User login
Biologics reduce exacerbations in severe asthma
, based on data from more than 2,000 individuals.
The development of biologics to target specific inflammatory pathways “has transformed the management of uncontrolled SA,” but data on the real-world use of biologics in severe asthma patients treated by subspecialists are limited, wrote Reynold A. Panettieri, Jr., MD, of Rutgers, State University of New Jersey, New Brunswick, and colleagues.
In a study published in the Annals of Allergy, Asthma & Immunology, the researchers reviewed data from CHRONICLE, an ongoing, prospective, real-world noninterventional study of adults aged 18 years and older with severe asthma in the United States.
The study population included 2,847 patients enrolled in the CHRONICLE study between February 2018 and February 2021; 68.8% were women, 74.6% were White. The patients ranged in age from 18 to 89 years, with a mean age of 54.2 years.
Biologic use was defined as patients who started or had ongoing use of biologics between 12 months before enrollment and the patient’s most recent data collection. Switches were defined as stopping one biologic and starting another within 6 months; stops were defined as discontinuing a biologic without switching to another within 6 months. A total of 66% of the patients were using biologics at the time of study enrollment. The most common biologic was omalizumab (47%), followed by benralizumab (27%), mepolizumab (26%), and dupilumab (18%).
Overall, 89% of the patients had ongoing biologic use, 16% had biologic switches, and 13% had stops.
Patients who started biologics or switched biologics had significant reductions in asthma exacerbations at 6 months, compared with nonbiologic users of 58% (1.80 vs. 0.76 per patient-year) and 49% (1.47 vs. 0.75 per patient-year), respectively (P < .001 for both). Asthma exacerbations declined by 70% among biologics users for whom data were available for 12 months before and 12 months after starting biologics.
Exacerbations decreased at 6 months after biologic initiation across all subgroups of patients, notably patients with pre-biologic FEV1 < 80% and patients with FEV1 ≥ 80% (66% and 53%, respectively); never smokers and current/former smokers (63% and 50%, respectively); and patients with COPD and without COPD (58% and 52%, respectively).
The researchers also found a greater reduction in exacerbations among patients who switched from anti-IgE therapy to anti–IL-5/IL-5R/IL-4R therapy, compared with those who switched among anti–IL-5/IL-5R/IL-4R therapies (58% vs. 46%).
Patients who stopped or switched biologics appeared to have more severe or treatment-refractory disease than those with ongoing biologic use, the researchers noted. The most common reason for stopping or switching was worsening symptoms.
The study findings were limited by several factors, including the focus only on adults in the United States with subspecialist-treated SA, which may limit generalizability to children or other populations, the researchers noted. Other limitations included the variation in clinical decisions and insurance coverage and the inability to conduct longitudinal assessments, they said.
The results demonstrate that starting or switching biologics was consistently associated with fewer exacerbations in severe asthma. However, more research is needed to determine why some patients were not receiving biologics because they were not considered clinically eligible by their subspecialist health care providers, the researchers concluded.
The current study and the CHRONICLE study were supported by AstraZeneca. Lead author Dr. Panettieri disclosed serving on the advisory boards for and receiving grant support from AstraZeneca, Sanofi, Genentech, Regeneron, and Novartis.
, based on data from more than 2,000 individuals.
The development of biologics to target specific inflammatory pathways “has transformed the management of uncontrolled SA,” but data on the real-world use of biologics in severe asthma patients treated by subspecialists are limited, wrote Reynold A. Panettieri, Jr., MD, of Rutgers, State University of New Jersey, New Brunswick, and colleagues.
In a study published in the Annals of Allergy, Asthma & Immunology, the researchers reviewed data from CHRONICLE, an ongoing, prospective, real-world noninterventional study of adults aged 18 years and older with severe asthma in the United States.
The study population included 2,847 patients enrolled in the CHRONICLE study between February 2018 and February 2021; 68.8% were women, 74.6% were White. The patients ranged in age from 18 to 89 years, with a mean age of 54.2 years.
Biologic use was defined as patients who started or had ongoing use of biologics between 12 months before enrollment and the patient’s most recent data collection. Switches were defined as stopping one biologic and starting another within 6 months; stops were defined as discontinuing a biologic without switching to another within 6 months. A total of 66% of the patients were using biologics at the time of study enrollment. The most common biologic was omalizumab (47%), followed by benralizumab (27%), mepolizumab (26%), and dupilumab (18%).
Overall, 89% of the patients had ongoing biologic use, 16% had biologic switches, and 13% had stops.
Patients who started biologics or switched biologics had significant reductions in asthma exacerbations at 6 months, compared with nonbiologic users of 58% (1.80 vs. 0.76 per patient-year) and 49% (1.47 vs. 0.75 per patient-year), respectively (P < .001 for both). Asthma exacerbations declined by 70% among biologics users for whom data were available for 12 months before and 12 months after starting biologics.
Exacerbations decreased at 6 months after biologic initiation across all subgroups of patients, notably patients with pre-biologic FEV1 < 80% and patients with FEV1 ≥ 80% (66% and 53%, respectively); never smokers and current/former smokers (63% and 50%, respectively); and patients with COPD and without COPD (58% and 52%, respectively).
The researchers also found a greater reduction in exacerbations among patients who switched from anti-IgE therapy to anti–IL-5/IL-5R/IL-4R therapy, compared with those who switched among anti–IL-5/IL-5R/IL-4R therapies (58% vs. 46%).
Patients who stopped or switched biologics appeared to have more severe or treatment-refractory disease than those with ongoing biologic use, the researchers noted. The most common reason for stopping or switching was worsening symptoms.
The study findings were limited by several factors, including the focus only on adults in the United States with subspecialist-treated SA, which may limit generalizability to children or other populations, the researchers noted. Other limitations included the variation in clinical decisions and insurance coverage and the inability to conduct longitudinal assessments, they said.
The results demonstrate that starting or switching biologics was consistently associated with fewer exacerbations in severe asthma. However, more research is needed to determine why some patients were not receiving biologics because they were not considered clinically eligible by their subspecialist health care providers, the researchers concluded.
The current study and the CHRONICLE study were supported by AstraZeneca. Lead author Dr. Panettieri disclosed serving on the advisory boards for and receiving grant support from AstraZeneca, Sanofi, Genentech, Regeneron, and Novartis.
, based on data from more than 2,000 individuals.
The development of biologics to target specific inflammatory pathways “has transformed the management of uncontrolled SA,” but data on the real-world use of biologics in severe asthma patients treated by subspecialists are limited, wrote Reynold A. Panettieri, Jr., MD, of Rutgers, State University of New Jersey, New Brunswick, and colleagues.
In a study published in the Annals of Allergy, Asthma & Immunology, the researchers reviewed data from CHRONICLE, an ongoing, prospective, real-world noninterventional study of adults aged 18 years and older with severe asthma in the United States.
The study population included 2,847 patients enrolled in the CHRONICLE study between February 2018 and February 2021; 68.8% were women, 74.6% were White. The patients ranged in age from 18 to 89 years, with a mean age of 54.2 years.
Biologic use was defined as patients who started or had ongoing use of biologics between 12 months before enrollment and the patient’s most recent data collection. Switches were defined as stopping one biologic and starting another within 6 months; stops were defined as discontinuing a biologic without switching to another within 6 months. A total of 66% of the patients were using biologics at the time of study enrollment. The most common biologic was omalizumab (47%), followed by benralizumab (27%), mepolizumab (26%), and dupilumab (18%).
Overall, 89% of the patients had ongoing biologic use, 16% had biologic switches, and 13% had stops.
Patients who started biologics or switched biologics had significant reductions in asthma exacerbations at 6 months, compared with nonbiologic users of 58% (1.80 vs. 0.76 per patient-year) and 49% (1.47 vs. 0.75 per patient-year), respectively (P < .001 for both). Asthma exacerbations declined by 70% among biologics users for whom data were available for 12 months before and 12 months after starting biologics.
Exacerbations decreased at 6 months after biologic initiation across all subgroups of patients, notably patients with pre-biologic FEV1 < 80% and patients with FEV1 ≥ 80% (66% and 53%, respectively); never smokers and current/former smokers (63% and 50%, respectively); and patients with COPD and without COPD (58% and 52%, respectively).
The researchers also found a greater reduction in exacerbations among patients who switched from anti-IgE therapy to anti–IL-5/IL-5R/IL-4R therapy, compared with those who switched among anti–IL-5/IL-5R/IL-4R therapies (58% vs. 46%).
Patients who stopped or switched biologics appeared to have more severe or treatment-refractory disease than those with ongoing biologic use, the researchers noted. The most common reason for stopping or switching was worsening symptoms.
The study findings were limited by several factors, including the focus only on adults in the United States with subspecialist-treated SA, which may limit generalizability to children or other populations, the researchers noted. Other limitations included the variation in clinical decisions and insurance coverage and the inability to conduct longitudinal assessments, they said.
The results demonstrate that starting or switching biologics was consistently associated with fewer exacerbations in severe asthma. However, more research is needed to determine why some patients were not receiving biologics because they were not considered clinically eligible by their subspecialist health care providers, the researchers concluded.
The current study and the CHRONICLE study were supported by AstraZeneca. Lead author Dr. Panettieri disclosed serving on the advisory boards for and receiving grant support from AstraZeneca, Sanofi, Genentech, Regeneron, and Novartis.
FROM THE ANNALS OF ALLERGY, ASTHMA & IMMUNOLOGY
Mepolizumab curbed corticosteroid use for severe asthma
Use of mepolizumab significantly reduced the need for maintenance oral corticosteroids in adults with severe asthma, based on data from more than 800 individuals.
Many patients with severe asthma require bursts of systemic corticosteroids (SCS) or maintenance oral corticosteroids (mOCS) for disease control, but these strategies are associated with side effects that can increase the disease burden, wrote Charles Pilette, MD, of Cliniques Universitaires Saint-Luc, Brussels, and colleagues.
Previous studies have shown that the humanized, monoclonal anti-interleukin (IL)–5 antibody mepolizumab, which is approved for the treatment of severe asthma, reduced use of SCS and has shown effectiveness in less homogeneous populations, but robust, real-world data on the occurrence and magnitude of these effects are lacking, the researchers said.
In a study known as REALITI-A, the researchers enrolled 822 adults with asthma diagnoses from 82 centers in Europe, Canada, and the United States who initiated mepolizumab at a subcutaneous dose of 100 mg. The study endpoints included daily use of oral corticosteroids at baseline and 1 year, percentage reduction in oral corticosteroid use from baseline, patients discontinuing oral corticosteroids; the primary outcome was the rate of clinically significant exacerbations (CSEs). CSEs were defined as the need for OCS for at least 3 days/parenteral administration, and/or an emergency department or hospital admission before and after treatment. The mean age of the participants was 54 years, 63% were women, and 60% were never-smokers. The mean asthma duration was 19.7 years.
A total of 319 patients (39%), used mOCS at baseline, and dose information was available for 298.
Real-world outcomes
At 1 year, the median mOCS dose in the study population was reduced by 75%, and 64% reduced their mOCS dose by at least 50% from baseline.
In addition, the proportion of patients who discontinued daily mOCS increased from 29% during week 25-28 to 43% during week 53-56.
Overall, 80% of patients remained on mepolizumab at 1 year. Lack of efficacy and patient decision were the top two reasons for discontinuation (6% and 4%, respectively).
The primary outcome of rate of CSE decreased by a clinically significant rate ratio of 0.29 (P < .001).
“The requirement for SCS bursts was also reduced, as observed by a decreased rate of CSEs,” the researchers wrote in their discussion. The results were consistent for patients receiving lower (less than 10 mg/day) or higher (10 mg/day or more) mOCS doses at baseline, they said. No unexpected safety signals were noted during the study period.
“Furthermore, , or those requiring hospitalization or an ER visit, improved symptom control, and lower work productivity and activity impairment,” they added.
The study findings were limited by several factors including the observational design, lack of mepolizumab comparator, and open-label data capture, the researchers noted. However, the results were consistent with similar studies, and support the use of mepolizumab as part of the standard of care for clinically effective disease control in severe asthma patients, they concluded.
The study was funded by GlaxoSmithKline. Lead author Dr. Pilette disclosed fees for advisory boards, speaker meetings, and 42 research grants from GSK, AstraZeneca, Chiesi, Novartis, Teva, and ALK-Abello.
Use of mepolizumab significantly reduced the need for maintenance oral corticosteroids in adults with severe asthma, based on data from more than 800 individuals.
Many patients with severe asthma require bursts of systemic corticosteroids (SCS) or maintenance oral corticosteroids (mOCS) for disease control, but these strategies are associated with side effects that can increase the disease burden, wrote Charles Pilette, MD, of Cliniques Universitaires Saint-Luc, Brussels, and colleagues.
Previous studies have shown that the humanized, monoclonal anti-interleukin (IL)–5 antibody mepolizumab, which is approved for the treatment of severe asthma, reduced use of SCS and has shown effectiveness in less homogeneous populations, but robust, real-world data on the occurrence and magnitude of these effects are lacking, the researchers said.
In a study known as REALITI-A, the researchers enrolled 822 adults with asthma diagnoses from 82 centers in Europe, Canada, and the United States who initiated mepolizumab at a subcutaneous dose of 100 mg. The study endpoints included daily use of oral corticosteroids at baseline and 1 year, percentage reduction in oral corticosteroid use from baseline, patients discontinuing oral corticosteroids; the primary outcome was the rate of clinically significant exacerbations (CSEs). CSEs were defined as the need for OCS for at least 3 days/parenteral administration, and/or an emergency department or hospital admission before and after treatment. The mean age of the participants was 54 years, 63% were women, and 60% were never-smokers. The mean asthma duration was 19.7 years.
A total of 319 patients (39%), used mOCS at baseline, and dose information was available for 298.
Real-world outcomes
At 1 year, the median mOCS dose in the study population was reduced by 75%, and 64% reduced their mOCS dose by at least 50% from baseline.
In addition, the proportion of patients who discontinued daily mOCS increased from 29% during week 25-28 to 43% during week 53-56.
Overall, 80% of patients remained on mepolizumab at 1 year. Lack of efficacy and patient decision were the top two reasons for discontinuation (6% and 4%, respectively).
The primary outcome of rate of CSE decreased by a clinically significant rate ratio of 0.29 (P < .001).
“The requirement for SCS bursts was also reduced, as observed by a decreased rate of CSEs,” the researchers wrote in their discussion. The results were consistent for patients receiving lower (less than 10 mg/day) or higher (10 mg/day or more) mOCS doses at baseline, they said. No unexpected safety signals were noted during the study period.
“Furthermore, , or those requiring hospitalization or an ER visit, improved symptom control, and lower work productivity and activity impairment,” they added.
The study findings were limited by several factors including the observational design, lack of mepolizumab comparator, and open-label data capture, the researchers noted. However, the results were consistent with similar studies, and support the use of mepolizumab as part of the standard of care for clinically effective disease control in severe asthma patients, they concluded.
The study was funded by GlaxoSmithKline. Lead author Dr. Pilette disclosed fees for advisory boards, speaker meetings, and 42 research grants from GSK, AstraZeneca, Chiesi, Novartis, Teva, and ALK-Abello.
Use of mepolizumab significantly reduced the need for maintenance oral corticosteroids in adults with severe asthma, based on data from more than 800 individuals.
Many patients with severe asthma require bursts of systemic corticosteroids (SCS) or maintenance oral corticosteroids (mOCS) for disease control, but these strategies are associated with side effects that can increase the disease burden, wrote Charles Pilette, MD, of Cliniques Universitaires Saint-Luc, Brussels, and colleagues.
Previous studies have shown that the humanized, monoclonal anti-interleukin (IL)–5 antibody mepolizumab, which is approved for the treatment of severe asthma, reduced use of SCS and has shown effectiveness in less homogeneous populations, but robust, real-world data on the occurrence and magnitude of these effects are lacking, the researchers said.
In a study known as REALITI-A, the researchers enrolled 822 adults with asthma diagnoses from 82 centers in Europe, Canada, and the United States who initiated mepolizumab at a subcutaneous dose of 100 mg. The study endpoints included daily use of oral corticosteroids at baseline and 1 year, percentage reduction in oral corticosteroid use from baseline, patients discontinuing oral corticosteroids; the primary outcome was the rate of clinically significant exacerbations (CSEs). CSEs were defined as the need for OCS for at least 3 days/parenteral administration, and/or an emergency department or hospital admission before and after treatment. The mean age of the participants was 54 years, 63% were women, and 60% were never-smokers. The mean asthma duration was 19.7 years.
A total of 319 patients (39%), used mOCS at baseline, and dose information was available for 298.
Real-world outcomes
At 1 year, the median mOCS dose in the study population was reduced by 75%, and 64% reduced their mOCS dose by at least 50% from baseline.
In addition, the proportion of patients who discontinued daily mOCS increased from 29% during week 25-28 to 43% during week 53-56.
Overall, 80% of patients remained on mepolizumab at 1 year. Lack of efficacy and patient decision were the top two reasons for discontinuation (6% and 4%, respectively).
The primary outcome of rate of CSE decreased by a clinically significant rate ratio of 0.29 (P < .001).
“The requirement for SCS bursts was also reduced, as observed by a decreased rate of CSEs,” the researchers wrote in their discussion. The results were consistent for patients receiving lower (less than 10 mg/day) or higher (10 mg/day or more) mOCS doses at baseline, they said. No unexpected safety signals were noted during the study period.
“Furthermore, , or those requiring hospitalization or an ER visit, improved symptom control, and lower work productivity and activity impairment,” they added.
The study findings were limited by several factors including the observational design, lack of mepolizumab comparator, and open-label data capture, the researchers noted. However, the results were consistent with similar studies, and support the use of mepolizumab as part of the standard of care for clinically effective disease control in severe asthma patients, they concluded.
The study was funded by GlaxoSmithKline. Lead author Dr. Pilette disclosed fees for advisory boards, speaker meetings, and 42 research grants from GSK, AstraZeneca, Chiesi, Novartis, Teva, and ALK-Abello.
FROM JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
Frequent asthma deteriorations? Check for bronchiectasis
, according to the authors of a retrospective study in the Journal of Allergy and Clinical Immunology: In Practice. While bronchiectasis is known to worsen the clinical and functional outcomes in patients with asthma, data regarding the long-term effects of bronchiectasis on the clinical course of asthma have been limited, stated corresponding author Jung-Kyu Lee, MD, division of pulmonary and critical care medicine, Seoul (Republic of Korea) Metropolitan Government – Seoul National University.
Moderate to severe acute clinical deterioration risks were increased among the 251 patients (mean age 66.6 years, 77.2% men) with bronchiectasis out of 667 asthma patients included in the study. All studied patients underwent chest computed tomography and pulmonary function tests from 2013 to 2019 at two tertiary hospitals in Seoul. The primary outcome, annual incidence of moderate to severe acute exacerbations requiring additional treatment (systemic steroids, antibiotics, or both), was significantly higher in patients with bronchiectasis after a mean follow-up period of 3.96 years. Compared with patients who did not exhibit bronchiectasis, the annual rates of severe exacerbations (0.15 ± 0.43 vs. 0.08 ± 0.27; P = .010), moderate to severe (0.47 ± 0.79 vs. 0.34 ± 0.63; P = .018), and acute exacerbations during the follow-up period (49.8% vs. 39.4%; P = .009) were all significantly higher. There was no difference in the proportion of frequent exacerbators between the two groups, however. Severe acute exacerbations leading to hospitalizations, also, were more frequent in the group with bronchiectasis.
Risk factors explored
Significant factors conferring greater risk of severe and moderate to severe acute exacerbations in multivariable analysis included low body mass index, low baseline forced expiratory volume in 1 second (FEV1), high use of inhaled corticosteroids, high medication possession, and high neutrophil/lymphocyte ratios. The existence of bronchiectasis remained an independent risk factor for severe and moderate to severe acute exacerbations despite adjustment for all other factors. While bronchiectasis score showed no association with annual rate of acute exacerbation, progression of bronchiectasis confirmed on follow-up CT was associated with increased risks of severe and moderate to severe acute exacerbation.
Included patients had a diagnosis of asthma confirmed by variable expiratory airflow limitation with pulmonary function tests (that is, positive bronchodilator response, positive bronchial provocation test, or excessive variation in lung function between visits). Past histories of tuberculosis and nontuberculous mycobacterial lung disease, lower absolute and predicted values of both baseline FEV1 and forced vital capacity were more common among patients with bronchiectasis.
Dividing the study population into a group that had at least one moderate to severe acute exacerbation during the follow-up period and a group that did not, the researchers identified characteristics shared by exacerbators: a greater proportion were women, they had lower forced vital capacity and lung-diffusing capacity for carbon monoxide, higher blood FVC and blood neutrophil/lymphocyte ratio, and more medication use (inhaled corticosteroids, long-acting antimuscarinic agent, leukotriene-receptor antagonist, and methylxanthine), compared with the nonexacerbators. More bronchiectasis, more severe bronchiectasis (higher bronchiectasis score), and more progression of bronchiectasis were common among the exacerbators.
Higher acute exacerbation risks accompanied bronchiectasis, at 1.47-fold for moderate, 1.72-fold for severe, and 1.50-fold for moderate to severe exacerbations. Higher risk for severe and moderate to severe exacerbations was conferred by bronchiectasis progression, also.
The researchers pointed to contradictory effects of inhaled corticosteroid use, noting both corticosteroids’ essential role in controlling airway inflammation and hyperresponsiveness, exacerbations, and lung-function decline in asthma patients and that longer or greater inhaled corticosteroid use is associated with both clinical deterioration in asthma and bronchiectasis, and exacerbation history. For bronchiectasis, however, inhaled corticosteroid use offers no benefit while increasing susceptibility to infection and its risks through partial immunosuppression.
“Considering these contradictory effects of inhaled corticosteroid use, further research is needed regarding its risks and benefits in asthma patients with bronchiectasis, including differences in the benefit of inhaled corticosteroid use according to patient phenotype,” Dr. Kim and his colleagues concluded.
The role of corticosteroids
“One of the more important points discussed in this observational cohort study is the role of inhaled corticosteroid use in bronchiectasis,” said Mary Jo Farmer, MD, PhD, director of pulmonary hypertension services, Baystate Health, and assistant professor of medicine, University of Massachusetts – Baystate, both in Springfield, in an interview with this news organization. She cited a review finding no significant benefit versus placebo in spirometry, exacerbation rate, or sputum volume in the Cochrane Database of Systematic Reviews and another suggesting that quality of life was improved with inhaled corticosteroid use in individuals with blood eosinophils greater than 3%, compared with those not using inhaled corticosteroids or having lower eosinophil counts in the European Respiratory Journal. She cited also higher percentages (48% versus 23%) of adrenal insufficiency in bronchiectasis patients among those taking inhaled corticosteroids versus those not taking them.
Dr. Farmer added, “According to the 2018 Cochrane review of inhaled corticosteroid treatment for non–cystic fibrosis bronchiectasis, results from most randomized, placebo-controlled trials have been disappointing in terms of effects on most endpoints such as pulmonary function and exacerbation frequency. As such, the European Respiratory Society guidelines for the management of adult bronchiectasis advise against prescribing inhaled corticosteroids to patients with bronchiectasis, unless otherwise indicated by either an asthma or chronic obstructive pulmonary disease diagnosis. Also, inhaled corticosteroid treatment in asthma and COPD is associated with common side effects such as oral candidiasis, dysphonia and, in some cases, systemic corticosteroid effects. The rate of adverse events from inhaled corticosteroid treatment of bronchiectasis, however, is largely unknown.Dr. Lee and Dr. Farmer reported no relevant financial relationships. The study was independently supported.
, according to the authors of a retrospective study in the Journal of Allergy and Clinical Immunology: In Practice. While bronchiectasis is known to worsen the clinical and functional outcomes in patients with asthma, data regarding the long-term effects of bronchiectasis on the clinical course of asthma have been limited, stated corresponding author Jung-Kyu Lee, MD, division of pulmonary and critical care medicine, Seoul (Republic of Korea) Metropolitan Government – Seoul National University.
Moderate to severe acute clinical deterioration risks were increased among the 251 patients (mean age 66.6 years, 77.2% men) with bronchiectasis out of 667 asthma patients included in the study. All studied patients underwent chest computed tomography and pulmonary function tests from 2013 to 2019 at two tertiary hospitals in Seoul. The primary outcome, annual incidence of moderate to severe acute exacerbations requiring additional treatment (systemic steroids, antibiotics, or both), was significantly higher in patients with bronchiectasis after a mean follow-up period of 3.96 years. Compared with patients who did not exhibit bronchiectasis, the annual rates of severe exacerbations (0.15 ± 0.43 vs. 0.08 ± 0.27; P = .010), moderate to severe (0.47 ± 0.79 vs. 0.34 ± 0.63; P = .018), and acute exacerbations during the follow-up period (49.8% vs. 39.4%; P = .009) were all significantly higher. There was no difference in the proportion of frequent exacerbators between the two groups, however. Severe acute exacerbations leading to hospitalizations, also, were more frequent in the group with bronchiectasis.
Risk factors explored
Significant factors conferring greater risk of severe and moderate to severe acute exacerbations in multivariable analysis included low body mass index, low baseline forced expiratory volume in 1 second (FEV1), high use of inhaled corticosteroids, high medication possession, and high neutrophil/lymphocyte ratios. The existence of bronchiectasis remained an independent risk factor for severe and moderate to severe acute exacerbations despite adjustment for all other factors. While bronchiectasis score showed no association with annual rate of acute exacerbation, progression of bronchiectasis confirmed on follow-up CT was associated with increased risks of severe and moderate to severe acute exacerbation.
Included patients had a diagnosis of asthma confirmed by variable expiratory airflow limitation with pulmonary function tests (that is, positive bronchodilator response, positive bronchial provocation test, or excessive variation in lung function between visits). Past histories of tuberculosis and nontuberculous mycobacterial lung disease, lower absolute and predicted values of both baseline FEV1 and forced vital capacity were more common among patients with bronchiectasis.
Dividing the study population into a group that had at least one moderate to severe acute exacerbation during the follow-up period and a group that did not, the researchers identified characteristics shared by exacerbators: a greater proportion were women, they had lower forced vital capacity and lung-diffusing capacity for carbon monoxide, higher blood FVC and blood neutrophil/lymphocyte ratio, and more medication use (inhaled corticosteroids, long-acting antimuscarinic agent, leukotriene-receptor antagonist, and methylxanthine), compared with the nonexacerbators. More bronchiectasis, more severe bronchiectasis (higher bronchiectasis score), and more progression of bronchiectasis were common among the exacerbators.
Higher acute exacerbation risks accompanied bronchiectasis, at 1.47-fold for moderate, 1.72-fold for severe, and 1.50-fold for moderate to severe exacerbations. Higher risk for severe and moderate to severe exacerbations was conferred by bronchiectasis progression, also.
The researchers pointed to contradictory effects of inhaled corticosteroid use, noting both corticosteroids’ essential role in controlling airway inflammation and hyperresponsiveness, exacerbations, and lung-function decline in asthma patients and that longer or greater inhaled corticosteroid use is associated with both clinical deterioration in asthma and bronchiectasis, and exacerbation history. For bronchiectasis, however, inhaled corticosteroid use offers no benefit while increasing susceptibility to infection and its risks through partial immunosuppression.
“Considering these contradictory effects of inhaled corticosteroid use, further research is needed regarding its risks and benefits in asthma patients with bronchiectasis, including differences in the benefit of inhaled corticosteroid use according to patient phenotype,” Dr. Kim and his colleagues concluded.
The role of corticosteroids
“One of the more important points discussed in this observational cohort study is the role of inhaled corticosteroid use in bronchiectasis,” said Mary Jo Farmer, MD, PhD, director of pulmonary hypertension services, Baystate Health, and assistant professor of medicine, University of Massachusetts – Baystate, both in Springfield, in an interview with this news organization. She cited a review finding no significant benefit versus placebo in spirometry, exacerbation rate, or sputum volume in the Cochrane Database of Systematic Reviews and another suggesting that quality of life was improved with inhaled corticosteroid use in individuals with blood eosinophils greater than 3%, compared with those not using inhaled corticosteroids or having lower eosinophil counts in the European Respiratory Journal. She cited also higher percentages (48% versus 23%) of adrenal insufficiency in bronchiectasis patients among those taking inhaled corticosteroids versus those not taking them.
Dr. Farmer added, “According to the 2018 Cochrane review of inhaled corticosteroid treatment for non–cystic fibrosis bronchiectasis, results from most randomized, placebo-controlled trials have been disappointing in terms of effects on most endpoints such as pulmonary function and exacerbation frequency. As such, the European Respiratory Society guidelines for the management of adult bronchiectasis advise against prescribing inhaled corticosteroids to patients with bronchiectasis, unless otherwise indicated by either an asthma or chronic obstructive pulmonary disease diagnosis. Also, inhaled corticosteroid treatment in asthma and COPD is associated with common side effects such as oral candidiasis, dysphonia and, in some cases, systemic corticosteroid effects. The rate of adverse events from inhaled corticosteroid treatment of bronchiectasis, however, is largely unknown.Dr. Lee and Dr. Farmer reported no relevant financial relationships. The study was independently supported.
, according to the authors of a retrospective study in the Journal of Allergy and Clinical Immunology: In Practice. While bronchiectasis is known to worsen the clinical and functional outcomes in patients with asthma, data regarding the long-term effects of bronchiectasis on the clinical course of asthma have been limited, stated corresponding author Jung-Kyu Lee, MD, division of pulmonary and critical care medicine, Seoul (Republic of Korea) Metropolitan Government – Seoul National University.
Moderate to severe acute clinical deterioration risks were increased among the 251 patients (mean age 66.6 years, 77.2% men) with bronchiectasis out of 667 asthma patients included in the study. All studied patients underwent chest computed tomography and pulmonary function tests from 2013 to 2019 at two tertiary hospitals in Seoul. The primary outcome, annual incidence of moderate to severe acute exacerbations requiring additional treatment (systemic steroids, antibiotics, or both), was significantly higher in patients with bronchiectasis after a mean follow-up period of 3.96 years. Compared with patients who did not exhibit bronchiectasis, the annual rates of severe exacerbations (0.15 ± 0.43 vs. 0.08 ± 0.27; P = .010), moderate to severe (0.47 ± 0.79 vs. 0.34 ± 0.63; P = .018), and acute exacerbations during the follow-up period (49.8% vs. 39.4%; P = .009) were all significantly higher. There was no difference in the proportion of frequent exacerbators between the two groups, however. Severe acute exacerbations leading to hospitalizations, also, were more frequent in the group with bronchiectasis.
Risk factors explored
Significant factors conferring greater risk of severe and moderate to severe acute exacerbations in multivariable analysis included low body mass index, low baseline forced expiratory volume in 1 second (FEV1), high use of inhaled corticosteroids, high medication possession, and high neutrophil/lymphocyte ratios. The existence of bronchiectasis remained an independent risk factor for severe and moderate to severe acute exacerbations despite adjustment for all other factors. While bronchiectasis score showed no association with annual rate of acute exacerbation, progression of bronchiectasis confirmed on follow-up CT was associated with increased risks of severe and moderate to severe acute exacerbation.
Included patients had a diagnosis of asthma confirmed by variable expiratory airflow limitation with pulmonary function tests (that is, positive bronchodilator response, positive bronchial provocation test, or excessive variation in lung function between visits). Past histories of tuberculosis and nontuberculous mycobacterial lung disease, lower absolute and predicted values of both baseline FEV1 and forced vital capacity were more common among patients with bronchiectasis.
Dividing the study population into a group that had at least one moderate to severe acute exacerbation during the follow-up period and a group that did not, the researchers identified characteristics shared by exacerbators: a greater proportion were women, they had lower forced vital capacity and lung-diffusing capacity for carbon monoxide, higher blood FVC and blood neutrophil/lymphocyte ratio, and more medication use (inhaled corticosteroids, long-acting antimuscarinic agent, leukotriene-receptor antagonist, and methylxanthine), compared with the nonexacerbators. More bronchiectasis, more severe bronchiectasis (higher bronchiectasis score), and more progression of bronchiectasis were common among the exacerbators.
Higher acute exacerbation risks accompanied bronchiectasis, at 1.47-fold for moderate, 1.72-fold for severe, and 1.50-fold for moderate to severe exacerbations. Higher risk for severe and moderate to severe exacerbations was conferred by bronchiectasis progression, also.
The researchers pointed to contradictory effects of inhaled corticosteroid use, noting both corticosteroids’ essential role in controlling airway inflammation and hyperresponsiveness, exacerbations, and lung-function decline in asthma patients and that longer or greater inhaled corticosteroid use is associated with both clinical deterioration in asthma and bronchiectasis, and exacerbation history. For bronchiectasis, however, inhaled corticosteroid use offers no benefit while increasing susceptibility to infection and its risks through partial immunosuppression.
“Considering these contradictory effects of inhaled corticosteroid use, further research is needed regarding its risks and benefits in asthma patients with bronchiectasis, including differences in the benefit of inhaled corticosteroid use according to patient phenotype,” Dr. Kim and his colleagues concluded.
The role of corticosteroids
“One of the more important points discussed in this observational cohort study is the role of inhaled corticosteroid use in bronchiectasis,” said Mary Jo Farmer, MD, PhD, director of pulmonary hypertension services, Baystate Health, and assistant professor of medicine, University of Massachusetts – Baystate, both in Springfield, in an interview with this news organization. She cited a review finding no significant benefit versus placebo in spirometry, exacerbation rate, or sputum volume in the Cochrane Database of Systematic Reviews and another suggesting that quality of life was improved with inhaled corticosteroid use in individuals with blood eosinophils greater than 3%, compared with those not using inhaled corticosteroids or having lower eosinophil counts in the European Respiratory Journal. She cited also higher percentages (48% versus 23%) of adrenal insufficiency in bronchiectasis patients among those taking inhaled corticosteroids versus those not taking them.
Dr. Farmer added, “According to the 2018 Cochrane review of inhaled corticosteroid treatment for non–cystic fibrosis bronchiectasis, results from most randomized, placebo-controlled trials have been disappointing in terms of effects on most endpoints such as pulmonary function and exacerbation frequency. As such, the European Respiratory Society guidelines for the management of adult bronchiectasis advise against prescribing inhaled corticosteroids to patients with bronchiectasis, unless otherwise indicated by either an asthma or chronic obstructive pulmonary disease diagnosis. Also, inhaled corticosteroid treatment in asthma and COPD is associated with common side effects such as oral candidiasis, dysphonia and, in some cases, systemic corticosteroid effects. The rate of adverse events from inhaled corticosteroid treatment of bronchiectasis, however, is largely unknown.Dr. Lee and Dr. Farmer reported no relevant financial relationships. The study was independently supported.
FROM JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE
Antibiotics during pregnancy may increase child’s risk for asthma and other atopic diseases
, a systematic review and meta-analysis reports.
“Antibiotic use during pregnancy is significantly associated with the development of asthma in children. Additionally prenatal antibiotic exposure is also associated with disorders present in the atopic march including atopic sensitization, dermatitis/eczema, food allergy, allergic rhinitis, and wheeze,” lead study author Alissa Cait, PhD, of Malaghan Institute of Medical Research in Wellington, New Zealand, and colleagues write in Allergy.
“Antibiotics account for 80% of prescribed medications during pregnancy, and it is estimated that 20%-25% of pregnant women receive at least one course of an antibiotic during this time period,” they add.
The researchers evaluated prenatal antibiotic exposure and the risk for childhood wheeze or asthma, as well as for diseases associated with the atopic march, by searching standard medical databases for controlled trials in English, German, French, Dutch, or Arabic involving the use of any antibiotic at any time during pregnancy and for atopic disease incidence in children with asthma or wheeze as primary outcome. They excluded reviews, preclinical data, and descriptive studies.
From the 6,060 citations the search returned, 11 prospective and 16 retrospective studies met the authors’ selection criteria. For each study, they evaluated risk of bias using the Newcastle-Ottawa Quality Assessment Scale, and they rated certainty of the evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) protocol.
The studies, published between 2002 and 2020, were conducted in Europe, North America, Asia, and South America. Exposure to antibiotics during the prenatal period was assessed through unsupervised questionnaires, interviews by medical professionals, or extraction from official medical databases.
The results showed that:
- Antibiotic use during pregnancy was linked with increased relative risk of developing wheeze (relative risk, 1.51; 95% confidence interval, 1.17-1.94) or asthma (RR, 1.28; 95% CI, 1.22-1.34) during childhood.
- Antibiotic use during pregnancy also increased a child’s risk for eczema or dermatitis (RR, 1.28; 95% CI, 1.06-1.53) and allergic rhinitis (RR, 1.13; 95% CI, 1.02-1.25).
- Food allergy increased in one study (RR, 1.81; 95% CI, 1.11-2.95).
Quality of studies
“These results have importance for antibiotic stewardship throughout the prenatal period,” the authors write. However, due to issues including high heterogeneity, publication bias, and lack of population numbers in some studies, the overall quality of the evidence presented in the studies was low. Other limitations include mainly White and European study populations, underpowered studies, and study protocol inconsistencies.
“Though there is evidence that antibiotic treatment during pregnancy is a driver of the atopic march, due to a large heterogeneity between studies more research is needed to draw firm conclusions on this matter,” the authors add. “Future studies should employ and report more direct and objective measurement methods rather than self-reported questionnaires.”
Dustin D. Flannery, DO, MSCE, a neonatologist and clinical researcher in perinatal infectious diseases and neonatal antimicrobial resistance and stewardship at Children’s Hospital of Philadelphia, said in an email that the study was well done.
He noted, though, that “although the study reports an association, it cannot prove causation. The relationship between prenatal antibiotics and childhood allergic disorders is likely multifactorial and quite complex.”
He joins the authors in recommending further related research. “Due to the variation in how exposures and outcomes were defined across the studies, more rigorous research will be needed in this area.”
Despite the study’s limitations, “given that some studies have found associations between prenatal antibiotic exposure and childhood atopic and allergic disorders, including asthma, while other studies have not, this systematic review and meta-analysis asks an important question,” Dr. Flannery, who was not involved in the study, said in an interview.
“Investigators found a strong association between prenatal antibiotic exposure and risk of childhood asthma and other disorders,” he said. “This finding supports efforts to safely reduce antibiotic use during pregnancy.”
The study was supported by the Deutsche Forschungsgemeinschaft and by the Konrad Adenauer Foundation. The authors and Dr. Flannery have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a systematic review and meta-analysis reports.
“Antibiotic use during pregnancy is significantly associated with the development of asthma in children. Additionally prenatal antibiotic exposure is also associated with disorders present in the atopic march including atopic sensitization, dermatitis/eczema, food allergy, allergic rhinitis, and wheeze,” lead study author Alissa Cait, PhD, of Malaghan Institute of Medical Research in Wellington, New Zealand, and colleagues write in Allergy.
“Antibiotics account for 80% of prescribed medications during pregnancy, and it is estimated that 20%-25% of pregnant women receive at least one course of an antibiotic during this time period,” they add.
The researchers evaluated prenatal antibiotic exposure and the risk for childhood wheeze or asthma, as well as for diseases associated with the atopic march, by searching standard medical databases for controlled trials in English, German, French, Dutch, or Arabic involving the use of any antibiotic at any time during pregnancy and for atopic disease incidence in children with asthma or wheeze as primary outcome. They excluded reviews, preclinical data, and descriptive studies.
From the 6,060 citations the search returned, 11 prospective and 16 retrospective studies met the authors’ selection criteria. For each study, they evaluated risk of bias using the Newcastle-Ottawa Quality Assessment Scale, and they rated certainty of the evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) protocol.
The studies, published between 2002 and 2020, were conducted in Europe, North America, Asia, and South America. Exposure to antibiotics during the prenatal period was assessed through unsupervised questionnaires, interviews by medical professionals, or extraction from official medical databases.
The results showed that:
- Antibiotic use during pregnancy was linked with increased relative risk of developing wheeze (relative risk, 1.51; 95% confidence interval, 1.17-1.94) or asthma (RR, 1.28; 95% CI, 1.22-1.34) during childhood.
- Antibiotic use during pregnancy also increased a child’s risk for eczema or dermatitis (RR, 1.28; 95% CI, 1.06-1.53) and allergic rhinitis (RR, 1.13; 95% CI, 1.02-1.25).
- Food allergy increased in one study (RR, 1.81; 95% CI, 1.11-2.95).
Quality of studies
“These results have importance for antibiotic stewardship throughout the prenatal period,” the authors write. However, due to issues including high heterogeneity, publication bias, and lack of population numbers in some studies, the overall quality of the evidence presented in the studies was low. Other limitations include mainly White and European study populations, underpowered studies, and study protocol inconsistencies.
“Though there is evidence that antibiotic treatment during pregnancy is a driver of the atopic march, due to a large heterogeneity between studies more research is needed to draw firm conclusions on this matter,” the authors add. “Future studies should employ and report more direct and objective measurement methods rather than self-reported questionnaires.”
Dustin D. Flannery, DO, MSCE, a neonatologist and clinical researcher in perinatal infectious diseases and neonatal antimicrobial resistance and stewardship at Children’s Hospital of Philadelphia, said in an email that the study was well done.
He noted, though, that “although the study reports an association, it cannot prove causation. The relationship between prenatal antibiotics and childhood allergic disorders is likely multifactorial and quite complex.”
He joins the authors in recommending further related research. “Due to the variation in how exposures and outcomes were defined across the studies, more rigorous research will be needed in this area.”
Despite the study’s limitations, “given that some studies have found associations between prenatal antibiotic exposure and childhood atopic and allergic disorders, including asthma, while other studies have not, this systematic review and meta-analysis asks an important question,” Dr. Flannery, who was not involved in the study, said in an interview.
“Investigators found a strong association between prenatal antibiotic exposure and risk of childhood asthma and other disorders,” he said. “This finding supports efforts to safely reduce antibiotic use during pregnancy.”
The study was supported by the Deutsche Forschungsgemeinschaft and by the Konrad Adenauer Foundation. The authors and Dr. Flannery have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
, a systematic review and meta-analysis reports.
“Antibiotic use during pregnancy is significantly associated with the development of asthma in children. Additionally prenatal antibiotic exposure is also associated with disorders present in the atopic march including atopic sensitization, dermatitis/eczema, food allergy, allergic rhinitis, and wheeze,” lead study author Alissa Cait, PhD, of Malaghan Institute of Medical Research in Wellington, New Zealand, and colleagues write in Allergy.
“Antibiotics account for 80% of prescribed medications during pregnancy, and it is estimated that 20%-25% of pregnant women receive at least one course of an antibiotic during this time period,” they add.
The researchers evaluated prenatal antibiotic exposure and the risk for childhood wheeze or asthma, as well as for diseases associated with the atopic march, by searching standard medical databases for controlled trials in English, German, French, Dutch, or Arabic involving the use of any antibiotic at any time during pregnancy and for atopic disease incidence in children with asthma or wheeze as primary outcome. They excluded reviews, preclinical data, and descriptive studies.
From the 6,060 citations the search returned, 11 prospective and 16 retrospective studies met the authors’ selection criteria. For each study, they evaluated risk of bias using the Newcastle-Ottawa Quality Assessment Scale, and they rated certainty of the evidence using the Grading of Recommendations Assessment, Development, and Evaluation (GRADE) protocol.
The studies, published between 2002 and 2020, were conducted in Europe, North America, Asia, and South America. Exposure to antibiotics during the prenatal period was assessed through unsupervised questionnaires, interviews by medical professionals, or extraction from official medical databases.
The results showed that:
- Antibiotic use during pregnancy was linked with increased relative risk of developing wheeze (relative risk, 1.51; 95% confidence interval, 1.17-1.94) or asthma (RR, 1.28; 95% CI, 1.22-1.34) during childhood.
- Antibiotic use during pregnancy also increased a child’s risk for eczema or dermatitis (RR, 1.28; 95% CI, 1.06-1.53) and allergic rhinitis (RR, 1.13; 95% CI, 1.02-1.25).
- Food allergy increased in one study (RR, 1.81; 95% CI, 1.11-2.95).
Quality of studies
“These results have importance for antibiotic stewardship throughout the prenatal period,” the authors write. However, due to issues including high heterogeneity, publication bias, and lack of population numbers in some studies, the overall quality of the evidence presented in the studies was low. Other limitations include mainly White and European study populations, underpowered studies, and study protocol inconsistencies.
“Though there is evidence that antibiotic treatment during pregnancy is a driver of the atopic march, due to a large heterogeneity between studies more research is needed to draw firm conclusions on this matter,” the authors add. “Future studies should employ and report more direct and objective measurement methods rather than self-reported questionnaires.”
Dustin D. Flannery, DO, MSCE, a neonatologist and clinical researcher in perinatal infectious diseases and neonatal antimicrobial resistance and stewardship at Children’s Hospital of Philadelphia, said in an email that the study was well done.
He noted, though, that “although the study reports an association, it cannot prove causation. The relationship between prenatal antibiotics and childhood allergic disorders is likely multifactorial and quite complex.”
He joins the authors in recommending further related research. “Due to the variation in how exposures and outcomes were defined across the studies, more rigorous research will be needed in this area.”
Despite the study’s limitations, “given that some studies have found associations between prenatal antibiotic exposure and childhood atopic and allergic disorders, including asthma, while other studies have not, this systematic review and meta-analysis asks an important question,” Dr. Flannery, who was not involved in the study, said in an interview.
“Investigators found a strong association between prenatal antibiotic exposure and risk of childhood asthma and other disorders,” he said. “This finding supports efforts to safely reduce antibiotic use during pregnancy.”
The study was supported by the Deutsche Forschungsgemeinschaft and by the Konrad Adenauer Foundation. The authors and Dr. Flannery have disclosed no relevant financial relationships.
A version of this article first appeared on Medscape.com.
FROM ALLERGY
Food allergy test breakthrough: Less risk, more useful results
What would you do if you believed you had a serious health issue, but the best way to find out for sure might kill you?
That’s the reality for patients who wish to confirm or rule out a food allergy, says Sindy Tang, PhD, an associate professor of mechanical engineering at Stanford (Calif.) University.
And it’s the reason Dr. Tang and her colleagues are developing a food allergy test that’s not only safer, but also more reliable than today’s tests. In a paper in the journal Lab on a Chip, Dr. Tang and her colleagues outline the basis for this future test, which isolates a food allergy marker from the blood using a magnetic field.
How today’s food allergy tests fall short
The gold standard for food allergy diagnosis is something called the oral food challenge. That’s when the patient eats gradually increasing amounts of a problem food – say, peanuts – every 15 to 30 minutes to see if symptoms occur. This means highly allergic patients may risk anaphylaxis, an allergic reaction that causes inflammation so severe that breathing becomes restricted and blood pressure drops. Because of that, a clinical team must be at the ready with treatments like oxygen, epinephrine, or albuterol.
“The test is very accurate, but it’s also potentially unsafe and even fatal in rare cases,” Dr. Tang says. “That’s led to many sham tests advertised online that claim to use hair samples for food tests, but those are inaccurate and potentially dangerous, since they may give someone a false sense of confidence about a food they should avoid.”
Less risky tests are available, such as skin-prick tests – those involve scratching a small amount of the food into a patient’s arm – as well as blood tests that measure allergen-specific antibodies.
“Unfortunately, both of those are not that accurate and have high false-positive rates,” Dr. Tang says. “The best method is the oral food challenge, which many patients are afraid to do, not surprisingly.”
The future of food allergy testing: faster, safer, more reliable
In their study, the Stanford researchers focused on a type of white blood cell known as basophils, which release histamine when triggered by allergens. By using magnetic nanoparticles that bind to some blood cells but not basophils, they were able to separate basophils from the blood with a magnetic field in just 10 minutes.
Once isolated, the basophils are exposed to potential allergens. If they react, that’s a sign of an allergy.
Basophils have been isolated in labs before but not nearly this quickly and efficiently, Dr. Tang says.
“For true basophil activation, you need the blood to be fresh, which is challenging when you have to send it to a lab,” Dr. Tang says. “Being able to do this kind of test within a clinic or an in-house lab would be a big step forward.”
Next steps
While this represents a breakthrough in basophil activation testing, more research is needed to fully develop the system for clinical use. It must be standardized, automated, and miniaturized, the researchers say.
That said, the results give hope to those with food allergies that tomorrow’s gold-standard test will require only a blood sample without an emergency team standing by.
A version of this article first appeared on WebMD.com.
What would you do if you believed you had a serious health issue, but the best way to find out for sure might kill you?
That’s the reality for patients who wish to confirm or rule out a food allergy, says Sindy Tang, PhD, an associate professor of mechanical engineering at Stanford (Calif.) University.
And it’s the reason Dr. Tang and her colleagues are developing a food allergy test that’s not only safer, but also more reliable than today’s tests. In a paper in the journal Lab on a Chip, Dr. Tang and her colleagues outline the basis for this future test, which isolates a food allergy marker from the blood using a magnetic field.
How today’s food allergy tests fall short
The gold standard for food allergy diagnosis is something called the oral food challenge. That’s when the patient eats gradually increasing amounts of a problem food – say, peanuts – every 15 to 30 minutes to see if symptoms occur. This means highly allergic patients may risk anaphylaxis, an allergic reaction that causes inflammation so severe that breathing becomes restricted and blood pressure drops. Because of that, a clinical team must be at the ready with treatments like oxygen, epinephrine, or albuterol.
“The test is very accurate, but it’s also potentially unsafe and even fatal in rare cases,” Dr. Tang says. “That’s led to many sham tests advertised online that claim to use hair samples for food tests, but those are inaccurate and potentially dangerous, since they may give someone a false sense of confidence about a food they should avoid.”
Less risky tests are available, such as skin-prick tests – those involve scratching a small amount of the food into a patient’s arm – as well as blood tests that measure allergen-specific antibodies.
“Unfortunately, both of those are not that accurate and have high false-positive rates,” Dr. Tang says. “The best method is the oral food challenge, which many patients are afraid to do, not surprisingly.”
The future of food allergy testing: faster, safer, more reliable
In their study, the Stanford researchers focused on a type of white blood cell known as basophils, which release histamine when triggered by allergens. By using magnetic nanoparticles that bind to some blood cells but not basophils, they were able to separate basophils from the blood with a magnetic field in just 10 minutes.
Once isolated, the basophils are exposed to potential allergens. If they react, that’s a sign of an allergy.
Basophils have been isolated in labs before but not nearly this quickly and efficiently, Dr. Tang says.
“For true basophil activation, you need the blood to be fresh, which is challenging when you have to send it to a lab,” Dr. Tang says. “Being able to do this kind of test within a clinic or an in-house lab would be a big step forward.”
Next steps
While this represents a breakthrough in basophil activation testing, more research is needed to fully develop the system for clinical use. It must be standardized, automated, and miniaturized, the researchers say.
That said, the results give hope to those with food allergies that tomorrow’s gold-standard test will require only a blood sample without an emergency team standing by.
A version of this article first appeared on WebMD.com.
What would you do if you believed you had a serious health issue, but the best way to find out for sure might kill you?
That’s the reality for patients who wish to confirm or rule out a food allergy, says Sindy Tang, PhD, an associate professor of mechanical engineering at Stanford (Calif.) University.
And it’s the reason Dr. Tang and her colleagues are developing a food allergy test that’s not only safer, but also more reliable than today’s tests. In a paper in the journal Lab on a Chip, Dr. Tang and her colleagues outline the basis for this future test, which isolates a food allergy marker from the blood using a magnetic field.
How today’s food allergy tests fall short
The gold standard for food allergy diagnosis is something called the oral food challenge. That’s when the patient eats gradually increasing amounts of a problem food – say, peanuts – every 15 to 30 minutes to see if symptoms occur. This means highly allergic patients may risk anaphylaxis, an allergic reaction that causes inflammation so severe that breathing becomes restricted and blood pressure drops. Because of that, a clinical team must be at the ready with treatments like oxygen, epinephrine, or albuterol.
“The test is very accurate, but it’s also potentially unsafe and even fatal in rare cases,” Dr. Tang says. “That’s led to many sham tests advertised online that claim to use hair samples for food tests, but those are inaccurate and potentially dangerous, since they may give someone a false sense of confidence about a food they should avoid.”
Less risky tests are available, such as skin-prick tests – those involve scratching a small amount of the food into a patient’s arm – as well as blood tests that measure allergen-specific antibodies.
“Unfortunately, both of those are not that accurate and have high false-positive rates,” Dr. Tang says. “The best method is the oral food challenge, which many patients are afraid to do, not surprisingly.”
The future of food allergy testing: faster, safer, more reliable
In their study, the Stanford researchers focused on a type of white blood cell known as basophils, which release histamine when triggered by allergens. By using magnetic nanoparticles that bind to some blood cells but not basophils, they were able to separate basophils from the blood with a magnetic field in just 10 minutes.
Once isolated, the basophils are exposed to potential allergens. If they react, that’s a sign of an allergy.
Basophils have been isolated in labs before but not nearly this quickly and efficiently, Dr. Tang says.
“For true basophil activation, you need the blood to be fresh, which is challenging when you have to send it to a lab,” Dr. Tang says. “Being able to do this kind of test within a clinic or an in-house lab would be a big step forward.”
Next steps
While this represents a breakthrough in basophil activation testing, more research is needed to fully develop the system for clinical use. It must be standardized, automated, and miniaturized, the researchers say.
That said, the results give hope to those with food allergies that tomorrow’s gold-standard test will require only a blood sample without an emergency team standing by.
A version of this article first appeared on WebMD.com.
NIAID trial to test asthma drug in disadvantaged urban children
The Prevention of Asthma Exacerbations Using Dupilumab in Urban Children and Adolescents (PANDA) trial was launched in order to examine the effects of treatment on children with poorly controlled allergic asthma who live in low-income urban environments in the United States, according to the National Institute of Allergy and Infectious Diseases.
Black and Hispanic children who live in these environments are at particularly high risk for asthma and are prone to attacks. These children and adolescents often have many allergies and are exposed to both high levels of indoor allergens and traffic-related pollution, which can make their asthma even more difficult to control, according to a June 2 NIAID press release.
PANDA is a multicenter, double-blind, placebo-controlled, randomized trial of dupilumab adjunctive therapy for the reduction of asthma exacerbations in urban children and adolescents 6-17 years with T2-high exacerbation-prone asthma. Approximately 240 participants will be randomized 2:1 to one of two study arms: 1) guidelines-based asthma treatment plus dupilumab, or 2) guidelines-based asthma treatment plus placebo. The planned study treatment will continue for 1 year with an additional 3 months of follow-up following completion of study treatment, according to the study details.
In an earlier study, NIAID-supported investigators identified numerous networks of genes that are activated together and are associated with asthma attacks in minority children and adolescents living in low-income urban settings
“We need to find out how well approved asthma drugs work for disadvantaged children of color living in urban areas, and whether biological markers can help predict how the drugs affect their asthma,” NIAID director Anthony S. Fauci, MD, said in the release. “The PANDA trial is an important step toward these goals.”
Participant criteria for the study include children of either sex, ages 6-17 years, who live in prespecified urban areas. Participants must have a diagnosis of asthma and must have had at least two asthma exacerbations in the prior year (defined as a requirement for systemic corticosteroids and/or hospitalization). At the screening visit, participants must have the following requirements for asthma controller medication: For children ages 6-11 years: treatments with at least fluticasone 250 mcg dry powder inhaler (DPI) one puff twice daily or its equivalent; for children ages 12 years and older, treatment with at least fluticasone 250 mcg plus long-acting beta agonist (LABA) DPI one puff twice daily or its equivalent.
ClinicalTrials.gov Identifier: NCT05347771Location: The NIAID-funded Childhood Asthma in Urban Settings (CAUSE) Network is conducting the study at seven medical centers located in Aurora, Colo.; Boston; Chicago; Cincinnati; New York, and Washington, D.C.
Sponsor: NIAID, Regeneron Pharmaceuticals and Sanofi are cofunding the phase 2 trial.
Study start date: April 2022
Expected completion Date: March 31, 2025
The Prevention of Asthma Exacerbations Using Dupilumab in Urban Children and Adolescents (PANDA) trial was launched in order to examine the effects of treatment on children with poorly controlled allergic asthma who live in low-income urban environments in the United States, according to the National Institute of Allergy and Infectious Diseases.
Black and Hispanic children who live in these environments are at particularly high risk for asthma and are prone to attacks. These children and adolescents often have many allergies and are exposed to both high levels of indoor allergens and traffic-related pollution, which can make their asthma even more difficult to control, according to a June 2 NIAID press release.
PANDA is a multicenter, double-blind, placebo-controlled, randomized trial of dupilumab adjunctive therapy for the reduction of asthma exacerbations in urban children and adolescents 6-17 years with T2-high exacerbation-prone asthma. Approximately 240 participants will be randomized 2:1 to one of two study arms: 1) guidelines-based asthma treatment plus dupilumab, or 2) guidelines-based asthma treatment plus placebo. The planned study treatment will continue for 1 year with an additional 3 months of follow-up following completion of study treatment, according to the study details.
In an earlier study, NIAID-supported investigators identified numerous networks of genes that are activated together and are associated with asthma attacks in minority children and adolescents living in low-income urban settings
“We need to find out how well approved asthma drugs work for disadvantaged children of color living in urban areas, and whether biological markers can help predict how the drugs affect their asthma,” NIAID director Anthony S. Fauci, MD, said in the release. “The PANDA trial is an important step toward these goals.”
Participant criteria for the study include children of either sex, ages 6-17 years, who live in prespecified urban areas. Participants must have a diagnosis of asthma and must have had at least two asthma exacerbations in the prior year (defined as a requirement for systemic corticosteroids and/or hospitalization). At the screening visit, participants must have the following requirements for asthma controller medication: For children ages 6-11 years: treatments with at least fluticasone 250 mcg dry powder inhaler (DPI) one puff twice daily or its equivalent; for children ages 12 years and older, treatment with at least fluticasone 250 mcg plus long-acting beta agonist (LABA) DPI one puff twice daily or its equivalent.
ClinicalTrials.gov Identifier: NCT05347771Location: The NIAID-funded Childhood Asthma in Urban Settings (CAUSE) Network is conducting the study at seven medical centers located in Aurora, Colo.; Boston; Chicago; Cincinnati; New York, and Washington, D.C.
Sponsor: NIAID, Regeneron Pharmaceuticals and Sanofi are cofunding the phase 2 trial.
Study start date: April 2022
Expected completion Date: March 31, 2025
The Prevention of Asthma Exacerbations Using Dupilumab in Urban Children and Adolescents (PANDA) trial was launched in order to examine the effects of treatment on children with poorly controlled allergic asthma who live in low-income urban environments in the United States, according to the National Institute of Allergy and Infectious Diseases.
Black and Hispanic children who live in these environments are at particularly high risk for asthma and are prone to attacks. These children and adolescents often have many allergies and are exposed to both high levels of indoor allergens and traffic-related pollution, which can make their asthma even more difficult to control, according to a June 2 NIAID press release.
PANDA is a multicenter, double-blind, placebo-controlled, randomized trial of dupilumab adjunctive therapy for the reduction of asthma exacerbations in urban children and adolescents 6-17 years with T2-high exacerbation-prone asthma. Approximately 240 participants will be randomized 2:1 to one of two study arms: 1) guidelines-based asthma treatment plus dupilumab, or 2) guidelines-based asthma treatment plus placebo. The planned study treatment will continue for 1 year with an additional 3 months of follow-up following completion of study treatment, according to the study details.
In an earlier study, NIAID-supported investigators identified numerous networks of genes that are activated together and are associated with asthma attacks in minority children and adolescents living in low-income urban settings
“We need to find out how well approved asthma drugs work for disadvantaged children of color living in urban areas, and whether biological markers can help predict how the drugs affect their asthma,” NIAID director Anthony S. Fauci, MD, said in the release. “The PANDA trial is an important step toward these goals.”
Participant criteria for the study include children of either sex, ages 6-17 years, who live in prespecified urban areas. Participants must have a diagnosis of asthma and must have had at least two asthma exacerbations in the prior year (defined as a requirement for systemic corticosteroids and/or hospitalization). At the screening visit, participants must have the following requirements for asthma controller medication: For children ages 6-11 years: treatments with at least fluticasone 250 mcg dry powder inhaler (DPI) one puff twice daily or its equivalent; for children ages 12 years and older, treatment with at least fluticasone 250 mcg plus long-acting beta agonist (LABA) DPI one puff twice daily or its equivalent.
ClinicalTrials.gov Identifier: NCT05347771Location: The NIAID-funded Childhood Asthma in Urban Settings (CAUSE) Network is conducting the study at seven medical centers located in Aurora, Colo.; Boston; Chicago; Cincinnati; New York, and Washington, D.C.
Sponsor: NIAID, Regeneron Pharmaceuticals and Sanofi are cofunding the phase 2 trial.
Study start date: April 2022
Expected completion Date: March 31, 2025
‘Smart inhalers’ may help diagnose and treat asthma – if used
After years going on and off medications for occasional asthma symptoms, things went downhill for Brian Blome in November 2020. The retired carpenter started feeling short of breath and wheezing during bike rides. At home, he struggled with chores.
“I was having a hard time climbing a flight of stairs, just doing laundry,” said Mr. Blome, who lives in the Chicago suburb of Palatine.
To get things under control, he saw an allergist and started regular medications – two tablets, two nasal sprays, and inhaled corticosteroids each day, plus an albuterol inhaler for flare-ups.
The inhalers have an extra feature: an electronic monitor that attaches to the device and automatically tracks where and when the medication is used. Bluetooth sends this information to an app on the patient’s mobile phone and to a dashboard where the medical team can see, at a glance, when symptoms are popping up and how regularly medications are taken – leading to the devices often being called “smart inhalers.”
At the 2022 American Academy of Allergy, Asthma, and Immunology conference in Phoenix, researchers explained how digital monitoring devices can help diagnose and treat hard-to-control asthma, potentially reducing the need for oral steroids or biologic therapies.
Even though electric monitors have been on the market for years, their use has been slow to catch on because of uncertainties around insurance coverage, liability, and how to manage and best use the data. One recent study said these devices cost $100-$500, but that price depends on many things, such as insurance.
About 17% of adult asthma patients have “difficult-to-control” asthma, meaning they limit their activity because of breathing symptoms and use reliever medications multiple times a week.
But research suggests that correcting inhaling technique and sticking to the use of the medications can cut that 17% down to just 3.7%, said Mr. Blome’s allergist, Giselle Mosnaim, MD, of NorthShore University HealthSystem in Glenview, Ill. Dr. Mosnaim spoke about digital monitoring at a conference session on digital technologies for asthma management.
A study of more than 5,000 asthma patients “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” she said. It also shows that, despite new devices and new technologies, “we still have poor inhaler technique.”
Yet adherence is poorly gauged by doctors and patient self-reporting. “The ideal measure of adherence should be objective, accurate, and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Improving use
Patients not following instructions or guidelines “is something we saw nonstop with kids,” said Caroline Moassessi, founder of the allergy and asthma blog Gratefulfoodie.com who formerly served on a regional board of the American Lung Association. She’s also the mother of two asthmatic children, now in college, who years ago used electronic medication monitors as part of a research trial.
They were “unimpressed – mostly since I think they thought their asthma was controlled,” she said. “When patients are not in crisis, they don’t manage their asthma well.”
Even in research studies such as the one Rachelle Ramsey, PhD, presented at the conference, it’s not only hard to determine if better adherence leads to improved health, but when.
“For example, does your adherence this week impact your asthma control this week, or does it impact your asthma control next week? Or is it even further out? Do you need to have some level of adherence over the course of a month in order to have better outcomes at the end of that month?” said Dr. Ramsey, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center. “I think it’s a little complicated.”
That said, results from several small studies do show a connection between remote monitoring and better clinical outcomes. One study enrolled asthma patients in the United Kingdom, and another was done by Dr. Mosnaim with Chicago-area patients.
In the U.K. quality improvement project, nurses asked patients with difficult-to-control asthma if they knew how to use their inhalers and were following treatment guidelines.
Those who said “yes” were invited to swap their steroid/inhalers for a controller fitted with a device that tracks use and measures acoustics to test inhaler technique. After 28 days of monitoring, many people in the study had better clinical outcomes.
And after 3 months of digital monitoring, patients didn’t use their rescue medication quite as often.
Mr. Blome has seen a marked improvement in his asthma since starting regular appointments and getting back on daily medications a year and a half ago. He says that now and then, he has wheezing and shortness of breath, usually while biking or exercising. But those symptoms aren’t as severe or frequent as before.
From a doctor’s perspective, “digital inhaler systems allow me to discern patterns in order to determine what triggers his asthma symptoms and to adjust medications at different times of the year,” Dr. Mosnaim said.
Electronic systems can monitor pollen counts and air quality as well as how often a patient uses a quick reliever medication. Thus, she said, tracking these measures year-round could raise attention to impending asthma attacks and suggest when to increase the dose of controller medications or add other treatments.
A version of this article first appeared on WebMD.com.
After years going on and off medications for occasional asthma symptoms, things went downhill for Brian Blome in November 2020. The retired carpenter started feeling short of breath and wheezing during bike rides. At home, he struggled with chores.
“I was having a hard time climbing a flight of stairs, just doing laundry,” said Mr. Blome, who lives in the Chicago suburb of Palatine.
To get things under control, he saw an allergist and started regular medications – two tablets, two nasal sprays, and inhaled corticosteroids each day, plus an albuterol inhaler for flare-ups.
The inhalers have an extra feature: an electronic monitor that attaches to the device and automatically tracks where and when the medication is used. Bluetooth sends this information to an app on the patient’s mobile phone and to a dashboard where the medical team can see, at a glance, when symptoms are popping up and how regularly medications are taken – leading to the devices often being called “smart inhalers.”
At the 2022 American Academy of Allergy, Asthma, and Immunology conference in Phoenix, researchers explained how digital monitoring devices can help diagnose and treat hard-to-control asthma, potentially reducing the need for oral steroids or biologic therapies.
Even though electric monitors have been on the market for years, their use has been slow to catch on because of uncertainties around insurance coverage, liability, and how to manage and best use the data. One recent study said these devices cost $100-$500, but that price depends on many things, such as insurance.
About 17% of adult asthma patients have “difficult-to-control” asthma, meaning they limit their activity because of breathing symptoms and use reliever medications multiple times a week.
But research suggests that correcting inhaling technique and sticking to the use of the medications can cut that 17% down to just 3.7%, said Mr. Blome’s allergist, Giselle Mosnaim, MD, of NorthShore University HealthSystem in Glenview, Ill. Dr. Mosnaim spoke about digital monitoring at a conference session on digital technologies for asthma management.
A study of more than 5,000 asthma patients “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” she said. It also shows that, despite new devices and new technologies, “we still have poor inhaler technique.”
Yet adherence is poorly gauged by doctors and patient self-reporting. “The ideal measure of adherence should be objective, accurate, and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Improving use
Patients not following instructions or guidelines “is something we saw nonstop with kids,” said Caroline Moassessi, founder of the allergy and asthma blog Gratefulfoodie.com who formerly served on a regional board of the American Lung Association. She’s also the mother of two asthmatic children, now in college, who years ago used electronic medication monitors as part of a research trial.
They were “unimpressed – mostly since I think they thought their asthma was controlled,” she said. “When patients are not in crisis, they don’t manage their asthma well.”
Even in research studies such as the one Rachelle Ramsey, PhD, presented at the conference, it’s not only hard to determine if better adherence leads to improved health, but when.
“For example, does your adherence this week impact your asthma control this week, or does it impact your asthma control next week? Or is it even further out? Do you need to have some level of adherence over the course of a month in order to have better outcomes at the end of that month?” said Dr. Ramsey, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center. “I think it’s a little complicated.”
That said, results from several small studies do show a connection between remote monitoring and better clinical outcomes. One study enrolled asthma patients in the United Kingdom, and another was done by Dr. Mosnaim with Chicago-area patients.
In the U.K. quality improvement project, nurses asked patients with difficult-to-control asthma if they knew how to use their inhalers and were following treatment guidelines.
Those who said “yes” were invited to swap their steroid/inhalers for a controller fitted with a device that tracks use and measures acoustics to test inhaler technique. After 28 days of monitoring, many people in the study had better clinical outcomes.
And after 3 months of digital monitoring, patients didn’t use their rescue medication quite as often.
Mr. Blome has seen a marked improvement in his asthma since starting regular appointments and getting back on daily medications a year and a half ago. He says that now and then, he has wheezing and shortness of breath, usually while biking or exercising. But those symptoms aren’t as severe or frequent as before.
From a doctor’s perspective, “digital inhaler systems allow me to discern patterns in order to determine what triggers his asthma symptoms and to adjust medications at different times of the year,” Dr. Mosnaim said.
Electronic systems can monitor pollen counts and air quality as well as how often a patient uses a quick reliever medication. Thus, she said, tracking these measures year-round could raise attention to impending asthma attacks and suggest when to increase the dose of controller medications or add other treatments.
A version of this article first appeared on WebMD.com.
After years going on and off medications for occasional asthma symptoms, things went downhill for Brian Blome in November 2020. The retired carpenter started feeling short of breath and wheezing during bike rides. At home, he struggled with chores.
“I was having a hard time climbing a flight of stairs, just doing laundry,” said Mr. Blome, who lives in the Chicago suburb of Palatine.
To get things under control, he saw an allergist and started regular medications – two tablets, two nasal sprays, and inhaled corticosteroids each day, plus an albuterol inhaler for flare-ups.
The inhalers have an extra feature: an electronic monitor that attaches to the device and automatically tracks where and when the medication is used. Bluetooth sends this information to an app on the patient’s mobile phone and to a dashboard where the medical team can see, at a glance, when symptoms are popping up and how regularly medications are taken – leading to the devices often being called “smart inhalers.”
At the 2022 American Academy of Allergy, Asthma, and Immunology conference in Phoenix, researchers explained how digital monitoring devices can help diagnose and treat hard-to-control asthma, potentially reducing the need for oral steroids or biologic therapies.
Even though electric monitors have been on the market for years, their use has been slow to catch on because of uncertainties around insurance coverage, liability, and how to manage and best use the data. One recent study said these devices cost $100-$500, but that price depends on many things, such as insurance.
About 17% of adult asthma patients have “difficult-to-control” asthma, meaning they limit their activity because of breathing symptoms and use reliever medications multiple times a week.
But research suggests that correcting inhaling technique and sticking to the use of the medications can cut that 17% down to just 3.7%, said Mr. Blome’s allergist, Giselle Mosnaim, MD, of NorthShore University HealthSystem in Glenview, Ill. Dr. Mosnaim spoke about digital monitoring at a conference session on digital technologies for asthma management.
A study of more than 5,000 asthma patients “showed that, if you have critical errors in inhaler technique, this leads to worse asthma outcomes and increased asthma exacerbations,” she said. It also shows that, despite new devices and new technologies, “we still have poor inhaler technique.”
Yet adherence is poorly gauged by doctors and patient self-reporting. “The ideal measure of adherence should be objective, accurate, and unobtrusive to minimize impact on patient behavior and allow reliable data collection in real-world settings,” Dr. Mosnaim said. “So electronic medication monitors are the gold standard.”
Improving use
Patients not following instructions or guidelines “is something we saw nonstop with kids,” said Caroline Moassessi, founder of the allergy and asthma blog Gratefulfoodie.com who formerly served on a regional board of the American Lung Association. She’s also the mother of two asthmatic children, now in college, who years ago used electronic medication monitors as part of a research trial.
They were “unimpressed – mostly since I think they thought their asthma was controlled,” she said. “When patients are not in crisis, they don’t manage their asthma well.”
Even in research studies such as the one Rachelle Ramsey, PhD, presented at the conference, it’s not only hard to determine if better adherence leads to improved health, but when.
“For example, does your adherence this week impact your asthma control this week, or does it impact your asthma control next week? Or is it even further out? Do you need to have some level of adherence over the course of a month in order to have better outcomes at the end of that month?” said Dr. Ramsey, a pediatric research psychologist at Cincinnati Children’s Hospital Medical Center. “I think it’s a little complicated.”
That said, results from several small studies do show a connection between remote monitoring and better clinical outcomes. One study enrolled asthma patients in the United Kingdom, and another was done by Dr. Mosnaim with Chicago-area patients.
In the U.K. quality improvement project, nurses asked patients with difficult-to-control asthma if they knew how to use their inhalers and were following treatment guidelines.
Those who said “yes” were invited to swap their steroid/inhalers for a controller fitted with a device that tracks use and measures acoustics to test inhaler technique. After 28 days of monitoring, many people in the study had better clinical outcomes.
And after 3 months of digital monitoring, patients didn’t use their rescue medication quite as often.
Mr. Blome has seen a marked improvement in his asthma since starting regular appointments and getting back on daily medications a year and a half ago. He says that now and then, he has wheezing and shortness of breath, usually while biking or exercising. But those symptoms aren’t as severe or frequent as before.
From a doctor’s perspective, “digital inhaler systems allow me to discern patterns in order to determine what triggers his asthma symptoms and to adjust medications at different times of the year,” Dr. Mosnaim said.
Electronic systems can monitor pollen counts and air quality as well as how often a patient uses a quick reliever medication. Thus, she said, tracking these measures year-round could raise attention to impending asthma attacks and suggest when to increase the dose of controller medications or add other treatments.
A version of this article first appeared on WebMD.com.
Food allergy risk not greater in C-section infants
Cesarean births are not likely linked to an elevated risk of food allergy during the first year of life, an Australian study found.
Published online in the Journal of Allergy and Clinical Immunology, the findings may help assess the risks and benefits of cesarean delivery and reassure women who require it that their babies are not more likely to develop food allergy, according to Rachel L. Peters, PhD, an epidemiologist at the Murdoch Child Research Institute (MCRI) in Melbourne, and colleagues.

Dr. Peters’ group undertook the analysis to clarify a possible association between mode of delivery and food allergy risk, which has remained unclear owing to the absence of studies with both challenge-proven food allergy outcomes and detailed information on the type and timing of cesarean delivery.
“The infant immune system undergoes rapid development during the neonatal period,” Dr. Peters said in an MCRI press release, and the mode of delivery may interfere with the normal development of the immune system. “Babies born by cesarean have less exposure to the bacteria from the mother’s gut and vagina, which influence the composition of the baby’s microbiome and immune system development. However, this doesn’t appear to play a major role in the development of food allergy,” she said.
The HealthNuts study
In the period 2007-2011, the longitudinal population-based HealthNuts cohort study enrolled 5,276 12-month-olds who underwent skin prick testing and oral food challenge for sensitization to egg, peanut, sesame, and either shellfish or cow’s milk. It linked the resulting data to additional birth statistics from the Victorian Perinatal Data Collection when children turned 6.
Birth data were obtained on 2,045 babies, and in this subgroup with linked data, 30% were born by cesarean – similar to the 31.7% of U.S. cesarean births in 2019 – and 12.7% of these had food allergy versus 13.2% of those delivered vaginally.
Compared with vaginal birth, C-section was not associated with the risk of food allergy (adjusted odds ratio [aOR] 0.95, 95% confidence interval [CI], 0.70-0.30).
Nor did the timing of the C-section have an effect. Cesarean delivery either before labor or after onset of labor was not associated with the risk of food allergy (aOR, 0.83, 95% CI, 0.55-1.23) and aOR, 1.13, 95% CI, 0.75-1.72), respectively.
Compared with vaginal delivery, elective or emergency cesarean was not associated with food allergy risk (aOR, 1.05, 95% CI, 0.71-1.55, and aOR, 0.86, 95% CI, 0.56-1.31).
Similarly, no evidence emerged of an effect modification by breastfeeding, older siblings, pet dog ownership, or maternal allergy.
“This study is helpful because in addition to blood and skin tests, it also used food challenge, which is the gold standard,” Terri Brown-Whitehorn, MD, an attending physician in the division of allergy and immunology at Children’s Hospital of Philadelphia, said in an interview. “If no actual food is given, the other tests could lead to false positives.”

Dr. Brown-Whitehorn, who was not involved in the MCRI research, said the findings are not likely to affect most decisions about C-sections because most are not voluntary. “But if a mother had a first baby by emergency cesarean section, she might be given the option of having the next one by the same method.”
She said the current advice is to introduce even high-risk foods to a child’s diet early on to ward off the development of food allergies.
According to the microbial exposure hypothesis, it was previously thought that a potential link between cesarean birth and allergy might reflect differences in early exposure to maternal flora beneficial to the immune system in the vagina during delivery. A C-section might bypass the opportunity for neonatal gut colonization with maternal gut and vaginal flora, thereby raising allergy risk. A 2018 meta-analysis, for example, suggested cesarean birth could raise the risk for food allergies by 21%.
In other research from HealthNuts, 30% of child peanut allergy and 90% of egg allergy appear to resolve naturally by age 6. These numbers are somewhat higher than what Dr. Brown-Whitehorn sees. “We find that about 20% of peanut allergies and about 70% or 80% – maybe a bit less – of egg allergies resolve by age 6.”
This research was supported by the National Health & Medical Research Council of Australia, the Ilhan Food Allergy Foundation, AnaphylaxiStop, the Charles and Sylvia Viertel Medical Research Foundation, the Victorian Government’s Operational Infrastructure Support Program, and the Melbourne Children’s Clinician-Scientist Fellowship.
Dr. Peters disclosed no competing interests. Several coauthors reported research support or employment with private companies and one is the inventor of an MCRI-held patent. Dr. Brown-Whitehorn had no competing interests to disclose.
Cesarean births are not likely linked to an elevated risk of food allergy during the first year of life, an Australian study found.
Published online in the Journal of Allergy and Clinical Immunology, the findings may help assess the risks and benefits of cesarean delivery and reassure women who require it that their babies are not more likely to develop food allergy, according to Rachel L. Peters, PhD, an epidemiologist at the Murdoch Child Research Institute (MCRI) in Melbourne, and colleagues.
Dr. Peters’ group undertook the analysis to clarify a possible association between mode of delivery and food allergy risk, which has remained unclear owing to the absence of studies with both challenge-proven food allergy outcomes and detailed information on the type and timing of cesarean delivery.
“The infant immune system undergoes rapid development during the neonatal period,” Dr. Peters said in an MCRI press release, and the mode of delivery may interfere with the normal development of the immune system. “Babies born by cesarean have less exposure to the bacteria from the mother’s gut and vagina, which influence the composition of the baby’s microbiome and immune system development. However, this doesn’t appear to play a major role in the development of food allergy,” she said.
The HealthNuts study
In the period 2007-2011, the longitudinal population-based HealthNuts cohort study enrolled 5,276 12-month-olds who underwent skin prick testing and oral food challenge for sensitization to egg, peanut, sesame, and either shellfish or cow’s milk. It linked the resulting data to additional birth statistics from the Victorian Perinatal Data Collection when children turned 6.
Birth data were obtained on 2,045 babies, and in this subgroup with linked data, 30% were born by cesarean – similar to the 31.7% of U.S. cesarean births in 2019 – and 12.7% of these had food allergy versus 13.2% of those delivered vaginally.
Compared with vaginal birth, C-section was not associated with the risk of food allergy (adjusted odds ratio [aOR] 0.95, 95% confidence interval [CI], 0.70-0.30).
Nor did the timing of the C-section have an effect. Cesarean delivery either before labor or after onset of labor was not associated with the risk of food allergy (aOR, 0.83, 95% CI, 0.55-1.23) and aOR, 1.13, 95% CI, 0.75-1.72), respectively.
Compared with vaginal delivery, elective or emergency cesarean was not associated with food allergy risk (aOR, 1.05, 95% CI, 0.71-1.55, and aOR, 0.86, 95% CI, 0.56-1.31).
Similarly, no evidence emerged of an effect modification by breastfeeding, older siblings, pet dog ownership, or maternal allergy.
“This study is helpful because in addition to blood and skin tests, it also used food challenge, which is the gold standard,” Terri Brown-Whitehorn, MD, an attending physician in the division of allergy and immunology at Children’s Hospital of Philadelphia, said in an interview. “If no actual food is given, the other tests could lead to false positives.”
Dr. Brown-Whitehorn, who was not involved in the MCRI research, said the findings are not likely to affect most decisions about C-sections because most are not voluntary. “But if a mother had a first baby by emergency cesarean section, she might be given the option of having the next one by the same method.”
She said the current advice is to introduce even high-risk foods to a child’s diet early on to ward off the development of food allergies.
According to the microbial exposure hypothesis, it was previously thought that a potential link between cesarean birth and allergy might reflect differences in early exposure to maternal flora beneficial to the immune system in the vagina during delivery. A C-section might bypass the opportunity for neonatal gut colonization with maternal gut and vaginal flora, thereby raising allergy risk. A 2018 meta-analysis, for example, suggested cesarean birth could raise the risk for food allergies by 21%.
In other research from HealthNuts, 30% of child peanut allergy and 90% of egg allergy appear to resolve naturally by age 6. These numbers are somewhat higher than what Dr. Brown-Whitehorn sees. “We find that about 20% of peanut allergies and about 70% or 80% – maybe a bit less – of egg allergies resolve by age 6.”
This research was supported by the National Health & Medical Research Council of Australia, the Ilhan Food Allergy Foundation, AnaphylaxiStop, the Charles and Sylvia Viertel Medical Research Foundation, the Victorian Government’s Operational Infrastructure Support Program, and the Melbourne Children’s Clinician-Scientist Fellowship.
Dr. Peters disclosed no competing interests. Several coauthors reported research support or employment with private companies and one is the inventor of an MCRI-held patent. Dr. Brown-Whitehorn had no competing interests to disclose.
Cesarean births are not likely linked to an elevated risk of food allergy during the first year of life, an Australian study found.
Published online in the Journal of Allergy and Clinical Immunology, the findings may help assess the risks and benefits of cesarean delivery and reassure women who require it that their babies are not more likely to develop food allergy, according to Rachel L. Peters, PhD, an epidemiologist at the Murdoch Child Research Institute (MCRI) in Melbourne, and colleagues.
Dr. Peters’ group undertook the analysis to clarify a possible association between mode of delivery and food allergy risk, which has remained unclear owing to the absence of studies with both challenge-proven food allergy outcomes and detailed information on the type and timing of cesarean delivery.
“The infant immune system undergoes rapid development during the neonatal period,” Dr. Peters said in an MCRI press release, and the mode of delivery may interfere with the normal development of the immune system. “Babies born by cesarean have less exposure to the bacteria from the mother’s gut and vagina, which influence the composition of the baby’s microbiome and immune system development. However, this doesn’t appear to play a major role in the development of food allergy,” she said.
The HealthNuts study
In the period 2007-2011, the longitudinal population-based HealthNuts cohort study enrolled 5,276 12-month-olds who underwent skin prick testing and oral food challenge for sensitization to egg, peanut, sesame, and either shellfish or cow’s milk. It linked the resulting data to additional birth statistics from the Victorian Perinatal Data Collection when children turned 6.
Birth data were obtained on 2,045 babies, and in this subgroup with linked data, 30% were born by cesarean – similar to the 31.7% of U.S. cesarean births in 2019 – and 12.7% of these had food allergy versus 13.2% of those delivered vaginally.
Compared with vaginal birth, C-section was not associated with the risk of food allergy (adjusted odds ratio [aOR] 0.95, 95% confidence interval [CI], 0.70-0.30).
Nor did the timing of the C-section have an effect. Cesarean delivery either before labor or after onset of labor was not associated with the risk of food allergy (aOR, 0.83, 95% CI, 0.55-1.23) and aOR, 1.13, 95% CI, 0.75-1.72), respectively.
Compared with vaginal delivery, elective or emergency cesarean was not associated with food allergy risk (aOR, 1.05, 95% CI, 0.71-1.55, and aOR, 0.86, 95% CI, 0.56-1.31).
Similarly, no evidence emerged of an effect modification by breastfeeding, older siblings, pet dog ownership, or maternal allergy.
“This study is helpful because in addition to blood and skin tests, it also used food challenge, which is the gold standard,” Terri Brown-Whitehorn, MD, an attending physician in the division of allergy and immunology at Children’s Hospital of Philadelphia, said in an interview. “If no actual food is given, the other tests could lead to false positives.”
Dr. Brown-Whitehorn, who was not involved in the MCRI research, said the findings are not likely to affect most decisions about C-sections because most are not voluntary. “But if a mother had a first baby by emergency cesarean section, she might be given the option of having the next one by the same method.”
She said the current advice is to introduce even high-risk foods to a child’s diet early on to ward off the development of food allergies.
According to the microbial exposure hypothesis, it was previously thought that a potential link between cesarean birth and allergy might reflect differences in early exposure to maternal flora beneficial to the immune system in the vagina during delivery. A C-section might bypass the opportunity for neonatal gut colonization with maternal gut and vaginal flora, thereby raising allergy risk. A 2018 meta-analysis, for example, suggested cesarean birth could raise the risk for food allergies by 21%.
In other research from HealthNuts, 30% of child peanut allergy and 90% of egg allergy appear to resolve naturally by age 6. These numbers are somewhat higher than what Dr. Brown-Whitehorn sees. “We find that about 20% of peanut allergies and about 70% or 80% – maybe a bit less – of egg allergies resolve by age 6.”
This research was supported by the National Health & Medical Research Council of Australia, the Ilhan Food Allergy Foundation, AnaphylaxiStop, the Charles and Sylvia Viertel Medical Research Foundation, the Victorian Government’s Operational Infrastructure Support Program, and the Melbourne Children’s Clinician-Scientist Fellowship.
Dr. Peters disclosed no competing interests. Several coauthors reported research support or employment with private companies and one is the inventor of an MCRI-held patent. Dr. Brown-Whitehorn had no competing interests to disclose.
FROM JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY
NAVIGATOR steers uncontrolled asthma toward calmer seas
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.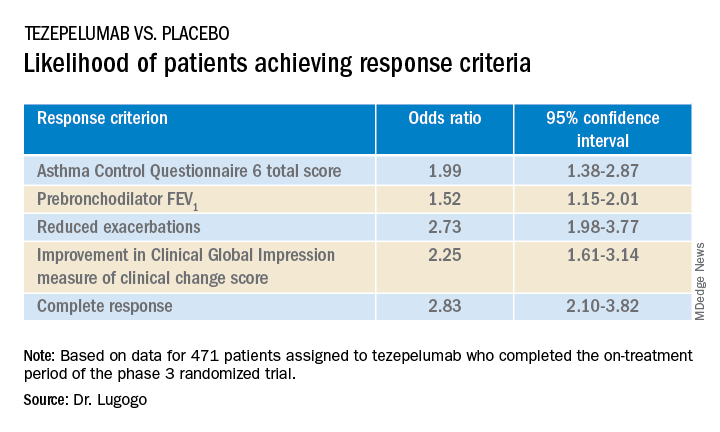
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
SAN FRANCISCO – Nearly half of all patients with severe, uncontrolled asthma who received a full course of the biologic agent tezepelumab (Tezspire) in the NAVIGATOR trial had a complete response to treatment at 1 year, results of a prespecified exploratory analysis indicated.
Among 471 patients assigned to tezepelumab who completed the on-treatment period of the phase 3 randomized trial, 46% had a complete response at 52 weeks, compared with 24% of patients assigned to placebo.
Complete response was defined as reduction in exacerbations of at least 50% over the previous year, improvement from baseline in Asthma Control Questionnaire 6 (ACQ-6) total score of at least 0.5 points, improvement in prebronchodilator forced expiratory volume in 1 second (pre-BD FEV1), and physician-assessed Clinical Global Impression measure of clinical change (CGI-C) score.
“These data further support the efficacy of tezepelumab in a broad population of patients with severe, uncontrolled asthma,” said Njira Lugogo, MD, of the division of pulmonary and critical care medicine at the University of Michigan, Ann Arbor.
Dr. Lugogo presented results of the exploratory analysis at the American Thoracic Society’s international conference.
Exacerbations reduced, lung function improved
Primary results from NAVIGATOR, published in The New England Journal of Medicine, showed that patients with severe, uncontrolled asthma randomly assigned to tezepelumab had fewer exacerbations and better lung function, asthma control, and health-related quality of life compared with patients assigned to placebo.
The investigators noted that approximately 10% of patients with asthma have symptoms and exacerbations despite maximal standard-of-care controller therapy.
Tezepelumab is a human monoclonal antibody that inhibits action of thymic stromal lymphopoietin (TSLP), an epithelial cytokine that is released in response to airborne triggers of asthma. TSLP is a major contributor to initiation and persistence of airway inflammation, Dr. Lugogo said.
The on-treatment analysis looked at all patients in the trial who completed 52 weeks of treatment and had complete data for all criteria studied.
The odds ratios (OR) for patients on tezepelumab achieving each of the response criteria are shown in the table.
Exacerbations explored
In a separate presentation, Christopher S. Ambrose, MD, MBA, of AstraZeneca in Gaithersburg, Md., presented information from investigator-narrative descriptions of all hospitalization events related to asthma exacerbations (mild, moderate, or severe) that occurred while the investigator was blinded to each patient’s treatment assignment in NAVIGATOR.
In all, 39 of 531 patients (7.3%) assigned to placebo had a total of 78 exacerbations requiring hospitalization, compared with 13 of 528 patients (2.5%) assigned to tezepelumab. The latter group had a total of 14 exacerbations requiring hospitalization during the study.
Among hospitalized patients, 32 of the 39 assigned to placebo had severe, incapacitating exacerbations, compared with 5 of 13 assigned to tezepelumab.
Reported symptoms were generally similar between hospitalized patients in the two treatment groups, although there appeared to be trends toward lower incidence of dyspnea, fever, and tachycardia with tezepelumab.
Health care resource utilization, a surrogate marker for disease burden, was substantially lower for patients assigned to tezepelumab.
Infections were the most common triggers of exacerbations in both groups.
“These data provide further evidence that tezepelumab can reduce the burden of disease of severe uncontrolled asthma, both to patients and to health care systems,” Dr. Ambrose said.
Head-to-head studies needed
Although there have been no head-to-head comparisons of biologic agents for asthma to date, results of these studies suggest that tezepelumab has efficacy similar to that of other agents for reducing exacerbation, said Fernando Holguin, MD, MPH, from the University of Colorado at Denver, Aurora, who comoderated the oral session where the data were presented but was not involved in the study.
Biologic agents appear to be slightly more effective against type 2 inflammation in asthma, “but in general I think we give it to a broader severe population, so that’s exciting,” he told this news organization.
Comoderator Amisha Barochia, MBBS, MHS, of the National Institutes of Health, Bethesda, Md., told this news organization that head-to-head trials of biologic agents would provide important clinical information going forward.
“Should we switch to a different biologic or add a second biologic? Those are questions we need answers for,” she said.
The NAVIGATOR trial is funded by AstraZeneca and Amgen. Dr. Lugogo disclosed financial relationships with both companies. Dr. Holguin and Dr. Barochia have disclosed no financial relationships relevant to the studies presented.
A version of this article first appeared on Medscape.com.
AT ATS 2022
More evidence links asthma severity to age of onset
A recently published multinational cohort study may be the largest to date that’s found the age of asthma onset is an integral factor in defining the severity of disease and the frequency of comorbidities.
“It’s very simple to ask your patient: ‘Did you have asthma as a child? When did your asthma start?’ ” coauthor Guy Brusselle, MD, a professor at the University of Ghent (Belgium), said in an interview. “You do not need expensive investigations, CT scans or proteomics or genomics; just two simple questions.”
The retrospective cohort study, published in the Journal of Allergy and Clinical Immunology: In Practice, combined national electronic health records databases from five different countries – the United Kingdom, Spain, Italy, the Netherlands, and Denmark – that included 586,436 adult asthma patients. The study divided the patients into three subtypes: childhood-onset asthma, meaning a diagnosis before age 18 (n = 81,691); adult-onset disease, defined as a diagnosis between ages 18 and 40 (n = 218,184); and late onset, defined as a diagnosis made after age 40 (n = 286,561).
Dr. Brusselle said the study found stark differences in characteristics between the three subtypes, including an increasing risk for women with later age of onset. Across the five databases, females comprised approximately 45% of those with childhood-onset asthma, but about 60% of those with later-onset disease, Dr. Brusselle said.
As for characteristics of asthma, 7.2% of the cohort (n = 42,611) had severe asthma, but the proportion was highest in late-onset asthma, 10% versus 5% in adult onset and 3% in childhood onset. The percentage of uncontrolled asthma followed a similar trend: 8%, 6%, and 0.4% in the respective treatment groups.
The most common comorbidities were atopic disorders (31%) and overweight/obesity (50%). The prevalence of atopic disorders was highest in the childhood-onset group, 45% versus 35%, and 25% in the adult-onset and late-onset patients. However, the trend for overweight/obesity was reversed: 30%, 43%, and 61%, respectively.
“The larger differences were when late-onset asthma was compared to adult-onset asthma with respect to comorbidities,” Dr. Brusselle said. “The late-onset asthma patients more frequently had nasal polyposis.” These patients typically lose their sense of smell, as in COVID-19. However, in nasal polyposis the loss is chronic rather than transient.
Pulmonologists should be attuned to the prevalence of overweight/obesity in the late-onset group, Dr. Brusselle said. “We know that obesity is an important risk factor for diabetes, and then obesity is also associated with gastroesophageal reflux – and we know that gastroesophageal reflux is a risk factor for asthma exacerbations.”
Smaller studies have arrived at the same conclusions regarding the relationships between asthma severity and age of onset, Dr. Brusselle said. What’s notable about this study is its size and the consistency of findings across different national databases.
“In childhood onset you need to watch for different allergies – atopic dermatitis and allergic rhinitis – but in late-onset asthma look for obesity, diabetes and reflux disease, and nasal polyposis,” he said.
Sally E. Wenzel, MD, professor at the University of Pittsburgh and director of the Asthma and Environmental Lung Health Institute at the University of Pittsburgh Medical Center, concurred that the size of this study makes it noteworthy.
“It’s certainly far and away the largest study of its kind that’s ever been done, and it’s multinational,” she said in an interview. “Just doing a study like this with thousands and thousands of patients is a step in the right direction. That’s probably what’s very unique about it, to bring all of these clinical cohorts as it were together and to look at what is the relationship of the age of onset.”
She also said the study is unique in how it delineates the groups by age of onset.
“In addition to this concept that there’s a difference in asthma by the age that you got diagnosed with it, I think it’s also important to just remember that when any physician, be they a specialist or nonspecialist, sees a patient with asthma, they should ask them when did their symptoms develop,” she said. “These are really simple questions that don’t take any sophisticated training and don’t take any sophisticated instruments to measure, but they can be really helpful.”
GlaxoSmithKline supplied a grant for the study. Dr. Brusselle disclosed relationships with AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Novartis, Sanofi, and Teva. A study coauthor is an employee of GSK. Dr. Wenzel reported no disclosures.
A version of this article first appeared on Medscape.com.
A recently published multinational cohort study may be the largest to date that’s found the age of asthma onset is an integral factor in defining the severity of disease and the frequency of comorbidities.
“It’s very simple to ask your patient: ‘Did you have asthma as a child? When did your asthma start?’ ” coauthor Guy Brusselle, MD, a professor at the University of Ghent (Belgium), said in an interview. “You do not need expensive investigations, CT scans or proteomics or genomics; just two simple questions.”
The retrospective cohort study, published in the Journal of Allergy and Clinical Immunology: In Practice, combined national electronic health records databases from five different countries – the United Kingdom, Spain, Italy, the Netherlands, and Denmark – that included 586,436 adult asthma patients. The study divided the patients into three subtypes: childhood-onset asthma, meaning a diagnosis before age 18 (n = 81,691); adult-onset disease, defined as a diagnosis between ages 18 and 40 (n = 218,184); and late onset, defined as a diagnosis made after age 40 (n = 286,561).
Dr. Brusselle said the study found stark differences in characteristics between the three subtypes, including an increasing risk for women with later age of onset. Across the five databases, females comprised approximately 45% of those with childhood-onset asthma, but about 60% of those with later-onset disease, Dr. Brusselle said.
As for characteristics of asthma, 7.2% of the cohort (n = 42,611) had severe asthma, but the proportion was highest in late-onset asthma, 10% versus 5% in adult onset and 3% in childhood onset. The percentage of uncontrolled asthma followed a similar trend: 8%, 6%, and 0.4% in the respective treatment groups.
The most common comorbidities were atopic disorders (31%) and overweight/obesity (50%). The prevalence of atopic disorders was highest in the childhood-onset group, 45% versus 35%, and 25% in the adult-onset and late-onset patients. However, the trend for overweight/obesity was reversed: 30%, 43%, and 61%, respectively.
“The larger differences were when late-onset asthma was compared to adult-onset asthma with respect to comorbidities,” Dr. Brusselle said. “The late-onset asthma patients more frequently had nasal polyposis.” These patients typically lose their sense of smell, as in COVID-19. However, in nasal polyposis the loss is chronic rather than transient.
Pulmonologists should be attuned to the prevalence of overweight/obesity in the late-onset group, Dr. Brusselle said. “We know that obesity is an important risk factor for diabetes, and then obesity is also associated with gastroesophageal reflux – and we know that gastroesophageal reflux is a risk factor for asthma exacerbations.”
Smaller studies have arrived at the same conclusions regarding the relationships between asthma severity and age of onset, Dr. Brusselle said. What’s notable about this study is its size and the consistency of findings across different national databases.
“In childhood onset you need to watch for different allergies – atopic dermatitis and allergic rhinitis – but in late-onset asthma look for obesity, diabetes and reflux disease, and nasal polyposis,” he said.
Sally E. Wenzel, MD, professor at the University of Pittsburgh and director of the Asthma and Environmental Lung Health Institute at the University of Pittsburgh Medical Center, concurred that the size of this study makes it noteworthy.
“It’s certainly far and away the largest study of its kind that’s ever been done, and it’s multinational,” she said in an interview. “Just doing a study like this with thousands and thousands of patients is a step in the right direction. That’s probably what’s very unique about it, to bring all of these clinical cohorts as it were together and to look at what is the relationship of the age of onset.”
She also said the study is unique in how it delineates the groups by age of onset.
“In addition to this concept that there’s a difference in asthma by the age that you got diagnosed with it, I think it’s also important to just remember that when any physician, be they a specialist or nonspecialist, sees a patient with asthma, they should ask them when did their symptoms develop,” she said. “These are really simple questions that don’t take any sophisticated training and don’t take any sophisticated instruments to measure, but they can be really helpful.”
GlaxoSmithKline supplied a grant for the study. Dr. Brusselle disclosed relationships with AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Novartis, Sanofi, and Teva. A study coauthor is an employee of GSK. Dr. Wenzel reported no disclosures.
A version of this article first appeared on Medscape.com.
A recently published multinational cohort study may be the largest to date that’s found the age of asthma onset is an integral factor in defining the severity of disease and the frequency of comorbidities.
“It’s very simple to ask your patient: ‘Did you have asthma as a child? When did your asthma start?’ ” coauthor Guy Brusselle, MD, a professor at the University of Ghent (Belgium), said in an interview. “You do not need expensive investigations, CT scans or proteomics or genomics; just two simple questions.”
The retrospective cohort study, published in the Journal of Allergy and Clinical Immunology: In Practice, combined national electronic health records databases from five different countries – the United Kingdom, Spain, Italy, the Netherlands, and Denmark – that included 586,436 adult asthma patients. The study divided the patients into three subtypes: childhood-onset asthma, meaning a diagnosis before age 18 (n = 81,691); adult-onset disease, defined as a diagnosis between ages 18 and 40 (n = 218,184); and late onset, defined as a diagnosis made after age 40 (n = 286,561).
Dr. Brusselle said the study found stark differences in characteristics between the three subtypes, including an increasing risk for women with later age of onset. Across the five databases, females comprised approximately 45% of those with childhood-onset asthma, but about 60% of those with later-onset disease, Dr. Brusselle said.
As for characteristics of asthma, 7.2% of the cohort (n = 42,611) had severe asthma, but the proportion was highest in late-onset asthma, 10% versus 5% in adult onset and 3% in childhood onset. The percentage of uncontrolled asthma followed a similar trend: 8%, 6%, and 0.4% in the respective treatment groups.
The most common comorbidities were atopic disorders (31%) and overweight/obesity (50%). The prevalence of atopic disorders was highest in the childhood-onset group, 45% versus 35%, and 25% in the adult-onset and late-onset patients. However, the trend for overweight/obesity was reversed: 30%, 43%, and 61%, respectively.
“The larger differences were when late-onset asthma was compared to adult-onset asthma with respect to comorbidities,” Dr. Brusselle said. “The late-onset asthma patients more frequently had nasal polyposis.” These patients typically lose their sense of smell, as in COVID-19. However, in nasal polyposis the loss is chronic rather than transient.
Pulmonologists should be attuned to the prevalence of overweight/obesity in the late-onset group, Dr. Brusselle said. “We know that obesity is an important risk factor for diabetes, and then obesity is also associated with gastroesophageal reflux – and we know that gastroesophageal reflux is a risk factor for asthma exacerbations.”
Smaller studies have arrived at the same conclusions regarding the relationships between asthma severity and age of onset, Dr. Brusselle said. What’s notable about this study is its size and the consistency of findings across different national databases.
“In childhood onset you need to watch for different allergies – atopic dermatitis and allergic rhinitis – but in late-onset asthma look for obesity, diabetes and reflux disease, and nasal polyposis,” he said.
Sally E. Wenzel, MD, professor at the University of Pittsburgh and director of the Asthma and Environmental Lung Health Institute at the University of Pittsburgh Medical Center, concurred that the size of this study makes it noteworthy.
“It’s certainly far and away the largest study of its kind that’s ever been done, and it’s multinational,” she said in an interview. “Just doing a study like this with thousands and thousands of patients is a step in the right direction. That’s probably what’s very unique about it, to bring all of these clinical cohorts as it were together and to look at what is the relationship of the age of onset.”
She also said the study is unique in how it delineates the groups by age of onset.
“In addition to this concept that there’s a difference in asthma by the age that you got diagnosed with it, I think it’s also important to just remember that when any physician, be they a specialist or nonspecialist, sees a patient with asthma, they should ask them when did their symptoms develop,” she said. “These are really simple questions that don’t take any sophisticated training and don’t take any sophisticated instruments to measure, but they can be really helpful.”
GlaxoSmithKline supplied a grant for the study. Dr. Brusselle disclosed relationships with AstraZeneca, Boehringer Ingelheim, Chiesi, GSK, Novartis, Sanofi, and Teva. A study coauthor is an employee of GSK. Dr. Wenzel reported no disclosures.
A version of this article first appeared on Medscape.com.
FROM THE JOURNAL OF ALLERGY AND CLINICAL IMMUNOLOGY: IN PRACTICE