other sessions throughout the conference, which is “the best way of addressing health equity instead of trying to just designate a session,” she said.
Dr. Mendizabal hopes that plenaries like this one and the weaving of health equity issues into presentations throughout neurology conferences continue.
“After the racial reckoning in 2020, there was a big impetus and a big wave of energy in addressing health disparities in the field, and I hope that that momentum is not starting to wane,” Dr. Mendizabal said. “It’s important because not talking about is not going to make this issue go away.”
Dr. Hamilton agreed that it is important that the conversation continue and that physicians recognize the importance of understanding health care disparities and determinants of health, regardless of where they fall on the political spectrum or whether they choose to get involved in policy or advocacy.
“Irrespective of whether you think race or ethnicity or socioeconomic status are political issues or not, it is the case that you’re obligated to have an objective understanding of the factors that contribute to your patient’s health and as points of intervention,” Dr. Hamilton said. “So even if you don’t want to sit down and jot off that email to your senator, you still have to take these factors into account when you’re treating the person who’s sitting right in front of you, and that’s not political. That’s the promise of being a physician.”
Dr. Amezcua has received personal compensation for consulting, speaking, or serving on steering committees or advisory boards for Biogen Idec, Novartis, Genentech, and EMD Serono, and she has received research support from Biogen Idec and Bristol Myers Squibb Foundation. Dr. Kind reported support from the Alzheimer’s Association. Dr. Diaz-Ortiz is coinventor of a provisional patent submitted by the University of Pennsylvania that relates to a potential therapeutic in Parkinson’s disease. Mr. Lusk reported fellowship support from American Heart Association and travel support from the American Neurological Association. No other speakers or sources had relevant disclosures.
Black and Latinx older adults are up to three times as likely to develop Alzheimer’s disease than non-Latinx White adults and tend to experience onset at a younger age with more severe symptoms, according to Monica Rivera-Mindt, PhD, a professor of psychology at Fordham University and the Icahn School of Medicine at Mount Sinai, New York. Looking ahead, that means by 2030, nearly 40% of the 8.4 million Americans affected by Alzheimer’s disease will be Black and/or Latinx, she said. These facts were among the stark disparities in health care outcomes Dr. Rivera-Mindt discussed in her presentation on brain health equity at the 2022 annual meeting of the American Neurological Association.
Dr. Rivera-Mindt’s presentation opened the ANA’s plenary session on health disparities and inequities. The plenary, “Advancing Neurologic Equity: Challenges and Paths Forward,” did not simply enumerate racial and ethnic disparities that exist with various neurological conditions. Rather it went beyond the discussion of what disparities exist into understanding the roots of them as well as tips, tools, and resources that can aid clinicians in addressing or ameliorating them.
Roy Hamilton, MD, an associate professor of neurology and physical medicine and rehabilitation at the University of Pennsylvania, Philadelphia, said. “If clinicians are unaware of these disparities or don’t have any sense of how to start to address or think about them, then they’re really missing out on an important component of their education as persons who take care of patients with brain disorders.”
Dr. Hamilton, who organized the plenary, noted that awareness of these disparities is crucial to comprehensively caring for patients.
Missed opportunities
“We’re talking about disadvantages that are structural and large scale, but those disadvantages play themselves out in the individual encounter,” Dr. Hamilton said. “When physicians see patients, they have to treat the whole patient in front of them,” which means being aware of the risks and factors that could affect a patient’s clinical presentation. “Being aware of disparities has practical impacts on physician judgment,” he said.
For example, recent research in multiple sclerosis (MS) has highlighted how clinicians may be missing diagnosis of this condition in non-White populations because the condition has been regarded for so long as a “White person’s” disease, Dr. Hamilton said. In non-White patients exhibiting MS symptoms, then, clinicians may have been less likely to consider MS as a possibility, thereby delaying diagnosis and treatment.
Those patterns may partly explain why the mortality rate for MS is greater in Black patients, who also show more rapid neurodegeneration than White patients with MS, Lilyana Amezcua, MD, an associate professor of neurology at the University of Southern California, Los Angeles, reported in the plenary’s second presentation.
Transgender issues
The third session, presented by Nicole Rosendale, MD, an assistant professor of neurology at the University of California, San Francisco, and director of the San Francisco General Hospital neurology inpatient services, examined disparities in neurology within the LGBTQ+ community through representative case studies and then offered specific ways that neurologists could make their practices more inclusive and equitable for sexual and gender minorities.
Her first case study was a 52-year-old man who presented with new-onset seizures, right hemiparesis, and aphasia. A brain biopsy consistent with adenocarcinoma eventually led his physician to discover he had metastatic breast cancer. It turned out the man was transgender and, despite a family history of breast cancer, hadn’t been advised to get breast cancer screenings.
“Breast cancer was not initially on the differential as no one had identified that the patient was transmasculine,” Dr. Rosendale said. A major challenge to providing care to transgender patients is a dearth of data on risks and screening recommendations. Another barrier is low knowledge of LGBTQ+ health among neurologists, Dr. Rosendale said while sharing findings from her 2019 study on the topic and calling for more research in LGBTQ+ populations.
Dr. Rosendale’s second case study dealt with a nonbinary patient who suffered from debilitating headaches for decades, first because they lacked access to health insurance and then because negative experiences with providers dissuaded them from seeking care. In data from the Center for American Progress she shared, 8% of LGB respondents and 22% of transgender respondents said they had avoided or delayed care because of fear of discrimination or mistreatment.
“So it’s not only access but also what experiences people are having when they go in and whether they’re actually even getting access to care or being taken care of,” Dr. Rosendale said. Other findings from the CAP found that:
- 8% of LGB patients and 29% of transgender patients reported having a clinician refuse to see them.
- 6% of LGB patients and 12% of transgender patients reported that a clinician refused to give them health care.
- 9% of LGB patients and 21% of transgender patients experienced harsh or abusive language during a health care experience.
- 7% of LGB patients and nearly a third (29%) of transgender patients experienced unwanted physical contact, such as fondling or sexual assault.
Reducing the disparities
Adys Mendizabal, MD, an assistant professor of neurology at the Institute of Society and Genetics at the University of California, Los Angeles, who attended the presentation, was grateful to see how the various lectures enriched the discussion beyond stating the fact of racial/ethnic disparities and dug into the nuances on how to think about and address these disparities. She particularly appreciated discussion about the need to go out of the way to recruit diverse patient populations for clinical trials while also providing them care.
“It is definitely complicated, but it’s not impossible for an individual neurologist or an individual department to do something to reduce some of the disparities,” Dr. Mendizabal said. “It starts with just knowing that they exist and being aware of some of the things that may be impacting care for a particular patient.”
Tools to counter disparity
In the final presentation, Amy Kind, MD, PhD, the associate dean for social health sciences and programs at the University of Wisconsin–Madison, rounded out the discussion by exploring social determinants of health and their influence on outcomes.
“Social determinants impact brain health, and brain health is not distributed equally,” Dr. Kind told attendees. “We have known this for decades, yet disparities persist.”
Dr. Kind described the “exposome,” a “measure of all the exposures of an individual in a lifetime and how those exposures relate to health,” according to the CDC, and then introduced a tool clinicians can use to better understand social determinants of health in specific geographic areas. The Neighborhood Atlas, which Dr. Kind described in the New England Journal of Medicine in 2018, measures 17 social determinants across small population-sensitive areas and provides an area deprivation index. A high area deprivation index is linked to a range of negative outcomes, including reshopitalization, later diagnoses, less comprehensive diagnostic evaluation, increased risk of postsurgical complications, and decreased life expectancy.
“One of the things that really stood out to me about Dr. Kind’s discussion of the use of the area deprivation index was the fact that understanding and quantifying these kinds of risks and exposures is the vehicle for creating the kinds of social changes, including policy changes, that will actually lead to addressing and mitigating some of these lifelong risks and exposures,” Dr. Hamilton said. “It is implausible to think that a specific group of people would be genetically more susceptible to basically every disease that we know,” he added. “It makes much more sense to think that groups of individuals have been subjected systematically to conditions that impair health in a variety of ways.”
Not just race, ethnicity, sex, and gender
Following the four presentations from researchers in health inequities was an Emerging Scholar presentation in which Jay B. Lusk, an MD/MBA candidate at Duke University, Durham, N.C., shared new research findings on the role of neighborhood disadvantage in predicting mortality from coma, stroke, and other neurologic conditions. His findings revealed that living in a neighborhood with greater deprivation substantially increased risk of mortality even after accounting for individual wealth and demographics.
Maria Eugenia Diaz-Ortiz, PhD, of the department of neurology, University of Pennsylvania, Philadelphia, said she found the five presentations to be an excellent introduction to people like herself who are in the earlier stages of learning about health equity research.
“I think they introduced various important concepts and frameworks and provided tools for people who don’t know about them,” Dr. Diaz-Ortiz said. “Then they asked important questions and provided some solutions to them.”
Dr. Diaz-Ortiz also appreciated seemingly minor but actually important details in how the speakers presented themselves, such as Dr. Rivera-Mindt opening with a land acknowledgment and her disclosures of “positionality.” The former recognized the traditional Native American custodians of the land on which she lives and works, and the latter revealed details about her as an individual – such as being the Afro-Latinx daughter of immigrants yet being cisgender, able-bodied, and U.S.-born – that show where she falls on the axis of adversity and axis of privilege.
Implications for research
The biggest takeaway for Dr. Diaz-Ortiz, however, came from the first Q&A session when someone asked how to increase underrepresented populations in dementia research. Dr. Rivera-Mindt described her experience engaging these communities by employing “community-based participatory research practices, which involves making yourself a part of the community and making the community active participants in the research,” Dr. Diaz-Ortiz said. “It’s an evidence-based approach that has been shown to increase participation in research not only in her work but in the work of others.”
Preaching to the choir
Dr. Diaz-Ortiz was pleased overall with the plenary but disappointed in its placement at the end of the meeting, when attendance is always lower as attendees head home.
“The people who stayed were people who already know and recognize the value of health equity work, so I think that was a missed opportunity where the session could have been included on day one or two to boost attendance and also to educate like a broader group of neurologists,” Dr. Diaz-Ortiz said in an interview.
Dr. Mendizabal felt similarly, appreciating the plenary but noting it was “definitely overdue” and that it should not be the last session. Instead, sessions on health equity should be as easy as possible to attend to bring in larger audiences. “Perhaps having that session on a Saturday or Sunday would have a higher likelihood of greater attendance than on a Tuesday,” she said. That said, Dr. Mendizabal also noticed that greater attention to health care disparities was woven into many other sessions throughout the conference, which is “the best way of addressing health equity instead of trying to just designate a session,” she said.
Dr. Mendizabal hopes that plenaries like this one and the weaving of health equity issues into presentations throughout neurology conferences continue.
“After the racial reckoning in 2020, there was a big impetus and a big wave of energy in addressing health disparities in the field, and I hope that that momentum is not starting to wane,” Dr. Mendizabal said. “It’s important because not talking about is not going to make this issue go away.”
Dr. Hamilton agreed that it is important that the conversation continue and that physicians recognize the importance of understanding health care disparities and determinants of health, regardless of where they fall on the political spectrum or whether they choose to get involved in policy or advocacy.
“Irrespective of whether you think race or ethnicity or socioeconomic status are political issues or not, it is the case that you’re obligated to have an objective understanding of the factors that contribute to your patient’s health and as points of intervention,” Dr. Hamilton said. “So even if you don’t want to sit down and jot off that email to your senator, you still have to take these factors into account when you’re treating the person who’s sitting right in front of you, and that’s not political. That’s the promise of being a physician.”
Dr. Amezcua has received personal compensation for consulting, speaking, or serving on steering committees or advisory boards for Biogen Idec, Novartis, Genentech, and EMD Serono, and she has received research support from Biogen Idec and Bristol Myers Squibb Foundation. Dr. Kind reported support from the Alzheimer’s Association. Dr. Diaz-Ortiz is coinventor of a provisional patent submitted by the University of Pennsylvania that relates to a potential therapeutic in Parkinson’s disease. Mr. Lusk reported fellowship support from American Heart Association and travel support from the American Neurological Association. No other speakers or sources had relevant disclosures.
FROM ANA 2022