User login
HHS funds experimental flu drug for hospital patients
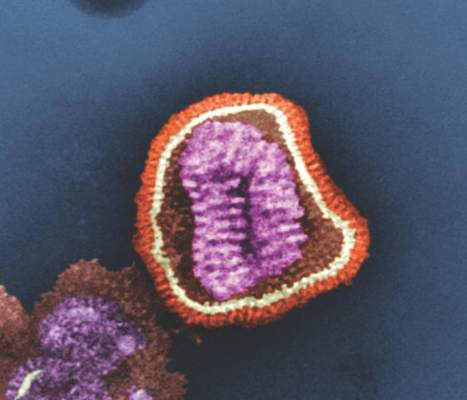
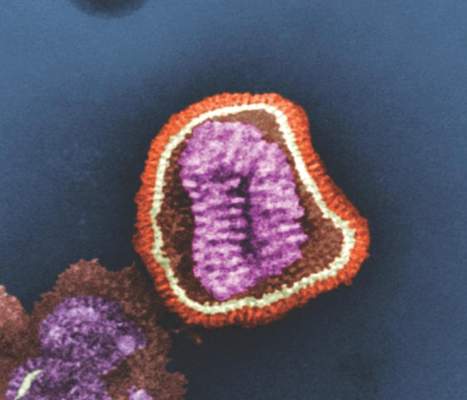
The U.S. Department of Health & Human Services’ Office of the Assistant Secretary for Preparedness and Response (ASPR) will provide “technical assistance and funding” to Janssen Pharmaceuticals for the development of an influenza antiviral drug that could be more potent and have a longer treatment window than do existing influenza drugs, according a statement from HHS.
The experimental drug, which Janssen intends to use to treat hospitalized patients with influenza, is called JNJ-872, also known as VX787, and may be the first in an entirely new class of influenza antivirals.
ASPR’s Biomedical Advanced Research and Development Authority (BARDA) specifically will provide up to $103.5 million over the next 4 years and 3 months to Janssen, and the contract leaves open the possibility of BARDA providing additional funding, capped at $131 million, for this project. BARDA’s contribution is part of its program for “advanced research and development, innovation, acquisition, and manufacturing of vaccines, drugs, diagnostic tools, and nonpharmaceutical products for public health emergency threats.”
Janssen will use the funds to conduct late stage clinical development of JNJ-872, which includes phase III studies in high-risk populations and hospitalized patients, and the final development of a validated commercial-scale manufacturing process. The pharmaceutical company will also explore the feasibility of an innovative approach to manufacturing, which allows for the continuous flow of materials throughout the manufacturing process, unlike the traditional manufacturing process, which is riddled with interruptions.
“BARDA’s goal for supporting JNJ-872 is development of a product that can be used not only to treat hospitalized influenza patients but also to treat patients for whom influenza poses high risks, such as the elderly, pediatrics, and those with chronic conditions such as COPD and heart disease ...,” the statement indicated.
The U.S. Department of Health & Human Services’ Office of the Assistant Secretary for Preparedness and Response (ASPR) will provide “technical assistance and funding” to Janssen Pharmaceuticals for the development of an influenza antiviral drug that could be more potent and have a longer treatment window than do existing influenza drugs, according a statement from HHS.
The experimental drug, which Janssen intends to use to treat hospitalized patients with influenza, is called JNJ-872, also known as VX787, and may be the first in an entirely new class of influenza antivirals.
ASPR’s Biomedical Advanced Research and Development Authority (BARDA) specifically will provide up to $103.5 million over the next 4 years and 3 months to Janssen, and the contract leaves open the possibility of BARDA providing additional funding, capped at $131 million, for this project. BARDA’s contribution is part of its program for “advanced research and development, innovation, acquisition, and manufacturing of vaccines, drugs, diagnostic tools, and nonpharmaceutical products for public health emergency threats.”
Janssen will use the funds to conduct late stage clinical development of JNJ-872, which includes phase III studies in high-risk populations and hospitalized patients, and the final development of a validated commercial-scale manufacturing process. The pharmaceutical company will also explore the feasibility of an innovative approach to manufacturing, which allows for the continuous flow of materials throughout the manufacturing process, unlike the traditional manufacturing process, which is riddled with interruptions.
“BARDA’s goal for supporting JNJ-872 is development of a product that can be used not only to treat hospitalized influenza patients but also to treat patients for whom influenza poses high risks, such as the elderly, pediatrics, and those with chronic conditions such as COPD and heart disease ...,” the statement indicated.
The U.S. Department of Health & Human Services’ Office of the Assistant Secretary for Preparedness and Response (ASPR) will provide “technical assistance and funding” to Janssen Pharmaceuticals for the development of an influenza antiviral drug that could be more potent and have a longer treatment window than do existing influenza drugs, according a statement from HHS.
The experimental drug, which Janssen intends to use to treat hospitalized patients with influenza, is called JNJ-872, also known as VX787, and may be the first in an entirely new class of influenza antivirals.
ASPR’s Biomedical Advanced Research and Development Authority (BARDA) specifically will provide up to $103.5 million over the next 4 years and 3 months to Janssen, and the contract leaves open the possibility of BARDA providing additional funding, capped at $131 million, for this project. BARDA’s contribution is part of its program for “advanced research and development, innovation, acquisition, and manufacturing of vaccines, drugs, diagnostic tools, and nonpharmaceutical products for public health emergency threats.”
Janssen will use the funds to conduct late stage clinical development of JNJ-872, which includes phase III studies in high-risk populations and hospitalized patients, and the final development of a validated commercial-scale manufacturing process. The pharmaceutical company will also explore the feasibility of an innovative approach to manufacturing, which allows for the continuous flow of materials throughout the manufacturing process, unlike the traditional manufacturing process, which is riddled with interruptions.
“BARDA’s goal for supporting JNJ-872 is development of a product that can be used not only to treat hospitalized influenza patients but also to treat patients for whom influenza poses high risks, such as the elderly, pediatrics, and those with chronic conditions such as COPD and heart disease ...,” the statement indicated.
Send patients reminders for flu vaccines, study says
ATLANTA – Mobile reminders from health care providers to their patients, notifying them to get influenza vaccinations, significantly increases the likelihood that those patients will get vaccinated, according to a study by Dr. Katherine A. Benedict and coinvestigators in the Enteric Diseases Epidemiology Branch at the Centers for Disease Control and Prevention. Dr. Benedict presented findings of the research at the International Conference on Emerging Infectious Diseases.
The researchers used data from the March 2012 National Flu Survey, a CDC “random digit dial telephone survey” of influenza vaccination trends in adults 18 years of age and older. They analyzed the data to determine whether or not patients received reminders, recommendations, or offers for influenza vaccinations from their health care providers since July 1, 2011. They did a logistic regression analysis to determine if there was any relationship between influenza vaccination rates and receipt of recommendations from health care providers.

Almost 73% of adults reported visiting a physician at least once since July 1, 2011, the start of data collection for the March 2012 study cycle, with 17.2% reporting that they received a reminder from their doctors to get a flu vaccine. Overall, 45.5% of adults ultimately got vaccinated, with 75.6% of those who reported receiving a reminder saying that they also were offered vaccinations by their doctors.
Adults who received recommendations for influenza vaccination from their health care providers were most likely to get vaccinated, and had an unadjusted prevalence ratio of 2.09. Next likely were those who received vaccination offers (PR = 1.90), and those who simply received reminders (PR = 1.33). Furthermore, those between 50 and 64 years old were found more likely to receive a recommendation or offer – PR = 1.23 and PR = 1.09, respectively – than were those in the 18- to 49-year age range (PR = 1.06 for recommendation, PR = 0.99 for offer).
The takeaway from this, according to the investigators, is that reminders should be sent at least once at the beginning of each influenza season. Prevalence ratios were consistently higher for patients with more frequent visits to their health care providers, meaning that continued interaction with and communication from doctors increases the likelihood of vaccination. Dr. Benedict also recommended sending additional reminders throughout the season, and that patients should either seek out or be referred to doctors who offer influenza vaccinations themselves.
Dr. Benedict did not report any relevant financial disclosures.
ATLANTA – Mobile reminders from health care providers to their patients, notifying them to get influenza vaccinations, significantly increases the likelihood that those patients will get vaccinated, according to a study by Dr. Katherine A. Benedict and coinvestigators in the Enteric Diseases Epidemiology Branch at the Centers for Disease Control and Prevention. Dr. Benedict presented findings of the research at the International Conference on Emerging Infectious Diseases.
The researchers used data from the March 2012 National Flu Survey, a CDC “random digit dial telephone survey” of influenza vaccination trends in adults 18 years of age and older. They analyzed the data to determine whether or not patients received reminders, recommendations, or offers for influenza vaccinations from their health care providers since July 1, 2011. They did a logistic regression analysis to determine if there was any relationship between influenza vaccination rates and receipt of recommendations from health care providers.
Almost 73% of adults reported visiting a physician at least once since July 1, 2011, the start of data collection for the March 2012 study cycle, with 17.2% reporting that they received a reminder from their doctors to get a flu vaccine. Overall, 45.5% of adults ultimately got vaccinated, with 75.6% of those who reported receiving a reminder saying that they also were offered vaccinations by their doctors.
Adults who received recommendations for influenza vaccination from their health care providers were most likely to get vaccinated, and had an unadjusted prevalence ratio of 2.09. Next likely were those who received vaccination offers (PR = 1.90), and those who simply received reminders (PR = 1.33). Furthermore, those between 50 and 64 years old were found more likely to receive a recommendation or offer – PR = 1.23 and PR = 1.09, respectively – than were those in the 18- to 49-year age range (PR = 1.06 for recommendation, PR = 0.99 for offer).
The takeaway from this, according to the investigators, is that reminders should be sent at least once at the beginning of each influenza season. Prevalence ratios were consistently higher for patients with more frequent visits to their health care providers, meaning that continued interaction with and communication from doctors increases the likelihood of vaccination. Dr. Benedict also recommended sending additional reminders throughout the season, and that patients should either seek out or be referred to doctors who offer influenza vaccinations themselves.
Dr. Benedict did not report any relevant financial disclosures.
ATLANTA – Mobile reminders from health care providers to their patients, notifying them to get influenza vaccinations, significantly increases the likelihood that those patients will get vaccinated, according to a study by Dr. Katherine A. Benedict and coinvestigators in the Enteric Diseases Epidemiology Branch at the Centers for Disease Control and Prevention. Dr. Benedict presented findings of the research at the International Conference on Emerging Infectious Diseases.
The researchers used data from the March 2012 National Flu Survey, a CDC “random digit dial telephone survey” of influenza vaccination trends in adults 18 years of age and older. They analyzed the data to determine whether or not patients received reminders, recommendations, or offers for influenza vaccinations from their health care providers since July 1, 2011. They did a logistic regression analysis to determine if there was any relationship between influenza vaccination rates and receipt of recommendations from health care providers.
Almost 73% of adults reported visiting a physician at least once since July 1, 2011, the start of data collection for the March 2012 study cycle, with 17.2% reporting that they received a reminder from their doctors to get a flu vaccine. Overall, 45.5% of adults ultimately got vaccinated, with 75.6% of those who reported receiving a reminder saying that they also were offered vaccinations by their doctors.
Adults who received recommendations for influenza vaccination from their health care providers were most likely to get vaccinated, and had an unadjusted prevalence ratio of 2.09. Next likely were those who received vaccination offers (PR = 1.90), and those who simply received reminders (PR = 1.33). Furthermore, those between 50 and 64 years old were found more likely to receive a recommendation or offer – PR = 1.23 and PR = 1.09, respectively – than were those in the 18- to 49-year age range (PR = 1.06 for recommendation, PR = 0.99 for offer).
The takeaway from this, according to the investigators, is that reminders should be sent at least once at the beginning of each influenza season. Prevalence ratios were consistently higher for patients with more frequent visits to their health care providers, meaning that continued interaction with and communication from doctors increases the likelihood of vaccination. Dr. Benedict also recommended sending additional reminders throughout the season, and that patients should either seek out or be referred to doctors who offer influenza vaccinations themselves.
Dr. Benedict did not report any relevant financial disclosures.
AT ICEID 2015
Key clinical point: Sending patients reminders to get their influenza vaccinations can significantly increase the likelihood that these patients will actually go out and get the vaccine.
Major finding: Adults who received a recommendation for influenza vaccination were more likely to get vaccinated, with an adjusted prevalence ratio (APR) of 1.15.
Data source: Retrospective review of adults 18 years and older in the March 2012 National Flu Survey.
Disclosures: Dr. Benedict did not report any relevant financial disclosures.

VIDEO: CDC urges flu shots for all eligible patients
WASHINGTON – While influenza vaccination rates have increased in recent years, work still needs to be done to achieve the Centers for Disease Control and Prevention’s goal of at least 70% vaccination.
“Vaccination is the single-most-important step people can take to protect themselves from influenza,” Dr. Tom Frieden, CDC director said at a press conference called by his agency and the National Foundation for Infectious Diseases (NFID). He urged people to get their influenza vaccination and make sure their children do as well.
The CDC estimates that 47% of U.S. residents aged 6 months or older received an influenza vaccination in the last flu season. The only age group that meets the federal 70% benchmark is the 6-23 months age group, with about 75% coverage. Children aged 2-4 years have a vaccination rate of 68%; adults aged 65 years and older have a vaccination rate of 67%; and 62% of children aged 5-12 years get vaccinated. The lowest vaccination rate is among adults aged 18-49 years, of whom only 40% get vaccinated.
Dr. Frieden was joined at the press event by Dr. William Schaffner, NFID medical director; Dr. Wendy Sue Swanson of Seattle Children’s Hospital; and Dr. Kathleen Neuzil, director of the Center for Vaccine Development at the University of Maryland, Baltimore.
In this interview, Dr. Neuzil discusses which strains of influenza are expected to be dominant in the coming flu season, whether to expect a strain mutation similar to what happened last season, the importance of getting children vaccinated, and pneumococcal vaccination for children and older adults.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – While influenza vaccination rates have increased in recent years, work still needs to be done to achieve the Centers for Disease Control and Prevention’s goal of at least 70% vaccination.
“Vaccination is the single-most-important step people can take to protect themselves from influenza,” Dr. Tom Frieden, CDC director said at a press conference called by his agency and the National Foundation for Infectious Diseases (NFID). He urged people to get their influenza vaccination and make sure their children do as well.
The CDC estimates that 47% of U.S. residents aged 6 months or older received an influenza vaccination in the last flu season. The only age group that meets the federal 70% benchmark is the 6-23 months age group, with about 75% coverage. Children aged 2-4 years have a vaccination rate of 68%; adults aged 65 years and older have a vaccination rate of 67%; and 62% of children aged 5-12 years get vaccinated. The lowest vaccination rate is among adults aged 18-49 years, of whom only 40% get vaccinated.
Dr. Frieden was joined at the press event by Dr. William Schaffner, NFID medical director; Dr. Wendy Sue Swanson of Seattle Children’s Hospital; and Dr. Kathleen Neuzil, director of the Center for Vaccine Development at the University of Maryland, Baltimore.
In this interview, Dr. Neuzil discusses which strains of influenza are expected to be dominant in the coming flu season, whether to expect a strain mutation similar to what happened last season, the importance of getting children vaccinated, and pneumococcal vaccination for children and older adults.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
WASHINGTON – While influenza vaccination rates have increased in recent years, work still needs to be done to achieve the Centers for Disease Control and Prevention’s goal of at least 70% vaccination.
“Vaccination is the single-most-important step people can take to protect themselves from influenza,” Dr. Tom Frieden, CDC director said at a press conference called by his agency and the National Foundation for Infectious Diseases (NFID). He urged people to get their influenza vaccination and make sure their children do as well.
The CDC estimates that 47% of U.S. residents aged 6 months or older received an influenza vaccination in the last flu season. The only age group that meets the federal 70% benchmark is the 6-23 months age group, with about 75% coverage. Children aged 2-4 years have a vaccination rate of 68%; adults aged 65 years and older have a vaccination rate of 67%; and 62% of children aged 5-12 years get vaccinated. The lowest vaccination rate is among adults aged 18-49 years, of whom only 40% get vaccinated.
Dr. Frieden was joined at the press event by Dr. William Schaffner, NFID medical director; Dr. Wendy Sue Swanson of Seattle Children’s Hospital; and Dr. Kathleen Neuzil, director of the Center for Vaccine Development at the University of Maryland, Baltimore.
In this interview, Dr. Neuzil discusses which strains of influenza are expected to be dominant in the coming flu season, whether to expect a strain mutation similar to what happened last season, the importance of getting children vaccinated, and pneumococcal vaccination for children and older adults.
The video associated with this article is no longer available on this site. Please view all of our videos on the MDedge YouTube channel
AT A CDC/NFID PRESS CONFERENCE
Uptick in health care workers getting flu shots in 2014-2015 season
Overall, 77.3% of health care personnel reported receiving an influenza vaccination during the 2014-2015 season, with the highest vaccination coverage was reported in work sites with employer requirements for vaccination, according to an investigation published in MMWR (2015 Sep 18;64[36]:993-9).
Vaccination data came from an opt-in Internet panel survey conducted by Abt Associates for the Centers for Disease Control and Prevention, and included questions on demographic characteristics, occupation, work setting, self-reported influenza vaccination, and employer vaccination policies. Results from 1,914 survey responses were analyzed. The overall health care personnel (HCP) influenza vaccination coverage estimate for the 2014-2015 season was 77.3%, compared with 75.2% for the 2013-2014 season. When compared with the 2013-2014 season, coverage in 2014-2015 was higher among pharmacists (95.3% vs. 85.7%), assistants/aides (64.4% vs. 57.7%), and nonclinical personnel (75.2% vs. 68.6%). Coverage among other clinical personnel decreased from 87.4% in 2013-2014 to 81.3% in 2014-2015, while other categories experienced little change between the two time periods.
The team of researchers, led by Carla L. Black, Ph.D., of the National Center for Immunization and Respiratory Diseases, CDC, noted that among HCP whose employers did not require vaccination, vaccination coverage among those who worked in locations where their employer made vaccination available on-site at no cost for more than 1 day was 83.9%, compared with coverage of 73.6% among those who worked in locations where their employer made vaccination available at no cost for 1 day only, and 59.5% among those who worked in locations where their employer did not provide influenza vaccination on-site at no cost but actively promoted vaccination through other mechanisms.
“These findings support recommendations for a comprehensive strategy that includes easy access to vaccination at no cost on multiple days, along with promotion of vaccination, to increase HCP influenza vaccination coverage,” the authors wrote.
Read the full report here: http://www.cdc.gov/mmwr/.
Overall, 77.3% of health care personnel reported receiving an influenza vaccination during the 2014-2015 season, with the highest vaccination coverage was reported in work sites with employer requirements for vaccination, according to an investigation published in MMWR (2015 Sep 18;64[36]:993-9).
Vaccination data came from an opt-in Internet panel survey conducted by Abt Associates for the Centers for Disease Control and Prevention, and included questions on demographic characteristics, occupation, work setting, self-reported influenza vaccination, and employer vaccination policies. Results from 1,914 survey responses were analyzed. The overall health care personnel (HCP) influenza vaccination coverage estimate for the 2014-2015 season was 77.3%, compared with 75.2% for the 2013-2014 season. When compared with the 2013-2014 season, coverage in 2014-2015 was higher among pharmacists (95.3% vs. 85.7%), assistants/aides (64.4% vs. 57.7%), and nonclinical personnel (75.2% vs. 68.6%). Coverage among other clinical personnel decreased from 87.4% in 2013-2014 to 81.3% in 2014-2015, while other categories experienced little change between the two time periods.
The team of researchers, led by Carla L. Black, Ph.D., of the National Center for Immunization and Respiratory Diseases, CDC, noted that among HCP whose employers did not require vaccination, vaccination coverage among those who worked in locations where their employer made vaccination available on-site at no cost for more than 1 day was 83.9%, compared with coverage of 73.6% among those who worked in locations where their employer made vaccination available at no cost for 1 day only, and 59.5% among those who worked in locations where their employer did not provide influenza vaccination on-site at no cost but actively promoted vaccination through other mechanisms.
“These findings support recommendations for a comprehensive strategy that includes easy access to vaccination at no cost on multiple days, along with promotion of vaccination, to increase HCP influenza vaccination coverage,” the authors wrote.
Read the full report here: http://www.cdc.gov/mmwr/.
Overall, 77.3% of health care personnel reported receiving an influenza vaccination during the 2014-2015 season, with the highest vaccination coverage was reported in work sites with employer requirements for vaccination, according to an investigation published in MMWR (2015 Sep 18;64[36]:993-9).
Vaccination data came from an opt-in Internet panel survey conducted by Abt Associates for the Centers for Disease Control and Prevention, and included questions on demographic characteristics, occupation, work setting, self-reported influenza vaccination, and employer vaccination policies. Results from 1,914 survey responses were analyzed. The overall health care personnel (HCP) influenza vaccination coverage estimate for the 2014-2015 season was 77.3%, compared with 75.2% for the 2013-2014 season. When compared with the 2013-2014 season, coverage in 2014-2015 was higher among pharmacists (95.3% vs. 85.7%), assistants/aides (64.4% vs. 57.7%), and nonclinical personnel (75.2% vs. 68.6%). Coverage among other clinical personnel decreased from 87.4% in 2013-2014 to 81.3% in 2014-2015, while other categories experienced little change between the two time periods.
The team of researchers, led by Carla L. Black, Ph.D., of the National Center for Immunization and Respiratory Diseases, CDC, noted that among HCP whose employers did not require vaccination, vaccination coverage among those who worked in locations where their employer made vaccination available on-site at no cost for more than 1 day was 83.9%, compared with coverage of 73.6% among those who worked in locations where their employer made vaccination available at no cost for 1 day only, and 59.5% among those who worked in locations where their employer did not provide influenza vaccination on-site at no cost but actively promoted vaccination through other mechanisms.
“These findings support recommendations for a comprehensive strategy that includes easy access to vaccination at no cost on multiple days, along with promotion of vaccination, to increase HCP influenza vaccination coverage,” the authors wrote.
Read the full report here: http://www.cdc.gov/mmwr/.
FROM MORBIDITY AND MORTALITY WEEKLY REPORT
ICEID: Population-level data support ACIP flu vaccine recommendations
ATLANTA – Expanded influenza vaccination coverage among children between 2002 and 2012 appears to have provided direct benefit with respect to influenza-related hospitalizations among vaccinated children, according to an analysis of vaccination and hospitalization data.
Additionally, the coverage among children appears to have provided indirect benefits in adults, Cecile Viboud, Ph.D. of the National Institutes of Health, Bethesda, Md., reported at the International Conference on Emerging Infectious Diseases.

Between 2006-2007 and 2010-2011, the U.S. Advisory Committee on Immunization Practices (ACIP) broadened vaccination recommendations to include not only children aged 6-23 months, but also those aged 24-59 months, then those aged 5-18 years, and eventually all those over age 6 months. Consequently, the vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 (and to about 70% in those under age 5 years). Modeling of weekly influenza-related hospitalization outcomes (pneumonia and influenza outcomes and respiratory and circulatory outcomes) provided solid evidence of a direct and significant protective effect of vaccination both in children under age 5 years and in those aged 5-19 years. This finding was consistent across disease outcomes, and remained significant in those under age 5 after adjusting for state, but the association was weaker with stratification by season, Dr. Viboud noted.
Further, hospitalization rates among working-age adults and seniors aged 65-74 years declined with increasing pediatric vaccine coverage, suggesting an indirect protective effect in that population, she said, noting that the vaccination rate among older adults remained stable across the study period.
No evidence was seen for an indirect protective effect among adults over age 74 years, she said.
Dr. Viboud and her colleagues used age-specific annual vaccination rates derived from the National Immunization Survey and the Behavioral Risk Factor Surveillance System. Age-specific rates of influenza-associated hospitalizations were estimated for each season during 1989-2012 by modeling weekly pneumonia and influenza outcomes plus respiratory and circulatory outcomes from the State Inpatient Databases of the Agency for Healthcare Research & Quality.
“In a nutshell, we see strong statistical evidence for the direct protective effects of the influenza vaccination program in children on the basis of analyses of population-level hospitalization data, which supports the expansion of the ACIP flu vaccine recommendations in the past decade,” Dr. Viboud said in an interview. “We also find weak evidence of herd immunity effects, whereby hospitalization rates are reduced in adults. That the evidence is weak is perhaps not surprising given that vaccine uptake in children remains moderate (60% in most highly vaccinated states) and vaccine effectiveness is modest at 40%-60% depending on the season. Independent information from mathematical transmission models confirms that herd immunity benefits are expected to be low given these levels of vaccine coverage.”
The indirect effects may become clearer with increasing vaccine uptake, she added.
Dr. Viboud reported having no disclosures.
ATLANTA – Expanded influenza vaccination coverage among children between 2002 and 2012 appears to have provided direct benefit with respect to influenza-related hospitalizations among vaccinated children, according to an analysis of vaccination and hospitalization data.
Additionally, the coverage among children appears to have provided indirect benefits in adults, Cecile Viboud, Ph.D. of the National Institutes of Health, Bethesda, Md., reported at the International Conference on Emerging Infectious Diseases.
Between 2006-2007 and 2010-2011, the U.S. Advisory Committee on Immunization Practices (ACIP) broadened vaccination recommendations to include not only children aged 6-23 months, but also those aged 24-59 months, then those aged 5-18 years, and eventually all those over age 6 months. Consequently, the vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 (and to about 70% in those under age 5 years). Modeling of weekly influenza-related hospitalization outcomes (pneumonia and influenza outcomes and respiratory and circulatory outcomes) provided solid evidence of a direct and significant protective effect of vaccination both in children under age 5 years and in those aged 5-19 years. This finding was consistent across disease outcomes, and remained significant in those under age 5 after adjusting for state, but the association was weaker with stratification by season, Dr. Viboud noted.
Further, hospitalization rates among working-age adults and seniors aged 65-74 years declined with increasing pediatric vaccine coverage, suggesting an indirect protective effect in that population, she said, noting that the vaccination rate among older adults remained stable across the study period.
No evidence was seen for an indirect protective effect among adults over age 74 years, she said.
Dr. Viboud and her colleagues used age-specific annual vaccination rates derived from the National Immunization Survey and the Behavioral Risk Factor Surveillance System. Age-specific rates of influenza-associated hospitalizations were estimated for each season during 1989-2012 by modeling weekly pneumonia and influenza outcomes plus respiratory and circulatory outcomes from the State Inpatient Databases of the Agency for Healthcare Research & Quality.
“In a nutshell, we see strong statistical evidence for the direct protective effects of the influenza vaccination program in children on the basis of analyses of population-level hospitalization data, which supports the expansion of the ACIP flu vaccine recommendations in the past decade,” Dr. Viboud said in an interview. “We also find weak evidence of herd immunity effects, whereby hospitalization rates are reduced in adults. That the evidence is weak is perhaps not surprising given that vaccine uptake in children remains moderate (60% in most highly vaccinated states) and vaccine effectiveness is modest at 40%-60% depending on the season. Independent information from mathematical transmission models confirms that herd immunity benefits are expected to be low given these levels of vaccine coverage.”
The indirect effects may become clearer with increasing vaccine uptake, she added.
Dr. Viboud reported having no disclosures.
ATLANTA – Expanded influenza vaccination coverage among children between 2002 and 2012 appears to have provided direct benefit with respect to influenza-related hospitalizations among vaccinated children, according to an analysis of vaccination and hospitalization data.
Additionally, the coverage among children appears to have provided indirect benefits in adults, Cecile Viboud, Ph.D. of the National Institutes of Health, Bethesda, Md., reported at the International Conference on Emerging Infectious Diseases.
Between 2006-2007 and 2010-2011, the U.S. Advisory Committee on Immunization Practices (ACIP) broadened vaccination recommendations to include not only children aged 6-23 months, but also those aged 24-59 months, then those aged 5-18 years, and eventually all those over age 6 months. Consequently, the vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 (and to about 70% in those under age 5 years). Modeling of weekly influenza-related hospitalization outcomes (pneumonia and influenza outcomes and respiratory and circulatory outcomes) provided solid evidence of a direct and significant protective effect of vaccination both in children under age 5 years and in those aged 5-19 years. This finding was consistent across disease outcomes, and remained significant in those under age 5 after adjusting for state, but the association was weaker with stratification by season, Dr. Viboud noted.
Further, hospitalization rates among working-age adults and seniors aged 65-74 years declined with increasing pediatric vaccine coverage, suggesting an indirect protective effect in that population, she said, noting that the vaccination rate among older adults remained stable across the study period.
No evidence was seen for an indirect protective effect among adults over age 74 years, she said.
Dr. Viboud and her colleagues used age-specific annual vaccination rates derived from the National Immunization Survey and the Behavioral Risk Factor Surveillance System. Age-specific rates of influenza-associated hospitalizations were estimated for each season during 1989-2012 by modeling weekly pneumonia and influenza outcomes plus respiratory and circulatory outcomes from the State Inpatient Databases of the Agency for Healthcare Research & Quality.
“In a nutshell, we see strong statistical evidence for the direct protective effects of the influenza vaccination program in children on the basis of analyses of population-level hospitalization data, which supports the expansion of the ACIP flu vaccine recommendations in the past decade,” Dr. Viboud said in an interview. “We also find weak evidence of herd immunity effects, whereby hospitalization rates are reduced in adults. That the evidence is weak is perhaps not surprising given that vaccine uptake in children remains moderate (60% in most highly vaccinated states) and vaccine effectiveness is modest at 40%-60% depending on the season. Independent information from mathematical transmission models confirms that herd immunity benefits are expected to be low given these levels of vaccine coverage.”
The indirect effects may become clearer with increasing vaccine uptake, she added.
Dr. Viboud reported having no disclosures.
AT ICEID 2015
Key clinical point: Expanded influenza vaccination coverage in children provided direct benefits with respect to hospitalizations.
Major finding: Vaccine coverage rate increased from less than 5% in 2002 to about 52% in 2012 .
Data source: An analysis of vaccination and hospitalization data.
Disclosures: Dr. Viboud reported having no disclosures.

Flu vaccine and heart attacks
As we head into influenza season, we are likely steeling our nerves for the inevitable debate with some of our patients about receiving the influenza vaccination.
We are used to hearing patients say, “I have never had it, and I have never gotten the flu,” or (my favorite), “Last time I got the shot, I got the flu.” Arguments that – while defying chance, logic, and science in general – keep us rooted in the daily joys of clinical practice.
Some handy influenza facts:
1. In well-matched years, the number needed to treat (NNT) to prevent one flu-like illness is 33.
2. In unmatched years, the NNT is 100.
We should be adding to this discussion some information about the observed association between the influenza vaccine and acute myocardial infarction (AMI). If compelling arguments about preventing flu-like symptoms don’t carry the day, maybe preventing heart attack will.
Dr. Michelle Barnes and her colleagues at UNSW Australia, Sydney, published the results of a systematic review of case-control studies evaluating the association between the influenza vaccine and AMI (Heart, 2015 Aug. 26. doi:10.1136/heartjnl-2015-307691). In this study, the investigators identified 16 studies on AMI and influenza vaccination or influenza infection.
The odds of influenza infection, influenza-like illness, or respiratory infection were significantly greater in patients with AMI (odds ratio, 2.01; 95% confidence interval: 1.47-2.76). Influenza vaccine was associated with a lower risk of AMI (OR, 0.71; 95% CI: 0.56-0.91).
This is the first meta-analysis compiling all case-control data on the relationship between AMI and the influenza vaccine. Overall, cases had double the risk of influenza or respiratory tract infection, compared with controls.
Influenza has been hypothesized to cause coronary artery occlusion through stenosis of subcritical atherosclerotic plaque, and it has been shown to promote atherogenesis in animal models. The connection between AMI and influenza was first observed in the 1930s during the flu season.
But medicine has a short memory, and our patients sometimes do as well. So, it is time we remind them about this link and encourage them to get their flu shots.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article. Follow him on Twitter @jonebbert.
As we head into influenza season, we are likely steeling our nerves for the inevitable debate with some of our patients about receiving the influenza vaccination.
We are used to hearing patients say, “I have never had it, and I have never gotten the flu,” or (my favorite), “Last time I got the shot, I got the flu.” Arguments that – while defying chance, logic, and science in general – keep us rooted in the daily joys of clinical practice.
Some handy influenza facts:
1. In well-matched years, the number needed to treat (NNT) to prevent one flu-like illness is 33.
2. In unmatched years, the NNT is 100.
We should be adding to this discussion some information about the observed association between the influenza vaccine and acute myocardial infarction (AMI). If compelling arguments about preventing flu-like symptoms don’t carry the day, maybe preventing heart attack will.
Dr. Michelle Barnes and her colleagues at UNSW Australia, Sydney, published the results of a systematic review of case-control studies evaluating the association between the influenza vaccine and AMI (Heart, 2015 Aug. 26. doi:10.1136/heartjnl-2015-307691). In this study, the investigators identified 16 studies on AMI and influenza vaccination or influenza infection.
The odds of influenza infection, influenza-like illness, or respiratory infection were significantly greater in patients with AMI (odds ratio, 2.01; 95% confidence interval: 1.47-2.76). Influenza vaccine was associated with a lower risk of AMI (OR, 0.71; 95% CI: 0.56-0.91).
This is the first meta-analysis compiling all case-control data on the relationship between AMI and the influenza vaccine. Overall, cases had double the risk of influenza or respiratory tract infection, compared with controls.
Influenza has been hypothesized to cause coronary artery occlusion through stenosis of subcritical atherosclerotic plaque, and it has been shown to promote atherogenesis in animal models. The connection between AMI and influenza was first observed in the 1930s during the flu season.
But medicine has a short memory, and our patients sometimes do as well. So, it is time we remind them about this link and encourage them to get their flu shots.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article. Follow him on Twitter @jonebbert.
As we head into influenza season, we are likely steeling our nerves for the inevitable debate with some of our patients about receiving the influenza vaccination.
We are used to hearing patients say, “I have never had it, and I have never gotten the flu,” or (my favorite), “Last time I got the shot, I got the flu.” Arguments that – while defying chance, logic, and science in general – keep us rooted in the daily joys of clinical practice.
Some handy influenza facts:
1. In well-matched years, the number needed to treat (NNT) to prevent one flu-like illness is 33.
2. In unmatched years, the NNT is 100.
We should be adding to this discussion some information about the observed association between the influenza vaccine and acute myocardial infarction (AMI). If compelling arguments about preventing flu-like symptoms don’t carry the day, maybe preventing heart attack will.
Dr. Michelle Barnes and her colleagues at UNSW Australia, Sydney, published the results of a systematic review of case-control studies evaluating the association between the influenza vaccine and AMI (Heart, 2015 Aug. 26. doi:10.1136/heartjnl-2015-307691). In this study, the investigators identified 16 studies on AMI and influenza vaccination or influenza infection.
The odds of influenza infection, influenza-like illness, or respiratory infection were significantly greater in patients with AMI (odds ratio, 2.01; 95% confidence interval: 1.47-2.76). Influenza vaccine was associated with a lower risk of AMI (OR, 0.71; 95% CI: 0.56-0.91).
This is the first meta-analysis compiling all case-control data on the relationship between AMI and the influenza vaccine. Overall, cases had double the risk of influenza or respiratory tract infection, compared with controls.
Influenza has been hypothesized to cause coronary artery occlusion through stenosis of subcritical atherosclerotic plaque, and it has been shown to promote atherogenesis in animal models. The connection between AMI and influenza was first observed in the 1930s during the flu season.
But medicine has a short memory, and our patients sometimes do as well. So, it is time we remind them about this link and encourage them to get their flu shots.
Dr. Ebbert is professor of medicine, a general internist at the Mayo Clinic in Rochester, Minn., and a diplomate of the American Board of Addiction Medicine. The opinions expressed are those of the author and do not necessarily represent the views and opinions of the Mayo Clinic. The opinions expressed in this article should not be used to diagnose or treat any medical condition nor should they be used as a substitute for medical advice from a qualified, board-certified practicing clinician. Dr. Ebbert has no relevant financial disclosures about this article. Follow him on Twitter @jonebbert.
