User login
Holding RA, SpA Drugs Did Not Improve Antibody Response to COVID Vaccine
WASHINGTON — There is no benefit to interrupting treatment with many of the available targeted synthetic or biologic disease-modifying antirheumatic drugs for rheumatoid arthritis (RA) or spondyloarthritis (SpA) at the time of a repeat COVID-19 vaccine dose, new research found.
In the multicenter, randomized controlled COVID Vaccine Response (COVER) trial of 577 patients with RA or SpA taking either abatacept, Janus kinase (JAK) inhibitors, interleukin (IL)–17 inhibitors, or tumor necrosis factor (TNF) inhibitors, holding those drugs for 2 weeks at the time of COVID-19 vaccination supplemental doses didn’t improve antibody response to the vaccine but did lead to disease flares. Most participants had significant antibody responses to the vaccine, regardless of whether their medication had been held or continued, Jeffrey R. Curtis, MD, the Harbert-Ball Professor of Medicine, Epidemiology, and Computer Science at the University of Alabama at Birmingham, reported at the annual meeting of the American College of Rheumatology (ACR).
Guidelines issued by ACR in 2023 recommended holding abatacept for the COVID vaccine but said that “the task force failed to reach consensus” on whether or not to temporarily interrupt the other medications following primary vaccination or supplemental/booster dosing.
Curtis, who was an author on those guidelines, said in an interview, “to date, we haven’t known whether it might be a good idea to hold certain drugs at the time patients receive their next dose of the COVID vaccine. ... That’s because without direct evidence, you have people trading opinions based on extrapolated data.”
The inability to measure cell-mediated immunity and only humoral (ie, antibody-based) immunity is a limitation in COVER. “Nevertheless, based on what we know now, it isn’t advisable to hold any of the four drug classes that we studied at the time patients receive their next COVID vaccine dose. This finding is in contrast to data from a different trial showing that holding methotrexate for 2 weeks does appear to help in response to COVID-19 vaccination, as well as influenza vaccine,” Curtis said.
Asked to comment, session moderator Elena Myasoedova, MD, PhD, consultant rheumatologist and director of the Inflammatory Arthritis Clinic at the Mayo Clinic, Rochester, Minnesota, said in an interview: “This has been an area of clinical uncertainty. It raises a lot of questions from patients and from physicians alike as to whether or not to hold the medication because the implications are flares, and that’s impactful for patients. Patients care about their RA status and how it is controlled, and if there is no difference, then there is no reason to change the medication regimen.”
To Hold or Not to Hold: COVER Shows It Makes Little Difference to Vaccine Response
In COVER, 128 patients were taking abatacept, 96 IL-17 inhibitors, 237 JAK inhibitors, and 116 TNF inhibitors. The study was conducted within 30 sites of the Excellence Network in Rheumatology, a rheumatology practice–based research network launched in 2021. Participants were identified and enrolled at clinic visits immediately prior to receiving their COVID-19 boosters (in routine settings).
All had previously received two or more doses of the mRNA vaccines made by Pfizer or Moderna. Blood was drawn, and they were randomized 1:1 to either continue or hold their disease medication for 2 weeks following the booster. Blood was collected again at 6 weeks post vaccine.
Anti–receptor-binding domain (RBD) IgG antibody titers increased significantly in all drug categories across both study arms, with no differences between the hold vs continue medication groups, even after adjustments for age, sex, body mass index, methotrexate use, steroid use, and time from booster to measurement. All groups also showed increases in geometric mean fold rise of more than 3%.
Subgroup analyses showed no major differences between antibody responses in the hold vs continue groups. The anti-RBD IgG response was lower for abatacept and JAK inhibitors than for the other two drugs, but there was still no significant benefit to holding them for 2 weeks post vaccination.
Holding Drugs Leads to Disease Flares
On the flip side, there were significant differences between the two groups in their responses to the question: “Did you experience any flare or worsening of your autoimmune disease following your recent COVID-19 booster dose?” Overall, 27% of the hold group responded that they had, compared with just 13% of the continue group (P < .05). This difference was greatest in the JAK inhibitor group (33% vs 9%; P < .05).
Among those reporting flares or worsening disease, both the severity and the duration of the flares were about the same. “Interestingly, the duration is beyond a week for the majority of patients. The reason that’s important is, any symptoms that are so-called flare might simply be reactogenicity symptoms, and that might be confused for flare or disease worsening, but you see that a majority of patients actually have those symptoms extending beyond the week. Most of them are worsening in arthritis, as you might expect,” Curtis said in his presentation.
Asked what they did about the flare, only a minority of patients reported contacting a healthcare provider. In all, 68% of the hold group and 78% of the continue group took no action. That’s good in the sense that most of the flares weren’t severe, but it has implications for research, Curtis pointed out.
“A lot of times in the vaccine literature, people do retrospective chart review by looking to see what the doctor said as to whether the patient had a flare. And what this would tell you is patients may be reporting a lot of flares that their doctor doesn’t know anything about. So if you really want to know whether people are having a flare, even a mild flare, you really have to collect prospective data.”
COVID is Not the Last Pandemic
“These results are reassuring, although I think we need a bit more data on abatacept,” Myasoedova said, adding, “I was also interested in the outcomes, such as severe infections, that actually happened to these patients. What we see in the labs in their immune response is one thing, but then also important is what actually evolves in terms of the outcomes, especially with abatacept.”
Overall, she said, “I think it’s reassuring and definitely informs clinical practice going forward. But then probably we’ll learn more. What we’re hearing is COVID is not the last pandemic.”
The COVER trial receives support from AbbVie, BMS, Eli Lilly, Novartis, and Pfizer. Curtis has received research grants and consulting fees from AbbVie, Amgen, BMS, GSK, Eli Lilly, Novartis, Pfizer, Sanofi, and UCB. Myasoedova has no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — There is no benefit to interrupting treatment with many of the available targeted synthetic or biologic disease-modifying antirheumatic drugs for rheumatoid arthritis (RA) or spondyloarthritis (SpA) at the time of a repeat COVID-19 vaccine dose, new research found.
In the multicenter, randomized controlled COVID Vaccine Response (COVER) trial of 577 patients with RA or SpA taking either abatacept, Janus kinase (JAK) inhibitors, interleukin (IL)–17 inhibitors, or tumor necrosis factor (TNF) inhibitors, holding those drugs for 2 weeks at the time of COVID-19 vaccination supplemental doses didn’t improve antibody response to the vaccine but did lead to disease flares. Most participants had significant antibody responses to the vaccine, regardless of whether their medication had been held or continued, Jeffrey R. Curtis, MD, the Harbert-Ball Professor of Medicine, Epidemiology, and Computer Science at the University of Alabama at Birmingham, reported at the annual meeting of the American College of Rheumatology (ACR).
Guidelines issued by ACR in 2023 recommended holding abatacept for the COVID vaccine but said that “the task force failed to reach consensus” on whether or not to temporarily interrupt the other medications following primary vaccination or supplemental/booster dosing.
Curtis, who was an author on those guidelines, said in an interview, “to date, we haven’t known whether it might be a good idea to hold certain drugs at the time patients receive their next dose of the COVID vaccine. ... That’s because without direct evidence, you have people trading opinions based on extrapolated data.”
The inability to measure cell-mediated immunity and only humoral (ie, antibody-based) immunity is a limitation in COVER. “Nevertheless, based on what we know now, it isn’t advisable to hold any of the four drug classes that we studied at the time patients receive their next COVID vaccine dose. This finding is in contrast to data from a different trial showing that holding methotrexate for 2 weeks does appear to help in response to COVID-19 vaccination, as well as influenza vaccine,” Curtis said.
Asked to comment, session moderator Elena Myasoedova, MD, PhD, consultant rheumatologist and director of the Inflammatory Arthritis Clinic at the Mayo Clinic, Rochester, Minnesota, said in an interview: “This has been an area of clinical uncertainty. It raises a lot of questions from patients and from physicians alike as to whether or not to hold the medication because the implications are flares, and that’s impactful for patients. Patients care about their RA status and how it is controlled, and if there is no difference, then there is no reason to change the medication regimen.”
To Hold or Not to Hold: COVER Shows It Makes Little Difference to Vaccine Response
In COVER, 128 patients were taking abatacept, 96 IL-17 inhibitors, 237 JAK inhibitors, and 116 TNF inhibitors. The study was conducted within 30 sites of the Excellence Network in Rheumatology, a rheumatology practice–based research network launched in 2021. Participants were identified and enrolled at clinic visits immediately prior to receiving their COVID-19 boosters (in routine settings).
All had previously received two or more doses of the mRNA vaccines made by Pfizer or Moderna. Blood was drawn, and they were randomized 1:1 to either continue or hold their disease medication for 2 weeks following the booster. Blood was collected again at 6 weeks post vaccine.
Anti–receptor-binding domain (RBD) IgG antibody titers increased significantly in all drug categories across both study arms, with no differences between the hold vs continue medication groups, even after adjustments for age, sex, body mass index, methotrexate use, steroid use, and time from booster to measurement. All groups also showed increases in geometric mean fold rise of more than 3%.
Subgroup analyses showed no major differences between antibody responses in the hold vs continue groups. The anti-RBD IgG response was lower for abatacept and JAK inhibitors than for the other two drugs, but there was still no significant benefit to holding them for 2 weeks post vaccination.
Holding Drugs Leads to Disease Flares
On the flip side, there were significant differences between the two groups in their responses to the question: “Did you experience any flare or worsening of your autoimmune disease following your recent COVID-19 booster dose?” Overall, 27% of the hold group responded that they had, compared with just 13% of the continue group (P < .05). This difference was greatest in the JAK inhibitor group (33% vs 9%; P < .05).
Among those reporting flares or worsening disease, both the severity and the duration of the flares were about the same. “Interestingly, the duration is beyond a week for the majority of patients. The reason that’s important is, any symptoms that are so-called flare might simply be reactogenicity symptoms, and that might be confused for flare or disease worsening, but you see that a majority of patients actually have those symptoms extending beyond the week. Most of them are worsening in arthritis, as you might expect,” Curtis said in his presentation.
Asked what they did about the flare, only a minority of patients reported contacting a healthcare provider. In all, 68% of the hold group and 78% of the continue group took no action. That’s good in the sense that most of the flares weren’t severe, but it has implications for research, Curtis pointed out.
“A lot of times in the vaccine literature, people do retrospective chart review by looking to see what the doctor said as to whether the patient had a flare. And what this would tell you is patients may be reporting a lot of flares that their doctor doesn’t know anything about. So if you really want to know whether people are having a flare, even a mild flare, you really have to collect prospective data.”
COVID is Not the Last Pandemic
“These results are reassuring, although I think we need a bit more data on abatacept,” Myasoedova said, adding, “I was also interested in the outcomes, such as severe infections, that actually happened to these patients. What we see in the labs in their immune response is one thing, but then also important is what actually evolves in terms of the outcomes, especially with abatacept.”
Overall, she said, “I think it’s reassuring and definitely informs clinical practice going forward. But then probably we’ll learn more. What we’re hearing is COVID is not the last pandemic.”
The COVER trial receives support from AbbVie, BMS, Eli Lilly, Novartis, and Pfizer. Curtis has received research grants and consulting fees from AbbVie, Amgen, BMS, GSK, Eli Lilly, Novartis, Pfizer, Sanofi, and UCB. Myasoedova has no disclosures.
A version of this article first appeared on Medscape.com.
WASHINGTON — There is no benefit to interrupting treatment with many of the available targeted synthetic or biologic disease-modifying antirheumatic drugs for rheumatoid arthritis (RA) or spondyloarthritis (SpA) at the time of a repeat COVID-19 vaccine dose, new research found.
In the multicenter, randomized controlled COVID Vaccine Response (COVER) trial of 577 patients with RA or SpA taking either abatacept, Janus kinase (JAK) inhibitors, interleukin (IL)–17 inhibitors, or tumor necrosis factor (TNF) inhibitors, holding those drugs for 2 weeks at the time of COVID-19 vaccination supplemental doses didn’t improve antibody response to the vaccine but did lead to disease flares. Most participants had significant antibody responses to the vaccine, regardless of whether their medication had been held or continued, Jeffrey R. Curtis, MD, the Harbert-Ball Professor of Medicine, Epidemiology, and Computer Science at the University of Alabama at Birmingham, reported at the annual meeting of the American College of Rheumatology (ACR).
Guidelines issued by ACR in 2023 recommended holding abatacept for the COVID vaccine but said that “the task force failed to reach consensus” on whether or not to temporarily interrupt the other medications following primary vaccination or supplemental/booster dosing.
Curtis, who was an author on those guidelines, said in an interview, “to date, we haven’t known whether it might be a good idea to hold certain drugs at the time patients receive their next dose of the COVID vaccine. ... That’s because without direct evidence, you have people trading opinions based on extrapolated data.”
The inability to measure cell-mediated immunity and only humoral (ie, antibody-based) immunity is a limitation in COVER. “Nevertheless, based on what we know now, it isn’t advisable to hold any of the four drug classes that we studied at the time patients receive their next COVID vaccine dose. This finding is in contrast to data from a different trial showing that holding methotrexate for 2 weeks does appear to help in response to COVID-19 vaccination, as well as influenza vaccine,” Curtis said.
Asked to comment, session moderator Elena Myasoedova, MD, PhD, consultant rheumatologist and director of the Inflammatory Arthritis Clinic at the Mayo Clinic, Rochester, Minnesota, said in an interview: “This has been an area of clinical uncertainty. It raises a lot of questions from patients and from physicians alike as to whether or not to hold the medication because the implications are flares, and that’s impactful for patients. Patients care about their RA status and how it is controlled, and if there is no difference, then there is no reason to change the medication regimen.”
To Hold or Not to Hold: COVER Shows It Makes Little Difference to Vaccine Response
In COVER, 128 patients were taking abatacept, 96 IL-17 inhibitors, 237 JAK inhibitors, and 116 TNF inhibitors. The study was conducted within 30 sites of the Excellence Network in Rheumatology, a rheumatology practice–based research network launched in 2021. Participants were identified and enrolled at clinic visits immediately prior to receiving their COVID-19 boosters (in routine settings).
All had previously received two or more doses of the mRNA vaccines made by Pfizer or Moderna. Blood was drawn, and they were randomized 1:1 to either continue or hold their disease medication for 2 weeks following the booster. Blood was collected again at 6 weeks post vaccine.
Anti–receptor-binding domain (RBD) IgG antibody titers increased significantly in all drug categories across both study arms, with no differences between the hold vs continue medication groups, even after adjustments for age, sex, body mass index, methotrexate use, steroid use, and time from booster to measurement. All groups also showed increases in geometric mean fold rise of more than 3%.
Subgroup analyses showed no major differences between antibody responses in the hold vs continue groups. The anti-RBD IgG response was lower for abatacept and JAK inhibitors than for the other two drugs, but there was still no significant benefit to holding them for 2 weeks post vaccination.
Holding Drugs Leads to Disease Flares
On the flip side, there were significant differences between the two groups in their responses to the question: “Did you experience any flare or worsening of your autoimmune disease following your recent COVID-19 booster dose?” Overall, 27% of the hold group responded that they had, compared with just 13% of the continue group (P < .05). This difference was greatest in the JAK inhibitor group (33% vs 9%; P < .05).
Among those reporting flares or worsening disease, both the severity and the duration of the flares were about the same. “Interestingly, the duration is beyond a week for the majority of patients. The reason that’s important is, any symptoms that are so-called flare might simply be reactogenicity symptoms, and that might be confused for flare or disease worsening, but you see that a majority of patients actually have those symptoms extending beyond the week. Most of them are worsening in arthritis, as you might expect,” Curtis said in his presentation.
Asked what they did about the flare, only a minority of patients reported contacting a healthcare provider. In all, 68% of the hold group and 78% of the continue group took no action. That’s good in the sense that most of the flares weren’t severe, but it has implications for research, Curtis pointed out.
“A lot of times in the vaccine literature, people do retrospective chart review by looking to see what the doctor said as to whether the patient had a flare. And what this would tell you is patients may be reporting a lot of flares that their doctor doesn’t know anything about. So if you really want to know whether people are having a flare, even a mild flare, you really have to collect prospective data.”
COVID is Not the Last Pandemic
“These results are reassuring, although I think we need a bit more data on abatacept,” Myasoedova said, adding, “I was also interested in the outcomes, such as severe infections, that actually happened to these patients. What we see in the labs in their immune response is one thing, but then also important is what actually evolves in terms of the outcomes, especially with abatacept.”
Overall, she said, “I think it’s reassuring and definitely informs clinical practice going forward. But then probably we’ll learn more. What we’re hearing is COVID is not the last pandemic.”
The COVER trial receives support from AbbVie, BMS, Eli Lilly, Novartis, and Pfizer. Curtis has received research grants and consulting fees from AbbVie, Amgen, BMS, GSK, Eli Lilly, Novartis, Pfizer, Sanofi, and UCB. Myasoedova has no disclosures.
A version of this article first appeared on Medscape.com.
FROM ACR 2024
Pemphigus, Bullous Pemphigoid Risk Increased After COVID-19 Infection
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
TOPLINE:
according to a study that also found that vaccination against COVID-19 is associated with a reduced risk for these conditions.
METHODOLOGY:
- Researchers conducted a population-based retrospective cohort study using data from the TriNetX Analytics Network, encompassing over 112 million electronic health records in the United States.
- The study compared the risk for AIBD within 3 months among individuals who had COVID-19 infection and no COVID-19 vaccination 6 months prior to the infection (n = 4,787,106), individuals who had COVID-19 vaccination but did not have COVID-19 infection (n = 3,466,536), and individuals who did not have COVID-19 infection or vaccination (n = 5,609,197).
- The mean age of the three groups was 44.9, 52.3, and 49.3 years, respectively.
- Propensity score matching included 4,408,748 individuals each for the comparison between COVID-19 infection and controls, 3,465,420 for COVID-19 vaccination and controls, and 3,362,850 for COVID-19 infection and vaccination. The mean follow-up ranged from 72.2 to 76.3 days.
TAKEAWAY:
- Individuals with COVID-19 infection showed a 50.8% increased risk for AIBD within 3 months (P < .001) compared with those without infection or vaccination. The risk was more pronounced for pemphigus (hazard ratio [HR], 2.432; P < .001) than bullous pemphigoid (HR, 1.376; P = .036).
- On the contrary, individuals who had the COVID-19 vaccination showed almost half the risk for AIBD (HR, 0.514; P < .001). The risk reduction was significant for pemphigus (HR, 0.477; P = .030), but not for bullous pemphigoid (HR, 0.846).
- When the infection and vaccination groups were compared, COVID-19 infection increased AIBD risk by more than threefold (HR, 3.130; P < .001), with a particularly high risk for pemphigus (HR, 5.508; P < .001). A significant risk was also seen for bullous pemphigoid (HR, 1.587; P = .008).
IN PRACTICE:
“The findings underscore the importance of vaccination not only in preventing severe COVID-19 outcomes but also in potentially protecting against autoimmune complications,” the authors wrote, adding that “this potential dual benefit of vaccination should be a key message in public health campaigns and clinical practice to enhance vaccine uptake and ultimately improve health outcomes.”
SOURCE:
The study was led by Philip Curman, MD, PhD, of the Dermato-Venereology Clinic at Karolinska University Hospital, Stockholm, Sweden, and was published online on November 7 in the Journal of the American Academy of Dermatology.
LIMITATIONS:
The retrospective design has inherent biases, there is potential underreporting of COVID-19 cases and vaccinations, and there is misallocation of individuals. Unmeasured confounding factors may be present.
DISCLOSURES:
This study was funded by grant from the State of Schleswig-Holstein. Two authors were employees of TriNetX. Some authors received financial support and travel grants from various sources, including TriNetX. Additional disclosures are noted in the article.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
COVID on the Floor Linked to Outbreaks on Two Hospital Wards
The viral burden of SARS-CoV-2 on floors, even in healthcare worker–only areas, was strongly associated with COVID-19 outbreaks in two acute-care hospitals, according to a new study from Ontario, Canada.
With every 10-fold increase in viral copies, the chance of an impending outbreak of COVID-19 rose 22-fold.
“These data add to the mounting evidence that built environment detection for SARS-CoV-2 may provide an additional layer of monitoring and could help inform local infection prevention and control measures,” they wrote.
The study was published online in Infection Control & Hospital Epidemiology.
Preventing Future Suffering
The current study builds on the researchers’ previous work, which found the same correlation between viral load on floors and COVID outbreaks in long-term care homes.
Currently, the best-known method of environmental surveillance for COVID is wastewater detection. “Swabbing the floors would be another approach to surveillance,” senior author Caroline Nott, MD, infectious disease physician at the Ottawa Hospital, said in an interview.
“We do have environmental surveillance with wastewater, but while this may tell you what’s going on in the city, it doesn’t tell you what is going on in a particular ward of a hospital, for instance,” she added.
Nott and her colleagues believe that swabbing, which is easy and relatively inexpensive, will become another tool to examine the built environment. “Instead of having to close a whole hospital, for example, we could just close one room instead of an entire ward if swabbing showed a high concentration of COVID,” Nott said.
The current study was conducted at two hospitals in Ontario between July 2022 and March 2023. The floors of healthcare worker–only areas on four inpatient adult wards were swabbed. These areas included changing rooms, meeting rooms, staff washrooms, nursing stations, and interdisciplinary team rooms.
SARS-CoV-2 RNA was detected on 537 of 760 floor swabs (71%). The overall positivity rate in the first hospital was 90% (n = 280). In the second hospital, the rate was 60% (n = 480).
Four COVID-19 outbreaks occurred in the first acute care hospital, and seven outbreaks occurred at the second hospital. Outbreaks occurred mostly among hospitalized patients (140 cases), but also in four hospital workers.
COVID-19 still requires vigilance, said Nott. “We weren’t prepared for COVID, and so as a result, many people died or have suffered long-term effects, especially vulnerable people like those being treated in hospital or in long-term care facilities. We want to develop methods to prevent similar suffering in the future, whether it’s a new COVID variant or a different pathogen altogether.”
Changing Surveillance Practice?
“This is a good study,” Steven Rogak, PhD, professor of mechanical engineering at the University of British Columbia (UBC) in Vancouver, Canada, said in an interivew. “The fundamental idea is that respiratory droplets and aerosols will deposit on the floor, and polymerase chain reaction [PCR] tests of swabs will provide a surrogate measurement of what might have been inhaled. There are solid statistics that it worked for the hospitals studied,” said Rogak, who studies aerosols at UBC’s Energy and Aerosols Laboratory. Rogak did not participate in the study.
“The authors note several limitations, including that increased healthcare worker testing may have been triggered by the higher values of PCR counts from the floor swabs. But this doesn’t seem to be a problem to me, because if the floor swabs motivate the hospital to test workers more, and that results in identifying outbreaks sooner, then great,” he said.
“Another limitation is that if the hospital has better HVAC or uses air purifiers, it could remove the most infectious aerosols, but the large droplets that fall quickly to the ground would remain, and this would still result in high PCR counts from floor swabs. In this case, perhaps the floor swabs would be a poorer indication of impending outbreaks,” said Rogak.
Determining the best timing and location for floor swabbing might be challenging and specific to the particular hospital, he added. ”For example, you would not want to take swabs from floors right after they are cleaned. Overall, I think this method deserves further development, and it could become a standard technique, but the details might require refinement for widespread application.”
Adrian Popp, MD, chair of the Infectious Disease Service at Huntington Hospital–Northwell Health in New York, said that, although interesting, the study would not change his current practice.
“I’m going to start testing the environment in different rooms in the hospital, and yes, I might find different amounts of COVID, but what does that mean? If pieces of RNA from COVID are on the floor, the likelihood is that they’re not infectious,” Popp said in an interview.
“Hospital workers do get sick with COVID, and sometimes they are asymptomatic and come to work. Patients may come into the hospital for another reason and be sick with COVID. There are many ways people who work in the hospital, as well as the patients, can get COVID. To me, it means that in that hospital and community there is a lot of COVID, but I can’t tell if there is causation here. Who is giving COVID to whom? What am I supposed to do with the information?”
The study was supported by the Northern Ontario Academic Medicine Association Clinical Innovation Opportunities Fund, the Ottawa Hospital Academic Medical Organization Innovation Fund, and a Canadian Institutes of Health Research Operating Grant. One author was a consultant for ProofDx, a startup company creating a point-of-care diagnostic test for COVID-19, and is an advisor for SIGNAL1, a startup company deploying machine-learning models to improve inpatient care. Nott, Rogak, and Popp reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The viral burden of SARS-CoV-2 on floors, even in healthcare worker–only areas, was strongly associated with COVID-19 outbreaks in two acute-care hospitals, according to a new study from Ontario, Canada.
With every 10-fold increase in viral copies, the chance of an impending outbreak of COVID-19 rose 22-fold.
“These data add to the mounting evidence that built environment detection for SARS-CoV-2 may provide an additional layer of monitoring and could help inform local infection prevention and control measures,” they wrote.
The study was published online in Infection Control & Hospital Epidemiology.
Preventing Future Suffering
The current study builds on the researchers’ previous work, which found the same correlation between viral load on floors and COVID outbreaks in long-term care homes.
Currently, the best-known method of environmental surveillance for COVID is wastewater detection. “Swabbing the floors would be another approach to surveillance,” senior author Caroline Nott, MD, infectious disease physician at the Ottawa Hospital, said in an interview.
“We do have environmental surveillance with wastewater, but while this may tell you what’s going on in the city, it doesn’t tell you what is going on in a particular ward of a hospital, for instance,” she added.
Nott and her colleagues believe that swabbing, which is easy and relatively inexpensive, will become another tool to examine the built environment. “Instead of having to close a whole hospital, for example, we could just close one room instead of an entire ward if swabbing showed a high concentration of COVID,” Nott said.
The current study was conducted at two hospitals in Ontario between July 2022 and March 2023. The floors of healthcare worker–only areas on four inpatient adult wards were swabbed. These areas included changing rooms, meeting rooms, staff washrooms, nursing stations, and interdisciplinary team rooms.
SARS-CoV-2 RNA was detected on 537 of 760 floor swabs (71%). The overall positivity rate in the first hospital was 90% (n = 280). In the second hospital, the rate was 60% (n = 480).
Four COVID-19 outbreaks occurred in the first acute care hospital, and seven outbreaks occurred at the second hospital. Outbreaks occurred mostly among hospitalized patients (140 cases), but also in four hospital workers.
COVID-19 still requires vigilance, said Nott. “We weren’t prepared for COVID, and so as a result, many people died or have suffered long-term effects, especially vulnerable people like those being treated in hospital or in long-term care facilities. We want to develop methods to prevent similar suffering in the future, whether it’s a new COVID variant or a different pathogen altogether.”
Changing Surveillance Practice?
“This is a good study,” Steven Rogak, PhD, professor of mechanical engineering at the University of British Columbia (UBC) in Vancouver, Canada, said in an interivew. “The fundamental idea is that respiratory droplets and aerosols will deposit on the floor, and polymerase chain reaction [PCR] tests of swabs will provide a surrogate measurement of what might have been inhaled. There are solid statistics that it worked for the hospitals studied,” said Rogak, who studies aerosols at UBC’s Energy and Aerosols Laboratory. Rogak did not participate in the study.
“The authors note several limitations, including that increased healthcare worker testing may have been triggered by the higher values of PCR counts from the floor swabs. But this doesn’t seem to be a problem to me, because if the floor swabs motivate the hospital to test workers more, and that results in identifying outbreaks sooner, then great,” he said.
“Another limitation is that if the hospital has better HVAC or uses air purifiers, it could remove the most infectious aerosols, but the large droplets that fall quickly to the ground would remain, and this would still result in high PCR counts from floor swabs. In this case, perhaps the floor swabs would be a poorer indication of impending outbreaks,” said Rogak.
Determining the best timing and location for floor swabbing might be challenging and specific to the particular hospital, he added. ”For example, you would not want to take swabs from floors right after they are cleaned. Overall, I think this method deserves further development, and it could become a standard technique, but the details might require refinement for widespread application.”
Adrian Popp, MD, chair of the Infectious Disease Service at Huntington Hospital–Northwell Health in New York, said that, although interesting, the study would not change his current practice.
“I’m going to start testing the environment in different rooms in the hospital, and yes, I might find different amounts of COVID, but what does that mean? If pieces of RNA from COVID are on the floor, the likelihood is that they’re not infectious,” Popp said in an interview.
“Hospital workers do get sick with COVID, and sometimes they are asymptomatic and come to work. Patients may come into the hospital for another reason and be sick with COVID. There are many ways people who work in the hospital, as well as the patients, can get COVID. To me, it means that in that hospital and community there is a lot of COVID, but I can’t tell if there is causation here. Who is giving COVID to whom? What am I supposed to do with the information?”
The study was supported by the Northern Ontario Academic Medicine Association Clinical Innovation Opportunities Fund, the Ottawa Hospital Academic Medical Organization Innovation Fund, and a Canadian Institutes of Health Research Operating Grant. One author was a consultant for ProofDx, a startup company creating a point-of-care diagnostic test for COVID-19, and is an advisor for SIGNAL1, a startup company deploying machine-learning models to improve inpatient care. Nott, Rogak, and Popp reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
The viral burden of SARS-CoV-2 on floors, even in healthcare worker–only areas, was strongly associated with COVID-19 outbreaks in two acute-care hospitals, according to a new study from Ontario, Canada.
With every 10-fold increase in viral copies, the chance of an impending outbreak of COVID-19 rose 22-fold.
“These data add to the mounting evidence that built environment detection for SARS-CoV-2 may provide an additional layer of monitoring and could help inform local infection prevention and control measures,” they wrote.
The study was published online in Infection Control & Hospital Epidemiology.
Preventing Future Suffering
The current study builds on the researchers’ previous work, which found the same correlation between viral load on floors and COVID outbreaks in long-term care homes.
Currently, the best-known method of environmental surveillance for COVID is wastewater detection. “Swabbing the floors would be another approach to surveillance,” senior author Caroline Nott, MD, infectious disease physician at the Ottawa Hospital, said in an interview.
“We do have environmental surveillance with wastewater, but while this may tell you what’s going on in the city, it doesn’t tell you what is going on in a particular ward of a hospital, for instance,” she added.
Nott and her colleagues believe that swabbing, which is easy and relatively inexpensive, will become another tool to examine the built environment. “Instead of having to close a whole hospital, for example, we could just close one room instead of an entire ward if swabbing showed a high concentration of COVID,” Nott said.
The current study was conducted at two hospitals in Ontario between July 2022 and March 2023. The floors of healthcare worker–only areas on four inpatient adult wards were swabbed. These areas included changing rooms, meeting rooms, staff washrooms, nursing stations, and interdisciplinary team rooms.
SARS-CoV-2 RNA was detected on 537 of 760 floor swabs (71%). The overall positivity rate in the first hospital was 90% (n = 280). In the second hospital, the rate was 60% (n = 480).
Four COVID-19 outbreaks occurred in the first acute care hospital, and seven outbreaks occurred at the second hospital. Outbreaks occurred mostly among hospitalized patients (140 cases), but also in four hospital workers.
COVID-19 still requires vigilance, said Nott. “We weren’t prepared for COVID, and so as a result, many people died or have suffered long-term effects, especially vulnerable people like those being treated in hospital or in long-term care facilities. We want to develop methods to prevent similar suffering in the future, whether it’s a new COVID variant or a different pathogen altogether.”
Changing Surveillance Practice?
“This is a good study,” Steven Rogak, PhD, professor of mechanical engineering at the University of British Columbia (UBC) in Vancouver, Canada, said in an interivew. “The fundamental idea is that respiratory droplets and aerosols will deposit on the floor, and polymerase chain reaction [PCR] tests of swabs will provide a surrogate measurement of what might have been inhaled. There are solid statistics that it worked for the hospitals studied,” said Rogak, who studies aerosols at UBC’s Energy and Aerosols Laboratory. Rogak did not participate in the study.
“The authors note several limitations, including that increased healthcare worker testing may have been triggered by the higher values of PCR counts from the floor swabs. But this doesn’t seem to be a problem to me, because if the floor swabs motivate the hospital to test workers more, and that results in identifying outbreaks sooner, then great,” he said.
“Another limitation is that if the hospital has better HVAC or uses air purifiers, it could remove the most infectious aerosols, but the large droplets that fall quickly to the ground would remain, and this would still result in high PCR counts from floor swabs. In this case, perhaps the floor swabs would be a poorer indication of impending outbreaks,” said Rogak.
Determining the best timing and location for floor swabbing might be challenging and specific to the particular hospital, he added. ”For example, you would not want to take swabs from floors right after they are cleaned. Overall, I think this method deserves further development, and it could become a standard technique, but the details might require refinement for widespread application.”
Adrian Popp, MD, chair of the Infectious Disease Service at Huntington Hospital–Northwell Health in New York, said that, although interesting, the study would not change his current practice.
“I’m going to start testing the environment in different rooms in the hospital, and yes, I might find different amounts of COVID, but what does that mean? If pieces of RNA from COVID are on the floor, the likelihood is that they’re not infectious,” Popp said in an interview.
“Hospital workers do get sick with COVID, and sometimes they are asymptomatic and come to work. Patients may come into the hospital for another reason and be sick with COVID. There are many ways people who work in the hospital, as well as the patients, can get COVID. To me, it means that in that hospital and community there is a lot of COVID, but I can’t tell if there is causation here. Who is giving COVID to whom? What am I supposed to do with the information?”
The study was supported by the Northern Ontario Academic Medicine Association Clinical Innovation Opportunities Fund, the Ottawa Hospital Academic Medical Organization Innovation Fund, and a Canadian Institutes of Health Research Operating Grant. One author was a consultant for ProofDx, a startup company creating a point-of-care diagnostic test for COVID-19, and is an advisor for SIGNAL1, a startup company deploying machine-learning models to improve inpatient care. Nott, Rogak, and Popp reported having no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM INFECTION CONTROL & HOSPITAL EPIDEMIOLOGY
How Much Does Long COVID Cost Society? New Data Shed Light
Long COVID, a major public health crisis, is also becoming a significant economic crisis. A new study in Nature reports that the global annual economic impact of long COVID has hit $1 trillion — or about 1% of the global economy.
Long COVID is estimated to affect 6%-7% of adults. Those afflicted are often unable to work for extended periods, and some simply stop working altogether.
Besides damaging individual lives, long COVID is having wide-ranging impacts on health systems and economies worldwide, as those who suffer from it have large absences from work, leading to lower productivity. Even those who return to work after weeks, months, or even up to a year out of work may come back with worse productivity and some functional impairment — as a few of the condition’s common symptoms include fatigue and brain fog.
Experts say more is needed not only in terms of scientific research into new treatments for long COVID but also from a public policy perspective.
Long COVID’s impact on the labor force is already having ripple effects throughout the economy of the United States and other countries. Earlier this year, the US Government Accountability Office stated long COVID potentially affects up to 23 million Americans, with as many as a million people out of work. The healthcare industry is particularly hard hit.
The latest survey from the National Center for Health Statistics estimated 17.3%-18.6% of adults have experienced long COVID. This isn’t the same as those who have it now, only a broad indicator of people who’ve ever experienced symptoms.
Public health experts, economists, researchers, and physicians say they are only beginning to focus on ways to reduce long COVID’s impact.
They suggest a range of potential solutions to address the public health crisis and the economic impacts — including implementing a more thorough surveillance system to track long COVID cases, building better ventilation systems in hospitals and buildings to reduce the spread of the virus, increasing vaccination efforts as new viral strains continuously emerge, and more funding for long COVID research to better quantify and qualify the disease’s impact.
Shaky Statistics, Inconsistent Surveillance
David Smith, MD, an infectious disease specialist at the University of California, San Diego, said more needs to be done to survey, quantify, and qualify the impacts of long COVID on the economy before practical solutions can be identified.
“Our surveillance system sucks,” Smith said. “I can see how many people test positive for COVID, but how many of those people have long COVID?”
Long COVID also doesn’t have a true definition or standard diagnosis, which complicates surveillance efforts. It includes a spectrum of symptoms such as shortness of breath, chronic fatigue, and brain fog that linger for 2-3 months after an acute infection. But there’s no “concrete case definition,” Smith said. “And not everybody’s long COVID is exactly the same as everybody else’s.”
As a result, epidemiologists can’t effectively characterize the disease, and health economists can’t measure its exact economic impact.
Few countries have established comprehensive surveillance systems to estimate the burden of long COVID at the population level.
The United States currently tracks new cases by measuring wastewater levels, which isn’t as comprehensive as the tracking that was done during the pandemic. But positive wastewater samples can’t tell us who is infected in an area, nor can it distinguish whether a visitor/tourist or resident is mostly contributing to the wastewater analysis — an important distinction in public health studies.
Wastewater surveillance is an excellent complement to traditional disease surveillance with advantages and disadvantages, but it shouldn’t be the sole way to measure disease.
What Research Best Informs the Debate?
A study by Economist Impact — a think tank that partners with corporations, foundations, NGOs, and governments to help drive policy — estimated between a 0.5% and 2.3% gross domestic product (GDP) loss across eight separate countries in 2024. The study included the United Kingdom and United States.
Meanwhile, Australian researchers recently detailed how long COVID-related reductions in labor supply affected its productivity and GDP from 2022 to 2024. The study found that long COVID could be costing the Australian economy about 0.5% of its GDP, which researchers deemed a conservative estimate.
Public health researchers in New Zealand used the estimate of GDP loss in Australia to measure their own potential losses and advocated for strengthening occupational support across all sectors to protect health.
But these studies can’t quite compare with what would have to be done for the United States economy.
“New Zealand is small ... and has an excellent public health system with good delivery of vaccines and treatments…so how do we compare that to us?” Smith said. “They do better in all of their public health metrics than we do.”
Measuring the Economic Impact
Gopi Shah Goda, PhD, a health economist and senior fellow in economic studies at the Brookings Institution, co-authored a 2023 study that found COVID-19 reduced the US labor force by about 500,000 people.
Plus, workers who missed a full week due to COVID-19 absences became 7% less likely to return to the labor force a year later compared with workers who didn’t miss work for health reasons. That amounts to 0.2% of the labor force, a significant number.
“Even a small percent of the labor force is a big number…it’s like an extra year of populating aging,” Goda said.
“Some people who get long COVID might have dropped out of the labor force anyway,” Goda added.
The study concluded that average individual earnings lost from long COVID were $9000, and the total lost labor supply amounted to $62 billion annually — about half the estimated productivity losses from cancer or diabetes.
But research into long COVID research continues to be underfunded compared with other health conditions, experts noted.
Cancer and diabetes both receive billions of research dollars annually from the National Institutes of Health. Long COVID research gets only a few million, according to Goda.
Informing Public Health Policy
When it comes to caring for patients with long COVID, the big issue facing every nation’s public policy leaders is how best to allocate limited health resources.
“Public health never has enough money ... Do they buy more vaccines? Do they do educational programs? Who do they target the most?” Smith said.
Though Smith thinks the best preventative measure is increased vaccination, vaccination rates remain low in the United States.
“Unfortunately, as last fall demonstrated, there’s a lot of vaccine indifference and skepticism,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University School of Medicine, Nashville, Tennessee.
Over the past year, only 14% of eligible children and 22% of adults received the 2023-2024 COVID vaccine boosters.
Schaffner said public health experts wrestle with ways to assure the public vaccines are safe and effective.
“They’re trying to provide a level of comfort that [getting vaccinated] is the socially appropriate thing to do,” which remains a significant challenge, Schaffner said.
Some people don’t have access to vaccines and comprehensive medical services because they lack insurance, Medicaid, and Medicare. And the United States still doesn’t distribute vaccines as well as other countries, Schaffner added.
“In other countries, every doctor’s office gets vaccines for free ... here, we have a large commercial enterprise that basically runs it…there are still populations who aren’t reached,” he said.
Long COVID clinics that have opened around the country have offered help to some patients with long COVID. A year and a half ago, Yale University, New Haven, Connecticut, established its Long COVID Care Center. Stanford University, Stanford, California, opened its Long COVID Clinic back in 2021. Vanderbilt University now has its own, as well — the Adult Post-COVID Clinic.
But these clinics have faced declining federal resources, forcing some to close and others to face questions about whether they will be able to continue to operate without more aggressive federal direction and policy planning.
“With some central direction, we could provide better supportive care for the many patients with long COVID out there,” Schaffner said.
For countries with universal healthcare systems, services such as occupational health, extended sick leave, extended time for disability, and workers’ compensation benefits are readily available.
But in the United States, it’s often left to the physicians and their patients to figure out a plan.
“I think we could make physicians more aware of options for their patients…for example, regularly check eligibility for workers compensation,” Schaffner said.
A version of this article first appeared on Medscape.com.
Long COVID, a major public health crisis, is also becoming a significant economic crisis. A new study in Nature reports that the global annual economic impact of long COVID has hit $1 trillion — or about 1% of the global economy.
Long COVID is estimated to affect 6%-7% of adults. Those afflicted are often unable to work for extended periods, and some simply stop working altogether.
Besides damaging individual lives, long COVID is having wide-ranging impacts on health systems and economies worldwide, as those who suffer from it have large absences from work, leading to lower productivity. Even those who return to work after weeks, months, or even up to a year out of work may come back with worse productivity and some functional impairment — as a few of the condition’s common symptoms include fatigue and brain fog.
Experts say more is needed not only in terms of scientific research into new treatments for long COVID but also from a public policy perspective.
Long COVID’s impact on the labor force is already having ripple effects throughout the economy of the United States and other countries. Earlier this year, the US Government Accountability Office stated long COVID potentially affects up to 23 million Americans, with as many as a million people out of work. The healthcare industry is particularly hard hit.
The latest survey from the National Center for Health Statistics estimated 17.3%-18.6% of adults have experienced long COVID. This isn’t the same as those who have it now, only a broad indicator of people who’ve ever experienced symptoms.
Public health experts, economists, researchers, and physicians say they are only beginning to focus on ways to reduce long COVID’s impact.
They suggest a range of potential solutions to address the public health crisis and the economic impacts — including implementing a more thorough surveillance system to track long COVID cases, building better ventilation systems in hospitals and buildings to reduce the spread of the virus, increasing vaccination efforts as new viral strains continuously emerge, and more funding for long COVID research to better quantify and qualify the disease’s impact.
Shaky Statistics, Inconsistent Surveillance
David Smith, MD, an infectious disease specialist at the University of California, San Diego, said more needs to be done to survey, quantify, and qualify the impacts of long COVID on the economy before practical solutions can be identified.
“Our surveillance system sucks,” Smith said. “I can see how many people test positive for COVID, but how many of those people have long COVID?”
Long COVID also doesn’t have a true definition or standard diagnosis, which complicates surveillance efforts. It includes a spectrum of symptoms such as shortness of breath, chronic fatigue, and brain fog that linger for 2-3 months after an acute infection. But there’s no “concrete case definition,” Smith said. “And not everybody’s long COVID is exactly the same as everybody else’s.”
As a result, epidemiologists can’t effectively characterize the disease, and health economists can’t measure its exact economic impact.
Few countries have established comprehensive surveillance systems to estimate the burden of long COVID at the population level.
The United States currently tracks new cases by measuring wastewater levels, which isn’t as comprehensive as the tracking that was done during the pandemic. But positive wastewater samples can’t tell us who is infected in an area, nor can it distinguish whether a visitor/tourist or resident is mostly contributing to the wastewater analysis — an important distinction in public health studies.
Wastewater surveillance is an excellent complement to traditional disease surveillance with advantages and disadvantages, but it shouldn’t be the sole way to measure disease.
What Research Best Informs the Debate?
A study by Economist Impact — a think tank that partners with corporations, foundations, NGOs, and governments to help drive policy — estimated between a 0.5% and 2.3% gross domestic product (GDP) loss across eight separate countries in 2024. The study included the United Kingdom and United States.
Meanwhile, Australian researchers recently detailed how long COVID-related reductions in labor supply affected its productivity and GDP from 2022 to 2024. The study found that long COVID could be costing the Australian economy about 0.5% of its GDP, which researchers deemed a conservative estimate.
Public health researchers in New Zealand used the estimate of GDP loss in Australia to measure their own potential losses and advocated for strengthening occupational support across all sectors to protect health.
But these studies can’t quite compare with what would have to be done for the United States economy.
“New Zealand is small ... and has an excellent public health system with good delivery of vaccines and treatments…so how do we compare that to us?” Smith said. “They do better in all of their public health metrics than we do.”
Measuring the Economic Impact
Gopi Shah Goda, PhD, a health economist and senior fellow in economic studies at the Brookings Institution, co-authored a 2023 study that found COVID-19 reduced the US labor force by about 500,000 people.
Plus, workers who missed a full week due to COVID-19 absences became 7% less likely to return to the labor force a year later compared with workers who didn’t miss work for health reasons. That amounts to 0.2% of the labor force, a significant number.
“Even a small percent of the labor force is a big number…it’s like an extra year of populating aging,” Goda said.
“Some people who get long COVID might have dropped out of the labor force anyway,” Goda added.
The study concluded that average individual earnings lost from long COVID were $9000, and the total lost labor supply amounted to $62 billion annually — about half the estimated productivity losses from cancer or diabetes.
But research into long COVID research continues to be underfunded compared with other health conditions, experts noted.
Cancer and diabetes both receive billions of research dollars annually from the National Institutes of Health. Long COVID research gets only a few million, according to Goda.
Informing Public Health Policy
When it comes to caring for patients with long COVID, the big issue facing every nation’s public policy leaders is how best to allocate limited health resources.
“Public health never has enough money ... Do they buy more vaccines? Do they do educational programs? Who do they target the most?” Smith said.
Though Smith thinks the best preventative measure is increased vaccination, vaccination rates remain low in the United States.
“Unfortunately, as last fall demonstrated, there’s a lot of vaccine indifference and skepticism,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University School of Medicine, Nashville, Tennessee.
Over the past year, only 14% of eligible children and 22% of adults received the 2023-2024 COVID vaccine boosters.
Schaffner said public health experts wrestle with ways to assure the public vaccines are safe and effective.
“They’re trying to provide a level of comfort that [getting vaccinated] is the socially appropriate thing to do,” which remains a significant challenge, Schaffner said.
Some people don’t have access to vaccines and comprehensive medical services because they lack insurance, Medicaid, and Medicare. And the United States still doesn’t distribute vaccines as well as other countries, Schaffner added.
“In other countries, every doctor’s office gets vaccines for free ... here, we have a large commercial enterprise that basically runs it…there are still populations who aren’t reached,” he said.
Long COVID clinics that have opened around the country have offered help to some patients with long COVID. A year and a half ago, Yale University, New Haven, Connecticut, established its Long COVID Care Center. Stanford University, Stanford, California, opened its Long COVID Clinic back in 2021. Vanderbilt University now has its own, as well — the Adult Post-COVID Clinic.
But these clinics have faced declining federal resources, forcing some to close and others to face questions about whether they will be able to continue to operate without more aggressive federal direction and policy planning.
“With some central direction, we could provide better supportive care for the many patients with long COVID out there,” Schaffner said.
For countries with universal healthcare systems, services such as occupational health, extended sick leave, extended time for disability, and workers’ compensation benefits are readily available.
But in the United States, it’s often left to the physicians and their patients to figure out a plan.
“I think we could make physicians more aware of options for their patients…for example, regularly check eligibility for workers compensation,” Schaffner said.
A version of this article first appeared on Medscape.com.
Long COVID, a major public health crisis, is also becoming a significant economic crisis. A new study in Nature reports that the global annual economic impact of long COVID has hit $1 trillion — or about 1% of the global economy.
Long COVID is estimated to affect 6%-7% of adults. Those afflicted are often unable to work for extended periods, and some simply stop working altogether.
Besides damaging individual lives, long COVID is having wide-ranging impacts on health systems and economies worldwide, as those who suffer from it have large absences from work, leading to lower productivity. Even those who return to work after weeks, months, or even up to a year out of work may come back with worse productivity and some functional impairment — as a few of the condition’s common symptoms include fatigue and brain fog.
Experts say more is needed not only in terms of scientific research into new treatments for long COVID but also from a public policy perspective.
Long COVID’s impact on the labor force is already having ripple effects throughout the economy of the United States and other countries. Earlier this year, the US Government Accountability Office stated long COVID potentially affects up to 23 million Americans, with as many as a million people out of work. The healthcare industry is particularly hard hit.
The latest survey from the National Center for Health Statistics estimated 17.3%-18.6% of adults have experienced long COVID. This isn’t the same as those who have it now, only a broad indicator of people who’ve ever experienced symptoms.
Public health experts, economists, researchers, and physicians say they are only beginning to focus on ways to reduce long COVID’s impact.
They suggest a range of potential solutions to address the public health crisis and the economic impacts — including implementing a more thorough surveillance system to track long COVID cases, building better ventilation systems in hospitals and buildings to reduce the spread of the virus, increasing vaccination efforts as new viral strains continuously emerge, and more funding for long COVID research to better quantify and qualify the disease’s impact.
Shaky Statistics, Inconsistent Surveillance
David Smith, MD, an infectious disease specialist at the University of California, San Diego, said more needs to be done to survey, quantify, and qualify the impacts of long COVID on the economy before practical solutions can be identified.
“Our surveillance system sucks,” Smith said. “I can see how many people test positive for COVID, but how many of those people have long COVID?”
Long COVID also doesn’t have a true definition or standard diagnosis, which complicates surveillance efforts. It includes a spectrum of symptoms such as shortness of breath, chronic fatigue, and brain fog that linger for 2-3 months after an acute infection. But there’s no “concrete case definition,” Smith said. “And not everybody’s long COVID is exactly the same as everybody else’s.”
As a result, epidemiologists can’t effectively characterize the disease, and health economists can’t measure its exact economic impact.
Few countries have established comprehensive surveillance systems to estimate the burden of long COVID at the population level.
The United States currently tracks new cases by measuring wastewater levels, which isn’t as comprehensive as the tracking that was done during the pandemic. But positive wastewater samples can’t tell us who is infected in an area, nor can it distinguish whether a visitor/tourist or resident is mostly contributing to the wastewater analysis — an important distinction in public health studies.
Wastewater surveillance is an excellent complement to traditional disease surveillance with advantages and disadvantages, but it shouldn’t be the sole way to measure disease.
What Research Best Informs the Debate?
A study by Economist Impact — a think tank that partners with corporations, foundations, NGOs, and governments to help drive policy — estimated between a 0.5% and 2.3% gross domestic product (GDP) loss across eight separate countries in 2024. The study included the United Kingdom and United States.
Meanwhile, Australian researchers recently detailed how long COVID-related reductions in labor supply affected its productivity and GDP from 2022 to 2024. The study found that long COVID could be costing the Australian economy about 0.5% of its GDP, which researchers deemed a conservative estimate.
Public health researchers in New Zealand used the estimate of GDP loss in Australia to measure their own potential losses and advocated for strengthening occupational support across all sectors to protect health.
But these studies can’t quite compare with what would have to be done for the United States economy.
“New Zealand is small ... and has an excellent public health system with good delivery of vaccines and treatments…so how do we compare that to us?” Smith said. “They do better in all of their public health metrics than we do.”
Measuring the Economic Impact
Gopi Shah Goda, PhD, a health economist and senior fellow in economic studies at the Brookings Institution, co-authored a 2023 study that found COVID-19 reduced the US labor force by about 500,000 people.
Plus, workers who missed a full week due to COVID-19 absences became 7% less likely to return to the labor force a year later compared with workers who didn’t miss work for health reasons. That amounts to 0.2% of the labor force, a significant number.
“Even a small percent of the labor force is a big number…it’s like an extra year of populating aging,” Goda said.
“Some people who get long COVID might have dropped out of the labor force anyway,” Goda added.
The study concluded that average individual earnings lost from long COVID were $9000, and the total lost labor supply amounted to $62 billion annually — about half the estimated productivity losses from cancer or diabetes.
But research into long COVID research continues to be underfunded compared with other health conditions, experts noted.
Cancer and diabetes both receive billions of research dollars annually from the National Institutes of Health. Long COVID research gets only a few million, according to Goda.
Informing Public Health Policy
When it comes to caring for patients with long COVID, the big issue facing every nation’s public policy leaders is how best to allocate limited health resources.
“Public health never has enough money ... Do they buy more vaccines? Do they do educational programs? Who do they target the most?” Smith said.
Though Smith thinks the best preventative measure is increased vaccination, vaccination rates remain low in the United States.
“Unfortunately, as last fall demonstrated, there’s a lot of vaccine indifference and skepticism,” said William Schaffner, MD, an infectious disease specialist at Vanderbilt University School of Medicine, Nashville, Tennessee.
Over the past year, only 14% of eligible children and 22% of adults received the 2023-2024 COVID vaccine boosters.
Schaffner said public health experts wrestle with ways to assure the public vaccines are safe and effective.
“They’re trying to provide a level of comfort that [getting vaccinated] is the socially appropriate thing to do,” which remains a significant challenge, Schaffner said.
Some people don’t have access to vaccines and comprehensive medical services because they lack insurance, Medicaid, and Medicare. And the United States still doesn’t distribute vaccines as well as other countries, Schaffner added.
“In other countries, every doctor’s office gets vaccines for free ... here, we have a large commercial enterprise that basically runs it…there are still populations who aren’t reached,” he said.
Long COVID clinics that have opened around the country have offered help to some patients with long COVID. A year and a half ago, Yale University, New Haven, Connecticut, established its Long COVID Care Center. Stanford University, Stanford, California, opened its Long COVID Clinic back in 2021. Vanderbilt University now has its own, as well — the Adult Post-COVID Clinic.
But these clinics have faced declining federal resources, forcing some to close and others to face questions about whether they will be able to continue to operate without more aggressive federal direction and policy planning.
“With some central direction, we could provide better supportive care for the many patients with long COVID out there,” Schaffner said.
For countries with universal healthcare systems, services such as occupational health, extended sick leave, extended time for disability, and workers’ compensation benefits are readily available.
But in the United States, it’s often left to the physicians and their patients to figure out a plan.
“I think we could make physicians more aware of options for their patients…for example, regularly check eligibility for workers compensation,” Schaffner said.
A version of this article first appeared on Medscape.com.
FROM NATURE
Maternal COVID-19 May Not Harm Baby’s Neural Development
TOPLINE:
Fetuses exposed in utero to SARS-CoV-2 are not at an increased risk for neurodevelopmental problems in early childhood.
METHODOLOGY:
- This prospective study aimed to assess whether in utero exposure to SARS-CoV-2, which causes COVID-19, is associated with abnormal neurodevelopment among children at ages 12, 18, and 24 months.
- It included 2003 pregnant individuals (mean age, 33.3 years) from the ASPIRE cohort who were enrolled before 10 weeks’ gestation and followed through 24 months post partum; 10.8% of them were exposed to SARS-CoV-2 during pregnancy, as determined via self-reported data or dried blood spot cards.
- The birth mothers were required to complete the Ages & Stages Questionnaires, Third Edition (ASQ-3), a validated screening tool for neurodevelopmental delays, at 12, 18, and 24 months postpartum.
- Neurodevelopmental outcomes were available for 1757, 1522, and 1523 children at ages 12, 18, and 24 months, respectively.
- The primary outcome was a score below the cutoff on the ASQ-3 across any of the following developmental domains: Communication, gross motor, fine motor, problem-solving, and social skills.
TAKEAWAY:
- The prevalence of abnormal ASQ-3 scores did not differ between children who were exposed to SARS-CoV-2 in utero and those who were not, at ages 12 (P = .39), 18 (P = .58), and 24 (P = .45) months.
- No association was observed between in utero exposure to SARS-CoV-2 and abnormal ASQ-3 scores among children in any of the age groups.
- The lack of an association between exposure to SARS-CoV-2 during pregnancy and abnormal neurodevelopment remained unchanged even when factors such as preterm delivery and the sex of the infant were considered.
- Supplemental analyses found no difference in risk based on the trimester of infection, presence of fever, or incidence of breakthrough infection following vaccination.
IN PRACTICE:
“In this prospective cohort study of pregnant individuals and offspring, in utero exposure to maternal SARS-CoV-2 infection was not associated with abnormal neurodevelopmental screening scores of children through age 24 months. These findings are critical considering the novelty of the SARS-CoV-2 virus to the human species, the global scale of the initial COVID-19 outbreak, the now-endemic nature of the virus indicating ongoing relevance for pregnant individuals,” the authors of the study wrote.
“While the scientific consensus resists a link between in utero COVID-19 exposure and impaired offspring neurodevelopment, the question remains whether societal responses to the pandemic impacted developmental trajectories,” the researchers added. “Certain studies comparing infants from a pandemic cohort with historic controls have raised concerns about lower ASQ-3 scores among children living during the pandemic. Critically, socioeconomic factors influence vulnerability, not only to infection itself but also regarding the ability to deploy resources in times of stress (eg, school closures) to mitigate sources of developmental harm. Our data support this theory, with the observed independent protective association of increasing household income with childhood ASQ-3 scores. Additional research is warranted to clarify the potential impact of societal measures on early development and the differential impact of these measures on different communities.”
SOURCE:
The study was led by Eleni G. Jaswa, MD, MSc, of the Department of Obstetrics, Gynecology & Reproductive Sciences at the University of California, San Francisco. It was published online in JAMA Network Open.
LIMITATIONS:
Limitations of the research included the use of self-reported data and dried blood spot cards for determining exposure to SARS-CoV-2, which may have led to misclassification. The ASQ-3 is a modestly sensitive tool for detecting developmental delays that may have affected the study’s power to detect associations. The sample size of this study, while larger than many, may still have been underpowered to detect small differences in neurodevelopmental outcomes.
DISCLOSURES:
The ASPIRE cohort was supported by research grants provided to the University of California, San Francisco, and by the Start Small Foundation, the California Breast Cancer Research Program, the COVID Catalyst Award, and other sources. Some authors reported receiving grants, royalties, and personal fees, serving on medical advisory boards, and having other ties with several institutions.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Fetuses exposed in utero to SARS-CoV-2 are not at an increased risk for neurodevelopmental problems in early childhood.
METHODOLOGY:
- This prospective study aimed to assess whether in utero exposure to SARS-CoV-2, which causes COVID-19, is associated with abnormal neurodevelopment among children at ages 12, 18, and 24 months.
- It included 2003 pregnant individuals (mean age, 33.3 years) from the ASPIRE cohort who were enrolled before 10 weeks’ gestation and followed through 24 months post partum; 10.8% of them were exposed to SARS-CoV-2 during pregnancy, as determined via self-reported data or dried blood spot cards.
- The birth mothers were required to complete the Ages & Stages Questionnaires, Third Edition (ASQ-3), a validated screening tool for neurodevelopmental delays, at 12, 18, and 24 months postpartum.
- Neurodevelopmental outcomes were available for 1757, 1522, and 1523 children at ages 12, 18, and 24 months, respectively.
- The primary outcome was a score below the cutoff on the ASQ-3 across any of the following developmental domains: Communication, gross motor, fine motor, problem-solving, and social skills.
TAKEAWAY:
- The prevalence of abnormal ASQ-3 scores did not differ between children who were exposed to SARS-CoV-2 in utero and those who were not, at ages 12 (P = .39), 18 (P = .58), and 24 (P = .45) months.
- No association was observed between in utero exposure to SARS-CoV-2 and abnormal ASQ-3 scores among children in any of the age groups.
- The lack of an association between exposure to SARS-CoV-2 during pregnancy and abnormal neurodevelopment remained unchanged even when factors such as preterm delivery and the sex of the infant were considered.
- Supplemental analyses found no difference in risk based on the trimester of infection, presence of fever, or incidence of breakthrough infection following vaccination.
IN PRACTICE:
“In this prospective cohort study of pregnant individuals and offspring, in utero exposure to maternal SARS-CoV-2 infection was not associated with abnormal neurodevelopmental screening scores of children through age 24 months. These findings are critical considering the novelty of the SARS-CoV-2 virus to the human species, the global scale of the initial COVID-19 outbreak, the now-endemic nature of the virus indicating ongoing relevance for pregnant individuals,” the authors of the study wrote.
“While the scientific consensus resists a link between in utero COVID-19 exposure and impaired offspring neurodevelopment, the question remains whether societal responses to the pandemic impacted developmental trajectories,” the researchers added. “Certain studies comparing infants from a pandemic cohort with historic controls have raised concerns about lower ASQ-3 scores among children living during the pandemic. Critically, socioeconomic factors influence vulnerability, not only to infection itself but also regarding the ability to deploy resources in times of stress (eg, school closures) to mitigate sources of developmental harm. Our data support this theory, with the observed independent protective association of increasing household income with childhood ASQ-3 scores. Additional research is warranted to clarify the potential impact of societal measures on early development and the differential impact of these measures on different communities.”
SOURCE:
The study was led by Eleni G. Jaswa, MD, MSc, of the Department of Obstetrics, Gynecology & Reproductive Sciences at the University of California, San Francisco. It was published online in JAMA Network Open.
LIMITATIONS:
Limitations of the research included the use of self-reported data and dried blood spot cards for determining exposure to SARS-CoV-2, which may have led to misclassification. The ASQ-3 is a modestly sensitive tool for detecting developmental delays that may have affected the study’s power to detect associations. The sample size of this study, while larger than many, may still have been underpowered to detect small differences in neurodevelopmental outcomes.
DISCLOSURES:
The ASPIRE cohort was supported by research grants provided to the University of California, San Francisco, and by the Start Small Foundation, the California Breast Cancer Research Program, the COVID Catalyst Award, and other sources. Some authors reported receiving grants, royalties, and personal fees, serving on medical advisory boards, and having other ties with several institutions.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
TOPLINE:
Fetuses exposed in utero to SARS-CoV-2 are not at an increased risk for neurodevelopmental problems in early childhood.
METHODOLOGY:
- This prospective study aimed to assess whether in utero exposure to SARS-CoV-2, which causes COVID-19, is associated with abnormal neurodevelopment among children at ages 12, 18, and 24 months.
- It included 2003 pregnant individuals (mean age, 33.3 years) from the ASPIRE cohort who were enrolled before 10 weeks’ gestation and followed through 24 months post partum; 10.8% of them were exposed to SARS-CoV-2 during pregnancy, as determined via self-reported data or dried blood spot cards.
- The birth mothers were required to complete the Ages & Stages Questionnaires, Third Edition (ASQ-3), a validated screening tool for neurodevelopmental delays, at 12, 18, and 24 months postpartum.
- Neurodevelopmental outcomes were available for 1757, 1522, and 1523 children at ages 12, 18, and 24 months, respectively.
- The primary outcome was a score below the cutoff on the ASQ-3 across any of the following developmental domains: Communication, gross motor, fine motor, problem-solving, and social skills.
TAKEAWAY:
- The prevalence of abnormal ASQ-3 scores did not differ between children who were exposed to SARS-CoV-2 in utero and those who were not, at ages 12 (P = .39), 18 (P = .58), and 24 (P = .45) months.
- No association was observed between in utero exposure to SARS-CoV-2 and abnormal ASQ-3 scores among children in any of the age groups.
- The lack of an association between exposure to SARS-CoV-2 during pregnancy and abnormal neurodevelopment remained unchanged even when factors such as preterm delivery and the sex of the infant were considered.
- Supplemental analyses found no difference in risk based on the trimester of infection, presence of fever, or incidence of breakthrough infection following vaccination.
IN PRACTICE:
“In this prospective cohort study of pregnant individuals and offspring, in utero exposure to maternal SARS-CoV-2 infection was not associated with abnormal neurodevelopmental screening scores of children through age 24 months. These findings are critical considering the novelty of the SARS-CoV-2 virus to the human species, the global scale of the initial COVID-19 outbreak, the now-endemic nature of the virus indicating ongoing relevance for pregnant individuals,” the authors of the study wrote.
“While the scientific consensus resists a link between in utero COVID-19 exposure and impaired offspring neurodevelopment, the question remains whether societal responses to the pandemic impacted developmental trajectories,” the researchers added. “Certain studies comparing infants from a pandemic cohort with historic controls have raised concerns about lower ASQ-3 scores among children living during the pandemic. Critically, socioeconomic factors influence vulnerability, not only to infection itself but also regarding the ability to deploy resources in times of stress (eg, school closures) to mitigate sources of developmental harm. Our data support this theory, with the observed independent protective association of increasing household income with childhood ASQ-3 scores. Additional research is warranted to clarify the potential impact of societal measures on early development and the differential impact of these measures on different communities.”
SOURCE:
The study was led by Eleni G. Jaswa, MD, MSc, of the Department of Obstetrics, Gynecology & Reproductive Sciences at the University of California, San Francisco. It was published online in JAMA Network Open.
LIMITATIONS:
Limitations of the research included the use of self-reported data and dried blood spot cards for determining exposure to SARS-CoV-2, which may have led to misclassification. The ASQ-3 is a modestly sensitive tool for detecting developmental delays that may have affected the study’s power to detect associations. The sample size of this study, while larger than many, may still have been underpowered to detect small differences in neurodevelopmental outcomes.
DISCLOSURES:
The ASPIRE cohort was supported by research grants provided to the University of California, San Francisco, and by the Start Small Foundation, the California Breast Cancer Research Program, the COVID Catalyst Award, and other sources. Some authors reported receiving grants, royalties, and personal fees, serving on medical advisory boards, and having other ties with several institutions.
This article was created using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
Heart Attack, Stroke Survivors at High Risk for Long COVID
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Primary care doctors and specialists should advise patients who have already experienced a heart attack or stroke that they are at a higher risk for long COVID and need to take steps to avoid contracting the virus, according to new research.
The study, led by researchers at Columbia University, New York City, suggests that anyone with cardiovascular disease (CVD) — defined as having experienced a heart attack or stroke — should consider getting the updated COVID vaccine boosters. They also suggest patients with CVD take other steps to avoid an acute infection, such as avoiding crowded indoor spaces.
There is no specific test or treatment for long COVID, which can become disabling and chronic. Long COVID is defined by the failure to recover from acute COVID-19 in 90 days.
The scientists used data from nearly 5000 people enrolled in 14 established, ongoing research programs, including the 76-year-old Framingham Heart Study. The results of the analysis of the “mega-cohort” were published in JAMA Network Open.
Most of the 14 studies already had 10-20 years of data on the cardiac health of thousands of enrollees, said Norrina B. Allen, one of the authors and a cardiac epidemiologist at Northwestern University Feinberg School of Medicine in Chicago, Illinois.
“This is a particularly strong study that looked at risk factors — or individual health — prior to developing COVID and their impact on the likely of recovering from COVID,” she said.
In addition to those with CVD, women and adults with preexisting chronic illnesses took longer to recover.
More than 20% of those in the large, racially and ethnically diverse US population–based study did not recover from COVID in 90 days. The researchers found that the median self-reported time to recovery from acute infection was 20 days.
While women and those with chronic illness had a higher risk for long COVID, vaccination and infection with the Omicron variant wave were associated with shorter recovery times.
These findings make sense, said Ziyad Al-Aly, MD, chief of research at Veterans Affairs St. Louis Health Care System and clinical epidemiologist at Washington University in St. Louis, Missouri.
“We also see that COVID-19 can lead to new-onset cardiovascular disease,” said Al-Aly, who was not involved in the study. “There is clearly a (link) between COVID and cardiovascular disease. These two seem to be intimately intertwined. In my view, this emphasizes the importance of targeting these individuals for vaccination and potentially antivirals (when they get infected) to help reduce their risk of adverse events and ameliorate their chance of full and fast recovery.”
The study used data from the Collaborative Cohort of Cohorts for COVID-19 Research. The long list of researchers contributing to this study includes epidemiologists, biostatisticians, neurologists, pulmonologists, and cardiologists. The data come from a list of cohorts like the Framingham Heart Study, which identified key risk factors for CVD, including cholesterol levels. Other studies include the Atherosclerosis Risk in Communities study, which began in the mid-1980s. Researchers there recruited a cohort of 15,792 men and women in rural North Carolina and Mississippi and suburban Minneapolis. They enrolled a high number of African American participants, who have been underrepresented in past studies. Other cohorts focused on young adults with CVD and Hispanics, while another focused on people with chronic obstructive pulmonary disease.
Lead author Elizabeth C. Oelsner, MD, of Columbia University Irving Medical Center in New York City, said she was not surprised by the CVD-long COVID link.
“We were aware that individuals with CVD were at higher risk of a more severe acute infection,” she said. “We were also seeing evidence that long and severe infection led to persistent symptoms.”
Oelsner noted that many patients still take more than 3 months to recover, even during the Omicron wave.
“While that has improved over the course of the pandemic, many individuals are taking a very long time to recover, and that can have a huge burden on the patient,” she said.
She encourages healthcare providers to tell patients at higher risk to take steps to avoid the virus, including vaccination and boosters.
A version of this article first appeared on Medscape.com.
Sperm Appear to Have a Nonreproductive Function
Brazilian researchers have identified a previously unrecognized function of sperm that is unrelated to reproduction. A study of 13 patients admitted to the Hospital das Clínicas da Universidade de São Paulo with moderate to severe COVID-19 showed that male gametes released extracellular traps (in a process called ETosis) in response to the infection. This immune response, which is common to macrophages and neutrophils, had never been observed in mammalian reproductive cells.
“It opens up a new line of research,” said Jorge Hallak, a professor at the University of São Paulo School of Medicine, São Paulo, Brazil, and first author of the article published in Andrology. “This may be an innovative mechanism, or it may have always existed, and no one knew.”
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in cells more than 3 months after infection in 11 participants, although polymerase chain reaction tests were negative. These findings suggest the potential for drafting a protocol or guidance on when to attempt a pregnancy. “My concern is with assisted reproduction, in which, in general, only one basic spermogram is done, without diagnostic investigation or serology for coronavirus,” said Hallak.
Symptomatic infections hinder the reproductive process because symptoms such as high fever impair cell function by triggering increased DNA fragmentation, reduced mitochondrial activity, decreased acrosome reaction, and cell death, thus affecting sperm count and gamete mobility.
The new findings indicate that the impact of SARS-CoV-2 infection can continue for as long as 90 days after symptoms and signs disappear and affect sperm count and gamete quality for even longer. “With the sperm selection technique, you are at risk of taking a cell with viruses and injecting it into the egg. It is not known what changes this may cause to the embryo,” said Hallak.
The expert emphasized that the finding contributes to the understanding of reproductive difficulties that previously had no plausible explanation. It serves as a warning against negligence in the evaluation of men in assisted reproductive treatments.
Daniel Zylberstein, urologist and member of the Brazilian Association of Assisted Reproduction, who did not participate in the research, noted that the result comes from a small study that should be expanded to try to develop guidance for doctors.
“There is still no protocol for these cases. The ideal approach would be to wait for complete spermatogenesis, which takes about 3 months, before putting patients on treatment. This often does not happen, and treatment begins shortly after clinical recovery. In the case of moderate to severe COVID-19, this period should be longer than 90 days,” he said.
The study suggests establishing a quarantine period for reproduction until the sperm are free of the virus, said Zylberstein. “With infected sperm, it makes no sense to start reproductive treatment. This sperm is spending energy to fight the pathogen. Assisted reproduction is expensive and exhaustive and may not have the expected outcome because of SARS-CoV-2 infectivity.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Brazilian researchers have identified a previously unrecognized function of sperm that is unrelated to reproduction. A study of 13 patients admitted to the Hospital das Clínicas da Universidade de São Paulo with moderate to severe COVID-19 showed that male gametes released extracellular traps (in a process called ETosis) in response to the infection. This immune response, which is common to macrophages and neutrophils, had never been observed in mammalian reproductive cells.
“It opens up a new line of research,” said Jorge Hallak, a professor at the University of São Paulo School of Medicine, São Paulo, Brazil, and first author of the article published in Andrology. “This may be an innovative mechanism, or it may have always existed, and no one knew.”
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in cells more than 3 months after infection in 11 participants, although polymerase chain reaction tests were negative. These findings suggest the potential for drafting a protocol or guidance on when to attempt a pregnancy. “My concern is with assisted reproduction, in which, in general, only one basic spermogram is done, without diagnostic investigation or serology for coronavirus,” said Hallak.
Symptomatic infections hinder the reproductive process because symptoms such as high fever impair cell function by triggering increased DNA fragmentation, reduced mitochondrial activity, decreased acrosome reaction, and cell death, thus affecting sperm count and gamete mobility.
The new findings indicate that the impact of SARS-CoV-2 infection can continue for as long as 90 days after symptoms and signs disappear and affect sperm count and gamete quality for even longer. “With the sperm selection technique, you are at risk of taking a cell with viruses and injecting it into the egg. It is not known what changes this may cause to the embryo,” said Hallak.
The expert emphasized that the finding contributes to the understanding of reproductive difficulties that previously had no plausible explanation. It serves as a warning against negligence in the evaluation of men in assisted reproductive treatments.
Daniel Zylberstein, urologist and member of the Brazilian Association of Assisted Reproduction, who did not participate in the research, noted that the result comes from a small study that should be expanded to try to develop guidance for doctors.
“There is still no protocol for these cases. The ideal approach would be to wait for complete spermatogenesis, which takes about 3 months, before putting patients on treatment. This often does not happen, and treatment begins shortly after clinical recovery. In the case of moderate to severe COVID-19, this period should be longer than 90 days,” he said.
The study suggests establishing a quarantine period for reproduction until the sperm are free of the virus, said Zylberstein. “With infected sperm, it makes no sense to start reproductive treatment. This sperm is spending energy to fight the pathogen. Assisted reproduction is expensive and exhaustive and may not have the expected outcome because of SARS-CoV-2 infectivity.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
Brazilian researchers have identified a previously unrecognized function of sperm that is unrelated to reproduction. A study of 13 patients admitted to the Hospital das Clínicas da Universidade de São Paulo with moderate to severe COVID-19 showed that male gametes released extracellular traps (in a process called ETosis) in response to the infection. This immune response, which is common to macrophages and neutrophils, had never been observed in mammalian reproductive cells.
“It opens up a new line of research,” said Jorge Hallak, a professor at the University of São Paulo School of Medicine, São Paulo, Brazil, and first author of the article published in Andrology. “This may be an innovative mechanism, or it may have always existed, and no one knew.”
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was identified in cells more than 3 months after infection in 11 participants, although polymerase chain reaction tests were negative. These findings suggest the potential for drafting a protocol or guidance on when to attempt a pregnancy. “My concern is with assisted reproduction, in which, in general, only one basic spermogram is done, without diagnostic investigation or serology for coronavirus,” said Hallak.
Symptomatic infections hinder the reproductive process because symptoms such as high fever impair cell function by triggering increased DNA fragmentation, reduced mitochondrial activity, decreased acrosome reaction, and cell death, thus affecting sperm count and gamete mobility.
The new findings indicate that the impact of SARS-CoV-2 infection can continue for as long as 90 days after symptoms and signs disappear and affect sperm count and gamete quality for even longer. “With the sperm selection technique, you are at risk of taking a cell with viruses and injecting it into the egg. It is not known what changes this may cause to the embryo,” said Hallak.
The expert emphasized that the finding contributes to the understanding of reproductive difficulties that previously had no plausible explanation. It serves as a warning against negligence in the evaluation of men in assisted reproductive treatments.
Daniel Zylberstein, urologist and member of the Brazilian Association of Assisted Reproduction, who did not participate in the research, noted that the result comes from a small study that should be expanded to try to develop guidance for doctors.
“There is still no protocol for these cases. The ideal approach would be to wait for complete spermatogenesis, which takes about 3 months, before putting patients on treatment. This often does not happen, and treatment begins shortly after clinical recovery. In the case of moderate to severe COVID-19, this period should be longer than 90 days,” he said.
The study suggests establishing a quarantine period for reproduction until the sperm are free of the virus, said Zylberstein. “With infected sperm, it makes no sense to start reproductive treatment. This sperm is spending energy to fight the pathogen. Assisted reproduction is expensive and exhaustive and may not have the expected outcome because of SARS-CoV-2 infectivity.”
This story was translated from the Medscape Portuguese edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article appeared on Medscape.com.
FROM ANDROLOGY
Maternal Immunization to Prevent Serious Respiratory Illness
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.

Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.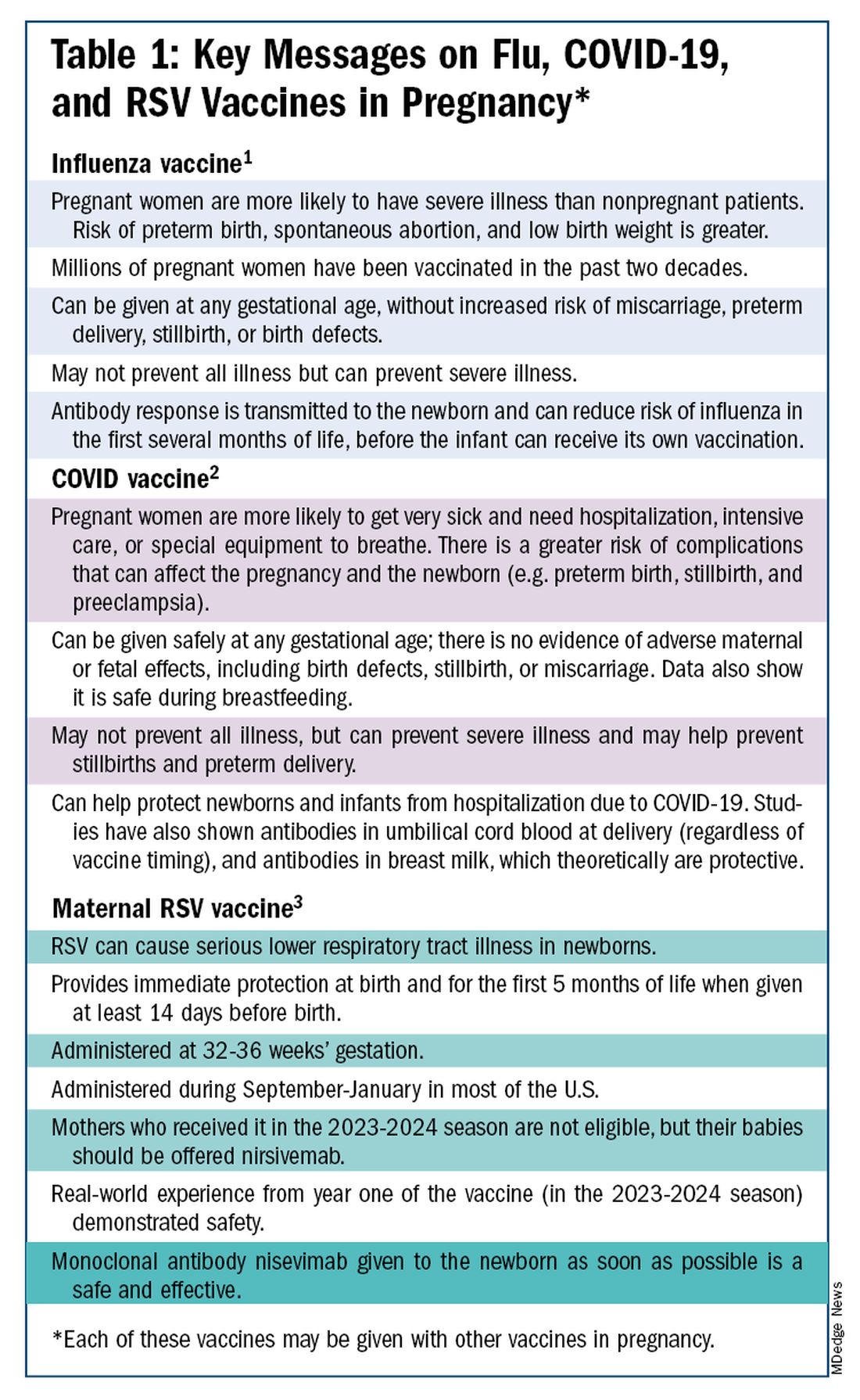
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.

With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)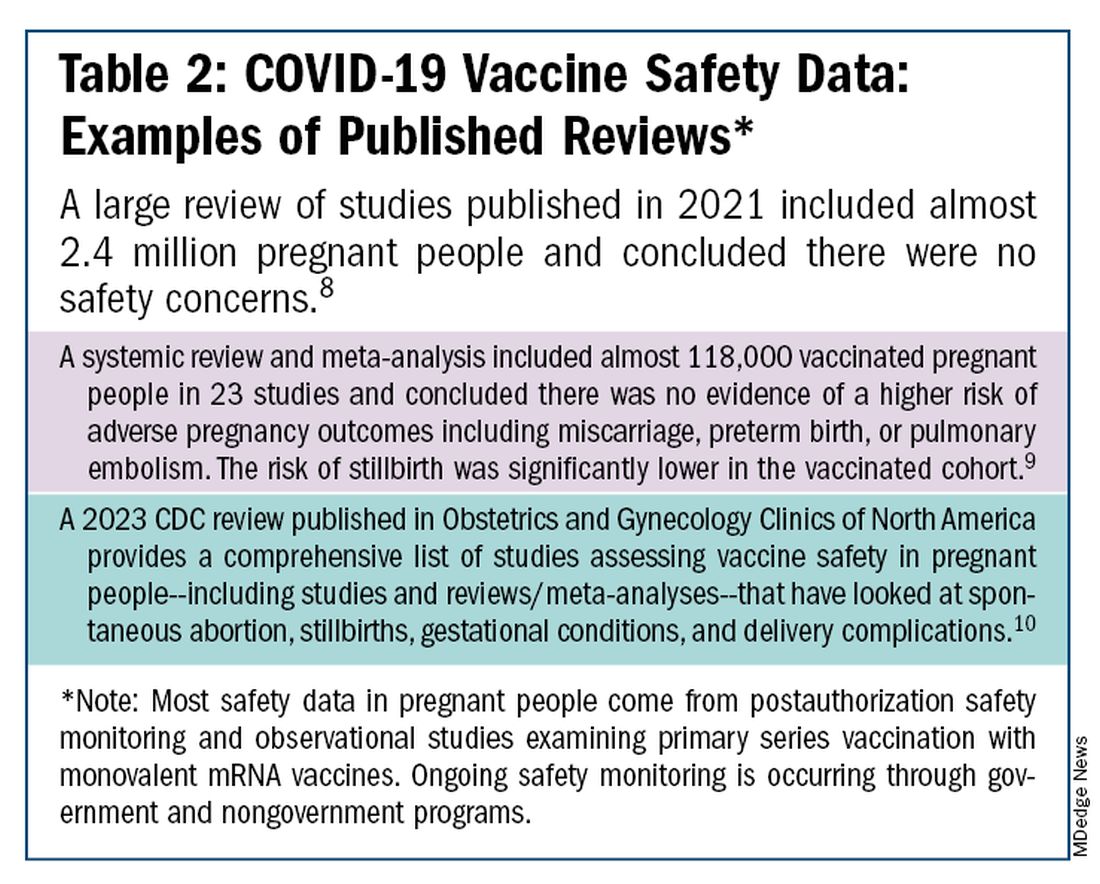
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Editor’s Note: Sadly, this is the last column in the Master Class Obstetrics series. This award-winning column has been part of Ob.Gyn. News for 20 years. The deep discussion of cutting-edge topics in obstetrics by specialists and researchers will be missed as will the leadership and curation of topics by Dr. E. Albert Reece.
Introduction: The Need for Increased Vigilance About Maternal Immunization
Viruses are becoming increasingly prevalent in our world and the consequences of viral infections are implicated in a growing number of disease states. It is well established that certain cancers are caused by viruses and it is increasingly evident that viral infections can trigger the development of chronic illness. In pregnant women, viruses such as cytomegalovirus can cause infection in utero and lead to long-term impairments for the baby.
Likewise, it appears that the virulence of viruses is increasing, whether it be the respiratory syncytial virus (RSV) in children or the severe acute respiratory syndrome (SARS) coronaviruses in adults. Clearly, our environment is changing, with increases in population growth and urbanization, for instance, and an intensification of climate change and its effects. Viruses are part of this changing background.
Vaccines are our most powerful tool to protect people of all ages against viral threats, and fortunately, we benefit from increasing expertise in vaccinology. Since 1974, the University of Maryland School of Medicine has a Center for Vaccine Development and Global Health that has conducted research on vaccines to defend against the Zika virus, H1N1, Ebola, and SARS-CoV-2.
We’re not alone. Other vaccinology centers across the country — as well as the National Institutes of Health at the national level, through its National Institute of Allergy and Infectious Diseases — are doing research and developing vaccines to combat viral diseases.
In this column, we are focused on viral diseases in pregnancy and the role that vaccines can play in preventing serious respiratory illness in mothers and their newborns. I have invited Laura E. Riley, MD, the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine, to address the importance of maternal immunization and how we can best counsel our patients and improve immunization rates.
As Dr. Riley explains, we are in a new era, and it behooves us all to be more vigilant about recommending vaccines, combating misperceptions, addressing patients’ knowledge gaps, and administering vaccines whenever possible.
Dr. Reece is the former Dean of Medicine & University Executive VP, and The Distinguished University and Endowed Professor & Director of the Center for Advanced Research Training and Innovation (CARTI) at the University of Maryland School of Medicine, as well as senior scientist at the Center for Birth Defects Research.
The alarming decline in maternal immunization rates that occurred in the wake of the COVID-19 pandemic means that, now more than ever, we must fully embrace our responsibility to recommend immunizations in pregnancy and to communicate what is known about their efficacy and safety. Data show that vaccination rates drop when we do not offer vaccines in our offices, so whenever possible, we should administer them as well.
The ob.gyn. is the patient’s most trusted person in pregnancy. When patients decline or express hesitancy about vaccines, it is incumbent upon us to ask why. Oftentimes, we can identify areas in which patients lack knowledge or have misperceptions and we can successfully educate the patient or change their perspective or misunderstanding concerning the importance of vaccination for themselves and their babies. (See Table 1.) We can also successfully address concerns about safety.
The safety of COVID-19 vaccinations in pregnancy is now backed by several years of data from multiple studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
Data also show that pregnant patients are more likely than patients who are not pregnant to need hospitalization and intensive care when infected with SARS-CoV-2 and are at risk of having complications that can affect pregnancy and the newborn, including preterm birth and stillbirth. Vaccination has been shown to reduce the risk of severe illness and the risk of such adverse obstetrical outcomes, in addition to providing protection for the infant early on.
Similarly, influenza has long been more likely to be severe in pregnant patients, with an increased risk of poor obstetrical outcomes. Vaccines similarly provide “two for one protection,” protecting both mother and baby, and are, of course, backed by many years of safety and efficacy data.
With the new maternal respiratory syncytial virus (RSV) vaccine, now in its second year of availability, the goal is to protect the baby from RSV-caused serious lower respiratory tract illness. The illness has contributed to tens of thousands of annual hospitalizations and up to several hundred deaths every year in children younger than 5 years — particularly in those under age 6 months.
The RSV monoclonal antibody nirsevimab is available for the newborn as an alternative to maternal immunization but the maternal vaccine is optimal in that it will provide immediate rather than delayed protection for the newborn. The maternal vaccine is recommended during weeks 32-36 of pregnancy in mothers who were not vaccinated during last year’s RSV season. With real-world experience from year one, the available safety data are reassuring.
Counseling About Influenza and COVID-19 Vaccination
The COVID-19 pandemic took a toll on vaccination interest/receptivity broadly in pregnant and nonpregnant people. Among pregnant individuals, influenza vaccination coverage declined from 71% in the 2019-2020 influenza season to 56% in the 2021-2022 season, according to data from the Centers for Disease Control and Prevention’s Vaccine Safety Datalink.4 Coverage for the 2022-2023 and 2023-2024 influenza seasons was even worse: well under 50%.5
Fewer pregnant women have received updated COVID-19 vaccines. Only 13% of pregnant persons overall received the updated 2023-2024 COVID-19 booster vaccine (through March 30, 2024), according to the CDC.6
Maternal immunization for influenza has been recommended in the United States since 2004 (part of the recommendation that everyone over the age of 6 months receive an annual flu vaccine), and flu vaccines have been given to millions of pregnant women, but the H1N1 pandemic of 2009 reinforced its value as a priority for prenatal care. Most of the women who became severely ill from the H1N1 virus were young and healthy, without co-existing conditions known to increase risk.7
It became clearer during the H1N1 pandemic that pregnancy itself — which is associated with physiologic changes such as decreased lung capacity, increased nasal congestion and changes in the immune system – is its own significant risk factor for severe illness from the influenza virus. This increased risk applies to COVID-19 as well.
As COVID-19 has become endemic, with hospitalizations and deaths not reaching the levels of previous surges — and with mask-wearing and other preventive measures having declined — patients understandably have become more complacent. Some patients are vaccine deniers, but in my practice, these patients are a much smaller group than those who believe COVID-19 “is no big deal,” especially if they have had infections recently.
This is why it’s important to actively listen to concerns and to ask patients who decline a vaccination why they are hesitant. Blanket messages about vaccine efficacy and safety are the first step, but individualized, more pointed conversations based on the patient’s personal experiences and beliefs have become increasingly important.
I routinely tell pregnant patients about the risks of COVID-19 and I explain that it has been difficult to predict who will develop severe illness. Sometimes more conversation is needed. For those who are still hesitant or who tell me they feel protected by a recent infection, for instance, I provide more detail on the unique risks of pregnancy — the fact that “pregnancy is different” — and that natural immunity wanes while the protection afforded by immunization is believed to last longer. Many women are also concerned about the safety of the COVID-19 vaccine, so having safety data at your fingertips is helpful. (See Table 2.)
The fact that influenza and COVID-19 vaccination protect the newborn as well as the mother is something that I find is underappreciated by many patients. Explaining that infants likely benefit from the passage of antibodies across the placenta should be part of patient counseling.
Counseling About RSV Vaccination
Importantly, for the 2024-2025 RSV season, the maternal RSV vaccine (Abrysvo, Pfizer) is recommended only for pregnant women who did not receive the vaccine during the 2023-2024 season. When more research is done and more data are obtained showing how long the immune response persists post vaccination, it may be that the US Food and Drug Administration (FDA) will approve the maternal RSV vaccine for use in every pregnancy.
The later timing of the vaccination recommendation — 32-36 weeks’ gestation — reflects a conservative approach taken by the FDA in response to data from one of the pivotal trials showing a numerical trend toward more preterm deliveries among vaccinated compared with unvaccinated patients. This imbalance in the original trial, which administered the vaccine during 24-36 weeks of gestation, was seen only in low-income countries with no temporal association, however.
In our experience at two Weill Cornell Medical College–associated hospitals we did not see this trend. Our cohort study of almost 3000 pregnant patients who delivered at 32 weeks’ gestation or later found no increased risk of preterm birth among the 35% of patients who received the RSV vaccine during the 2023-2024 RSV season. We also did not see any difference in preeclampsia, in contrast with original trial data that showed a signal for increased risk.11
When fewer than 2 weeks have elapsed between maternal vaccination and delivery, the monoclonal antibody nirsevimab is recommended for the newborn — ideally before the newborn leaves the hospital. Nirsevimab is also recommended for newborns of mothers who decline vaccination or were not candidates (e.g. vaccinated in a previous pregnancy), or when there is concern about the adequacy of the maternal immune response to the vaccine (e.g. in cases of immunosuppression).
While there was a limited supply of the monoclonal antibody last year, limitations are not expected this year, especially after October.
The ultimate goal is that patients choose the vaccine or the immunoglobulin, given the severity of RSV disease. Patient preferences should be considered. However, given that it takes 2 weeks after vaccination for protection to build up, I stress to patients that if they’ve vaccinated themselves, their newborn will leave the hospital with protection. If nirsevimab is relied upon, I explain, their newborn may not be protected for some period of time.
Take-home Messages
- When patients decline or are hesitant about vaccines, ask why. Listen actively, and work to correct misperceptions and knowledge gaps.
- Whenever possible, offer vaccines in your practice. Vaccination rates drop when this does not occur.
- COVID-vaccine safety is backed by many studies showing no increase in birth defects, preterm delivery, miscarriage, or stillbirth.
- Pregnant women are more likely to have severe illness from the influenza and SARS-CoV-2 viruses. Vaccines can prevent severe illness and can protect the newborn as well as the mother.
- Recommend/administer the maternal RSV vaccine at 32-36 weeks’ gestation in women who did not receive the vaccine in the 2023-2024 season. If mothers aren’t eligible their babies should be offered nirsevimab.
Dr. Riley is the Given Foundation Professor and Chair of Obstetrics and Gynecology at Weill Cornell Medicine and the obstetrician and gynecologist-in-chief at New York Presbyterian Hospital. She disclosed that she has provided one-time consultations to Pfizer (Abrysvo RSV vaccine) and GSK (cytomegalovirus vaccine), and is providing consultant education on CMV for Moderna. She is chair of ACOG’s task force on immunization and emerging infectious diseases, serves on the medical advisory board for MAVEN, and serves as an editor or editorial board member for several medical publications.
References
1. ACOG Committee Opinion No. 741: Maternal Immunization. Obstet Gynecol. 2018;131(6):e214-e217.
2. Centers for Disease Control and Prevention. COVID-19 Vaccination for People Who are Pregnant or Breastfeeding. https://www.cdc.gov/covid/vaccines/pregnant-or-breastfeeding.html.
3. ACOG Practice Advisory on Maternal Respiratory Syncytial Virus Vaccination, September 2023. (Updated August 2024).4. Irving S et al. Open Forum Infect Dis. 2023;10(Suppl 2):ofad500.1002.
5. Flu Vaccination Dashboard, CDC, National Center for Immunization and Respiratory Diseases.
6. Weekly COVID-19 Vaccination Dashboard, CDC. https://www.cdc.gov/covidvaxview/weekly-dashboard/index.html
7. Louie JK et al. N Engl J Med. 2010;362:27-35. 8. Ciapponi A et al. Vaccine. 2021;39(40):5891-908.
9. Prasad S et al. Nature Communications. 2022;13:2414. 10. Fleming-Dutra KE et al. Obstet Gynecol Clin North Am 2023;50(2):279-97. 11. Mouen S et al. JAMA Network Open 2024;7(7):e2419268.
Public Health, Not Politics, Should Drive Mask Policies, Says Ethicist
This transcript has been edited for clarity.
I recently saw a ban that has me very worried, concerned, and strongly in opposition.
Basically, the standard kind of medical mask would be captured, although I think their aim in doing this was to try to discourage people at political protests from being able to wear masks and hide their identity. They’re basically trying to discourage that. This is particularly triggered by, I think, protests about the invasion of Israel, the war that resulted in Gaza, and the demonstrations that have gone on around the country, with many people masked.
There may be issues about what is acceptable to wear when you go to a demonstration. I don’t claim to know about the civil rights of that.
In a time at which COVID-19 is flourishing, really on the rebound, expanding fast, and still causing 600 deaths a week; the flu season is going to be upon us soon enough; and there are also concerns about the possibility of avian flu jumping into the human population, it is absolutely the wrong time to single out those who are trying to mask for health reasons.
Basically, there are two strong reasons. One, there are people out there who wear a medical mask or mask for a medical reason because they have an underlying disease. They may have had a transplant or they may feel they’re immunocompromised for some reason. They worry that, if they don’t wear a mask, they’re going to get an infection from something like COVID-19 or flu, which could really be super-dangerous for them.
The other reason people mask is to protect their family members. They may have someone who’s immunocompromised in the family, or they’re doing it kindly and altruistically to protect the rest of us and to stop viruses from circulating.
These bans are not taking into account public health. They’re being brought forward in the midst of political heat about demonstrations and political issues. I think they should be opposed. I do not think they should be enacted.
I think the medical rights of people with disabilities and immunologic disorders, and those who want to mask to prevent getting sick at a time at which infectious diseases are still circulating and killing people, ought to take priority. Public health, in this case, should drive our policies about masks.
Dr. Caplan, director, Division of Medical Ethics, New York University Langone Medical Center, New York, NY, served on Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I recently saw a ban that has me very worried, concerned, and strongly in opposition.
Basically, the standard kind of medical mask would be captured, although I think their aim in doing this was to try to discourage people at political protests from being able to wear masks and hide their identity. They’re basically trying to discourage that. This is particularly triggered by, I think, protests about the invasion of Israel, the war that resulted in Gaza, and the demonstrations that have gone on around the country, with many people masked.
There may be issues about what is acceptable to wear when you go to a demonstration. I don’t claim to know about the civil rights of that.
In a time at which COVID-19 is flourishing, really on the rebound, expanding fast, and still causing 600 deaths a week; the flu season is going to be upon us soon enough; and there are also concerns about the possibility of avian flu jumping into the human population, it is absolutely the wrong time to single out those who are trying to mask for health reasons.
Basically, there are two strong reasons. One, there are people out there who wear a medical mask or mask for a medical reason because they have an underlying disease. They may have had a transplant or they may feel they’re immunocompromised for some reason. They worry that, if they don’t wear a mask, they’re going to get an infection from something like COVID-19 or flu, which could really be super-dangerous for them.
The other reason people mask is to protect their family members. They may have someone who’s immunocompromised in the family, or they’re doing it kindly and altruistically to protect the rest of us and to stop viruses from circulating.
These bans are not taking into account public health. They’re being brought forward in the midst of political heat about demonstrations and political issues. I think they should be opposed. I do not think they should be enacted.
I think the medical rights of people with disabilities and immunologic disorders, and those who want to mask to prevent getting sick at a time at which infectious diseases are still circulating and killing people, ought to take priority. Public health, in this case, should drive our policies about masks.
Dr. Caplan, director, Division of Medical Ethics, New York University Langone Medical Center, New York, NY, served on Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape.
A version of this article appeared on Medscape.com.
This transcript has been edited for clarity.
I recently saw a ban that has me very worried, concerned, and strongly in opposition.
Basically, the standard kind of medical mask would be captured, although I think their aim in doing this was to try to discourage people at political protests from being able to wear masks and hide their identity. They’re basically trying to discourage that. This is particularly triggered by, I think, protests about the invasion of Israel, the war that resulted in Gaza, and the demonstrations that have gone on around the country, with many people masked.
There may be issues about what is acceptable to wear when you go to a demonstration. I don’t claim to know about the civil rights of that.
In a time at which COVID-19 is flourishing, really on the rebound, expanding fast, and still causing 600 deaths a week; the flu season is going to be upon us soon enough; and there are also concerns about the possibility of avian flu jumping into the human population, it is absolutely the wrong time to single out those who are trying to mask for health reasons.
Basically, there are two strong reasons. One, there are people out there who wear a medical mask or mask for a medical reason because they have an underlying disease. They may have had a transplant or they may feel they’re immunocompromised for some reason. They worry that, if they don’t wear a mask, they’re going to get an infection from something like COVID-19 or flu, which could really be super-dangerous for them.
The other reason people mask is to protect their family members. They may have someone who’s immunocompromised in the family, or they’re doing it kindly and altruistically to protect the rest of us and to stop viruses from circulating.
These bans are not taking into account public health. They’re being brought forward in the midst of political heat about demonstrations and political issues. I think they should be opposed. I do not think they should be enacted.
I think the medical rights of people with disabilities and immunologic disorders, and those who want to mask to prevent getting sick at a time at which infectious diseases are still circulating and killing people, ought to take priority. Public health, in this case, should drive our policies about masks.
Dr. Caplan, director, Division of Medical Ethics, New York University Langone Medical Center, New York, NY, served on Johnson & Johnson’s Panel for Compassionate Drug Use (unpaid position), and is a contributing author and adviser for Medscape.
A version of this article appeared on Medscape.com.
Six Tips on Coronavirus Testing for Doctors and Patients
according to the Robert Koch Institute, Germany. If a patient has a fever and cough and feels exhausted, it could be COVID-19. What significance do rapid tests have? And when should doctors advise their patients about them?
When to Test
People at a higher risk for severe COVID-19 benefit from tests. This population includes the following groups:
- Older patients
- Immunocompromised patients
- Patients with respiratory diseases
- Patients with cardiovascular diseases
- Patients with liver and kidney diseases
- Patients with neurological diseases
- Patients with obesity
If doctors detect SARS-CoV-2 infection early, they can prescribe Paxlovid, for example, to reduce morbidity and mortality risks. Conversely, people without specific risks should test themselves if they plan to visit vulnerable individuals.
Detecting New Variants
A comprehensive study from the fall of 2022 provides evidence that antigen tests targeting the nucleocapsid (N) protein of SARS-CoV-2 also detect new variants.
The researchers built a library of various versions of the SARS-CoV-2 N protein. Their collection included nearly 8000 individual amino acid substitutions, representing more than 99.5% of all statistically possible mutations of the N protein.
They then examined how these N proteins interacted with 17 antibodies used in 11 commercially available antigen rapid tests.
All antibodies were able to recognize altered N proteins. Since the researchers successfully investigated diagnostic antibodies against nearly all possible N-protein mutations, rapid tests should be able to detect future virus variants. However, sensitivity and specificity may still change.
Test Timing
Uncertainty about what time of day to test can be mitigated by performing multiple COVID-19 rapid tests over time. The Food and Drug Administration (FDA) and similar organizations make this recommendation. Studies of symptomatic individuals show that serial tests increase accuracy.
In the early stages of infection, swabs may contain too little virus material because of widespread immunity against SARS-CoV-2. That is, they may contain inadequate levels of the relevant antigen. Especially in asymptomatic individuals or patients in the incubation phase, a single test may therefore yield a false-negative result. Therefore, the FDA recommends conducting at least two additional tests 48 hours apart in case of a negative test result.
Costs of Rapid Tests
The days of free tests are long gone. In Germany, the distribution of free preventive coronavirus tests was discontinued on March 1, 2023.
Test kits are still available in pharmacies or drugstores. In packages with 5-10 tests, the individual test costs between €0.90 and €1.50, depending on the provider. If a patient still has old rapid coronavirus tests in his or her medicine cabinet, are they still suitable?
Expired Tests
Properly stored tests that have not passed their expiration dates can still be used. But microbiologist and pathologist Daniel Rhoads, MD, from the Cleveland Clinic in Ohio warns against expired rapid tests.
The chemicals may have decomposed, the solvent may have evaporated, or antibodies may have lost their effectiveness, thus making false negative results more likely. “These are proteins that can decompose over time,” said Dr. Rhoads.
Ordering PCR Tests
The polymerase chain reaction (PCR) test remains the gold standard for diagnosing COVID-19. It is still available within statutory health insurance coverage. As Germany’s National Association of Statutory Health Insurance Physicians observes, form Muster 10 is used to order the test in that country.
The fee for the swab is included in the insured patient’s basic flat rate. Laboratories bill the PCR test using fee schedule position (GOP) 32816, according to the Uniform Value Scale (EBM).
There is no possibility for billing rapid tests for SARS-CoV-2 in medical practices within the EBM. A laboratory-based SARS-CoV-2 antigen detection test (GOP 32779) can be requested via the Muster 10 form.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
according to the Robert Koch Institute, Germany. If a patient has a fever and cough and feels exhausted, it could be COVID-19. What significance do rapid tests have? And when should doctors advise their patients about them?
When to Test
People at a higher risk for severe COVID-19 benefit from tests. This population includes the following groups:
- Older patients
- Immunocompromised patients
- Patients with respiratory diseases
- Patients with cardiovascular diseases
- Patients with liver and kidney diseases
- Patients with neurological diseases
- Patients with obesity
If doctors detect SARS-CoV-2 infection early, they can prescribe Paxlovid, for example, to reduce morbidity and mortality risks. Conversely, people without specific risks should test themselves if they plan to visit vulnerable individuals.
Detecting New Variants
A comprehensive study from the fall of 2022 provides evidence that antigen tests targeting the nucleocapsid (N) protein of SARS-CoV-2 also detect new variants.
The researchers built a library of various versions of the SARS-CoV-2 N protein. Their collection included nearly 8000 individual amino acid substitutions, representing more than 99.5% of all statistically possible mutations of the N protein.
They then examined how these N proteins interacted with 17 antibodies used in 11 commercially available antigen rapid tests.
All antibodies were able to recognize altered N proteins. Since the researchers successfully investigated diagnostic antibodies against nearly all possible N-protein mutations, rapid tests should be able to detect future virus variants. However, sensitivity and specificity may still change.
Test Timing
Uncertainty about what time of day to test can be mitigated by performing multiple COVID-19 rapid tests over time. The Food and Drug Administration (FDA) and similar organizations make this recommendation. Studies of symptomatic individuals show that serial tests increase accuracy.
In the early stages of infection, swabs may contain too little virus material because of widespread immunity against SARS-CoV-2. That is, they may contain inadequate levels of the relevant antigen. Especially in asymptomatic individuals or patients in the incubation phase, a single test may therefore yield a false-negative result. Therefore, the FDA recommends conducting at least two additional tests 48 hours apart in case of a negative test result.
Costs of Rapid Tests
The days of free tests are long gone. In Germany, the distribution of free preventive coronavirus tests was discontinued on March 1, 2023.
Test kits are still available in pharmacies or drugstores. In packages with 5-10 tests, the individual test costs between €0.90 and €1.50, depending on the provider. If a patient still has old rapid coronavirus tests in his or her medicine cabinet, are they still suitable?
Expired Tests
Properly stored tests that have not passed their expiration dates can still be used. But microbiologist and pathologist Daniel Rhoads, MD, from the Cleveland Clinic in Ohio warns against expired rapid tests.
The chemicals may have decomposed, the solvent may have evaporated, or antibodies may have lost their effectiveness, thus making false negative results more likely. “These are proteins that can decompose over time,” said Dr. Rhoads.
Ordering PCR Tests
The polymerase chain reaction (PCR) test remains the gold standard for diagnosing COVID-19. It is still available within statutory health insurance coverage. As Germany’s National Association of Statutory Health Insurance Physicians observes, form Muster 10 is used to order the test in that country.
The fee for the swab is included in the insured patient’s basic flat rate. Laboratories bill the PCR test using fee schedule position (GOP) 32816, according to the Uniform Value Scale (EBM).
There is no possibility for billing rapid tests for SARS-CoV-2 in medical practices within the EBM. A laboratory-based SARS-CoV-2 antigen detection test (GOP 32779) can be requested via the Muster 10 form.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.
according to the Robert Koch Institute, Germany. If a patient has a fever and cough and feels exhausted, it could be COVID-19. What significance do rapid tests have? And when should doctors advise their patients about them?
When to Test
People at a higher risk for severe COVID-19 benefit from tests. This population includes the following groups:
- Older patients
- Immunocompromised patients
- Patients with respiratory diseases
- Patients with cardiovascular diseases
- Patients with liver and kidney diseases
- Patients with neurological diseases
- Patients with obesity
If doctors detect SARS-CoV-2 infection early, they can prescribe Paxlovid, for example, to reduce morbidity and mortality risks. Conversely, people without specific risks should test themselves if they plan to visit vulnerable individuals.
Detecting New Variants
A comprehensive study from the fall of 2022 provides evidence that antigen tests targeting the nucleocapsid (N) protein of SARS-CoV-2 also detect new variants.
The researchers built a library of various versions of the SARS-CoV-2 N protein. Their collection included nearly 8000 individual amino acid substitutions, representing more than 99.5% of all statistically possible mutations of the N protein.
They then examined how these N proteins interacted with 17 antibodies used in 11 commercially available antigen rapid tests.
All antibodies were able to recognize altered N proteins. Since the researchers successfully investigated diagnostic antibodies against nearly all possible N-protein mutations, rapid tests should be able to detect future virus variants. However, sensitivity and specificity may still change.
Test Timing
Uncertainty about what time of day to test can be mitigated by performing multiple COVID-19 rapid tests over time. The Food and Drug Administration (FDA) and similar organizations make this recommendation. Studies of symptomatic individuals show that serial tests increase accuracy.
In the early stages of infection, swabs may contain too little virus material because of widespread immunity against SARS-CoV-2. That is, they may contain inadequate levels of the relevant antigen. Especially in asymptomatic individuals or patients in the incubation phase, a single test may therefore yield a false-negative result. Therefore, the FDA recommends conducting at least two additional tests 48 hours apart in case of a negative test result.
Costs of Rapid Tests
The days of free tests are long gone. In Germany, the distribution of free preventive coronavirus tests was discontinued on March 1, 2023.
Test kits are still available in pharmacies or drugstores. In packages with 5-10 tests, the individual test costs between €0.90 and €1.50, depending on the provider. If a patient still has old rapid coronavirus tests in his or her medicine cabinet, are they still suitable?
Expired Tests
Properly stored tests that have not passed their expiration dates can still be used. But microbiologist and pathologist Daniel Rhoads, MD, from the Cleveland Clinic in Ohio warns against expired rapid tests.
The chemicals may have decomposed, the solvent may have evaporated, or antibodies may have lost their effectiveness, thus making false negative results more likely. “These are proteins that can decompose over time,” said Dr. Rhoads.
Ordering PCR Tests
The polymerase chain reaction (PCR) test remains the gold standard for diagnosing COVID-19. It is still available within statutory health insurance coverage. As Germany’s National Association of Statutory Health Insurance Physicians observes, form Muster 10 is used to order the test in that country.
The fee for the swab is included in the insured patient’s basic flat rate. Laboratories bill the PCR test using fee schedule position (GOP) 32816, according to the Uniform Value Scale (EBM).
There is no possibility for billing rapid tests for SARS-CoV-2 in medical practices within the EBM. A laboratory-based SARS-CoV-2 antigen detection test (GOP 32779) can be requested via the Muster 10 form.
This story was translated from the Medscape German edition using several editorial tools, including AI, as part of the process. Human editors reviewed this content before publication. A version of this article first appeared on Medscape.com.