User login
For MD-IQ use only
Can immune checkpoint inhibitors treat PML?
investigators reported in the New England Journal of Medicine.
Three research teams described 10 cases in which patients with PML received pembrolizumab or nivolumab.
In one study, researchers administered pembrolizumab to eight adults with PML. Five patients had clinical improvement or stabilization, whereas 3 patients did not. Among the patients with clinical improvement, treatment led to reduced JC viral load in cerebrospinal fluid (CSF) and increased CD4+ and CD8+ anti–JC virus activity in vitro. Among patients without clinical improvement, treatment did not meaningfully change viral load or antiviral cellular immune response.
In a separate letter, researchers in Germany described an additional patient with PML who had clinical stabilization and no disease progression on MRI after treatment with pembrolizumab.
In another letter, researchers in France described a patient with PML whose condition improved after treatment with nivolumab.
“Do pembrolizumab and nivolumab fit the bill for treatment of PML? The current reports are encouraging but suggest that the presence of JC virus–specific T cells in the blood is a prerequisite for their use,” said Igor J. Koralnik, MD, of the department of neurological sciences at Rush University Medical Center in Chicago, in an accompanying editorial. “A controlled trial may be needed to determine whether immune checkpoint inhibitors are indeed able to keep JC virus in check in patients with PML.”
Reinvigorating T cells
Both monoclonal antibodies target programmed cell death protein 1 (PD-1), which inhibits T-cell proliferation and cytokine production when it binds its associated ligand, Dr. Koralnik said. Pembrolizumab and nivolumab block this inhibition and have been used to spur T-cell activity against tumors in patients with cancer.
PML, an often fatal brain infection caused by the JC virus in patients with immunosuppression, has no specific treatment. Management hinges on “recovery of the immune system, either by treating the underlying cause of immunosuppression or by discontinuing the use of immunosuppressive medications,” said Dr. Koralnik.
Pembrolizumab
Prior studies have found that PD-1 expression is elevated on T lymphocytes of patients with PML. To determine whether PD-1 blockade with pembrolizumab reinvigorates anti–JC virus immune activity in patients with PML, Irene Cortese, MD, of the National Institutes of Health’s Neuroimmunology Clinic and her research colleagues administered pembrolizumab at a dose of 2 mg/kg of body weight every 4-6 weeks to eight adults with PML. The patients received 1-3 doses, and each patient had a different underlying condition.
In all patients, treatment induced down-regulation of PD-1 expression on lymphocytes in CSF and peripheral blood, and five of the eight patients had clinical stabilization or improvement. Of the other three patients who did not improve, one had stabilized prior to treatment and remained stable. The other two patients died from PML.
Additional reports
Separately, Sebastian Rauer, MD, of Albert Ludwigs University in Freiburg, Germany, and his colleagues reported that a patient with PML whose symptoms culminated in mutism in February 2018 began speaking again after receiving five infusions of pembrolizumab over 10 weeks. “In addition, the size and number of lesions on MRI decreased, and JCV was no longer detectable in CSF,” Dr. Rauer and his colleagues wrote. “The patient has remained stable as of the end of March 2019, with persistent but abating psychomotor slowing, aphasia, and disorientation.”
Finally, Ondine Walter, of Toulouse (France) University Hospital and colleagues described the case of a 60-year-old woman with PML who received nivolumab on a compassionate-use basis. Two weeks after treatment, JC viral load in CSF and blood had decreased. “Starting 8 weeks after the initiation of nivolumab therapy, the patient’s neurologic symptoms and signs stabilized, and subsequently she showed improved alertness, and the ptosis and hemiplegia abated.”
Reason for caution
Prior studies, however, give reasons for caution when considering the potential use of immune checkpoint inhibitors to treat PML, Dr. Koralnik noted. In one case, a patient developed an inflammatory form of PML known as immune reconstitution inflammatory syndrome after receiving nivolumab (J Neurovirol. 2019 March 12. doi: 10.1007/s13365-019-00738-x). In addition, researchers have reported a case of PML that occurred after 1 year of nivolumab treatment, and four cases of PML related to nivolumab have been reported in pharmacovigilance databases (Emerg Infect Dis. 2018;24:1594-6). The cost and safety profiles of the medications also may be considerations, Dr. Koralnik said.
The study by Dr. Cortese and colleagues was funded by the National Institutes of Health, and the authors had no relevant disclosures. Some of the research letter authors disclosed grants and personal fees from pharmaceutical companies.
SOURCES: Cortese I et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMoa1815039; Rauer S et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMc1817193; Walter O et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMc1816198; Koralnik IJ. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMe1904140.
investigators reported in the New England Journal of Medicine.
Three research teams described 10 cases in which patients with PML received pembrolizumab or nivolumab.
In one study, researchers administered pembrolizumab to eight adults with PML. Five patients had clinical improvement or stabilization, whereas 3 patients did not. Among the patients with clinical improvement, treatment led to reduced JC viral load in cerebrospinal fluid (CSF) and increased CD4+ and CD8+ anti–JC virus activity in vitro. Among patients without clinical improvement, treatment did not meaningfully change viral load or antiviral cellular immune response.
In a separate letter, researchers in Germany described an additional patient with PML who had clinical stabilization and no disease progression on MRI after treatment with pembrolizumab.
In another letter, researchers in France described a patient with PML whose condition improved after treatment with nivolumab.
“Do pembrolizumab and nivolumab fit the bill for treatment of PML? The current reports are encouraging but suggest that the presence of JC virus–specific T cells in the blood is a prerequisite for their use,” said Igor J. Koralnik, MD, of the department of neurological sciences at Rush University Medical Center in Chicago, in an accompanying editorial. “A controlled trial may be needed to determine whether immune checkpoint inhibitors are indeed able to keep JC virus in check in patients with PML.”
Reinvigorating T cells
Both monoclonal antibodies target programmed cell death protein 1 (PD-1), which inhibits T-cell proliferation and cytokine production when it binds its associated ligand, Dr. Koralnik said. Pembrolizumab and nivolumab block this inhibition and have been used to spur T-cell activity against tumors in patients with cancer.
PML, an often fatal brain infection caused by the JC virus in patients with immunosuppression, has no specific treatment. Management hinges on “recovery of the immune system, either by treating the underlying cause of immunosuppression or by discontinuing the use of immunosuppressive medications,” said Dr. Koralnik.
Pembrolizumab
Prior studies have found that PD-1 expression is elevated on T lymphocytes of patients with PML. To determine whether PD-1 blockade with pembrolizumab reinvigorates anti–JC virus immune activity in patients with PML, Irene Cortese, MD, of the National Institutes of Health’s Neuroimmunology Clinic and her research colleagues administered pembrolizumab at a dose of 2 mg/kg of body weight every 4-6 weeks to eight adults with PML. The patients received 1-3 doses, and each patient had a different underlying condition.
In all patients, treatment induced down-regulation of PD-1 expression on lymphocytes in CSF and peripheral blood, and five of the eight patients had clinical stabilization or improvement. Of the other three patients who did not improve, one had stabilized prior to treatment and remained stable. The other two patients died from PML.
Additional reports
Separately, Sebastian Rauer, MD, of Albert Ludwigs University in Freiburg, Germany, and his colleagues reported that a patient with PML whose symptoms culminated in mutism in February 2018 began speaking again after receiving five infusions of pembrolizumab over 10 weeks. “In addition, the size and number of lesions on MRI decreased, and JCV was no longer detectable in CSF,” Dr. Rauer and his colleagues wrote. “The patient has remained stable as of the end of March 2019, with persistent but abating psychomotor slowing, aphasia, and disorientation.”
Finally, Ondine Walter, of Toulouse (France) University Hospital and colleagues described the case of a 60-year-old woman with PML who received nivolumab on a compassionate-use basis. Two weeks after treatment, JC viral load in CSF and blood had decreased. “Starting 8 weeks after the initiation of nivolumab therapy, the patient’s neurologic symptoms and signs stabilized, and subsequently she showed improved alertness, and the ptosis and hemiplegia abated.”
Reason for caution
Prior studies, however, give reasons for caution when considering the potential use of immune checkpoint inhibitors to treat PML, Dr. Koralnik noted. In one case, a patient developed an inflammatory form of PML known as immune reconstitution inflammatory syndrome after receiving nivolumab (J Neurovirol. 2019 March 12. doi: 10.1007/s13365-019-00738-x). In addition, researchers have reported a case of PML that occurred after 1 year of nivolumab treatment, and four cases of PML related to nivolumab have been reported in pharmacovigilance databases (Emerg Infect Dis. 2018;24:1594-6). The cost and safety profiles of the medications also may be considerations, Dr. Koralnik said.
The study by Dr. Cortese and colleagues was funded by the National Institutes of Health, and the authors had no relevant disclosures. Some of the research letter authors disclosed grants and personal fees from pharmaceutical companies.
SOURCES: Cortese I et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMoa1815039; Rauer S et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMc1817193; Walter O et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMc1816198; Koralnik IJ. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMe1904140.
investigators reported in the New England Journal of Medicine.
Three research teams described 10 cases in which patients with PML received pembrolizumab or nivolumab.
In one study, researchers administered pembrolizumab to eight adults with PML. Five patients had clinical improvement or stabilization, whereas 3 patients did not. Among the patients with clinical improvement, treatment led to reduced JC viral load in cerebrospinal fluid (CSF) and increased CD4+ and CD8+ anti–JC virus activity in vitro. Among patients without clinical improvement, treatment did not meaningfully change viral load or antiviral cellular immune response.
In a separate letter, researchers in Germany described an additional patient with PML who had clinical stabilization and no disease progression on MRI after treatment with pembrolizumab.
In another letter, researchers in France described a patient with PML whose condition improved after treatment with nivolumab.
“Do pembrolizumab and nivolumab fit the bill for treatment of PML? The current reports are encouraging but suggest that the presence of JC virus–specific T cells in the blood is a prerequisite for their use,” said Igor J. Koralnik, MD, of the department of neurological sciences at Rush University Medical Center in Chicago, in an accompanying editorial. “A controlled trial may be needed to determine whether immune checkpoint inhibitors are indeed able to keep JC virus in check in patients with PML.”
Reinvigorating T cells
Both monoclonal antibodies target programmed cell death protein 1 (PD-1), which inhibits T-cell proliferation and cytokine production when it binds its associated ligand, Dr. Koralnik said. Pembrolizumab and nivolumab block this inhibition and have been used to spur T-cell activity against tumors in patients with cancer.
PML, an often fatal brain infection caused by the JC virus in patients with immunosuppression, has no specific treatment. Management hinges on “recovery of the immune system, either by treating the underlying cause of immunosuppression or by discontinuing the use of immunosuppressive medications,” said Dr. Koralnik.
Pembrolizumab
Prior studies have found that PD-1 expression is elevated on T lymphocytes of patients with PML. To determine whether PD-1 blockade with pembrolizumab reinvigorates anti–JC virus immune activity in patients with PML, Irene Cortese, MD, of the National Institutes of Health’s Neuroimmunology Clinic and her research colleagues administered pembrolizumab at a dose of 2 mg/kg of body weight every 4-6 weeks to eight adults with PML. The patients received 1-3 doses, and each patient had a different underlying condition.
In all patients, treatment induced down-regulation of PD-1 expression on lymphocytes in CSF and peripheral blood, and five of the eight patients had clinical stabilization or improvement. Of the other three patients who did not improve, one had stabilized prior to treatment and remained stable. The other two patients died from PML.
Additional reports
Separately, Sebastian Rauer, MD, of Albert Ludwigs University in Freiburg, Germany, and his colleagues reported that a patient with PML whose symptoms culminated in mutism in February 2018 began speaking again after receiving five infusions of pembrolizumab over 10 weeks. “In addition, the size and number of lesions on MRI decreased, and JCV was no longer detectable in CSF,” Dr. Rauer and his colleagues wrote. “The patient has remained stable as of the end of March 2019, with persistent but abating psychomotor slowing, aphasia, and disorientation.”
Finally, Ondine Walter, of Toulouse (France) University Hospital and colleagues described the case of a 60-year-old woman with PML who received nivolumab on a compassionate-use basis. Two weeks after treatment, JC viral load in CSF and blood had decreased. “Starting 8 weeks after the initiation of nivolumab therapy, the patient’s neurologic symptoms and signs stabilized, and subsequently she showed improved alertness, and the ptosis and hemiplegia abated.”
Reason for caution
Prior studies, however, give reasons for caution when considering the potential use of immune checkpoint inhibitors to treat PML, Dr. Koralnik noted. In one case, a patient developed an inflammatory form of PML known as immune reconstitution inflammatory syndrome after receiving nivolumab (J Neurovirol. 2019 March 12. doi: 10.1007/s13365-019-00738-x). In addition, researchers have reported a case of PML that occurred after 1 year of nivolumab treatment, and four cases of PML related to nivolumab have been reported in pharmacovigilance databases (Emerg Infect Dis. 2018;24:1594-6). The cost and safety profiles of the medications also may be considerations, Dr. Koralnik said.
The study by Dr. Cortese and colleagues was funded by the National Institutes of Health, and the authors had no relevant disclosures. Some of the research letter authors disclosed grants and personal fees from pharmaceutical companies.
SOURCES: Cortese I et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMoa1815039; Rauer S et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMc1817193; Walter O et al. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMc1816198; Koralnik IJ. N Engl J Med. 2019 Apr 10. doi: 10.1056/NEJMe1904140.
FROM THE NEW ENGLAND JOURNAL OF MEDICINE
Volunteerism: How and why to do it, according to Dr. Eileen Barrett
PHILADELPHIA –
“I think what we get out of it is the feeling of our commitment to our sense of purpose and mission, and you just feel great when you’re giving, and then you meet these really remarkable people who do really, really remarkable things. ... It’s tremendously inspiring,” Dr. Barrett said in a video interview at the annual meeting of the American College of Physicians. She is a hospitalist at the University of New Mexico, Albuquerque, and serves on the ACP Board of Regents.
In addition, Dr. Barrett has done disaster relief work in West Africa, provided patient care to refugees in a hospital on the Thailand side of the Thailand-Myanmar border, and even helped bring organization to a public radio station in rural New Mexico.
She also described some opportunities available to internists who are trying to get their feet wet in volunteering that are available through the organizations, Health Volunteers Overseas and the Maven Project.
PHILADELPHIA –
“I think what we get out of it is the feeling of our commitment to our sense of purpose and mission, and you just feel great when you’re giving, and then you meet these really remarkable people who do really, really remarkable things. ... It’s tremendously inspiring,” Dr. Barrett said in a video interview at the annual meeting of the American College of Physicians. She is a hospitalist at the University of New Mexico, Albuquerque, and serves on the ACP Board of Regents.
In addition, Dr. Barrett has done disaster relief work in West Africa, provided patient care to refugees in a hospital on the Thailand side of the Thailand-Myanmar border, and even helped bring organization to a public radio station in rural New Mexico.
She also described some opportunities available to internists who are trying to get their feet wet in volunteering that are available through the organizations, Health Volunteers Overseas and the Maven Project.
PHILADELPHIA –
“I think what we get out of it is the feeling of our commitment to our sense of purpose and mission, and you just feel great when you’re giving, and then you meet these really remarkable people who do really, really remarkable things. ... It’s tremendously inspiring,” Dr. Barrett said in a video interview at the annual meeting of the American College of Physicians. She is a hospitalist at the University of New Mexico, Albuquerque, and serves on the ACP Board of Regents.
In addition, Dr. Barrett has done disaster relief work in West Africa, provided patient care to refugees in a hospital on the Thailand side of the Thailand-Myanmar border, and even helped bring organization to a public radio station in rural New Mexico.
She also described some opportunities available to internists who are trying to get their feet wet in volunteering that are available through the organizations, Health Volunteers Overseas and the Maven Project.
REPORTING FROM INTERNAL MEDICINE 2019

2018 at a glance: Recently approved therapies in oncology
Advances in genomics and technology perpetually change and improve therapies in oncology. Enhanced comprehension of cellular signaling, division, and replication has created a platform to selectively restrict neoplastic growth while preserving the integrity of benign cells.
This article reviews therapies that were newly approved in 2018, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
Click on the PDF above to download the full article and charts in an easy-to-print format.
Apalutamide (Erleada)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 240 mg orally, once daily.
Adverse Events (AEs): Hyperkalemia and increased risks of seizures, falls, and fractures.
Phase 3 SPARTAN trial (NCT01946204): 40.5-month metastasis-free survival rate, compared with 16.2 months in the placebo group.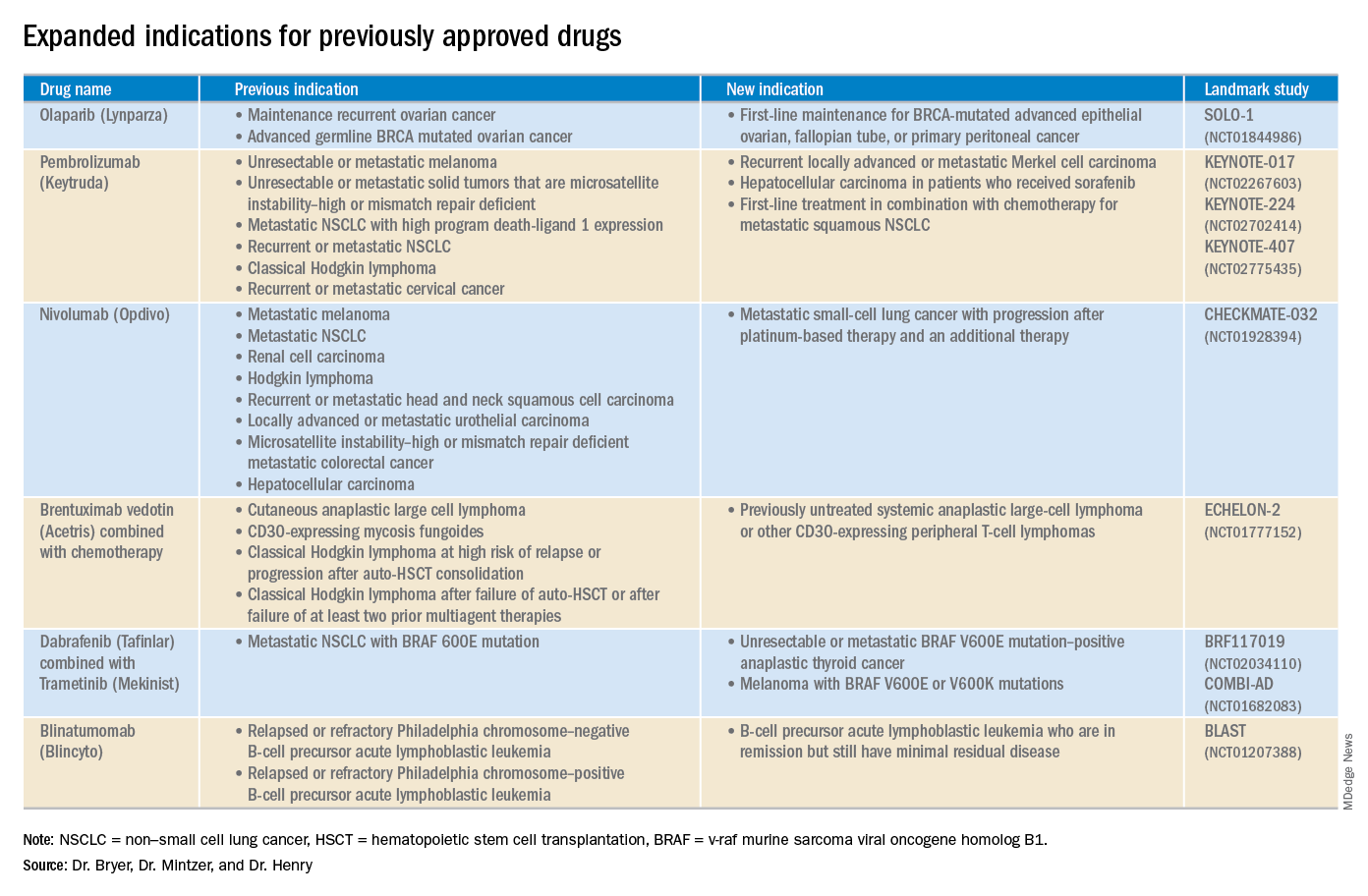
Cemiplimab (Libtayo)
Class: Antibody against programmed cell death protein-1 (PD-1).
Disease: Metastatic cutaneous squamous cell carcinoma (CSCC) or locally advanced CSCC that is ineligible for curative surgery/radiation.
Dose: 350 mg intravenous infusion every 3 weeks.
AEs: Pneumonitis, autoimmune myocarditis, hepatitis, and aseptic meningitis.
1423 and 1540 trials (NCT02383212 and NCT02760498): 47.2% of patients who received cemiplimab had complete disappearance of the tumor or a decrease in tumor size.
Dacomitinib (Vizimpro)
Class: Second-generation tyrosine kinase inhibitor.
Disease: Metastatic non–small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletion or exon 21 L858R substitution mutation.
Dose: 45 mg orally once daily.
AEs: Dermatotoxicity and diarrhea.
ARCHER1050 trial (NCT01774721): Patients who received dacomitinib demonstrated an improved overall survival, with a median of 34.1 months, compared with 26.8 months with gefitinib.
Duvelisib (Copiktra)
Class: Dual inhibitor of phosphatidylinositol 3-kinase delta and gamma.
Disease: Relapsed or refractory chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma, or relapsed or refractory follicular lymphoma after at least two prior systemic therapies.
Dose: 25 mg orally twice daily.
AEs: Infection, diarrhea or colitis, and pneumonia.
Phase 3 DUO trial (NCT02004522): Progression-free survival in the duvelisib arm was 7.3 months longer than that in the ofatumumab arm. The overall response rate for patients receiving duvelisib was 78%, compared with 39% for those receiving ofatumumab.
Gilteritinib (Xospata)
Class: Inhibits the FLT3 internal tandem duplication (ITD) and FLT3 tyrosine kinase domain (TKD).
Disease: Relapsed or refractory acute myeloid leukemia (AML) with an FLT3 mutation.
Dose: 120 mg orally daily.
ADMIRAL trial (NCT02421939): 21% of the patients who received gilteritinib exhibited complete remission or complete remission with partial hematologic recovery.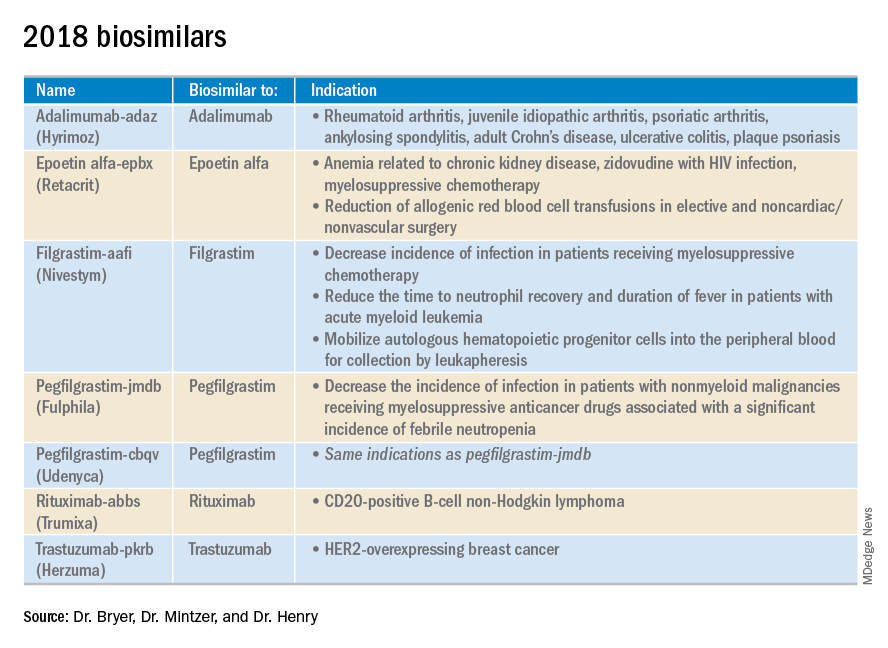
Glasdegib (Daurismo)
Class: Hedgehog pathway inhibitor.
Disease: Adults over age 75 years with newly diagnosed AML and other medical comorbidities that preclude them from intensive chemotherapy.
Dose: The recommended dose is 100 mg orally continuously in 28-day cycles.
AE: QT prolongation and embryo-fetal toxicity
Phase 2 BRIGHT 1003 trial (NCT01546038): 3.9-month overall survival advantage for glasdegib plus cytarabine, compared with cytarabine alone. Overall, 15% of the glasdegib plus low dose cytarabine arm achieved complete remission, compared with the 1% complete remission rate in patients who received cytarabine alone.
Iobenguane I 131 (Azedra)
Class: Radiopharmaceutical agent; induces cell death within the noradrenaline transporter.
Disease: Iobenguane scan–positive, unresectable, locally advanced or metastatic pheochromocytoma or paraganglioma
Dose: Initial intravenous dosimetric dose, followed by two therapeutic doses.
AE: Pancytopenia and elevated international normalized ratio (INR).
IB12B trial (NCT00874614): One-quarter of patients receiving this therapy had at least a 50% reduction in the dose and number of antihypertensives for at least 6 months; almost all patients had a tumor response.
Ivosidenib (Tibsovo)
Class: Small-molecule inhibitor of mutant isocitrate dehydrogenase (IDH1).
Disease: Refractory AML and an IDH1 mutation
Dose: 500 mg orally daily.
AG120-C-001 trial (NCT02074839): Overall response rate of 41.6% in patients who received ivosidenib, with a 30.4% rate of complete remission or complete remission with partial hematologic recovery.
Larotrectinib (Vitrakvi)
Class: Oral tyrosine kinase inhibitor.
Disease: Advanced solid tumors harboring a neurotrophic tyrosine receptor kinase (NTRK) gene fusion.
Dose: 100 mg orally twice daily.
LOXO-TRK-14001, SCOUT, and NAVIGATE trials (NCT02122913, NCT02637687, and NCT02576431): Patients who received larotrectinib had durable responses regardless of patient age, tumor type, and fusion status.
Lutetium Lu 177 dotatate (Lutathera)
Class: Radiolabeled somatostatin analogue.
Disease: Somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs).
Dose: Intravenous infusion 7.4 GBq (200 mCi) every 8 weeks for a total of four doses.
NETTER-1 trial (NCT01578239): 65% of adults who received lutetium Lu 177 showed improved progression-free survival at 20 months, compared with just 10.8% in the control group.
Mogamulizumab (Poteligeo)
Class: Monoclonal antibody that binds to a protein (CC chemokine receptor type 4).
Disease: Relapsed or refractory mycosis fungoides or Sézary syndrome.
Dose: Intravenous infusion 1 mg/kg.
AE: Dermatologic toxicity.
MAVORIC trial (NCT01728805): Patients who received mogamulizumab had improved progression-free survival (median 7.7 months), compared with those taking vorinostat (median 3.1 months).
Moxetumomab pasudotox-tdfk (Lumoxiti)
Class: CD22-directed cytotoxin fused with a fragment of Pseudomonas exotoxin A.
Disease: Relapsed or refractory hairy cell leukemia previously treated with at least two prior systemic therapies, including a purine nucleoside analogue.
Dose: Intravenously as 0.04 mg/kg.
AE: Hemolytic uremic syndrome.
1053 trial (NCT01829711): 30% of the patients who received moxetumomab pasudotox-tdfk had a durable complete response confirmed by maintenance hematologic remission.
Talazoparib (Talzenna)
Class: Poly (ADP-ribose) polymerase (PARP) inhibitor.
Disease: gBRCAm HER2-negative locally advanced or metastatic breast cancer.
Dose: 1 mg orally per day.
EMBRACA trial (NCT01945775): Patients who received talazoparib demonstrated significantly longer progression-free survival, with a median of 8.6 months versis 5.6 months in the control arm.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mentzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and a professor of medicine at the University of Pennsylvania.
Advances in genomics and technology perpetually change and improve therapies in oncology. Enhanced comprehension of cellular signaling, division, and replication has created a platform to selectively restrict neoplastic growth while preserving the integrity of benign cells.
This article reviews therapies that were newly approved in 2018, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
Click on the PDF above to download the full article and charts in an easy-to-print format.
Apalutamide (Erleada)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 240 mg orally, once daily.
Adverse Events (AEs): Hyperkalemia and increased risks of seizures, falls, and fractures.
Phase 3 SPARTAN trial (NCT01946204): 40.5-month metastasis-free survival rate, compared with 16.2 months in the placebo group.
Cemiplimab (Libtayo)
Class: Antibody against programmed cell death protein-1 (PD-1).
Disease: Metastatic cutaneous squamous cell carcinoma (CSCC) or locally advanced CSCC that is ineligible for curative surgery/radiation.
Dose: 350 mg intravenous infusion every 3 weeks.
AEs: Pneumonitis, autoimmune myocarditis, hepatitis, and aseptic meningitis.
1423 and 1540 trials (NCT02383212 and NCT02760498): 47.2% of patients who received cemiplimab had complete disappearance of the tumor or a decrease in tumor size.
Dacomitinib (Vizimpro)
Class: Second-generation tyrosine kinase inhibitor.
Disease: Metastatic non–small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletion or exon 21 L858R substitution mutation.
Dose: 45 mg orally once daily.
AEs: Dermatotoxicity and diarrhea.
ARCHER1050 trial (NCT01774721): Patients who received dacomitinib demonstrated an improved overall survival, with a median of 34.1 months, compared with 26.8 months with gefitinib.
Duvelisib (Copiktra)
Class: Dual inhibitor of phosphatidylinositol 3-kinase delta and gamma.
Disease: Relapsed or refractory chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma, or relapsed or refractory follicular lymphoma after at least two prior systemic therapies.
Dose: 25 mg orally twice daily.
AEs: Infection, diarrhea or colitis, and pneumonia.
Phase 3 DUO trial (NCT02004522): Progression-free survival in the duvelisib arm was 7.3 months longer than that in the ofatumumab arm. The overall response rate for patients receiving duvelisib was 78%, compared with 39% for those receiving ofatumumab.
Gilteritinib (Xospata)
Class: Inhibits the FLT3 internal tandem duplication (ITD) and FLT3 tyrosine kinase domain (TKD).
Disease: Relapsed or refractory acute myeloid leukemia (AML) with an FLT3 mutation.
Dose: 120 mg orally daily.
ADMIRAL trial (NCT02421939): 21% of the patients who received gilteritinib exhibited complete remission or complete remission with partial hematologic recovery.
Glasdegib (Daurismo)
Class: Hedgehog pathway inhibitor.
Disease: Adults over age 75 years with newly diagnosed AML and other medical comorbidities that preclude them from intensive chemotherapy.
Dose: The recommended dose is 100 mg orally continuously in 28-day cycles.
AE: QT prolongation and embryo-fetal toxicity
Phase 2 BRIGHT 1003 trial (NCT01546038): 3.9-month overall survival advantage for glasdegib plus cytarabine, compared with cytarabine alone. Overall, 15% of the glasdegib plus low dose cytarabine arm achieved complete remission, compared with the 1% complete remission rate in patients who received cytarabine alone.
Iobenguane I 131 (Azedra)
Class: Radiopharmaceutical agent; induces cell death within the noradrenaline transporter.
Disease: Iobenguane scan–positive, unresectable, locally advanced or metastatic pheochromocytoma or paraganglioma
Dose: Initial intravenous dosimetric dose, followed by two therapeutic doses.
AE: Pancytopenia and elevated international normalized ratio (INR).
IB12B trial (NCT00874614): One-quarter of patients receiving this therapy had at least a 50% reduction in the dose and number of antihypertensives for at least 6 months; almost all patients had a tumor response.
Ivosidenib (Tibsovo)
Class: Small-molecule inhibitor of mutant isocitrate dehydrogenase (IDH1).
Disease: Refractory AML and an IDH1 mutation
Dose: 500 mg orally daily.
AG120-C-001 trial (NCT02074839): Overall response rate of 41.6% in patients who received ivosidenib, with a 30.4% rate of complete remission or complete remission with partial hematologic recovery.
Larotrectinib (Vitrakvi)
Class: Oral tyrosine kinase inhibitor.
Disease: Advanced solid tumors harboring a neurotrophic tyrosine receptor kinase (NTRK) gene fusion.
Dose: 100 mg orally twice daily.
LOXO-TRK-14001, SCOUT, and NAVIGATE trials (NCT02122913, NCT02637687, and NCT02576431): Patients who received larotrectinib had durable responses regardless of patient age, tumor type, and fusion status.
Lutetium Lu 177 dotatate (Lutathera)
Class: Radiolabeled somatostatin analogue.
Disease: Somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs).
Dose: Intravenous infusion 7.4 GBq (200 mCi) every 8 weeks for a total of four doses.
NETTER-1 trial (NCT01578239): 65% of adults who received lutetium Lu 177 showed improved progression-free survival at 20 months, compared with just 10.8% in the control group.
Mogamulizumab (Poteligeo)
Class: Monoclonal antibody that binds to a protein (CC chemokine receptor type 4).
Disease: Relapsed or refractory mycosis fungoides or Sézary syndrome.
Dose: Intravenous infusion 1 mg/kg.
AE: Dermatologic toxicity.
MAVORIC trial (NCT01728805): Patients who received mogamulizumab had improved progression-free survival (median 7.7 months), compared with those taking vorinostat (median 3.1 months).
Moxetumomab pasudotox-tdfk (Lumoxiti)
Class: CD22-directed cytotoxin fused with a fragment of Pseudomonas exotoxin A.
Disease: Relapsed or refractory hairy cell leukemia previously treated with at least two prior systemic therapies, including a purine nucleoside analogue.
Dose: Intravenously as 0.04 mg/kg.
AE: Hemolytic uremic syndrome.
1053 trial (NCT01829711): 30% of the patients who received moxetumomab pasudotox-tdfk had a durable complete response confirmed by maintenance hematologic remission.
Talazoparib (Talzenna)
Class: Poly (ADP-ribose) polymerase (PARP) inhibitor.
Disease: gBRCAm HER2-negative locally advanced or metastatic breast cancer.
Dose: 1 mg orally per day.
EMBRACA trial (NCT01945775): Patients who received talazoparib demonstrated significantly longer progression-free survival, with a median of 8.6 months versis 5.6 months in the control arm.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mentzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and a professor of medicine at the University of Pennsylvania.
Advances in genomics and technology perpetually change and improve therapies in oncology. Enhanced comprehension of cellular signaling, division, and replication has created a platform to selectively restrict neoplastic growth while preserving the integrity of benign cells.
This article reviews therapies that were newly approved in 2018, as well as those previously approved whose indications were expanded this past year. The list highlights the most clinically important approvals, as well as adverse events that are unique or especially severe.
Click on the PDF above to download the full article and charts in an easy-to-print format.
Apalutamide (Erleada)
Class: Androgen receptor inhibitor.
Disease: Nonmetastatic castration-resistant prostate cancer.
Dose: 240 mg orally, once daily.
Adverse Events (AEs): Hyperkalemia and increased risks of seizures, falls, and fractures.
Phase 3 SPARTAN trial (NCT01946204): 40.5-month metastasis-free survival rate, compared with 16.2 months in the placebo group.
Cemiplimab (Libtayo)
Class: Antibody against programmed cell death protein-1 (PD-1).
Disease: Metastatic cutaneous squamous cell carcinoma (CSCC) or locally advanced CSCC that is ineligible for curative surgery/radiation.
Dose: 350 mg intravenous infusion every 3 weeks.
AEs: Pneumonitis, autoimmune myocarditis, hepatitis, and aseptic meningitis.
1423 and 1540 trials (NCT02383212 and NCT02760498): 47.2% of patients who received cemiplimab had complete disappearance of the tumor or a decrease in tumor size.
Dacomitinib (Vizimpro)
Class: Second-generation tyrosine kinase inhibitor.
Disease: Metastatic non–small cell lung cancer (NSCLC) with epidermal growth factor receptor (EGFR) exon 19 deletion or exon 21 L858R substitution mutation.
Dose: 45 mg orally once daily.
AEs: Dermatotoxicity and diarrhea.
ARCHER1050 trial (NCT01774721): Patients who received dacomitinib demonstrated an improved overall survival, with a median of 34.1 months, compared with 26.8 months with gefitinib.
Duvelisib (Copiktra)
Class: Dual inhibitor of phosphatidylinositol 3-kinase delta and gamma.
Disease: Relapsed or refractory chronic lymphocytic leukemia (CLL), small lymphocytic lymphoma, or relapsed or refractory follicular lymphoma after at least two prior systemic therapies.
Dose: 25 mg orally twice daily.
AEs: Infection, diarrhea or colitis, and pneumonia.
Phase 3 DUO trial (NCT02004522): Progression-free survival in the duvelisib arm was 7.3 months longer than that in the ofatumumab arm. The overall response rate for patients receiving duvelisib was 78%, compared with 39% for those receiving ofatumumab.
Gilteritinib (Xospata)
Class: Inhibits the FLT3 internal tandem duplication (ITD) and FLT3 tyrosine kinase domain (TKD).
Disease: Relapsed or refractory acute myeloid leukemia (AML) with an FLT3 mutation.
Dose: 120 mg orally daily.
ADMIRAL trial (NCT02421939): 21% of the patients who received gilteritinib exhibited complete remission or complete remission with partial hematologic recovery.
Glasdegib (Daurismo)
Class: Hedgehog pathway inhibitor.
Disease: Adults over age 75 years with newly diagnosed AML and other medical comorbidities that preclude them from intensive chemotherapy.
Dose: The recommended dose is 100 mg orally continuously in 28-day cycles.
AE: QT prolongation and embryo-fetal toxicity
Phase 2 BRIGHT 1003 trial (NCT01546038): 3.9-month overall survival advantage for glasdegib plus cytarabine, compared with cytarabine alone. Overall, 15% of the glasdegib plus low dose cytarabine arm achieved complete remission, compared with the 1% complete remission rate in patients who received cytarabine alone.
Iobenguane I 131 (Azedra)
Class: Radiopharmaceutical agent; induces cell death within the noradrenaline transporter.
Disease: Iobenguane scan–positive, unresectable, locally advanced or metastatic pheochromocytoma or paraganglioma
Dose: Initial intravenous dosimetric dose, followed by two therapeutic doses.
AE: Pancytopenia and elevated international normalized ratio (INR).
IB12B trial (NCT00874614): One-quarter of patients receiving this therapy had at least a 50% reduction in the dose and number of antihypertensives for at least 6 months; almost all patients had a tumor response.
Ivosidenib (Tibsovo)
Class: Small-molecule inhibitor of mutant isocitrate dehydrogenase (IDH1).
Disease: Refractory AML and an IDH1 mutation
Dose: 500 mg orally daily.
AG120-C-001 trial (NCT02074839): Overall response rate of 41.6% in patients who received ivosidenib, with a 30.4% rate of complete remission or complete remission with partial hematologic recovery.
Larotrectinib (Vitrakvi)
Class: Oral tyrosine kinase inhibitor.
Disease: Advanced solid tumors harboring a neurotrophic tyrosine receptor kinase (NTRK) gene fusion.
Dose: 100 mg orally twice daily.
LOXO-TRK-14001, SCOUT, and NAVIGATE trials (NCT02122913, NCT02637687, and NCT02576431): Patients who received larotrectinib had durable responses regardless of patient age, tumor type, and fusion status.
Lutetium Lu 177 dotatate (Lutathera)
Class: Radiolabeled somatostatin analogue.
Disease: Somatostatin receptor–positive gastroenteropancreatic neuroendocrine tumors (GEP-NETs).
Dose: Intravenous infusion 7.4 GBq (200 mCi) every 8 weeks for a total of four doses.
NETTER-1 trial (NCT01578239): 65% of adults who received lutetium Lu 177 showed improved progression-free survival at 20 months, compared with just 10.8% in the control group.
Mogamulizumab (Poteligeo)
Class: Monoclonal antibody that binds to a protein (CC chemokine receptor type 4).
Disease: Relapsed or refractory mycosis fungoides or Sézary syndrome.
Dose: Intravenous infusion 1 mg/kg.
AE: Dermatologic toxicity.
MAVORIC trial (NCT01728805): Patients who received mogamulizumab had improved progression-free survival (median 7.7 months), compared with those taking vorinostat (median 3.1 months).
Moxetumomab pasudotox-tdfk (Lumoxiti)
Class: CD22-directed cytotoxin fused with a fragment of Pseudomonas exotoxin A.
Disease: Relapsed or refractory hairy cell leukemia previously treated with at least two prior systemic therapies, including a purine nucleoside analogue.
Dose: Intravenously as 0.04 mg/kg.
AE: Hemolytic uremic syndrome.
1053 trial (NCT01829711): 30% of the patients who received moxetumomab pasudotox-tdfk had a durable complete response confirmed by maintenance hematologic remission.
Talazoparib (Talzenna)
Class: Poly (ADP-ribose) polymerase (PARP) inhibitor.
Disease: gBRCAm HER2-negative locally advanced or metastatic breast cancer.
Dose: 1 mg orally per day.
EMBRACA trial (NCT01945775): Patients who received talazoparib demonstrated significantly longer progression-free survival, with a median of 8.6 months versis 5.6 months in the control arm.
Dr. Bryer is a resident in the department of internal medicine at the University of Pennsylvania, Philadelphia. Dr. Mentzer is chief of hematology-oncology at Pennsylvania Hospital and professor of medicine at the University of Pennsylvania. Dr. Henry is a hematologist-oncologist at Pennsylvania Hospital and a professor of medicine at the University of Pennsylvania.
Nontraditional specialty physicians supplement hospitalist staffing
More HMGs cover inpatient and ED settings
Our profession continues to experience steady growth, and demand for hospitalist physicians exceeds supply. In a recent article in The Hospitalist, Andrew White, MD, SFHM, highlighted the fact that most hospital medicine groups (HMGs) are constantly recruiting and open positions are not uncommon.

When we think about recruitment and staffing, I bet many of us think principally of physicians trained in the general medicine specialties of internal medicine, family medicine, and pediatrics. Yet, to help meet demand for hospital-based clinicians, HMGs sometimes turn to physicians certified in emergency medicine, critical care, geriatric medicine, palliative care, and other fields.
To gain a better understanding of the diversity within our profession, the Society of Hospital Medicine’s State of Hospital Medicine survey asked HMGs whether they employ at least one physician in these various specialties. Results published in the recently released 2018 State of Hospital Medicine (SoHM) Report show significant differences among groups, affected by location, group size, and type of employer.
At the core of our profession are physicians trained in internal medicine, present in 99.2% of adult medicine HMGs throughout the United States. No surprise given that our field was founded by internists and remains a popular career choice for IM residency graduates. Family physicians follow, with the highest percentage of groups employing at least one FP located in the southern United States at 70.3% and lowest in the west at 54.7%. Small-sized groups – fewer than 10 full-time equivalents (FTEs) – were also more likely to employ FPs.
This speaks to the challenge – often faced by smaller hospitals – of covering both adult and pediatric patient populations and limited workforce availability. Pediatrics- and internal medicine/pediatrics–trained physicians help meet this need and were prevalent within small-sized groups. Another distinction found in the report is that, while 92.1% of multistate hospitalist management companies employed family physicians, only 28.8% of academic university settings did so. Partly because of Accreditation Council for Graduate Medical Education requirements for IM-certified teaching attending for internal medicine residents, FP and other specialties are filling some non–teaching hospitalist positions within our academic programs.
What may be surprising is that emergency medicine and critical care had the largest increase in representation in hospital medicine. The two specialties showed similar growth trends, with a larger presence in the South and Midwest states and 56% of multistate hospitalist management companies employing them. Small- to medium-sized groups of up to 20 FTEs were also more likely to have physicians from these fields, with up to 44% of groups doing so. This is a significant change from 2016, when less than 3.4% of all HMGs overall had a physician certified in emergency or critical care medicine.
This finding seems to coincide with the growth in hospital medicine groups who are covering both ED and inpatient services. For small and rural hospitals, it has become necessary and beneficial to have physicians capable of covering both clinical settings.
Contrast this with geriatric medicine and palliative care. Here, we saw these two specialties to be present in our academic institutions at 26.8% and 22.5%, respectively. Large-sized HMGs were more likely to employ them, whereas their presence in multistate management groups or private multispecialty/primary care groups was quite low. Compared with our last survey in 2016, their overall prevalence in HMGs hasn’t changed significantly. Whether this will be different in the future with our aging population will be interesting to follow.
Published biannually, the SoHM report provides insight into these and other market-based dynamics that shape hospital medicine. The demand for hospital-based clinicians and the demands of acute inpatient care are leading to the broad and inclusive nature of hospital medicine. Our staffing will continue to be met not only by internal medicine and family medicine physicians but also through these other specialties joining our ranks and adding diversity to our profession.
Dr. Sites is the executive medical director of acute medicine at Providence St. Joseph Health, Oregon, and a member of SHM’s Practice Analysis Committee. She leads the hospital medicine programs and is involved in strategy development and alignment of acute inpatient medicine services at eight member hospitals. She has been a practicing hospitalist for 20 years and volunteers on medical mission trips to Guatemala annually.
More HMGs cover inpatient and ED settings
More HMGs cover inpatient and ED settings
Our profession continues to experience steady growth, and demand for hospitalist physicians exceeds supply. In a recent article in The Hospitalist, Andrew White, MD, SFHM, highlighted the fact that most hospital medicine groups (HMGs) are constantly recruiting and open positions are not uncommon.
When we think about recruitment and staffing, I bet many of us think principally of physicians trained in the general medicine specialties of internal medicine, family medicine, and pediatrics. Yet, to help meet demand for hospital-based clinicians, HMGs sometimes turn to physicians certified in emergency medicine, critical care, geriatric medicine, palliative care, and other fields.
To gain a better understanding of the diversity within our profession, the Society of Hospital Medicine’s State of Hospital Medicine survey asked HMGs whether they employ at least one physician in these various specialties. Results published in the recently released 2018 State of Hospital Medicine (SoHM) Report show significant differences among groups, affected by location, group size, and type of employer.
At the core of our profession are physicians trained in internal medicine, present in 99.2% of adult medicine HMGs throughout the United States. No surprise given that our field was founded by internists and remains a popular career choice for IM residency graduates. Family physicians follow, with the highest percentage of groups employing at least one FP located in the southern United States at 70.3% and lowest in the west at 54.7%. Small-sized groups – fewer than 10 full-time equivalents (FTEs) – were also more likely to employ FPs.
This speaks to the challenge – often faced by smaller hospitals – of covering both adult and pediatric patient populations and limited workforce availability. Pediatrics- and internal medicine/pediatrics–trained physicians help meet this need and were prevalent within small-sized groups. Another distinction found in the report is that, while 92.1% of multistate hospitalist management companies employed family physicians, only 28.8% of academic university settings did so. Partly because of Accreditation Council for Graduate Medical Education requirements for IM-certified teaching attending for internal medicine residents, FP and other specialties are filling some non–teaching hospitalist positions within our academic programs.
What may be surprising is that emergency medicine and critical care had the largest increase in representation in hospital medicine. The two specialties showed similar growth trends, with a larger presence in the South and Midwest states and 56% of multistate hospitalist management companies employing them. Small- to medium-sized groups of up to 20 FTEs were also more likely to have physicians from these fields, with up to 44% of groups doing so. This is a significant change from 2016, when less than 3.4% of all HMGs overall had a physician certified in emergency or critical care medicine.
This finding seems to coincide with the growth in hospital medicine groups who are covering both ED and inpatient services. For small and rural hospitals, it has become necessary and beneficial to have physicians capable of covering both clinical settings.
Contrast this with geriatric medicine and palliative care. Here, we saw these two specialties to be present in our academic institutions at 26.8% and 22.5%, respectively. Large-sized HMGs were more likely to employ them, whereas their presence in multistate management groups or private multispecialty/primary care groups was quite low. Compared with our last survey in 2016, their overall prevalence in HMGs hasn’t changed significantly. Whether this will be different in the future with our aging population will be interesting to follow.
Published biannually, the SoHM report provides insight into these and other market-based dynamics that shape hospital medicine. The demand for hospital-based clinicians and the demands of acute inpatient care are leading to the broad and inclusive nature of hospital medicine. Our staffing will continue to be met not only by internal medicine and family medicine physicians but also through these other specialties joining our ranks and adding diversity to our profession.
Dr. Sites is the executive medical director of acute medicine at Providence St. Joseph Health, Oregon, and a member of SHM’s Practice Analysis Committee. She leads the hospital medicine programs and is involved in strategy development and alignment of acute inpatient medicine services at eight member hospitals. She has been a practicing hospitalist for 20 years and volunteers on medical mission trips to Guatemala annually.
Our profession continues to experience steady growth, and demand for hospitalist physicians exceeds supply. In a recent article in The Hospitalist, Andrew White, MD, SFHM, highlighted the fact that most hospital medicine groups (HMGs) are constantly recruiting and open positions are not uncommon.
When we think about recruitment and staffing, I bet many of us think principally of physicians trained in the general medicine specialties of internal medicine, family medicine, and pediatrics. Yet, to help meet demand for hospital-based clinicians, HMGs sometimes turn to physicians certified in emergency medicine, critical care, geriatric medicine, palliative care, and other fields.
To gain a better understanding of the diversity within our profession, the Society of Hospital Medicine’s State of Hospital Medicine survey asked HMGs whether they employ at least one physician in these various specialties. Results published in the recently released 2018 State of Hospital Medicine (SoHM) Report show significant differences among groups, affected by location, group size, and type of employer.
At the core of our profession are physicians trained in internal medicine, present in 99.2% of adult medicine HMGs throughout the United States. No surprise given that our field was founded by internists and remains a popular career choice for IM residency graduates. Family physicians follow, with the highest percentage of groups employing at least one FP located in the southern United States at 70.3% and lowest in the west at 54.7%. Small-sized groups – fewer than 10 full-time equivalents (FTEs) – were also more likely to employ FPs.
This speaks to the challenge – often faced by smaller hospitals – of covering both adult and pediatric patient populations and limited workforce availability. Pediatrics- and internal medicine/pediatrics–trained physicians help meet this need and were prevalent within small-sized groups. Another distinction found in the report is that, while 92.1% of multistate hospitalist management companies employed family physicians, only 28.8% of academic university settings did so. Partly because of Accreditation Council for Graduate Medical Education requirements for IM-certified teaching attending for internal medicine residents, FP and other specialties are filling some non–teaching hospitalist positions within our academic programs.
What may be surprising is that emergency medicine and critical care had the largest increase in representation in hospital medicine. The two specialties showed similar growth trends, with a larger presence in the South and Midwest states and 56% of multistate hospitalist management companies employing them. Small- to medium-sized groups of up to 20 FTEs were also more likely to have physicians from these fields, with up to 44% of groups doing so. This is a significant change from 2016, when less than 3.4% of all HMGs overall had a physician certified in emergency or critical care medicine.
This finding seems to coincide with the growth in hospital medicine groups who are covering both ED and inpatient services. For small and rural hospitals, it has become necessary and beneficial to have physicians capable of covering both clinical settings.
Contrast this with geriatric medicine and palliative care. Here, we saw these two specialties to be present in our academic institutions at 26.8% and 22.5%, respectively. Large-sized HMGs were more likely to employ them, whereas their presence in multistate management groups or private multispecialty/primary care groups was quite low. Compared with our last survey in 2016, their overall prevalence in HMGs hasn’t changed significantly. Whether this will be different in the future with our aging population will be interesting to follow.
Published biannually, the SoHM report provides insight into these and other market-based dynamics that shape hospital medicine. The demand for hospital-based clinicians and the demands of acute inpatient care are leading to the broad and inclusive nature of hospital medicine. Our staffing will continue to be met not only by internal medicine and family medicine physicians but also through these other specialties joining our ranks and adding diversity to our profession.
Dr. Sites is the executive medical director of acute medicine at Providence St. Joseph Health, Oregon, and a member of SHM’s Practice Analysis Committee. She leads the hospital medicine programs and is involved in strategy development and alignment of acute inpatient medicine services at eight member hospitals. She has been a practicing hospitalist for 20 years and volunteers on medical mission trips to Guatemala annually.
Interventional endoscopic ultrasonography is hitting its stride

SAN FRANCISCO – Interventional endoscopic ultrasonography (EUS) recently has brought transluminal stent placement to problems like walled off pancreatic necroses, Joo Ha Hwang, MD, PhD, professor of medicine at Stanford (Calif.) University, said in an interview at the AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology. He sees EUS taking over surgical territory beyond the usual biopsies in the gastrointestinal and biliary tracts and soon moving into tumor treatment in these areas. The field is “rapidly expanding,” he said, and the value of these minimally invasive procedures means that the field will soon need to train more interventional endoscopists.
SAN FRANCISCO – Interventional endoscopic ultrasonography (EUS) recently has brought transluminal stent placement to problems like walled off pancreatic necroses, Joo Ha Hwang, MD, PhD, professor of medicine at Stanford (Calif.) University, said in an interview at the AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology. He sees EUS taking over surgical territory beyond the usual biopsies in the gastrointestinal and biliary tracts and soon moving into tumor treatment in these areas. The field is “rapidly expanding,” he said, and the value of these minimally invasive procedures means that the field will soon need to train more interventional endoscopists.
SAN FRANCISCO – Interventional endoscopic ultrasonography (EUS) recently has brought transluminal stent placement to problems like walled off pancreatic necroses, Joo Ha Hwang, MD, PhD, professor of medicine at Stanford (Calif.) University, said in an interview at the AGA Tech Summit, sponsored by the AGA Center for GI Innovation and Technology. He sees EUS taking over surgical territory beyond the usual biopsies in the gastrointestinal and biliary tracts and soon moving into tumor treatment in these areas. The field is “rapidly expanding,” he said, and the value of these minimally invasive procedures means that the field will soon need to train more interventional endoscopists.
REPORTING FROM 2019 AGA TECH SUMMIT
Anastrozole-fulvestrant in breast cancer and daily aspirin to prevent HCC
Welcome to the first edition of “How I will treat my next patient,” a regular column analyzing the practical clinical relevance of the latest literature. In this first column, I will take a look at two interesting studies – a combination hormonal treatment for metastatic ER-positive breast cancer and aspirin therapy for prevention of hepatocellular cancer.
Anastrozole plus fulvestrant

In a large SWOG trial for postmenopausal patients with stage IV, hormonally responsive breast cancer whose metastatic disease could be treated with frontline hormonal therapy, long-term survival analysis showed that the combination of anastrozole plus fulvestrant was superior to anastrozole alone, with essentially no increase in toxicity.
The study – “Overall Survival With Fulvestrant Plus Anastrozole in Metastatic Breast Cancer” – was published in the New England Journal of Medicine (2019;380:1226-34).
The overall survival difference was not only statistically and clinically significant, but impressively so among patients who had not received prior adjuvant hormonal therapy. That is despite the fact that 45% of patients who were assigned to initial treatment with anastrozole received single agent fulvestrant at first relapse.
What this means in practice
Because of the generally negative results of combined hormonal therapy in comparison with sequential use of the same agents and the potency of CDK4/6 inhibitors in combination with hormonal agents in the frontline setting, many oncologists have forgotten the initial publication of this regimen in 2012. In that study, the combination demonstrated improved progression-free survival over anastrozole alone, particularly in the subset of patients who presented with stage IV breast cancer as their initial presentation.
Although the benefits for CDK4/6 inhibitors as an addition to hormonal therapy are truly impressive, the practical aspects of utilizing the CDK4/6 inhibitors may be prohibitive for a small subset of our most vulnerable, medically underserved patients. Specifically, these are patients who are unable to return for frequent blood counts in the initial few months of therapy, patients with limited financial resources who cannot afford the out-of-pocket costs of an expensive oral medication and required laboratory testing, those with difficulty adhering to oral medication regimens, or those with constitutional neutropenia.
Not coincidentally, many of these patients are exactly the ones who present with stage IV disease as their initial manifestation of breast cancer. For such patients, the combination of anastrozole plus fulvestrant is an attractive alternative and may offer competitive survival benefits. This is not “yesterday’s therapy” in the era of CDK4/6 inhibitors, but rather represents a valuable option for treatment in at-risk populations.
When I see my next patient who presents with stage IV breast cancer, I will consider combined hormonal therapy among the various available treatment options.
Aspirin to prevent HCC
Investigators at Taichung (Taiwan) Veterans General Hospital recently analyzed 16 years of data from a cohort of more than 10,000 patients with chronic hepatitis B virus (HBV) infection and found statistically significantly fewer cases of hepatocellular cancer (HCC) in patients who took antiviral antinucleoside analogue therapy, statins, and aspirin.
The study – “Association of Daily Aspirin Therapy With Risk of Hepatocellular Carcinoma in Patients With Chronic Hepatitis B” – was published in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2018.8342).
Although there were more impressive reductions in relative risk of HCC among statin and antinucleoside analogue users, the authors highlighted that HCC developed in 5.20% of the approximately 2,100 chronic aspirin users and in 7.87% of nonusers – a 29% relative reduction in risk in this cohort study. Toxicity, including upper GI bleeding, was low.
What this means in practice
This is a hypothesis-generating analysis at best. Although the authors highlight possible mechanisms by which aspirin use could lead to reduction in HCC among patients with chronic inflammatory conditions affecting the liver, the study produces more questions than it answers (dose, chronicity of use, duration of protection, biomarkers for benefit).
Owing to the simplicity and low cost of the intervention, it may be worth studying prospectively in chronic HBV-infected patients and other populations at risk for HCC, but the intervention should not be adopted at this point based on an international cohort study.
The practicality of conducting such a large, complicated, prospective study of a widely available medication that has widely publicized additional health benefits is an open question.
When I see my next patient with a high risk for HCC, I won’t prescribe aspirin for chemoprevention.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers, and in expanding access to clinical trials to medically underserved populations.
Welcome to the first edition of “How I will treat my next patient,” a regular column analyzing the practical clinical relevance of the latest literature. In this first column, I will take a look at two interesting studies – a combination hormonal treatment for metastatic ER-positive breast cancer and aspirin therapy for prevention of hepatocellular cancer.
Anastrozole plus fulvestrant
In a large SWOG trial for postmenopausal patients with stage IV, hormonally responsive breast cancer whose metastatic disease could be treated with frontline hormonal therapy, long-term survival analysis showed that the combination of anastrozole plus fulvestrant was superior to anastrozole alone, with essentially no increase in toxicity.
The study – “Overall Survival With Fulvestrant Plus Anastrozole in Metastatic Breast Cancer” – was published in the New England Journal of Medicine (2019;380:1226-34).
The overall survival difference was not only statistically and clinically significant, but impressively so among patients who had not received prior adjuvant hormonal therapy. That is despite the fact that 45% of patients who were assigned to initial treatment with anastrozole received single agent fulvestrant at first relapse.
What this means in practice
Because of the generally negative results of combined hormonal therapy in comparison with sequential use of the same agents and the potency of CDK4/6 inhibitors in combination with hormonal agents in the frontline setting, many oncologists have forgotten the initial publication of this regimen in 2012. In that study, the combination demonstrated improved progression-free survival over anastrozole alone, particularly in the subset of patients who presented with stage IV breast cancer as their initial presentation.
Although the benefits for CDK4/6 inhibitors as an addition to hormonal therapy are truly impressive, the practical aspects of utilizing the CDK4/6 inhibitors may be prohibitive for a small subset of our most vulnerable, medically underserved patients. Specifically, these are patients who are unable to return for frequent blood counts in the initial few months of therapy, patients with limited financial resources who cannot afford the out-of-pocket costs of an expensive oral medication and required laboratory testing, those with difficulty adhering to oral medication regimens, or those with constitutional neutropenia.
Not coincidentally, many of these patients are exactly the ones who present with stage IV disease as their initial manifestation of breast cancer. For such patients, the combination of anastrozole plus fulvestrant is an attractive alternative and may offer competitive survival benefits. This is not “yesterday’s therapy” in the era of CDK4/6 inhibitors, but rather represents a valuable option for treatment in at-risk populations.
When I see my next patient who presents with stage IV breast cancer, I will consider combined hormonal therapy among the various available treatment options.
Aspirin to prevent HCC
Investigators at Taichung (Taiwan) Veterans General Hospital recently analyzed 16 years of data from a cohort of more than 10,000 patients with chronic hepatitis B virus (HBV) infection and found statistically significantly fewer cases of hepatocellular cancer (HCC) in patients who took antiviral antinucleoside analogue therapy, statins, and aspirin.
The study – “Association of Daily Aspirin Therapy With Risk of Hepatocellular Carcinoma in Patients With Chronic Hepatitis B” – was published in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2018.8342).
Although there were more impressive reductions in relative risk of HCC among statin and antinucleoside analogue users, the authors highlighted that HCC developed in 5.20% of the approximately 2,100 chronic aspirin users and in 7.87% of nonusers – a 29% relative reduction in risk in this cohort study. Toxicity, including upper GI bleeding, was low.
What this means in practice
This is a hypothesis-generating analysis at best. Although the authors highlight possible mechanisms by which aspirin use could lead to reduction in HCC among patients with chronic inflammatory conditions affecting the liver, the study produces more questions than it answers (dose, chronicity of use, duration of protection, biomarkers for benefit).
Owing to the simplicity and low cost of the intervention, it may be worth studying prospectively in chronic HBV-infected patients and other populations at risk for HCC, but the intervention should not be adopted at this point based on an international cohort study.
The practicality of conducting such a large, complicated, prospective study of a widely available medication that has widely publicized additional health benefits is an open question.
When I see my next patient with a high risk for HCC, I won’t prescribe aspirin for chemoprevention.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers, and in expanding access to clinical trials to medically underserved populations.
Welcome to the first edition of “How I will treat my next patient,” a regular column analyzing the practical clinical relevance of the latest literature. In this first column, I will take a look at two interesting studies – a combination hormonal treatment for metastatic ER-positive breast cancer and aspirin therapy for prevention of hepatocellular cancer.
Anastrozole plus fulvestrant
In a large SWOG trial for postmenopausal patients with stage IV, hormonally responsive breast cancer whose metastatic disease could be treated with frontline hormonal therapy, long-term survival analysis showed that the combination of anastrozole plus fulvestrant was superior to anastrozole alone, with essentially no increase in toxicity.
The study – “Overall Survival With Fulvestrant Plus Anastrozole in Metastatic Breast Cancer” – was published in the New England Journal of Medicine (2019;380:1226-34).
The overall survival difference was not only statistically and clinically significant, but impressively so among patients who had not received prior adjuvant hormonal therapy. That is despite the fact that 45% of patients who were assigned to initial treatment with anastrozole received single agent fulvestrant at first relapse.
What this means in practice
Because of the generally negative results of combined hormonal therapy in comparison with sequential use of the same agents and the potency of CDK4/6 inhibitors in combination with hormonal agents in the frontline setting, many oncologists have forgotten the initial publication of this regimen in 2012. In that study, the combination demonstrated improved progression-free survival over anastrozole alone, particularly in the subset of patients who presented with stage IV breast cancer as their initial presentation.
Although the benefits for CDK4/6 inhibitors as an addition to hormonal therapy are truly impressive, the practical aspects of utilizing the CDK4/6 inhibitors may be prohibitive for a small subset of our most vulnerable, medically underserved patients. Specifically, these are patients who are unable to return for frequent blood counts in the initial few months of therapy, patients with limited financial resources who cannot afford the out-of-pocket costs of an expensive oral medication and required laboratory testing, those with difficulty adhering to oral medication regimens, or those with constitutional neutropenia.
Not coincidentally, many of these patients are exactly the ones who present with stage IV disease as their initial manifestation of breast cancer. For such patients, the combination of anastrozole plus fulvestrant is an attractive alternative and may offer competitive survival benefits. This is not “yesterday’s therapy” in the era of CDK4/6 inhibitors, but rather represents a valuable option for treatment in at-risk populations.
When I see my next patient who presents with stage IV breast cancer, I will consider combined hormonal therapy among the various available treatment options.
Aspirin to prevent HCC
Investigators at Taichung (Taiwan) Veterans General Hospital recently analyzed 16 years of data from a cohort of more than 10,000 patients with chronic hepatitis B virus (HBV) infection and found statistically significantly fewer cases of hepatocellular cancer (HCC) in patients who took antiviral antinucleoside analogue therapy, statins, and aspirin.
The study – “Association of Daily Aspirin Therapy With Risk of Hepatocellular Carcinoma in Patients With Chronic Hepatitis B” – was published in JAMA Internal Medicine (doi: 10.1001/jamainternmed.2018.8342).
Although there were more impressive reductions in relative risk of HCC among statin and antinucleoside analogue users, the authors highlighted that HCC developed in 5.20% of the approximately 2,100 chronic aspirin users and in 7.87% of nonusers – a 29% relative reduction in risk in this cohort study. Toxicity, including upper GI bleeding, was low.
What this means in practice
This is a hypothesis-generating analysis at best. Although the authors highlight possible mechanisms by which aspirin use could lead to reduction in HCC among patients with chronic inflammatory conditions affecting the liver, the study produces more questions than it answers (dose, chronicity of use, duration of protection, biomarkers for benefit).
Owing to the simplicity and low cost of the intervention, it may be worth studying prospectively in chronic HBV-infected patients and other populations at risk for HCC, but the intervention should not be adopted at this point based on an international cohort study.
The practicality of conducting such a large, complicated, prospective study of a widely available medication that has widely publicized additional health benefits is an open question.
When I see my next patient with a high risk for HCC, I won’t prescribe aspirin for chemoprevention.
Dr. Lyss has been a community-based medical oncologist and clinical researcher for more than 35 years, practicing in St. Louis. His clinical and research interests are in the prevention, diagnosis, and treatment of breast and lung cancers, and in expanding access to clinical trials to medically underserved populations.
Dr. Douglas Paauw: Consider rechallenging patients with penicillin allergy
PHILADELPHIA – As fluoroquinolone warnings stack up, internists seeking treatment alternatives should consider rechallenging patients with penicillin allergy or referring those patients for testing, said Douglas S. Paauw, MD, during a presentation.

This was one of the pieces of advice provided by Dr. Paauw, professor of medicine in the division of general internal medicine at the University of Washington, Seattle, at the annual meeting of the American College of Physicians.
“The FDA [Food and Drug Administration] has been just killing trees, sending us letters over the last 5-10 years, with fluoroquinolone warnings,” said Dr. Paauw, referencing previous warnings describing risks of tendon rupture, peripheral neuropathy, hypoglycemia, mental health side effects, and more.
“I think the buzz in 2019 is that we should not overreact to a history of penicillin allergy,” he said.
As many as 98% of patients who have reported penicillin allergy don’t have true allergy and can safely receive penicillin, he explained.
“If they don’t have an allergy, make sure you get it out of the electronic record,” Dr. Paauw also advised.
The latest warning on fluoroquinolones from the FDA, issued in Dec. 20, 2018, said that clinicians should avoid prescribing these antibiotics in patients who have, or are at risk of, aortic aneurysm. This comprises a very large proportion of patients in an internist’s practice, Dr. Paauw noted. The warning specifically singled out elderly patients as being in the at-risk population, along with patients who have peripheral atherosclerotic vascular diseases, hypertension, or genetic conditions such as Marfan syndrome or Ehlers-Danlos syndrome, he added.
Dr. Paauw further supported his suggestions by describing two relevant studies.
In one of those studies, which was published this year in an allergy and asthma journal, 20 subjects with a history of penicillin allergy agreed to direct oral amoxicillin rechallenge by an allergist, he said. None of those 20 patients were observed to have developed immediate or delayed hypersensitivity reactions, investigators reported. That study included a total of 50 adults with a penicillin allergy label, of whom 24 (48%) had the label removed from their medical records.
In another recent and reassuring study, penicillin allergy testing was conducted in 100 children with parent-reported penicillin allergy that was considered low risk based on reported symptoms, Dr. Paauw said. Of that group, all 100 children were found to be negative for true penicillin allergy.
Dr. Paauw had no relevant disclosures.
SOURCE: Paauw DS. Annual Meeting of the American College of Physicians, Presentation MTP 013.
PHILADELPHIA – As fluoroquinolone warnings stack up, internists seeking treatment alternatives should consider rechallenging patients with penicillin allergy or referring those patients for testing, said Douglas S. Paauw, MD, during a presentation.
This was one of the pieces of advice provided by Dr. Paauw, professor of medicine in the division of general internal medicine at the University of Washington, Seattle, at the annual meeting of the American College of Physicians.
“The FDA [Food and Drug Administration] has been just killing trees, sending us letters over the last 5-10 years, with fluoroquinolone warnings,” said Dr. Paauw, referencing previous warnings describing risks of tendon rupture, peripheral neuropathy, hypoglycemia, mental health side effects, and more.
“I think the buzz in 2019 is that we should not overreact to a history of penicillin allergy,” he said.
As many as 98% of patients who have reported penicillin allergy don’t have true allergy and can safely receive penicillin, he explained.
“If they don’t have an allergy, make sure you get it out of the electronic record,” Dr. Paauw also advised.
The latest warning on fluoroquinolones from the FDA, issued in Dec. 20, 2018, said that clinicians should avoid prescribing these antibiotics in patients who have, or are at risk of, aortic aneurysm. This comprises a very large proportion of patients in an internist’s practice, Dr. Paauw noted. The warning specifically singled out elderly patients as being in the at-risk population, along with patients who have peripheral atherosclerotic vascular diseases, hypertension, or genetic conditions such as Marfan syndrome or Ehlers-Danlos syndrome, he added.
Dr. Paauw further supported his suggestions by describing two relevant studies.
In one of those studies, which was published this year in an allergy and asthma journal, 20 subjects with a history of penicillin allergy agreed to direct oral amoxicillin rechallenge by an allergist, he said. None of those 20 patients were observed to have developed immediate or delayed hypersensitivity reactions, investigators reported. That study included a total of 50 adults with a penicillin allergy label, of whom 24 (48%) had the label removed from their medical records.
In another recent and reassuring study, penicillin allergy testing was conducted in 100 children with parent-reported penicillin allergy that was considered low risk based on reported symptoms, Dr. Paauw said. Of that group, all 100 children were found to be negative for true penicillin allergy.
Dr. Paauw had no relevant disclosures.
SOURCE: Paauw DS. Annual Meeting of the American College of Physicians, Presentation MTP 013.
PHILADELPHIA – As fluoroquinolone warnings stack up, internists seeking treatment alternatives should consider rechallenging patients with penicillin allergy or referring those patients for testing, said Douglas S. Paauw, MD, during a presentation.
This was one of the pieces of advice provided by Dr. Paauw, professor of medicine in the division of general internal medicine at the University of Washington, Seattle, at the annual meeting of the American College of Physicians.
“The FDA [Food and Drug Administration] has been just killing trees, sending us letters over the last 5-10 years, with fluoroquinolone warnings,” said Dr. Paauw, referencing previous warnings describing risks of tendon rupture, peripheral neuropathy, hypoglycemia, mental health side effects, and more.
“I think the buzz in 2019 is that we should not overreact to a history of penicillin allergy,” he said.
As many as 98% of patients who have reported penicillin allergy don’t have true allergy and can safely receive penicillin, he explained.
“If they don’t have an allergy, make sure you get it out of the electronic record,” Dr. Paauw also advised.
The latest warning on fluoroquinolones from the FDA, issued in Dec. 20, 2018, said that clinicians should avoid prescribing these antibiotics in patients who have, or are at risk of, aortic aneurysm. This comprises a very large proportion of patients in an internist’s practice, Dr. Paauw noted. The warning specifically singled out elderly patients as being in the at-risk population, along with patients who have peripheral atherosclerotic vascular diseases, hypertension, or genetic conditions such as Marfan syndrome or Ehlers-Danlos syndrome, he added.
Dr. Paauw further supported his suggestions by describing two relevant studies.
In one of those studies, which was published this year in an allergy and asthma journal, 20 subjects with a history of penicillin allergy agreed to direct oral amoxicillin rechallenge by an allergist, he said. None of those 20 patients were observed to have developed immediate or delayed hypersensitivity reactions, investigators reported. That study included a total of 50 adults with a penicillin allergy label, of whom 24 (48%) had the label removed from their medical records.
In another recent and reassuring study, penicillin allergy testing was conducted in 100 children with parent-reported penicillin allergy that was considered low risk based on reported symptoms, Dr. Paauw said. Of that group, all 100 children were found to be negative for true penicillin allergy.
Dr. Paauw had no relevant disclosures.
SOURCE: Paauw DS. Annual Meeting of the American College of Physicians, Presentation MTP 013.
REPORTING FROM INTERNAL MEDICINE 2019
Geroscience brings bench science to the real-world problems of aging
NEW ORLEANS – Patients ask their doctors whether dietary manipulation can extend lifespan and promote healthy aging. Right now, basic scientists and clinicians from many disciplines are teaming up under the broad umbrella of the field of geroscience to try to answer these and other concerns relevant to an aging population.
“The idea here is that, instead of going after each disease one at a time, as we do ... [we] instead go after disease vulnerability – and this is something that is shared, as a function of age,” Rozalyn Anderson, PhD, said of this new discipline. The work touches on disparate diseases such as cancer, dementia, and diabetes, she pointed out during a video interview at the annual meeting of the Endocrine Society.
“I separate these things out into ‘front-end’ and ‘back-end,’ work,” said Dr. Anderson of the University of Wisconsin-Madison’s aging and caloric restriction program. She explained that the caloric restriction she researches is back-end work to support the rapidly evolving field of nutritional modulation of aging.
When the basic science builds the framework, physicians and scientists can turn to front-end research, looking at humans to see which dietary manipulations are effective – and which are achievable.
“Take a paradigm that works, and then try to understand how it works,” said Dr. Anderson. “So [for example], we have this paradigm, and it’s tremendously effective in rodents. It’s effective in flies, in worms, in yeast, in spiders, in dogs – and in nonhuman primates.” Then, she and her team try to pull out clues “about the biology of aging itself, and what creates disease vulnerability as a function of age,” she said.
“The most important thing of all is that we can modify aging. This is not a foregone conclusion – no one would have believed it. But even in a primate species, we can change how they age. And the way in which we change is through nutrition.”
Dr Anderson added that “the paradigm of caloric restriction is tremendously effective, but [in reality], people are not going to do it.” It’s simply not practical to ask individuals to restrict calories by 30% or more over a lifespan, so “.”
Dr. Anderson reported no relevant conflicts of interest or disclosures.
NEW ORLEANS – Patients ask their doctors whether dietary manipulation can extend lifespan and promote healthy aging. Right now, basic scientists and clinicians from many disciplines are teaming up under the broad umbrella of the field of geroscience to try to answer these and other concerns relevant to an aging population.
“The idea here is that, instead of going after each disease one at a time, as we do ... [we] instead go after disease vulnerability – and this is something that is shared, as a function of age,” Rozalyn Anderson, PhD, said of this new discipline. The work touches on disparate diseases such as cancer, dementia, and diabetes, she pointed out during a video interview at the annual meeting of the Endocrine Society.
“I separate these things out into ‘front-end’ and ‘back-end,’ work,” said Dr. Anderson of the University of Wisconsin-Madison’s aging and caloric restriction program. She explained that the caloric restriction she researches is back-end work to support the rapidly evolving field of nutritional modulation of aging.
When the basic science builds the framework, physicians and scientists can turn to front-end research, looking at humans to see which dietary manipulations are effective – and which are achievable.
“Take a paradigm that works, and then try to understand how it works,” said Dr. Anderson. “So [for example], we have this paradigm, and it’s tremendously effective in rodents. It’s effective in flies, in worms, in yeast, in spiders, in dogs – and in nonhuman primates.” Then, she and her team try to pull out clues “about the biology of aging itself, and what creates disease vulnerability as a function of age,” she said.
“The most important thing of all is that we can modify aging. This is not a foregone conclusion – no one would have believed it. But even in a primate species, we can change how they age. And the way in which we change is through nutrition.”
Dr Anderson added that “the paradigm of caloric restriction is tremendously effective, but [in reality], people are not going to do it.” It’s simply not practical to ask individuals to restrict calories by 30% or more over a lifespan, so “.”
Dr. Anderson reported no relevant conflicts of interest or disclosures.
NEW ORLEANS – Patients ask their doctors whether dietary manipulation can extend lifespan and promote healthy aging. Right now, basic scientists and clinicians from many disciplines are teaming up under the broad umbrella of the field of geroscience to try to answer these and other concerns relevant to an aging population.
“The idea here is that, instead of going after each disease one at a time, as we do ... [we] instead go after disease vulnerability – and this is something that is shared, as a function of age,” Rozalyn Anderson, PhD, said of this new discipline. The work touches on disparate diseases such as cancer, dementia, and diabetes, she pointed out during a video interview at the annual meeting of the Endocrine Society.
“I separate these things out into ‘front-end’ and ‘back-end,’ work,” said Dr. Anderson of the University of Wisconsin-Madison’s aging and caloric restriction program. She explained that the caloric restriction she researches is back-end work to support the rapidly evolving field of nutritional modulation of aging.
When the basic science builds the framework, physicians and scientists can turn to front-end research, looking at humans to see which dietary manipulations are effective – and which are achievable.
“Take a paradigm that works, and then try to understand how it works,” said Dr. Anderson. “So [for example], we have this paradigm, and it’s tremendously effective in rodents. It’s effective in flies, in worms, in yeast, in spiders, in dogs – and in nonhuman primates.” Then, she and her team try to pull out clues “about the biology of aging itself, and what creates disease vulnerability as a function of age,” she said.
“The most important thing of all is that we can modify aging. This is not a foregone conclusion – no one would have believed it. But even in a primate species, we can change how they age. And the way in which we change is through nutrition.”
Dr Anderson added that “the paradigm of caloric restriction is tremendously effective, but [in reality], people are not going to do it.” It’s simply not practical to ask individuals to restrict calories by 30% or more over a lifespan, so “.”
Dr. Anderson reported no relevant conflicts of interest or disclosures.
REPORTING FROM ENDO 2019

Using humor in clinical practice
A patient in Seattle reported drinking alcohol on only two occasions during the year: when it rains – and when it doesn’t.
Various benefits of humor have been studied as part of the treatment modality. Humor can be a powerful resource, but it remains a complex process, and its proper use in clinical practice requires careful consideration. Despite having demonstrated the ability to relieve stress in patients and among medical professionals,1 humor has not gained widespread acceptance.

Humor has been shown to help build relationships, and establish trust and support for favorable health outcomes. It increases patients’ satisfaction, decreases medical malpractice claims, and has the potential to reduce cultural differences and hierarchy between patients and health care practitioners.2 The Accreditation Council of Graduate Medical Education values interpersonal and communication skills as being among the core competencies to be imparted to physicians in training.

Currently, there is no standard methodology for using humor in practice, as each clinical setting and circumstance can vary widely. Whichever setting you find yourself in, however, you might 1-3
Explore the benefits of humor in your clinical practice
Consider humor an integral part of your professionalism. Initiate it where you have assessed it is appropriate.
Understand your audience
Assess your patients’ capability of understanding or appreciating your humor. Do not force it on patients. Be respectful of their perspectives and mindful of cultural differences.
Reciprocate humor
If patients take the humor route to lighten what might be a tense encounter, respond to their attempt and join them in bringing levity into the mix.
Use humor to support patients
Humor can take many forms. It can be subtle and does not always require a punchline. Patients may use it to express concerns or even fear. Health care providers can use it as support and to demonstrate caring, reflecting anxieties likely displayed or revealed by patients.
Avoid certain forms of humor
Avoid using self-disparaging or gallows humor. Humor between health care providers and patients should never be sarcastic, ethnic, or sexist.
Pay attention to how your patients use humor
Explore the possible meanings of your patients’ attempts at humor and what concerns they might be seeking to express. Use your findings to discuss deeper issues.
Incorporate humor into your teaching
Students, too, can benefit from the therapeutic potential of humor. Use humor to dispel or lessen your students’ fears or anxieties. It can help in the learning process and memory. Creating a cheery ambience can help lessen nervousness, ease coping, and reduce burnout.
References
1. South Med J. 2003 Dec;96(12):1257-61.
2. J Am Board Fam Med. 2018 Mar-Apr;31(2):270-8.
3. Health Expect. 2014 Jun;17(3):332-44.
Dr. Lamba is a psychiatrist and medical director at Bayridge Hospital in Lynn, Mass. Dr. Rana is assistant professor of pediatrics at Boston University.
A patient in Seattle reported drinking alcohol on only two occasions during the year: when it rains – and when it doesn’t.
Various benefits of humor have been studied as part of the treatment modality. Humor can be a powerful resource, but it remains a complex process, and its proper use in clinical practice requires careful consideration. Despite having demonstrated the ability to relieve stress in patients and among medical professionals,1 humor has not gained widespread acceptance.
Humor has been shown to help build relationships, and establish trust and support for favorable health outcomes. It increases patients’ satisfaction, decreases medical malpractice claims, and has the potential to reduce cultural differences and hierarchy between patients and health care practitioners.2 The Accreditation Council of Graduate Medical Education values interpersonal and communication skills as being among the core competencies to be imparted to physicians in training.
Currently, there is no standard methodology for using humor in practice, as each clinical setting and circumstance can vary widely. Whichever setting you find yourself in, however, you might 1-3
Explore the benefits of humor in your clinical practice
Consider humor an integral part of your professionalism. Initiate it where you have assessed it is appropriate.
Understand your audience
Assess your patients’ capability of understanding or appreciating your humor. Do not force it on patients. Be respectful of their perspectives and mindful of cultural differences.
Reciprocate humor
If patients take the humor route to lighten what might be a tense encounter, respond to their attempt and join them in bringing levity into the mix.
Use humor to support patients
Humor can take many forms. It can be subtle and does not always require a punchline. Patients may use it to express concerns or even fear. Health care providers can use it as support and to demonstrate caring, reflecting anxieties likely displayed or revealed by patients.
Avoid certain forms of humor
Avoid using self-disparaging or gallows humor. Humor between health care providers and patients should never be sarcastic, ethnic, or sexist.
Pay attention to how your patients use humor
Explore the possible meanings of your patients’ attempts at humor and what concerns they might be seeking to express. Use your findings to discuss deeper issues.
Incorporate humor into your teaching
Students, too, can benefit from the therapeutic potential of humor. Use humor to dispel or lessen your students’ fears or anxieties. It can help in the learning process and memory. Creating a cheery ambience can help lessen nervousness, ease coping, and reduce burnout.
References
1. South Med J. 2003 Dec;96(12):1257-61.
2. J Am Board Fam Med. 2018 Mar-Apr;31(2):270-8.
3. Health Expect. 2014 Jun;17(3):332-44.
Dr. Lamba is a psychiatrist and medical director at Bayridge Hospital in Lynn, Mass. Dr. Rana is assistant professor of pediatrics at Boston University.
A patient in Seattle reported drinking alcohol on only two occasions during the year: when it rains – and when it doesn’t.
Various benefits of humor have been studied as part of the treatment modality. Humor can be a powerful resource, but it remains a complex process, and its proper use in clinical practice requires careful consideration. Despite having demonstrated the ability to relieve stress in patients and among medical professionals,1 humor has not gained widespread acceptance.
Humor has been shown to help build relationships, and establish trust and support for favorable health outcomes. It increases patients’ satisfaction, decreases medical malpractice claims, and has the potential to reduce cultural differences and hierarchy between patients and health care practitioners.2 The Accreditation Council of Graduate Medical Education values interpersonal and communication skills as being among the core competencies to be imparted to physicians in training.
Currently, there is no standard methodology for using humor in practice, as each clinical setting and circumstance can vary widely. Whichever setting you find yourself in, however, you might 1-3
Explore the benefits of humor in your clinical practice
Consider humor an integral part of your professionalism. Initiate it where you have assessed it is appropriate.
Understand your audience
Assess your patients’ capability of understanding or appreciating your humor. Do not force it on patients. Be respectful of their perspectives and mindful of cultural differences.
Reciprocate humor
If patients take the humor route to lighten what might be a tense encounter, respond to their attempt and join them in bringing levity into the mix.
Use humor to support patients
Humor can take many forms. It can be subtle and does not always require a punchline. Patients may use it to express concerns or even fear. Health care providers can use it as support and to demonstrate caring, reflecting anxieties likely displayed or revealed by patients.
Avoid certain forms of humor
Avoid using self-disparaging or gallows humor. Humor between health care providers and patients should never be sarcastic, ethnic, or sexist.
Pay attention to how your patients use humor
Explore the possible meanings of your patients’ attempts at humor and what concerns they might be seeking to express. Use your findings to discuss deeper issues.
Incorporate humor into your teaching
Students, too, can benefit from the therapeutic potential of humor. Use humor to dispel or lessen your students’ fears or anxieties. It can help in the learning process and memory. Creating a cheery ambience can help lessen nervousness, ease coping, and reduce burnout.
References
1. South Med J. 2003 Dec;96(12):1257-61.
2. J Am Board Fam Med. 2018 Mar-Apr;31(2):270-8.
3. Health Expect. 2014 Jun;17(3):332-44.
Dr. Lamba is a psychiatrist and medical director at Bayridge Hospital in Lynn, Mass. Dr. Rana is assistant professor of pediatrics at Boston University.
2019 Legislative Goals: Implementation of VA Mission Act Top Priority
As nurses who are often the first face that a veteran sees, members of NOVA (Nurses Organization of Veterans Affairs) are committed to enhancing access, coordinating care, and improving health care at the US Department of Veterans Affairs (VA). NOVA also is the voice of VA nurses on Capitol Hill. Every year, the leadership and legislative committee members provide a list of critical issues identified in their Legislative Priority Goals. For 2019, the goals are divided into 3 areas of concern that either require legislation, funding, or implementation at the regulatory level within the VA.
At the top of the list is implementation of the VA Mission Act and its community care network. The 2018 VA Mission Act (Section 101 of Public Law 115-182) mandated the VA to consolidate existing community care programs and rewrite eligibility rules. Currently, the VA has at least 7 separate community care programs, including the Veterans Choice Program, which gives veterans who live ≥ 40 miles from a VA facility or have a wait time of ≥ 30 days an option to receive care in the local community with VA picking up the bill. Proposed access standards for the new program—Veterans Community Care Program (VCCP)—were made public in January 2019 and would allow veterans with ≥ 30-minute drive time and/or a wait time of ≥ 20 days for primary care or mental health appointments at a VA facility to use outside care. For specialty care eligibility, the drive time would increase to ≥ 60 minutes and ≥ 28 days for an appointment at a VA facility.
NOVA understands the need for community care partners: They are a crucial part of an integrated network designed to provide care for services that are not readily available within the Veterans Health Administration (VHA), but care that veterans receive in the community must be equal to VHA care. Equal care will require training and strict quality measures and standards verified for the VCCP providers. The VA also must remain the primary provider of care and the coordinator of care for all enrolled veterans.
NOVA identified 6 goals for VA Mission Act implementation. These include the following:
- Require that training, competency, and quality standards for VCCP providers are equal to those of VHA providers;
- Request third-party administrator to verify that providers meet those standards before assigning to VCCP panel;
- Simplify eligibility/access rules for community care without depleting VA funds;
- Ensure that VHA continues to be the first point of access and coordinator of all health care for enrolled veterans;
- Implement a care coordination system allowing veterans to return with ease to the VA when resources are available; and
- Employ mandatory training for VHA personnel and all community providers to improve the coordination of care, understanding of military culture, and health care needs across networks.
Other priorities include staffing/recruitment and retention—a longstanding issue within many VA facilities. Currently, the VHA has > 40,000 unfilled positions. It is no secret that the VA has had difficulty hiring essential staff at many levels. Complexities of job site databases and excessive time required to complete on-boarding, shortages in human resources personnel, and less than competitive salaries all add to the growing backlog. The inability for the VA to hire and train providers negatively impacts the access to VHA care and spurs increases in veterans using private sector care.
The VA modernization must include an electronic health record designed to support VHA’s model of health care delivery. It is crucial that Congress ensure proper IT funding to improve patient safety, software usability, and standardization of patient health care records across VHA.
VA nurses are the largest sector of employees within VHA with > 90,000 currently taking care of veterans. As VA continues its modernization, NOVA asks that nursing leadership be at the forefront of all strategic decision making.
In March, NOVA nurses shared their thoughts and views with members of Congress. They also continued discussions with the administration and VA leadership about how we can work together toward common goals—whether that be educating the next generation of nurses, providing innovative health care solutions, or engaging veterans in how they envision their health care in the future. Visit www.vanurse.org for more information about NOVA, the Legislative Priority Goals, or to become a member.
As nurses who are often the first face that a veteran sees, members of NOVA (Nurses Organization of Veterans Affairs) are committed to enhancing access, coordinating care, and improving health care at the US Department of Veterans Affairs (VA). NOVA also is the voice of VA nurses on Capitol Hill. Every year, the leadership and legislative committee members provide a list of critical issues identified in their Legislative Priority Goals. For 2019, the goals are divided into 3 areas of concern that either require legislation, funding, or implementation at the regulatory level within the VA.
At the top of the list is implementation of the VA Mission Act and its community care network. The 2018 VA Mission Act (Section 101 of Public Law 115-182) mandated the VA to consolidate existing community care programs and rewrite eligibility rules. Currently, the VA has at least 7 separate community care programs, including the Veterans Choice Program, which gives veterans who live ≥ 40 miles from a VA facility or have a wait time of ≥ 30 days an option to receive care in the local community with VA picking up the bill. Proposed access standards for the new program—Veterans Community Care Program (VCCP)—were made public in January 2019 and would allow veterans with ≥ 30-minute drive time and/or a wait time of ≥ 20 days for primary care or mental health appointments at a VA facility to use outside care. For specialty care eligibility, the drive time would increase to ≥ 60 minutes and ≥ 28 days for an appointment at a VA facility.
NOVA understands the need for community care partners: They are a crucial part of an integrated network designed to provide care for services that are not readily available within the Veterans Health Administration (VHA), but care that veterans receive in the community must be equal to VHA care. Equal care will require training and strict quality measures and standards verified for the VCCP providers. The VA also must remain the primary provider of care and the coordinator of care for all enrolled veterans.
NOVA identified 6 goals for VA Mission Act implementation. These include the following:
- Require that training, competency, and quality standards for VCCP providers are equal to those of VHA providers;
- Request third-party administrator to verify that providers meet those standards before assigning to VCCP panel;
- Simplify eligibility/access rules for community care without depleting VA funds;
- Ensure that VHA continues to be the first point of access and coordinator of all health care for enrolled veterans;
- Implement a care coordination system allowing veterans to return with ease to the VA when resources are available; and
- Employ mandatory training for VHA personnel and all community providers to improve the coordination of care, understanding of military culture, and health care needs across networks.
Other priorities include staffing/recruitment and retention—a longstanding issue within many VA facilities. Currently, the VHA has > 40,000 unfilled positions. It is no secret that the VA has had difficulty hiring essential staff at many levels. Complexities of job site databases and excessive time required to complete on-boarding, shortages in human resources personnel, and less than competitive salaries all add to the growing backlog. The inability for the VA to hire and train providers negatively impacts the access to VHA care and spurs increases in veterans using private sector care.
The VA modernization must include an electronic health record designed to support VHA’s model of health care delivery. It is crucial that Congress ensure proper IT funding to improve patient safety, software usability, and standardization of patient health care records across VHA.
VA nurses are the largest sector of employees within VHA with > 90,000 currently taking care of veterans. As VA continues its modernization, NOVA asks that nursing leadership be at the forefront of all strategic decision making.
In March, NOVA nurses shared their thoughts and views with members of Congress. They also continued discussions with the administration and VA leadership about how we can work together toward common goals—whether that be educating the next generation of nurses, providing innovative health care solutions, or engaging veterans in how they envision their health care in the future. Visit www.vanurse.org for more information about NOVA, the Legislative Priority Goals, or to become a member.
As nurses who are often the first face that a veteran sees, members of NOVA (Nurses Organization of Veterans Affairs) are committed to enhancing access, coordinating care, and improving health care at the US Department of Veterans Affairs (VA). NOVA also is the voice of VA nurses on Capitol Hill. Every year, the leadership and legislative committee members provide a list of critical issues identified in their Legislative Priority Goals. For 2019, the goals are divided into 3 areas of concern that either require legislation, funding, or implementation at the regulatory level within the VA.
At the top of the list is implementation of the VA Mission Act and its community care network. The 2018 VA Mission Act (Section 101 of Public Law 115-182) mandated the VA to consolidate existing community care programs and rewrite eligibility rules. Currently, the VA has at least 7 separate community care programs, including the Veterans Choice Program, which gives veterans who live ≥ 40 miles from a VA facility or have a wait time of ≥ 30 days an option to receive care in the local community with VA picking up the bill. Proposed access standards for the new program—Veterans Community Care Program (VCCP)—were made public in January 2019 and would allow veterans with ≥ 30-minute drive time and/or a wait time of ≥ 20 days for primary care or mental health appointments at a VA facility to use outside care. For specialty care eligibility, the drive time would increase to ≥ 60 minutes and ≥ 28 days for an appointment at a VA facility.
NOVA understands the need for community care partners: They are a crucial part of an integrated network designed to provide care for services that are not readily available within the Veterans Health Administration (VHA), but care that veterans receive in the community must be equal to VHA care. Equal care will require training and strict quality measures and standards verified for the VCCP providers. The VA also must remain the primary provider of care and the coordinator of care for all enrolled veterans.
NOVA identified 6 goals for VA Mission Act implementation. These include the following:
- Require that training, competency, and quality standards for VCCP providers are equal to those of VHA providers;
- Request third-party administrator to verify that providers meet those standards before assigning to VCCP panel;
- Simplify eligibility/access rules for community care without depleting VA funds;
- Ensure that VHA continues to be the first point of access and coordinator of all health care for enrolled veterans;
- Implement a care coordination system allowing veterans to return with ease to the VA when resources are available; and
- Employ mandatory training for VHA personnel and all community providers to improve the coordination of care, understanding of military culture, and health care needs across networks.
Other priorities include staffing/recruitment and retention—a longstanding issue within many VA facilities. Currently, the VHA has > 40,000 unfilled positions. It is no secret that the VA has had difficulty hiring essential staff at many levels. Complexities of job site databases and excessive time required to complete on-boarding, shortages in human resources personnel, and less than competitive salaries all add to the growing backlog. The inability for the VA to hire and train providers negatively impacts the access to VHA care and spurs increases in veterans using private sector care.
The VA modernization must include an electronic health record designed to support VHA’s model of health care delivery. It is crucial that Congress ensure proper IT funding to improve patient safety, software usability, and standardization of patient health care records across VHA.
VA nurses are the largest sector of employees within VHA with > 90,000 currently taking care of veterans. As VA continues its modernization, NOVA asks that nursing leadership be at the forefront of all strategic decision making.
In March, NOVA nurses shared their thoughts and views with members of Congress. They also continued discussions with the administration and VA leadership about how we can work together toward common goals—whether that be educating the next generation of nurses, providing innovative health care solutions, or engaging veterans in how they envision their health care in the future. Visit www.vanurse.org for more information about NOVA, the Legislative Priority Goals, or to become a member.