User login
Experimental Topical Drug Shows Promise for Atopic Dermatitis and Plaque Psoriasis
, results from a phase 2a study showed.

PDE4 inhibitors are a promising therapeutic target for inflammatory diseases because “they can increase cyclic adenosine monophosphate levels and subsequently reduce the production of proinflammatory cytokines,” lead study author Lawrence F. Eichenfield, MD, of the dermatology department at the University of California, San Diego, and colleagues wrote. The paper was published online in JAMA Dermatology.
Currently Available Treatments
For plaque psoriasis, the FDA approved the topical PDE4 inhibitor roflumilast in 2022. The oral PDE4 inhibitor apremilast has shown to be effective for plaque psoriasis and is well tolerated, and “it has been associated with gastrointestinal adverse events (AEs) such as nausea and diarrhea,” the researchers wrote.
For AD, crisaborole is the only approved topical PDE4 treatment, and it is associated with application site burning and stinging, they wrote.
An Experimental Alternative
The new study tested a topical PDE4 inhibitor known as PF-07038124, which is being developed by Pfizer. It is designed to be “a potent, oxaborole-based PDE4 inhibitor [that shows] immunomodulatory activity in T-cell–based assays, contributing to inhibition of [interleukin]-4 and IL-13; thus, it could provide therapeutic benefit in the treatment of AD and plaque psoriasis,” the authors wrote.
The phase 2a study was conducted from December 21, 2020, to August 18, 2021. Researchers at 34 sites in four countries randomized 104 patients with mild to moderate AD (70) or plaque psoriasis (34) to receive PF-07038124 as a 0.001% topical ointment or a vehicle only once daily for 6 weeks.
The primary end point was the percent change from baseline in the Eczema Area and Severity Index (EASI) total score among patients with AD and in the Psoriasis Area and Severity Index (PASI) score among patients with plaque psoriasis at week 6. Safety measures of interest included treatment-emergent adverse events.
Overall, the mean age of the 104 patients was 43 years, 52.9%, were women, 3.8% were Asian, 12.5% were Black, and 83.7% were White. Most had moderate disease.
At week 6 in patients with AD, the PF-07038124 group showed statistically significantly greater improvement in the EASI total score, compared with vehicle group (−74.9% vs −35.5% respectively; least squares mean [LSM] difference, −39.4%; 90% CI, −58.8% to−20.1%]; P < .001).
Similarly, at week 6 in patients with plaque psoriasis, the PF-07038124 group demonstrated a significantly greater improvement in the PASI total score, compared with the vehicle group (LSM, −4.8; 90% CI, −6.2 to −3.4] vs 0.1; 90% CI, −1.5 to 1.7), for a difference of −4.9; 90% CI, −7.0 to −2.8; P < .001.
In safety outcomes, treatment-emergent adverse events were reported in 16 people receiving PF-07038124 and 26 people receiving a vehicle. The treatment-related adverse events were reported only in the vehicle groups across all indications, while no patients in the PF-07038124 groups experienced pain or skin reactions at the application sites.
The researchers acknowledged certain limitations of the trial, including its small size and the 6-week treatment period. “Unlike crisaborole, topical PF-07038124 was not associated with application site burning and stinging,” they noted. “To confirm persistence of efficacy and the safety profile of PF-07038124, long-term data should be collected in larger studies.”
Pfizer supported the study. Dr. Eichenfield reported receiving personal fees from Pfizer during the conduct of the study. He also has received grant support from, is consultant to, and/or is a member of the advisory board for many other pharmaceutical companies. Several other study authors reported similar disclosures.
, results from a phase 2a study showed.
PDE4 inhibitors are a promising therapeutic target for inflammatory diseases because “they can increase cyclic adenosine monophosphate levels and subsequently reduce the production of proinflammatory cytokines,” lead study author Lawrence F. Eichenfield, MD, of the dermatology department at the University of California, San Diego, and colleagues wrote. The paper was published online in JAMA Dermatology.
Currently Available Treatments
For plaque psoriasis, the FDA approved the topical PDE4 inhibitor roflumilast in 2022. The oral PDE4 inhibitor apremilast has shown to be effective for plaque psoriasis and is well tolerated, and “it has been associated with gastrointestinal adverse events (AEs) such as nausea and diarrhea,” the researchers wrote.
For AD, crisaborole is the only approved topical PDE4 treatment, and it is associated with application site burning and stinging, they wrote.
An Experimental Alternative
The new study tested a topical PDE4 inhibitor known as PF-07038124, which is being developed by Pfizer. It is designed to be “a potent, oxaborole-based PDE4 inhibitor [that shows] immunomodulatory activity in T-cell–based assays, contributing to inhibition of [interleukin]-4 and IL-13; thus, it could provide therapeutic benefit in the treatment of AD and plaque psoriasis,” the authors wrote.
The phase 2a study was conducted from December 21, 2020, to August 18, 2021. Researchers at 34 sites in four countries randomized 104 patients with mild to moderate AD (70) or plaque psoriasis (34) to receive PF-07038124 as a 0.001% topical ointment or a vehicle only once daily for 6 weeks.
The primary end point was the percent change from baseline in the Eczema Area and Severity Index (EASI) total score among patients with AD and in the Psoriasis Area and Severity Index (PASI) score among patients with plaque psoriasis at week 6. Safety measures of interest included treatment-emergent adverse events.
Overall, the mean age of the 104 patients was 43 years, 52.9%, were women, 3.8% were Asian, 12.5% were Black, and 83.7% were White. Most had moderate disease.
At week 6 in patients with AD, the PF-07038124 group showed statistically significantly greater improvement in the EASI total score, compared with vehicle group (−74.9% vs −35.5% respectively; least squares mean [LSM] difference, −39.4%; 90% CI, −58.8% to−20.1%]; P < .001).
Similarly, at week 6 in patients with plaque psoriasis, the PF-07038124 group demonstrated a significantly greater improvement in the PASI total score, compared with the vehicle group (LSM, −4.8; 90% CI, −6.2 to −3.4] vs 0.1; 90% CI, −1.5 to 1.7), for a difference of −4.9; 90% CI, −7.0 to −2.8; P < .001.
In safety outcomes, treatment-emergent adverse events were reported in 16 people receiving PF-07038124 and 26 people receiving a vehicle. The treatment-related adverse events were reported only in the vehicle groups across all indications, while no patients in the PF-07038124 groups experienced pain or skin reactions at the application sites.
The researchers acknowledged certain limitations of the trial, including its small size and the 6-week treatment period. “Unlike crisaborole, topical PF-07038124 was not associated with application site burning and stinging,” they noted. “To confirm persistence of efficacy and the safety profile of PF-07038124, long-term data should be collected in larger studies.”
Pfizer supported the study. Dr. Eichenfield reported receiving personal fees from Pfizer during the conduct of the study. He also has received grant support from, is consultant to, and/or is a member of the advisory board for many other pharmaceutical companies. Several other study authors reported similar disclosures.
, results from a phase 2a study showed.
PDE4 inhibitors are a promising therapeutic target for inflammatory diseases because “they can increase cyclic adenosine monophosphate levels and subsequently reduce the production of proinflammatory cytokines,” lead study author Lawrence F. Eichenfield, MD, of the dermatology department at the University of California, San Diego, and colleagues wrote. The paper was published online in JAMA Dermatology.
Currently Available Treatments
For plaque psoriasis, the FDA approved the topical PDE4 inhibitor roflumilast in 2022. The oral PDE4 inhibitor apremilast has shown to be effective for plaque psoriasis and is well tolerated, and “it has been associated with gastrointestinal adverse events (AEs) such as nausea and diarrhea,” the researchers wrote.
For AD, crisaborole is the only approved topical PDE4 treatment, and it is associated with application site burning and stinging, they wrote.
An Experimental Alternative
The new study tested a topical PDE4 inhibitor known as PF-07038124, which is being developed by Pfizer. It is designed to be “a potent, oxaborole-based PDE4 inhibitor [that shows] immunomodulatory activity in T-cell–based assays, contributing to inhibition of [interleukin]-4 and IL-13; thus, it could provide therapeutic benefit in the treatment of AD and plaque psoriasis,” the authors wrote.
The phase 2a study was conducted from December 21, 2020, to August 18, 2021. Researchers at 34 sites in four countries randomized 104 patients with mild to moderate AD (70) or plaque psoriasis (34) to receive PF-07038124 as a 0.001% topical ointment or a vehicle only once daily for 6 weeks.
The primary end point was the percent change from baseline in the Eczema Area and Severity Index (EASI) total score among patients with AD and in the Psoriasis Area and Severity Index (PASI) score among patients with plaque psoriasis at week 6. Safety measures of interest included treatment-emergent adverse events.
Overall, the mean age of the 104 patients was 43 years, 52.9%, were women, 3.8% were Asian, 12.5% were Black, and 83.7% were White. Most had moderate disease.
At week 6 in patients with AD, the PF-07038124 group showed statistically significantly greater improvement in the EASI total score, compared with vehicle group (−74.9% vs −35.5% respectively; least squares mean [LSM] difference, −39.4%; 90% CI, −58.8% to−20.1%]; P < .001).
Similarly, at week 6 in patients with plaque psoriasis, the PF-07038124 group demonstrated a significantly greater improvement in the PASI total score, compared with the vehicle group (LSM, −4.8; 90% CI, −6.2 to −3.4] vs 0.1; 90% CI, −1.5 to 1.7), for a difference of −4.9; 90% CI, −7.0 to −2.8; P < .001.
In safety outcomes, treatment-emergent adverse events were reported in 16 people receiving PF-07038124 and 26 people receiving a vehicle. The treatment-related adverse events were reported only in the vehicle groups across all indications, while no patients in the PF-07038124 groups experienced pain or skin reactions at the application sites.
The researchers acknowledged certain limitations of the trial, including its small size and the 6-week treatment period. “Unlike crisaborole, topical PF-07038124 was not associated with application site burning and stinging,” they noted. “To confirm persistence of efficacy and the safety profile of PF-07038124, long-term data should be collected in larger studies.”
Pfizer supported the study. Dr. Eichenfield reported receiving personal fees from Pfizer during the conduct of the study. He also has received grant support from, is consultant to, and/or is a member of the advisory board for many other pharmaceutical companies. Several other study authors reported similar disclosures.
FROM JAMA DERMATOLOGY
Expert Frames Factors to Consider Among Atopic Dermatitis Treatment Options
With so many treatment options available for atopic dermatitis (AD) and more in the pipeline, one common question Raj Chovatiya, MD, PhD, hears from his fellow dermatologists is: How do I choose the right therapy for my patients?
“There isn’t going to be a one-size-fits-all approach, and it may be impossible to differentiate, given that these agents are not likely to be studied head-to-head,” Dr. Chovatiya, assistant professor in the department of dermatology at Northwestern University, Chicago, said during the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.

He shared . These include:
- Severity of disease (mild vs moderate vs severe).
- Extent of disease (low vs high body surface area).
- Rapidity of drug onset (hours vs days vs weeks).
- Depth of response based on different endpoints such as itch and number of lesions.
- Long-term efficacy (durability on treatment vs off treatment).
- Adverse events (cutaneous vs systemic).
- Black box warnings (present vs absent).
- Tolerance (selective areas vs the entire skin).
- Vehicle (ointment vs cream).
- Patient preference. “This may be the biggest driver; what do patients want?” Dr. Chovatiya said.
- Access to the drug. Is it easily obtainable for the patient?
He concluded his remarks by posing a question to attendees: “Are we closer to living in a topical steroid–free world for AD? Is that what we want?” he asked. “I wholeheartedly say that’s what we’ve been working toward all these years, and we should keep up the good fight. We have more data for targeted therapy to treat very specific disease with very specific outcomes and endpoints, because I think that’s [what] we all dream about in dermatology.”
Dr. Chovatiya disclosed that he is speaker for and/or a consultant and advisory board member to many pharmaceutical companies.
With so many treatment options available for atopic dermatitis (AD) and more in the pipeline, one common question Raj Chovatiya, MD, PhD, hears from his fellow dermatologists is: How do I choose the right therapy for my patients?
“There isn’t going to be a one-size-fits-all approach, and it may be impossible to differentiate, given that these agents are not likely to be studied head-to-head,” Dr. Chovatiya, assistant professor in the department of dermatology at Northwestern University, Chicago, said during the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.
He shared . These include:
- Severity of disease (mild vs moderate vs severe).
- Extent of disease (low vs high body surface area).
- Rapidity of drug onset (hours vs days vs weeks).
- Depth of response based on different endpoints such as itch and number of lesions.
- Long-term efficacy (durability on treatment vs off treatment).
- Adverse events (cutaneous vs systemic).
- Black box warnings (present vs absent).
- Tolerance (selective areas vs the entire skin).
- Vehicle (ointment vs cream).
- Patient preference. “This may be the biggest driver; what do patients want?” Dr. Chovatiya said.
- Access to the drug. Is it easily obtainable for the patient?
He concluded his remarks by posing a question to attendees: “Are we closer to living in a topical steroid–free world for AD? Is that what we want?” he asked. “I wholeheartedly say that’s what we’ve been working toward all these years, and we should keep up the good fight. We have more data for targeted therapy to treat very specific disease with very specific outcomes and endpoints, because I think that’s [what] we all dream about in dermatology.”
Dr. Chovatiya disclosed that he is speaker for and/or a consultant and advisory board member to many pharmaceutical companies.
With so many treatment options available for atopic dermatitis (AD) and more in the pipeline, one common question Raj Chovatiya, MD, PhD, hears from his fellow dermatologists is: How do I choose the right therapy for my patients?
“There isn’t going to be a one-size-fits-all approach, and it may be impossible to differentiate, given that these agents are not likely to be studied head-to-head,” Dr. Chovatiya, assistant professor in the department of dermatology at Northwestern University, Chicago, said during the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.
He shared . These include:
- Severity of disease (mild vs moderate vs severe).
- Extent of disease (low vs high body surface area).
- Rapidity of drug onset (hours vs days vs weeks).
- Depth of response based on different endpoints such as itch and number of lesions.
- Long-term efficacy (durability on treatment vs off treatment).
- Adverse events (cutaneous vs systemic).
- Black box warnings (present vs absent).
- Tolerance (selective areas vs the entire skin).
- Vehicle (ointment vs cream).
- Patient preference. “This may be the biggest driver; what do patients want?” Dr. Chovatiya said.
- Access to the drug. Is it easily obtainable for the patient?
He concluded his remarks by posing a question to attendees: “Are we closer to living in a topical steroid–free world for AD? Is that what we want?” he asked. “I wholeheartedly say that’s what we’ve been working toward all these years, and we should keep up the good fight. We have more data for targeted therapy to treat very specific disease with very specific outcomes and endpoints, because I think that’s [what] we all dream about in dermatology.”
Dr. Chovatiya disclosed that he is speaker for and/or a consultant and advisory board member to many pharmaceutical companies.
FROM RAD 2023
‘Milestone’ Study Zeros in on 5-Year Safety Data From Upadacitinib Trials
, underscoring the medication’s stable safety profile over an extended duration.
Those are among the key findings from an integrated analysis of long-term upadacitinib use presented by Christopher G. Bunick, MD, PhD, during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis Virtual Conference. Upadacitinib (Rinvoq) is an oral Janus kinase (JAK) inhibitor, approved by the Food and Drug Administration for adults and pediatric patients aged 12 years of age and older with refractory, moderate to severe AD in January 2022.
“What makes this study special is that these patients are followed for 260 weeks, or 5 years, and it encompasses over 7,000 patient-years of exposure,” said Dr. Bunick, associate professor of dermatology at Yale University, New Haven, Connecticut. “This is a milestone because it’s the longest safety study ever published for any systemic drug for AD.”

He and his colleagues evaluated the safety data for up to 5 years of upadacitinib 15 mg and 30 mg use in adolescents and adults with moderate to severe AD, based on the results of integrated data from three ongoing global multicenter phase 3 trials: Measure Up 1, Measure Up 2, and AD Up. Patients in the trials were randomized 1:1:1 to receive oral upadacitinib 15 mg, upadacitinib 30 mg, or placebo once daily alone (Measure Up 1 and 2) or with concomitant topical corticosteroids (AD Up). At week 16, patients receiving 15 mg or 30 mg upadacitinib during the double-blind period continued their assigned treatment in the blinded extension (BE) period, whereas patients receiving placebo were randomized 1:1 to receive either 15 mg or 30 mg upadacitinib in the BE period. The integrated analysis included 2683 patients (529 adolescents and 2154 adults) who received at least one dose of upadacitinib. Of these, 1337 received the 15-mg dose, while 1346 received the 30-mg dose. The researchers analyzed treatment-emergent events of special interest as exposure-adjusted rates per 100 patient-years (PY) for the entire treatment period to adjust for potentially different follow-up durations.
According to Dr. Bunick, researchers often refer to “100 patient-years” in safety analyses to measure how common certain events are. “It is a straightforward way to convey the collective experience of the study’s participants over time,” he told this news organization. “For instance, if 100 patients are each monitored for 1 year, or 50 patients for 2 years each, both scenarios amount to 100 patient-years. This metric allows clinicians to understand how often certain adverse events occur across a diverse group over a specific time frame, providing a clear picture of long-term safety.”
Upadacitinib trials in atopic dermatitis have included diverse patient groups with varying risk factors. “Patients were not cherry-picked,” he said. “What I mean by that is that about 50% of patients enrolled in these trials had, at baseline, at least one cardiovascular risk factor: about 30% used tobacco; 10% had hypertension, and 5% had a history of a cardiovascular event.” In addition, about 15% were over age 50 with one cardiovascular risk factor and about 20% had a body mass index (BMI) greater than 30 kg/m2. Among women in the study, about 20% were on oral contraceptives, yet none developed a venous thromboembolism (VTE).
In the integrated analysis, the rate of treatment-emergent adverse events that led to discontinuation of upadacitinib was about 4.2 events per 100 PY, “meaning that this medicine shows durability,” Dr. Bunick said. “Very few people are discontinuing due to adverse events.”
Serious and opportunistic infections ranged from 1.6 to 2.8 events per 100 PY, but these were stable across the 1- to 5-year time points. The rates of active TB were less than 0.1 per 100 PY, while the rates of herpes zoster ranged from 3.5 to 5.5 events per 100 PY. “The key take-home point here is that 5% or less of the patients at baseline had received the shingles vaccine, so it’s very important to talk to patients about receiving the shingles vaccine before they go on upadacitinib,” Dr. Bunick advised, because “this could reduce risk of herpes zoster occurring in upadacitinib-treated patients substantially.”
In other findings, incidence rates of nonmelanoma skin cancer (NMSC) ranged between 0.3 and 0.4 per 100 PY, while the rate of malignancy excluding NMSC ranged between 0.3 and 0.4 per 100 PY. Meanwhile, the rates of gastrointestinal perforations and VTE stood at 0.1 per 100 PY or lower, and MACE incidence rates ranged from 0.1 to 0.2 per 100 PY.
During his presentation, Dr. Bunick compared findings related to malignancy (excluding NMSC), MACE, and VTE to other published real-world background rates observed in moderate to severe AD populations. He noted that, while the malignancy rate in the current trial ranged from 0.3 to 0.4 per 100 PY, an observational study of more than 66,000 AD patients in the United Kingdom reported a malignancy (excluding NMSC) background incidence rate of 0.33 per 100 PY, and SEER data estimate that the malignancy incidence rate in the US general population is 0.45 per 100 PY. “Therefore, patients on upadacitinib at the 5-year mark are right at the AD population baseline risk,” he said.
And while the incidence rate of MACE in the current trial ranged from less than 0.1 to 0.2 per 100 PY, the background incidence rate of MACE in a Danish observational study of more than 2,500 patients with moderate to severe AD was 0.63 per 100 PY. “This suggests that there may be an anti-inflammatory and even a cardiovascular protective effect for patients on upadacitinib,” Dr. Bunick said.
As for VTE, the incidence rate in the current trial was 0.1 per 100 PY, but VTE background incidence rate observed in a moderate to severe AD population in the United States is 0.31 per 100 PY. “Again, this suggests anti-inflammatory and cardiovascular protective effects of upadacitinib in AD patients at the 5-year mark,” he said. “Reporting of MACE, VTE, and malignancy (excluding NMSC) in upadacitinib phase 3 clinical trials for AD generally reflects the background observations of these events in the AD population.”
He acknowledged certain limitations of the study, including the fact that observational data may overestimate the risk of adverse events.
Discussing the incidence rates for MACE, VTE, and malignancy in upadacitinib AD trials, Dr. Bunick remarked, “these are rock-bottom rates that have been low through 5 years of treatment.”
Dr. Bunick disclosed that he has received grant or research support from AbbVie (the manufacturer of upadacitinib), Almirall, Ortho Dermatologics, Timber, and Palvella. He is also a consultant and/or an adviser to AbbVie, Almirall, Apogee, Connect Bropharma, Arcutis, Eli Lilly, Novartis, Pfizer, Sanofi-Regeneron, Ortho Dermatologics, Leo Pharma, and UCB.
, underscoring the medication’s stable safety profile over an extended duration.
Those are among the key findings from an integrated analysis of long-term upadacitinib use presented by Christopher G. Bunick, MD, PhD, during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis Virtual Conference. Upadacitinib (Rinvoq) is an oral Janus kinase (JAK) inhibitor, approved by the Food and Drug Administration for adults and pediatric patients aged 12 years of age and older with refractory, moderate to severe AD in January 2022.
“What makes this study special is that these patients are followed for 260 weeks, or 5 years, and it encompasses over 7,000 patient-years of exposure,” said Dr. Bunick, associate professor of dermatology at Yale University, New Haven, Connecticut. “This is a milestone because it’s the longest safety study ever published for any systemic drug for AD.”
He and his colleagues evaluated the safety data for up to 5 years of upadacitinib 15 mg and 30 mg use in adolescents and adults with moderate to severe AD, based on the results of integrated data from three ongoing global multicenter phase 3 trials: Measure Up 1, Measure Up 2, and AD Up. Patients in the trials were randomized 1:1:1 to receive oral upadacitinib 15 mg, upadacitinib 30 mg, or placebo once daily alone (Measure Up 1 and 2) or with concomitant topical corticosteroids (AD Up). At week 16, patients receiving 15 mg or 30 mg upadacitinib during the double-blind period continued their assigned treatment in the blinded extension (BE) period, whereas patients receiving placebo were randomized 1:1 to receive either 15 mg or 30 mg upadacitinib in the BE period. The integrated analysis included 2683 patients (529 adolescents and 2154 adults) who received at least one dose of upadacitinib. Of these, 1337 received the 15-mg dose, while 1346 received the 30-mg dose. The researchers analyzed treatment-emergent events of special interest as exposure-adjusted rates per 100 patient-years (PY) for the entire treatment period to adjust for potentially different follow-up durations.
According to Dr. Bunick, researchers often refer to “100 patient-years” in safety analyses to measure how common certain events are. “It is a straightforward way to convey the collective experience of the study’s participants over time,” he told this news organization. “For instance, if 100 patients are each monitored for 1 year, or 50 patients for 2 years each, both scenarios amount to 100 patient-years. This metric allows clinicians to understand how often certain adverse events occur across a diverse group over a specific time frame, providing a clear picture of long-term safety.”
Upadacitinib trials in atopic dermatitis have included diverse patient groups with varying risk factors. “Patients were not cherry-picked,” he said. “What I mean by that is that about 50% of patients enrolled in these trials had, at baseline, at least one cardiovascular risk factor: about 30% used tobacco; 10% had hypertension, and 5% had a history of a cardiovascular event.” In addition, about 15% were over age 50 with one cardiovascular risk factor and about 20% had a body mass index (BMI) greater than 30 kg/m2. Among women in the study, about 20% were on oral contraceptives, yet none developed a venous thromboembolism (VTE).
In the integrated analysis, the rate of treatment-emergent adverse events that led to discontinuation of upadacitinib was about 4.2 events per 100 PY, “meaning that this medicine shows durability,” Dr. Bunick said. “Very few people are discontinuing due to adverse events.”
Serious and opportunistic infections ranged from 1.6 to 2.8 events per 100 PY, but these were stable across the 1- to 5-year time points. The rates of active TB were less than 0.1 per 100 PY, while the rates of herpes zoster ranged from 3.5 to 5.5 events per 100 PY. “The key take-home point here is that 5% or less of the patients at baseline had received the shingles vaccine, so it’s very important to talk to patients about receiving the shingles vaccine before they go on upadacitinib,” Dr. Bunick advised, because “this could reduce risk of herpes zoster occurring in upadacitinib-treated patients substantially.”
In other findings, incidence rates of nonmelanoma skin cancer (NMSC) ranged between 0.3 and 0.4 per 100 PY, while the rate of malignancy excluding NMSC ranged between 0.3 and 0.4 per 100 PY. Meanwhile, the rates of gastrointestinal perforations and VTE stood at 0.1 per 100 PY or lower, and MACE incidence rates ranged from 0.1 to 0.2 per 100 PY.
During his presentation, Dr. Bunick compared findings related to malignancy (excluding NMSC), MACE, and VTE to other published real-world background rates observed in moderate to severe AD populations. He noted that, while the malignancy rate in the current trial ranged from 0.3 to 0.4 per 100 PY, an observational study of more than 66,000 AD patients in the United Kingdom reported a malignancy (excluding NMSC) background incidence rate of 0.33 per 100 PY, and SEER data estimate that the malignancy incidence rate in the US general population is 0.45 per 100 PY. “Therefore, patients on upadacitinib at the 5-year mark are right at the AD population baseline risk,” he said.
And while the incidence rate of MACE in the current trial ranged from less than 0.1 to 0.2 per 100 PY, the background incidence rate of MACE in a Danish observational study of more than 2,500 patients with moderate to severe AD was 0.63 per 100 PY. “This suggests that there may be an anti-inflammatory and even a cardiovascular protective effect for patients on upadacitinib,” Dr. Bunick said.
As for VTE, the incidence rate in the current trial was 0.1 per 100 PY, but VTE background incidence rate observed in a moderate to severe AD population in the United States is 0.31 per 100 PY. “Again, this suggests anti-inflammatory and cardiovascular protective effects of upadacitinib in AD patients at the 5-year mark,” he said. “Reporting of MACE, VTE, and malignancy (excluding NMSC) in upadacitinib phase 3 clinical trials for AD generally reflects the background observations of these events in the AD population.”
He acknowledged certain limitations of the study, including the fact that observational data may overestimate the risk of adverse events.
Discussing the incidence rates for MACE, VTE, and malignancy in upadacitinib AD trials, Dr. Bunick remarked, “these are rock-bottom rates that have been low through 5 years of treatment.”
Dr. Bunick disclosed that he has received grant or research support from AbbVie (the manufacturer of upadacitinib), Almirall, Ortho Dermatologics, Timber, and Palvella. He is also a consultant and/or an adviser to AbbVie, Almirall, Apogee, Connect Bropharma, Arcutis, Eli Lilly, Novartis, Pfizer, Sanofi-Regeneron, Ortho Dermatologics, Leo Pharma, and UCB.
, underscoring the medication’s stable safety profile over an extended duration.
Those are among the key findings from an integrated analysis of long-term upadacitinib use presented by Christopher G. Bunick, MD, PhD, during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis Virtual Conference. Upadacitinib (Rinvoq) is an oral Janus kinase (JAK) inhibitor, approved by the Food and Drug Administration for adults and pediatric patients aged 12 years of age and older with refractory, moderate to severe AD in January 2022.
“What makes this study special is that these patients are followed for 260 weeks, or 5 years, and it encompasses over 7,000 patient-years of exposure,” said Dr. Bunick, associate professor of dermatology at Yale University, New Haven, Connecticut. “This is a milestone because it’s the longest safety study ever published for any systemic drug for AD.”
He and his colleagues evaluated the safety data for up to 5 years of upadacitinib 15 mg and 30 mg use in adolescents and adults with moderate to severe AD, based on the results of integrated data from three ongoing global multicenter phase 3 trials: Measure Up 1, Measure Up 2, and AD Up. Patients in the trials were randomized 1:1:1 to receive oral upadacitinib 15 mg, upadacitinib 30 mg, or placebo once daily alone (Measure Up 1 and 2) or with concomitant topical corticosteroids (AD Up). At week 16, patients receiving 15 mg or 30 mg upadacitinib during the double-blind period continued their assigned treatment in the blinded extension (BE) period, whereas patients receiving placebo were randomized 1:1 to receive either 15 mg or 30 mg upadacitinib in the BE period. The integrated analysis included 2683 patients (529 adolescents and 2154 adults) who received at least one dose of upadacitinib. Of these, 1337 received the 15-mg dose, while 1346 received the 30-mg dose. The researchers analyzed treatment-emergent events of special interest as exposure-adjusted rates per 100 patient-years (PY) for the entire treatment period to adjust for potentially different follow-up durations.
According to Dr. Bunick, researchers often refer to “100 patient-years” in safety analyses to measure how common certain events are. “It is a straightforward way to convey the collective experience of the study’s participants over time,” he told this news organization. “For instance, if 100 patients are each monitored for 1 year, or 50 patients for 2 years each, both scenarios amount to 100 patient-years. This metric allows clinicians to understand how often certain adverse events occur across a diverse group over a specific time frame, providing a clear picture of long-term safety.”
Upadacitinib trials in atopic dermatitis have included diverse patient groups with varying risk factors. “Patients were not cherry-picked,” he said. “What I mean by that is that about 50% of patients enrolled in these trials had, at baseline, at least one cardiovascular risk factor: about 30% used tobacco; 10% had hypertension, and 5% had a history of a cardiovascular event.” In addition, about 15% were over age 50 with one cardiovascular risk factor and about 20% had a body mass index (BMI) greater than 30 kg/m2. Among women in the study, about 20% were on oral contraceptives, yet none developed a venous thromboembolism (VTE).
In the integrated analysis, the rate of treatment-emergent adverse events that led to discontinuation of upadacitinib was about 4.2 events per 100 PY, “meaning that this medicine shows durability,” Dr. Bunick said. “Very few people are discontinuing due to adverse events.”
Serious and opportunistic infections ranged from 1.6 to 2.8 events per 100 PY, but these were stable across the 1- to 5-year time points. The rates of active TB were less than 0.1 per 100 PY, while the rates of herpes zoster ranged from 3.5 to 5.5 events per 100 PY. “The key take-home point here is that 5% or less of the patients at baseline had received the shingles vaccine, so it’s very important to talk to patients about receiving the shingles vaccine before they go on upadacitinib,” Dr. Bunick advised, because “this could reduce risk of herpes zoster occurring in upadacitinib-treated patients substantially.”
In other findings, incidence rates of nonmelanoma skin cancer (NMSC) ranged between 0.3 and 0.4 per 100 PY, while the rate of malignancy excluding NMSC ranged between 0.3 and 0.4 per 100 PY. Meanwhile, the rates of gastrointestinal perforations and VTE stood at 0.1 per 100 PY or lower, and MACE incidence rates ranged from 0.1 to 0.2 per 100 PY.
During his presentation, Dr. Bunick compared findings related to malignancy (excluding NMSC), MACE, and VTE to other published real-world background rates observed in moderate to severe AD populations. He noted that, while the malignancy rate in the current trial ranged from 0.3 to 0.4 per 100 PY, an observational study of more than 66,000 AD patients in the United Kingdom reported a malignancy (excluding NMSC) background incidence rate of 0.33 per 100 PY, and SEER data estimate that the malignancy incidence rate in the US general population is 0.45 per 100 PY. “Therefore, patients on upadacitinib at the 5-year mark are right at the AD population baseline risk,” he said.
And while the incidence rate of MACE in the current trial ranged from less than 0.1 to 0.2 per 100 PY, the background incidence rate of MACE in a Danish observational study of more than 2,500 patients with moderate to severe AD was 0.63 per 100 PY. “This suggests that there may be an anti-inflammatory and even a cardiovascular protective effect for patients on upadacitinib,” Dr. Bunick said.
As for VTE, the incidence rate in the current trial was 0.1 per 100 PY, but VTE background incidence rate observed in a moderate to severe AD population in the United States is 0.31 per 100 PY. “Again, this suggests anti-inflammatory and cardiovascular protective effects of upadacitinib in AD patients at the 5-year mark,” he said. “Reporting of MACE, VTE, and malignancy (excluding NMSC) in upadacitinib phase 3 clinical trials for AD generally reflects the background observations of these events in the AD population.”
He acknowledged certain limitations of the study, including the fact that observational data may overestimate the risk of adverse events.
Discussing the incidence rates for MACE, VTE, and malignancy in upadacitinib AD trials, Dr. Bunick remarked, “these are rock-bottom rates that have been low through 5 years of treatment.”
Dr. Bunick disclosed that he has received grant or research support from AbbVie (the manufacturer of upadacitinib), Almirall, Ortho Dermatologics, Timber, and Palvella. He is also a consultant and/or an adviser to AbbVie, Almirall, Apogee, Connect Bropharma, Arcutis, Eli Lilly, Novartis, Pfizer, Sanofi-Regeneron, Ortho Dermatologics, Leo Pharma, and UCB.
FROM RAD 2023
What’s the Real Prevalence of Conjunctivitis in AD Patients Treated With Dupilumab?
Those are key findings from an analysis of published trials of dupilumab for AD and other conditions that study author Matthew Zirwas, MD, presented during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.
Adults with AD have a significant and disease severity–dependent increased risk of developing ocular surface diseases, including conjunctivitis and keratitis, compared with the general population and independent of any drug effect, according to Dr. Zirwas, a dermatologist with Probity Medical Research of Columbus, Ohio.

Dupilumab inhibits signaling of interleukin (IL)-4 and IL-13, which drive type 2 inflammatory diseases such as AD, asthma, chronic rhinosinusitis with nasal polyposis (CRSwNP), eosinophilic esophagitis (EoE), prurigo nodularis (PN), and chronic spontaneous urticaria (CSU).
In randomized, placebo-controlled trials of dupilumab in patients with moderate to severe AD, conjunctivitis was reported in more patients who received dupilumab treatment than in placebo-treated patients.
“When it comes to dupilumab-induced conjunctivitis, we have a good idea of the etiology, but the question of how frequently it occurs versus how frequently the conjunctivitis is unrelated to dupilumab is an interesting one,” he said. “How often is it clinically meaningful? What is it that is so unique about AD patients? We’ve all heard that it is a unique adverse event that only happens to people with AD and not to people using dupilumab for other indications. Where it gets interesting to me is how do we differentiate the cases that are dupilumab induced versus the cases that are just part of the underlying AD process?”
For their analysis, Dr. Zirwas and co-authors reviewed the incidence of conjunctivitis adverse events in patients from 15 completed, randomized, double-blind placebo-controlled trials evaluating dupilumab in AD, asthma, CRSwNP, EoE, PN, and CSU, along with the severity and resolution of conjunctivitis events in adults with AD.
Of the 15 trials, 7 were conducted in patients with AD: 4 in adults, 1 in adolescents, 1 in school-aged children, and 1 in preschoolers. One of the AD trials, LIBERTY AD CHRONOS, extends 52 weeks. The remaining eight trials of patients with asthma, CRSwNP, EoE, PN, and CSU lasted 24-52 weeks.
In the non-AD trials, the researchers observed that conjunctivitis rates were generally in the 1%-3% range, with less pronounced or no differences between the dupilumab and placebo groups. In the AD trials, conjunctivitis rates were higher in patients receiving dupilumab, compared with those receiving placebo across age groups.
In the 16-week SOLO 1 & 2 and AD-1021 monotherapy trials, 12 conjunctivitis events occurred in 517 patients who received placebo (2%), compared with 103 of 1047 patients (9.84%) who received dupilumab. Of the dupilumab-associated conjunctivitis cases, 80 (78%) patients recovered by the end of the trials. Of the 23 cases of conjunctivitis that did not recover or dropped out of the trial, 15 were among the 529 patients who received 300 mg dupilumab once every 2 weeks (q2w) (3%) and eight were among the 518 who received 300 mg dupilumab once weekly (qw) (2%).
In the 52-week LIBERTY AD CHRONOS trial, 29 conjunctivitis events occurred in 315 patients who received placebo plus topical corticosteroid (TCS) (9%), compared with 113 of 425 patients (27%) who received dupilumab plus TCS. Of these, 103 (91%) recovered by the end of the trial. Of the 11 patients with conjunctivitis who did not recover or dropped out of the trial, 3 were among the 110 patients who received 300 mg dupilumab q2w plus TCS (3%), and 8 were among the 315 who received 300 mg dupilumab qw plus TCS (3%).
“When I look at all of this data, I think that about 2% of people treated with dupilumab are going to get clinically very meaningful conjunctivitis that may be therapy limiting,” Dr. Zirwas concluded. “The vast majority of those cases appear to happen in the first 16 weeks. This is just not something we see in cases of patients treated with dupilumab treated for other reasons.”
Following his presentation, a meeting attendee asked Dr. Zirwas if conjunctivitis occurs more often in patients with facial dermatitis. “My perception is that it happens more often in people who have facial or eyelid dermatitis, but I’ve seen it in plenty of people who didn’t have any facial or eyelid dermatitis,” he said. “I have seen more conjunctivitis in people with more severe AD and more severe atopic comorbidities. That is anecdotal. The data that I have seen has been back and forth on this topic.”
Dr. Zirwas disclosed that he is a speaker and consultant for Sanofi, Regeneron, Leo, Lilly, Galderma, Pfizer, and AbbVie. Several of his co-authors work for Regeneron Pharmaceuticals.
Those are key findings from an analysis of published trials of dupilumab for AD and other conditions that study author Matthew Zirwas, MD, presented during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.
Adults with AD have a significant and disease severity–dependent increased risk of developing ocular surface diseases, including conjunctivitis and keratitis, compared with the general population and independent of any drug effect, according to Dr. Zirwas, a dermatologist with Probity Medical Research of Columbus, Ohio.
Dupilumab inhibits signaling of interleukin (IL)-4 and IL-13, which drive type 2 inflammatory diseases such as AD, asthma, chronic rhinosinusitis with nasal polyposis (CRSwNP), eosinophilic esophagitis (EoE), prurigo nodularis (PN), and chronic spontaneous urticaria (CSU).
In randomized, placebo-controlled trials of dupilumab in patients with moderate to severe AD, conjunctivitis was reported in more patients who received dupilumab treatment than in placebo-treated patients.
“When it comes to dupilumab-induced conjunctivitis, we have a good idea of the etiology, but the question of how frequently it occurs versus how frequently the conjunctivitis is unrelated to dupilumab is an interesting one,” he said. “How often is it clinically meaningful? What is it that is so unique about AD patients? We’ve all heard that it is a unique adverse event that only happens to people with AD and not to people using dupilumab for other indications. Where it gets interesting to me is how do we differentiate the cases that are dupilumab induced versus the cases that are just part of the underlying AD process?”
For their analysis, Dr. Zirwas and co-authors reviewed the incidence of conjunctivitis adverse events in patients from 15 completed, randomized, double-blind placebo-controlled trials evaluating dupilumab in AD, asthma, CRSwNP, EoE, PN, and CSU, along with the severity and resolution of conjunctivitis events in adults with AD.
Of the 15 trials, 7 were conducted in patients with AD: 4 in adults, 1 in adolescents, 1 in school-aged children, and 1 in preschoolers. One of the AD trials, LIBERTY AD CHRONOS, extends 52 weeks. The remaining eight trials of patients with asthma, CRSwNP, EoE, PN, and CSU lasted 24-52 weeks.
In the non-AD trials, the researchers observed that conjunctivitis rates were generally in the 1%-3% range, with less pronounced or no differences between the dupilumab and placebo groups. In the AD trials, conjunctivitis rates were higher in patients receiving dupilumab, compared with those receiving placebo across age groups.
In the 16-week SOLO 1 & 2 and AD-1021 monotherapy trials, 12 conjunctivitis events occurred in 517 patients who received placebo (2%), compared with 103 of 1047 patients (9.84%) who received dupilumab. Of the dupilumab-associated conjunctivitis cases, 80 (78%) patients recovered by the end of the trials. Of the 23 cases of conjunctivitis that did not recover or dropped out of the trial, 15 were among the 529 patients who received 300 mg dupilumab once every 2 weeks (q2w) (3%) and eight were among the 518 who received 300 mg dupilumab once weekly (qw) (2%).
In the 52-week LIBERTY AD CHRONOS trial, 29 conjunctivitis events occurred in 315 patients who received placebo plus topical corticosteroid (TCS) (9%), compared with 113 of 425 patients (27%) who received dupilumab plus TCS. Of these, 103 (91%) recovered by the end of the trial. Of the 11 patients with conjunctivitis who did not recover or dropped out of the trial, 3 were among the 110 patients who received 300 mg dupilumab q2w plus TCS (3%), and 8 were among the 315 who received 300 mg dupilumab qw plus TCS (3%).
“When I look at all of this data, I think that about 2% of people treated with dupilumab are going to get clinically very meaningful conjunctivitis that may be therapy limiting,” Dr. Zirwas concluded. “The vast majority of those cases appear to happen in the first 16 weeks. This is just not something we see in cases of patients treated with dupilumab treated for other reasons.”
Following his presentation, a meeting attendee asked Dr. Zirwas if conjunctivitis occurs more often in patients with facial dermatitis. “My perception is that it happens more often in people who have facial or eyelid dermatitis, but I’ve seen it in plenty of people who didn’t have any facial or eyelid dermatitis,” he said. “I have seen more conjunctivitis in people with more severe AD and more severe atopic comorbidities. That is anecdotal. The data that I have seen has been back and forth on this topic.”
Dr. Zirwas disclosed that he is a speaker and consultant for Sanofi, Regeneron, Leo, Lilly, Galderma, Pfizer, and AbbVie. Several of his co-authors work for Regeneron Pharmaceuticals.
Those are key findings from an analysis of published trials of dupilumab for AD and other conditions that study author Matthew Zirwas, MD, presented during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.
Adults with AD have a significant and disease severity–dependent increased risk of developing ocular surface diseases, including conjunctivitis and keratitis, compared with the general population and independent of any drug effect, according to Dr. Zirwas, a dermatologist with Probity Medical Research of Columbus, Ohio.
Dupilumab inhibits signaling of interleukin (IL)-4 and IL-13, which drive type 2 inflammatory diseases such as AD, asthma, chronic rhinosinusitis with nasal polyposis (CRSwNP), eosinophilic esophagitis (EoE), prurigo nodularis (PN), and chronic spontaneous urticaria (CSU).
In randomized, placebo-controlled trials of dupilumab in patients with moderate to severe AD, conjunctivitis was reported in more patients who received dupilumab treatment than in placebo-treated patients.
“When it comes to dupilumab-induced conjunctivitis, we have a good idea of the etiology, but the question of how frequently it occurs versus how frequently the conjunctivitis is unrelated to dupilumab is an interesting one,” he said. “How often is it clinically meaningful? What is it that is so unique about AD patients? We’ve all heard that it is a unique adverse event that only happens to people with AD and not to people using dupilumab for other indications. Where it gets interesting to me is how do we differentiate the cases that are dupilumab induced versus the cases that are just part of the underlying AD process?”
For their analysis, Dr. Zirwas and co-authors reviewed the incidence of conjunctivitis adverse events in patients from 15 completed, randomized, double-blind placebo-controlled trials evaluating dupilumab in AD, asthma, CRSwNP, EoE, PN, and CSU, along with the severity and resolution of conjunctivitis events in adults with AD.
Of the 15 trials, 7 were conducted in patients with AD: 4 in adults, 1 in adolescents, 1 in school-aged children, and 1 in preschoolers. One of the AD trials, LIBERTY AD CHRONOS, extends 52 weeks. The remaining eight trials of patients with asthma, CRSwNP, EoE, PN, and CSU lasted 24-52 weeks.
In the non-AD trials, the researchers observed that conjunctivitis rates were generally in the 1%-3% range, with less pronounced or no differences between the dupilumab and placebo groups. In the AD trials, conjunctivitis rates were higher in patients receiving dupilumab, compared with those receiving placebo across age groups.
In the 16-week SOLO 1 & 2 and AD-1021 monotherapy trials, 12 conjunctivitis events occurred in 517 patients who received placebo (2%), compared with 103 of 1047 patients (9.84%) who received dupilumab. Of the dupilumab-associated conjunctivitis cases, 80 (78%) patients recovered by the end of the trials. Of the 23 cases of conjunctivitis that did not recover or dropped out of the trial, 15 were among the 529 patients who received 300 mg dupilumab once every 2 weeks (q2w) (3%) and eight were among the 518 who received 300 mg dupilumab once weekly (qw) (2%).
In the 52-week LIBERTY AD CHRONOS trial, 29 conjunctivitis events occurred in 315 patients who received placebo plus topical corticosteroid (TCS) (9%), compared with 113 of 425 patients (27%) who received dupilumab plus TCS. Of these, 103 (91%) recovered by the end of the trial. Of the 11 patients with conjunctivitis who did not recover or dropped out of the trial, 3 were among the 110 patients who received 300 mg dupilumab q2w plus TCS (3%), and 8 were among the 315 who received 300 mg dupilumab qw plus TCS (3%).
“When I look at all of this data, I think that about 2% of people treated with dupilumab are going to get clinically very meaningful conjunctivitis that may be therapy limiting,” Dr. Zirwas concluded. “The vast majority of those cases appear to happen in the first 16 weeks. This is just not something we see in cases of patients treated with dupilumab treated for other reasons.”
Following his presentation, a meeting attendee asked Dr. Zirwas if conjunctivitis occurs more often in patients with facial dermatitis. “My perception is that it happens more often in people who have facial or eyelid dermatitis, but I’ve seen it in plenty of people who didn’t have any facial or eyelid dermatitis,” he said. “I have seen more conjunctivitis in people with more severe AD and more severe atopic comorbidities. That is anecdotal. The data that I have seen has been back and forth on this topic.”
Dr. Zirwas disclosed that he is a speaker and consultant for Sanofi, Regeneron, Leo, Lilly, Galderma, Pfizer, and AbbVie. Several of his co-authors work for Regeneron Pharmaceuticals.
FROM RAD 2023
‘Real-World’ Registry Study of Upadacitinib Supports Clinical Trial Data
, results from an analysis of registry data showed.
“We know from clinical trials that upadacitinib is effective, but we have very little real-world experience on its effectiveness,” presenting study author Melinda Gooderham, MD, medical director of the Skin Center for Dermatology in Peterborough, Ontario, Canada, said during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.

For the analysis, she and her coauthors evaluated the real-world clinical and patient-reported outcomes of 335 adults enrolled in the CorEvitas AD Registry from July 21, 2020, through Aug. 7, 2023. They included patients who were on upadacitinib for at least 4 weeks and persisted on the drug until the time of evaluation.
The CorEvitas AD Registry is a prospective, non-interventional registry of adults diagnosed with AD by a dermatologist or qualified dermatology practitioner. Outcomes measures included the proportion of patients who achieved skin clearance as defined by a Validated Investigators Global Assessment Scale for Atopic Dermatitis (vIGA) score of 0 or 1, an Eczema Area and Severity Index (EASI) score of 3 or less, a Peak Pruritus Numeric Rating Scale (PP-NRS) score of 0 or 1, Patient-Oriented Eczema Measure (POEM) scores of 0-2, Dermatology Life Quality Index (DLQI) scores of 0 or 1, or an Atopic Dermatitis Control Tool (ADCT) score of <7.
The researchers evaluated cross-sectional data from three different cohorts: data from the last registry visit (the overall cohort), data from a visit within 1 month to less than 5 months of upadacitinib initiation (the 1-5 months cohort), and data from a visit within 5-9 months following upadacitinib initiation (the 5-9 months cohort). They also conducted subgroup analyses of patients with prior use of biologics for AD (bio-experience) and those with no such history (bio-naive). Safety events were not assessed in this analysis.
The mean age of the 335 patients was 45.6 years, 51.6% were female, 64.2% were White, 64.2% were based in the United States and the rest were based in Canada. Most patients (70.8%) were treated with the 15-mg dose of upadacitinib. The median duration of treatment was 6.9 months. Slightly more than one-quarter of patients (28.1%) reported concomitant use of topical corticosteroids for AD, while 45.4% reported prior use of dupilumab and 6% reported prior use of tralokinumab.
Dr. Gooderham reported that 57.5% of patients in the total cohort total cohort achieved clear or almost clear skin (a vIGA-AD score of 0 or 1), with slight differences between the bio-naive (60.6%) and bio-experienced (54.1%) subgroups.
The other outcomes were similarly close between the 176 bio-naive and 159 bio-experienced patients. Specifically, 74.8% in the total cohort, 79.4% in the bio-naive subgroup, and 69.6% in the bio-experienced subgroup achieved an EASI score of 3 or less. In the measure of the worst itch in the past 24 hours, 45.3%, 47.7%, and 42.8% respectively achieved a PP-NRS of 0 or 1. In the patient-reported disease burden, 36.4%, 41%, and 31.4% achieved a POEM score of 0-2. In the quality of life measure, 39.8%, 42.8%, and 36.5% achieved a DLQI score of 0 or 1. In the measure of disease control, 69.3%, 70.5%, and 67.9% achieved an ADCT score of <7. In a combination of skin clearance and itch control, 40.9%, 43.2%, and 38.4% of the total cohort, bio-naive, and bio-experienced respectively achieved both an EASI score of 3 or less and a PP-NRS of 0 or 1.
The study outcomes were similar between the 1-5 months cohort and the 5-9 months cohort, but there was a trend toward more clearance the longer patients were on therapy.
“The findings suggest that low levels of disease severity are observed in patients on upadacitinib in a real-world setting,” Dr. Gooderham concluded. “This confirms what we see in the clinical trials.”
She disclosed that she is a consultant to, a speaker for, and/or a member of the advisory board for many pharmaceutical companies, including AbbVie.
, results from an analysis of registry data showed.
“We know from clinical trials that upadacitinib is effective, but we have very little real-world experience on its effectiveness,” presenting study author Melinda Gooderham, MD, medical director of the Skin Center for Dermatology in Peterborough, Ontario, Canada, said during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.
For the analysis, she and her coauthors evaluated the real-world clinical and patient-reported outcomes of 335 adults enrolled in the CorEvitas AD Registry from July 21, 2020, through Aug. 7, 2023. They included patients who were on upadacitinib for at least 4 weeks and persisted on the drug until the time of evaluation.
The CorEvitas AD Registry is a prospective, non-interventional registry of adults diagnosed with AD by a dermatologist or qualified dermatology practitioner. Outcomes measures included the proportion of patients who achieved skin clearance as defined by a Validated Investigators Global Assessment Scale for Atopic Dermatitis (vIGA) score of 0 or 1, an Eczema Area and Severity Index (EASI) score of 3 or less, a Peak Pruritus Numeric Rating Scale (PP-NRS) score of 0 or 1, Patient-Oriented Eczema Measure (POEM) scores of 0-2, Dermatology Life Quality Index (DLQI) scores of 0 or 1, or an Atopic Dermatitis Control Tool (ADCT) score of <7.
The researchers evaluated cross-sectional data from three different cohorts: data from the last registry visit (the overall cohort), data from a visit within 1 month to less than 5 months of upadacitinib initiation (the 1-5 months cohort), and data from a visit within 5-9 months following upadacitinib initiation (the 5-9 months cohort). They also conducted subgroup analyses of patients with prior use of biologics for AD (bio-experience) and those with no such history (bio-naive). Safety events were not assessed in this analysis.
The mean age of the 335 patients was 45.6 years, 51.6% were female, 64.2% were White, 64.2% were based in the United States and the rest were based in Canada. Most patients (70.8%) were treated with the 15-mg dose of upadacitinib. The median duration of treatment was 6.9 months. Slightly more than one-quarter of patients (28.1%) reported concomitant use of topical corticosteroids for AD, while 45.4% reported prior use of dupilumab and 6% reported prior use of tralokinumab.
Dr. Gooderham reported that 57.5% of patients in the total cohort total cohort achieved clear or almost clear skin (a vIGA-AD score of 0 or 1), with slight differences between the bio-naive (60.6%) and bio-experienced (54.1%) subgroups.
The other outcomes were similarly close between the 176 bio-naive and 159 bio-experienced patients. Specifically, 74.8% in the total cohort, 79.4% in the bio-naive subgroup, and 69.6% in the bio-experienced subgroup achieved an EASI score of 3 or less. In the measure of the worst itch in the past 24 hours, 45.3%, 47.7%, and 42.8% respectively achieved a PP-NRS of 0 or 1. In the patient-reported disease burden, 36.4%, 41%, and 31.4% achieved a POEM score of 0-2. In the quality of life measure, 39.8%, 42.8%, and 36.5% achieved a DLQI score of 0 or 1. In the measure of disease control, 69.3%, 70.5%, and 67.9% achieved an ADCT score of <7. In a combination of skin clearance and itch control, 40.9%, 43.2%, and 38.4% of the total cohort, bio-naive, and bio-experienced respectively achieved both an EASI score of 3 or less and a PP-NRS of 0 or 1.
The study outcomes were similar between the 1-5 months cohort and the 5-9 months cohort, but there was a trend toward more clearance the longer patients were on therapy.
“The findings suggest that low levels of disease severity are observed in patients on upadacitinib in a real-world setting,” Dr. Gooderham concluded. “This confirms what we see in the clinical trials.”
She disclosed that she is a consultant to, a speaker for, and/or a member of the advisory board for many pharmaceutical companies, including AbbVie.
, results from an analysis of registry data showed.
“We know from clinical trials that upadacitinib is effective, but we have very little real-world experience on its effectiveness,” presenting study author Melinda Gooderham, MD, medical director of the Skin Center for Dermatology in Peterborough, Ontario, Canada, said during a late-breaking abstract session at the Revolutionizing Atopic Dermatitis (RAD) Virtual Conference.
For the analysis, she and her coauthors evaluated the real-world clinical and patient-reported outcomes of 335 adults enrolled in the CorEvitas AD Registry from July 21, 2020, through Aug. 7, 2023. They included patients who were on upadacitinib for at least 4 weeks and persisted on the drug until the time of evaluation.
The CorEvitas AD Registry is a prospective, non-interventional registry of adults diagnosed with AD by a dermatologist or qualified dermatology practitioner. Outcomes measures included the proportion of patients who achieved skin clearance as defined by a Validated Investigators Global Assessment Scale for Atopic Dermatitis (vIGA) score of 0 or 1, an Eczema Area and Severity Index (EASI) score of 3 or less, a Peak Pruritus Numeric Rating Scale (PP-NRS) score of 0 or 1, Patient-Oriented Eczema Measure (POEM) scores of 0-2, Dermatology Life Quality Index (DLQI) scores of 0 or 1, or an Atopic Dermatitis Control Tool (ADCT) score of <7.
The researchers evaluated cross-sectional data from three different cohorts: data from the last registry visit (the overall cohort), data from a visit within 1 month to less than 5 months of upadacitinib initiation (the 1-5 months cohort), and data from a visit within 5-9 months following upadacitinib initiation (the 5-9 months cohort). They also conducted subgroup analyses of patients with prior use of biologics for AD (bio-experience) and those with no such history (bio-naive). Safety events were not assessed in this analysis.
The mean age of the 335 patients was 45.6 years, 51.6% were female, 64.2% were White, 64.2% were based in the United States and the rest were based in Canada. Most patients (70.8%) were treated with the 15-mg dose of upadacitinib. The median duration of treatment was 6.9 months. Slightly more than one-quarter of patients (28.1%) reported concomitant use of topical corticosteroids for AD, while 45.4% reported prior use of dupilumab and 6% reported prior use of tralokinumab.
Dr. Gooderham reported that 57.5% of patients in the total cohort total cohort achieved clear or almost clear skin (a vIGA-AD score of 0 or 1), with slight differences between the bio-naive (60.6%) and bio-experienced (54.1%) subgroups.
The other outcomes were similarly close between the 176 bio-naive and 159 bio-experienced patients. Specifically, 74.8% in the total cohort, 79.4% in the bio-naive subgroup, and 69.6% in the bio-experienced subgroup achieved an EASI score of 3 or less. In the measure of the worst itch in the past 24 hours, 45.3%, 47.7%, and 42.8% respectively achieved a PP-NRS of 0 or 1. In the patient-reported disease burden, 36.4%, 41%, and 31.4% achieved a POEM score of 0-2. In the quality of life measure, 39.8%, 42.8%, and 36.5% achieved a DLQI score of 0 or 1. In the measure of disease control, 69.3%, 70.5%, and 67.9% achieved an ADCT score of <7. In a combination of skin clearance and itch control, 40.9%, 43.2%, and 38.4% of the total cohort, bio-naive, and bio-experienced respectively achieved both an EASI score of 3 or less and a PP-NRS of 0 or 1.
The study outcomes were similar between the 1-5 months cohort and the 5-9 months cohort, but there was a trend toward more clearance the longer patients were on therapy.
“The findings suggest that low levels of disease severity are observed in patients on upadacitinib in a real-world setting,” Dr. Gooderham concluded. “This confirms what we see in the clinical trials.”
She disclosed that she is a consultant to, a speaker for, and/or a member of the advisory board for many pharmaceutical companies, including AbbVie.
FROM RAD 2023
What Makes Patients Vulnerable to Delusions of Parasitosis?
, reported researchers in a small retrospective case-control study.
Delusions of parasitosis (DOP) affects mostly middle-aged women and has associations with renal failure and some medications, wrote corresponding author Colleen Reisz, MD, a dermatologist with the department of internal medicine at the University of Missouri–Kansas City School of Medicine, and her coauthors. The study was published online December 15, 2023, in the Journal of the American Academy of Dermatology.
“We hypothesize that vulnerability to DOP emerges when multiple factors combine, such as age, sex, medications, and changes in [drug] clearance capacity,” Dr. Reisz and her coauthors wrote. “Changes in health care, such as the dramatic increase in stimulant prescriptions and alternatives to opioids in pain management, may be contributing to off target drug effects on the brain.”
To test their hypothesis, the researchers conducted a case-control study of biometric and pharmaceutical data from 34 patients with DOP which they compared to an age-matched control group of 53 women presenting with a dermatitis above the clavicle from a general dermatology practice between 2012 and 2020. They de-identified the data and performed statistical analysis on variables that included biometric data and intake of pharmaceuticals and nutraceuticals. Polypharmacy was defined as five or more drugs.
Of the 34 patients with DOP, 27 were women with a mean age of 58 years and 7 were men with a mean age of 60 years. Dr. Reisz and her colleagues observed statistical significance between cases and controls in terms of polypharmacy (P = .011), attention-deficit/hyperactivity disorder medications (P < .001), selective serotonin reuptake inhibitors (P = .005), opioids (P = .003), and gabapentin (P = .003).
In other findings, half of DOP cases presented with samples of perceived parasitic material, and four associated the perceived infestation with a single emotion-laden event. This prompted the researchers “to consider that DOP may share mechanisms with fear conditioning and extinction,” they wrote. “Fear conditioning refers to the process of memory acquisition and extinction. This process is essential for survival and has been studied in posttraumatic stress disorder.”
They acknowledged certain limitations of the study, including its retrospective single-center design and the lack of control for factors such as socioeconomic background and level of education.
“Patients with DOP should undergo detailed drug histories and examination of clearance profiles, especially renal function,” the researchers concluded.
Evan A. Rieder, MD, a New York City–based dermatologist and psychiatrist who was asked to comment on the study, said that delusional infestation is one of the most difficult medical conditions to treat and study.

“Though the numbers of cases in this research letter are small, they are instructive in demonstrating a high burden of polypharmacy including psychostimulants, opioids, and SSRIs in such patients,” he told this news organization. “Dermatologists should be performing detailed drug histories, obtaining comprehensive lab work, and considering the effects of medications — both illicit and prescribed — on clinical presentations. While in many cases, delusional patients refuse to consent to psychopharmacologic medications (or treatment in general), the elimination or decrease in dose of certain problematic medications may be helpful in and of themselves.”
The researchers reported having no financial disclosures. Dr. Rieder disclosed that he is a consultant for AbbVie, L’Oréal, Pierre Fabre, Procter & Gamble, and Unilever.
, reported researchers in a small retrospective case-control study.
Delusions of parasitosis (DOP) affects mostly middle-aged women and has associations with renal failure and some medications, wrote corresponding author Colleen Reisz, MD, a dermatologist with the department of internal medicine at the University of Missouri–Kansas City School of Medicine, and her coauthors. The study was published online December 15, 2023, in the Journal of the American Academy of Dermatology.
“We hypothesize that vulnerability to DOP emerges when multiple factors combine, such as age, sex, medications, and changes in [drug] clearance capacity,” Dr. Reisz and her coauthors wrote. “Changes in health care, such as the dramatic increase in stimulant prescriptions and alternatives to opioids in pain management, may be contributing to off target drug effects on the brain.”
To test their hypothesis, the researchers conducted a case-control study of biometric and pharmaceutical data from 34 patients with DOP which they compared to an age-matched control group of 53 women presenting with a dermatitis above the clavicle from a general dermatology practice between 2012 and 2020. They de-identified the data and performed statistical analysis on variables that included biometric data and intake of pharmaceuticals and nutraceuticals. Polypharmacy was defined as five or more drugs.
Of the 34 patients with DOP, 27 were women with a mean age of 58 years and 7 were men with a mean age of 60 years. Dr. Reisz and her colleagues observed statistical significance between cases and controls in terms of polypharmacy (P = .011), attention-deficit/hyperactivity disorder medications (P < .001), selective serotonin reuptake inhibitors (P = .005), opioids (P = .003), and gabapentin (P = .003).
In other findings, half of DOP cases presented with samples of perceived parasitic material, and four associated the perceived infestation with a single emotion-laden event. This prompted the researchers “to consider that DOP may share mechanisms with fear conditioning and extinction,” they wrote. “Fear conditioning refers to the process of memory acquisition and extinction. This process is essential for survival and has been studied in posttraumatic stress disorder.”
They acknowledged certain limitations of the study, including its retrospective single-center design and the lack of control for factors such as socioeconomic background and level of education.
“Patients with DOP should undergo detailed drug histories and examination of clearance profiles, especially renal function,” the researchers concluded.
Evan A. Rieder, MD, a New York City–based dermatologist and psychiatrist who was asked to comment on the study, said that delusional infestation is one of the most difficult medical conditions to treat and study.
“Though the numbers of cases in this research letter are small, they are instructive in demonstrating a high burden of polypharmacy including psychostimulants, opioids, and SSRIs in such patients,” he told this news organization. “Dermatologists should be performing detailed drug histories, obtaining comprehensive lab work, and considering the effects of medications — both illicit and prescribed — on clinical presentations. While in many cases, delusional patients refuse to consent to psychopharmacologic medications (or treatment in general), the elimination or decrease in dose of certain problematic medications may be helpful in and of themselves.”
The researchers reported having no financial disclosures. Dr. Rieder disclosed that he is a consultant for AbbVie, L’Oréal, Pierre Fabre, Procter & Gamble, and Unilever.
, reported researchers in a small retrospective case-control study.
Delusions of parasitosis (DOP) affects mostly middle-aged women and has associations with renal failure and some medications, wrote corresponding author Colleen Reisz, MD, a dermatologist with the department of internal medicine at the University of Missouri–Kansas City School of Medicine, and her coauthors. The study was published online December 15, 2023, in the Journal of the American Academy of Dermatology.
“We hypothesize that vulnerability to DOP emerges when multiple factors combine, such as age, sex, medications, and changes in [drug] clearance capacity,” Dr. Reisz and her coauthors wrote. “Changes in health care, such as the dramatic increase in stimulant prescriptions and alternatives to opioids in pain management, may be contributing to off target drug effects on the brain.”
To test their hypothesis, the researchers conducted a case-control study of biometric and pharmaceutical data from 34 patients with DOP which they compared to an age-matched control group of 53 women presenting with a dermatitis above the clavicle from a general dermatology practice between 2012 and 2020. They de-identified the data and performed statistical analysis on variables that included biometric data and intake of pharmaceuticals and nutraceuticals. Polypharmacy was defined as five or more drugs.
Of the 34 patients with DOP, 27 were women with a mean age of 58 years and 7 were men with a mean age of 60 years. Dr. Reisz and her colleagues observed statistical significance between cases and controls in terms of polypharmacy (P = .011), attention-deficit/hyperactivity disorder medications (P < .001), selective serotonin reuptake inhibitors (P = .005), opioids (P = .003), and gabapentin (P = .003).
In other findings, half of DOP cases presented with samples of perceived parasitic material, and four associated the perceived infestation with a single emotion-laden event. This prompted the researchers “to consider that DOP may share mechanisms with fear conditioning and extinction,” they wrote. “Fear conditioning refers to the process of memory acquisition and extinction. This process is essential for survival and has been studied in posttraumatic stress disorder.”
They acknowledged certain limitations of the study, including its retrospective single-center design and the lack of control for factors such as socioeconomic background and level of education.
“Patients with DOP should undergo detailed drug histories and examination of clearance profiles, especially renal function,” the researchers concluded.
Evan A. Rieder, MD, a New York City–based dermatologist and psychiatrist who was asked to comment on the study, said that delusional infestation is one of the most difficult medical conditions to treat and study.
“Though the numbers of cases in this research letter are small, they are instructive in demonstrating a high burden of polypharmacy including psychostimulants, opioids, and SSRIs in such patients,” he told this news organization. “Dermatologists should be performing detailed drug histories, obtaining comprehensive lab work, and considering the effects of medications — both illicit and prescribed — on clinical presentations. While in many cases, delusional patients refuse to consent to psychopharmacologic medications (or treatment in general), the elimination or decrease in dose of certain problematic medications may be helpful in and of themselves.”
The researchers reported having no financial disclosures. Dr. Rieder disclosed that he is a consultant for AbbVie, L’Oréal, Pierre Fabre, Procter & Gamble, and Unilever.
FROM THE JOURNAL OF THE AMERICAN ACADEMY OF DERMATOLOGY
FDA Approves Topical Gel For Wounds Associated With JEB and DEB
The FDA has approved a topical gel containing birch triterpenes for the treatment of partial thickness wounds in patients 6 months and older with junctional epidermolysis bullosa (JEB) and dystrophic epidermolysis bullosa (DEB).
The gel is marketed under the name Filsuvez. It is the first approved treatment for wounds associated with JEB and the second for patients with DEB, following the approval of Vyjuvek (Krystal Biotech), a topical gene therapy gel, in May 2023.
First developed by Amryt Pharma and intended for home use, Filsuvez is now marketed by Chiesi Global Rare Diseases, which acquired Amryt in January 2023. The gel is applied topically to the wound at each dressing change.
The approval of Filsuvez is based on results from the Efficacy and Safety Study of Oleogel-S10 in Epidermolysis Bullosa (EASE), a randomized, placebo-controlled study of 223 people, the largest-ever phase 3 clinical trial for the treatment of EB, according to the Chiesi news release. The gel was well tolerated and met the primary endpoint with statistical significance, with 41.3% of patients achieving first complete target wound closure within 45 days (compared with 28.9% on placebo).
“I am so excited to say that this is another hurdle cleared and milestone achieved for the EB Community,” Brett Kopelan, executive director at debra of America said in a blog post. “We are now on the road to being able to treat EB more effectively, and to make the worst disease you’ve never heard of chronic, but livable, by making use of multiple therapeutic options in conjunction with each other.”
The FDA has approved a topical gel containing birch triterpenes for the treatment of partial thickness wounds in patients 6 months and older with junctional epidermolysis bullosa (JEB) and dystrophic epidermolysis bullosa (DEB).
The gel is marketed under the name Filsuvez. It is the first approved treatment for wounds associated with JEB and the second for patients with DEB, following the approval of Vyjuvek (Krystal Biotech), a topical gene therapy gel, in May 2023.
First developed by Amryt Pharma and intended for home use, Filsuvez is now marketed by Chiesi Global Rare Diseases, which acquired Amryt in January 2023. The gel is applied topically to the wound at each dressing change.
The approval of Filsuvez is based on results from the Efficacy and Safety Study of Oleogel-S10 in Epidermolysis Bullosa (EASE), a randomized, placebo-controlled study of 223 people, the largest-ever phase 3 clinical trial for the treatment of EB, according to the Chiesi news release. The gel was well tolerated and met the primary endpoint with statistical significance, with 41.3% of patients achieving first complete target wound closure within 45 days (compared with 28.9% on placebo).
“I am so excited to say that this is another hurdle cleared and milestone achieved for the EB Community,” Brett Kopelan, executive director at debra of America said in a blog post. “We are now on the road to being able to treat EB more effectively, and to make the worst disease you’ve never heard of chronic, but livable, by making use of multiple therapeutic options in conjunction with each other.”
The FDA has approved a topical gel containing birch triterpenes for the treatment of partial thickness wounds in patients 6 months and older with junctional epidermolysis bullosa (JEB) and dystrophic epidermolysis bullosa (DEB).
The gel is marketed under the name Filsuvez. It is the first approved treatment for wounds associated with JEB and the second for patients with DEB, following the approval of Vyjuvek (Krystal Biotech), a topical gene therapy gel, in May 2023.
First developed by Amryt Pharma and intended for home use, Filsuvez is now marketed by Chiesi Global Rare Diseases, which acquired Amryt in January 2023. The gel is applied topically to the wound at each dressing change.
The approval of Filsuvez is based on results from the Efficacy and Safety Study of Oleogel-S10 in Epidermolysis Bullosa (EASE), a randomized, placebo-controlled study of 223 people, the largest-ever phase 3 clinical trial for the treatment of EB, according to the Chiesi news release. The gel was well tolerated and met the primary endpoint with statistical significance, with 41.3% of patients achieving first complete target wound closure within 45 days (compared with 28.9% on placebo).
“I am so excited to say that this is another hurdle cleared and milestone achieved for the EB Community,” Brett Kopelan, executive director at debra of America said in a blog post. “We are now on the road to being able to treat EB more effectively, and to make the worst disease you’ve never heard of chronic, but livable, by making use of multiple therapeutic options in conjunction with each other.”
Paradoxical Eczema Risk Low With Biologic Psoriasis Treatments
examined in a large observational analysis.
Using data from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR) database, Ali Al-Janabi, MA, from the University of Manchester (England) and associates found that 273 (1%) of approximately 25,000 drug exposures in 13,699 biologic-treated patients with psoriasis were associated with paradoxical eczema.
The incidence of paradoxical eczema was found to vary by class. The highest rate was seen for IL-17 inhibitors, at 1.22 per 100,000 person-years, and the lowest rate was seen with IL-23 inhibitors, at 0.56 per 100,000 person-years. The respective incidence rates for tumor necrosis factor (TNF) inhibitors and IL-12/IL-23 inhibitors were a respective 0.94 and 0.80 per 100,000 person-years.
“Compared with TNF inhibitors, IL-23 inhibitor exposure was associated with significantly lower risk of paradoxical eczema,” the BADBIR Study Group reported in JAMA Dermatology. Indeed, patients treated with IL-23 inhibitors were 61% less likely than were those taking TNF-inhibitors to experience a paradoxical eczema event.
“These findings remained when restricting the analysis to first-line biologic exposures and were specific to this eczema phenotype” the group said.
Cautious Interpretation
As the corresponding author for the work, Mr. Al-Janabi observed in an email that the research needs to be replicated, and the findings need to be interpreted with caution.
“As well as usual clinical variables influencing biologic selection, clinicians could consider IL-23 inhibitors in patients with previous atopic dermatitis, hay fever, or paradoxical eczema episodes, as this class was associated with the lowest risk of paradoxical eczema,” he suggested.
A prior history of atopic dermatitis (AD) and hay fever appears to be particularly relevant, as both substantially upped the chances that paradoxical eczema would occur, with hazard ratios of 12.40 and 3.78, respectively. Increasing age also increased the risk, albeit slightly (hazard ratio [HR], 1.02 per year), and there was an apparent lower risk (HR, 0.60) comparing men and women.
The BADBIR Study Group authors believe that, to the best of their knowledge, this is the first study to compare paradoxical eczema risk by biologic class. “Based on clinical experience and prevalence of eczematous reactions reported in some IL-17 inhibitor clinical trials, we suspected an association between IL-17 inhibitor exposure and paradoxical eczema,” they wrote.
“While the incidence of paradoxical eczema was numerically highest among IL-17 inhibitor exposures, it was not significantly different from the incidence among TNF inhibitor exposures.” The low overall incidence of paradoxical eczema “may be reassuring for patients and clinicians,” they added, “but it is possible that the incidence was underestimated due to underreporting or exclusion of adverse events with insufficient detail.”
Details of the Analysis, Other Findings
To explore the risk of paradoxical eczema by biologic class and identify possible risk factors, the BADBIR Study Group performed a prospective cohort study using data held within the BADBIR database between September 2007 and December 2022.
Adults over the age of 18 year or older with plaque psoriasis and who had been treated with at least one of the following biologics were eligible for inclusion: the TNF inhibitors adalimumab, certolizumab pegol, etanercept, and infliximab; the IL-17 inhibitors bimekizumab, brodalumab, ixekizumab, and secukinumab; the IL-12/23 inhibitor ustekinumab; and the IL-23 inhibitors guselkumab, risankizumab, and tildrakizumab.
Patient records and adverse event data were reviewed to determine the incidence of paradoxical eczema events, using terms such as eczema, eczematized, eczematous, atopy, atopic, and dermatitis.
Of 24,952 drug exposures analyzed, the majority (11,819) were for TNF inhibitors, followed by IL-17 inhibitors (4,776), IL-12/23 inhibitors (6,423), and finally, IL-23 inhibitors (1,934).
Mr. Al-Janabi and coauthors reported that the median time to onset of paradoxical eczema events was 294 days — approximately 9.8 months. The earliest that these events were recorded was at 120 days (4 months), and the latest at 699 days (almost 2 years).
The face and neck were the most common sites affected (26% of exposures), with other sites including the limbs (23%), the trunk (13%), and hands or feet (12%). Itching (18%), redness (7%), and dryness (4%) were the most commonly reported symptoms.
The researchers noted that 21 patients had skin biopsies taken and “all showed spongiosis or a feature of eczema, with 1 having overlapping features of psoriasis.”
In the majority (92 %) of cases, patients experienced only one eczema event. Of the 20 patients who had more than one event, just over one-fifth of repeat events occurred after receiving the same biologic as for the index event. A quarter of events occurred after a different biologic of the same class had been used, and just over half of events occurred after a different class of biologic had been given.
Strengths and Limitations
The “large sample size and inclusion of multiple lines of exposure per participant” are strengths of the study, said the researchers. “We included data for all currently available biologics, originating from more than 160 dermatology centers in the UK and Ireland.”
They added, however, that the “main limitation is the small numbers of observations within certain subgroups, such as specific biologic exposures or participants in ethnic minority groups, restricting generalizability of our findings and the interpretation of some subgroup analyses.”
Moreover, the small number of paradoxical eczema events seen may have resulted in imprecise effect estimates, they observe, noting that the number of exposures to IL-23 inhibitors was low compared with other classes.
“Future studies with more exposures and paradoxical eczema events would enable a more robust analysis of individual drugs and patient subgroups,” the authors concluded.
The study was funded by the Medical Research Council. BADBIR is coordinated by The University of Manchester, and funded by the British Association of Dermatologists (BAD). The BAD receives income from AbbVie, Almirall, Amgen, Celgene, Janssen, LEO Pharma, Lilly, Novartis, Samsung Bioepis, Sandoz Hexal AG, and UCB Pharma for providing pharmacovigilance services. This income finances a separate contract between the BAD and The University of Manchester, which coordinates BADBIR. Mr. Al-Janabi reported receiving grants from the Medical Research Council during the conduct of the study; nonfinancial support from UCB, Almirall, and Janssen; and personal fees from UCB outside the submitted work.
examined in a large observational analysis.
Using data from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR) database, Ali Al-Janabi, MA, from the University of Manchester (England) and associates found that 273 (1%) of approximately 25,000 drug exposures in 13,699 biologic-treated patients with psoriasis were associated with paradoxical eczema.
The incidence of paradoxical eczema was found to vary by class. The highest rate was seen for IL-17 inhibitors, at 1.22 per 100,000 person-years, and the lowest rate was seen with IL-23 inhibitors, at 0.56 per 100,000 person-years. The respective incidence rates for tumor necrosis factor (TNF) inhibitors and IL-12/IL-23 inhibitors were a respective 0.94 and 0.80 per 100,000 person-years.
“Compared with TNF inhibitors, IL-23 inhibitor exposure was associated with significantly lower risk of paradoxical eczema,” the BADBIR Study Group reported in JAMA Dermatology. Indeed, patients treated with IL-23 inhibitors were 61% less likely than were those taking TNF-inhibitors to experience a paradoxical eczema event.
“These findings remained when restricting the analysis to first-line biologic exposures and were specific to this eczema phenotype” the group said.
Cautious Interpretation
As the corresponding author for the work, Mr. Al-Janabi observed in an email that the research needs to be replicated, and the findings need to be interpreted with caution.
“As well as usual clinical variables influencing biologic selection, clinicians could consider IL-23 inhibitors in patients with previous atopic dermatitis, hay fever, or paradoxical eczema episodes, as this class was associated with the lowest risk of paradoxical eczema,” he suggested.
A prior history of atopic dermatitis (AD) and hay fever appears to be particularly relevant, as both substantially upped the chances that paradoxical eczema would occur, with hazard ratios of 12.40 and 3.78, respectively. Increasing age also increased the risk, albeit slightly (hazard ratio [HR], 1.02 per year), and there was an apparent lower risk (HR, 0.60) comparing men and women.
The BADBIR Study Group authors believe that, to the best of their knowledge, this is the first study to compare paradoxical eczema risk by biologic class. “Based on clinical experience and prevalence of eczematous reactions reported in some IL-17 inhibitor clinical trials, we suspected an association between IL-17 inhibitor exposure and paradoxical eczema,” they wrote.
“While the incidence of paradoxical eczema was numerically highest among IL-17 inhibitor exposures, it was not significantly different from the incidence among TNF inhibitor exposures.” The low overall incidence of paradoxical eczema “may be reassuring for patients and clinicians,” they added, “but it is possible that the incidence was underestimated due to underreporting or exclusion of adverse events with insufficient detail.”
Details of the Analysis, Other Findings
To explore the risk of paradoxical eczema by biologic class and identify possible risk factors, the BADBIR Study Group performed a prospective cohort study using data held within the BADBIR database between September 2007 and December 2022.
Adults over the age of 18 year or older with plaque psoriasis and who had been treated with at least one of the following biologics were eligible for inclusion: the TNF inhibitors adalimumab, certolizumab pegol, etanercept, and infliximab; the IL-17 inhibitors bimekizumab, brodalumab, ixekizumab, and secukinumab; the IL-12/23 inhibitor ustekinumab; and the IL-23 inhibitors guselkumab, risankizumab, and tildrakizumab.
Patient records and adverse event data were reviewed to determine the incidence of paradoxical eczema events, using terms such as eczema, eczematized, eczematous, atopy, atopic, and dermatitis.
Of 24,952 drug exposures analyzed, the majority (11,819) were for TNF inhibitors, followed by IL-17 inhibitors (4,776), IL-12/23 inhibitors (6,423), and finally, IL-23 inhibitors (1,934).
Mr. Al-Janabi and coauthors reported that the median time to onset of paradoxical eczema events was 294 days — approximately 9.8 months. The earliest that these events were recorded was at 120 days (4 months), and the latest at 699 days (almost 2 years).
The face and neck were the most common sites affected (26% of exposures), with other sites including the limbs (23%), the trunk (13%), and hands or feet (12%). Itching (18%), redness (7%), and dryness (4%) were the most commonly reported symptoms.
The researchers noted that 21 patients had skin biopsies taken and “all showed spongiosis or a feature of eczema, with 1 having overlapping features of psoriasis.”
In the majority (92 %) of cases, patients experienced only one eczema event. Of the 20 patients who had more than one event, just over one-fifth of repeat events occurred after receiving the same biologic as for the index event. A quarter of events occurred after a different biologic of the same class had been used, and just over half of events occurred after a different class of biologic had been given.
Strengths and Limitations
The “large sample size and inclusion of multiple lines of exposure per participant” are strengths of the study, said the researchers. “We included data for all currently available biologics, originating from more than 160 dermatology centers in the UK and Ireland.”
They added, however, that the “main limitation is the small numbers of observations within certain subgroups, such as specific biologic exposures or participants in ethnic minority groups, restricting generalizability of our findings and the interpretation of some subgroup analyses.”
Moreover, the small number of paradoxical eczema events seen may have resulted in imprecise effect estimates, they observe, noting that the number of exposures to IL-23 inhibitors was low compared with other classes.
“Future studies with more exposures and paradoxical eczema events would enable a more robust analysis of individual drugs and patient subgroups,” the authors concluded.
The study was funded by the Medical Research Council. BADBIR is coordinated by The University of Manchester, and funded by the British Association of Dermatologists (BAD). The BAD receives income from AbbVie, Almirall, Amgen, Celgene, Janssen, LEO Pharma, Lilly, Novartis, Samsung Bioepis, Sandoz Hexal AG, and UCB Pharma for providing pharmacovigilance services. This income finances a separate contract between the BAD and The University of Manchester, which coordinates BADBIR. Mr. Al-Janabi reported receiving grants from the Medical Research Council during the conduct of the study; nonfinancial support from UCB, Almirall, and Janssen; and personal fees from UCB outside the submitted work.
examined in a large observational analysis.
Using data from the British Association of Dermatologists Biologics and Immunomodulators Register (BADBIR) database, Ali Al-Janabi, MA, from the University of Manchester (England) and associates found that 273 (1%) of approximately 25,000 drug exposures in 13,699 biologic-treated patients with psoriasis were associated with paradoxical eczema.
The incidence of paradoxical eczema was found to vary by class. The highest rate was seen for IL-17 inhibitors, at 1.22 per 100,000 person-years, and the lowest rate was seen with IL-23 inhibitors, at 0.56 per 100,000 person-years. The respective incidence rates for tumor necrosis factor (TNF) inhibitors and IL-12/IL-23 inhibitors were a respective 0.94 and 0.80 per 100,000 person-years.
“Compared with TNF inhibitors, IL-23 inhibitor exposure was associated with significantly lower risk of paradoxical eczema,” the BADBIR Study Group reported in JAMA Dermatology. Indeed, patients treated with IL-23 inhibitors were 61% less likely than were those taking TNF-inhibitors to experience a paradoxical eczema event.
“These findings remained when restricting the analysis to first-line biologic exposures and were specific to this eczema phenotype” the group said.
Cautious Interpretation
As the corresponding author for the work, Mr. Al-Janabi observed in an email that the research needs to be replicated, and the findings need to be interpreted with caution.
“As well as usual clinical variables influencing biologic selection, clinicians could consider IL-23 inhibitors in patients with previous atopic dermatitis, hay fever, or paradoxical eczema episodes, as this class was associated with the lowest risk of paradoxical eczema,” he suggested.
A prior history of atopic dermatitis (AD) and hay fever appears to be particularly relevant, as both substantially upped the chances that paradoxical eczema would occur, with hazard ratios of 12.40 and 3.78, respectively. Increasing age also increased the risk, albeit slightly (hazard ratio [HR], 1.02 per year), and there was an apparent lower risk (HR, 0.60) comparing men and women.
The BADBIR Study Group authors believe that, to the best of their knowledge, this is the first study to compare paradoxical eczema risk by biologic class. “Based on clinical experience and prevalence of eczematous reactions reported in some IL-17 inhibitor clinical trials, we suspected an association between IL-17 inhibitor exposure and paradoxical eczema,” they wrote.
“While the incidence of paradoxical eczema was numerically highest among IL-17 inhibitor exposures, it was not significantly different from the incidence among TNF inhibitor exposures.” The low overall incidence of paradoxical eczema “may be reassuring for patients and clinicians,” they added, “but it is possible that the incidence was underestimated due to underreporting or exclusion of adverse events with insufficient detail.”
Details of the Analysis, Other Findings
To explore the risk of paradoxical eczema by biologic class and identify possible risk factors, the BADBIR Study Group performed a prospective cohort study using data held within the BADBIR database between September 2007 and December 2022.
Adults over the age of 18 year or older with plaque psoriasis and who had been treated with at least one of the following biologics were eligible for inclusion: the TNF inhibitors adalimumab, certolizumab pegol, etanercept, and infliximab; the IL-17 inhibitors bimekizumab, brodalumab, ixekizumab, and secukinumab; the IL-12/23 inhibitor ustekinumab; and the IL-23 inhibitors guselkumab, risankizumab, and tildrakizumab.
Patient records and adverse event data were reviewed to determine the incidence of paradoxical eczema events, using terms such as eczema, eczematized, eczematous, atopy, atopic, and dermatitis.
Of 24,952 drug exposures analyzed, the majority (11,819) were for TNF inhibitors, followed by IL-17 inhibitors (4,776), IL-12/23 inhibitors (6,423), and finally, IL-23 inhibitors (1,934).
Mr. Al-Janabi and coauthors reported that the median time to onset of paradoxical eczema events was 294 days — approximately 9.8 months. The earliest that these events were recorded was at 120 days (4 months), and the latest at 699 days (almost 2 years).
The face and neck were the most common sites affected (26% of exposures), with other sites including the limbs (23%), the trunk (13%), and hands or feet (12%). Itching (18%), redness (7%), and dryness (4%) were the most commonly reported symptoms.
The researchers noted that 21 patients had skin biopsies taken and “all showed spongiosis or a feature of eczema, with 1 having overlapping features of psoriasis.”
In the majority (92 %) of cases, patients experienced only one eczema event. Of the 20 patients who had more than one event, just over one-fifth of repeat events occurred after receiving the same biologic as for the index event. A quarter of events occurred after a different biologic of the same class had been used, and just over half of events occurred after a different class of biologic had been given.
Strengths and Limitations
The “large sample size and inclusion of multiple lines of exposure per participant” are strengths of the study, said the researchers. “We included data for all currently available biologics, originating from more than 160 dermatology centers in the UK and Ireland.”
They added, however, that the “main limitation is the small numbers of observations within certain subgroups, such as specific biologic exposures or participants in ethnic minority groups, restricting generalizability of our findings and the interpretation of some subgroup analyses.”
Moreover, the small number of paradoxical eczema events seen may have resulted in imprecise effect estimates, they observe, noting that the number of exposures to IL-23 inhibitors was low compared with other classes.
“Future studies with more exposures and paradoxical eczema events would enable a more robust analysis of individual drugs and patient subgroups,” the authors concluded.
The study was funded by the Medical Research Council. BADBIR is coordinated by The University of Manchester, and funded by the British Association of Dermatologists (BAD). The BAD receives income from AbbVie, Almirall, Amgen, Celgene, Janssen, LEO Pharma, Lilly, Novartis, Samsung Bioepis, Sandoz Hexal AG, and UCB Pharma for providing pharmacovigilance services. This income finances a separate contract between the BAD and The University of Manchester, which coordinates BADBIR. Mr. Al-Janabi reported receiving grants from the Medical Research Council during the conduct of the study; nonfinancial support from UCB, Almirall, and Janssen; and personal fees from UCB outside the submitted work.
FROM JAMA DERMATOLOGY
How to Reduce Cardiovascular Morbidity and Mortality in Psoriasis and PsA
Patients with psoriatic disease have significantly higher risks of myocardial infarction, stroke, and cardiovascular mortality than does the general population, yet research consistently paints what dermatologist Joel M. Gelfand, MD, calls an “abysmal” picture: Only a minority of patients with psoriatic disease know about their increased risks, only a minority of dermatologists and rheumatologists screen for cardiovascular risk factors like lipid levels and blood pressure, and only a minority of patients diagnosed with hyperlipidemia are adequately treated with statin therapy.
In the literature and at medical meetings, Dr. Gelfand and others who have studied cardiovascular disease (CVD) comorbidity and physician practices have been urging dermatologists and rheumatologists to play a more consistent and active role in primary cardiovascular prevention for patients with psoriatic disease, who are up to 50% more likely than patients without it to develop CVD and who tend to have atherosclerosis at earlier ages.
According to the 2019 joint American Academy of Dermatology (AAD)–National Psoriasis Foundation (NPF) guidelines for managing psoriasis “with awareness and attention to comorbidities,” this means not only ensuring that all patients with psoriasis receive standard CV risk assessment (screening for hypertension, diabetes, and hyperlipidemia), but also recognizing that patients who are candidates for systemic therapy or phototherapy — or who have psoriasis involving > 10% of body surface area — may benefit from earlier and more frequent screening.
CV risk and premature mortality rises with the severity of skin disease, and patients with psoriatic arthritis (PsA) are believed to have risk levels similar to patients with moderate-severe psoriasis, cardiologist Michael S. Garshick, MD, director of the cardio-rheumatology program at New York University Langone Health, said in an interview.

In a recent survey study of 100 patients seen at NYU Langone Health’s psoriasis specialty clinic, only one-third indicated they had been advised by their physicians to be screened for CV risk factors, and only one-third reported having been told of the connection between psoriasis and CVD risk. Dr. Garshick shared the unpublished findings at the annual research symposium of the NPF in October.
Similarly, data from the National Ambulatory Medical Care Survey shows that just 16% of psoriasis-related visits to dermatology providers from 2007 to 2016 involved screening for CV risk factors. Screening rates were 11% for body mass index, 7.4% for blood pressure, 2.9% for cholesterol, and 1.7% for glucose, Dr. Gelfand and coauthors reported in 2023. .
Such findings are concerning because research shows that fewer than a quarter of patients with psoriasis have a primary care visit within a year of establishing care with their physicians, and that, overall, fewer than half of commercially insured adults under age 65 visit a primary care physician each year, according to John S. Barbieri, MD, of the department of dermatology at Brigham and Women’s Hospital in Boston. He included these findings when reporting in 2022 on a survey study on CVD screening.

In many cases, dermatologists and rheumatologists may be the primary providers for patients with psoriatic disease. So, “the question is, how can the dermatologist or rheumatologist use their interactions as a touchpoint to improve the patient’s well-being?” Dr. Barbieri said in an interview.
For the dermatologist, educating patients about the higher CVD risk fits well into conversations about “how there may be inflammation inside the body as well as in the skin,” he said. “Talk about cardiovascular risk just as you talk about PsA risk.” Both specialists, he added, can incorporate blood pressure readings and look for opportunities to measure lipid levels and hemoglobin A1c (HbA1c). These labs can easily be integrated into a biologic work-up.
“The hard part — and this needs to be individualized — is how do you want to handle [abnormal readings]? Do you want to take on a lot of the ownership and calculate [10-year CVD] risk scores and then counsel patients accordingly?” Dr. Barbieri said. “Or do you want to try to refer, and encourage them to work with their PCP? There a high-touch version and a low-touch version of how you can turn screening into action, into a care plan.”
Beyond traditional risk elevation, the primary care hand-off
Rheumatologists “in general may be more apt to screen for cardiovascular disease” as a result of their internal medicine residency training, and “we’re generally more comfortable prescribing ... if we need to,” said Alexis R. Ogdie, MD, a rheumatologist at the Hospital of the University of Pennsylvania, Philadelphia, and director of the Penn Psoriatic Arthritis Clinic.

Referral to a preventive cardiologist for management of abnormal lab results or ongoing monitoring and prevention is ideal, but when hand-offs to primary care physicians are made — the more common scenario — education is important. “A common problem is that there is underrecognition of the cardiovascular risk being elevated in our patients,” she said, above and beyond risk posed by traditional risk factors such as dyslipidemia, hypertension, metabolic syndrome, and obesity, all of which have been shown to occur more frequently in patients with psoriatic disease than in the general population.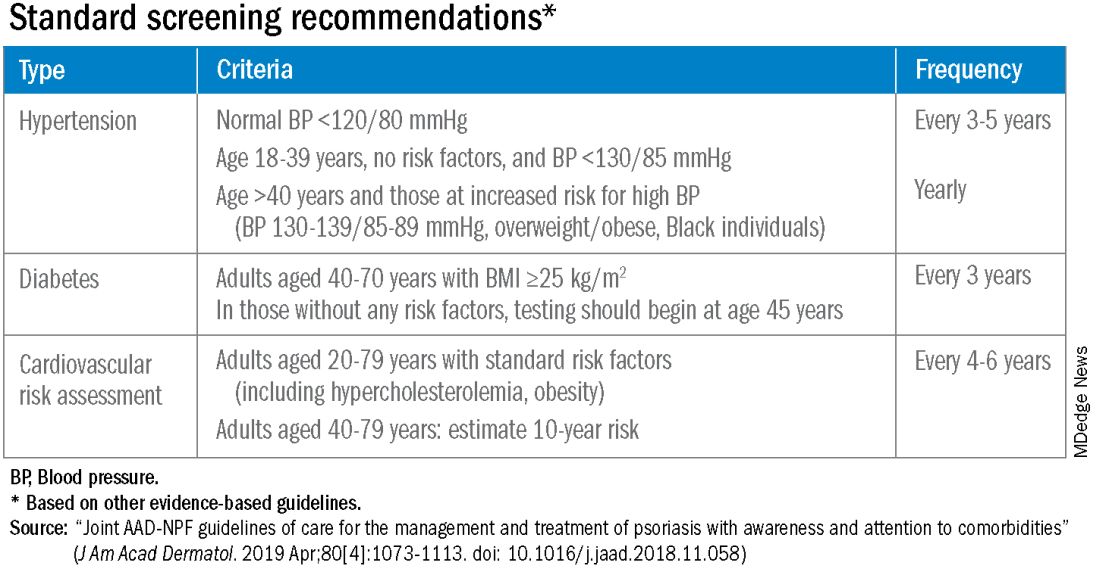
Risk stratification guides CVD prevention in the general population, and “if you use typical scores for cardiovascular risk, they may underestimate risk for our patients with PsA,” said Dr. Ogdie, who has reported on CV risk in patients with PsA. “Relative to what the patient’s perceived risk is, they may be treated similarly (to the general population). But relative to their actual risk, they’re undertreated.”
The 2019 AAD-NPF psoriasis guidelines recommend utilizing a 1.5 multiplication factor in risk score models, such as the American College of Cardiology’s Atherosclerotic Cardiovascular Disease (ASCVD) Risk Estimator, when the patient has a body surface area >10% or is a candidate for systemic therapy or phototherapy.
Similarly, the 2018 American Heart Association (AHA)-ACC Guideline on the Management of Blood Cholesterol defines psoriasis, along with RA, metabolic syndrome, HIV, and other diseases, as a “cardiovascular risk enhancer” that should be factored into assessments of ASCVD risk. (The guideline does not specify a psoriasis severity threshold.)
“It’s the first time the specialty [of cardiology] has said, ‘pay attention to a skin disease,’ ” Dr. Gelfand said at the NPF meeting.
Using the 1.5 multiplication factor, a patient who otherwise would be classified in the AHA/ACC guideline as “borderline risk,” with a 10-year ASCVD risk of 5% to <7.5%, would instead have an “intermediate” 10-year ASCVD risk of ≥7.5% to <20%. Application of the AHA-ACC “risk enhancer” would have a similar effect.
For management, the main impact of psoriasis being considered a risk enhancer is that “it lowers the threshold for treatment with standard cardiovascular prevention medications such as statins.”
In general, “we should be taking a more aggressive approach to the management of traditional cardiovascular risk factors” in patients with psoriatic disease, he said. Instead of telling a patient with mildly elevated blood pressure, ‘I’ll see you in a year or two,’ or a patient entering a prediabetic stage to “watch what you eat, and I’ll see you in a couple of years,” clinicians need to be more vigilant.

“It’s about recognizing that these traditional cardiometabolic risk factors, synergistically with psoriasis, can start enhancing CV risk at an earlier age than we might expect,” said Dr. Garshick, whose 2021 review of CV risk in psoriasis describes how the inflammatory milieu in psoriasis is linked to atherosclerosis development.
Cardiologists are aware of this, but “many primary care physicians are not. It takes time for medical knowledge to diffuse,” Dr. Gelfand said. “Tell the PCP, in notes or in a form letter, that there is a higher risk of CV disease, and reference the AHA/ACC guidelines,” he advised. “You don’t want your patient to go to their doctor and the doctor to [be uninformed].”
‘Patients trust us’
Dr. Gelfand has been at the forefront of research on psoriasis and heart disease. A study he coauthored in 2006, for instance, documented an independent risk of MI, with adjusted relative risks of 1.29 and 3.10 for a 30-year-old patient with mild or severe disease, respectively, and higher risks for a 60-year-old. In 2010, he and coinvestigators found that severe psoriasis was an independent risk factor for CV mortality (HR, 1.57) after adjusting for age, sex, smoking, diabetes, hypertension, and hyperlipidemia.
Today, along with Dr. Barbieri, Dr. Ogdie, and others, he is studying the feasibility and efficacy of a proposed national, “centralized care coordinator” model of care whereby dermatologists and rheumatologists would educate the patient, order lipid and HbA1c measurements as medically appropriate, and then refer patients as needed to a care coordinator. The care coordinator would calculate a 10-year CVD risk score and counsel the patient on possible next steps.
In a pilot study of 85 patients at four sites, 92% of patients followed through on their physician’s recommendations to have labs drawn, and 86% indicated the model was acceptable and feasible. A total of 27% of patients had “newly identified, previously undiagnosed, elevated cardiovascular disease risk,” and exploratory effectiveness results indicated a successful reduction in predicted CVD risk in patients who started statins, Dr. Gelfand reported at the NPF meeting.
With funding from the NPF, a larger, single-arm, pragmatic “CP3” trial (NCT05908240) is enrolling 525 patients with psoriasis at 10-20 academic and nonacademic dermatology sites across the United States to further test the model. The primary endpoint will be the change in LDL cholesterol measured at 6 months among people with a 10-year risk ≥5%. Secondary endpoints will cover improvement in disease severity and quality of life, behavior modification, patient experience, and other issues.
“We have only 10-15 minutes [with patients] ... a care coordinator who is empathetic and understanding and [informed] could make a big difference,” Dr. Gelfand said at the NPF meeting. If findings are positive, the model would be tested in rheumatology sites as well. The hope, he said, is that the NPF would be able to fund an in-house care coordinator(s) for the long-term.
Notably, a patient survey conducted as part of exploratory research leading up to the care coordinator project showed that patients trust their dermatologist or rheumatologist for CVD education and screening. Among 160 patients with psoriasis and 162 patients with PsA, 76% and 90% agreed that “I would like it if my dermatologist/rheumatologist educated me about my risk of heart disease,” and 60% and 75%, respectively, agree that “it would be convenient for me to have my cholesterol checked by my dermatologist/rheumatologist.”
“Patients trust us,” Dr. Gelfand said at the NPF meeting. “And the pilot study shows us that patients are motivated.”
Taking an individualized, holistic, longitudinal approach
“Sometimes you do have to triage bit,” Dr. Gelfand said in an interview. “For a young person with normal body weight who doesn’t smoke and has mild psoriasis, one could just educate and advise that they see their primary care physician” for monitoring.
“But for the same patient who is obese, maybe smokes, and doesn’t have a primary care physician, I’d order labs,” he said. “You don’t want a patient walking out the door with an [undiagnosed] LDL of 160 or hypertension.”
Age is also an important consideration, as excess CVD risk associated with autoimmune diseases like psoriasis rises with age, Dr. Gelfand said during a seminar on psoriasis and PsA held at NYU Langone in December. For a young person, typically, “I need to focus on education and lifestyle … setting them on a healthy lifestyle trajectory,” he said. “Once they get to 40, from 40 to 75 or so, that’s a sweet spot for medical intervention to lower cardiovascular risk.”
Even at older ages, however, lipid management is not the be-all and end-all, he said in the interview. “We have to be holistic.”
One advantage of having highly successful therapies for psoriasis, and to a lesser extent PsA, is the time that becomes available during follow-up visits — once disease is under control — to “focus on other things,” he said. Waiting until disease is under control to discuss diet, exercise, or smoking, for instance, makes sense anyway, he said. “You don’t want to overwhelm patients with too much to do at once.”
Indeed, said dermatologist Robert E. Kalb, MD, of the Buffalo Medical Group in Buffalo, NY, “patients have an open mind [about discussing cardiovascular disease risk], but it is not high on their radar. Most of them just want to get their skin clear.” (Dr. Kalb participated in the care coordinator pilot study, and said in an interview that since its completion, he has been more routinely ordering relevant labs.)
Rheumatologists are less fortunate with highly successful therapies, but “over the continuum of care, we do have time in office visits” to discuss issues like smoking, exercise, and lifestyle, Dr. Ogdie said. “I think of each of those pieces as part of our job.”
In the future, as researchers learn more about the impact of psoriasis and PsA treatments on CVD risk, it may be possible to tailor treatments or to prescribe treatments knowing that the therapies could reduce risk. Observational and epidemiologic data suggest that tumor necrosis factor-alpha inhibitor therapy over 3 years reduces the risk of MI, and that patients whose psoriasis is treated have reduced aortic inflammation, improved myocardial strain, and reduced coronary plaque burden, Dr. Garshick said at the NPF meeting.
“But when we look at the randomized controlled trials, they’re actually inconclusive that targeting inflammation in psoriatic disease reduces surrogates of cardiovascular disease,” he said. Dr. Garshick’s own research focuses on platelet and endothelial biology in psoriasis.
Dr. Barbieri reported he had no relevant disclosures. Dr. Garshick reported consulting fees from Bristol-Myers Squibb, Kiniksa, Horizon Therapeutics, and Agepha. Dr. Ogdie reported financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, Takeda, and UCB. Dr. Gelfand reported serving as a consultant for AbbVie, Artax, Bristol-Myers Squibb, GlaxoSmithKline, and other companies.
Patients with psoriatic disease have significantly higher risks of myocardial infarction, stroke, and cardiovascular mortality than does the general population, yet research consistently paints what dermatologist Joel M. Gelfand, MD, calls an “abysmal” picture: Only a minority of patients with psoriatic disease know about their increased risks, only a minority of dermatologists and rheumatologists screen for cardiovascular risk factors like lipid levels and blood pressure, and only a minority of patients diagnosed with hyperlipidemia are adequately treated with statin therapy.
In the literature and at medical meetings, Dr. Gelfand and others who have studied cardiovascular disease (CVD) comorbidity and physician practices have been urging dermatologists and rheumatologists to play a more consistent and active role in primary cardiovascular prevention for patients with psoriatic disease, who are up to 50% more likely than patients without it to develop CVD and who tend to have atherosclerosis at earlier ages.
According to the 2019 joint American Academy of Dermatology (AAD)–National Psoriasis Foundation (NPF) guidelines for managing psoriasis “with awareness and attention to comorbidities,” this means not only ensuring that all patients with psoriasis receive standard CV risk assessment (screening for hypertension, diabetes, and hyperlipidemia), but also recognizing that patients who are candidates for systemic therapy or phototherapy — or who have psoriasis involving > 10% of body surface area — may benefit from earlier and more frequent screening.
CV risk and premature mortality rises with the severity of skin disease, and patients with psoriatic arthritis (PsA) are believed to have risk levels similar to patients with moderate-severe psoriasis, cardiologist Michael S. Garshick, MD, director of the cardio-rheumatology program at New York University Langone Health, said in an interview.
In a recent survey study of 100 patients seen at NYU Langone Health’s psoriasis specialty clinic, only one-third indicated they had been advised by their physicians to be screened for CV risk factors, and only one-third reported having been told of the connection between psoriasis and CVD risk. Dr. Garshick shared the unpublished findings at the annual research symposium of the NPF in October.
Similarly, data from the National Ambulatory Medical Care Survey shows that just 16% of psoriasis-related visits to dermatology providers from 2007 to 2016 involved screening for CV risk factors. Screening rates were 11% for body mass index, 7.4% for blood pressure, 2.9% for cholesterol, and 1.7% for glucose, Dr. Gelfand and coauthors reported in 2023. .
Such findings are concerning because research shows that fewer than a quarter of patients with psoriasis have a primary care visit within a year of establishing care with their physicians, and that, overall, fewer than half of commercially insured adults under age 65 visit a primary care physician each year, according to John S. Barbieri, MD, of the department of dermatology at Brigham and Women’s Hospital in Boston. He included these findings when reporting in 2022 on a survey study on CVD screening.
In many cases, dermatologists and rheumatologists may be the primary providers for patients with psoriatic disease. So, “the question is, how can the dermatologist or rheumatologist use their interactions as a touchpoint to improve the patient’s well-being?” Dr. Barbieri said in an interview.
For the dermatologist, educating patients about the higher CVD risk fits well into conversations about “how there may be inflammation inside the body as well as in the skin,” he said. “Talk about cardiovascular risk just as you talk about PsA risk.” Both specialists, he added, can incorporate blood pressure readings and look for opportunities to measure lipid levels and hemoglobin A1c (HbA1c). These labs can easily be integrated into a biologic work-up.
“The hard part — and this needs to be individualized — is how do you want to handle [abnormal readings]? Do you want to take on a lot of the ownership and calculate [10-year CVD] risk scores and then counsel patients accordingly?” Dr. Barbieri said. “Or do you want to try to refer, and encourage them to work with their PCP? There a high-touch version and a low-touch version of how you can turn screening into action, into a care plan.”
Beyond traditional risk elevation, the primary care hand-off
Rheumatologists “in general may be more apt to screen for cardiovascular disease” as a result of their internal medicine residency training, and “we’re generally more comfortable prescribing ... if we need to,” said Alexis R. Ogdie, MD, a rheumatologist at the Hospital of the University of Pennsylvania, Philadelphia, and director of the Penn Psoriatic Arthritis Clinic.
Referral to a preventive cardiologist for management of abnormal lab results or ongoing monitoring and prevention is ideal, but when hand-offs to primary care physicians are made — the more common scenario — education is important. “A common problem is that there is underrecognition of the cardiovascular risk being elevated in our patients,” she said, above and beyond risk posed by traditional risk factors such as dyslipidemia, hypertension, metabolic syndrome, and obesity, all of which have been shown to occur more frequently in patients with psoriatic disease than in the general population.
Risk stratification guides CVD prevention in the general population, and “if you use typical scores for cardiovascular risk, they may underestimate risk for our patients with PsA,” said Dr. Ogdie, who has reported on CV risk in patients with PsA. “Relative to what the patient’s perceived risk is, they may be treated similarly (to the general population). But relative to their actual risk, they’re undertreated.”
The 2019 AAD-NPF psoriasis guidelines recommend utilizing a 1.5 multiplication factor in risk score models, such as the American College of Cardiology’s Atherosclerotic Cardiovascular Disease (ASCVD) Risk Estimator, when the patient has a body surface area >10% or is a candidate for systemic therapy or phototherapy.
Similarly, the 2018 American Heart Association (AHA)-ACC Guideline on the Management of Blood Cholesterol defines psoriasis, along with RA, metabolic syndrome, HIV, and other diseases, as a “cardiovascular risk enhancer” that should be factored into assessments of ASCVD risk. (The guideline does not specify a psoriasis severity threshold.)
“It’s the first time the specialty [of cardiology] has said, ‘pay attention to a skin disease,’ ” Dr. Gelfand said at the NPF meeting.
Using the 1.5 multiplication factor, a patient who otherwise would be classified in the AHA/ACC guideline as “borderline risk,” with a 10-year ASCVD risk of 5% to <7.5%, would instead have an “intermediate” 10-year ASCVD risk of ≥7.5% to <20%. Application of the AHA-ACC “risk enhancer” would have a similar effect.
For management, the main impact of psoriasis being considered a risk enhancer is that “it lowers the threshold for treatment with standard cardiovascular prevention medications such as statins.”
In general, “we should be taking a more aggressive approach to the management of traditional cardiovascular risk factors” in patients with psoriatic disease, he said. Instead of telling a patient with mildly elevated blood pressure, ‘I’ll see you in a year or two,’ or a patient entering a prediabetic stage to “watch what you eat, and I’ll see you in a couple of years,” clinicians need to be more vigilant.
“It’s about recognizing that these traditional cardiometabolic risk factors, synergistically with psoriasis, can start enhancing CV risk at an earlier age than we might expect,” said Dr. Garshick, whose 2021 review of CV risk in psoriasis describes how the inflammatory milieu in psoriasis is linked to atherosclerosis development.
Cardiologists are aware of this, but “many primary care physicians are not. It takes time for medical knowledge to diffuse,” Dr. Gelfand said. “Tell the PCP, in notes or in a form letter, that there is a higher risk of CV disease, and reference the AHA/ACC guidelines,” he advised. “You don’t want your patient to go to their doctor and the doctor to [be uninformed].”
‘Patients trust us’
Dr. Gelfand has been at the forefront of research on psoriasis and heart disease. A study he coauthored in 2006, for instance, documented an independent risk of MI, with adjusted relative risks of 1.29 and 3.10 for a 30-year-old patient with mild or severe disease, respectively, and higher risks for a 60-year-old. In 2010, he and coinvestigators found that severe psoriasis was an independent risk factor for CV mortality (HR, 1.57) after adjusting for age, sex, smoking, diabetes, hypertension, and hyperlipidemia.
Today, along with Dr. Barbieri, Dr. Ogdie, and others, he is studying the feasibility and efficacy of a proposed national, “centralized care coordinator” model of care whereby dermatologists and rheumatologists would educate the patient, order lipid and HbA1c measurements as medically appropriate, and then refer patients as needed to a care coordinator. The care coordinator would calculate a 10-year CVD risk score and counsel the patient on possible next steps.
In a pilot study of 85 patients at four sites, 92% of patients followed through on their physician’s recommendations to have labs drawn, and 86% indicated the model was acceptable and feasible. A total of 27% of patients had “newly identified, previously undiagnosed, elevated cardiovascular disease risk,” and exploratory effectiveness results indicated a successful reduction in predicted CVD risk in patients who started statins, Dr. Gelfand reported at the NPF meeting.
With funding from the NPF, a larger, single-arm, pragmatic “CP3” trial (NCT05908240) is enrolling 525 patients with psoriasis at 10-20 academic and nonacademic dermatology sites across the United States to further test the model. The primary endpoint will be the change in LDL cholesterol measured at 6 months among people with a 10-year risk ≥5%. Secondary endpoints will cover improvement in disease severity and quality of life, behavior modification, patient experience, and other issues.
“We have only 10-15 minutes [with patients] ... a care coordinator who is empathetic and understanding and [informed] could make a big difference,” Dr. Gelfand said at the NPF meeting. If findings are positive, the model would be tested in rheumatology sites as well. The hope, he said, is that the NPF would be able to fund an in-house care coordinator(s) for the long-term.
Notably, a patient survey conducted as part of exploratory research leading up to the care coordinator project showed that patients trust their dermatologist or rheumatologist for CVD education and screening. Among 160 patients with psoriasis and 162 patients with PsA, 76% and 90% agreed that “I would like it if my dermatologist/rheumatologist educated me about my risk of heart disease,” and 60% and 75%, respectively, agree that “it would be convenient for me to have my cholesterol checked by my dermatologist/rheumatologist.”
“Patients trust us,” Dr. Gelfand said at the NPF meeting. “And the pilot study shows us that patients are motivated.”
Taking an individualized, holistic, longitudinal approach
“Sometimes you do have to triage bit,” Dr. Gelfand said in an interview. “For a young person with normal body weight who doesn’t smoke and has mild psoriasis, one could just educate and advise that they see their primary care physician” for monitoring.
“But for the same patient who is obese, maybe smokes, and doesn’t have a primary care physician, I’d order labs,” he said. “You don’t want a patient walking out the door with an [undiagnosed] LDL of 160 or hypertension.”
Age is also an important consideration, as excess CVD risk associated with autoimmune diseases like psoriasis rises with age, Dr. Gelfand said during a seminar on psoriasis and PsA held at NYU Langone in December. For a young person, typically, “I need to focus on education and lifestyle … setting them on a healthy lifestyle trajectory,” he said. “Once they get to 40, from 40 to 75 or so, that’s a sweet spot for medical intervention to lower cardiovascular risk.”
Even at older ages, however, lipid management is not the be-all and end-all, he said in the interview. “We have to be holistic.”
One advantage of having highly successful therapies for psoriasis, and to a lesser extent PsA, is the time that becomes available during follow-up visits — once disease is under control — to “focus on other things,” he said. Waiting until disease is under control to discuss diet, exercise, or smoking, for instance, makes sense anyway, he said. “You don’t want to overwhelm patients with too much to do at once.”
Indeed, said dermatologist Robert E. Kalb, MD, of the Buffalo Medical Group in Buffalo, NY, “patients have an open mind [about discussing cardiovascular disease risk], but it is not high on their radar. Most of them just want to get their skin clear.” (Dr. Kalb participated in the care coordinator pilot study, and said in an interview that since its completion, he has been more routinely ordering relevant labs.)
Rheumatologists are less fortunate with highly successful therapies, but “over the continuum of care, we do have time in office visits” to discuss issues like smoking, exercise, and lifestyle, Dr. Ogdie said. “I think of each of those pieces as part of our job.”
In the future, as researchers learn more about the impact of psoriasis and PsA treatments on CVD risk, it may be possible to tailor treatments or to prescribe treatments knowing that the therapies could reduce risk. Observational and epidemiologic data suggest that tumor necrosis factor-alpha inhibitor therapy over 3 years reduces the risk of MI, and that patients whose psoriasis is treated have reduced aortic inflammation, improved myocardial strain, and reduced coronary plaque burden, Dr. Garshick said at the NPF meeting.
“But when we look at the randomized controlled trials, they’re actually inconclusive that targeting inflammation in psoriatic disease reduces surrogates of cardiovascular disease,” he said. Dr. Garshick’s own research focuses on platelet and endothelial biology in psoriasis.
Dr. Barbieri reported he had no relevant disclosures. Dr. Garshick reported consulting fees from Bristol-Myers Squibb, Kiniksa, Horizon Therapeutics, and Agepha. Dr. Ogdie reported financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, Takeda, and UCB. Dr. Gelfand reported serving as a consultant for AbbVie, Artax, Bristol-Myers Squibb, GlaxoSmithKline, and other companies.
Patients with psoriatic disease have significantly higher risks of myocardial infarction, stroke, and cardiovascular mortality than does the general population, yet research consistently paints what dermatologist Joel M. Gelfand, MD, calls an “abysmal” picture: Only a minority of patients with psoriatic disease know about their increased risks, only a minority of dermatologists and rheumatologists screen for cardiovascular risk factors like lipid levels and blood pressure, and only a minority of patients diagnosed with hyperlipidemia are adequately treated with statin therapy.
In the literature and at medical meetings, Dr. Gelfand and others who have studied cardiovascular disease (CVD) comorbidity and physician practices have been urging dermatologists and rheumatologists to play a more consistent and active role in primary cardiovascular prevention for patients with psoriatic disease, who are up to 50% more likely than patients without it to develop CVD and who tend to have atherosclerosis at earlier ages.
According to the 2019 joint American Academy of Dermatology (AAD)–National Psoriasis Foundation (NPF) guidelines for managing psoriasis “with awareness and attention to comorbidities,” this means not only ensuring that all patients with psoriasis receive standard CV risk assessment (screening for hypertension, diabetes, and hyperlipidemia), but also recognizing that patients who are candidates for systemic therapy or phototherapy — or who have psoriasis involving > 10% of body surface area — may benefit from earlier and more frequent screening.
CV risk and premature mortality rises with the severity of skin disease, and patients with psoriatic arthritis (PsA) are believed to have risk levels similar to patients with moderate-severe psoriasis, cardiologist Michael S. Garshick, MD, director of the cardio-rheumatology program at New York University Langone Health, said in an interview.
In a recent survey study of 100 patients seen at NYU Langone Health’s psoriasis specialty clinic, only one-third indicated they had been advised by their physicians to be screened for CV risk factors, and only one-third reported having been told of the connection between psoriasis and CVD risk. Dr. Garshick shared the unpublished findings at the annual research symposium of the NPF in October.
Similarly, data from the National Ambulatory Medical Care Survey shows that just 16% of psoriasis-related visits to dermatology providers from 2007 to 2016 involved screening for CV risk factors. Screening rates were 11% for body mass index, 7.4% for blood pressure, 2.9% for cholesterol, and 1.7% for glucose, Dr. Gelfand and coauthors reported in 2023. .
Such findings are concerning because research shows that fewer than a quarter of patients with psoriasis have a primary care visit within a year of establishing care with their physicians, and that, overall, fewer than half of commercially insured adults under age 65 visit a primary care physician each year, according to John S. Barbieri, MD, of the department of dermatology at Brigham and Women’s Hospital in Boston. He included these findings when reporting in 2022 on a survey study on CVD screening.
In many cases, dermatologists and rheumatologists may be the primary providers for patients with psoriatic disease. So, “the question is, how can the dermatologist or rheumatologist use their interactions as a touchpoint to improve the patient’s well-being?” Dr. Barbieri said in an interview.
For the dermatologist, educating patients about the higher CVD risk fits well into conversations about “how there may be inflammation inside the body as well as in the skin,” he said. “Talk about cardiovascular risk just as you talk about PsA risk.” Both specialists, he added, can incorporate blood pressure readings and look for opportunities to measure lipid levels and hemoglobin A1c (HbA1c). These labs can easily be integrated into a biologic work-up.
“The hard part — and this needs to be individualized — is how do you want to handle [abnormal readings]? Do you want to take on a lot of the ownership and calculate [10-year CVD] risk scores and then counsel patients accordingly?” Dr. Barbieri said. “Or do you want to try to refer, and encourage them to work with their PCP? There a high-touch version and a low-touch version of how you can turn screening into action, into a care plan.”
Beyond traditional risk elevation, the primary care hand-off
Rheumatologists “in general may be more apt to screen for cardiovascular disease” as a result of their internal medicine residency training, and “we’re generally more comfortable prescribing ... if we need to,” said Alexis R. Ogdie, MD, a rheumatologist at the Hospital of the University of Pennsylvania, Philadelphia, and director of the Penn Psoriatic Arthritis Clinic.
Referral to a preventive cardiologist for management of abnormal lab results or ongoing monitoring and prevention is ideal, but when hand-offs to primary care physicians are made — the more common scenario — education is important. “A common problem is that there is underrecognition of the cardiovascular risk being elevated in our patients,” she said, above and beyond risk posed by traditional risk factors such as dyslipidemia, hypertension, metabolic syndrome, and obesity, all of which have been shown to occur more frequently in patients with psoriatic disease than in the general population.
Risk stratification guides CVD prevention in the general population, and “if you use typical scores for cardiovascular risk, they may underestimate risk for our patients with PsA,” said Dr. Ogdie, who has reported on CV risk in patients with PsA. “Relative to what the patient’s perceived risk is, they may be treated similarly (to the general population). But relative to their actual risk, they’re undertreated.”
The 2019 AAD-NPF psoriasis guidelines recommend utilizing a 1.5 multiplication factor in risk score models, such as the American College of Cardiology’s Atherosclerotic Cardiovascular Disease (ASCVD) Risk Estimator, when the patient has a body surface area >10% or is a candidate for systemic therapy or phototherapy.
Similarly, the 2018 American Heart Association (AHA)-ACC Guideline on the Management of Blood Cholesterol defines psoriasis, along with RA, metabolic syndrome, HIV, and other diseases, as a “cardiovascular risk enhancer” that should be factored into assessments of ASCVD risk. (The guideline does not specify a psoriasis severity threshold.)
“It’s the first time the specialty [of cardiology] has said, ‘pay attention to a skin disease,’ ” Dr. Gelfand said at the NPF meeting.
Using the 1.5 multiplication factor, a patient who otherwise would be classified in the AHA/ACC guideline as “borderline risk,” with a 10-year ASCVD risk of 5% to <7.5%, would instead have an “intermediate” 10-year ASCVD risk of ≥7.5% to <20%. Application of the AHA-ACC “risk enhancer” would have a similar effect.
For management, the main impact of psoriasis being considered a risk enhancer is that “it lowers the threshold for treatment with standard cardiovascular prevention medications such as statins.”
In general, “we should be taking a more aggressive approach to the management of traditional cardiovascular risk factors” in patients with psoriatic disease, he said. Instead of telling a patient with mildly elevated blood pressure, ‘I’ll see you in a year or two,’ or a patient entering a prediabetic stage to “watch what you eat, and I’ll see you in a couple of years,” clinicians need to be more vigilant.
“It’s about recognizing that these traditional cardiometabolic risk factors, synergistically with psoriasis, can start enhancing CV risk at an earlier age than we might expect,” said Dr. Garshick, whose 2021 review of CV risk in psoriasis describes how the inflammatory milieu in psoriasis is linked to atherosclerosis development.
Cardiologists are aware of this, but “many primary care physicians are not. It takes time for medical knowledge to diffuse,” Dr. Gelfand said. “Tell the PCP, in notes or in a form letter, that there is a higher risk of CV disease, and reference the AHA/ACC guidelines,” he advised. “You don’t want your patient to go to their doctor and the doctor to [be uninformed].”
‘Patients trust us’
Dr. Gelfand has been at the forefront of research on psoriasis and heart disease. A study he coauthored in 2006, for instance, documented an independent risk of MI, with adjusted relative risks of 1.29 and 3.10 for a 30-year-old patient with mild or severe disease, respectively, and higher risks for a 60-year-old. In 2010, he and coinvestigators found that severe psoriasis was an independent risk factor for CV mortality (HR, 1.57) after adjusting for age, sex, smoking, diabetes, hypertension, and hyperlipidemia.
Today, along with Dr. Barbieri, Dr. Ogdie, and others, he is studying the feasibility and efficacy of a proposed national, “centralized care coordinator” model of care whereby dermatologists and rheumatologists would educate the patient, order lipid and HbA1c measurements as medically appropriate, and then refer patients as needed to a care coordinator. The care coordinator would calculate a 10-year CVD risk score and counsel the patient on possible next steps.
In a pilot study of 85 patients at four sites, 92% of patients followed through on their physician’s recommendations to have labs drawn, and 86% indicated the model was acceptable and feasible. A total of 27% of patients had “newly identified, previously undiagnosed, elevated cardiovascular disease risk,” and exploratory effectiveness results indicated a successful reduction in predicted CVD risk in patients who started statins, Dr. Gelfand reported at the NPF meeting.
With funding from the NPF, a larger, single-arm, pragmatic “CP3” trial (NCT05908240) is enrolling 525 patients with psoriasis at 10-20 academic and nonacademic dermatology sites across the United States to further test the model. The primary endpoint will be the change in LDL cholesterol measured at 6 months among people with a 10-year risk ≥5%. Secondary endpoints will cover improvement in disease severity and quality of life, behavior modification, patient experience, and other issues.
“We have only 10-15 minutes [with patients] ... a care coordinator who is empathetic and understanding and [informed] could make a big difference,” Dr. Gelfand said at the NPF meeting. If findings are positive, the model would be tested in rheumatology sites as well. The hope, he said, is that the NPF would be able to fund an in-house care coordinator(s) for the long-term.
Notably, a patient survey conducted as part of exploratory research leading up to the care coordinator project showed that patients trust their dermatologist or rheumatologist for CVD education and screening. Among 160 patients with psoriasis and 162 patients with PsA, 76% and 90% agreed that “I would like it if my dermatologist/rheumatologist educated me about my risk of heart disease,” and 60% and 75%, respectively, agree that “it would be convenient for me to have my cholesterol checked by my dermatologist/rheumatologist.”
“Patients trust us,” Dr. Gelfand said at the NPF meeting. “And the pilot study shows us that patients are motivated.”
Taking an individualized, holistic, longitudinal approach
“Sometimes you do have to triage bit,” Dr. Gelfand said in an interview. “For a young person with normal body weight who doesn’t smoke and has mild psoriasis, one could just educate and advise that they see their primary care physician” for monitoring.
“But for the same patient who is obese, maybe smokes, and doesn’t have a primary care physician, I’d order labs,” he said. “You don’t want a patient walking out the door with an [undiagnosed] LDL of 160 or hypertension.”
Age is also an important consideration, as excess CVD risk associated with autoimmune diseases like psoriasis rises with age, Dr. Gelfand said during a seminar on psoriasis and PsA held at NYU Langone in December. For a young person, typically, “I need to focus on education and lifestyle … setting them on a healthy lifestyle trajectory,” he said. “Once they get to 40, from 40 to 75 or so, that’s a sweet spot for medical intervention to lower cardiovascular risk.”
Even at older ages, however, lipid management is not the be-all and end-all, he said in the interview. “We have to be holistic.”
One advantage of having highly successful therapies for psoriasis, and to a lesser extent PsA, is the time that becomes available during follow-up visits — once disease is under control — to “focus on other things,” he said. Waiting until disease is under control to discuss diet, exercise, or smoking, for instance, makes sense anyway, he said. “You don’t want to overwhelm patients with too much to do at once.”
Indeed, said dermatologist Robert E. Kalb, MD, of the Buffalo Medical Group in Buffalo, NY, “patients have an open mind [about discussing cardiovascular disease risk], but it is not high on their radar. Most of them just want to get their skin clear.” (Dr. Kalb participated in the care coordinator pilot study, and said in an interview that since its completion, he has been more routinely ordering relevant labs.)
Rheumatologists are less fortunate with highly successful therapies, but “over the continuum of care, we do have time in office visits” to discuss issues like smoking, exercise, and lifestyle, Dr. Ogdie said. “I think of each of those pieces as part of our job.”
In the future, as researchers learn more about the impact of psoriasis and PsA treatments on CVD risk, it may be possible to tailor treatments or to prescribe treatments knowing that the therapies could reduce risk. Observational and epidemiologic data suggest that tumor necrosis factor-alpha inhibitor therapy over 3 years reduces the risk of MI, and that patients whose psoriasis is treated have reduced aortic inflammation, improved myocardial strain, and reduced coronary plaque burden, Dr. Garshick said at the NPF meeting.
“But when we look at the randomized controlled trials, they’re actually inconclusive that targeting inflammation in psoriatic disease reduces surrogates of cardiovascular disease,” he said. Dr. Garshick’s own research focuses on platelet and endothelial biology in psoriasis.
Dr. Barbieri reported he had no relevant disclosures. Dr. Garshick reported consulting fees from Bristol-Myers Squibb, Kiniksa, Horizon Therapeutics, and Agepha. Dr. Ogdie reported financial relationships with AbbVie, Amgen, Bristol-Myers Squibb, Celgene, Eli Lilly, Gilead, GlaxoSmithKline, Janssen, Novartis, Pfizer, Takeda, and UCB. Dr. Gelfand reported serving as a consultant for AbbVie, Artax, Bristol-Myers Squibb, GlaxoSmithKline, and other companies.
Roflumilast foam gets nod as new option for seborrheic dermatitis
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.
The in a press release.
The 0.3% foam, marketed as Zoryve, applied once-daily, is indicated for patients aged 9 years and older with seborrheic dermatitis, and can be used anywhere on the body, including areas with hair, with no limits on duration of use, according to the company, Arcutis. A 0.3% cream formulation of roflumilast was previously approved by the FDA for the topical treatment of plaque psoriasis in patients aged 6 years and older.
Approval was based on data from the phase 3 STRATUM trial and an accompanying phase 2 study known as Trial 203. These studies included a total of 683 adults and youth aged 9 years and older with seborrheic dermatitis. Participants were randomized to roflumilast or a placebo.
At 8 weeks, 79.5 % of patients on roflumilast met the primary efficacy endpoint of Investigator Global Assessment (IGA) scores of 0 or 1 (clear or almost clear) compared with 58.0% of patients on placebo (P < .001); the results were similar in the phase 2 Trial 203 (73.1% vs. 40.8%, respectively; P < .001). Overall, more than 50% of the patients on roflumilast achieved a clear score.
Patients in the roflumilast group also showed significant improvement in all secondary endpoints, including itching, scaling, and erythema, according to the company.
In the STRATUM study, 62.8% of roflumilast-treated patients and 40.6% of placebo patients achieved a 4-point or more reduction in itch based on the Worst Itch Numerical Rating Score (P =.0001), and 28% of roflumilast-treated patients reported significant itch improvement within the first 48 hours of use, compared with 13% of placebo patients (P = .0024).
Over a treatment period of up to 1 year, no treatment-related severe adverse events were reported in the phase 2 and 3 studies. The incidence of treatment emergent adverse events was similar between the treatment and placebo groups, and the most common adverse events (occurring in 1% of more of patients) across both studies were nasopharyngitis (1.5%), nausea (1.3%), and headache (1.1%).
Roflumilast foam is scheduled to be available by the end of January 2024, according to the company. The product is for topical use only, and contraindicated for individuals with severe liver impairment.