User login
For MD-IQ use only
Report card may foretell achalasia surgery outcomes
BALTIMORE – The Eckardt score has been established as a tool to evaluate outcomes of surgery for achalasia, but researchers have developed a report card that uses multiple variables that may provide a more accurate picture of surgical outcomes, according to results of study reported at the annual meeting of the Society of American Gastrointestinal Endoscopic Surgeons.
“The use of an accurate score to assess outcomes after achalasia surgery shows outstanding results,” said Ealaf Shemmeri, MD, of Swedish Medical Center in Seattle. “Using patient-reported symptoms, objective measures, and rates of reinterventions organized into a report card provides a more comprehensive and informative view.”
The Eckardt score evaluates four symptoms to evaluate outcomes of surgery to treat achalasia: weight loss, retrosternal pain, regurgitation, and dysphagia. “However, it does not address the other changes that can occur after myotomy, including the quality of swallowing and the onset of reflux disease,” she said. “Thus, there is a need for a more comprehensive assessment of quality after achalasia treatment.”
So the Swedish investigators set out to devise a report card that provides “a comprehensive and informative assessment” of surgical myotomy outcomes, she said. This involved a retrospective, single-center chart review of 185 patients who had surgical myotomy for primary achalasia from 2005 to 2017.
To determine patient-reported outcomes, the report card defines success as an Eckardt score below 3, Dakkak dysphagia score above 40, and GERD-HRQL (health-related quality of life) score below 10. The objective measures consisted of DeMeester (pH) score below 14.72, no column at 5 minutes on timed barium swallow, normalized integrated relaxation pressure less than 15 on manometry, and absence of esophagitis on endoscopy. For the third pillar of the report card, no reintervention was recorded as a success, Dr. Shemmeri said.
Regarding the etiology of achalasia in the study population, 42 had type 1, 109 had type 2, and 34 had type 3. A total of 71 patients had per oral endoscopic myotomy and 114 had Heller myotomy, 92 with Dor fundoplication and 20 with Toupet. Major perioperative complications included four per oral endoscopic myotomy patients who developed a leak requiring intervention. Six patients required return to the operating room for persistent dysphagia, Dr. Shemmeri said.
After the procedures, 93% of study patients reported an Eckardt score less than 3. However, only 45% have a Dakkak dysphagia score greater than 40 and 71% had a GERD-HRQL score less than 10, Dr. Shemmeri said. The objective measures told a similar story: Integrated relaxation pressure normalized in 80%, barium clearance was achieved in 61%, normal esophageal mucosa was recorded in 71%, “but pH testing was normal only 50% of the time,” Dr. Shemmeri said.
“The final success of not needing intervention is 79%,” she said. At this point in the study, 139 patients were available for follow-up. Among the 29 who needed reintervention, 19 had dilation below 20 mm Hg, 3 underwent pneumatic dilation, and 2 had botulinum toxin. Two patients required a redo myotomy, two had antireflux surgery, and one had an esophagectomy.
“When you only focus on a singular outcome, you can miss the whole story that occurs after myotomy,” Dr. Shemmeri said. “Providing a comprehensive tool gives you the ability to identify areas for improvement in your achalasia practice. Its simplicity allows it to be applied in various settings.” In the academic setting, it can be a tool for evaluating technologies and approaches for postmyotomy management. In hospitals and surgeons’ practices, it can aid in quality improvement, comparative outcomes research, and in evaluating operative approaches to myotomy.
The outcomes highlight the high prevalence of GERD, thus stressing the importance of pH testing after myotomy, Dr. Shemmeri said. Her study team recommends pH testing at 6-month follow-up because patients may not always self-report the extent of esophagitis present. Coauthor Brian Louie, MD, also of Swedish Medical Center, added during the discussion that ongoing follow-up of achalasia patients is necessary to address issues patients encounter with their swallowing over time.
Dr. Shemmeri had no relevant financial relationships to disclose. Dr. Louie reported relationships with Boston Scientific, ERBE, and Olympus.
SOURCE: Shemmeri E et al. SAGES 2019, Presentation S085.
BALTIMORE – The Eckardt score has been established as a tool to evaluate outcomes of surgery for achalasia, but researchers have developed a report card that uses multiple variables that may provide a more accurate picture of surgical outcomes, according to results of study reported at the annual meeting of the Society of American Gastrointestinal Endoscopic Surgeons.
“The use of an accurate score to assess outcomes after achalasia surgery shows outstanding results,” said Ealaf Shemmeri, MD, of Swedish Medical Center in Seattle. “Using patient-reported symptoms, objective measures, and rates of reinterventions organized into a report card provides a more comprehensive and informative view.”
The Eckardt score evaluates four symptoms to evaluate outcomes of surgery to treat achalasia: weight loss, retrosternal pain, regurgitation, and dysphagia. “However, it does not address the other changes that can occur after myotomy, including the quality of swallowing and the onset of reflux disease,” she said. “Thus, there is a need for a more comprehensive assessment of quality after achalasia treatment.”
So the Swedish investigators set out to devise a report card that provides “a comprehensive and informative assessment” of surgical myotomy outcomes, she said. This involved a retrospective, single-center chart review of 185 patients who had surgical myotomy for primary achalasia from 2005 to 2017.
To determine patient-reported outcomes, the report card defines success as an Eckardt score below 3, Dakkak dysphagia score above 40, and GERD-HRQL (health-related quality of life) score below 10. The objective measures consisted of DeMeester (pH) score below 14.72, no column at 5 minutes on timed barium swallow, normalized integrated relaxation pressure less than 15 on manometry, and absence of esophagitis on endoscopy. For the third pillar of the report card, no reintervention was recorded as a success, Dr. Shemmeri said.
Regarding the etiology of achalasia in the study population, 42 had type 1, 109 had type 2, and 34 had type 3. A total of 71 patients had per oral endoscopic myotomy and 114 had Heller myotomy, 92 with Dor fundoplication and 20 with Toupet. Major perioperative complications included four per oral endoscopic myotomy patients who developed a leak requiring intervention. Six patients required return to the operating room for persistent dysphagia, Dr. Shemmeri said.
After the procedures, 93% of study patients reported an Eckardt score less than 3. However, only 45% have a Dakkak dysphagia score greater than 40 and 71% had a GERD-HRQL score less than 10, Dr. Shemmeri said. The objective measures told a similar story: Integrated relaxation pressure normalized in 80%, barium clearance was achieved in 61%, normal esophageal mucosa was recorded in 71%, “but pH testing was normal only 50% of the time,” Dr. Shemmeri said.
“The final success of not needing intervention is 79%,” she said. At this point in the study, 139 patients were available for follow-up. Among the 29 who needed reintervention, 19 had dilation below 20 mm Hg, 3 underwent pneumatic dilation, and 2 had botulinum toxin. Two patients required a redo myotomy, two had antireflux surgery, and one had an esophagectomy.
“When you only focus on a singular outcome, you can miss the whole story that occurs after myotomy,” Dr. Shemmeri said. “Providing a comprehensive tool gives you the ability to identify areas for improvement in your achalasia practice. Its simplicity allows it to be applied in various settings.” In the academic setting, it can be a tool for evaluating technologies and approaches for postmyotomy management. In hospitals and surgeons’ practices, it can aid in quality improvement, comparative outcomes research, and in evaluating operative approaches to myotomy.
The outcomes highlight the high prevalence of GERD, thus stressing the importance of pH testing after myotomy, Dr. Shemmeri said. Her study team recommends pH testing at 6-month follow-up because patients may not always self-report the extent of esophagitis present. Coauthor Brian Louie, MD, also of Swedish Medical Center, added during the discussion that ongoing follow-up of achalasia patients is necessary to address issues patients encounter with their swallowing over time.
Dr. Shemmeri had no relevant financial relationships to disclose. Dr. Louie reported relationships with Boston Scientific, ERBE, and Olympus.
SOURCE: Shemmeri E et al. SAGES 2019, Presentation S085.
BALTIMORE – The Eckardt score has been established as a tool to evaluate outcomes of surgery for achalasia, but researchers have developed a report card that uses multiple variables that may provide a more accurate picture of surgical outcomes, according to results of study reported at the annual meeting of the Society of American Gastrointestinal Endoscopic Surgeons.
“The use of an accurate score to assess outcomes after achalasia surgery shows outstanding results,” said Ealaf Shemmeri, MD, of Swedish Medical Center in Seattle. “Using patient-reported symptoms, objective measures, and rates of reinterventions organized into a report card provides a more comprehensive and informative view.”
The Eckardt score evaluates four symptoms to evaluate outcomes of surgery to treat achalasia: weight loss, retrosternal pain, regurgitation, and dysphagia. “However, it does not address the other changes that can occur after myotomy, including the quality of swallowing and the onset of reflux disease,” she said. “Thus, there is a need for a more comprehensive assessment of quality after achalasia treatment.”
So the Swedish investigators set out to devise a report card that provides “a comprehensive and informative assessment” of surgical myotomy outcomes, she said. This involved a retrospective, single-center chart review of 185 patients who had surgical myotomy for primary achalasia from 2005 to 2017.
To determine patient-reported outcomes, the report card defines success as an Eckardt score below 3, Dakkak dysphagia score above 40, and GERD-HRQL (health-related quality of life) score below 10. The objective measures consisted of DeMeester (pH) score below 14.72, no column at 5 minutes on timed barium swallow, normalized integrated relaxation pressure less than 15 on manometry, and absence of esophagitis on endoscopy. For the third pillar of the report card, no reintervention was recorded as a success, Dr. Shemmeri said.
Regarding the etiology of achalasia in the study population, 42 had type 1, 109 had type 2, and 34 had type 3. A total of 71 patients had per oral endoscopic myotomy and 114 had Heller myotomy, 92 with Dor fundoplication and 20 with Toupet. Major perioperative complications included four per oral endoscopic myotomy patients who developed a leak requiring intervention. Six patients required return to the operating room for persistent dysphagia, Dr. Shemmeri said.
After the procedures, 93% of study patients reported an Eckardt score less than 3. However, only 45% have a Dakkak dysphagia score greater than 40 and 71% had a GERD-HRQL score less than 10, Dr. Shemmeri said. The objective measures told a similar story: Integrated relaxation pressure normalized in 80%, barium clearance was achieved in 61%, normal esophageal mucosa was recorded in 71%, “but pH testing was normal only 50% of the time,” Dr. Shemmeri said.
“The final success of not needing intervention is 79%,” she said. At this point in the study, 139 patients were available for follow-up. Among the 29 who needed reintervention, 19 had dilation below 20 mm Hg, 3 underwent pneumatic dilation, and 2 had botulinum toxin. Two patients required a redo myotomy, two had antireflux surgery, and one had an esophagectomy.
“When you only focus on a singular outcome, you can miss the whole story that occurs after myotomy,” Dr. Shemmeri said. “Providing a comprehensive tool gives you the ability to identify areas for improvement in your achalasia practice. Its simplicity allows it to be applied in various settings.” In the academic setting, it can be a tool for evaluating technologies and approaches for postmyotomy management. In hospitals and surgeons’ practices, it can aid in quality improvement, comparative outcomes research, and in evaluating operative approaches to myotomy.
The outcomes highlight the high prevalence of GERD, thus stressing the importance of pH testing after myotomy, Dr. Shemmeri said. Her study team recommends pH testing at 6-month follow-up because patients may not always self-report the extent of esophagitis present. Coauthor Brian Louie, MD, also of Swedish Medical Center, added during the discussion that ongoing follow-up of achalasia patients is necessary to address issues patients encounter with their swallowing over time.
Dr. Shemmeri had no relevant financial relationships to disclose. Dr. Louie reported relationships with Boston Scientific, ERBE, and Olympus.
SOURCE: Shemmeri E et al. SAGES 2019, Presentation S085.
REPORTING FROM SAGES 2019
Long-term antibiotic use may heighten stroke, CHD risk
, according to a study in the European Heart Journal.
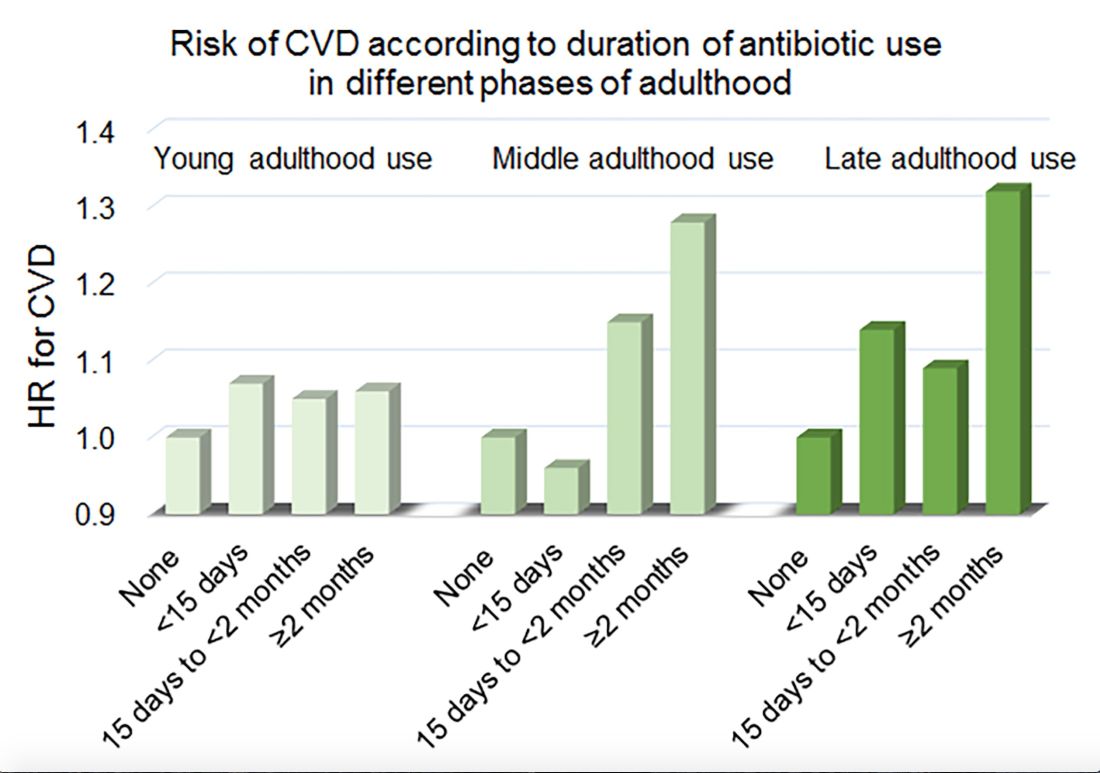
Women in the Nurses’ Health Study who used antibiotics for 2 or more months between ages 40 and 59 years or at age 60 years and older had a significantly increased risk of cardiovascular disease, compared with those who did not use antibiotics. Antibiotic use between 20 and 39 years old was not significantly related to cardiovascular disease.
Prior research has found that antibiotics may have long-lasting effects on gut microbiota and relate to cardiovascular disease risk.
“Antibiotic use is the most critical factor in altering the balance of microorganisms in the gut,” said lead investigator Lu Qi, MD, PhD, in a news release. “Previous studies have shown a link between alterations in the microbiotic environment of the gut and inflammation and narrowing of the blood vessels, stroke, and heart disease,” said Dr. Qi, who is the director of the Tulane University Obesity Research Center in New Orleans and an adjunct professor of nutrition at Harvard T.C. Chan School of Public Health in Boston.
To evaluate associations between life stage, antibiotic exposure, and subsequent cardiovascular disease, researchers analyzed data from 36,429 participants in the Nurses’ Health Study. The women were at least 60 years old and had no history of cardiovascular disease or cancer when they completed a 2004 questionnaire about antibiotic usage during young, middle, and late adulthood. The questionnaire asked participants to indicate the total time using antibiotics with eight categories ranging from none to 5 or more years.
The researchers defined incident cardiovascular disease as a composite endpoint of coronary heart disease (nonfatal myocardial infarction or fatal coronary heart disease) and stroke (nonfatal or fatal). They calculated person-years of follow-up from the questionnaire return date until date of cardiovascular disease diagnosis, death, or end of follow-up in 2012.
Women with longer duration of antibiotic use were more likely to use other medications and have unfavorable cardiovascular risk profiles, including family history of myocardial infarction and higher body mass index. Antibiotics most often were used to treat respiratory infections. During an average follow-up of 7.6 years, 1,056 participants developed cardiovascular disease.
In a multivariable model that adjusted for demographics, diet, lifestyle, reason for antibiotic use, medications, overweight status, and other factors, long-term antibiotic use – 2 months or more – in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Although antibiotic use was self-reported, which could lead to misclassification, the participants were health professionals, which may mitigate this limitation, the authors noted. Whether these findings apply to men and other populations requires further study, they said.
Because of the study’s observational design, the results “cannot show that antibiotics cause heart disease and stroke, only that there is a link between them,” Dr. Qi said. “It’s possible that women who reported more antibiotic use might be sicker in other ways that we were unable to measure, or there may be other factors that could affect the results that we have not been able take account of.”
“Our study suggests that antibiotics should be used only when they are absolutely needed,” he concluded. “Considering the potentially cumulative adverse effects, the shorter time of antibiotic use the better.”
The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
SOURCE: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
, according to a study in the European Heart Journal.
Women in the Nurses’ Health Study who used antibiotics for 2 or more months between ages 40 and 59 years or at age 60 years and older had a significantly increased risk of cardiovascular disease, compared with those who did not use antibiotics. Antibiotic use between 20 and 39 years old was not significantly related to cardiovascular disease.
Prior research has found that antibiotics may have long-lasting effects on gut microbiota and relate to cardiovascular disease risk.
“Antibiotic use is the most critical factor in altering the balance of microorganisms in the gut,” said lead investigator Lu Qi, MD, PhD, in a news release. “Previous studies have shown a link between alterations in the microbiotic environment of the gut and inflammation and narrowing of the blood vessels, stroke, and heart disease,” said Dr. Qi, who is the director of the Tulane University Obesity Research Center in New Orleans and an adjunct professor of nutrition at Harvard T.C. Chan School of Public Health in Boston.
To evaluate associations between life stage, antibiotic exposure, and subsequent cardiovascular disease, researchers analyzed data from 36,429 participants in the Nurses’ Health Study. The women were at least 60 years old and had no history of cardiovascular disease or cancer when they completed a 2004 questionnaire about antibiotic usage during young, middle, and late adulthood. The questionnaire asked participants to indicate the total time using antibiotics with eight categories ranging from none to 5 or more years.
The researchers defined incident cardiovascular disease as a composite endpoint of coronary heart disease (nonfatal myocardial infarction or fatal coronary heart disease) and stroke (nonfatal or fatal). They calculated person-years of follow-up from the questionnaire return date until date of cardiovascular disease diagnosis, death, or end of follow-up in 2012.
Women with longer duration of antibiotic use were more likely to use other medications and have unfavorable cardiovascular risk profiles, including family history of myocardial infarction and higher body mass index. Antibiotics most often were used to treat respiratory infections. During an average follow-up of 7.6 years, 1,056 participants developed cardiovascular disease.
In a multivariable model that adjusted for demographics, diet, lifestyle, reason for antibiotic use, medications, overweight status, and other factors, long-term antibiotic use – 2 months or more – in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Although antibiotic use was self-reported, which could lead to misclassification, the participants were health professionals, which may mitigate this limitation, the authors noted. Whether these findings apply to men and other populations requires further study, they said.
Because of the study’s observational design, the results “cannot show that antibiotics cause heart disease and stroke, only that there is a link between them,” Dr. Qi said. “It’s possible that women who reported more antibiotic use might be sicker in other ways that we were unable to measure, or there may be other factors that could affect the results that we have not been able take account of.”
“Our study suggests that antibiotics should be used only when they are absolutely needed,” he concluded. “Considering the potentially cumulative adverse effects, the shorter time of antibiotic use the better.”
The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
SOURCE: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
, according to a study in the European Heart Journal.
Women in the Nurses’ Health Study who used antibiotics for 2 or more months between ages 40 and 59 years or at age 60 years and older had a significantly increased risk of cardiovascular disease, compared with those who did not use antibiotics. Antibiotic use between 20 and 39 years old was not significantly related to cardiovascular disease.
Prior research has found that antibiotics may have long-lasting effects on gut microbiota and relate to cardiovascular disease risk.
“Antibiotic use is the most critical factor in altering the balance of microorganisms in the gut,” said lead investigator Lu Qi, MD, PhD, in a news release. “Previous studies have shown a link between alterations in the microbiotic environment of the gut and inflammation and narrowing of the blood vessels, stroke, and heart disease,” said Dr. Qi, who is the director of the Tulane University Obesity Research Center in New Orleans and an adjunct professor of nutrition at Harvard T.C. Chan School of Public Health in Boston.
To evaluate associations between life stage, antibiotic exposure, and subsequent cardiovascular disease, researchers analyzed data from 36,429 participants in the Nurses’ Health Study. The women were at least 60 years old and had no history of cardiovascular disease or cancer when they completed a 2004 questionnaire about antibiotic usage during young, middle, and late adulthood. The questionnaire asked participants to indicate the total time using antibiotics with eight categories ranging from none to 5 or more years.
The researchers defined incident cardiovascular disease as a composite endpoint of coronary heart disease (nonfatal myocardial infarction or fatal coronary heart disease) and stroke (nonfatal or fatal). They calculated person-years of follow-up from the questionnaire return date until date of cardiovascular disease diagnosis, death, or end of follow-up in 2012.
Women with longer duration of antibiotic use were more likely to use other medications and have unfavorable cardiovascular risk profiles, including family history of myocardial infarction and higher body mass index. Antibiotics most often were used to treat respiratory infections. During an average follow-up of 7.6 years, 1,056 participants developed cardiovascular disease.
In a multivariable model that adjusted for demographics, diet, lifestyle, reason for antibiotic use, medications, overweight status, and other factors, long-term antibiotic use – 2 months or more – in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Although antibiotic use was self-reported, which could lead to misclassification, the participants were health professionals, which may mitigate this limitation, the authors noted. Whether these findings apply to men and other populations requires further study, they said.
Because of the study’s observational design, the results “cannot show that antibiotics cause heart disease and stroke, only that there is a link between them,” Dr. Qi said. “It’s possible that women who reported more antibiotic use might be sicker in other ways that we were unable to measure, or there may be other factors that could affect the results that we have not been able take account of.”
“Our study suggests that antibiotics should be used only when they are absolutely needed,” he concluded. “Considering the potentially cumulative adverse effects, the shorter time of antibiotic use the better.”
The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
SOURCE: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
FROM THE EUROPEAN HEART JOURNAL
Key clinical point: Among middle-aged and older women, 2 or more months’ exposure to antibiotics is associated with an increased risk of coronary heart disease or stroke.
Major finding: Long-term antibiotic use in late adulthood was associated with significantly increased risk of cardiovascular disease (hazard ratio, 1.32), as was long-term antibiotic use in middle adulthood (HR, 1.28).
Study details: An analysis of data from nearly 36,500 women in the Nurses’ Health Study.
Disclosures: The study was supported by National Institutes of Health grants, the Boston Obesity Nutrition Research Center, and the United States–Israel Binational Science Foundation. One author received support from the Japan Society for the Promotion of Science. The authors had no conflicts of interest.
Source: Heianza Y et al. Eur Heart J. 2019 Apr 24. doi: 10.1093/eurheartj/ehz231.
Perceived Physical Functioning Predicts Mortality
Researchers from Erasmus University, The Netherlands, and Monash University, Australia, say theirs is the first study to determine the independent association of various measures of subjective health with mortality. Previously, few studies had showed an effect of physical functioning independent of other subjective measures.
The researchers evaluated data on 5,538 adults who took part in the Rotterdam Study and who were followed for a mean of 12 years. One-third had cardiovascular disease; 8% had chronic obstructive pulmonary disease, and 38% had joint problems.
The researchers investigated 6 different measures of subjective health and how they related to all-cause mortality. They conceptualized subjective health—often associated with health and well-being—as a continuum with physical functioning at one end and mental health at the other. Physical functioning included basic activities of daily living (BADL), such as eating and grooming. Instrumental activities of daily living (IADL) included the cognitive attributes of performing self-reliant daily tasks, such as meal preparation and shopping. The researchers assessed mental health with scales measuring positive and negative effects as well as somatic symptoms (the physical manifestations of dysthymia) and quality of life.
“Importantly,” the researchers say, any of those indicators is affected strongly by both physical and mental aspects of health. For example, physical and functional decline are related to higher scores on dysthymia questionnaires.
During 48,534 person-years of follow-up, 2,021 people died. Only impairment in physical functioning assessed by either self-report of BADL or IADL was related to mortality. Quality of life, positive affect, somatic symptoms, and negative affect did not predict mortality once self-rated physical functioning was accounted for.
Clinically speaking, the researchers say, it might be good to focus interventions aimed at improving survival on subjective indicators of physical well-being: in other words, activities of daily living and what it takes to perform them.
Researchers from Erasmus University, The Netherlands, and Monash University, Australia, say theirs is the first study to determine the independent association of various measures of subjective health with mortality. Previously, few studies had showed an effect of physical functioning independent of other subjective measures.
The researchers evaluated data on 5,538 adults who took part in the Rotterdam Study and who were followed for a mean of 12 years. One-third had cardiovascular disease; 8% had chronic obstructive pulmonary disease, and 38% had joint problems.
The researchers investigated 6 different measures of subjective health and how they related to all-cause mortality. They conceptualized subjective health—often associated with health and well-being—as a continuum with physical functioning at one end and mental health at the other. Physical functioning included basic activities of daily living (BADL), such as eating and grooming. Instrumental activities of daily living (IADL) included the cognitive attributes of performing self-reliant daily tasks, such as meal preparation and shopping. The researchers assessed mental health with scales measuring positive and negative effects as well as somatic symptoms (the physical manifestations of dysthymia) and quality of life.
“Importantly,” the researchers say, any of those indicators is affected strongly by both physical and mental aspects of health. For example, physical and functional decline are related to higher scores on dysthymia questionnaires.
During 48,534 person-years of follow-up, 2,021 people died. Only impairment in physical functioning assessed by either self-report of BADL or IADL was related to mortality. Quality of life, positive affect, somatic symptoms, and negative affect did not predict mortality once self-rated physical functioning was accounted for.
Clinically speaking, the researchers say, it might be good to focus interventions aimed at improving survival on subjective indicators of physical well-being: in other words, activities of daily living and what it takes to perform them.
Researchers from Erasmus University, The Netherlands, and Monash University, Australia, say theirs is the first study to determine the independent association of various measures of subjective health with mortality. Previously, few studies had showed an effect of physical functioning independent of other subjective measures.
The researchers evaluated data on 5,538 adults who took part in the Rotterdam Study and who were followed for a mean of 12 years. One-third had cardiovascular disease; 8% had chronic obstructive pulmonary disease, and 38% had joint problems.
The researchers investigated 6 different measures of subjective health and how they related to all-cause mortality. They conceptualized subjective health—often associated with health and well-being—as a continuum with physical functioning at one end and mental health at the other. Physical functioning included basic activities of daily living (BADL), such as eating and grooming. Instrumental activities of daily living (IADL) included the cognitive attributes of performing self-reliant daily tasks, such as meal preparation and shopping. The researchers assessed mental health with scales measuring positive and negative effects as well as somatic symptoms (the physical manifestations of dysthymia) and quality of life.
“Importantly,” the researchers say, any of those indicators is affected strongly by both physical and mental aspects of health. For example, physical and functional decline are related to higher scores on dysthymia questionnaires.
During 48,534 person-years of follow-up, 2,021 people died. Only impairment in physical functioning assessed by either self-report of BADL or IADL was related to mortality. Quality of life, positive affect, somatic symptoms, and negative affect did not predict mortality once self-rated physical functioning was accounted for.
Clinically speaking, the researchers say, it might be good to focus interventions aimed at improving survival on subjective indicators of physical well-being: in other words, activities of daily living and what it takes to perform them.
Best of RIV highlights practical, innovative projects
Delirium, alcohol detox, and med rec
A project to improve how hospitalists address inpatient delirium, which has led to reductions in length of stay and cost, took center stage in the Best of RIV plenary session at HM19 in March.

The project, conducted at the University of California, San Francisco (UCSF), was presented alongside projects on alcohol detox at the Cleveland Veterans Affairs Medical Center and on medication reconciliation at Brigham and Women’s Hospital in Boston.
“The plenary is the top three of the 1,000 that are out there – so, impressive work,” said Benji Mathews, MD, SFHM, the chair of the Research, Innovations and Vignettes competition.
At UCSF, the project was meant to tackle the huge problem of delirium in the hospital, said Catherine Lau, MD, SFHM, associate professor of medicine there. Each year delirium affects more than 7 million people who are hospitalized, and hospital-acquired delirium is linked with prolonged stays and more emergency department visits and hospital readmissions. But research has found that as many as a third of these hospital-acquired cases can be prevented, Dr. Lau said.
New admissions and transfers – a total of more than 2,800 patients – were assessed for delirium risk, and those deemed high risk were entered into a delirium care plan, aimed at prevention with nonpharmacologic steps such as maximizing their mobility and helping them sleep at night.
All patients also were screened on every nursing shift for delirium, and those diagnosed with the disorder were placed in the delirium care plan, with notification of the patient’s team for treatment.
The average length of stay decreased by 0.8 days (P less than .001), with a decrease of 1.9 days in patients with delirium, compared with outcomes for nearly 2,600 patients before the intervention was implemented, Dr. Lau said. Researchers also found a decrease in $850 spent per patient (P less than .001), with a direct savings to the hospital of a total of $997,000, she said. The 30-day readmission rate also fell significantly, from 18.9% to 15.9% (P = .03).
The screening itself seemed to be the most important factor in the project, Dr. Lau said.
“Just the recognition that their patient was at risk for delirium or actually had delirium really raised awareness,” she said.

The project on alcohol detox used careful risk assessments at emergency department discharge, e-consults, protocols to limit benzodiazepine prescribing, and telephone follow-up to reduce hospital admissions and 30-day readmissions, as well as length of stay.
Researchers used scores on CIWA – a 10-question measurement of the severity of someone’s alcohol withdrawal – and history of complicated alcohol-use withdrawal to determine whether ED patients should be admitted to the floor or sent home with or without prescriptions for gabapentin and lorazepam, said Robert Patrick, MD, a hospitalist at the Cleveland VA.
Perhaps the most innovative feature of the program was using systolic blood pressure and heart rate in addition to CIWA to determine whether someone should receive a benzodiazepine, he said. Someone with a CIWA of 9-12, for instance, would be prescribed one of these drugs only if their vitals were elevated, Dr. Patrick said.
He encouraged other hospitalists to try a similar program at their centers.
“You don’t have to be at a VA to do this,” he said. “And most importantly, you don’t have to have a cooperative ED to do this. You can do this just within your hospitalist group.”
In another presentation, Jeffrey Schnipper MD, MPH, FHM, associate professor of medicine at Harvard Medical School, Boston, described the results from a project in which SHM’s MARQUIS program – an evidence-based “toolkit” on medication reconciliation – was implemented at 18 hospitals. The kit offers a plan to get the best possible medication history, give medication counseling on discharge, and identify patients at risk for medication discrepancies. The 18 sites were coached, with areas of improvement identified.
By months 13-18 of the study period, the number of medication discrepancies had fallen to 0.93 per patient for those who’d received at least one form of intervention, compared with 2.69 per patient among those who’d received none.
“The MARQUIS interventions, including the toolkit and mentored implementation,” Dr. Schnipper said, “are associated with a marked reduction in medication discrepancies.”
Delirium, alcohol detox, and med rec
Delirium, alcohol detox, and med rec
A project to improve how hospitalists address inpatient delirium, which has led to reductions in length of stay and cost, took center stage in the Best of RIV plenary session at HM19 in March.
The project, conducted at the University of California, San Francisco (UCSF), was presented alongside projects on alcohol detox at the Cleveland Veterans Affairs Medical Center and on medication reconciliation at Brigham and Women’s Hospital in Boston.
“The plenary is the top three of the 1,000 that are out there – so, impressive work,” said Benji Mathews, MD, SFHM, the chair of the Research, Innovations and Vignettes competition.
At UCSF, the project was meant to tackle the huge problem of delirium in the hospital, said Catherine Lau, MD, SFHM, associate professor of medicine there. Each year delirium affects more than 7 million people who are hospitalized, and hospital-acquired delirium is linked with prolonged stays and more emergency department visits and hospital readmissions. But research has found that as many as a third of these hospital-acquired cases can be prevented, Dr. Lau said.
New admissions and transfers – a total of more than 2,800 patients – were assessed for delirium risk, and those deemed high risk were entered into a delirium care plan, aimed at prevention with nonpharmacologic steps such as maximizing their mobility and helping them sleep at night.
All patients also were screened on every nursing shift for delirium, and those diagnosed with the disorder were placed in the delirium care plan, with notification of the patient’s team for treatment.
The average length of stay decreased by 0.8 days (P less than .001), with a decrease of 1.9 days in patients with delirium, compared with outcomes for nearly 2,600 patients before the intervention was implemented, Dr. Lau said. Researchers also found a decrease in $850 spent per patient (P less than .001), with a direct savings to the hospital of a total of $997,000, she said. The 30-day readmission rate also fell significantly, from 18.9% to 15.9% (P = .03).
The screening itself seemed to be the most important factor in the project, Dr. Lau said.
“Just the recognition that their patient was at risk for delirium or actually had delirium really raised awareness,” she said.
The project on alcohol detox used careful risk assessments at emergency department discharge, e-consults, protocols to limit benzodiazepine prescribing, and telephone follow-up to reduce hospital admissions and 30-day readmissions, as well as length of stay.
Researchers used scores on CIWA – a 10-question measurement of the severity of someone’s alcohol withdrawal – and history of complicated alcohol-use withdrawal to determine whether ED patients should be admitted to the floor or sent home with or without prescriptions for gabapentin and lorazepam, said Robert Patrick, MD, a hospitalist at the Cleveland VA.
Perhaps the most innovative feature of the program was using systolic blood pressure and heart rate in addition to CIWA to determine whether someone should receive a benzodiazepine, he said. Someone with a CIWA of 9-12, for instance, would be prescribed one of these drugs only if their vitals were elevated, Dr. Patrick said.
He encouraged other hospitalists to try a similar program at their centers.
“You don’t have to be at a VA to do this,” he said. “And most importantly, you don’t have to have a cooperative ED to do this. You can do this just within your hospitalist group.”
In another presentation, Jeffrey Schnipper MD, MPH, FHM, associate professor of medicine at Harvard Medical School, Boston, described the results from a project in which SHM’s MARQUIS program – an evidence-based “toolkit” on medication reconciliation – was implemented at 18 hospitals. The kit offers a plan to get the best possible medication history, give medication counseling on discharge, and identify patients at risk for medication discrepancies. The 18 sites were coached, with areas of improvement identified.
By months 13-18 of the study period, the number of medication discrepancies had fallen to 0.93 per patient for those who’d received at least one form of intervention, compared with 2.69 per patient among those who’d received none.
“The MARQUIS interventions, including the toolkit and mentored implementation,” Dr. Schnipper said, “are associated with a marked reduction in medication discrepancies.”
A project to improve how hospitalists address inpatient delirium, which has led to reductions in length of stay and cost, took center stage in the Best of RIV plenary session at HM19 in March.
The project, conducted at the University of California, San Francisco (UCSF), was presented alongside projects on alcohol detox at the Cleveland Veterans Affairs Medical Center and on medication reconciliation at Brigham and Women’s Hospital in Boston.
“The plenary is the top three of the 1,000 that are out there – so, impressive work,” said Benji Mathews, MD, SFHM, the chair of the Research, Innovations and Vignettes competition.
At UCSF, the project was meant to tackle the huge problem of delirium in the hospital, said Catherine Lau, MD, SFHM, associate professor of medicine there. Each year delirium affects more than 7 million people who are hospitalized, and hospital-acquired delirium is linked with prolonged stays and more emergency department visits and hospital readmissions. But research has found that as many as a third of these hospital-acquired cases can be prevented, Dr. Lau said.
New admissions and transfers – a total of more than 2,800 patients – were assessed for delirium risk, and those deemed high risk were entered into a delirium care plan, aimed at prevention with nonpharmacologic steps such as maximizing their mobility and helping them sleep at night.
All patients also were screened on every nursing shift for delirium, and those diagnosed with the disorder were placed in the delirium care plan, with notification of the patient’s team for treatment.
The average length of stay decreased by 0.8 days (P less than .001), with a decrease of 1.9 days in patients with delirium, compared with outcomes for nearly 2,600 patients before the intervention was implemented, Dr. Lau said. Researchers also found a decrease in $850 spent per patient (P less than .001), with a direct savings to the hospital of a total of $997,000, she said. The 30-day readmission rate also fell significantly, from 18.9% to 15.9% (P = .03).
The screening itself seemed to be the most important factor in the project, Dr. Lau said.
“Just the recognition that their patient was at risk for delirium or actually had delirium really raised awareness,” she said.
The project on alcohol detox used careful risk assessments at emergency department discharge, e-consults, protocols to limit benzodiazepine prescribing, and telephone follow-up to reduce hospital admissions and 30-day readmissions, as well as length of stay.
Researchers used scores on CIWA – a 10-question measurement of the severity of someone’s alcohol withdrawal – and history of complicated alcohol-use withdrawal to determine whether ED patients should be admitted to the floor or sent home with or without prescriptions for gabapentin and lorazepam, said Robert Patrick, MD, a hospitalist at the Cleveland VA.
Perhaps the most innovative feature of the program was using systolic blood pressure and heart rate in addition to CIWA to determine whether someone should receive a benzodiazepine, he said. Someone with a CIWA of 9-12, for instance, would be prescribed one of these drugs only if their vitals were elevated, Dr. Patrick said.
He encouraged other hospitalists to try a similar program at their centers.
“You don’t have to be at a VA to do this,” he said. “And most importantly, you don’t have to have a cooperative ED to do this. You can do this just within your hospitalist group.”
In another presentation, Jeffrey Schnipper MD, MPH, FHM, associate professor of medicine at Harvard Medical School, Boston, described the results from a project in which SHM’s MARQUIS program – an evidence-based “toolkit” on medication reconciliation – was implemented at 18 hospitals. The kit offers a plan to get the best possible medication history, give medication counseling on discharge, and identify patients at risk for medication discrepancies. The 18 sites were coached, with areas of improvement identified.
By months 13-18 of the study period, the number of medication discrepancies had fallen to 0.93 per patient for those who’d received at least one form of intervention, compared with 2.69 per patient among those who’d received none.
“The MARQUIS interventions, including the toolkit and mentored implementation,” Dr. Schnipper said, “are associated with a marked reduction in medication discrepancies.”
Top 10 things physician advisors want hospitalists to know
The practice of hospital medicine is rapidly changing. Higher-acuity patients are being admitted to hospitals already struggling with capacity, and hospitalists are being instructed to pay attention to length of stay, improve their documentation and billing, and participate in initiatives to improve hospital throughput, all while delivering high-quality patient care.

As hospitalists and SHM members who are also physician advisors, we have a unique understanding of these pressures. In this article, we answer common questions we receive from hospitalists regarding utilization management, care coordination, clinical documentation, and CMS regulations.
Why do physician advisors exist, and what do they do?
A physician advisor is hired by the hospital to act as a liaison between the hospital administration, clinical staff, and support personnel in order to ensure regulatory compliance, advise physicians on medical necessity, and assist hospital leadership in meeting overall organizational goals related to the efficient utilization of health care services.1
Given their deep knowledge of hospital systems and processes, and ability to collaborate and teach, hospitalists are well-positioned to serve in this capacity. Our primary goal as physician advisors is to help physicians continue to focus on the parts of medicine they enjoy – clinical care, education, quality improvement, research etc. – by helping to demystify complex regulatory requirements and by creating streamlined processes to make following these requirements easier.
Why does this matter?
We understand that regulatory and hospital systems issues such as patient class determination, appropriate clinical documentation, and hospital throughput and capacity management can feel tedious, and sometimes overwhelming, to busy hospitalists. While it is easy to attribute these problems solely to hospitals’ desire for increased revenue, these issues directly impact the quality of care we provide to their patients.

In addition, our entire financial system is predicated on appropriate health care resource utilization, financial reimbursement, demonstration of medical acuity, and our impact on the care of a patient. Thus, our ability to advocate for our patients and for ourselves is directly connected with this endeavor. Developing a working knowledge of regulatory and systems issues allows hospitalists to be more engaged in leadership and negotiations and allows us to advocate for resources we deem most important.
Why are clinical documentation integrity teams so important?
Accurately and specifically describing how sick your patients are helps ensure that hospitals are reimbursed appropriately, coded data is accurate for research purposes, quality metrics are attributed correctly, and patients receive the correct diagnoses.
Clarification of documentation and/or addressing “clinical validity” of a given diagnosis (e.g., acute hypoxic respiratory failure requires both hypoxia and respiratory distress) may support an increase or result in a decrease in hospital reimbursement. For example, if the reason for a patient’s admission is renal failure, renal failure with true acute hypoxic respiratory failure will be reimbursed at a rate 40% higher than renal failure without the documentation of other conditions that reflect how ill the patient really is. The patient with acute hypoxic respiratory failure (or other major comorbid condition) is genuinely sicker, thus requiring more time (length of stay) and resources (deserved higher reimbursement).
What is the two-midnight rule, and why does it matter?
In October of 2013, the Centers for Medicare & Medicaid Services initiated the two-midnight rule, which states a Medicare patient can be an “inpatient” class if the admitting provider determines that 1) the patient requires medically necessary care which cannot be provided outside the hospital and 2) the patient is expected to stay at least 2 midnights in the hospital.
If, at the time of admission, an admitting provider thinks it is likely that the patient may be discharged prior to 2 midnights, then outpatient care with “observation” designation is appropriate. Incorrect patient class assignment may result in significant adverse consequences for hospitals, including improper patient billing, decreased hospital reimbursement, substantial risk for external auditing, violation of Medicare conditions of participation, and even loss of accreditation.
Who can I talk to if I have a question about a patient’s class? What should I do if I disagree with the class assigned to my patient?
The Utilization Management team typically consists of nurses and physician advisors specifically trained in UM. This team functions as a liaison between providers and payers (particularly Medicare and Medicaid) regarding medical necessity, appropriateness of care received, and efficiency of health care services.
When it comes to discussions about patient class, start by learning more about why the determination was made. The most common reason for patient class disagreements is simply that the documentation does not reflect the severity of illness or accurately reflect the care the patient is receiving. Your documentation should communicate that your patient needs services that only the hospital can provide, and/or they need monitoring that must be done in the hospital to meet the medical necessity criteria that CMS requires for a patient to be “inpatient” class.
If you disagree with a determination provided by the UM nurse and/or physician advisor, then the case will be presented to the hospital UM committee for further review. Two physicians from the UM committee must review the case and provide their own determinations of patient status, and whichever admission determination has two votes is the one that is appropriate.
How do I talk to patients about class determinations?
As media coverage continues about the two-midnight rule and the impact this has on patients, providers should expect more questions about class determination from their patients.
An AARP Bulletin article from 2012 advised patients to “ask [their] own doctor whether observation status is justified … and if not ask him or her to call the hospital to explain the medical reasons why they should be admitted as inpatient.”2 Patients should be informed that providers understand the implications of patient class determinations and are making these decisions as outlined by CMS.
We recommend informing patients that the decision about whether a patient is “inpatient” or “outpatient with observation” class is complex and involves taking into consideration a patient’s medical history, the severity of their current medical condition, need for diagnostic testing, and degree of health resource utilization, as well as a provider’s medical opinion of the risk of an adverse event occurring.
Is it true that observation patients receive higher hospital bills?
It is a common misperception that a designation of “observation” class means that a patient’s medical bill will be higher than “inpatient” class. In 2016, CMS changed the way observation class patients are billed so that, in most scenarios, patients do not receive a higher hospital bill when placed in “observation” class.
How do I approach a denial from a payer?
Commercial payers review all hospitalizations for medical necessity and appropriateness of care received during a patient’s hospitalization. If you receive notice that all or part of your patient’s hospital stay was denied coverage, you have the option of discussing the case with the medical director of the insurance company – this is called a peer-to-peer discussion.

We recommend reviewing the patient’s case and your documentation of the care you provided prior to the peer to peer, especially since these denials may come weeks to months after you have cared for the patient. Begin your conversation by learning why the insurance company denied coverage of the stay and then provide an accurate portrayal of the acuity of illness of the patient, and the resources your hospital used in caring for them. Consider consulting with your hospital’s physician advisor for other high-yield tips.
How can care management help with ‘nonmedical’ hospitalizations?
Care managers are your allies for all patients, especially those with complex discharge needs. Often patients admitted for “nonmedical” reasons do not have the ability to discharge to a skilled nursing facility, long-term care facility, or home due to lack of insurance coverage or resources and/or assistance. Care managers can help you creatively problem solve and coordinate care. Physician advisors are your allies in helping create system-level interventions that might avert some of these “nonmedical” admissions. Consider involving both care managers and physician advisors early in the admission to help navigate social complexities.
How can hospitalists get involved?
According to CMS, the decision on “whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital … can typically be made in less than 48 hours, usually in less than 24 hours.”3 In reality, this is not black and white. The “2 midnights” has brought a host of new challenges for hospitals, hospitalists, and patients to navigate. The Society of Hospital Medicine released an Observation White Paper in 2017 challenging the status quo and proposing comprehensive observation reform.4
We encourage hospital medicine providers to more routinely engage with their institutional physician advisors and consider joining the SHM Public Policy Committee to become more involved in advocacy, and/or consider becoming a physician advisor.
Dr. Singh is physician advisor for Utilization & CM in the division of hospital medicine at the University of Colorado at Denver, Aurora. Dr. Patel is a hospitalist and assistant professor of medicine at the university. Dr. Anoff is director of clinical operations and director of nights for the Hospital Medicine Group at the University of Colorado at Denver. Dr. Stella is a hospitalist at Denver Health and Hospital Authority and an associate professor of medicine at the university.
References
1. What is a physician advisor? 2017 Oct 9.
2. Barry P. Medicare: Inpatient or outpatient. AARP Bulletin. 2012 Oct.
3. Goldberg TH. The long-term and post-acute care continuum. WV Med J. 2014 Nov-Dec;10(6):24-30.
4. Society of Hospital Medicine Public Policy Committee. The hospital observation care problem. Perspectives and solutions from the Society of Hospital Medicine. 2017 Sep.
The practice of hospital medicine is rapidly changing. Higher-acuity patients are being admitted to hospitals already struggling with capacity, and hospitalists are being instructed to pay attention to length of stay, improve their documentation and billing, and participate in initiatives to improve hospital throughput, all while delivering high-quality patient care.
As hospitalists and SHM members who are also physician advisors, we have a unique understanding of these pressures. In this article, we answer common questions we receive from hospitalists regarding utilization management, care coordination, clinical documentation, and CMS regulations.
Why do physician advisors exist, and what do they do?
A physician advisor is hired by the hospital to act as a liaison between the hospital administration, clinical staff, and support personnel in order to ensure regulatory compliance, advise physicians on medical necessity, and assist hospital leadership in meeting overall organizational goals related to the efficient utilization of health care services.1
Given their deep knowledge of hospital systems and processes, and ability to collaborate and teach, hospitalists are well-positioned to serve in this capacity. Our primary goal as physician advisors is to help physicians continue to focus on the parts of medicine they enjoy – clinical care, education, quality improvement, research etc. – by helping to demystify complex regulatory requirements and by creating streamlined processes to make following these requirements easier.
Why does this matter?
We understand that regulatory and hospital systems issues such as patient class determination, appropriate clinical documentation, and hospital throughput and capacity management can feel tedious, and sometimes overwhelming, to busy hospitalists. While it is easy to attribute these problems solely to hospitals’ desire for increased revenue, these issues directly impact the quality of care we provide to their patients.
In addition, our entire financial system is predicated on appropriate health care resource utilization, financial reimbursement, demonstration of medical acuity, and our impact on the care of a patient. Thus, our ability to advocate for our patients and for ourselves is directly connected with this endeavor. Developing a working knowledge of regulatory and systems issues allows hospitalists to be more engaged in leadership and negotiations and allows us to advocate for resources we deem most important.
Why are clinical documentation integrity teams so important?
Accurately and specifically describing how sick your patients are helps ensure that hospitals are reimbursed appropriately, coded data is accurate for research purposes, quality metrics are attributed correctly, and patients receive the correct diagnoses.
Clarification of documentation and/or addressing “clinical validity” of a given diagnosis (e.g., acute hypoxic respiratory failure requires both hypoxia and respiratory distress) may support an increase or result in a decrease in hospital reimbursement. For example, if the reason for a patient’s admission is renal failure, renal failure with true acute hypoxic respiratory failure will be reimbursed at a rate 40% higher than renal failure without the documentation of other conditions that reflect how ill the patient really is. The patient with acute hypoxic respiratory failure (or other major comorbid condition) is genuinely sicker, thus requiring more time (length of stay) and resources (deserved higher reimbursement).
What is the two-midnight rule, and why does it matter?
In October of 2013, the Centers for Medicare & Medicaid Services initiated the two-midnight rule, which states a Medicare patient can be an “inpatient” class if the admitting provider determines that 1) the patient requires medically necessary care which cannot be provided outside the hospital and 2) the patient is expected to stay at least 2 midnights in the hospital.
If, at the time of admission, an admitting provider thinks it is likely that the patient may be discharged prior to 2 midnights, then outpatient care with “observation” designation is appropriate. Incorrect patient class assignment may result in significant adverse consequences for hospitals, including improper patient billing, decreased hospital reimbursement, substantial risk for external auditing, violation of Medicare conditions of participation, and even loss of accreditation.
Who can I talk to if I have a question about a patient’s class? What should I do if I disagree with the class assigned to my patient?
The Utilization Management team typically consists of nurses and physician advisors specifically trained in UM. This team functions as a liaison between providers and payers (particularly Medicare and Medicaid) regarding medical necessity, appropriateness of care received, and efficiency of health care services.
When it comes to discussions about patient class, start by learning more about why the determination was made. The most common reason for patient class disagreements is simply that the documentation does not reflect the severity of illness or accurately reflect the care the patient is receiving. Your documentation should communicate that your patient needs services that only the hospital can provide, and/or they need monitoring that must be done in the hospital to meet the medical necessity criteria that CMS requires for a patient to be “inpatient” class.
If you disagree with a determination provided by the UM nurse and/or physician advisor, then the case will be presented to the hospital UM committee for further review. Two physicians from the UM committee must review the case and provide their own determinations of patient status, and whichever admission determination has two votes is the one that is appropriate.
How do I talk to patients about class determinations?
As media coverage continues about the two-midnight rule and the impact this has on patients, providers should expect more questions about class determination from their patients.
An AARP Bulletin article from 2012 advised patients to “ask [their] own doctor whether observation status is justified … and if not ask him or her to call the hospital to explain the medical reasons why they should be admitted as inpatient.”2 Patients should be informed that providers understand the implications of patient class determinations and are making these decisions as outlined by CMS.
We recommend informing patients that the decision about whether a patient is “inpatient” or “outpatient with observation” class is complex and involves taking into consideration a patient’s medical history, the severity of their current medical condition, need for diagnostic testing, and degree of health resource utilization, as well as a provider’s medical opinion of the risk of an adverse event occurring.
Is it true that observation patients receive higher hospital bills?
It is a common misperception that a designation of “observation” class means that a patient’s medical bill will be higher than “inpatient” class. In 2016, CMS changed the way observation class patients are billed so that, in most scenarios, patients do not receive a higher hospital bill when placed in “observation” class.
How do I approach a denial from a payer?
Commercial payers review all hospitalizations for medical necessity and appropriateness of care received during a patient’s hospitalization. If you receive notice that all or part of your patient’s hospital stay was denied coverage, you have the option of discussing the case with the medical director of the insurance company – this is called a peer-to-peer discussion.
We recommend reviewing the patient’s case and your documentation of the care you provided prior to the peer to peer, especially since these denials may come weeks to months after you have cared for the patient. Begin your conversation by learning why the insurance company denied coverage of the stay and then provide an accurate portrayal of the acuity of illness of the patient, and the resources your hospital used in caring for them. Consider consulting with your hospital’s physician advisor for other high-yield tips.
How can care management help with ‘nonmedical’ hospitalizations?
Care managers are your allies for all patients, especially those with complex discharge needs. Often patients admitted for “nonmedical” reasons do not have the ability to discharge to a skilled nursing facility, long-term care facility, or home due to lack of insurance coverage or resources and/or assistance. Care managers can help you creatively problem solve and coordinate care. Physician advisors are your allies in helping create system-level interventions that might avert some of these “nonmedical” admissions. Consider involving both care managers and physician advisors early in the admission to help navigate social complexities.
How can hospitalists get involved?
According to CMS, the decision on “whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital … can typically be made in less than 48 hours, usually in less than 24 hours.”3 In reality, this is not black and white. The “2 midnights” has brought a host of new challenges for hospitals, hospitalists, and patients to navigate. The Society of Hospital Medicine released an Observation White Paper in 2017 challenging the status quo and proposing comprehensive observation reform.4
We encourage hospital medicine providers to more routinely engage with their institutional physician advisors and consider joining the SHM Public Policy Committee to become more involved in advocacy, and/or consider becoming a physician advisor.
Dr. Singh is physician advisor for Utilization & CM in the division of hospital medicine at the University of Colorado at Denver, Aurora. Dr. Patel is a hospitalist and assistant professor of medicine at the university. Dr. Anoff is director of clinical operations and director of nights for the Hospital Medicine Group at the University of Colorado at Denver. Dr. Stella is a hospitalist at Denver Health and Hospital Authority and an associate professor of medicine at the university.
References
1. What is a physician advisor? 2017 Oct 9.
2. Barry P. Medicare: Inpatient or outpatient. AARP Bulletin. 2012 Oct.
3. Goldberg TH. The long-term and post-acute care continuum. WV Med J. 2014 Nov-Dec;10(6):24-30.
4. Society of Hospital Medicine Public Policy Committee. The hospital observation care problem. Perspectives and solutions from the Society of Hospital Medicine. 2017 Sep.
The practice of hospital medicine is rapidly changing. Higher-acuity patients are being admitted to hospitals already struggling with capacity, and hospitalists are being instructed to pay attention to length of stay, improve their documentation and billing, and participate in initiatives to improve hospital throughput, all while delivering high-quality patient care.
As hospitalists and SHM members who are also physician advisors, we have a unique understanding of these pressures. In this article, we answer common questions we receive from hospitalists regarding utilization management, care coordination, clinical documentation, and CMS regulations.
Why do physician advisors exist, and what do they do?
A physician advisor is hired by the hospital to act as a liaison between the hospital administration, clinical staff, and support personnel in order to ensure regulatory compliance, advise physicians on medical necessity, and assist hospital leadership in meeting overall organizational goals related to the efficient utilization of health care services.1
Given their deep knowledge of hospital systems and processes, and ability to collaborate and teach, hospitalists are well-positioned to serve in this capacity. Our primary goal as physician advisors is to help physicians continue to focus on the parts of medicine they enjoy – clinical care, education, quality improvement, research etc. – by helping to demystify complex regulatory requirements and by creating streamlined processes to make following these requirements easier.
Why does this matter?
We understand that regulatory and hospital systems issues such as patient class determination, appropriate clinical documentation, and hospital throughput and capacity management can feel tedious, and sometimes overwhelming, to busy hospitalists. While it is easy to attribute these problems solely to hospitals’ desire for increased revenue, these issues directly impact the quality of care we provide to their patients.
In addition, our entire financial system is predicated on appropriate health care resource utilization, financial reimbursement, demonstration of medical acuity, and our impact on the care of a patient. Thus, our ability to advocate for our patients and for ourselves is directly connected with this endeavor. Developing a working knowledge of regulatory and systems issues allows hospitalists to be more engaged in leadership and negotiations and allows us to advocate for resources we deem most important.
Why are clinical documentation integrity teams so important?
Accurately and specifically describing how sick your patients are helps ensure that hospitals are reimbursed appropriately, coded data is accurate for research purposes, quality metrics are attributed correctly, and patients receive the correct diagnoses.
Clarification of documentation and/or addressing “clinical validity” of a given diagnosis (e.g., acute hypoxic respiratory failure requires both hypoxia and respiratory distress) may support an increase or result in a decrease in hospital reimbursement. For example, if the reason for a patient’s admission is renal failure, renal failure with true acute hypoxic respiratory failure will be reimbursed at a rate 40% higher than renal failure without the documentation of other conditions that reflect how ill the patient really is. The patient with acute hypoxic respiratory failure (or other major comorbid condition) is genuinely sicker, thus requiring more time (length of stay) and resources (deserved higher reimbursement).
What is the two-midnight rule, and why does it matter?
In October of 2013, the Centers for Medicare & Medicaid Services initiated the two-midnight rule, which states a Medicare patient can be an “inpatient” class if the admitting provider determines that 1) the patient requires medically necessary care which cannot be provided outside the hospital and 2) the patient is expected to stay at least 2 midnights in the hospital.
If, at the time of admission, an admitting provider thinks it is likely that the patient may be discharged prior to 2 midnights, then outpatient care with “observation” designation is appropriate. Incorrect patient class assignment may result in significant adverse consequences for hospitals, including improper patient billing, decreased hospital reimbursement, substantial risk for external auditing, violation of Medicare conditions of participation, and even loss of accreditation.
Who can I talk to if I have a question about a patient’s class? What should I do if I disagree with the class assigned to my patient?
The Utilization Management team typically consists of nurses and physician advisors specifically trained in UM. This team functions as a liaison between providers and payers (particularly Medicare and Medicaid) regarding medical necessity, appropriateness of care received, and efficiency of health care services.
When it comes to discussions about patient class, start by learning more about why the determination was made. The most common reason for patient class disagreements is simply that the documentation does not reflect the severity of illness or accurately reflect the care the patient is receiving. Your documentation should communicate that your patient needs services that only the hospital can provide, and/or they need monitoring that must be done in the hospital to meet the medical necessity criteria that CMS requires for a patient to be “inpatient” class.
If you disagree with a determination provided by the UM nurse and/or physician advisor, then the case will be presented to the hospital UM committee for further review. Two physicians from the UM committee must review the case and provide their own determinations of patient status, and whichever admission determination has two votes is the one that is appropriate.
How do I talk to patients about class determinations?
As media coverage continues about the two-midnight rule and the impact this has on patients, providers should expect more questions about class determination from their patients.
An AARP Bulletin article from 2012 advised patients to “ask [their] own doctor whether observation status is justified … and if not ask him or her to call the hospital to explain the medical reasons why they should be admitted as inpatient.”2 Patients should be informed that providers understand the implications of patient class determinations and are making these decisions as outlined by CMS.
We recommend informing patients that the decision about whether a patient is “inpatient” or “outpatient with observation” class is complex and involves taking into consideration a patient’s medical history, the severity of their current medical condition, need for diagnostic testing, and degree of health resource utilization, as well as a provider’s medical opinion of the risk of an adverse event occurring.
Is it true that observation patients receive higher hospital bills?
It is a common misperception that a designation of “observation” class means that a patient’s medical bill will be higher than “inpatient” class. In 2016, CMS changed the way observation class patients are billed so that, in most scenarios, patients do not receive a higher hospital bill when placed in “observation” class.
How do I approach a denial from a payer?
Commercial payers review all hospitalizations for medical necessity and appropriateness of care received during a patient’s hospitalization. If you receive notice that all or part of your patient’s hospital stay was denied coverage, you have the option of discussing the case with the medical director of the insurance company – this is called a peer-to-peer discussion.
We recommend reviewing the patient’s case and your documentation of the care you provided prior to the peer to peer, especially since these denials may come weeks to months after you have cared for the patient. Begin your conversation by learning why the insurance company denied coverage of the stay and then provide an accurate portrayal of the acuity of illness of the patient, and the resources your hospital used in caring for them. Consider consulting with your hospital’s physician advisor for other high-yield tips.
How can care management help with ‘nonmedical’ hospitalizations?
Care managers are your allies for all patients, especially those with complex discharge needs. Often patients admitted for “nonmedical” reasons do not have the ability to discharge to a skilled nursing facility, long-term care facility, or home due to lack of insurance coverage or resources and/or assistance. Care managers can help you creatively problem solve and coordinate care. Physician advisors are your allies in helping create system-level interventions that might avert some of these “nonmedical” admissions. Consider involving both care managers and physician advisors early in the admission to help navigate social complexities.
How can hospitalists get involved?
According to CMS, the decision on “whether patients will require further treatment as hospital inpatients or if they are able to be discharged from the hospital … can typically be made in less than 48 hours, usually in less than 24 hours.”3 In reality, this is not black and white. The “2 midnights” has brought a host of new challenges for hospitals, hospitalists, and patients to navigate. The Society of Hospital Medicine released an Observation White Paper in 2017 challenging the status quo and proposing comprehensive observation reform.4
We encourage hospital medicine providers to more routinely engage with their institutional physician advisors and consider joining the SHM Public Policy Committee to become more involved in advocacy, and/or consider becoming a physician advisor.
Dr. Singh is physician advisor for Utilization & CM in the division of hospital medicine at the University of Colorado at Denver, Aurora. Dr. Patel is a hospitalist and assistant professor of medicine at the university. Dr. Anoff is director of clinical operations and director of nights for the Hospital Medicine Group at the University of Colorado at Denver. Dr. Stella is a hospitalist at Denver Health and Hospital Authority and an associate professor of medicine at the university.
References
1. What is a physician advisor? 2017 Oct 9.
2. Barry P. Medicare: Inpatient or outpatient. AARP Bulletin. 2012 Oct.
3. Goldberg TH. The long-term and post-acute care continuum. WV Med J. 2014 Nov-Dec;10(6):24-30.
4. Society of Hospital Medicine Public Policy Committee. The hospital observation care problem. Perspectives and solutions from the Society of Hospital Medicine. 2017 Sep.
Employee Wellness Programs: Location, Location, Location
Employee wellness programs (EWPs) have a good track record, with plenty of affirmative research showing benefits: lowered stress levels, fewer sick days, reduced absenteeism, health care savings. Studies have found that for every dollar spent on an EWP, medical costs fall by $3 to $6. Moreover, studies have found that organizations that invest in EWPs have higher rates of employee satisfaction, morale, and retention.
But does one size of EWP fit all needs? Not according to researchers from Northern Arizona University. They studied factors that go in to successful EWPs and suggest that geography should play a big part in decision making: from whether to have an EWP to what it should offer. Take Houston, Texas, for instance, where influenza lasts longer than in most other places. Geographic and climatologic variables, the researchers say, like those necessitate “tailored wellness responses,” such as spending more money on outreach and educational programs to make sure people are prepared for seasonal outbreaks.
The researchers endorse the idea of “individualism in city preferences”—that is, that cities maximize their wellness offerings by taking advantage of the characteristics of the spaces, cultures, and lifestyles unique to them. The researchers note that cities with high incidence of obesity, such as Memphis, Tennessee, and Louisville, Kentucky, tend to put more money into weight-loss programs. Cities with more elderly workers, like Phoenix, Arizona, and Jacksonville, Florida, have “robust programs” for managing chronic diseases associated with age. Stress management may be a priority in impoverished areas. Similarly, EWPs need to factor in geography to make sure the programs meet local needs. Some cities have more and longer days with sunshine: How much of the year can people be active outside? Some have farmland nearby: EWPs can encourage eating healthy locally sourced foods. It is significant, the researchers say, that EWPs in “lower obesity” regions have a proportionately higher intake of activities associated with the outdoors.
Geography is only one consideration among many, the researchers emphasize. City leadership and commitment and incentive structures lead to recreational investments and investments in healthy-living infrastructures, which in turn, lead to higher livability rankings and quality-of-life indexes, workforce productivity, and attracting new business. Those lead to more community involvement, cohesion, and reduced reliance on public health care facilities. And ultimately, the researchers say, the components of a successful EWP all lead to a positive impact on health and longevity.
Employee wellness programs (EWPs) have a good track record, with plenty of affirmative research showing benefits: lowered stress levels, fewer sick days, reduced absenteeism, health care savings. Studies have found that for every dollar spent on an EWP, medical costs fall by $3 to $6. Moreover, studies have found that organizations that invest in EWPs have higher rates of employee satisfaction, morale, and retention.
But does one size of EWP fit all needs? Not according to researchers from Northern Arizona University. They studied factors that go in to successful EWPs and suggest that geography should play a big part in decision making: from whether to have an EWP to what it should offer. Take Houston, Texas, for instance, where influenza lasts longer than in most other places. Geographic and climatologic variables, the researchers say, like those necessitate “tailored wellness responses,” such as spending more money on outreach and educational programs to make sure people are prepared for seasonal outbreaks.
The researchers endorse the idea of “individualism in city preferences”—that is, that cities maximize their wellness offerings by taking advantage of the characteristics of the spaces, cultures, and lifestyles unique to them. The researchers note that cities with high incidence of obesity, such as Memphis, Tennessee, and Louisville, Kentucky, tend to put more money into weight-loss programs. Cities with more elderly workers, like Phoenix, Arizona, and Jacksonville, Florida, have “robust programs” for managing chronic diseases associated with age. Stress management may be a priority in impoverished areas. Similarly, EWPs need to factor in geography to make sure the programs meet local needs. Some cities have more and longer days with sunshine: How much of the year can people be active outside? Some have farmland nearby: EWPs can encourage eating healthy locally sourced foods. It is significant, the researchers say, that EWPs in “lower obesity” regions have a proportionately higher intake of activities associated with the outdoors.
Geography is only one consideration among many, the researchers emphasize. City leadership and commitment and incentive structures lead to recreational investments and investments in healthy-living infrastructures, which in turn, lead to higher livability rankings and quality-of-life indexes, workforce productivity, and attracting new business. Those lead to more community involvement, cohesion, and reduced reliance on public health care facilities. And ultimately, the researchers say, the components of a successful EWP all lead to a positive impact on health and longevity.
Employee wellness programs (EWPs) have a good track record, with plenty of affirmative research showing benefits: lowered stress levels, fewer sick days, reduced absenteeism, health care savings. Studies have found that for every dollar spent on an EWP, medical costs fall by $3 to $6. Moreover, studies have found that organizations that invest in EWPs have higher rates of employee satisfaction, morale, and retention.
But does one size of EWP fit all needs? Not according to researchers from Northern Arizona University. They studied factors that go in to successful EWPs and suggest that geography should play a big part in decision making: from whether to have an EWP to what it should offer. Take Houston, Texas, for instance, where influenza lasts longer than in most other places. Geographic and climatologic variables, the researchers say, like those necessitate “tailored wellness responses,” such as spending more money on outreach and educational programs to make sure people are prepared for seasonal outbreaks.
The researchers endorse the idea of “individualism in city preferences”—that is, that cities maximize their wellness offerings by taking advantage of the characteristics of the spaces, cultures, and lifestyles unique to them. The researchers note that cities with high incidence of obesity, such as Memphis, Tennessee, and Louisville, Kentucky, tend to put more money into weight-loss programs. Cities with more elderly workers, like Phoenix, Arizona, and Jacksonville, Florida, have “robust programs” for managing chronic diseases associated with age. Stress management may be a priority in impoverished areas. Similarly, EWPs need to factor in geography to make sure the programs meet local needs. Some cities have more and longer days with sunshine: How much of the year can people be active outside? Some have farmland nearby: EWPs can encourage eating healthy locally sourced foods. It is significant, the researchers say, that EWPs in “lower obesity” regions have a proportionately higher intake of activities associated with the outdoors.
Geography is only one consideration among many, the researchers emphasize. City leadership and commitment and incentive structures lead to recreational investments and investments in healthy-living infrastructures, which in turn, lead to higher livability rankings and quality-of-life indexes, workforce productivity, and attracting new business. Those lead to more community involvement, cohesion, and reduced reliance on public health care facilities. And ultimately, the researchers say, the components of a successful EWP all lead to a positive impact on health and longevity.
Gut bacterium R. gnavus linked to lupus flares
SAN FRANCISCO –
Not only that, but those patients also had highly elevated antibodies to an endotoxin-like antigen released by one particular R. gnavus strain.
That antigen is “very proinflammatory, very immunogenic. We are wondering if this is actually [what drives] the immune activation that results in immune complexes in the glomeruli” of patients with lupus nephritis, said investigator Gregg Silverman, MD, a professor of medicine and pathology and head of the laboratory of B-cell immunobiology at New York University.
R. gnavus is an obligate anaerobe found in the guts of most people, but in lupus, it might be a problem.
“We are finding a very specific relationship with lupus patients and this bacteria – and this particular antibody,” Dr. Silverman explained in an interview at an international congress on systemic lupus erythematosus. “There’s an expansion of this particular bug, but also a contraction of others” as disease activity progresses.
“It speaks to an imbalance,” he added, and it suggests a role for probiotics or even fecal transplants to restore order.
“What if instead of killing the immune system” in lupus treatment, “we should be reducing or removing a single bacterium or a single molecule?” he asked.
Dr. Silverman is one of many researchers working to unravel the role of the human microbiome in both disease and health. His findings are preliminary, and, as he cautioned, correlation is not causation. But the implications are remarkable, Dr. Silverman noted.
SAN FRANCISCO –
Not only that, but those patients also had highly elevated antibodies to an endotoxin-like antigen released by one particular R. gnavus strain.
That antigen is “very proinflammatory, very immunogenic. We are wondering if this is actually [what drives] the immune activation that results in immune complexes in the glomeruli” of patients with lupus nephritis, said investigator Gregg Silverman, MD, a professor of medicine and pathology and head of the laboratory of B-cell immunobiology at New York University.
R. gnavus is an obligate anaerobe found in the guts of most people, but in lupus, it might be a problem.
“We are finding a very specific relationship with lupus patients and this bacteria – and this particular antibody,” Dr. Silverman explained in an interview at an international congress on systemic lupus erythematosus. “There’s an expansion of this particular bug, but also a contraction of others” as disease activity progresses.
“It speaks to an imbalance,” he added, and it suggests a role for probiotics or even fecal transplants to restore order.
“What if instead of killing the immune system” in lupus treatment, “we should be reducing or removing a single bacterium or a single molecule?” he asked.
Dr. Silverman is one of many researchers working to unravel the role of the human microbiome in both disease and health. His findings are preliminary, and, as he cautioned, correlation is not causation. But the implications are remarkable, Dr. Silverman noted.
SAN FRANCISCO –
Not only that, but those patients also had highly elevated antibodies to an endotoxin-like antigen released by one particular R. gnavus strain.
That antigen is “very proinflammatory, very immunogenic. We are wondering if this is actually [what drives] the immune activation that results in immune complexes in the glomeruli” of patients with lupus nephritis, said investigator Gregg Silverman, MD, a professor of medicine and pathology and head of the laboratory of B-cell immunobiology at New York University.
R. gnavus is an obligate anaerobe found in the guts of most people, but in lupus, it might be a problem.
“We are finding a very specific relationship with lupus patients and this bacteria – and this particular antibody,” Dr. Silverman explained in an interview at an international congress on systemic lupus erythematosus. “There’s an expansion of this particular bug, but also a contraction of others” as disease activity progresses.
“It speaks to an imbalance,” he added, and it suggests a role for probiotics or even fecal transplants to restore order.
“What if instead of killing the immune system” in lupus treatment, “we should be reducing or removing a single bacterium or a single molecule?” he asked.
Dr. Silverman is one of many researchers working to unravel the role of the human microbiome in both disease and health. His findings are preliminary, and, as he cautioned, correlation is not causation. But the implications are remarkable, Dr. Silverman noted.
REPORTING FROM LUPUS 2019

Short Takes
Short Takes
Both sleep quantity and quality is disturbed in hospitalized patients
A cross-sectional, observational, single-day study of over 2,000 hospitalized patients showed that, on average, these patients received 83 minutes less sleep time than at home. Quality of sleep – as measured by the Consensus Sleep Diary (CSD) and the Dutch-Flemish Patient-Reported-Outcomes Measurement Information System (PROMIS) Sleep Disturbance item bank – was also significantly disturbed. Sleep disruptions were most commonly caused by noise from other patients and by being awakened by hospital staff.
Citation: Wesselius H et al. Quality and quantity of sleep and factors associated with sleep disturbance in hospitalized patients. JAMA Intern Med. 2018 Jul 16. doi: 10.1001/jamainternmed.2018.2669.
Health care costs and mortality improve in Medicare beneficiaries who receive transitional care management (TCM) service
In a retrospective cohort analysis of Medicare Fee-for-Service beneficiaries, the adjusted total Medicare costs (average, $3,358 vs. $3,033) and mortality (1.6% vs 1.0%) were higher among those beneficiaries who did not receive TCM services, compared with those who did receive TCM services, in the 31-60 days following an eligible discharge; however, use of this service by clinicians remained very low.
Citation: Bindman AB et al. Changes in health care costs and mortality associated with transitional care management services after a discharge among Medicare beneficiaries. JAMA Intern Med. 2018 Jul 30. doi: 10.1001/jamainternmed.2018.2572.

Unsafe zolpidem use is common
In a review of the 2015 US Medical Expenditure Panel Survey, investigators found that up to 77% of patients prescribed zolpidem reported being prescribed longer durations and higher doses, as well as the drug being prescribed alongside other CNS depressants, despite known risks and recommended prescription and Food and Drug Administration guidelines.
Citation: Moore T et al. Assessment of patterns of potentially unsafe use of zolpidem. JAMA Intern Med. 2018 Jul 16. doi: 10.1001/jamainternmed.2018.3031.
Short Takes
Short Takes
Both sleep quantity and quality is disturbed in hospitalized patients
A cross-sectional, observational, single-day study of over 2,000 hospitalized patients showed that, on average, these patients received 83 minutes less sleep time than at home. Quality of sleep – as measured by the Consensus Sleep Diary (CSD) and the Dutch-Flemish Patient-Reported-Outcomes Measurement Information System (PROMIS) Sleep Disturbance item bank – was also significantly disturbed. Sleep disruptions were most commonly caused by noise from other patients and by being awakened by hospital staff.
Citation: Wesselius H et al. Quality and quantity of sleep and factors associated with sleep disturbance in hospitalized patients. JAMA Intern Med. 2018 Jul 16. doi: 10.1001/jamainternmed.2018.2669.
Health care costs and mortality improve in Medicare beneficiaries who receive transitional care management (TCM) service
In a retrospective cohort analysis of Medicare Fee-for-Service beneficiaries, the adjusted total Medicare costs (average, $3,358 vs. $3,033) and mortality (1.6% vs 1.0%) were higher among those beneficiaries who did not receive TCM services, compared with those who did receive TCM services, in the 31-60 days following an eligible discharge; however, use of this service by clinicians remained very low.
Citation: Bindman AB et al. Changes in health care costs and mortality associated with transitional care management services after a discharge among Medicare beneficiaries. JAMA Intern Med. 2018 Jul 30. doi: 10.1001/jamainternmed.2018.2572.
Unsafe zolpidem use is common
In a review of the 2015 US Medical Expenditure Panel Survey, investigators found that up to 77% of patients prescribed zolpidem reported being prescribed longer durations and higher doses, as well as the drug being prescribed alongside other CNS depressants, despite known risks and recommended prescription and Food and Drug Administration guidelines.
Citation: Moore T et al. Assessment of patterns of potentially unsafe use of zolpidem. JAMA Intern Med. 2018 Jul 16. doi: 10.1001/jamainternmed.2018.3031.
Both sleep quantity and quality is disturbed in hospitalized patients
A cross-sectional, observational, single-day study of over 2,000 hospitalized patients showed that, on average, these patients received 83 minutes less sleep time than at home. Quality of sleep – as measured by the Consensus Sleep Diary (CSD) and the Dutch-Flemish Patient-Reported-Outcomes Measurement Information System (PROMIS) Sleep Disturbance item bank – was also significantly disturbed. Sleep disruptions were most commonly caused by noise from other patients and by being awakened by hospital staff.
Citation: Wesselius H et al. Quality and quantity of sleep and factors associated with sleep disturbance in hospitalized patients. JAMA Intern Med. 2018 Jul 16. doi: 10.1001/jamainternmed.2018.2669.
Health care costs and mortality improve in Medicare beneficiaries who receive transitional care management (TCM) service
In a retrospective cohort analysis of Medicare Fee-for-Service beneficiaries, the adjusted total Medicare costs (average, $3,358 vs. $3,033) and mortality (1.6% vs 1.0%) were higher among those beneficiaries who did not receive TCM services, compared with those who did receive TCM services, in the 31-60 days following an eligible discharge; however, use of this service by clinicians remained very low.
Citation: Bindman AB et al. Changes in health care costs and mortality associated with transitional care management services after a discharge among Medicare beneficiaries. JAMA Intern Med. 2018 Jul 30. doi: 10.1001/jamainternmed.2018.2572.
Unsafe zolpidem use is common
In a review of the 2015 US Medical Expenditure Panel Survey, investigators found that up to 77% of patients prescribed zolpidem reported being prescribed longer durations and higher doses, as well as the drug being prescribed alongside other CNS depressants, despite known risks and recommended prescription and Food and Drug Administration guidelines.
Citation: Moore T et al. Assessment of patterns of potentially unsafe use of zolpidem. JAMA Intern Med. 2018 Jul 16. doi: 10.1001/jamainternmed.2018.3031.
May 2019 – ICYMI
Gastroenterology
How to write an effective business plan in medicine. Jazayeri A; Park KT. 2019 April;156(5):1243-7.
doi.org/10.1053/j.gastro.2019.03.003 https://www.gastrojournal.org/article/S0016-5085(19)32513-2/fulltext
How to deliver safer and effective patient care: Tips for team leaders and educators. Shah BJ. 2019 March;156(4):852-5.
doi.org/10.1053/j.gastro.2019.02.017 https://www.gastrojournal.org/article/S0016-5085(19)30390-7/fulltext
AGA Clinical Practice Update on diagnosis and monitoring of celiac disease – changing utility of serology and histologic measures: expert review. Husby S; Murray JA; Kattzka DA. 2019 March;156(4):885-9.
doi.org/10.1053/j.gastro.2018.12.010 https://www.gastrojournal.org/article/S0016-5085(18)35408-8/fulltext
How to get involved in global health. Proctor DD. 2019 Feb;156(3):542-4.
doi.org/10.1053/j.gastro.2019.01.012 https://www.gastrojournal.org/article/S0016-5085(19)30033-2/fulltext
AGA Clinical Practice Guidelines on the management of mild-to-moderate ulcerative colitis. Ko CW; Singh S; Feuerstein JD; Falck-Yytter C; Falck-Ytter Y; Cross RK; on behalf of the American Gastroenterological Association Institute Clinical Guidelines Committee. 2019 Feb;156(3);748-64.
doi.org/10.1053/j.gastro.2018.12.009 https://www.gastrojournal.org/article/S0016-5085(18)35407-6/fulltext
Clin Gastro Hepatol
Translating best practices to meaningful quality measures: From measure conceptualization to implementation. Adams MA; Allen JI; Saini SD. 2019 April;17(5):805-8.
doi.org/10.1016/j.cgh.2018.10.027 https://www.cghjournal.org/article/S1542-3565(18)31149-2/fulltext
Switching between biologics and biosimilars in inflammatory bowel diseases. Raffals LE; Nguyen GC; Rubin DT. 2019 April;17(5):818-23.
doi.org/10.1016/j.cgh.2018.08.064 https://www.cghjournal.org/article/S1542-3565(18)30943-1/fulltext
Preventive medicine in inflammatory bowel disease. Weaver KN; Long MD. 2019 April;17(5):824-8.
doi.org/10.1016/j.cgh.2018.11.054 https://www.cghjournal.org/article/S1542-3565(18)31331-4/fulltext
Innovating in your practice: Overcoming barriers to create new opportunities. Muthusamy VR; Komanduri S. 2019 March;17(4):580-3.
doi.org/10.1016/j.cgh.2018.09.016 https://www.cghjournal.org/article/S1542-3565(18)30978-9/fulltext
Incorporating advanced practice providers into gastroenterology practice. Nandwani MDR; Clarke JO. 2019 Feb;17(3):365-9.
doi.org/10.1016/j.cgh.2018.09.015 https://www.cghjournal.org/article/S1542-3565(18)30977-7/fulltext
AGA Clinical Practice Update on functional gastrointestinal symptoms in patients with inflammatory bowel disease: expert review. Colombel J-F; Shin A; Gibson PR. 2019 Feb;17(3):380-90.
doi.org/10.1016/j.cgh.2018.08.001 https://www.cghjournal.org/article/S1542-3565(18)30810-3/fulltext
Gastroenterology
How to write an effective business plan in medicine. Jazayeri A; Park KT. 2019 April;156(5):1243-7.
doi.org/10.1053/j.gastro.2019.03.003 https://www.gastrojournal.org/article/S0016-5085(19)32513-2/fulltext
How to deliver safer and effective patient care: Tips for team leaders and educators. Shah BJ. 2019 March;156(4):852-5.
doi.org/10.1053/j.gastro.2019.02.017 https://www.gastrojournal.org/article/S0016-5085(19)30390-7/fulltext
AGA Clinical Practice Update on diagnosis and monitoring of celiac disease – changing utility of serology and histologic measures: expert review. Husby S; Murray JA; Kattzka DA. 2019 March;156(4):885-9.
doi.org/10.1053/j.gastro.2018.12.010 https://www.gastrojournal.org/article/S0016-5085(18)35408-8/fulltext
How to get involved in global health. Proctor DD. 2019 Feb;156(3):542-4.
doi.org/10.1053/j.gastro.2019.01.012 https://www.gastrojournal.org/article/S0016-5085(19)30033-2/fulltext
AGA Clinical Practice Guidelines on the management of mild-to-moderate ulcerative colitis. Ko CW; Singh S; Feuerstein JD; Falck-Yytter C; Falck-Ytter Y; Cross RK; on behalf of the American Gastroenterological Association Institute Clinical Guidelines Committee. 2019 Feb;156(3);748-64.
doi.org/10.1053/j.gastro.2018.12.009 https://www.gastrojournal.org/article/S0016-5085(18)35407-6/fulltext
Clin Gastro Hepatol
Translating best practices to meaningful quality measures: From measure conceptualization to implementation. Adams MA; Allen JI; Saini SD. 2019 April;17(5):805-8.
doi.org/10.1016/j.cgh.2018.10.027 https://www.cghjournal.org/article/S1542-3565(18)31149-2/fulltext
Switching between biologics and biosimilars in inflammatory bowel diseases. Raffals LE; Nguyen GC; Rubin DT. 2019 April;17(5):818-23.
doi.org/10.1016/j.cgh.2018.08.064 https://www.cghjournal.org/article/S1542-3565(18)30943-1/fulltext
Preventive medicine in inflammatory bowel disease. Weaver KN; Long MD. 2019 April;17(5):824-8.
doi.org/10.1016/j.cgh.2018.11.054 https://www.cghjournal.org/article/S1542-3565(18)31331-4/fulltext
Innovating in your practice: Overcoming barriers to create new opportunities. Muthusamy VR; Komanduri S. 2019 March;17(4):580-3.
doi.org/10.1016/j.cgh.2018.09.016 https://www.cghjournal.org/article/S1542-3565(18)30978-9/fulltext
Incorporating advanced practice providers into gastroenterology practice. Nandwani MDR; Clarke JO. 2019 Feb;17(3):365-9.
doi.org/10.1016/j.cgh.2018.09.015 https://www.cghjournal.org/article/S1542-3565(18)30977-7/fulltext
AGA Clinical Practice Update on functional gastrointestinal symptoms in patients with inflammatory bowel disease: expert review. Colombel J-F; Shin A; Gibson PR. 2019 Feb;17(3):380-90.
doi.org/10.1016/j.cgh.2018.08.001 https://www.cghjournal.org/article/S1542-3565(18)30810-3/fulltext
Gastroenterology
How to write an effective business plan in medicine. Jazayeri A; Park KT. 2019 April;156(5):1243-7.
doi.org/10.1053/j.gastro.2019.03.003 https://www.gastrojournal.org/article/S0016-5085(19)32513-2/fulltext
How to deliver safer and effective patient care: Tips for team leaders and educators. Shah BJ. 2019 March;156(4):852-5.
doi.org/10.1053/j.gastro.2019.02.017 https://www.gastrojournal.org/article/S0016-5085(19)30390-7/fulltext
AGA Clinical Practice Update on diagnosis and monitoring of celiac disease – changing utility of serology and histologic measures: expert review. Husby S; Murray JA; Kattzka DA. 2019 March;156(4):885-9.
doi.org/10.1053/j.gastro.2018.12.010 https://www.gastrojournal.org/article/S0016-5085(18)35408-8/fulltext
How to get involved in global health. Proctor DD. 2019 Feb;156(3):542-4.
doi.org/10.1053/j.gastro.2019.01.012 https://www.gastrojournal.org/article/S0016-5085(19)30033-2/fulltext
AGA Clinical Practice Guidelines on the management of mild-to-moderate ulcerative colitis. Ko CW; Singh S; Feuerstein JD; Falck-Yytter C; Falck-Ytter Y; Cross RK; on behalf of the American Gastroenterological Association Institute Clinical Guidelines Committee. 2019 Feb;156(3);748-64.
doi.org/10.1053/j.gastro.2018.12.009 https://www.gastrojournal.org/article/S0016-5085(18)35407-6/fulltext
Clin Gastro Hepatol
Translating best practices to meaningful quality measures: From measure conceptualization to implementation. Adams MA; Allen JI; Saini SD. 2019 April;17(5):805-8.
doi.org/10.1016/j.cgh.2018.10.027 https://www.cghjournal.org/article/S1542-3565(18)31149-2/fulltext
Switching between biologics and biosimilars in inflammatory bowel diseases. Raffals LE; Nguyen GC; Rubin DT. 2019 April;17(5):818-23.
doi.org/10.1016/j.cgh.2018.08.064 https://www.cghjournal.org/article/S1542-3565(18)30943-1/fulltext
Preventive medicine in inflammatory bowel disease. Weaver KN; Long MD. 2019 April;17(5):824-8.
doi.org/10.1016/j.cgh.2018.11.054 https://www.cghjournal.org/article/S1542-3565(18)31331-4/fulltext
Innovating in your practice: Overcoming barriers to create new opportunities. Muthusamy VR; Komanduri S. 2019 March;17(4):580-3.
doi.org/10.1016/j.cgh.2018.09.016 https://www.cghjournal.org/article/S1542-3565(18)30978-9/fulltext
Incorporating advanced practice providers into gastroenterology practice. Nandwani MDR; Clarke JO. 2019 Feb;17(3):365-9.
doi.org/10.1016/j.cgh.2018.09.015 https://www.cghjournal.org/article/S1542-3565(18)30977-7/fulltext
AGA Clinical Practice Update on functional gastrointestinal symptoms in patients with inflammatory bowel disease: expert review. Colombel J-F; Shin A; Gibson PR. 2019 Feb;17(3):380-90.
doi.org/10.1016/j.cgh.2018.08.001 https://www.cghjournal.org/article/S1542-3565(18)30810-3/fulltext
Physicians discuss bringing cultural humility to medicine
PHILADELPHIA – during a panel discussion moderated by Sarah Candler, MD, an internist in Houston.
Dr. Candler, former chair, Council of Resident and Fellow Members, Board of Regents, American College of Physicians, began the discussion by asking Dr. DeLisser, to describe his role in teaching medical students about the social determinants of health, at the annual Internal Medicine meeting of the ACP.
Dr. DeLisser, associate dean for professionalism and humanism at the University of Pennsylvania, Philadelphia, said he focuses on a number of issues, including social medicine, cultural competency, and cultural humility.
“We look at health care disparities and try to do a lot of innovation around service learning that will bring our students into the community, one to learn about these determinants but more importantly to be able to see how these issues can be addressed both on a provider level but also on a more structural systemic level,” he noted.
Dr. Poorman, an internist at the University of Washington, later discussed the importance of practicing cultural humility as it related to her experience providing care to migrant workers while she was a medical school student.
Dr. Candler, an internist in Houston, concluded the discussion by describing some of the ACP’s newest resources designed to address the social determinants of health for specific groups of patients.
The full panel discussion was recorded as a video.
PHILADELPHIA – during a panel discussion moderated by Sarah Candler, MD, an internist in Houston.
Dr. Candler, former chair, Council of Resident and Fellow Members, Board of Regents, American College of Physicians, began the discussion by asking Dr. DeLisser, to describe his role in teaching medical students about the social determinants of health, at the annual Internal Medicine meeting of the ACP.
Dr. DeLisser, associate dean for professionalism and humanism at the University of Pennsylvania, Philadelphia, said he focuses on a number of issues, including social medicine, cultural competency, and cultural humility.
“We look at health care disparities and try to do a lot of innovation around service learning that will bring our students into the community, one to learn about these determinants but more importantly to be able to see how these issues can be addressed both on a provider level but also on a more structural systemic level,” he noted.
Dr. Poorman, an internist at the University of Washington, later discussed the importance of practicing cultural humility as it related to her experience providing care to migrant workers while she was a medical school student.
Dr. Candler, an internist in Houston, concluded the discussion by describing some of the ACP’s newest resources designed to address the social determinants of health for specific groups of patients.
The full panel discussion was recorded as a video.
PHILADELPHIA – during a panel discussion moderated by Sarah Candler, MD, an internist in Houston.
Dr. Candler, former chair, Council of Resident and Fellow Members, Board of Regents, American College of Physicians, began the discussion by asking Dr. DeLisser, to describe his role in teaching medical students about the social determinants of health, at the annual Internal Medicine meeting of the ACP.
Dr. DeLisser, associate dean for professionalism and humanism at the University of Pennsylvania, Philadelphia, said he focuses on a number of issues, including social medicine, cultural competency, and cultural humility.
“We look at health care disparities and try to do a lot of innovation around service learning that will bring our students into the community, one to learn about these determinants but more importantly to be able to see how these issues can be addressed both on a provider level but also on a more structural systemic level,” he noted.
Dr. Poorman, an internist at the University of Washington, later discussed the importance of practicing cultural humility as it related to her experience providing care to migrant workers while she was a medical school student.
Dr. Candler, an internist in Houston, concluded the discussion by describing some of the ACP’s newest resources designed to address the social determinants of health for specific groups of patients.
The full panel discussion was recorded as a video.
REPORTING FROM INTERNAL MEDICINE 2019
