User login
Does the use of frankincense make sense in dermatology?
The Boswellia serrata exudate or gum (known in India as “guggulu”) that forms an aromatic resin traditionally used as incense – and known as frankincense (especially when retrieved from Boswellia species found in Eritrea and Somalia but also from the Indian variety) – has been considered for thousands of years to possess therapeutic properties. It is used in Ayurvedic medicine, as well as in traditional medicine in China and the Middle East, particularly for its anti-inflammatory effects to treat chronic conditions.1-8 In fact, such essential oils have been used since 2800 BC to treat various inflammatory conditions, including skin sores and wounds, as well as in perfumes and incense.2,9 In the West, use of frankincense dates back to thousands of years as well, more often found in the form of incense for religious and cultural ceremonies.7 Over the past 2 decades, .3 This column focuses on some of the emerging data on this ancient botanical agent.

Chemical constituents
Terpenoids and essential oils are the primary components of frankincense and are known to impart anti-inflammatory and anticancer activity. The same is true for myrrh, which has been combined with frankincense in traditional Chinese medicine as a single medication for millennia, with the two acting synergistically and considered still to be a potent combination in conferring various biological benefits.7
In 2010, in a systematic review of the anti-inflammatory and anticancer activities of Boswellia species and their chemical ingredients, Efferth and Oesch found that frankincense blocks the production of leukotrienes, cyclooxygenase (COX) 1 and 2, as well as 5-lipoxygenase; and oxidative stress. It also contributes to regulation of immune cells from the innate and acquired immune systems and exerts anticancer activity by influencing signaling transduction responsible for cell cycle arrest, as well as inhibition of proliferation, angiogenesis, invasion, and metastasis. The investigators also reported on clinical trial results that have found efficacy of frankincense and its constituents in ameliorating symptoms of psoriasis and erythematous eczema, among other disorders.3
Anti-inflammatory activity
Li et al. completed a study in 2016 to identify the active ingredients responsible for the anti-inflammatory and analgesic effects of frankincense. They found that alpha-pinene, linalool, and 1-octanol were key contributors. These constituents were noted for suppressing COX-2 overexpression in mice, as well as nociceptive stimulus-induced inflammatory infiltrates.10
Noting the increasing popularity of frankincense essential oil in skin care, despite a paucity of data, in 2017, Han et al. evaluated the biological activities of the essential oil in pre-inflamed human dermal fibroblasts using 17 key protein biomarkers. Frankincense essential oil displayed significant antiproliferative activity and suppressed collagen III, interferon gamma-induced protein 10, and intracellular adhesion molecule 1. The investigators referred to the overall encouraging potential of frankincense essential oil to exert influence over inflammation and tissue remodeling in human skin and called for additional research into its mechanisms of action and active constituents.11
Anticancer activity
The main active ingredient in frankincense, boswellic acid, has been shown to promote apoptosis, suppress matrix metalloproteinase secretion, and hinder migration in metastatic melanoma cell lines in mice.6,12
In 2019, Hakkim et al. demonstrated that frankincense essential oil yielded substantial antimelanoma activity in vitro and in vivo and ameliorated hepatotoxicity caused by acetaminophen.13
There is one case report in the literature on the use of frankincense as a treatment for skin cancer. A 56-year-old man received frankincense oil multiple times a day for 4 months to treat a nodular basal cell carcinoma on one arm (which resolved) and an infiltrative BCC on the chest (some focal residual tumor remained).6,14 Topical frankincense or boswellic acid has been given a grade D recommendation for treating skin cancer, however, because of only one level-of-evidence-5 study.6
Antimicrobial activity
In 2012, de Rapper et al. collected samples of three essential oils of frankincense (Boswellia rivae, Boswellia neglecta, and Boswellia papyrifera) and two essential oil samples of myrrh and sweet myrrh from different regions of Ethiopia to study their anti-infective properties alone and in combination. The investigators observed synergistic and additive effects, particularly between B. papyrifera and Commiphora myrrha. While noting the long history of the combined use of frankincense and myrrh essential oils since 1500 BC, the investigators highlighted their study as the first antimicrobial work to verify the effectiveness of this combination, validating the use of this combination to thwart particular pathogens.15
Just 2 years ago, Ljaljević Grbić et al. evaluated the in vitro antimicrobial potential of the liquid and vapor phases of B. carteri and C. myrrha (frankincense and myrrh, respectively) essential oils, finding that frankincense demonstrated marked capacity to act as a natural antimicrobial agent.9
Transdermal delivery
In 2017, Zhu et al. showed that frankincense and myrrh essential oils promoted the permeability of the Chinese herb Chuanxiong and may facilitate drug elimination from the epidermis via dermal capillaries by dint of improved cutaneous blood flow, thereby augmenting transdermal drug delivery.16 The same team also showed that frankincense and myrrh essential oils, by fostering permeation by enhancing drug delivery across the stratum corneum, can also alter the structure of the stratum corneum.17
Conclusion
The use of frankincense in traditional medicine has a long and impressive track record. Recent research provides reason for optimism, and further investigating the possible incorporation of this botanical agent into modern dermatologic therapies appears warranted. Clearly, however, much more research is needed.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Kimmatkar N et al. Phytomedicine. 2003 Jan;10(1):3-7.
2. Ammon HP. Wien Med Wochenschr. 2002;152(15-16):373-8.
3. Efferth T & Oesch F. Semin Cancer Biol. 2020 Feb 4;S1044-579X(20)30034-1.
4. Banno N et al. J Ethnopharmacol. 2006 Sep 19;107(2):249-53.
5. Poeckel D & Werz O. Curr Med Chem. 2006;13(28):3359-69.
6. Li JY, Kampp JT. Dermatol Surg. 2019 Jan;45(1):58-67.
7. Cao B et al. Molecules. 2019 Aug 24;24(17): 3076.
8. Mertens M et al. Flavour Fragr J. 2009;24:279-300.
9. Ljaljević Grbić M et al. J Ethnopharmacol. 2018 Jun 12;219:1-14.
10. Li XJ et al. J Ethnopharmacol. 2016 Feb 17;179:22-6.
11. Han X et al. Biochim Open. 2017 Feb 3;4:31-5.
12. Zhao W et al. Cancer Detect Prev. 2003;27:67-75.
13. Hakkim FL et al. Oncotarget. 2019 May 28;10(37):3472-90.
14. Fung K et al. OA Altern Med 2013;1:14.
15. de Rapper S et al. Lett Appl Microbiol. 2012 Apr;54(4):352-8.
16. Zhu XF et al. Zhongguo Zhong Yao Za Zhi. 2017 Feb;42(4):680-5.
17. Guan YM et al. Zhongguo Zhong Yao Za Zhi. 2017 Sep;42(17):3350-5.
The Boswellia serrata exudate or gum (known in India as “guggulu”) that forms an aromatic resin traditionally used as incense – and known as frankincense (especially when retrieved from Boswellia species found in Eritrea and Somalia but also from the Indian variety) – has been considered for thousands of years to possess therapeutic properties. It is used in Ayurvedic medicine, as well as in traditional medicine in China and the Middle East, particularly for its anti-inflammatory effects to treat chronic conditions.1-8 In fact, such essential oils have been used since 2800 BC to treat various inflammatory conditions, including skin sores and wounds, as well as in perfumes and incense.2,9 In the West, use of frankincense dates back to thousands of years as well, more often found in the form of incense for religious and cultural ceremonies.7 Over the past 2 decades, .3 This column focuses on some of the emerging data on this ancient botanical agent.
Chemical constituents
Terpenoids and essential oils are the primary components of frankincense and are known to impart anti-inflammatory and anticancer activity. The same is true for myrrh, which has been combined with frankincense in traditional Chinese medicine as a single medication for millennia, with the two acting synergistically and considered still to be a potent combination in conferring various biological benefits.7
In 2010, in a systematic review of the anti-inflammatory and anticancer activities of Boswellia species and their chemical ingredients, Efferth and Oesch found that frankincense blocks the production of leukotrienes, cyclooxygenase (COX) 1 and 2, as well as 5-lipoxygenase; and oxidative stress. It also contributes to regulation of immune cells from the innate and acquired immune systems and exerts anticancer activity by influencing signaling transduction responsible for cell cycle arrest, as well as inhibition of proliferation, angiogenesis, invasion, and metastasis. The investigators also reported on clinical trial results that have found efficacy of frankincense and its constituents in ameliorating symptoms of psoriasis and erythematous eczema, among other disorders.3
Anti-inflammatory activity
Li et al. completed a study in 2016 to identify the active ingredients responsible for the anti-inflammatory and analgesic effects of frankincense. They found that alpha-pinene, linalool, and 1-octanol were key contributors. These constituents were noted for suppressing COX-2 overexpression in mice, as well as nociceptive stimulus-induced inflammatory infiltrates.10
Noting the increasing popularity of frankincense essential oil in skin care, despite a paucity of data, in 2017, Han et al. evaluated the biological activities of the essential oil in pre-inflamed human dermal fibroblasts using 17 key protein biomarkers. Frankincense essential oil displayed significant antiproliferative activity and suppressed collagen III, interferon gamma-induced protein 10, and intracellular adhesion molecule 1. The investigators referred to the overall encouraging potential of frankincense essential oil to exert influence over inflammation and tissue remodeling in human skin and called for additional research into its mechanisms of action and active constituents.11
Anticancer activity
The main active ingredient in frankincense, boswellic acid, has been shown to promote apoptosis, suppress matrix metalloproteinase secretion, and hinder migration in metastatic melanoma cell lines in mice.6,12
In 2019, Hakkim et al. demonstrated that frankincense essential oil yielded substantial antimelanoma activity in vitro and in vivo and ameliorated hepatotoxicity caused by acetaminophen.13
There is one case report in the literature on the use of frankincense as a treatment for skin cancer. A 56-year-old man received frankincense oil multiple times a day for 4 months to treat a nodular basal cell carcinoma on one arm (which resolved) and an infiltrative BCC on the chest (some focal residual tumor remained).6,14 Topical frankincense or boswellic acid has been given a grade D recommendation for treating skin cancer, however, because of only one level-of-evidence-5 study.6
Antimicrobial activity
In 2012, de Rapper et al. collected samples of three essential oils of frankincense (Boswellia rivae, Boswellia neglecta, and Boswellia papyrifera) and two essential oil samples of myrrh and sweet myrrh from different regions of Ethiopia to study their anti-infective properties alone and in combination. The investigators observed synergistic and additive effects, particularly between B. papyrifera and Commiphora myrrha. While noting the long history of the combined use of frankincense and myrrh essential oils since 1500 BC, the investigators highlighted their study as the first antimicrobial work to verify the effectiveness of this combination, validating the use of this combination to thwart particular pathogens.15
Just 2 years ago, Ljaljević Grbić et al. evaluated the in vitro antimicrobial potential of the liquid and vapor phases of B. carteri and C. myrrha (frankincense and myrrh, respectively) essential oils, finding that frankincense demonstrated marked capacity to act as a natural antimicrobial agent.9
Transdermal delivery
In 2017, Zhu et al. showed that frankincense and myrrh essential oils promoted the permeability of the Chinese herb Chuanxiong and may facilitate drug elimination from the epidermis via dermal capillaries by dint of improved cutaneous blood flow, thereby augmenting transdermal drug delivery.16 The same team also showed that frankincense and myrrh essential oils, by fostering permeation by enhancing drug delivery across the stratum corneum, can also alter the structure of the stratum corneum.17
Conclusion
The use of frankincense in traditional medicine has a long and impressive track record. Recent research provides reason for optimism, and further investigating the possible incorporation of this botanical agent into modern dermatologic therapies appears warranted. Clearly, however, much more research is needed.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Kimmatkar N et al. Phytomedicine. 2003 Jan;10(1):3-7.
2. Ammon HP. Wien Med Wochenschr. 2002;152(15-16):373-8.
3. Efferth T & Oesch F. Semin Cancer Biol. 2020 Feb 4;S1044-579X(20)30034-1.
4. Banno N et al. J Ethnopharmacol. 2006 Sep 19;107(2):249-53.
5. Poeckel D & Werz O. Curr Med Chem. 2006;13(28):3359-69.
6. Li JY, Kampp JT. Dermatol Surg. 2019 Jan;45(1):58-67.
7. Cao B et al. Molecules. 2019 Aug 24;24(17): 3076.
8. Mertens M et al. Flavour Fragr J. 2009;24:279-300.
9. Ljaljević Grbić M et al. J Ethnopharmacol. 2018 Jun 12;219:1-14.
10. Li XJ et al. J Ethnopharmacol. 2016 Feb 17;179:22-6.
11. Han X et al. Biochim Open. 2017 Feb 3;4:31-5.
12. Zhao W et al. Cancer Detect Prev. 2003;27:67-75.
13. Hakkim FL et al. Oncotarget. 2019 May 28;10(37):3472-90.
14. Fung K et al. OA Altern Med 2013;1:14.
15. de Rapper S et al. Lett Appl Microbiol. 2012 Apr;54(4):352-8.
16. Zhu XF et al. Zhongguo Zhong Yao Za Zhi. 2017 Feb;42(4):680-5.
17. Guan YM et al. Zhongguo Zhong Yao Za Zhi. 2017 Sep;42(17):3350-5.
The Boswellia serrata exudate or gum (known in India as “guggulu”) that forms an aromatic resin traditionally used as incense – and known as frankincense (especially when retrieved from Boswellia species found in Eritrea and Somalia but also from the Indian variety) – has been considered for thousands of years to possess therapeutic properties. It is used in Ayurvedic medicine, as well as in traditional medicine in China and the Middle East, particularly for its anti-inflammatory effects to treat chronic conditions.1-8 In fact, such essential oils have been used since 2800 BC to treat various inflammatory conditions, including skin sores and wounds, as well as in perfumes and incense.2,9 In the West, use of frankincense dates back to thousands of years as well, more often found in the form of incense for religious and cultural ceremonies.7 Over the past 2 decades, .3 This column focuses on some of the emerging data on this ancient botanical agent.
Chemical constituents
Terpenoids and essential oils are the primary components of frankincense and are known to impart anti-inflammatory and anticancer activity. The same is true for myrrh, which has been combined with frankincense in traditional Chinese medicine as a single medication for millennia, with the two acting synergistically and considered still to be a potent combination in conferring various biological benefits.7
In 2010, in a systematic review of the anti-inflammatory and anticancer activities of Boswellia species and their chemical ingredients, Efferth and Oesch found that frankincense blocks the production of leukotrienes, cyclooxygenase (COX) 1 and 2, as well as 5-lipoxygenase; and oxidative stress. It also contributes to regulation of immune cells from the innate and acquired immune systems and exerts anticancer activity by influencing signaling transduction responsible for cell cycle arrest, as well as inhibition of proliferation, angiogenesis, invasion, and metastasis. The investigators also reported on clinical trial results that have found efficacy of frankincense and its constituents in ameliorating symptoms of psoriasis and erythematous eczema, among other disorders.3
Anti-inflammatory activity
Li et al. completed a study in 2016 to identify the active ingredients responsible for the anti-inflammatory and analgesic effects of frankincense. They found that alpha-pinene, linalool, and 1-octanol were key contributors. These constituents were noted for suppressing COX-2 overexpression in mice, as well as nociceptive stimulus-induced inflammatory infiltrates.10
Noting the increasing popularity of frankincense essential oil in skin care, despite a paucity of data, in 2017, Han et al. evaluated the biological activities of the essential oil in pre-inflamed human dermal fibroblasts using 17 key protein biomarkers. Frankincense essential oil displayed significant antiproliferative activity and suppressed collagen III, interferon gamma-induced protein 10, and intracellular adhesion molecule 1. The investigators referred to the overall encouraging potential of frankincense essential oil to exert influence over inflammation and tissue remodeling in human skin and called for additional research into its mechanisms of action and active constituents.11
Anticancer activity
The main active ingredient in frankincense, boswellic acid, has been shown to promote apoptosis, suppress matrix metalloproteinase secretion, and hinder migration in metastatic melanoma cell lines in mice.6,12
In 2019, Hakkim et al. demonstrated that frankincense essential oil yielded substantial antimelanoma activity in vitro and in vivo and ameliorated hepatotoxicity caused by acetaminophen.13
There is one case report in the literature on the use of frankincense as a treatment for skin cancer. A 56-year-old man received frankincense oil multiple times a day for 4 months to treat a nodular basal cell carcinoma on one arm (which resolved) and an infiltrative BCC on the chest (some focal residual tumor remained).6,14 Topical frankincense or boswellic acid has been given a grade D recommendation for treating skin cancer, however, because of only one level-of-evidence-5 study.6
Antimicrobial activity
In 2012, de Rapper et al. collected samples of three essential oils of frankincense (Boswellia rivae, Boswellia neglecta, and Boswellia papyrifera) and two essential oil samples of myrrh and sweet myrrh from different regions of Ethiopia to study their anti-infective properties alone and in combination. The investigators observed synergistic and additive effects, particularly between B. papyrifera and Commiphora myrrha. While noting the long history of the combined use of frankincense and myrrh essential oils since 1500 BC, the investigators highlighted their study as the first antimicrobial work to verify the effectiveness of this combination, validating the use of this combination to thwart particular pathogens.15
Just 2 years ago, Ljaljević Grbić et al. evaluated the in vitro antimicrobial potential of the liquid and vapor phases of B. carteri and C. myrrha (frankincense and myrrh, respectively) essential oils, finding that frankincense demonstrated marked capacity to act as a natural antimicrobial agent.9
Transdermal delivery
In 2017, Zhu et al. showed that frankincense and myrrh essential oils promoted the permeability of the Chinese herb Chuanxiong and may facilitate drug elimination from the epidermis via dermal capillaries by dint of improved cutaneous blood flow, thereby augmenting transdermal drug delivery.16 The same team also showed that frankincense and myrrh essential oils, by fostering permeation by enhancing drug delivery across the stratum corneum, can also alter the structure of the stratum corneum.17
Conclusion
The use of frankincense in traditional medicine has a long and impressive track record. Recent research provides reason for optimism, and further investigating the possible incorporation of this botanical agent into modern dermatologic therapies appears warranted. Clearly, however, much more research is needed.
Dr. Baumann is a private practice dermatologist, researcher, author, and entrepreneur who practices in Miami. She founded the Cosmetic Dermatology Center at the University of Miami in 1997. Dr. Baumann has written two textbooks and a New York Times Best Sellers book for consumers. Dr. Baumann has received funding for advisory boards and/or clinical research trials from Allergan, Galderma, Revance, Evolus, and Burt’s Bees. She is the CEO of Skin Type Solutions Inc., a company that independently tests skin care products and makes recommendations to physicians on which skin care technologies are best. Write to her at [email protected].
References
1. Kimmatkar N et al. Phytomedicine. 2003 Jan;10(1):3-7.
2. Ammon HP. Wien Med Wochenschr. 2002;152(15-16):373-8.
3. Efferth T & Oesch F. Semin Cancer Biol. 2020 Feb 4;S1044-579X(20)30034-1.
4. Banno N et al. J Ethnopharmacol. 2006 Sep 19;107(2):249-53.
5. Poeckel D & Werz O. Curr Med Chem. 2006;13(28):3359-69.
6. Li JY, Kampp JT. Dermatol Surg. 2019 Jan;45(1):58-67.
7. Cao B et al. Molecules. 2019 Aug 24;24(17): 3076.
8. Mertens M et al. Flavour Fragr J. 2009;24:279-300.
9. Ljaljević Grbić M et al. J Ethnopharmacol. 2018 Jun 12;219:1-14.
10. Li XJ et al. J Ethnopharmacol. 2016 Feb 17;179:22-6.
11. Han X et al. Biochim Open. 2017 Feb 3;4:31-5.
12. Zhao W et al. Cancer Detect Prev. 2003;27:67-75.
13. Hakkim FL et al. Oncotarget. 2019 May 28;10(37):3472-90.
14. Fung K et al. OA Altern Med 2013;1:14.
15. de Rapper S et al. Lett Appl Microbiol. 2012 Apr;54(4):352-8.
16. Zhu XF et al. Zhongguo Zhong Yao Za Zhi. 2017 Feb;42(4):680-5.
17. Guan YM et al. Zhongguo Zhong Yao Za Zhi. 2017 Sep;42(17):3350-5.
Early Pilomatrix Carcinoma: A Case Report With Emphasis on Molecular Pathology and Review of the Literature
Pilomatrix carcinoma is a rare adnexal tumor with origin from the germinative matrical cells of the hair follicle. Clinically, it presents as a solitary lesion commonly found in the head and neck region as well as the upper back. The tumors cannot be distinguished by their clinical appearance only and frequently are mistaken for cysts. Histopathologic examination provides the definitive diagnosis in most cases. These carcinomas are aggressive neoplasms with a high probability of local recurrence and distant metastasis. Assessment of the Wnt signaling pathway components such as β-catenin, lymphoid enhancer-binding factor 1 (LEF-1), and caudal-related homeobox transcription factor 2 (CDX-2) potentially can be used for diagnostic purposes and targeted therapy.
We report a rare and unique case of early pilomatrix carcinoma with intralesional melanocytes. We review the molecular pathology and pathogenesis of these carcinomas as well as the significance of early diagnosis.
Case Report
A 73-year-old man with a history of extensive sun exposure presented with a 1-cm, raised, rapidly growing, slightly irregular, purple lesion on the right forearm of 3 months’ duration with tendency to bleed. He did not have a history of skin cancers and was otherwise healthy. Excision was recommended due to the progressive and rapid growth of the lesion.
Histopathologic Findings—Gross examination revealed a 0.9×0.7-cm, raised, slightly irregular lesion located 1 mm away from the closest peripheral margin. Histologically, the lesion was a relatively circumscribed, dermal-based basaloid neoplasm with slightly ill-defined edges involving the superficial and deep dermis (Figure 1A). The neoplasm was formed predominantly of sheets of basaloid cells and small nests of ghost cells, in addition to some squamoid and transitional cells (Figure 1B). The basaloid cells exhibited severe nuclear atypia, pleomorphism, increased nuclear to cytoplasmic ratio (Figure 1C), minimal to moderate amounts of eosinophilic cytoplasm, enlarged nuclei, prominent nucleoli, and coarse chromatin pattern. Abundant mitotic activity and apoptotic bodies were present as well as focal area of central necrosis (Figure 1C). Also, melanophages and a multinucleated giant cell reaction was noted. Elastic trichrome special stain highlighted focal infiltration of the neoplastic cells into the adjacent desmoplastic stroma. Melanin stain was negative for melanin pigment within the neoplasm. Given the presence of severely atypical basaloid cells along with ghost cells indicating matrical differentiation, a diagnosis of pilomatrix carcinoma was rendered.
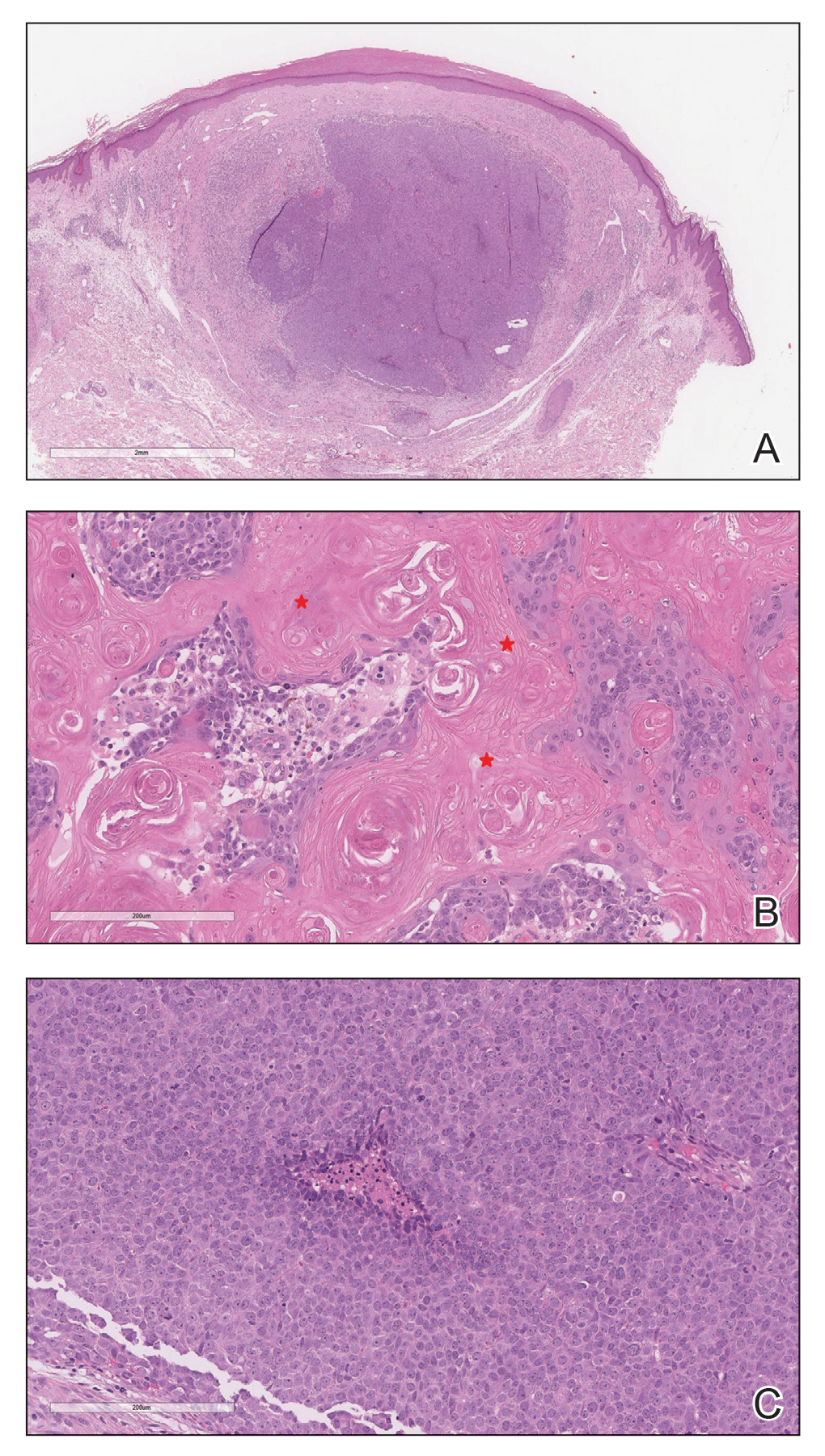
Immunohistochemistry—The neoplastic cells were diffusely positive for p63, CDX-2 (Figure 2A), β-catenin (Figure 2B), and CD10 (Figure 2C), and focally and weakly positive for cytokeratin (CK) 5, BerEP4 (staining the tumor periphery), androgen receptor, and CK18 (a low-molecular-weight keratin). They were negative for monoclonal carcinoembryonic antigen, epithelial membrane antigen, CK7, CK20, CD34, SOX-10, CD56, synaptophysin, and chromogranin. Cytokeratin 14 was positive in the squamoid cells but negative in the basaloid cells. SOX-10 and melanoma cocktail immunostains demonstrated few intralesional dendritic melanocytes.

Comment
Pilomatrix carcinoma is a rare malignant cutaneous adnexal neoplasm with origin from the germinative matrix of the hair bulb region of hair follicles. Pilomatrix carcinoma was first reported in 1980.1,2 These tumors are characterized by rapid growth and aggressive behavior. Their benign counterpart, pilomatrixoma, is a slow-growing, dermal or subcutaneous tumor that rarely recurs after complete excision.
As with pilomatrixoma, pilomatrix carcinomas are asymptomatic and present as solitary dermal or subcutaneous masses3,4 that most commonly are found in the posterior neck, upper back, and preauricular regions of middle-aged or elderly adults with male predominance.5 They range in size from 0.5 to 20 cm with a mean of 4 cm that is slightly larger than pilomatrixoma. Pilomatrix carcinomas predominantly are firm tumors with or without cystic components, and they exhibit a high probability of recurrence and have risk for distant metastasis.6-15
The differential diagnosis includes epidermal cysts, pilomatrixoma, basal cell carcinoma with matrical differentiation, trichoblastoma/trichoblastic carcinoma, and trichilemmal carcinoma. Pilomatrix carcinomas frequently are mistaken for epidermal cysts on clinical examination. Such a distinction can be easily resolved by histopathologic evaluation. The more challenging differential diagnosis is with pilomatrixoma. Histologically, pilomatrixomas consist of a distinct population of cells including basaloid, squamoid, transitional, and shadow cells in variable proportions. The basaloid cells transition to shadow cells in an organized zonal fashion.16 Compared to pilomatrixomas, pilomatrix carcinomas often show predominance of the basaloid cells; marked cytologic atypia and pleomorphism; numerous mitotic figures; deep infiltrative pattern into subcutaneous fat, fascia, and skeletal muscle; stromal desmoplasia; necrosis; and neurovascular invasion (Tables 1 and 2). Furthermore, the shadow cells tend to form a small nested pattern in pilomatrix carcinoma instead of the flat sheetlike pattern usually observed in pilomatrixoma.16 Basal cell carcinoma with matrical differentiation can pose a diagnostic challenge in the differential diagnosis; basal cell carcinoma usually exhibits a peripheral palisade of the basaloid cells accompanied by retraction spaces separating the tumor from the stroma. Trichoblastoma/trichoblastic carcinoma with matrical differentiation can be distinguished by its exuberant stroma, prominent primitive hair follicles, and papillary mesenchymal bodies. Trichilemmal carcinomas are recognized by their connection to the overlying epidermis, peripheral palisading, and presence of clear cells, while pilomatrix carcinoma lacks connection to the surface epithelium.

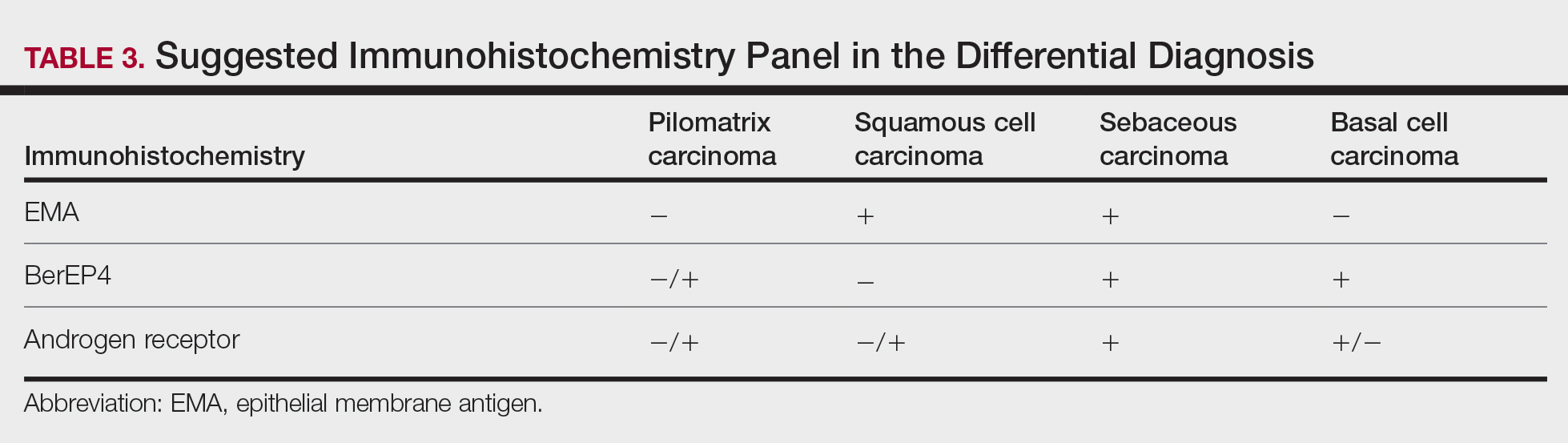
Immunohistochemical stains have little to no role in the differential diagnosis, and morphology is the mainstay in making the diagnosis. Rarely, pilomatrix carcinoma can be confused with poorly differentiated sebaceous carcinoma and poorly differentiated squamous cell carcinoma. Although careful scrutiny of the histologic features may help identify mature sebocytes in sebaceous carcinoma, evidence of keratinization in squamous cell carcinoma and ghost cells in pilomatrix carcinoma, using a panel of immunohistochemical stains can be helpful in reaching the final diagnosis (Table 3).

The development of hair matrix tumors have been known to harbor mutations in exon 3 of the catenin beta-1 gene, CTNNB1, that encodes for β-catenin, a downstream effector in the Wnt signaling pathway responsible for differentiation, proliferation, and adhesion of epithelial stem cells.17-21 In a study conducted by Kazakov et al,22 DNA was extracted from 86 lesions: 4 were pilomatrixomas and 1 was a pilomatrix carcinoma. A polymerase chain reaction assay revealed 8 pathogenic variants of the β-catenin gene. D32Y (CTNNB1):c.94G>T (p.Asp32Tyr) and G34R (CTNNB1):c.100G>C (p.Gly34Arg) were the mutations present in pilomatrixoma and pilomatrix carcinoma, respectively.22 In addition, there are several proteins that are part of the Wnt pathway in addition to β-catenin—LEF-1 and CDX-2.
Tumminello and Hosler23 found that pilomatrixomas and pilomatrix carcinomas were positive for CDX-2, β-catenin, and LEF-1 by immunohistochemistry. These downstream molecules in the Wnt signaling pathway could have the potential to be used as diagnostic and prognostic markers.2,13,15,23
Although the pathogenesis is unclear, there are 2 possible mechanisms by which pilomatrix carcinomas develop. They can either arise as de novo tumors, or it is possible that initial mutations in β-catenin result in the formation of pilomatrixomas at an early age that may undergo malignant transformation in elderly patients over time with additional mutations.2
Our case was strongly and diffusely positive for β-catenin in a nuclear and cytoplasmic pattern and CDX-2 in a nuclear pattern, supporting the role of the Wnt signaling pathway in such tumors. Furthermore, our case demonstrated the presence of few intralesional normal dendritic melanocytes, a rare finding1,24,25 but not unexpected, as melanocytes normally are present within the hair follicle matrix.
Pilomatrix carcinomas are aggressive tumors with a high risk for local recurrence and tendency for metastasis. In a study of 13 cases of pilomatrix carcinomas, Herrmann et al13 found that metastasis was significantly associated with local tumor recurrence (P<.0413). They concluded that the combination of overall high local recurrence and metastatic rates of pilomatrix carcinoma as well as documented tumor-related deaths would warrant continued patient follow-up, especially for recurrent tumors.13 Rapid growth of a tumor, either de novo or following several months of stable size, should alert physicians to perform a diagnostic biopsy.
Management options of pilomatrix carcinoma include surgery or radiation with close follow-up. The most widely reported treatment of pilomatrix carcinoma is wide local excision with histologically confirmed clear margins. Mohs micrographic surgery is an excellent treatment option.2,13-15 Adjuvant radiation therapy may be necessary following excision. Currently there is no consensus on surgical management, and standard excisional margins have not been defined.26 Jones et al2 concluded that complete excision with wide margins likely is curative, with decreased rates of recurrence, and better awareness of this carcinoma would lead to appropriate treatment while avoiding unnecessary diagnostic tests.2
Conclusion
We report an exceptionally unique case of early pilomatrix carcinoma with a discussion on the pathogenesis and molecular pathology of hair matrix tumors. A large cohort of patients with longer follow-up periods and better molecular characterization is essential in drawing accurate information about their prognosis, identifying molecular markers that can be used as therapeutic targets, and determining ideal management strategy.
- Jani P, Chetty R, Ghazarian DM. An unusual composite pilomatrix carcinoma with intralesional melanocytes: differential diagnosis, immunohistochemical evaluation, and review of the literature. Am J Dermatopathol. 2008;30:174-177.
- Jones C, Twoon M, Ho W, et al. Pilomatrix carcinoma: 12-year experience and review of the literature. J Cutan Pathol. 2018;45:33-38.
- Forbis R, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol. 1961;83:606.
- Elder D, Elenitsas R, Ragsdale BD. Tumors of epidermal appendages. In: Elder D, Elenitsas R, Jaworsky C, eds. Lever’s Histopathology of the Skin. 8th ed. Lippincott Raven; 1997:757-759.
- Aherne NJ, Fitzpatrick DA, Gibbons D, et al. Pilomatrix carcinoma presenting as an extra axial mass: clinicopathological features. Diagn Pathol. 2008;3:47.
- Papadakis M, de Bree E, Floros N, et al. Pilomatrix carcinoma: more malignant biological behavior than was considered in the past. Mol Clin Oncol. 2017;6:415-418.
- LeBoit PE, Parslow TG, Choy SH. Hair matrix differentiation: occurrence in lesions other than pilomatricoma. Am J Dermatopathol. 1987;9:399-405.
- Campoy F, Stiefel P, Stiefel E, et al. Pilomatrix carcinoma: role played by MR imaging. Neuroradiology. 1989;31:196-198.
- Tateyama H, Eimoto T, Tada T, et al. Malignant pilomatricoma: an immunohistochemical study with antihair keratin antibody. Cancer. 1992;69:127-132.
- O’Donovan DG, Freemont AJ, Adams JE, et al. Malignant pilomatrixoma with bone metastasis. Histopathology. 1993;23:385-386.
- Cross P, Richmond I, Wells S, et al. Malignant pilomatrixoma with bone metastasis. Histopathology. 1994;24:499-500.
- Niedermeyer HP, Peris K, Höfler H. Pilomatrix carcinoma with multiple visceral metastases: report of a case. Cancer. 1996;77:1311-1314.
- Herrmann JL, Allan A, Trapp KM, et al. Pilomatrix carcinoma: 13 new cases and review of the literature with emphasis on predictors of metastasis. J Am Acad Dermatol. 2014;71:38-43.
- Xing L, Marzolf SA, Vandergriff T, et al. Facial pilomatrix carcinomas treated with Mohs micrographic surgery. JAAD Case Rep. 2018;4:253-255.
- Fernandez-Flores A, Cassarino DS. Sarcomatoid pilomatrix carcinoma. J Cutan Pathol. 2018;45:508-514.
- Sau P, Lupton GP, Graham JH. Pilomatrix carcinoma. Cancer. 1993;71:2491-2498.
- Chan E, Gat U, McNiff JM, et al. A common human skin tumour is caused by activating mutations in β-catenin. Nat Genet. 1999;21:410-413.
- Huelsken J, Vogel R, Erdmann B, et al. β-catenin controls hair follicle morphogenesis and stem cell differentiation in the skin. Cell. 2001;105:533-545.
- Kikuchi A. Tumor formation by genetic mutations in the components of the Wnt signaling pathway. Cancer Sci. 2003;94:225-229.
- Durand M, Moles J. Beta-catenin mutations in a common skin cancer: pilomatricoma. Bull Cancer. 1999;86:725-726.
- Lazar AJF, Calonje E, Grayson W, et al. Pilomatrix carcinomas contain mutations in CTNNB1, the gene encoding beta-catenin. J Cutan Pathol. 2005;32:148-157.
- Kazakov DV, Sima R, Vanecek T, et al. Mutations in exon 3 of the CTNNB1 gene (β-catenin gene) in cutaneous adnexal tumors. Am J Dermatopathol. 2009;31:248-255.
- Tumminello K, Hosler GA. CDX2 and LEF-1 expression in pilomatrical tumors and their utility in the diagnosis of pilomatrical carcinoma. J Cutan Pathol. 2018;45:318-324.
- Rodic´ N, Taube JM, Manson P, et al Locally invasive dermal squamomelanocytic tumor with matrical differentiation: a peculiar case with review of the literature. Am J Dermatopathol. 2013;35:E72-E76.
- Perez C, Debbaneh M, Cassarino D. Preference for the term pilomatrical carcinoma with melanocytic hyperplasia: letter to the editor. J Cutan Pathol. 2017;44:655-657.
- Herrmann JL, Allan A, Trapp KM, et al. Pilomatrix carcinoma: 13 new cases and review of the literature with emphasis on predictors of metastasis. J Am Acad Dermatol. 2014;71:38-43.
Pilomatrix carcinoma is a rare adnexal tumor with origin from the germinative matrical cells of the hair follicle. Clinically, it presents as a solitary lesion commonly found in the head and neck region as well as the upper back. The tumors cannot be distinguished by their clinical appearance only and frequently are mistaken for cysts. Histopathologic examination provides the definitive diagnosis in most cases. These carcinomas are aggressive neoplasms with a high probability of local recurrence and distant metastasis. Assessment of the Wnt signaling pathway components such as β-catenin, lymphoid enhancer-binding factor 1 (LEF-1), and caudal-related homeobox transcription factor 2 (CDX-2) potentially can be used for diagnostic purposes and targeted therapy.
We report a rare and unique case of early pilomatrix carcinoma with intralesional melanocytes. We review the molecular pathology and pathogenesis of these carcinomas as well as the significance of early diagnosis.
Case Report
A 73-year-old man with a history of extensive sun exposure presented with a 1-cm, raised, rapidly growing, slightly irregular, purple lesion on the right forearm of 3 months’ duration with tendency to bleed. He did not have a history of skin cancers and was otherwise healthy. Excision was recommended due to the progressive and rapid growth of the lesion.
Histopathologic Findings—Gross examination revealed a 0.9×0.7-cm, raised, slightly irregular lesion located 1 mm away from the closest peripheral margin. Histologically, the lesion was a relatively circumscribed, dermal-based basaloid neoplasm with slightly ill-defined edges involving the superficial and deep dermis (Figure 1A). The neoplasm was formed predominantly of sheets of basaloid cells and small nests of ghost cells, in addition to some squamoid and transitional cells (Figure 1B). The basaloid cells exhibited severe nuclear atypia, pleomorphism, increased nuclear to cytoplasmic ratio (Figure 1C), minimal to moderate amounts of eosinophilic cytoplasm, enlarged nuclei, prominent nucleoli, and coarse chromatin pattern. Abundant mitotic activity and apoptotic bodies were present as well as focal area of central necrosis (Figure 1C). Also, melanophages and a multinucleated giant cell reaction was noted. Elastic trichrome special stain highlighted focal infiltration of the neoplastic cells into the adjacent desmoplastic stroma. Melanin stain was negative for melanin pigment within the neoplasm. Given the presence of severely atypical basaloid cells along with ghost cells indicating matrical differentiation, a diagnosis of pilomatrix carcinoma was rendered.
Immunohistochemistry—The neoplastic cells were diffusely positive for p63, CDX-2 (Figure 2A), β-catenin (Figure 2B), and CD10 (Figure 2C), and focally and weakly positive for cytokeratin (CK) 5, BerEP4 (staining the tumor periphery), androgen receptor, and CK18 (a low-molecular-weight keratin). They were negative for monoclonal carcinoembryonic antigen, epithelial membrane antigen, CK7, CK20, CD34, SOX-10, CD56, synaptophysin, and chromogranin. Cytokeratin 14 was positive in the squamoid cells but negative in the basaloid cells. SOX-10 and melanoma cocktail immunostains demonstrated few intralesional dendritic melanocytes.
Comment
Pilomatrix carcinoma is a rare malignant cutaneous adnexal neoplasm with origin from the germinative matrix of the hair bulb region of hair follicles. Pilomatrix carcinoma was first reported in 1980.1,2 These tumors are characterized by rapid growth and aggressive behavior. Their benign counterpart, pilomatrixoma, is a slow-growing, dermal or subcutaneous tumor that rarely recurs after complete excision.
As with pilomatrixoma, pilomatrix carcinomas are asymptomatic and present as solitary dermal or subcutaneous masses3,4 that most commonly are found in the posterior neck, upper back, and preauricular regions of middle-aged or elderly adults with male predominance.5 They range in size from 0.5 to 20 cm with a mean of 4 cm that is slightly larger than pilomatrixoma. Pilomatrix carcinomas predominantly are firm tumors with or without cystic components, and they exhibit a high probability of recurrence and have risk for distant metastasis.6-15
The differential diagnosis includes epidermal cysts, pilomatrixoma, basal cell carcinoma with matrical differentiation, trichoblastoma/trichoblastic carcinoma, and trichilemmal carcinoma. Pilomatrix carcinomas frequently are mistaken for epidermal cysts on clinical examination. Such a distinction can be easily resolved by histopathologic evaluation. The more challenging differential diagnosis is with pilomatrixoma. Histologically, pilomatrixomas consist of a distinct population of cells including basaloid, squamoid, transitional, and shadow cells in variable proportions. The basaloid cells transition to shadow cells in an organized zonal fashion.16 Compared to pilomatrixomas, pilomatrix carcinomas often show predominance of the basaloid cells; marked cytologic atypia and pleomorphism; numerous mitotic figures; deep infiltrative pattern into subcutaneous fat, fascia, and skeletal muscle; stromal desmoplasia; necrosis; and neurovascular invasion (Tables 1 and 2). Furthermore, the shadow cells tend to form a small nested pattern in pilomatrix carcinoma instead of the flat sheetlike pattern usually observed in pilomatrixoma.16 Basal cell carcinoma with matrical differentiation can pose a diagnostic challenge in the differential diagnosis; basal cell carcinoma usually exhibits a peripheral palisade of the basaloid cells accompanied by retraction spaces separating the tumor from the stroma. Trichoblastoma/trichoblastic carcinoma with matrical differentiation can be distinguished by its exuberant stroma, prominent primitive hair follicles, and papillary mesenchymal bodies. Trichilemmal carcinomas are recognized by their connection to the overlying epidermis, peripheral palisading, and presence of clear cells, while pilomatrix carcinoma lacks connection to the surface epithelium.
Immunohistochemical stains have little to no role in the differential diagnosis, and morphology is the mainstay in making the diagnosis. Rarely, pilomatrix carcinoma can be confused with poorly differentiated sebaceous carcinoma and poorly differentiated squamous cell carcinoma. Although careful scrutiny of the histologic features may help identify mature sebocytes in sebaceous carcinoma, evidence of keratinization in squamous cell carcinoma and ghost cells in pilomatrix carcinoma, using a panel of immunohistochemical stains can be helpful in reaching the final diagnosis (Table 3).
The development of hair matrix tumors have been known to harbor mutations in exon 3 of the catenin beta-1 gene, CTNNB1, that encodes for β-catenin, a downstream effector in the Wnt signaling pathway responsible for differentiation, proliferation, and adhesion of epithelial stem cells.17-21 In a study conducted by Kazakov et al,22 DNA was extracted from 86 lesions: 4 were pilomatrixomas and 1 was a pilomatrix carcinoma. A polymerase chain reaction assay revealed 8 pathogenic variants of the β-catenin gene. D32Y (CTNNB1):c.94G>T (p.Asp32Tyr) and G34R (CTNNB1):c.100G>C (p.Gly34Arg) were the mutations present in pilomatrixoma and pilomatrix carcinoma, respectively.22 In addition, there are several proteins that are part of the Wnt pathway in addition to β-catenin—LEF-1 and CDX-2.
Tumminello and Hosler23 found that pilomatrixomas and pilomatrix carcinomas were positive for CDX-2, β-catenin, and LEF-1 by immunohistochemistry. These downstream molecules in the Wnt signaling pathway could have the potential to be used as diagnostic and prognostic markers.2,13,15,23
Although the pathogenesis is unclear, there are 2 possible mechanisms by which pilomatrix carcinomas develop. They can either arise as de novo tumors, or it is possible that initial mutations in β-catenin result in the formation of pilomatrixomas at an early age that may undergo malignant transformation in elderly patients over time with additional mutations.2
Our case was strongly and diffusely positive for β-catenin in a nuclear and cytoplasmic pattern and CDX-2 in a nuclear pattern, supporting the role of the Wnt signaling pathway in such tumors. Furthermore, our case demonstrated the presence of few intralesional normal dendritic melanocytes, a rare finding1,24,25 but not unexpected, as melanocytes normally are present within the hair follicle matrix.
Pilomatrix carcinomas are aggressive tumors with a high risk for local recurrence and tendency for metastasis. In a study of 13 cases of pilomatrix carcinomas, Herrmann et al13 found that metastasis was significantly associated with local tumor recurrence (P<.0413). They concluded that the combination of overall high local recurrence and metastatic rates of pilomatrix carcinoma as well as documented tumor-related deaths would warrant continued patient follow-up, especially for recurrent tumors.13 Rapid growth of a tumor, either de novo or following several months of stable size, should alert physicians to perform a diagnostic biopsy.
Management options of pilomatrix carcinoma include surgery or radiation with close follow-up. The most widely reported treatment of pilomatrix carcinoma is wide local excision with histologically confirmed clear margins. Mohs micrographic surgery is an excellent treatment option.2,13-15 Adjuvant radiation therapy may be necessary following excision. Currently there is no consensus on surgical management, and standard excisional margins have not been defined.26 Jones et al2 concluded that complete excision with wide margins likely is curative, with decreased rates of recurrence, and better awareness of this carcinoma would lead to appropriate treatment while avoiding unnecessary diagnostic tests.2
Conclusion
We report an exceptionally unique case of early pilomatrix carcinoma with a discussion on the pathogenesis and molecular pathology of hair matrix tumors. A large cohort of patients with longer follow-up periods and better molecular characterization is essential in drawing accurate information about their prognosis, identifying molecular markers that can be used as therapeutic targets, and determining ideal management strategy.
Pilomatrix carcinoma is a rare adnexal tumor with origin from the germinative matrical cells of the hair follicle. Clinically, it presents as a solitary lesion commonly found in the head and neck region as well as the upper back. The tumors cannot be distinguished by their clinical appearance only and frequently are mistaken for cysts. Histopathologic examination provides the definitive diagnosis in most cases. These carcinomas are aggressive neoplasms with a high probability of local recurrence and distant metastasis. Assessment of the Wnt signaling pathway components such as β-catenin, lymphoid enhancer-binding factor 1 (LEF-1), and caudal-related homeobox transcription factor 2 (CDX-2) potentially can be used for diagnostic purposes and targeted therapy.
We report a rare and unique case of early pilomatrix carcinoma with intralesional melanocytes. We review the molecular pathology and pathogenesis of these carcinomas as well as the significance of early diagnosis.
Case Report
A 73-year-old man with a history of extensive sun exposure presented with a 1-cm, raised, rapidly growing, slightly irregular, purple lesion on the right forearm of 3 months’ duration with tendency to bleed. He did not have a history of skin cancers and was otherwise healthy. Excision was recommended due to the progressive and rapid growth of the lesion.
Histopathologic Findings—Gross examination revealed a 0.9×0.7-cm, raised, slightly irregular lesion located 1 mm away from the closest peripheral margin. Histologically, the lesion was a relatively circumscribed, dermal-based basaloid neoplasm with slightly ill-defined edges involving the superficial and deep dermis (Figure 1A). The neoplasm was formed predominantly of sheets of basaloid cells and small nests of ghost cells, in addition to some squamoid and transitional cells (Figure 1B). The basaloid cells exhibited severe nuclear atypia, pleomorphism, increased nuclear to cytoplasmic ratio (Figure 1C), minimal to moderate amounts of eosinophilic cytoplasm, enlarged nuclei, prominent nucleoli, and coarse chromatin pattern. Abundant mitotic activity and apoptotic bodies were present as well as focal area of central necrosis (Figure 1C). Also, melanophages and a multinucleated giant cell reaction was noted. Elastic trichrome special stain highlighted focal infiltration of the neoplastic cells into the adjacent desmoplastic stroma. Melanin stain was negative for melanin pigment within the neoplasm. Given the presence of severely atypical basaloid cells along with ghost cells indicating matrical differentiation, a diagnosis of pilomatrix carcinoma was rendered.
Immunohistochemistry—The neoplastic cells were diffusely positive for p63, CDX-2 (Figure 2A), β-catenin (Figure 2B), and CD10 (Figure 2C), and focally and weakly positive for cytokeratin (CK) 5, BerEP4 (staining the tumor periphery), androgen receptor, and CK18 (a low-molecular-weight keratin). They were negative for monoclonal carcinoembryonic antigen, epithelial membrane antigen, CK7, CK20, CD34, SOX-10, CD56, synaptophysin, and chromogranin. Cytokeratin 14 was positive in the squamoid cells but negative in the basaloid cells. SOX-10 and melanoma cocktail immunostains demonstrated few intralesional dendritic melanocytes.
Comment
Pilomatrix carcinoma is a rare malignant cutaneous adnexal neoplasm with origin from the germinative matrix of the hair bulb region of hair follicles. Pilomatrix carcinoma was first reported in 1980.1,2 These tumors are characterized by rapid growth and aggressive behavior. Their benign counterpart, pilomatrixoma, is a slow-growing, dermal or subcutaneous tumor that rarely recurs after complete excision.
As with pilomatrixoma, pilomatrix carcinomas are asymptomatic and present as solitary dermal or subcutaneous masses3,4 that most commonly are found in the posterior neck, upper back, and preauricular regions of middle-aged or elderly adults with male predominance.5 They range in size from 0.5 to 20 cm with a mean of 4 cm that is slightly larger than pilomatrixoma. Pilomatrix carcinomas predominantly are firm tumors with or without cystic components, and they exhibit a high probability of recurrence and have risk for distant metastasis.6-15
The differential diagnosis includes epidermal cysts, pilomatrixoma, basal cell carcinoma with matrical differentiation, trichoblastoma/trichoblastic carcinoma, and trichilemmal carcinoma. Pilomatrix carcinomas frequently are mistaken for epidermal cysts on clinical examination. Such a distinction can be easily resolved by histopathologic evaluation. The more challenging differential diagnosis is with pilomatrixoma. Histologically, pilomatrixomas consist of a distinct population of cells including basaloid, squamoid, transitional, and shadow cells in variable proportions. The basaloid cells transition to shadow cells in an organized zonal fashion.16 Compared to pilomatrixomas, pilomatrix carcinomas often show predominance of the basaloid cells; marked cytologic atypia and pleomorphism; numerous mitotic figures; deep infiltrative pattern into subcutaneous fat, fascia, and skeletal muscle; stromal desmoplasia; necrosis; and neurovascular invasion (Tables 1 and 2). Furthermore, the shadow cells tend to form a small nested pattern in pilomatrix carcinoma instead of the flat sheetlike pattern usually observed in pilomatrixoma.16 Basal cell carcinoma with matrical differentiation can pose a diagnostic challenge in the differential diagnosis; basal cell carcinoma usually exhibits a peripheral palisade of the basaloid cells accompanied by retraction spaces separating the tumor from the stroma. Trichoblastoma/trichoblastic carcinoma with matrical differentiation can be distinguished by its exuberant stroma, prominent primitive hair follicles, and papillary mesenchymal bodies. Trichilemmal carcinomas are recognized by their connection to the overlying epidermis, peripheral palisading, and presence of clear cells, while pilomatrix carcinoma lacks connection to the surface epithelium.
Immunohistochemical stains have little to no role in the differential diagnosis, and morphology is the mainstay in making the diagnosis. Rarely, pilomatrix carcinoma can be confused with poorly differentiated sebaceous carcinoma and poorly differentiated squamous cell carcinoma. Although careful scrutiny of the histologic features may help identify mature sebocytes in sebaceous carcinoma, evidence of keratinization in squamous cell carcinoma and ghost cells in pilomatrix carcinoma, using a panel of immunohistochemical stains can be helpful in reaching the final diagnosis (Table 3).
The development of hair matrix tumors have been known to harbor mutations in exon 3 of the catenin beta-1 gene, CTNNB1, that encodes for β-catenin, a downstream effector in the Wnt signaling pathway responsible for differentiation, proliferation, and adhesion of epithelial stem cells.17-21 In a study conducted by Kazakov et al,22 DNA was extracted from 86 lesions: 4 were pilomatrixomas and 1 was a pilomatrix carcinoma. A polymerase chain reaction assay revealed 8 pathogenic variants of the β-catenin gene. D32Y (CTNNB1):c.94G>T (p.Asp32Tyr) and G34R (CTNNB1):c.100G>C (p.Gly34Arg) were the mutations present in pilomatrixoma and pilomatrix carcinoma, respectively.22 In addition, there are several proteins that are part of the Wnt pathway in addition to β-catenin—LEF-1 and CDX-2.
Tumminello and Hosler23 found that pilomatrixomas and pilomatrix carcinomas were positive for CDX-2, β-catenin, and LEF-1 by immunohistochemistry. These downstream molecules in the Wnt signaling pathway could have the potential to be used as diagnostic and prognostic markers.2,13,15,23
Although the pathogenesis is unclear, there are 2 possible mechanisms by which pilomatrix carcinomas develop. They can either arise as de novo tumors, or it is possible that initial mutations in β-catenin result in the formation of pilomatrixomas at an early age that may undergo malignant transformation in elderly patients over time with additional mutations.2
Our case was strongly and diffusely positive for β-catenin in a nuclear and cytoplasmic pattern and CDX-2 in a nuclear pattern, supporting the role of the Wnt signaling pathway in such tumors. Furthermore, our case demonstrated the presence of few intralesional normal dendritic melanocytes, a rare finding1,24,25 but not unexpected, as melanocytes normally are present within the hair follicle matrix.
Pilomatrix carcinomas are aggressive tumors with a high risk for local recurrence and tendency for metastasis. In a study of 13 cases of pilomatrix carcinomas, Herrmann et al13 found that metastasis was significantly associated with local tumor recurrence (P<.0413). They concluded that the combination of overall high local recurrence and metastatic rates of pilomatrix carcinoma as well as documented tumor-related deaths would warrant continued patient follow-up, especially for recurrent tumors.13 Rapid growth of a tumor, either de novo or following several months of stable size, should alert physicians to perform a diagnostic biopsy.
Management options of pilomatrix carcinoma include surgery or radiation with close follow-up. The most widely reported treatment of pilomatrix carcinoma is wide local excision with histologically confirmed clear margins. Mohs micrographic surgery is an excellent treatment option.2,13-15 Adjuvant radiation therapy may be necessary following excision. Currently there is no consensus on surgical management, and standard excisional margins have not been defined.26 Jones et al2 concluded that complete excision with wide margins likely is curative, with decreased rates of recurrence, and better awareness of this carcinoma would lead to appropriate treatment while avoiding unnecessary diagnostic tests.2
Conclusion
We report an exceptionally unique case of early pilomatrix carcinoma with a discussion on the pathogenesis and molecular pathology of hair matrix tumors. A large cohort of patients with longer follow-up periods and better molecular characterization is essential in drawing accurate information about their prognosis, identifying molecular markers that can be used as therapeutic targets, and determining ideal management strategy.
- Jani P, Chetty R, Ghazarian DM. An unusual composite pilomatrix carcinoma with intralesional melanocytes: differential diagnosis, immunohistochemical evaluation, and review of the literature. Am J Dermatopathol. 2008;30:174-177.
- Jones C, Twoon M, Ho W, et al. Pilomatrix carcinoma: 12-year experience and review of the literature. J Cutan Pathol. 2018;45:33-38.
- Forbis R, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol. 1961;83:606.
- Elder D, Elenitsas R, Ragsdale BD. Tumors of epidermal appendages. In: Elder D, Elenitsas R, Jaworsky C, eds. Lever’s Histopathology of the Skin. 8th ed. Lippincott Raven; 1997:757-759.
- Aherne NJ, Fitzpatrick DA, Gibbons D, et al. Pilomatrix carcinoma presenting as an extra axial mass: clinicopathological features. Diagn Pathol. 2008;3:47.
- Papadakis M, de Bree E, Floros N, et al. Pilomatrix carcinoma: more malignant biological behavior than was considered in the past. Mol Clin Oncol. 2017;6:415-418.
- LeBoit PE, Parslow TG, Choy SH. Hair matrix differentiation: occurrence in lesions other than pilomatricoma. Am J Dermatopathol. 1987;9:399-405.
- Campoy F, Stiefel P, Stiefel E, et al. Pilomatrix carcinoma: role played by MR imaging. Neuroradiology. 1989;31:196-198.
- Tateyama H, Eimoto T, Tada T, et al. Malignant pilomatricoma: an immunohistochemical study with antihair keratin antibody. Cancer. 1992;69:127-132.
- O’Donovan DG, Freemont AJ, Adams JE, et al. Malignant pilomatrixoma with bone metastasis. Histopathology. 1993;23:385-386.
- Cross P, Richmond I, Wells S, et al. Malignant pilomatrixoma with bone metastasis. Histopathology. 1994;24:499-500.
- Niedermeyer HP, Peris K, Höfler H. Pilomatrix carcinoma with multiple visceral metastases: report of a case. Cancer. 1996;77:1311-1314.
- Herrmann JL, Allan A, Trapp KM, et al. Pilomatrix carcinoma: 13 new cases and review of the literature with emphasis on predictors of metastasis. J Am Acad Dermatol. 2014;71:38-43.
- Xing L, Marzolf SA, Vandergriff T, et al. Facial pilomatrix carcinomas treated with Mohs micrographic surgery. JAAD Case Rep. 2018;4:253-255.
- Fernandez-Flores A, Cassarino DS. Sarcomatoid pilomatrix carcinoma. J Cutan Pathol. 2018;45:508-514.
- Sau P, Lupton GP, Graham JH. Pilomatrix carcinoma. Cancer. 1993;71:2491-2498.
- Chan E, Gat U, McNiff JM, et al. A common human skin tumour is caused by activating mutations in β-catenin. Nat Genet. 1999;21:410-413.
- Huelsken J, Vogel R, Erdmann B, et al. β-catenin controls hair follicle morphogenesis and stem cell differentiation in the skin. Cell. 2001;105:533-545.
- Kikuchi A. Tumor formation by genetic mutations in the components of the Wnt signaling pathway. Cancer Sci. 2003;94:225-229.
- Durand M, Moles J. Beta-catenin mutations in a common skin cancer: pilomatricoma. Bull Cancer. 1999;86:725-726.
- Lazar AJF, Calonje E, Grayson W, et al. Pilomatrix carcinomas contain mutations in CTNNB1, the gene encoding beta-catenin. J Cutan Pathol. 2005;32:148-157.
- Kazakov DV, Sima R, Vanecek T, et al. Mutations in exon 3 of the CTNNB1 gene (β-catenin gene) in cutaneous adnexal tumors. Am J Dermatopathol. 2009;31:248-255.
- Tumminello K, Hosler GA. CDX2 and LEF-1 expression in pilomatrical tumors and their utility in the diagnosis of pilomatrical carcinoma. J Cutan Pathol. 2018;45:318-324.
- Rodic´ N, Taube JM, Manson P, et al Locally invasive dermal squamomelanocytic tumor with matrical differentiation: a peculiar case with review of the literature. Am J Dermatopathol. 2013;35:E72-E76.
- Perez C, Debbaneh M, Cassarino D. Preference for the term pilomatrical carcinoma with melanocytic hyperplasia: letter to the editor. J Cutan Pathol. 2017;44:655-657.
- Herrmann JL, Allan A, Trapp KM, et al. Pilomatrix carcinoma: 13 new cases and review of the literature with emphasis on predictors of metastasis. J Am Acad Dermatol. 2014;71:38-43.
- Jani P, Chetty R, Ghazarian DM. An unusual composite pilomatrix carcinoma with intralesional melanocytes: differential diagnosis, immunohistochemical evaluation, and review of the literature. Am J Dermatopathol. 2008;30:174-177.
- Jones C, Twoon M, Ho W, et al. Pilomatrix carcinoma: 12-year experience and review of the literature. J Cutan Pathol. 2018;45:33-38.
- Forbis R, Helwig EB. Pilomatrixoma (calcifying epithelioma). Arch Dermatol. 1961;83:606.
- Elder D, Elenitsas R, Ragsdale BD. Tumors of epidermal appendages. In: Elder D, Elenitsas R, Jaworsky C, eds. Lever’s Histopathology of the Skin. 8th ed. Lippincott Raven; 1997:757-759.
- Aherne NJ, Fitzpatrick DA, Gibbons D, et al. Pilomatrix carcinoma presenting as an extra axial mass: clinicopathological features. Diagn Pathol. 2008;3:47.
- Papadakis M, de Bree E, Floros N, et al. Pilomatrix carcinoma: more malignant biological behavior than was considered in the past. Mol Clin Oncol. 2017;6:415-418.
- LeBoit PE, Parslow TG, Choy SH. Hair matrix differentiation: occurrence in lesions other than pilomatricoma. Am J Dermatopathol. 1987;9:399-405.
- Campoy F, Stiefel P, Stiefel E, et al. Pilomatrix carcinoma: role played by MR imaging. Neuroradiology. 1989;31:196-198.
- Tateyama H, Eimoto T, Tada T, et al. Malignant pilomatricoma: an immunohistochemical study with antihair keratin antibody. Cancer. 1992;69:127-132.
- O’Donovan DG, Freemont AJ, Adams JE, et al. Malignant pilomatrixoma with bone metastasis. Histopathology. 1993;23:385-386.
- Cross P, Richmond I, Wells S, et al. Malignant pilomatrixoma with bone metastasis. Histopathology. 1994;24:499-500.
- Niedermeyer HP, Peris K, Höfler H. Pilomatrix carcinoma with multiple visceral metastases: report of a case. Cancer. 1996;77:1311-1314.
- Herrmann JL, Allan A, Trapp KM, et al. Pilomatrix carcinoma: 13 new cases and review of the literature with emphasis on predictors of metastasis. J Am Acad Dermatol. 2014;71:38-43.
- Xing L, Marzolf SA, Vandergriff T, et al. Facial pilomatrix carcinomas treated with Mohs micrographic surgery. JAAD Case Rep. 2018;4:253-255.
- Fernandez-Flores A, Cassarino DS. Sarcomatoid pilomatrix carcinoma. J Cutan Pathol. 2018;45:508-514.
- Sau P, Lupton GP, Graham JH. Pilomatrix carcinoma. Cancer. 1993;71:2491-2498.
- Chan E, Gat U, McNiff JM, et al. A common human skin tumour is caused by activating mutations in β-catenin. Nat Genet. 1999;21:410-413.
- Huelsken J, Vogel R, Erdmann B, et al. β-catenin controls hair follicle morphogenesis and stem cell differentiation in the skin. Cell. 2001;105:533-545.
- Kikuchi A. Tumor formation by genetic mutations in the components of the Wnt signaling pathway. Cancer Sci. 2003;94:225-229.
- Durand M, Moles J. Beta-catenin mutations in a common skin cancer: pilomatricoma. Bull Cancer. 1999;86:725-726.
- Lazar AJF, Calonje E, Grayson W, et al. Pilomatrix carcinomas contain mutations in CTNNB1, the gene encoding beta-catenin. J Cutan Pathol. 2005;32:148-157.
- Kazakov DV, Sima R, Vanecek T, et al. Mutations in exon 3 of the CTNNB1 gene (β-catenin gene) in cutaneous adnexal tumors. Am J Dermatopathol. 2009;31:248-255.
- Tumminello K, Hosler GA. CDX2 and LEF-1 expression in pilomatrical tumors and their utility in the diagnosis of pilomatrical carcinoma. J Cutan Pathol. 2018;45:318-324.
- Rodic´ N, Taube JM, Manson P, et al Locally invasive dermal squamomelanocytic tumor with matrical differentiation: a peculiar case with review of the literature. Am J Dermatopathol. 2013;35:E72-E76.
- Perez C, Debbaneh M, Cassarino D. Preference for the term pilomatrical carcinoma with melanocytic hyperplasia: letter to the editor. J Cutan Pathol. 2017;44:655-657.
- Herrmann JL, Allan A, Trapp KM, et al. Pilomatrix carcinoma: 13 new cases and review of the literature with emphasis on predictors of metastasis. J Am Acad Dermatol. 2014;71:38-43.
Practice Points
- Clinicians and pathologists should be aware of pilomatrix carcinoma to facilitate early detection.
- Early diagnosis and prompt treatment of pilomatrix carcinoma is crucial in lowering recurrence rate and avoiding a poor outcome.
- Caudal-related homeobox transcription factor 2 and β-catenin components of the Wnt signaling pathway play an important role in the pathogenesis of pilomatrix carcinoma.
- Although controversial, wide local excision is the treatment of choice for pilomatrix carcinoma.

TANS Syndrome: Tanorexia, Anorexia, and Nonmelanoma Skin Cancer
The term tanorexia describes compulsive use of a tanning bed, a disorder often identified in White patients. This compulsion is driven by underlying psychological distress that typically correlates with another psychiatric disorder, such as anxiety, body dysmorphic disorder, or an eating disorder. 1 Severe anorexia combined with excessive indoor tanning led to a notable burden of cutaneous squamous cell carcinomas (SCCs) and keratoacanthomas in one of our patients. We discuss the management and approach to patient care in this difficult situation, which we have coined TANS syndrome (for T anorexia, A norexia, and N onmelanoma s kin cancer).
A Patient With TANS Syndrome
A 35-year-old cachectic woman, who appeared much older than her chronologic age, presented for management of numerous painful bleeding skin lesions. Diffuse, erythematous, tender nodules with central keratotic cores, some several centimeters in diameter, were scattered on the abdomen, chest, and extremities (Figure 1); similar lesions were noted on the neck (Figure 2). Numerous erythematous scaly papules and plaques consistent with actinic keratoses were noted throughout the body.

The patient reported that the cutaneous SCCs presented over the last few years, whereas her eating disorder began in adolescence and persisted despite multiple intensive outpatient and inpatient programs. The patient adamantly refused repeat hospitalization, against repeated suggestions by health care providers and her family. Comorbidities related to her anorexia included severe renal insufficiency, iron deficiency anemia, hypertriglyceridemia, kwashiorkor, and pellagra.

Within the last year, the patient had several biopsies showing SCC, keratoacanthoma type. The largest tumors had been treated by Mohs micrographic surgery, excision, and electrodesiccation or curettage. Adjuvant therapy over the last 2 years consisted of tazarotene cream 0.1%, imiquimod cream 5%, oral nicotinamide 500 mg twice daily, and acitretin 10 to 20 mg daily. Human papillomavirus 9-valent vaccine, recombinant, also had been tried as a chemopreventive and treatment, based on a published report of 2 patients in whom keratinocytic carcinomas decreased after such vaccination.2 The dose of acitretin was kept low because of the patient’s severe renal insufficiency and lack of supporting data for its use in this setting. Despite these modalities, our patient continued to develop new cutaneous SCCs.
We considered starting intralesional methotrexate but deferred this course of action, given the patient’s deteriorating renal function. Our plan was to initiate intralesional 5-fluorouracil; however, the patient was admitted to the hospital and subsequently died due to cardiovascular complications of anorexia.
UV Radiation in the Setting of Immune Compromise
Habitual tanning bed use has been recognized as a psychologic addiction.3,4 After exposure to UV radiation, damaged DNA upregulates pro-opiomelanocortin, which posttranslationally generates β-endorphins to elevate mood.3,5
Tanning beds deliver a higher dose of UVA radiation than UVB radiation and cause darkening of pigmentation by oxidation of preformed melanin and redistribution of melanosomes.3 UVA radiation (320–400 nm) emitted from a tanning bed is 10- to 15-times higher than the radiation emitted by the midday sun and causes DNA damage through generation of reactive oxygen species. UVA penetrates the dermis; its harmful effect on DNA contributes to the pathogenesis of melanoma.
UVB radiation (290–320 nm) is mainly restricted to the epidermis and is largely responsible for erythema of the skin. UVB specifically causes direct damage to DNA by forming pyrimidine dimers, superficially causing sunburn. Excessive exposure to UVB radiation increases the risk for nonmelanoma skin cancer.6
Severe starvation and chronic malnutrition, as seen in anorexia nervosa, also are known to lead to immunosuppression.7 Exposure to UV radiation has been shown to impair the function of antigen-presenting cells, cytokines, and suppressor T cells, and is classified as a Group 1 carcinogen by the World Health Organization.3,8 Combining a compromised immune system in anorexia with DNA damage from frequent indoor tanning provides a dangerous milieu for carcinogenesis.8 Without immune surveillance, as occurs with adequate nutrition, treatment of cutaneous SCC is, at best, challenging.
Primary care physicians, dermatologists, psychiatrists, nutritionists, and public health officials should educate high-risk patients to prevent TANS syndrome.
- Petit A, Karila L, Chalmin F, et al. Phenomenology and psychopathology of excessive indoor tanning. Int J Dermatol. 2014;53:664-672. doi:10.1111/ijd.12336
- Nichols AJ, Allen AH, Shareef S, et al. Association of human papillomavirus vaccine with the development of keratinocyte carcinomas. JAMA Dermatol. 2017;153:571-574. doi:10.1001/jamadermatol.2016.5703
- Madigan LM, Lim HW. Tanning beds: impact on health, and recent regulations. Clin Dermatol. 2016;34:640-648. doi:10.1016/j.clindermatol.2016.05.016
- Schwebel DC. Adolescent tanning, disordered eating, and risk taking. J Dev Behav Pediatr. 2014;35:225-227. doi:10.1097/DBP.0000000000000045
- Friedman B, English JC 3rd, Ferris LK. Indoor tanning, skin cancer and the young female patient: a review of the literature. J Pediatr Adolesc Gynecol. 2015;28:275-283. doi:10.1016/j.jpag.2014.07.015
- Armstrong BK, Kricker A. Epidemiology of UV induced skin cancer. J Photochem Photobiol B. 2001;63:8-18. doi:10.1016/s1011-1344(01)00198-1
- Hanachi M, Bohem V, Bemer P, et al. Negative role of malnutrition in cell-mediated immune response: Pneumocystis jirovecii pneumonia (PCP) in a severely malnourished, HIV-negative patient with anorexia nervosa. Clin Nutr ESPEN. 2018;25:163-165. doi:10.1016/j.clnesp.2018.03.121
- Schwarz T, Beissert S. Milestones in photoimmunology. J Invest Dermatol. 2013;133:E7-E10. doi:10.1038/skinbio.2013.177
The term tanorexia describes compulsive use of a tanning bed, a disorder often identified in White patients. This compulsion is driven by underlying psychological distress that typically correlates with another psychiatric disorder, such as anxiety, body dysmorphic disorder, or an eating disorder. 1 Severe anorexia combined with excessive indoor tanning led to a notable burden of cutaneous squamous cell carcinomas (SCCs) and keratoacanthomas in one of our patients. We discuss the management and approach to patient care in this difficult situation, which we have coined TANS syndrome (for T anorexia, A norexia, and N onmelanoma s kin cancer).
A Patient With TANS Syndrome
A 35-year-old cachectic woman, who appeared much older than her chronologic age, presented for management of numerous painful bleeding skin lesions. Diffuse, erythematous, tender nodules with central keratotic cores, some several centimeters in diameter, were scattered on the abdomen, chest, and extremities (Figure 1); similar lesions were noted on the neck (Figure 2). Numerous erythematous scaly papules and plaques consistent with actinic keratoses were noted throughout the body.
The patient reported that the cutaneous SCCs presented over the last few years, whereas her eating disorder began in adolescence and persisted despite multiple intensive outpatient and inpatient programs. The patient adamantly refused repeat hospitalization, against repeated suggestions by health care providers and her family. Comorbidities related to her anorexia included severe renal insufficiency, iron deficiency anemia, hypertriglyceridemia, kwashiorkor, and pellagra.
Within the last year, the patient had several biopsies showing SCC, keratoacanthoma type. The largest tumors had been treated by Mohs micrographic surgery, excision, and electrodesiccation or curettage. Adjuvant therapy over the last 2 years consisted of tazarotene cream 0.1%, imiquimod cream 5%, oral nicotinamide 500 mg twice daily, and acitretin 10 to 20 mg daily. Human papillomavirus 9-valent vaccine, recombinant, also had been tried as a chemopreventive and treatment, based on a published report of 2 patients in whom keratinocytic carcinomas decreased after such vaccination.2 The dose of acitretin was kept low because of the patient’s severe renal insufficiency and lack of supporting data for its use in this setting. Despite these modalities, our patient continued to develop new cutaneous SCCs.
We considered starting intralesional methotrexate but deferred this course of action, given the patient’s deteriorating renal function. Our plan was to initiate intralesional 5-fluorouracil; however, the patient was admitted to the hospital and subsequently died due to cardiovascular complications of anorexia.
UV Radiation in the Setting of Immune Compromise
Habitual tanning bed use has been recognized as a psychologic addiction.3,4 After exposure to UV radiation, damaged DNA upregulates pro-opiomelanocortin, which posttranslationally generates β-endorphins to elevate mood.3,5
Tanning beds deliver a higher dose of UVA radiation than UVB radiation and cause darkening of pigmentation by oxidation of preformed melanin and redistribution of melanosomes.3 UVA radiation (320–400 nm) emitted from a tanning bed is 10- to 15-times higher than the radiation emitted by the midday sun and causes DNA damage through generation of reactive oxygen species. UVA penetrates the dermis; its harmful effect on DNA contributes to the pathogenesis of melanoma.
UVB radiation (290–320 nm) is mainly restricted to the epidermis and is largely responsible for erythema of the skin. UVB specifically causes direct damage to DNA by forming pyrimidine dimers, superficially causing sunburn. Excessive exposure to UVB radiation increases the risk for nonmelanoma skin cancer.6
Severe starvation and chronic malnutrition, as seen in anorexia nervosa, also are known to lead to immunosuppression.7 Exposure to UV radiation has been shown to impair the function of antigen-presenting cells, cytokines, and suppressor T cells, and is classified as a Group 1 carcinogen by the World Health Organization.3,8 Combining a compromised immune system in anorexia with DNA damage from frequent indoor tanning provides a dangerous milieu for carcinogenesis.8 Without immune surveillance, as occurs with adequate nutrition, treatment of cutaneous SCC is, at best, challenging.
Primary care physicians, dermatologists, psychiatrists, nutritionists, and public health officials should educate high-risk patients to prevent TANS syndrome.
The term tanorexia describes compulsive use of a tanning bed, a disorder often identified in White patients. This compulsion is driven by underlying psychological distress that typically correlates with another psychiatric disorder, such as anxiety, body dysmorphic disorder, or an eating disorder. 1 Severe anorexia combined with excessive indoor tanning led to a notable burden of cutaneous squamous cell carcinomas (SCCs) and keratoacanthomas in one of our patients. We discuss the management and approach to patient care in this difficult situation, which we have coined TANS syndrome (for T anorexia, A norexia, and N onmelanoma s kin cancer).
A Patient With TANS Syndrome
A 35-year-old cachectic woman, who appeared much older than her chronologic age, presented for management of numerous painful bleeding skin lesions. Diffuse, erythematous, tender nodules with central keratotic cores, some several centimeters in diameter, were scattered on the abdomen, chest, and extremities (Figure 1); similar lesions were noted on the neck (Figure 2). Numerous erythematous scaly papules and plaques consistent with actinic keratoses were noted throughout the body.
The patient reported that the cutaneous SCCs presented over the last few years, whereas her eating disorder began in adolescence and persisted despite multiple intensive outpatient and inpatient programs. The patient adamantly refused repeat hospitalization, against repeated suggestions by health care providers and her family. Comorbidities related to her anorexia included severe renal insufficiency, iron deficiency anemia, hypertriglyceridemia, kwashiorkor, and pellagra.
Within the last year, the patient had several biopsies showing SCC, keratoacanthoma type. The largest tumors had been treated by Mohs micrographic surgery, excision, and electrodesiccation or curettage. Adjuvant therapy over the last 2 years consisted of tazarotene cream 0.1%, imiquimod cream 5%, oral nicotinamide 500 mg twice daily, and acitretin 10 to 20 mg daily. Human papillomavirus 9-valent vaccine, recombinant, also had been tried as a chemopreventive and treatment, based on a published report of 2 patients in whom keratinocytic carcinomas decreased after such vaccination.2 The dose of acitretin was kept low because of the patient’s severe renal insufficiency and lack of supporting data for its use in this setting. Despite these modalities, our patient continued to develop new cutaneous SCCs.
We considered starting intralesional methotrexate but deferred this course of action, given the patient’s deteriorating renal function. Our plan was to initiate intralesional 5-fluorouracil; however, the patient was admitted to the hospital and subsequently died due to cardiovascular complications of anorexia.
UV Radiation in the Setting of Immune Compromise
Habitual tanning bed use has been recognized as a psychologic addiction.3,4 After exposure to UV radiation, damaged DNA upregulates pro-opiomelanocortin, which posttranslationally generates β-endorphins to elevate mood.3,5
Tanning beds deliver a higher dose of UVA radiation than UVB radiation and cause darkening of pigmentation by oxidation of preformed melanin and redistribution of melanosomes.3 UVA radiation (320–400 nm) emitted from a tanning bed is 10- to 15-times higher than the radiation emitted by the midday sun and causes DNA damage through generation of reactive oxygen species. UVA penetrates the dermis; its harmful effect on DNA contributes to the pathogenesis of melanoma.
UVB radiation (290–320 nm) is mainly restricted to the epidermis and is largely responsible for erythema of the skin. UVB specifically causes direct damage to DNA by forming pyrimidine dimers, superficially causing sunburn. Excessive exposure to UVB radiation increases the risk for nonmelanoma skin cancer.6
Severe starvation and chronic malnutrition, as seen in anorexia nervosa, also are known to lead to immunosuppression.7 Exposure to UV radiation has been shown to impair the function of antigen-presenting cells, cytokines, and suppressor T cells, and is classified as a Group 1 carcinogen by the World Health Organization.3,8 Combining a compromised immune system in anorexia with DNA damage from frequent indoor tanning provides a dangerous milieu for carcinogenesis.8 Without immune surveillance, as occurs with adequate nutrition, treatment of cutaneous SCC is, at best, challenging.
Primary care physicians, dermatologists, psychiatrists, nutritionists, and public health officials should educate high-risk patients to prevent TANS syndrome.
- Petit A, Karila L, Chalmin F, et al. Phenomenology and psychopathology of excessive indoor tanning. Int J Dermatol. 2014;53:664-672. doi:10.1111/ijd.12336
- Nichols AJ, Allen AH, Shareef S, et al. Association of human papillomavirus vaccine with the development of keratinocyte carcinomas. JAMA Dermatol. 2017;153:571-574. doi:10.1001/jamadermatol.2016.5703
- Madigan LM, Lim HW. Tanning beds: impact on health, and recent regulations. Clin Dermatol. 2016;34:640-648. doi:10.1016/j.clindermatol.2016.05.016
- Schwebel DC. Adolescent tanning, disordered eating, and risk taking. J Dev Behav Pediatr. 2014;35:225-227. doi:10.1097/DBP.0000000000000045
- Friedman B, English JC 3rd, Ferris LK. Indoor tanning, skin cancer and the young female patient: a review of the literature. J Pediatr Adolesc Gynecol. 2015;28:275-283. doi:10.1016/j.jpag.2014.07.015
- Armstrong BK, Kricker A. Epidemiology of UV induced skin cancer. J Photochem Photobiol B. 2001;63:8-18. doi:10.1016/s1011-1344(01)00198-1
- Hanachi M, Bohem V, Bemer P, et al. Negative role of malnutrition in cell-mediated immune response: Pneumocystis jirovecii pneumonia (PCP) in a severely malnourished, HIV-negative patient with anorexia nervosa. Clin Nutr ESPEN. 2018;25:163-165. doi:10.1016/j.clnesp.2018.03.121
- Schwarz T, Beissert S. Milestones in photoimmunology. J Invest Dermatol. 2013;133:E7-E10. doi:10.1038/skinbio.2013.177
- Petit A, Karila L, Chalmin F, et al. Phenomenology and psychopathology of excessive indoor tanning. Int J Dermatol. 2014;53:664-672. doi:10.1111/ijd.12336
- Nichols AJ, Allen AH, Shareef S, et al. Association of human papillomavirus vaccine with the development of keratinocyte carcinomas. JAMA Dermatol. 2017;153:571-574. doi:10.1001/jamadermatol.2016.5703
- Madigan LM, Lim HW. Tanning beds: impact on health, and recent regulations. Clin Dermatol. 2016;34:640-648. doi:10.1016/j.clindermatol.2016.05.016
- Schwebel DC. Adolescent tanning, disordered eating, and risk taking. J Dev Behav Pediatr. 2014;35:225-227. doi:10.1097/DBP.0000000000000045
- Friedman B, English JC 3rd, Ferris LK. Indoor tanning, skin cancer and the young female patient: a review of the literature. J Pediatr Adolesc Gynecol. 2015;28:275-283. doi:10.1016/j.jpag.2014.07.015
- Armstrong BK, Kricker A. Epidemiology of UV induced skin cancer. J Photochem Photobiol B. 2001;63:8-18. doi:10.1016/s1011-1344(01)00198-1
- Hanachi M, Bohem V, Bemer P, et al. Negative role of malnutrition in cell-mediated immune response: Pneumocystis jirovecii pneumonia (PCP) in a severely malnourished, HIV-negative patient with anorexia nervosa. Clin Nutr ESPEN. 2018;25:163-165. doi:10.1016/j.clnesp.2018.03.121
- Schwarz T, Beissert S. Milestones in photoimmunology. J Invest Dermatol. 2013;133:E7-E10. doi:10.1038/skinbio.2013.177
Practice Points
- Primary care physicians, dermatologists, psychiatrists, nutritionists, and public health officials should educate high-risk patients to prevent TANS syndrome.
- Combining a compromised immune system in anorexia with DNA damage from frequent indoor tanning provides a dangerous milieu for carcinogenesis.
- Comorbidities related to TANS syndrome make it challenging to effectively treat cutaneous squamous cell carcinoma.

In and out surgeries become the norm during pandemic
Urologist Ronney Abaza, MD, a robotic surgery specialist in Dublin, Ohio, and colleagues, reviewed robotic surgeries at their hospital during COVID-19 restrictions on surgery in Ohio between March 17 and June 5, 2020, and compared them with robotic procedures before COVID-19 and after restrictions were lifted. They published their results in Urology.
Since 2016, the hospital has offered the option of same-day discharge (SDD) to all robotic urologic surgery patients, regardless of procedure or patient-specific factors.
Among patients who had surgery during COVID-19 restrictions, 98% (87/89 patients) opted for SDD versus 52% in the group having surgery before the restrictions (P < .00001). After the COVID-19 surgery restrictions were lifted, the higher rate of SDD remained at 98%.
“There were no differences in 30-day complications or readmissions between SDD and overnight patients,” the authors write.
The right patient, the right motivation for successful surgery
Brian Lane, MD, PhD, a urologic oncologist with Spectrum Health in Grand Rapids, Michigan, told this news organization that, for nephrectomies, uptake of same-day discharge will continue to be slow.
“You have to have the right patient, the right patient motivation, and the surgery has to go smoothly,” he said. “If you start sending everyone home the same day, you will certainly see readmissions,” he said.
Dr. Lane is part of the Michigan Urologic Surgery Improvement Collaborative and he said the group recently looked at same-day discharge outcomes after robotic prostatectomies with SDD as compared with 1-2 nights in the hospital.
The work has not yet been published but, “There was a slight signal that there were increased readmissions with same-day discharge vs. 0-1 day,” he said.
A paper on outcomes of same-day discharge in total knee arthroplasty in the Journal of Bone & Joint Surgery found a higher risk of perioperative complications “including component failure, surgical site infection, knee stiffness, and deep vein thrombosis.” Researchers compared outcomes between 4,391 patients who underwent outpatient TKA and 128,951 patients who underwent inpatient TKA.
But for other many surgeries, same-day discharge numbers are increasing without worsening outcomes.
A paper in the Journal of Robotic Surgery found that same-day discharge following robotic-assisted endometrial cancer staging is “safe and feasible.”
Stephen Bradley, MD, MPH, with the Minneapolis Heart Institute in Minneapolis, and colleagues write in the Journal of the American College of Cardiology: Cardiovascular Interventions that they found a large increase in the use of same-day discharge after elective percutaneous coronary intervention (PCI) was not associated with worse 30-day mortality rates or readmission.
In that study, 114,461 patients were discharged the same day they underwent PCI. The proportion of patients who had a same-day discharge increased from 4.5% in 2009 to 28.6% in the fourth quarter of 2017.
Risk-adjusted 30-day mortality did not change in that time, while risk-adjusted rehospitalization decreased over time and more quickly when patients had same-day discharge.
Deepak L. Bhatt, MD, MPH, and Jonathan G. Sung, MBCHB, both of Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, wrote in an accompanying article that, “Advances in the devices and techniques of PCI have improved the safety and efficacy of the procedure. In selected patients, same-day discharge has become possible, and overnight in-hospital observation can be avoided. By reducing unnecessary hospital stays, both patients and hospitals could benefit.”
Evan Garden, a medical student at Icahn School of Medicine at Mount Sinai in New York, presented findings at the American Urological Association 2021 annual meeting that show patients selected for same-day discharge after partial or radical nephrectomy did not have increased rates of postoperative complications or readmissions in the immediate postoperative period, compared with standard discharge of 1-3 days.
Case studies in nephrectomy
While several case studies have looked at the feasibility and safety of performing partial and radical nephrectomy with same-day discharge in select cases, “this topic has not been addressed on a national level,” Mr. Garden said.
Few patients who have partial or radical nephrectomies have same-day discharges. The researchers found that fewer than 1% of patients who have either procedure in the sample studied were discharged the same day.
Researchers used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, a nationally representative deidentified database that prospectively tracks patient characteristics and 30-day perioperative outcomes for major inpatient and outpatient surgical procedures at more than 700 hospitals.
They extracted all minimally invasive partial and radical nephrectomies from 2012 to 2019 and refined the cohort to 28,140 patients who were theoretically eligible for same-day discharge: Of those, 237 (0.8%) had SSD, and 27,903 (99.2%) had a standard-length discharge (SLD).
The team found that there were no differences in 30-day complications or readmissions between same-day discharge (Clavien-Dindo [CD] I/II, 4.22%; CD III, 0%; CD IV, 1.27%; readmission, 4.64%); and SLD (CD I/II, 4.11%; CD III, 0.95%; CD IV, 0.79%; readmission, 3.90%; all P > .05).
Controlling for demographic and clinical variables, SDD was not associated with greater risk of 30-day complications or readmissions (CD I/II: odds ratio, 1.08; 95% confidence interval, 0.57-2.048; P = .813; CD IV: OR 1.699; 95% CI, 0.537-5.375; P = .367; readmission: OR, 1.254; 95% CI, 0.681-2.31; P = .467).
Mr. Garden and coauthors report no relevant financial relationships.
Dr. Lane reports no relevant financial relationships.
Urologist Ronney Abaza, MD, a robotic surgery specialist in Dublin, Ohio, and colleagues, reviewed robotic surgeries at their hospital during COVID-19 restrictions on surgery in Ohio between March 17 and June 5, 2020, and compared them with robotic procedures before COVID-19 and after restrictions were lifted. They published their results in Urology.
Since 2016, the hospital has offered the option of same-day discharge (SDD) to all robotic urologic surgery patients, regardless of procedure or patient-specific factors.
Among patients who had surgery during COVID-19 restrictions, 98% (87/89 patients) opted for SDD versus 52% in the group having surgery before the restrictions (P < .00001). After the COVID-19 surgery restrictions were lifted, the higher rate of SDD remained at 98%.
“There were no differences in 30-day complications or readmissions between SDD and overnight patients,” the authors write.
The right patient, the right motivation for successful surgery
Brian Lane, MD, PhD, a urologic oncologist with Spectrum Health in Grand Rapids, Michigan, told this news organization that, for nephrectomies, uptake of same-day discharge will continue to be slow.
“You have to have the right patient, the right patient motivation, and the surgery has to go smoothly,” he said. “If you start sending everyone home the same day, you will certainly see readmissions,” he said.
Dr. Lane is part of the Michigan Urologic Surgery Improvement Collaborative and he said the group recently looked at same-day discharge outcomes after robotic prostatectomies with SDD as compared with 1-2 nights in the hospital.
The work has not yet been published but, “There was a slight signal that there were increased readmissions with same-day discharge vs. 0-1 day,” he said.
A paper on outcomes of same-day discharge in total knee arthroplasty in the Journal of Bone & Joint Surgery found a higher risk of perioperative complications “including component failure, surgical site infection, knee stiffness, and deep vein thrombosis.” Researchers compared outcomes between 4,391 patients who underwent outpatient TKA and 128,951 patients who underwent inpatient TKA.
But for other many surgeries, same-day discharge numbers are increasing without worsening outcomes.
A paper in the Journal of Robotic Surgery found that same-day discharge following robotic-assisted endometrial cancer staging is “safe and feasible.”
Stephen Bradley, MD, MPH, with the Minneapolis Heart Institute in Minneapolis, and colleagues write in the Journal of the American College of Cardiology: Cardiovascular Interventions that they found a large increase in the use of same-day discharge after elective percutaneous coronary intervention (PCI) was not associated with worse 30-day mortality rates or readmission.
In that study, 114,461 patients were discharged the same day they underwent PCI. The proportion of patients who had a same-day discharge increased from 4.5% in 2009 to 28.6% in the fourth quarter of 2017.
Risk-adjusted 30-day mortality did not change in that time, while risk-adjusted rehospitalization decreased over time and more quickly when patients had same-day discharge.
Deepak L. Bhatt, MD, MPH, and Jonathan G. Sung, MBCHB, both of Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, wrote in an accompanying article that, “Advances in the devices and techniques of PCI have improved the safety and efficacy of the procedure. In selected patients, same-day discharge has become possible, and overnight in-hospital observation can be avoided. By reducing unnecessary hospital stays, both patients and hospitals could benefit.”
Evan Garden, a medical student at Icahn School of Medicine at Mount Sinai in New York, presented findings at the American Urological Association 2021 annual meeting that show patients selected for same-day discharge after partial or radical nephrectomy did not have increased rates of postoperative complications or readmissions in the immediate postoperative period, compared with standard discharge of 1-3 days.
Case studies in nephrectomy
While several case studies have looked at the feasibility and safety of performing partial and radical nephrectomy with same-day discharge in select cases, “this topic has not been addressed on a national level,” Mr. Garden said.
Few patients who have partial or radical nephrectomies have same-day discharges. The researchers found that fewer than 1% of patients who have either procedure in the sample studied were discharged the same day.
Researchers used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, a nationally representative deidentified database that prospectively tracks patient characteristics and 30-day perioperative outcomes for major inpatient and outpatient surgical procedures at more than 700 hospitals.
They extracted all minimally invasive partial and radical nephrectomies from 2012 to 2019 and refined the cohort to 28,140 patients who were theoretically eligible for same-day discharge: Of those, 237 (0.8%) had SSD, and 27,903 (99.2%) had a standard-length discharge (SLD).
The team found that there were no differences in 30-day complications or readmissions between same-day discharge (Clavien-Dindo [CD] I/II, 4.22%; CD III, 0%; CD IV, 1.27%; readmission, 4.64%); and SLD (CD I/II, 4.11%; CD III, 0.95%; CD IV, 0.79%; readmission, 3.90%; all P > .05).
Controlling for demographic and clinical variables, SDD was not associated with greater risk of 30-day complications or readmissions (CD I/II: odds ratio, 1.08; 95% confidence interval, 0.57-2.048; P = .813; CD IV: OR 1.699; 95% CI, 0.537-5.375; P = .367; readmission: OR, 1.254; 95% CI, 0.681-2.31; P = .467).
Mr. Garden and coauthors report no relevant financial relationships.
Dr. Lane reports no relevant financial relationships.
Urologist Ronney Abaza, MD, a robotic surgery specialist in Dublin, Ohio, and colleagues, reviewed robotic surgeries at their hospital during COVID-19 restrictions on surgery in Ohio between March 17 and June 5, 2020, and compared them with robotic procedures before COVID-19 and after restrictions were lifted. They published their results in Urology.
Since 2016, the hospital has offered the option of same-day discharge (SDD) to all robotic urologic surgery patients, regardless of procedure or patient-specific factors.
Among patients who had surgery during COVID-19 restrictions, 98% (87/89 patients) opted for SDD versus 52% in the group having surgery before the restrictions (P < .00001). After the COVID-19 surgery restrictions were lifted, the higher rate of SDD remained at 98%.
“There were no differences in 30-day complications or readmissions between SDD and overnight patients,” the authors write.
The right patient, the right motivation for successful surgery
Brian Lane, MD, PhD, a urologic oncologist with Spectrum Health in Grand Rapids, Michigan, told this news organization that, for nephrectomies, uptake of same-day discharge will continue to be slow.
“You have to have the right patient, the right patient motivation, and the surgery has to go smoothly,” he said. “If you start sending everyone home the same day, you will certainly see readmissions,” he said.
Dr. Lane is part of the Michigan Urologic Surgery Improvement Collaborative and he said the group recently looked at same-day discharge outcomes after robotic prostatectomies with SDD as compared with 1-2 nights in the hospital.
The work has not yet been published but, “There was a slight signal that there were increased readmissions with same-day discharge vs. 0-1 day,” he said.
A paper on outcomes of same-day discharge in total knee arthroplasty in the Journal of Bone & Joint Surgery found a higher risk of perioperative complications “including component failure, surgical site infection, knee stiffness, and deep vein thrombosis.” Researchers compared outcomes between 4,391 patients who underwent outpatient TKA and 128,951 patients who underwent inpatient TKA.
But for other many surgeries, same-day discharge numbers are increasing without worsening outcomes.
A paper in the Journal of Robotic Surgery found that same-day discharge following robotic-assisted endometrial cancer staging is “safe and feasible.”
Stephen Bradley, MD, MPH, with the Minneapolis Heart Institute in Minneapolis, and colleagues write in the Journal of the American College of Cardiology: Cardiovascular Interventions that they found a large increase in the use of same-day discharge after elective percutaneous coronary intervention (PCI) was not associated with worse 30-day mortality rates or readmission.
In that study, 114,461 patients were discharged the same day they underwent PCI. The proportion of patients who had a same-day discharge increased from 4.5% in 2009 to 28.6% in the fourth quarter of 2017.
Risk-adjusted 30-day mortality did not change in that time, while risk-adjusted rehospitalization decreased over time and more quickly when patients had same-day discharge.
Deepak L. Bhatt, MD, MPH, and Jonathan G. Sung, MBCHB, both of Brigham and Women’s Hospital Heart & Vascular Center, Harvard Medical School, Boston, wrote in an accompanying article that, “Advances in the devices and techniques of PCI have improved the safety and efficacy of the procedure. In selected patients, same-day discharge has become possible, and overnight in-hospital observation can be avoided. By reducing unnecessary hospital stays, both patients and hospitals could benefit.”
Evan Garden, a medical student at Icahn School of Medicine at Mount Sinai in New York, presented findings at the American Urological Association 2021 annual meeting that show patients selected for same-day discharge after partial or radical nephrectomy did not have increased rates of postoperative complications or readmissions in the immediate postoperative period, compared with standard discharge of 1-3 days.
Case studies in nephrectomy
While several case studies have looked at the feasibility and safety of performing partial and radical nephrectomy with same-day discharge in select cases, “this topic has not been addressed on a national level,” Mr. Garden said.
Few patients who have partial or radical nephrectomies have same-day discharges. The researchers found that fewer than 1% of patients who have either procedure in the sample studied were discharged the same day.
Researchers used the American College of Surgeons National Surgical Quality Improvement Program (NSQIP) database, a nationally representative deidentified database that prospectively tracks patient characteristics and 30-day perioperative outcomes for major inpatient and outpatient surgical procedures at more than 700 hospitals.
They extracted all minimally invasive partial and radical nephrectomies from 2012 to 2019 and refined the cohort to 28,140 patients who were theoretically eligible for same-day discharge: Of those, 237 (0.8%) had SSD, and 27,903 (99.2%) had a standard-length discharge (SLD).
The team found that there were no differences in 30-day complications or readmissions between same-day discharge (Clavien-Dindo [CD] I/II, 4.22%; CD III, 0%; CD IV, 1.27%; readmission, 4.64%); and SLD (CD I/II, 4.11%; CD III, 0.95%; CD IV, 0.79%; readmission, 3.90%; all P > .05).
Controlling for demographic and clinical variables, SDD was not associated with greater risk of 30-day complications or readmissions (CD I/II: odds ratio, 1.08; 95% confidence interval, 0.57-2.048; P = .813; CD IV: OR 1.699; 95% CI, 0.537-5.375; P = .367; readmission: OR, 1.254; 95% CI, 0.681-2.31; P = .467).
Mr. Garden and coauthors report no relevant financial relationships.
Dr. Lane reports no relevant financial relationships.
Sunscreen, other sun-protective habits not linked with poorer bone health, fractures
Using , according to a new study that included more than 3,000 men and women.

“We have objective data for the first time, and in a large-scale representative population of the U.S. adults, to indicate sun protection is not associated with negative bone-related outcomes,” said study lead author Mohsen Afarideh, MD, MPH, a postdoctoral research fellow at the autoimmune skin diseases unit at the University of Pennsylvania, Philadelphia.
The study, published online in JAMA Dermatology, goes a step further than previous research by others that has found sunscreen use does not compromise vitamin D synthesis and has little effect on circulating 25-hydroxyvitamin D levels.
In the new study, researchers looked at three sun-protective behaviors – sunscreen use, staying in the shade, wearing long sleeves – and their effects on bone mineral density and the risk of fractures.
While the effects of sun-protective habits on blood levels of vitamin D and BMD scores are important, ‘’what we are more interested to know is if the sun-protective behaviors actually cause or increase the risk of fracture,” Dr. Afarideh said in an interview. “The answer to that is a firm ‘No.’ These data are very reassuring and will help clinicians to keep recommending sun protection to the public.”
Study details
Dr. Afarideh and his colleagues from the Mayo Clinic in Rochester, Minn., looked at data from the National Health and Nutrition Examination Survey (NHANES) from 2017 to 2018, obtaining final information on 3,403 men and women, ages 20-59, who completed a dermatology questionnaire The men and women reported on the three sun-protective habits, and noted whether they followed these practices always or most of the time, sometimes, or never or rarely.
The frequency of the three behaviors was not widespread. Frequent staying in the shade was reported by 31.6% of the sample, wearing long sleeves by 11.8%, and sunscreen use by 26.1%.
The researchers also had data on the participants’ bone mineral density (BMD) scores along with dietary information such as milk consumption, vitamin D supplement use, taking steroid drugs, and exercise activity.
“Moderate sunscreen use was linked with a slightly lower lumbar BMD score,” Dr. Afarideh said, which was “the only significant association that could be interpreted as concerning.” And this was more likely to be seen in older respondents, he said.
However, otherwise they found the practice of the three behaviors was not associated with lower total or site-specific BMD z scores, nor was it linked with an increased risk of osteoporotic fractures. (The BMD z score compares an individual’s bone density to the average bone density of someone their same age and gender.)
The focus on fracture risk is the more important outcome, Dr. Afarideh said. And they found no increased risk overall of osteoporotic fractures in those who practiced sun-protective behaviors.
Moderate to frequent staying in the shade was actually linked with a reduced prevalence of spine fractures in the multivariate model (odds ratio, 0.19; 95% confidence interval, 0.04-0.86, P = .02). The researchers say that may be attributable to these respondents also being careful in other areas of life, such as avoiding falls and not participating in high-risk activities that would increase the chance of fractures. “However, this is just an assumption,” Dr. Afarideh said.
Expert perspectives
Other dermatologists not involved in the new research said the study results provide some “real-world” information that’s valuable for clinicians to share with patients.
“I think this is an important study on multiple levels,” said Henry W. Lim, MD, a former president of the American Academy of Dermatology who is a member of the department of dermatology and senior vice president of academic affairs at Henry Ford Health System, Detroit. “It is a well-done study, involving a large number. It is a real-life situation, asking people their photo protective behaviors and then looking at their bone mineral density.” The bottom line, he said: “Bone health is not affected by photo protection habits in real life.”
The findings are important but not surprising, said Antony R. Young, PhD, emeritus professor of experimental photobiology at St. John’s Institute of Dermatology, King’s College, London, who has researched sunscreens and vitamin D status. “My study showed that correct sunscreen use, albeit with a relatively low SPF of 15, did prevent sunburn in a high UVR [ultraviolet radiation] environment but did allow very good vitamin D synthesis. I think this is because the necessary dose of UVB is very low.”
Michele Green, MD, a New York dermatologist and clinical staff member at Lenox Hill Hospital there, said she often hears concerns about bone health from patients. “Every week, patients ask, ‘Why would I wear sunblock? Don’t I need sun for bone health? Don’t I need it for vitamin D?’’’
Now, she said, ‘’Dermatologists can point to the study and say ‘Don’t worry.’ It clarifies that using sunscreen won’t cause you to have osteoporosis.’’
Dr. Afarideh, who was a postdoctoral research fellow at the Mayo Clinic, and his coauthors, Megha M. Tollefson, MD, and Julio C. Sartori-Valinotti, of the Mayo Clinic, and Dr. Green had no disclosures. Dr. Lim and Dr. Young consult for the sunscreen industry.
Using , according to a new study that included more than 3,000 men and women.
“We have objective data for the first time, and in a large-scale representative population of the U.S. adults, to indicate sun protection is not associated with negative bone-related outcomes,” said study lead author Mohsen Afarideh, MD, MPH, a postdoctoral research fellow at the autoimmune skin diseases unit at the University of Pennsylvania, Philadelphia.
The study, published online in JAMA Dermatology, goes a step further than previous research by others that has found sunscreen use does not compromise vitamin D synthesis and has little effect on circulating 25-hydroxyvitamin D levels.
In the new study, researchers looked at three sun-protective behaviors – sunscreen use, staying in the shade, wearing long sleeves – and their effects on bone mineral density and the risk of fractures.
While the effects of sun-protective habits on blood levels of vitamin D and BMD scores are important, ‘’what we are more interested to know is if the sun-protective behaviors actually cause or increase the risk of fracture,” Dr. Afarideh said in an interview. “The answer to that is a firm ‘No.’ These data are very reassuring and will help clinicians to keep recommending sun protection to the public.”
Study details
Dr. Afarideh and his colleagues from the Mayo Clinic in Rochester, Minn., looked at data from the National Health and Nutrition Examination Survey (NHANES) from 2017 to 2018, obtaining final information on 3,403 men and women, ages 20-59, who completed a dermatology questionnaire The men and women reported on the three sun-protective habits, and noted whether they followed these practices always or most of the time, sometimes, or never or rarely.
The frequency of the three behaviors was not widespread. Frequent staying in the shade was reported by 31.6% of the sample, wearing long sleeves by 11.8%, and sunscreen use by 26.1%.
The researchers also had data on the participants’ bone mineral density (BMD) scores along with dietary information such as milk consumption, vitamin D supplement use, taking steroid drugs, and exercise activity.
“Moderate sunscreen use was linked with a slightly lower lumbar BMD score,” Dr. Afarideh said, which was “the only significant association that could be interpreted as concerning.” And this was more likely to be seen in older respondents, he said.
However, otherwise they found the practice of the three behaviors was not associated with lower total or site-specific BMD z scores, nor was it linked with an increased risk of osteoporotic fractures. (The BMD z score compares an individual’s bone density to the average bone density of someone their same age and gender.)
The focus on fracture risk is the more important outcome, Dr. Afarideh said. And they found no increased risk overall of osteoporotic fractures in those who practiced sun-protective behaviors.
Moderate to frequent staying in the shade was actually linked with a reduced prevalence of spine fractures in the multivariate model (odds ratio, 0.19; 95% confidence interval, 0.04-0.86, P = .02). The researchers say that may be attributable to these respondents also being careful in other areas of life, such as avoiding falls and not participating in high-risk activities that would increase the chance of fractures. “However, this is just an assumption,” Dr. Afarideh said.
Expert perspectives
Other dermatologists not involved in the new research said the study results provide some “real-world” information that’s valuable for clinicians to share with patients.
“I think this is an important study on multiple levels,” said Henry W. Lim, MD, a former president of the American Academy of Dermatology who is a member of the department of dermatology and senior vice president of academic affairs at Henry Ford Health System, Detroit. “It is a well-done study, involving a large number. It is a real-life situation, asking people their photo protective behaviors and then looking at their bone mineral density.” The bottom line, he said: “Bone health is not affected by photo protection habits in real life.”
The findings are important but not surprising, said Antony R. Young, PhD, emeritus professor of experimental photobiology at St. John’s Institute of Dermatology, King’s College, London, who has researched sunscreens and vitamin D status. “My study showed that correct sunscreen use, albeit with a relatively low SPF of 15, did prevent sunburn in a high UVR [ultraviolet radiation] environment but did allow very good vitamin D synthesis. I think this is because the necessary dose of UVB is very low.”
Michele Green, MD, a New York dermatologist and clinical staff member at Lenox Hill Hospital there, said she often hears concerns about bone health from patients. “Every week, patients ask, ‘Why would I wear sunblock? Don’t I need sun for bone health? Don’t I need it for vitamin D?’’’
Now, she said, ‘’Dermatologists can point to the study and say ‘Don’t worry.’ It clarifies that using sunscreen won’t cause you to have osteoporosis.’’
Dr. Afarideh, who was a postdoctoral research fellow at the Mayo Clinic, and his coauthors, Megha M. Tollefson, MD, and Julio C. Sartori-Valinotti, of the Mayo Clinic, and Dr. Green had no disclosures. Dr. Lim and Dr. Young consult for the sunscreen industry.
Using , according to a new study that included more than 3,000 men and women.
“We have objective data for the first time, and in a large-scale representative population of the U.S. adults, to indicate sun protection is not associated with negative bone-related outcomes,” said study lead author Mohsen Afarideh, MD, MPH, a postdoctoral research fellow at the autoimmune skin diseases unit at the University of Pennsylvania, Philadelphia.
The study, published online in JAMA Dermatology, goes a step further than previous research by others that has found sunscreen use does not compromise vitamin D synthesis and has little effect on circulating 25-hydroxyvitamin D levels.
In the new study, researchers looked at three sun-protective behaviors – sunscreen use, staying in the shade, wearing long sleeves – and their effects on bone mineral density and the risk of fractures.
While the effects of sun-protective habits on blood levels of vitamin D and BMD scores are important, ‘’what we are more interested to know is if the sun-protective behaviors actually cause or increase the risk of fracture,” Dr. Afarideh said in an interview. “The answer to that is a firm ‘No.’ These data are very reassuring and will help clinicians to keep recommending sun protection to the public.”
Study details
Dr. Afarideh and his colleagues from the Mayo Clinic in Rochester, Minn., looked at data from the National Health and Nutrition Examination Survey (NHANES) from 2017 to 2018, obtaining final information on 3,403 men and women, ages 20-59, who completed a dermatology questionnaire The men and women reported on the three sun-protective habits, and noted whether they followed these practices always or most of the time, sometimes, or never or rarely.
The frequency of the three behaviors was not widespread. Frequent staying in the shade was reported by 31.6% of the sample, wearing long sleeves by 11.8%, and sunscreen use by 26.1%.
The researchers also had data on the participants’ bone mineral density (BMD) scores along with dietary information such as milk consumption, vitamin D supplement use, taking steroid drugs, and exercise activity.
“Moderate sunscreen use was linked with a slightly lower lumbar BMD score,” Dr. Afarideh said, which was “the only significant association that could be interpreted as concerning.” And this was more likely to be seen in older respondents, he said.
However, otherwise they found the practice of the three behaviors was not associated with lower total or site-specific BMD z scores, nor was it linked with an increased risk of osteoporotic fractures. (The BMD z score compares an individual’s bone density to the average bone density of someone their same age and gender.)
The focus on fracture risk is the more important outcome, Dr. Afarideh said. And they found no increased risk overall of osteoporotic fractures in those who practiced sun-protective behaviors.
Moderate to frequent staying in the shade was actually linked with a reduced prevalence of spine fractures in the multivariate model (odds ratio, 0.19; 95% confidence interval, 0.04-0.86, P = .02). The researchers say that may be attributable to these respondents also being careful in other areas of life, such as avoiding falls and not participating in high-risk activities that would increase the chance of fractures. “However, this is just an assumption,” Dr. Afarideh said.
Expert perspectives
Other dermatologists not involved in the new research said the study results provide some “real-world” information that’s valuable for clinicians to share with patients.
“I think this is an important study on multiple levels,” said Henry W. Lim, MD, a former president of the American Academy of Dermatology who is a member of the department of dermatology and senior vice president of academic affairs at Henry Ford Health System, Detroit. “It is a well-done study, involving a large number. It is a real-life situation, asking people their photo protective behaviors and then looking at their bone mineral density.” The bottom line, he said: “Bone health is not affected by photo protection habits in real life.”
The findings are important but not surprising, said Antony R. Young, PhD, emeritus professor of experimental photobiology at St. John’s Institute of Dermatology, King’s College, London, who has researched sunscreens and vitamin D status. “My study showed that correct sunscreen use, albeit with a relatively low SPF of 15, did prevent sunburn in a high UVR [ultraviolet radiation] environment but did allow very good vitamin D synthesis. I think this is because the necessary dose of UVB is very low.”
Michele Green, MD, a New York dermatologist and clinical staff member at Lenox Hill Hospital there, said she often hears concerns about bone health from patients. “Every week, patients ask, ‘Why would I wear sunblock? Don’t I need sun for bone health? Don’t I need it for vitamin D?’’’
Now, she said, ‘’Dermatologists can point to the study and say ‘Don’t worry.’ It clarifies that using sunscreen won’t cause you to have osteoporosis.’’
Dr. Afarideh, who was a postdoctoral research fellow at the Mayo Clinic, and his coauthors, Megha M. Tollefson, MD, and Julio C. Sartori-Valinotti, of the Mayo Clinic, and Dr. Green had no disclosures. Dr. Lim and Dr. Young consult for the sunscreen industry.
FROM JAMA DERMATOLOGY

Some diuretics tied to increased skin cancer risk
The findings were originally reported in two Danish case-control studies in which physicians reported a fourfold increased risk of squamous cell carcinoma, and a moderate increased risk of basal cell carcinoma and cutaneous malignant melanoma in patients who used hydrochlorothiazide long-term.
And, while the new study did not find an increased risk of basal cell carcinoma and cutaneous malignant melanoma among long-term users of hydrochlorothiazide, they suggest that bendroflumethiazide “may be a safer alternative for patients at increased risk of skin cancer.” The long-term use of indapamide was associated with a moderately increased risk of cutaneous malignant melanoma but did not alter the risk of either squamous cell or basal cell carcinoma
“Our results suggest that bendroflumethiazide may be a safer alternative to hydrochlorothiazide and indapamide, especially for patients at increased risk of skin cancer, but future studies are needed to rule out a causal association between bendroflumethiazide and cutaneous malignant melanoma,” wrote authors who were led by Christoph R. Meier, PhD, a professor in pharmacy with University Hospital Basel (Switzerland) and a contributor to the Boston Collaborative Drug Surveillance Program.
This study adds to existing evidence that there is a dose-dependent increased risk of squamous cell carcinoma in users of high cumulative doses of hydrochlorothiazide, compared with non–hydrochlorothiazide users.
The study, an observational cohort study, was published earlier this year. It is based on data from the U.K.-based Clinical Practice Research Datalink. It included 271,154 new users of thiazides and thiazidelike diuretics, the majority at 87.6% having been prescribed bendroflumethiazide, 5.8% indapamide, and 3.6% hydrochlorothiazide. Outcomes were compared to those observed in 275,263 users of calcium channel blockers.
“The three primary outcomes of interest were a first-time diagnosis of cutaneous malignant melanoma, basal cell carcinoma, or squamous cell carcinoma,” the authors wrote.
Incidence rates and incidence rate ratios were estimated for both short-term and long-term users of thiazidelike diuretics and calcium channel blockers, while a propensity score (PS) analysis was done in order to control for 23 baseline covariates. The mean follow-up after PS weighting was 3.9 years for indapamide users and 5.5 years for hydrochlorothiazide users. Overall, the incidence rate ratios of squamous cell carcinoma were not markedly increased for either short-term or long-term users of thiazidelike diuretics, the authors reported.
In contrast, the incidence rate ratios of squamous cell carcinoma for hydrochlorothiazide users were increased by 29% for short-term users at an IRR of 1.29 while they were increased by almost twofold for long-term hydrochlorothiazide users at an IRR of 1.95.
Long-term use of hydrochlorothiazide was again associated with a 64% increased risk of basal cell carcinoma, compared with users of a renin-angiotensin inhibitor at a weighted IRR of 1.64.
In contrast, weighted incident rate ratios for basal cell carcinoma for both short-term and long-term thiazide users were not significantly different and results were similar for patients who took hydrochlorothiazide, indapamide, or bendroflumethiazide.
Weighted overall incident rate ratios for cutaneous malignant melanoma were not significantly different for either short-term or long-term users of thiazidelike diuretics, compared with calcium channel blocker users.
However, there was a 43% increased risk of cutaneous malignant melanoma among long-term indapamide users at a weighted IRR of 1.43, compared with calcium channel blocker users, the authors reported.
“Given the biological plausibility and the severe clinical implications of cutaneous malignant melanoma, this finding should be considered carefully,” they cautioned.
Limitations to the study include the fact that the database analyzed does not have information on sun exposure, skin characteristics, or socioeconomic status which may affect the amount of sun exposure participants received.
The authors had no conflicts of interest to declare.
The findings were originally reported in two Danish case-control studies in which physicians reported a fourfold increased risk of squamous cell carcinoma, and a moderate increased risk of basal cell carcinoma and cutaneous malignant melanoma in patients who used hydrochlorothiazide long-term.
And, while the new study did not find an increased risk of basal cell carcinoma and cutaneous malignant melanoma among long-term users of hydrochlorothiazide, they suggest that bendroflumethiazide “may be a safer alternative for patients at increased risk of skin cancer.” The long-term use of indapamide was associated with a moderately increased risk of cutaneous malignant melanoma but did not alter the risk of either squamous cell or basal cell carcinoma
“Our results suggest that bendroflumethiazide may be a safer alternative to hydrochlorothiazide and indapamide, especially for patients at increased risk of skin cancer, but future studies are needed to rule out a causal association between bendroflumethiazide and cutaneous malignant melanoma,” wrote authors who were led by Christoph R. Meier, PhD, a professor in pharmacy with University Hospital Basel (Switzerland) and a contributor to the Boston Collaborative Drug Surveillance Program.
This study adds to existing evidence that there is a dose-dependent increased risk of squamous cell carcinoma in users of high cumulative doses of hydrochlorothiazide, compared with non–hydrochlorothiazide users.
The study, an observational cohort study, was published earlier this year. It is based on data from the U.K.-based Clinical Practice Research Datalink. It included 271,154 new users of thiazides and thiazidelike diuretics, the majority at 87.6% having been prescribed bendroflumethiazide, 5.8% indapamide, and 3.6% hydrochlorothiazide. Outcomes were compared to those observed in 275,263 users of calcium channel blockers.
“The three primary outcomes of interest were a first-time diagnosis of cutaneous malignant melanoma, basal cell carcinoma, or squamous cell carcinoma,” the authors wrote.
Incidence rates and incidence rate ratios were estimated for both short-term and long-term users of thiazidelike diuretics and calcium channel blockers, while a propensity score (PS) analysis was done in order to control for 23 baseline covariates. The mean follow-up after PS weighting was 3.9 years for indapamide users and 5.5 years for hydrochlorothiazide users. Overall, the incidence rate ratios of squamous cell carcinoma were not markedly increased for either short-term or long-term users of thiazidelike diuretics, the authors reported.
In contrast, the incidence rate ratios of squamous cell carcinoma for hydrochlorothiazide users were increased by 29% for short-term users at an IRR of 1.29 while they were increased by almost twofold for long-term hydrochlorothiazide users at an IRR of 1.95.
Long-term use of hydrochlorothiazide was again associated with a 64% increased risk of basal cell carcinoma, compared with users of a renin-angiotensin inhibitor at a weighted IRR of 1.64.
In contrast, weighted incident rate ratios for basal cell carcinoma for both short-term and long-term thiazide users were not significantly different and results were similar for patients who took hydrochlorothiazide, indapamide, or bendroflumethiazide.
Weighted overall incident rate ratios for cutaneous malignant melanoma were not significantly different for either short-term or long-term users of thiazidelike diuretics, compared with calcium channel blocker users.
However, there was a 43% increased risk of cutaneous malignant melanoma among long-term indapamide users at a weighted IRR of 1.43, compared with calcium channel blocker users, the authors reported.
“Given the biological plausibility and the severe clinical implications of cutaneous malignant melanoma, this finding should be considered carefully,” they cautioned.
Limitations to the study include the fact that the database analyzed does not have information on sun exposure, skin characteristics, or socioeconomic status which may affect the amount of sun exposure participants received.
The authors had no conflicts of interest to declare.
The findings were originally reported in two Danish case-control studies in which physicians reported a fourfold increased risk of squamous cell carcinoma, and a moderate increased risk of basal cell carcinoma and cutaneous malignant melanoma in patients who used hydrochlorothiazide long-term.
And, while the new study did not find an increased risk of basal cell carcinoma and cutaneous malignant melanoma among long-term users of hydrochlorothiazide, they suggest that bendroflumethiazide “may be a safer alternative for patients at increased risk of skin cancer.” The long-term use of indapamide was associated with a moderately increased risk of cutaneous malignant melanoma but did not alter the risk of either squamous cell or basal cell carcinoma
“Our results suggest that bendroflumethiazide may be a safer alternative to hydrochlorothiazide and indapamide, especially for patients at increased risk of skin cancer, but future studies are needed to rule out a causal association between bendroflumethiazide and cutaneous malignant melanoma,” wrote authors who were led by Christoph R. Meier, PhD, a professor in pharmacy with University Hospital Basel (Switzerland) and a contributor to the Boston Collaborative Drug Surveillance Program.
This study adds to existing evidence that there is a dose-dependent increased risk of squamous cell carcinoma in users of high cumulative doses of hydrochlorothiazide, compared with non–hydrochlorothiazide users.
The study, an observational cohort study, was published earlier this year. It is based on data from the U.K.-based Clinical Practice Research Datalink. It included 271,154 new users of thiazides and thiazidelike diuretics, the majority at 87.6% having been prescribed bendroflumethiazide, 5.8% indapamide, and 3.6% hydrochlorothiazide. Outcomes were compared to those observed in 275,263 users of calcium channel blockers.
“The three primary outcomes of interest were a first-time diagnosis of cutaneous malignant melanoma, basal cell carcinoma, or squamous cell carcinoma,” the authors wrote.
Incidence rates and incidence rate ratios were estimated for both short-term and long-term users of thiazidelike diuretics and calcium channel blockers, while a propensity score (PS) analysis was done in order to control for 23 baseline covariates. The mean follow-up after PS weighting was 3.9 years for indapamide users and 5.5 years for hydrochlorothiazide users. Overall, the incidence rate ratios of squamous cell carcinoma were not markedly increased for either short-term or long-term users of thiazidelike diuretics, the authors reported.
In contrast, the incidence rate ratios of squamous cell carcinoma for hydrochlorothiazide users were increased by 29% for short-term users at an IRR of 1.29 while they were increased by almost twofold for long-term hydrochlorothiazide users at an IRR of 1.95.
Long-term use of hydrochlorothiazide was again associated with a 64% increased risk of basal cell carcinoma, compared with users of a renin-angiotensin inhibitor at a weighted IRR of 1.64.
In contrast, weighted incident rate ratios for basal cell carcinoma for both short-term and long-term thiazide users were not significantly different and results were similar for patients who took hydrochlorothiazide, indapamide, or bendroflumethiazide.
Weighted overall incident rate ratios for cutaneous malignant melanoma were not significantly different for either short-term or long-term users of thiazidelike diuretics, compared with calcium channel blocker users.
However, there was a 43% increased risk of cutaneous malignant melanoma among long-term indapamide users at a weighted IRR of 1.43, compared with calcium channel blocker users, the authors reported.
“Given the biological plausibility and the severe clinical implications of cutaneous malignant melanoma, this finding should be considered carefully,” they cautioned.
Limitations to the study include the fact that the database analyzed does not have information on sun exposure, skin characteristics, or socioeconomic status which may affect the amount of sun exposure participants received.
The authors had no conflicts of interest to declare.
FROM BRITISH JOURNAL OF DERMATOLOGY
Uncertainty looms large in treatment options for high-risk cutaneous SCC
say the authors of a clinical review recently published in the journal Head and Neck.
The review, led by Jason G. Newman, MD, director of head and neck surgery at Penn Medicine, Philadelphia, includes evidence-based research findings from the last 10 years which describe the possible roles for adjuvant radiation, chemotherapy, immunotherapy, and/or targeted therapy in the management of high-risk cSCC.
Dr. Newman and colleagues wrote that more data – and high-quality data – are needed for physicians to determine with more confidence which adjuvant therapies would be best for specific patients with high-risk cSCC. But without that data, uncertainty in treatment decisions will persist.
“The requirements for and efficacy of adjuvant therapies in cutaneous squamous cell carcinoma are unclear, and the gap in evidence for practice decisions regarding adjuvant therapy in patients with high-risk cSCC has been apparent for more than a decade,” they wrote.
While surgical excision with clear margins of the primary cSCC lesion remains the standard of care, certain high-risk factors necessitate adjuvant therapy, the authors wrote. However, since the evidence consists of small retrospective studies with conflicting results, it is unclear which patients might benefit from adjuvant therapy. This review included recent and current trials in cutaneous SCC and the role of immune checkpoint inhibitors.
According to the review, adjuvant radiation therapy is usually considered with high-risk features, such as perineural invasion, lymph node metastasis and extracapsular/extranodal extension, if the patient is otherwise at high risk for metastasis or recurrence, or if further surgery is not possible.
The National Comprehensive Cancer Network, the American College of Radiology, and the American Society for Radiation Oncology do not recommend adjuvant radiation therapy for most patients with cSCC. However, adjuvant radiation therapy with or without systemic therapy may be considered in locally advanced disease, when further surgery is not an option, or if there is regional lymph node metastasis, but multidisciplinary consultation is recommended.
Regarding checkpoint inhibitors, the NCCN, ACR, and ASTRO do not recommend the use of systemic therapy for local disease amenable to surgery. Potential use of a checkpoint inhibitor with radiation therapy in a clinical trial is recommended for residual disease in locally advanced cSCC as palliative care when other options are not available. While the use of cemiplimab or pembrolizumab are preferred in regional recurrence when curative surgery and radiation therapy are not an option, a targeted therapy can be considered if this is not feasible.
“Given the current activity of checkpoint inhibition in this disease, enthusiasm for the addition of cytotoxic chemotherapeutic agents in the adjuvant setting may be on the decline,” the authors wrote. “Multidisciplinary approaches will most likely continue to be recommended in complicated cases, including those involving immunosuppression.”
The authors said that further study is needed on prognostic testing, such as gene expression profile testing or sentinel lymph node biopsy, as such testing early in disease could identify patients who would likely benefit from adjuvant therapy. They added that the need to identify patients at early stages of disease who are at high risk for metastasis continues to remain critical.
say the authors of a clinical review recently published in the journal Head and Neck.
The review, led by Jason G. Newman, MD, director of head and neck surgery at Penn Medicine, Philadelphia, includes evidence-based research findings from the last 10 years which describe the possible roles for adjuvant radiation, chemotherapy, immunotherapy, and/or targeted therapy in the management of high-risk cSCC.
Dr. Newman and colleagues wrote that more data – and high-quality data – are needed for physicians to determine with more confidence which adjuvant therapies would be best for specific patients with high-risk cSCC. But without that data, uncertainty in treatment decisions will persist.
“The requirements for and efficacy of adjuvant therapies in cutaneous squamous cell carcinoma are unclear, and the gap in evidence for practice decisions regarding adjuvant therapy in patients with high-risk cSCC has been apparent for more than a decade,” they wrote.
While surgical excision with clear margins of the primary cSCC lesion remains the standard of care, certain high-risk factors necessitate adjuvant therapy, the authors wrote. However, since the evidence consists of small retrospective studies with conflicting results, it is unclear which patients might benefit from adjuvant therapy. This review included recent and current trials in cutaneous SCC and the role of immune checkpoint inhibitors.
According to the review, adjuvant radiation therapy is usually considered with high-risk features, such as perineural invasion, lymph node metastasis and extracapsular/extranodal extension, if the patient is otherwise at high risk for metastasis or recurrence, or if further surgery is not possible.
The National Comprehensive Cancer Network, the American College of Radiology, and the American Society for Radiation Oncology do not recommend adjuvant radiation therapy for most patients with cSCC. However, adjuvant radiation therapy with or without systemic therapy may be considered in locally advanced disease, when further surgery is not an option, or if there is regional lymph node metastasis, but multidisciplinary consultation is recommended.
Regarding checkpoint inhibitors, the NCCN, ACR, and ASTRO do not recommend the use of systemic therapy for local disease amenable to surgery. Potential use of a checkpoint inhibitor with radiation therapy in a clinical trial is recommended for residual disease in locally advanced cSCC as palliative care when other options are not available. While the use of cemiplimab or pembrolizumab are preferred in regional recurrence when curative surgery and radiation therapy are not an option, a targeted therapy can be considered if this is not feasible.
“Given the current activity of checkpoint inhibition in this disease, enthusiasm for the addition of cytotoxic chemotherapeutic agents in the adjuvant setting may be on the decline,” the authors wrote. “Multidisciplinary approaches will most likely continue to be recommended in complicated cases, including those involving immunosuppression.”
The authors said that further study is needed on prognostic testing, such as gene expression profile testing or sentinel lymph node biopsy, as such testing early in disease could identify patients who would likely benefit from adjuvant therapy. They added that the need to identify patients at early stages of disease who are at high risk for metastasis continues to remain critical.
say the authors of a clinical review recently published in the journal Head and Neck.
The review, led by Jason G. Newman, MD, director of head and neck surgery at Penn Medicine, Philadelphia, includes evidence-based research findings from the last 10 years which describe the possible roles for adjuvant radiation, chemotherapy, immunotherapy, and/or targeted therapy in the management of high-risk cSCC.
Dr. Newman and colleagues wrote that more data – and high-quality data – are needed for physicians to determine with more confidence which adjuvant therapies would be best for specific patients with high-risk cSCC. But without that data, uncertainty in treatment decisions will persist.
“The requirements for and efficacy of adjuvant therapies in cutaneous squamous cell carcinoma are unclear, and the gap in evidence for practice decisions regarding adjuvant therapy in patients with high-risk cSCC has been apparent for more than a decade,” they wrote.
While surgical excision with clear margins of the primary cSCC lesion remains the standard of care, certain high-risk factors necessitate adjuvant therapy, the authors wrote. However, since the evidence consists of small retrospective studies with conflicting results, it is unclear which patients might benefit from adjuvant therapy. This review included recent and current trials in cutaneous SCC and the role of immune checkpoint inhibitors.
According to the review, adjuvant radiation therapy is usually considered with high-risk features, such as perineural invasion, lymph node metastasis and extracapsular/extranodal extension, if the patient is otherwise at high risk for metastasis or recurrence, or if further surgery is not possible.
The National Comprehensive Cancer Network, the American College of Radiology, and the American Society for Radiation Oncology do not recommend adjuvant radiation therapy for most patients with cSCC. However, adjuvant radiation therapy with or without systemic therapy may be considered in locally advanced disease, when further surgery is not an option, or if there is regional lymph node metastasis, but multidisciplinary consultation is recommended.
Regarding checkpoint inhibitors, the NCCN, ACR, and ASTRO do not recommend the use of systemic therapy for local disease amenable to surgery. Potential use of a checkpoint inhibitor with radiation therapy in a clinical trial is recommended for residual disease in locally advanced cSCC as palliative care when other options are not available. While the use of cemiplimab or pembrolizumab are preferred in regional recurrence when curative surgery and radiation therapy are not an option, a targeted therapy can be considered if this is not feasible.
“Given the current activity of checkpoint inhibition in this disease, enthusiasm for the addition of cytotoxic chemotherapeutic agents in the adjuvant setting may be on the decline,” the authors wrote. “Multidisciplinary approaches will most likely continue to be recommended in complicated cases, including those involving immunosuppression.”
The authors said that further study is needed on prognostic testing, such as gene expression profile testing or sentinel lymph node biopsy, as such testing early in disease could identify patients who would likely benefit from adjuvant therapy. They added that the need to identify patients at early stages of disease who are at high risk for metastasis continues to remain critical.
FROM HEAD AND NECK
Immunocompromised people face highest risk of cutaneous SCC metastasis
However, no study has thoroughly evaluated the prognostic factors associated with metastasis until now.
In the Journal of Otolaryngology – Head & Neck Surgery, researchers wrote that immunocompromised individuals, such as solid organ transplant patients, make up 73.3% of all patients with cutaneous SCC who are at risk of metastasis and decreased overall survival.
Led by Alex M. Mlynarek, MD, a specialist in head and neck oncology and microvascular reconstruction at McGill University, Montreal, the finding is based on a systematic literature review of 40 studies involving 8,535 patients.
“The prognostic factors for head and neck cutaneous squamous cell carcinoma that were most consistently reported as significant in the literature are a state of immunosuppression, tumor depth, margins involved, number of lymph nodes affected by carcinoma, parotideal disease, and age,” Dr. Mlynarek and colleagues wrote.
Cutaneous SCC is the second most common nonmelanoma skin cancer with an increase of 263% between 2000 and 2010, shows research from the Mayo Clinic Rochester Epidemiology Project.
Patients in this study with tumors that are 6 mm or greater, or whose tumor invaded fat tissue, were found to have a poor prognosis followed by patients with perineural and lymphovascular invasion and in particular, patients with a poorer grade of cellular differentiation. The number of lymph nodes was significant at 70%, with more than two nodes involved linked to a worse the prognosis, followed by 66.7% for margins involved with carcinoma and 50% for tumor depth.
“The majority of patients with cutaneous SCC undergoes electrodesiccation and curettage, cryosurgery, or Mohs surgery, and have an excellent prognosis,” the authors wrote. “However, there is a subset of patients in which these therapies are unsuccessful and where cutaneous SCC appears to be far more aggressive, often resulting in metastasis and recurrence.”
Age was shown to be a significant factor in 53.3% of the studies, but the extent of its effect on prognosis was questionable.
Sentinel lymph node biopsy is commonly used to stage melanoma and has been used in oral SCC.
“A patient post biopsy with either two major criteria or one major and two minor criteria should be considered as a candidate for sentinel lymph node biopsy,” the authors wrote, adding that the findings were consistent with those for cutaneous SCC generally, not specified to the head and neck.
Limitations of the systematic review include potential selection bias as the majority of the studies were based in Australia and most studies were not specified to cutaneous SCC of the head and neck region.
“Given the low rate of metastasis from head and neck cutaneous SCC lesions, it can be challenging to identify the patients who are at high risk of having metastatic disease,” the authors wrote. “We believe this review could help identify patients that would require a closer follow-up and those that could possibly profit from a sentinel lymph node biopsy.”
No disclosures were disclosed for the authors.
However, no study has thoroughly evaluated the prognostic factors associated with metastasis until now.
In the Journal of Otolaryngology – Head & Neck Surgery, researchers wrote that immunocompromised individuals, such as solid organ transplant patients, make up 73.3% of all patients with cutaneous SCC who are at risk of metastasis and decreased overall survival.
Led by Alex M. Mlynarek, MD, a specialist in head and neck oncology and microvascular reconstruction at McGill University, Montreal, the finding is based on a systematic literature review of 40 studies involving 8,535 patients.
“The prognostic factors for head and neck cutaneous squamous cell carcinoma that were most consistently reported as significant in the literature are a state of immunosuppression, tumor depth, margins involved, number of lymph nodes affected by carcinoma, parotideal disease, and age,” Dr. Mlynarek and colleagues wrote.
Cutaneous SCC is the second most common nonmelanoma skin cancer with an increase of 263% between 2000 and 2010, shows research from the Mayo Clinic Rochester Epidemiology Project.
Patients in this study with tumors that are 6 mm or greater, or whose tumor invaded fat tissue, were found to have a poor prognosis followed by patients with perineural and lymphovascular invasion and in particular, patients with a poorer grade of cellular differentiation. The number of lymph nodes was significant at 70%, with more than two nodes involved linked to a worse the prognosis, followed by 66.7% for margins involved with carcinoma and 50% for tumor depth.
“The majority of patients with cutaneous SCC undergoes electrodesiccation and curettage, cryosurgery, or Mohs surgery, and have an excellent prognosis,” the authors wrote. “However, there is a subset of patients in which these therapies are unsuccessful and where cutaneous SCC appears to be far more aggressive, often resulting in metastasis and recurrence.”
Age was shown to be a significant factor in 53.3% of the studies, but the extent of its effect on prognosis was questionable.
Sentinel lymph node biopsy is commonly used to stage melanoma and has been used in oral SCC.
“A patient post biopsy with either two major criteria or one major and two minor criteria should be considered as a candidate for sentinel lymph node biopsy,” the authors wrote, adding that the findings were consistent with those for cutaneous SCC generally, not specified to the head and neck.
Limitations of the systematic review include potential selection bias as the majority of the studies were based in Australia and most studies were not specified to cutaneous SCC of the head and neck region.
“Given the low rate of metastasis from head and neck cutaneous SCC lesions, it can be challenging to identify the patients who are at high risk of having metastatic disease,” the authors wrote. “We believe this review could help identify patients that would require a closer follow-up and those that could possibly profit from a sentinel lymph node biopsy.”
No disclosures were disclosed for the authors.
However, no study has thoroughly evaluated the prognostic factors associated with metastasis until now.
In the Journal of Otolaryngology – Head & Neck Surgery, researchers wrote that immunocompromised individuals, such as solid organ transplant patients, make up 73.3% of all patients with cutaneous SCC who are at risk of metastasis and decreased overall survival.
Led by Alex M. Mlynarek, MD, a specialist in head and neck oncology and microvascular reconstruction at McGill University, Montreal, the finding is based on a systematic literature review of 40 studies involving 8,535 patients.
“The prognostic factors for head and neck cutaneous squamous cell carcinoma that were most consistently reported as significant in the literature are a state of immunosuppression, tumor depth, margins involved, number of lymph nodes affected by carcinoma, parotideal disease, and age,” Dr. Mlynarek and colleagues wrote.
Cutaneous SCC is the second most common nonmelanoma skin cancer with an increase of 263% between 2000 and 2010, shows research from the Mayo Clinic Rochester Epidemiology Project.
Patients in this study with tumors that are 6 mm or greater, or whose tumor invaded fat tissue, were found to have a poor prognosis followed by patients with perineural and lymphovascular invasion and in particular, patients with a poorer grade of cellular differentiation. The number of lymph nodes was significant at 70%, with more than two nodes involved linked to a worse the prognosis, followed by 66.7% for margins involved with carcinoma and 50% for tumor depth.
“The majority of patients with cutaneous SCC undergoes electrodesiccation and curettage, cryosurgery, or Mohs surgery, and have an excellent prognosis,” the authors wrote. “However, there is a subset of patients in which these therapies are unsuccessful and where cutaneous SCC appears to be far more aggressive, often resulting in metastasis and recurrence.”
Age was shown to be a significant factor in 53.3% of the studies, but the extent of its effect on prognosis was questionable.
Sentinel lymph node biopsy is commonly used to stage melanoma and has been used in oral SCC.
“A patient post biopsy with either two major criteria or one major and two minor criteria should be considered as a candidate for sentinel lymph node biopsy,” the authors wrote, adding that the findings were consistent with those for cutaneous SCC generally, not specified to the head and neck.
Limitations of the systematic review include potential selection bias as the majority of the studies were based in Australia and most studies were not specified to cutaneous SCC of the head and neck region.
“Given the low rate of metastasis from head and neck cutaneous SCC lesions, it can be challenging to identify the patients who are at high risk of having metastatic disease,” the authors wrote. “We believe this review could help identify patients that would require a closer follow-up and those that could possibly profit from a sentinel lymph node biopsy.”
No disclosures were disclosed for the authors.
FROM THE JOURNAL OF OTOLARYNGOLOGY – HEAD AND NECK SURGERY
Watchful waiting sometimes best for asymptomatic basal cell carcinoma
“Patient preferences, treatment goals, and the option for proceeding with a watchful waiting approach should be discussed as part of personalized shared decision-making,” wrote Marieke van Winden, MD, MSc, of Radboud University Medical Center in Nijmegen, the Netherlands, and colleagues. “In patients with a limited life expectancy and asymptomatic low-risk tumors, the time to benefit from treatment might exceed life expectancy, and watchful waiting should be discussed as a potentially appropriate approach.”
As little research has been undertaken on watchful waiting in patients with BCC, the expected tumor growth, progression and the chance of developing symptoms while taking this approach are poorly understood. Patients with limited life expectancy might not live long enough to develop BCC symptoms and may benefit more from watchful waiting than active treatment, authors of the study wrote.
This observational cohort study evaluated the reasons for watchful waiting, along with the natural course of 280 BCCs in 89 patients (53% men, median age 83 years) who chose this approach. Patients had one or more untreated BCCs for at least 3 months and the median follow-up was 9 months. The researchers also looked at the reasons for initiating later treatment.
Patient-related factors, including limited life expectancy, comorbidity prioritizations, and frailty, were the most important reasons to choose watchful waiting in 83% of patients, followed by tumor-related factors in 55% of patients. Of the tumors, 47% increased in size. The estimated tumor diameter increase in 1 year was 4.46 mm for infiltrative/micronodular BCCs and 1.06 mm for nodular, superficial, or clinical BCCs. Tumor growth was not associated with initial tumor size and location.
The most common reasons to initiate active treatment were tumor burden, resolved reasons for watchful waiting, and reevaluation of patient-related factors.
“All patients should be followed up regularly to determine whether a watchful waiting approach is still suited and if patients still prefer watchful waiting to reconsider the consequences of refraining from treatment,” the authors wrote.
In an accompanying editorial, Mackenzie R. Wehner, MD, MPhil, of the University of Texas MD Anderson Cancer Center in Houston, said that, while the observational and retrospective design was a limitation of the study, this allowed the authors to observe patients avoiding or delaying treatment for BCC in real clinical practice.
The study “shows that few patients developed new symptoms, and few patients who decided to treat after a delay had more invasive interventions than originally anticipated, an encouraging result as we continue to study the option and hone the details of active surveillance in BCC,” Dr. Wehner wrote. “It is important to note that the authors did not perform actual active surveillance. This study did not prospectively enroll patients and see them in follow-up at set times, nor did it have prespecified end points for recommending treatment.”
“Before evidence-based active surveillance in BCC can become a viable option, prospective studies of active surveillance, with specified follow-up times and clear outcome measures, are needed,” Dr. Wehner wrote.
Dr. van Winden did not report any conflicts of interest.
“Patient preferences, treatment goals, and the option for proceeding with a watchful waiting approach should be discussed as part of personalized shared decision-making,” wrote Marieke van Winden, MD, MSc, of Radboud University Medical Center in Nijmegen, the Netherlands, and colleagues. “In patients with a limited life expectancy and asymptomatic low-risk tumors, the time to benefit from treatment might exceed life expectancy, and watchful waiting should be discussed as a potentially appropriate approach.”
As little research has been undertaken on watchful waiting in patients with BCC, the expected tumor growth, progression and the chance of developing symptoms while taking this approach are poorly understood. Patients with limited life expectancy might not live long enough to develop BCC symptoms and may benefit more from watchful waiting than active treatment, authors of the study wrote.
This observational cohort study evaluated the reasons for watchful waiting, along with the natural course of 280 BCCs in 89 patients (53% men, median age 83 years) who chose this approach. Patients had one or more untreated BCCs for at least 3 months and the median follow-up was 9 months. The researchers also looked at the reasons for initiating later treatment.
Patient-related factors, including limited life expectancy, comorbidity prioritizations, and frailty, were the most important reasons to choose watchful waiting in 83% of patients, followed by tumor-related factors in 55% of patients. Of the tumors, 47% increased in size. The estimated tumor diameter increase in 1 year was 4.46 mm for infiltrative/micronodular BCCs and 1.06 mm for nodular, superficial, or clinical BCCs. Tumor growth was not associated with initial tumor size and location.
The most common reasons to initiate active treatment were tumor burden, resolved reasons for watchful waiting, and reevaluation of patient-related factors.
“All patients should be followed up regularly to determine whether a watchful waiting approach is still suited and if patients still prefer watchful waiting to reconsider the consequences of refraining from treatment,” the authors wrote.
In an accompanying editorial, Mackenzie R. Wehner, MD, MPhil, of the University of Texas MD Anderson Cancer Center in Houston, said that, while the observational and retrospective design was a limitation of the study, this allowed the authors to observe patients avoiding or delaying treatment for BCC in real clinical practice.
The study “shows that few patients developed new symptoms, and few patients who decided to treat after a delay had more invasive interventions than originally anticipated, an encouraging result as we continue to study the option and hone the details of active surveillance in BCC,” Dr. Wehner wrote. “It is important to note that the authors did not perform actual active surveillance. This study did not prospectively enroll patients and see them in follow-up at set times, nor did it have prespecified end points for recommending treatment.”
“Before evidence-based active surveillance in BCC can become a viable option, prospective studies of active surveillance, with specified follow-up times and clear outcome measures, are needed,” Dr. Wehner wrote.
Dr. van Winden did not report any conflicts of interest.
“Patient preferences, treatment goals, and the option for proceeding with a watchful waiting approach should be discussed as part of personalized shared decision-making,” wrote Marieke van Winden, MD, MSc, of Radboud University Medical Center in Nijmegen, the Netherlands, and colleagues. “In patients with a limited life expectancy and asymptomatic low-risk tumors, the time to benefit from treatment might exceed life expectancy, and watchful waiting should be discussed as a potentially appropriate approach.”
As little research has been undertaken on watchful waiting in patients with BCC, the expected tumor growth, progression and the chance of developing symptoms while taking this approach are poorly understood. Patients with limited life expectancy might not live long enough to develop BCC symptoms and may benefit more from watchful waiting than active treatment, authors of the study wrote.
This observational cohort study evaluated the reasons for watchful waiting, along with the natural course of 280 BCCs in 89 patients (53% men, median age 83 years) who chose this approach. Patients had one or more untreated BCCs for at least 3 months and the median follow-up was 9 months. The researchers also looked at the reasons for initiating later treatment.
Patient-related factors, including limited life expectancy, comorbidity prioritizations, and frailty, were the most important reasons to choose watchful waiting in 83% of patients, followed by tumor-related factors in 55% of patients. Of the tumors, 47% increased in size. The estimated tumor diameter increase in 1 year was 4.46 mm for infiltrative/micronodular BCCs and 1.06 mm for nodular, superficial, or clinical BCCs. Tumor growth was not associated with initial tumor size and location.
The most common reasons to initiate active treatment were tumor burden, resolved reasons for watchful waiting, and reevaluation of patient-related factors.
“All patients should be followed up regularly to determine whether a watchful waiting approach is still suited and if patients still prefer watchful waiting to reconsider the consequences of refraining from treatment,” the authors wrote.
In an accompanying editorial, Mackenzie R. Wehner, MD, MPhil, of the University of Texas MD Anderson Cancer Center in Houston, said that, while the observational and retrospective design was a limitation of the study, this allowed the authors to observe patients avoiding or delaying treatment for BCC in real clinical practice.
The study “shows that few patients developed new symptoms, and few patients who decided to treat after a delay had more invasive interventions than originally anticipated, an encouraging result as we continue to study the option and hone the details of active surveillance in BCC,” Dr. Wehner wrote. “It is important to note that the authors did not perform actual active surveillance. This study did not prospectively enroll patients and see them in follow-up at set times, nor did it have prespecified end points for recommending treatment.”
“Before evidence-based active surveillance in BCC can become a viable option, prospective studies of active surveillance, with specified follow-up times and clear outcome measures, are needed,” Dr. Wehner wrote.
Dr. van Winden did not report any conflicts of interest.
FROM JAMA DERMATOLOGY
PDT for actinic keratoses continues to be refined
.

“We have conventional PDT, daylight PDT; we can combine with a range of topicals, and we can combine a range of different physical treatment procedures in order to provide better and individualized treatment regimens for our patients,” Merete Haedersdal, MD, PhD, DMSc, professor of dermatology at the University of Copenhagen, said during a course on laser and aesthetic skin therapy.
In Europe, PDT consists of a three-step procedure: curettage of AKs, application of photosensitizer on the skin (typically methyl aminolevulinate, versus aminolevulinic acid, used more often in the United States), and illumination with red light (versus blue light, used more often in the United States), which causes a photochemical reaction.
“It’s a photochemical-reaction concept with which we can achieve up to 90% cure rates of AKs at 3 months,” Dr. Haedersdal said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine.
PDT is also used in Europe for select patients with Bowen’s disease (yielding a 90% cure rate at 3 months, 70% at 2 years); superficial basal cell carcinoma (yielding a 90% cure rate at 3 months, 75% at 5 years), and nodular BCC (yielding a 90% cure rate at 3 months, 75% at 5 years.
“With conventional PDT, whether it’s blue light, red light, MAL, or ALA, we have beautiful cosmesis, but we also have a challenge, which is pain,” she said. This is behind the motivation to look at other ways to provide PDT.
Daylight PDT, which was pioneered by Dr. Haedersdal’s mentor, Hans Christian Wulf, MD, DMSc, PharmD, professor of dermatology at the University of Copenhagen, provides 80%-90% clearance of thin AKs, lower clearance of thick AKs – and is a nearly pain-free procedure because of continuous photoactivation of protoporphyrin IX, with a Visual Analog Scale in the range of 1-3. “Globally, thousands of patients have been treated [with daylight PDT], which is backed up in the literature with more than 150 publications,” she said.
According to Dr. Haedersdal, MAL cream with daylight activation for treatment of AK was approved in Colombia and Mexico in 2013; in Australia, Brazil, and Costa Rica in 2014; and in Chile, Europe, and New Zealand in 2015. “I do hope that one day you will have daylight PDT approved in the United States,” she said.
The suggested protocol for daylight PDT starts by applying a sunscreen with an organic filter. After about 15 minutes, the lesion or lesions are prepared, and MAL is applied with no occlusion. Patients should start their exposure to daylight within 30 minutes of application, remaining outdoors for 2 hours of continuous exposure, either at a dedicated space located on the ground of the hospital or clinic or at their home. After 2 hours, patients wipe off the remaining cream and are advised to stay indoors for the rest of the day.
“Ideal candidates are those who have large skin areas that can be easily exposed to sunlight,” such as the scalp and lower legs, said Dr. Haedersdal, who is also a visiting scientist at the Wellman Center for Photomedicine, Boston. “If patients are treated in areas covered by clothing, it can be greasy and sticky with the cream. In these cases, you can cover the area with Tegaderm, which allows for 99% light transmission. Daylight can shine through and the Tegaderm can be removed after the procedure.”
On rainy days between April 1 and October 1 in Copenhagen, she said, daylight PDT is provided in a greenhouse in the hospital garden, with a heater and blankets for patients when the temperature falls below 10° C.
The amount of light required for a treatment effect is 5,000-10,000 lux, and the number of lux on a sunny day in Denmark is about 100,000, she said. “That means that all year round in countries south of latitude 45 degrees N, patients can be treated with daylight PDT.”
To intensify the treatment efficacy of conventional PDT and daylight PDT, especially in those with severely photodamaged skin, combining treatment with a physical pretreatment technique such as curettage, ablative fractional laser, microdermabrasion, microneedling, and nonablative fractional laser is another strategy. A small randomized controlled trial found that ablative fractional laser treatment extended notable relative effectiveness, compared with other physical enhancement techniques.
Dr. Haedersdal and colleagues published a study that compared pretreatment with ablative fractional laser and microdermabrasion pads before daylight PDT for AKs in field-cancerized skin. They found that with a single treatment, combination therapy with ablative fractional laser before daylight PDT led to significantly greater efficacious AK clearance and skin rejuvenation, compared with treatment with microdermabrasion.
“We don’t know why this is, but we believe it may be due to the fact that with the laser, we have a photothermal response, which in combination with the photochemical response from the photodynamic therapy induces a synergistic effect,” she said.
A range of topical treatments can also be given in combination with PDT. In a meta-analysis of 10 randomized controlled trials, German researchers evaluated the efficacy of PDT combined with imiquimod cream, 5-fluorouracil cream, tazarotene gel, and calcipotriol ointment. They concluded that the combination of PDT with another topical drug intervention improves AK clearance rates, compared with monotherapy.
More recently, the same authors summarized the current knowledge on the efficacy and safety of local combination therapies for the treatment of patients with AK in a review article, which Dr. Haedersdal said provides a nice overview of this topic.
Dr. Haedersdal disclosed that she has received equipment from Cherry Imaging, Cynosure-Hologic, MiraDry, and PerfAction Technologies. She has also received research grants from Leo Pharma, Lutronic, Mirai Medical, Novoxel, and Venus Concept.
.
“We have conventional PDT, daylight PDT; we can combine with a range of topicals, and we can combine a range of different physical treatment procedures in order to provide better and individualized treatment regimens for our patients,” Merete Haedersdal, MD, PhD, DMSc, professor of dermatology at the University of Copenhagen, said during a course on laser and aesthetic skin therapy.
In Europe, PDT consists of a three-step procedure: curettage of AKs, application of photosensitizer on the skin (typically methyl aminolevulinate, versus aminolevulinic acid, used more often in the United States), and illumination with red light (versus blue light, used more often in the United States), which causes a photochemical reaction.
“It’s a photochemical-reaction concept with which we can achieve up to 90% cure rates of AKs at 3 months,” Dr. Haedersdal said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine.
PDT is also used in Europe for select patients with Bowen’s disease (yielding a 90% cure rate at 3 months, 70% at 2 years); superficial basal cell carcinoma (yielding a 90% cure rate at 3 months, 75% at 5 years), and nodular BCC (yielding a 90% cure rate at 3 months, 75% at 5 years.
“With conventional PDT, whether it’s blue light, red light, MAL, or ALA, we have beautiful cosmesis, but we also have a challenge, which is pain,” she said. This is behind the motivation to look at other ways to provide PDT.
Daylight PDT, which was pioneered by Dr. Haedersdal’s mentor, Hans Christian Wulf, MD, DMSc, PharmD, professor of dermatology at the University of Copenhagen, provides 80%-90% clearance of thin AKs, lower clearance of thick AKs – and is a nearly pain-free procedure because of continuous photoactivation of protoporphyrin IX, with a Visual Analog Scale in the range of 1-3. “Globally, thousands of patients have been treated [with daylight PDT], which is backed up in the literature with more than 150 publications,” she said.
According to Dr. Haedersdal, MAL cream with daylight activation for treatment of AK was approved in Colombia and Mexico in 2013; in Australia, Brazil, and Costa Rica in 2014; and in Chile, Europe, and New Zealand in 2015. “I do hope that one day you will have daylight PDT approved in the United States,” she said.
The suggested protocol for daylight PDT starts by applying a sunscreen with an organic filter. After about 15 minutes, the lesion or lesions are prepared, and MAL is applied with no occlusion. Patients should start their exposure to daylight within 30 minutes of application, remaining outdoors for 2 hours of continuous exposure, either at a dedicated space located on the ground of the hospital or clinic or at their home. After 2 hours, patients wipe off the remaining cream and are advised to stay indoors for the rest of the day.
“Ideal candidates are those who have large skin areas that can be easily exposed to sunlight,” such as the scalp and lower legs, said Dr. Haedersdal, who is also a visiting scientist at the Wellman Center for Photomedicine, Boston. “If patients are treated in areas covered by clothing, it can be greasy and sticky with the cream. In these cases, you can cover the area with Tegaderm, which allows for 99% light transmission. Daylight can shine through and the Tegaderm can be removed after the procedure.”
On rainy days between April 1 and October 1 in Copenhagen, she said, daylight PDT is provided in a greenhouse in the hospital garden, with a heater and blankets for patients when the temperature falls below 10° C.
The amount of light required for a treatment effect is 5,000-10,000 lux, and the number of lux on a sunny day in Denmark is about 100,000, she said. “That means that all year round in countries south of latitude 45 degrees N, patients can be treated with daylight PDT.”
To intensify the treatment efficacy of conventional PDT and daylight PDT, especially in those with severely photodamaged skin, combining treatment with a physical pretreatment technique such as curettage, ablative fractional laser, microdermabrasion, microneedling, and nonablative fractional laser is another strategy. A small randomized controlled trial found that ablative fractional laser treatment extended notable relative effectiveness, compared with other physical enhancement techniques.
Dr. Haedersdal and colleagues published a study that compared pretreatment with ablative fractional laser and microdermabrasion pads before daylight PDT for AKs in field-cancerized skin. They found that with a single treatment, combination therapy with ablative fractional laser before daylight PDT led to significantly greater efficacious AK clearance and skin rejuvenation, compared with treatment with microdermabrasion.
“We don’t know why this is, but we believe it may be due to the fact that with the laser, we have a photothermal response, which in combination with the photochemical response from the photodynamic therapy induces a synergistic effect,” she said.
A range of topical treatments can also be given in combination with PDT. In a meta-analysis of 10 randomized controlled trials, German researchers evaluated the efficacy of PDT combined with imiquimod cream, 5-fluorouracil cream, tazarotene gel, and calcipotriol ointment. They concluded that the combination of PDT with another topical drug intervention improves AK clearance rates, compared with monotherapy.
More recently, the same authors summarized the current knowledge on the efficacy and safety of local combination therapies for the treatment of patients with AK in a review article, which Dr. Haedersdal said provides a nice overview of this topic.
Dr. Haedersdal disclosed that she has received equipment from Cherry Imaging, Cynosure-Hologic, MiraDry, and PerfAction Technologies. She has also received research grants from Leo Pharma, Lutronic, Mirai Medical, Novoxel, and Venus Concept.
.
“We have conventional PDT, daylight PDT; we can combine with a range of topicals, and we can combine a range of different physical treatment procedures in order to provide better and individualized treatment regimens for our patients,” Merete Haedersdal, MD, PhD, DMSc, professor of dermatology at the University of Copenhagen, said during a course on laser and aesthetic skin therapy.
In Europe, PDT consists of a three-step procedure: curettage of AKs, application of photosensitizer on the skin (typically methyl aminolevulinate, versus aminolevulinic acid, used more often in the United States), and illumination with red light (versus blue light, used more often in the United States), which causes a photochemical reaction.
“It’s a photochemical-reaction concept with which we can achieve up to 90% cure rates of AKs at 3 months,” Dr. Haedersdal said during the meeting, which was sponsored by Harvard Medical School, Massachusetts General Hospital, and the Wellman Center for Photomedicine.
PDT is also used in Europe for select patients with Bowen’s disease (yielding a 90% cure rate at 3 months, 70% at 2 years); superficial basal cell carcinoma (yielding a 90% cure rate at 3 months, 75% at 5 years), and nodular BCC (yielding a 90% cure rate at 3 months, 75% at 5 years.
“With conventional PDT, whether it’s blue light, red light, MAL, or ALA, we have beautiful cosmesis, but we also have a challenge, which is pain,” she said. This is behind the motivation to look at other ways to provide PDT.
Daylight PDT, which was pioneered by Dr. Haedersdal’s mentor, Hans Christian Wulf, MD, DMSc, PharmD, professor of dermatology at the University of Copenhagen, provides 80%-90% clearance of thin AKs, lower clearance of thick AKs – and is a nearly pain-free procedure because of continuous photoactivation of protoporphyrin IX, with a Visual Analog Scale in the range of 1-3. “Globally, thousands of patients have been treated [with daylight PDT], which is backed up in the literature with more than 150 publications,” she said.
According to Dr. Haedersdal, MAL cream with daylight activation for treatment of AK was approved in Colombia and Mexico in 2013; in Australia, Brazil, and Costa Rica in 2014; and in Chile, Europe, and New Zealand in 2015. “I do hope that one day you will have daylight PDT approved in the United States,” she said.
The suggested protocol for daylight PDT starts by applying a sunscreen with an organic filter. After about 15 minutes, the lesion or lesions are prepared, and MAL is applied with no occlusion. Patients should start their exposure to daylight within 30 minutes of application, remaining outdoors for 2 hours of continuous exposure, either at a dedicated space located on the ground of the hospital or clinic or at their home. After 2 hours, patients wipe off the remaining cream and are advised to stay indoors for the rest of the day.
“Ideal candidates are those who have large skin areas that can be easily exposed to sunlight,” such as the scalp and lower legs, said Dr. Haedersdal, who is also a visiting scientist at the Wellman Center for Photomedicine, Boston. “If patients are treated in areas covered by clothing, it can be greasy and sticky with the cream. In these cases, you can cover the area with Tegaderm, which allows for 99% light transmission. Daylight can shine through and the Tegaderm can be removed after the procedure.”
On rainy days between April 1 and October 1 in Copenhagen, she said, daylight PDT is provided in a greenhouse in the hospital garden, with a heater and blankets for patients when the temperature falls below 10° C.
The amount of light required for a treatment effect is 5,000-10,000 lux, and the number of lux on a sunny day in Denmark is about 100,000, she said. “That means that all year round in countries south of latitude 45 degrees N, patients can be treated with daylight PDT.”
To intensify the treatment efficacy of conventional PDT and daylight PDT, especially in those with severely photodamaged skin, combining treatment with a physical pretreatment technique such as curettage, ablative fractional laser, microdermabrasion, microneedling, and nonablative fractional laser is another strategy. A small randomized controlled trial found that ablative fractional laser treatment extended notable relative effectiveness, compared with other physical enhancement techniques.
Dr. Haedersdal and colleagues published a study that compared pretreatment with ablative fractional laser and microdermabrasion pads before daylight PDT for AKs in field-cancerized skin. They found that with a single treatment, combination therapy with ablative fractional laser before daylight PDT led to significantly greater efficacious AK clearance and skin rejuvenation, compared with treatment with microdermabrasion.
“We don’t know why this is, but we believe it may be due to the fact that with the laser, we have a photothermal response, which in combination with the photochemical response from the photodynamic therapy induces a synergistic effect,” she said.
A range of topical treatments can also be given in combination with PDT. In a meta-analysis of 10 randomized controlled trials, German researchers evaluated the efficacy of PDT combined with imiquimod cream, 5-fluorouracil cream, tazarotene gel, and calcipotriol ointment. They concluded that the combination of PDT with another topical drug intervention improves AK clearance rates, compared with monotherapy.
More recently, the same authors summarized the current knowledge on the efficacy and safety of local combination therapies for the treatment of patients with AK in a review article, which Dr. Haedersdal said provides a nice overview of this topic.
Dr. Haedersdal disclosed that she has received equipment from Cherry Imaging, Cynosure-Hologic, MiraDry, and PerfAction Technologies. She has also received research grants from Leo Pharma, Lutronic, Mirai Medical, Novoxel, and Venus Concept.
FROM A LASER & AESTHETIC SKIN THERAPY COURSE