User login
RA risk raised by work-related inhaled agents
Exposure to inhaled agents in the workplace could be putting people at risk of developing rheumatoid arthritis, according to research published in Annals of the Rheumatic Diseases.
In an analysis of data from the long-running Swedish Epidemiological Investigation of RA (EIRA) population-based cohort study, there was a 21% increased risk of RA and a 25% increased risk of anti–citrullinated protein antibody (ACPA)–positive RA associated with exposure to any occupationally inhaled agent.
“We have investigated a number of occupational airborne exposures and found that exposure for those agents infer a high risk for RA,” Lars Klareskog, MD, PhD, senior professor of rheumatology at the Karolinska Institute and Karolinska University Hospital (Solna) in Stockholm, said in an interview.
Dr. Klareskog, who is one of the lead authors of the published work, added that the risk is particularly high in individuals who had a genetic susceptibility and in those who smoked.
“The importance of this is that it further demonstrates that exposures to the lung may trigger immune reactions associated with the major subset of rheumatoid arthritis,” Dr. Klareskog said. “Second, it shows that those exposed to these agents should be very keen to not smoke.” “These findings further implicate the respiratory tract mucosa in ACPA-positive RA pathogenesis,” agreed Vanessa L. Kronzer, MD, of the Mayo Clinic in Rochester, Minn., and Jeffrey A. Sparks, MD, MMSc, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
They also “impress the need for public policy initiatives related to occupational inhalants to prevent RA,” they suggested in an editorial.
Multiple occupational inhalable exposures assessed
In the analysis, the researchers assessed exposure to 32 inhalable agents in people with (n = 4,033) and without RA (n = 6,485). The list of agents considered included detergents, diesel engine exhaust, fine particulate matter, solvents, and agricultural chemicals.
A total of 17 agents showed a positive association with an increased risk of ACPA-positive RA. Dr. Kronzer and Dr. Sparks noted that breathing in insecticides and fungicides at work was associated with the highest odds ratios for having ACPA-positive RA (both 2.38).
“Importantly, both the number and duration of exposures exhibited a dose-response effect on RA risk,” the editorialists said.
They also picked out that there was “a gene-environment interaction for RA risk for certain inhalants,” including diesel engine exhaust, asbestos, carbon monoxide, and quartz dust.
Smoking amplified the risk for ACPA-positive RA associated with certain agents, such as detergents, and adding in genetic susceptibility for a third exposure increased the risk still further.
A key message is that there are many agents that can affect the airways and increase the risk of RA rather than there being a specific one, Dr. Klareskog said.
“On one hand, it’s a message of public health,” he said. Many public health authorities are aware of the potential risks of inhaled agents on the lung, “but this just adds another dimension that it’s bad also for rheumatoid arthritis.” Thus, greater efforts to help protect people from being exposed at work may be needed.
From the individual’s perspective, “if you have RA or other immune diseases in your family, then you may know that you’re at increased risk,” Dr. Klareskog said. The message here is perhaps to “be aware, [protect yourself], and stop smoking.”
The EIRA study was supported by funding from the Swedish Research Foundation for Health, Working Life, and Welfare, the Swedish Research Council, the AFA foundation, Region Stockholm, King Gustaf V’s 80-year foundation, and the Swedish Rheumatic Foundation. Dr. Klareskog and coauthors had no competing interests to disclose. Dr. Kronzer and Dr. Sparks had no disclosures of relevance to their comments.
Exposure to inhaled agents in the workplace could be putting people at risk of developing rheumatoid arthritis, according to research published in Annals of the Rheumatic Diseases.
In an analysis of data from the long-running Swedish Epidemiological Investigation of RA (EIRA) population-based cohort study, there was a 21% increased risk of RA and a 25% increased risk of anti–citrullinated protein antibody (ACPA)–positive RA associated with exposure to any occupationally inhaled agent.
“We have investigated a number of occupational airborne exposures and found that exposure for those agents infer a high risk for RA,” Lars Klareskog, MD, PhD, senior professor of rheumatology at the Karolinska Institute and Karolinska University Hospital (Solna) in Stockholm, said in an interview.
Dr. Klareskog, who is one of the lead authors of the published work, added that the risk is particularly high in individuals who had a genetic susceptibility and in those who smoked.
“The importance of this is that it further demonstrates that exposures to the lung may trigger immune reactions associated with the major subset of rheumatoid arthritis,” Dr. Klareskog said. “Second, it shows that those exposed to these agents should be very keen to not smoke.” “These findings further implicate the respiratory tract mucosa in ACPA-positive RA pathogenesis,” agreed Vanessa L. Kronzer, MD, of the Mayo Clinic in Rochester, Minn., and Jeffrey A. Sparks, MD, MMSc, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
They also “impress the need for public policy initiatives related to occupational inhalants to prevent RA,” they suggested in an editorial.
Multiple occupational inhalable exposures assessed
In the analysis, the researchers assessed exposure to 32 inhalable agents in people with (n = 4,033) and without RA (n = 6,485). The list of agents considered included detergents, diesel engine exhaust, fine particulate matter, solvents, and agricultural chemicals.
A total of 17 agents showed a positive association with an increased risk of ACPA-positive RA. Dr. Kronzer and Dr. Sparks noted that breathing in insecticides and fungicides at work was associated with the highest odds ratios for having ACPA-positive RA (both 2.38).
“Importantly, both the number and duration of exposures exhibited a dose-response effect on RA risk,” the editorialists said.
They also picked out that there was “a gene-environment interaction for RA risk for certain inhalants,” including diesel engine exhaust, asbestos, carbon monoxide, and quartz dust.
Smoking amplified the risk for ACPA-positive RA associated with certain agents, such as detergents, and adding in genetic susceptibility for a third exposure increased the risk still further.
A key message is that there are many agents that can affect the airways and increase the risk of RA rather than there being a specific one, Dr. Klareskog said.
“On one hand, it’s a message of public health,” he said. Many public health authorities are aware of the potential risks of inhaled agents on the lung, “but this just adds another dimension that it’s bad also for rheumatoid arthritis.” Thus, greater efforts to help protect people from being exposed at work may be needed.
From the individual’s perspective, “if you have RA or other immune diseases in your family, then you may know that you’re at increased risk,” Dr. Klareskog said. The message here is perhaps to “be aware, [protect yourself], and stop smoking.”
The EIRA study was supported by funding from the Swedish Research Foundation for Health, Working Life, and Welfare, the Swedish Research Council, the AFA foundation, Region Stockholm, King Gustaf V’s 80-year foundation, and the Swedish Rheumatic Foundation. Dr. Klareskog and coauthors had no competing interests to disclose. Dr. Kronzer and Dr. Sparks had no disclosures of relevance to their comments.
Exposure to inhaled agents in the workplace could be putting people at risk of developing rheumatoid arthritis, according to research published in Annals of the Rheumatic Diseases.
In an analysis of data from the long-running Swedish Epidemiological Investigation of RA (EIRA) population-based cohort study, there was a 21% increased risk of RA and a 25% increased risk of anti–citrullinated protein antibody (ACPA)–positive RA associated with exposure to any occupationally inhaled agent.
“We have investigated a number of occupational airborne exposures and found that exposure for those agents infer a high risk for RA,” Lars Klareskog, MD, PhD, senior professor of rheumatology at the Karolinska Institute and Karolinska University Hospital (Solna) in Stockholm, said in an interview.
Dr. Klareskog, who is one of the lead authors of the published work, added that the risk is particularly high in individuals who had a genetic susceptibility and in those who smoked.
“The importance of this is that it further demonstrates that exposures to the lung may trigger immune reactions associated with the major subset of rheumatoid arthritis,” Dr. Klareskog said. “Second, it shows that those exposed to these agents should be very keen to not smoke.” “These findings further implicate the respiratory tract mucosa in ACPA-positive RA pathogenesis,” agreed Vanessa L. Kronzer, MD, of the Mayo Clinic in Rochester, Minn., and Jeffrey A. Sparks, MD, MMSc, of Brigham and Women’s Hospital and Harvard Medical School, both in Boston.
They also “impress the need for public policy initiatives related to occupational inhalants to prevent RA,” they suggested in an editorial.
Multiple occupational inhalable exposures assessed
In the analysis, the researchers assessed exposure to 32 inhalable agents in people with (n = 4,033) and without RA (n = 6,485). The list of agents considered included detergents, diesel engine exhaust, fine particulate matter, solvents, and agricultural chemicals.
A total of 17 agents showed a positive association with an increased risk of ACPA-positive RA. Dr. Kronzer and Dr. Sparks noted that breathing in insecticides and fungicides at work was associated with the highest odds ratios for having ACPA-positive RA (both 2.38).
“Importantly, both the number and duration of exposures exhibited a dose-response effect on RA risk,” the editorialists said.
They also picked out that there was “a gene-environment interaction for RA risk for certain inhalants,” including diesel engine exhaust, asbestos, carbon monoxide, and quartz dust.
Smoking amplified the risk for ACPA-positive RA associated with certain agents, such as detergents, and adding in genetic susceptibility for a third exposure increased the risk still further.
A key message is that there are many agents that can affect the airways and increase the risk of RA rather than there being a specific one, Dr. Klareskog said.
“On one hand, it’s a message of public health,” he said. Many public health authorities are aware of the potential risks of inhaled agents on the lung, “but this just adds another dimension that it’s bad also for rheumatoid arthritis.” Thus, greater efforts to help protect people from being exposed at work may be needed.
From the individual’s perspective, “if you have RA or other immune diseases in your family, then you may know that you’re at increased risk,” Dr. Klareskog said. The message here is perhaps to “be aware, [protect yourself], and stop smoking.”
The EIRA study was supported by funding from the Swedish Research Foundation for Health, Working Life, and Welfare, the Swedish Research Council, the AFA foundation, Region Stockholm, King Gustaf V’s 80-year foundation, and the Swedish Rheumatic Foundation. Dr. Klareskog and coauthors had no competing interests to disclose. Dr. Kronzer and Dr. Sparks had no disclosures of relevance to their comments.
FROM ANNALS OF THE RHEUMATIC DISEASES
U.S. sees most flu hospitalizations in a decade
But the number of deaths and outpatient visits for flu or flu-like illnesses was down slightly from the week before, the CDC said in its weekly FluView report.
There were almost 26,000 new hospital admissions involving laboratory-confirmed influenza over those 7 days, up by over 31% from the previous week, based on data from 5,000 hospitals in the HHS Protect system, which tracks and shares COVID-19 data.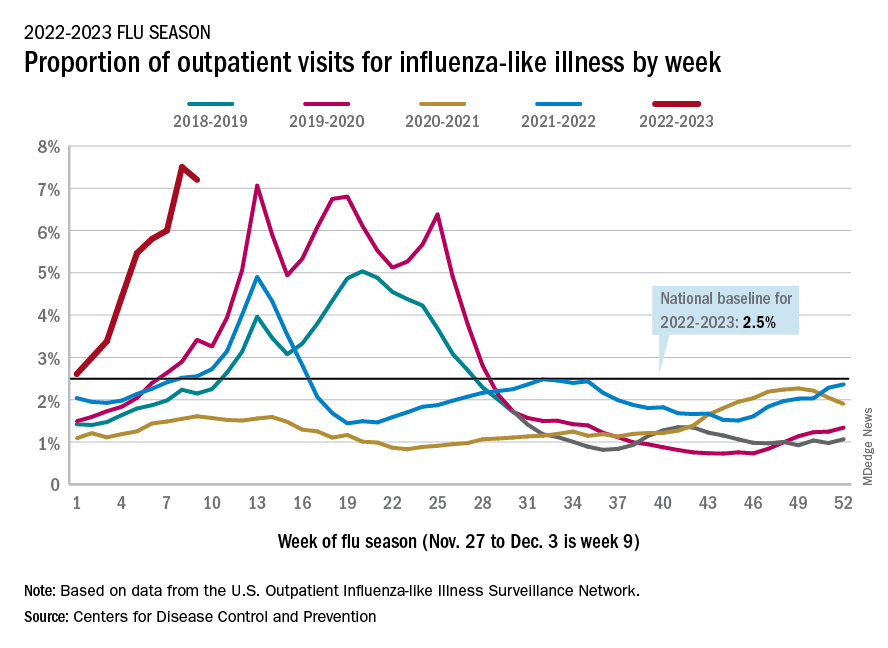
The cumulative hospitalization rate for the 2022-2023 season is 26.0 per 100,000 people, the highest seen at this time of year since 2010-2011, the CDC said, based on data from its Influenza Hospitalization Surveillance Network, which includes hospitals in select counties in 13 states.
At this point in the 2019-2020 season, just before the COVID-19 pandemic began, the cumulative rate was 3.1 per 100,000 people, the CDC’s data show.
On the positive side, the proportion of outpatient visits for influenza-like illness dropped slightly to 7.2%, from 7.5% the week before. But these cases from the CDC’s Outpatient Influenza-like Illness Surveillance Network are not laboratory confirmed, so the data could include people with the flu, COVID-19, or respiratory syncytial virus.
The number of confirmed flu deaths for the week of Nov. 27 to Dec. 3 also fell slightly from the last full week of November, 246 vs. 255, but the number of pediatric deaths rose from 2 to 7, and total deaths in children are already up to 21 for 2022-2023. That’s compared to 44 that were reported during all of the 2021-2022 season, the CDC said.
“So far this season, there have been at least 13 million illnesses, 120,000 hospitalizations, and 7,300 deaths from flu,” the agency estimated.
A version of this article first appeared on Medscape.com.
But the number of deaths and outpatient visits for flu or flu-like illnesses was down slightly from the week before, the CDC said in its weekly FluView report.
There were almost 26,000 new hospital admissions involving laboratory-confirmed influenza over those 7 days, up by over 31% from the previous week, based on data from 5,000 hospitals in the HHS Protect system, which tracks and shares COVID-19 data.
The cumulative hospitalization rate for the 2022-2023 season is 26.0 per 100,000 people, the highest seen at this time of year since 2010-2011, the CDC said, based on data from its Influenza Hospitalization Surveillance Network, which includes hospitals in select counties in 13 states.
At this point in the 2019-2020 season, just before the COVID-19 pandemic began, the cumulative rate was 3.1 per 100,000 people, the CDC’s data show.
On the positive side, the proportion of outpatient visits for influenza-like illness dropped slightly to 7.2%, from 7.5% the week before. But these cases from the CDC’s Outpatient Influenza-like Illness Surveillance Network are not laboratory confirmed, so the data could include people with the flu, COVID-19, or respiratory syncytial virus.
The number of confirmed flu deaths for the week of Nov. 27 to Dec. 3 also fell slightly from the last full week of November, 246 vs. 255, but the number of pediatric deaths rose from 2 to 7, and total deaths in children are already up to 21 for 2022-2023. That’s compared to 44 that were reported during all of the 2021-2022 season, the CDC said.
“So far this season, there have been at least 13 million illnesses, 120,000 hospitalizations, and 7,300 deaths from flu,” the agency estimated.
A version of this article first appeared on Medscape.com.
But the number of deaths and outpatient visits for flu or flu-like illnesses was down slightly from the week before, the CDC said in its weekly FluView report.
There were almost 26,000 new hospital admissions involving laboratory-confirmed influenza over those 7 days, up by over 31% from the previous week, based on data from 5,000 hospitals in the HHS Protect system, which tracks and shares COVID-19 data.
The cumulative hospitalization rate for the 2022-2023 season is 26.0 per 100,000 people, the highest seen at this time of year since 2010-2011, the CDC said, based on data from its Influenza Hospitalization Surveillance Network, which includes hospitals in select counties in 13 states.
At this point in the 2019-2020 season, just before the COVID-19 pandemic began, the cumulative rate was 3.1 per 100,000 people, the CDC’s data show.
On the positive side, the proportion of outpatient visits for influenza-like illness dropped slightly to 7.2%, from 7.5% the week before. But these cases from the CDC’s Outpatient Influenza-like Illness Surveillance Network are not laboratory confirmed, so the data could include people with the flu, COVID-19, or respiratory syncytial virus.
The number of confirmed flu deaths for the week of Nov. 27 to Dec. 3 also fell slightly from the last full week of November, 246 vs. 255, but the number of pediatric deaths rose from 2 to 7, and total deaths in children are already up to 21 for 2022-2023. That’s compared to 44 that were reported during all of the 2021-2022 season, the CDC said.
“So far this season, there have been at least 13 million illnesses, 120,000 hospitalizations, and 7,300 deaths from flu,” the agency estimated.
A version of this article first appeared on Medscape.com.
As COVID treatments dwindle, are new ones waiting in the wings?
It was the last monoclonal antibody treatment standing. But less than 10 months after the U.S. Food and Drug Administration gave bebtelovimab its emergency use authorization (EUA) to fight COVID-19, it earlier this month de-authorized it, just as it had for other monoclonal antibody treatments, and for the same reason:
Bebtelovimab couldn’t neutralize the Omicron subvariants BQ.1 and BQ.1.1, the cause of nearly 60% of COVID cases nationally as of November 30.
Next on the chopping block, some predict, will be Evusheld, the combination of tixagevimab and cilgavimab given as a preventive monoclonal antibody to people who are immunocompromised and at high risk of contracting COVID and to those who can’t take the vaccine. In October, the FDA warned that Evusheld was not neutralizing circulating COVID variants.
As the options for treating and preventing COVID decline, will companies rally quickly to develop new ones, or cut their losses in developing treatments that may work for only a few months, given the speed of viral mutations?
But although monoclonal antibody treatments are off the table, at least for now, antiviral drugs – including Paxlovid – are still very much available, and some say underused.
Others suggest it’s time to resurrect interest in convalescent plasma, a treatment used early in the pandemic before drugs or vaccines were here and still authorized for use in those who are immunosuppressed or receiving immunosuppressive treatment.
And on the prevention front, staying up to date with booster vaccines, masking, and taking other precautions should be stressed more, others say, regardless of the number of treatment options, and especially now, as cases rise and people gather for the winter holidays.
‘A major setback’
The bebtelovimab de-authorization was “a major setback,” but an understandable one, said Arturo Casadevall, MD, PhD, professor and chair of molecular microbiology and immunology at the Johns Hopkins Bloomberg School of Public Health in Baltimore. “Monoclonal antibodies are great drugs. We are in an unfortunate situation in that they are vulnerable to changes in the virus” and can’t offer long-lasting protection.
Supplies of bebtelovimab will be retained, according to the FDA, in case variants susceptible to it return.
“What happened to bebtelovimab is no surprise,” agreed Amesh Adalja, MD, senior scholar at Johns Hopkins Center for Health Security. “This is what is going to happen when you are targeting a virus that mutates a lot.”
Monoclonal antibodies work by binding to the spike protein on the virus surface to prevent it from entering cells.
However, Dr. Adalja doesn’t view the disappearance of monoclonal antibody treatments as a major setback. Monoclonal antibodies were not the primary way COVID was treated, he said.
While he does believe it’s important that more monoclonal antibody treatments be developed, “I think it’s important to remember we still have Paxlovid while everyone is lamenting the loss of bebtelovimab.’’
Antivirals: What’s here, what’s coming
Compared with monoclonal antibodies, “Paxlovid remains a much easier drug to give,” Dr. Adalja told this news organization, because it is taken orally, not intravenously.
And it’s effective. In a recent study, researchers found that adults diagnosed with COVID given Paxlovid within 5 days of diagnosis had a 51% lower hospitalization rate within the next 30 days than those not given it. Another study shows it could also reduce a person’s risk of developing long COVID by 26%.
Paxlovid is underused, Dr. Adalja said, partly because the rebound potential got more press than the effectiveness. When a celebrity got rebound from Paxlovid, he said, that would make the news, overshadowing the research on its effectiveness.
Besides Paxlovid, the antivirals remdesivir (Veklury), given intravenously for 3 days, and molnupiravir (Lagevrio), taken orally, are also still available. Antivirals work by targeting specific parts of the virus to prevent it from multiplying.
In the lab, remdesivir, molnupiravir, and another antiviral, nirmatrelvir, all appear to be effective against both BQ.1.1 (a BA.5 subvariant) and XBB (a BA.2 subvariant), both rapidly rising in the United States, according to a report last week in the New England Journal of Medicine.
The researchers also tested several monoclonal antibodies and found they did not neutralize either of the subvariants BQ.1.1 and XBB.
A new oral antiviral, Xocova (ensitrelvir fumaric acid), from Japanese manufacturer Shionogi, received emergency approval in Japan on November 22. It’s taken once a day for 5 days. The goal is to expand access to it globally, according to the company.
Pardes Biosciences launched a phase 2 trial in September for its oral antiviral drug (PBI-0451), under study as a treatment and preventive for COVID. It expects data by the first quarter of 2023.
Pfizer, which makes Paxlovid, has partnered with Clear Creek Bio to develop another oral antiviral COVID drug.
Other approaches
A receptor protein known as ACE2 (angiotensin-converting enzyme 2) is the main “doorway” that SARS-CoV-2 uses to enter and infect cells.
Dana-Farber Cancer Institute scientists are developing a “decoy” drug that works by mimicking the ACE2 receptor on the surface of cells; when the virus tries to bind to it, the spike protein is destroyed. Human trials have not yet started.
Other researchers are investigating whether an already-approved drug used to treat a liver disease, Actigall (UDCA/ursodeoxycholic acid), could protect against COVID infection by reducing ACE2.
So far, the researchers have found in early research that people taking UDCA for liver conditions were less likely than those not taking the drug to have severe COVID. They also found that UDCA reduced SARS-CoV-2 infection in human lungs maintained outside the body.
Monoclonal antibody treatments?
After the FDA decision to withdraw the bebtelovimab EUA, which Eli Lilly said it agreed with, the company issued a statement, promising it wasn’t giving up on monoclonal antibody treatments.
“Lilly will continue to search and evaluate monoclonal antibodies to identify potential candidates for clinical development against new variants,” it read in part.
AstraZeneca, which makes Evusheld, is also continuing to work on monoclonal antibody development. According to a spokesperson, “We are also developing a new long-acting antibody combination – AZD5156 – which has been shown in the lab to neutralize emerging new variants and all known variants to date. We are working to accelerate the development of AZD5156 to make it available at the end of 2023.”
The AstraZeneca spokesperson said he could share no more information about what the combination would include.
A convalescent plasma comeback?
Although Paxlovid can help, there are many contraindications to it, such as drug-drug interactions, Dr. Casadevall told this news organization. And now that the monoclonal antibody treatments have been paused, convalescent plasma “is the only antibody-based therapy that is reliably available. Convalescent plasma includes thousands of different antibodies.”
With his colleagues, Dr. Casadevall evaluated plasma samples from 740 patients. Some had received booster vaccines and been infected with Omicron, others had received boosters and not been infected, and still others had not been vaccinated and became infected.
In a report (not yet peer-reviewed), they found the plasma from those who had been infected or boosted within the past 6 months neutralized the new Omicron variants BQ.1.1, XBB.1, and BF.7.
A push for boosters, masks
To get through the coming months, taking precautions like masking and distancing and staying up to date on booster vaccinations, especially for older adults, can make a difference, other experts say.
In a Twitter thread in early December, Peter Hotez, MD, PhD, professor of pediatrics and molecular virology and microbiology at Baylor College of Medicine, Houston, urged people to take COVID seriously as holiday parties and gatherings occur.
“The single most impactful thing you can do is get your bivalent booster,” he tweeted, as well as give your kids the booster, citing preliminary research that the bivalent mRNA booster broadens immunity against the Omicron subvariants.
For seniors, he said, ‘‘if you get breakthrough COVID, [it’s] really important to get Paxlovid.” Masks will help not only for COVID but also influenza, respiratory syncytial virus (RSV), and other conditions.
Mitigation measures have largely been abandoned, according to Eric Topol, MD, director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape. In an op-ed in the Los Angeles Times, and on his Twitter feed, he reminds people about masking and urges people to get the bivalent booster.
According to the Centers for Disease Control and Prevention, as of Dec. 8, only 13.5% of people aged 5 and older have gotten an updated booster, despite research that shows an increase in antibodies to BQ.1.1. Recent research has found that the bivalent booster increases antibodies to BQ.1.1 by up to 10-fold, Dr. Topol said.
Dr. Adalja is on advisory boards for Shionogi, GSK, and Pardes. Dr. Casadevall reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It was the last monoclonal antibody treatment standing. But less than 10 months after the U.S. Food and Drug Administration gave bebtelovimab its emergency use authorization (EUA) to fight COVID-19, it earlier this month de-authorized it, just as it had for other monoclonal antibody treatments, and for the same reason:
Bebtelovimab couldn’t neutralize the Omicron subvariants BQ.1 and BQ.1.1, the cause of nearly 60% of COVID cases nationally as of November 30.
Next on the chopping block, some predict, will be Evusheld, the combination of tixagevimab and cilgavimab given as a preventive monoclonal antibody to people who are immunocompromised and at high risk of contracting COVID and to those who can’t take the vaccine. In October, the FDA warned that Evusheld was not neutralizing circulating COVID variants.
As the options for treating and preventing COVID decline, will companies rally quickly to develop new ones, or cut their losses in developing treatments that may work for only a few months, given the speed of viral mutations?
But although monoclonal antibody treatments are off the table, at least for now, antiviral drugs – including Paxlovid – are still very much available, and some say underused.
Others suggest it’s time to resurrect interest in convalescent plasma, a treatment used early in the pandemic before drugs or vaccines were here and still authorized for use in those who are immunosuppressed or receiving immunosuppressive treatment.
And on the prevention front, staying up to date with booster vaccines, masking, and taking other precautions should be stressed more, others say, regardless of the number of treatment options, and especially now, as cases rise and people gather for the winter holidays.
‘A major setback’
The bebtelovimab de-authorization was “a major setback,” but an understandable one, said Arturo Casadevall, MD, PhD, professor and chair of molecular microbiology and immunology at the Johns Hopkins Bloomberg School of Public Health in Baltimore. “Monoclonal antibodies are great drugs. We are in an unfortunate situation in that they are vulnerable to changes in the virus” and can’t offer long-lasting protection.
Supplies of bebtelovimab will be retained, according to the FDA, in case variants susceptible to it return.
“What happened to bebtelovimab is no surprise,” agreed Amesh Adalja, MD, senior scholar at Johns Hopkins Center for Health Security. “This is what is going to happen when you are targeting a virus that mutates a lot.”
Monoclonal antibodies work by binding to the spike protein on the virus surface to prevent it from entering cells.
However, Dr. Adalja doesn’t view the disappearance of monoclonal antibody treatments as a major setback. Monoclonal antibodies were not the primary way COVID was treated, he said.
While he does believe it’s important that more monoclonal antibody treatments be developed, “I think it’s important to remember we still have Paxlovid while everyone is lamenting the loss of bebtelovimab.’’
Antivirals: What’s here, what’s coming
Compared with monoclonal antibodies, “Paxlovid remains a much easier drug to give,” Dr. Adalja told this news organization, because it is taken orally, not intravenously.
And it’s effective. In a recent study, researchers found that adults diagnosed with COVID given Paxlovid within 5 days of diagnosis had a 51% lower hospitalization rate within the next 30 days than those not given it. Another study shows it could also reduce a person’s risk of developing long COVID by 26%.
Paxlovid is underused, Dr. Adalja said, partly because the rebound potential got more press than the effectiveness. When a celebrity got rebound from Paxlovid, he said, that would make the news, overshadowing the research on its effectiveness.
Besides Paxlovid, the antivirals remdesivir (Veklury), given intravenously for 3 days, and molnupiravir (Lagevrio), taken orally, are also still available. Antivirals work by targeting specific parts of the virus to prevent it from multiplying.
In the lab, remdesivir, molnupiravir, and another antiviral, nirmatrelvir, all appear to be effective against both BQ.1.1 (a BA.5 subvariant) and XBB (a BA.2 subvariant), both rapidly rising in the United States, according to a report last week in the New England Journal of Medicine.
The researchers also tested several monoclonal antibodies and found they did not neutralize either of the subvariants BQ.1.1 and XBB.
A new oral antiviral, Xocova (ensitrelvir fumaric acid), from Japanese manufacturer Shionogi, received emergency approval in Japan on November 22. It’s taken once a day for 5 days. The goal is to expand access to it globally, according to the company.
Pardes Biosciences launched a phase 2 trial in September for its oral antiviral drug (PBI-0451), under study as a treatment and preventive for COVID. It expects data by the first quarter of 2023.
Pfizer, which makes Paxlovid, has partnered with Clear Creek Bio to develop another oral antiviral COVID drug.
Other approaches
A receptor protein known as ACE2 (angiotensin-converting enzyme 2) is the main “doorway” that SARS-CoV-2 uses to enter and infect cells.
Dana-Farber Cancer Institute scientists are developing a “decoy” drug that works by mimicking the ACE2 receptor on the surface of cells; when the virus tries to bind to it, the spike protein is destroyed. Human trials have not yet started.
Other researchers are investigating whether an already-approved drug used to treat a liver disease, Actigall (UDCA/ursodeoxycholic acid), could protect against COVID infection by reducing ACE2.
So far, the researchers have found in early research that people taking UDCA for liver conditions were less likely than those not taking the drug to have severe COVID. They also found that UDCA reduced SARS-CoV-2 infection in human lungs maintained outside the body.
Monoclonal antibody treatments?
After the FDA decision to withdraw the bebtelovimab EUA, which Eli Lilly said it agreed with, the company issued a statement, promising it wasn’t giving up on monoclonal antibody treatments.
“Lilly will continue to search and evaluate monoclonal antibodies to identify potential candidates for clinical development against new variants,” it read in part.
AstraZeneca, which makes Evusheld, is also continuing to work on monoclonal antibody development. According to a spokesperson, “We are also developing a new long-acting antibody combination – AZD5156 – which has been shown in the lab to neutralize emerging new variants and all known variants to date. We are working to accelerate the development of AZD5156 to make it available at the end of 2023.”
The AstraZeneca spokesperson said he could share no more information about what the combination would include.
A convalescent plasma comeback?
Although Paxlovid can help, there are many contraindications to it, such as drug-drug interactions, Dr. Casadevall told this news organization. And now that the monoclonal antibody treatments have been paused, convalescent plasma “is the only antibody-based therapy that is reliably available. Convalescent plasma includes thousands of different antibodies.”
With his colleagues, Dr. Casadevall evaluated plasma samples from 740 patients. Some had received booster vaccines and been infected with Omicron, others had received boosters and not been infected, and still others had not been vaccinated and became infected.
In a report (not yet peer-reviewed), they found the plasma from those who had been infected or boosted within the past 6 months neutralized the new Omicron variants BQ.1.1, XBB.1, and BF.7.
A push for boosters, masks
To get through the coming months, taking precautions like masking and distancing and staying up to date on booster vaccinations, especially for older adults, can make a difference, other experts say.
In a Twitter thread in early December, Peter Hotez, MD, PhD, professor of pediatrics and molecular virology and microbiology at Baylor College of Medicine, Houston, urged people to take COVID seriously as holiday parties and gatherings occur.
“The single most impactful thing you can do is get your bivalent booster,” he tweeted, as well as give your kids the booster, citing preliminary research that the bivalent mRNA booster broadens immunity against the Omicron subvariants.
For seniors, he said, ‘‘if you get breakthrough COVID, [it’s] really important to get Paxlovid.” Masks will help not only for COVID but also influenza, respiratory syncytial virus (RSV), and other conditions.
Mitigation measures have largely been abandoned, according to Eric Topol, MD, director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape. In an op-ed in the Los Angeles Times, and on his Twitter feed, he reminds people about masking and urges people to get the bivalent booster.
According to the Centers for Disease Control and Prevention, as of Dec. 8, only 13.5% of people aged 5 and older have gotten an updated booster, despite research that shows an increase in antibodies to BQ.1.1. Recent research has found that the bivalent booster increases antibodies to BQ.1.1 by up to 10-fold, Dr. Topol said.
Dr. Adalja is on advisory boards for Shionogi, GSK, and Pardes. Dr. Casadevall reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
It was the last monoclonal antibody treatment standing. But less than 10 months after the U.S. Food and Drug Administration gave bebtelovimab its emergency use authorization (EUA) to fight COVID-19, it earlier this month de-authorized it, just as it had for other monoclonal antibody treatments, and for the same reason:
Bebtelovimab couldn’t neutralize the Omicron subvariants BQ.1 and BQ.1.1, the cause of nearly 60% of COVID cases nationally as of November 30.
Next on the chopping block, some predict, will be Evusheld, the combination of tixagevimab and cilgavimab given as a preventive monoclonal antibody to people who are immunocompromised and at high risk of contracting COVID and to those who can’t take the vaccine. In October, the FDA warned that Evusheld was not neutralizing circulating COVID variants.
As the options for treating and preventing COVID decline, will companies rally quickly to develop new ones, or cut their losses in developing treatments that may work for only a few months, given the speed of viral mutations?
But although monoclonal antibody treatments are off the table, at least for now, antiviral drugs – including Paxlovid – are still very much available, and some say underused.
Others suggest it’s time to resurrect interest in convalescent plasma, a treatment used early in the pandemic before drugs or vaccines were here and still authorized for use in those who are immunosuppressed or receiving immunosuppressive treatment.
And on the prevention front, staying up to date with booster vaccines, masking, and taking other precautions should be stressed more, others say, regardless of the number of treatment options, and especially now, as cases rise and people gather for the winter holidays.
‘A major setback’
The bebtelovimab de-authorization was “a major setback,” but an understandable one, said Arturo Casadevall, MD, PhD, professor and chair of molecular microbiology and immunology at the Johns Hopkins Bloomberg School of Public Health in Baltimore. “Monoclonal antibodies are great drugs. We are in an unfortunate situation in that they are vulnerable to changes in the virus” and can’t offer long-lasting protection.
Supplies of bebtelovimab will be retained, according to the FDA, in case variants susceptible to it return.
“What happened to bebtelovimab is no surprise,” agreed Amesh Adalja, MD, senior scholar at Johns Hopkins Center for Health Security. “This is what is going to happen when you are targeting a virus that mutates a lot.”
Monoclonal antibodies work by binding to the spike protein on the virus surface to prevent it from entering cells.
However, Dr. Adalja doesn’t view the disappearance of monoclonal antibody treatments as a major setback. Monoclonal antibodies were not the primary way COVID was treated, he said.
While he does believe it’s important that more monoclonal antibody treatments be developed, “I think it’s important to remember we still have Paxlovid while everyone is lamenting the loss of bebtelovimab.’’
Antivirals: What’s here, what’s coming
Compared with monoclonal antibodies, “Paxlovid remains a much easier drug to give,” Dr. Adalja told this news organization, because it is taken orally, not intravenously.
And it’s effective. In a recent study, researchers found that adults diagnosed with COVID given Paxlovid within 5 days of diagnosis had a 51% lower hospitalization rate within the next 30 days than those not given it. Another study shows it could also reduce a person’s risk of developing long COVID by 26%.
Paxlovid is underused, Dr. Adalja said, partly because the rebound potential got more press than the effectiveness. When a celebrity got rebound from Paxlovid, he said, that would make the news, overshadowing the research on its effectiveness.
Besides Paxlovid, the antivirals remdesivir (Veklury), given intravenously for 3 days, and molnupiravir (Lagevrio), taken orally, are also still available. Antivirals work by targeting specific parts of the virus to prevent it from multiplying.
In the lab, remdesivir, molnupiravir, and another antiviral, nirmatrelvir, all appear to be effective against both BQ.1.1 (a BA.5 subvariant) and XBB (a BA.2 subvariant), both rapidly rising in the United States, according to a report last week in the New England Journal of Medicine.
The researchers also tested several monoclonal antibodies and found they did not neutralize either of the subvariants BQ.1.1 and XBB.
A new oral antiviral, Xocova (ensitrelvir fumaric acid), from Japanese manufacturer Shionogi, received emergency approval in Japan on November 22. It’s taken once a day for 5 days. The goal is to expand access to it globally, according to the company.
Pardes Biosciences launched a phase 2 trial in September for its oral antiviral drug (PBI-0451), under study as a treatment and preventive for COVID. It expects data by the first quarter of 2023.
Pfizer, which makes Paxlovid, has partnered with Clear Creek Bio to develop another oral antiviral COVID drug.
Other approaches
A receptor protein known as ACE2 (angiotensin-converting enzyme 2) is the main “doorway” that SARS-CoV-2 uses to enter and infect cells.
Dana-Farber Cancer Institute scientists are developing a “decoy” drug that works by mimicking the ACE2 receptor on the surface of cells; when the virus tries to bind to it, the spike protein is destroyed. Human trials have not yet started.
Other researchers are investigating whether an already-approved drug used to treat a liver disease, Actigall (UDCA/ursodeoxycholic acid), could protect against COVID infection by reducing ACE2.
So far, the researchers have found in early research that people taking UDCA for liver conditions were less likely than those not taking the drug to have severe COVID. They also found that UDCA reduced SARS-CoV-2 infection in human lungs maintained outside the body.
Monoclonal antibody treatments?
After the FDA decision to withdraw the bebtelovimab EUA, which Eli Lilly said it agreed with, the company issued a statement, promising it wasn’t giving up on monoclonal antibody treatments.
“Lilly will continue to search and evaluate monoclonal antibodies to identify potential candidates for clinical development against new variants,” it read in part.
AstraZeneca, which makes Evusheld, is also continuing to work on monoclonal antibody development. According to a spokesperson, “We are also developing a new long-acting antibody combination – AZD5156 – which has been shown in the lab to neutralize emerging new variants and all known variants to date. We are working to accelerate the development of AZD5156 to make it available at the end of 2023.”
The AstraZeneca spokesperson said he could share no more information about what the combination would include.
A convalescent plasma comeback?
Although Paxlovid can help, there are many contraindications to it, such as drug-drug interactions, Dr. Casadevall told this news organization. And now that the monoclonal antibody treatments have been paused, convalescent plasma “is the only antibody-based therapy that is reliably available. Convalescent plasma includes thousands of different antibodies.”
With his colleagues, Dr. Casadevall evaluated plasma samples from 740 patients. Some had received booster vaccines and been infected with Omicron, others had received boosters and not been infected, and still others had not been vaccinated and became infected.
In a report (not yet peer-reviewed), they found the plasma from those who had been infected or boosted within the past 6 months neutralized the new Omicron variants BQ.1.1, XBB.1, and BF.7.
A push for boosters, masks
To get through the coming months, taking precautions like masking and distancing and staying up to date on booster vaccinations, especially for older adults, can make a difference, other experts say.
In a Twitter thread in early December, Peter Hotez, MD, PhD, professor of pediatrics and molecular virology and microbiology at Baylor College of Medicine, Houston, urged people to take COVID seriously as holiday parties and gatherings occur.
“The single most impactful thing you can do is get your bivalent booster,” he tweeted, as well as give your kids the booster, citing preliminary research that the bivalent mRNA booster broadens immunity against the Omicron subvariants.
For seniors, he said, ‘‘if you get breakthrough COVID, [it’s] really important to get Paxlovid.” Masks will help not only for COVID but also influenza, respiratory syncytial virus (RSV), and other conditions.
Mitigation measures have largely been abandoned, according to Eric Topol, MD, director of the Scripps Research Translational Institute, La Jolla, Calif., and editor-in-chief of Medscape. In an op-ed in the Los Angeles Times, and on his Twitter feed, he reminds people about masking and urges people to get the bivalent booster.
According to the Centers for Disease Control and Prevention, as of Dec. 8, only 13.5% of people aged 5 and older have gotten an updated booster, despite research that shows an increase in antibodies to BQ.1.1. Recent research has found that the bivalent booster increases antibodies to BQ.1.1 by up to 10-fold, Dr. Topol said.
Dr. Adalja is on advisory boards for Shionogi, GSK, and Pardes. Dr. Casadevall reports no relevant financial relationships.
A version of this article first appeared on Medscape.com.
How a cheap liver drug may be the key to preventing COVID
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
As soon as the pandemic started, the search was on for a medication that could stave off infection, or at least the worst consequences of infection.
One that would be cheap to make, safe, easy to distribute, and, ideally, was already available. The search had a quest-like quality, like something from a fairy tale. Society, poisoned by COVID, would find the antidote out there, somewhere, if we looked hard enough.
You know the story. There were some pretty dramatic failures: hydroxychloroquine, ivermectin. There were some successes, like dexamethasone.
I’m not here today to tell you that the antidote has been found – no, it takes large randomized trials to figure that out. But
How do you make a case that an existing drug – UDCA, in this case – might be useful to prevent or treat COVID? In contrast to prior basic-science studies, like the original ivermectin study, which essentially took a bunch of cells and virus in a tube filled with varying concentrations of the antiparasitic agent, the authors of this paper appearing in Nature give us multiple, complementary lines of evidence. Let me walk you through it.
All good science starts with a biologically plausible hypothesis. In this case, the authors recognized that SARS-CoV-2, in all its variants, requires the presence of the ACE2 receptor on the surface of cells to bind.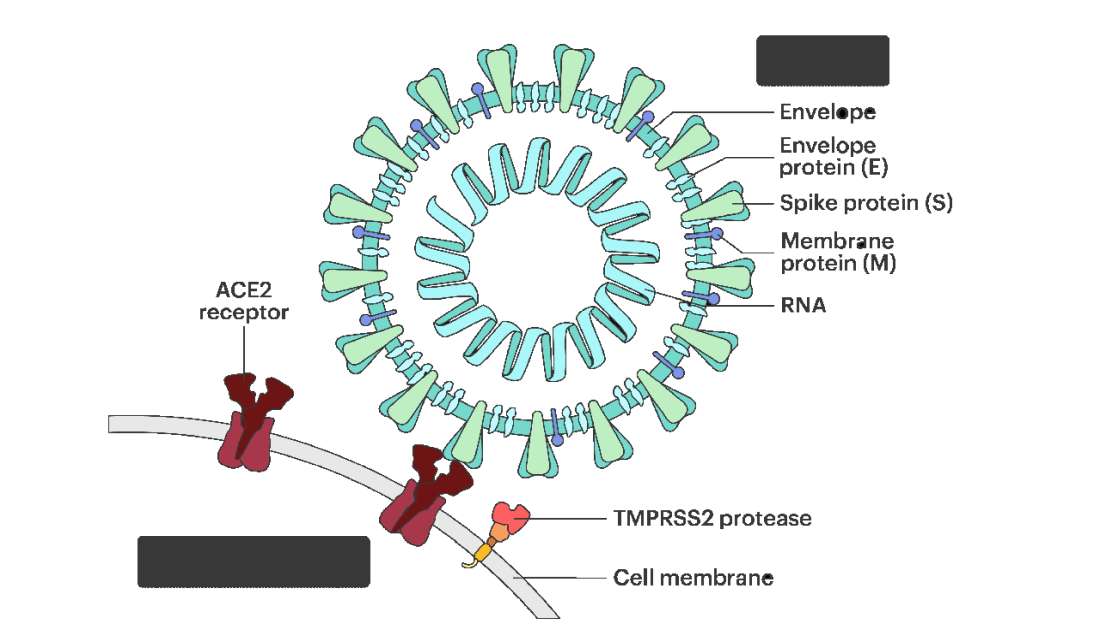
That is the doorway to infection. Vaccines and antibodies block the key to this door, the spike protein and its receptor binding domain. But what if you could get rid of the doors altogether?
The authors first showed that ACE2 expression is controlled by a certain transcription factor known as the farnesoid X receptor, or FXR. Reducing the binding of FXR should therefore reduce ACE2 expression.
As luck would have it, UDCA – Actigall – reduces the levels of FXR and thus the expression of ACE2 in cells.
Okay. So we have a drug that can reduce ACE2, and we know that ACE2 is necessary for the virus to infect cells. Would UDCA prevent viral infection?
They started with test tubes, showing that cells were less likely to be infected by SARS-CoV-2 in the presence of UDCA at concentrations similar to what humans achieve in their blood after standard dosing. The red staining here is spike protein; you can see that it is markedly lower in the cells exposed to UDCA.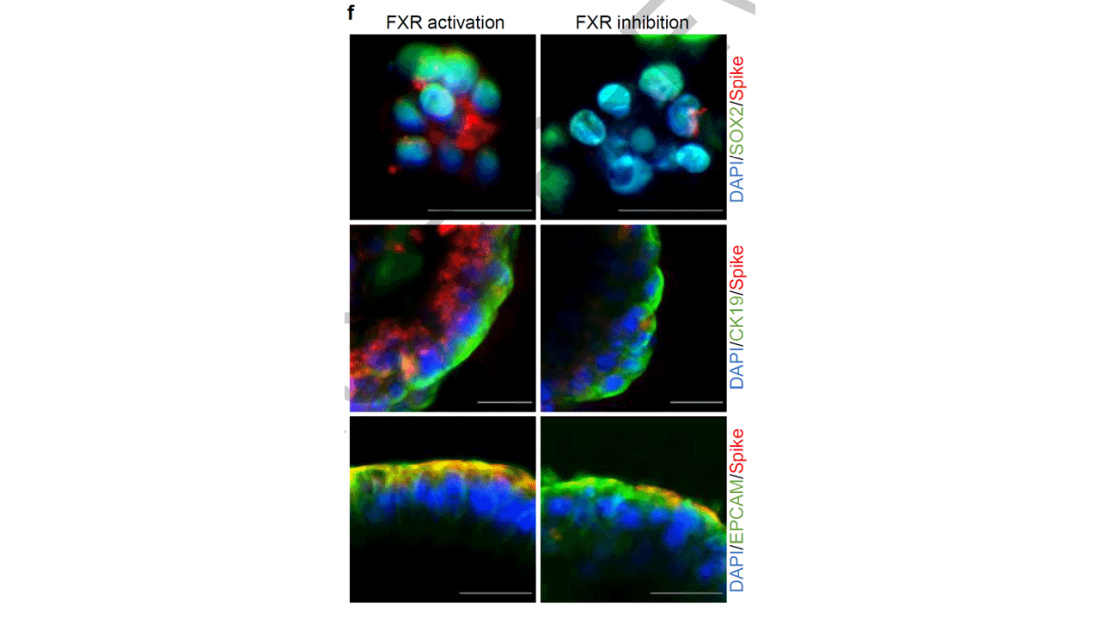
So far, so good. But test tubes aren’t people. So they moved up to mice and Syrian golden hamsters. These cute fellows are quite susceptible to human COVID and have been a model organism in countless studies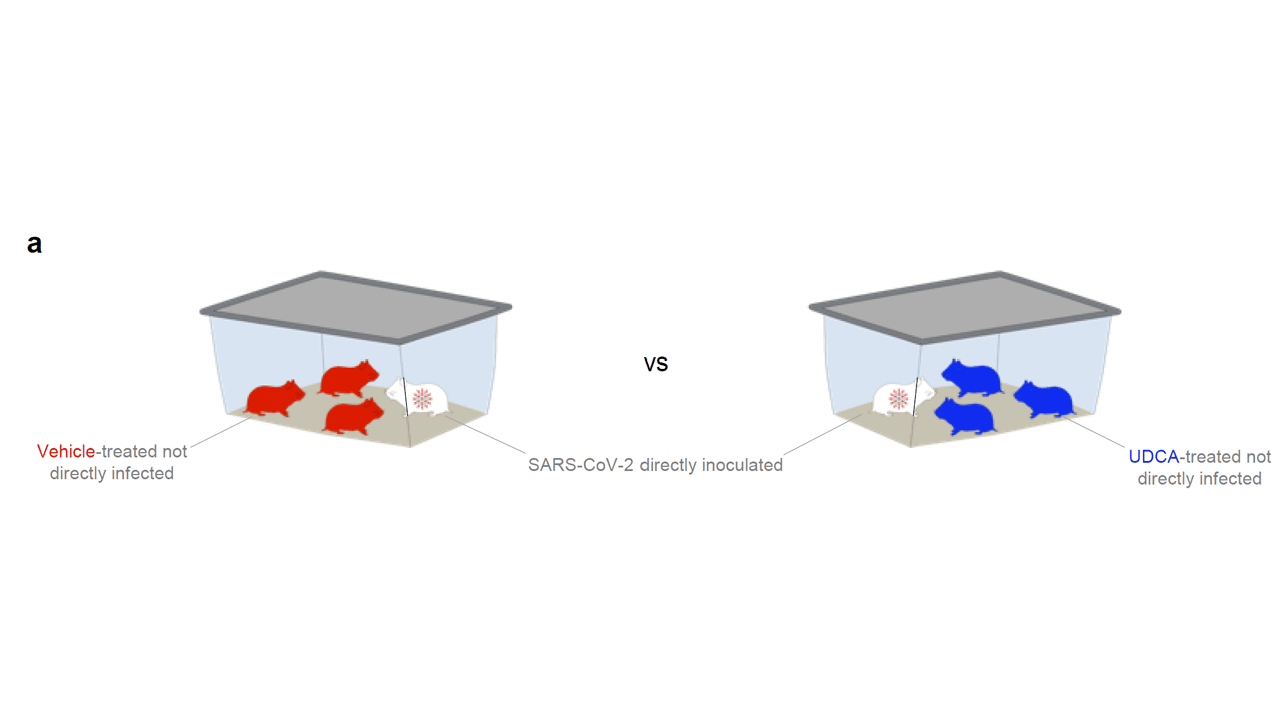
Mice and hamsters treated with UDCA in the presence of littermates with COVID infections were less likely to become infected themselves compared with mice not so treated. They also showed that mice and hamsters treated with UDCA had lower levels of ACE2 in their nasal passages.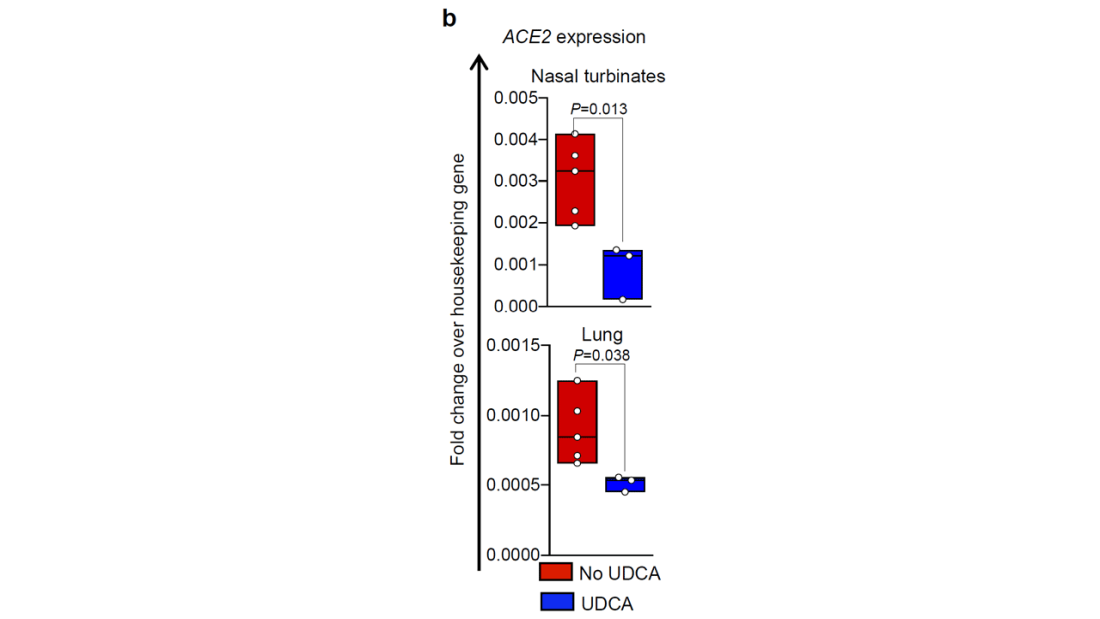
Of course, mice aren’t humans either. So the researchers didn’t stop there.
To determine the effects of UDCA on human tissue, they utilized perfused human lungs that had been declined for transplantation. The lungs were perfused with a special fluid to keep them viable, and were mechanically ventilated. One lung was exposed to UDCA and the other served as a control. The authors were able to show that ACE2 levels went down in the exposed lung. And, importantly, when samples of tissue from both lungs were exposed to SARS-CoV-2, the lung tissue exposed to UDCA had lower levels of viral infection.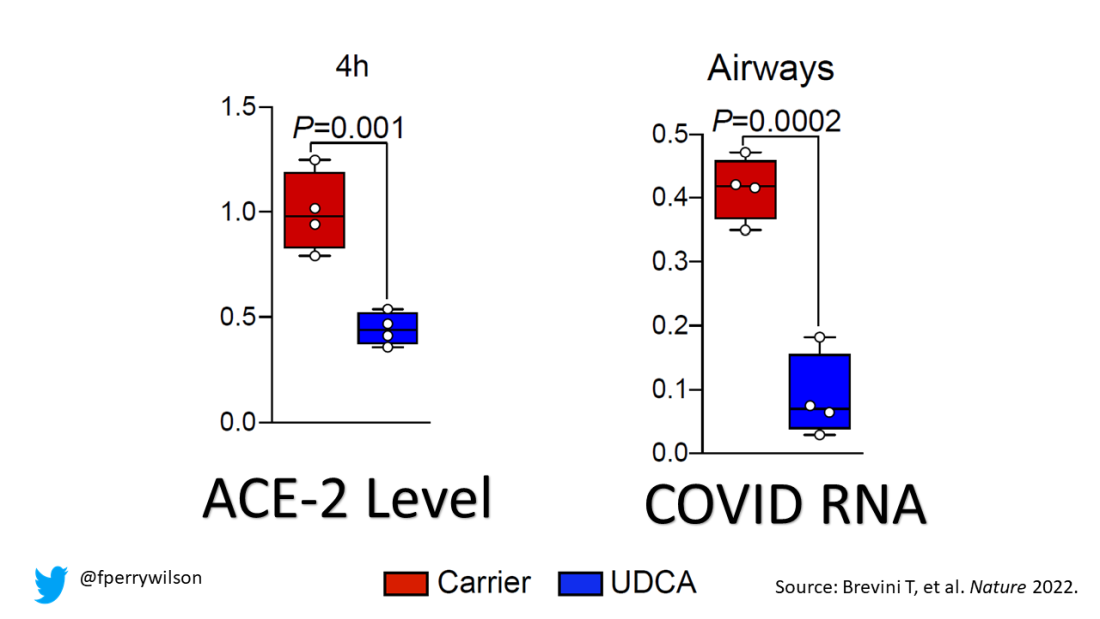
They didn’t stop there.
Eight human volunteers were recruited to take UDCA for 5 days. ACE2 levels in the nasal passages went down over the course of treatment. They confirmed those results from a proteomics dataset with several hundred people who had received UDCA for clinical reasons. Treated individuals had lower ACE2 levels.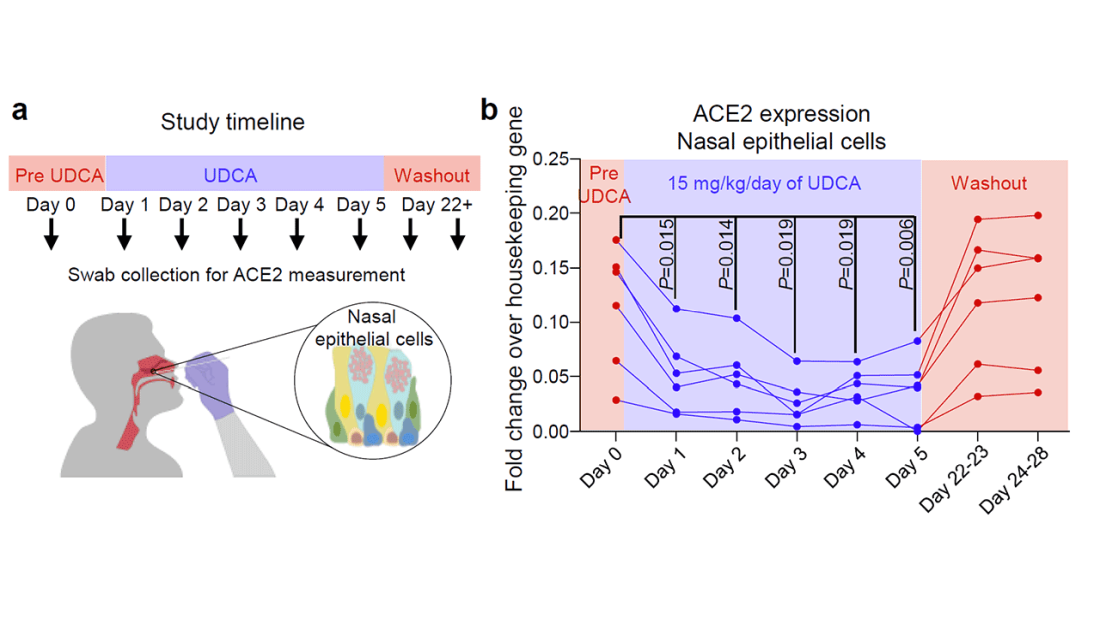
Finally, they looked at the epidemiologic effect. They examined a dataset that contained information on over 1,000 patients with liver disease who had contracted COVID-19, 31 of whom had been receiving UDCA. Even after adjustment for baseline differences, those receiving UDCA were less likely to be hospitalized, require an ICU, or die.
Okay, we’ll stop there. Reading this study, all I could think was, Yes! This is how you generate evidence that you have a drug that might work – step by careful step.
But let’s be careful as well. Does this study show that taking Actigall will prevent COVID? Of course not. It doesn’t show that it will treat COVID either. But I bring it up because the rigor of this study stands in contrast to those that generated huge enthusiasm earlier in the pandemic only to let us down in randomized trials. If there has been a drug out there this whole time which will prevent or treat COVID, this is how we’ll find it. The next step? Test it in a randomized trial.
For Medscape, I’m Perry Wilson.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He disclosed no relevant financial relationships.
A version of this video transcript first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
As soon as the pandemic started, the search was on for a medication that could stave off infection, or at least the worst consequences of infection.
One that would be cheap to make, safe, easy to distribute, and, ideally, was already available. The search had a quest-like quality, like something from a fairy tale. Society, poisoned by COVID, would find the antidote out there, somewhere, if we looked hard enough.
You know the story. There were some pretty dramatic failures: hydroxychloroquine, ivermectin. There were some successes, like dexamethasone.
I’m not here today to tell you that the antidote has been found – no, it takes large randomized trials to figure that out. But
How do you make a case that an existing drug – UDCA, in this case – might be useful to prevent or treat COVID? In contrast to prior basic-science studies, like the original ivermectin study, which essentially took a bunch of cells and virus in a tube filled with varying concentrations of the antiparasitic agent, the authors of this paper appearing in Nature give us multiple, complementary lines of evidence. Let me walk you through it.
All good science starts with a biologically plausible hypothesis. In this case, the authors recognized that SARS-CoV-2, in all its variants, requires the presence of the ACE2 receptor on the surface of cells to bind.
That is the doorway to infection. Vaccines and antibodies block the key to this door, the spike protein and its receptor binding domain. But what if you could get rid of the doors altogether?
The authors first showed that ACE2 expression is controlled by a certain transcription factor known as the farnesoid X receptor, or FXR. Reducing the binding of FXR should therefore reduce ACE2 expression.
As luck would have it, UDCA – Actigall – reduces the levels of FXR and thus the expression of ACE2 in cells.
Okay. So we have a drug that can reduce ACE2, and we know that ACE2 is necessary for the virus to infect cells. Would UDCA prevent viral infection?
They started with test tubes, showing that cells were less likely to be infected by SARS-CoV-2 in the presence of UDCA at concentrations similar to what humans achieve in their blood after standard dosing. The red staining here is spike protein; you can see that it is markedly lower in the cells exposed to UDCA.
So far, so good. But test tubes aren’t people. So they moved up to mice and Syrian golden hamsters. These cute fellows are quite susceptible to human COVID and have been a model organism in countless studies
Mice and hamsters treated with UDCA in the presence of littermates with COVID infections were less likely to become infected themselves compared with mice not so treated. They also showed that mice and hamsters treated with UDCA had lower levels of ACE2 in their nasal passages.
Of course, mice aren’t humans either. So the researchers didn’t stop there.
To determine the effects of UDCA on human tissue, they utilized perfused human lungs that had been declined for transplantation. The lungs were perfused with a special fluid to keep them viable, and were mechanically ventilated. One lung was exposed to UDCA and the other served as a control. The authors were able to show that ACE2 levels went down in the exposed lung. And, importantly, when samples of tissue from both lungs were exposed to SARS-CoV-2, the lung tissue exposed to UDCA had lower levels of viral infection.
They didn’t stop there.
Eight human volunteers were recruited to take UDCA for 5 days. ACE2 levels in the nasal passages went down over the course of treatment. They confirmed those results from a proteomics dataset with several hundred people who had received UDCA for clinical reasons. Treated individuals had lower ACE2 levels.
Finally, they looked at the epidemiologic effect. They examined a dataset that contained information on over 1,000 patients with liver disease who had contracted COVID-19, 31 of whom had been receiving UDCA. Even after adjustment for baseline differences, those receiving UDCA were less likely to be hospitalized, require an ICU, or die.
Okay, we’ll stop there. Reading this study, all I could think was, Yes! This is how you generate evidence that you have a drug that might work – step by careful step.
But let’s be careful as well. Does this study show that taking Actigall will prevent COVID? Of course not. It doesn’t show that it will treat COVID either. But I bring it up because the rigor of this study stands in contrast to those that generated huge enthusiasm earlier in the pandemic only to let us down in randomized trials. If there has been a drug out there this whole time which will prevent or treat COVID, this is how we’ll find it. The next step? Test it in a randomized trial.
For Medscape, I’m Perry Wilson.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He disclosed no relevant financial relationships.
A version of this video transcript first appeared on Medscape.com.
Welcome to Impact Factor, your weekly dose of commentary on a new medical study. I’m Dr F. Perry Wilson of the Yale School of Medicine.
As soon as the pandemic started, the search was on for a medication that could stave off infection, or at least the worst consequences of infection.
One that would be cheap to make, safe, easy to distribute, and, ideally, was already available. The search had a quest-like quality, like something from a fairy tale. Society, poisoned by COVID, would find the antidote out there, somewhere, if we looked hard enough.
You know the story. There were some pretty dramatic failures: hydroxychloroquine, ivermectin. There were some successes, like dexamethasone.
I’m not here today to tell you that the antidote has been found – no, it takes large randomized trials to figure that out. But
How do you make a case that an existing drug – UDCA, in this case – might be useful to prevent or treat COVID? In contrast to prior basic-science studies, like the original ivermectin study, which essentially took a bunch of cells and virus in a tube filled with varying concentrations of the antiparasitic agent, the authors of this paper appearing in Nature give us multiple, complementary lines of evidence. Let me walk you through it.
All good science starts with a biologically plausible hypothesis. In this case, the authors recognized that SARS-CoV-2, in all its variants, requires the presence of the ACE2 receptor on the surface of cells to bind.
That is the doorway to infection. Vaccines and antibodies block the key to this door, the spike protein and its receptor binding domain. But what if you could get rid of the doors altogether?
The authors first showed that ACE2 expression is controlled by a certain transcription factor known as the farnesoid X receptor, or FXR. Reducing the binding of FXR should therefore reduce ACE2 expression.
As luck would have it, UDCA – Actigall – reduces the levels of FXR and thus the expression of ACE2 in cells.
Okay. So we have a drug that can reduce ACE2, and we know that ACE2 is necessary for the virus to infect cells. Would UDCA prevent viral infection?
They started with test tubes, showing that cells were less likely to be infected by SARS-CoV-2 in the presence of UDCA at concentrations similar to what humans achieve in their blood after standard dosing. The red staining here is spike protein; you can see that it is markedly lower in the cells exposed to UDCA.
So far, so good. But test tubes aren’t people. So they moved up to mice and Syrian golden hamsters. These cute fellows are quite susceptible to human COVID and have been a model organism in countless studies
Mice and hamsters treated with UDCA in the presence of littermates with COVID infections were less likely to become infected themselves compared with mice not so treated. They also showed that mice and hamsters treated with UDCA had lower levels of ACE2 in their nasal passages.
Of course, mice aren’t humans either. So the researchers didn’t stop there.
To determine the effects of UDCA on human tissue, they utilized perfused human lungs that had been declined for transplantation. The lungs were perfused with a special fluid to keep them viable, and were mechanically ventilated. One lung was exposed to UDCA and the other served as a control. The authors were able to show that ACE2 levels went down in the exposed lung. And, importantly, when samples of tissue from both lungs were exposed to SARS-CoV-2, the lung tissue exposed to UDCA had lower levels of viral infection.
They didn’t stop there.
Eight human volunteers were recruited to take UDCA for 5 days. ACE2 levels in the nasal passages went down over the course of treatment. They confirmed those results from a proteomics dataset with several hundred people who had received UDCA for clinical reasons. Treated individuals had lower ACE2 levels.
Finally, they looked at the epidemiologic effect. They examined a dataset that contained information on over 1,000 patients with liver disease who had contracted COVID-19, 31 of whom had been receiving UDCA. Even after adjustment for baseline differences, those receiving UDCA were less likely to be hospitalized, require an ICU, or die.
Okay, we’ll stop there. Reading this study, all I could think was, Yes! This is how you generate evidence that you have a drug that might work – step by careful step.
But let’s be careful as well. Does this study show that taking Actigall will prevent COVID? Of course not. It doesn’t show that it will treat COVID either. But I bring it up because the rigor of this study stands in contrast to those that generated huge enthusiasm earlier in the pandemic only to let us down in randomized trials. If there has been a drug out there this whole time which will prevent or treat COVID, this is how we’ll find it. The next step? Test it in a randomized trial.
For Medscape, I’m Perry Wilson.
F. Perry Wilson, MD, MSCE, is an associate professor of medicine and director of Yale’s Clinical and Translational Research Accelerator. He disclosed no relevant financial relationships.
A version of this video transcript first appeared on Medscape.com.
Know the right resuscitation for right-sided heart failure
Amado Alejandro Baez, MD, said in a presentation at the 2022 scientific assembly of the American College of Emergency Physicians.
The patient arrived on day 20 after a radical cystoprostatectomy. He had driven 4 hours from another city for a urology follow-up visit. On arrival, he developed respiratory distress symptoms and presented to the emergency department, said Dr. Baez, professor of emergency medicine and epidemiology at the Medical College of Georgia/Augusta University and triple-board certified in EMS, emergency medicine, and critical care.
The patient developed a massive pulmonary embolism with acute cor pulmonale (right-sided heart failure). An electrocardiogram showed an S1Q3T3, demonstrating the distinctive nature of right ventricular failure, said Dr. Baez.
Research has demonstrated the differences in physiology between the right and left ventricles, he said.
Dr. Baez highlighted some of the features of right ventricle (RV) failure and how to manage it. Notably, the RV is thinner and less resilient. “RV failure patients may fall off the Starling curve,” in contrast to patients with isolated left ventricle (LV) failure.
RV pressure overload is associated with a range of conditions, such as pericardial disease, pulmonary embolism, acute respiratory distress syndrome, and pulmonary arterial hypertension. When combined with RV overload, patients may develop intracardiac shunting or coronary heart disease, Dr. Baez said. Decreased contractility associated with RV failure can result from sepsis, right ventricular myocardial infarction, myocarditis, and arrhythmia.
Dr. Baez cited the 2018 scientific statement from the American Heart Association on the evaluation and management of right-sided heart failure. The authors of the statement noted that the complicated geometry of the right heart makes functional assessment a challenge. They wrote that various hemodynamic and biochemical markers can help guide clinical assessment and therapeutic decision-making.
Increased RV afterload drives multiple factors that can ultimately lead to cardiogenic shock and death, said Dr. Baez. These factors include decreased RV oxygen delivery, decreased RV coronary perfusion, decreased systemic blood pressure, and low carbon monoxide levels. RV afterload also leads to decreased RV contractility, an increase in RV oxygen demand, and tension in the RV wall, and it may contribute to tricuspid valve insufficiency, neurohormonal activation, and RV ischemia.
Treatment strategies involve improving symptoms and stopping disease progression, said Baez. In its scientific statement, the AHA recommends steps for assessing RV and LV function so as to identify RV failure as soon as possible, he said. After excluding pericardial disease, the AHA advises diagnosis and treatment of etiology-specific causes, such as right ventricular MI, pulmonary embolism, and sepsis. For arrhythmias, it recommends maintaining sinus rhythm when possible and considering a pacemaker to maintain atrioventricular synchrony and to avoid excessive bradycardia.
In its statement, the AHA also recommends optimizing preload with right arterial pressure/central venous pressure of 8-12 mm Hg, said Dr. Baez. Preload optimization combined with afterload reduction and improved contractility are hallmarks of care for patients with RV failure.
Avoiding systemic hypotension can prevent sequelae, such as myocardial ischemia and further hypotension, he said.
Optimization of fluid status is another key to managing RV failure, said Dr. Baez. Right heart coronary perfusion pressure can be protected by maintaining mean arterial pressure, and consideration should be given to reducing the RV afterload. Other strategies include inotropic medications and rhythm stabilization.
In general, for RV failure patients, “correct hypoxia, hypercarbia, and acidosis and avoid intubation when possible,” he said. Extracorporeal membrane oxygenation (ECMO) may be an option, depending on how many mechanical ventilator settings need to be adjusted.
In a study by Dr. Baez and colleagues published in Critical Care Medicine, the authors presented a Bayesian probability model for plasma lactate and severity of illness in cases of acute pulmonary embolism. “This Bayesian model demonstrated that the combination of shock index and lactate yield superior diagnostic gains than those compare to the sPESI and lactate,” Dr. Baez said.
The care model needs to be specific to the etiology, he added. Volume management in congested pulmonary hypertension involves a “squeeze and diurese” strategy.
According to the Internet Book of Critical Care, for patients with mean arterial pressure (MAP) of 60 mm Hg, central venous pressure (CVP) of 25 mm Hg, renal perfusion pressure of 25 mm Hg, and no urine output, a vasopressor should be added to treatment, Dr. Baez said. In cases in which the MAP 75 mm Hg, the CVP is 25 mm Hg, the renal perfusion pressure is 50 mm Hg, and the patient has good urine output, vasopressors should be continued and fluid should be removed through use of a diuretic. For patients with a MAP of 75 mm Hg, a CVP of 12 mm Hg, and renal perfusion pressure of 63 mm Hg who have good urine output, the diuretic and the vasopressor should be discontinued.
Dr. Baez also reviewed several clinical studies of the utility of acute mechanical circulatory support systems for RV failure.
In two small studies involving a heart pump and a right ventricular assistive device, the 30-day survival rate was approximately 72%-73%. A study of 179 patients involving ECMO showed an in-hospital mortality rate of 38.6%, he said.
Overall, “prompt diagnosis, hemodynamic support, and initiation of specific treatment” are the foundations of managing RV failure, he concluded.
Dr. Baez disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Amado Alejandro Baez, MD, said in a presentation at the 2022 scientific assembly of the American College of Emergency Physicians.
The patient arrived on day 20 after a radical cystoprostatectomy. He had driven 4 hours from another city for a urology follow-up visit. On arrival, he developed respiratory distress symptoms and presented to the emergency department, said Dr. Baez, professor of emergency medicine and epidemiology at the Medical College of Georgia/Augusta University and triple-board certified in EMS, emergency medicine, and critical care.
The patient developed a massive pulmonary embolism with acute cor pulmonale (right-sided heart failure). An electrocardiogram showed an S1Q3T3, demonstrating the distinctive nature of right ventricular failure, said Dr. Baez.
Research has demonstrated the differences in physiology between the right and left ventricles, he said.
Dr. Baez highlighted some of the features of right ventricle (RV) failure and how to manage it. Notably, the RV is thinner and less resilient. “RV failure patients may fall off the Starling curve,” in contrast to patients with isolated left ventricle (LV) failure.
RV pressure overload is associated with a range of conditions, such as pericardial disease, pulmonary embolism, acute respiratory distress syndrome, and pulmonary arterial hypertension. When combined with RV overload, patients may develop intracardiac shunting or coronary heart disease, Dr. Baez said. Decreased contractility associated with RV failure can result from sepsis, right ventricular myocardial infarction, myocarditis, and arrhythmia.
Dr. Baez cited the 2018 scientific statement from the American Heart Association on the evaluation and management of right-sided heart failure. The authors of the statement noted that the complicated geometry of the right heart makes functional assessment a challenge. They wrote that various hemodynamic and biochemical markers can help guide clinical assessment and therapeutic decision-making.
Increased RV afterload drives multiple factors that can ultimately lead to cardiogenic shock and death, said Dr. Baez. These factors include decreased RV oxygen delivery, decreased RV coronary perfusion, decreased systemic blood pressure, and low carbon monoxide levels. RV afterload also leads to decreased RV contractility, an increase in RV oxygen demand, and tension in the RV wall, and it may contribute to tricuspid valve insufficiency, neurohormonal activation, and RV ischemia.
Treatment strategies involve improving symptoms and stopping disease progression, said Baez. In its scientific statement, the AHA recommends steps for assessing RV and LV function so as to identify RV failure as soon as possible, he said. After excluding pericardial disease, the AHA advises diagnosis and treatment of etiology-specific causes, such as right ventricular MI, pulmonary embolism, and sepsis. For arrhythmias, it recommends maintaining sinus rhythm when possible and considering a pacemaker to maintain atrioventricular synchrony and to avoid excessive bradycardia.
In its statement, the AHA also recommends optimizing preload with right arterial pressure/central venous pressure of 8-12 mm Hg, said Dr. Baez. Preload optimization combined with afterload reduction and improved contractility are hallmarks of care for patients with RV failure.
Avoiding systemic hypotension can prevent sequelae, such as myocardial ischemia and further hypotension, he said.
Optimization of fluid status is another key to managing RV failure, said Dr. Baez. Right heart coronary perfusion pressure can be protected by maintaining mean arterial pressure, and consideration should be given to reducing the RV afterload. Other strategies include inotropic medications and rhythm stabilization.
In general, for RV failure patients, “correct hypoxia, hypercarbia, and acidosis and avoid intubation when possible,” he said. Extracorporeal membrane oxygenation (ECMO) may be an option, depending on how many mechanical ventilator settings need to be adjusted.
In a study by Dr. Baez and colleagues published in Critical Care Medicine, the authors presented a Bayesian probability model for plasma lactate and severity of illness in cases of acute pulmonary embolism. “This Bayesian model demonstrated that the combination of shock index and lactate yield superior diagnostic gains than those compare to the sPESI and lactate,” Dr. Baez said.
The care model needs to be specific to the etiology, he added. Volume management in congested pulmonary hypertension involves a “squeeze and diurese” strategy.
According to the Internet Book of Critical Care, for patients with mean arterial pressure (MAP) of 60 mm Hg, central venous pressure (CVP) of 25 mm Hg, renal perfusion pressure of 25 mm Hg, and no urine output, a vasopressor should be added to treatment, Dr. Baez said. In cases in which the MAP 75 mm Hg, the CVP is 25 mm Hg, the renal perfusion pressure is 50 mm Hg, and the patient has good urine output, vasopressors should be continued and fluid should be removed through use of a diuretic. For patients with a MAP of 75 mm Hg, a CVP of 12 mm Hg, and renal perfusion pressure of 63 mm Hg who have good urine output, the diuretic and the vasopressor should be discontinued.
Dr. Baez also reviewed several clinical studies of the utility of acute mechanical circulatory support systems for RV failure.
In two small studies involving a heart pump and a right ventricular assistive device, the 30-day survival rate was approximately 72%-73%. A study of 179 patients involving ECMO showed an in-hospital mortality rate of 38.6%, he said.
Overall, “prompt diagnosis, hemodynamic support, and initiation of specific treatment” are the foundations of managing RV failure, he concluded.
Dr. Baez disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
Amado Alejandro Baez, MD, said in a presentation at the 2022 scientific assembly of the American College of Emergency Physicians.
The patient arrived on day 20 after a radical cystoprostatectomy. He had driven 4 hours from another city for a urology follow-up visit. On arrival, he developed respiratory distress symptoms and presented to the emergency department, said Dr. Baez, professor of emergency medicine and epidemiology at the Medical College of Georgia/Augusta University and triple-board certified in EMS, emergency medicine, and critical care.
The patient developed a massive pulmonary embolism with acute cor pulmonale (right-sided heart failure). An electrocardiogram showed an S1Q3T3, demonstrating the distinctive nature of right ventricular failure, said Dr. Baez.
Research has demonstrated the differences in physiology between the right and left ventricles, he said.
Dr. Baez highlighted some of the features of right ventricle (RV) failure and how to manage it. Notably, the RV is thinner and less resilient. “RV failure patients may fall off the Starling curve,” in contrast to patients with isolated left ventricle (LV) failure.
RV pressure overload is associated with a range of conditions, such as pericardial disease, pulmonary embolism, acute respiratory distress syndrome, and pulmonary arterial hypertension. When combined with RV overload, patients may develop intracardiac shunting or coronary heart disease, Dr. Baez said. Decreased contractility associated with RV failure can result from sepsis, right ventricular myocardial infarction, myocarditis, and arrhythmia.
Dr. Baez cited the 2018 scientific statement from the American Heart Association on the evaluation and management of right-sided heart failure. The authors of the statement noted that the complicated geometry of the right heart makes functional assessment a challenge. They wrote that various hemodynamic and biochemical markers can help guide clinical assessment and therapeutic decision-making.
Increased RV afterload drives multiple factors that can ultimately lead to cardiogenic shock and death, said Dr. Baez. These factors include decreased RV oxygen delivery, decreased RV coronary perfusion, decreased systemic blood pressure, and low carbon monoxide levels. RV afterload also leads to decreased RV contractility, an increase in RV oxygen demand, and tension in the RV wall, and it may contribute to tricuspid valve insufficiency, neurohormonal activation, and RV ischemia.
Treatment strategies involve improving symptoms and stopping disease progression, said Baez. In its scientific statement, the AHA recommends steps for assessing RV and LV function so as to identify RV failure as soon as possible, he said. After excluding pericardial disease, the AHA advises diagnosis and treatment of etiology-specific causes, such as right ventricular MI, pulmonary embolism, and sepsis. For arrhythmias, it recommends maintaining sinus rhythm when possible and considering a pacemaker to maintain atrioventricular synchrony and to avoid excessive bradycardia.
In its statement, the AHA also recommends optimizing preload with right arterial pressure/central venous pressure of 8-12 mm Hg, said Dr. Baez. Preload optimization combined with afterload reduction and improved contractility are hallmarks of care for patients with RV failure.
Avoiding systemic hypotension can prevent sequelae, such as myocardial ischemia and further hypotension, he said.
Optimization of fluid status is another key to managing RV failure, said Dr. Baez. Right heart coronary perfusion pressure can be protected by maintaining mean arterial pressure, and consideration should be given to reducing the RV afterload. Other strategies include inotropic medications and rhythm stabilization.
In general, for RV failure patients, “correct hypoxia, hypercarbia, and acidosis and avoid intubation when possible,” he said. Extracorporeal membrane oxygenation (ECMO) may be an option, depending on how many mechanical ventilator settings need to be adjusted.
In a study by Dr. Baez and colleagues published in Critical Care Medicine, the authors presented a Bayesian probability model for plasma lactate and severity of illness in cases of acute pulmonary embolism. “This Bayesian model demonstrated that the combination of shock index and lactate yield superior diagnostic gains than those compare to the sPESI and lactate,” Dr. Baez said.
The care model needs to be specific to the etiology, he added. Volume management in congested pulmonary hypertension involves a “squeeze and diurese” strategy.
According to the Internet Book of Critical Care, for patients with mean arterial pressure (MAP) of 60 mm Hg, central venous pressure (CVP) of 25 mm Hg, renal perfusion pressure of 25 mm Hg, and no urine output, a vasopressor should be added to treatment, Dr. Baez said. In cases in which the MAP 75 mm Hg, the CVP is 25 mm Hg, the renal perfusion pressure is 50 mm Hg, and the patient has good urine output, vasopressors should be continued and fluid should be removed through use of a diuretic. For patients with a MAP of 75 mm Hg, a CVP of 12 mm Hg, and renal perfusion pressure of 63 mm Hg who have good urine output, the diuretic and the vasopressor should be discontinued.
Dr. Baez also reviewed several clinical studies of the utility of acute mechanical circulatory support systems for RV failure.
In two small studies involving a heart pump and a right ventricular assistive device, the 30-day survival rate was approximately 72%-73%. A study of 179 patients involving ECMO showed an in-hospital mortality rate of 38.6%, he said.
Overall, “prompt diagnosis, hemodynamic support, and initiation of specific treatment” are the foundations of managing RV failure, he concluded.
Dr. Baez disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ACEP 2022
Paxlovid has been free so far. Next year, sticker shock awaits
Nearly 6 million Americans have taken Paxlovid for free, courtesy of the federal government. The Pfizer pill has helped prevent many people infected with COVID-19 from being hospitalized or dying, and it may even reduce the risk of developing long COVID.
And that means fewer people will get the potentially lifesaving treatments, experts said.
“I think the numbers will go way down,” said Jill Rosenthal, director of public health policy at the Center for American Progress, a left-leaning think tank. A bill for several hundred dollars or more would lead many people to decide the medication isn’t worth the price, she said.
In response to the unprecedented public health crisis caused by COVID, the federal government spent billions of dollars on developing new vaccines and treatments, to swift success: Less than a year after the pandemic was declared, medical workers got their first vaccines. But as many people have refused the shots and stopped wearing masks, the virus still rages and mutates. In 2022 alone, 250,000 Americans have died from COVID, more than from strokes or diabetes.
But soon the Department of Health & Human Services will stop supplying COVID treatments, and pharmacies will purchase and bill for them the same way they do for antibiotic pills or asthma inhalers. Paxlovid is expected to hit the private market in mid-2023, according to HHS plans shared in an October meeting with state health officials and clinicians. Merck’s Lagevrio, a less-effective COVID treatment pill, and AstraZeneca’s Evusheld, a preventive therapy for the immunocompromised, are on track to be commercialized sooner, sometime in the winter.
The U.S. government has so far purchased 20 million courses of Paxlovid, priced at about $530 each, a discount for buying in bulk that Pfizer CEO Albert Bourla called “really very attractive” to the federal government in a July earnings call. The drug will cost far more on the private market, although in a statement to Kaiser Health News, Pfizer declined to share the planned price. The government will also stop paying for the company’s COVID vaccine next year – those shots will quadruple in price, from the discount rate the government pays of $30 to about $120.
Mr. Bourla told investors in November that he expects the move will make Paxlovid and its COVID vaccine “a multibillion-dollars franchise.”
Nearly 9 in 10 people dying from the virus now are 65 or older. Yet federal law restricts Medicare Part D – the prescription drug program that covers nearly 50 million seniors – from covering the COVID treatment pills. The medications are meant for those most at risk of serious illness, including seniors.
Paxlovid and the other treatments are currently available under an emergency use authorization from the FDA, a fast-track review used in extraordinary situations. Although Pfizer applied for full approval in June, the process can take anywhere from several months to years. And Medicare Part D can’t cover any medications without that full stamp of approval.
Paying out-of-pocket would be “a substantial barrier” for seniors on Medicare – the very people who would benefit most from the drug, wrote federal health experts.
“From a public health perspective, and even from a health care capacity and cost perspective, it would just defy reason to not continue to make these drugs readily available,” said Dr. Larry Madoff, medical director of Massachusetts’s Bureau of Infectious Disease and Laboratory Sciences. He’s hopeful that the federal health agency will find a way to set aside unused doses for seniors and people without insurance.
In mid-November, the White House requested that Congress approve an additional $2.5 billion for COVID therapeutics and vaccines to make sure people can afford the medications when they’re no longer free. But there’s little hope it will be approved – the Senate voted that same day to end the public health emergency and denied similar requests in recent months.
Many Americans have already faced hurdles just getting a prescription for COVID treatment. Although the federal government doesn’t track who’s gotten the drug, a Centers for Disease Control and Prevention study using data from 30 medical centers found that Black and Hispanic patients with COVID were much less likely to receive Paxlovid than White patients. (Hispanic people can be of any race or combination of races.) And when the government is no longer picking up the tab, experts predict that these gaps by race, income, and geography will widen.
People in Northeastern states used the drug far more often than those in the rest of the country, according to a KHN analysis of Paxlovid use in September and October. But it wasn’t because people in the region were getting sick from COVID at much higher rates – instead, many of those states offered better access to health care to begin with and created special programs to get Paxlovid to their residents.
About 10 mostly Democratic states and several large counties in the Northeast and elsewhere created free “test-to-treat” programs that allow their residents to get an immediate doctor visit and prescription for treatment after testing positive for COVID. In Massachusetts, more than 20,000 residents have used the state’s video and phone hotline, which is available 7 days a week in 13 languages. Massachusetts, which has the highest insurance rate in the country and relatively low travel times to pharmacies, had the second-highest Paxlovid usage rate among states this fall.
States with higher COVID death rates, like Florida and Kentucky, where residents must travel farther for health care and are more likely to be uninsured, used the drug less often. Without no-cost test-to-treat options, residents have struggled to get prescriptions even though the drug itself is still free.
“If you look at access to medications for people who are uninsured, I think that there’s no question that will widen those disparities,” Ms. Rosenthal said.
People who get insurance through their jobs could face high copays at the register, too, just as they do for insulin and other expensive or brand-name drugs.
Most private insurance companies will end up covering COVID therapeutics to some extent, said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms. After all, the pills are cheaper than a hospital stay. But for most people who get insurance through their jobs, there are “really no rules at all,” she said. Some insurers could take months to add the drugs to their plans or decide not to pay for them.
And the additional cost means many people will go without the medication. “We know from lots of research that when people face cost sharing for these drugs that they need to take, they will often forgo or cut back,” Ms. Corlette said.
One group doesn’t need to worry about sticker shock. Medicaid, the public insurance program for low-income adults and children, will cover the treatments in full until at least early 2024.
HHS officials could set aside any leftover taxpayer-funded medication for people who can’t afford to pay the full cost, but they haven’t shared any concrete plans to do so. The government purchased 20 million courses of Paxlovid and 3 million of Lagevrio. Fewer than a third have been used, and usage has fallen in recent months, according to KHN’s analysis of the data from HHS.
Sixty percent of the government’s supply of Evusheld is also still available, although the COVID prevention therapy is less effective against new strains of the virus. The health department in one state, New Mexico, has recommended against using it.
HHS did not make officials available for an interview or answer written questions about the commercialization plans.
The government created a potential workaround when they moved bebtelovimab, another COVID treatment, to the private market this summer. It now retails for $2,100 per patient. The agency set aside the remaining 60,000 government-purchased doses that hospitals could use to treat uninsured patients in a convoluted dose-replacement process. But it’s hard to tell how well that setup would work for Paxlovid: Bebtelovimab was already much less popular, and the FDA halted its use on Nov. 30 because it’s less effective against current strains of the virus.
Federal officials and insurance companies would have good reason to make sure patients can continue to afford COVID drugs: They’re far cheaper than if patients land in the emergency room.
“The medications are so worthwhile,” said Dr. Madoff, the Massachusetts health official. “They’re not expensive in the grand scheme of health care costs.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Nearly 6 million Americans have taken Paxlovid for free, courtesy of the federal government. The Pfizer pill has helped prevent many people infected with COVID-19 from being hospitalized or dying, and it may even reduce the risk of developing long COVID.
And that means fewer people will get the potentially lifesaving treatments, experts said.
“I think the numbers will go way down,” said Jill Rosenthal, director of public health policy at the Center for American Progress, a left-leaning think tank. A bill for several hundred dollars or more would lead many people to decide the medication isn’t worth the price, she said.
In response to the unprecedented public health crisis caused by COVID, the federal government spent billions of dollars on developing new vaccines and treatments, to swift success: Less than a year after the pandemic was declared, medical workers got their first vaccines. But as many people have refused the shots and stopped wearing masks, the virus still rages and mutates. In 2022 alone, 250,000 Americans have died from COVID, more than from strokes or diabetes.
But soon the Department of Health & Human Services will stop supplying COVID treatments, and pharmacies will purchase and bill for them the same way they do for antibiotic pills or asthma inhalers. Paxlovid is expected to hit the private market in mid-2023, according to HHS plans shared in an October meeting with state health officials and clinicians. Merck’s Lagevrio, a less-effective COVID treatment pill, and AstraZeneca’s Evusheld, a preventive therapy for the immunocompromised, are on track to be commercialized sooner, sometime in the winter.
The U.S. government has so far purchased 20 million courses of Paxlovid, priced at about $530 each, a discount for buying in bulk that Pfizer CEO Albert Bourla called “really very attractive” to the federal government in a July earnings call. The drug will cost far more on the private market, although in a statement to Kaiser Health News, Pfizer declined to share the planned price. The government will also stop paying for the company’s COVID vaccine next year – those shots will quadruple in price, from the discount rate the government pays of $30 to about $120.
Mr. Bourla told investors in November that he expects the move will make Paxlovid and its COVID vaccine “a multibillion-dollars franchise.”
Nearly 9 in 10 people dying from the virus now are 65 or older. Yet federal law restricts Medicare Part D – the prescription drug program that covers nearly 50 million seniors – from covering the COVID treatment pills. The medications are meant for those most at risk of serious illness, including seniors.
Paxlovid and the other treatments are currently available under an emergency use authorization from the FDA, a fast-track review used in extraordinary situations. Although Pfizer applied for full approval in June, the process can take anywhere from several months to years. And Medicare Part D can’t cover any medications without that full stamp of approval.
Paying out-of-pocket would be “a substantial barrier” for seniors on Medicare – the very people who would benefit most from the drug, wrote federal health experts.
“From a public health perspective, and even from a health care capacity and cost perspective, it would just defy reason to not continue to make these drugs readily available,” said Dr. Larry Madoff, medical director of Massachusetts’s Bureau of Infectious Disease and Laboratory Sciences. He’s hopeful that the federal health agency will find a way to set aside unused doses for seniors and people without insurance.
In mid-November, the White House requested that Congress approve an additional $2.5 billion for COVID therapeutics and vaccines to make sure people can afford the medications when they’re no longer free. But there’s little hope it will be approved – the Senate voted that same day to end the public health emergency and denied similar requests in recent months.
Many Americans have already faced hurdles just getting a prescription for COVID treatment. Although the federal government doesn’t track who’s gotten the drug, a Centers for Disease Control and Prevention study using data from 30 medical centers found that Black and Hispanic patients with COVID were much less likely to receive Paxlovid than White patients. (Hispanic people can be of any race or combination of races.) And when the government is no longer picking up the tab, experts predict that these gaps by race, income, and geography will widen.
People in Northeastern states used the drug far more often than those in the rest of the country, according to a KHN analysis of Paxlovid use in September and October. But it wasn’t because people in the region were getting sick from COVID at much higher rates – instead, many of those states offered better access to health care to begin with and created special programs to get Paxlovid to their residents.
About 10 mostly Democratic states and several large counties in the Northeast and elsewhere created free “test-to-treat” programs that allow their residents to get an immediate doctor visit and prescription for treatment after testing positive for COVID. In Massachusetts, more than 20,000 residents have used the state’s video and phone hotline, which is available 7 days a week in 13 languages. Massachusetts, which has the highest insurance rate in the country and relatively low travel times to pharmacies, had the second-highest Paxlovid usage rate among states this fall.
States with higher COVID death rates, like Florida and Kentucky, where residents must travel farther for health care and are more likely to be uninsured, used the drug less often. Without no-cost test-to-treat options, residents have struggled to get prescriptions even though the drug itself is still free.
“If you look at access to medications for people who are uninsured, I think that there’s no question that will widen those disparities,” Ms. Rosenthal said.
People who get insurance through their jobs could face high copays at the register, too, just as they do for insulin and other expensive or brand-name drugs.
Most private insurance companies will end up covering COVID therapeutics to some extent, said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms. After all, the pills are cheaper than a hospital stay. But for most people who get insurance through their jobs, there are “really no rules at all,” she said. Some insurers could take months to add the drugs to their plans or decide not to pay for them.
And the additional cost means many people will go without the medication. “We know from lots of research that when people face cost sharing for these drugs that they need to take, they will often forgo or cut back,” Ms. Corlette said.
One group doesn’t need to worry about sticker shock. Medicaid, the public insurance program for low-income adults and children, will cover the treatments in full until at least early 2024.
HHS officials could set aside any leftover taxpayer-funded medication for people who can’t afford to pay the full cost, but they haven’t shared any concrete plans to do so. The government purchased 20 million courses of Paxlovid and 3 million of Lagevrio. Fewer than a third have been used, and usage has fallen in recent months, according to KHN’s analysis of the data from HHS.
Sixty percent of the government’s supply of Evusheld is also still available, although the COVID prevention therapy is less effective against new strains of the virus. The health department in one state, New Mexico, has recommended against using it.
HHS did not make officials available for an interview or answer written questions about the commercialization plans.
The government created a potential workaround when they moved bebtelovimab, another COVID treatment, to the private market this summer. It now retails for $2,100 per patient. The agency set aside the remaining 60,000 government-purchased doses that hospitals could use to treat uninsured patients in a convoluted dose-replacement process. But it’s hard to tell how well that setup would work for Paxlovid: Bebtelovimab was already much less popular, and the FDA halted its use on Nov. 30 because it’s less effective against current strains of the virus.
Federal officials and insurance companies would have good reason to make sure patients can continue to afford COVID drugs: They’re far cheaper than if patients land in the emergency room.
“The medications are so worthwhile,” said Dr. Madoff, the Massachusetts health official. “They’re not expensive in the grand scheme of health care costs.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
Nearly 6 million Americans have taken Paxlovid for free, courtesy of the federal government. The Pfizer pill has helped prevent many people infected with COVID-19 from being hospitalized or dying, and it may even reduce the risk of developing long COVID.
And that means fewer people will get the potentially lifesaving treatments, experts said.
“I think the numbers will go way down,” said Jill Rosenthal, director of public health policy at the Center for American Progress, a left-leaning think tank. A bill for several hundred dollars or more would lead many people to decide the medication isn’t worth the price, she said.
In response to the unprecedented public health crisis caused by COVID, the federal government spent billions of dollars on developing new vaccines and treatments, to swift success: Less than a year after the pandemic was declared, medical workers got their first vaccines. But as many people have refused the shots and stopped wearing masks, the virus still rages and mutates. In 2022 alone, 250,000 Americans have died from COVID, more than from strokes or diabetes.
But soon the Department of Health & Human Services will stop supplying COVID treatments, and pharmacies will purchase and bill for them the same way they do for antibiotic pills or asthma inhalers. Paxlovid is expected to hit the private market in mid-2023, according to HHS plans shared in an October meeting with state health officials and clinicians. Merck’s Lagevrio, a less-effective COVID treatment pill, and AstraZeneca’s Evusheld, a preventive therapy for the immunocompromised, are on track to be commercialized sooner, sometime in the winter.
The U.S. government has so far purchased 20 million courses of Paxlovid, priced at about $530 each, a discount for buying in bulk that Pfizer CEO Albert Bourla called “really very attractive” to the federal government in a July earnings call. The drug will cost far more on the private market, although in a statement to Kaiser Health News, Pfizer declined to share the planned price. The government will also stop paying for the company’s COVID vaccine next year – those shots will quadruple in price, from the discount rate the government pays of $30 to about $120.
Mr. Bourla told investors in November that he expects the move will make Paxlovid and its COVID vaccine “a multibillion-dollars franchise.”
Nearly 9 in 10 people dying from the virus now are 65 or older. Yet federal law restricts Medicare Part D – the prescription drug program that covers nearly 50 million seniors – from covering the COVID treatment pills. The medications are meant for those most at risk of serious illness, including seniors.
Paxlovid and the other treatments are currently available under an emergency use authorization from the FDA, a fast-track review used in extraordinary situations. Although Pfizer applied for full approval in June, the process can take anywhere from several months to years. And Medicare Part D can’t cover any medications without that full stamp of approval.
Paying out-of-pocket would be “a substantial barrier” for seniors on Medicare – the very people who would benefit most from the drug, wrote federal health experts.
“From a public health perspective, and even from a health care capacity and cost perspective, it would just defy reason to not continue to make these drugs readily available,” said Dr. Larry Madoff, medical director of Massachusetts’s Bureau of Infectious Disease and Laboratory Sciences. He’s hopeful that the federal health agency will find a way to set aside unused doses for seniors and people without insurance.
In mid-November, the White House requested that Congress approve an additional $2.5 billion for COVID therapeutics and vaccines to make sure people can afford the medications when they’re no longer free. But there’s little hope it will be approved – the Senate voted that same day to end the public health emergency and denied similar requests in recent months.
Many Americans have already faced hurdles just getting a prescription for COVID treatment. Although the federal government doesn’t track who’s gotten the drug, a Centers for Disease Control and Prevention study using data from 30 medical centers found that Black and Hispanic patients with COVID were much less likely to receive Paxlovid than White patients. (Hispanic people can be of any race or combination of races.) And when the government is no longer picking up the tab, experts predict that these gaps by race, income, and geography will widen.
People in Northeastern states used the drug far more often than those in the rest of the country, according to a KHN analysis of Paxlovid use in September and October. But it wasn’t because people in the region were getting sick from COVID at much higher rates – instead, many of those states offered better access to health care to begin with and created special programs to get Paxlovid to their residents.
About 10 mostly Democratic states and several large counties in the Northeast and elsewhere created free “test-to-treat” programs that allow their residents to get an immediate doctor visit and prescription for treatment after testing positive for COVID. In Massachusetts, more than 20,000 residents have used the state’s video and phone hotline, which is available 7 days a week in 13 languages. Massachusetts, which has the highest insurance rate in the country and relatively low travel times to pharmacies, had the second-highest Paxlovid usage rate among states this fall.
States with higher COVID death rates, like Florida and Kentucky, where residents must travel farther for health care and are more likely to be uninsured, used the drug less often. Without no-cost test-to-treat options, residents have struggled to get prescriptions even though the drug itself is still free.
“If you look at access to medications for people who are uninsured, I think that there’s no question that will widen those disparities,” Ms. Rosenthal said.
People who get insurance through their jobs could face high copays at the register, too, just as they do for insulin and other expensive or brand-name drugs.
Most private insurance companies will end up covering COVID therapeutics to some extent, said Sabrina Corlette, a research professor at Georgetown University’s Center on Health Insurance Reforms. After all, the pills are cheaper than a hospital stay. But for most people who get insurance through their jobs, there are “really no rules at all,” she said. Some insurers could take months to add the drugs to their plans or decide not to pay for them.
And the additional cost means many people will go without the medication. “We know from lots of research that when people face cost sharing for these drugs that they need to take, they will often forgo or cut back,” Ms. Corlette said.
One group doesn’t need to worry about sticker shock. Medicaid, the public insurance program for low-income adults and children, will cover the treatments in full until at least early 2024.
HHS officials could set aside any leftover taxpayer-funded medication for people who can’t afford to pay the full cost, but they haven’t shared any concrete plans to do so. The government purchased 20 million courses of Paxlovid and 3 million of Lagevrio. Fewer than a third have been used, and usage has fallen in recent months, according to KHN’s analysis of the data from HHS.
Sixty percent of the government’s supply of Evusheld is also still available, although the COVID prevention therapy is less effective against new strains of the virus. The health department in one state, New Mexico, has recommended against using it.
HHS did not make officials available for an interview or answer written questions about the commercialization plans.
The government created a potential workaround when they moved bebtelovimab, another COVID treatment, to the private market this summer. It now retails for $2,100 per patient. The agency set aside the remaining 60,000 government-purchased doses that hospitals could use to treat uninsured patients in a convoluted dose-replacement process. But it’s hard to tell how well that setup would work for Paxlovid: Bebtelovimab was already much less popular, and the FDA halted its use on Nov. 30 because it’s less effective against current strains of the virus.
Federal officials and insurance companies would have good reason to make sure patients can continue to afford COVID drugs: They’re far cheaper than if patients land in the emergency room.
“The medications are so worthwhile,” said Dr. Madoff, the Massachusetts health official. “They’re not expensive in the grand scheme of health care costs.”
KHN (Kaiser Health News) is a national newsroom that produces in-depth journalism about health issues. Together with Policy Analysis and Polling, KHN is one of the three major operating programs at KFF (Kaiser Family Foundation). KFF is an endowed nonprofit organization providing information on health issues to the nation.
GOLD Report 2023: Important updates and revisions
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) Report is revised annually and is used widely throughout the world as a tool for implementing effective management.
Among the updates in the 2023 GOLD Report, the section on diagnostic criteria added a proposed new category “PRISm,” denoting “preserved ratio impaired spirometry,” encompassing individuals who present with structural lung lesions (for example, emphysema) and/or other physiological abnormalities such as low-normal forced expiratory volume in 1 second (FEV1), gas trapping, hyperinflation, reduced lung diffusing capacity and/or rapid FEV1 decline, but without airflow obstruction (FEV1/FEV ≥ 0.7 post bronchodilation). Some of these “pre-COPD” (chronic obstructive pulmonary disease) individuals, who have a normal ratio but abnormal spirometry are at risk over time of developing airflow obstruction. The best treatment for them, beyond smoking cessation, needs to be determined through research, the report states.
Clinical updates
The GOLD 2023 Report also offers proposed clinical guidance, in the absence of high-quality clinical trial evidence, on initial pharmacologic management of COPD. The proposal is based on individual assessment of symptoms and exacerbation risk following use of the ABE Assessment Tool, a revised version of the ABCD Assessment Tool that recognizes the clinical relevance of exacerbations independent of symptom level.
These updates to information and figures pertaining to initial pharmacological treatment and follow-up pharmacological treatment revise the positioning of LABA (long-acting beta2 agonists) plus LAMA (long-acting muscarinic agonists) and LABA/ICS (inhaled corticosteroids). Among GOLD group A patients with 0 or 1 moderate exacerbations that do not lead to hospital admission, a bronchodilator is recommended.
The recommendation for group B patients is LABA/LAMA with the caveat that single inhaler therapy may be more convenient and effective than multiple inhalers. For group E patients with two or more moderate exacerbations or one or more leading to hospitalization, LABA/LAMA is recommended (with the same inhaler therapy caveat). With blood eosinophil levels at 300 or higher, LABA/LAMA/ICS may be considered.
Commenting on the combination recommendations in a press release, Antonio Anzueto, MD, professor of medicine, pulmonary critical care, University of Texas Health, San Antonio, stated: “From a physician’s perspective, we are always grateful to receive well-vetted and informed recommendations on how we can best utilize available treatment options to provide the most benefit to our patients. The new 2023 GOLD recommendations represent a meaningful change for the treatment of COPD by prioritizing the utilization of a fixed LAMA/LABA combination.”
More interventions
In a section on therapeutic interventions to reduce COPD mortality, the report lists studies showing mortality benefits for fixed-dose inhaled triple combinations (LABA + LAMA + ICS) versus dual inhaled long-acting bronchodilations, and for smoking cessation and pulmonary rehabilitation.
Also new is a strong emphasis on inhaler choice, education, and technique training with assessment of inhaler technique and adherence urged as a prerequisite to judging whether current therapy as insufficient. The report summarizes principles guiding inhaler type selection.
The report also added a section on chronic bronchitis, defining it as a common but variable condition in COPD patients with cough and expectorated sputum on a regular basis over a defined period in the absence of other conditions plausibly causing symptoms.
The fact that chronic bronchitis is sometimes found in never-smokers suggests the involvement of other factors such as exposure to inhaled dusts, biomass fuels, chemical fumes, or domestic heating and cooking fuels, according to the report. Gastroesophageal reflux may also be associated with chronic bronchitis.
The report discusses various taxonomic terms for different types of COPD, such as COPD-G for genetically determined COPD, COPD-D for those with abnormal lung development, and COPD-C for COPD associated with cigarette smoking, etc.
Change in exacerbations
The report also revises the definition of a COPD exacerbation as “an event characterized by increased dyspnea and/or cough and sputum that worsens in less than 14 days which may be accompanied by tachypnea and/or tachycardia and is often associated with increased local and system inflammation caused by infection, pollution, or other insult to the airways.” To overcome limitations conferred by the current grading of COPD exacerbations, the 2023 report proposes a four-step point-of-contact diagnosis and assessment tool.
Telemedicine
Given the constraints brought on by COVID-19 on top of the generally sparse availability of programs and facilities for delivering well-proven pulmonary rehabilitation methods, tele-rehabilitation has been proposed as an alternative to traditional approaches. While the evidence base is still evolving and best practices have not yet been established, the GOLD Report calls for better understanding of barriers to tele-rehabilitation success.
Comorbidities update
The GOLD Report chapter on COPD and comorbidities was also updated, and lists cardiovascular disease, lung cancer, osteoporosis, depression/anxiety, and gastroesophageal reflux disease as common comorbid conditions which may affect prognosis and, in the case of cancer, mortality. The report urges simplicity of treatment to minimize polypharmacy. While annual low-dose CT is recommended for COPD caused by smoking, it is not recommended for COPD caused by smoking; data are insufficient to establish benefit over harm.
While the GOLD Report “COVID-19 and COPD” chapter summarizes current evidence stating that individuals with COPD do not seem to be at substantially greater risk of infection with SARS-CoV-2, it underscores that they are at higher risk of hospitalization for COVID-19 and may be at higher risk for developing severe disease and death.
Many other topics are included in the updated report, among them screening, imaging, vaccinations, adherence to therapy, and surgical and bronchoscopic interventions. In its closing section, the GOLD Report 2023 reiterates its mission, stating: “The GOLD initiative will continue to work with National Leaders and other interested health care professionals to bring COPD to the attention of governments, public health officials, health care workers, and the general public, to raise awareness of the burden of COPD and to develop programs for early detection, prevention and approaches to management.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) Report is revised annually and is used widely throughout the world as a tool for implementing effective management.
Among the updates in the 2023 GOLD Report, the section on diagnostic criteria added a proposed new category “PRISm,” denoting “preserved ratio impaired spirometry,” encompassing individuals who present with structural lung lesions (for example, emphysema) and/or other physiological abnormalities such as low-normal forced expiratory volume in 1 second (FEV1), gas trapping, hyperinflation, reduced lung diffusing capacity and/or rapid FEV1 decline, but without airflow obstruction (FEV1/FEV ≥ 0.7 post bronchodilation). Some of these “pre-COPD” (chronic obstructive pulmonary disease) individuals, who have a normal ratio but abnormal spirometry are at risk over time of developing airflow obstruction. The best treatment for them, beyond smoking cessation, needs to be determined through research, the report states.
Clinical updates
The GOLD 2023 Report also offers proposed clinical guidance, in the absence of high-quality clinical trial evidence, on initial pharmacologic management of COPD. The proposal is based on individual assessment of symptoms and exacerbation risk following use of the ABE Assessment Tool, a revised version of the ABCD Assessment Tool that recognizes the clinical relevance of exacerbations independent of symptom level.
These updates to information and figures pertaining to initial pharmacological treatment and follow-up pharmacological treatment revise the positioning of LABA (long-acting beta2 agonists) plus LAMA (long-acting muscarinic agonists) and LABA/ICS (inhaled corticosteroids). Among GOLD group A patients with 0 or 1 moderate exacerbations that do not lead to hospital admission, a bronchodilator is recommended.
The recommendation for group B patients is LABA/LAMA with the caveat that single inhaler therapy may be more convenient and effective than multiple inhalers. For group E patients with two or more moderate exacerbations or one or more leading to hospitalization, LABA/LAMA is recommended (with the same inhaler therapy caveat). With blood eosinophil levels at 300 or higher, LABA/LAMA/ICS may be considered.
Commenting on the combination recommendations in a press release, Antonio Anzueto, MD, professor of medicine, pulmonary critical care, University of Texas Health, San Antonio, stated: “From a physician’s perspective, we are always grateful to receive well-vetted and informed recommendations on how we can best utilize available treatment options to provide the most benefit to our patients. The new 2023 GOLD recommendations represent a meaningful change for the treatment of COPD by prioritizing the utilization of a fixed LAMA/LABA combination.”
More interventions
In a section on therapeutic interventions to reduce COPD mortality, the report lists studies showing mortality benefits for fixed-dose inhaled triple combinations (LABA + LAMA + ICS) versus dual inhaled long-acting bronchodilations, and for smoking cessation and pulmonary rehabilitation.
Also new is a strong emphasis on inhaler choice, education, and technique training with assessment of inhaler technique and adherence urged as a prerequisite to judging whether current therapy as insufficient. The report summarizes principles guiding inhaler type selection.
The report also added a section on chronic bronchitis, defining it as a common but variable condition in COPD patients with cough and expectorated sputum on a regular basis over a defined period in the absence of other conditions plausibly causing symptoms.
The fact that chronic bronchitis is sometimes found in never-smokers suggests the involvement of other factors such as exposure to inhaled dusts, biomass fuels, chemical fumes, or domestic heating and cooking fuels, according to the report. Gastroesophageal reflux may also be associated with chronic bronchitis.
The report discusses various taxonomic terms for different types of COPD, such as COPD-G for genetically determined COPD, COPD-D for those with abnormal lung development, and COPD-C for COPD associated with cigarette smoking, etc.
Change in exacerbations
The report also revises the definition of a COPD exacerbation as “an event characterized by increased dyspnea and/or cough and sputum that worsens in less than 14 days which may be accompanied by tachypnea and/or tachycardia and is often associated with increased local and system inflammation caused by infection, pollution, or other insult to the airways.” To overcome limitations conferred by the current grading of COPD exacerbations, the 2023 report proposes a four-step point-of-contact diagnosis and assessment tool.
Telemedicine
Given the constraints brought on by COVID-19 on top of the generally sparse availability of programs and facilities for delivering well-proven pulmonary rehabilitation methods, tele-rehabilitation has been proposed as an alternative to traditional approaches. While the evidence base is still evolving and best practices have not yet been established, the GOLD Report calls for better understanding of barriers to tele-rehabilitation success.
Comorbidities update
The GOLD Report chapter on COPD and comorbidities was also updated, and lists cardiovascular disease, lung cancer, osteoporosis, depression/anxiety, and gastroesophageal reflux disease as common comorbid conditions which may affect prognosis and, in the case of cancer, mortality. The report urges simplicity of treatment to minimize polypharmacy. While annual low-dose CT is recommended for COPD caused by smoking, it is not recommended for COPD caused by smoking; data are insufficient to establish benefit over harm.
While the GOLD Report “COVID-19 and COPD” chapter summarizes current evidence stating that individuals with COPD do not seem to be at substantially greater risk of infection with SARS-CoV-2, it underscores that they are at higher risk of hospitalization for COVID-19 and may be at higher risk for developing severe disease and death.
Many other topics are included in the updated report, among them screening, imaging, vaccinations, adherence to therapy, and surgical and bronchoscopic interventions. In its closing section, the GOLD Report 2023 reiterates its mission, stating: “The GOLD initiative will continue to work with National Leaders and other interested health care professionals to bring COPD to the attention of governments, public health officials, health care workers, and the general public, to raise awareness of the burden of COPD and to develop programs for early detection, prevention and approaches to management.
The Global Initiative for Chronic Obstructive Lung Disease (GOLD) Report is revised annually and is used widely throughout the world as a tool for implementing effective management.
Among the updates in the 2023 GOLD Report, the section on diagnostic criteria added a proposed new category “PRISm,” denoting “preserved ratio impaired spirometry,” encompassing individuals who present with structural lung lesions (for example, emphysema) and/or other physiological abnormalities such as low-normal forced expiratory volume in 1 second (FEV1), gas trapping, hyperinflation, reduced lung diffusing capacity and/or rapid FEV1 decline, but without airflow obstruction (FEV1/FEV ≥ 0.7 post bronchodilation). Some of these “pre-COPD” (chronic obstructive pulmonary disease) individuals, who have a normal ratio but abnormal spirometry are at risk over time of developing airflow obstruction. The best treatment for them, beyond smoking cessation, needs to be determined through research, the report states.
Clinical updates
The GOLD 2023 Report also offers proposed clinical guidance, in the absence of high-quality clinical trial evidence, on initial pharmacologic management of COPD. The proposal is based on individual assessment of symptoms and exacerbation risk following use of the ABE Assessment Tool, a revised version of the ABCD Assessment Tool that recognizes the clinical relevance of exacerbations independent of symptom level.
These updates to information and figures pertaining to initial pharmacological treatment and follow-up pharmacological treatment revise the positioning of LABA (long-acting beta2 agonists) plus LAMA (long-acting muscarinic agonists) and LABA/ICS (inhaled corticosteroids). Among GOLD group A patients with 0 or 1 moderate exacerbations that do not lead to hospital admission, a bronchodilator is recommended.
The recommendation for group B patients is LABA/LAMA with the caveat that single inhaler therapy may be more convenient and effective than multiple inhalers. For group E patients with two or more moderate exacerbations or one or more leading to hospitalization, LABA/LAMA is recommended (with the same inhaler therapy caveat). With blood eosinophil levels at 300 or higher, LABA/LAMA/ICS may be considered.
Commenting on the combination recommendations in a press release, Antonio Anzueto, MD, professor of medicine, pulmonary critical care, University of Texas Health, San Antonio, stated: “From a physician’s perspective, we are always grateful to receive well-vetted and informed recommendations on how we can best utilize available treatment options to provide the most benefit to our patients. The new 2023 GOLD recommendations represent a meaningful change for the treatment of COPD by prioritizing the utilization of a fixed LAMA/LABA combination.”
More interventions
In a section on therapeutic interventions to reduce COPD mortality, the report lists studies showing mortality benefits for fixed-dose inhaled triple combinations (LABA + LAMA + ICS) versus dual inhaled long-acting bronchodilations, and for smoking cessation and pulmonary rehabilitation.
Also new is a strong emphasis on inhaler choice, education, and technique training with assessment of inhaler technique and adherence urged as a prerequisite to judging whether current therapy as insufficient. The report summarizes principles guiding inhaler type selection.
The report also added a section on chronic bronchitis, defining it as a common but variable condition in COPD patients with cough and expectorated sputum on a regular basis over a defined period in the absence of other conditions plausibly causing symptoms.
The fact that chronic bronchitis is sometimes found in never-smokers suggests the involvement of other factors such as exposure to inhaled dusts, biomass fuels, chemical fumes, or domestic heating and cooking fuels, according to the report. Gastroesophageal reflux may also be associated with chronic bronchitis.
The report discusses various taxonomic terms for different types of COPD, such as COPD-G for genetically determined COPD, COPD-D for those with abnormal lung development, and COPD-C for COPD associated with cigarette smoking, etc.
Change in exacerbations
The report also revises the definition of a COPD exacerbation as “an event characterized by increased dyspnea and/or cough and sputum that worsens in less than 14 days which may be accompanied by tachypnea and/or tachycardia and is often associated with increased local and system inflammation caused by infection, pollution, or other insult to the airways.” To overcome limitations conferred by the current grading of COPD exacerbations, the 2023 report proposes a four-step point-of-contact diagnosis and assessment tool.
Telemedicine
Given the constraints brought on by COVID-19 on top of the generally sparse availability of programs and facilities for delivering well-proven pulmonary rehabilitation methods, tele-rehabilitation has been proposed as an alternative to traditional approaches. While the evidence base is still evolving and best practices have not yet been established, the GOLD Report calls for better understanding of barriers to tele-rehabilitation success.
Comorbidities update
The GOLD Report chapter on COPD and comorbidities was also updated, and lists cardiovascular disease, lung cancer, osteoporosis, depression/anxiety, and gastroesophageal reflux disease as common comorbid conditions which may affect prognosis and, in the case of cancer, mortality. The report urges simplicity of treatment to minimize polypharmacy. While annual low-dose CT is recommended for COPD caused by smoking, it is not recommended for COPD caused by smoking; data are insufficient to establish benefit over harm.
While the GOLD Report “COVID-19 and COPD” chapter summarizes current evidence stating that individuals with COPD do not seem to be at substantially greater risk of infection with SARS-CoV-2, it underscores that they are at higher risk of hospitalization for COVID-19 and may be at higher risk for developing severe disease and death.
Many other topics are included in the updated report, among them screening, imaging, vaccinations, adherence to therapy, and surgical and bronchoscopic interventions. In its closing section, the GOLD Report 2023 reiterates its mission, stating: “The GOLD initiative will continue to work with National Leaders and other interested health care professionals to bring COPD to the attention of governments, public health officials, health care workers, and the general public, to raise awareness of the burden of COPD and to develop programs for early detection, prevention and approaches to management.
Study comparing surgical and N95 masks sparks concern
The study’s senior author is John Conly, MD, an infectious disease specialist and professor at the University of Calgary (Alta.), and Alberta Health Services. The findings are not consistent with those of many other studies on this topic.
Commenting about Dr. Conly’s study, Eric Topol, MD, editor-in-chief of Medscape, wrote: “It’s woefully underpowered but ruled out a doubling of hazard for use of medical masks.”
The study, which was partially funded by the World Health Organization, was published online in Annals of Internal Medicine.
This is not the first time that Dr. Conly, who also advises the WHO, has been the subject of controversy. He previously denied that COVID-19 is airborne – a position that is contradicted by strong evidence. In 2021, Dr. Conly made headlines with his controversial claim that N95 respirators can cause harms, including oxygen depletion and carbon dioxide retention.
A detailed examination by the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota, Minneapolis, pointed out numerous scientific flaws in the study, including inconsistent use of both types of masks. The study also examined health care workers in four very different countries (Canada, Israel, Egypt, and Pakistan) during different periods of the pandemic, which may have affected the results. Furthermore, the study did not account for vaccination status and lacked a control group. CIDRAP receives funding from 3M, which makes N95 respirators.
In a commentary published alongside the study, Roger Chou, MD, professor of medicine at Oregon Health & Science University, Portland, said that the results were “not definitive,” with “a generous noninferiority threshold” that is actually “consistent with up to a relative 70% increased risk ... which may be unacceptable to many health workers.”
Lead study author Mark Loeb, MD, professor of infectious diseases at McMaster University, Hamilton, Ont., defended the findings. “The confidence intervals around this, that is, what the possible results could be if the trial was repeated many times, range from −2.5% to 4.9%,” he told this news organization. “This means that the risk of a COVID-19 infection in those using the medical masks could have ranged from anywhere from 2.5% reduction in risk to a 4.9% increase in risk. Readers and policy makers can decide for themselves about this.”
“There is no point continuing to run underpowered, poorly designed studies that are designed to confirm existing biases,” Raina MacIntyre, PhD, professor of global biosecurity and head of the Biosecurity Program at the Kirby Institute, Sydney, said in an interview. “The new study in Annals of Internal Medicine is entirely consistent with our finding that to prevent infection, you need an N95, and it needs to be worn throughout the whole shift. A surgical mask and intermittent use of N95 are equally ineffective. This should not surprise anyone, given a surgical mask is not designed as respiratory protection but is designed to prevent splash or spray of liquid on the face. Only a respirator is designed as respiratory protection through both the seal around the face and the filter of the face piece to prevent inhalation of virus laden aerosols, but you need to wear it continually in a high-risk environment like a hospital.”
“It makes zero sense to do a randomized trial on something you can measure directly,” said Kimberly Prather, PhD, an atmospheric chemist, professor, and director of the NSF Center for Aerosol Impacts on Chemistry of the Environment at the University of California, San Diego. “In fact, many studies have shown aerosols leaking out of surgical masks. Surgical masks are designed to block large spray droplets. Aerosols (0.5-3 mcm), which have been shown to contain infectious SARS-CoV-2 virus, travel with the air flow, and escape.”
“This study ... will be used to justify policies of supplying health care workers, and perhaps patients and visitors, too, with inadequate protection,” Trish Greenhalgh, MD, professor of primary care health sciences at the University of Oxford (England), told this news organization.
“These authors have been pushing back against treating COVID as airborne for 3 years,” David Fisman, MD, an epidemiologist and infectious disease specialist at the University of Toronto, said in an interview. “So, you’ll see these folks brandishing this very flawed trial to justify continuing the infection control practices that have been so disastrous throughout the pandemic.”
The study was funded by the World Health Organization, the Canadian Institutes of Health Research, and the Juravinski Research Institute. Dr. Conly reported receiving grants from the Canadian Institutes for Health Research, Pfizer, and the WHO. Dr. Chou disclosed being a methodologist for WHO guidelines on infection prevention and control measures for COVID-19. Dr. Loeb disclosed payment for expert testimony on personal protective equipment from the government of Manitoba and the Peel District School Board. Dr. MacIntyre has led a large body of research on masks and respirators in health workers, including four randomized clinical trials. She is the author of a book, “Dark Winter: An insider’s guide to pandemics and biosecurity” (Syndey: NewSouth Publishing, 2022), which covers the history and politics of the controversies around N95 and masks. Dr. Prather reported no disclosures. Dr. Greenhalgh is a member of Independent SAGE and an unpaid adviser to the philanthropic fund Balvi. Dr. Fisman has served as a paid legal expert for the Ontario Nurses’ Association in their challenge to Directive 5, which restricted access to N95 masks in health care. He also served as a paid legal expert for the Elementary Teachers’ Federation of Ontario in its efforts to make schools safer in Ontario.
A version of this article first appeared on Medscape.com.
The study’s senior author is John Conly, MD, an infectious disease specialist and professor at the University of Calgary (Alta.), and Alberta Health Services. The findings are not consistent with those of many other studies on this topic.
Commenting about Dr. Conly’s study, Eric Topol, MD, editor-in-chief of Medscape, wrote: “It’s woefully underpowered but ruled out a doubling of hazard for use of medical masks.”
The study, which was partially funded by the World Health Organization, was published online in Annals of Internal Medicine.
This is not the first time that Dr. Conly, who also advises the WHO, has been the subject of controversy. He previously denied that COVID-19 is airborne – a position that is contradicted by strong evidence. In 2021, Dr. Conly made headlines with his controversial claim that N95 respirators can cause harms, including oxygen depletion and carbon dioxide retention.
A detailed examination by the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota, Minneapolis, pointed out numerous scientific flaws in the study, including inconsistent use of both types of masks. The study also examined health care workers in four very different countries (Canada, Israel, Egypt, and Pakistan) during different periods of the pandemic, which may have affected the results. Furthermore, the study did not account for vaccination status and lacked a control group. CIDRAP receives funding from 3M, which makes N95 respirators.
In a commentary published alongside the study, Roger Chou, MD, professor of medicine at Oregon Health & Science University, Portland, said that the results were “not definitive,” with “a generous noninferiority threshold” that is actually “consistent with up to a relative 70% increased risk ... which may be unacceptable to many health workers.”
Lead study author Mark Loeb, MD, professor of infectious diseases at McMaster University, Hamilton, Ont., defended the findings. “The confidence intervals around this, that is, what the possible results could be if the trial was repeated many times, range from −2.5% to 4.9%,” he told this news organization. “This means that the risk of a COVID-19 infection in those using the medical masks could have ranged from anywhere from 2.5% reduction in risk to a 4.9% increase in risk. Readers and policy makers can decide for themselves about this.”
“There is no point continuing to run underpowered, poorly designed studies that are designed to confirm existing biases,” Raina MacIntyre, PhD, professor of global biosecurity and head of the Biosecurity Program at the Kirby Institute, Sydney, said in an interview. “The new study in Annals of Internal Medicine is entirely consistent with our finding that to prevent infection, you need an N95, and it needs to be worn throughout the whole shift. A surgical mask and intermittent use of N95 are equally ineffective. This should not surprise anyone, given a surgical mask is not designed as respiratory protection but is designed to prevent splash or spray of liquid on the face. Only a respirator is designed as respiratory protection through both the seal around the face and the filter of the face piece to prevent inhalation of virus laden aerosols, but you need to wear it continually in a high-risk environment like a hospital.”
“It makes zero sense to do a randomized trial on something you can measure directly,” said Kimberly Prather, PhD, an atmospheric chemist, professor, and director of the NSF Center for Aerosol Impacts on Chemistry of the Environment at the University of California, San Diego. “In fact, many studies have shown aerosols leaking out of surgical masks. Surgical masks are designed to block large spray droplets. Aerosols (0.5-3 mcm), which have been shown to contain infectious SARS-CoV-2 virus, travel with the air flow, and escape.”
“This study ... will be used to justify policies of supplying health care workers, and perhaps patients and visitors, too, with inadequate protection,” Trish Greenhalgh, MD, professor of primary care health sciences at the University of Oxford (England), told this news organization.
“These authors have been pushing back against treating COVID as airborne for 3 years,” David Fisman, MD, an epidemiologist and infectious disease specialist at the University of Toronto, said in an interview. “So, you’ll see these folks brandishing this very flawed trial to justify continuing the infection control practices that have been so disastrous throughout the pandemic.”
The study was funded by the World Health Organization, the Canadian Institutes of Health Research, and the Juravinski Research Institute. Dr. Conly reported receiving grants from the Canadian Institutes for Health Research, Pfizer, and the WHO. Dr. Chou disclosed being a methodologist for WHO guidelines on infection prevention and control measures for COVID-19. Dr. Loeb disclosed payment for expert testimony on personal protective equipment from the government of Manitoba and the Peel District School Board. Dr. MacIntyre has led a large body of research on masks and respirators in health workers, including four randomized clinical trials. She is the author of a book, “Dark Winter: An insider’s guide to pandemics and biosecurity” (Syndey: NewSouth Publishing, 2022), which covers the history and politics of the controversies around N95 and masks. Dr. Prather reported no disclosures. Dr. Greenhalgh is a member of Independent SAGE and an unpaid adviser to the philanthropic fund Balvi. Dr. Fisman has served as a paid legal expert for the Ontario Nurses’ Association in their challenge to Directive 5, which restricted access to N95 masks in health care. He also served as a paid legal expert for the Elementary Teachers’ Federation of Ontario in its efforts to make schools safer in Ontario.
A version of this article first appeared on Medscape.com.
The study’s senior author is John Conly, MD, an infectious disease specialist and professor at the University of Calgary (Alta.), and Alberta Health Services. The findings are not consistent with those of many other studies on this topic.
Commenting about Dr. Conly’s study, Eric Topol, MD, editor-in-chief of Medscape, wrote: “It’s woefully underpowered but ruled out a doubling of hazard for use of medical masks.”
The study, which was partially funded by the World Health Organization, was published online in Annals of Internal Medicine.
This is not the first time that Dr. Conly, who also advises the WHO, has been the subject of controversy. He previously denied that COVID-19 is airborne – a position that is contradicted by strong evidence. In 2021, Dr. Conly made headlines with his controversial claim that N95 respirators can cause harms, including oxygen depletion and carbon dioxide retention.
A detailed examination by the Center for Infectious Disease Research and Policy (CIDRAP) at the University of Minnesota, Minneapolis, pointed out numerous scientific flaws in the study, including inconsistent use of both types of masks. The study also examined health care workers in four very different countries (Canada, Israel, Egypt, and Pakistan) during different periods of the pandemic, which may have affected the results. Furthermore, the study did not account for vaccination status and lacked a control group. CIDRAP receives funding from 3M, which makes N95 respirators.
In a commentary published alongside the study, Roger Chou, MD, professor of medicine at Oregon Health & Science University, Portland, said that the results were “not definitive,” with “a generous noninferiority threshold” that is actually “consistent with up to a relative 70% increased risk ... which may be unacceptable to many health workers.”
Lead study author Mark Loeb, MD, professor of infectious diseases at McMaster University, Hamilton, Ont., defended the findings. “The confidence intervals around this, that is, what the possible results could be if the trial was repeated many times, range from −2.5% to 4.9%,” he told this news organization. “This means that the risk of a COVID-19 infection in those using the medical masks could have ranged from anywhere from 2.5% reduction in risk to a 4.9% increase in risk. Readers and policy makers can decide for themselves about this.”
“There is no point continuing to run underpowered, poorly designed studies that are designed to confirm existing biases,” Raina MacIntyre, PhD, professor of global biosecurity and head of the Biosecurity Program at the Kirby Institute, Sydney, said in an interview. “The new study in Annals of Internal Medicine is entirely consistent with our finding that to prevent infection, you need an N95, and it needs to be worn throughout the whole shift. A surgical mask and intermittent use of N95 are equally ineffective. This should not surprise anyone, given a surgical mask is not designed as respiratory protection but is designed to prevent splash or spray of liquid on the face. Only a respirator is designed as respiratory protection through both the seal around the face and the filter of the face piece to prevent inhalation of virus laden aerosols, but you need to wear it continually in a high-risk environment like a hospital.”
“It makes zero sense to do a randomized trial on something you can measure directly,” said Kimberly Prather, PhD, an atmospheric chemist, professor, and director of the NSF Center for Aerosol Impacts on Chemistry of the Environment at the University of California, San Diego. “In fact, many studies have shown aerosols leaking out of surgical masks. Surgical masks are designed to block large spray droplets. Aerosols (0.5-3 mcm), which have been shown to contain infectious SARS-CoV-2 virus, travel with the air flow, and escape.”
“This study ... will be used to justify policies of supplying health care workers, and perhaps patients and visitors, too, with inadequate protection,” Trish Greenhalgh, MD, professor of primary care health sciences at the University of Oxford (England), told this news organization.
“These authors have been pushing back against treating COVID as airborne for 3 years,” David Fisman, MD, an epidemiologist and infectious disease specialist at the University of Toronto, said in an interview. “So, you’ll see these folks brandishing this very flawed trial to justify continuing the infection control practices that have been so disastrous throughout the pandemic.”
The study was funded by the World Health Organization, the Canadian Institutes of Health Research, and the Juravinski Research Institute. Dr. Conly reported receiving grants from the Canadian Institutes for Health Research, Pfizer, and the WHO. Dr. Chou disclosed being a methodologist for WHO guidelines on infection prevention and control measures for COVID-19. Dr. Loeb disclosed payment for expert testimony on personal protective equipment from the government of Manitoba and the Peel District School Board. Dr. MacIntyre has led a large body of research on masks and respirators in health workers, including four randomized clinical trials. She is the author of a book, “Dark Winter: An insider’s guide to pandemics and biosecurity” (Syndey: NewSouth Publishing, 2022), which covers the history and politics of the controversies around N95 and masks. Dr. Prather reported no disclosures. Dr. Greenhalgh is a member of Independent SAGE and an unpaid adviser to the philanthropic fund Balvi. Dr. Fisman has served as a paid legal expert for the Ontario Nurses’ Association in their challenge to Directive 5, which restricted access to N95 masks in health care. He also served as a paid legal expert for the Elementary Teachers’ Federation of Ontario in its efforts to make schools safer in Ontario.
A version of this article first appeared on Medscape.com.
FROM ANNALS OF INTERNAL MEDICINE
Have long COVID? Newest booster vaccines may help you
Yet at 58, the Arizona writer is in no hurry to get the latest vaccine booster. “I just don’t want to risk getting any sicker,” she said.
Ms. Dishner has had two doses of vaccine plus two boosters. Each time, she had what regulators consider to be mild reactions, including a sore arm, slight fever, nausea, and body aches. Still, there’s some evidence that the newest booster, which protects against some of the later variants, could help people like Ms. Dishner in several ways, said Ziyad Al-Aly, MD, a clinical epidemiologist and prolific long COVID researcher at Washington University in St. Louis.
“A bivalent booster might actually [help with] your long COVID,” he said.
There may be other benefits. “What vaccines or current vaccine boosters do is reduce your risk of progression to severe COVID-19 illness,” Dr. Al-Aly said. “You are avoiding hospital stays or even worse; you’re avoiding potentially fatal outcomes after infection. And that’s really worth it. Who wants to be in the hospital this Christmas holiday?”
Each time people are infected with SARS-CoV-2, the virus that causes COVID-19, they have a fresh risk of not only getting severely ill or dying, but of developing long COVID, Dr. Al-Aly and colleagues found in a study published in Nature Medicine. “If you dodged the bullet the first time and did not get long COVID after the first infection, if you get reinfected, you’re trying your luck again,” Dr. Al-Aly said. “I would advise people not to get reinfected, which is another reason to get the booster.”
In a recent review in The Lancet eClinicalMedicine, an international team of researchers looked at 11 studies that sought to find out if vaccines affected long COVID symptoms. Seven of those studies found that people’s symptoms improved after they were vaccinated, and four found that symptoms mostly remained the same. One found symptoms got worse in some patients.
A study of 28,000 people published in the British Medical Journal found more evidence that vaccination may help ease symptoms. “Vaccination may contribute to a reduction in the population health burden of long COVID,” the team at the United Kingdom’s Office for National Statistics concluded. Most studies found vaccination reduced the risk of getting long COVID in the first place.
Vaccines prompt the body to produce antibodies, which stop a microbe from infecting cells. They also prompt the production of immune cells called T cells, which continue to hunt down and attack a pathogen even after infection.
A booster dose could help rev up that immune response in a patient with long COVID, said Stephen J. Thomas, MD, an infectious disease specialist at Upstate Medical Center in Syracuse, N.Y., and the center’s lead principal investigator for Pfizer/BioNTech’s COVID-19 2020 vaccine trial.
Some scientists believe long COVID might be caused when the virus persists in parts of the body where the immune system isn’t particularly active. Although they don’t fully understand the workings of the many and varied long COVID symptoms, they have a good idea about why people with long COVID often do better after receiving a vaccine or booster.
“The theory is that by boosting, the immune system may be able to ‘mop up’ those virus stragglers that have remained behind after your first cleanup attempt,” Dr. Thomas said.
“The vaccine is almost lending a hand or helping your immune response to clear that virus,” Dr. Al-Aly said.
It could be difficult for long COVID patients to make an informed decision about boosters, given the lack of studies that focus exclusively on the relationship between long COVID and boosters, according to Scott Roberts, MD, associate medical director for infection prevention at Yale New Haven (Conn.) Hospital.
Dr. Roberts recommended that patients speak with their health care providers and read about the bivalent booster on trusted sites such as those sponsored by the Food and Drug Administration and the Centers for Disease Control and Prevention. Long COVID patients should get the latest boosters, especially as there’s no evidence they are unsafe for them. “The antibody response is appropriately boosted, and there is a decent chance this will help reduce the impact of long COVID as well,” he said. “Waiting will only increase the risk of getting infected and increase the chances of long COVID.”
Only 12% of Americans 5 years and older have received the updated booster, according to the CDC, although it’s recommended for everyone. Just over 80% of Americans have gotten at least one vaccine dose. Dr. Thomas understands why the uptake has been so low: Along with people like Ms. Dishner, who fear more side effects or worse symptoms, there are those who believe that hybrid immunity – vaccination immunity plus natural infection – is superior to vaccination alone and that they don’t need a booster.
Studies show that the bivalent boosters, which protect against older and newer variants, can target even the new, predominant COVID-19 strains. Whether that is enough to convince people in the no-booster camp who lost faith when their vaccinated peers started getting COVID-19 is unclear, although, as Dr. Al-Aly has pointed out, vaccinations help keep people from getting so sick that they wind up in the hospital. And, with most of the population having received at least one dose of vaccine, most of those getting infected will naturally come from among the vaccinated.
Thomas describes the expectation that vaccines would prevent everyone from getting sick as “one of the major fails” of the pandemic.
Counting on a vaccine to confer 100% immunity is “a very high bar,” he said. “I think that’s what people expected, and when they weren’t seeing it, they kind of said: ‘Well, what’s the point? You know, things are getting better. I’d rather take my chances than keep going and getting boosted.’ ”
One point – and it’s a critical one – is that vaccination immunity wanes. Plus new variants arise that can evade at least some of the immunity provided by vaccination. That’s why boosters are built into the COVID vaccination program.
While it’s not clear why some long COVID patients see improvements in their symptoms after being vaccinated or boosted and others do not, Dr. Al-Aly said there’s little evidence vaccines can make long COVID worse. “There are some reports out there that some people with long COVID, when they got a vaccine or booster, their symptoms got worse. You’ll read anecdotes on this side,” he said, adding that efforts to see if this is really happening have been inconclusive.
“The general consensus is that vaccines really save lives,” Dr. Al-Aly said. “Getting vaccinated, even if you are a long COVID patient, is better than not getting vaccinated.”
A version of this article first appeared on WebMD.com.
Yet at 58, the Arizona writer is in no hurry to get the latest vaccine booster. “I just don’t want to risk getting any sicker,” she said.
Ms. Dishner has had two doses of vaccine plus two boosters. Each time, she had what regulators consider to be mild reactions, including a sore arm, slight fever, nausea, and body aches. Still, there’s some evidence that the newest booster, which protects against some of the later variants, could help people like Ms. Dishner in several ways, said Ziyad Al-Aly, MD, a clinical epidemiologist and prolific long COVID researcher at Washington University in St. Louis.
“A bivalent booster might actually [help with] your long COVID,” he said.
There may be other benefits. “What vaccines or current vaccine boosters do is reduce your risk of progression to severe COVID-19 illness,” Dr. Al-Aly said. “You are avoiding hospital stays or even worse; you’re avoiding potentially fatal outcomes after infection. And that’s really worth it. Who wants to be in the hospital this Christmas holiday?”
Each time people are infected with SARS-CoV-2, the virus that causes COVID-19, they have a fresh risk of not only getting severely ill or dying, but of developing long COVID, Dr. Al-Aly and colleagues found in a study published in Nature Medicine. “If you dodged the bullet the first time and did not get long COVID after the first infection, if you get reinfected, you’re trying your luck again,” Dr. Al-Aly said. “I would advise people not to get reinfected, which is another reason to get the booster.”
In a recent review in The Lancet eClinicalMedicine, an international team of researchers looked at 11 studies that sought to find out if vaccines affected long COVID symptoms. Seven of those studies found that people’s symptoms improved after they were vaccinated, and four found that symptoms mostly remained the same. One found symptoms got worse in some patients.
A study of 28,000 people published in the British Medical Journal found more evidence that vaccination may help ease symptoms. “Vaccination may contribute to a reduction in the population health burden of long COVID,” the team at the United Kingdom’s Office for National Statistics concluded. Most studies found vaccination reduced the risk of getting long COVID in the first place.
Vaccines prompt the body to produce antibodies, which stop a microbe from infecting cells. They also prompt the production of immune cells called T cells, which continue to hunt down and attack a pathogen even after infection.
A booster dose could help rev up that immune response in a patient with long COVID, said Stephen J. Thomas, MD, an infectious disease specialist at Upstate Medical Center in Syracuse, N.Y., and the center’s lead principal investigator for Pfizer/BioNTech’s COVID-19 2020 vaccine trial.
Some scientists believe long COVID might be caused when the virus persists in parts of the body where the immune system isn’t particularly active. Although they don’t fully understand the workings of the many and varied long COVID symptoms, they have a good idea about why people with long COVID often do better after receiving a vaccine or booster.
“The theory is that by boosting, the immune system may be able to ‘mop up’ those virus stragglers that have remained behind after your first cleanup attempt,” Dr. Thomas said.
“The vaccine is almost lending a hand or helping your immune response to clear that virus,” Dr. Al-Aly said.
It could be difficult for long COVID patients to make an informed decision about boosters, given the lack of studies that focus exclusively on the relationship between long COVID and boosters, according to Scott Roberts, MD, associate medical director for infection prevention at Yale New Haven (Conn.) Hospital.
Dr. Roberts recommended that patients speak with their health care providers and read about the bivalent booster on trusted sites such as those sponsored by the Food and Drug Administration and the Centers for Disease Control and Prevention. Long COVID patients should get the latest boosters, especially as there’s no evidence they are unsafe for them. “The antibody response is appropriately boosted, and there is a decent chance this will help reduce the impact of long COVID as well,” he said. “Waiting will only increase the risk of getting infected and increase the chances of long COVID.”
Only 12% of Americans 5 years and older have received the updated booster, according to the CDC, although it’s recommended for everyone. Just over 80% of Americans have gotten at least one vaccine dose. Dr. Thomas understands why the uptake has been so low: Along with people like Ms. Dishner, who fear more side effects or worse symptoms, there are those who believe that hybrid immunity – vaccination immunity plus natural infection – is superior to vaccination alone and that they don’t need a booster.
Studies show that the bivalent boosters, which protect against older and newer variants, can target even the new, predominant COVID-19 strains. Whether that is enough to convince people in the no-booster camp who lost faith when their vaccinated peers started getting COVID-19 is unclear, although, as Dr. Al-Aly has pointed out, vaccinations help keep people from getting so sick that they wind up in the hospital. And, with most of the population having received at least one dose of vaccine, most of those getting infected will naturally come from among the vaccinated.
Thomas describes the expectation that vaccines would prevent everyone from getting sick as “one of the major fails” of the pandemic.
Counting on a vaccine to confer 100% immunity is “a very high bar,” he said. “I think that’s what people expected, and when they weren’t seeing it, they kind of said: ‘Well, what’s the point? You know, things are getting better. I’d rather take my chances than keep going and getting boosted.’ ”
One point – and it’s a critical one – is that vaccination immunity wanes. Plus new variants arise that can evade at least some of the immunity provided by vaccination. That’s why boosters are built into the COVID vaccination program.
While it’s not clear why some long COVID patients see improvements in their symptoms after being vaccinated or boosted and others do not, Dr. Al-Aly said there’s little evidence vaccines can make long COVID worse. “There are some reports out there that some people with long COVID, when they got a vaccine or booster, their symptoms got worse. You’ll read anecdotes on this side,” he said, adding that efforts to see if this is really happening have been inconclusive.
“The general consensus is that vaccines really save lives,” Dr. Al-Aly said. “Getting vaccinated, even if you are a long COVID patient, is better than not getting vaccinated.”
A version of this article first appeared on WebMD.com.
Yet at 58, the Arizona writer is in no hurry to get the latest vaccine booster. “I just don’t want to risk getting any sicker,” she said.
Ms. Dishner has had two doses of vaccine plus two boosters. Each time, she had what regulators consider to be mild reactions, including a sore arm, slight fever, nausea, and body aches. Still, there’s some evidence that the newest booster, which protects against some of the later variants, could help people like Ms. Dishner in several ways, said Ziyad Al-Aly, MD, a clinical epidemiologist and prolific long COVID researcher at Washington University in St. Louis.
“A bivalent booster might actually [help with] your long COVID,” he said.
There may be other benefits. “What vaccines or current vaccine boosters do is reduce your risk of progression to severe COVID-19 illness,” Dr. Al-Aly said. “You are avoiding hospital stays or even worse; you’re avoiding potentially fatal outcomes after infection. And that’s really worth it. Who wants to be in the hospital this Christmas holiday?”
Each time people are infected with SARS-CoV-2, the virus that causes COVID-19, they have a fresh risk of not only getting severely ill or dying, but of developing long COVID, Dr. Al-Aly and colleagues found in a study published in Nature Medicine. “If you dodged the bullet the first time and did not get long COVID after the first infection, if you get reinfected, you’re trying your luck again,” Dr. Al-Aly said. “I would advise people not to get reinfected, which is another reason to get the booster.”
In a recent review in The Lancet eClinicalMedicine, an international team of researchers looked at 11 studies that sought to find out if vaccines affected long COVID symptoms. Seven of those studies found that people’s symptoms improved after they were vaccinated, and four found that symptoms mostly remained the same. One found symptoms got worse in some patients.
A study of 28,000 people published in the British Medical Journal found more evidence that vaccination may help ease symptoms. “Vaccination may contribute to a reduction in the population health burden of long COVID,” the team at the United Kingdom’s Office for National Statistics concluded. Most studies found vaccination reduced the risk of getting long COVID in the first place.
Vaccines prompt the body to produce antibodies, which stop a microbe from infecting cells. They also prompt the production of immune cells called T cells, which continue to hunt down and attack a pathogen even after infection.
A booster dose could help rev up that immune response in a patient with long COVID, said Stephen J. Thomas, MD, an infectious disease specialist at Upstate Medical Center in Syracuse, N.Y., and the center’s lead principal investigator for Pfizer/BioNTech’s COVID-19 2020 vaccine trial.
Some scientists believe long COVID might be caused when the virus persists in parts of the body where the immune system isn’t particularly active. Although they don’t fully understand the workings of the many and varied long COVID symptoms, they have a good idea about why people with long COVID often do better after receiving a vaccine or booster.
“The theory is that by boosting, the immune system may be able to ‘mop up’ those virus stragglers that have remained behind after your first cleanup attempt,” Dr. Thomas said.
“The vaccine is almost lending a hand or helping your immune response to clear that virus,” Dr. Al-Aly said.
It could be difficult for long COVID patients to make an informed decision about boosters, given the lack of studies that focus exclusively on the relationship between long COVID and boosters, according to Scott Roberts, MD, associate medical director for infection prevention at Yale New Haven (Conn.) Hospital.
Dr. Roberts recommended that patients speak with their health care providers and read about the bivalent booster on trusted sites such as those sponsored by the Food and Drug Administration and the Centers for Disease Control and Prevention. Long COVID patients should get the latest boosters, especially as there’s no evidence they are unsafe for them. “The antibody response is appropriately boosted, and there is a decent chance this will help reduce the impact of long COVID as well,” he said. “Waiting will only increase the risk of getting infected and increase the chances of long COVID.”
Only 12% of Americans 5 years and older have received the updated booster, according to the CDC, although it’s recommended for everyone. Just over 80% of Americans have gotten at least one vaccine dose. Dr. Thomas understands why the uptake has been so low: Along with people like Ms. Dishner, who fear more side effects or worse symptoms, there are those who believe that hybrid immunity – vaccination immunity plus natural infection – is superior to vaccination alone and that they don’t need a booster.
Studies show that the bivalent boosters, which protect against older and newer variants, can target even the new, predominant COVID-19 strains. Whether that is enough to convince people in the no-booster camp who lost faith when their vaccinated peers started getting COVID-19 is unclear, although, as Dr. Al-Aly has pointed out, vaccinations help keep people from getting so sick that they wind up in the hospital. And, with most of the population having received at least one dose of vaccine, most of those getting infected will naturally come from among the vaccinated.
Thomas describes the expectation that vaccines would prevent everyone from getting sick as “one of the major fails” of the pandemic.
Counting on a vaccine to confer 100% immunity is “a very high bar,” he said. “I think that’s what people expected, and when they weren’t seeing it, they kind of said: ‘Well, what’s the point? You know, things are getting better. I’d rather take my chances than keep going and getting boosted.’ ”
One point – and it’s a critical one – is that vaccination immunity wanes. Plus new variants arise that can evade at least some of the immunity provided by vaccination. That’s why boosters are built into the COVID vaccination program.
While it’s not clear why some long COVID patients see improvements in their symptoms after being vaccinated or boosted and others do not, Dr. Al-Aly said there’s little evidence vaccines can make long COVID worse. “There are some reports out there that some people with long COVID, when they got a vaccine or booster, their symptoms got worse. You’ll read anecdotes on this side,” he said, adding that efforts to see if this is really happening have been inconclusive.
“The general consensus is that vaccines really save lives,” Dr. Al-Aly said. “Getting vaccinated, even if you are a long COVID patient, is better than not getting vaccinated.”
A version of this article first appeared on WebMD.com.
FROM NATURE MEDICINE
Pediatric emergencies associated with unnecessary testing: AAP
Children seen for these conditions in emergency settings and even in primary care offices could experience avoidable pain, exposure to harmful radiation, and other harms, according to the group.
“The emergency department has the ability to rapidly perform myriad diagnostic tests and receive results quickly,” said Paul Mullan, MD, MPH, chair of the AAP’s Section of Emergency Medicine’s Choosing Wisely task force. “However, this comes with the danger of diagnostic overtesting.”
The five recommendations are as follows:
- Radiographs should not be obtained for children with bronchiolitis, croup, asthma, or first-time wheezing.
- Laboratory tests for screening should not be undertaken in the medical clearance process of children who require inpatient psychiatric admission unless clinically indicated.
- Laboratory testing or a CT scan of the head should not be ordered for a child with an unprovoked, generalized seizure or a simple febrile seizure whose mental status has returned to baseline.
- Abdominal radiographs should not be obtained for suspected constipation.
- Comprehensive viral panel testing should not be undertaken for children who are suspected of having respiratory viral illnesses.
The AAP task force partnered with Choosing Wisely Canada to create the recommendations. The list is the first of its kind to be published jointly by two countries, according to the release.
“We hope this Choosing Wisely list will encourage clinicians to rely on their clinical skills and avoid unnecessary tests,” said Dr. Mullan, who is also a physician at Children’s Hospital of the King’s Daughters and professor of pediatrics at Eastern Virginia Medical School, Norfolk.
A version of this article first appeared on Medscape.com.
Children seen for these conditions in emergency settings and even in primary care offices could experience avoidable pain, exposure to harmful radiation, and other harms, according to the group.
“The emergency department has the ability to rapidly perform myriad diagnostic tests and receive results quickly,” said Paul Mullan, MD, MPH, chair of the AAP’s Section of Emergency Medicine’s Choosing Wisely task force. “However, this comes with the danger of diagnostic overtesting.”
The five recommendations are as follows:
- Radiographs should not be obtained for children with bronchiolitis, croup, asthma, or first-time wheezing.
- Laboratory tests for screening should not be undertaken in the medical clearance process of children who require inpatient psychiatric admission unless clinically indicated.
- Laboratory testing or a CT scan of the head should not be ordered for a child with an unprovoked, generalized seizure or a simple febrile seizure whose mental status has returned to baseline.
- Abdominal radiographs should not be obtained for suspected constipation.
- Comprehensive viral panel testing should not be undertaken for children who are suspected of having respiratory viral illnesses.
The AAP task force partnered with Choosing Wisely Canada to create the recommendations. The list is the first of its kind to be published jointly by two countries, according to the release.
“We hope this Choosing Wisely list will encourage clinicians to rely on their clinical skills and avoid unnecessary tests,” said Dr. Mullan, who is also a physician at Children’s Hospital of the King’s Daughters and professor of pediatrics at Eastern Virginia Medical School, Norfolk.
A version of this article first appeared on Medscape.com.
Children seen for these conditions in emergency settings and even in primary care offices could experience avoidable pain, exposure to harmful radiation, and other harms, according to the group.
“The emergency department has the ability to rapidly perform myriad diagnostic tests and receive results quickly,” said Paul Mullan, MD, MPH, chair of the AAP’s Section of Emergency Medicine’s Choosing Wisely task force. “However, this comes with the danger of diagnostic overtesting.”
The five recommendations are as follows:
- Radiographs should not be obtained for children with bronchiolitis, croup, asthma, or first-time wheezing.
- Laboratory tests for screening should not be undertaken in the medical clearance process of children who require inpatient psychiatric admission unless clinically indicated.
- Laboratory testing or a CT scan of the head should not be ordered for a child with an unprovoked, generalized seizure or a simple febrile seizure whose mental status has returned to baseline.
- Abdominal radiographs should not be obtained for suspected constipation.
- Comprehensive viral panel testing should not be undertaken for children who are suspected of having respiratory viral illnesses.
The AAP task force partnered with Choosing Wisely Canada to create the recommendations. The list is the first of its kind to be published jointly by two countries, according to the release.
“We hope this Choosing Wisely list will encourage clinicians to rely on their clinical skills and avoid unnecessary tests,” said Dr. Mullan, who is also a physician at Children’s Hospital of the King’s Daughters and professor of pediatrics at Eastern Virginia Medical School, Norfolk.
A version of this article first appeared on Medscape.com.